CADTH Reimbursement Review
Abemaciclib (Verzenio)
Sponsor: Eli Lilly Canada Inc.
Therapeutic area: Adjuvant treatment of hormone receptor–positive, human epidermal growth factor receptor 2–negative early breast cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AI
aromatase inhibitor
ALN
axillary lymph node
ASCO
American Society of Clinical Oncology
CBCN
Canadian Breast Cancer Network
CDK
cyclin-dependent kinase
CI
confidence interval
DFS
disease-free survival
DRFS
distant relapse–free survival
DVT
deep vein thrombosis
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EQ-5D-5L
5-Level EQ-5D
ER
estrogen receptor
ET
endocrine therapy
FACT-B
Functional Assessment of Cancer Therapy – Breast
GnRH
gonadotropin-releasing hormone
HER2
human epidermal growth factor receptor 2
HR
hormone receptor
HRQoL
health-related quality of life
IDFS
invasive disease–free survival
IHC
immunohistochemistry
IKWG
International Ki-67 in Breast Cancer Working Group
ILD
interstitial lung disease
IQWiG
Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen [Institute for Quality and Efficiency in Health Care]
ITT
intention to treat
MID
minimal important difference
OS
overall survival
PR
progesterone receptor
PRO
patient-reported outcome
SAE
serious adverse event
SAP
statistical analysis plan
SD
standard deviation
STEEP
Standardized Definitions for Efficacy End Points
TEAE
treatment-emergent adverse event
VTE
venous thromboembolism
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Abemaciclib (Verzenio), 50 mg, 100 mg, 150 mg, 200 mg oral tablet |
Indication | In combination with endocrine therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 test score ≥ 20% |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | January 12, 2022 |
Sponsor | Eli Lilly Canada Inc. |
HR = hormone receptor; NOC = Notice of Compliance.
Introduction
Breast cancer is the most commonly diagnosed cancer among women in Canada, and the second most common cancer in men and women combined. In 2020, 27,700 women were diagnosed with breast cancer, representing about 25% of new cancer cases in Canada.1 Breast cancer is the second leading cause of cancer deaths among women, accounting for 14% of all cancer deaths.1 The 5-year net survival rate for breast cancer is more than 85% among women diagnosed before 85 years of age, after which it drops to approximately 73%.1
Patients with breast cancer are stratified and treated based on the expression status of certain tumour receptors that serve as important prognostic and predictive biomarkers, including estrogen receptor (ER) and progesterone receptor (PR). Hormone receptor (HR)–positive breast cancers that have ERs or PRs or both are the most prevalent type of breast cancer, accounting for 70% to 80% of all breast cancers.2 Overexpression of the human epidermal growth factor receptor 2 (HER2) oncogene — which belongs to the epidermal growth factor receptor (EGFR/HER) family and enables constitutive activation of growth factor that signals and triggers breast cancer cell survival, proliferation, and invasion — is associated with poor prognosis.3 Approximately 85% of patients with breast cancer do not have tumours that overexpress HER2 and are HER2-negative. HR-positive, HER2-negative tumours are the most common subtype of breast cancer, accounting for approximately 70% of breast cancers.4 More than 90% of patients with breast cancer are diagnosed with early-stage disease, which is defined as not having spread beyond the breast tissue or nearby lymph nodes.3 Unlike patients with distant metastatic disease, early-stage breast cancer is potentially curable. In patients with HR-positive, HER2-negative early breast cancer, the 5-year survival rate is 94.3%.5
Although many people with HR-positive, HER2-negative disease will not experience recurrence or have distant recurrence with standard therapies alone — mainly endocrine therapy (ET) — around 7% to 11% of people with early breast cancer experience a local recurrence during the first 5 years after treatment. Nearly 30% of patients eventually experience disease relapse with metastases following treatment with curative intent, often with distant metastases, at which time their prognosis is poor.6 Risk factors for recurrence include large tumour size, a higher degree of involvement of axillary lymph nodes (ALNs), a high histologic grade, positive or close margins, age, HR and HER2 status (positive), and high tumour proliferation rate (Ki-67).7-11 Ki-67 immunohistochemistry (IHC) testing is a prognostic factor for the risk of recurrence.12,13 However, the use of IHC Ki-67 testing in Canadian clinical practice is currently limited due to variability in routine testing and a lack of standardized laboratory assays.
The objective of this review was to evaluate the efficacy and safety of abemaciclib in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 test score of 20% or more.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups, Rethink Breast Cancer (Rethink) and the Canadian Breast Cancer Network (CBCN) submitted patient input for this review. Respondents from Rethink stated that a breast cancer diagnosis and treatment had a devasting and traumatic impact on a young person’s life and many patients express a willingness to take on whatever treatments are needed to lower the chance of recurrence. Patients who had experience with abemaciclib indicated that they were willing to endure the additional side effects of a stronger therapy to ensure that they were doing everything they could to treat what they know is an aggressive form of breast cancer. The CBCN respondents reported that the following factors were the most important ones when considering treatment options: having the most effective treatment possible, reducing the risk of recurrence, maintaining quality of life, having manageable side effects, and having affordable and accessible treatments. Maintaining mobility, productivity, and an ability to continue childcare duties were also highlighted by survey respondents as important when deciding on treatment options. CBCN respondents noted that patients have an expectation that abemaciclib will provide a possibility for improving their rate of invasive disease–free survival (IDFS) and reduce their risk of recurrence, allowing them to live a better quality of life.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH noted that very few treatments developed in recent years have improved survival or quality of life in the adjuvant breast cancer setting; therefore, there is a need for treatments to reduce recurrence risk and improve survival outcomes. Tolerability issues such as arthralgias and mood disturbances are common with ET, particularly in young and premenopausal women. Drugs that can prolong the time to recurrence without compromising quality of life are highly desired. The clinical experts noted that abemaciclib is a new indication in this setting. For eligible patients, abemaciclib would be added to standard adjuvant ET with or without ovarian suppression.
Clinician Group Input
Clinician group input was received from the Ontario Health–Cancer Care Ontario Breast Cancer Drug Advisory Committee, with 3 clinicians contributing to the submission. The clinician group noted that up to 30% of patients with high-risk clinical and/or pathologic features may experience distant recurrence and stated that there is a need for superior treatment options to prevent early recurrence and improve survival. Patients most likely to benefit from abemaciclib would be those with HR-positive, HER2-negative early breast cancer at high risk of recurrence who are node-positive, as per inclusion criteria of the monarchE trial. Patients who are least suitable for abemaciclib would be those excluded from enrolment as per monarchE trial eligibility criteria. Abemaciclib would be used in addition to ET in high-risk patients following surgery and chemotherapy (if applicable). The clinician group input strongly recommended against the inclusion of high Ki-67 levels as the sole criteria for drug eligibility, noting that Ki-67 was prognostic and not predictive and that it is not a standard pathology test for breast cancer in Ontario.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for abemaciclib:
considerations for the initiation of therapy
considerations for the discontinuation of therapy
care provision issues
system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Study
A single sponsor-submitted pivotal study was included in the systematic review. The monarchE trial is an ongoing, open-label, phase III randomized controlled trial that compared the efficacy and safety of abemaciclib in combination with ET to ET alone in the adjuvant treatment of patients with HR-positive, HER2-negative, node-positive early breast cancer who completed definitive locoregional therapy and were at high risk of recurrence based on clinicopathologic features or a high (20% or higher) Ki-67 index. The primary efficacy end point was IDFS, and the secondary end points included distant relapse–free survival (DRFS) and overall survival (OS). A total of 5,637 patients in 38 countries, including |||||||| patients from Canada, were randomized to treatment with either abemaciclib plus ET or ET alone. Patients with at least 1 positive lymph node were recruited into 2 cohorts: patients in Cohort 1 (n = 5,120) were eligible based on high-risk clinicopathologic features (i.e., ≥ 4 positive ALNs, or 1 positive ALN to 3 positive ALNs and at least 1 of the following: tumour size ≥ 5 cm or histologic grade 3) and Cohort 2 (n = 517) included patients at high risk of recurrence based on high levels of Ki-67 (≥ 20%). In Cohort 1, a total of 3,917 (76%) patients had Ki-67 testing results available and of these, 2,003 patients (51%) had a high Ki-67 index; this patient population is aligned with the Health Canada–approved indication and the current reimbursement request. Cohort 1 patients with a Ki-67 index of 20% or more were predominantly female (||||||||) with a mean age of |||||||| years (standard deviation [SD] = ||||||||) and an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 (||||||||); |||||||| of patients were postmenopausal.
Efficacy Results
The results of the efficacy outcomes of OS, IDFS, and DRFS included in the main body of this report are for the “Ki-67 High” population, which is aligned with the Health Canada–approved indication and the current reimbursement request.
Overall Survival
At the interim analysis 1 for OS (April 1, 2021), OS data were immature. There were 95 deaths (42 in the abemaciclib + ET arm and 53 in the ET arm) in the Cohort 1 Ki-67 High population. The hazard ratio between treatment arms was 0.767 (95% confidence interval [CI], 0.511 to 1.152).
Invasive Disease–Free Survival
At the interim analysis (March 16, 2020), |||||||| IDFS events were observed (|||||||| in the abemaciclib + ET arm and |||||||| in the ET arm). The hazard ratio between treatment arms was |||||||| (95% CI, |||||||| to ||||||||; P = ||||||||).
At the final IDFS analysis (July 8, 2020), with a median follow-up of 19.1 months, |||||||| IDFS events were observed (|||||||| in the abemaciclib + ET arm and ||| in the ET arm). The hazard ratio between treatment arms was 0.643 (95% CI, 0.475 to 0.872; P = 0.0042). The 2-year IDFS rates in the abemaciclib plus ET arm versus the ET arm were 91.3% versus 86.1%, respectively.
At the additional follow-up analysis (April 1, 2021), with a median follow-up of 27 months, 262 IDFS events were observed (104 in the abemaciclib + ET arm and 158 in the ET arm). The hazard ratio between treatment arms was 0.63 (95% CI, 0.49 to 0.80). The 3-year IDFS rates in the abemaciclib plus ET arm versus the ET arm were 86.1% versus 79.0%, respectively.
Distant Relapse–Free Survival
At the interim analysis (March 16, 2020), a total of |||||||| events were observed (|||||||| in the abemaciclib + ET arm and |||||||| in the ET arm). The hazard ratio between treatment arms was |||||||| (95% CI, ||||||||). The 2-year DRFS rates in the abemaciclib plus ET arm versus the ET arm were |||||||| versus ||||||||, respectively.
At the final primary outcome (IDFS) analysis (July 8, 2020), a total of |||||||| events were observed (|||||||| in the abemaciclib + ET arm and |||||||| in the ET arm). The hazard ratio between treatment arms was |||||||| (95% CI, |||||||| to ||||||||). The 2-year DRFS rates in the abemaciclib plus ET arm versus the ET arm were |||||||| versus ||||||||, respectively.
At the additional follow-up analysis (April 1, 2021), a total of 220 events were observed (85 in the abemaciclib + ET arm and 135 in the ET arm). The hazard ratio between treatment arms was 0.599 (95% CI, 0.456 to 0.787). The 3-year DRFS rate in the abemaciclib plus ET arm versus the ET arm was 87.8% versus 82.6%, respectively.
Health-Related Quality of Life
The mean scores for the Functional Assessment of Cancer Therapy – Breast Cancer (FACT-B) and EQ-5D 5-Level (EQ-5D-5L) scales were similar in the 2 treatment arms and changes from baseline scores, in both arms, were less than the minimal important difference (MID) of the baseline SD.
Health Care Resource Utilization
As of the final primary outcome (IDFS) analysis (July 8, 2020), |||||||| of patients in the abemaciclib plus ET arm and |||||||| of patients in the ET arm reported at least 1 hospitalization. The majority of patients were hospitalized due to ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Transfusions were reported for |||||||||||||||| of patients in the abemaciclib plus ET arm and |||||||||||||||| of patients in the ET arm. |||||||||||||||||||||||| was the most commonly reported adverse event (AE) requiring a transfusion (|||||||| of patients in the abemaciclib + ET arm and |||||||||||||||| of patients in the ET arm).
Table 2: Summary of Key Efficacy Results From the monarchE Study — Cohort 1 Ki-67 High Population
Event | Treatment, n (%) | Treatment effecta | ||
|---|---|---|---|---|
Abemaciclib + ET N = 1,017 | ET N = 986 | Hazard ratio (95% CI)b,c | 2-sided P valueb,d | |
IDFS | ||||
Interim analysise | |||||||| | |||||||| | |||||||| | |||||||| |
Final analysisf | |||||||| | |||||||| | 0.643 (0.475 to 0.872) | 0.00422 |
Additional follow-up analysisg | 104 (10.2) | 158 (16.0) | 0.626 (0.488 to 0.803) | 0.0002h |
DRFS | ||||
Interim analysise | |||||||| | |||||||| | |||||||| | |||||||| |
Final analysisf | |||||||| | |||||||| | |||||||| | |||||||| |
Additional follow-up analysisg | 85 (8.4) | 135 (13.7) | 0.599 (0.456 to 0.787) | 0.0002i |
OS | ||||
Additional follow-up (i.e., interim analysis 1 for OS)g | |||||||| | |||||||| | |||||||| | |||||||| |
CI = confidence interval; DRFS = distant relapse–free survival; ET = endocrine therapy; IDFS = invasive disease–free survival; OS = overall survival.
Note: The median estimates were not reached for IDFS, DRFS, and OS due to the corresponding event rates.
aTreatment effects in terms of hazard ratio estimates and P values are computed based on comparator ET.
bThis was stratified by geographical region, prior treatment, and menopausal status.
cA stratified Cox proportional hazards model with treatment as a factor was used to estimate the hazard ratio between treatment arms and corresponding 95% CI.
dThis was estimated using the log-rank test.
eThe data cut-off date was March 16, 2020.
fThe data cut-off date was July 8, 2020.
gThe data cut-off date was April 1, 2021.
hThis was tested outside the statistical hierarchy (after the end point was met).
iThis was not pre-specified for this population and unadjusted for multiple comparisons.
Sources: Clinical Study Reports for Verzenio (interim analysis 2), Verzenio (final IDFS [primary outcome] analysis), and Verzenio (overall survival interim analysis 1).14-16
Table 3: Summary of Key Harms Results From the monarchE Study — Safety Population
Harm, n (%) | Abemaciclib + ET arm N = 2,791 | ET arm N = 2,800 |
|---|---|---|
Patients with ≥ 1 TEAE | 2,733 (97.9) | 2,441 (87.2) |
Patients with ≥ 1 grade 3 or higher TEAE | 1,323 (47.4) | 397 (14.2) |
Patients with ≥ 1 SAE | 372 (13.3) | 219 (7.8) |
Patients who discontinued study treatment due to an AE | 172 (6.2) | 23 (0.8) |
Patients who died due to an AE | 15 (0.5) | 16 (0.6) |
Notable harms | ||
Diarrhea | 2,304 (82.6) | 218 (7.8) |
ILD/pneumonitis | 43 (1.5) | 10 (0.4) |
VTE | 67 (2.4) | 16 (0.6) |
Neutropenia | 1,262 (45.2) | 145 (5.2) |
AE = adverse event; ET = endocrine therapy; IDFS = invasive disease–free survival; ILD = interstitial lung disease; SAE = serious adverse event; TEAE = treatment-emergent adverse event; VTE = venous thromboembolism.
Source: Clinical Study Report for Verzenio (final IDFS [primary outcome] analysis).15
Harms Results
As of the final primary outcome (IDFS) analysis (July 8, 2020), 97.9% of patients in the abemaciclib plus ET arm and 87.2% of patients in the ET arm experienced at least 1 treatment-emergent adverse event (TEAE). The most frequent TEAEs were diarrhea (82.6%), neutropenia (45.2%), and fatigue (39.2%) in the abemaciclib plus ET arm, and arthralgia (33.1%), hot flush (21.8%), and fatigue (16.6%) in the ET arm. Serious adverse events (SAEs) occurred in 13.3% of patients in the abemaciclib plus ET arm and 7.8% of patients in the ET arm. The most frequently reported SAEs in both arms were pneumonia (0.9% in the abemaciclib plus ET arm and 0.5% in the ET arm). Grade 3 or higher TEAEs occurred in 47.4% of patients in the abemaciclib plus ET arm and 14.2% of patients in the ET arm. The most frequently reported grade 3 or higher TEAEs in the abemaciclib plus ET arm were neutropenia (19.1%), leukopenia (10.9%), and diarrhea (7.7%). The most common grade 3 or higher TEAEs in the ET arm were neutropenia (0.7%), arthralgia (0.7%), and lymphopenia (0.5%). A total of 481 (17.2%) patients discontinued abemaciclib due to AEs. The 3 most common reasons for discontinuations of abemaciclib were diarrhea (5.1%), fatigue (1.9%), and neutropenia (0.9%).
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Diarrhea was reported for 82.6% of patients in the abemaciclib plus ET arm and 7.8% of patients in the ET arm.
Neutropenia was reported for 45.2% of patients in the abemaciclib plus ET arm and 5.2% of patients in the ET arm. Venous thromboembolisms (VTEs) were reported in 2.4% of patients in the abemaciclib plus ET arm and 0.6% of patients in the ET arm.
Interstitial lung disease (ILD) or pneumonitis was reported for 1.5% of patients in the abemaciclib plus ET arm and 0.4% of patients in the ET arm.
Critical Appraisal
The monarchE study was a randomized, open-label trial. Since Ki-67 index was not a stratification factor, the population of interest (Cohort 1 Ki-67 High) cannot be considered to have been truly randomized, and analyses of this population are therefore at risk of confounding due to potential prognostic imbalances across treatment groups. However, this risk is likely to be low since available baseline characteristics appeared well balanced. Although patient blinding would have been impractical and challenging given the differences in the 2 study treatment regimens and different known toxicity profiles, performance and detection bias that may result from lack of blinding of patients and investigators to assigned study treatments cannot be ruled out. The primary outcome (IDFS) was investigator-assessed but based on objective criteria and, thus, unlikely to be greatly affected by the lack of investigator blinding. The subjective patient-reported outcomes (PROs) may, however, have been affected by this source of bias, as well as a high rate of attrition at later follow-up times. The primary and secondary efficacy end points of IDFS and DRFS are considered appropriate for the disease setting but OS data remain immature. Given that the correlation of disease-free survival (DFS) surrogates with OS is debatable, it is unclear if improvements in IDFS observed in patients in the abemaciclib plus ET arm of the trial would translate into OS benefits.
The trial included a heterogenous population of patients with early breast cancer, and a wide range of clinical presentations of high recurrence risk were well represented. The clinical experts consulted noted that the trial population was about a decade younger than patients with early breast cancer encountered in clinical practice — potentially explained by high-risk features being more prevalent in younger patients. The inclusion of younger and healthier patients may have led to a more favourable toxicity profile where more AEs were manageable, and reversible. Unlike the monarchE trial that implemented standardized Ki-67 central testing, Ki-67 testing is not routinely performed in clinical practice and its reproducibility is affected by several factors, including time and method of biopsy, specimen preparation, and assay used.
Conclusions
Based on data from the monarchE trial, abemaciclib plus ET demonstrated a statistically significant and clinically meaningful benefit compared to ET alone in improving IDFS in people with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score of 20% or more. DRFS was tested outside the statistical hierarchy but appeared to be supportive of the primary efficacy results. It is not yet clear whether IDFS benefits will translate to improved OS as the data remain immature; follow-up is ongoing. The safety profile of abemaciclib was consistent with the known adverse effects profile of abemaciclib. Effects on health-related quality of life (HRQoL) and health resource utilization remain uncertain due to high attrition and a lack of between-group statistical testing for these outcomes. Although a much longer follow-up time will likely be needed to determine the efficacy of abemaciclib plus ET in terms of OS, given the slow event rate in this setting, abemaciclib in addition to ET in this new indication could help optimize adjuvant treatment to improve outcomes in terms of disease recurrence. Uncertainties remain regarding the validity and generalizability of Ki-67 testing and practical considerations for its implementation in clinical practice in terms of determining patient eligibility for abemaciclib treatment.
Introduction
Disease Background
Breast cancer is the most commonly diagnosed cancer among women in Canada, and the second most common cancer in men and women combined.1 In 2020, 27,700 women were diagnosed with breast cancer, representing about 25% of new cancer cases in Canada.1 Breast cancer is the second leading cause of cancer deaths among women, accounting for 14% of all cancer deaths.1 It is estimated that about 1 in 8 (12%) women living in Canada will develop breast cancer during their lifetime and 1 in 34 (3%) will die of it.1 The 5-year net survival for breast cancer is more than 85% among women diagnosed before 85 years of age, after which it drops to about 73%.1 In men, the incidence of breast cancer is less than 1% per year, with 260 new cases diagnosed in 2021 in Canada.1 Breast cancer risk is influenced by several factors, including aging, family history, reproductive status (e.g., late menopause), hormone exposures (e.g., estrogen), and lifestyle factors such as alcohol intake and physical inactivity.5
Patients with breast cancer are stratified and treated based on the expression status of certain tumour receptors that have been shown to be important prognostic and predictive biomarkers. These include ER and PR; HR-positive breast cancers are those that express ER or PR or both.3 These tumours are the most prevalent type of breast cancer, accounting for 70% to 80% of all breast cancers, and can often be treated successfully with a variety of drugs that modulate ER or reduce estrogen, known as ET or anti-estrogen therapy.2 Overexpression of the HER2 oncogene — which belongs to the EGFR/HER family and enables constitutive activation of growth factor that signals and triggers breast cancer cell survival, proliferation, and invasion — is associated with poor prognosis.3 Approximately 85% of patients with breast cancer do not have tumours that overexpress HER2 and are HER2-negative.3 HR-positive, HER2-negative tumours are the most common subtype of breast cancer, accounting for approximately 70% of cases.4
Anatomical staging of breast cancer is based on the size and extent of the breast tumour (T), the extent of regional lymph node involvement (N), and the presence or absence of distant metastases (M). These features are assigned individual scores and then combined to identify the stage (i.e., TNM staging).17 More than 90% of patients with breast cancer are diagnosed with early-stage disease, which is defined as not having spread beyond the breast tissue or nearby lymph nodes.3 Early breast cancer includes ductal carcinoma in situ (stage 0) and stage I to stage IIIA, but may also include only invasive cancers within stage I to stage IIIC, excluding stage 0.3 Unlike patients with distant metastatic disease, early-stage breast cancer is potentially curable. In patients with HR-positive, HER2-negative early breast cancer, the 5-year survival rate is 94.3%.5
Although many patients with HR-positive, HER2-negative disease will not experience recurrence or have distant recurrence with standard therapies alone, around 7% to 11% of patients with early breast cancer experience a local recurrence during the first 5 years after treatment.6 Nearly 30% of patients eventually experience disease relapse with metastases following treatment with curative intent, often with distant metastases, at which time their prognosis is poor.6 Larger tumour size (> 2 cm), a higher number of lymph nodes affected, and/or patients receiving ET for a short period of time after surgery are associated with a higher risk of late recurrence (after 5 years).18 The risk of breast cancer recurrence is frequently predicted based on TNM staging, HR status, and genomic profiling.3 The clinical experts consulted by CADTH noted that some multiparameter gene expression assays such as the Oncotype Dx test may be used to guide adjuvant treatment decisions. Risk factors for recurrence include large tumour size, a higher degree of involvement of ALNs, a high histologic grade, positive or close margins, age, HR and HER2 status (positive), and a high tumour proliferation rate (Ki-67).7-11 Ki-67 IHC testing is used in diagnostic work-up of a variety of tumours, including breast cancer. Ki-67 is a marker of cellular proliferation and is a prognostic factor for the risk of recurrence during the first 5 years following primary breast cancer treatment.10 Although there is no uniformly accepted threshold of Ki-67 levels indicative of a high risk of recurrence, the International Ki-67 in Breast Cancer Working Group (IKWG) consensus was that Ki-67 expression of more than 30% can be used to identify high-risk patients.19 However, the use of IHC Ki-67 testing in Canadian clinical practice is currently limited due to geographical variability in routine testing and a lack of standardized laboratory assays.
Standards of Therapy
Patients diagnosed with HR-positive, HER2-negative early breast cancer are typically treated with curative intent with definitive surgery (lumpectomy and/or mastectomy), which may be preceded by neoadjuvant chemotherapy and/or ET and followed by a combination of adjuvant ET with or without radiotherapy and chemotherapy. Premenopausal women may receive concurrent ovarian suppression or ablation (bilateral salpingo-oophorectomy) to improve outcomes. Adjuvant bisphosphonate may be considered in postmenopausal women.20,21
Adjuvant ET is the standard of care for the systemic treatment of patients with HR-positive, HER2-negative early breast cancer.18,20,21 Regimens may include tamoxifen and/or 1 of 3 aromatase inhibitors (AIs): anastrozole, letrozole, or exemestane. The choice of endocrine drug is primarily determined by the patient’s menopausal status.18,20,21 Following primary local therapy, ET is administered for at least 5 years and for up to 10 years; extended ET (10 years) is recommended for patients with node-positive tumours.18,20,21 The clinical experts consulted by CADTH noted common tolerability issues with ET, such as low-estrogen symptoms, arthralgias, and mood disturbances, particularly in young or premenopausal women. Based on input received from the clinical experts consulted by CADTH, in patients with breast cancer gene–positive (BRCA-positive) tumours, there may be a future role for adjuvant olaparib; however, this regimen has not been reviewed by CADTH in the suggested setting and is currently not reimbursed. Treatment of men with breast cancer is similar to that of postmenopausal women. In men, the use of androgen suppression with gonadotropin-releasing hormone (GnRH) agonists could be considered.18
Neoadjuvant treatments have the goal of improving surgical outcomes, while adjuvant treatments are intended to eradicate micrometastatic disease and prevent distant recurrence. Patients considered at high risk of recurrence generally receive more extensive and aggressive adjuvant treatment with ET and chemotherapy. The clinical experts consulted by CADTH noted that most patients with 4 or more positive lymph nodes will receive chemotherapy unless contraindicated. Given the increased risk of recurrence in patients with high-risk clinicopathologic features, the clinical experts consulted by CADTH agreed that optimizing adjuvant therapy to prevent or delay recurrence and prolong survival with an acceptable toxicity profile and improvement in quality of life are the most important treatment goals.
Drug
Abemaciclib (Verzenio) is an orally available, selective, and potent ATP-competitive inhibitor of cyclin-dependent kinases (CDKs) 4 and 6 that blocks retinoblastoma (Rb) protein phosphorylation; this prevents cancer cell proliferation by arresting the cell cycle in the G1 phase, thereby suppressing DNA synthesis and inhibiting cancer cell growth.18 Longer treatment with abemaciclib can lead to prolonged antitumour effects by inducing senescence, apoptosis, and modification of cellular mechanism.18,22
Abemaciclib received a Notice of Compliance from Health Canada on January 12, 2022, for use in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of recurrence based on clinicopathological features and a Ki-67 score of at least 20%.18 The sponsor’s requested reimbursement criteria for abemaciclib are as per the Health Canada–approved indication. Abemaciclib is the first and only CDK4 and CDK6 inhibitor approved for the adjuvant treatment of early breast cancer in Canada.
In October 2021, the US FDA approved abemaciclib with ET (tamoxifen or an AI) for adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence and with a Ki-67 score of 20% or more, as determined by an FDA-approved test.23 Abemaciclib is the first CDK4 and CDK6 inhibitor approved for adjuvant treatment of breast cancer in the US.23 In February 2022, the European Medicines Agency’s Committee for Medicinal Products for Human Use recommended abemaciclib in combination with ET as adjuvant treatment for patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk for recurrence.24
Abemaciclib is supplied as tablets (50 mg, 100 mg, 150 mg, and 200 mg) for oral administration.25 The recommended dosage of abemaciclib in combination with ET for early breast cancer is 150 mg taken orally twice daily until completion of either 2 years of treatment or until disease recurrence or unacceptable toxicity.25
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Two patient groups, Rethink and the CBCN, submitted patient input for this review. Rethink gathered data through general observations and meetings with patients with breast cancer as well as via telephone interviews with 2 patients who had experience taking abemaciclib for HR-positive, HER2-negative, high-risk early breast cancer, and 1 patient to whom abemaciclib had been prescribed, but who had not initiated treatment with it yet. CBCN conducted an online survey, with responses from 103 patients in Canada with early-stage HR-positive, HER2-negative breast cancer. Most participants in the CBCN survey indicated having been diagnosed with stage II cancer, followed by those diagnosed with stage I, and stage III cancer. Few respondents to the survey did not specify their cancer stage. None of the 103 participants had direct experience with abemaciclib treatment.
According to Rethink, a breast cancer diagnosis and treatment has a devasting and traumatic impact on a young person’s life and many patients express a willingness to take on whatever treatments are needed to lower the chance of recurrence. Rethink indicated that most of their patients are diagnosed at a younger age, which can lead to age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, childcare, an impact on relationships, body image, dating and sexuality, feeling isolated from peers, career hiatuses, and financial insecurity. Most CBCN survey respondents reported having undergone surgery (91%), radiation therapy (57%), chemotherapy (53%), and ET (77%) as part of their overall breast cancer treatment. According to CBCN, side effects of HR-positive breast cancer and the therapies used to treat this disease include hot flashes, night sweats, vaginal dryness, gastrointestinal symptoms, nausea, vomiting, constipation, weakness, fatigue, and a risk of blood clots.
Rethink indicated that the 2 patients who had experience with abemaciclib indicated that they were willing to endure the additional side effects of a stronger therapy to ensure they were doing everything they could to treat what they know is an aggressive form of breast cancer. Both patients reported an overall positive experience taking abemaciclib and would recommend it to other patients. One patient reported being tired as a side effect of abemaciclib treatment.
According to the CBCN patient input received, survey respondents reported that the following factors were the most important when considering treatment options: having the most effective treatment possible, reducing the risk of recurrence, maintaining quality of life, having manageable side effects, and having affordable and accessible treatments. Maintaining mobility, productivity, and an ability to continue childcare duties were also highlighted by survey respondents as important when deciding on treatment options. CBCN noted that patients have an expectation that abemaciclib will provide a possibility for improving their rate of IDFS and reduce their risk of recurrence, allowing them to live a better quality of life. A copy of the 2 original full patient inputs is presented in the Stakeholder Input section of the CADTH report.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of breast cancer.
Unmet Needs
The clinical experts consulted by CADTH noted that there is a significant recurrence risk in patients with high-risk clinicopathologic features. DFS is prolonged with extended adjuvant ET (though it is largely driven by a decrease in second cancers rather than recurrence), but no clear benefit in OS is observed. It was further noted by the clinical experts that very few treatments developed in recent years have improved survival or quality of life in the adjuvant breast cancer setting and, therefore, there is a need for treatments that improve survival outcomes. Tolerability issues such as low-estrogen symptoms, arthralgias, and mood disturbances are common with current treatments, particularly in young and premenopausal women. Drugs that can prolong time to recurrence without compromising quality of life are highly desired.
Place in Therapy
The clinical experts indicated that the mechanism of action of abemaciclib is new in this setting. As it is a new indication, abemaciclib is not reserved for patients who are intolerant to other treatments. It was also noted by the clinical experts that for eligible patients, abemaciclib would be added to standard adjuvant ET (tamoxifen or AI such as letrozole, anastrozole, or exemestane with or without ovarian suppression). The experts agreed that it would not be appropriate to try other treatments before initiating abemaciclib treatment because there is no comparable alternative to abemaciclib in this setting.
Patient Population
The clinical experts consulted by CADTH agreed that eligible patients would be those who meet the monarchE trial inclusion criteria. Namely, these are high-risk patients, both male and female, with HR-positive, HER2-negative breast cancer (with “high risk” defined as grade 3, ≥ 4 ipsilateral axillary positive nodes, and tumour ≥ 5 cm or high ki-67 [≥ 20%]), and patients who have had surgery and, as indicated, radiotherapy and/or adjuvant or neoadjuvant chemotherapy. It was noted by the clinical experts that Ki-67 testing required to define high-risk patients is available in most centres but not routinely performed on all cases. The clinical experts noted that problems with Ki-67 test standardization may complicate the composite definition of high risk. The clinical experts highlighted that, based on the monarchE trial data, certain lower-risk patient subgroups — including those with smaller tumour size (2 cm to 5 cm), grade 1 tumours, and stage IIA disease — appear to derive less benefit in terms of IDFS.
Assessing Response to Treatment
The clinical experts consulted by CADTH noted that since the current indication is for the adjuvant setting, where patients are free of detectable tumours, treatment “response” cannot be assessed. It was agreed by the clinical experts that treatment benefit would be measured by the absence of recurrence and death. The clinical experts noted that the primary outcome of IDFS in the monarchE trial is an accepted end point in recent clinical trials in this setting. Importantly, data on OS, HRQoL, and long-term IDFS are needed to determine the efficacy of abemaciclib in this setting.
Discontinuing Treatment
The clinical experts consulted by CADTH noted that disease progression and severe or intolerable toxicity would be factors to consider when deciding to discontinue treatment with abemaciclib.
Prescribing Conditions
The clinical experts consulted by CADTH noted that abemaciclib treatment requires ongoing monitoring and should be prescribed by a medical oncologist or a general practitioner in oncology in an outpatient clinic setting.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Clinician group input was received from the Ontario Health–Cancer Care Ontario Breast Cancer Drug Advisory Committee, with 3 clinicians contributing to the submission. The clinician group noted that up to 30% of patients with high-risk clinical and/or pathologic features may experience distant recurrence and stated that there is a need for superior treatment options to prevent early recurrence and improve survival. Patients most likely to benefit from abemaciclib would be those with HR-positive, HER2-negative early breast cancer at high risk of recurrence who are node-positive as per the inclusion criteria of the monarchE trial. Patients who are least suitable for abemaciclib would be those excluded from enrolment as per the monarchE trial eligibility criteria. Abemaciclib would be used in addition to ET in high-risk patients following surgery and chemotherapy (if applicable). The clinician group noted that clinicians with experience treating breast cancer, access to laboratory blood work, and expert pharmacy support would be required to diagnose, treat, and monitor patients. The group also stated that monitoring for hematologic toxicity, diarrhea, and extra visits would be required to assess patients for toxicity. The clinician group input strongly recommended against the inclusion of high Ki-67 as the sole criteria for drug eligibility, noting that Ki-67 was a prognostic factor for recurrence in the target setting and not predictive of treatment effect and that it is not a standard pathology test for breast cancer in Ontario.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
In the trial, patients must have been assigned within 16 months of definitive breast cancer surgery. What is the maximum allowable time frame since surgery to be eligible for abemaciclib? | According to the inclusion criteria of the monarchE trial, patients had to be randomized within 16 months from the time of definitive breast cancer surgery. The clinical experts felt that the trial inclusion criteria were reasonable. |
Can patients be re-treated again with CDK4 and CDK6 inhibitors in the metastatic setting? If yes, what is the minimum disease-free interval requirement? | CDK4 and CDK6 inhibitors are currently approved and funded in the metastatic breast cancer setting (first-line or second-line). Re-treatment with a CDK4 and CDK6 inhibitor may be reasonable if disease recurrence is > 12 months post-completion of adjuvant abemaciclib. |
Considerations for discontinuation of therapy | |
If a patient experiences an interruption within the 2 years from starting treatment, do you give a total of 2 years of abemaciclib or complete 2 years of abemaciclib from the start of treatment? | It would be reasonable to resume treatment with abemaciclib for 2 years total post-interruption for toxicity. However, resuming treatment post-interruption may not be appropriate in all cases and is likely up to the discretion of the treating physician. |
Care provision issues | |
Ki-67 testing may not be routinely performed on breast cancer samples. Is Ki-67 testing required to be completed on patients who may be eligible for abemaciclib? | Ki67 testing should be performed since Ki-67 was 1 of the inclusion criteria and the benefit is claimed based on a Ki-67 threshold. |
System and economic issues | |
The addition of abemaciclib to endocrine therapy could have a substantial impact on budget. | For pERC consideration. |
pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee.
Clinical Evidence
The clinical evidence included in the CADTH review of abemaciclib includes the following 3 sections: a systematic review of pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol; indirect evidence from the sponsor (if submitted) and indirect evidence selected from the literature that met the selection criteria specified in the review; and sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To evaluate the efficacy and safety of abemaciclib in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki67 score of 20% or more
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criterion | Description |
|---|---|
Population | Adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki67 test score ≥ 20% Subgroups of interest:
|
Intervention | ET + abemaciclib 150 mg administered orally twice daily for 2 years |
Comparators |
|
Outcomes | Efficacy and patient-reported outcomes
Harms outcomes
Notable harms
|
Study designs | Published and unpublished phase III and phase IV randomized controlled trials |
AI = aromatase inhibitor; BSO = bilateral salpingo-oophorectomy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ET = endocrine therapy; HRQoL = health-related quality of life; OFS = ovarian function suppression; SERM = selective estrogen receptor modulator; vs. = versus.
The literature search was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.26
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the US National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was Verzenio (abemaciclib). Clinical trials registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on April 21, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on August 10, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist.27 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 633 studies were identified from the literature for inclusion in the systematic review (Figure 1). Seven reports of a single study (monarchE) were included.14-16,18,28-30 The included study is summarized in Table 6.
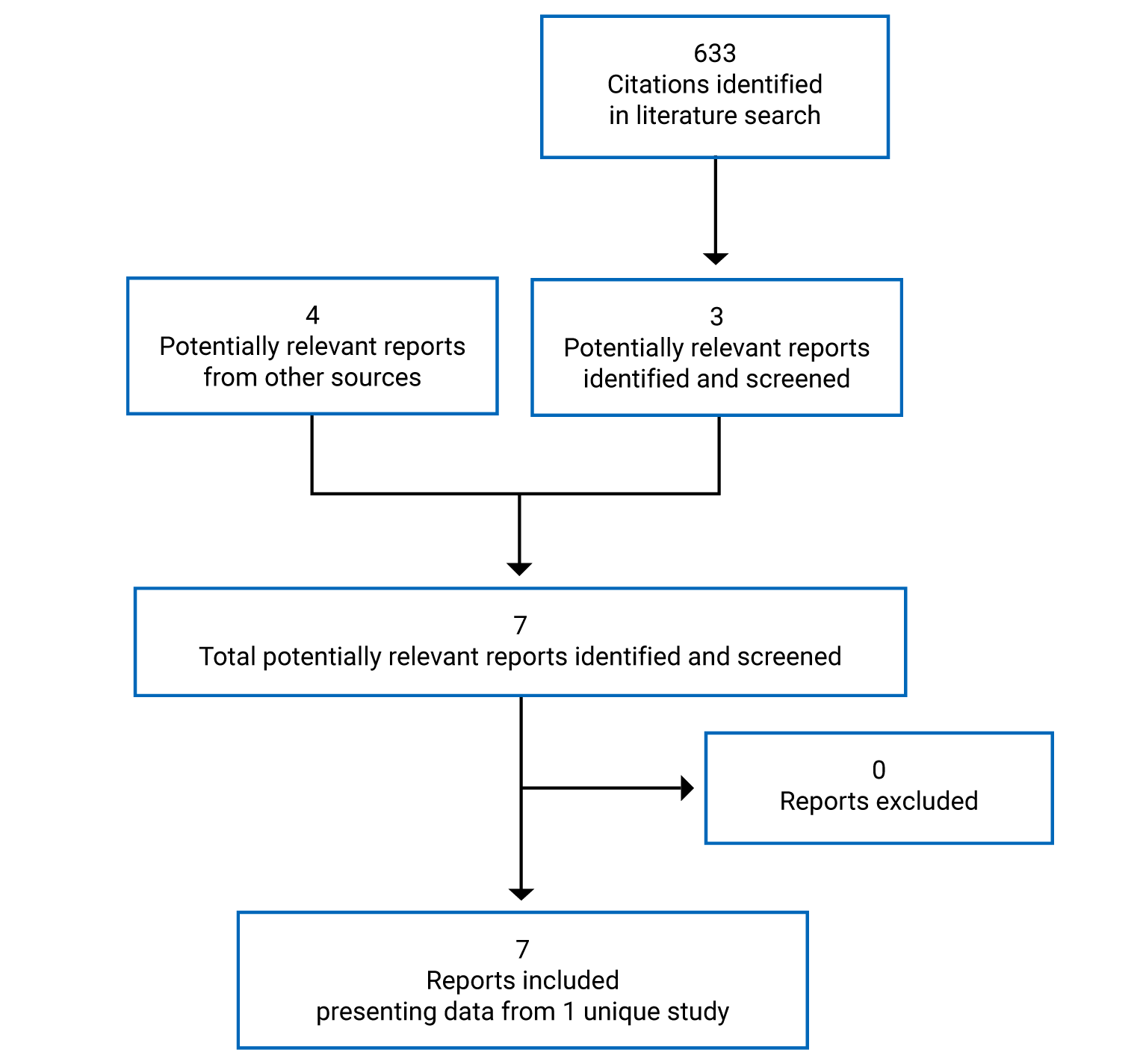
Table 6: Details of the monarchE Study
Detail | Design and population |
|---|---|
Study design | Phase III, open-label, multi-centre RCT |
Locations | 603 sites in 38 countries (Argentina, Australia, Austria, Belgium, Brazil, Canada [|| patients], China, Czech Republic, Denmark, Finland, France, Germany, Greece, Hong Kong, Hungary, India, Israel, Italy, Japan, South Korea, Mexico, the Netherlands, New Zealand, Poland, Portugal, Puerto Rico, Romania, Russia, Saudi Arabia, Singapore, South Africa, Spain, Sweden, Taiwan, Turkey (Türkiye), Ukraine, the UK, and the US) |
Study duration | July 12, 2017, to ongoing |
Data cut-off date | IDFS interim analysis 2: March 16, 2020 IDFS preplanned primary outcome final analysis (at approximately 390 IDFS events): July 8, 2020 OS interim analysis conducted at regulatory request: April 1, 2021 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Number of patients randomized (randomization ratio) | 5,637 (1:1) |
Main inclusion criteria |
|
Main exclusion criteria |
|
Drugs | |
Intervention | Abemaciclib 150 mg orally twice daily with at least 6 hours between doses (up to 2 years or until discontinuation criteria are met) combined with standard adjuvant ET (of physician’s choice) until discontinuation criteria are met (≥ 5 years) |
Comparator | Standard adjuvant ET (of physician’s choice) until discontinuation criteria are met (≥ 5 years) |
Duration | |
Phases | |
Screening | Cohort 1 = 3 months; Cohort 2 = 6 months |
Open-label | Standard adjuvant ET (of physician’s choice) until discontinuation criteria are met (≥ 5 years) in both treatment arms and abemaciclib daily (2 years) |
Follow-up | Visits every 6 months until year 5 and then annually from year 6 to year 10 |
Outcomes | |
Primary end point | IDFS in the ITT population |
Secondary end points |
|
Safety end points |
|
Notes | |
Publications | Johnston et al. (2020)30 Harbeck et al. (2021)29 Rugo et al. (2022)28 |
AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; DCIS = ductal carcinoma in situ; DRFS = distant relapse–free survival; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ET = endocrine therapy; EQ-5D-5L = EQ-5D Five-Level; FACIT = Functional Assessment of Chronic Illness Therapy; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue; FACT-B = Functional Assessment of Cancer Therapy – Breast; FACT-ES = Functional Assessment of Cancer Therapy – Endocrine Symptoms; GnRH = gonadotropin-releasing hormone; HRQoL = health-related quality of life; ITT = intention to treat; IDFS = invasive disease–free survival; OS = overall survival; RCT = randomized controlled trial; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Source: Clinical Study Report for Verzenio (interim analysis 2).14
Description of the monarchE Study
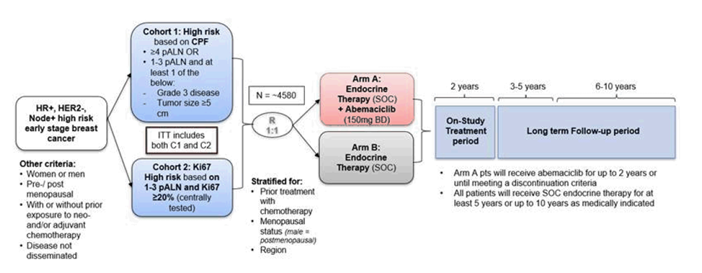
The monarchE study is a multi-centre, randomized, open-label, phase III study that compares the efficacy of abemaciclib plus standard adjuvant ET to ET alone in patients with node-positive, invasive, resected, HR-positive, HER2-negative early breast cancer who completed definitive locoregional therapy, with or without neoadjuvant or adjuvant chemotherapy, and whose cancer was at high risk of disease recurrence. The trial was conducted across 603 sites in 38 countries; || patients were recruited in Canada. The primary outcome was IDFS in the intention-to-treat (ITT) population.
Treatment with abemaciclib was given for up to 2 years or until discontinuation criteria were met, whichever occurred first. The duration of 2 years was selected based on previous studies that showed patients with early breast cancer taking ET experienced an initial peak of recurrence at 2 years of treatment. The goal of monarchE was to treat through the first peak of recurrence. The choice of ET, such as tamoxifen or an AI, was at the investigator’s discretion and was taken as prescribed during the on-study treatment period, year 1 and year 2. In year 3 and beyond, ET was continued for a total duration of at least 5 years and up to 10 years, if deemed medically appropriate.
Randomization and treatment allocation: An interactive web response system was used to randomly assign patients in a 1:1 ratio within each cohort to either up to 2 years of oral abemaciclib at 150 mg twice daily and ET or ET alone using the following stratification factors: prior treatment (neoadjuvant chemotherapy versus adjuvant chemotherapy versus no chemotherapy), menopausal status (premenopausal versus postmenopausal), and region (North America or Europe versus Asia versus other). Patients receiving standard adjuvant ET at the time of study entry may not have received more than 12 weeks of standard adjuvant ET after completion of their last non-ET (surgery, chemotherapy, or radiation) before randomization. Randomization had to occur within a maximum of 16 months following the definitive breast cancer surgery. Patients were randomized into 2 cohorts: Cohort 1 included patients at high risk of recurrence based on high-risk clinicopathologic features and Cohort 2 included patients at high risk of recurrence based on a high Ki-67 index (≥ 20%).
Blinding: This was an open-label study; patients were aware of their assigned treatment group and all staff at each investigative site involved in treating and caring for study patients had full knowledge of the patient’s treatment assignment. An open-label design was chosen because toxicities and laboratory abnormalities related to abemaciclib treatment, such as diarrhea, neutropenia, and creatinine increase, had the potential to unblind the study. The sponsor was blinded to treatment group assignment until the study reached a positive outcome. An independent data monitoring committee was responsible for reviewing the unblinded safety and efficacy analyses.
Study phases: The screening phase was 3 months for Cohort 1 and 6 months for Cohort 2. The treatment phase started with the first dose of treatment following randomization (i.e., abemaciclib and ET or ET alone in the intervention and control arms, respectively). The first dose of abemaciclib plus ET was initiated no later than 3 days following randomization. During year 1 and year 2 (the on-study treatment period), patients returned to a clinic every 2 weeks (15 days ± 3 days) for the first 2 months, monthly (30 days ± 5 days) starting with month 3 to month 6, and every 3 months thereafter (every 90 days ± 10 days until visit 27). After a short-term follow-up visit that took place 30 days after discontinuation or after completion of the on-study treatment period, all patients entered the long-term follow-up period that will continue for up to 10 years or until study completion, with long-term follow-up visits occurring approximately every 6 months until the completion of year 5 and then yearly starting in year 6 (Figure 2).
Protocol Amendments
There were modifications to the statistical analysis plan (SAP) for the study that were documented in the SAP amendments. Amendments (from least to most recent) included the following: the exclusion of patients with a history of VTE and safety guidance in reference to VTEs and increased alanine transaminase (October 11, 2018); the inclusion of dose suspension recommendations for patients undergoing surgery (June 29, 2018); the inclusion of Cohort 2 in the ITT population and updates for the eligibility of patients with positive anterior margins of the primary breast tumours (December 19, 2018); and the addition of ILD or pneumonitis as a new AE (June 29, 2019). The most recent amendment (version 5, June 5, 2020) was made after the database lock for the second interim analysis for efficacy. The most important amendment to the SAP concerned analysis of OS. At the FDA’s request in November 2020, an OS interim analysis was added to the protocol-specified main OS analyses. This additional interim OS analysis with the April 1, 2021, data cut-off date was documented in an SAP addendum approved in December 2020. The number of OS events at final OS analysis was increased from 390 to 650 and an additional OS interim analysis (July 2023) was added to allow a yearly assessment of benefit-risk within the first few years of long-term follow-up. In the originally planned final OS analysis, the median follow-up in the study population would have been less than 4 years; this was later deemed insufficient to adequately characterize OS in patients receiving adjuvant breast cancer therapy as the minimum standard time for follow-up is considered to be 5 years. Therefore, the amendment to the OS analyses was to ensure that OS can be characterized for at least 5 years, consistent with expectations from the medical and scientific community.
Figure 2: monarchE Study Design
BD = twice daily; C1 = Cohort 1; C2 = Cohort 2; CPF = clinical and/or pathological features; HER2– = HER2-negative; HR+ = HR-positive; ITT = intention to treat; pALN = positive axillary lymph node; pt = patient; R = randomization; SOC = standard of care.
Source: Clinical Study Report for Verzenio (interim analysis 2).14
Populations
Inclusion and Exclusion Criteria
Eligible patients were 18 years or older, with confirmed HR-positive, HER2-negative, resected invasive early breast cancer without metastases, who had undergone definitive surgery of primary breast tumour and randomized within 16 months of surgery, had an ECOG PS of 0 or 1, and adequate organ function. To be enrolled in 1 of the cohorts, patients had to fulfill 1 of the following criteria: 1) pathological tumour involvement in 4 or more positive ipsilateral ALNs, or 2) pathological tumour involvement in 1 ipsilateral ALN to 3 ipsilateral ALNs and either grade 3 disease, or primary tumour size of 5 cm or more. Patients eligible based on 1 to 3 positive ALNs (not grade 3 and not primary tumour size of 5 cm or more) who had a Ki-67 index of 20% or more were also eligible (Cohort 2). Patients were ineligible if they had metastatic disease, node-negative or inflammatory breast cancer, a previous history of breast cancer (with the exception of ipsilateral ductal carcinoma in situ treated by locoregional therapy alone at least 5 years ago), a history of any other cancer (except nonmelanoma skin cancer or carcinoma in situ of the cervix), concurrent exogenous reproductive hormone therapy, prior ET for breast cancer, or raloxifene or previous exposure to CDK4 and CDK6 inhibitors (Table 6).
The inclusion criteria for selecting the patient population at high risk of recurrence were based on unpublished efficacy outcome data from the West German Study Group PlanB trial and the NSABP B-28 trial. Among a subset of the PlanB patient population that satisfied the monarchE criteria for high-risk disease, the estimated 5-year IDFS rate was 82.5% (95% CI, 77.8% to 87.2%), suggesting that approximately 17.5% of those patients who were at high risk of recurrence would develop invasive recurrence events within the first 5 years.29
Patients were enrolled into 2 cohorts.
Cohort 1 (high risk based on clinicopathologic features): Patients were eligible based on clinicopathologic features such as the degree of ALN involvement, tumour size, grade, or a combination of any of those. This included patients with 4 or more positive ALNs, or 1 positive ALN to 3 positive ALNs and at least 1 of the following: a tumour size of 5 cm or more or histologic grade 3. Patients in Cohort 1 were not required to submit a tissue sample to the study’s central laboratory for Ki-67 testing before randomization, but a sample was requested, where available, to support the secondary analysis related to Ki-67.
Cohort 2 (high risk based on Ki-67 index): Patients were eligible based on having 1 positive ALN to 3 positive ALNs, and a centrally determined high Ki-67 index (≥ 20%). These patients would not have been eligible based on eligibility requirements for Cohort 1. Patients in Cohort 2 were required to submit an untreated breast tissue sample to the study’s central laboratory for central determination of Ki-67 status to deduce eligibility (tissue was to be submitted within 1 month of signing the consent). The sample was tested using the investigational in vitro diagnostic medical device pharmDx Ki-67 Kit, manufactured by Dako.
The ITT population includes all randomized patients in Cohort 1 and Cohort 2. The Cohort 1 Ki-67 High population includes all randomized patients in Cohort 1 with a centrally assessed Ki-67 score of 20% or more, which is aligned with both the Health Canada–approved indicated population and the current reimbursement request. Therefore, this CADTH clinical review focuses on efficacy results based on Cohort 1 patients with Ki-67 of 20% or more (Cohort 1 Ki-67 High population) in the main body of the report. The study was planned and powered based on the ITT population and the statistical testing hierarchy included the ITT population, the ITT Ki-67 High population (Cohort 1 + Cohort 2), and the Cohort 1 Ki-67 High population for IDFS. Some efficacy data from the ITT and ITT Ki-67 analysis populations are presented in Appendix 2 to provide fuller context.
Baseline Characteristics
Cohort 1 patients with a Ki-67 score of 20% or more (39.1% of the 5,120 patients randomized into Cohort 1) were predominantly female (99.2%) with a mean age of 51.6 years (SD = 11.1) and an ECOG PS of 0 (86.3%). More than half of the patients (54.4%) were postmenopausal. Most patients were diagnosed with invasive ductal breast carcinoma (75.5%) with a primary tumour size of 2 cm or more but less than 5 cm determined by pathology (52.9%). Almost all patients had positive ALNs (99.9%) — 57% of patients had 4 or more ALNs and 42.9% of patients had 1 positive ALN to 3 positive ALNs. The majority of patients (95.2%) had received prior radiotherapy — 36.9% of patients had received neoadjuvant chemotherapy and 60.2% of patients had received adjuvant chemotherapy (Table 7). Despite Ki-67 score (≥ 20% versus < 20%) not being a stratification factor (and therefore the population not being truly randomized), the available baseline characteristics appeared well balanced across groups.
The Cohort 1 Ki-67 High population had a lower incidence of invasive lobular breast carcinoma than the ITT population (6.5% versus 12.8%, respectively), with a corresponding higher incidence of invasive ductal breast carcinoma. The percentage of patients with histopathological grade 3 tumours at diagnosis was also higher in this population compared to the ITT population (58.0% versus 38.2%, respectively).
Table 7: Summary of Baseline Characteristics — Cohort 1 Ki-67 High Population
Characteristic | Abemaciclib + ET arm N = 1,017 | ET arm N = 986 | Total N = 2,003 |
|---|---|---|---|
Age (years), mean (SD) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Sex, female n (%) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Region, n (%) | |||
North America/Europe | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Asia | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Other | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Menopausal status, n (%) | |||
Premenopausal | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Postmenopausal | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Baseline ECOG PS, n (%) | |||
0 | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
1 | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Initial pathological diagnosis, n (%) | |||
Invasive ductal breast carcinoma | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Breast cancer | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Invasive lobular breast carcinoma | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Mucinous breast carcinoma | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Invasive papillary breast carcinoma | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Inflammatory carcinoma of the breast | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Medullary carcinoma of the breast | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Tubular breast carcinoma | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Paget disease of nipple | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Metastatic breast carcinoma | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Primary tumour size by pathology after definitive surgery, n | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
< 20 mm | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
≥ 20 mm but < 50 mm | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
≥ 50 mm | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Number of positive lymph nodes, n (%) | |||
0 | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
1 to 3 | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
4 to 9 | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
≥ 10 | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Histopathological diagnosis grade, n | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
G1: Favourable | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
G2: Moderately favourable | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
G3: Unfavourable | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
GX: Cannot be assessed | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Disease stage at initial diagnosis, n | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Stage IA | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Stage IIA | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Stage IIB | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Stage IIIA | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Stage IIIB | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Stage IIIC | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Progesterone receptor status, n | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Positive | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Negative | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Unknown | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Prior chemotherapy, n (%) | |||
Neoadjuvant chemotherapy | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Adjuvant chemotherapy | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
No chemotherapy | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Prior radiotherapy | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Interventions
Abemaciclib Plus Endocrine Therapy Arm
Treatment consisted of abemaciclib 150 mg administered orally, twice daily, with at least 6 hours separating doses. Treatment with abemaciclib was given for up to 2 years or until discontinuation criteria were met. Standard adjuvant ET of a physician’s choice, such as letrozole, anastrozole, exemestane, or tamoxifen with or without GnRH agonist, was taken as prescribed during the on-study treatment period (year 1 to year 2). In year 3 and beyond, standard adjuvant ET was continued to complete at least 5 years and up to 10 years if this was medically appropriate. Treatment with ET was given until discontinuation criteria were met. Adjuvant treatment with fulvestrant was not allowed at any time during the study.
If a patient discontinued only 1 of the combination drugs (abemaciclib or ET) before completion of the 2-year on-study treatment period for a reason other than an IDFS event, the patient had to continue the other drug until completion of the 2-year on-study treatment period or until other discontinuation criteria were met, whichever occurred first. The study protocol included instructions for mandated abemaciclib dose modifications (holds and reductions) to manage AEs, with a maximum of 2 dose reductions. Patients requiring more than 2 dose reductions were required to discontinue abemaciclib. Study treatment could be held for up to 28 days to permit sufficient time for recovery from toxicity. For patients not recovering from toxicity within 28 days, a delay of more than 28 days was permitted after agreement with the investigator and the sponsor, abemaciclib dose adjustment was considered. Dose adjustment for ET was determined by the investigator and when applicable. A switch to another ET regimen was permitted per the physician’s choice as part of standard of care.
Endocrine Therapy Arm
Standard adjuvant ET of a physician’s choice, such as letrozole, anastrozole, exemestane, or tamoxifen with or without GnRH agonist, was taken as prescribed during the on-study treatment period (year 1 to year 2). In year 3 and beyond, standard adjuvant ET was continued to complete at least 5 years and up to 10 years if this was medically appropriate. Treatment with ET was given until discontinuation criteria were met. Adjuvant treatment with fulvestrant was not allowed at any time during the study. Dose adjustment for ET was determined by the investigator and when applicable. A switch to another ET regimen was permitted per the physician’s choice as part of standard of care.
Concomitant Treatments
All concomitant medications and supportive care therapies were documented at each visit. In general, the list of prohibited medications that affected patient eligibility or participation in the study were limited to ET for breast cancer prevention, concurrent exogenous reproductive hormone therapy, and recent experimental treatment in a clinical trial. Concurrent treatment with standard of care bone-modifying drugs such as bisphosphonates and denosumab was permitted. With the exception of standard ET for breast cancer, no other anticancer therapy was permitted while patients were on study treatment. Patients could receive full supportive care to maximize quality of life (e.g., antiemetics, standard of care bone-modifying drugs) based on the judgment of the treating physician. Patients in the abemaciclib plus ET arm received instructions on the management of diarrhea and were prescribed antidiarrheal therapy (e.g., loperamide) on their first visit.
Study Treatment Discontinuation
Patients would be discontinued from study treatment in the following circumstances.
The patient was enrolled in any other clinical trial involving an investigational product or any other type of medical research judged not to be scientifically or medically compatible with this study.
Investigator decision: If the investigator decided that the patient should be discontinued from the study or study treatment, or if the patient, for any reason, required treatment with another therapeutic drug that had been demonstrated to be effective for treatment of the study indication, discontinuation from the study drug occurred before introduction of the new drug.
Patient decision: If the patient requested to be withdrawn from the study or study treatment, this was done.
Sponsor decision: The sponsor could stop the study or the patient’s participation in the study for medical, safety, regulatory, or other reasons consistent with applicable laws, regulations, and good clinical practice.
The patient became pregnant during the study.
The patient was significantly non-compliant with study procedures and/or treatment.
The patient experienced any of the IDFS events as per Standardized Definitions for Efficacy End Points (STEEP) in adjuvant breast cancer trials criteria.
There was unacceptable toxicity.
Outcomes
The efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial included in this review are summarized as follows.
Efficacy
The primary end point was IDFS in the ITT population. The secondary efficacy end points were DRFS in the ITT population, OS in the ITT population, and IDFS in the Ki-67 High population (Cohort 1 + Cohort 2) and the Ki-67 High population (Cohort 1). Other secondary end points included HRQoL and health care resource utilization assessed in the safety population.
IDFS was defined per the STEEP criteria33 and measured from the date of randomization to the date of first occurrence of the following factors:
ipsilateral invasive breast tumour recurrence — local recurrence, defined as invasive breast cancer in the ipsilateral breast parenchyma or invasive breast cancer in the skin of the breast or the chest wall occurring after a lumpectomy and/or mastectomy
regional invasive breast cancer recurrence — defined as the development of a tumour in the axilla, regional lymph nodes (internal mammary, supraclavicular, infraclavicular), and the soft tissue of the ipsilateral breast following surgery
distant recurrence — defined as evidence of tumour in all areas other than the ones qualifying for local or regional recurrence as described previously
death attributable to any cause, including breast cancer, non-breast cancer, or unknown cause
contralateral invasive breast cancer
second primary non-breast invasive cancer.
Confirmation by biopsy or imaging was required, when possible. During treatment and follow-up, imaging was to be performed per the investigator’s judgment and according to routine standard practice. All imaging was done locally and, therefore, no central imaging assessments were performed. All patients who experienced local recurrence continued to be followed for distant recurrence. Patients for whom no event had been observed were censored at the date of their last post-baseline assessment for disease recurrence or date of randomization if no post-baseline assessment for disease recurrence had occurred. For patients who experienced an IDFS event other than distant recurrence or death, assessments continued to be performed until there was an event of distant recurrence, death, or study completion, whichever occurred first.
DRFS was defined as the time from randomization to distant recurrence or death attributable to any cause, whichever occurred first. Patients for whom no event was observed were censored on the day of their last assessment for recurrence or date of randomization if no post-baseline assessment for recurrence occurred.
The OS time was measured from the date of randomization to the date of death from any cause. For each patient who was not known to have died as of the data cut-off date for a particular analysis time point, OS was censored for that analysis at the date of the last contact before the data cut-off date.
During year 1 and year 2 (the on-study treatment period), patients returned to a clinic every 2 weeks (15 days ± 3 days) for the first 2 months, monthly (30 days ± 5 days) starting with month 3 to month 6, and every 3 months thereafter (every 90 days ± 10 days until visit 27). Phone visits were conducted monthly between the every 3 month visits. Patients had a short-term follow-up visit that took place approximately 30 days after 1 of the following time points, whichever occurred first: after the completion of the 2-year on-study treatment period, or after discontinuation criteria were met and a decision was made for the patient to discontinue all study treatment before the completion of the 2-year on-study treatment period. After the short-term follow-up visit, all patients entered the long-term follow-up period, which began the day after the short-term follow-up visit and that will continue for up to 10 years or until study completion, whichever occurs first. Long-term follow-up visits occur approximately every 6 months until the completion of year 5 and then yearly starting in year 6.
The PRO assessment aimed at assessing the effects of treatment on patient-reported HRQoL and AEs. The FACT-B 37-item questionnaire was used to evaluate the 2 treatment arms in terms of general oncology and breast cancer self-reported HRQoL. The summary scores are presented for the FACT-B total score (a score range of 0 to 148), physical well-being (a score range of 0 to 28), social well-being (a score range of 0 to 28), emotional well-being (a score range of 0 to 24), and functional well-being (a score range of 0 to 28), as well as the breast cancer subscale (a score range of 0 to 40) and trial outcome index (a score range of 0 to 96).
The EQ-5D-5L questionnaire was used to evaluate patients’ health status to inform decision modelling for health economic evaluation. The EQ-5D-5L index values are summary scores based on a scale anchored at 0 being equivalent to death and 1 being full health. Negative values are deemed health states worse than death. The index values were calculated as per the EQ-5D-5L guidance using the published UK value set. The EQ Visual Analogue Scale (EQ VAS) is a measure of the patients’ self-reported health “today” (i.e., on the day of self-assessment) on a scale of 0 to 100, where 0 is the worst health you can imagine and 100 is the best health you can imagine. The EQ VAS score, based on the patient’s self-rated health today, serves to compliment the EQ-5D-5L single index score.
Health care resource utilization included self-reported hospitalizations and transfusions.
After the baseline assessment, PRO questionnaires were next administered to patients at visit 6, visit 9, visit 15, and visit 21 (18 months). Questionnaires were given at visit 27 (24 months) and follow-up visits but were not included in analyses due to less than 25% of patients having an assessment at those visits. Thus, the timing of assessments did not capture the effects of any AEs the patient might have experienced during the first 3 months.
Safety
AEs were graded according to the Common Terminology Criteria for Adverse Events version 4.0. TEAEs were defined as events that first occurred or worsened in severity while on therapy and until 30 days after treatment discontinuation, or serious events beyond 30 days of treatment discontinuation that were related to study treatment. SAEs were reported as treatment-emergent events on study and during the long-term follow-up period (up to 5 years after randomization). SAEs included AEs with an outcome of death, initial or prolonged hospitalization, or life-threatening events. All SAEs in both arms were and will continue to be collected from randomization through year 5. AEs leading to dose adjustments and discontinuation from study treatment due to AEs or death were also recorded. Second primary non-breast neoplasms were captured as AEs (in addition to being captured within the primary end point). Patients were followed up beyond 30 days post–study treatment discontinuation for SAEs regardless of causality to detect any long-term serious toxicities that are likely to be relevant for the adjuvant setting.
Statistical Analysis
Sample Size Calculations
The study was powered at approximately 85% to detect the superiority of abemaciclib plus ET versus ET alone in terms of IDFS in the ITT population, assuming a hazard ratio of 0.73 at a cumulative 2-sided alpha of 0.05, with a 5-year IDFS rate of 82.5% in the control arm, and a dropout probability rate of 10% over the first 5 years following randomization. This required approximately 390 events in the ITT population at the time of the primary analysis. Notably, the study was not powered for the reimbursement population of interest, which was the Cohort 1 Ki-67 High population.
Analyses of Outcomes
The IDFS analysis to test the superiority of abemaciclib with ET to ET alone was performed on the ITT population and used the log-rank test stratified by randomization factors. The 2 planned efficacy interim analyses and 1 planned final analysis for IDFS were to be performed after approximately 195 events, 293 events, and 390 events had been observed in the ITT population. The second efficacy interim analysis at approximately 293 IDFS events included both an efficacy criterion for statistical significance and a futility boundary. The cumulative 1-sided alpha was controlled at 0.025, with an alpha split of 0.00000001 for the first futility analysis and 0.02499999 for the planned efficacy analyses. The cumulative 1-sided type I error rate of 0.02499999 for the 2 planned efficacy interim analyses and 1 planned final analysis was maintained using the Lan-DeMets method (DeMets and Lan 1994).34 Specifically, the alpha spent at each efficacy interim analysis was based on the exact number of IDFS events observed using the O’Brien-Fleming type stopping boundary.
A sequential gatekeeping strategy was used to control the family-wise type I error at 0.025 (1-sided) for IDFS in the ITT, Ki-67 High, and Cohort 1 Ki-67 High populations. IDFS was tested hierarchically in the order of the ITT, Ki-67 High, then Cohort 1 Ki-67 High populations, each gated after the former population. IDFS in the Ki-67 High population was tested only if IDFS in the ITT population was significant, and IDFS in the Cohort 1 Ki-67 High population was tested only if IDFS in the Ki-67 High population was significant.
The Kaplan-Meier method was used to estimate the IDFS curve for each treatment arm. The difference between IDFS rates for each arm was reported with 95% CIs estimated by normal approximation. A stratified Cox proportional hazards model with treatment as a factor was used to estimate the hazard ratio between the 2 treatment arms and the corresponding CI and Wald P value.
Similar analyses were performed on DRFS but there was no alpha control to account for the risk of type I error.
For OS, a sequential gatekeeping strategy was used to test treatment effect on OS in the ITT population, to maintain the experiment-wise type I error rate. That is, only if the tests of IDFS in the ITT, Ki-67 High, and Cohort 1 Ki-67 High populations were all significant, OS (in the ITT population) would be hierarchically tested. Of note, analyses of OS in other populations (i.e., Ki-67 High population and Cohort 1 Ki-67 High population) were not part of the testing hierarchy and were not planned a priori. Analysis of OS in Cohort 1 Ki-67 High population, which is the focus of this CADTH review, was not controlled for multiplicity. At each analysis, the treatment effect on OS was tested using a 1-sided log-rank test stratified by randomization factors. The Kaplan-Meier method was used to estimate the OS curve for each treatment arm. The OS rates for each arm were compared using a normal approximation for the difference between the rates. A stratified Cox proportional hazards model with treatment as a factor was used to estimate the hazard ratio between the 2 treatment arms and the corresponding CI and Wald P values. The follow-up time for OS was defined from the date of randomization and used the inverse of censoring rules for OS. The median follow-up time was calculated using the Kaplan-Meier method. Per the last addendum to the SAP, the final OS analysis was defined as observing approximately 650 OS events, or 10 years after the last patient is randomized, whichever occurs first. The cumulative 1-sided type I error rate of 0.025 was maintained using the Lan-DeMets method34; the alpha spent at each interim analysis was calculated based on the actual number of events using the O’Brien-Fleming type stopping boundary.
The stratification factors for the analysis of primary and secondary end points were prior treatment (neoadjuvant chemotherapy versus adjuvant chemotherapy versus no chemotherapy), menopausal status (premenopausal versus postmenopausal), and region (North America or Europe versus Asia versus other). If a patient received both neoadjuvant and adjuvant chemotherapy, the patient was stratified as neoadjuvant chemotherapy. Male patients were stratified as postmenopausal at the time of randomization.
For HRQoL scores, a mixed effects model for repeated measures was applied to compare treatment arms by assessment with respect to each of the summary scores and select items. An effect size of one-half SD (SD = 0.5) was used to represent an MID. PRO data were analyzed at the pre-specified primary outcome analysis (data cut-off date: July 8, 2020).
AEs were summarized by maximum toxicity regardless of causality. TEAEs were summarized by system organ class and by decreasing frequency of preferred term within the system organ class. Preferred terms identified as clinically identical or synonymous were grouped together under a single consolidated PT. Descriptive statistics were used to summarize safety data.
With the exception of dates, missing data were not imputed.
Sensitivity Analyses
The following sensitivity analyses were performed on IDFS, DRFS, and OS: a log-rank test without stratification by randomization factors was performed to test the superiority of abemaciclib plus ET to ET alone on the ITT population, an unstratified Cox proportional hazards model with treatment as a factor was used to estimate the hazard ratio between the 2 treatment arms, and censoring for control arm patients receiving a CDK4 and CDK6 inhibitor was done. If a patient in the control arm received a CDK4 and CDK6 inhibitor before their first IDFS event, IDFS was censored at the date of the last disease assessment before the CDK4 and CDK6 inhibitor start date.
Subgroup Analyses
Subgroup analyses of IDFS in the ITT population were performed for preplanned subgroups according to menopausal status, primary tumour size, tumour grade, number of positive lymph nodes, PR status, and ECOG PS at baseline; these were subgroups of interest identified in the CADTH systematic review protocol. A similar statistical analysis approach to the main IDFS analysis was used. There was no multiplicity control. As such, all subgroup analyses were exploratory in nature.
Analyses
There were or are 6 planned interim analyses and 1 final analysis to test the null hypothesis, which occurred or will occur at the following time points:
IDFS efficacy interim analysis 1 — approximately 195 IDFS events (the data cut-off date: September 27, 2019)
IDFS efficacy interim analysis 2 — approximately 293 IDFS events (the data cut-off date: March 16, 2020)
final IDFS analysis — approximately 390 IDFS events (the data cut-off date: July 8, 2020)
OS interim analysis 1 (an additional follow-up analysis conducted at regulatory request; the data cut-off date: April 1, 2021).
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Analysis Populations
The ITT population (N = 5,637) includes all randomized patients in Cohort 1 (N = 5,120) and Cohort 2 (N = 517). This was the primary analysis population for all efficacy analyses, including the primary end point (IDFS) and a key gated secondary end point (OS). The study was powered based on this population. The safety population included all patients in Cohort 1 and Cohort 2 who received any quantity of study treatment, regardless of the arm to which they were randomized. The safety population was used for the primary analysis of dosing and/or exposure, safety, and resource utilization. The Ki-67 High population included all randomized patients in Cohort 1 and Cohort 2 with a centrally assessed Ki-67 index of 20% or more and the Cohort 1 Ki-67 High population included all randomized patients in Cohort 1 with a centrally assessed Ki-67 index of 20% or more; gated secondary efficacy analyses were performed on these 2 cohorts. The Ki-67 Low population included all randomized patients in Cohort 1 and Cohort 2 with a centrally assessed Ki-67 index of less than 20%. Cohort 1 Ki-67 Low population included all randomized patients in Cohort 1 with a centrally assessed Ki-67 index of less than 20%; exploratory efficacy analyses were performed on this population. Cohort 2 included patients randomized based on a centrally determined Ki-67 index of 20% or more (Table 8).
In line with the approved Health Canada indication and the current reimbursement request, data from the Cohort 1 Ki-67 High population are reported in the main body of this CADTH report.
Analysis population, n (%) | Abemaciclib + ET arm | ET arm | Total |
|---|---|---|---|
ITT | 2,808 | 2,829 | 5,637 |
Safety | 2,791 | 2,800 | 5,591 |
Ki-67 High (C1 + C2)a | 1,262 | 1,236 | 2,498 |
Ki-67 Low (C1 + C2)b | 953 | 974 | 1,927 |
C1 | 2,555 | 2,565 | 5,120 |
C1 Ki-67 Higha | 1,017 | 986 | 2,003 |
C1 Ki-67 Lowb | 946 | 968 | 1,914 |
C2 | 253 | 264 | 517 |
C1 = Cohort 1; C2 = Cohort 2; ET = endocrine therapy; IDFS = invasive disease–free survival; ITT = intention to treat.
Note: Not all patients had a Ki-67 test or available test results.
aPatients with Ki-67 score ≥ 20%.
bPatients with Ki-67 score < 20%.
Source: Clinical Study Report for Verzenio (final IDFS [primary outcome] analysis).15
Results
Patient Disposition
A total of 7,372 patients entered the study at 611 sites in 38 countries. A total of 1,872 patients were not randomized due to screen failures. The main reasons for screen failure were inclusion or exclusion criteria not having been met (n = 1,427; 76.2%), withdrawal by patient (n = 364; 19.4%), physician decision (n = 75; 4.0%), and AEs (n = 6; 0.3%). Per protocol, patients who were screen failures could be rescreened; of these, 151 patients were rescreened, and 141 (93.4%) patients were then randomized into the study. Four patients entered the study with consent but did not complete screening and were not randomized. A total of 5,637 patients were randomized (|| patients in Canada) and included in the ITT population (Cohort 1 and Cohort 2), with 2,808 patients randomized to receive abemaciclib plus ET and 2,829 patients randomized to receive ET alone. A total of 5,120 patients were enrolled into Cohort 1. Of these, 3,917 (76%) patients had Ki-67 testing results available; among these, 2,003 (51%) patients had a Ki-67 score of 20% or more.
The end of the study treatment period was planned at 2 years (27 visits), according to the schedule of assessments. Patients performing the total number of visits of the treatment period were considered to have completed the study treatment period. Patients who discontinued abemaciclib, yet continued on ET, were considered still on study treatment. At the time of the primary outcome analysis (with a data cut-off date of July 8, 2020), 26.9% of patients in the abemaciclib plus ET arm and 28.2% of patients in the ET arm had completed the 2-year on-study treatment period. At the additional follow-up analysis (April 1, 2021), 73% of patients who had remained in the study had completed the study treatment phase (Table 9).
Table 9: Patient Disposition — Cohort 1 Ki-67 High Population
Disposition | Abemaciclib + ET arm (N = 1,017) | ET arm (N = 986) | Total (N = 2,003) |
|---|---|---|---|
At the primary outcome analysis (July 8, 2020) | |||
Randomized but not treated, n (%) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
On treatment, n (%) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Off treatment, n (%) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Reason for treatment discontinuation | |||
Adverse event | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Completed | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Death | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Disease relapse | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Lost to follow-up | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Non-compliance with study drug | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Physician decision | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Protocol deviation | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Withdrawal by patient | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Post-treatment discontinuation follow-up | |||
No | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Yes | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
At the additional follow-up analysis (April 1, 2021) | |||
Randomized but not treated, n (%) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
On treatment, n (%) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Off treatment, n (%) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Reason for treatment discontinuation | |||
Adverse event | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Completed | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Death | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Disease relapse | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Lost to follow-up | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Non-compliance with study drug | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Physician decision | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Protocol deviation | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Withdrawal by patient | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Post-treatment discontinuation follow-up | |||
No | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Yes | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
ET = endocrine therapy
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Protocol Deviations
At the time of final IDFS analysis, 141 (2.5%) patients were reported to have 1 or more important protocol deviations, which included 74 (2.6%) patients in the abemaciclib plus ET arm and 67 (2.4%) patients in the ET arm (ITT population). The most commonly reported protocol deviations were deviations from inclusion or exclusion criteria, and criteria not met (2.2% in the abemaciclib + ET arm and 2.1% in the ET arm). Protocol deviations were evenly distributed between the 2 treatment arms and were considered unlikely to jeopardize the integrity of the data.
Exposure to Study Treatments
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Table 10 ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Table 11.
Table 10: Exposure to Study Treatments — Cohort 1 Ki-67 High Population
Exposure | Abemaciclib + ET arm (N = 1,016) | ET arm (N = 984) | |
|---|---|---|---|
Abemaciclib | ET | ||
Cycles received per patient, mean (SD)a | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Duration of therapy (weeks), mean (SD) | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Patients who received treatment for ≥ n cycles, n (%) | |||
≥ 1 cycle | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
≥ 6 cycles | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
≥ 12 cycles | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
≥ 18 cycles | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
≥ 24 cycles | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
≥ 26 cycles | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
ET = endocrine therapy; SD = standard deviation.
Note: Based on the safety population within Cohort 1 Ki-67 High (i.e., patients who received at least 1 dose of study treatment)
aA cycle is defined as every 30 days of treatment.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 11: Summary of Endocrine Therapies — Cohort 1 Ki-67 High Population
Therapy, n (%) | Abemaciclib + ET arm (N = 1,016) | ET arm (N = 984) | ||
|---|---|---|---|---|
At start of study | Any time | At start of study | Any time | |
Aromatase inhibitors | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Anastrozole | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Exemestane | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Letrozole | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Anti-estrogens | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Tamoxifen | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Toremifene | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
GnRH analogues | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Goserelin | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Leuprorelin | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
Triptorelin | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |
ET = endocrine therapy; GnRH = gonadotropin-releasing hormone.
Note: Based on the safety population within Cohort 1 Ki-67 High (i.e., patients who received at least 1 dose of study treatment).
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Prior and Concomitant Therapy
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Table 12 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Table 13.
Subsequent Anticancer Therapy
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Table 14.
Table 12: Prior Anticancer Therapy for Breast Cancer — Cohort 1 Ki-67 High Population
Prior anticancer therapy, n (%) | Abemaciclib + ET arm (N = 1,017) | ET arm (N = 986) |
|---|---|---|
Surgical procedure, curative intent | |||||||||||||||| | |||||||||||||||| |
Radiotherapy | |||||||||||||||| | |||||||||||||||| |
Neoadjuvant | |||||||||||||||| | |||||||||||||||| |
Adjuvant | |||||||||||||||| | |||||||||||||||| |
Systemic therapy | |||||||||||||||| | |||||||||||||||| |
Neoadjuvant | |||||||||||||||| | |||||||||||||||| |
Chemotherapy | |||||||||||||||| | |||||||||||||||| |
ET | |||||||||||||||| | |||||||||||||||| |
Other | |||||||||||||||| | |||||||||||||||| |
Target therapy | |||||||||||||||| | |||||||||||||||| |
Adjuvant | |||||||||||||||| | |||||||||||||||| |
Chemotherapy | |||||||||||||||| | |||||||||||||||| |
ET | |||||||||||||||| | |||||||||||||||| |
Other | |||||||||||||||| | |||||||||||||||| |
ET = endocrine therapy.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 13: Concomitant Medications — Cohort 1 Ki-67 High Population
Medication, n (%) | Abemaciclib + ET arm (N = 1,016) | ET arm (N = 984) |
|---|---|---|
General concomitant medications | |||||||||||||||| | |||||||||||||||| |
Adverse event | |||||||||||||||| | |||||||||||||||| |
Loperamide | |||||||||||||||| | |||||||||||||||| |
Paracetamol | |||||||||||||||| | |||||||||||||||| |
Ibuprofen | |||||||||||||||| | |||||||||||||||| |
Amoxicillin; clavulanic acid | |||||||||||||||| | |||||||||||||||| |
Amoxicillin | |||||||||||||||| | |||||||||||||||| |
Prophylaxis | |||||||||||||||| | |||||||||||||||| |
Calcium carbonate; cholecalciferol | |||||||||||||||| | |||||||||||||||| |
Vitamin D | |||||||||||||||| | |||||||||||||||| |
Cholecalciferol | |||||||||||||||| | |||||||||||||||| |
Influenza vaccine | |||||||||||||||| | |||||||||||||||| |
Medical history events | |||||||||||||||| | |||||||||||||||| |
Levothyroxine | |||||||||||||||| | |||||||||||||||| |
Paracetamol | |||||||||||||||| | |||||||||||||||| |
Metformin | |||||||||||||||| | |||||||||||||||| |
Bone-modifying drugs | |||||||||||||||| | |||||||||||||||| |
Zoledronic acid | |||||||||||||||| | |||||||||||||||| |
Denosumab | |||||||||||||||| | |||||||||||||||| |
Alendronic acid | |||||||||||||||| | |||||||||||||||| |
Ibandronic acid | |||||||||||||||| | |||||||||||||||| |
Risedronic acid | |||||||||||||||| | |||||||||||||||| |
Clodronic acid | |||||||||||||||| | |||||||||||||||| |
ET = endocrine therapy.
Note: Based on the safety population within Cohort 1 Ki-67 High (i.e., patients who received at least 1 dose of study treatment).
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 14: Post-Discontinuation Therapy — Cohort 1 Ki-67 High Population
Therapy | Abemaciclib + ET arm (N = 1,017) | ET arm (N = 986) |
|---|---|---|
Surgical procedure | |||||||||||||||| | |||||||||||||||| |
Radiotherapy | |||||||||||||||| | |||||||||||||||| |
Systemic therapy | |||||||||||||||| | |||||||||||||||| |
Chemotherapy | |||||||||||||||| | |||||||||||||||| |
ET | |||||||||||||||| | |||||||||||||||| |
Anastrozole | |||||||||||||||| | |||||||||||||||| |
Exemestane | |||||||||||||||| | |||||||||||||||| |
Fulvestrant | |||||||||||||||| | |||||||||||||||| |
Goserelin | |||||||||||||||| | |||||||||||||||| |
Letrozole | |||||||||||||||| | |||||||||||||||| |
Leuprorelin | |||||||||||||||| | |||||||||||||||| |
Tamoxifen | |||||||||||||||| | |||||||||||||||| |
Toremifene | |||||||||||||||| | |||||||||||||||| |
Triptorelin | |||||||||||||||| | |||||||||||||||| |
Other | |||||||||||||||| | |||||||||||||||| |
Atezolizumab | |||||||||||||||| | |||||||||||||||| |
Dendritic cells cytokine-induced killer cells | |||||||||||||||| | |||||||||||||||| |
Immunotherapy | |||||||||||||||| | |||||||||||||||| |
Pertuzumab | |||||||||||||||| | |||||||||||||||| |
Zoledronic acid | |||||||||||||||| | |||||||||||||||| |
Target therapy | |||||||||||||||| | |||||||||||||||| |
Abemaciclib | |||||||||||||||| | |||||||||||||||| |
Alpelisib | |||||||||||||||| | |||||||||||||||| |
Bevacizumab | |||||||||||||||| | |||||||||||||||| |
Neratinib | |||||||||||||||| | |||||||||||||||| |
Olaparib | |||||||||||||||| | |||||||||||||||| |
Palbociclib | |||||||||||||||| | |||||||||||||||| |
Ribociclib | |||||||||||||||| | |||||||||||||||| |
Talazoparib | |||||||||||||||| | |||||||||||||||| |
Trastuzumab | |||||||||||||||| | |||||||||||||||| |
Trastuzumab emtansine | |||||||||||||||| | |||||||||||||||| |
Xentuzumab | |||||||||||||||| | |||||||||||||||| |
ET = endocrine therapy.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported as follows. Refer to Appendix 2 for detailed efficacy data.
Overall Survival
At the interim analysis 1 for OS (i.e., additional follow-up analysis, with a data cut-off date of April 1, 2021), data were immature, with a |||||||||||||||| event rate. There were ||||||||| deaths in the Cohort 1 Ki-67 High population (|||||||||||||||| in the abemaciclib + ET arm and |||||||||||||||| in the ET arm). The hazard ratio between treatment arms was |||||||||||||||| (95% CI, ||||||||||||||||) (Table 15 and Figure 3).
Table 15: Overall Survival — Cohort 1 Ki-67 High Population
Survival | Abemaciclib + ET arm N = 1,017 | ET arm N = 986 | |
|---|---|---|---|
Number of events, n (%) | |||||||||||||||| | |||||||||||||||| | |
Number of patients censored, n (%) | |||||||||||||||| | |||||||||||||||| | |
Alive, n (%) | |||||||||||||||| | |||||||||||||||| | |
Lost to follow-up, n (%) | |||||||||||||||| | |||||||||||||||| | |
Withdrawal by patient, n (%) | |||||||||||||||| | |||||||||||||||| | |
Treatment effect/difference — P value (2-sided) log-ranka | |||||||||||||||| | ||
Hazard ratio (95% CI)c | |||||||||||||||| | ||
Survival rate, % (95% CI)d | |||
12 months | |||||||||||||||| | |||||||||||||||| | |
Treatment effect/difference — P valuea,e | |||||||||||||||| | ||
24 months | |||||||||||||||| | |||||||||||||||| | |
Treatment effect/difference — P valuea,e | |||||||||||||||| | ||
36 months | |||||||||||||||| | |||||||||||||||| | |
Treatment effect/difference — P valuea,e | |||||||||||||||| | ||
CI = confidence interval; ET = endocrine therapy; OS = overall survival.
Notes: The data cut-off date: April 1, 2021.
The median estimate for OS was not reached due to low event rates.
aTested outside the preplanned statistical hierarchy and unadjusted for multiple comparisons.
bStratified by geographical region, prior treatment, menopausal status.
cEstimated using a Cox proportional hazards model.
d95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
eComputed based on comparator ET.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In its regulatory submission to Health Canada, the sponsor was requested to provide an additional unplanned OS analysis in the Cohort 1 population according to Ki-67 index (i.e., ≥ 20% versus < 20%) at the primary outcome (IDFS) analysis (with a data cut-off date of July 8, 2020). Data provided by the sponsor are presented in Table 30, Appendix 2. These data form the basis for the current approved indication of abemaciclib for early breast cancer (i.e., patients with high-risk clinicopathologic features and a Ki-76 index ≥ 20%). Briefly, although the OS data were highly immature, the OS analysis by Ki-67 index in Cohort 1 showed a hazard ratio of |||||||||||||||| (95% CI, ||||||||||||||||) in the Ki-67 of 20% or more population and a hazard ratio of |||||||||||||||| (95% CI, ||||||||||||||||) in the Ki-67 of less than 20% population (n = 1,913).18
Figure 3: Kaplan-Meier Plot of Overall Survival — Cohort 1 Ki-67 High Population

Note: This figure has been redacted as per sponsor’s request.
Invasive Disease–Free Survival
At the interim analysis (March 16, 2020) with a median follow-up of 15 months, |||||||||||||||| IDFS events were observed in the Cohort 1 Ki-67 High population (|||||||||| events in the abemaciclib + ET arm and |||||||||||||||| events in the ET arm). ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The hazard ratio estimate between treatment arms was |||||||||||||||| (95% CI, ||||||||||||||||). The 2-year IDFS rates in the abemaciclib plus ET arm versus the ET arm were |||||||||||||||| versus |||||||||||||||| (Table 16).
At the final IDFS analysis (July 8, 2020), with a median follow-up of 19.1 months, ||| IDFS events were observed (|| events in the abemaciclib + ET arm and ||| events in the ET arm). The hazard ratio between treatment arms was 0.643 (95% CI, 0.475 to 0.872; P = 0.0042). The 2-year IDFS rates in the abemaciclib plus ET arm versus the ET arm were 91.3% versus 86.1%, respectively (Table 17 and Figure 4).
At the additional follow-up analysis (April 1, 2021), IDFS was assessed as post hoc analyses. With a median follow-up of 27 months, 262 IDFS events were observed (104 events in the abemaciclib + ET arm and 158 events in the ET arm). The hazard ratio between treatment arms was 0.63 (95% CI, 0.49 to 0.80). The 3-year IDFS rates in the abemaciclib plus ET arm versus the ET arm were 86.1% versus 79.0%, respectively (Table 18 and Figure 5).
IDFS in the ITT population and the ITT Ki-67 High population at the final IDFS analysis are included in Table 26 and Table 27 in Appendix 2.
Table 16: Invasive Disease–Free Survival, Interim Analysis — Cohort 1 Ki-67 High Population
Survival | Abemaciclib + ET arm N = 1,017 | ET arm N = 986 |
|---|---|---|
Number of events, n (%) | |||||||||||||||| | |||||||||||||||| |
Deaths without invasive disease, n (%) | |||||||||||||||| | |||||||||||||||| |
Invasive disease, n (%) | |||||||||||||||| | |||||||||||||||| |
Number of patients censored, n (%) | |||||||||||||||| | |||||||||||||||| |
Invasive disease before randomization, n (%) | |||||||||||||||| | |||||||||||||||| |
No post-baseline assessment, n (%) | |||||||||||||||| | |||||||||||||||| |
No documented invasive disease, n (%) | |||||||||||||||| | |||||||||||||||| |
Restricted mean (95% CI) with restriction time = 24.95 monthsa | |||||||||||||||| | |||||||||||||||| |
Treatment effect/difference — P value (2-sided)b | |||||||||||||||| | |
P value (2-sided) log-rank | |||||||||||||||| | |
Hazard ratio (95% CI)e | |||||||||||||||| | |
IDFS rate, % (95% CI)f | ||
12 months | |||||||||||||||| | |||||||||||||||| |
Treatment effect/difference — P value (2-sided) | |||||||||||||||| | |
24 months | |||||||||||||||| | |||||||||||||||| |
Treatment effect/difference — P value (2-sided) | |||||||||||||||| | |
CI = confidence interval; ET = endocrine therapy; IDFS = invasive disease–free survival.
Note: The data cut-off date was March 16, 2020. Tests were performed after failure of the statistical hierarchy.
aRestriction time is defined by the latest time where the standard error of the survival estimates is 0.075 or less.
bTreatment effect, difference, and P values were computed based on comparator ET.
cThe 2-sided P value was based on normal approximation.
dStratified by geographical region, prior treatment, and menopausal status.
eEstimated using a Cox proportional hazards model.
fThe 95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 17: Invasive Disease–Free Survival, Final Analysis — Cohort 1 Ki-67 High Population
Survival | Abemaciclib + ET arm N = 1,017 | ET arm N = 986 |
|---|---|---|
Number of events, n (%) | |||||||||||||||| | |||||||||||||||| |
Deaths without invasive disease, n (%) | |||||||||||||||| | |||||||||||||||| |
Invasive disease, n (%) | |||||||||||||||| | |||||||||||||||| |
Number of patients censored, n (%) | |||||||||||||||| | |||||||||||||||| |
Invasive disease before randomization, n (%) | |||||||||||||||| | |||||||||||||||| |
No post-baseline assessment, n (%) | |||||||||||||||| | |||||||||||||||| |
No documented invasive disease, n (%) | |||||||||||||||| | |||||||||||||||| |
Restricted mean (95% CI) with restriction time = 30.7 monthsa | |||||||||||||||| | |||||||||||||||| |
Treatment effect/difference (95% CI) — P value (2-sided)b | |||||||||||||||| | |
P value (2-sided) log-rank | |||||||||||||||| | |
Hazard ratio (95% CI)e | |||||||||||||||| | |
IDFS rate, % (95% CI)f | ||
12 months | |||||||||||||||| | |||||||||||||||| |
Treatment effect/difference — P value (2-sided) | |||||||||||||||| | |
24 months | |||||||||||||||| | |||||||||||||||| |
Treatment effect/difference — P value (2-sided) | |||||||||||||||| | |
CI = confidence interval; ET = endocrine therapy; IDFS = invasive disease–free survival.
Note: The data cut-off date was July 8, 2020.
aRestriction time is defined by the latest time where the standard error of the survival estimates is 0.075 or less.
bTreatment effect, difference, and P values were computed based on comparator ET.
cThe 2-sided P value was based on normal approximation.
dStratified by geographical region, prior treatment, and menopausal status.
eEstimated using a Cox proportional hazards model.
fThe 95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 18: Invasive Disease–Free Survival, Additional Follow-Up Analysis — Cohort 1 Ki-67 High Population
Survival | Abemaciclib + ET arm (N = 1,017) | ET arm (N = 986) |
|---|---|---|
Number of events, n (%) | 104 (10.2) | 158 (16.0) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |
Hazard ratio (95% CI)c | Stratifieda,b = 0.626 (0.488 to 0.803); Unstratified = 0.631 (0.493 to 0.809) | |
IDFS rate, % (95% CI)d,e | ||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |
24 months | 91.5 (89.5 to 93.1) | 86.4 (84.0 to 88.4) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |
36 months | 86.1 (82.8 to 88.8) | 79.0 (75.3 to 82.3) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |
CI = confidence interval; ET = endocrine therapy; IDFS = invasive disease–free survival.
Note: Date cut-off date: April 1, 2021.
aStratified by geographical region, prior treatment, menopausal status.
bTesting was performed outside the statistical hierarchy (after end point was met).
cEstimated using a Cox proportional hazards model.
d95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
eTreatment effect, difference, and P values are computed based on comparator ET.
Source: Clinical Study Report for Verzenio (overall survival interim analysis 1).16
Figure 4: Kaplan-Meier Plot of Invasive Disease–Free Survival, Final Analysis — Cohort 1 Ki-67 High Population

Note: This figure has been redacted as per sponsor’s request.
Figure 5: Kaplan-Meier Plot of Invasive Disease–Free Survival, Additional Follow-Up Analysis — Cohort 1 Ki-67 High Population
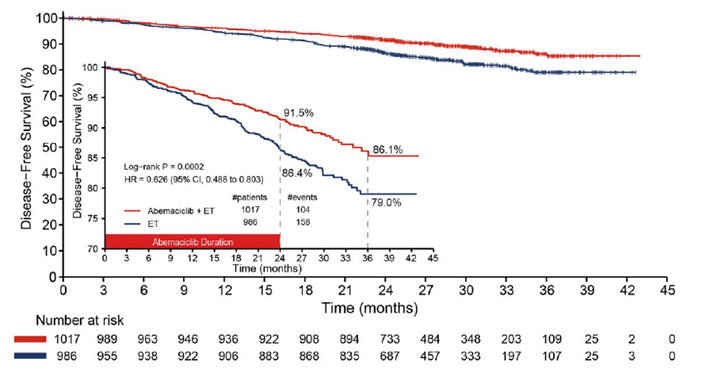
CI = confidence interval; ET = endocrine therapy; HR = hazard ratio.
Notes: Date cut-off date: April 1, 2021.
The P value is based on testing outside of the statistical hierarchy.
Source: Clinical Study Report for Verzenio (overall survival interim analysis 1).16
Subgroup Analyses
In the subgroup analyses, point estimates for hazard ratio were overall supportive of IDFS benefit with abemaciclib in the ITT population. Some subgroups had small sample sizes and wide overlapping 95% CIs. No statistically significant interactions were observed, suggesting a consistent treatment benefit across all subgroups (Table 28, Appendix 2).
Distant Relapse–Free Survival
At the interim analysis (March 16, 2020), a total of ||||||||||||||| events were observed (|||||||||| patients in the abemaciclib + ET arm and |||||||| patients in the ET arm). The hazard ratio between treatment arms was ||||||||||||||||||||||||||||||||||||||||||||||||. The 2-year DRFS rates in the abemaciclib plus ET arm versus the ET arm were ||||||||||||||||| versus ||||||||||||||||||, respectively (Table 19).
Table 19: Distant Relapse–Free Survival, Interim Analysis — Cohort 1 Ki-67 High Population
Survival | Abemaciclib + ET arm N = 1,017 | ET arm N = 986 |
|---|---|---|
Number of events, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Deaths without distant relapse, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Distant relapse, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Number of patients censored, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Distant relapse before randomization, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
No post-baseline assessment, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
No documented distant relapse, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Restricted mean (95% CI) with restriction time = 24.99 monthsa | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Treatment effect/difference (95% CI) — P value (2-sided) | |||||||||||||||||||||||| | |
P value (2-sided) log-rank | |||||||||||||||||||||||| | |
Hazard ratio (95% CI)d | |||||||||||||||||||||||| | |
DRFS rate, % (95% CI)e | ||
12 months | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided) | |||||||||||||||||||||||| | |
24 months | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided) | |||||||||||||||||||||||| | |
CI = confidence interval; DRFS = distant relapse–free survival; ET = endocrine therapy.
Note: Data cut-off date: March 16, 2020. Analyses were not pre-specified and not adjusted for multiple comparisons; therefore, there is an increased risk of type I error.
aRestricted time is defined by the latest time where the standard error of the survival estimates is ≤ 0.075.
b2-sided P value based on normal approximation.
cStratified by geographical region, prior treatment, menopausal status.
dEstimated using a Cox proportional hazards model.
e95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 20: Distant Relapse–Free Survival, Final Primary Outcome Analysis — Cohort 1 Ki-67 High Population
Survival | Abemaciclib + ET arm N = 1,017 | ET arm N = 986 |
|---|---|---|
Number of events, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Deaths without distant relapse, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Distant relapse, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Number of patients censored, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Distant relapse before randomization, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
No post-baseline assessment, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
No documented distant relapse, n (%) | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Restricted mean (95% CI) with restriction time = 30.67 monthsa | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Treatment effect/difference (95% CI) — P value (2-sided)b | |||||||||||||||||||||||| | |
P value (2-sided) log-rank | |||||||||||||||||||||||| | |
Hazard ratio (95% CI)e | |||||||||||||||||||||||| | |
DRFS rate, % (95% CI)f | ||
12 months | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided)b | |||||||||||||||||||||||| | |
24 months | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided)b | |||||||||||||||||||||||| | |
30 months | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided)b | |||||||||||||||||||||||| | |
CI = confidence interval; ET = endocrine therapy, DRFS = distant relapse–free survival.
Note: The data cut-off date was July 8, 2020.
aRestricted mean time is defined by the latest time where the standard error of the survival estimates is ≤ 0.075.
bAnalyses were not pre-specified and not adjusted for multiple comparisons and therefore there is an increased risk of type I error.
c2-sided P value based on normal approximation.
dStratified by geographical region, prior treatment, menopausal status.
eEstimated using a Cox proportional hazards model.
f95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
At the final primary outcome (IDFS) analysis (July 8, 2020), a total of |||||||||||||| events were observed (|||||||| patients in the abemaciclib + ET arm and |||||||||||| patients in the ET arm). The hazard ratio between treatment arms was ||||||||||||||||||||||||||||||||||||||||||||||||. The 2-year DRFS rates in the abemaciclib plus ET arm versus the ET arm were ||||||||||||| versus ||||||||||||||||||||||||, respectively (Table 20 and Figure 6).
At the additional follow-up analysis (April 1, 2021), a total of 220 events were observed (85 patients in the abemaciclib + ET arm and 135 patients in the ET arm). The hazard ratio between treatment arms was 0.599 (95% CI, 0.456 to 0.787). The 3-year DRFS rates in the abemaciclib plus ET arm versus the ET arm were 87.8% versus 82.6%, respectively (Table 21).
Figure 6: Kaplan-Meier Plot of Distant Relapse–Free Survival, Final Primary Outcome Analysis — Cohort 1 Ki-67 High Population

Note: This figure has been redacted as per sponsor’s request.
Table 21: Distant Relapse–Free Survival, Additional Follow-Up Analysis — Cohort 1 Ki-67 High Population
Survival | Abemaciclib + ET arm (N = 1,017) | ET arm (N = 986) |
|---|---|---|
Number of events, n (%) | 85 (8.4) | 135 (13.7) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |
DRFS rate, % (95% CI)d | ||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||| | |
36 months | 87.8 (84.4 to 90.5) | 82.6 (79.2 to 85.5) |
Treatment effect/difference — P value (2-sided)c | 5.2 (0.8 to 9.5) P = 0.0190 | |
CI = confidence interval; ET = endocrine therapy; DRFS = distant relapse–free survival.
Note: The data cut-off date was April 1, 2021.
aAnalyses were not pre-specified and not adjusted for multiple comparisons; therefore, there is an increased risk of type I error.
bStratified by geographical region, prior treatment, menopausal status.
cEstimated using a Cox proportional hazards model.
d95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
eThe 2-sided P value based on normal approximation.
Source: Clinical Study Report for Verzenio (overall survival interim analysis 1).16
Health-Related Quality of Life
In the monarchE study, HRQoL data were assessed in the safety population only. As such, the results reported as follows are not based on the population of interest for this CADTH report (i.e., Cohort 1 Ki-67 High population).
FACT-B: At baseline, ||||||||| (|||||||||) patients in the abemaciclib plus ET arm and ||||||||| (|||||||||) patients in the ET arm completed the questionnaire; a total of ||||||||| (|||||||||) patients did not complete the questionnaire due to patient refusal, study site failure to administer, translation not being available, and other or missing reasons. At visit 21, ||||||||| patients in the abemaciclib plus ET arm and the ET arm, respectively, had completed questionnaires, representing ||||||||| and ||||||||| of patients with data at baseline; a total of ||||||||| (|||||||||) patients were non-compliant. The mean scores and changes from baseline scores were similar in both arms. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
EQ-5D-5L: Questionnaire completion rates were ||||||||| and ||||||||| in the abemaciclib plus ET arm and the ET arm, respectively, at baseline, and ||||||||| and |||||||||, respectively, at visit 21 (of patients who reached visit 21). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Health Care Resource Utilization
As of the final primary outcome (IDFS) analysis (July 8, 2020), a total of ||||||||| patients reported at least 1 hospitalization, including ||||||||| (||||||||| patients in the abemaciclib plus ET arm and ||||||||| (|||||||||) patients in the ET arm. The majority of patients were hospitalized due to ||||||||||||||||||||||||||||||||||||||||||||||||||||||. The median duration of hospitalization was |||||||||||||||||||||||||||||||||||||||||||||||||||||| in both treatment arms.
At least 1 transfusion during the study treatment period and within 30 days of study treatment discontinuation was received by ||||||||| patients, including ||||||||| (|||||||||) patients in the abemaciclib plus ET arm and ||||||||| (|||||||||) patients in the ET arm. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| was the most commonly reported AE requiring a transfusion, with ||||||||| (|||||||||) patients in the abemaciclib plus ET arm and ||||||||| (|||||||||) patients in the ET arm.
Harms
Adverse Events
At the final IDFS analysis (July 8, 2020), a total of 5,174 patients experienced at least 1 TEAE (97.9% in the abemaciclib plus ET arm and 87.2% in the ET arm) (Table 22). TEAEs by maximum Common Terminology Criteria for Adverse Events grade and PT that occurred in 10% or more of patients in either arm are summarized in Table 23. The most frequent TEAEs were diarrhea (82.6%), neutropenia (45.2%), and fatigue (39.2%) in the abemaciclib plus ET arm, and arthralgia (33.1%), hot flush (21.8%), and fatigue (16.6%) in the ET arm. Grade 3 or higher AEs occurred in 47.4% of patients in the abemaciclib plus ET arm, and in 14.2% of patients in the ET arm. The most frequently reported grade 3 or higher TEAEs in the abemaciclib plus ET arm were neutropenia (19.1%), leukopenia (10.9%), and diarrhea (7.7%). The most common grade 3 or higher TEAEs in the ET arm were neutropenia and arthralgia (0.7%) and lymphopenia (0.5%).
Serious Adverse Events
At least 1 SAE occurred in 13.3% of patients in the abemaciclib plus ET arm and 7.8% of patients in the ET arm. The most frequently reported SAE in both arms was pneumonia (0.9% and 0.5%, respectively) (Table 24).
The most common SAEs in the abemaciclib plus ET arm by system organ class were infections and infestations (4.5% in the abemaciclib plus ET arm versus 2.5% in the ET arm) followed by gastrointestinal disorders (1.9% in the abemaciclib plus ET arm versus 0.6% in the ET arm).
During the long-term follow-up period, ||||||||| patients with at least 1 SAE were reported (||||||||| [|||||||||] patients in the abemaciclib + ET arm, ||||||||| [|||||||||] patients in the ET arm). The SAEs included |||| fatal cases: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 22: Summary of Adverse Events — Safety Population
Adverse event, n (%)a | Abemaciclib + ET arm N = 2,791 | ET arm N = 2,800 |
|---|---|---|
Patients with ≥ 1 TEAE | 2,733 (97.9) | 2,441 (87.2) |
Patients with ≥ 1 grade 3 or higher TEAE | 1,323 (47.4) | 397 (14.2) |
Patients with ≥ 1 SAE | 372 (13.3) | 219 (7.8) |
Patients who discontinued study treatment due to an AE | 172 (6.2) | 23 (0.8) |
Patients who discontinued study treatment due to a SAE | 23 (0.8) | 9 (0.3) |
Patients who died due to an AEb | 15 (0.5) | 16 (0.6) |
||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; ET = endocrine therapy; IDFS = invasive disease–free survival; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Note: Data cut-off date: July 8, 2020. AEs were graded per CTCAE version 4.0.
aPatients may be counted in more than 1 category.
bDeaths were also included as SAEs and discontinuations due to AEs.
Source: Clinical Study Report for Verzenio (final IDFS [primary outcome] analysis).15
Table 23: Treatment-Emergent Adverse Events by Maximum CTCAE Grade Reported in 10% or More of Patients in Either Treatment Arm by Preferred Term — Safety Population
Preferred term, n (%) | Abemaciclib + ET arm (N = 2,791) | ET arm (N = 2,800) | ||
|---|---|---|---|---|
CTCAE ≥ grade 3 | CTCAE any grade | CTCAE ≥ grade 3 | CTCAE Any grade | |
Diarrhea | 215 (7.7) | 2,304 (82.6) | 5 (0.2) | 218 (7.8) |
Neutropenia | 533 (19.1) | 1,262 (45.2) | 20 (0.7) | 145 (5.2) |
Fatigue | 78 (2.8) | 1,094 (39.2) | 4 (0.1) | 464 (16.6) |
Leukopenia | 305 (10.9) | 1,038 (37.2) | 10 (0.4) | 177 (6.3) |
Abdominal pain | 37 (1.3) | 959 (34.4) | 9 (0.3) | 251 (9.0) |
Nausea | 13 (0.5) | 795 (28.5) | 1 (0.0) | 232 (8.3) |
Anemia | 51 (1.8) | 656 (23.5) | 10 (0.4) | 94 (3.4) |
Arthralgia | 7 (0.3) | 614 (22.0) | 20 (0.7) | 928 (33.1) |
Headache | 6 (0.2) | 500 (17.9) | 4 (0.1) | 387 (13.8) |
Vomiting | 13 (0.5) | 466 (16.7) | 2 (0.1) | 122 (4.4) |
Hot flush | 4 (0.1) | 405 (14.5) | 10 (0.4) | 611 (21.8) |
Lymphopenia | 147 (5.3) | 377 (13.5) | 13 (0.5) | 94 (3.4) |
||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Thrombocytopenia | 33 (1.2) | 353 (12.6) | 3 (0.1) | 45 (1.6) |
Decreased appetite | 16 (0.6) | 320 (11.5) | 2 (0.1) | 61 (2.2) |
Lymphedema | 2 (0.1) | 310 (11.1) | 0 (0.0) | 227 (8.1) |
Urinary tract infection | 13 (0.5) | 306 (11.0) | 6 (0.2) | 191 (6.8) |
Constipation | 1 (0.0) | 304 (10.9) | 1 (0.0) | 154 (5.5) |
Upper respiratory tract infection | 6 (0.2) | 293 (10.5) | 0 (0.0) | 226 (8.1) |
ALT, increased | 68 (2.4) | 291 (10.4) | 16 (0.6) | 136 (4.9) |
||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
AST, increased | 49 (1.8) | 281 (10.1) | 14 (0.5) | 120 (4.3) |
Alopecia | 0 (0.0) | 280 (10.0) | 0 (0.0) | 62 (2.2) |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; CTCAE = Common Terminology Criteria for Adverse Events; ET = endocrine therapy; IDFS = invasive disease–free survival.
Note: Data cut-off date: July 8, 2020.
Source: Clinical Study Report for Verzenio (final IDFS [primary outcome] analysis).15
Table 24: Treatment-Emergent Serious Adverse Events Occurring in 5 or More Patients in Any Arm — Safety Population
System organ class preferred term, n (%)a | Abemaciclib + ET arm (N = 2,791) | ET arm (N = 2,800) |
|---|---|---|
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||| | ||||||||| |
Elevated transaminases | ||||||||| | ||||||||| |
ET = endocrine therapy; ILD = interstitial lung disease; VTE = venous thromboembolism.
Note: The data cut-off date was July 8, 2020. MedDRA Version 23.0.
a“Composite terms” are defined as a grouping of terms from 1 or more preferred terms that are treatment-emergent events and are related to a defined medical condition or area of interest.
Source: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
At the additional follow-up (with a data cut-off date of April 1, 2021), safety results were generally consistent with the safety results reported at the final IDFS analysis. A higher incidence of grade 3 or higher AEs and SAEs was observed in the abemaciclib plus ET arm than in the ET arm (50% versus 15% for grade 3 or higher AEs, respectively, and 15% versus 9% for grade 3 or higher SAEs, respectively). In total, 181 (6.5%) patients in the abemaciclib plus ET arm and 30 (1.1%) patients in the ET arm discontinued from the 2-year treatment period due to AEs.
Dose Modifications of Abemaciclib Due to Adverse Events
Abemaciclib dose modifications due to AEs were common (patients with ≥ 1 dose reduction [42.5%] and omission). ||||||||||||||||||||||||||||||||||||||||| of the patients with a dose omission due to an AE reported only 1 occurrence; |||||||| of the patients with a dose reduction due to an AE reported only 1 occurrence; ||||||||||||||||| had 2 dose reductions due to AEs (up to 2 dose reductions were allowed, per protocol). The most frequent reason for dose modifications of abemaciclib was ||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Most dose reductions occurred early during study treatment, with ||||||||||||||||| of the treated patients in the abemaciclib plus ET arm experiencing dose reductions due to AEs within the second month. Reductions were below || per month after 4 months, and dropped below ||||||||||||||||| after 6 months, and below ||||||||||||||||| after 15 months of treatment. Dose reductions were higher for low-grade events (grade 1 or grade 2) in the first month (|||||||||||||||||) but then ||||||||||||||||| of the dose reductions occurred for events of grade 3 or higher throughout the treatment period, per protocol.
Discontinuation Due to Adverse Events
A total of 481 (17.2%) patients discontinued abemaciclib due to AEs, ||||||||| of whom remained on ET when abemaciclib was discontinued. Of these ||||||||||||| patients, ||||||||||||| patients later also discontinued ET due to an AE before completing the 2-year on-study treatment period. The 3 most common reasons for discontinuation of abemaciclib were diarrhea (5.1%), fatigue (1.9%), and neutropenia (0.9%). Low-grade AEs (grade 1 and grade 2) were the cause of discontinuation in 321 of the 481 (66.7%) patients who discontinued abemaciclib. One-third of the discontinuations (n = 160) were due to AEs of grade 3 or higher. The highest number of discontinuations due to any AE occurred during the first month of treatment (77 of the 481 [16.0%] total abemaciclib discontinuations due to AEs). These were mostly due to low-grade (grade 1 or grade 2) events and the frequency of discontinuations diminished over time. Approximately 40% of total abemaciclib discontinuations due to AEs occurred during the first 3 months of treatment. The majority of discontinuations (60.1%), including those due to diarrhea, fatigue, and neutropenia, occurred within the first 6 months of treatment. The percentage of patients discontinuing each month diminished over time, with 1.0% or fewer patients discontinuing each month after month 6.
Deaths
At the time of final IDFS analysis, there were ||||||||||||| (|||||||||||||) deaths in the abemaciclib plus ET arm and ||||||||||||| (|||||||||||||) deaths in the ET arm in the safety population.
There were ||||||||||||| (|||||||||||||) deaths due to AEs in the abemaciclib plus ET arm compared to ||||||||||||| (|||||||||||||) deaths in the ET arm on-study treatment, or within 30 days of all treatment discontinuation. There were ||||||||||||| (|||||||||||||) deaths due to AEs in the abemaciclib plus ET arm (|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||) and 1 death in the ET arm (||||||||||||||||||||||||||||||||||||||||||||||||||||), which occurred more than 30 days after discontinuation of all study treatment.
Notable Harms
Interstitial Lung Disease or Pneumonitis
The most frequently reported ILD or pneumonitis preferred terms were pneumonitis reported in 1.5% and 0.4% of patients in the abemaciclib plus ET and ET arms, respectively, and radiation pneumonitis reported in ||||||||||||| and ||||||||||||| of patients in the abemaciclib plus ET and ET arms, respectively. ILD and pneumonitis events of grade 3 or higher occurred in 11 (0.4%) patients in the abemaciclib plus ET arm and in 1 (< 0.1%) patient in the ET arm.
Diarrhea
The most frequently reported AE in the abemaciclib arm was diarrhea (82.6%); most of these events were low grade (44.8% = grade 1; 30.1% = grade 2; 7.7% = grade 3 or higher). In all, 6.1% of patients discontinued abemaciclib or all treatment in the abemaciclib plus ET arm due to diarrhea. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. In the ET arm, 7.8% of patients experienced diarrhea.
Increased Aminotransferases
In the abemaciclib plus ET arm, 12.8% of patients experienced a TEAE of elevated transaminases, with 3.1% of patients experiencing events of grade 3 or higher. In the ET arm, 6.5% of patients experienced TEAE elevated transaminases, with 0.9% being grade 3 or higher events. SAEs of elevated transaminases occurred in 0.4% of patients in the abemaciclib plus ET arm and 0.1% of patients in the ET arm.
Neutropenia
In the abemaciclib plus ET arm, 1,262 (45.2%) patients experienced a TEAE of neutropenia, with 552 (19.8%) patients experiencing grade 2 and 533 (19.1%) patients experiencing events of grade 3 or higher. Grade 4 neutropenia events occurred in 18 (0.6%) patients and SAEs in 3 (0.1%) patients. In the ET arm, 145 (5.2%) patients experienced TEAE neutropenia, with the majority being grade 1 or grade 2 events.
Infections and Infestations
The frequency of any grade of infection and grade 3 or higher infections was higher in the abemaciclib plus ET arm (47.7% versus 4.7%, respectively) compared to the ET arm (36.4% versus 2.6%, respectively). The most frequent (> 5%) infections by PT in the abemaciclib plus ET arm and the ET arm were upper respiratory tract infections (10.5% versus 8.1%, respectively), urinary tract infection (11.0% versus 6.8%, respectively), and nasopharyngitis (8.7% versus 7.0%, respectively).
Serious infections were reported for 4.5% of patients in the abemaciclib plus ET arm and 2.5% of patients in the ET arm. Pneumonia was the most frequently reported serious infection in both arms (0.9% in the abemaciclib plus ET arm and 0.5% in the ET arm).
Venous Thromboembolisms
VTE events compromising pulmonary embolism and deep vein thrombi (DVTs) were reported in 2.4% of patients in the abemaciclib plus ET arm and 0.6% of patients in the ET arm. In the abemaciclib plus ET arm, DVT was reported in 1.6% of patients and pulmonary embolism was reported in 1% of patients. In the ET arm, DVT was reported in 0.5% of patients and pulmonary embolism in 0.1% of patients.
Second Malignancy
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Fatigue
Fatigue was reported for 39.2% of patients in the abemaciclib plus ET arm and 16.6% of patients in the ET arm. Grade 3 or higher fatigue was reported for 2.8% of patients and 0.1% of patients in the abemaciclib plus ET arm and ET arm, respectively. Fatigue was 1 of the most common reasons for dose modifications of abemaciclib; there were dose omissions in 4.8% of patients and dose reductions in 4.4% of patients.
Critical Appraisal
Internal Validity
In the monarchE study, treatment assignment was based on a central randomization scheme that would ensure concealment of the randomized groups until allocation. However, the Ki-67 index was not a stratification factor; therefore, the population of interest (Cohort 1 Ki-67 High) cannot be considered to have been truly randomized. In addition, Ki-67 status in Cohort 1 was tested retrospectively (thus, this may have been affected by variability in testing times and methods), and data were not available for the full cohort. Analyses of this population subgroup could therefore be subject to confounding due to known or unknown prognostic imbalances across groups. The extent of potential confounding due to unknown prognostic factors or effect modifiers cannot be known, but the balanced available baseline characteristics across treatment arms suggests that concern for potential confounding may be minimal.18 The clinical experts consulted indicated that the high-risk criteria used in the monarchE study appeared reasonable. However, the 20% threshold for Ki-67 index used to categorize patients into high and low recurrence risk is not the threshold recommended by the recent IKWG guidelines.19 Ki-67 testing is not routinely performed in clinical practice and its reproducibility is affected by several factors, including time and method of biopsy, specimen preparation, and assay used. A discussion of Ki-67 testing and issues surrounding its validity and reliability can be found in Appendix 4.
Following allocation, the trial was open label. Although patient blinding would have been impractical and challenging given the differences in the 2 study treatment regimens and different known toxicity profiles, performance and detection bias that may have resulted from lack of blinding of patients and investigators to assigned study treatments cannot be ruled out. For example, a patient’s knowledge of their assigned treatment could result in the overestimation or underestimation of safety end points and PROs like symptoms and HRQoL. PROs are particularly susceptible to bias from a lack of blinding of patients to their treatment. Investigator knowledge of the treatment group could have also resulted in different concomitant supportive care being offered to patients in the 2 treatment arms. However, the main difference in concomitant treatments was from more loperamide use in the abemaciclib arm to manage diarrhea; this is a known AE related to abemaciclib treatment. The primary outcome (IDFS) was investigator-assessed but based on objective criteria (STEEP) and, thus, unlikely to be greatly affected by the lack of investigators blinding.
Sample size was adequate, and the study was powered (based on the ITT population) to test its primary end point. The primary end point was met, but the study was not powered for the population of interest in this CADTH review (i.e., the Cohort 1 Ki-67 High population). The statistical approach of gatekeeping to sequentially test the primary and secondary end points was acceptable to account for multiple testing across these analyses. However, some analyses conducted on ITT subpopulations such as DRFS and OS in the Cohort 1 Ki-67 High population that are the focus of this CADTH report were not gated end points. Analyses in the Cohort 1 Ki-67 High population including IDFS at the additional analysis (April 1, 2021) were not preplanned and not controlled for multiple comparisons. As such, the analyses for these end points are at increased risk of type I error (i.e., false-positive findings).
The primary and secondary efficacy end points of IDFS and DRFS are considered appropriate for the disease setting. IDFS is widely used and accepted for regulatory drug approvals, especially in the early breast cancer setting with low event rates.18 As is common in oncology trials, the results for IDFS are the results of an interim analysis; therefore, there is some risk that the effect is overestimated. However, concern for this is reduced because the observed treatment effect appears to be clearly clinically important and maintained in the later additional analysis. IDFS and DRFS are considered early indicators of a patient’s survival, especially for less advanced conditions in which longer survival is expected. OS data in the monarchE study remain immature, which is expected in this disease setting with longer survival prognosis. An understanding of the efficacy of abemaciclib and ET with regard to OS will require a larger number of events and a longer follow-up. The correlation of DFS surrogates with OS remains debatable and requires further investigation. Evidence from the literature is limited, with some studies suggesting that the correlation between DFS may not be strong enough to be used as a predictor of OS in adjuvant breast cancer trials.35 Moreover, estimates of acceptable correlation from other treatments and disease stages may not be generalizable to treatment with abemaciclib in this setting. Therefore, it is unclear if improvements in IDFS that were observed in patients in the abemaciclib plus ET arm of the monarchE trial would translate into OS benefits. Appendix 3 describes the DFS outcome measure and summarizes evidence that examines the validity of DFS as a surrogate for OS in patients with early-stage breast cancer.
Data for some end points, specifically HRQoL and health care resource utilization, were unavailable for the population of interest in this CADTH review. It is not clear if the findings for these outcomes would be similar to those reported for the overall safety population. Moreover, there was a substantial attrition rate for HRQoL assessments over time, with approximately 50% of patients contributing to these assessments at visit 21. No HRQoL data were captured for the first 3 months; this may have been an important time point in terms of changes in quality of life after initiation of new treatment.
External Validity
The monarchE trial included a heterogenous population of patients with early breast cancer and a wide range of clinical presentations were well represented. The clinical experts consulted by CADTH noted that patients in the trial are about a decade younger than patients with early breast cancer encountered in clinical practice, who are generally diagnosed and treated in their early to mid 60s. This discrepancy, however, may be explained by high-risk features potentially being more prevalent in younger patients. The inclusion of younger and healthier patients may have led to a more favourable toxicity profile where more AEs were manageable, and reversible. In terms of clinicopathologic features used for eligibility, the clinical experts noted that for patients who received neoadjuvant therapy, the monarchE study allowed the tumour size to be based on imaging; however, lymph node involvement could have been assessed cytologically and may have produced different results. If multiple lymph nodes were sampled in the trial to determine eligibility, it should be noted that this is not done in routine clinical practice. The clinical experts noted that the ET regimens used in the trial and their distribution are representative of ET regimens used in the Canadian clinical setting.
The Ki-67 IHC is a marker of cell proliferation and considered an important prognostic factor in early breast cancer. In the monarchE study, Ki-67 assessment was performed by the investigational (central) test using standardized laboratory procedures for tissue handling, preparation, and assays to ensure consistency. The clinical experts consulted by CADTH and the clinician group input stated that Ki-67 testing is not broadly practised in the Canadian clinical setting and expressed concerns regarding the reliability of Ki-67 IHC analyses. Unlike a clinical trial setting with centralized testing, the variability in sample preparation methods between different laboratories and different scoring methods between observers reduce the reproducibility of Ki-67 IHC in clinical practice. The clinical experts noted the many internal and external factors that can impact Ki-67 values. For example, tumour heterogeneity and samples from core biopsy and surgery can produce different Ki-67 test values, particularly in patients who undergo neoadjuvant treatment. There are other uncertainties regarding the use of Ki-67 testing in clinical practice and its implementation as a criterion to select eligible patients for treatment. For example, the clinical experts questioned at what time point to conduct the Ki-67 IHC test as biomarkers can change drastically at different time points, and what to do in case of multiple testing results with different values, or if a patient’s test is borderline for the eligibility cut-off (19% instead of 20%). Whether the 20% cut-off value for Ki-67 to categorize recurrence risk as high or low can meaningfully and consistently distinguish patients’ recurrence risk is also debated, and the extent to which Ki-67 is predictive of treatment response is unclear. It is important to note that in the monarchE study, the Ki-67 index was used only as an additional prognostic factor to determine the risk of recurrence. It was not considered as a companion diagnostic for predicting response to treatment.18 However, regulatory bodies (the FDA, Health Canada) considered that the benefit-risk ratio of adding abemaciclib to ET was only favourable in patients with a Ki-67 index of 20% or higher, in addition to high-risk clinicopathologic features.18,23 A detailed discussion of Ki-67 testing is included in Appendix 4.
Indirect Evidence
A focused literature search for indirect treatment comparisons dealing with breast cancer was run in MEDLINE All (1946–) on April 20, 2022. No limits were applied to the search. No indirect evidence was identified from the literature and no indirect treatment comparison was submitted by the sponsor.
Other Relevant Evidence
No other relevant evidence was submitted by the sponsor or identified from the literature.
Discussion
Summary of Available Evidence
The monarchE trial that forms the evidence base for this review is an ongoing, open-label, phase III randomized controlled trial that compared the efficacy and safety of abemaciclib in combination with ET to ET alone in the adjuvant treatment of patients with HR-positive, HER2-negative, node-positive early breast cancer who completed definitive locoregional therapy and were at high risk of recurrence based on clinicopathologic features or the Ki-67 index. The primary efficacy end point was IDFS, and the secondary end points included DRFS and OS. A total of 5,637 patients in 38 countries, including ||||||||| patients from Canada, were randomized to treatment with either abemaciclib plus ET or ET alone. Patients with at least 1 positive lymph node were recruited into 2 cohorts: Cohort 1 or Cohort 2. Patients in Cohort 1 (n = 5,120) were eligible based on high-risk clinicopathologic features (i.e., ≥ 4 positive ALNs, or 1 positive ALN to 3 positive ALNs and at least 1 of the following: tumour size ≥ 5 cm or histologic grade 3). Patients in Cohort 2 (n = 517) were patients at high risk of recurrence based on high levels of the Ki-67 index (Ki-67 index ≥ 20%). In Cohort 1, 3,917 (76%) patients had Ki-67 testing information available and of these, 2,003 patients (51%) had a high Ki-67 index; this patient population is aligned with the Health Canada–approved indication and the current reimbursement request. Cohort 1 patients with a Ki-67 index of 20% or more were predominantly female (99.2%) with a mean age of 51.6 years (SD = 11.1) and an ECOG PS of 0 (86.3%); 54.4% were postmenopausal.
Interpretation of Results
Efficacy
In the monarchE trial, abemaciclib combined with ET resulted in an improvement in IDFS in patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of early recurrence. This treatment benefit extended to the subpopulation of patients with high recurrence risk based on high-risk clinicopathologic features and a Ki-67 index of 20% or more (Cohort 1 Ki-67 High population); this aligns with the Health Canada indication for abemaciclib in the adjuvant treatment of early breast cancer and the current reimbursement request. At the final IDFS primary end point analysis with a median follow-up of 19.1 months, IDFS showed a statistically significant and clinically meaningful difference between the 2 treatment arms in favour of abemaciclib plus ET among the Cohort 1 Ki-67 High population (hazard ratio = 0.643; 95% CI, 0.475 to 0.872; P = 0.0042). The 2-year IDFS rate in the abemaciclib plus ET arm was higher than in the ET arm (91.3% versus 86.1%, respectively). This treatment benefit was maintained at the additional follow-up analysis with a median follow-up of 27 months and 90% of patients having completed or discontinued from the study treatment period (hazard ratio = 0.63; 95% CI, 0.49 to 0.80). The 3-year IDFS rates in the abemaciclib plus ET arm versus the ET arm were 86.1% versus 79.0%, respectively. The DRFS secondary end point was not preplanned for the Cohort 1 Ki-67 High population and was tested outside the statistical hierarchy, precluding definitive conclusions due to the increased risk of false-positive results. However, the findings for DRFS were supportive of the IDFS treatment effect (hazard ratio = 0.571; 95% CI, 0.410 to 0.793); findings at the additional follow-up analysis were similar (hazard ratio = 0.599; 95% CI, 0.456 to 0.787).
OS data remain immature at the most recent analysis in the Cohort 1 Ki-67 High population (and in the ITT population). OS is an event-driven secondary end point with a longer expected maturity in the adjuvant setting. At OS interim analysis 1, there were ||||||||| deaths (||||||||| in the abemaciclib + ET arm and ||||||||| in the ET arm) in the Cohort 1 Ki-67 High population with a hazard ratio of ||||||||||||| (95% CI, |||||||||||||). Therefore, no conclusions can be drawn regarding the efficacy of abemaciclib plus ET with respect to OS at this time and reaching statistical significance for OS will require a considerable number of events and a much longer follow-up. In addition to requiring long follow-up time, interpretation of OS in terms of treatment effect is less clear than in the advanced or metastatic settings. Given these caveats, as Health Canada reviewers have noted, it should be considered that the objective of this trial of demonstrating the benefit in preventing or delaying disease progression in the first 2 years of treatment was achieved.18
Although the efficacy data from the monarchE study demonstrate consistent treatment benefit of abemaciclib plus ET as measured by IDFS and DRFS across all Ki-67 populations in Cohort 1, the data suggest that patients most likely to develop recurrence (i.e., Cohort 1 with a Ki-67 score ≥ 20%) may draw the greatest benefit from the treatment. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Health Canada reviewers concluded that the interpretation of the effect of abemaciclib plus ET on OS is limited and it is not possible to anticipate that the preliminary OS benefit observed in Cohort 1 with Ki-67 of 20% or more will precede an OS benefit in the entire population of Cohort 1, as a persistent negative OS effect cannot be ruled out.18 Consequently, taking into account the benefit-harm-uncertainty assessment, Health Canada recommended that the indication be restricted to those patients in whom the greatest benefit was observed — namely, patients with HR-positive, HER2-negative, node-positive early breast cancer with high risk of disease recurrence based on high-risk clinicopathologic features and a Ki-67 index of 20% or more, despite no significant interaction effects between groups.
HRQoL was identified by both patients and clinical experts as an important aspect of treatment for patients with early breast cancer. Based on the patient group input, most patients are willing to accept treatment side effects if the treatment could lower the risk of disease recurrence. As treatment in the adjuvant setting is with curative intent, it is less amenable than the advanced and/or metastatic setting to improving disease-related symptoms and HRQoL. PRO data suggest that the addition of abemaciclib to ET did not result in any clinically meaningful differences in HRQoL. The interpretation of results (i.e., the ability to assess trends over time [over the treatment period] and to make comparisons across treatment groups) is limited by the significant decline in patients available to provide assessment over time and the lack of formal statistical testing.
Harms
The safety profile of abemaciclib plus ET is well established in the advanced breast cancer setting. Data from the monarchE trial show a similar safety profile of adjuvant abemaciclib in the early breast cancer setting. Overall, the most common AEs experienced on abemaciclib plus ET were predictable and according to the clinical experts consulted, clinically manageable in most patients. Most patients in both treatment arms experienced AEs (97.9% in the abemaciclib + ET arm and 87.2% in the ET arm). A higher proportion of patients in the abemaciclib plus ET arm experienced grade 3 or higher AEs compared to the ET arm (47.4% versus 14.2%, respectively) and SAEs (13.3% versus 7.8%, respectively). The most common AEs in the abemaciclib plus ET arm were diarrhea, neutropenia, fatigue, leukopenia, abdominal pain, nausea, and anemia. Most of these AEs were mild to moderate and the highest incidence of severe events (≥ grade 3) was seen for neutropenia and leukopenia (19.1% and 10.9%, respectively). The most common AEs in the ET arm were arthralgia, hot flush, and fatigue. At the additional follow-up with more than 2 years of follow-up data and more than 90% of patients off the study treatment, the safety results were consistent with the safety results reported at the final IDFS analysis. A higher incidence of grade 3 or higher AEs and SAEs were observed in the abemaciclib plus ET arm than in the ET arm (50% in the abemaciclib plus ET arm versus 15% in the ET arm and 15% in the abemaciclib plus ET arm versus 9% in the ET arm at additional follow-up), with the difference driven mainly by a higher incidence of grade 3 or higher diarrhea, neutropenia, and fatigue in the abemaciclib plus ET population. Similar to the metastatic setting, notable AEs identified in the monarchE study included neutropenia, diarrhea, VTE, and ILD or pneumonitis. Although some AEs — including neutropenia and diarrhea — had faster onset, their incidence and severity decreased over time. The clinical experts consulted indicated that, overall, the type and distribution of AEs observed in the monarchE trial were not unexpected compared to clinical practice.
The proportion of patients who discontinued treatment permanently because of AEs was higher in the abemaciclib plus ET arm compared to the ET arm (6.2% versus 0.8%, respectively). However, the AE profile was notably different in the 2 treatment arms. Most patients in the abemaciclib plus ET arm experienced diarrhea (82.6% in the abemaciclib plus ET arm compared to 7.8% in the ET arm). The majority of patients in the abemaciclib plus ET arm who discontinued abemaciclib or all treatment discontinued due to diarrhea (6.1%). In most cases, discontinuation was due to low-grade events (grade < 2) and occurred during the first 3 months of treatment with no prior dose reduction before discontinuing abemaciclib. After 3 months, the proportion of patients who discontinued treatment decreased monthly and reached 1.0% or less after 6 months. The clinical experts consulted indicated that diarrhea is a known AE experienced by patients on abemaciclib and is managed effectively in most patients in clinical practice. However, given the prolonged duration of adjuvant therapy, persistent AEs such as diarrhea can be particularly bothersome for these young patients with active lives, leading to treatment fatigue and discontinuation of treatment for some. Of note, patient groups indicated that, overall, they were willing to endure the additional side effects of abemaciclib.
Infections were commonly observed in both arms and were mostly low grade, although the incidence of any grade and severe infections was higher in the abemaciclib plus ET arm. The most frequent type of infections reported in both arms were upper respiratory tract infections (abemaciclib + ET arm = 10.5%; ET arm = 8.1%), urinary tract infections (abemaciclib + ET arm = 11.0%; ET arm = 6.8%), and nasopharyngitis (abemaciclib + ET arm = 8.7%; ET arm = 7.0%). However, none of these infections was associated with neutropenia. The incidence of VTE was higher in the abemaciclib plus ET arm (2.4% in the abemaciclib plus ET arm versus 0.6% in the ET arm). The clinical experts noted that VTEs have been reported with other CDK4 and CDK6 inhibitors in combination with ET and the proportion of patients who experienced VTE in the monarchE study is similar to what would be expected in clinical practice. Fatigue was also commonly reported in the monarchE study, with a higher proportion of patients in the abemaciclib arm (39.2% in the abemaciclib plus ET arm versus 16.6% in the ET arm). Although fatigue was mild in most cases, it was 1 of the most common reasons for dose modifications (9.2%) and treatment discontinuation (1.9%). These AEs are well-known for abemaciclib and are labelled in prominent sections of the product monograph.18
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. No specific patterns in etiology or a temporal relationship with exposure was reported for deaths caused by AEs and a cause-effect relationship could not be established due to multiple confounding factors.
Conclusions
Based on data from the monarchE trial, abemaciclib plus ET demonstrated a statistically significant and clinically meaningful benefit compared to ET alone in improving IDFS in people with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score of 20% or more. DRFS was not a pre-specified end point for the Cohort 1 Ki-67 High population and tested outside the statistical hierarchy but appeared to be supportive of the primary efficacy results. It is not yet clear whether IDFS benefits will translate to improved OS as the data remain immature, and follow-up is ongoing. The safety profile of abemaciclib was consistent with the known adverse effects profile of abemaciclib. Effects on HRQoL and health resource utilization remain uncertain due to high attrition and a lack of between-group statistical testing for these outcomes. Although a much longer follow-up time will likely be needed to determine the efficacy of abemaciclib plus ET in terms of OS, given the slow event rate in this setting, the addition of abemaciclib to ET in this new indication could help optimize adjuvant treatment to improve outcomes in terms of disease recurrence. Uncertainties remain regarding the validity and generalizability of Ki-67 testing and practical considerations for its implementation in clinical practice in determining patient eligibility for abemaciclib treatment.
References
1.Canadian Cancer Statistics Advisory Committee, Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian Cancer Statistics 2021. Toronto (ON): Canadian Cancer Society; 2021: https://cancer.ca/Canadian-Cancer-Statistics-2021-EN. Accessed 2022 May 20.
2.Kohler BA, Sherman RL, Howlader N, et al. Annual Report to the Nation on the Status of Cancer, 1975-2011, Featuring Incidence of Breast Cancer Subtypes by Race/Ethnicity, Poverty, and State. J Natl Cancer Inst. 2015;107(6):djv048. PubMed
3.Harbeck N, Penault-Llorca F, Cortes J, et al. Breast cancer. Nat Rev Dis Primers. 2019;5(1):66. PubMed
4.Cardoso F, Spence D, Mertz S, et al. Global analysis of advanced/metastatic breast cancer: Decade report (2005-2015). Breast. 2018;39:131-138. PubMed
5.Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Female Breast Cancer Subtypes. Bethesda (MD): National Cancer Institute: https://seer.cancer.gov/statfacts/html/breast-subtypes.html. Accessed 2022 May 23.
6.Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in premenopausal women with oestrogen receptor-positive early-stage breast cancer treated with ovarian suppression: a patient-level meta-analysis of 7030 women from four randomised trials. Lancet Oncol. 2022;23(3):382-392. PubMed
7.Pan H, Gray R, Braybrooke J, et al. 20-Year Risks of Breast-Cancer Recurrence after Stopping Endocrine Therapy at 5 Years. N Engl J Med. 2017;377(19):1836-1846. PubMed
8.Stuart-Harris R, Dahlstrom JE, Gupta R, Zhang Y, Craft P, Shadbolt B. Recurrence in early breast cancer: Analysis of data from 3,765 Australian women treated between 1997 and 2015. Breast. 2019;44:153-159. PubMed
9.Song F, Zhang J, Li S, et al. ER-positive breast cancer patients with more than three positive nodes or grade 3 tumors are at high risk of late recurrence after 5-year adjuvant endocrine therapy. Onco Targets Ther. 2017;10:4859-4867. PubMed
10.Fasching PA, Gass P, Haberle L, et al. Prognostic effect of Ki-67 in common clinical subgroups of patients with HER2-negative, hormone receptor-positive early breast cancer. Breast Cancer Res Treat. 2019;175(3):617-625. PubMed
11.Cefaro GA, Genovesi D, Trignani M, M DIN. Human epidermal growth factor receptor-2 positivity predicts locoregional recurrence in patients with T1-T2 breast cancer. Anticancer Res. 2014;34(3):1207-1212. PubMed
12.Liang Q, Ma D, Gao RF, Yu KD. Effect of Ki-67 Expression Levels and Histological Grade on Breast Cancer Early Relapse in Patients with Different Immunohistochemical-based Subtypes. Sci Rep. 2020;10(1):7648. PubMed
13.Burstein HJ, Curigliano G, Loibl S, et al. Estimating the benefits of therapy for early-stage breast cancer: the St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann Oncol. 2019;30(10):1541-1557. PubMed
14.Clinical Study Report: I3Y-MC-JPCF. Version 1. monarchE: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Toronto (ON): Eli Lilly Canada Inc.; 2020 Sep 25.
15.Clinical Study Report: I3Y-MC-JPCF. Version 2. monarchE: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Toronto (ON): Eli Lilly Canada Inc.; 2020 Dec 15.
16.Clinical Study Report: I3Y-MC-JPCF. Version 3. monarchE: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Toronto (ON): Eli Lilly Canada Inc.; 2021 Jun 28.
17.Sawaki M, Shien T, Iwata H. TNM classification of malignant tumors (Breast Cancer Study Group). Jpn J Clin Oncol. 2019;49(3):228-231. PubMed
18.Health Canada reviewer's report: Verzenio (abemaciclib) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc.; 2022 Apr 07.
19.Nielsen TO, Leung SCY, Rimm DL, et al. Assessment of Ki67 in Breast Cancer: Updated Recommendations From the International Ki67 in Breast Cancer Working Group. J Natl Cancer Inst. 2021;113(7):808-819. PubMed
20.Guideline Resource Unit. Systemic therapy for early breast cancer - quick reference guide. (Clinical practice guideline BR-014 – version 6). Edmonton (AB): Cancer Care Alberta; 2021: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-systemic-therapy-early-breast.pdf. Accessed 2022 Jul 19.
21.Breast Disease Site Group. Practice Guideline: Disease Management. Provincial Consensus Recommendations for Adjuvant Systemic Therapy for Breast Cancer. Winnipeg (MB): CancerCare Manitoba; 2017: https://ext-opencms.cancercare.mb.ca/export/sites/default/For-Health-Professionals/.galleries/files/treatment-guidelines-rro-files/practice-guidelines/breast/Adjuvant_Breast_Guideline_July_2017.pdf. Accessed 2022 Jul 19.
22.National Center for Biotechnology Information. PubChem Compound Summary for CID 46220502: abemaciclib. Bethesda (MD): National Library of Medicine; 2022: https://pubchem.ncbi.nlm.nih.gov/compound/Abemaciclib. Accessed 2022 May 23.
23.U.S. Food and Drug Administration (FDA). FDA approves abemaciclib with endocrine therapy for early breast cancer. 2021; https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-abemaciclib-endocrine-therapy-early-breast-cancer. Accessed 2022 May 23.
24.Product information: Verzenios (abemaciclib). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2022: https://www.ema.europa.eu/en/documents/product-information/verzenios-epar-product-information_en.pdf. Accessed 2022 Jun 15.
25.Verzenio (abemaciclib): 50 mg, 100 mg, 150 mg, or 200 mg oral tablets [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Jan 10.
26.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
27.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Apr 08.
28.Rugo HS, O'Shaughnessy J, Boyle F, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: safety and patient-reported outcomes from the monarchE study. Ann Oncol. 2022;33(6):616-627. PubMed
29.Harbeck N, Rastogi P, Martin M, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: updated efficacy and Ki-67 analysis from the monarchE study. Ann Oncol. 2021;32(12):1571-1581. PubMed
30.Johnston SRD, Harbeck N, Hegg R, et al. Abemaciclib Combined With Endocrine Therapy for the Adjuvant Treatment of HR+, HER2-, Node-Positive, High-Risk, Early Breast Cancer (monarchE). J Clin Oncol. 2020;38(34):3987-3998. PubMed
31.Elston CW, Ellis IO. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: experience from a large study with long-term follow-up. Histopathology. 1991;19(5):403-410. PubMed
32.Eli Lilly Canada Inc. response to May 27, 2022 DRR request for additional information regarding Verzenio (abemaciclib) DRR review [internal additional sponsor's information]. Toronto (ON): Eli Lilly Canada Inc.; 2022.
33.Hudis CA, Barlow WE, Costantino JP, et al. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: the STEEP system. J Clin Oncol. 2007;25(15):2127-2132. PubMed
34.DeMets DL, Lan KK. Interim analysis: the alpha spending function approach. Stat Med. 1994;13(13-14):1341-1352; discussion 1353-1346. PubMed
35.Gyawali B, Hey SP, Kesselheim AS. Evaluating the evidence behind the surrogate measures included in the FDA's table of surrogate endpoints as supporting approval of cancer drugs. EClinicalMedicine. 2020;21:100332. PubMed
36.Webster K, Cella D, Yost K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: properties, applications, and interpretation. Health Qual Life Outcomes. 2003;1:79. PubMed
37.Hahn EA, Segawa E, Kaiser K, Cella D, Smith BD. Validation of the Functional Assessment of Cancer Therapy-Breast (FACT-B) quality of life instrument. J Clin Oncol. 2015;33(15_suppl):e17753-e17753.
38.Brady MJ, Cella DF, Mo F, et al. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J Clin Oncol. 1997;15(3):974-986. PubMed
39.Eton DT, Cella D, Yost KJ, et al. A combination of distribution- and anchor-based approaches determined minimally important differences (MIDs) for four endpoints in a breast cancer scale. J Clin Epidemiol. 2004;57(9):898-910. PubMed
40.EQ-5D-5L User Guide. Basic information on how to use the EQ-5D-5L instrument. Rotterdam (NL): EuroQol Research Foundation; 2019: https://euroqol.org/publications/user-guides/. Accessed 2022 Jun 02.
41.Lee CF, Ng R, Luo N, et al. The English and Chinese versions of the five-level EuroQoL Group's five-dimension questionnaire (EQ-5D) were valid and reliable and provided comparable scores in Asian breast cancer patients. Support Care Cancer. 2013;21(1):201-209. PubMed
42.Kimman ML, Dirksen CD, Lambin P, Boersma LJ. Responsiveness of the EQ-5D in breast cancer patients in their first year after treatment. Health Qual Life Outcomes. 2009;7:11. PubMed
43.Conner-Spady B, Cumming C, Nabholtz JM, Jacobs P, Stewart D. Responsiveness of the EuroQol in breast cancer patients undergoing high dose chemotherapy. Qual Life Res. 2001;10(6):479-486. PubMed
44.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
45.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
46.Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics: Guidance for Industry. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2018: https://www.fda.gov/media/71195/download. Accessed 2022 May 25.
47.U.S. Food and Drug Administration (FDA). Table of surrogate endpoints that were the basis of drug approval or licensure. 2022; https://www.fda.gov/drugs/development-resources/table-surrogate-endpoints-were-basis-drug-approval-or-licensure. Accessed 2022 May 04.
48.U.S. Food and Drug Administration (FDA). FDA facts: biomarkers and surrogate endpoints. 2017; https://www.fda.gov/about-fda/innovation-fda/fda-facts-biomarkers-and-surrogate-endpoints. Accessed 2022 May 04.
49.Saad ED, Squifflet P, Burzykowski T, et al. Disease-free survival as a surrogate for overall survival in patients with HER2-positive, early breast cancer in trials of adjuvant trastuzumab for up to 1 year: a systematic review and meta-analysis. Lancet Oncol. 2019;20(3):361-370. PubMed
50.Committee For Medicinal Products For Human Use. Guideline on the clinical evaluation of anticancer medicinal products. Amsterdam (NL): European Medicines Agency; 2019: https://www.ema.europa.eu/documents/scientific-guideline/draft-guideline-evaluation-anticancer-medicinal-products-man-revision-6_en.pdf. Accessed 2022 May 25.
51.Validity of surrogate endpoints in oncology, version 1.1. (IQWiG Reports – Commission No. A10-05). Cologne (DE): Institute for Quality and Efficiency in Health Care (IQWiG); 2011: https://www.iqwig.de/download/a10-05_executive_summary_v1-1_surrogate_endpoints_in_oncology.pdf. Accessed 2022 May 26.
52.Haslam A, Hey SP, Gill J, Prasad V. A systematic review of trial-level meta-analyses measuring the strength of association between surrogate end-points and overall survival in oncology. Eur J Cancer. 2019;106:196-211. PubMed
53.Buyse M, Saad ED, Burzykowski T, Regan MM, Sweeney CS. Surrogacy Beyond Prognosis: The Importance of “Trial-Level” Surrogacy. Oncologist. 2022;27(4):266-271. PubMed
54.Buyse M, Molenberghs G, Burzykowski T, Renard D, Geys H. The validation of surrogate endpoints in meta-analyses of randomized experiments. Biostatistics. 2000;1(1):49-67. PubMed
55.Ng R, Pond GR, Tang PA, MacIntosh PW, Siu LL, Chen EX. Correlation of changes between 2-year disease-free survival and 5-year overall survival in adjuvant breast cancer trials from 1966 to 2006. Ann Oncol. 2008;19(3):481-486. PubMed
56.U.S. Food and Drug Administration (FDA). Ki-67 IHC MIB-1 pharmDx (Dako Omnis) - P210026. 2021; https://www.fda.gov/medical-devices/recently-approved-devices/ki-67-ihc-mib-1-pharmdx-dako-omnis-p210026. Accessed 2022 May 10.
57.Inwald EC, Klinkhammer-Schalke M, Hofstadter F, et al. Ki-67 is a prognostic parameter in breast cancer patients: results of a large population-based cohort of a cancer registry. Breast Cancer Res Treat. 2013;139(2):539-552. PubMed
58.Dowsett M, Nielsen TO, A'Hern R, et al. Assessment of Ki67 in breast cancer: recommendations from the International Ki67 in Breast Cancer working group. J Natl Cancer Inst. 2011;103(22):1656-1664. PubMed
59.Yerushalmi R, Woods R, Ravdin PM, Hayes MM, Gelmon KA. Ki67 in breast cancer: prognostic and predictive potential. Lancet Oncol. 2010;11(2):174-183. PubMed
60.Smith I, Robertson J, Kilburn L, et al. Long-term outcome and prognostic value of Ki67 after perioperative endocrine therapy in postmenopausal women with hormone-sensitive early breast cancer (POETIC): an open-label, multicentre, parallel-group, randomised, phase 3 trial. Lancet Oncol. 2020;21(11):1443-1454. PubMed
61.Andre F, Ismaila N, Allison KH, et al. Biomarkers for Adjuvant Endocrine and Chemotherapy in Early-Stage Breast Cancer: ASCO Guideline Update. J Clin Oncol. 2022;40(16):1816-1837. PubMed
62.Nielsen TO, Jensen MB, Burugu S, et al. High-Risk Premenopausal Luminal A Breast Cancer Patients Derive no Benefit from Adjuvant Cyclophosphamide-based Chemotherapy: Results from the DBCG77B Clinical Trial. Clin Cancer Res. 2017;23(4):946-953. PubMed
63.Hofmann D, Nitz U, Gluz O, et al. WSG ADAPT - adjuvant dynamic marker-adjusted personalized therapy trial optimizing risk assessment and therapy response prediction in early breast cancer: study protocol for a prospective, multi-center, controlled, non-blinded, randomized, investigator initiated phase II/III trial. Trials. 2013;14:261. PubMed
64.Mengel M, von Wasielewski R, Wiese B, Rudiger T, Muller-Hermelink HK, Kreipe H. Inter-laboratory and inter-observer reproducibility of immunohistochemical assessment of the Ki-67 labelling index in a large multi-centre trial. J Pathol. 2002;198(3):292-299. PubMed
65.Davey MG, Hynes SO, Kerin MJ, Miller N, Lowery AJ. Ki-67 as a Prognostic Biomarker in Invasive Breast Cancer. Cancers (Basel). 2021;13(17):4455. PubMed
66.Owens R, Gilmore E, Bingham V, et al. Comparison of different anti-Ki67 antibody clones and hot-spot sizes for assessing proliferative index and grading in pancreatic neuroendocrine tumours using manual and image analysis. Histopathology. 2020;77(4):646-658. PubMed
67.Parry S, Dowsett M, Dodson A. UK NEQAS ICC & ISH Ki-67 Data Reveal Differences in Performance of Primary Antibody Clones. Appl Immunohistochem Mol Morphol. 2021;29(2):86-94. PubMed
68.Polewski MD, Nielsen GB, Gu Y, et al. A Standardized Investigational Ki-67 Immunohistochemistry Assay Used to Assess High-Risk Early Breast Cancer Patients in the monarchE Phase 3 Clinical Study Identifies a Population With Greater Risk of Disease Recurrence When Treated With Endocrine Therapy Alone. Appl Immunohistochem Mol Morphol. 2022;30(4):237-245. PubMed
69.Coates AS, Winer EP, Goldhirsch A, et al. Tailoring therapies--improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann Oncol. 2015;26(8):1533-1546. PubMed
70.Leung SCY, Nielsen TO, Zabaglo LA, et al. Analytical validation of a standardised scoring protocol for Ki67 immunohistochemistry on breast cancer excision whole sections: an international multicentre collaboration. Histopathology. 2019;75(2):225-235. PubMed
71.Boyaci C, Sun W, Robertson S, Acs B, Hartman J. Independent Clinical Validation of the Automated Ki67 Scoring Guideline from the International Ki67 in Breast Cancer Working Group. Biomolecules. 2021;11(11):30. PubMed
72.Acs B, Pelekanou V, Bai Y, et al. Ki67 reproducibility using digital image analysis: an inter-platform and inter-operator study. Lab Invest. 2019;99(1):107-117. PubMed
73.Giordano SH, Freedman RA, Somerfield MR, Optimal Adjuvant Chemotherapy and Targeted Therapy Guideline Expert Panel. Abemaciclib With Endocrine Therapy in the Treatment of High-Risk Early Breast Cancer: ASCO Optimal Adjuvant Chemotherapy and Targeted Therapy Guideline Rapid Recommendation Update. J Clin Oncol. 2022;40(3):307-309. PubMed
74.NCCN Guidelines. Breast Cancer, version 2.2022. Plymouth Meeting (PA): National Comprehensive Cancer Network (NCCN); 2021: https://www.nccn.org/. Accessed 2022 Apr 11.
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: August 30, 2021
Alerts: Biweekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
exp breast neoplasms/
((breast* or mamma or mammar* or lobular*) adj5 (cancer* or carcinoid* or carcinoma* or carcinogen* or adenocarcinoma* or adeno-carcinoma* or malignan* or neoplas* or sarcoma* or tumo?r* or mass*)).ti,ab,kf.
or/1-2
network meta-analysis/
(meta-analysis/ or meta-analysis as topic/ or "meta analysis (topic)"/) and network.ti,ab,kf.
((indirect or indirect treatment or mixed treatment or bayesian) adj3 comparison*).ti,ab,kf.
(network* adj3 (meta-analy* or metaanaly*)).ti,ab,kf.
(multi* adj3 treatment adj3 comparison*).ti,ab,kf.
(mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf.
umbrella review*.ti,ab,kf.
nma.ti,ab,kf.
(Multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
(Multiparamet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
MPES.ti,ab,kf.
or/4-15
3 and 16
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search – Studies with results | Verzenio OR Verzenios OR abemaciclib OR bemaciclib OR ABE OR LY-2835219 OR LY2835219 OR LY-2385219 OR LY2385219 OR LY-2835210 OR LY2835210 OR 60UAB198HK | Breast Cancer]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms – (Verzenio OR Verzenios OR abemaciclib OR bemaciclib OR ABE OR LY-2835219 OR LY2835219 OR LY-2385219 OR LY2385219 OR LY-2835210 OR LY2835210 OR 60UAB198HK) AND breast cancer]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms – abemaciclib]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms – (Verzenio OR abemaciclib) AND breast cancer]
Grey Literature
Search dates: April 8, 2022, to April 21, 2022
Keywords: [Verzenio OR abemaciclib OR breast cancer]
Limits: Publication years: 1996–present
Updated: Search updated prior to the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC)
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Detailed Outcome Data
Note this appendix has not been copy-edited.
Table 26: Invasive Disease–Free Survival, Final Analysis — Intention-to-Treat Population
Survival | Abemaciclib + ET N = 2,808 | ET N = 2,829 |
|---|---|---|
Number of events, n (%) | 163 (5.8) | 232 (8.2) |
|||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Treatment effect/difference — P value (c)b | ||||||||||||||||||||||||| | |
P value (2-sided) log-rank | Stratified:d P = 0.00089 (|||||||||||||||||||||||||) | |
Hazard ratio (95% CI)e | Stratified:d 0.713 (0.583 to 0.871), ||||||||||||||||||||||||| | |
IDFS rate, % (95% CI)f | ||
12 months | 96.5 (95.7 to 97.1) | 95.7 (94.9 to 96.4) |
Treatment effect/difference — P value (2-sided) | 0.8 (–0.2 to 1.8), P = 0.1276 | |
24 months | 92.3 (90.9 to 93.5) | 89.3 (87.7 to 90.7) |
Treatment effect/difference — P value (2-sided) | 3.0 (1.1 to 5.0), P = 0.0025 | |
CI = confidence interval; ET = endocrine therapy; IDFS = invasive disease–free survival; ITT = intention to treat.
Note: Data cut-off date: July 8, 2020.
aRestriction time is defined by the latest time where the standard error of the survival estimates is ≤ 0.075.
bTreatment Effect/Difference/P values are computed based on comparator ET.
c2-sided P value based on normal approximation.
dStratified by IWRS Geographical Region, IWRS Prior Treatment, IWRS Menopausal Status.
eEstimated using a Cox proportional hazards model.
f95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Source: Clinical Study Report for Verzenio (final IDFS [primary outcome] analysis).15
Table 27: Invasive Disease–Free Survival, Final Analysis — Ki-67 High Population
Survival | Abemaciclib + ET N = 1,262 | ET N = 1,236 |
|---|---|---|
Number of events, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Deaths without invasive disease, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Invasive disease, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Number of patients censored, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Invasive disease prior to randomization, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
No post-baseline assessment, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
No documented invasive disease, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Restricted mean (95% CI) with restriction time = 30.7 monthsa | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided)b | ||||||||||||||||||||||||| | |
P value (2-sided) log-rank | ||||||||||||||||||||||||| | |
Hazard ratio (95% CI)e | ||||||||||||||||||||||||| | |
IDFS rate, % (95% CI)f | ||
12 months | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided) | ||||||||||||||||||||||||| | |
24 months | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided) | ||||||||||||||||||||||||| | |
CI = confidence interval; ET = endocrine therapy; IDFS = invasive disease–free survival; ITT = intention to treat.
Note: Data cut-off date: July 8, 2020.
aRestriction time is defined by the latest time where the standard error of the survival estimates is ≤ 0.075.
bTreatment effect, difference, and P values are computed based on comparator ET.
c2-sided P value based on normal approximation.
dStratified by geographical region, prior treatment, and menopausal Status.
eEstimated using a Cox proportional hazards model.
f95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Source: Clinical Study Report for Verzenio (final IDFS [primary outcome] analysis).15
Table 28: Invasive Disease–Free Survival by Subgroup — Intention-to-Treat Population
Subgroup survival | 2-year IDFS rate | Hazard ratio (95% CI) | Interaction P value | |
|---|---|---|---|---|
Abemaciclib + ET N = 2,808 | ET N = 2,829 | |||
Menopausal status | ||||
Premenopausal | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Postmenopausal | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
Primary tumour size | ||||
< 20 mm | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
≥ 20 mm but < 50 mm | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
≥ 50 mm | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
Tumour grade | ||||
G1: Favourable | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
G2: Moderately favourable | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
G3: Unfavourable | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
Number of positive lymph nodes | ||||
1 to 3 | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
4 to 9 | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
10 or more | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
Progesterone receptor | ||||
Negative | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Positive | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
Baseline ECOG PS | ||||
0 | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
1 | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ET = endocrine therapy, IDFS = invasive disease–free survival.
Note: Data cut-off date: July 8, 2020.
Source: Clinical Study Report for Verzenio (final IDFS [primary outcome] analysis).15
Table 29: Overall Survival — Intention-to-Treat Population
Survival | Abemaciclib + ET N = 2,802 | ET N = 2,829 |
|---|---|---|
Number of events, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Deaths, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Number of patients censored, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Alive, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Lost to follow-up, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Withdrawal by patient, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
P value (2-sided) log-rank | ||||||||||||||||||||||||| | |
Hazard ratio (95% CI)b | ||||||||||||||||||||||||| | |
OS time survival rate, % (95% CI)c | ||
12 months | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided) d | ||||||||||||||||||||||||| | |
24 months | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided) d | ||||||||||||||||||||||||| | |
36 months | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| |
Treatment effect/difference — P value (2-sided) d | ||||||||||||||||||||||||| | |
CI = confidence interval; ET = endocrine therapy; ITT = intention to treat.
Note: Data cut-off date: April 1, 2021.
aStratified by geographical region, prior treatment, and menopausal status.
bEstimated using a Cox proportional hazards model.
c95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
dTreatment Effect/Difference/P values are computed based on comparator ET.
Source: Clinical Study Report for Verzenio (overall survival interim analysis 1).16
Table 30: Summary of Overall Survival, Cohort 1, By Ki-67 Index — 20% or More Versus Less Than 20%
Cohort survival | Abemaciclib + ET | ET | Treatment effect | ||
|---|---|---|---|---|---|
Stratified hazard ratio (95% CI)a, b, c | 2-sided P valuea | ||||
Cohort 1 Ki-67 High (≥ 20%) | |||||
Total subgroup population, N | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | — | ||
Number of deaths, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
Cohort 1 Ki-67 Low (< 20%) | |||||
Total subgroup population, N | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | — | ||
Number of deaths, n (%) | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | ||||||||||||||||||||||||| | |
CI = confidence interval; ET = endocrine therapy.
Note: Data cut-off date: July 8, 2020.
aThe analyses were not adjusted for multiple comparisons, therefore at increased risk of type I error.
bStratified by geographical region, prior treatment, and menopausal status.
cEstimated using a Cox proportional hazards model.
Source: Health Canada reviewer’s report.18
Appendix 3: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
FACT-B
EQ-5D-5L
Findings
The findings about the validity, reliability, responsiveness, and MID of each outcome measure are summarized in Table 31.
Table 31: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Functional Assessment of Cancer Therapy-Breast (FACT-B); version 4 | Disease-specific HRQoL questionnaire including 27 items from the FACT-G related to physical, social/family, emotional, and functional well-being as well as a breast cancer-specific 10-item subscale.36 | Validity: In studies of breast cancer: moderate correlations between most FACT-B version 3 subscales and the Body Image Scale (r = –0.34 to –0.55)37; most subscales differentiated groups by ECOG PSR or extent of disease indicating discriminant validity.38 Reliability: Good internal consistency reliability with alpha > 0.7 for most subscales in a study of patients with advanced breast cancer.37 Alpha coefficients ranged from 0.63 to 0.86 for all subscales and 0.90 for the total score and good test-retest reliability with a correlation coefficient of 0.85 for the total score in a study of patients with breast cancer.38 Responsiveness: Among 47 patients with breast cancer tested at 2-month intervals, a significant sensitivity to change in PSR was found for the FACT-B total score, the physical and function well-being subscales, and the breast cancer subscale. Sensitivity to change as measured by the FLIC was found in the FACT-B and FACT-G total score and the physical, function, and emotional subscales.38 | In patients with advanced breast cancer, an MID has been defined as a 7-point to 8-point change on the total FACT-B score using anchor and distribution-based methods.39 |
EQ-5D-5L | Generic preference based HRQoL scale consisting of an EQ VAS with values between 100 (best imaginable health) and 0 (worst imaginable health) as judged by the patient. A composite index score of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/ depression. Five response levels for each dimension ranging from experiencing no problems to extreme problems.40 In the monarchE trial the index values were calculated using the published UK value set.15 | Validity: In a study of English-speaking Asian patients with breast cancer: FACT-B total score moderately correlated with the utility index (r = 0.56) and with the EQ VAS (r = 0.61) indicating convergent validity41 Reliability: Strong test-retest reliability in aforementioned study of patients with breast cancer with an ICC of 0.83 (95% CI, 0.76 to 0.89) for the EQ VAS and 0.81 (95% CI, 0.73 to 0.87) for the utility index.41 Responsiveness: Demonstrated in patients with breast cancer following curative treatment; however, small changes in health were not recognized as being meaningful.42,43 | MID for the index score was estimated to range from 0.037 to 0.056 in the general Canadian population.44 MID for the EQ VAS among various types of cancer using both anchor and distribution-based methods ranged from 7 to 12.45 An MID specific to patients with breast cancer was not identified. |
ECOG = Eastern Cooperative Oncology Group; EQ-5D-5L = EQ-5D Five-Level; FACIT-F = Functional Assessment of Chronic Illness Therapy - Fatigue; FACT-B = Functional Assessment of Cancer Therapy - Breast; FACT-ES = Functional Assessment of Cancer Therapy - Endocrine Symptoms; FACT-G = Functional Assessment of Cancer Therapy-General; HRQoL = Health-related quality of life; FLIC = Functional Living Index-Cancer; GHS = Global Health Status; ICC = intraclass correlation coefficient; MID = minimal important difference; POMS = Profile of Mood States; PSR = performance status rating.
The following section describes the DFS outcome measure and summarizes evidence that examines the validity of DFS as surrogate for OS in patients with early-stage breast cancer. Studies discussed in this section were identified through a literature search and by reviewing bibliographies of key papers.
In the monarchE trial,15 IDFS was the primary outcome used to evaluate efficacy of abemaciclib plus ET compared to those treated with ET alone in the ITT population (all randomized patients in Cohort 1 and Cohort 2). Secondary objectives included the assessment of IDFS in the Cohort 1 Ki-67H population of the monarchE trial. IDFS events in the trial were defined as local, regional, contralateral, distant, second primary non-breast invasive cancers, and death as defined by the STEEP system (version 1).33 The STEEP system definition of IDFS specifically excludes all in situ cancer events (ipsilateral or contralateral DCIS, ipsilateral or contralateral LCIS and all in situ cancers of non-breast sites) and was proposed as an alternative to DFS which had been inconsistently defined across previous clinical trials.33 The identification of IDFS events in the monarchE trial (that were not defined by death) was based on the location of the recurrent disease as recorded by the investigator.15 During the on-study treatment period patients were evaluated for recurrence at every clinic visit (biweekly for the first 2 months, monthly during months 3 to 6, and every 3 months thereafter) and at every telephone visit (monthly between every 3 month clinic visits) until distant disease recurrence or death.15
Guideline Recommendations
In a guidance document assessing end points used in clinical trials for cancer drugs and biologics, the FDA noted the benefits and drawbacks to using DFS as a primary end point.46 Advantages of the DFS outcome include being an objective measure based on quantitative assessment, being evaluable sooner (especially when the survival period is expected to be prolonged), and needing a smaller sample size compared with studies using OS as an end point.46 Using DFS as an end point has disadvantages such as variable definitions across studies, the potential for assessment bias especially in open-label studies, inclusion of non-cancer deaths, and achieving a balanced timing of assessments across treatment groups is essential.46 The FDA guidelines recommend that sponsors clearly define the end point, outline the schedule for assessments, include an estimation of the treatment effect size, and ensure blinding of treatment assignments to help reduce the potential for bias.46 According to the FDA guidance, the Oncology Drug Advisory Committee agreed in December 2003, that DFS prolongation represented clinical benefit if the magnitude of this benefit outweighed the toxicity of the adjuvant treatment.46 According to the FDA, DFS has served as the key outcome for FDA’s Accelerated or Traditional Approvals for adjuvant breast cancer hormonal therapy, adjuvant colon cancer, adjuvant cytotoxic breast cancer, adjuvant therapy for stage III non–small cell lung cancer, melanoma, renal cell cancer, and gastrointestinal stromal tumour.47 The FDA guidance noted that while reasonable likely surrogate end points that have not been validated (i.e., not shown to reliably predict, or correlate with, clinical benefit) may be used under the FDA’s Accelerated Approval program to shorten the time to patient access, sponsors must verify the predicted clinical benefit with post-approval clinical trials.46,48
The FDA’s guidance on the trial design indicates that DFS is a suitable surrogate for OS for accelerated or regular approval for breast cancer treatments and has been used has the primary basis of approval for adjuvant hormonal and cytotoxic therapies.46 The FDA does not discuss the validity of DFS as surrogate end point for OS in their guidance.46 Gyawali et al. (2020) evaluated the evidence for surrogate end points listed in the FDA table of surrogate end points for breast cancer and found no strong correlation between treatment effects on DFS and OS despite being listed as appropriate for traditional approval.35 The only exception was DFS in HER2 positive early breast cancer which had strong correlation with OS according to 1 systematic review.35,49
The European Medicines Agency guidance noted that while a benefit in OS is the most convincing outcome, other possible primary end points include progression-free survival, DFS, and PROs.50 The European Medicines Agency guidance states that while DFS is considered a benefit to a patient regardless of cure, OS data should be reported in the adjuvant setting, as adjuvant therapy may limit treatment options upon disease recurrence. In established areas of adjuvant therapy (e.g., breast cancer, colorectal cancer) and if a favourable benefit-risk ratio exists based on DFS, safety and survival data, and progression-free survival results for next-line therapy are available, the reporting of mature survival data may be delayed until after licensing.50
There are several methods used to assess validity of surrogate outcomes, particularly correlation-based approaches.51 In order to examine the validity of surrogate end points for OS, it has been suggested to evaluate the strength of correlation between OS and the surrogate outcome.35,52 For the purpose of assessing the validity of surrogates for regulatory approval, focus has been placed on trial-level surrogacy (i.e., the correlation of the group-level treatment effect on the surrogate outcome with the treatment effect on OS).52 In contrast, correlations that assess the prognostic validity of a surrogate in individual patients (e.g., correlations of median DFS with median OS), cannot confirm the validity of a surrogate for predicting treatment effects on OS.35 Buyse et al., (2022) similarly suggested that individual-level surrogacy cannot determine how changes in the surrogate will result in changes in OS in a group of patients, therefore the use of trial-level surrogacy is necessary to determine if the effect of treatment on the surrogate can be used to predict the effect of treatment on OS.53
The Institute of Quality and Efficacy in Health Care (IQWiG) suggested that an observed correlation between the surrogate outcome and the clinical end point on its own, cannot adequately demonstrate the validity of a surrogate.51 Instead, comprehensive data are required, preferable a meta-analysis of several randomized trials showing robust results. A requirement for large datasets was also suggested by Buyse et al. (2000), noting that multiple randomized studies are required to obtain precise estimates and to distinguish individual-level from trial-level associations between the end points and effects of interest.54 In the guidance of the IQWiG, it is cautioned that the validity of a surrogate is likely both disease-specific and intervention-specific and that conclusions about the validity of a surrogate cannot be easily applied across different indications or interventions.51 Buyse et al. similarly noted that trial-level surrogacy results in 1 setting may not necessarily apply to a future trial examining a different question. For instance, the effects of a new drug with a novel mechanism of action may have considerably different direct and indirect effects on survival than previous treatments. The IQWiG guidance further suggests that a correlation between the surrogate and a clinical end point could be characterized as strong if the correlation coefficient is at least 0.85, as low if the correlation coefficient is 0.7 or less, and as medium if the correlation coefficient is between 0.85 and 0.7.
Selected Evidence for DFS as a Surrogate Outcome for OS in Breast Cancer
Ng et al. (2008) conducted a systematic review to assess trial-level associations by examining 126 adjuvant breast cancer trials conducted between 1966 to 2006 with more than 100 patients per treatment group to evaluate whether differences between treatment and control groups in 2-year DFS was a significant predictor of difference in 5-year OS.55 Comparisons were made between control groups and other experimental groups due to potential correlations between treatment comparisons within trials with multiple groups. The authors used a meta-analytic validation approach,54 in which linear regression weighted according to the sample size of individual trials was used to calculate correlation coefficients, the proportion of variation, and predicted estimates of 95% prediction intervals. The review found a moderate correlation coefficient of 0.65 (P < 0.001) between 2-year DFS difference and 5-year OS difference after adjusting for all other predictors (i.e., menopausal status, intervention, nodal status, hormonal status, and the year accrual was completed). Less than half the variation of the differences in 5-year OS was explained by the model with an R2 value of 0.42. When examining various predicted differences in 5-year OS for a range of 2-year DFS differences and trial sample sizes, the 95% prediction intervals were very wide. For example, for a future trial with 1,000 patients where the 2-year DFS for the experimental group was 10% higher than the control arm; the 95% prediction interval for 5-year OS difference would range from –0.2% to 11%. Therefore, the authors concluded that the correlation between the 2-year DFS difference and the difference in 5-year OS was not strong enough for DFS to be used as a surrogate for OS. The authors noted limitations including the fact that breast cancer is a heterogenous disease with many factors not captured in their analyses such as HER2 status. Most of the trials included in the systematic review used treatments developed before 2008 and had small improvements in DFS and OS compared to their control. This resulted in limited variability in the DFS differences which reduced the power to detect correlations between differences in DFS and OS.55 It should be noted that this review is missing numerous more recent trials and the treatment landscape has changed since its publication with potential improvements in adjuvant treatments.
A more recent systematic review and meta-analysis by Saad et al. (2019) assessed trial- and patient-level data from 8 randomized controlled trials to determine the correlation of treatment effects on DFS with those on OS in patients with HER2-positive early breast cancer.49 In all 8 trials, trastuzumab was the anti-HER2 antibody examined with data for a total of 21,480 patients who were enrolled between 1999 to 2012. Each trial had at least 1 control group with chemotherapy, a lower total dose or duration of trastuzumab, or observation alone. Trials had slight differences in their definitions for DFS, and therefore DFS in the analysis referred to any type of recurrence (invasive or non-invasive) or death from any cause. The Spearman's correlation coefficient was used to determine the association between DFS and OS at the patient level and a linear regression model weighted by the number of deaths was used to determine the coefficient of determination to ascertain the association between log hazard ratios for DFS and OS at the trial-level. The results found strong associations between DFS and OS at the patient level with R = 0.90 (95% CI, 0.89 to 0.90), unadjusted for prognostic factors. Strong associations between DFS and OS were found at the trial-level with R2 = 0.75 (95% CI, 0.50 to 1.00) for the full-set of 12 contrasts and R2 = 0.85 (95% CI, 0.67 to 1.00) when excluding 1 outlying trial, comparing 11 contrasts. The review concluded that DFS is an appropriate surrogate measure for the long-term outcome OS in adjuvant studies for HER2-positive early breast cancer.49 It should be noted that this review only examined the use of trastuzumab among patients with HER2-positive early breast cancer which may not be generalizable to the current reimbursement request.
Conclusion
Two systematic reviews were summarized, which assessed the appropriateness of DFS as a surrogate outcome for OS in early-stage breast cancer. Ng et al. found a moderate correlation between 2-year DFS difference and 5-year OS difference with wide 95% prediction intervals, suggesting that the correlation was not strong enough for DFS to be used as a predictor of OS in adjuvant breast cancer trials.55 Limitations of this review included the significant heterogeneity across trials in terms of patient populations (i.e., node, hormonal, and menopausal status) and interventions (i.e., chemotherapy, hormonal treatment, and immunotherapy) examined. Also, differing definitions used for DFS across trials were noted with 30% of studies not specifying their definition for DFS. Of the trial that did define DFS, 31% did not include contralateral breast cancer, and 30% did not include all deaths, both of which were used in the monarchE trial definition for IDFS.15,55 Therefore, generalizability of results of the review to the monarchE patient group is uncertain. A strength of the Saad et al. review was the inclusion of a large dataset with trial-level correlations which provides support for DFS as a surrogate for OS in adjuvant studies for HER2-positive breast cancer.49 However, it has been noted that the validity of a surrogate is likely both disease-specific and intervention-specific as the validity of a surrogate cannot be easily applied across different indications or interventions.51 The review by Saad et al. was specific to HER2-postive breast cancer and therefore these correlations cannot be directly applied to the patient population in the monarchE trial.15,49 No study was identified that investigated patient-level and/or trial-level surrogacy of DFS with abemaciclib plus ET in the present target population; therefore, it cannot be determined to what extent, if any, the improvements in IDFS observed in patients in the abemaciclib plus ET group of the monarchE trial15 would translate into OS benefits.
Appendix 4: Summary of Ki-67 Testing in Breast Cancer
Note this appendix has not been copy-edited.
Material considered in this section is provided as supporting information. The information has not been systematically reviewed.
Aim
To summarize the use, limitations, and guideline recommendations for Ki-67 testing in patients with breast cancer.
Findings
Background
In the monarchE trial, Ki-67 levels were measured in a central laboratory with the use of a standardized IHC assay; the Ki-67 pharmDx Kit15 (Dako Omnis).56 The monarchE trial used a Ki-67 score of 20% or more as its cut-off for determining a high risk of recurrence.
The clinical experts consulted by CADTH for this review stated that Ki-67 testing is not broadly practised in the Canadian clinical setting and expressed concerns regarding the reliability of Ki-67 IHC analyses.
Overview of Ki-67
The Ki-67 antigen is a marker of cellular proliferation that can be detected and quantified by IHC. Various studies have found that the Ki-67 antigen acts as a prognostic biomarker of tumour progression or recurrence, including early-stage breast cancer.57-60 For example, in a 2013 retrospective cohort study of 3,658 patients in Germany with breast cancer, in multivariate analysis (including clinical and histopathological parameters) Ki-67 had an independent prognostic effect on both DFS (Ki-67 > 45% compared to ≤ 15%, hazard ratio = 1.96 [95% CI, 1.31 to 2.91; P = 0.001]) and OS (Ki-67 > 45% compared to ≤ 15%, hazard ratio = 2.06 [95% CI, 1.30 to 3.28; P = 0.002]).57 Ki-67 has been examined in the neoadjuvant ET setting to guide adjuvant therapy recommendations for postmenopausal women.61 For instance, in the POETIC trial,60 postmenopausal patients with ER-positive, HER2-negative, stage I to stage III breast cancer with Ki-67 levels of less than 10% before any systemic therapy and after 2 weeks of neoadjuvant AI therapy had a 5-year recurrence risk of 4.3% (95% CI, 2.9% to 6.3%) while patients with Ki-67 index of 10% or more at both time points had a 5-year recurrence risk of 21.5% (95% CI, 17.1% to 27.0%).60 It should be noted that various clinical studies have used different Ki-67 cut-offs which limits their interpretability and the use of Ki-67 in the neoadjuvant setting is still investigational.19,61
There is limited evidence indicating that Ki-67 may be predictive of whether certain cancer treatments in patients with breast cancer are likely to be efficacious and may provide indication of whether the therapy is actively working. For instance, lower levels of Ki-67 may be associated with lesser or no benefit of cytotoxic chemotherapy.19,62 Further research in this area is being conducted.19,63
Ki-67 Testing and Standardization
IHC analyses are used to assess tumour cell proliferation in breast tissue.19 The Ki-67 score in IHC-stained slides is the percentage of positively stained cells among the total number of cancer cells examined in a number of regions.64 Variability in sample preparation methods between different laboratories and different scoring methods between observers limits the reproducibility of Ki-67 IHC.19 The expression of Ki-67 has been difficult to standardize,61 as many factors can affect the results of analyses such as preanalytical considerations (type of specimen, fixation, and means of storage), analytical considerations (antigen retrieval, selection of an antibody, the detection system used, and the completeness of counterstaining), and scoring considerations (method of scoring, area of slide read, global versus hot spots, how many cells to be counted, digital imaging, and data cut-offs).19,65
In 2019, the IKWG aimed to develop internationally acceptable methods for IHC processes (preanalytical and analytical) and reporting (scoring) with their recommendations published in July 2021.19 In regard to IHC processes, the IKWG stated that core biopsies are preferred, and high temperature antigen retrieval is mandatory. For antibody selection, MIB1 is currently the most commonly used antibody and other common antibodies used include SP6, 30-9, K2, and MM1.19 Certain antibodies have been found to work better on specific staining platforms such as the 30-9 for the Ventana Ultra or K2 and MM1 for the Leica Bond III.19,66 A 2021 study examining Ki-67 staining data from 374 laboratories found that higher quality staining results occurred when Agilent Dako antigen retrieval, detection, and staining platforms were used for MIB-1 clones and Leica Biosystems platforms were used for MM1 clones, respectively.67 In terms of detection system used, the IKWG stated that polymer detection on automated platforms has replaced avidin-biotin systems which have demonstrated lower sensitivity.19 They recommend that all negative nuclei should be counterstained to prevent a falsely high Ki-67 score.19
The monarchE trial assessed Ki-67 using the Ki-67 pharmDx kit on the Omnis platform.68 It is important to consider the assay performance and concordance of the results from the trial as compared with other assays on the market which have yet to be determined. According to a clinical expert consulted on this review, the Agilent Ki-67 pharmDx assay performed on the Omnis platform is not available in Canada and is also not widely available in the US. According to the clinical expert, it is not clear at this time how the 20% cut-off would be applied to other antibodies and kits from other vendors.
There is no consistent cut-off for the Ki-67 score used in clinical studies.19 The monarchE trial used a Ki-67 cut-off of 20% or more for determining a high risk of recurrence which was proposed by the St. Gallen International Expert Consensus in 2015.15,69 A majority of the expert panel agreed to a Ki-67 cut-off within the range of 20 to 29% to define luminal B-like tumours, but one-fifth of the panel believed that Ki-67 should not be used at all to make this distinction.69 The IKWG developed a standardized method for visual scoring of Ki-67 in breast cancer which requires calibration training for colour threshold and tumour cell selection, software installation to download and install the Ki-67 counting app, and a median of 9 minutes to score each case.19 They found that the global average scoring across the entire IHC-stained slide rather than examining selected “hot spots” on the slide resulted in higher reproducibility.70 Although the differences between methods were not statistically significant, the intraclass correlation coefficient for the global method met the pre-specified success criterion whereas the hot spot approach did not.70 In developing this standardized scoring method, the IKWG found considerable inter-observer variability in Ki-67 scores ranging from greater than 5% to less than 30%, and therefore recommended cut-off scores of 5% or less for low Ki-67 and 30% or more for high Ki-67 to be used in non-trial health settings which differs from the 20% or more cut-off used in the monarchE trial.19,61
The IKWG noted that developments in automated scoring methods may assist with addressing the current variability in IHC Ki-67 scoring.19 One such method mentioned in the IKWG guidelines includes an open-source digital image analysis platform named QuPath. A recent study assessed the reproducibility of QuPath to determine Ki-67 scoring following IKWG guidelines in a cohort of 157 patients with ER-positive breast cancer71 Results found high inter-observer reproducibility between the 4 different algorithms developed and the reference standard (obtained by a separate QuPath algorithm on a subset of 30 patients) with an ICC of 0.938 (95% CI, 0.920 to 0.952).71 A prior study examining the Ki-67 scoring using the QuPath platform found similar results.72
The April 2022 American Society of Clinical Oncology (ASCO) guidelines update notes that there were analytical differences in the way that Ki-67 was measured in the monarchE trial compared to the recommendations made by the IKWG.73 The differences were mainly related to what constitutes a positive nucleus.68 The criteria of what constitutes a positive nucleus used in the monarchE trial include: the signal must be unequivocally brown, corresponding to a nucleus; the staining must cover the whole chromatin distribution within the nucleus; and staining must be corresponding to nonapoptotic cell.68 The IKWG defines a nucleus as positive if it is not blue.19 Grey staining nuclei were considered negative in the monarchE trial.68
Ki-67 Recommended Use
The IKWG recommendations stated that the clinical utility for the use of Ki-67 IHC is evident for anatomically favourable ER-positive, HER2-negative patients to identify those who may not need adjuvant chemotherapy as there is limited evidence for other intended uses, such as in neoadjuvant ET.19 Similarly, the National Comprehensive Care Network Version 2.2022 guidelines published in December 2021 stated that there is currently no conclusive evidence that Ki-67 alone assists with selecting the type of ET for a patient and the National Comprehensive Care Network Breast Cancer Panel does not currently recommend assessment of Ki-67.74 The guidelines recommended that for “patients with HR-positive/HER2-negative, high-risk breast cancer (i.e., those with ≥ 4 positive lymph nodes, or 1–3 positive lymph nodes with 1 or more of the following: Grade 3 disease, tumour size ≥ 5 cm, or a Ki-67 score of ≥ 20%) 2 years of adjuvant abemaciclib can be considered in combination with endocrine therapy.”74
The ASCO updated guidelines recommended that patients with high-risk node-positive breast cancer and a Ki-67 score of 20% or more (determined by an FDA-approved test) can be offered 2 years of abemaciclib plus ET.61 The ASCO guidelines noted that the potential benefits (improved IDFS) to patients should be compared against potential harms (treatment toxicity and financial cost).61
Conclusion
The literature has shown that the Ki-67 antigen is an independent prognostic biomarker in early-stage breast cancer.57-60 The use of IHC testing for Ki-67currently lacks reproducibility, particularly across laboratories.19 Current IKWG guidelines that aimed to standardize the Ki-67 testing processes and scoring methods to address these limitations are promising. The IKWG recommended cut-off scores of 5% or less for low Ki-67 and 0% or more for high Ki-67 to be used in routine health settings for anatomically favourable ER-positive and HER-negative patients to identify those who do not need adjuvant chemotherapy.19 The reasoning was that there is considerable inter-observer variability in Ki-67 scores ranging from greater than 5% to less than 30%, In the ASCO guidelines, patients with high-risk node-positive breast cancer and a Ki-67 score of 20% or more (determined by an FDA-approved test) can be offered 2 years of abemaciclib plus ET.61 Additional work is required to identify correlates of pharmDx 20% or more cut-off with other Ki-67 assays and platforms on the market. Continued efforts to automate scoring may assist with addressing the issue of inter-rater variability in IHC Ki-67 testing.19,71
Pharmacoeconomic Review
Abbreviations
ABE
abemaciclib
BIA
budget impact analysis
CDK
cyclin-dependent kinase
ET
endocrine therapy
HER2
human epidermal growth factor receptor 2
HR
hormone receptor
ICER
incremental cost-effectiveness ratio
IDFS
invasive disease–free survival
ITT
intention to treat
LY
life-year
OS
overall survival
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Abemaciclib (Verzenio), 50 mg, 100 mg, 150 mg, 200 mg oral tablet |
Submitted price | Abemaciclib, 50 mg: $98.4714 per tablet Abemaciclib, 100 mg: $99.9704 per tablet Abemaciclib, 150 mg: $98.4714 per tablet Abemaciclib, 200 mg: $99.9704 per tablet |
Indication | Indicated in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score ≥ 20% |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | January 12, 2022 |
Reimbursement request | As per indication |
Sponsor | Eli Lilly Canada Inc. |
Submission history | Previously reviewed: Yes Indication: Advanced or metastatic breast cancer
|
ET = endocrine therapy; HER2 = human epidermal growth factor receptor 2; HR = hormone receptor; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence and with a Ki-67 test score ≥ 20% |
Treatment | ABE plus ET (ET consisted of anastrozole, exemestane, letrozole, or tamoxifen) |
Comparator | ET |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (49 years) |
Key data source | monarchE trial (Ki-67 ≥ 20% subgroup of Cohort 1) |
Submitted results | ICER = $42,008 per QALY (incremental costs = $78,094; incremental QALYs = 1.859) |
Key limitations | The sponsor used a “fixed payoff” approach that could not be fully validated by CADTH. Patients with metastatic recurrence after ABE + ET or ET alone were assigned a fixed number of LYs calculated using the results of pharmacoeconomic models that were not provided to CADTH as part of the current review. The sponsor’s base case predicts a survival advantage with ABE + ET compared to ET alone (incremental gain = 3.60 LYs) over a 49-year horizon; however, no difference in survival was observed in the monarchE trial. Clinical experts consulted by CADTH indicated that it is highly uncertain whether delayed disease progression will translate to gains in OS. Given the sponsor’s fixed payoff approach, CADTH was unable to validate the survival benefit predicted for patients in the metastatic health state, introducing additional uncertainty into the sponsor’s base case. The long-term impact of ABE + ET on IDFS is highly uncertain. Overall, 97% of the total incremental QALYs predicted by the sponsor’s analysis are accrued in the invasive disease–free health state, and all incremental QALYs were accrued through extrapolation. The extrapolation curve chosen by the sponsor for IDFS resulted in the incremental effectiveness of ABE + ET vs. ET alone increasing after patients discontinued ABE, which clinical experts considered highly uncertain. The sponsor assumed that the effectiveness of ABE + ET would begin to wane after 8 years (i.e., 6 years after the ABE stopping rule was imposed) and that waning would continue for a period of 19 years. The sponsor supported the assumptions using evidence from a separate class of drug with a different mechanism of action. Clinical experts consulted by CADTH considered this assumption to be implausible. The sponsor assumed that patients with metastatic recurrence after adjuvant ABE + ET would not receive subsequent treatment with a CDK4 and CDK6 inhibitor. Clinical experts consulted by CADTH indicated that a proportion of patients with ET-sensitive disease (with recurrence at least 6 months after adjuvant ABE + ET treatment) would receive a CDK4 and CDK6 inhibitor as part of standard of care for metastatic recurrence. The assumption that no patients receive CDK4 and CDK6 inhibitors after ABE + ET likely underestimates the cost of treating metastatic recurrence and biases the ICER in favour of ABE + ET. |
CADTH reanalysis results | Given the modelling approach adopted by the sponsor, the cost-effectiveness of ABE + ET is highly uncertain. CADTH undertook reanalyses that adopted an alternative extrapolation assumption for IDFS, and that used alternative assumptions about treatment effectiveness waning. CADTH was unable to fully validate the submitted model owing to the use of a fixed payoff approach that relied on external models not provided to CADTH. CADTH’s base-case estimate of cost-effectiveness, therefore, remains highly uncertain. Based on CADTH reanalyses, ABE + ET remained more costly and more effective than ET alone: ICER = $78,438 per QALY (incremental costs = $81,924; incremental QALYs = 1.04). A price reduction of at least 24% for ABE would be required for ABE + ET to be considered optimal at a WTP threshold of $50,000 per QALY compared to ET alone. This estimate is subject to the high degree of uncertainty due to the limitations described earlier — most notably, the fixed payoff approach — and further price reduction may be warranted. CADTH notes that all of the predicted benefit with ABE + ET is accrued in the extrapolation period, and it is uncertain whether this benefit would be realized in practice. |
ABE = abemaciclib; CDK = cyclin-dependent kinase; ET = endocrine therapy; HER2 = human epidermal growth factor receptor 2; HR = hormone receptor; ICER = incremental cost-effectiveness ratio; IDFS = invasive disease–free survival; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year; vs. = versus; WTP = willingness to pay.
Conclusions
The CADTH clinical review found that data from the Cohort 1 Ki-67 High (≥ 20%) subpopulation in the monarchE trial suggests that treatment with adjuvant abemaciclib (ABE) plus endocrine therapy (ET) may be associated with improved invasive disease–free survival (IDFS) among patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score of 20% or more. The effects of ABE plus ET on overall survival (OS) are highly uncertain, given that the OS data from the monarchE trial are immature and that, in the Ki-67 High subpopulation of Cohort 1, ||||| ||| || |||||||||| || OS between patients who received ABE plus ET or ET alone based on the first OS interim analysis. The sponsor’s model predicts increased OS with ABE plus ET (3.6 life-years [LYs]) on the basis of OS data from the ongoing monarchE trial and on the basis of LYs estimated in external models (i.e., for patients with metastatic recurrence). OS data from the monarchE study are immature, and the extrapolation of short-term trial data over a 49-year horizon introduces considerable uncertainty. Further, while IDFS benefit was observed in the monarchE trial with ABE plus ET, it is highly uncertain whether this will translate to an increase in OS.
In addition to the limitations with the clinical data, CADTH identified several key limitations in the economic analysis submitted by the sponsor. Importantly, the sponsor’s model relied on data from 2 external models to predict outcomes for patients with metastatic recurrence; the output of these models could not be validated by CADTH and the resulting LYs, quality-adjusted life-years (QALYs), and costs (and hence the ICER) should be considered highly uncertain. In CADTH reanalyses, an alternative extrapolation for IDFS and alternative assumptions about treatment effectiveness waning were considered. CADTH found adjuvant treatment with ABE plus ET is more costly (incremental costs = $81,924) and more effective (incremental QALYs = 1.04) compared with ET alone, resulting in an ICER of $78,438 per QALY. A price reduction of 24% for abemaciclib would be necessary to achieve an ICER of $50,000 per QALY for ABE plus ET compared with ET alone. The CADTH analysis allows for a survival benefit for ABE plus ET of 1.94 years, despite the current clinical evidence, which may be optimistic. The high degree of uncertainty contributed by the sponsor’s “fixed payoff” approach and the unknown relationship between IDFS and OS suggest that a greater price reduction may be needed to achieve cost-effectiveness.
While clinical experts consulted by CADTH considered the long-term IDFS and effectiveness waning assumptions adopted in the CADTH base case to be more plausible than those assumed by the sponsor, experts cautioned that, beyond the trial duration, the effectiveness and durability of the effect of abemaciclib is highly uncertain and may be overestimated. As shown by CADTH scenario analysis exploring a shorter time horizon (5 years), the ICER is highly sensitive to assumptions about long-term efficacy beyond the available evidence. Further, the pharmacoeconomic model predicted that ABE plus ET was more costly and less effective than (“dominated by”) ET alone, suggesting that even the on-trial benefit is subject to a high degree of uncertainty. Thus, the ICER predicted by the CADTH base case should be considered highly uncertain and may be underestimated.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Two patient groups, Canadian Breast Cancer Network and Rethink Breast Cancer, provided input for this review. The Canadian Breast Cancer Network collected information in 2017 through a patient survey comprising responses from 103 Canadian patients with early-stage, HR-positive, HER2-negative breast cancer. Rethink Breast Cancer conducted interviews in March 2022 with 2 patients with HR-positive, HER2-negative, high-risk early-stage breast cancer who had experience with abemaciclib. Patients described physical symptoms associated with early-stage breast cancer (e.g., fatigue), psychosocial effects associated with fear of death and risk of recurrence (e.g., anxiety, distress, depression), and adverse side effects associated with chemotherapy and radiation (e.g., nausea, vomiting, neuropathy). Patients noted that important outcomes of treatment include delaying disease recurrence, achieving long-term remission, and improving survival, as well as reducing side effects, preserving independence, and maintaining productivity and quality of life. Patients noted the lack of adjuvant therapeutic options that could be used in combination with ET to reduce the risk of recurrence following surgical resection and chemotherapy. The 2 patients with abemaciclib experience described mild to moderate side effects, including fatigue, diarrhea, cramping, and bloating.
Registered clinician input was received from the Ontario Health–Cancer Care Ontario Breast Cancer Drug Advisory Committee. Clinicians indicated that the current pathway of care for patients with HR-positive, HER2-negative, early-stage breast cancer varies depending on risk of recurrence but includes combinations of surgery, radiotherapy, adjuvant and neoadjuvant chemotherapy, and ET. Clinicians indicated that adjuvant ET is standard treatment of HR-positive, HER2-negative, early-stage breast cancer; however, a proportion of patients with high-risk clinical and/or pathologic features may experience distant recurrence and additional treatment options are needed to prevent early recurrence and the development of metastases. Clinicians indicated that adjuvant abemaciclib in combination with ET would supplement the current management of HR-positive, HER2-negative, early-stage breast cancer following surgery but would not replace current therapies. Clinicians noted that, although OS is the gold standard therapeutic target, IDFS is an important clinical outcome. Clinicians recommended against the inclusion of a high Ki-67 score as a criterion for drug eligibility, noting that the test is prognostic and not predictive.
CADTH participating drug plans noted considerations related to the budget impact of reimbursing abemaciclib and whether abemaciclib will change the place in therapy of comparator drugs, as well as considerations related to Ki-67 testing. The drug plans noted that, at present, Ki-67 testing is not routinely performed on breast cancer samples.
Several of these concerns were addressed in the sponsor’s model:
IDFS and OS were included in the model.
The use of a cost-utility approach accounts for some issues related to quality of life; however, it is unclear if all quality-of-life concerns noted to be important to patients were captured in the health state utility values adopted by the sponsor.
Costs and quality-of-life decrements related to adverse events were included.
Costs related to Ki-67 testing were included.
CADTH was unable to address the following concerns raised from stakeholder input:
Changes to the place in therapy of comparators could not be addressed.
The sponsor’s modelling approach precluded full validation of the model findings related to OS.
Economic Review
The current review is for abemaciclib (Verzenio) in combination with ET for the adjuvant treatment of HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score of 20% or more.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis1 of adjuvant abemaciclib in combination with ET compared with ET alone in adults (≥ 18 years) with HR-positive, HER2-negative, node-positive, early-stage breast cancer who are at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score of 20% or more, which is aligned with the Health Canada indication.2 The efficacy of ABE plus ET and ET alone was informed by the monarchE trial — specifically, the high Ki-67 subgroup of Cohort 1. In the pharmacoeconomic model, ET was assumed by the sponsor to include anastrozole, letrozole, tamoxifen, and exemestane, which is in line with the treatments used as part of ET in the monarchE trial.3 However, the relative proportion of each treatment adopted for the pharmacoeconomic model is not aligned with observations from the Cohort 1 high Ki-67 subgroup.
Abemaciclib is available as 50 mg, 100 mg, 150 mg, and 200 mg tablets.2 Health Canada’s recommended dosage of abemaciclib when taken in combination with ET for early breast cancer is 150 mg twice daily, until the completion of either 2 years of therapy or until disease recurrence or unacceptable toxicity.2 At the sponsor’s submitted price of $98.47 per 150 mg tablet,4 the per-patient 28-day cost of abemaciclib is $5,514 (annual cost = $71,884). When used in combination with ET, the per-patient 28-day drug acquisition costs were as follows: abemaciclib plus letrozole is $5,553 (letrozole alone = $38.58), abemaciclib plus anastrozole is $5,541 (anastrozole alone = $27), abemaciclib plus tamoxifen is $5,524 (tamoxifen alone = $10), and abemaciclib plus exemestane is $5,552 (exemestane alone = $37.14) (Table 8). The annual cost of ET is $341, calculated by the sponsor on the basis of the expected frequency of use of each of letrozole (41%), anastrozole (25%), and tamoxifen (34%).5
The analysis was performed from the perspective of the Canadian publicly funded health care system. Costs and clinical outcomes (LYs and QALYs) were simulated over a lifetime time horizon of 49 years (28-day cycle) and discounted at an annual rate of 1.5% per annum.1
Model Structure
The sponsor submitted a Markov model with 5 health states: invasive disease–free, non-metastatic recurrence, metastatic recurrence, remission, and death (Figure 1).1 Patients entered the model in the invasive disease–free state and received ABE plus ET or ET alone. Abemaciclib (as part of abemaciclib + ET) could be received for a maximum of 2 years and ET (in both arms) could be received for up to 5 years, with discontinuation before 2 years (abemaciclib) or 5 years (ET) based on time to treatment discontinuation (TTD) in the monarchE trial. In each cycle, patients could remain in the invasive disease–free state, experience a metastatic recurrence or a non-metastatic recurrence, or die. Patients with metastatic recurrence moved to the ET-resistant or the ET-sensitive substate of the metastatic recurrence state, depending on the timing of metastatic recurrence (≤ 12 months or > 12 months, respectively). Patients in the metastatic recurrence health state were assigned a fixed number of LYs based on external models developed by the sponsor for other submissions to CADTH pan-Canadian Oncology Drug Review (the fixed payoff approach).6,7 These LYs were multiplied by costs and utilities to determine total costs and QALYs for patients in the metastatic recurrence states. Patients with a non-metastatic recurrence moved to the non-metastatic recurrence health state and were assumed to have either a second primary neoplasm or locoregional and/or contralateral disease; those with a second primary neoplasm were assumed to incur only the cost of diagnosis (the cost of treating the secondary primary neoplasm was not included). Patients with non-metastatic locoregional and/or contralateral recurrence were assumed to receive treatment (based on type and location of the disease) for 12 months (unless death occurred before 12 months), and to subsequently move to the remission health state. Patients in the remission state were at risk of death from non-early breast cancer and remained at risk of recurrence and were assumed to remain in remission unless a recurrence occurred (assumed to be incurable). Treatment effectiveness waning (for abemaciclib + ET) was assumed to begin at year 8 and to last for a period of 19 years.
Model Inputs
Baseline patient characteristics (|||| |||||| |||| ||| ||||| ||||||) were based on Cohort 1 (Ki-67 ≥ 20%) of the monarchE trial. In the monarchE study, patients received ABE plus ET or ET alone, with ET consisting of physicians’ choice of “standard endocrine therapy.” Cohort 1 included patients based on high-risk clinicopathologic features, and Ki-67 results were obtained retrospectively for a proportion of patients who had Ki-67 testing results available. Those with a high Ki-67 score (≥ 20%) make up the Cohort 1 Ki-67 High group.
Clinical efficacy parameters to inform the economic model (IDFS, TTD, OS without distant recurrence) were based on data from the high K1-67 (≥ 20%) subgroup of Cohort 1 of the monarchE trial. Kaplan-Meier estimates of IDFS, TTD, and OS (without distant recurrence) from the trial period were used to fit parametric survival curves to extrapolate the observed trial data (median follow-up = 27 months) over the entire model horizon (49 years) for ABE plus ET and ET alone. The sponsor fit a single curve for abemaciclib plus ET and ET alone for IDFS and OS (without distant recurrence), which included an adjustment factor for treatment effect (i.e., hazard ratio). The sponsor adopted a log-logistic distribution for IDFS, a hazard spline 1-knot distribution for TTD, and a Weibull distribution for OS (without distant recurrence). As noted previously, the sponsor adopted a fixed payoff approach to determine LYs, QALYs, and costs for patients with metastatic recurrence. The disease course for patients with ET-resistant and ET-sensitive metastatic recurrence was based on data from the MONARCH 2 and MONARCH 3 models,6,7 which included HR-positive, HER2-negative, locally advanced or metastatic breast cancer patients who progressed on or immediately after prior ET (MONARCH 2) or HR-positive, HER2-negative, locoregionally recurrent or metastatic patients with no prior systemic therapy (MONARCH 3).1
Health state utility values were adopted from multiple sources. For the invasive disease–free health state, utility values were based on observations from the monarchE trial (intention-to-treat [ITT] population; EQ-5D 5-Level (EQ-5D-5L), cross-walked to EQ-5D-3L; UK tariff).1 For the non-metastatic recurrence health state, utilities were adopted from the National Institute for Health and Care Excellence appraisal of neratinib,8 which adopted utility values from the literature.9 Utility values for patients in the metastatic health state were based on EQ-5D-5L data from the MONARCH 2 trial7 (using the TA239 regression model), while the utility estimate for patients with ET-sensitive disease were based on EQ-5D data collected in the MONARCH 3 trial (using the MONARCH 3 regression model).6 Utility values for patients in the pre-metastatic states were age-adjusted.10 The sponsor’s model incorporated grade 3 and higher adverse events experienced by at least 1% of the full monarchE population (ITT population). Adverse events were associated with a 1-time cost and utility decrement and were assumed to occur during the first model cycle. Disutility values for adverse events were obtained from multiple sources, including the MONARCH 2 and MONARCH 3 trials and the literature.
The sponsor’s model included costs related to drug acquisition, Ki-67 testing, administration costs for chemotherapy drugs in the non-metastatic recurrence health state, disease management, adverse events, and terminal care. The cost of Ki-67 testing ($19.10) was obtained from the publication Répertoire québécois et système de mesure des procédures de biologie médicale and was applied to 100% of patients receiving ABE plus ET and 19% of patients receiving ET alone. Drug acquisition costs for abemaciclib were based on the sponsor’s submitted price,1 while acquisition costs for anastrozole, exemestane, letrozole, and tamoxifen (as part of ET) were obtained from the Ontario Drug Benefit Formulary. Dosages for drugs included as part of ET were based on their respective product monographs. No administration costs were applied for oral drugs; administration costs for chemotherapy (received in the non-metastatic recurrence health state) were obtained from the Ontario Ministry of Health and Long-Term Care.11 For patients in the invasive disease–free health state, disease management costs included general practitioner visits and mammograms, with the frequency of each being obtained from the National Institute for Health and Care Excellence appraisal of neratinib8 and costed by use of the Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act.11 For patients in the non-metastatic recurrence health state, resource use included oncologist visits, mammograms, echocardiography, radionuclide lymphangiography, CT, mastectomy, breast reconstruction, and radiotherapy (costs from the Ontario Case Costing Initiative12 and the Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act).11 Patients with a second primary neoplasm were assumed to incur the cost of 1 multidisciplinary team meeting (i.e., for diagnosis, with costs from the Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act11); no further costs were applied to these patients. Patients in the remission health state incurred costs related to oncologist and general practitioner visits, mammography, echocardiography, and radionuclide lymphangiography. For patients with metastatic disease, costs were based on whether the patient had ET-resistant or ET-sensitive recurrence, with the per-cycle cost of each resource used multiplied by the applicable number of cycles based on mean progression-free survival (PFS), post-progression survival (PPS), and time on treatment based on data from the MONARCH 2 and MONARCH 3 models.6,7 The cost of terminal care ($18,309) per patient was obtained from the literature.13 Costs associated with the management of adverse events were applied as a 1-time cost in the first model cycle, based on the incidence in the monarchE trial (ITT population) and costs obtained from the Ontario Case Costing Initiative.12
Summary of Sponsor’s Economic Evaluation Results
The sponsor’s base case was run probabilistically (1,000 iterations). The deterministic and probabilistic results were similar. The probabilistic findings are presented as follows. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Base-Case Results
In the sponsor’s base-case analysis, ABE plus ET was associated with an incremental cost of $78,094 and 1.86 QALYs compared with ET alone over a 49-year horizon, resulting in an incremental cost-effectiveness ratio (ICER) of $42,008 per QALY (Table 3). In the sponsor’s base case, ABE plus ET had a 79% probability of being cost-effective compared to ET alone at a willingness-to-pay (WTP) threshold of $50,000 per QALY.
Results were driven by predicted differences in total LYs between ABE plus ET and ET alone (incremental LYs = 3.60 years) and the increased drug acquisition costs associated with abemaciclib (incremental costs = $116,997). The sponsor’s model estimated that, in the first 2 years (i.e., approximately equal to the median duration of follow-up as per the additional follow-up data cut 1 analysis), patients on ET alone accrued more QALYs than those who received ABE plus ET (ABE plus ET = 1.58 QALYs; ET alone = 1.63 QALYs) and that ABE plus ET was associated with higher costs compared to ET alone (ABE plus ET = $131,569; ET alone = $19,343). As such, ABE plus ET was dominated by ET alone (higher costs, lower QALYs) during the period where direct comparative evidence exists. This indicates that all of the incremental benefits associated with ABE plus ET compared to ET alone in the sponsor’s base-case analysis were accrued in the post-trial period via extrapolation.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. ET ($/QALY) |
|---|---|---|---|---|---|
ET | 127,634 | Reference | 10.77 | Reference | Reference |
ABE + ET | 205,727 | 78,094 | 12.63 | 1.86 | 42,008 |
ABE = abemaciclib; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted sensitivity and scenario analyses, including adopting alternative time horizons, alternative extrapolations for IDFS and OS, and alternative structural assumptions (e.g., stopping rules). Most scenarios had no notable impact on the ICER, with the exception of adopting an alternative time horizon. When a shorter time horizon was selected, the ICER increased to $241,868 per QALY (10-year horizon), $73,576 per QALY (20-year horizon), and $51,879 (30-year horizon).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Limitations with the sponsor’s modelling approach. The sponsor’s model included invasive disease–free survival (IDFS) health states in which patients were assumed to have no invasive disease or to have a metastatic or non-metastatic recurrence. For the IDFS and non-metastatic recurrence states, the sponsor adopted a typical Markov cohort approach in which patients accrue costs, LYs, and QALYs based on the duration of time spent in each state. In contrast, for the metastatic recurrence state (which was further divided as ET-resistant or ET-sensitive based on the timing of recurrence since prior adjuvant ET), the sponsor adopted a fixed payoff approach. Using this approach, the sponsor assigned each patient who entered this state a fixed number of LYs and multiplied this by costs and utility values to determine total costs and QALYs. To determine the LYs (and hence costs and QALYs), the sponsor used previous economic models built to assess the cost-effectiveness of abemaciclib in the metastatic breast cancer setting.6,7 This fixed payoff approach was described by clinical experts consulted by the sponsor as a “black box approach to modelling,” meaning that the method by which results were produced were opaque1 CADTH agrees with this assessment, as the models used by the sponsor to estimate LYs, QALYs, and costs for patients with metastatic disease were not provided to CADTH as part of the review process. Thus, CADTH was unable to validate the model’s predicted outcomes for patients in the metastatic recurrence health state. CADTH further notes that these external models were partitioned survival models, which are subject to inherent modelling limitations, and any assumptions made during the development of these models are carried through to the current submission.
CADTH further notes that the models used to determine the “payoff” for patients in the metastatic health state were informed by data from the MONARCH 2 trial (which assessed abemaciclib in combination with fulvestrant after progression on or after prior ET) and the MONARCH 3 trial (which assessed abemaciclib in the first-line metastatic setting). Because individual patient data were not used in the current model, the sponsor incorporated an assumption that all patients in the metastatic state would remain alive until the mean LY point was reached in the MONARCH 2 and MONARCH 3 populations. There were important differences in patient populations between the MONARCH 2 and MONARCH 3 trials and the monarchE trial, including an 8-year and 11-year difference in age between the patients enrolled in the monarchE trials compared to the MONARCH 2 and MONARCH 3 trials, respectively. Because the MONARCH 2 and MONARCH 3 trials were not submitted to CADTH as part of this review, the data incorporated in the economic models from these trials have not been appraised by CADTH as part of this submission.
CADTH was unable to address this limitation and was unable to validate the outcomes predicted for patients in the metastatic recurrence health state. As such, the predicted incremental LYs, QALYs, and costs for ABE plus ET versus ET alone (and hence the ICER) should be viewed as highly uncertain.
The impact of abemaciclib on OS is highly uncertain. The sponsor’s base case predicts a survival advantage with ABE plus ET compared to ET alone (incremental gain = 3.60 LYs). As noted in the CADTH clinical report, the monarchE trial was not powered to detect differences in OS between abemaciclib plus ET compared to ET alone in the Ki-67 High subpopulation. As of the first OS interim analysis (additional follow-up with a data cut-off date of April 1, 2021), the OS data remain immature, and |||||||| || ||||||||||| |||||||||| || OS between ABE plus ET and ET alone (hazard ratio |||||, 95% CI ||||| || |||||) for patients in the high Ki-67 subpopulation of Cohort 1. Clinical experts consulted by CADTH indicated that it is highly uncertain whether delayed disease recurrence (reflected by IDFS), as observed in the high Ki-67 Cohort 1 group, will translate to gains in OS.
There is additional uncertainty associated with the predicted OS associated with ABE plus ET owing to the modelling approach adopted by the sponsor. The sponsor’s model incorporates OS data from the monarchE trial only for patients without distant recurrence, while a fixed payoff approach (described previously) was adopted for patients with metastatic recurrence. This approach is subject to extensive limitations, as outlined earlier. For the OS data incorporated in the current model (i.e., OS for patients without distant relapse), the sponsor selected the Weibull distribution for ABE plus ET and ET alone (single model with treatment coefficient) on the basis of “the best BIC [Bayesian information criterion] value and good AIC [Akaike information criterion] values.”1 However, statistical fit speaks only to fit of the predicted data to the observed data within the trial period, not to the validity of predicted data for the extrapolated period. CADTH notes that there were several extrapolation curves with comparable AIC and BIC values; however, selecting alternative curves for OS for patients without distant recurrence had little impact on the ICER, likely owing to the modelling approach adopted by the sponsor.
CADTH was unable to address this limitation owing to the structure of the sponsor’s model.
The impact of ABE plus ET on long-term IDFS is highly uncertain. The sponsor used parametric modelling to extrapolate IDFS beyond the observable time points in the monarchE trial (median follow-up of 27 months for the high Ki-67 Cohort 1 group) to a lifetime horizon (49 years). The extrapolation curve chosen by the sponsor (along with other modelling assumptions such as treatment effectiveness waning; refer to the following) resulted in an incremental gain of 1.80 QALYs in the invasive disease–free health state with abemaciclib plus ET, which reflects 97% of the total incremental QALYs accrued over the model horizon. CADTH notes that the gains in predicted incremental QALYs are generated exclusively through extrapolation: in the first 2 years of the model — approximately aligned with the median follow-up time — more QALYs were accrued by patients who received ET alone compared to those who received abemaciclib plus ET (ABE plus ET = 1.58 QALYs; ET alone = 1.63 QALYs). The sponsor submitted multiple extrapolation curves for IDFS and selected the log-logistic curve for extrapolation of IDFS for ABE plus ET and ET alone (a single model with a treatment coefficient). Based on the selected log-logistic curve, the sponsor’s model predicts that ABE plus ET will continue to become more effective compared to ET alone after the discontinuation of abemaciclib. That is, based on the log-logistic extrapolation of observed data from the Ki-67 High Cohort 1 subgroup of the monarchE trial, the incremental difference in IDFS at 2 years is approximately 5 percentage points while after 10 years, the incremental difference in IDFS is 12 percentage points. Clinical experts consulted by CADTH for this review considered this to be a very optimistic assumption, and experts indicated a lack of evidence provided as part of the review to support the assumption that abemaciclib will continue to become more effective once patients have discontinued treatment (i.e., when patients are on ET alone).
In CADTH reanalyses, alternative parametric extrapolation curves for IDFS were adopted (ABE plus ET = exponential; ET alone = log-normal). Based on these extrapolations, the difference in IDFS between ABE plus ET and ET alone after 2 years of treatment is approximately 5 percentage points; after 10 years, the difference remains approximately 5 percentage points. While clinical experts consulted by CADTH for this review considered this to be a more plausible scenario, they noted that it is also possible that there is no incremental difference in IDFS at 5 years or later time points. As such, it is possible that the CADTH base case overestimates the long-term incremental IDFS benefit with abemaciclib plus ET, and consequently underestimates the ICER.
Waning of treatment effectiveness of abemaciclib is highly uncertain. In the pharmacoeconomic model, the sponsor assumes that treatment waning for ABE plus ET will start at year 8 and gradually wane linearly until year 27. Implicit in this assumption is that the treatment effect of abemaciclib will continue to be experienced for at least 6 years after discontinuation (as the maximum duration of abemaciclib treatment in the monarchE trial was 2 years) and that, when waning starts, it will take approximately 19 years for the effects of ABE plus ET to fully dissipate. Clinical experts consulted by CADTH for this review indicated that they are unaware of data for abemaciclib to support these assumptions and that it is equally plausible that effectiveness waning would start immediately after patients stop taking abemaciclib. It was additionally considered unlikely by the clinical experts that waning would last for 19 years.
The sponsor’s assumptions about when waning would initiate were based on data from the Arimidex, Tamoxifen, Alone or in Combination (ATAC) trial,14 which reported follow-up data for anastrozole and tamoxifen for up to 10 years among HR-positive patients (HER2 status was not reported). Clinical experts consulted by CADTH indicated that it is not appropriate to use data from anastrozole and tamoxifen to infer effectiveness waning for abemaciclib plus ET because of different mechanisms of action and patient populations (i.e., the ATAC trial has not reported on HER2 or Ki-67 status). For the end of the waning period, the sponsor assumed that this would occur when the IDFS rate is equal to the background mortality rate. Clinical experts consulted by CADTH noted that assuming a 19-year waning period was overly generous and unlikely to occur in practice.
The effectiveness waning assumptions adopted by the sponsor were found to be lacking face validity by clinical experts consulted by CADTH. In the absence of data to support the long-term effectiveness waning for abemaciclib, experts considered it equally likely that waning would begin as soon as abemaciclib was discontinued. In the CADTH reanalysis, treatment waning was assumed to start at month 25 (i.e., at the end of the maximum treatment duration in the monarchE trial), and that waning would continue until year 5.
Costs associated with metastatic recurrence are highly uncertain. The sponsor’s model predicts that ABE plus ET will generate cost savings in the metastatic recurrence health state (incremental costs = –$60,706 versus ET alone). Given the sponsor’s use of a fixed payoff approach, this value is highly uncertain. How total costs are calculated in the model is not transparently described. Generally, the per-cycle cost of each resource (e.g., stratified by progression-free or post-progression status, first-line or second-line treatment) was multiplied by a set number of cycles, which was informed by the mean number of LYs accrued in the progression-free state or the post-progression state, as predicted by the sponsor’s external MONARCH 3 model (for ET-sensitive disease) and MONARCH 2 model (for ET-resistant disease).6,7 Drug costs for patients in the metastatic recurrence state were based on regimens received in the MONARCH 2 trial for ET-resistant disease and in the MONARCH 3 trial for those with ET-sensitive disease, as well as on “the primary publications used in the NMA [network meta-analysis].”1 This NMA was not provided by the sponsor and the relevance of its findings to the current submission have not been appraised by CADTH. Clinical experts consulted by CADTH for this review indicated that the proportion of patients with metastatic ET-sensitive disease assumed by the sponsor to receive a cyclin-dependent kinase 4 (CDK4) and CDK6 inhibitor (0%) does not align with Canadian clinical practice and that patients whose disease recurred after at least 12 months would be considered for a CDK4 and CDK6 inhibitor, as CDK4 and CDK6 inhibitors are standard of care for the primary treatment of metastatic breast cancer. Given the higher price of CDK4 and CDK6 inhibitors compared to the other included treatments for metastatic recurrence and the incremental difference in CDK4 and CDK6 inhibitor usage assumed between who initially received ABE plus ET (0%) or ET alone (76%), this is an influential parameter in the model.
CADTH was unable to validate the costs predicted by the sponsor’s analysis owing to the use of external models. In scenario analysis, CADTH adopted alternative assumptions regarding the usage of CDK4 and CDK6 inhibitors among patients with metastatic recurrence.
The model lacked transparency. In addition to the lack of transparency noted previously (i.e., the use of a “black box” fixed payoff modelling approach for the metastatic health state), the sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors.
CADTH was unable to address this limitation and notes that a thorough validation of the sponsor’s model was not possible.
Additional limitations were identified but were not considered to be key limitations.
The ET basket of treatments does not represent current Canadian clinical practice. The sponsor compared the effectiveness of ABE plus ET to ET alone, with ET assumed to be consisting of 41% letrozole, 25% anastrozole, 0% exemestane, and 34% tamoxifen. This assumed distribution was not justified by the sponsor and is not aligned with the relative usage of each agent as part of ET in the monarchE trial. For example, in the Cohort 1 Ki-67 High subgroup of the monarchE trial, exemestane was received as part of ET by ||||% of participants. Clinical experts consulted by CADTH for this review indicated that the assumption that 0% of patients would receive exemestane is not aligned with Canadian clinical practice. Experts indicated that approximately two-thirds of patients would receive an aromatase inhibitor (letrozole, anastrozole, or exemestane) and one-third would receive tamoxifen; however, clinical experts noted that the relative usage of individual aromatase inhibitors was uncertain.
While the composition of the ET basket adopted by the sponsor is not reflective of Canadian practice, this limitation is expected to have little impact on the ICER, given the comparable price of letrozole, anastrozole, and exemestane (Table 8). The effectiveness data incorporated in the sponsor’s pharmacoeconomic model is based on data from the monarchE trial, which included exemestane as part of ET.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients enrolled in the monarchE trial were assumed to be representative of patients in Canada who would be eligible for ABE + ET (||| |||| |||||| ||||| ||||||| |||| ||| |||| ||||||| |||| ||| ||). | Reasonable, although clinical experts noted that the patients enrolled in the monarchE trial were generally younger than those seen in Canadian clinical practice by approximately 10 years. |
The effectiveness of ABE (IDFS, OS for patients without distant recurrence) was based on the Ki-67 High (≥ 20%) subgroup of Cohort 1 of the monarchE trial. | Appropriate, based on the Health Canada indication for abemaciclib. The full Cohort 1 population included patients at high risk of disease recurrence based on clinicopathologic features and/or Ki-67 ≥ 20%. Of patients in Cohort 1 who had samples available for Ki-67 testing, approximately 51% had high Ki-67; the effectiveness data for the economic model were based on this subgroup. |
The probability of having a metastatic recurrence for patients in the remission health state was assumed to be equal to the risk of having a second primary malignancy. | Uncertain. The sponsor based the probability of a metastatic recurrence for patients in remission on a retrospective cohort study of secondary malignancy after adjuvant therapy among women with stage I or stage II breast cancer.15 Clinical experts consulted by CADTH for this review indicated that secondary malignancy is conceptually distinct from disease recurrence and that it may be inappropriate to assume the same risk. |
Ki-67 testing was assumed to be received by 100% of patients in the ABE + ET arm and 19% of patients in the ET arm. | Uncertain. Clinical experts consulted by CADTH indicated that should ABE become reimbursed, all potentially eligible patients (i.e., those at high risk of recurrence based on clinical features) would undergo Ki-67 testing. Given that having a high Ki-67 score is required for ABE use as per the Health Canada product monograph,2 it is assumed that 100% of patients who receive ABE + ET are tested for Ki-67. It is uncertain what percentage of patients would be tested and found to have Ki-67 < 20% (and thus be ineligible) in clinical practice. The sponsor estimated this to be 19% of patients who receive ET, based on a survey of physicians conducted by the sponsor. |
Health state utility values were acquired from multiple sources. | Uncertain. The sponsor adopted utility values from the monarchE trial, the MONARCH 2 trial and the MONARCH 3 trial, and the published literature, and treatment-specific utilities were incorporated within some health states. Incorporating utilities from a variety of sources, which were measured and valued in different ways in different patient populations, adds uncertainty to the analysis. While adopting treatment-specific utilities is inappropriate based on CADTH economic guidelines, the ICER is not sensitive to this assumption. |
Adverse events were assumed to occur once during the first model cycle. | Inappropriate. The sponsor’s model included grade ≥ 3 adverse events (≥ 1% incidence) based on the observed frequency in the monarchE trial (ITT population), applied in the first model cycle. The sponsor selected an arbitrary threshold to capture the impact of adverse events rather than selecting the most clinically meaningful adverse events to include within the model. This approach may underestimate the impact of rare adverse events, and it is uncertain whether patients are at risk of adverse events only once. |
ABE = abemaciclib; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; IDFS = invasive disease–free survival; ITT = intention to treat; OS = overall survival.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH reanalyses addressed key limitations of the submitted economic model as described in Table 5. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. IDFS parametric extrapolation | Log-logistic, applied to both ABE + ET and ET alone | ABE + ET: Exponential ET alone: Log-normal |
2. Treatment waning | Treatment waning starts at year 8 and continues to wane until year 27 (total waning period 19 years) | Treatment waning starts at month 25 and waning continues until year 5 (for total waning period of 35 months) |
CADTH base case | Reanalysis 1 + 2 | |
ABE = abemaciclib; ET = endocrine therapy; IDFS = invasive disease–free survival.
CADTH undertook a stepped analysis, incorporating each change proposed in Table 5 to the sponsor’s base case to highlight the impact of each change (Table 6; disaggregated results are presented in Appendix 4).
In CADTH’s base case, ABE plus ET was associated with higher costs (incremental = $81,924) and higher QALYs (incremental = 1.04) than ET alone over a 49-year horizon. The ICER for ABE and ET versus ET alone was $78,438 per QALY. There is a 7% probability that ABE plus ET is optimal compared with ET alone at a WTP threshold of $50,000 per QALY.
The drug acquisition costs for abemaciclib are greater than the total incremental cost (incremental costs for ABE plus ET = $116,998); as such, the cost of abemaciclib is a key driver of the ICER. The model predicts that these costs will be offset by savings in the metastatic recurrence health state (incremental cost savings = $56,794). Owing to the sponsor’s use of a fixed payoff approach, CADTH was unable to validate this outcome. As highlighted in the CADTH scenario analyses, whether this savings is realized depends on the treatments used to treat metastatic recurrence and whether these vary between patients who initially received ABE plus ET or ET alone.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base casea | ET | 128,505 | 10.98 | Reference |
ABE + ET | 206,706 | 12.80 | 42,805 | |
CADTH reanalysis 1a | ET | 123,028 | 12.52 | Reference |
ABE + ET | 205,391 | 13.75 | 66,820 | |
CADTH reanalysis 2a | ET | 128,505 | 10.98 | Reference |
ABE + ET | 207,890 | 11.85 | 91,996 | |
CADTH base case 1 + 2 (deterministic) | ET | 123,028 | 12.52 | Reference |
ABE + ET | 205,451 | 13.47 | 86,216 | |
CADTH base case 1 + 2 (probabilistic) | ET | 122,578 | 12.16 | Reference |
ABE + ET | 204,502 | 13.21 | 78,438 |
ABE = abemaciclib; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: CADTH notes the discrepancy between the estimated QALYs between the deterministic and probabilistic case. The use of the “fixed payoff” approach prevented CADTH from determining the source of this discrepancy.
aDeterministic analysis.
Scenario Analysis Results
CADTH undertook a series of price reduction analyses on the price of abemaciclib based on the sponsor’s submitted base case and CADTH’s exploratory reanalysis (Table 7). Based on the CADTH base-case analysis, a price reduction for abemaciclib of 24% would be required for ABE plus ET to be considered cost-effective compared to ET alone at a WTP threshold of $50,000 per QALY. Given that the estimates of incremental costs and incremental LYs (and hence QALYs) are highly uncertain based on the modelling approach adopted by the sponsor and may not be representative of the true incremental effect of abemaciclib plus ET, the true price reduction required for abemaciclib to be cost-effective is highly uncertain.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for ABE + ET vs. ET alone ($) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 42,805 | 78,438 |
10% | 36,405 | 66,208 |
20% | 30,005 | 53,978 |
30% | 23,604 | 41,748 |
40% | 17,204 | 29,518 |
50% | 10,804 | 17,288 |
60% | 4,404 | 5,058 |
70% | ABE + ET dominant | ABE + ET dominant |
80% | ABE + ET dominant | ABE + ET dominant |
90% | ABE + ET dominant | ABE + ET dominant |
100% | ABE + ET dominant | ABE + ET dominant |
ABE = abemaciclib; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; vs. = versus.
Several scenario and sensitivity analyses were conducted on the CADTH exploratory reanalysis. These scenario analyses explored the impact of the following model parameters and assumptions:
the loss of treatment effectiveness as soon as abemaciclib is discontinued, using a sponsor-provided option to do so
adopting an equal distribution of treatments received for patients with ET-sensitive metastatic recurrence, regardless of whether the initial treatment was ABE plus ET or ET alone
a time horizon of 5 years
a time horizon of 10 years.
The results of these analyses are presented in Table 12. The ICER is highly sensitive to the time horizon of the analysis, as well as the duration of treatment effectiveness and assumptions about what treatments are received by patients with metastatic recurrence. Notably, when treatment effectiveness is assumed to be lost as soon as abemaciclib is discontinued (i.e., effectiveness does not slowly wane after abemaciclib is discontinued), the ICER was $127,953 per QALY for ABE plus ET versus ET alone. Further, when a 5-year horizon was adopted, the ICER was $5,777,555 per QALY for abemaciclib plus ET, illustrating the influence of the extrapolated data on the ICER.
Issues for Consideration
Clinical experts consulted by CADTH for this review and drug plan input indicated that, at present, Ki-67 testing is not routinely performed in all Canadian jurisdictions. Should abemaciclib become reimbursed, clinical experts consulted by CADTH expect that all patients at high risk of recurrence based on clinical characteristics will undergo Ki-67 testing. This is reflected in CADTH’s reanalysis of the budget impact of reimbursing abemaciclib and is a key driver of the budget impact.
The EQ-5D measure used to calculate QALYs does not directly capture the impact that diarrhea has on patient utility. This is notable, as 97.9% of patients who received ABE plus ET in the safety population of the monarchE trial reported at least 1 adverse event, with 82.6% of patients reporting diarrhea, for example, compared to 7.8% of patients in the ET alone group. Clinical experts consulted by CADTH noted that diarrhea can be managed and may not have a meaningful impact on patient preference for treatment. However, the cost-effectiveness of abemaciclib is likely lower in patients with underlying gastrointestinal issues or other conditions where diarrhea cannot be managed easily. CADTH was not able to reflect this effect in its analysis.
Overall Conclusions
The CADTH clinical review found that data from the Cohort 1 Ki-67 High (≥ 20%) subpopulation in the monarchE trial suggests that treatment with adjuvant ABE plus ET may be associated with improved IDFS among patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score of 20% or more. The effects of ABE plus ET on OS are highly uncertain, given that the OS data from the monarchE trial are immature and that, in the Ki-67 High subpopulation of Cohort 1, ||||| ||| || |||||||||| || OS between patients who received ABE plus ET or ET alone based on the first OS interim analysis. The sponsor’s model predicts increased OS with ABE plus ET (3.60 LYs) on the basis of OS data from the ongoing monarchE trial and on the basis of LYs estimated in external models (i.e., for patients with metastatic recurrence). OS data from the monarchE study are immature, and the extrapolation of short-term trial data over a 49-year horizon introduces considerable uncertainty. Further, while IDFS benefit was observed in the monarchE trial with abemaciclib plus ET, it is highly uncertain whether this will translate to an increase in OS.
In addition to the limitations with the clinical data, CADTH identified several key limitations in the economic analysis submitted by the sponsor. Importantly, the sponsor’s model relies on data from 2 external models to predict outcomes for patients with metastatic recurrence; the output of these models could not be validated by CADTH and the resulting LYs, QALYs, and costs (and hence the ICER) should be considered highly uncertain. In CADTH reanalyses, an alternative extrapolation for IDFS and alternative assumptions about treatment effectiveness waning were considered. CADTH found adjuvant treatment with ABE plus ET is more costly (incremental costs = $81,924) and more effective (incremental QALYs = 1.04) compared with ET alone, resulting in an ICER of $78,438 per QALY. A price reduction of 24% for abemaciclib would be necessary to achieve an ICER of $50,000 per QALY for ABE plus ET compared with ET alone. The CADTH analysis allows for a survival benefit for ABE plus ET of 1.94 years, despite the current clinical evidence, which may be optimistic. The high degree of uncertainty contributed by the sponsor’s fixed payoff approach and the unknown relationship between IDFS and OS suggest that a greater price reduction may be needed to achieve cost-effectiveness.
While clinical experts consulted by CADTH considered the long-term IDFS and effectiveness waning assumptions adopted in the CADTH base case to be more plausible than those assumed by the sponsor, experts cautioned that, beyond the trial duration, the effectiveness and durability of the effect of abemaciclib is highly uncertain and may be overestimated. As shown by CADTH scenario analysis exploring a shorter time horizon (5 years), the ICER is sensitive to assumptions about long-term efficacy beyond the available evidence. Thus, the ICER predicted by the CADTH base case should be considered highly uncertain and may be underestimated.
The cost-effectiveness of ABE plus ET depends on 3 principal factors: the long-term IDFS of abemaciclib plus ET, whether improved IDFS translates into OS benefits, and whether the predicted savings are realized among patients who have a metastatic recurrence after adjuvant abemaciclib plus ET. Plausible changes in any of these factors would result in a higher ICER, and the need for a higher price reduction. Should the long-term effectiveness of ABE plus ET be lower than predicted from the extrapolation of 2 years of data observed from the monarchE trial, the ICER will be higher than in the CADTH base case. Incremental QALYs estimated during the period of the trial were lower for ABE plus ET than for ET alone, suggesting that even the on-trial benefit is highly uncertain. While clinical experts consulted by CADTH indicated improved IDFS is an important goal, they noted that it is highly uncertain whether improved IDFS will lead to an improvement in OS. Similarly, should the predicted savings among patients with metastatic disease not be realized in clinical practice (e.g., should patients with ET-sensitive disease receive a CDK4 and CDK6 inhibitor as part of subsequent therapy), the ICER will be higher, and a greater price reduction would be required.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc.; 2022 Apr 07.
2.Verzenio (abemaciclib): 50 mg, 100 mg, 150 mg, or 200 mg oral tablets [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Jan 10.
3.Clinical Study Report: I3Y-MC-JPCF. Version 1. monarchE: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Toronto (ON): Eli Lilly Canada Inc.; 2020 Sep 25.
4.Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets [internal sponsor's package]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Apr 07.
5.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc.; 2022 Apr 07.
6.A cost-effectiveness analysis of abemaciclib in the treatment of advanced breast cancer in the MONARCH 3 indication: Canadian pCODR technical report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc.; 2018 Nov 09.
7.A cost-effectiveness analysis of abemaciclib in the treatment of advanced or metastatic breast cancer in the MONARCH 2 indication: pCODR technical report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc.; 2018 Nov 27.
8.National Institute for Health and Care Excellence. Neratinib for extended adjuvant treatment of hormone receptor-positive, HER2-positive early stage breast cancer after adjuvant trastuzumab. (Technology appraisal guidance TA612) 2019; https://www.nice.org.uk/guidance/ta612. Accessed 2022 Jun 06.
9.Lidgren M, Wilking N, Jonsson B, Rehnberg C. Health related quality of life in different states of breast cancer. Qual Life Res. 2007;16(6):1073-1081. PubMed
10.Ara R, Brazier JE. Using health state utility values from the general population to approximate baselines in decision analytic models when condition-specific data are not available. Value Health. 2011;14(4):539-545. PubMed
11.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Jun 07.
12.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Jun 07.
13.Yu M, Guerriere DN, Coyte PC. Societal costs of home and hospital end-of-life care for palliative care patients in Ontario, Canada. Health Soc Care Community. 2015;23(6):605-618. PubMed
14.Cuzick J, Sestak I, Baum M, et al. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol. 2010;11(12):1135-1141. PubMed
15.Hamilton SN, Tyldesley S, Li D, Olson R, McBride M. Second malignancies after adjuvant radiation therapy for early stage breast cancer: is there increased risk with addition of regional radiation to local radiation? Int J Radiat Oncol Biol Phys. 2015;91(5):977-985. PubMed
16.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Jun 07.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Adjuvant Treatment of HR-Positive, HER2-Negative Early Breast Cancer
Treatment | Strength | Dosage form | Price ($) | Recommended dosage | Daily cost ($) | Cost per 28-day cycle ($) |
|---|---|---|---|---|---|---|
Abemaciclib (Verzenio)a | 50 mg 100 mg 150 mg 200 mg | Tablet | 98.4714a 99.9704 98.4714 99.9704 | 150 mg twice daily | 196.94 | 5,514 |
Abemaciclib + anastrozole | 197.90 | 5,541 | ||||
Abemaciclib + exemestane | 198.27 | 5,552 | ||||
Abemaciclib + letrozole | 198.32 | 5,553 | ||||
Abemaciclib + tamoxifen | 197.29 | 5,524 to 5,534 | ||||
Endocrine therapy | ||||||
Anastrozole (generics) | 1 mg | Tablet | 0.9522 | 1 mg daily | 0.95 | 27 |
Exemestane (generics) | 25 mg | Tablet | 1.3263 | 25 mg daily | 1.33 | 37 |
Letrozole (generics) | 2.5 mg | Tablet | 1.3780 | 2.5 mg daily | 1.38 | 39 |
Tamoxifen (generics) | 10 mg 20 mg | Tablet | 0.1750 0.3500 | 20 to 40 mg daily | 0.35 to 0.70 | 10 to 20 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed June 2022), unless otherwise indicated, and do not include dispensing fees. Recommended dosage for endocrine therapy drugs based on Cancer Care Ontario monographs.
aPrice submitted by sponsor.4 Recommended dosage based on the product monograph.2
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | Modelled population is based on the high Ki-67 (≥ 20%) subgroup of Cohort 1 of the monarchE trial, which reflects the Health Canada indication for abemaciclib. |
Model has been adequately programmed and has sufficient face validity | No | Costs and outcomes for patients in the metastatic recurrence health state were adopted from models used for prior sponsor submissions.6,7 These models were not provided to CADTH as part of the review and have not been appraised for validity. |
Model structure is adequate for decision problem | No | While the model structure is generally adequate (i.e., the included health states are appropriate for the indication), the sponsor has adopted a “fixed payoff” approach to modelling costs, life-years, and QALYs for the metastatic recurrence health state. Because this approach is based on external models not provided to CADTH, CADTH is unable to validate the output of these models and the relevance to the current decision problem. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | The sponsor has assumed a standard error of +/–20% of the mean value for variables where they could have specified from standard error from trial data (e.g., some utility values, resource use, the proportion of patients who receive specific treatments in the metastatic state). Some inputs were inappropriately considered variable (administration costs, resource use costs). |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Parameter uncertainty was not adequately considered. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The model is poorly organized and difficult to maneuver. The “fixed payoff” approach was not transparently described. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
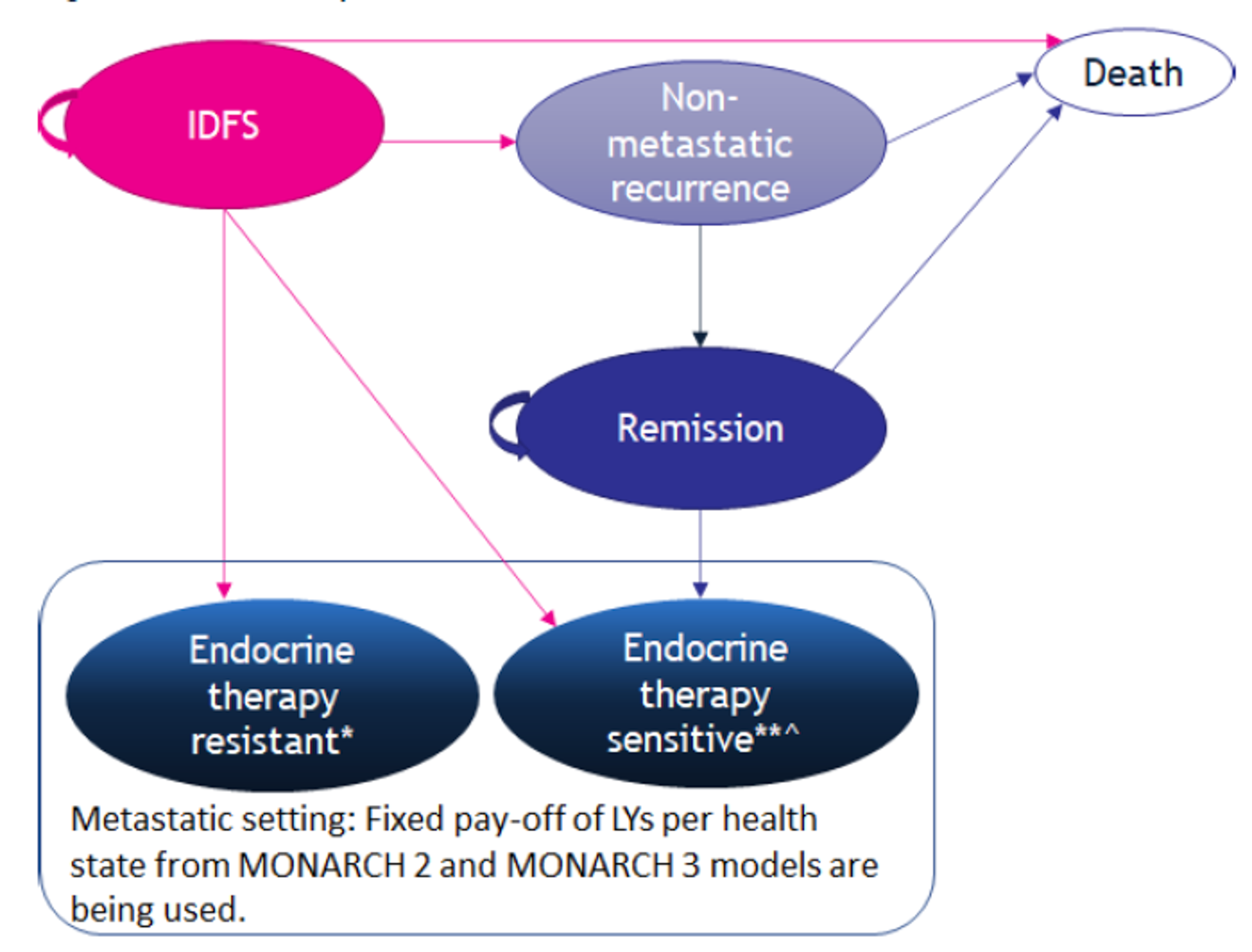
ET = endocrine therapy; IDFS = invasive disease–free survival; LY = life-year.
Notes: ET-resistant: Disease recurrence while receiving or within 12 months of completing prior adjuvant ET.
ET-sensitive: Disease recurrence at least 12 months after completion of prior adjuvant ET.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | ABE + ET | ET | Incremental |
|---|---|---|---|
Discounted LYs | |||
Invasive disease–free | 16.69 | 13.38 | 3.31 |
Non-metastatic recurrence | 0.23 | 0.17 | 0.06 |
Remission | 1.93 | 1.52 | 0.42 |
Metastatic recurrence: ET-resistant | 0.69 | 1.03 | –0.33 |
Metastatic recurrence: ET-sensitive | 2.94 | 2.80 | 0.15 |
Total | 22.49 | 18.89 | 3.60 |
Discounted QALYs | |||
Invasive disease–free | 10.00 | 8.20 | 1.80 |
Non-metastatic recurrence | 0.13 | 0.10 | 0.02 |
Remission | 0.99 | 0.81 | 0.18 |
Metastatic recurrence: ET-resistant | 0.32 | 0.53 | −0.21 |
Metastatic recurrence: ET-sensitive | 1.20 | 1.13 | 0.06 |
Total | 12.63 | 10.77 | 1.86 |
Discounted costs ($) | |||
Pre-metastatic remission | 154,508 | 17,326 | 137,182 |
Drug acquisition | 118,261 | 1,264 | 116,997 |
Treatment-specific costs | 4,696 | 2,314 | 2,381 |
Background therapy | 31,440 | 13,660 | 17,779 |
Drug-related costs in non-metastatic remission | 112 | 88 | 24 |
Disease management, pre-metastatic | 6,897 | 5,529 | 1,368 |
Metastatic setting | 25,962 | 86,160 | –60,199 |
Metastatic recurrence: ET-resistant | 5,387 | 32,051 | –26,663 |
Metastatic recurrence: ET-sensitive | 20,574 | 54,110 | –33,535 |
Drug administration/monitoring | 19 | 4 | 15 |
Terminal care | 13,824 | 14,718 | –894 |
Adverse events | 4,518 | 3,896 | 621 |
Total | 205,727 | 127,634 | 78,094 |
ICER ($/QALY) | 42,008 | ||
ABE = abemaciclib; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 11: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | ABE + ET | ET | Incremental |
|---|---|---|---|
Discounted LYs | |||
Invasive disease–free | 18.21 | 16.53 | 1.68 |
Non-metastatic recurrence | 0.22 | 0.17 | 0.05 |
Remission | 1.83 | 1.42 | 0.41 |
Metastatic recurrence: ET-resistant | 0.69 | 0.92 | −0.23 |
Metastatic recurrence: ET-sensitive | 2.91 | 2.89 | 0.02 |
Total | 23.87 | 21.93 | 1.94 |
Discounted QALYs | |||
Invasive disease–free | 10.68 | 9.74 | 0.94 |
Non-metastatic recurrence | 0.12 | 0.10 | 0.03 |
Remission | 0.93 | 0.74 | 0.19 |
Metastatic recurrence: ET-resistant | 0.32 | 0.47 | –0.15 |
Metastatic recurrence: ET-sensitive | 1.16 | 1.12 | 0.04 |
Total | 13.21 | 12.16 | 1.04 |
Discounted costs ($) | |||
Pre-metastatic remission | 154,507 | 17,245 | 137,262 |
Drug acquisition | 118,261 | 1,263 | 116,998 |
Treatment-specific costs | 4,786 | 2,355 | 2,431 |
Background therapy | 31,351 | 13,542 | 17,809 |
Drug-related costs in non-metastatic remission | 109 | 86 | 24 |
Disease management, pre-metastatic | 6,737 | 5,459 | 1,278 |
Metastatic setting | 25,339 | 82,133 | –56,794 |
Metastatic recurrence: ET-resistant | 5,385 | 28,570 | –23,185 |
Metastatic recurrence: ET-sensitive | 19,954 | 53,563 | –33,609 |
Drug administration/monitoring | 19 | 4 | 15 |
Terminal care | 13,453 | 13,985 | –532 |
Adverse events | 4,446 | 3,752 | 694 |
Total | 204,502 | 122,578 | 81,924 |
ICER ($/QALY) | 78,438 | ||
ABE = abemaciclib; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 12: CADTH Scenario Analyses
Scenario | CADTH base case | CADTH scenario |
|---|---|---|
Scenario analyses | ||
1. ABE treatment effectiveness | Effectiveness waning begins at month 25 and lasts until year 5 (maximum ABE treatment duration: 24 months) | Effectiveness is lost as soon as ABE is discontinued, using a sponsor-provided option to do so |
2. ABE treatment effectiveness | Effectiveness waning begins at month 25 and lasts until year 5 (maximum ABE treatment duration: 24 months) | Effectiveness waning begins at month 36 and lasts until year 8 |
3. Treatments received in the by patients with ET-sensitive metastatic recurrence | Patients with ET-sensitive recurrence whose initial treatment was ABE + ET were assumed to not receive subsequent treatment with a CDK4 and CDK6 inhibitor; 76% of patients whose initial treatment was ET were assumed to receive subsequent CDK4 and CDK6 inhibitor treatment | An equal distribution of subsequent treatment was adopted for patients with ET-sensitive metastatic recurrence, regardless of whether initial treatment was ABE + ET or ET |
4. Analysis horizon | 49 years | 5 years |
5. Analysis horizon | As previously mentioned | 10 years |
ABE = abemaciclib; ET = endocrine therapy.
Table 13: CADTH Scenario Analyses Results (Deterministic)
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
CADTH base case | |||
ET | 123,028 | 12.52 | Reference |
ABE + ET | 205,451 | 13.47 | 86,216 |
Scenario 1: ABE effectiveness waning starting at discontinuation | |||
ET | 123,028 | 12.52 | Reference |
ABE + ET | 205,680 | 13.16 | 127,953 |
Scenario 2: ABE effectiveness waning starting at year 3 | |||
ET | 123,028 | 12.52 | Reference |
ABE + ET | 205,243 | 13.73 | 67,659 |
Scenario 3: Treatments received in the ET-sensitive state | |||
ET | 123,028 | 12.52 | Reference |
ABE + ET | 244,439 | 13.50 | 122,854 |
Scenario 4: 5-year analysis horizon | |||
ET | 43,382 | 3.65 | Reference |
ABE + ET | 144,151 | 3.67 | 5,777,555 |
Scenario 5: 10-year analysis horizon | |||
ET | 67,060 | 6.19 | Reference |
ABE + ET | 159,373 | 6.43 | 382,103 |
ABE = abemaciclib; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: CADTH base-case and scenario analyses are deterministic.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA)5 assessed the expected budgetary impact resulting from reimbursing adjuvant abemaciclib for the Health Canada indication (for use in combination with ET, for the adjuvant treatment of adult patients with HR-positive, HER2-negative early breast cancer at high risk of recurrence [Ki-67 ≥ 20%]).2 The BIA was undertaken from the perspective of the Canadian public drug plans over a 3-year horizon (2023 to 2025) using an epidemiological approach. The sponsor’s analysis included drug acquisition costs, wholesaler mark-up, and dispensing fees; the cost of Ki-67 testing was excluded. Data to inform the model were obtained from various sources, including the published literature, the sponsor’s internal data, and input from clinical experts consulted by the sponsor.
In the model, abemaciclib (150 mg twice daily) was assumed to be received for a maximum of 2 years, after which time patients were assumed to receive ET alone for the remainder of the model horizon.5 Discontinuation of abemaciclib before 2 years was based on discontinuation rates from the monarchE trial, with 41% of patients assumed to receive 2 full years of abemaciclib treatment. ET was assumed to be consisting of anastrozole (25%), letrozole (40.7%), and tamoxifen (34.3%), and was assumed to be administered for the full BIA time horizon. Drug costs were obtained from the sponsor’s submission for abemaciclib4 or from the Ontario Drug Benefit Formulary.16 In the new drug scenario, the sponsor assumed that ABE plus ET will displace ET, with uptake base on internal forecast data and market research. Key inputs to the BIA are documented in Table 16.
Key assumptions included:
12% of HR-positive, HER2-negative early breast cancer patients are at high risk of recurrence, based on monarchE ITT population (i.e., those with ≥ 4 positive lymph nodes, or 1 to 3 positive lymph nodes with 1 or more of the following: Grade 3 disease, tumour size ≥ 5 cm, or a Ki-67 score ≥ 20%).
50% of patients deemed to be at high risk of recurrence undergo Ki-67 testing, and 50% of tested patients have high Ki-67 (≥ 20%).
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
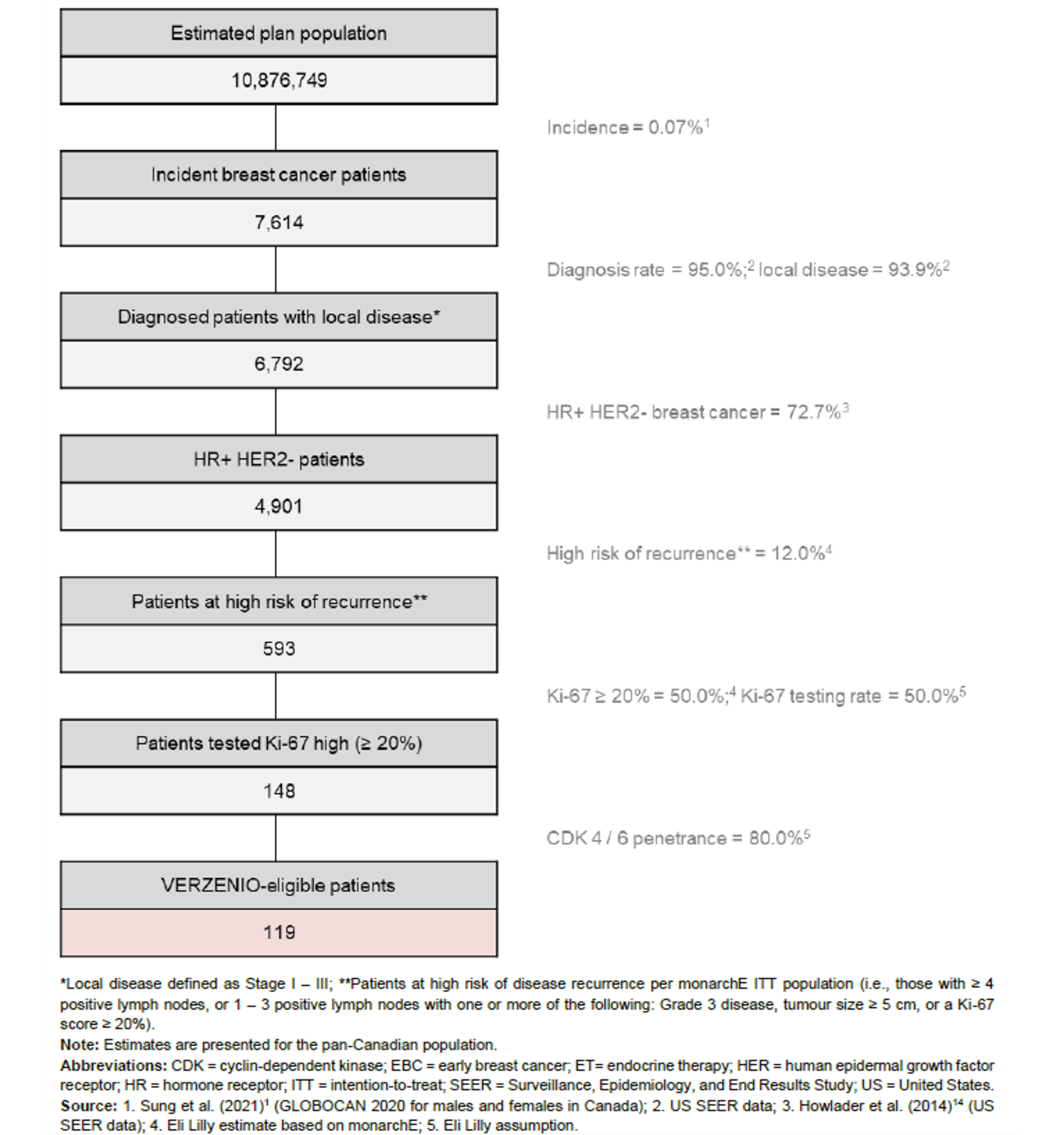
Note: “119 Verzenio-eligible patients” reflects the sponsor’s estimated number of patients eligible for abemaciclib plus endocrine therapy (abemaciclib + endocrine therapy) in the baseline year (year 0). The number of eligible patients for year 1, year 2, and year 3 was 238, 360, and 483, respectively.
Source: Sponsor’s submission.5
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1 / year 2 / year 3) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 238/360/483 |
Market uptake (reference scenario, 3 years) | |
ABE + ET | 0% / 0% / 0% |
ETa | 100% / 100% / 100% |
Market uptake (new drug scenario, 3 years) | |
ABE + ET | 48.4% / 49.7% / 49.9% |
ET | 51.6% / 50.3% / 50.1% |
Annual cost of treatment (per patient) | |
ABE + ETb | 72,224 |
ET | 341 |
ABE = abemaciclib: ET = endocrine therapy.
aAssumed to be consisting of anastrozole 25%, exemestane 0%, letrozole 40.7%, and tamoxifen 34.3%.
bABE was assumed to be received for a maximum of 2 years, after which time costs for ET alone were incurred. The cost of ABE was based on the sponsor’s submitted price for the 150 mg tablet ($98.47). The sponsor’s base case assumes 100% usage of the 150 mg tablet.5
Summary of the Sponsor’s Budget Impact Analysis Results
Results of the sponsor’s analysis suggest that the reimbursement of abemaciclib for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score of 20% or more will be associated with a 3-year cost of $15,033,295 (year 1 = $3,533,136; year 2 = $5,476,728; year 3 = $6,023,431).
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of eligible patients is uncertain. While the sponsor’s modelled BIA population generally reflects the Health Canada indicated population (patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence based on clinicopathologic features and Ki-67 ≥ 20%), the sponsor restricted the BIA population to patients “with ≥ 4 positive lymph nodes, or 1 – 3 positive lymph nodes with 1 or more of the following: Grade 3 disease, tumour size ≥ 5 cm, or a Ki-67 score ≥ 20%.”5 As part of this derivation, the sponsor assumed that 12% of patients with HR-positive, HER2-negative early breast cancer would be at high risk of recurrence based on clinicopathologic features, based on data from the monarchE trial. It is uncertain whether the proportion of patients defined as “high risk” based on the eligibility criteria for the global monarchE trial are directly applicable in the Canadian context (data not provided for Canadian monarchE study sites), and the inclusion of only patients defined as high risk based on the monarchE eligibility criteria may underestimate the number of eligible patients in clinical practice (i.e., the Health Canada indication does not restrict the usage of abemaciclib based on the number of positive nodes or tumour size).
The sponsor further estimated that 50% of patients deemed “high risk” would undergo Ki-67 testing and that 50% would have Ki-67 of 20% or more. As such, Ki-67 score is potentially incorporated twice in the derivation of the eligible population, which may artificially reduce the number of eligible patients.
In scenario analyses, CADTH explored the impact of assuming that a higher proportion of patients will meet the Health Canada indication of “high risk based on clinicopathological features.”
The proportion of Ki-67 High patients is uncertain. The sponsor assumed that 50% of patients at high risk of disease recurrence would undergo Ki-67 testing. Clinical experts consulted by CADTH for this review indicated that, at present, few patients undergo Ki-67 testing and that this may vary by study centre. Experts indicated, however, should abemaciclib become reimbursed, all high-risk patients (i.e., those potentially eligible for abemaciclib + ET) would likely undergo Ki-67 testing. The sponsor further assumed that, of those tested, 50% would have a Ki-67 score of 20% or more. Clinical experts indicated that there is considerable uncertainty around this value, as Ki-67 testing is not routinely performed in clinical practice in Canada, resulting in a lack of Canadian data. In the monarchE trial, of the Cohort 1 patients who underwent Ki-67 testing, approximately 51% were reported to have high Ki-67 (≥ 20%). Clinical experts additionally noted that there is considerable variation in Ki-67 testing, including variation between centres, as well as issues regarding reproducibility (e.g., variation in test results between tests performed on the same sample or on samples from the same patient at different times). In the sponsor’s submitted cost-utility analysis, all patients in the ABE plus ET group were assumed to have undergone Ki-67 testing, along with 19% of patients in the ET group.1
In the CADTH reanalysis, all potentially eligible patients were assumed to undergo Ki-67 testing. In scenario analyses, CADTH adopted alternative estimates for the proportion of patients with high Ki-67.
Market share of comparators is uncertain. To inform the market share of anastrozole, exemestane, letrozole, and tamoxifen as part of ET in the reference scenario, the sponsor states that they “considered a weighted average of aromatase inhibitors (anastrozole, exemestane, and letrozole) and tamoxifen based on observed utilization in monarchE (25%, 0.0%, 40.7%, 34.3%, respectively)”. Clinical experts consulted by CADTH indicated that this distribution of treatments does not reflect Canadian clinical practice, and that exemestane is used in their practices. As noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, in the Cohort 1 Ki-67 High subpopulation of the monarchE trial, exemestane was received as part of ET by 11.5% of participants. Clinical experts consulted by CADTH for this review indicated approximately two-thirds of patients would receive an aromatase inhibitor (letrozole, anastrozole, or exemestane) and one-third would receive tamoxifen; however, clinical experts noted that the relative usage of individual aromatase inhibitors was uncertain.
While the composition of the ET basket, and hence the market share assumptions, likely do not reflect Canadian clinical practice, these assumptions have little impact on the budget impact estimate, given that the same distribution was applied in the reference and new drug scenario and that abemaciclib is given in addition to ET (i.e., no displacement occurs).
The full cost of ABE plus ET may be underestimated: In the model, the sponsor assumed that patients become eligible for ABE plus ET treatment over the entire calendar year (i.e., instead of assuming all patients are eligible at the start of the year). While this approach potentially provides a more accurate estimate of costs that are incurred at any 1 time during the 3-year period, this approach likely underestimates the budget impact of ABE plus ET in the final analysis year. For example, although the sponsor notes that 483 patients are eligible for abemaciclib in year 3 of the analysis, the full cost of ABE plus ET for this year will be captured only for patients who initiate treatment in January of that year. This approach additionally makes the BIA substantially more complex and difficult to validate.
CADTH was unable to address this limitation owing to the structure of the sponsor’s model. As such, the incremental budget impact in year 3 (and hence the 3-year total budget impact) may be underestimated.
Additional limitations were identified, but were not considered to be key limitations:
The baseline year (year 0) does not reflect the period before abemaciclib is publicly reimbursed. The baseline year is intended to reflect the 12-month period before the public reimbursement of the drug under review, and no uptake should be assumed during that period. In the BIA, the sponsor assumed that uptake of ABE plus ET would begin early in the baseline year (2022), after the Health Canada Notice of Compliance was received. CADTH was unable to correct this error owing to the model structure, but notes that this error has no impact on the estimated 3-year budget impact (as the 3-year budget impact incudes year 1, year 2, and year 3 only).
The ET basket of treatments does not represent current Canadian clinical practice. As noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation, the assumption that ET would consist of 41% letrozole, 25% anastrozole, 0% exemestane, and 34% tamoxifen was not justified by the sponsor, and clinical experts consulted by CADTH for this review indicated that the composition of the ET basket is not aligned with clinical practice in Canada. Experts indicated that approximately two-thirds of patients would receive an aromatase inhibitor (letrozole, anastrozole, or exemestane) and one-third would receive tamoxifen; however, experts noted that the relative usage of individual aromatase inhibitors was uncertain. While the composition of the ET basket likely does not reflect Canadian clinical practice, these assumptions have little impact on the budget impact estimate, given that the same distribution was applied in the reference and new drug scenario and that abemaciclib is given in addition to ET (i.e., no displacement occurs).
CADTH Reanalyses of the Budget Impact Analysis
CADTH conducted reanalyses of the BIA, by revising the proportion of patients who undergo Ki-67 testing (Table 16).
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Proportion of patients who undergo Ki-67 testing | 50% | 100% |
CADTH base case | Reanalysis 1 | |
The results of the CADTH step-wise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18.
Based on the CADTH base case, the budget impact of the reimbursement of abemaciclib for use in combination with ET as adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathologic features and a Ki-67 score of 20% or more is expected to be $7,066,272 in year 1, $10,953,457 in year 2, and $12,046,862 in year 3, with a 3-year total of $30,066,591.
The budget impact is sensitive to uncertainty in number of patients deemed to be at high risk based on clinicopathologic features, Ki-67 test positivity rates, and assumptions about the market uptake.
Table 17: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | 15,033,295 |
CADTH reanalysis 1 | 30,066,591 |
CADTH base case (reanalysis 1) | 30,066,591 |
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 18:
Assuming that 20% of patients are at high risk of recurrence.
Assuming a 60% test positivity for Ki-67.
Assuming a 40% test positivity for Ki-67.
Assuming that all patients receive abemaciclib for 2 years.
Assuming a peak market share of 60% for abemaciclib plus ET.
Price of abemaciclib reduced by 24%.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysisa | Scenario | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|
Submitted base case | Reference | 91,297 | 151,369 | 212,167 | 454,833 |
New drug | 3,624,433 | 5,628,097 | 6,235,598 | 15,488,128 | |
Budget impact | 3,533,136 | 5,476,728 | 6,023,431 | 15,033,295 | |
CADTH base case | Reference | 182,594 | 302,738 | 424,334 | 909,666 |
New drug | 7,248,867 | 11,256,194 | 12,471,196 | 30,976,257 | |
Budget impact | 7,066,272 | 10,953,457 | 12,046,862 | 30,066,591 | |
CADTH scenario analysis: 20% at high-risk of recurrence | Reference | 301,788 | 500,376 | 701,381 | 1,503,545 |
New drug | 11,989,424 | 18,618,357 | 20,629,273 | 51,237,055 | |
Budget impact | 11,687,636 | 18,117,981 | 19,927,892 | 49,733,510 | |
CADTH scenario analysis: 60% Ki-67 test positivity | Reference | 219,113 | 363,285 | 509,201 | 1,091,599 |
New drug | 8,698,640 | 13,507,433 | 14,965,435 | 37,171,508 | |
Budget impact | 8,479,527 | 13,144,148 | 14,456,234 | 36,079,909 | |
CADTH scenario analysis: 40% Ki-67 test positivity | Reference | 146,076 | 242,190 | 339,467 | 727,733 |
New drug | 5,799,093 | 9,004,956 | 9,976,957 | 24,781,005 | |
Budget impact | 5,653,018 | 8,762,765 | 9,637,489 | 24,053,273 | |
CADTH scenario analysis: All patients receive ABE for 2 years | Reference | 182,594 | 302,738 | 424,334 | 909,666 |
New drug | 9,336,254 | 16,288,630 | 18,436,092 | 44,060,977 | |
Budget impact | 9,153,660 | 15,985,893 | 18,011,758 | 43,151,311 | |
CADTH scenario analysis: peak market share of ABE + ET assumed to be 60% | Reference | 182,594 | 302,738 | 424,334 | 909,666 |
New drug | 8,662,121 | 13,446,886 | 14,880,568 | 36,989,575 | |
Budget impact | 8,479,527 | 13,144,148 | 14,456,234 | 36,079,909 | |
CADTH scenario analysis: 24% price reduction for abemaciclib | Reference | 182,594 | 302,738 | 424,334 | 909,666 |
New drug | 5,556,002 | 8,632,074 | 9,585,122 | 23,773,198 | |
Budget impact | 5,373,408 | 8,329,336 | 9,160,788 | 22,863,532 |
ABE = abemaciclib; ET = endocrine therapy.
aEstimates for year 0 (baseline year) are not presented owing to errors in the sponsor’s submitted model. CADTH notes that this had no impact on the estimated budget impact in year 1 to year 3.
Stakeholder Input
Patient Input
Rethink Breast Cancer
About Rethink Breast Cancer
Rethink Breast Cancer (Rethink) is a Canadian charity known for making positive change. Rethink educates, empowers and advocates for system changes to improve the experience and outcomes of those with breast cancer, focusing on historically underserved groups: people diagnosed at a younger age, those with metastatic breast cancer and people systemically marginalized due to race, income or other factors. We foster spaces to connect, listen, empower and rethink breast cancer, together. Rethink’s strategic priorities and organizational direction are guided by the unique, unmet needs identified by breast cancer patients and their families.
Programs and Activities
Rethink Breast Cancer builds community, bringing patients with various stages of breast cancer together through our private and public social spaces as well as in-person events
Rethink runs patient retreats and facilitates peer-support
Rethink creates and runs education forums and conferences
Rethink creates support and education tools, resources and content
Rethink funds and supports breast cancer research You can find out more by visiting:
Rethink Breast Cancer Instagram Rethink Breast Cancer Website
Information Gathering
For over 20 years, Rethink has been working closely with breast cancer patients in Canada. We learn from and listen to the community to understand their values, priorities and pain points to help drive change and system improvements. Each year, we learn from the patients we serve, survey and collaborate with. We learn from the 40 individuals that we work extremely closely with as key patient advisors; the 100 patients that share their stories on our blog; the 500 patients that participate in our virtual support groups; the 1,600 members of our private peer- support network; the 30,000 people that have joined our Instagram community; and the 150,000 individuals reached each month through the reach of that channel. We listen, learn, engage and have conversations in all these spaces.
Rethink Breast Cancer has several important patient advisory boards and working groups that offer experience-focused insights on issues related to those affected by and concerned about breast cancer, including:
Metastatic Breast Cancer Advisory Board
Early Breast Cancer Advisory Board
Equity, Diversity and Inclusion working group
Triple Negative Breast Cancer working group (all stages)
For this submission, we have drawn on our general observations and insights gathered through programming and meetings with breast cancer patients as described above. Rethink also conducted in-depth telephone interviews in March 2022 with two patients who have experience with abemaciclib for HR+, HER2- high risk early breast cancer, and one patient who has been prescribed it by her oncologist but, two months later, was still waiting to start it.
Disease Experience
Most people in the Rethink community are diagnosed at a younger age. When young people get breast cancer it may be more aggressive, which can lead to tougher treatments. In addition, those diagnosed in their 20s, 30s and early 40s face age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, childcare, impact on relationships, body image, dating and sexuality, feeling isolated from peers who don’t have cancer, career hiatuses, and financial insecurity. The physical and emotional toll that a breast cancer diagnosis and treatment takes on a young person’s life is devastating and traumatic.
When it comes to those in the community who have been told their breast cancer is at a high risk of recurrence, treatment is less about controlling an aspect of the illness and more a deep desire to take on whatever treatment(s) are needed to decrease the chance of recurrence and metastatis. They are facing mortality prematurely and many express a goal to treat aggressively to optimize treatment. Those we interviewed in March for this submission shared:
“I think when anyone gets a cancer diagnosis, you’re always scared of the illness coming back. Especially when I have young kids that I want to be there for, and I have a lot of things I want to do myself. It’s not only my kids, but also my life too. I want to be able to enjoy it. Because I feel that I’m doing anything and everything that’s available out there to have a lower chance of recurrence, it gives me peace of mind. It gives me less anxiety in my life.” —Negar
“I am generally a fan of treatment - the more aggressive the better. In fact, after having chemo done, I advocated to have a total axillary LN dissection, and I also had my ovaries out last year. Again, I don't mind treatment at all, even the side effects that come with it - I'm more concerned about the prospect of mortality.” — Ada
“I want to try anything to prevent recurrence, I want to add it to my exercise routine and healthy diet in my bag of tricks.” — Jessica
Experiences With Currently Available Treatments
Current treatment for HR positive HER2 negative early breast cancer depends on the details of the persons diagnosis and the characteristics revealed on their pathology report. It is usually treated with a combination of surgery, chemotherapy, radiation therapy, and hormonal therapy, which can reduce the risk of early-stage breast cancer coming back. Some patients will opt for an oophorectomy. These treatments are all incredibly difficult with both physical and emotional impacts that require a lot of support and care. Peer support is incredibly helpful as is professional support. Being well prepared for what you are about to endure is essential and oncology nurses and a peer community are extremely helpful in this regard both with short term and long-term side effect management. Difficulty coping with the side-effects of hormone therapy is frequently discussed in our community.
Improved Outcomes
Each individual patient brings their own personal values and goals to their discussions with their oncology team. Communication and trust in their team is essential. In our experience working closely with many young high risk breast cancer patients, we find most are willing to trade toxicity for confidence in knowing they’ve “thrown everything they could” at the cancer. In other words, they will choose to endure additional side-effects and impacts on quality of life from the toxicity of a stronger therapy to ensure they are doing everything they can to treat what they know is an aggressive form of breast cancer. That was a take-away from the patients we interviewed for this submission who are on Verzenio and the one that has been prescribed it and is waiting. We’ve also had patients in the community reaching out to our organization, asking when it will be available in Canada for early breast cancer.
Experience With Drug Under Review
Rethink conducted in depth phone interviews with two patients with high-risk early breast cancer who have experience with abemaciblib (Verzenio). We also interviewed one person whose only experience with Verzenio was that she’d been prescribed it by her oncologist over two months ago and was still waiting to start it as she deals with navigating the challenges of her insurance’s heavy co-pay.
Patient 1 Interview: Negar
My name is Negar. I’m located in Vancouver, BC. At the end of my pathology report, I was Stage 2B. I was 39 at the time. I had three tumours. I found it myself. We never had any family history. The lump was moving. My family physician was sure that it wasn’t cancer, but she just wanted to make sure and have peace of mind, so she sent me for testing and here I am. I did surgery first and then 8 rounds of chemo, 25 rounds of radiation. I did an oophorectomy. At the beginning I was going to do Zoladex, but I talked with my doctors, after 10 years I’ll be almost 50 so there was no point for me to stay on Zoladex, so I did an oophorectomy in March.
In regards to my treatment path, I wouldn’t say hell, although I had days that looked like hell. I was lucky I caught it early. I had node involvement and normally when there’s a lymph node involvement it spreads quickly after that. It was a lot of ups and downs; I still have a lot of that. Sometimes I think I came to terms with it, but I don’t think I have yet. It was very scary as I have 2 young children. I was working full time. I always say it was my prime time with my kids and my work, but I had to put everything on pause. It’s a scary, scary situation to be in because you see so many people that had the same diagnosis, they got the same care, but they had a recurrence. So, when my doctor talked about Verzenio although the side effects are not something that I look forward to, but again it’s bringing the possibility of recurrence lower, so I take it.
I was really lucky that my oncologist referred me – I think the manufacturer is the one paying for me, I’m not paying out of pocket. Here it’s $13,000 per month and I definitely cannot afford that. I was very concerned about the cost. Maybe if I didn’t have kids, it would be a totally different experience. I had a cousin; she was like my sister. She was 5 years younger than me. She passed away from ovarian cancer in 2019, so we had that scare in our family. Not in a blaming way, but one thing that everyone thought is that she didn’t take the cancer seriously. So, from the minute I was diagnosed, I was quite proactive on finding the best solution. When I was talking with my oncologist, I already had done tons of research on breast cancer, what treatments are available, my second opinion from MD Anderson, etc. So, when the Verzenio got approved by Health Canada, I knew about it, I read about it, I did research. I follow quite a few of women with breast cancer on Instagram and I saw them talking about it and the cost of it. So, the cost was something that I was concerned about. $13,000 a month is a lot of money. Both my husband and I are making good money, but this is still a lot of money per month. We thought, we’re going to try to do this, and even if we have to remortgage our house to get the money from the equity in our house to pay for the treatments, we’re going to do it.
My oncologist was on board for me taking this medication and said there’s ways it can be covered. Thankfully I was approved for it. So, I feel very blessed and lucky that this treatment was available to me for free. I understand some provinces don’t cover oral chemo and it’s scary. Especially with cancer, time is of the essence. You need to be very quick. You cannot wait a year for this to become available because in that year, the cancer might spread and turn metastatic.
I feel so lucky that I have access to it at no cost. But the side effects, I haven’t had severe ones yet. I’m very tired, but I’ll take being tired rather than the cancer coming back. I think when anyone gets a cancer diagnosis, you’re always scared of the illness coming back. Especially when I have young kids that I want to be there for, and I have a lot of things I want to do myself. It’s not only my kids, but also my life too. I want to be able to enjoy it. Because I feel that I’m doing anything and everything that’s available out there to have a lower chance of recurrence, it gives me peace of mind. It gives me less anxiety in my life.
I would absolutely recommend Verzenio to other patients in my position. This is $13,000 per month. But what if the illness relapses? If you compare the amount of emotional distress and money that they’re going to put the family through with loss of life, other chemo, hospice, etc. so many things. When I got diagnosed with breast cancer in Canada, I felt so lucky because finances weren’t something I had to worry about. Of course, we were losing my income, but I didn’t have any extra costs. But this is the extra cost. If the Canada doesn’t fund this, I cannot imagine this stress in having the thought that something was available to me, and I wasn’t able to access this because I didn’t have the financial resources. It’s not fair.
Patient 2 Interview: Ada
I am 36 years old and was diagnosed with breast cancer when I was 33 years old. I had hormone positive and receptor negative type. I had my double mastectomy first, and my lump was 4.3cm! with 3/4 sentinel lymph nodes positive. I live in Richmond BC. I'm a social worker at a very large long term care home in Richmond. Being sick during the COVID 19 pandemic meant that I wasn't able to be at work during a time when they really needed staff and that was hard. I have a 4-year-old and 6-year-old now.
I didn't mind the treatment because for me, having treatment was taking action. I don't mind treatment at all, even the side effects that come with it - I'm more concerned about the prospect of mortality. My oncologist, who I trust, thought Verzenio would be good for me, so I didn't even hesitate to say yes. As long as it doesn't make my Anastrazole less effective, then I'm game - always.
The Lilley program is paying for my Verzenio. My extended health from work doesn't cover it. The pharmacy that it comes from has been good too. I just don't like that they deliver it
monthly because it's a hassle to coordinate, and I'm always worried that something will happen where I don't get my next delivery. I was expecting to get diarrhea my first week, so I took Imodium but then I ended up with constipation for like a week. Now my body has gotten used to it. I still get the occasional cramping or bloating, but nothing I can't tolerate. I would say though, for people just starting on Verzenio that I think once your body adjusts to it, it gets better. The first couple of weeks can be rough.
I would recommend Verzenio. Patients should never have to worry about getting their medications through bureaucratic processes. Please make life easier for patients than they already are. Provinces should fund this medication and make it easy for those who fit the criteria to get it.
Patient 3 Interview: Jessica
I am currently 41 years old, having just passed the one-year anniversary of my diagnosis in April 2021. I live in Ottawa with my husband and our 7-month-old son. I work at Global Affairs Canada in the Foreign Service, so I was actually diagnosed in Brazil and came home immediately to start treatment. I was also 15 weeks pregnant while diagnosed.
I’m not sure where to begin. Diagnosed with IDC, stage 2B, HR+, PR+, HER-. I started Chemo in April, AC-T dose dense protocol. I finished in August and had a few weeks to recover before my son was induced at 38 weeks which resulted in a c-section. From there I had a lumpectomy, balancing reduction and a SLND a little over a week after the birth of my baby. My margins did not come back clear and there was a significant number of affected lymph nodes. The pathology report was fairly damming. My Ki score was very high. I had surgery again a few weeks after the first, this time a mastectomy and a complete lymph node dissection. I followed with 15 rounds of radiation. I have been, and continue to be, terrified I will not be able to watch my son grow-up. It is my constant worry.
My oncologist told me about the success of the Monarch E studies and the announcement in the US came right around the same time as my pathology report. It gave me hope that my cancer, at very high risk for recurrence, could be kept at bay. I want to try it because I want to try anything to prevent recurrence, I want to add it to my exercise routine and healthy diet in my bag of tricks.
I am still waiting to access Verzenio. My oncologist prescribed it two months ago. I do have private insurance but the additional 20% is still quite steep. My understanding is that the hospital is trying to sort out the payment plans.
It is not an easy treatment and there are many side effects, but it could allow people like me to do everything possible to prevent recurrence. From a purely financial perspective, the medication is expensive, but the cost of treating MBC, or even just a second early-stage cancer, paired with 20 potential years of lost employment/productivity is a heavy burden as well.
Companion Diagnostic Test
Nothing to report on this topic.
Anything Else?
We’d like to emphasize that young, high-risk breast cancer patients want more effective tools in their toolbox that will help improve their chances against this challenging disease that’s turned their life-plans upside-down.
As we ponder “anything else,” we think about the MBC community that we know so well—and their loved ones. We think about those we’ve lost. Too, too many at such a young age over the years. Their families will never be the same. We also think about the MBC community that we see currently thriving. The CDK 4/6 inhibitors have been more of a game-changer in our community than we could have ever imagined. That said, moving the needle on MBC outcomes is still not the same as a cure. Verzenio as an option for those with HR+ HER2- breast cancer that is at a high risk of recurrence can give patients a tangible way to help achieve their goal of a cure.
And, finally, as we have been in the thick of #BitterestPill, an advocacy campaign calling for equal funding for Take Home Cancer Treatments in Ontario, we think about the delays, dollars, distress and discrimination that the current program in Ontario entails, which negatively impacts patient outcomes. Many in our community are underinsured and uninsured and our hearts go out to Jessica, who has been waiting two months to start the Verzenio she was prescribed by her oncologist because of the cost of her insurance co-pay. Too many are impacted by a policy that’s needed updating for over a decade!
Rethink Breast Cancer Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for Rethink Breast Cancer
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eli Lilly 2021 | — | — | X | — |
Eli Lily 2020 | — | — | X | — |
Canadian Breast Cancer Network
About the Canadian Breast Cancer Network
The Canadian Breast Cancer Network (CBCN) is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all Canadians affected by breast cancer through the promotion of information, education and advocacy activities. www.cbcn.ca
The Canadian Breast Cancer Network is committed to strict adherence to the Code of Conduct Governing Corporate Funding.
Information Gathering
Information for this submission was collected via:
CBCN’s 2017 Lived Experience Breast Cancer Patient Survey: An online survey was distributed in English and French to patients living with breast cancer. No patients surveyed had direct experience with the treatment under review. Survey questions comprised of a combination of scoring options and free form commentary. Patients were contacted through the membership databases of CBCN and other patient organizations.
Patient Respondents Profile: 278 early-stage, breast cancer patients responded to the survey in English and French. In this submission, CBCN specifically utilizes the data provided by 103 Canadian, early- stage, HR-positive, HER2-negative breast cancer patients who responded to our survey.
The respondents mostly (91) identified as female and primarily (89) spoke English as a first-language, with 4 speaking French as a first language, and 2 respondents selecting other as their first language (split between Hungarian and Italian), and 8 respondents undeclared. The majority of respondents were from Ontario (27) and Saskatchewan (21), 9 from British Columbia, 9 from Manitoba, 8 from Nova Scotia, 3 from New Brunswick, 4 from Quebec, 4 from Newfoundland and Labrador, 4 from Alberta and 1 from Prince Edward Island, 1 from Northwest Territories and 1 from Yukon. The remainder did not specify their province of residence.
Most of the respondents (41) were between the ages of 40-49 when diagnosed, 37 respondents were in the 50-59 age range, 14 were 60-69 years, 8 were between 30-39 years, 2 were 70-79, and 1 were between 20-29 years of age.
Most respondents were in a relationship (75), while 15 declared themselves as single, and the rest did not specify their relationship status. Most of the patients (70) had children, with the majority (42) with children 20 years or older, 28 had children between the ages of 13-19, 16 had children between 6-12 years of age 3 had children 2-5 years of age, and none had children below 1 year.
Printed sources: A review was conducted of current studies and grey literature to identify issues and issues and experiences that are commonly shared among many women living with breast cancer.
Disease Experience
A diagnosis of early-stage, hormone receptor (HR)-positive breast cancer has a significant impact on the day-to-day life of the patient. The diagnosis of HR-positive breast cancer, as well as the treatments that are used, impact both the emotional and physical well-being of a patient.
HR-positive, HER2-negative breast cancer is the most common form of breast cancer, affecting 70 percent of patients. The majority (90 percent) of these patients are diagnosed in non-metastatic, early stages (stages I-III). The median overall survival among patients with stage IV HR+/HER2− disease ranges from four to five years. Roughly 20 percent of HR-positive patients have high-risk disease and will develop a recurrence, either locally in the breast or elsewhere in the body over the first 10 years of treatment.
Treatment of HR+/HER2− breast cancer has mainly focused on hormone-blocking endocrine therapy. For early-stage, HR-positive, HER2-negative breast cancer, this includes at least 5 years of tamoxifen or aromatase inhibition with anastrozole, exemestane, or letrozole in post-menopausal or ovarian suppressed women. Extended adjuvant therapy is recommended for women at high risk of recurrence. The decision to add adjuvant chemotherapy is informed by a combination of clinical and genomic risk assessment, as well as patient preference. Standard surgical approaches include mastectomy or lumpectomy, typically followed by radiation.
Despite the effectiveness of standard endocrine therapy, as many as 41 percent of women diagnosed with HR-positive, early-stage BC will experience distant (or metastatic) recurrence. Recent studies have revealed that for patients with high-risk HR-positive, HER2-negative breast cancer, the risk of recurrence is even greater, especially during the first few years on adjuvant endocrine therapy. High risk, early breast cancers are also known to show a degree of resistance to hormone therapy, relapsing early, despite treatment with endocrine therapy. It is therefore of critical importance for patients to have targeted therapies available to them to reduce the risk of disease recurrence.
The primary aspect to control for patients with early-stage, high-risk HR-positive breast cancer is reducing the risk of recurrence and disease progression to improve patients’ overall survival. Several factors are known to increase the risk of recurrence in these patients, including lymph node involvement, tumor size, and tumor grade which can indicate aggressiveness of the cancer. Another key factor used in risk-calculation clinically, is the percentage of Ki-67 protein expression, which is associated with cell division. However the Ki-67 index marker is not routinely determined for all HR-positive breast cancer patients currently.
Some of the side effects of HR-positive breast cancer and the therapies used to manage this disease include: Hot flashes, night sweats, and vaginal dryness are common side effects of all hormone therapies. Many patients also experience gastro-intestinal symptoms, as well as nausea, vomiting, and constipation, weakness and fatigue, and an associated risk of blood clots. Many of these symptoms have the ability to impact daily life, primarily: fatigue, pain and nausea. Therefore it is important for patients to have access to therapies that will extend their life expectancy without significantly increasing side effects that will negatively impact their daily lives.
Despite the efficacy of adjuvant endocrine therapy, adherence rates range from 41 percent to 72 percent. Aromatase inhibitor adherence in particular is sub-optimal, ranging from 50 percent to 91 percent over 5 years of therapy and only 40 percent to 60 percent of women complete the recommended course of aromatase inhibitors. Early discontinuation or non-adherence to adjuvant endocrine therapy is associated with increased mortality
Experiences With Currently Available Treatments
Goals of Current Therapy
Managing early-stage, high-risk, HR-positive, HER2-negative breast cancer is always a challenge-particularly in terms of adherence to endocrine therapy. As these breast cancers have been clinically demonstrated to have a higher risk of recurrence than other tumors, the goal of therapy is to target cancer cells in the body and reduce the risk of disease recurrence. Currently, most patients receive a combination surgery, radiation, endocrine therapy and possibly chemotherapy.
This was reinforced in our 2017 survey, most of the HR-positive, HER2-negative, early- stage breast cancer patients had been or were currently being treated with a combination of surgery, radiation, chemotherapy and hormone therapy.
Respondents in our 2017 Survey indicated that the following key factors influenced their decision-making around treatments:
Effectiveness of the treatment – how well the treatment stabilized their disease and delayed progression of their cancer.
Reducing the risk of recurrence without sacrificing quality of life – being able to maintain productive, active lives with minimal disruption to daily routines and avoiding relapse of their cancer.
Side effect management – minimizing risk while stabilizing their disease.
Cost and accessibility of treatments – affordability and ease of accessing treatments.
Patient Values in Determining Treatment Options:
In our survey of HR-positive, HER2-negative, early-stage breast cancer patients, the majority of respondents (43) were diagnosed with Stage 2 cancer , 36 were diagnosed Stage 1, 14 were diagnosed with Stage 3, 10 did not specify their stage. Most patients had undergone surgery (94), radiation therapy (58) chemotherapy (54) and endocrine therapy (79) as part of their overall breast cancer treatment. Of the patients taking hormone therapy, 12 stated that they discontinued hormone therapy, with 11 citing side effects as the primary reason for non-adherence.
Treatment Efficacy
When asked about deciding on treatment options, patients cited the following as most important to them:
The effectiveness of the treatment was ranked the most important for patients in deciding on treatment options, with 79 patients declaring it very important to them.
78 patients responded that effectiveness of their treatment was the single most important factor in making decisions about their treatment.
9 patients stated that potential side-effects were the single most important factor for them in making decisions about their treatment, and 3 patients stated that assessing risks versus benefits was the most important factor for making decisions about their treatment.
“To do everything I could to eradicate the cancer and decrease recurrence rate.” — Patient respondent
“For me it was all about effectiveness.” — Patient respondent
Reducing the risk of recurrence was also ranked highly as a priority for patients with 79 patients stating it was very important to them and 11 stated it was important in their treatment deliberation.
“I just wanted to do everything possible to prevent the cancer from returning”. — Patient respondent
“The main concern was to have the treatment get rid of any remaining cancer cells and to prevent a recurrence.” — Patient respondent
“I wanted to do everything in my power to make sure the cancer did not come back.” — Patient respondent
Quality of Life
Maintaining quality of life was also crucial for patients, with 49 patients declaring it very important, 32 stating it was important and 5 stating it was somewhat important.
“Making my body whole again in order to live the life I want to live” — Patient respondent
“What will be the impact on my quality of life on AI’s?” — Patient respondent
Maintaining mobility was also essential for patients, with 40 patients stating it was very important to them and 29 stating it was important.
Maintaining productivity was also a key concern, with 20 patients stating it was very important, 29 patients stating it was important and 31 stating it was a somewhat important factor in their treatment decision-making.
Patient Willingness to Tolerate Treatment Side Effects
Minimal side effects was cited by 23 patients as very important, 42 patients as important and 19 patients as somewhat important. Eight patients also stated that side effect management was the single most important factor in making decisions about their treatment.
“I think the most important factors for me are that the treatment actually works and that the cancer won't come back. I don't want a lot of side effects either, but I take the good with the bad”. — Patient respondent
“The side effects of the treatment vs their effectiveness at preventing future reoccurrence.
I chose not to have chemo for this reason”. — Patient respondent
“Although I was given a pamphlet about chemo side effects, they were dismissed by my oncologist as rare. I had every side effect in the book and had to postpone treatment three times. Also had to abort taxol. I now have cataracts, heart damage, esophagus damage and terrible chemo brain.” — Patient respondent
Factors Influencing Accessibility
Finally, ability to continue childcare duties was ranked by 13 patients as very important, 8 patients as important, and 57 patients as not important. CBCN would like to note that the majority of patients who responded to our survey had children over the age of 20 years, and as such it is understandable that for these respondents, childcare was not a concern during their treatment. However, for patients with younger children, childcare would be a much more critical factor in determining treatment options.
“I am a mother. I need to do everything I can in order to increase my chances of survival.“ — Patient respondent
“I wish I could have more support with my home life. Dealing with cancer and taking care of kids and other domestic work-it’s not easy.” — Patient respondent
The Financial Burden of Treating and Managing Breast Cancer
The financial burden associated with living with breast cancer extends far beyond any loss of income during a temporary or permanent absence from employment. In addition to the loss of income during illness, breast cancer patients can incur substantial costs associated with treatment and disease management.
Research on the financial impact of breast cancer on patients identified the following:
80% of breast cancer patients report a financial impact due to their illness.
44% of patients have used their savings, and 27% have taken on debt to cover costs (Janet Dunbrack, Breast Cancer: Economic Impact and Labour Force Re-entry. Canadian Breast Cancer Network, 2010)
These findings were consistent with the responses in our current survey of 103 HR- positive, HER2-negative, early stage breast cancer patients:
Nineteen respondents stated that they had experienced a very large financial impact as result of their diagnosis, and 42 stated that they had experienced some financial impact from their diagnosis.
While at the time of their diagnosis, most respondents (49) were employed full- time, 10 were employed part –time, 4 were employed but on disability, 4 were self- employed, and 13 were retired, their employment status changed significantly following breast cancer. At the time of our survey, only 24 patient respondents remained employed full-time, 8 were employed but on disability, 7 were employed part-time, 23 were retired, and 5 were on disability and 3 were caregivers at home, 8 were unemployed and 1 was on government assistance. This small snapshot, highlights the significant financial burden placed on early-stage breast cancer patients and their families while undergoing a breast cancer diagnosis.
“Financial security is a big issue. With no income and so far no government assistance my retirement savings have been impacted. Also, I am uncertain of when I will be able to begin searching for a job again or when I will be successful in my search. you don’t need this stress on top of everything else.“ — Patient respondent
Other barriers included access to private insurance coverage and support medications: While 82 of the patients surveyed reported having private insurance coverage, several (10) also reported challenges accessing medications not publicly reimbursed. Many patients (32) stated that they had been prescribed support medications as part of their treatment and 14 patients stated that their support medications were not provincially reimbursed. Instead, respondents stated that they had to use private insurance (18 respondents) or pay out of pocket (7 respondents) to access medications they had been prescribed. Three patients also accessed manufacturer assistance programs to cover the costs of treatments.
“Although I had access to health insurance through work it was not 100% and included a cap on spending.” — Patient Respondent
“I had to get approval for the anti-nausea medications. It was horrible after my first chemo treatment to not have anti-nausea medications”. — Patient Respondent
“My only comment is that I was fortunate to have private coverage I'm not sure what others do that do not.” — Patient Respondent
Improved Outcomes
For HR-positive, HER2-negative, early-stage breast cancer patients, reducing the risk of recurrence is of critical concern. Patients have an expectation that Verzenio will provide a possibility for improving their rate of invasive disease-free survival and reduce their risk of recurrence allowing them to live a better quality of life. This is based on the data from the international Phase 3 MonarchE study, which showed that abemaciclib reduced the risk for invasive recurrence by 25.3% compared with endocrine therapy alone. In addition, the 2-year invasive disease-free survival (DFS) rates were 92.2% with abemaciclib versus 88.7% with endocrine therapy alone. Patients treated with abemaciclib plus endocrine therapy had a 31.3 percent reduction in risk of distant recurrence or death compared to patients treated with endocrine therapy alone. The greatest reduction in sites of metastatic disease with abemaciclib was seen in bone and liver, followed by the brain, lymph nodes, pleura, and central nervous system. Patients are aware that more than 86% of people treated with abemaciclib and endocrine therapy had not experienced a recurrence after 3 years compared with 79% of those treated with endocrine therapy alone.
Patients understand that Verzenio was approved as adjuvant treatment for people with HR-positive, high-risk, early-stage breast cancer in the U.S. in 2021. Given the propensity for patients with this type of breast cancer to face recurrence, and progression to metastatic disease, there is an understanding that these patients have an unmet medical need for treatments, such as abemaciclib, that improve long-term outcomes. The breast cancer patient community has expressed general concern that treatments that have been accepted internationally as standard of care for early-stage breast cancer and having demonstrated value and clinical benefit for patients, may not be publicly accessible in Canada. Patients want to feel confident that they will be receiving treatment and care that is on par with international standards and protocols.
It is also of utmost importance to breast cancer patients that adjuvant access to HR- positive-directed agents, like abemaciclib, should not end up limiting access to these agents in the metastatic setting. Should patients be treated with HR directed therapies in the earlier stage setting, and subsequently progress to a metastatic setting, it is vital that they remain eligible to benefit from these targeted HR directed therapies for their metastatic disease.
Adverse Effects
The Phase 3 MonarchE trial showed that the Verzenio regimen had a tolerable and manageable safety profile. The most common adverse reactions (≥20%) were diarrhea, infections, neutropenia, fatigue, leukopenia, nausea, anemia, and headache.
Impact of Treatment Options to Patients
In treating the cancer and reducing the risk of recurrence, this treatment can relieve cancer-related symptoms, and improve a patient’s quality of life. When living with no or with minimal cancer-related symptoms, and with minimal side effects from the treatment, patients are able to reduce the impact of cancer on their ability to care for children and dependents, continue with their employment and earn income, spend time with loved ones and participate in their life in a meaningful way by engaging in social activities, travelling, maintaining friendships, and pursuing personal interests.
Experience With Drug Under Review
Given that this treatment is not yet widely accessible in Canada, CBCN was unfortunately unable to connect with, and interview, breast cancer patients with experience on the treatment.
Companion Diagnostic Test
At this time, Ki-67 index marker testing is only available through select clinical testing programs and is not implemented routinely in breast cancer care in Canada.
Accessing testing and treatment is of great importance for hormone-receptor-positive breast cancer patients. It is imperative that all HR-positive, HER2-negative breast cancer patients who could benefit from this therapy are being identified and offered testing to assess their eligibility for adjuvant treatment with Verzenio. It is critical that access to adequate marker testing does not create a barrier for access to effective therapies for cancer patients.
Anything Else?
Is there anything else specifically related to this drug review that CADTH reviewers or the expert committee should know?
While CBCN was not able to interview patients with direct experience of the treatment, it is vital to note what the breast cancer patient community feels about the value and benefit of abemaciclib in the early-stage setting.
Of particular note is the fact that Verzenio represents a major advancement in the treatment of early-stage, HR-positive, HER2-negative breast cancer. This is of significant relevance and importance to high-risk patients who face greater risk of recurrence and resistance to hormone therapies alone. Since Verzenio demonstrated an ability to delay cancer recurrence and improve the curation of cancer free survival from 79% at 3 years to 86%, it has the potential to become a new standard of care for this patient population, and should be regarded as filling a gap in our current treatment protocol for high-risk, HR-positive, HER2-negative patients.
Canadian Breast Cancer Network Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
CBCN did connect with the manufacturer, Eli Lilly Canada, to try and connect us with patients with experience on the treatment.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
All other research, interviews and outreach to patients was conducted independently by the Canadian Breast Cancer Network, as was the compilation of information and data for the writing of this submission.
The Canadian Breast Cancer Network is committed to adhering to the Code of Conduct Governing Corporate Funding
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosure for the Canadian Breast Cancer Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Eli Lilly Canada | — | — | — | — |
Clinician Input
Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee
About the Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Discussed jointly at a DAC meeting.
Current Treatments and Treatment Goals
Standard treatment varies depending on risk of recurrence but includes combinations of surgery, radiotherapy, adjuvant/ neoadjuvant chemotherapy, and endocrine therapy (ET). Adjuvant ET is standard treatment of HR+, HER2- early breast cancer (EBC) and has been associated with a significant reduction in risk of recurrence and death. There is a lack of access to Ki67 testing within Canada.
Abemaciclib is an oral, continuously dosed, CDK4/6 inhibitor approved for HR+, HER2- advanced breast cancer (ABC). Efficacy and safety of abemaciclib in ABC supported evaluation in the adjuvant setting.
Treatment goals would be improved survival and decrease risk of recurrence.
Treatment Gaps (Unmet Needs)
Despite the advances of treatment in HR+, HER2- BC, up to 30% of patients with high-risk clinical and/or pathologic features may experience distant recurrence. Superior treatment options are needed to prevent early recurrence and development of metastases for this group of patients.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Abemaciclib would be used in addition to ET in high-risk patients following surgery and chemotherapy (if applicable).
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients best suited would be HR+, HER2- early breast cancer (EBC) at high risk of recurrence who are node positive. Patients best suited would align with the inclusion criteria from the clinical trial.
Patients least suitable would be patients listed in the exclusion criteria from the clinical trial.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
No extra imaging is needed but patients would need extra monitoring for hematologic toxicity, diarrhea, and extra visits would be required. Patients should be assessed for toxicity.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Disease progression and toxicity.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Experience with treating breast cancer patients, access to laboratory blood work, and expert pharmacy support.
Additional Information
We have significant concerns about the inclusion of patients with high Ki 67. All patients benefit from this drug. Ki 67 was prognostic and not predictive. Additionally, the methodology is challenging for Ki 67 requirement and not standard. Lastly, Ki 67 is not a standard pathology test for breast cancer in Ontario.
We strongly recommend against the inclusion of high Ki 67 as the sole criteria for drug eligibility.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, For perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Dr. Andrea Eisen
Position: OH-CCO Breast Cancer Drug Advisory Committee Lead
Date: 8/4/2022
Table 3: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee Clinician 1
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Orit Freedman
Position: OH-CCO Breast Cancer Drug Advisory Committee Member
Date: 8/4/2022
Table 4: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee for Clinician 2
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Phillip Blanchette
Position: OH-CCO Breast Cancer Drug Advisory Committee Member
Date: 8/4/2022
Table 5: Conflict of Interest Declaration for Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee Clinician 3
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.