CADTH Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Early-stage triple-negative breast cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
ALT
alanine aminotransferase
APaT
all participants as treated
ASCO
American Society of Clinical Oncology
CAP
College of American Pathologists
CBCN
Canadian Breast Cancer Network
CI
confidence interval
CPS
combined positive score
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EFS
event-free survival
EORTC QLQ-BR23
European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
ER
estrogen receptor
HR
hazard ratio
HRQoL
health-related quality of life
IA
interim analysis
ITT
intention to treat
LS
least squares
MID
minimal important difference
NACT
neoadjuvant chemotherapy
NMA
network meta-analysis
NOC
Notice of Compliance
OH-CCO
Ontario Health–Cancer Care Ontario
OS
overall survival
pCR
pathological complete response
PD-L1
programmed death ligand 1
PR
progesterone receptor
QoL
quality of life
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
RR
risk ratio
SAP
statistical analysis plan
TNBC
triple-negative breast cancer
TOHCC
The Ottawa Hospital Cancer Centre
VAS
Visual Analogue Scale
ypT0/Tis
no invasive residual disease in breast or nodes; noninvasive breast residuals allowed
ypT0/Tis ypN0
no invasive residual disease in breast or nodes; noninvasive breast residuals allowed
ypT0 ypN0
no invasive or noninvasive residual disease in breast or nodes
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 200 mg IV every 3 weeks or 400 mg IV every 6 weeks |
Indication1 | For the treatment of adult patients with high-risk, early-stage triple-negative breast cancer in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery |
Reimbursement request | For the treatment of adult patients with high-risk, early-stage triple-negative breast cancer in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgerya |
Health Canada approval status | NOC |
Health Canada review pathway | Priority |
NOC date | April 12, 2022 |
Sponsor | Merck Canada Inc. |
NOC = Notice of Compliance.
aThe reimbursement request was submitted for CADTH review pre-NOC, and the request aligned with the proposed Health Canada indication.
Source: Sponsor-submitted reimbursement package.2
Introduction
Breast cancer is the most frequently diagnosed cancer in females in Canada, with projected estimates of about 27,700 new cases in 2021. It was estimated that 5,400 females would die from the disease in the same year. Fewer males are affected, with an estimated 290 new cases and 55 related deaths in 2021.3 Triple-negative breast cancer (TNBC) is an invasive form of breast cancer, affecting 10% to 20% of patients.4,5 It is most common in women younger than 40 years; African-American women; and women with a BRCA1 mutation.5,6 It is well established that patients with the BRCA1 mutation are more likely to develop TNBC than patients with other mutations.5,7,8 Triple-negative breast cancer is distinguished by the absence of an estrogen receptor (ER) and a progesterone receptor (PR) and by no expression of the HER2-negative gene.6,8,9 The clinician groups consulted highlighted that patients with TNBC have a higher risk of recurrence and death than patients with other types of breast cancer. The clinician groups noted that patients with a pathological complete response (pCR) have on average a 5-year disease-free survival of 85% to 90% for localized disease,6 while those with no pCR have a higher recurrence rate. Most patients with breast cancer, including TNBC, present with no symptoms at early stages of the disease. Breast changes such as firm or hard lumps, a lump in the armpit, changes in breast size and shape, changes to the nipple, and discharge from the nipples are some common symptoms reported. Additional symptoms—such as bone pain, weight loss, nausea, appetite loss, shortness of breath, cough, headache, double vision, and muscle weakness—may manifest with tumour size increase or spread to other organs.6,9
The standard approach for early-stage TNBC is neoadjuvant chemotherapy (NACT) for cT1c or greater tumours. According to the experts consulted, this approach allows for clinical downstaging (better chance of clear margins, breast-conserving surgery, and potential avoidance of completion axillary node dissection) and prognostication (patients achieving pCR having excellent long-term outcomes). Several NACT regimens are available in practice. The clinical experts and clinician groups highlighted that the sequential use of anthracycline-taxane (or taxane-anthracycline) combination chemotherapy (standard: every 3 weeks; dose dense: every 2 weeks) was standard of practice across jurisdictions in Canada. The clinical experts consulted also noted that dose-dense AC (doxorubicin-cyclophosphamide) every 2 weeks for 4 cycles followed by paclitaxel every 2 weeks for 4 cycles, with carboplatin often added, is the preferred NACT regimen in Canadian practice.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of pembrolizumab for the treatment of adult patients with early-stage TNBC in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input, clinician group input, and input from clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups, the Canadian Breast Cancer Network (CBCN) and Rethink Breast Cancer, provided input for this review. The CBCN patient input was based on an online survey (the CBCN’s 2017 Lived Experience Breast Cancer Patient Survey), telephone interviews, and a literature review of current studies and grey literature. The Rethink Breast Cancer input was based on general observations and insights gathered through various ongoing initiatives (including patients’ blogs, virtual support groups, working groups, and patient advisory boards), through telephone interviews with 2 patients and a caregiver to 1 of the patients, and through a focus group with 7 patients from the TNBC working group.
Respondents from both patient groups highlighted that TNBC is a rare subtype of breast cancer that is relatively more aggressive and has a higher rate of recurrence and poorer prognosis than other breast cancers. Respondents in both groups expressed lack of access to effective treatment as an unmet need. Respondents from the CBCN highlighted the need for treatment options that will reduce the risk of disease recurrence, delay disease progression, control disease, improve quality of life (QoL), and reduce severity of side effects from treatments. Respondents from Rethink Breast Cancer indicated that they are willing to tolerate additional side effects and reduced QoL in exchange for a treatment that can control TNBC.
Respondents in both patient groups who had received pembrolizumab stated that the treatment was effective and improved their QoL, with tolerable or minimal side effects. The most common adverse events (AEs) reported by patients who had experience with pembrolizumab included fatigue, colitis, and diarrhea. Respondents in both groups noted challenges in differentiating whether the side effects were due to pembrolizumab or to chemotherapy, given that they received treatments concurrently. One patient in the Rethink Breast Cancer group reported that pembrolizumab had effectively reduced their tumour size but that they had experienced AEs such as hives, skin conditions, and thyroid issues, while other patients noted experiencing minimal side effects with pembrolizumab. One caregiver mentioned that, overall, pembrolizumab treatment had been a positive experience, with side effects being somewhat of a challenge. Patient respondents who had received pembrolizumab indicated that they would recommend pembrolizumab to other patients with TNBC.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Pathological complete response, overall survival (OS), and event-free survival (EFS) were considered clinically meaningful outcomes by the clinical experts consulted during the CADTH review. The experts highlighted that the treatment goal for high-risk, early-stage TNBC is to reduce the risk of breast cancer recurrence and improve survival in patients. The clinical experts stated that pCR is associated with improvement in disease-free survival in TNBC, that not all patients respond to current treatment options, and that pCR rates are approximately 50% in patients receiving chemotherapy. The clinical experts indicated that staging approaches and routine breast tumour biopsy characterization of ER, PR, and HER2 status are currently in place to identify patients in Canada.
The experts generally agreed that the use of immunotherapy will cause a paradigm shift in practice for the treatment of TNBC. The clinical experts advised that patients who meet the inclusion criteria outlined in the KEYNOTE-522 study would be best suited for treatment. In the opinion of the experts, patients with pre-existing serious autoimmune diseases may not be eligible for this regimen. The experts added that patients with T1a/T1B N0 (node 0) are also not eligible due to the early-stage disease (regardless of coexisting autoimmune conditions), as these patients will likely have surgery upfront. In addition, the experts indicated that patients with less serious autoimmune conditions and patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 2 should weigh the pros and cons of the new regimen while considering older standard options in lower risk TNBC cases. The experts highlighted that there are currently no biomarkers to assess treatment response early on in patients with TNBC. The experts noted that in practice settings, patients will undergo a physical exam before each cycle in the neoadjuvant setting and that imaging scans may be used to rule out disease progression and review the patient’s fit for surgery.
According to the clinical experts, disease progression (tumour enlargement unless pseudoprogression is suspected) and the occurrence of AEs, particularly autoimmune toxicities (any grade 4 treatment-related AEs or grade 2 to 3 AEs not improving to grade 1 with supportive care or dose modifications), would be considered when deciding treatment discontinuation.
Clinician Group Input
Two clinician group inputs were provided: 1 from the Ontario Health–Cancer Care Ontario (OH-CCO) Breast Cancer Drug Advisory Committee (based on input from 2 clinicians) and 1 from The Ottawa Hospital Cancer Centre (TOHCC) Breast Disease Site Group (based on input from 15 medical oncologists). The OH-CCO’s Drug Advisory Committee provides timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. TOHCC aims to provide each person affected by cancer with world-class care, exceptional service, and compassion.
Both clinician groups identified NACT and then adjuvant chemotherapy as the current Canadian treatment paradigm for patients with TNBC. Both groups considered achieving long-term cure, improving OS and EFS, and delaying disease progression as important treatment goals. Both groups identified the lack of effective treatment options for patients with TNBC, limited pCR rates, the highest recurrence and death rates among the types of breast cancer, and the overall death rates among patients with breast cancer as unmet needs. Both groups anticipate that pembrolizumab will fit into the current treatment paradigm as a new treatment standard for TNBC. Both groups agreed that it would not be appropriate to recommend patients with TNBC to try other treatments before initiating pembrolizumab. Both clinician groups consulted considered tumour shrinkage (clinically or radiographically), improvement in pCR, and EFS as clinically meaningful outcomes when assessing treatment response.
The views of the clinician groups were, overall, consistent with the clinical experts consulted by CADTH.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Clinical Evidence
Pivotal Study
Description of Study
KEYNOTE-522 is an ongoing, phase III, randomized, multi-centre, double-blind, placebo-controlled trial. The primary objective of KEYNOTE-522 is to evaluate pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared with placebo plus chemotherapy as neoadjuvant therapy followed by continued placebo as adjuvant therapy for patients with high-risk, early-stage TNBC. The study was initiated in March 2017 and has 194 participating centres across 21 countries in North America (7 centres in Canada), South America, Europe, Asia, and Australia.10
Enrolled patients were male or female, 18 years and older, and newly diagnosed; had a locally advanced, centrally confirmed TNBC, as defined by the most recent American Society of Clinical Oncology (ASCO)–College of American Pathologists (CAP) guidelines; were previously untreated; and had a locally advanced nonmetastatic (M0) TNBC as per the current American Joint Committee on Cancer (AJCC) staging criteria for breast cancer, assessed by an investigator based on radiological and/or clinical assessment (T1c, N1 to N2; T2 to T4d; N0 to N2).10
Pathological complete response using the absence of invasive cancer in the breast irrespective of no invasive residual disease in breast or nodes; noninvasive breast residuals allowed (no invasive residual disease in breast or nodes; noninvasive breast residuals allowed [ypT0/Tis ypN0] definition; assessed by a local pathologist) and EFS (assessed by an investigator) were co-primary outcomes investigated in the KEYNOTE-522 trial. Overall survival, safety, and tolerability, and health-related QoL (HRQoL) (using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 [EORTC QLQ-C30], the European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire [EORTC QLQ-BR23], and the EQ-5D-5L questionnaire) were other secondary and exploratory outcomes investigated.
Patients were randomized in a 2:1 ratio based on 3 stratification factors: nodal status (positive versus negative); tumour size (T1/T2 versus T3/T4); and choice of carboplatin regimen (every 3 weeks or weekly).
By the fourth interim analysis (IA4) data cut-off (March 23, 2021), 1,608 patients had been screened and 1,174 randomized to 1 of the 2 trial arms. In total, 784 patients received pembrolizumab plus chemotherapy treatment, and 390 patients received placebo plus chemotherapy. The majority of the patients enrolled were female (1 man was enrolled), younger than 65 years, White, and pre-menopausal and had an ECOG PS of 0. More than 80% of patients were programmed death ligand 1 (PD-L1) positive. In the neoadjuvant phase, more patients in the pembrolizumab plus chemotherapy arm (24.2%) had discontinued study intervention than in the placebo plus chemotherapy arm (14.9%). In the adjuvant phase, the most common reason for discontinuation was AEs (5.4%) in the pembrolizumab group and relapse or recurrence (4.6%) or withdrawal by participant (4.4%) in the placebo group.10
Efficacy
Overall, almost all patients in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (99.2%) and all patients in the placebo plus chemotherapy followed by placebo arm (100%) reported at least 1 AE by the March 23, 2021, data cut-off. Adverse events of grade 3 or higher were slightly higher (82.4%) in the pembrolizumab plus chemotherapy followed by pembrolizumab arm than in the placebo plus chemotherapy followed by placebo arm (78.7%). The most common AEs in both arms were nausea, alopecia, anemia, and neutropenia.10
Adverse events of grade 3 to 5 reported in at least 5% of patients were also generally similar in both treatment arms and included neutropenia (35.23% versus 34.4%), decreased neutrophil count (19% versus 23.7%), anemia (19.5% versus 15.7%), febrile neutropenia (18.4% versus 16.2%), and decreased white blood cell count (6.4% versus 2.8%) in the pembrolizumab plus chemotherapy followed by pembrolizumab arm versus the placebo plus chemotherapy followed by placebo arm. Overall, AEs resulting in death in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (0.9%) were consistent with the placebo plus chemotherapy followed by placebo arm (0.3%). Adverse events leading to discontinuation of any study intervention in the combined neoadjuvant and adjuvant phases was higher in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (29.9%) than in the placebo plus chemotherapy followed by placebo arm (15.4%). Overall, the incidence of AEs leading to dose reduction of chemotherapy was generally similar between the pembrolizumab plus chemotherapy followed by pembrolizumab arm (12.8%) and the placebo plus chemotherapy followed by placebo arm (11.3%).10
Notable harms were more common in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (43.6%) than in the placebo plus chemotherapy followed by placebo arm (21.9%). The most common notable harms reported in the 2 study arms are presented in Table 2.10
Table 2 presents a summary of key results from the KEYNOTE-522 study.
Overall Survival
By the IA4 data cut-off (March 23, 2021), 135 out of 297 pre-specified events had occurred, representing approximately 45% of the information fraction for OS for the final analyses. The median OS was not estimable, and the hazard ratio (HR) obtained in the comparison of pembrolizumab plus chemotherapy followed by pembrolizumab versus placebo plus chemotherapy followed by placebo was 0.72 (95% confidence interval [CI], 0.51 to 1.02; P [1 sided] = 0.0321377).10
Pathological Complete Response Rate (Using ypT0/Tis ypN0)
At the IA1 data cut-off (September 24, 2018), the pCR rate was 64.8% (95% CI, 59.9% to 69.5%) in patients receiving pembrolizumab plus chemotherapy in the neoadjuvant phase and 51.2% (95% CI, 44.1% to 58.3%) in patients receiving placebo plus chemotherapy. At IA2 (April 24, 2019), the treatment difference in pCR rate (pembrolizumab plus chemotherapy versus placebo plus chemotherapy) was 9.2% (95% CI, 2.8% to 15.6%; P = 0.00221). The pCR rate (95% CI) for pembrolizumab plus chemotherapy in the neoadjuvant phase was 64.0% (95% CI, 60.2% to 67.6%), compared to 54.7% (95% CI, 49.1% to 60.1%) for placebo plus chemotherapy. At IA4 (March 23, 2021), the pCR rate in the patients receiving pembrolizumab plus chemotherapy in the neoadjuvant phase was 63% (95% CI, 59.5% to 66.4%) and in patients receiving placebo plus chemotherapy was 55% (95% CI, 50.6% to 60.6%). The pCR rate was not formally tested in IA4.10
Event-Free Survival
At the IA4 data cut-off (March 23, 2021), the median EFS was not estimable in either study arm. The EFS HR between the 2 arms was 0.63 (95% CI, 0.48 to 0.82; P [1 sided] = 0.0003093). The findings were consistent with data observed across IAs (in IA2, the EFS HR was 0.63 [95% CI, 0.43 to 0.93]; in IA3, the EFS HR was 0.65 [95% CI, 0.48 to 0.88]). Five pre-specified sensitivity analyses were conducted for EFS in the intention-to-treat (ITT) population. The results of the sensitivity analyses were consistent with the primary analysis (sensitivity analysis 1: the EFS HR was 0.64 [95% CI, 0.48 to 0.84]; sensitivity analysis 2: the EFS HR was 0.63 [95% CI, 0.48 to 0.82]; sensitivity analysis 3: the EFS HR was 0.65 [95% CI, 0.50 to 0.85]; sensitivity analysis 4: the EFS HR was 0.63 [95% CI, 0.48 to 0.84]; sensitivity analysis 5: the EFS HR was 0.63 [95% CI, 0.48 to 0.82]).10
Health-Related QoL
Multiplicity adjustments for type I error rate were not conducted for HRQoL outcomes, and P values were nominal. The findings were considered exploratory.
European Organisation for Research and Treatment of Cancer QLQ-C30
Neoadjuvant phase: Compliance rates in the neoadjuvant phase were similar at baseline for EORTC QLQ-C30 in both the pembrolizumab plus chemotherapy arm and the placebo plus chemotherapy arm among all patients (92.0% versus 95.8%). After 21 weeks of follow-up in the neoadjuvant phase, the completion rate among all patients was 80.7% in each arm. The mean change from baseline in global health status–QoL score was –11.24 (95% CI, –12.82 to –9.66) versus –10.20 (95% CI, –12.30 to –8.10) in the pembrolizumab plus chemotherapy versus the placebo plus chemotherapy arms at the IA4 data cut-off (March 23, 2021). The physical functioning scale difference in least squares (LS) mean scores in patients receiving pembrolizumab plus chemotherapy compared to placebo plus chemotherapy was –2.85 (95% CI, –5.11 to –0.60). The LS mean differences in change from baseline between groups for global health status–QoL score and functional scores were –1.04 (95% CI, –3.46 to 1.38) and –2.85 (95% CI, –5.11 to –0.60), respectively. The LS mean difference between groups for emotional functioning was –0.69 (95% CI, –3.13 to 1.75).10
Adjuvant phase: Compliance rates in the adjuvant phase were similar at baseline for EORTC QLQ-C30 in both the pembrolizumab and placebo arms among all participants (90.7% versus 91.9%) at the March 23, 2021, data cut-off. After 24 weeks of follow-up in the adjuvant phase, the compliance rate among patients was 82.4% versus 80.8% in the pembrolizumab versus placebo arms. Scores obtained in the different subscales in the pembrolizumab arm versus the placebo arm at the IA4 data cut-off (March 23, 2021) were as follows: global health status–QoL (mean change from baseline: 2.47 [95% CI, 1.05 to 3.88] versus 2.88 [95% CI, 1.05 to 4.71]); physical functioning (mean change from baseline: 1.60 [95% CI, 0.46 to 2.75] versus 3.18 [95% CI, 1.70 to 4.66]); and emotional functioning scales (mean change from baseline: –1.53 [95% CI, –3.03 to –0.03] versus –0.92 [95% CI, –2.88 to 1.04]). The LS mean differences between groups for global health status–QoL score, physical functioning, and emotional functioning were –0.41 (95% CI, –2.60 to 1.77), –1.57 (95% CI, –3.36 to 0.21), and –0.60 (95% CI, –2.99 to 1.79), respectively.10
European Organisation for Research and Treatment of Cancer QLQ-BR23
Neoadjuvant phase: Compliance rates in the neoadjuvant phase were similar at baseline for EORTC QLQ-BR23 in both the pembrolizumab plus chemotherapy arm and the placebo plus chemotherapy arm among all participants (91.6% versus 94.8%) at the March 23, 2021, data cut-off. After 21 weeks of follow-up in the neoadjuvant phase, the compliance rate for all patients was 80.5% versus 80.4% in the pembrolizumab plus chemotherapy arm versus the placebo plus chemotherapy arm. The mean change from baseline scores obtained in the pembrolizumab plus chemotherapy arm versus the placebo plus chemotherapy arm was –9.92 (95% CI, –11.34 to –8.49) versus –9.78 (95% CI, –11.53 to –8.03). The LS mean difference between groups for the EORTC QLQ-BR23 Breast Symptoms score was –0.13 (95% CI, –1.92 to 1.65).10
Adjuvant phase: Compliance rates in the adjuvant phase were similar at baseline for EORTC QLQ-BR23 in both the pembrolizumab and placebo arms among all participants (90.5% and 92.2%, respectively) at the March 23, 2021, data cut-off. After 24 weeks of follow-up, the compliance rate was 82.2% and 80.7% in the pembrolizumab and placebo arms, respectively. The mean change from baseline scores obtained in the pembrolizumab arm when compared to the placebo arm was –5.73 (95% CI, –7.32 to –4.15) versus –6.02 (95% CI, –8.04 to –4.01). The LS mean difference between groups for the EORTC QLQ-BR23 Breast Symptoms score was 0.29 (95% CI, –2.05 to 2.63).10
EQ Visual Analogue Scale
Neoadjuvant phase: Compliance rates in the neoadjuvant phase were similar at baseline for the EQ Visual Analogue Scale (VAS) in both the pembrolizumab plus chemotherapy arm and the placebo plus chemotherapy arm among all participants (92.8% versus 96.3%, respectively) at the March 23, 2021, data cut-off. After 21 weeks of follow-up in the neoadjuvant phase, the compliance rate was 80.8% versus 81.0% in the pembrolizumab plus chemotherapy arm and the placebo plus chemotherapy arm, respectively. The mean change from baseline in EQ VAS scores in the pembrolizumab plus chemotherapy arm versus the placebo plus chemotherapy arm was –8.98 (95% CI, –10.48 to –7.47) versus –7.36 (95% CI, – 9.34 to –5.38). The LS mean difference between groups for the EQ VAS score was –1.61 (95% CI, –3.87 to 0.64).10
Adjuvant phase: Compliance rates in the adjuvant phase were similar at baseline for EQ VAS in both the pembrolizumab and placebo arms among all participants (91.7% versus 91.9%). After 24 weeks of follow-up in the adjuvant phase, the compliance rate was 82.2% versus 80.3% in the pembrolizumab versus placebo arms. The mean change from baseline in EQ VAS scores in the pembrolizumab arm was 1.83 (95% CI, 0.66 to 3.00) compared to 2.42 (95% CI, 0.91 to 3.93) in the placebo arm. The LS mean difference between groups for the EQ VAS was –0.59 (95% CI, –2.40 to 1.23).10
Harms
Overall, almost all patients in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (99.2%) and all patients in the placebo plus chemotherapy followed by placebo arm (100%) reported at least 1 AE by the March 23, 2021, data cut-off. Adverse events of grade 3 or higher were slightly higher (82.4%) in the pembrolizumab plus chemotherapy followed by pembrolizumab arm than in the placebo plus chemotherapy followed by placebo arm (78.7%). The most common AEs in both arms were nausea, alopecia, anemia, and neutropenia.10
Adverse events of grade 3 to 5 reported in at least 5% of patients were also generally similar in both treatment arms and included neutropenia (35.23% versus 34.4%), decreased neutrophil count (19% versus 23.7%), anemia (19.5% versus 15.7%), febrile neutropenia (18.4% versus 16.2%), and decreased white blood cell count (6.4% versus 2.8%) in the pembrolizumab plus chemotherapy followed by pembrolizumab arm versus the placebo plus chemotherapy followed by placebo arm. Overall, AEs resulting in death in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (0.9%) were consistent with the placebo plus chemotherapy followed by placebo arm (0.3%). Adverse events leading to discontinuation of any study intervention in the combined neoadjuvant and adjuvant phases was higher in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (29.9%) than in the placebo plus chemotherapy followed by placebo arm (15.4%). Overall, the incidence of AEs leading to dose reduction of chemotherapy was generally similar between the pembrolizumab plus chemotherapy followed by pembrolizumab arm (12.8%) and the placebo plus chemotherapy followed by placebo arm (11.3%).10
Notable harms were more common in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (43.6%) than in the placebo plus chemotherapy followed by placebo arm (21.9%). The most common notable harms reported in the 2 study arms are presented in Table 2.10
Table 2: Summary of Key Results From Pivotal Study
Outcomes | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo |
|---|---|---|
OS | ||
Number of events, n (%) | 80 (10.2) | 55 (14.1) |
Number censored, n (%) | 704 (89.8) | 335 (85.9) |
Median OS (95% CI) | NE (NE to NE) | NE (NE to NE) |
Pembrolizumab plus chemotherapy followed by pembrolizumab vs. placebo plus chemotherapy followed by placebo | ||
Hazard ratio (95% CI)a | 0.72 (0.51 to 1.02) | |
P valueb | 0.032138 | |
pCR by ypT0/Tis ypN0 (co-primary outcome) at IA1 | ||
n | 401 | 201 |
Number of pCR | 260 | 103 |
pCR rate, % (95% CI) | 64.8 (59.9 to 69.5) | 51.2 (44.1 to 58.3) |
Percent difference in pembrolizumab plus chemotherapy vs. placebo plus chemotherapy | ||
Estimate (95% CI)c | 13.6 (5.4 to 21.8) | |
P valued | 0.00055 | |
pCR (by ypT0/Tis ypN0) at IA4 | ||
n | 784 | 390 |
Number of pCR | 494 | 217 |
pCR rate, % (95% CI) | 63 (59.5 to 66.4) | 55 (50.6 to 60.6) |
Percent difference in pembrolizumab plus chemotherapy vs. placebo plus chemotherapy | ||
Estimate (95% CI)c | 7.5 (1.6 to 13.4) | |
EFS (co-primary outcome) | ||
Number of events, n (%) | 123 (15.7) | 93 (23.8) |
Secondary primary malignancy | 6 (0.8) | 4 (1.0) |
Local PD precludes surgery | 3 (0.4) | 4 (1) |
Local PD precludes definitive surgery | 1 (0.1) | 4 (1) |
Distant PD | 4 (0.5) | 1 (0.3) |
Positive margin at last surgery | 6 (0.8) | 10 (2.6) |
Local recurrence | 28 (3.6) | 17 (4.4) |
Distant recurrence | 60 (7.7) | 51 (13.1) |
Death | 15 (1.9) | 6 (1.5) |
Kaplan–Meier estimates, monthse | ||
Median (95% CI) | NE (NE to NE) | NE (NE to NE) |
Pembrolizumab plus chemotherapy followed by pembrolizumab vs. placebo plus chemotherapy followed by placebo | ||
Hazard ratio (95% CI)a | 0.63 (0.48 to 0.82) | |
P valueb | 0.0003093 | |
Harms, n (%) | ||
One or more AEs | 777 (99.2) | 389 (100.0) |
Toxicity grade 3 to 5 AEs | 645 (82.4) | 306 (78.7) |
SAEs | 341 (43.6) | 111 (28.5) |
Any dose modificationf due to an AE | 644 (82.2) | 306 (78.7) |
Discontinued any drug due to an AE | 234 (29.9) | 60 (15.4) |
Notable harms, n (%) | ||
Colitis | 13 (1.7) | 3 (0.8) |
Hyperthyroidism | 41 (5.2) | 7(1.8) |
Hypophysitis | 15 (1.9) | 1 (0.3) |
Hypothyroidism | 118 (15.1) | 22 (5.7) |
Infusion reactions | 141 (18.0) | 45 (11.6) |
Nephritis | 7 (0.9) | 0 (0.0) |
Pneumonitis | 17 (2.2) | 6 (1.5) |
Severe skin reactions | 45 (5.7) | 4 (1.0) |
Type 1 diabetes mellitus | 4 (0.5) | 0 (0.3) |
AE = adverse event; CI = confidence interval; EFS = event-free survival; IA = interim analysis; NE = not estimable; OS = overall survival; pCR = pathological complete response; PD = progressed disease; SAE = serious adverse event; vs. = versus; ypT0/Tis ypN0 = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed.
Note: Data cut-off: March 23, 2021 (IA4), and September 24, 2018 (IA1).
aBased on Cox regression model with the Efron method of tie handling, with treatment as a covariate, stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly).
bOne-sided P value based on log-rank test stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly).
cBased on Miettinen and Nurminen method, stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly).
dOne-sided P value for testing H0: difference in % = 0 vs. H1: difference in % > 0.
eFrom product limit (Kaplan–Meier) method for censored data.
fDefined as an action taken of dose reduced, drug interrupted, or drug withdrawn. Grades are based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 4.0.
Source: Clinical Study Report.10
Critical Appraisal
KEYNOTE-522 is a randomized, double-blind, multi-centre, phase III trial. A 2:1 randomization scheme was implemented that allowed more patients in the pembrolizumab plus chemotherapy followed by pembrolizumab arm than in the placebo plus chemotherapy followed by placebo arm. The baseline and demographic characteristics of patients were considered well balanced in both study arms, and the risk of selection bias was considered low. The double-blind trial design lowered the risk of performance bias from the assessment of pCR, EFS, and OS outcomes. Subjective outcomes like HRQoL and safety also had a low risk of bias due to the double-blind nature of the trial. Overall survival, EFS, pCR, and HRQoL were considered clinically meaningful outcomes investigated in the trial by the clinical experts, clinician groups, and patient groups consulted during the review. All interim and subgroup analyses were pre-specified in the statistical plan. Multiplicity adjustments for type I error were conducted for pCR, EFS, and OS according to a pre-specified statistical hierarchy plan. Subgroup and HRQoL analyses were not adjusted for type I error; therefore, the findings were considered exploratory. The magnitude of benefit of pembrolizumab plus chemotherapy followed by pembrolizumab in the adjuvant phase in improving HRQoL is uncertain due to the lack of multiplicity adjustments to account for type I error in the analyses conducted.
The reimbursement request was submitted for CADTH review pre–Notice of Compliance (NOC), and the request aligned with the proposed Health Canada indication (indicated for the treatment of adult patients with early-stage TNBC in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery). The inclusion and exclusion criteria of the KEYNOTE-522 study were considered appropriate, and the baseline and demographic characteristics were considered generalizable to Canadian practice by the clinical experts consulted. Most patients enrolled had an ECOG PS of 0 or 1. The clinical experts agreed that they may consider administering pembrolizumab to patients with an ECOG PS of 2 but would not offer treatment to patients with an ECOG PS of 3 or greater. Therefore, the magnitude of benefit of pembrolizumab in patients who did not meet the inclusion criteria outlined in the KEYNOTE-522 study is uncertain. The dosage of pembrolizumab aligns with the Health Canada NOC indication, and the clinical experts anticipate dose modifications in practice to manage treatment-related toxicity. The choice of comparator for both neoadjuvant and adjuvant phases in the KEYNOTE-522 study was considered appropriate by the experts, given that the study was initiated before capecitabine or olaparib were available for public funding. Pathological complete response, EFS, and OS are validated outcomes recommended by the FDA for trials that include patients with TNBC.11,12 The clinical experts considered the outcomes important for patients with TNBC in Canadian practice. Some patients enrolled in the KEYNOTE-522 study were possibly more exposed to frequent assessments than patients in real-world practice. This may impact the generalizability of the findings to patients in real-world practice. The experts noted that patients are assessed before every cycle in the real world and may not necessarily undergo routine breast MRIs.
Indirect Treatment Comparison
Direct head-to-head clinical trials assessing pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared to other treatments for adult patients with early-stage TNBC are limited. The sponsor did not provide any indirect evidence for this review. Published indirect evidence was considered and summarized for this review to address the lack of direct evidence for relevant comparators.
Description and Methods of Published NMA
One published network meta-analysis (NMA) by Miyashita et al. (2020)13 was summarized for this review to supplement the assessment of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared to other treatments for adult patients with early-stage TNBC. The published NMA did not assess adjuvant treatment of TNBC. The published NMA included 13 randomized controlled trials (RCTs) and 3,008 patients with TNBC.
Eligible studies included patients with TNBC who received treatment that included anthracycline, bevacizumab, pembrolizumab, platinum salts, or other therapies (i.e., chemotherapies aside from the previously noted therapies of interest). The dosing of these interventions was not specified. Outcomes of interest included the rate of pCR (defined as ypT0/is and ypN0) or toxicities, specifically febrile neutropenia, grade 3 or greater thrombocytopenia, nausea/vomiting, and diarrhea. The systematic review only included RCTs and did not report any additional criteria regarding the study design.
Information about the statistical model selected for the NMA was limited. The authors reported that a random effects model was used for the NMA. Heterogeneity within the network was estimated using the I2 statistic, where an I2 value greater than 50% was considered an indicator of substantial heterogeneity. Inconsistency was evaluated using Q statistics.
Efficacy Results
The analysis of the rate of pCR suggested a higher rate of pCR for treatments that include anthracycline plus pembrolizumab plus platinum salts relative to anthracycline (risk ratio [RR] = 0.58; 95% CI, 0.43 to 0.77) and anthracycline plus platinum salts (RR = 0.79; 95% CI, 0.63 to 0.99). Conclusions could not be drawn for comparisons with anthracycline plus pembrolizumab or for comparison with platinum salts alone due to serious imprecision in the effect estimates.
Harms Results
The analysis of tolerability outcomes in the published NMA that are reported here are specific to the neoadjuvant setting. The analysis of the rate of febrile neutropenia suggested a higher rate of febrile neutropenia than is seen with anthracycline (RR = 0.53; 95% CI, 0.33 to 0.86). Conclusions could not be drawn for comparisons with anthracycline plus pembrolizumab, with anthracycline plus platinum salts, with platinum salts, or with other therapies (“C” node) due to serious imprecision in the effect estimates.
Regarding the analysis of the rate of grade 3 or greater nausea/vomiting, conclusions could not be drawn for comparisons with anthracycline alone, anthracycline in combination with platinum salts, or platinum salts alone due to serious imprecision in the effect estimates. No conclusions could be drawn for comparisons within the analysis of the rate of grade 3 or greater diarrhea due to serious imprecision in the effect estimates.
Critical Appraisal
The results of the published NMA by Miyashita et al. (2020)13 were associated with a number of limitations due to the lack of important details about the included trials and the methodology used to perform the NMA. As such, the appropriateness of conducting the NMA is uncertain. Most of the trials contributing to the network were at high risk of bias and are only applicable to the neoadjuvant phase of treatment. There was uncertainty regarding the plausibility of the transitivity assumption as sufficient assessment of potential effect modifiers was not reported. Results that were reported were associated with serious imprecision that limited the ability to draw conclusions for most of the comparisons in the network. Additionally, construction of treatment nodes used in the NMA preclude the ability to draw conclusions regarding comparisons of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy to other specific treatment options for TNBC. Overall, the findings of the NMA are uncertain.
Conclusions
One pivotal study (KEYNOTE-522) and 1 published NMA provided evidence for this CADTH review. No additional evidence directly comparing pembrolizumab plus chemotherapy in the neoadjuvant setting and pembrolizumab in the adjuvant setting with other standard therapies for early-stage TNBC was identified. The pCR rate and EFS were co-primary end points assessed in the KEYNOTE-522 study. Pathological complete response, EFS, OS, and HRQoL (including safety outcomes) investigated in the KEYNOTE-522 trial were considered clinically meaningful by the clinical experts, and they align with outcomes highlighted as important by the patient groups. The median OS and median EFS were not estimable at IA4; thus, there is uncertainty in the effect of the intervention for OS and EFS. The clinical experts considered differences in the pCR rate and percent change, as well as EFS, between the 2 arms clinically meaningful to clinicians and patients in clinical practice. The HRQoL assessments were considered exploratory due to the lack of multiplicity adjustments in the analyses. Both clinical experts and clinician groups stated that neoadjuvant therapy is current standard for TNBC and that pembrolizumab would be the preferred treatment option if it were to receive public funding. The clinical experts considered the safety profile of pembrolizumab plus chemotherapy followed by pembrolizumab manageable in practice. The experts stated that most oncologists have experience using pembrolizumab for other indications and are familiar with AEs due to pembrolizumab. Immune-related AEs are anticipated following the use of pembrolizumab. Both clinical experts and clinician groups considered toxicity and disease progression as important factors when deciding treatment discontinuation in patients. The KEYNOTE-522 study is a randomized, phase III, double-blinded design, and adjustments of multiplicity for type I error were conducted in the analyses of key outcomes OS, PFS, and pCR. The OS findings are interim, with other analyses planned after a pre-specified number of events have occurred. The clinical experts considered the baseline and demographic characteristics of the KEYNOTE-522 study generalizable to Canadian practice.
One published NMA by Miyashita et al. (2020)13 was summarized for this review to supplement the assessment of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared to other treatments for adult patients with early-stage TNBC. The NMA presented findings of pCR and grade 3 AEs specific to the neoadjuvant setting, which was a key limitation identified. Other methodological limitations—such as the lack of important details reported in the NMA methodology; high risk of bias in the studies included; the lack of information about the characteristics of the trials included in the network; and the imprecision of the estimates reported—precluded definitive conclusions of the findings observed for the different chemotherapy regimens and combinations assessed within the study.
Introduction
Disease Background
Breast cancer is the most frequently diagnosed cancer in females in Canada, with projected estimates of about 27,700 new cases in 2021. It was estimated that 5,400 females would die from the disease in the same year. Fewer males are affected, with an estimated 290 new cases and 55 related deaths in 2021. The predicted 5-year survival is 89% for females and 76% for males.3 Identified risk factors include lifestyle choices such as alcohol use, limited physical activity, not having children, not breastfeeding, birth control use, menopausal hormone therapy, and breast implants; age; inherited gene changes (BRCA1 and BRCA2); family history of breast cancer; personal history of breast cancer; race; and ethnicity.6,9
Triple-negative breast cancer is an invasive form of breast cancer affecting 10% to 20% of patients.4,5 It is most common among women younger than 40 years; African-American women; and women who have a BRCA1 mutation.5,6 It is well established that patients with the BRCA1 mutation are more likely to develop TNBC than patients with other mutations.5,7,8 Triple-negative breast cancer is distinguished by the absence of an ER and a PR and by no expression of the HER2-negative gene.6,8,9 The clinician groups consulted during the review highlighted that patients with TNBC have a higher risk of recurrence and death than patients with other types of breast cancer. The clinician groups also noted that patients with a pCR have on average a 5-year disease-free survival of 85% to 90% for localized disease,6 while those with no pCR have a higher recurrence rate. More than 50% of patients with early-stage (stage I to III) TNBC are bound to experience recurrence, of which 37% will die in the first 5 years following surgery.4
Most patients with breast cancer, including TNBC, present with no symptoms at early stages of the disease. Breast changes such as firm or hard lumps, a lump in the armpit, changes in breast size and shape, changes to the nipple, and discharge from the nipples are some common symptoms reported. Additional symptoms—including bone pain, weight loss, nausea, appetite loss, shortness of breath, cough, headache, double vision, and muscle weakness—may manifest with tumour size increase or spread to other organs.6,9
Breast cancers can be diagnosed during screening exams using mammograms. In most Canadian provinces and territories, organized screening via mammography at 2- to 3-year intervals is available for women 50 to 74 years of age at an average risk of breast cancer.14,15 Imaging techniques available include breast ultrasound and radionuclide imaging. Other diagnostic methods include tissue biopsy examinations, hormone receptor status testing, HER2 status testing, complete blood count, blood chemistry tests, tumour marker tests, X-rays, bone scans, and ductography.6,8,9
Standards of Therapy
The clinical experts and clinician groups consulted during the CADTH review indicated that the standard approach for early-stage TNBC is NACT for cT1c or greater tumours. In the clinical experts’ opinion, this approach allows for clinical downstaging (better chance of clear margins, breast-conserving surgery, and potential avoidance of completion axillary node dissection) and prognostication (those with pCR having excellent long-term outcomes; those without pCR having higher risk of disease recurrence) and can inform post-operative adjuvant chemotherapy decisions (e.g., oral capecitabine for 6 to 8 cycles for those without pCR). Both clinical experts and clinician groups highlighted that pCR is the universally accepted treatment goal for neoadjuvant therapy.
Several NACT regimens are available in practice. The clinical experts and clinician groups consulted during the review highlighted that the sequential use of anthracycline-taxane (or taxane-anthracycline) combination chemotherapy (standard: every 3 weeks; dose dense: every 2 weeks) was standard of practice across jurisdictions in Canada. The experts also noted that carboplatin is increasingly added to the taxane portion of treatment. In patients with BRCA-positive mutations, olaparib will be likely used in the adjuvant setting. As noted by the experts, 4 cycles of dose-dense AC (doxorubicin, cyclophosphamide) twice weekly followed by 4 cycles of paclitaxel twice weekly, with carboplatin often added, is the preferred NACT regimen. When carboplatin is added, dosing can be weekly for 12 cycles or once every 3 weeks for 4 cycles, as highlighted by the experts.
Preferred treatment options outlined in the National Comprehensive Cancer Network guidelines for patients with HER-negative TNBC include anthracyclines (doxorubicin or liposomal doxorubicin), taxanes (paclitaxel), and antimetabolites (capecitabine or gemcitabine). In patients with BRCA1 or BRCA2 mutations, olaparib or talazoparib, as well as platinum (carboplatin or cisplatin), are preferred options.8,10
Drug
Pembrolizumab is an immunoglobulin G4 monoclonal antibody against the programmed cell death protein 1. By inhibiting the programmed cell death protein 1 receptor from binding to its ligands expressed on T-cells, pembrolizumab restores the cytotoxic T-cell effector function. Combinations of pembrolizumab and chemotherapy were studied in an effort to enhance the antitumour activity of a single agent by creating a tumour microenvironment that stimulates responses to immunotherapy.10
The Health Canada–recommended dosage of pembrolizumab for adults with early-stage TNBC is either 200 mg IV every 3 weeks or 400 mg IV every 6 weeks, for a total of 1 year of treatment. It is recommended that patients be treated with neoadjuvant pembrolizumab in combination with NACT for 8 doses of 200 mg every 3 weeks or 4 doses of 400 mg every 6 weeks or until disease progression that precludes definitive surgery or unacceptable toxicity. This should be followed by adjuvant treatment with pembrolizumab as monotherapy for 9 doses of 200 mg every 3 weeks or 5 doses of 400 mg every 6 weeks or until disease recurrence or unacceptable toxicity. Patients who experience disease progression that precludes definitive surgery or unacceptable toxicity related to pembrolizumab as neoadjuvant treatment in combination with NACT should not receive pembrolizumab monotherapy as adjuvant treatment.10 Key characteristics of pembrolizumab, carboplatin, and paclitaxel are shown in Table 3.
Pembrolizumab underwent a priority review at Health Canada and obtained an NOC on April 13, 2022, for the treatment of adult patients with high-risk, early-stage TNBC in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery.1 The reimbursement request is for the treatment of adult patients with early-stage TNBC in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery. This submission was submitted for CADTH review pre-NOC, and the reimbursement request aligned with the proposed Health Canada indication. The proposed pre-NOC indication differs from the approved indication in the addition of “high-risk” patients to align the population with the KEYNOTE-522 trial population. Pembrolizumab has been previously reviewed by CADTH for other indications.
Table 3: Key Characteristics of Pembrolizumab, Carboplatin, and Paclitaxel
Detail | Pembrolizumab10 | Carboplatin16 | Paclitaxel17 |
|---|---|---|---|
Mechanism of action | Pembrolizumab is a high-affinity antibody against PD-1, which exerts dual ligand blockade of the PD-1 pathway, including PD-L1 and PD-L2, on antigen-presenting or tumour cells. By inhibiting the PD-1 receptor from binding to its ligands, pembrolizumab reactivates tumour-specific cytotoxic T lymphocytes in the tumour microenvironment. | Carboplatin is a synthetic analogue of cisplatin. Like cisplatin, carboplatin interferes with DNA intrastrand and interstrand crosslinks in cells exposed to the drug. DNA reactivity has been correlated with cytotoxicity. | Paclitaxel is a novel antimicrotubule agent that promotes the assembly of microtubules from tubulin dimers and stabilizes microtubules by preventing depolymerization. This stability results in the inhibition of the normal dynamic reorganization of the microtubule network, which is essential for vital interphase and mitotic cellular functions. In addition, paclitaxel induces abnormal arrays or “bundles” of microtubules throughout the cell cycle and multiple asters of microtubules during mitosis. In vitro, paclitaxel exhibits cytotoxic activity against a wide variety of both human and rodent tumour cell lines. |
Indicationa | For the treatment of adult patients with high-risk, early-stage triple-negative breast cancer in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery. | For the treatment of ovarian cancer of epithelial origin in first-line therapy, and in second-line therapy after other treatments have failed. | Adjuvant treatment of node-positive breast cancer, administered sequentially to standard combination therapy. Second-line treatment of metastatic breast cancer resistant to the usual treatments. |
Route of administration | IV | IV | IV |
Recommended dose | 200 mg IV fixed-dose, every 3 weeks | 400 mg/m2 as a single 15-to 60-minute infusion | Administered intravenously by continuous infusion over 3 hours at a dose of 175 mg/m2 at 21-day intervals |
Serious adverse effects or safety issues | Immune-mediated adverse reactions such as endocrinopathies, nephritis, and renal dysfunction; hepatitis; colitis; pneumonitis; severe skin reactions; thyroid disorders; type 1 diabetes mellitus; hypophysis; and adrenal insufficiency |
|
|
Other | Drug received NOC for new indication on April 12, 2022, | NA | NA |
NA = not applicable; NOC = Notice of Compliance; PD-1 = programmed cell death protein 1; PD-L = programmed death ligand.
aHealth Canada–approved indication.
Source: Pembrolizumab product monograph1; carboplatin product monograph16; paclitaxel product monograph.17
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full patient group input is included in the Stakeholder section of this review.
Two patient groups, the CBCN and Rethink Breast Cancer provided input for this review. The CBCN is a patient-directed charity and a member of the Canadian Cancer Action Network whose mission is to ensure the best quality of care for all Canadians affected by breast cancer through the promotion of information, education, and advocacy activities. Rethink Breast Cancer is a Canadian charity committed to educating, empowering, and advocating for system changes to improve the experience and outcomes of patients with breast cancer, especially for those in underserved groups such as those diagnosed at a younger age, those with metastatic breast cancer, and those who are systemically marginalized due to race, income, or other factors.
The patient input received by the CBCN was based on an online survey (the CBCN’s 2017 Lived Experience Breast Cancer Patient Survey), key informant telephone interviews, and a literature review of current studies and grey literature. Responses from 24 survey participants and 2 telephone interviewees were included in the patient input. All respondents included in the patient input indicated having had a diagnosis of TNBC. Most survey respondents (54%) were diagnosed with stage II TNBC; 8 and 2 respondents, respectively, were diagnosed with stage III and stage I TNBC. None of the survey respondents reported having experience with pembrolizumab treatment. Two patients being interviewed by telephone reported having received pembrolizumab treatment for TNBC, which was diagnosed at stage II and stage IIb in each of the 2 patients, respectively. The input from Rethink Breast Cancer was based on general observations and insights gathered through various ongoing initiatives (including patients’ blogs, virtual support groups, working groups, and patient advisory boards), as well as telephone interviews with 2 patients and with a caregiver to 1 of the patients, and from a focus group with 7 patients from the TNBC working group. Two patients and 1 caregiver interviewed reported having experience with pembrolizumab treatment for TNBC. Both patient interviewees reported being diagnosed with stage III TNBC.
Both patient groups indicated that, given the limited treatment options available, the diagnosis of TNBC has devastating and traumatic impacts on patients’ lives. The input provided by Rethink Breast Cancer indicated that, especially for patients who are diagnosed at a young age, TNBC may have detrimental effects on their well-being in terms of fertility, childcare, relationships, body image, social activities, employment, and mental health. Patients from the CBCN reported that the cost related to managing and treating TNBC would have negative financial impacts. The CBCN indicated that 7 and 12 survey respondents, respectively, had experienced a very large or some financial impact due to their TNBC diagnosis. Some survey respondents reported having difficulties accessing benefit programs that would help reduce the financial burden.
Respondents in the CBCN patient group expected new treatments to improve the following key outcomes: risk of recurrence, delay in disease progression, disease control, QoL, and severity of side effects. Patient respondents in the Rethink Breast Cancer group indicated that they were willing to tolerate additional side effects and detrimental impacts to their QoL in exchange for a new treatment that would be effective in controlling their TNBC. Additionally, patients from both patient groups perceived having access to effective treatments as a challenge and expressed their hope and desire to ensure that patients with TNBC can access effective treatments.
Patient respondents who had direct experience with pembrolizumab treatment indicated that, overall, pembrolizumab was an effective treatment, improved their QoL, and had tolerable or minimal side effects. Respondents in the CBCN input indicated that pembrolizumab was an effective treatment in terms of reducing the risk of recurrence, achieving a pCR, and having tolerable side effects. Key side effects highlighted by respondents in the CBCN included general fatigue, colitis, and diarrhea. Respondents in both patient groups noted similar challenges in attributing whether side effects were due to either pembrolizumab or chemotherapy as they received both treatments concurrently. One patient respondent in the Rethink Breast Cancer group reported that pembrolizumab had effectively reduced the tumour size but that they had experienced side effects such as hives, skin conditions, and thyroid issues. Other patient respondents mentioned having experienced minimal side effects while receiving pembrolizumab. One caregiver cited that, overall, the use of pembrolizumab treatment had been a positive experience, with side effects being somewhat of a challenge. In addition, the caregiver highlighted that ensuring a patient is comfortable, confident, and reassured with the treatment received is of critical concern to caregivers. All patients who had received pembrolizumab indicated they would recommend pembrolizumab to other patients with TNBC.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of TNBC.
Unmet Needs
Pathological complete response, OS, and EFS were considered important outcomes by the clinical experts consulted. The experts noted that pCR is associated with improvement in disease-free survival in TNBC. The clinical experts emphasized that not all patients respond to current treatment options and that pCR rates are approximately 50% in patients receiving chemotherapy. The clinical experts stated that recurrence rates are higher in patients with TNBC than in those with other forms of breast cancer and that the risks of recurrence and death are higher in patients who do not achieve a pCR following treatment.
Place in Therapy
According to the clinical experts, the approval of immunotherapy will cause a paradigm shift in practice for the treatment of TNBC. The experts noted that although carboplatin was administered in the KEYNOTE-522 trial and is increasingly being used in neoadjuvant settings, there is some variation in its administration across jurisdictions in Canada. The experts noted that in the KEYNOTE-522 trial, carboplatin and paclitaxel cycles were administered before the doxorubicin and cyclophosphamide cycles, which is the opposite order to standard practice in Canada. In the opinion of the experts, the new treatment regimen would likely become the new standard of care for patients with TNBC, as currently no adjuvant therapy is administered in the setting of pCR in TNBC.
The clinical experts advised that it would not be appropriate for patients to try other treatments before initiating pembrolizumab combined with chemotherapy. The experts stated that pembrolizumab combined with chemotherapy would be required to be used first, as patients only have “1 chance” at receiving an appropriate neoadjuvant therapy to maximize their chance of pCR. According to the experts, the best therapy that suits a patient’s medical needs and tolerance is prioritized in practice settings.
Patient Population
The clinical experts advised that patients best suited for treatment with pembrolizumab combined with chemotherapy are those that meet the inclusion criteria of the KEYNOTE-522 study. Typically, this will include patients 18 years and older diagnosed with nonmetastatic TNBC, with any clinically node-positive or node-negative patients, if the primary tumour size is cT2 (2 cm) or greater, and with an ECOG PS of 0 to 1.
The experts stated that patients will be routinely identified in practice during consultations with a medical oncologist. The experts indicated that standard breast cancer clinical staging approaches (with no additional testing required) and routine breast tumour biopsy characterization of ER, PR, and HER2 status are used to identify patients. One expert highlighted that jurisdictions with low uptake of neoadjuvant therapy for TNBC may require reminders to their surgical practitioners to refer patients for the therapy, although the anticipated need to inform physicians is low, stated the expert, as neoadjuvant therapy for TNBC with T1c or greater and node-positive disease is standard of care.
The clinical experts advised that patients with pre-existing serious autoimmune diseases, regardless of tumour size or nodes, may not be eligible for this regimen. Patients with T1a/T1B N0 (node 0) are also not eligible due to the early-stage disease (regardless of coexisting autoimmune conditions). According to the experts, these patients will likely have surgery upfront. The experts stated that patients with less serious autoimmune conditions may need to weigh the pros and cons of using pembrolizumab while considering older standard regimens in lower risk TNBC cases.
Assessing Response to Treatment
The experts indicated that there are no biomarkers to select TNBC cases early on during treatment. The experts noted that PD-L1 status has been predictive of benefit in metastatic cases but not in early disease.
The clinical experts stated that patients undergo a physical exam before each cycle, and sometimes imaging scans may be considered during treatments to rule out primary disease progression and to review possible candidacy for breast-sparing surgery. The experts considered evidence of tumour shrinkage, either clinically or radiographically, upon receiving treatment as a clinically meaningful response to treatment. According to the experts, the greater the response (particularly pCR), the better the long-term prognosis. Typically, patients will be assessed before each cycle in the neoadjuvant setting.
Discontinuing Treatment
The clinical experts stated that disease progression (tumour enlargement unless pseudoprogression is suspected) and the occurrence of AEs, particularly autoimmune toxicities (any grade 4 treatment-related AE or grade 2 to 3 AE not improving to grade 1 with supportive care or dose modifications), would be considered when deciding treatment discontinuation.
Prescribing Conditions
The clinical experts advised that chemotherapy infusion units with experience in administering cytotoxic agents and immunotherapy would be appropriate for administering the treatment regimen. The experts advised that a medical oncologist would usually initiate therapy and that treatment monitoring could be performed by either the treating oncologist or extender (e.g., family practitioner in oncology, nurse practitioner, or clinical nurse specialist).
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full clinician group input is included in the Stakeholder section of this review.
Two clinician group inputs were provided: 1 from OH-CCO Breast Cancer Drug Advisory Committee (based on input from 2 clinicians) and 1 from TOHCC Breast Disease Site Group (based on input from 15 medical oncologists). The OH-CCO’s Drug Advisory Committee provides timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. TOHCC aims to provide each person affected by cancer with world-class care, exceptional service, and compassion.
The OH-CCO and TOHCC clinician groups identified NACT and then adjuvant chemotherapy as the current Canadian treatment paradigm for patients with TNBC. Both groups considered achieving long-term cure, improving OS and EFS, and delaying disease progression as important treatment goals. Both groups identified the lack of effective treatment options for patients with TNBC, limited pCR rates, and the highest recurrence and death rates (among forms of breast cancer) as unmet needs. Both groups anticipate that pembrolizumab would fit into the current treatment paradigm as a new treatment standard for TNBC. However, the OH-CCO group mentioned that there is a lack of evidence on combining pembrolizumab with different agents, such as adjuvant capecitabine or adjuvant olaparib, or on comparing treatment effectiveness with different agents. In addition, at least 35% of patients with TNBC would receive capecitabine as the standard of care after the neoadjuvant treatment, whereas adjuvant capecitabine was not allowed in the KEYNOTE-522 trial. The TOHCC group highlighted that the carboplatin and paclitaxel cycles were given before the doxorubicin and cyclophosphamide cycles in the KEYNOTE-522 trial, which is the opposite order to Canadian standard practice.
Both groups agreed that it would be not appropriate to recommend patients with TNBC to try other treatments before initiating pembrolizumab as studies have shown that, in the advanced disease setting, delaying pembrolizumab while giving chemotherapy leads to worse outcomes and patients only have “1 chance” to receive the optimal evidence-based neoadjuvant and adjuvant regimen to achieve cure and prevent systemic recurrences. The clinician groups agreed that high-risk patients with TNBC who meet the eligibility criteria in the KEYNOTE-522 trial would be best suited for the pembrolizumab treatment and that patients with an ECOG PS of 2 to 4 or who have contraindications, such as serious pre-existing autoimmune disorders, would be least suitable for the pembrolizumab treatment.
Both clinician groups consulted considered tumour shrinkage (clinically or radiographically), improved pCR, and EFS as clinically meaningful outcomes to assess treatment response. Both clinician groups described that patients will be assessed for a response based physical examination and radiographic imaging before every cycle of treatment. Both clinician groups highlighted that disease progression or serious AEs (any grade 4 treatment-related AE or grade 2 to 3 AE not improving to grade 1 with supportive care or dose modifications) will be considered when deciding treatment discontinuation. The 2 groups identified hospitals or chemotherapy infusion units with experience in administering cytotoxic agents and immunotherapy as appropriate settings for treatment with pembrolizumab.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
KEYNOTE-522 used chemotherapy with paclitaxel-carboplatin for 4 cycles (12 weeks), then doxorubicin-cyclophosphamide for 4 cycles (12 weeks). This regimen is 1 of many chemotherapy options available for neoadjuvant chemotherapy. Most chemotherapy regimens available in Canada for neoadjuvant use for early-stage TNBC are anthracycline and taxane based. What chemotherapy regimens are appropriate for neoadjuvant use in combination with pembrolizumab? | According to the experts, any anthracycline- and taxane-based protocol theoretically will be appropriate. But dose-dense protocols have evidence supporting greater efficacy in TNBC and therefore improved survival. In the opinion of the experts, if a patient had contraindications to anthracycline, a taxane-based chemotherapy protocol could be used. The experts highlighted that most clinicians will likely maintain the ACT regimen. The experts noted that oncologists may switch the sequence to taxane and carboplatin first, and then anthracycline, to correspond to administration in KEYNOTE-522. According to the experts, some clinicians may elect to give the ACT in a dose-dense manner and keep pembrolizumab to every 3 weeks. Another alternative could be weekly paclitaxel with carboplatin for 12 weeks then AC, as AC weekly paclitaxel is superior to ACT. The experts noted that although epirubicin and docetaxel could be administered interchangeably with doxorubicin and paclitaxel, it is not clear if the protocol could be interchanged and offer the same pCR rates. |
Many chemotherapy regimens for neoadjuvant chemotherapy use dose-dense scheduling (every-14-day cycles for anthracycline-based treatments instead of every-21-day cycles).
| The experts mentioned that they suspect most clinicians will attempt to use dose-dense administration, when possible, given the evidence of better outcomes in TNBC with dose-dense treatment than with every-3-week treatment. Dose-dense ACT would likely be the best appropriate option. Options may include weekly taxane for 12 weeks with weekly carboplatin (or carboplatin every 3 weeks) and pembrolizumab every 3 weeks, then dose-dense AC every 2 weeks with pembrolizumab every 3 weeks. In the opinion of the experts, taxanes and carboplatin will likely be administered as per the clinical trial; however, dose-dense protocols may be considered, either as dose-dense ACT or as dose-dense taxane-AC; carboplatin would have to be integrated for the taxane component (so 8 weeks). Carboplatin is not usually given dose dense, so patients may receive less carboplatin than in KEYNOTE-522 if a completely dose-dense AC-taxane or taxane-AC protocol is attempted. Pembrolizumab could continue every 3 weeks. The experts also noted that they may consider giving pembrolizumab every 6 weeks with a dose-dense (every-2-week) chemotherapy schedule. |
KEYNOTE-522 allowed for either weekly or every-3-week dosing schedules of carboplatin. The pCR rate was higher in the patient group that received weekly carboplatin dosing. Which dosing schedule of carboplatin is most appropriate for this combination (every 3 weeks vs. weekly)? | The experts noted that in practice, weekly will be easier to implement as they can use dose-dense AC and then switch to weekly paclitaxel with weekly carboplatin. The experts also noted that this sequence is better tolerated by patients, and it is easier to identify neuropathy earlier to adjust therapy. According to the experts, both dosing schedules are appropriate; however, the preference should be for a weekly administration given the higher pCR rate, with the option for every 3 weeks if for medical reasons a weekly administration is not possible. |
Patients in KEYNOTE-522 were not permitted to have capecitabine maintenance following surgery.
| The clinical experts noted that, unfortunately, the major gap is data availability. The experts noted that it is unclear what should be done (i.e., no capecitabine at all, even if no pCR, or attempt capecitabine with the pembrolizumab, or stop the pembrolizumab and switch to capecitabine). The experts highlighted that similar issues exist with adjuvant olaparib. |
Considerations for initiation of therapy | |
KEYNOTE-522 enrolled patients with untreated, nonmetastatic TNBC (T1c, N1 to 2 or T2 to 4, N0 to2 [per AJCC]) independent of PD-L1 status.
| According to the clinical experts, the staging in KEYNOTE-522 is appropriate. The experts also noted that PD-L1 status is not required for neoadjuvant therapy with pembrolizumab with chemotherapy. |
KEYNOTE-522 did not include patients with stage I disease with triple-negative phenotype.
| In the opinion of the clinical experts, the potential for indication creep is certainly possible; however, most clinicians will not offer carboplatin to patients with stage I disease. For those patients receiving upfront surgery, adjuvant chemotherapy is not routinely offered for T1a or T1b node-negative disease. However, this is discussed with motivated patients, particularly those with T1bN0 disease. According to the experts, the clinical stage of the disease is the biggest driver of treatment selection. The experts also noted that T1a/b node-negative tumours are usually resected upfront, even if triple negative. Patients generally have favourable outcomes. There is a risk of overtreatment in these cases. |
Considerations for continuation or renewal of therapy | |
Total duration of pembrolizumab-based therapy in KEYNOTE-522 was 1 year (combined 17 doses including 8 cycles in neoadjuvant setting and 9 cycles in adjuvant setting). Pembrolizumab was permitted to be administered concurrently with any adjuvant radiation therapy or could be delayed until completion of radiation therapy.
| In the opinion of the experts consulted, if there is a delay for surgery, it is reasonable to continue single-agent pembrolizumab until surgery. As noted by the experts, for patients who may require delays in pembrolizumab doses (e.g., post-operative recovery, holding pembrolizumab therapy during radiation), it will likely be applicable case by case, although most of the time, it will be reasonable to resume therapy for a total of 17 doses. According to the experts, if there are extenuating delays, they would consider stopping therapy early. The experts noted that there are no data to guide the decision-making; rather, looking at the clinical situation of the patient will guide the decision. For example, it may be worthwhile to review guidelines and efficacy in other solid tumours that use adjuvant pembrolizumab for their practice recommendations. |
Considerations for prescribing of therapy | |
The pembrolizumab dosage in KEYNOTE-522 was 200 mg intravenously every 21 days for 17 doses.
| This approach seemed reasonable to the experts consulted given the clear interchangeable use in dosing for other tumour sites. |
Generalizability | |
Should patients with an ECOG PS of 2 or greater be eligible for pembrolizumab in this indication? | The experts noted that they would not offer pembrolizumab to patients with an ECOG PS of 3 or greater. An ECOG PS of 2 may be reasonable; however, other comorbidities would also have to be taken into consideration. |
Patients on active treatment with a time-limited opportunity to switch to pembrolizumab: Should patients currently receiving neoadjuvant chemotherapy in early-stage TNBC be eligible to have pembrolizumab added? | The experts generally agreed with this approach. However, the experts noted that if patients have completed neoadjuvant therapy, they would not offer pembrolizumab as single agent in the adjuvant setting. |
AC = anthracycline-cyclophosphamide; ACT = anthracycline plus cyclophosphamide plus taxane; AJCC = American Joint Committee on Cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; pCR = pathological complete response; PD-L1 = programmed death ligand 1; TNBC = triple-negative breast cancer.
Clinical Evidence
The clinical evidence included in the review of pembrolizumab (Keytruda) is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence selected from the literature that met the selection criteria specified in the review.
Systematic Review: Pivotal and Protocol Selected Studies
Objectives
To perform a systematic review of the beneficial and harmful effects of pembrolizumab (200 mg administered intravenously every 3 weeks or 400 mg every 6 weeks) for the treatment of adult patients with early-stage TNBC in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
The systematic review protocol presented here was established before the granting of an NOC from Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adult patients with early-stage TNBC (previously untreated, locally advanced nonmetastatic TNBC) Subgroups:
|
Intervention | Pembrolizumab in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery:
|
Comparators | Neoadjuvant systemic therapy:
Adjuvant:
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase III and IV RCTs |
AE = adverse event; HRQoL = health-related quality of life; PD-L1 = programmed death ligand 1; RCT = randomized controlled trial; SAE = serious adverse event; TEAE = treatment-emergent adverse event; TNBC = triple-negative breast cancer; WDAE = withdrawal due to adverse event.
aDraft product monograph states: “For the neoadjuvant and adjuvant treatment of early-stage TNBC, patients should be treated with neoadjuvant pembrolizumab in combination with chemotherapy for 8 doses of 200 mg every 3 weeks or 4 doses of 400 mg every 6 weeks or until disease progression that precludes definitive surgery or unacceptable toxicity, followed by adjuvant treatment with pembrolizumab as monotherapy for 9 doses of 200 mg every 3 weeks or 5 doses of 400 mg every 6 weeks or until disease recurrence or unacceptable toxicity. Patients who experience disease progression that precludes definitive surgery or unacceptable toxicity related to pembrolizumab as neoadjuvant treatment in combination with chemotherapy should not receive pembrolizumab monotherapy as adjuvant treatment.”
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS (Peer Review of Electronic Search Strategies) checklist.18
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Keytruda (pembrolizumab) and TNBC. Clinical trial registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register. No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on March 8, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on July 13, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.19 Included in this search were the websites of regulatory agencies (the FDA and the European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented through review of bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Findings From the Literature
Three reports of a single study were identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6. A list of excluded studies is presented in Appendix 2.
Description of Study
KEYNOTE-522 is an ongoing, phase III, randomized, multi-centre, double-blind, placebo-controlled trial. The primary objective of KEYNOTE-522 is to evaluate the rate of pCR for pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared with placebo plus chemotherapy as neoadjuvant therapy followed by continued placebo as adjuvant therapy for patients with high-risk, early-stage TNBC.10
Two primary outcomes, pCR rate (using the no invasive residual disease in breast or nodes; noninvasive breast residuals allowed [ypT0/Tis ypN0] definition) assessed by local pathologist and EFS assessed by investigator, were defined in the study. Overall survival, pCR rate (using no invasive or noninvasive residual disease in breast or nodes [ypT0 ypN0] and no invasive residual disease in breast or nodes; noninvasive breast residuals allowed [ypT0/Tis] definitions), pCR rate in PD-L1 (positive) tumours (combined positive score [CPS] ≥ 1), EFS assessed by the investigator in patients with PD-L1 (positive) tumours (CPS ≥ 1), OS in PD-L1 (positive) tumours (CPS ≥ 1), safety and tolerability, and HRQoL (using the EORTC QLQ-C30, the EORTC QLQ-BR23, and the EQ-5D-5L questionnaire) were some secondary and exploratory outcomes investigated in the study.
Enrolled patients were randomized via an interactive voice response system or integrated web response system in a 2:1 ratio to 1 of the 2 study arms based on 3 stratification factors:
Nodal status: positive versus negative
Tumour size: T1 or T2 versus T3 or T4
Choice of carboplatin regimen: every 3 weeks or weekly
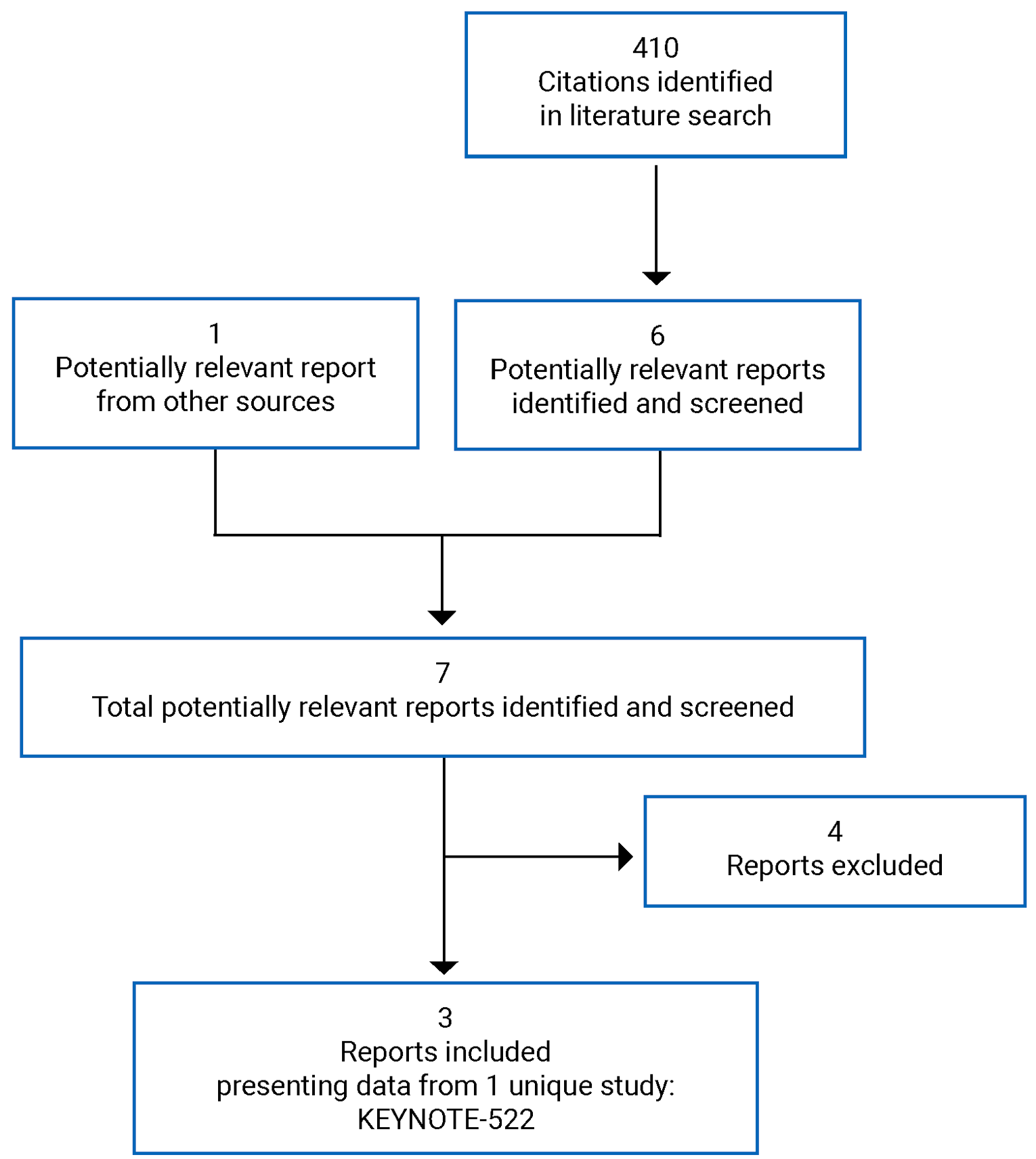
Table 6: Details of Included Study
Detail | Description |
|---|---|
Design and population | |
Study design | Multi-centre, double-blind, parallel-arm, randomized, phase III trial |
Locations | 194 centres in 21 countries: North America (7 sites in Canada), South America, Europe, Asia, and Australia |
Study duration |
|
Data cut-off date |
|
Randomized (N) |
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Neoadjuvant phase: pembrolizumab plus chemotherapy Adjuvant phase: pembrolizumab Pembrolizumab: 200 mg fixed-dose, IV, q.3.w., in the neoadjuvant and adjuvant treatment phases Chemotherapy (treatment 1):
Followed by (treatment 2):
|
Comparator | Neoadjuvant phase: placebo plus chemotherapy Adjuvant phase: placebo Placebo: normal saline, IV, q.3.w., in the neoadjuvant and adjuvant treatment phases Chemotherapy (treatment 1):
Followed by (treatment 2):
|
Duration | |
Screening phase | 28 days |
Neoadjuvant phase |
|
Adjuvant phase | Adjuvant treatment: cycles 1 to 9; 27 weeks |
Outcomes | |
Primary end points |
|
Secondary and exploratory end points | Secondary end points
Exploratory end points
|
Notes | |
Publications | Schmid et al. (2020)20 Schmid et al. (2022)21 |
AC = doxorubicin plus cyclophosphamide; AE = adverse events; AJCC = American Joint Committee on Cancer; ASCO = American Society of Clinical Oncology; AUC = area under the curve; BCS = breast-conserving surgery; CAP = College of American Pathologists; CHF = congestive heart failure; CPS = combined positive score; DRFS = distant recurrence-free survival; EC = epirubicin plus cyclophosphamide; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EFS = event-free survival; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FTV = functional tumour volume; HRQoL = health-related quality of life; IA = interim analysis; LLN = lower limit of normal; LVEF = left ventricular ejection fraction; NYHA = New York Heart Association; ORR = objective response rate; OS = overall survival; pCR = pathological complete response; PD-L1 = programmed death ligand 1; q.3.w. = every 3 weeks; RCB = residual cancer burden; RECIST = Response Evaluation Criteria in Solid Tumours; SAE = serious adverse event; TIL = tumour-infiltrating T lymphocytes; TNBC = triple-negative breast cancer; ypTO ypNO = no invasive or noninvasive residual disease in breast or nodes; ypT0/Tis ypN0 = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed.
Note: Data cut-off: March 23, 2021.
Source: Clinical Study Report.10
By the IA4 data cut-off (March 23, 2021), 1,608 patients had been screened, of which 1,174 were randomized to 1 of the 2 study arms (refer to Figure 2). In total, 784 patients were randomized to receive pembrolizumab plus chemotherapy and 390 to receive placebo plus chemotherapy. The majority of the patients enrolled were female (1 man was enrolled), younger than 65 years, White, and pre-menopausal and had an ECOG PS of 0. More than 80% of patients were PD-L1 positive.10
The KEYNOTE-522 trial was initiated in March 2017 and has 194 participating centres across 21 countries in North America (7 sites in Canada), South America, Europe, Asia, and Australia. The last patient was randomized into the study in September 2018. Patients and investigators were blinded to study treatments administered during the trial. The study was conducted in 2 phases: the neoadjuvant phase and the adjuvant phase, as shown in Figure 2.
Study phases
The screening phase took place approximately 28 days before randomization and treatment allocation. Patients were evaluated to determine if they met the inclusion criteria outlined in the protocol.
Following randomization, patients entered the neoadjuvant treatment phase, during which they were treated with the assigned therapy (pembrolizumab plus chemotherapy or placebo plus chemotherapy) for 12 weeks. Assessments and procedures were performed on day 1 of each cycle before the dosing of any study treatment (or before weekly dosing of paclitaxel), unless otherwise specified. Each treatment cycle lasted 3 weeks (21 days). Definitive surgery such as breast-conserving surgery or mastectomy with sentinel lymph node biopsy, with or without axillary lymph node dissection, was performed as part of the local standard of care approximately 3 weeks to 6 weeks following the completion or early discontinuation of the treatments in the neoadjuvant phase.
Figure 2: KEYNOTE-522 Study Design
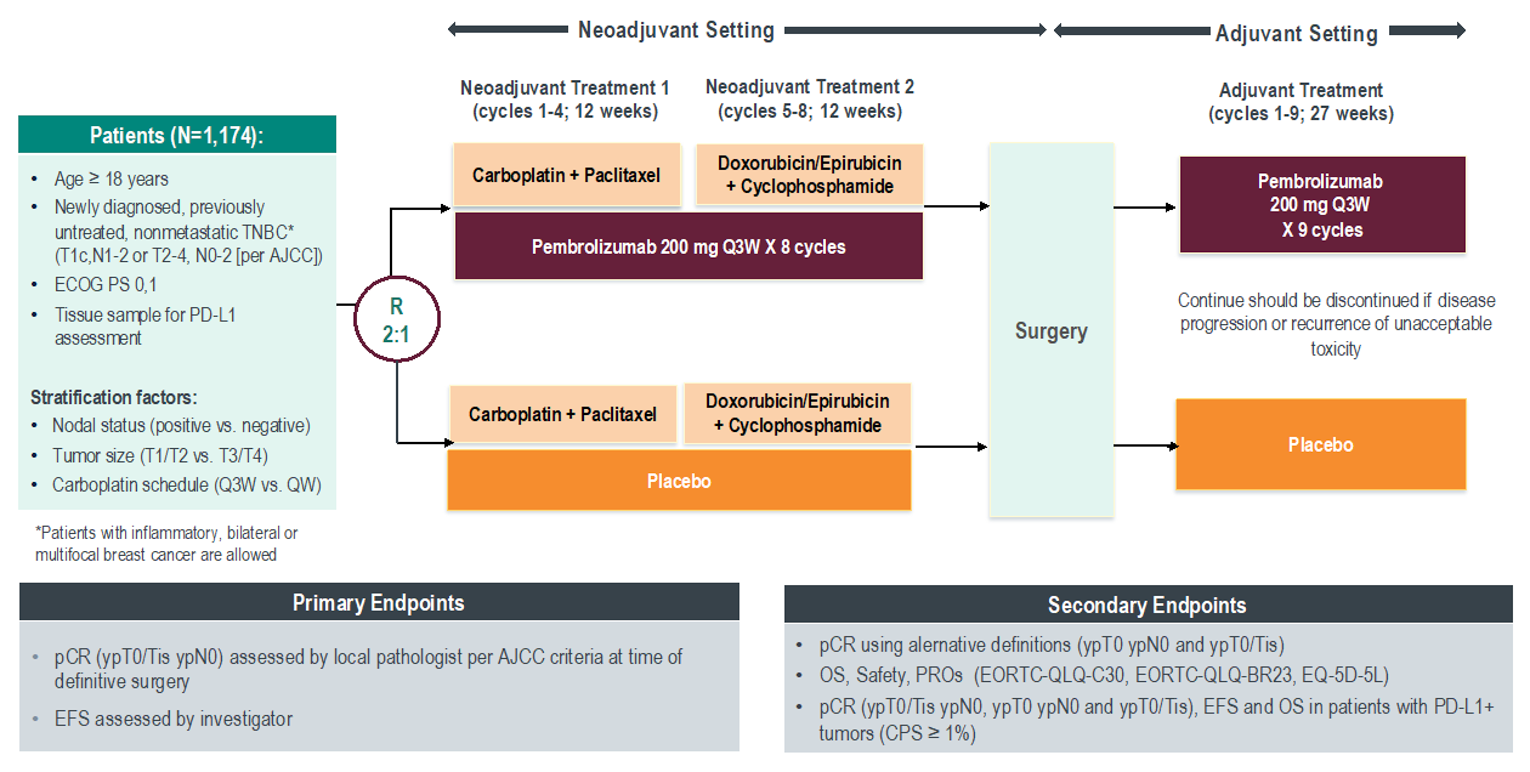
AJCC = American Joint Committee on Cancer; AUC = area under the curve; CPS = combined positive score; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EFS = event-free survival; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; OS = overall survival; pCR = pathological complete response; PD-L1 = programmed death ligand 1; PRO = patient-reported outcome; Q3W = every 3 weeks; QW = every week; TNBC = triple-negative breast cancer; vs. = versus.
Note: Data cut-off date: March 23, 2021. Neoadjuvant chemotherapy as follows: carboplatin AUC5 every 3 weeks or AUC1.5 every week plus paclitaxel 80 mg/m2 every week in the first 12 weeks and then doxorubicin 60 mg/m2 or epirubicin 90 mg/m2 every 3 weeks plus cyclophosphamide 600 mg/m2 every 3 weeks in the subsequent 12 weeks.
pCR (ypT0/Tis ypN0) = no residual invasive cancer on hematoxylin and eosin evaluation of the complete resected breast specimen and all sampled regional lymph nodes following completion of neoadjuvant systemic therapy at time of definitive surgery (noninvasive breast residuals [i.e., in situ cancer] allowed).
EFS = time from randomization to the first occurrence of any of the following events: progression of disease that precludes definitive surgery, local or distant recurrence, second primary malignancy, or death due to any cause.
pCR (ypT0 ypN0) = no residual invasive and in situ cancer on hematoxylin and eosin evaluation of the complete resected breast specimen and all sampled regional lymph nodes following completion of neoadjuvant systemic therapy at time of definitive surgery.
pCR (ypT0/Tis) = no residual invasive cancer in the breast irrespective of ductal carcinoma in situ or nodal involvement following completion of neoadjuvant systemic therapy at time of definitive surgery.
Source: Sponsor-submitted reimbursement package2; Schmid et al. (2020).22
Following surgery, patients entered the adjuvant treatment phase (30 days to 60 days after definitive surgery). Post-operative radiation therapy was acceptable in accordance with the standard of care, as applicable, and administered before or concurrently with systemic adjuvant treatment. If the patient was found to have disease progression before surgery, they were not allowed to proceed with the adjuvant treatment phase. Participants received either pembrolizumab or placebo every 3 weeks for 9 cycles (each cycle lasting 21 days).
Study treatment continued until completion of treatment (17 cycles [approximately 1 year] of pembrolizumab or placebo), disease progression in the neoadjuvant phase, recurrence (local or distance) after surgery, unacceptable AE(s), intercurrent illness that prevented further administration of treatment, investigator’s decision to withdraw the participant from treatment, pregnancy of the patient, noncompliance with treatment or procedure requirements, consent withdrawal, loss to follow-up, death, or administrative reasons that required treatment discontinuation.10
Post-Treatment Visits
Early Discontinuation Visit
An early discontinuation visit was conducted for patients who discontinued all protocol-specified treatments after the first treatment, cycle 1, through the adjuvant treatment phase. Early discontinuation procedures were recommended if the discontinuation visit occurred 30 days from the last dose of study treatment, at the time of the mandatory safety follow-up visit.
Safety Follow-Up Visits
Mandatory safety follow-up visits were conducted approximately 30 days (± 3 days) following the end of the neoadjuvant treatment phase, definitive surgery, and adjuvant treatment phase. In the event of an early discontinuation visit, a 30-day safety follow-up visit (30 days ± 3 days) was performed.
Long-Term Follow-Up for Disease Status and Survival
Long-term follow-up was planned every 3 months (± 1 month), then every 6 months (± 1 month) in years 3 to 4, and annually after 5 years for assessment of recurrent disease; or for metastatic disease for the first 2 years following adjuvant treatment. Any additional tests, investigations, or imaging assessments for recurrent or metastatic disease (e.g., bone or liver scan) were conducted at the discretion of the patient’s treating physician, and per local standard of care, or at the time of symptoms.
Treatment phase
Patients who discontinued treatment received follow-up by telephone every 6 months (± 1 month) for OS until consent withdrawal from trial, loss to follow-up, death, or end of the study, whichever came first.10
Populations
Inclusion and Exclusion Criteria
To be eligible, patients 18 years and older were required to have centrally confirmed TNBC, as defined by the most recent ASCO–CAP guidelines; have previously untreated, locally advanced nonmetastatic (M0) TNBC, defined per current AJCC staging criteria for breast cancer as assessed by the investigator based on radiological and/or clinical assessment (T1c, N1 to N2; T2 to T4d, N0 to N2); provide a core needle biopsy consisting of at least 2 separate tumour cores from the primary tumour at screening; have an ECOG PS of 0 or 1 within 10 days of treatment initiation; have adequate organ function; and have left ventricular ejection fraction of at least 50% or at least an institution lower limit of normal as assessed by echocardiogram or multigated acquisition scan.10
Patients were excluded from the study if they had received prior chemotherapy, targeted therapy, and radiation therapy within the past 12 months; had a history of (noninfectious) pneumonitis that required steroids or current pneumonitis; or had significant cardiovascular disease such as a history of myocardial infarction, acute coronary syndrome, or coronary angioplasty, stenting, or bypass grafting within the last 6 months, or congestive heart failure of New York Heart Association class II to IV, or a history of congestive heart failure of New York Heart Association class III or IV.10
Table 7: Summary of Baseline Characteristics at IA4—Intention-to-Treat Population
Characteristic | Pembrolizumab plus chemotherapy followed by pembrolizumab n = 784 | Placebo plus chemotherapy followed by placebo n = 390 |
|---|---|---|
Sex, n (%) | ||
Male | 1 (0.1) | 0 (0.0) |
Female | 783 (99.9) | 390 (100) |
Age, years, n (%) | ||
< 65 | 700 (89.3) | 342 (87.7) |
≥ 65 | 84 (10.7) | 48 (12.3) |
Median (range) | 49 (22 to 80) | 48 (24 to 79) |
Race, n (%)a | ||
American Indian or Alaska Native | 14 (1.8) | 7 (1.8) |
Asian | 149 (19.0) | 89 (22.8) |
Black or African-American | 38 (4.8) | 15 (3.8) |
Multiple | 13 (1.7) | 6 (1.5) |
White | 504 (64.3) | 24 (62.1) |
Missing | 65 (8.3) | 31 (7.9) |
Geographic region, n (%) | ||
North America | 166 (21.2) | 78 (20.0) |
Europe | 388 (49.5) | 180 (46.2) |
Australia | 23 (2.9) | 16 (4.1) |
Asia | 166 (21.2) | 91 (23.3) |
Rest of world | 41 (5.2) | 25 (6.4) |
ECOG PS, n (%) | ||
0 | 678 (86.5) | 341 (87.4) |
1 | 106 (13.5) | 49 (12.6) |
Menopausal status, n (%)b | ||
Pre-menopausal | 438 (55.9) | 221 (56.7) |
Post-menopausal | 345 (44.0) | 169 (43.3) |
Missing | 1 (0.1) | 0 (0.0) |
Choice of carboplatin, planned, n (%) | ||
Carboplatin q.3.w. | 335 (42.7) | 167 (42.8) |
Carboplatin weekly | 449 (57.3) | 223 (57.2) |
Primary tumour, planned, n (%) | ||
Tumour size T1/T2 | 580 (74.0) | 290 (74.4) |
Tumour size T3/T4 | 204 (26.0) | 100 (25.6) |
Nodal involvement, planned, n (%) | ||
Nodal status positive | 405 (51.7) | 200 (51.3) |
Nodal status negative | 379 (48.3) | 190 (48.7) |
Metastases, n (%) | ||
M0 | 784 (100.0) | 390 (100.0) |
Overall stage, n (%) | ||
Stage I | 0 (0.0) | 1 (0.3) |
Stage II | 590 (75.3) | 291(74.6) |
Stage III | 194 (24.7) | 98 (25.1) |
PD-L1 CPS 1 cut-off, n (%) | ||
PD-L1 CPS ≥ 1 | 656 (83.7) | 317 (81.3) |
PD-L1 CPS < 1 | 128 (16.3) | 69 (17.7) |
Unknown | 0 (0) | 4 (1.0) |
PD-L1 CPS 10 cut-off, n (%) | ||
PD-L1 CPS ≥ 10 | 393 (50.1) | 177 (45.4) |
PD-L1 CPS < 10 | 391 (49.9) | 209 (53.6) |
Unknown | 0 (0) | 4 (1) |
PD-L1 CPS 20 cut-off, n (%) | ||
PD-L1 CPS ≥ 20 | 247 (31.5) | 121 (31) |
PD-L1 CPS < 20 | 537 (68.5) | 265 (67.9) |
Unknown | 0 (0) | 4 (1) |
HER2 status, n (%)c | ||
0 to 1+ by IHC | 595 (75.9) | 286 (73.3) |
2+ by IHC (but FISH negative) | 188 (24.0) | 104 (26.7) |
CPS = combined positive score; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FISH = fluorescence in situ hybridization; IA = interim analysis; IHC = immunohistochemistry; M0 = nonmetastatic; PD-L1 = programmed death ligand 1; q.3.w. = every three weeks.
Note: Data cut-off: March 23, 2021.
aMissing values in race and ethnicity are mainly because France is not permitted to report this information.
bMissing value in menopausal status is from 1 male participant.
cMissing value in HER2 status is from the participant with missing IHC but with a FISH-negative result.
Source: Clinical Study Report.10
Baseline Characteristics
At the time of IA4, all patients (except for 1 in the pembrolizumab plus chemotherapy arm) were female and most were younger than 65 years, White, non-Hispanic or Latino, and pre-menopausal and had an ECOG PS of 0. Most patients (> 80%) had a tumour tissue PD-L1 expression score that was a CPS of 1 or higher. All patients enrolled had nonmetastatic disease, with the majority in both study arms having stage II disease. Table 7 presents the baseline and demographic characteristics of patients enrolled in the KEYNOTE-522 study at IA4.10
Interventions
Patients were randomized in a 2:1 ratio to 1 of the 2 study arms.
Arm 1
Pembrolizumab plus chemotherapy (pembrolizumab every 3 weeks, plus paclitaxel weekly, plus carboplatin every 3 weeks or weekly for 4 cycles, followed by pembrolizumab plus doxorubicin or epirubicin plus cyclophosphamide every 3 weeks for 4 cycles) as neoadjuvant therapy before surgery, followed by 9 cycles of pembrolizumab every 3 weeks as adjuvant therapy post-surgery.
Arm 2
Placebo plus chemotherapy (placebo every 3 weeks, plus paclitaxel weekly, plus carboplatin every 3 weeks or weekly for 4 cycles, followed by placebo plus doxorubicin or epirubicin plus cyclophosphamide every 3 weeks for 4 cycles) as neoadjuvant therapy before surgery, followed by 9 cycles of placebo every 3 weeks as adjuvant therapy post-surgery.10
Treatment Administration
Each cycle referred to in this section is 21 days.
Pembrolizumab: Administered at a 200 mg fixed dose via IV every 3 weeks, in the neoadjuvant and adjuvant treatment phases. The expected duration for the treatment was 12 months. A fixed-dose regimen was implemented to simplify the dosing regimen to be more convenient for physicians and to reduce potential for dosing errors.
Placebo: Composed of normal saline plus dextrose administered via IV every 3 weeks in the neoadjuvant and adjuvant treatment phases.
Chemotherapy (treatment 1):
Carboplatin: Area under the curve 5 (IV, every 3 weeks, on day 1 of cycles 1 to 4 of the paclitaxel and carboplatin regimen) or area under the curve 1.5 (IV, weekly, on days 1, 8, and 15 of cycles 1 to 4 of the paclitaxel and carboplatin regimen).
Paclitaxel: Administered at 80 mg/m2, IV, weekly, on days 1, 8, and 15 of cycles 1 to 4 of the paclitaxel and carboplatin regimen.
Followed by (treatment 2):
Doxorubicin: 60 mg/m2, IV, every 3 weeks, on day 1 of cycles 1 to 4 of the doxorubicin plus cyclophosphamide or epirubicin plus cyclophosphamide regimen, or
Epirubicin: 90 mg/m2, IV, every 3 weeks, on day 1 of cycles 1 to 4 of the doxorubicin plus cyclophosphamide or epirubicin plus cyclophosphamide regimen, plus
Cyclophosphamide: 600 mg/m2, IV, every 3 weeks, on day 1 of cycles 1 to 4 of the doxorubicin plus cyclophosphamide or epirubicin plus cyclophosphamide regimen.
Dose Modification
In the event of drug-related toxicity, including severe or life-threatening AEs, pembrolizumab was withheld. Dosing interruptions were permitted in the case of medical or surgical events or logistical reasons not related to study therapy (e.g., elective surgery, unrelated medical events, patient vacation, or holidays). Patients were to resume study therapy within 6 weeks of the scheduled interruption, unless otherwise discussed with the sponsor. Dose modification strategies for other chemotherapy agents were allowed in the study protocol. Local guidelines and practices were recommended if dosing was different from the sponsor’s recommendations. In the event that a dose delay did not lead to chemotherapy discontinuation, patients were allowed to resume treatment with the next scheduled dose in the regimen and continue on treatment to complete the full number of cycles per protocol.10
Treatment Discontinuation Criteria
Patients were allowed to discontinue 1 or more components of the study treatment at the discretion of the investigator in case of untoward effects. During the first part of the combination therapy, if 1 or more than 1 component of the regimen was discontinued due to toxicity, the investigator was required to consult and select 1 of many options outlined in the protocol for the patient at the investigator’s discretion.10 The investigator or sponsor was allowed to discontinue study treatment if the treatment was considered inappropriate, if the trial plan was violated, or for administrative or other safety reasons. A patient had to discontinue treatment but was permitted to remain in the trial and continue to receive follow-up and monitoring in the trial for the following reasons:
Request from the patient or patient’s legally acceptable representative to discontinue treatment
Unacceptable adverse experiences
Intercurrent illness that prevents further administration of treatment
Investigator’s decision to withdraw the patient from study treatment due to disease progression or other reasons
Confirmed positive serum pregnancy test
Noncompliance with trial treatment or procedure requirements
If the discontinuation from treatment was considered permanent, the patient was not allowed to restart treatment.10
Withdrawal From the Trial
Patients were allowed to withdraw from the trial if the patient or patient’s legally acceptable representative withdrew consent. Patients who withdrew from the trial were not permitted to receive treatment and were not followed at scheduled protocol visits. The patient underwent an early discontinuation visit procedure at the time of discontinuation.10
Concomitant Medications
All concomitant medications were documented, including all prescription and over-the-counter medications, herbal supplements, and IV medications and fluids. Reported concomitant interventions and concomitant use of steroid interventions were generally balanced between treatment groups. Supportive care was permitted for managing drug-related toxicities. Any supportive therapy or vaccination allowed during the trial was at the discretion of the investigator and/or the patient’s primary physician. Treatments considered necessary for patients’ welfare were allowed at the discretion of the investigator. Medications prohibited during the trial included immunotherapy, chemotherapy, or investigational agents not specified in the protocol; radiation therapy (except for radiation therapy post-surgery according to the standard of care, that is, in cases of breast-conserving surgery or large primary tumour or for patients with positive lymph nodes); live vaccines within 30 days before the first dose of trial treatment and during the trial (except for inactivated seasonal influenza vaccines); and glucocorticoids for any purpose other than to modulate the symptoms for an immune-related AE or for use as a pre-medication for chemotherapeutic agents specified in the protocol. Table 8 presents information on participants with specific concomitant medications (incidence > 0% in 1 or more treatment groups).10
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized below. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 3.
Table 8: Participants With Specific Concomitant Medication at IA4—All Participants as Treated Population
Medication | Pembrolizumab plus chemotherapy followed by pembrolizumab n = 783 | Placebo plus chemotherapy followed by placebo n = 389 |
|---|---|---|
Patients with at least 1 concomitant medication, n (%) | 770 (98.3) | 378 (97.2) |
Systemic hormonal preparations, excluding sex hormones and insulins, n (%) | ||
Corticosteroids for systemic use | 770 (98.3) | 378 (97.2) |
Alimentary tract and metabolism, n (%) | ||
Antidiarrheals, intestinal anti-inflammatory or anti-infective agents | 181 (23.1) | 83 (21.3) |
Antiemetics and antinauseants | 773 (98.7) | 382 (98.2) |
Bile and liver therapy | 47 (6.0) | 22 (5.7) |
Digestives, including enzymes | 13 (1.7) | 7 (1.8) |
Drugs for acid-related disorders | 751 (95.9) | 373 (95.9) |
Drugs for constipation | 236 (30.1) | 121 (31.1) |
Drugs for functional gastrointestinal disorders | 384 (49.0) | 190 (48.8) |
Drugs used in diabetes | 64 (8.2) | 29 (7.5) |
Mineral supplements | 214 (27.3) | 79 (20.3) |
Other alimentary tract and metabolism products | 38 (4.9) | 19 (4.9) |
Stomatological preparations | 60 (7.7) | 37 (9.5) |
Vitamins | 255 (32.6) | 123 (31.6) |
Anti-infectives for systemic use, n (%) | 625 (79.8) | 308 (79.2) |
Antimycobacterials | 5 (0.6) | 3 (0.8) |
Antimycotics for systemic use | 91 (11.6) | 23 (5.9) |
Antivirals for systemic use | 85 (10.9) | 53 (13.6) |
Immune sera and immunoglobulins, n (%) | 3 (0.4) | 1 (0.3) |
Vaccines | 45 (5.7) | 26 (6.7) |
Antineoplastic agents | 13 (1.7) | 4 (1.0) |
Endocrine therapy | 56 (7.2) | 28 (7.2) |
Immunostimulants | 553 (70.6) | 271 (69.7) |
Immunosuppressants | 16 (2.0) | 3 (0.8) |
Antiparasitic products, insecticides, and repellents, n (%) | ||
Anthelmintics | 5 (0.6) | 4 (1.0) |
Antiprotozoals | 4 (0.5) | 1 (0.3) |
Blood and blood-forming organs, n (%) | ||
Antianemic preparations | 196 (25.0) | 110 (28.3) |
Antihemorrhagics | 36 (4.6) | 9 (2.3) |
Antithrombotic agents | 245 (31.3) | 106 (27.2) |
Blood substitutes and perfusion solutions | 409 (52.2) | 178 (45.8) |
Cardiovascular system, n (%) | ||
Agents acting on the renin-angiotensin system | 136 (17.4) | 64 (16.5) |
IA = interim analysis.
Note: Every participant is counted a single time for each applicable specific concomitant medication. A participant with multiple concomitant medications within a medication category is counted a single time for that category. Database cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | KEYNOTE-522 trial end point | Definition | Included in hierarchical multiple testing procedure |
|---|---|---|---|
OS | Secondary | Defined as the time from randomization to death due to any cause. Patients without documented death at the time of the analysis will be censored at the date of the last follow-up. | Yes |
pCR rate | Primary | pCR rate (ypT0/Tis ypN0) was defined as the proportion of patients without residual invasive cancer on hematoxylin and eosin evaluation of the complete resected breast specimen and all sampled regional lymph nodes following completion of neoadjuvant systemic therapy by AJCC staging criteria (7th edition) assessed by the local pathologist at the time of definitive surgery. | Yes |
pCR rate | Secondary | pCR rate (ypT0 ypN0) was defined as the proportion of participants without residual invasive and in situ cancer on hematoxylin and eosin evaluation of the complete resected breast specimen and all sampled regional lymph nodes following completion of neoadjuvant systemic therapy by AJCC staging criteria assessed by the local pathologist at the time of definitive surgery. | No |
EFS | Primary | Defined as the time from randomization to any of the following events: progression of disease that precludes surgery; local or distant recurrence; second primary malignancy (breast or other cancers); or death due to any cause. | Yes |
HRQoL | Exploratory | EORTC QLQ-C30, EORTC QLQ-BR23, and the EQ-5D-5L questionnaire were used to measure HRQoL. | No |
Symptom severity | Not reported | Not applicable | Not applicable |
Safety | Safety | Safety parameters—such as incidence of AE or SAEs (including fatal SAEs), irAEs and laboratory abnormalities, rates of dose interruption and discontinuation due to AEs, and events of clinical interest—are important end points for safety and tolerability evaluations. | No |
AE = adverse event; AJCC = American Joint Committee on Cancer; EFS = event-free survival; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; irAE = immune-related adverse event; OS = overall survival; pCR = pathological complete response; SAE = serious adverse event; ypTO ypNO = no invasive or noninvasive residual disease in breast or nodes; ypT0/Tis ypN0 = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed.
Source: Clinical Study Report.10
Efficacy Measurement for Primary and Secondary Outcomes
Imaging (e.g., CT, MRI, bone scan) was performed at the discretion of the investigator, as per the local standard of care. Disease assessments were performed per Response Evaluation Criteria in Solid Tumours (RECIST) version 1.1, if applicable.
Definitive Surgery
Patients underwent definitive surgery as per local standard of care, 3 weeks to 6 weeks after the completion of neoadjuvant treatments. Breast tissues obtained during surgery were staged according to the AJCC guidelines and assessed for surgical margins by a local pathologist.
Pathologists reviewing and interpreting surgical specimens for pCR assessment were blinded to treatment assignment. All pathologists received formal training, and a procedure manual was provided that outlined standard guidelines for localization of tumour bed, handling of lymph nodes, and pathological evaluation of specimens. Regional pathologist(s) served as adjudicators or consultants for cases for which the site pathologist was uncertain of the pCR outcome. Tissue samples of patients who did not achieve a pCR were collected and submitted to designated central laboratories for translational research.
Disease Progression Determination
Breast MRI was performed in patients with locally advanced TNBC who chose to participate for more accurate clinical staging of the primary tumour and axilla lymphadenopathy and to ensure the primary tumour and regional lymph node staging fulfilled the protocol-required criteria. Breast MRI and MRI were scheduled for patients who provided consent to participate in these assessments as follows:
At screening (before first dose of study drug)
After the neoadjuvant treatment phase, treatment 1 cycle 4
After the neoadjuvant treatment phase, treatment 2 cycle 4 (before definitive surgery)
Breast MRI performed as part of the routine clinical management was acceptable for initial screening tumour imaging if it had diagnostic quality and had been performed within 28 days before the first dose of the trial treatment.2
For the patients who chose to receive breast MRIs at protocol-specified time points, measurement of the baseline lesions, changes from the baseline, and objective response were assessed by the investigator per RECIST 1.1. Central confirmation assessment of complete response or partial response were not conducted. Imaging assessments for recurrent or metastatic disease were conducted at the discretion of the treating physician, per local standard of care, or at the time of symptoms.2
Health-Related QoL
Health-related QoL measures were assessed using the EORTC QLQ-C30, the EORTC QLQ-BR23, and the EQ-5D-5L questionnaire. A detailed discussion and critical appraisal of EORTC QLQ-C30 and EORTC QLQ-BR23 is available in Appendix 3. Patients completed the questionnaires at the following pre-specified time points:
Neoadjuvant treatment phase:
On day 1 of cycle 1 of treatment 1
On day 1 of cycles 1 and 4 of treatment 2
Adjuvant treatment phase:
On day 1 of cycles 1, 5, and 9
At the early discontinuation visit
At long-term follow-up visits (after the adjuvant treatment phase, questionnaires were completed every 12 months for 2 years or until progression, whichever was earlier)2
The EORTC QLQ-C30 is a multidimensional, cancer-specific, self-administered measure of HRQoL. The EORTC QLQ-C30 is composed of both multi-item scales and single-item measures. These include 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a global health status–QoL scale, and 5 single items assessing additional symptoms commonly reported by cancer patients (dyspnea, loss of appetite, insomnia, constipation, and diarrhea), as well as perceived financial impact of the disease.23 The EORTC QLQ-C30 uses a 1-week recall period to assess functional status and symptoms. All scales and single-item measures are scored from 0 to 100. Scale sum scores are transformed such that a high score on the functional scales represents a high (or healthy) level of functioning, a high score on the symptom scales represents a high level of symptomatology, and a high score on the global health status–QoL scale represents a high HRQoL.24
The EORTC QLQ-BR23 includes an additional 23 items that are specific to breast cancer, with 5 multi-item scales assessing systemic therapy side effects, arm symptoms, breast symptoms, body image, and sexual functioning, as well as single items assessing sexual enjoyment, hair loss, and future perspective.25 All scales range in score from 0 to 100, and higher scores represent higher response. Thus, a high score for functioning represents high functioning, while a high symptom score represents a high symptom burden. The EORTC QLQ-BR23 is not a free-standing instrument as it does not measure a multi-dimensional construct of body image; instead, the EORTC QLQ-BR23 is administered in conjunction with the EORTC QLQ-C30.25
The EQ-5D-5L questionnaire consists of 2 separate elements. The first is the utility score (or descriptive system), which captures health states across 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each unique health state is defined by combining response levels from each of the 5 dimensions. The second component, the EQ VAS, records the respondent’s self-rated health on a vertical VAS ranging from 0 to 100, where the end points are labelled “best imaginable health state” (100) and “worst imaginable health state” (0).2
Harms Outcomes
Safety parameters such as incidence of AEs, serious AEs including fatal serious AEs, immune-related AEs, laboratory abnormalities, rates of dose interruption and discontinuation due to AEs, and events of clinical interest were monitored throughout the trial.2
Statistical Analysis
Sample Size and Power Calculation
A total sample size of 1,150 was initially planned for the study. The sample size was determined based on the EFS.2
Pathological Complete Response Rate: ypT0/Tis ypN0
Pathological complete response rate using the ypT0/Tis ypN0 definition was a co-primary end point of the KEYNOTE-522 trial. The pCR analysis was planned after enrolment was completed, when at least 1,000 patients had completed surgery (if they continued treatment), after approximately 6 months of neoadjuvant treatment. A sample size of about 1,000 was needed to achieve approximately 95% power to detect a true pCR rate difference of 15% between pembrolizumab plus chemotherapy and placebo plus chemotherapy at an alpha of 0.5% (1 sided). The sample size calculation was based on the following assumptions:
Alpha of 0.5% is allocated to the pCR hypothesis.
The underlying pCR is 50% in the placebo plus chemotherapy arm, and there is a 15% increase in pCR in the pembrolizumab plus chemotherapy arm (pCR of 65%) in patients with locally advanced TNBC.
The dropout rate is approximately 10%.2
In addition, a Hwang-Shih-DeCani alpha-spending function with gamma parameter (0) was used to assign group sequential boundaries that controlled the type I error.2 The assumptions for a pCR rate of 50% in the placebo plus chemotherapy arm was based on estimates observed by Sikov et al. (2015)26 and von Minckwitz et al. (2014).27
Event-Free Survival
Event-free survival was a co-primary end point of the KEYNOTE-522 trial. The final analysis of the trial is EFS event driven and planned after approximately 327 EFS events have been observed, unless the study is terminated early. A pre-specified alpha level of 2% (1 sided) and a sample size of 1,150 were needed to achieve approximately 80% power to detect EFS in patients with locally advanced TNBC, assuming that the true HR (pembrolizumab versus placebo) was 0.71. This value was based on evidence published in a meta-analysis by Cortazar et al. (2014)28 that suggested that approximately 50% of patients may become disease-free in the long-term. The sponsor applied a cure rate model to accommodate decreases in failure over time.2 The calculations were based on the following assumptions:
Event-free survival follows a Poisson mixture model (cure rate model with decreasing failure rate) distribution with an approximately 78% EFS rate at 36 months and an approximately 50% cure rate in the placebo arm.
There is an enrolment period of 18 months and at least 84 months of follow-up.
There is a yearly dropout rate of 2% and an additional approximately 3% to 5% dropout rate after surgery.
The EFS control rate of 78% was estimated from an updated report of the sponsor.2 In addition, the Lan-DeMets O’Brien-Fleming approximation alpha-spending function was applied to assign group sequential boundaries that control type I error.2
Overall Survival
Overall survival was a secondary end point assessed in the KEYNOTE-522 trial. In the event that the null hypothesis for EFS was rejected at any IA, the final OS analysis was planned as an event-driven outcome, after approximately 297 OS events have occurred, unless the study was terminated early. A pre-specified alpha of 2% (1 sided) and a sample size of approximately 1,150 were required for approximately 79.7% power to detect OS events in patients with locally advanced TNBC, assuming that the true HR (pembrolizumab versus placebo) was 0.70. The sponsor applied a cure rate model for decreases in failure over time based on evidence published in a meta-analysis by Cortazar et al. (2014)28 that suggested that approximately 50% of patients may become disease-free in the long-term.2 The sponsor’s calculations were based on the following assumptions:
Overall survival follows a Poisson mixture model (cure rate model with decreasing failure rate) distribution with an approximately 81% OS rate at 36 months and an approximately 50% cure rate in the placebo arm.
There is an enrolment period of 18 months and at least 84 months of follow-up.
There is a yearly dropout rate of 3%.
A Lan-DeMets O’Brien-Fleming approximation alpha-spending function was used to assign group sequential boundaries that control the type I error.2
Analyses, Multiple Testing Procedure, and Alpha Spending
Dual hypothesis testing was conducted in the KEYNOTE-522 trial, and multiplicity adjustments were conducted for 2 primary objectives (EFS and pCR) and 1 secondary hypothesis (OS), as presented in Figure 3.
Figure 3: Multiplicity Strategy for the KEYNOTE-522 Trial
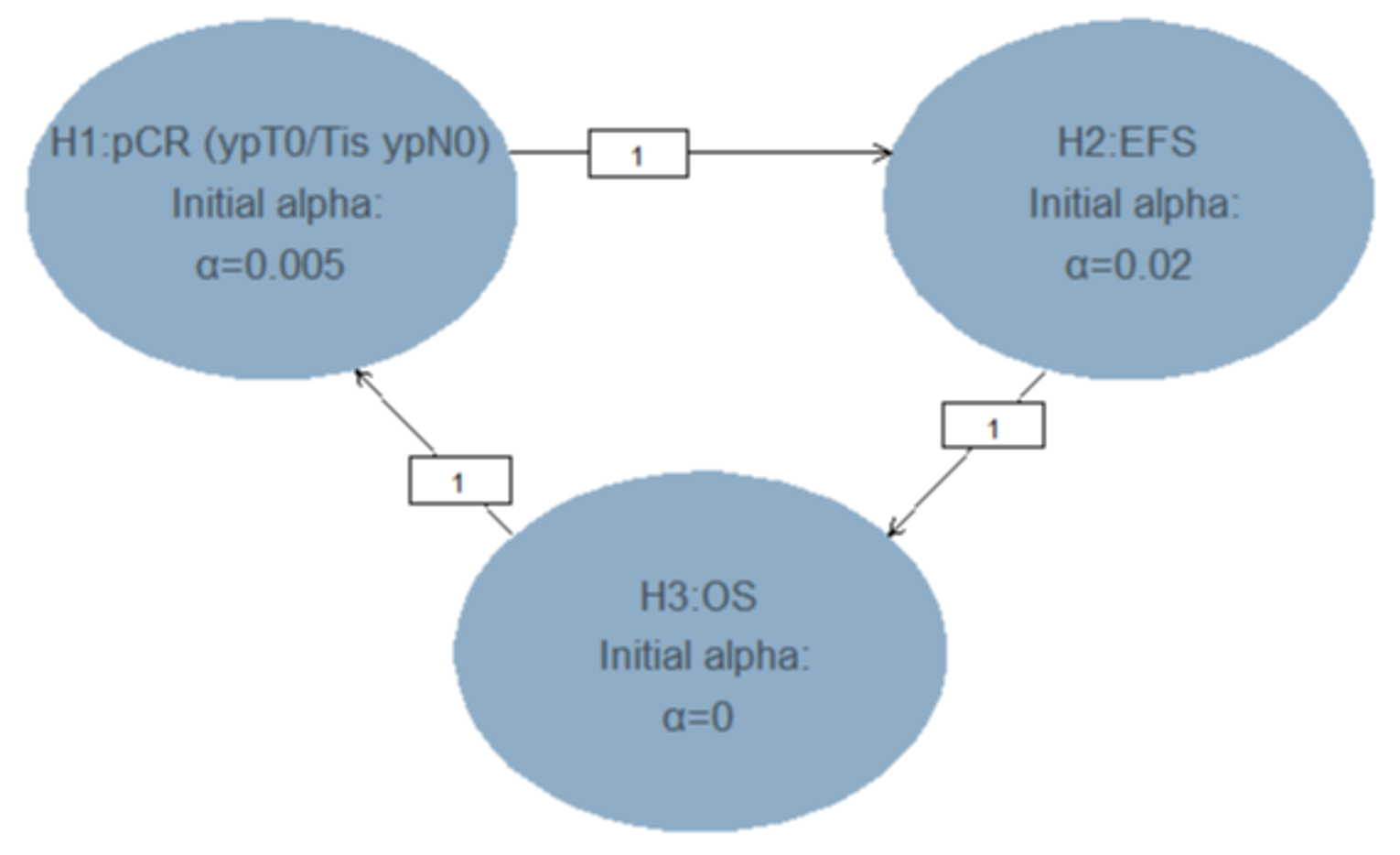
EFS = event-free survival; H = hypothesis; OS = overall survival; pCR = pathological complete response; ypT0/Tis ypN0 = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed
Source: Sponsor-submitted reimbursement package.2
The dual primary hypotheses tested the superiority of pembrolizumab compared to placebo in pCR (ypT0/Tis ypN0) or EFS in patients with locally advanced TNBC. The secondary hypothesis tested the superiority of OS in patients with locally advanced TNBC. The overall type I error was controlled at an alpha level of 2.5% (1 sided); 0.5% initially allocated to the pCR (ypT0/Tis ypN0) hypothesis, and 2.0% initially allocated to the EFS hypothesis. The study was considered a success if pCR (ypT0/Tis ypN0) or EFS demonstrated a statistically significant difference at either preplanned IAs or the full analysis under multiplicity control.2
The graphical method by Maurer and Bretz was used; this method allowed the study hypotheses to be tested more than once, and in the situation where the null hypothesis was rejected, the alpha allocated to that hypothesis was reallocated to other hypothesis tests.2
Planned Analyses
Two IAs were planned for the pCR (ypT0/Tis ypN0) rate, while EFS analyses were planned annually after 2 years of study initiation. Seven efficacy IAs were planned in addition to the final analysis for the KEYNOTE-522 trial. No futility boundary was defined as the sponsor had no plans to stop the study for futility. Table 10 presents all preplanned IAs.2
Primary Outcome Analyses
Pathological Complete Response Rate
The stratified Miettinen and Nurminen method was used to compare the pCR rates between the 2 treatment arms based on 3 definitions. The difference in pCR rate and its 95% CI from the stratified Miettinen and Nurminen method with strata weighting by sample size was reported for patients with locally advanced TNBC and for patients with PD-L1 (positive) tumours. The stratification factors used for randomization were applied during the analysis.2
In the primary pCR analysis, as per clinical judgment, patients who used the same neoadjuvant regimens but different doses or schedules from those specified in the study may not have been considered as using new anticancer therapy in neoadjuvant treatment before definitive surgery.
Sensitivity analyses were conducted for pCR rates using the Cochran-Mantel-Haenszel test, and associated odds ratios and 95% CIs were calculated.2
Table 10: Planned Interim Analyses, End Points Evaluated, and Drivers of Timing
Analysis | Criteria for conduct of analysis | End point(s) | Data cut-off date | Estimated time after first patient randomized | Primary purpose of analysis |
|---|---|---|---|---|---|
IA1: interim pCR analysis | Enrolment is completed, and at least 500 patients have completed surgery after approximately 6 months neoadjuvant treatment | pCR (ypT0/Tis ypN0) | September 24, 2018 | ~18 months | pCR IA |
IA2: interim EFS analysis and final pCR analysis | Approximately 24 months after first patient is randomized | EFS pCR (ypT0/Tis ypN0) | April 24, 2019 | ~24 months | EFS IA pCR final analysis |
IA3: interim EFS analysis | Approximately 36 months after first patient is randomized | EFS pCR | NR | ~36 months | EFS IA |
IA4: interim EFS analysis | Approximately 48 months after the first patient is randomized | EFS OS pCR | March 23, 2021 | ~48 months | EFS IA |
IA5: interim EFS analysis | Approximately 60 months after the first patient is randomized | EFS | TBD | ~60 months | EFS IA |
IA6: interim EFS analysis | Approximately 72 months after the first patient is randomized | EFS | TBD | ~72 months | EFS IA |
IA7: interim EFS analysis | Approximately 84 months after the first patient is randomized | EFS | TBD | ~84 months | EFS IA |
FA: final EFS analysis | Approximately 327 EFS events have been observed | EFS | TBD | ~102 months | EFS FA |
EFS = event-free survival; FA = final analysis; IA = interim analysis; NR = not reported; OS = overall survival; pCR = pathological complete response; TBD = to be determined; ypT0/Tis ypN0 = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed.
Source: Sponsor-submitted reimbursement package.2
Event-Free Survival
The Kaplan–Meier method was used to estimate the EFS curve for each treatment group. The treatment difference in EFS was assessed using the stratified log-rank test. A stratified Cox proportional hazard model using the Efron method of tie handling was used to assess the magnitude of the treatment difference (i.e., HR) between the 2 treatments. The HR with the 95% CI and Kaplan–Meier estimates with the corresponding 95% CIs at 2 years, 3 years, and 5 years were reported. The stratification factors used for randomization were applied to both the stratified log-rank test and the stratified Cox model.2
For the primary analysis, the true date of event was approximated as the date of the first assessment for which the event was objectively documented. Patients who did not experience an event at the time of data analysis were censored at the date they were last known to be alive and event free (Table 11).
The proportional hazards assumption was examined using a graphical and analytical approach. A plot of the log[-log] of the survival function versus time for EFS was planned for the comparison of the pembrolizumab plus chemotherapy and placebo plus chemotherapy arms. In the event of a violation of the proportional hazard assumption, a sensitivity analysis was planned based on a 2-step weighted Cox model approach, as described by Mehrotra et al. (2012).29 Sensitivity analyses were planned based on the censoring rules presented in Table 11.
Table 11: Censoring Rules for the Primary Analysis and Sensitivity Analyses 1 and 2 of EFS
Situation | Primary analysis | Sensitivity analysis 1a | Sensitivity analysis 2b |
|---|---|---|---|
EFS event documented after ≤ 1 missed disease assessment and before new anticancer therapy, if any | Progressed at date of documented EFS event | Progressed at date of documented EFS event | Progressed at date of documented EFS event |
EFS event immediately after ≥ 2 consecutive missed disease assessments or after new anticancer therapy, if any | Progressed at date of documented EFS event | Censored at last disease assessment before the earlier date of ≥ 2 consecutive missed disease assessments and new anticancer therapy, if any | Progressed at date of documented EFS event if no new anticancer therapy; progressed at date of new anticancer therapy if there is new anticancer therapy |
No EFS event, and new anticancer treatment not initiated | Censored at last disease assessment | Censored at last disease assessment | Censored at last disease assessment |
No EFS event; new anticancer treatment initiated | Censored at last disease assessment | Censored at last disease assessment before new anticancer treatment | Progressed at the date of new anticancer therapy |
EFS = event-free survival.
aThe new anticancer therapy in sensitivity analysis 1 is defined as any post-surgery new oncology drugs or post-surgery radiation to treat metastatic disease.
bThe new anticancer therapy in sensitivity analysis 2 is defined as the radiation and/or oncology drugs to treat metastatic disease.
Source: Sponsor-submitted reimbursement package.2
Subgroup Analyses
To determine whether the treatment effect was consistent across various subgroups, the estimate of the between-group treatment effect (with a nominal 95% CI) for the primary end points was estimated and plotted within each category of the following classification variables in patients with locally advanced TNBC and in patients with PD-L1 (positive) tumours (CPS ≥ 1)2:
Nodal status: positive versus negative.
Tumour size: T1/T2 versus T3/T4.
Choice of carboplatin: every 3 weeks versus weekly.
Tumour PD-L1 status using different cut-off values for CPS (applies to all patients with locally advanced TNBC): CPS greater than or equal to 1 versus CPS less than 1; CPS greater than or equal to 10 versus CPS less than 10; CPS greater than or equal to 20 versus CPS less than 20.
Overall stage: stage II versus stage III.
Menopausal status (for women only): pre- versus post-menopausal.
Age: younger than 65 years versus 65 years and older.
Geographic region: Europe, Israel, North America, and Australia versus Asia versus rest of world.
Ethnic origin: Hispanic versus non-Hispanic.
ECOG PS: 0 versus 1.
HER2 status: immunohistochemistry of 2 or higher (but fluorescence in situ hybridization negative) versus immunohistochemistry of 0 to 1 or higher.
Lactate dehydrogenase greater than the upper limit of normal versus less than or equal to the upper limit of normal.
Secondary Outcome Analyses
Overall Survival
The Kaplan–Meier method was used to estimate the OS survival curves. The treatment difference in survival was assessed using a stratified log-rank test. A stratified Cox proportional hazard model with the Efron method of tie handling was used to assess the magnitude of the treatment difference. The HR and its 95% CI from the stratified Cox model, with a single treatment covariate, was reported for patients with locally advanced TNBC and for individuals with PD-L1 (positive) tumours. The stratification factors used for randomization were applied, as stratification factors to both the stratified log-rank test and the stratified Cox model. Kaplan–Meier estimates and the corresponding 95% CIs at 3 years and 5 years were provided for OS.2
The secondary hypothesis of OS in patients with locally advanced TNBC was tested according to the hypotheses testing plan as described in the statistical analysis plan (SAP). The study initially allocated an alpha of zero, 1 sided, to test OS. And OS was tested only when the null hypothesis for EFS was rejected. Boundaries were defined at each planned IA, derived using a cure model and a Lan-DeMets O’Brien-Fleming spending function. The spending time was defined as 1 for the final analysis. In the event that EFS, but not OS, was found to be positive at any interim, OS continued to be followed.2
Crossover between study arms was not permitted in the KEYNOTE-522 trial. Adjustment for the effect of crossover on OS was performed as an exploratory analysis using the rank-preserving structural failure time 2-stage model as proposed by Robins and Tsiatis.2
Analysis Populations
Efficacy analysis populations: The ITT population was analyzed for primary efficacy analyses. All randomized patients were included in this population in the treatment group to which they were randomized.
Safety analysis populations: The all participants as treated (APaT) population was used for the analysis of safety data in the KEYNOTE-522 trial. The APaT population consisted of all randomized patients who received at least 1 study treatment. Patients were included in the treatment group corresponding to the study treatment they actually received for the analysis of safety data using the APaT population. Patients who received an incorrect study treatment for the entire treatment period were included in the treatment group corresponding to the study treatment actually received. Any patient who received an incorrect study treatment for 2 cycles but received the correct treatment for all other cycles was assessed according to the correct treatment group, and a narrative was provided for events that occurred during the cycle for which the patient was incorrectly dosed. At least 1 laboratory or vital sign measurement obtained subsequent to at least 1 study treatment was required for inclusion in the analysis of each specific parameter.2
Patient-reported outcomes analysis populations: Patient-reported outcomes analyses (for HRQoL) were based on the full analysis set population, defined as randomized patients who had at least 1 patient-reported outcomes assessment and received at least 1 study treatment.2
Protocol Amendments
The original protocol was approved on December 6, 2016. Four protocol amendments were made before the IA4 data cut-off.
Amendment 1 (December 16, 2016): The protocol was amended to clarify the dose modification guidelines provided for paclitaxel and carboplatin and to incorporate mandatory overdose language for the pembrolizumab program.
Amendment 2 (May 1, 2018): The protocol was amended to adjust the timing of IA1 to occur after at least 500 patients have or would have completed surgery; to add a second IA (IA2) for pCR; and to increase the sample size from approximately 855 to approximately 1,150 based on a revision to the assumed EFS rate at 36 months in the control arm.
Amendment 3 (October 17, 2018): The protocol was amended to add an analysis of EFS at IA2 and to adjust the timing of IA2.
Amendment 4 (February 26, 2020): The protocol was amended to clarify an adjustment of efficacy boundaries at IAs for EFS based on the actual number of events observed.10
Results
Patient Disposition
By the IA4 data cut-off (March 23, 2021), 1,608 patients had been screened, 434 participants had failed screening, and 1,174 patients had been successfully randomized in a 2:1 ratio to receive either pembrolizumab plus chemotherapy followed by pembrolizumab (n = 784) or placebo plus chemotherapy followed by placebo (n = 390). Overall, 1,172 patients (99.8%) received at least 1 study intervention. By the IA4 cut-off date, no patient was on any study intervention. Table 12 summarizes patient disposition in the ITT population at IA4.10
In the neoadjuvant phase, more patients in the pembrolizumab plus chemotherapy arm (24.2%) had discontinued the study intervention than in the placebo plus chemotherapy arm (14.9%). In the adjuvant phase, the most common reason for discontinuation was AEs (5.4%) in the pembrolizumab group and relapse or recurrence (4.6%) and withdrawal by participant (4.4%) in the placebo arm. The median duration of follow-up for the ITT population was similar between the 2 treatment groups (37.8 [range = 2.7 to 48.0] months versus 37.6 [range = 3.4 to 47.6] months in the pembrolizumab plus chemotherapy followed by pembrolizumab arm versus the placebo plus chemotherapy followed by placebo arm).10
Table 12: Patient Disposition at IA4—ITT Population
Details | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo |
|---|---|---|
Screened, n | 1,608 | |
Randomized, n | 1,174 | |
Randomized, n | 784 | 390 |
Treated patients, n (%) | 783 (99.9) | 389 (99.7) |
Patients who had surgery but did not receive study medication | 5 (0.6) | 0 (0.0) |
Patients who were on treatments | 0 (0.0) | 0 (0.0) |
Patients who completed all treatmentsa | 487 (62.1) | 283 (72.6) |
Patients who discontinued from all treatments | 291 (37.1) | 106 (27.2) |
Discontinued in neoadjuvant phase, n (%)b | 190 (24.2) | 58 (14.9) |
Adverse event | 112 (14.3) | 20 (5.1) |
Clinical progression | 2 (0.3) | 3 (0.8) |
Physician decision | 32 (4.1) | 15 (3.8) |
Progressive disease | 8 (1.0) | 7 (1.8) |
Relapse or recurrencec | 7 (0.9) | 3 (0.8) |
Withdrawal by patient | 29 (3.7) | 10 (2.6) |
Discontinued in adjuvant phase, n (%)d | 101 (12.9) | 48 (12.3) |
Adverse event | 42 (5.4) | 10 (2.6) |
Physician decision | 17 (2.2) | 3 (0.8) |
Relapse or recurrence | 20 (2.6) | 18 (4.6) |
Withdrawal by patient | 22 (2.8) | 17 (4.4) |
Patients with surgery, n (%) | 768 (98.0) | 381 (97.7) |
IA = interim analysis; ITT = intention to treat.
Note: Data cut-off date: March 23, 2021.
aPatients who had completed all treatments included participants who completed adjuvant treatment.
bPatients discontinued in neoadjuvant phase included participants who discontinued on or after neoadjuvant treatment 1, on or after neoadjuvant treatment 2, or on or after definitive surgery.
cPatients discontinued due to relapse or recurrence in the neoadjuvant phase are participants who had surgery but did not receive adjuvant treatment.
dPatients discontinued in adjuvant phase included participants who discontinued on or after adjuvant radiation only or on adjuvant treatment.
Source: Clinical Study Report.10
Premature Unblinding
In total, 81 (6.9%) of the 1,174 patients enrolled were prematurely unblinded due to the following reasons:
Sponsor-approved nonemergency unblinding requests for patients who had disease progression or recurrence, knowing their study treatment would guide future treatment plans (n = 57)
Inadvertent unblinding of investigator site and/or sponsor personnel (n = 5)
Emergency unblinding (n = 19)10
Protocol Deviations
Important protocol deviations are highlighted in Table 13.
Exposure to Study Treatments
Neoadjuvant phase
The median duration of exposure to study treatment for all drugs in the neoadjuvant phase was similar in both arms: pembrolizumab plus chemotherapy (22.1 weeks [range = 0.1 to 34.1 weeks]) and placebo plus chemotherapy (22.1 weeks [range = 0.1 to 31.1 weeks]).10
Adjuvant phase
The median duration of exposure to study treatment in the adjuvant phase was similar between the pembrolizumab plus chemotherapy group (24.1 weeks [range = 0.1 to 37.7 weeks]) and the placebo plus chemotherapy group (24.1 weeks [range = 0.1 to 39.7 weeks]). Table 14 presents a summary of drug exposure in the neoadjuvant and adjuvant phases.10
Table 13: Summary of Protocol Deviations Considered to Be Clinically Important by Trial Investigators at IA4—ITT Population
Detail | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo |
|---|---|---|
Participants in population, n | 784 | 390 |
Patients with 1 or more clinically important protocol deviations, n (%) | 28 (3.6) | 8 (2.1) |
Discontinuation criteria, n (%) | 1 (0.1) | 0 (0.0) |
Patient developed trial-specific discontinuation criteria but was not discontinued from the trial | 1 (0.1) | 0 (0.0) |
Inclusion or exclusion criteria, n (%) | 14 (1.8) | 7 (1.8) |
Inclusion 3: Patients who do not have centrally confirmed TNBC, as defined by the most recent ASCO–CAP guidelines | 1 (0.1) | 0 (0.0) |
Inclusion 4: Patients who do not have previously untreated locally advanced nonmetastatic (M0) TNBC, defined as combined primary tumour and regional lymph node staging per AJCC staging criteria for breast cancer | 12 (1.5) | 7 (1.8) |
Inclusion 8: Patients who do not have left ventricular ejection fraction of ≥ 50% or ≥ institution lower limit of normal as assessed by echocardiogram or multigated acquisition scan performed at screening | 1 (0.1) | 0 (0.0) |
Safety reporting, n (%) | 2 (0.3) | 0 (0.0) |
Patients had a reportable safety event and/or follow-up safety event information that was not reported per the timelines outlined in the protocol | 2 (0.3) | 0 (0.0) |
Study intervention, n (%) | 11 (1.4) | 1 (0.3) |
Patients were dispensed study intervention other than what was assigned in the allocation schedule (i.e., incorrect medication or potential cross-treatment) | 11 (1.4) | 1 (0.3) |
AJCC = American Joint Committee on Cancer; ASCO = American Society of Clinical Oncology; CAP = College of American Pathologists; IA = interim analysis; ITT = intention to treat; TNBC = triple-negative breast cancer.
Note: Every patient is counted a single time for each applicable row and column. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Table 14: Summary of Drug Exposure in the Neoadjuvant and Adjuvant phase at IA4—APaT Population
Detail | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo |
|---|---|---|
Neoadjuvant phase | ||
Patients, n | 783 | 389 |
All drugs | ||
Patients, n | 778 | 389 |
Number of weeks on therapy, median (range) | 22.1 (0.1 to 34.1) | 22.1 (0.1 to 31.1) |
Pembrolizumab 200 mg q.3.w. number of weeks on therapy | ||
n | 778 | NA |
Median (range) | 22 (0.1 to 31.6) | NA |
Number of administrations | 778 | NA |
Median (range) | 8 (1 to 8) | NA |
Placebo q.3.w. number of weeks on therapy | ||
n | NA | 389 |
Median (range) | NA | 22.1 (0.1 to 31.1) |
Number of administrations | NA | 389 |
Median (range) | NA | 8 (1 to 8) |
Carboplatin weekly number of weeks on therapy | ||
n | 444 | 220 |
Median (range) | 11.1 (2 to 26.1) | 11.1 (2.3 to 17.1) |
Number of administrations | 444 | 220 |
Median (range) | 12 (3 to 12) | 12 (3 to 12) |
Carboplatin q.3.w. number of weeks on therapy | ||
n | 334 | 164 |
Median (range) | 9.6 (0.1 to 16.4) | 9.4 (3 to 15.1) |
Number of administrations | 334 | 167 |
Median (range) | 4 (1 to 4) | 4 (2 to 4) |
Paclitaxel weekly number of weeks on therapy | ||
n | 778 | 389 |
Median (range) | 11.3 (0.1 to 26.1) | 11.3 (0.1 to 17.1) |
Number of administrations | 778 | 389 |
Median (range) | 12 (1 to 13) | 12 (1 to 12) |
Doxorubicin q.3.w. number of weeks on therapy | ||
n | 488 | 247 |
Median (range) | 9.1 (0.1 to 13.1) | 9.1 (0.1 to 13.3) |
Number of administrations | 488 | 247 |
Median (range) | 4 (1 to 4) | 4 (1 to 4) |
Epirubicin q.3.w. number of weeks on therapy | ||
n | 238 | 122 |
Median (range) | 9.1 (0.1 to 13.1) | 9.1 (0.1 to 13.1) |
Number of administrations | 238 | 122 |
Median (range) | 4.0 (1 to 5) | 4.0 (1 to 4) |
Cyclophosphamide q.3.w. number of weeks on therapy | ||
n | 726 | 369 |
Median (range) | 9.1 (0.1 to 13.1) | 9.1 (0.1 to 13.3) |
Number of administrations | 726 | 369 |
Median (range) | 4 (1 to 4) | 4 (1 to 4) |
Adjuvant phase | ||
n | 588 | 331 |
All drugs number of weeks on therapy | 558 | 320 |
Median (range) | 24.1 (0.1 to 37.7) | 24.1 (0.1 to 39.7) |
Pembrolizumab 200 mg q.3.w. number of weeks on therapy | ||
n | 558 | NA |
Median (range) | 24.1 (0.1 to 37.7) | NA |
Number of administrations | 558 | NA |
Median (range) | 9 (1 to 9) | NA |
Placebo q.3.w. number of weeks on therapy | ||
n | NA | 320 |
Median (range) | NA | 24.1 (0.1 to 39.7) |
Number of administrations | NA | 320 |
Median (range) | NA | 9 (1 to 9) |
APaT = all participants as treated; IA = interim analysis; NA = not applicable; q.3.w. = every 3 weeks.
Note: Patients who did not have neoadjuvant treatments but had surgery are included in the APaT population in the neoadjuvant phase. Patients who had post-surgery radiation therapy but did not have adjuvant treatment are included in the APaT population in the adjuvant phase. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below.
Overall Survival
By the IA4 data cut-off (March 23, 2021), 135 of 297 predefined events had occurred, representing approximately 45% of the information fraction required for OS. The OS hypothesis was tested at an alpha level of 2.5% following the successful achievement of EFS analysis according to the multiplicity strategy outlined in the sponsor’s SAP. The median OS was not estimable, and the HR obtained in the comparison between the 2 arms stratified by nodal status, tumour size, and choice of carboplatin schedule was 0.72 (95% CI, 0.51 to 1.02; P [1 sided] = 0.0321377).10
The success criterion for the secondary OS hypothesis was not met because the P value did not cross the multiplicity-adjusted, 1-sided pre-specified P value boundary (0.00085861) defined for statistical significance. Table 15 and Figure 4 present the OS findings in the ITT population at the IA4 data cut-off. Overall survival continues to be followed in the KEYNOTE-522 study.10
Table 15: Overall Survival at IA4—ITT Population
Detail | Pembrolizumab plus chemotherapy followed by pembrolizumab n = 784 | Placebo plus chemotherapy followed by placebo n = 390 |
|---|---|---|
Number of events, n (%) | 80 (10.2) | 55 (14.1) |
Number of censored, n (%) | 704 (89.8) | 335 (85.9) |
Kaplan–Meier estimates, monthsa | ||
Median (95% CI) | NE (NE, NE) | NE (NE, NE) |
Q1 to Q3 | NR, NR | NR, NR |
Pembrolizumab plus chemotherapy followed by pembrolizumab vs. placebo plus chemotherapy followed by placebo | ||
Hazard ratio (95% CI)b | 0.72 (0.51 to 1.02) | |
P valuec | 0.032137 | |
Event rate per 100 person-months | 0.3 | 0.4 |
OS rate at 6 months, % (95% CI) | 99.2 (98.3 to 99.7) | 99.7 (98.2 to 100.0) |
OS rate at 12 months, % (95% CI) | 97.2 (95.8 to 98.1) | 98.7 (96.9 to 99.5) |
OS rate at 18 months, % (95% CI) | 95.0 (93.2 to 96.3) | 93.8 (91.0 to 95.8) |
OS rate at 24 months, % (95% CI) | 92.3 (90.2 to 94.0) | 91.0 (87.7 to 93.5) |
OS rate at 30 months, % (95% CI) | 91.3 (89.1 to 93.1) | 88.7 (85.1 to 91.5) |
OS rate at 36 months, % (95% CI) | 89.7 (87.3 to 91.7) | 86.9 (83.0 to 89.9) |
OS rate at 42 months, % (95% CI) | 89.2 (86.7 to 91.3) | 84.1 (79.5 to 87.7) |
CI = confidence interval; IA = interim analysis; ITT = intention to treat; NACT = neoadjuvant chemotherapy; NE = not estimable; NR = not reached; OS = overall survival; vs. = versus.
Note: Data cut-off date: March 23, 2021.
aFrom product-limit (Kaplan–Meier) method for censored data.
bBased on Cox regression model with the Efron method of tie handling, with treatment as a covariate, stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4) and choice of carboplatin (every three weeks vs. weekly).
cOne-sided P value based on log-rank test stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly). The multiplicity-adjusted, 1-sided, pre-specified P value boundary for statistical significance was P = 0.00085861.
Source: Clinical Study Report.10
Figure 4: Kaplan–Meier Estimates of Overall Survival at IA4—ITT Population
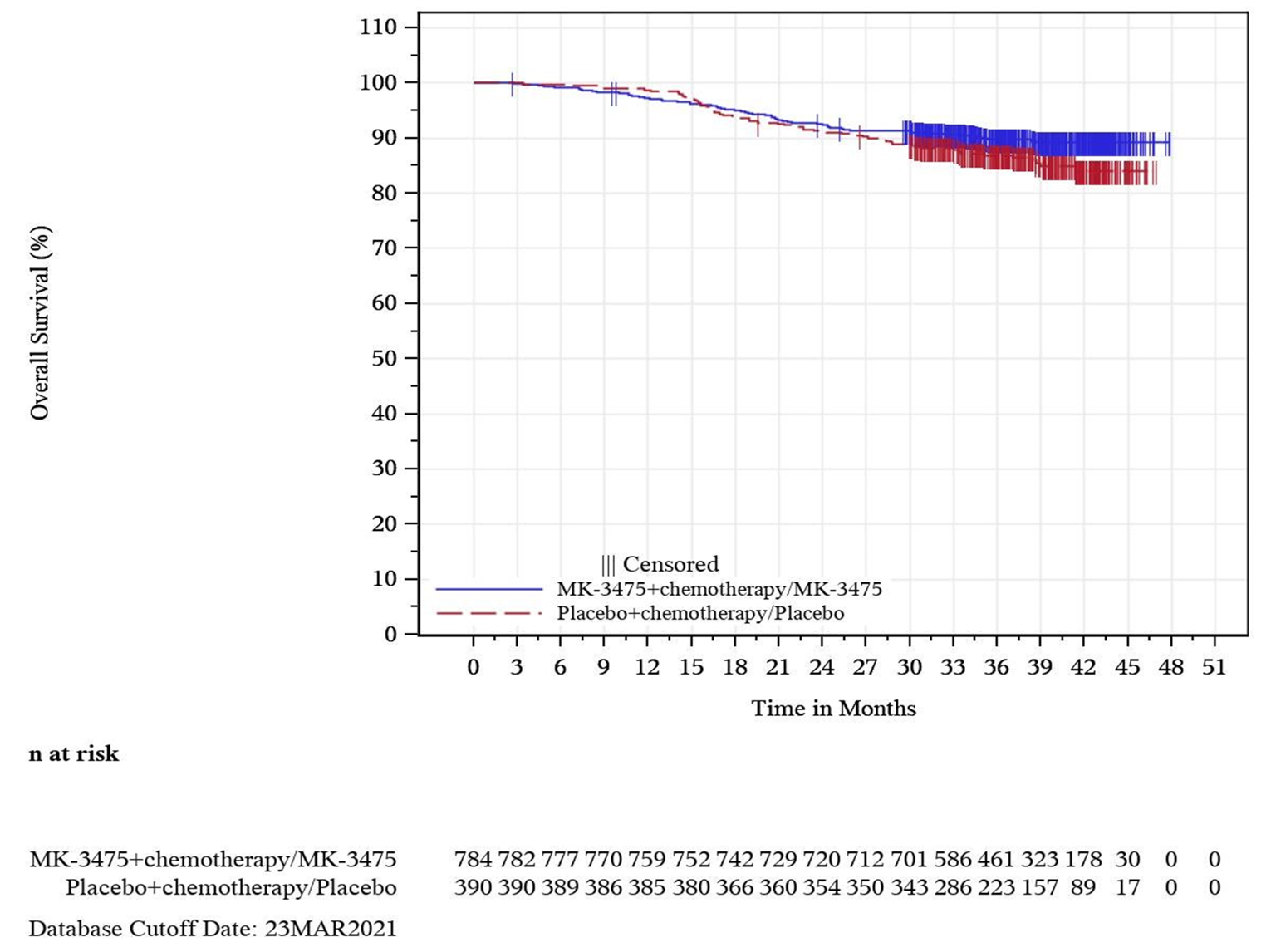
IA = interim analysis; ITT = intention to treat; MK-3475 = pembrolizumab.
Note: Data cut-off date: March 23, 2021.
Source: Clinical study Report.10
Pathological Complete Response Rate (ypT0/Tis ypN0)
The pCR rate at the IA1 data cut-off (September 24, 2018) was 64.8% (95% CI, 59.9% to 69.5%) in the group receiving pembrolizumab plus chemotherapy in the neoadjuvant phase and 51.2% (95% CI, 44.1% to 58.3%) in the group receiving placebo plus chemotherapy. The difference in pCR rate between groups was 13.6% (95% CI, 5.4% to 21.8%; P = 0.00055).
At IA2 (April 24, 2019), the treatment difference in the pCR rate (pembrolizumab plus chemotherapy versus placebo plus chemotherapy) was 9.2% (95% CI, 2.8% to 15.6%; P = 0.00221). The pCR rate (95% CI) for pembrolizumab plus chemotherapy at the neoadjuvant phase was 64.0% (95% CI, 60.2% to 67.6%) compared to 54.7% (95% CI, 49.1% to 60.1%) for placebo plus chemotherapy.
A supportive analysis of the primary pCR end point was conducted with all randomized participants at IA4. The pCR rate in patients receiving pembrolizumab plus chemotherapy was 63% (95% CI, 59.5% to 66.4%) in the neoadjuvant phase, and in patients receiving placebo plus chemotherapy the pCR rate was 55% (95% CI, 50.6% to 60.6%). Pathological complete response was not tested formally based on the statistical hierarchy at IA4 in the ITT population. The difference in pCR rate between groups was 7.5% (95% CI, 1.6% to 13.4%).10 The pCR rates observed in both study arms at IA1 and IA4 are presented in Table 16.
Pathological Complete Response Rate Using Alternative Definitions
The pCR rates using the ypT0 ypN0 and ypT0/Tis definitions are presented in Table 17. The pCR rates were consistent with the primary findings (using the ypT0/Tis ypN0 definition).10
Subgroup Analyses
Table 18 presents the pCR in the subgroups10 identified in the CADTH protocol.
Event-Free Survival
At the IA4 data cut-off (March 23, 2021), a total of 123 events (15.7%) had occurred in the pembrolizumab plus chemotherapy followed by pembrolizumab arm and 93 events (23.8%) in the placebo plus chemotherapy followed by placebo arm.10 The median EFS was not estimable in either study arm at the IA4 data cut-off (March 23, 2021). The EFS HR stratified by nodal status, tumour size, and choice of carboplatin schedule obtained between the 2 study arms was 0.63 (95% CI, 0.48 to 0.82; P [1 sided] = 0.0003093). The number of patients with reported distant recurrence was 7.7% in the pembrolizumab plus chemotherapy followed by pembrolizumab arm compared to 13.1% in the placebo plus chemotherapy followed by placebo arm.
Table 16: Pathological Complete Response (ypT0/Tis ypN0) at IA1 and IA4—ITT Population
Detail | Pembrolizumab plus chemotherapy | Placebo plus chemotherapy |
|---|---|---|
IA1 cut-off | ||
n | 401 | 201 |
Number of pCR | 260 | 103 |
pCR rate, % (95% CI) | 64.8 (59.9 to 69.5) | 51.2 (44.1 to 58.3) |
Difference between pembrolizumab plus chemotherapy vs. placebo plus chemotherapy, % | ||
Estimate (95% CI)a | 13.6 (5.4 to 21.8) | |
P valueb | 0.00055 | |
IA4 cut-offc | ||
n | 784 | 390 |
Number of pCR | 494 | 217 |
pCR rate, % (95% CI) | 63 (59.5 to 66.4) | 55 (50.6 to 60.6) |
Difference between pembrolizumab plus chemotherapy vs. placebo plus chemotherapy, % | ||
Estimate (95% CI)a | 7.5 (1.6 to 13.4) | |
CI = confidence interval; IA = interim analysis; ITT = intention to treat; n = number of participants; pCR = pathological complete response; vs. = versus; ypTO/Tis ypNO = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed.
Note: Data cut-off date: September 24, 2018; March 23, 2021.
aBased on Miettinen and Nurminen method stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly).
bOne-sided P value for testing hypothesis 0: difference in percentage = 0, vs. hypothesis 1: difference in percentage greater than 0.
cAt IA4, pCR was not formally tested according to the statistical plan.
Source: Clinical Study Report.10
Table 17: Analysis of pCR using the ypT0 ypN0 and ypT0/Tis definitions IA4—ITT population
Detail | Pembrolizumab plus chemotherapy | Placebo plus chemotherapy |
|---|---|---|
Analysis of pCR (using the ypT0 ypN0 definition) | ||
n | 784 | 390 |
Number of pCR | 453 | 196 |
pCR rate, % (95% CI) | 57.8 (54.2 to 61.3) | 50.3 (45.2 to 55.3) |
Difference between pembrolizumab plus chemotherapy vs. placebo plus chemotherapy, % | ||
Estimate (95% CI)a | 7.6 (1.6 to 13.6) | |
Analysis of pCR using the ypT0/Tis definition | ||
n | 784 | 390 |
Number of pCR | 516 | 228 |
pCR rate, % (95% CI) | 65.8 (62.4 to 69.1) | 58.5 (53.4 to 63.4) |
Difference between pembrolizumab plus chemotherapy vs. placebo plus chemotherapy, % | ||
Estimate (95% CI)a | 7.4 (1.7 to 13.3) | |
CI = confidence interval; IA = interim analysis; ITT = intention to treat; pCR = pathological complete response; vs. = versus; ypTO/Tis = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed; ypTO ypNO = no invasive or noninvasive residual disease in breast or nodes.
Note: Data cut-off date: March 23, 2021.
aBased on Miettinen and Nurminen method stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly).
Source: Clinical Study Report.10
Table 18: Pathological Complete Response (ypT0/Tis ypN0) by Subgroups at IA4—ITT Population
Subgroup | Pembrolizumab plus chemotherapy | Placebo plus chemotherapy | Pembrolizumab plus chemotherapy vs. placebo plus chemotherapy | ||||
|---|---|---|---|---|---|---|---|
n | Number of events | pCR rate, % (95% CI) | n | Number of events | pCR rate, % (95% CI) | Hazard ratio (95% CI)a | |
PD-L1 status | |||||||
PD-L1 CPS ≥ 1 | 656 | 436 | 66.5 (62.7 to 70.1) | 317 | 187 | 59 (53.4 to 64.5) | 7.8 (1.4 to 14.2) |
PD-L1 CPS < 1 | 128 | 58 | 45.3 (36.5 to 54.3) | 69 | 27 | 39.1 (27.6 to 51.6) | 7.1 (–7.8 to 21.1) |
Nodal status | |||||||
Positive | 408 | 255 | 62.5 (57.6 to 67.2) | 196 | 99 | 50.5 (43.3 to 57.7) | 12 (3.6 to 20.4) |
Negative | 376 | 239 | 36.6 (58.5 to 68.4) | 194 | 118 | 60.8 (53.6 to 67.7) | 2.7 (–5.6 to 11.2) |
Tumour size | |||||||
T1/T2 | 581 | 393 | 67.6 (63.7 to 71.4) | 290 | 175 | 60.3 (54.5 to 66) | 7.3 (0.6 to 14.1) |
T3/T4 | 203 | 101 | 49.8 (42.7 to 56.8) | 100 | 42 | 42.0 (32.2 to 52.3) | 7.8 (–4.2 to 19.3) |
Carboplatin schedule | |||||||
Every 3 weeks | 334 | 214 | 64.1 (58.7 to 69.2) | 167 | 100 | 59.9 (52 to 67.4) | 4.2 (–4.7 to 13.3) |
Weekly | 444 | 280 | 63.1 (58.4 to 67.6) | 220 | 117 | 53.2 (46.4 to 59.9) | 9.9 (1.9 to 17.8) |
CI = confidence interval; CPS = combined positive score; IA = interim analysis; ITT = intention to treat; pCR = pathological complete response; PD-L1 = programmed death ligand 1; vs. = versus; ypT0/Tis ypN0 = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed.
Note: Multiplicity adjustments were not conducted in the subgroup analyses to adjust type I error. Data cut-off date: March 23, 2021.
aFor overall population and the PD-L1 subgroup, analysis is based on the Miettinen and Nurminen method, stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4) and choice of carboplatin (every 3 weeks vs. weekly). For other subgroups, analysis is based on an unstratified Miettinen and Nurminen method.
Source: Clinical Study Report.10
The study met the success criterion for EFS at IA4 (the P value crossed the pre-specified boundary for statistical significance [0.00516941]).10The findings were consistent with data observed across IAs (at IA2 [data cut-off: April 24, 2019], EFS HR values were 0.63 [95% CI, 0.43 to 0.93]; at IA3, EFS HR was 0.65 [95% CI, 0.48 to 0.88]). Table 19 and Figure 5 present the findings of EFS at IA4 in the ITT population.
Table 19: Event-Free Survival at IA4—ITT Population
Detail | Pembrolizumab plus chemotherapy followed by pembrolizumab n = 784 | Placebo plus chemotherapy followed by placebo n = 390 |
|---|---|---|
Number of events, n (%) | 123 (15.7) | 93 (23.8) |
Secondary primary malignancy | 6 (0.8) | 4 (1.0) |
Local PD precludes surgery | 3 (0.4) | 4 (1) |
Local PD precludes definitive surgery | 1 (0.1) | 4 (1) |
Distant PD | 4 (0.5) | 1 (0.3) |
Positive margin at last surgery | 6 (0.8) | 10 (2.6) |
Local recurrence | 28 (3.6) | 17 (4.4) |
Distant recurrence | 60 (7.7) | 51 (13.1) |
Death | 15 (1.9) | 6 (1.5) |
Number of patients censored, n (%) | 661 (84.3) | 297 (76.2) |
Kaplan–Meier estimates, monthsa Median (95% CI) | NE (NE to NE) | NE (NE to NE) |
Q1 to Q3 | NR, NR | 41.9, NR |
Pembrolizumab plus chemotherapy followed by pembrolizumab vs. placebo plus chemotherapy followed by placebo | ||
Hazard ratio (95% CI)b | 0.63 (0.48 to 0.82) | |
P valuec | 0.0003093 | |
Event rate per 100 person-months | 0.5 | 0.7 |
EFS rate at 6 months, % (95% CI) | 98.3 (97.2 to 99.0) | 98.5 (96.6 to 99.3) |
EFS rate at 12 months, % (95% CI) | 93.3 (91.4 to 94.9) | 92.5 (89.4 to 94.7) |
EFS rate at 18 months, % (95% CI) | 90.0 (87.7 to 91.9) | 85.8 (81.9 to 88.9) |
EFS rate at 24 months, % (95% CI) | 87.8 (85.3 to 89.9) | 81.0 (76.8 to 84.6) |
EFS rate at 30 months, % (95% CI) | 85.8 (83.1 to 88.0) | 78.2 (73.7 to 82.0) |
EFS rate at 36 months, % (95% CI) | 84.5 (81.7 to 86.9) | 76.8 (72.2 to 80.7) |
EFS rate at 42 months, % (95% CI) | 83.5 (80.5 to 86.0) | 74.9 (69.8 to 79.2) |
CI = confidence interval; EFS = event-free survival; IA = interim analysis; ITT = intention to treat; NE = not estimable; NR = not reached; PD = progressive disease; Q = quarter; vs = vs.
Note: Data cut-off date: March 23, 2021.
aFrom product-limit (Kaplan–Meier) method for censored data.
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly).
cOne-sided P value based on log-rank test stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly).
Source: Clinical Study Report.10
Figure 5: Kaplan–Meier Estimates of Event-Free Survival at IA4—ITT Population
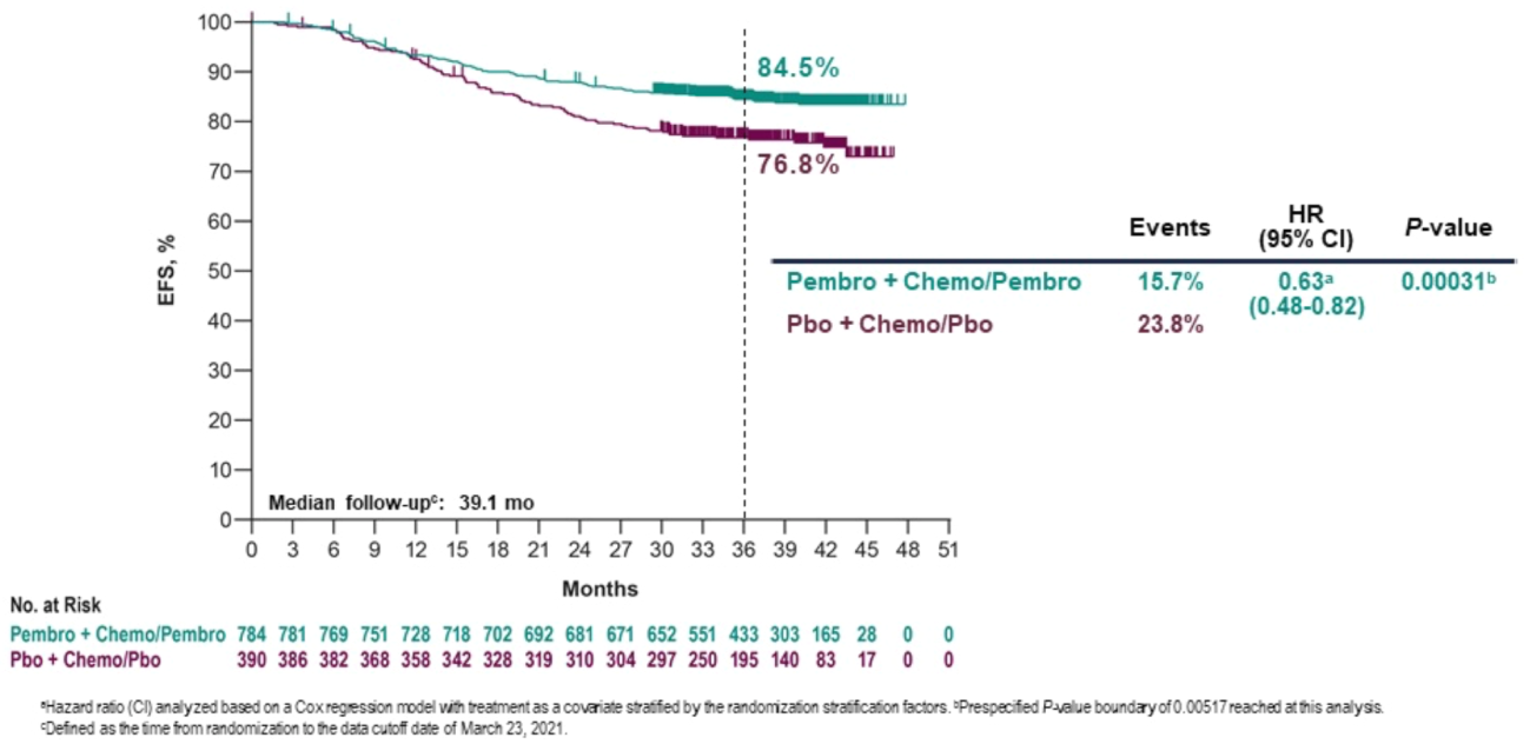
Chemo = chemotherapy; CI = confidence interval; EFS = event-free survival; HR = hazard ratio; IA = interim analysis; ITT = intention to treat; Pembro = pembrolizumab; Pbo = placebo.
Note: Data cut-off date: March 23, 2021.
Source: Sponsor-submitted reimbursement package.2
Sensitivity Analyses for EFS
Five pre-specified sensitivity analyses were conducted for EFS in the ITT population. The results of the sensitivity analyses were consistent with the primary analysis.
Sensitivity analysis 1: This analysis was similar to the primary analysis, except different censoring rules were applied (any events after 2 consecutive missed disease assessments or after initiation of post-surgery new anticancer therapy were censored at last disease assessment before the earlier date of ≥ 2 consecutive missed disease assessments and initiation of post-surgery new anticancer therapy, and if there were no events before new anticancer therapy, patients were censored at last disease assessment before initiation of post-surgery new anticancer treatment). The EFS HR was 0.64 (95% CI, 0.48 to 0.84).
Sensitivity analysis 2: Similar to the primary analysis, except that new anticancer therapy to treat metastatic disease was also considered in defining an EFS event. The EFS HR was 0.63 (95% CI, 0.48 to 0.82).
Sensitivity analysis 3: Similar to the primary analysis, except that positive margins at a patient’s last surgery were excluded from the EFS event definition. The EFS HR was 0.65 (95% CI, 0.50 to 0.85).
Sensitivity analysis 4: Similar to the primary analysis, except that both positive margins at a patient’s last surgery and second primary malignancy were excluded from the EFS event definition. The EFS HR was 0.63 (95% CI, 0.48 to 0.84).
Sensitivity analysis 5: Similar to the primary analysis, except that second breast primary malignancy was included in the EFS event definition. The EFS HR was 0.63 (95% CI, 0.48 to 0.82).10
Subgroup Analyses10
Table 20 presents findings of EFS in the subgroups identified in the CADTH review protocol.
Health-Related QoL
The findings presented are for the March 23, 2021, data cut-off using the full analysis set population.
European Organisation for Research and Treatment of Cancer QLQ-C30
Neoadjuvant phase: Compliance rates in the neoadjuvant phase were similar at baseline for EORTC QLQ-C30 in both the pembrolizumab plus chemotherapy and the placebo plus chemotherapy arms (92.0% versus 95.8%). After 21 weeks of follow-up in the neoadjuvant phase, the completion rate among all patients was 80.7% versus 80.7% in the pembrolizumab plus chemotherapy and placebo plus chemotherapy arms, respectively. The LS mean difference between groups for global health status–QoL score and physical functioning score was –1.04 (95% CI, –3.46 to 1.38) and –2.85 (95% CI, –5.11 to –0.60), respectively. The LS mean difference between groups for emotional functioning was –0.69 (95% CI, –3.13 to 1.75) at the March 23, 2021, data cut-off. Table 21, Figure 6, and Figure 7 summarize the change from neoadjuvant baseline in EORTC QLQ-C30 global health status–QoL, emotional functioning, and physical functioning at neoadjuvant week 21.10
Table 20: Event-Free Survival by Subgroups at IA4—ITT Population
Subgroup | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo | Pembrolizumab plus chemotherapy followed by pembrolizumab vs. placebo plus chemotherapy followed by placebo, HR (95% CI)a | ||
|---|---|---|---|---|---|
n | Number of events (%) | n | Number of events (%) | ||
PD-L1 status | |||||
PD-L1 CPS ≥ 1 | 656 | 98 (14.9) | 317 | 68 (21.5) | 0.67 (0.49 to 0.92) |
PD-L1 CPS < 1 | 128 | 25 (19.5) | 69 | 25 (36.2) | 0.48 (0.28 to 0.85) |
Nodal status | |||||
Positive | 408 | 80 (19.1) | 196 | 57 (29.1) | 0.65 (0.46 to 0.91) |
Negative | 376 | 43 (11.4) | 194 | 36 (18.6) | 0.58 (0.37 to 0.91) |
Tumour size | |||||
T1/T2 | 581 | 64 (11.0) | 290 | 59 (20.3) | 0.51 (0.36 to 0.73) |
T3/T4 | 203 | 59 (29.1) | 100 | 34 (34) | 0.84 (0.55 to 1.28) |
Carboplatin schedule | |||||
Every 3 weeks | 334 | 50 (15) | 167 | 37 (21.5) | 0.65 (0.42 to 0.90) |
Weekly | 444 | 71 (16) | 220 | 56 (25.5) | 0.60 (0.42 to 0.86) |
CI = confidence interval; CPS = combined positive score; HR = hazard ratio; IA = interim analysis; ITT = intention to treat; PD-L1 = programmed death ligand 1; vs. = versus; ypT0/Tis ypN0 = no invasive residual disease in breast or nodes; noninvasive breast residuals allowed.
Note: Multiplicity adjustments were not conducted in the subgroup analyses to adjust for type I error. Data cut-off date: March 23, 2021.
aFor the overall population and the PD-L1 subgroup, analysis is based on the Miettinen and Nurminen method, stratified by nodal status (positive vs. negative), tumour size (T1/T2 vs. T3/T4), and choice of carboplatin (every 3 weeks vs. weekly). For other subgroups, analysis is based on an unstratified Miettinen and Nurminen method.
Source: Clinical Study Report.10
Table 21: Summary of Change From Neoadjuvant Baseline in EORTC QLQ-C30 Global Health Status–QoL, Physical Functioning, and Emotional Functioning at Neoadjuvant Week 21—FAS Population
Category | Pembrolizumab plus chemotherapy | Placebo plus chemotherapy |
|---|---|---|
Baseline, na | 701 | 366 |
EORTC QLQ-C30 global health status–QoL, mean (SD) | 77.08 (18.493) | 78.96 (17.124) |
EORTC QLQ-C30 physical functioning, mean (SD) | 91.89 (12.796) | 91.51 (13.134) |
EORTC QLQ-C30 emotional functioning, mean (SD) | 76.14 (19.495) | 75.20 (20.694) |
Neoadjuvant week 21, na | 615 | 309 |
EORTC QLQ-C30 global health status–QoL, mean (SD) | 66.79 (19.386) | 68.26 (17.816) |
EORTC QLQ-C30 physical functioning, mean (SD) | 77.01 (18.987) | 79.18 (17.129) |
EORTC QLQ-C30 emotional functioning, mean (SD) | 74.61 (20.785) | 74.95 (21.635) |
Change from neoadjuvant baseline at neoadjuvant week 21, nb | 762 | 383 |
EORTC QLQ-C30 global health status–QoL, LS mean (95% CI)c | –11.24 | –10.20 |
EORTC QLQ-C30 physical functioning, LS mean (95% CI)c | –15.37 | –12.52 |
EORTC QLQ-C30 emotional functioning, LS mean (95% CI)c | –1.31 (–2.82 to 0.21) | –0.62 (–2.67 to 1.44) |
Pairwise comparison, difference in LS means (95% CI) | ||
EORTC QLQ-C30 global health status–QoL | –1.04 (–3.46 to 1.38) | |
P valued | 0.3985 | |
EORTC QLQ-C30 physical functioning | –2.85 (–5.11 to –0.60) | |
P valued | 0.0133 | |
EORTC QLQ-C30 emotional functioning | –0.69 (–3.13 to 1.75) | |
P valued | 0.5796 | |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; QoL = quality of life; SD = standard deviation.
Note: A high score in a functional scale represents a high (or healthy) level of functioning, a high score in the global health status–QoL represents a high QoL, and a high score for a symptom scale or item represents a high level of symptomatology or problems. Data cut-off date: March 23, 2021.
aFor neoadjuvant baseline and neoadjuvant week 21, n is the number of participants in each treatment group with nonmissing assessments at the specific time point.
bFor change from neoadjuvant baseline, n is the number of participants in the analysis population in each treatment group.
cBased on Constrained' longitudinal data analysis (cLDA) model with the patient-reported outcome score as the response variable, and with treatment by time point interaction, stratification factors (nodal status [positive vs. negative], tumour size [T1/T2 vs. T3/T4], and choice of carboplatin [every 3 weeks vs. weekly]) as covariates.
dP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report.10
Figure 6: Change From Neoadjuvant Baseline for EORTC QLQ-C30 Global Health Status–QoL and Functional Scales at Neoadjuvant Week 21—FAS Population
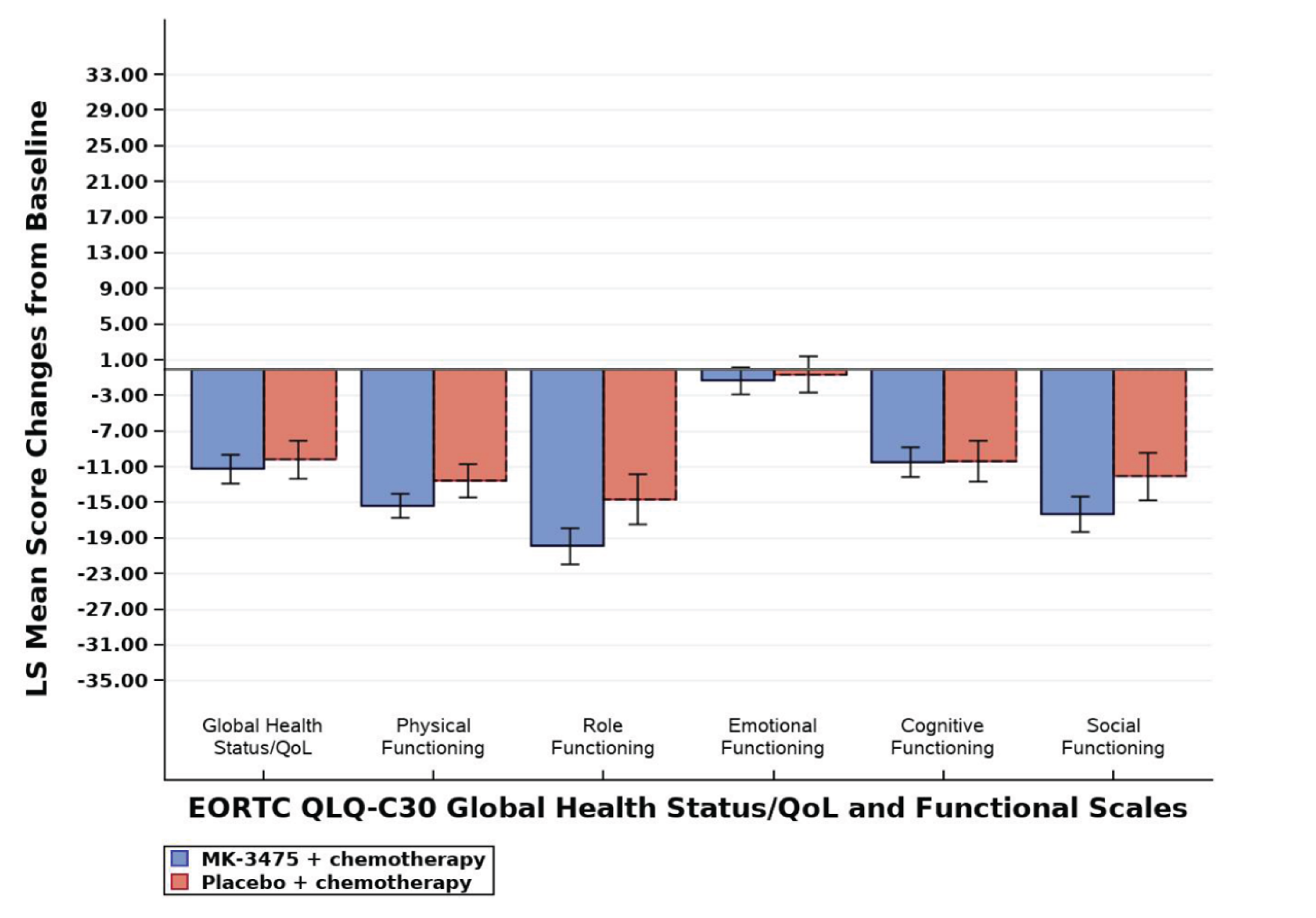
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; MK-3475 = pembrolizumab; QoL = quality of life.
Note: For global health status–QoL score and all functional scales, a higher score denotes better health-related QoL or function. For symptoms scales, a higher score denotes worse symptoms. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Figure 7: Change From Neoadjuvant Baseline for EORTC QLQ-C30 Symptom Scales or Items at Neoadjuvant Week 21—FAS Population
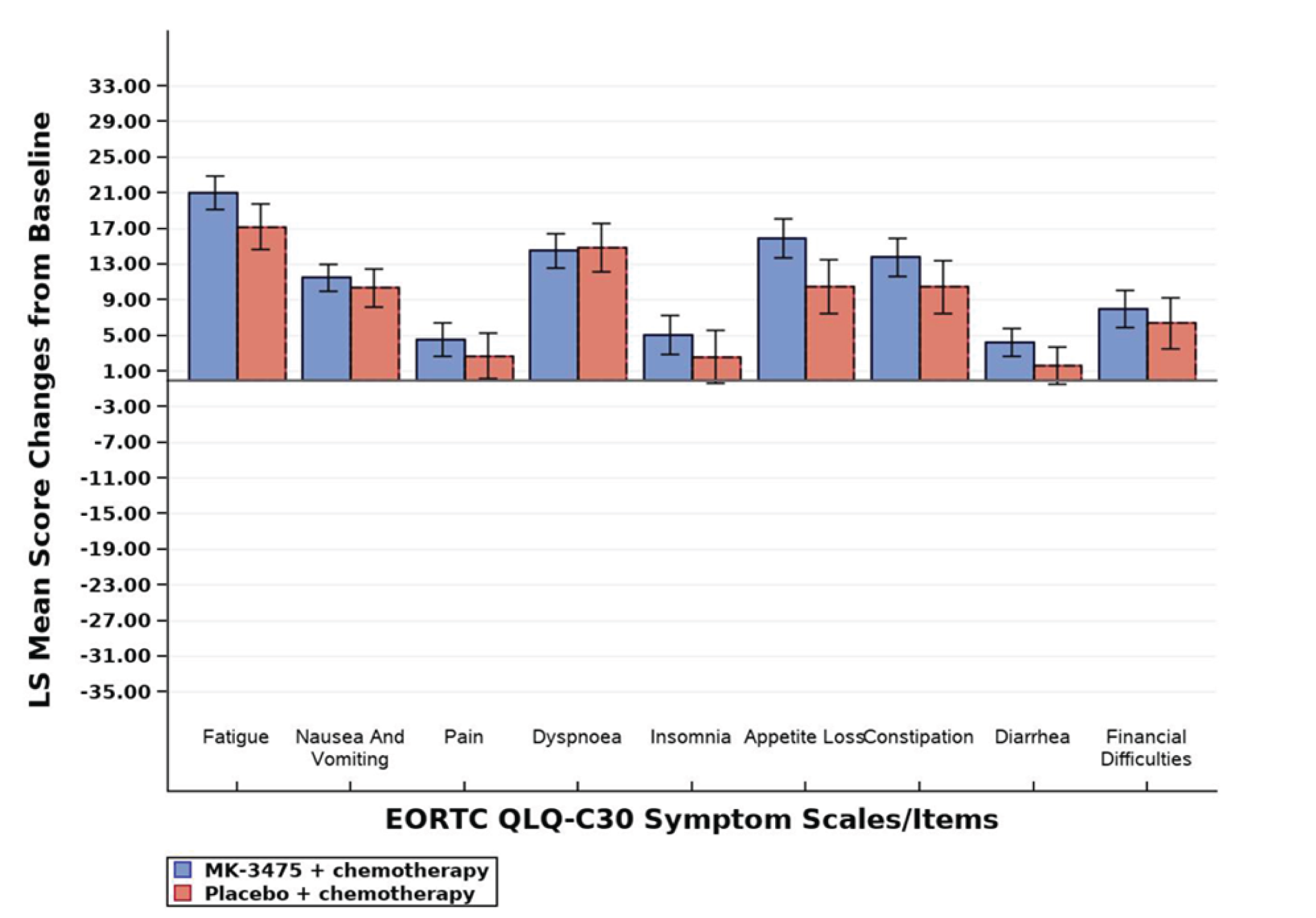
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; MK-3475 = pembrolizumab.
Note: For global health status–QoL score and all functional scales, a higher score denotes better health-related QoL or function. For symptoms scales, a higher score denotes worse symptoms. Database cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Adjuvant phase: Compliance rates in the adjuvant phase were similar at baseline for EORTC QLQ-C30 in both the pembrolizumab and placebo arms (90.7% versus 91.9%) at the March 23, 2021, data cut-off. After 24 weeks of follow-up in the adjuvant phase, the compliance rate among patients was 82.4% versus 80.8% in the pembrolizumab versus placebo arms. The LS mean difference between groups for global health status–QoL score, physical functioning, and emotional functioning was –0.41 (95% CI, –2.60 to 1.77), –1.57 (95% CI, –3.36 to 0.21), and –0.60 (95% CI, –2.99 to 1.79), respectively, at the March 23, 2021, data cut-off. Table 22, Figure 8, and Figure 9 summarize the change from adjuvant baseline in EORTC QLQ-C30 global health status–QoL, physical functioning, and emotional functioning at adjuvant week 24.10
Table 22: Summary of Change From Adjuvant Baseline in EORTC QLQ-C30 Global Health Status–QoL, Physical Functioning, and Emotional Functioning at Adjuvant Week 24—FAS Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo |
|---|---|---|
Baseline, na | 489 | 283 |
EORTC QLQ-C30 global health status–QoL, mean (SD) | 73.82 (15.68) | 73.14 (18.15) |
EORTC QLQ-C30 physical functioning, mean (SD) | 83.3 (15.32) | 81.63 (16.61) |
EORTC QLQ-C30 emotional functioning, mean (SD) | 81.75 (17.72) | 78.98 (20.81) |
Adjuvant week 24, na | 444 | 249 |
EORTC QLQ-C30 global health status–QoL, mean (SD) | 76.26 (16.67) | 76.24 (16.56) |
EORTC QLQ-C30 physical functioning, mean (SD) | 84.82 (15.68) | 85.38 (15.03) |
EORTC QLQ-C30 emotional functioning, mean (SD) | 79.62 (19.64) | 78.41 (20.44) |
Change from adjuvant baseline at adjuvant week 24, nb | 539 | 308 |
EORTC QLQ-C30 global health status–QoL, LS mean (95% CI)c | 2.47 | 2.88 |
EORTC QLQ-C30 physical functioning, LS mean (95% CI)c | 1.60 | 3.18 |
EORTC QLQ-C30 emotional functioning, LS mean (95% CI)c | –1.53 | –0.92 |
Pairwise comparison, difference in LS mean (95% CI) | ||
EORTC QLQ-C30 global health status–QoL | –0.41 (–2.60 to 1.77) | |
P valued | 0.7107 | |
EORTC QLQ-C30 physical functioning | –1.57 (–3.36 to 0.21) | |
P valued | 0.0839 | |
EORTC QLQ-C30 emotional functioning | –0.60 (–2.99 to 1.79) | |
P valued | 0.6209 | |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; QoL = quality of life; SD = standard deviation.
Note: A high score in a functional scale represents a high (or healthy) level of functioning, a high score in the global health status–QoL represents a high QoL, and a high score for a symptom scale or item represents a high level of symptomatology or problems. Data cut-off date: March 23, 2021.
aFor neoadjuvant baseline and neoadjuvant week 21, n is the number of participants in each treatment group with nonmissing assessments at the specific time point.
bFor change from neoadjuvant baseline, n is the number of participants in the analysis population in each treatment group.
cBased on Constrained' longitudinal data analysis (cLDA) model with the patient-reported outcome score as the response variable, and with treatment by time point interaction, stratification factors (nodal status [positive vs. negative], tumour size [T1/T2 vs. T3/T4], and choice of carboplatin [every 3 weeks vs. weekly]) as covariates.
dP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report.10
Figure 8: Change From Adjuvant Baseline for EORTC QLQ-C30 Global Health Status–QoL and Functional Scales at Adjuvant Week 24—FAS Population
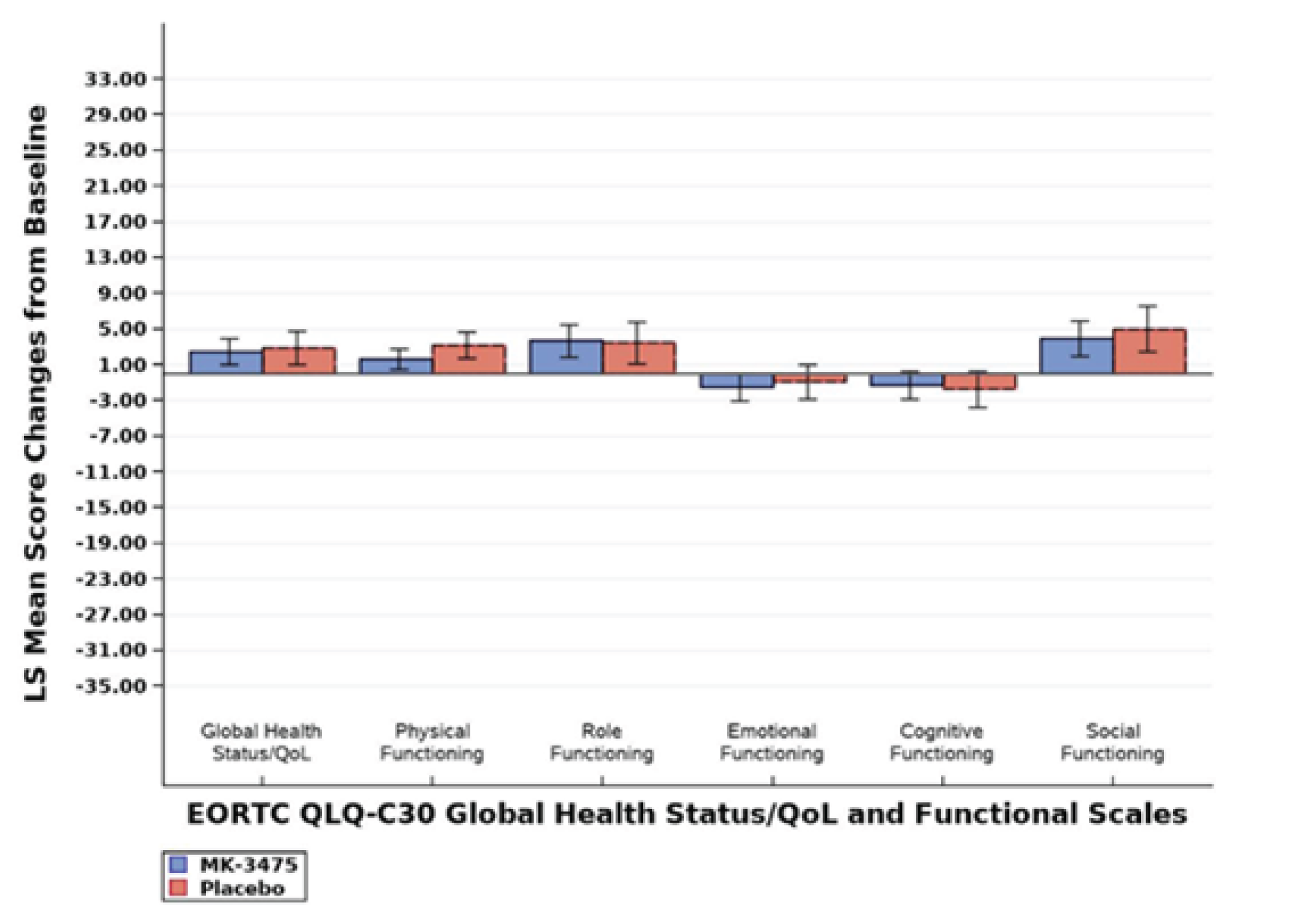
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; MK-3475 = pembrolizumab; QoL = quality of life.
Note: For global health status–QoL score and all functional scales, a higher score denotes better health-related QoL or function. For symptom scales, a higher score denotes worse symptoms. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Figure 9: Change From Adjuvant Baseline for EORTC QLQ-C30 Symptom Scales or Items at Adjuvant Week 24—FAS Population
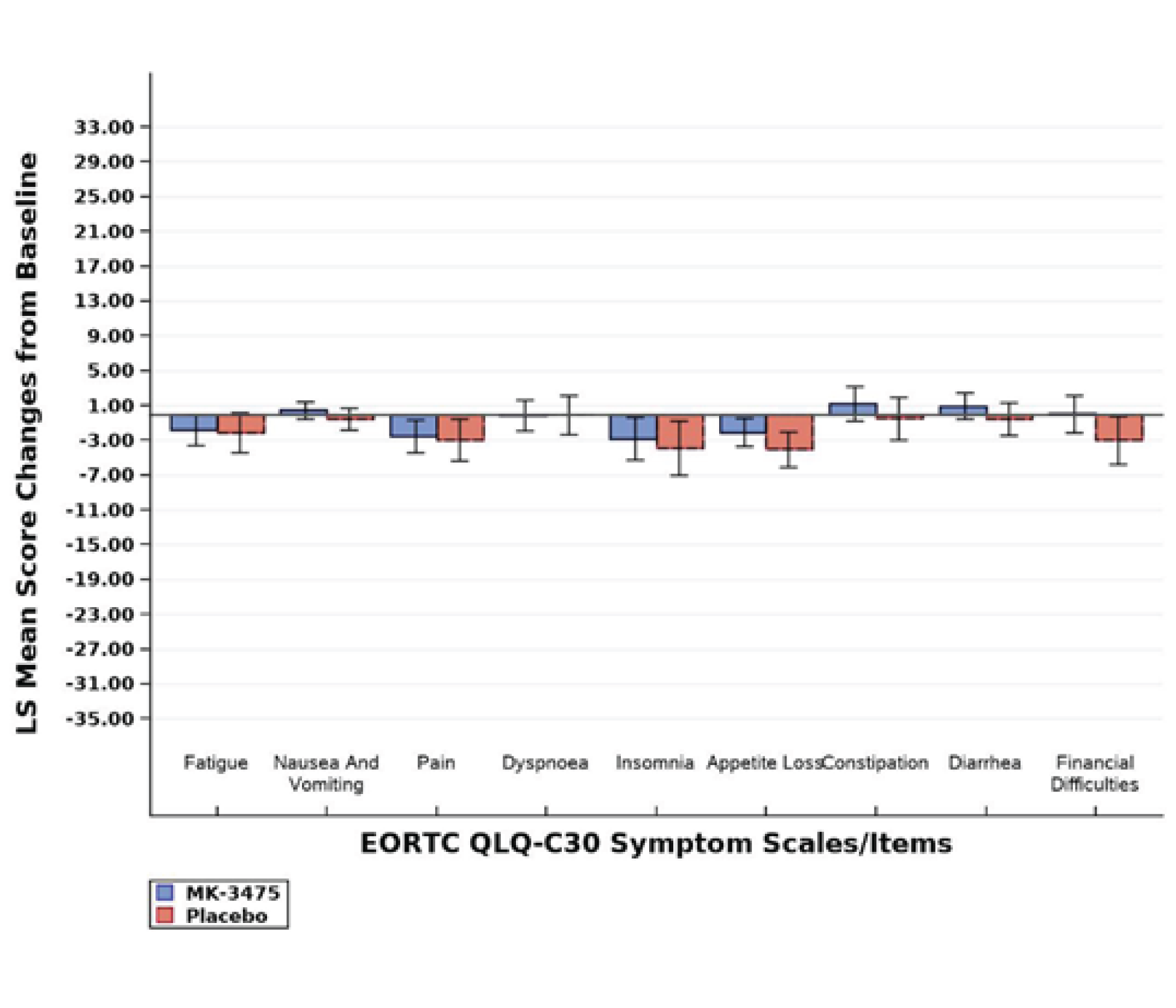
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; MK-3475 = pembrolizumab.
Note: For global health status–quality of life score and all functional scales, a higher score denotes better health-related quality of life or function. For symptoms scales, a higher score denotes worse symptoms. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Table 23: Summary of Change From Neoadjuvant Baseline in EORTC QLQ-BR23 Breast Symptoms at Neoadjuvant Week 21—FAS Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo |
|---|---|---|
Baseline, na | 695 | 361 |
Mean (SD) | 18.67 (20.36) | 18.47 (19.32) |
Neoadjuvant week 21, na | 611 | 307 |
Mean (SD) | 8.82 (12.92) | 8.5 (14.03) |
Change from neoadjuvant baseline at neoadjuvant week 21, nb | 796 | 382 |
LS mean (95% CI)c | –9.92 (–11.34 to –8.49) | –9.78 (–11.53 to –8.03) |
Difference in LS means | –0.13 | |
95% CI | –1.92 to 1.65 | |
P valued | 0.884 | |
CI = confidence interval; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; FAS = full analysis set; LS = least squares; SD = standard deviation.
Note: A high score in a functional scale represents a high (or healthy) level of functioning, a high score in the global health status–quality of life represents a high quality of life, and a high score for a symptom scale or item represents a high level of symptomatology or problems. Data cut-off date: March 23, 2021.
aFor neoadjuvant baseline and neoadjuvant week 21, n is the number of participants in each treatment group with nonmissing assessments at the specific time point.
bFor change from neoadjuvant baseline, n is the number of participants in the analysis population in each treatment group.
cBased on Constrained' longitudinal data analysis (cLDA) model with the patient-reported outcome score as the response variable, and with treatment by time point interaction, stratification factors (nodal status [positive vs. negative], tumour size [T1/T2 vs. T3/T4], and choice of carboplatin [every 3 weeks vs. weekly]) as covariates.
dP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report.10
European Organisation for Research and Treatment of Cancer QLQ-BR23
Neoadjuvant phase: Compliance rates in the neoadjuvant phase were similar at baseline for the EORTC QLQ-BR23 in both the pembrolizumab plus chemotherapy and placebo plus chemotherapy arms (91.6% versus 94.8%) at the March 23, 2021, data cut-off. After 21 weeks of follow-up in the neoadjuvant phase, the compliance rate for all patients was 80.5% versus 80.4% in the pembrolizumab plus chemotherapy arm versus the placebo plus chemotherapy arm. The LS mean difference between groups for the EORTC QLQ-BR23 Breast Symptoms score was –0.13 (95% CI, –1.92 to 1.65). Table 23 summarizes change from the neoadjuvant baseline in EORTC QLQ-BR23 Breast Symptoms score at neoadjuvant week 21. Figure 10 and Figure 11 summarize the change from the neoadjuvant baseline in EORTC QLQ-BR23 functional and symptom scales or items at neoadjuvant week 21.10
Adjuvant phase: Compliance rates in the adjuvant phase were similar at baseline for EORTC QLQ-BR23 in both the pembrolizumab and placebo arms (90.5% versus 92.2%, respectively) at the March 23, 2021, data cut-off. After 24 weeks of follow-up, the compliance rate was 82.2% versus 80.7% in the pembrolizumab and placebo arms, respectively. The LS mean difference between groups for the EORTC QLQ-BR23 Breast Symptoms score was 0.29 (95% CI, –2.05 to 2.63). Table 24 summarizes change from adjuvant baseline in EORTC QLQ-BR23 Breast Symptoms score at adjuvant week 24. Figure 12 and Figure 13 summarize the change from adjuvant baseline in EORTC QLQ-BR23 functional and symptom scales or items at adjuvant week 24.10
Figure 10: Change From Neoadjuvant Baseline for EORTC QLQ-BR23 Functional Scales or Items at Neoadjuvant Week 21—FAS Population
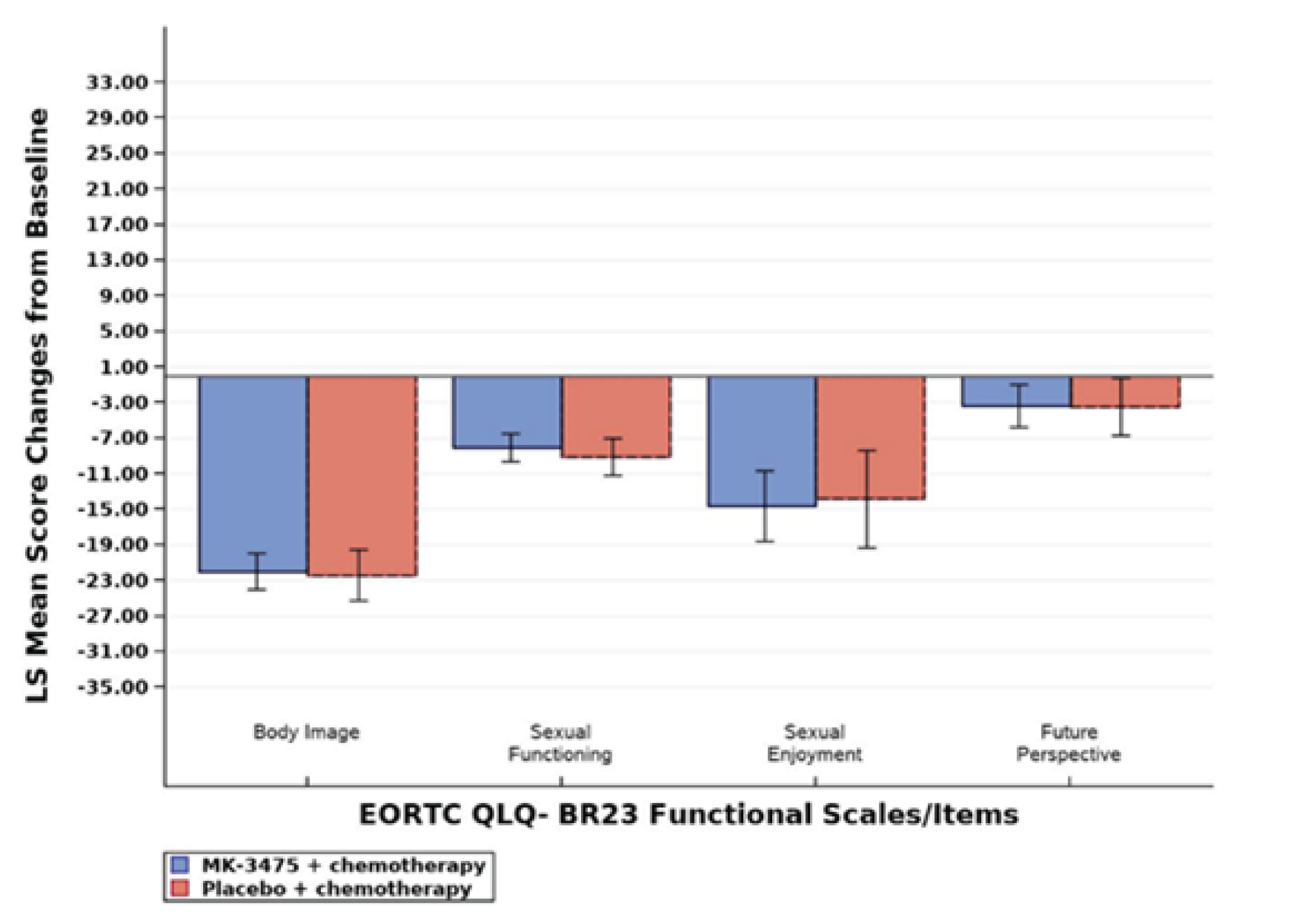
EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; FAS = full analysis set; LS = least squares; MK-3475 = pembrolizumab.
Note: For global health status–quality of life score and all functional scales, a higher score denotes better health-related quality of life or function. For symptom scales, a higher score denotes worse symptoms. If the patient did not lose any hair, then “upset by hair loss” is imputed as the lowest score (0). Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Figure 11: Change From Neoadjuvant Baseline for EORTC QLQ-BR23 Symptom Scales or Items at Neoadjuvant Week 21—FAS Population
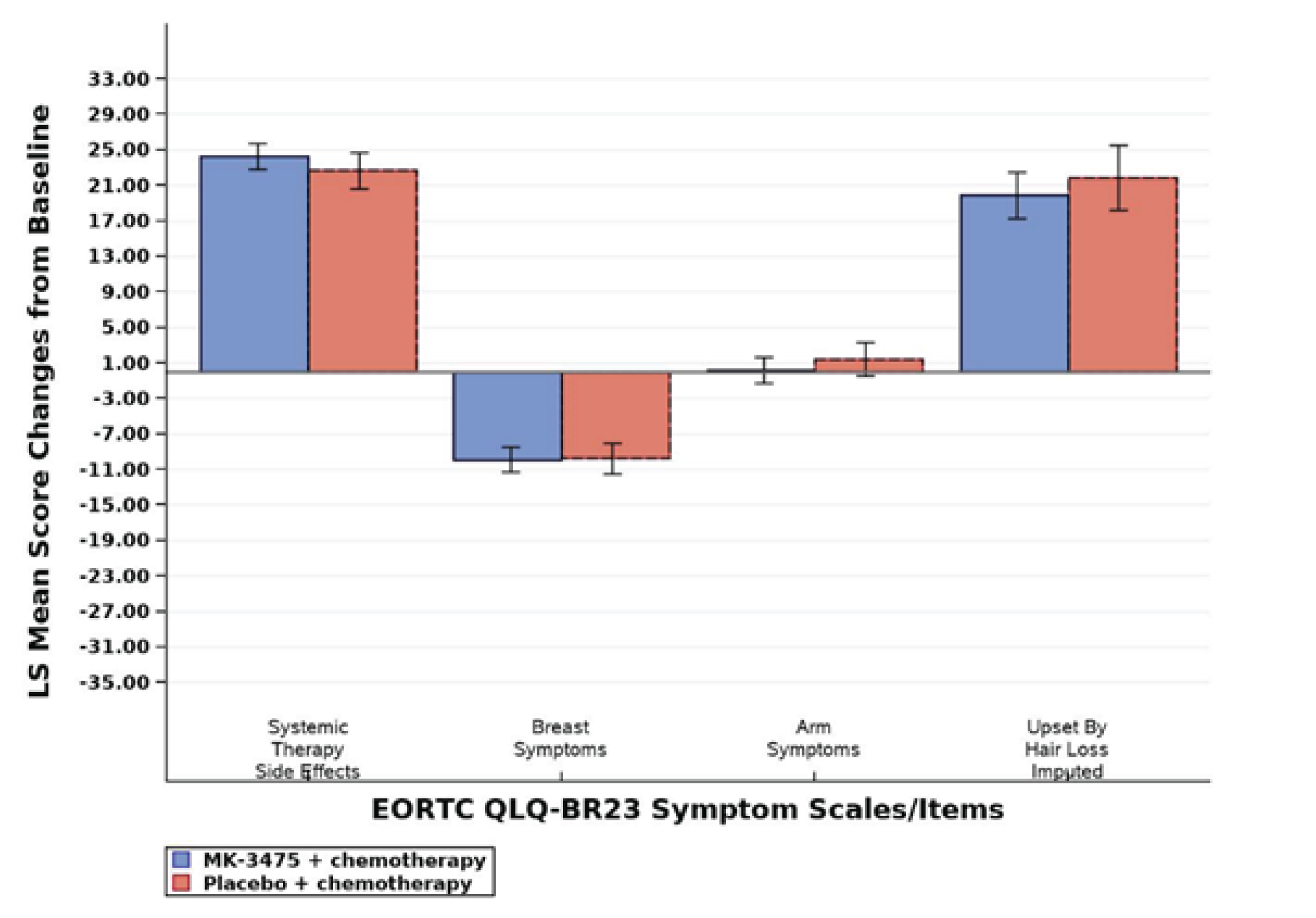
EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; FAS = full analysis set; LS = least squares; MK-3475 = pembrolizumab.
Note: For global health status–quality of life score and all functional scales, a higher score denotes better health-related quality of life or function. For symptoms scales, a higher score denotes worse symptoms. If the patient did not lose any hair, then “upset by hair loss” is imputed as the lowest score (0). Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Table 24: Summary of Change From Adjuvant Baseline in EORTC QLQ-BR23 Breast Symptoms at Adjuvant Week 24—FAS Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo |
|---|---|---|
Baseline, na | 487 | 282 |
Mean (SD) | 22.23 (18.71) | 23.02 (20.24) |
Adjuvant week 24, na | 442 | 247 |
Mean (SD) | 16.84 (17.19) | 16.70 (18.14) |
Change from adjuvant baseline at adjuvant week 24, nb | 538 | 306 |
LS mean (95% CI) c | –5.73 (–7.32 to –4.15) | –6.02 (–8.04 to –4.01) |
Difference in LS means | 0.29 | |
95% CI | –2.05 to 2.63 | |
P valued | 0.8077 | |
CI = confidence interval; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; FAS = full analysis set; LS = least squares; SD = standard deviation.
Note: A high score in a functional scale represents a high (or healthy) level of functioning, a high score in the global health status–quality of life represents a high quality of life, and a high score for a symptom scale or item represents a high level of symptomatology or problems. Data cut-off date: March 23, 2021.
aFor neoadjuvant baseline and neoadjuvant week 21, n is the number of participants in each treatment group with nonmissing assessments at the specific time point.
bFor change from neoadjuvant baseline, nis the number of participants in the analysis population in each treatment group.
cBased on Constrained' longitudinal data analysis (cLDA) model with the patient-reported outcome score as the response variable, and with treatment by time point interaction, stratification factors (nodal status [positive vs. negative], tumour size [T1/T2 vs. T3/T4], and choice of carboplatin [every 3 weeks vs. weekly]) as covariates.
dP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report.10
EQ Visual Analogue Scale
Neoadjuvant phase: Compliance rates in the neoadjuvant phase were similar at baseline for the EQ VAS in both the pembrolizumab plus chemotherapy and placebo plus chemotherapy arms (92.8% versus 96.3%, respectively) at the March 23, 2021, data cut-off. After 21 weeks of follow-up in the neoadjuvant phase, the compliance rate was 80.8% versus 81.0% in the pembrolizumab plus chemotherapy arm versus the placebo plus chemotherapy arm. The LS mean difference between groups for the EQ VAS score was –1.61 (95% CI, –3.87 to 0.64). Table 25 summarizes change from neoadjuvant baseline in EQ VAS at neoadjuvant week 21, and Figure 14 summarizes the change from neoadjuvant baseline in EQ VAS across time at neoadjuvant week 21.10
Adjuvant phase: Compliance rates in the adjuvant phase were similar at baseline for the EQ VAS in both the pembrolizumab and placebo arms (91.7% versus 91.9%). After 24 weeks of follow-up in the adjuvant phase, the compliance rate was 82.2% versus 80.3% in the pembrolizumab and placebo arms, respectively. The LS mean difference between groups for the EQ VAS was –0.59 (95% CI, –2.40 to 1.23). Table 26 summarizes change from adjuvant baseline in EQ VAS at adjuvant week 24, and Figure 15 summarizes the change from adjuvant baseline in EQ VAS across time observed at adjuvant week 24.10
Figure 12: Change From Adjuvant Baseline for EORTC QLQ-BR23 Functional Scales or Items at Adjuvant Week 24—FAS Population
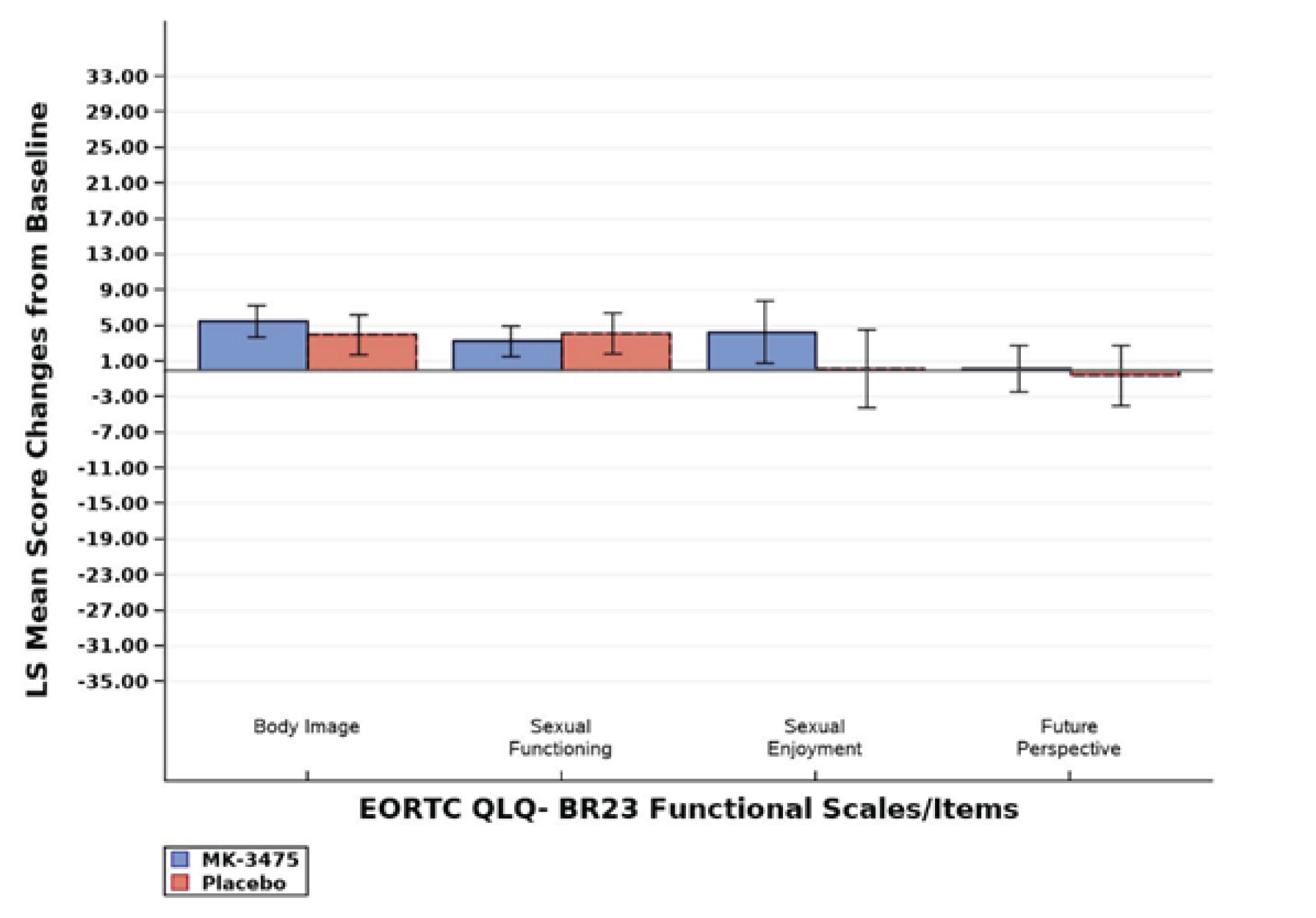
EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; FAS = full analysis set; LS = least squares; MK-3475 = pembrolizumab.
Note: For global health status–quality of life score and all functional scales, a higher score denotes better health-related quality of life or function. For symptoms scales, a higher score denotes worse symptoms. If the patient did not lose any hair, then “upset by hair loss” is imputed as the lowest score (0). Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Figure 13: Change From Adjuvant Baseline for EORTC QLQ-BR23 Symptom Scales or Items at Adjuvant Week 24—FAS Population
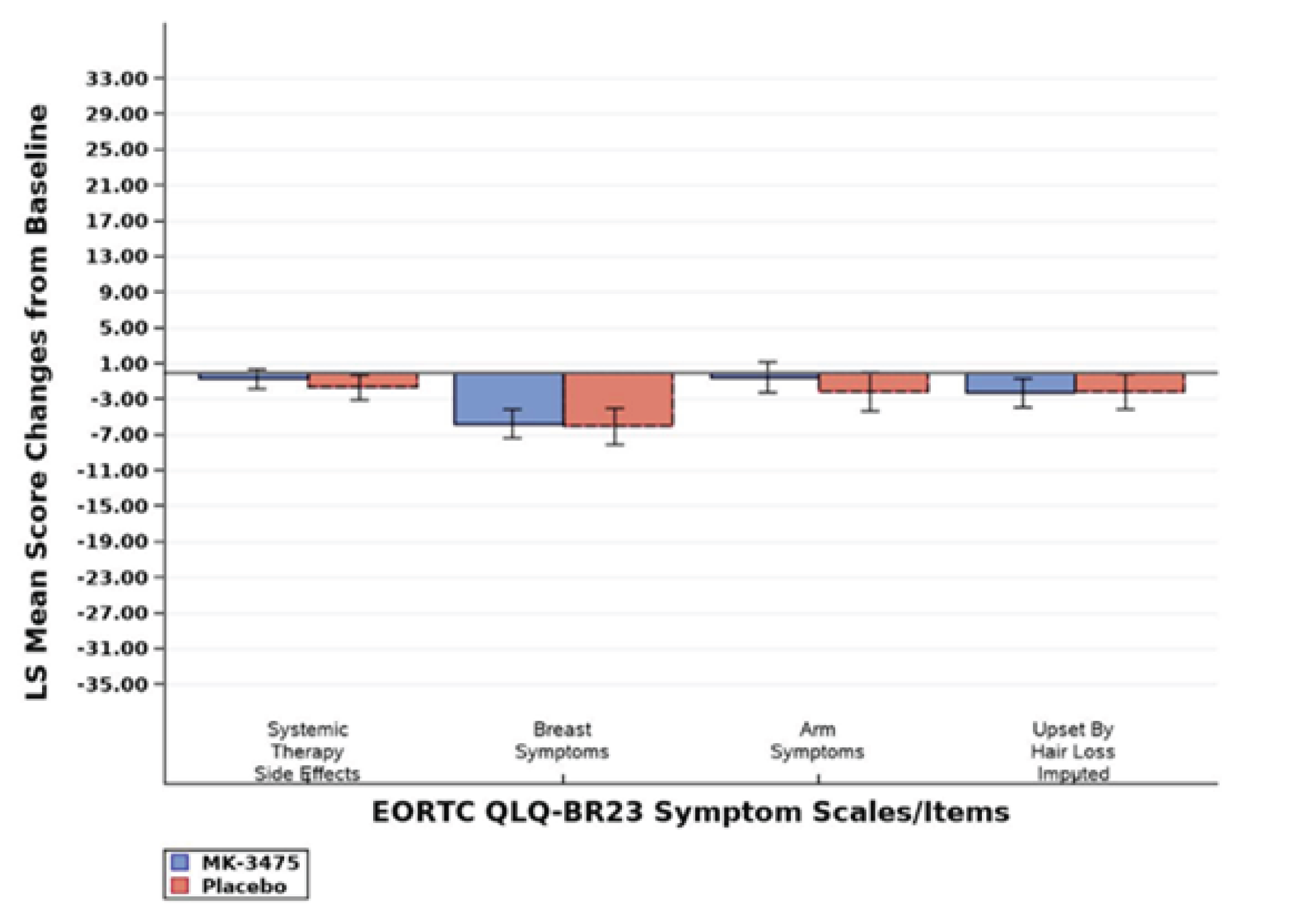
EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Breast Cancer–Specific Quality of Life Questionnaire; FAS = full analysis set; LS = least squares; MK-3475 = pembrolizumab.
Note: For global health status–quality of life score and all functional scales, a higher score denotes better health-related quality of life or function. For symptom scales, a higher score denotes worse symptoms. If the patient did not lose any hair, then “upset by hair loss” is imputed as the lowest score (0). Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Table 25: Summary of Change From Neoadjuvant Baseline in EQ VAS at Neoadjuvant Week 21—FAS Population
Category | Pembrolizumab plus chemotherapy | Placebo plus chemotherapy |
|---|---|---|
Baseline, na | 707 | 369 |
Mean (SD) | 81.1 (18.07) | 82.6 (16.98) |
Neoadjuvant week 21, na | 616 | 311 |
Mean (SD) | 72.76 (18.14) | 74.99 (16.37) |
Change from neoadjuvant baseline at neoadjuvant week 21, nb | 762 | 384 |
LS mean (95% CI)c | –8.98 (–10.48 to –7.47) | –7.36 (–9.34 to –5.38) |
Difference in LS means | –1.61 | |
95% CI | –3.87 to 0.64 | |
P valued | 0.1605 | |
CI = confidence interval; EQ VAS = EQ Visual Analogue Scale; FAS = full analysis set; LS = least squares; SD = standard deviation.
Note: Data cut-off date: March 23, 2021.
aFor neoadjuvant baseline and neoadjuvant week 21, nis the number of participants in each treatment group with nonmissing assessments at the specific time point.
bFor change from neoadjuvant baseline, nis the number of participants in the analysis population in each treatment group.
cBased on Constrained’ longitudinal data analysis (cLDA) model with the patient-reported outcome score as the response variable, and with treatment by time point interaction, stratification factors (nodal status [positive vs. negative], tumour size [T1/T2 vs. T3/T4], and choice of carboplatin [every 3 weeks vs. weekly]) as covariates.
dP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report.10
Table 26: Summary of Change From Adjuvant Baseline in EQ VAS at Adjuvant Week 24—FAS Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab | Placebo plus chemotherapy followed by placebo |
|---|---|---|
Baseline, na | 495 | 285 |
Mean (SD) | 78.43 (14.58) | 78.79 (14.54) |
Adjuvant week 24, na | 444 | 249 |
Mean (SD) | 80.58 (14.86) | 81.2 (13.35) |
Change from adjuvant baseline at adjuvant week 24, nb | 540 | 310 |
LS mean (95% CI)c | 1.83 (0.66 to 3.00) | 2.42 (0.91 to 3.93) |
Difference in LS means | –0.59 | |
95% CI | –2.40 to 1.23 | |
P valued | 0.5257 | |
CI = confidence interval; EQ VAS = EQ Visual Analogue Scale; FAS = full analysis set; LS = least squares; SD = standard deviation.
Note: Data cut-off date: March 23, 2021.
aFor neoadjuvant baseline and neoadjuvant week 21, nis the number of participants in each treatment group with nonmissing assessments at the specific time point.
bFor change from neoadjuvant baseline, n is the number of participants in the analysis population in each treatment group.
cBased on Constrained' longitudinal data analysis (cLDA) model with the patient-reported outcome score as the response variable, and with treatment by time point interaction, stratification factors (nodal status [positive vs. negative], tumour size [T1/T2 vs. T3/T4], and choice of carboplatin [every 3 weeks vs. weekly]) as covariates.
dP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report.10
Figure 14: Empirical Mean Change From Neoadjuvant Baseline in EQ VAS Across Time—FAS Population
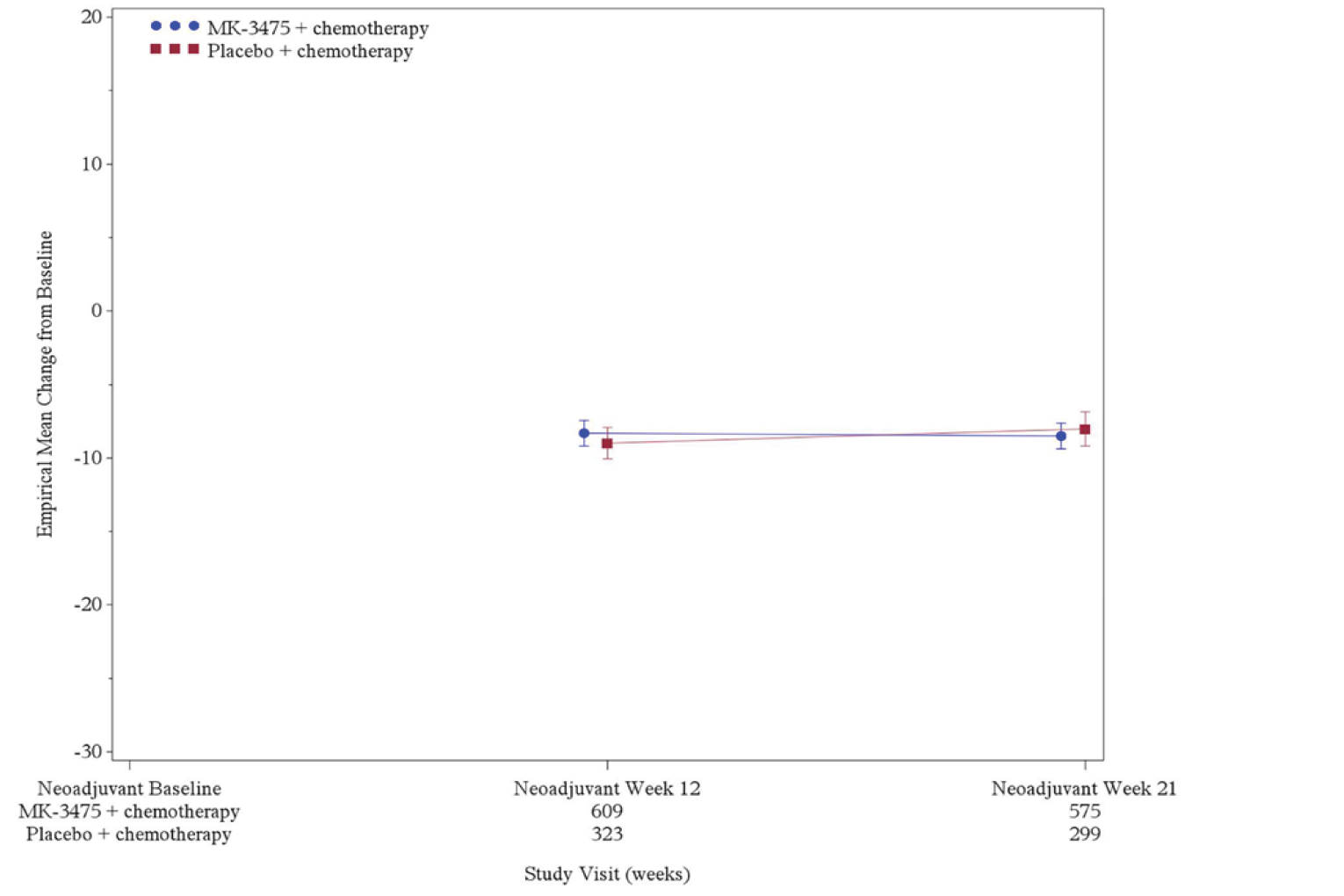
EQ VAS = EQ Visual Analogue Scale; FAS = full analysis set; MK-3475 = pembrolizumab.
Note: Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Harms
Only those harms identified in the CADTH review protocol are reported below. The safety evaluation of all participants in combined phases (neoadjuvant and adjuvant) obtained at the IA4 (March 23, 2021) data cut-off are presented in Table 27.
Adverse Events
Overall, 99.2% of patients enrolled in the pembrolizumab plus chemotherapy followed by pembrolizumab arm and 100% in the placebo plus chemotherapy followed by placebo arm reported at least 1 AE by the March 23, 2021, data cut-off. Adverse events of grade 3 or higher occurred in 82.4% of patients in the pembrolizumab plus chemotherapy followed by pembrolizumab arm and 78.7% in the placebo plus chemotherapy followed by placebo arm. Table 27 presents an overview of AEs in the pembrolizumab plus chemotherapy followed by pembrolizumab arm and the placebo plus chemotherapy followed by placebo arm.10
The most frequently reported AEs (occurring in > 30% of patients) in the pembrolizumab plus chemotherapy followed by pembrolizumab arm were nausea, alopecia, anemia, neutropenia, fatigue, constipation, diarrhea, vomiting, and increased alanine aminotransferase (ALT). In the placebo plus chemotherapy followed by placebo arm, nausea, alopecia, anemia, neutropenia, fatigue, constipation, diarrhea, and arthralgia were the most frequently reported AEs. Overall, incidences of the most frequently reported AEs (incidence ≥ 30%) were generally similar between the 2 treatment groups. More patients receiving pembrolizumab in the adjuvant phase had serious AEs than did patients receiving placebo in the adjuvant phase.
More deaths due to AEs were reported in the pembrolizumab plus chemotherapy followed by pembrolizumab arm than in the placebo plus chemotherapy followed by placebo arm. More patients discontinued treatment due to an AE in the pembrolizumab plus chemotherapy followed by pembrolizumab arm than in the placebo plus chemotherapy followed by placebo arm. Table 28 summarizes AEs occurring in at least 10% of patients receiving pembrolizumab plus chemotherapy followed by pembrolizumab and placebo plus chemotherapy followed by placebo in the KEYNOTE-522 trial.10
Figure 15: Empirical Mean Change From Adjuvant Baseline in EQ VAS Across Time—FAS Population
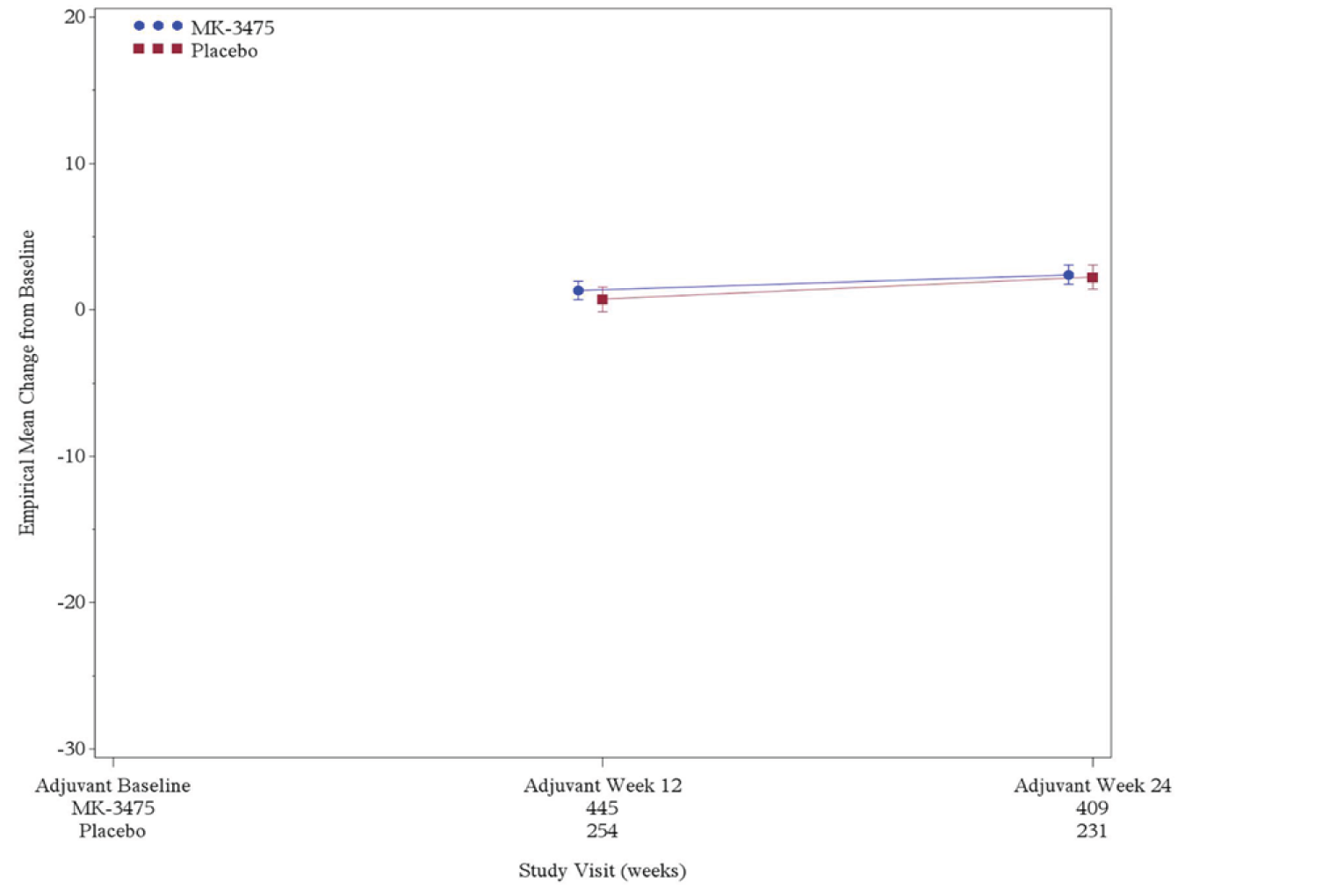
EQ VAS = EQ Visual Analogue Scale; FAS = full analysis set; MK-3475 = pembrolizumab.
Note: Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Table 27: Summary of Adverse Events Occurring in the Combined Neoadjuvant and Adjuvant phase at IA4—APaT Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab (N = 783) | Placebo plus chemotherapy followed by placebo (N = 389) |
|---|---|---|
One or more adverse events, n (%) | 777 (99.2) | 389 (100.0) |
Toxicity grade 3 to 5 adverse events, n (%) | 645 (82.4) | 306 (78.7) |
Serious adverse events, n (%) | 341 (43.6) | 111 (28.5) |
Any dose modificationa due to an adverse event, n (%) | 644 (82.2) | 306 (78.7) |
Pembrolizumab or placebo | 530 (67.7) | 239 (61.4) |
Paclitaxel | 517 (66) | 248 (63.8) |
Carboplatin | 434 (55.4) | 201 (51.7) |
Doxorubicin | 157 (20.1) | 81 (20.8) |
Epirubicin | 82 (10.5) | 40 (10.3) |
Cyclophosphamide | 232 (29.6) | 119 (30.6) |
Died, n (%) | 7 (0.9) | 1 (0.3) |
Discontinued any drug due to an adverse event, n (%) | 234 (29.9) | 60 (15.4) |
Pembrolizumab or placebo | 157 (20.1) | 31 (8) |
Paclitaxel | 82 (10.5) | 26 (6.7) |
Carboplatin | 76 (9.7) | 12 (3.1) |
Doxorubicin | 26 (3.3) | 8 (2.1) |
Epirubicin | 16 (2) | 4 (1) |
Cyclophosphamide | 41 (5.2) | 12 (3.1) |
Discontinued any drug due to a serious adverse event, n (%) | 94 (12) | 15 (3.9) |
Pembrolizumab or placebo | 81 (10.3) | 14 (3.6) |
Paclitaxel | 23 (2.9) | 1 (0.3) |
Carboplatin | 22 (2.8) | 0 (0) |
Doxorubicin | 18 (2.3) | 3 (0.8) |
Epirubicin | 7 (0.9) | 3 (0.8) |
Cyclophosphamide | 24 (3.1) | 6 (1.5) |
APaT = all participants as treated; IA = interim analysis.
Note: Included adverse events starting from the first treatment including definitive surgery and radiation therapy and up to 30 days after the last treatment including definitive surgery and radiation therapy for the nonserious adverse events and up to 90 days after the last treatment including definitive surgery and radiation therapy for the serious adverse events. Medical Dictionary for Regulatory Activities–preferred terms “neoplasm progression,” “malignant neoplasm progression,” and “disease progression” not related to the drug are excluded. Data cut-off date: March 23, 2021.
aDefined as an action taken of dose reduced, drug interrupted, or drug withdrawn. Grades are based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 4.0.
Source: Clinical Study Report.10
Table 28: Summary of Adverse Events Occurring in at Least 10% of Patients in the Combined Neoadjuvant and Adjuvant phases at IA4—APaT Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab (N = 783) | Placebo plus chemotherapy followed by placebo (N = 389) |
|---|---|---|
One or more adverse events, n (%) | 777 (99.2) | 389 (100) |
Nausea | 522 (66.7) | 257 (66.1) |
Alopecia | 477 (60.9) | 226 (58.1) |
Anemia | 463 (59.1) | 229 (58.9) |
Neutropenia | 376 (48) | 190 (48.8) |
Fatigue | 365 (46.6) | 168 (43.2) |
Constipation | 328 (41.9) | 150 (38.6) |
Diarrhea | 318 (40.6) | 133 (34.2) |
Vomiting | 244 (31.2) | 108 (27.8) |
Headache | 234 (29.9) | 113 (29) |
Alanine aminotransferase increased | 238 (30.4) | 108 (27.8) |
Arthralgia | 225 (28.7) | 120 (30.8) |
Asthenia | 219 (28) | 111 (28.5) |
Rash | 234 (29.9) | 92 (23.7) |
Neutrophil count decreased | 191 (24.4) | 113 (29) |
Pyrexia | 221 (28.2) | 72 (18.5) |
Cough | 193 (24.6) | 86 (22.1) |
Aspartate aminotransferase increased | 187 (23.9) | 77 (19.8) |
Neuropathy peripheral | 163 (20.8) | 90 (23.1) |
Decreased appetite | 178 (22.7) | 65 (16.7) |
Insomnia | 161 (20.6) | 74 (19) |
Peripheral sensory neuropathy | 156 (19.9) | 72 (18.5) |
Myalgia | 153 (19.5) | 73 (18.8) |
Febrile neutropenia | 151 (19.3) | 66 (17) |
Pruritus | 147 (18.8) | 56 (14.4) |
Stomatitis | 141 (18) | 58 (14.9) |
Radiation skin injury | 114 (14.6) | 73 (18.8) |
Hot flush | 117 (14.9) | 69 (17.7) |
Urinary tract infection | 123 (15.7) | 62 (15.9) |
Epistaxis | 117 (14.9) | 63 (16.2) |
Dizziness | 118 (15.1) | 60 (15.4) |
Thrombocytopenia | 110 (14) | 68 (17.5) |
Dysgeusia | 128 (16.3) | 49 (12.6) |
White blood cell count decreased | 113 (14.4) | 56 (14.4) |
Dyspepsia | 111 (14.2) | 56 (14.4) |
Abdominal pain | 112 (14.3) | 49 (12.6) |
Mucosal inflammation | 112 (14.3) | 49 (12.6) |
Back pain | 97 (12.4) | 63 (16.2) |
Upper respiratory tract infection | 106 (13.5) | 47 (12.1) |
Dyspnea | 99 (12.6) | 50 (12.9) |
Leukopenia | 98 (12.5) | 51 (13.1) |
Hypothyroidism | 118 (15.1) | 22 (5.7) |
Pain in extremity | 91 (11.6) | 49 (12.6) |
Erythema | 81 (10.3) | 36 (9.3) |
Nasopharyngitis | 65 (8.3) | 52 (13.4) |
Platelet count decreased | 78 (10) | 37 (9.5) |
Abdominal pain upper | 80 (10.2) | 34 (8.7) |
Hypokalemia | 88 (11.2) | 24 (6.2) |
Bone pain | 70 (8.9) | 39 (10) |
Breast pain | 64 (8.2) | 43 (11.1) |
Infusion-related reaction | 79 (10.1) | 27 (6.9) |
Gastroesophageal reflux disease | 57 (7.3) | 43 (11.1) |
APaT = all participants as treated; IA = interim analysis.
Note: Every participant is counted a single time for each applicable specific adverse event. A specific adverse event appears in this report only if its incidence in 1 or more of the columns meets the incidence criterion in the report title, after rounding. Included are adverse events starting from the first treatment including definitive surgery and radiation therapy and up to 30 days after the last treatment including definitive surgery and radiation therapy for the nonserious adverse events and up to 90 days after the last treatment including definitive surgery and radiation therapy for the serious adverse events. Medical Dictionary for Regulatory Activities–preferred terms “neoplasm progression,” “malignant neoplasm progression,” and “disease progression” not related to the drug are excluded. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Grade 3 to 5 Adverse Events
The incidence of grade 3 to 5 AEs reported in at least 5% of patients in either treatment group by the IA4 data cut-off (March 23, 2021) are presented in Table 29. The overall incidence of grade 3 to 5 AEs during the combined phases was similar in the 2 treatment arms (82.4% of patients receiving pembrolizumab plus chemotherapy followed by pembrolizumab versus 78.7% receiving placebo plus chemotherapy followed by placebo). The most frequent grade 3 to 5 AEs (occurring in ≥ 5% of patients in either arm) reported in both arms included neutropenia, decreased neutrophil count, anemia, febrile neutropenia, and decreased white blood cell count. In the pembrolizumab plus chemotherapy followed by pembrolizumab arm, the incidence of increased ALT (6.4%) was higher than in the placebo plus chemotherapy followed by placebo arm (2.8%).10
Mortality
By the March 23, 2021, data cut-off, deaths due to AEs, other than “neoplasm progression,” “malignant neoplasm progression,” and “disease progression,” were included in the frequency counts for fatal AEs.
The overall incidence of AEs resulting in death in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (0.9%) was consistent with the placebo plus chemotherapy followed by placebo arm (0.3%). Table 30 summarizes AEs resulting in death reported in patients receiving either study treatment.10
Table 29: Grade 3 to 5 Adverse Events Occurring in at Least 5% of Patients in the Combined Neoadjuvant and Adjuvant phases at IA4—APaT Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab (N = 783) | Placebo plus chemotherapy followed by placebo (N = 389) |
|---|---|---|
One or more grade 3 to 5 adverse events, n (%) | 645 (82.4) | 306 (78.7) |
Neutropenia | 276 (35.2) | 134 (34.4) |
Neutrophil count decreased | 149 (19) | 92 (23.7) |
Anemia | 153 (19.5) | 61 (15.7) |
Febrile neutropenia | 144 (18.4) | 63 (16.2) |
White blood cell count decreased | 61 (7.8) | 21 (5.4) |
Alanine aminotransferase increased | 50 (6.4) | 11 (2.8) |
APaT = all participants as treated; IA = interim analysis.
Note: Every participant is counted a single time for each applicable specific adverse event. A specific adverse event appears in this report only if its incidence in 1 or more of the columns meets the incidence criterion in the report title, after rounding. Included are adverse events starting from the first treatment including definitive surgery and radiation therapy and up to 30 days after the last treatment including definitive surgery and radiation therapy for the nonserious adverse events and up to 90 days after the last treatment including definitive surgery and radiation therapy for the serious adverse events. Grades are based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 4.0. Medical Dictionary for Regulatory Activities–preferred terms “neoplasm progression,” “malignant neoplasm progression,” and “disease progression” not related to the drug are excluded. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Table 30: Deaths due to AEs Occurring in Patients in the Combined Neoadjuvant and Adjuvant phases at IA4—APaT Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab (N = 783) | Placebo plus chemotherapy followed by placebo (N = 389) |
|---|---|---|
One or more deaths due to adverse events, n (%) | 7 (0.9) | 1 (0.3) |
Death | 1 (0.1) | 0 (0.0) |
Encephalitis autoimmune | 1 (0.1) | 0 (0.0) |
Multiple organ dysfunction syndrome | 1 (0.1) | 0 (0.0) |
Myocardial infarction | 1 (0.1) | 0 (0.0) |
Pneumonia | 1 (0.1) | 0 (0.0) |
Pneumonitis | 1 (0.1) | 0 (0.0) |
Pulmonary embolism | 1 (0.1) | 0 (0.0) |
Sepsis | 1 (0.1) | 0 (0.0) |
Septic shock | 0 (0.0) | 1 (0.3) |
Shock | 1 (0.1) | 0 (0.0) |
AE = adverse event; APaT = all participants as treated; IA = interim analysis.
Note: Every participant is counted a single time for each applicable specific adverse event. Included are adverse events starting from the first treatment including definitive surgery and radiation therapy and up to 30 days after the last treatment including definitive surgery and radiation therapy for the nonserious adverse events and up to 90 days after the last treatment including definitive surgery and radiation therapy for the serious adverse events. Grades are based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 4.0. Medical Dictionary for Regulatory Activities–preferred terms “neoplasm progression,” “malignant neoplasm progression,” and “disease progression” not related to the drug are excluded. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Discontinuations due to Adverse Events
By the March 23, 2021, data cut-off, the overall incidence of AEs resulting in the discontinuation of any study intervention during the combined phases was higher in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (29.9%) than in the placebo plus chemotherapy followed by placebo arm (15.4%). The most frequently reported AEs (incidence ≥ 1%) resulting in discontinuation of any study intervention in the pembrolizumab plus chemotherapy followed by pembrolizumab arm were increased ALT (3.1%), neutropenia (2.0%), increased aspartate aminotransferase (1.8%), febrile neutropenia (1.5%), infusion-related reaction (1.3%), and peripheral neuropathy (1.0%). For the placebo plus chemotherapy followed by placebo arm, the most frequently reported AEs (incidence ≥ 1%) resulting in discontinuation of any study intervention were neutropenia (1.5%), peripheral neuropathy (1.3%), and increased ALT (1.3%).10 Discontinuations due to AEs were higher in the pembrolizumab plus chemotherapy followed by pembrolizumab arm than in the placebo plus chemotherapy followed by placebo arm.
Dose Reduction due to AEs
As no dose reductions were allowed for pembrolizumab (200 mg once every 3 weeks) or placebo; all dose reductions occurred in chemotherapy during the neoadjuvant phase. The overall incidences of AEs resulting in dose reduction of chemotherapy were generally similar between the pembrolizumab plus chemotherapy (12.8%) and placebo plus chemotherapy arms (11.3%). The most frequently reported AEs (incidence ≥ 1%) resulting in dose reduction of chemotherapy in the pembrolizumab plus chemotherapy followed by pembrolizumab arm were febrile neutropenia (3.3%), neutropenia (2.8%), and decreased neutrophil count (1.1%). For the placebo plus chemotherapy followed by placebo arm, the most frequently reported AEs (incidence ≥ 1%) resulting in dose reduction of chemotherapy were febrile neutropenia (2.6%), neutropenia (2.3%), and decreased neutrophil count (1.5%).10
Notable Harms
The overall incidence of notable harms identified during the combined phases was higher in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (43.6%) than in the placebo plus chemotherapy followed by placebo arm (21.9%). Table 31 presents a summary of the proportion of patients reporting AEs identified in the CADTH review protocol in the pembrolizumab plus chemotherapy followed by pembrolizumab arm versus the placebo plus chemotherapy followed by placebo arm.10
Table 31: Notable Harms Occurring in Patients in the Combined Neoadjuvant and Adjuvant phases at IA4—APaT Population
Category | Pembrolizumab plus chemotherapy followed by pembrolizumab (N = 783) | Placebo plus chemotherapy followed by placebo (N = 389) |
|---|---|---|
Patients in population with 1 or more adverse events, n (%) | 341 (43.6) | 85 (21.9) |
Grade 3 | 97 (12.4) | 8 (2.1) |
Grade 4 | 18 (2.3) | 0 (0) |
Grade 5 | 2 (0.3) | 0 (0) |
Adrenal insufficiency, n (%) | 20 (2.6) | 0 (0.0) |
Grade 3 | 7 (0.9) | 0 (0) |
Grade 4 | 1 (0.1) | 0 (0) |
Colitis, n (%) | 13 (1.7) | 3 (0.8) |
Autoimmune colitis (grade 3) | 1 (0.1) | 0 (0) |
Colitis, n (%) | 8 (1) | 3 (0.8) |
Grade 3 | 4 (0.5) | 1 (0.3) |
Grade 4 | 1 (0.1) | 0 (0) |
Encephalitis autoimmune, n (%) | 2 (0.3) | 0 (0) |
Grade 3 | 1 (0.1) | 0 (0) |
Grade 5 | 1 (0.1) | 0 (0) |
Hypothyroidism | 118 (15.1) | 22 (5.7) |
Grade 3 | 4 (0.5) | 0 (0) |
Infusion reactions, n (%) | 141 (18) | 45 (11.6) |
Anaphylactic reaction | 4 (0.5) | 3 (0.8) |
Grade 3 | 0 (0) | 1 (0.3) |
Grade 4 | 2 (0.3) | 0 (0) |
Cytokine release syndrome (grade 4) | 3 (0.4) | 0 (0) |
Drug hypersensitivity | 20 (2.6) | 8 (2.1) |
Grade 3 | 3 (0.4) | 1 (0.3) |
Hypersensitivity | 40 (5.1) | 10 (2.6) |
Grade 3 | 3 (0.4) | 1 (0.3) |
Infusion-related reaction | 79 (10.1) | 27 (6.9) |
Grade 3 | 9 (1.1) | 2 (0.5) |
Serum sickness (grade 3) | 1 (0.1) | 0 (0) |
Nephritis, n (%) | 7 (0.9) | 0 (0.0) |
Nephritis (grade 3) | 2 (0.3) | 0 (0) |
Tubulointerstitial nephritis | 4 (0.5) | 0 (0) |
Grade 3 | 3 (0.4) | 0 (0) |
Grade 4 | 1 (0.1) | 0 (0) |
Pneumonitis, n (%) | 17 (2.2) | 6 (1.5) |
Grade 3 | 6 (0.8) | 2 (0.5) |
Grade 5 | 1 (0.1) | 0 (0) |
Severe skin reactions, n (%) | 45 (5.7) | 4 (1) |
Dermatitis bullous | 5 (0.6) | 1 (0.3) |
Grade 3 | 1 (0.1) | 0 (0) |
Dermatitis exfoliative generalized | 3 (0.4) | 1 (0.3) |
Grade 3 | 1 (0.1) | 0 (0) |
Erythema multiforme | 5 (0.6) | 1 (0.3) |
Grade 3 | 1 (0.1) | 0 (0) |
Grade 4 | 1 (0.1) | 0 (0) |
Pruritus (grade 3) | 2 (0.3) | 0 (0) |
Rash (grade 3) | 14 (1.8) | 1 (0.3) |
Rash maculopapular (grade 3) | 15 (1.9) | 0 (0) |
Rash pustular (grade 3) | 1 (0.1) | 0 (0) |
Stevens-Johnson syndrome (grade 4) | 1 (0.1) | 0 (0) |
Toxic skin eruption (grade 3) | 1 (0.1) | 0 (0) |
Type 1 diabetes mellitus, n (%) | 4 (0.5) | 0 (0.3) |
Diabetic ketoacidosis (grade 4) | 1 (0.1) | 0 (0) |
Type 1 diabetes mellitus | 3 (0.4) | 0 (0) |
Grade 3 | 2 (0.3) | 0 (0) |
Grade 4 | 1 (0.1) | 0 (0) |
APaT = all participants as treated; IA = interim analysis.
Note: Every participant is counted a single time for each applicable specific adverse event. A participant with multiple adverse events within a bolded term is counted a single time for that bolded term. “Infusion-related reaction” includes infusion-related reactions due to pembrolizumab and chemotherapy, for example paclitaxel.
Included are adverse events starting from the first treatment including definitive surgery and radiation therapy and up to 30 days after the last treatment including definitive surgery and radiation therapy for the nonserious adverse events and up to 90 days after the last treatment including definitive surgery and radiation therapy for the serious adverse events. Data cut-off date: March 23, 2021.
Source: Clinical Study Report.10
Critical Appraisal
Internal Validity
KEYNOTE-522 is a randomized, double-blind, placebo-controlled, phase III study. A 2:1 randomization scheme was implemented centrally using an interactive voice response system–integrated web response system, stratified by 3 factors: nodal status (positive versus negative), tumour size (T1/T2 versus T3/T4), and choice of carboplatin regimen (every 3 weeks versus weekly). The baseline and demographic characteristics of patients were well balanced between the 2 groups, and the risk of selection bias was considered low.
Patients, investigators, and pathologists were blinded to the treatment regimens in the KEYNOTE-522 trial. The preparation and dispensing of pembrolizumab and placebo was performed by an unblinded member of the trial site personnel who was not involved in trial assessments. The incidence of AEs, particularly immune-related reactions resulting from the use of pembrolizumab, may have revealed the treatments administered to patients and investigators. However, how often this may have occurred is uncertain. More patients (24.2%) receiving pembrolizumab plus chemotherapy in the neoadjuvant phase had discontinued the study intervention than had patients receiving placebo plus chemotherapy (14.9%). The most common cause of discontinuations was AEs. Most discontinuations in the neoadjuvant phase for patients receiving pembrolizumab plus chemotherapy treatment were due to AEs (14.3%), physician decision (4.1%), and patient withdrawal from study (3.7%). Similarly, more patients receiving pembrolizumab discontinued in the adjuvant phase than did patients receiving placebo. The most common reasons for discontinuations in patients receiving pembrolizumab were AEs (5.4%), relapse or recurrence (2.6%), and patient withdrawal (2.8%). Safety outcomes may have been overestimated in patients receiving pembrolizumab compared to patients receiving placebo. The extent and direction of bias due to treatment knowledge is uncertain.
Pathologists reviewing and interpreting specimens for pCR following surgery were blinded for treatment assessment. Event-free survival was assessed per RECIST 1.1 guidelines, which are validated for tumour assessments. The assessment of EFS may also have been influenced by treatment knowledge, given that it was assessed by investigator. However, the double-blind nature of the trial reduced the risk of assessment bias. In the case of unblinding, there is a potential for detection bias by the investigator that may impact the findings of EFS at assessment, likely favouring the pembrolizumab plus chemotherapy arm, although the extent of any bias is uncertain. There is also a potential risk of performance bias for other subjective outcomes, such as HRQoL and safety, although the direction and extent of any bias is uncertain.
Pathological complete response, EFS, OS, HRQoL, and safety outcomes were considered relevant according to the clinical experts consulted. Overall survival and pCR are validated outcomes for oncology trials, and EFS has been validated as a surrogate end point for accelerated or regular approval by regulatory agencies for trials in breast cancer.11,12,30,31 Censoring rules for EFS and sensitivity analyses were reported in the SAP. Crossing over from 1 study arm to the other was not permitted during the trial, which preserved treatment differences observed in the randomized arms for OS. A Cox proportional hazard model, which relies on the assumption of proportional hazard in both treatment groups was used to assess OS and EFS survival curves. The visual assessment of the Kaplan–Meier curve for EFS did not suggest any violation of the proportional hazard, suggesting that the EFS HRs were accurate, given that the ratio of HR was approximately constant throughout the trial. The visual assessment of the Kaplan–Meier curve for OS suggests that the proportional hazard assumption may have been violated at given points (at 15.5 months and meet at 22 months) where both curves crossed in the trial. The violation of the proportional hazard assumption in the OS curves adds uncertainty to the interpretation of the OS HR finding reported at IA4 since it differs over time throughout the trial. In addition, the median OS and EFS was not estimable at IA4 due to data immaturity, which adds uncertainty to the findings observed.
Health-related QoL was assessed using the EORTC QLQ-C30, the EORTC QLQ-BR23, and the EQ-5D-5L questionnaire. The EORTC QLQ-C30 is a cancer-specific instrument that has been validated in many cancer populations. The EORTC QLQ-BR23 is a modified version designed for breast cancer patients. These questionnaires were considered validated in patients with TNBC. Health-related QoL reporting is subjective, and there is always a potential for unblinding; however, the risk of performance bias is low. Because the EORTC QLQ-BR23 is more tailored to breast cancer patients, it focuses on identifying treatment-related side effects. Construct validity was assessed, and minimal important differences (MIDs) were derived using anchor-based approaches. Approximately 20% of patients had missing data at follow-up for HRQoL measures. The sponsor described methods to address missing data for HRQoL. These methods were considered appropriate but conservative by the CADTH review team. Thus, there remains a potential for attrition bias, which introduces uncertainty into the findings given that many patients who received pembrolizumab plus chemotherapy in the neoadjuvant setting discontinued (the majority due to AEs) and did not receive treatment in the adjuvant phase. In addition, multiplicity adjustments were not conducted to account for the type I error rate, so the findings were considered exploratory (hence, conclusions could not be drawn).
The study was powered to detect a true pCR rate of 15% between pembrolizumab plus chemotherapy versus placebo plus chemotherapy at an alpha level of 0.5% (1 sided), with an underlying assumption of a pCR rate of 50% in the placebo plus chemotherapy arm. The clinical experts considered the effect size clinically meaningful. The study was also powered to detect a true HR of 0.71 between pembrolizumab plus chemotherapy versus placebo plus chemotherapy for EFS at an alpha level of 2% (1 sided). The sponsor provided a rationale for the margins defined for pCR and EFS in the SAP. The clinical experts considered the pre-specified HR between the 2 study arms clinically meaningful.
There was a low risk of bias due to selective reporting as all the outcomes pre-specified in the protocol were reported. All IAs were pre-specified in the protocol, and stopping rules were adequately outlined in the SAP. The approaches used to preserve alpha and the power in the IAs were considered appropriate. Efficacy analyses were conducted using the ITT populations, which maintains randomization and minimizes the risk of bias that may be introduced by comparing groups that differ in prognostic factors. Health-related QoL analyses were based on the full analysis set. Interim analyses were planned and performed by an independent data monitoring committee.
The type I error rate was adjusted during the analyses of pCR, EFS, and OS using the overall family-wise error rate approach. Sensitivity analyses and adjustments for covariates were conducted for pCR and EFS, and the findings were consistent with the primary analysis of the ITT population. Pathological complete response assessed at IA4 was not formally tested based on the statistical hierarchy; thus, the findings at IA4 were considered exploratory.
All subgroup analyses were pre-specified in the protocol. The subgroup analyses may not have been powered to detect a difference between the 2 treatment arms. In addition, multiplicity adjustments were not conducted to account for the type I error rate; thus, the findings were considered exploratory. Some CIs observed in the analyses were imprecise and included the null value. There were also no between-group tests conducted for the subgroup analyses.
Protocol deviations and premature unblinding were reported for patients receiving either 1 of the study treatments in the KEYNOTE-522 study (6.9% of patients experienced premature unblinding in total). The proportion of patients with significant protocol deviations was slightly higher in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (3.6%) than in the placebo plus chemotherapy followed by placebo arm (2.1%). The most common reasons were violation of inclusion criteria and patients being dispensed study interventions other than what was assigned in the trial schedule. Patients who had unblinded treatments continued to be monitored in the trial. Patients who were unblinded in both the neoadjuvant and adjuvant phases were required to end all study treatment and entered the early discontinuation phase; they were then followed for 6 months via phone.
The SAP outlined the methods used to account for missing data for the primary outcomes, secondary outcomes, and safety outcomes. The treatment duration for each treatment administered in the neoadjuvant setting was comparable in both arms since patients in both groups received similar treatment regimens of chemotherapy in addition to pembrolizumab or placebo. In the adjuvant phase, treatment duration did not differ as patients received pembrolizumab or placebo for a similar number of cycles.
External Validity
The reimbursement request is for the treatment of adult patients with early-stage TNBC in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery. The reimbursement request was submitted for CADTH review pre-NOC, and the request aligned with the proposed Health Canada indication.
KEYNOTE-522 was conducted in a multinational setting, with 194 sites in 21 countries (7 sites in Canada). The inclusion and exclusion criteria of KEYNOTE-522 were considered appropriate by the clinical experts. KEYNOTE-522 excluded patients who had received prior therapy (chemotherapy, radiation, or targeted therapy), patients with significant cardiovascular disease, and patients who had a history of pneumonitis or current pneumonitis. Thus, the magnitude of benefit of pembrolizumab plus chemotherapy to patients in real-world practice presenting with 1 or more characteristics identified in the exclusion criteria in the KEYNOTE-522 study is uncertain. In addition, more than 25% of patients screened in the KEYNOTE-522 trial were not enrolled, suggesting that the participants in the trial may not be fully representative of the patient population in real-world settings. The experts highlighted that in current practice, patients are not routinely required to have a left ventricular ejection fraction of at least 50% or greater than or equal to the institution lower limit of normal as assessed by echocardiogram or multigated acquisition scan to be eligible to receive treatment. Both experts agreed that they would not offer pembrolizumab to patients with an ECOG PS of 3 or greater. However, the experts noted that they would offer pembrolizumab to patients with an ECOG PS of 2, while considering factors such as comorbidities. The clinical experts considered the baseline characteristics generalizable to patients in the Canadian setting.
The dosage of pembrolizumab aligns with the Health Canada NOC indication. Dose modifications were allowed for all study drugs used in the KEYNOTE-522 trial, except pembrolizumab (it was recommended that pembrolizumab be withheld in case of drug-related toxicities), and outlined in the protocol. The clinical experts considered the chemotherapy regimens administered during the trial appropriate and reflective of Canadian practice. However, the clinical experts noted that some dose and cycle schedules implemented in the KEYNOTE-522 study were different from Canadian practice. The experts noted that carboplatin and paclitaxel cycles were administered before the doxorubicin and cyclophosphamide cycles in the KEYNOTE-522 study, which is the opposite order to some jurisdictions in Canadian practice. The experts highlighted that clinicians may maintain an anthracycline plus cyclophosphamide plus taxane schedule, or they may switch the sequence to taxanes and carboplatin first and then anthracycline-cyclophosphamide to correspond to the administration implemented in KEYNOTE-522. The sponsor-submitted indication states that pembrolizumab in combination with chemotherapy is recommended for high-risk patients with early-stage TNBC. The sponsor did not specify the chemotherapy regimen in the indication. It is therefore uncertain whether the addition of pembrolizumab to chemotherapy agents not used in the KEYNOTE-522 trial will result in similar benefits as those seen for the chemotherapy agents (including dosing and cycles of administration) used in the KEYNOTE-522 trial.
The clinical experts agreed that dose adjustments anticipated in practice would be similar to those implemented in the KEYNOTE-522 trial. The clinical experts also highlighted that drug discontinuations are expected in practice, although clinicians will generally encourage patients to complete all cycles of chemotherapy by implementing dose reductions in situations of toxicity.
The clinical experts noted that the choice of NACT used in the KEYNOTE-522 study was appropriate and reflective of treatments administered in neoadjuvant setting. The clinician group input from the Drug Advisory Committee of the OH-CCO noted that capecitabine and olaparib (for patients with a BRCA1 or 2 mutation) are currently available for patients in the adjuvant setting in Canada. The clinical experts consulted indicated that, since the publication of CREATE-X, capecitabine has been employed as a standard adjuvant option in TNBC if there is no pCR.32 The clinical experts stated that at the time of trial initiation, the CREATE-X study had not been published and so capecitabine would not have been considered as comparator, and the use of olaparib in patients with a BRCA1 or 2 mutation in the adjuvant setting is recent (reported in 2021).33 Thus, the use of placebo in the adjuvant setting was considered appropriate in the absence of the standard of care therapies highlighted. The Drug Advisory Committee of OH-CCO indicated that it is unclear how pembrolizumab will fit with capecitabine or Olaparib given that capecitabine was not allowed in the KEYNOTE-522 trial. The clinician group highlighted uncertainty associated with choosing the best-suited drug in the adjuvant setting owing to lack of evidence relating to combining the agents or the comparative efficacy of the agents in the patient population.
The clinical experts considered the duration of follow-up implemented in the KEYNOTE-522 study appropriate. The clinical experts noted that the concomitant medications allowed in the KEYNOTE-522 study were also commonly used in Canadian practice. The experts did not identify any major concerns or discrepancies between the trial and real-world settings in terms of concomitant medication use and duration of follow-up.
Pathological complete response, EFS, and OS are validated outcomes recommended by regulatory agencies for trials that include patients with TNBC. The clinical experts considered the outcomes important for patients with TNBC in Canadian practice.
Concomitant medications commonly used by patients in the trial were generally considered appropriate by the clinical experts consulted.
Some patients in the KEYNOTE-522 study were possibly exposed to frequent assessments compared to patients in real-world practice. This may impact the generalizability of the findings to patients in real-world practice. Both the clinical experts and clinician groups consulted indicated that patients in real-world practice are assessed before every cycle of treatment (physical and clinical exams conducted) and that frequent breast scans and MRIs are not routine in practice.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
Direct head-to-head clinical trials assessing pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared to other treatments for adult patients with early-stage TNBC are limited. Indirect evidence was considered and summarized for this review to address the lack of direct evidence for relevant comparators.
The sponsor did not provide any indirect evidence for this review. A focused literature search for NMAs dealing with TNBC was run in MEDLINE All (1946–) on March 8, 2022. No search limits were applied. Indirect treatment comparisons were selected for full-text review using the same criteria as for the systematic review (Table 5). Two published NMAs were identified from the NMA literature search and reviewed (Miyashita et al. [2020]13 and Li et al. [2022]34). The published NMA by Li et al.34 was excluded because the results were limited to a ranking of comparisons (pairwise comparisons between pembrolizumab and other active treatments were not available). In total, 1 published NMA, by Miyashita et al. (2020),13 was summarized for this review.
Description and Methods of Published NMA
Objectives
The objective of the published NMA was to define the overall most effective neoadjuvant systemic therapy for TNBC by comparing the efficacy and safety of different regimens containing anthracycline, bevacizumab, pembrolizumab, and platinum salts in patients with TNBC.
Study Selection Methods
The authors performed a systematic review to select studies for inclusion in the NMA. Eligible studies included patients with TNBC who received neoadjuvant treatment that included different combinations of medications of special interest (anthracycline, bevacizumab, pembrolizumab, or platinum salts) or chemotherapy without the medications of special interest. The dosing of these interventions was not specified. Outcomes of interest included the rate of pCR (defined as ypT0/is and ypN0) or toxicities, specifically febrile neutropenia, grade 3 or greater thrombocytopenia, nausea/vomiting, and diarrhea. The systematic review only included RCTs and did not report any additional criteria regarding the study design.
The literature search was conducted in March 2020 using MEDLINE, Embase, and Web of Science and supplemented by manual searches of secondary sources including references of initially identified articles and reviews. Articles were screened and selected independently by 2 reviewers. A third author was consulted to resolve any discrepancies between the 2 reviewers. Information about the data extraction process was not reported.
The Cochrane risk of bias tool (version 1)35 was used to assess the risk of bias in the RCTs included in the NMA. The risk of bias was indicated by labelling RCTs as having high, low, or unclear risk of bias. Studies were not excluded based on the risk of bias. A quality assessment of included studies was not reported.
Published NMA Analysis Methods
Information about the statistical model selected for the NMA was limited. The authors reported that a random effects model was used for the NMA. Heterogeneity within the network was estimated using the I2 statistic, where an I2 value greater than 50% was considered an indicator of substantial heterogeneity. Inconsistency was evaluated using Q statistics.
No further information regarding the NMA methods or assessment of heterogeneity or inconsistency was provided.
No sensitivity analyses were reported. Some of the trials included patients with and without TNBC. In these trials, patients with TNBC were equally randomized across groups and were investigated in subgroup analyses for the pCR outcome. Only patients with TNBC were included in the analysis of pCR in the NMA. All patients, regardless of diagnosis, were included in the analysis of safety outcomes.
Interventions of included trials were grouped into 8 categories corresponding to the therapies involved, representing up to 8 treatment nodes in each of the analyses. The categories (treatment nodes) were as follows:
anthracycline
anthracycline plus bevacizumab
anthracycline plus B plus platinum salts
anthracycline plus pembrolizumab
anthracycline plus platinum salts
anthracycline plus pembrolizumab plus platinum salts
not a medication of special interest to the published NMA
platinum salts.
The anthracycline plus pembrolizumab plus platinum salts category included evidence from 1 trial for 1 treatment, which was the intervention of interest to this review (pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy).
Results of Published NMA
Summary of Included Studies
A total of 1,476 articles were identified in the systematic review, 673 of which were assessed for eligibility. Thirteen RCTs were included in the NMA. The eligible studies included a total of 3,008 patients with TNBC, with the number of patients included in each study ranging from 49 to 602. The published NMA reported a summary of the main characteristics of the trial included in the NMA (refer to publication for characteristics of included trials13). This summary included the publication year, treatment regimens, study design, number of patients, age of patients, stage of cancer, and definition of TNBC used. Additional information about the included studies was not reported. The year of publication ranged from 2012 to 2020. Most of the trials were open label (92%) and multi-centre (77%). The pivotal trial for pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy was the only double-blind trial included in the NMA. The authors of the published NMA reported that the age and stage of patients and the definition of TNBC that was used were similar among the included trials.
Most of the studies included in the NMA had a high risk of bias due to inadequate blinding (> 75%), and approximately half the studies had a high risk of bias due to the inadequate random sequence generation and/or allocation concealment. Additionally, some of the studies were at a high risk of bias due to selective reporting (< 25%), incomplete outcome data (< 25%), and other sources of bias (< 25%).
Results
The analysis of pCR, febrile neutropenia, nausea/vomiting, and diarrhea include 19, 15, 17, and 14 comparisons, respectively. The analysis of thrombocytopenia did not include the treatments that include the anthracycline plus pembrolizumab plus platinum salts treatment node; the reason for this was not reported. The anthracycline plus pembrolizumab plus platinum salts node was connected to the networks through the anthracycline plus pembrolizumab node. Please refer to the publication for a graphical depiction of the evidence networks.13
A summary of the results for the comparison of treatments that include anthracycline plus pembrolizumab plus platinum salts in terms of rate of pCR, febrile neutropenia, grade 3 or greater nausea/vomiting, and grade 3 or greater diarrhea is provided in Table 32. The relative risks for pCR and harms for relevant comparators relative to anthracycline plus pembrolizumab plus platinum salts are shown. The authors reported that the NMAs did not exhibit significant heterogeneity or inconsistency based on the I2 and Q statistics.
Table 32: Results for Comparisons of Treatment to Anthracycline Plus Pembrolizumab Plus Platinum Salts, Miyashita et al. (2020) NMA
Outcome or treatment | Rate of pCR | Rate of febrile neutropenia | Rate of grade 3+ nausea/vomiting | Rate of grade 3+ diarrhea |
|---|---|---|---|---|
Relative risk (95% CI) | Relative risk (95% CI) | Relative risk (95% CI) | Relative risk (95% CI) | |
Number of studies (patients), model | 13 studies (3,008), RE model | NR (NR), RE model | NR (NR), RE model | NR (NR), RE model |
Anthracycline | 0.58 (0.43 to 0.77) | 0.53 (0.33 to 0.86) | 0.45 (0.15 to 1.34) | 0.38 (0.09 to 1.57) |
Anthracycline plus pembrolizumab | 1.52 (0.83 to 2.77) | 0.64 (0.23 to 1.83) | — | — |
Anthracycline plus platinum salts | 0.79 (0.63 to 0.99) | 0.83 (0.60 to 1.14) | 0.46 (0.19 to 1.12) | 0.59 (0.22 to 1.59) |
Platinum salts | 1.07 (0.57 to 2.01) | 0.24 (0.01 to 4.80) | 0.17 (0.02 to 1.31) | 0.06 (0.00 to 2.18) |
Comment | No significant heterogeneity (I2 = 18.7%; P = 0.15) or inconsistency (P = 0.58) | No significant heterogeneity (I2 = 0%; P = 0.48) or inconsistency (P = 0.55) | No significant heterogeneity (I2 = 0%; P = 0.97) or inconsistency (P = 0.91) | No significant heterogeneity (I2 = 0%; P = 0.72) or inconsistency (P = 0.91) |
CI = confidence interval; NA = not applicable; NMA = network meta-analysis; NR = not reported; pCR = pathological complete response; RE = random effects.
Source: Miyashita et al. (2020).13
The analysis of the rate of pCR suggested a higher rate of pCR for anthracycline plus pembrolizumab plus platinum salts relative to anthracycline (relative risk = 0.58; 95% CI, 0.43 to 0.77) and anthracycline plus platinum salts (relative risk = 0.79; 95% CI, 0.63 to 0.99). Conclusions could not be drawn for comparisons with anthracycline plus pembrolizumab or with platinum salts alone due to serious imprecision in the effect estimates.
The analysis of the rate of febrile neutropenia suggested a higher rate of febrile neutropenia for anthracycline plus pembrolizumab plus platinum salts when compared to anthracycline (relative risk = 0.53; 95% CI, 0.33 to 0.86). Conclusions could not be drawn for comparisons with anthracycline plus pembrolizumab, anthracycline plus platinum salts, or platinum salts alone due to serious imprecision in the effect estimates.
Regarding the analysis of the rate of grade 3 or greater nausea/vomiting, conclusions could not be drawn for comparisons with anthracycline alone or in combination platinum salts, or with platinum salts alone, due to serious imprecision in the effect estimates. A comparison to anthracycline plus pembrolizumab was not included in this analysis.
No conclusions could be drawn for comparisons within the analysis of the rate of grade 3 or greater diarrhea due to serious imprecision in the effect estimates.
Critical Appraisal of Published NMA
The NMA by Miyashita et al. (2020) was associated with a number of limitations due to the lack of important details about the included trials and methodology used to perform the NMA. The systematic review informing the NMA was limited to RCTs in which patients received treatment that included anthracycline, bevacizumab, pembrolizumab, or platinum salts, which did not capture studies of comparisons to some of the treatments of interest to this review. The trials that were included and informed the NMA were at high risk of bias, particularly due to blinding, randomization, and/or allocation concealment. The authors did not report on potential effect modifiers, and few characteristics of the included trials were reported. The authors stated that the age and stage of patients and the definition of TNBC that was used were similar among the included trials, but the assessment of potential effect modifiers did not extend beyond this. For example, no information was provided about dosage used, duration of follow-up, treatment duration, route of administration, or supportive care provided. Therefore, it is unclear whether the transitivity assumption was plausible (i.e., whether the trials were jointly randomizable). A statistical assessment of methodological heterogeneity was performed using the I2 statistic, which did not indicate significant heterogeneity in any of the analyses. The Q statistics were used to evaluate inconsistency. Additional information about the assessment of inconsistency was not provided. As tests for inconsistency have low power and may fail to detect inconsistency or incoherence, the absence of statistically significant inconsistency is not evidence for the absence of inconsistency. As a result, consistency in the networks is uncertain. No information was provided about an assessment of model fit, and no justification for the use of a random effects model was provided. Additional information about the statistical model used for the NMA was not reported; therefore, its appropriateness is uncertain.
The NMA was constructed using nodes that related to the interventions of interest to the published NMA (i.e., anthracycline, bevacizumab, pembrolizumab, and platinum salts). In doing so, the network did not account for differences in dose intensity or the administration schedule, and it combined different medications within the same node. Further, the NMA was focused on the neoadjuvant treatment phase, so the results of the network do not inform comparisons of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy to other specific treatment options (i.e., the results are only applicable to the neoadjuvant treatment phase). In addition, details about the node construction were limited. For example, the number of studies and number of patients included in the analysis of toxicity outcomes were not clearly reported. No information was provided regarding the exclusion of treatments that include anthracycline plus pembrolizumab plus platinum salts from the NMA of the rate of grade 3 or greater thrombocytopenia.
The lack of information about the characteristics of the trials, the treatments included in the network, and the node construction also hinders the assessment of generalizability of the results of the NMA to treatments used for the treatment of TNBC in Canadian clinical practice.
Summary
One published NMA by Miyashita et al. (2020)13 was summarized for this review to supplement the assessment of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared to other treatments for adult patients with early-stage TNBC. The NMA included 13 articles and 3,008 patients with TNBC. The NMA grouped treatments based on the inclusion of anthracycline, bevacizumab, pembrolizumab, and platinum salts and constructed the network based on these treatment groups (nodes). The analysis of the rate of pCR suggested a higher rate of pCR with treatments that include anthracycline plus pembrolizumab plus platinum salts relative to treatments that include anthracycline and treatments that include anthracycline plus platinum salts. The analysis of the rate of febrile neutropenia suggested a higher rate of febrile neutropenia with anthracycline plus pembrolizumab plus platinum salts compared to treatments that include anthracycline. The analysis of the rate of grade 3 or greater nausea/vomiting and the rate of grade 3 or greater diarrhea suggested no difference was observed between treatments . The results of the NMA published NMA by Miyashita et al. (2020) were associated with a number of limitations due to the lack of important details about the included trials and methodology used to perform the NMA. As such, there is low confidence in the results, and they should be interpreted with caution. Additionally, construction of treatment nodes used in the NMA preclude the ability to draw conclusions regarding comparisons of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy to other specific treatment options for TNBC.
Discussion
Summary of Available Evidence
The CADTH systematic review included 1 pivotal trial (KEYNOTE-522) submitted by the sponsor and 1 published NMA identified via the searches. Additional input from 2 patient groups, 2 clinician groups, and 2 clinician experts was also considered during the review.
KEYNOTE-522 is an ongoing, phase III, randomized, multi-centre, double-blind, placebo-controlled trial. The primary objective is to evaluate pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared with placebo plus chemotherapy as neoadjuvant therapy followed by continued placebo as adjuvant therapy for patients with high-risk, early-stage TNBC. KEYNOTE-522 was initiated in March 2017 with 194 participating centres across 21 countries in North America (7 centres in Canada), South America, Europe, Asia, and Australia.10
Enrolled patients were male or female; were 18 years and older; were newly diagnosed; had a locally advanced, centrally confirmed TNBC, as defined by the most recent ASCO–CAP guidelines; were previously untreated; and had a locally advanced nonmetastatic (M0) TNBC as per the current AJCC staging criteria for breast cancer assessed by an investigator based on radiological and/or clinical assessment (T1c, N1 to N2; T2 to T4d, N0 to N2). Patients were randomized in a 2:1 ratio into 1 of the 2 trial arms based on 3 stratification factors: nodal status (positive versus negative), tumour size (T1/T2 versus T3/T4), and choice of carboplatin regimen (every 3 weeks or weekly). Co-primary end points investigated in the KEYNOTE-522 trial were pCR rate (using the ypT0/Tis ypN0 definition) assessed by a local pathologist and EFS assessed by an investigator. Overall survival, HRQoL, and safety outcomes were some secondary and exploratory outcomes assessed in the trial.10 These outcomes were considered clinically meaningful by the clinical experts, clinician groups, and patient groups consulted during the CADTH review.
By the IA4 data cut-off (March 23, 2021), 1,608 patients had been screened and 1,174 were randomized to 1 of the 2 trial arms via a centralized interactive voice response system–integrated web response system. In total, 784 patients received pembrolizumab plus chemotherapy treatment followed by pembrolizumab, and 390 patients received placebo plus chemotherapy followed by placebo. The majority of the patients enrolled were female (1 man enrolled), were younger than 65 years, were White, were pre-menopausal, and had an ECOG PS of 0. More than 80% of patients randomized had PD-L1-positive status.10
Interpretation of Results
Efficacy
The CADTH review protocol identified OS, pCR, EFS, HRQoL, safety, and reduction in symptom severity as important outcomes for patients, clinicians, and drug plans. All outcomes (except symptom severity) were pre-specified in the KEYNOTE-522 protocol before the IA4 data cut-off (March 23, 2021), and the findings are presented in this review. The type I error rate was adequately accounted for during the analyses of EFS, OS, and pCR using the family-wise error rate. The stopping rules were presented in the SAP. Sensitivity analyses were conducted for EFS, and the results were consistent with the primary analyses. The HRQoL and subgroup analyses conducted were not controlled for multiple comparisons, so there is an increased risk of type I error; thus, conclusions could not be drawn for these outcomes.
The median OS was not estimable at the IA4 data cut-off (March 23, 2021) due to data immaturity, limiting the ability to draw conclusions for this outcome. The HR obtained in the comparison of pembrolizumab plus chemotherapy followed by pembrolizumab versus placebo plus chemotherapy followed by placebo was 0.72 (95% CI, 0.51 to 1.02). The final OS analysis is planned to take place alongside the final EFS analysis once a pre-specified number of events have accrued in both study arms.
The pCR rate was achieved at the IA1 data cut-off (September 21, 2018). The pCR rate was 64.8% (95% CI, 59.9% to 69.5%) in the pembrolizumab plus chemotherapy arm and 51.2% (95% CI, 44.1% to 58.3%) in the placebo plus chemotherapy arm. The percent difference estimated between pembrolizumab plus chemotherapy and placebo plus chemotherapy was 13.6% (95% CI, 5.4% to 21.8%; P [1 sided] = 0.00055). At IA2 (April 24, 2019), the treatment difference in pCR rate (pembrolizumab plus chemotherapy versus placebo plus chemotherapy) was 9.2% (95% CI, 2.8% to 15.6%; P = 0.00221). The pCR rate for pembrolizumab plus chemotherapy at the neoadjuvant phase was 64.0% (95% CI, 60.2% to 67.6%), compared to 54.7% (95% CI, 49.1% to 60.1%) for placebo plus chemotherapy. The pCR rate obtained at the IA4 data cut-off (March 23, 2021) was consistent with IA1, although not tested according to the statistical hierarchy. Thus, pCR rate findings at IA4 are considered exploratory. The clinical experts consulted during the review considered the pCR rate in the pembrolizumab plus chemotherapy arm clinically meaningful. Pathological complete response has been approved as a surrogate outcome for OS by different regulatory agencies, including the FDA.
Event-free survival was assessed as a co-primary outcome in the KEYNOTE-522 trial. Event-free survival has been validated by regulatory agencies, including the FDA, as an important outcome to be investigated in trials with patients with TNBC.11,12,30,31 The median EFS was not estimable at IA4 (March 23, 2021) due to data immaturity. The HR obtained in the comparison of the pembrolizumab plus chemotherapy followed by pembrolizumab arm versus the placebo plus chemotherapy followed by placebo arm was 0.63 (95% CI, 0.48 to 0.82). The clinical experts consulted considered the finding clinically meaningful. The number of patients with reported distant recurrence was 7.7% in the pembrolizumab plus chemotherapy followed by pembrolizumab arm, compared to 13.1% in the placebo plus chemotherapy followed by placebo arm. The clinical experts considered the findings clinically meaningful since distant recurrence implies metastatic disease.
The clinician and patient groups consulted during the CADTH review highlighted improvement in HRQoL as an important treatment goal for patients with early-stage TNBC. Health-related QoL was measured using 3 questionnaires (EORTC QLQ-C30, EORTC QLQBR23, and EQ-5D-5L). Because the analyses of HRQoL were not adjusted for multiple comparisons, conclusions could not be drawn for this outcome. The experts expressed that they expect decreases in HRQoL in practice in this curative setting.
All subgroup analyses were pre-specified before the interim data cut-offs; however, multiplicity adjustments were not conducted to adjust for alpha inflation. The findings were considered exploratory; thus, no definitive conclusions were made.
The KEYNOTE-522 study eligibility criteria included only patients with an ECOG PS of 0 or 1. As a result, the benefit and safety of pembrolizumab plus chemotherapy in the neoadjuvant setting followed by pembrolizumab in the adjuvant setting is unknown in patients with an ECOG PS greater than 1 in the real-world setting, particularly in patients with an ECOG PS of 2, who may be considered for therapy. The clinical experts consulted generally agreed that patients with early-stage TNBC with an ECOG PS of 2 would benefit from the treatment with pembrolizumab, although they would not consider patients with an ECOG PS of 3 or greater eligible to receive pembrolizumab treatment.
As highlighted by the clinical experts, anthracycline-taxane combination chemotherapy regimens are usually used to treat patients with early-stage TNBC, most commonly a dose-dense AC (doxorubicin, cyclophosphamide) every 2 weeks for 4 cycles followed by paclitaxel every 2 weeks for 4 cycles, with carboplatin often added. The experts also noted that pCR is a widely accepted goal for neoadjuvant therapy, and these chemotherapy agents are all supported by international guidelines. When carboplatin is added, it can be weekly for 12 cycles or every 3 weeks for 4 cycles. The experts also noted that patients with a BRCA1- or 2-positive mutation may likely receive olaparib in the adjuvant setting based on the results obtained in the OLYMPIA study. The experts noted that in the KEYNOTE-522 trial, carboplatin and paclitaxel cycles were administered before the doxorubicin and cyclophosphamide cycles, which is the opposite order to standard practice in Canada. They further highlighted that most clinicians will likely adhere to anthracycline-cyclophosphamide-taxane; however, they may switch the sequence to taxane and carboplatin first, and then anthracycline, to correspond to the treatment administration of the KEYNOTE-522 trial.
One published NMA by Miyashita et al. (2020)13 was summarized for this review to supplement the assessment of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared to other treatments for adult patients with early-stage TNBC. The NMA included 13 articles and 3,008 patients with TNBC. The NMA grouped treatments based on the inclusion of anthracycline, bevacizumab, pembrolizumab, and platinum salts and constructed the network based on these treatment groups (nodes). The analysis of the rate of pCR suggested a higher rate of pCR with treatments that include anthracycline plus pembrolizumab plus platinum salts relative to treatments that include anthracycline and treatments that included anthracycline plus platinum salts.
Harms
Overall, almost all patients enrolled in both study arms of KEYNOTE-522 (99.2% in the pembrolizumab plus chemotherapy followed by pembrolizumab arm and 100.0% in the placebo plus chemotherapy followed by placebo arm) reported at least 1 AE by the IA4 (March 23, 2021) data cut-off. Adverse events of grade 3 or greater were slightly higher in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (82.4%) than in the placebo plus chemotherapy followed by placebo arm (78.7%). The most common AEs in both arms were nausea, alopecia, anemia, and neutropenia.10 There were more serious AEs reported in patients receiving pembrolizumab plus chemotherapy followed by pembrolizumab (approximately 15% more) than in patients receiving placebo plus chemotherapy followed by placebo.
Adverse events of grade 3 to 5 commonly reported in at least 5% of patients were generally similar in both treatment arms. These AEs included neutropenia (35.2% versus 34.4%), decreased neutrophil count (19% versus 23.7%), anemia (19.5% versus 15.7%), febrile neutropenia (18.4% versus 16.2%), and decreased white blood cell count (6.4% versus 2.8%) in the pembrolizumab plus chemotherapy followed by pembrolizumab arm and the placebo plus chemotherapy followed by placebo arm, respectively. Overall, AEs resulting in death in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (0.9%) were consistent with the placebo plus chemotherapy followed by placebo arm (0.3%). Adverse events leading to discontinuation of any study intervention in the combined neoadjuvant and adjuvant phases were higher in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (29.9%) than in the placebo plus chemotherapy followed by placebo arm (15.4%). Overall, the incidence of AEs leading to dose reduction of chemotherapy was generally similar between the pembrolizumab plus chemotherapy (12.8%) and the placebo plus chemotherapy (11.3%) arms.10
Notable harms were more common in the pembrolizumab plus chemotherapy followed by pembrolizumab arm (43.6%) than in the placebo plus chemotherapy followed by placebo arm (21.9%). The most common notable harms were adrenal insufficiency (2.6% versus 0.0%), colitis (1.7% versus 0.8%), hyperthyroidism (5.2% versus 1.8%), hypophysitis (1.9% versus 0.3%), hypothyroidism (15.1% versus 5.7%), infusion-related reactions (18% versus 11.6%), nephritis (0.9% versus 0.0%), pneumonitis (2.2% versus 1.5%), severe skin reactions (5.7% versus 1%), and type 1 diabetes mellitus (0.5% versus 0.3%) in the pembrolizumab plus chemotherapy followed by pembrolizumab arm versus the placebo plus chemotherapy followed by placebo arm.10 The clinical experts noted that they would expect more AEs in the pembrolizumab group given that an additional treatment has been added to the regimen. They also noted that in practice they would try to keep patients on treatment as much as possible (e.g., by using dose adjustments).
The published indirect treatment comparison by Miyashita et al. (2020),13 which assessed the rate of febrile neutropenia, suggested a higher rate of febrile neutropenia with anthracycline plus pembrolizumab plus platinum salts when compared to treatments that included anthracycline. The analysis of the rate of grade 3 or greater nausea/vomiting and the rate of grade 3 or greater diarrhea suggested no difference was observed between treatments. No definitive conclusions could be drawn from the findings due to imprecision in the estimates obtained and other methodological limitations identified in NMA (the lack of important details about the included trials and methodology used to perform the NMA). As such, there is low confidence in the results, and they should be interpreted with caution. Additionally, construction of treatment nodes used in the NMA preclude the ability to draw conclusions regarding comparisons of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy to other specific treatment options for TNBC.
The clinical experts consulted agreed that the toxicity profile of pembrolizumab plus chemotherapy followed by pembrolizumab was manageable in practice, and they highlighted the importance of immune-related AEs associated with the use of pembrolizumab. The experts noted that pembrolizumab is currently being used in practice for other indications and that AEs, particularly immune-related AEs specific to pembrolizumab, are already known to clinicians. Therefore, the therapy can be managed in practice, and no extra activities to manage AEs are needed.
Conclusions
One pivotal study (KEYNOTE-522) and 1 published NMA provided evidence for this CADTH review. No additional evidence directly comparing pembrolizumab plus chemotherapy in the neoadjuvant setting and pembrolizumab in the adjuvant setting with other standard therapies for early-stage TNBC was identified. The pCR rate and EFS were co-primary end points assessed in the KEYNOTE-522 study. Pathological complete response, EFS, OS, and HRQoL (including safety outcomes) investigated in the KEYNOTE-522 trial were considered clinically meaningful by the clinical experts, and they align with outcomes highlighted as important by the patient groups. The median OS and median EFS were not estimable at IA4; thus, there is uncertainty in the effect of the intervention for OS and EFS. The clinical experts considered the pCR rate (and percent change) and EFS between the 2 arms clinically meaningful to clinicians and patients in clinical practice. The HRQoL assessments were considered exploratory due to the lack of multiplicity adjustments in the analyses. Both clinical experts and clinician groups stated that neoadjuvant therapy is current standard for TNBC and that pembrolizumab would be the preferred treatment option if it were to receive public funding. The clinical experts considered the safety profile of pembrolizumab plus chemotherapy followed by pembrolizumab manageable in practice. The experts stated that most oncologists have experience using pembrolizumab for other indications and are familiar with AEs due to pembrolizumab. Immune-related AEs are anticipated following the use of pembrolizumab. Clinical experts and clinician groups both considered toxicity and disease progression as important factors when deciding treatment discontinuation in patients. The KEYNOTE-522 study is a randomized, phase III, double-blinded design, and adjustments of multiplicity for the type I error were conducted in the analyses of key outcomes OS, PFS, and pCR. The OS findings are interim, with other analyses planned after a pre-specified number of events have occurred. The clinical experts considered the baseline and demographic characteristics of the KEYNOTE-522 study generalizable to Canadian practice.
One published NMA, by Miyashita et al. (2020), was summarized for this review to supplement the assessment of pembrolizumab plus chemotherapy as neoadjuvant therapy followed by continued pembrolizumab monotherapy as adjuvant therapy compared to other treatments for adult patients with early-stage TNBC. The NMA presented findings of pCR and grade 3 AEs specific to the neoadjuvant setting, which was a key limitation identified. Other methodological limitations—such as the lack of important details reported in the NMA methodology; high risk of bias in the studies included; lack of information about the characteristics of the trials included in the network; and imprecision of the estimates reported—precluded definitive conclusions of the findings observed for the different chemotherapy regimens and combinations assessed within the study.
References
1.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial. Antineoplastic agent, monoclonal antibody [product monograph]. Kirkland (QC): Merck Canada Inc.; 2022 Apr 5.
2.Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial [internal sponsor's package]. Kirkland (QC): Merck Canada Inc.; 2022 Feb 17.
3.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics. 2021; https://cancer.ca/Canadian-Cancer-Statistics-2021-EN. Accessed 2022 Apr 25.
4.Costa RLB, Gradishar WJ. Triple-negative breast cancer: current practice and future directions. J Oncol Pract. 2017;13(5):301-303. PubMed
5.Brouckaert O, Wildiers H, Floris G, Neven P. Update on triple-negative breast cancer: prognosis and management strategies. Int J Womens Health. 2012;4:511-520. PubMed
6.American Cancer Society. Types of cancer: triple-negative breast cancer. 2022; https://www.cancer.org/cancer/breast-cancer/about/types-of-breast-cancer/triple-negative.html#written_by. Accessed 2022 Apr 25.
7.Gierach GL, Burke A, Anderson WF. Epidemiology of triple negative breast cancers. Breast Dis. 2010;32(1-2):5-24. PubMed
8.National Comprehensive Cancer Network. NCCN guidelines for patients. 2022; https://www.nccn.org/patients/guidelines/content/PDF/stage_iv_breast-patient.pdf. Accessed 2022 Apr 25.
9.Canadian Cancer Society. Breast cancer. 2022; https://cancer.ca/en/cancer-information/cancer-types/breast. Accessed 2022 Apr 25.
10.Clinical Study Report: P522V03MK3475. A phase III, randomized, double-blind study to evaluate pembrolizumab plus chemotherapy vs placebo plus chemotherapy as neoadjuvant therapy and pembrolizumab vs placebo as adjuvant therapy for triple negative breast cancer (TNBC) [internal sponsor's report]. Kenilworth (NJ): Merck Sharp & Dohme Corp.; 2021 Jul 26.
11.Clinical trial endpoints for the approval of cancer drugs and biologics: guidance for industry. Silver Spring (MD): U.S. Food and Drug Administration; 2018: https://www.fda.gov/media/71195/download?msclkid=13ae9943b6a611ec8c85e1611aaf5d94. Accessed 2022 Apr 25.
12.Pathological complete response in neoadjuvant treatment of high-risk early-stage breast cancer: use as an endpoint to support accelerated approval guidance for industry. Silver Spring (MD): U.S. Food and Drug Administration; 2020: https://www.fda.gov/media/83507/download. Accessed 2022 Apr 25.
13.Miyashita H, Satoi S, Cruz C, Malamud SC. Neo-adjuvant therapy for triple-negative breast cancer: Insights from a network meta-analysis. Breast J. 2020;26(9):1717-1728. PubMed
14.Klarenbach S, Sims-Jones N, Lewin G, et al. Recommendations on screening for breast cancer in women aged 40–74 years who are not at increased risk for breast cancer. CMAJ. 2018;190(49):E1441-1451. https://www.cmaj.ca/content/cmaj/190/49/E1441.full.pdf. Accessed 2022 May 16. PubMed
15.Breast cancer screening in Canada - 2019/2020. Environmental scan. Toronto (ON): Canadian Partnership Against Cancer; 2021: https://s22457.pcdn.co/wp-content/uploads/2021/01/breast-cancer-screening-environmental-scan-2019-2020-Jan132021-EN.pdf. Accessed 2022 May 16.
16.Carboplatin injection (Teva Standard): 10 mg/mL; Antineoplastic agent [product monograph]. Toronto (ON): Teva Canada Limited; 2013 Nov 5.
17.TAXOL (paclitaxel): injection, 6 mg/mL; Antineoplastic agent [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2010 Feb 22.
18.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
19.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Jun 14.
20.Schmid P, Cortes L, Pusztai L. Pembrolizumab plus neoadjuvant chemotherapy improves pathologic complete response rates in triple-negative breast cancer. J Clin Outcomes Manag. 2020;27(2):53-55.
21.Schmid P, Cortes J, Dent R, et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386(6):556-567. PubMed
22.Schmid P, Salgado R, Park YH, et al. Pembrolizumab plus chemotherapy as neoadjuvant treatment of high-risk, early-stage triple-negative breast cancer: results from the phase 1b open-label, multicohort KEYNOTE-173 study. Ann Oncol. 2020;31(5):569-581. PubMed
23.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
24.Fayers P, Bottomley A. Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur J Cancer. 2002;38 Suppl 4:S125-133. PubMed
25.Sprangers MA, Groenvold M, Arraras JI, et al. The European Organization for Research and Treatment of Cancer breast cancer-specific quality-of-life questionnaire module: first results from a three-country field study. J Clin Oncol. 1996;14(10):2756-2768. PubMed
26.Sikov WM, Berry DA, Perou CM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol. 2015;33(1):13-21. PubMed
27.von Minckwitz G, Schneeweiss A, Loibl S, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trial. Lancet Oncol. 2014;15(7):747-756. PubMed
28.Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164-172. PubMed
29.Mehrotra DV, Su S-C, Li X. An efficient alternative to the stratified Cox model analysis. Stat Med. 2012;31(17):1849-1856. PubMed
30.Gion M, Pérez-García JM, Llombart-Cussac A, Sampayo-Cordero M, Cortés J, Malfettone A. Surrogate endpoints for early-stage breast cancer: a review of the state of the art, controversies, and future prospects. Ther Adv Med Oncol. 2021;13:17588359211059587. PubMed
31.Huang M, O'Shaughnessy J, Zhao J, et al. Association of pathologic complete response with long-term survival outcomes in triple-negative breast cancer: a meta-analysis. Cancer Res. 2020;80(24):5427-5434. PubMed
32.Masuda N, Lee S-J, Ohtani S, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med. 2017;376(22):2147-2159. PubMed
33.Tutt ANJ, Garber JE, Kaufman B, et al. Adjuvant olaparib for patients with BRCA1- or BRCA2-mutated breast cancer. N Engl J Med. 2021;384(25):2394-2405. PubMed
34.Li J, Chen L, Tan W, et al. Platinum is essential in neoadjuvant treatment of triple-negative breast cancer: a network meta-analysis. Cancer Biol. 2022;16:16. PubMed
35.Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. PubMed
36.Ali MA, Aiman W, Shah SS, Hussain M, Kashyap R. Efficacy and safety of pembrolizumab based therapies in triple-negative breast cancer: A systematic review of clinical trials. Critical Reviews in Oncology-Hematology. 2021;157:103197. PubMed
37.Balibegloo M, Nejadghaderi SA, Sadeghalvad M, et al. Adverse events associated with immune checkpoint inhibitors in patients with breast cancer: A systematic review and meta-analysis. Int Immunopharmacol. 2021;96:107796. PubMed
38.Sher AF, Golshani GM, Wu S. Fatal adverse events associated with pembrolizumab in cancer patients: a meta-analysis. Cancer Invest. 2020;38(2):130-138. PubMed
39.Tarantino P, Gandini S, Trapani D, Criscitiello C, Curigliano G. Immunotherapy addition to neoadjuvant chemotherapy for early triple negative breast cancer: A systematic review and meta-analysis of randomized clinical trials. Critical Reviews in Oncology-Hematology. 2021;159:103223. PubMed
40.Letellier ME, Dawes D, Mayo N. Content verification of the EORTC QLQ-C30/EORTC QLQ-BR23 with the International Classification of Functioning, Disability and Health. Qual Life Res. 2015;24(3):757-768. PubMed
41.McLachlan SA, Devins GM, Goodwin PJ. Validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30) as a measure of psychosocial function in breast cancer patients. Eur J Cancer. 1998;34(4):510-517. PubMed
42.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. PubMed
43.Groenvold M, Klee MC, Sprangers MA, Aaronson NK. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol. 1997;50(4):441-450. PubMed
44.Musoro JZ, Coens C, Fiteni F, et al. Minimally Important Differences for interpreting EORTC QLQ-C30 scores in patients with advanced breast cancer. JNCI Cancer Spectr. 2019;3(3):pkz037. PubMed
45.Ousmen A, Conroy T, Guillemin F, et al. Impact of the occurrence of a response shift on the determination of the minimal important difference in a health-related quality of life score over time. Health Qual Life Outcomes. 2016;14(1):167. PubMed
46.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
47.Cocks K, King MT, Velikova G, Martyn St-James M, Fayers PM, Brown JM. Evidence-based guidelines for determination of sample size and interpretation of the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. J Clin Oncol. 2011;29(1):89-96. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: March 8, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475 or DPT0O3T46P).ti,ab,kf,ot,hw,rn,nm.
exp breast neoplasms/
(((breast* or mamma or mammar* or lobular*) adj5 (cancer* or carcinoid* or carcinoma* or carcinogen* or adenocarcinoma* or adeno-carcinoma* or malignan* or metasta* or neoplas* or sarcoma* or tumo?r* or mass* or triple-negative)) or mBC or m-BC or LABC or TNBC or mTNBC).ti,ab,kf,ot,hw.
2 or 3
1 and 4
5 use medall
*pembrolizumab/
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475).ti,ab,kf,dq.
7 or 8
exp breast tumor/
(((breast* or mamma or mammar* or lobular*) adj5 (cancer* or carcinoid* or carcinoma* or carcinogen* or adenocarcinoma* or adeno-carcinoma* or malignan* or metasta* or neoplas* or sarcoma* or tumo?r* or mass* or triple-negative)) or mBC or m-BC or LABC or TNBC or mTNBC).ti,ab,kf,dq.
10 or 11
9 and 12
13 use oemezd
14 not (conference abstract or conference review).pt.
6 or 15
remove duplicates from 16
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search – Studies with results | Keytruda OR pembrolizumab) AND (triple-negative breast cancer OR TNBC)]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms – pembrolizumab AND triple-negative breast cancer]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms – pembrolizumab AND triple-negative breast cancer]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms – pembrolizumab AND triple-negative breast cancer]
Grey Literature
Search dates: February 28, 2022 – March 2, 2022
Keywords: [Keytruda OR pembrolizumab) AND (triple-negative breast cancer OR TNBC)]
Limits: No publication date limits
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals.
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for Exclusion |
|---|---|
Ali MA, Aiman W, Shah SS, Hussain M, Kashyap R. Efficacy and safety of pembrolizumab based therapies in triple-negative breast cancer: A systematic review of clinical trials. Critical Reviews in Oncology-Hematology. 2021;157:103197.36 | Not RCT (Review Article) |
Balibegloo M, Nejadghaderi SA, Sadeghalvad M, et al. Adverse events associated with immune checkpoint inhibitors in patients with breast cancer: A systematic review and meta-analysis. Int Immunopharmacol. 2021;96:107796.37 | Not relevant comparator |
Schmid P, Cortes L, Pusztai L. Pembrolizumab plus Neoadjuvant Chemotherapy Improves Pathologic Complete Response Rates in Triple-Negative Breast Cancer. J Clin Outcomes Manag. 2020;27(2):53 to 55.20 | Not RCT (Commentary) |
Sher AF, Golshani GM, Wu S. Fatal Adverse Events Associated with Pembrolizumab in Cancer Patients: A Meta-Analysis. Cancer Invest. 2020;38(2):130 to 138.38 | Not relevant intervention |
Tarantino P, Gandini S, Trapani D, Criscitiello C, Curigliano G. Immunotherapy addition to neoadjuvant chemotherapy for early triple negative breast cancer: A systematic review and meta-analysis of randomized clinical trials. Critical Reviews in Oncology-Hematology. 2021;159:103223.39 | Not relevant intervention |
Appendix 3: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and minimal important difference [MID])
European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30)
The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Breast Cancer–Specific Quality of Life Questionnaire-23 item (EORTC QLQ-BR23)
Findings
Table 35: Summary of Outcome Measures and their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A 30-item, patient-reported, cancer-specific, HRQoL questionnaire using 4- and 7-point Likert scales.23 | Validity Content validity: When mapping to the WHO’s ICF framework, 25 of the 30 items in the EORTC QLQ-C30 were endorsed by the experts.40 Discriminant validity: As represented by correlation with external parameters such as ECOG performance status (Spearman’s rank correlation values ranging from 0.02 to 0.56) in patients with metastatic breast cancer.41 Convergent validity: As represented by correlation with scores on the Profile of Mood States and Psychosocial Adjustment to Illness Scale, was also deemed to be acceptable (Spearman’s rank correlation values ranging from 0.02 to 0.76) in patients with metastatic breast cancer.41 Reliability Inter-rater reliability: As represented by patient-observer agreement on the EORTC QLQ-C30 questionnaire, the median kappa coefficient for agreement across the 30 items in the EORTC QLQ-C30 was 0.86 with a range of 0.48 to 1.00 in patients with metastatic breast cancer, representing substantial to near-perfect agreement for most items.42,43 Responsiveness No literature was identified that assessed responsiveness in patients with breast cancer. | For patients with breast cancer, MIDs for within-group changes ranged from 5 to 14 points for improvements and from −14 to −4 points for deterioration across the individual scales. For between-group differences, MIDs ranged from 4 to 11 points for improvements and from −18 to −4 points for deterioration across the individual scales.44 |
EORTC QLQ-BR23 | A 23-items patient-reported, breast cancer–specific, HRQoL questionnaire using scales range in score from 0 to 100.25 | Validity Content validity: When mapping to the WHO’s ICF framework, 21 of the 23 items in the EORTC QLQ-BR23 were endorsed by the experts.40 Convergent validity: The EORTC QLQ-BR23 demonstrated weak to moderate item-scale correlations (ranging from 0.09 to 0.90) for all scales in patients with breast cancer.25 Discriminant validity: In patients with breast cancer, the EORTC QLQ-BR23 demonstrated the ability to discriminate between patients from mutually exclusive subgroups with medium to large effect sizes (ranging from 0.42 to 1.1).25 Reliability Internal consistency was adequate in patients with breast cancer. Cronbach alpha coefficients for the multi-item scales of the EORTC QLQ-BR23 ranged from 0.46 to 0.94 across all samples.25 Responsiveness No literature was identified that assessed responsiveness in patients with breast cancer. | In patients with breast cancer or suspicious breast cancer, the minimal of observed MID at 6 months (ranging from 0.4 to 4) was smaller in case of deterioration for EORTC QLQ-BR23 compared to 3 months (ranging from 7 to 20). Similar trend was observed in the case of improvement, where the observed MID was 2 or less at 6 months (ranging from 0.7 to 2) while the observed at 3 months was greater than or equal to 2 (ranging from 2 to 15).45 |
ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-BR23 = The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Breast Cancer–Specific Quality of Life Questionnaire-23 item; HRQoL = health-related quality of life; ICF = International Classification of Functioning; MID = minimal important difference.
The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30)
Description and Scoring
The EORTC QLQ-C30 is 1 of the most used patient-reported outcome measures in oncology clinical trials. It is a multidimensional, cancer-specific, self-administered, measure of HRQoL.23
The EORTC QLQ-C30 is composed of both multi-item scales and single-item measures. These include 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a global health status/HRQoL scale, and 6 single items assessing additional symptoms commonly reported by cancer patients (dyspnea, loss of appetite, insomnia, constipation, and diarrhea) as well as perceived financial impact of the disease.23
The EORTC QLQ-C30 uses a 1-week recall period to assess functional status and symptoms. All scales and single-item measures are scored from 0 to 100. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. For the 2 items that form the global HRQoL scale, the response format is a 7-point Likert-type scale with anchors at 1 = “very poor” and 7 = “excellent.” Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Scale sum scores are transformed such that a high score on the functional scales represents a high/healthy level of functioning, a high score on the symptom scales represents a high level of symptomatology, and a high score on the global health status/HRQoL scale represents a high HRQoL.24
According to the EORTC QLQ-C30 scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least half of the items. The values for missing items are interpolated with the average of the respondent-completed items.24
Assessment of Validity, Reliability, and Responsiveness
One study40 assessed the content validity of the EORTC QLQ-C30 based on the opinions of 21 experts. When mapping to the WHO’s International Classification of Functioning (ICF) framework, 25 of the 30 items in the EORTC QLQ-C30 were endorsed by the experts: 15 items mapping to impairment of body function, 7 mapping to activity limitations/participation restrictions, and 1 item mapping to both components. There were only 2 items of the EORTC QLQ-C30 tapped content outside of functioning: Item 29 mapping to perceived health and item 30 mapping to global quality of health. The authors stated that the fact that most items from the EORTC QLQ-C30 can be linked to the ICF framework means that the instrument’s content reflects functioning, which is a key component of HRQoL.40
No studies were identified that investigated the validity, reliability, or responsiveness of the EORTC QLQ-C30 among patients with early-stage TNBC. Among patients with metastatic breast cancer, a 1997 study investigated the inter-rater reliability using patient-observer agreement on the EORTC QLQ-C30 questionnaire. The median kappa coefficient for agreement across the 30 items in the EORTC QLQ-C30 was 0.86 with a range of 0.48 to 1.00,43 representing substantial to near-perfect agreement for most items.42 Another study41 investigated the discriminative and convergent validity of the psychosocial subscales of EORTC QLQ-C30 in patients with breast cancer. The study found acceptable discriminative validity represented by correlation with external parameters such as ECOG performance status (Spearman’s rank correlation values ranging from 0.02 to 0.56). A correlation of 0.2 represented significance at the 0.01 level. The convergent validity, as represented by correlation with scores on the Profile of Mood States and Psychosocial Adjustment to Illness Scale, was also deemed to be acceptable (Spearman’s rank correlation values ranging from 0.08 to 0.76).41
Minimal Important Difference
One study from 1998,46 conducted in patients with breast cancer and small-cell lung cancer, estimated that a change in score on any scale of the EORTC QLQ-C30 of 10 points would be clinically significant. This estimate was based on an anchor-based approach to estimate the MID in which patients who reported “a little” change (for better or worse) on the subjective significance questionnaire had corresponding changes on a function or symptom scale of the EORTC QLQ-C30 of approximately 5 to 10 points. Patients who reported a “moderate” change had corresponding changes in the EORTC QLQ-C30 of about 10 to 20 points, and those who reported “very much” change had corresponding changes in the EORTC QLQ-C30 of more than 20 points.46
A more recent study from 201944 aimed to estimate the MID for the EORTC QLQ-C30 in patients with advanced breast cancer. This study used anchor-based and distribution-based approaches, using performance status and selected AEs as the anchor variables. MIDs for within-group changes ranged from 5 to 14 points for improvements and from −14 to −4 points for deterioration across the individual scales. For between-group differences, MIDs ranged from 4 to 11 points for improvements and from −18 to −4 points for deterioration across the individual scales.44 A 2011 report combined a systematic review, expert opinions, and meta-analysis to estimate large, medium and small differences for EORTC QLQ-C30 scores and recommended that small and medium differences corresponded with changes from 3 to 6 and 9 to 19 points, respectively, depending on the subscale.47 In addition, A study from 201645 aimed to investigate the effect of response shift on MID over time for the EORTC QLQ-BR23 in patients with breast cancer or suspicious breast cancer. Three hundred 81 patients recruited from 4 hospitals and care centres participated in this study with a mean age of 58.4 years (SD = 11 years). This study used an anchor-based approach using deterioration improvement as the anchor variables. The minimal of observed MID at 6 months (ranging from 0.5 to 10) was smaller in case of deterioration for EORTC QLQ-C30 compared to 3 months (ranging from 5 to 26). With regards to improvement, the observed MID at 6 months (ranging from 0.8 to 7) was similar to the observed MID at 3 months (ranging from 0.3 to 10).45
The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Breast Cancer–Specific Quality of Life Questionnaire-23 item (EORTC QLQ-BR23)
Description and Scoring
The EORTC QLQ-BR23 includes an additional 23 items that are specific to breast cancer, with 5 multi-item scales assessing systemic therapy side effects, arm symptoms, breast symptoms, body image, and sexual functioning, as well as single items assessing sexual enjoyment, hair loss, and future perspective.25 All scales range in score from 0 to 100, and higher scores represent higher response thus a high score for functioning represents high functioning while a high symptom score represents a high symptom burden. The EORTC QLQ-BR23 should not be administered as a freestanding instrument as it does not measure a multidimensional construct of body image; instead, the EORTC QLQ-BR23 should be administered in conjunction with the EORTC QLQ-C30.25
Assessment of Validity, Reliability, and Responsiveness
One study40 assessed the content validity of the EORTC QLQ-BR23 based on the opinions of 13 experts. When mapping to the WHO’s International Classification of Functioning (ICF) framework, 21 of the 23 items in the EORTC QLQ-BR23 were endorsed by the experts: 20 at the impairment level and 1 at the activity and participation level. The authors stated that the fact that most items from the EORTC QLQ-BR23 can be linked to the ICF framework means that the instrument’s content reflects functioning, which is a key component of HRQoL.
Construct validity was assessed by investigating convergent validity and known-groups validity in 1 study25 of 496 patients aged 25 to 83 years with breast cancer from 3 countries (Netherlands, Spain, and the US). Overall, the EORTC QLQ-BR23 had weak to moderate item-scale correlations (ranging from 0.09 to 0.90) for all scales, among them, the body image and sexual functioning scales had demonstrated moderated to strong item-scale correlations (ranging from 0.30 to 0.83 for body image and from 0.77 to 0.90 for sexual functioning) across all samples. With regards to known-groups validity, the EORTC QLQ-BR23 demonstrated the ability to discriminate between patients from mutually exclusive subgroups differing in disease stage, previous surgery, performance status, and treatment modality. The study reported medium to large effect sizes (ranging from 0.42 to 1.1) of the significant group differences in sexual functioning, future perspective, arm symptoms and systemic therapy side effects between patients from the abovementioned mutually exclusive subgroups.25
Internal consistency reliability was also investigated in the same study.25 Cronbach alpha coefficients for the multi-item scales of the EORTC QLQ-BR23 were, in general, lowest in the Spanish sample (ranging from 0.46 to 0.94), and highest in the American sample (range, 0.70 to 0.91), with the coefficients of the Dutch sample holding an intermediate position (range, 0.57 to 0.89).25
Minimal Important Difference (MID)
MIDs for EORTC QLQ-BR23 were also investigated in the same study that investigated the effect of response shift on MID over time for the EORTC QLQ-C30 in patients with breast cancer or suspicious breast cancer.45 The study used an anchor-based approach using deterioration and improvement as the anchor variables. The minimal of observed MID at 6 months (ranging from 0.4 to 4) was smaller in case of deterioration for EORTC QLQ-BR23 compared to 3 months (ranging from 7 to 20). A similar trend was observed in the case of improvement, where the observed MID at 6 months ranged from 0.7 to 2, while the observed MID at 3 months ranged from 2 to 15.45
Pharmacoeconomic Review
Abbreviations
AE
adverse event
DM
distant metastases
EFS
event-free survival
ICER
incremental cost-effectiveness ratio
LRR
locoregional recurrence
OS
overall survival
QALY
quality-adjusted life-year
RDI
relative dose intensity
TNBC
triple-negative breast cancer
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 200 mg IV every 3 weeks or 400 mg IV every 6 weeks |
Indication | For the treatment of adult patients with high-risk, early-stage triple-negative breast cancer in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgery |
Health Canada approval status | NOC |
Health Canada review pathway | Priority |
NOC date | April 12, 2022 |
Reimbursement request | For the treatment of adult patients with early-stage triple-negative breast cancer in combination with chemotherapy as neoadjuvant treatment and then continued as monotherapy as adjuvant treatment after surgerya |
Sponsor | Merck Canada Inc. |
Submission history | Pembrolizumab has been reviewed for numerous indications at CADTH This is the first submission reviewed for triple-negative breast cancer |
NOC = Notice of Compliance.
aThe reimbursement request was submitted for CADTH review pre-NOC, and the request aligned with the proposed Health Canada indication.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost–utility analysis based on a Markov model |
Target population | Patients with high-risk, early-stage TNBC |
Treatments | Pembrolizumab regimen: in combination with chemotherapy as neoadjuvant therapy followed by pembrolizumab as a single agent as adjuvant therapy |
Comparator | Chemotherapy as neoadjuvant therapy followed by no additional adjuvant therapy |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs, LYs |
Time horizon | Lifetime = 51 years |
Key data source | The KEYNOTE-522 phase III, randomized, double-blind clinical trial of pembrolizumab plus chemotherapy vs. placebo plus chemotherapy as neoadjuvant therapy followed by pembrolizumab vs. placebo as adjuvant therapy for early-stage TNBC patients |
Submitted results | ICER for pembrolizumab regimen vs. chemotherapy (probabilistic analysis): $25,249 per QALY (incremental costs of $103,349 and incremental QALYs of 4.09) |
Key limitations |
|
CADTH reanalysis results | For CADTH reanalysis, the following changes were made: a treatment waning effect was implemented; more appropriate survival estimates were assumed for LRR and DM; relative dose intensity was set to 100% for all drugs; an alternative survival function was adopted; and programming errors were fixed. The CADTH base case included a fixed-dose regimen for pembrolizumab. A scenario analysis adopted a weight-based dose for pembrolizumab.
|
DM = distant metastases; ICER = incremental cost-effectiveness ratio; LRR = locoregional recurrence; LY = life-year; QALY = quality-adjusted life-year; TNBC = triple-negative breast cancer.
Conclusions
The CADTH clinical review noted that evidence from 1 pivotal study (KEYNOTE-522) suggests that pembrolizumab plus chemotherapy as neoadjuvant and adjuvant therapy has a clinically meaningful impact on event-free survival (EFS) and overall survival (OS) compared to placebo plus chemotherapy as neoadjuvant therapy alone, according to clinical experts. The median OS and median EFS were not estimable at the fourth interim analysis; thus, there is uncertainty in the effect of the intervention for OS and EFS.
CADTH undertook reanalyses to address several key limitations identified in the sponsor’s model. CADTH revised the sponsor’s model to incorporate a treatment waning effect; used more appropriate survival estimates for locoregional recurrence (LRR) and distant metastases (DM); set relative dose intensity to 100% for all drugs; used alternative survival functions for EFS; and fixed programming errors within the model. For the CADTH base case, the incremental cost-effectiveness ratio (ICER) of the pembrolizumab regimen compared to chemotherapy alone was $81,408 per quality-adjusted life-year (QALY) (incremental costs: $106,930; incremental QALYs: 1.31) in the Health Canada–indicated population.
CADTH notes that the majority of QALY benefit is derived from additional survival (model predicts an additional 1.52 additional life-years). This additional survival benefit is derived through the prevention of LRR and DM, which reduce life expectancy. The extent of OS benefit depends on:
how many LRR and DM events are prevented, rather than delayed
the impact LRR and DM have on life expectancy.
Regarding the first point, given the length of follow-up obtained from the trial, including the time spent off treatment, clinical experts felt that pembrolizumab could prevent some LRR and DM events from occurring relative to chemotherapy alone. Regarding the second point, as part of the CADTH reanalysis, more appropriate assumptions regarding life expectancy outcomes for those who experience LRR or DM were used based on Canadian data. If LRR or DM are only delayed and not prevented, then the cost-effectiveness of pembrolizumab is greatly diminished. Therefore, although the analysis models a plausible estimate of long-term survival, longer term data would help validate the survival outcomes predicted by the model.
Based on the CADTH reanalysis, the price of pembrolizumab would need to be reduced by 36% for it to be cost-effective at a $50,000 per QALY threshold. If pembrolizumab was provided through weight-based dosing, assuming equal effectiveness as in the trial, the ICER would decrease to $67,657 per QALY. This is because with vial sharing, pembrolizumab can be given at a lower cost than a fixed-based dose, and as efficacy is assumed to be equivalent, this leads to a lower ICER. Under these assumptions, the price of pembrolizumab would need to be reduced by 24% for it to be cost-effective. Substantially higher price reductions would be required if pembrolizumab did not translate into additional survival gains for patients. CADTH notes that the OS findings are interim, with other analyses planned after a pre-specified number of events have occurred. Additional data on OS could be used to validate findings from the model.
CADTH notes that KEYNOTE-522 did not compare pembrolizumab adjuvant therapy with capecitabine adjuvant therapy, which became the standard of care for patients with residual invasive triple-negative breast cancer (TNBC) following surgery after the start of KEYNOTE-522. The cost-effectiveness of pembrolizumab versus capecitabine as an adjuvant therapy is unknown and cannot be addressed, given the clinical evidence base available. The CADTH assessment of cost-effectiveness is dependent on the generalizability of the KEYNOTE trial to current practice.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from 2 patient groups: the Canadian Breast Cancer Network and Rethink Breast Cancer. Both are national charities dedicated to educating and empowering patients with breast cancer and ensuring the best quality of care for those patients. Patient input was based on an online survey (including 24 Canadian participants with early-stage TNBC), interviews, and a focus group. Patient input highlighted as key aspects of TNBC the impact of the disease on day-to-day life, including effects on emotional and physical well-being. Treatment for TNBC usually involves chemotherapy, surgery, and radiation. Both groups highlighted that there were fewer treatment options available for TNBC than for other forms of breast cancer, despite TNBC being more aggressive. The majority of patients were seeking new treatments that reduce risk of recurrence and prolong long-term survival. Most patients indicated that the balance between effectiveness and side effects for a good quality of life was essential to them, particularly regarding the ability to maintain their productivity and mobility. Patient input also pointed to the increased financial burden of treating and managing TNBC, mainly related to out-of-pocket spending, such as medication costs. Four patients had experience with pembrolizumab as neoadjuvant or adjuvant therapy. All patients found pembrolizumab to be an effective treatment. Pembrolizumab’s side effects for 1 patient led to discontinuation of treatment, however pembrolizumab was discontinued after achievement of pathological complete response and having the risk–benefit of therapy reassessed. All patients agreed that most of the side effects were tolerable, given the benefit achieved with pembrolizumab. Two patients also found it hard to attribute side effects specifically to pembrolizumab and not to the other chemotherapy agents.
Clinician input was received from 2 groups: the Ontario Health–Cancer Care Ontario Breast Cancer Drug Advisory Committee and The Ottawa Hospital Cancer Centre Breast Disease Site Group. Clinician groups identified the following as the current Canadian treatment pathway for patients with TNBC: neoadjuvant chemotherapy, surgery, and then adjuvant chemotherapy with capecitabine (if there is residual disease) or olaparib (for BRCA1 or 2 mutation carriers). Clinician input noted that it is unclear how pembrolizumab would fit with the other available adjuvant therapies as part of the clinical practice guidelines, since there were no studies evaluating the combination of adjuvant pembrolizumab plus capecitabine or olaparib. In addition, using pembrolizumab in early treatment might impact subsequent therapy options for advanced or metastatic breast cancer. Both groups mentioned achieving long-term cure, improving OS and EFS, and delaying disease progression as treatment goals. It was noted that the subgroup of patients with the greatest unmet need would be TNBC patients with higher risk of recurrence.
The CADTH participating drug plan highlighted several implementation and economic considerations, including the potential of using other neoadjuvant or adjuvant regimens (e.g., dose-dense scheduling for anthracycline-based therapies or use of capecitabine as maintenance therapy after surgery) or distinct neoadjuvant regimen scheduling (e.g., pembrolizumab every 6 weeks, carboplatin weekly). The drug plan considered whether patients would be eligible to receive pembrolizumab as adjuvant therapy if they did not receive it during the neoadjuvant course, or as neoadjuvant therapy after having already initiated neoadjuvant treatment. Furthermore, the drug plan considered the possibility of pembrolizumab being used in patients with an Eastern Cooperative Oncology Group Performance Status of 2 or greater or in patients with stage I TNBC. Finally, concerns were raised regarding uncertainty of treatment duration for patients who have a delay between completion of chemotherapy and access to surgery or delays in pembrolizumab doses after surgery (e.g., post-operative recovery).
Several of these concerns were addressed in the sponsor’s model:
EFS and health state utilities capturing TNBC quality of life were included.
AEs associated with pembrolizumab were included in the pharmacoeconomic analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
The impact of using pembrolizumab alongside other neoadjuvant therapies; this was not reviewed in KEYNOTE-522.
Comparison of pembrolizumab to other adjuvant therapies after surgery.
Economic Review
The current review is for pembrolizumab (Keytruda) in addition to chemotherapy as a neoadjuvant therapy, followed by pembrolizumab as an adjuvant therapy for early-stage TNBC patients.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The submitted analysis is a cost–utility analysis comparing pembrolizumab plus chemotherapy versus chemotherapy as neoadjuvant therapy followed by pembrolizumab versus placebo as adjuvant therapy for early-stage TNBC patients.1 As per the clinical trial, the analysis incorporates a dose of pembrolizumab of 200 mg every 3 weeks, with up to 8 doses in the neoadjuvant phase and 9 doses in the adjuvant phase.2,3 For the neoadjuvant phase, pembrolizumab is given in combination with paclitaxel (80 mg/m2 once weekly for the duration of neoadjuvant treatment) and carboplatin (for area under the curve 5, once every 3 weeks, or for area under the curve 1.5, once weekly in the first 12 weeks), followed by cyclophosphamide (600 mg/m2 once every 3 weeks in the subsequent 12 weeks) and 4 cycles of either doxorubicin (60 mg/m2) or epirubicin (90 mg/m2).
The pembrolizumab regimen was compared to chemotherapy in the neoadjuvant setting followed by no adjuvant therapy. The schedule of chemotherapy in the neoadjuvant setting was the same as the regimen given in combination with pembrolizumab above.
Pembrolizumab is available in a 100 mg vial at a cost of $4,400. Thus, the cost per dose is $8,800, with a maximum cost of $70,400 in the neoadjuvant setting and an additional $79,200 in the adjuvant setting. Combined with chemotherapy, the cost per 3-week cycle is $9,000 up to week 12 in the neoadjuvant setting, $9,445 for the remainder of the neoadjuvant setting, and $8,800 for the adjuvant setting, assuming full dose intensity. The total potential cost is $152,977. The cost per 3-week cycle for the chemotherapy regimen is $200 up to week 12 in the neoadjuvant setting, $645 for the remainder of the neoadjuvant setting, and $0 for the adjuvant setting, leading to a total potential cost of $3,340. In the sponsor’s analysis, the costs of all therapies were adjusted to be lower by assuming reduced dose intensity.
Administration costs are applied to all comparators based on administration time and an assumed cost of $40 per hour.
Analysis takes the form of a health care system perspective with a 51-year time horizon and an equivalent annual discount rate of 1.5% for all outcomes.
Model Structure
The model takes the form of a Markov model with weekly cycles. The health states incorporated are as follows: an event-free state (meaning alive with no LRR or DM), LRR, DM, and death. The analysis models the transition from event-free to LRR, DM, or death, from LRR to DM or death, and from DM to death. Figure 1 in Appendix 3 outlines these transitions. This structure is appropriate for the context of the decision problem.
Model Inputs
Transition probabilities were primarily derived from the KEYNOTE-522 phase III, randomized, double-blind clinical trial.2,3 The trial was a comparison of pembrolizumab plus chemotherapy versus placebo plus chemotherapy as neoadjuvant therapy, followed by pembrolizumab versus placebo as adjuvant therapy for early-stage TNBC patients. Analysis is based on data from an interim analysis. The probabilities of transition from LRR to DM or death and from DM to death were obtained for both comparators directly from the clinical trial and assumed to hold for the time horizon of the model. The regimen-specific transitions from event-free were based on extrapolating data from the trial for EFS. The proportion of events that were LRR, DM, or death were assumed to vary by regimen. These were estimated for the first year of the trial and for subsequent years. The first-year proportions are applied to year 1 of the models, and the subsequent years’ proportions applied to year 2 onwards for the full-time horizon.
To estimate the long-term probabilities of having an event from the event-free state, EFS for both the pembrolizumab regimen and the chemotherapy regimen was estimated using the patient-level data from the KEYNOTE-522 trial.2,3 Data were fit to a variety of parametric models and then extrapolated for the overall time horizon. Methods were similar to those recommended by the National Institute for Health and Care Excellence Decision Support Unit.4
Separate survival models were estimated for both regimens, as the proportional hazards assumption was demonstrated to be invalid. Piecewise models were considered to have a better fit with the data than standard parametric models. The models incorporated Kaplan–Meier data for the first 50 weeks, and then data beyond 50 weeks were fit to standard survival functions. Survival functions were based primarily on statistical fit, although visual inspection and clinical plausibility were also listed as factors, though the approach taken for those 2 criteria was unclear. For the pembrolizumab regimen, a generalized gamma model was used, and for the chemotherapy regimen, a log-normal model was adopted.
The probability of death was adjusted to allow for all-cause mortality.5 However, the method adopted did not ensure that mortality was at least as high as all-cause mortality.
Adverse events (AEs) were incorporated at model onset as 1-off disutilities and costs. AE were considered if they were grade 3 or higher and had an incidence of at least 5% in 1 or both regimens.
Utility data were derived from the KEYNOTE-522 study through the EQ-5D-5L utility instrument and a Canadian 5L tariff. Utility values were estimated for the event-free state, LRR, and DM and were assumed the same for both regimens. The disutility associated with AEs was incorporated by assuming the same AE duration for all AEs (12.5 weeks) and by estimating a common disutility for AEs.
Analysis incorporated the following range of costs: drug acquisition costs, drug administration costs, AE costs, radiation costs, surgery costs, management of patients who are event-free, management of patients with LRR, management of patients with DM, therapy costs with DM, and terminal care costs. Data sources appear appropriate.6-9
Summary of Sponsor’s Economic Evaluation Results
The sponsor submitted a probabilistic analysis based on 5,000 replications. The results of the probabilistic analyses were broadly in line with the deterministic analyses.
Base-Case Results
The sponsor’s economic evaluation base-case analysis estimated the incremental cost per QALY gained for the pembrolizumab regimen versus the chemotherapy regimen as $25,249 (Table 3). The submitted analysis is based on the publicly available prices of the comparator treatments and assumes reduced dose intensity and a fixed-dose regimen of pembrolizumab.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs, $ | Total QALYs | ICER vs. chemotherapy, $/QALY |
|---|---|---|---|
Chemotherapy | 56,744 | 15.09 | Reference |
Pembrolizumab + chemotherapy | 160,094 | 19.18 | 25,249 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Disaggregated results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
A wide range of scenario analyses were conducted. Scenario analysis found that the results were sensitive to assumptions concerning the survival functions and the inclusion of waning of treatment effect.
CADTH Appraisal of the Sponsor’s Economic Evaluation
Waning of treatment effect: In the sponsor’s submitted model, incremental QALY and life-year gains for pembrolizumab versus chemotherapy over the lifetime time horizon were 4.26 and 4.96, respectively. The QALY and life-year gains at 2 years after the curtailment of treatment were 0.005 and 0.001, respectively. Hence, less than 0.5% of gains occur during the treatment period. By plotting the QALY gains from pembrolizumab on an annual basis, as forecasted by the sponsor’s model, it is apparent that the annual QALY gains increase with time after treatment curtailment, with a peak at 18 years (Figure 2, Appendix 3). At 40 years, there is assumed to still be an annual gain in QALYs of 0.05. This is because if a drug leads to the patient’s cancer being cured, versus progression to LRR or DM, then this will incur benefits that will continue to accrue for the lifetime of that patient. If you compared 2 identical patients, 1 whose cancer was cured and 1 who progressed to DM, then the immediate short-term QALY differences would be small, but over time—as the risk of death with DM would become substantially higher and quality of life worse—incremental QALYs would increase.
Given the above, assumptions relating to continued treatment effects may have a substantial impact on the study results. In Figure 3, Appendix 3, the dots represent the relative risk of having an event with pembrolizumab versus chemotherapy over 6-month periods based on the raw data from the clinical trial. Data are simply (1 – the survival at time t + 1) / (survival at time t). The data suggest that pembrolizumab has an effect after the first 6 months, but this effect declines after 24 months, once patients are no longer on pembrolizumab. Data from 36 months to 39 months are limited but suggest limited relative effects beyond 36 months. This suggests that pembrolizumab prevents disease progression in the first 2 years to 3 years post–treatment initiation, and then beyond this there are no further reductions in disease progression.
The relative risk of having an event every 6 months for pembrolizumab versus chemotherapy derived from the sponsor’s model is not consistent with the findings above from the clinical trial (refer to Figure 3). Rather, the effect appears to grow larger (the relative effect increases) up to 2 years and then gets smaller from 24 months to 30 months. Then, rather than show a declining effect, the effect size starts to increase, with the maximum effect of pembrolizumab versus chemotherapy occurring at 13 years. The clinical experts agreed that it was unlikely that pembrolizumab would continue to influence the probability of having an event after 5 years. At 5 years, rates of disease progression were thought to be very similar between those who received pembrolizumab and those who did not, as any new progression would likely be unrelated to the original treated tumour site.
Given the above, to provide a more appropriate measure of the long-term health benefits from pembrolizumab, CADTH used the functionality within the model provided by the sponsor to include waning of treatment effect, assuming that waning begins at 36 months and that by 60 months the probability of having a new event will be the same regardless of initial treatment. This assumption does not mean that treatment with pembrolizumab will not lead to further benefits after 60 months, as prevention of events in the first 60 months will lead to fewer costs and greater QALYs for the remainder of the patient’s life.
Choice of survival functions: Analysis adopts a piecemeal survival function for the time to events for both pembrolizumab and chemotherapy. The generalized gamma function is chosen for pembrolizumab and the log-normal functional form for chemotherapy. This is based on visual inspection and statistical fit, as measured by the Akaike information criterion and the Bayesian information criterion. Separate survival functions, rather than a joint model, were justified by the failure of the proportional hazards assumption. For pembrolizumab, the log-normal distribution was the second-best fitting model.
Visual inspection and statistical fit only relate to interpolation (how well a model fits the data we have) but not to extrapolation (what will happen in the period we do not have data for). The appropriateness of the extrapolation for chemotherapy is further assessed by reviewing external data, but such data relate to only approximately 5 years. The appropriateness of extrapolation for pembrolizumab was assessed by asking key opinion leaders to assess the validity of the EFS function for pembrolizumab. No further information is provided about this process, but what is important to assess is the long-term relative effect of pembrolizumab versus chemotherapy. It is unlikely that the relative effects within the sponsor’s model, as highlighted in Figure 3, of increasing effects up to 13 years, were validated. The sponsor does provide a scenario analysis where the log-normal survival function is used for both regimens, and this nearly doubled the estimated ICER. This would appear a legitimate analysis given the little difference in statistical fit between functions.
The revisions relating to waning of treatment effect address concerns over the extrapolation of long-term EFS for pembrolizumab relative to chemotherapy. For consistency, the CADTH base case followed the sponsor’s scenario analysis, whereby the same form of survival function for both treatments is adopted: piecemeal at 50 weeks, with log-normal function thereafter.
The probability of events within the LRR and DM states: CADTH notes concerns within the model over the long-term survival of patients experiencing LRR and DM. Within the sponsor’s model, survival at 2 years, 5 years, and 10 years post-LRR were 48%, 10%, and 0.4%. CADTH noted that recent data from British Columbia (patients diagnosed from 2005 to 2013) suggests OS after LRR for TNBC patients is 24.2% after 10 years for patients not experiencing death or DM within the first 120 days.10 The clinical experts expressed agreement that these data were an appropriate basis for calibration of the model.
Within the sponsor’s model, survival at 2 years and 5 years post-DM were 18% and 1%. CADTH consulted with the clinical experts, who suggested that survival at 2 years post-DM would be less than 50%, with survival at 5 years being below 10%. The clinical experts suggested this was an appropriate basis for calibration of the model. CADTH recognizes that the sponsor used data from its trial within the model but feels the data were immature with respect to survival post-recurrence and did not hold face validity given external evidence.
CADTH weighted the probabilities of developing DM from LRR and the probabilities of death from LRR and DM such that they replicated the assumptions above.
Error in programming mortality: In the sponsor’s model there is an error in the calculation of the probability of death in patients in the event-free state. This leads to scenarios where the probability of dying is less than the population death rate. This would mean that an individual with TNBC post-surgical resection who does not experience LRR or DM would have a lower probability of dying than the general Canadian population. This is an unintentional outcome from the sponsor’s programming. Further details regarding this error are provided in Appendix 4.
CADTH adopted revised formulas for the cycle-specific probability of death.
Relative dose intensity: The sponsor’s base case incorporates reduced dose intensities for all therapies (i.e., for neoadjuvant, adjuvant, LRR, and DM therapies). Consistent with previous reviews, given the inability to link reduced dose intensity with outcomes, the CADTH base case does not incorporate reduced dose intensity. A reduction in relative dose intensity (RDI) can be derived from a delayed dose, a missed dose, or a reduction in dose. When considering wastage, each component can have a very different influence on drug costs. Likewise, it is unclear how treatment discontinuation influences RDI.
CADTH uses the functionality within the sponsor’s model to exclude reduced dose intensity.
Weight-based dosing for pembrolizumab: The pembrolizumab dosage in KEYNOTE-522 was a fixed dose of 200 mg intravenously every 21 days. After consultation, CADTH notes that in line with other indications for pembrolizumab, jurisdictions would likely implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks, with the possibility of extended dosing intervals to every 6 weeks (4 mg/kg up to a 400 mg cap). The clinical experts agreed that this approach seemed reasonable, given the clear interchangeable use in dosing for other tumour sites. However, CADTH notes that it is not possible to make the direct assumption that the use of weight-based dosing will lead to the same outcomes as fixed dose. As patients will be exposed to a lower dose, this may improve the AE profile, reducing the rate of discontinuation. This may in turn impact treatment efficacy. In the absence of any data to explore these outcomes, a scenario analysis was conducted assuming equivalent efficacy but a lower treatment cost.
CADTH conducted a scenario analysis using weight-based dosing based on an average weight of 69.7 kg.
Disutility implied by high rates of discontinuation: CADTH notes that there are high rates of discontinuation with pembrolizumab due to AEs and patient choice. During the neoadjuvant phase, 26.4% of patients did not receive all doses of treatment (207 out of 784). Of the 487 who received all doses of neoadjuvant therapy, 19 did not proceed to adjuvant therapy and a further 71 did not receive all doses. The proportion of patients who received all doses of adjuvant and neoadjuvant therapy is unknown given the data available, but it was no more than 62.1%. AE, withdrawal by patient, and physician decision account for 87.2% of withdrawals. Clinical progression, disease progression, or recurrence account for the other 12.8%.
The sponsor’s model reflects the impact of disease progression and recurrence, but it is unclear if it adequately reflects the AE profile with pembrolizumab or the reasons for withdrawal by the patient or physician. The incremental effect of AEs from pembrolizumab versus chemotherapy is a decrease in QALYs of 0.0004. It is unclear whether this truly represents the loss of quality of life suggested by the high rates of discontinuation, but CADTH was unable to adjust the analysis to reflect the potential of this or to reflect the reasons for withdrawal by patient or physician decision.
To explore the impact of a worse AE profile, CADTH conducted a sensitivity analysis in which the incremental effect of pembrolizumab on the disutility from AEs was 0.03, as opposed to 0.0004.
Generalizability of the KEYNOTE-522 trial: KEYNOTE-522 did not compare pembrolizumab adjuvant therapy with capecitabine adjuvant therapy, which became the standard of care for patients with residual invasive TNBC following surgery after the start of KEYNOTE-522. The degree of incremental benefit and cost derived from the model assumes that no other adjuvant therapy is given. The cost-effectiveness of pembrolizumab relative to capecitabine is unknown. It is unclear whether pembrolizumab would displace or be given alongside capecitabine and, in either case, how this would influence the EFS and OS of a pembrolizumab regimen.
CADTH was unable to address this limitation and notes that the cost-effectiveness of pembrolizumab versus capecitabine is unknown.
CADTH notes that the model was well designed and transparent, enabling a robust validation to be undertaken. The sponsor’s original model contained 120,977 uses of IFERROR statements. As IFERROR statements should not be needed to operate a model, CADTH requested that the sponsor remove these throughout the model, otherwise it would limit CADTH’s ability to fully validate the model. CADTH notes that the sponsor removed these without any impact on the model functionality or results. The revised model is used within this report.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Table 4: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Probability of death | Sponsor’s adjustment for all-cause mortality was inappropriate and led to probabilities lower than the general population | CADTH revised analysis ensured probabilities were no lower than the general population |
Changes to derive the CADTH base case | ||
2. Waning of treatment effect | Sponsor assumed no waning of treatment effect | Based on evidence from the KEYNOTE-522 trial and the clinical experts’ opinions, CADTH assumed that treatment effect, with respect to the probability of an event, waned beginning after 3 years, with the same probability of an event after 5 years |
3. Choice of survival functions | Sponsor assumed a piecewise function with a generalized gamma model for the pembrolizumab regimen and a piecewise function with log-normal model for chemotherapy | CADTH assumed a piecewise function with log-normal model for both regimens |
4. Probability of events within the LRR and DM states | Sponsor used data from the KEYNOTE-522 trial to model probabilities | Given concerns over the short life expectancy assumed in both states, CADTH adopted revised probabilities to reflect the current literature and the clinical experts’ opinions |
5.Dose intensity | Sponsor assumed reduced dose intensity with all therapies | CADTH assumed full dose intensity with all therapies |
6.Weight-based dosing | Pembrolizumab dose was based on fixed dose | Pembrolizumab dose was based on weight-based dosing |
CADTH base-case analysis | — | 1 + 2 + 3 + 4 + 5 |
CADTH scenario analysis (weight-based dose) | — | 1 + 2 + 3 + 4 + 5 + 6 |
DM = distant metastases; LRR = locoregional recurrence.
The CADTH base-case analysis also found that pembrolizumab as a neoadjuvant and adjuvant therapy was associated with more QALYs (16.29 versus 14.97) and increased costs ($175,870 versus $68,940), leading to an ICER of $81,408.
In the CADTH base case, the QALY and life-year gains at 5 years are 0.09 and 0.08, respectively. Over the lifetime time horizon, these values increase to 1.32 and 1.51, suggesting that even when waning of treatment effect is adopted, less than 10% of benefit is accumulated in the initial period, where treatment impacts transition probabilities. This is illustrated in Figure 4, which contrasts the QALY gains from the sponsor’s model with the final QALY gains from the CADTH analysis assuming a waning treatment effect.
Incremental costs for pembrolizumab were due to the increased drug costs from pembrolizumab, which were partially offset by reduced DM treatment costs. The incremental QALYs were primarily due to increased time in the event-free state, which was partially offset by reduced times in the LRR and DM states (Appendix 4).
In the CADTH base-case analysis, the probability of pembrolizumab being cost-effective at a threshold of $50,000 per QALY was 11.4%.
Table 5: Summary of the Stepped Analysis of the CADTH Reanalysis
Stepped analysis | Pembrolizumab vs. chemotherapy | ||
|---|---|---|---|
Incremental costs, $ | Incremental QALYs | ICER, $/QALY | |
Sponsor’s base casea | 103,349 | 4.09 | 25,249 |
CADTH reanalysis 1b | 103,668 | 4.42 | 23,453 |
CADTH reanalysis 2b | 108,016 | 1.65 | 65,549 |
CADTH reanalysis 3b | 107,231 | 2.25 | 47,591 |
CADTH reanalysis 4b | 99,028 | 3.18 | 31,102 |
CADTH reanalysis 5b | 106,978 | 4.26 | 25,118 |
CADTH base-case analysis 1 + 2 + 3 + 4 + 5a | 106,930 | 1.31 | 81,408 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aAnalysis based on probabilistic analysis.
bAnalysis based on deterministic analyses.
Scenario and Sensitivity Analysis Results
The above analyses are based on publicly available prices of the comparator treatments and on a fixed-dose regimen for pembrolizumab. Within the scenario analysis incorporating weight-based dosing for pembrolizumab, the incremental costs with pembrolizumab were $89,042 and the incremental QALYs were 1.31. This leads to a lower ICER of $67,657. The probability that pembrolizumab is cost-effective based on a threshold of $50,000 per QALY increased to 22%.
A sensitivity analysis was conducted that increased the QALY decrement due to AEs up to 0.03. This analysis was conducted to demonstrate the sensitivity of the results to dramatic shifts in AE disutility. In this analysis, the ICER increases to $83,539 per QALY (incremental costs: $106,930; incremental QALYs: 1.28). This demonstrates that if pembrolizumab generates the additional survival gains as predicted by the model, then even substantial changes in AEs will have a small impact on the cost-effectiveness conclusions.
Table 6 provides an analysis of the impact of a price reduction for pembrolizumab on the estimated ICERs for both the sponsor’s submission and the CADTH base-case and scenario analyses.
Based on the sponsor’s analysis, at the list price, pembrolizumab is cost-effective, assuming a threshold of $50,000 per QALY, and no price reduction is required. Based on the CADTH base-case analysis, a price reduction for pembrolizumab of 36% is required for the ICER to be reduced to $50,000 per QALY. Based on the CADTH scenario analysis, a price reduction of 24% is required for the ICER to be reduced to $50,000 per QALY.
The above analyses are based on publicly available prices of the comparator treatments and exclude any current effective price for pembrolizumab.
Table 6: CADTH Price Reduction Analyses
Price reduction, % | ICERs for pembrolizumab vs. chemotherapy | ||
|---|---|---|---|
Sponsor base case, $ | CADTH case, flat-based dose, $ | CADTH scenario analysis, weight-based dose, $ | |
No price reduction | 24,346 | 81,408 | 67,657 |
10 | 22,554 | 72,711 | 60,333 |
20 | 22,554 | 64,013 | 53,010 |
24 | 19,860 | 60,534 | 50,000 |
30 | 18,782 | 55,316 | 45,687 |
36 | 17,165 | 50,000 | 41,293 |
40 | 15,548 | 46,619 | 38,364 |
50 | 14,470 | 37,922 | 31,041 |
60 | 11,776 | 29,225 | 23,718 |
70 | 9,081 | 20,528 | 16,395 |
80 | 6,386 | 11,831 | 9,072 |
90 | 3,692 | 3,134 | 1,749 |
100 | Dominant | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio.
Overall Conclusions
The CADTH clinical review noted that evidence from 1 pivotal study (KEYNOTE-522) suggests that pembrolizumab plus chemotherapy as neoadjuvant and adjuvant therapy has a clinically meaningful impact on EFS and OS compared to placebo plus chemotherapy as neoadjuvant therapy alone, according to clinical experts. The median OS and median EFS were not estimable at the fourth interim analysis; thus, there is uncertainty in the effect of the intervention for OS and EFS.
CADTH undertook reanalyses to address several key limitations identified in the sponsor’s model. CADTH revised the sponsor’s model to incorporate a treatment waning effect; used more appropriate survival estimates for LRR and DM; set RDI to 100% for all drugs; used alternative survival functions for EFS; and fixed programming errors within the model. For the CADTH base case, the ICER of the pembrolizumab regimen compared to chemotherapy alone was $81,408 per QALY (incremental costs: $106,930; incremental QALYs: 1.31) in the Health Canada–indicated population.
CADTH notes that the majority of QALY benefit is derived from additional survival (model predicts an additional 1.52 additional life-years). This additional survival benefit is derived through the prevention of LRR and DM, which reduce life expectancy. The extent of OS benefit depends on:
how many LRR and DM events are prevented, rather than delayed
the impact LRR and DM have on life expectancy.
Regarding the first point, given the length of follow-up obtained from the trial, including the time spent off treatment, clinical experts felt that pembrolizumab could prevent some LRR and DM events from occurring relative to chemotherapy alone. Regarding the second point, as part of the CADTH reanalysis, more appropriate assumptions regarding life expectancy outcomes for those who experience LRR or DM were used based on Canadian data. If LRR or DM were only delayed and not prevented, then the cost-effectiveness of pembrolizumab is greatly diminished. Therefore, although the analysis models a plausible estimate of long-term survival, longer term data would help validate the survival outcomes predicted by the model.
Based on the CADTH reanalysis, the price of pembrolizumab would need to be reduced by 36% for it to be cost-effective at a $50,000 per QALY threshold. If pembrolizumab were provided through weight-based dosing, assuming equal effectiveness as in the trial, the ICER would decrease to $67,657 per QALY. This is because with vial sharing, pembrolizumab can be given at a lower cost than at a fixed-based dose, and as efficacy is assumed to be equivalent, this leads to a lower ICER. Under these assumptions, the price of pembrolizumab would need to be reduced by 24% for it to be cost-effective. Substantially higher price reductions would be required if pembrolizumab did not translate into additional survival gains for patients. CADTH notes that the OS findings are interim, with other analyses planned after a pre-specified number of events have occurred. Additional data on OS could be used to validate findings from the model.
CADTH notes that KEYNOTE-522 did not compare pembrolizumab adjuvant therapy with capecitabine adjuvant therapy, which became the standard of care for patients with residual invasive TNBC following surgery after the start of KEYNOTE-522. The cost-effectiveness of pembrolizumab versus capecitabine as an adjuvant therapy is unknown and cannot be addressed given the clinical evidence base available. The CADTH assessment of cost-effectiveness is dependent on the generalizability of the KEYNOTE trial to current practice.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada Inc. 2022 Feb 17.
2.Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N Engl J Med. 2020;382(9):810-821. PubMed
3.Schmid P, Cortes J, Dent R, et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386(6):556-567. PubMed
4.Latimer NR. Survival analysis for economic evaluations alongside clinical trials - extrapolation with patient-level data. NICE DSU technical support document no. 14. London (United Kingdom): National Institute for Health and Care Exellence (NICE); 2013: . Accessed 2022 Jun 17.
5.Statistics Canada. Table 13-10-0392-01: Deaths and age-specific mortality rates, by selected grouped causes. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039201. Accessed 2022 Jun 17.
6.Brezden-Masley C, Fathers KE, Coombes ME, Pourmirza B, Xue C, Jerzak KJ. A population-based comparison of treatment patterns, resource utilization, and costs by cancer stage for Ontario patients with triple-negative breast cancer. Cancer Med. 2020;9(20):7548-7557. PubMed
7.Mittmann N, Liu N, Cheng SY, et al. Health system costs for cancer medications and radiation treatment in Ontario for the 4 most common cancers: a retrospective cohort study. CMAJ Open. 2020;8(1):E191-e198. PubMed
8.Beauchemin C, Letarte N, Mathurin K, Yelle L, Lachaine J. A global economic model to assess the cost-effectiveness of new treatments for advanced breast cancer in Canada. J Med Econ. 2016;19(6):619-629. PubMed
9.Wehler E, Zhao Z, Pinar Bilir S, Munakata J, Barber B. Economic burden of toxicities associated with treating metastatic melanoma in eight countries. Eur J Health Econ. 2017;18(1):49-58. PubMed
10.Allen K, Lohrisch CA, Le D, et al. Survival following locoregional recurrence in breast cancer by clinical subtype. J Clin Oncol. 2021;39(15_suppl):543-543.
11.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada Inc. 2022 Feb 17.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CADTH Cost Comparison Table for Neoadjuvant Treatments for TNBC
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Cost per 28-day cyclea ($) |
|---|---|---|---|---|---|---|
Pembrolizumab | 100 mg/4mL | 100 mg | 4,400.0000b | 200mg, every 3 weeks | 419 | 11,733 |
400mg, every 6 weeks | ||||||
Protocol used in the trial (similar to CRBPPACL(W) followed by AC) | ||||||
Carboplatin (generics) | 10 mg/mL | 50 mg 150 mg 450 mg 600 mg | 70.0000 210.0000 600.0000 775.0000 | AUC 5 on Day 1 every 3 weeks for 4 cyclesd | 40 | 1,127 |
Or, AUC 1.5 on day 1 every week for 12 weeks | 40 | 1,120 | ||||
Paclitaxel (Taxol) | 6 mg/mL | 30 mg vial 96 mg vial 150 mg vial 300 mg vial | 300.0000 1,196.8000 1,870.0000 3,740.0000 | 80 mg/m2 on Day 1 every 3 weeks for 4 cycles | 278 | 7,779 |
Carboplatin (AUC 5 every 3 weeks) + Paclitaxel per 28-days | 8,906 | |||||
Carboplatin (AUC 1.5 weekly) + Paclitaxel per 28-days | 8,899 | |||||
Doxorubicin (generics) | 2 mg/mL | 10 mg vial 50 mg vial 200 mg vial | 50.0000 255.0000 770.0000 | After CP: 60 mg/m2 IV on Day 1 once every 3 weeks for 4 cycles | 27 | 747 |
Epirubicin | 2 mg/mL | 50 mg vial 200 mg vial | 194.8900 803.6400 | Or, 90 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 38 | 1,072 |
Cyclophosphamide (generics) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial | 91.3100 165.5200 304.4000 | 600 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 12 | 514 |
Doxorubicin + Cyclophosphamide per 28-days | 1,096 | |||||
Epirubicin + Cyclophosphamide per 28-days | 1,421 | |||||
AC-PACL (DD) | ||||||
Doxorubicin (generics) | 2 mg/mL | 10 mg vial 50 mg vial 200 mg vial | 50.0000 255.0000 770.0000 | 60 mg/m2 IV on Day 1 every 2 weeks for 4 cycles | 40 | 1,120 |
Cyclophosphamide (generics) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial | 91.3100 165.5200 304.4000 | 600 mg/m2 IV on Day 1 every 2 weeks for 4 cycles | 19 | 524 |
Paclitaxel (Taxol) | 6 mg/mL | 30 mg vial 96 mg vial 150 mg vial 300 mg vial | 374.0000 1,196.8000 1,870.0000 3,740.0000 | After AC is complete: 175 mg/m2 on Day 1 every 2 weeks for 4 cycles | 294 | 8,228 |
AC-PACL(DD) per 28-days | 9,872 | |||||
AC-PACL (W) | ||||||
Doxorubicin (generics) | 2 mg/mL | 10 mg vial 50 mg vial 200 mg vial | 50.0000 255.0000 770.0000 | 60 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 27 | 747 |
Cyclophosphamide (generics) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial | 91.3100 165.5200 304.4000 | 600 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 12 | 349 |
Paclitaxel (Taxol) | 6 mg/mL | 30 mg vial 96 mg vial 150 mg vial 300 mg vial | 300.0000 1,196.8000 1,870.0000 3,740.0000 | After AC is complete: 80 mg/m2 every week for 12 weeks | 278 | 7,779 |
AC-PACL(W), per 28-days | 8,875 | |||||
AC-D/TAC | ||||||
Doxorubicin (generics) | 2 mg/mL | 10 mg vial 50 mg vial 200 mg vial | 50.0000 255.0000 770.0000 | 60 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 27 | 747 |
Cyclophosphamide (generics) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial | 91.3100 165.5200 304.4000 | 600 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 12 | 349 |
Docetaxel (generics) | 10 mg/mL 10 mg/mL 20 mg/mL 20 mg/mL 20 mg/mL | 80 mg vial 160 mg vial 20 mg vial 80 mg vial 160 mg vial | 970.2000 1,850.0000 249.0000 497.0000 990.0000 | After AC is complete: 100 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 59 | 1,652 |
AC-D, per 28-days | 2,748 | |||||
TC with carboc | ||||||
Docetaxel (generics) | 10 mg/mL 10 mg/mL 20 mg/mL 20 mg/mL 20 mg/mL | 80 mg vial 160 mg vial 20 mg vial 80 mg vial 160 mg vial | 970.2000 1,850.0000 249.0000 497.0000 990.0000 | 75 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 47 | 1,327 |
Carboplatin (generics) | 10 mg/mL | 50 mg 150 mg 450 mg 600 mg | 70.0000 210.0000 600.0000 775.0000 | AUC 6 on Day 1 every 3 weeks for 4 cyclesd | 47 | 1,313 |
TC | 2,640 | |||||
TC with cyclophophamidec | ||||||
Docetaxel (generics) | 10 mg/mL 10 mg/mL 20 mg/mL 20 mg/mL 20 mg/mL | 80 mg vial 160 mg vial 20 mg vial 80 mg vial 160 mg vial | 970.2000 1,850.0000 249.0000 497.0000 990.0000 | 100 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 59 | 1,652 |
Cyclophosphamide (generics) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial | 91.3100 165.5200 304.4000 | 600 mg/m2 IV on Day 1 every 3 weeks for 4 cycles | 12 | 349 |
TC | 2,001 | |||||
FEC-D | ||||||
Fluorouracil (generics) | 50 mg/mL | 500 mg vial | 160.9000 | 500 mg/m2 IV on Day 1 every 3 weeks for 3 cycles | 8 | 214 |
Epirubicin | 2 mg/mL | 50 mg vial 200 mg vial | 194.8900 803.6400 | 100 mg/m2 IV on Day 1 every 3 weeks for 3 cycles | 38 | 1,072 |
Cyclophosphamide (generics) | 20 mg/mL | 500 mg vial 1,000 mg vial 2000 mg vial | 91.3100 165.5200 304.4000 | 500 mg/m2 IV on Day 1 every 3 weeks for 3 cycles | 16 | 450 |
Docetaxel (generics) | 10 mg/mL 10 mg/mL 20 mg/mL 20 mg/mL 20 mg/mL | 80 mg vial 160 mg vial 20 mg vial 80 mg vial 160 mg vial | 970.2000 1,850.0000 249.0000 497.0000 990.0000 | After FEC is complete: 100 mg/m2 IV on Day 1 every 3 weeks for 3 cycles | 59 | 1,652 |
FEC-D, per 28 days | 3,388 | |||||
Note: All prices are wholesale prices from the IQVIA Delta PA database (accessed March 2022), unless otherwise indicated, and do not include dispensing or administration fees but do assume wastage of excess medication in vials. Doses are from the Cancer Care Ontario Drug Formulary regimen database.
Mean patient body weight was assumed to be 69.7 kg, while mean body surface area was 1.8 m2. For the purposes of calculating glomerular filtration rate, patient age was assumed to be 49 and serum creatinine was 0.8871.
A = doxorubicin; AUC = product of serum concentration (mg/mL) and time (min); C = cyclophosphamide; CRBP = carboplatin; D = docetaxel; DD = dose dense; F = fluorouracil; E = epirubicin; GFR = glomerular filtration rate; IV = IV; PACL = paclitaxel; SC = subcutaneous.
aCost standardized to 28-day cycles to allow for comparison among regimens of different cycle lengths.
bSponsor’s submitted price.
cRegimen indicated for treating patients who are not eligible to receive anthracyclines.
Table 8: CADTH Cost Comparison Table for Adjuvant Treatments for Triple-Negative Breast Cancer (TNBC)
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Cost per 28-day cycle ($) |
|---|---|---|---|---|---|---|
Pembrolizumab | 100 mg/4mL | 100 mg | 4,400.0000a | 200mg, every 3 weeks 400, every 6 weeks | 419 | 11,733 |
Other regimens | ||||||
Capecitabineb | 150 mg 500 mg | 150 mg tab 500 mg tab | 0.4575 1.5250 | 1,250 mg/m2 twice a day from days 1 to 14 every 21 days | 9 | 256 |
Olaparibc,d | 100 mg 150 mg | 100 mg tab 150 mg tab | 66.6173 66.6173 | 300 mg twice a day for 52 weeks | 267 | 7,461 |
Note: All prices are wholesale prices from the IQVIA Delta PA database (accessed March 2022), unless otherwise indicated, and do not include dispensing or administration fees but do assume wastage of excess medication in vials. Doses are from the Cancer Care Ontario Drug Formulary regimen database.
Mean patient body weight was assumed to be 69.7 kg, while mean body surface area was 1.8 m2.
aSponsor’s submitted price.
bIndicated for treatment of patients with residual disease after surgery.
cIndicated for treatment of patients with BRCA mutation (not funded).
dPrices from the Ontario Exceptional Access Program.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Commentsa |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | — |
Model has been adequately programmed and has sufficient face validity | Yes | — |
Model structure is adequate for decision problem | Yes | — |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | — |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | — |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | — |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
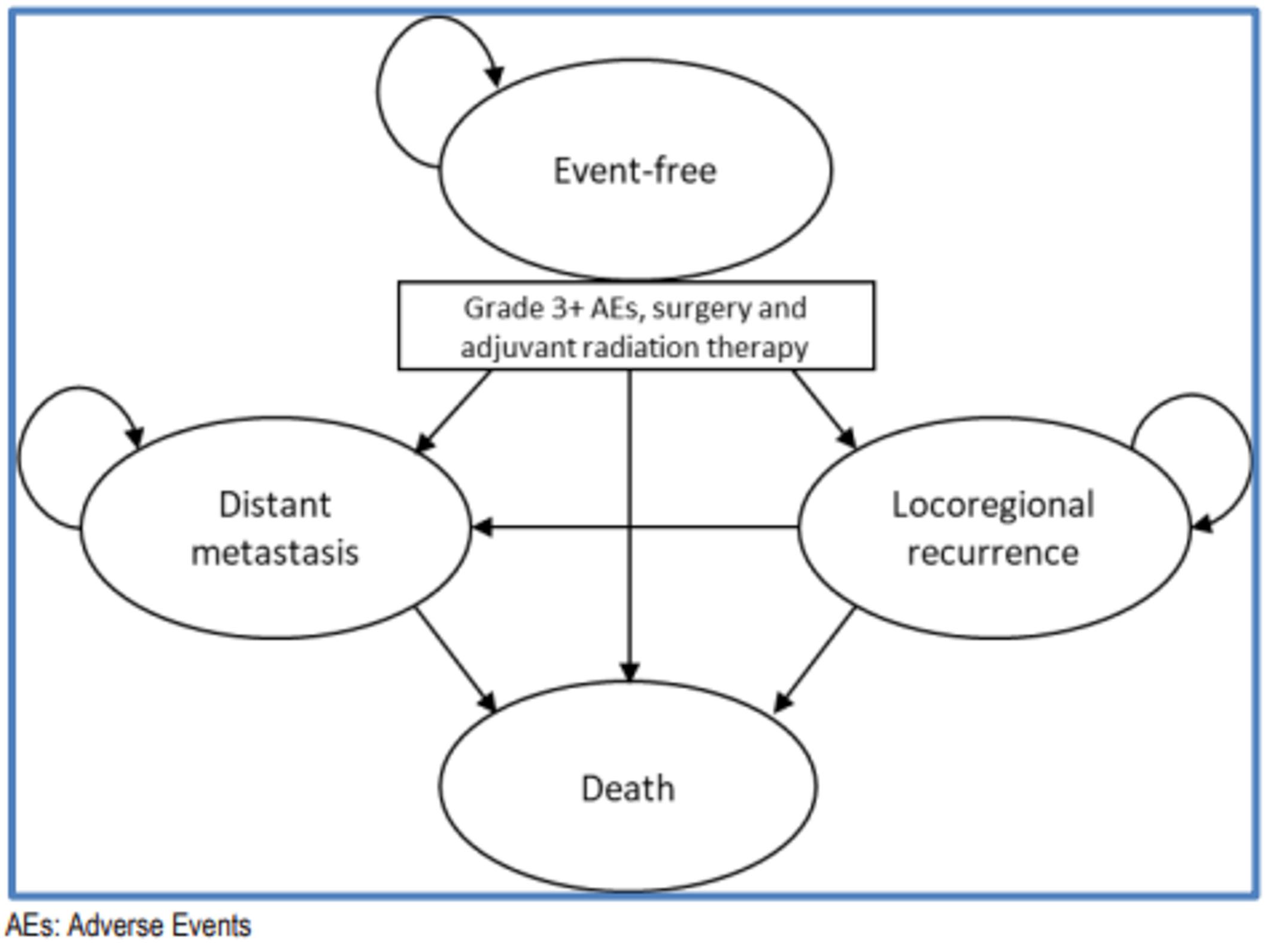
Figure 2: Annual QALY Gains with Pembrolizumab from Sponsor’s Model
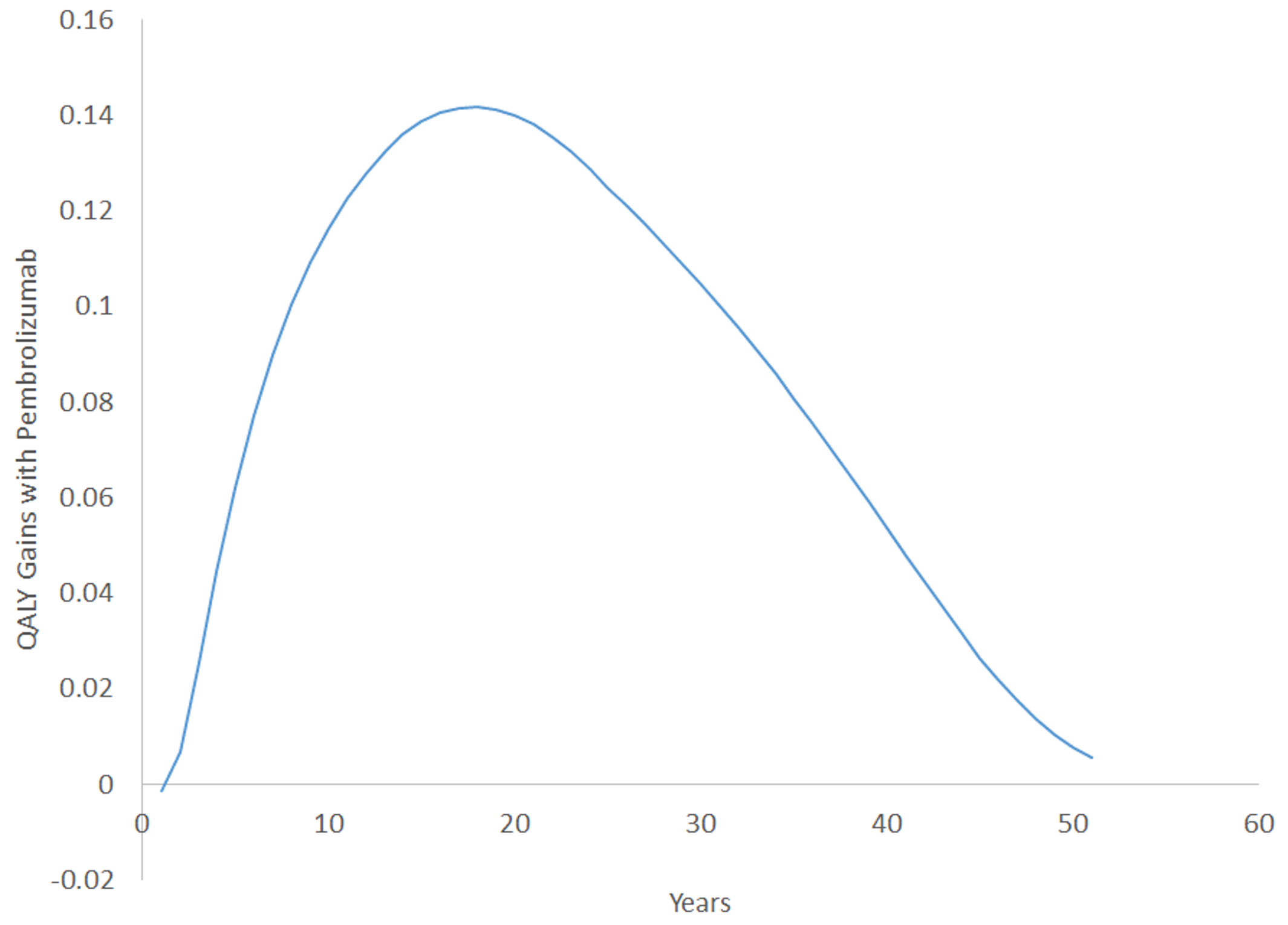
Source: CADTH calculation based on sponsor’s base-case analysis.
Figure 3: Ratio of Probabilities of Having an Event for the Pembrolizumab Regimen to Chemotherapy
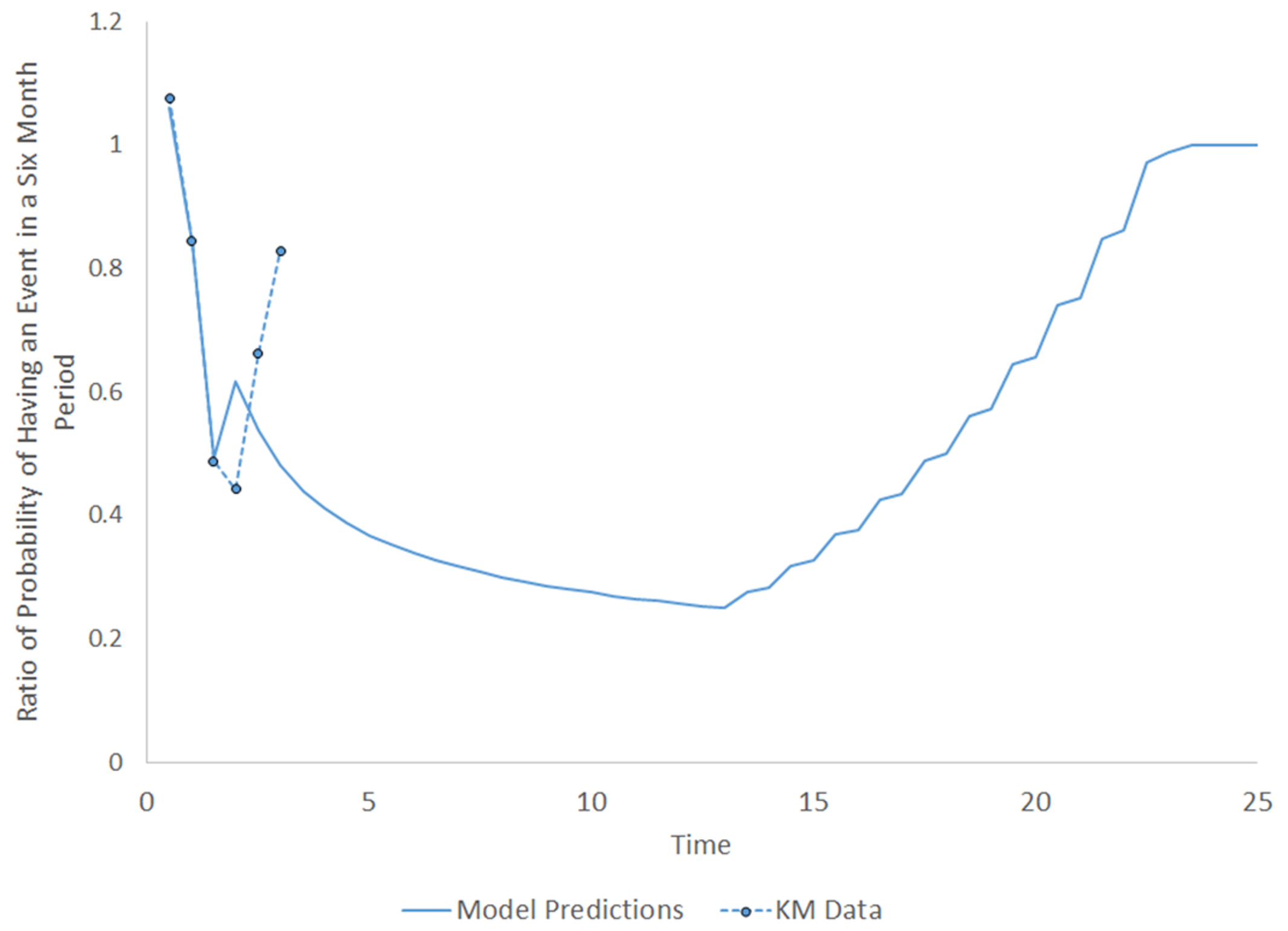
Source: CADTH calculation based on sponsor’s base-case analysis and the KEYNOTE-522 trial.
Table 10: Sponsor’s Disaggregated Results
Cost, QALY, and LYs | Pembrolizumab plus chemotherapy | Chemotherapy |
|---|---|---|
Total costs (2020 CAD) | 160,094 | 56,744 |
Neoadjuvant treatment costs | 65,773 | 3,857 |
Drug acquisition costs | 64,889 | 3,110 |
Drug administration costs | 883 | 747 |
Adjuvant treatment costs | 48,120 | 0 |
Drug acquisition costs | 48,010 | 0 |
Drug administration costs | 110 | 0 |
Surgery costs | 1,840 | 1,835 |
Radiation costs | 14,123 | 14,586 |
Metastatic treatment costs | 3,214 | 7,058 |
Disease management costs | 5,101 | 5,391 |
Event-free | 4,441 | 3,916 |
Locoregional recurrence | 210 | 428 |
Distant metastasis | 449 | 1,047 |
Terminal care costs | 20,371 | 22,758 |
Adverse event costs | 1,552 | 1,260 |
Total QALYs | 19.18 | 15.09 |
Event-free | 18.92 | 14.49 |
On treatment | 0.84 | 0.90 |
AE-related QALY decrement | −0.01 | −0.00 |
Off treatment | 18.08 | 13.60 |
Locoregional recurrence | 0.09 | 0.19 |
Distant metastasis | 0.17 | 0.41 |
Within the trial period | 2.55 | 2.52 |
After the trial period | 16.63 | 12.57 |
Total Life-Years | 22.65 | 17.89 |
Event-free | 22.29 | 17.08 |
Locoregional recurrence | 0.12 | 0.24 |
Distant metastasis | 0.24 | 0.57 |
Source: Sponsor’s pharmacoeconomic submission, probabilistic analysis.
Appendix 4: Additional Details on the CADTH Base-Case and Scenario Analyses
Note that this appendix has not been copy-edited.
Figure 4: Annual QALY Gains with Pembrolizumab: Comparison of Sponsor’s Model and CADTH Base-Case Assumption Relating to Waning of Treatment Effect
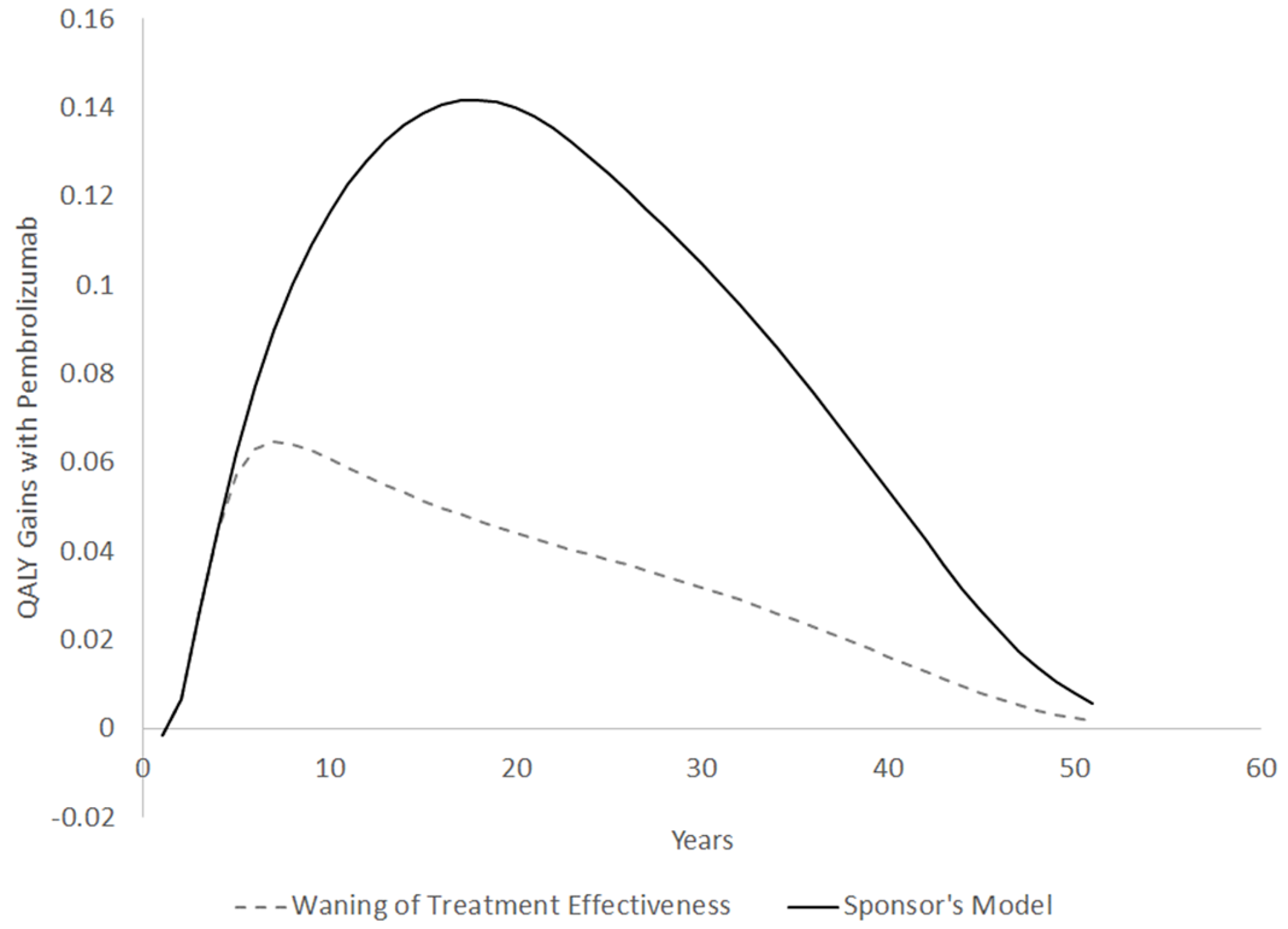
Source: CADTH calculation based on sponsor’s base-case analysis.
Table 11: CADTH Base-Case Analysis Disaggregated Results
Cost, QALY, and LYs | Pembrolizumab plus chemotherapy | Chemotherapy |
|---|---|---|
Total costs (2020 CAD) | 175,870 | 68,940 |
Neoadjuvant treatment costs | 69,620 | 3,882 |
Drug acquisition costs | 68,739 | 3,137 |
Drug administration costs | 881 | 745 |
Adjuvant treatment costs | 48,632 | 0 |
Drug acquisition costs | 48,523 | 0 |
Drug administration costs | 110 | 0 |
Surgery costs | 1,843 | 1,839 |
Radiation costs | 14,141 | 14,620 |
Metastatic treatment costs | 11,203 | 17,467 |
Disease management costs | 6,752 | 7,011 |
Event-free | 4,259 | 3,887 |
Locoregional recurrence | 1,140 | 1,383 |
Distant metastasis | 1,353 | 1,742 |
Terminal care costs | 22,121 | 22,858 |
Adverse event costs | 1,558 | 1,262 |
Total QALYs | 16.29 | 14.97 |
Event-free | 15.22 | 13.64 |
On treatment | 0.84 | 0.90 |
AE-related QALY decrement | −0.01 | −0.00 |
Off treatment | 14.39 | 12.75 |
Locoregional recurrence | 0.52 | 0.64 |
Distant metastasis | 0.54 | 0.70 |
Within the trial period | 2.60 | 2.57 |
After the trial period | 13.69 | 12.41 |
Total Life-Years | 19.35 | 17.85 |
Event-free | 17.94 | 16.07 |
Locoregional recurrence | 0.65 | 0.79 |
Distant metastasis | 0.76 | 0.98 |
Table 12: CADTH Scenario Analysis, Using Weight-Based Pembrolizumab Costs, Disaggregated Results
Cost, QALY, and LYs | Pembrolizumab plus chemotherapy | Chemotherapy |
|---|---|---|
Total costs (2020 CAD) | 158,412 | 69,010 |
Neoadjuvant treatment costs | 59,572 | 3,892 |
Drug acquisition costs | 58,690 | 3,147 |
Drug administration costs | 882 | 745 |
Adjuvant treatment costs | 41,204 | 0 |
Drug acquisition costs | 41,094 | 0 |
Drug administration costs | 110 | 0 |
Surgery costs | 1,834 | 1,830 |
Radiation costs | 14,111 | 14,577 |
Metastatic treatment costs | 11,246 | 17,562 |
Disease management costs | 6,773 | 7,029 |
Event-free | 4,272 | 3,897 |
Locoregional recurrence | 1,135 | 1,377 |
Distant metastasis | 1,366 | 1,755 |
Terminal care costs | 22,119 | 22,865 |
Adverse event costs | 1,553 | 1,254 |
Total QALYs | 16.30 | 14.98 |
Event-free | 15.23 | 13.64 |
On treatment | 0.84 | 0.90 |
AE-related QALY decrement | −0.01 | −0.00 |
Off treatment | 14.40 | 12.75 |
Locoregional recurrence | 0.52 | 0.64 |
Distant metastasis | 0.54 | 0.70 |
Within the trial period | 2.60 | 2.57 |
After the trial period | 13.70 | 12.41 |
Total Life-Years | 19.37 | 17.85 |
Event-free | 17.95 | 16.07 |
Locoregional recurrence | 0.65 | 0.79 |
Distant metastasis | 0.77 | 0.99 |
Additional details regarding mortality programming error in the sponsor’s model.
The formulas in the sponsors model for estimating the probability of death is:
= MAX(Pop DEATH rate - prob LRR - prob DM, prob ANY EVENT * prob DEATH| Event))
Formulas for mortality from LRR are similar.
The formula should be:
= MAX(Pop DEATH rate, prob ANY EVENT * prob DEATH| Event))
Similar formulas need to be adopted for the probability of death with LRR.
= MAX(Pop DEATH rate, prob DEATH| LRR))
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) assessed pembrolizumab in combination with chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment after surgery, in early-stage TNBC.11 The analysis was taken from the perspective of the Canadian public drug plans using a top-down epidemiology approach, with drug and administration costs considered. A 3-year time horizon was used, from April 2023 to March 2026. The eligible population was estimated based on data from Canadian Cancer Statistics and adjusted using epidemiology estimates from various sources including published literature and Statistics Canada, to limit for type of breast cancer and cancer stage (Figure 2). Key inputs to the BIA are documented in Table 15.
The reference case scenario included neoadjuvant and adjuvant chemotherapy, with anthracycline-/taxane-based chemotherapy being the current standard of care for neoadjuvant therapy. However, because the sponsor considered that the addition of pembrolizumab to the current standard of care would not modify or replace the agents currently in use, reference case scenario was set as to zero (i.e., status Quo) and the new drug scenario included only pembrolizumab costs. The market share estimates were based on sponsor’s assumptions. Within the market shares for the reference and new drug scenarios, the sponsor assumed 10% of patients would be participating in clinical trials. The submitted BIA also included costs of subsequent treatments for advanced TNBC for both reference and new drug scenarios. The costs were sources from multiple sources including IQVIA Delta PA database, pCODR reports, and the literature. The subsequent treatments consisted in a weighted bucket of therapies which varied depending on whether patients received pembrolizumab or not in the neoadjuvant setting. The market share for each 1 of the subsequent treatment options was based on sponsor’s estimates. The duration of therapy with all treatments was estimated from parametric distributions fitted to Kaplan–Meier time-on-treatment data from KN522 clinical trial.
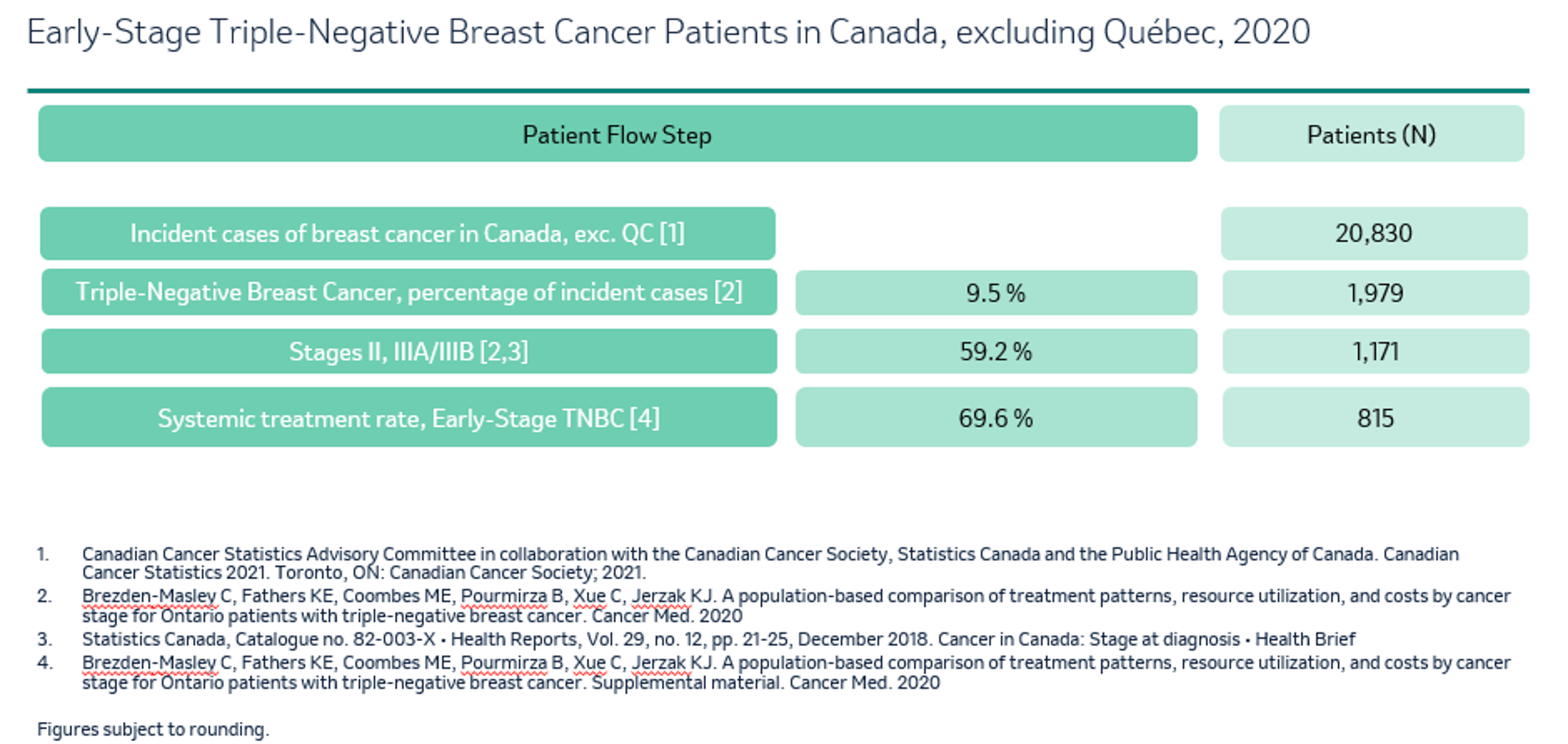
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1, year 2, and year 3; if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 860 / 874 / 887 |
Market Uptake (3 years) | |
Uptake (reference scenario) SoC Clinical trial protocol | 90% / 90% / 90% 10% / 10% / 10% |
Uptake (new drug scenario) Pembrolizumab + SoC SoC Clinical trial protocol | ||||| | ||||| | ||||||||||| | ||||| | ||||||||||| | ||||| | ||||| ||||| | ||||| | ||||||||||| | ||||| | ||||||||||| | ||||| | ||||| ||||| | ||||| | ||||||||||| | ||||| | ||||||||||| | ||||| | ||||| |
Cost of treatment (per patient) | |
Cost of treatment over one cycle (3 weeks) Pembrolizumab + SoC SoC Clinical trial protocol | $8,360 $0 $0 |
Cost of subsequent therapies per cycle Gemcitabine-Carboplatin Paclitaxel Nab-Paclitaxel Capecitabine | $52 $47 $4,066 $94 |
SoC: standard of care.
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding pembrolizumab for the treatment of early-stage TNBC was $10,134,447, $48,998,818, $75,183,850 for year 1, 2, and 3, respectively. The 3-year total was $134,317,115.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The sponsor’s assumption regarding patient enrolment in clinical trials as a comparator is uncertain: The sponsor assumed that 10% of patients were enrolled in clinical trials and as a result received trial medications – not incurring treatment/ drug costs. This artificially decreases the estimated market size, omitting treatment costs incurred by patients in clinical trials and underestimating the budget impact. Likewise, if pembrolizumab was approved this may decrease clinical trial use as patient’s would forgo an effective therapy to be placed on the trial. Clinical experts consulted for this review noted that patient enrolment in clinical trials can vary significantly by province.
In CADTH reanalysis, clinical trials were removed from the market mix; the market share of clinical trials was re-distributed over other comparators based on feedback from clinical experts.
The market uptake for pembrolizumab may be underestimated: In its BIA, the sponsor estimated that ||||% of patients would have pembrolizumab prescribed in the first year. According to the clinical experts consulted for this review, pembrolizumab is expected to have a faster uptake, especially as it is a drug that is well known by the oncologists. The final expected uptake was felt to be as high as 95% with uptake after a year reaching 55%. Although it was agreed that initial uptake would be faster than what was presumed by the sponsor it was noted that there is some uncertainty regarding final uptake percentages among all clinicians in Canada.
CADTH changed the base case to address this limitation, with market uptake rates starting from 55% in the first year, reaching 95% in year 2. A scenario analysis was conducted that assumed a peak 80% uptake.
Weight-based dosing for pembrolizumab: Pembrolizumab dosing in KEYNOTE-522 was a fixed dose of 200 mg intravenously every 21 days. After consultation, CADTH notes that in line with other indications for pembrolizumab, jurisdictions would likely implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks with the possibility of extended dosing intervals of every 6 weeks (4mg/kg up to a 400mg cap). The clinical experts agreed that this approach seemed reasonable, given the interchangeable use in dosing for other tumour sites.
CADTH assumed pembrolizumab would be provided using a weight-based dosing based on an average weight of 69.7kg. A scenario analysis was conducted using a flat-based dose as per the KEYNOTE-522 trial.
Use of RDI is inappropriate: The sponsor’s base case incorporates reduced dose intensities for all therapies (i.e., for neoadjuvant, adjuvant, subsequent therapies). Consistent with previous reviews, given the inability to link reduced dose intensity with outcomes, the CADTH base case does not incorporate reduced dose intensity. CADTH notes RDI estimates derived from the trial apply to a fixed-based dose and therefore would not be applicable to a weight-based dose.
CADTH uses the functionality within the sponsor’s model to exclude reduced dose intensity.
Budget impact of patients diagnosed in years 1 to 3 not fully captured: To provide a more exact estimate over 3 years the sponsor assumed those diagnosed with TNBC (stage II to III) would be spread evenly over the year. Although the sponsor notes that 887 patients are diagnosed in the final year of the analysis only full neoadjuvant/adjuvant costs will be captured for those diagnosed in the first week (as costs are incurred over a year). Although this approach potentially provides a more accurate estimate of costs that are incurred in a 3-year period the analysis omits a substantial impact on the budget that will be incurred in year 4. Likewise, this approach makes the BIA sufficiently more complex and difficult to validate.
Given complexities in the sponsor’s modelling approach CADTH conducted a scenario analysis which estimated the full neoadjuvant/adjuvant costs for all incident patients diagnosed in years 1 to 3. To calculate this budget impact CADTH assumed in the new drug scenario: 860, 874, and 887 patients would be diagnosed in years 1 to 3 respectively. In year 1 55% (473 patients) would receive pembrolizumab, in year 2 95% (830 patients) would receive pembrolizumab and in year 3 95% (843 patients) would receive pembrolizumab. The rest would receive standard of care. In the reference scenario CADTH assumes 100% of patients in all years receive standard of care.
The total cost of adjuvant and neoadjuvant therapy, using a weight-based dose, was taken from the sponsor’s cost–utility analysis and was estimated to be $99,784 for those receiving pembrolizumab + chemotherapy. The cost of neoadjuvant SoC costs was taken from the sponsor model and estimated to be $3,147 chemotherapy costs alone). The sponsor excludes standard of care costs from its analysis as they are incurred regardless of whether pembrolizumab is funded. Given slight differences in treatment discontinuation they are included here for additional accuracy.
For simplicity CADTH has not included subsequent therapy costs in this analysis though notes the difference in subsequent therapy costs likely be under $1 million using the sponsor’s estimates.
Additional limitations were identified but were not considered to be key limitations. These limitations include:
NIHB population was not submitted although subsequent treatment includes drugs funded by NIHB: Subsequent treatments include drugs funded by NIHB. Therefore, the NIHB population should have been submitted to demonstrate the expected budget impact introduced by funding the drug under review. CADTH notes that the use of pembrolizumab may reduce subsequent therapy costs and this impact would be small.
Indication creep: Clinical experts discussed that there is potential for indication creep, however, most clinicians will not offer carboplatin to patients with stage I disease. For those patients receiving upfront surgery, adjuvant chemotherapy is not routinely offered for T1a or T1b N0 disease. If indication creep were to occur, then the budget impact would be inflated.
CADTH Reanalyses of the BIA
CADTH’s base case revised the proportion of patients on clinical trials, market uptake, RDI, and assumed a weight-based dosing for pembrolizumab.
Table 15: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case (none) | ||
Changes to derive the CADTH base case | ||
1. Proportion of patients on clinical trials and market uptake | Proportion of patients on trials: 10% Market uptake: 27.2% / 73.6% / 80.0% | Proportion of patients on trials: 0% Market uptake: ||| | ||| | ||| |
2. Use of relative dose intensity | Yes | No |
3. Weight-based dosage | Fixed dose of 200mg every 3 weeks or 400 every 6 weeks | Dosage of 2mg/kg every 3 weeks (or 4mg/kg every 6 weeks) considering mean weight of 69.65 kg based on KEYNOTE-522 trial, with no wastage |
CADTH base case | Reanalysis 1 + 2 + 3 | |
The results of the CADTH step-wise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17.
Based on the BIA base case, the expected budget impact for funding pembrolizumab for the treatment of pembrolizumab for neoadjuvant and adjuvant TNBC is expected to be $15,210,765 in year 1, $55,163,378 in year 2, and $67,716,386 in year 3, with a 3-year budget impact of $138,090,529.
Table 16: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $134,317,115 |
CADTH reanalysis 1 | $188,275,760 |
CADTH reanalysis 2 | $141,389,234 |
CADTH reanalysis 3 | $93,582,635 |
CADTH base case (1 + 2 + 3) | $138,090,529 |
BIA = budget impact analysis.
Table 17: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $7,064 | $71,503 | $175,613 | $279,767 | $526,882 |
New drug | $7,064 | $10,205,949 | $49,174,430 | $75,463,618 | $134,843,997 | |
Budget impact | $0 | $10,134,447 | $48,998,818 | $75,183,850 | $134,317,115 | |
CADTH reanalysis 1 | Reference | $7,064 | $71,503 | $175,613 | $279,767 | $526,882 |
New drug | $7,064 | $20,817,264 | $75,394,948 | $92,590,430 | 188,802,642 | |
Budget impact | $0 | $20,745,761 | $75,219,335 | $92,310,663 | $188,275,760 | |
CADTH reanalysis 2 | Reference | $7,560 | $76,874 | $189,735 | $303,229 | $569,837 |
New drug | $7,560 | $10,744,751 | $51,768,163 | $79,446,157 | $141,959,071 | |
Budget impact | $0 | $10,667,877 | $51,578,428 | $79,142,928 | $141,389,234 | |
CADTH reanalysis 3 | Reference | $7,064 | $71,503 | $175,613 | $279,767 | $526,882 |
New drug | $7,064 | $7,130,499 | $34,310,608 | $52,668,411 | $94,109,518 | |
Budget impact | $0 | $7,058,996 | $34,134,996 | $52,388,644 | $93,582,635 | |
CADTH base case | Reference | $7,560 | $76,874 | $189,735 | $303,229 | $569,837 |
New drug | $7,560 | $15,287,639 | $55,353,112 | $68,019,615 | $138,660,366 | |
Budget impact | $0 | $15,210,765 | $55,163,378 | $67,716,386 | $138,090,529 |
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 18:
Alternative market uptake (55% / 80% / 80%).
Consider wastage at 50% using the sponsor provided option to do so.
Fixed pembrolizumab dose of 200mg every 3 weeks (400mg every 6 weeks) using the sponsor provided option to do so.
Incidence of breast cancer to occur at the beginning of each year using CADTH calculations.
Results of CADTH’s scenario analyses demonstrate that the estimated budget impact is highly sensitive to the changes in dosing and wastage. CADTH notes that scenario analysis 4 indicates that the current analysis does not account for a substantial amount of budget impact that will occur in year 4. It was unclear whether this increase was due entirely to the timing of when individuals were diagnosed due to the complexity in the sponsor’s model.
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
CADTH scenario 1: alternative market uptake (55% / 80% / 80%) | Reference | $7,560 | $76,874 | $189,735 | $303,229 | $569,837 |
New drug | $7,560 | $16,204,786 | $49,398,273 | $57,365,052 | $122,968,111 | |
Budget impact | $0 | $16,127,912 | $49,208,538 | $57,061,824 | $122,398,274 | |
CADTH scenario 2: wastage 50% | Reference | $7,560 | $76,874 | $189,735 | $303,229 | $569,837 |
New drug | $7,560 | $18,601,118 | $67,361,220 | $82,747,397 | $168,709,734 | |
Budget impact | $0 | $18,524,244 | $67,171,485 | $82,444,168 | $168,139,897 | |
CADTH scenario 3: fixed pembrolizumab dose | Reference | $7,560 | $76,874 | $189,735 | $303,229 | $569,837 |
New drug | $7,560 | $21,914,597 | $79,369,328 | $97,475,178 | $198,759,102 | |
Budget impact | $0 | $21,837,723 | $79,179,593 | $97,171,950 | $198,189,265 | |
CADTH scenario 4: incidence of cases to occur at start of each year | Referencea | $2,706,420 | $2,706,420 | $2,750,478 | $2,791,389 | $8,248,287 |
New drug | $2,706,420 | $48,415,721 | $82,988,179 | $84,222,557 | $215,626,457 | |
Budget impact | $0 | $45,709,301 | $ 80,237,701 | $ 81,431,168 | $ 207,378,170 |
a – standard of care (SoC) costs are included in both the reference and new drug scenario here whereas they are excluded in the sponsor’s analysis. This is the reason why the reference costs are higher in this scenario analysis. As SoC costs are also included in the new drug scenario as well the impact on the budget impact will only be slight. In other scenarios the costs in the reference arm relate only to subsequent therapy costs.
Stakeholder Input
Patient Input
Canadian Breast Cancer Network
About the Canadian Breast Cancer Network
The Canadian Breast Cancer Network (CBCN) is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all Canadians affected by breast cancer through the promotion of information, education and advocacy activities.
As a member of the Canadian Cancer Action Network, the Canadian Breast Cancer Network is committed to adhering to the Code of Conduct Governing Corporate Funding.
Information Gathering
Information for this submission was collected via:
CBCN’s 2017 Lived Experience Breast Cancer Patient Survey: An online survey was distributed in English and French to patients living with breast cancer. No patients surveyed had direct experience with the treatment under review. Survey questions comprised of a combination of scoring options and free form commentary. Patients were contacted through the membership databases of CBCN and other patient organizations.
Patient respondents profile: 24 Canadians with early-stage triple negative breast cancer patients participated in the survey. The majority of respondents were from Ontario (9) and Newfoundland and Labrador (4). The rest of the respondents were from British Columbia (3), Saskatchewan (2), Nova Scotia (2), Alberta (2), Prince Edward Island (1) and New Brunswick (1). All participants identified as female and as heterosexual. 92% of participants identified English as their first language. 1 reported her first language as Dutch and another reported her first language as Spanish.
Most of the respondents were first diagnosed when they were between the ages of 30 and 39 (9) and between the ages of 50 and 59 (9). 5 participants were first diagnosed when they were between 40-49 years old and 1 respondent was first diagnosed between 70 and 79 years old.
18 participants reported that they were in a relationship and 5 reported that they were single. 71% of all respondents had children at the time of their diagnosis. At the time of their diagnosis, participants reported having a child or children that were between the ages of 0 and 1 (7), 2 and 5 (4), 6 and 12 (3), 13 and 19 (5) and 20 and older (7). 2 participants reported that they were pregnant at the time of their diagnosis.
Key informant interviews: Phone interviews were conducted in March of 2022 with two Canadian breast cancer patients living with early-stage triple negative breast cancer that had direct experience with the treatment under review.
Printed sources: A review was conducted of current studies and grey literature to identify issues and experiences that are commonly shared among many women living with breast cancer.
Disease Experience
A diagnosis of early-stage, triple negative breast cancer (TNBC) has a significant impact on the day-to-day life of the patient. The diagnosis of TNBC, as well as the treatments that are used, impact both the emotional and physical well-being of a patient.
Triple negative breast cancers are cancers whose growth is not driven by estrogen, progesterone or by the overexpression of HER2 (human epidermal growth factor receptor) proteins. Approximately 10 to 20% of breast cancers are triple negative. Tumor grade informs about how much cancer cells resemble normal, healthy breast cells in both look and growth patterns from a scale of 1 to 3, with higher grades indicating less normalcy. TNBC is often diagnosed as a grade 3.
Triple negative breast cancers are most common in women with BRCA mutations (particularly those with a BRCA1 mutation) and those with non-BRCA gene mutations. Studies have found that approximately 70% of individuals with altered BRCA genes who were diagnosed with breast cancer had their cancers diagnosed as triple negative. This subtype of breast cancer has also been found to be higher in young people as well as in Black and Hispanic women.
Triple negative breast cancers are considered to be more aggressive and have poorer prognosis than other breast cancers because they grow and spread faster, have limited treatment options, and because of their high likeliness to recur following treatment. A 2019 study found that around 40% of early-stage TNBC will recur after being treated with the standard of care. Treating TNBC early-on is critical as the first few years after a TNBC diagnosis is associated with lower survival rates. While TNBC is less likely to recur 5 years after diagnosis, it is likely to recur in the first 5 years post diagnosis, with peak incidence being at around 3 years.
In our 2017 Lived Experience Breast Cancer Patient Survey (2017 Survey), the majority of TNBC patients’ cancers (54%) were diagnosed as Stage II, 8 were diagnosed with Stage III TNBC and 2 were diagnosed with Stage I TNBC. 71% of TNBC patients in our survey (the majority) had grade 3 breast cancer and 7 did not know their grade. None of the early-stage TNBC patients in our 2017 Survey had a breast cancer recurrence.
Experiences With Currently Available Treatments
The Goals of Current Therapy
In terms of treatment options, hormonal therapies that treat hormone receptor-positive cancers and targeted therapies that treat HER2-positive cancers are usually ineffective in treating TNBC. Currently, treatment for TNBC is very limited and usually involves chemotherapy, surgery, and radiation. The effectiveness of chemotherapy has been found to vary with tumor grade; grade 3 tumors usually benefit the most from chemotherapy.1 Neoadjuvant chemotherapy, where chemotherapy is administered preoperatively to first shrink the tumor varies across Canada and it use in treating early-stage TNBC is very inconsistent. This may be due to restricted access to neoadjuvant treatment in certain parts of the country. Neoadjuvant therapies for treating breast cancer is often recommended over adjuvant therapies, where treatment is administered after surgery, because a reduction in the size of the tumour may make the disease operable, and in other cases allow for breast-conserving surgery, thereby reducing the need for more complicated procedures like mastectomy and breast reconstruction and their associated risks. Preoperative therapy can also provide a real-time evaluation of tumor response to allow discontinuation of ineffective therapies, and can provide vital prognostic information as a supplement to conventional prognostic data (ie tumour staging, grade, receptor status etc). That being said, adjuvant chemotherapy is not without its benefits as it helps to destroy any remaining cancer cells, an important step in TNBC treatment due to its high rate of recurrence.
In our 2017 Survey, all TNBC patients had received chemotherapy as part of their overall breast cancer treatment. The majority also underwent surgery (96%), with 4 of these 23 patients requiring more than one surgery to remove the cancer. 83% of all TNBC patients also received radiation therapy and 2 patients reported receiving hormone therapy.
Key Factors for Decision-Making Around Treatment
Respondents in our 2017 Survey discussed the importance of the following factors in influencing their decision-making around treatments:
Effectiveness of the treatment – how well the treatment stabilized their disease, delayed progression of their disease, and reduced risk of recurrence.
Reducing the risk of recurrence without sacrificing quality of life – being able to maintain productive, active lives with minimal disruption to daily routines and avoiding relapse of their cancer.
Side effect management – minimizing risk while stabilizing their disease.
Ease and accessibility of treatments – Ease of accessing treatments.
Treatment Efficacy and Effectiveness
When asked about treatment decision-making, 100% of all TNBC patients in our 2017 Survey ranked reducing the risk of the cancer coming back as a very important factor. The importance of this was also stated anecdotally:
“I wanted a treatment that had the best chance of beating the cancer the first time.”
Additionally, TNBC patients in our 2017 Survey reported the following:
The effectiveness of the treatment was ranked as one of the most important factors for patients in deciding on treatment options. 96% of patients ranked it as very important.
92% of patients responded that effectiveness of their treatment was the single most important factor in making decisions about their treatment.
“Success rates for the treatment type, ability to talk to other patients using the same treatment and their experiences.”
“I am concerned about long term survival as a survivor of Triple Negative Breast Cancer.”
“When you're told you have cancer, all of a sudden you realize how great a life you have and that you do want to live... a long time. My family (husband, mother), I wanted to be with them for a lot more years.”
“Effectiveness and the best chance of PCR [pathological complete response] after chemo.”
“Survival. At what ever cost necessary[.]”
Quality of Life
Ensuring a good balance between effectiveness of treatment and side effects from treatments with a good quality of life was essential to patients. 58% of TNBC patients ranked quality of life as a very important factor in treatment decision-making and 25% ranked it as an important factor.
Maintaining productivity and mobility was essential for patients. 9 TNBC patients stated that productivity was an important factor in treatment decision-making and 9 TNBC patients stated that it was a somewhat important factor. Mobility as a factor in making decisions about treatments was ranked as important by half of all TNBC patients and ranked as very important by 33% of all TNBC patients.
The importance of productivity and mobility in terms of ability to continue childcare duties also played a role in treatment decision-making:
3 TNBC patients ranked childcare as an important factor;
5 TNBC patients ranked it as a somewhat important factor;
And 4 TNBC patients ranked it as a very important factor.
“I was pregnant so I did not want to impact my unborn baby. I also wanted to have enough energy to be able to deliver naturally.”
While 12 (50% of all participants) patients ranked childcare as not important, 7 of the these patients had children over the age of 20 years. All 7 of these patients who had children 20 years or older at the time of their diagnosis were also the same who reported that childcare was not an important treatment-decision making factor. The other 5 who ranked childcare as not important had also reported not having children at the time of their diagnosis. As such, it is understandable that for these two sets of respondents, childcare was not a concern during their treatment, however for patients with younger children, childcare was a concern in determining treatment options.
Patient Willingness to Tolerate Treatment Side Effects
Minimal side effects as a factor in making decisions about treatments was cited as important by 29% of TNBC patients, as somewhat important by 29% TNBC of patients, and as very important by 29% TNBC of patients.
Factors Influencing Accessibility
Having minimal medical appointments also played a role in TNBC patients’ treatment decision-making:
3 patients ranked minimal medical appointments as an important factor;
8 patients ranked it as a somewhat important factor;
And 2 patients ranked it as a very important factor.
TNBC patients also spoke on the accessibility of treatments and its impact on treatment decision-making:
“I've heard of many other women with the same diagnosis in other countries receive the addition of another chemo drug and my Oncologist said I can't have it.”
“I'm concerned we don't have enough influence or treatment options in Canada.”
“Originally my [treatments] were not presented as options. I would have liked to know I had a choice beforehand.”
The Financial Burden of Treating and Managing Breast Cancer
The financial burden associated with living with breast cancer extends far beyond any loss of income during a temporary or permanent absence from employment. In addition to the loss of income during illness, breast cancer patients can incur substantial costs associated with treatment and disease management.
Research on the financial impact of breast cancer on patients identified the following:
80% of breast cancer patients report a financial impact due to their illness.
44% of patients have used their savings, and 27% have taken on debt to cover costs.2
The negative financial impact of a breast cancer diagnosis were consistent with the responses in our 2017 Survey with TNBC patients:
7 respondents stated that they had experienced a very large financial impact as result of their diagnosis, and 12 stated that they had experienced some financial impact from their diagnosis.
Of the 22 patients who had private insurance coverage at the time of their diagnosis, 5 had challenges accessing it and 2 had a claim denied.
4 patients were prescribed cancer medications that weren’t covered through the public health care system.
Of the 22 patients who were prescribed support medications, 16 were prescribed support medications that weren’t covered through the public health care system.
1 patient stated that the cost of cancer medications stopped her from taking them and 2 patients stated that the cost of support medications stopped them from taking their support medications.
3 patients were able to access all the financial support that they needed, 4 were able to access some of the financial support that they needed, and 4 were unable to access any financial support.
At the time of their diagnosis, the majority of participants (58%) were employed full-time, 3 were self-employed, 2 were employed part-time, 2 were caregivers, 1 was on maternity leave, 1 was a homemaker and 1 was retired. By the time of our survey
9 were employed full-time;
5 were retired;
2 were employed but on disability;
2 were caregivers;
1 was on government assistance;
1 was on maternity leave;
1 was a homemaker;
1 was on long-term disability;
And 1 was working two part-time jobs.
The financial impact of a triple negative breast cancer diagnosis was also extensively written about in the open-ended responses:
“I worry that if I have a cancer recurrence and anything happens to my insurance, I will be in trouble - not able to pay for medications.”
“Last thing you need to worry about is finances when you are fighting for your life. I'm a single person and found it challenging on a reduced income.”
“I would have found a way to pay for them, even if they weren't covered. However, it made me realize I am lucky to have insurance, there are many who don't, I don't know what they do.”
“I was self employed and didn't have EI benefits assistance. I am excluded from all programs I have tried to access.”
“I'm extremely grateful for MSP, but cancer treatment still gets pretty expensive. I was also annoyed that cipro was prescribed as an antibiotic for 6 months, which was very expensive. I (fortunately?) reacted badly to it and was switched to another antibiotic after 2 months which was a tenth of the cost. Options should have been presented to me up front since I was paying for it.”
“As a teacher I didn't qualify for sick benefits during the summer months benefits get cut off on last day of school but can resume in September when school reopens.”
“I was self employed and did not qualify for any kind of financial assistance.”
“I was off work for 9 months. I used all my short term disability benefits from work, 15 weeks of EI and a few weeks of long term disability and a gradual return to work. I was very ill and unable to look after myself during treatment and my spouse had to take every other week off without pay to look after me. We used much of our savings to supplement our loss of income during that time.”
This small snapshot, provides a glimpse into the financial burden placed on early-stage, triple negative breast cancer patients and their families due to their diagnosis. It also illustrates how a breast cancer diagnosis can cause long lasting physical impacts, in turn causing financial disruptions which can be incredibly burdensome depending on one’s situation.
Improved Outcomes
For early-stage TNBC patients, reducing the risk of recurrence, treatment effectiveness and efficacy, and quality of life are of critical concern. Patients have an expectation that Keytruda will provide a possibility for improving their rate of invasive disease-free survival and reduce their risk of recurrence, allowing them to live a better quality of life.
Pembrolizumab (Keytruda) is an anti-programmed death 1 (PD-1) monoclonal antibody shown to have antitumor activity with mainly low-grade toxic effects in patients with metastatic TNBC, especially as a first-line treatment.3,4,5
KEYNOTE-5226 is a phase 3 clinical trial that explored pembrolizumab in the neoadjuvant and adjuvant setting amongst early triple negative breast cancer patients. Results from this and other studies with pembrolizumab suggest that immune checkpoint inhibitors added to neoadjuvant chemotherapy may increase the percentage of patients with triple negative breast cancer who have pathological complete response (pCR). Pathological complete response is important because patients who achieve it following neoadjuvant therapy have longer EFS and overall survival (OS), and also have potentially increased likelihood of tumor resectability and breast conservation.7,8,9,10
Key characteristics of patients in KEYNOTE-522 at baseline:
In the pembrolizumab-chemotherapy group:
656 patients (83.7%) were PD-L1-positive; 127 patients (16.2%) were PD-L1-negative
449 patients (57.5%) were administered carboplatin on a weekly schedule; 335 patients (42.7%) received carboplatin every 3 weeks
405 patients (51.7%) had positive nodal involvement; 379 patients (48.3%) had negative nodal involvement
590 patients (75.3%) had stage II TNBC; 194 patients (24.7%) had stage III TNBC
Key characteristics of patients in KEYNOTE-522 at baseline cont’d:
In the placebo-chemotherapy group:
317 patients (81.3%) were PD-L1-positive; 69 (17.7%) were PD-L1-negative
223 patients (57.2%) were administered carboplatin on a weekly schedule; 167 patients (42.8%) received carboplatin every 3 weeks
200 patients (51.3%) had positive nodal involvement; 190 patients (48.7%) had negative nodal involvement
291 patients (74.6%) had stage II TNBC; 98 patients (25.1%) had stage III TNBC
KEYNOTE-522 included 1,174 patients with previously untreated stage II or stage III triple negative breast cancer who were stratified by nodal status (positive versus negative), tumor size (T1, T2, T3, or T4), and schedule of carboplatin administration (weekly or every 3 weeks) and then randomly assigned to one of two groups in a 2:1 ratio. In the first neoadjuvant phase, the pembrolizumab-chemotherapy group, or treatment group, (n = 784 patients) received neoadjuvant therapy with four cycles of pembrolizumab every 3 weeks plus paclitaxel and carboplatin. The placebo-chemotherapy group, or control group, (n = 390 patients) received placebo plus paclitaxel and carboplatin every 3 weeks. In a second neoadjuvant phase, patients received four cycles of doxorubicin–cyclophosphamide or epirubicin–cyclophosphamide for both groups plus pembrolizumab (for the pembrolizumab-chemotherapy group/pembrolizumab arm/treatment group) or placebo (for the placebo-chemotherapy group/placebo arm/control group). This was followed by surgery and then up to 9 cycles of adjuvant pembrolizumab (pembrolizumab arm) or placebo (placebo arm).
The primary end points for analysis were pCR at the time of surgery and event-free survival (EFS) in an intention-to-treat population.
Primary results from KEYNOTE-522 showed that among the first 602 patients in the study, pCR in the pembrolizumab arm was 64.8% (95% confidence interval [CI], 59.9 to 69.5) (260 of 401 patients) and 51.2% (95% CI, 44.1 to 58.3) (103 of 201 patients) in the placebo arm. The difference between these two treatment groups was 13.6 percentage points (95% CI, 5.4 to 21.8), which was found to be significantly significant, P<0.001. The percentage of patients in the placebo arm who achieved pCR in this study was similar to the percentage reported in other studies of platinum-containing neoadjuvant therapy in patients with early-stage breast cancer.
The pCR benefits of pembrolizumab plus chemotherapy were fairly consistent across various subgroups of patients in the study, including PD-L1-expression subgroups. In the PD-L1-positive subgroup of the first 602 randomized patients, patients who achieved pCR were 68.9% (230 of 334 patients) in the treatment group and 54.9% (90 of 164 patients) in the control group. In the PD-L1- negative subgroup, patients who achieved pCR were 45.3% (29 of 64 patients) in the treatment group and 30.3% (10 of 33 patients) in the control group.
Similarly, neoadjuvant pembrolizumab in combination with chemotherapy led to a higher pCR benefit compared to chemotherapy alone in patients with stage III TNBC and/or node positive TNBC. This benefit was also shown in patients who received less than planned chemotherapy. Results from the preliminary analysis of the first 602 randomized patients showed that pCR among node positive patients in the pembrolizumab group occurred in 64.8% of node positive patients (136 of 210 patients) and in 44.1% of node positive patients (45 of 102 patients) in the control group. This was a difference of 20.6% (95% CI, 8.9 to 31.9). Results from this preliminary analysis also showed that among patients who received carboplatin on a weekly basis, pCR occurred in 154 of 231 patients (66.7%) in the treatment group and in 56 of 116 patients (48.3%) in the control group with a difference of 18.4% (95% CI, 7.4 to 29.1) between the two groups.
A median follow-up of 15.5 months showed that 7.4% of patients in the treatment group and 11.8% of patients in the control group had disease progression precluding definitive surgery, had local or distant recurrence or a secondary primary tumor, or died from any cause (hazard ratio, 0.63; 95% CI, 0.43 to 0.93, in favor of the pembrolizumab arm).
First EFS event measured at second interim analysis found that among all 1,174 patients, 58 patients in the pembrolizumab arm experienced an event. This included PD precluding surgery (n=2), PD precluding definitive surgery (n=1), distant PD (n=4), positive margin at last surgery (n=7), local recurrence (n=9), distant recurrence (n=27) and death (n=8). 46 patients in the placebo arm experienced an event, including PD precluding surgery (n=3), distant PD (n=1), positive margin at last surgery (n=10), local recurrence (n=6), distant recurrence (n=23) and death (n=3). With 104 events (of 327 expected at the final analysis), Kaplan–Meier estimates of the percentage of patients at 18 months who were alive without disease progression precluding definitive surgery, without local or distant recurrence, and without a second primary tumor were 91.3% (95% CI, 88.8 to 93.3) in the treatment group and 85.3% (95% CI, 80.3 to 89.1) in the control group.
Adverse Effects
The majority of adverse events of interest and treatment-related adverse events (TRAEs) occurred during the neoadjuvant phase. Adverse events that occurred among patients in the pembrolizumab arm were consistent with the known safety profiles of platinum- containing neoadjuvant chemotherapy for patients with early TNBC and with the known safety profiles of pembrolizumab as a monotherapy. Adding pembrolizumab was not shown to increase chemotherapy-related toxic effects such as myelosuppression, nausea and vomiting, renal insufficiency, and neuropathy.
Results from all patients during the neoadjuvant phase at second interim analysis showed that 38.9% of patients in the treatment group experienced adverse events of interest while 18.3% of patients in the control group experienced the same. Adverse events of grade 3 or higher was experienced by 12.9% of patients in the treatment group and 1.8% in the control group. Adverse events of interest of grade 3 or higher than occurred in 10 or more patients were severe skin reactions (3.8% of patients), infusion reactions (2.6% of patients), and adrenal insufficiency (1.3% of patients) in the treatment group. The most common adverse events of grade 3 or higher that occurred in both the treatment and control group (neutropenia, anemia, decreased neutrophil count, and febrile neutropenia) were consistent with those usually seen with platinum-based chemotherapy.11,12
32.5% of patients in the pembrolizumab group experienced serious TRAEs, while 19.5% of patients in the control group experienced the same. The most common TRAEs in the treatment group and placebo group were febrile neutropenia (14.6% and 12.1%, respectively), anemia (2.6% and 2.1%, respectively), and pyrexia (2.6% and 0.3%, respectively). TRAEs led to discontinuation in 23.3% of patients in the treatment group and in 12.3% of patients in the control group.
TRAEs across all treatments during the neoadjuvant phase at the second interim analysis of any grade occurred in 99.0% of the 781 patients in the pembrolizumab group and 99.7% of the 389 patients in the placebo group. TRAEs of grade 3 or higher in this analysis occurred in 76.8% of patients in the treatment group and in 72.2% of patients in the placebo group. TRAEs of any grade across all treatments during the adjuvant phase at the second interim analysis were experienced by 48.1% of the 547 patients in the pembrolizumab arm who had started adjuvant therapy and by 43.0% of the 314 patients in the control arm who had started adjuvant therapy. TRAEs of grade 3 or higher were experienced in 5.7% of patients in the treatment group and in 1.9% of patients in the control group. Adverse events of interest of any grade occurred in 8.2% of patients and those of grade 3 or higher occurred in 2.0% of patients in the treatment group. In the control group, adverse events of interest of any grade occurred in 5.7% of patients and those of grade 3 or higher occurred in 0.3% of patients.
While the incidence of TRAEs was higher in the treatment group compared to the control group, it did not impact the administration of neoadjuvant chemotherapy. This is of importance as administration of less doses of neoadjuvant chemotherapy than planned is correlated with worse long-term outcomes.13 Similarly, while incidence of adverse effects was higher in the treatment group than in the control group, their occurrence was largely due to infusion and skin reactions, both due to pembrolizumab and chemotherapy.
Impact of Treatment Options to Patients
In treating triple negative breast cancer and reducing the risk of recurrence, Keytruda can relieve cancer-related symptoms and improve a patient’s quality of life. When living with no or with minimal cancer-related symptoms, and with minimal side effects from the treatment, patients are able to reduce the impact of cancer on their ability to care for children and dependents, continue with their employment and earn income, spend time with loved ones and participate in their life in a meaningful way by engaging in social activities, travelling, maintaining friendships, and pursuing personal interests.
Experience With Drug Under Review
Patient Profiles
CBCN connected with two Canadian patients who had experience with the treatment.
Patient 1: Is 36 years old and was diagnosed in July 2021 at 35 years old. She was diagnosed with Stage IIb triple negative breast cancer with a BRCA1 gene mutation. The current therapy was offered to her as an addition to her other treatments and she is paying for it out-of-pocket. She has been previously treated with chemotherapy: Adriamycin, Carboplatin, and Taxol. She underwent a bilateral mastectomy (one prophylactic, one to remove the cancer) and will be having radiation therapy as part of her treatment.
Patient 2: Is 52 years old and was diagnosed in August 2017 with stage II triple negative breast cancer. She accessed this therapy through a clinical trial that was mentioned and recommended to her by her oncology team. She has been treated with chemotherapy and she underwent a partial mastectomy and radiation.
The Impact of the Treatment on the Disease
Both patients spoke of the positive impact that being on Keytruda had on their cancer and found it to be an effective treatment for triple negative breast cancer.
“I go back to living my life and there’s no more future cancer treatment. Unless I get an event or recurrence of the cancer, which has been substantially downgraded because of the treatment, because of the chemo, because of the [pembrolizumab].” – Patient 1
“I believe that I am here talking to you today because of having had access to that drug.” – Patient 2
“Next August I will make my five years from diagnosis. Come September, I will be on the survivor side. And I believe it’s attributed to [pembrolizumab].” – Patient 2
Both patients also spoke about the promising statistics of Keytruda on giving them hope, despite being diagnosed with a rare and aggressive breast cancer known to have a high recurrence rate. This was expressed when both patients spoke about pCR, which was discussed at length, and which played a big part in their treatment decision-making process to be on Keytruda.
“[You’re] talking about a 10 percent difference in some cases, which may not seem like a lot, but when you’re looking at your whole life, 10 percent is huge… Pathological complete response is the ultimate goal, in my opinion. When going through cancer treatment, that’s what you ultimately want at the time of surgery.” – Patient 1
“And because of that, well, what I believe, based on what I’ve read and the research that I’ve done before I decided to take the drug, that it does help in overall survivorship. It puts me in a different prognostic category, especially if I get that pathological complete response.” – Patient 1
“Absolutely it [PCR] was a relevant factor because of the statistics with my cancer in terms of the recurrence rate. And having access to [pembrolizumab], the way that they explained to me how it works in the body was part of the decision-making plan.” – Patient 2
Additionally, both patients spoke about achieving pCR while on treatment.
“I attribute the fact that I got that pathological complete response and now I can go back to living my life because of [pembrolizumab].” – Patient 1
“Yes, I had one. After my surgery, and that was when I knew that my outcome was pretty great.” – Patient 2
Assessing Risks Associated with the Treatment
While both patients had vastly different experiences of side effects from being on Keytruda, they expressed that the risks assumed from being on the therapy and the side effects that they experienced were worth the benefits of the drug, especially being able to achieve pCR.
“I wouldn’t change it at all, mainly because I was able to have that treatment, have the pathological complete response through surgery. – Patient 1
“I would honestly say that in my experience, there were no unacceptable side effects with [pembrolizumab].”- Patient 2
In terms of specific side effects, patient 1 reported experiencing minor side effects, general fatigue, colitis, and diarrhea. The fatigue she experienced, she attributed to general cancer treatment and not specifically to Keytruda. Which of the other minor side effects came from what treatment, since she was also on Taxol and carboplatin, was hard to distinguish. However, when she was on Keytruda alone, she experienced minimal side effects during the weeks following the treatment and only recently experienced diarrhea and colitis. She ended up stopping her treatments on Keytruda due to the diarrhea and colitis, however, she pointed out that part of the reason she stopped her treatment was because she had already achieved pCR and the benefit of adding a “two percent or four percent increase in overall event-free survivorship” was not worth the risk of colitis for her after that. And although the side effect led her to stopping the treatment, she expressed that it was manageable.
“So it’s certainly not pleasant but other than that, very manageable. Worth the risk, I guess, in my opinion.” – Patient 1
She was able to address the side effects of fatigue and colitis. With fatigue, she mentioned needing to just “take care of yourself and get as much rest as possible as your body’s going through all of these changes”. Prednisone was used to treat her colitis. Overall, for patient 1, the risk versus benefit of treatment and what it acceptable and not acceptable occurs when the treatment causes more harm than good with unmanageable side effects that are not worth the risks.
“I think when [pembrolizumab] starts attacking the immune system, as it can by virtue of the drug, once it turns on your body, I think that’s the point that it’s no longer acceptable. Saying that, if I had not [gotten] the pathological complete response, and I had the colitis that I currently have as a result of [pembrolizumab], with the guidance of my oncologist, I would probably have continued taking it and weighed that risk/benefit to see if it was worth continuing and managing the colitis while on it.” – Patient 1
Patient 2 also experienced fatigue which she also attributed not to Keytruda but to a year of chemotherapy, surgery, and radiation. Similar to patient 1, it was hard for her to distinguish which side effects came from which treatment. However, her oncologist attributed any other side effect that she did experience to chemotherapy. And although she was on a clinical trial and could have been on a placebo, her doctors were certain that she was on Keytruda due to the rash she always got on her face the day following treatment. This was the only side effect attributed to Keytruda. She expressed that the rash was more than manageable and was so minor that it did not require treatment.
“I got a rash. It was more unsightly. There was no discomfort associated with it at all.” – Patient 2
“In my case there was really nothing to be done about the side effects associated with [pembrolizumab]. It was rest, and the rash would just go away on its own after a day.” – Patient 2
Alternatives to the Treatment
When speaking about alternatives to Keytruda as a treatment, both patients expressed that they saw it less as being an option to other treatments and more of it being an additional treatment for TNBC. Had they not been offered the immunotherapy Keytruda, they would have gone with the regular standard of care for early-stage TNBC: chemotherapy, surgery and radiation. Patient 1 expressed that if she had only been offered the standard of care and did not achieve pCR, then she would have also used PARP inhibitors.
Both understood that the aggressive nature of TNBC and it’s high rates of recurrence meant that treatment options were limited. Because of this, they were thankful to have an additional treatment whose data showed promising results for pCR, effectiveness, and overall outcomes. This factored into their decisions to be on this treatment.
“So I chose to do that mainly because of the statistical evidence of survivorship and the physical evidence of pathological complete response, which was incredibly important to me, especially given the triple negative breast cancer. My understanding of triple negative breast cancer is that five years after treatment is done it’s very crucial not to get a recurrence, and [pembrolizumab] offered significant statistical evidence that it would help me achieve that pathological complete response.” – Patient 1
“I had read great things about immunotherapy: the notion of it being a targeted therapy with very strong outcomes and fewer side effects, so I would say that about sums up my reasons for being part of this clinical trial and having access to the [pembrolizumab].” – Patient 2
“And it was highly recommended to me by my oncology team that I seriously consider this clinical trial because it would—you know, the addition of [pembrolizumab] to my treatment plan, they convinced me, would improve my outcome significantly because triple negative breast cancer has one of the highest rates of recurrence of any of the cancers.” – Patient 2
The side effects of Keytruda, as an immunotherapy, was also preferable to the side effects of chemotherapy for patient 2. She expressed her hopes that immunotherapy could one day replace chemotherapy in treating cancer.
“For me it was just a rash. That was it. A little fatigue, but other than that, a rash, a little fatigue, that’s it. A cakewalk compared to the horrors of chemotherapy. For me, anyways. I experienced many side effects from chemotherapy, and the immunotherapy was, as I said, it was at one point going to replace chemotherapy in some patients. That’s the best news ever for cancer patients.” – Patient 2
“[If] it ever became a question that [pembrolizumab] would replace some of the requirements of chemotherapy, then that is the best news ever for cancer patients, that is for sure.” – Patient 2
The Social and Financial Impact of the Treatment
Both patients appreciated the great quality of life afforded to them through Keytruda. Patient 1 rated her quality of life on Keytruda as a seven or eight out of ten and patient 2 rated her quality of life on Keytruda as a nine out of ten. Both patients could not comment on the impact of Keytruda on their general productivity when it was taken in addition to chemotherapy as its associated side effects got in the way. However, when they were both exclusively on Keytruda, they saw an improvement in their productivity.
“[When] I was just exclusively on [pembrolizumab], and having just the normal side effects, my day-to-day activities were normal, and I felt that I could do things like I actually hadn’t been able to do when I initially was on chemo with no immunotherapy.” – Patient 1
“I do do some administrative work virtually. I had been able to maintain that minimally.” – Patient 1
“[The six months that I had [pembrolizumab] alone, definitely because the side effects were so few, I was able to return to a normal life for me.” – Patient 2
Both patients were parents to younger children and being on Keytruda meant being able to be there for their children.
“I was still taking [pembrolizumab] in January and I was able to be home with both children and do at-home learning with my son and caring for my daughter, who is two. I mean, I was tired, as most people probably would be anyways, but it was manageable. But overall, like when I was on full chemotherapy treatment, I certainly had help with childcare.” – Patient 1
“At the time I had[,] when I was diagnosed[,] an 8-year-old and a 12-year-old. And I was able to be a parent to them much better when I was on [pembrolizumab] than when I was on chemotherapy. Other than a little fatigue, I was able to carry on pretty normally with the [pembrolizumab]” – Patient 2
For patient 2, being on Keytruda did not have too big of an impact on her family members but patient 1 spoke in great details about the hope and that it meant for her and her family.
“I will say that this treatment has probably affected my family in a positive way. And I say that because of the fact that it gave me more hope during treatment knowing that I was having it, knowing that I was doing everything that I could do to get rid of the cancer in my body and because of that, that desire, that fact that I wasn’t feeling hopeless was helpful to my family and anyone giving care to me because I kept a very positive attitude. I felt that I had everything that I could have to attack that cancer and there was nothing more I could do. So having that fight and having all the equipment to fight that cancer was positive and it left my family feeling good because I wasn’t in despair.” – Patient 1
Being on Keytruda meant a great deal to both patients personally and they attributed the treatment to their current outcomes. When asked what being on Keytruda meant to them personally, both women were thankfully to have had access to the treatment and expressed their desire to ensure that other patients like them are able to also access Keytruda.
“For me personally, it is something that I hope every woman or man who develops triple negative breast cancer in this country has the ability to have, because it gave me a hope, an added hope due to the seriousness of the triple negative breast cancer diagnosis. And when you have everything you can use to combat cancer, especially this particular cancer, it means your life. It means the world to me. I think to have an access program to help fund this for other people would be huge because triple negative breast cancer historically has not had the best prognosis, and I think that [pembrolizumab] is really changing that from what I see from the studies that I’ve seen and the clinical trials that I’ve read. And personally from my own experience. I’m sitting here for all intents and purposes[,] cancer-free, and I do attribute that to [pembrolizumab]. You can’t ask for more. When you have a cancer diagnosis, I don’t think you can ask for more than life, and I think [pembrolizumab] gives you that hope.” – Patient 1
“The world. I truly believe that I am on this phone call with you today because of it. So I wish for fellow cancer patients to have access to this treatment because I believe it is much kinder, I believe it’s so much easier to tolerate. Night and day from chemotherapy to [pembrolizumab]. So we have a future where this is the future of cancer care, I think that it is amazing news for anyone diagnosed with this dreadful disease.” – Patient 2
Neither patient spoke about what having access to Keytruda meant to them financially. Patient 2 was accessing it through a clinical trial and patient 1 was paying privately out-of-pocket to access it but was passionate about there being some type of funding and access program so that others who are unable to access it due to financial reasons or otherwise can have access to it.
“I’m passionate about it just because it was the added tool in my toolbox to combat cancer and it shouldn’t be exclusive to those who can maybe either fund it privately or crowdfund it. I’ve seen that[,] where people have done the GoFundMe pages too. I think it’s something that should be available to any man or woman who’s been diagnosed with triple negative breast cancer. I feel very strongly about that. I think that in today’s day and age, we should all have the opportunity to be able to fight cancer with whatever we can, whatever’s available.” – Patient 1
Companion Diagnostic Test
Not applicable
Anything Else?
Not applicable
References
Prognosis of triple-negative breast cancer. verywellhealth. Accessed February 28, 2022. https://www.verywellhealth.com/triple- negative-breast-cancer-prognosis-4778440
Dunbrack, J. Breast Cancer: Economic Impact and Labour Force Re-entry. Canadian Breast Cancer Network. (2010).
Adams, S. et al. Pembrolizumab monotherapy for previously untreated, PD-L1-positive, metastatic triple-negative breast cancer: cohort B of the phase II KEYNOTE-086 study. Ann Oncol. 30(3), 405-411 (2019). https://doi.org/10.1093/annonc/mdy518
Adams, S. et al. Pembrolizumab monotherapy for previously treated metastatic triple-negative breast cancer: cohort A of the phase II KEYNOTE-086 study. Ann Oncol. 30(3), 397-404 (2019). https://doi.org/10.1093/annonc/mdy517
Nanda, R. et al. Pembrolizumab in patients with advanced triple-negative breast cancer: phase Ib KEYNOTE-012 study. J Clin Oncol. 34(21), 2460-2467 (2016). https://ascopubs.org/doi/abs/10.1200/JCO.2015.64.8931
Schmid, P. et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N Engl J Med. 382(9), 810-821 (2020). https://doi.org/10.1056/NEJMoa1910549
Cortazar, P. et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 384(9938), 164–172 (2014). https://doi.org/10.1016/S0140-6736(13)62422-8
Huang, M. et al. Evaluation of pathological complete response as a trial-level surrogate for long-term survival outcomes among triple-negative breast cancer patients receiving neoadjuvant therapy. Presented at ESMO Breast Cancer, Berlin, (2019).
Sikov, W.M. et al. CALGB (Alliance) 40603: Long-term outcomes (LTOs) after neoadjuvant chemotherapy (NACT) +/− carboplatin (Cb) and bevacizumab (Bev) in triple-negative breast cancer (TNBC). J Clin Oncol. Advanced online publication (2022). https://doi.org/10.1200/JCO.21.01506
Spring, L.M. et al. Pathological complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and mortality, stratified by breast cancer subtypes and adjuvant chemotherapy usage: individual patient-level meta-analyses of over 27,000 patients. Clin Cancer Res. 26(12), 2838-2848 (2019). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7299787/
Hassett, M.J. et al. Frequency and cost of chemotherapy-related serious adverse effects in a population sample of women with breast cancer. J Natl Cancer Inst. 98(16), 1108-1117 (2006). https://doi.org/10.1093/jnci/djj305
Rashid, N. et al. Clinical impact of chemotherapy-related adverse events in patients with metastatic breast cancer in an integrated health care system. J Manag Care Spec Pharm. 21(10), 863–871 (2015). https://doi.org/10.18553/jmcp.2015.21.10.863
Sikov, W.M. et al. CALGB (Alliance) 40603: Long-term outcomes (LTOs) after neoadjuvant chemotherapy (NACT) +/− carboplatin (Cb) and bevacizumab (Bev) in triple-negative breast cancer (TNBC). J Clin Oncol. Advanced online publication (2022). https://doi.org/10.1200/JCO.21.01506
Patient Group Conflict of Interest Declaration — Canadian Breast Cancer Network
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
CBCN did connect with the manufacturer, Merck, to identify clinicians that could connect us with patients with experience on the treatment.
All other research, interviews and outreach to patients was conducted independently by the Canadian Breast Cancer Network, as was the compilation of information and data for the writing of this submission.
As a member of the Canadian Cancer Action Network, the Canadian Breast Cancer Network is committed to adhering to the Code of Conduct Governing Corporate Funding.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No. The Canadian Breast Cancer Network compiled and wrote this submission independently.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Conflict of Interest Declaration for the Canadian Breast Cancer Network
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck Canada | — | — | — | X |
Rethink Breast Cancer
About Rethink Breast Cancer (Rethink)
Rethink Breast Cancer (Rethink) is a Canadian charity known for making positive change. Rethink educates, empowers and advocates for system changes to improve the experience and outcomes of those with breast cancer, focusing on historically underserved groups: people diagnosed at a younger age, those with metastatic breast cancer and people systemically marginalized due to race, income or other factors. We foster spaces to connect, listen, empower, and rethink breast cancer, together. Rethink’s strategic priorities and organizational direction are guided by the unique, unmet needs identified by breast cancer patients and their families.
Programs and Activities
Rethink Breast Cancer builds community, bringing patients with various stages of breast cancer together through our private and public social spaces as well as in-person events
Rethink runs patient retreats and facilitates peer-support
Rethink creates and runs education forums and conferences
Rethink creates support and education tools, resources and content
Rethink funds and supports breast cancer research
You can find out more by visiting:
Rethink Breast Cancer Instagram
Information Gathering
CADTH is interested in hearing from a wide range of patients and caregivers in this patient input submission. Describe how you gathered the perspectives: for example, by interviews, focus groups, or survey; personal experience; or a combination of these. Where possible, include when the data were gathered; if data were gathered in Canada or elsewhere; demographics of the respondents; and how many patients, caregivers, and individuals with experience with the drug in review contributed insights. We will use this background to better understand the context of the perspectives shared.
For over 20 years, Rethink has been working closely with breast cancer patients in Canada. We learn from and listen to the community to understand their values, priorities and pain points to help drive change and system improvements. Each year, we learn from the patients we serve, survey and collaborate with. We learn from the 40 individuals that we work extremely closely with as key patient advisors; the 100 patients that share their stories on our blog; the 500 patients that participate in our virtual support groups; the 1,600 members of our private peer-support network; the 30,000 people that have joined our Instagram community; and the 150,000 individuals reached each month through the reach of that channel. We listen, learn, engage and have conversations in all these spaces.
Rethink Breast Cancer has several important patient advisory boards and working groups that offer experience-focused insights on issues related to those affected by and concerned about breast cancer, including:
Metastatic Breast Cancer Advisory Board
Early Breast Cancer Advisory Board
Equity, Diversity and Inclusion working group
Triple Negative Breast Cancer working group (all stages)
For this submission, we have drawn on our general observations and insights gathered through programming and meetings with breast cancer patients as described above. Rethink also conducted in-depth telephone interviews in February 2022 with two patients who are both stage 3 triple negative breast cancer patients who have experience with pembrolizumab and one caregiver to one of the patients interviewed. We also held a focus group with 7 patients from our Triple Negative Breast Cancer Working Group on March 3, 2022.
Disease Experience
CADTH involves clinical experts in every review to explain disease progression and treatment goals. Here we are interested in understanding the illness from a patient’s perspective. Describe how the disease impacts patients’ and caregivers’ day-to-day life and quality of life. Are there any aspects of the illness that are more important to control than others?
Most people in the Rethink community are diagnosed at a younger age. When young people get breast cancer it may be more aggressive, which can lead to tougher treatments. In addition, those diagnosed in their 20s, 30s and early 40s face age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, childcare, impact on relationships, body image, dating and sexuality, feeling isolated from peers who don’t have cancer, career hiatuses, and financial insecurity. The physical and emotional toll that a breast cancer diagnosis and treatment takes on a young person’s life is devastating and traumatic. Of all breast cancers diagnosed in Canada, up to 15% will have a subtype known as triple negative breast cancer (TNBC) that is a more aggressive form, often occurring in young people, and has a high risk of recurrence or presentation as Stage IV at diagnosis.
When it comes to TNBC, it’s less about controlling an aspect of the illness and more a deep desire for their treatment to work well enough that they make it through that first-year danger zone post active treatment. That they beat the odds despite having one of the most aggressive types of breast cancer, a subtype that is more likely to spread and more likely to reoccur than other types. The subtype that only accounts for 15% of all breast cancer cases but a much higher percentage of breast cancer deaths. They know that their tumor lacks the three most common receptors that most breast cancer therapies target, and therefore there haven’t been targeted treatment options available.
“Because I have TNBC, the common breast cancer maintenance meds wouldn’t do anything, so I’m just being told to go live my life and try and put cancer on a shelf for now – although that’s easier said than done. Anxiety still makes it hard to fall asleep. Fear jolts me up in the middle of the night as I think about what the next few years may hold.” – Patient
Experiences With Currently Available Treatments
CADTH examines the clinical benefit and cost-effectiveness of new drugs compared with currently available treatments. We can use this information to evaluate how well the drug under review might address gaps if current therapies fall short for patients and caregivers. Describe how well patients and caregivers are managing their illnesses with currently available treatments (please specify treatments). Consider benefits seen, and side effects experienced and their management. Also consider any difficulties accessing treatment (cost, travel to clinic, time off work) and receiving treatment (swallowing pills, infusion lines).
Triple negative breast cancer is usually treated with a combination of surgery, radiation therapy, and chemotherapy. Chemotherapy is often given before surgery. The patient learns stage and grade and begins talking through their treatment plan with their oncologist. In Canada, right now, patients are immediately tested for BRCA if diagnosed under 35 or if you’re TNBC age 60 or under.
As mentioned, it can be upsetting for patients to find out that they’ve been diagnosed with a type of breast cancer that is more aggressive than other types. As they join patient communities online, like ours, they begin learning about the experiences of others with breast cancer, start learning about subtypes, share treatment plans, read blog posts about targeted treatments for other subtypes and can feel that their particular type of breast cancer doesn’t have the same transformative targeted treatments as those who benefit from, say, Herceptin. If they are then also BRCA, that adds a layer of concern for family while also going through their own treatment.
This can leave them feeling isolated from the broader breast cancer community, compounding the cancer-related anxiety they already feel.
Improved Outcomes
CADTH is interested in patients’ views on what outcomes we should consider when evaluating new therapies. What improvements would patients and caregivers like to see in a new treatment that is not achieved in currently available treatments? How might daily life and quality of life for patients, caregivers, and families be different if the new treatment provided those desired improvements? What trade-offs do patients, families, and caregivers consider when choosing therapy?
Each individual patient brings their own personal values and goals to their discussions with their oncology team. Communication and trust in their team is essential. In our experience working closely with many young triple negative breast cancer patients, we find most, especially those with Stage 3 TNBC, are willing to trade toxicity for confidence in knowing they’ve “thrown everything they could” at the cancer. In other words, they will choose to endure additional side-effects and impacts on quality of life from the toxicity of a stronger therapy to ensure they are doing everything they can to treat what they know is an aggressive form of breast cancer.
Experience With Drug Under Review
CADTH will carefully review the relevant scientific literature and clinical studies. We would like to hear from patients about their individual experiences with the new drug. This can help reviewers better understand how the drug under review meets the needs and preferences of patients, caregivers, and families. How did patients have access to the drug under review (for example, clinical trials, private insurance)? Compared to any previous therapies patients have used, what were the benefits experienced? What were the disadvantages? How did the benefits and disadvantages impact the lives of patients, caregivers, and families? Consider side effects and if they were tolerated or how they were managed. Was the drug easier to use than previous therapies? If so, how? Are there subgroups of patients within this disease state for whom this drug is particularly helpful? In what ways? If applicable, please provide the sequencing of therapies that patients would have used prior to and after in relation to the new drug under review. Please also include a summary statement of the key values that are important to patients and caregivers with respect to the drug under review.
Rethink conducted phone interviews with two patients with stage 3 triple negative breast cancer who have experience with pembrolizumab (Keytruda). We also interviewed one of the caregivers to one of the patients we interviewed.
Patient 1 Interview
“I was diagnosed in 2019 and I was pregnant at that time. I joined a lot of cancer communities on Facebook, all over the world, and this drug was already available in the US for clinical trials, so I had heard of it and a lot of breast cancer patients had already been on it, so I’ve been following Keytruda for a while. When I spoke to my oncologist about it, it wasn’t available to me. There was no clinical trial at that time. So, I went through my chemotherapy and I gave birth, and then I had more chemo after that. In the beginning of 2020, I finished my chemo and then I had my double mastectomy surgery, removed my breasts, then I went through 25 radiation treatments and then I went on chemo pills. When I finished all my treatment and I was on my chemo pills, that’s when my oncologist said there’s going to be a few clinical trials coming out soon for Keytruda for TNBC, which is my cancer. She referred me to a doctor where the clinical trial was. I started the trial December of 2020, a clinical trial for TNBC early-stage. I was selected to receive the drug and started it on December 24, 2020.
“I had a lot of the side effects from Keytruda, my oncologist told me some of her patients don’t have any side effects, majority of them have thyroid issues, and I had hives and skin conditions and thyroid issues. But I would say it is minor, any issues that I’ve had so far, I was never hospitalized. To be honest, if I were to recommend this drug for patients who are TNBC like me, I would say go ahead and do it and just tolerate whatever side effects you get because this drug is so helpful in decreasing recurrence. And TNBC has the highest recurrence rate. I’ve just lost a family member from TNBC a couple weeks ago. She was diagnosed a year after me, but she couldn’t get into the clinical trial I was in because at that time I think it had already spread. I knew about this drug when I was first diagnosed and I knew I wanted to be on this drug, just because I’ve heard so many good things about it. There are side effects, yes, but these are tolerable side effects. There are treatments for these side effects, it’s not something that is bad that you’d be hospitalized for.
“It was very important for me to get access to Keytruda. I’d recommend people to either get on a clinical trial or try to find a way to get access to this drug because to me I feel like, obviously this is new for TNBC, but it’s an extra treatment for this disease. TNBC has just a standard treatment because there’s not enough research and drugs to treat it like the other types of breast cancer. Ours is very standard, it’s just chemo and radiation, pills, that’s about it. There’s really nothing on the long-term. With Keytruda, if they’re able to treat or help with the recurrence for TNBC, I’d recommend it 100% to get it. With TNBC, my oncologist advised me to go maximum with whatever treatment is out there. And that’s what I did. I didn’t have to get both of my breasts taken out, but I did because of the recurrence rate. I don’t want the recurrence. I would totally recommend Keytruda, and if we can get access to the drug, it would be great. When I was going through chemo and I knew about this drug, I was really sad and disappointed that it wasn’t available for us here. It was really sad. I thought, ok if I’m done my chemo, I’m done my chemo pills, my radiation, what do I do next? What is going to happen? When the opportunity came up for me to do the clinical trial, I was so excited for it. It’s sad that not everyone could have gotten into this trial. I feel like Canada is so behind in all the drugs. In the US, this is already given to patients during their chemo.”
Patient 1’s Caregiver and Husband
“It was a sigh of relief to know she was getting the treatment, even though the side effects were somewhat of a challenge.
“Whatever benefitted my wife and made her feel more secure throughout this journey was what was important. It’s the responsibility of the caregiver to ensure the person receiving treatment is as comfortable, confident and reassured with whatever decision they make as possible. For what this treatment is, it’s been nothing, but a benefit.”
Patient 2 Interview
“I’ve been very fortunate and very grateful that the side effects from my treatment so far have been pretty mild. I do have side effects, but they’ve been manageable using over-the-counter drugs or prescription medication. I feel pretty good overall. The outcome from what my oncologist has expressed that after my first cycle of treatment there was a noticeable change in the size of the tumour. At the time of my CT scan, I started with a 2.8cm tumour and at the end of cycle one it had gone down to about 1-1.5cm. My oncologist was floored, we were both so excited. To my understanding, my oncologist didn’t expect to see that kind of result so quickly. She indicated she believes it is because of the Keytruda. The only cancer symptom I had was finding the lump and after the biopsy it just felt uncomfortable on that side. My oncologist believes that Keytruda helped shrink my tumour down, which relieved my pain and discomfort. It wasn’t putting pressure on me anymore.
“At first, I was terrified because Keytruda is newer and it deals with the immune system and there are risks associated with that, and I personally have a lot of allergies and I’m very sensitive to medication, so of course, my concerns with it were, “Can my body tolerate this? Am I going to have a reaction? How will it affect me in the long run?” That said, I’m so glad that it was an option for me, because I know in one of my online support groups, there are women who hear about it and don’t have that option and they want to know why. They want to be able to make the best decision for their health long-term and to get through this especially with the triple negative. Even though it was a little scary for me at first, I’m so glad it was an option because I feel like it gives me a little more peace of mind and a little more confidence going into this, and obviously I’ve had positive results so far. I feel like if it doesn’t need to be a mandatory thing, women should at least have the option to explore it and be able to see if that’s going to help them get through this.
“I was very fearful about it, but I’ve had a good experience and I really feel for the people who don’t have that option to explore Keytruda in their treatment plan. I just think that it could really be a game-changer in terms of triple negative and why not let people have that option to be able to have that in their toolbox while they’re fighting this, you know? As of right now I have really positive things to say about it and I hope access to it can change for people who don’t have that access. I really think it’s important.”
Companion Diagnostic Test
Nothing to report on this topic.
Anything Else?
We’d like to emphasize that the triple negative breast cancer community has been underserved for a very long time. At the recent meeting with our TNBC Working Group, what was most striking was them expressing a strong sense of isolation from the rest of the breast cancer community. This intense isolation comes from being diagnosed with a breast cancer that Is:
less common
more aggressive
has a very different treatment path than other subtypes
has fewer treatments than other forms of breast cancer, despite being more aggressive
Many in the TNBC community self-identify as “TNBC Thrivers” to feel empowered - they are determined to “thrive” despite the odds. We’ve noticed that as patients with TNBC are finding each other online and forming TNBC Thriver sub-communities, the sense of community and belonging is empowering; yet; by being in community with other “TNBC Thrivers” they are shaken and re-traumatized by the deaths of their young fellow “Thrivers.” We see them posting “Their story is not my story” as a way to cope and a way to feel hope that they won’t be next. The TNBC community wants more research done on their subtype and they want more effective tools in their toolbox that will help improve their chances against this challenging disease that’s turned their life-plans upside-down.
As we ponder “anything else,” we think about the TNBC Thrivers we know—both early TNBC and those who are now metastatic TNBC—and their loved ones. We know their cancer stories and we know, at least partly, their personal life stories too. We see their family pictures on Facebook and Instagram. We know what they have at stake. We know the feeling we get when we see their updates about being 2 years cancer free or 5 years cancer free. And we know how we feel if they’ve become metastatic and live scan to scan posting about their stability, or, their heartbreak over progression. And, we think of the TNBC Thrivers we’ve lost. Too, too many over the years. Their families will never be the same. Keytruda as an option for those with stage 3 TNBC can give patients a tangible way to help ensure that indeed “Their story won’t be my story.”
Patient Group Conflict of Interest Declaration — Rethink Breast Cancer (Rethink)
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Conflict of Interest Declaration for Rethink Breast Cancer (Rethink)
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | — | — | X | — |
Clinician Input
Ontario Health (Cancer Care Ontario) Breast Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Breast Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Discussed jointly at a DAC meeting.
Current Treatments
These patients receive neoadjuvant chemotherapy and then adjuvant capecitabine if there is residual disease. On the horizon in this similar setting, there are BRCA carriers and there are neratinib.
Treatment Goals
The most important goals that an ideal treatment would address would be event-free survival, prolong life, delay disease progression, and improve overall survival.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Not all patients benefit from the current available treatments. TNBC patients have a significantly high rate of relapse and death. Better treatment options are needed for this patient population.
Which patients have the greatest unmet need for an intervention such as the drug under review?
The greatest unmet need for an intervention would be higher risk TNBC patients with higher risk of recurrence.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Pembrolizumab for TNBC would fit into the current treatment paradigm as a new treatment standard, but it is unclear how it would fit with other available treatment such as adjuvant capecitabine or adjuvant Olaparib (for BRCA 1/ 2 mutation carriers). There are no data about combining these treatments. The DAC is unsure if pembrolizumab could be combined with current treatment paradigms or if the clinician would choose which drug is best suited for the patient. There is a lack of evidence on combining different agents and comparing different agents. In the KEYNOTE trial adjuvant capecitabine was not allowed. At least 35% of the patients would have been received capecitabine as the standard after the neoadjuvant treatment.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Neoadjuvant chemotherapy is the current standard of care for TNBC. Patients would try other treatments if pembrolizumab were not available. If pembrolizumab were available, it would be the preferred treatment.
How would this drug affect the sequencing of therapies for the target condition?
See previous comments.
Which patients would be best suited for treatment with the drug under review?
High risk TNBC patients would be best suited for treatment. The Breast DAC agrees with the eligibility criteria in the study.
How would patients best suited for treatment with the drug under review be identified?
Standard pathology and clinical assessment. Based on the study data, there is no requirement for PDL-1 testing.
Which patients would be least suitable for treatment with the drug under review?
Based on the trial criteria and patients that have contraindications to receiving immunotherapy.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
No, it is not possible to identify those patients. Based on the updated analysis in the study, most subgroups benefits from the treatment (Figure 2).
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
pCR, event-free survival and overall survival. During the neoadjuvant treatment phase, clinical and radiologic assessments.
What would be considered a clinically meaningful response to treatment?
A clinically meaningful response would be tumor response within the breast, pCR rate and event-free survival.
How often should treatment response be assessed?
As per current clinical standards. Typically, patients have clinical assessment before every cycle of treatment.
What factors should be considered when deciding to discontinue treatment?
Toxicity and disease progression.
What settings are appropriate for treatment with the drug under review?
Hospital (outpatient clinic) with expertise in immunotherapy.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
N/A
Additional Information
The placebo arm in the study is not the current standard of care within Ontario. The DAC believes there should be flexibility with using Ontario’s current standard chemotherapy options with the addition of Pembrolizumab, based on the study results of the effectiveness of pembrolizumab. The approval of this would lead to the implementation of a new standard of chemotherapy within Ontario.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Breast Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Andrea Eisen
Position: OH-CCO Breast Cancer Drug Advisory Committee Lead
Date: 11/02/2022
Table 3: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Breast Drug Advisory Committee Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Phillip Blanchette
Position: OH-CCO Breast Cancer Drug Advisory Committee Member
Date: 11/02/2022
Table 4: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Breast Drug Advisory Committee Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
The Ottawa Hospital Cancer Centre – Breast Disease Site Group (Medical Oncology) and Additional Canadian Breast Medical Oncologists
About The Ottawa Hospital Cancer Centre – Breast Disease Site Group (Medical Oncology) and Additional Canadian Breast Medical Oncologists
We are medical oncologists treating breast cancer at the Ottawa Hospital Cancer Centre, Cross Cancer Institute (Edmonton), British Columbia Cancer Agency, Mount Sinai Hospital, London Health Science Centre, Sault Area Hospital (Sault Ste Marie ON), St Joseph’s Health Centre (Toronto), Tom Baker Cancer Centre (Calgary), Sunnybrook Odette Cancer Centre (Toronto), St. John NB, Dalhousie University Halifax NS, Memorial University St John’s NL.
Information Gathering
Ongoing review of emerging data relevant to this file, including from ASCO and ESMO conferences in 2021, and the associated publication of the KN522 data. Local and regional consensus meetings/rounds and shared input into this submission’s content.
Current Treatments
Current Canadian treatment paradigm: For patients with triple negative (ER/PR/HER2 negative) breast cancer, neoadjuvant chemotherapy is the preferred approach for cT1c or greater tumours. This approach is preferred to: allow for clinical downstaging (better chance of clear margins, breast conservation surgery, and potential avoidance of completion axillary node dissection), prognostication (pathologic complete response [pCR] having excellent long term outcomes, whereas non-pCR having higher risk of disease recurrence), and to use pathological response at surgery (pathologic complete response or not) to inform potential further postoperative adjuvant chemotherapy decisions (e.g. oral capecitabine for 6-8 cycles for non-pCR).
Sequential anthracycline-taxane (or taxane-anthracycline) combination chemotherapy (standard q3wk or q2wk dose dense) regimens are usually used, with carboplatin increasingly added to the taxane portion of treatment. Pathologic complete response is universally accepted as a desirable goal of neoadjuvant therapy and these agents are all supported by international guidelines.
TNBC patients treated with neoadjuvant chemotherapy who have residual disease have a poor 5-year survival rates of 50%. This poor survival rate has remained unchanged until the KN522 trial.
Treatment Goals
The most important goal of treatment is to achieve long term cure, i.e., reduction in the risk of recurrent cancer (usually metastatic and incurable).
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Not all TNBCs respond to currently used standard chemotherapy treatments
TNBC currently remains the deadliest type of breast cancer (highest risk of recurrence and death, stage for stage), and occurs more commonly in younger patients
Unlike other breast cancer types (ER+ or HER2+), there are no other standard targeted treatments currently funded
Recurrence rates are highest for TNBC, compared with the other types
pCR (pathologic complete response rates) remain limited with current approaches, occurring in 45-50% of patients.
These patients have an average 5 year disease free survival of 85-90%, but those without pCR have recurrence rates that are much higher.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Patients meeting the eligibility criteria for KN522 would need this treatment approach: female or male adults with TNBC, cT1cN+ or any cT2 or larger, ECOG performance status 0-1 and without contraindications to immunotherapy
Most patients with early stage TNBC would thus be appropriate for consideration
This treatment approach would improve the long-term event free survival of this population and, since most events are metastatic/incurable relapses, save lives
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The KN522 regimen includes carboplatin chemotherapy for all patients. This is commonly added to the taxane portion of neoadjuvant chemotherapy currently. In the new regimen, the carboplatin/paclitaxel cycles are given before the doxorubicin/cyclophosphamide cycles. While the sequence may differ currently between jurisdictions, the chemotherapy agents remain the same.
Pembrolizumab would be added for all fit patients meeting the KN522 eligibility criteria, preop for 24 wk then postop adjuvantly for 27 weeks completing one year in total
This regimen would become the new favoured routine protocol for this patient population, a shift from our current paradigm
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
For patients eligible for KN522, it would not be appropriate to start another regimen beforehand. Patients only have “one chance” to receive the optimal evidence-based regimen neoadjuvantly/ adjuvantly to achieve cure and prevent systemic recurrences (which are uniformly fatal). Indeed, repeated studies in the advanced disease setting have shown that delaying pembrolizumab while giving chemotherapy leads to worse patient outcomes. Patients with pre-existing serious autoimmune diseases might not be candidates, and those with less serious autoimmune conditions would weigh the pros and cons while considering older standard regimens in lower risk TNBC cases.
How would this drug affect the sequencing of therapies for the target condition?
Should incurable metastatic relapse occur, after neo/adjuvant pembrolizumab using the KN522 regimen, we would not routinely retreat with pembrolizumab for metastatic disease at this time as there is no supporting data, although there may be in the future. For patients not treated with neo/adjuvant pembrolizumab, based on KN355, we would use pembrolizumab with chemo in the first line relapsed setting for tumours with PD-L1 expression of greater or equal to 10%. In that metastatic setting, the benefits would only be palliative, and patients would eventually succumb to cancer progression. Thus, for early breast cancer the ideal time to treat would be in the curative neoadjuvant setting.
Which patients would be best suited for treatment with the drug under review?
Stages: any clinically node positive patients or node negative if primary tumour size cT2 or greater (2 cm)
ECOG performance status 0-1
Female or male patients (age 18 or older) with newly diagnosed non metastatic triple negative breast cancer
How would patients best suited for treatment with the drug under review be identified?
Patients would be identified routinely as they are currently using standard breast cancer clinical staging approaches (no additional testing required) and routine breast tumour biopsy characterization of ER/PR/HER2 status (all negative). They would not be difficult to identify and PD-L1 biomarker testing is not required in this neoadjuvant setting.
Which patients would be least suitable for treatment with the drug under review?
ECOG performance status 2-4
Serious pre-existing autoimmune disorders which might cause serious or life-threatening harm if exacerbated by immunotherapy (in practice, neurologic conditions such as multiple sclerosis or myasthenia gravis are concerning)
Patients with other autoimmune disorders (inflammatory bowel disease, rheumatoid arthritis for example) where their tumours are small, and the benefits of therapy might be counterbalanced by the risk of exacerbation of their underlying conditions
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
There is no current biomarker to select amongst TNBC cases. The triple negative phenotype involved is indeed the only tumour biomarker profile required (ER/PR/HER2 negative)
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Patients are assessed before every cycle with physical examination, and imaging scans may occur at the end of neoadjuvant treatment to assess response.
What would be considered a clinically meaningful response to treatment?
Tumour shrinkage clinically/ radiographically on treatment is a marker but the greater the response (esp PCR) the better the long- term prognosis. Ideally a PCR is achieved but any decrease in disease may be clinically meaningful.
How often should treatment response be assessed?
Patients would be clinically assessed before each cycle of treatment and radiographic assessment may be considered if there are concerns based on clinical examinations or for preoperative planning post neoadjuvant treatment completion.
What factors should be considered when deciding to discontinue treatment?
Disease progression (tumour enlargement)
Certain severe adverse events occur, particularly autoimmune toxicities (as per the KN522 protocol, any grade 4 treatment related adverse event or grade 2-3 not improving to grade 1 with supportive care or dose modifications)
What settings are appropriate for treatment with the drug under review?
Chemotherapy infusion units with experience administering cytotoxic agents and immunotherapy
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Not applicable
Additional Information
Outcomes have remained largely stagnant in this not uncommon aggressive breast cancer subtype for many years. While major improvements have been realized in HER2+ and high risk ER+ early breast cancers, there have been little improvement for TNBC until KN522. Patients and clinicians have been excited about the benefits seen and are eager to offer pembrolizumab in this neo/adjuvant setting as soon as possible. The absolute event free survival benefit of 7% is practice changing and the regimen has an acceptable toxicity profile.
Conflict of Interest Declarations — The Ottawa Hospital Cancer Centre – Breast Disease Site Group (Medical Oncology) and Additional Canadian Breast Medical Oncologists
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr Sandeep Sehdev
Position: MD FRCPC Medical Oncologist, Assistant Professor, The Ottawa Hospital Cancer Centre, lead of breast cancer disease site group
Date: 07-Feb-2022
Table 5: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | — | X | — | — |
Declaration for Clinician 2
Name: Dr Silvana Spadafora
Position: Regional Lead for Systemic Therapy for North East, Ontario Health, Medical Oncology, Algoma District Cancer Program (Sault Ste Marie)
Date: 20-FEB-2022
Table 6: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Pfizer, Merck, Novartis, Gilead, Bayer, AstraZeneca, Lilly | X | — | — | — |
Declaration for Clinician 3
Name: Dr Dorothy Lo
Position: Medical Oncologist, St Joseph’s Health Centre, Toronto ON. Lead, COMET (Community Oncologists of Metropolitan Toronto)
Date: 23-FEB-2022
Table 7: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
Declaration for Clinician 4
Name: Dr Jan-Willem Henning
Position: Medical Oncologist, Breast and Sarcoma Tumour Groups, Tom Baker Cancer Centre, Calgary AB, Cumming School of Medicine, U of Calgary. Medical Co-Lead, Sarcoma Tumour Group and Adolescent and Young Adult Southern Alberta Program, Alberta Health Services, Cancer Care Alberta
Date: 18-FEB-2022
Table 8: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
Declaration for Clinician 5
Name: Dr Christine Brezden-Masley MD PhD FRCPC
Position: Medical Oncologist, Mt Sinai Hospital, Assoc Prof U of Toronto, Medical Director, Cancer Program and Sinai Health System, Director Marvelle Koffler Breast Centre, President Canadian Cardio-Oncology Network
Date: 19-FEB- 2022
Table 9: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
Declaration for Clinician 6
Name: Dr Mark Clemons
Position: Medical Oncologist, Ottawa Hospital Cancer Centre, Professor U of Ottawa
Date: 8-FEB-2022
Table 10: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
None | — | — | — | — |
Declaration for Clinician 7
Name: Dr Anil Joy
Position: Medical Oncologist, Cross Cancer Institute, Edmonton AB. Professor, U of Alberta. Previous consultant for Medical Council of Canada, grant reviewer for Cdn Breast Cancer Foundation and NCIC (National Cancer Institute of Canada). Medical Director (Edmonton) of Alberta Cancer Research Biobank.
Date: 19-FEB-2022
Table 11: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
Declaration for Clinician 8
Name: Dr Jawaid Younus
Position: Medical Oncologist, London Regional Cancer Centre, London ON. Assistant Prof, Western University.
Date: 19-FEB-2022
Table 12: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 8
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
Declaration for Clinician 9
Name: Dr Karen Gelmon
Position: Medical Oncologist, Professor, Univ of British Columbia, BC Cancer Agency, Vancouver BC
Date: 8-FEB-2022
Table 13: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 9
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
AstraZeneca | — | X | — | — |
Lilly | X | — | — | — |
Novartis | — | X | — | — |
Pfizer | X | — | — | — |
Roche | X | — | — | — |
Seagen | X | — | — | — |
Gilead | X | — | — | — |
Ayala | X | — | — | — |
Declaration for Clinician 10
Name: Dr Amirrtha Srikanthan
Position: Medical Oncologist, Ottawa Hospital Cancer Centre, Assistant Professor U of Ottawa
Date: 8-FEB-2022
Table 14: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 10
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
None | — | — | — | — |
Declaration for Clinician 11
Name: Dr Daniel Rayson
Date: 28-FEB-2022
Table 15: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 11
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
Declaration for Clinician 12
Name: Dr Amy Groom
Position: MD, FRCPC, Medical Oncologist, Saint John Regional Hospital, Assistant Professor of Medicine Dalhousie University, Assistant Professor of Medicine, Memorial University
Date: 28-FEB-2022
Table 16: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 12
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
Declaration for Clinician 13
Name: Dr Katarzyna Jerzak
Position: Medical Oncologist, Sunnybrook Odette Cancer Centre; Assoc Scientist Sunnybrook Research Institute; Assistant Professor Dept of Medicine, U of Toronto
Date: 28-FEB-2022
Table 17: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 13
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
Declaration for Clinician 14
Name: Dr Terry Ng
Position: MD FRCPC, Assistant Professor, U of Ottawa, Medical Oncologist (Ottawa Hospital Cancer Centre)
Date: 28-FEB-2022
Table 18: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 14
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Knight | X | — | — | — |
Novartis | X | — | — | — |
ARIAD/Takeda | X | — | — | — |
Boehringer-Ingelheim | X | — | — | — |
Declaration for Clinician 15
Name: Dr Daniel Rayson
Position: Medical Oncologist, Professor of Medicine, Dalhousie University
Date: 28-FEB-2022
Table 19: Conflict of Interest Declaration for Ottawa Hospital Cancer Centre – Breast Disease Site Group and Additional Oncologists Clinician 15
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Merck | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.