CADTH Reimbursement Review
Lutetium (177Lu) oxodotreotide (Lutathera)
Sponsor: Advanced Accelerator Applications
Therapeutic area: Gastroenteropancreatic neuroendocrine tumours
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
177Lu
lutetium-177
68Ga
gallium-68
AAA
Advanced Accelerator Applications
AE
adverse event
AMSMNQ
Association des médecins spécialistes en médecine nucléaire du Québec
BOR
best overall response
CANM
Canadian Association of Nuclear Medicine
CHU
Centre hospitalier universitaire
CI
confidence interval
CNETS
Canadian Neuroendocrine Tumour Society
CTCAE
Common Terminology Criteria for Adverse Events
CUP
Compassionate Use Program
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ
European Organisation for Research and Treatment of Cancer – Quality of Life questionnaire
ESS
effective sample size
FAS
full analysis set
GEPNET
gastroenteropancreatic neuroendocrine tumour
GI
gastrointestinal
HRQoL
health-related quality of life
ITC
indirect treatment comparison
LAR
long-acting release
LOCF
last observation carried forward
MAIC
matching-adjusted indirect comparison
MDS
myelodysplastic syndrome
mFAS
modified full analysis set
NCI
National Cancer Institute
NET
neuroendocrine tumour
OH-CCO
Ontario Health Cancer Care Ontario
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
PKI
protein kinase inhibitor
pNET
pancreatic neuroendocrine tumours
PRRT
peptide receptor radionuclide therapy
RECIST
Response Evaluation Criteria in Solid Tumors
SAE
serious adverse event
SAS
safety analysis set
SD
standard deviation
SMAB
Scientific and Medical Advisory Board
SSA
somatostatin analogue
SSR
somatostatin receptor
TEAE
treatment-emergent adverse event
TKI
tyrosine kinase inhibitor
TTP
time to tumour progression
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Lutetium oxodotreotide |
|---|---|
Drug product | Lutetium oxodotreotide (Lutathera), 370 MBq/mL at calibration, sterile solution for IV infusion |
Indication | Lutathera is indicated for the treatment of unresectable or metastatic, well-differentiated, SSR-positive GEPNETs in adults with progressive disease |
Reimbursement request | For the treatment of unresectable or metastatic, well-differentiated, SSR-positive pancreatic NETs (pNETs) in adults whose disease has progressed after treatment with an SSA, unless there is a contraindication or intolerance |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | January 9, 2019 |
Sponsor | As per application overview |
GEP = gastroenteropancreatic; NET = neuroendocrine tumour; NOC = Notice of Compliance; SSA = somatostatin analogue; SSR = somatostatin receptor.
Introduction
Neuroendocrine tumours (NETs) are a heterogenous group of cancers that arise from the secretory cells of the diffuse neuroendocrine system.1 Pancreatic neuroendocrine tumours (pNETs) are a subset of gastroenteropancreatic (GEP) NETs (GEPNETs). Somatostatin receptors (SSRs) are expressed in the majority (> 80%) of well-differentiated NETs.2 GEPNETs are the second most prevalent type of digestive cancer.1 The annual incidence of pNETs is less than 1 per 100,000 persons.3 Compared to other types of NETs, pNETs have a worse prognosis, typically resulting in less than 5 years’ survival.3 Due to the heterogenous nature of pNETs, patients may not follow the same disease trajectory. Diagnosis of pNETs is typically through biopsy. Staging of disease is typically conducted using imaging — usually CT or MRI scans, although gallium PET scans are becoming a more standard form of imaging for this group of patients.
For localized solid tumours, surgery is typically the initial treatment option. For patients with metastatic disease, systemic drug therapies are used, although surgery can play a role as well. Somatostatin analogues (SSAs) are the usual first-line therapy for patients with unresectable metastatic disease or with hormonal overproduction syndromes. SSAs that patients may receive include octreotide and lanreotide. For patients who have progressed while receiving SSAs, treatment options include everolimus, sunitinib, and capecitabine plus temozolomide. The clinical experts consulted by CADTH for this review stated that currently available treatment options for patients with pNETs are palliative in nature. They may increase the length and the quality of life; however, patients are expected to eventually progress on these therapies. The clinical experts also identified surgery, radiofrequency ablation, and liver embolization therapy for patients with liver-dominant metastatic pNETs. Radiolabelled SSAs have also been developed for SSR-positive well-differentiated NETs that have progressed after first-line therapy with SSAs; this type of therapy is part of a group of treatments called peptide receptor radionuclide therapy (PRRT).2 The clinical experts consulted by CADTH for this review stated that the choice between PRRT and other therapies is not necessarily difficult, although it is not guided by strong evidence. PRRT is better tolerated than currently available options. In addition, the dosing schedule of PRRT is preferred by patients because it involves only 4 sessions, compared to higher numbers of sessions for other options; sessions result in fatigue and loss of appetite. While PRRT is not funded for patients with pNETs in most of Canada, it is funded in Quebec, which introduces issues of inequity among patients in Canada with pNETs.
Lutetium-177 (177Lu) oxodotreotide is a radiolabelled SSA that binds to SSRs. 177Lu oxodotreotide is administered intravenously at a recommended dose of 7.4 GBq (200 mCi) over 30 minutes every 8 weeks, for a total of 4 doses. 177Lu oxodotreotide is administered alongside octreotide long-acting release (LAR), which continues monthly for up to 18 months. 177Lu oxodotreotide received a Notice of Compliance from Health Canada on January 9, 2019. The indication approved by Health Canada is for the treatment of unresectable or metastatic, well-differentiated, SSR-positive GEPNETs in adults with progressive disease. CADTH reviewed this Health Canada–approved indication in 2019 and the CADTH pan-Canadian Oncology Drug Review Expert Review Committee (pERC) provided a positive recommendation for patients with SSR-positive midgut NETs whose disease had progressed on an SSA and was unresectable; however, the recommendation did not support treatment for patients with SSR-positive foregut and hindgut NETs whose disease had progressed and was unresectable. The previous CADTH review for 177Lu oxodotreotide did not support use among patients with pNETs, as these patients were excluded from the pivotal NETTER-1 trial. The sponsor’s reimbursement request for this current CADTH reassessment is for adult patients with unresectable or metastatic, well-differentiated, SSR-positive pNET tumours whose disease has progressed after treatment with an SSA, unless there is a contraindication or intolerance.
The objective of this review is to perform a systematic review of the beneficial and harmful effects of 177Lu oxodotreotide at 7.4 GBq (200 mCi) as an IV infusion over 30 minutes every 8 weeks, for a total of 4 doses, for the treatment of unresectable or metastatic, well-differentiated, SSR-positive pNETs in adults whose disease has progressed after treatment with an SSA, unless there is a contraindication or intolerance.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
CADTH received 1 submission from the Canadian Neuroendocrine Tumour Society (CNETS) for the review of 177Lu oxodotreotide for patients with GEPNETs. The information used to inform the submission was based on an online questionnaire that was promoted on the CNETS website and across its social media platforms from February 25 to March 25, 2022, to patients with neuroendocrine cancer. A total of 57 patients responded to the survey, including 21 (37%) patients with pNETs and 36 (63%) patients with gastrointestinal (GI)-NETs; 33 (58%) patients reported having experience with 177Lu oxodotreotide.
Survey respondents reported that their NET cancer negatively affected their quality of life. Symptoms of fatigue, weakness, and diarrhea had an extremely high impact on quality of life. The most commonly used therapies for the management of NET cancer reported by respondents were SSA therapies, surgery, and PRRT. Respondents indicated that benefits of currently available treatments included temporarily slowing the progression of the disease and achieving symptom control, while the challenges were long recovery times, debilitating side effects, and complications. None of the respondents reported that current treatments had cured or stopped the progression of their NET cancer. Respondents described current treatments as effective for control of symptoms (e.g., bloating, diarrhea, constipation, and energy levels), and as slightly effective or ineffective for stopping disease progression, shrinking or stopping tumour growth, or preventing metastasis. According to respondents, common barriers to access included lack of private-payer coverage, personal financial difficulties, inaccessibility through their physician, or lack of funding for their specific type of NET cancer.
All 33 respondents with experience with 177Lu oxodotreotide agreed that its side effects were tolerable or manageable and the treatment experience was easier than the lengthy recovery from surgery or the debilitating side effects from chemotherapy. The most commonly reported benefits of 177Lu oxodotreotide included reduced progression of disease (69%), tumour shrinkage (59%), and decrease in disease symptoms (45%), while the most commonly reported side effects were increased fatigue (58%), and nausea and vomiting (27%).
The majority (98%) of respondents indicated that disease progression is the most important outcome of NET cancer to control, followed by fatigue (36%), diarrhea (35%), and flushing (29%). Overall, patients reported a need for equitable access to 177Lu oxodotreotide for NET cancer to overcome challenges, including the lack of funding for their type of NETs and the need to travel long distances to access treatment.
Clinician Input
Input from Clinical Experts Consulted by CADTH
CADTH gathered input from 2 clinical specialists with expertise in the diagnosis and management of pNETs. The clinical experts highlighted an unmet need for treatments that extend patient’s lives and improve their quality of life. As patients eventually become refractory to all currently available treatment options, the clinical experts stated that sequencing of 177Lu oxodotreotide would be individualized to each patient’s circumstance. In most instances, patients should have progressed on SSAs before receiving 177Lu oxodotreotide. The clinical experts stated that identifying patients eligible for 177Lu oxodotreotide will require gallium PET scans. They specified that eligibility should not be based on strict criteria for Ki-67 index, as there is too much variability in Ki-67 among different specimens from the same patient. In addition, there is subjectivity in interpreting the specimens, which can result in variability in determining eligibility based on Ki-67. The patient’s response to therapy can be assessed through clinical assessment, radiographic information, and analysis of biomarkers (i.e., 5-hydroxyindoleacetic acid). They advised that clinical assessments be conducted every few months initially and before every cycle of PRRT, and that radiographic assessments be conducted every 3 to 6 months initially, depending on the clinical needs of the patient. Discontinuation of therapy is based on serious toxicities, including permanent renal toxicities and bone marrow toxicity (e.g., myelodysplastic syndrome [MDS]), and disease progression. Administration of 177Lu oxodotreotide requires referral to a tertiary centre with dedicated nuclear medicine and/or radiation oncology.
Clinician Group Input
Seven clinician groups provided input to CADTH for the review of 177Lu oxodotreotide. These included:
2 clinicians from the Ontario Health Cancer Care Ontario (OH-CCO) Gastrointestinal Cancer Drug Advisory Committee
1 clinician from the Canadian Association of Nuclear Medicine (CANM)
9 clinicians from the CNETS Scientific and Medical Advisory Board (SMAB)
1 clinician from the Centre hospitalier universitaire (CHU) de Québec, Université Laval Research Centre — Oncology Axis; the Hôtel-Dieu de Québec — Nuclear Medicine Department; the Fondation du CHU de Québec — Research Chair in Theranostics; and the Association des médecins spécialistes en médecine nucléaire du Québec (AMSMNQ).
The clinician groups identified the following unmet needs in patients with NETs, including pNETs: currently available treatments are not effective for all patients, are not well tolerated, and can lead to the development of resistance; also, disease can become refractory to current treatments. Further, the clinician groups expressed the need for treatments to slow the progression of the disease, control hormonal symptoms, and improve progression-free survival (PFS).
Clinicians from CANM; CNETS SMAB; CHU de Québec, Université Laval Research Centre — Oncology Axis; the Hôtel-Dieu de Québec — Nuclear Medicine Department; the Fondation du CHU de Québec — Research Chair in Theranostics; and AMSMNQ indicated that Lutathera should be second-line treatment for patients with NETs, including pNETs, who have progressed on a somatostatin analogue. In contrast, OH-CCO indicated Lutathera should be a fourth-line treatment option following SSAs, everolimus, and sunitinib.
Drug Program Input
The drug programs identified the following jurisdictional implementation issues: relevant comparators, considerations for initiation of therapy, considerations for discontinuation of therapy, considerations for prescribing of therapy, funding algorithm, care provision issues, and system and economic issues. The clinical experts consulted by CADTH weighed evidence from the key study submitted by the sponsor and clinical expertise to provide responses to the drug program implementation questions (Table 4).
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The NETTER-R study was a non-interventional, non-comparative, post-authorization retrospective registry study to assess long-term efficacy and safety of treatment with 177Lu oxodotreotide in patients with SSR-positive pNETs who had unresectable or metastatic, progressive disease based on radiological, biochemical, or clinical assessment. The approximate number of patients to be enrolled was based on the number of potentially eligible patients included in the compassionate use program (CUP) and those identified by investigators who were receiving commercial 177Lu oxodotreotide at the selected study sites. To be included in the study, patients must have been treated with 177Lu oxodotreotide either through the Advanced Accelerator Applications (AAA) Lutathera CUP, which was approved in 10 European countries since 2011 to 2012, or with a commercial drug. The study included 110 patients from Spain, France, and the UK who met the pre-specified criteria for inclusion. Most of the patients with pNETs who received treatment in this study were part of the CUP in 1 of the European Neuroendocrine Tumor Society Centers participating in this program. The retrospective data collection from medical records began on October 31, 2018, at the first study site. Data were tentatively collected at follow-up visits every 3 months, depending on the standard care in local practice and source document availability at the sites. The primary objective of the NETTER-R study was to determine the efficacy of 177Lu oxodotreotide in patients with pNET according to a set of pre-specified eligibility criteria. The secondary objective of the study was to determine the safety and tolerability of 177Lu oxodotreotide.4 All inclusion criteria and none of the exclusion criteria had to be met in order for patients to be eligible for the NETTER-R study. Eligibility criteria included patients with SSR-positive, unresectable or metastatic, well-differentiated pNETs with progressive disease who had been treated with 177Lu oxodotreotide. Patients were not eligible if they were diagnosed with NETs of other origins.5
Patients in the NETTER-R study had a mean age of 58 years (||||||||; range, 28.0 to 89.0 years). Relatively equal proportions of male (53%) and female (47%) patients were enrolled. |||| of patients were white (||||). The primary sites of metastases before patients started treatment with 177Lu oxodotreotide were the liver (96%), lymph nodes (43%), bone (29%), and lungs (4%). The liver tumour burden was 10% to 25% in 29% of patients, and more than 25% or more than 2 metastatic organs in 36% of patients. More than half of patients had nonfunctional tumours (57%), 30% of patients had functional tumour status, and the remainder lacked an assessment of tumour functionality (11%). Most patients had a Ki-67 index of 3% to 20% (66%), while 24% had a Ki-67 index of 2% or less. Most patients had a histopathological intermediate (grade 2; 65%) or low (grade 1; 27%) grade of disease.6 Many patients received an octreotide scan (||||) or a gallium-68 (68Ga) PET scan (||||). Of patients with Eastern Cooperative Oncology Group Performance Status (ECOG PS) assessed, most patients had an ECOG PS of 0 (||||) or 1 (||||).5 Most patients had received prior anticancer treatments (92%) and had received a mean 4.7 prior or concomitant therapies. Of patients, 91% had received prior anticancer therapy for NET disease; patients mostly received chemotherapy (||||), radiotherapy (||||), or other therapies (91%).5 Seventy percent had received prior somatostatins and analogues, mainly lanreotide or octreotide (||| ||||). Thirty-eight percent had received prior tyrosine kinase inhibitors (TKIs), mainly everolimus (33%) or sunitinib (20%). Just more than |||| of patients (||||) had received prior surgical and medical procedures; patients most commonly underwent pancreatic operation (||||), followed by liver operation (||||) and radiotherapy (||||).
Efficacy Results
Overall Survival
A median follow-up time of 24.5 months was reported. There were 55 patients (50%) who experienced an overall survival (OS) event (i.e., death due to any cause) in the NETTER-R study. The median OS was 41.4 months (95% confidence interval [CI], 28.6 to 50.2). Half of all patients were censored for the analysis of OS.
Progression-Free Survival
Results for the primary end point of PFS were based on Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. In the primary analysis of PFS, there were 41 PFS events (66%), of which most were progression (||||), and |||| were deaths (||||). The median PFS was 24.8 months (95% CI, 17.5 to 34.5). PFS was also assessed using the RECIST version 1.1 criteria, based on investigator’s opinion as a secondary end point. PFS based on investigator’s opinion 1 was based on tumour assessments and other radiological assessments. PFS based on investigator’s opinion 2 was based on other radiological, clinical, biomarker, and metabolic assessments. The additional analyses of PFS were consistent with the primary analysis of PFS.
Objective Response Rate
Objective response rate (ORR), based on the primary analysis, was assessed in 62 patients. The ORR was 40.3% (95% CI, 28.1 to 53.6). None of the patients had a complete response, according to RECIST version 1.1 criteria. Partial response was reported in 40.3% of patients. Stable disease and progressive disease were reported for 35.5% and 21.0% of patients, respectively. Results for ORR based on investigators’ opinion 1 and 2 were consistent with the primary analysis of ORR, although the response was slightly better for ORR assessed by investigator’s opinion 2.
Duration of Response
The median duration of response (DOR) was 60.7 months (95% CI, 13.1 to 62.1). At the time of the analysis, there were 8 PFS events observed. The DOR based on investigator’s opinion 1 and 2 were both shorter than the primary analysis of DOR. The median DOR based on investigator’s opinion 1 was 31.1 months (95% CI, 16.8 to 62.1) with |||| PFS events, while the DOR based on investigator’s opinion 2 was 28.3 months (95% CI, 16.8 to 60.7) with |||| PFS events.
Time to Tumour Progression
There was a total of |||| (||||) time to tumour progression (TTP) events, with a median TTP of 29.5 months (95% CI, 21.4 to 67.6; Figure 9). As with PFS, TTP was assessed based on investigator’s opinion 1 and 2, the results of which were both consistent with the primary analysis of TTP.
Health-Related Quality of Life
|||||| ||| |||||| ||||||||||||| |||||||||||||| | ||||| || || |||||||| ||||||||| ||| ||||||| ||||||||| ||||||||||||| |||| || |||||||||||| ||||||||| ||||||||| ||||||||| || ||||| ||||||||| ||| |||||| ||| ||||| |||||| || |||||||| || |||||||||| ||| ||| |||| ||||||| || ||| |||| || ||||| |||| ||| |||| || ||||||| |||| |||| ||||||||| |||||| |||||||| ||||| |||||||| || |||||| |||||||||||||| |||| ||||| || |||||||| |||| ||||| || ||| ||||| |||||||||| ||| ||||||| ||||||| || ||| |||||||| |||| |||||||||| |||| ||||| |||| ||||||| |||| || ||||||||| | ||||| || || |||||||| ||||||| |||||||| |||||| |||||||| ||||||||| |||| || |||||| ||| ||||| ||||||||| ||||||||| |||||||| || |||||||||||| ||||||| ||| |||||||| ||||| |||||||||||||| ||||||| ||| ||| |||||| ||| |||||||| ||| ||||||||||||| ||||| ||| || ||||||||||| || |||| |||| ||| ||||||||| |||| ||| |||| |||||||| || ||||||||| ||||| |||| ||||||| | ||| | |||||||| ||| |||||||| |||| ||| |||| ||||||||||||||||
Harms Results
Adverse Events
Adverse events (AEs) were reported in 79 patients (72%). The most common AEs included nausea (28%), fatigue (23%), abdominal pain (16%), vomiting (||||), upper abdominal pain (||||), anemia (||||), diarrhea, lymphopenia, and thrombocytopenia (||| ||||). Grade 3 or 4 AEs were reported in 30 patients (27%). The incidence of grade 3 or 4 AEs was generally infrequent, with each event occurring in less than 5% of patients. The most common grade 3 or 4 AEs were lymphopenia (||||), abdominal pain, ascites, hypercalcemia, and liver abscess (|| ||||).
Serious Adverse Events
Serious adverse events (SAEs) were reported in 29 patients (26%). SAEs were infrequently reported, occurring in less than 3% of patients. The most common SAEs were liver abscess, ascites, and hypercalcemia (|||| ||||).
Withdrawals Due to Adverse Events and Dose Modifications
There were no treatment-emergent AEs (TEAEs) that resulted in treatment discontinuation. TEAEs leading to dose modification were infrequent, occurring in 10 patients (9%). The most common TEAEs that led to dose modifications were lymphopenia and nausea (|| ||||).
Mortality
There was a total of ||||| deaths (|||) due to AEs in the NETTER-R study. The causes of death were reported to be abdominal abscess, hepatorenal syndrome and metabolic encephalopathy, hepatic encephalopathy, ascites, and lower respiratory tract infection and pulmonary embolism.
Notable Harms
Notable harms were detailed in the CADTH systematic review protocol and included myelotoxicity, renal toxicity, transformation to leukemia or MDS, nausea and/or vomiting, and fatigue.
Hematological toxicities were reported among || patients (|||). Hematological toxicities were mostly grade 1 or 2 (||||), with 5 patients with grade 3 events. Nausea and fatigue were the 2 most commonly reported AEs in the NETTER-R study, occurring in 31 patients (28%) and 25 patients (23%), respectively. Renal toxicity was infrequently reported among 6 patients (6%); of these, 3 patients had grade 1 or 2 events and 3 patients had grade 3 events. There were no reports of secondary hematological malignancies (acute leukemia or MDS) in any patient.
Table 2: Summary of Key Results From Pivotal and Protocol-Selected Studies
Result | 177Lu oxodotreotide |
|---|---|
Overall survival — FAS N = 110 | |
Number of events, n (%) | 55 (50.0) |
Number censored (alive at last contact), n (%) | 55 (50.0) |
Alive, n (%) | 51 (46.4) |
Lost to follow-up, n (%) | 4 (3.6) |
Median, months (95% CI)a | 41.4 (28.6 to 50.2) |
Progression-free survival — RECIST version 1.1 | |
Patients with post-baseline scan per RECIST version 1.1 in modified FAS N = 62 | |
Number of events, n (%) | 41 (66.1) |
Documented progression | || ||||||| |
Death | | ||||||| |
Number censored, n (%) | 21 (33.9) |
No post-baseline tumour assessments | 2 (3.2) |
No documented progression | 19 (30.6) |
Median, months (95% CI)a | 24.8 (17.5 to 34.5) |
Duration of response N = 8 | |
Median DOR, months (95% CI) | 60.7 (13.1 to 62.1) |
Objective response rate — RECIST version 1.1 | |
Patients with post-baseline scan per RECIST version 1.1 in modified FAS N = 62 | |
Objective response, n (%) (95% CI) | 25 (40.3) (28.1 to 53.6) |
Best overall response, n (%) | |
Best response | 62 |
Complete response | 0 |
Partial response | 25 (40.3) |
Stable disease | 22 (35.5) |
Progressive disease | 13 (21.0) |
Not evaluable | 2 (3.2) |
Time to progression — RECIST version 1.1 | |
Patients with post-baseline scan per RECIST 1.1 in modified FAS N = 62 | |
Number of events, n (%) | 32 (51.6) |
Documented progression | 32 (51.6) |
Number censored, n (%) | 30 (48.4) |
No post-baseline tumour assessments | 2 (3.2) |
No documented progression | 19 (30.6) |
Death without documented PD | 9 (14.5) |
Median, months (95% CI) | 29.5 (21.4 to 67.6) |
Harms, n (%) (safety analysis set) N = 110 | |
AEs | 79 (71.8) |
Patients with any grade 3 or 4 AE | 30 (27.2) |
SAEs | 29 (26.4) |
AEs leading to dose modifications | 10 (9.1) |
AEs leading to treatment discontinuation | 0 |
Deaths | | |||||| |
Notable harms | |
Hematological toxicity | || ||||||| |
Renal toxicity | 6 (5.5) |
Transformation to leukemia, MDS | 0 |
Nausea and/or vomiting | 31 (28.2) |
Fatigue | 25 (22.7) |
Renal toxicity | 6 (5.5) |
AE = adverse event; CI = confidence interval; DOR = duration of response; FAS = full analysis set; MDS = myelodysplastic syndrome; PD = progressive disease; RECIST = Response Evaluation Criteria in Solid Tumors; SAE = serious adverse event.
aEstimated by the Kaplan-Meier method.
Source: NETTER-R Clinical Study Report.5
Critical Appraisal
NETTER-R was a retrospective, non-comparative, registry-based, observational study. Without a comparison group, the safety and effectiveness of 177Lu oxodotreotide relative to currently available therapies is unknown. Moreover, due to lack of an adequate control group, the estimate of long-term efficacy was compromised. In particular, no causal inference could be made as to whether the treatment effect (e.g., changes on PFS or OS) could be completely attributable to 177Lu oxodotreotide or could be due to temporality changes in other factors, including concomitant therapies or natural course of disease. In a retrospective observational cohort study of drug effectiveness based on existing medical records, lack of a sound study design to make an adjustment or control of potential bias has been recognized as fatal limitation by various real-world evidence study guidance documents.
The CADTH team considered that the retrospective design of the NETTER-R study could have allowed for a matched comparator group of patients who had received relevant comparator therapies, such as everolimus or sunitinib. The clinical experts consulted by CADTH for this review agreed that a retrospective study with a matched analysis incorporating a comparator group would have improved the strength of evidence for this funding request for 177Lu oxodotreotide for treatment of pNETs. It was also acknowledged that a matched analysis would depend on whether such data were available.
There was a large amount of censoring for all efficacy analyses. For example, in the estimate of PFS, about 1-third of patients were censored at the date of their last evaluable tumour assessment if they had not experienced disease progression or if they had not died at the time of data collection, in the context of time-to-event analyses. Similarly, in the assessment of OS, half of the patients were censored on their last date of contact if they were still alive or if their status was unknown. The large amount of censoring (e.g., non-informative) for most efficacy outcomes (i.e., OS, PFS, DOR, TTP) would have resulted in biased estimates of the absolute changes over time, as illustrated by the Kaplan-Meier curves, on those efficacy outcomes and would have further introduced uncertainty concerning the true effect of 177Lu oxodotreotide on OS and progression of patients with pNETs.
The median follow-up time of the NETTER-R study was 24.5 months. The clinical experts consulted by CADTH for this review commented that, while no control group was part of the study, efficacy results for PFS and OS showed benefit to patients treated with 177Lu oxodotreotide. However, longer-term data may have benefited the study by providing evidence of the impact of treatment with 177Lu oxodotreotide over a longer period.
The NETTER-R study was conducted in Europe, with patients enrolled from the UK, France, and Spain. Consultation with clinical experts engaged by CADTH for this review suggested that eligibility criteria and baseline characteristics were generally representative of patients in Canada who might be treated in clinical practice, although centres in European countries may have more experience administering PRRT than those in Canada. The clinical experts commented that 1 patient in the NETTER-R study received dactolisib as a prior therapy, which is not approved by Health Canada and not used among patients in Canada. The impact of this is expected to be low. It was also noted that eligibility criteria of the NETTER-R study specified inclusion of patients with unresectable or metastatic pNETs. The clinical experts confirmed that inclusion of these patients would be unlikely to affect study outcomes. pNETs are a heterogeneous group of tumours that result in aggressive disease, and results of treatment with 177Lu oxodotreotide based on the NETTER-R study will likely apply to these patients as well.
Regarding prior therapies received by patients, 70% of patients received prior treatment with SSAs and 30% did not. The funding request by the sponsor specifies that a patient’s disease must have progressed after prior treatment with an SSA unless an SSA was contraindicated or the patient was intolerant to SSAs. Further, the NETTER-R study did not specify that patients must have had prior treatment with SSAs. While this is not in exact alignment with the funding request, CADTH’s consultation with clinical experts for this review confirmed that results of the NETTER-R study would still be generalizable to most patients in Canadian clinical practice.
The NETTER-R study did not include a comparator group. Consultation with clinical experts for this review suggested that a randomized trial may not have been possible, as it would have been unlikely for patients to have accepted assignment to a treatment group that did not include 177Lu oxodotreotide. In addition, treatment with PRRT has been accepted in Europe and in the US, based on data from the NETTER-1 study that was extrapolated to patients with pNETs.
Indirect Comparisons
Description of Studies
Sponsor’s Indirect Treatment Comparison
The aim of the sponsor’s indirect treatment comparison (ITC) was to compare 177Lu oxodotreotide to relevant comparators. Due to the lack of published clinical trial data, the sponsor conducted matching-adjusted indirect comparisons (MAICs) comparing 177Lu oxodotreotide to everolimus and sunitinib. The RADIANT-3 trial, comparing everolimus to placebo, and NCT00428597, comparing sunitinib to placebo, were compared with the NETTER-R study though MAICs. Comparison of key eligibility across the trials suggested that characteristics were comparable across the trials. The median age was similar across all studies (between 56 and 58 years of age), with similar proportions of male and female participants. The majority of patients across all trials had an ECOG PS of 1 or 2, although the proportion of patients with an ECOG PS of 1 was greater in the RADIANT-3 and NCT00428597 studies (> 60%) than in the NETTER-R study (33%). Similar proportions of patients in the NETTER-R and NCT00428597 studies had a time from disease progression to randomization or receipt of study treatment of 3 to 12 months (26% versus 28%, respectively). There were some differences noted across the populations of the included studies. Specifically, there were differences in the proportions of patients with organ involvement, time from disease progression to randomization of receipt of study treatment, and prior therapies. Classification of tumour functionality was not reported consistently across the trials.
Khan et al. (2021)
The aim of the ITC by Khan et al. (2021)7 was to use MAICs to indirectly compare PFS in patients with GI-NETs or pNETs, and OS in patients with pNETs, after treatment with 177Lu oxodotreotide, everolimus, sunitinib, or best supportive care across different studies. Khan et al. (2021) compared 177Lu oxodotreotide to everolimus and sunitinib using data from the ERASMUS, RADIANT-3, and NCT00428597 studies. The authors concluded that there were no differences in key covariates among the ERASMUS, RADIANT-3, and NCT00428597 studies. Age, ECOG PS, previous chemotherapy, and previous radiotherapy were reported to be statistically significantly associated with PFS and OS in the ERASMUS study at the 20% level and were adjusted for in the MAICs.
Efficacy Results
Sponsor’s Indirect Treatment Comparison
Progression-Free Survival: The median PFS of 177Lu oxodotreotide before adjustment was |||| |||||| |||| ||| |||| || |||||. After adjustment, the median PFS of 177Lu oxodotreotide was |||| |||||| |||| ||| |||| || |||||, which was longer than the median PFS of everolimus at |||| |||||| |||| ||| |||| || |||||. The hazard ratio (HR) for PFS between 177Lu oxodotreotide and everolimus favoured treatment with 177Lu oxodotreotide (|||||||| ||| ||| |||| || ||||).
The median PFS of 177Lu oxodotreotide before adjustment was |||| |||||| |||| ||| ||||| || |||||. After adjustment, the median PFS of 177Lu oxodotreotide remained the same, at |||| |||||| |||| ||| ||||| || |||||, which was longer than the median PFS of sunitinib at |||| |||||| |||| ||| |||| || |||. The HR for PFS also favoured 177Lu oxodotreotide over sunitinib (|||||||| ||| ||| |||| || ||||).
Overall Survival: The median OS of 177Lu oxodotreotide before adjustment was |||| |||||| |||| ||| |||| || |||||. After adjustment, the median PFS of 177Lu oxodotreotide was |||| |||||| |||| ||| |||| || |||. The median OS of everolimus was ||| ||||||||| |||| ||| |||| || |||. The 95% CI of HR for OS between 177Lu oxodotreotide and everolimus ||||||| ||| |||| |||||, although the point estimate was in favour of 177Lu oxodotreotide over everolimus (|||||||| ||| ||| |||| || ||||).
The median OS of 177Lu oxodotreotide before adjustment was |||| |||||| |||| ||| |||| || |||||. After adjustment, the median OS of 177Lu oxodotreotide remained the same, at |||| |||||| |||| ||| |||| || |||, which was longer than the median OS of sunitinib at |||| |||||| |||| ||| |||| || |||||. The HR for OS failed to show a statistically significant difference in favour of 177Lu oxodotreotide over sunitinib (|||||||| ||| ||| |||| || ||||).
Khan et al. (2021)
Progression-Free Survival: The MAIC suggested that PFS improved more in patients treated with 177Lu oxodotreotide than in those treated with sunitinib (HR = 0.36; 95% CI, 0.18 to 0.70) and everolimus (HR = 0.46; 95% CI, 0.30 to 0.71). Results of the sensitivity analyses also supported improvement with 177Lu oxodotreotide over sunitinib and everolimus.
Overall Survival: The MAIC suggested that OS was improved more in patients treated with 177Lu oxodotreotide compared with sunitinib (HR = 0.42; 95% CI, 0.25 to 0.72) and everolimus (HR = 0.53; 95% CI, 0.33 to 0.87). Results of the sensitivity analyses also supported improvement with 177Lu oxodotreotide over sunitinib and everolimus.
Harms Results
No analyses for harms were conducted in either ITC.
Critical Appraisal
Sponsor’s Indirect Treatment Comparison
Patient demographic and disease characteristics across the 3 studies were mostly similar. However, there were some differences regarding organ involvement, time from initial diagnosis, time between disease progression and randomization, tumour functionality, and prior treatments. There may be residual confounding bias because the matching adjustment was limited to a number of pre-identified covariates. As mentioned, the MAICs chosen for comparisons between 177Lu oxodotreotide and everolimus or sunitinib were designed based on the combination of covariates that resulted in the highest effective sample size (ESS). The ESS for the MAICs between 177Lu oxodotreotide versus everolimus and 177Lu oxodotreotide versus sunitinib were ||| and |||, respectively. The reductions in ESS for these MAICs may indicate that there was little overlap between the individual patient-level data of the NETTER-R study and the RADIANT-3 and NCT00428597 studies, with less overlap between the NETTER-R and RADIANT-3 studies than between the NETTER-R and NCT00428597 studies. The lack of high overlap between patients across the studies may indicate heterogeneity across patient characteristics, which may, in turn, suggest additional unknown prognostic and predictive factors and introduce bias in the comparisons of efficacy between 177Lu oxodotreotide and everolimus or sunitinib.
The results of the MAICs suggested that 177Lu oxodotreotide was favoured over everolimus and sunitinib for PFS but not for OS. The median OS was not reached in either the RADIANT-3 and NCT00428597 studies. Therefore, the interpretability of the efficacy analyses of the sponsor’s MAICs, in particular for OS, is limited.
In general, the MAICs rely on statistical assumptions and a limited list of known predictive and prognostic covariates, which are difficult to confirm. The MAICs reduced the sample size significantly by excluding more than half of the patients in the NETTER-R study, which compromised the generalizability and reliability of the results.
Khan et al. (2021)
Some differences in baseline characteristics were observed across the included studies. There were some differences noted in patient’s sex, tumour functionality, and previous treatments. These characteristics were not included in the matching between the ERASMUS and the NCT00428597 and RADIANT-3 studies. After matching, these characteristics were not well-balanced. The differences in patient characteristics may affect the validity of the comparisons between 177Lu oxodotreotide and everolimus and sunitinib.
The authors conducted matching with key covariates between the ERASMUS study and the comparator studies (NCT00428597 and RADIANT-3). The ESS after matching with the sunitinib comparator group in the NCT00428597 study was 77% of the initial sample. However, the ESS was much lower (35%) after matching with the everolimus group in the RADIANT-3 study. The characteristics of patients that were unadjusted for were not well-balanced, as illustrated by the differences in the patients’ sex, previous surgery, and tumour functionality. Therefore, any unknown covariates are likely not balanced across studies. There is likely little patient overlap between the ERASMUS and comparator studies, although this is more the case with the RADIANT-3 study.
As mentioned previously, OS was not reached in either the RADIANT-3 and NCT00428597 studies. Therefore, the efficacy analyses for OS based on immature data may suffer from high uncertainty.
Other Relevant Evidence
Three separate non-comparative observational studies by Fröss-Baron et al. (2021),8 Marinova et al. (2018),9 and Zandee et al. (2019)10 are briefly summarized here to provide additional efficacy and safety data on 177Lu oxodotreotide in patients with pNETs.
Description of Studies
Fröss-Baron et al. (2021)8 Study
Fröss-Baron et al. (2021)8 conducted a retrospective study to determine the efficacy (PFS and OS) and safety of 177Lu oxodotreotide in 102 adult patients with metastatic and/or locally advanced pNETs who have been previously treated with chemotherapy. Patients in Sweden treated with 177Lu oxodotreotide between 2005 and 2014 were identified using hospital records, and medical and radiological reports were retrospectively examined. Patients received 7.4 GBq 177Lu oxodotreotide per cycle with an intended 6- to 8-week interval between each cycle.
Marinova et al. (2018)9 Study
Marinova et al. (2018)9 conducted a retrospective study to determine the change in health-related quality of life (HRQoL) and symptom burden in 68 adult patients with pNETs following treatment with 177Lu oxodotreotide. Patients treated with 177Lu oxodotreotide between 2007 and 2015 at a hospital in Germany were identified, and data were retrospectively analyzed. Briefly, inclusion criteria for the study were that unresectable metastatic pNETs were confirmed with histopathology, the patient had an ECOG PS of 0 to 2, the intended number of cycles were administered, follow-up was completed at 3 months after the last cycle, and the European Organisation for Research and Treatment of Cancer – Quality of Life of Cancer Patients questionnaire, Version 3.0 (EORTC QLQ-C30) was completed before the first cycle and at least once after the last cycle. Patients received a mean activity of 7.6 GBq (standard deviation [SD] = not reported) 177Lu oxodotreotide per cycle. Change in HRQoL and symptom status were evaluated according to the EORTC QLQ-C30. Higher scores on the Global Health Status and functional scales indicate better function, and higher scores on the symptom scales and single items indicate significant symptoms. Patients completed the EORTC QLQ-C30 at baseline and every 3 months following each treatment cycle for up to 12 months.
Zandee et al. (2019)10 Study
Zandee et al. (2019)10 conducted a retrospective study to determine the efficacy and safety of 177Lu oxodotreotide in 34 adult patients with functional pNETs — 14 patients with insulinoma, 8 with glucagonoma, 7 with gastrinoma, and 5 with VIPoma. Patients treated with 177Lu oxodotreotide between 2000 and 2017 at a centre in the Netherlands were identified. Patients received up to 4 cycles of 7.4 GBq 177Lu oxodotreotide per cycle, with an intended interval of 6 to 10 weeks and an intended cumulative activity of 27.8 to 29.6 GBq. Patients were admitted for clinical observation or treatment of hormonal syndrome, per protocol. The study aimed to evaluate symptomatic, biochemical, and radiological response, as well as toxicity. Hematology, kidney, and liver function tests were completed following each cycle and at follow-up visits (6 weeks, 3 months, and 6 months following the last cycle, and every 6 months thereafter). CT or MRI imaging was completed within 3 months of the first cycle and at each follow-up visit. Patients completed the EORTC QLQ-C30 at all visits.
Efficacy Results
Fröss-Baron et al. (2021)8 Study
The median follow-up period was 34 months (range, 4 to 160), and survival data for patients (46.1%) were based on the Swedish National Health Registry up to 2018. PFS was calculated using the Kaplan-Meier method and was based on the first date of treatment to the date of radiologically confirmed progression, per RECIST version 1.1, or death from any cause. OS was calculated using the Kaplan-Meier method and was based on the first day of treatment with 177Lu oxodotreotide to the day of death or the last day of follow-up. The median PFS was 24 months (95% CI, 17 to 28), and the median OS was 42 months (95% CI, 29 to 61). During follow-up, 63 (61.8%) patients died; tumour progression was reported as the cause of death in 60 patients. Tumour response was assessed with RECIST version 1.1 criteria in 100 patients. Complete response was reported in 4 (4.0%) patients, partial response in 45 (45.0%) patients, stable disease in 44 (44.0%) patients, and progressive disease in 7 (7.0%) patients. Forty-nine percent of patients reached objective response, which was defined as patients with complete or partial response. The median time to best response was 14.8 months (range, 3 to 108). Disease control, which was defined as complete response, partial response, or stable disease, was reported in 91.0% of 92 patients with progressive disease at baseline.
Marinova et al. (2018)9 Study
The primary analysis using the EORTC QLQ-C30 was according to data collected at baseline and 3 months following the last cycle (follow-up). The mixed longitudinal (panel) model was used to evaluate the data, and a non-parametric Skilling-Mack test was used to verify the unbalanced panel data; a value of less than 0.05 was considered statistically significant. An increase in the mean Global Health Status score was reported (P = 0.008); the mean score was 58.2 (95% CI, 53.1 to 63.2) at baseline and 69.3 (95% CI, 61.4 to 77.2) at follow-up. An increase in the mean social functioning score was reported (P = 0.049); the mean score was 63.9 (95% CI, 56.7 to 71.2) at baseline and 70.9 (95% CI, 61.1 to 80.7) at follow-up. A decrease in the mean fatigue symptom score was reported (P = 0.029); the mean score was 42.4 (95% CI, 36.3 to 48.4) at baseline and 32.0 (95% CI, 22.2 to 41.7) at follow-up. A decrease in the mean appetite loss symptom score was reported (P = 0.015); the mean score was 25.7 (95% CI, 19.5 to 31.9) at baseline and 11.6 (95% CI, 0.7 to 22.5) at follow-up. The differences in change from baseline in the mean scores on the remaining functional and symptom scales were not considered statistically significant. Further, the investigators reported a significantly greater improvement (magnitude of benefit was not reported) on the diarrhea and dyspnea symptom scale scores in patients with functional versus nonfunctional pNETs. The subanalysis of EORTC QLQ-C30 was based on data collected at baseline and at 3 months following the first, second, and third cycle. Changes from baseline in the EORTC QLQ-C30 in the subanalysis were generally consistent with those observed in the primary analysis.
Zandee et al. (2019)10 Study
The median follow-up period was 39.3 months (range, NR). PFS was calculated using the Kaplan-Meier method and was based on the time from the first cycle of 177Lu oxodotreotide to objective progression, change to a new line of therapy, or death from any cause. The median PFS was 18.1 months (interquartile range, 3.3 to 35.7). A primary event was reported in 31 patients, of whom 24 had progressive disease, 5 changed to a new line of therapy, and 2 died. Tumour response was evaluated with RECIST version 1.1 criteria in 34 patients. Complete response was reported in 1 (2.9%) patient, partial response in 19 (55.9%) patients, stable disease in 8 (23.6%) patients, and progressive disease in 6 (17.6%) patients. Disease control, which was defined as patients with complete response, partial response, or stable disease, was reported in 18 of the 23 patients with progressive disease at baseline.
HRQoL was assessed in 22 patients using the EORTC QLQ-C30 by comparing the scores 3 months after the last cycle (follow-up) to those at baseline. A paired t-test and the Wilcoxon signed-rank test were used for normally distributed and non-normally distributed variables in the comparison of continuous variables, respectively. An increase in the mean Global Health Score/Quality of Life was reported (P = 0.002); the mean score was 61.7 (95% CI, NR) at baseline and 79.5 (95% CI, NR) at follow-up. An increase in the mean physical functioning score was reported (P = 0.008); the mean score was 79.7 (95% CI, NR) at baseline and 90.0 (95% CI, NR) at follow-up. An increase in the mean role functioning score was reported (P = 0.006); the mean score was 62.7 (95% CI, NR) at baseline and 90.3 (95% CI, NR) at follow-up. An increase in the mean emotional functioning score was reported (P = 0.002); the mean score was 74.1 (95% CI, NR) at baseline and 84.5 (95% CI, NR) at follow-up. An increase in the mean social functioning score was reported (P = 0.047); the mean score was 77.3 (95% CI, NR) at baseline and 85.6 (95% CI, NR) at follow-up. A decrease in the mean fatigue symptom score was reported (P = 0.02); the mean score was 27.3 (95% CI, NR) at baseline and 17.2 (95% CI, NR) at follow-up. The difference in change from baseline in the mean scores on the remaining functional and symptom scales were not considered statistically significant.
Harms Results
Fröss-Baron et al. (2021)8 Study
Bone marrow, liver, and kidney toxicity were defined by the Common Terminology Criteria for Adverse Events (CTCAE) version 3.0. Grade 3 or 4 bone marrow toxicity was reported in 11 (10.8%) patients. Grade 3 toxicity of white blood cells and/or granulocytes was reported in 5 (4.9%) patients, grade 3 or 4 toxicity of platelets was reported in 5 (4.9%) patients, and grade 3 toxicity of hemoglobin was reported in 2 (1.9%) patients. Grade 4 (lethal) thrombocytopenia and acute myeloid leukemia were reported in 1 (1.0%) patient each. Fatal liver toxicity was reported in 1 (1.0%) patient; the cause of death was also considered related to tumour progression. Grade 3 or 4 nephrotoxicity was not observed. Treatment discontinuations were due to the following: termination according to the dosimetry-guided protocol was applied to 51 (50.0%) patients, disease progression in 17 (16.7%) patients, bone marrow toxicity in 11 (10.8%) patients, the standard 4-cycle protocol was applied to 9 (8.8%) patients, reduced tumour load in 3 (2.9%) patients, deterioration in 2 (1.9%) patients, death in 2 (1.9%) patients, and a combination of factors not specified in 7 (6.8%) patients.
Marinova et al. (2018)9 Study
No analyses for harms were conducted.
Zandee et al. (2019)10 Study
Nausea, vomiting, and pain were reported in 22 (17.6%), 6 (4.8%), and 10 (8.0%) of the 125 cycles administered in total, respectively. Toxicity was defined according to the CTCAE 4.03 criteria. Grade 3 anemia and grade 3 thrombocytopenia were reported in 1 (2.9%) patient each, and grade 3 leukopenia was reported in 3 (8.8%) patients. Hormonal crisis, which was defined as an acute complication of hormonal secretion following treatment with 177Lu oxodotreotide and requiring medical care, was reported in 3 (8.8%) patients, and late toxicity with myelodysplastic syndrome was reported in 1 (2.9%) patient. There were several reasons that patients did not receive the intended cumulative activity of 29.6 GBq 177Lu oxodotreotide. A reduced cumulative activity of 18.5 to 25.9 GBq 177Lu oxodotreotide was administered in 5 (14.7%) patients due to hepatotoxicity. Only 1 cycle was administered in 3 (8.8%) patients each due to noncompliance, unexplained progressive cognitive decline, and patient withdrawal. Only 3 cycles were provided to 1 (2.9%) patient due to clinical progression, and the last patient case was not reported.
Critical Appraisal
In the absence of an active comparator or placebo group, the interpretation of the efficacy and safety results from the 3 non-comparative observational studies8-10 is limited. The interpretation of treatment benefit is further limited by the retrospective nonrandomized study design and a relatively small sample size. This is compounded by the relatively large number of patients who were excluded from the analysis due to their incomplete questionnaires, as indicated in the study conducted by Marinova et al. (2018).9 However, the clinical experts consulted by CADTH indicated that patients with NETs in general were rare, and Zandee et al. (2019)10 also indicated that pNETs were rare. Although treatment with 177Lu oxodotreotide can be ascertained by the use of hospital records, data were sourced from 1 hospital in either Sweden,8 Germany,9 or Netherlands10 and retrospectively analyzed. The use of a single source for the recruitment of patients may introduce the risk of selection bias, because patients under the care of 1 team may share common characteristics, including treatment history, disease severity, and level of supportive care, which can bias the estimation of treatment effect and limit the external validity of the results. Notably, the place of 177Lu oxodotreotide in the treatment sequence varied within the cohort and was preceded by various therapies, which the clinical experts suggested can bias the median OS. Marinova et al. (2018)9 indicated that they used the validated German version of EORTC QLQ-C30 but did not identify a clinically meaningful difference; Zandee et al. (2019)10 also did not identify a clinically meaningful difference. Although patients did not undergo further therapies after treatment with 177Lu oxodotreotide and follow-up,9 it was unclear whether patients received any concomitant therapy that could bias the reporting on the HRQoL questionnaire.
A number of baseline characteristics of the cohorts in the studies, specifically the mean age,8-10 proportion of patients with liver metastases,8,10 and the proportion of patients with an ECOG status of 0,8,9 were similar to those of the NETTER-R5 study, which the clinical experts consulted by CADTH suggested were representative of patients seen in clinical practice in Canada. (A detailed description of the patient population in NETTER-R is presented in the Systematic Review section.) The retrospective studies included patients with experience with various treatments; therefore, 177Lu oxodotreotide was in various lines in the treatment sequence, preceded by different therapies. Only 56.9%, 36.8%, and 64.7% of patients received an SSA before treatment with 177Lu oxodotreotide in the studies by Fröss-Baron et al. (2021),8 Marinova et al. (2018),9 and Zandee et al. (2019),10 respectively, and thus match the reimbursement request for this review. Further, the number of cycles administered and the intervals between the cycles, such as the application of the dosimetry-guided protocol8 and the use of 3-month intervals,9 varied among studies. Last, Zandee et al. (2019)10 included patients with functional pNETs, specifically patients with insulinoma, glucagonoma, gastrinoma, and VIPoma, but did not include patients with nonfunctional pNETs.
Conclusions
The NETTER-R study was provided in this reassessment of 177Lu oxodotreotide for treatment of patients with pNETs. The previous recommendation for 177Lu oxodotreotide did not support use for patients with pNETs because they were excluded from the pivotal NETTER-1 study. Due to the small sample size, lack of comparator group, retrospective design, and missing data, the results of the NETTER-R study are difficult to interpret and cannot be used to draw firm conclusions about the relative benefits of 177Lu oxodotreotide in the treatment of pNETs. Evidence from other observational studies by Fröss-Baron et al. (2021),8 Marinova et al. (2018),9 and Zandee et al. (2019)10 were largely consistent with NETTER-R but were associated with the same level of uncertainty. Indirect evidence available from the sponsor and the literature provided comparative results between 177Lu oxodotreotide with everolimus and sunitinib and suggested improved efficacy with 177Lu oxodotreotide over everolimus and sunitinib. The indirect evidence had methodological limitations, which introduced uncertainty in the interpretation of the comparative data. Based on the totality of the evidence and their experience treating patients with pNETs, clinical experts agreed that 177Lu oxodotreotide would be a safe and effective regimen, preferred over everolimus or sunitinib. Direct comparative evidence may help reduce uncertainty and inform whether 177Lu oxodotreotide would be beneficial for patients with pNETs.
Introduction
Disease Background
NETs are a heterogenous group of cancers that arise from the secretory cells of the diffuse neuroendocrine system.1 Almost half of NETs are in the bowels and pancreas. These NETs often present with distant metastases.11 pNETs are a subset of GEPNETs. pNETs share some common features with GI-NETs, such as an overexpression of SSRs, expression of certain neuroendocrine markers (i.e., chromogranin A), and localization methods used for treatment of both GI-NETs and pNETs.12 GEPNETs can present as hormonally functional or nonfunctional tumours, which indicates whether the NETs are hormone-producing or non–hormone-producing, respectively. Depending on the functionality, the tumours may present with distinct clinical features based on their site of origin. pNETs typically present as silent hormonally, but can produce many peptide hormones, including insulin, gastrin, and glucagon, which cause insulinoma syndrome, gastrinoma syndrome, and glucagonoma syndromes, respectively.1 SSRs are expressed in the majority (> 80%) of well-differentiated NETs.2
GEPNETs are the second most prevalent type of digestive cancer.1 The annual incidence of pNETs is less than 1 per 100,000 persons.3 The median OS for patients with NETs, irrespective of the type of NET and grade of disease, is estimated to be approximately 9 years.11 Compared to other types of NETs, advanced pNETs have a worse prognosis, typically resulting in less than 5 years’ survival.3
According to clinical experts consulted by CADTH for this review, diagnosis of pNETs is typically through biopsy. Staging of disease is typically conducted using imaging — usually CT or MRI scans, although 68Ga-PET scans are becoming a more standard form of imaging for this group of patients. The clinical experts highlighted the importance of tissue diagnosis and reliance on tertiary care centres for the diagnosis and management of pNETs.
Standards of Therapy
Management of NET is often influenced by the disease grade, stage of disease, and underlying pathobiology of the neuroendocrine cell type or its direction of differentiation.11 Input from the clinical experts consulted by CADTH for this review highlighted that management of NETs requires a multidisciplinary team and that some care may involve tertiary care centres. Due to the heterogenous nature of pNETs, patients may not follow the same disease trajectory. For localized solid tumours, surgery is typically the initial treatment option. For patients with metastatic disease, systemic drug therapies are used, although surgery can play a role as well. SSAs are the usual first-choice therapy for patients with unresectable metastatic disease or with hormonal overproduction syndromes. SSAs may include octreotide or lanreotide. For patients who have progressed on SSAs, treatment options may include everolimus, sunitinib, and capecitabine plus temozolomide. The clinical experts consulted by CADTH for this review stated that currently available treatment options for patients with pNETs are palliative in nature. They may increase the length and the quality of life. However, patients are expected to eventually progress on these therapies. The clinical experts also identified surgery, radiofrequency ablation, and liver embolization therapy for patients with liver-dominant metastatic pNETs.
Radiolabelled SSAs have also been developed for SSR-positive well-differentiated NETs that have progressed after first-line therapy with SSAs; this type of therapy is part of a group of treatments called PRRT.2 PRRT consists of a radioisotope linked to another molecule that targets peptide receptors on cancer cells, allowing targeted delivery of radiation. 177Lu oxodotreotide is considered PRRT and has been studied since the 1990s.2 The clinical experts consulted by CADTH for this review stated that the decision between PRRT and other therapies can be challenging. In addition, the administration schedule of PRRT is more convenient for patients because it is limited to 4 sessions, compared to other, lengthier treatment options that result in toxicity issues, such as fatigue and loss of appetite. While PRRT is not funded for patients with pNETs in most of Canada, it is funded in Quebec, which introduces issues of inequity among patients in Canada with pNETs, according to the clinical experts.
Drug
177Lu oxodotreotide is a radiolabelled SSA that binds to SSRs. 177Lu oxodotreotide has the highest affinity for subtype 2 SSRs (SSRT2). Binding of 177Lu oxodotreotide to cells that express SSRs, which include malignant tumours expressing SSRs, results in cellular damage in SSR-positive cells as well as in neighbouring cells.13 177Lu oxodotreotide is administered IV at a recommended dose of 7.4 GBq (200 mCi) over 30 minutes every 8 weeks, for a total of 4 doses. 177Lu oxodotreotide is administered alongside octreotide LAR, which continues monthly.
177Lu oxodotreotide received a Notice of Compliance from Health Canada on January 9, 2019. The indication approved by Health Canada is for the treatment of unresectable or metastatic, well-differentiated, SSR-positive GEPNETs in adults with progressive disease. CADTH reviewed this Health Canada–approved indication in 2019 and pERC provided a positive recommendation for patients with SSR-positive midgut NETs whose disease had progressed on an SSA and was unresectable; however, the recommendation did not support treatment for patients with SSR-positive foregut and hindgut NETs whose disease had progressed and was unresectable. The previous CADTH review for 177Lu oxodotreotide did not support use among patients with pNETs, as these patients were excluded from the pivotal NETTER-1 trial. The sponsor’s reimbursement request for this current CADTH reassessment is for adult patients with unresectable or metastatic, well-differentiated, SSR-positive pNET tumours whose disease has progressed after treatment with an SSA, unless there is a contraindication or intolerance.
Table 3: Key Characteristics of 177Lu Oxodotreotide, Everolimus, and Sunitinib
Characteristic | 177Lu oxodotreotide | Everolimus | Sunitinib | Chemotherapy |
|---|---|---|---|---|
Mechanism of action | 177Lu binds to cells expressing somatostatin receptors, which include malignant somatostatin receptor–positive tumours. Upon binding, 177Lu releases beta particles that result in the formation of free radicals and induce cellular damage. | Everolimus is an mTOR (mammalian target of rapamycin) inhibitor. Inhibition of mTOR leads to reduced cell proliferation and results in antitumour activity. | Sunitinib is a small molecule that inhibits receptor tyrosine kinases (RTKs), which can be involved in the growth of tumours. The inhibition of RTKs results in inhibition of cell function and tumour growth. | Temozolomide: an alkylating agent with antitumour activity once it is chemically converted in systemic circulation, which leads to cytotoxic lesions Capecitabine: an antineoplastic agent in the fluoropyrimidine carbamate class. Capecitabine is selectively activated to 5-fluorouracil, which is then metabolized to other compounds that lead to cell damage in tumour and normal cells |
Indicationa | The treatment of unresectable or metastatic, well-differentiated, somatostatin receptor–positive GEPNETs in adults with progressive disease | The treatment of well-differentiated pNETs in patients with unresectable, locally advanced or metastatic disease that has progressed within the last 12 months | The treatment of patients with unresectable, locally advanced or metastatic, well-differentiated pNETs, whose disease is progressive | NA |
Route of administration | IV | Oral | Oral | Temozolomide: Oral Capecitabine: Oral |
Recommended dose | 7.4 GBq (200 mCi) over 30 minutes every 8 weeks for a total of 4 doses | 10 mg once daily | 37.5 mg once daily | Temozolomide: 200 mg/m2 once daily for 5 days per cycle Capecitabine: 750 mg/m2 twice daily for 14 days per cycle |
Serious adverse effects or safety issues | Serious warnings and precautions
| Serious warnings and precautions
| Serious warnings and precautions
| Temozolomide: Serious warnings and precautions
Capecitabine: Serious warnings and precautions
|
Other | None | The effectiveness in pNETs is based on demonstrated PFS benefit in a phase III placebo-controlled study in patients with documented progressive disease within 12 months of randomization; no evidence of an OS benefit and HRQoL was not measured | Approval for pNETs is based on progression-free survival in patients with good performance status (ECOG 0 or 1) | None |
177Lu = 177lutetium; ECOG = Eastern Cooperative Oncology Group; GEPNET = gastroenteropancreatic neuroendocrine tumour; HRQoL = health-related quality of life; LVEF = left ventricular ejection fraction; MDS = myelodysplastic syndrome; NA = not applicable; OS = overall survival; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour.
aHealth Canada–approved indication.
Source: Lutathera product monograph,13 Afinitor Disperz product monograph,14 Sutent product monograph,15 Temodal product monograph,16 and Xeloda product monograph.17
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Group and Information Gathered
One patient group, CNETS, provided input on 177Lu oxodotreotide for the treatment of GEPNETs. CNETS is an organization that helps to improve the quality of life and survival for patients with NETs by raising awareness of the condition and the latest available diagnostics and treatments. In addition, CNETS helps to ensure that patients, caregivers, health care professionals, and others have the information they need regarding medical and scientific research, treatment, and support. CNETS helps patients navigate the health care system to obtain the best care options. CNETS helps to provide support and education about NETs and advocates on behalf of individual patients and for policies to support NET patients.
CNETS obtained information from NET patients using an online questionnaire that was promoted on the CNETS website and social media (i.e., Facebook). The survey was conducted from February 25, 2022, to March 25, 2022, and contained quantitative and qualitative questions, including open-ended questions for patients to provide their own experiences. A total of 57 respondents with NETs completed the online survey, including 21 (37%) patients with pNETs and 36 (63%) patients with GI-NETs; 19 (33%) respondents were male and 38 (67%) were female. Most respondents were between 50 and 79 years of age (n = 50; range, 29 to 80). Respondents included individuals residing across Canada, with most being from Ontario (47%), as well as 3 respondents from outside of Canada.
Disease Experience
Respondents reported that their condition had a generally negative impact on their quality of life. When asked to rate how symptoms of NETs affected day-to-day life, respondents indicated that fatigue, weakness, and diarrhea had the most negative impact on their quality of life. Further, the impact on respondent’s energy levels and emotions, as well as the requirements for travel, were reported as having an extremely high negative impact on their quality of life. Other important considerations included effects on their social life, their ability to work, and their ability to participate in leisure activities. Comments from respondents also highlighted the negative impact of fatigue and pain due to NETs, as well as the impacts of surgery.
CNETS also reported experiences of 1,928 NET patients from a global survey conducted by the International Neuroendocrine Cancer Alliance and Novartis Pharmaceuticals Corporation; of the patients included, 22% were reported to have pNETs. The global survey indicated that decreased energy levels and emotional issues were common concerns among patients. Most respondents to the global survey (80%) reported being unable to work due to NETs. Other issues reported by respondents included impacts on their diet and physical activity, and greater time and money spent on appointments.
Experience with Treatment
The most common treatments respondents reported were SSAs (i.e., octreotide, lanreotide; 80%), surgery (64%), and PRRT (60%). Other treatments included liver-directed therapies (e.g., embolization; 29%), ablative techniques (i.e., radiofrequency ablation, cryotherapy; 22%), chemotherapy (22%), radiation therapy (15%), biologically targeted therapies (i.e., everolimus, sunitinib; 13%), immunotherapies (4%), and others (9%). According to CNETS, respondents reported that treatments temporarily slowed disease progression and controlled symptoms. However, treatments were also associated with long recovery times, debilitating side effects, and complications. No therapies were reported to stop progression of their NET cancer. Patients described treatments for control of symptoms such as bloating, diarrhea, constipation, and energy levels as effective. Treatments for the condition (i.e., surgery, embolization, radiation, chemotherapy, and biologic drugs) were reported to be slightly effective or not effective at stopping disease progression and preventing spread to other organs. Some patients also reported difficulties in accessing and receiving treatments due to lack of private insurance, financial difficulties, inability to access their therapy through their physician, lack of funding for a specific treatment for their type of NET cancer, and inability to travel to where the drug is administered. In fact, respondents provided many comments on needing to travel long distances to receive treatment.
A total of 33 respondents (60%) reported having been treated, or current treatment, with 177Lu oxodotreotide. Respondents reported accessing 177Lu oxodotreotide through various clinical trials across the country, provincial reimbursement, compassionate access, and private insurance. According to CNETS, respondents reported that they could tolerate or manage side effects of treatment with 177Lu oxodotreotide. Compared to other treatment options, such surgery, respondents indicated that treatment with 177Lu oxodotreotide involved a quicker recovery and had less debilitating side effects. Respondents reported that benefits from treatment with 177Lu oxodotreotide included slower progression of their disease (69%), tumour shrinkage (59%), decrease in disease symptoms (45%), and overall improved well-being (41%). Side effects associated with treatment with 177Lu oxodotreotide included increased fatigue (58%), nausea and vomiting (27%), increased diarrhea (8%), and increased pain (4%). Many respondents (38%) also reported “other” side effects; respondents’ comments highlighted side effects related to fatigue and neurocognitive issues. Respondents’ comments were generally positive toward 177Lu oxodotreotide, with patients highlighting the effectiveness of this treatment in controlling their NET cancer.
Improved Outcomes
When asked what aspects of NET cancer are most important to control, almost all (98%) respondents reported a need to control disease progression. Other answers included a need to control fatigue, diarrhea, flushing, and wheezing. Respondents also commented on other aspects of disease that they would like greater management of, including energy levels, shortness of breath, high blood pressure, and cardiac symptoms.
CNETS also highlighted the 68Ga-dotatate PET scan companion diagnostic test to 177Lu oxodotreotide. CNETS stated that the 68Ga-PET scan has advantages over the octreotide scan because it has higher-resolution images, detects smaller lesions, provides better guidance to treatment and dosage, exposes patients to less radiation, has greater efficiency and cost-effectiveness, is easier to access, and is more convenient for patients.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of pNETs.
Unmet Needs
The clinical experts highlighted an unmet need for treatments that extent patients’ lives and improve their quality of life. Because patients eventually become refractory to all currently available treatment options, the clinical experts indicated that 177Lu oxodotreotide is another treatment option that is also highly tolerated.
Place in Therapy
The clinical experts stated that sequencing of 177Lu oxodotreotide is individualized to each patient’s circumstance. In most instances, patients should have progressed on SSAs before receiving 177Lu oxodotreotide. However, the clinical experts stated that recommending use of other treatments before 177Lu oxodotreotide would not be appropriate, given that each patient’s treatment options may be individualized to their needs. In some cases of locally advanced pNETs, 177Lu oxodotreotide may be used as an induction (preoperative) strategy.
Patient Population
The clinical experts stated that identifying patients eligible for 177Lu oxodotreotide requires gallium PET scans. They specified that eligibility should not be based on strict criteria for Ki-67 index, as there is too much variability in Ki-67 among different specimens from the same patient. In addition, there is subjectivity in interpreting the specimens, which can result in variability in determining eligibility based on Ki-67. The clinical experts indicated fluorodeoxyglycose PET scans are not widely available but could be used.
Assessing Response to Treatment
Patients’ response to therapy is assessed through clinical assessment, radiographic information, and analysis of biomarkers (i.e., 5-hydroxyindoleacetic acid), according to the clinical experts. Clinical assessments were advised every few months initially and before every cycle of PRRT. Radiographic assessments were advised every 3 to 6 months initially, depending on the clinical needs of the patients.
Discontinuing Treatment
The clinical experts stated discontinuation of therapy is based on serious toxicities, including permanent renal toxicities and bone marrow toxicity (e.g., MDS), and disease progression.
Prescribing Conditions
The clinical experts stated that administration of 177Lu oxodotreotide requires referral to a tertiary referral centre with dedicated nuclear medicine and/or radiation oncology. |
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Four groups provided clinician input on the review of 177Lu oxodotreotide for the treatment of pNETs:
OH-CCO’s Gastrointestinal Cancer Drug Advisory Committee (prepared by 2 clinicians)
CANM (prepared by 1 clinician)
the CNETS SMAB and other neuroendocrine cancer treating clinicians (prepared by 9 clinicians)
a collaboration between the CHU de Québec, Université Laval Research Centre — Oncology Axis; Hôtel-Dieu de Québec, Nuclear Medicine Department; Fondation du CHU de Québec — Research Chair in Theranostics; and AMSMNQ (prepared by 1 clinician).
The OH-CCO Gastrointestinal Cancer Drug Advisory Committee provides timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. CANM aims to achieve excellence in the practice of diagnostic and therapeutic nuclear medicine by promoting the continued professional competence of nuclear medicine specialists, establishing guidelines of clinical practice, and encouraging biomedical research. The CHU de Québec, Université Laval Research Centre — Oncology Axis is composed of researchers and students who aim to bring clarity and resolution to complex problems related to cancer for the benefit of patients and society. The Hôtel-Dieu de Québec, Nuclear Medicine Department is composed of world-renowned research groups in theranostics in patients with NETs, using PRRT. It includes the highest concentration of physicians with the most post-graduate and post-residency training in nuclear oncology and theranostics in Canada. The Fondation du CHU de Québec — Research Chair in Theranostics was launched on June 8, 2021, at the CHU de Québec to further advancements in clinical research based on research projects and experience with 177Lu octreotate and PRRT. The Quebec association of nuclear medicine specialists (AMSMNQ) is a non-profit organization representing all 116 board-certified nuclear medicine specialists in the province of Quebec, advocating for better and equal access to nuclear medicine for patients, and the development of clinical guidelines for the appropriate use of technology in nuclear medicine in Quebec. CNETS includes a SMAB, composed of leading Canadian neuroendocrine cancer multidisciplinary clinicians and scientists who provide expert scientific, clinical, and strategic advice to the CNETS board of directors. The SMAB works alongside the patient group to support best practices across the spectrum of research pillars, partnerships, advocacy, and scientific and medical matters relevant to the organization’s mission. As part of its mandate, CNETS is committed to raising awareness about the disease and the latest evidence concerning diagnosis and treatment, and ensuring that patients, caregivers, and health care professionals have the information they need in the areas of medical and scientific research, treatment, and support.
Unmet Needs
All clinician groups highlighted a need for treatments that improve OS, slow the progression of disease, and control hormonal symptoms. The clinician groups stated that most NETs eventually progress, with metastases to multiple organ systems, eventually causing death. CANM stated that PFS is a key metric in assessing NET therapies. Over time, nearly all patients will develop resistance to treatments. They highlighted that there are limited effective treatment options after standard first-line treatment with SSAs. AMSMNQ stated that, once the disease is considered metastatic and/or unresectable, all further treatments are considered palliative. The goals of treatment become to reduce symptoms, prevent complications, and prolong patient survival, by delaying disease progression and death. However, currently available treatments, such as everolimus and sunitinib, have many significant side effects and complications and are poorly tolerated
Also, many pNETs produce excess hormones, including insulin and gastrin, which can have devastating clinical implications, such as dangerous bouts of marked hypoglycemia (insulinomas) and severe gastritis (gastrinomas). Therefore, CANM highlighted the importance of maintaining or improving quality of life for these patients. CANM also highlighted that patients with metastatic NETs of pancreatic origin that progress on SSAs have a high unmet need for treatment.
Place in Therapy
In general, there was disagreement among the clinician groups regarding the optimal place in therapy for 177Lu oxodotreotide.
The OH-CCO Gastrointestinal Cancer Drug Advisory Committee stated that there are 4 established lines of therapy for patients with pNETs. Treatments available to patients include SSAs, capecitabine plus temozolomide, everolimus, and sunitinib. The OH-CCO Gastrointestinal Cancer Drug Advisory Committee acknowledged that, while the patient population of pNETs in the Ontario is small (representing between 10% to 20% of NET cases), there is high demand for therapies from both clinicians and patients. The OH-CCO Gastrointestinal Cancer Drug Advisory Committee suggested that 177Lu oxodotreotide would fit as a fourth-line therapy.
CANM described first-line therapy for metastatic pNETs as non-radiolabelled SSAs, such as octreotide or lanreotide. It was acknowledged that most patients would eventually progress and require other therapies to control symptoms and slow the progression of their disease. Other treatment options include targeted therapies, such as everolimus or sunitinib. CANM stated that everolimus and sunitinib were effective and have a worse side effect profile than 177Lu oxodotreotide. Targeted therapies were also stated to be more expensive, especially with longer use, than 177Lu oxodotreotide, which is delivered to patients 4 times under the current therapeutic regimen.
CANM stated that chemotherapy is ineffective for treatment of most NETs, which are low-grade, although a small proportion of high-grade NETs may be treated with chemotherapy regimens (e.g., capecitabine plus temozolomide). High-grade NETs do not express SSRs, making treatment with SSAs, such as 177Lu oxodotreotide, ineffective. CANM, CNETS SMAB, and AMSMNQ agreed that 177Lu oxodotreotide would be an optimal second-line treatment for patients with NETs who had progressed on SSAs. The impact of 177Lu oxodotreotide on treatment sequencing is minimal, according to these 3 clinician groups, as 177Lu oxodotreotide is the preferred second-line treatment for patients who have progressed on SSAs.
Patient Population
All clinician groups agreed that patients with advanced, unresectable or metastatic pNETs who had progressed after first-line treatment with SSAs and who had demonstrated SSR positivity via imaging with a 68Ga-dotatate PET scan or indium-111 (111In)-octreotide scan would be best suited for 177Lu oxodotreotide. Imaging includes a combination of anatomic imaging (CT or MRI) as well as functional imaging (i.e., 68Ga-dotatate PET scan). CANM also stated that, depending on the level of local expertise assessment of potential therapy for NETs, multidisciplinary tumour boards can be helpful in deciding when 177Lu oxodotreotide is best used for patients’ treatment.
According to CANM, patients least suitable for treatment include those who do not express SSRs. CANM stated that NETs often demonstrate significant variability among metastases, even within the same patient. Therefore, 68Ga-dotatate PET scans are important for identifying patients most likely to exhibit a response to treatment, according to these experts. If 68Ga-PET scans are not available, indium-111 (111In)-octreotide scanning was acknowledged to be a suitable surrogate test, and it is more widely available.
Assessing Response to Treatment
The clinician groups agreed that patients’ response to treatment is assessed based on symptoms, quality of life, and the size of measurable lesions. Progression could be identified based on a combination of clinical symptoms, biochemical monitoring of hormonal levels, imaging monitoring of disease bulk, or involvement of important organs or structures. A clinically meaningful response to treatment considers improvement or stability of symptoms and/or disease bulk.
According to CANM, there is no consensus among clinicians about the optimum follow-up for patients. CANM stated that, when 177Lu oxodotreotide treatment has been administered to patients with midgut NETs, both functional and anatomic imaging is generally conducted every 4 to 6 months following the completion of the 4 treatments of 177Lu oxodotreotide. For monitoring thereafter, anatomic imaging was suggested every 4 to 6 months, with functional imaging as indicated on an individual basis.
Discontinuing Treatment
All clinician groups stated that treatment should be discontinued when patients experience disease progression or unacceptable toxicity (e.g., myelosuppression and renal dysfunction). Treatment may also be discontinued based on patient preference.
Prescribing Conditions
CANM highlighted that 177Lu oxodotreotide is a radioactive therapy that can be administered only in select centres with appropriate training and with certification by the Canadian Nuclear Safety Commission. Appropriate training in handling radioisotopes and therapy administration, including all relevant radiation precautions and medical concerns for this specific treatment, are required for all personnel involved in the treatment (i.e., physicians, nurses, and nuclear medicine technologists). There was general agreement among all clinician groups that administration of 177Lu oxodotreotide would require a multidisciplinary team to optimize benefits and risks of the intervention. Therefore, it is expected that 177Lu oxodotreotide will be administered at limited sites. The clinician groups also stated that 177Lu oxodotreotide therapy can be administered on an outpatient basis in the majority of patients.
Additional Considerations
CNETS SMAB and AMSMNQ noted that there is currently inequity in treatment options for patients across Canada and internationally. 177Lu oxodotreotide is available for patients with pNETs in Europe, the UK, and Australia, as well as in Quebec. AMSMNQ also acknowledged that approximately 30% of patients receiving treatment with 177Lu oxodotreotide at their centre are Canadians from outside of the province of Quebec.
Many clinician groups also pointed out the favourable toxicity profile of 177Lu oxodotreotide and the improved effect of treatment on PFS compared to other treatments for pNETs. AMSMNQ also stated that it had conducted a phase II trial at the CHU de Québec, which assessed the safety and efficacy of personalized dosimetry for PRRT.18 There were 52 patients who had completed 4 cycles, of which 13 were patients with pNETs; of these patients with pNETs, 11 (85%) had a partial or minor response.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
NETTER-R is a phase IV, non-interventional retrospective registry study of patients with pancreatic neuroendocrine tumours who have been treated with 177Lu oxodotreotide. Relevant comparators for 177Lu oxodotreotide may include sunitinib, everolimus, or temozolomide plus capecitabine. | For pERC consideration |
Considerations for initiation of therapy | |
Can patients treated with octreotide LAR 60 mg be eligible for treatment with 177Lu oxodotreotide? Can patients previously treated with lanreotide be eligible for treatment with 177Lu oxodotreotide? | The clinical experts agreed that patients who were treated with octreotide LAR 60 mg or lanreotide would be eligible for treatment with 177Lu oxodotreotide. |
PAG noted that CADTH previously did not recommend 177Lu oxodotreotide re-treatment for adult patients with SSR-positive midgut neuroendocrine tumours. Should 177Lu oxodotreotide re-treatment be funded for patients with unresectable or metastatic SSR-positive pancreatic neuroendocrine tumours? | The clinical experts agreed that, once patients complete 4 doses of 177Lu oxodotreotide, they are typically not re-treated with that therapy. However, some patients may be considered for re-treatment if they were free of disease for 2 years or longer. |
Considerations for discontinuation of therapy | |
The sponsor’s request is for 177Lu oxodotreotide used after progression on an SSA, unless there is a contraindication or intolerance. Can pERC clarify what would constitute a contraindication or intolerance to an SSA? | The clinical experts stated that contraindications to SSAs would include an anaphylactic reaction, or consistent, reproducible, and severe diarrhea after an injection; such diarrhea takes time to resolve (i.e., greater than 1 week) or results in abdominal pain. In general, true contraindications are expected to be rare. |
Considerations for prescribing of therapy | |
7.4 GBq (200 mCi) of 177Lu oxodotreotide is infused IV over 30 minutes every 8 weeks for a maximum of 4 doses. | For pERC consideration |
Administration of 177Lu oxodotreotide is restricted to specialized centres that have the infrastructure to handle, prepare, administer, and dispose of lutetium in a safe manner. Patients may have to travel long distances to access treatment. In some jurisdictions, patients may need to be referred out of province. | For pERC consideration |
Funding algorithm | |
What is the optimal place in therapy for 177Lu oxodotreotide? Under what clinical circumstances would 177Lu oxodotreotide be preferred over everolimus, sunitinib, or temozolomide plus capecitabine? | The NETTER-R study was retrospective and did not include a comparator group. The sponsor provided an ITC that compared 177Lu oxodotreotide to everolimus and sunitinib. While there were significant uncertainties concerning the results of the ITCs, the results suggested that 177Lu oxodotreotide would be more efficacious than everolimus and sunitinib. The clinical experts agreed that 177Lu oxodotreotide would be a preferred regimen over everolimus and sunitinib, as 177Lu oxodotreotide is better tolerated, and, while there is no direct evidence, 177Lu oxodotreotide is expected to be more efficacious than other currently available treatment options. However, temozolomide plus capecitabine may be preferred over 177Lu oxodotreotide for patients with grade 3 well-differentiated pNETs. |
Care provision issues | |
177Lu oxodotreotide has a shelf life of 72 hours, which may result in wastage if the patient cannot receive a scheduled dose for any reason. | For pERC consideration |
Administration of an amino acid solution is required before, during, and after each 177Lu oxodotreotide dose. The compounded solution is prepared within the hospital or procured externally. An antiemetic is also given before the amino acid solution. Octreotide LAR 30 mg IM also needs to be administered between 4 to 24 hours after each 177Lu oxodotreotide dose and then every 4 weeks after completing 177Lu oxodotreotide, until disease progression or for up to 18 months following treatment initiation. Is there evidence to support alternative SSA schedules relative to 177Lu oxodotreotide? | The clinical experts acknowledged that there can be variability in the schedule of administration of SSAs relative to 177Lu oxodotreotide, depending on the institution. The clinical experts agreed that scheduling SSA therapy after PRRT can be challenging in practice, and alternative administration schedules relative to 177Lu oxodotreotide may be appropriate. |
Access to functional imaging (e.g., 68Ga-PET) is needed to confirm SSR positivity. Does the patient require imaging after each 177Lu oxodotreotide dose, and when should imaging be done? | The clinical experts commented that there may be some variation in imaging for patients. A 68Ga-PET scan is required before starting treatment with 177Lu oxodotreotide. 68Ga-PET scans are not typically conducted after each cycle of treatment with 177Lu oxodotreotide. However, SPECT scans should be conducted after each cycle to confirm treatment uptake and to assess whether patient’s disease has progressed. CT imaging is also used as another strategy for surveillance after cycles. The clinical experts also commented that FDG PET scans may also be used to help identify when patients are progressing to higher-grade disease, although this type of imaging may not be as commonly available. |
System and economic issues | |
The budget impact would be influenced by the actual place in therapy for 177Lu oxodotreotide (use in earlier lines vs. later lines). There may be potential “indication creep” if 177Lu oxodotreotide is preferred over an SSA, as 177Lu oxodotreotide may be better tolerated. | For pERC consideration |
Additional resources and coordination among nuclear medicine, radiation oncology, and medical oncology teams are required for imaging, blood work monitoring, and management of adverse events. Inpatient administration may also be required. | For pERC consideration |
In most jurisdictions, oversight and funding of radiopharmaceuticals is through other areas of the Ministry, outside of the drug programs. Inpatient funding may also be covered through a different Ministry budget. | For pERC consideration |
177Lu = lutetium-177; 68Ga = gallium-68; FDG = fluorodeoxyglucose; IM = intramuscularly; LAR = long-acting release; PAG = Provincial Advisory Group; pERC = pCODR Expert Review Committee; pNET = pancreatic neuroendocrine tumour; PRRT = peptide receptor radionuclide therapy; SPECT = single-photon emission CT; SSA = somatostatin analogue; SSR = somatostatin receptor.
Clinical Evidence
The clinical evidence included in the review of 177Lu oxodotreotide is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of177Lu oxodotreotide at 7.4 GBq (200 mCi) as an IV infusion over 30 minutes every 8 weeks for a total of 4 doses. 177Lu oxodotreotide is being reviewed for the treatment of unresectable or metastatic, well-differentiated, SSR-positive pNETs in adults whose disease has progressed after treatment with an SSA, unless there is a contraindication or intolerance.
Methods
Studies selected for inclusion in the systematic review include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adult patients with unresectable or metastatic, well-differentiated, somatostatin receptor–positive pancreatic neuroendocrine tumours whose disease has progressed after treatment with a somatostatin analogue |
Intervention | 177Lu oxodotreotide administered in 4 doses, for a total dose of 29.6 GBq (800 mCi), via IV infusion, in weeks 0, 8, 16, and 24 in combination with octreotide 30 mg long-acting release, which continues monthly up to 18 months |
Comparators |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase III and IV RCTs |
177Lu = 177lutetium; AE = adverse event; DOR = duration of response; HRQoL = health-related quality of life; MDS = myelodysplastic syndrome; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; TTP = time to tumour progression; WDAE = withdrawal due to adverse event.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.19
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were lutetium Lu 177 oxodotreotide and pancreatic neuroendocrine tumours. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on April 21, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on August 10, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.20 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
Findings From the Literature
A total of 1 study was identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6. A list of excluded studies is presented in Appendix 2.
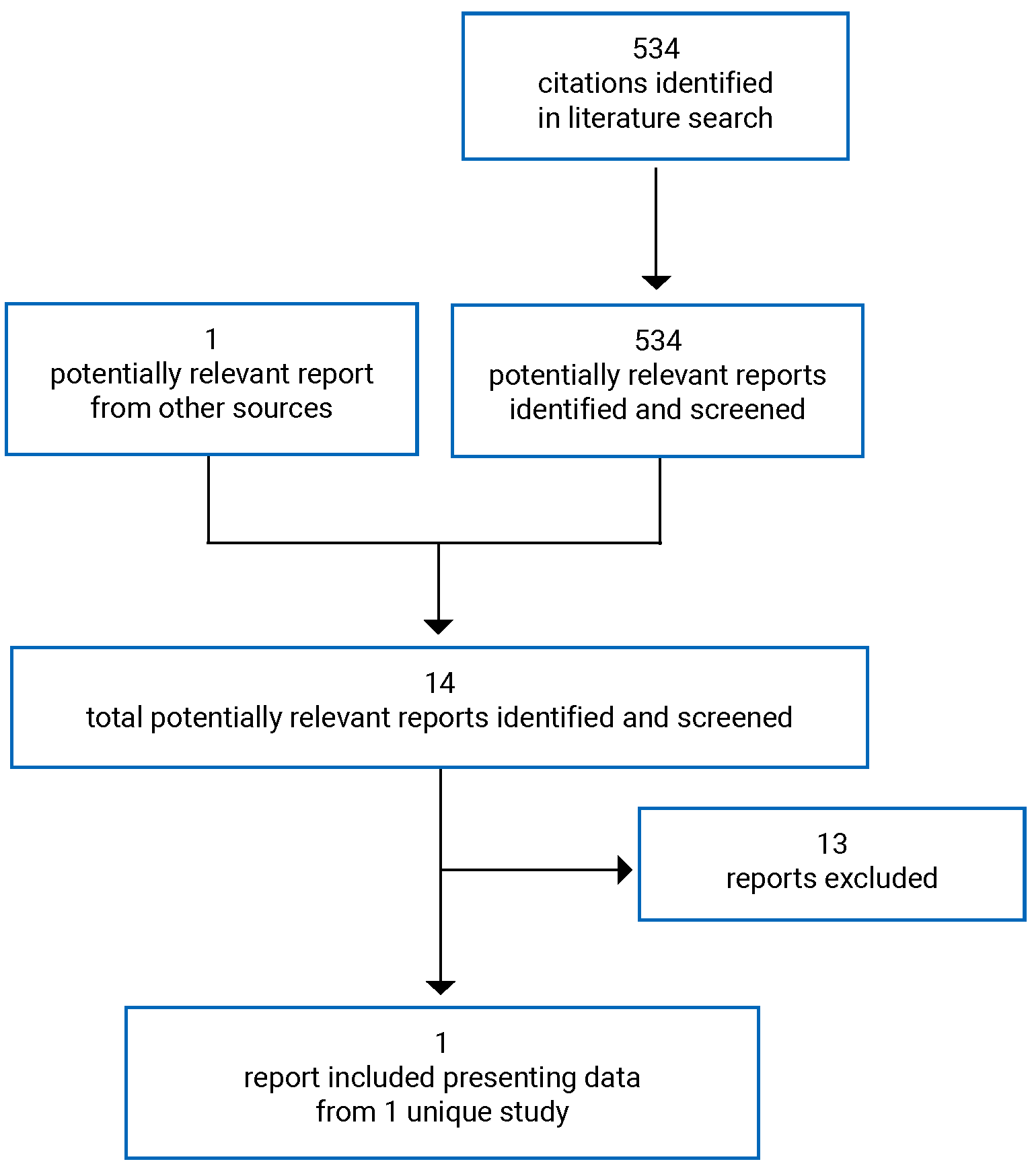
Table 6: Details of Included Studies
Detail | NETTER-R |
|---|---|
Design and population | |
Study design | Retrospective registry study |
Locations | Europe (UK, Spain, France) |
Patient enrolment dates | NA |
Enrolled (N) | 110 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | 177Lu oxodotreotide was administered in 4 infusions of 7,400 MBq each. |
Comparator | NA |
Outcomes | |
Primary end point | PFS |
Secondary and exploratory end points | Secondary:
|
Notes | |
Publications | Clement et al., 202221 |
111In = indium-111; 177Lu = 177lutetium; 68Ga = gallium-68; DOR = duration of response; HRQoL = health-related quality of life; NA = not applicable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour; SSR = somatostatin receptor; TTP = time to tumour progression.
Source: NETTER-R Clinical Study Report.5
Description of Studies
In a previous CADTH review for 177Lu oxodotreotide, the recommendation did not support use of 177Lu oxodotreotide among patients with pNETs, since these patients were excluded from the pivotal study (NETTER-1 trial). The NETTER-R post-marketing study was provided for this reassessment for 177Lu oxodotreotide for patients with pNETs. The NETTER-R study was a non-interventional, non-comparative, post-authorization retrospective registry study to assess long-term efficacy and safety of treatment with 177Lu oxodotreotide in patients with SSR-positive pNETs who had unresectable or metastatic, progressive disease. Progressive disease was assessed both radiologically and clinically, through investigator opinion. Approximately 120 patients across 3 countries were planned to be enrolled for data collection; specifically, 85 patients from 3 sites in the UK, 25 patients from 4 sites in France, and 15 patients from 4 sites in Spain. In fact, the study included 110 patients who met the pre-specified criteria for inclusion (Table 6). The approximate number of patients planned to be enrolled was based on the number of potentially eligible patients included in the CUP and those identified by investigators who were receiving commercial 177Lu oxodotreotide at the selected study. To be included in the study, patients must have been treated with 177Lu oxodotreotide either through the AAA Lutathera CUP, which was approved in 10 European countries since 2011 to 2012, or with a commercial drug. Patients’ paper-based and electronic medical records were collected in 3 of the countries where the CUP was in place, including the UK, France, and Spain. Most of the patients with pNETs who received treatment in this study were part of the CUP in 1 of the European Neuroendocrine Tumor Society Centers participating in this program. The retrospective data collection from medical records began on October 31, 2018, at the first study site. Data were tentatively collected at follow-up visits every 3 months, depending on the standard care in local practice and source document availability at the sites.
The primary objective of the NETTER-R study was to determine the efficacy of 177Lu oxodotreotide, in patients with pNET according to a set of pre-specified eligibility criteria. The secondary objective of the study was to determine the safety and tolerability of 177Lu oxodotreotide.4
Populations
Inclusion and Exclusion Criteria
A complete list of eligibility criteria is reported in Table 6; to be eligible for the NETTER-R study, patients had to meet all eligibility criteria and none of the exclusion criteria. Eligibility criteria included patients with SSR-positive, unresectable or metastatic, well-differentiated pNETs with progressive disease who had been treated with 177Lu oxodotreotide. Patients were not eligible if they were diagnosed with NETs of other origins.5
Baseline Characteristics
A summary of baseline characteristics of patients in the NETTER-R study are reported in Table 7. A total of 110 patients were enrolled, with a mean age of 58 years (||||||||; range, 28.0 to 89.0 years). Relatively equal proportions of males (53%) and females (47%) were enrolled. |||| of patients were white (|||), although for many patients, race was not reported (43%). The primary sites of metastases before patients started treatment with 177Lu oxodotreotide were the liver (96%), lymph nodes (43%), bone (29%), and lungs (4%). The liver tumour burden was from 10% to 25% in 29% of patients and more than 25% or more than 2 metastatic organs in 36% of patients. More than half of patients had nonfunctional tumours (57%), 30% of patients had functional tumour status, and the remainder lacked an assessment of tumour functionality (11%). Most patients had a Ki-67 index of 3% to 20% (66%) and 24% had a Ki-67 index of 2% or less. Most had a histopathological intermediate (grade 2; 65%) or low (grade 1; 27%) grade of disease. The majority of patients (74.5%) had an inoperable tumour, leaving approximately 1-quarter of patients (25.5%) who did not have an inoperable tumour; based on the eligibility criteria, patients with operable tumours should not have been included in the NETTER-R study. The sponsor clarified that patients with advanced pNETs with uncontrolled symptoms are considered for debulking surgery; patients who underwent debulking surgery were not excluded from the trial and were aligned with the indication for 177Lu oxodotreotide approved in Europe.6 Many patients received an Octreoscan (|||) or a 68Ga-PET scan (|||). Of patients with ECOG PS assessed, most patients had an ECOG PS of 0 (|||) or 1 (|||).5
Most patients had received prior anticancer treatments (92%), with a mean 4.7 prior or concomitant therapies. Prior anticancer therapy specifically for pNET disease was received by 91% of patients; these patients received mainly chemotherapy (|||), radiotherapy (|||), or other therapies (91%).5 Seventy percent of patients had received prior somatostatins and analogues, mainly lanreotide or octreotide (||| ||||). Prior TKIs were received by 38% of patients, mainly everolimus (33%) or sunitinib (20%). Slightly more than |||| of patients (|||) had received prior surgical and medical procedures. Patients most commonly underwent a pancreatic operation (|||), with others having a liver operation (|||), or radiotherapy (|||).
Table 7: Summary of Patient Characteristics (Full Analysis Set)
Characteristic | 177Lu oxodotreotide N = 110 |
|---|---|
Age (years) | |
Mean (SD) | 58.0 (12.17) |
Range | 28 to 89 |
Sex, n (%) | |
Male | 58 (52.7) |
Female | 52 (47.3) |
Race, n (%) | |
Black or African American | | |||||| |
Asian | | |||||| |
White | || ||||||| |
Not reported | || ||||||| |
Patients with prior/concomitant anticancer therapy | |
n | 103 |
Mean, (SD) | 4.7 (2.87) |
Time to 177Lu oxodotreotide treatment (months) | |
First GEPNET diagnosis (months) | |
n | 110 |
Mean (SD) | 58.1 (47.56) |
First metastasis (months) | |
n | 106 |
Mean (SD) | 45.6 (34.90) |
First progression (months) | |
n | 105 |
Mean (SD) | 27.2 (25.99) |
Last progression (months) | |
n | 105 |
Mean (SD) | 4.3 (3.11) |
Site of metastasis before starting 177Lu oxodotreotide, n (%) | |
Liver | 105 (95.5) |
Lymph nodes | 47 (42.7) |
Bone | 32 (29.1) |
Lungs | 4 (3.6) |
Peritoneal | 2 (1.8) |
Peritoneum | 2 (1.8) |
Othera | 7 (6.4) |
Liver tumour burden before starting 177Lu oxodotreotide, n (%) | |
Liver burden < 10% | 9 (8.2) |
Liver burden ≥ 10% to ≤ 25% | 32 (29.1) |
Liver burden > 25% or more than 2 metastatic organs | 39 (35.5) |
Missing | 30 (27.3) |
Tumour status, n (%) | |
Functional | 33 (30.0) |
Nonfunctional | 63 (57.3) |
Not assessed | 12 (10.9) |
Missing | 2 (1.8) |
Is the tumour inoperable? n (%) | |
Yes | 82 (74.5) |
No | 28 (25.5) |
Missing | 0 |
Ki-67 index, n (%) | |
≤ 2% | 26 (23.6) |
3% to 20% | 73 (66.4) |
> 20% | 3 (2.7) |
Missing | 8 (7.3) |
Histopathological grade at diagnosis, n (%) | |
Grade 1: low-grade | 30 (27.3) |
Grade 2: intermediate-grade | 71 (64.5) |
Grade 3: high-grade | 3 (2.7) |
Missing | 6 (5.5) |
Tumour uptake, n (%) | |
Octreotide scan | || ||||||| |
Grade 0 | |||||||| |
Grade 1 | | |||||| |
Grade 2 | || ||||||| |
Grade 3 | || ||||||| |
Grade 4 | || ||||||| |
Missing | | |||||| |
68Ga-PET | || ||||||| |
Grade 0 | |||||||| |
Grade 1 | |||||||| |
Grade 2 | |||||||| |
Grade 3 | | |||||| |
Grade 4 | || ||||||| |
Missing | || ||||||| |
Otherb | | |||||| |
Grade 0 | |||||||| |
Grade 1 | |||||||| |
Grade 2 | |||||||| |
Grade 3 | |||||||| |
Grade 4 | |||||||| |
Missing | | |||||| |
Was the ECOG performed? n (%) | |
Yes | 59 (53.6) |
No | 50 (45.5) |
ECOG PS, n (%),c | |
0 | || ||||||| |
1 | || ||||||| |
2 | | |||||| |
3 | | |||||| |
4 | |||||||| |
5 | |||||||| |
ECG evaluationd | |
N | 6 |
Normal, n (%) | 6 (100.0) |
Abnormal, not clinically significant, n (%) | 0 |
Abnormal, clinically significant, n (%) | 0 |
Target lesions: Were any target lesions identified? n (%) | |
Yes | 75 (68.2) |
No | 35 (31.8) |
Missing | 0 (0.0) |
Number of target lesions | |
n | 75 |
Sum of longest diameters for target lesions (short axis for lymph nodes) (mm), mean (SD) | 110.9 (67.70) |
Were any non-target lesions identified? n (%) | |
Yes | 48 (43.6) |
No | 62 (56.4) |
Missing | 0 |
177Lu = 177lutetium; 68Ga = gallium-68; ECG = electrocardiogram; ECOG = Eastern Cooperative Oncology Group; GEPNET = gastroenteropancreatic neuroendocrine tumour; PS = performance status; SD = standard deviation.
aIncludes celiac, ileal mass, mesenteric, pancreas, pelvis, pleura and spleen (n = 1 for each).
bTumour uptake other than 68Ga-PET and octreotide scan.
cPercentages are based on the population who have performed the ECOG test.
dPercentages are based on the population who have performed the ECG test.
Source: NETTER-R Clinical Study Report.5
Table 8: Prior Therapies (Full Analysis Set)
Characteristic | 177Lu oxodotreotide N = 110 |
|---|---|
Patient with prior medication or therapy to treat cancer? n (%) | |
Yes | 101 (91.8) |
No | 9 (8.2) |
Patient with prior anticancer therapy for pNET disease? n (%) | |
Yes | 100 (90.9) |
No | 10 (9.1) |
Treatment type | |
Radiotherapy | || ||||||| |
Radiometabolic | 2 (1.8) |
Chemotherapy | || ||||||| |
Other | 100 (90.9) |
Patients with any prior medication, n (%) | 109 (99.1) |
Prior somatostatin and analogues, n (%) | 77 (70.0) |
Lanreotide | || ||||||| |
Octreotide | || ||||||| |
Somatostatin | 8 (7.3) |
Prior protein kinase inhibitors, n (%) | 42 (38.2) |
Everolimus | 36 (32.7) |
Sunitinib | 22 (20.0) |
Dactolisib | 1 (0.9) |
Surgical and medical procedures, n (%) | || ||||||| |
Pancreatic operation | || ||||||| |
Liver operation | || ||||||| |
Radiotherapy | | |||||| |
Source: NETTER-R Clinical Study Report.5
Treatments
177Lu oxodotreotide was administered in 4 infusions of 7,400 MBq each. The study included patients with pNETs who received any dosage of 177Lu oxodotreotide (regardless of the duration and number of doses administered) and discontinued the treatment for any reason. Patients could withdraw from the protocol at any time without giving a reason for doing so. Information on concomitant therapies and surgeries was also captured.
Outcomes
The efficacy end points identified in the CADTH review protocol that were assessed in the included study are provided in Table 9. These end points are further summarized in this section. Tumour response was based on local investigator assessment. Attempts were made to retrospectively collect radiological response according to RECIST version 1.1 and according to other local assessments, if available, including biochemical, clinical, and/or metabolic assessments (based on somatostatin receptor imaging; e.g., octreotide scan, Tektrotyd, 68Ga-PET). For efficacy assessments based on tumour assessments (i.e., PFS, ORR, DOR, TTP), 2 versions of the end points were derived: 1 version included only RECIST version 1.1 tumour assessments, while the other version included all assessments available (i.e., including biochemical, metabolic, clinical, and radiological assessments, if different from RECIST 1.1) and was labelled as investigator opinion.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | Definition in NETTER-R |
|---|---|
Primary | |
PFS as documented by the local investigator based on radiological assessment | The time from treatment start to documented disease progression or death due to any cause |
Secondary | |
AE | Incidence and frequency of AEs according to the NCI CTCAE version 4.03 |
OS | The time from the date of first 177Lu oxodotreotide treatment to the date of death due to any cause |
PFS by local investigator, based on biochemical, metabolic, and/or clinical assessments | The time from treatment start to documented disease progression or death due to any cause |
ORR | The proportion of patients with partial or complete response at the time of the statistical analysis Best response was defined as the best tumour assessment outcome (partial or complete response, stable disease, or progressive disease) a patient reached after treatment with 177Lu oxodotreotide and before progressing or starting a new anticancer therapy, whichever came first |
DOR | The time from initially meeting the criteria for response (partial or complete) until the time of disease progression |
TTP | The time from treatment start to tumour progression |
AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; DOR = duration of response; NCI = National Cancer Institute; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; TTP = time to tumour progression.
Source: NETTER-R Clinical Study Report.5
Statistical Analysis
Descriptive statistic and graphical presentations of data were the primary focus of the statistical analysis. Continuous variables were presented as the number of non-missing values, mean, SD, median, range, and quartiles. Descriptive statistics for categorical variables included counts and percentages per category, and 95% CIs were computed where appropriate. Exploratory analyses were performed to explore the impact on the outcomes of population characteristics that were thought to bias any comparisons of results from the NETTER-R study with those of other studies.
Outcomes analyzed in the NETTER-R study, along with their definitions, are summarized in Table 9.
Progression-Free Survival
A summary of the number of patients with PFS events was reported, along with summary statistics obtained from the Kaplan-Meier estimates, including median PFS with 95% CIs and 25th and 75th percentiles, and PFS probabilities at key time points after their first dose, if relevant, along with 95% CIs. A Kaplan-Meier plot was produced. Patients were censored at the date of their last evaluable tumour assessment if they had not experienced disease progression or died by the time of data collection, in the context of time-to-event analyses. Patients were also censored at their treatment start date if they did not have any post-baseline assessments. Two sensitivity analyses were performed: 1 that censored PFS for cases if 2 adjacent tumour assessments were more than 9 months apart, and another that censored patients on the date of their last available assessment before new anticancer therapy (if they received a new anticancer therapy before disease progression).4
Objective Response Rate
The data cut-off date was the last data point collected, provided that enough efficacy data were available. ORRs and 95% CIs were presented descriptively.4
Base response rates were presented descriptively using frequencies and percentages. A summary of the number of unconfirmed responses who will fall under the stable disease category was also provided. The best overall response (BOR) was derived following these 2 steps:
All available post-baseline tumour assessments that were on or before the minimum on non-missing dates were kept among first radiological progressive disease, start date of new anticancer therapy, and cut-off date. When all 3 dates were missing, all available post-baseline tumour assessments were included. If patients had at least 1 post-baseline tumour assessment with an overall response of complete response, then the BOR equated to complete response; further, if a patient had at least 1 post-baseline tumour assessment an overall response of partial response, then BOR equated to partial response; and if a patient had at least 1 post-baseline tumour assessment with an overall response of stable disease, the BOR equated to stable disease.
If BOR could not be obtained based on the previous step, the following step was conducted to capture BOR:
If a patient had at least 1 radiological progressive disease, BOR equated to progressive disease; otherwise, if a patient had at least 1 available post-baseline target or non-target lesion, then BOR equated to not evaluable or to “No post-baseline scan.”
Duration of Response
The Kaplan-Meier method was used to assess median DOR and its associated 95% CI. A Kaplan-Meier plot was also produced. Patients were censored on the date of their last adequate radiological assessment if they never had documented progression.
Time to Tumour Progression
TTP was analyzed in the same manner as PFS, except that patients who died without measured progression were not considered a progression event; instead, these patients were censored at their date of last tumour assessment. The median TTP, 95% CI, 25th and 75th percentile, and TTP probabilities at key time points after patient’s first dose, if relevant, with 95% CIs, were provided using the Kaplan-Meier method. A Kaplan-Meier plot was produced.
Overall Survival
The analysis of OS consisted of summary statistics, along with data obtained from Kaplan-Meier estimates, including the median OS with associated 95% CIs, 25th and 75th percentiles, and survival probabilities at key time points. A Kaplan-Meier plot was produced. Patients were censored on their last date of contact if they were still alive or if their status was unknown.
Safety
AEs were coded using the available version of MedDRA (version 20.1 or later). Frequencies and proportions were reported for AEs.
Missing Data
No imputation was performed for missing data.4
Analysis Populations
A summary of analysis sets used in the NETTER-R study is reported in Table 10. The full analysis set (FAS) was used for efficacy analyses, while the safety analysis set (SAS) was used for safety analyses.4 An addendum was made to the statistical analysis plan of the NETTER-R study, which included a post hoc analysis using the modified FAS (mFAS) for efficacy end points. Patients who would were excluded from the FAS due to a lack of adequate post-baseline imaging were included in the mFAS. However, both the FAS and mFAS were considered interchangeable, as all 110 patients were included in both. PFS, ORR, and TTP were analyzed using the mFAS.
Table 10: Analysis Sets in the NETTER-R Study
Analysis set | Description |
|---|---|
Full analysis set (FAS) | All eligible patients who had received at least 1 dose of 177Lu oxodotreotide and who had performed at least 1 efficacy assessment after baseline |
Modified FAS (mFAS) | All patients who received at least 1 dose of 177Lu oxodotreotide and provided data for at least 1 efficacy end point, including OS |
Safety analysis set (SAS) | All patients who received at least 1 dose of 177Lu oxodotreotide |
Source: NETTER-R Protocol.4
Results
Patient Disposition
A summary of the patient disposition of the NETTER-R study is provided in Table 11. A total of 110 patients were enrolled, including 66 patients from the UK, 21 from France, and 23 from Spain. Of these, 76% completed the treatment with 177Lu oxodotreotide. The primary reasons for stopping treatment were disease progression (10%), death (6%), the patient’s best interest in the opinion of the investigator (|||), other (|||), and AEs (1%).
Disposition | Total N = 110 |
|---|---|
Completed treatment, n (%) | 84 (76.4) |
Primary reason for end of treatment phase, n (%) | |
AEs | 1 (0.9)a |
Best patient’s interest in the investigator’s opinion | ||| (||||) |
Death | 7 (6.4) |
Disease progression | 11 (10.0) |
Other | ||| (||||) |
Missing | 0 |
FAS, N (%) | 110 (100.0) |
mFAS, N (%) | 110 (100.0) |
OS, N (%) | 110 (100.0) |
PFS, ORR, TTP, DOR by RECIST version 1.1, N | 62 |
PFS, ORR, TTP, DOR by Investigator opinion 1, N | 83 |
PFS, ORR, TTP, DOR by Investigator opinion 2, N | 100 |
Safety, N (%) | 110 (100.0) |
AE = adverse event; DOR = duration of response; FAS = full analysis set; mFAS = modified full analysis set; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors; TTP = time to tumour progression.
aFor Patient A-LUT-ES02 to 0097 to 0003, the reason for end of treatment phase was not consistent with the action taken field for AEs in the case report form. Therefore, this patient is not counted for the analysis of TEAEs leading to discontinuation.
Source: NETTER-R Clinical Study Report.5
Protocol Deviations
| ||||| || |||| |||||||| |||||| ||| | ||||| |||||||| |||||||||. These protocol deviations were due to not meeting inclusion or exclusion criteria, mainly having no progressive disease at baseline visit (in 4 patients), baseline tumour SSR uptake equal to grade 1 (in 3 patients), and having a tumour that was not well-differentiated (in 2 patients). According to the sponsor, the major protocol deviations did not lead to exclusion of patients from the FAS or the SAS.5
||||| |||||||| |||||||||| |||| |||||||| || || ||||||| ||||||||. The most common reasons for minor protocol deviations involved baseline diagnoses; specifically, 21 patients (19.1%) had missing baseline tumour uptake, 6 patients (5.5%) did not have information on well-differentiated tumour, and 5 patients (4.5%) had unknown tumour uptake. Other minor protocol deviations, such as deviations due to visit dates out of the scheduled time window or lab parameters not evaluated, were also reported in a limited number of patients (n < 3).5
Exposure to Study Treatments
A summary of study treatment exposure is provided in Table 12. All 110 patients (100.0%) patients received 177Lu oxodotreotide under the AAA CUP in Europe. Most patients received 4 doses of 177Lu oxodotreotide (70%), with some patients (11% and 12%) receiving 3 or 2 doses, respectively. The cumulative dose of 177Lu oxodotreotide received was high, with most patients receiving from 720 to 880 mCi (66%), and a third of patients receiving less than 720 mCi. The average dose per administration of 177Lu oxodotreotide was 199.8 mCi (SD = 15.80), which is in line with the standard dose of 177Lu oxodotreotide of 200 mCi ± 10%. The mean total duration of first to last dose of 177Lu oxodotreotide was 8.8 months (SD = 4.15), which is also in line with a standard course of 4 administrations of 177Lu oxodotreotide within 12 months. In general, dose intensity results for 177Lu oxodotreotide in the NETTER-R study suggests that a full dose of 177Lu oxodotreotide is tolerable.5
After the initial treatment period, there were 12 patients who received additional doses of 177Lu oxodotreotide; 3 patients had received 1 additional dose, 7 patients received 2 additional doses, and additional 3 and 4 doses were given to 1 patient each. The average dose per administration was 187 mCi among these patients, with a mean duration from first to last administration of 6.4 months (SD = 5.11).
Table 12: Exposure to Study Drug (Safety Analysis Set)
Dosage variable | Treatment period N = 110 | Re-treatment period N = 12 |
|---|---|---|
Cumulative dose, n (%) | ||
< 720 mCi | 35 (31.8) | 11 (91.7) |
≥ 720 to < 880 mCi | 72 (65.5) | 1 (8.3) |
≥ 880 mCi | 3 (2.7) | 0 |
Number of dose administrations in categories, n (%) | ||
1 dose | 7 (6.4) | 3 (25.0) |
2 doses | 13 (11.8) | 7 (58.3) |
3 doses | 12 (10.9) | 1 (8.3) |
4 doses | 77 (70.0) | 1 (8.3) |
5 doses | 1 (0.9) | 0 |
Average dose per administration, mCi | ||
Mean (SD) | 199.8 (15.80) | 187.3 (34.95) |
Number of administrations | ||
Mean (SD) | 3.5 (0.95) | 2.0 (0.85) |
Total duration from first to last administration (months) | ||
Mean (SD) | 8.8 (4.15) | 6.4 (5.11) |
SD = standard deviation.
Source: NETTER-R Clinical Study Report.5
Concomitant Medications
A summary of concomitant medications taken by patients in the NETTER-R study is provided in Table 13. Concomitant therapies were received by ||| of patients. The most common type of concomitant therapy was other (|||) and chemotherapy (|||), with few patients (||||) receiving radiotherapy. Patients receiving other therapies mostly received somatostatin and analogues (|||).5
Dose Modifications
Dose modifications are provided in Table 14. |||||||| ||||| |||| ||| |||| |||||||||||||| |||| ||||||||||||| |||| |||||||| || || |||||||| |||||| |||| |||||||| |||||||| ||| || |||||||| ||||| ||||| |||| |||||||| |||||||| ||| ||| |||||||| ||||.
Table 13: Concomitant Therapies (Safety Analysis Set)
Therapy | 177Lu oxodotreotide N = 110 |
|---|---|
Patient with medication or therapy to treat cancer? | |
Yes | || ||||||| |
No | || ||||||| |
Patient with anticancer therapy for study NET disease? | |
Yes | || ||||||| |
No | || ||||||| |
Treatment type | |
Radiotherapy | | |||||| |
Radiometabolic | ||||||||| |
Chemotherapy | || ||||||| |
Other | || ||||||| |
NET = neuroendocrine tumour.
Source: NETTER-R Clinical Study Report.5
Table 14: Dose Modifications (Safety Analysis Set)
Dose modification | 177Lu oxodotreotide N = 110 |
|---|---|
|||||||| |||| |||| ||||||||||||| | || ||||||| |
|||| || |||| ||||||||||||| | |
|||| |||||||| | || ||||||| |
||||| | | |||||| |
|||||| | | |||||| |
|||| |||||||| | | |||||| |
||||| | | |||||| |
|||||| | | |||||| |
| |||| |||||||||||| |||||||| |||| |||||||| ||| |||| ||||||||| || |||| ||||| || |||| ||||||||||||| | ||||||| || ||||||| |||| ||||||| |||| |||||||| || ||||||| || |||| |||| ||| |||||||||||| ||||| | ||| ||||| ||| |||| |||| |||||||| || ||||||| || |||| |||| ||| |||||||||||| ||||| ||| |||| ||| ||||||||| |||| |||| ||| |||||||| |||| |||| ||| |||| |||||||| ||||| ||||||||| |||| |||| ||| |||||||| ||||| || || |||| |||| ||||| ||| |||| ||||||||
Source: NETTER-R Clinical Study Report.5
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported in this section. All analyses are considered descriptive. Refer to Appendix 3 for detailed efficacy data.
Overall Survival
Detailed outcome data for OS are provided in Table 15. A median follow-up time of 24.5 months was reported. There were 55 patients (50%) who experienced an OS event in the NETTER-R study. The median OS was 41.4 months (95% CI, 28.6 to 50.2; Figure 2). Half of patients were censored for the analysis of OS.
Table 15: Overall Survival (Full Analysis Set)
Survival variables | 177Lu oxodotreotide N = 110 |
|---|---|
Number of events, n (%) | 55 (50.0) |
Number censored (alive at last contact), n (%) | 55 (50.0) |
Alive, n (%) | 51 (46.4) |
Lost to follow-up, n (%) | 4 (3.6) |
Median, months (95% CI)a | 41.4 (28.6 to 50.2) |
6-month survival rate, % (95% CI)a | 92.7 (86.0 to 96.3) |
12-month survival rate, % (95% CI)a | 82.2 (73.6 to 88.3) |
24-month survival rate, % (95% CI)a | 68.2 (58.0 to 76.4) |
36-month survival rate, % (95% CI)a | 53.8 (42.8 to 63.7) |
48-month survival rate, % (95% CI)a | 44.6 (32.9 to 55.5) |
60-month survival rate, % (95% CI)a | 35.6 (23.9 to 47.6) |
72-month survival rate, % (95% CI)a | 32.4 (20.4 to 44.9) |
84-month survival rate, % (95% CI)a | 27.8 (15.3 to 41.8) |
96-month survival rate, % (95% CI)a | 20.8 (8.0 to 37.8) |
CI = confidence interval.
aEstimated by the Kaplan-Meier method.
Notes: OS is defined as the time from the date of treatment start to the date of death due to any cause.
Data cut-off date: October 27, 2020.
Source: NETTER-R Clinical Study Report.5
Figure 2: Kaplan-Meier Plot of Overall Survival (Full Analysis Set)
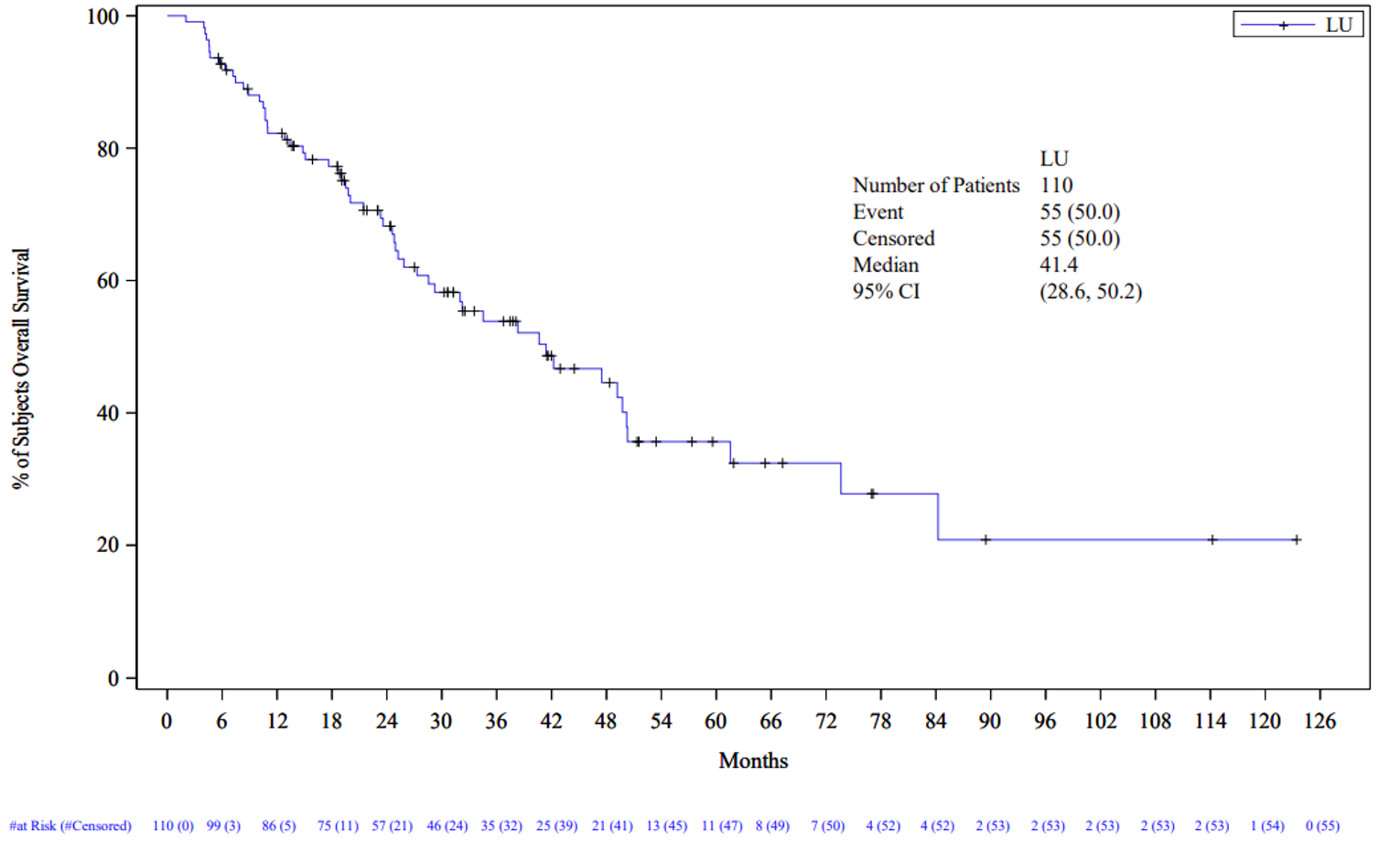
LU = 177Lu oxodotreotide.
Notes: Overall survival is defined as the time from treatment start to the date of death due to any cause, unless censored.
Data cut-off date: October 27, 2020.
Source: NETTER-R Clinical Study Report.5
Progression-Free Survival
Results for the primary end point of PFS were based on RECIST version 1.1 in the mFAS (Table 16). Results using the FAS were nearly identical. In the primary analysis of PFS, there were 41 PFS events (66%), of which most were progression (|||), and |||| were deaths (|||). The median PFS was 24.8 months (95% CI, 17.5 to 34.5). PFS was also assessed using the RECIST version 1.1 criteria based on investigator’s opinion as a secondary end point (Figure 3). PFS based in investigator’s opinion 1 was based on tumour assessments and other radiological assessments. PFS based on investigator’s opinion 2 was based on other radiological, clinical, biomarker, and metabolic assessments. The additional analyses of PFS were consistent with the primary analysis of PFS (Figure 4; Figure 5).
Sensitivity analyses are not reported here but were consistent with the primary analyses of PFS.
Table 16: Progression-Free Survival — RECIST Version 1.1 (Patients With Post-Baseline Scan per RECIST 1.1 in Modified FAS)
Variable | 177Lu oxodotreotide N = 62 | 177Lu oxodotreotide Investigator opinion 1 N = 83 | 177Lu oxodotreotide Investigator opinion 2 N = 100 |
|---|---|---|---|
Number of events, n (%) | 41 (66.1) | 56 (67.5) | 64 (64.0) |
Documented progression | ||| (|||||) | 44 (53.0) | 49 (49.0) |
Death | ||| (|||||) | 12 (14.5) | 15 (15.0) |
Number censored, n (%) | 21 (33.9) | 27 (32.5) | 36 (36.0) |
No post-baseline tumour assessments | 2 (3.2) | 27 (32.5) | 36 (36.0) |
No documented progression | 19 (30.6) | NA | NA |
Median, months (95% CI)a | 24.8 (17.5 to 34.5) | 24.0 (19.8 to 31.3) | 24.0 (19.8 to 29.7) |
6-month survival rate, % (95% CI)a | 84.8 (72.8 to 91.8) | 86.6 (77.1 to 92.4) | 85.9 (77.3 to 91.4) |
12-month survival rate, % (95% CI)a | 71.1 (57.7 to 81.0) | 72.9 (61.8 to 81.2) | 70.9 (60.6 to 78.9) |
24-month survival rate, % (95% CI)a | 51.9 (37.3 to 64.6) | 49.7 (37.5 to 60.8) | 49.0 (37.6 to 59.5) |
36-month survival rate, % (95% CI)a | 35.9 (22.0 to 50.0) | 32.8 (21.3 to 44.8) | 31.1 (20.2 to 42.6) |
48-month survival rate, % (95% CI)a | 29.4 (16.1 to 43.9) | 25.5 (14.7 to 37.8) | 24.7 (14.5 to 36.3) |
60-month survival rate, % (95% CI)a | 25.7 (13.0 to 40.5) | 19.4 (9.4 to 32.1) | 19.9 (10.5 to 31.5) |
72-month survival rate, % (95% CI)a | 12.8 (3.7 to 27.9) | 11.7 (3.6 to 24.9) | 12.0 (3.9 to 24.9) |
CI = confidence interval.
aEstimated by the Kaplan-Meier method.
Note: Long-time elapsed missing assessments are defined as more than 9 months after the last radiological assessment (i.e., 270 days following the previous visit).
Source: NETTER-R Clinical Study Report.5
Figure 3: Kaplan-Meier Plot of PFS — RECIST 1.1 (Patients With Post-Baseline Scan per RECIST 1.1 in Modified FAS)
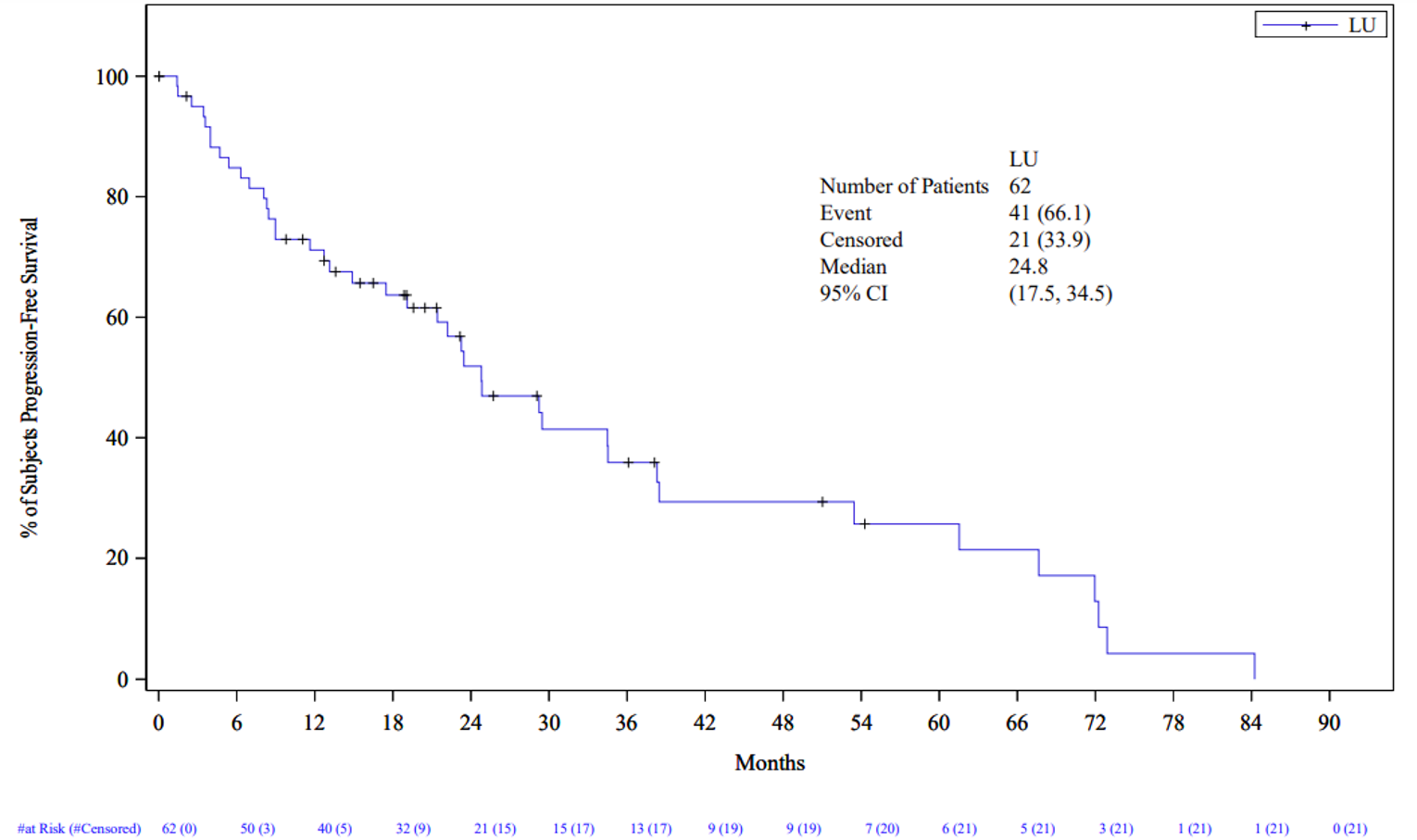
LU = 177Lu oxodotreotide.
Notes: Progression-free survival is defined as the time from treatment start to documented assessed disease progression, per RECIST version 1.1, or death due to any cause, unless censored.
Data cut-off date: October 27, 2020.
Source: NETTER-R Clinical Study Report.5
Figure 4: Kaplan-Meier Plot of PFS — Based on RECIST 1.1 or Radiological Assessments (Investigator Opinion 1) (Patients With Post-Baseline Scan Per Investigator Opinion 1 in Modified FAS) — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Figure 5: Kaplan-Meier Plot of PFS — Based on RECIST 1.1, or Radiological, Clinical, Metabolic, or Biomarker Assessments (Investigator Opinion 2) (Patients With Post-Baseline Tumour Assessment per Investigator Opinion 2 in Modified FAS) — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Objective Response Rate
ORR based on the primary analysis was assessed in 62 patients. The ORR was 40.3% (95% CI, 28.1 to 53.6). None of the patients had a complete response, according to RECIST version 1.1 criteria. Partial response was reported in 40.3% of patients. Stable disease and progressive disease were reported for 35.5% and 21.0% of patients, respectively. As with PFS, ORR was also assessed using the RECIST version 1.1 criteria based on investigator’s opinion as a secondary end point. Results for ORR, based on investigators’ opinions 1 and 2, were consistent with the primary analysis of ORR, although the response was slightly better for ORR assessed by investigator’s opinion 2 (Table 17).
Table 17: Overall Tumour Response or Objective Response — RECIST 1.1 (Patients With Post-Baseline Scan per RECIST 1.1 in Modified FAS)
Detail | ORR – RECIST version 1.1 Patients with post-baseline scan per RECIST version 1.1 in modified FAS N = 62 n (%) | ORR – RECIST version 1.1 or other radiological assessments (investigator’s opinion 1) (Patients with post-baseline scan per Investigator’s opinion 1 in modified FAS) N = 83 n (%) | ORR – RECIST version 1.1 or other radiological assessments, or clinical, metabolic, or biomarker assessments (investigator’s opinion 2) (Patients with post-baseline scan per Investigator’s opinion 2 in modified FAS) N = 100 n (%) |
|---|---|---|---|
Best response | 62 | 83 | 100 |
Complete response | 0 | 0 | 2 (2.0) |
Partial response | 25 (40.3) | 36 (43.4) | 52 (52.0) |
Stable disease | 22 (35.5) | 31 (37.3) | 34 (34.0) |
Progressive disease | 13 (21.0) | 16 (19.3) | 12 (12.0) |
Not evaluable | 2 (3.2) | 0 | 0 |
Objective response | 25 (40.3) | 36 (43.4) | 54 (54.0) |
95% CI | (28.1 to 53.6) | (32.5 to 54.7) | (43.7 to 64.0) |
Source: NETTER-R Clinical Study Report.5
Duration of Response
The median DOR was 60.7 months (95% CI, 13.1 to 62.1; Figure 6). At the time of the analysis, there were 8 PFS events observed. As with PFS, DOR was assessed via investigators’ opinions 1 and 2. The DOR based on investigators’ opinions 1 and 2 was shorter than the primary analysis of DOR. The median DOR based on investigator’s opinion 1 was 31.1 months (95% CI, 16.8 to 62.1; Figure 7), with ||| PFS events, while the DOR based on investigator’s opinion 2 was 28.3 months (95% CI, 16.8 to 60.7; Figure 8), with ||| PFS events.
Figure 6: Kaplan-Meier Plot of Duration of Response — RECIST 1.1 Patients With Post-Baseline Scan per RECIST 1.1 in Modified FAS — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Figure 7: Kaplan-Meier Plot of Duration of Response Based on RECIST Version 1.1, or Radiological Assessments (Investigator’s Opinion 1) Patients With Post-Baseline Scan per Investigator’s Opinion 1 in Modified FAS — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Figure 8: Kaplan-Meier Plot of Duration of Response Based on RECIST Version 1.1, or Radiological, Clinical, Metabolic, or Biomarker Assessments (Investigator’s Opinion 2) Patients With Post-Baseline Tumour Assessment Per Investigator’s Opinion 2 in Modified FAS — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Time to Tumour Progression
Results for TTP are reported in Table 18. There was a total of ||| (|||) TTP events, with a median TTP of 29.5 months (95% CI, 21.4 to 67.6; Figure 9). As with PFS, TTP was assessed via investigators’ opinions 1 (Figure 10) and 2 (Figure 11), the results of which were both consistent with the primary analysis of TTP.
Table 18: Time to Tumour Progression — RECIST Version 1.1
Detail | TTP — RECIST version 1.1 Patients with post-baseline scan per RECIST 1.1 in modified FAS N = 62 n (%) | TTP — RECIST version 1.1 or other radiological assessments (Investigator’s opinion 1) Patients with post-baseline scan per investigator’s opinion 1 in modified FAS N = 83 n (%) | TTP — RECIST version 1.1 or other radiological assessments, or clinical, metabolic, or biomarker assessments (investigator’s opinion 2) Patients with post-baseline scan per investigator’s opinion 2 in modified FAS N = 100 n (%) |
|---|---|---|---|
Number of events, n (%) | || ||||||| | || ||||||| | || ||||||| |
Documented progression | || ||||||| | || ||||||| | || ||||||| |
Number censored, n (%) | || ||||||| | || ||||||| | || ||||||| |
No post-baseline tumour assessments | | |||||| | |||||||| | — |
No documented progression | || ||||||| | || ||||||| | || ||||||| |
Death without documented PD | | ||||||| | || ||||||| | || ||||||| |
Median (months) 95% CI | 29.5 (21.4 to 67.6) | 27.9 (21.4 to 37.2) | 29.2 (21.4 to 32.3) |
FAS = full analysis set; PD = progressive disease; TTP = time to tumour progression.
Source: NETTER-R Clinical Study Report.5
Figure 9: Kaplan-Meier Plot of Time to Tumour Progression RECIST 1.1 (Patients With Post-Baseline Scan per RECIST 1.1 in Modified FAS) — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Figure 10: Kaplan-Meier Plot of Time to Tumour Progression RECIST 1.1, or Radiological Assessments (Investigator’s Opinion 1) (Patients With Post-Baseline Scan per Investigator’s Opinion 1 in Modified FAS) — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Figure 11: Kaplan-Meier Plot of Time to Tumour Progression RECIST 1.1, or Radiological, Clinical, Metabolic, or Biomarker Assessments (Investigator’s Opinion 2) RECIST 1.1, or Radiological, Clinical, Metabolic, or Biomarker Assessments (Investigator’s Opinion 2) — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Health-Related Quality of Life
|||||| ||| |||||| ||||||||||||| ||||||||||||| || ||||| || || |||||||| ||||||||| ||| ||||||| ||||||||| ||||||||||||| |||| || |||||||||||| ||||||||| ||||||||| ||||||||| || ||||| ||||||||| ||| |||||| ||| ||||| |||||| || |||||||| || |||||||||| ||| ||| |||| ||||||| || ||| |||| || ||||| |||| ||| |||| || ||||||| |||| |||| ||||||||| |||||| |||||||| ||||| |||||||| || |||||| |||||||||||||| |||| ||||| || |||||||| |||| ||||| || ||| ||||| |||||||||| ||| ||||||| ||||||| || ||| |||||||| |||| |||||||||| |||| ||||| |||| ||||||| |||| || ||||||||| | ||||| || || |||||||| ||||||| |||||||| |||||| |||||||| ||||||||| |||| || |||||| ||| ||||| ||||||||| ||||||||| |||||||| || ||||||||||5 ||||||| ||| |||||||| ||||| ||||||||||||| |||||||| ||| ||| |||||| ||| |||||||| ||| ||||||||||||| ||||| ||| || ||||||||||| || |||| |||| ||| ||||||||| |||| ||| |||| |||||||| || ||||||||| ||||| |||| ||||||| | ||| | |||||||| ||| |||||||| |||| ||| |||| ||||||||||||||5
Harms
Only those harms identified in the review protocol are reported in this section. Refer to Table 19 for detailed harms data.
Adverse Events
AEs were reported in 79 patients (72%). The most common AEs included nausea (28%), fatigue (23%), abdominal pain (16%), vomiting (|||), upper abdominal pain (|||), anemia (|||), diarrhea, lymphopenia, and thrombocytopenia (||| ||||). Grade 3 or 4 AEs were reported in 30 patients (27%). The incidence of grade 3 or 4 AEs was generally infrequent, with each event occurring in less than 5% of patients. The most common grade 3 or 4 AEs were lymphopenia (||||), abdominal pain, ascites, hypercalcemia, and liver abscess (|| ||||).
Serious Adverse Events
SAEs were reported in 29 patients (26%). SAEs were infrequently reported; no SAE occurred in more than 3% of patients. The most common SAEs were liver abscess, ascites, and hypercalcemia (|||| ||||).
Withdrawals Due to Adverse Events and Dose Modifications
No TEAEs resulted in treatment discontinuation. TEAEs leading to dose modification were infrequent, occurring in 10 patients (9%). The most common TEAEs that led to dose modifications were lymphopenia and nausea (|| ||||).
Mortality
There was a total of |||| deaths (||||) due to AEs in the NETTER-R study. The causes of death were reported to be abdominal abscess, hepatorenal syndrome and metabolic encephalopathy, hepatic encephalopathy, ascites, and lower respiratory tract infection and pulmonary embolism.
Notable Harms
Notable harms were detailed in the CADTH systematic review protocol and included myelotoxicity, renal toxicity, transformation to leukemia or MDS, nausea and/or vomiting, and fatigue.
Hematological toxicities were reported among ||| patients (||||). Hematological toxicities were mostly grade 1 or 2 (||||), with 5 patients experiencing grade 3 events. Nausea and fatigue were the 2 most commonly reported AEs in the NETTER-R study, occurring in 31 patients (28%) and 25 patients (23%), respectively. Renal toxicity was reported among 6 patients (6%); of these, 3 patients had grade 1 or 2 events and 3 patients had grade 3 events. There were no reports of secondary hematological malignancies (acute leukemia or MDS) in any patient.
Table 19: Summary of Harms (Safety Analysis Set)
Harm | 177Lu oxodotreotide N = 110 |
|---|---|
Patients with ≥ 1 AE, n (%) | 79 (71.8) |
Most common AEs, n (%)a | |
Nausea | 31 (28.2) |
Fatigue | 25 (22.7) |
Abdominal pain | 18 (16.4) |
Vomiting | || ||||||| |
Abdominal pain, upper | || ||||||| |
Anemia | || ||||||| |
Diarrhea | || ||||||| |
Lymphopenia | || ||||||| |
Thrombocytopenia | || ||||||| |
Constipation | || |||||| |
Hypertension | | |||||| |
Pyrexia | | |||||| |
Asthenia | | |||||| |
Leukopenia | | |||||| |
White blood cell count decreased | | |||||| |
Ascites | | |||||| |
Decreased appetite | | |||||| |
Lymphocyte count decreased | | |||||| |
Edema, peripheral | | |||||| |
Patients with any grade 3 or 4 AE, n (%)b | 30 (27.2) |
Most common grade ≥ 3 AE, n (%) | |
Lymphopenia | | |||||| |
Abdominal pain | | |||||| |
Ascites | | |||||| |
Hypercalcemia | | |||||| |
Liver abscess | | |||||| |
Patients with ≥ 1 SAE | |
Patients with ≥ 1 SAE, n (%) | 29 (26.4) |
Most common events,a n (%) | |
Liver abscess | | |||||| |
Ascites | | |||||| |
Hypercalcemia | | |||||| |
Sepsis | 2 (1.8) |
Abdominal pain | 2 (1.8) |
Duodenal ulcer | 2 (1.8) |
Nausea | 2 (1.8) |
Upper gastrointestinal hemorrhage | 2 (1.8) |
Hypoglycemia | 2 (1.8) |
Pyrexia | 2 (1.8) |
AEs leading to dose modifications, n (%) | 10 (9.1) |
Most common AEs leading to dose modifications, n (%) | |
Lymphopenia | | |||||| |
Nausea | | |||||| |
AEs leading to treatment discontinuation, n (%) | 0 |
Deaths | | |||||| |
Deaths, n (%)c | |
Infections and infestations | 5 (4.5) |
Abdominal abscess | 2 (1.8) |
Lower respiratory tract infection | 1 (0.9) |
Nervous system disorders | 1 (0.9) |
Hepatic encephalopathy | 2 (1.8) |
Metabolic encephalopathy | 1 (0.9) |
Gastrointestinal disorders | 1 (0.9) |
Ascites | 1 (0.9) |
Hepatobiliary disorders | 1 (0.9) |
Hepatorenal syndrome | 1 (0.9) |
Respiratory, thoracic, and mediastinal disorders | 1 (0.9) |
Pulmonary embolism | 1 (0.9) |
Notable harms, n (%) | |
Hematological toxicity | || ||||||| |
Renal toxicity | 6 (5.5) |
Transformation to leukemia, MDS | 0 |
Nausea and/or vomiting | 31 (28.2) |
Fatigue | 25 (22.7) |
AE = adverse event; MDS = myelodysplastic syndrome; SAE = serious adverse event.
aFrequency > 4%.
bFrequency > 2%.
cAt each level of summarization, a subject is counted only once.
Source: NETTER-R Clinical Study Report.5
Critical Appraisal
Internal Validity
The NETTER-R study was a retrospective, non-comparative, registry-based, observational study. Without a comparison group, the safety and effectiveness of 177Lu oxodotreotide relative to currently available therapies is unknown. Moreover, due to lack of an adequate control group, the estimate of long-term efficacy was compromised. In particular, no causal inference could be made concerning whether the treatment effect (e.g., changes on PFS or OS) could be completely attributable to 177Lu oxodotreotide or to temporality changes in other factors, including concomitant therapies, subsequent therapies, or natural course of disease. In a retrospective, observational cohort study of drug effectiveness based on existing medical records, lack of a sound study design to make an adjustment or control of potential bias has been recognized as fatal limitation by various real-world evidence study guidance documents.
The CADTH team considered that the retrospective design of the NETTER-R study could have allowed for a matched comparator group of patients who had received relevant comparator therapies, such as everolimus or sunitinib. The clinical experts consulted by CADTH for this review agreed that a retrospective study with a matched analysis incorporating a comparator group would have improved the strength of evidence for this funding request for pNETs. It was also acknowledged that a matched analysis would depend on whether such data were available.
There was a large amount of censoring for all efficacy analyses. For example, in the estimate of PFS, about 1-third of patients were censored at the date of their last evaluable tumour assessment if they had not experienced disease progression or if they had not died at the time of data collection, in the context of time-to-event analyses. Similarly, in the assessment of OS, half of the patients were censored on their last date of contact if they were still alive or if their status was unknown. The large amount of censoring (e.g., non-informative) for most efficacy outcomes (i.e., OS, PFS, DOR, TTP) would have resulted in biased estimates of the absolute changes over time, as illustrated by the Kaplan-Meier curves, in those efficacy outcomes and would have further introduced uncertainty concerning the true effect of 177Lu oxodotreotide on OS and progression of patients with pNETs.
The median follow-up time of the NETTER-R study was 24.5 months. The clinical experts consulted by CADTH for this review commented that, while no control group was part of the study, efficacy results for PFS and OS showed benefit to patients treated with 177Lu oxodotreotide. However, longer-term data may have benefited the study by providing evidence of the impact of treatment with 177Lu oxodotreotide over a longer period.
||||| |||| | ||||| || |||| |||||||| |||||| ||| ||| | ||||| |||||||| ||||||||| || ||| |||||||| |||||. The major protocol deviations were due to patients not meeting eligibility criteria specified for the study. The sponsor reported that the major protocol deviations did not result in exclusion of these patients from the efficacy and safety analyses sets. As the NETTER-R study was retrospective in nature, the inclusion of patients who did not meet study eligibility criteria could have been avoided. However, since there were few patients with major protocol deviations, the impact is expected to be low.
External Validity
The NETTER-R study was conducted in Europe, with patients enrolled from the UK, France, and Spain. Consultation with clinical experts engaged by CADTH for this review suggested that eligibility criteria and baseline characteristics were generally representative of patients in Canada who might be treated in clinical practice, although European countries may have more experience administering PRRT than Canada. The clinical experts commented that, while 1 patient received dactolisib as a prior therapy in the NETTER-R study, this treatment is not approved by Health Canada and not used among patients in Canada; the impact of this is expected to be low, since only 1 patient received this treatment. Eligibility criteria of the NETTER-R study specified that patients with unresectable or metastatic pNETs be included in the study. The clinical experts confirmed that inclusion of these patients would be unlikely to affect study outcomes; pNETs are a heterogenous group of tumours that result in aggressive disease, and results of treatment with 177Lu oxodotreotide based on the NETTER-R study will likely apply to these patients as well.
Regarding prior therapies received by patients, 70% of patients received prior treatment with SSAs, leaving 30% of patients who had not received prior treatment with SSAs. The funding request by the sponsor specifies that patient’s disease must have progressed after prior treatment with an SSA unless there was a contraindication or intolerance. Further, the NETTER-R study did not specify that patients must have had prior treatment with SSAs. While this is not in exact alignment with the funding request, consultation by CADTH with clinical experts for this review confirmed that results of the NETTER-R study would still be generalizable to most patients in Canadian clinical practice.
The NETTER-R study did not include a comparator group. Consultation with clinical experts for this review suggested that a randomized trial may not have been possible, because patients would have been unlikely to have accepted assignment to a treatment group that did not include 177Lu oxodotreotide. In addition, treatment with PRRT has been accepted in Europe and in the US, based on data from the NETTER-1 study, which was extrapolated to patients with pNETs.
Information regarding subsequent therapies was not reported for the NETTER-R study. Due to lack of information, it is impossible to know whether the choices of subsequent therapies reflect Canadian treatment practices for patients with pNETs and how subsequent therapies may have affected patients’ OS.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to summarize and critically appraise available indirect evidence comparing 177Lu oxodotreotide to other relevant treatments (identified in the CADTH protocol) for patients with pNETs.
A focused literature search for network meta-analyses dealing with GEPNETS was run in MEDLINE All (1946–) on April 20, 2022. No limits were applied to the search. Of 183 records identified by the CADTH literature search, 1 published ITC by Khan et al. (2021)7 was included.
Description of Indirect Comparisons
Selection criteria for studies to be included in the sponsor’s ITC and published ITC are described in Table 20.
Table 20: Study Selection Criteria and Methods for ITCs
Detail | Sponsor’s ITC | Khan et al., 2021 |
|---|---|---|
Population | Adult patients with inoperable GEPNETsa | Adult patients with inoperable GEPNETs |
Intervention | 177Lu oxodotreotide | 177Lu oxodotreotide |
Comparator | GI-NETs
pNETs
Additional comparators
| GI-NETs
pNETs
|
Outcome | To be considered for the ITC:
Additional outcomes for consideration:
|
|
Study design |
|
|
Publication characteristics | Studies were limited to those published in English from September 20, 2017, onward. Studies must also have reported at least 1 relevant outcome for > 15 patients. | Not reported |
Exclusion criteria |
| Not reported |
Databases searched |
|
|
Selection process | Screening for title and abstract and full-text review was conducted by 2 reviewers. Discrepancies were settled through discussion. | Screening for title and abstract and full-text review was conducted by 2 reviewers. Discrepancies were settled through discussion. |
Data extraction process | Outcome data were extracted from included studies and recorded in predefined data extraction forms. | Outcome data were extracted from included studies and recorded in predefined data extraction forms. |
Quality assessment | Methodological quality was assessed using the risk-of-bias assessment recommended by NICE in Appendix C of the guidelines manual [PMG6], the Centre for Review and Dissemination (2009), and The Cochrane Collaboration (2011). | Not reported |
AE = adverse event; GEPNET = gastroenteropancreatic neuroendocrine tumour;; GI-NET = gastrointestinal neuroendocrine tumour; HRQoL = health-related quality of life; ICTRP = International Clinical Trials Registry Platform; ITC = indirect treatment comparison; NET = neuroendocrine tumour; NICE = UK National Institute for Health and Care Excellence; NIH = US National Institutes of Health; OS = overall survival; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour; SSA = somatostatin analogue; WHO = WHO.
aPatients can only receive Lutathera (177Lu oxodotreotide) if they are SSR-positive; however, this is not a requirement patients have to fulfill to receive alternative therapies, and therefore it has not been included in the description of the patient population for this systematic review.
bTreatments can be used individually or in combination with SSAs.
Source: Sponsor’s ITC,6,22 Khan et al. (2021).7
Methods of the Sponsor’s ITC
Objectives
The aim of the sponsor’s ITC was to compare 177Lu oxodotreotide to relevant comparators. Specifically, the sponsor conducted MAICs comparing 177Lu oxodotreotide to everolimus and sunitinib.
Study Selection Methods
To identify relevant studies for the sponsor’s ITC, a literature search was conducted based on eligibility criteria reported in Table 20. Databases used for identification of relevant studies were searched using the Ovid platform. In addition, studies were also identified through clinical trial registries. The reference lists of studies were hand-searched to identify any additional published or unpublished material. Full-text review for potentially relevant studies was conducted by 2 independent researchers. Data were extracted for included studies based on predefined forms.22 The literature search was initially conducted in 2017 and then updated twice, in 2020 and 2021.6 Only 2 studies included outcomes data for patients with pNET, including the RADIANT-3 and NCT00428597 studies. These 2 studies were compared with the NETTER-R study.22
ITC Analysis Methods
Due to a lack of available networks of relevant studies (randomized controlled trials), a network meta-analysis was not feasible. Therefore, the sponsor conducted MAICs by matching and adjusting for patient demographic and disease characteristics between the study populations.22 Patient-level data from the NETTER-R study were used along with Kaplan-Meier data from the RADIANT-3 (everolimus) and NCT00428597 (sunitinib) studies for the MAICs of OS and PFS comparing 177Lu oxodotreotide with everolimus and sunitinib. The Kaplan-Meier data from the RADIANT-3 and NCT00428597 studies were digitized, and the Guyot method was used to reconstruct individual event times and censoring times.22 Hazard ratios were estimated through weighted Cox proportional hazards models.22
The method for estimation of model parameters was based on a method of moments approach outlined in Signorovitch et al. (2010).23 Weights were applied for baseline characteristics, based on guidelines developed by the Decision Support Unit commission by the UK National Institute for Health and Care Excellence. The weighting scheme was based on regression models. The effect of weights was assessed through analysis of distribution of patient characteristics. The ESS was assessed as a measure of the extent of the population matching.22 All analyses were conducted in R version 4.0.5 or above by 1 statistician and checked by another statistician.
Identification of Covariates
The sponsor removed from the analyses of OS and PFS patients in the NETTER-R study who would not have been included in the comparator studies because they would not have met eligibility criteria related to the key covariates identified by the sponsor. These included bone metastasis, prior radiotherapy, ECOG PS, lung metastasis, number of disease sites as 1 and 2, surgery, lymph metastasis, time from initial diagnosis ≤ 24 months, median age of 58 years, sex, liver metastasis, and radiofrequency ablation. The list of key covariates was confirmed by the sponsor through consultation with clinical experts who identified covariates of prognostic importance in the treatment of pNETs. A detailed description of eligibility and baseline characteristics across studies is reported in this section.22
The key covariates for inclusion into the ITC were determined by ranking P values from univariate analysis for OS and PFS for baseline characteristics. Cox proportional hazards models were used for continuous variables, and log-rank tests were used for categorical variables. Covariates were considered for inclusion in the models if they were statistically significant at the 20% level; covariates with an ESS of less than 75% of the initial population size were excluded if they were not statistically significant at the 10% level (starting from the covariates with the largest P values). Kaplan-Meier plots and log-cumulative hazard plots were used to visualize the results. Scenario analyses were also conducted to determine which combination of covariates resulted in the highest ESS value.22
For the MAIC between 177Lu oxodotreotide and everolimus, the following covariates were included: ECOG PS, prior radiotherapy, bone metastasis, and liver metastasis. The sponsor noted that the P value for liver metastasis was low but included liver metastasis in the MAIC, since the proportion of patients with liver metastasis was almost the same before matching when the 2 trials (NETTER-R and RADIANT-3) were compared. The ESS for this MAIC was 51 patients, accounting for 46% of the total number of available patients for analysis (N = 110).22
For the MAIC between 177Lu oxodotreotide and sunitinib, the following covariates were included: ECOG PS, prior radiotherapy, median time from initial diagnosis of 2.4 years, and prior radiofrequency ablation. The ESS for this MAIC was 74 patients, accounting for 67% of the total number of available patients for this analysis (N = 110).22
Results of the Sponsor’s ITC
Summary of Included Studies
A total of 2 studies were retrieved from the sponsor’s systematic literature review for inclusion in the ITC: the RADIANT-3 trial, comparing everolimus to placebo, and NCT00428597 comparing sunitinib to placebo. These 2 studies were compared with the NETTER-R study though the MAIC.
The sponsor compared eligibility criteria across the 3 studies included in their MAIC. A list of key eligibility criteria from the 3 studies is reported in Table 21. The studies had somewhat varied inclusion and exclusion criteria. However, in general, the studies recruited patients with measurable pancreatic disease and excluded patients with uncontrolled comorbid conditions. The sponsor concluded that the eligibility criteria of the RADIANT-3 and NCT00428597 studies were fairly similar to those of the NETTER-R study. Consultation by CADTH with clinical experts for this review confirmed that characteristics were comparable across the trials.
Table 21: Eligibility Criteria Across Studies Included in the Sponsor's ITC
Parameters | NETTER-R | RADIANT-3 | NCT00428597 |
|---|---|---|---|
Disease | pNETs | Advanced pNETs | Advanced pancreatic islet cell tumours |
Inclusion criteria |
|
|
|
Exclusion criteria |
|
|
|
177Lu = lutetium-177; ITC = indirect treatment comparison; NET = neuroendocrine tumour; pNET = pancreatic neuroendocrine tumour; PS = performance score; SSA = somatostatin analogue; TKI = tyrosine kinase inhibitor; VEGF = vascular endothelial growth factor; WHO = WHO.
Source: Sponsor’s ITC.22
The end points of interest across these 3 studies were OS and PFS. The definition of PFS was assumed to be the same across the trials. PFS was assessed using RECIST version 1.0 criteria in the RADIANT-3 trial, while the version of RECIST was not specified in the NCT00248597 trial. The NETTER-R used RECIST version 1.1 for assessment of PFS.
Baseline Characteristics
A summary of baseline characteristic across the intervention groups of the trials is reported in Table 22. The median age was similar across all studies (between 56 and 58 years of age), with similar proportions of males and females. The majority of patients across all trials had an ECOG PS of 1 or 2, although the proportion of patients with an ECOG PS of 1 was greater in the RADIANT-3 and NCT00428597 (> 60%) than the NETTER-R study (|||).
While patients in the NCT00428597 study did not report whether patients with organ involvement were enrolled, patients in the NETTER-R and RADIANT-3 had high proportions of liver (> 90%) and lymph node (33% to 43%) involvement. Patients in the RADIANT-3 also had higher proportions of pancreas (44%) and lung (14%) involvement, while patients in the NETTER-R study had greater proportions of bone involvement (29.1%). The time from initial diagnosis was similar for both the RADIANT-3 and NETTER-R studies; similar information was not reported for the NCT00428597 study, although the median time from initial diagnosis was 2.4 months (range, 0.1 to 25.6). Similar proportions of patients in the NETTER-R and NCT00428597 study had a time from disease progression to randomization or receipt of study treatment of 3 to 12 months (26% versus 28%, respectively). However, more patients in the RADIANT-3 trial had a time from disease progression to randomization of less than 3 months, while more patients in the NETTER-R study had a time from disease progression to randomization or receipt of study treatment of greater than 12 months. Classification of tumour functionality was not reported consistently across the trials.
There were differences in the types of previous treatments received by patients across the trials. There were few patients who had prior radiotherapy, chemoembolization, and radiofrequency ablation. However, more patients in the NCT00428597 study had prior surgery (88%) than in the NETTER-R study (30%), and more patients in the NETTER-R study (62%) had prior chemotherapy than in the NCT00428597 study (n = 0). Prior SSA was reported in 70% of patients in the NETTER-R study, 25% of patients in the NCT00428597 study, and 49% of patients in the RADIANT-3 study.
The baseline characteristics pre- and post-matching for the MAICs with everolimus and sunitinib are provided in Table 23 and Table 24. The matching was considered successful.
Table 22: Baseline Characteristics Across Studies Included in the Sponsor's ITC
Parameters | NETTER-R 177Lu oxodotreotide group N = 110 | RADIANT-3 Everolimus group N = 207 | NCT00428597 Sunitinib group N = 86 |
|---|---|---|---|
Age, years | |||
Mean | 58 | NA | NA |
Median (range) | 58 (28 to 89) | 58 (23 to 87) | 56 (25 to 84) |
Sex, n (%) | |||
Male | 58 (52.7) | 110 (53) | 42 (49) |
Female | 52 (47.3) | 97 (47) | 44 (51) |
ECOG PS, n (%) | |||
0 | || |||| | 139 (67) | 53 (62) |
1 | || |||| | 62 (30) | 33 (38) |
2 | | ||| | 6 (3) | 0 |
3 | | ||| | 0 | 0 |
4 | |||| | 0 | 0 |
NA | || |||| | 0 | 0 |
Organ involved, n (%) | |||
Liver | 105 (95.5) | 190 (92) | NR |
Pancreas | | ||||| | 92 (44) | NR |
Lymph nodes | 47 (42.7) | 68 (33) | NR |
Lung | 4 (3.6) | 28 (14) | NR |
Bones | 32 (29.1) | 13 (6) | NR |
Time from initial diagnosis, n (%) | |||
≤ 6 months | | |||||| | 24 (12) | NR |
> 6 months to ≤ 2 years | || ||||||| | 65 (31) | NR |
2 years to ≤ 5 years | || ||||||| | 54 (26) | NR |
> 5 years | || ||||||| | 64 (31) | NR |
NA | | |||||| | NR | NR |
Median, years | |||| | NR | 2.4 (0.1 to 25.6) |
Time from disease progression to randomization, n (%) | |||
≤ 1 month | | |||||| | 73 (35) | NR |
> 1 month to ≤ 2 months | | |||||| | 43 (21) | NR |
> 3 months to ≤ 3 months | | |||||| | 30 (14) | NR |
> 3 months to ≤ 12 months | || ||||||| | 58 (28) | NR |
> 12 months | || ||||||| | 3 (1) | NR |
NA | | |||||| | NR | NR |
Tumour functionality, n (%) | |||
Nonfunctional | 63 (57.3) | NR | NR |
Functional | 33 (30) | NR | NR |
Not assessed | 12 (10.9) | NR | NR |
NA | 2 (1.8) | NR | NR |
Gastrinoma | NR | NR | 9 (10) |
Glucagonoma | NR | NR | 3 (3) |
Insulinoma | NR | NR | 2 (2) |
VIPoma | NR | NR | 0 |
Somatostatinoma | NR | NR | 1 (1) |
Other/unknown | NR | NR | 29 (34) |
Nonfunctional | NR | NR | 42 (49) |
Previous treatment, n (%) | |||
Surgery | 33 | NR | 76 (88) |
Radiotherapy | ||||| | NR | 9 (10) |
Chemoembolization | ||||| | NR | 7 (8) |
Radiofrequency ablation | 10 | NR | 3 (3) |
Chemotherapy | 68 | NR | — |
Percutaneous ethanol injection | NR | NR | 1 (1) |
SSA | NR | NR | 30 (25) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; NA = not available; NR = not reported; SSA = somatostatin analogue.
Source: Sponsor’s ITC.22
Table 23: Comparison of Baseline Characteristics for NETTER-R (Pre- and Post-MAIC) With Radiant-3 Trial
Parameters | Value | NETTER-R Pre-match | NETTER-R Post-match | RADIANT-3 Everolimus |
|---|---|---|---|---|
||||| | ||||| | |||| | |||| | |||| |
ECOG PS | ||||
||||| | |||| | |||| | |||| | |||| |
Previous radiotherapy | ||||
||||| | |||| | |||| | |||| | |||| |
||||| | |||| | |||| | |||| | |||| |
Bone metastasis | ||||
||||| | |||| | |||| | |||| | |||| |
||||| | |||| | |||| | |||| | |||| |
Liver metastasis | ||||
||||| | |||| | ||||| | |||| | |||| |
||||| | |||| | ||||| | |||| | |||| |
|||| | ||||||| ||||||||||| |||||||| |||||| || | ||||||||||| |||||||
Source: Sponsor’s ITC.22
Table 24: Comparison of Baseline Characteristics for NETTER-R (Pre- and Post-MAIC) With NCT00428597 (Sunitinib) Trial
Parameters | Value | NETTER-R Pre-Match | NETTER-R Post-Match | RADIANT-3 Everolimus |
|---|---|---|---|---|
||||| | ||||| | |||| | |||| | |||| |
ECOG PS | ||||
||||| | |||| | |||| | |||| | |||| |
Previous radiotherapy | ||||
||||| | |||| | |||| | |||| | ||||| |
||||| | |||| | |||| | |||| | ||||| |
Radiofrequency ablation | ||||
||||| | |||| | |||| | |||| | |||| |
||||| | |||| | ||||| | |||| | ||||| |
Median time from initial diagnosis of 2.4 years | ||||
||||| | ||||| | |||| | |||| | |||| |
||| | ||||||||| |||| | ||||||| ||||||||||| |||||||| |||||| || | ||||||||||| |||||||
Source: Sponsor’s ITC.22
Risk of Bias
The sponsor did not report the results of their risk-of-bias assessment, conducted for their ITC.
Results
The results of the survival analysis, based on the NETTER-R patient-level data and reconstructed data for the comparators, as well as the median PFS and OS based on reconstructed Kaplan-Meier data, are reported in Table 25.
Table 25: Hazard Ratios Estimated From Matching-Adjusted Indirect Comparisons
Comparison | PFS | OS |
|---|---|---|
177Lu vs. everolimus | ||
Median, months (95% CI) | ||
177Lu oxodotreotide (before MAIC) | |||| ||||||||||| | |||| ||||||||||| |
177Lu oxodotreotide (post-MAIC) | |||| ||||||||||| | |||| ||||||||| |
Everolimus | |||| ||||||||||| | || ||||||||| |
HR (95% CI) | |||| ||||||||||| | |||| ||||||||||| |
177Lu vs. sunitinib | ||
Median, months (95% CI) | ||
177Lu oxodotreotide (before MAIC) | |||| |||||||||||| | |||| ||||||||||| |
177Lu oxodotreotide (post-MAIC) | |||| |||||||||||| | |||| ||||||||| |
Sunitinib | |||| ||||||||| | |||| ||||||||||| |
HR (95% CI) | |||| ||||| | ||||| | |||| ||||||||||| |
177Lu = lutetium-177; CI = confidence interval; HR = hazard ratio; MAIC = matching-adjusted indirect comparison; NE = not estimable; OS = overall survival; PFS = progression-free survival.
Source: Sponsor’s ITC.22
Progression-Free Survival
The Kaplan-Meier curves for the MAIC for PFS between 177Lu oxodotreotide and everolimus and 177Lu oxodotreotide and sunitinib are depicted in Figure 12 and Figure 13.
The median PFS of 177Lu oxodotreotide before adjustment was |||| |||||| |||| ||| |||| || |||||. After adjustment, the median PFS of 177Lu oxodotreotide was |||| |||||| |||| ||| |||| || |||||, which was longer than the median PFS of everolimus at |||| |||||| |||| ||| |||| || |||||. The HR for PFS between 177Lu oxodotreotide and everolimus favoured treatment with 177Lu oxodotreotide (|||||||| ||| ||| |||| || ||||).
The median PFS of 177Lu oxodotreotide before adjustment was |||| |||||| |||| ||| ||||| || |||||. After adjustment, the median PFS of 177Lu oxodotreotide remained the same at |||| |||||| |||| ||| ||||| || |||||, which was longer than the median PFS of sunitinib at |||| |||||| |||| ||| |||| || |||. The HR for PFS also favoured 177Lu oxodotreotide over sunitinib ||||||||| ||| ||| |||| || |||||.
Figure 12: Progression-Free Survival for Everolimus Versus 177Lu Oxodotreotide Pre- and Post-MAIC — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: Sponsor’s ITC.22
Figure 13: Progression-Free Survival for Sunitinib Versus 177Lu Oxodotreotide Pre- and Post-MAIC — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: Sponsor’s ITC.22
Overall Survival
The Kaplan-Meier curves for the MAIC for OS between 177Lu oxodotreotide and everolimus and 177Lu oxodotreotide and sunitinib are depicted in Figure 14 and Figure 15.
The median OS of 177Lu oxodotreotide before adjustment was |||| |||||| |||| ||| |||| || |||||. After adjustment, the median PFS of 177Lu oxodotreotide was |||| |||||| |||| ||| |||| || |||. The median OS of everolimus was ||| ||||||||| |||| ||| |||| || |||. The 95% CI of HR for OS between 177Lu oxodotreotide and everolimus ||||||| ||| |||| |||||, although the point estimate was in favour of 177Lu oxodotreotide over everolimus ||||||||| ||| ||| |||| || |||||.
The median OS of 177Lu oxodotreotide before adjustment was |||| |||||| |||| ||| |||| || |||||. After adjustment, the median OS of 177Lu oxodotreotide remained the same at |||| |||||| |||| ||| |||| || |||, which was longer than the median OS of sunitinib at |||| |||||| |||| ||| |||| || |||||. The HR for OS failed to show a statistically significant difference in favour of 177Lu oxodotreotide over sunitinib ||||||||| ||| ||| |||| || |||||.
Figure 14: Overall Survival for Everolimus Versus 177Lu Oxodotreotide Pre- and Post-MAIC — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: Sponsor’s ITC.22
Figure 15: Overall Survival for Sunitinib and 177Lu Oxodotreotide Pre- and Post-MAIC — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: Sponsor’s ITC.22
Critical Appraisal of the Sponsor’s ITC
The sponsor reported that it had conducted a quality assessment of studies included in its ITC. However, the results of the quality assessment were not reported, although it is likely that the quality level of evidence was not consistent among the 3 studies used in the MAICs. This is likely due to the fact that the NETTER-R study was a retrospective, single-group study, whereas the RADIANT-3 and NCT00428597 studies were phase III randomized trials.
Patient demographic and disease characteristics across the 3 studies were mostly similar. However, there were some differences regarding organ involvement, time from initial diagnosis, time between disease progression and randomization, tumour functionality, and prior treatments. Residual confounding bias may exist, as the matching adjustment was limited to a number of pre-identified covariates. As mentioned, the MAICs chosen for comparisons between 177Lu oxodotreotide and everolimus or sunitinib were designed based on the combination of covariates that resulted in the highest ESS. The ESS for the MAICs between 177Lu oxodotreotide versus everolimus and 177Lu oxodotreotide versus sunitinib were ||| and |||, respectively. The reductions in ESS for these MAICs may indicate that there was little overlap between the individual patient-level data of the NETTER-R study and the RADIANT-3 and NCT00428597 studies, with less overlap between the NETTER-R and RADIANT-3 studies than between NETTER-R and NCT00428597 studies. The lack of high overlap between patients across the studies may serve as an indicator of heterogeneity across patient characteristics, which may suggest additional unknown prognostic and predictive factors and introduce bias into the comparisons of efficacy between 177Lu oxodotreotide and everolimus or sunitinib.
The results of the MAICs suggested that 177Lu oxodotreotide was favoured over everolimus and sunitinib for PFS but not for OS. It should be noted that the median OS was not reached in either the RADIANT-3 and NCT00428597 studies. Therefore, the efficacy analyses of the sponsor’s MAICs, in particular for OS, is of limited interpretability.
In general, the MAICs rely on statistical assumptions and a limited list of known predictive and prognostic covariates, which are difficult to confirm. The MAIC has resulted in a significant reduction of sample size by excluding more than half of NETTER-R patients, which would have compromised the generalizability and reliability of the results.
Methods of Khan et al. (2021)7
Objectives
The aim of the ITC by Khan et al. (2021) was to use MAICs to indirectly compare PFS in patients with GI-NETs or pNETs, and OS in patients with pNETs, after treatment with 177Lu oxodotreotide, everolimus, sunitinib, or best supportive care across different studies.
Study Selection Methods
Some details of the literature searched conducted by Khan et al. (2021) are reported in Table 20. The literature search was performed in 2015 and then updated in 2018. A total of 3 studies were considered relevant for inclusion in the MAICs conducted by Khan et al. (2021) (ERASMUS, RADIANT-3, and NCT00428597).
ITC Analysis Methods
Data for OS and PFS for patients with pNETs were obtained from the RADIANT-3 and NCT00428597 studies. The authors reported that the definitions of OS and PFS were the same in all studies.
As the RADIANT-3 and NCT00428597 studies had published Kaplan-Meier data, the data were digitized, and the Guyot method was used to reconstruct individual even times and censoring times. Individual patient-level data were available from the ERASMUS study. To identify the covariates for inclusion in the MAICs, covariates that were reported in the ERASMUS study and at least 1 of the RADIANT-3 and NCT00428597 studies were compiled in a list. An investigation was made into the relationship of each covariate with OS and PFS for subgroups of patients with both pNETs and GI-NETs in the ERASMUS study; a log-rank test was used for categorical variables and a Cox proportional hazards model was used for continuous variables. Results were visualized using Kaplan-Meier plots and log-cumulative hazard plots. Covariates found to be statistically significant at the 20% level with OS or PFS were included in the MAICs if they were reported for the comparator study.
Logistic regression analysis was used to estimate the weight for each patient in the ERASMUS study, describing the propensity to enrol in the ERASMUS study versus the relevant comparator in the comparator trial. The balancing of the covariates was checked to ensure that the weighting procedure was conducted correctly; the distribution of weights was summarized using medians, ranges, and histograms. The ESS was also calculated; models with large reductions in ESS were not reported.
The median time-to-event and Kaplan-Meier curves were used to describe OS and PFS in the original ERASMUS population and the reweighted population. Data from the reweighted ERASMUS population and from each comparator treatment group were combined in Cox proportional hazards regression models to estimate hazard ratios.
Sensitivity analyses were conducted to assess the sensitivity of the results to a number of key assumptions underlying the MAICs.
All analyses were conducted using T version 3.3.2 and were in accordance with the UK National Institute for Health and Care Excellence Decision Support Unit guidelines.
Results of ITC by Khan et al. (2021)
Summary of Included Studies
The authors conducted MAICs for patients with GI-NETs and pNETs. Only the results pertaining to patients with pNETs are reported here.
The authors concluded that there were no differences in key covariates among the ERASMUS, RADIANT-3, and NCT00428597 studies. Age, ECOG PS, previous chemotherapy, and previous radiotherapy were reported to be statistically significantly associated with PFS and OS in the ERASMUS study at the 20% level and were adjusted for in the MAICs. A summary of baseline characteristics pre- and post-matching with the NCT00428597 and RADIANT-3 studies are reported in Figure 16 and Figure 17. Matching was considered successful; however, the ESS was greatly reduced for the ERASMUS study. Covariates that were not adjusted for were not well-balanced. There were more male patients in the ERASMUS study than in the NCT00428597 study. Fewer patients in the ERASMUS study had received prior surgery compared to the NCT00428597 study, and fewer patients in the ERASMUS study had nonfunctional tumours compared to the NCT00428597 study. The results pre- and post-matching with the RADIANT-3 study were similar. The ESS after matching with the RADIANT-3 study was much lower than with the NCT00428597 study, which may suggest low population overlap. The covariates that were not adjusted were also not well-balanced.
Figure 16: Patient Characteristics in the ERASMUS Study Before and After Matching to the NCT00428597 Study
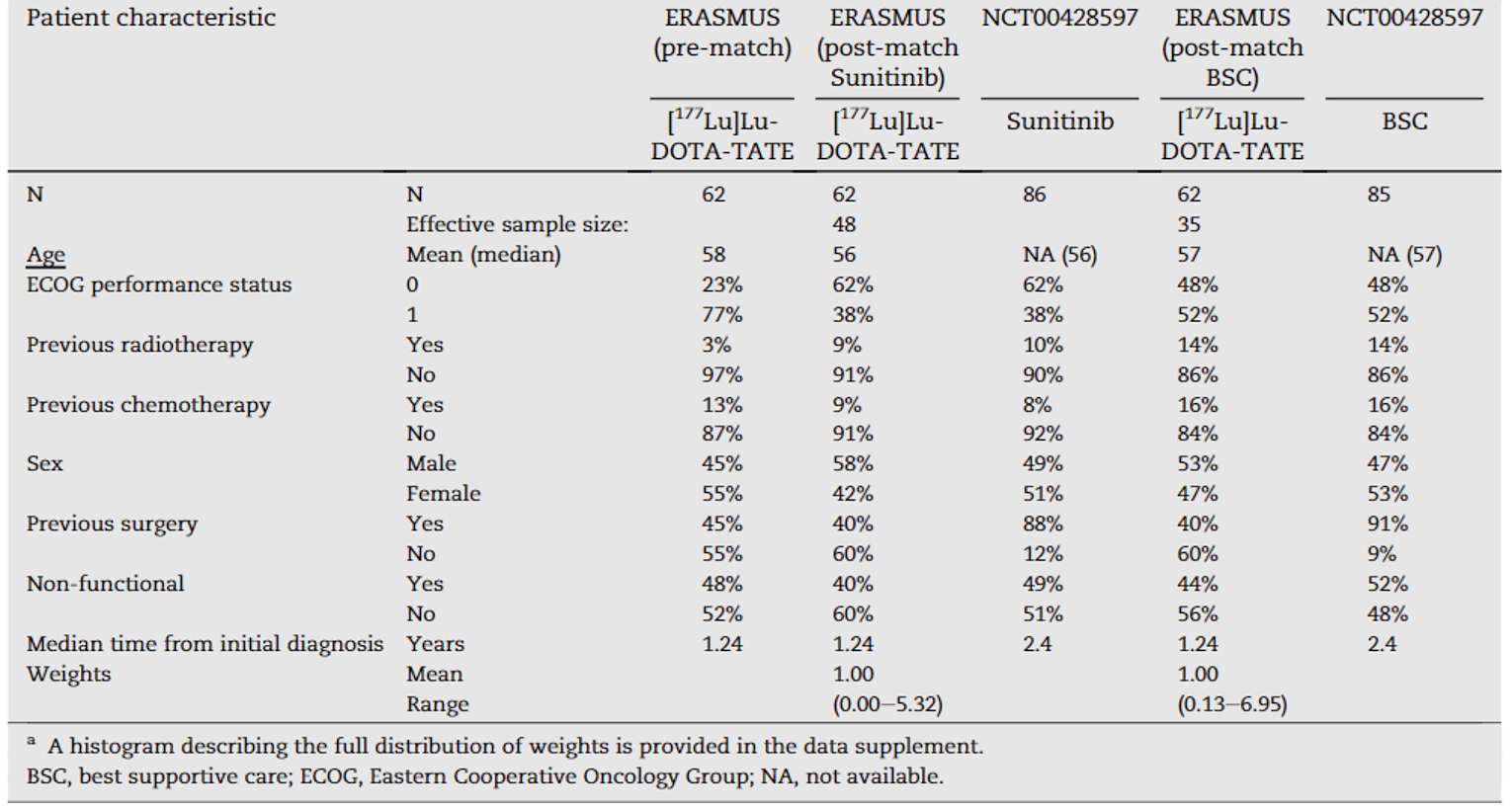
Source: Khan et al. (2021).7 Copyright 2021 Elsevier Ltd. Reprinted in accordance with CC BY-NC-ND.
Figure 17: Patient Characteristics in the ERASMUS Study Before and After Matching to RADIANT-3
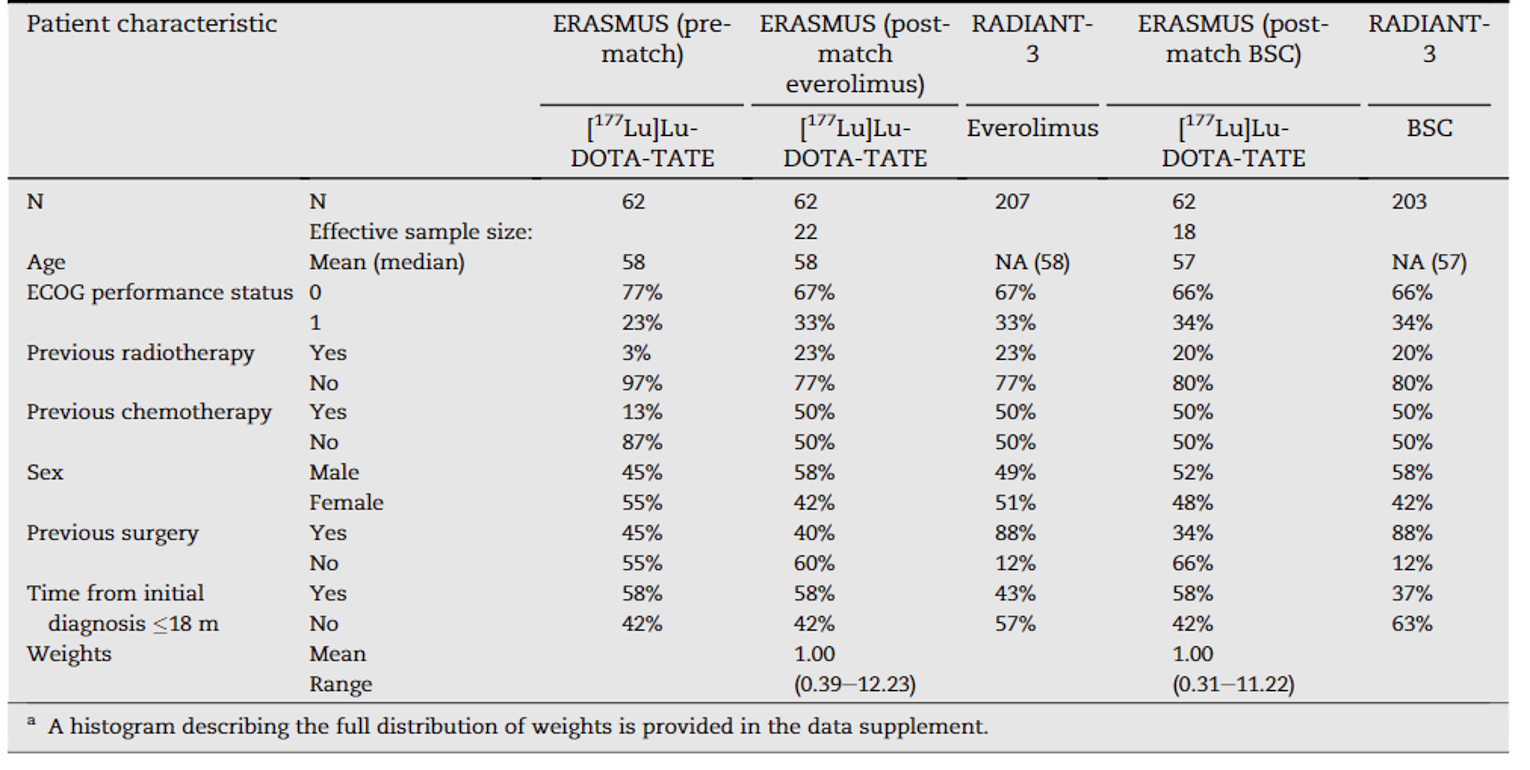
BSC = best supportive care; ECOG = Eastern Cooperative Oncology Group; NA = not available.
Source: Khan et al. (2021).7 Copyright 2021 Elsevier Ltd. Reprinted in accordance with CC BY-NC-ND.
Results
Progression-Free Survival
Results for analyses of PFS are reported in Figure 18. The MAIC suggested that PFS improved more in patients treated with 177Lu oxodotreotide than in those treated with sunitinib (HR = 0.36; 95% CI, 0.18 to 0.70) and everolimus (HR = 0.46; 95% CI, 0.30 to 0.71). Results of the sensitivity analyses also supported improvement with 177Lu oxodotreotide over sunitinib and everolimus.
Figure 18: Hazard Ratios Estimated From Matching-Adjusted Indirect Comparisons for PFS in pNETs
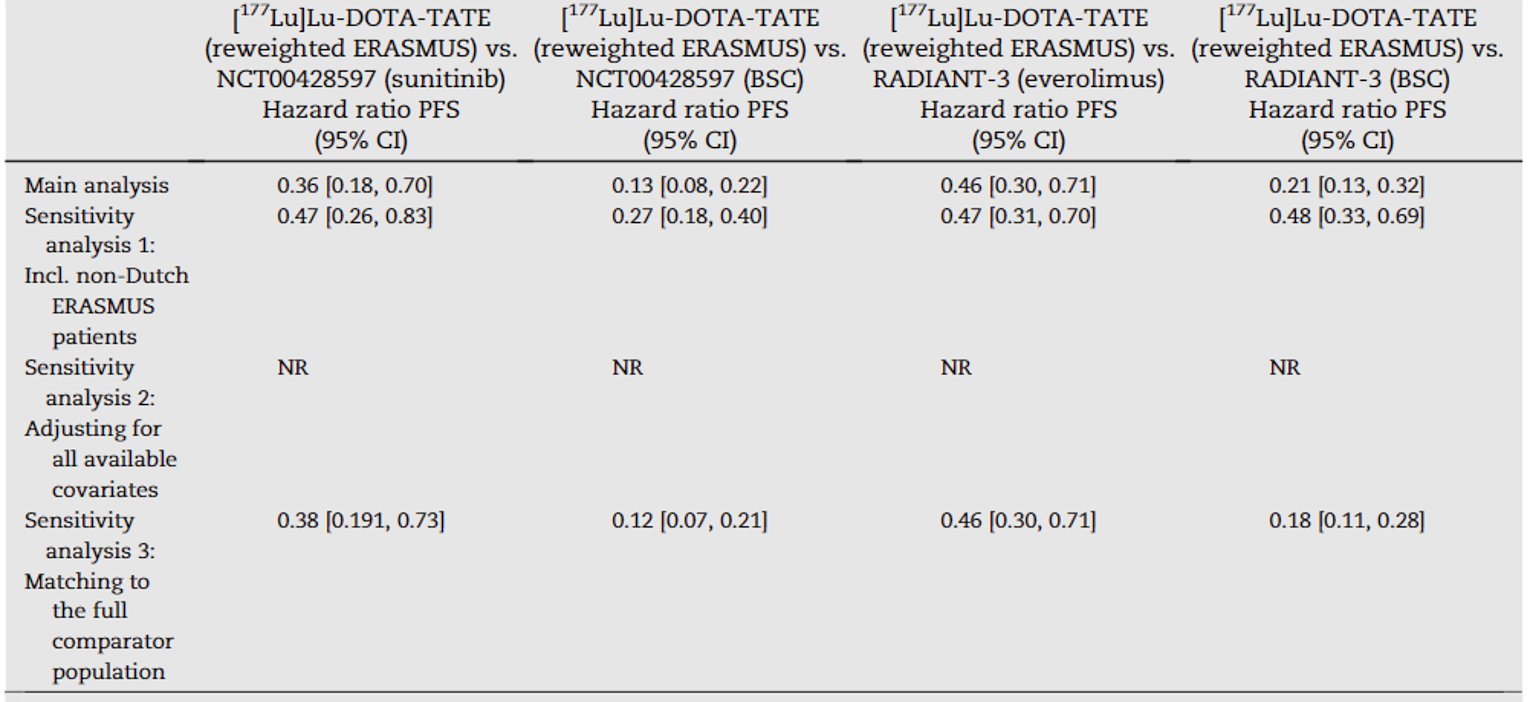
BSC = best supportive care; CI = confidence interval; PFS = progression-free survival; pNET = pancreatic neuroendocrine tumour; NR = not reported.
Source: Khan et al. (2021).7 Copyright 2021 Elsevier Ltd. Reprinted in accordance with CC BY-NC-ND.
Overall Survival
Results for analyses of OS are reported in Figure 19. The MAIC suggested that OS improved more in patients treated with 177Lu oxodotreotide than in those treated with sunitinib (HR = 0.42; 95% CI, 0.25 to 0.72) and everolimus (HR = 0.53; 95% CI, 0.33 to 0.87). Results of the sensitivity analyses also supported improvement with 177Lu oxodotreotide over sunitinib and everolimus.
Figure 19: Hazard Ratios Estimated From Matching-Adjusted Indirect Comparisons for OS in pNETs
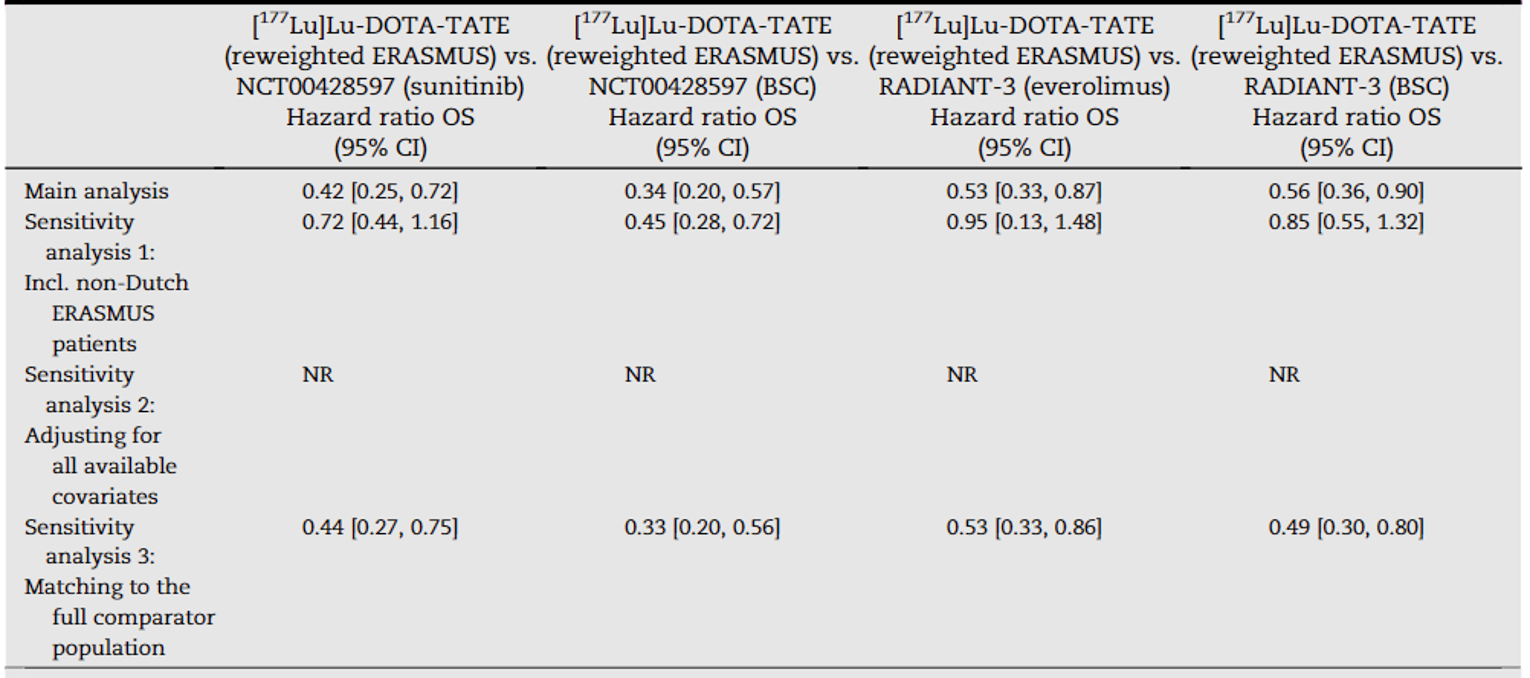
BSC = best supportive care; CI = confidence interval; OS = overall survival; pNET = pancreatic neuroendocrine tumour; NR = not reported.
Source: Khan et al. (2021).7 Copyright 2021 Elsevier Ltd. Reprinted in accordance with CC BY-NC-ND.
Critical Appraisal of ITC by Khan et al. (2021)
Some differences in baseline characteristics were observed across the included studies. There were some differences noted in patient’s sex, tumour functionality, and previous treatments. These characteristics were not included in the matching between the ERASMUS study and the NCT00428597 and RADIANT-3 studies. After matching, these characteristics were not well-balanced. These differences in patient characteristics may affect the validity of the comparisons between 177Lu oxodotreotide and everolimus and sunitinib.
The authors conducted matching with key covariates between the ERASMUS study and the comparator studies (NCT00428597 and RADIANT-3). The ESS after matching with the sunitinib comparator group in the NCT00428597 study was 77% of the initial sample. However, the ESS was much lower (35%) after matching with the everolimus group in the RADIANT-3 study. Characteristics of patients that were unadjusted for were not well-balanced, as illustrated by the differences in patient’s sex, previous surgery, and tumour functionality. Therefore, any unknown covariates are likely not balanced across studies. There is likely little patient overlap between the ERASMUS and comparator studies, although this is more the case with the RADIANT-3 study.
As mentioned previously, OS was not reached in either the RADIANT-3 and NCT00428597 studies. Therefore, the efficacy analyses for OS based on immature data may suffer from high uncertainty.
Details regarding the risk-of-bias assessment were not reported. Therefore, the quality of the studies included is not known; the risk of bias in each study is important for consideration, as the quality of the study may reveal important insights regarding study methodology and impact of these biases on the ITC study outcomes.
Other Relevant Evidence
This section includes submitted long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
Three separate non-comparative observational studies by Fröss-Baron et al. (2021),8 Marinova et al. (2018),9 and Zandee et al. (2019)10 are briefly summarized here to provide additional efficacy and safety data on 177Lu oxodotreotide in patients with pNETs. Only those efficacy outcomes identified in the review protocol are reported here.
Description of Studies
Fröss-Baron et al. (2021)8 Study
Fröss-Baron et al. (2021)8 conducted a retrospective study to determine the efficacy and safety of 177Lu oxodotreotide in 102 adult patients with metastatic and/or locally advanced pNETs who had been previously treated with chemotherapy. Patients in Sweden treated with 177Lu oxodotreotide between 2005 and 2014 were identified using hospital records, and medical and radiological reports were retrospectively examined. Patients received 7.4 GBq 177Lu oxodotreotide per cycle, with an intended 6- to 8- week interval between each cycle. The standard 4-cycle protocol was applied to the first 12 patients, and the dosimetry-guided protocol (greater than 4 cycles) was applied to the following 90 patients. Notably, patients with functional pNETs continued to receive therapy with an SSA during treatment with 177Lu oxodotreotide. The study aimed to analyze PFS, OS, toxicity, and their determinants. CT or MRI imaging was completed at baseline, before every second cycle, 3 months after the last cycle, and every 6 months thereafter, until disease progression was documented, per RECIST version 1.1. Apart from patients with early progression or death, all patients had at least 12 months of follow-up.
The majority of patients (64 [62.7%]) were male, and the mean age was 57.1 years (SD = not reported; range, 29 to 79). A total of 72 patients (70.6%) had a nonfunctional tumour, and 97 patients (95.1%) had liver metastases. Most patients (76 [74.5%]) had a Ki-67 index of 3% to 20%, and most patients (56 [54.9%]) had an ECOG PS of 0. All patients received 1 to 3 lines of chemotherapy, and 58 patients (56.9%) received an SSA before 177Lu oxodotreotide. For most patients (92 [90.2%]), treatment with 177Lu oxodotreotide was indicated due to tumour progression. A mean activity of 32 GBq (SD = 10.9; range, 7.4 to 74) was administered in a median of 4 cycles (range, 1 to 10), with 44 patients (43.1%) having received more than 4 cycles.
Marinova et al. (2018)9 Study
Marinova et al. (2018)9 conducted a retrospective study to determine the change in HRQoL and symptom burden in 68 adult patients with pNETs following treatment with 177Lu oxodotreotide. Patients treated with 177Lu oxodotreotide between 2007 and 2015 at a hospital in Germany were identified, and data were retrospectively analyzed. Briefly, inclusion criteria for the study were that unresectable metastatic pNETs were confirmed with histopathology, the patient had an ECOG PS of 0 to 2, the intended number of cycles were administered, follow-up was completed at 3 months after the last cycle, and the EORTC QLQ-C30 was completed before the first cycle and at least once after the last cycle. Patients received a mean activity of 7.6 GBq (SD = NR) 177Lu oxodotreotide per cycle. Change in HRQoL and symptom status were evaluated according to the EORTC QLQ-C30. EORTC QLQ-C30 is a 30-item, self-reported questionnaire used to assess HRQoL in patients with cancer. It consists of single- and multi-item measures, and scores can range from 0 to 100. Higher scores on the Global Health Status and functional scales indicate better function, and higher scores on the symptom scales and single items indicate significant symptoms. Patients completed the EORTC QLQ-C30 at baseline and every 3 months following each treatment cycle for up to 12 months.
Most (37 [54.4%]) patients were male, and the mean age was 61.4 years (SD = NR; range, 14 to 85). The majority (46 [67.6%]) of patients had a nonfunctional tumour. Most (40 [58.8%]) patients had a Ki-67 index of 3% to 20%, and most (39 [57.4%]) patients had an ECOG PS of 0. A total of 26 (38.2%) and 25 (36.8%) patients received chemotherapy and SSAs as therapies before 177Lu oxodotreotide, respectively. Most (49 [72.1%]) patients had a documented morphological or clinical progression before the first treatment cycle. A total of 53 (77.9%) patients received all 4 cycles; with the exception of 2 reported deaths, treatment discontinuation was decided by an interdisciplinary tumour board. A median cumulative activity of 28.2 GBq (range, NR) was administered in intervals of 3 months and up to 4 cycles. Notably, patients did not receive further therapies during treatment with 177Lu oxodotreotide and follow-up.
Zandee et al. (2019)10 Study
Zandee et al. (2019)10 conducted a retrospective study to determine the efficacy and safety of 177Lu oxodotreotide in 34 adult patients with functional pNETs — 14 patients with insulinoma, 8 with glucagonoma, 7 with gastrinoma, and 5 with VIPoma. Patients treated with 177Lu oxodotreotide between 2000 and 2017 at a centre in the Netherlands were identified. Patients received up to 4 cycles of 7.4 GBq 177Lu oxodotreotide per cycle, with an intended interval of 6 to 10 weeks and an intended cumulative activity of 27.8 to 29.6 GBq. Patients were admitted for clinical observation or treatment of hormonal syndrome, per protocol. The study aimed to evaluate symptomatic, biochemical, and radiological response, as well as toxicity. Hematology, kidney, and liver function tests were completed following each cycle and at follow-up visits (6 weeks, 3 months, and 6 months following the last cycle, and every 6 months thereafter). CT or MRI imaging was completed within 3 months of the first cycle and at each follow-up visit. Patients completed the EORTC QLQ-C30 at all visits.
The mean age was 59.0 years (SD = 11.3), and 17 (50%) patients were male. All patients had metastatic pNETs, and 33 patients (97.1%) had liver metastases. Most patients (18 [52.9%]) had a grade 2 tumour, according to the European Neuroendocrine Tumor Society criteria. The majority of patients (22 [64.7%]) had received an SSA as previous treatment. Most patients (14 [41.2%]) received 177Lu oxodotreotide due to tumour progression only. Notably, 2 patients were receiving concomitant treatment with capecitabine in a clinical trial. The majority of patients (24 [70.6%]) received the intended cumulative activity of 29.6 GBq 177Lu oxodotreotide.
Summary of Findings
Fröss-Baron et al. (2021)8 Study
The median follow-up period was 34 months (range, 4 to 160), and survival data for patients (46.1%) were based on the Swedish National Health Registry up to 2018. PFS was calculated using the Kaplan-Meier method and was based on the first date of treatment to the date of radiologically confirmed progression, per RECIST version 1.1, or death from any cause. OS was calculated using the Kaplan-Meier method and was based on the first day of treatment with 177Lu oxodotreotide to the day of death or the last day of follow-up. The median PFS was 24 months (95% CI, 17 to 28), and the median OS was 42 months (95% CI, 29 to 61). During follow-up, 63 (61.8%) patients died; tumour progression was reported as the cause of death in 60 patients.
Tumour response was assessed with RECIST version 1.1 criteria in 100 patients. Complete response was reported in 4 (4.0%) patients, partial response in 45 (45.0%) patients, stable disease in 44 (44.0%) patients, and progressive disease in 7 (7.0%) patients. Forty-nine percent of patients reached objective response, which was defined as patients with complete or partial response. The median time to best response was 14.8 months (range, 3 to 108). Disease control, which was defined as complete response, partial response, or stable disease, was reported in 91.0% of 92 patients with progressive disease at baseline.
Bone marrow, liver, and kidney toxicity were defined by the CTCAE version 3.0. Grade 3 or 4 bone marrow toxicity was reported in 11 (10.8%) patients. Grade 3 toxicity of white blood cells and/or granulocytes was reported in 5 (4.9%) patients, grade 3 or 4 toxicity of platelets was reported in 5 (4.9%) patients, and grade 3 toxicity of hemoglobin was reported in 2 (1.9%) patients. Grade 4 (lethal) thrombocytopenia and acute myeloid leukemia were reported in 1 (1.0%) patient each. Fatal liver toxicity was reported in 1 (1.0%) patient; the cause of death was also considered related to tumour progression. Grade 3 or 4 nephrotoxicity was not observed.
Treatment discontinuations were due to the following: termination according to the dosimetry-guided protocol was applied to 51 (50.0%) patients, disease progression in 17 (16.7%) patients, bone marrow toxicity in 11 (10.8%) patients, the standard 4-cycle protocol was applied to 9 (8.8%) patients, reduced tumour load in 3 (2.9%) patients, deterioration in 2 (1.9%) patients, death in 2 (1.9%) patients, and a combination of factors not specified in 7 (6.8%) patients.
Marinova et al. (2018)9 Study
The primary analysis using the EORTC QLQ-C30 was according to data collected at baseline and 3 months following the last cycle (follow-up). The mixed longitudinal (panel) model was used to evaluate the data, and a non-parametric Skilling-Mack test was used to verify the unbalanced panel data; a value of less than 0.05 was considered statistically significant. An increase in the mean Global Health Status score was reported (P = 0.008); the mean score was 58.2 (95% CI, 53.1 to 63.2) at baseline and 69.3 (95% CI, 61.4 to 77.2) at follow-up. An increase in the mean social functioning score was reported (P = 0.049); the mean score was 63.9 (95% CI, 56.7 to 71.2) at baseline and 70.9 (95% CI, 61.1 to 80.7) at follow-up. A decrease in the mean fatigue symptom score was reported (P = 0.029); the mean score was 42.4 (95% CI, 36.3 to 48.4) at baseline and 32.0 (95% CI, 22.2 to 41.7) at follow-up. A decrease in the mean appetite loss symptom score was reported (P = 0.015); the mean score was 25.7 (95% CI, 19.5 to 31.9) at baseline and 11.6 (95% CI, 0.7 to 22.5) at follow-up. The differences in change from baseline in the mean scores on the remaining functional and symptom scales were not considered statistically significant. Further, the investigators reported a significantly greater improvement (magnitude of benefit was not reported) on the diarrhea and dyspnea symptom scale scores in patients with functional versus nonfunctional pNETs. The subanalysis of EORTC QLQ-C30 was based on data collected at baseline and at 3 months following the first, second, and third cycle. Changes from baseline in the EORTC QLQ-C30 in the subanalysis were generally consistent with those observed in the primary analysis.
Zandee et al. (2019)10 Study
The median follow-up period was 39.3 months (range, NR). PFS was calculated using the Kaplan-Meier method and was based on the time from the first cycle of 177Lu oxodotreotide to objective progression, change to a new line of therapy, or death from any cause. The median PFS was 18.1 months (interquartile range, 3.3 to 35.7). A primary event was reported in 31 patients, of whom 24 had progressive disease, 5 changed to a new line of therapy, and 2 died.
Tumour response was evaluated with RECIST version 1.1 criteria in 34 patients. Complete response was reported in 1 (2.9%) patient, partial response in 19 (55.9%) patients, stable disease in 8 (23.6%) patients, and progressive disease in 6 (17.6%) patients. Disease control, which was defined as patients with complete response, partial response, or stable disease, was reported in 18 of the 23 patients with progressive disease at baseline.
Symptomatic response was reported in 17 of the 23 patients with uncontrolled symptoms at baseline, of whom 6 experienced a reduction in hypoglycemic events, 4 experienced a reduction in diarrhea, 5 experienced a reduction in skin lesions or weight increase, and 2 experienced a reduction in pyrosis or diarrhea.
HRQoL was assessed in 22 patients using the EORTC QLQ-C30 by comparing the scores 3 months after the last cycle (follow-up) to those at baseline. A paired t-test and the Wilcoxon signed-rank test were used for normally distributed and non-normally distributed variables in the comparison of continuous variables, respectively. An increase in the mean Global Health Score/Quality of Life was reported (P = 0.002); the mean score was 61.7 (95% CI, NR) at baseline and 79.5 (95% CI, NR) at follow-up. An increase in the mean physical functioning score was reported (P = 0.008); the mean score was 79.7 (95% CI, NR) at baseline and 90.0 (95% CI, NR) at follow-up. An increase in the mean role functioning score was reported (P = 0.006); the mean score was 62.7 (95% CI, NR) at baseline and 90.3 (95% CI, NR) at follow-up. An increase in the mean emotional functioning score was reported (P = 0.002); the mean score was 74.1 (95% CI, NR) at baseline and 84.5 (95% CI, NR) at follow-up. An increase in the mean social functioning score was reported (P = 0.047); the mean score was 77.3 (95% CI, NR) at baseline and 85.6 (95% CI, NR) at follow-up. A decrease in the mean fatigue symptom score was reported (P = 0.02); the mean score was 27.3 (95% CI, NR) at baseline and 17.2 (95% CI, NR) at follow-up. The difference in change from baseline in the mean scores on the remaining functional and symptom scales were not considered statistically significant.
Nausea, vomiting, and pain were reported in 22 (17.6%), 6 (4.8%), and 10 (8.0%) of the 125 cycles administered in total, respectively. Toxicity was defined according to the CTCAE 4.03 criteria. Grade 3 anemia and grade 3 thrombocytopenia were reported in 1 (2.9%) patient each, and grade 3 leukopenia was reported in 3 (8.8%) patients. Hormonal crisis, which was defined as an acute complication of hormonal secretion following treatment with 177Lu oxodotreotide and requiring medical care, was reported in 3 (8.8%) patients and late toxicity with myelodysplastic syndrome was reported in 1 (2.9%) patient.
There were several reasons that patients did not receive the intended cumulative activity of 29.6 GBq 177Lu oxodotreotide. A reduced cumulative activity of 18.5 to 25.9 GBq 177Lu oxodotreotide was administered in 5 (14.7%) patients due to hepatotoxicity. Only 1 cycle was administered in 3 (8.8%) patients each due to noncompliance, unexplained progressive cognitive decline, and patient withdrawal. Only 3 cycles were provided to 1 (2.9%) patient due to clinical progression, and the last patient case was not reported.
Critical Appraisal
In the absence of an active comparator or placebo group, the interpretation of the efficacy and safety results from the 3 non-comparative observational studies8-10 is limited. The interpretation of treatment benefit is further limited by the retrospective nonrandomized study design and a relatively small sample size. This is compounded by the relatively large number of patients who were excluded from the analysis due to their incomplete questionnaires as indicated in the study conducted by Marinova et al. (2018).9 However, the clinical experts consulted by CADTH indicated that patients with NETs in general were rare, and Zandee et al. (2019)10 also indicated that pNETs were rare. Although treatment with 177Lu oxodotreotide can be ascertained by the use of hospital records, data were sourced from 1 hospital in either Sweden,8 Germany,9 or Netherlands10 and retrospectively analyzed. The use of a single source for the recruitment of patients may introduce the risk of selection bias, because patients under the care of 1 team may share common characteristics, including treatment history, disease severity, and level of supportive care, which can bias the estimation of treatment effect and limit the external validity of the results. Notably, the place of 177Lu oxodotreotide in the treatment sequence varied within the cohort and was preceded by various therapies, which the clinical experts suggested can bias the median OS. Marinova et al. (2018)9 indicated that they used the validated German version of EORTC QLQ-C30 but did not identify a clinically meaningful difference; Zandee et al. (2019)10 also did not identify a clinically meaningful difference. Although patients did not undergo further therapies after treatment with 177Lu oxodotreotide and follow-up,9 it was unclear whether patients received any concomitant therapy that could bias the reporting on the HRQoL questionnaire.
A number of baseline characteristics of the cohorts in the studies, specifically the mean age,8-10 proportion of patients with liver metastases,8,10 and the proportion of patients with an ECOG status of 0,8,9 were similar to those of the NETTER-R5 study, which the clinical experts consulted by CADTH suggested were representative of patients seen in clinical practice in Canada. (A detailed description of the patient population in NETTER-R is presented in the Systematic Review section.) The retrospective studies included patients with experience with various treatments; therefore, 177Lu oxodotreotide was in various lines in the treatment sequence, preceded by different therapies. Only 56.9%, 36.8%, and 64.7% of patients received an SSA before treatment with 177Lu oxodotreotide in the study conducted by Fröss-Baron et al. (2021),8 Marinova et al. (2018),9 and Zandee et al. (2019),10 respectively, and thus match the reimbursement request for this review. Further, the number of cycles administered and the intervals between the cycles, such as the application of the dosimetry-guided protocol8 and the use of 3-month intervals,9 varied among studies. Last, Zandee et al. (2019)10 included patients with functional pNETs, specifically patients with insulinoma, glucagonoma, gastrinoma, and VIPoma, but did not include patients with nonfunctional pNETs.
Discussion
Summary of Available Evidence
One non-interventional, non-comparative, post-authorization retrospective registry study (N = 110) (NETTER-R),5 1 sponsor-provided ITC,22 1 published ITC,7 and 3 studies providing supplemental information (Fröss-Baron et al. (2021)8 [N = 102], Marinova et al. (2018)9 [N = 68], and Zandee et al. (2019)10 [N = 34]) contributed evidence to this report. Patients assessed in the NETTER-R study included those with SSR-positive, unresectable or metastatic, well-differentiated pNETs who had progressive disease and were treated with 177Lu oxodotreotide. Patients were not eligible if they were diagnosed with NETs of other origins. The primary end point was PFS. The study by Fröss-Baron et al. (2021)8 was a retrospective study that assessed the efficacy and safety of 177Lu oxodotreotide in patients in Sweden with metastatic and/or locally advanced pNETs, who had been previously treated with chemotherapy. The study by Marinova et al. (2018)9 was a retrospective analysis assessing the change in HRQoL and symptom burden in German patients with pNETs who had been treated with 177Lu oxodotreotide. The study by Zandee et al. (2019)10 was a retrospective analysis of efficacy and safety of patients in the Netherlands with pNETs treated with 177Lu oxodotreotide.
Patients included in the NETTER-R study had a mean age of 58 years (||||||||; range, 28.0 to 89.0 years), with relatively equal proportions of males (53%) and females (47%). |||| of patients were white (|||). The primary sites of metastases before the patients started treatment with 177Lu oxodotreotide were the liver (96%), lymph nodes (43%), bone (29%), and lungs (4%). The liver tumour burden was from 10% to 25% in 29% of patients and more than 25% or more than 2 metastatic organs in 36%. More than half of patients had nonfunctional tumours (57%), 30% of patients had functional tumour status, and the remainder lacked assessment of tumour functionality (11%). Most patients had inoperable tumours (75%). Most patients had a Ki-67 index of 3% to 20% (66%), and 24% had a Ki-67 index of 2% or less. Most had a histopathological intermediate (grade 2; 65%) or low (grade 1; 27%) grade of disease. The. Of patients with ECOG PS assessed, most had an ECOG PS of 0 (|||) or 1 (|||).5 Most patients completed a standard regimen of 177Lu oxodotreotide.
Interpretation of Results
Efficacy
The NETTER-R study demonstrated a median OS of 41.4 months (95% CI, 28.6 to 50.2), and a median PFS of 24.8 months (95% CI, 17.5 to 34.5). Due to the nature of the study, all statistical analyses of the NETTER-R study were considered descriptive. In addition, the NETTER-R study lacked a comparative group. The lack of formal statistical analyses and a comparator group introduces difficulty in interpreting the efficacy of 177Lu oxodotreotide and ascribing the latter as the causal factor for the observed outcomes. The clinical experts consulted by CADTH for this review confirmed that the PFS and OS observed in the NETTER-R study were clinically meaningful. While the interpretability of results of the NETTER-R is limited, the clinical experts commented that the observed PFS and OS were impressive and longer than those expected for patients with pNETs not treated with 177Lu oxodotreotide. While there is no comparator group, the clinical experts commented that OS and PFS of patients in Canada treated with regimens currently available in clinical practice are not as long as what is suggested with treatment with 177Lu oxodotreotide, based on results of the NETTER-R study. The clinical experts also commented that other secondary end points of the NETTER-R study, including ORR, DOR, and TTP, were also clinically meaningful.
The NETTER-1 study was considered the pivotal trial in the previous CADTH review of 177Lu oxodotreotide; NETTER-1 compared 177Lu oxodotreotide to high-dose long-acting octreotide. As patients with pNETs were not included in the NETTER-1 study, they were excluded from the reimbursement recommendation issued by CADTH. To address this gap, the sponsor submitted evidence based on the NETTER-R post-marketing study. Only patients with GI-NETs, specifically of the midgut, were included in the NETTER-1 trial. The primary end point of the NETTER-1 trial was PFS, and a secondary end point was OS. At the time of the initial CADTH review, the median PFS and OS were not reached in patients who received 177Lu oxodotreotide in the NETTER-1 trial. Results of the final analysis of the NETTER-1 trial were based on a median follow-up of more than 76 months. The median OS was 48.0 months (95% CI, 37.4 to 55.2) in the 177Lu oxodotreotide group compared to 36.3 months (95% CI, 25.9 to 51.7) in the control group (HR = 0.84; 95% CI, 0.60 to 1.17; unstratified 2-sided log-rank P value = 0.30).24,25 OS results can be considered numerically similar in NETTER-1 and NETTER-R studies, although it is impossible to directly compare these populations and studies, and results are associated with serious imprecision, as demonstrated by the wide 95% CI. Both studies have limitations, such as subsequent treatments affecting analysis of OS, that introduce complexities when interpreting efficacy data, in particular for patients with pNETs in the NETTER-R study.
Everolimus and sunitinib were identified as relevant comparators for patients in Canada with pNETs. However, as mentioned, the NETTER-R study was a single-group study. The sponsor-provided indirect comparative evidence through MAICs that compared 177Lu oxodotreotide to everolimus and sunitinib for PFS and OS. Additional published indirect evidence was also found in the literature. Khan et al. (2021)7 conducted similar analyses using MAICs to compare 177Lu oxodotreotide to everolimus and sunitinib for PFS and OS. Both sets of MAICs favoured treatment with 177Lu oxodotreotide over sunitinib and everolimus in terms of PFS. The sponsor’s MAIC in terms of OS did not achieve statistical significant differences between 177Lu oxodotreotide and everolimus or sunitinib, while MAICs published by Khan et al. (2021)7 did suggest greater improvement with 177Lu oxodotreotide over both everolimus and sunitinib. This may be explained by the use of different studies for the 177Lu oxodotreotide arms of the MAICs (the NETTER-R study for the sponsor’s ITC, and the ERASMUS study for the published ITC). Nevertheless, both the sponsor-provided and published MAICs faced similar limitations, which may have affected the validity of the results, including potential residual confounding and reduced sample sizes from matching. In particular for OS, the sponsor-provided MAICs and the published MAICs included the RADIANT-3 and NCT00428597 studies, which reported immature OS data. Therefore, all sets of indirect comparisons were faced with limitations, which introduce considerable uncertainty in the evidence comparing 177Lu oxodotreotide to everolimus and sunitinib.
Capecitabine plus temozolomide was also considered a relevant comparator, according to the clinical experts consulted by CADTH, but was not included in an ITC. Therefore, the relative efficacy and safety of 177Lu oxodotreotide versus this drug combination is unknown.
HRQoL was considered an important outcome for patients by clinician and patient groups who provided input, as well as clinicians consulted by CADTH for this review. HRQoL results were not available for the NETTER-R study. Based on the analysis conducted by Marinova et al. (2018),9 there was improvement in HRQoL from baseline to 3 months’ follow-up after the last cycle of treatment with 177Lu oxodotreotide. There was a statistically significant increase in the Global Health Status and the mean social functioning score. However, there was a statistically significant decrease in the mean fatigue symptom score and mean appetite loss symptom score. The authors also reported significant improvement in diarrhea and dyspnea symptoms in patients with functional pNETs versus patients with nonfunctional pNETs.9 In the study by Zandee et al. (2019)10 in 22 patients, HRQoL was also assessed using the EORTC QLQ-C30. The authors reported an increase in the mean Global Health Score (P = 0.002), which is in line with results from the study by Marinova et al. (2018).9 The patient group (CNETS) highlighted diarrhea and fatigue as important symptoms to control, because they have a negative impact on patients’ quality of life. These symptoms were also included as notable harms in the CADTH systematic literature review protocol. There are limitations to these studies, including a retrospective design with analyses that are likely underpowered and descriptive. The HRQoL results of the studies by Marinova et al. (2018)9 and Zandee et al. (2019)10 align with the efficacy analyses of the NETTER-R study, which demonstrate longer PFS and OS for patients with pNETs than might be expected with other treatments, according to clinical experts consulted by CADTH for this review.
As mentioned in the Critical Appraisal section for the NETTER-R study, it is unlikely that the sponsor could have conducted a randomized study in patients with pNETs who had received prior therapy, because patients may be hesitant to agree to receive an alternative therapy to PRRT. In addition, 177Lu oxodotreotide is used in Europe, Australia, and the US on the basis of results from the NETTER-1 study that were extrapolated to patients with pNETs. The NETTER-1 study did not enrol patients with pNETs but enrolled patients with other types of GEPNETs. The clinical experts consulted by CADTH for this review suggested that the division between pNETs and non-pNETs may not be an important consideration. While pNETs tend to be more aggressive and have a poorer survival outlook compared to other NETs, the clinical experts suggested that there is little basis for treatment with 177Lu oxodotreotide in patients with pNETs to differ from treatment for patients with other NETs. Overall, the clinical experts endorsed that 177Lu oxodotreotide would be efficacious in patients with pNETs.
Harms
The dose intensity of 177Lu oxodotreotide in the NETTER-R study suggested that most patients received all 4 doses (70%) of 177Lu oxodotreotide and that most patients could tolerate near the full dose of 177Lu oxodotreotide. The average dose per administration of 177Lu oxodotreotide was 199.8 mCi (SD = 15.80), which is in line with a standard dose of 177Lu oxodotreotide, at 200 mCi ± 10%. The clinical experts consulted by CADTH, as well as the clinician groups providing input for this review, reported that clinicians and patients generally agree that the toxicity of 177Lu oxodotreotide is tolerable. As most patients in the NETTER-R study could receive most doses of 177Lu oxodotreotide, and few discontinued due to AEs, there is evidence that the tolerability of 177Lu oxodotreotide is high. Input from the patient group also reported that, among 33 patients who had received 177Lu oxodotreotide, they found that side effects of treatment were manageable and less debilitating, with a quicker recovery time, than standard therapies for pNETs.
Notable harms included in the CADTH systematic review protocol, in consultation with clinical experts, included myelotoxicity, renal toxicity, transformation to leukemia, nausea and/or vomiting, and fatigue. Input from the patient group reported that side effects from 177Lu oxodotreotide included fatigue, nausea and vomiting, diarrhea, and pain. While there is no comparator group in the NETTER-R study to provide a relative toxicity profile, the NETTER-R study did report nausea (28%), fatigue (23%), abdominal pain (16%), vomiting (|||), upper abdominal pain (|||), and anemia (|||) as the most commonly reported AEs, supporting input provided by the patient group. Hematological toxicities were also reported in 26% of patients. Renal toxicities were highlighted as being of concern for patients with pNETs, although the NETTER-R study reported few patients with renal toxicities (6%). No patients had a secondary transformation to leukemia or MDS. The clinical experts consulted by CADTH for this review stated that the lack of secondary hematological malignancies was unexpected, as this is a harm typically noted among this patient population, but the outcome is possible and may further indicate the favourable toxicity profile of 177Lu oxodotreotide.
Neither ITCs reviewed in this report conducted analyses for safety. Therefore, the toxicity profile of 177Lu oxodotreotide relative to everolimus and sunitinib is not known.
Conclusions
The NETTER-R study was provided in this reassessment of 177Lu oxodotreotide for treatment of patients with pNETs. The previous recommendation for 177Lu oxodotreotide did not support use for patients with pNETs because they were excluded from the pivotal NETTER-1 study. Due to the small sample size, lack of comparator group, retrospective design, and missing data, the results of the NETTER-R study are difficult to interpret and cannot be used to draw firm conclusions about the relative benefits of 177Lu oxodotreotide in the treatment of pNETs. Evidence from other observational studies by Fröss-Baron et al. (2021),8 Marinova et al. (2018),9 and Zandee et al. (2019)10 were largely consistent with NETTER-R but were associated with the same level of uncertainty. Indirect evidence available from the sponsor and the literature provided comparative results between 177Lu oxodotreotide with everolimus and sunitinib and suggested improved efficacy of 177Lu oxodotreotide over everolimus and sunitinib. The indirect evidence had methodological limitations that introduced uncertainty in the interpretation of the comparative data. Based on the totality of the evidence and their experience treating patients with pNETs, clinical experts agreed that 177Lu oxodotreotide would be a safe and effective regimen, preferred over everolimus or sunitinib. Direct comparative evidence may help reduce uncertainty and inform whether 177Lu oxodotreotide would be beneficial for patients with pNETs.
References
1.Cives M, Strosberg JR. Gastroenteropancreatic Neuroendocrine Tumors. CA Cancer J Clin. 2018;68(6):471-487. PubMed
2.Das S, Al-Toubah T, El-Haddad G, Strosberg J. (177)Lu-DOTATATE for the treatment of gastroenteropancreatic neuroendocrine tumors. Expert Rev Gastroenterol Hepatol. 2019;13(11):1023-1031. PubMed
3.Dasari A, Shen C, Halperin D, et al. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017;3(10):1335-1342. PubMed
4.Drug Reimbursement Review sponsor submission: Lutathera (lutetium (177Lu) oxodotreotide), 370 mMBq/mL at calibration [internal sponsor's package]. Mississauga (ON): Advanced Accelerator Applications Canada Inc.; 2022 Apr 1.
5.Clinical Study Report: A-LUT-T-E01-401/CAAA601A12401. An international, non-interventional, post-authorization retrospective registry of subjects treated with Lutathera (lutetium (177Lu) oxodotreotide), to assess the efficacy and safety of Lutathera for the treatment of pancreatic neuroendocrine tumors (pNETS) - NETTER-R [internal sponsor's report]. Basel (CH): Advanced Accelerator Applications; 2020 Jun 1.
6.Advanced Accelerator Applications response to May 25, 2022 DRR request for additional information regarding Lutathera DRR review [internal additional sponsor's information]. Toronto (ON): Advanced Accelerator Applications; 2022.
7.Khan MS, Stamp E, Sammon C, Brabander T, de Herder WW, Pavel ME. Matching-adjusted indirect treatment comparison of [(177)Lu]Lu-DOTA-TATE, everolimus and sunitinib in advanced, unresectable gastroenteropancreatic neuroendocrine tumours: Relative effectiveness of [(177)Lu]Lu-DOTA-TATE in gastroenteropancreatic neuroendocrine tumours. EJC Suppl. 2021;16:5-13. PubMed
8.Fross-Baron K, Garske-Roman U, Welin S, et al. 177Lu-DOTATATE Therapy of Advanced Pancreatic Neuroendocrine Tumors Heavily Pretreated with Chemotherapy: Analysis of Outcome, Safety, and Their Determinants. Neuroendocrinology. 2021;111(4):330-343. PubMed
9.Marinova M, Mucke M, Mahlberg L, et al. Improving quality of life in patients with pancreatic neuroendocrine tumor following peptide receptor radionuclide therapy assessed by EORTC QLQ-C30. Eur J Nucl Med Mol Imaging. 2018;45(1):38-46. PubMed
10.Zandee WT, Brabander T, Blazevic A, et al. Symptomatic and Radiological Response to 177Lu-DOTATATE for the Treatment of Functioning Pancreatic Neuroendocrine Tumors. J Clin Endocrinol Metab. 2019;104(4):1336-1344. PubMed
11.Clift AK, Kidd M, Bodei L, et al. Neuroendocrine Neoplasms of the Small Bowel and Pancreas. Neuroendocrinology. 2020;110(6):444-476. PubMed
12.Ito T, Igarashi H, Jensen RT. Pancreatic neuroendocrine tumors: clinical features, diagnosis and medical treatment: advances. Best Pract Res Clin Gastroenterol. 2012;26(6):737-753. PubMed
13.Lutathera® (lutetium [177Lu] oxodotreotide): Sterile Solution for Intravenous Infusion 370 MBq/mL at calibration [product monograph]. Milburn (NJ): Advanced Accelerator Applications USA, Inc.; 2021 May 13.
14.Afinitor Disperz (everolimus): tablets for oral suspension, 2 mg, 3 mg and 5 mg, oral [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2021 Nov 30: https://www.ask.novartispharma.ca/download.htm?res=afinitor_scrip_e.pdf&resTitleId=705#:~:text=AFINITOR%C2%AE%20(everolimus)%20is%20indicated%20for%3A&text=the%20treatment%20of%20postmenopausal%20women,treatment%20with%20letrozole%20or%20anastrozole. Accessed 2022 Apr 22.
15.Sutent (sunitinib capsules): 12.5 mg, 25 mg, 37.5§ mg, 50 mg sunitinib per capsule (as sunitinib malate) [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2019 Jul 11: https://www.pfizer.ca/sites/default/files/201908/SUTENT_PM_DC_E_226908_11July2019.pdf. Accessed 2022 Apr 22.
16.Temodal (temozolomide): 5 mg, 20 mg, 100 mg, 140 mg and 250 mg capsules [product monograph]. Kirkland (QC): Merck Canada Inc.; 2017 Jun 23: https://pdf.hres.ca/dpd_pm/00039947.PDF Accessed 2022 Apr 21.
17.Xeloda (capecitabine tablets): tablets 150 mg and 500 mg [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; 2022 Apr 4: https://www.rochecanada.com/PMs/Xeloda/Xeloda_PM_E.pdf. Accessed 2022 Apr 21.
18.Del Prete M, Buteau FA, Arsenault F, et al. Personalized (177)Lu-octreotate peptide receptor radionuclide therapy of neuroendocrine tumours: initial results from the P-PRRT trial. Eur J Nucl Med Mol Imaging. 2019;46(3):728-742. PubMed
19.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
20.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Apr 21.
21.Clement D, Navalkissoor S, Srirajaskanthan R, et al. Efficacy and safety of (177)LuDOTATATE in patients with advanced pancreatic neuroendocrine tumours: data from the NETTER-R international, retrospective study. Eur J Nucl Med Mol Imaging. 2022;07:07.
22.A matching adjusted indirect comparison of Lutathera, everolimus and sunitinib in conjunction with the treatment of pancreatic neuroendocrine tumours (P-NETs) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lutathera, 370 MBq/mL, IV. Toronto (Ontario): Advanced Accelerator Applications; 2022 January 24.
23.Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics. 2010;28(10):935-945. PubMed
24.Strosberg JR, Caplin ME, Kunz PL, et al. Final overall survival in the phase 3 NETTER-1 study of lutetium-177-DOTATATE in patients with midgut neuroendocrine tumors. J Clin Oncol. 2021;39(15_suppl):4112-4112.
25.Strosberg JR, Caplin ME, Kunz PL, et al. 177Lu-Dotatate plus long-acting octreotide versus high-dose long-acting octreotide in patients with midgut neuroendocrine tumours (NETTER-1): final overall survival and long-term safety results from an open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021;22(12):1752-1763. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: April 21, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Humans
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Lutathera* or lutate or AE221IM3BB or 177Lu-dota* or 177Ludota* or 177Lutetium).ti,ab,kf,ot,hw,nm,rn.
((177* or 177-Lu* or 177Lu* or Lu-177* or Lu177* or 177lutetium* or 177-lutetium* or Lu) adj5 (octreotate or dota-tate or dotatate or ludotatate or oxodotreotide)).ti,ab,kf,ot,hw,nm,rn.
((177* or 177-Lu* or 177Lu* or Lu-177* or Lu177*) adj5 lutetium*).ti,ab,kf,ot,hw,nm,rn.
or/1-3
(exp Neuroendocrine tumors/ and ((pancreat* or pancreas* or GEP-NET? or GEPNET? or P-NET? or PNET? or gastroenteropancreatic* or islet or foregut or fore-gut or midgut or mid-gut or hindgut or hind-gut).ti,ab,kf. or exp pancreas/)) or exp Pancreatic Neoplasms/
((alpha cell or beta cell or diarrheogenic or foregut or fore-gut or midgut or mid-gut or hindgut or hind-gut or gastroenteropancreatic* or pancreat* or pancreas* or islet) adj3 (adenoma? or argentaffinoma* or cancer* or carcinoid* or carcinoma? or gastrinoma? or malignanc* or neoplas* or neoplasm* or NET or NETs or paraganglioma* or polypeptidoma or sarcoma* or tumor* or tumour*)).ti,ab,kf.
((endocrine adj2 neoplasia*) or glucagonoma? or insulinoma* or MEN1 or P-NET? or PNET? or GEP-NET? or GEPNET? or somatostatinoma* or Verner-Morrison or VIPoma* or (Wermer adj2 Syndrome) or Zolinger-Ellison).ti,ab,kf.
or/5-7
4 and 8
9 use medall
*oxodotreotide lutetium lu 177/
(Lutathera* or lutate or AE221IM3BB or 177Lu-dota* or 177Ludota* or 177Lutetium).ti,ab,kf,dq.
((177* or 177-Lu* or 177Lu* or Lu-177* or Lu177* or 177lutetium* or 177-lutetium* or Lu) adj5 (octreotate or dota-tate or dotatate or ludotatate or oxodotreotide)).ti,ab,kf,dq.
((177* or 177-Lu* or 177Lu* or Lu-177* or Lu177*) adj5 lutetium*).ti,ab,kf,dq.
or/11-14
exp gastroenteropancreatic neuroendocrine tumor/ or exp pancreas cancer/ or exp pancreas disease/
((alpha cell or beta cell or diarrheogenic or foregut or fore-gut or midgut or mid-gut or hindgut or hind-gut or gastroenteropancreatic* or pancreat* or pancreas* or islet) adj3 (adenoma? or argentaffinoma* or cancer* or carcinoid* or carcinoma? or gastrinoma? or malignanc* or neoplas* or neoplasm* or NET or NETs or paraganglioma* or polypeptidoma or sarcoma* or tumor* or tumour*)).ti,ab,kf,dq.
((endocrine adj2 neoplasia*) or glucagonoma? or insulinoma* or MEN1 or P-NET? or PNET? or GEP-NET? or GEPNET? or somatostatinoma* or Verner-Morrison or VIPoma* or (Wermer adj2 Syndrome) or Zolinger-Ellison).ti,ab,kf,dq.
or/16-18
15 and 19
20 use oemezd
(conference review or conference abstract).pt.
21 not 22
10 or 23
exp animals/
exp animal experimentation/ or exp animal experiment/
exp models animal/
nonhuman/
exp vertebrate/ or exp vertebrates/
or/25-29
exp humans/
exp human experimentation/ or exp human experiment/
or/31-32
30 not 33
24 not 34
remove duplicates from 35
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | lutathera, lutetium, 177 Lu]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- lutathera, lutetium, 177 Lu]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- lutathera, lutetium, 177 Lu]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- lutathera, lutetium, 177 Lu]
Grey Literature
Search dates: April 8, 2022, to April 14, 2022
Keywords: lutathera, lutetium, 177 Lu, P-NETs, pancreatic neuroendocrine tumour*
Limits: none
Updated: Search updated before the meeting of CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC).
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for Exclusion |
|---|---|
Fröss-Baron K, Garske-Roman U, Welin S, et al. 177Lu-DOTATATE Therapy of Advanced Pancreatic Neuroendocrine Tumors Heavily Pretreated with Chemotherapy: Analysis of Outcome, Safety, and Their Determinants. Neuroendocrinology. 2021;111(4):330 to 43. | Wrong study population |
Kudo A, Tateishi U, Yoshimura R, et al. Safety and response after peptide receptor radionuclide therapy with (177) Lu-DOTATATE for neuroendocrine tumours in phase 1/2 prospective Japanese trial. J Hepatobiliary Pancreat Sci. 2021;14:14. | Wrong study population |
Satapathy S, Mittal BR. 177Lu-DOTATATE peptide receptor radionuclide therapy vs. Everolimus in advanced pancreatic neuroendocrine tumours: a systematic review and meta-analysis. Nucl Med Commun. 2019;40(12):1195 to 203. | Systematic review |
Demirci E, Kabasakal L, Toklu T, et al. 177Lu-DOTATATE therapy in patients with neuroendocrine tumours including high-grade (WHO G3) neuroendocrine tumours: response to treatment and long-term survival update. Nucl Med Commun. 2018;39(8):789 to 96. | Wrong study population |
Ezziddin S, Khalaf F, Vanezi M, et al. Outcome of peptide receptor radionuclide therapy with 177Lu-octreotate in advanced grade 1/2 pancreatic neuroendocrine tumours. Eur J Nucl Med Mol Imaging. 2014;41(5):925 to 33. | Wrong study population |
Teunissen JJ, Kwekkeboom DJ, Krenning EP. Quality of life in patients with gastroenteropancreatic tumours treated with [177Lu-DOTA0,Tyr3]octreotate. J Clin Oncol. 2004;22(13):2724 to 9. | Wrong study population |
Abou Jokh Casas E, Pubul Nunez V, et al. Evaluation of (177)Lu-Dotatate treatment in patients with metastatic neuroendocrine tumours and prognostic factors. World J Gastroenterol. 2020;26(13):1513 to 24. | Wrong study population |
Heckert JM, Kipnis ST, Kumar S, et al. Abnormal Pretreatment Liver Function Tests Are Associated with Discontinuation of Peptide Receptor Radionuclide Therapy in a US-Based Neuroendocrine Tumor Cohort. Oncologist. 2020;25(7):572 to 8. | Wrong study population |
Zandee WT, Brabander T, Blazevic A, et al. Symptomatic and Radiological Response to 177Lu-DOTATATE for the Treatment of Functioning Pancreatic Neuroendocrine Tumors. J Clin Endocrinol Metab. 2019;104(4):1336 to 44. | Wrong study population |
Kipnis ST, Hung M, Kumar S, et al. Laboratory, Clinical, and Survival Outcomes Associated With Peptide Receptor Radionuclide Therapy in Patients With Gastroenteropancreatic Neuroendocrine Tumors. JAMA Netw. 2021;4(3):e212274. | Wrong study population |
Ezziddin S, Attassi M, Yong-Hing CJ, et al. Predictors of long-term outcome in patients with well-differentiated gastroenteropancreatic neuroendocrine tumours after peptide receptor radionuclide therapy with 177Lu-octreotate. J Nucl Med. 2014;55(2):183 to 90. | Wrong study population |
Marinova M, Mucke M, Mahlberg L, et al. Improving quality of life in patients with pancreatic neuroendocrine tumour following peptide receptor radionuclide therapy assessed by EORTC QLQ-C30. Eur J Nucl Med Mol Imaging. 2018;45(1):38 to 46. | Wrong study population |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 20: Kaplan-Meier Plot of Progression-Free Survival — RECIST 1.1 — Sensitivity Analysis Patients With Post-Baseline Scan per RECIST 1.1 in Modified FAS — Redacted

Figure contained confidential information and was removed at the request of the sponsor.
Source: NETTER-R Clinical Study Report.5
Table 28: PFS — RECIST 1.1 (Sensitivity Analysis) (Patients With Post-Baseline Scan per RECIST 1.1 in Modified FAS)
Outcome | 177Lu oxodotreotide N = 62 |
|---|---|
Number of events, n (%) | || ||||||| |
Documented progression | || ||||||| |
Death | | ||||||| |
Number Censored, n (%) | || ||||||| |
No post-Baseline tumour assessments | | |||||| |
No documented progression | || ||||||| |
Adjacent tumour assessments more than 9 months apart | | ||||||| |
Start of New Anticancer Therapy | | |||||| |
Median (months) 95% CIa | |||| |||||| ||||| |
6 month Survival Rate (%) (95% CI) | |||| |||||| ||||| |
12 month Survival Rate (%) (95% CI) | |||| |||||| ||||| |
24 month Survival Rate (%) (95% CI) | |||| |||||| ||||| |
36 month Survival Rate (%) (95% CI) | |||| |||||| ||||| |
48 month Survival Rate (%) (95% CI) | |||| |||||| ||||| |
60 month Survival Rate (%) (95% CI) | |||| |||||| ||||| |
72 month Survival Rate (%) (95% CI) | |||| ||||| ||||| |
aEstimated by the Kaplan-Meier method.
Note: Long-time elapsed missing assessments is defined as more than 9 months after the last radiological assessment (i.e., 270 days following the previous visit).
Subgroup Analysis for OS
Risk factors for PRRT were also assessed, but were inconsistently reported for some patients. The sponsor reported that the drug category was at times incorrectly understood including SSAs or protein kinase inhibitor (PKI) treatments as “chemotherapy.” Therefore, results for subgroup analyses related to risk factors for PRRT are not reported in this CADTH report.
Table 29: Subgroup Analyses for OS (FAS)
Characteristic | OS – RECIST version 1.1 N = 110 | |
|---|---|---|
n | Median, months (95% CI) | |
Age | ||
18 to < 65 years | |||| | |||| |||||| ||||| |
≥ 65 years | |||| | |||| |||||| ||||| |
18 to < 75 years | |||| | |||| |||||| ||||| |
≥ 75 years | |||| | |||| |||||| ||| |
Sex | ||
Female | |||| | |||| |||||| ||||| |
Male | |||| | |||| |||||| ||||| |
NE = not estimable; OS = overall survival.
Source: NETTER-R Clinical Study Report.5
Subgroup Analysis for PFS
Risk factors for PRRT were also assessed, but were inconsistently reported for some patients. The sponsor reported that the drug category was at times incorrectly understood including SSAs or PKI treatments as “chemotherapy.” Therefore, results for subgroup analyses related to risk factors for PRRT are not reported in this CADTH report.
Table 30: Subgroup Analyses for PFS
Characteristic | PFS – RECIST version 1.1 Patients with post-baseline scan per RECIST 1.1 in modified FAS | PFS – RECIST version 1.1 or other radiological assessments (Investigator’s opinion 1) (Patients with post-baseline scan per Investigator’s opinion 1 in modified FAS) | PFS – RECIST version 1.1 or other radiological assessments, or clinical, or metabolic, or biomarker assessments (Investigator’s opinion 2) (Patients with post-baseline scan per Investigator’s opinion 2 in modified FAS) | |||
|---|---|---|---|---|---|---|
n | Median, months (95% CI) | n | Median, months (95% CI) | n | Median, months (95% CI) | |
Age | ||||||
18 to < 65 years | |||| | |||| |||||| ||||| | |||| | |||| |||||| ||||| | |||| | |||| |||||| ||||| |
≥ 65 years | |||| | |||| ||||| ||||| | |||| | |||| |||||| ||||| | |||| | |||| |||||| ||||| |
18 to < 75 years | |||| | |||| |||||| ||||| | |||| | |||| |||||| ||||| | |||| | |||| |||||| ||||| |
≥ 75 years | ||| | ||| ||||||| | ||| | |||| ||||| ||| | ||| | |||| ||||| ||| |
Sex | ||||||
Female | |||| | |||| |||||| ||||| | |||| | |||| |||||| ||||| | |||| | |||| |||||| ||||| |
Male | |||| | |||| ||||| ||||| | |||| | |||| |||||| ||||| | |||| | |||| |||||| ||||| |
FAS = full analysis set; NE = not estimable; PFS = progression-free survival.
Source: NETTER-R Clinical Study Report.5
Subgroup Analysis for ORR
Risk factors for PRRT were also assessed, but were inconsistently reported for some patients. The sponsor reported that the drug category was at times incorrectly understood including SSAs or PKI treatments as “chemotherapy.” Therefore, results for subgroup analyses related to risk factors for PRRT are not reported in this CADTH report.
Table 31: Subgroup Analyses for ORR
Characteristic | ORR – RECIST version 1.1 Patients with post-baseline scan per RECIST 1.1 in modified FAS | ORR – RECIST version 1.1 or other radiological assessments (Investigator’s opinion 1) (Patients with post-baseline scan per Investigator’s opinion 1 in modified FAS) | ORR – RECIST version 1.1 or other radiological assessments, or clinical, or metabolic, or biomarker assessments (Investigator’s opinion 2) (Patients with post-baseline scan per Investigator’s opinion 2 in modified FAS) | |||
|---|---|---|---|---|---|---|
n | ORR (95% CI) | n | ORR (95% CI) | n | ORR (95% CI) | |
Age | ||||||
18 to < 65 years | |||| | ||||| |||||| ||||| | |||| | ||||| |||||| ||||| | |||| | ||||| |||||| ||||| |
≥ 65 years | |||| | ||||| |||||| ||||| | |||| | ||||| |||||| ||||| | |||| | ||||| ||||| ||||| |
18 to < 75 years | |||| | ||||| |||||| ||||| | |||| | ||||| |||||| ||||| | |||| | ||||| |||||| ||||| |
≥ 75 years | |||| | ||||| ||||| ||||| | |||| | ||||| ||||| ||||| | |||| | ||||| ||||| ||||| |
Sex | ||||||
Female | |||| | ||||| |||||| ||||| | |||| | |||| | |||||| ||||| | |||| | |||| | |||||| ||||| |
Male | |||| | ||||| |||||| ||||| | |||| | |||| | |||||| ||||| | |||| | |||| | |||||| ||||| |
FAS = full analysis set; NE = not estimable; ORR = objective response rate.
Source: NETTER-R Clinical Study Report.5
Pharmacoeconomic Review
Abbreviations
177Lu
lutetium-177
AE
adverse event
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer – Quality of Life questionnaire
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
MAIC
matching-adjusted indirect comparison
NET
neuroendocrine tumour
OS
overall survival
PFS
progression-free survival
pNET
pancreatic neuroendocrine tumour
PRRT
peptide receptor radionuclide therapy
PSM
partitioned survival model
QALY
quality-adjusted life-year
RDI
relative dose intensity
RECIST
Response Evaluation Criteria in Solid Tumors
SSA
somatostatin analogue
TTO
time trade-off
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Lutetium oxodotreotide (Lutathera) 370 MBq/mL at calibration, sterile solution for IV infusion |
Submitted price | Lutetium oxodotreotide, 7.4 GBq (200 mCi): $35,000 per pack |
Indication | Treatment of unresectable or metastatic, well-differentiated, somatostatin receptor-positive gastroenteropancreatic neuroendocrine tumours in adults with progressive disease |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | January 9, 2019 |
Reimbursement request | For the treatment of unresectable or metastatic, well-differentiated, somatostatin receptor-positive pancreatic neuroendocrine tumours in adults whose disease has progressed after treatment with a somatostatin analogue, unless there is a contraindication or intolerance |
Sponsor | Advanced Accelerator Applications |
Submission history | Previously reviewed: Yes Indication: Gastroenteropancreatic neuroendocrine tumours Recommendation date: August 1, 2019 Recommendation: Recommended on the conditions of cost-effectiveness being improved to an acceptable level |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Partitioned survival model Cost-utility analysis |
Target population | Adult patients with unresectable or metastatic, well-differentiated, somatostatin receptor-positive pancreatic neuroendocrine tumours whose disease has progressed after treatment with a somatostatin analogue |
Treatment | Lutetium (177Lu) oxodotreotide |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 20 years |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
177Lu = lutetium-177; AE = adverse event; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; LY = life-year; PFS = progression-free survival; MAIC = matching-adjusted indirect comparison; OS = overall survival; QALY = quality-adjusted life-year; RDI = relative dose intensity; WTP = willingness to pay.
Conclusions
There has been no head-to-head evidence comparing lutetium-177 (177Lu) oxodotreotide to everolimus or sunitinib. Therefore, the sponsor used unanchored matching-adjusted indirect comparisons (MAICs) alongside the NETTER-R study, which was a retrospective single-group study. The clinical report found that the NETTER-R study, due to various limitations and missing data, had results that were difficult to interpret and that cannot be used to draw firm conclusions about the relative benefits of 177Lu in the treatment of pancreatic neuroendocrine tumours (pNETs). The sponsor’s MAICs suggested that 177Lu oxodotreotide was associated with improved progression-free survival (PFS) but comparable overall survival (OS) compared to everolimus or sunitinib. However, the sponsor-submitted indirect treatment comparisons (ITCs) had limitations that may affect the validity and increase the uncertainty of the study results.
CADTH identified several key limitations of the sponsor’s economic analyses, in particular, the lack of robust evidence on the comparative clinical efficacy of 177Lu oxodotreotide, the uncertainty associated with long-term benefits of 177Lu oxodotreotide, and the incorrect estimation of 177Lu oxodotreotide and comparator costs and quality-adjusted life-years (QALYs). Due to the methodological concerns about the NETTER-R study and the submitted ITCs, the comparative clinical effects of 177Lu oxodotreotide are highly uncertain. As a result, CADTH was unable to conduct a base case and instead carried out exploratory reanalyses.
In CADTH’s reanalyses, the acquisition and administration costs of octreotide long-acting release 30 mg were corrected to reflect the 177Lu oxodotreotide product monograph. For the comparison with sunitinib, CADTH also replaced the unit cost of sunitinib with the publicly available drug price. For both reanalyses, CADTH assumed the same proportion of patients requiring octreotide long-acting release and a single set of health utility values across comparators; CADTH applied health utility decrements due to adverse events (AEs) during treatment duration; CADTH used the median treatment duration to calculate drug acquisition and AE costs of comparators; and CADTH used alternative parametric survival models to predict OS curves.
In CADTH’s reanalyses, the incremental cost-effectiveness ratio (ICER) for 177Lu oxodotreotide compared with everolimus was $120,931 per QALY. A price reduction of at least 41% was required to make 177Lu oxodotreotide cost-effective at a willingness to pay (WTP) of $50,000 per QALY. Compared with sunitinib, the ICER for 177Lu oxodotreotide was $466,632 per QALY, and a price reduction of at least 63% was required for 177Lu oxodotreotide to be a cost-effective option.
Scenario analyses highlighted that assumptions on costing, treatment waning, and health utility values were key drivers of CADTH’s reanalyses for both comparators. CADTH was unable to address the uncertainty regarding the comparative clinical efficacy of 177Lu oxodotreotide or the potential survival bias because of the sponsor’s model structure. In the absence of comparative clinical information, sequential analysis could not be conducted to determine the most cost-effective treatment option for the modelled population. As a result, greater price reductions may be required to ensure the cost-effectiveness of 177Lu oxodotreotide.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process—specifically, information that pertains to the economic submission.
Patient input, received from the Canadian Neuroendocrine Tumour Society, was collected through a survey of patients with neuroendocrine cancer (N = 57) in and outside of Canada from February 25, 2022, to March 25, 2022. The respondents included 21 patients with pNETs and 36 patients with gastrointestinal NETs. Patients reported symptoms that affected quality of life, including fatigue and weakness, diarrhea, side effects of surgery with ablation, pain, impaired cognitive ability, appetite changes, back pain, isolation, lack of energy, and inability to travel. Patients noted that NET negatively affects their quality of life and ability to work. Current treatments included somatostatin analogue (SSA) therapies (octreotide, lanreotide), surgery, peptide receptor radionuclide therapy (PRRT), liver-directed therapies (embolization), ablative techniques (radiofrequency ablation, cryotherapy), chemotherapy, radiation therapies, biologically targeted therapies (everolimus, sunitinib), and immunotherapies. These treatments have helped temporarily slow disease progression and control symptoms but have long recovery times, debilitating side effects, and complications. There is a need for therapies that cure disease or halt progression. Patients who had experience with the drug under review reported slower disease progression and tumour shrinkage. Almost half of these patients reported side effects such as increased fatigue, nausea and/or vomiting, diarrhea, and pain, which were generally considered tolerable.
Clinician input was received from a group comprised of researchers, specialists, and clinicians treating neuroendocrine cancer, collected via interviews with national and international clinicians, Drug Advisory Committee meetings, literature reviews of available evidence, and attendance at conferences. The input noted that current treatments available in Canada for patients with metastatic or unresectable disease include biologic therapy (SSAs such as octreotide, octreotide long-acting release, and lanreotide), targeted agents (everolimus and sunitinib), combination chemotherapy (capecitabine plus temozolomide regimen and platinum-based chemotherapy), and PRRT with 177Lu oxodotreotide. Clinicians noted that the goal of treatment is to slow disease progression, prolong PFS, minimize treatment toxicities, reduce societal burden of disease, and control hormonal symptoms caused by insulinomas and severe gastritis. Clinicians noted 177Lu oxodotreotide will be used to treat patients with unresectable or metastatic, well-differentiated, somatostatin receptor-positive gastroenteropancreatic NETs, including pNETs, who experience disease progression on currently available first-line therapies. 177Lu oxodotreotide is not suitable for patients with octreotide non-avid disease, high-grade or poorly differentiated tumours, significant renal impairment or bone marrow dysfunction, or those who have previously received PRRT with no clinical benefit.
Drug plan input received for this review noted that relevant comparators may include sunitinib, everolimus, or combination temozolomide plus capecitabine. The plans indicated issues with therapy access and care provision, noting that administration of 177Lu oxodotreotide is restricted to specialized centres that have the infrastructure to handle, prepare, administer, and dispose of lutetium safely. This may require patients to travel long distances to access treatment. The plans also noted that drug wastage is a concern, because 177Lu oxodotreotide has a shelf life of 72 hours. Further, 177Lu oxodotreotide may be used earlier in the treatment paradigm, and chosen over an SSA, if it is better tolerated.
Several of these concerns were addressed in the sponsor’s model:
The sponsor included everolimus and sunitinib as comparators in the submitted economic evaluations. The comparative treatment efficacy for 177Lu oxodotreotide and each comparator was derived using MAICs.
The sponsor’s model considered the impact of 177Lu oxodotreotide and comparators on progression, survival, and quality of life.
The sponsor considered health care utilization and associated costs used to monitor pNETs. Costs and health utility decrements due to AEs were also accounted for in the sponsor’s model.
In addition, CADTH addressed some of these concerns:
Drug wastage was considered by assuming a relative dose intensity (RDI) of 100% in a scenario analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
Cost-effectiveness of 177Lu oxodotreotide compared to a combination of capecitabine plus temozolomide was unknown due to the lack of comparative efficacy data.
Economic Review
The current review is a reassessment for 177Lu oxodotreotide (Lutathera), solely in the reimbursement request population, for the treatment of unresectable or metastatic, well-differentiated, somatostatin receptor-positive pNETs in adults whose disease has progressed after treatment with an SSA. The previous recommendation for 177Lu did not support use for patients with pNETs, as they were excluded from the pivotal NETTER-1 study.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted 2 cost-utility analyses of 177Lu oxodotreotide. In 1 analysis, the sponsor compared 177Lu oxodotreotide with everolimus, and, in another analysis, the sponsor compared 177Lu oxodotreotide with sunitinib. The modelled population was adult patients with unresectable or metastatic, well-differentiated, somatostatin receptor-positive pNETs whose disease has progressed after treatment with an SSA. The population was in line with the reimbursement request and representative of a subset of the Health Canada–approved indication.
177Lu oxodotreotide is available as 370 MBq/mL in a single-dose vial (10 mCi/mL). According to the product monograph, the recommended dosage is 7.4 GBq (200 mCi) as an IV infusion over 30 minutes every 8 weeks for a total of 4 doses, administered on weeks 0, 8, 16, and 24. The cost of 177Lu oxodotreotide is $35,000 per vial, equating to an average monthly cost of $23,333. The sponsor assumed a ||||| RDI in its drug cost calculation. The sponsor’s analysis also assumed a monthly cost of $4,823 for everolimus (91.3% RDI) and $5,470 for sunitinib (86% RDI).
The clinical outcomes were QALYs and life-years. The economic analysis was undertaken over a time horizon of 20 years from the perspective of a Canadian publicly funded health care system. Costs and QALYs were discounted at a rate of 1.5% per annum.
Model Structure
The sponsor used a partitioned survival model (PSM) with 3 health states: PFS, post-progression survival, and death (Appendix 3; Figure 1). The proportion of patients who were progression-free, who experienced post-progression, or who were dead at any time over the model horizon was derived from non-mutually exclusive survival curves. All patients entered in the PFS state and were assumed to receive treatments (177Lu oxodotreotide, everolimus, or sunitinib). Patients could discontinue treatment but remain in the PFS health state until disease progression. At the end of each monthly cycle, the proportion of patients with post-progression survival or death was derived based on the area under the survival curves. Specifically, OS was partitioned to estimate the proportion of patients in the death state, while the PFS was used to estimate the proportion of patients in the PFS health state. The difference between the OS curve and PFS curve was partitioned at each time point to estimate the proportion of patients in the post-progression survival health state. Disease progression was determined by investigator assessment according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 criterion.1,2
Model Inputs
The modelled population reflected the baseline patient characteristics of the enrolled population in the NETTER-R study, an international, retrospective, single-arm study of patients treated with 177Lu oxodotreotide as per the European label in the UK, France, and Spain.1,2 The sponsor’s model assumed a median age of 58 years and a median weight of 68.9 kg.
Transitions from the pre-progression health state to post-progression survival health state was informed by PFS curves obtained from the NETTER-R study. At baseline, 96.4% of patients had progressive disease. The median follow-up after the first cycle of 177Lu oxodotreotide was 24.5 months (range = 2.0 to 123.4 months). The sponsor derived the relative treatment benefits of 177Lu oxodotreotide versus each comparator from an unanchored MAIC, which used patient-level data obtained from the NETTER- R study and aggregated data from published relevant trials (RADIANT-3 study for everolimus and NCT00428597 for sunitinib).3,4 Weighted Cox proportional hazards models were fitted to estimate hazard ratios (HRs), which were applied to PFS and OS of 177Lu oxodotreotide predicted from the NETTER-R study. The joint parametric survival models were used to represent the relative PFS and OS benefits of 177Lu oxodotreotide and each comparator.4 The gamma and exponential models were used to predict long-term PFS of 177Lu oxodotreotide for the comparison with everolimus and sunitinib, respectively. A log-logistic model was used to predict OS of 177Lu oxodotreotide for both everolimus and sunitinib comparisons.
The model accounted for AEs of grade 3 or higher. Health-state–specific utility values were assumed to be independent of treatments; however, the sponsor used different values and data sources for each analysis. For everolimus, the sponsor mapped European Organisation for Research and Treatment of Cancer – Quality of Life questionnaire (EORTC QLQ-C30) scores reported in the ERASMUS study to EQ-5D values; the utility values for pre-progression and post-progression health states were 0.800 (standard error [SE] = 0.081) and 0.790 (SE = 0.079), respectively.5 The ERASMUS study was a randomized controlled trial comparing the efficacy and safety of 177Lu oxodotreotide in 1,214 progressed patients with gastroenteropancreatic NETs and bronchial NETs in the Netherlands.6 For sunitinib, the sponsor obtained utility values from a UK study that reviewed published literature and conducted in-depth interviews with patients and clinical experts to elicit utility values using a time trade-off (TTO) method for patients with NETs.7 According to this UK study, the utility values for pre-progression and post-progression health states were 0.768 (SE = 0.077) and 0.613 (SE = 0.061). The sponsor’s analyses adjusted utility decrements due to grade 3 or 4 AEs, which were obtained from the published literature.
Costs included drugs (acquisition and administration), monitoring, AEs, and palliative care. Drug acquisition costs for each treatment were sourced from the Ontario Drug Benefit formulary and published Canadian literature. Drug costs for 177Lu oxodotreotide included the drug ingredient and supportive medications, which consisted of octreotide long-acting release 30 mg for up to a maximum of 24 months during pre-progression. The sponsor assumed that 10% of patients without and with disease progression may receive octreotide 30 mg subcutaneously for symptom management. This dosing regimen was validated by Canadian expert clinicians. Drug administration costs included costs of pharmacist preparation, chair time, hourly wages of pharmacist and nurse, and overhead facility costs. The sponsor further assumed that 5% of patients receiving 177Lu oxodotreotide were admitted to a hospital. Resource utilization to monitor pNETs in the model was informed by the NETTER-1 trial and input from Canadian clinicians. The sponsor’s model assumed that all patients would receive octreotide 30 mg after disease progression. A palliative care cost was applied to patients who died. The cost estimate was obtained from a published cost-effectiveness of everolimus for the treatment of advanced NETs of gastrointestinal or lung origin in Canada, but this cost-effectiveness study did not provide a source for the palliative care cost.8
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically with 2,000 iterations. Deterministic and probabilistic results were consistent for a comparison of 177Lu oxodotreotide with everolimus but not for a comparison with sunitinib. CADTH noted that the probabilistic ICER of 177Lu oxodotreotide compared to sunitinib was 22% lower than the deterministic ICER ($27,006 versus $34,791 per QALY). The probabilistic findings are presented in this section.
Base-Case Results
In the sponsor’s base-case analysis over a 20-year time horizon, 177Lu oxodotreotide was associated with an ICER of $45,077 and $27,006 per QALY compared to everolimus and sunitinib, respectively (Table 3). At a WTP of $50,000 per QALY, the probability of 177Lu oxodotreotide being cost-effective was 69.7% compared to everolimus and 73.9% compared to sunitinib.
The main cost drivers were parametric survival models for PFS and OS data prediction, followed by assumptions concerning the duration of therapy and the use of short- and long-acting octreotide. At the end of the model time horizon (i.e., 20 years), 8.4% of patients in the comparison of 177Lu oxodotreotide and everolimus and 7.5% of patients in the comparison of 177Lu oxodotreotide and sunitinib were still alive. A breakdown of the sponsor-submitted results for the base-case population by trial duration (i.e., 7 years) and extrapolated period shows that 42.4% of the expected QALY gains of 177Lu oxodotreotide versus everolimus and 44.5% of the expected QALY gains of 177Lu oxodotreotide versus sunitinib come from the time beyond the NETTER-R’s retrospective registry study period (i.e., 13 years).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER ($/QALY) |
|---|---|---|---|---|---|---|---|
177Lu oxodotreotide vs. everolimus | |||||||
Everolimus | 164,677 | Reference | 4.53 | Reference | 2.74 | Reference | Reference |
177Lu oxodotreotide | 237,010 | 72,333 | 6.62 | 2.09 | 4.35 | 1.60 | 45,077 |
177Lu oxodotreotide vs. sunitinib | |||||||
Sunitinib | 190,585 | Reference | 5.03 | Reference | 3.60 | Reference | Reference |
177Lu oxodotreotide | 209,207 | 18,622 | 5.69 | 0.66 | 4.29 | 0.69 | 27,006 |
177Lu = lutetium-177; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.
Sensitivity and Scenario Analysis Results
The sponsor performed scenario analyses by varying the time horizon; changing discount rates; changing assumptions regarding duration of therapy, parametric survival models for PFS and OS prediction, and 177Lu oxodotreotide’s dosing (i.e., assuming an RDI of 100%); and using an alternative data source for utility data. Key drivers of the cost-effectiveness of 177Lu oxodotreotide versus everolimus included parametric survival models for PFS and OS prediction (log-logistic = $27,586 per QALY) and a shorter time horizon (5 years = $73,138 per QALY). Cost-effectiveness of 177Lu oxodotreotide versus sunitinib was also driven by parametric survival models for PFS and OS predictions (177Lu oxodotreotide was dominant) and duration of therapy (extrapolated treatment duration using an exponential distribution = $111,555 per QALY).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations of the sponsor’s analysis that have notable implications for the economic analysis:
Comparative clinical efficacy of 177Lu oxodotreotide to everolimus or sunitinib is highly uncertain. There has been no head-to-head evidence comparing 177Lu oxodotreotide to everolimus or sunitinib. Therefore, the sponsor used unanchored MAICs alongside the NETTER-R study, which was a retrospective single-group study. The clinical report found that the NETTER-R study, due to various limitations and missing data, had results that were difficult to interpret and that cannot be used to draw firm conclusions about the relative benefits of 177Lu in the treatment of pNETs. The sponsor’s MAICs suggested that 177Lu oxodotreotide was associated with improved PFS but comparable OS compared to everolimus or sunitinib. However, there are methodological concerns about the internal validity of the comparative efficacy derived from unanchored MAICs, as noted in the clinical report. In summary, the analyses adjusted for a limited number of baseline characteristics, and there were some differences regarding organ involvement, time from initial diagnosis, time between disease progression and randomization, tumour functionality, and prior treatments. CADTH also noted the methodological heterogeneity due to a potentially different definition of PFS used in the NCT00428597 trial and the NETTER-R study, as the RADIANT-3 trial used RECIST version 1.0 criteria, while the NCT00428597 trial did not specify the version of the RECIST criteria used for defining PFS. Additionally, the median OS was not reached in either the RADIANT-3 or NCT00428597 studies. As a result of the limitations of the MAICs, the estimated treatment benefits of 177Lu oxodotreotide from unanchored MAICs were subject to residual confounding and are highly uncertain. The use of aggregate data for the trials in MAICs also precludes the use of established methods to verify the model’s fit and calibration. The submitted MAICs should therefore be interpreted with caution.
Due to the lack of a sequential analysis, the interpretation of the economic value of 177Lu oxodotreotide was restricted to each comparator (either everolimus or sunitinib). As a result, the most cost-effective treatment for unresectable or metastatic, well-differentiated, somatostatin receptor-positive pNETs in adults with progressive disease remains unknown.
While the submitted MAICs showed the potential PFS and OS benefits of 177Lu oxodotreotide, there was no clear mechanism by which 177Lu oxodotreotide would continue to provide clinical benefit after progression. The sponsor’s use of a PSM structure introduces structural assumptions about the relationship between PFS and OS that could not be adjusted for in the CADTH reanalysis. These assumptions may produce a post-progression survival bias that favours 177Lu oxodotreotide. Due to the structural independence between PFS and OS end points assumed in the sponsor’s model, extrapolations for each end point may reflect within-trial trends in the rates of progression and death.
Additional uncertainty concerning comparative efficacy was contributed by the sponsor’s use of a joint model to predict PFS and OS data during and after the NETTER-R study duration. This approach forced CADTH to use the same survival model for 177Lu oxodotreotide and comparator despite its poor goodness of fit. More important, the sponsor used the weighted Cox proportional hazards models to estimate HRs but did not describe whether proportional hazards assumptions were met. It was therefore questionable whether the estimated PFS and OS benefits would be constant and sustained over the model’s time horizon.
CADTH was unable to determine the extent to which the implied post-progression benefit was due to treatment versus due to structural bias within the PSM; CADTH could not address this in its reanalysis. CADTH’s reanalyses used alternative survival models to predict OS data and performed scenario analyses in which alternative distributions for PFS and OS were explored.
CADTH was unable to address the limitation regarding the joint model because of the sponsor’s model structure. However, in the reanalyses, CADTH applied a treatment-waning effect on PFS and OS benefits of 177Lu oxodotreotide after 36 months. After this period, the PFS and OS hazard rates of 177Lu oxodotreotide were adjusted by the hazard rates of each comparator.
Long-term treatment benefits of 177Lu oxodotreotide were associated with high uncertainty. The sponsor used the best fitted survival models to predict long-term PFS and OS data for 177Lu oxodotreotide and comparators, but CADTH noted that the parametric survival models did not fit PFS and OS data well when interpolated. The sponsor indicated that sustained efficacy of 177Lu oxodotreotide was supported by the extended Kaplan–Meier OS curve reported in a study conducted by Brabander et al., which included 1,214 patients who were treated with 177Lu oxodotreotide from January 2000 to January 2015 at a single institution in Rotterdam, the Netherlands.9 However, CADTH noticed that the population enrolled in Brabander et al. might be healthier than those who participated in the NETTER-R study because a lower proportion of patients had progressive disease at the baseline (54% versus 96%). It was therefore questionable whether the long-term treatment benefits of 177Lu oxodotreotide shown in Brabander et al. would be generalizable to the modelled population.
CADTH was unable to fully assess this limitation. CADTH applied a treatment-waning effect after 3 years as part of its reanalyses and assessed the impact of alternative parametric survival models to extrapolate PFS and OS data within scenario analyses. The use of a 3-year treatment-waning assumption was supported by the PFS and OS curves of 177Lu oxodotreotide reported in the NETTER-R study, which started to flatten after 36 months, which does not reflect the sponsor’s assumption of a constant and sustained benefit over time.
Total costs and QALYs of 177Lu oxodotreotide and comparators were incorrectly estimated. The sponsor’s analyses assumed that 75% of patients received octreotide long-acting release 30 mg during 177Lu oxodotreotide treatment for up to 24 months. This assumption did not align with the 177Lu oxodotreotide product monograph, which states that octreotide long-acting release 30 mg should be administered after each 177Lu oxodotreotide dose and continued until disease progression or for up to 18 months following treatment initiation. This means that the cost of octreotide long-acting release 30 mg should be applied to all patients during this period. The sponsor’s models further assumed that patients who were progression-free would receive octreotide long-acting release 30 mg for 24 months, while 100% of patients experiencing disease progression would receive this medication until progression or death. This assumption was inconsistent with clinical practice. According to the clinical experts consulted by CADTH, most patients would receive octreotide long-acting release 30 mg indefinitely (until progression or death). Applying the cost of long-acting octreotide 30 mg to 24 months for patients without disease progression was likely to underestimate the incremental cost of 177Lu oxodotreotide because more patients receiving 177Lu oxodotreotide were progression-free compared to those receiving each comparator.
In addition, the sponsor used PFS curves to represent treatment duration for everolimus and sunitinib and to estimate the proportion of patients who experienced AEs. This approach likely overestimates the treatment costs but underestimates the QALYs of the comparators, resulting in optimistic ICERs for 177Lu oxodotreotide, given that it is administered for a fixed number of doses (4 doses). According to clinical experts consulted by CADTH, patients receiving everolimus or sunitinib may discontinue these drugs or experience dose interruptions due to their toxicity; therefore, treatment duration for each comparator was expected to be shorter than the time to progression.
CADTH’s reanalyses corrected the cost calculation for 177Lu oxodotreotide by conservatively assuming that 100% of patients in the 177Lu oxodotreotide arm received octreotide long-acting release 30 mg during 177Lu oxodotreotide treatment and continued until 24 months; after this period, 75% were assumed to receive octreotide long-acting release 30 mg until progression or death. For everolimus and sunitinib, the same proportion of patients who were progression-free (75%) were assumed to receive octreotide long-acting release 30 mg until progression or death. For patients experiencing disease progression, CADTH retained the sponsor’s assumption and assumed that octreotide long-acting release 30 mg was given to all patients who were alive.
In its reanalysis, CADTH used time to treatment discontinuation curves predicted from the median treatment duration reported in relevant trials (RADIANT-3 trial for everolimus and A6181111 for sunitinib) to calculate the acquisition costs and health utility decrements due to AEs of everolimus and sunitinib.4
Health utility estimates lacked face validity. In the NETTER-R study, a limited number of participants completed a health-related quality of life questionnaire; therefore, the sponsor obtained health utility data from the published literature. The sponsor did not, however, justify why different data sources and health utility values were used for the comparisons of 177Lu oxodotreotide versus everolimus and 177Lu oxodotreotide versus sunitinib. For the comparison with everolimus, the sponsor obtained health utility values for pre-progression and post-progression from a vignette-based TTO study conducted in a UK general population. For the comparison with sunitinib, the same health state utility values were based on a study by Soare et al. that mapped EORTC QLQ-C30 data to EQ-5D-3L utility values.5 The clinical experts consulted by CADTH advised that quality of life is expected to depend on disease progression but should not vary by the type of initial treatments.
Given the feedback from the clinical experts and the inconsistency in values used, CADTH used the health utility values derived from Soare et al. in the reanalyses for both pairwise comparisons, because it provided health utility values specific to patients with pNETs in both base-case analyses. Health utility values obtained from the UK vignette-based TTO study were highly dependent on the description of the health states and might incorrectly estimate utility values. It should be noted that clinical experts consulted by CADTH questioned the face validity of health utility values of pre- and post-progression health states reported in Soare et al., as they were nearly identical (0.800 versus 0.790). In addition, CADTH also noted additional uncertainty due to the use of a health utility mapping method. The validity of the mapping algorithm depends on the overlap between measures considered in the EORTC QLQ-C30 and EQ-5D questionnaires and the statistical performance of the mapping algorithm. Therefore, CADTH conducted a scenario analysis using the health state utility values from the vignette-based TTO study.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
5% of patients receiving octreotide long-acting release would be admitted to the hospital. | Acceptable. This assumption was expected to have minimal impact on ICERs, as the same proportion was applied to patients receiving 177Lu oxodotreotide and comparators. |
10% of patients receiving 177Lu oxodotreotide or a comparator would receive subcutaneous octreotide. | This assumption was deemed acceptable by clinical experts consulted by CADTH; however, the proportion is likely to vary by centre. Notably, this assumption would have minimal impact on ICERs, as the same proportion was applied to patients receiving 177Lu oxodotreotide and comparators. |
The sponsor applied RDI obtained from relevant studies in the calculation of treatment costs. For the sponsor’s base case, the RDIs for 177Lu oxodotreotide, everolimus, and sunitinib were |||||, 86.0%, and 91.3%, respectively. | Clinical experts consulted by CADTH found this assumption acceptable but raised a minor concern that RDI for sunitinib was higher than what is observed in clinical practice. CADTH performed a scenario analysis to assess the impact of this assumption by assuming a 100% RDI for all treatments. |
The sponsor assumed that palliative care was associated with an additional cost of $4,838.52 and a utility decrement of 0.15 for each model cycle. | It was unclear whether the cost and utility decrement were specific to the modelled population. CADTH was unable to verify the sources for these values. However, this assumption was expected to have minimal impact on the ICERs. |
The sponsor’s base cases assumed that patients experiencing disease progression would receive octreotide long-acting release only as a subsequent therapy. | Inappropriate. Clinical experts consulted by CADTH advised that subsequent therapies after disease progression would depend on the initial treatment and may involve other targeted therapies, such as everolimus and sunitinib, chemotherapy, and a hepatic-directed therapy, including radioembolization and cytoreductive surgery or ablative therapy. However, the experts concurred with the sponsor that it would be challenging to measure the distribution of these subsequent treatments, as treatments likely varied by centre and by physician and patient preference. CADTH was unable to explore the impact of subsequent treatments on the ICERs due to data limitations. |
177Lu = lutetium-177; ICER = incremental cost-effectiveness ratio; RDI = relative dose intensity.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH could not address several key limitations associated with the sponsor’s economic evaluation, primarily the lack of robust evidence on the comparative efficacy for 177Lu oxodotreotide. Due to these limitations, all reanalyses undertaken by CADTH are considered exploratory.
CADTH corrected the sponsor’s models by correcting the acquisition and administration costs of octreotide long-acting release 30 mg to match its dosing schedule in the 177Lu oxodotreotide product monograph. For the comparison with sunitinib, CADTH also replaced the unit cost of sunitinib with the publicly available drug price. For both analyses, CADTH’s reanalyses assumed that 75% of patients who were progression-free receiving octreotide long-acting release 30 mg until progression or death, applying health utility decrements due to AEs during treatment duration, using the median treatment duration reported in the relevant trial (RADIANT-3 trial for everolimus and A4181111 trial for sunitinib) to represent treatment duration and to calculate drug acquisition and AE costs for comparators, using alternative parametric survival models to predict the OS curve. For the comparison with everolimus, CADTH replaced health utility values for pre-progression and post-progression health states with those used in the comparison with sunitinib. CADTH also increased the number of simulations to 5,000 to improve the stability of the cost-effectiveness results. Table 5 details the changes made to derive the CADTH’s base cases, and the summary results of the CADTH’s reanalyses are presented in Table 6. Additional results are shown in Appendix 4.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s reanalyses | ||
1. Daily cost of sunitinib was incorrect. | Comparison with sunitinib Daily cost of sunitinib: $193.25 | Comparison with sunitinib Daily cost of sunitinib: $195.37 |
2. The administration cost of octreotide long-acting release 30 mg used in the pre- and post-progression health states were inconsistent. | Comparison with everolimus Pre-progression health state: administration fee plus hotel cost Post-progression health state: administration fee Comparison with sunitinib Pre-progression health state: administration fee plus hotel cost Post-progression health state: administration fee | Comparison with everolimus No change Post-progression health state: administration fee plus hotel cost Comparison with sunitinib No change Post-progression health state: administration fee plus hotel cost |
3. The cost of octreotide long-acting release 30 mg in the 177Lu oxodotreotide arm was incorrectly estimated. | Comparison with everolimus 75% of patients were assumed to receive octreotide long-acting release 30 mg during 4 doses of 177Lu oxodotreotide treatment and continue for 24 months. Comparison with sunitinib 75% of patients were assumed to receive octreotide long-acting release 30 mg during 4 doses of 177Lu oxodotreotide treatment and continue for 24 months. | Comparison with everolimus 100% of patients were assumed to receive octreotide long-acting release 30 mg during 4 doses of 177Lu oxodotreotide treatment and continue for 24 months. Comparison with sunitinib 100% of patients were assumed to receive octreotide long-acting release 30 mg during 4 doses of 177Lu oxodotreotide treatment and continue for 24 months. |
Changes to derive the CADTH base case | ||
1. Comparative efficacy of 177Lu oxodotreotide was highly uncertain due the lack of robust clinical evidence. | PFS and OS benefits of 177Lu oxodotreotide vs. comparator were assumed to be constant and sustained over the model’s time horizon. | PFS and OS benefits of 177Lu oxodotreotide vs. comparator were assumed to wane and match the comparator’s level after 36 months. |
2. The proportion of patients who were progression-free and received octreotide long-acting release 30 mg and the treatment duration of octreotide long-acting release 30 mg did not align with clinical practice. | Comparison with everolimus 75% of patients receiving 177Lu oxodotreotide or everolimus who were progression-free were assumed to receive octreotide long-acting release 30 mg for 24 months. Comparison with sunitinib 75% of patients receiving 177Lu oxodotreotide and 50% of patients receiving sunitinib who were progression-free were assumed to receive octreotide long-acting release 30 mg for 24 months. | Comparison with everolimus 75% of patients receiving 177Lu oxodotreotide or everolimus who were progression-free were assumed to continue long-acting octreotide 30 mg until progression or death. Comparison with sunitinib 75% of patients receiving 177Lu oxodotreotide and 75% of patients receiving sunitinib who were progression-free were assumed to continue octreotide long-acting release 30 mg until progression or death. |
3. Health-state–specific utility values lacked face validity. | Comparison with everolimus Pre-progression: 0.768 Post-progression: 0.612 Comparison with sunitinib Pre-progression: 0.805 Post-progression: 0.790 | Comparison with everolimus Pre-progression: 0.805 Post-progression: 0.790 Comparison with sunitinib No change |
4. QALYs of comparators were incorrectly estimated. | Comparison with everolimus Utility decrements were applied to every model cycle. Comparison with sunitinib Utility decrements were applied to every model cycle. | Comparison with everolimus Utility decrements were applied during treatment duration. Comparison with sunitinib Utility decrements were applied during treatment duration. |
5. Total costs of comparators were incorrectly estimated. | Comparison with everolimus A PFS curve was used to represent treatment duration and to calculate acquisition drug and AE costs. Comparison with sunitinib A PFS curve was used to represent treatment duration and calculate acquisition drug and AE costs. | Comparison with everolimus A median treatment duration reported in the RADIANT-3 trial was used to represent treatment duration and to calculate drug and AE costs. Comparison with sunitinib A median treatment duration reported in the A4181111 trial was used to represent treatment duration and calculate drug and AE costs. |
6. Long-term OS data were highly uncertain. | Comparison with everolimus Log-logistic distribution Comparison with sunitinib Log-logistic distribution | Comparison with everolimus Gompertz distribution Comparison with sunitinib Weibull distribution |
CADTH reanalyses | — | 1 + 2 + 3 + 4 + 5 + 6 |
177Lu = lutetium-177; AE = adverse event; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year.
Results from CADTH reanalyses showed that 177Lu oxodotreotide was associated with higher costs ($94,549) and improved QALYs (0.78), resulting in ICERs of $120,931 per QALY compared to everolimus. The probability that 177Lu oxodotreotide is cost-effective was 0% at a WTP threshold of $50,000 per QALY. Compared to sunitinib, results from CADTH’s reanalysis suggested that 177Lu oxodotreotide was more costly ($93,727) and more effective (0.38 QALYs), with an ICER of 466,632. The probability that 177Lu oxodotreotide is cost-effective was 0% at the WTP threshold of $50,000 per QALY.
Table 6: Summary of the CADTH Reanalysis Results
Drug | Total costs ($) | Total QALYs | ICER vs. reference ($/QALY) | Sequential ICER ($/QALY) |
|---|---|---|---|---|
177Lu oxodotreotide vs. everolimus | ||||
Sponsor’s corrected base case | ||||
Everolimus | 169,523 | 2.77 | Reference | Reference |
177Lu oxodotreotide | 247,835 | 4.38 | 48,886 | 48,886 |
CADTH reanalysis | ||||
Everolimus | 139,374 | 2.67 | Reference | Reference |
177Lu oxodotreotide | 233,923 | 3.45 | 120,931 | 120,931 |
177Lu oxodotreotide vs. sunitinib | ||||
Sponsor’s corrected base case | ||||
Sunitinib | 196,325 | 3.58 | Reference | Reference |
177Lu oxodotreotide | 216,124 | 4.21 | 31,490 | 31,490 |
CADTH reanalysis | ||||
Sunitinib | 136,460 | 3.27 | Reference | Reference |
177Lu oxodotreotide | 228,331 | 3.46 | 466,632 | 466,632 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
A series of scenario analyses was conducted to explore the impact of the following model parameters and assumptions: assumptions regarding treatment dosages (i.e., RDI assumption) and administration location, a proportion of subcutaneous octreotide used for symptom management, a proportion of patients receiving long-acting octreotide 30 mg, treatment duration, treatment-waning assumption, and parametric survival models for PFS and OS predictions. CADTH also explored the impact of health utility values by applying treatment-specific health utility values derived from an alternate source.
Results from scenario analyses (Appendix 4, Table 13 and Table 14) demonstrated that the ICERs of 177Lu oxodotreotide were mostly sensitive to assumptions regarding costing (RDI and treatment duration), treatment waning, and health utility values. For the comparison between 177Lu oxodotreotide and everolimus, the ICERs of 177Lu oxodotreotide ranged between $69,816 per QALY and $159,338 per QALY. Similarly, for the comparison with sunitinib, the ICERs of 177Lu oxodotreotide ranged between $172,745 per QALY and $578,680 per QALY. Cost-effectiveness findings were found to be robust to the choices of parametric survival models used to predict long-term PFS and OS curves.
A price-reduction analysis based on the sponsor’s corrected and CADTH reanalyses (Table 7) indicated that, at a WTP threshold of $50,000 per QALY, a price reduction of up to 41% is required for 177Lu oxodotreotide to be considered cost-effective compared to everolimus. A larger price reduction (63%) is required for 177Lu oxodotreotide to be considered cost-effective compared to sunitinib. A price-reduction analysis of the sponsor’s 2 base cases was not performed, given that 177Lu oxodotreotide was deemed cost-effective at the submitted price.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICER 177Lu oxodotreotide vs. everolimus | ICER 177Lu oxodotreotide vs. sunitinib | ||
|---|---|---|---|---|
Price reduction | Sponsor’s base case | CADTH reanalysis | Sponsor’s base case | CADTH reanalysis |
No price reduction | $45,077 | $120,931 | $27,006 | $466,632 |
10% | — | $103,941 | — | $390,084 |
20% | — | $85,649 | — | $352,755 |
30% | — | $68,552 | — | $258,884 |
40% | — | $51,631 | — | $214,382 |
41% | — | $49,513 | — | $196,361 |
50% | — | — | — | $145,196 |
60% | — | — | — | $76,009 |
63% | — | — | — | $49,074 |
177Lu = lutetium-177; ICER = incremental cost-effectiveness ratio.
Issues for Consideration
Clinical experts consulted by CADTH indicated that lanreotide is also available in Canada. This SSA can also be used as the first-line or subsequent treatment in patients with somatostatin receptor-positive pNETs. The impact of this SSA on the cost-effectiveness of 177Lu oxodotreotide remains unknown, as it was not considered in the sponsor’s and CADTH’s reanalyses. However, its impact on the ICER of 177Lu oxodotreotide is expected to be minimal, because octreotide long-acting release and lanreotide are deemed interchangeable, according to the National Comprehensive Cancer Network guidelines.
A combination of capecitabine plus temozolomide is publicly funded and considered a relevant comparator but was not included in the sponsor’s and CADTH’s reanalyses. Based on the feedback from clinical experts consulted by CADTH, it is reasonable to exclude this comparator, as the treatment is not commonly used and not expected to be displaced by 177Lu oxodotreotide.
177Lu oxodotreotide is a radiopharmaceutical that has specific handling requirements. It has a limited shelf life of 72 hours, and accessibility may be of concern. The impact of drug wastage from missed doses has not been considered in this review, and the budget impact may have been underestimated. Drug plans also noted that 177Lu oxodotreotide may be restricted to specialized centres that have the infrastructure to handle, prepare, administer, and dispose of lutetium in a safe manner. This may require patients to travel long distances to access treatment.
Overall Conclusions
There has been no head-to-head evidence comparing 177Lu oxodotreotide to everolimus or sunitinib; therefore, the sponsor used unanchored MAICs alongside the NETTER-R study, which was a retrospective single-group study. The clinical report found that the NETTER-R study, due to various limitations and missing data, had results difficult to interpret that cannot be used to draw firm conclusions about the relative benefits of 177Lu oxodotreotide in the treatment of pNETs. The sponsor’s MAICs suggested that 177Lu oxodotreotide was associated with improved PFS but comparable OS compared to everolimus or sunitinib. However, the sponsor-submitted ITCs had limitations that may impact the validity and increase the uncertainty of the study results.
CADTH identified several key limitations of the sponsor’s economic analyses, in particular, the lack of robust evidence of the comparative clinical efficacy of 177Lu oxodotreotide, the uncertainty associated with long-term benefits of 177Lu oxodotreotide, and incorrect estimation of 177Lu oxodotreotide and comparator costs and QALYs. Due to the methodological concerns with the NETTER-R study and the submitted ITCs, the comparative clinical effects of 177Lu oxodotreotide are highly uncertain. As a result, CADTH was unable to conduct a base case and instead conducted exploratory reanalyses.
For CADTH reanalyses, the acquisition and administration costs of octreotide long-acting release 30 mg were corrected to reflect the 177Lu oxodotreotide product monograph. For the comparison with sunitinib, CADTH also replaced the unit cost of sunitinib with the publicly available drug price. For both reanalyses, CADTH assumed the same proportion of patients requiring octreotide long-acting release and a single set of health utility values across comparators; applied health utility decrements due to AEs during treatment duration; used the median treatment duration to calculate drug acquisition and AE costs of comparators; and used alternative parametric survival models to predict OS curves.
In CADTH’s reanalyses, the ICER for 177Lu oxodotreotide compared with everolimus was $120,931 per QALY. A price reduction of at least 41% was required to make 177Lu oxodotreotide cost-effective at a WTP of $50,000 per QALY. Compared with sunitinib, the ICER for 177Lu oxodotreotide was $466,632 per QALY, and a price reduction of at least 63% was required for 177Lu oxodotreotide to be a cost-effective option.
Scenario analyses highlighted that assumptions on costing, treatment waning, and health utility values were the key drivers of CADTH’s reanalyses for both comparators. CADTH was unable to address the uncertainty regarding the comparative clinical efficacy of 177Lu oxodotreotide or the potential survival bias due to the sponsor’s model structure. In the absence of comparative clinical information, sequential analysis could not be conducted to determine the most cost-effective treatment option for the modelled population. As a result, greater price reductions may be required to ensure the cost-effectiveness of 177Lu oxodotreotide.
References
1.Pharmacoeconomic evaluation [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Lutathera (lutetium (177Lu) oxodotreotide), 370 mMBq/mL at calibration [internal sponsor’s package]. Mississauga (ON): Advanced Accelerator Applications Canada Inc.; 2022 Apr 1.
2.Clement D, Navalkissoor S, Srirajaskanthan R, et al. Efficacy and safety of (177)Lu-DOTATATE in patients with advanced pancreatic neuroendocrine tumours: data from the NETTER-R international, retrospective study. Eur J Nucl Med Mol Imaging. 2022. PubMed
3.Yao JC, Shah MH, Ito T, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med. 2011;364(6):514-523. PubMed
4.Faivre S, Niccoli P, Castellano D, et al. Sunitinib in pancreatic neuroendocrine tumors: updated progression-free survival and final overall survival from a phase III randomized study. Ann Oncol. 2017;28(2):339-343. PubMed
5.Soare IA, Leeuwenkamp O, Longworth L. Estimation of Health-Related Utilities for (177)Lu-DOTATATE in GEP-NET Patients Using Utilities Mapped from EORTC QLQ-C30 to EQ-5D-3L and QLU-C10D Utilities. Pharmacoecon Open. 2021;5(4):715-725. PubMed
6.Strosberg J, El-Haddad G, Wolin E, et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N Engl J Med. 2017;376(2):125-135. PubMed
7.Swinburn P, Wang J, Chandiwana D, Mansoor W, Lloyd A. Elicitation of health state utilities in neuroendocrine tumours. J Med Econ. 2012;15(4):681-687. PubMed
8.Chau I, Casciano R, Willet J, Wang X, Yao JC. Quality of life, resource utilisation and health economics assessment in advanced neuroendocrine tumours: a systematic review. Eur J Cancer Care (Engl). 2013;22(6):714-725. PubMed
9.Brabander T, van der Zwan WA, Teunissen JJM, et al. Long-Term Efficacy, Survival, and Safety of [(177)Lu-DOTA(0),Tyr(3)]octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors. Clin Cancer Res. 2017;23(16):4617-4624. PubMed
10.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Apr 22.
11.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2022: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2022 Apr 22.
12.Sandoz everolimus (everolimus tablets): 2.5 mg, 5 mg, and 10 mg [product monograph]. Boucherville (QC): Sandoz Canada Inc.; 2020 Jan 27: https://www.sandoz.ca/sites/www.sandoz.ca/files/Sandoz%20Everolimus%20Product%20Monograph.pdf. Accessed 2022 Jun 6.
13.Taro-Sunitinib (sunitinib capsules): 12.5 mg, 25 mg, 37.5 mg, 50 mg sunitinib per capsule (as sunitinib malate) [product monograph]. Brampton (ON): Taro Pharmaceuticals Inc; 2022.
14.Cancer Care Ontario. Drug formulary: CAPETMZL. 2021; https://www.cancercareontario.ca/en/drugformulary/regimens/46796. Accessed 2022 Jun 6.
15.Cancer Care Ontario: funded evidence-informed regimens. 2022; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2022 Jun 6.
16.Budget Impact Analysis [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Lutathera (lutetium (177Lu) oxodotreotide), 370 mMBq/mL at calibration [internal sponsor’s package]. Mississauga (ON): Advanced Accelerator Applications Canada Inc.; 2022 Apr 1.
17.Hallet J, Law CH, Cukier M, Saskin R, Liu N, Singh S. Exploring the rising incidence of neuroendocrine tumors: a population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer. 2015;121(4):589-597. PubMed
18.Halfdanarson TR, Rabe KG, Rubin J, Petersen GM. Pancreatic neuroendocrine tumors (PNETs): incidence, prognosis and recent trend toward improved survival. Ann Oncol. 2008;19(10):1727-1733. PubMed
19.pan-Canadian Oncology Drug Review final economic guidance report: lutetium Lu 177 dotatate (Lutathera) for gastroenteropancreatic neuroendocrine tumors. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10142LutetiumLu177dotatateGEP-NET_fnEGR_NOREDACT-ABBREV_Post_01Aug2019_final.pdf. Accessed 2022 Jun 6.
20.Drug Reimbursement Review sponsor submission: Lutathera (lutetium (177Lu) oxodotreotide), 370 mMBq/mL at calibration [internal sponsor’s package]. Mississauga (ON): Advanced Accelerator Applications Canada Inc.; 2022 Apr 1.
21.Lutathera (lutetium (177Lu) oxodotreotide): 370 MBq/mL at calibration [product monograph]. Milburn (NJ): Advanced Accelerator Applications USA Inc.; 2021 May 13.
22.Raymond E, Dahan L, Raoul JL, et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med. 2011;364(6):501-513. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Unresectable Locally Advanced Or Metastatic, Well-Differentiated Pancreatic Neuroendocrine Tumours
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Average daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Lutetium (177Lu) oxodotreotide) | 370 MBq/mL or 10 mCi/mL (7.4 GBq) | Vial IV infusion | 35,000.0000 | 7.4 GBq (200 mCi) every 8 weeks for a total of 4 doses | 625.00 | 17,500 |
Kinase inhibitors | ||||||
Everolimus | 2.5 mg 5 mg 10 mg | Tablet | 172.2559 | 10 mg once daily | 172.26 | 4,823 |
Sunitinib | 12.5 mg 25 mg 37.5 mg 50 mg | Capsule | 65.124 130.247 NAb 260.495 | 37.5 mg taken orally once daily | 195.37 | 5,470 |
Chemotherapy | ||||||
Capecitabine | 150 mg 500 mg | Tablet | 0.4570 1.5250 | 750 mg/m2 twice daily on Days 1 to 14 every 4 weeks | 4.42 | 124 |
Temozolomide | 5 mg 20 mg 100 mg 140 mg 250 mg | Capsule | 3.9000 15.6000 78.0030 109.2050 195.0020 | 200 mg/m2 daily on Days 10 to 14 every 4 weeks | 50.14 | 1,404 |
Capecitabine + Temozolomide | 54.56 | 1,528 | ||||
Note: All prices are from the Ontario Drug Benefit formulary (accessed April 24, 2022),10 unless otherwise indicated, and do not include dispensing fees. The cost of sunitinib is obtained from Ontario Exceptional Access Program drug list (accessed April 24, 2022).11 Dosing obtained from Cancer Care Ontario formulary and respective product monographs.12-15
bProduct strength is approved but not marketed in Canada.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | A combination of capecitabine and temozolomide is considered a relevant comparator but was not included in the sponsor’s base-case analyses. Based on the feedback from clinical experts consulted by CADTH, it is reasonable to exclude this comparator as the treatment is not commonly used and not expected to displace 177Lu oxodotreotide. |
Model has been adequately programmed and has sufficient face validity | No | CADTH identified errors in the drug cost calculations. The sponsor’s models were not flexible to modify some input parameters, such as treatment effect of 177Lu oxodotreotide, because they were hardcoded and not transparent. See CADTH appraisal section. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | CADTH identified limitations with the use of PFS data to represent treatment duration, the transparency of costs, and the inconsistency of using some parameters, such as the percentage of patients receiving long-acting octreotide and health-state–specific utility values, across comparators. See CADTH appraisal section. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | A dosing schedule of long-acting octreotide in combination with 177Lu oxodotreotide was not clearly described. Additionally, CADTH was unable to verify data sources used to inform costs and health utility decrement associated with palliative care. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
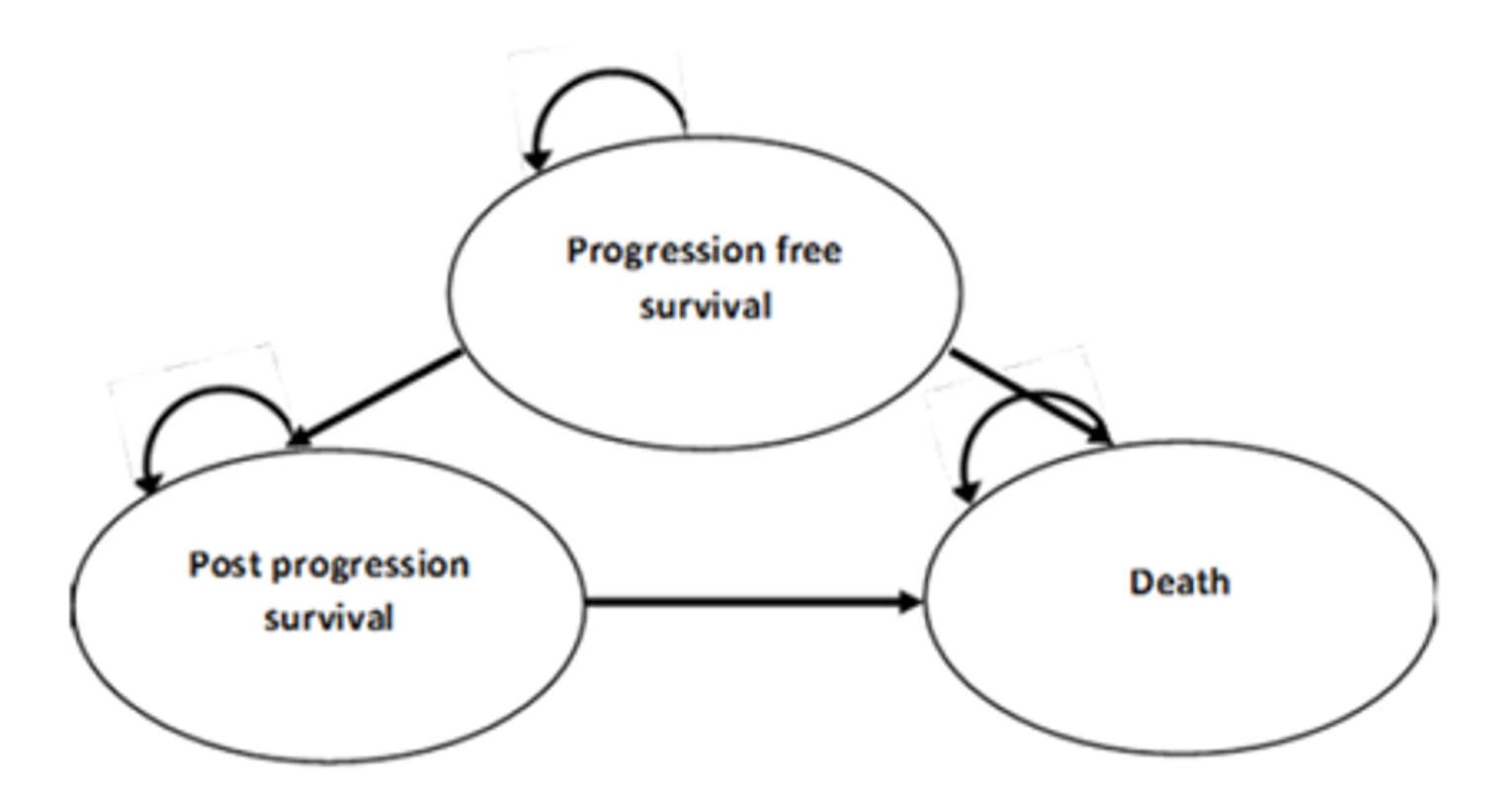
Detailed Results of the Sponsor’s Base Case
Figure 2: Predicted PFS Data — 177Lu Oxodotreotide (Compared to Everolimus) — Redacted

Figure was redacted per the sponsor’s request.
Source: Sponsor’s pharmacoeconomic submission.
Figure 3: Predicted OS Data — 177Lu Oxodotreotide (Compared to Everolimus) — Redacted

Figure was redacted per the sponsor’s request.
Source: Sponsor’s pharmacoeconomic submission.
Figure 4: Predicted PFS Data — Everolimus (Compared to Everolimus)
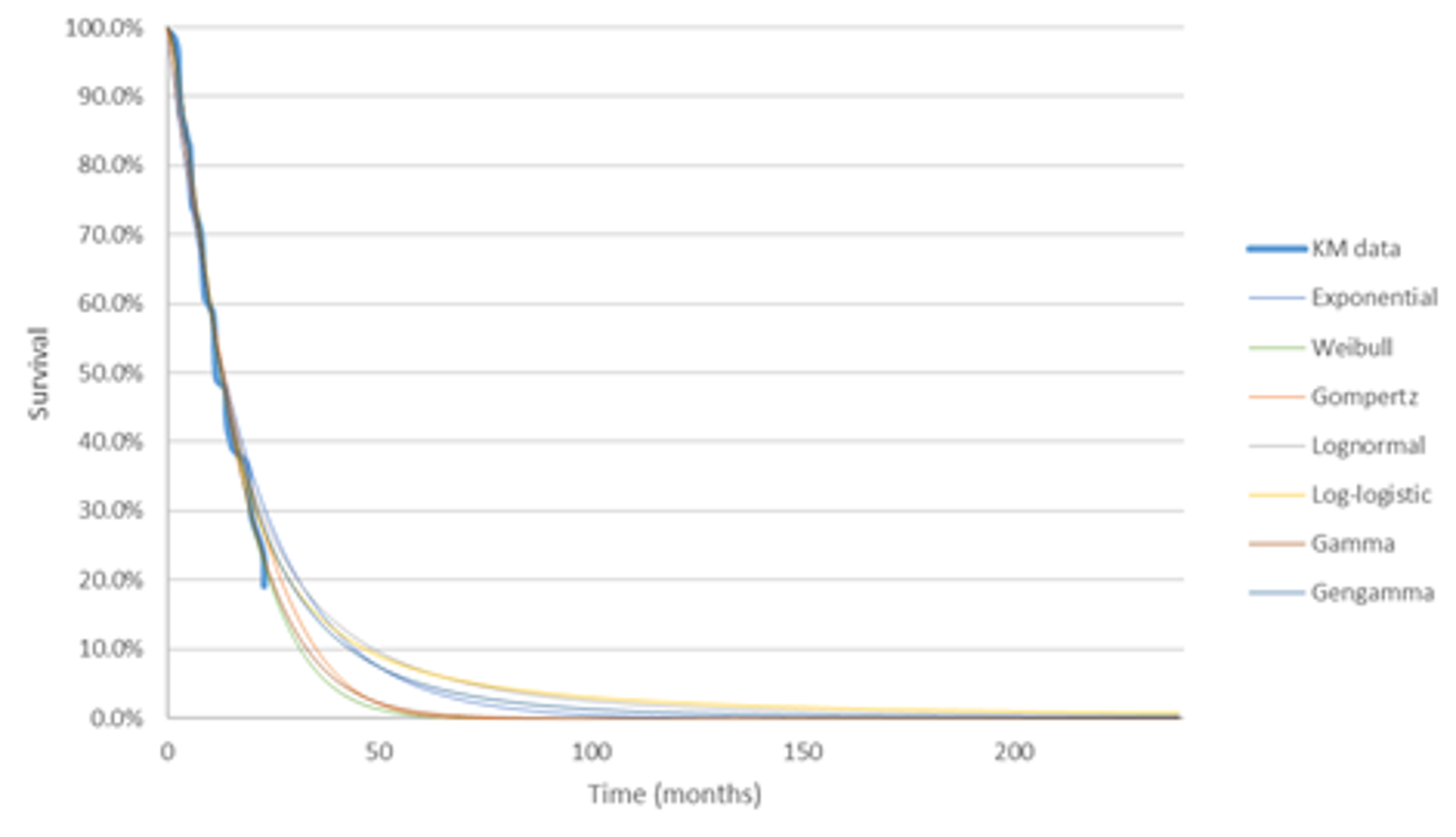
Source: Sponsor’s pharmacoeconomic submission.
Figure 5: Predicted OS Data — Everolimus (Compared to Everolimus)
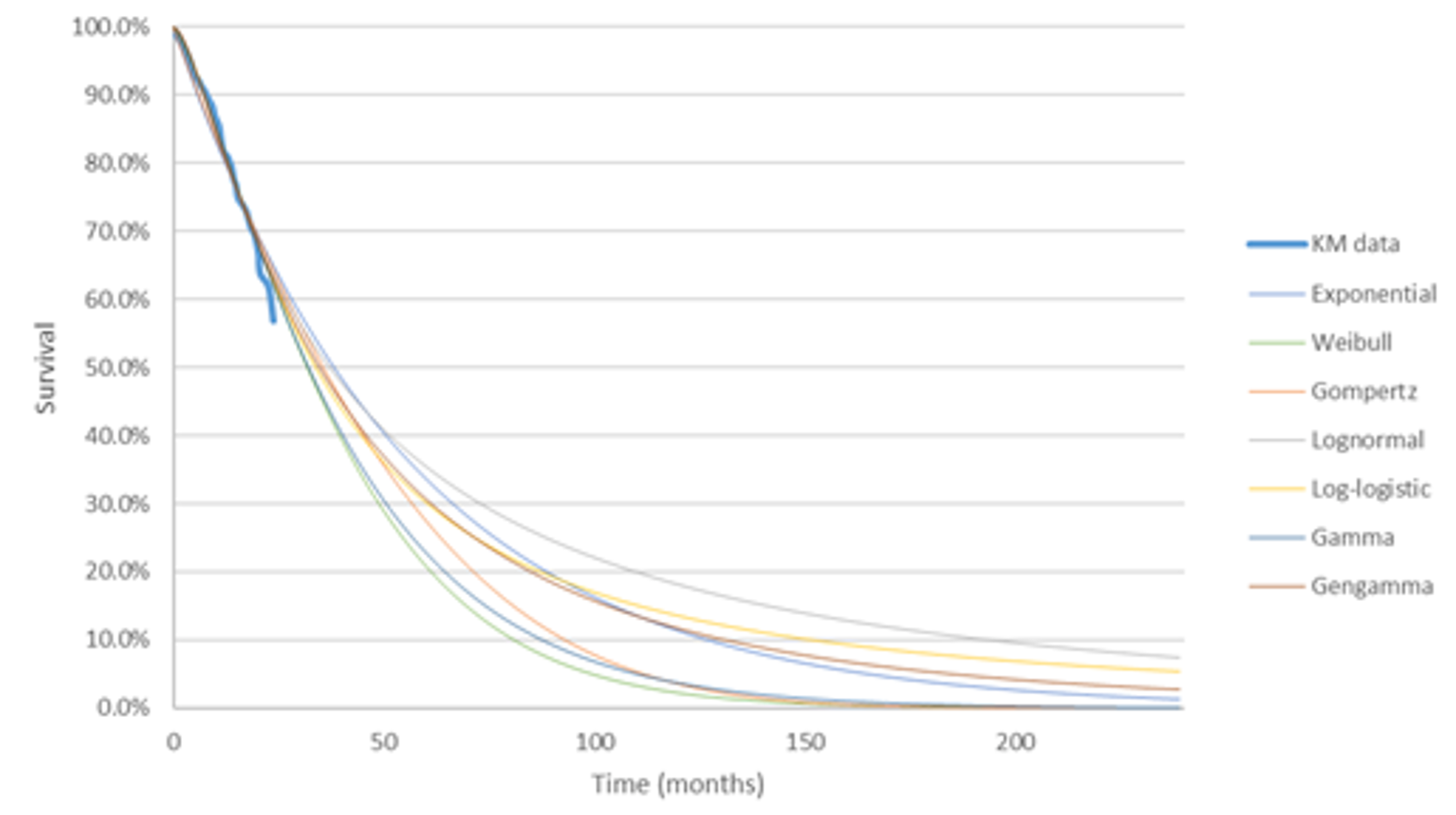
Source: Sponsor’s pharmacoeconomic submission.
Figure 6: Predicted PFS Data — 177Lu Oxodotreotide (Compared to Sunitinib) — Redacted

Figure was redacted as per the sponsor’s request.
Source: Sponsor’s pharmacoeconomic submission.
Figure 7: Predicted OS Data — 177Lu Oxodotreotide (Compared to Sunitinib) — Redacted

Figure was redacted as per the sponsor’s request.
Source: Sponsor’s pharmacoeconomic submission.
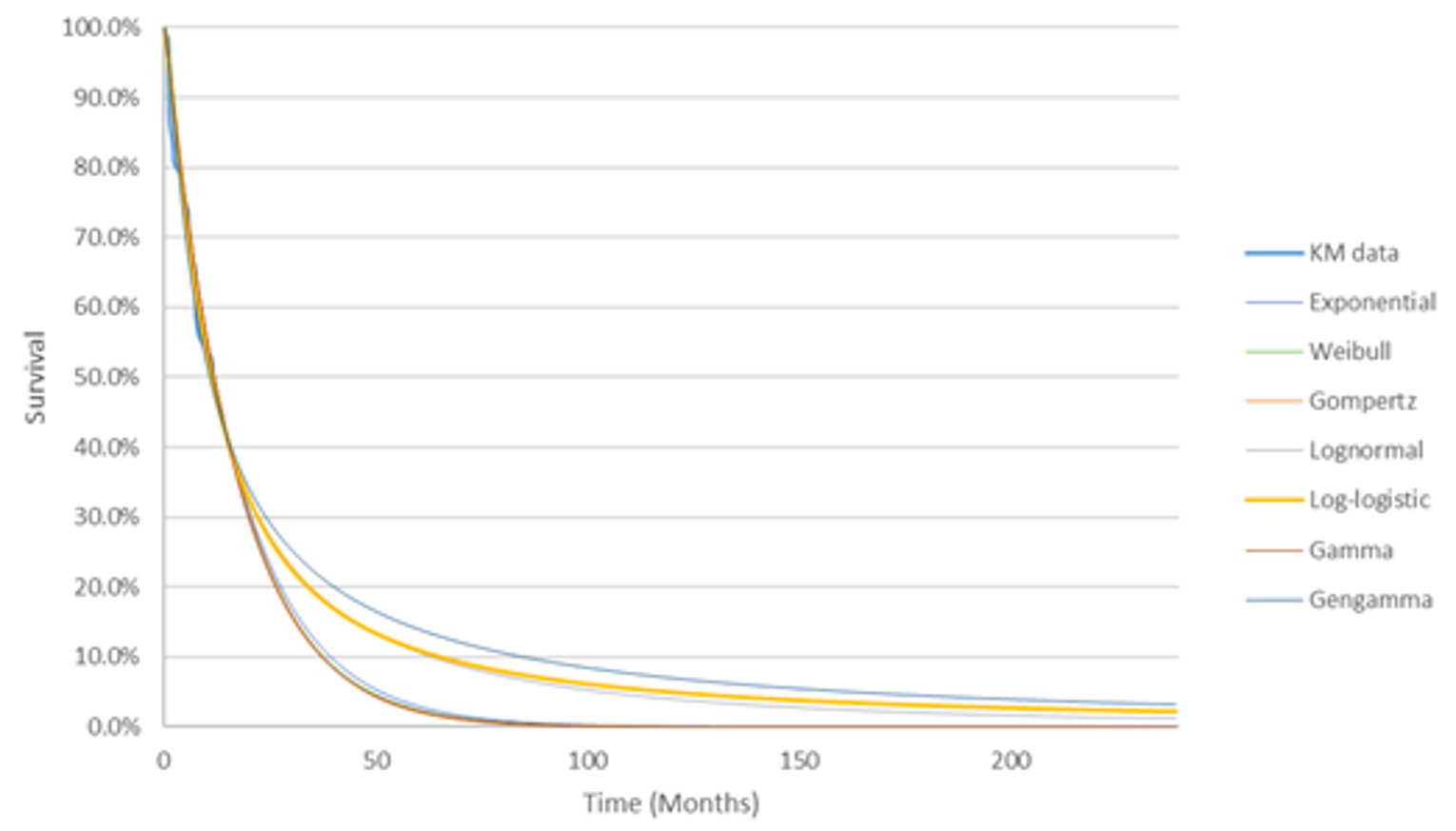
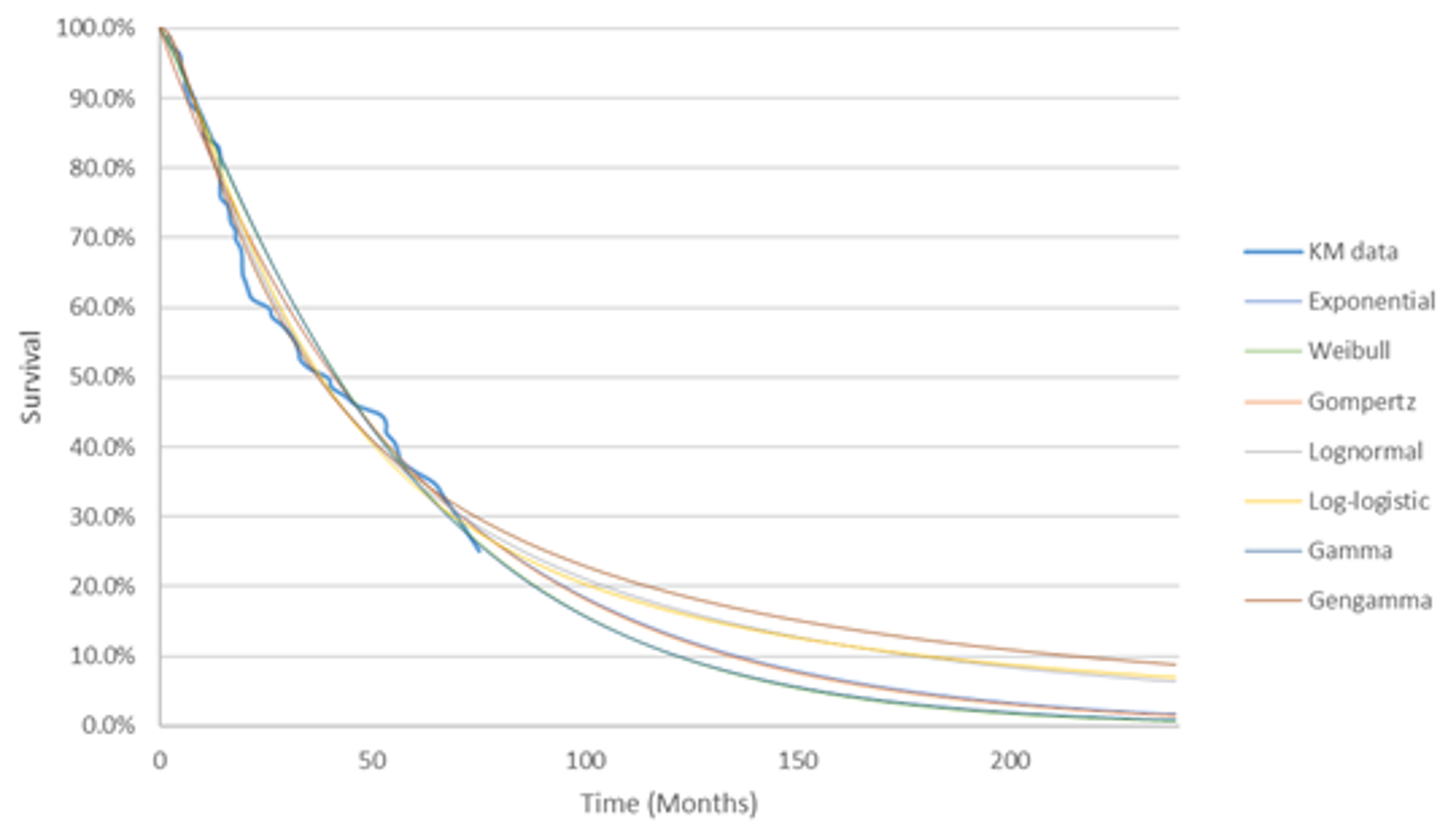
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 10: Disaggregated Summary of CADTH’s Economic Evaluation Results (177Lu Oxodotreotide Versus Everolimus)
Parameter | 177Lu oxodotreotide | Everolimus | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 4.59 | 3.74 | 0.85 |
By health state | |||
Pre-progression | 2.55 | 1.41 | 1.14 |
Post-progression | 2.04 | 2.33 | –0.29 |
Discounted QALYs | |||
Total | 3.45 | 2.67 | 0.78 |
By health state | |||
Pre-progression | 2.04 | 1.04 | 1.00 |
Post-progression | 1.55 | 1.77 | –0.22 |
Palliative | –0.13 | –0.14 | 0.01 |
Discounted costs ($) | |||
Total | 233,923 | 139,374 | 94,549 |
Acquisition | 218,428 | 127,408 | 91,020 |
Administration | 9,113 | 5,255 | 3,858 |
Adverse events | 66 | 667 | –601 |
Monitoring | 1,847 | 1,504 | 343 |
Palliative | 4,470 | 4,539 | –70 |
ICER ($/QALY) | 120,931 | ||
177Lu oxodotreotide = lutetium oxodotreotide; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Table 11: Disaggregated Summary of CADTH’s Economic Evaluation Results (177Lu Oxodotreotide Versus Sunitinib)
Parameter | 177Lu oxodotreotide | Sunitinib | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 4.60 | 4.46 | 0.14 |
By health state | |||
Pre-progression | 2.50 | 1.52 | 0.98 |
Post-progression | 2.10 | 2.94 | –0.84 |
Discounted QALYs | |||
Total | 3.46 | 3.27 | 0.20 |
By health state | |||
Pre-progression | 2.01 | 1.17 | 0.83 |
Post-progression | 1.59 | 2.23 | –0.64 |
Palliative | –0.13 | –0.14 | 0.00 |
Discounted costs ($) | |||
Total | 228,331 | 136,460 | 91,871 |
Acquisition | 212,932 | 123,245 | 89,687 |
Administration | 9,011 | 6,329 | 2,683 |
Adverse events | 63 | 608 | –545 |
Monitoring | 1,855 | 1,798 | 57 |
Palliative | 4,470 | 4,480 | –11 |
ICER ($/QALY) | 466,632 | ||
177Lu oxodotreotide = lutetium oxodotreotide; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Table 12: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
177Lu oxodotreotide vs. everolimus | ||||
Sponsor’s base case | Everolimus | 164,677 | 2.74 | Reference |
177Lu oxodotreotide | 237,010 | 4.35 | 45,077 | |
Sponsor’s corrected base case | Everolimus | 169,523 | 2.77 | Reference |
177Lu oxodotreotide | 247,835 | 4.38 | 48,886 | |
CADTH reanalysis 1 | Everolimus | $165,277 | 2.77 | Reference |
177Lu oxodotreotide | $232,030 | 3.77 | $66,929 | |
CADTH reanalysis 2 | Everolimus | 173,631 | 2.78 | Reference |
177Lu oxodotreotide | 272,074 | 4.34 | 62,883 | |
CADTH reanalysis 3 | Everolimus | 169,089 | 3.27 | Reference |
177Lu oxodotreotide | 247,985 | 4.99 | 78,896 | |
CADTH reanalysis 4 | Everolimus | 170,239 | 2.85 | Reference |
177Lu oxodotreotide | 248,319 | 4.40 | 50,546 | |
CADTH reanalysis 5 | Everolimus | 153,400 | 2.77 | Reference |
177Lu oxodotreotide | 248,935 | 4.35 | 60,400 | |
CADTH reanalysis 6 | Everolimus | 152,308 | 2.26 | Reference |
177Lu oxodotreotide | 229,111 | 3.81 | 49,355 | |
CADTH base case (1 to 6) | Everolimus | 139,374 | 2.67 | Reference |
177Lu oxodotreotide | 233,923 | 3.45 | 120,931 | |
177Lu oxodotreotide vs. sunitinib | ||||
Sponsor’s base case | Sunitinib | 190,585 | 3.60 | Reference |
177Lu oxodotreotide | 209,207 | 4.29 | 27,006 | |
Sponsor’s corrected base case | Sunitinib | 196,325 | 3.58 | Reference |
177Lu oxodotreotide | 216,124 | 4.21 | 31,490 | |
CADTH reanalysis 1 | Sunitinib | 190,364 | 3.60 | Reference |
177Lu oxodotreotide | 218,269 | 4.07 | 59,042 | |
CADTH reanalysis 2 | Sunitinib | 208,567 | 3.57 | Reference |
177Lu oxodotreotide | 243,589 | 4.18 | 57,750 | |
CADTH reanalysis 3 | Sunitinib | 196,626 | 3.59 | Reference |
177Lu oxodotreotide | 215,419 | 4.18 | 31,864 | |
CADTH reanalysis 4 | Sunitinib | 196,947 | 3.71 | Reference |
177Lu oxodotreotide | 215,512 | 4.21 | 37,450 | |
CADTH reanalysis 5 | Sunitinib | 136,279 | 3.59 | Reference |
177Lu oxodotreotide | 216,267 | 4.18 | 134,447 | |
CADTH reanalysis 6 | Sunitinib | 183,824 | 3.14 | Reference |
177Lu oxodotreotide | 200,578 | 3.62 | 34,873 | |
CADTH base case (1 to 6) | Sunitinib | 136,460 | 3.27 | Reference |
177Lu oxodotreotide | 228,331 | 3.46 | 466,632 | |
177Lu oxodotreotide = lutetium oxodotreotide; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analyses
CADTH conducted several additional scenario analyses to assess the uncertainty surrounding the model structure and parameters used in the sponsor’s analyses and found consistent results for the comparisons of 177Lu oxodotreotide with both comparators (everolimus or sunitinib). CADTH found that increased ICERs were associated with using higher utility values for pre-progression and post-progression health states and applying a treatment-waning assumption. By contrast, smaller ICERs were associated with increasing an RDI and using PFS curves to represent treatment duration for comparators.
Table 13: Summary of CADTH Scenario Analyses — 177Lu Oxodotreotide Versus Everolimus
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
Sponsor’s corrected base case | |||
Everolimus | 169,523 | 2.77 | Reference |
177Lu oxodotreotide | 247,835 | 4.38 | 48,886 |
CADTH reanalysis | |||
Everolimus | 139,374 | 2.67 | Reference |
177Lu oxodotreotide | 233,923 | 3.45 | 120,931 |
CADTH’s scenario analysis 1: Assuming an outpatient administration for all treatments | |||
Everolimus | 134,115 | 2.66 | Reference |
177Lu oxodotreotide | 227,555 | 3.44 | 119,171 |
CADTH’s scenario analysis 2: Assuming a 100% RDI | |||
Everolimus | 148,853 | 2.66 | Reference |
177Lu oxodotreotide | $33,748 | 3.44 | 108,546 |
CADTH’s scenario analysis 3: Assuming 50% of patients who were progression-free received octreotide 30 mg LAR | |||
Everolimus | 130,984 | 2.64 | Reference |
177Lu oxodotreotide | 229,930 | 3.43 | 125,750 |
CADTH’s scenario analysis 4: Assuming 100% of patients who were progression-free received octreotide 30 mg LAR | |||
Everolimus | 146,591 | 2.66 | Reference |
177Lu oxodotreotide | 236,801 | 3.45 | 114,836 |
CADTH’s scenario analysis 5: Assuming 5% of patients required octreotide SC for symptom management | |||
Everolimus | 139,372 | 2.69 | Reference |
177Lu oxodotreotide | 233,722 | 3.47 | 119,843 |
CADTH’s scenario analysis 6: Assuming 10% of patients required octreotide SC for symptom management | |||
Everolimus | 139,349 | 2.65 | Reference |
177Lu oxodotreotide | 234,137 | 3.44 | 121,154 |
CADTH’s scenario analysis 7: Using PFS to calculate treatment duration | |||
Everolimus | 155,610 | 2.71 | Reference |
177Lu oxodotreotide | 233,853 | 3.46 | 105,468 |
CADTH’s scenario analysis 8: Using alternative (higher) health-state–specific utility values | |||
Everolimus | 139,238 | 2.28 | Reference |
177Lu oxodotreotide | 233,805 | 3.06 | 120,897 |
CADTH’s scenario analysis 9: Using Gompertz distribution to predict long-term PFS curves | |||
Everolimus | 138,947 | 2.68 | Reference |
177Lu oxodotreotide | 232,260 | 3.44 | 121,721 |
CADTH’s scenario analysis 10: Using log-normal distribution to predict long-term PFS curves | |||
Everolimus | 138,020 | 2.68 | Reference |
177Lu oxodotreotide | 231,309 | 3.46 | 119,421 |
CADTH’s scenario analysis 11: Using exponential distribution to predict long-term OS curves | |||
Everolimus | 153,062 | 3.22 | Reference |
177Lu oxodotreotide | 247,901 | 4.03 | 116,640 |
CADTH’s scenario analysis 12: Using gamma distribution to predict long-term OS curves | |||
Everolimus | 132,249 | 2.42 | Reference |
177Lu oxodotreotide | 229,533 | 3.29 | $112,176 |
CADTH’s scenario analysis 13: Using log-logistic distribution to predict long-term OS curves | |||
Everolimus | 156,600 | 3.29 | Reference |
177Lu oxodotreotide | 259,672 | 4.37 | $95,658 |
CADTH’s scenario analysis 14: No treatment waning | |||
Everolimus | 139,565 | 2.68 | Reference |
177Lu oxodotreotide | 255,130 | 4.33 | 69,816 |
CADTH’s scenario analysis 15: Applying a treatment-waning assumption after 24 months | |||
Everolimus | 138,126 | 2.65 | Reference |
177Lu oxodotreotide | 229,000 | 3.22 | 159,338 |
CADTH’s scenario analysis 16: Applying a treatment-waning assumption after 48 months | |||
Everolimus | 139,008 | 2.65 | Reference |
177Lu oxodotreotide | 237,333 | 3.61 | 102,212 |
177Lu oxodotreotide = lutetium oxodotreotide; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SC = subcutaneous.
Table 14: Summary of CADTH Scenario Analyses — 177Lu Oxodotreotide Versus Sunitinib
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
Sponsor’s corrected base case | |||
Sunitinib | 196,325 | 3.58 | Reference |
177Lu oxodotreotide | 216,124 | 4.21 | 31,490 |
CADTH’s reanalysis | |||
Sunitinib | 136,460 | 3.27 | Reference |
177Lu oxodotreotide | 228,331 | 3.46 | 466,632 |
CADTH’s scenario analysis 1: Assuming an outpatient administration for all treatments | |||
Sunitinib | 130,576 | 3.27 | Reference |
177Lu oxodotreotide | 222,403 | 3.46 | 463,240 |
CADTH’s scenario analysis 2: Assuming a 100% RDI | |||
Sunitinib | 140,417 | 3.27 | Reference |
177Lu oxodotreotide | 228,487 | 3.46 | 451,162 |
CADTH’s scenario analysis 3: Assuming 50% of patients who were progression-free received octreotide 30 mg LAR | |||
Sunitinib | 128,202 | 3.26 | Reference |
177Lu oxodotreotide | 224,564 | 3.46 | 476,584 |
CADTH’s scenario analysis 4: Assuming 100% of patients who were progression-free received octreotide 30 mg LAR | |||
Sunitinib | 144,384 | 3.26 | Reference |
177Lu oxodotreotide | 232,265 | 3.46 | 438,490 |
CADTH’s scenario analysis 5: Assuming 5% of patients required octreotide SC for symptom management | |||
Sunitinib | 136,093 | 3.27 | Reference |
177Lu oxodotreotide | 227,819 | 3.46 | 471,169 |
CADTH’s scenario analysis 6: Assuming 15% of patients required octreotide SC for symptom management | |||
Sunitinib | 136,636 | 3.25 | Reference |
177Lu oxodotreotide | 229,002 | 3.45 | 451,779 |
CADTH’s scenario analysis 7: Using PFS to calculate treatment duration | |||
Sunitinib | 197,038 | 3.28 | Reference |
177Lu oxodotreotide | 228,366 | 3.46 | 172,745 |
CADTH’s scenario analysis 8: Using (lower) alternative health-state–specific utility values | |||
Sunitinib | 136,617 | 2.78 | Reference |
177Lu oxodotreotide | 228,564 | 3.07 | 324,279 |
CADTH’s scenario analysis 9: Using Gompertz distribution to predict long-term PFS curves | |||
Sunitinib | 136,634 | 3.27 | Reference |
177Lu oxodotreotide | 228,971 | 3.47 | 461,234 |
CADTH’s scenario analysis 10: Using log-logistic distribution to predict long-term PFS curves | |||
Sunitinib | 133,388 | 3.30 | Reference |
177Lu oxodotreotide | 224,541 | 3.52 | 417,412 |
CADTH’s scenario analysis 11: Using gamma distribution to predict long-term OS curves | |||
Sunitinib | 135,989 | 3.24 | Reference |
177Lu oxodotreotide | 228,102 | 3.44 | 456,185 |
CADTH’s scenario analysis 12: Using Gompertz distribution to predict long-term OS curves | |||
Sunitinib | 140,657 | 3.42 | Reference |
177Lu oxodotreotide | 235,091 | 3.70 | 330,708 |
CADTH’s scenario analysis 13: Using log-logistic distribution to predict long-term OS curves | |||
Sunitinib | 148,315 | 3.69 | Reference |
177Lu oxodotreotide | 244,754 | 4.05 | 270,662 |
CADTH’s scenario analysis 14 No treatment waning | |||
Sunitinib | 136,583 | 3.26 | Reference |
177Lu oxodotreotide | 229,589 | 3.65 | 240,352 |
CADTH’s scenario analysis 15 Applying a treatment-waning assumption after 24 months | |||
Sunitinib | 136,553 | 3.25 | Reference |
177Lu oxodotreotide | 229,398 | 3.41 | 578,680 |
CADTH’s scenario analysis 16 Applying a treatment-waning assumption after 48 months | |||
Sunitinib | 136,239 | 3.25 | Reference |
177Lu oxodotreotide | 228,564 | 3.50 | 373,463 |
177Lu oxodotreotide = lutetium oxodotreotide; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SC = subcutaneous.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA),16 assessing the expected budgetary impact of the introduction of 177Lu oxodotreotide for the treatment of unresectable or metastatic, well-differentiated, somatostatin receptor-positive pancreatic neuroendocrine tumours (pNETs) in adults whose disease has progressed after treatment with a SSA, unless there is a contraindication or intolerance. The analysis was done from the perspective of a Canadian public drug plans over a 3-year time horizon; the base year was assumed to be 2022 and the 3-year time horizon ran from 2023 to 2025. Key inputs to the BIA are documented in Table 16.
The sponsor estimated the population size using an epidemiology-based approach, with data obtained from published literature and the NETTER-R trial to estimate the number of patients eligible for treatment with 177Lu oxodotreotide.17-20 The comparators included everolimus and sunitinib. Comparators’ costs were obtained from the Ontario Drug Benefit formulary and the Ontario Exceptional Drug List, and dosing regimens were obtained from product monographs.10-13,21 Total costs were calculated by multiplying drug cost per administration with the number of doses administered over the treatment duration. The sponsor adopted the median treatment duration for comparators in published trials.3,22 The total cost per treatment was adjusted by a RDI of ||||| for 177Lu oxodotreotide, 86% for everolimus and 91.3% for sunitinib. The sponsor assumed treatment with SSAs such as octreotide and lanreotide did not differ based on choice of second-line therapy and as such the cost of SSAs were excluded.
If reimbursed, the sponsor assumed 177Lu oxodotreotide ||||| ||||||| |||||||| market shares of everolimus and sunitinib in jurisdictions where both comparators have public drug plan coverage. In jurisdictions where 1 of the comparators, everolimus or sunitinib, is not covered, 177Lu oxodotreotide was assumed to |||||||| |||||| ||||| || ||| |||| |||| |||||| ||||||||.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1/Year 2/Year 3 if appropriate) |
|---|---|
Target population | |
NETs Incidence (per 100,000 persons) | 5.86 |
Average growth rate | 1.71% |
Proportion of pancreatic NETs | 9.40% |
Total advanced unresectable tumours | 80.00% |
Locally advanced unresectable tumours | 20.00% |
Metastatic unresectable tumours | 60.00% |
Somatostatin receptor-positive patients | 90.00% |
Prior somatostatin analogue use | |||||| |
Number of patients eligible for drug under review | || | || | || |
Market uptake (3 years) | |
Uptake (reference scenario)a | |
177Lu oxodotreotide | 0% /0% / 0% |
Everolimus | 50% / 50% / 50% |
Sunitinib | 50% / 50% / 50% |
Uptake (new drug scenario)b | |
177Lu oxodotreotide | 20% / 40% / 50% |
Everolimus | 40% / 30% / 25% |
Sunitinib | 40% / 30% / 25% |
Cost of treatment | |
Cost of treatment over cyclec | |
177Lu oxodotreotide | |||||||||| |
Everolimus | $8,295.84 |
Sunitinib | $9,880.28 |
NET = neuroendocrine tumour, Lu = lutetium.
a||||||||| ||| |||||| ||||| || |||||||||| ||| ||||||||| |||||||||||||| || ||| |||||||| || ||| |||||||||| || ||||||||||||| ||||| |||| ||| |||||||||| || ||||||| ||||| ||| |||||| |||| |||| |||||| ||||||||| |||||| |||||| |||||||| ||| |||| |||| |||||| |||||||| ||| |||| || |||||| |||||| |||||||||| || ||| |||||||||| ||||||||| ||||||| ||||||||||||| ||||| |||||||||| ||| | |||||| |||||| ||||| |||| |||||||||| || |||| |||| |||||| ||||| ||| ||||||| ||||||
b||||||||| ||| |||||| ||||| || |||||||||| ||| ||||||||| |||||||||||||| || ||| |||||||| || ||| |||||||||| |||||||| ||||| ||| |||| |||||||||| || ||||| |||||||||||||| || ||||||||| ||||||||| ||| | |||||| ||||| || || || |||| || | ||| || ||| |||||||||| ||| | |||||| ||||| || ||| || |||| || ||| || |||| | ||| ||| || |||| || || |||||| |||||| ||||||| |||||||||| ||| | |||||| ||||| || || || |||| || | ||| || ||| ||||||||| ||| | |||||| ||||| || ||| || |||| || ||| || |||| | ||| ||| || |||| || || |||||||| |||||||||| ||| | |||||| ||||| || ||| || |||| || ||| || |||| | ||| ||| || |||| || ||| ||||||||| ||| | |||||| ||||| || ||| || |||| || ||| || |||| | ||| ||| || |||| || || |||| ||||||| |||||||||| ||| | |||||| ||||| || ||| || |||| || ||| || |||| | ||| ||| || |||| || ||| ||||||||| ||| | |||||| ||||| || ||| || |||| || ||| || |||| | ||| ||| || |||| ||
cTreatment cost is per person cost over a cycle of 56 days, adjusted by RDI.
Summary of the Sponsor’s BIA Results
The sponsor estimated the budget impact of reimbursing 177Lu oxodotreotide for the treatment of unresectable or metastatic, well-differentiated, somatostatin receptor-positive pNETs in adults whose disease has progressed after treatment with a SSA, unless there is a contraindication or intolerance. The 3-year budget impact was $8,291,662 (Year 1: $1,483,970; Year 2: $3,004,752; Year 3: $3,802,939).
CADTH Appraisal of the Sponsor’s BIA
CADTH identified a key limitation to the sponsor’s analysis that have notable implications on the results of the BIA:
Use of RDI to estimate actual drug costs is not appropriate: The consideration of RDI is problematic as this parameter can be influenced by several factors. For example, the dose received by a patient may differ from the full planned dose of the drug due to dose delays, missed doses, dose reductions to manage toxicity, or subsequent dose re-escalation. Each of these reasons have differing impacts on drug costs. Furthermore, prescriptions for 177Lu oxodotreotide may be filled and reimbursed regardless of treatment adherence. Overall, without explicitly modelling dose delays and reductions for the patient population, multiplying RDI estimates by drug acquisition costs creates additional uncertainty and likely underestimates the drug cost incurred by payers.
In the CADTH reanalysis, an RDI of 100% was applied for all drugs.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by assuming 100% of RDI for all drugs.
Table 17: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. RDI | 177Lu oxodotreotide: ||||| Everolimus: 86% Sunitinib: 91.3% | 177Lu oxodotreotide: 100% Everolimus: 100% Sunitinib: 100% |
CADTH base case | Reanalysis 1 | |
BIA = budget impact analysis; RDI = relative dose intensity.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19.
Assuming 100% RDI for 177Lu oxodotreotide and comparators decreased the estimated 3-year budget impact to $7,934,115.
Table 18: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | 3-year total |
|---|---|
Submitted base case | $8,291,662 |
CADTH reanalysis 1 | $7,934,115 |
CADTH base case | $7,934,115 |
BIA = budget impact analysis.
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 19. The scenario analysis involved:
Assuming a relative 25% increase in the sponsor’s assumed market share of 177Lu oxodotreotide (25% in year 1, 50% in year 2 and 62.5% in year 3).
Assuming a public health care payer perspective (including costs of administration, AEs, and supportive medicine).
Assuming 177Lu oxodotreotide has a price reduction of 41% and 63%, the price reductions recommended in the CADTH reanalysis at which 177Lu oxodotreotide would be considered cost-effective when compared to everolimus and sunitinib, respectively.
Table 19: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | 3-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $2,226,298 | $2,255,142 | $2,284,037 | $2,313,492 | $6,852,670 |
New drug | $2,226,298 | $3,739,112 | $5,288,789 | $6,116,431 | $15,144,332 | |
Budget impact | $0 | $1,483,970 | $3,004,752 | $3,802,939 | $8,291,662 | |
CADTH base case | Reference | $2,551,553 | $2,584,614 | $2,617,732 | $2,651,489 | $7,853,834 |
New drug | $2,551,553 | $4,004,626 | $5,492,929 | $6,290,394 | $15,787,949 | |
Budget impact | $0 | $1,420,013 | $2,875,197 | $3,638,906 | $7,934,115 | |
CADTH scenario analysis: 25% increase in market share of 177Lu oxodotreotide | Reference | $2,551,553 | $2,584,614 | $2,617,732 | $2,651,489 | $7,853,834 |
New drug | $2,551,553 | $4,359,630 | $6,211,728 | $7,200,121 | $17,771,478 | |
Budget impact | $0 | $1,775,016 | $3,593,996 | $4,548,632 | $9,917,644 | |
CADTH scenario analysis: Health care payer perspective | Reference | $2,551,553 | $2,584,614 | $2,617,732 | $2,651,489 | $7,853,834 |
New drug | $2,551,553 | $4,053,963 | $5,592,836 | $6,416,852 | $16,063,652 | |
Budget impact | $0 | $1,469,350 | $2,975,104 | $3,765,363 | $8,209,817 | |
CADTH scenario analysis: 177Lu oxodotreotide price reduction of 41% | Reference | $2,551,553 | $2,584,614 | $2,617,732 | $2,651,489 | $7,853,834 |
New drug | $2,551,553 | $3,210,483 | $3,884,790 | $4,254,888 | $11,350,161 | |
Budget impact | $0 | $625,869 | $1,267,058 | $1,603,399 | $3,496,326 | |
CADTH scenario analysis: 177Lu oxodotreotide price reduction of 63% | Reference | $2,551,553 | $2,584,614 | $2,617,732 | $2,651,489 | $7,853,834 |
New drug | $2,551,553 | $2,784,357 | $3,021,886 | $3,162,665 | $8,968,908 | |
Budget impact | $0 | $199,743 | $404,154 | $511,176 | $1,115,074 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Canadian Neuroendocrine Tumour Society
About the Canadian Neuroendocrine Tumour Society
The Canadian Neuroendocrine Tumour Society (CNETS) is widely recognized by patients and the medical community across Canada as an organization that helps improve the quality of life and survival for NET patients by raising awareness of the disease and the latest available diagnostics and treatments; making sure that patients, caregivers, health care professionals and others have the information they need in the areas of medical and scientific research, treatment and support; and by supporting patients and helping them navigate the best care options.
CNETS provides support and education for Canadians on all aspects of Neuroendocrine Tumours (NETs). We help Canadian NET patients seek and obtain personalized diagnostic and therapeutic options. We also advocate on behalf of individual patients and for policies to support NET patients. The organization does its work in collaboration with medical and scientific experts, stakeholders, and partner associations.
CNETS website: www.cnets.ca
Facebook: https://www.facebook.com/cnetscanada (2,978 likes/followers)
Twitter: https://twitter.com/CNETSCanada (1,383 followers)
Information Gathering
As a registered patient group with CADTH, CNETS has provided feedback on prior drug submissions for Neuroendocrine (NET) cancer. We understand that input from patients is vital to the CADTH review process as it ensures that patient and caregiver values are considered appropriately during a drug/ radiopharmaceutical review. The pERC considers patient perspectives as evidence during the review, deliberation, and recommendation for public drug insurance plan listings.
CNETS used an online questionnaire (SurveyMonkey) to collect both qualitative and quantitative information from Neuroendocrine cancer patients for our submission on the reassessment of Lutathera for the treatment of unresectable or metastatic, well-differentiated, somatostatin receptor-positive pancreatic neuroendocrine tumours in adults whose disease has progressed after treatment with a somatostatin analogue, unless there is a contraindication or intolerance.
The online survey was promoted on the CNETS website, Facebook page and Facebook closed support group. The survey included many open-ended questions where patients could provide their own impact statements. Survey respondents were informed that their information would remain confidential and anonymized.
The online survey was open from February 25th to March 25th, 2022. On closing CNETS received a total of fifty-seven (57) responses.
Demographics:
57 Neuroendocrine cancer (NET) patients provided input into CNETS submission on the reassessment of Lutathera.
21 (36.84%) Pancreatic NET patients
36 (63.16%) Gastrointestinal NET patients
19 (33.33%) Male, 38 (66.67%) Female
Age ranges: 20-29 (1), 30-39 (0), 40-49 (5), 50-59 (12), 60-69 (25), 70-79 (13), 80-89 (1). The youngest patient is 29 and the oldest is 80.
Patients are from British Columbia 8 (14.04%), Alberta 5 (8.77%), Manitoba 3 (5.26%), Ontario 27 (47.37%), Quebec 5 (8.77%), Nova Scotia 2 (3.51%), New Brunswick 2 (3.51%), Newfoundland 1 (1.75%), Yukon 1 (1.75%), Outside of Canada 3 (5.26%)
33 patients were treated or currently on treatment with Lutathera
Disease Experience
Impact of NETs on Quality of Life
The majority of Neuroendocrine (NET) cancer patients report a negative impact on their quality of life.
Background (Global NET Patient Survey)
The International Neuroendocrine Cancer Alliance (INCA) and Novartis Pharmaceuticals Corporation collaborated on the first global survey to gather data on the NET patient experience. The goal of the Global NET Survey was to “increase understanding of the experiences, needs and challenges of NET patients, and to provide insights and learnings among countries and regions to advance NET care.”
1928 NET patients responded to the survey worldwide. The study found that most NET patients’ quality of life was negatively affected.
The study results showed that decreased energy levels and emotional health issues were very common among respondents. Patients also had to make necessary lifestyle changes around diet, physical activity, and spend more time and money on appointments. Their work life was also negatively affected. 80% of those patients not working were not able to work because of their NET. A further 50% of those patients working had to often miss work because of their disease.
The May-June 2017 issue of The Pancreas, Journal of neuroendocrine tumors and pancreatic diseases and sciences, published the article “Patient-Reported Experience of Diagnosis, Management, and Burden of Neuroendocrine Tumors: Results From a Large Patient Survey in the United States, spreading among medical community the US results of the Global NET Patient Survey”
CNETS Survey – Disease Impact on Quality of Life
The 57 patients who completed the online survey were asked to rate how symptoms and the disease impacts their day-to-day life and overall quality of life on a scale of 1 – No impact to 5 – Extremely high impact.
Impact of NET cancer symptoms on quality of life
Patients were asked to rate the impact of seven common NET cancer symptoms on their quality of life. Fatigue & weakness, and diarrhea were identified as the top two symptom categories that have a high to extremely high impact on quality of life.
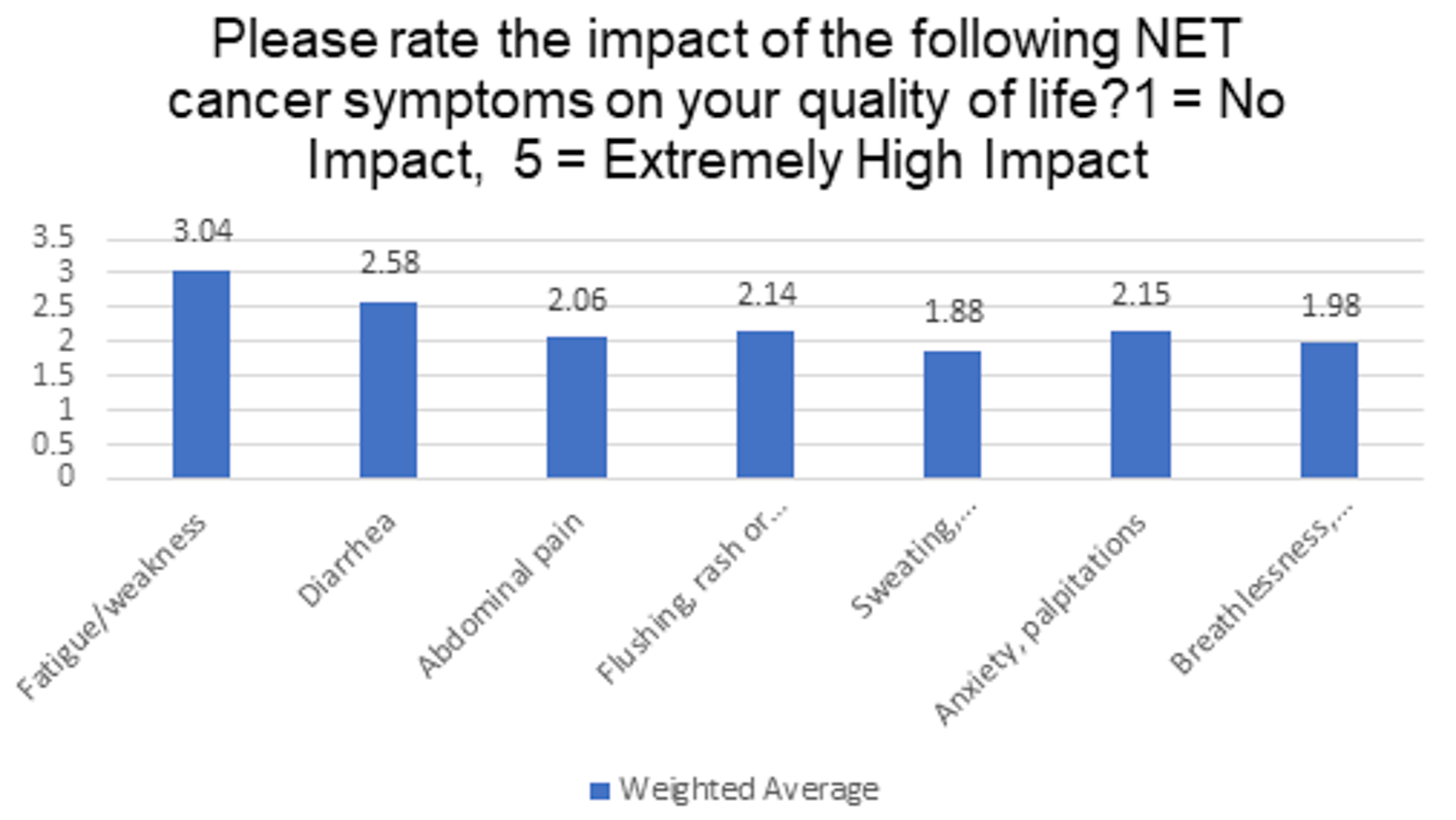
Patients were asked to rate the impact of NET cancer on quality of life indicators. Energy, Emotional & Travel were identified as indicators that have a high to extremely high impact on quality of life.
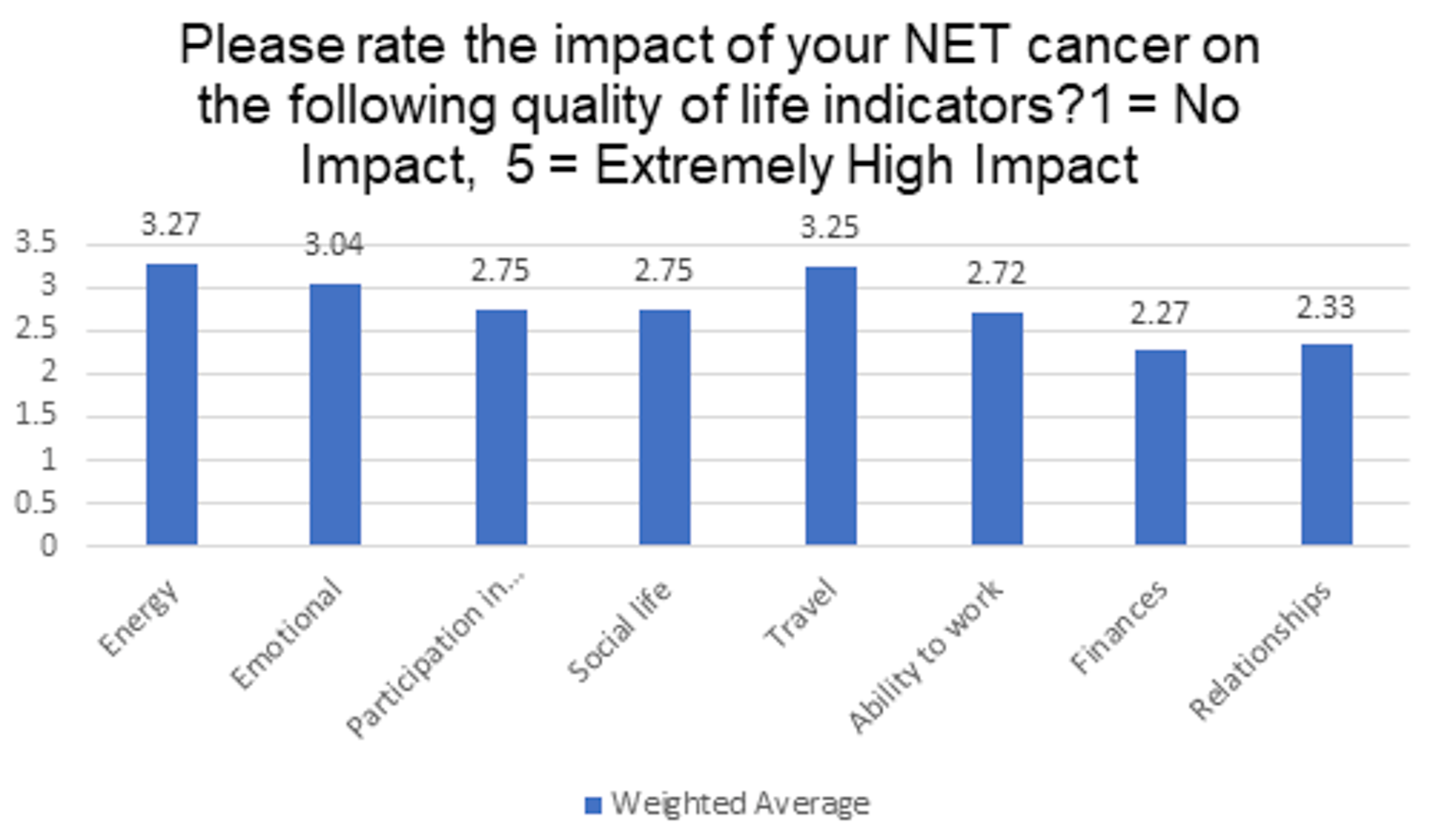
Patients were asked what other symptoms or conditions related to NET cancer affected their quality of life?
“Surgery with ablation recovery was long and difficult, more so than resection. Elevated bp has persisted since day of surgery for which I take drugs but my kidneys are damaged.”
Pain. “I want to decrease morphine intake”.
“Cognitive abilities, itching and dry skin, confusion, memory, food intake/triggers, unexplained weight loss, isolation.”
“Hair loss, diet concerns, Covid, pain control, intimacy, appetite”
Such low energy!! I am a different person now….quite sad!”
“This is a little difficult to pinpoint as I also have metastatic breast cancer which has now impacted the abdominal region making it uncertain as to what is causing what symptoms at times. However, thanks to the monthly Lanreotide injections and Lutetium 177 treatments, most NETS symptoms have been well managed for several years.”
“General 'fog' and forgetfulness”
“…joint pain, gallbladder sludge/stones which result in chronic back pain.”
“Neurocognitive impact: on memory ability to work, participate in activities.”
“Back pain due to tumors on spine”
“Cognitive issues”
“Complete lack of life, I know I'm eighty, was always up & away. I hardly leave the house, as I get defeated after walking fifty paces. I have become a burden.”
“Extensive resection, surgery and radiation have affected energy, emotional stability, travel, exercise. Not having access to doctors with NET expertise is very trying.
“Bloating and weight gain”
Experiences With Currently Available Treatments
Patients were asked what therapies / treatments have you used to manage NET cancer?
Table 1: Therapies and Treatments Used to Manage NET Cancer
Answer Choices | Responses | |
|---|---|---|
Somatostatin Analog Therapies (Sandostatin, Lanreotide) | 80.00% | 44 |
Surgery | 63.64% | 35 |
Peptide Receptor Radionuclide Therapy (PRRT) | 60.00% | 33 |
Liver Directed Therapies (Embolization) | 29.09% | 16 |
Ablative Techniques (Radiofrequency Ablation, Cryotherapy) | 21.82% | 12 |
Chemotherapy | 21.82% | 12 |
Radiation Therapies | 14.55% | 8 |
Biologically Targeted Therapies (Everolimus, Sunitinib) | 12.73% | 7 |
Immunotherapies | 3.64% | 2 |
Other (please specify) | 9.09% | 5 |
Answered | 55 | |
Skipped | 2 | |
Patients were asked to describe benefits and challenges of current NET cancer treatments.
Patients described a wide range in both challenges and benefits of the current therapies for patients. At the very best, some patients said the treatments have helped temporarily slow disease progression and help control symptoms. On the downside, patients indicated the treatments cause long recovery times, debilitating side effects, and complications. No patient reported that the current therapies cured or stopped progression of their NET cancer.
The patients surveyed described current treatments for symptom control including, bloating, diarrhea, constipation, and energy levels as being effective. Most patients described current treatments for the disease including surgery, embolization, radiation, chemotherapy, and biologics, as slightly or not effective at stopping disease progression, shrinking / stopping tumour growth and preventing the spread to other organs.
Selected quotes of benefits and challenges of NET cancer treatments from survey:
Ablative Techniques
“Post-Ablation Syndrome – 2 weeks of high fevers”
“Did not slow growth/surgery after resection was difficult”
“Extreme shoulder pain after second ablation”
“Effective but invasive with complications”
“Time consuming, painful, negligible benefit”
Biologically Targeted Therapies
“I had an extremely negative experience with Everolimus. Wicked diarrhea, Extreme loss of weight and energy. Also developed ground glass symptoms in my lungs. I was taken of the drug after about two months. I believe that if I had stayed on Everolimus for a couple more months that would have killed me.”
“Feeling unwell, failed treatment, disease progressed.”
Chemotherapy
“No benefits for me but lots of side effects”
“The negative side effects include significant loss of energy and appetite and taste, dried out flaking and cracked skin particularly on my feet and hands and the inside of my mouth, brain fog, general lousy feeling”
“Intolerable side effects”
“Feeling unwell, fatigue and nausea- very minor stability with tumour control”
Liver Directed Therapies
“Really knocked the tumours down for a little while. Took several weeks before I was able to get back to work.”
“Bland embolization’s stopped the growth for a few months”
“Not sure of long-term effectiveness, had two separate sessions, spent 5 days in the hospital after each time.”
“Embolization… makes me very sick but I’m hoping to gain some time”
Somatostatin Analog Therapies
“Started on the injectable about 37 years ago. Very well tolerated. Started on LAR about 14 years ago. Can't say enough about it. Fantastic for controlling symptoms.”
“I am taking Sandostatin for the past 6 years. Not much side effects. Only I am tired 2-3 days after every injection”
“Lanreotide gave me nausea, vomiting & vertigo for 1 week out of every 4 weeks taking the injection, I had no symptoms previously, tumour was found by chance.”
“Helping control symptoms but injections are painful and lifelong treatment.”
“Challenges: cost of drug, administration of drug (when I was hospitalized for a long period of time it was challenging to obtain the medication and get a nurse who could administer the medication. Bruising/pain at injection site; Benefits: hope is that it has slowed progression of tumours, helped to manage flushing symptoms.”
Surgery
“Difficult three-month recovery”
“January 6, 2017 I underwent cancer rectal surgery. I had an ileostomy bag for 9 months and then had reversal surgery. This was how the Neuroendocrine cancer was detected. 3 lymph nodes got away and resulted with a lesion on my ilium bone which was dormant for a few years. In January 2021 new cancer lesions had spread to my spine.”
“Benefits: removed primary tumour and lymph nodes, thereby slowing progression of disease; repaired heart valves affected by disease thereby reducing some symptoms of shortness of breath/preventing heart failure; through liver transplant removed tumour burden in the liver thereby extending my life. Without these surgeries I do not believe I would be alive today. Challenges: surgery complications (ie. hematoma, blood clots),”
“Removed the bulk of the tumours from the mesentery. and primary site in the gut. Trouble with post op infections.”
“Extensive surgery & recovery - resection of liver, removal of gallbladder and appendix, 16 lymph nodes”
Patients were asked to check all the difficulties they had in accessing and receiving treatments.
Table 2: Difficulties in Accessing and Receiving Treatments
Answer Choices | Responses | |
|---|---|---|
Do not have private payer coverage | 29.63% | 8 |
Financial difficulties | 22.22% | 6 |
Unable to access the therapy through my physician | 22.22% | 6 |
Not funded for my NET cancer | 22.22% | 6 |
Unable to travel to location where the drug is administered | 18.52% | 5 |
Not indicated for my NET cancer | 11.11% | 3 |
Other (please specify) | 44.44% | 12 |
Answered | 27 | |
Skipped | 30 | |
Other Difficulties
“Unsure if the treatment would be funded.”
“Had to wait for a year to get into treatment study.”
“Travel and access to maintenance scans”
“I live 8 hours away from Toronto where I get all my care.”
“Our provincial government was reluctant to approve funding for my PRRT due to the fact I have hind gut cancer. However, on the final letter for funding and approval, the provincial government approved my treatment (An answer to prayer)!”
“I have to travel 450 km from my place to the treatment city.”
“Canada (Ontario) lags behind other countries in terms of treatment and accessibility to scans such as Gallium 68.”
“Navigating the health care system to get to the right doctors who can support me with the various therapies I have had. Getting access to a Gallium 68 scan is extremely difficult!”
“Have to travel long distances for treatments.”
“Just the time required.”
“Have to travel a long distance for surgery.”
“Do not like driving 3 hours to see the doctor for 2 minutes to pick up my chemo pills.”
Improved Outcomes
Patients were asked about improved outcomes and what aspects of NET cancer are most important to control
Table 3: Outcomes and Aspects of NET Cancer Most Important to Control
Answer Choices | Responses | |
|---|---|---|
Disease progression | 98.18% | 54 |
Fatigue | 36.36% | 20 |
Diarrhea | 34.55% | 19 |
Flushing | 29.09% | 16 |
Wheezing | 7.27% | 4 |
Other (please specify) | 12.73% | 7 |
Answered | 55 | |
Skipped | 2 | |
98% of the patients who completed the online survey indicated the most important aspect of their disease to control is disease progression.
36% of patients said that second most important aspect to control is fatigue. 35% of patients indicated diarrhea and 29% of patients indicated flushing as important aspects to control.
Experience With Drug Under Review
60% of patients surveyed were treated or currently on treatment with Lutetium oxodotreotide (Lutathera®)
All patients treated or on treatment with Lutetium oxodotreotide (Lutathera®) said they were able to tolerate or manage the side effects of the treatment, having little or no impact on their quality of life. Patients also expressed that the treatment was far easier than the lengthy recovery from surgery (ablative, debulking, resection) or the debilitating side effects from chemotherapy.
Patients were asked if they were treated or currently being treated with Lutetium oxodotreotide (Lutathera®)
Table 4: Currently Being Treated with Lutetium Oxodotreotide
Answer Choices | Responses | |
|---|---|---|
Yes | 60.00% | 33 |
No | 40.00% | 22 |
Answered | 55 | |
Skipped | 2 | |
Patients were asked how they were able to access Lutetium oxodotreotide (Lutathera®)
Table 5: Access to Lutetium Oxodotreotide
Answer Choices | Responses | |
|---|---|---|
Clinical trials (various sites across the country) | 32.14% | 9 |
Provincial reimbursement | 28.57% | 8 |
Compassionate access | 10.71% | 3 |
Private Payer (Private Insurance) | 3.57% | 1 |
Out of pocket | 0.00% | 0 |
Other (please specify) | 0.00% | 0 |
Answered | 28 | |
Skipped | 29 | |
Patients were asked what were the benefits from treatment with Lutetium oxodotreotide (Lutathera®)
Table 6: Benefits of Treatment With Lutetium Oxodotreotide
Answer Choices | Responses | |
|---|---|---|
Reduction in the progression of my disease | 68.97% | 20 |
Tumour shrinkage | 58.62% | 17 |
Decrease in disease symptoms | 44.83% | 13 |
Improved wellness | 41.38% | 12 |
Other (please specify) | 13.79% | 4 |
Answered | 29 | |
Skipped | 28 | |
Other Benefits
“Stable disease.”
“All of the above choices are benefits I have received with my treatment.”
“The incredible support of the NETS team in providing knowledge and support.”
“Not measurable/evaluated yet due to ongoing treatment.” (4 respondents)
Patients were asked what were the negative effects from treatment with Lutetium oxodotreotide (Lutathera®)
Table 7: Negative Effects of Treatment With Lutetium Oxodotreotide
Answer Choices | Responses | |
|---|---|---|
Increased fatigue | 57.69% | 15 |
Nausea/vomiting | 26.92% | 7 |
Increased diarrhea | 7.69% | 2 |
Increased pain | 3.85% | 1 |
Infections | 0.00% | 0 |
Other (please specify) | 38.46% | 10 |
Answered | 26 | |
Skipped | 31 | |
Other Negative Effects
“Just being radioactive.”
“Low energy.”
"Unexplained weight loss”
“Fatigue for a short period right after treatment”
“Hair loss” (2 respondents)
“Neurocognitive issues worsened, some hair loss.”
“Headaches, less energy.”
"Myelosuppression.”
“Severe weakness, dizziness, lack of appetite.”
Patients were asked to describe the overall impact treatment with Lutetium oxodotreotide (Lutathera®) has had on their health and well-being?
Selected quotes and impact statements from the online survey:
“The results that I saw with PRRT were remarkable. Some of my tumors shrunk while others seem to have entirely disappeared.”
“Finally, after 7 treatments symptoms seem to have subsided”
“Killed more tumours. Better health and sense of well-being. “
“This was an amazing treatment and virtually eliminated almost all of the symptoms of the NET cancer.”
“PRRT treatment stopped the growth of tumors for more than two years. Not much side effects.”
“Tumor on pancreas reduced by 1 cm from 3 cm, challenge was travelling to another province for treatment.”
“Grateful for tumor shrinkage, dreading travel for treatment and feeling unwell and tired for 2-3 weeks afterwards.”
“My tumors were growing every 3 months and either slowed or stopped - I think that means overall my health is better for it.”
“Tolerated it well, have had stable disease since 2018.”
“Seemed to knock out more of the smaller tumours. Well tolerated. No missed work time..”
“Benefits: increased energy for up to a year after, stopped the carcinoid crisis and fewer flushing episodes and less triggers with food. Tumor growth slowed. I had debilitating anxiety and it stopped after the first treatment of four. Considered stable! Challenges: having to isolate away from family after treatment - had to rent space.”
“The overall impact of treatment with PRRT has been a miracle and very emotional to me. From not being approved for out of province treatment and then to finally being approved has been a roller coaster ride. My 15 cancer lesions on the spine are shrinking and new bone growth is being created in their place. A miracle for sure! As of today, it has given me a new outlook on the quality of life I can enjoy moving forward into the future. I will have my 4th treatment in 4 weeks. Knowing that the Quebec medical team will be monitoring me for 5 years after this last treatment, gives me peace of mind and reassurance that I will continue to be looked after.”
“It has been great. While I was getting the treatments, I had 6 years of really good health. I was able to do all the things I would normally do. The Sandostatin injections have not been as effective in controlling all the symptoms.”
“Major change. More energy, less pain, able to do social and family activities. Home activities (cleaning, errands, driving. Personnel activities: walking, yoga.”
“Again, hard to know exactly with two active cancers but my general feeling is that it was very helpful in managing the NET and has helped immensely with a pretty good quality of life the past few years.”
“Extremely positive impact: slowed down disease progression.”
“Really not sure but neuro cog issues may be worsened.”
“I was having recurring issues with palpitations, shortness of breath and flushing in 2019, the treatment took all of that away.
“I think too early to tell but so far, easily tolerated.”
“Most impactful and best long-term response with the least lasting side effects.”
“My symptoms improved, I had close to 5 years of progression free time. But I developed myelosuppression.”
“Feeling much better and am more active.”
“Great impact for tumors in my liver.”
“Best treatment.”
Patients were asked if they had any other comments or feedback on treatment with Lutetium oxodotreotide (Lutathera®)
Responses
“All NET patients should be able to access this revolutionary treatment.”
“Very positive experience.”
“Just glad it was available.“
“Seems to be the only treatment available for me so was happy to get into the study.”
“If I could use Lutetium as an adjunct therapy during times of disease progression, I'll be asking for it. I was able to get back to running and cycling afterwards. Please find a way to quicken the process for patient access - each day is a gift.”
“More centres should have it along with the important gallium scan.”
“Very happy this treatment was available to me (midgut). We must make this available for all NET patients.”
“I am sure that data related to the success of PRRT is quite evident. To me, that would indicate just how readily available this treatment should be for all Canadians regardless of which province they live in. The wait time should not be drawn out until the patient is extremely/gravely ill with cancer.
“It was very successful for me.”
“I am very thankful that my Oncologist was able to get me into the clinical trial - I learned a lot through it as the medical team was wonderful in answering questions which provided me the ability to play a bigger role in my own healing/treatment and I believe that positively impacted my mental 'strength of being' as well as benefited in slowing the disease progression. Building emotional, mental and physical strength together is an important piece of cancer survival.”
“I would like to see Lutathera offered as a "maintenance" thereby for patients such that a patient could be eligible for this treatment every few years (or as necessary) to keep the disease from progressing.”
“Must be funded as standard of care for all Canadians that need cancer treatment for NETs.”
Companion Diagnostic Test
The companion diagnostic test to Lutetium oxodotreotide (Lutathera®) treatment is the Ga68 PET scan. Although this is our submission for Lutathera treatment, CNETS has been extensively advocating for access to the Ga68 Scan as a standard of care in diagnosing NET cancer. The 68Ga PET scan advantages over Octreoscan include higher resolution images, detection of smaller lesions, better guidance to treatment and dosing, exposure to less radiation, greater efficiency, cost effectiveness, access, and patient convenience since it involves a two-three-hour procedure.
Anything Else?
Equitable access to PRRT/Lutathera treatment for NET cancer in Canada has been very slow. Our NET patient community was hopeful that this treatment was going to be reimbursed for all GEP-NET patients in 2018.
In August 2018, CNETS provided patient group input for the pCODR review of Lutetium oxodotreotide (Lutathera®), indicated for Gastroenteropancreatic neuroendocrine tumours (GEP-NETs). We received feedback from 69 NET patients, including 53 patients across the range of GEP-NET types on their experience of Lutathera treatment. The tremendous patient feedback informed our request that pERC issue a positive recommendation for treatment with Lutetium oxodotreotide (Lutathera®) for Gastroenteropancreatic neuroendocrine tumours (GEP-NETs) and immediately reimburse the treatment of somatostatin receptor-positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs), including foregut, midgut, and hindgut neuroendocrine tumors in adults.
CNETS was very disappointed in the narrow recommendation, which excluded so many NET patients who could benefit from with Lutetium oxodotreotide (Lutathera®) treatment. The pCODR Expert Review Committee (pERC) noted in their clinical report, fully one-third of respondents were P-NETs patients. Patients of all types consistently reported favourable outcomes and a positive treatment experience.
CNETS asked pERC to reconsider their narrow recommendation and look at patient testimonies, and also consider the results of the ERASMUS trial, which showed that Lutathera is effective in a variety of NETs.
Unfortunately, pERC did not reconsider their initial recommendation and NET patients who could benefit from treatment with Lutetium oxodotreotide (Lutathera®) have been denied access to this treatment for another three plus years. As outlined within the survey question on accessing treatments, NET patients have endured lack of access, financial challenges, lack of indication/funding for their type of NETs and challenges with travelling to access treatment.
As evidenced in the patient input, we received in 2018 and again in 2022, for many NET cancer patients, treatment with Lutetium oxodotreotide (Lutathera®) has been a “game changer”, with the benefits hugely outweighing the risks. Respondents provided heartfelt and compelling comments with respect to the need for broader access to this treatment.
Ninety-eight percent of respondents to our 2022 survey indicated that controlling disease progression was their highest priority outcome of treatment and approximately sixty-nine percent of respondents who were treated with Lutetium oxodotreotide (Lutathera®) indicated they experienced reduction in disease progression, and approximately fifty-nine percent experienced tumour shrinkage.
Based on the input from the NET community, represented herein, and overwhelming positive outcomes, CNETS urges a positive recommendation for the reassessment of Lutathera for the treatment of unresectable or metastatic, well-differentiated, somatostatin receptor-positive pancreatic neuroendocrine tumours in adults whose disease has progressed after treatment with a somatostatin analogue, unless there is a contraindication or intolerance.
Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 8: Financial Disclosures for the Canadian Neuroendocrine Tumour Society
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | — | X | — | — |
Ipsen Biopharmaceuticals | — | — | X | — |
Advanced Accelerator Applications (AAA) A Novartis Company | — | — | X | — |
Pfizer | X | — | — | — |
Sanofi | X | — | — | — |
Clinician Input
Ontario Health Cancer Care Ontario Gastrointestinal Cancer Drug Advisory Committee
About the Ontario Health Cancer Care Ontario Gastrointestinal Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
This input was jointly discussed at a DAC meeting
Current Treatments and Treatment Goals
Currently, there are four established lines of therapy for patients with pNETS. Somatastatin-analogs, tem-cap com, everolimus and sunitinib would be drugs available. The patient population within the province is quite small, about 10-20% of NETs would be pNETs. There is high demand for therapies by clinicians and patients.
Treatment Gaps (Unmet Needs)
Treatments are needed to improve survival.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
There currently are 4 established lines of therapy. Somatostatin-analogues, everolimus, sunitinib, and cap-tem combination are the current available treatments. 177Lu would fit in the 4th line therapy.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients with advanced, unresectable, metastatic pNETs being treatment with palliative intent.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
N/A
What factors should be considered when deciding to discontinue treatment with the drug under review?
Disease progression or toxicity.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
PRT programs within the province that can administer radio-pharmaceuticals.
Additional Information
N/A
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Erin Kennedy
Position: Ontario Health Cancer Care Ontario Gastrointestinal Cancer Drug Advisory Committee Lead
Date: 4/8/2022
Table 9: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario Gastrointestinal Cancer Drug Advisory Committee Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Tim Asmis
Position: Ontario Health Cancer Care Ontario Gastrointestinal Cancer Drug Advisory Committee Member
Date: 4/8/2022
Table 10: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario Gastrointestinal Cancer Drug Advisory Committee Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Canadian Association of Nuclear Medicine
About the Canadian Association of Nuclear Medicine
The Canadian Association of Nuclear Medicine strives for excellence in the practice of diagnostic and therapeutic nuclear medicine by promoting the continued professional competence of nuclear medicine specialists, establishing guidelines of clinical practice, and encouraging biomedical research. We work with all professionals in nuclear medicine to ensure that Canadians have access to the highest quality nuclear medicine services.
Information Gathering
Information was gathered through personal experience contributing to care of patients with neuroendocrine tumours (NETs). This includes co-leading discussions for a decade at local Neuroendocrine Tumour board on when best to offer Lutathera (or its predecessor offered in some centres under a CTA) to NET patients, including pancreatic NETs, viz-a-viz other therapies. This has been supplemented by attendance at conferences and literature review. Since November 2020 I have been personally using Lutathera to treat patients with NETs of midgut origin (currently approved indication).
Current Treatments
Response: First line treatment for metastatic pancreatic NETs is a (non-radiolabeled) somatostatin analog such as Sandostatin or Somatuline. However, many patients will eventually progress requiring a change in therapy to control symptoms and/or slow the progression of the metastatic disease. Targeted therapies such as Everolimus (m-TORC 1 inhibitor) and Sunitinib (tyrosine kinase inhibitor) are available. However, they are much less desirable than Lutathera due to lower effectiveness (consider Progression Free Survival) and a worse side effect profile. These targeted therapies are expensive, more so with longer use (versus Lutathera which is delivered 4 times maximum under the current therapeutic regimen).
Chemotherapy is ineffective in most NETs, which are low grade. However, the small portion of NETs which are high grade are treated with chemotherapy such as capecitabine and temozolamide. These higher grade NETs usually do not significantly express somatostatin receptors and hence are not amenable to treatment with Lutathera, a somatostatin analog.
Treatment Goals
Response: The key goals in treatment of pancreatic NETs are:
Slow the progress of disease. Most NETs, even low grade, will invariably progress with metastases to multiple organ systems and may ultimately lead to death. Progression Free survival is a key metric in assessing NET therapies.
Control hormonal symptoms. Many pancreatic NETs produce excess hormones such as insulin and gastrin which can have devasting clinical implications including dangerous bouts of marked hypoglycemia (insulinomas) and severe gastritis (gastrinomas). As such maintaining or improving quality of life is extremely important in these patients.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Response: There are unmet needs regarding both of the major treatment goals discussed in Section 4. In terms of slowing the progress of the disease, Progression Free Survival is considerably longer with Lutathera than the available targeted therapies.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Response: Patients with metastatic NET of pancreatic origin progressing on a (non-radiolabeled) somatostatin analog.
Place In Therapy
How would the drug under review fit into the current treatment paradigm?
Response: Lutathera is the optimum second line treatment for NET patients who have progressed on a (non-radiolabeled) somatostatin analog. The ability to assess all sites of metastatic disease for the therapeutic target in vivo (Section 6.7) and the greater effectiveness (eg Progression Free Survival) versus targeted therapies make this the preferred treatment.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective. If so, please describe which treatments should be tried, in what order, and include a brief rationale.
Response: It is entirely appropriate for patients to first undergo treatment with a (non-radiolabeled) somatostatin analog such as Sandostatin or Somatuline. Lutathera is being considered in patients who have progressed on a somatostatin analog.
How would this drug affect the sequencing of therapies for the target condition?
Response: Little effect in the sequencing. Lutathera is the preferred second line treatment for NET patients who have progressed on a somatostatin analog.
Which patients would be best suited for treatment with the drug under review?
Response: Best suited patients for Lutathera are those who:
have progressed, either in symptom control or metastatic aggregate tumour volume, in spite of treatment with a somatostatin analog.
have demonstrated somastostatin receptor positivity on much of their metastatic disease via imaging with a 68Ga-DOTATATE PET scan or In-Octreotide scan as discussed in Section 6.7.
How would patients best suited for treatment with the drug under review be identified?
Response: While NETs can be challenging to initially diagnosis, for consideration of Lutathera the diagnosis would have been made and would have been known for quite some time as Lutathera is being considered in the setting of disease progression. Progression can be a combination of:
clinical symptoms, typically due either to hormonal production or physical bulk of disease
biochemical monitoring of hormonal levels
imaging monitoring of disease bulk or involvement of important organs or structures. Imaging includes a combination of anatomic imaging (CT, MRI) and functional imaging such as 68Ga-DOTATATE PET.
Depending on the level of local expertise in NETs assessment of potential therapy candidates at multi-disciplinary tumour boards can be helpful to decide when Lutathera is best invoked in the patient’s care.
Which patients would be least suitable for treatment with the drug under review?
Response: Those who do not have confirmation of targeting of most metastases via a 68Ga-DOTATATE PET scan: refer to next section.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review? If so, how would these patients be identified?
Response: Yes, and in fact this is one of the major benefits of this treatment. Potential patients undergo molecular imaging with an analogous radiopharmaceutical to confirm tumour target for therapy. Lutathera (177Lu-DOTATATE) is predicated on the uptake of DOTATATE, a somatostatin analog, by NETs due to the high expression of somatostatin receptors by most (though not all) NETs. Confirmation of targeting is best performed through Positron Emission Tomography (PET) scanning with 68Ga-DOTATATE, a PET radiopharmaceutical that uses the identical tumour-seeking molecule DOTATATE. Uptake of the diagnostic (68Ga-DOTATATE) on a PET scan displays the exact distribution of the therapeutic (177Lu-DOTATATE). This is important, as NETs often demonstrate significant variability amongst different metastases even within the same patient. Few systemic therapies are afforded such a strong pre-therapy confirmation of anticipated delivery of the therapeutic to sites of disease. If 68Ga-DOTATATE PET scanning is not available, 111In-Octreotide scanning, which is more widely available, is a reasonable surrogate.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response: Monitoring metrics are essentially as per the selection metrics in 6.5, namely:
clinical symptoms, typically due either to hormonal production or physical bulk of disease
biochemical monitoring of hormonal levels
imaging monitoring of disease bulk or involvement of important organs or structures.
What would be considered a clinically meaningful response to treatment?
Response: As the anticipated course of the untreated disease is gradual progression, either improvement or stability of symptoms and/or disease bulk are considered a meaningful response to treatment.
How often should treatment response be assessed?
Response: Specific monitoring during the course of the treatment is not necessary, though imaging can be obtained if a complication or progression is suspected. Some centres will image the Lutathera distribution in the body after each treatment as 177Lutetium emits gamma rays amenable to imaging, in addition to the beta particles which perform the therapy. This however is not mandatory.
There is no consensus on optimum follow up. At our centre, for Lutathera performed for treatment of NETs of midgut origin (currently approved indication) we suggest imaging follow up with functional imaging (68Ga-DOTATATE PET) and anatomic imaging (CT) at 4-6 months following completion of the 4 Lutathera treatments. For monitoring thereafter we suggest anatomic imaging at 4-6 month intervals, with functional imaging as indicated on an individual basis.
What factors should be considered when deciding to discontinue treatment?
Response: Discontinuation should be considered when significant adverse events occur which do not recover after an appropriate pause in the regimen. These are detailed in the product monograph and include myelosuppression (majority of patients, but usually mild or moderate, and transient) and renal dysfunction (mostly mild or subclinical).
What settings are appropriate for treatment with the drug under review?
Response: Lutathera is a radioactive therapy and can only be administered in select centres with appropriate training and certification by the Canadian Nuclear Safety Commission. All personnel involved in the treatment, including physicians, nurses, and nuclear medicine technologists, must have appropriate training in radioisotope handling and therapy administration, including all relevant radiation precautions and medical concerns for this specific treatment. In light of this it is anticipated that Lutathera will only be administered at limited sites.
Lutathera can be performed on an outpatient basis in the vast majority of patients.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Response: N/A.
Additional Information
Response: I highly endorse approval for this indication given the unique ability to identify targeting in vivo with 68Ga-DOTATATE PET scans, the high effectiveness of the therapy as evidenced by the Progression Free Survival, and the good side effect profile.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Steven Burrell, MD
Position: Head of Nuclear Medicine, QEII Health Sciences Centre, Halifax NS.
Date: 07-04-2021
Table 11: Conflict of Interest Declaration for CANM Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Advanced Accelerators Applications | X | — | — | — |
CHU de Québec – Université Laval Research Center – Oncology Axis; Hôtel-Dieu de Québec – Nuclear Medicine Department; Fondation du CHU de Québec – Research Chair in Theranostics; Association des Médecins Spécialistes en Médecine Nucléaire du Québec
About CHU de Québec – Université Laval Research Center – Oncology Axis; Hôtel-Dieu de Québec – Nuclear Medicine Department; Fondation du CHU de Québec – Research Chair in Theranostics; Association des Médecins Spécialistes en Médecine Nucléaire du Québec
The CHU de Québec – Université Laval Research Center – Oncology Axis regroups more than 200 researchers and students, whose mission is to bring clarity and resolution to complex problems related to cancer, for the benefit of patients and society. In the field of neuroendocrine tumors, the Oncology Axis brings together surgeons, medical oncologists, endocrinologists, nuclear medicine consultants along with nurses and research clerical staff to better understand neuroendocrine tumors. We consider the CHU de Québec as an excellence center, treating patients from all over Canada, with many patients coming from British Columbia, Manitoba, New-Bruswick and Newfoundland. We aim at improving the health of patients by providing the right treatment to the right patient, at the right time for the right dosage. Using a personalized approach, we develop a tailored diagnostic and therapeutic sequence to one of the largest cohorts of neuroendocrine tumor patients in Canada.
CHU de Québec - Université Laval Research Center - Oncology
The Hôtel-Dieu de Québec – Nuclear Medecine Department is home of one of the world-renowned research groups in theranostics, diagnostic and therapeutic interventions in neuroendocrine tumor patients using PRRT. It is without a doubt the nuclear medicine department bearing the highest concentration of physicians with the most post-graduate and post-residency training in nuclear oncology and theranostics in Canada. Namely, the department is headed by the visionary Dr François-Alexandre Buteau (MD, FRCPC, Fellowship at the Cross Cancer Institute, Alberta) and the research program is headed by Dr Jean-Mathieu Beauregard (MD, MSc, FRCPC, Fellowship at the Peter Maccallum Cancer Centre, Melbourne). Both Dr Buteau and Beauregard are supported by Dr Alexis Beaulieu (MD, FRCPC, Fellowship at the Peter Maccallum Cancer Centre, Melbourne), Dr Frédéric Arsenault (MD, MSc, FRCPC, Fellowship in nuclear oncology, CHU de Québec) and Dr Geneviève April (MD, FRCPC, Fellowship at the CHU de Sainte-Justine, Mother and Child Hospital in Montreal). Soon after her residency completion, Dr Melanie Desaulniers (MD) will join our team of physicians prior to completing her fellowship in theranostics at Zentralklinik Bad Berka, Germany.
CHU de Québec - PRRT Clinical Trial
The Fondation du CHU de Québec – Research Chair in Theranostics is the first of its kind at the CHU de Québec and in Canada, announced on June 8th, 2021. Having the development of health research in mind, this chair will fuel further advancements in clinical research by targeting highly efficient research projects with direct patient benefits, based on our experience with Lutetium-177-octreotate and PRRT, showing promising repercussions. This chair is a catalyst for life changing treatments and innovations to patients, a reflection of the successful treatments administered to neuroendocrine tumor patients with PRRT.
Research Chair in Theranostics
Finally, the Association des Médecins Spécialistes en médecine Nucléaire du Québec, for the Québec Association of Nuclear Medicine consultants (AMSMNQ) is a non-profit organization representing all of 116 board-certified nuclear medicine consultants in the province of Québec, advocating for a better and equal access to nuclear medicine for patients, and the consultation and development of clinical guidelines for the appropriate use of technology in nuclear medicine in Québec.
Québec Association of Nuclear Medicine Association (AMSMNQ)
Information Gathering
All of the information gathered and included in the submission was obtained from our own experience at our world-renowned nuclear medicine and theranostics department (both published and unpublished data) and with regular patients from all over Canada. We have one of the largest cohorts of patients that underwent PRRT with lutetium octreotate from November 2012 to March 2022 in Canada. All data is compiled, anonymized and kept in protected servers from willing recruited patients throughout Canada.
Current Treatments and Treatment Goals
Neuroendocrine tumors regroup more than a dozen different diseases, each with their own specificity according to their cellular origin and biology. What identifies a NET is a tumor that derives from cells originating from the neural crest, and most show an overexpression of somatostatin receptors to the surface of the tumor, making it a perfect target to both diagnose and treat the disease.
The first line of therapy to consider with NETs patients is through surgery. When diagnosed early, a surgical approach can be performed with an intent to cure. With an advanced, unresectable or metastatic disease, then the surgical gesture will aim at debulking the tumor, or addressing complications caused either by the tumor, its metastases or complications from previous treatments. These complications include and are not limited to pain, bowel obstruction and cholecystitis.
Once the disease is considered metastatic and/or unresectable, all further treatments are then considered palliative. The aim is then to reduce symptoms, prevent complications, and ultimately prolong patient survival, by delaying disease progression, coma and death.
The first systemic treatment prescribed to patients is a somatostatin analogue, most often long-acting analogues (Sandostatin LAR of Lanreotide). The goals of somatostatin analogues are to reduce the patients’ symptoms (diarrhea, flushing, shortness of breath), and to delay disease progression. Somatostatin analogues has an antiproliferative activity as demonstrated in the Clarinet Clinical Trial comparing Lanreotide to placebo. There is a reported 3% disease response rate in the literature.
Because of lack of availability in all medical centres in Canada, when patients should undergo PRRT according to the body of literature in the field, patients will undergo biotherapies consisting of Everolimus and Sunitinib, with many significant side effects and complications.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
For patients with metastatic neuroendocrine tumors of pancreatic origin (PanNET), there are many unmet needs regarding treatment options, the therapeutic profile, but most importantly there are definitive inequities to access to PRRT (Peptide Receptor Radionuclide Therapy) for patients throughout Canada.
Currently, for patients with well-differentiated PanNET throughout Canada (except for the Province of Québec), three treatment options are available: A surgical approach, somatostatin analogues (short- or long-acting), and biotherapies comprised of Everolimus (mTOR inhibitor) and Sunitinib (receptor tyrosine kinase inhibitor).
Patients with secretory or functional PanNET fail to respond to available treatments. Examples such as Insulinomas, Glucagonomas, VIPomas, ACTHomas, Somatostatinomas still secrete active proteins and hormones to life-threatening levels even after all available treatment options.
Patients become refractory to current treatment options. As PanNET is an heterogenous and polyclonal disease, some clones will resist and proliferate under current treatments.
Current treatment options aren’t well tolerated. Sandostatin LAR is an intramuscular injection in the gluteus muscles, up to 30-40% injections end up subcutaneous because of the depth of the muscles. Some patients need to have up to three deep injections every 2 weeks, associated with pain, paresis and paresthesia. Everolimus and Sunitinib have many side effects that include change or unpleasant taste, nausea, diarrhea, throat pain and sores, rash, joint pain, blisters or rash on hands or feet, numbness or tingling sensations of the arms or legs. Such side effects lower the compliance to medication.
In the Province of Québec, Lutathera is now recommended and reimbursed for its full clinical indication (unresectable or metastatic, well-differentiated somatostatin receptor positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs) in adults with progressive disease. Currently Lutathera is limited to 4 injections of 7.4 GBq every 8 weeks, and clinical trial are needed to confirm efficacy of additional cycles (Consolidation and Salvage cycles).
PRRT in its first form using Indium-111-pentetroctreotide was pioneered back in 1992 at Erasmus Medical Centre, Rotterdam. Toxicity was high, and the clinical outcome did not meet expectations. Then came Yttrium-90-octreotide, with great clinical outcomes, but the Yttium-90 electron range and energy better suited for high disease burden, and the medullary and renal toxicity was to be considered. Finally in the early 2000’s came Lutetium-177-octreotate, with significant clinical results when used in patients with Gastroenteropancreatic Neuroendocine Tumors (GEPNET). Side effects are mild and alleviated when administered in conjunction with kidney-protective agents (namely an amino acid infusion of lysine and Arginine). The patients that responded less to PRRT were the patients with low grade midgut NET, that the NETTER-1 clinical trial demonstrated significant benefits to OS and PFS, that should translate as even better results to PanNETs.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The only treatment to consider before PRRT using Lutathera is administration of long-acting somatostatin analogues, as recommended by NCCN, the expert panel evaluating neuroendocrine tumor in the province of Quebec and the strong recommendation from the NETTER-1 study.
Considering the NETTER-1 study, the PFS and OS gain over control arm, the gain in quality of life and control over functioning tumors, Lutathera is currently in the treatment paradigm for GEP-NET as a standard of care since. Just like immunotherapy, because of it’s unique mechanism of action and because we can image and diagnose with the use of somatostatin receptor PET-CT, PRRT using Lutathera (Lutetium-177-octreotate) should be indicated for:
All patients with a well differentiated neuroendocrine tumor (including PanNET);
Significant overexpression of somatostatin receptor as demonstrated on SSTr PET-CT (or octreoscan);
Performance index score of Karnofsky equal or greater than 60%.
When we look at our centre experience since 2012:
we count 30% of patients coming from out of province of Québec;
All these patients seek and find a treatment that are tailored to their unmet needs in their respective province. We advocate for patients of Canada to have access to PRRT. Prior to 2012 patients had to travel to Germany or Australia to have access;
This treatment was administered to patients under special access program or a CTA;
In the province of Québec, PRRT using Lutathera is now considered a standard of care for well differentiated GEP-NET showing progression under somatostatin analogues (2nd line of treatment), independently of tumor grade, origin and extent.
Finally, the authorization and reimbursement of Lutathera for all it’s clinical indications (GEP-NET) approved by Health Canada for all Canadian citizens in need of this treatment would insure a universal access to patients in their own medical community, ensuring the absence of inequities in GEP-NET patients where there are currently 2 classes of citizens (Québec residents getting Lutathera available in more than 5 teaching hospitals, and the rest of Canada having to travel to Québec, USA, Germany or Australia to get access to what is considered standard of care).
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
The treatment has three objectives:
Limit or stop progression of the disease
Limit or reduce the clinical sign and symptoms of the disease
Limit or reduce hormonal secretion
Which patients would most benefit from treatment:
Patients with known neuroendocrine tumor
Progression of the disease after somatostatin analogues (SSAs)
Disease showing significant overexpression of somatostatin receptor, as demonstrated by somatostatin receptor PET-CT or SPECT-CT.
Patient’s ECOG = 0 – 2
How we identify patients best suited for treatment:
Medical consultation to assess patient’s fitness to treatment (ECOG = 0 – 2) and to discuss treatment’s rationale, risks and benefits, along with radioprotection information.
Disease characterization assessed by a nuclear medicine or radiation oncologist administering PRRT using PET-CT (Gallium-68 octreotate or octreoscan), with optional FDG PET-CT. Patient with discordant disease or non-octreotate avid should be considered non-eligible for PRRT.
Disease progression proven on conventional imaging (CT, MRI) or functional imaging (PET-CT, SPECT-CT).
Disease will go underdiagnosed (downstaged or not diagnosed) if only traditional imaging (CT or MRI) or SPECT-CT is used instead of PET-CT imaging.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The outcomes used in clinical practice to determine patient’s response to treatment are as follow:
Symptoms are objectively and\or subjectively less (decrease in frequency, intensity and duration) or stable
Increase in quality of life
The measurable lesions that were increasing in size prior to treatment stopped progressing (PFS)
These outcomes are in line with the one typically used in clinical trials when considering neuroendocrine tumors.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Disease progression under treatment as demonstrated by:
Deterioration of symptoms
Disease progression as proven by post-treatment functional imaging
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
The patient’s eligibility to PRRT using Lutathera should be accessed by either a nuclear medicine consultant or radiation oncologist that administers such treatments, And the treatment is administered to teaching hospitals on an outpatient basis, after insuring the safety to administer such a treatment.
Additional Information
In our phase II clinical trial at the CHU de Québec assessing safety and efficacy of personalized dosimetry for PRRT, out of 52 patients who had completed all 4 induction cycles at the time of analysis, 13 patients had PanNET, and 85% (11 patients) had partial or minor response, compared to 59% of overall patients. In our cohort, patients with PanNET showed better response when compared to midgut NETs, and midgut NETs response to treatment was well established in the NETTER-1 clinical trial.
Del Prete, M., Buteau, FA., Arsenault, F. et al. Personalized 177Lu-octreotate peptide receptor radionuclide therapy of neuroendocrine tumours: initial results from the P-PRRT trial. Eur J Nucl Med Mol Imaging 46, 728–742 (2019). https://doi.org/10.1007/s00259-018-4209-7
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Frederic Arsenault
Position: Nuclear Medicine consultant – CHU de Québec.
Date: 31-03-2022
Table 12: Conflict of Interest Declaration for CHU de Québec Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AAA inc. | X | — | — | — |
Ipsen inc. | X | — | — | — |
Canadian Neuroendocrine Tumour Society Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians
About the Canadian Neuroendocrine Tumour Society Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians
The Canadian Neuroendocrine Tumour Society, known as CNETS, includes a Scientific & Medical Advisory Board (SMAB). The SMAB members, composed of leading Canadian neuroendocrine cancer multi-disciplinary clinicians and scientists, provide expert scientific, clinical and strategic advice to the CNETS Board of Directors. The SMAB works alongside the patient group to support best practices across the spectrum of research pillars, partnerships, advocacy and scientific and medical matters relevant to organization’s mission.
CNETS is a national oncology patient organization providing support and education on all aspects of Neuroendocrine Tumours (NETs) for people living in Canada. As part of its mandate, CNETS is committed to raising awareness about the disease and the latest evidence around diagnosis and treatment, and ensuring that patients, caregivers, and healthcare professionals have the information they need in the areas of medical and scientific research, treatment and support.
More information about CNETS can be found on the CNETS website.
Information Gathering
Information was gathered through clinician first-hand experience in the treatment of neuroendocrine tumours, a literature review of available evidence and discussion with national and international clinical experts.
Current Treatments and Treatment Goals
This application is for patients with unresectable or metastatic, well-differentiated, somatostatin receptor-positive gastroenteropancreatic neuroendocrine tumours (GEP-NETs).
Although curative-intent surgery is the cornerstone of initial treatment in Canada, many patients present with unresectable local-regional or metastatic disease, or develop metastatic disease following initial surgery. For these patients, non-curative debulking surgery is often considered but most will require systemic medical treatment for the ongoing management of disease. In the metastatic setting, patients can have symptoms impacting quality of life and functional status due to tumor bulk, organ dysfunction and/or secretory syndromes as a result of hormones and peptides produced by the malignancy.
In Canada, medical therapies for unresectable or metastatic, somatostatin receptor-positive GEP-NETs, including pancreatic NETs (pNETs), generally include biologic therapy, targeted agents, combination chemotherapy, and peptide receptor radionuclide therapy (PRRT) with Lutetium oxodotreotide.
Biologic therapy includes the somatostatin analogs (SSAs), Octreotide LAR and Lanreotide, which have been shown to significantly improve Progression-Free Survival (PFS) and can dramatically improve hormonal syndromes associated with secretory disease.
Targeted agents include everolimus, a mammalian Target of Rapamycin (mTOR) inhibitor, and sunitinib, a tyrosine kinase inhibitor. Both of these agents have been shown to improve PFS in large phase III, placebo-controlled randomized clinical trials but are also associated with a variety of toxicities sometimes limiting therapy and often resulting in a deterioration in quality of life.
Combination chemotherapy is generally reserved for patients with rapidly proliferating well-differentiated disease or those with high-grade poorly differentiated GEP-NETs. Options include the capecitabine and temozolomide (CAP/TEM) regimen for the first group of patients and is a regimen which has demonstrated high objective response rates and improved progression-free survival (PFS) compared to other cytotoxic treatments. For poorly differentiated neuroendocrine carcinomas (NECs), platinum-based chemotherapy regimens can elicit disease response, but duration of responses are relatively short.
PRRT with Lutetium oxodotreotide is an approved and funded second-line systemic therapy after disease progression on standard dose SSAs for patients with unresectable or metastatic midgut NETs across Canada. In the province of Quebec, patients with GEP-NETs, including pNETs, also have access to Lutetium oxodotreotide. For midgut NETs, PRRT with Lutetium oxodotreotide has been shown to significantly improve PFS and quality of life compared to an escalated dose of SSA for patients with metastatic midgut NETs with disease progression on standard-dose SSAs. In several large patient cohorts examining the efficacy of PRRT specifically for pNETS, as well as for patients with non-GEP NETS, PFS has been observed to be within the same range as that seen for patients with midgut NETs. Lutetium oxodotreotide is better tolerated than currently available targeted therapies in Canada and is associated with a clinically significant longer PFS of 24-30 months compared to PFS estimates of 11-12 months for targeted therapies.
Overall goals in the treatment of GEP-NETs, including pNETs, are to improve Progression-Free Survival (PFS) and enhance Quality of Life. Important quality of life goals include minimizing symptom burden, reducing treatment frequency, minimizing treatment adverse effects and reducing caregiver burden.
References
Singh, Simron, et al. "Diagnosis and management of gastrointestinal neuroendocrine tumors: an evidence-based Canadian consensus." Cancer Treatment Reviews 47 (2016): 32-45.
Singh, Simron, et al. "Consensus recommendations for the diagnosis and management of pancreatic neuroendocrine tumors: guidelines from a Canadian National Expert Group." Annals of Surgical Oncology 22.8 (2015): 2685-2699.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There are patients with unresectable or metastatic GEP-NETs, including pNETs, for whom biologic therapy, targeted agents, and combination chemotherapy have proven to be ineffective or are poorly tolerated with or without refractory disease. Additionally, over time, all patients generally develop resistance to biologic therapy, targeted agents and combination chemotherapy.
Sequential systemic therapies can significantly prolong PFS for many of these patients although publicly reimbursed treatment options remain limited. Following disease progression on standard first-line SSA, there are limited well-tolerated options. With effective therapies many patients can continue to have productive lives with minimization of treatment toxicities. The safety and tolerability profile of PRRT with Lutetium oxotreotide is more favorable than currently employed second-line treatment options for a diverse group of NETs and thus meets the relevant goals of both prolonging PFS and minimizing treatment toxicities and societal burden for this patient population.
Internationally, PRRT with Lutetium oxotreotide is reimbursed for patients with GEP-NETs, including pNETs, in many jurisdictions including Europe, the United States and Australia. Currently in Canada, there is interprovincial inequity as the province of Quebec currently funds this treatment for GEP-NETs, including pNETs, whereas Lutetium oxotreotide is only available for patients with midgut NETs in the rest of the country.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Lutetium oxodotreotide would be used for the treatment of patients with unresectable or metastatic, well-differentiated, somatostatin receptor-positive GEP-NETs, including pNETs who experience disease progression on available first-line treatment. This indication mirrors the current indication for this therapy in the more limited midgut NET patient population.
Availability of this therapy would be expected to significantly impact both PFS and quality of life for this patient population compared to currently available second-line therapies.
The unique radiopharmaceutical properties of lutetium oxodotreotide as well as the lack of cross-resistance to other systemic therapies for this disease represents a different and complementary mechanism of action to those of all other systemic treatments for NETs.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients best suited for treatment with lutetium oxodotreotide are patients with unresectable or metastatic, well-differentiated, somatostatin receptor-positive GEP-NETs, including pNETs, who experience disease progression on currently available first-line therapies. The companion diagnostic test includes either an Octreoscan or Gallium 68 DOTATATE PET scan, both of which are currently funded across Canada and are already in use for the diagnosis and evaluation of NETs of multiple origins.
The patient population is selective as all would have to have disease demonstrating somatostatin-receptor avidity on currently available nuclear medicine imaging, either Octreoscan or Gallium-68 DOATATATE PET scan.
Lutetium oxodotreotide is less suitable in patients who have not tried existing first-line treatments, such as SSAs.
Lutetium oxodotreotide is not suitable for patients with Octreotide non-avid disease, high-grade or poorly differentiated tumours, significant renal impairment or bone marrow dysfunction and those that have previously received PRRT with no clinical benefit.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The primary outcome of Progression-Free Survival (PFS) is the standard metric of clinical benefit in both clinical trials and routine clinical management of patients with NETs of all origins. An expected median PFS of 24-30 months with Lutetium oxodotreotide is a highly clinically meaningful response which is longer than expectations for any currently available second line therapy. For those with symptoms related to hormonal or peptide secretion by the disease, clinical symptom control and biochemical response is also assessed on a continuous basis and improvement correlated highly with improved quality of life.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Factors include disease progression as determined on cross-sectional imaging, treatment-induced toxicities, lack of symptom control and/or patient preference.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
This treatment would be available in major neuroendocrine treatment centres, and requires a multidisciplinary team, including medical, surgical, nuclear medicine teams (or in some centers the combination of radiology and radiation oncology), to optimize benefits and risks of the intervention. The treatment would be administered on an outpatient basis within the hospital center.
Additional Information
Peptide Receptor Radionuclide Therapy (PRRT), including lutetium oxodotreotide, is now a standard of care treatment in the management of neuroendocrine tumours internationally. It has been utilized for over a decade in Australia following the promising results from European centers of prolonging progression-free survival. Many patients previously seen in Canada have had to travel to these countries for therapy
The collective experience of Canadian medical professionals who are involved in treating patients with progressive, unresectable or metastatic, well-differentiated, somatostatin receptor-positive gastroenteropancreatic neuroendocrine tumours (GEP-NETs), is that Lutetium oxotreotide provides significant clinical benefits across patients with SSTR-expressing GEP-NETs, including pNETs. These benefits include objective disease response, improvement in symptom burden, stabilization or improvement in quality of life and prolongation of progression-free survival. The current Canadian landscape is one of inequity due to lack of access to this therapy for non-midgut NETs outside of the province of Quebec where it is currently funded.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Janice L. Pasieka
Position: Clinical Professor of Surgery and Oncology
Date: 16-03-2022
Table 13: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
IPSEN | X | — | — | — |
NOVARTIS | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Jean-Mathieu Beauregard
Position: Nuclear Medicine Physician, CHU de Québec-Université Laval
Date: 06-04-2022
Table 14: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AAA/Novartis (Ad Board) | X | — | — | — |
IPSEN (Education Program) | X | — | — | — |
Declaration for Clinician 3
Name: Dr. Shereen Ezzat
Position: Professor of Medicine
Date: <05-04-2022>
Table 15: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Rachel Goodwin
Position: Medical Oncologist, The Ottawa Hospital Cancer Centre
Date: 29-03-2022
Table 16: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Ipsen: for Independent NET REB lead research projects | — | — | — | X |
AAA: Consultation Board | X | — | — | — |
Novartis: Consultation Board | X | — | — | — |
Declaration for Clinician 5
Name: Dr. Sharlene Gill
Position: Medical Oncologist, BC Cancer - Vancouver
Date: 23-03-2022
Table 17: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Ipsen | — | X | — | — |
AAA | X | — | — | — |
Declaration for Clinician 6
Name: Dr. Daniel Rayson
Position: Attending medical oncologist and Professor of Medicine, QEII Health Sciences Center and Dalhousie University, Halifax, NS
Date: 05-04-2022
Table 18: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Ipsen Canada | — | X | — | — |
AAA Canada | X | — | — | — |
Declaration for Clinician 7
Name: Dr. J. Dean Ruether
Position: Interim Senior Medical Director, Cancer Care Alberta, Alberta Health Services
Date: 06-04-2022
Table 19: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 8
Name: Dr. Radhika Yelamanchili
Position: Medical Oncologist, Walker Family Cancer Centre
Date: 31-03-2022
Table 20: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 8
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AAA | X | — | — | — |
Declaration for Clinician 9
Name: Dr. David Laidley
Position: Nuclear Medicine Physician, Assistant Professor Western University
Date: 23-03-2022
Table 21: Conflict of Interest Declaration for CNETS Scientific and Medical Advisory Board and Other Neuroendocrine Cancer Treating Clinicians — Clinician 9
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | X | — | — | — |
Ipsen | X | — | — | — |
Bayer | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.