CADTH Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Advanced endometrial cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ASaT
all subjects as-treated
PD-1
programmed death receptor 1
CCRAN
Colorectal Cancer Resource & Action Network
CCS
Canadian Cancer Society
CCSN
Canadian Cancer Survivor Network
CI
confidence interval
CNS
central nervous system
CR
complete response
dMMR
deficient mismatch repair
DOR
duration of response
ECHO
Endometrial Cancer Health Outcomes
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-EN24
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Endometrial Cancer Module
EQ VAS
EQ visual analogue scale
EQ-5D-3L
3-Level EQ-5D
ESMO
European Society for Medical Oncology
ESS
effective sample size
FACT-B
Functional Assessment of Cancer Therapy–Breast
FACT-G
Functional Assessment of Cancer Therapy–General
FIGO
International Federation of Gynecology and Obstetrics
GHS
global health status
HR
hazard ratio
HRQoL
health-related quality of life
IHC
immunohistochemistry
IPD
individual patient-level data
ITC
indirect treatment comparison
ITT
intention to treat
KN-158
KEYNOTE-158
KN-775
KEYNOTE-775
MAIC
matching-adjusted indirect comparison
MID
minimal important difference
MMR
mismatch repair
MSI
microsatellite instability
MSI-H
microsatellite instability–high
MSI-L
microsatellite instability–low
MSS
microsatellite stable
NE
not estimable
ORR
objective response rate
OS
overall survival
PCR
polymerase chain reaction
PD-L1
programmed cell death 1 ligand 1
PD-L2
programmed cell death 2 ligand 2
pERC
CADTH pan-Canadian Oncology Review Expert Review Committee
PFS
progression-free survival
pMMR
proficient mismatch repair
PR
partial response
QoL
quality of life
RECIST
Response Evaluation Criteria in Solid Tumours
RCT
randomized controlled trial
RR
response ratio
rwORR
real-world overall response
rwPFS
real-world progression-free survival
SAE
serious adverse event
SD
standard deviation
TEAE
treatment-emergent adverse event
TPC
treatment of physician’s choice
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Pembrolizumab; powder for solution for infusion 50 mg or solution for infusion 100 mg/4 mL vial IV infusion over 30 minutes |
Indication | For the treatment of adult patients with unresectable or metastatic microsatellite instability–high or mismatch repair–deficient endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options, as monotherapy |
Reimbursement request | As per indication |
Health Canada approval status | NOC/c |
Health Canada review pathway | Standard review pathway |
NOC date | April 18, 2019 |
Sponsor | Merck Canada Inc. |
NOC = Notice of Compliance; NOC/c = Notice of Compliance with conditions.
Introduction
Endometrial cancer is the most common gynecological cancer in Canada.1 Endometrial cancer usually occurs in patients older than 50 years, with an average age of diagnosis at 60 years.2 Diagnosis of endometrial cancer commonly occurs at an early stage for approximately 80% of patients.1,3,4 The prognosis of endometrial cancer depends primarily on the tumour stage, histology of the tumour, and grade. In terms of histology, there are 2 subtypes. Type I endometrial cancers are low-grade (grade 1 or grade 2) endometrioid tumours and represent 80% of patients.1,3,5 Type II accounts for 10% to 20% of endometrial cancers and includes grade 3 endometrioid tumours as well as tumours of nonendometrioid cancers.1,3,6 The 5-year survival for type I endometrial cancer is around 80% to 90%, while the 5-year survival for type II endometrial cancer is about 20%. The prognosis of patients with recurrent endometrial cancer is poor, with a median survival of about 12 months.7 Molecular testing of cancer biomarkers during endometrial biopsy assists in identifying treatment options and risk stratification.1 Two molecular cancer biomarkers commonly assessed are microsatellite instability (MSI) and mismatch repair (MMR) protein expression.8 Based on the variability of DNA microsatellite lengths, endometrial cancer can be classified into the categories of microsatellite instability–high (MSI-H), microsatellite instability–low (MSI-L), and microsatellite stable (MSS).8,9 Based on the DNA MMR status, endometrial cancer can be classified into deficient mismatch repair (dMMR) and proficient mismatch repair (pMMR). In clinical practice and in clinical trials, the terms dMMR and MSI-H are often used interchangeably, while non–MSI-H and pMMR are also interchangeable.8-11
Treatment options for endometrial cancer are dependent on stage and pathologic factors after initial surgery and are based on estimated risk of disease recurrence.12-14 Individuals diagnosed with advanced or recurrent endometrial cancer may require adjuvant radiotherapy and/or chemotherapy, which is dependent on the extent and location of spread and/or pathologic risk factors. The current standard of care for patients with advanced or recurrent disease is platinum-based chemotherapy as a doublet or single drug.15,16 The most common platinum-based therapies are carboplatin and paclitaxel.12,15-17 However, for patients with advanced or recurrent endometrial cancer who have progressed on or after platinum-based chemotherapy, there is currently no established standard effective or curative second-line therapy.12,16 In clinical practice, these patients are typically re-treated with platinum-based chemotherapy, but the response is poor. The response rates observed among all available treatment options range between 10% and 15%.16 The clinical experts consulted by CADTH indicated that there is a great unmet need for effective therapies with acceptable toxicity profiles for patients with dMMR or MSI-H recurrent or advanced endometrial cancer that has progressed on or following treatment with a platinum-containing regimen.
Pembrolizumab is an inhibitor of PD-1. The recommended dose for pembrolizumab is 200 mg every 3 weeks or 400 mg every 6 weeks administered as an IV infusion until disease progression or unacceptable toxicity, or up to 24 months. Health Canada has issued market authorization for pembrolizumab in various indications such as classical Hodgkin lymphoma, primary mediastinal B-cell lymphoma, urothelial carcinoma, melanoma, non–small cell lung carcinoma, renal cell carcinoma, head and neck squamous cell carcinoma, and colorectal cancer.9 The Health Canada–approved indication of interest for this review is pembrolizumab as monotherapy for the treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options.9 The CADTH reimbursement request aligns with this Health Canada indication (refer to Table 3).
The objective of this clinical review is to review the beneficial and harmful effects of pembrolizumab monotherapy for the treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options.
Following the issuance of the draft CADTH pan-Canadian Oncology Drug Review Expert Review Committee (pERC) recommendation for pembrolizumab in May 2022, the following additional information was provided to CADTH:
One unanchored matching-adjusted indirect comparison (MAIC) was submitted by the sponsor. The objective of the unanchored MAIC was to evaluate the relative efficacy of pembrolizumab monotherapy in female patients with advanced, recurrent, or metastatic endometrial carcinoma with dMMR (MSI-H) who had been treated with at least 1 prior platinum-based chemotherapy regimen against standard of care treatment (treatment of physician’s choice [TPC], which was doxorubicin or paclitaxel). Overall survival (OS), progression-free survival (PFS), and objective response rate (ORR) were the outcomes investigated in the unanchored MAIC. These data were not included in the original submission to CADTH as the sponsor indicated it was not available until after the draft CADTH recommendation had been issued. Based on the evidence included in the original submission, pERC was unable to determine the comparative efficacy of pembrolizumab with conventional chemotherapy with respect to survival outcomes due to the limitations identified for the original sponsor-submitted indirect treatment comparison (ITC). As such, the lack of comparative efficacy data was identified as an important gap in the evidence and the additional information from the unanchored MAIC submitted by the sponsor has been summarized as an addendum to the CADTH report in Appendix 3.
An updated analysis of outcomes from the KEYNOTE-158 (KN-158) study, including PFS, ORR, and OS, as well as safety outcomes, was submitted. The updated analysis was descriptive and based on a data cut-off that occurred on January 12, 2022. One of the limitations identified for the evidence included in the original submission was the short follow-up period of the KN-158 study. The updated analysis was submitted by the sponsor to address this gap in the evidence and, as such, this information has been summarized as an addendum to the CADTH report in Appendix 7.
The sponsor submitted a multicentre, retrospective, medical chart review (cohort) study by Kelkar et al. (2022)18 (the Endometrial Cancer Health Outcomes [ECHO] study). The sponsor indicated that the real-world evidence provided by the ECHO study may address the gap in evidence comparing pembrolizumab to other treatments for patients with dMMR endometrial cancer, which was not included in the original submission to CADTH. As such, the study by Kelkar et al. (2022)18 has been summarized and critically appraised as part of the sponsor’s request for reconsideration, available in Appendix 8.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
This section was prepared by CADTH staff based on the input provided by patient groups.
The input from patient advocacy groups for pembrolizumab monotherapy for the treatment of advanced endometrial cancer was provided by Colorectal Cancer Resource & Action Network (CCRAN), in collaboration with Canadian Cancer Society (CCS) and Canadian Cancer Survivor Network (CCSN). CCRAN is a Canadian not-for-profit patient advocacy group focusing on patients with colorectal cancer, with an extended mandate to support other cancer populations — either those who lack capacity or representative patient groups.
The information provided by CCS was collected through an online survey, conducted between October 22 and November 3, 2021, with 22 responses from Canada (20 patients and 2 caregivers). CCSN conducted an outreach survey on December 5, 2021, and provided feedback from 1 Canadian patient with endometrial cancer. CCRAN provided additional feedback from 1 caregiver and 3 patients with advanced endometrial cancer via telephone interviews that took place from December 1 to December 14, 2021, in Canada.
The 3 patient groups reported that patients with endometrial cancer experience physical symptoms (e.g., vaginal bleeding, pelvic pain, diarrhea, nausea, fatigue) and psychological symptoms (e.g., feeling isolated and lonely). Some of the patients expressed substantial frustration related to their long diagnostic journey, noting that it might have contributed to their advanced stage diagnosis and disease progression. Endometrial cancer negatively influences the quality of life (QoL) of patients and their families. Many patients report issues with work, daily chores, and socialization. Caregivers and family members have to take on additional responsibilities and deal with emotional tolls such as stress and anxiety.
Regarding current treatment, patients reported a variety of options, including surgery, chemotherapy, and hormonal therapy. The CCSN survey and CCRAN interviews captured a general lack of efficacy and debilitating side effects of standard of care treatments indicated for the management of advanced endometrial cancer.
One Canadian patient had experience with pembrolizumab monotherapy as a second-line treatment through a private insurance plan for 5 months. The patient reported the monotherapy provided significant resolution of cancer-induced symptoms, disease regression, and superior QoL. In addition, the patient reported being able to resume daily activities at home and spend time with and care for their loved ones. The patient did not report any adverse effects associated with the treatment under review.
Key outcomes identified by the patient advocacy groups as important to patients with endometrial cancer include the following: improved symptoms, cancer control, fewer side effects, good QoL, and extension of survival.
Overall, the CCRAN patient group indicated that there is an urgent unmet need for the treatment of patients with advanced endometrial cancer. The group emphasized that patients need access to treatments with fewer side effects that would extend and improve the quality of their lives. CCRAN strongly supported the use of pembrolizumab monotherapy as a second-line treatment option for patients with MSI-H (dMMR) endometrial cancer whose tumour is inoperable, or metastatic or recurrent.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted for this review indicated that there is a lack of treatment options and no standard second-line therapy for individuals with metastatic or recurrent endometrial cancer. Both clinical experts noted that most patients undergoing current therapies show low response rates, short duration of response (DOR), and disease progression. This represents a critical unmet need in this patient population.
The clinical experts indicated that patients with endometrial cancer who have progressed on platinum chemotherapy currently receive cytotoxic treatments such as carboplatin and paclitaxel, doxorubicin, or pegylated liposomal doxorubicin. Additional chemotherapeutic drugs that can be taken into consideration occasionally include topotecan, gemcitabine, pemetrexed ifosfamide, and hormonal treatments (megestrol acetate, tamoxifen). The aforementioned treatments are not considered curative and have low expected response rates and short DORs. Both clinical experts indicated that pembrolizumab would become standard second-line therapy for patients with dMMR endometrial cancer after recurrence or failure of typical platinum-based regimens. This pembrolizumab treatment would address the underlying disease process. The clinical experts felt that it would be preferable to initiate treatment with the drug under review before other therapies. Clinical experts indicated that there is currently no evidence to support re-treatment with the same drug in the case of relapse.
The clinical experts agreed that all patients with dMMR or MSI-H endometrial carcinoma who experience recurrent or progressive disease following platinum-containing chemotherapy and have good performance status would most benefit from pembrolizumab treatment (i.e., Eastern Cooperative Oncology Group Performance Status [ECOG PS] of 0 or 1). Although not supported by clinical trial evidence, the experts also indicated that the treatment might be extended to patients with ECOG PS of 2 if the patient is appropriately informed and motivated. The experts noted that there is currently a lack of data on the treatment response among patients with other histologic types of endometrial cancer (carcinosarcoma, endometrial leiomyosarcoma, and endometrial stromal sarcomas). One expert indicated that the presence of unstable central nervous system (CNS) metastases should be treated first with neurosurgical resection and/or cranial irradiation, before considering treatment with pembrolizumab. Regarding the identification of patients, 1 clinical expert mentioned that standard practice includes a clinical examination by an oncologist, diagnostic imaging, and biopsies. The other expert noted that biomarker testing for MMR status via immunohistochemistry (IHC) staining is applied across many centres in Canada. The clinical experts indicated that treatment with pembrolizumab would be least suitable in patients with poor performance status (ECOG PS score of 3 or 4). In addition, 1 expert also added that patients with multiple lines of prior chemotherapies and patients with an intolerance or contraindications to pembrolizumab would be least suited to receive the drug under review.
According to the clinical experts, the evaluation of treatment response in clinical practice is performed through an assessment of clinical symptoms, imaging (e.g., CT, MRI), and physical exam findings. One expert noted that the treatment benefit for most biologics would include the absence of progression and good tolerance to treatment. Both experts agreed that improved PFS and OS, maintained or improved health-related quality of life (HRQoL), and symptom control can be considered clinically meaningful responses to the treatment under review. An assessment of treatment response should be conducted every 12 weeks to 16 weeks (i.e., every 3 months to 4 months).
According to the clinical experts, treatment with pembrolizumab should be discontinued in case of disease progression (confirmed clinically or on imaging), the appearance of serious immune adverse events (AEs), or intolerable treatment toxicities.
The clinical experts indicated that treatment administration and the monitoring of patients with endometrial cancer should be undertaken by a specialist; namely, a gynecologist oncologist or medical oncologist. Treatment monitoring can potentially be conducted by a general practitioner oncologist, but under the overview of 1 of the specialists. The experts recommended pembrolizumab be administered in an infusion setting, either in hospital or in oncology centre clinics with appropriate monitoring capabilities. In terms of companion diagnostics, 1 expert noted that detection of dMMR status through IHC staining would be required. In reference to dosing, clinical experts noted that fixed dosing would be applied for pembrolizumab. One clinical expert expressed that less frequent administrations (i.e., 400 mg every 6 weeks) would be better for patients, clinicians, and health centres.
One clinical expert expressed concerns with the high costs of the treatment under review and indicated that the costs might improve with increased availability of other PD-1 inhibitors on the market.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
One joint clinician input was provided by 7 physicians on behalf of the Ontario Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee. The clinician group noted the absence of currently available therapies for patients with recurrent or progressive endometrial cancer. The group recognized the unmet needs of this patient population, indicating that most patients remain unresponsive to available treatments and highlighting a need for better tolerated treatment options. Prolonged life, delayed disease progression, symptomatic relief, partial response (PR), full response, and improved HRQoL were identified as the most important treatment goals. In terms of assessing response to treatment, the clinician group stated that imaging, clinical exam, and symptomatic improvement should be assessed in clinical practice. Lastly, outpatient hospital settings were noted as appropriate treatment settings for these patients.
Of note, 5 of the 7 physicians provided CADTH with a Conflict of Interest declaration within the clinician group input.
Drug Program Input
The Provincial Advisory Group identified the following jurisdictional implementation issues: considerations for the initiation of therapy, considerations for the prescribing of therapy, generalizability issues, and care provision issues. The clinical experts consulted by CADTH weighed evidence from the KN-158 study and other clinical considerations to provide responses to the Provincial Advisory Group’s drug program implementation questions. Refer to Table 4 for more details.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The KN-158 study (i.e., cohort D and cohort K of the KN-158 study)19 is a single-arm, phase II, open-label, nonrandomized trial in patients with advanced MSI-H or dMMR endometrial cancer. The trial was conducted in 38 centres in 15 countries (including the US, Canada [3 centres], the UK, France, Germany, Australia, and other European, Central American, South American, and Asian countries). Enrolment started on February 1, 2016, and is still ongoing. The data cut-off date was October 5, 2020, and the estimated study completion date is June 18, 2026.20 The objective of study KN-158 was to assess the efficacy and safety of pembrolizumab monotherapy for the treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options.
A total of 90 patients were included in the trial. Patients included were 18 years and older with incurable dMMR or MSI-H advanced (metastatic and unresectable, or unresectable) endometrial carcinoma and had failed prior standard first-line treatments. The primary outcome was ORR, which was defined as the proportion of patients in the analysis population who have a complete response (CR) or PR. Response for the primary analysis was determined by independent central radiologic review, with confirmatory assessment as required per the Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1). The DOR, OS, and PFS were assessed as secondary outcomes. HRQoL was assessed as an exploratory outcome (but results were not presented in the KN-158 Clinical Study Report).
Efficacy Results
The key efficacy findings of the KN-158 study are summarized in Table 2. At the time of the data cut-off, the median duration of follow-up was 16.5 months (range, 0.5 months to 56.1 months) and the median duration of treatment was 8.3 months (range, 0.03 months to 26.88 months). By the time of the data cut-off, 35.7% of patients had died and based on Kaplan-Meier estimation, the median OS was not reached (lower bound of 95% confidence interval [CI] = 27.2 months). The OS probabilities of patients at 12 months, 24 months, 36 months, and 48 months were 69.4%, 64%, 60.1%, and 60.1%, respectively.
By the time of the data cut-off, there had been 29 (36.7%) PFS events, and based on Kaplan-Meier estimation, the median PFS was 13.1 months (95% CI, 4.3 months to 34.4 months). The PFS rates at 12 months, 24 months, and 48 months were 51.0%, 41.3%, and 37.0%, respectively.
A total of 38 of 79 patients (48.1%; 95% CI, 36.7% to 59.6%) achieved an objective response. Among these patients, based on the Kaplan-Meier method, the median DOR was not reached (range, 2.9 months to 49.7 months). Extended response durations of more than 12 months, 24 months, and 36 months were observed in 88.1%, 72.9%, and 68.1% of responders, respectively.
Patient-reported (HRQoL) outcomes were available in a sponsor-submitted conference abstract presented at the European Society for Medical Oncology (ESMO) Congress 2021.19 Following treatment with pembrolizumab, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) global health status (GHS), EORTC QLQ-C30 symptom score, and 3-Level EQ-5D (EQ-5D-3L) visual analogue scale (VAS) appeared to be maintained or improved, based on the change from baseline to week 9.
Harms Results
The key harms findings of the KN-158 study are shown in Table 2. Of the 90 patients who received at least 1 dose of pembrolizumab, 95.6% experienced at least 1 treatment-emergent adverse event (TEAE). The most common AEs (those that occurred in at least 25% of patients) were fatigue (33.3%), diarrhea (32.2%), pruritus (28.9%), arthralgia (27.8%), and nausea (27.8%) (refer to Table 28). A total of 37.8% of patients experienced a serious adverse event (SAE). Each SAE was reported in 1 patient21 except for ascites, chest pain, pneumonia, pyelonephritis, sepsis, and urinary tract infection, which were each reported for 2 (2.2%) patients. AEs leading to study drug discontinuation were reported in 6.7% of patients. These included an increase in transaminases, arthritis, enterocolitis, drug-induced liver injury, and rash. Each occurred in 1 (1.1%) patient except transaminase increase, which occurred in 2 (2.2%) patients.
No deaths due to AEs were reported. Regarding notable harms (i.e., AEs of special interest for this review as identified in the review protocol), hypothyroidism occurred in 14.4% of patients, followed by hyperthyroidism (7.8%), colitis (3.3%), type 1 diabetes mellitus (2.2%), pneumonitis (1.1%), adrenal insufficiency (1.1%), and hepatitis (1.1%). No hypophysitis or nephritis were reported.
Table 2: Summary of Key Results From Pivotal and Protocol-Selected Studies
Outcome | Study KN-158 |
|---|---|
Efficacy (efficacy analysis population) N = 79 | |
OS | |
Death, n (%) | 29 (36.7) |
Median survival (months), median (95% CI)a | NR (27.2 to NR) |
OS rate, %a | |
6 months | 82.3 |
12 months | 69.4 |
18 months | 67.9 |
24 months | 64.0 |
36 months | 60.1 |
48 months | 60.1 |
PFS | |
PFS events, (%) | 45 (57.0) |
Person-months | 1,238 |
Event rate per 100 person-months, % | 3.6 |
Median PFS (months), median (95% CI)a | 13.1 (4.3 to 34.4) |
PFS rate, %a | |
6 months | 59.5 |
12 months | 51.0 |
18 months | 45.4 |
24 months | 41.3 |
36 months | 37.0 |
48 months | 37.0 |
ORRb | |
Objective response (CR + PR), n (%; 95% CI) | 38 (48.1; 36.7 to 59.6) |
CR | 11 (13.9; 7.2 to 23.5) |
PR | 27 (34.2; 23.9 to 45.7) |
DOR,c N | 38 |
Duration (months), median (range)a | NR (2.9 to 49.7) |
≥ 12 months, n (%)a | 24 (88.1) |
≥ 24 months, n (%)a | 18 (72.9) |
≥ 36 months, n (%)a | 12 (68.1) |
Harms (safety analysis population) N = 129 | |
Safety analysis population, N | 129 |
Patients with at least 1 AE, n (%) | 86 (95.6) |
Patients with at least 1 SAE, n (%) | 34 (37.8) |
Patients with an AE leading to discontinuation from the treatment, n (%) | 6 (6.7) |
Death due to AEs, n (%) | 0 (0) |
Notable harms, n (%) | |
Adrenal insufficiency | 1 (1.1) |
Colitis | 3 (3.3) |
Hepatitis | 1 (1.1) |
Hyperthyroidism | 7 (7.8) |
Hypophysitis | 0 (0.0) |
Hypothyroidism | 13 (14.4) |
Nephritis | 0 (0.0) |
Pneumonitis | 1 (1.1) |
Type 1 diabetes mellitus | 2 (2.2) |
AE = adverse event; CI = confidence interval; CR = complete response; DOR = duration of response; KN-158 = KEYNOTE-158; NR = not reached; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; SAE = serious adverse event.
Note: Non-SAEs were followed up to 30 days after last dose and SAEs were followed up to 90 days after last dose are included.
aFrom product-limit (Kaplan-Meier) method for censored data.
b95% CI based on the binomial exact CI method.
cIncluded patients with confirmed CR or PR.
Source: KN-158 Clinical Study Report.21
Critical Appraisal
The main limitation of the included pivotal study (KN-158) was the single-arm study design, which does not include a comparator group. Such a design, in addition to a lack of consideration of confounding variables, precludes causal inferences (i.e., the outcomes cannot be directly attributed to pembrolizumab). Without an active comparator or standard of care, nor any statistical hypothesis testing, it is not possible to assess the relative therapeutic benefit or safety of pembrolizumab against other available treatments (such as chemotherapy in this population). Though inclusion and exclusion criteria were stated, selection procedures were not described; therefore, the potential for selection bias cannot be excluded.
As all results are part of an interim analysis, there is some risk that the efficacy of pembrolizumab has been overestimated. The median OS was not reached at the time of cut-off, the survival data from the trial were immature, and 36.7% of patients had died by the time of the data cut-off. An updated analysis of OS was provided as part of the sponsor’s request for reconsideration. A summary of the updated analysis based on a data cut-off of January 12, 2022, is available in Appendix 7. Descriptive results for OS were included, which indicate median OS was reached. Also of note, the efficacy assessment in study KN-158 was not based on the intention-to-treat (ITT) population. The efficacy analyses were based on the all subjects as-treated (ASaT) [from original source] population for efficacy analysis, defined as patients who received at least 1 dose of study intervention and had been enrolled at least 26 weeks before the data cut-off date. Finally, no formal statistical significance and hypothesis testing were conducted in the analysis; causal inferences could not be made, and this limited the ability to draw robust conclusions regarding efficacy or safety from the findings.
Overall, according to the clinical experts consulted by CADTH, the population enrolled in the trial was consistent with the population expected to be treated in Canadian clinical practice. No major generalizability issues were noted regarding the findings from the pivotal study. Although patients with CNS metastases, endometrial sarcomas, or ECOG PS scores of 2 or more were not included in the study, the clinical experts indicated that the patients with CNS metastases still might benefit from the pembrolizumab treatment after they are treated with radiotherapy first. Similarly, patients with carcinosarcomas and patients with an ECOG PS score of 2 may also benefit from the pembrolizumab treatment in this clinical setting.
Indirect Comparisons
Description of Studies
The sponsor submitted an unadjusted (naive) ITC that compared the efficacy of pembrolizumab monotherapy with doxorubicin or paclitaxel in patients with advanced MSI-H or dMMR endometrial cancer and at least 1 prior line of therapy. This analysis estimated the relative time to OS or PFS using individual treatment group data from 2 separate studies (the KN-158 study and the KEYNOTE-775 [KN-775] study), based on nonparametric Kaplan-Meier methods and unstratified Cox proportional hazards models.
Efficacy Results
For pembrolizumab versus chemotherapy, the hazard ratio (HR) for time to OS was 0.34 (95% CI, 0.20 to 0.56; P < 0.001) and the HR for PFS was 0.42 (95% CI, 0.27 to 0.64; P < 0.001).
Harms Results
The ITC did not assess safety outcomes.
Critical Appraisal
Limitations of the ITC include the lack of justification for the selection of the chemotherapy arm of study KN-775 as the comparator group and for the analytical methods used. The exploration of between-study differences and potential biases was limited by missing information on patient and study characteristics for the 2 data sources. Considering that prognostic factors and effect modifiers are likely imbalanced between treatment groups, the results of the unanchored, unadjusted ITC is subject to an unknown amount of bias. Thus, the findings of the ITC are highly uncertain and conclusions regarding the efficacy of pembrolizumab monotherapy versus chemotherapy cannot be established.
The ITC did not assess harms data; thus, the comparative safety of pembrolizumab versus chemotherapy is unknown. Other outcomes of importance to patients, such as HRQoL, were not investigated.
Conclusions
One sponsor-submitted pivotal single-arm, open-label, multicentre, phase II trial (cohort D and cohort K in the KN-158 study)21 provided evidence regarding the efficacy and safety of pembrolizumab in the treatment of adult patients with dMMR or MSI-H recurrent or advanced endometrial carcinoma that had progressed on or following prior systemic treatments. There was uncertainty around the magnitude of the clinical benefit attributable to pembrolizumab, given the limitations inherent to the single-arm trial design and the lack of formal hypothesis testing. The sponsor also submitted a naive ITC comparing pembrolizumab with doxorubicin or paclitaxel. However, no robust conclusion could be drawn on the comparative efficacy and safety of pembrolizumab versus chemotherapy (i.e., doxorubicin and paclitaxel) due to several methodological limitations. While a well-designed randomized controlled trial (RCT) would be ideal and preferred to confirm the comparative clinical benefit of pembrolizumab over chemotherapy, the clinical experts consulted by CADTH indicated that the efficacy outcomes (OS, PFS, ORR, and DOR) observed in the KN-158 trial appeared favourable compared with that observed with chemotherapy (e.g., doxorubicin and paclitaxel) in clinical practice and are potentially clinically meaningful for this patient population The safety profile of pembrolizumab observed in this study appeared consistent with the known safety profile of pembrolizumab, and no additional safety signals were identified.
Introduction
Disease Background
Endometrial cancer arises from the cells of the uterine lining. It is the most common gynecological cancer in Canada.1 More than 95% of all uterine cancers are endometrial.3 Uterine cancer is ranked as the 17th leading cause of cancer death in Canada.3,22 CCS estimated that 8,000 women would be diagnosed with uterine cancer in 2021 and 1,400 women would die of the disease.22,23 Endometrial cancer most often occurs in patients older than 50 years, with an average age of diagnosis at 60 years.2 Diagnosis of endometrial cancer commonly occurs at an early stage for approximately 80% of patients due to early presenting symptoms of uterine bleeding.1,3,4 The most common method of diagnosis of endometrial cancer is endometrial biopsy, followed by endometrial curettage and hysterectomy specimen.1 The International Federation of Gynecological and Obstetrics (FIGO) criteria is commonly used to determine the disease stage of endometrial cancer, which is based on the size of the tumour and the extent to which the tumour has spread to lymph nodes or distant sites (i.e., metastasis).24 Generally, the higher the stage number, the more that the cancer has spread.25 Tumour stage is fixed regardless of tumour type.1 The prognosis of endometrial cancer depends primarily on the tumour stage, histology of the tumour, and grade. Prognosis by FIGO stage is 80% to 90% for stage I, 70% to 80% for stage II, and 20% to 60% for stage III and stage IV.1 In terms of histology, there are 2 subtypes. Type I endometrial cancers are low-grade (grade 1 or grade 2) endometrioid tumours and represent 80% of patients.1,3,5 Type II accounts for 10% to 20% of endometrial cancers and includes grade 3 endometrioid tumours as well as tumours of nonendometrioid histology such as serous clear cell, mucinous, squamous, transitional cell, mesonephric carcinosarcoma, and undifferentiated.1,3,6 The 5-year survival for type I endometrial cancer is around 80% to 90%, while the 5-year survival for type II endometrial cancer is as low as 20%. Other notable prognostic factors that may predict prognosis for endometrial cancer include race, age, uterine tumour location, peritoneal cytology results, and lymph vascular space invasion.1
Molecular testing of cancer biomarkers during endometrial biopsy assists in decision-making about treatment options and risk stratification.1 Two molecular cancer biomarkers are commonly assessed in patients with endometrial cancer. One is MSI, which evaluates DNA hypermutability. The other is MMR protein expression, which evaluates the functional status of the MMR DNA repair pathway.8 Tumours can be classified as MSI-H, which exhibit 30% to 40% or greater microsatellite marker instability; MSI-L, which exhibit instability at less than 30% to 40% of loci; and MSS, which exhibit no unstable markers.26 Based on the MMR status, endometrial cancer can be classified into dMMR and pMMR. IHC is used to test for dMMR, whereby the cells’ ability to repair DNA mistakes is impaired. The tumour is immunohistochemically assessed for the loss of at least 1 of the following MMR proteins: MLH1, MSH2, MSH6, and/or PMS2.27-29 MSI status can be determined by the analysis of 5 tumour microsatellite loci using polymerase chain reaction (PCR)-based assays (either the 5 mononucleotide loci [BAT25, BAT26, NR21, NR24, and Mono27] or the 5 mixed mononucleotide and dinucleotide loci [BAT25, BAT26, Di 5S346, Di 2S123, and Di 17S250]).30 If MMR status cannot be determined from tumour samples, the sample may undergo genetic testing using next generation sequencing to identify MSI status. Although MSI and MMR are 2 distinct biomarkers, they are both signs of an altered MMR pathway. The defect or absence of MMR protein causes DNA hypermutation and high levels of MSI in sections of the DNA.29 In clinical trials, the terms dMMR and MSI-H are often used interchangeably. Non–MSI-H (including MSI-stable and MSI-L) and pMMR are also interchangeable.8-11 Clinical experts CADTH consulted for this review agreed that dMMR and MSI-H are commonly used interchangeably in clinical practice. MSI-H or dMMR endometrial cancer is associated with a higher neoantigen load and increased PD-1–expressing tumour-infiltrating lymphocytes and programmed cell death 1 ligand 1 (PD-L1)–expressing intraepithelial and peritumoral immune cells compared with MSS endometrial cancers.31 Thus, MSI-H or dMMR tumour status is predictive of clinical benefit from PD-1 inhibitors. MSI-H or dMMR represents approximately 25% to 31% of primary endometrial cancers and 13% to 30% of recurrent endometrial cancers.32-36
Recurrence occurs in approximately 13% to 20% of patients with endometrial cancer, with rates varying greatly by FIGO stage at diagnosis, being highest among patients with stage IV endometrial cancer (more than 65%).7,12,37 The prognosis of patients with recurrent endometrial cancer is poor, with a median survival of about 12 months.7
Standards of Therapy
Treatment options for endometrial cancer are dependent on stage and pathologic factors after initial surgery and are based on estimated risk of disease recurrence. Early stage endometrial cancer and/or type I tumour endometrial cancers can be cured through surgery alone.12-14 Individuals diagnosed with advanced or recurrent endometrial cancer may require adjuvant radiotherapy and/or chemotherapy, which is dependent on the extent and location of spread and/or pathologic risk factors. Cancer Care Ontario and Alberta Health Services recommendations favour combination chemotherapy over single-drug chemotherapy for individuals with advanced or recurrent endometrial cancer, as combination therapy elicits a higher response rate with less toxicity.12,15 The current standard of care for patients with advanced or recurrent disease is platinum-based chemotherapy as a doublet or single drug,15 a standard echoed by the European Society of Gynaecological Oncology, the European Society of Radiotherapy and Oncology, and the European Society of Pathology.16 The most common platinum-based therapy is carboplatin and paclitaxel.12,15-17 For a subset of patients with low-grade recurrent or metastatic endometrial cancer who are estrogen or progesterone receptor–positive or for patients with poor tolerance to systemic therapy, hormonal therapy such as megestrol, letrozole, and medroxyprogesterone may be used.15
For patients with newly diagnosed advanced or recurrent endometrial cancer, response rates for standard first-line treatment range from 40% to 62%.38-41 However, for patients with advanced or recurrent endometrial cancer who have progressed on or after platinum-based chemotherapy, there is currently no established standard effective or curative second-line therapy.12,16 Patients with recurrent endometrial cancer are typically re-treated with either platinum-based chemotherapy or doxorubicin, but the response is poor. The response rates observed among all available treatment options range between 10% and 15%.16 The clinical experts consulted by CADTH noted that median survival ranges from 12 months to 15 months after re-treatment. Various single-drug chemotherapies may be administered to patients who are resistant or refractory to platinum-based chemotherapy, with response rates typically below 15% and no known clear survival benefit.42 Hormonal treatments may also be used for disease control but are not considered curative.
The clinical experts consulted by CADTH for this review indicated that there is a great unmet need for effective therapies with acceptable toxicity profiles that achieve disease control, reduce disease-related symptoms, improve HRQoL, prevent disease progression, and prolong survival among patients with recurrent or advanced endometrial cancer that has progressed on or following prior treatment with a platinum-containing regimen. There is currently no standard effective second-line therapy for recurrent or refractory disease and commonly used therapies are noncurative. The clinical experts anticipated more promising benefits with biomarker-driven treatments for patients with MSI-H or dMMR endometrial cancers.
Drug
Pembrolizumab is a selective humanized monoclonal antibody that enhances immune system detection of tumours and facilitates tumour regression via the PD-1 pathway. The Health Canada–recommended dose is 200 mg every 3 weeks or 400 mg every 6 weeks administered as an IV infusion until disease progression or unacceptable toxicity, or up to 24 months. Health Canada has issued market authorization for pembrolizumab in various indications such as classical Hodgkin lymphoma, primary mediastinal B-cell lymphoma, urothelial carcinoma, melanoma, non–small cell lung carcinoma, renal cell carcinoma, head and neck squamous cell carcinoma, and colorectal cancer.9
The Health Canada–approved indication of interest for this review is pembrolizumab as monotherapy for the treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options.9 The CADTH reimbursement request aligns with this Health Canada indication (refer to Table 3).
Table 3: Key Characteristics of Pembrolizumab
Characteristic | Pembrolizumab |
|---|---|
Mechanism of action | Exerts dual ligand blockade of the PD-1 pathway on antigen or tumour cells and reactivates tumour-specific cytotoxic T-lymphocytes in the tumour microenvironment |
Indicationa | The treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options, as monotherapy. |
Route of administration | IV |
Recommended dosage | 200 mg, IV, over 30 minutes every 3 weeks until disease progression or unacceptable toxicity, or up to 24 months in patients without disease progression |
Serious adverse effects or safety issues |
|
dMMR = deficient mismatch repair; MSI-H = microsatellite instability–high.
aHealth Canada–approved indication.
Source: Health Canada product monograph.9
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
The input from patient advocacy groups for pembrolizumab monotherapy for the treatment of advanced endometrial cancer was provided by CCRAN, in collaboration with CCS and CCSN. CCRAN is a Canadian not-for-profit patient advocacy group focusing on patients with colorectal cancer, with an extended mandate to support other cancer populations — either those who lack capacity or representative patient groups.
The information provided by CCS was collected through an online survey, conducted between October 22 and November 3, 2021, with 22 responses from Canada (20 patients and 2 caregivers). CCSN conducted an outreach survey on December 5, 2021, and provided feedback from 1 patient with endometrial cancer who lived in Canada. CCRAN provided additional feedback from 1 caregiver and 3 patients with advanced endometrial cancer via telephone interviews that took place from December 1 to December 14, 2021, in Canada.
The 3 patient groups reported that patients with endometrial cancer experience physical symptoms (e.g., vaginal bleeding, pelvic pain, diarrhea, nausea, fatigue) and psychological symptoms (e.g., feeling isolated and lonely). Some of the patients expressed substantial frustration related to their long diagnostic journey, noting that it might have contributed to their advanced stage of diagnosis and disease progression. Endometrial cancer negatively influences the QoL of patients and their families. Many patients report issues with work, daily chores, and socialization. Caregivers and family members have to take on additional responsibilities and deal with emotional tolls such as stress and anxiety.
Regarding current treatment, patients reported a variety of options, including surgery, chemotherapy, and hormonal therapy. The CCSN survey and CCRAN interviews captured a general lack of efficacy and debilitating side effects of standard of care treatments indicated for the management of advanced endometrial cancer.
One patient living in Canada had experience with pembrolizumab monotherapy as a second-line treatment through a private insurance plan for 5 months. The patient reported that the monotherapy provided significant resolution of cancer-induced symptoms, disease regression, and superior QoL. In addition, the patient reported being able to resume daily activities at home and to spend time with and care for their loved ones. The patient did not report any AEs associated with the treatment under review.
Key outcomes identified by the patient advocacy groups as important to patients with endometrial cancer include the following: improved symptoms, cancer control, fewer side effects, good QoL, and extension of survival.
Overall, the CCRAN patient group indicated that there is an urgent unmet need for the treatment of patients with advanced endometrial cancer. The group emphasized that patients need access to treatments with fewer side effects that would extend and improve the quality of their life. CCRAN strongly supported the use of pembrolizumab monotherapy as a second-line treatment option for patients with MSI-H (dMMR) cancer whose tumour is inoperable, or metastatic or recurrent.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of endometrial cancer.
Unmet Needs
Currently, there is a lack of treatment options and no standard second-line therapy for individuals with metastatic or recurrent endometrial cancer. Both clinical experts noted that most patients undergoing current therapies show low response rates, short DOR, and disease progression. This represents a critical unmet need in this patient population.
Place in Therapy
Patients with endometrial cancer who have progressed on platinum chemotherapy currently receive cytotoxic treatments such as carboplatin and paclitaxel, doxorubicin, or pegylated liposomal doxorubicin. Additional chemotherapeutic drugs that can be taken into consideration occasionally include topotecan, gemcitabine, pemetrexed ifosfamide, and hormonal treatments (megestrol acetate, tamoxifen). The described treatments are not considered curative and have low expected response rates and short DORs.
Both clinical experts indicated that pembrolizumab would become standard second-line therapy for patients with dMMR endometrial cancer after recurrence or failure of typical platinum-based regimens. This pembrolizumab treatment would address the underlying disease process. The clinical experts felt it would be preferable to initiate treatment with the drug under review before other therapies in the same setting.
Clinical experts indicated that there is currently no evidence to support re-treatment with the same drug in the case of relapse.
Patient Population
Clinical experts agreed that all patients with dMMR or MSI-H endometrial carcinoma who experience recurrent or progressive disease following platinum-containing chemotherapy and have good performance status would most benefit from pembrolizumab treatment (i.e., ECOG PS of 0 or 1). Although not supported by clinical trial evidence, the experts also indicated that the treatment might be extended to patients with ECOG PS of 2 if the patient is appropriately informed and motivated. The experts noted that there is currently a lack of data on the treatment response among patients with other histologic types of uterine malignancies (carcinosarcoma, endometrial leiomyosarcoma, and endometrial stromal sarcomas). One expert indicated that unstable CNS metastases should be treated first with neurosurgical resection and/or cranial irradiation before considering treatment with pembrolizumab.
Regarding the identification of patients, 1 clinical expert mentioned that standard practice includes a clinical examination by an oncologist, diagnostic imaging, and biopsies. The other expert noted that biomarker testing for MMR status via IHC staining is applied across many centres in Canada. MSI testing might be expensive to the patient currently.
The clinical experts reported that treatment with pembrolizumab would be least suitable in patients with poor performance status (ECOG PS of 3 or 4). In addition, 1 expert also added that patients with multiple lines of prior chemotherapies and with poor performance status (ECOG PS of 3 or 4). would be least suited to receive the drug under review.
Assessing Response to Treatment
According to the clinical experts, the evaluation of treatment response in clinical practice is performed through an assessment of clinical symptoms, imaging (e.g., CT, MRI), and physical exam findings. One expert noted that treatment benefit for most biologics would include the absence of progression and good tolerance to treatment.
Both experts agreed that improved PFS and OS, maintained or improved QoL, and symptoms control can be considered clinically meaningful responses to the treatment under review. The assessment of treatment response should be conducted every 12 weeks to 16 weeks (every 3 months to 4 months).
Discontinuing Treatment
According to the clinical experts, treatment with pembrolizumab should be discontinued in the case of disease progression (confirmed clinically or on imaging), the appearance of serious immune AEs, or intolerable treatment toxicities.
Prescribing Conditions
Clinical experts consulted by CADTH indicated that treatment administration and the monitoring of patients with endometrial cancer should be undertaken by a specialist; namely, a gynecologist oncologist or medical oncologist. Treatment monitoring can potentially be conducted by a general practitioner oncologist, provided it is under the supervision of 1 of the specialists.
The experts recommend pembrolizumab be administered in an infusion setting, either in hospital or in oncology centre clinics with appropriate monitoring capabilities. In terms of companion diagnostics, the clinical experts noted that the detection of dMMR status through either IHC for dMMR, PCR for MSI-H, or next generation sequencing for dMMR would be required.
In reference to dosing, clinical experts consulted by CADTH noted that fixed dosing would be applied for pembrolizumab. One clinical expert expressed that less frequent administrations (i.e., 400 mg every 6 weeks) would be better for patients, clinicians, and health centres.
Additional Considerations
One clinical expert expressed concerns with the high costs of the treatment under review and indicated that the costs might decrease with increased availability of other PD-L1 inhibitors on the market.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
One joint clinician input was provided by 7 physicians on behalf of the Ontario Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee. The clinician group noted the absence of currently available therapies for patients with recurrent or progressive endometrial cancer. The group recognized the unmet needs of this patient population, indicating most patients remain unresponsive to available treatments and highlighting a need for better tolerated treatment options. Prolonged life, delayed disease progression, symptomatic relief, PR, full response, and improved HRQoL were identified as the most important treatment goals. In terms of assessing response to treatment, the clinician group stated that imaging, clinical exam, and symptomatic improvement should be assessed in clinical practice. Lastly, outpatient hospital settings were noted as appropriate treatment settings for these patients.
Of note, 5 out of 7 physicians provided CADTH with a Conflict of Interest declaration within the clinician group input.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
What is the guidance on the maximum number of prior lines of platinum therapy to be eligible for pembrolizumab treatment? | Clinical experts expressed uncertainty regarding the number of previous platinum-based treatments for the pembrolizumab monotherapy. While patients are unlikely to have more than 3 previous treatments, such patients should not be disqualified if they have good fitness and expect benefits. Clinical experts suggested that pembrolizumab might be preferable to a different treatment after platinum because of the toxicity of alternative chemotherapy options (such as doxorubicin). |
What is the guidance on re-treatment? | The clinical experts indicated that re-treatment with the same regimen is a valid question. However, there is no data to show what the response would be. In general, using the same medications in a relapsed setting could be considered, although relapses are usually in short intervals and responses poor. The longer the interval between treatment termination and reintroduction, the more likely a response would be seen. |
Considerations for prescribing of therapy | |
Jurisdictions may implement weight-based dosing up to a maximum dose for pembrolizumab (i.e., 2 mg/kg up to a maximum of 200 mg every 3 weeks). Should pembrolizumab 4 mg/kg (up to a maximum of 400 mg IV every 6 weeks) be an option? | The clinical experts indicated that weight-based dosing is only seen in pediatric patients. All adult regimens have had fixed doses as indicated previously. Experts mentioned that for patients who are very underweight, weight-based dosing might be appropriate. The clinical experts noted that less frequent administrations (i.e., 400 mg every 6 weeks) would be better for patients, clinicians, and health centres. |
Generalizability | |
Can pembrolizumab monotherapy used in MSI-H or dMMR endometrial cancer be extended to patients with ECOG PS > 1? | The clinical experts believe that the treatments could be extended to ECOG PS 2 in an appropriately informed and motivated patient. This drug should likely not be used in patients with ECOG PS score of 3 or 4. |
The KN-158 study (pembrolizumab monotherapy) excluded patients with sarcomas and mesenchymal tumours. Can PEM monotherapy be extended to patients with endometrial sarcomas? | The clinical experts indicated that the evidence to date is in carcinomas, so they are not aware of benefit in pure sarcomas. However, since carcinosarcomas are a combination, theoretically, pembrolizumab monotherapy may be extended to patients with carcinosarcomas, although there is no supporting research evidence at the moment. |
The KN-158 study (pembrolizumab monotherapy) excluded patients with active CNS metastases. Can pembrolizumab be extended to patients with active CNS metastases? | The clinical experts indicated that unstable CNS metastasis should be treated with typical methods; presently, that is neurosurgical resection and/or cranial irradiation. Subsequently, pembrolizumab treatment may be considered. |
Can pERC clarify the instances wherein time-limited funding would be applicable? | One expert indicated that patients who had started next-line therapy after platinum-based chemotherapy should be given the choice to switch to pembrolizumab on a time-limited basis. However, the preference would be to continue with the current regimen and switch to pembrolizumab when progression occurs, particularly if patients are responding to current treatment. |
Care provision issues | |
MSI and/or MMR testing is needed to confirm eligibility for single-drug pembrolizumab monotherapy. Is there a standardized definition of MSI-H or dMMR to guide implementation of eligibility criteria? | The clinical experts indicated that MMR testing is based on IHC staining of the tumour as a screening test. PCR testing for MSI-H is the next test and, if positive, Lynch syndrome is considered and investigated. These probably are the standard tests across Canada. |
When should testing for MSI-H or dMMR take place in patients with endometrial cancer? | The dMMR status needs to be determined before considering pembrolizumab monotherapy. |
CNS = central nervous system; dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IHC = immunohistochemistry; KN-158 = KEYNOTE-158; MMR = mismatch repair; MSI = microsatellite instability; MSI-H = microsatellite instability–high; PCR = polymerase chain reaction; PEM = pembrolizumab; pERC = CADTH pCODR Expert Review Committee.
Clinical Evidence
The clinical evidence included in the review of pembrolizumab is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review (if available).
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of pembrolizumab monotherapy for the treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with unresectable or MSI-H (dMMR) endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options Subgroups:
|
Intervention | Pembrolizumab for IV infusion over 30 minutes; 200 mg every 3 weeks or 400 mg every 6 weeks until unacceptable toxicity or disease progression, or for up to 24 months or 35 doses for 200 mg or 18 doses for 400 mg, whichever is longer |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and phase IV RCTs |
AE = adverse event; DOR = duration of response; dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HRQoL = health-related quality of life; FIGO = International Federation of Gynecology and Obstetrics; ICU = intensive care unit; MSI-H = microsatellite instability–high; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Note: Dostarlimab is approved by Health Canada for the treatment of patients with MSI-H or dMMR endometrial carcinoma. However, the drug is not currently reimbursed for this indication and submissions are under review by CADTH as of February 2021. Therefore, it is not considered as a comparator in the present protocol.
aIndicates patient-important outcomes identified in patient input.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.43
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. The search strategy comprised both controlled vocabulary, such as the US National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Keytruda and pembrolizumab, and endometrial cancer. Clinical trials registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on January 21, 2022. Regular alerts updated the search until the meeting of pERC on May 11, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.44 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol shown in Table 5. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for network meta-analyses dealing with endometrial cancer was run in MEDLINE All (1946–) on January 20, 2022. No limits were applied to the search.
Findings From the Literature
A total of 1 study21 was identified from the literature for inclusion in the systematic review (Figure 1). Detailed information on the included study is summarized in Table 6. A list of excluded studies is presented in Appendix 2.
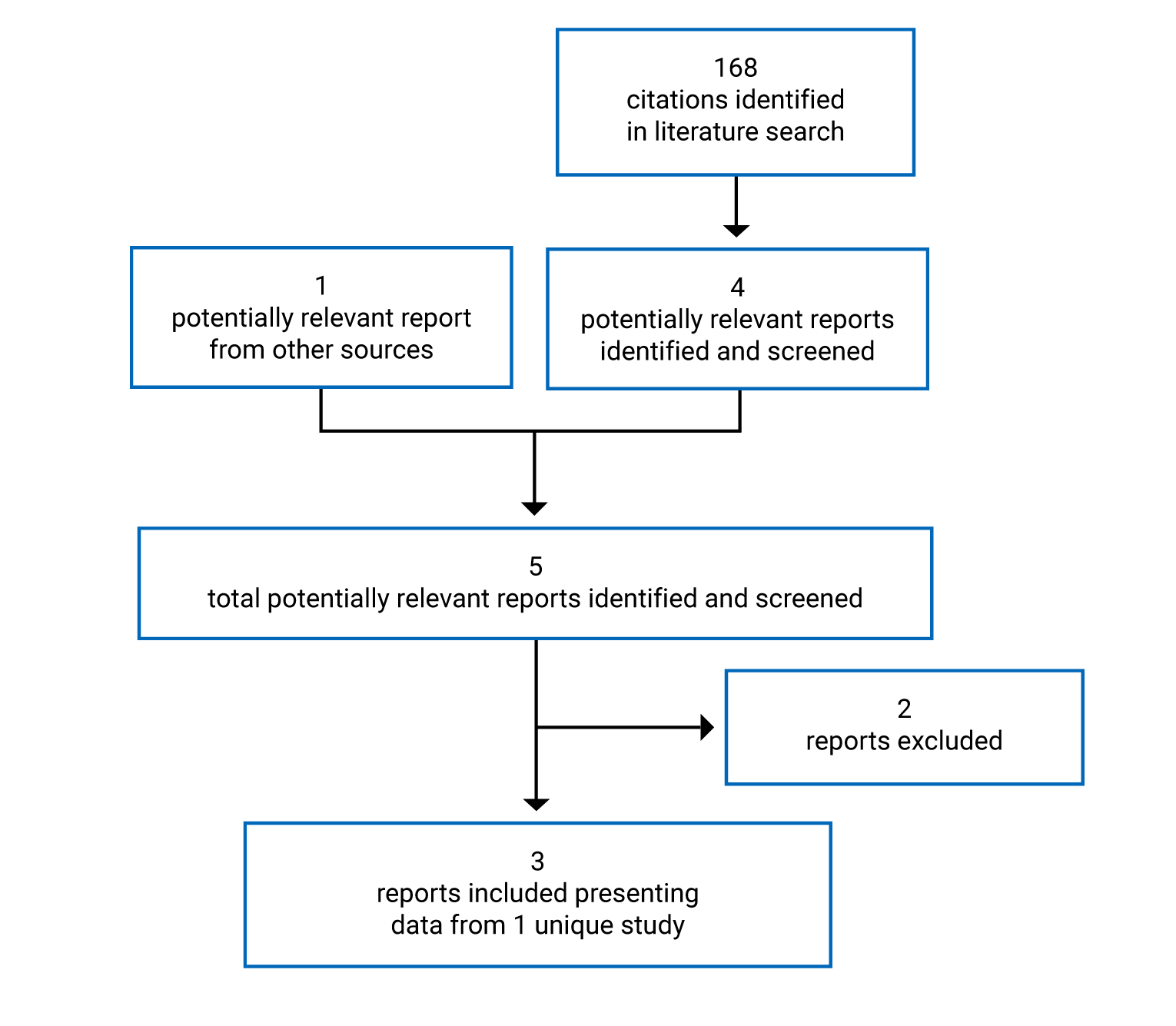
Table 6: Details of Included Studies
Detail | Study KN-158 (cohort D and cohort K)a |
|---|---|
Designs and populations | |
Study design | Nonrandomized, multicentre, single-arm, open-label, phase II trial |
Locations | 38 centres in 15 countries that enrolled 90 patients with advanced MSI-H or dMMR endometrial carcinoma in cohort D and cohort K. The study was conducted in the US, Canada (3 centres), the UK, France, Germany, Australia, and other European, Central American, South American, and Asian countries. |
Patient enrolment dates | First patient’s first visit: February 1, 2016 Ongoing study, data cut-off: October 5, 2020 |
Randomized (N) | 90 |
Inclusion criteria | Key inclusion criteria were that patients:
|
Exclusion criteria | Key exclusion criteria were that patients:
|
Drugs | |
Intervention | Pembrolizumab 200 mg q.3.w. IV infusion over 30 minutes, on day 1 of each 3-week cycle, for up to 35 cycles (approximately 2 years)
|
Comparator(s) | None |
Duration | |
Phase | |
Screening | Up to 42 days |
Open-label | Up to 35 cycles (about 2 years), documented disease progression, unacceptable AE, intercurrent illness preventing further treatment administration, investigator decision, or patient withdrawal of consent, whichever came first |
Follow-up | Follow-up duration was defined as the time from first dose to the date of death or the database cut-off date if the participant was still alive. Median follow-up duration = 16.5 months (range, 0.5 months to 56.1 months) |
Outcomes | |
Primary end point | ORR |
Secondary and exploratory end points | Secondary
Exploratory
|
Notes | |
Publications | O’Malley et al. (2022)10 Marabelle et al. (2020)45 |
AE = adverse event; CNS = central nervous system; CR = complete response; dMMR = deficient mismatch repair; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HRQoL = health-related quality of life; IRC = independent central radiologic review; irRECIST = immune-related Response Evaluation Criteria in Solid Tumours; KN-158 = KEYNOTE-158; mAb = monoclonal antibody; MSI-H = microsatellite instability–high; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PD-L1 = programmed cell death 1 ligand 1; PD-L2 = programmed cell death 2 ligand 2; PR = partial response; PRO = patient-reported outcome; q.3.w. = once every 3 weeks; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event.
Note: In O’Malley (2022),10 it was reported that as of October 5, 2020, the median time from first dose to data cut-off was 42.6 months (range, 6.4 months to 56.1 months).
aInformation extracted focused on endometrial patients with dMMR or MSI-H status from cohort D and cohort K in study KN-158 only. In this report, “study KN-158” alludes to cohort D and cohort K in the KN-158 study, unless otherwise specified.
bPatient-reported HRQoL was listed as an outcome in the protocol. However, no PRO or HRQoL outcome results were reported in the Clinical Study Report. Rather, the patient-reported HRQoL findings were presented at the European Society for Medical Oncology Congress 2021.19
Source: KN-158 Clinical Study Report.21
Description of Study
The KN-158 study (specifically cohort D and cohort K for this review)21 is an ongoing, nonrandomized, multicentre, single-arm, open-label, phase II trial. The key objective of this study is to evaluate the efficacy and safety of pembrolizumab in patients with previously treated advanced endometrial cancer who were MSI-H or dMMR.
The trial was conducted in 38 global sites in 15 countries (Canada [3 sites], the US, and 13 other countries in Europe, South America, Central America, and Asia). The key characteristics of the study design are summarized in Table 6 and Figure 2.
The enrolment for this study started on February 1, 2016, and is still ongoing.20 The cut-off date for the included study was October 5, 2020 (11th interim analysis). The estimated study completion date is June 18, 2026. As of the cut-off date, a total of 90 patients were included in this study and all 90 patients received at least 1 dose of pembrolizumab. The primary outcome was ORR. The secondary outcomes were DOR, PFS, OS, and safety. HRQoL was an exploratory outcome.
Important protocol deviations were reported by 4 (4.4%) patients in the study. These were categorized as a reportable safety event and/or follow-up safety event information that was not reported per the timelines outlined in the protocol. None of the deviations were considered to be clinically important.
Figure 2: KN-158 Overall Study Design
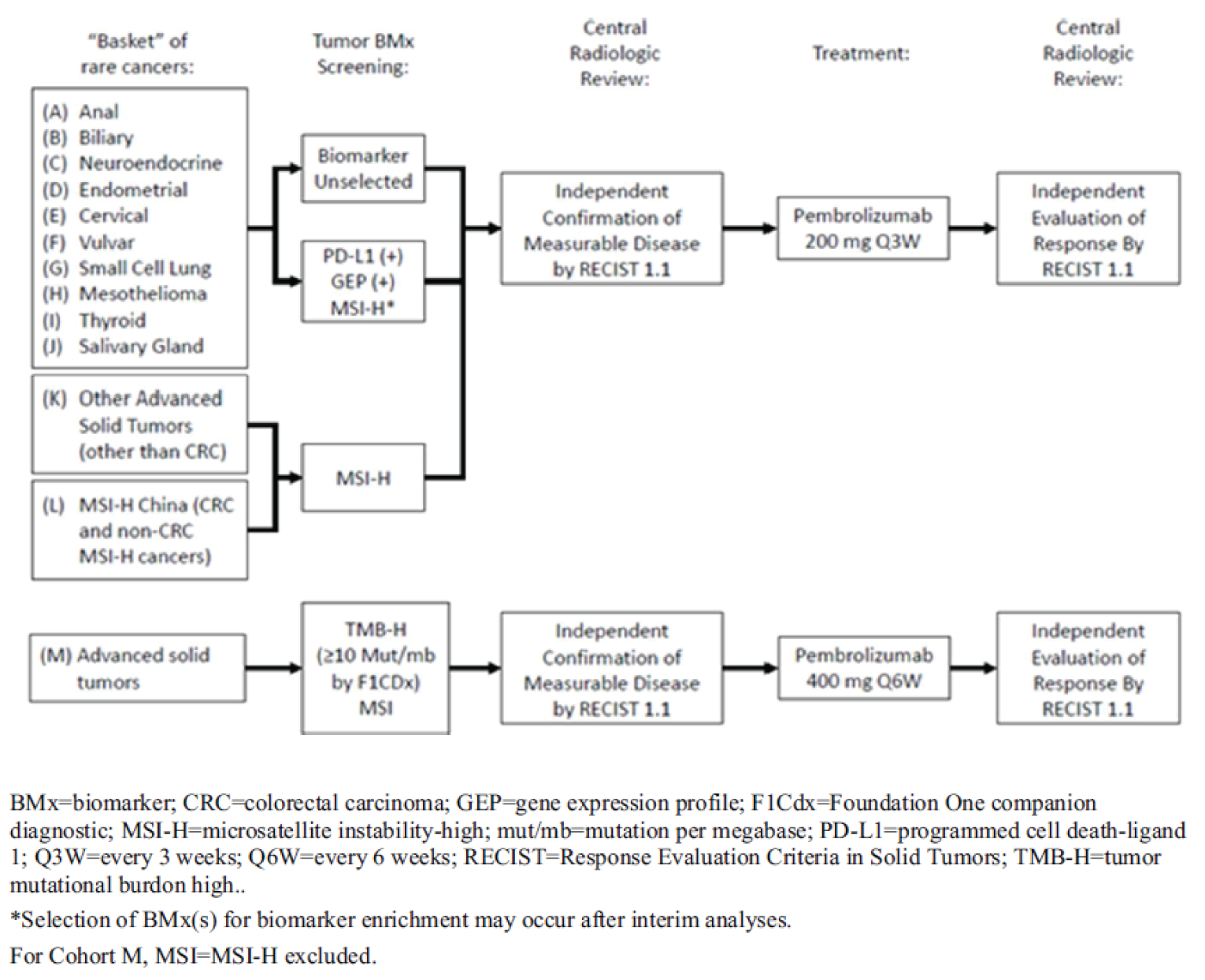
Note: Only cohort D and cohort K patients with mismatch repair–deficient endometrial cancer were reported in this CADTH review.
Source: KN-158 Clinical Study Report.21
Populations
Inclusion and Exclusion Criteria
Eligible patients were adults (18 years and older) with advanced (metastatic and/or unresectable) endometrial carcinoma which was MSI-H, was incurable, and for which prior standard first-line treatment had failed. Patients were required to have an ECOG PS score of 0 or 1. The main exclusion criteria included patients who had sarcoma and mesenchymal tumours, active CNS metastases and/or carcinomatous meningitis, or prior therapy with an anti–PD-1, anti–PD-L1, anti–programmed cell death 2 ligand 2 (PD-L2), or any other immune-modulating monoclonal antibody.
Baseline Characteristics
The main baseline demographics and disease characteristics of the 90 patients in the trial are summarized in Table 7.
The median age was 64.0 years (range, 42 years to 86 years). Patients either had a baseline ECOG PS of 0 (38.9%) or 1 (61.1%). In the study, 75 (83.3%) patients were white and 7 (7.8%) patients were Asian, 61 (67.8%) patients reported a prior history of radiation therapy, 78 (86.7%) patients had had surgery treatment for cancer, and 86 (95.6%) patients had had metastatic cancer.
A total of 46 (51.1%) patients had previously received 1 line of systemic treatment and 20 (22.2%) patients had received 2 lines of prior systematic therapies. A total of 23 (25.6%) patients had received 3 or more lines of prior systemic therapies. Among patients who had received prior systemic treatment, 82 (91.1%) patients had received carboplatin, 12 (13.3%) patients had received cisplatin, 21 (23.4%) patients had received doxorubicin or doxorubicin hydrochloride, 81 (90.0%) patients had received paclitaxel, and 26 (28.9%) patients had received hormonal therapy (refer to Table 22).
In cohort D, the MSI-H or dMMR status was determined retrospectively by PCR assays at a central laboratory while in cohort K, the MSI-H or dMMR status was assessed retrospectively by PCR and/or IHC at a local laboratory.46 MSI-H or dMMR status was determined by examining either the loss of protein expression by IHC of 4 MMR enzymes or the analysis of 5 tumour microsatellite loci using PCR-based assays.30
Table 7: Summary of Baseline Characteristics — All Participants As-Treated Population in Study KN-158 (Cohort D and Cohort K)
Characteristic | Pembrolizumab group N = 90 |
|---|---|
Sex, n (%) | |
Female | 90 (100.0) |
Age (years), n (%) | |
< 65 | 47 (52.2) |
≥ 65 | 43 (47.8) |
Median (range) | 64.0 (42 to 86) |
Race, n (%) | |
Asian | 7 (7.8) |
White | 75 (83.3) |
Other | 8 (8.8) |
Missing | 2 (2.2) |
Geographic region, n (%) | |
US | 18 (20.0) |
Non-US | 72 (80.0) |
ECOG PS, n (%) | |
0 | 35 (38.9) |
1 | 55 (61.1) |
Metastatic staging, n (%) | |
M0 | 4 (4.4) |
M1 | 86 (95.6) |
Brain metastases present | |
No | 90 (100.0) |
Number of prior lines of therapy, n (%) | |
0 | 1 (1.1) |
1 | 46 (51.1) |
2 | 20 (22.2) |
3 | 14 (15.6) |
4 | 6 (6.7) |
5 or more | 3 (3.3) |
Sum of target lesions measurable at baseline (mm) | |
Patients with data, n | 86 |
Median (range) | 70.9 (11.8 to 282.8) |
Prior radiation therapy, n (%) | |
Yes | 61 (67.8) |
No | 29 (32.2) |
Prior surgery, n (%) | |
Yes | 78 (86.7) |
No | 12 (13.3) |
PD-L1 status, n (%) | |
Positive | 17 (18.9) |
Negative | 6 (6.7) |
Not evaluable | 1 (1.1) |
Missing | 66 (73.3) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; KN-158 = KEYNOTE-158; PD-L1 = programmed cell death 1 ligand 1.
Note: The all participants as-treated population included all allocated patients who received at least 1 dose of study treatment.
Source: KN-158 Clinical Study Report.21
Interventions
All patients (N = 90) received pembrolizumab 200 mg as a 30-minute IV infusion on day 1 of each 3-week cycle, for 35 cycles (approximately 2 years), on an outpatient basis. Treatment continued until documented disease progression, unacceptable AE, intercurrent illness preventing further treatment administration, investigator decision, or patient withdrawal of consent. The discontinuation of treatment could be considered for patients who attained a CR and who had been treated with at least 8 administrations of pembrolizumab, 2 of which were beyond the date where initial CR was declared. Patients who discontinued pembrolizumab with CR, PR, or stable disease were eligible for up to 17 cycles (approximately 1 year) of re-treatment (second course) with pembrolizumab after disease progression if safety criteria were met.
Pembrolizumab was withheld or discontinued for drug-related toxicities and severe or life-threatening AEs. Pembrolizumab was permanently discontinued for any severe or grade 3 (grade 2 for pneumonitis) drug-related AE that recurred, or any life-threatening event. Dosing interruptions were permitted for medical or surgical events or logistical reasons not related to study therapy. Patients were to be placed back on therapy within 3 weeks, unless otherwise discussed with the sponsor. No dose reductions were permitted during the trial.
Concomitant Medications
Treatments considered necessary for the patient’s welfare were allowed at the discretion of the investigator and were recorded. Patients were prohibited from receiving the following therapies during the screening and treatment phases of the trial (including during re-treatment for relapse): antineoplastic systemic chemotherapy or biological therapy, immunotherapy not specified in the protocol, chemotherapy not specified in the protocol, investigational drugs other than pembrolizumab, radiation therapy, glucocorticoids for any purpose other than to modulate symptoms from suspected immunologic etiology, live vaccines (including 30 days before the first dose of pembrolizumab). The exclusion criteria describe other medications that were prohibited in this trial. There were no prohibited therapies during the posttreatment follow-up phase. Patients were allowed to receive rescue medications and supportive care as deemed necessary by the treating investigator. This included oral or IV treatment with corticosteroids as well as additional anti-inflammatory drugs.
Subsequent Cancer Therapy
New antineoplastic therapies initiated after the last dose of trial treatment were reviewed and documented. If the new therapy was initiated within 30 days after the last dose of trial treatment, the 30-day safety follow-up visit needed to occur before the first dose of the new treatment. Following the initiation of new antineoplastic therapy, the patient moved into the survival follow-up. The sponsor reported that 10 (11%) patients received 1 subsequent oncologic therapy after discontinuing from study treatment, 4 (4.4%) patients received 2 subsequent oncologic therapies, and 2 (2.2%) patients received 3 subsequent oncologic therapies after discontinuing from study treatment.47
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial included in this review is provided in Table 8. A detailed discussion on the validity of the outcome measures for HRQoL is provided in Appendix 6.
The primary outcome of the KN-158 study was ORR, which was defined as the proportion of patients in the analysis population who had a CR or PR at any time during the trial. Response for the primary analysis was determined by independent central radiologic review, with confirmatory assessment as required per RECIST 1.1. Patients with unknown or missing information were considered to be nonresponders.
The secondary outcomes were DOR, PFS, and OS. DOR was defined as the time from the first documented evidence of CR or PR until the first documented sign of disease progression or death due to any cause, whichever occurred first. PFS was defined as the time from the date of the first dose of study medication to the first documented disease progression per RECIST 1.1 based on blinded central imaging vendor review or death due to any cause, whichever occurred first. OS was defined as the time from the date of the first dose of study medication to death due to any cause.
AEs were assessed throughout the study and for 30 days after the end of treatment (90 days for serious AEs) and were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0.10
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | Types of outcomes assessed in Study KN-158 (cohort D and cohort K) | Description |
|---|---|---|
Efficacy outcomes | ||
OS | Secondary | OS was defined as the time from the date of the first dose of study medication to death due to any cause. Patients without documented death at the time of analysis were censored at the date of last known contact. |
PFS | Secondary | PFS was defined as the time from the date of the first dose of study medication to the first documented disease progression per RECIST 1.1 based on blinded central imaging vendor review or death due to any cause, whichever occurred first. If a patient did not have a documented date of progression or death, PFS was censored at the date of the last adequate assessment. |
ORR | Primary | ORR was defined as the proportion of patients in the analysis population who had a CR or PR. Response for the primary analysis was determined by independent central radiologic review, with confirmatory assessment as required per RECIST 1.1. |
DOR | Secondary | DOR was defined in the subset of patients with a CR or PR, based on RECIST 1.1, as assessed by independent central radiologic review, as the time from the first documented evidence of CR or PR until the first documented sign of disease progression or death due to any cause, whichever occurred first. Patients who were alive, had not progressed, had not initiated new anticancer treatment, and had not been determined to be lost to follow-up were considered ongoing responders at the time of analysis. |
HRQoL EORTC QLQ-C30 EORTC QLQ-C30 functional and symptom scales and items EQ-5D-3L VAS | Exploratory19 | A self-reported instrument designed to measure the physical, psychological, and social functions of patients with cancers. The EORTC QLQ-C30 incorporates 5 functional scales (physical, role, cognitive, emotional and social); 3 symptom scales (fatigue, pain, and nausea/ vomiting); a global health and quality-of-life scale; and single items that assess additional symptoms commonly reported by patients with cancer (dyspnea, appetite loss, sleep disturbance, constipation, and diarrhea), as well as the perceived financial impact of the disease and treatment.48-50 EQ-5D-3L VAS, a vertical visual analogue scale with anchors of 100 (best imaginable health) and 0 (worst imaginable health) on which patients provide a global assessment of their health.51-54 |
Harms outcomes | ||
AEs, SAEs, WDAEs, notable harms, deaths | Exploratory | The assessment of safety was based on frequency of AEs, SAEs, WDAEs (AEs leading to discontinuation of study drug), AEs leading to dose modification (delay and/or reduction), and notable harms. Analyses were conducted using the 30-day safety window for general AEs and the 90-day safety window for SAEs from the date of the last dose received. AEs were graded using CTCAE (version 4.0) criteria. |
AE = adverse event; CR = complete response; CTCAE = Common Terminology Criteria for Adverse Events; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-3L = 3-level EQ-5D; HRQoL = health-related quality of life; KN-158 = KEYNOTE-158; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; VAS = visual analogue scale; WDAE = withdrawal due to adverse event.
Note: Patient-reported outcomes and HRQoL outcomes (i.e., EORTC QLQ-C30 and EQ-5D) were listed in the protocol; however, no results were reported in the KN-158 Clinical Study Report. The results were presented in a conference abstract submitted by the sponsor.19
Source: KN-158 Clinical Study Report.21
Statistical Analysis
No formal hypothesis testing was planned in this trial. The protocol indicated that the trial incorporated an adaptive design in which multiple interim analyses could be performed for the overall KN-158 study (i.e., regardless of the type of tumour or MMR status). However, no specific information on the interim analysis was provided for the population of interest in this review (i.e., patients with endometrial cancer who were MSI-H or dMMR). The general guidance for evaluation criteria for the interim analysis for the overall KN-158 trial is presented in Table 25 in Appendix 4. The primary end point (ORR) was used for all interim analyses. Results presented herein are from interim analysis 11.
Efficacy outcomes were assessed in patients who received 1 dose or more of pembrolizumab and had been enrolled 26 weeks or longer before data cut-off (to allow sufficient time for responses to occur and be assessed). Safety was assessed in all patients who received 1 dose or more of pembrolizumab. The point estimate and exact Clopper-Pearson 95% CIs were provided for ORR. The Kaplan-Meier method was used to estimate DOR, PFS, and OS. The censoring rules for DOR are presented in Table 24 in Appendix 4.
Power Calculation
Sample size and power calculations were not performed. The study plan was to enrol a minimum of 200 patients and a maximum of 1,595 patients over 126 months, with approximately 50 patients in each tumour type subgroup, and up to 350 patients in MSI-H subgroup K.
Primary Analysis
Statistical analysis methods for the efficacy outcomes are shown in Table 9. Cumulative data were reviewed by the study team on an ongoing basis with no multiplicity control.
Primary Outcome: Objective Response Rate
The point estimate and 95% CI for ORR were assessed using the Clopper-Pearson exact method based on a binomial distribution.
Secondary Outcomes: Duration of Response, Progression-Free Survival, and Overall Survival
The median (95% CI) DOR, PFS, and OS were estimated and plotted using the Kaplan-Meier product-limit method. Event rates over time were also estimated using the Kaplan-Meier method.
Exploratory Patient-Reported Outcome and Health-Related Quality of Life Outcome
Changes from baseline in the EORTC QLQ-C30 GHS and QoL scores and in the EQ-5D-3L VAS scores were summarized over time. The results were not provided in the KN-158 Clinical Study Report.21 However, the results were presented in ESMO conference abstracts included in the sponsor’s submissions.19,47 HRQoL was analyzed in all patients who completed at least 1 assessment and received at least 1 dose of study treatment; changes from baseline were analyzed in patients who also had both a baseline and postbaseline HRQoL assessment.
Subgroup and Sensitivity Analyses
Subgroup analysis was conducted only for ORR. The subgroup analysis of interest defined in the review protocol was based on the number and type of prior systemic therapies (i.e., < 2 and ≥ 2). No subgroup analyses were conducted for OS, PFS, and DOR.
No sensitivity analyses were conducted for any outcomes.
Safety Outcomes
Only descriptive statistics of safety were presented, with evidence summarized based on frequencies and the proportion of total patients. Separate summaries were provided for all AEs, SAEs, and AEs leading to discontinuation and dose modification. The incidence of deaths and their primary cause were summarized.
Table 9: Statistical Analysis of Efficacy End Points
End point | Statistical method or model | Missing data approach | Adjustment factors | Sensitivity analyses |
|---|---|---|---|---|
ORR | Exact test of binomial parameter, 95% CI calculated using the Clopper-Pearson method | Patients with missing data were considered nonresponders | None | None |
DOR | Summary statistics (median and quartiles) using the Kaplan-Meier method | Nonresponders were excluded | None | None |
OS | Summary statistics (median and quartiles) using the Kaplan-Meier method | Censored at last assessment | None | None |
PFS | Summary statistics (median and quartiles) using the Kaplan-Meier method | Censored at last assessment | None | None |
CI = confidence interval; DOR = duration of response; KN-158 = KEYNOTE-158; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Source: KN-158 Clinical Study Report.21
Analysis Populations
The efficacy analyses were based on the ASaT population for efficacy analysis (N = 79), defined as patients who received at least 1 dose of study intervention and had been enrolled at least 26 weeks (i.e., 6 months) before the data cut-off. A total of 79 patients with advanced MSI-H or dMMR endometrial carcinoma were included in the ASaT population for efficacy analysis.
The analysis for HRQoL was based on the full analysis set population (N = 63), defined as patients in the primary efficacy population with at least 1 HRQoL assessment available.19,21,47
Safety analyses were based on the ASaT population, which included all 90 patients who received at least 1 dose of study intervention.
Results
Patient Disposition
Patient disposition for the KN-158 study (cohort D and cohort K) is presented in Table 10. The number of patients screened in this population (i.e., those with endometrial cancer who were MSI-H or dMMR) was not reported. All patients included in this population (N = 90) received at least 1 dose of pembrolizumab.
At the time of the data cut-off date, a total of 18 (20.0%) patients had completed the treatment and 52 (57.8%) patients had discontinued from the treatment. The main reasons for discontinuation of treatment were disease progression (N = 30; 33.3%), clinical progression (N = 7; 7.8%), AE (N = 6; 6.7%), withdrawal by patients (N = 5; 5.6%), CR (N = 2; 2.2%), and physician decision (N = 2; 2.2%). A total of 20 (22.2%) patients were still receiving the treatment at the time of data cut-off.
Table 10: Patient Disposition — All Participants As-Treated Population in Study KN-158 (Cohort D and Cohort K)
Characteristic | Pembrolizumab group (N = 90) |
|---|---|
Screened, N | NR |
Total number of patients included in this population, N | 90 |
Status for study medication in trial,a n (%) | |
Started | 90 (100.0) |
Completed | 18 (20.0) |
Discontinued | 52 (57.8) |
Adverse event | 6 (6.7) |
Clinical progression | 7 (7.8) |
Complete response | 2 (2.2) |
Physician decision | 2 (2.2) |
Progressive disease | 30 (33.3) |
Withdrawal by patient | 5 (5.6) |
Treatment ongoing | 20 (22.2) |
Status for trial, n (%) | |
Discontinued | 32 (35.6) |
Death | 29 (32.2) |
Withdrawal by patient | 3 (3.3) |
Ongoing In trial | 58 (64.4) |
ITT, N | Not performed |
ASaT for efficacy analysis,b N | 79 |
Full analysis | 63 |
PP, N | Not performed |
Safety analysis,c N | 90 |
ASaT = all subjects as-treated; ITT = intention to treat; KN-158 = KEYNOTE-158; NR = not reported; PP = per protocol.
aEach patient was counted once for patient study medication disposition based on the latest corresponding disposition record.
bA total of 79 patients was included in the all patients as-treated for efficacy analysis, which was defined as all patients who received at least 1 dose of study intervention and had been enrolled at least 26 weeks before the data cut-off date.
cThe safety analysis population included all patients who received at least 1 treatment.
Source: KN-158 Clinical Study Report.21
Exposure to Study Treatments
The median duration of exposure to pembrolizumab was 8.3 months (range, 0.03 months to 26.88 months), and the median number of administrations was 12.5 (range, 1.00 to 35.00). As of the data cut-off date, 56.7% of patients had received pembrolizumab for at least 6 months, 37.8% of patients had received pembrolizumab for at least 12 months, and 26.7% of patients had received pembrolizumab for at least 18 months (refer to Table 26 in Appendix 4).
The median duration of follow-up of patients in the ASaT population for efficacy analysis (N = 79) as of the data cut-off date was 16.5 months (range, 0.5 months to 56.1 months). Twenty-nine of 38 responders had at least 12 months of follow-up from the time of response onset; 8 ongoing responders had less than 12 months of follow-up.21
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported as follows. Refer to Appendix 4 for detailed efficacy data.
Overall Survival
The results for OS are summarized in Table 11 and Figure 3. In total, there were 29 (36.7%) deaths. The survival probabilities of patients at 12 months, 24 months, 36 months, and 48 months were 69.4%, 64%, 60.1%, and 60.1%, respectively. The median OS was not reached (lower bound of 95% CI = 27.2 months).
Figure 3: Kaplan-Meier Estimates of Overall Survival — All Participants As-Treated Population for Efficacy Analysis
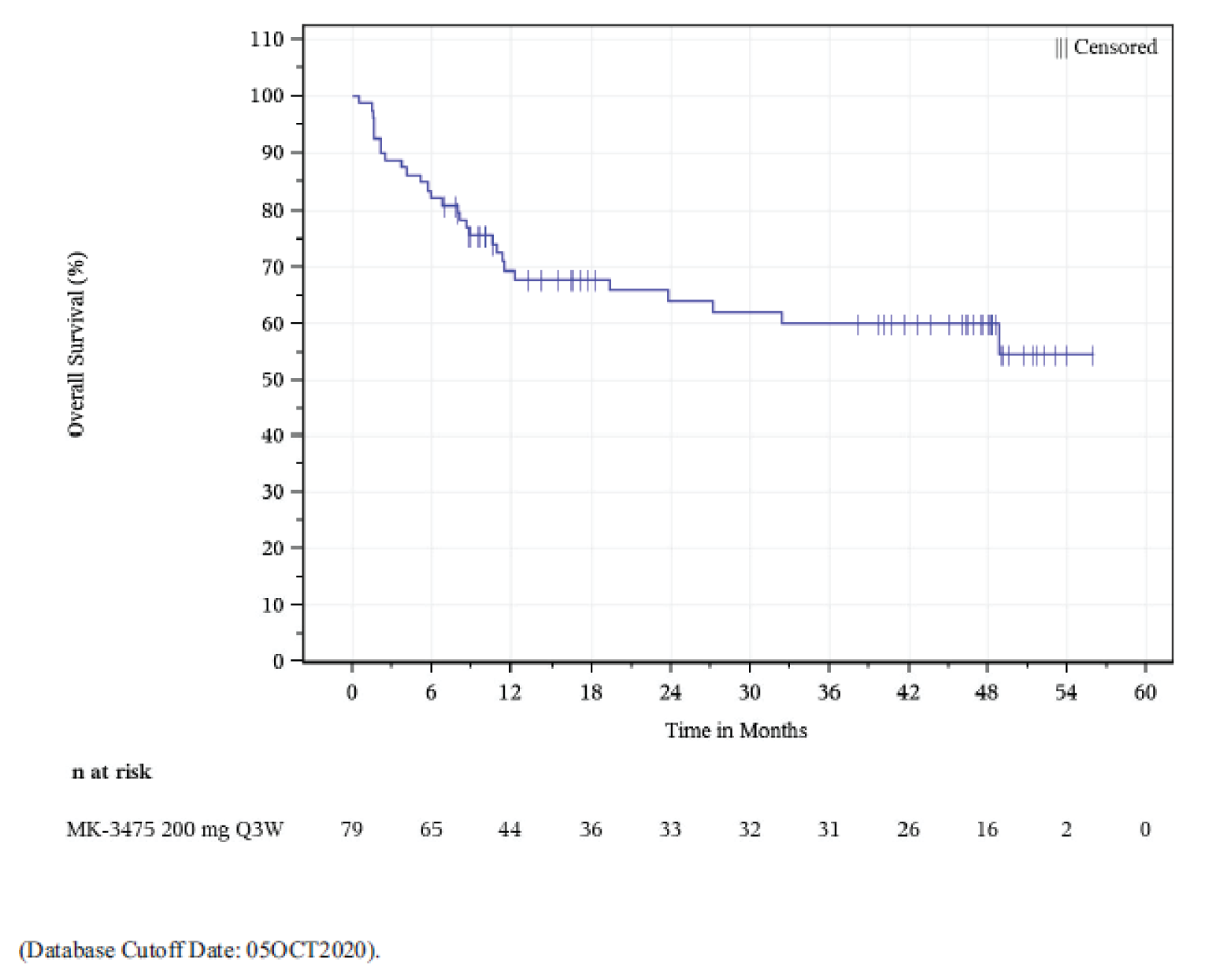
ASaT = all subjects as-treated; KN-158 = KEYNOTE-158; MSI-H = microsatellite instability–high; Q3W = once every 3 weeks.
Source: KN-158 Clinical Study Report.21
Progression-Free Survival
The results for PFS are summarized in Table 11 and Figure 4. By the date of the data cut-off, 45 (57.0%) patients had had a PFS event. The median PFS was 13.1 months (95% CI, 4.3 months to 34.4 months). PFS rates at 12 months, 24 months, and 48 months were 51.0%, 41.3%, and 37.0%, respectively.
Figure 4: Kaplan-Meier Estimates of Progression-Free Survival — All Participants As-Treated Population for Efficacy Analysis
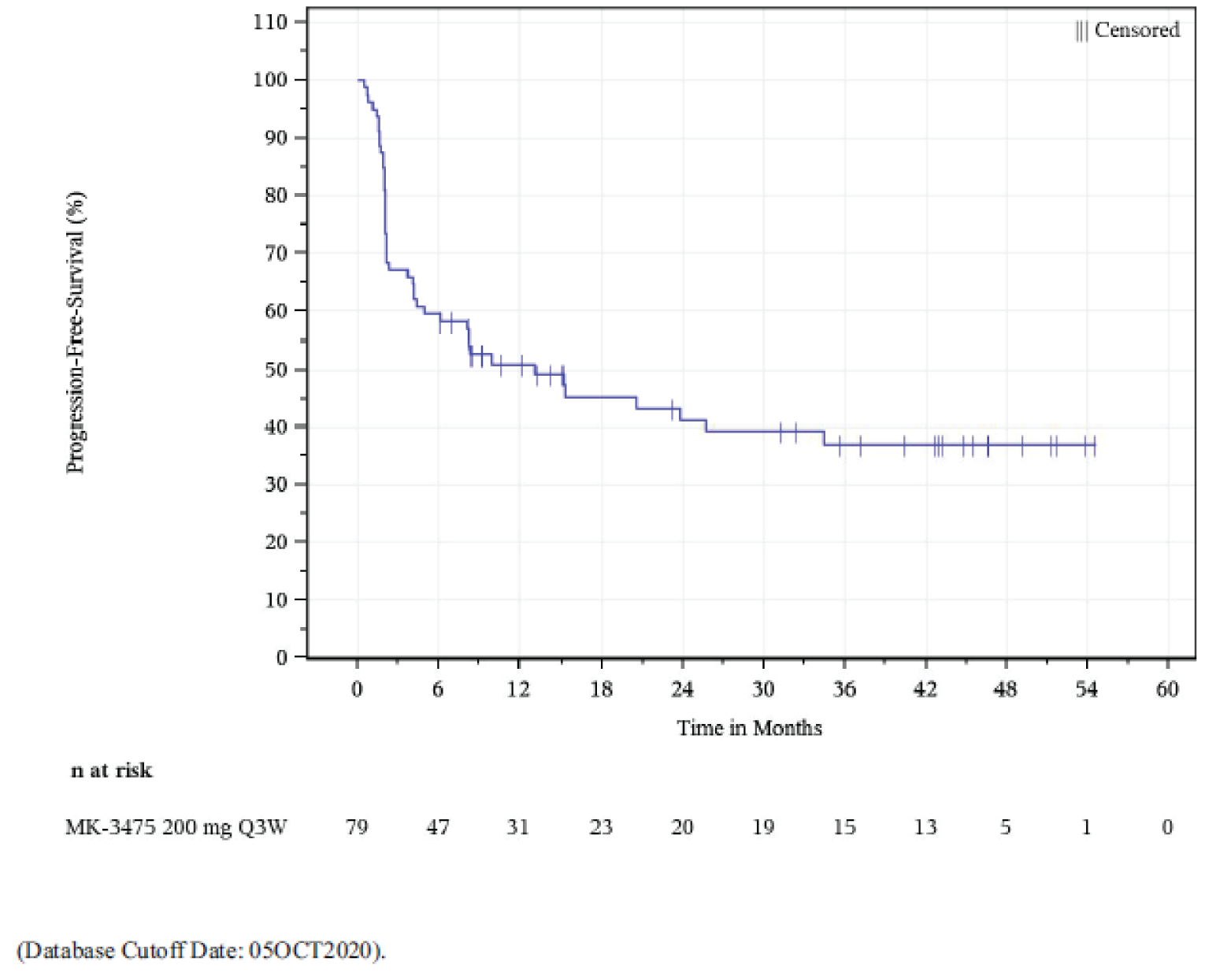
ASaT = all subjects as-treated; KN-158 = KEYNOTE-158; MSI-H = microsatellite instability–high; Q3W = once every 3 weeks; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: KN-158 Clinical Study Report.21
Health-Related Quality of Life
The findings for HRQoL were not reported in the KN-158 Clinical Study Report. However, the sponsor submitted a conference abstract presented at ESMO Congress 2021.19 The results presented in the abstract are briefly summarized in Appendix 5. It was reported that with the treatment of pembrolizumab, scores for EORTC QLQ-C30 GHS, EORTC QLQ-C30 function and symptom scales, and EQ-5D-3L VAS reported in the KN-158 study appeared to be maintained or improved based on the mean change from baseline to week 9. These comparisons were not tested statistically; however, the CIs at each time point were wide and overlapping.
Symptom Reduction
Symptom reduction was not assessed in this study. However, symptoms such as pain are 1 of the 5 dimensions of the EQ-5D-3L. No findings related to individual dimension-level assessment (such as pain) were reported.
Objective Response Rate
The results of ORR (per radiology assessment) are presented in Table 11. In patients who had been enrolled at least 26 weeks before the data cut-off date, 38 of 79 patients achieved an objective response resulting in an ORR of 48.1% (95% CI, 36.7% to 59.6%). Eleven patients (13.9%, 95% CI, 7.2% to 23.5%) achieved CR and 27 patients (34.2%, 95% CI, 23.9% to 45.7%) achieved PR.
Subgroup analysis showed that the ORR was 52.6% (95% CI, 35.8% to 69.0%) in patients with fewer than 2 lines of prior systemic treatment and was 43.9% (95% CI, 28.5% to 60.3%) in patients with 2 or more lines of prior systemic treatments. The ORR was 52% (95% CI, 38% to 65%) in the 56 patients with prior radiation therapy and 39% (95% CI, 20% to 61%) in the 23 patients with no prior radiation therapy.10,21
Duration of Response
The results of DOR are presented in Table 11, Table 27 in Appendix 4, and Figure 5.
Among responders (N = 38), 9 (23.7%) patients experienced disease progression or died. Twenty-nine (76.3%) patients were censored, primarily because they had ongoing response (n = 21; 55.3%) or had their last assessment 5 months or more before the data cut-off (n = 7; 18.4%). One patient had started a new anticancer treatment (refer to Table 28 in Appendix 4).
Based on the product-limit (Kaplan-Meier) method for censored data, the median DOR was not reached (range, 2.9 to 49.7 at last assessment). By the Kaplan-Meier estimation, extended response durations of at least 12 months, 24 months, and 36 months were observed in 88.1%, 72.9%, and 68.1% of responders, respectively.
Health Care Utilization
Health care utilization (e.g., hospital admission, hospital days, intensive care unit admission, intensive care unit days, emergency department visits) was not an outcome assessed in study KN-158.21,47
Table 11: Summary of Key Results From Pivotal and Protocol-Selected Studies — Efficacy Analysis Population
Outcome | Study KN-158 (cohort D and cohort K) (N = 79) |
|---|---|
Efficacy | N = 79 |
OS | |
Death, n (%) | 29 (36.7) |
Median survival (95% CI), monthsa | NR (27.2 to NR) |
OS rate, %a | |
6 months | 82.3 |
12 months | 69.4 |
18 months | 67.9 |
24 months | 64.0 |
30 months | 62.0 |
36 months | 60.1 |
42 months | 60.1 |
48 months | 60.1 |
PFS | |
Number of PFS events, n (%) | 45 (57.0) |
Person-months | 1,238 |
Event rate per 100 person-months (%) | 3.6 |
Median PFS (95% CI), monthsa | 13.1 (4.3 to 34.4) |
PFS rate, %a | |
6 months | 59.5 |
12 months | 51.0 |
18 months | 45.4 |
24 months | 41.3 |
30 months | 39.3 |
36 months | 37.0 |
42 months | 37.0 |
48 months | 37.0 |
ORR, n (%; 95% CI)b | |
Objective response (CR + PR) | 38 (48.1; 35.7 to 59.6) |
CR | 11 (13.9; 7.2 to 23.5) |
PR | 27 (34.2; 23.9 to 45.7) |
Stable disease | 14 (17.7; 10.0 to 27.9) |
Progressive disease | 23 (29.1; 19.4 to 40.4) |
Nonevaluable | 1 (1.3; 0.0 to 6.9) |
No assessment | 3 (3.8; 0.8 to 10.7) |
DORc (N = 38) | |
Median (range), monthsa | NR (2.9 to 49.7) |
≥ 12 months, n (%)a | 24 (88.1) |
≥ 24 months, n (%)a | 18 (72.9) |
≥ 36 months, n (%)a | 12 (68.1) |
CI = confidence interval; CR = complete response; DOR = duration of response; KN-158 = KEYNOTE-158; NR = not reached. ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response.
Notes: The sponsor provided updated ORR results based on the cut-off date of April 5, 2021, in which all 90 patients were included. The ORR was reported in 44 (48.9%) patients. The overall ORR as of April 5, 2021, was consistent with the findings as of October 5, 2020.47
Database cut-off date: October 5, 2020.
aFrom the product-limit (Kaplan-Meier) method for censored data.
bMeasured among patients with confirmed CR or PR.
cBased on the binomial exact CI method.
Source: KN-158 Clinical Study Report.21
Figure 5: Kaplan-Meier Estimates of Objective Response Duration in Responders (N = 38) Per Central Radiology Assessment
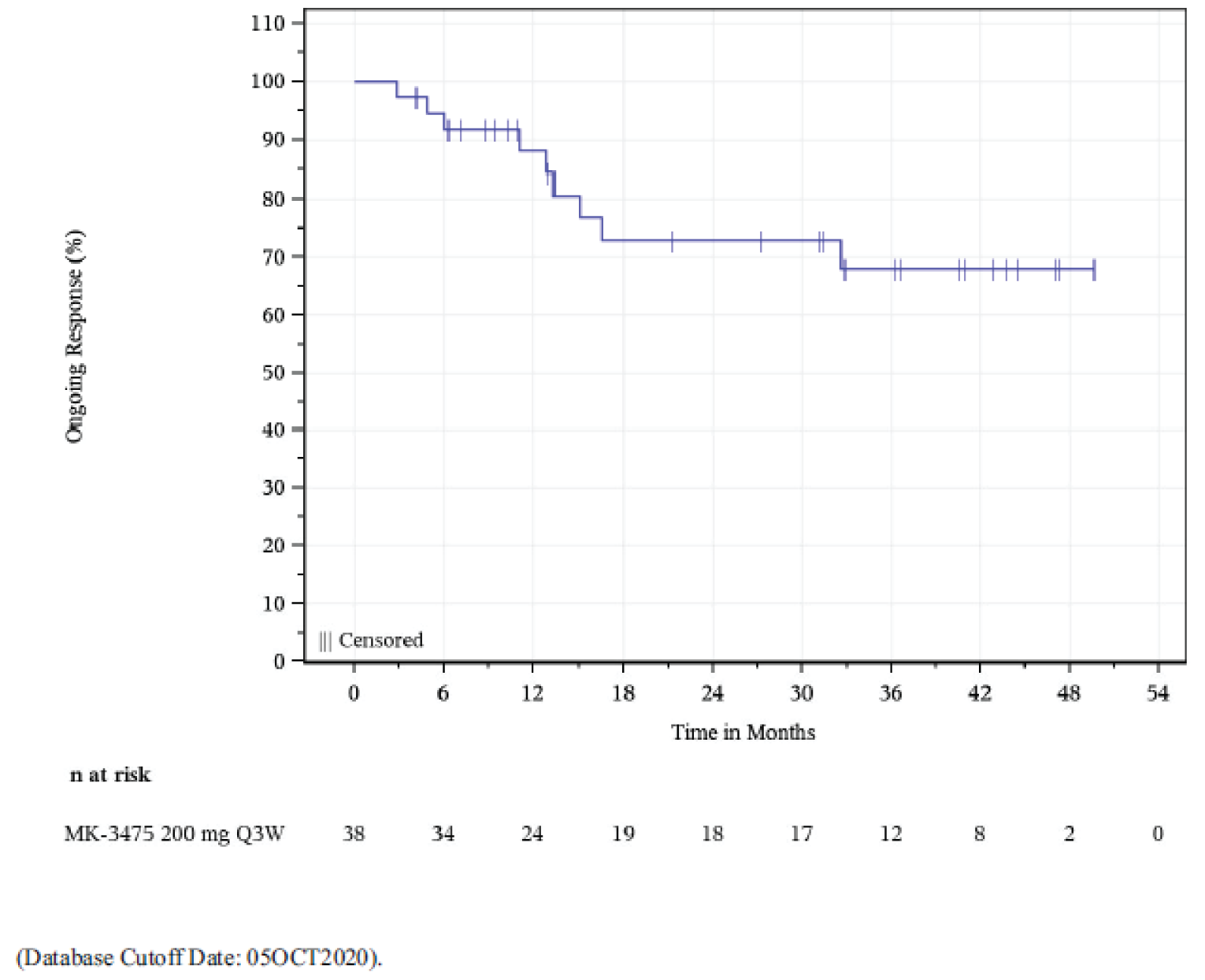
KN-158 = KEYNOTE-158; MSI-H = microsatellite instability–high; Q3W = once every 3 weeks; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: KN-158 Clinical Study Report.21
Harms
Only those harms identified in the review protocol are reported as follows. Refer to Table 12 and, in Appendix 4, Table 29, Table 30, and Table 31 for detailed harms data.
Adverse Events
A total of 86 (95.6%) of patients experienced at least 1 TEAE. The most common AEs (those which occurred in at least 25% of patients) were fatigue (n = 30; 33.3%), diarrhea (n = 29, 32.2%), pruritus (n = 26, 28.9%), arthralgia (n = 25; 27.8%), and nausea (n = 25; 27.8%). (Table 29). Grade 3 or higher AEs occurred in 47 (52.2%) of patients.
Serious Adverse Events
A total of 37.8% of patients experienced an SAE (refer to Table 12). Each SAE was reported in 1 patient,21 except for ascites, chest pain, pneumonia, pyelonephritis, sepsis, and urinary tract infection, which were each reported for 2 (2.2%) patients (refer to Table 30 in Appendix 4).
Withdrawals Due to Adverse Events
A total of 6 (6.7%) patients experienced AEs leading to study drug discontinuation (refer to Table 12).
AEs resulting in treatment discontinuation were increased transaminases, arthritis, enterocolitis, drug-induced liver injury, and rash. Each occurred in 1 (1.1%) patient, except increased transaminases, which occurred in 2 (2.2%) patients (refer to Table 31).
Mortality
No patients died due to an AE. Refer to Table 12.
Notable Harms
Hypothyroidism occurred in 14.4% of patients, followed by hyperthyroidism (7.8%), colitis (3.3%), type 1 diabetes mellitus (2.2%), pneumonitis (1.1%), adrenal insufficiency (1.1%), and hepatitis (1.1%). No hypophysitis or nephritis were reported (refer to Table 12).
AE | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 90) |
|---|---|
Patients with at least 1 TEAE, n (%) | 86 (95.6) |
Patients with at least 1 SAE, n (%) | 34 (37.8) |
Patients with dose interruptionc due to an AE, n (%) | 30 (33.3) |
Patients with an AE leading to discontinuation from the treatment, n (%) | 6 (6.7) |
Patients who discontinued drug due to an SAE, n (%) | 2 (2.2) |
Death,a n (%) | 0 (0.0) |
Notable harms, n (%) | |
Adrenal insufficiency | 1 (1.1) |
Colitis | 3 (3.3) |
Hepatitis | 1 (1.1) |
Hyperthyroidism | 7 (7.8) |
Hypophysitis | 0 (0.0) |
Hypothyroidism | 13 (14.4) |
Nephritis | 0 (0.0) |
Pneumonitis | 1 (1.1) |
Type 1 diabetes mellitus | 2 (2.2) |
AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; KN-158 = KEYNOTE-158; NCI = National Cancer Institute; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Notes: Non-SAEs followed for up to 30 days from the last dose and SAEs followed for up to 90 days from the last dose are included.
Database cut-off date: October 5, 2020.
aDeath due to AEs.
Source: KN-158 Clinical Study Report.21
Critical Appraisal
Internal Validity
The main limitation of the included pivotal study (study KN-158) was the single-arm study design, which does not include a comparator group. Such a design, in addition to lacking consideration of confounding variables, precludes causal inferences (i.e., the outcomes cannot be directly attributed to pembrolizumab). Without an active comparator or standard of care, nor any statistical hypothesis testing, it is not possible to assess the relative therapeutic benefit or safety of pembrolizumab against other available treatments (such as chemotherapy in this population). Though inclusion and exclusion criteria were stated, selection procedures were not described; therefore, the potential for selection bias cannot be excluded.
In addition, study KN-158 was an open-label trial and the study investigators and patients were aware of their treatment status. This increases the risk of detection and performance biases, which have the potential to influence outcome reporting. However, OS, PFS, ORR, and DOR are all objective response measurements, which were assessed per RECIST 1.1 criteria by independent central radiologic review. The central radiology review was blinded to biomarker results to minimize any bias in response assessments.21 Therefore, the open-label design is less of a concern for objective responses such as OS, PFS, ORR, and DOR, and more of a concern for subjective end points such as safety and HRQoL. The direction of anticipated bias related to these outcomes is unclear.
Based on the study design, patients who discontinued pembrolizumab with CR, PR, or stable disease were eligible for up to 17 cycles (approximately 1 year) of re-treatment (second course) with pembrolizumab after disease progression if safety criteria were met. It was reported that 2 patients received second-course pembrolizumab;10 in addition, other potential subsequent treatments appeared to have been allowed.47 It is therefore possible that OS data were confounded by the fact that some patients potentially received subsequent anticancer therapy after disease progression. This may result in bias of OS results.
As all results are part of an interim analysis, there is some risk that the efficacy of pembrolizumab has been overestimated. The median OS had not been reached at the time of the data cut-off, the survival data from the trial were immature, and 36.7% of patients had died by the time of the data cut-off. The DOR was assessed among those patients with CR or PR (N = 38). However, it should be noted that among the 38 responders, only 9 (23.7%) patients experienced disease progression or died. Since 21 (55.3%) patients were censored because they were still in the status of ongoing response, it is possible that the actual DOR differs from the current estimate. Furthermore, the efficacy assessment was not based on the ITT population and instead included patients who had received at least 1 dose of study intervention and had been enrolled at least 26 weeks before the data cut-off. Of note, an updated analysis of OS was provided as part of the sponsor’s request for reconsideration. A summary of the updated analysis based on a data cut-off of January 12, 2022, is available in Appendix 7. Descriptive results for OS were included, which indicate the median OS was reached. Based on the updated analysis, 41 (43.6%) patients had died and the median survival was 65.4 months (95% CI, 29.5% to NR).
In the opinion of the clinical experts consulted by CADTH, as long as patients have a known dMMR or MSI-H tumour status, pembrolizumab would be appropriate to administer after any of the prior platinum-based chemotherapies received by patients in the trial. The majority of patients (n = 66; 73.3%) in the KN-158 trial had received 2 or fewer prior lines of systemic therapy before trial enrolment, and (n = 23; 25.6% of patients had received 3 or more lines of prior systemic therapy. One (1.1%) patient did not receive any prior systemic therapy, which was a violation of the protocol. This aligns with the results of the ORR subgroup analysis, whereby the ORR was higher in patients with 1 line of prior anticancer therapy versus patients who received 2 or more lines of prior anticancer therapy (52.6% versus 43.9%). However, the sample size was small in each subgroup and no statistical comparisons between subgroups were performed. This may limit the credibility of the findings, which may be considered to be exploratory. The clinical experts noted that experience from clinical practice suggests that pembrolizumab may have a lower magnitude of treatment benefit in patients having experienced more lines of systemic therapy; however, patients would be eligible to receive the pembrolizumab treatment if they had failed up to 3 prior lines of platinum-based chemotherapy.
External Validity
Overall, according to the clinical experts consulted by CADTH, the inclusion and exclusion criteria of study KN-158 were reasonable and the baseline patient characteristics, concomitant medications, and prohibited medications were reflective of patients they see in clinical practice for the indication under review. Of the 90 patients included, the majority were white (83.3%) and non-US patients (80%). The number of patients living in Canada included in the study was not reported. However, the clinical experts CADTH consulted for this review indicated that they did not expect any significant difference among varying races or geographic regions in terms of the response to PD-1 inhibitors such as pembrolizumab for endometrial carcinoma. There were no barriers to identifying patients who would most benefit from the treatment, given that testing for MMR and MSI status is standard practice in Canada.
Patients with CNS metastases, endometrial sarcomas, and/or an ECOG PS of greater than 1 were excluded from this study; therefore, there is uncertainty in whether the findings may be generalized to these populations. The clinical experts consulted by CADTH indicated that it may be reasonable to expect patients with CNS metastases controlled by radiation, patients with carcinosarcomas, and patients with ECOG PS of 0 or 1 could benefit from treatment with pembrolizumab.
No subgroup analysis was performed for OS, PFS, and DOR. And no subgroups based on ECOG PS status (i.e., ECOG PS of 0 or 1) or histology of tumour type (e.g., type I, type II or endometrioid, nonendometrioid) analysis were conducted for ORR. Therefore, there was a lack of clarity about which of these groups might benefit more or less from the treatment. Additional subgroups of interest, noted in the CADTH protocol, were not explored.
Symptoms associated with endometrial cancer (including pain, fatigue, anxiety, distress, and depression) can result in decreased HRQoL.19 Symptom reduction was identified as an important outcome to patients in the CADTH review protocol. Individual symptom severity was not assessed as a distinct outcome in the KN-158 study. These symptoms were assessed with EORTC QLQ-C30 functional and symptom scales and items.
Finally, the magnitude of the treatment effect estimates observed in a relatively small study sample (N = 79) may not be replicable in a larger study sample or generalizable to the target population in real-world clinical practice. However, the sponsor indicated that real-world evidence recently presented as a conference abstract demonstrated that the magnitude of the pembrolizumab effect was consistent with the results of study KN-158 in the treatment of patients with MSI-H or dMMR advanced endometrial cancer.55
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
No direct comparative data for the use of pembrolizumab as monotherapy in patients with MSI-H or dMMR advanced endometrial cancer were identified in the systematic review; thus, a search for indirect evidence was conducted.
A focused literature search for ITCs dealing with endometrial cancer was run in MEDLINE All (1946–) on January 20, 2022. No limits were applied to the search. The search results were screened by 1 researcher for ITCs that met the patient, intervention, comparator, and outcome criteria in the review protocol (Table 5). In addition, the ITC submitted by the sponsor was evaluated.47,56
No other relevant ITCs were found in the literature search; thus, this appraisal focuses on the sponsor-submitted ITC that was used to inform the pharmacoeconomic analysis.
Description of Indirect Comparisons
The sponsor submitted an unadjusted ITC that compared pembrolizumab monotherapy to doxorubicin or paclitaxel in patients with advanced MSI-H or dMMR endometrial cancer.
Methods of Sponsor-Submitted Indirect Treatment Comparison
Objectives
The objective of the sponsor-submitted ITC was to evaluate the efficacy of pembrolizumab monotherapy in patients with MSI-H or dMMR advanced endometrial carcinoma compared with patients who received standard care (doxorubicin or paclitaxel).
Study Selection Methods
The ITC was based on the endometrial cancer subgroup from study KN-158 (i.e., cohort D and cohort K from the uncontrolled open-label study described herein), compared with the dMMR subgroup of patients from the standard of care treatment group of study KN-775 (an open-label, phase III RCT). The report did not provide any rationale for the selected control group used in the ITC, nor for whether other studies or comparators may have been used to inform the ITC. There was no assessment of the risk of bias of the source studies.
Table 13 provides a description of the patients, interventions, and outcomes of each treatment group that was used to inform the analysis. Data for the KN-775 study were extracted from conference proceedings presented by Makker et al. (2021)57 at the International Gynecologic Cancer Society 2021 Annual Global Meeting. OS and PFS data were obtained from digitized Kaplan-Meier curves from this publication (the software used was not reported). From the ITC report, it appears that the analysts had access to individual patient data from study KN-158, but this is not explicitly stated.
Table 13: Description of Patients, Interventions, and Outcomes Included in Indirect Treatment Comparison
Characteristic | Pembrolizumab group (N = 79) | TPC group (N = 65) |
|---|---|---|
Population | MSI-H or dMMR advanced endometrial cancer and at least 1 prior therapy (cohort D and cohort K of study KN-158) | Advanced, metastatic, or recurrent dMMR endometrial cancer; 1 prior platinum-based therapy;a ECOG PS of 0 or 1 (subgroup of study KN-775) |
Intervention | Pembrolizumab 200 mg IV every 3 weeks (duration of treatment not reported) |
|
Outcomes | ||
Overall survival | Time from the date of the first dose to the date of death due to any cause Patients without event were censored on day of last contact, or study cut-off (October 5, 2020) | Time from the date of randomization to the date of death due to any cause. Patients who were lost to follow-up and those who were alive at the date of data cut-off (October 26, 2020) were censored at the date the patient was last known alive, or date of data cut-off, whichever occurred first. |
PFS | Time from the date of the first dose to the date of the first documentation of disease progression according to RECIST 1.1 (assessed by independent central radiologic review) or death due to any cause. Patients without event (death, progression, or new treatment) were censored on the day of last contact. Patients requiring new anticancer treatment were censored at the last assessment before the start of new therapy. | Time from the date of randomization to the date of the first documentation of disease progression, as determined by blinded independent central review of objective radiographic disease progression per RECIST 1.1 or death due to any cause (whichever occurred first) Of note: 3 different censoring rules were used in study KN-775. Although not explicitly stated in Makker et al. (2021),57 CADTH assumed the data reported were based on primary analysis in which patients without an event were censored at the day of last contact, or the date before starting new anticancer therapy. For patients with an event but who had missed 1 disease assessment, progression was based on the documented progression or death date. For patients who had missed 2 or more consecutive disease assessments or who had started new therapy, progression was based on the date of the last disease assessment before missed visits or starting new anticancer therapy. |
Analysis population | The all patients as-treated population for efficacy analysis (i.e., patients who had received at least 1 dose of pembrolizumab and had been enrolled at least 6 months before the data cut-off) | All patients randomized |
Follow-up duration | NR | NR |
dMMR = deficient mismatch repair ; ECOG PS = Eastern Cooperative Oncology Group Performance Status; KN-158 = KEYNOTE-158; KN-775 = KEYNOTE-775; MSI-H = microsatellite instability–high; NR = not reported; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; TPC = treatment of physician’s choice.
aMay have received up to 2 prior platinum-based chemotherapy regimens if 1 course was given in the neoadjuvant or adjuvant setting.
Sources: Sponsor submission,47 Makker et al. (2021),57 and Makker et al. (2022).58
Indirect Treatment Comparison Analysis Methods
Unanchored, unadjusted ITCs for the time to OS and PFS were calculated based on the treatment group data from the 2 source studies (study KN-158 and study KN-775). Survival curves for each treatment group were estimated using nonparametric Kaplan-Meier methods and were presented graphically. The HR for pembrolizumab versus standard care (paclitaxel or doxorubicin) was estimated using an unstratified Cox proportional hazards model, with treatment differences tested using the Wald test. Table 13 provides the outcome definition, censoring rules, and analysis population for the pembrolizumab group; limited data were available for study KN-775.
The authors of the ITC stated that statistical methods to account for differences between studies in the patient or study design characteristics was not possible due to the small samples size in each treatment group.
Results of Sponsor-Submitted Indirect Treatment Comparison
Summary of Included Studies
The ITC included data from 79 patients with MSI-H advanced endometrial cancer who received pembrolizumab and 65 patients with dMMR advanced endometrial cancer who received either doxorubicin (n = 50; 77%) or paclitaxel (n = 13; 20%) (2 patients received neither treatment) (Table 14). The authors of the ITC only presented baseline characteristics for which data were available in both studies being compared. The median age of patients was similar in both groups (patients receiving pembrolizumab = 64 years [range, 42 years to 86 years]; patients receiving chemotherapy = 63 years [range, 38 years to 85 years]). Differences were noted in other baseline characteristics such as the distribution of races, ECOG PS score, and number of prior therapies. Most patients who received pembrolizumab were white (86%), with relatively few patients who were Asian (5%), Black (4%), or other races (5%). In contrast, 54% of patients in the chemotherapy group were white, 19% of patients were Asian, 8% of patients were Black, and 20% of patients were other races. The majority of patients who received pembrolizumab had an ECOG PS score of 1 (61%), compared with 48% of patients in the chemotherapy group (the remaining patients had an ECOG PS score of 0). The proportion of patients in the pembrolizumab and chemotherapy groups who had 1 prior line of therapy was 48% versus 78%, or who had 2 or more lines of therapy was 52% versus 22%, respectively.
Table 14: Baseline Characteristics of Patients Included in Indirect Treatment Comparison
Characteristic | Pembrolizumab group (N = 79) | TPC group (paclitaxel or doxorubicin) (N = 65) |
|---|---|---|
Median age, years (range) | 64 (42 to 86) | 63 (38 to 85) |
Race group, n (%) | ||
Asian | 4 (5) | 12 (19) |
Black | 3 (4) | 5 (8) |
White | 68 (86) | 35 (54) |
Other | 4 (5) | 13 (20) |
ECOG PS, n (%) | ||
0 | 31 (39) | 34 (52) |
1 | 48 (61) | 31 (48) |
Number of prior lines of therapy, n (%) | ||
1 | 38 (48) | 51 (78) |
2 or more | 41 (52) | 14 (22) |
Number of patients (%) who received prior neoadjuvant or adjuvant treatment | 23 (29) | 32 (49) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; TPC = treatment of physician’s choice.
Source: Sponsor submission.47
There was no information on the analysis population or methods used to estimate OS or PFS in the chemotherapy group. No information on follow-up duration was reported for either study. According to the Clinical Study Reports for study KN-158 and study KN-775, the median follow-up duration was longer for the pembrolizumab group versus the chemotherapy group (pembrolizumab group = 16.5 months [range, 0.5 months to 56.1 months]; chemotherapy group = 8.8 months [range, 1.0 months to 23.8 months]) based on the as-treated efficacy population in study KN-158 (N = 79) and the ITT population for the dMMR subgroup of study KN-775 (N = 65).21,59
Results
Among patients who received pembrolizumab, 29 (36.7%) patients died, compared with 42 (64.6%) patients who received chemotherapy. Based on the unadjusted ITC, the HR for the time to OS was 0.34 (95% CI, 0.20 to 0.56; P < 0.001) for pembrolizumab versus chemotherapy (Table 15).
For the analysis of time to PFS, 45 (57.0%) patients versus 48 (73.8%) patients progressed or died in the pembrolizumab versus chemotherapy groups, with an estimated HR of 0.42 (95% CI, 0.27 to 0.64, P < 0.001).
The Kaplan-Meier curves for OS and PFS are shown in Figure 6 and Figure 7.
Table 15: Summary of Indirect Treatment Comparison Results
Outcome | Pembrolizumab group (N = 79) | TPC group (paclitaxel or doxorubicin) (N = 65) | Pembrolizumab vs. TPC | |||
|---|---|---|---|---|---|---|
Patients with event, n (%) | Median time, months (95% CI)a | Patients with event, n (%) | Median time, months (95% CI)a | HR (95% CI)b | P valuec | |
OS | 29 (36.7) | Not reached (27.2 to NE) | 42 (64.6) | 8.6 (5.5 to 12.9) | 0.34 (0.20 to 0.56) | < 0.001 |
PFS | 45 (57.0) | 13.1 (4.3 to 34.4) | 48 (73.8) | 3.7 (3.1 to 4.4) | 0.42 (0.27 to 0.64) | < 0.001 |
CI = confidence interval; HR = hazard ratio; NE = not estimable; OS = overall survival; PFS = progression-free survival; TPC = treatment of physician’s choice; vs. = versus.
aBased on Kaplan-Meier method for censored data.
bUnstratified Cox proportional hazards model.
cTwo-sided P value using Wald test.
Source: Sponsor submission.47
Critical Appraisal of Sponsor-Submitted Indirect Treatment Comparison
The sponsor-submitted ITC compared the efficacy of pembrolizumab versus chemotherapy, based on subgroup data from 2 open-label clinical trials (study KN-158 and study KN-775). The authors provided no justification for selecting the chemotherapy group of study KN-775 as the control group, and it is unclear if there were other potentially relevant clinical trials that may have also been used to inform the ITC. The sponsor submitted a feasibility assessment, which included a literature review; however, there was no discussion if any of the 30 trials identified were considered as relevant comparators in the ITC for pembrolizumab monotherapy. Moreover, there was no assessment of the risk of bias in the 2 source studies, which were both open-label studies. In response to these critical appraisal points, the sponsor stated that they were unaware of any other RCTs reporting the efficacy of chemotherapy in patients with advanced and recurrent MSI-H or dMMR endometrial cancer who progressed on previous chemotherapy.
Figure 6: Kaplan-Meier Curve of Overall Survival From ITC Analysis
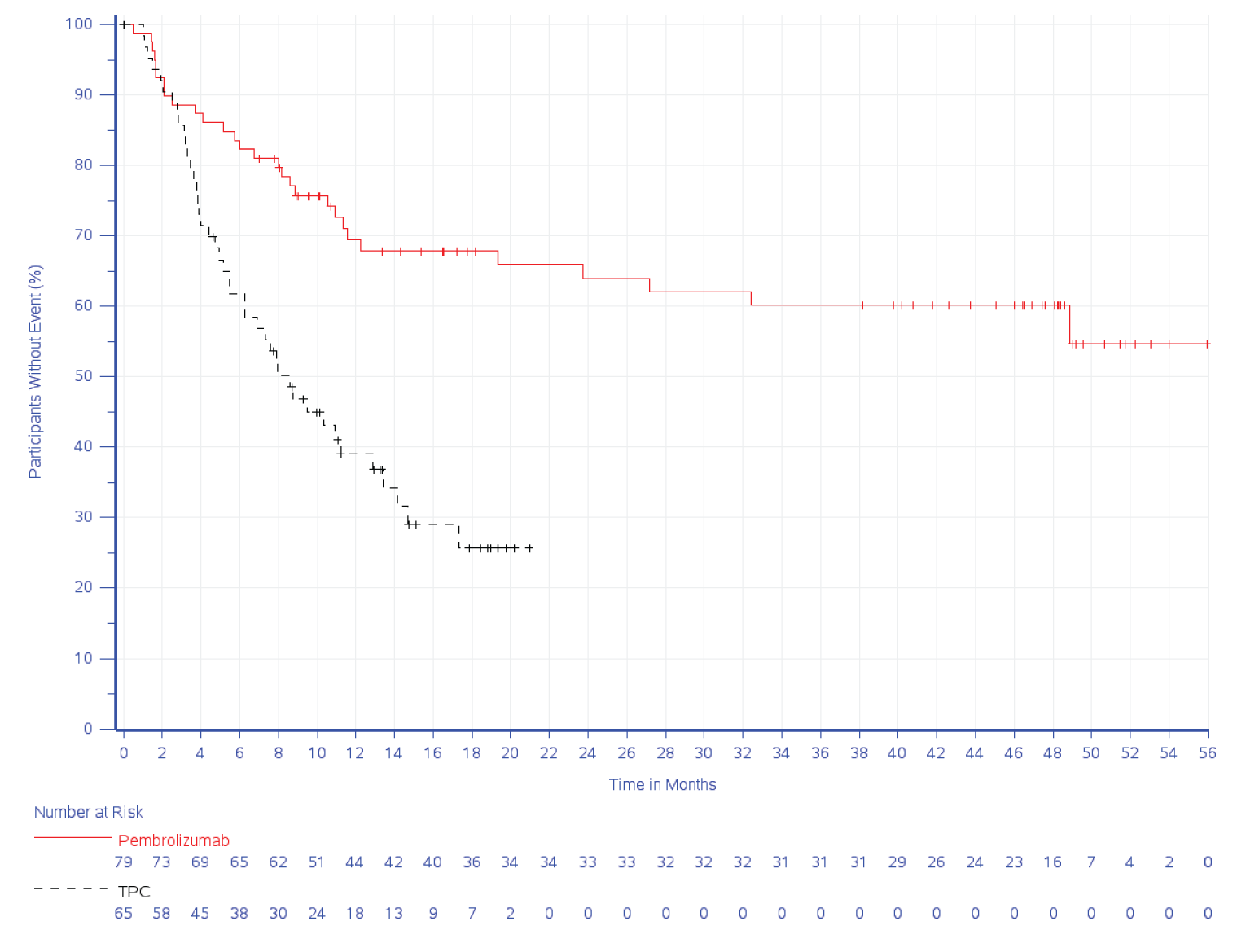
ITC = indirect treatment comparison; TPC = treatment of physician’s choice.
Source: Sponsor submission.47
Data for study KN-775 were extracted from a conference proceeding, which was missing key information, such as the analysis population, length of follow-up, outcomes definitions, analysis methods, and censoring rules. The sponsor has stated that some of the missing information on the analysis methods was available from the published study report by Makker et al. (2022).58 In addition, limited patient characteristic data were provided for both studies. Due to the lack of information, it was difficult to assess if the study and patient characteristics were comparable between studies. In this ITC, differences were observed between groups at baseline in the racial distribution, ECOG PS, and prior therapies, which may be prognostic or effect modifying factors. Thus, the limited data available suggests these patients may not be comparable at the start of follow-up. Information on other potentially important characteristics identified in the CADTH protocol, like FIGO stage and tumour histology, were not reported; therefore, it is not possible to know if the groups were comparable on these characteristics.
Figure 7: Kaplan-Meier Curve of Progression-Free Survival From ITC Analysis
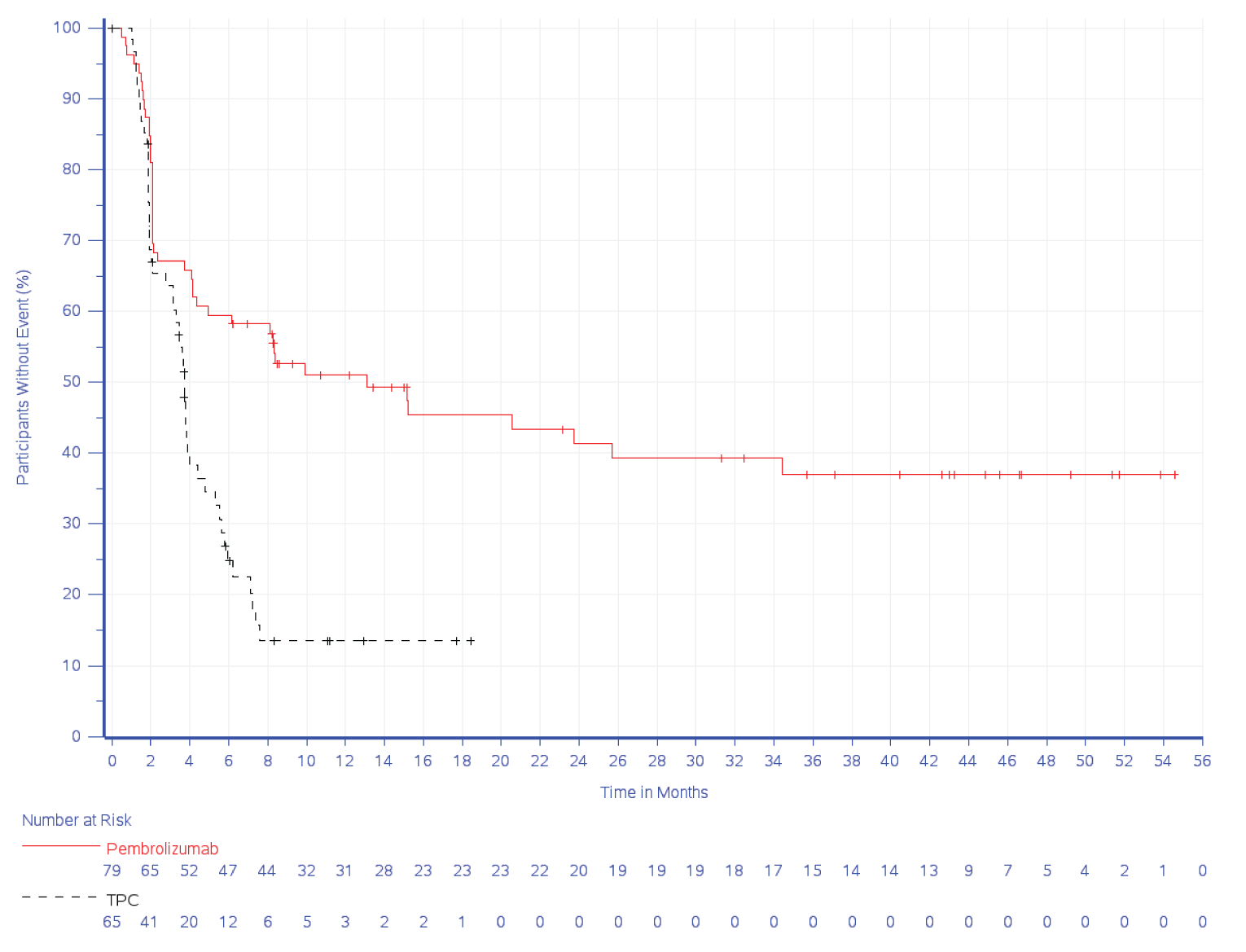
ITC = indirect treatment comparison; TPC = treatment of physician’s choice.
Source: Sponsor submission.47
Regarding the methods used to conduct the ITC, the authors provided no justification for the approach taken. The data from the 2 different clinical trials were analyzed as if they had been obtained from 1 study, without any statistical adjustment to control for between-study differences in patient or study characteristics. The investigators stated that due to the small sample size, it was not possible to use methods to attempt to control for imbalances between treatment groups. While it may not have been feasible to conduct an adjusted analysis, a more comprehensive evaluation of potential sources of heterogeneity was warranted to justify the analysis methods used. In order for an unadjusted ITC to show valid estimates, all known and unknown prognostic factors and effect modifiers must be distributed equally between the 2 groups. This assumption is largely considered impossible to meet (and differences between the 2 study groups were observed), and the failure of this assumption leads to an unknown amount of bias in the unanchored estimate. Additionally, differences in study design between the 2 data sources cannot be adjusted for within the indirect comparison.
Due to the limitations of the unadjusted ITC, which is at risk of an unknown amount and direction of bias, the findings were highly uncertain and, thus, no conclusions can be drawn on the comparative efficacy of pembrolizumab compared to chemotherapy (paclitaxel or doxorubicin) in patients with MSI-H or dMMR advanced endometrial cancer. The ITC did not assess any harms data; thus, the comparative safety of pembrolizumab is unknown. Other outcomes of importance to patients, such as HRQoL, were also not investigated.
Summary
The sponsor submitted an unadjusted (naive) ITC that compared the efficacy of pembrolizumab with doxorubicin or paclitaxel in patients with advanced MSI-H or dMMR endometrial cancer. This analysis estimated the relative time to OS or PFS based on individual treatment group data from 2 separate studies using nonparametric Kaplan-Meier methods and unstratified Cox proportional hazards models. For pembrolizumab versus chemotherapy, the HR for time to OS was 0.34 (95% CI, 0.20 to 0.56; P < 0.001) and the HR for PFS was 0.42 (95% CI, 0.27 to 0.64; P < 0.001).
Limitations of the ITC included the lack of justification for the selection of the chemotherapy group of KN-775 as the comparator group, and for the analytical methods used. The exploration of between-study differences and potential biases was further limited by missing information on patient and study characteristics for the 2 data sources. Considering that prognostic factors and effect modifiers are likely imbalanced between treatment groups, the results of the unanchored, unadjusted ITC is subject to an unknown amount and direction of bias. Thus, the findings of the ITC are highly uncertain and may be rated as very low quality.
Other Relevant Evidence
No other relevant study was identified in this review.
Discussion
Summary of Available Evidence
The CADTH clinical review report included inputs from patient groups, clinician groups, clinical experts, and drug programs. The evidence included 1 pivotal single-arm, phase II, open-label, nonrandomized trial (KN-158) and a sponsor-submitted unadjusted (naive) ITC that compared the efficacy of pembrolizumab with doxorubicin or paclitaxel in patients with advanced MSI-H or dMMR endometrial cancer. No other relevant studies were identified.
This CADTH review focused on cohort D and cohort K of study KN-158, which aligned with the Health Canada indication and the sponsor’s reimbursement request. KN-158 (cohort D and cohort K) is a single-arm, open-label, nonrandomized, multicentre phase II trial to assess pembrolizumab monotherapy for the treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options. The study is ongoing, and the results herein are from an interim analysis based on the October 5, 2020, data cut-off. A total of 90 patients were included in the trial. Patients included were aged 18 years or older with incurable dMMR or MSI-H advanced endometrial carcinoma and had failed prior standard first-line treatments.
The primary outcome of the study was ORR per RECIST 1.1; secondary outcomes included DOR, OS, and PFS. HRQoL was an exploratory outcome mentioned in the sponsor’s research protocol, but the findings of HRQoL were not reported in the KN-158 Clinical Study Report. Instead, these were presented briefly in a conference abstract. The main limitations of the pivotal study were its single-arm design, its lack of consideration of confounding variables, and the absence of statistical hypothesis testing.
In the absence of comparative evidence, the sponsor submitted an unadjusted (naive) ITC that compared the efficacy of pembrolizumab with doxorubicin or paclitaxel in patients with advanced MSI-H or dMMR endometrial cancer. This analysis estimated the OS or PFS based on individual treatment group data from 2 separate studies using nonparametric Kaplan-Meier methods and unadjusted Cox proportional hazards models. The lack of adjustment for key prognostic factors and effect modifiers in this analysis violates the assumptions of the indirect comparison and introduces an unknown amount and direction of bias.
Interpretation of Results
Efficacy
The interpretation of time-to-event outcomes is limited in a single-arm trial, as without a comparison group and no consideration of confounding variables, the observed efficacy results could be potentially confounded. As noted in the FDA guidance for industry,60 because of variability in the natural history of many forms of cancer, a randomized trial is required to further evaluate time-to-event end points, such as OS or PFS. The median OS was not reached at the time of data cut-off, and the survival data from the trial were immature. While Kaplan-Meier estimates were provided at different time points, these data may potentially overestimate the efficacy of the treatment, given the immaturity of the data. Similar limitations also apply to the interpretation of PFS. In addition, there was no formal hypothesis testing done in the KN-158 trial. Given that the trial was not designed to detect differences in treatment effects across subgroups, no conclusions should be made on the basis of prespecified subgroup results. Therefore, the findings of the OS and PFS reported in study KN-158 should be interpreted while also considering the limitations discussed previously. However, the clinical experts indicated that the efficacy findings (OS, PFS, ORR, and DOR) in the KN-158 trial appeared favourable compared with what they have observed with other currently available chemotherapies (e.g., doxorubicin, paclitaxel) in this population.
Stakeholder input from the patient advocacy groups, clinician groups, and the clinical experts consulted by CADTH highlighted HRQoL as an important outcome and treatment goal for patients. Although they were designated as patient-reported outcomes in the sponsor’s protocol, the HRQoL outcomes were not reported in the KN-158 Clinical Study Report. Rather, they were presented in a conference abstract. Change from baseline to 9 weeks was not tested statistically; thus, no conclusions could be drawn, but it is notable that estimates at each time point appeared to be affected by wide variation. Nevertheless, the clinical experts consulted by CADTH expressed that they would not expect to see a substantial HRQoL improvement in patients with advanced or recurrent endometrial carcinoma treated with pembrolizumab. Rather, at most, the pembrolizumab treatment may slow down the deterioration of HRQoL (although this was not demonstrated in the pivotal study).
The clinical experts indicated that ORR is an important outcome in this patient population. In the experience of the clinical experts, the improved ORR (based on radiographic evaluation) is usually correlated with improvement of other clinical outcomes, such as PFS, OS, or slower decline in ECOG PS, delay in clinical symptoms, and worsening of HRQoL deterioration, although they are not always absolutely proportionally correlated. None of these potential effects could be substantiated from the trial data.
According to the clinical experts consulted by CADTH, patients recruited in the KN-158 trial were considered representative of patients in Canadian clinical practice. There were no major concerns of generalizability of the findings to Canadian practice. The clinical experts anticipated that because of its mechanism of action and acceptable safety profile, they would expect to see a benefit of treatment with pembrolizumab for all patients with dMMR or MSI-H endometrial cancer, regardless of the number of previous lines of systemic therapy.
The sponsor submitted an unanchored and unadjusted ITC, in which findings are highly uncertain and may be rated as very low quality. No conclusion could be drawn on the comparative efficacy comparing pembrolizumab with chemotherapy (i.e., doxorubicin and paclitaxel) based on the sponsor’s submitted ITC.
Harms
The safety profile of pembrolizumab has been well established in previous clinical trials in the treatment of various cancers, including endometrial cancer.21 In study KN-158, a total of 86 (95.6%) patients experienced at least 1 TEAE and 47 (52.2%) of these were grade 3 or higher TEAEs. The treatment discontinuation rate due to TEAEs was relatively low (6.7%) and no deaths occurred due to TEAEs. The frequency of any grade of TEAEs, SAEs, and notable AEs reported in this trial appeared similar to the known safety profile of pembrolizumab. No additional safety signals were identified with pembrolizumab monotherapy in the treatment of adult patients with unresectable or metastatic dMMR or MSI-H endometrial cancer whose tumours had progressed following prior therapy and who had no satisfactory alternative treatment options. The clinical experts consulted by CADTH agreed that the pembrolizumab safety profile observed in this study seemed generally manageable and consistent with the known safety profile of pembrolizumab.
There was no direct evidence from an RCT, nor any indirect evidence identified in this review to inform conclusions about the safety of pembrolizumab compared to alternative treatment options. The clinical experts consulted by CADTH indicated that the overall safety profile seemed favourable compared with currently available chemotherapy options (i.e., doxorubicin and paclitaxel) observed in clinical practice.
Conclusions
One sponsor-submitted pivotal single-arm, open-label, multicentre, phase II trial (cohort D and cohort K in the KN-158 study)21 provided evidence regarding the efficacy and safety of pembrolizumab in the treatment of adult patients with dMMR or MSI-H recurrent or advanced endometrial carcinoma that had progressed on or following prior systemic treatments. There was uncertainty around the magnitude of the clinical benefit attributable to pembrolizumab given the limitations inherent to the single-arm trial design and the lack of formal hypothesis testing. The sponsor also submitted a naive ITC comparing pembrolizumab with doxorubicin or paclitaxel. However, no robust conclusion could be drawn on the comparative efficacy and safety of pembrolizumab versus chemotherapy (i.e., doxorubicin and paclitaxel) due to several methodological limitations. While a well-designed RCT would be ideal and preferred to confirm the comparative clinical benefit of pembrolizumab over chemotherapy, the clinical experts consulted by CADTH indicated that the efficacy outcomes observed in the KN-158 trial (OS, PFS, ORR, and DOR) appeared favourable compared with that observed with chemotherapy in clinical practice (e.g., doxorubicin and paclitaxel) and are potentially clinically meaningful for this patient population The safety profile of pembrolizumab observed in this study appeared consistent with the known safety profile of pembrolizumab, and no additional safety signals were identified.
References
1.Steven C Plaxe, Arno J Mundt, . Overview of endometrial carcinoma. In: Barbara Goff M, Don S Dizon M, Deputy Editors:Sadhna R Vora M, Alana Chakrabarti, MD, eds2021: .
2.Uterine cancer: risk factors and prevention. In: Alexandria (VA): American Society of Clinical Oncology; 2020: https://www.cancer.net/cancer-types/uterine-cancer/risk-factors-and-prevention. Accessed 2022 Feb 28.
3.Cancerous tumours of the uterus. In: Toronto (ON): Canadian Cancer Society; 2021: https://cancer.ca/en/cancer-information/cancer-types/uterine/what-is-uterine-cancer/cancerous-tumours. Accessed 2022 Feb 28.
4.Ott PA, Bang YJ, Berton-Rigaud D, et al. Safety and antitumor activity of pembrolizumab in advanced programmed death ligand 1-positive endometrial cancer: results from the KEYNOTE-028 study. Obstet Gynecol Surv. 2018;73(1):26-27.
5.Endometrial cancer: detection, diagnosis, staging, survival rates. In: Atlanta (GA): American Cancer Society; 2021: https://www.cancer.org/cancer/endometrial-cancer/detection-diagnosis-staging/survival-rates.html1. Accessed 2022 Feb 28.
6.Plaxe SC, Mundt AJ. Overview of endometrial carcinoma. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022 Feb 28: https://www.uptodate.com. Accessed 2022 Feb 28.
7.Fung-Kee-Fung M, Dodge J, Elit L, et al. Follow-up after primary therapy for endometrial cancer: a systematic review. Gynecol Oncol. 2006;101(3):520-529. PubMed
8.Kurnit KC, Westin SN, Coleman RL. Microsatellite instability in endometrial cancer: new purpose for an old test. Cancer. 2019;125(13):2154-2163. PubMed
9.PrKeytruda® (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial [draft product monograph]. In: Kirckland (QC): Merck Canada; 2021 Jun 2.
10.O'Malley DM, Bariani GM, Cassier PA, et al. Pembrolizumab in patients with microsatellite instability-high advanced endometrial cancer: results from the KEYNOTE-158 study. J Clin Oncol. 2022;40(7):752-761. PubMed
11.Lorusso D, Colombo N, Casado Herraez A, et al. Health-related quality of life in advanced endometrial cancer patients treated with lenvatinib + pembrolizumab or treatment of physician’s choice [poster]. Presented at the American Society of Clinical Oncology Annual Meeting; Jun 4-8, 2021; Virtual format. In.
12.Endometrial cancer. In: (Clinical practice guideline GYNE-002. Version 5). Edmonton (AB): Alberta Health Services; 2015: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gyne002-endometrial.pdf. Accessed 2022 Feb 28.
13.Genital tract cancers in females: endometrial cancer. In: BC guidelines. Victoria (BC): Province of British Columbia; 2014: https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/endometrial-cancer. Accessed 2022 Feb 28.
14.Treatment option overview for endometrial cancer. In: Bethesda (MD): National Cancer Institute; 2021: https://www.cancer.gov/types/uterine/hp/endometrial-treatment-pdq#_36. Accessed 2022 Mar 2.
15.Systemic therapy for advanced or recurrent endometrial cancer and advanced or recurrent uterine papillary serous carcinoma. In: Toronto (ON): Cancer Care Ontario; 2019: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/501. Accessed 2022 Feb 28.
16.Concin N, Matias-Guiu X, Vergote I, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12-39. PubMed
17.Campos SM, Cohn DE. Treatment of metastatic endometrial cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021 Nov 8: https://www.uptodate.com. Accessed 2022 Feb 28.
18.Kelkar S, Prabhu V, Corman S, et al. Treatment patterns and real-world clinical outcomes in patients with advanced endometrial cancer who 2 are microsatellite instability (MSI)-high or are mismatch repair deficient (dMMR) in the United States Draft manuscript. 2022.
19.O'Malley D, Bariani GM, Cassier PA, et al. Health-related quality of life with pembrolizumab monotherapy in patients with previously treated advanced microsatellite instability high (MSI-H)/mismatch repair deficient (dMMR) endometrial cancer: results from KEYNOTE-158 [poster]. Presented at the European Society for Medical Oncology (ESMO) Congress 2021; Sep 16‒21, 2021; Virtual Meeting. In.
20.Merck Sharp & Dohme Corp. NCT02628067: Study of pembrolizumab (MK-3475) in participants with advanced solid tumors (MK-3475-158/KEYNOTE-158). In: ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2015 Dec 11: https://clinicaltrials.gov/ct2/show/NCT02628067. Accessed 2022 Feb 22.
21.Clinical Study Report: P158V10MK3475. A clinical trial of pembrolizumab (MK-3475) evaluating predictive biomarkers in subjects with advanced solid tumors (KEYNOTE-158) [internal sponsor's report]. In: Kenilworth (NJ): Merck Sharp & Dohme; 2021.
22.Cancer-specific stats 2021. In: Toronto (ON): Canadian Cancer Society; 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021_cancer-specific-stats.pdf?rev=bbadfd869b66415e97be9655a842858c&hash=3E552CE702E1BD7657E4E91FB7BA624B&_ga=2.72656595.1540445839.1639772303-397212376.1636582496. Accessed 2022 Feb 28.
23.Uterine cancer statistics. In: Toronto (ON): Canadian Cancer Society; 2021: https://cancer.ca/en/cancer-information/cancer-types/uterine/statistics. Accessed 2022 Feb 28.
24.Endometrial cancer stages. In: Atlanta (GA): American Cancer Society; 2019: https://www.cancer.org/cancer/endometrial-cancer/detection-diagnosis-staging/staging.html. Accessed 2022 Feb 28.
25.Stages of uterine cancer. In: Toronto (ON): Canadian Cancer Society; 2021: https://cancer.ca/en/cancer-information/cancer-types/uterine/staging. Accessed 2022 Feb 28.
26.Boland CR, Thibodeau SN, Hamilton SR, et al. A National Cancer Institute Workshop on Microsatellite Instability for cancer detection and familial predisposition: development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res. 1998 Nov 15;59(22). PubMed
27.McEachron J, Zhou N, Spencer C, et al. Adjuvant chemoradiation associated with improved outcomes in patients with microsatellite instability-high advanced endometrial carcinoma. Int J Gynecol Cancer. 2021;31(2):203-208. PubMed
28.Pakish JB, Zhang Q, Chen Z, et al. Immune microenvironment in microsatellite-instable endometrial cancers: hereditary or sporadic origin matters. Clin Cancer Res. 2017;23(15):4473-4481. PubMed
29.Meyer LA, Broaddus RR, Lu KH. Endometrial cancer and Lynch syndrome: clinical and pathologic considerations. Cancer Control. 2009;16(1):14-22. PubMed
30.Marabelle A, Le DT, Ascierto PA, et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair-deficient cancer: results from the phase II KEYNOTE-158 study. J Clin Oncol. 2020;38(1):1-10. PubMed
31.Howitt BE, Shukla SA, Sholl LM, et al. Association of polymerase e-mutated and microsatellite-instable endometrial cancers with neoantigen load, number of tumor-infiltrating lymphocytes, and expression of PD-1 and PD-L1. JAMA Oncol. 2015;1(9):1319-1323. PubMed
32.Green AK, Feinberg J, Makker V. A review of immune checkpoint blockade therapy in endometrial cancer. Am Soc Clin Oncol Educ Book. 2020;40:1-7. PubMed
33.Lorenzi M, Amonkar M, Zhang J, Mehta S, Liaw K-L. Epidemiology of microsatellite instability high (MSI-H) and deficient mismatch repair (dMMR) in solid tumors: a structured literature review. J Oncol. 2020:1807929.
34.Zhao P, Li L, Jiang X, Li Q. Mismatch repair deficiency/microsatellite instability-high as a predictor for anti-PD-1/PD-L1 immunotherapy efficacy. J Hematol Oncol. 2019;12(1):54. PubMed
35.Ryan NAJ, Glaire MA, Blake D, Cabrera-Dandy M, Evans DG, Crosbie EJ. The proportion of endometrial cancers associated with Lynch syndrome: a systematic review of the literature and meta-analysis. Genet Med. 2019;21(10):2167-2180. PubMed
36.Bonneville R, Krook MA, Kautto EA, et al. Landscape of microsatellite instability across 39 cancer types. JCO Precis Oncol. 2017;2017.
37.Sorbe B, Juresta C, Ahlin C. Natural history of recurrences in endometrial carcinoma. Oncol Lett. 2014;8(4):1800-1806. PubMed
38.Sovak MA, Dupont J, Hensley ML, et al. Paclitaxel and carboplatin in the treatment of advanced or recurrent endometrial cancer: a large retrospective study. Int J Gynecol Cancer. 2007;17(1):197-203. PubMed
39.Sorbe B, Andersson H, Boman K, Rosenberg P, Kalling M. Treatment of primary advanced and recurrent endometrial carcinoma with a combination of carboplatin and paclitaxel-long-term follow-up. Int J Gynecol Cancer. 2008;18(4):803-808. PubMed
40.Makker V, Hensley ML, Zhou Q, Iasonos A, Aghajanian CA. Treatment of advanced or recurrent endometrial carcinoma with doxorubicin in patients progressing after paclitaxel/carboplatin: Memorial Sloan-Kettering Cancer Center experience from 1995 to 2009. Int J Gynecol Cancer. 2013;23(5):929-934. PubMed
41.Miller DS, Filiaci VL, Mannel RS, et al. Carboplatin and paclitaxel for advanced endometrial cancer: final overall survival and adverse event analysis of a phase III trial (NRG Oncology/GOG0209). J Clin Oncol. 2020;38(33):3841-3850. PubMed
42.Brooks RA, Fleming GF, Lastra RR, et al. Current recommendations and recent progress in endometrial cancer. CA Cancer J Clin. 2019;69(4):258-279. PubMed
43.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
44.Grey matters: a practical tool for searching health-related grey literature. In: Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Jan 22.
45.Marabelle A, Le DT, Ascierto PA, et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/ mismatch repair-deficient cancer: results from the phase II KEYNOTE-158 study. J Clin Oncol. 2020;38(1):1-10. PubMed
46.O'Malley DO, Marabelle A, De Jesus-Acosta A, et al. Pembrolizumab in patients with MSI-H advanced endometrial cancer from the KEYNOTE-158 study [abstract]. Ann Oncol. 2019;30(Suppl 5):v425-v426.
47.Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial with levantinib [internal sponsor's package]. In: Kirkland (QC): Merck Canada; 2022 Mar 4.
48.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
49.Davda J, Kibet H, Achieng E, Atundo L, Komen T. Assessing the acceptability, reliability, and validity of the EORTC Quality of Life Questionnaire (QLQ-C30) in Kenyan cancer patients: a cross-sectional study. J Patient Rep Outcomes. 2021;5(1):4. PubMed
50.EORTC quality of life. https://qol.eortc.org/. Accessed 2022 Mar 9.
51.EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
52.Ameri H, Yousefi M, Yaseri M, Nahvijou A, Arab M, Akbari Sari A. Mapping the cancer-specific QLQ-C30 onto the generic EQ-5D-5L and SF-6D in colorectal cancer patients. Expert Rev Pharmacoecon Outcomes Res. 2019;19(1):89-96. PubMed
53.Sinnott PL, Joyce VR, Barnett PG. Preference measurement in economic analysis. Guidebook. In: Menlo Park (CA): Health Economics Research Center; 2007: https://www.herc.research.va.gov/files/BOOK_419.pdf. Accessed 2022 Mar 3.
54.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
55.Kelkar S, Corman S, Macahling C, et al. Treatment patterns, real-world outcomes, and resource use in patients with microsatellite-instability high or deficient mismatch repair advanced endometroial cancer [abstract]. Int J Gynecol Cancer. 2021;31(Suppl 3):A121.
56.Keytruda (MK-3475) MSI-H endometrial carcinoma Indirect Treatment Comparison KN158 vs. KN775 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada; 2022 Jan 6. In.
57.Makker V, Colombo N, Casado Herraez A, et al. Randomized phase 3 study of lenvatinib plus pembrolizumab for advanced endometrial cancer: subgroup analysis of patients with DNA mismatch repair-deficient tumors [abstract]. Int J Gynecol Cancer. 2021;31(Suppl 4):A1-A2.
58.Makker V, Colombo N, Casado Herráez A, et al. Lenvatinib plus pembrolizumab for advanced endometrial cancer. N Engl J Med. 2022;386(5):437-448. PubMed
59.Clinical Study Report: P775V01MK3475. A multicenter, open-label, randomized, phase 3 trial to compare the efficacy and safety of lenvatinib in combination with pembrolizumab versus treatment of physician’s choice in participants with advanced endometrial cancer [internal sponsor's report]. In: Woodcliff Lake (NJ): Eisai; 2021.
60.Clinical trial endpoints for the approval of cancer drugs and biologics: guidance for industry. In: Silver Spring (MD): U.S. Food and Drug Administration; 2018: https://www.fda.gov/downloads/Drugs/Guidances/ucm071590.pdf. Accessed 2022 Mar 7.
61.Bellone S, Roque DM, Siegel ER, et al. A phase 2 evaluation of pembrolizumab for recurrent Lynch-like versus sporadic endometrial cancers with microsatellite instability. Cancer. 2021;128(6):1206-1218. PubMed
62.Ott PA, Bang YJ, Berton-Rigaud D, et al. Safety and antitumor activity of pembrolizumab in advanced programmed death ligand 1-positive endometrial cancer: results from the KEYNOTE-028 study. J Clin Oncol. 2017;35(22):2535-2541. PubMed
63.Keytruda (MK-3475), MSI-H Endometrial Carcinoma, Indirect Treatment Comparisons KN158 vs. KN775 [internal sponsor's report]. In: Kirkland (QC): Merck Canada; 2022 Jul.
64.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for Population-Adjusted Indirect Comparisons in Health Technology Appraisal. Med Decis Making. 2018;38(2):200-211. PubMed
65.Phillippo DM AA, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submissions to NICE. Vol 18. Decision Support Unit, ScHARR, University of Sheffield: NICE Decision Support Unit; 2016.
66.Guyot P, Ades AE, Ouwens MJNM, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9. PubMed
67.15. Makker V, Taylor MH, Aghajanian C, et al. Lenvatinib Plus Pembrolizumab in Patients With Advanced Endometrial Cancer. J Clin Oncol. 2020;38(26):2981-2992.
68.Osoba D, Zee B, Pater J, Warr D, Kaizer L, Latreille J. Psychometric properties and responsiveness of the EORTC quality of Life Questionnaire (QLQ-C30) in patients with breast, ovarian and lung cancer. Qual Life Res. 1994;3(5):353-364. PubMed
69.Zhao H, Kanda K. Translation and validation of the standard Chinese version of the EORTC QLQ-C30. Qual Life Res. 2000;9(2):129-137. PubMed
70.Butler L, Bacon M, Carey M, Zee B, Tu D, Bezjak A. Determining the relationship between toxicity and quality of life in an ovarian cancer chemotherapy clinical trial. J Clin Oncol. 2004;22(12):2461-2468. PubMed
71.Bedard G, Zeng L, Zhang L, et al. Minimal important differences in the EORTC QLQ-C30 in patients with advanced cancer. Asia Pac J Clin Oncol. 2014;10(2):109-117. PubMed
72.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
73.Lang HC, Chuang L, Shun SC, Hsieh CL, Lan CF. Validation of EQ-5D in patients with cervical cancer in Taiwan. Support Care Cancer. 2010;18(10):1279-1286. PubMed
74.Kim SH, Jo MW, Lee JW, Lee HJ, Kim JK. Validity and reliability of EQ-5D-3L for breast cancer patients in Korea. Health Qual Life Outcomes. 2015;13:203. PubMed
75.Zeng X, Sui M, Liu B, et al. Measurement properties of the EQ-5D-5L and EQ-5D-3L in six commonly diagnosed cancers. Patient. 2021;14(2):209-222. PubMed
76.Doherty MK, Leung Y, Su J, et al. Health utility scores from EQ-5D and health-related quality of life in patients with esophageal cancer: a real-world cross-sectional study. Dis Esophagus. 2018;31(12). PubMed
77.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
78.Bjordal K, de Graeff A, Fayers PM, et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer. 2000;36(14):1796-1807. PubMed
79.Bergman B, Sullivan M, Sörenson S. Quality of life during chemotherapy for small cell lung cancer. II. A longitudinal study of the EORTC Core Quality of Life Questionnaire and comparison with the Sickness Impact Profile. Acta Oncol. 1992;31(1):19-28. PubMed
80.Bjordal K, Kaasa S. Psychometric validation of the EORTC Core Quality of Life Questionnaire, 30-item version and a diagnosis-specific module for head and neck cancer patients. Acta Oncol. 1992;31(3):311-321. PubMed
81.Greimel E, Nordin A, Lanceley A, et al. Psychometric validation of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Endometrial Cancer Module (EORTC QLQ-EN24). Eur J Cancer. 2011;47(2):183-190. PubMed
82.Gallardo-Rincon D, Toledo-Leyva A, Bahena-Gonzalez A, et al. Validation of the QLQ-EN24 instrument for the assessment of health-related quality of life for women with endometrial cancer in Mexico. Arch Gynecol Obstet. 2021;304(3):773-782. PubMed
83.Descriptive Summaries Based on Participants Treated with Pembrolizumab Database Cutoff Date 12-Jan-2022 Version 0.1.
84.Completed 7 tables with the updated data (cut-off on Jan 12, 2022) [internal additional sponsor's information]. In: Kirkland (QC): Merck Canada.
85.Pembrolizumab for microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) advanced endometrial cancer: long-term follow-up results from KEYNOTE-158. [internal additional sponsor's information]. In: Kirkland (QC): Merck Canada.
86.Merck Canada response to June 27, 2022 request for additional information for RfR updated clinical study report: A Clinical Trial of Pembrolizumab (MK-3475) Evaluating Predictive Biomarkers in Subjects with Advanced Solid Tumors (KEYNOTE-158) received on July 11, 2022 and July 25, 2022. [internal additional sponsor's information].
Appendix 1: Literature Search Strategy
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: January 21, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit retrieval by study type.
Limits: Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(pembrolizumab* or Keytruda* or SCH-900475 or SCH900475 or MK-3475 or MK3475 or lambrolizumab* or HSDB8257 or HSDB 8257 or Merck 3475 or DPT0O3T46P).ti,ab,ot,kf,hw,nm,rn.
exp Endometrial neoplasms/
((endometri* or uterus or uterine) adj3 (cancer* or carcinoma* or neoplas* or sarcoma* or tumo?r* or adenocarcinoma* or carcinosarcoma*)).ti,ab,kf.
1 and (2 or 3)
4 use medall
*pembrolizumab/
(pembrolizumab* or Keytruda* or SCH-900475 or SCH900475 or MK-3475 or MK3475 or lambrolizumab* or HSDB8257 or HSDB 8257 or Merck 3475).ti,ab,kf,dq.
6 or 7
exp Endometrium tumor/
((endometri* or uterus or uterine) adj3 (cancer* or carcinoma* or neoplas* or sarcoma* or tumo?r* or adenocarcinoma* or carcinosarcoma*)).ti,ab,kf,dq.
9 or 10
8 and 11
12 use oemezd
12 not (conference abstract or conference review).pt.
5 or 14
remove duplicates from 15
Clinical Trials Registries
ClinicalTrials.gov
Produced by the U.S. National Library of Medicine. Targeted search used to capture registered clinical trials.
Search -- pembrolizumab | "Endometrial Neoplasms"
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
Search terms – pembrolizumab AND endometrial
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search terms – pembrolizumab AND endometrial
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Search terms – pembrolizumab AND endometrial
Grey Literature
Search dates: January 13 to 18, 2022
Keywords: Keytruda/pembrolizumab, endometrial cancer
Limits: Conference abstracts excluded
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Appendix 2: Excluded Studies
Reference | Reason for exclusion |
|---|---|
Bellone S, Roque DM, Siegel ER, et al. A phase 2 evaluation of pembrolizumab for recurrent Lynch-like versus sporadic endometrial cancers with microsatellite instability. Cancer. 2021;07:07.61 | Study design not of interest (phase II, single-arm study) |
Ott PA, Bang YJ, Berton-Rigaud D, et al. Safety and Antitumor Activity of Pembrolizumab in Advanced Programmed Death Ligand 1-Positive Endometrial Cancer: Results From the KEYNOTE-028 Study. J Clin Oncol. 2017;35(22):2535-2541.62 | Study design not of interest (phase Ib, single-arm study) |
Appendix 3: Summary of Sponsor-Submitted Matching-Adjusted Indirect Comparison
Note this appendix has not been copy-edited.
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to summarize and critically appraise the methods and findings of the sponsor-submitted unanchored MAIC comparing pembrolizumab monotherapy with other comparators relevant for the treatment of advanced, recurrent, or metastatic endometrial MSI-H carcinoma in female patients that have received at least 1 prior line of therapy.
Due to the lack of direct evidence comparing pembrolizumab monotherapy with other existing treatments for patients with advanced, recurrent, or metastatic endometrial MSI-H carcinoma that have received at least 1 prior line of therapy, the sponsor submitted an unanchored MAIC which indirectly compares the efficacy of pembrolizumab monotherapy against standard of care (TPC, which consisted of doxorubicin or paclitaxel).
The sponsor’s rationale for using an unanchored MAIC was the single-arm design of the KN-158 trial and the lack of a head-to-head RCT estimating the relative safety and efficacy of pembrolizumab monotherapy against relevant comparators. In the absence of a common comparator, aggregated data from the DNA dMMR subpopulation of a selected comparator trial (KN-775) was matched with individual patient-level data (IPD) from the index trial (KN-158; cohort D and cohort K) in order to evaluate the relative efficacy of pembrolizumab against TPC.
Description of Indirect Comparisons
Methods of Matching-Adjusted Indirect Comparisons
Objectives
The objective of the sponsor-submitted unanchored MAIC63 was to evaluate the relative efficacy of pembrolizumab monotherapy in female patients with advanced, recurrent, or metastatic endometrial carcinoma with dMMR (MSI-H) (cohort D and cohort K of the KN-158 trial) against standard of care treatment (TPC) which consisted of doxorubicin or paclitaxel) in DNA dMMR subpopulation (from the KN-775 trial). OS, PFS, and ORR were outcomes investigated in the unanchored MAIC.
Systematic Literature Review
The sponsor did not provide a systematic review for the unanchored MAIC, and the submitted technical report did not provide a rationale for selecting the comparator trial (KN-775). However, through communications with the sponsor, they asserted that a systematic review was not needed because, to their knowledge, no RCT data exists regarding the efficacy of chemotherapy for patients with dMMR or MSI-H endometrial cancer besides KN-775. The index trial (KN-158) was a nonrandomized, single-arm, multisite, open-label trial of pembrolizumab in patients with multiple types of advanced (unresectable and/or metastatic) rare cancers. Patients in cohort K received pembrolizumab 200 mg IV once every 3 weeks as monotherapy and had the following tumour type: any advanced solid tumour, with the exception of colorectal carcinoma, which is MSI-H. Cohort D and cohort K were of interest for the MAIC.
The comparator trial, KN-775 trial was a randomized phase III, multicentre, open-label trial that enrolled female patients, 18 years or older with advanced, recurrent, or metastatic endometrial cancer who had been treated with at least 1 prior platinum-based chemotherapy regimen. The dMMR subpopulation from this trial was used in the MAIC. The potential risk of bias of this trial was not reported.
MAIC Analysis Methods
Table 18 presents the analysis methods of the sponsor-submitted unanchored MAIC.63
Sources of Data
The sponsor-submitted unanchored MAIC followed the guidelines outlined in the National Institute for Health and Care Excellence guidance document for conducting MAICs.64,65 The relative efficacy of pembrolizumab monotherapy against TPC in females with endometrial MSI-H carcinoma had been treated with at least 1 prior platinum-based chemotherapy regimen was assessed for OS, PFS, and ORR using aggregate data from KN-775 trial (subpopulation with dMMR) and IPD from KN-158 (cohort D and cohort K).
The standard of care group in the KN-775 trial were of interest for the unanchored MAIC. The all-participants-as-treated population set, consisting of patients who had received at least a dose of study treatment in the KN-158 trial, was used to extract IDP data. Aggregated data of the KN-775 trial was retrieved from an abstract by Makker et al. (2022),58 consisting of a subset of patients with dMMR. According to the sponsor, the analysis population of the KN-775 trial was not clearly stated in the published analysis, therefore data were used as presented. Kaplan-Meier curves from the KN-775 trial were extracted using a digital software. The number of at-risk patients over time and the digitized Kaplan-Meier curves were extracted, while pseudo IPD were generated using the approach described by Guyot et al (2012).66
The sponsor provided definitions of each outcome for the target population trial (KN-158) and the comparator population (KN-775). The sponsor considered definitions of outcomes (OS, PFS, and ORR) in both trials comparable, including the PFS censoring rules.
Variable Identification for Weighting
Key baseline prognostic factors and effect modifiers selected as matching variables for the analysis were based on clinical input; it is unclear how this clinical input was generated.
Matching variables derived from both trials, were compared before and after matching. Key baseline variables identified included age (median), race (Asian, Black, white, other), ECOG PS (0 versus 1), number of prior lines of therapy (1 versus ≥ 2), and histology status (endometrioid carcinoma, others).
Propensity Score Estimation and Calculation of Weights
An arm-to-arm matching (i.e., weighted statistics in the IPD trial set matched with reported statistics of comparator group in KN-775) was performed. Weights were considered missing and not accounted for in the calculation of treatment effect if there were any missing values of effect modifiers. A propensity score logistic regression model, based on the method of moments, was used to estimate weights for the propensity to be enrolled in the index trial (KN-158 trial) versus the comparator trial (KN-775), with effect modifiers used as predictive covariates in the model.
The impact of matching more effect modifiers on the effective sample size (ESS) was assessed using a histogram of the individual weights and a calculated ESS. The calculated ESS was presented to support the evaluation of the existence of extreme individual weights and cross-trial differences.
Derivation of Weighted Effect Estimates
Weighting statistics were used to derive the adjusted treatment effect of pembrolizumab monotherapy versus TPC after matching. For OS and PFS, an unstratified Cox proportional hazards model with only treatment as a covariate and Efron’s method of tie handling was fitted using pseudo IPDs with universal weights of 1 from the TPC group in the KN-775 trial group and IPDs from the KN-158 trial with weights from the previous matching step. HRs with their corresponding 95% CI were estimated using a sandwich (empirical) covariance matrix before and after matching. The Wald test from the unstratified Cox model was used to estimate treatment differences between the 2 treatments and a 2-sided score test was used in case a 0 event was observed in 1 of the treatment groups. Kaplan-Meier curves were presented for the TPC group in the KN-775 trial and for pembrolizumab monotherapy from the KN-158 (with unweighted and weighted data, respectively).
Analyses considering time varying HRs were not performed due to the limited sample size within the endometrial carcinoma subpopulation of KN-158 which could have caused parametrization issues.
For ORR, a weighted response ratio (RR) approach, with no stratification, was used to estimate the magnitude of the treatment difference between pembrolizumab monotherapy and TPC based on the derived pseudo IPD, with a universal weight of 1 for TPC group (in the KN-775) and IPD from the KN-158 trial with weights from the previous matching step. The statistical significance of the difference in treatments was estimated using the Wald test from the Mantel-Haenszel or Peto odds ratio model. The 95% CI for RR were calculated using a robust sandwich estimator. Statistical methods to account for differences between study characteristics, study design, inclusion/exclusion criteria, were not used, due to the low patient numbers in each treatment group.
Sensitivity Analyses
Sensitivity analyses were conducted for all end points to investigate any differences in results when adjustments were made for a different set of 5 baseline characteristics: age (median), race (Asian, Black, white, other), ECOG PS (0 versus 1), number of prior lines of therapy (1 versus ≥ 2), and histology status (endometrioid carcinoma, others).
Table 18: Matching-Adjusted Indirect Comparison Analysis Methods
Characteristics | MAIC |
|---|---|
Analysis methods | Unanchored MAIC |
Justification |
|
Differences in inclusion/exclusion criteria | NR |
Variable identification approach | Clinical expertise |
Covariates used in the matching adjustment |
|
Outcomes |
|
Follow-up time points | NR |
Sensitivity analyses | Use of different characteristics for matching: median age, race, ECOG PS, number of prior lines of therapy, prior adjuvant/neoadjuvant therapy (yes, no) |
Subgroup analysis | None |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Source: Sponsor-submitted unanchored matching-adjusted indirect comparison.63
Results of MAIC
Baseline Characteristics
Table 19 presents baseline characteristics on the KN-158 trial and the comparator trial.
The ESS after matching the index trial (KN-158) with the comparator trial (KN-775) was ||||||, representing a |||||| reduction of the initial sample size of 94. The sponsor conducted 2 feasibility assessments to assess the impact of some baseline characteristics on the MAIC. The ESS after matching for 4 baseline characteristics (age, race, ECOG PS group, number of prior therapies) was |||||||||||| representing a |||||| reduction in the initial sample size of 94; and ESS was ||||||, representing a |||||| reduction of the initial sample size, after adjusting for 3 baseline characteristics (race, ECOG PS group, number of prior therapies).
Table 19: Baseline Characteristics of the Unanchored Matching-Adjusted Indirect Comparison of Pembrolizumab Versus TPC — All Participants As-Treated Population
Characteristic | TPC (study KN-775) (Nb = 65) | Study KN-158a | |
|---|---|---|---|
Before matching (Nc = 94) | After matching |||||||||||| | ||
Age (years), median | 63.0 | 64.0 | |||||||||||| |
ECOG PS (%) | |||
0 | 52.3 | 44.7 | |||||||||||| |
1 | 47.7 | 55.3 | |||||||||||| |
Race (%) | |||
Asian | 18.5 | 7.4 | |||||||||||| |
Black | 7.7 | 3.2 | |||||||||||| |
White | 53.8 | 84.0 | |||||||||||| |
Other | 20.0 | 5.3 | |||||||||||| |
Prior lines of therapy (%) | |||
1 | 78.5 | 52.1 | |||||||||||| |
≥ 2 | 21.5 | 47.9 | |||||||||||| |
Histology (%) | |||
Endometrial | 86.2 | 66.0 | |||||||||||| |
Other | 13.8 | 34.0 | |||||||||||| |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability–high; TPC = treatment of physician's choice (doxorubicin or paclitaxel).
Note: Selected comparators: TPC based on Makker et al. (2021).
aDatabase cut-off date: January 12, 2022.
bNumber of participants: Based on Makker et al. (2021).
cNumber of participants: Based on KEYNOTE 158, the all participants as-treated population, MSI-H with Endometrial Carcinoma (cohort D and cohort K), at least 1 line of prior therapy.
dEffective sample size computed as the square of the summed weights divided by the sum of the squared weights; Weighted according to matched baseline characteristics of selected comparators.
Source: Sponsor-submitted unanchored matching-adjusted indirect comparison.63
Risk-of-Bias Results
The sponsor did not provide a quality assessment of the included studies in the unanchored MAIC.
Overall Survival
The estimated HR between pembrolizumab monotherapy and TPC before matching was 0.34 (95% CI, 0.21 to 0.54; P < 0.001) and after matching, the HR was 0.24 (95% CI, 0.13 to 0.45; P < 0.001). Table 20 presents OS findings between the 2 treatments in the unanchored analysis.
Sensitivity analyses were performed before and after matching. The estimated HR between pembrolizumab monotherapy and TPC before matching was 0.34 (95% CI, 0.21 to 0.54; P < 0.001) and 0.24 (95% CI, 0.13 to 0.46; P < 0.001) after matching. The sensitivity analysis was consistent with the main analysis.
Progression-Free Survival
The estimated HR between pembrolizumab monotherapy and TPC before matching was 0.42 (95% CI, 0.28 to 0.64; P < 0.001) and 0.31 (95% CI, 0.19 to 0.53; P < 0.001) after matching. Table 19 presents PFS findings between the 2 treatments in the unanchored analysis.
A sensitivity analysis of PFS was performed and consistent with the main analysis: the estimated HR between pembrolizumab monotherapy and TPC before matching was 0.42 (95% CI, 0.28 to 0.64; P < 0.001) and 0.33 (95% CI, 0.20 to 0.56; P <0.001) after matching.
Table 20: OS and PFS Before and After Matching in the Unanchored Matching-Adjusted Indirect Comparison of Pembrolizumab Versus TPC — All Participants As-Treated Population
Characteristics | Pembrolizumab (study KN-158)a | TPC (study KN-775) | Pembrolizumab vs. TPC | |||||
|---|---|---|---|---|---|---|---|---|
Nb | Participants with event, | Median timec in months (95% CI) | Nd | Participants with event, | Median timec in months (95% CI) | Hazard ratio (95% CI)e | P valuee,f | |
OS | ||||||||
Before matching | 94 | 41 (43.6) | 65.4 (29.5 to NR) | 65d | 42 (64.6) | 8.6 (5.5 to 12.9) | 0.34 (0.21 to 0.54) | < 0.001 |
After matchingg | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 0.24 (0.13 to 0.45) | < 0.001 |
PFS | ||||||||
Before matching | 94 | 58 (61.7) | 13.1 (4.3 to 25.7) | 65 | 48 (73.8) | 3.7 (3.1 to 4.4) | 0.42 (0.28 to 0.64) | < 0.001 |
After matchingg | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 0.31 (0.19 to 0.53) | < 0.001 |
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability–high; NR = not reached; TPC = treatment of physician's choice (doxorubicin or paclitaxel); vs. = versus.
Note: Selected comparators: TPC based on Makker et al. (2021).
aDatabase cut-off date: January 12, 2022.
bNumber of participants: Based on KEYNOTE 158, the all participants as-treated population, MSI-H with Endometrial Carcinoma (cohort D and cohort K), at least 1 line of prior therapy.
cFrom product-limit (Kaplan-Meier) method for censored data.
dNumber of participants: Based on Makker et al. (2021).
eBased on Cox regression model with treatment as a covariate.
fTwo-sided P value using Wald test (score test in case of 0 event in 1 treatment group).
gMatching was done on the following covariates: Age (Median), ECOG PS, Race, Prior Lines of Therapy, and Histology Status.
hSample size after matching computed as the sum of the weights.
Source: Sponsor-submitted unanchored matching-adjusted indirect comparison.63
Objective Response Rate
The estimated RR between pembrolizumab monotherapy and TPC before matching was 4.06 (95% CI, 2.06 to 8.02; P < 0.001) and 4.50 (95% CI, 2.22 to 9.10; P < 0.001) after matching. Table 21 presents the ORR analyses between pembrolizumab and TPC before and after matching.
The sensitivity analyses for ORR showed an estimated RR of 4.06 (95% CI, 2.06 to 8.02; P < 0.001) before matching and 4.27 (95% CI, 2.11 to 8.64; P < 0.001) after matching, consistent with the main analysis.
Table 21: ORR Analysis Before and After Matching in the Unanchored Matching-Adjusted Indirect Comparison of Pembrolizumab Versus TPC — All Participants As-Treated Population
Characteristic | Pembrolizumab (study KN-158)a | TPC (study KN-775)b | Pembrolizumaba vs. TPCb | |||
|---|---|---|---|---|---|---|
N | Participants with event, n (%) | N | Participants with event, n (%) | Response ratio (95% CI)c | P valued | |
Before matching | 94 | 47 (50.00) | 65 | 8 (12.31) | 4.06 (2.06 to 8.02) | < 0.001 |
After matchinge | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | 4.50 (2.22 to 9.10) | < 0.001 |
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability–high; TPC = treatment of physician's choice (doxorubicin or paclitaxel); vs. = versus.
Note: Selected comparators: TPC based on Makker et al. (2021).
aNumber of participants: Based on KEYNOTE 158, the all participants as-treated population, MSI-H with Endometrial Carcinoma (cohort D and cohort K), at least 1 line of prior therapy; Database cut-off date: January 12, 2022.
bNumber of participants: Based on Makker et al. (2021).
cBased on a robust sandwich estimator using PROC GENMOD in SAS.
dTwo-sided P value based on Wald test.
eMatching was done on the following covariates: Age (Median), ECOG PS, Race, Prior Lines of Therapy, Histology.
fEffective sample size after matching computed as the sum of the weights.
Source: Sponsor-submitted unanchored matching-adjusted indirect comparison.63
Critical Appraisal of MAIC
The sponsor provided a relevant rationale for using an unanchored MAIC over other ITC approaches; however, the selection of the comparator trial was not based on a systematic review process; therefore, it was not possible to assess whether important comparator trials were missed. As per the summary of the MAIC submitted by the sponsor, the reference provided for the comparator trial was available only as a conference abstract.67 Due to the limited methodology and information available in the conference abstract, it is likely that some important information may have been missing. Additionally, risk of bias of the trial was not reported and it is likely that it could not be adequately assessed based on the abstract. The unanchored MAIC methods for the analyses of outcomes were consistent with the National Institute for Health and Care Excellence methodological guidance document for MAIC analyses.64,65
A key underlying assumption of a MAIC is that all effect modifiers and prognostic variables are balanced across the groups being compared. In the sponsor-submitted unanchored MAIC, key important effect modifiers and prognostic factors were identified prior to the analyses based on clinical expertise. However, the process of selecting these factors which were not included in the sponsor’s analysis due to data unavailability in the comparator trial publications was not clearly described. Ideally, these would have been determined through a combination of quantitative evidence from external sources, systematic reviews, and clinical expert opinion. The sponsor noted that MAIC adjustments were made for all confirmed prognostic factors and effect modifiers that were available within the trial; however, there is the possibility that not all effect modifiers and prognostic factors were considered in the unanchored MAIC analyses because the data were unavailable in the trial. The CADTH review protocol identified FIGO (International Federation of Gynecology and Obstetrics) stage and the type of prior treatments as potential prognostic and/or effect modifying variables, which were not included in the sponsor’s analysis. In addition, the sponsor did not provide an assessment of the risk of residual bias due to potentially missing prognostic factors in the unanchored MAIC estimates, thus it must be assumed that the residual bias may be substantial. In addition, MAICs are unable to account for unknown cross-trial differences (i.e., study design features).
It was unlikely that effect modifiers relevant to the selected population were balanced between the 2 trials given that only 5 variables selected from both trials were used for matching in the MAIC. The small sample size of the index trial used in the MAIC would have limited the adjustment for multiple variables that may be important for the given patient population. As such, the small number of factors adjusted for in the sponsor’s MAIC may have biased the findings presented In addition, the ability to adjust for multiple patient characteristics depends on a sufficient number of patients in the trial set with IPD, which was lacking in the sponsor-submitted MAIC. Although the sponsor made efforts to balance effect modifiers and prognostic values between the 2 trials, the were no attempts made to adjust for differences in study characteristics, study design, inclusion/exclusion criteria, due to the low patient numbers in each treatment group . Although the sponsor mentioned that the outcome definitions were comparable in both trials, the censoring rules for PFS were not the same and could have impacted the PFS findings. However, it is unlikely that the differences in censoring rules between the 2 trials introduced bias in favour of pembrolizumab.
The statistical models used to determine PFS, and OS were adequately described by the sponsor; however, it was unclear whether the proportional hazard assumptions for PFS were met. The sensitivity analyses also showed that the Kaplan-Meier curves for OS and PFS were not parallel, suggesting that the proportional hazard assumption was not met. Sensitivity analyses were conducted for OS, PFS, and ORR by adjusting all 5 effect modifiers (age, race, ECOG PS, number of prior lines of therapy, and prior adjuvant/ neoadjuvant therapy). The sponsor did not provide analyses considering time varying HRs due to the limited sample size within the endometrial carcinoma subpopulation of KN-158 which could potentially cause parametrization issues.
The sponsor provided a before and after comparison of baseline characteristics of patients between the 2 trials, including the sensitivity analyses. The CADTH team noted important differences in the KN-158 trial for some baseline characteristics which may impact the generalizability of the findings (the population was reflective of a subgroup of the comparator trial, rather than those enrolled in KN-158). The ESS represented |||||||||||| reduction in the already small sample size in KN-158 which may be indicative an important loss of precision and a large influence of subsets of patients in KN-158. The effect and 95% CI could be considered fragile/potentially unstable.
Other important outcomes identified in the CADTH review protocol such as HRQoL, DOR, symptom reduction, and harms were not assessed.
Summary
Due to the lack of direct comparative evidence that compared pembrolizumab monotherapy with other existing treatments, the sponsor submitted an unanchored MAIC, which evaluated the relative efficacy of pembrolizumab monotherapy in female patients with advanced, recurrent, or metastatic endometrial carcinoma with dMMR that have received at least 1 prior line of therapy. The KN-158 trial was a single-arm trial, requiring that the sponsor match IPD data with aggregate data from a comparator trial (subset of the TPC group in the KN-775 trial) to evaluate the relative efficacy of pembrolizumab against TPC. Five effect modifiers (age, race, ECOG PS, number of prior lines of therapy, and histology status) were used as matching variables between the KN-158 and the KN-775 trials in the MAIC. After matching for baseline characteristics, findings from the primary analyses suggested that the efficacy of pembrolizumab monotherapy was better than TPC for OS, PFS, and ORR end points. Sensitivity analyses using a different set of variables for matching for all outcomes were consistent with the primary analyses. However, several limitations were identified in the unanchored MAIC which affects the internal and external validity of the findings. Due to the limitations identified from the unanchored MAIC, no definitive conclusions could be drawn of the relative efficacy of pembrolizumab in female patients with advanced, recurrent, or metastatic endometrial carcinoma with dMMR that have received at least 1 prior line of therapy.
Appendix 4: Detailed Outcome Data
Note this appendix has not been copy-edited.
Table 22: Prior Medications (Incidence Greater Than 0%) Oncologic Therapies
Characteristic | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 90) |
|---|---|
Patients with 1 or more prior medications, n (%) | 89 (98.9) |
Antineoplastic and immunomodulating drugs, n (%) | |
Antineoplastic drugs | 85 (94.4) |
Antineoplastic (unspecified) | 1 (1.1) |
Bevacizumab | 4 (4.4) |
Capivasertib | 1 (1.1) |
Carboplatin | 82 (91.1) |
Cisplatin | 12 (13.3) |
Cyclophosphamide | 2 (2.2) |
Docetaxel | 2 (2.2) |
Doxorubicin | 14 (15.6) |
Doxorubicin hydrochloride | 7 (7.8) |
Dual Akt kinase inhibitor and ERK inhibitor (unspecified), n (%) | 1 (1.1) |
Epirubicin hydrochloride | 1 (1.1) |
Gedatolisib | 1 (1.1) |
Gemcitabine | 5 (5.6) |
Ifosfamide | 1 (1.1) |
Lurbinectedin | 1 (1.1) |
Paclitaxel | 81 (90) |
Palbociclib | 1 (1.1) |
Sapanisertib | 1 (1.1) |
Selumetinib | 1 (1.1) |
Topotecan | 1 (1.1) |
Vinorelbine tartrate | 1 (1.1) |
Endocrine therapy, n (%) | 26 (28.9) |
Immunosuppressants, n (%) | 2 (2.2) |
Sex hormones and modulators of the genital system | 2 (2.2) |
Note: Every patient is counted a single time for each applicable specific prior medication. A patient with multiple prior medications within a medication category is counted a single time for that category.
Source: KN-158 Clinical Study Report.21
Table 23: Concomitant Medications Used
Characteristic | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 90) |
|---|---|
Antineoplastic and immunomodulating drugs (i.e., methotrexate), n, (%) | 1 (1.1) |
Endocrine therapy, n, (%) | 2 (2.2) |
Immunosuppressants, n, (%) | 3 (3.3) |
Corticosteroids for systemic use, n, (%) | 3 6 (40.0) |
Source: KN-158 Clinical Study Report.21
Table 24: Censoring Rules for Duration of Response
Situation | Date of progression or censoring | Outcome |
|---|---|---|
No progression nor death, no new anticancer therapy initiated | Last adequate disease assessment | Censor (nonevent) |
No progression nor death, new anticancer therapy initiated | Last adequate disease assessment before new anticancer therapy initiated | Censor (nonevent) |
Death or progression after ≥ 2 missed adequate disease assessments | Last adequate disease assessment prior to the after ≥ 2 missed adequate disease assessments | Censor (nonevent) |
Death or progression after ≤ 1 missed adequate disease assessments | PD or death | End of response (Event) |
PD = progression of the disease.
Note: Patients were considered to have an ongoing response if censored, alive, have not progressed, and have not started a new anticancer therapy and have not been lost to follow-up (i.e., Situation 1 in the first row of the table). Patients are considered lost to follow-up if there was no scan within 22 weeks of the data cut-off.
Source: KN-158 Clinical Study Report.21
Table 25: General Guidance for Evaluation Criteria for Interim Analysis
Population | Cut-off | Evaluation and enrolment |
|---|---|---|
All comers pooled across all tumour types | Observed ORR ≥ 15% | Consult with health authorities to discuss the opportunity for a regulatory submission or plan for confirmation in future enrolment cohorts. |
Observed ORR < 15% | Start/continue enrolling biomarker positive patients across all tumour types. | |
Biomarker-selected patients pooled across all tumour types | Observed ORR ≥ 25% | Consult with health authorities to discuss the opportunity for a regulatory submission or plan for confirmation in future enrolment cohorts. |
Observed ORR < 25% | Continue enrolling all comers. | |
All comers within an individual tumour type | Observed ORR ≥ 15% | Consult with health authorities to discuss the opportunity for a regulatory submission or plan for confirmation in future enrolment cohorts. |
Observed ORR < 15% | Start/continue enrolling biomarker positive patients within the individual tumour type. | |
Biomarker-selected patients within an individual tumour type | Observed ORR ≥ 25% | Consult with health authorities to discuss the opportunity for a regulatory submission or plan for confirmation in future enrolment cohorts. |
Observed ORR < 25% | Continue enrolling all comers. |
ORR = objective response rate.
Source: KN-158 Clinical Study Report.21
Table 26: Summary of Drug Exposure — Safety Population
Drug exposure | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 90) |
|---|---|
Study duration on therapy (months), median (range) | 8.30 (0.03 to 26.88) |
Number of administrations, median (range) | 12.50 (1.00 to 35.00) |
Duration of treatment for pembrolizumab (months), n (%) | |
> 0 | 90 (100.0) |
≥ 6 | 51 (56.7) |
≥ 12 | 34 (37.8) |
≥ 18 | 24 (26.7) |
≥ 21 | 23 (25.6) |
Note: Database cut-off date: October 5, 2020.
Source: KN-158 Clinical Study Report.21
Table 27: Summary of Time to Response and Duration of Response in Responders (Per Central Radiology Assessment)
Response | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 79) |
|---|---|
Number of patients with responsea | 38 |
Time to response (months), median (range) | 2.3 (1.3 to 10.6) |
Response durationb (months), median (range) | NR (2.9 to 49.7+) |
Patients with extended response duration, n (%)b | |
≥ 6 months | 34 (91.8) |
≥ 12 months | 24 (88.1) |
≥ 18 months | 19 (72.9) |
≥ 24 months | 18 (72.9) |
≥ 30 months | 17 (72.9) |
≥ 36 months | 12 (68.1) |
DOR = duration of response; NR = not reached.
Notes: The sponsor provided updated DOR results based on the cut-off date of April 5, 2021, in which all 90 patients were included. The DOR results as of April 5, 2021, were consistent with the findings as of October 5, 2020.47
"+" indicates there is no progressive disease by the time of last disease assessment (i.e., the response was still ongoing).
Database cut-off date: October 5, 2020.
aIncludes patients with confirmed complete response or partial response.
bFrom product-limit (Kaplan-Meier) method for censored data.
Source: KN-158 Clinical Study Report.21
Table 28: Censored Information for Duration of Response Assessment (Per Central Radiology Assessment)
Duration of response information | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 79) |
|---|---|
Number of patients with responsea | 38 |
Patients who progressed or died,b n (%) | 9 (23.7) |
Censored patients, n (%) | 29 (76.3) |
Patients who missed 2 or more consecutive disease assessments | 0 (0.0) |
Patients who started new anticancer treatment | 1 (2.6) |
Patients who were lost to follow-up | 0 (0.0) |
Patients whose last adequate assessment was ≥ 5 months prior to data cut-off date | 7 (18.4) |
Ongoing responsec | 21 (55.3) |
Notes: For censored patients who met multiple criteria for censoring and do not have ongoing response, patients were included in the censoring criterion that occurred earliest.
Database cut-off date: October 5, 2020.
aIncludes patients with a confirmed complete response or partial response.
bIncludes patients who progressed or died without previously missing 2 or more consecutive disease assessments.
cIncludes patients who are alive, have not progressed, have not initiated new anticancer treatment, are not lost to follow-up, and whose last disease assessment was less than 5 months prior to data cut-off date.
Source: KN-158 Clinical Study Report.21
Table 29: Adverse Events Occurred in 10% or More of Patients — Safety Population
Adverse events | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 90) |
|---|---|
Total N in the analysis | 90 |
With 1 or more AEs, n (%) | 86 (95.6) |
AEs (> 10%), n (%) | |
Fatigue | 30 (33.3) |
Diarrhea | 29 (32.2) |
Pruritus | 26 (28.9) |
Arthralgia | 25 (27.8) |
Nausea | 25 (27.8) |
Decreased appetite | 21 (23.3) |
Urinary tract infection | 20 (22.2) |
Vomiting | 20 (22.2) |
Back pain | 16 (17.8) |
Constipation | 14 (15.6) |
Rash | 14 (15.6) |
Anemia | 13 (14.4) |
Hypothyroidism | 13 (14.4) |
Cough | 12 (13.3) |
Abdominal pain | 11 (12.2) |
Dyspnea | 11 (12.2) |
Headache | 11 (12.2) |
Insomnia | 11 (12.2) |
Dizziness | 10 (11.1) |
AE = adverse event.
Notes: Every patient is counted a single time for each applicable row and column.
A specific AE appears on this report only if its incidence in 1 or more of the columns meets the incidence criterion in the report title, after rounding.
Nonserious AEs up to 30 days of last dose and serious AEs up to 90 days of last dose are included.
Database cut-off date: October 5, 2020.
Source: KN-158 Clinical Study Report.21
Table 30: Serious Adverse Events Occurred in More Than 2% of Patients — Safety Population
AE | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 90) |
|---|---|
Total N in the analysis | 90 |
Patients with 1 or more AEs, n (%) | 34 (37.8) |
SAEs, n (%) | |
Ascites | 2 (2.2) |
Chest pain | 2 (2.2) |
Pneumonia | 2 (2.2) |
Pyelonephritis | 2 (2.2) |
Sepsis | 2 (2.2) |
Urinary tract infection | 2 (2.2) |
AE = adverse event.
Notes: Every patient is counted a single time for each applicable row and column.
A specific AE appears on this report only if its incidence in 1 or more of the columns meets the incidence criterion in the report title, after rounding. Nonserious AEs up to 30 days of last dose and serious AEs up to 90 days of last dose are included.
Database cut-off date: October 5, 2020.
Source: KN-158 Clinical Study Report.21
Table 31: Adverse Events Resulting in Treatment Discontinuation (Incidence Greater Than 0%) — Safety Population
AE | Study KN-158 (cohort D and cohort K) Pembrolizumab (N = 90) |
|---|---|
# of patients in the analysis, N | 90 |
Patients with 1 or more AEs resulting in treatment discontinuation, n (%) | 6 (6.7) |
AEs leading treatment discontinuation, n (%) | |
Enterocolitis | 1 (1.1) |
Drug-induced liver injury | 1 (1.1) |
Transaminases increased | 2 (2.2) |
Arthritis | 1 (1.1) |
Rash | 1 (1.1) |
AE = adverse event.
Notes: Every patient is counted a single time for each applicable row and column.
A specific AE appears on this report only if its incidence in 1 or more of the columns meets the incidence criterion in the report title, after rounding. Nonserious AEs up to 30 days of last dose and serious AEs up to 90 days of last dose are included.
Database cut-off date: October 5, 2020.
Source: KN-158 Clinical Study Report.21
Appendix 5: Patient-Reported Health-Related Quality of Life Outcomes Presented in ESMO Congress 2021
Note this appendix has not been copy-edited.
HRQoL outcomes presented in ESMO Congress 2021 was submitted by the sponsor for this submission.19,47 The objective of this appendix is to summarize the prespecified exploratory HRQoL outcomes.
Outcomes Assessed
EORTC QLQ-C30 GHS
QLQ-C30 functional and symptom scales/items
EuroQol visual analogue scale (EQ-5D VAS)
The EORTC QLQ-C30 and EQ-5D were administered at baseline, every cycle for the first 4 cycles, then every 3 cycles until 9 months, then every 4 cycles during study treatment until disease progression, at the treatment discontinuation visit, and at the 30-day safety follow-up visit; the EQ-5D-3L questionnaire was administered first, followed by EORTC QLQ-C30; Questionnaires were administered before treatment administration, AE evaluation, and tumour imaging.
Statistical Analysis
HRQoL was analyzed in all patients who completed at least 1 assessment and received at least 1 dose of study treatment; changes from baseline were analyzed in patients who also had both a baseline and postbaseline HRQoL assessment.
Changes from baseline in the EORTC QLQ-C30 GHS/QoL and EQ- VAS scores were summarized over time through final assessment at week 111.
Result
As of the data cut-off date, among 90 patients enrolled, 76 patients completed at least 1 QLQ-C30 questionnaire and among those 63 had no missing change from baseline data to week 9 at the data cut-off; 79 patients completed at least 1 EQ-5D-3L questionnaire, and among those 65 had no missing change from baseline data at the data cut-off. The HRQoL results are presented in Table 32.
For the EORTC QLQ-C30 GHS/QoL scale, there were 63 patients with nonmissing change from baseline to week 9 at the data cut-off; among these the mean change from baseline (95% CI) was 6.08 (0.71 to 11.46). For the EORTC QLQ-C30 function and symptom scales, there were 63 patients with nonmissing change from baseline to week 9 at the data cut-off; among these QLQ-C30 function and symptom scale scores appeared maintained or improved from baseline to week 9. Data were presented in figures and not extractable.19,47 For the EQ- VAS, there were 65 patients with nonmissing change from baseline to week 9 at the data cut-off; among these the mean change from baseline (95% CI) was 6.00 (2.25 to 9.75).It should be noted that the change from baseline to week 111 were presented in figures, Figure 8, Figure 9, and Figure 10, from which the data were not extractable.
Table 32: Health-Related Quality of Life Results — Full Analysis Set
Outcome | Study KN-158 (cohort D and cohort K) (N = 79) |
|---|---|
EORTC QLQ-C30 global health status | |
n | 63 |
Global health status scores at baseline, mean (95%CI) | 65.61 (NR) |
Global health status score at week 9, mean (95%CI) | 71.69 (NR) |
Global health status score mean change from baseline to week 9 (95% CI) | 6.08 (0.71 to 11.46) |
EORTC QLQ-C30 functional scalea | Not extractable |
EORTC QLQ-C30 symptom scalea | Not extractable |
EQ-5D-3L VAS | |
n | 63 |
VAS scores at baseline mean (95%CI) | 69.68 (NR) |
VAS score at week 9, mean (95%CI) | 75.68 (NR) |
VAS score mean change from baseline to week 9 (95%CI) | 6.00 (2.25 to 9.75). |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; HRQoL = health-related quality of life; NR = not reported.
Notes: Results of HRQoL (EORTC QLQ-C30 global health status, EORTC QLQ-C30 function scale, EORTC QLQ-C30 symptom scale, EQ-5D-3L-VAS) were not reported in the Clinical Study Report.21 The results were presented in ESMO conference abstracts included in the sponsor’s submissions.19,47
FAS: HRQoL FAS population, defined as the patients in the primary efficacy population with at least 1 HRQoL assessment available.21
aData were presented in figures and not extractable. The figures cannot be copied to this summary, either.
Sources: Sponsor submissions.19,47
Figure 8: Mean Change From Baseline in EORTC QLQ-C30 Global Health Status/QoL by Study Visit Over Time — Full Analysis Population
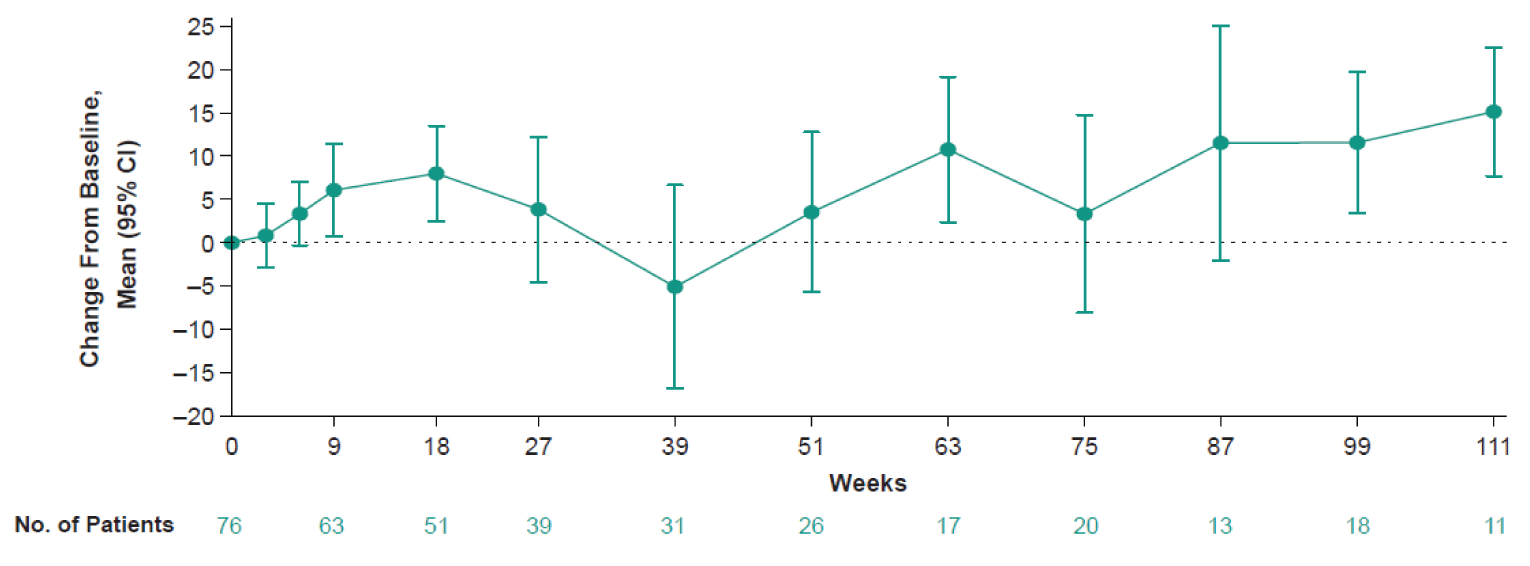
* Two patients experienced a sudden decrease in EORTC QLQ-C30 global health status/QoL at week 39: changes from baseline were –100 (patient died approximately 3 months later) and –75.
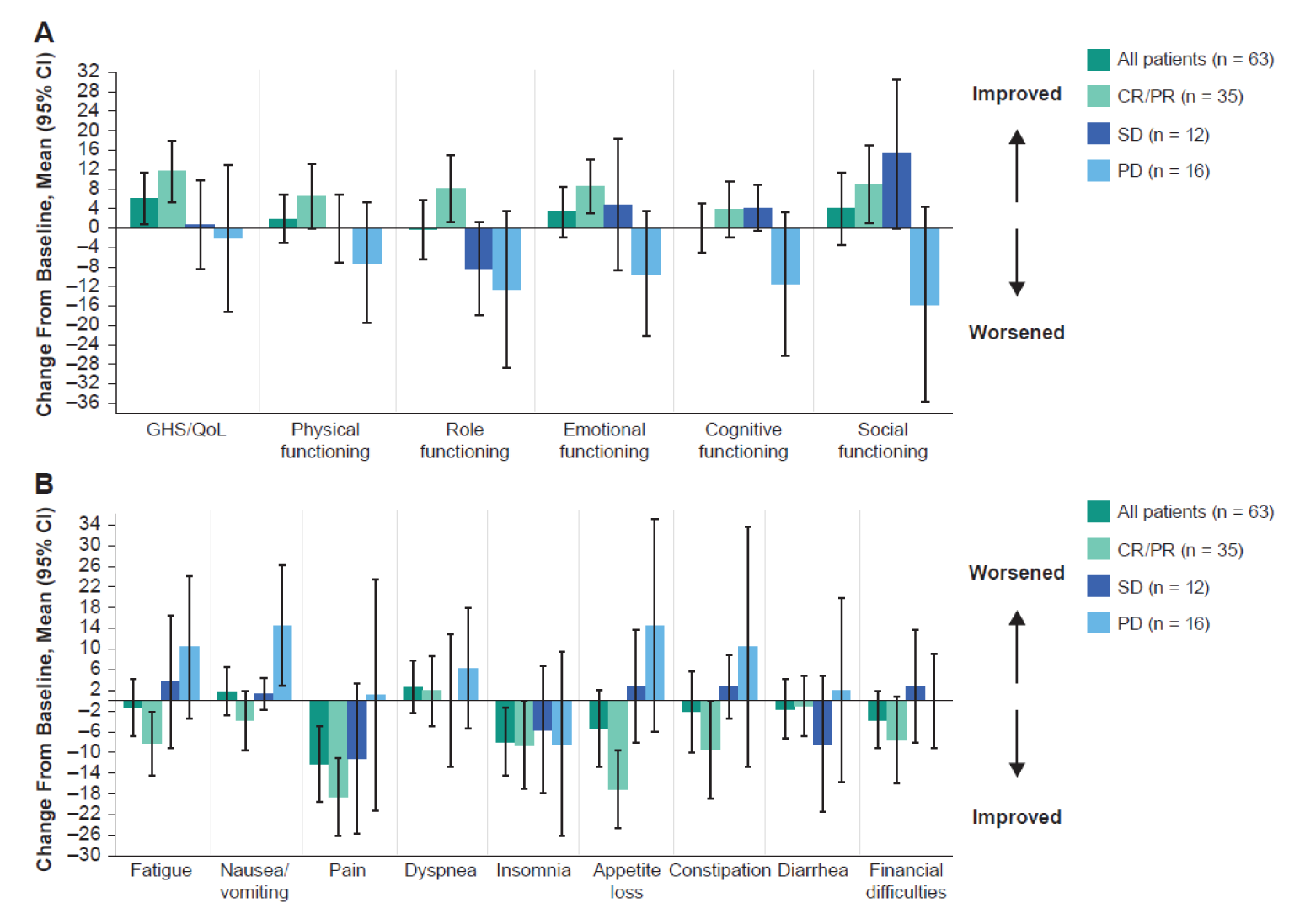
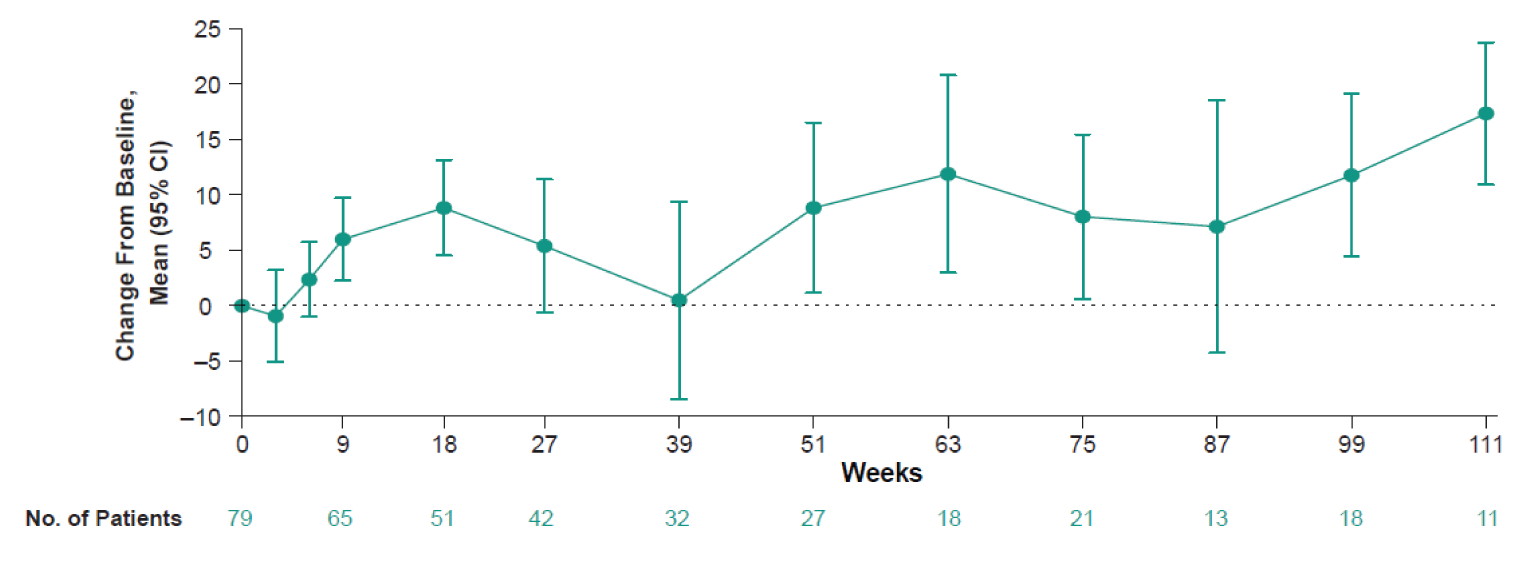
Appendix 6: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and minimal important difference [MID]):
EORTC QLQ-C30 version 3.0
EQ-5D-3L version 2.0
Findings
Table 33: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A self-reported instrument designed to measure the physical, psychological, and social functions of patients with cancers. The EORTC QLQ-C30 incorporates 5 functional scales (Physical, Role, Cognitive, Emotional and Social); 3 symptom scales (fatigue, pain, and nausea/vomiting), a global health and quality-of-life scale; and single items that assess additional symptoms commonly reported by patients with cancer (dyspnea, appetite loss, sleep disturbance, constipation, and diarrhea), as well as the perceived financial impact of the disease and treatment.48-50 | Validity: Construct, criterion, and discriminant validity were demonstrated in patients with ovarian and gestational trophoblastic disease cancers.68,69 The EORTC QLQ-30 was found to adequately assess the effect of expected toxicities on patients’ HRQoL during and following treatment.70 No reported validation studies were found for patients with EC. Reliability: Minimum reliability with Cronbach alpha > 0.70 was met in 7 of 9 subscales of the Chinese version of the tool in patients with gestational trophoblastic disease, ovarian cancer, and other types of gynecological cancers.69 Responsiveness: There were no data available for responsiveness in patients with EC. | Among patients with various advanced cancers71,72:
No reported MID was found for patients with EC. |
EQ-5D-3L version 2.0 | A generic preference-based self-reported HRQoL instrument that has been applied to a wide range of health conditions and treatments. The EQ-5D-3L assesses 5 domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each domain has 3 levels: no problems, some problems, and severe problems. The EQ-5D-3L also includes an EQ VAS, a vertical visual analogue scale with anchors of 100 (best imaginable health) and 0 (worst imaginable health), on which patients provide a global assessment of their health.51,54 | The validation of EQ-5D-3L is available across countries around the world and for various conditions.51,54 Validity: Among patients with cervical cancer, convergent validity was demonstrated through moderate to strong correlations between EQ-5D index and all EORTC QLQ-C30 scales (Spearman’s rank correlation range from 0.32 to 0.62), and moderate to strong correlations between EQ VAS and EORTC QLQ-C30 global QoL, physical, fatigue, and pain scales (Spearman’s rank correlation range from 0.35 to 0.62). Discriminant validity was observed for the EQ VAS and the remaining EORTC QLQ-C30 (Spearman’s rank correlation range from 0.22 to 0.31).73 Among patients with breast cancer, construct validity was demonstrated in relation to the FACT-B questionnaire (highest correlation for physical well-being) (Pearson r = 0.553) and lowest for social well-being (Pearson r = 0.199).74 Reliability: Among patients with breast cancer, test-retest reliability ranged from 0.32 to 0.70 (Cohen kappa). ICCs assessing internal consistency reliability for EQ-5D-3L index and EQ VAS scores were 0.70 and 0.48, respectively.74 Among 90 patients with cancer, test-retest reliability ranged from 0.78 to 0.84 (Cohen kappa) for EQ-5D index scores (ICC = 0.952; 95% CI, 0.928 to 0.968).75 Responsiveness: There were no data available for responsiveness in patients with EC.76 | For cancers (not specified for endometrial cancer)77: MID (UK algorithm): 0.10 to 0.12 based on PS range and 0.09 to 0.10 based on FACT-G score MID (US algorithm): 0.07 to 0.09 grouped by PS and 0.06 to 0.07 grouped by FACT-G score MIDs for VAS: 8 - 12 using PS and 7 - 10 using FACT-G quintiles No reported MID was found for patients with EC. |
MID = minimal important difference; CIN = cervical intraepithelial neoplasia; EC = endometrial cancer; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ VAS = EuroQol Visual Analogue Scale; FACT-B = Functional Assessment of Cancer Therapy–Breast; FACT-G = Functional Assessment of Cancer Therapy–General; FACT-E = Functional Assessment of Cancer Therapy Scale-Esophageal Cancer; HRQoL = health-related quality of life; HUS = health utility score; ICC = intraclass correlation coefficient; PS = performance status.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
Description
The EORTC QLQ-C30 is a self-reported instrument designed to measure the physical, psychological, and social function of patients with cancer.50 The EORTC QLQ-C30 consists of 30 items that are scored to create 5 multiitem functional scales, 3 multiitem symptom scales, 6 single-item symptom scales, and 2 global QoL scales (Table 34). Version 3.0 of the questionnaire is the most current version and has been in use since December of 1997.50,78 It is intended for use in the adult population only.50
Table 34: EORTC QLQ-C30 Scales
Functional scales (15 questions) | Symptom scales (7 questions) | Single-item symptom scales (6 questions) | Global quality of life (2 questions) |
|---|---|---|---|
Physical function (5) Role function (2) Cognitive function (2) Emotional function (4) Social function (2) | Fatigue (3) Pain (2) Nausea and vomiting (2) | Dyspnea (1) Insomnia (1) Appetite loss (1) Constipation (1) Diarrhea (1) Financial impact (1) | Global Quality of Life (2) |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30.
Scoring
The EORTC QLQ-C30 uses a 1-week recall period to assess self-reported function and symptoms.50 Twenty-eight questions are scored on a 4-point Likert scale (1: not at all; 2: a little; 3: quite a bit; 4: very much). The 2 questions that make up the global HRQoL scale are scored on a 7-point Likert scale with anchors at 1 (“very poor”) and 7 (“excellent”).
Raw scores for each scale are computed as the average of the items that contribute to a particular scale.50 This scaling approach is based on the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of 1 unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better HRQoL. Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and HRQoL scales would reflect an improvement. According to the EORTC QLQ-C30 scoring algorithm, if there are missing items for a scale (i.e., the patient did not provide a response), the score for the scale can still be computed if there are responses for at least one-half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.
Psychometric Properties
The EORTC QLQ-C30 was originally validated in patients with lung cancer and head and neck cancer from various European and North American countries, as well as from Australia.48,79,80 The scales of the EORTC QLQ-C30 have been found to assess distinct components of HRQoL, can distinguish between patients with different performance status and degrees of weight loss, and is responsive to change over time.48,79,80
A literature search was conducted to identify validation information of the EORTC QLQ-C30 in patients with endometrial cancer and none were identified. Of note, there is a validated version of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire that was developed specifically for endometrial cancer: European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire - Endometrial Cancer Module (EORTC QLQ-EN24).81 The EORTC QLQ-EN24 was designed to assess disease and treatment specific aspects of the HRQoL of patients with endometrial cancer. A validation study of the Mexican-Spanish version of the EORTC QLQ-EN24 in 189 patients with endometrial cancer included a brief validation of the QLQ-C30.82 The study confirmed the internal consistency and reliability of the QLQ-C30 and found that its convergent and discriminant validity (Cronbach alpha range, 0.77 to 0.89) was consistent with its original report.82
In a validation study of the EORTC QLQ-C30 (English or French versions), patients with breast cancer (n = 121), ovarian cancer (n = 111), lung cancer (n = 160), and a heterogenous group of other cancers (n = 121) completed the questionnaire before and on day 8 of chemotherapy.68 The item-domain Pearson correlations of the EORTC QLQ-C30 were not different across the primary tumour sites (i.e., breast, ovary, or lung). The Pearson correlations for all items, except for item 5 (whether the responders needed help with eating, dressing, washing, or using the toilet) and the physical function domain (r = –0.3), were more highly correlated within their own domain than with any other domains (r = –0.65 to 0.95 within the domains). At day 8 of chemotherapy, the item-domain Pearson correlation for item 5 and the physical function domain was 0.49 for the entire group and ranged from –0.38 for ovarian cancer to –0.55 for breast cancer. These higher values at day 8 suggest that item 5 was more relevant in the week after chemotherapy than before chemotherapy.68 Similarly, items asking about vomiting showed a higher correlation with domains for nausea/vomiting on day 8 after chemotherapy (r = 0.89) than before chemotherapy (r = 0.74). The questionnaire also demonstrated good internal consistency reliability for most domains at baseline and at day 8 (Cronbach alpha > 0.70). However, values were less than 0.70 at baseline and day 8 for role function (0.66 and 0.53, respectively) and cognitive function (0.63 and 0.58, respectively). Examination of the discrimination of the domain scores according to metastatic disease (i.e., individuals with distant metastases or individuals with disease confined to the primary site and regional lymph nodes) found No significant differences in mean scores of emotional function, cognitive function, and nausea/vomiting at baseline and day 8. However, the mean scores for each of the other domains differed between the groups at baseline, with patients with localized disease tending to have better physical function, role function, social function, less fatigue, and pain and better global HRQoL. At day 8, only social function and fatigue were shown to be no longer significant. Patients with lung and ovarian cancer reported lower scores for all these domains, with patients with ovarian cancer reporting the lowest scores for all domains. After chemotherapy, many of the differences seen at baseline between the groups were no longer evident. At day 8, patients with ovarian cancer had the smallest magnitude of change, with little-to-no change in role function, social function, and global HRQoL, while being the only cancer group reporting a significant improvement in pain.68
An analysis of data from a Canadian RCT of paclitaxel and cisplatin versus cyclophosphamide and cisplatin in the treatment of 153 patients with epithelial ovarian cancer found the EORTC QLQ-C30 adequately assessed the effect of expected toxicities on patients HRQoL during and after treatment.70 At baseline, prior to the initiation of treatment, there was close agreement in the “mild or none” category between the symptoms recorded on case report forms and paired EORTC QLQ-C30 questions, calculated by dividing 2 times the number of patients classified in the mild or none category with both toxicity and QoL assessments, with the sum of patients classified as mild or none based on toxicity and QoL assessment only. The greatest degree of agreement ranged between 0.80 (95% CI, 0.75 to 0.86) to 0.98 (95% CI, 0.92 to 0.99). The pairing of lethargy with Question 18, and mood with Question 22 were slightly weaker in agreement compared to the other pairs at 0.72 and 0.73, respectively. The weakest pairs were constipation with Question 16, and lethargy with Question 18 at 0.44 and 0.44, respectively. During treatment and at the end of cycles 3 and 6, all but 1 symptom and HRQoL pairs demonstrated marked agreement ranging from 0.71 to 0.93. The one exception was the pair assessing symptom hair loss and Question 42 with a degree of agreement of 0.50 and 0.37 at cycles 3 and 6, respectively. A regression model predicting global HRQoL scores based on baseline grades of the most frequently observed toxicities and scores corresponding to HRQoL question found that the questions related to motor weakness (question 12), anorexia (question 13), mood (question 24), gastrointestinal pain (question 40) and vomiting (question 15) explained 60% of the variance in baseline global HRQoL on the EROTC QLQ-C30. When patients were off chemotherapy, 78% of symptoms and HRQoL pairs had a high level of agreement (> 0.80).
Minimal Important Difference
A literature search was conducted to identify the MID of the EORTC QLQ-C30 in patients with endometrial cancer and none were identified. The following is a summary of the MID of the EORTC QLQ-C30 in patients with cancer in general.
Change in the EORTC QLQ-C30 may be interpreted in terms of small, moderate, or large changes in HRQoL.72 A study of patients with breast cancer and small cell lung cancer estimated that a clinically relevant change in score on any of the EORTC QLQ-C30 scales to be 10 points.72 Using an anchor-based approach to estimate the MID in which patients who reported “a little” change (for better or worse) on the subjective significance questionnaire had corresponding changes on a function or symptom scale of the EORTC QLQ-C30 of approximately 5 to 10 points. Patients who reported a “moderate” change had corresponding changes in the EORTC QLQ-C30 of about 10 to 20 points, and those who reported being “very much” changed had corresponding changes of more than 20 points.
A Canadian study estimated the MID for the EORTC QLQ-C30 among 369 patients with advanced cancer, the most common cancer being breast cancer, followed by lung, prostate, gastrointestinal, renal cell, and other cancers.71 Patients completed the questionnaire at baseline and 1 month postradiation. MIDs were estimated using both an anchor- and distribution-based methods for improvement and deterioration. In the anchor-based approach, the 2 anchors of overall health and overall HRQoL were used, both taken directly from the EORTC QLQ-C30 (questions 29 and 30). Improvement and deterioration were categorized as an increase or decrease of 2 units to account for the natural fluctuation of patient scoring. With these 2 anchors, the estimated MIDs across all EORTC QLQ-C30 scales ranged from 9.1 units (cognitive functioning) to 23.5 units (role functioning) for improvement, and from 7.2 units (physical functioning) to 13.5 units (role functioning) for deterioration. Distribution-based estimates were closest to 0.5 standard deviation (SD).
EQ-5D-3L
Description
The EQ-5D-3L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments.51,54 The first of 2 parts of the EQ-5D-3L is a descriptive system that classifies respondents (aged 12 years and older) into 1 of 243 distinct health states. The descriptive system consists of the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 possible levels (1, 2, or 3) representing “no problems,” “some problems,” and “extreme problems,” respectively. Respondents are asked to choose 1 level that reflects their own health state for each of the 5 dimensions. A scoring function can be used to assign a value (EQ- 5D-3L index score) to self-reported health states from a set of population-based preference weights.51,54 The second part is a vertical, calibrated 20 cm visual analogue scale (EQ VAS) that has end points labelled 0 and 100, with anchors of ‘worst imaginable health state’ and ‘best imaginable health state,’ respectively. Respondents are asked to rate their own health by drawing a line from an anchor box to the point on the EQ VAS which best represents their own health on that day. Hence, the EQ-5D-3L produces 3 types of data for each respondent:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 11121, 33211
A population preference-weighted health index score based on the descriptive system
A self-reported current health status based on the EQ VAS that is used to assess the overall health of the respondent rather than selected dimensions of individuals’ health
The EQ-5D-3L index score is generated by applying a multiattribute utility function to the descriptive system. Different utility functions are available that reflect the preferences of specific populations (e.g., US, UK). The lowest possible overall score (corresponding to severe problems on all 5 attributes) varies depending on the utility function that is applied to the descriptive system (e.g., −0.59 for the UK algorithm, −0.109 for the US algorithm). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.
Psychometric Properties
A literature search was conducted to identify validation information of the EQ-5D-3L in patients with endometrial carcinoma and none were identified. The following is a summary of the psychometric property of the EQ-5D-3L in patients with different cancers.
Among 530 patients with cervical cancer in Taiwan, the EQ-5D-3L was found to be both a reliable and valid assessment of HRQoL.73 The intraclass correlation for test-retest reliability after a median 11 (range, 2 to 15) days was 0.83; Cohen kappa values for the different dimensions ranged from 0.54 to 0.73. EQ-5D-3L convergent and discriminant validities were examined by comparing to the EORTC QLQ-30, and using clinical indicators of the functional performance according to the Karnofsky performance scale as discriminators. The EQ-5D was moderately or strongly correlated with all EORTC QLQ-C30 functioning scales (Spearman’s rank correlation coefficient = 0.36 to 0.51), except the social functioning scale (coefficient, 0.32), and its index and VAS scores were higher for patients with higher Karnofsky performance scale score and disease-free status (p < 0.001).73
Psychometric properties of EQ-5D-3L were assessed in a sample of 827 postoperative patients with breast cancer from Korea.74 Construct validity, evaluated by Pearson correlation between the EQ-5D-3L index and EQ VAS score, and the Functional Assessment of Cancer Therapy–Breast (FACT-B) scores, showed the highest correlations in physical well-being (r = 0.553 for EQ-5D-3L index and r = 0.447 for EQ VAS score) and lowest correlations in social well-being (r = 0.199 for EQ-5D-3L index and r = 0.170 for EQ VAS score). Observed test-retest reliability (1 week between tests) ranged from 0.32 to 0.70 (using Cohen kappa values), while the intraclass correlation coefficient for EQ-5D-3L index and EQ VAS scores were 0.70 and 0.48, respectively. Discriminant validity was tested using the known groups approach, which assessed differences in the EQ-5D-3L index and EQ VAS score according to patient demographic and clinical characteristics. The results revealed higher scores among patients who were educated, patients undergoing current radiotherapy, and unmarried individuals.74 Significant differences were not seen by age, type of surgery (mastectomy vs. breast-conserving), stage at diagnosis, nor current treatment with chemotherapy. Discriminant validity of the instrument was further assessed through a comparison of mean values of FACT-B subscale scores across individuals without problems and individuals with moderate/severe problems in each EQ-5D-3L dimension, using the Student’s t-test. As the authors expected, all FACT-B subscale scores as well as combined index scores were significantly larger across all EQ-5D-3L dimensions, when comparing individuals without problems to those with any problems.74
A study conducted on 416 patients with different types of cancer, including lung, breast, colorectal, liver, gastric, or thyroid cancer, evaluated psychometric properties of EQ-5D-3L, EQ-5D Five-Level, and Functional Assessment of Cancer Therapy–General (FACT-G) questionnaires.75 Among 90 patients with cancer who completed both the baseline and follow-up survey, results of the test-retest reliability for each dimension of EQ-5D-3L showed a Cohen kappa range from 0.781 to 0.840, and an intraclass correlation coefficient value of 0.952 (95% CI, 0.928 to 0.968). Satisfactory convergent validity was observed by presenting Spearman’s correlation between EQ-5D scales and FACT-G in the total population. In order to assess known group validity, the EQ-5D dimension responses and indices were compared across subgroups of patients with different ECOG PS and cancer stage. For the entire sample, a downward trend of index scores was observed as the ECOG PS decreased and cancer stage increased.75
Minimal Important Difference
A literature search was conducted to identify MID of the EQ-5D-3L in patients with endometrial cancer and none were identified. The following is a summary of MID of the EQ-5D-3L in patients with other cancers.
Pickard et al. conducted a retrospective analysis on cross-sectional data collected from 534 patients with cancer.77 A range of MIDs in EQ-5D index-based utility (UK and US) scores and VAS scores were estimated using both anchor-based (ECOG PS and FACT-G total score–based quintiles) and distribution-based (0.5 SD and standard error of the measure) approaches. Important differences in EQ-5D utility and VAS scores were similar for all cancers (not including endometrial cancer). For UK-utility scores, MID estimates based on PS ranged from 0.10 to 0.12 and were 0.09 to 0.10 using FACT-G quintiles for all cancers (not including endometrial cancer). For US-utility scores, MIDs ranged 0.07 to 0.09 grouped by PS and when based on FACT-G quintiles, MIDs were 0.06 to 0.07 in all cancers (not including endometrial cancer). MIDs for VAS scores ranged from 8 to 12 (PS) and 7 to 10 (FACT-G quintiles).77
Appendix 7: Sponsor-Provided New Data of Study KN-158 From Request for Reconsideration (Cut-Off Date: January 12, 2022)
Note this appendix has not been copy-edited.
To support the request for reconsideration (RfR), the sponsor provided a descriptive analyses of patients with MSI-H or dMMR endometrial carcinoma receiving pembrolizumab monotherapy (i.e., cohort D and cohort K of study KN-158).83-86 The updated efficacy and safety data are presented in Table 35, Figure 11, Figure 12, and Figure 13. The baseline characteristics were similar except that more patients had an ECOG PS score of 0 in the updated analysis (42 out of 94 patients, 44.7%) compared with that in the original analysis (35 out of 90, 38.9%). The patient disposition, drug exposure and censoring rules for DOR are presented in Table 36, Table 37 and Table 38, respectively. The use of prior medication, concomitant medication, and subsequent anticancer drug use appeared similar to that reported in the original analysis.
The updated results for PFS and ORR (Cut-off date: January 12, 2022, with the median follow-up time of 24.2 months, range from 0.5 months to 71.4 months) appeared consistent with the data originally included in the submission for this review (Cut-off date: October 5, 2020, with the median follow-up time of 16.5 months, range from 0.5 months to 56.1 months). The updated median OS was 65.4 months (95% CI, 29.5 to NR) compared to the original median OS (NR [95% CI, 27.2 to NR] reported in the cut-off date of October 5, 2020, with the median follow-up time of 16.5 months [range, 0.5 months to 56.1 months]).
The safety profile was aligned with the original analysis and no additional safety signals were observed. The updated data further confirmed the potential durable response of OS, PFS, ORR in patients with advanced endometrial carcinoma that is MSI-H or dMMR, who have PD following prior systemic therapy and are not candidates for curative surgery or radiation. However, there was uncertainty regarding the magnitude of clinical benefit directly attributable to pembrolizumab due to the nonrandomized, noncomparative, open-label study design, the small sample size, and lack of formal hypothesis testing of the submitted evidence. The lack of comparator or adjustment for confounding precludes causal inferences.
Table 35: Summary of Key Results From Pivotal and Protocol-Selected Studies
Outcome | Study KN-158 (cohort D and cohort K) Pembrolizumab | |
|---|---|---|
(N = 90) Reported in Original Clinical Study Report (cut-off date: October 5, 2020) | (N = 94) Updated Data for RfR (cut-off date: January 12, 2022) | |
Efficacy (efficacy analysis population) | N = 79 | N = 94 |
OS | ||
Death, n (%) | 29 (36.7) | 41 (43.6) |
Median survival (95% CI),a months | NR (27.2 to NR) | 65.4 (29.5 to NR) |
OS rate, % a | ||
6 months | 82.3 | 82.9 |
12 months | 69.4 | 70.0 |
18 months | 67.9 | NR |
24 months | 64.0 | 64.2 |
36 months | 60.1 | 59.2 |
48 months | 60.1 | 59.2 |
60 months | 60.1 | 51.3 |
PFS | ||
Number (%) of PFS events | 45 (57.0) | 58 (61.7) |
Person-months | 1,238 | 1,733 |
Event rate per 100 person-months (%) | 3.6 | 3.3 |
Median PFS (95% CI), monthsa | 13.1 (4.3 to 34.4) | 13.1 (4.3 to 25.7) |
PFS rate, % a | ||
6 months | 59.5 | 58.3 |
12 months | 51.0 | 50.3 |
18 months | 45.4 | NR |
24 months | 41.3 | 40.5 |
36 months | 37.0 | 36.6 |
48 months | 37.0 | 36.6 |
60 months | 37.0 | 31.5 |
ORR, n (%; 95% CI)b | ||
Objective response (CR + PR) | 38 (48.1; 36.7 to 59.6) | 47 (50.0; 39.5 to 60.5) |
CR | 11 (13.9; 7.2 to 23.5) | 15 (16.0; 9.2 to 25.0) |
PR | 27 (34.2; 23.9 to 45.7) | 32 (34.0; 24.6 to 44.5) |
DORc | N = 38 | N = 47 |
Median (range),a months | NR (2.9 to 49.7) | 63.2 (2.9 to 63.2) |
≥ 12 months, n (%)a | 24 (88.1) | 34 (86.8) |
≥ 24 months, n (%)a | 18 (72.9) | 18 (70.7) |
≥ 36 months, n (%)a | 12 (68.1) | 15 (66.3) |
≥ 48 months, n (%) | NR | 13 (66.3) |
≥ 60 months, n (%) | NR | 5 (66.3) |
Harms (safety analysis population) | N = 90 | N = 94 |
Patients with at least 1 AE, n (%) | 86 (95.6) | 92 (97.9) |
Patients with at least 1 SAE, n (%) | 34 (37.8) | 38 (40.4) |
Patients with an AE leading to discontinuation from the treatment, n (%) | 6 (6.7) | 8 (8.5) |
Death due to AEs | 0 (0.0) | 0 (0.0) |
Notable harms | ||
Adrenal insufficiency | 1 (1.1) | 1 (1.1) |
Colitis | 3 (3.3) | 4 (4.3) |
Hepatitis | 1 (1.1) | 1 (1.1) |
Hyperthyroidism | 7 (7.8) | 7 (7.4) |
Hypophysitis | 0 (0.0) | 0 (0.0) |
Hypothyroidism | 13 (14.4) | 15 (16.0) |
Nephritis | 0 (0.0) | 0 (0.0) |
Pneumonitis | 1 (1.1) | 2 (2.1) |
Type 1 diabetes mellitus | 2 (2.2) | 2 (2.1) |
AE = adverse event; CI = confidence interval; CR = complete response; DOR = duration of response; NR = not reached; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response. RfR = request for reconsideration; SAE = serious adverse event.
Note: Nonserious AEs were followed up to 30 days of last dose and SAEs were followed up to 90 days of last dose are included.
aFrom product-limit (Kaplan-Meier) method for censored data.
b95% CI based on the binomial exact CI method.
cIncluded patients with confirmed CR or PR.
Sources: KN-158 Clinical Study Report.21 The sponsor updated analysis on January 22, 2022.86
Figure 11: Kaplan-Meier Estimates of Overall Survival — All Participants As-Treated Population
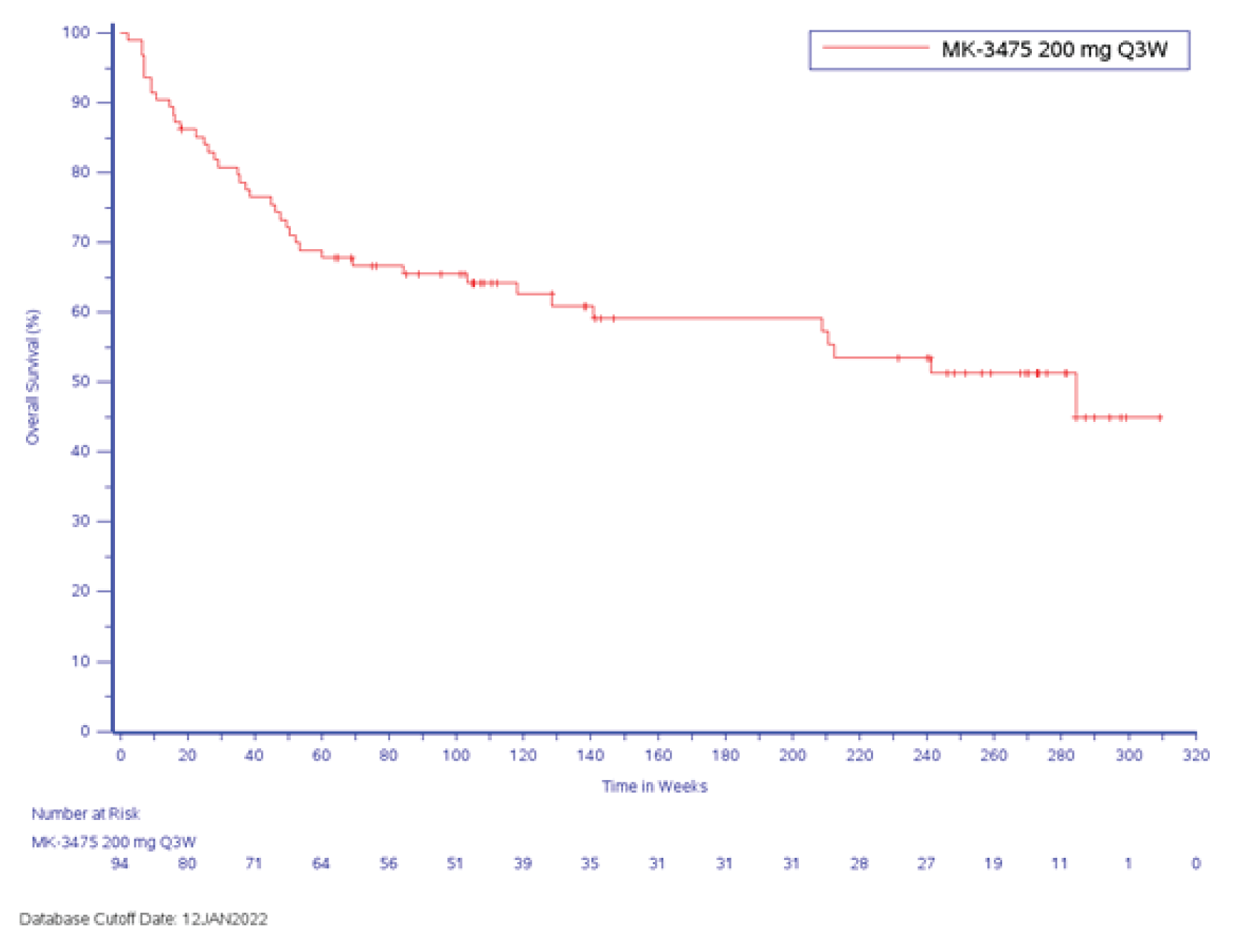
Source: Additional information from the sponsor was received on July 25, 2022.86
Figure 12: Kaplan-Meier Estimates of Progression-Free Survival Based on IRC Assessment (All Participants As-Treated Population)
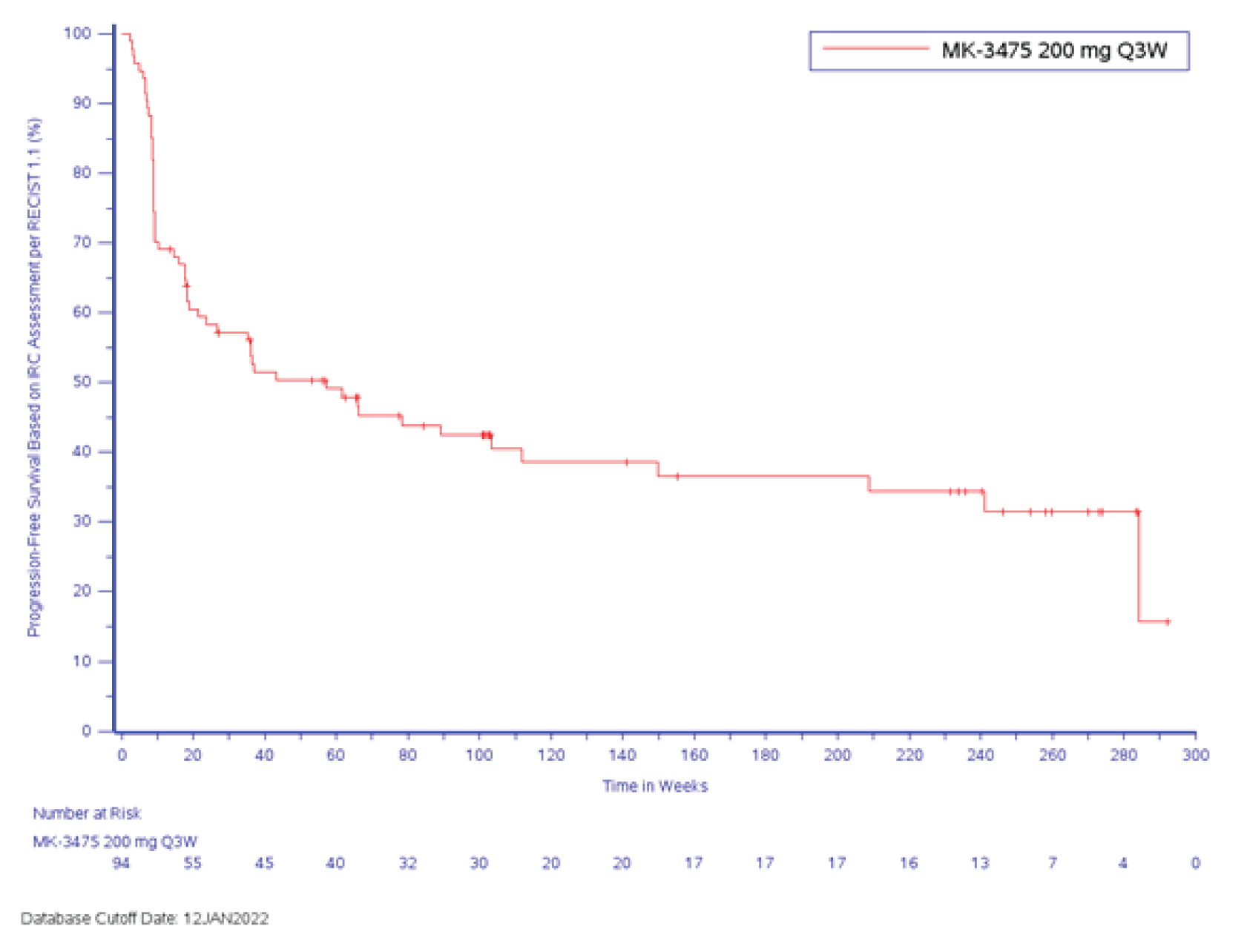
Source: Additional information from the sponsor was received on July 25, 2022.86
Figure 13: Kaplan-Meier Estimates of Duration of Response (All Participants As-Treated Population)
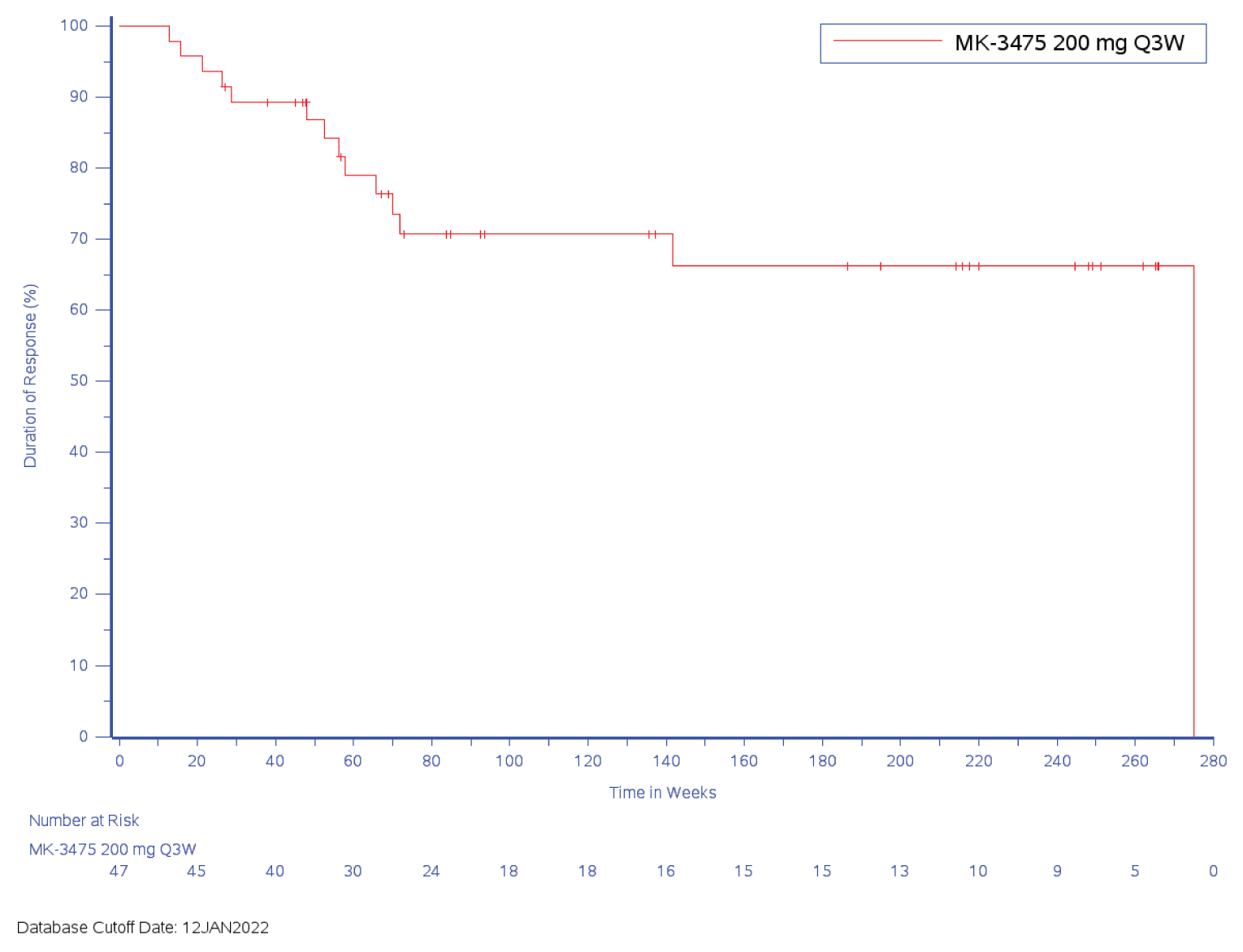
Source: Additional information from the sponsor was received on July 25, 2022.86
Table 36: Patient Disposition — All Participants As-Treated Population
Characteristic | Study KN-158 (cohort D and cohort K) Pembrolizumab | |
|---|---|---|
(N = 90) Reported in Original Clinical Study Report (cut-off date: October 5, 2020) | (N = 94) Updated Data for RfR (cut-off date: January 12, 2022) | |
Screened, N | NR | NR |
Total # of patients included in this population, N | 90 | 94 |
Status for study medication in triala, n (%) | ||
Started | 90 (100.0) | 94 (100.0) |
Completed | 18 (20.0) | 22 (23.4) |
Discontinued | 52 (57.8) | 67 (71.3) |
Adverse event | 6 (6.7) | 9 (9.6) |
Clinical progression | 7 (7.8) | 7 (7.4) |
Complete response | 2 (2.2) | 3 (3.2) |
Physician decision | 2 (2.2) | 1 (1.1) |
Progressive disease | 30 (33.3) | 42 (44.7) |
Withdrawal by patient | 5 (5.6) | 5 (5.3) |
Treatment ongoing | 20 (22.2) | 5 (5.3) |
Status for trial, n (%) | ||
Discontinued | 32 (35.6) | 43 (45.7) |
Death | 29 (32.2) | 39 (41.5) |
Withdrawal by patient | 3 (3.3) | 4 (4.3) |
Ongoing In trial | 58 (64.4) | 51 (54.3) |
ITT, N | Not performed | NR |
ASaT for efficacy analysis b, N | 79 | NR |
Full analysis | 63 | NR |
PP, N | Not performed | NR |
Safety analysis,c N | 90 | NR |
ASaT = all subjects as-treated; ITT = intention to treat; NA = not applicable; NR = not reported; PP = per-protocol; RfR = request for reconsideration.
aEach patient was counted once for patient study medication disposition based on the latest corresponding disposition record.
bA total of 79 patients included in the all patients as-treated for efficacy analysis, which was defined as all patients who received at least 1 dose of study intervention and had been enrolled at least 26 weeks before the data cut-off.
cThe safety analysis population included all patients who received at least 1 treatment.
Sources: KN-158 Clinical Study Report.21 The sponsor updated analysis on January 22, 2022.86
Table 37: Summary of Drug Exposure (Safety Population)
Characteristic | Study KN-158 (cohort D and cohort K) Pembrolizumab | |
|---|---|---|
(N = 90) Reported in Original Clinical Study Report (cut-off date: October 5, 2020) | (N = 94) Updated Data (cut-off date: January 12, 2022) | |
Follow-up time, median (range), months | 16.5 (0.5 to 56.1) | 24.2 (0.5, 71.4) |
Subsequent cancer therapy after discontinuing from study treatment; | ||
1 subsequent oncologic therapy | 10 (11%) | 12 (12.8%) |
2 subsequent oncologic therapies | 4 (4.4%) | 4 (4.3%) |
3 subsequent oncologic therapies | 2(2.2%) | 1 (1.1%) |
> 3 subsequent oncologic therapies | NR | 3 (3.2%) |
Study duration on therapy (months) | ||
Median (range) | 8.30 (0.03 to 26.88) | 11.02 (0.03 to 26.88) |
Number of administrations | ||
Median (range) | 12.50 (1.00 to 35.00) | 15.00 (1.00 to 35.00) |
Duration of treatment for pembrolizumab (months) | ||
> 0 | 90 (100.0) | 94 (100.0) |
≥ 6 | 51 (56.7) | 59 (62.8) |
≥ 12 | 34 (37.8) | 47 (50.0) |
≥ 18 | 24 (26.7) | 33 (35.1) |
≥ 21 | 23 (25.6) | 29 (30.9) |
Note: Database cut-off date: October 5, 2020.
Sources: KN-158 Clinical Study Report.21 The sponsor updated analysis on January 22, 2022.86
Table 38: Censored Information for Duration of Response Assessment (Per Central Radiology Assessment)
Characteristic | Study KN-158 (cohort D and cohort K) Pembrolizumab | |
|---|---|---|
(N = 90) Reported in Original Clinical Study Report (cut-off date: October 5, 2020) | (N = 94) Updated Data (cut-off date: January 12, 2022) | |
Number of patients with responsea | 38 | 47 |
Patients who progressed or died,b n (%) | 9 (23.7) | 14 (29.8) |
Censored patients, n (%) | 29 (76.3) | 33 (70.2) |
Patients who missed 2 or more consecutive disease assessments | 0 (0.0) | 2 (4.3) |
Patients who started new anticancer treatment | 1 (2.6) | 1 (2.1) |
Patients who were lost to follow-up | 0 (0.0) | 0 (0.0) |
Patients whose last adequate assessment was ≥ 5 months prior to data cut-off date | 7 (18.4) | 7 (14.9) |
Ongoing responsec | 21 (55.3) | 23 (48.9) |
Notes: For censored patients who met multiple criteria for censoring and do not have ongoing response, patients were included in the censoring criterion that occurred earliest.
Database cut-off date: October 5, 2020.
aIncludes patients with a confirmed complete response or partial response.
bIncludes patients who progressed or died without previously missing 2 or more consecutive disease assessments.
cIncludes patients who are alive, have not progressed, have not initiated new anticancer treatment, are not lost to follow-up, and whose last disease assessment was less than 5 months prior to data cut-off date.
Sources: KN-158 Clinical Study Report.21 The sponsor updated analysis on January 22, 2022.86
Appendix 8: Summary and Critical Appraisal of Real-World Evidence Study by Kelkar et al. (2022)
Note this appendix has not been copy-edited.
As part of the sponsor’s request for reconsideration of the draft recommendation from pERC, the sponsor submitted a real-world evidence study by Kelkar et al. (2022). The sponsor indicated that this study may address the gap in evidence comparing pembrolizumab to other treatments for patients with dMMR EC, which was not included in the original submission to CADTH. As such, the study by Kelkar et al. (2022)18 has been summarized and critically appraised as part of the sponsor’s request for reconsideration.
The purpose of the study by Kelkar et al. (2022), herein referred to as the ECHO study, was “to describe treatment patterns and real-world clinical outcomes in patients with MSI-H or dMMR advanced endometrial cancer who have progressed following prior systemic therapy in the US from mid-2016 to mid-2019.”
Methods
The ECHO study was a multicentre, retrospective, medical chart review (cohort) study. Data informing the real-world evidence study were based on de-identified data from medical records of eligible patients provided by physicians that were recruited from a health care database (Definitive Healthcare National Database). Eligible patients were aged at least 18 years, diagnosed with advanced endometrial cancer between July 1, 2016, and December 31, 2018, and not candidates for curative surgery. Patients also must have had a known tumour status of MSI-H or dMMR, received at least 1 systemic therapy after diagnosis, had disease progression between July 1, 2016, and June 30, 2019, and were not currently enrolled in an endometrial cancer clinical trial.
De-identified patient data included age, comorbidities, race, body mass index, ECOG PS, disease stage, histology, and MSI/MMR testing information (type of test, result). Details of treatment including drugs, dosage, frequency, and discontinuation, as well as best overall response to treatment were also included. Treatment response to second-line therapy was categorized as CR, PR, stable disease, or disease progression. CR and PR informed the real-world overall response (rwORR) to treatment outcome. The measurement of response was variable, and could have been assessed using Response Evaluation Criteria in Solid Tumours (RECIST) (78%), immune-related RECIST( imRECIST) (11%), or clinical assessment (11%). Real-world progression-free survival (rwPFS) was defined as the time from initiation of second-line therapy to an increase in tumour size, cancer stage, discontinuation of a line of therapy due to disease progression, or death. OS was defined as the time form date of initiation of second-line therapy to death.
The findings were summarized descriptively. Kaplan-Meier curves medians as well as estimated event probabilities at various time points were reported for OS and PFS. For time-to-event outcomes, patients were censored at the last recent contact documented in the medical chart. There were no formal comparisons between groups.
Results
A total of 48 physicians participated in this study, providing medical chart data for 124 eligible patients which was abstracted for the ECHO study. Among these, the most common (105 patients, 85%) first-line therapy was carboplatin/paclitaxel. As second-line therapy, 21 (17%) had initiated chemotherapy with or without bevacizumab and 103 (83%) initiated immunotherapy. Further, the majority (12 patients, 57%) of patients who received chemotherapy with or without bevacizumab received doxorubicin/doxorubicin liposomal monotherapy, and 92 (89%) patients who initiated immunotherapy received pembrolizumab.
The mean age was 61.4 (SD = 9.5) years at diagnosis, 78% were white, 13% were Black, and the most prevalent comorbidity was diabetes (34% of patients). At diagnosis, the majority of patients had Stage IIIB-IV advanced endometrial cancer (86%) and an ECOG PS of 1 or 2 (77%). The sponsor reported that patient demographics and characteristics were similar for patients who received chemotherapy with or without bevacizumab and those who received immunotherapy.
In the chemotherapy ± bevacizumab group, 95.2% of patients discontinued after a median of 4 months (95% CI, 2.0 to 6.0), while in the immunotherapy group 50.5% of patients discontinued after a median of 21 months (95% CI, 15.0 to not estimable [NE]). Within the immunotherapy group, patients who were treated with pembrolizumab had a median time to discontinuation of 24 months (95% CI, 15.0 to NE). Patients who received doxorubicin/doxorubicin liposomal monotherapy discontinued after a median of 2 months (95% CI, 2.0 to 5.0).
Overall Survival
Median OS was 7.0 months (95% CI, 5.0 to 18.0) in patients who received chemotherapy with or without bevacizumab and median OS was not reached (95% CI, 30.0 to NE) in patients who received immunotherapy. The median OS reported for patients who received doxorubicin/doxorubicin liposomal monotherapy was 4.5 months (95% CI, 4.0 to 18.0) and for patients who received pembrolizumab, median OS was 30.0 months (95% CI, 30.0 to NE). The estimated probability of survival at 6, 12, and 24 months after initiation of second-line therapy was 93.4%, 77.4%, and 62.0%, respectively, for patients who received pembrolizumab.
Progression-Free Survival
Median rwPFS was estimated to be 4.0 months (95% CI, 2.0 to 9.0) for patients who received chemotherapy with or without bevacizumab and 29.0 months (95% CI, 18.0 to NE) for patients who received immunotherapy. For patients that received doxorubicin/doxorubicin liposomal monotherapy, rwPFS was 2.0 months (95% CI, 2.0 to 9.0) and for patients who received pembrolizumab, rwPFS was 29.0 months (95% CI, 18.0 to NE). Further, the estimated probability rwPFS at 6, 12, and 24 months after initiation of second-line therapy for patients who received pembrolizumab was 83.4%, 69.9%, and 55.5%, respectively.
Overall Response Rate
The physician-reported rwORR was 23.8% (4.8% had CR and 19.0% had PR) in patients who received chemotherapy with or without bevacizumab and was 78.6% (29.1% had CR and 49.5% had PR) in patients who received immunotherapy. For patients that received pembrolizumab, the rwORR was 80.4%. No patients who received doxorubicin/doxorubicin liposomal monotherapy responded to treatment.
Duration of Response
The DOR was 4 months (95% CI, 4.0 to 14.0) among those who received chemotherapy ± bevacizumab and was 26 months (95% CI, 26.0 to NE) among those who received immunotherapy. The median time to rwORR was 3 months among those who received pembrolizumab.
Critical Appraisal
There is a risk of selection bias related to both the selection of the physicians and the patients. This risk of bias is of unknown magnitude and direction, but likely high given the lack of information available (i.e., the population of eligible physicians and response rate is not reported, and patients were required to have received MSI/MMR tumour testing). The data informing this study are based on US medical records, therefore it is unclear how generalizable the results are to Canadian clinical practice. The results were descriptive and there was no hypothesis testing or control for patient characteristics. The risk of confounding is high as it was not considered in either the design or analysis of the study. No formal comparisons were made within the study; therefore, it is not possible to draw conclusions about comparative efficacy (vs. chemotherapy). It is unclear why some patients received immunotherapy (pembrolizumab) and others received an alternative second-line therapy. Moreover, whether there was a difference in these patients might relate to differences in outcomes, which is another issue of confounding for the results.
As for the relevance of comparators included in the ECHO study, bevacizumab was not considered a relevant comparator for Canada in this review. Doxorubicin/doxorubicin liposomal monotherapy was of interest; however, this comparator group represented a small number and proportion of patients included in the analysis (n = 12 or 10% of all included patients). As such, the estimates obtained from comparator groups are likely unreliable.
OS was estimated from the date of initiation to the date of death and is an objective outcome, therefore bias in measurement of the outcome is not concerning. Very limited information is available on how other outcomes were measured and there was potential for variability across hospitals and clinicians for response and progression outcomes. It is also unclear how many patients may have been lost to follow-up and how many patients were censored, as this was not addressed in the report. Consequently, it is not clear how much this affected the findings. Another consideration is that the data were collected from the charts unblinded; therefore, there is a potential for bias being introduced in the collection of the outcome data. The extent of missing data in the patient charts is unknown, and data extraction errors may have occurred; the degree to which this may have affected the findings is unclear.
Summary
The ECHO study was summarized as part of the sponsor’s request for reconsideration as the sponsor indicated this may address the gap in evidence regarding the comparison of pembrolizumab to other treatments for patients with dMMR EC. This multicentre, retrospective, medical chart review study reported OS observed in patients that received pembrolizumab as second-line treatment for advanced endometrial cancer, which was consistent with the updated analysis of KN-158 (data cut-off of January 12, 2022) submitted by the sponsor (Appendix 7). Results for PFS, ORR, and DOR from the ECHO study suggested favourable results for patients that received pembrolizumab; however, these results are subject to limitations such as likely selection bias, potential for bias in outcome measurement, variability between hospitals and clinicians, lack of information on missing data and loss to follow, and potential data extraction errors which may have resulted in poor data quality. All results reported in the ECHO study were descriptive and did not include hypothesis testing, therefore, how treatment with pembrolizumab compares to other treatments for patients with dMMR endometrial cancer remains unclear.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
dMMR
mismatch repair deficient
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
KM
Kaplan-Meier
KN-158
KEYNOTE-158
KN-775
KEYNOTE-775
MSI-H
microsatellite instability–high
OS
overall survival
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
ToT
time on treatment
TPC
treatment of physician’s choice
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab; powder for solution for infusion 50 mg or solution for infusion 100 mg/4 mL vial IV infusion over 30 minutes |
Submitted price | Pembrolizumab, 100 mg, solution: $4,400.00 per 100 mg/4 mL vial for IV infusion |
Indication | For the treatment of adult patients with unresectable or metastatic microsatellite instability–high or mismatch repair–deficient endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options, as monotherapy |
Health Canada approval status | NOC/c |
Health Canada review pathway | Standard |
NOC date | April 18, 2019 |
Reimbursement request | As per indication |
Sponsor | Merck Canada Inc. |
Submission history | Previously reviewed: Yes Pembrolizumab (Keytruda) has been reviewed for multiple indications at CADTH. The following indications were reviewed in 2020 and 2021. Indication: Esophageal carcinoma, gastroesophageal junction adenocarcinoma
Indication: Classical Hodgkin lymphoma
Indication: Metastatic or unresectable recurrent head and neck squamous cell carcinoma
Indication: Advanced renal cell carcinoma
|
dMMR = deficient mismatch repair; MSI-H = microsatellite instability–high; NOC/c = Notice of Compliance with conditions.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Second-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy |
Treatment | Pembrolizumab |
Comparators | TPC (doxorubicin or paclitaxel) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (20 years) |
Key data source | KEYNOTE-158, a nonrandomized, open-label, multisite phase II study |
Submitted results | ICER for pembrolizumab was $39,879 per QALY (incremental costs = $154,373; incremental LYs = 6.04; incremental QALYs = 3.87) compared with TPC |
Key limitations |
|
CADTH reanalysis results |
|
dMMR = mismatch repair deficient; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; LY = life-year; MSI-H = microsatellite instability–high; OS = overall survival; TPC = treatment of physician’s choice; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year.
Conclusions
The sponsor’s economic evaluation was informed by results from the KEYNOTE-158 (KN-158) trial — a single-arm phase I trial that aimed to assess the efficacy and safety of pembrolizumab among adult patients with mismatch repair–deficient (dMMR) or microsatellite instability–high (MSI-H) recurrent or advanced endometrial carcinoma. According to the CADTH clinical review, there was uncertainty around the magnitude of the clinical benefit given the single-arm trial design, which does not support the development of causal inferences. The clinical review also categorized the sponsor’s submitted indirect treatment comparison (ITC) as very low quality due to serious methodological limitations. No robust conclusions can be made concerning the comparative efficacy of pembrolizumab versus physician’s choice of chemotherapy (TPC), and incremental effectiveness is therefore unknown.
Due to this lack of robust comparative clinical evidence and other methodological limitations within the sponsor’s economic model, CADTH was not able to derive a base-case reanalysis. The sponsor’s choice of a partitioned survival model (PSM) may overestimate incremental quality-adjusted life-years (QALYs), and the long-term extrapolations of overall survival (OS) and progression-free survival (PFS) are highly uncertain and are based on assumptions that lack face validity or evidentiary support. The sponsor’s model is highly sensitive to extrapolations of OS. The sponsor’s base-case results indicate that 96% of the incremental benefit of pembrolizumab was obtained beyond the observation period of the single-arm trial period (16.5 months), and cost-effectiveness results vary widely based on the chosen extrapolation function.
Based on the CADTH exploratory analysis, treatment with pembrolizumab was associated with an incremental cost-effectiveness ratio (ICER) of $60,933 per QALY compared to TPC, and a price reduction of 18% would be needed for pembrolizumab to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY. This estimate is subject to the limitations within the sponsor’s submission. Most crucially, the lack of direct evidence or robust indirect evidence and the high degree of uncertainty around the extrapolation functions used to extrapolate OS beyond the period of the trial produces a bias that favours pembrolizumab. As such, an additional price reduction may be warranted.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process (specifically, information that pertains to the economic submission).
One patient group, the Colorectal Cancer Resource & Action Network, a collaboration between the Canadian Cancer Society and the Canadian Cancer Survivor Network, provided input for the current review. Patient input emphasized that there are limited treatment options in general for patients with advanced endometrial cancer, which are associated with significant treatment-related toxicities or adverse effects, including fatigue, constipation, peripheral neuropathy (numbness, tingling, and pain in the nerves), and changes in libido or sexual function. Importantly, patient input reported that the overall lack of efficacy associated with standard of care chemotherapies compromised their everyday quality of life due to toxic side effects. Additionally, patients reported that their activities or tasks of daily living were moderately to significantly impacted, including exercise, work, travel, and household chores, and this affected their quality of life. Patients indicated that drug affordability, improved efficacy (e.g., OS), disease regression, a reduction in side effects and toxicities (none or minimal), and an improved quality of life were important treatment goals and the most clinically meaningful outcomes. Commonly reported symptoms in the advanced disease setting included pelvic and abdominal discomfort, bloating, or presence of a mass, gastrointestinal or genitourinary symptoms, or constitutional symptoms. Patients with experience being on pembrolizumab monotherapy indicated that they had previously exhausted all standard of care therapies for the management of advanced endometrial cancer, and while on pembrolizumab monotherapy, their quality of life improved remarkably as they were able to resume a normal life without interruptions while under therapy, experienced no adverse events, had significant disease regression, had delayed disease progression, and experienced short infusion time, unlike other standard chemotherapies.
One clinician group provided input for this review: the Ontario Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee. They reiterated the same treatment goals that were expressed by patients as being most important: prolonged life, delayed disease progression, symptomatic relief, partial response, full response, improved health-related quality of life (HRQoL), and decreased treatment toxicity. Importantly, registered clinicians indicated that there is currently no standard of care for the indicated population, as most patients do not respond to the limited number of available treatments. Place in therapy was noted to be the same for pembrolizumab monotherapy and pembrolizumab in combination with lenvatinib, as there is no established second-line treatment paradigm and would replace potential treatment with carboplatin or paclitaxel, or doxorubicin. Both pembrolizumab monotherapy and pembrolizumab in combination with lenvatinib were indicated to be the preferred options for post–platinum therapy.
Feedback from the drug plans reiterated the input from patients and registered clinicians — that, currently, there is no standard of care treatment for patients who progress on platinum-containing regimens. Drug plans noted that pembrolizumab is currently under review for patients with dMMR or MSI-H endometrial cancer who have progressed on or after platinum-based treatment. Drug plans anticipated the potential for indication creep for patients who may be eligible, such as for those patients with carcinosarcoma and sarcoma (i.e., leiomyosarcoma and stromal sarcomas), patients with unstable central nervous system metastases, and patients with an Eastern Cooperative Oncology Group Performance Status of 1 or greater who are eligible for pembrolizumab monotherapy. Drug plans anticipate that drug wastage is likely for pembrolizumab and raised concerns about whether weight-based dosing of pembrolizumab would be applicable to Canadian clinical practice for the given indication.
Several of these concerns were addressed in the sponsor’s model:
PFS and OS were modelled for the overall population. HRQoL was incorporated into the model by progression status.
One-off costs of dMMR or MSI-H testing were included.
CADTH was unable to address the following concerns raised from stakeholder input:
Within the economic model, the sponsor incorporated a fixed dosing approach (i.e., 200 mg every 3 weeks) for pembrolizumab as per the Health Canada indication and product monograph for pembrolizumab, which was implemented in the KN-158 trial. The sponsor did not include an option to assess the effects of weight-based dosing for pembrolizumab and, as such, CADTH was unable to explore this option further. However, drug wastage of comparator treatments was incorporated, as appropriate. The cost-effectiveness of weight-based dosing for pembrolizumab remains unknown.
Economic Review
The current review is for pembrolizumab (Keytruda) for adult patients with recurrent or advanced dMMR or MSI-H endometrial cancer.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Pembrolizumab is indicated as monotherapy for the treatment of adult patients with unresectable or metastatic dMMR or MSI-H endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options.1
The sponsor submitted a cost-utility analysis to assess the cost-effectiveness of pembrolizumab compared with a mixed basket comparator, which is TPC (doxorubicin or paclitaxel). The modelled population is consistent with the reimbursement request and is aligned with the population of the KN-158 trial, a nonrandomized, multicentre, single-arm, open-label, phase II trial.1,2
Pembrolizumab is supplied in single-use vials at a submitted price of $4,400.00 per injectable 4 mL vial (100 mg/mL). The recommended dose for pembrolizumab is 200 mg every 3 weeks until unacceptable toxicity or disease progression, or for up to 24 months in patients without disease progression.3 The dosages of all comparator treatments were based on the recommended dosages in their respective product monographs: for doxorubicin, it was 60 mg/m2 every 21 days and for paclitaxel, it was 80 mg/m2 every 21 days.4,5
The sponsor’s calculated cost of pembrolizumab (including administration costs and wastage) is $8,800 per treatment course. The sponsor estimated the costs of each comparator per treatment course (doxorubicin = $780.00 per treatment course; paclitaxel = $36.56 per treatment course), which were calculated based on the consideration of partial (i.e., 50%) wastage and as a sum of 2 different formulations.
The clinical outcomes of interest were QALYs and life-years. The economic analysis was undertaken over a lifetime horizon (20 years) from the perspective of a Canadian publicly funded health care payer. Costs and outcomes were discounted at a rate of 1.5% annually.1
Model Structure
A PSM was submitted to capture the long-term costs and effects associated with the natural history of recurrent or advanced dMMR or MSI-H endometrial cancer over the model’s time horizon.1 The model consisted of 3 primary health states: PFS, progressive disease, and death. The proportion of patients who were progression-free, experienced progressive disease, or were dead at any time over the model’s time horizon was derived from nonmutually exclusive Kaplan-Meier (KM) survival curves. The modelled time cycle was 1 week. OS and PFS curves were derived from the KN-158 trial for pembrolizumab and the treatment of physician’s choice (doxorubicin or paclitaxel), and were used to determine the proportion of patients in each health state.1 These nonmutually exclusive survival curves were used to inform the proportion of patients who were in PFS, progressive disease, or death states at any time over the model’s time horizon. Specifically, all patients entered the model in the progression-free state; the proportion of progression-free patients was derived as the area under the PFS curve while the proportion of patients with progressed disease was derived by the difference in the area under the curve between the OS and PFS curves.1 Progression in the KN-158 trial was defined as the time from allocation to the first documented disease progression according to Response Evaluation Criteria in Solid Tumours Version 1.1, as assessed by independent central radiologic review or death due to any cause, whichever occurred first.2 OS was defined as the time from the date of allocation to the date of death due to any cause.2 Time on treatment (ToT) was calculated for pembrolizumab using the KN-158 trial data to identify the proportion of patients who were alive and who remained on treatment for the full duration of the treatment cycle.1
Model Inputs
The patient cohort consisted of adult patients with recurrent or advanced dMMR or MSI-H endometrial cancer, whose baseline characteristics mainly reflected the pivotal trial, KN-158.2 The median age of patients in the model was 62.80 years, with a mean weight of ███████, and a body surface area of █████.1
Key clinical efficacy inputs (i.e., OS and PFS) and ToT for pembrolizumab were based on the results of the KN-158 trial (i.e., data cut-off of October 5, 2020). KM estimates of PFS, OS, and TTD for pembrolizumab from the trial period (median follow-up = 16.5 months) were used to extrapolate the treatment effect beyond the observed trial data via parametric survival curves over the entire model time horizon (20 years).1 The sponsor fitted several parametric survival functions to the OS and PFS data of pembrolizumab to extrapolate its long-term efficacy. To determine the best fitting distribution, diagnostic plots, goodness-of-fit statistics, visual inspection, and clinical expectations were assessed regarding long-term progression risk and survival. The chosen parametric survival distribution for both OS and PFS of pembrolizumab was the log-normal distribution. ToT data for pembrolizumab was obtained from the KN-158 trial, and the parametric survival distribution chosen to extrapolate ToT for pembrolizumab over the lifetime was the exponential distribution.1
The comparative efficacy of pembrolizumab versus chemotherapy comparator treatments within TPC (doxorubicin and paclitaxel) was derived from an unadjusted, unanchored, naive ITC submitted by the sponsor via hazard ratios for OS and PFS. The inverse of these hazard ratios (reflecting the comparative efficacy of TPC versus pembrolizumab) under the assumption of proportional hazards were applied to the pembrolizumab survival data to generate OS and PFS curves for TPC. The ToT curve for TPC was generated by applying the same hazard ratio for the PFS of TPC.1
Health state utility values were estimated by a regression model that adjusted for baseline utility and progression status using patients’ HRQoL data collected in the KN-158 trial via the 5-Level EQ-5Dquestionnaire and values based on the UK population. Utility data were fit to a series of linear mixed-effects regression models, and in the economic base case, the sponsor used the regression model that accounted for the effect of adverse events and progression status (PFS or PD). The sponsor incorporated utility values in the base case that differed by health state and whether patients were on or off treatment. The utility weight assigned to the PFS health state (0.764) for patients on or off treatment was greater than the utility weight assigned to the progressed disease health state (0.702) (for patients who had progressed and were on or off subsequent treatment); the same utility weights were applied for both treatments.1
The model included drug acquisition and administration costs, costs associated with subsequent treatment, dMMR or MSI-H endometrial cancer screening, adverse events, resource use for each health state, and terminal care. Drug acquisition costs for pembrolizumab, doxorubicin, and subsequent therapies were obtained from the IQVIA database6 while those for paclitaxel were sourced from Institut national d’excellence en santé et en services sociaux.7 Drug administration costs for therapies administered by IV infusion (pembrolizumab, paclitaxel, and doxorubicin) were assumed to be based on a cost-effectiveness study of systemic therapies for metastatic pancreatic cancer.8,9 The majority of adverse events costs were informed by the Ontario Case Costing Initiative10 while other costs were derived from published literature.11,12 Costs associated with screening for dMMR or MSI-H were obtained from a previous CADTH Optimal Use Report on patients with colorectal cancer requiring dMMR testing.13
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented as follows.
Base-Case Results
In the sponsor’s base case, pembrolizumab was associated with an incremental cost of $154,373 and 3.87 incremental QALYs over a 20-year time horizon (refer to probabilistic results in Table 3), which resulted in an ICER of $39,879 per QALY. In the sponsor’s base case, 25% of patients who received pembrolizumab and 2% of patients who received TPC (both paclitaxel and doxorubicin) were alive at the 20-year time horizon.1
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER vs. TPC (doxorubicin or paclitaxel) ($/QALY) |
|---|---|---|---|---|---|---|---|
TPC | 34,970 | Reference | 2.55 | Reference | 1.74 | Reference | Reference |
Pembrolizumab | 189,343 | 154,373 | 8.58 | 6.04 | 5.61 | 3.87 | 39,879 |
ICER = incremental cost-effectiveness ratio; LY = life-year; TPC = treatment of physician’s choice; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Results were driven by the sponsor’s assumptions about the long-term efficacy of OS that predicted substantial differences in total life-years and the increased drug acquisition costs associated with pembrolizumab.1 The sponsor did not report the incremental benefit (QALYs) derived over the trial period compared to the extrapolated period in its submitted model. CADTH calculated this incremental benefit based on the sponsor’s submitted model and determined that approximately 96% of the incremental benefit associated with pembrolizumab was derived from the extrapolated period.
Sensitivity and Scenario Analysis Results
The sponsor conducted several sensitivity and scenario analyses, the majority of which did not impact model results. These included varying the discount rate to 0% and 3%; testing alternate time horizon periods (15 years, 30 years, and 40 years, respectively); incorporating adverse events disutilities; removing costs associated with adverse events, MSI-H testing costs, and subsequent treatments; applying alternate estimates of patients who would be eligible for subsequent treatment; and applying treatment waning effects to a range of patients. The sponsor’s base-case results were most sensitive to scenarios that fitted various parametric functions for PFS and OS of pembrolizumab to the KM data at various data cut-off points. The ICER was most sensitive to the scenario that explored the OS of pembrolizumab with a KM plus generalized gamma distribution fit at 26 weeks (ICER = $167,864 per QALY) and explored the OS of pembrolizumab with a KM plus log-logistic distribution fit at 52 weeks (ICER = $46,046 per QALY).1
CADTH Appraisal of the Sponsor’s Economic Evaluation
The comparative clinical efficacy and safety of pembrolizumab to TPC is unknown. The CADTH clinical review identified several methodological limitations with the study design of the KN-158 trial and findings from the sponsor’s ITC analysis. The sponsor’s pivotal trial was a nonrandomized, open-label, single-arm trial that aimed to demonstrate the efficacy (i.e., OS and PFS) and safety of pembrolizumab. A key limitation of the KN-158 trial was the absence of a comparator arm, which makes it difficult to interpret efficacy and safety outcomes, as these cannot be definitively attributed to pembrolizumab. Additionally, it was not designed to estimate efficacy compared to chemotherapy directly. Instead, naive indirect comparisons were made between dMMR or MSI-H patients in the KN-158 trial and the subgroup of patients in the KEYNOTE-775 (KN-775) trial. Importantly, the OS and PFS data from the pivotal trial are immature and were not adjusted for potential confounding factors. This may potentially overestimate the efficacy of the treatment.
In the absence of comparative clinical evidence from the pivotal trial, the sponsor undertook an unanchored, unadjusted, naive ITC to assess the cost-effectiveness of pembrolizumab with doxorubicin or paclitaxel using individual treatment group data from 2 separate studies (KN-158 and KN-775). The CADTH clinical review rated the ITC evidence as being very low quality, identifying several methodological concerns with the ITC, including uncontrolled heterogeneity, a failure to conduct a risk of bias assessment from the chosen studies, a lack of data on patient characteristics, and a failure to identify prognostic factors and effect modifiers that were likely imbalanced between groups. Altogether, important methodological limitations of the sponsor’s ITC contributed to an unknown amount and direction of bias such that no formal conclusion could be drawn on the comparative efficacy comparing pembrolizumab with TPC.
CADTH was not able to address the lack of direct comparative evidence or the limitations of the indirect evidence in reanalysis. The comparative effectiveness and cost-effectiveness of pembrolizumab compared with TPC is unknown.
The sponsor’s application of a hazard ratio based on the assumption of proportional hazards, to model the comparative efficacy of TPC, is inappropriate. In the economic model, the sponsor extrapolated lifetime OS and PFS curves for TPC by applying the inverse of the hazard ratios for OS and PFS to the respective KM curves for pembrolizumab from the KN-158 trial. In addition to the many limitations identified previously with the sponsor’s ITC analysis upon which this hazard ratio is based, the sponsor further assumed that the relationship between the hazard rates for pembrolizumab (an immunotherapy) and comparator treatments (chemotherapies using doxorubicin and paclitaxel) could be described by the proportional hazards assumption over the lifetime horizon. This assumption is inappropriate for several reasons. First, it is unlikely that the long-term extrapolations of OS and PFS for pembrolizumab and TPC would follow a parallel trajectory (response pattern) over time, as suggested by the assumption of proportional hazards, as they neither belong to the same drug class nor have the same mechanism of action.14 Second, the input from clinician groups consulted for this review indicated that the survival seen with pembrolizumab seemed incompatible with what would be expected with chemotherapy in practice as pembrolizumab is known to provide a high response rate in long-term responders compared to current chemotherapy treatments that do not provide a durable response and have a high toxicity profile. Lastly, the clinical experts consulted by CADTH indicated that the extrapolated OS and PFS estimates for TPC were overestimated and did not align with the natural history of patients seen in clinical practice in Canada. Based on the commonly used second-line chemotherapies in Canadian clinical practice, the clinical experts consulted by CADTH estimated that fewer than 5% of patients who received TPC would likely remain alive at 5 years and about 2% would be in PFS. QALYs for TPC are likely overestimated as a result of this limitation. This limitation produces a bias that favours TPC (i.e., a bias against pembrolizumab).
CADTH requested the sponsor to provide additional information on testing for the proportional hazard assumption. In its response, the sponsor noted that a visual assessment of the log-cumulative hazard plots was performed, which illustrated that the shape of the KM survival curves from 2 separate studies (KN-158 and KN-775) are not parallel (and indicate separation over time). No formal statistical testing of the proportional hazards assumption was undertaken, and the sponsor acknowledged that the proportional hazards assumption may not be valid. The sponsor further indicated that a limitation of its approach may be the small sample size of patients with dMMR or MSI-H endometrial cancer who received TPC in study KN-775, and this may preclude any definitive conclusions about the incremental OS and PFS of pembrolizumab versus TPC in this group. In an exploratory analysis, CADTH applied the hazard ratio for TPC versus pembrolizumab to the parametric distribution selected for OS and PFS of pembrolizumab, which suggests that TPC will follow a parallel trajectory to pembrolizumab no matter which extrapolation is selected for pembrolizumab.
The PSM structure applied in the economic analysis suggests a postprogression survival benefit, which does not align with clinical expectations. The sponsor’s base-case results suggest that pembrolizumab is associated with a longer survival after disease progression. Specifically, the sponsor’s results imply that patients receiving pembrolizumab would experience a postprogression survival benefit of 3.32 life-years (nearly 55% of the incremental survival). This benefit would be accrued after patients have experienced disease progression and have discontinued pembrolizumab (Table 13). The CADTH clinical review team noted that there is no evidence of a clear mechanism by which pembrolizumab would continue to provide clinical benefit for patients with progressive disease given that the KN-158 trial was a single-arm study and, therefore, a treatment effect between groups could not be assessed. The sponsor’s use of a PSM introduces structural assumptions about the relationship between PFS and OS that likely do not accurately reflect causal relationships within the disease pathway. These assumptions may produce a postprogression survival bias that favours pembrolizumab. Due to the structural independence between OS and PFS end points assumed in a PSM, extrapolations for each end point may reflect within-trial trends in the rates of progression and death. Lastly, the clinical experts consulted by CADTH observed that the sponsor’s extrapolated results for pembrolizumab (based on immature data from the trial observed period) yielded higher survival in the indicated patient population at 5 years and 10 years than that expected in the indicated population. This further indicated that the suggested postprogression benefit of pembrolizumab is not clinically plausible.
CADTH requested the sponsor to provide additional evidence to support the implied postprogression benefit (3.32 incremental life-years; 1.99 incremental QALYs compared with TPC). However, the sponsor did not provide appropriate clinical evidence from the KN-158 trial to substantiate this claim. The sponsor acknowledged that PFS data from the KN-158 trial are not mature with 41% survival at 24 months and 27% survival at 36 months and 48 months. The sponsor further asserted that even though the median OS had not been reached at the data cut-off of 42.6 months, the lower bound of the 95% confidence interval for the median OS (27.2 months) was indicative of a postprogression survival benefit since this lower bound surpassed the median PFS reached at 13.1 months (95% confidence interval, 4.3 months to 34.4 months). Additionally, the sponsor deferred to its extrapolated OS curves (i.e., log-normal distribution) to illustrate a postprogression benefit for pembrolizumab over the time horizon based on immature data. CADTH was unable to determine the extent to which the implied postprogression benefit was due to the effect of treatment with pembrolizumab, structural bias within PSM, or limitations in the comparator efficacy evidence.
Long-term extrapolations of the clinical efficacy for pembrolizumab (OS and PFS) are likely overestimated. The sponsor fitted several parametric survival curves to extrapolate OS and PFS for patients who received pembrolizumab over the lifetime time horizon (20 years) based on the observed period of the single-arm trial, KN-158 (median duration of follow-up = 16.5 months). The OS data informing pembrolizumab transition probabilities were considered immature as the median OS was not reached at the time of the available data cut-off (October 5, 2020). The clinical experts consulted by CADTH further indicated that the estimates of OS projected by the sponsor’s extrapolations beyond the observed period of the KN-158 trial were unrealistically high and did not align with the anticipated prognosis for this patient population based on their clinical expectations. Similar concerns were raised for PFS. Overall, the CADTH clinical review did not find evidence within the KN-158 trial to support the sponsor’s survival extrapolations and further indicated that the immature OS and PFS data from the single-arm trial may overestimate the efficacy of pembrolizumab and introduces considerable additional uncertainty into the long-term extrapolations.
Incremental QALYs for pembrolizumab are likely overestimated as a result of this limitation. CADTH explored alternative assumptions in an exploratory analysis (refer to Appendix 4).
Health state utility values lacked face validity and were derived using uncertain methodology. In the sponsor’s base case, utility values for patients in the progressed disease health state (0.702) were similar to those of patients who were in the progression-free health state (0.764). The clinical experts consulted by CADTH indicated that patient quality of life typically worsens with disease progression. As such, health state utility values for the progressed disease health state lack face validity and likely overestimate patients’ quality of life postprogression, in favour of pembrolizumab. The magnitude of bias in favour of pembrolizumab remains unknown, resulting in additional uncertainty with regard to the impact of health state utility values on the ICER.
CADTH explored alternative assumptions in an exploratory analysis (refer to Appendix 4).
Drug pricing for TPC did not reflect the lowest publicly available list prices, and treatment costs were calculated by summing the costs for more than 1 formulation in consideration of partial (50%) drug wastage. In the economic model, the sponsor selected drug costs for paclitaxel that were sourced from Institut national d’excellence en santé et en services sociaux7 while the price for doxorubicin was not based on the lowest publicly available pricing in the IQVIA DeltaPA database.6 Additionally, the sponsor applied a drug wastage setting that only accounted for partial drug wastage or vial sharing (i.e., 50% of the remaining vial quantity would be shared between patients and the remainder would result in product loss) for comparator treatments administered by IV injection. In consideration of partial wastage, the sponsor further calculated drug costs for paclitaxel and doxorubicin by calculating the average cost of the 2 modelled formulations of each treatment, rather than selecting the treatment that was least costly. These issues underestimate the drug costs for TPC and bias the results in favour of pembrolizumab. However, the clinical experts consulted by CADTH indicated that the policies around vial sharing may vary across Canadian jurisdictions and that partial or full drug wastage might be an area of uncertainty.
CADTH explored alternative assumptions and addressed corrections for drug prices in a scenario analysis (refer to Appendix 4).
The impact of adverse events on patients’ quality of life is uncertain. The sponsor incorporated adverse events utility data collected in the KN-775 trial to model the impact of adverse events on patients’ quality of life in the current review. However, CADTH was unable to validate the details for either of the sponsor’s methodological approaches to account for their impact (i.e., the inclusion of a coefficient for adverse events in regression analyses or applying adverse events disutilities) as the sponsor’s submission was not sufficiently transparent. Additionally, the CADTH clinical review indicated that the comparative safety of pembrolizumab is unknown as the sponsor’s ITC did not assess any harms data or other outcomes of importance to patients. As such, the impact of adverse events on cost-effectiveness results is unknown.
CADTH was unable to address this in reanalysis.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Baseline characteristics of patient population. | Appropriate. The clinical experts consulted by CADTH indicated that the baseline patient characteristics of patients in the KN-158 trial were representative of dMMR or MSI-H endometrial cancer patients in Canadian clinical practice and expressed no concerns of generalizability of the study findings. |
A lifetime time horizon of 20 years. | Appropriate as this time horizon is adequate to capture all lifetime associated costs and outcomes for the indicated population. |
The sponsor’s choice of chemotherapy treatments as part of the TPC group includes doxorubicin and paclitaxel. The sponsor further assumed that 25% of patients would receive paclitaxel and 75% would be on doxorubicin. | Appropriate. The clinical experts consulted by CADTH indicated that the distribution of treatment use for patients who received paclitaxel and doxorubicin in the economic model aligned with the distribution of treatment use in Canadian clinical practice. Importantly, there is no true standard of care for second-line treatment in the indicated population. |
The distribution of subsequent therapies in the model were assumed to be based on the distribution of subsequent treatment use in the KN-775 trial, a multicentre, open-label, randomized, phase III trial of pembrolizumab plus lenvatinib.1 | Appropriate, according to the clinical experts consulted by CADTH. |
The sponsor assumed that 28% and 48% of patients who progressed on pembrolizumab and TPC, respectively, would likely receive subsequent therapies, based on the KN-775 trial. | Inappropriate. The clinical experts consulted by CADTH indicated that a higher proportion of patients (approximately 60%) would be eligible to receive subsequent therapy following treatment with pembrolizumab. While the sponsor’s assumption likely underestimates the proportion of patients who receive subsequent therapy following initial treatment with pembrolizumab, this parameter has minimal to no impact on model results. |
Patients who received paclitaxel within TPC were assumed to be treated with it indefinitely over the lifetime time horizon. | Inappropriate. In the sponsor’s base case, patients who received paclitaxel within TPC were assumed to receive paclitaxel indefinitely over the lifetime time horizon (20 years), which overestimated costs of this chemotherapy. The clinical experts consulted by CADTH indicated that this was unlikely, and patients were likely to receive paclitaxel up to 2 years, and further expressed that this was an area of uncertainty. |
The probabilities of grade ≥ 3 AEs were derived from the KN-158 trial for pembrolizumab reflecting those that occurred in greater than 2% of patients.1 | Appropriate. |
In the economic model, the sponsor did not apply treatment waning effects for pembrolizumab over the lifetime time horizon.1 | Appropriate. The sponsor provided justification in its submission that pembrolizumab has previously been shown to have a sustained a long-term effect on overall survival in patients with endometrial cancer after they discontinued pembrolizumab at 2 years. The clinical experts consulted by CADTH affirmed this, based on their clinical knowledge and on literature demonstrating longer-term immunotherapeutic effects of pembrolizumab after treatment discontinuation. |
dMMR or MSI-H screening costs were included as 1-time costs. | Appropriate. |
AE = adverse event; dMMR = deficient mismatch repair; KN-158 = KEYNOTE-158; KN-775 = KEYNOTE-775; MSI-H = microsatellite instability–high; TPC = treatment of physician’s choice.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
As noted earlier, there are key limitations associated with the model structure and with available clinical data for pembrolizumab and comparative efficacy versus relevant chemotherapies. The use of the PSM in the current review is inappropriate, given that PSMs rely on mature OS data to produce reliable cost-effectiveness estimates. CADTH notes that the sponsor’s model predicts improbable estimates of incremental QALYs gained after disease progression, which was not supported by trial data. Importantly, the comparator population was based on data from the sponsor’s submitted ITC, using individual treatment group data from 2 separate studies (KN-158 and KN-775), which has significant limitations. As such, the comparative effectiveness and safety of pembrolizumab to relevant comparators is highly uncertain. The result of these limitations is that the costs and QALYs associated with the use of pembrolizumab are highly uncertain. CADTH reanalyses cannot address this uncertainty in the clinical evidence. Consequently, CADTH was unable to conduct any base-case reanalysis of the sponsor’s model.
Scenario Analysis Results
A CADTH base-case reanalysis was not performed. Price reduction analyses were not required on the sponsor’s submitted base case, given that pembrolizumab is cost-effective within the conventional threshold of $50,000 per QALY compared to TPC. However, the sponsor’s base-case results are subject to the key limitations of the sponsor’s model, noted previously, and are based on publicly available prices of the comparator chemotherapies (Appendix 4). It is important to note that the sponsor’s estimated incremental OS is likely not representative of the true incremental benefit of pembrolizumab, which is based on single-arm trial results and unanchored, unadjusted, and naive comparative evidence that is subject to an unknown amount of bias, and has overestimated and produced highly uncertain survival estimates, among other limitations. As such, the directionality of bias within the sponsor’s submission is in favour of pembrolizumab, and the long-term incremental benefit of pembrolizumab versus comparator treatments is unknown.
Although CADTH did not conduct any formal reanalyses of the sponsor’s model, an exploratory analysis was undertaken to explore the impact that changes to model assumptions had on the ICER. CADTH observes that the key limitations of the sponsor’s base-case analysis noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation section apply to this exploratory analysis, including the fundamental limitation that there is no direct evidence to support the comparative efficacy of pembrolizumab to relevant chemotherapies. As such, this exploratory analysis should not be interpreted as a CADTH base case, as there remains uncertainty regarding the true effect of pembrolizumab. The key insight from this exploratory analysis is that the validity of the cost-effectiveness estimate for pembrolizumab is highly sensitive to the choice of extrapolation function. Given that the near entirety of incremental benefit is estimated through extrapolation and built upon evidence from an ITC with serious methodological concerns, all estimates of cost-effectiveness are therefore highly uncertain. Details of this exploratory analysis are provided in Appendix 4.
Issues for Consideration
Dostarlimab is indicated for this patient population; however, it is currently not funded in Canada although it has received regulatory approval. The cost-effectiveness of pembrolizumab compared with dostarlimab is unknown.
Based on clinical experts’ responses to drug plan feedback for the given indication, there is the potential for indication creep among patients who may be eligible, such as those with carcinosarcoma and sarcoma (i.e., leiomyosarcoma and stromal sarcomas), as well as patients with unstable central nervous system metastases. Potential indication creep may be possible as eligible patients with an Eastern Cooperative Oncology Group Performance Status of 1 or greater are eligible for pembrolizumab. Thus, off-label usage of pembrolizumab among patients with advanced or recurrent endometrial cancer is likely to result in an increased budget impact. The cost-effectiveness of pembrolizumab in these patients is unknown.
Based on drug plan feedback, dMMR or MSI-H testing is not a standard or reflexive test across jurisdictions. The clinical experts consulted by CADTH indicated that dMMR or MSI-H testing should occur for all patients with endometrial cancer at any stage at the time of diagnosis, and that it is easily performed at low cost.
The submitted economic model did not include an option to assess a weight-based dosing regimen for pembrolizumab, but rather, 1 fixed-dose regimen (i.e., 200 mg every 3 weeks) based on the anticipated Health Canada indication and the KN-158 trial’s study protocol. The clinical experts consulted by CADTH for this review noted that pembrolizumab would be administered on a fixed-dose basis in adult patients except for patients who were very underweight. The impact of weight-based dosing in this population on the cost-effectiveness of pembrolizumab is likely negligible.
Overall Conclusions
The CADTH review of the clinical evidence found no direct comparative evidence between pembrolizumab and TPC (doxorubicin or paclitaxel) for adult patients with recurrent or advanced dMMR or MSI-H endometrial carcinoma. While the safety profile of pembrolizumab in the KN-158 trial appeared consistent with the known safety profile of pembrolizumab, there was uncertainty around the magnitude of benefit of pembrolizumab given the limitations inherent to the single-arm trial design. No robust conclusions can be drawn on the comparative efficacy comparing pembrolizumab with TPC due to the very low methodological quality of the sponsor’s submitted ITC. The comparative safety of pembrolizumab to TPC is also unknown as the ITC did not assess any harms data. While clinical experts consulted by CADTH indicated that the trial outcomes appeared favourable compared to TPC, the magnitude of comparative efficacy of pembrolizumab relative to any currently reimbursed chemotherapies remains highly uncertain.
The pharmacoeconomic results are informed by results from the KN-158 trial and the ITC results. Given that, according to the CADTH clinical review, no robust conclusions can be made concerning the comparative efficacy of pembrolizumab versus TPC, the incremental effectiveness is therefore unknown.
In addition to this lack of robust comparative evidence, CADTH identified other methodological limitations within the pharmacoeconomic model: the sponsor made assumptions about the long-term patient survival that lacked face validity and were not supported by evidence. The sponsor’s choice of a PSM may overestimate incremental QALYs, and the long-term extrapolations of OS and PFS are highly uncertain. The sponsor’s base case was also based on an assumption that the response patterns of pembrolizumab and TPC are parallel over the lifetime horizon, which does not align with what is known about the durability of response for immunotherapies compared with chemotherapies in other cancers.14 CADTH conducted exploratory analysis, the results of which suggest that the model is highly sensitive to long-term extrapolations of OS. The sponsor’s base-case results indicate that 96% of the incremental benefit of pembrolizumab was obtained beyond the observation period of the single-arm trial period (16.5 months), where cost-effectiveness results vary widely based on the chosen extrapolation function. CADTH, in its exploratory analysis, estimated an ICER of $60,933 per QALY and that a price reduction of 18% would be needed for pembrolizumab to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY. However, this estimate is subject to the limitations within the sponsor’s submission — most crucially, the lack of direct evidence or robust indirect evidence and the high degree of uncertainty concerning long-term extrapolation. CADTH’s exploratory analysis results still suggested a large survival benefit for patients (3.91 incremental QALYs), estimated through using highly uncertain data and a methodological approach that adds considerable uncertainty. Due to the high degree of unquantified uncertainty around incremental effectiveness, an additional price reduction may be warranted.
Treatment of dMMR or MSI-H endometrial cancer with pembrolizumab increases costs compared to other currently available treatments. Clinical experts consulted by CADTH suggested that these patients may experience clinical benefit due to the safety profile of pembrolizumab. Given the identified limitations with the sponsor’s submission, CADTH could not estimate the magnitude of potential patient benefit. Due to the methodological limitations identified within the model and clinical evidence, the cost-effectiveness of pembrolizumab monotherapy is unknown.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial[internal sponsor's package]. Toronto (ON): Merck; 2022 Jan 6. .
2.Clinical Study Report: P158V10MK3475. A clinical trial of pembrolizumab (MK-3475) evaluating predictive biomarkers in subjects with advanced solid tumors (KEYNOTE-158) [internal sponsor's report]. Kenilworth (NJ): Merck Sharp & Dohme; 2021.
3.Merck Canada Inc. Product Monograph including patient medication information: Keytruda Pembrolizumab. 2021.
4.Cancer Care Ontario. Product Monograph - Doxorubicin. 2020.
5.Cancer Care Ontario. Product Monograph - Paclitaxel. 2020: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/50491#DrugRegimen.
7.Institut national d'excellence en santé et en services sociaux (INESSS). Avis au ministre - Avastin. . 2016: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Aout_2016/Avastin_2016_06.pdf.
8.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
9.Bank of Canada. Consumer Price Index, 2000 to Present. 2021: https://www.bankofcanada.ca/rates/price-indexes/cpi/. . Accessed November 15, 2021.
10.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 1800 Jan 1.
11.Dranitsaris G, Maroun J, Shah A. Severe chemotherapy-induced diarrhea in patients with colorectal cancer: a cost of illness analysis. Support Care Cancer. 2005;13(5):318-324. PubMed
12.Lathia N, Mittmann N, DeAngelis C, et al. Evaluation of direct medical costs of hospitalization for febrile neutropenia. Cancer. 2010;116(3):742-748. PubMed
13.CADTH. CADTH OPTIMAL USE REPORT DNA Mismatch Repair Deficiency Tumour Testing for Patients With Colorectal Cancer: Recommendations. 2016: https://www.cadth.ca/sites/default/files/pdf/OP0522_dMMR_Report_Recommendations.pdf.
14.Monnickendam G, Zhu M, McKendrick J, Su Y. Measuring Survival Benefit in Health Technology Assessment in the Presence of Nonproportional Hazards. Value Health. 2019;22(4):431-438. PubMed
15.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/. Accessed Feb 28 2022.
16.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 1800 Jan 1.
17.Cancer Care Ontario: funded evidence-informed regimens. 2022; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 1800 Jan 1.
19.Merck. pembrolizumab PM. 2021.
25.CCO. CRBPDOCE Regimen. 2022.
27.INC P. Medroxyprogesterone PM. 2004.
31.Limited TC. Letrozole PM. 2010.
33.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Drug name, doses and administration. City (PROV): Sponsor name; 1800 Jan 1.
34.Statistics CC. Committee Canadian Cancer Statistics Advisory. 2018.
35.Society CC. Canadian Cancer Society’s Advisory Committee. Canadian Cancer Statistics 2019. 2019.
36.Cancer.Net. Uterine Cancer - Statistics. 2021.
37.Cancer SA. Key Statistics for Endometrial Cancer. 2021.
38.Brenner D. R. WHK, Demers A. A., et al. Projected estimates of cancer in Canada in 2020. . CMAJ. 2020;9. PubMed
39.Authority PHS. Endometrium. 2018.
40.Committee CCSsA. Canadian Cancer Statistics 2021. 2021.
41.INESSS. GIOTRIFMC – Cancer du poumon non à petites cellules. 2014.
42.INESSS. XTRAITS D’AVIS DONT LA PUBLICATION AVAIT ÉTÉ REPORTÉE. 2016.
43.Reaume M. N. LNB, Mittmann N., et al. . Economic analysis of a randomized phase III trial of gemcitabine plus vinorelbine compared with cisplatin plus vinorelbine or cisplatin plus gemcitabine for advanced non-small-cell lung cancer (Italian GEMVIN3/NCIC CTG BR14 trial). . Lung Cancer. 2013. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in Table 5 have been deemed to be appropriate based on feedback from clinical expert(s) and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in Table 4 and as such, the table may not represent the actual costs to public drug plans.
Table 5: CADTH Cost Comparison Table for dMMR or MSI-H Endometrial Cancer
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Pembrolizumab (Keytruda)a | 100 mg/4mL | Vial IV Infusion | 4,400.0000 | 200 mg q.3.w. | 419.05 | 11,733 |
Single-drug chemotherapies | ||||||
Carboplatin | 50 mg 150 mg 450 mg 600 mg | Vial | 70.0000 210.0000 599.9985 775.00 | AUC 4 to 6 (600 mg to 900 mg) on day 1 q.3.w.b | 36.90 to 56.90 | 1,033 to 1,593 |
Cisplatin | 1 mg/mL | 50 mL 100 mL Vial | 323.0000 270.0000 | 50 mg/m2 to 75 mg/m2 on day 1 q.3.w.c | 12.86 to 19.29 | 360 to 540 |
Paclitaxel | 6 mg/mL | 5 16 25 50 Vial | 300.0000 1,196.8000 1,870.0000 3,740.0000 | 80 mg/m2 on day 1, day 8, day 15, and day 22 q.4.w.d | 214.29 | 6,000 |
Doxorubicin | 2 mg/mL | 5 mL 25 mL 50 mL 100 mL Vial | 50.4500 252.2500 1,304.2000 770.0000 | 50 mg/m2 to 60 mg/m2 on day 1 q.3.w.e | 26.43 | 740 |
Platinum-based chemotherapies | ||||||
Carboplatin + paclitaxelf | ||||||
Carboplatin | 50 mg 150 mg 450 mg 600 mg | Vial | 70.0000 210.0000 599.9985 840.0000 | AUC 4 to 6 (600 to 900 mg) on day 1 q.3.w. | 36.90 to 56.90 | 1,033 to 1,593 |
Paclitaxel | 6 mg/mL | 5 16 25 50 Vial | 300.0000 1,196.8000 1,870.0000 3,740.0000 | 175 mg /m2 on day 1 q.3.w. | 157.14 | 4,400 |
Carboplatin + paclitaxel | 194.04 to 214.04 | 5,433 to 5,993 | ||||
Carboplatin + docetaxelg | ||||||
Carboplatin | 50 mg 150 mg 450 mg 600 mg | Vial | 70.0000 210.0000 599.9985 840.0000 | AUC 5 to 6 (750 to 900 mg) q.3.w. | 46.90 to 56.90 | 1,313 to 1,593 |
Docetaxel | 20 mg 80 mg 160 mg | Vial | 249.0000 497.0000 925.000 990.0000 1,940.4000 1,850.0000 | 75 mg/m2 q.3.w. | 59.24 | 1,659 |
Carboplatin + docetaxel | 106.14 to 116.14 | 2,972 to 3,252 | ||||
Cisplatin + doxorubicinh | ||||||
Cisplatin | 1 mg/mL (50 mL) [50 mg] 1 mg/mL (100 mL) [100 mg] | Vial | 323.0000 (6.4600 per mL) 270.0000 (2.7000 per mL) | 50 mg/m2 on day 1 q.3.w. | 12.86 | 360 |
Doxorubicin | 2 mg/mL | 5 mL 25 mL 50 mL 100 mL Vial | 50.4500 252.2500 1,304.2000 770.0000 | 50 to 60 mg/m2 on day 1 q.3.w. | 26.43 | 740 |
Cisplatin + doxorubicin | 39.29 | 1,100 | ||||
Hormone therapies | ||||||
Medroxyprogesterone | 2.5 mg 5 mg 10 mg 100 mg 150 mg/mL | Tablet Vial | 0.1183 0.2365 0.1670 1.2057 31.6900 | 200 to 400 mg once dailyi | 2.41 to 4.82 | 68 to 135 |
Megestrol | 40 mg 160 mg | Tablet | 1.3340 5.8151 | 160-200 mg once dailyj | 5.34 to 6.67 | 149 to 187 |
Tamoxifen | 10 mg 20 mg | Tablet | 0.1750 0.3500 | 20 mg twice dailyk | 0.35 | 10 |
Letrozole (generic) | 2.5 mg | Tablet | 1.3780 | 2.5 mg dailyl | 1.38 | 39 |
Exemestane (generic) | 25 mg | Tablet | 1.3263 5.7533 | 25 mg dailym | 1.33 | 37 |
AUC = area under the curve; q.3.w. = once every 3 weeks; q.4.w. = once every 4 weeks; q.6.w. = once every 6 weeks.
Note: Prices of chemotherapies were obtained from the DeltaPA IQVIA database15 (accessed February 28, 2022), and the prices of hormone therapies were obtained from the Ontario Drug Benefit Formulary16 (accessed February 28, 2022), unless otherwise indicated, and do not include dispensing fees. Cost calculations assume a body surface area of 1.80 m2 where applicable. Wastage of excess medication in vials is included in costs. Recommended dosage is based on Cancer Care Ontario monographs,17 unless otherwise indicated. For all target AUC calculations, dose calculations followed guidance from the Cancer Care Ontario product monograph for Carboplatin: Target AUC is 4 to 6. Carboplatin is dosed according to the following formula: Maximum carboplatin dose (mg) = target AUC (mg/mL per min) X (125 + 25); maximum dose is based on a capped GFR estimate at 125 mL/min for patients with normal renal function.18
aPembrolizumab price is based on the sponsor’s submission;1 dosage is based on the draft product monograph. Pembrolizumab treatment is capped at 24 months (35 doses of 200 mg or 18 doses of 400 mg).19
bCarboplatin product monograph.20
cCisplatin product monograph.21
dPaclitaxel product monograph.22
eDoxorubicin product monograph.23
fCarboplatin plus paclitaxel product monograph.24
gCarboplatin plus docetaxel product monograph.25
hCarboplatin plus doxorubicin product monograph.26
IMedroxyprogesterone acetate product monograph.27,28
jMegestrol product monograph.29
kTamoxifen product monograph.30
lLetrozole product monograph.31
mExemestane product monograph.32
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | No | Refer to key limitations for the sponsor’s inappropriate use of partitioned survival modelling approach. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The sponsor’s submitted model did not reflect the settings reported in its economic submission base case. The presentation of both the combination therapy and monotherapy in a single document was not clear and disorganized as information was difficult to locate. The approach used to estimate the impact of AEs on patient utility was insufficiently described. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
Figure 1: Sponsor’s Estimates of Long-Term Progression-Free Survival for Pembrolizumab
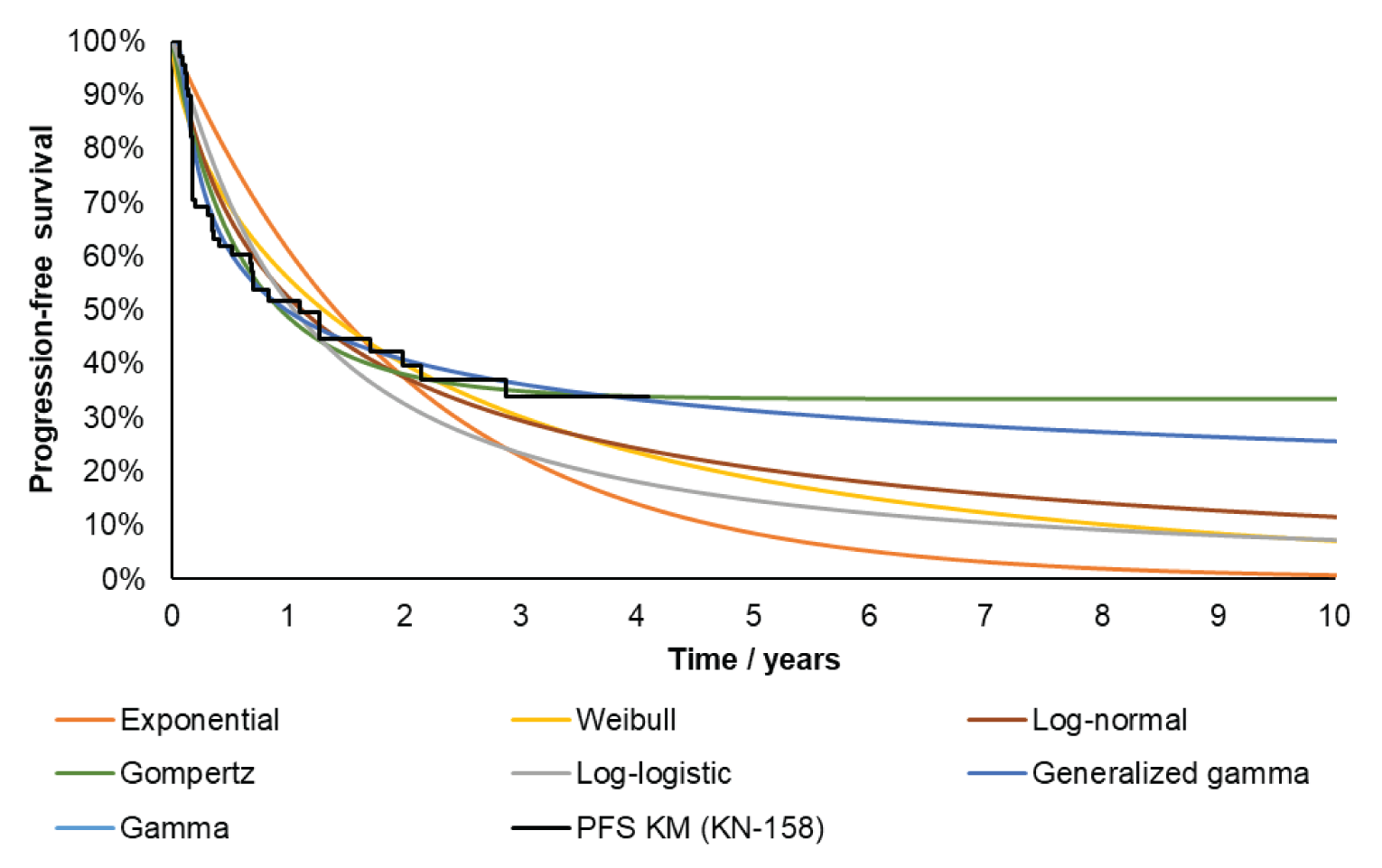
Note: The log-normal distribution was used in the sponsor’s base case for the PFS of pembrolizumab.
Source: Sponsor’s submitted economic model.1
Figure 2: Sponsor’s Estimates of Long-Term Overall Survival for Pembrolizumab
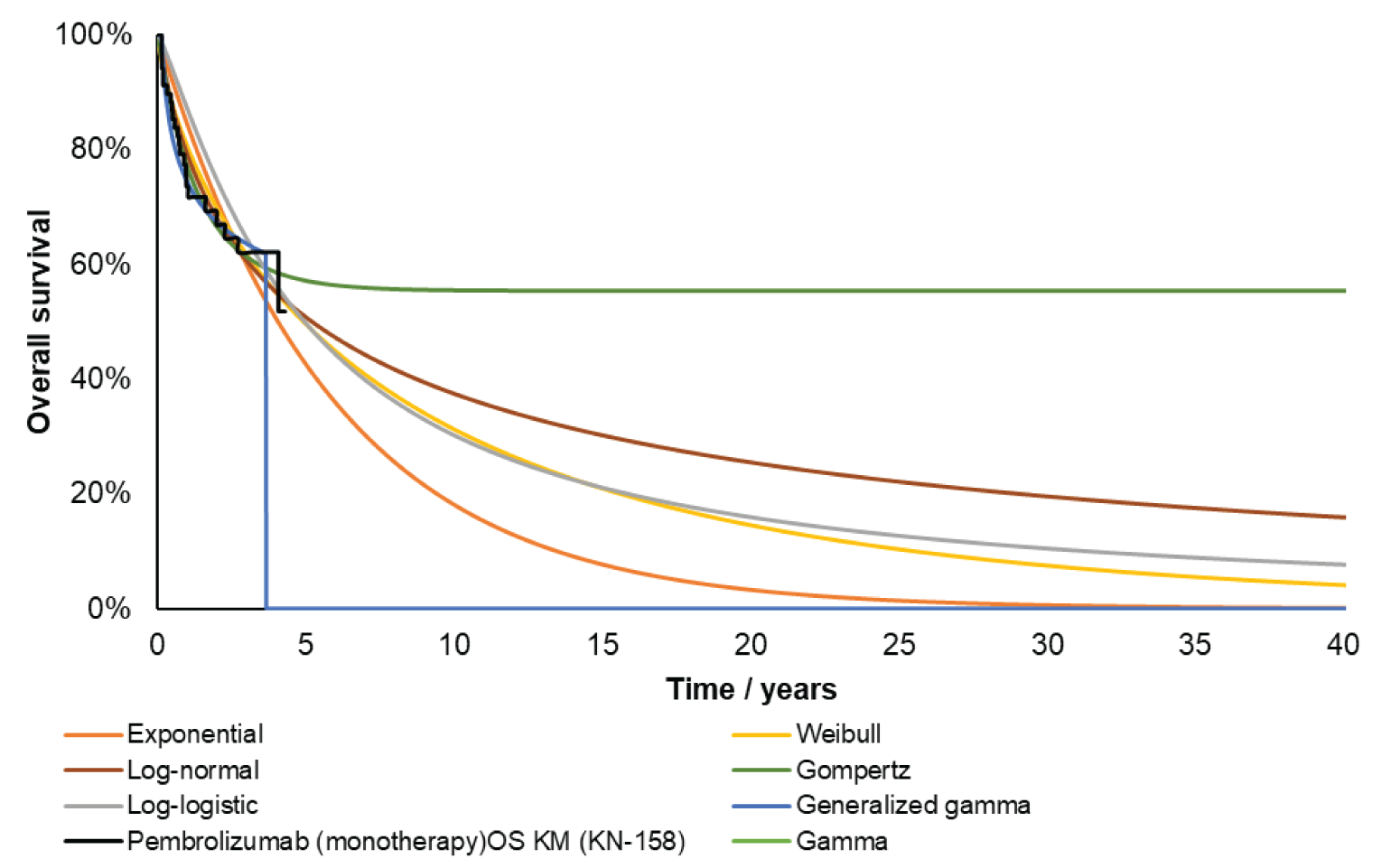
Note: The log-normal distribution was used in the sponsor’s base case for the OS of pembrolizumab.
Source: Sponsor’s submitted economic model.1
Detailed Results of the Sponsor’s Base Case
Table 7: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Pembrolizumab | TPC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 8.58 | 2.55 | 2.71 |
Progression-free | 3.61 | 0.90 | 3.32 |
Progressed disease | 4.97 | 1.65 | 6.04 |
Discounted QALYs | |||
Total | 5.61 | 1.74 | 3.87 |
Progression-free | 2.55 | 0.67 | 1.88 |
Progressed disease | 3.07 | 1.08 | 1.99 |
Discounted costs ($) | |||
Total | 40,381 | 205,171 | 164,790 |
Acquisition | 3,124 | 166,359 | 163,235 |
Administration | 1,492 | 3,286 | 1,794 |
Adverse events | 5,265 | 7,419 | 2,153 |
Disease management | 2,476 | 5,289 | 2,813 |
One-off progression | 218 | 182 | –36 |
Subsequent treatment | 4,615 | 1,212 | –3,403 |
End-of-life | 23,192 | 21,425 | –1,766 |
Testing | 0 | 0 | 0 |
ICER ($ per QALY) | 39,879 | ||
ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year; vs = versus; TPC = treatment of physician’s choice (doxorubicin or paclitaxel).
Note: Probabilistic results reported in Table 7.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Scenario Analyses
While CADTH did not conduct any formal reanalyses of the sponsor’s model, the economic review team performed an exploratory analysis to explore the impact of several key limitations on the ICER which included applying an alternate parametric survival distribution for OS; applying an alternate parametric survival distribution for PFS; and revising the pricing of paclitaxel and doxorubicin while allowing for full drug wastage.
Of note, the fundamental limitations in the sponsor’s model persist within this exploratory analysis. There is no direct evidence to support the comparative efficacy of pembrolizumab to TPC. While there is indirect evidence to suggest that pembrolizumab may improve OS and PFS compared with TPC, no strong conclusions can be drawn due to many limitations in the ITC. Therefore, this exploratory analysis should not be interpreted as a formal CADTH reanalysis to which credence should be given to the results; in particular, it is unlikely that the incremental QALY benefit estimated as part of this exploratory analysis represents the true effect of pembrolizumab, and it is unlikely that the corresponding ICER reflects the true cost-effectiveness of pembrolizumab. Instead, the key insight from this exploratory analysis is that the cost-effectiveness estimate of pembrolizumab highly uncertain.
The cost-effectiveness of pembrolizumab compared with TPC is unknown. Due to several limitations of the KM data for OS and PFS informed by the available clinical evidence in addition to the many limitations associated with the sponsor’s ITC, and feedback from the clinical experts consulted by CADTH pertaining to the clinical plausibility of the long-term extrapolations for OS and PFS in the sponsor’s base case, CADTH selected alternate survival distributions for OS and PFS as part of the exploratory analysis. Specifically, CADTH selected OS and PFS curves that produced the most plausible survival estimates for TPC (existing treatments), which were nevertheless still overestimated. The proportional hazard assumption was applied to the TPC curve to estimate the relative efficacy of pembrolizumab. When alternative parametric survival distributions were chosen for OS and PFS the predicted incremental QALYs were 38% lower than in the sponsor’s base case, resulting in a higher estimated ICER ($61,200 per QALY). Altogether, results of the CADTH exploratory analysis suggest that 93% of the incremental benefit of pembrolizumab was accrued beyond the observation period of the single-arm trial (16.5 months). Even with selecting the most plausible survival estimates in the sponsor’s model, the percentage of incremental QALYs estimated beyond the trial period remained similar to sponsor’s base case. This highlights that the cost-effectiveness estimates produced by both the sponsor’s model and the exploratory analysis are highly sensitive to assumptions about the long-term efficacy of pembrolizumab that are not supported by trial evidence.
Table 8: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH exploratory value or assumption |
|---|---|---|
1. Extrapolation of OS curves for pembrolizumab | OS: KM + log-logistic | OS: Exponential |
2. Extrapolation of PFS curves for pembrolizumab | PFS: Generalized gamma | PFS: Exponential |
3. Drug wastage and drug pricing | None |
|
CADTH exploratory analysis | Reanalyses 1 + 2 + 3 | |
KM = Kaplan-Meier; OS = overall survival; PFS = progression-free survival.
Table 9: Summary of the Stepped Analysis of the CADTH Exploratory Analysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base casea | TPC | 34,970 | 1.74 | Reference |
Pembrolizumab | 189,343 | 5.61 | 39,879 | |
CADTH reanalysis 1 | TPC | 36,065 | 1.42 | Reference |
Pembrolizumab | 193,507 | 3.92 | 63,097 | |
CADTH reanalysis 2 | TPC | 34,923 | 1.71 | Reference |
Pembrolizumab | 186,742 | 5.54 | 39,629 | |
CADTH reanalysis 3 | TPC | 43,448 | 1.70 | Reference |
Pembrolizumab | 191,464 | 5.62 | 37,826 | |
CADTH exploratory analysis (deterministic) | TPC | 44,968 | 1.42 | Reference |
Pembrolizumab | 192,189 | 3.84 | 60,933 | |
CADTH exploratory analysis (probabilistic) | TPC | 44,878 | 1.44 | Reference |
Pembrolizumab | 191,584 | 3.84 | 61,200 |
ICER = incremental cost-effectiveness ratio; TPC = treatment of physician’s choice; QALY = quality-adjusted life-year.
aProbabilistic results are reported for the sponsor’s base case while remaining analyses are deterministically presented, unless otherwise indicated. The CADTH exploratory reanalysis includes key limitations identified by CADTH that were modifiable in the sponsor’s economic model.
CADTH undertook several scenario analyses on the CADTH exploratory analysis to determine the impact of alternative assumptions on the exploratory analysis of cost-effectiveness for pembrolizumab compared with TPC. This included:
Alternate health state utility values sourced from a NICE TA528, which were reported by progression status and are 0.812 for the progression-free health state and 0.728 for the progressed disease health state.1
The CADTH exploratory analysis remained robust to the scenario that explored alternate health state utility values from NICE TA528.
Table 10: Summary of CADTH Exploratory Scenario Analyses
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER vs. TPC ($/QALY) |
|---|---|---|---|---|---|---|---|
Sponsor’s submitted base case | |||||||
TPC | 34,854 | Reference | 2.49 | Reference | 1.70 | Reference | Reference |
Pembrolizumab | 189,876 | 155,022 | 8.59 | 6.10 | 5.62 | 3.91 | 39,616 |
CADTH’s exploratory analysis | |||||||
TPC | 44,968 | Reference | 2.00 | Reference | 1.42 | Reference | Reference |
Pembrolizumab | 192,189 | 147,221 | 5.67 | 3.67 | 3.84 | 2.42 | 60,933 |
CADTH scenario: Alternate health state utility values from NICE TA528 | |||||||
TPC | 44,968 | Reference | 2.00 | Reference | 1.49 | Reference | Reference |
Pembrolizumab | 192,189 | 147,221 | 5.67 | 3.67 | 4.02 | 2.53 | 58,236 |
ICER = incremental cost-effectiveness ratio; PLD = Pegylated liposomal doxorubicin; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: The sponsor’s base-case results and CADTH’s exploratory analysis results are presented probabilistically while all scenarios are deterministic.
Table 11: Price Reduction Analyses of Sponsor’s Base Case and CADTH Exploratory Analysis
Price reduction | ICERs for pembrolizumab vs. TPC ($/QALY) | |
|---|---|---|
Sponsor’s base case | CADTH exploratory analysis | |
No price reduction | 39,616 | 60,933 |
10% | 35,779 | 54,731 |
18% | 32,709 | 49,770 |
20% | 31,941 | 48,529 |
ICER = incremental cost-effectiveness ratio; NA = not applicable; vs. = versus.
Note: All analyses in this table are deterministic and are subject to limitations within the sponsor’s economic model.
Price Reduction Analysis
As no formal CADTH reanalysis was performed, price reduction analyses were conducted using only the CADTH exploratory analysis. This deterministic analysis was subject to the key limitations of the sponsor’s model as noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation section. Based on the CADTH exploratory deterministic analysis, a reduction in the price of pembrolizumab by 18% would be required for pembrolizumab to be cost-effective at a willingness-to-pay threshold of $50,000 per QALY compared to TPC. It is important to note that this price reduction estimate is based on estimates of incremental life-years (and hence QALYs) that are highly uncertain and may not be representative of the true incremental effect of pembrolizumab. Consequently, the price reduction required for pembrolizumab to be cost-effective remains unknown.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 12: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA)33 estimating the incremental budget impact of reimbursing pembrolizumab monotherapy for use by patients aged 18 years and older with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy. The BIA was undertaken from the perspective of the Canadian public drug plans over a 3-year time horizon, and the sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec). Key inputs to the BIA are documented in Table 13.
The sponsor estimated the number of eligible patients using an epidemiologic approach with data obtained from various sources33-39 including: Canadian Cancer Society statistics40 and sponsor-conducted opinion survey of Canadian medical oncologists (N = 10).33 The sponsor adopted an average annual growth rate of 5.44% in estimating the total number of uterine cases over the time horizon.34,35,38 The sponsor estimated that 90% of these uterine cancers occur in the endometrium36 and 8% of endometrium carcinoma are advanced or metastatic cases.39 The sponsor assumed 84% of patients are referred to a medical oncologist or gynecologic oncologist, 87% receive first-line treatment and 63% move on to receive second-line treatment.33 The sponsor assumed 67% of patients who had received second-line treatment relapse and progress to advanced stages33 The sponsor also assumed the dMMR or MSI-H testing rate increased linearly from 70% at baseline to 90% by year 3.33 The proportion of patients with endometrial cancer categorized as MSI-H or dMMR tumours was 15.7% based on the KN755 trial.33
The BIA outcomes were estimated using the number of patients expected to be treated each week, which was modelled to increase over time. The treatment costs accrued by pembrolizumab monotherapy and comparators were based on KM ToT data in the KN775 and KN158 trials. The market share of pembrolizumab monotherapy increased from 0% to ███ over a ███████████████ based on a linear model. Drug costs were obtained from publicly available drug reviews41-43 and IQVIA DeltaPA database.6 No drug wastage was assumed.
Table 13: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of patients with uterine cancers | 7,040 / 7,930 / 8,93340 |
Proportion of endometrial cancer | |
Proportion of advanced or metastatic disease | |
Referral rate to medical oncologists or gynecologic oncologists | 84%33 |
First-line treatment rate by medical oncologists and gynecologic oncologists | 87%33 |
Second-line treatment rate | 63%33 |
Diagnosed earlier and progressed to advanced disease (includes recurrent disease) | 67%33 |
dMMR or MSI-H testing rate (from baseline to peak) | 70% to 90%33 |
Proportion of patients with dMMR or MSI-H EC | 15.7%33 |
Market uptake (3 years) | |
Uptake (reference scenario) Pembrolizumab Paclitaxel Doxorubicin Docetaxel Ifosfamide Gemcitabine Clinical trials | 0% / 0% / 0% 19% / 19% / 19% 56% / 56% / 56% 7% / 7% / 7% 0% / 0% / 0% 10% / 10% / 10% 8% / 8% / 8% |
Uptake (new drug scenario) Pembrolizumab Paclitaxel Doxorubicin Docetaxel Ifosfamide Gemcitabine Clinical trials | ███████% / ███████ % / ███████ % ███████% / ███████ % / ███████ % ███████% / ███████ % / ███████ % ███████% / ███████ % / ███████ % ███████% / ███████ % / ███████ % ███████% / ███████ % / ███████ % ███████% / ███████ % / ███████ % |
Cost of 1L treatment (per patient)a | |
Cost of treatment over cycle Pembrolizumab q.3.w. Pembrolizumab q.3.w. Lenvatinib (20 mg) Lenvatinib (14 mg) Lenvatinib (10 mg) Lenvatinib (8 mg) Lenvatinib (4 mg) Paclitaxel Doxorubicin Docetaxel Ifosfamide Gemcitabine Clinical trials | $8,800.00 $17,600.00 $1,159.48 $772.94 $501.48 $456.00 $228.00 $24.86 $408.87 $128.60 $126.96 $4.51 $0.00 |
Cost of 2L treatment (per patient)a | |
Carboplatin Paclitaxel Doxorubicin | $66.28 $24.86 $408.87 |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability–high; q.3.w. = once every 3 weeks.
Note: Cost estimation assumed average weight of 70.5 kg, body surface area of 1.77 m2 and no drug wastage.
aTreatment duration is 35 maximum cycles for pembrolizumab (200 mg q.3.w.) and 8 maximum cycles for doxorubicin. Paclitaxel accrues costs over the time horizon.
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor estimated the net 3-year budget impact of introducing pembrolizumab monotherapy for treatment of patients aged 18 years and older with unresectable or metastatic dMMR or MSI-H endometrial cancer whose tumours have progressed following prior therapy to be $14,867,554 (year 1: $1,125,165; year 2: $5,483,039; year 3: $8,259,350).
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Unit costs of paclitaxel and doxorubicin were inaccurate: The sponsor submitted BIA33 obtained drug costs of paclitaxel and doxorubicin using published literature42 and IQVIA DeltaPA database,6 respectively. However, these estimates do not match the most recent cost estimates CADTH obtained using the IQVIA DeltaPA database.15
In CADTH reanalysis, the cost per milligram of paclitaxel and doxorubicin was updated to the most recent prices in the IQVIA DeltaPA database.15
There is uncertainty in market share of pembrolizumab and comparators: In the submitted BIA,33 the sponsor assumed treatments that accrue market share include paclitaxel, doxorubicin, docetaxel, gemcitabine and clinical trials. In the economic evaluation,1 the comparator is TPC, which consists of 25% paclitaxel and 75% doxorubicin. The sponsor’s assumptions on market share captured by relevant treatments differ between the cost-utility analysis and BIA; the cost-utility analysis does not include docetaxel and gemcitabine as comparators. The clinical experts consulted for this review by CADTH suggested docetaxel is rarely used to treat patients with dMMR or MSI-H endometrial cancer. Further, gemcitabine may have a market share up to 3% in second-line setting and the introduction of pembrolizumab would decrease the market share of gemcitabine. The sponsor also assumed clinical trials capture 8% of market share and accrue no drug costs. The sponsor’s approach to include clinical trials in the market mix artificially decreases the estimated market size, disregarding the treatment costs incurred by those in clinical trials and underestimating the budget impact.
In CADTH reanalysis, the market share at baseline was revised based on feedback from clinical experts consulted for this review and excluded clinical trials. The reimbursement of pembrolizumab displaced the market share of paclitaxel, doxorubicin, and gemcitabine proportionally to the sponsor’s assumptions on market share displacement.
The proportion of advanced or metastatic endometrial cancer is uncertain: In estimating the number of eligible patients, the sponsor estimated 8% of all endometrial cancers are advanced or metastatic (which included stage IIIc, stage IVa, and stage IVb tumours).44 However, the clinical experts consulted for this review suggested the proportion of advanced or metastatic endometrial cancer may be in the range of 25% to 30%. Advanced or metastatic endometrial cancer refer to cancers that have spread into the surrounding tissues and organs.44 CADTH noted uncertainty in the proportion of endometrial cancer classified as advanced or have metastasized in published literature. In another report by Alberta Health Services,45 approximately 30% of patients with endometrial cancer were reported to present with stage III and IV tumours. As such, there is uncertainty in the proportion of advanced or metastatic endometrial cancer and may have been underestimated.
In a scenario analysis, the impact of uncertainty in the estimated proportion of advanced or metastatic endometrial cancers was explored by adopting a value of 25% based on the feedback received from clinical experts.
There is uncertainty in market uptake of pembrolizumab: The sponsor assumed that pembrolizumab monotherapy uptake is linear. The clinical experts consulted by CADTH considered the speed of uptake to be rapid if it becomes available in the MSI-H/dMMR population. The budget impact is sensitive to the rate of market uptake, which is based on the sponsor’s assumptions.
CADTH explored the impact of market uptake of pembrolizumab in scenario analyses:
Assuming rapid uptake of pembrolizumab initially and plateauing off at 52 weeks (uptake curve: logarithmic)
Assuming rapid uptake of pembrolizumab after a delay and plateauing off at 52 weeks (uptake curve: exponential)
Inclusion of dMMR or MSI-H testing costs: The sponsor’s base case included the cost of dMMR or MSI-H testing. As the analysis is focused on treatments funded by the drug plans, the cost of dMMR or MSI-H testing is not relevant to the drug plan perspective. The dMMR or MSI-H testing costs are, however, relevant to the health care payer perspective.
In CADTH reanalysis, the cost of dMMR or MSI-H testing was excluded. CADTH explored the impact of including the costs of dMMR or MSI-H testing under the health care payer perspective in a scenario analysis.
The budget impact model has limited transparency and flexibility: The sponsor’s submitted BIA model is complex, using circular referencing and hard coding which increases validity issues when making changes to the model and ensuring consistency throughout the budget impact model. Furthermore, the model lacks transparency and has limited flexibility to allow the reviewers to assess the impact of changing the sponsor’s base assumptions on estimated budgetary impact.
CADTH could not address this limitation. CADTH notes that the results presented should be treated with a degree of caution as the validity of the model calculations could not be thoroughly appraised.
CADTH Reanalyses of the Budget Impact Analysis
CADTH revised the sponsor’s base case by updating paclitaxel and doxorubicin costs, revising market share of pembrolizumab and comparators based on clinical experts, excluding clinical trial from the market mix, and excluding dMMR or MSI-H testing costs.
Table 14: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Update costs per mg | Paclitaxel: $0.1756 Doxorubicin: $3.8500 | Paclitaxel: $10.0000 Doxorubicin: $5.0000 |
2. Market share assumptions (base year / year 1 / year 2 / year 3) | █████████████████████ █████████████████████ █████████████████████ █████████████████████ █████████████████████ █████████████████████ █████████████████████ | Pembrolizumab: 0% / 43% / 80% / 80% Paclitaxel: 25% / 14% / 5% / 5% Doxorubicin: 72% / 41% / 14% / 14% Docetaxel: 0% / 0% / 0% / 0% Ifosfamide: 0% / 0% / 0% / 0% Gemcitabine: 3% / 2% / 1% / 1% Clinical trials: 0% / 0% / 0% / 0% |
3. dMMR or MSI-H testing costs | Include | Exclude |
CADTH base case | Reanalysis 1 + 2 + 3 | |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability–high.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 15 and a more detailed breakdown is presented in Table 16.
Based on the CADTH base case, the budget impact of the reimbursement of introducing pembrolizumab monotherapy for treatment of patients with unresectable or metastatic dMMR or MSI-H endometrial cancer in second- or subsequent-line of therapy is expected to be $1,572,345 in year 1, $7,858,502 in year 2, and $11,969,306 in year 3, with a 3-year total of $21,400,154. The budget impact is sensitive to uncertainty in the estimated proportion of advanced or metastatic endometrial cancer and pembrolizumab dosing (flat vs weight-based dosing).
Table 15: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | 3-year total |
|---|---|
Submitted base case | $14,867,554 |
CADTH reanalysis 1 | $14,405,568 |
CADTH reanalysis 2 | $22,677,471 |
CADTH reanalysis 3 | $14,615,674 |
CADTH base case | $21,400,154 |
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 16.
Assuming 25% of patients with endometrial cancers are advanced or metastatic.
Assuming rapid uptake of pembrolizumab and plateauing off at 52 weeks (uptake curve is logarithmic based).
Assuming rapid uptake of pembrolizumab after a delay and plateauing off at 52 weeks (uptake curve is exponential based).
Including dMMR or MSI-H testing costs.
Price reduction by 18%.
Table 16: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | 3-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $256,008 | $465,976 | $667,734 | $879,705 | $2,013,415 |
New drug | $256,008 | $1,591,141 | $6,150,773 | $9,139,055 | $16,880,969 | |
Budget impact | $0 | $1,125,165 | $5,483,039 | $8,259,350 | $14,867,554 | |
CADTH base case | Reference | $521,610 | $792,914 | $851,265 | $898,732 | $2,542,910 |
New drug | $521,610 | $2,365,259 | $8,709,767 | $12,868,038 | $23,943,064 | |
Budget impact | $0 | $1,572,345 | $7,858,502 | $11,969,306 | $21,400,154 | |
CADTH scenario analysis: 25% advanced or metastatic rate | Reference | $1,630,032 | $2,477,855 | $2,660,202 | $2,808,536 | $7,946,593 |
New drug | $1,630,032 | $7,391,434 | $27,218,022 | $40,212,618 | $74,822,074 | |
Budget impact | $0 | $4,913,579 | $24,557,820 | $37,404,082 | $66,875,481 | |
CADTH scenario analysis: Logarithmic market uptake of pembrolizumab | Reference | $521,610 | $792,914 | $851,265 | $898,732 | $2,542,910 |
New drug | $521,610 | $3,495,953 | $9,803,931 | $13,128,504 | $26,428,388 | |
Budget impact | $0 | $2,703,039 | $8,952,667 | $12,229,772 | $23,885,478 | |
CADTH scenario analysis: Exponential market uptake of pembrolizumab | Reference | $521,610 | $792,914 | $851,265 | $898,732 | $2,542,910 |
New drug | $521,610 | $1,316,007 | $7,255,162 | $12,422,042 | $20,993,212 | |
Budget impact | $0 | $523,094 | $6,403,897 | $11,523,311 | $18,450,302 | |
CADTH scenario analysis: Including dMMR or MSI-H testing costs | Reference | $521,610 | $792,914 | $851,265 | $898,732 | $2,542,910 |
New drug | $521,610 | $2,365,259 | $8,709,767 | $12,868,038 | $23,943,064 | |
Budget impact | $0 | $1,599,530 | $7,941,451 | $12,111,053 | $21,652,034 | |
CADTH scenario analysis: 18% price reduction | Reference | $521,610 | $792,914 | $851,265 | $898,732 | $2,542,910 |
New drug | $521,610 | $2,057,585 | $7,202,827 | $10,607,811 | $19,868,223 | |
Budget impact | $521,610 | $2,057,585 | $7,202,827 | $10,607,811 | $19,868,223 |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability–high.
Stakeholder Input
Patient Input
Colorectal Cancer Resource & Action Network, in collaboration with the Canadian Cancer Society and the Canadian Cancer Survivor Network
About Colorectal Cancer Resource & Action Network
The Colorectal Cancer Resource & Action Network (herein ‘CCRAN’) led a collective patient input submission on Pembrolizumab monotherapy and Pembrolizumab in combination with Lenvatinib for the treatment of advanced endometrial cancer. The following patient advocacy groups thoughtfully collaborated with CCRAN to provide meaningful and compelling patient input:
Canadian Cancer Society (CCS)
Canadian Cancer Survivor Network (CCSN)
All patient groups are registered with CADTH.
Please note: CCRAN is a national not for profit patient advocacy group championing the health and wellbeing of Canadians touched by colorectal cancer and those at risk of developing the disease. CCRAN has recently expanded its patient-focused mandate to serve a population of patients with cancer outside of the colorectal cancer space by providing HTA patient and clinician input submissions within the oncology space for:
patient groups who do not have the capacity to perform these submissions; and/or
a drug therapy wherein there currently is no representative patient group (such as the drug therapy currently under review).
Information Gathering
To ensure the advanced endometrial cancer patient perspective was captured for this critically important therapeutic under review, CCRAN employed a multi-faceted outreach approach. On November 11, 2021, we reached out to 12 Canadian clinicians via email who treat advanced endometrial cancer patients requesting assistance identifying patients who had/have experience with Pembrolizumab + Lenvatinib who would be willing to participate in a telephone interview to share that experience for an HTA patient input submission being made to two expert committees in Canada. That same email was followed up on November 28th, 2021. On December 6th, 2021, the President (Dr. Helen MacKay) of The Society of Gynecologic Oncology of Canada (‘GOC’) was respectfully contacted with the same request. The GOC kindly sent a mass email authored by the GOC President on CCRAN’s behalf to the members of the GOC on December 9th, 2021, requesting assistance with patient recruitment.
Additionally, a connection was made between CCRAN and the Mission Coordinator from the Canadian Cancer Society (CCS) on November 29, 2021, ensuring CCS support the inclusion of the endometrial cancer patient’s values and preferences in this submission through a recent online survey they conducted regarding the endometrial cancer patient’s:
Experience with respect to the diagnosis of their endometrial cancer
Experience with respect to their endometrial cancer journey
Experience with respect to the drug therapies administered prior to the therapy under review.
The online survey was administered from October 22nd to November 3rd, 2021, wherein 22 survey respondents provided input.
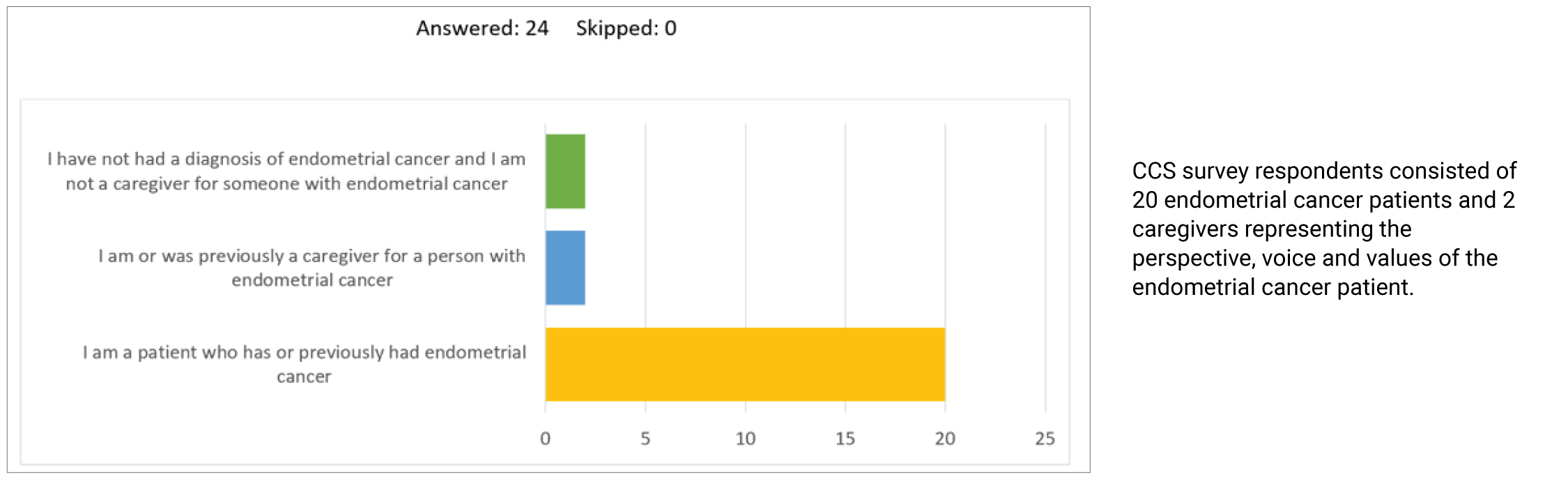
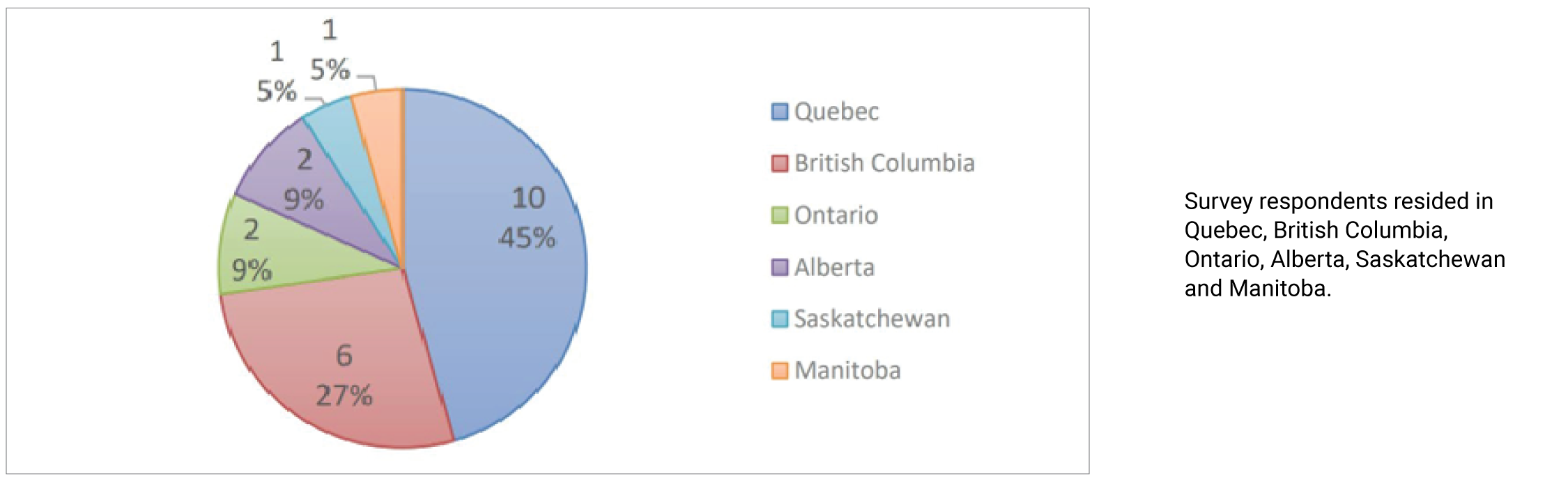
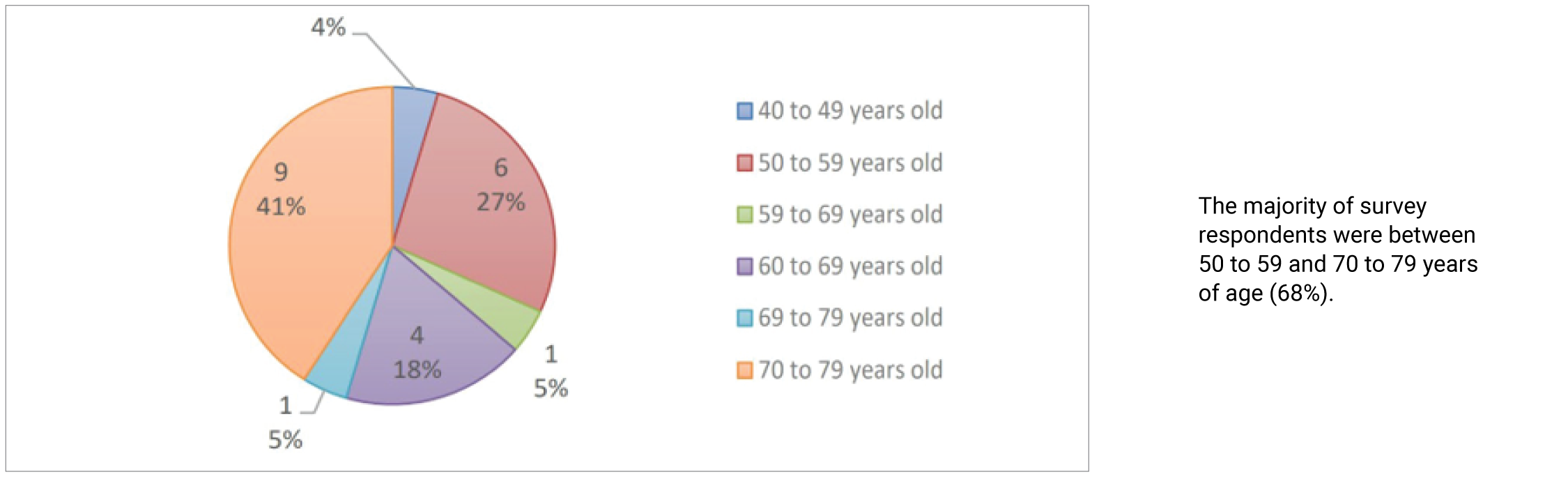
The CCS survey findings will be referenced throughout this submission for they reflect the perspectives of the endometrial cancer patient population. CCS also sent out mass emails on behalf of CCRAN requesting advanced endometrial cancer patients who have experience with the therapy under review contact CCRAN for a telephone interview to kindly share that experience. Emails were also shared by the CCS with Cancer Connection Forum and with McGill University Health Center’s Gynecological Unit. Additional outreach efforts were made on behalf of CCRAN to the following American and European based organizations with similar requests:
Force: www.facingourrisk.org; Cancer Care: www.cancercare.org; ESGO https://engage.esgo.org
One additional outreach effort was made to the Canadian Cancer Survivor Network (CCSN) on December 5, 2021, who employed an online survey as well, resulting in one endometrial cancer patient having experience with the therapy under review.
It was the clinician and GOC outreach efforts that resulted in 1 caregiver and 3 advanced endometrial cancer patient telephone interviews. Telephone interviews were conducted by CCRAN between December 1st and December 14th, 2021, inclusive, with each patient providing firsthand compelling, relevant and high-quality input regarding their:
experience with respect to the diagnosis of their cancer
disease experience
experience with respect to previous therapies administered prior to Pembrolizumab + Lenvatinib and
experience with respect to Pembrolizumab + Lenvatinib.
The mean age of the patients was 62 years, and the median age was 64 years at the time of their diagnosis. The qualitative data from the interviews is summarized and represented entirely, which will serve, for the most part, as the basis for this qualitative submission, in addition to the survey findings furnished by CCS, and the one survey result supplied by CCSN.
Disease Experience
Endometrial cancer is the most common gynecological malignancy in Canada and our interviewed patients were surprised to learn from their treating oncologists that its incidence is increasing. Sadly, no specific screening is recommended in the general population which may account, in part, for the advanced disease case counts, which are associated with a poor prognosis, primarily because patients with advanced endometrial carcinoma have limited treatment options.
Most women with endometrial cancer will present with abnormal bleeding, irregular cycles and/or excessive bleeding in the premenopausal female, or any bleeding in the post-menopausal setting. In the advanced disease setting, women may complain of pelvic and abdominal discomfort, bloating, or presence of a mass, gastrointestinal or genitourinary symptoms, or constitutional symptoms. According to the qualitative data, all four patients had been experiencing incessant vaginal bleeding for a period of at least 6 months to >2 years. Patient B reported having experienced a mucus-type vaginal discharge accompanied by significant abdominal discomfort in addition to her vaginal bleeding. Three of the four patients (Patients A, B, and D) expressed significant frustration and profound disappointment over their ongoing symptoms whose cause could not be identified for quite some time, despite repeated diagnostics, which they believe contributed to their disease progression and diagnosis of advanced stage disease.
“I had been symptomatic for years, whose cause couldn’t be understood or identified. I just kept bleeding and bleeding. The ultrasounds couldn’t pick anything up and then I had a CT scan that sort of picked up something, so I went on to have a D&C which picked up my cancer…I was then scheduled for my surgery. And I have to tell you that 10 minutes before I went into my surgery, I found out that I had metastatic disease to my lungs. It was so shocking and disappointing. How awful for me.” — Patient D
The Canadian Cancer Society (CCS) Survey findings (n=22) clearly demonstrated the impact of the disease on the patient’s day to day activities and ultimately their quality of life. Q3 of the survey asked, “How much of an impact do symptoms associated with endometrial cancer have on your day-to-day activities and quality of life?” Patients diagnosed with endometrial cancer were asked to select all that apply from a list of tasks. Those tasks scoring highest in the moderate to significant impact range included the ability to:
conduct household chores
exercise
travel and
work
Figure 4: Impact Symptoms Associated With Endometrial Cancer Have on Day-to-Day Activities and Quality of Life
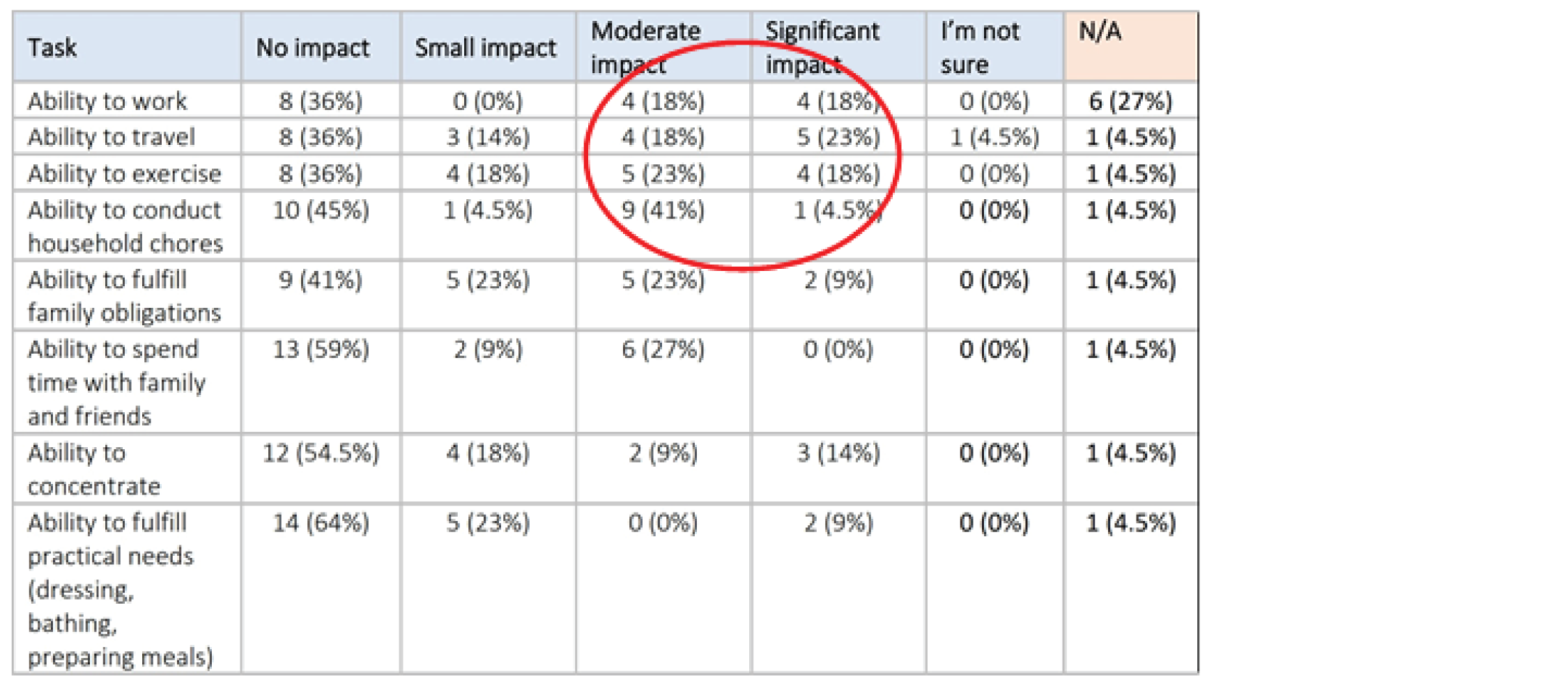
The CCSN survey respondent also expressed concerns regarding her day-to-day living. She identified “living with uncertainty, feeling isolated or lonely” and that she experienced “diarrhea, occasional interstitial cystitis, and herpes outbreaks” which compromised her quality of life.
Interviewed Patients B and D both shared that they had cancer induced symptoms with which they had struggled. Patient B had endured pelvic pain and constipation; while Patient D was fraught with fatigue, nausea, and a lack of appetite (Q17).
The four interviewed patients articulately and vividly described the toll a diagnosis of advanced endometrial cancer plays on the caregiver. Th diagnosis can be equally frightening for the caregiver, who is typically the spouse, but can be anyone – a family member, friend or loved one. The caregiver may take on many roles in the course of the patient’s journey. They will assume the role of medical translator, information specialist, housekeeper/meal preparation, financial advisor, psychosocial expert, and so much more. Quite often the caregiver’s function is overshadowed or under- valued; in large part because the focus is typically on the patient, thus discounting the essential role played and meaningful contribution delivered by the caregiver. Our interviewed patients painfully described the stress, and debilitating anxiety a caregiver undergoes once a diagnosis of advanced endometrial cancer is delivered to the family. They explain (Q22):
“Yes, it was life-altering. We have been through a major trauma, even to this day, it still affects us. The impact is lifelong. Both my sister and I were quite young. She and I would take turns taking my mom to her appointments. We would do research …. We struggled with the side effects of the treatments, learning how to give her injections every day for her thrombosis. …dreadful disease.” — Caregiver A
“My husband has always been there but emotionally; it has been very draining and stressful for him. He had to become Dr. Google overnight. He came to all my appointments and to the 6 cycles of chemo and had to deal with all the chemo side effects which were brutal. Then covid kicked in and he couldn’t come with me so that was so very stressful for him. So, he sat in his car and waited for me the whole time. He was there the whole time for me, including during surgery. And he has his own health issues…” — Patient B
“My husband was there taking care of me, doing housework, cooking, I guess just taking on the bulk of responsibilities because I couldn’t do it. But then in 2019, he had a stroke and now he is different and compromised, it is difficult for him. He had to do rehabilitation because of his stroke. He really cannot help me. I had to make arrangements for him and for me. For example, who will go first, him or me? It is a terrible situation. His stroke may not have been caused by my diagnosis, but my diagnosis may have impacted his health to the point where it could have contributed to his poor health…. Cancer does atrocious things to not only the patient but to their family members.” — Patient D
Experiences With Currently Available Treatments
Patients with advanced endometrial carcinoma have limited treatment options. If diagnosed with an early stage of the disease, patients will undergo surgery to remove the uterus (and perhaps the cervix), fallopian tubes and regional lymph nodes. Radiation therapy may also be indicated to kill cancer cells in addition to hormonal therapy to block cancer growth. Carboplatin in combination with paclitaxel are standard chemotherapy treatments indicated for endometrial cancer in both the adjuvant setting and first line treatment of metastatic endometrial cancer. These therapies, particularly the latter, are associated with treatment induced toxicities that compromise patients’ quality of life and fail to extend patients’ longevity in a meaningful way.
The CCS survey findings (Q8) captured the impact of treatment-induced toxicities as reported below in the figure. Previously administered treatments included surgery, chemotherapy (Caelyx, Carbotaxol) and hormonal therapy (Anastrozole). Surveyed patients selected “changes in libido or sexual function” as the most significant side effect resulting from their previous treatment(s) with 10 responses appearing in the moderate to significant impact range. Fatigue (9), constipation (6), and peripheral neuropathy (5) followed, as highlighted in the table.
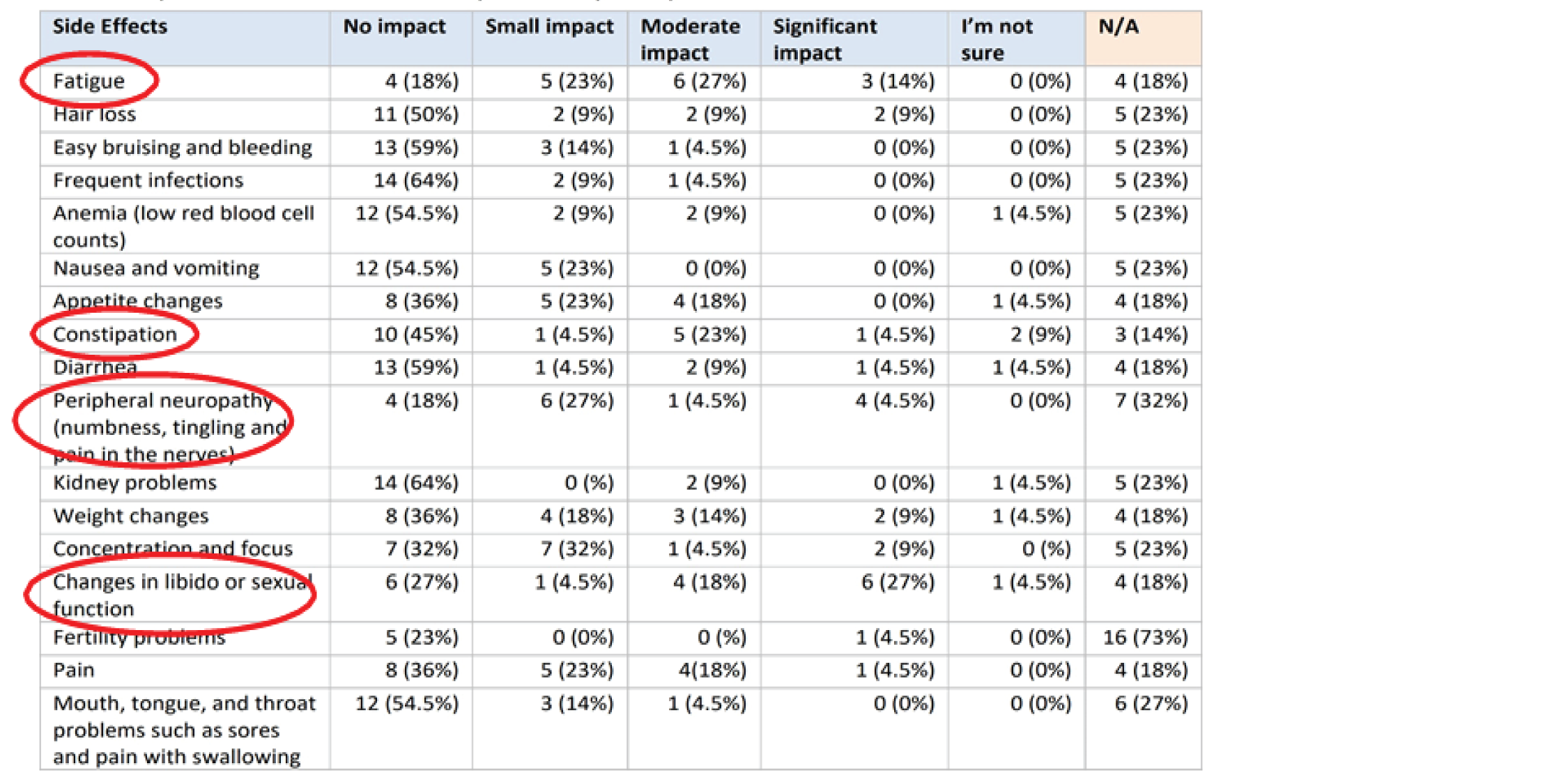
CCS captured patient input through firsthand testimonials as well which described the harsh and debilitating side effects these patients endured as they underwent standard of care treatments indicated for the management of their advanced endometrial cancer. These testimonials also highlight the overall lack of efficacy associated with these standard of care therapies that compromised their everyday quality of life. Appearing below is one of the testimonials CCS secured outside of the Survey:
“The first line of chemotherapy gave me very bad side effects, pain and complications. They gave me first and second line chemotherapy sessions, both had very bad side effects and were not effective.…. At that point, they gave me radiation to shrink the tumour, and yet that was only for one small tumour that I had…. My abdominal pain became worse and worse. The pain medications were not effective.” CCS Patient Testimonial
Interviewed patients provided thoughtful input regarding their treatment journeys. Caregiver A summarized her mother’s experience as quite ghastly. Her mother underwent surgical resection and then received radiation therapy which she tolerated quite well, and it controlled her cancer for approximately 3.5 years but spinal and bone metastases eventually ensued. She was prescribed Nexavar to which there was no response. Her mother was then prescribed second line Carbotaxol but could only endure 2 cycles due to “horrible side effects” that were debilitating and unmanageable. Her mother then succumbed to the disease.
Patient B underwent surgical resection for her cancer but shortly after her surgery (3 months) she was diagnosed with a mass that was strangulating her left ureter as well as metastases to her spleen, liver and peritoneum. She was prescribed 6 cycles of Carbotaxol to which there was little response. Her left kidney failed due to hydronephrosis. She was then recommended the therapy under review (Pembrolizumab + Lenvatinib).
After undergoing surgical resection for her cancer, Patient C endured 6 toxic cycles of Carbotaxol and 3 treatments of brachytherapy for any remnant microscopic disease. Sadly, she was diagnosed with a recurrence in her peritoneum and spine for which she was prescribed more Carbotaxol (6 cycles). She initially experienced a partial response to the Carbotaxol and eventually progression. She was then prescribed hormonal therapy, Letrazole in combination with Vitamin D but that too showed progressive disease. She then started Doxorubicin (6 cycles) but had to stop due to diminished quality of life and eventually progressive disease developed and was recommended Pembrolizumab + Lenvatinib).
Patient D was diagnosed with metastatic disease (lungs) as she was being wheeled into surgery. She was prescribed Carbotaxol. She could only endure one cycle of the carboplatin due to extreme neuropathy. She then continued on with the paclitaxel only, which regressed the lung metastases but was ineffective against the abdominal disease which was discovered post op. She was recommended Pembrolizumab monotherapy.
Carbotaxol was accessed by all four of our interviewed patients (Patients A, B, C and D) as a treatment option for women with advanced endometrial cancer. All four patients reported debilitating side effects while being on Carbotaxol despite having spent a relatively short period of time on the drug therapy (<2 months, 4 months, 6 months, 5 months respectively), and sadly none of the patients reported having benefited from the treatment. Patient reported side effects from Carbotaxol therapy included: neuropathy, fatigue, nausea, lack of energy, headaches, hypothermia, cramping in extremities, abdominal pain, hair loss and diarrhea. Patients were disheartened to learn of the lack of response and their quality of life was significantly impacted to the point where they were unable to function because they were physically unwell and debilitated. They were quite emphatic about their experience with Carbotaxol, despite the fact that it was short lived. In their words (Q8A-C):
“…her life started to deteriorate. So, when she started Nexavar, her quality of life got worse. She could no longer socialize or travel. And Carbotaxol was the worst of them all. Horrible side effects. Her outlook even became negative. She even stopped working. And it was so difficult to watch from a caregiver’s perspective.” — Caregiver A
“I had typical side effects while I was on the Carbotaxol. I had hair loss…. I had absolutely no energy. The coldness and chills were horrible. I couldn’t do any housework or shopping. I had to have everything delivered because that was very challenging for me due to fatigue and exhaustion. My energy level was so low, and I was so weak. I tried to stock my house with products and food. My husband did the cooking and cleaning. Thank goodness. How do single women get through this? I can’t imagine.” — Patient B
“When I was on the Carbotaxol, my quality of life was really not so good, actually, it was pretty terrible. It was because of the pain in my hands. They were like electroshock waves were going through them. They were also numb at the same time. It was hard to explain. I hated it so much. I still have the pain to this day. The doxorubicin was not painful, but my heart is not the same anymore. I am at a lower level today and as a result I have to be careful with activity like running, walking etc…. My heart is 70% at its pumping capacity now because of doxorubicin. Isn’t that awful?” — Patient C
“I was totally dependent on my husband while on Carbotaxol. He would have to give me showers, dry my hair, I couldn’t dry myself after a shower, he had to help me dress myself, I couldn’t cook, I couldn’t clean the house, I was a total clean freak and I had to abandon that. I couldn’t do anything around the house. I couldn’t leave the house for weeks and weeks because I had no energy due to the chemo. I couldn’t do grocery shopping or any type of shopping. I wasn’t engaged in life at all. There was no socializing for me at all. I couldn’t even go to church or see my kids and grandkids who I cherished so much. The side effects of chemo were so brutal. I had nausea, fatigue, no energy at all, I had headaches which bound me to bed, I was useless. I slept a lot. All these were so severe 80% of the time. They had to take me off the carboplatin because of the neuropathy. What sort of life is this to lead?” — Patient D
Improved Outcomes
Q10 of the CCS survey asked, “What improvements would you like to see in new treatments that are not achieved in currently available treatments?” Open ended survey replies included: fewer side effects such as skin issues, fatigue, bladder control, stamina, vaginal bleeding after intercourse, vaginal dryness, hair loss, pain, concentration problems (chemotherapy fog) and arthritis. Respondents also indicated they would like to see more drug affordability as the cancer journey can become quite expensive while undergoing treatment, as usual everyday activities may become interrupted, requiring additional expenditures to help cover or assume those activities.
All interviewed patients provided their perspective on the improvements (Q25) they would wish to see associated with a new drug therapy – improvements they believe are currently not available with standard of care therapies for the management of advanced endometrial cancer. They passionately expressed the following: a desire to access a therapy that would promote good quality of life while effectively regressing their disease.
“I would like to see an extension in life and of course a reduction in side effects that will permit a patient from living their life with some degree of normalcy or a good degree of quality of life.” — Caregiver A
“Treatments should have better side effects for everyone.” — Patient C
These interviewed patients focused heavily on being able to access a drug therapy that could be free of debilitating side effects, allowing them the ability to live their lives with some degree of normalcy. One patient (Patient B) also emphasized the need to access therapies that can be easily administered, in the comfort of their own home: an oral therapy that would minimize visits to the cancer centre. In patients’ own words:
“I would say that all therapies should come in a pill form, have no side effects or minimal side effects, and it should shrink the disease big time!” — Patient B
“I would probably like to see a better quality of life – so I guess no side effects, because of what I went through. A better drug on the market because of the damage I underwent. It was horrible what I went through. Cancer is not so easy so it would be helpful to go through it with a drug that provides a good quality of life.” — Patient D
Furthermore, the three interviewed patients (Patients B, C and D) maintain the therapy under review currently possesses these desired improvements and were extremely grateful to have been able to access this therapy (Q26). According to their explicit and detailed input, it has prolonged their life significantly with minimal to no side effects, promoting excellent quality of life. Their lives have been truly ameliorated, such that they have been able to resume normal daily activities, spend quality time with friends and family (pandemic notwithstanding), permitting them the freedom to “living life again”. In their own words, patients provided the following input regarding the current therapy (Pembrolizumab monotherapy and Pembrolizumab + Lenvatinib) possessing the desired improvements:
“Yes, I do! Look at my results! My disease was so stubborn, but this therapy has reduced my disease considerably and the side effects have been so great and so very minimal for me. My quality of life has been excellent.” — Patient B
“Yes! it’s fantastic, I do not feel any side effects at all. I would say it has been constructive being on this immunotherapy vs having been on previous therapies like chemo which I would consider as destructive.” — Patient C
“Yes, I certainly do. It has given me all of that and so much more because I am myself again. I have my life back. I believe that says it all.” — Patient D
Experience With Drug Under Review
The treatment-related experiences were captured for three interviewed Canadian patients who are currently undergoing the therapy under review. One additional patient provided input regarding her experience with the therapy through the CCSN online survey. In total, four patients provided compelling input (Patient B and C provided input regarding Pembrolizumab + Lenvatinib; Patient D provided input regarding Pembrolizumab monotherapy; and the CCSN patient provided input regarding Pembrolizumab + Lenvatinib), all of whom underscored the dire need to improve therapeutics for the management of advanced endometrial cancer because patients diagnosed with recurrent or metastatic endometrial cancer have limited treatment options. And the options that are available to them are not only short lived but riddled with debilitating side effects. The following four patients were diagnosed with metastatic, chemotherapy resistant endometrial cancers treated with pembrolizumab + Lenvatinib who, having achieved long term durable responses, wished to share their experiences for the purposes of informing your deliberative processes:
Patient B was a 51-year-old female who underwent surgical resection of her endometrial cancer. Three months post op, she was diagnosed with a mass that was strangulating her left ureter as well as metastases to her spleen, liver and peritoneum. She was prescribed 6 cycles of Carbotaxol to which there was little response. Her left kidney failed due to hydronephrosis. She was then recommended Pembrolizumab in combination with Lenvatinib in October 2019 as part of a clinical study in second line therapy.
Patient C was a 64-year-old female who underwent surgical resection, endured 6 toxic cycles of Carbotaxol and 3 treatments of brachytherapy. She was diagnosed with recurrent disease in her peritoneum and spine for which she was prescribed first line Carbotaxol (6 cycles). Progression ensued. Hormonal therapy (Letrazole) + Vitamin D was then prescribed as part of second line therapy to which there was no response. Third line therapy followed consisting of Doxorubicin (6 cycles) to which she responded poorly and experienced diminished quality of life. In August 2021, the patient accessed Pembrolizumab + Lenvatinib through a private pay plan as part of fourth line therapy.
Patient D is a 69-year-old female who learned of her metastatic disease to her lungs as she was being wheeled into surgery. She was prescribed first line Carbotaxol post op. She could only endure one cycle of the carboplatin due to significant neuropathy but did continue with the paclitaxel portion, which regressed the lung metastases but was ineffective against the abdominal disease, which appeared while on the paclitaxel. She was then recommended Pembrolizumab monotherapy as part of second line and began treatment in June 2021, accessed through her husband’s private insurance plan.
The CCSN patient accessed standard of care therapies such as Carbotaxol as well as complementary therapies and alternative medicines that were somewhat effective but due to progressive disease, did go on to access Pembrolizumab + Lenvatinib through a clinical trial. The Pembrolizumab + Lenvatinib provided tumour shrinkage and slowed progression of disease according to the patient input. It did, however, cause undesirable treatment induced side effects such as diarrhea and herpes outbreaks.
The three interviewed patients accessed the therapy under review with great anticipation and hope because they had either exhausted standard of care therapies for the management of their cancer (Patient C) or had been recommended to enroll in a clinical trial that could prove helpful in the treatment of their cancer (Patient B) or could molecularly target their particular cancer: MSI-High Cancer (Patient D). Two of the three interviewed patients (Patients C, D) experienced no side effects whatsoever from their Pembrolizumab + Lenvatinib and Pembrolizumab monotherapy treatments respectively (Q15A).
“No, not at all. It has been amazing. I am a little tired because of the previous therapies I was on, but no, no side effects at all, whatsoever.” — Patient C
“Nope, no side effects whatsoever.” — Patient D
Patient B experienced two treatment-induced side effects: diarrhea and mild fatigue, both of which are well managed and easily controlled. She was prescribed loperamide to control the diarrhea and Synthroid for the fatigue, both of which are no longer issues.
“The main side effect I have experienced is irritable bowel syndrome (diarrhea) for which I was prescribed loperamide. And I had some fatigue at the end of the treatment, in August so they put me on Synthroid. The diarrhea was mild because if I watch what I eat, it is ok. I get to manage it very well. And the fatigue is mild as well. That’s pretty much it.” — Patient B
And the CCSN patient reported the following treatment-induced side effects: fatigue, diarrhea, and urinary tract infection. She does report there has been tumour shrinkage and that the therapy has “slowed progression of disease”. Interviewed patients were asked to rate their quality of life while on the therapy under review (Q16). All three patients provided high scores: 9, 8, and 10, generating an average score of 9, and two patients provided comments with their scores:
“My life has definitely been better since being on this therapy both from a quality-of-life perspective and from a survival perspective.” — Patient B
“I feel so good while on this therapy. I am as I am right now, all the time.” — Patient D
All three interviewed patients maintain that Pembrolizumab + Lenvatinib or Pembrolizumab monotherapy has delivered a remarkable response wherein their disease has regressed significantly in addition to having provided them with an excellent quality of life (Q19). The objective findings from diagnostics such as imaging (CT – except for Patient C) and labs support their improved overall well-being. Clinically, they feel better! In the patients’ own words:
“First, I felt better. I had no more cancer symptoms. I could go to the bathroom. I had no more constipation, and I had no more pain in my pelvis. And the tingling resolved. And the CT scan showed that I was responding to the therapy. They were taking measurements every time I had a CT scan. My cancer shrank by 70%! and now there is so much scar tissue. It is pretty much dead in there. I am so lucky to have been on this therapy. It has been so wonderful for me.” — Patient B
“I had 2 CT scans so far that confirmed response. The first CT scan showed lots of improvement in all tumours including my belly. The second one showed more improvement in all tumours too. I also feel so well. That’s a sign that the treatment is working. I have no more cancer symptoms. I could go on taking this therapy with no side effects forever.” — Patient D
All three interviewed patients cited how much easier the therapy under review was to use when compared to previously administered therapies, resulting in a superior quality of life (Q21). For patients who accessed Pembrolizumab + Lenvatinib: patients appreciated the opportunity to access an oral therapy (Lenvatinib) which is easily administered in the comfort of their own homes, thereby avoiding a long and grueling stay and infusion time at the cancer centre.
Patients also appreciated the short infusion time associated with Pembrolizumab (30-45 minutes), administered every 3 weeks, which is unlike the infusion times associated with previously administered standard of care therapies for advanced endometrial cancer (Carbotaxol and Doxorubicin).
“Yes, it has. When I was on the Carbotaxol, I used to have to sit in an infusion chair for 8 hours a day at the hospital and I have no more veins because of it. I now require a portacath because of that now. What a horrible therapy. But now, because of this immunotherapy, it is done in a 45-minute infusion, and I have no side effects. And the other half of the therapy I get to take at home. And the other beauty of it is, there is no Decadron anymore, woohoo! So no more discomfort. I am so happy about that. I love this treatment. It is wonderful and I have no pain. It is fantastic to take. And I get an oral therapy at home. What more can you ask for as a cancer patient?”
Two of the three interviewed patients (B and D) struggled with cancer induced symptoms prior to starting the therapy under review and in each case the therapy provided significant resolution of those symptoms. In Patient B’s case, her pelvic and abdominal disease regressed after starting Pembrolizumab + Lenvatinib which in turn resolved her pelvic pain and constipation. Patient D had been experiencing fatigue, nausea, lethargy and lack of appetite, due entirely to the disease in her abdomen but these symptoms completely resolved after commencing Pembrolizumab monotherapy. The therapy has regressed the disease in both these patients to the point where symptoms have completely ameliorated (Q17). Patients expressed how grateful they were to be rid of those cancer induced symptoms:
“…. I don’t have any of those symptoms anymore. The therapy shrank my cancer and took all those symptoms away.” — Patient B
“Pembrolizumab helped to resolve all of them. It was a miracle. I don’t have any of them anymore. Apparently, a lot of those symptoms were because of the disease in my belly. But the disease in my belly has shrunk so much, it is not giving me problems anymore or symptoms. They are completely gone.” — Patient D
Interviewed patients have been undergoing the therapy under review for, what is in some cases, an extended period of time, reflective of sustained and durable responses: 26 months, 4 months, 5 months. Efficacy was radiographically and clinically confirmed in each patient’s case (save Patient C who was scheduled to undergo imaging within a few weeks of their telephone interview, but the patient was quite emphatic that based on how they were feeling clinically and their labs, response was imminent and would correlate with CT scan findings (Q19).
Patients B, C and D were quite expressive and became emotional when describing what impact the therapy has had on their lives and what they have managed to accomplish or fulfill. They expressed profound disappointment with having accessed previous therapies that failed to successfully treat their cancer and caused indescribable pain, suffering and anguish, enduring unimaginable and debilitating side effects. But the therapy under review has been and continues to be their lifeline, a “miracle” drug (Patient D), a “God-sent” (Patient C), without which they would not be alive today. They credit their longevity and ability to function at an almost normal level entirely to Pembrolizumab + Lenvatinib or Pembrolizumab monotherapy. Patients were able to resume what most would consider to be a normal lifestyle while undergoing therapy, but wished to note that this was quite extraordinary for a cancer patient based on their experience with previously administered therapies. Interviewed patients reported significant improvements in health status while undergoing the therapy under review (both Pembrolizumab + Lenvatinib and Pembrolizumab monotherapy) with respect to physical function and overall quality of life. They were able to resume responsibilities such as grocery shopping, housework, cooking, baking, caring for their loved ones – responsibilities most healthy Canadians take for granted (Q24). But Patient C no longer takes these simple chores for granted in the setting of a cancer diagnosis. She is grateful to be able to perform them while actively undergoing cancer therapy. Patients were also able to fulfill and accomplish a great deal while on the therapy. They mention being able to travel, resume their studies, spend quality time with family and cherished friends, complete their sailing certification, rejoin the YMCA to rebuild muscle mass, engage in social media, and so much more. Patients can not only function, but they can thrive.
This life altering therapy has been repeatedly referred to as a “gift” and a “miracle” or that which has provided patients with great “hope” because it has offered them significant life extending properties while improving the patient’s quality of life. Additionally, it is worth noting that adverse events resulting in permanent discontinuation of the drug occurred in none of the patients; dosage interruptions due to an adverse reaction occurred in none of the patients; one patient (C) experienced a dose reduction (14mg to 10mg/day) in the Lenvatinib in the first few days of starting therapy due to headaches but has never experienced any issues since (Q20). Patients were overcome with gratitude and emotion throughout the interviews when speaking of their experience with the therapy under review:
“Do you really want an answer? (volume increased 5x). 1000% of course, I am so grateful for this therapy. Of course, of course, of course. I couldn’t afford to pay for this on my own, so I am so terribly appreciative of this. This therapy is my hope for a great extension in life. It is my way of continuing to live. Is it going to change for me? Will I be able to accept it for free in the future? I am so scared I might run out of luck in that respect and be forced to pay for it which is why I am participating today. I pray that I will be able to accept this therapy for free and that others who qualify will be able to accept it for free as well so they can benefit like me.” Patient C
“If I had not accessed this therapy, my life would have spiraled out of control and inevitably, to death. I have been able to travel, take an interest in my studies and my loving family again. Nothing is more important than family. I have nephews who have moved into the city who are spending Christmas eve with us, and I am looking forward to spending time with them which is so special to me and important to me. I have 2 nieces and 2 nephews in Ontario who I am seeing that I get to see because this therapy is making it possible to do so. These are special times because I am well enough to do it – all because of the therapy. These are not remarkable events, but they are nevertheless remarkable to me.” Patient B
Companion Diagnostic Test
Both mismatch repair deficiency (dMMR) and high microsatellite instability (MSI-H) have been proposed as predictive biomarkers of response to the immune checkpoint inhibitor Pembrolizumab. Approximately 16% of patients diagnosed with recurrent endometrial cancer have tumours with high levels of MSI-H and dMMR (jco.19.02627 (1).pdf) and these patients could benefit from Pembrolizumab monotherapy. Patients need to provide a tissue sample for biomarker analysis (that can be done through IHC or PCR) to help guide treatment. Our interviewed patients were not aware of any specific testing requirements to help determine their biomarker status that would identify them from potentially benefiting from Pembrolizumab monotherapy (Q11A). They were, however, aware of a myriad of testing they had to undergo, to which they happily subjected themselves because they had either exhausted therapeutic options or progressed on standard of care therapies.
“I don’t really know, and I didn’t really ask. All I know is that my tissue went to a tissue bank for testing and my oncologist spoke to me about it.” — Patient B
None of our interviewed patients incurred any out-of-pocket expenses for any diagnostic testing they required to qualify for their therapy (Q11D). Based on previous submissions made by CCRAN, patients’ MSI/MMR status could be determined through IHC testing at their local treatment centre and patients are typically grateful to access the test.
For those who qualify for the immunotherapy based on the identification of a unique biomarker, patients may be able to experience a life prolonging therapy with minimal to no side effects, allowing them to resume their day-to-day activities. For patients whose endometrial tumours are identified to be microsatellite stable (MSS) and mismatch repair proficient (pMMR), they too are able to avail themselves of a life-prolonging therapy that includes pembrolizumab in combination with lenvatinib based on patient input. The combination therapy, according to our interviewed patients (B and C, and CCSN patient), has demonstrated great efficacy in the treatment of their recurrent/metastatic disease. Upfront testing will identify the patients who qualify for monotherapy vs combination therapy and will ultimately change the treatment paradigm and guide treatment decisions. The result, according to patient input, will be improved quality of life due to fewer treatment induced toxicities, disease regression, an oral therapy permitting at home use, and reduced infusion time. For patients who are identified with the unique biomarker (MSI-H/dMMR), the therapy delivers on the promise of precision medicine guiding treatment decisions for advanced endometrial cancer.
Anything Else?
The standard of care for patients with advanced or recurrent endometrial cancer is multiagent systemic chemotherapy, which includes Carbotaxol in the first line setting. In addition to being quite toxic, this combination therapy has, according to our patient input, low response rates which creates an urgent, unmet need to provide treatment options that yield better outcomes for this patient population: outcomes that include fewer side effects contributing to an improved quality of life, an extension in progression free survival and overall survival.
The patients who received Pembrolizumab monotherapy or Pembrolizumab + Lenvatinib reported significant improvements in health status with respect to physical function and overall quality of life. According to patients, the therapy has fewer side effects compared to previously administered therapies. Patients expressed their profound gratitude for having been able to access the therapy under review because for the most part, it has delivered a robust, durable, safe and effective response compared to previously accessed therapies with a substantially favorable toxicity profile. This was repeatedly stressed throughout the captured data. They also appreciated the shorter infusion time of the therapy and the convenient use of an oral therapy, easily administered at home. Patients stated they wish to continue to avail themselves of the therapy and wish same for others who qualify.
The use of Pembrolizumab monotherapy in the MSI-H/dMMR patient and Pembrolizumab + Lenvatinib in the MSS/pMMR patients demonstrated a level of benefit unlike any other previously accessed treatment. These patients were permitted to resume a “normal, active lifestyle” which patients’ credit entirely to the therapy. They were once again engaged in life in a meaningful way – contributing members of society, their families and their communities. The use of the therapy under review helps to address the urgent, unmet need that currently exists in the management of metastatic/recurrent endometrial cancer.
If publicly funded:
Pembrolizumab would be an extremely important therapeutic option for patients whose progressive disease test positive for MSI-H/dMMR and whose disease has been deemed to be inoperable or metastatic/recurrent, and
Pembrolizumab + Lenvatinib would be an equally important therapeutic option for the MSS/pMMR patient population whose progressive disease has been deemed to be inoperable or metastatic/recurrent.
Funding these therapies in the appropriate settings (based on the identification of a unique biomarker), aligns well with the patient perspectives captured within this submission. Interviewed patients and their caregivers strongly supported the need for a positive funding recommendation be issued for Pembrolizumab monotherapy and Pembrolizumab + Lenvatinib for the treatment of MSI-H/dMMR and MSS/pMMR advanced endometrial cancer. The interviewed advanced endometrial patient population whose voice was captured and submitted herein underscores that the therapy under review aligns well with the identified need for a new, effective, quickly and easily administered, less toxic treatment option that is capable of maintaining a high quality of life. Survey data provided by CCS for this submission further underscores that patients and caregivers are asking for treatments that are more effective, but with non- debilitating side effects so they can lead a better quality of life, with the longest remission possible and fewer visits to the clinic.
Conflict of Interest Declaration — Colorectal Cancer Resource & Action Network
To maintain the objectivity and credibility of the CADTH CDR and pCODR programs, all patients in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for the Colorectal Cancer Resource & Action Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | — | — | X | — |
Conflict of Interest Declaration — Canadian Cancer Society
To maintain the objectivity and credibility of the CADTH CDR and pCODR programs, all patients in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
The network of the Division of Gynecologic Oncology at McGill University Health Center provided the testimonials which were written by patients. One nurse assisted a caregiver by writing down his verbal testimonial as indicated in the testimonial itself. They also shared our survey directly with patients.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for the Canadian Cancer Society
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | — | — | — | X |
Conflict of Interest Declaration — Canadian Cancer Survivor Network
To maintain the objectivity and credibility of the CADTH CDR and pCODR programs, all patients in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 3: Financial Disclosures for the Canadian Cancer Survivor Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | — | — | X | — |
Clinician Input
Ontario Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee
About Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug- related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
This input was jointly discussed with the listed DAC members.
Current Treatments
Pembrolizumab monotherapy: This therapy would be for individuals with mismatch repair deficiency (MMRd)/MSI-H endometrial cancer (EC) that has progressed after chemotherapy (after adjuvant chemotherapy in advanced stage or after chemotherapy for recurrent disease). Currently there are no agents that have specific approval for treatment of recurrent/progressive EC. At time of recurrence there are limited chemotherapy options and trial of carboplatin/taxol retreatment or Adriamycin at progression is current standard of care. The response to these limited chemotherapy options is poor. There are limited options with clinical trial enrolment for patients with advanced EC. There is currently no evidence for another line of therapy and therefore best supportive care would be an option. There are no special access programs for this population of patients. There is a limited subset of patients that are ER/PR positive that would be eligible for hormonal therapy (ex. Letrozole). The hormonal therapy available has limited low-level data and not Health Canada approved indication.
Lenvatinib in combination with Pembrolizumab: Currently there are no agents that have specific approval for treatment of recurrent/progressive EC. At time of recurrence there are limited chemotherapy options and trial of carboplatin/taxol retreatment or Adriamycin at progression is current standard of care. The response to these limited chemotherapy options is poor. There are limited options with clinical trial enrolment for patients with advanced EC. There is currently no evidence for another line of therapy and therefore best supportive care would be an option. There are no special access programs for this population of patients. There are a limited subset of patients that are ER/PR positive that would be eligible for hormonal therapy (ex. Letrozole). The hormonal therapy available has limited low-level data and not Health Canada approved indication.
Treatment Goals
Pembrolizumab monotherapy: The most important goals would be prolonged life, delay disease progression, symptomatic relief, partial response, full response, improved health-related quality or life, and decreased treatment toxicity.
Lenvatinib in combination with Pembrolizumab: The most important goals would be prolonged life, delay disease progression, symptomatic relief, partial response, full response, and improved health-related quality or life.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Pembrolizumab monotherapy: Currently there are no agents that have specific approval for treatment of recurrent/progressive MMRd/MSI-H endometrial cancer. At time of recurrence there are limited chemotherapy options and trial of carboplatin/taxol followed by Adriamycin at progression. There is currently no standard of care for these patients. Most patients do not response to available treatments and become refractory to current treatment options. Treatments are needed that are better tolerated.
Lenvatinib in combination with Pembrolizumab: Currently there are no agents that have specific approval for treatment of recurrent/progressive endometrial cancer. At time of recurrence there are limited chemotherapy options and trial of carboplatin/taxol followed by Adriamycin at progression. There is currently no standard of care for these patients. Most patients do not response to available treatments and become refractory to current treatment options. Treatments are needed that are better tolerated.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Pembrolizumab monotherapy: Patients with MMRd/MSI-H EC would have the greatest unmet need. There is current no options for MMRd/MSI-H endometrial cancer in the recurrent setting after platinum-based therapy.
Lenvatinib in combination with Pembrolizumab: There are current no options for endometrial cancer in the recurrent setting after platinum-based therapy. All patients with recurrent/progressive endometrial cancer post-platinum therapy would have the greatest unmet need.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Pembrolizumab monotherapy: There is no established second line treatment paradigm for these patients. It would replace potential retreatment with carboplatin/taxol or adriamycin.
Lenvatinib in combination with Pembrolizumab: There is no established second line treatment paradigm for these patients. It would replace potential retreatment with carboplatin/taxol or adriamycin.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Pembrolizumab monotherapy: No, we would not recommend other treatments since there are no other approved second line therapies for patient population. This would be the preferred option post platinum therapy at time of recurrence after failing chemotherapy.
Lenvatinib in combination with Pembrolizumab: No, we would not recommend other treatments since there are no other approved second line therapies for patient population. This would be the preferred option post platinum therapy at time of recurrence after failing chemotherapy.
How would this drug affect the sequencing of therapies for the target condition?
Pembrolizumab monotherapy: There is no current second line option and this would provide patients a second-line option. After failing platinum-based therapy, proceed to pembrolizumab monotherapy.
Lenvatinib in combination with Pembrolizumab: There is no current second line option and this would provide patients a second-line options. After failing platinum-based therapy, proceed to pembrolizumab in combo with lenvatinib.
Which patients would be best suited for treatment with the drug under review?
Pembrolizumab monotherapy: Individuals with MMRd)/MSI-H endometrial cancer (EC) that have progressed after platinum-based chemotherapy (after adjuvant chemotherapy in advanced stage or after chemotherapy for recurrent disease).
Lenvatinib in combination with Pembrolizumab: All EC patients that have recurred or progressed after platinum-based chemotherapy.
How would patients best suited for treatment with the drug under review be identified?
Pembrolizumab monotherapy: MMRd/MSI-H and evidence of recurrence on imaging (CT, MRI, PET Scan), biopsy, and examination. Immunohistochemisty for MMR is performed reflexively on all newly diagnosed cases of EC in Ontario and therefore MMRd patients are easily identified at time of recurrence/progression.
Lenvatinib in combination with Pembrolizumab: Evidence of recurrence on imaging (CT, MRI, PET Scan), biopsy, and examination.
Which patients would be least suitable for treatment with the drug under review?
Pembrolizumab monotherapy: Patients that are contraindication to immunotherapy, chemo-naïve, and MMR intact.
Lenvatinib in combination with Pembrolizumab: Patients that are contraindication to immunotherapy or Lenvatinib and chemo-naïve.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Pembrolizumab monotherapy: Yes. Reflex MMR testing.
Lenvatinib in combination with Pembrolizumab: While a greater benefit from treatment was seen in MMRd, all patients regardless of MMR status should achieve benefit.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Pembrolizumab monotherapy: Imaging, clinical exam, and symptomatic improvement.
Lenvatinib in combination with Pembrolizumab: Imaging, clinical exam, and symptomatic improvement.
What would be considered a clinically meaningful response to treatment?
Pembrolizumab monotherapy: Reduction in the frequency or severity of symptoms, improvement of symptoms, disease response or stability.
Lenvatinib in combination with Pembrolizumab: Reduction in the frequency or severity of symptoms, improvement of symptoms, disease response or stability.
How often should treatment response be assessed?
Pembrolizumab monotherapy: As per standard of care.
Lenvatinib in combination with Pembrolizumab: As per standard of care.
What factors should be considered when deciding to discontinue treatment?
Pembrolizumab monotherapy: Disease progression or intolerable side effects.
Lenvatinib in combination with Pembrolizumab: Disease progression or intolerable side effects.
What settings are appropriate for treatment with the drug under review?
Pembrolizumab monotherapy: Hospital (outpatient clinic)
Lenvatinib in combination with Pembrolizumab: Hospital (outpatient clinic)
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Not applicable.
Additional Information
Pembrolizumab monotherapy: This therapy provides high response rate in long term responders. The current chemotherapy does not provide a durable response. More tolerable toxicity profile compared to alternatives.
Lenvatinib in combination with Pembrolizumab: This therapy provides high response rate in long term responders. The current chemotherapy does not provide a durable response. More tolerable toxicity profile compared to alternatives.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Gynecology Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all patients in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
The DAC received secretariat support from Ontario Health-Cancer Care Ontario provincial drug reimbursement specialist.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Dr. Sarah Ferguson
Position: OH-CCO Gynecological Drug Advisory Committee Lead
Date: 08/12/2021
Table 4: COI Declaration for OH-CCO Gynecology Cancer Drug Advisory Committee — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Stephen Welch
Position: OH-CCO Gynecological Drug Advisory Committee Member
Date: 08/12/2021
Table 5: COI Declaration for OH-CCO Gynecology Cancer Drug Advisory Committee — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck (Advisory Board) — No COI | — | — | — | — |
Eisai Limited (Advisory Board) — No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Josee-Lyne Ethier
Position: OH-CCO Gynecological Drug Advisory Committee Lead
Date: 08/12/2021
Table 6: COI Declaration for OH-CCO Gynecology Cancer Drug Advisory Committee — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck (Advisory Board) — No COI | — | — | — | — |
Merck (Speaker) — No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Julie Ann Francis
Position: OH-CCO Gynecological Drug Advisory Committee Lead
Date: 08/12/2021
Table 7: COI Declaration for OH-CCO Gynecology Cancer Drug Advisory Committee — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Dr. Leah Jutzi
Position: OH-CCO Gynecological Drug Advisory Committee Lead
Date: 08/12/2021
Table 8: COI Declaration for OH-CCO Gynecology Cancer Drug Advisory Committee — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.