CADTH Reimbursement Review
Atezolizumab (Tecentriq)
Sponsor: Hoffmann-La Roche Ltd.
Therapeutic area: Extensive-stage small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
CI
confidence interval
CR
complete response
CrI
credible interval
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-LC13
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13
ES-SCLC
extensive-stage small cell lung cancer
FE
fixed effect
GHS
global health status
HR
hazard ratio
HRQoL
health-related quality of life
ICI
immune checkpoint inhibitor
ITC
indirect treatment comparison
ITT
intention to treat
LCC
Lung Cancer Canada
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
OR
odds ratio
ORR
objective response rate
OS
overall survival
PCI
prophylactic cranial irradiation
PD-1
programmed cell death protein 1
PD-L1
programmed death ligand −1
PFS
progression-free survival
PICO
population, interventions, comparisons, outcomes
PR
partial response
PRO
patient-reported outcome
QoL
quality of life
RCT
randomized controlled trial
RE
random effect
RECIST
Response Evaluation Criteria in Solid Tumours
SAE
serious adverse event
SCLC
small cell lung cancer
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Atezolizumab for injection (Tecentriq), solution for IV infusion, 1,200 mg/20 mL |
Indication | In combination with carboplatin and etoposide for the first-line treatment of adult patients with extensive-stage small cell lung cancer |
Reimbursement request | Tecentriq for the first-line treatment of patients with extensive-stage small cell lung cancer in combination with a platinum-based chemotherapy and etoposide. Maintenance Tecentriq should be continued until loss of clinical benefit or unacceptable toxicity. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | August 8, 2019 |
Sponsor | Hoffmann-La Roche Ltd. |
NOC = notice of compliance.
Introduction
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer-related death in Canada.1 In 2021, an estimated 29,600 Canadians were diagnosed with lung cancer, representing approximately 13% of all new cancer cases, and an estimated 21,000 Canadians died from lung cancer.1 The main known risk factor for lung cancer is tobacco smoking, including exposure to second-hand smoke. Non–small cell lung cancer (NSCLC) is the predominant subtype of lung cancer, accounting for approximately 85% of cases. Small cell lung cancer (SCLC) accounts for about 15% of cases and is distinguished from NSCLC by its rapid growth, early development of metastatic disease, and initial responsiveness to platinum-based chemotherapy.2 SCLC is classified into 2 stages. The first, limited-stage disease, is confined to 1 hemithorax, with no extrathoracic metastases, except for ipsilateral supraclavicular lymph nodes (provided they can be included in the same radiation port as the tumour), and primary tumour and regional nodes that can be adequately encompassed in a radiation port.3,4 The second, extensive-stage disease, is defined as disease that cannot be classified as limited, including malignant pleural or pericardial effusions, contralateral hilar or supraclavicular lymph nodes, and hematogenous metastases.3,4 Approximately 2-thirds of patients with SCLC have extensive-stage disease at diagnosis, which is associated with particularly poor prognosis.5 Extensive-stage SCLC (ES-SCLC) has a median survival of 7 months to 10 months and a 1-year overall survival (OS) rate of 40% (with treatment).1,6
Despite the considerable response rates observed with first-line chemotherapy regimens, response is not durable, and most patients with ES-SCLC relapse within 1 year of treatment completion.7 Subsequent treatment options for patients with relapsed disease are few, due to the limited efficacy of chemotherapy and other regimens in later lines and the low performance status of many patients with relapsed disease. In addition, brain metastases are common in SCLC, with about 10% of patients presenting with brain metastases at the time of diagnosis; an additional 40% to 50% of patients subsequently develop brain metastases, which further contributes to poor prognosis.8,9 In the first-line setting, the most important goals of treatment are prolonging survival and improving quality of life (QoL) (reduction in symptom severity, ability to maintain independence in daily activities, and so forth). Patients with ES-SCLC have a significant need for better first-line therapies with more durable response to prolong survival beyond 2 years and preserve QoL.
Until recently, the standard first-line treatment of patients with ES-SCLC was a platinum agent (cisplatin or carboplatin) and etoposide chemotherapy.10 Despite a median survival limited to approximately 10 months, there has been no considerable improvement in OS in more than 20 years. Recently, immune checkpoint inhibitors (ICIs) added to platinum and etoposide chemotherapy have demonstrated benefit in this setting. Two ICIs, durvalumab and atezolizumab, are approved in Canada, in combination with etoposide and either carboplatin or cisplatin for the first-line treatment of patients with ES-SCLC. However, neither is currently publicly funded. Durvalumab received a CADTH recommendation to reimburse in July 2021, but the Health Technology Assessment process is not yet complete, and price negotiations are ongoing with the pan-Canadian Pharmaceutical Alliance. A reimbursement request for atezolizumab in combination with carboplatin and etoposide for the treatment of ES-SCLC was previously submitted to CADTH and did not receive a recommendation to reimburse. This current CADTH Reimbursement Review for atezolizumab in combination with a platinum-based chemotherapy and etoposide is for of a resubmission filed by the sponsors for the aforementioned indication.
Atezolizumab (Tecentriq) is a humanized monoclonal anti–programmed death ligand 1 that inhibits programmed death ligand1 (PD-L1) engagement with programmed cell death protein 1 (PD-1) and B7.1. Health Canada has approved atezolizumab in combination with carboplatin and etoposide for the first-line treatment of adult patients with ES-SCLC. The sponsor’s funding request differs from the approved Health Canada indication: “for the first-line treatment of patients with extensive-stage small cell lung cancer (ES-SCLC) in combination with a platinum-based chemotherapy and etoposide. Maintenance Tecentriq should be continued until loss of clinical benefit or unacceptable toxicity.”
The objective of this review was to evaluate the efficacy and safety of atezolizumab in combination with carboplatin and etoposide for the first-line treatment of patients with ES-SCLC.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
The patient and caregiver input received for this review was collected by Lung Cancer Canada (LCC) from interviews with patients with SCLC and their caregivers, gathered from December 2021 to February 2022, as well as information from previous LCC submissions. Six respondents with SCLC had experience with atezolizumab (in combination with chemotherapy or as a single treatment), 4 of whom had extensive-stage disease. Five patients had access to atezolizumab through clinical trial and 1 through a compassionate access program. Four of these respondents resided in Ontario, 1 resided in British Columbia, and 1 resided in Quebec. Respondents indicated that a diagnosis of SCLC and the subsequent treatment had a major impact on the lives of patients and their family members. They reported that they expect the following key outcomes from any new drug or treatment: relief from disease symptoms, manageability of side effects, improved QoL, ability to maintain independence and functionality, greater access across jurisdictions, disease stability, longer periods of remission, and prolonged survival. Patients with SCLC have had a very high unmet need, as there had been no new treatment options for SCLC in 30 years until 2021, when durvalumab was approved for treatment of ES-SCLC. Six respondents who had received or were continuing to receive atezolizumab indicated that this drug had promising and durable treatment results with tolerable side effects. They also mentioned that atezolizumab had helped them regain independence, functionality, and livelihood, which reduced the burden on their caregivers and loved ones.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH noted that ES-SCLC has a relatively short median OS (10 months). Although patients typically have an initial response to treatment, most patients relapse within 6 months with poor prognosis. Given most patients’ poor performance status and poor response to subsequent therapies, first-line treatment options that increase survival are highly desired. The combination of immunotherapy and chemotherapy is widely accepted as the new standard of care for the management of ES-SCLC. The addition of durvalumab or atezolizumab to a platinum agent and etoposide would be the most appropriate initial therapy for ES-SCLC. The clinical experts consulted also indicated that there is no specific subgroup of patients best suited for treatment with atezolizumab plus carboplatin and etoposide, and all patients with ES-SCLC should be treated with combination immunotherapy and chemotherapy in the first-line setting, irrespective of symptoms, as ES-SCLC is an aggressive disease and requires prompt treatment. Response to treatment is typically assessed every 3 cycles while on chemotherapy, using radiographic imaging with a CT scan, and every 3 months thereafter.
Clinician Group Input
Clinician input was received from the Ontario Health (Cancer Care Ontario) Drug Advisory Committee and from LCC. The clinician groups noted that patients with ES-SCLC have a high unmet need for more effective therapies since most patients progress in a short period of time despite a high response rate to initial therapy. Atezolizumab would be used as initial systemic therapy in patients with ES-SCLC in combination with 4 cycles of platinum and etoposide, followed by maintenance atezolizumab until disease progression. Atezolizumab will be an alternative option to durvalumab (if durvalumab is indeed added to the provincial or territorial public formularies across Canada following negotiations with the pan-Canadian Pharmaceutical Alliance) in the first-line treatment of patients with ES-SCLC. It would fit into the current treatment paradigm only as an agent to be started concurrently with first-line platinum and etoposide chemotherapy, with the intention of continuing until disease progression, intolerance, or a patient’s choice to discontinue therapy. Patients with symptomatic brain metastases would need to receive treatment for their brain metastases before starting systemic therapy. The clinician groups believed that no specific subgroups of patients are more likely to benefit from the addition of atezolizumab to platinum-based chemotherapy and etoposide; therefore, they felt the treatment should be considered for any patient with ES-SCLC and an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 2 or better.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH Reimbursement Review process. The following were identified as key factors that could impact the implementation of a CADTH recommendation for atezolizumab:
considerations for initiation of therapy
considerations for prescription of therapy
considerations for discontinuation of therapy
generalizability of trial populations to the broader populations in the jurisdictions
system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
IMpower133 is a randomized, multi-centre, double-blind, placebo-controlled, phase III study designed to evaluate the efficacy and safety of treatment with atezolizumab plus carboplatin and etoposide compared with treatment with placebo plus carboplatin and etoposide in patients with chemotherapy-naive ES-SCLC.11 The trial was conducted in 106 sites across 21 countries (none in Canada). The co-primary end points were investigator-assessed progression-free survival (PFS) and OS. The key secondary end points were investigator-assessed objective response rate (ORR) and investigator-assessed duration of response (DOR). Patient-reported outcomes (PROs) included health-related QoL (HRQoL). The clinical cut-off date for the primary analysis (primary PFS analysis and interim OS analysis) was April 24, 2018. The clinical cut-off date for the updated analysis (final analysis of OS) was January 24, 2019. Overall, the mean age of the patients was 63.7 years (standard deviation [SD] = 8.9); 64.8% were male, and 79.9% were White. Patients had to have an ECOG PS of 0 or 1, and approximately 64% of the patients in both treatment arms had an ECOG PS of 1. Of the 526 patients screened, 403 were randomized: 201 patients to the atezolizumab arm and 202 patients to the placebo arm. The median duration of follow-up was 13.9 months at the data cut-off date of April 24, 2018 (PFS analysis; interim OS analysis), and 22.9 months at the data cut-off date of January 24, 2019 (final OS analysis).
Efficacy Results
Progression-Free Survival
At the data cut-off date for PFS analysis (April 24, 2018), the median PFS was 5.2 months (95% confidence interval [CI], 4.4 to 5.6) in the atezolizumab arm and 4.3 months (95% CI, 4.2 to 4.5) in the placebo arm. The stratified hazard ratio (HR) for disease progression or death was 0.77 (95% CI, 0.62 to 0.96; P = 0.0170).
Overall Survival
At the time of the OS interim analysis (data cut-off date: April 24, 2018), patients had a median survival follow-up time of 13.9 months. The median OS was 12.3 months (95% CI, 10.8 to 15.9) in the atezolizumab arm and 10.3 months (95% CI, 9.3 to 11.3) in the placebo arm. The stratified HR for death was 0.70 (95% CI, 0.54 to 0.91; P = 0.007).
At the final OS analysis (data cut-off date: January 24, 2019), the median survival follow-up time was 22.9 months. The median OS was 12.3 months (95% CI, 10.8 to 15.8) in the atezolizumab arm and 10.3 months (95% CI, 9.3 to 11.3) in the placebo arm. The stratified HR for death was 0.75 (95% CI, 0.60 to 0.95; P = 0.015). The 2-year event-free rates were 22.0% in the atezolizumab arm and 16.8% in the placebo arm.
Objective Response Rate
The investigator-assessed, confirmed ORR was 60.2% in the atezolizumab arm and 64.4% in the placebo arm; 2.5% and 1.0% of patients in the atezolizumab and placebo arms, respectively, had a complete response (CR). At the updated analysis, the confirmed investigator-assessed, ORR was 60.2% (95% CI, 53.1 to 67.0) in the atezolizumab arm and 64.4% (95% CI, 57.3 to 71.0) in the placebo arm; 3.5% and 1.0% of patients in the atezolizumab and placebo arms, respectively, had a CR.
Duration of Response
The median DOR (confirmed) was 4.2 months (range = 1.4 to 24.3) in the atezolizumab arm and 3.9 months (range = 2.0 to 24.2) in the placebo arm. At data cut-off (April 24, 2018), 14.9% of patients in the atezolizumab arm and 5.4% of patients in the placebo arm had ongoing response. At the updated analysis, the median DOR was 4.2 months (95% CI, 4.1 to 4.5) in the atezolizumab arm and 3.9 months (95% CI, 3.1 to 4.2) in the placebo arm.
Harms Results
The majority of patients in both treatment arms — 100% in the atezolizumab arm and 96.4% in the placebo arm — experienced at least 1 adverse event (AE) of any grade. In the atezolizumab arm, the most common AE of any grade by preferred term experienced by at least 10% of patients were anemia (43.4%), nausea (37.9%), and neutropenia (37.4%). In the chemotherapy arm, the most common AEs of any grade by preferred term experienced by at least 10% of patients were anemia (35.2%), neutropenia (35.2%), and alopecia (34.7%).
Grade 3 or 4 AEs occurred in 67.7% of patients in the atezolizumab arm and 63.3% of patients in the placebo arm. The most common grade 3 or 4 AEs reported in at least 5% of patients in the atezolizumab and placebo arms were neutropenia (22.7% versus 25.0%), decreased neutrophil count (15.7% versus 16.8%), anemia (15.7% versus 13.3%), thrombocytopenia (10.1% versus 8.7%), and hyponatremia (4.5% versus 6.6%).
In the atezolizumab arm, 38.9% of patients had at least 1 serious AE (SAE). In the placebo arm, 35.2% of patients experienced at least 1 SAE. The most common SAEs experienced by at least 1% of patients in either the atezolizumab or the chemotherapy arm were pneumonia (4.5% versus 3.6%), neutropenia (3.5% versus 4.1%), febrile neutropenia (2.5% versus 4.6%), and thrombocytopenia (2.5% versus 2.0%).
Withdrawal from any study treatment due to AEs was reported for 12.1% of patients in the atezolizumab arm and 3.1% of patients in the chemotherapy arm. In the atezolizumab arm, 11.6% of patients experienced AEs leading to discontinuation of atezolizumab, and in the placebo arm 2.6% of patients had AEs leading to discontinuation of placebo. The main reasons for permanently discontinuing atezolizumab in 21 patients in the atezolizumab arm were infusion-related reactions and gastrointestinal disorders.
Grade 5 fatal AEs occurred in 4 patients (2.0%) in the atezolizumab arm and included pneumonia, respiratory failure, death, and neutropenia. Grade 5 fatal AEs occurred in 11 patients (5.6%) in the placebo arm and included pneumonia, pulmonary sepsis, sepsis, septic shock, acute respiratory failure, hemoptysis, cardiopulmonary failure, pericardial effusion, and general physical health deterioration. The only grade 5 AE (by preferred term) that occurred in more than 1 patient was pneumonia (1 patient in the atezolizumab arm and 3 patients in the placebo arm). Of the grade 5 events, 3 events in each arm were considered related to at least 1 component of study treatment. In the atezolizumab arm, a grade 5 death was considered related to all study treatment; there was also 1 case of grade 5 pneumonia and 1 case of grade 5 neutropenia that were both considered related to both carboplatin and etoposide. In the placebo arm, a grade 5 septic shock was considered related to all study treatment, a grade 5 pneumonia was considered related to placebo, and a grade 5 cardiopulmonary failure was considered related to carboplatin.
Immune-related AEs were reported for 41.4% of patients in the atezolizumab arm and 24.5% of patients in the placebo arm. Rash (both treatment arms) and hypothyroidism (atezolizumab arm) were the most common (≥ 10% incidence) and most differentially reported (≥ 5% difference between treatment arms) immune-related AEs during treatment. Immune-related infusion-related reaction events were experienced by 5.6% of patients (n = 11) in the atezolizumab arm and 5.1% of patients (n = 10) in the placebo arm. The majority of these events were grade 1 or 2 (atezolizumab arm: n = 7 [3.5%]; placebo arm: n = 9 [4.6%]). Four patients (2.0%) in the atezolizumab arm and 1 patient (0.5%) in the placebo arm had grade 3 or 4 infusion-related reactions.
Table 2: Summary of Key Results From the IMpower133 Study
Outcomes | Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) |
|---|---|---|
PFS | ||
Median (95% CI), months | 5.2 (4.4 to 5.6) | 4.3 (4.2 to 4.5) |
Stratified HR (95% CI)a | 0.772 (0.624 to 0.955) | |
P valueb | 0.0170a | |
OS, interim analysis | ||
Median (95% CI), months | 12.3 (10.8 to 15.9) | 10.3 (9.3 to 11.3) |
Stratified HR (95% CI)a | 0.701 (0.541 to 0.909) | |
P valueb | 0.0069a | |
OS, final analysis | ||
Median (95% CI), months | 12.3 (10.8 to 15.8) | 10.3 (9.3 to 11.3) |
Stratified HR (95% CI)a | 0.755 (0.601 to 0.949) | |
P valueb | 0.0154b | |
Objective confirmed response, CR or PR | ||
ORR, n (%) | 121 (60.2) | 130 (64.4) |
95% CI for response ratec | 53.07 to 67.02 | 57.33 to 70.95 |
Difference in response rates (95% CId) | –4.16 (–14.11 to 5.79) | |
P valueb | 0.3839 | |
Duration of response | ||
Median (range), months | 4.2 (1.4 to 24.3) | 3.9 (2.0 to 24.2) |
Median time to event (95% CI), months | 4.2 (4.1 to 4.5) | 3.9 (3.1 to 4.2) |
Stratified HR (95% CI)a | 0.700 (0.53 to 0.92) | |
P valueb | 0.0109 | |
Harms, safety population, n (%) | ||
AEs | 198 (100) | 189 (96.4) |
Grades 3 to 4 | 134 (67.7) | 124 (63.3) |
SAEs | 77 (38.9) | 69 (35.2) |
AEs leading to withdrawal from any treatment | 24 (12.1) | 6 (3.1) |
AEs leading to withdrawal from atezolizumab or placebo | 23 (11.6) | 5 (2.6) |
Deaths due to AEs | 4 (2.0) | 11 (5.6) |
Notable harms, safety population, n (%) | ||
Immune-related AEs | 82 (41.4) | 48 (24.5) |
Infusion-related AEs | 11 (5.6) | 10 (5.1) |
AE = adverse event; CE = carboplatin and etoposide; CI = confidence interval; CR = complete response; HR = hazard ratio; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; SAE = serious adverse event.
aStratified by sex (male vs. female) and Eastern Cooperative Oncology Group Performance Status (0 vs. 1).
bLog-rank test.
cClopper-Pearson interval.
dWald with continuity correction.
Source: Clinical Study Report for IMpower133 study12; Update Clinical Study Report for IMpower133 study.13
Critical Appraisal
The baseline demographic and disease characteristics were roughly balanced between the 2 treatment arms. Response outcomes (ORR and DOR) were assessed by investigators per Response Evaluation Criteria in Solid Tumours (RECIST) Version 1.1. Although the trial was double blinded and the investigators were blinded to treatment assignment, risk of bias cannot be ruled out. For example, nearly half the patients in the atezolizumab arm experienced immune-related AEs or other events. These events may have made the investigator aware of the patient’s treatment assignment. Therefore, for all investigator-assessed outcomes there may be a degree of subjectivity that could have biased the results. In addition, although the proportion of patients receiving concomitant and supportive care for symptom control was largely similar in the 2 treatment arms, which may have led to comparable PROs, including QoL outcomes, as observed in the trial, this may not mean that the 2 trial regimens truly have comparable safety and impact on QoL. Interim and final analyses were planned a priori and adequately described. The interim analysis applied the Lan-DeMets alpha spending function with the O’Brien-Fleming stopping boundary, which is deemed conservative in controlling type I error when claiming a treatment effect based on interim analysis. The updated final analysis results of OS were consistent with the interim analysis results.
The patient population in the IMpower133 study generally reflects patients in Canadian clinical practice in this setting. However, some patient groups were not represented, including those with an ECOG PS of 2 and patients with active untreated metastases. The proportion of patients with brain metastases (9%) was lower than that observed in clinical practice (10% to 20%), but this is likely due to the specific inclusion requirements for these patients (e.g., only supratentorial and cerebellar metastases, and no ongoing requirement for corticosteroids as therapy for central nervous system disease). Due to the small number of patients in some subgroups, including brain metastases at baseline, subgroup analyses failed to demonstrate similar effects in patients with brain metastases as in patients free of brain metastases. The comparator in the IMpower133 trial (carboplatin and etoposide) is relevant to the Canadian context as platinum (carboplatin or cisplatin) and etoposide chemotherapy is the current standard of care.
Indirect Comparisons
Description of Studies
One sponsor-submitted indirect treatment comparison (ITC)14 and 9 published ITCs retrieved from literature were summarized and appraised for this CADTH review.
The sponsor-submitted ITC provided estimates of PFS, OS, ORR, and incidence of SAEs for atezolizumab plus carboplatin and etoposide and for competing interventions, platinum doublet therapies, and immunotherapies used for the first-line treatment of ES-SCLC. The results of comparisons between atezolizumab plus carboplatin and etoposide versus etoposide and carboplatin, etoposide and cisplatin, and durvalumab plus carboplatin (or cisplatin) and etoposide were considered relevant for the purpose of this CADTH review.
The sponsor’s base-case analysis for each outcome included adjusted or stratified HRs reported across the trials in the relevant evidence network. Additional scenario analyses were conducted to investigate the choice of platinum agent for the analyses of PFS and OS and to explore the effect on OS of 1 study with outlier ECOG PS data.
Efficacy Results
This section will focus on the findings of the sponsor-submitted network meta-analysis (NMA).14
Progression-Free Survival
The results of the base-case analysis showed that atezolizumab plus carboplatin and etoposide was associated with longer PFS than carboplatin (or cisplatin) and etoposide (HR = 0.77; 95% credible interval [CrI], 0.62 to 0.96). Similar findings were observed in the scenario analyses that included unadjusted or unstratified HRs (scenario 1: HR = 0.76; 95% CrI, 0.62 to 0.94) or that considered etoposide and carboplatin as distinct nodes (scenario 2: HR = 0.77; 95% CrI, 0.62 to 0.95).
The results of the base-case analysis for the comparison of atezolizumab plus carboplatin and etoposide versus durvalumab plus carboplatin (or cisplatin) and etoposide showed no statistically significant difference in PFS based on the CrI which included the null, and the point estimate that was close to the null value (HR = 0.97; 95% CrI, 0.73 to 1.28). Similar findings were observed in the scenario analyses that included unadjusted or unstratified HRs (scenario 1: HR = 0.95; 95% CrI, 0.72 to 1.26).
Overall Survival
The results of the base-case analysis suggested that atezolizumab plus carboplatin and etoposide may be associated with improvement in OS, when compared with etoposide and carboplatin (or cisplatin) (HR = 0.75; 95% CrI, 0.60 to 0.95). Similar findings were obtained in the other 3 scenario analyses, which included unadjusted or unstratified HRs (scenario 1: HR = 0.71; 95% CrI, 0.55 to 0.92), investigated the robustness of the results to the exclusion of a study with outlier ECOG PS data (i.e., the Hermes 2008 study) (scenario 2: HR = 0.75; 95% CrI, 0.60 to 0.95), or considered etoposide and cisplatin as distinct nodes (scenario 3: HR = 0.75; 95% CrI, 0.60 to 0.95).
The results of the base-case analysis for the comparison of atezolizumab plus carboplatin and etoposide versus durvalumab plus carboplatin (or cisplatin) and etoposide showed no statistically significant difference in OS based on the CrI which included the null, and the point estimate that was close to the null value (HR = 1.01; 95% CrI, 0.75 to 1.36). Similar findings were obtained in the other 3 scenario analyses, which included unadjusted or unstratified HRs (scenario 1: HR = 0.95; 95% CrI, 0.69 to 1.31), investigated the robustness of the results to exclusion of the Hermes 2008 study (scenario 2: HR = 1.01; 95% CrI, 0.75 to 1.35), or considered etoposide and cisplatin as distinct nodes (scenario 3: HR = 0.95; 95% CrI, 0.69 to 1.31).
Objective Response Rate
The comparison of atezolizumab plus carboplatin and etoposide versus durvalumab plus carboplatin (or cisplatin) and etoposide showed that atezolizumab plus etoposide and carboplatin was associated with lower odds of ORR (odds ratio [OR] = 0.54; 95% CrI, 0.32 to 0.94). The OR for the comparison of atezolizumab plus carboplatin and etoposide versus etoposide and carboplatin or cisplatin was estimated to be 0.84 (95% CrI, 0.56 to 1.25), and the OR for the comparison of atezolizumab plus carboplatin and etoposide versus etoposide and cisplatin was 0.70 (95% CrI, 0.37 to 1.35).
Harms Results
Serious Adverse Events
Two studies were used to inform the evidence network for SAEs. The OR observed in the comparison of atezolizumab plus carboplatin and etoposide versus durvalumab plus carboplatin (or cisplatin) and etoposide was estimated to be 1.37 (95% CrI, 0.79 to 2.37), and in the comparison of atezolizumab plus carboplatin and etoposide versus etoposide and cisplatin, the OR was 1.12 (95% CrI, 0.74 to 1.70). No statistically significant difference was observed based on the CrIs which included the null value, and the point estimates that were close to the null value (i.e., OR = 1).
Critical Appraisal
The sponsor’s systematic review methods for identifying and assessing studies included in the network were considered appropriate for identifying relevant studies. The PICO (population, interventions, comparisons, outcomes) criteria were pre-specified, and articles were reviewed by 2 independent reviewers while a second analyst extracted data. All relevant comparators identified in the CADTH review protocol that were considered relevant to the Canadian practice context were presented in the sponsor’s NMA. Outcomes presented in the trials included in the network analysis were considered relevant and clinically meaningful by the clinician experts consulted during the CADTH review. The population studied in all 8 trials included in the NMA was considered relevant for the reimbursement request. Most studies included untreated patients with ES-SCLC. One study (Skarlos 1994) recruited a different population in the trial but had a subgroup of patients with ES-SCLC. Information from the subgroup analysis was used to inform the network. Quality assessments were conducted using the validated 7-criteria checklist provided by the National Institute for Health and Care Excellence (NICE) single technology appraisal user guide.
A generalized linear regression model with a binomial likelihood, logit link model was used; this model was considered appropriate for the types of outcomes assessed in the network. The sponsor explored both fixed-effect (FE) and random-effect (RE) models in its base-case scenarios, and results from the FE model were presented. The sponsor provided a justified rationale for using the FE model over the RE model based on the model fit criteria, including a judgment on the similarities of the studies included in terms of effect modifiers.
The transitivity assumption was assessed by evaluating potential effect modifiers. There was considerable heterogeneity across trials, particularly in terms of ECOG PS. The Hermes 2008 trial enrolled less than 53% of patients with an ECOG PS of 0 or 1 in both treatment arms versus 100% in the CASPIAN, ECOG-ACRIN EA5161, IMpower133, and KEYNOTE-604 trials. In the Okamoto 2007 trial, patients with an ECOG PS of 0 to 2 were included if they were 70 years or older and those with an ECOG PS of 3 were included if they were younger than 70 years. There was inconsistency in the reporting of the number and type of metastatic sites across the trials. Heterogeneity in the use of subsequent anticancer therapy administered in the second line and higher to patients recruited in the studies was identified as a potential source of bias affecting OS assessment (non-protocol second- and third-line treatment was reported in the Hermes 2008, Okamoto 2007, and Schmittel 2011 trials); this may also affect the generalizability of the findings of the NMA to the Canadian setting. Variability was also observed in the dosing of etoposide plus carboplatin or cisplatin across the trials: 3 studies — CASPIAN, Schmittel 2011, and Skarlos 1994 — randomized patients to combination chemotherapy regimens for up to 4 to 6 cycles, whereas in the IMpower133 trial (including ECOG-ACRIN EA5161, KEYNOTE-604, Hermes 2008, and Okamoto 2007) patients were dosed with the comparator for up to 4 cycles. This may have impacted the findings of the ITC.
According to the sponsor’s ITC report, a meta-regression analysis to investigate inter-trial heterogeneity was not possible as there were insufficient studies (i.e., due to the presence of several single study connections between interventions). Scenario analyses related to certain characteristics of interest were included in the sponsor’s NMA report to address heterogeneity across the trials included in the network (e.g., removal of the Hermes 2008 trial, which was an outlier as it had the smallest proportion of patients with ECOG PS < 2 from the OS base-case analysis). According to the clinical expert consulted, ECOG PS and metastatic sites (liver and brain) were the most significant effect modifiers in the treatment of ES-SCLC patients. The sponsor acknowledged that additional scenario or subgroup analyses were feasible for PFS and OS; however, because relevant subgroup data are not currently available from the trials of the evidence networks investigating immunotherapies (i.e., the CASPIAN, ECOG-ACRIN EA5161, and KEYNOTE-6040 ongoing trials), not all possible subgroup analyses were included in the sponsor’s report. Therefore, the NMA results should be interpreted with caution due to limitations that may arise from between-study differences in some covariates and lack of sufficient evidence to minimize heterogeneity and inconsistency (e.g., by performing meta-regression analysis).
Other Relevant Evidence
No other relevant evidence was identified.
Conclusions
Based on clinical data from the IMpower133 study, atezolizumab in combination with carboplatin and etoposide demonstrated a statistically significant benefit compared to placebo in combination with carboplatin and etoposide in the first-line treatment of patients with ES-SCLC. The updated OS analysis, with a median of 22.9 months of follow-up, showed results consistent with those reported at the interim OS analysis, which suggests maintained clinical benefit for atezolizumab in combination with carboplatin and etoposide. Although the net gain of about 1 month in median PFS and 2 months in median OS observed with the addition of atezolizumab to carboplatin and etoposide is modest, it was considered by the clinical experts consulted by CADTH to be clinically meaningful in this setting where patients experience rapid tumour growth and fast clinical deterioration and have poor prognosis. The toxicity profile of atezolizumab was consistent with its immune-mediated mechanism of action, with no new safety concerns. Based on the results of the sponsor-submitted ITC, atezolizumab appears to demonstrate, in terms of improving PFS and OS, comparable benefit to durvalumab, the only other immunotherapy agent approved for the first-line treatment of ES-SCLC in Canada (but not currently funded by the drug plans in Canada). However, no firm conclusions could be drawn due to the small number of studies per comparison, leading to lower precision in effect estimates.
Introduction
Disease Background
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer-related death in Canada.1 In 2021, an estimated 29,600 Canadians were diagnosed with lung cancer, representing approximately 13% of all new cancer cases, and 21,000 Canadians died from lung cancer, representing 25% of all cancer deaths in 2021.1 It is estimated that 1 in 15 Canadians will develop lung cancer during their lifetime; 1 in 18 men and 1 in 20 women will die from it. The overall 5-year net survival for lung cancer from 2015 to 2017 was estimated to be 19% for men and 26% for women.1 The incidence of lung cancer begins to rise at 40 years of age and peaks between 65 and 84 years of age.15 The main known risk factors for lung cancer include tobacco smoking (including exposure to second-hand smoke) and exposure to asbestos, arsenic, radon, non-tobacco-related polycyclic aromatic hydrocarbons, and air pollution. The most common symptoms of lung cancer are cough, dyspnea, hemoptysis, chest pain, and systemic symptoms such as fatigue and weight loss. The diagnostic evaluation entails imaging that can include chest X-ray, CT scan, PET, MRI and bone scans, and tissue biopsy for histologic confirmation.
Lung cancer is histologically divided into NSCLC, which accounts for approximately 85% of cases, and SCLC which accounts for about 12% to 15% of cases, with more than 4,000 cases diagnosed annually across Canada.2,16 Small cell lung cancer has pathological, clinical, and molecular characteristics that are distinct from those of NSCLC. SCLC is a high-grade neuro-endocrine carcinoma arising predominantly in current or former smokers.9 It is marked by an exceptionally high proliferative rate and early development of widespread metastases.9,17 SCLC is primarily classified into limited-stage and extensive-stage disease. The Veterans Administration Lung Study Group 2-stage system has been routinely used for the clinical staging of SCLC since the late 1950s. Limited-stage disease is defined as a disease confined to 1 hemithorax (although local extension may be present); no extrathoracic metastases, except for ipsilateral supraclavicular lymph nodes, provided they can be included in the same radiation port as the tumour; and primary tumour and regional nodes that can be adequately encompassed in a radiation port.3,4 Extensive-stage disease is defined as disease that cannot be classified as limited, including malignant pleural or pericardial effusions, contralateral hilar or supraclavicular lymph nodes, and hematogenous metastases.3,4 More recently, the International Association for the Study of Lung Cancer has promoted the use of the tumour-node-metastasis staging classification to provide better anatomic discrimination for the measurement of outcomes, prognostic information, and more precise lymph node staging.9 However, patient selection in clinical trials has so far predominantly relied on the Veterans Administration Lung Study Group classification system. Approximately 2-thirds of patients with SCLC have extensive-stage disease at diagnosis, which is associated with particularly poor prognosis.5 Extensive-stage SCLC has a median survival of 7 months to 10 months (with treatment) and a 1-year OS rate of 40%.1,6 Survival beyond 2 years is generally no more than 15%, and the 5-year survival rate is less than 7%.18 In addition to extensive-stage disease, poor prognostic factors in SCLC include older age, male sex, impaired performance status, weight loss, elevated lactate dehydrogenase, and higher total gross tumour volume.19
As SCLC is a chemosensitive tumour, rapid responses with symptomatic improvement are often observed with platinum doublet chemotherapy. Evidence has shown that chemotherapy dramatically prolongs survival compared to best supportive care; 60% to 80% of patients with ES-SCLC respond to first-line chemotherapy.20 However, despite the remarkable response rates observed with first-line chemotherapy regimens, response is not durable. Most patients with ES-SCLC develop chemotherapy-resistant disease and relapse within 1 year of treatment completion.7 Prognosis continues to remain poor for those with relapsed disease, with a median survival of 5 months to 6 months.21 Subsequent therapy options for patients with relapsed disease are few due to limited efficacy of chemotherapy and other regimens in later lines and the low performance status of many patients with relapsed disease. In addition, brain metastases are common in SCLC, with about 10% of patients presenting with brain metastases at the time of diagnosis and an additional 40% to 50% of patients subsequently developing brain metastases, which further contributes to poor prognosis.8,9 Although prophylactic cranial irradiation (PCI) has been shown to improve systemic control of disease in some patients with ES-SCLC, it is associated with significant impairment in neurocognitive functioning, and the overall evidence for the effectiveness of this approach in improving OS in all patients with ES-SCLC with central nervous system metastases remains limited.22-24 In the first-line setting, the most important goals of treatment are prolonging survival and improving QoL (reducing symptom severity, maintaining independence in daily activities, and so forth).
Standards of Therapy
The standard first-line treatment for patients with newly diagnosed ES-SCLC consists of a platinum agent (cisplatin or carboplatin) with etoposide. The treatment landscape for SCLC had remained virtually unchanged for the past 3 decades. Recently, multiple phase III randomized controlled trials (RCTs) have demonstrated the benefits of adding an ICI to first-line chemotherapy in patients with newly diagnosed ES-SCLC.11,25,26 The addition of either of 2 anti-PD-L1 monoclonal antibodies, durvalumab or atezolizumab, to standard platinum-etoposide, with continuation of immunotherapy as maintenance, improved PFS and OS. In Canada, 2 ICIs — durvalumab and atezolizumab — are approved, in combination with etoposide and either carboplatin or cisplatin for the first-line treatment of patients with ES-SCLC. However, neither is currently publicly funded. Durvalumab received a CADTH recommendation to reimburse in July 2021, but the Health Technology Assessment process is not yet complete, and price negotiations are ongoing with the pan-Canadian Pharmaceutical Alliance. Durvalumab can currently be obtained only through the sponsor’s compassionate access program in some provinces. A reimbursement request for atezolizumab in combination with carboplatin and etoposide for the treatment of ES-SCLC was previously submitted to CADTH and did not receive a recommendation to reimburse. The current CADTH Reimbursement Review has been conducted for a resubmission filed by the sponsors for the aforementioned indication.
Drug
Atezolizumab (Tecentriq) is an engineered humanized immunoglobulin monoclonal antibody targeting PD-L1 and provides a dual blockade of interactions between PD-L1 and its receptors PD-1 and B7.1, restoring tumour-specific T-cell immunity.
In the US, the FDA has approved atezolizumab in combination with carboplatin and etoposide for the first-line treatment of adult patients with ES-SCLC. Atezolizumab has been approved for the same indication by the European Medicines Agency’s Committee for Medicinal Products for Human Use.
Health Canada has approved atezolizumab in combination with carboplatin and etoposide for the first-line treatment of adult patients with ES-SCLC. The sponsor’s reimbursement request differs from the approved Health Canada indication. The requested reimbursement is for the first-line treatment of patients with ES-SCLC in combination with a platinum-based chemotherapy and etoposide. Maintenance Tecentriq should be continued until loss of clinical benefit or unacceptable toxicity.
Atezolizumab for injection is supplied as a concentrate for solution for infusion in 60 mg/mL, 1,200 mg/20 mL, and 840 mg/14mL single-use vials. During the induction phase, the recommended dose of atezolizumab is 1,200 mg administered by IV infusion followed by carboplatin, and then etoposide administered by IV infusion on day 1. Etoposide is administered by IV infusion on days 2 and 3. This regimen is administered every 3 weeks for 4 cycles. The induction phase is followed by a maintenance phase without chemotherapy in which 1,200 mg of atezolizumab is administered by IV infusion every 3 weeks. Patients are treated with atezolizumab until loss of clinical benefit or unacceptable toxicity.27
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. Please refer to the Stakeholder Input for the full patient group input submitted to CADTH.
The patient and caregiver input received for this review was collected by LCC, a registered national charitable organization focused on lung cancer education, patient support, research, and advocacy. The input was sourced from interviews with patients with SCLC and caregiver testimonies gathered from December 2021 to February 2022, as well as information from previous LCC submissions. Six respondents with SCLC had experience with atezolizumab (in combination with chemotherapy or as a single treatment), 4 of whom had extensive-stage disease. Five patients had access to atezolizumab through clinical trial and 1 through a compassionate access program. Four of these respondents resided in Ontario, 1 in British Columbia, and 1 in Quebec.
Respondents indicated that a diagnosis of SCLC and the subsequent treatment had a major impact on the lives of patients and their family members. Several respondents reported that the diagnosis of SCLC was devastating to them and their family. Respondents indicated a varying range of SCLC symptoms that affected their daily activities. The daily activities that were most commonly impacted included the ability work, drive, travel, participate in activities they enjoy, and spend time with family and friends. Caregivers might need to retire or take time off work to provide care. Respondents reported that they expect the following key outcomes from any new drug or treatment: relief from disease symptoms, manageability of side effects, improved QoL, ability to maintain independence and functionality, greater access across jurisdictions, disease stability, longer periods of remission, and prolonged survival. According to the patient input received, the SCLC patient population has had a significant unmet need, as there had been no new treatment options for SCLC in 30 years, until 2021, when durvalumab was approved for treatment of ES-SCLC. Six respondents who had received or were continuing to receive atezolizumab indicated that this drug had had promising and durable treatment results with tolerable side effects. They also mentioned that atezolizumab had helped them regain independence, functionality, and livelihood, which reduced the burden on their caregivers and loved ones.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of SCLC.
Unmet Needs
The clinical experts consulted by CADTH noted that ES-SCLC is considered incurable, with a relatively short median OS (10 months). Although patients typically have initial response, the majority of patients will experience a relapse within 6 months. At relapse, outcomes are poor due both to patient-related factors, including poor performance status, and treatment-related factors such as poor response to subsequent therapies and significant toxicity. Therefore, first-line treatment options that increase expected survival are highly desired.
Place in Therapy
Atezolizumab is a monoclonal antibody against the PD-1/PD-L1 pathway, which would be used in combination with carboplatin and etoposide. This drug would be used in the first-line setting and would change the current treatment paradigm for SCLC. The clinical experts noted that there are numerous examples in other cancers, including NSCLC, demonstrating that the combination of chemotherapy and immunotherapy results in longer PFS and OS than with standard chemotherapy alone. The combination of immunotherapy and chemotherapy is widely accepted as the new standard of care for the management of ES-SCLC. The addition of durvalumab, or atezolizumab, to a platinum agent and etoposide would be the most appropriate initial therapy for ES-SCLC.
Patient Population
The clinical experts believed that no specific subgroup of patients is best suited for treatment with atezolizumab plus carboplatin and etoposide. They noted that data on various subgroups (e.g., age, sex, brain metastasis, PD-L1, and tumour mutational burden) were collected in the pivotal trials of atezolizumab and durvalumab (i.e., IMpower133 and CASPIAN), but none of the clinical characteristics studied as subgroups were found to be predictive or prognostic in this setting. In the absence of any contraindications (e.g., active or uncontrolled autoimmune conditions, or paraneoplastic autoimmune conditions requiring systemic therapy), atezolizumab should be offered to all patients with ES-SCLC (too extensive to be treated safely with curative intent radiotherapy). Patients should be treated irrespective of symptoms, as ES-SCLC is an aggressive disease and treatment needs to be started on an urgent basis. The clinical experts indicated that the diagnosis of ES-SCLC is easily made by oncologists involved in the treatment of SCLC. Diagnosis is routinely made by pathologists, and staging investigations are standardized to determine if limited- or extensive-stage disease exists. There is no population of pre-symptomatic patients who would be observed and not treated.
Assessing Response to Treatment
The clinical experts consulted by CADTH noted that there are currently no clinical features or biomarkers known to be predictive of response to treatment in patients with ES-SCLC. Thus, all patients should be treated with combination immunotherapy and chemotherapy in the first-line setting. Response to treatment is typically assessed every 3 cycles while on chemotherapy, using radiographic imaging with a CT scan, and every 3 months thereafter. It is challenging at an individual patient level to measure if survival is improved. Important outcomes to measure for individual patients are response rate, DOR, improvement in symptoms, and QoL.
Discontinuing Treatment
The decision to discontinue treatment with atezolizumab may be made after occurrence of disease progression or development of significant toxicity (i.e., grade 3 or higher or persistent grade 2 toxicity that is impacting function). The clinical experts also noted that it is important to recognize that some patients may have progression according to RECIST but might be benefiting from treatment. In these cases, it may be appropriate to continue treatment until it is clear that the treatment is failing.
Prescribing Conditions
Atezolizumab would typically be prescribed by medical oncologists. In some regions, pulmonologists who treat thoracic malignancies may also manage patients with ES-SCLC. No companion testing is required.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. Please refer to the Stakeholder Input section for the full clinical group input submitted to CADTH.
Clinician input was received from the Ontario Health (Cancer Care Ontario) Drug Advisory Committee, which provides evidence-based clinical and health system guidance on drug-related issues in support of Cancer Care Ontario’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program, and from LCC, a national charity with the objective of increasing awareness about lung cancer, supporting research and advocating access to treatments for patients with lung cancer. The clinician groups noted that the most important goal of treatment for ES-SCLC is improved OS. Moreover, since ES-SCLC is a cancer with a high propensity to spread to the brain, a systemic therapy with significant activity in the brain would be important to avoid brain irradiation and preserve functioning and QoL. Patients with ES-SCLC have a high unmet need for more effective therapies since most patients progress in a short period of time despite a high response rate to initial therapy. Atezolizumab would be used as initial systemic therapy in patients with ES-SCLC in combination with 4 cycles of platinum and etoposide, followed by maintenance atezolizumab until disease progression. The clinician groups noted that atezolizumab would be considered as an alternative option to durvalumab for the first-line treatment of patients with ES-SCLC. It would fit into the current treatment paradigm only as an agent to be started concurrently with first-line platinum and etoposide chemotherapy, with the intention of continuing until disease progression, intolerance, or a patient’s choice to discontinue therapy. Patients with symptomatic brain metastases should have treatment for their brain metastases before starting systemic therapy. The addition of atezolizumab to platinum and etoposide will not have any downstream impact on other treatment options. Progression after atezolizumab therapy would be treated with additional systemic chemotherapy or other regimens, including cyclophosphamide, Adriamycin, and vincristine, as per the current paradigm. The clinician groups also indicated that no specific subgroups of patients are more likely to benefit from the addition of atezolizumab; therefore, the treatment should be considered for any patient with ES-SCLC and an ECOG PS of 2 or better.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH Reimbursement Review process. The following were identified as key factors that could impact the implementation of a CADTH recommendation for atezolizumab.
The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The current funded standard of care is platinum-based chemotherapy plus etoposide. Durvalumab is not funded at this time. | For pERC consideration. |
In some jurisdictions cisplatin and etoposide is used rather than the platinum-based regimen used in the IMpower133 trial (i.e., carboplatin and etoposide). Is it reasonable to consider combination therapy with platinum-based chemotherapy and etoposide for the implementation of atezolizumab? | The clinical experts believed that carboplatin and cisplatin can be considered interchangeable in this setting. The results of the IMpower133 trial with respect to the efficacy of atezolizumab plus carboplatin and etoposide can be generalized to atezolizumab plus cisplatin and etoposide. |
Considerations for initiation of therapy | |
IMpower133 required patients to have an ECOG PS of 0 or 1. PAG is asking if the drug combination under review would be offered to patients with an ECOG PS of 2? | According to the clinical experts, there is no reason not to consider atezolizumab for patients with an ECOG PS of 2. This would be consistent with guideline recommendations for the treatment of patients with lung cancer. |
Is there evidence to treat patients requiring radiation for local symptomatic control, prophylactic cranial irradiation, or whole brain radiation with atezolizumab? | The clinical experts noted that radiation therapy should not be a barrier to accessing atezolizumab therapy. Patients could have received prior radiation therapy before entering the IMpower133 trial. |
If the patient’s disease progresses during a treatment break of atezolizumab maintenance, can atezolizumab be restarted or should the patient be re-treated with atezolizumab plus platinum and etoposide, followed by atezolizumab maintenance? | Re-treatment was not part of the planned therapy in the IMpower133 trial. The clinical experts consulted by CADTH noted that there was insufficient evidence to support re-treatment with atezolizumab. |
Considerations for discontinuation of therapy | |
Should patients be treated with atezolizumab until disease progression or until loss of clinical benefit? In clinical practice, what would be the stopping rules for atezolizumab? (For example, the usual stopping rule for immunotherapy is a 10% increase in total tumour burden, confirmed with a second CT scan 6 weeks to 8 weeks following the last scan if progression is suspected.) | The IMpower133 trial allowed treatment until disease progression but did allow treatment to continue in patients who had ongoing benefit. The clinical experts believed that it would be most appropriate to allow treatment until progression or loss of treatment benefit. Patients with ongoing benefit and evidence of disease progression according to RECIST should be allowed to continue treatment until the next disease reassessment. If there is further progression, treatment should be discontinued. |
Considerations for prescribing of therapy | |
In ES-SCLC, atezolizumab is in the same therapeutic space as durvalumab. Consider alignment of the prescribing criteria. | For pERC consideration. |
Generalizability of trial populations to the broader populations in the jurisdictions | |
Would pERC support use of atezolizumab in a second-line setting as monotherapy or in combination with topotecan following progression on platinum-based chemotherapy? | The clinical experts believed that atezolizumab would not be suited to second-line therapy since there are randomized clinical trial data showing atezolizumab is inferior to topotecan; they were aware of no evidence to support the use of combination therapy in second line. |
Could current patients receiving platinum-based chemotherapy (cisplatin or carboplatin plus etoposide) without progression have atezolizumab added? | The clinical experts consulted by CADTH believed that patients who are currently receiving platinum-etoposide chemotherapy should be allowed to receive add-on atezolizumab. |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ES-SCLC = extensive-stage small cell lung cancer; PAG = provincial advisory group; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; RECIST = Response Evaluation Criteria in Solid Tumours.
Clinical Evidence
The clinical evidence included in the review of atezolizumab is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review: Pivotal and Protocol-Selected Studies
Objectives
To evaluate the efficacy and safety of atezolizumab in combination with carboplatin and etoposide for the first-line treatment of patients with ES-SCLC.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 4. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 4: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Patients with extensive-stage small cell lung cancer Subgroups of interest:
|
Intervention | Four 21-day cycles of carboplatin (area under the curve of 5 mg/mL/min administered intravenously on day 1 of each cycle) and etoposide (100 mg/m2 of body surface area, administered intravenously on day 1 to day 3 of each cycle), plus atezolizumab (at dose of 1,200 mg, administered intravenously on day 1 of each cycle), followed by maintenance atezolizumab monotherapy until the occurrence of unacceptable toxicity or RECIST-defined disease progression |
Comparator | Carboplatin or cisplatin plus etoposidea Carboplatin or cisplatin plus etoposide plus durvalumabb |
Outcomes | Efficacy outcomes:
Harms outcomes:
Notable harms:
|
Study designs | Published and unpublished phase III and IV RCTs |
DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HRQoL = health-related quality of life; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trials; RECIST = Response Evaluation Criteria in Solid Tumours.
aCurrent standard of care.
bNot publicly funded. Available through compassionate access only.
cThese outcomes were identified as being of particular importance to patients in the input received by CADTH from patient groups.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS (Peer Review of Electronic Search Strategies) checklist.28
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as multi-file searches. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were atezolizumab and small cell lung cancer. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on February 22, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on July 13, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.29 Included in this search were the websites of regulatory agencies (the FDA and the European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented through the review of bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for NMAs dealing with atezolizumab or SCLC was run in MEDLINE All (1946–) on February 18, 2022. No search limits were applied.
Findings From the Literature
A total of 934 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 5. A list of excluded studies is presented in Appendix 2.
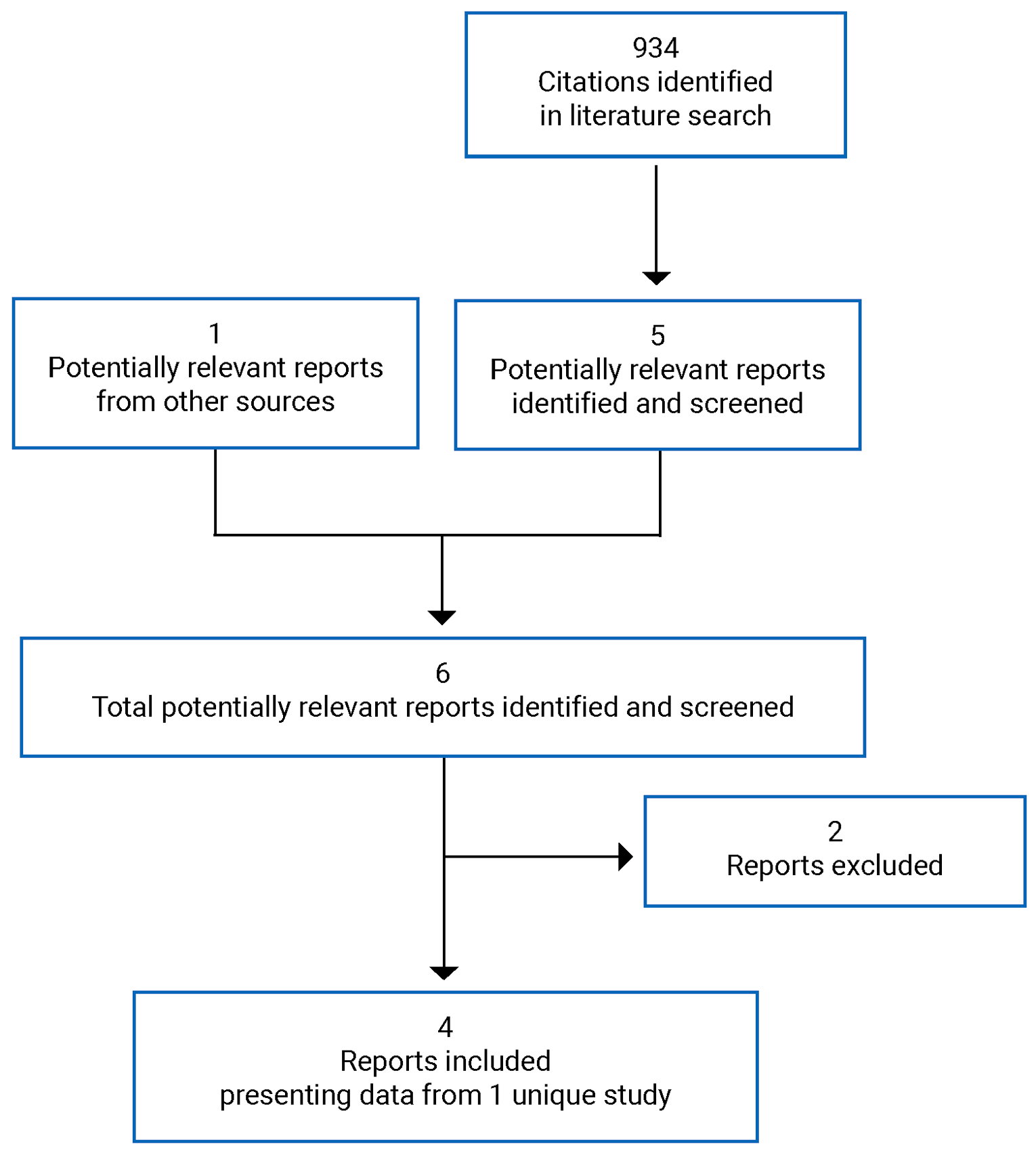
Table 5: Details of the IMpower133 Study
Detail | Description |
|---|---|
Designs and populations | |
Study design | Phase III, double-blind, placebo-controlled, multi-centre RCT |
Locations | 106 centres in 21 countries (US, Poland, Japan, Russia, Spain, Austria, Hungary, Czech Republic, South Korea, Italy, Serbia, Australia, Greece, UK, Germany, Taiwan, France, Chile, Brazil, Mexico, China) |
Study duration | Patient enrolment: June 6, 2016, to May 31, 2017 Study completion date: March 24, 2020 |
Data cut-off date | April 24, 2018 (primary PFS analysis, interim OS analysis) January 24, 2019 (final OS analysis: “updated analysis”) |
No. of patients randomized (randomization ratio) | 403 (1:1) |
Main inclusion criteria |
|
Main exclusion criteria |
|
Drugs | |
Intervention | Induction phase: Four cycles (1 cycle = 21 days) of atezolizumab plus chemotherapy administered in each cycle as follows:
Maintenance phase: Atezolizumab 1,200 mg (every 21-day cycle) until the occurrence of unacceptable toxic effects or disease progression according to RECIST 1.1 |
Comparator | Induction phase: Four cycles (1 cycle = 21 days) of placebo plus chemotherapy administered in each cycle as follows:
Maintenance phase: Placebo (every 21-day cycle) until the occurrence of unacceptable toxic effects or disease progression according to RECIST 1.1 |
Duration | |
Induction phase | Four 21-day cycles of atezolizumab or placebo plus carboplatin and etoposide |
Maintenance phase | Atezolizumab 1,200 mg or placebo every 21-day cycle until unacceptable toxic effects or disease progression according to RECIST 1.1 |
Follow-up phase | Follow-up completed (first clinical data cut-off: April 24, 2018, 11 months after the last patient was enrolled); follow-up visits were every 6 weeks for the first 48 weeks, starting from day 1 of cycle 1, and every 9 weeks thereafter |
Outcomes | |
Primary end points | OS and investigator-assessed PFS by RECIST 1.1 criteria |
Secondary end points |
|
Safety end points |
|
Notes | |
Publications | Horn et al. (2018)11 Liu et al. (2021)30 Mansfield et al. (2020)31 |
AE = adverse event; AUC = area under the curve; CNS = central nervous system; DOR: duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; ES-SCLC = extensive-stage small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SCLC = small cell lung cancer.
Source: Clinical Study Report for IMpower133 study.12
Description of the IMpower133 Study
IMpower133 is a randomized, multi-centre, double-blind, placebo-controlled phase III study designed to evaluate the efficacy and safety of treatment with atezolizumab plus carboplatin and etoposide compared with treatment with placebo plus carboplatin and etoposide in patients with chemotherapy-naive ES-SCLC. The study included a phase I safety run-in period to establish tolerability of the study treatment. The trial was conducted in 106 sites across 21 countries (none in Canada). The clinical cut-off date for the primary analysis (primary PFS analysis and interim OS analysis) was April 24, 2018. The clinical cut-off date for the updated analysis (final analysis of OS) was January 24, 2019. The trial was funded by Hoffmann-La Roche Ltd.
Randomization and treatment allocation: A total of 403 eligible patients were randomized (1:1) to receive either atezolizumab plus carboplatin and etoposide or placebo plus carboplatin and etoposide. Randomization was performed with the use of a permuted-block randomization method — the interactive voice or web response system IxRS — and was stratified according to sex, ECOG PS (0 versus 1), and presence of brain metastases (yes versus no). After written informed consent had been obtained, all screening procedures and assessments had been completed, and eligibility had been established, the study site obtained each patient’s identification number and treatment assignment from the IxRS for eligible patients.
Blinding: IMpower133 was a double-blind study. The sponsor, the study site personnel including the investigators, and the patients were blinded to treatment assignment.
Study phases: The induction phase of the study consisted of 4 cycles of atezolizumab or placebo plus chemotherapy, with each cycle being 21 days in duration. Following the induction phase, patients continued maintenance therapy with either atezolizumab or placebo (21-day cycles). The patients received their first dose of the study drug on the day of randomization if possible. If not possible, the first dose occurred within 5 days after randomization (Figure 2).
Figure 2: IMpower133 Study Schema
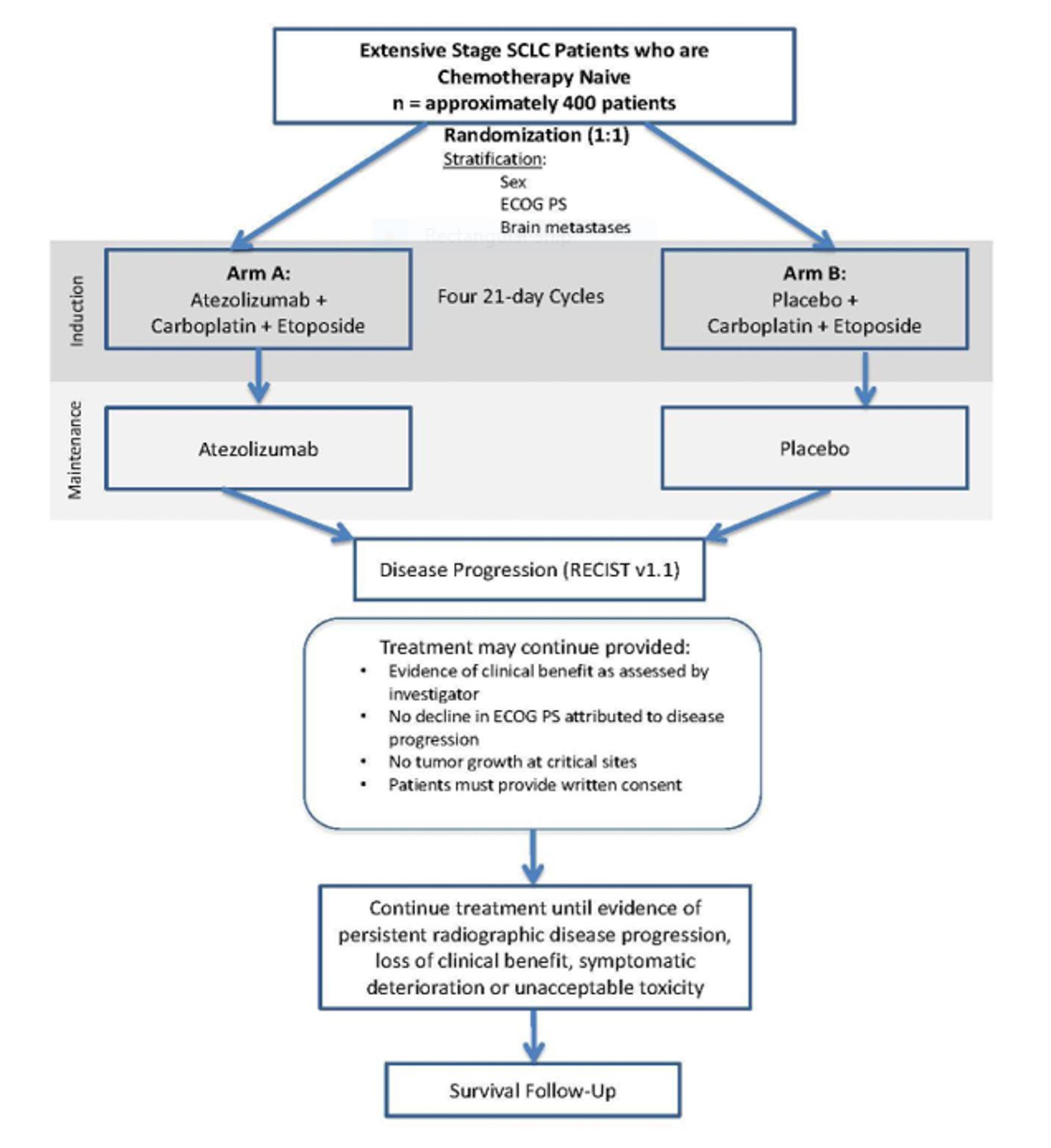
ECOG PS = Eastern Cooperative Oncology Group Performance Status; RECIST v1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SCLC = small cell lung cancer.
Source: Update Clinical Study Report for IMpower133 study.13
Protocol Amendments
Several changes were made to the original study protocol throughout the duration of the study. The main amendments (from most to least recent) were as follows. On August 29, 2017, modifications were made to the statistical analysis plan and the timing for the efficacy analyses for PFS and OS in the global study. The OS event-patient ratio for the interim OS analysis was increased from 45% to 55%; for the final OS analysis, the ratio was reduced from 74% to 70%. The second OS interim analysis, at the time when 258 OS events had occurred, was also removed. Consequently, 280 deaths were required for the final OS analysis, estimated to be achieved at approximately first patient randomized plus 31 months, compared to 298 OS events at 37 months under a 74% event-patient ratio. These changes were implemented to be consistent with other studies in the atezolizumab first-line lung cancer program. The multiplicity strategy was adjusted from splitting alpha to a group sequential Holm procedure so that alpha spent on PFS could be recycled to OS when PFS was significant, and vice versa, to most efficiently use alpha and maximize power. On August 25, 2016, the requirement for a tumour response assessment at the treatment discontinuation visit was removed. On June 8, 2016, it was added that in the case of an early termination of the study, patients who were deriving clinical benefit from treatment with atezolizumab would be permitted to continue treatment with atezolizumab at the discretion of the investigator.
Populations
Inclusion and Exclusion Criteria
Eligible patients were adults with histologically or cytologically confirmed ES-SCLC (defined according to the Veterans Administration Lung Study Group staging system), measurable ES-SCLC according to RECIST 1.1, and an ECOG PS of 0 or 1 who had not received previous systemic treatment for ES-SCLC. Patients with treated asymptomatic central nervous system metastases were eligible. Patients with a history of autoimmune disease and previous treatment with CD137 agonists or immune checkpoint blockade therapies were ineligible.
Baseline Characteristics
Between June 6, 2016, and May 31, 2017, a total of 403 patients who met the eligibility criteria were enrolled at 106 sites in 21 countries and were randomly assigned to receive chemotherapy with either atezolizumab (n = 201) or placebo (n = 202). In the intention-to-treat (ITT) population, most patients (79.9%) were White and most (64.8%) were male. More than half the patients (53.8%) were 65 years or younger, with a median (range) age of 64.0 (26 to 90) years. Almost 2-thirds of patients (65.3%) had an ECOG PS of 1. The majority of patients (97.0%) were either past or current smokers. Overall, 8.7% of patients had brain metastases and 37.0% of patients had liver metastases at enrolment. Most patients (93.1%) enrolled in the study were initially diagnosed with ES-SCLC; 6.7% were initially diagnosed with limited-stage SCLC before progressing to ES-SCLC. The median time from diagnosis of ES-SCLC to study enrolment was 0.7 months. Twenty-two patients in each treatment arm received PCI. The baseline demographic and disease characteristics were well balanced between the 2 treatment arms (Table 6).
Table 6: Summary of Baseline Characteristics
Characteristic | ITT population | |
|---|---|---|
Atezolizumab + CE (n = 201) | Placebo + CE (n = 202) | |
Age, years | ||
Mean (SD) | 63.8 (8.8) | 63.6 (9.0) |
≥ 65, n (%) | 90 (44.8) | 96 (47.5) |
Male sex, n (%) | 129 (64.2) | 132 (65.3) |
Race, n (%) | ||
White | 163 (81.1) | 159 (78.7) |
Asian | 33 (16.4) | 36 (17.8) |
Black | 1 (0.5) | 2 (1.0) |
American Indian or Alaska native | 0 | 1 (0.5) |
Unknown | 4 (2.0) | 4 (2.0) |
Geographical region, n (%) | ||
Asia-Pacific | 40 (19.9) | 40 (19.8) |
Europe and Middle East | 116 (57.7) | 107 (53.0) |
North America | 39 (19.4) | 51 (25.2) |
South America | 6 (3.0) | 4 (2.0) |
ECOG Performance Status, n (%) | ||
0 | 73 (36.3) | 67 (33.2) |
1 | 128 (63.7) | 135 (66.8) |
History of tobacco use, n (%) | ||
Never | 9 (4.5) | 3 (1.5) |
Current | 74 (36.8) | 75 (37.1) |
Previous | 118 (58.7) | 124 (61.4) |
Brain metastasis at enrolment, n (%) | 17 (8.5) | 18 (8.9) |
Liver metastasis at enrolment, n (%) | 77 (38.3) | 72 (35.6) |
Blood-based tumour mutational burden, n of total n (%) | ||
< 10 mutations/Mb | 71 of 173 (41.0) | 68 of 178 (38.2) |
≥ 10 mutations/Mb | 102 of 173 (59.0) | 110 of 178 (61.8) |
< 16 mutations/Mb | 133 of 173 (76.9) | 138 of 178 (77.5) |
≥ 16 mutations/Mb | 40 of 173 (23.1) | 40 of 178 (22.5) |
Time since ES-SCLC diagnosis, months, mean (SD) | 16.3 (19.8) | 15.7 (9.4) |
CE = carboplatin and etoposide; ECOG = Eastern Cooperative Oncology Group; ES-SCLC = extensive-stage small cell lung cancer; ITT = intention to treat; SD = standard deviation.
Source: Clinical Study Report for IMpower133 study.12
Interventions
Induction phase
Atezolizumab Plus Carboplatin and Etoposide
For patients randomly assigned to the atezolizumab plus carboplatin and etoposide arm, treatment in the induction phase consisted of 4 21-day cycles of carboplatin (area under the curve of 5 mg/mL/min administered intravenously on day 1 of each cycle) and etoposide (100 mg/m2 of body surface area administered intravenously on days 1 through 3 of each cycle), plus atezolizumab (at a dose of 1,200 mg, administered on day 1 of each cycle). Atezolizumab was provided as a sterile liquid in a single-use, 20 mL glass vial. The vial was designed to deliver 20 mL (1,200 mg) of atezolizumab solution but could contain more than the stated volume to enable delivery of the entire 20 mL.
Placebo Plus Carboplatin and Etoposide
For patients randomly assigned to the placebo plus carboplatin and etoposide arm, treatment in the induction phase consisted of 4 21-day cycles of carboplatin (area under the curve of 5 mg/mL/min administered intravenously on day 1 of each cycle) and etoposide (100 mg/m2 of body surface area administered intravenously on days 1 through 3 of each cycle), plus placebo (administered on day 1 of each cycle). Carboplatin and etoposide were used in the commercially available formulations.
Maintenance phase
In both treatment arms, the induction phase was followed by a maintenance phase during which patients received either atezolizumab (1,200 mg) or placebo according to their previous random assignment, until the occurrence of unacceptable toxic effects or disease progression according to RECIST 1.1 criteria. During the maintenance phase, PCI was permitted per local standard of care. Thoracic radiation with curative intent or the intent to eliminate residual disease was not permitted. Palliative thoracic radiation was allowed.
Concomitant Treatment
Concomitant treatment included any medication (e.g., prescription drugs, over-the-counter drugs, or homeopathic remedies and nutritional supplements) used by a patient from 7 days before screening until the treatment discontinuation visit. Pre-medication with antihistamines could be administered for any atezolizumab or placebo infusions after cycle 1.
Patient care with supportive therapies was managed as clinically indicated per local standards. Patients who experienced infusion-associated symptoms could be treated symptomatically with acetaminophen, ibuprofen, diphenhydramine, and/or famotidine or another H2 receptor antagonist per standard practice. Serious infusion-associated events — manifested by dyspnea, hypotension, wheezing, bronchospasm, tachycardia, reduced oxygen saturation, or respiratory distress — could be managed with supportive therapies (e.g., supplemental oxygen and Beta2-adrenergic agonists) as clinically indicated. Systemic corticosteroids and tumour necrosis factor alpha inhibitors could be administered at the discretion of the treating physician for the treatment of specific AEs when associated with atezolizumab therapy.
Study Treatment Discontinuation
Patients discontinued study treatment if they experienced symptomatic deterioration attributed to the following: disease progression as determined by the investigator after integrated assessment of radiographic data, biopsy results if available, and the patient’s clinical status; intolerable toxic effects related to atezolizumab (including immune-mediated AEs determined by the investigator to be unacceptable given the individual patient’s potential response to therapy and severity of the event); or intolerable toxic effects related to other components of the study treatment. If 1 component of study treatment was discontinued permanently because of tolerability concerns, the patient was allowed to continue with other components of study treatment until disease progression if agreed by the investigator and patient. In addition, radiographic progressive disease per RECIST 1.1, use of another non-protocol-specified anticancer therapy, or presence of any medical condition that could jeopardize the patient’s safety by continued treatment were grounds for discontinuation of study treatment.
Patients could be considered for treatment beyond radiographic progression per RECIST 1.1 at the discretion of the investigator and after discussion with the patient if the following criteria were met: evidence of clinical benefit as assessed by the investigator; no decline in ECOG PS that could be attributed to disease progression; and absence of tumour progression at critical anatomic sites (e.g., leptomeningeal disease) that could not be managed by protocol-allowed medical interventions. Patients were required to provide informed consent to acknowledge deferring other treatment options in favour of continuing study treatment at the time of initial progression. Patients were monitored clinically and with a follow-up scan after 6 weeks, or sooner if symptomatic deterioration occurred. Treatment was discontinued for unacceptable toxic effects or clinical deterioration due to disease progression.
Dose Modification or Interruption
No dose reductions for atezolizumab or placebo were permitted. Patients could temporarily suspend treatment with atezolizumab or placebo for up to 105 days beyond the last dose if they experienced an AE that required a dose to be withheld. If atezolizumab or placebo was withheld because of AEs for more than 105 days beyond the last dose, the patient was discontinued from atezolizumab or placebo treatment. If a patient had to be tapered off steroids used to treat AEs, atezolizumab could be withheld for additional time beyond 105 days from the last dose until steroids were discontinued or reduced to a prednisone dose (or dose equivalent) less than or equal to 10 mg/day. The acceptable length of interruption depended on agreement between the investigator and the medical monitor.
Dose modifications for carboplatin and etoposide were permitted for toxicity according to the prescribing information and local standard of care. Once reduced, the dose could not be increased back to 100%. Treatment with carboplatin or etoposide was recommended to be discontinued if a patient experienced any hematologic or non-hematologic grade 3 or 4 toxicity after 2 dose reductions or a treatment delay of more than 63 days due to toxicities.
Outcomes
The efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial included in this review are summarized below.
Efficacy
The primary end points were PFS and OS. PFS was defined as the time from randomization to the first occurrence of disease progression, as determined by the investigator using RECIST 1.1 criteria, or death from any cause, whichever occurred first. OS was defined as the time from randomization to death from any cause.
Key secondary end points included ORR and DOR. ORR was defined as CR or partial response (PR) as determined by the investigator according to RECIST 1.1. Confirmation of responses was not required per protocol, but confirmed response rates were reported. DOR was defined as the time interval from first occurrence of a documented objective response to the time of disease progression, as determined by the investigator using RECIST 1.1, or death from any cause, whichever came first.
Patients underwent tumour assessments at baseline and every 6 weeks (± 7 days) for 48 weeks following day 1 of cycle 1, regardless of treatment dose delays. After completion of the week 48 tumour assessment, tumour assessments were required every 9 weeks (± 7 days), regardless of treatment dose delays. Patients underwent tumour assessments until radiographic disease progression per RECIST 1.1, withdrawal of consent, study termination by the sponsor, or death, whichever occurred first. Patients who continued treatment beyond radiographic disease progression per RECIST 1.1 continued to undergo tumour assessments every 6 weeks (± 7 days), or sooner if symptomatic deterioration occurred. For these patients, tumour assessments continued every 6 weeks (± 7 days), regardless of time in the study, until study treatment was discontinued. Patients who discontinued treatment for reasons other than radiographic disease progression per RECIST 1.1 (e.g., toxicity or symptomatic deterioration) continued scheduled tumour assessments at the same frequency as would have been followed if the patient had remained on study treatment (i.e., every 6 weeks [± 7 days] for 48 weeks following cycle 1, day 1, and every 9 weeks [± 7 days] thereafter, regardless of treatment dose delays) until radiographic disease progression per RECIST 1.1, withdrawal of consent, study termination by the sponsor, or death, whichever occurred first, regardless of whether patients started a new anticancer therapy.
Patient-reported outcomes were evaluated as secondary and exploratory end points and measured using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13 (EORTC QLQ-LC13).
The EORTC QLQ-C30 instrument is a generic questionnaire consisting of 30 items developed to assess the symptoms and functioning of cancer patients. The instrument includes 5 functional scales, 4 symptom scales, 1 global health status (GHS) scale, and 1 financial impact score. Most items are scored 1 (“not at all”) to 4 (“very much”), except for the items contributing to the GHS scale, which are scored 1 (“very poor”) to 7 (“excellent”). The recall period for each question is “during the past week.” An outcome variable consisting of a score from 0 to 100 is derived for each of the symptom scales and items, according to the EORTC QLQ-C30 instructions. Higher scores on symptoms indicate a worse health state. Higher scores on the GHS and functioning scales indicate better health status or function.
The EORTC QLQ-LC13 is a questionnaire measuring lung cancer symptoms and side effects from conventional chemo- and radiotherapy. It comprises 13 questions assessing lung cancer symptoms (cough, hemoptysis, dyspnea, and site-specific pain), treatment-related side effects (sore mouth, dysphagia, peripheral neuropathy, and alopecia), and pain medication. Except for a multi-item scale for dyspnea, all are single items. An outcome variable consisting of a score from 0 to 100 is derived for each of the symptom scales and items, according to the EORTC QLQ-LC13 instructions. Higher scores on the symptom scales indicate greater symptom burden and therefore a worse health state.
The validity and reliability of both instruments have been established in populations of patients with lung cancer. However, there is a dearth of information with respect to their responsiveness in this setting. A detailed discussion and critical appraisal of the EORTC QLQ-30 and EORTC QLQ-LC13 is provided in Appendix 3.
The EORTC QLQ-C30 and EORTC QLQ-LC13 assessments were completed on day 1 of each 21-day treatment cycle at scheduled study visits during treatment, and at 3 months and 6 months after treatment discontinuation. The instruments, translated into the local language, were completed by patients on an electronic PRO device before administration of study treatment and before any other study assessments.
Time to deterioration in patient-reported lung cancer symptoms was defined as time from randomization to deterioration (10-point change) on each of the EORTC QLQ-C30 and EORTC QLQ-LC13 symptom subscales maintained for 2 assessments or reported at 1 assessment followed by death from any cause within 3 weeks.
Safety
Patient safety was assessed based on reported AEs, clinical laboratory data, vital signs, electrocardiogram, and physical examination. The incidence, nature, and severity of AEs were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events Version 4.0 and coded using the standard Medical Dictionary for Regulatory Activities version 21.0 terms. AEs of special interest were immune-related AEs, defined based on the mechanism of action of atezolizumab, organized by medical concepts. Patients were assessed for AEs before each dose, and dosing occurred only if the clinical assessment and local laboratory test values were acceptable. The investigators determined whether AEs were related to the trial regimen. AEs were recorded during the study and for up to 30 days after the last dose of the study (90 days for SAEs and AEs of special interest) or until the initiation of new systemic anticancer therapy after the last dose of study treatment, whichever occurred first. After that period, any SAEs or AEs of special interest were reported if they were considered related to prior exposure to study treatment by the investigators. Causality of the AEs was assessed by the investigators.
Statistical Analysis
Sample Size Calculations
The sample size of the trial was determined by the analysis of OS. To detect an improvement of HR equal to 0.68 in OS using a log-rank test, approximately 306 deaths in the ITT population were required to achieve a 91% power at a 2-sided significance level of 0.045. One OS interim analysis was performed when 238 OS events in the ITT population had occurred (data cut-off date: April 24, 2018), which was estimated to occur 25 months after the first patient was randomized, with a 2-sided alpha level of 0.0193 (stopping boundary), computed on the basis of the Lan-DeMets alpha spending function approximating the O’Brien-Fleming boundary.
The OS interim analysis was planned for when approximately 240 OS events in the ITT population had been observed. The pre-specified primary analysis of PFS was planned to be conducted at the time of the OS interim analysis and was estimated to occur when approximately 295 PFS events in the ITT population had occurred, which was expected at approximately 25 months after the first patient was randomized. This provided a 99% power to detect an improvement of HR equal to 0.55 in PFS at a 2-sided significance level of 0.005. The study planned to randomize 400 patients during the global enrolment phase.
The calculation of sample size and estimates of the analysis timelines were based on the following assumptions: PFS and OS are exponentially distributed; the median duration of PFS in the control arm is 6 months; the median duration of OS in the control arm is 10 months; the interim and final analyses of OS use the Lan-DeMets alpha spending function to approximate the O’Brien-Fleming boundary; and there is a dropout rate of 5% over 12 months for PFS and OS.
Analyses of Outcomes
For the primary analyses of PFS and OS, the Kaplan–Meier method was used to estimate median PFS and OS, and the Brookmeyer-Crowley methodology and log-log transformation for normal approximation were used to construct the 95% CIs for the median PFS and median OS in each treatment arm. For the PFS analysis, patients who did not experience disease progression or death at the time of analysis were censored at the time of the last tumour assessment. For the analysis of OS, data for patients who were alive were censored at the time of the last contact. For both PFS and OS analyses, patients with no post-baseline tumour assessment were censored at the date of randomization plus 1 day.
Treatment comparisons were based on the stratified log-rank test (stratified according to sex and ECOG PS score [0 versus 1]). The stratification factor that contained the level with the smallest size was dropped from the stratified analysis if at least 1 stratum had fewer than 10 events. This was pre-specified in the statistical analysis plan. As a result, the stratification factor of presence or absence of brain metastases was removed from the stratified analysis as it contained the level with the lowest number of patients. The HR and corresponding 95% CIs were estimated with the use of a stratified Cox regression model with the same stratification factors that were used in the stratified log-rank test.
To control the overall 2-sided type I error rate at 0.05, a group sequential weighted Holm procedure was used, for which the 2-sided significance levels of 0.005 and 0.045 were allocated to the primary comparisons for PFS and OS, respectively. The test that was significant could pass its alpha level to the test that was not statistically significant at the original allocated alpha level. If PFS in the ITT population was statistically significant at the 2-sided alpha level of 0.005, OS in the ITT population was tested at a 2-sided alpha level of 0.045. Similarly, if OS in the ITT population was statistically significant at the 2-sided alpha level of 0.045, PFS in the ITT population was tested at a 2-sided alpha level of 0.005.
The ORR was estimated using the Clopper-Pearson method for 95% CI of response rates. The 95% CI for the difference in ORRs between the 2 treatment arms was estimated using the normal approximation to the binomial distribution method.
The DOR was assessed for patients who had an objective response as determined by the investigator using RECIST 1.1. Patients whose disease has not progressed and who had not died at the time of analysis were censored at the time of last tumour assessment date. If no tumour assessments were performed after the date of the first occurrence of a CR or PR, DOR was censored at the date of the first occurrence of a CR or PR plus 1 day. Since DOR was based on a nonrandomized subset of patients (i.e., patients who achieved an objective response), formal hypothesis testing was not performed for this end point. Comparisons between treatment arms were made for descriptive purposes. A similar approach to the primary analyses of PFS was used for the DOR analysis.
HRQoL was pre-specified as a secondary and exploratory end point. Descriptive analysis included time to deterioration in lung cancer symptoms, change from baseline summaries, and cumulative distribution function curves of within-patient change from baseline.
All safety end points were reported using descriptive statistics.
Summaries of AEs by treatment group included the following:
The number and percentage of patients with at least 1 AE by standard of care and preferred term
AEs by severity (National Cancer Institute Common Terminology Criteria for Adverse Events Version 4.0), presented by standard of care and preferred term
AEs leading to treatment discontinuation
AEs related to study drug
AEs of special interest
Immune-related AEs (defined based on the mechanism of action of atezolizumab)
Infusion-related reactions
Deaths and SAEs were listed and summarized by treatment group. Events of National Cancer Institute Common Terminology Criteria for Adverse Events grade 3 and grade 4 severity were summarized by treatment group. Treatment-emergent AEs leading to permanent treatment discontinuation were listed and summarized by treatment group.
Subgroup Analyses
HRs for OS and PFS were evaluated by pre-planned subgroups according to ECOG PS and presence of brain metastases at baseline, which were subgroups of interest identified in the CADTH systematic review protocol. Between-group treatment effects, with a nominal 95% CI for these end points, were estimated within each category. There was no multiplicity control. As such, all subgroup analyses are exploratory in nature.
Sensitivity Analyses
The potential impact of missing scheduled tumour assessments on the primary analysis of PFS as determined by the investigator was assessed using a PFS event imputation rule: If a patient missed 2 or more assessments scheduled immediately before the date of the PFS event, the patient would be counted as having progressed on the date of the first of these missed assessments, and patients with a PFS event who missed 2 or more scheduled assessments immediately before the PFS event would be censored at the last tumour assessment before the missed visits. The imputation rule would be applied to patients in both treatment arms. Statistical analyses were similar to those used in the primary analysis of PFS. Analyses were also conducted to assess the impact of non-prior anticancer therapy on PFS for patients who switched to other treatment before a PFS event. The Kaplan–Meier method was used to estimate median PFS; 95% CIs for the median were computed using the method of Brookmeyer-Crowley, and HRs were estimated by Cox regression.
Interim Analyses
One interim efficacy analysis of OS was planned for when approximately 240 OS events had been observed. The interim analysis of OS (data cut-off date: April 24, 2018) was conducted when 238 of the planned 240 OS events had been observed.
The primary analysis of PFS was conducted at the time of the interim analysis of OS, and the exact timing of the analysis depended on when 240 OS events in the ITT population had occurred. No interim analysis of PFS was planned.
Updated Analyses
The final OS analysis was planned to be conducted when approximately 306 OS events in the ITT population had been observed, expected to occur at approximately 36 months after the first patient. The updated analysis of OS (data cut-off date: January 24, 2019) was conducted when 302 of the planned 306 OS events had occurred.
Analysis Populations
The ITT population (N = 403) was defined as all the randomized patients, regardless of whether the patient received the assigned treatment. The primary end points were assessed in the ITT population.
The safety population included all treated patients (N = 394), defined as patients who received any amount of any component of study treatment. For the safety analyses, patients who received any amount of atezolizumab were analyzed as part of the atezolizumab arm, even if atezolizumab was given in error.
Results
Patient Disposition
A total of 526 patients were screened; 123 patients failed screening based on information collected in the IxRS system. The most common reasons for screen failure were active or untreated central nervous system metastases (n = 25), withdrawal by patient (n = 13), and lack of evidence of histologically or cytologically confirmed ES-SCLC per the Veterans Administration Lung Study Group staging system (n = 10 patients). Of the 403 patients who were randomly assigned to receive atezolizumab (n = 201) or placebo (n = 202) plus carboplatin and etoposide, 9 did not receive any study treatment (4 patients in the atezolizumab arm and 5 patients in the placebo arm). As of the first clinical cut-off date (April 24, 2018), all 9 untreated patients had discontinued the study due to withdrawal by patient (n = 4), death (n = 4), or physician decision (n = 1). Treatment allocation was unblinded for 4 patients (2 patients in each arm) for safety reasons and for 6 patients (2 patients in the atezolizumab arm and 4 patients in the placebo arm) for other reasons, such as to inform subsequent treatment decisions after disease progression. These were cases of individual patient unblinding that occurred at the site level; the study sponsor continued to remain blinded to the treatment assignment. Patients who were unblinded were included in the analysis populations.
At the time of the primary clinical data cut-off, 124 patients (61.7%) in the atezolizumab arm and 142 (70.3%) in the placebo arm had discontinued the study. Withdrawal of consent was more common in the atezolizumab arm (9.0%) than the placebo arm (4.5%). At the time of the data cut-off date for the updated analysis, 161 patients (80.1%) in the atezolizumab arm and 172 (85.1%) in the placebo arm had discontinued the study. Overall, 14 patients (3.5%) were still on study treatment, and 56 (13.9%) were in follow-up (Table 7).
Treatment Beyond Progressive Disease
Forty-nine patients (24.4%) in the atezolizumab arm were treated beyond investigator-assessed disease progression per RECIST 1.1. The median duration of atezolizumab treatment following investigator-assessed disease progression was 0.7 months (range = 0 to 16). In the atezolizumab arm, 7 of 49 patients (14.3%) treated with atezolizumab beyond progressive disease were still receiving treatment at the time of the first clinical data cut-off date. In total, 85.7% of patients were withdrawn from atezolizumab treatment, mainly due to subsequent progressive disease (79.6%), symptomatic deterioration (4.1%), or withdrawal by patient (2.0%).
Patient status | Primary analysisa | Updated analysisb | ||||
|---|---|---|---|---|---|---|
Atezolizumab | Placebo | Total | Atezolizumab | Placebo | Total | |
Screened, N | 526 | |||||
Randomized, N | 201 | 202 | 403 | 201 | 202 | 403 |
Received treatment, n (%) | 197 (98.0) | 197 (97.5) | 394 (97.8) | 197 (98.0) | 197 (97.5) | 394 (97.8) |
Discontinued the study | 124 (61.7) | 142 (70.3) | 266 (66.0) | 161 (80.1) | 172 (85.1) | 333 (82.6) |
Died | 101 (50.2) | 132 (65.8) | 233 (57.8) | 138 (68.7) | 158 (78.2) | 296 (73.4) |
Lost to follow-up | 3 (1.5) | 1 (0.5) | 4 (1.0) | 3 (1.5) | 2 (1.0) | 5 (1.2) |
Withdrawal by physician | 2 (1.0) | 0 | 2 (0.5) | 2 (1.0) | 0 | 2 (0.5) |
Withdrawal of consent or patient decision | 18 (9.0) | 9 (4.5) | 27 (6.7) | 18 (9.0) | 12 (5.9) | 30 (7.1) |
On-study status, n (%) | 77 (38.3) | 60 (29.7) | 137 (34.0) | 40 (19.9) | 30 (14.9) | 70 (17.4) |
Alive, on study treatment | 23 (11.4) | 11 (5.4) | 34 (8.4) | 13 (6.5) | 1 (0.5) | 14 (3.5) |
Alive, in follow-up | 54 (26.9) | 49 (24.3) | 103 (25.6) | 27 (13.4) | 29 (14.4) | 56 (13.9) |
Included in safety analysis, n | 198c | 196 | 394 | 198c | 196 | 394 |
aData cut-off date: April 24, 2018.
bData cut-off date: January 24, 2019.
cOne patient randomized to the placebo arm received atezolizumab and was therefore counted in the atezolizumab arm in the safety population.
Source: Clinical Study Report for IMpower133 study12; Liu et al. (2021).30
Protocol Deviations
During the course of the study, 222 protocol deviations were reported for 118 patients in the atezolizumab arm and 104 patients in the placebo arm. Overall, 153 patients (38.0%) had at least 1 protocol deviation (39.3% and 36.6% in the atezolizumab and placebo arms, respectively). Major protocol deviations were described as procedural (e.g., error with stratification, omission of safety labs required by protocol, tumour assessment significantly out of window, or omission of tumour assessment); related to inclusion criteria (e.g., inclusion or exclusion tests not done or out of window, ineligible history or current SCLC stage, or inclusion lab values outside limit); or related to medication (e.g., significant deviation from planned study drug dose or received incorrect study drug or wrong dose) in 32.0% (atezolizumab: 32.3%; placebo: 31.7%), 6.0% (atezolizumab: 7.5%; placebo: 4.5%), and 4.0% (atezolizumab: 3.5%; placebo: 4.5%) of patients.
Exposure to Study Treatments
The safety population included 198 patients who received at least 1 dose of atezolizumab and 196 patients who received placebo. The median duration of treatment with atezolizumab was 4.7 months (range = 0 to 21). Patients received a median of 7 doses of atezolizumab (range = 1 to 30) and 6 doses of placebo. The median number of doses of chemotherapy was the same in the 2 treatment arms (carboplatin: 4 doses; etoposide: 12 doses). Median exposure to carboplatin and etoposide was 2.3 months in the atezolizumab arm and 2.2 months in the placebo arm. The median dose intensity of atezolizumab or placebo was 95% in both arms, while the mean dose intensity of carboplatin and etoposide, respectively, was 92.3% and 89.4% in the atezolizumab arm and 93.3% and 90.3% in the placebo arm. Most patients in the atezolizumab and placebo arms (80% and 90%, respectively) completed the planned 4 cycles of induction treatment (Table 8).
Table 8: Summary of Treatment Exposure — Safety Population
Treatment exposure | Atezolizumab + CE (N = 198) | Placebo + CE (N = 196) | ||||
|---|---|---|---|---|---|---|
Atezolizumab | Carboplatin | Etoposide | Placebo | Carboplatin | Etoposide | |
Median treatment duration, months | ||||||
Median | 4.7 | 2.3 | 2.3 | 4.1 | 2.2 | 2.2 |
0 to 3, n (%) | 47 (23.7) | 193 (97.5) | 191 (96.5) | 41 (20.9) | 191 (97.4) | 191 (97.4) |
3 to 6, n (%) | 87 (43.9) | 5 (2.5) | 7 (3.5) | 113 (57.7) | 5 (2.6) | 5 (2.6) |
6 to 12, n (%) | 41 (20.7) | 0 | 0 | 30 (15.3) | 0 | 0 |
> 12, n (%) | 23 (11.6) | 0 | 0 | 12 (6.1) | 0 | 0 |
Median dose intensity,a % | 94.9 | 92.3 | 89.4 | 94.7 | 93.3 | 90.3 |
Median doses, n | 7 | 4 | 12 | 6 | 4 | 12 |
Total cumulative dose, mg | ||||||
Mean (SD) | 10,193.0 (7,166.6) | 2,019.2 (642.2) | 1,965.8 (539.8) | 0 | 2,145.7 (645.0) | 2,034.5 (477.2) |
Median | 8,400.0 | 2,062.5 | 2,055.2 | 0 | 2,175 | 2,131.7 |
CE = carboplatin and etoposide; SD = standard deviation.
aDose intensity is the number of doses actually received divided by the expected number of doses.
Source: Clinical Study Report for IMpower133 study.12
Prior and Concomitant Treatments
At the time of study enrolment, 20 patients (5.0%) had received non-anthracycline chemotherapy: 8 patients (4.0%) in the atezolizumab arm and 12 patients (5.9%) in the placebo arm. All patients who received prior anticancer therapy had non-anthracycline chemotherapy, with the most common treatment being cisplatin or carboplatin plus etoposide and concurrent radiation. Overall, 14.4% of patients had undergone prior surgery for SCLC, with “other” surgeries (atezolizumab: 13.4%; placebo: 11.4%), metastasectomy (atezolizumab: 1.5%; placebo: 0.5%), lobectomy (atezolizumab: 1%; placebo: 0%), and thoracotomy (atezolizumab: 0.5%; placebo: 0.5%) being the most commonly reported procedures. Prior radiotherapy was reported for 12.4% and 13.9% of patients in the atezolizumab and placebo arms, respectively. A total of 13.2% of patients had received prior radiotherapy for SCLC, including patients in the extensive-stage setting (atezolizumab: 7.0% and placebo: 7.9%, including patients with prior radiotherapy to the brain [atezolizumab: 6.5%; placebo: 6.4%]), in the limited-stage setting (atezolizumab: 5.0%; placebo: 5.4%), and in other settings (atezolizumab: 1.0%; placebo: 1.5%) (Table 9).
At the time of study enrolment and before the randomization date, 90.6% of patients were receiving at least 1 concomitant medication (atezolizumab: 89.6%; placebo: 91.6%). The most commonly used classes of drugs (≥ 25% of patients in any arm) were opioid analgesics (atezolizumab: 29.4%; placebo: 33.2%), statins (atezolizumab: 25.4%; placebo: 27.7%), beta-adrenoceptor blocking agents (atezolizumab: 28.9%; placebo: 22.3%), bronchodilators and anti-asthmatics (atezolizumab: 21.9%; placebo: 28.7%), and proton pump inhibitors (atezolizumab: 21.4%; placebo: 26.7%).
Nearly all patients (97.0%) received at least 1 concomitant medication initiated on or after the randomization date (atezolizumab: 97.5%; placebo: 96.5%). The most commonly used classes of drugs (≥ 25% of patients in any arm) were 5-HT3 antagonists (atezolizumab: 77.6%; placebo: 73.8%), steroids (atezolizumab: 65.7%; placebo: 62.9%), colony-stimulating factors (atezolizumab: 41.8%; placebo: 42.1%), supplements (atezolizumab: 41.3%; placebo: 36.1%), antiemetics not elsewhere classified (atezolizumab: 39.3%; placebo: 35.1%), opioid analgesics (atezolizumab: 33.3%; placebo: 33.7%), nonsteroidal anti-inflammatories (atezolizumab: 24.9%; placebo: 27.2%), laxatives and stool softeners (atezolizumab: 25.4%; placebo: 24.8%), and antihistamines (atezolizumab: 26.4%; placebo: 19.8%).
There were no reported concomitant cancer-related surgeries during the study up to the clinical data cut-off date. No immunosuppressive agents, excluding corticosteroids, started on the day of or after atezolizumab or placebo treatment were reported during the study up to the clinical data cut-off date.
Overall, 7.9% of patients received on-study cancer radiotherapy, with bone (atezolizumab: 2.0%; placebo: 4.0%), brain (excluding PCI) (atezolizumab: 2.0%; placebo: 2.5%), and lung (atezolizumab: 1.5%; placebo: 2.0%) being the most common sites irradiated.
Overall, 10.9% of patients in each treatment arm received PCI during the maintenance phase, For patients who did not receive PCI, the reasons reported were as follows: not considered standard of care (atezolizumab: 52.2%; placebo: 46.5%), progressive disease (atezolizumab: 12.4%; placebo 18.3%), “other” reasons (atezolizumab: 13.4%; placebo: 16.8%), patient preference (atezolizumab: 7.0%; placebo: 3.0%), and clinical deterioration or comorbidities (atezolizumab: 4.0%; placebo: 3.0%).
Table 9: Prior Anticancer Treatments — ITT Population
Treatment | Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) |
|---|---|---|
Chemotherapy or non-anthracycline, n (%) | 8 (4.0) | 12 (5.9) |
Cisplatin, etoposide, plus concurrent radiation | 6 (3.0) | 7 (3.5) |
Carboplatin, etoposide, plus concurrent radiation | 2 (1.0) | 6 (3.0) |
Radiotherapy, n (%) | 25 (12.4) | 28 (13.9) |
Cancer-related surgery, n (%) | 33 (16.4) | 25 (12.4) |
CE = carboplatin and etoposide; ITT = intention to treat.
Source: Clinical Study Report for IMpower133 study.12
Subsequent Anticancer Treatments
In the ITT population, 51.7% of patients in the atezolizumab arm and 57.4% of patients in the placebo arm received at least 1 non-protocol or follow-up non-protocol anticancer therapy. The most common treatment received in the atezolizumab and placebo arms was non-anthracycline chemotherapy: 40.3% and 43.6%, respectively. In the atezolizumab and placebo arms, 3.0% and 7.4% of patients, respectively, received subsequent immunotherapy (Table 10).
Table 10: Treatments — ITT Population
Treatment | Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) | All patients (N = 403) |
|---|---|---|---|
Line of therapy, n (%) | |||
Maintenance | 2 (1.0) | 0 | 2 (0.5) |
Second | 101 (50.2) | 116 (57.4) | 217 (53.8) |
Third | 29 (14.4) | 38 (18.8) | 67 (16.6) |
Fourth | 3 (1.5) | 15 (7.4) | 18 (4.5) |
Missing | 0 | 1 (0.5) | 1 (0.2) |
Therapy type, n (%) | |||
Total number of patients with ≥ 1 treatment | 104 (51.7) | 116 (57.4) | 220 (54.6) |
Total number of treatments | 138 | 176 | 314 |
Chemotherapy, non-anthracycline | 81 (40.3) | 88 (43.6) | 169 (41.9) |
Chemotherapy, anthracycline | 31 (15.4) | 46 (22.8) | 77 (19.1) |
Immunotherapy | 6 (3.0) | 15 (7.4) | 21 (5.2) |
Other | 2 (1.0) | 2 (1.0) | 4 (1.0) |
Targeted therapy | 2 (1.0) | 1 (0.5) | 3 (0.7) |
CE = carboplatin and etoposide; ITT = intention to treat.
Note: Multiple cases within a specific line of therapy and regimen for a patient were counted once for the frequency of line of therapy or regimen name.
A patient was counted more than once if they received more than 1 therapy type under each line and regimen.
Source: Clinical Study Report for IMpower133 study.12
Efficacy
Progression-Free Survival
As of the data cut-off date (April 24, 2018), 171 patients (85.1%) in the atezolizumab arm and 189 patients (93.6%) in the placebo arm had disease progression or died. The median PFS was 5.2 (95% CI, 4.4 to 5.6) months in the atezolizumab arm and 4.3 (95% CI, 4.2 to 4.5) months in the placebo arm. The stratified HR for disease progression or death was 0.77 (95% CI, 0.62 to 0.96; P = 0.0170) (Table 11 and Figure 3).
The 6-month event-free rate in the atezolizumab and placebo arms was 30.86 (95% CI, 24.26 to 37.45) versus 22.39 (95% CI, 16.56 to 28.22). The 12-month event-free rate was 12.62 (95% CI, 7.85 to 17.40) in the atezolizumab arm and 5.35 (95% CI, 2.14 to 8.56) in the placebo arm (Table 11).
In the 2 subgroups of interest identified for this review (ECOG PS and brain metastases at baseline), while the overall PFS benefit with atezolizumab observed in the overall population was evident in patients with an ECOG PS of 1 and those without brain metastases, for those with an ECOG PS of 0 and those with brain metastases at baseline, the benefit of adding atezolizumab to carboplatin and etoposide in terms of PFS was uncertain (Table 12). The number of patients in these subgroups was low (ECOG PS of 0: n = 128; brain metastases at baseline: n = 33).
Sensitivity Analysis of PFS
The sensitivity analysis of PFS censored for missing scheduled tumour assessments was consistent with the primary analysis. The median PFS was 5.1 (95% CI, 4.3 to 5.6) months in the atezolizumab arm and 4.3 (95% CI, 4.2 to 4.5) months in the placebo arm. The stratified HR for disease progression or death was 0.77 (95% CI, 0.63 to 0.96; P = 0.0209).
The sensitivity analysis of PFS censoring at non-prior anticancer therapy showed similar results to those of the main analysis. The median PFS was 5.2 (95% CI, 4.4 to 5.6) months in the atezolizumab arm and 4.3 (95% CI, 4.2 to 4.5) months in the placebo arm. The stratified HR for disease progression or death was 0.78 (95% CI, 0.63 to 0.96; P = 0.0212).
Table 11: PFS — ITT Population
Co-primary efficacy end point: PFS | Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) |
|---|---|---|
Patients with event, n (%) | 171 (85.1) | 189 (93.6) |
Earliest contributing event | ||
Death | 19 | 20 |
Disease progression | 152 | 169 |
Patients without event, n (%) | 30 (14.9) | 13 (6.4) |
Median duration of PFS (95% CI), months | 5.2 (4.4 to 5.6) | 4.3 (4.2 to 4.5) |
Stratified HR (95% CI) | 0.772 (0.624 to 0.955) | |
P value (log-rank) | 0.0170a | |
Time point analysis | ||
6 months | ||
Event-free rate (95% CI), % | 30.86 (24.26 to 37.45) | 22.39 (16.56 to 28.22) |
Difference in event-free rate (95% CI) | 8.47 (–0.33 to17.27) | |
P value (z test) | 0.0593 | |
12 months | ||
Event-free rate (95% CI), % | 12.62 (7.85 to 17.40) | 5.35 (2.14 to 8.56) |
Difference in event-free rate (95% CI) | 7.27 (1.52 to 13.02) | |
P value (z test) | 0.0133 | |
CE = carboplatin and etoposide; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; PFS = progression-free survival.
aSince null hypothesis for overall survival was rejected at an overall 2-sided significance level of 0.045, PFS was tested at 2-sided type I error of 0.05.
Source: Clinical Study Report for IMpower133 study.12
Figure 3: Kaplan–Meier Curves for PFS — ITT Population
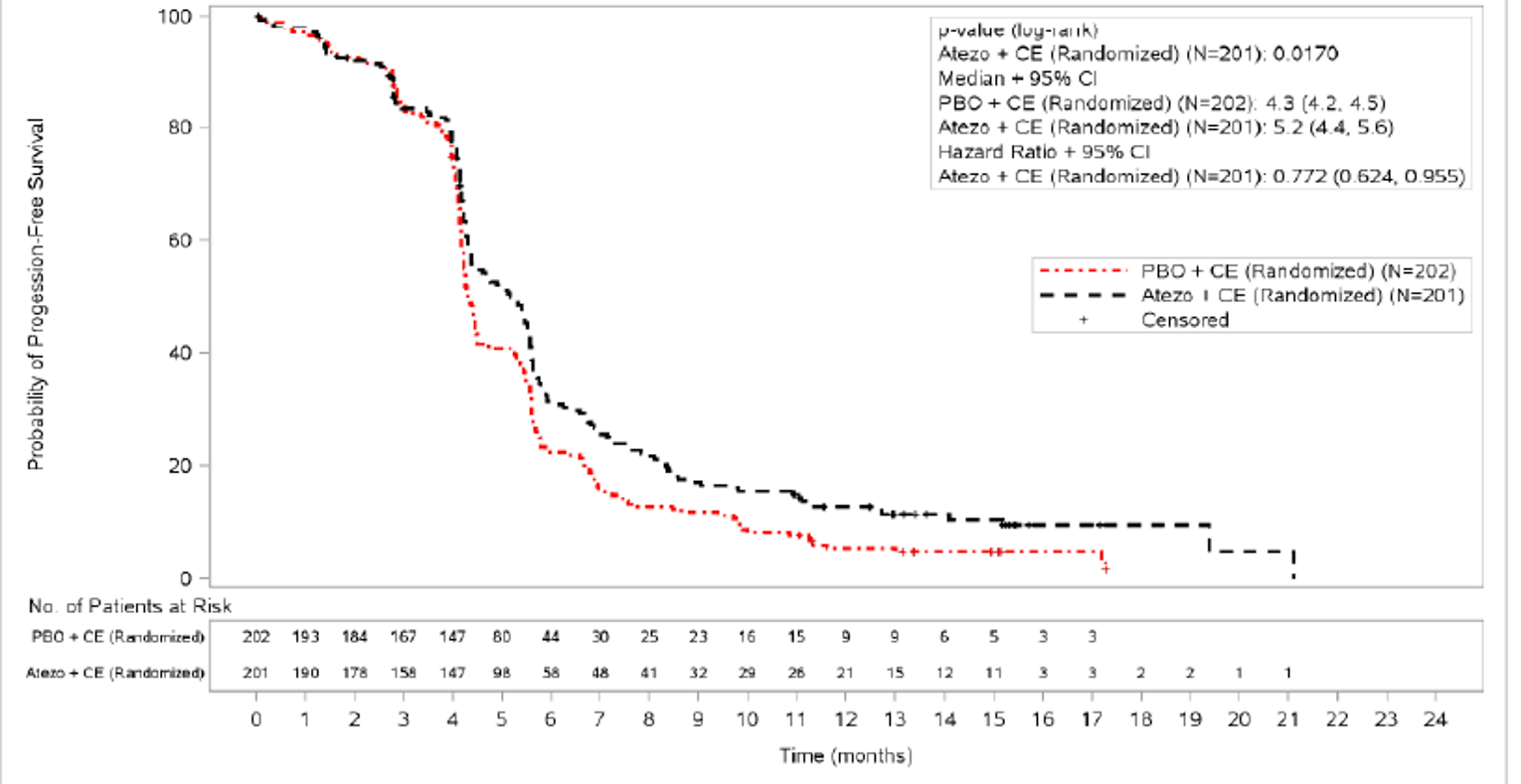
Atezo = atezolizumab; CE = carboplatin and etoposide; CI = confidence interval; ITT = intention to treat; PBO = placebo.
Source: Clinical Study Report for IMpower133 study.12
Table 12: PFS by Subgroup at Baseline — ITT Population
Subgroup | Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) | HR (95% Wald CI) | ||
|---|---|---|---|---|---|
Events | Median PFS, months | Events | Median PFS, months | ||
ECOG PS | |||||
0 (n = 140) | 64 | 4.9 | 64 | 4.3 | 0.84 (0.59 to 1.20) |
1 (n = 263) | 107 | 5.4 | 125 | 4.3 | 0.72 (0.55 to 0.94) |
Brain metastasis at baseline | |||||
Yes (n = 35) | 15 | 4.2 | 18 | 4.4 | 0.98 (0.49 to 2.00) |
No (n = 368) | 156 | 5.3 | 171 | 4.3 | 0.75 (0.60 to 0.93) |
CE = carboplatin and etoposide; CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; ITT = intention to treat; PFS = progression-free survival.
Note: Medians were estimated using the Kaplan–Meier method. Hazard ratios relative to placebo and the associated CIs were estimated using unstratified Cox regression.
Source: Clinical Study Report for IMpower133 study.12
Overall Survival
At the time of the OS interim analysis (data cut-off date: April 24, 2018), patients had a median survival follow-up time of 13.9 months. A total of 104 patients (51.7%) in the atezolizumab arm and 134 patients (66.3%) in the placebo arm had died. The median OS was 12.3 months (95% CI, 10.8 to 15.9) in the atezolizumab arm and 10.3 months (95% CI, 9.3 to 11.3) in the placebo arm. The stratified HR for death was 0.70 (95% CI, 0.54 to 0.91; P = 0.007). The 1-year OS rate was 51.7% in the atezolizumab arm and 38.2% in the placebo arm (Table 13 and Figure 4).
Co-primary efficacy end point: OS | Interim analysis | Updated analysis | ||
|---|---|---|---|---|
Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) | Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) | |
Patients with event, n (%) | 104 (51.7) | 134 (66.3) | 142 (70.6) | 160 (79.2) |
Median duration of survival, months (95% CI) | 12.3 (10.8 to 15.9) | 10.3 (9.3 to 11.3) | 12.3 (10.8 to 15.8) | 10.3 (9.3 to 11.3) |
Stratified HR (95% CI) | 0.701 (0.541 to 0.909) | 0.755 (0.601 to 0.949) | ||
P value (log-rank) | 0.0069a | 0.0154b | ||
Patients remaining at risk, n | 74 | 59 | 93 | 74 |
12-month event-free rate, % (95% CI) | 51.7 (44.4 to 59.0) | 38.2 (31.2 to 45.3) | 51.9 (44.6 to 59.1) | 39.0 (32.1 to 45.9) |
Patients remaining at risk, n | 5 | 3 | 61 | 39 |
18-month event-free rate, % (95% CI) | 25.0 (11.2 to 38.7) | 20.2 (11.1 to 29.4) | 34.0 (27.1 to 40.9) | 21.0 (15.2 to 26.8) |
Patients remaining at risk, n | NE | NE | 21 | 8 |
24-month event-free rate, % (95% CI) | NE (NE to NE) | NE (NE to NE) | 22.0 (15.7 to 28.3) | 16.8 (11.3 to 22.2) |
CE = carboplatin and etoposide; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; NE = not estimable; OS = overall survival.
aInterim analysis: OS was tested at 2-sided alpha of 0.0193 (with 238 observed OS events at the data cut-off date of April 24, 2018) to control the overall 2-sided type I error for OS at 0.045 by Lan-DeMets function approximating O’Brien-Fleming boundary.
bDescriptive purposes only.
Source: Update Clinical Study Report for IMpower133 study.13
Updated Analysis
At the final OS analysis (data cut-off date: January 24, 2019), median survival follow-up time was 22.9 months. The median duration of survival follow-up was 23.1 months (range = 0.0 to 29.5) in the atezolizumab arm and 22.6 months (range = 0.0 to 30.7) in the placebo arm.
The median OS was 12.3 months (95% CI, 10.8 to 15.8) in the atezolizumab arm and 10.3 months (95% CI, 9.3 to 11.3) in the placebo arm. The stratified HR for death was 0.75 (95% CI, 0.60 to 0.95; P = 0.015). Based on the landmark analysis, in the atezolizumab versus placebo arms, 34.0% versus 21.0% of patients were alive at 18 months and 22.0% versus 16.8% of patients were alive at 24 months (Table 13 and Table 5).
Of the 2 subgroups of interest identified for this review (ECOG PS and brain metastases at baseline), the OS benefit was consistent for patients with an ECOG PS of 0 and an ECOG PS of 1. With respect to brain metastases, an OS benefit was not observed in patients with brain metastases at baseline but was observed in patients without brain metastases at baseline (Table 14).
Objective Response Rate
The confirmed ORR was 60.2% in the atezolizumab arm and 64.4% in the placebo arm; 2.5% and 1.0% of patients in the atezolizumab and placebo arms, respectively, had a CR (Table 15).
At the updated analysis (data cut-off date: January 24, 2019), the confirmed ORR was 60.2% (95% CI, 53.1 to 67.0) in the atezolizumab arm and 64.4% (95% CI, 57.3 to 71.0) in the placebo arm; 3.5% and 1.0% of patients in the atezolizumab and placebo arms, respectively, had a CR.
Figure 4: Kaplan-Meier Curves for OS — ITT Population
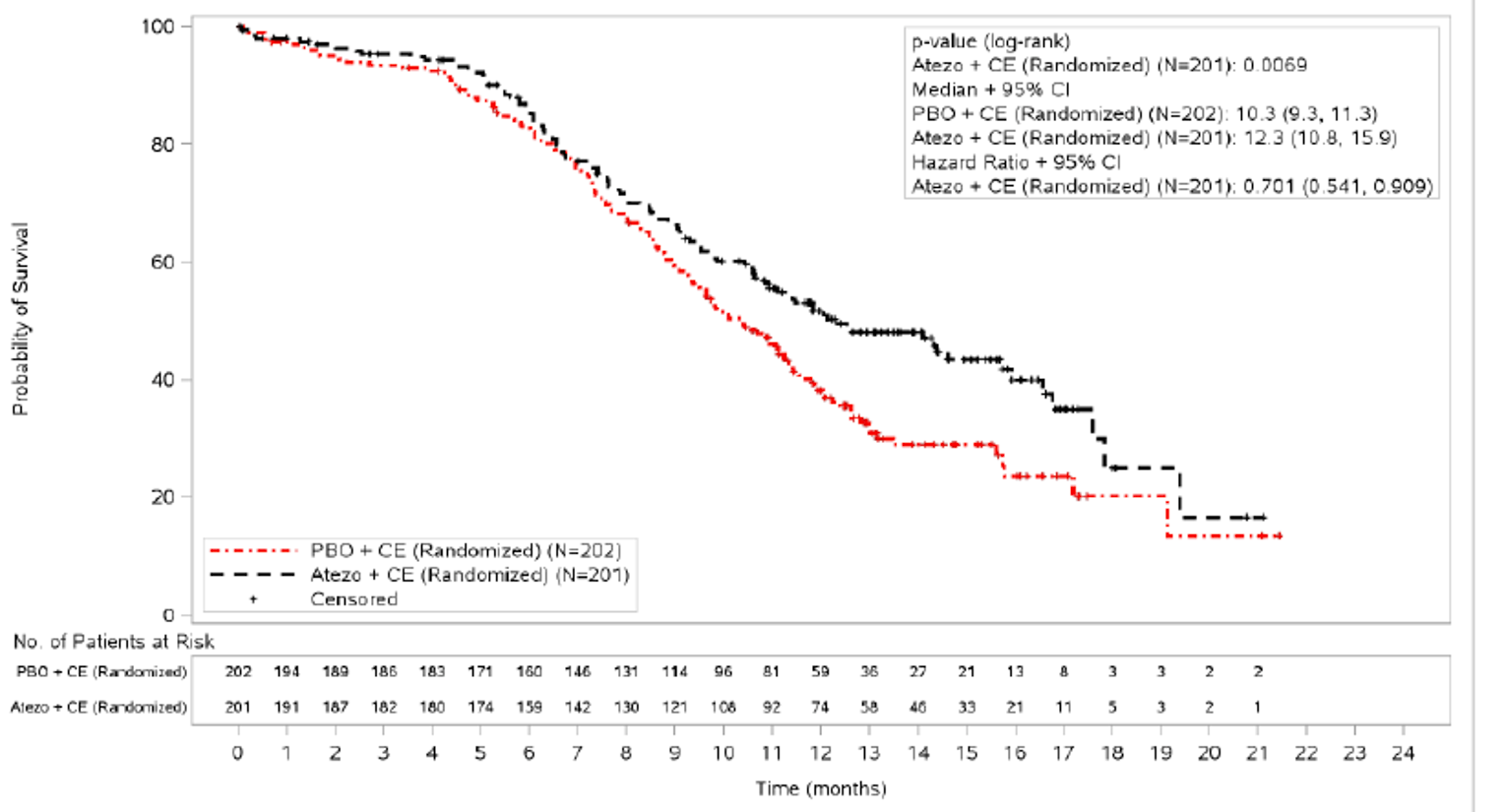
Atezo = atezolizumab; CE = carboplatin and etoposide; CI = confidence interval; ITT = intention to treat; PBO = placebo.
Note: Analyses were stratified by sex (male versus female) and Eastern Cooperative Oncology Group Performance Status (0 versus 1).
Source: Clinical Study Report for IMpower133 study.12
Table 14: OS by Subgroup at Baseline — ITT Population
Subgroup | Interim analysis | Updated analysis | ||||
|---|---|---|---|---|---|---|
Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) | HR (95% CI) | Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) | HR (95% CI) | |
Median OS, months | ||||||
ECOG PS | ||||||
0 | 16.6 | 12.4 | 0.79 (0.49 to 1.27) | 16.8 | 12.6 | 0.73 (0.48 to 1.10) |
1 | 11.4 | 9.3 | 0.68 (0.50 to 0.93) | 11.3 | 9.3 | 0.78 (0.60 to 1.03) |
Brain metastasis at baseline | ||||||
Yes | 8.5 | 9.7 | 1.07 (0.47 to 2.43) | 8.5 | 9.7 | 0.96 (0.46 to 2.01) |
No | 12.6 | 10.4 | 0.68 (0.52 to 0.89) | 12.6 | 10.4 | 0.74 (0.58 to 0.94) |
CE = carboplatin and etoposide; CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; ITT = intention to treat; OS = overall survival.
Note: Medians were estimated using the Kaplan–Meier method. Hazard ratios relative to placebo and the associated CIs were estimated using unstratified Cox regression.
Source: Clinical Study Report for IMpower133 study12; Updated Clinical Study Report for IMpower133 study.13
Table 15: Objective Response Rate — ITT Population
Measure | Atezolizumab + CE (n = 202) | Placebo + CE (n = 201) |
|---|---|---|
Objective confirmed response, n (%) | 121 (60.2) | 130 (64.4) |
95% CI for response ratea | 53.07 to 67.02 | 57.33 to 70.95 |
Difference in response rates (95% CIb) | –4.16 (–14.11 to 5.79) | |
P valuec | 0.3839 | |
Odds ratiod (95% CI) | 0.84 (0.56 to 1.25) | |
Complete response, n (%) | 5 (2.5) | 2 (1.0) |
95% CI | 0.81 to 5.71 | 0.12 to 3.53 |
Partial response, n (%) | 116 (57.7) | 128 (63.4) |
95% CI | 50.56 to 64.63 | 56.32 to 70.02 |
Stable disease, n (%) | 42 (20.9) | 43 (21.3) |
95% CI | 15.49 to 27.18 | 15.85 to 27.58 |
Progressive disease, n (%) | 22 (10.9) | 14 (6.9) |
95% CI | 6.99 to 16.10 | 3.84 to 11.36 |
Missing or unevaluable, n (%) | 16 (8.0) | 15 (7.4) |
CE = carboplatin and etoposide; CI = confidence interval; ITT = intention to treat.
Note: Objective response rate with confirmed response was assessed by investigator per Response Evaluation Criteria in Solid Tumours Version 1.1.
aClopper-Pearson interval.
bWald with continuity correction.
cCochran-Mantel-Haenszel test.
dStratified by sex (male vs. female) and Eastern Cooperative Oncology Group Performance Status (0 vs. 1).
Source: Clinical Study Report for IMpower133 study.12
Duration of Response
The median DOR (confirmed) was 4.2 months (range = 1.4 to 19.5) in the atezolizumab arm and 3.9 months (range = 2.0 to 16.1) in the placebo arm. At data cut-off (April 24, 2018), 14.9% of patients in the atezolizumab arm and 5.4% of patients in the placebo arm had ongoing response. Median time to event (progression) was 4.2 months (95% CI, 4.1 to 4.5) in the atezolizumab arm and 3.9 months (3.1 to 4.2) in the placebo arm (Table 16).
At the updated analysis, the median DOR was 4.2 months (range = 1.4 to 24.3) in the atezolizumab arm and 3.9 months (range = 2.0 to 24.2) in the placebo arm. As of the data cut-off date (January 24, 2019), 9.1% of patients in the atezolizumab arm and 2.3% of patients in the placebo arm had ongoing response.
Figure 5: Kaplan-Meier Curves for OS, Updated Analysis — ITT Population
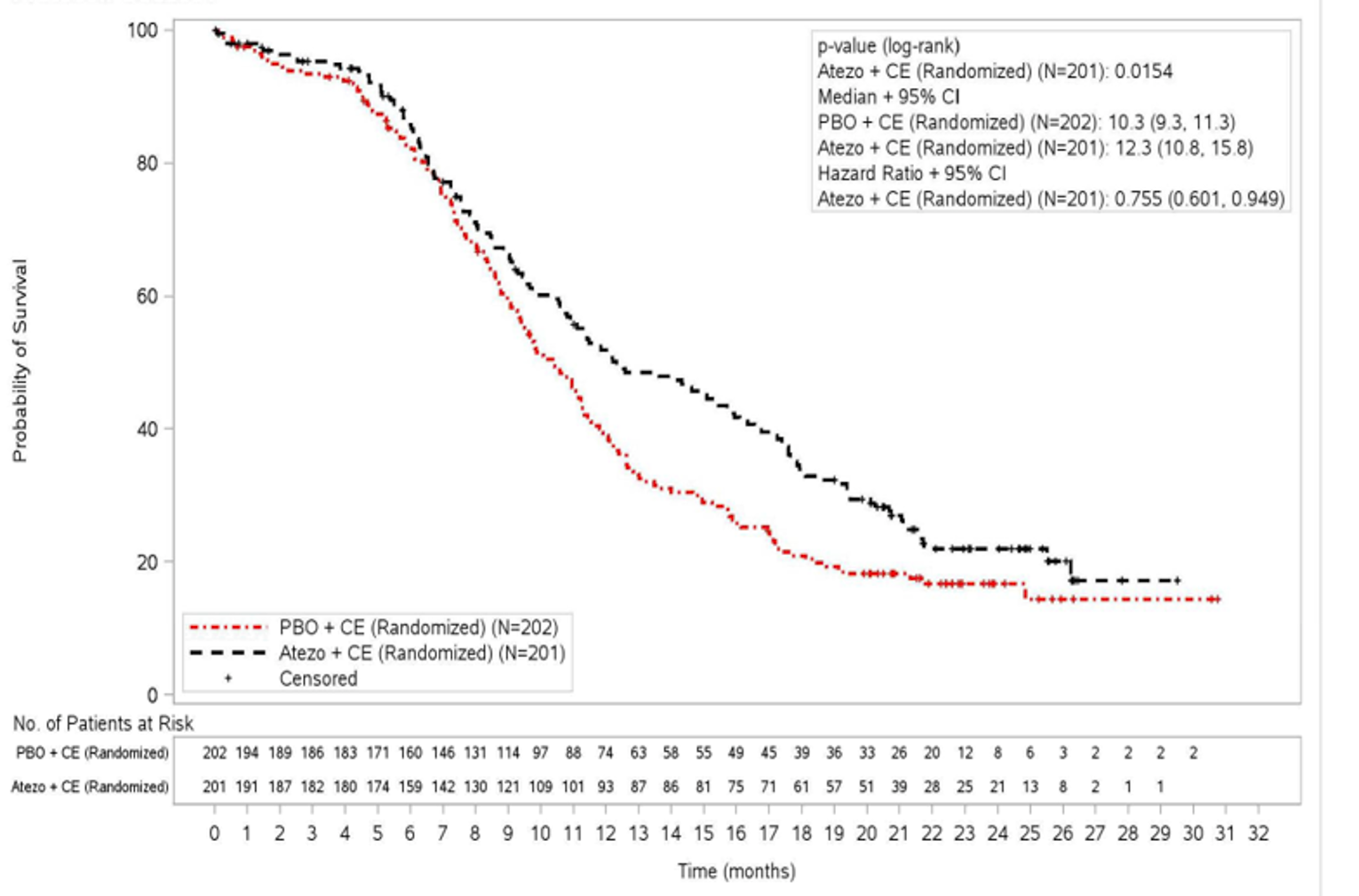
Atezo = atezolizumab; CE = carboplatin and etoposide; CI = confidence interval; ITT = intention to treat; PBO = placebo.
Note: Analyses were stratified by sex (male versus female) and Eastern Cooperative Oncology Group Performance Status (0 versus 1).
Source: Update Clinical Study Report for IMpower133 study.13
Table 16: Duration of Response — ITT Population Patients With Confirmed Response Assessed by Investigator per RECIST 1.1
Event | Atezolizumab + CE (n = 121) | Placebo + CE (n = 130) |
|---|---|---|
Patients with event, n (%) | 103 (85.1) | 123 (94.6) |
Earliest contributing event, n | ||
Death | 4 | 7 |
Disease progression | 99 | 116 |
Patients without event, n (%) | 18 (14.9) | 7 (5.4) |
Median time to event, months (95% CI)a | 4.2 (4.1 to 4.5) | 3.9 (3.1 to 4.2) |
Stratified HR (95% CI)b | 0.700 (0.53 to 0.92) | |
P value (log-rank) | 0.0109 | |
CE = carboplatin and etoposide; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
aKaplan–Meier estimates. The 95% CIs for medians were computed using the Brookmeyer-Crowley method.
bEstimated by Cox regression.
Source: Clinical Study Report for IMpower133 study.12
Time to Next Treatment
Time to next treatment was not an end point in the IMpower133 trial.
Health-Related Quality of Life
At baseline, 175 patients (87%) in the atezolizumab arm and 179 patients (89%) in the placebo arm completed the EORTC QLQ-C30, and 176 (88%) and 168 (83%), respectively, completed the EORTC QLQ-LC13. Completion rates remained above 80% up to week 36 in the atezolizumab arm and up to week 24 in the placebo arm. At week 54, 34 (8%) of the 403 randomized patients remained on study treatment and were eligible to complete PRO assessment.
Patients in the IMpower133 study generally reported worse disease-related symptoms (cough, chest pain, dyspnea, arm/shoulder pain, or pain in other parts) at baseline than are reported in the normative scores of patients with SCLC.31 Changes from baseline in treatment-related symptoms, including diarrhea, dysphagia, sore mouth, peripheral neuropathy, nausea/vomiting, and insomnia, were generally similar between treatment arms at most visits through week 54.31
Mean change from baseline in function scores (physical, cognitive, emotional, social, and role) were similar in both treatment arms through week 54, with a general trend for improvement of function (physical, emotional, and social) or maintenance of function (role and cognitive) (Figure 6).
Harms
Adverse Events
The majority of patients in both treatment arms — 100% in the atezolizumab arm and 96.4% in the placebo arm — experienced at least 1 AE of any grade (Table 17). In the atezolizumab arm, the most common AEs of any grade by preferred term experienced by at least 10% of patients were anemia (43.4%), nausea (37.9%), and neutropenia (37.4%). In the placebo arm, the most common AEs of any grade by preferred term experienced by at least 10% of patients were anemia (35.2%), neutropenia (35.2%), and alopecia (34.7%) (Table 18).
Grade 3 or 4 AEs, regardless of attribution, occurred in 67.7% of patients in the atezolizumab arm and 63.3% of patients in the placebo arm. The most common grade 3 or 4 AEs reported in at least 5% of patients in any treatment arm were neutropenia (22.7% versus 25.0% in the atezolizumab and placebo arms, respectively), decreased neutrophil count (15.7% versus 16.8%), anemia (15.7% versus 13.3%), thrombocytopenia (10.1% versus 8.7%), and hyponatremia (4.5% versus 6.6%).
Serious Adverse Events
In the atezolizumab arm, 37.4% of patients had at least 1 SAE. In the placebo arm, 34.7% of patients experienced at least 1 SAE (38.9% and 35.2% as of Jan 24, 2019 cut-off date). The most common SAEs experienced by at least 1% of patients in either the atezolizumab or placebo arm were pneumonia (4.5% versus 3.6%), neutropenia (3.5% versus 4.1%), febrile neutropenia (2.5% versus 4.6%), and thrombocytopenia (2.5% versus 2.0%) (Table 19).
Figure 6: Change From Baseline Through Week 54 in Function and in Health-Related Quality of Life
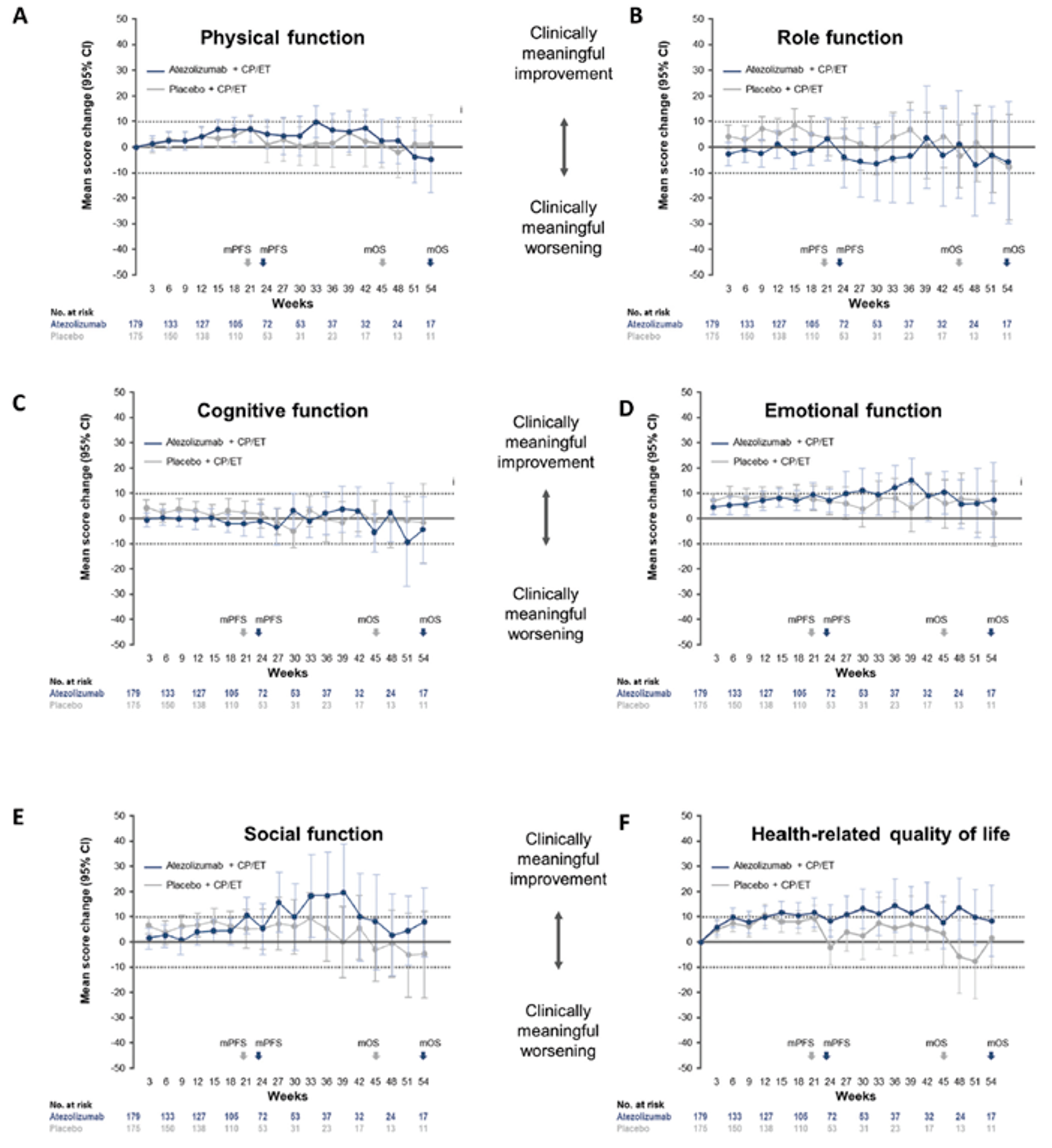
CI = confidence interval; CP = carboplatin; ET = etoposide; mOS = mean overall survival; mPFS = mean progression-free survival.
Source: Clinical Summary for IMpower133 study.12
Withdrawals Due to AEs
Withdrawal from any study treatment due to AEs was reported for 12.1% of patients in the atezolizumab arm and 3.1% of patients in the placebo arm. In the atezolizumab arm, 11.6% of patients experienced AEs leading to discontinuation of atezolizumab, and in the placebo arm, 2.6% of patients had AEs leading to discontinuation of placebo. The main reasons for permanently discontinuing atezolizumab in 21 patients in the atezolizumab arm were infusion-related reactions and gastrointestinal disorders.
In the atezolizumab arm, 70.2% of patients had AEs resulting in dose modification or interruption. In the placebo arm, 60.7% of patients had dose modification or interruption to their treatment due to AEs. Neutropenia was the most common AE leading to dose modification or interruption of any study treatment in both treatment arms. The most frequent AEs leading to dose modification or interruption of any study treatment reported in at least 2% patients were neutropenia, anemia, leukopenia, fatigue, pyrexia, and increased alanine aminotransferase incidence in the atezolizumab arm, whereas those more common in the placebo arm were decreased neutrophil, platelet, and white blood cell counts.
Table 17: Summary of AEs — Safety Population
Patients, n (%) | Atezolizumab + CE (N = 198) | Placebo + CE (N = 196) |
|---|---|---|
≥ 1 AE | 198 (100) | 189 (96.4) |
Grade 3 to 4 | 134 (67.7) | 124 (63.3) |
Grade 5 | 4 (2.0) | 11 (5.6) |
SAEs | 77 (38.9) | 69 (35.2) |
Immune-related AEs | 82 (41.4) | 48 (24.5) |
Treated with steroids or hormone replacement therapya | 40 (20.2) | 11 (5.6) |
AEs leading to withdrawal from any treatmentb | 24 (12.1) | 6 (3.1) |
AEs leading to withdrawal from atezolizumab or placebo | 23 (11.6) | 5 (2.6) |
AEs leading to withdrawal from carboplatin | 5 (2.5) | 1 (0.5) |
AEs leading to withdrawal from etoposide | 8 (4.0) | 2 (1.0) |
AEs leading to any dose modification or interruption | 139 (70.2) | 119 (60.7) |
AEs leading to dose modification from atezolizumab or placebo | 118 (59.6) | 102 (52.0) |
Treatment-related AEs | 188 (94.9) | 181 (92.3) |
Atezolizumab or placebo related | 130 (65.7) | 100 (51.0) |
Grade 3 to 4 | 113 (57.1) | 110 (56.1) |
Grade 5 | 3 (1.5) | 3 (1.5) |
AE = adverse event; CE = carboplatin and etoposide; SAE = serious adverse event.
Note: Clinical data cut-off date: January 24, 2019.
aAn event consistent with an immune-mediated mechanism of action requiring treatment with systemic corticosteroids or hormone replacement therapy.
bIncidence of treatment-related AEs and AEs leading to withdrawal from any treatment are for any treatment component.
Source: Clinical Summary for IMpower133 study12; Liu et al. (2021)30; Reck et al. (2019).32
Table 18: AEs by Preferred Term Occurring in at Least 10% of Patients in Either Treatment Arm — Safety Population
AEs | Atezolizumab + CE (N = 198) | Placebo + CE (N = 196) |
|---|---|---|
Patients with ≥ 1 AE, n (%) | 198 (100) | 189 (96.4) |
Total number of events | 2,166 | 1,861 |
MedDRA preferred term, n (%) | ||
Anemia | 86 (43.4) | 69 (35.2) |
Nausea | 75 (37.9) | 64 (32.7) |
Neutropenia | 74 (37.4) | 69 (35.2) |
Alopecia | 73 (36.9) | 68 (34.7) |
Decreased appetite | 54 (27.3) | 36 (18.4) |
Fatigue | 54 (27.3) | 49 (25.0) |
Constipation | 51 (25.8) | 58 (29.6) |
Vomiting | 39 (19.7) | 33 (16.8) |
Decreased neutrophil count | 37 (18.7) | 46 (23.5) |
Diarrhea | 35 (17.7) | 31 (15.8) |
Thrombocytopenia | 33 (16.7) | 31 (15.8) |
Asthenia | 25 (12.6) | 20 (10.2) |
Leukopenia | 25 (12.6) | 19 (9.7) |
Decreased platelet count | 25 (12.6) | 29 (14.8) |
Headache | 24 (12.1) | 23 (11.7) |
Dyspnea | 20 (10.1) | 18 (9.2) |
Hypothyroidism | 20 (10.1) | 1 (0.5) |
Pyrexia | 20 (10.1) | 16 (8.2) |
Decreased weight | 20 (10.1) | 10 (5.1) |
Arthralgia | 18 (9.1) | 13 (6.6) |
Cough | 18 (9.1) | 25 (12.8) |
Decreased white blood cell count | 18 (9.1) | 25 (12.8) |
AE = adverse event; CE = carboplatin and etoposide; MedDRA = Medical Dictionary for Regulatory Activities.
Source: Clinical Study Report for IMpower133 study.12
Table 19: Serious Adverse Events by Preferred Term Occurring in at Least 1% of Patients in Either Treatment Arm — Safety Population
SAEs | Atezolizumab + CE (N = 198) | Placebo + CE (N = 196) |
|---|---|---|
Patients with ≥ 1 SAE, n (%) | 74 (37.4) | 68 (34.7) |
Total number of events | 129 | 113 |
MedDRA preferred term, n (%) | ||
Pneumonia | 9 (4.5) | 7 (3.6) |
Neutropenia | 7 (3.5) | 8 (4.1) |
Febrile neutropenia | 5 (2.5) | 9 (4.6) |
Thrombocytopenia | 5 (2.5) | 4 (2.0) |
Anemia | 3 (1.5) | 2 (1.0) |
Diarrhea | 3 (1.5) | 1 (0.5) |
Fatigue | 3 (1.5) | 0 |
Syncope | 3 (1.5) | 0 |
Vomiting | 3 (1.5) | 3 (1.5) |
CE = carboplatin and etoposide; MedDRA = Medical Dictionary for Regulatory Activities; SAE = serious adverse event.
Note: Grade 5 adverse events due to progressive disease are excluded.
Source: Clinical Study Report for IMpower133 study.12
Death
As of the primary data cut-off date, 103 deaths had occurred in the atezolizumab arm (52.0% of patients), and 130 deaths had occurred in the placebo arm (66.3% of patients). The most common cause of death in both arms was progressive disease, which accounted for 87.4% of deaths in the atezolizumab arm and 88.5% of deaths in the placebo arm (Table 20).
Grade 5 AEs occurred in 4 patients (2.0%) in the atezolizumab arm, and included pneumonia, respiratory failure, death, and neutropenia. Grade 5 fatal AEs occurred in 11 patients (5.6%) in the placebo arm and included pneumonia, pulmonary sepsis, sepsis, septic shock, acute respiratory failure, hemoptysis, cardiopulmonary failure, pericardial effusion, and general physical health deterioration. The only grade 5 AE (by preferred term) that occurred in more than 1 patient was pneumonia (1 patient in the atezolizumab arm and 3 patients in the placebo arm).
Table 20: All Deaths and Primary Causes of Death — Safety Population
Deaths | Atezolizumab + CE (N = 198) | Placebo + CE (N = 196) |
|---|---|---|
All death, n (%) | 103 (52.0) | 130 (66.3) |
≤ 30 days from last study drug administration | 8 (4.0) | 13 (6.6) |
> 30 days from last study drug administration | 95 (48.0) | 117 (59.7) |
Primary cause of death, n (%) | ||
Adverse event | 4 (2.0) | 11 (5.6) |
Progressive disease | 90 (45.5) | 115 (58.7) |
Other | 9 (4.5) | 4 (2.0) |
CE = carboplatin and etoposide.
Note: “Other” primary causes of death include unrelated adverse events outside of reporting window.
Source: Clinical Study Report for IMpower133 study.12
Of the grade 5 events, 3 events in each arm were considered related to at least 1 component of study treatment. In the atezolizumab arm, 1 grade 5 death was considered related to all study treatment; there was also 1 case of grade 5 pneumonia and 1 case of grade 5 neutropenia that were both considered related to both carboplatin and etoposide. In the placebo arm, 1 case of grade 5 septic shock was considered related to all study treatment, 1 case of grade 5 pneumonia was considered related to placebo, and 1 case of grade 5 cardiopulmonary failure was considered related to carboplatin.
Notable Harms
Immune-Related AEs
Immune-related AEs were reported for 41.4% of patients in the atezolizumab arm and 24.5% of patients in the placebo arm (Table 21). Rash (both treatment arms) and hypothyroidism (atezolizumab arm) were the most common (≥ 10% incidence) and most differentially reported (≥ 5% difference between treatment arms) immune-related AEs during treatment. More patients in the atezolizumab arm experienced immune-related rash than in the placebo arm (20.2% versus 10.7%). The majority of rash AEs were grade 1 or 2 in severity; 2.0% of patients in the atezolizumab arm and no patients in the placebo arm experienced a grade 3 or 4 rash AE. One patient in each arm experienced an immune-relate rash that was experienced as serious. One patient in the atezolizumab arm had erythema, which led to atezolizumab withdrawal. Rash maculo-papular led to treatment modification or interruption in 2 patients (1.0%) in the atezolizumab arm and no patients in the placebo arm. Immune-related rash that required systemic corticosteroid treatment occurred in 2 patients (1.0%) in the atezolizumab arm and no patients in the placebo arm.
Immune-related hypothyroidism was reported for 12.6% of patients in the atezolizumab arm and 0.5% of patients in the placebo arm. The proportion of patients with immune-related hyperthyroidism in the atezolizumab and placebo arms was 5.6% and 2.6%, respectively. All hyperthyroidism AEs were grade 1 or 2 in severity, and none led to study treatment withdrawal. Hyperthyroidism led to treatment modification or interruption in 1 patient in each arm (0.5%).
Table 21: Adverse Events of Special Interest
Immune-related AEsa > 1% in either treatment group, n (%) | Atezolizumab + CE (N = 198) | Placebo + CE (N = 196) | ||
|---|---|---|---|---|
AE | Grade 1 to 2 | Grade 3 to 4 | Grade 1 to 2 | Grade 3 to 4 |
Rash | 36 (18.2) | 4 (2.0) | 21 (10.7) | 0 |
Hypothyroidism | 25 (12.6) | 0 | 1 (0.5) | 0 |
Hyperthyroidism | 11 (5.6) | 0 | 5 (2.6) | 0 |
Hepatitis | 12 (6.1) | 3 (1.5) | 9 (4.6) | 0 |
Pneumonitis | 4 (2.0) | 1 (0.5) | 3 (1.5) | 2 (1.0) |
Colitis | 1 (0.5) | 2 (1.0) | 0 | 0 |
Adrenal insufficiency | 0 | 0 | 3 (1.5) | 0 |
Infusion-related reaction | 7 (3.5) | 4 (2.0) | 9 (4.6) | 1 (0.5) |
AE = adverse event; CE = carboplatin and etoposide.
Note: Clinical data cut-off date: January 24, 2019.
aAn event consistent with an immune-mediated mechanism of action, not taking into account whether treatment was given for the event.
Source: Reck et al. (2019).32
Infusion-Related Reactions
Immune-related infusion-related reaction events were experienced by 5.6% of patients (n = 11) in the atezolizumab arm and 5.1% of patients (n = 10) in the placebo arm. The majority of these events were grade 1 or 2 (atezolizumab arm: n = 7 [3.5%]; placebo arm: n = 9 [4.6%]). Four patients (2.0%) in the atezolizumab arm and 1 patient (0.5%) in the placebo arm had grade 3 or 4 infusion-related reactions. One patient (0.5%) in the atezolizumab arm and 2 patients (1.0%) in the placebo arm experienced infusion-related reactions that were reported as serious. Five patients (2.5%) in the atezolizumab arm (versus none in the placebo arm) had an infusion-related reaction that led to withdrawal of any study treatment. Infusion-related reactions led to treatment modification or interruption in 7 patients (3.5%) in the atezolizumab arm and 6 patients (3.1%) in the placebo arm. An infusion-related reaction that required systemic corticosteroid treatment occurred in 5 patients (2.5%) in the atezolizumab arm and 3 patients (1.5%) in the placebo arm.
Critical Appraisal
Internal Validity
The baseline demographic and disease characteristics across treatment arms were roughly balanced between the 2 treatment arms. Protocol deviations were reported in approximately 30% to 40% of patients across the 2 treatment arms. Although the overall proportion of protocol deviations was comparable between the 2 treatment arms, the impact on outcome assessments remains. Concomitant anticancer therapies, including all second-, third-, and fourth-line therapies, were higher (roughly 12% in total) in the placebo arm than in the atezolizumab arm, which may have led to biased estimates of treatment effect against atezolizumab.
Response outcomes (ORR and DOR) were assessed by investigators per RECIST 1.1. While the trial was double blinded and the investigators were blinded to treatment assignment, risk of bias cannot be ruled out. For example, nearly half the patients in the atezolizumab arm experienced immune-related AEs or other events. These events may have made the investigator aware of the patient’s treatment assignment. Therefore, for all investigator-assessed outcomes a certain degree of subjectivity may exist, which may have biased the results. In addition, although the proportion of patients receiving concomitant and supportive care for symptom control was largely similar in the 2 treatment arms, which may have led to comparable PROs including QoL outcomes as observed in the trial, this may not mean that the 2 trial regimens truly have comparable safety and impact on QoL.
Interim and final analyses were planned a priori and adequately described. The interim analysis applied Lan-DeMets alpha spending function with the O’Brien-Fleming stopping boundary, which is deemed conservative in controlling type I error when claiming a treatment effect based on interim analysis. The updated final analysis results of OS were consistent with the interim analysis results.
Treatment of atezolizumab continued until disease progression per RECIST 1.1, treatment discontinuation or interruption due to AEs, and early withdrawals; immune-related AEs were particularly disproportional between treatment arms. Patients could be considered for treatment beyond radiographic disease progression if they had evidence of clinical benefit. During the maintenance phase, concomitant treatments including PCI and palliative thoracic radiation were permitted per local standard of care and approved indications. While treatment beyond progression would not affect PFS, it might impact OS estimates. The clinical experts consulted by CADTH noted that the concept of treatment beyond progression for select patients who show evidence of ongoing benefit with treatment has broad acceptance among oncologists in clinical practice; however, the IMpower133 trial was not designed to evaluate the effect of treatment beyond progression.
External Validity
The patient population in the IMpower133 study generally reflects patients in Canadian clinical practice in this setting. However, some patient groups were not represented, including those with an ECOG PS of 2 and patients with active untreated metastases. The clinical experts consulted by CADTH for this review indicated that patients with an ECOG PS of 2 should not be excluded from treatment with combination immunotherapy and chemotherapy, including atezolizumab plus carboplatin and etoposide. The exclusion of these patients from the IMpower133 trial limits the generalizability of clinical evidence with respect to the efficacy and safety of atezolizumab in these groups of patients. The proportion of patients with brain metastases (9%) was lower than that observed in clinical practice (10% to 20%), but this is likely due to the specific inclusion requirements for these patients (e.g., only supratentorial and cerebellar metastases, and no ongoing requirement for corticosteroids as therapy for central nervous system disease). Due to the small number of patients in some subgroups, including brain metastases at baseline, subgroup analyses failed to demonstrate similar effects in patients with brain metastases as in patients free of brain metastases. In addition, the study recruited patients mainly from Asia and Europe; no patients from Canada were recruited. However, the clinical experts consulted by CADTH noted that the lower-than-expected proportion of trial patients with brain metastases and the lack of representation of Canadian patients does not reduce the generalizability of the results to Canadian clinical practice.
The comparator in the IMpower133 trial (carboplatin and etoposide) is relevant to the Canadian context as platinum (carboplatin or cisplatin) and etoposide chemotherapy is the current standard of care. The clinical experts consulted by CADTH noted that in Canadian clinical practice, approximately 70% to 75% of patients with ES-SCLC receive carboplatin and etoposide. Although cisplatin is generally considered more effective, carboplatin is frequently substituted for cisplatin in clinical practice as it reduces the risk of toxicity, including nausea and vomiting, neuropathy, neutropenia, and infection. The clinical experts indicated that although cisplatin was not included in the IMpower133 trial, atezolizumab may be added to cisplatin and etoposide, as well as to carboplatin and etoposide. Thoracic radiation, a treatment used in some patients with ES-SCLC in clinical practice, was not allowed in the trial. The clinical experts noted that while up to 1-quarter of patients with ES-SCLC might have thoracic radiation, including for palliative reasons, the evidence to support the addition of thoracic radiation to systemic therapy in SCLC is inconclusive.33
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The IMpower133 study compared atezolizumab plus carboplatin and etoposide against placebo plus carboplatin and etoposide in patients with ES-SCLC. No direct comparative evidence was submitted that compared atezolizumab plus carboplatin and etoposide with other current standard of care treatments for ES-SCLC in Canada. The clinical experts consulted by CADTH identified carboplatin plus etoposide or cisplatin plus etoposide as standard of care therapies currently funded in Canada. In addition, the clinical experts noted that durvalumab plus etoposide and carboplatin (or cisplatin) was also a suitable comparator, although the combination may not currently be available through public drug plans in all Canadian jurisdictions. The objective of this section is to summarize and critically appraise available indirect evidence comparing atezolizumab plus carboplatin and etoposide against other relevant treatments for ES-SCLC.
In the absence of a head-to-head RCT comparing atezolizumab plus carboplatin and etoposide with a standard of care regimen, the sponsor submitted an ITC in the form of an NMA, which provides comparative evidence of the efficacy of atezolizumab plus carboplatin and etoposide against several comparators.
A supplemental literature search was conducted by CADTH to retrieve published ITCs for atezolizumab. A focused literature search for NMAs including atezolizumab as a treatment option for SCLC was run in MEDLINE All (1946–) on February 18, 2022. No search limits were applied. Nine ITCs were retrieved from the CADTH literature search.
Description of the Sponsor-Submitted NMA
Objectives
The primary objective of the sponsor-submitted NMA was to compare atezolizumab in combination with etoposide plus a platinum-based chemotherapy for the first-line treatment of ES-SCLC against relevant platinum doublet therapies and immunotherapies used in clinical practice.14
Study Selection Methods
The sponsor conducted a systematic review to select studies based on pre-specified PICO criteria, as outlined in Table 22. The systematic review including a feasibility assessment, ||| ||||||||| ||||||||| || |||| || ||||| ||| ||||||| || ||| ||||. The systematic review was restricted to phase II, III, and IV RCTs with active or placebo or best supportive care as controls, with no restriction on blinding, that were conducted in adult patients (≥ 18 years) with histologically or cytologically confirmed ES-SCLC and no prior systemic treatment for ES-SCLC. The sponsor considered different comparators in the systematic review, as presented in Table 22. The primary focus was to retrieve English-language publications or non–English-language publications with an English abstract. A grey literature search was conducted in congress proceedings and other available grey literature sites. Citations were screened by 2 independent analysts, and a second analyst extracted data. Risk of bias assessments of the studies included were conducted based on the 7-criteria checklist by the NICE single technology appraisal user guide.
Table 22: Study Selection Criteria and Methods for Sponsor-Submitted NMA
Item | Criteria |
|---|---|
Population | Adult patients (≥ 18 years) with histologically or cytologically confirmed ES-SCLC with no prior systemic treatment for ES-SCLC (similar to IMpower) |
Intervention | Atezolizumab plus carboplatin and etoposide |
Comparators | Cisplatin plus etoposide Carboplatin plus irinotecan Carboplatin plus paclitaxel Best supportive care Cancer immunotherapies:a
|
Outcomes | Efficacy:
Safety:
HRQoL:
|
Study design | Prospective RCTs (phase II to IV) with active or placebo or best supportive care controls with no restriction on blinding |
Publication characteristics | No restrictions for publication date or territory of interest; primary focus on English-language publications or non–English-language publications with an English abstract |
Exclusion criteria |
|
Databases searched | MEDLINE, MEDLINE Epub Ahead of Print (in-process and other non-indexed citations), Embase, and the Cochrane Library were interrogated on July 1, 2018. Additional searches of congress proceedings from the past 3 years (American Society of Clinical Oncology, European Society for Medical Oncology, American Association for Cancer Research); reference lists of included publications, Health Technology Assessment bodies, and the International Clinical Trials Registry Platform; and reference lists of eligible clinical studies or tagged systematic reviews and meta-analysis publications. An update to the original search (electronic database and congress proceedings) was conducted on May 8, 2020. |
Selection process | Citations were screened by 2 independent analysts; a second analyst checked and extracted data. |
Data extraction process | Records were reviewed based on title and abstract in the first instance, and those included were reviewed based on the full publication. A single reviewer extracted data, and all data inputs were independently checked against the source document by a second analyst. |
Quality assessment | Quality (risk of bias) assessment of RCTs was conducted using the 7-criteria checklist provided by the National Institute for Health and Care Excellence single technology appraisal user guide. |
ES-SCLC = extensive-stage small cell lung cancer; HRQoL = health-related quality of life; NMA = network meta-analysis; RCT = randomized controlled trial.
aThe immunotherapies were not considered interventions of interest for the original search. However, relevant search terms were included in the systematic review update search strategy (without a related date restriction).
Source: Sponsor-submitted NMA.14
The sponsor-submitted systematic review and feasibility assessment14 included a best-case evidence network (irrespective of inter-trial heterogeneity or reported outcomes) that considered platinum-based combination chemotherapy regimens and immunotherapy treatments. As the comparator arms of the 3 immunotherapy trials (the CASPIAN, ECOG-ACRIN EA5161, and KEYNOTE-604 trials) included etoposide administered in combination with cisplatin or carboplatin, a grouped node was required for inclusion of these trials in the network, irrespective of which chemotherapy was administered. The Skarlos 1994 and Okamoto 2007 trials, which compared etoposide plus carboplatin against etoposide plus cisplatin, were also kept in the best-case scenario network. In the feasibility assessment, outcome-specific evidence networks were explored for all primary and secondary outcomes of the IMpower133 trial. Connected networks were obtained for OS, PFS, ORR, and incidence of SAEs. However, an NMA was found not to be feasible for DOR, time in response, time to deterioration, and incidence of grade 3 to 5 AEs or treatment-related SAEs.
ITC Analysis Methods
Table 23 presents the ITC methods used in the sponsor-submitted NMA.14
Table 23: Sponsor-Submitted ITC Analysis Methods
ITC characteristics | Description |
|---|---|
ITC methods | A Bayesian approach with binomial likelihood was used to conduct the NMA. The MCMC method with 2 chains was used to estimate the relative treatment effects. Both FE and RE models were explored in the base-case analysis. The main results presented are based on the fixed-effect model. A GLM with a binomial likelihood, logit link model was constructed. The model assumes that all patients who report an outcome do so by a specific follow-up time and that further follow-up would make no difference to the relative treatment effect. For the multi-arm studies included in the network, correlations were incorporated using a multi-arm correction, and the δijk are assumed to come from a multivariate normal distribution with co-variances of δ2/2. |
Priors | Vague priors were used for the treatment effect sizes relative to treatment 1 (d1k) in the form of a normal distribution with d12~Normal (0,1002) (by Dias 2011). In the RE models explored, uniformly distributed prior distributions between 0 and 2 were used. Uniformly distributed priors between 0 and 5, as described by Dias 2011, were used. |
Assessment of model fit | The deviance information criterion was used to assess the model fit between the FE and RE models constructed. |
Assessment of consistency | The multi-arm study (CASPIAN) formed a loop in the network structure. Thus, no inconsistency was reported since it is not possible for the multi-arm study to be inconsistent with itself (there can therefore be no inconsistency within a multi‐arm trial). Heterogeneity was assessed by conducting subgroup analyses given the small number of studies included in the NMA. The sponsor conducted scenario analyses by removing some studies in the base-case analyses. Meta-regression could not be done because of the sparsity of the network. |
Assessment of convergence | Convergence for all models was assessed by analyzing history and density plots and Brooks-Gelman-Rubin diagnostic plots. Autocorrelation plots were also assessed to detect the presence of autocorrelation in the chains. Following the model convergence, inferences were made from data obtained by sampling for a further 20,000 iterations. |
Outcomes | Connected networks were available for OS, PFS, ORR, and the incidence of SAEs. PFS: 6 months, 1 year. OS: 6 months, 1 year, 2 years. |
Follow-up time points | Reported for specific outcomes (variable, depending on included trial):
|
Construction of nodes | Interventions were connected to the network diagram via etoposide plus cisplatin or carboplatin. The sponsor included a grouped node for 3 trials (CASPIAN, ECOG-ACRIN EAS161, and KEYNOTE-604) within the network that investigated immunotherapy treatments and etoposide administered in combination with cisplatin or carboplatin, which required an assumption of equivalence of carboplatin and cisplatin. The sponsor included 2 trials (Skarlos 1994 and Okamoto 2007) to the network even though they did not provide relevant data to the network. According to the sponsor, these trials were important for the conduct of subgroup analysis. |
Sensitivity analyses | Conducted by removing some studies from the network for some outcomes. |
Subgroup analysis | Subgroup analysis was conducted for trials investigating etoposide plus carboplatin only (i.e., aligned with IMpower133) (i.e., exploring the robustness of the assumption of equivalent efficacy of etoposide plus cisplatin vs. etoposide plus carboplatin). |
Methods for pairwise meta-analysis | NMA results were presented as median hazard ratios and associated 95% credible intervals, or median odds ratios and associated 95% credible intervals for time-to-event outcomes and binary outcomes, respectively. |
FE = fixed effect; GLM = generalized linear model; ITC = indirect treatment comparison; MCMC = Markov chain Monte Carlo; NMA = network meta-analysis; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RE = random effect; SAE = serious adverse event.
Source: Sponsor-submitted NMA.14
The sponsor-submitted NMA methodology used a Bayesian approach. Both FE and RE models were explored in the base-case scenarios to fit the model. All findings presented by the sponsor were based on the FE model, which assumes homogeneity of the underlying true treatment effects. The sponsor noted that the FE model gave a better fit to the data in terms of residual deviance (closer to the number of data points) in all base-case analyses than the RE model did. The sponsor highlighted that the results of the RE model were associated with high levels of uncertainty due to insufficient power in the analyses to accurately estimate between-study SD and that the relative treatment effects of treatment comparisons were not aligned with the trial-level estimates. Vague priors with a mean of 1 and variance of 100,2 as recommended by Dias (2011), were used to estimate the treatment effect sizes. The RE model constructed stated that uniformly distributed prior distributions, which ran between 0 and 5 as recommended by Dias 2011, should be used.
The sponsor included 1 3-armed trial (CASPIAN) in the network analyses of OS and PFS. Adjustments were made to account for the potential likelihood of correlation between treatments in trial-level data. According to the sponsor, the variance of the log-hazard for the baseline treatments in the 3-armed trial was unknown, and approximations were made based on the variances of the differences using methods described by Woods (2010).
Markov chain Monte Carlo simulations with 2 chains starting from different initial values of selected unknown parameters were used to construct the models in estimating the relative treatment effects. The binomial likelihood, logit link model was considered appropriate for the NMA by the sponsor. Model convergence for each model constructed was assessed by analyzing history and density plots and Brooks-Gelman-Rubin diagnostic plots. In addition, autocorrelation plots were assessed to detect the presence of autocorrelation in the chains. Following the model convergence, inferences were made from data obtained by sampling 20,000 iterations.
Heterogeneity was assessed across the trials included in the sponsor-submitted network by conducting subgroup analyses for selected outcomes. There were insufficient studies in the sponsor’s network to conduct a meta-regression. Scenario analyses were conducted for OS (with the removal of the Hermes 2008 trial from the base-case analysis) as the sponsor considered some studies as potential outliers due to differences in ECOG PS in the patients recruited.
The transitivity assumption was assessed by evaluating the effect of potential treatment effect modifiers across studies that may impact the ITC results. All trials reported a median age of patients ranging from 60 years to 74 years, with an overall median of 65 years across the trials. The Okamoto 2007 trial was conducted in an elderly, high-risk population and included patients with ages ranging from 55 years to 86 years (92% of patients were ≥ 70 years). In total, 54% of patients enrolled in the IMpower133 trial were younger than 65 years. Most patients recruited across the trials included in the sponsor’s network were male (mean = 68%; range = 44% to 91%). Baseline data on ethnicity were only available in the IMpower133 and CASPIAN trials, and the majority of patients were White or Asian. Variability was observed across and within trial arms for gender. Across the trials included in the network, the proportion of patients with an ECOG PS of 0 to 1 ranged from 52% to 100%, with a mean of 85%. In 3 studies that permitted the enrolment of patients with ECOG PS greater than 1 (Okamoto 2007, Hermes 2008, and Skarlos 1994), the majority of patients were classified as having an ECOG PS of 2, with only a small proportion reported as having an ECOG PS of 3. The sponsor observed variability in ECOG PS across and within trials investigating non-immunotherapy regimens. There were inconsistencies in the reporting of the number and type of metastatic sites across trials in the network, and the most common were brain and liver metastases. IMpower133 included a smaller proportion of patients with brain or liver metastases than the other trials in the network. According to the clinical experts consulted, it is not anticipated that smoking status will be a contributing effect modifier given that smoking is an established risk factor associated with SCLC.
Intervention nodes were connected to the network diagram through etoposide plus cisplatin or carboplatin. The sponsor included a grouped node within the network for 3 trials (CASPIAN, ECOG-ACRIN EAS161, and KEYNOTE-604) that required an assumption of equivalence of carboplatin and cisplatin.
Sensitivity analyses were conducted for the outcomes investigated. Analyses using the unadjusted HRs were conducted by the sponsor given that both adjusted (or stratified) and unadjusted (or unstratified) HRs were reported for some trials. The removal of Okamoto 2007 was suggested as a scenario for sensitivity analysis as the trial was considered a potential outlier.
The risk of bias was generally considered low or unclear across the studies for the remaining elements of bias assessment. The studies appeared sufficiently homogenous to combine in analyses.
Treatments
Indirect comparisons for atezolizumab plus carboplatin and etoposide were performed for the following interventions: irinotecan plus carboplatin, etoposide plus carboplatin, etoposide plus cisplatin, durvalumab plus etoposide and carboplatin (or cisplatin), durvalumab plus tremelimumab plus etoposide and carboplatin (or cisplatin), and nivolumab plus etoposide and carboplatin (or cisplatin).
Only comparisons between atezolizumab plus carboplatin and etoposide versus etoposide plus carboplatin, etoposide plus cisplatin, durvalumab plus etoposide and carboplatin (or cisplatin) were considered for this CADTH review.
End Points
The sponsor created several outcome-specific networks for OS, PFS, ORR, and SAEs.
Results of Sponsor-Submitted NMA
Summary of Included Studies
Ninety-one publications were identified by the sponsor, and a feasibility assessment was conducted to determine a best-case evidence network. Eight trials (IMpower133,11 Hermes 2008,34 Schmittel 2011,35 CASPIAN,25 KEYNOTE-604,26 Skarlos 1994,36 Okamoto 2007,37 and ECOG-ACRIN EA516138) formed a connected network. There were notable differences observed in the treatment pathway between IMpower133 and the “non-immunotherapy” trials of the best-case network (Skarlos 1994, Okamoto 2007, Hermes 2008, and Schmittel 2011). The CASPIAN, KEYNOTE-604, and ECOG-ACRIN EA5161 trials had a similar design to the IMpower133 trial in that randomized induction therapy was followed by maintenance therapy with placebo or immunotherapy.
Etoposide plus carboplatin or cisplatin was consistent as a comparator across the trials included in the network. Dosing regimens differed across some trials.
In 3 trials (CASPIAN, Schmittel 2011, and Skarlos 1994), dosing of etoposide plus carboplatin or cisplatin was performed for up to 6 cycles, and in 5 trials (including the ECOG-ACRIN EA5161 and KEYNOTE-604 trials, Hermes 2008, and Okamoto 2007) dosing of the comparator was for up to 4 cycles. The primary outcome was stated for all trials except Skarlos 1994. Table 24 summarizes the assessment of homogeneity within the sponsor-submitted NMA.
A summary of study design and patient baseline characteristics of the included trials is presented in Appendix 4. Of the 8 studies included in the sponsor’s network, 7 included patients 18 years and older with ES-SCLC. In Skarlos 1994, the authors recruited previously untreated SCLC patients, and a subgroup with ES-SCLC was available, which provided data for the analyses. All trials reported a median age of patients ranging from 60 years to 74 years, with an overall median of 65 years across the trials. The proportion of patients with an ECOG PS of 0 to 1 ranged from 52% to 100%, with a mean of 85% across the 8 trials included.
Table 24: Assessment of Homogeneity for Sponsor-Submitted NMA
Potential effect modifiers | Description and handling of potential effect modifiers |
|---|---|
Disease severity: risk status | In Okamoto 2007, the patients recruited were considered high-risk populations. The proportion of patients that had never smoked was reported across 4 trials. More than 91% of patients had a history of smoking. |
Disease severity: metastatic sites | The number of metastatic sites was inconsistent across studies; the most common sites were brain and liver. Fewer patients in the IMpower133 trial had brain or liver metastases than in other trials in the network. |
Disease severity: ECOG PS | Inconsistency was observed across and within trials included in the network. Hermes 2008 enrolled less than 53% of patients with an ECOG PS of 0 or 1 in both treatment arms; this enrolment was 100% in CASPIAN (performance status reported using WHO criteria), ECOG-ACRIN EA5161, IMpower133, and KEYNOTE-604. Okamoto 2007 included patients with an ECOG PS of 0 to 2 if they were 70 years or older and with an ECOG PS of 3 if they were younger than 70 years. |
Treatment history | All trials randomized patients before first-line therapy for ES-SCLC (except Skarlos 1994). Notable differences were observed in the treatment pathway between IMpower133 and the “non-immunotherapy” trials of the best-case network (Skarlos 1994, Okamoto 2007, Hermes 2008, and Schmittel 2011). All non-immunotherapy studies randomized patients to combination chemotherapy regimens for up to 4 to 6 cycles. Radiotherapy was permitted for stable disease, but maintenance therapy or second-line treatment was not allowed (in line with standard treatment for ES-SCLC: platinum-based chemotherapy administered for 4 to 6 cycles followed by active surveillance). In Okamoto 2007 and Hermes 2008, chemotherapy was allowed at relapse at physician discretion. Off-protocol second- and third-line treatment was reported in Hermes 2008, Okamoto 2007, and Schmittel 2011. IMpower133 also randomized patients to induction chemotherapy (in addition to placebo or atezolizumab) for up to 4 cycles. CASPIAN, KEYNOTE-604, and ECOG-ACRIN EA5161 had a similar design to IMpower133 in that randomized induction therapy was followed by maintenance therapy with placebo or immunotherapy. |
Clinical trial eligibility criteria | All trials involved adult patients with previously untreated ES-SCLC, except for Skarlos 1994, which enrolled 147 patients with SCLC and reported data for ES-SCLC as a subgroup (61 patients with ES-SCLC [30 and 31 patients in each arm]). The 7 trials that were conducted exclusively in ES-SCLC patients (IMpower133, Schmittel 2011, Okamoto 2007, Hermes 2008, KEYNOTE-604, ECOG-ACRIN EA5161, and CASPIAN) enrolled at least 160 patients. |
Dosing of comparators | Etoposide plus carboplatin or cisplatin as a comparator was consistent across the trials included in the network. Dosing regimens were reported. In 3 trials (CASPIAN, Schmittel 2011, and Skarlos 1994), dosing of etoposide plus carboplatin or cisplatin was up to 6 cycles. In 5 trials (including the ECOG-ACRIN EA5161 and KEYNOTE-604 trials, Hermes 2008, and Okamoto 2007), dosing of the comparator was for 4 cycles. |
Definitions of end points | The primary outcome was explicitly stated for all trials except Skarlos 1994. OS was consistent in 7 trials. CASPIAN: OS, PFS, ORR, AEs KEYNOTE-604: PFS, OS, ORR ECOG-ACRIN EA5161: PFS, OS, ORR IMpower133: Co-primary end point of PFS and OS, ORR, AEs Hermes 2008: OS Okamoto 2007: OS, PFS Schmittel 2011: PFS, ORR, OS Skarlos 1994: ORR |
Timing of end point evaluation or trial duration | Not reported |
Withdrawal frequency | Not reported |
Clinical trial setting | All the trials of the network were multi-centre (Europe, Asia, North America, and South America), and 4 of the trials were conducted in single territories. Hermes 2008 was conducted only in Norway and Sweden. CASPIAN, IMpower133, and KEYNOTE-604 were conducted internationally. |
Study design | All trials of the network were phase II or III, except 1 where the sponsor could not ascertain the phase. Three studies were double blinded (IMpower133 trial, CASPIAN, and KEYNOTE-604). Three were open label (Schmittel 2001, Hermes 2008, and ECOG-ACRIN EA5161). Two had unclear blinding status (Skarlos 1994 and Okamoto 2007). |
AE = adverse event; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ES-SCLC = extensive-stage small cell lung cancer; NMA = network meta-analysis; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Source: Sponsor-submitted NMA.14
Results
Only results of the FE model are presented in this section.
Progression-Free Survival
The sponsor conducted 3 scenario analyses: a base-case scenario (which included adjusted or stratified HRs reported across the trials); scenario 1 (which included the unadjusted or unstratified HRs reported); and scenario 2 (which consisted of an analysis where etoposide plus cisplatin, and etoposide plus carboplatin, were considered as distinct nodes).
Of the 8 trials selected, PFS data were available in 5 (CASPIAN, ECOG-ACRIN EA5161, KEYNOTE-604, Schmittel 2011, and IMpower133); these data were used to inform the base-case and scenario 1 network structure. Figure 7 presents the overall network diagram for the base case and scenario 1.
In the base-case and scenario analyses, atezolizumab plus carboplatin and etoposide was associated with longer PFS than carboplatin or cisplatin plus etoposide, and the comparisons were considered to be statistically meaningful as the 95% CrIs excluded the null value (refer to Table 25).
In the base-case and scenario analyses of the comparison of PFS for atezolizumab plus carboplatin and etoposide against durvalumab plus carboplatin (or cisplatin) and etoposide, no statistically significant difference was observed based on the CrI intervals, which included the null value, and the point estimates were close to null.

Confidential figure redacted at the request of the sponsor.
Source: Sponsor-submitted network meta-analysis.14
Table 25: Progression-Free Survival NMA Results for the Comparison of Atezolizumab Plus Carboplatin and Etoposide Versus Relevant Comparators — FE Model
Scenario | Atezolizumab plus carboplatin and etoposide vs. comparator | |
|---|---|---|
Etoposide plus carboplatin or cisplatin (carboplatin for scenario 2) HR (95% CrI) | Durvalumab plus carboplatin (or cisplatin) and etoposide HR (95% CrI) | |
Base casea | |||| ||||| || ||||| | |||| ||||| || ||||| |
Scenario 1b (unadjusted or unstratified HRs) | |||| ||||| || ||||| | |||| ||||| || ||||| |
Scenario 2c (choice of platinum agents considered as distinct nodes) | |||| ||||| || ||||| | |||||| |
CrI = credible interval; FE = fixed effect; HR = hazard ratio; NA = not applicable; NMA = network meta-analysis; PFS = progression-free survival.
Note: The 95% CrIs for atezolizumab plus carboplatin and etoposide against carboplatin (or cisplatin) and etoposide plus durvalumab included the null value.
aBase case: ||| |||||||| |||||||| |||| ||| ||||| ||| |||| || |||||||||| |||| ||| |||| |||||||
bScenario 1: ||| |||||||| |||||||| |||| ||| ||||| ||| |||| || |||||||||| |||| ||| |||| |||||||
cScenario 2: ||| |||||||| |||||||| |||| ||| ||||| ||| |||| || |||||||||| |||| ||||| |||| ||||||
Source: Sponsor-submitted NMA.14
Overall Survival
Seven studies (the CASPIAN, ECOG-ACRIN EA5161, KEYNOTE-604, and Impower133 trials; Hermes 2008; Okamoto 2007; and Schmittel 2011) were used to inform the network for OS. Four scenario analyses were conducted: a base case (adjusted or stratified HRs), scenario 1 (unadjusted or unstratified HRs), scenario 2 (Hermes 2008 trial excluded), and scenario 3 (etoposide plus cisplatin, and etoposide plus carboplatin, considered as distinct nodes). The evidence network for the base-case scenario is presented in Figure 8, and Table 26 presents the summary of the NMA results (HRs with their corresponding 95% CrIs) for the comparison of atezolizumab plus etoposide and carboplatin versus comparators from each scenario.
In all scenarios assessed, atezolizumab plus carboplatin and etoposide was favoured in terms of OS when compared with etoposide plus carboplatin or cisplatin (|||| ||||| ||| |||| |||| ||||| |||| || ||||); |||||||| || ||||||| |||| |||| |||| || ||||| and the 95% CrIs excluded the null value (refer to Table 26). The HRs presented in the base-case and scenario analyses of atezolizumab plus carboplatin and etoposide against durvalumab plus carboplatin (or cisplatin) and etoposide (|||| |||| ||||||||| ||||||| |||| |||| |||| || ||||) showed no statistically significant difference between the 2 combinations based on the CrI which included the null value, and the point estimates were close to the null.

Confidential figure redacted at the request of the sponsor.
Source: Sponsor-submitted network meta-analysis.14
Table 26: Overall Survival NMA Results for the Comparison of Atezolizumab Plus Carboplatin and Etoposide Versus Relevant Comparators – FE Model
Scenario | Atezolizumab plus carboplatin and etoposide vs. comparator | ||
|---|---|---|---|
Etoposide plus cisplatin HR (95% CrI) | Etoposide plus carboplatin or cisplatin (carboplatin for scenario 3) HR (95% CrI) | Durvalumab plus carboplatin (or cisplatin) and etoposide HR (95% CrI) | |
Base case | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| |
Scenario 1a (unadjusted or unstratified HRs) | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| |
Scenario 2b (exclusion of Hermes 2008) | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| |
Scenario 3c (choice of platinum agents considered as distinct nodes) | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| |
CrI = credible interval; FE = fixed effect; HR = hazard ratio; NMA = network meta-analysis.
Note: The 95% CrIs for comparison of atezolizumab plus carboplatin and cisplatin against etoposide plus cisplatin and etoposide and carboplatin (or cisplatin) plus durvalumab include the null value.
aScenario 1: ||| |||||||| |||||||| |||| ||| ||||| ||| |||| || |||||||||| |||| ||||| |||| |||||||
bScenario 2: ||| |||||||| |||||||| |||| ||| ||||| ||| |||| || |||||||||| |||| ||||| |||| ||||||
cScenario 3: ||| |||||||| |||||||| |||| ||| ||||| ||| |||| || |||||||||| |||| ||||| |||| ||||||
Source: Sponsor-submitted NMA.14
Objective Response Rate
Eight studies (the CASPIAN, ECOG-ACRIN EA5161, KEYNOTE-604, Okamoto 2007, Schmittel 2011, Hermes 2008, Skarlos 1994, and IMpower133 trials) were used to inform the network for ORR. The residual deviance from the model was 14.88, in comparison with 15 data points. Figure 9 presents the evidence network for ORR. The results of the analysis of ORR are presented in Table 27.
The OR reported for the comparison of atezolizumab plus carboplatin and etoposide against etoposide plus carboplatin or cisplatin was |||| |||| |||| |||| || ||||, and the OR for the comparison of the atezolizumab combination against etoposide plus cisplatin was |||| |||| |||| |||| || ||||. The comparison of atezolizumab plus carboplatin and etoposide against durvalumab plus carboplatin (or cisplatin) and etoposide was associated with a lower ORR (|||||||| ||| |||| |||| || ||||), which indicated that the atezolizumab combination may be associated with a statistically meaningful improvement in ORR as the 95% CrI did not include the null value, although the CrI was wide.

Confidential figure redacted at the request of the sponsor.
Source: Sponsor-submitted network meta-analysis.14
Table 27: Objective Response Rate NMA Results for the Comparison of Atezolizumab Plus Carboplatin and Etoposide Versus Relevant Comparators — FE Model
Treatment | Etoposide plus cisplatin OR (95% CrI) | Etoposide plus carboplatin or cisplatin OR (95% CrI) | Durvalumab plus carboplatin (or cisplatin) and etoposide OR (95% CrI) |
|---|---|---|---|
Atezolizumab plus carboplatin and etoposide | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| |
CrI = credible interval; FE = fixed effect; NMA = network meta-analysis; OR = odds ratio.
Note: The ORs (95% CrIs) are presented for treatment A (row) vs. treatment B (column).
Source: Sponsor-submitted NMA.14
Serious Adverse Events
Data from 2 studies (CASPIAN and IMpower133) were used to populate the SAE network.
Figure 10 provides the evidence network for SAEs, and Table 28 provides the ORs and corresponding 95% CrIs for the analysis. The OR was estimated to be |||| |||| |||| |||| || ||||| for the comparison between atezolizumab plus carboplatin and etoposide against durvalumab plus carboplatin (or cisplatin) and etoposide, and |||| |||| |||| |||| || ||||| for the comparison of the atezolizumab combination against etoposide plus cisplatin. The CrIs for both comparisons included the null value.

Confidential figure redacted at the request of the sponsor.
Source: Sponsor-submitted network meta-analysis.14
Table 28: Serious Adverse Event NMA Results for the Comparison of Atezolizumab Plus Carboplatin and Etoposide Versus Relevant Comparators — FE Model
Treatment | Etoposide plus cisplatin OR (95% CrI) | Durvalumab plus carboplatin (or cisplatin) and etoposide OR (95% CrI) |
|---|---|---|
Atezolizumab plus carboplatin and etoposide | |||| ||||| || ||||| | |||| ||||| || ||||| |
CrI = credible interval; FE = fixed effect; NMA = network meta-analysis; OR = odds ratio.
Note: The ORs (95% CrIs) are presented for treatment A (row) vs. treatment B (column).
Source: Sponsor-submitted NMA.14
Critical Appraisal of Sponsor-Submitted NMA
The sponsor’s systematic review methods for identifying and assessing studies included in the network were considered appropriate for identifying relevant studies. The PICO criteria were pre-specified, and articles were reviewed by 2 independent reviewers, while a second analyst extracted data. All relevant comparators identified in the CADTH review protocol that were considered relevant to the Canadian practice context were presented in the sponsor’s NMA. The outcomes presented in the trials included in the network analysis were considered relevant and clinically meaningful by the clinician experts consulted during the CADTH review. The population studied in all 8 trials was considered relevant for the reimbursement request. Most studies included untreated patients with ES-SCLC. One study (Skarlos 1994) recruited a different population in the trial but had a subgroup of patients with ES-SCLC. Information from the subgroup analysis was used to inform the network. Quality assessments were conducted using the validated 7-criteria checklist provided by the NICE single technology appraisal user guide.
A generalized linear regression model with a binomial likelihood, logit link model was used; the model was considered appropriate for the types of outcomes assessed in the network. The sponsor explored both FE and RE models in its base-case scenarios, and results from the FE model were presented. The sponsor provided a justified rationale for using the FE model over the RE model based on the model fit criteria, including a judgment on the similarities of the studies included in terms of effect modifiers.
The transitivity assumption was assessed by evaluating potential effect modifiers. There was considerable heterogeneity across trials, particularly in terms of ECOG PS. The Hermes 2008 trial enrolled less than 53% of patients with an ECOG PS of 0 or 1 in both treatment arms versus 100% in the CASPIAN, ECOG-ACRIN EA5161, IMpower133, and KEYNOTE-604 trials. In the Okamoto 2007 trial, in those aged 70 years and older, patients with an ECOG PS of 0 to 2 were included, whereas those with an ECOG PS of 3 were included if they were younger than 70 years of age. There was inconsistency in the reporting of the number and type of metastatic sites across the trials. Heterogeneity in the use of subsequent anticancer therapy administered to patients in the second line and higher recruited in the studies was identified as a potential source of bias affecting OS assessment (non-protocol second- and third-line treatment was reported in the Hermes 2008, Okamoto 2007, and Schmittel 2011 trials) and as potentially affecting the generalizability of the findings of the NMA to the Canadian setting. Variability was also observed in the dosing of etoposide plus carboplatin or cisplatin across the trials (3 studies — CASPIAN, Schmittel 2011, and Skarlos 1994 — randomized patients to combination chemotherapy regimens for up to 4 to 6 cycles, while in the IMpower133 trial [including ECOG-ACRIN EA5161, KEYNOTE-604, Hermes 2008, and Okamoto 2007], patients were dosed with the comparator for up to 4 cycles), and this may impact the findings of the ITC.
According to the sponsor’s ITC report, a meta-regression analysis was not possible to investigate inter-trial heterogeneity due to insufficient studies (i.e., the presence of several single study connections between interventions). Scenario analyses related to certain characteristics of interest were included in the sponsor’s NMA report to address heterogeneity across the trials included in the network (e.g., removal of the Hermes 2008 trial, which was an outlier due to having the smallest proportion of patients with ECOG PS < 2, from the OS base-case analysis). According to the clinical expert consulted, ECOG PS and metastatic sites (liver and brain) were the most significant effect modifiers in the treatment of ES-SCLC patients. The sponsor acknowledged that additional scenario or subgroup analyses were feasible for PFS and OS; however, because relevant subgroup data are not currently available from the trials of the evidence networks investigating immunotherapies (i.e., CASPIAN, ECOG-ACRIN EA5161, and KEYNOTE-6040 ongoing trials), not all possible subgroup analyses were included in the sponsor’s report. Therefore, the NMA results should be interpreted with caution due to limitations that may arise from between-study differences in some covariates and lack of sufficient evidence to minimize heterogeneity and inconsistency (e.g., a meta-regression analysis).
Description of Published Indirect Comparisons
Nine ITCs were retrieved from literature that assessed other treatment options in patients ES-SCLC.
Objectives
The objectives of the 9 ITCs retrieved from the CADTH literature search are outlined in Table 34 and Table 35.
Study Selection Methods
Table 34 and Table 35 in Appendix 3 present the study selection methods applied by the published ITCs to select studies for their network. All 9 studies included untreated patients with ES-SCLC, although 1 study (Gristina et al. [2021]) focused on patients with advanced or unresectable ES-SCLC with stage IVA or IVB disease. Chemotherapy (platinum-based agents) plus etoposide was the common comparator identified across the published ITCs. Eight studies in total presented data on OS, PFS, and AEs as the outcomes investigated. One study (Chen et al. [2017]) investigated AEs as the main outcome.
All 9 ITCs performed literature searches in electronic databases, some of which included PubMed and other grey literature websites. Most studies limited their search to English-language publications, and 3 studies reportedly had no language restrictions. Most studies had their literature search conducted independently by 2 reviewers and further validated by a third author. Most studies (8 in total) conducted risk of bias analysis across the studies included in the network using the Cochrane risk of bias tool; 1 study used the CONSORT checklist to assess bias.
Methods of Published Indirect Comparisons
ITC Analysis Methods
Table 36 and Table 37 in Appendix 4 provide a summary of the ITC methods used in the published ITCs.
Of the 9 published ITCs assessed in the CADTH review, 4 (Ando et al. [2021]39; Kang et al. [2021]40; Gristina et al. [2021]41; Zhou et al. [2020]42) used Bayesian methods to conduct the NMA, 3 (Chen et al. [2021]43; Chen HL et al. [2020]44; Wang et al. [2020]45) reported a frequentist approach, and the rest did not specify clearly the NMA methods used in the ITC. None of the studies reported the priors used in conducting the NMA. Only 1 study (Kang et al. [2021]40) reported information on the assessment of model fit. Consistency assessments were reported for some studies, most of which used the I2 statistics to assess heterogeneity between the trials included in the network. In other studies, consistency could not be assessed due to the absence of closed loops. Only 1 study (Ando et al. [2021]39) reported how convergence was assessed in the NMA. Three studies (Chen HL et al. [2020]44; Ando et al. [2021]39; Gristina et al. [2020]41) included subgroup analyses. In 4 studies (Chen et al. [2020]46; Zhou et al. [2020]42; Chen et al. [2017]47; Kang et al. [2021]40), the authors reported reasons why subgroup analyses could not be conducted. Only 3 studies (Ando et al. [2021]39; Chen et al. [2017]47; Kang et al. [2021]40) had conducted sensitivity analyses.
Results of Published Indirect Comparisons
Summary of Included Studies
The KEYNOTE-604, CASPIAN, IMpower133, and EA5161 trials were common studies included in the network structures across the 9 published ITCs assessed (refer to Table 34 and Table 35). These studies were also included in the sponsor-submitted NMA. In the ITC by Chen et al. (2020), the network geometry included 46 trials compared to the other ITCs retrieved and the sponsor-submitted NMA. The lowest number of studies included in the ITCs was observed in Wang et al. (2020) (4 studies). Given that most ITCs included studies that were also in the sponsor’s ITC, the baseline characteristics of those studies are also presented in Appendix 4.
Efficacy Outcomes
Progression-Free Survival
In Ando et al. (2021),39 the authors concluded that PFS was statistically different between the atezolizumab plus etoposide and platinum (HR = 0.71; 95% CrI, 0.53 to 0.93) and the durvalumab platinum-based chemotherapy plus etoposide (HR = 0.72; 95% CrI, 0.55 to 0.91) groups, respectively, compared to platinum plus irinotecan, as the CrIs for these comparisons excluded the null value.
The ITC by Chen et al. (2021)43 observed no statistically significant differences in PFS in the indirect comparison between atezolizumab and durvalumab (HR = 0.96; 95% CI, 0.72 to 1.29).
In the ITC by Gristina et al. (2021),41 the pooled results did not suggest a difference in terms of PFS (HR = 1.21; 95% CI, 0.98 to 1.49) between the anti-PD-1 class of therapies and chemotherapy.
The ITC by Chen et al. (2020)46 suggested that atezolizumab plus carboplatin and etoposide may be associated with an improvement in PFS compared with the common comparator carboplatin plus etoposide, considering the CIs that did not include the null value (HR = 0.77; 95% CI, 0.60 to 0.99).
Similarly, the ITC by Chen HL et al. (2020)44 showed an improvement in PFS with atezolizumab plus chemotherapy (HR = 0.77; 95% CI, 0.61 to 0.96) when compared with chemotherapy alone. No superior effects were observed in this ITC for the pairwise comparisons between the different ICIs.
In Wang et al. (2020),45 the pooled HR estimates showed that immunotherapy (including ipilimumab, atezolizumab, and durvalumab) plus chemotherapy significantly improved PFS (HR = 0.81; 95% CI, 0.74 to 0.88;) when compared against placebo plus chemotherapy.
In the ITC by Zhou et al. (2020),42 the addition of PD-L1 inhibitors (durvalumab and atezolizumab) to etoposide plus platinum chemotherapy resulted in an HR of 1.29 (95% CI, 0.96 to 1.75) for PFS, compared with etoposide plus platinum chemotherapy alone.
Overall Survival
In the ITC by Ando et al. (2021),39 the OS in the groups treated with atezolizumab plus etoposide and platinum-based chemotherapy, durvalumab plus etoposide and platinum-based chemotherapy, or pembrolizumab plus etoposide and platinum-based chemotherapy was found to be significantly higher than that in groups treated with etoposide plus platinum, with HRs of 0.71 (95% CrI, 0.54 to 0.91), 0.73 (95% CrI, 0.59 to 0.91), and 0.81 (95% CrI, 0.65 to 0.99), respectively. The OS of groups treated with atezolizumab plus etoposide and platinum-based chemotherapy or durvalumab plus etoposide and platinum-based chemotherapy was significantly higher than that of groups treated with platinum-amrubicin, with HRs of 0.73 (95% CrI, 0.52 to 0.99) and 0.757 (95% CrI, 0.56 to 0.99), respectively. No significant differences in OS were observed between each pair of 3 ICIs plus etoposide and platinum.
In the ITC by Chen et al. (2021),43 no significant difference in OS was observed in the indirect comparison between atezolizumab and durvalumab (HR = 0.93; 95% CI, 0.67 to 1.30).
The ITC by Gristina et al. (2021)41 reported an HR of 1.22 (95% CI, 0.97 to 1.53) for treatments in the anti-PD-1 class against chemotherapy.
In the ITC by Chen et al. (2020),46 findings in the comparison groups of atezolizumab plus platinum-based chemotherapy and etoposide (HR = 0.70; 95% CI, 0.52 to 0.94) versus platinum and etoposide plus durvalumab (HR = 0.73; 95% CI, 0.57 to 0.94) suggested improved OS for the atezolizumab combination.
The ITC by Chen HL et al. (2020)44 suggested an improvement in OS in the atezolizumab plus chemotherapy group (HR = 0.70; 95% CI, 0.54 to 0.91) compared with chemotherapy alone.
In the ITC by Wang et al. (2020),45 the pooled HR estimates suggested that immunotherapy (including ipilimumab, atezolizumab, and durvalumab) plus chemotherapy may improve the survival outcomes in terms of OS (HR = 0.84; 95% CI, 0.75 to 0.93) in comparison with chemotherapy plus placebo.
In the ITC by Zhou et al. (2020),42 the HR for OS was reported to be 1.40 (95% CI, 1.09 to 1.80) with the addition of PD-L1 inhibitors (durvalumab and atezolizumab) to etoposide-platinum chemotherapy compared with etoposide-platinum chemotherapy alone.
Objective Response Rate
In the ITC by Chen et al. (2021),43 the OR observed for ORR in the comparison of durvalumab versus atezolizumab (monotherapy) was 0.79 (95% CI, 0.64 to 0.98).
In the ITC by Chen HL et al. (2020),44 the authors observed no significant difference between any comparable ICIs except for durvalumab, which produced a noticeable benefit over atezolizumab.
In Wang et al. (2020),45 the pooled risk ratios for ORR in direct comparisons were 1.04 (95% CI, 0.94 to 1.16; P = 0.452) for immunotherapy (including ipilimumab, atezolizumab, and durvalumab) plus chemotherapy against placebo plus chemotherapy.
In the ITC by Zhou et al. (2020),42 no significant difference was observed in ORR by the authors between the etoposide-platinum chemotherapy with PD-L1 inhibitors (including atezolizumab and durvalumab), etoposide plus cisplatin, or carboplatin plus a PD-L1 inhibitor (OR = 0.86; 95% CI, 0.48 to 1.58), compared with etoposide plus cisplatin or carboplatin alone.
Safety Outcomes: AEs
In the ITC by Ando et al. (2021),39 the incidence of at least grade 3 AEs was significantly higher with ICIs plus etoposide and platinum than with irinotecan and platinum. There were no significant differences observed in grade 3 AEs between each pair of 3 ICIs plus etoposide and platinum.
In the ITC by Chen et al. (2021),43 the authors reported an OR of 0.22 (95% CI, 0.1 to 0.5) in the comparison between durvalumab versus atezolizumab (OR = 0.22; 95% CI, 0.10 to 0.50).
In the ITC by Gristina et al. (2021),41 no statistically meaningful differences were observed in AEs between the treatments included in the network compared with chemotherapy alone (risk ratio [RR] = 2.27; 95% CI, 1.02 to 5.1).
In the ITC by Chen HL et al. (2020),44 no significant differences were observed in the risk of grade 3 or 4 AEs for etoposide and platinum plus ICIs (nivolumab, atezolizumab, or durvalumab) compared with etoposide plus platinum alone.
In the ITC by Wang et al. (2020),45 the pooled relative risks of the direct comparisons in the network were 1.03 (95% CI, 0.98 to 1.08) for any grade AEs and 0.97 (95% CI, 0.89 to 1.05) for at least grade 3 AEs in the immunotherapy (including ipilimumab, atezolizumab, and durvalumab) plus chemotherapy groups against placebo plus chemotherapy.
In the ITC by Zhou et al. (2020),42 the addition of PD-L1 inhibitors to etoposide-platinum chemotherapy was reported to be associated with no meaningfully different toxic effects in general (OR = 1.14; 95% CI, 0.36 to 2.31) when compared with etoposide plus cisplatin or carboplatin, considering the wide CI for OR that includes the null value.
Critical Appraisal of Published Indirect Comparisons
The NMA methodology reported in the published ITCs did not include sufficient details to assess the credibility and validity of the ITCs. However, the CADTH review team attempted to identify commonalities and differences between the identified ITCs and the sponsor-submitted NMA. A summary is provided below.
In the ITC by Ando et al. (2021),39 variability was reported in the age and performance status of patients recruited across trials, although upon assessment of risk of bias, the authors concluded that heterogeneity had little impact on the final conclusions, and no significant inconsistency was detected in the global inconsistency test conducted.
The trials included in the ITC by Chen et al. (2021)43 were identical to the sponsor-submitted ITC. The authors reported a low risk of bias in their quality assessments in allocation concealment, random sequence generation, blinding of outcome assessments, and blinding of participants and personnel; however, they reported potential heterogeneity in the diversity of the racial population given that most of the studies included in the network recruited non-Asian populations.
The ITC by Gristina et al. (2021)41 included 4 of the 6 studies also included in the sponsor-submitted NMA. The authors conducted a risk of bias analysis using the CONSORT checklist, and the authors reported average quality results for the trials. The authors identified some issues with the trials in Gristina et al. (2021)41 that were related to the likelihood of performance bias and detection bias owing to the open-label nature of the trials.
The ITC by Chen et al. (2020)46 reported baseline characteristics for all 46 trials included in the network diagram. Six of the 46 trials also featured in the sponsor-submitted NMA. Forty of the 46 trials (87%) compared platinum plus etoposide with other regimens. The authors reported that comparisons between carboplatin and cisplatin were not robust because of the sparse network. In addition, most of the RCTs included only patients with ECOG PS 0 to 1 or 0 to 2.
In the ITC by Chen HL et al. (2020),44 4 of the 6 studies that were included in the network geometry were also included in the sponsor-submitted NMA. Baseline characteristics were presented, and the authors also performed quality assessments and reported heterogeneity in the RCTs included in the network diagram in terms of regimen for chemotherapy and criteria for treatment response or progression.
The ITC by Wang et al. (2020)45 also presented the baseline characteristics of patients included in the 4 RCTs in the network, 2 of them also presented in the sponsor’s NMA. The quality assessments conducted by the authors showed that all studies achieved randomization and had low-to-moderate risk of bias. The network geometry was considered sparse, and the authors concluded that more data were needed to supplement the findings.
The ITC by Zhou et al. (2020)42 included 14 studies, of which 4 featured in the sponsor’s NMA. The authors did not present the baseline characteristics, and the quality assessments showed low risk of detection and reporting bias. All trials that were included implemented blinding of patients and personnel; 8 studies were reported to have low risk of attrition bias. Subgroup analyses were not reported in the ITC, and some of the patients included in the RCTs had received second-line and later therapies. Adverse events data could not be investigated.
In the ITC by Chen et al. (2017),47 9 studies were included, of which 3 were similar to the RCTs in the sponsor’s NMA. Baseline characteristics were reported for the study, and the quality assessments showed low risk of attrition or reporting bias given that all studies included required the blinding of participants and personnel. The authors reported no heterogeneity in the RCTs following their assessment. The authors reported variability in the follow-up durations, pre-medication dosage, and racial differences. In addition, genetic variations between the comparisons could not be adjusted. The authors also reported a limited sample size, which would affect the precision of the results, and inconsistency could not be evaluated.
The ITC by Kang et al. (2021)40 included 5 trials in the network, of which 4 were identical to those included in the sponsor’s NMA. Risk of bias was assessed, and a key limitation identified was the absence of subgroup analyses.
Summary
Overall, heterogeneity was identified in the sponsor-submitted NMA, and comparisons had imprecise estimates (atezolizumab plus carboplatin and etoposide against durvalumab plus carboplatin (or cisplatin) and etoposide for PFS, OS, and ORR). The PFS and OS comparisons of atezolizumab plus carboplatin and etoposide against durvalumab plus carboplatin (or cisplatin) and etoposide showed no statistically significant differences based on the wide CrIs which included the null value, and the point estimates that were close to the null. Therefore, it is likely that the treatment effects for both regimens are comparable. However, no firm conclusion could be drawn due to the small number of studies per comparison, leading to a sparce network and lower precision of effect estimates.
The safety data were considered uncertain given that only 2 trials informed the network, and the estimates were imprecise (the 95% CrIs obtained were wide and included the null value).
The published ITCs had too little information related to the networks constructed to make definitive conclusions on the findings reported. The limitations identified were mainly related to the NMA methodology used, heterogeneity across the studies included in the networks, and heterogeneity in the baseline characteristics of patients within the included trials. Further, the findings on OS and PFS reported in most of the ITCs had imprecise estimates (wide 95% CIs which included the null). The CADTH review team considered that the findings from the ITCs published did not provide sufficient evidence to inform the comparison of the efficacy and safety of atezolizumab plus carboplatin and etoposide against relevant comparators.
Other Relevant Evidence
The sponsor submitted additional exploratory analyses from the IMpower133 trial, in conference abstract format, which included an analysis of long-term survivors (defined as patients who lived for at least 18 months after randomization). Of the 373 patients included in this analysis, more long-term survivors were treated with atezolizumab plus carboplatin (or cisplatin) and etoposide (33.5%) than with carboplatin or cisplatin plus etoposide (20.4%).48 An exploratory analysis that assessed the benefit of atezolizumab plus carboplatin and etoposide compared to carboplatin and etoposide alone in patients who reached the maintenance phase of the trial (i.e., patients who received at least the first dose of maintenance therapy regardless of the number of chemotherapy cycles received) showed that a similar proportion of patients received maintenance treatment in the 2 treatment arms (77% in the atezolizumab arm, and 81% in the placebo arm). The analysis suggested an OS and PFS benefit in the maintenance population in patients receiving atezolizumab plus carboplatin and etoposide versus carboplatin and etoposide alone (OS: HR = 0.59; 95% CI, 0.43 to 0.81; PFS: HR = 0.64; 95% CI, 0.50 to 0.82). The authors concluded that induction treatment with atezolizumab plus carboplatin and etoposide as well as maintenance with atezolizumab both appeared to contribute to the OS benefit observed in the IMpower133 trial.49 Another post hoc exploratory analysis showed that time to intra-cranial progression was delayed with atezolizumab plus carboplatin and etoposide (median time to intra-cranial progression [95% CI] = 20.2 months [11.0 to NE], when compared to carboplatin and etoposide alone (10.5 months [8.7 to 17.3]; HR = 0.66; 95% CI, 0.44 to 1.00).50
Discussion
Summary of Available Evidence
The evidence base for this review consists of 1 RCT, 1 ITC submitted by the sponsor, and 9 published ITCs. IMpower133 is a randomized, multi-centre, double-blind, placebo-controlled phase III study designed to evaluate the efficacy and safety of treatment with atezolizumab plus carboplatin and etoposide compared with treatment with placebo plus carboplatin and etoposide in patients with chemotherapy-naive ES-SCLC. The trial was conducted in 106 sites across 21 countries (none in Canada). The co-primary end points were investigator-assessed PFS and OS. The key secondary end points were investigator-assessed ORR and investigator-assessed DOR. Patient-reported outcomes included HRQoL. Overall, the mean age was 63.7 years (SD = 8.9); 64.8% of patients were male and 79.9% were White. Patients had to have an ECOG PS of 0 or 1, and approximately 64% of the patients in both treatment arms had an ECOG PS of 1. Of the 526 patients screened, 403 were randomized, 201 patients to the atezolizumab arm and 202 patients to the placebo arm.
The sponsor-submitted ITC compared atezolizumab in combination with etoposide and platinum-based chemotherapy for the first-line treatment of ES-SCLC with relevant platinum doublet therapies and immunotherapies used in clinical practice. Only comparisons of atezolizumab plus carboplatin and etoposide versus etoposide plus carboplatin, etoposide plus cisplatin, and durvalumab plus etoposide and carboplatin (or cisplatin) were considered for the CADTH review. However, uncertainty remains around the findings of the sponsor-submitted ITC due to heterogeneity between the included studies (e.g., patient characteristics across studies) and wide CrIs around the reported point estimates of comparative treatment effect. Few inferences can be made from the published ITCs due to important limitations related to the NMA methodology used and heterogeneity across the studies included in the networks and in the baseline characteristics of patients within the trials.
Interpretation of Results
Efficacy
In the IMpower133 study, the addition of atezolizumab to carboplatin and etoposide chemotherapy resulted in longer PFS and OS than was observed with placebo plus carboplatin and etoposide in the first-line treatment of patients with ES-SCLC. At the first data cut-off date (April 24, 2018), 233 death events (59%) and 360 PFS events (89%) had occurred and both co-primary end points of the study had been met. The OS showed a statistically significant difference between the 2 arms in favour of atezolizumab (median OS = 12.3 months) over placebo (median OS = 10.3 months), as indicated by a stratified HR of 0.701 (95% CI, 0.54 to 0.91; P = 0.0069). OS results from the placebo arm of the trial are in line with data from most published studies of platinum plus etoposide. The final OS analysis after a median follow-up of 22.9 months (data cut-off January 24, 2019; 302 out of 403 OS events = 75%) was consistent with the interim OS analysis. The median OS in both treatment arms was unchanged (12.3 months in the atezolizumab arm and 10.3 months in the placebo arm; HR = 0.76; 95% CI, 0.60 to 0.95; P = 0.0154). At 24 months, the survival rate was approximately 5% higher in the atezolizumab arm than in the placebo arm (22.0% versus 16.8%). This difference in survival rate at 2 years was noted as clinically important by the clinical experts consulted by CADTH. Subgroup analyses did not identify a particular group of patients with considerably higher or lower benefit from atezolizumab plus carboplatin and etoposide. Progression-free survival results were also in favour of atezolizumab, with a median investigator-assessed PFS of 5.2 months, versus 4.3 months in the placebo arm (HR = 0.772; 95% CI, 0.62 to 0.96; P = 0.0170). The clinical experts consulted by CADTH noted that although the net benefits of 2 months in OS and about 1 month in PFS are not striking, in the context of ES-SCLC, which is an aggressive disease with poor prognosis, these marginally improved OS and PFS effects are clinically meaningful.
The benefit of the addition of atezolizumab to carboplatin and etoposide was not substantially supported by secondary end points. The confirmed ORR was numerically higher in the placebo arm (64.4%, compared to 60.2% in the atezolizumab arm). However, this difference between treatment arms may reflect the initial high response rate to chemotherapy that is characteristic of patients with ES-SCLC. The median DOR was similar in both treatment arms (4.2 months versus 3.9 months in the atezolizumab and placebo arms, respectively). The clinical experts consulted indicated that durability of survival benefit as measured by survival rates is key in the setting of ES-SCLC, where most patients do not live longer than 8 months to 10 months with chemotherapy alone, and ORR does not capture this aspect of treatment effect. Landmark OS rates were numerically higher in the atezolizumab arm than in the placebo arm at 12 months (51.9% versus 39.0%), 18 months (34.0% versus 21.0%), and 24 months (22.0% versus 16.8%) after randomization. At 12 months, OS rates were approximately 13% higher, and at 24 months they were 5.2% higher in the atezolizumab arm than in the placebo arm. However, these results should be treated with caution as landmark analyses do not take censoring into account.
In the CASPIAN study evaluating the efficacy and safety of durvalumab in combination with carboplatin (or cisplatin) and etoposide for the first-line treatment of patients with ES-SCLC, the median OS was 13.0 months (95% CI, 11.5 to 14.8) in the durvalumab plus platinum-etoposide arm versus 10.3 months (95% CI, 9.3 to 11.2) in the platinum-etoposide arm (HR = 0.73; 95% CI, 0.59 to 0.91).25 As of the final analysis, the median OS was 12.9 months (95% CI, 11.3 to 14.7) in the durvalumab plus carboplatin (or cisplatin) and etoposide arm, compared to 10.5 months (95% CI, 9.3 to 11.2) in the platinum-etoposide arm (HR = 0.78; 95% CI, 0.64 to 0.94). The landmark analysis of OS at 12, 18, and 24 months in the CASPIAN study showed similar event-free rates as observed in the IMpower133 trial (52.8%, 32%, and 22.9%, respectively). The effect of durvalumab on OS appears to be comparable to the OS benefit observed with the addition of atezolizumab to carboplatin and etoposide.51 There is some suggestion from the ITC included in this review that atezolizumab plus carboplatin and etoposide may be similar to durvalumab plus carboplatin (or cisplatin) and etoposide in terms of OS benefit based on the HR; however, the 95% CrIs observed were imprecise.
Selected patients were allowed to continue treatment with atezolizumab monotherapy beyond radiographic progression. In the setting of ES-SCLC, given patients’ poor prognosis and the limited efficacy of later-line treatments, achieving clinically significant benefit from therapy in the first-line setting is important. In addition, there is a potential for pseudoprogression or tumour-immune infiltration. The clinical experts consulted by CADTH agreed that conventional response criteria may not adequately assess the activity of immunotherapy agents and that progressive disease may not necessarily imply therapeutic failure. While the rationale for implementing treatment beyond progression in the IMpower133 trial is acceptable and is endorsed by the clinical experts consulted, current data from the IMpower133 trial are insufficient to establish a clear benefit of treatment beyond progression.
An important aspect of treatment desired by both clinicians and patient groups consulted by CADTH was improvement in patients’ cancer symptoms and HRQoL. The overall HRQoL improved in both treatment arms. However, overall, there was no significant difference in any domain of HRQoL between the 2 treatment arms, suggesting that the addition of atezolizumab to chemotherapy neither improves nor impedes HRQoL.
Harms
Atezolizumab exhibited an acceptable toxicity profile, as expected from an anti-PD-1 checkpoint inhibitor. The incidence and severity of immune-related AEs were also reasonable, and AEs were consistent with atezolizumab’s immune-mediated mechanism of action. Adverse events were observed in almost all patients in the trial. Although the proportion of patients with grade 3 or 4 AEs was high, it was comparable between the 2 treatment arms (atezolizumab arm: 67.7%; placebo arm: 63.3%). The incidence of SAEs was also similar in the 2 treatment arms (atezolizumab arm: 38.9%; placebo arm: 35.2%). However, grade 5 fatal AEs were more common in the placebo arm than in the atezolizumab arm (5.6% versus 2.0%). More patients with AEs required treatment withdrawal in the atezolizumab arm (11.6%) than in the placebo arm (2.6%).
The most common AEs of any grade that occurred in the trial were anemia (39%), neutropenia (36%), alopecia (36%), nausea (35%), constipation (28%), and fatigue (26%), which is consistent with what is expected from carboplatin and etoposide chemotherapy, the backbone treatment in both treatment arms. Grade 3 or 4 AEs that occurred in the trial were in general also related to myelotoxicity and thus more likely related to carboplatin and etoposide backbone treatment. The incidence of grade 3 or 4 neutropenia was comparable in both arms (atezolizumab arm: 22.7%; placebo arm: 25.0%). The majority of SAEs were also related to myelotoxicity and were observed in a similar proportion of patients in the 2 treatment arms. The proportion of patients with febrile neutropenia was higher in the placebo arm (4.6%, versus 2.5% in the atezolizumab arm).
The proportion of patients with immune-related AEs was considerably higher in the atezolizumab arm than in the placebo arm (41.4% versus 24.5%). Approximately a quarter of the patients from each treatment arm required systemic corticosteroids. Of the immune-related AEs, the most frequent was rash, followed by thyroid disorders and hepatitis. The clinical experts consulted by CADTH indicated that the safety profile of carboplatin and etoposide in the trial is consistent with the known safety profile of these drugs in clinical practice. The incidence and type of immune-related AEs observed in the atezolizumab arm are also largely consistent with what is expected in clinical practice. Although the addition of atezolizumab to carboplatin and etoposide appears to increase the incidence of grade 3 or 4 AEs and SAEs, leading to a higher proportion of patients requiring treatment modification or withdrawal from treatment, the majority of AEs occurring with atezolizumab and other ICIs in this setting are amenable to timely detection and manageable with treatment.
The results of the ITC relating to the safety of atezolizumab with respect to other comparable regimens are highly uncertain as only 2 trials informed the network, and the estimates were imprecise. There is no evidence of differences in the safety profiles of atezolizumab plus carboplatin and etoposide versus durvalumab plus carboplatin (or cisplatin) and etoposide.
Conclusions
Based on clinical data from the IMpower133 study, atezolizumab in combination with carboplatin and etoposide demonstrated a statistically significant benefit compared to placebo in combination with carboplatin and etoposide in the first-line treatment of patients with ES-SCLC. The updated OS analysis with a median of 22.9 months of follow-up showed consistent results with those reported at the interim OS analysis and suggests maintained clinical benefit from atezolizumab in combination with carboplatin and etoposide. Although the net gain of about 1 month in median PFS and 2 months in median OS observed with the addition of atezolizumab to carboplatin and etoposide is modest, it was considered by the clinical experts consulted by CADTH to be clinically meaningful in this setting, where patients experience rapid tumour growth and fast clinical deterioration and have poor prognosis. The toxicity profile of atezolizumab was consistent with its immune-mediated mechanism of action, with no new safety concerns. In terms of improving OS, atezolizumab appears to demonstrate comparable benefit to durvalumab, the only other immunotherapy agent approved (but not currently funded by the drug plans) in Canada for this indication, and can be considered an alternative treatment in combination with carboplatin and etoposide chemotherapy for the first-line treatment of ES-SCLC in Canada.
References
1.Canadian Cancer Society. Lung and bronchus cancer statistics. 2021; https://cancer.ca/en/cancer-information/cancer-types/lung/statistics. Accessed 2022 Apr 1.
2.Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83(5):584-594. PubMed
3.Kalemkerian GP. Staging and imaging of small cell lung cancer. Cancer Imaging. 2012;11:253-258. PubMed
4.Kalemkerian GP, Gadgeel SM. Modern staging of small cell lung cancer. J Natl Compr Canc Netw. 2013;11(1):99-104. PubMed
5.Nicholson AG, Chansky K, Crowley J, et al. The International Association for the Study of Lung Cancer lung cancer staging project: Proposals for the revision of the clinical and pathologic staging of small cell lung cancer in the forthcoming eighth edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11(3):300-311.
6.Socinski MA, Smit EF, Lorigan P, et al. Phase III study of pemetrexed plus carboplatin compared with etoposide plus carboplatin in chemotherapy-naive patients with extensive-stage small-cell lung cancer. J Clin Oncol. 2009;27(28):4787-4792. PubMed
7.Small cell lung cancer, version 2.2022. (NCCN Clinical Practice Guidelines in Oncology). Plymouth Meeting (PA): National Comprehensive Cancer Network; 2021: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1462 (free registration required). Accessed 2022 Apr 1.
8.Auperin A, Arriagada R, Pignon JP, et al. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. Prophylactic Cranial Irradiation Overview Collaborative Group. N Engl J Med. 1999;341(7):476-484. PubMed
9.Rudin CM, Brambilla E, Faivre-Finn C, Sage J. Small-cell lung cancer. Nat Rev Dis Primers. 2021;7(1):3. PubMed
10.Ganti AKP, Loo BW, Bassetti M, et al. Small cell lung cancer, version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2021;19(12):1441-1464. https://jnccn.org/view/journals/jnccn/19/12/article-p1441.xml. Accessed 2022 Jun 10. PubMed
11.Horn L, Mansfield AS, Szczesna A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220-2229. PubMed
12.Clinical Study Report: Primary CSR Study GO30081 (IMpower133). A Phase I/III, randomized, double-blind, placebo-controlled study of carboplatin plus etoposide with or without atezolizumab (anti-PD-L1 antibody) in patients with untreated extensive-stage small cell lung cancer. Report No.1084268 [internal sponsor's report]. Mississauga (ON): F. Hoffmann-La Roche Ltd; 2018 Sep.
13.Clinical Study Report: Update CSR Study GO30081 (IMpower133). A Phase I/III, randomized, double-blind, placebo-controlled study of carboplatin plus etoposide with or without atezolizumab(anti-PD-L1 antibody) in patients with untreated extensive-stage small cell lung cancer. Report No.1093769 [internal sponsor's report]. Mississauga (ON): F. Hoffmann-La Roche Ltd; 2019 Jun.
14.Center for Drug Evaluation and Research. Cross-discipline team leader review. Tecentriq (atezolizumab), injection for intravenous administration. Company: Genentech, Inc. Application No.:761034. Approval date: 01/12/2016 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2016 Apr 8: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2016/761034Orig1s000CrossR.pdf. Accessed 2022 Feb 8.
15.Duma N, Santana-Davila R, Molina JR. Non-small cell lung cancer: Epidemiology, screening, diagnosis, and treatment. Mayo Clin Proc. 2019;94(8):1623-1640. PubMed
16.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics 2018. Toronto: Canadian Cancer Society; 2018: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf. Accessed 2022 Jun 10.
17.Karachaliou N, Pilotto S, Lazzari C, Bria E, de Marinis F, Rosell R. Cellular and molecular biology of small cell lung cancer: an overview. Transl Lung Cancer Res. 2016;5(1):2-15. PubMed
18.Bernhardt EB, Jalal SI. Small cell lung cancer. Cancer Treat Res. 2016;170:301-322. PubMed
19.Foster NR, Mandrekar SJ, Schild SE, et al. Prognostic factors differ by tumor stage for small cell lung cancer: a pooled analysis of North Central Cancer Treatment Group trials. Cancer. 2009;115(12):2721-2731. PubMed
20.Agra Y, Pelayo M, Sacristan M, Sacristan A, Serra C, Bonfill X. Chemotherapy versus best supportive care for extensive small cell lung cancer. Cochrane Database Syst Rev. 2003(4):CD001990. PubMed
21.Qin A, Kalemkerian GP. Cisplatin, etoposide, and irinotecan for relapsed small-cell lung cancer. Transl Cancer Res. 2016;5(Suppl 6):S1142-S1144. PubMed
22.Edelman MJ. Prophylactic cranial irradiation for small-cell lung cancer: time for a reassessment. Am Soc Clin Oncol Educ Book. 2020;40:24-28. PubMed
23.Slotman BJ, Mauer ME, Bottomley A, et al. Prophylactic cranial irradiation in extensive disease small-cell lung cancer: short-term health-related quality of life and patient reported symptoms: results of an international Phase III randomized controlled trial by the EORTC Radiation Oncology and Lung Cancer Groups. J Clin Oncol. 2009;27(1):78-84. PubMed
24.Yin X, Yan D, Qiu M, Huang L, Yan SX. Prophylactic cranial irradiation in small cell lung cancer: a systematic review and meta-analysis. BMC Cancer. 2019;19(1):95. PubMed
25.Paz-Ares L, Dvorkin M, Chen Y, et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929-1939. PubMed
26.Rudin CM, Awad MM, Navarro A, et al. Pembrolizumab or Placebo Plus Etoposide and Platinum as First-Line Therapy for Extensive-Stage Small-Cell Lung Cancer: Randomized, Double-Blind, Phase III KEYNOTE-604 Study. J Clin Oncol. 2020;38(21):2369-2379. PubMed
27.Tecentriq (atezolizumab): concentrate for solution for infusion, 60 mg/mL; 1200 mg/20 mL and 840 mg/14 mL single use vials [product monograph]. Mississauga (ON): Hoffmann-La Roche Ltd; 2022 Jan 14.
28.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
29.Grey matters: a tool for searching health-related grey literature. Ottawa (ON): CADTH; 2022: https://greymatters.cadth.ca/. Accessed 2022 Jun 10.
30.Liu SV, Reck M, Mansfield AS, et al. Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133). J Clin Oncol. 2021;39(6):619-630. PubMed
31.Mansfield AS, Kazarnowicz A, Karaseva N, et al. Safety and patient-reported outcomes of atezolizumab, carboplatin, and etoposide in extensive-stage small-cell lung cancer (IMpower133): a randomized phase I/III trial. Ann Oncol. 2020;31(2):310-317. PubMed
32.Reck M, Liu S, Mansfield AS, et al. IMPower 133: updated overall survival (OS) analysis of first-line (1L) atezolizumab + carboplatin + etoposide in extensive-stage SCLC (ES-SCLC) [conference paper presented at: ESMO 2019 Congress; 2019 Sep 27 - Oct 1; Barcelona, Spain]. Ann Oncol. 2019;30(suppl 5):v710-v717. https://oncologypro.esmo.org/meeting-resources/esmo-2019-congress/IMpower133-updated-overall-survival-OS-analysis-of-first-line-1L-atezolizumab-atezo-carboplatin-etoposide-in-extensive-stage-SCLC-ES-SCLC. Accessed 2022 Jun 10.
33.Ellis PM, Swaminath A, Pond GR. Patterns of relapse in small cell lung cancer: competing risks of thoracic versus CNS relapse. Curr Oncol. 2021;28(4):2778-2788. PubMed
34.Hermes A, Bergman B, Bremnes R, et al. Irinotecan plus carboplatin versus oral etoposide plus carboplatin in extensive small-cell lung cancer: a randomized phase III trial. J Clin Oncol. 2008;26(26):4261-4267. PubMed
35.Schmittel A, Sebastian M, Fischer von Weikersthal L, et al. A German multicenter, randomized phase III trial comparing irinotecan-carboplatin with etoposide-carboplatin as first-line therapy for extensive-disease small-cell lung cancer. Ann Oncol. 2011;22(8):1798-1804. PubMed
36.Skarlos DV, Samantas E, Kosmidis P, et al. Randomized comparison of etoposide-cisplatin vs. etoposide-carboplatin and irradiation in small-cell lung cancer. A Hellenic Co-operative Oncology Group study. Ann Oncol. 1994;5(7):601-607. PubMed
37.Okamoto H, Watanabe K, Kunikane H, et al. Randomised phase III trial of carboplatin plus etoposide vs split doses of cisplatin plus etoposide in elderly or poor-risk patients with extensive disease small-cell lung cancer: JCOG 9702. Br J Cancer. 2007;97(2):162-169. PubMed
38.Leal T, Wang Y, Dowlati A, et al. Randomized phase II clinical trial of cisplatin/carboplatin and etoposide (CE) alone or in combination with nivolumab as frontline therapy for extensive-stage small cell lung cancer (ES-SCLC): ECOG-ACRIN EA5161. J Clin Oncol. 2020;38(15_suppl):9000-9000.
39.Ando K, Manabe R, Kishino Y, et al. Comparative efficacy and safety of immunotherapeutic regimens with PD-1/PD-L1 inhibitors for previously untreated extensive-stage small cell lung cancer: a systematic review and network meta-analysis. Curr Oncol. 2021;28(2):1094-1113. PubMed
40.Kang S, Wang X, Zhang Y, Zhang B, Shang F, Guo W. First-Line Treatments for Extensive-Stage Small-Cell Lung Cancer With Immune Checkpoint Inhibitors Plus Chemotherapy: A Network Meta-Analysis and Cost-Effectiveness Analysis. Front Oncol. 2021;11:740091. PubMed
41.Gristina V, Galvano A, Castellana L, et al. Is there any room for PD-1 inhibitors in combination with platinum-based chemotherapy as frontline treatment of extensive-stage small cell lung cancer? A systematic review and meta-analysis with indirect comparisons among subgroups and landmark survival analyses. Ther Adv Med Oncol. 2021;13:17588359211018018. PubMed
42.Zhou T, Zhang Z, Luo F, et al. Comparison of First-Line Treatments for Patients With Extensive-Stage Small Cell Lung Cancer: A Systematic Review and Network Meta-analysis. JAMA netw. 2020;3(10):e2015748.
43.Chen J, Wang J, Xu H. Comparison of atezolizumab, durvalumab, pembrolizumab, and nivolumab as first-line treatment in patients with extensive-stage small cell lung cancer: A systematic review and network meta-analysis. Medicine. 2021;100(15):e25180. PubMed
44.Chen HL, Tu YK, Chang HM, et al. Systematic review and network meta-analysis of immune checkpoint inhibitors in combination with chemotherapy as a first-line therapy for extensive-stage small cell carcinoma. Cancers (Basel). 2020;12(12):03.
45.Wang BC, Xiao BY, Li PC, et al. Efficacy and safety of first-line immunotherapy in combination with chemotherapy for patients with extensive-stage small cell lung cancer: A systematic review and network meta-analysis. J Oncol. 2020;2020:2368164. PubMed
46.Chen H, Horita N, Ito K, et al. Systematic review of first-line chemotherapy for chemo-naive extensive-stage small-cell lung cancer: network meta-analysis. Ther Adv Med Oncol. 2020;12:1758835920965841. PubMed
47.Chen Y, Chen L, Zhong D. Comparing the adverse effects of platinum in combination with etoposide or irinotecan in previously untreated small-cell lung cancer patients with extensive disease: A network meta-analyses. Thorac Cancer. 2017;8(3):170-180. PubMed
48.Liu S, Horn L, Mok T, et al. IMpower133: characterization of long-term survivors treated first line with chemotherapy +/− atezolizumab in extensive-stage small cell lung cancer [conference abstract presented at ESMO Virtual Congress 2020; 2020 Sep 19 - Oct 18; Switzerland]. Ann Oncol. 2020;31(suppl 4):S974-S987. https://oncologypro.esmo.org/meeting-resources/esmo-virtual-congress-2020/impower133-characterisation-of-long-term-survivors-treated-first-line-with-chemotherapy-atezolizumab-in-extensive-stage-small-cell-lung-cancer. Accessed 2022 Jun 10.
49.Reck M, Horn L, Mok T, et al. IMpower133: exploratory analysis of maintenance therapy in patients with extensive-stage small cell lung cancer [conference paper]. Proceedings of the IASLC 2020 World Conference on Lung Cancer; 2020 Aug 9-12; Singapore. 2020; Abstract: https://library.iaslc.org/virtual-library-search?product_id=20&author=Reck&category=Small+Cell+Lung+Cancer%2FNET; Slides: https://dialogoroche.com.ar/content/dam/roche-dialogo/global-assets/downloadable-assets/oncology/roche-wclc-2020/presentaciones/WCLC-2020-presentation-reck-IMpower133-exploratory-analysis-of-maintenance-therapy-in-patients-with-extensive-stage-small-cell-lung-cancer.pdf. Accessed 2022 Jun 10.
50.Higgins K, Curran W, Liu S, Yu W, Brockman M, Johnson A. Patterns of disease progression after carboplatin/etoposide + atezolizumab in extensive-stage small cell lung cancer (ES-SCLC) [conference abstract at ASTRO’s 62nd Annual Meeting; 2020 Oct 23-29]. Int J Radiat Oncol Biol Phys. 2020;108(5):1398. PubMed
51.Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open. 2022;7(2):100408. PubMed
52.Nishio M, Sugawara S, Atagi S, et al. Subgroup analysis of Japanese patients in a phase III study of atezolizumab in extensive-stage small-cell lung cancer (IMpower133). Clin Lung Cancer. 2019;20(6):469-476.e461. PubMed
53.Nishio M, Saito H, Goto K, et al. IMpower132: Atezolizumab plus platinum-based chemotherapy vs chemotherapy for advanced NSCLC in Japanese patients. Cancer Sci. 2021;112(4):1534-1544. PubMed
54.Agrawal S, Kumar A, Srivastava V, Mishra BN. Cloning, expression, activity and folding studies of serine hydroxymethyltransferase: a target enzyme for cancer chemotherapy. J Mol Microbiol Biotechnol. 2003;6(2):67-75. PubMed
55.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
56.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30a(5):635-642. PubMed
57.Osoba D, Aaronson N, Zee B, Sprangers M, te Velde A. Modification of the EORTC QLQ-C30 (version 2.0) based on content validity and reliability testing in large samples of patients with cancer. The Study Group on Quality of Life of the EORTC and the Symptom Control and Quality of Life Committees of the NCI of Canada Clinical Trials Group. Qual Life Res. 1997;6(2):103-108. PubMed
58.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-1028. PubMed
59.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
60.Bedard G, Zeng L, Zhang L, et al. Minimal important differences in the EORTC QLQ-C30 in patients with advanced cancer. Asia Pac J Clin Oncol. 2014;10(2):109-117. PubMed
61.Bjordal K, de Graeff A, Fayers PM, et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer. 2000;36(14):1796-1807. PubMed
62.Zhang Z, Li M, Wang H, Agrawal S, Zhang R. Antisense therapy targeting MDM2 oncogene in prostate cancer: Effects on proliferation, apoptosis, multiple gene expression, and chemotherapy. Proc Natl Acad Sci U S A. 2003;100(20):11636-11641. PubMed
63.Maringwa JT, Quinten C, King M, et al. Minimal important differences for interpreting health-related quality of life scores from the EORTC QLQ-C30 in lung cancer patients participating in randomized controlled trials. Support Care Cancer. 2011;19(11):1753-1760. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid and in Endnote citation software.
Date of search: February 22, 2022.
Alerts: Biweekly search updates until project completion.
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(atezolizumab* or Tecentriq* or tecntriq or MPDL3280A or MPDL-3280A or RG7446 or RG-7446 or L01FF05 or 52CMI0WC3Y).ti,ab,kf,ot,hw,rn,nm.
Small Cell Lung Carcinoma/
(SCLC or SCLCs or ESSCLC? or ESCLC? or CSCLC?).ti,ab,kf.
((lung* or bronchial or pulmonary) adj4 ((small cell* or smallcell* or microcellular*) adj3 (cancer* or carcinoma* or neoplas* or tumour* or tumor* or malignan*))).ti,ab,kf.
(oat cell adj (cancer* or carcinoma* or neoplas* or tumour* or tumor* or malignan*)).ti,ab,kf.
or/2-5
1 and 6
(IMpower133 or NCT02763579).ti,ab,kf. use medall
7 or 8
use medall
*atezolizumab/ or (atezolizumab* or Tecentriq* or tecntriq or MPDL3280A or MPDL-3280A or RG7446 or RG-7446 or L01FF05).ti,ab,kf,dq.
small cell lung cancer/
(SCLC or SCLCs or ESSCLC? or ESCLC? or CSCLC?).ti,ab,kf,dq.
((lung* or bronchial or pulmonary) adj4 ((small cell* or smallcell* or microcellular*) adj3 (cancer* or carcinoma* or neoplas* or tumour* or tumor* or malignan*))).ti,ab,kf,dq.
(oat cell adj (cancer* or carcinoma* or neoplas* or tumour* or tumor* or malignan*)).ti,ab,kf,dq.
or/12-15
11 and 16
(IMpower133 or NCT02763579).ti,ab,kf,dq.
17 or 18
use oemezd
not (conference abstract or conference review).pt.
10 or 21
remove duplicates from 22
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
Search – (atezolizumab OR Tecentriq OR MPDL3280A OR MPDL-3280A OR RG7446 OR RG-7446 OR L01FF05 OR 52CMI0WC3Y) and Disease: (small cell OR smallcell OR SCLC OR ESSCLC OR ESCLC) AND (lung OR pulmonary OR bronchial)
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
Search - (atezolizumab OR Tecentriq OR MPDL3280A OR MPDL-3280A OR RG7446 OR RG-7446 OR L01FF05 OR 52CMI0WC3Y) AND (small cell OR smallcell OR SCLC OR ESCLC OR ESSCLC) NOT NCT*
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search terms – atezolizumab, Tecentriq, small cell lung cancer
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Search - (atezolizumab OR Tecentriq OR MPDL3280A OR MPDL-3280A OR RG7446 OR RG-7446 OR L01FF05 OR 52CMI0WC3Y) AND (small cell OR smallcell OR SCLC OR ESSCLC OR ESCLC) AND (lung OR pulmonary OR bronchial) NOT NCT*
Grey Literature
Search dates: February 8 to 15, 2022.
Keywords: Tecentriq, atezolizumab; small cell lung cancer.
Limits: no limits by date or language.
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Databases (free)
Internet Search
The complete search archive of sites consulted for this report is available on request.
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Nishio et al., 201952 | Subgroup not of interest |
Nishio et al., 202153 | Subgroup not of interest |
Appendix 3: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30)
QLQ LC13 Lung Cancer Supplement
The outcomes are evaluated in the included study and their properties are shown in : Summary of outcome measures and their measurement properties.
Findings
Table 31: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 and supplement QLQ LC13 | A generic, patient self-administered questionnaire, consisting of 30 items to measure the physical, psychological, and social functions of patients with cancer. The instrument consists of 30 items that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a global quality of life (QoL) scale.54,55 The QLQ C30 can be used with a supplement for patients with lung cancer (QLQ LC13) with 13 items, assessing lung cancer symptoms and treatment-related side effects.54,56 | There were observed strong inter-domain correlations between physical function and role function (r > 0.6), and between physical function and fatigue (r = –0.62) of the EORTC QLQ-30.57 The 6–minute walking score was found to be strongly correlated with the QLQ-30 physical functioning scale, moderately correlated with fatigue, role functioning and global QoL (r > 0.4), and weakly correlated with dyspnea (r = 0.21).58 In the same study, the hospital anxiety and depression (HADS) anxiety scale was found to be strongly correlated with the QLQ-30 emotional functioning scale (r = –0.75), and moderately correlated with global quality of life (r = –0.47). The HADS depression scale was found to have a moderate to strong correlation with all functioning scales, fatigue and appetite loss (r = 0.48 to 0.55).58 In terms of reliability, both QLQ-C30 and QLQ-LC13 demonstrated an adequate internal consistency for most multi-item scales (Cronbach Alpha > 0.70), except for the cognitive functioning scale (Cronbach Alpha = 0.57).58 | The MID estimates in patients with small cell lung cancer and breast cancer who reported “a little” change in the subjective significance questionnaire (SSQ) had corresponding changes in the QLQ-C30 of 5 to 10 points, those who reported a “moderate” change had corresponding changes of about 10 to 20 points, and those who reported “very much” change had corresponding changes of more than 20 points.59 In another study, MID estimates of the QLQ-30 ranged from a meaningful change for improvement of 9.1 units (cognitive functioning) to 23.5 units (pain), and a meaningful change for deterioration ranging from 7.2 units (physical functioning) to 13.5 units (role functioning). Distribution-based estimates were closest to 0.5 SD.60 |
MID = minimal important difference.
European Organization for Research and Treatment of Cancer, 30 Item Core Quality of Life Questionnaire (EORTC QLQ C-30) and Lung Cancer Supplement (LC13)
The EORTC QLQ C-30 (version 3) is a generic, patient self-administered questionnaire for evaluating the QoL of patients with cancer participating in clinical trials.54,55 This questionnaire is intended to be complemented by tumour-specific questionnaire modules or supplements, such as the 1 for patients with lung cancer, or QLQ-LC13.54,56
The EORTC QLQ-C30 consists of 30 items that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a global QoL scale (Table 32).54 Version 3.0 of the questionnaire is the most current version and has been in use since December of 1997.61 It is intended for use in the adult population only.54 The QLQ-C30 uses a 1-week recall period to assess function and symptoms.54 Twenty-eight questions are scored on a 4–point Likert with anchors at 1 (“not at all”) and 4 (“very much”). The 2 questions that make up the global QoL scale are scored on a 7–point Likert scale with anchors at 1 (“very poor”) and 7 (“excellent”).62 Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, and better HRQoL, while a higher score in the symptom scale means higher burden of symptoms and therefore a worse health state.58,62
The EORTC QLQ-LC13 is a questionnaire measuring lung cancer symptoms and side effects from conventional chemo- and radiotherapy. It comprises 13 questions of lung cancer-associated symptoms (e.g., coughing, dyspnea and pain) and side effects from conventional chemo- and radiotherapy (e.g., hair loss, neuropathy, sore mouth and dysphagia).56 All questions are scored on a 4–point Likert scale with anchors at 1 (“not at all”) and 4 (“very much”). The scoring approach for the QLQ-LC13 is identical in principle to that for the symptom scales/single items of the QLQ-C30. An outcome variable consists of a score from 0 to 100, with a higher score reflecting greater symptom burden and therefore a worse health state.62
Table 32: EORTC QLQ-C30 Scales
Functional scales (15 questions) | Symptom scales (7 questions) | Single-item symptom scales (6 questions) | Global Quality of Life (2 questions) |
|---|---|---|---|
Physical function (5) | Fatigue (3) | Dyspnea (1) | Global Quality of Life (2) |
Role function (2) | Pain (2) | Insomnia (1) | — |
Cognitive function (2) | Nausea and vomiting (2) | Appetite loss (1) | — |
Emotional function (4) | — | Constipation (1) | — |
Social function (2) | — | Diarrhea (1) | — |
— | — | Financial impact (1) | — |
Psychometric Properties
The validity and reliability of the QLQ-C30 has been assessed in several studies among patients with cancer, including lung cancer.55-58 In a validation study of the QLQ-C30, patients with lung cancer (n = 160) and a heterogenous group of other cancers (n = 375) completed the questionnaire at baseline and at day 8 after chemotherapy.57 Item-domain correlations were determined for the entire patient group at baseline and at day 8 after chemotherapy. At baseline, all items were strongly correlated within their own domain than with any other domains (r = −0.65 to 0.95), except for item 5 (whether the responders needed help with eating, dressing, washing, or using the toilet) and the physical function domain (r = −0.3). On day 8 after chemotherapy, the item-domain for item 5 and the physical function domain was higher (r = 0.49), indicating that item 5 was more relevant in the week after chemotherapy than before chemotherapy.57 Similarly, items asking about vomiting showed a higher correlation with domains for nausea/vomiting on day 8 after chemotherapy (r = 0.89) than before chemotherapy (r = 0.74). The questionnaire also demonstrated adequate internal consistency for most domains at baseline and at day 8 after chemotherapy (Cronbach Alpha > 0.70).57 There were observed strong inter-domain correlations between physical function and role function (r > 0.6), and between physical function and fatigue (r = –0.62). In the same study, the mean scores for physical, role and social functions, as well as for global QoL decreased significantly with decreasing ECOG Performance Status.57
In a study consisting of 112 patients with advanced lung cancer or pleural mesothelioma, criterion and concurrent validity of the QLQ-C30 was supported for most of the functioning and symptom scales, and global QoL.58 When used as a continuous score, the 6-minute walking score was found to be strongly correlated with the QLQ-C30 physical functioning, moderately to strongly correlated with fatigue, role functioning and global QoL (r > 0.4), and poorly correlated with dyspnea (r = 0.21). In the same study, the Hospital anxiety and depression (HADS) anxiety scale was found to be strongly correlated with the QLQ-30 emotional functioning (r = –0.75), and moderately correlated with global QoL (r = –0.47). The HADS depression scale has been found to have a moderate to strong correlation with all functioning scales, fatigue and appetite loss (r = 0.48 to 0.55).58 In terms of reliability, both QLQ-C30 and QLQ-LC13 demonstrated an adequate internal consistency for most multi-item scales (Cronbach Alpha > 0.70), except for the cognitive functioning scale (Cronbach Alpha = 0.57).58 The findings of another study demonstrate that the QLQ-30 and QLQ-LC13 items and scales pertaining to symptoms of lung cancer discriminate clearly between patient subgroups on the basis of ECOG Performance Status and disease stage, while items pertaining to treatment toxicity were found to discriminate between subgroups of patients receiving chemotherapy versus radiotherapy.56
Minimally Important Difference
Change in the EORTC QLQ-C30 may be interpreted in terms of small, moderate or large changes in HRQoL.59 A study of patients with SCLC and breast cancer estimated a clinically relevant change in score on any of the QLQ-C30 scales using an anchor-based approach.59 The MID estimates in patients who reported “a little” change (for better or worse) on the subjective significance questionnaire (SSQ) had corresponding changes on a function or symptom scale of the QLQ-C30 of approximately 5 to 10 points. Participants who reported a “moderate” change in the SSQ had corresponding changes in the QLQ-C30 of about 10 to 20 points, and those who reported “very much” change had corresponding changes of more than 20 points.59
Another study estimated the MID for the QLQ-C30 among 369 patients with advanced cancer (including lung cancer), using anchor and distribution-based methods for improvement and deterioration. Using 2 patient-based anchors (overall health and overall QoL), MID estimates of the QLQ-30 ranged from a meaningful change for improvement of 9.1 units (cognitive functioning) to 23.5 units (pain), and a meaningful change for deterioration ranging from 7.2 units (physical functioning) to 13.5 units (role functioning). Distribution-based estimates were closest to 0.5 SD.60
In another study, WHO performance status and weight change were used as clinical anchors to determine estimates of MIDs for the QLQ-C30 scales in 812 patients with NSCLC.63 The MID estimates for improvement (based on the performance status and weight gain) were physical functioning (9, 5); role functioning (14, 7); social functioning (5, 7); GHS (9, 4); fatigue (14,5); and pain (16, 2). The respective MID estimates for deterioration were physical (4, 6); role (5, 5); social (7, 9); GHS (4, 4); fatigue (6, 11); and pain (3, 7), based on the performance status and weight, respectively.63
Limitations
The reliability of social items such as social functioning and the social worker’s ratings of social support and activity still need more study and are yet to be proven. The difference in methodology and timing of the studies assessing these values can imply uncertainty in the body of evidence for the properties of the measurement scales.
Appendix 4: Additional Data
Table 33: Overview of Study Design and Patient Characteristics of Trials Included in the Sponsor-Submitted NMA
Study | Inclusion criteria | Treatment arms | N | Male, n (%) | Age, median (IQR) | ECOG PS or WHO PS, n (%) 0 | ECOG PS or WHO PS, n (%) 1 | Presence of brain metastases, n (%) | Non-protocol follow-up cancer therapies, n (%) |
|---|---|---|---|---|---|---|---|---|---|
CASPIAN Phase III, double-blind RCT 209 sites across Europe, Asia, North America and South America NCT03043872 |
| Induction
Maintenance
| 268 | (75.4) | 63 | (40.7)* | (59.3)* | (14.2) |
|
Induction
Maintenance
| 268 | 190 (70.9) | 62 | 99 (36.9)* | 169 (63.1)* | 28 (10.4) |
| ||
Induction
| 269 | 184 (68) | 63 | 90 (33.5)* | 179 (66.5)* | (10) |
| ||
KEYNOTE-604 Phase III, double-blind RCT 148 sites globally NCT03066778 |
| Induction
Maintenance
| 228 | 152 (66.7) | 64 | NR | 168 (73.7) | 33 (14.5) | PCI, 12% |
Induction
Maintenance
| 225 | 142 (63.1) | 65 | NR | 169 (75.1) | 22 (9.8) | PCI, 14% | ||
ECOG-ACRIN EA5161 Phase II, open-label RCT 781 sites US NCT03382561 |
| Induction
Maintenance
| 80 | 35 (44) | 65 | 23 (49) | NR | 11 (14) | NR |
Induction
Maintenance
| 80 | 36 (45) | 65 | 24 (51) | NR | 7 (9) | NR | ||
IMpower133 Phase III, double-blind RCT 135 sites globally NCT02763579 |
| Induction
Maintenance
Treat to PD or loss of clinical benefit | 201 | 130 (64.7) | 111 (55.2%) of patients aged < 65 | 73 (36.3) | 128 (63.7) | 16(8.0) |
|
Induction
Maintenance
(maintenance) Treat to PD or loss of clinical benefit | 202 | 132 (65.3) | 106 (52.5%) of patients aged < 65 | 72 (35.6) | 130 (64.4) | 16 (7.9) |
| ||
Hermes 2008 Phase III, open-label RCT Norway and Sweden |
(Brain metastases not an exclusion criteria) |
| 105 | 66 (63) | 67 | 5 | 6 (63) | NR | 49 patients received second-line chemotherapy (13 reinduction) |
| 104 | 72 (69) | 68 | 5 | 4 (52) | NR | 48 patients received second-line chemotherapy (17 reinduction) | ||
Okamoto 2007 Phase III RCT (Unclear blinding) Japan JCOG 9702 |
|
| 110 | 95 | 74 | NR | 81 | 18 | 68 (62%) patients received second-line chemotherapy after relapse |
| 110 | 98 | 73.5 | 81 | NR | 18 | 62 (56%) patients received second-line chemotherapy after relapse | ||
Schmittel 2011 Phase III, open-label RCT Germany NCT00168896 |
|
| 106 | 70 (66) | 60 | NR | NR | (25) | 13 patients received additional chemotherapy after disease progression (second and third line) |
| 110 | 71 (65) | 63 | NR | NR | 23 patients received additional chemotherapy after disease progression (second and third line) | |||
Skarlos 1994 RCT (unclear phase and blinding) Greece |
Data reported for ES-SCLC subgroup baseline characteristics provided for total SCLC trial population |
| 73 (30 ES-SCLC) | 66 | 60 | 6 | 52 | NR | NR |
| 74 (31 ES-SCLC) | 67 | 60 | 10 | 43 | NR | NR |
AUC = area under curve; BSA = body surface area; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ES-SCLC = extensive-stage SCLC; IQR = interquartile range; NR = not reported; PCI = prophylactic cranial irradiation; PD = progressed disease; PS = performance status; SCLC = small cell lung cancer; WHO = WHO.
Note: *WHO PS
Note that this appendix has not been copy-edited.
Source: Sponsor-submitted NMA4
Table 34: Study Selection Criteria and Methods for Published ITCs
Item | Ando et al., 2021 39 | Chen et al., 2021 43 | Gristina et al., 2021 41 | Chen et al., 2020 46 |
|---|---|---|---|---|
Objective | To compare the efficacy and safety of ICIs + etoposide + platinum (i.e., pembrolizumab + etoposide + platinum, durvalumab + etoposide + platinum, or atezolizumab + etoposide + platinum) and platinum–irinotecan (IP) in adult patients with previously untreated ES-SCLC and to compare the efficacy and safety of ICI-containing regimens (pembrolizumab + etoposide + platinum, durvalumab + etoposide + platinum, or atezolizumab + etoposide + platinum) with each other. | To compare the efficacy and safety profile of immune checkpoint inhibitors (ICIs), including atezolizumab, durvalumab, pembrolizumab, and nivolumab as first-line treatment in patients with ES-SCLC. | To assess different ICIs in combination with platinum-based CT in untreated ES-SCLC patients. | To assess the efficacy and safety of first-line chemotherapy regimens for chemo-naïve patients with extensive disease small cell lung cancer (ED-SCLC). |
Population | Untreated patients advanced SCLC, particularly ES-SCLC. | Untreated patients with ES-SCLC. | Patients with histological diagnosis of unresectable or advanced ES-SCLC (stage IVA/IVB according to the eighth TNM classification and clinical staging system) were included. | Chemo-naïve extensive-stage small cell lung cancer (ES-SCLC) patients. |
Intervention |
| Atezolizumab, durvalumab, pembrolizumab, and nivolumab. | Immunotherapies + chemotherapy (CT + IO) platinum-based CT plus single-agent IO regimens containing anti-PD-1 (nivolumab or pembrolizumab) or anti-PD-L1 (atezolizumab or durvalumab) (ipilimumab). | Molecular targeted agents and immune checkpoint inhibitors were considered chemotherapy along with cytotoxic medications. |
Comparator | Etoposide plus platinum | Etoposide plus platinum | Chemotherapy (including cisplatin or carboplatin in association with etoposide or paclitaxel) | Platinum + etoposide |
Outcome | OS and PFS incidence of ≥ grade 3 adverse events | PFS, OS, ORR, and AEs | PFS, OS, ORR, DOR, treatment related, disease control rate (DCR), adverse events (TRAEs) | OS, PFS, response rate. |
Study design | Phase III RCTs | Randomized, prospective, controlled studies (full publications and abstracts) | Phase II and III RCTs | RCTs (superiority, non-inferiority, phase II, phase III, non-blinded, single-blinded, and double-blinded trials) were included. |
List of studies included | 11 TRIALS KEYNOTE-604, CASPIAN, IMpower133, Sun et al., 2016 (NCT00660504), Satouchi et al., 2014 (JCOG0509), Kim et al. 2019 (NCT00 to 349492), Zatloukal et al.2010, Lara et al., 2009 (SWOG S0124), Hanna et al., 2006, Noda et al., 2002 (JCOG9511). |
| Six studies were included CA184 to 041; CA184 to 156; IMpower133; EA5161; KEYNOTE-604; CASPIAN | 46 studies included: Cheng., 2019; Weiss., 2019; Reck., 2019; Owonikoko., 2019 (ECOG-ACRIN2511); Paz-Ares., 2019 (CASPIAN); Kim., 2019; Horn., 2018 (IMpower133); Morikawa., 2017 (NJLCG0901); Jalal., 2017 (MATISSE); Seckl., 2017 (LUNGSTAR); Salgia., 2017 ; Tiseo., 2017 (GOIRC-AIFA FARM6PMFJM); Sanborn., 2017 (LUN06 to 113); Oh., 2016; Reck., 2016 Belani., 2016 (E1508); Sun, 2016; Shi., 2015; Lu., 2015; Beniwal_2015; Satouchi., 2014 (JCOG0509); Sekine., 2014; Langer., 2014; Fink., 2012 Obrien., 2011 (EORTC08062) Spigel., 2011 SALUTE; Schmittel., 2011; Zatloukal., 2010; Socinski., 2009; Lara., 2009 (SWOG0124); Lee., 2009; Rudin., 2008 (CALGB30103); Dimitroulis., 2008 Hermes., 2008; Sekine., 2008; Okamoto., 2007 (JCOG9702); Glisson., 2007 Socinski., 2006; Eckardt., 2006; Hanna., 2006; Schmittel., 2006; Greco., 2005 Quoix., 2005., Niell., 2005 (CALGB9732) Lyss., 2002 (CALGB9430); Noda., 2002 (JCOG9511) |
Publication characteristics |
| English-language publications retrieved with the deadline up to June 20, 2020 | English-only articles |
|
Exclusion criteria | Trials on children, observational studies, case reports, and non-RCTs were excluded. | Retrospective or single-arm research were excluded. Patients diagnosed with limited-stage SCLC or treatments as further-line options were excluded. Any review or systematic reviews, correspondence, case studies or comments were excluded. For repeated published research, or update reports for same studies, the most updating data were adopted. Non–English-language publications were also excluded. | Non-randomized, cohort, cross-sectional, retrospective and case-control studies, other reviews (systematic or not) and meta-analyses, duplicates including trials whose results for relevant outcomes were not available or ongoing trials or trials with fewer than 10 patients were excluded. | Phase II, phase III trials that randomized relapsed or responsive cases were excluded. Trials that did not report survival data were excluded. Trials with “first-generation” cytotoxic agents developed around 1950 namely methotrexate, mitomycin, vincristine, cyclophosphamide, doxorubicin, and ifosfamide were also excluded. Studies that reported multimodality treatments including chemoradiotherapy, radiotherapy, or surgery Studies that reported irregular regimens, such as alternative regimens were also excluded. |
Databases searched | PubMed, Embase, CENTRAL, and Scopus | MEDLINE, Cochrane library, and Embase were retrieved (Chen) with the deadline up to June 20, 2020. including fully published research and meeting abstracts belong to American Society of Clinical Oncology (ASCO) meeting, European Society for Medical Oncology (ESMO) congress, World Conference on Lung Cancer (WCLC), and American Association of Cancer Research (AACR). | MEDLINE (PubMed), Scopus, and Cochrane Library databases were collected until 20 March 2021. Abstracts were retrieved from the American Society of Clinical Oncology (ASCO) and the European Society of Medical Oncology (ESMO) as well as the National Institute of Health (NIH) website (www.clinicaltrials.gov) for as yet unpublished ongoing studies. | PubMed, Web of Science Core Collection, Cochrane advanced search, and Embase. Conference abstracts in English reported after 2015 were included. |
Selection process | Conducted independently by 2 researchers. Any disagreements that arose were resolved by discussions with a third author. The search was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement for Systematic Review and Meta-analysis and the PRISMA extension of the NMA. | Two authors extracted relevant data independently, and a third author consulted to resolve discrepancies when necessary. Viewpoints held by 2 investigators were considered for the final decision | Two authors independently selected trials based on an established inclusion and exclusion criteria. Papers were included in the final analysis if they met the pre-specified relevant outcomes. Disagreements were debated and solved by consulting a senior author. | Literature independently screened by 2 investigators. Papers identified by hand search were carefully evaluated before being added to the list of candidate articles. Any discrepancies were resolved through discussions between the 2 investigators. |
Data extraction process | Literature search was conducted independently by 2 researchers. | Two authors extracted relevant data independently, and a third author consulted to resolve discrepancies when necessary. Viewpoints held by 2 investigators would be the final decision. | Two authors independently selected trials. Disagreements were debated and solved by consulting a senior author. | Data were extracted from the included studies independently by 2 investigators Discrepancies were resolved through discussions between the 2 investigators. |
Quality assessment | Cochrane Collaboration risk of bias tool 2 (RoB2). | Cochrane Collaboration's tool for assessing risk of bias of RCTs was adopted for quality evaluation in the present study by the 2 reviewers. | CONSORT checklist statement using modified Jadad’s score. | Cochrane Risk of Bias tool. |
AE = adverse event; anti-PD-L1 = anti- programmed cell death-1 ligand 1; DCR = disease control rate; DOR = duration of response; ES-SCLC = extensive-stage small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RoB = risk of bias.
Table 35: Study Selection Criteria and Methods for Published ITCs
Item | Chen HL et al., 202044 | Wang et al., 202045 | Zhou et al., 202042 | Chen et al., 201747 | Kang et al., 202140 |
|---|---|---|---|---|---|
Objective | To assess the ranking of immune check point inhibitors (ICIs) in terms of overall survival (OS), progression-free survival (PFS), and objective response rate (ORR), as well as adverse events. | To assess the comparative effectiveness of different first-line treatment strategies for extensive-stage SCLC. | To assess and clarify which first-line combination regimen is associated with the best tumour response among patients with ES-SCLC. | To compare the toxicity of different therapies for patients with ED‐SCLC. | To evaluate the efficacy and cost-effectiveness of ICIs plus chemotherapy as a first-line treatment for ES-SCLC from the perspective of the Chinese health care system. |
Population | Untreated Patients with extensive-stage small cell lung cancer (ED-SCLC) | treatment-naive extensive-stage SCLC patients | Untreated patients with extensive-stage small cell lung cancer | Untreated patients with extensive-stage small‐cell lung cancer | Untreated patients with extensive-stage small cell lung cancer (ES-SCLC) |
Intervention | Nivolumab, atezolizumab, durvalumab, pembrolizumab, and ipilimumab. | Immune checkpoint inhibitors (including ipilimumab, atezolizumab, and durvalumab) + chemotherapy | chemotherapy-only regimens as well as chemotherapy plus either PD-L1 antibody, CTLA-4 antibody, or VEGF antibody as the first-line treatment (durvalumab, atezolizumab, or ipilimumab plus etoposide-platinum chemotherapy), and bevacizumab) | irinotecan with cisplatin (IP), etoposide with carboplatin (EC), irinotecan with carboplatin (IC), and etoposide with cisplatin (EP). | ICIs plus chemotherapy (atezolizumab plus chemotherapy, durvalumab plus chemotherapy, pembrolizumab plus chemotherapy, nivolumab plus chemotherapy, and ipilimumab plus chemotherapy) |
Comparator | Chemotherapy + etoposide | Chemotherapy + placebo Standard of care = Platinum-based combination chemotherapy Chemotherapy + (etoposide plus platinum (carboplatin or cisplatin) and paclitaxel plus carboplatin). | etoposide-based chemotherapy alone etoposide + platinum (cisplatin or carboplatin) | Etoposide with carboplatin | Standard platinum-based first-line chemotherapy |
Outcome | OS, PFS, ORR, AEs | OS, PFS, ORR, DCR, and AEs. | ORR, DCR, PFS, OS, AEs | Hematological and non‐hematological toxicities | OS, PFS |
Study design | Randomized phase II and phase III trials which reported on ICI plus etoposide and platinum treatment | RCTs | Phase II and III RCTs | Parallel RCTs | RCTs |
List of studies included | Six studies included: Keynote-604 (2020), EA5161 (2020), IMpower133 (2018), CASPIAN (2019), CA184 to 041 (2013), and CA184 to 156 (2016). | 4 studies: M. Reck (2013), M. Reck (2016), L. Horn (IMpower133 2018), L. Paz-Ares (CASPIAN 2019) | 14 studies included: Paz-Ares et al., 2019, Kim et al., 2019, Horn et al., 2018, Tiseo et al., 2017, Reck et al., 2016, Shi et al., 2015, Schmittel et al., 2011, Spigel et al., 2011, Zatloukal et al., 2010, Lara et al., 2009, Hermes et al., 2008, Hanna et al., 2006, Schmittel et al., 2006, Noda et al., 2002 | Nine studies included: Hermes 2008, Okamato 2007, Lara et al., 2009, Hanna et al., 2006, Noda et al., 2002, Pan et al., 2006 Schmittel et al., 2011, Zatloukal et al., 2010, Schmittel et al., 2006. | Five studies included: IMpower133, CASPIAN, KEYNOTE-604, CA184 to 156, and EA5161 trials. |
Publication characteristics | No language limitations were implemented. A controlled vocabulary search terms for PubMed (MeSH) and Embase (Emtree) was done. | No language limitations implemented. Additional clinical studies were checked through reference lists | Searches were conducted from database inception to December 2019. | No restrictions for language or duration of follow-up | RCTs deadline up to June 22, 2021. Restricted to English-language publications. |
Exclusion criteria | Title/abstract reviews that had incomplete RCTs non-completed phase II–III randomized control trials (RCTs) involving adults with ED-SCLC RCTs that did not involve newly diagnosed untreated patients with ED-SCLC RCTs that did not compare the efficacy and safety of an ICI combined with chemotherapy with chemotherapy alone. | Conference abstracts were not included due to the absence of full data and the potential publication bias. For duplicate studies, the data were available from the most recent and complete publication, and the other reports were used to verify the data. Non-prospective RCTs in full papers Studies that did not investigate newly diagnosed extensive-stage SCLC and previously untreated patients | Studies failing to meet the inclusion criteria were excluded. Inclusion criteria: Randomized clinical head-to-head phase II or III trials Studies that enrolled patients with either histologically or cytologically confirmed ES-SCLC Studies that compared 2 or more first-line treatments for patients with ES-SCLC, including immunotherapy plus chemotherapy and an etoposide-platinum chemotherapy regimen and studies that reported detailed outcomes and toxic effects including PFS, OS, objective response rate (ORR), disease control rate (DCR), and treatment-related adverse events (TRAEs) of grade 3 or higher. | Studies of patients who received surgery, radiotherapy, or chemotherapy before receiving first‐line chemotherapy. | Publications which were not written in English were ineligible, and only the latest data of the same trial were considered for the network meta-analysis. |
Databases searched | PubMed, Embase, Cochrane library ClinicalTrials.gov, the database of the American Society of Clinical Oncology (ASCO) and the dataset of European Medical Oncology (ESMO) from their conception until 30 September 2020. | PubMed, Web of Science, Embase, and Cochrane Library | PubMed, Embase, Cochrane Central Register of Controlled Trials, and Web of Science from database inception to December 2019 relevant abstracts and presentations presented in American Society of Clinical Oncology, the World Conference on Lung Cancer, and the European Society for Medical Oncology from 2010 to 2019. Manual search of reference lists of all available reviews was additionally performed to confirm the final selection. | EMBASE, PubMed, CENTRAL and clinicaltrials.gov | PubMed, Embase and the Cochrane Central Register of Controlled Trials Abstracts from European Society of Medical Oncology (ESMO), the American Society of Clinical Oncology (ASCO), the American Association for Cancer Research (AACR), and the World Conference on Lung Cancer (WCLC). |
Selection process | Two independent reviewers | Two authors independently reviewed and selected the eligible studies. Discrepancies were resolved by discussion. 2 authors assessed the risk of bias | Three reviewers independently carried out the literature retrieval. Disagreements were resolved in discussion, and consensus was reached. | Two authors independently made the preliminary selection according to citation title and abstract. | Independently screened studies were conducted by 2 reviewers. |
Data extraction process | Two independent reviewers extracted data and conducted quality assessment. Unresolved discrepancies in the data extraction or appraisal of the results were resolved by discussion with a third reviewer | 2 authors extracted the data independently | Data were independently extracted and collected by 2 reviewers following Cochrane Collaboration guidelines. All disagreements were resolved in discussion, and consensus was reached. | Two authors independently assessed the methodological quality of the included studies with the Cochrane risk of bias tool | Independently by 2 reviewers |
Quality assessment | Cochrane Collaboration’s Risk of Bias tool Review Manager version 5.1. | Cochrane Risk of Bias Tool in RevMan 5.3 software | Cochrane risk of bias tool | Cochrane risk of bias tool | Cochrane Collaboration’s tool in RevMan software (version 5.3) |
AE = adverse event; anti-PD-L1 = anti- programmed cell death-1 ligand 1; DCR = disease control rate; ES-SCLC = extensive-stage small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RoB = risk of bias.
Table 36: ITC Analysis Methods of the Published ITCs
Item | Ando et al., 2021 | Chen et al., 2021 | Gristina et al., 2021 | Chen et al., 2020 |
|---|---|---|---|---|
ITC methods | Bayesian model in accordance with the National Institute for Health and Care guidelines. Standard Bayesian model as described by Dias et al. which presupposes inconsistency and heterogeneity among the included studies. | Random effect model. (The authors did not clearly state whether a Bayesian or frequentist was used. Confidence intervals reported which may be suggestive of a frequentist approach). | Confidence intervals were reported; thus, a frequentist approach was used to conduct the NMA. The random effect–based model by Der Simonian and Laird; otherwise, the fixed effect–based model by Mantel-Haenszel was performed. | A Frequentist network meta-analysis approach with weighted least squares random model was considered. |
Priors | A noninformative prior distribution was adopted. The posterior distribution for effect size was estimated using the Gibbs sampling method based on the Markov Chain Monte Carlo method | NR | NR | NR |
Assessment of model fit | NR | NR | NR | NR |
Assessment of consistency | Heterogeneity among studies with direct comparisons was assessed by using I2 statistics. Heterogeneity was judged to be low when I2 was < 40%, moderate when I2 was ≥ 40% and < 60%, substantial when I2 was ≥ 60% and < 75%, and considerable when I2 was > 75%. global inconsistency in the overall network model was assessed by using the statistical global inconsistency test. heterogeneity of the direct comparison was calculated from the results of an integrated analysis of 5 studies. The results indicated that heterogeneity had little impact on the final conclusions | Based on the absence of a closed loop for the indirect comparison, consistency or inconsistency test was exempted. Heterogeneity assessment was not clearly reported. However, the authors noted that there could be heterogeneity based on diversity of racial population. | Heterogeneity between studies was explored through the Cochrane Q test and the inconsistency test (I2). A high degree of heterogeneity was diagnosed if the I2 test was greater than 50% or the P value was statistically significant. | Heterogeneity among studies with direct comparisons was assessed by using I2 statistics. |
Assessment of convergence | A total of to 50,000 iterations were used and they considered the first 10,000 as a burn-in sample to eliminate the effect of the initial value. The Brooks-Gelman-Rubin (BGR) diagnostic method was used to assess convergence for all comparisons both visual diagnosis and BGR diagnostics were conducted | NR | NR | NR |
Outcomes | OS, PFS, safety end points | PFS, OS, ORR, DCR, and AEs | ORR, DORR, DCR, PFS, OS, TRAEs and DR | OS, PFS, response rate |
Follow-up time points | NR | NR | NR | NR |
Construction of nodes | NR | NR | NR | The network graph of the main loop had 2 dominant hubs. Seven trials permitted selective administration of cisplatin (CDDP) and carboplatin (CBDCA) in all arms. Therefore, these trials composed an independent small loop. |
Sensitivity analyses | Sensitivity analysis was conducted by excluding the studies that showed heterogeneity. | NR | NR | NR |
Subgroup analysis | ECOG PS Geography: western vs Asian countries | NR | Sex, age, Eastern Cooperative Oncology Group (ECOG) Performance Status (PS), use of platinum salt, presence of brain and liver metastases and smoking status. | Not conducted due to insufficient sample size |
Methods for pairwise meta-analysis | Effect sizes were expressed as HR and RR with their 95% CrIs. when the 95% CrI did not include 1, the difference in the effect size between the treatment groups was considered statistically significant. | Comparisons of HRs, as well as variance estimates, were calculated from the reported CIs for PFS and OS by random effect model. | Hazard ratios (HRs) were considered to evaluate the association for PFS and OS, with the relative 95% confidence intervals (CI). | The authors pooled the logarithm of hazard ratio (HR) and its standard error. A league table of the HRos, HRpfs, ORrr, and their 95% confidence intervals (CI) was presented. |
AE = adverse event; CI = confidence interval; CrI = credible interval; DCR = disease control rate; DORR = duration of objective response rate; DR = discontinuation rate; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; ITC = indirect treatment comparison; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Table 37: ITC Analysis Methods of the Published ITCs
Item | Chen Hsiao-ling et al., 2020 | Wang et al., 2020 | Zhou et al., 2020 | Chen et al., 2017 | Kang et al., 2021 |
|---|---|---|---|---|---|
ITC methods | Network graphs for different outcomes were generated separately to determine which treatments were directly or indirectly comparable. A frequentist network meta-analysis Fixed-effect models were used, since in most cases the treatment of interest was evaluated in one trial and the number of included trials per comparison was too small to estimate between-study heterogeneity. | A frequentist model NMA. The random effect was applied. NMA based on random effect model a random-effects consistency model to pool evidence from direct and indirect comparisons. | Bayesian network meta-analysis. A random-effects hierarchical model which assumes that different comparisons for each survival outcome (i.e., PFS, OS) shared a common heterogeneity parameter was used. Markov chain Monte Carlo methods was implemented. | Not clear. Confidence intervals were reported suggesting a frequentist approach implemented. | Bayesian methods. A fixed-effect model was used for the analysis due to the absence of data to assess the heterogeneity between trials. |
Priors | NR | NR | NR | NR | NR |
Assessment of model fit | NR | NR | NR | NR | Visual inspection and Akaike information criterion (AIC) were used to judge the goodness of model fitting. |
Assessment of consistency | The authors reported that between-study heterogeneity could not be assessed because of small number of trials. 2 Studies ((CA184 to 041 and CA184 to 156) were excluded from the analysis due to heterogeneity. | Heterogeneity of the results using the chi-square (χ2) tests and quantified using I2 statistic percentages. | The sponsor considered the distribution that might affect outcomes to be similar in all of the pairwise comparisons according to the transitivity assumption. Inconsistency standard deviation and random-effects standard deviation were used to evaluate the inconsistency within the multiple treatment comparison. A 95% CI that includes 1 indicated a low risk of inconsistency. | Consistency could not be assessed, as only tree‐shaped networks were available. The transitivity assumption was made where the sponsor compared the baseline characteristics of each included study and performed data synthesis after verifying that the transitivity among different studies was good. A common within‐network between‐study variance was assumed, indicated by I2 calculated using the restricted maximum likelihood method. | Consistency test was exempted because of the deficiency of a closed loop for the indirect comparison. A fixed-effect model was used for the analysis due to the absence of data to assess the heterogeneity between trials. |
Assessment of convergence | NR | NR | NR | NR | NR |
Outcomes | OS, PFS, AEs and ORR | OS, PFS, ORR, DCR, and adverse events. | ORR, DCR, PFS, OS, TRAEs | AEs (Hematological and non‐hematological toxicities) | PFS and OS |
Follow-up time points | NR | NR | NR | NR | NR |
Construction of nodes | Networks were constructed such that all treatments were linked to chemotherapy treatment comparator. | Network diagram was constructed such that treatments of interest were linked to placebo | The network was designed to allow for multiple comparisons of different drugs added to chemotherapy and conventional therapy. Network diagram constructed such that etoposide + platin/carboplatin was the main connection for all treatment comparisons | The network geometry showed that no comparison was informed by either direct or indirect evidence. Data were synthesized to estimate the network estimates. | NR |
Sensitivity analyses | NR | NR | NR | The predictive interval (PrI) of each outcome was calculated and the authors excluded studies with a high risk of bias as sensitivity analyses. | Probabilistic sensitivity analyses were performed. |
Subgroup analysis | Sex Age Brain metastasis ECOG PS | NR | Not conducted | Not conducted because some comparisons only included one study. | Not conducted due to the inconsistency of the subgroup information across the clinical trials included in the ITC. |
Methods for pairwise meta-analysis | The effect sizes of the pairwise comparisons were summarized as surface under cumulative ranking curve (SUCRA) rankings and forest plots Response ratio was regarded as the effect size for the objective response rate and risk ratio was used for adverse events along with 95% confidence intervals (CIs). | Direct and indirect treatment effects were merged into a single effect size, and the relative effects between interventions were presented as risk ratios (RRs) and associated 95% CIs. | The hazard ratio (HR) for survival outcomes (OS and PFS), the odds ratio (OR) for binary outcomes (ORR and TRAEs grade 3 or higher), and their 95% CIs were used to measure outcomes and safety. The 95% CIs of either the pooled HR excluding 1 or a 2-sided P < 0.05 was considered statistically significant. | All outcomes were indicated with odds ratios (ORs) and the corresponding 95% confidence intervals (CIs) reported. A common within‐network between‐study variance was assumed, indicated by I2 calculated using the restricted maximum likelihood method (if a value of I2 exceeds 0.5, then significant heterogeneity is considered to exist between studies). | Different treatments were ranked in terms of the surface area under the cumulative ranking curve (SUCRA). |
AE = adverse event; CI = confidence interval; CrI = credible interval; DCR = disease control rate; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; ITC = indirect treatment comparison; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RR = risk ratio; TRAE = treatment-related adverse event.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
ES-SCLC
extensive-stage small cell lung cancer
NMA
network meta-analysis
pCPA
pan-Canadian Pharmaceutical Alliance
pERC
CADTH pan-Canadian Oncology Drug Review Expert Review Committee
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Atezolizumab for injection (Tecentriq), solution for IV infusion, 1,200 mg/20 mL |
Submitted price | Atezolizumab, 1,200 mg/20 mL (60 mg/mL): $6,776.00 per 1,200 mg vial |
Indication | In combination with carboplatin and etoposide for the first-line treatment of adult patients with extensive-stage small cell lung cancer |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | August 8, 2019 |
Reimbursement request | For the first-line treatment of patients with ES-SCLC in combination with a platinum-based chemotherapy and etoposide. Maintenance atezolizumab should be continued until loss of clinical benefit or unacceptable toxicity. |
Sponsor | Hoffmann-La Roche Ltd. |
Submission history | Previously reviewed: Yes Indication: Small cell lung cancer Recommendation date: January 30, 2020 Recommendation: Do not reimburse Indication: Non–small cell lung cancer Recommendation date: June 20, 2018 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Advanced or metastatic triple-negative breast cancer Recommendation: Withdrawn |
ES-SCLC = extensive-stage small cell lung cancer; NOC = notice of compliance.
Table 2: Summary of Economic Information
Component | Description |
|---|---|
Type of economic evaluation | Cost minimization analysis |
Target population | Adult patients with extensive-stage small cell lung cancer who were chemotherapy-naive for their extensive-stage disease |
Treatments |
|
Comparator | Durvalumab in combination with platinum-based chemotherapy and etoposide |
Perspective | Canadian publicly funded health care payer |
Time horizon | 1 year |
Key data source | A sponsor-commissioned indirect treatment comparison to establish the equivalent comparative efficacy and safety of atezolizumab in combination with carboplatin and etoposide vs. durvalumab in combination with platinum-based chemotherapy and etoposide |
Costs considered | Drug acquisition costs, drug administration costs, monitoring costs |
Submitted results |
|
Key limitations | In the absence of direct evidence comparing atezolizumab and durvalumab, both in combination with a platinum-based chemotherapy and etoposide, a sponsor-commissioned NMA was submitted; the NMA showed no clinically meaningful difference in the survival benefit between atezolizumab and durvalumab. However, the CADTH clinical review noted that the credible intervals were wide, which introduces some uncertainty into the conclusions that may be drawn. |
CADTH reanalysis results |
|
NMA = network meta-analysis.
Conclusions
The sponsor’s submitted cost minimization analysis assumes equivalent clinical efficacy and safety of atezolizumab and durvalumab therapy when used in combination with platinum-based chemotherapies. An assumption of comparable efficacy and safety is appropriate when considering atezolizumab in combination with carboplatin and etoposide. However, limitations identified by the CADTH clinical review of the sponsor’s submitted network meta-analysis (NMA) noted that this assumption was associated with some uncertainty.
Based on the assumption of equal efficacy and safety for atezolizumab and durvalumab, atezolizumab in combination with carboplatin and etoposide resulted in drug cost savings of $25,084 and total cost savings of $25,967 per patient when compared with durvalumab in combination with platinum-based chemotherapy for the first-line treatment of extensive-stage small cell lung cancer (ES-SCLC). Similar cost savings were observed when considering any platinum-based chemotherapy in combination with atezolizumab and etoposide.
The sponsor’s submitted cost minimization analysis assumes that durvalumab is publicly available. Durvalumab is undergoing active pan-Canadian Pharmaceutical Alliance (pCPA) negotiations at the time of this review. The cost-effectiveness of atezolizumab in combination with platinum-based chemotherapy and etoposide versus platinum-based chemotherapy and etoposide alone was not assessed for this review as this was not part of the submitted cost minimization analysis. Additionally, the CADTH pan-Canadian Oncology Drug Review Expert Review Committee (pERC) recommendation for durvalumab recommended a reduction in price of at least 88%. The submitted cost minimization analysis only takes into account publicly available list prices. The confidential price of durvalumab should be considered to ensure that the cost savings suggested by the sponsor are realized with atezolizumab.
Economic Review
The current review is for atezolizumab (Tecentriq) for the first-line treatment of adult patients with chemotherapy-naive ES-SCLC in combination with carboplatin and etoposide.
Economic Information
Summary of Sponsor’s Economic Information
The sponsor submitted a cost minimization analysis1 for atezolizumab in comparison with durvalumab, both in combination with a platinum-based chemotherapy and etoposide during the induction phase and followed by monotherapy in the maintenance phase, for the first-line treatment of adult patients with ES-SCLC. The sponsor submitted a request for deviation to limit its comparison to durvalumab, which was granted by CADTH. The sponsor submitted a base-case analysis aligned with its Health Canada indication, where atezolizumab was considered solely in combination with carboplatin and etoposide, and a scenario analysis aligned with its reimbursement request in which atezolizumab was considered in combination with either carboplatin or cisplatin plus etoposide.
The sponsor assumed no differences in clinical efficacy and safety between atezolizumab and durvalumab therapies based on a sponsor-commissioned NMA.2 As such, the analysis included only drug acquisition costs, treatment administration costs, and clinical consultation costs. The sponsor’s analysis was conducted from the perspective of the publicly funded health care payer over a time horizon of 1 year. As such, discounting was not applied.
Atezolizumab is available as a 1,200 mg concentrate in 20 mL vials (60 mg/mL) for solution for infusion.1 The recommended dose in the induction phase is 1,200 mg of atezolizumab, followed by carboplatin on day 1 and etoposide administered by IV infusion on days 1, 2, and 3, repeated every 3 weeks for a maximum of 4 cycles. This regimen is delivered for a maximum of 4 cycles.3 The maintenance phase consists of atezolizumab monotherapy at the recommended dosage of 1,200 mg of atezolizumab repeated every 3 weeks thereafter. The number of cycles of each drug for the atezolizumab combination therapy was based on the mean duration of treatment in the IMpower133 trial (4.7 months).4 The sponsor assumed identical treatment duration for atezolizumab- and durvalumab-based regimens. The number of cycles of each drug included in the sponsor’s analysis, corresponding to the assumed duration of treatment, was derived using the suggested dosing regimens from the product monograph.5,6 The sponsor assumed platinum-based chemotherapy consisted of 70% carboplatin use and 30% cisplatin when both therapies were options. The sponsor assumed there would be no drug wastage and 100% adherence.
When considering the sponsor’s analysis based on the Health Canada indication, and atezolizumab at a price of $6,776.00 per 20 mL vial, atezolizumab in combination with carboplatin and etoposide was associated with total drug costs of $50,867 per patient and total treatment costs of $53,787 per patient. The sponsor’s analysis considered durvalumab at a price of $3,911.11 per 10 mL vial. Treatment with durvalumab in combination with platinum-based chemotherapy and etoposide was associated with total drug costs of $75,951 per patient and total treatment costs of $79,754 per patient. In comparison with durvalumab combination therapy, atezolizumab combination therapy was associated with drug cost savings of $25,084 and total cost savings of $25,967.
Similar cost savings were estimated in an analysis aligned with the reimbursement request; treatment with atezolizumab combination therapy was associated with incremental cost savings of $25,938 per patient compared with durvalumab combination therapy, both with platinum-based chemotherapy as backbone during the induction phase.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total drug costs, $ | Incremental drug costs, $ | Total costs, $ | Incremental costs, $ |
|---|---|---|---|---|
Health Canada indication | ||||
Durvalumab plus platinum chemotherapy and etoposide | 75,951 | Reference | 79,754 | Reference |
Atezolizumab plus carboplatin and etoposide | 50,867 | –25,084 | 53,787 | –25,967 |
Reimbursement request | ||||
Durvalumab plus platinum chemotherapy and etoposide | 75,951 | Reference | 79,754 | Reference |
Atezolizumab plus platinum chemotherapy and etoposide | 50,439 | –25,512 | 53,816 | –25,938 |
Note: The negative incremental costs represent cost savings.
Source: Sponsor’s economic submission.1
CADTH Appraisal of the Sponsor’s Economic Information
CADTH identified the following key limitation to the sponsor’s analysis that has notable implications on the economic analysis:
There is uncertainty in the assumption of equivalent clinical efficacy and safety between atezolizumab and durvalumab: In the absence of a direct head-to-head comparison between atezolizumab and durvalumab therapy, both in combination with a platinum-based chemotherapy and etoposide, the sponsor commissioned an NMA assessing the comparative efficacy and safety of atezolizumab and durvalumab. The NMA results showed no statistically significant difference in progression-free survival and overall survival between atezolizumab and durvalumab therapy, indicating they are likely comparable. However, the CADTH clinical review noted that the 95% credible intervals for these outcomes were wide, highlighting that some uncertainty remains in the sponsor’s assumption of equivalent clinical efficacy between atezolizumab and durvalumab therapy. The clinical experts consulted by CADTH for this review noted that there is no evidence to suggest a clinically meaningful difference between the efficacy, safety, and duration of therapy with atezolizumab, when used in combination with carboplatin and etoposide, and durvalumab when used in combination with a platinum-based chemotherapy and etoposide. Should there be differences in either of these parameters from the assumptions made by the sponsor in its submission, the cost-effectiveness of atezolizumab for ES-SCLC would be uncertain.
CADTH was unable to address this limitation in reanalyses.
CADTH Reanalyses of the Economic Information
CADTH did not undertake a reanalysis of the sponsor’s submission. The limitations identified by CADTH could not be addressed and were related to the underlying assumption of equivalent efficacy and safety of atezolizumab and durvalumab, as well as to the generalizability of the efficacy of atezolizumab in combination with carboplatin and etoposide to the use of atezolizumab in combination with cisplatin and etoposide.
Under an assumption of equivalent clinical efficacy and safety of atezolizumab and durvalumab, CADTH accepted the sponsor’s submitted analysis. Atezolizumab in combination with carboplatin and etoposide resulted in estimated cost savings of $25,938 per patient compared to durvalumab in combination with platinum-based chemotherapy and etoposide. Similar cost savings were observed when considering the sponsor’s reimbursement request.
Issues for Consideration
CADTH has previously reviewed atezolizumab for first-line treatment of ES-SCLC: CADTH has previously reviewed atezolizumab for first-line treatment of ES-SCLC, with a recommendation published in January 2020.7 pERC did not recommend reimbursement of atezolizumab in combination with a platinum-based chemotherapy and etoposide as pERC was unable to conclude that there was a clinically meaningful net benefit associated with atezolizumab in combination with platinum-based chemotherapy and etoposide in comparison with platinum-based chemotherapy and etoposide alone. pERC also concluded that atezolizumab in combination with platinum-based chemotherapy and etoposide was not cost-effective at its submitted price in comparison with platinum-based chemotherapy and etoposide alone. The cost-effectiveness of atezolizumab in combination with platinum-based chemotherapy and etoposide in comparison with platinum-based chemotherapy and etoposide alone was not assessed in this review.
pCPA negotiations for durvalumab are ongoing, and analyses are based on publicly available list prices: The sponsor’s submitted cost minimization analysis was focused on a comparison of atezolizumab versus durvalumab, both in combination with platinum-based chemotherapy and etoposide, and assumes durvalumab is publicly available. The pCPA negotiations for durvalumab are ongoing.8 This means that durvalumab has not yet been listed, and the price has not been determined. The sponsor’s analyses are based on publicly available list prices for all comparators. The pERC recommendation for durvalumab included a reduction in price of at least 88%. The relevance of the sponsor’s submitted cost minimization analysis depends on the availability of durvalumab, as well as the negotiated price of durvalumab. This introduces notable uncertainty into the cost savings estimated for atezolizumab. CADTH considered a scenario in the budget impact analysis (BIA) where durvalumab was unavailable.
Durvalumab and atezolizumab follow different maintenance dosing schedules: Atezolizumab maintenance dosing is once every 21 days, whereas durvalumab maintenance dosing is once every 28 days. As a result, there is a difference in the number of cycles required of each drug for a given time period when assuming equal duration of treatment. This will have an impact on total treatment costs and should be considered when determining the relative costs of atezolizumab in comparison with durvalumab. This may be of concern when considering scenarios where the drug price for durvalumab is different from the publicly available list price.
Durvalumab dosing is assumed to be flat: The sponsor’s analysis assumed flat dosing for durvalumab, but the product monograph allows for weight-based dosing for patients weighing less than 30 kg. In this review, the sponsor assumed all patients eligible for treatment would receive flat dosing. The results of this analysis are not applicable to patients who weigh less than 30 kg or are receiving weight-based dosing.
Conclusions
The sponsor’s submitted cost minimization analysis assumes equivalent clinical efficacy and safety of atezolizumab and durvalumab therapy when used in combination with platinum-based chemotherapies. Based on the CADTH clinical review and consultation with clinical experts, an assumption of comparable efficacy and safety is appropriate when considering atezolizumab in combination with carboplatin and etoposide. However, limitations identified by the CADTH clinical review of the sponsor’s submitted NMA noted that this assumption was associated with some uncertainty.
Based on the assumption of equal efficacy and safety for atezolizumab and durvalumab, atezolizumab in combination with carboplatin and etoposide resulted in drug cost savings of $25,084 and total cost savings of $25,967 per patient when compared with durvalumab in combination with platinum-based chemotherapy for the first-line treatment of ES-SCLC. Similar cost savings were observed when considering any platinum-based chemotherapy in combination with atezolizumab and etoposide.
The sponsor’s submitted cost minimization analysis assumes that durvalumab is publicly available. Durvalumab is undergoing active pCPA negotiations at the time of this review. The cost-effectiveness of atezolizumab in combination with platinum-based chemotherapy and etoposide in comparison with platinum-based chemotherapy and etoposide alone was not assessed for this review as this was not part of the submitted cost minimization analysis. Additionally, the pERC recommendation for durvalumab recommended a reduction in price of at least 88%. The submitted cost minimization analysis only takes into account publicly available list prices. The confidential price of durvalumab should be considered to ensure the cost savings suggested by the sponsor are realized with atezolizumab.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tecentriq (atezolizumab), concentrate for solution for infusion, 60mg/mL; 1200 mg/20mL and 840 mg/14mL single use vials. Mississauga (ON): Hoffmann-La Roche Limited (Roche); 2022.
2.Atezolizumab in untreated extensive-stage small cell lung cancer: network meta-analysis report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tecentriq (atezolizumab), concentrate for solution for infusion, 60mg/mL; 1200 mg/20mL and 840 mg/14mL single use vials. Mississauga (ON): Hoffmann-La Roche Limited (Roche); 2022. 2021.
3.CRBPETOP+ATEZ provider monograph. Toronto: Cancer Care Ontario; 2020: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/62091#DrugRegimen. Accessed 2022 Feb 27.
4.Clinical Study Report: Primary CSR Study GO30081 (IMpower133). A Phase I/III, randomized, double-blind, placebo-controlled study of carboplatin plus etoposide with or without atezolizumab (anti-PD-L1 antibody) in patients with untreated extensive-stage small cell lung cancer. Report No.1084268 [internal sponsor's report]. Mississauga (ON): F. Hoffmann-La Roche Ltd; 2018 Sep.
5.CRBPETOP+DURV provider monograph. Toronto: Cancer Care Ontario; 2021: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/68436#DrugRegimen. Accessed 2022 Feb 27.
6.CISPETOP+DURV provider monograph. Toronto: Cancer Care Ontario; 2021: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/68431#DrugRegimen. Accessed 2022 Feb 27.
7.Drug Reimbursement Review: Tecentriq (atezolizumab) for small cell lung cancer. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/tecentriq-small-cell-lung-cancer. Accessed 2022 Apr 19.
8.pan-Canadian Pharmaceutical Alliance. Imfinzi (durvalumab). 2022; https://www.pcpacanada.ca/negotiation/21550. Accessed 2022 Mar 17.
9.CARBOplatin provider monograph. Toronto: Cancer Care Ontario; 2022: https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/43796#Dosing. Accessed 2022 Apr 4.
10.ATEZ(MNT) provider monograph. Toronto: Cancer Care Ontario; 2022: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/62101#DrugRegimen. Accessed 2022 Feb 27.
11.DURV(MNT) provider monograph. Toronto: Cancer Care Ontario; 2022: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/68426#DrugRegimen. Accessed 2022 Feb 27.
12.Budget Impact Analysis: Budget Impact Report for Tecentriq® (atezolizumab) for the first-line treatment of patients with extensive stage small cell lung cancer (ES-SCLC) in combination with a platinum-based chemotherapy and etoposide [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tecentriq (atezolizumab), concentrate for solution for infusion, 60mg/mL; 1200 mg/20mL and 840 mg/14mL single use vials. Mississauga (ON): Hoffmann-La Roche Limited (Roche); 2022.
13.Canadian cancer statistics: a 2020 special report on lung cancer. Ottawa (ON): Canadian Cancer Society, Statistics Canada, the Public Health Agency of Canada, in collaboration with the provincial and territorial cancer registries; 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2020-statistics/canadian-cancer-statistics/2020-special-report/res-cancerstatistics-canadiancancerstatistics-2020_special-report_en.pdf. Accessed 2022 Mar 7.
14.Province-specific statistics. In: Canadian Cancer Statistics 2021. Ottawa (ON): Canadian Cancer Society, Public Health Agency of Canada, in collaboration with the provincial and territorial cancer registries: https://cancer.ca/en/research/cancer-statistics/canadian-cancer-statistics. Accessed 2022 Mar 7.
15.Imfinzi (durvalumab for injection), concentrate for solution for infusion, 50 mg/mL, intravenous [product monograph]. Mississauga (ON): AstraZeneca Canada; 2021: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/imfinzi-product-monograph-en.pdf. Accessed 2021 Nov 1.
16.Etoposide injection USP (etoposide), 20 mg/mL [product monograph]. Boucherville (QC): Sandoz Canada; 2015 May 21: https://www.sandoz.ca/sites/www.sandoz.ca/files/Etoposide%20Product%20Monograph.pdf. Accessed 2021 Nov 1.
17.Cisplatin injection BP, sterile solution, 1 mg/mL (50 mg and 100 mg cisplatin per vial) [product monograph]. Kirkland (QC): Pfizer Canada; 2020 Apr 3: https://www.pfizer.ca/sites/default/files/202004/Cisplatin_PM_E_235278_2020-04-03.pdf. Accessed 2021 Nov 1.
18.Carboplatin injection BP, sterile solution, 10 mg / mL [product monograph]. Kirkland (QC): Pfizer Canada; 2019: https://www.pfizer.ca/sites/default/files/202001/Carboplatin_PM_E_231317_16Dec2019.pdf. Accessed 2021 Nov 1.
19.CRBPETOP+DURV regimen. Toronto: Cancer Care Ontario; 2021: https://www.cancercareontario.ca/en/drugformulary/regimens/68436. Accessed 2021 Nov 1.
20.CISPETOP+DURV regimen. Toronto: Cancer Care Ontario; 2021: https://www.cancercareontario.ca/en/drugformulary/regimens/68431. Accessed 2021 Nov 1.
21.CRBPETOP+ATEZ regimen. Toronto: Cancer Care Ontario; 2020: https://www.cancercareontario.ca/en/drugformulary/regimens/62091. Accessed 2021 Nov 1.
22.CADTH Reimbursement Recommendation. Durvalumab (Imfinzi) for first-line treatment of adult patients with ES-SCLC in combination with etoposide and either carboplatin or cisplatin. Canadian Journal of Health Technologies. 2021. https://www.cadth.ca/sites/default/files/pcodr/Reviews2021/PC0234%20Imfinzi%20-%20Draft%20CADTH%20Recommendation%20For%20posting%20June%2010,%202021.pdf. Accessed 2022 Apr 4.
23.Doherty J, Dawe DE, Pond GR, Ellis PM. The effect of age on referral to an oncologist and receipt of chemotherapy among small cell lung cancer patients in Ontario, Canada. J Geriatr Oncol. 2019;10(3):449-458. PubMed
Appendix 1: Additional Economic Information
Note that this appendix has not been copy-edited.
Cost Comparison Table
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table, and as such, the table may not represent the actual costs to public drug plans.
Table 4: CADTH Cost Comparison Table for First-Line Treatment of Adult Patients With ES-SCLC
Treatment | Strength/ concentration | Form | Price per vial ($) | Recommended dosage | Average daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Atezolizumab (Tecentriq) | 60 mg/mL | 14 mL 20 mL Vial for IV infusion | 4,732.0000a 6,776.0000a | Induction dosage: 1,200 mg on day 1 Q3W in combination with chemotherapy for 4 cycles Maintenance dosage: After 4 cycles,1,200 mg on day 1 Q3W as monotherapy | 322.67 | 9,035 |
Carboplatin (generics) | 10 mg/mL | 5 mL 15 mL 45 mL 60 mL Vial for IV infusion | 70.0000 210.0000 599.9985 775.0000 | AUC 5 (maximum of 750 mg) on day 1 Q3W for 4 cycles | 46.90 | 1,313 |
Cisplatin (generics) | 1 mg/mL | 50 mL 100 mL Vial for IV infusion | 135.0000 270.0000 | 75 mg/m2 on day 1 Q3W for 4 cycles | 19.29 | 540 |
Etoposide (generics) | 20 mg/mL | 5 mL 10 mL 25 mL 50 mL Injection | 75.0000 150.0000 375.0000 750.0000 | 100 mg/m2 on days 1 to 3 Q3W for 4 cycles | 21.43 | 600 |
Carboplatin + atezolizumab | — | — | — | — | 369.57 | 10,348 |
Cisplatin + atezolizumab | — | — | — | — | 341.95 | 9,575 |
Atezolizumab (monotherapy) | — | — | — | — | 322.67 | 9,035 |
Durvalumab + chemotherapy | ||||||
Durvalumab (Imfinzi) | 50 mg/mL | 2.4 mL 10 mL Concentrate solution for infusion | 938.6700 3,911.1100 | Induction dosage: 1,500 mg in combination with chemotherapy Q3W for 4 cycles Maintenance dosage: 1,500 mg Q4W as monotherapy | 558.73 419.05 | 15,645 11,733 |
Carboplatin (generics) | 10 mg/mL | 5 mL 15 mL 45 mL 60 mL Vial for IV infusion | 70.0000 210.0000 599.9985 775.0000 | AUC 5 to 6 (maximum of 750 mg to 900 mg) on day 1 Q3W for 4 cyclesb | 46.90 to 56.90 | 1,313 to 1,593 |
Cisplatin (generics) | 1 mg/mL | 50 mL 100 mL Vial for IV infusion | 135.0000 270.0000 | 75 mg/m2 to 80 mg/m2 on day 1 Q3W for 4 cyclesb | 19.29 | 540 |
Etoposide (generics) | 20 mg/mL | 5 mL 10 mL 25 mL 50 mL Injection | 75.0000 150.0000 375.0000 750.0000 | 80 mg/m2 to 100 mg/m2 on days 1 to 3 Q3W for 4 cyclesb | 21.43 | 600 |
Carboplatin + durvalumab | 615.87 | 17,244 | ||||
Cisplatin + durvalumab | 578.02 | 16,185 | ||||
Durvalumab (monotherapy) | 419.05 | 11,733 | ||||
AUC = target area under the concentration vs. time curve; Q3W = every 3 weeks; Q4W = every 4 weeks.
Note: All prices are IQVIA Delta PA database wholesale list prices (accessed February 28, 2022), unless otherwise indicated, and do not include dispensing fees or administration. Assumes a patient weighing 70 kg, with a body surface area of 1.8 m2 and a glomerular filtration rate of 125 mL/min.9 Wastage of excess medication in vials is also assumed. Recommended dosage is based on Cancer Care Ontario monographs,3,5,6,10,11 unless otherwise indicated. Total cost estimates per regimen are based on the cheapest combination of the component drugs.
aSponsor’s submitted price.
bPatients with a body weight less than 30 kg must receive weight-based dosing at 20 mg/kg on the same schedule, until their weight increases to more than 30 kg.
Additional Details on the Sponsor’s Submission
No additional information from the sponsor’s submitted pharmacoeconomic evaluation was considered in the review of atezolizumab.
Additional Details on the CADTH Reanalyses and Additional Analyses
CADTH did not conduct any additional pharmacoeconomic analyses in the review of atezolizumab.
Appendix 2: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 5: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a BIA,12 assessing the expected budgetary impact of the introduction of atezolizumab, in combination with carboplatin and etoposide during the induction phase, followed by atezolizumab monotherapy, for the first-line treatment of adult patients with ES-SCLC. The sponsor’s base-case analysis was aligned with the Health Canada indication for atezolizumab. The sponsor submitted a scenario analysis based on the sponsor’s reimbursement request where atezolizumab is considered in combination with any platinum-based chemotherapy and etoposide during the induction phase. The analyses were done from the perspective of the Canadian public drug plans, over a 3-year time horizon; the base year was assumed to be 2022 and the 3-year time horizon ran from 2023 to 2025. Current treatments evaluated in the reference scenario included durvalumab in combination with platinum-based chemotherapy and etoposide, platinum-based chemotherapy in combination with etoposide, mono-chemotherapy, and patient participation in clinical trials.
The sponsor estimated the eligible patient population size using an epidemiology-based approach, with data obtained from published literature and Canadian Cancer Statistics to estimate the number of new (incident) patients eligible for treatment.13,14 In the new drug scenario, the sponsor assumed that atezolizumab would split the market evenly with durvalumab therapy. Patients accrued drug acquisition costs in the incident year only. Drug costs were based on the recommended dosing regimens as per the Cancer Care Ontario formulary and anticipated duration of therapy, which was based on the IMPower133 trial for atezolizumab regimen.4,15-21 The sponsor assumed duration of therapy was the same for the rest of the included therapies. Key inputs to the BIA are documented in Table 6.
Table 6: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3, if appropriate) |
|---|---|
Target population | |
Lung cancer patients | 21,032 / 21,266 / 21,500 |
Proportion of lung cancer patients with SCLC | 12% |
Proportion of SCLC patients with extensive-stage disease | 67% |
Proportion of patients who receive treatment | 80% |
Number of patients eligible for drug under review | 1,353 / 1,368 / 1,383 |
Market uptake (3 years) | |
Uptake (reference scenario) Durvalumab + platinum chemotherapy + etoposide Platinum chemotherapy Mono-chemotherapy Clinical trials | ||| / ||| / ||| ||| / ||| / ||| |||| / |||| / |||| |||| / |||| / |||| |
Uptake (new drug scenario) Atezolizumab + carboplatin + etoposide Durvalumab + platinum chemotherapy + etoposide Platinum chemotherapy Mono-chemotherapy Clinical trials | ||| / ||| / ||||| ||| / ||| / ||||| |||| / |||| / |||| |||| / |||| / |||| |||| / |||| / |||| |
Cost of treatment (per patient)a | |
Cost of treatment over cycle Atezolizumab + carboplatin + etoposide Atezolizumab + cisplatin + etoposide Durvalumab + carboplatin + etoposide Durvalumab + cisplatin + etoposide Carboplatin + etoposide Cisplatin + etoposide | $7,670 $7,313 $12,628 $12,271 $894 $537 |
Cost of administration (per patient) | |
Cost of initial administration Atezolizumab Durvalumab Carboplatin Cisplatin Etoposide Cost of subsequent administrations Atezolizumab Durvalumab Carboplatin Cisplatin Etoposide | $218 $218 $54 $435 $109 $109 $218 $54 $435 $109 |
SCLC = small cell lung cancer.
aThe sponsor assumed body surface areas of 1.86 m2, and vial sharing with 4.37% wastage in estimating treatment costs.
Note: No costs were included for mono-chemotherapy and clinical trials.
Summary of the Sponsor’s BIA Results
From the Canadian public drug plan perspective, the sponsor estimated the net 3-year budget impact of introducing atezolizumab in combination with carboplatin and etoposide during the induction phase, followed by atezolizumab monotherapy for the first-line treatment adult patients with ES-SCLC to be cost savings of $30,049,695 (Year 1: $8,482,973; Year 2: $10,293,220; Year 3: $11,273,502). The 3-year budgetary impact increased to estimated cost savings of $30,621,947 when administration costs were included under the health care perspective.
Based on the sponsor’s reimbursement request, atezolizumab in combination with platinum-based chemotherapy (70% carboplatin and 30% cisplatin) and etoposide, followed by atezolizumab monotherapy resulted in cost savings of $8,627,891 in year 1, $10,469,064 in year 2 and $11,466,092 in year 3, for a total 3-year budget impact of $30,563,048.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The sponsor’s assumption regarding participation in clinical trials as a relevant comparator with market share is inappropriate: The sponsor assumed patient participation in clinical trials captured |||| of market share and accrued no costs. Participation in clinical trials is uncertain and the sponsor’s inclusion of clinical trials in the market mix artificially decreases the estimated population size, disregarding the treatment costs incurred by drug plans and underestimating the budget impact. The clinical expert consulted for this review noted individuals healthy enough to enter clinical trials would be eligible for immunotherapy.
In CADTH reanalysis, clinical trials were removed from the market mix; the market share of clinical trials was redistributed to available immunotherapies.
The proportion of patients assumed to be treated is uncertain: In the submitted BIA, the sponsor assumed 80% of patients with ES-SCLC receive first-line treatment based on CADTH’s review of durvalumab.22 However, the durvalumab review noted this assumption is associated with uncertainty and may range from 70% to 80%. The clinical expert consulted for this review by CADTH noted that the proportion of patients receiving treatment may be in the range of 75% based on a population-based retrospective cohort study investigating treatment patterns among small cell lung cancer patients in Ontario, Canada.23
In CADTH scenario, it was assumed that 75% of patients receive treatment based on clinical expert opinion.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by redistributing market share of clinical trials over immunotherapies based on feedback from clinical experts.
Table 7: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Market share assumptions (year 1/year 2/year 3) | Reference scenario: Atezolizumab + platinum chemotherapy + etoposide: 0% / 0% / 0% Durvalumab + platinum chemotherapy + etoposide: ||| / ||| / ||| Platinum chemotherapy: ||| / ||| / ||| Mono-chemotherapy: |||| / |||| / |||| Clinical trials: |||| / |||| / |||| New drug scenario: Atezolizumab + platinum chemotherapy + etoposide: |||| / |||| / ||||| Durvalumab + platinum chemotherapy + etoposide: |||| / |||| / ||||| Platinum chemotherapy: ||||| / ||||| / ||||| Mono-chemotherapy: |||| / |||| / |||| Clinical trials: |||| / |||| / |||| | Reference scenario: Atezolizumab + platinum chemotherapy + etoposide: 0% / 0% / 0% Durvalumab + platinum chemotherapy + etoposide: 55% / 65% / 70% Platinum chemotherapy: 40% / 30% / 25% Mono-chemotherapy: 5% / 5% / 5% Clinical trials: 0% / 0% / 0% New drug scenario: Atezolizumab + platinum chemotherapy + etoposide: 27.5% / 32.5% / 35% Durvalumab + platinum chemotherapy + etoposide: 27.5% / 32.5% / 35% Platinum chemotherapy: 40% / 40% / 30% / 25% Mono-chemotherapy: 5% / 5% / 5% Clinical trials: 0% / 0% / 0% |
CADTH base case | Reanalysis 1 | |
In the CADTH reanalysis, the 3-year budget impact of reimbursing atezolizumab from the public drug plan perspective for the first-line treatment of adult patients with ES-SCLC was estimated to be cost savings of $33,180,266 (year 1: $9,490,680; year 2: $11,341,486; year 3: $12,348,099).
The results of the CADTH step-wise reanalysis is presented in summary format in Table 8 and a more detailed breakdown is presented in Table 9.
Table 8: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total | |
|---|---|---|
Health Canada indication | Reimbursement request | |
Submitted base case | -$30,049,695 | -$30,563,048 |
CADTH reanalysis 1 | -$32,622,953 | -$33,180,266 |
CADTH base case | -$32,622,953 | -$33,180,266 |
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case aligned with Health Canada indication. Results are provided in Table 9. The scenario analysis involved:
assuming 75% of patients receive treatment
assuming durvalumab therapy does not have a market share since negotiations with pCPA are ongoing; the share of durvalumab therapy was redistributed to platinum-based chemotherapy in the reference scenario and to atezolizumab in the new drug scenario
adopting a health care payer perspective (including administration costs).
The estimated budget impact was sensitive to uncertainty in the market share of durvalumab. Similar results were estimated in analyses aligned with the sponsor’s reimbursement request.
Table 9: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current year) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $5,705,239 | $53,935,737 | $64,278,641 | $69,908,722 | $188,123,100 |
New drug | $5,705,239 | $45,452,764 | $53,985,421 | $58,635,221 | $158,073,406 | |
Budget impact | $0.00 | –$8,482,973 | –$10,293,220 | –$11,273,502 | –$30,049,695 | |
CADTH base case | Reference | $5,705,239 | $59,072,871 | $69,473,130 | $75,160,282 | $203,706,283 |
New drug | $5,705,239 | $49,741,601 | $58,322,142 | $63,019,588 | $171,083,330 | |
Budget impact | $0.00 | –$9,331,270 | –$11,150,989 | –$12,140,694 | –$32,622,953 | |
CADTH scenario analysis: assuming 75% treated | Reference | $5,348,662 | $55,380,816 | $65,131,060 | $70,462,764 | $190,974,640 |
New drug | $5,348,662 | $46,632,751 | $54,677,008 | $59,080,863 | $160,390,622 | |
Budget impact | $0.00 | –$8,748,066 | –$10,454,052 | –$11,381,901 | –$30,584,018 | |
CADTH scenario analysis: assuming durvalumab does not have a market share | Reference | $5,705,239 | $6,090,446 | $6,158,445 | $6,226,106 | $18,474,998 |
New drug | $5,705,239 | $40,410,331 | $47,171,153 | $50,878,894 | $138,460,377 | |
Budget impact | $0.00 | $34,319,884 | $41,012,708 | $44,652,787 | $119,985,380 | |
CADTH scenario analysis: health care payer perspective | Reference | $7,538,080 | $62,016,583 | $72,631,190 | $78,444,775 | $213,092,548 |
New drug | $7,538,080 | $52,507,613 | $61,267,847 | $66,072,879 | $179,848,339 | |
Budget impact | $0.00 | –$9,508,970 | –$11,363,343 | –$12,371,896 | –$33,244,209 |
Stakeholder Input
Patient Input
Lung Cancer Canada
About Lung Cancer Canada
Lung Cancer Canada is a registered national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research, and advocacy. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only organization in Canada focused exclusively on lung cancer.
https://www.lungcancercanada.ca/
Lung Cancer Canada is registered with CADTH.
Information Gathering
Data Collection: The information discussed throughout this submission consists of the thoughts and experiences of small cell lung cancer patients and caregivers. They were collected through interviews Lung Cancer Canada had with the patients, as well as information from previous LCC submissions. All interviews were conducted between December 2021 and February 2022.
Demographic Data: Small cell lung cancer (SCLC) represents a minority of the lung cancer patient population, representing only about 10-15% of all lung cancer patients. All the patients discussed in this submission have small cell lung cancer and have experience with atezolizumab (in combination with chemotherapy or as a single treatment). Specific treatment experience can be found in section 6.
||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
|---|---|---|---|---|---|---|
||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| | ||||||||| |
Note: Additional redacted rows have been deleted.
Disease Experience
65-year-old DR had retired early in 2017 after working at a local trucking company for nearly 30 years, which was keeping her active and on her feet most of the day, but because she also had fibromyalgia, it slowly started to limit her mobility and made it hard to move around as much as she needed to. 2 years into retirement in mid-2019 after the onset of non-stop coughing fits, DR visited the hospital knowing that something did not feel right. She had tests done that revealed two tumours: a benign tumour on her left adrenal gland and an aggressive cancerous tumour in her lung. Her doctors gave her a prognosis of about 1 year with treatment and without it, less than 6 months. DR was shocked to say the least, because they had always been keeping fairly active, maintained a healthy diet, and often enjoyed the outdoors with her family, so being given an advanced cancer diagnosis was probably the last thing she’d expect. Because DR also had a number of other health issues develop after her initial cancer diagnosis, such as a blood clot in her left arm and a cholecystectomy, she had to undergo a number of lifestyle changes in addition to the side effects and burdens from the cancer treatments. As a result of a gallbladder surgery, she became diabetic and had to be placed on a strict diet, during which she lost almost 50 pounds, as well as being left with limited movement in her left hand, which she is still recovering from to this day almost a year later. All of these impacted her experience and tolerance for further cancer treatments. By the time she was about to start her first line treatment with chemotherapy, she was already in a negative mindset because of the slew of other health issues that had arose, and was not optimistic she’d live to see another Christmas. DR started her initial cancer treatments with chemotherapy after recovering from the blood clot, then radiation, which was difficult for her while also recovering from the gallbladder surgery. She then started atezolizumab immunotherapy in early 2021, which was met with a very good response, and she has been slowly regaining her strength and functionality to this day. Atezolizumab has allowed her to maintain her independence, she drives herself to immunotherapy appointments alone, and runs errands with her husband on a regular basis; it has not held her back from enjoying her life now, and attributes her success to atezolizumab, which has helped her regain her confidence and livelihood. Her experiences with chemotherapy and radiation are detailed further in this submission, but with the success of atezolizumab, DR is virtually cancer-free as of February 2022.
TD was a 54-year-old teacher and led a very active lifestyle with her family, being a long-distance runner and was kept busy in the classroom. When she developed a new cough in January 2020, doctors found significant tumors in her right lung, which sent her into a tailspin while she was waiting for biopsies and scans to know what was happening. After a few months, she was diagnosed with extensive SCLC with metastases to her pancreas and lymph nodes. She said, “This diagnosis was devastating to me and my family.” Her oncologist said that with chemotherapy, she could live up to one year, but her weakened body may not withstand the treatment. Once she learned about the promising atezolizumab from her oncologist, a treatment that could extend her life, there posed a significant barrier to access this treatment because the cost was not publicly covered, and this is a major determinant that many Canadians patients diagnosed with lung cancer face. With a 14-year-old son, even a few months to celebrate another birthday was worth fighting for, and knowing atezolizumab was out there, getting access to it was worth a try. TD was unable to secure coverage for atezolizumab, the immunotherapy recommended to her and approved by Health Canada. She applied to a compassionate program and was able to get a fraction of the cost of the drug funded. Her friends launched a GoFundMe page to raise funds to help mitigate this burden and help her access the drug. A diagnosis of lung cancer is devastating enough, and patients like TD should not have to add the extra burden of worrying about the ability to access viable treatment options that can help prolong their lives and improve overall survival.
Atezolizumab is a PD-1/PD-L1 immune checkpoint inhibitor that has seen incredibly promising results in patients with extensive stage |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Data from the IMpower 133 trial has shown efficacy in extending median overall survival and progression-free survival in the atezolizumab group compared to chemotherapy alone, at 2 months longer and 0.9 months longer respectively (Frampton, 2020). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Lung cancer is the most common cancer and by far the leading killer of all cancers in Canada. It accounts for 25% of all cancer deaths and the five-year survival rate is 22%, with even lower rates for cases in advanced stages (Canadian Cancer Statistics, 2021). Though small cell lung cancer (SCLC) accounts for only 10-15% of all lung cancer cases, it is much more aggressive of the two types with a high symptom burden and poorer outcomes, yet there are major gaps and fewer treatment options available for those with SCLC. Compared to non-small cell lung cancer, SCLC spreads much more rapidly, and thus, by the time patients experience symptoms like coughing up blood, persistent cough, weight loss, and shortness of breath, their cancer has likely already metastasized and therefore making recovery less likely. Median survival for those with extensive-stage SCLC is less than a year, at 7-11 months at best with treatment, according to the Canadian Cancer Society. The SCLC patient population has a very high unmet need, as there have been no new treatment options approved in this paradigm in the last three decades until the last 12 months, with the approval of durvalumab for the ES-SCLC indication. With the very few options available for this population, atezolizumab will serve as an alternative to durvalumab, being one of the first treatments made publicly available for Canadian patients with extensive-stage SCLC. Though chemotherapy currently represents the standard of care for these patients, it has been seen to be very limited in its potential. Receiving a lung cancer diagnosis is already quite devastating, but with recent developments in research and healthcare, new treatments like atezolizumab are now available and can make all the difference for cancer patients. With these new treatments, patients can live longer, manage their symptoms, be independent, have a good quality of life, and even go back to work. Patients already have a huge burden coping with their lung cancer diagnosis; the battle to survive this disease should be made easier by ensuring the availability of treatments that work beyond what is already the standard in Canada. For patients with extensive stage SCLC where the treatment goal is to relieve symptoms, maintain disease stability and prolong life, atezolizumab has the potential to achieve this.
Experiences With Currently Available Treatments
Currently, the standard of care for those with extensive stage small cell lung cancer consists of chemotherapy and radiation, though immunotherapy has recently taken a more prominent role in the treatment paradigm for these patients.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| MD was diagnosed with extensive stage small cell lung cancer back in March 2021 after scans found masses in his lung and brain. He first had surgery to remove the brain tumour, but this left him with decreased functionality and thus, increased dependence on his wife, his primary caregiver, for daily activities, including driving. He then started chemotherapy sessions, which was very taxing on his health. He attended treatment 3 days in a row every 3 weeks, had to take anti-nausea pills both before and after each session to minimize the side effects commonly associated with chemotherapy treatments ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| have any major adverse reactions to the treatment other than hair loss. Since then, he started on atezolizumab and has been on it since July 2021.
For 67-year-old MB who was had just retired from her job as a cashier when she was diagnosed with extensive SCLC in May 2020, her initial journey was a rocky start. After developing pneumonia and being in the hospital for 9 days, she was short of breath and struggled with fatigue most of the day and started chemotherapy soon after being released. She also took anti-nausea pills to suppress it, lost her hair, and continued to struggle with fatigue. It was very taxing on her mental and emotional health, however, and was very hard throughout the 5 rounds of treatment she did. She had to terminate chemotherapy when one of her PICC lines became infected and led to a staph infection. She then started radiation treatments.
TD attended her initial chemotherapy appointments with her husband wheeling her in as she was already very weak, and the treatments were very difficult. However, she began to see slivers of light improvement, that is, until she learned about atezolizumab immunotherapy treatments from her oncologist, which ultimately made a “night and day” difference in her life.
With SCLC being EH’s second cancer diagnosis in his lifetime, he was somewhat mentally prepared for the treatments that were to come. After he was diagnosed in 2018, he first underwent chemotherapy treatments for 1.5 years. However, he had no side effects from chemotherapy at all other than hiccups, but no nausea, vomiting, or fatigue, which he was surprised to find. When he finished his treatments 3 years ago, he was placed on atezolizumab, and is currently still on this treatment to this day.
Radiation: Once MB recovered from the staph infection, she then had 10 rounds of radiation targeted to her metastases in her liver, chest lymph node, and brain, which was very tiring, but she had no major effects from radiation as well. After her final radiation treatment in early December 2021, she started atezolizumab and has been on it ever since.
When RS was diagnosed by chance 2.5 years ago, she had virtually no symptoms or indicators of feeling unwell other than inflammation in one eye. After blood tests, biopsies, and scans revealed localized small cell lung cancer, she started chemotherapy and atezolizumab 6 weeks after diagnosis due to inflammation from the biopsy. After only 3 treatments, she was switched to radiotherapy after scans showed shrinkage of her tumour. Radiation was also successful and also slowly shrunk the tumours even further, until there were almost no spots left. After 15 radiation treatments, she was able to switch back to atezolizumab immunotherapy in 2020, which she has been on ever since.
While EH was also on atezolizumab, he also had 5 rounds of radiation in 2021. By this time, most of his cancer was already gone apart from a small speck on the thyroid, which was not responsive to chemotherapy or atezolizumab. His only side effect from radiation was fatigue, as he was constantly tired and could fall asleep almost anywhere yet had no other side effects. It was very tolerable for him and allowed him to carry on his day-to-day life with almost no issues. He continued with only atezolizumab immunotherapy after radiation was done and is still currently on it.
Improved Outcomes
Advancements in SCLC research have been slow and limited in the past three decades, and outcomes for patients have remained poor in comparison to the rapid developments that have been made in recent years for NSCLC. Around 13% of all people diagnosed with lung cancer have small cell, and the lack of treatment advances for this population have been disappointing, until now. With immunotherapy, the first-line treatment options for SCLC patients have been limited to the standard of care, which is platinum chemotherapy (carboplatin or cisplatin) with etoposide. The addition of atezolizumab will bring significant change to the treatment paradigm for SCLC as patients value being able to have additional treatment options in the market as a first line option or an alternative in case their current therapy is not effective or there are comorbidities that prevent them from accessing certain treatments. For new therapy, patients most value:
Improvements in managing their symptoms while having manageable side effects
Being able to have a full and worthwhile quality of life
Being able to maintain their independence and functionality to minimize the burden on their caregivers and loved ones
Delaying disease progression and settling patients into long-term remission for improved survivorship
Table 2: Experience With Drug Under Review
Patient | Year diagnosed | Drug access method | Period on atezolizumab | Duration on atezolizumab | Currently on atezolizumab? |
|---|---|---|---|---|---|
||||||||| | 2020 | Clinical trial | Dec 2021 - present | 2 months | Yes |
||||||||| | 2021 | Clinical trial/insurance | July 2021 - present | 7 months | Yes |
TD | 2020 | Compassionate program and GoFundMe | June 2020 – Unknown | Unknown, at least 1 year | Unknown |
||||||||| | 2019 | Clinical trial | June 2020 – present | 1.5 years | Yes |
||||||||| | 2018 | Clinical trial | Mid-2019 – present | Approx. 2.5 years | Yes |
||||||||| | 2019 | Clinical trial | Early 2021 – present | 1 year | Yes |
There have been very limited advancements in recent decades for patients with SCLC, and it is imperative to consider the high unmet need of this population, as the ultimate treatment goal for these patients is to maintain disease stability, manage and minimize symptoms, and allow them to live a worthwhile quality of life. Atezolizumab has the ability to achieve this for SCLC patients with advanced disease, and as discussed below, this treatment has seen to be life-changing for patients and will have numerous positive impacts for others as well.
Atezolizumab is very effective in treating the cancer and maintaining a stable disease
Throughout RS’s cancer journey for the past 2.5 years, she had a slew of chemotherapy, radiation, and atezolizumab immunotherapy treatments to target her small cell lung cancer. When she was diagnosed, she had no symptoms and only found out about her cancer through bloodwork due to inflammation in one of her eyes, which further lead to scans and biopsies confirming her SCLC. Initially, her doctors explained it was a very aggressive tumour and were not necessarily aiming for remission as their end goal. They started her on the atezolizumab immunotherapy and chemotherapy treatment since atezolizumab had just started a trial in their area, which she was on for only 3 treatments before switching to radiation due to the onset of COVID-19 in 2020. However, even during the 3 atezolizumab/chemotherapy treatments, scans had already shown improvements and shrinkage in her tumor. When she started sole atezolizumab immunotherapy again about 6 months later, there was even more improvement at every scan, where there was always something diminishing with less white spots and tumours continuously shrinking. RS’s most recent scan in October 2021 revealed the tumor had shrunk enough that there is virtually no evidence of disease (NED) now. RS is still on atezolizumab to this day and continues to maintain NED status.
DR started chemotherapy for 6 months, which was tolerable for her, though she lost her sense of smell ever since. However, after she had completed chemotherapy, DR had another coughing fit, during which she ended up likely coughing up the tumour, and scans after that incident revealed the tumour was virtually gone from its original position, leaving only a small scar. As precaution, her oncologist continued with a course of radiation for 12 treatments, then switched over to immunotherapy with atezolizumab in early 2021 to ensure any remnants of her cancer were treated and has been on it ever since. With this year of atezolizumab treatment, DR has not seen any further growth from the spot her initial lung tumour was and has virtually no evidence of disease.
At diagnosis in March 2021, MD had been feeling “off” and unlike himself, and after a trip to the emergency room revealed extensive stage small cell lung cancer that had metastasized to his brain, MD was tasked to start treatment for his cancer right away, starting with brain surgery. On top of the cancer, he also has Crohn’s disease as well, which made his stools abnormal and watery, and terrible indigestion and heartburn. However, once he started atezolizumab in July 2021, it helped clear up his Crohn’s almost immediately with normal stools, no heartburn or GI issues that he had before. He received immunotherapy treatments once every 3 weeks and did not have any major side effects other than phlegm and Charlie horses. MD said his lung tumour has shrunk by 80% within the 5 months he was on atezolizumab, which is incredible. He has been able to carry on with his daily life, drive himself, go shopping, and maintain his independence.
EH had no symptoms of feeling unwell when an incidental finding of SCLC was discovered in 2018, which also had spread to his thyroid. After undergoing chemotherapy for 1.5 years and atezolizumab ever since, most of his cancer was already gone, apart from a small speck on the thyroid. EH did a few rounds of radiation to further shrink this, which was successful. He still continues to be on atezolizumab as of February 2022 and is free of disease with virtually no visible signs of cancer in his scans.
In TD’s case, her initial chemotherapy treatments after being diagnosed in May 2020 were difficult and only saw slight improvements in her cancer. However, when her oncologist recommended atezolizumab with immunotherapy, she saw the clear night and day difference it made in her health and her condition improved a lot. By summer, her recent CT scan revealed the cancerous nodes in her lungs and pelvis had reduced by almost 50%, and ones in her breast and pancreas had nearly cleared. She could breathe better too, the tumor in her lung no longer pressing on a pulmonary artery. It skyrocketed her quality of life, improved her symptoms, and she was astonished by how much of an improvement atezolizumab has made.
Atezolizumab is a durable form of treatment
As seen above, many of these patients have seen long lasting and very durable results with atezolizumab, all of whom are still on it today. 3 of these patients have been on the treatment for at least a year, 2 of whom have extensive stage disease. The drastic improvements in their symptoms and tumours have been astonishing, and many of them have almost no signs of tumours. From the IMpower 133 trial, the median overall survival with atezolizumab/carboplatin and etoposide patients was 12.3 months, compared to 10.3 months with the control group. This translates directly to what these patients have been on here, such as EH, MD, MB, RS, and DR, and yet some have exceeded these results, most notably EH, who has been on atezolizumab (both on its own and alongside chemotherapy) for almost 3 years. The quality of life these patients also have is great, and they are able to continue to do many day-to-day activities independently. Some are even able to travel across the country while on atezolizumab, and the fulfillment they feel with being able to return to the hobbies and activities they love is what this treatment can provide for patients like EH who have been on the treatment long-term.
Atezolizumab has minimal and manageable side effects
Common side effects that have been attributed to atezolizumab as per the IMpower133 study include nausea, vomiting, constipation, diarrhea, rash, headache, decreased appetite, and shortness of breath, which had impacts on patients’ quality of life. 29% of patients in the study had grade 5 adverse events, and 5% of patients had adverse events leading to discontinuation of treatment (Mansfield et al., 2020). However, the incidences of these adverse events were reported in the study to have gradually decreased from the induction to maintenance phases and are considered to be relatively minor in comparison to the side effects experienced with the current standard of care treatments.
Both RS and DR experienced virtually no side effects during their atezolizumab treatments, though RS did have a minor rash a few times, but attributed it to dry skin as it did not affect her daily life. One patient had to pause treatment after developing flaky skin around their eyes and nose, and a rash over much of their body. This was treated with prednisone throughout this pause, which cleared up the rash for her, and they were able to resume treatment with atezolizumab. Others also reported breaking out in rash around their face and back, fatigue, some joint pain and aches in the area where they have spread and feeling sick or nauseous at times. For another patient, he had 8 treatments with atezolizumab before a rash appeared on his right chest, and after biopsy, it was discovered the cancer had spread to his skin, so he had to terminate treatment. Some patients reported effects to their GI tract, including abdominal pain, constipation, gas, diarrhea, cramps, as well as dry mouth. However, for the most part, many patients reported that the side effects of atezolizumab were generally minimal and much more tolerable and less aggressive compared to chemotherapy, and some did not experience any side effects at all, including DR and RS, who have been on atezolizumab for about 1 and 2 years respectively, and counting.
Atezolizumab has shown to maintain and improve the quality-of-life patients had prior to treatment
Eight years ago, EH was an incredibly active person working as a professional charter tour bus driver who had driven across North America numerous times during the 51 years of his career. He was constantly on-the-go and travelling, but when he got the news of being diagnosed with prostate cancer in June 2014 on top of his COPD, he decided to retire and care for his health. While he underwent treatment, he continued to live normally almost without any impediments, yet when he was diagnosed with cancer again for a second time in 2018 with limited stage SCLC, his wife also made the decision to retire as EH needed a caregiver for what was to come. The treatments that EH has had for his SCLC have been very tolerable, with very minimal side effects other than fatigue and hiccups and has continued to lead a quality and worthwhile life that is comparable to what he had prior to his 8-year long journey with cancer. He continues to travel around British Columbia with his wife, going on long road trips, and lives a fulfilling life in retirement thanks to atezolizumab.
Ever since RS had started her atezolizumab treatments 2 years ago, she has been living her daily life that is very comparable to what she had before diagnosis. She has always been active and on her feet most of the day from being a waitress for 45 years, retiring just before she was diagnosed with cancer 2 years ago. Aside from a small break when she had inflammation from the initial biopsy, she has continued to live her life as normal throughout the last 2 years doing all her errands herself, such as driving around, shopping and socializing with friends, and exercising. Grocery shopping, shoveling the snow, going for a walk, getting on the train into the city to meet and get coffee with friends has always been part of her routine since she retired, and this has not changed one bit since she was diagnosed. She had next to no side effects with any of her treatments, including atezolizumab, and continues to have virtually no symptoms of the cancer. While she is still currently on atezolizumab, her most recent scan in October 2021 showed almost no white spots or signs of cancer, and this has really attributed to her positivity and gratitude. Being able to maintain the same quality of life because of atezolizumab as a cancer patient and survivor, RS has never really lost her sense of independence or functionality and has continued to pursue a positive outlook all throughout her journey with cancer.
Prior to atezolizumab, TD had mets to her pancreas and lymph nodes, which left her weak and with little energy. Once TD began three-week cycles of chemotherapy and atezolizumab together, her appetite returned quickly and was even up and running again in no time. She no longer needed her wheelchair and was able to breathe better. In her words, atezolizumab elicited a clear “night and day” difference in her quality of life. She was able to become more independent, rely less on her caregivers, and be there for her children. Being a teacher and long-distance runner in excellent shape prior to diagnosis, lung cancer did not often cross her mind, so having atezolizumab as an option for her when she felt hopeless was almost like a miracle. It allowed her to return to a quality of life that is comparable to pre-diagnosis. In an interview with Lung Cancer Canada, TD says, “[Cancer] is devastating as a parent, because you want to protect your children. But what happens if I’m not here? Even an extra two months was everything to me. I have so much to live for, everybody does”.
Atezolizumab allowed patients to regain their independence and functionality
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| MD was an extremely healthy and active person most of his life, and was in the navy for over 30 years, so when he was diagnosed with SCLC in March 2021, it came to him as a shock. After undergoing chemotherapy for 3 days in a row every 3 weeks and 30 sessions of radiation treatments nearly every day for several weeks, in addition to surgery to remove a tumour in his brain, functionality-wise it was very hard on him, and was unable to do many activities he used to love, including hunting, sports, exercising, fishing, and hiking. He was out of breath every time he walked upstairs, was not able to drive himself, relied on his wife for errands and house chores, and hadn’t been able to socialize with friends much. However, once he started atezolizumab, he slowly started regaining his energy and functionality while recovering and returned to a level of functionality that allows him to get by in his daily life. He was able to walk upstairs with less difficulty, take walks outside, drive, run errands like grocery shopping, and even start shoveling the snow in his driveway, which seemed like an impossible task only a few months prior during his previous treatments. Although his wife had stayed incredibly supportive during MD’s entire cancer journey, he was able to regain a sense of independence and rely on her much less to get by day-to-day. He’s still currently unable to do many sports and hobbies he used to prior to diagnosis; however, atezolizumab was an incredible step forward in his journey that he hopes one day, will allow him to return to enjoying the outdoor sports he used to love.
Atezolizumab addresses the high unmet need in extensive stage SCLC patients
Patients with small cell lung cancer only makes up a minority of those with lung cancer in Canada, yet it is the most aggressive type of cancer between the two most common types. There have not been any advancements in treatments available for small cell patients in the last 30 years, and this brings forth a large gap in treatments available for these SCLC patients once they progress on the standard of care. However, these experiences from patients with extensive-stage SCLC on atezolizumab have shown otherwise. Atezolizumab has shown to work and improve disease conditions, allow patients a quality of life that is meaningful and worthwhile, a chance for them to be together with family, and for many, live a life that is comparable to pre-diagnosis.
Companion Diagnostic Test
Atezolizumab for SCLC does not require any biomarker testing.
Anything Else?
Patients with extensive SCLC have a large unmet met need due to a high symptom burden, rapid spread and progression of the disease resulting in poorer outcomes. There are also few viable treatment options, quite unlike those with NSCLC who have a wider range of options. Atezolizumab in combination with chemotherapy is a viable option that has been shown to work in this group of patients. This benefit is highlighted in the updated overall survival analysis in the IMpower133 trial, which showed a continued benefit with this form of treatment.
The previous submission for this treatment was provided a negative recommendation by pERC as it was unable to conclude there was a meaningful clinical benefit. Now and with more mature data from the IMpower 133 phase III study and RWE as evident from the patient experiences in this submission, this form of treatment has shown to be not just clinically beneficial and durable, but also aligns with patients’ values by allowing patients to maintain a good quality of life, has manageable side effects, and gives patients an additional treatment option that can allow them to live longer.
With the recent approval of durvalumab, it should be noted that this form of treatment has yet to be made publicly available which still leaves many patients without treatment access. Atezolizumab would be an additional option for patients without access to durvalumab, or as serve as an alternative to durvalumab.
LCC believes this form of treatment should be adopted as a standard of care in the first line treatment of patients with extensive SCLC. These group of patients cannot afford to wait and deserve to have access to treatments that can help prolong and maintain their lives now. LCC hopes CADTH provides a positive recommendation for this submission.
References
Mansfield, A. S., Każarnowicz, A., Karaseva, N., Sánchez, A., De Boer, R., Andric, Z., ... & Califano, R. (2020). Safety and patient-reported outcomes of atezolizumab, carboplatin, and etoposide in extensive-stage small-cell lung cancer (IMpower133): a randomized phase I/III trial. Annals of Oncology, 31(2), 310-317. DOI: 10.1016/j.annonc.2019.10.021
Frampton, J. E. (2020). Atezolizumab: A Review in Extensive-Stage SCLC. Drugs, 80(15), 1587-1594. DOI: 10.1007/s40265-020-01398-6
Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 3: Financial Disclosures for Lung Cancer Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Roche | X | — | — | — |
Clinician Input
Ontario Health Lung Cancer Drug Advisory Committee
About Ontario Health Lung Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
The comments contained in this input were collected via emails.
Current Treatments
Current treatment would be a platinum agent plus etoposide for 4 to 6 cycles. While atezolizumab and durvalumab are Health Canada approved, they are not publicly funded thus there is little to no access for patients. There may be a few patients accessing atezolizumab or durvalumab in combination with platinum chemotherapy through private insurers. There is a high response rate to platinum and etoposide of 60-70%. However, median PFS is only about 4 months with median OS around 10 months. Only 15% of patients survive beyond two years. Supportive management alone has a median OS of approximately 6-8 weeks
Treatment Goals
The most important goal would be more effective therapy. The primary goal would be improved overall survival. Other important goals would be higher response rates and longer control of the cancer (PFS). Improvement is symptoms and QoL is also important but this is generally linked to effective therapy. More effective therapy is generally associated with better QoL. Lastly it is important that these therapies have tolerable profile of side effects.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, describe goals (needs) that are not being met by currently available treatments.
Despite high response rates to initial therapy, many patients progress in a short period of time. Less than half the patients live beyond one year with few surviving beyond two years. Therefore, there is a high unmet need for more effective therapies that result in longer disease control and better OS.
Which patients have the greatest unmet need for an intervention such as the drug under review?
All patients with ES SCLC have high unmet need. The only factors that predict worse outcome are factors associated with a higher tumor burden, so it is not possible to identify subgroups of greater need.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Atezolizumab would be used as initial systemic therapy in patients with ES SCLC in combination with 4 cycles of platinum and etoposide, followed by maintenance atezolizumab until disease progression. The goals of adding atezolizumab to platinum and etoposide would be to improve PFS and OS. In particular the hope is that the addition of atezolizumab will increase the proportion of patients living beyond 18-24 months.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
The current standard of care is platinum and etoposide. This has been the case for the last three decades. No other agents apart from immune checkpoint inhibitors have demonstrated improved OS as initial therapy for ES SCLC. It would not be appropriate to recommend the addition of other therapy apart from an immune checkpoint inhibitor.
How would this drug affect the sequencing of therapies for the target condition?
The addition of atezolizumab to platinum and etoposide will not have any downstream impact on other treatment options. Second line therapy would remain either retreatment with platinum and etoposide, or CAV. Topotecan is another option although not funded in all jurisdictions.
Which patients would be best suited for treatment with the drug under review?
All patients with ES SCLC are in need of improved therapies. It is not possible to identify subgroups that are more likely to benefit from the addition of atezolizumab. Therefore this treatment would be considered for any patient with ES SCLC and ECOG PS of 2 or greater.
How would patients best suited for treatment with the drug under review be identified?
ES SCLC is a common condition that medical oncologists see and treat on a regular basis. These patients would be identified at the time of initial consultation with a medical oncologist. There are no specific issues for consideration.
Which patients would be least suitable for treatment with the drug under review?
All patients with ES SCLC and ECOG PS of two or better would be candidates for therapy with platinum etoposide and atezolizumab, unless they have specific contraindications to an immune checkpoint inhibitor. Patients with symptomatic brain metastases should have treatment for their brain metastases prior to commencing their systemic therapy.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
As discussed above there are no predictive biomarkers of benefit for the addition of atezolizumab to chemotherapy.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Tumor shrinkage on imaging studies would typically be used to determine if a patient is responding to therapy. Improvement in patients’ symptoms would also be looked for as a measure of treatment benefit. Freedom from progression is also important in this population.
What would be considered a clinically meaningful response to treatment?
A meaningful response to treatment would be tumour shrinkage, improved symptoms and/or performance status and freedom from progression.
How often should treatment response be assessed?
Typically, after every three cycles of chemotherapy. For patients receiving platinum etoposide and atezolizumab, treatment would continue until disease progression. After six months or so, the frequency of imaging may be extended to every four cycles of therapy.
What factors should be considered when deciding to discontinue treatment?
In the Impower133 trial treatment continued until disease progression. In clinical practice, the reasons to discontinue treatment would be unequivocal disease progression, the development of grade 3 immune related AEs, or patient choice.
What settings are appropriate for treatment with the drug under review?
Treatment would be administered under the supervision of a medical oncologist in any facility accredited to administer anti cancer systemic therapy.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
N/A
Additional Information
There have been no significant treatment advances in ES SCLC in more than three decades. The addition of atezolizumab represents a modest but real improvement in survival for a group of patients with high unmet need.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the Lung DAC in completing this input submission.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Natasha Leighl
Position: Ontario Health Lung Drug Advisory Committee
Date: 18-02-2022
Table 4: Conflict of Interest Declaration for Ontario Health Lung Cancer Drug Advisory Committee Clinician 1
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
N/A | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Andrew Robinson
Position: Ontario Health Lung Drug Advisory Committee
Date: 18-02-2022
Table 5: Conflict of Interest Declaration for Ontario Health Lung Cancer Drug Advisory Committee Clinician 2
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
N/A | — | — | — | — |
Lung Cancer Canada
About Lung Cancer Canada
Lung Cancer Canada (LCC) is a national charity with the purpose of increasing awareness about lung cancer, providing support and education to lung cancer patients and their families, to support research and to advocate for access to the best care for all lung cancer patients in all provinces and territories.
Through the LCC Medical Advisory Committee (MAC), we have been providing clinician input for submissions of new lung cancer drugs to the HTA process for many years. The LCC MAC is made up of clinicians and key opinion leaders in the field of lung cancer across the country.
Information Gathering
Information is from publicly available sources, primarily published manuscripts and conference presentations, together with experience of the members of the clinician group. Specific references are listed in the below text. This submission is entirely independent of the manufacturer (Roche).
Current Treatments
Small cell lung cancer (SCLC) represents approximately 12% of all lung cancers in Canada. Most patients present at late stage; in 67% of patients the cancer has spread outside the lung and regional lymph nodes (Extensive Stage or stage IV) (Canadian Cancer Statistics – A 2020 special report on lung cancer. Available at https://cancer.ca/Canadian-Cancer-Statistics-2020-EN).
SCLC is characterized by a high response rate to initial therapy with cytotoxic chemotherapy, however, this benefit is generally short lived, and patients typically relapse within six months. Less than 10% of patients treated with chemotherapy remain progression free at 12 months, which results in a poor overall survival rate. The median overall survival (OS) is 8-10 months in patients with extensive stage (ES) SCLC treated with chemotherapy alone. Long term survivors are exceedingly rare; historically with chemotherapy alone, 2-year survival for ES SCLC was <5%, and 5-year survival was <2%.
Patients with ES SCLC have a high tumour burden and are usually highly symptomatic at presentation. In responding patients, chemotherapy is very effective in reducing symptoms and improving quality of life (QOL), however, at the time of progression, there is often a rapid and profound increase in symptoms with a concomitant deterioration of QOL.
Until recently, the standard of care with four to six cycles of intravenous etoposide-platinum (EP) doublet chemotherapy had not changed in more than 30 years. Recent data has emerged however, supporting the addition of immunotherapy to standard of care chemotherapy for patients with extensive stage SCLC. The addition of the immunotherapy checkpoint inhibitor durvalumab, a monoclonal antibody targeting PD-L1, was shown to provide improvements in OS, progression free survival (PFS) and patient reported outcomes when compared to standard EP chemotherapy alone in the randomized phase III CASPIAN study (Goldman et al, Lancet Oncology 2020 Dec).
The improved outcomes seen in the CASPIAN study were felt to be clinically relevant in terms of both magnitude and duration. This led to a positive CADTH recommendation for funding by public drug plans for the treatment of adult patients with extensive-stage small cell lung cancer (ES-SCLC) if certain conditions were met, including a reduction in the price of durvalumab. Currently, the health technology assessment process is not completed for durvalumab for this indication, with price negotiations ongoing with PCPA. Thus, the addition of durvalumab to EP chemotherapy (D+EP) is not yet available in Canadian provinces through provincial/territorial drug formularies. That being said, this combination of D+EP is considered to be the standard of care for all eligible extensive stage small cell lung cancer patients who have received no prior therapy. D+EP is in widespread use throughout Canada with access being provided through a patient support program. This program allows enrollment of extensive stage small cell lung cancer patients with an ECOG performance status of 3 or better, and provides durvalumab to be delivered concurrently with EP chemotherapy starting with the first cycle for those starting with an ECOG performance status of 0-2, and allows for the addition of durvalumab beginning with the second cycle for those patients who had an initial ECOG PS of 3 at the time of enrollment, but who had achieved an ECOG performance status of 2 or better at the time of the second cycle.
Current standard of care therapy with D+EP both improves symptoms and prolongs survival. In the latest update of outcomes from CASPIAN study presented at the 2020 ASCO annual meeting (Paz-Arez et al, Journal of Clinical Oncology May 20, 2020, abstract 9002), OS was significantly improved in the group of patients getting D+EP vs EP along with a hazard ratio (HR) of 0.71 (0.60-0.86) with a corresponding improvement in median OS from 10.5 months with EP alone to 12.9 months in the D+EP experimental arm. OS rates at key landmark time points after a median follow up time of 39.4 months illustrated the durability of this response, with 12-month, 18-month, 24-month and 36-month survival rates in the D+EP population reported at 52.8%, 32%, 22.9% and 17.6% respectively. Thus, the “tail of the curve” shape of the survival curve representing durable and long-lasting responses for some patients that has been seen in other tumour types sensitive to immunotherapy checkpoint inhibitors has been illustrated to be relevant in ES-SCLC as well. Patient reported also support combination therapy with D+EP with a longer time to deterioration in physical and cognitive functioning in patients receiving D+EP vs EP alone.
After chemotherapy, thoracic irradiation and PCI may be considered. The role of radiation post chemotherapy is not clear when the chemotherapy has been delivered concurrently with immunotherapy. Specifically, no trials of immunotherapy checkpoint inhibitors given with EP allowed patients to receive thoracic irradiation after chemotherapy, and in the CASPIAN trial, only the control EP arm was allowed to receive PCI. Thus, there is no good guidance at present for how radiation may or should be sequenced with systemic therapy in patients receiving D+EP.
Treatment Goals
Prolongation of overall survival is always the primary goal of treatment for ES SCLC. Untreated patients have a median survival of only six weeks.
Secondary objectives include response rate, improvement in symptoms, and QOL. These outcomes translate into benefits very important to patients and caregivers, including increased functioning and decreased caregiver burden.
Finally, ES SCLC is a cancer with a high propensity to spread to the brain. A systemic therapy with significant activity in brain would be important to preclude or delay significant symptoms and decreased functioning/QOL related to progression in the brain, and the side effects with needing to have brain irradiation, especially whole brain irradiation.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Atezolizumab would be an additional option for patients without access to durvalumab, or as an alternative to durvalumab.
As outlined in section 3, access to immunotherapy concurrently delivered with EP is limited at present to access via a patient support program that provides access to durvalumab. Assuming that negotiations with PCPA are successful, however, one would assume that ultimately durvalumab will be listed on many provincial/territorial public drug formularies. Historically we do know that some provinces do not list recommended cancer therapies, generally due to budget constraints (Srikanthan et al, Current Oncology 2017, 24 (5), 295–301).
Given the comparable outcome data for the addition of atezolizumab to EP (A+EP) shown by mature data from the IMpower133 trial (Liu et al, Journal of Clinical Oncology, January 2021) as outlined below in section 6.9, atezolizumab may provide a more cost effective but equally effective option and hence could be more readily adopted by a larger number of provinces/territories.
Patients with ES SCLC have a significant chance of developing brain metastases. Approximately 20% of patients with ES SCLC have brain metastases as presentation (Goncalves et al, Cancer April 2016). In patients treated with chemotherapy alone, the brain is a common site of disease relapse as chemotherapy generally has little to no effect in the CNS due to limited penetration through the blood brain barrier. The cumulative risk of developing symptomatic brain metastases in patients without CNS disease at presentation who are treated with chemotherapy alone is 40% (Slotman et al, NEJM 2007).
Brain metastases have a negative impact on QoL and carry a poor prognosis. Only a small number of ES SCLC patients will be candidates for surgical resection and/or stereotactic brain radiation. The majority will be treated with whole brain radiation (WBRT), which carries significant short-term and long-term toxicity, such as immediate memory loss, loss of higher cortical function and fatigue, can negatively impair the functional status, independence and QoL of patients.
In contrast to the CASPIAN study of D+EP, the IMpower133 trial of A+EP allowed PCI to be delivered to both the study and control arms as per local practice. While there has been a trend towards less uptake of PCI in the modern era where many patients and oncologists elect for serial brain surveillance with MRI imaging, this is not always feasible from a resource perspective, especially for those patients who live in areas where access to MRI is limited due to geographic or resource limitations. Thus, for a patient in whom PCI may be considered to be an appropriate intervention post chemotherapy, oncologists can proceed with greater certainty with the safety data gained from the IMpower133 trial if that patient were to receive atezolizumab concurrently with chemotherapy.
Which patients have the greatest unmet need for an intervention such as the drug under review?
For Canadian patients with ES SCLC who live in areas where durvalumab will be added to their provincial/territorial public formularies across Canada, strictly speaking, this will not be an unmet need. The drug under review, atezolizumab, will offer an alternative option, as opposed to an additional option.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Targeting the immune system is a new treatment paradigm for cancer in general and lung cancer in particular. The addition of immunotherapy to chemotherapy has been shown to lead to meaningful benefits in outcomes in the ES SCLC lung cancer population with D+EP worthy of funding in a Canadian health care context. The mature results from IMpower133 have shown the combination of A+EP work in a similar complementary manner.
Atezolizumab would be the second drug approved that addresses the underlying disease process by significantly extending survival.
Studies of immunotherapy checkpoint inhibitors given sequentially after initial EP chemotherapy in first line, or at the time of progression in later lines of therapy have not indicated these are successful treatment strategies. Thus, atezolizumab would fit into the current treatment paradigm only as an agent to be started concurrently with first line EP chemotherapy, with the intention of continuing until disease progression, intolerance or a patient’s choice to discontinue therapy.
It would not be expected to cause a shift in the current treatment paradigm which already recommends for first line therapy with D+EP, but rather would provide an alternative option to D+EP for initial therapy in that paradigm.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
It would not be appropriate to recommend that patients try other treatments before initiating treatment with A+EP. As per section 6.1, studies of immunotherapy in which the checkpoint inhibitor was not started concurrently with first line EP chemotherapy have not shown efficacy. There are no studies that show that immunotherapy, including atezolizumab, is effective either as a single agent or in combination with other treatments in the second line setting in ES SCLC. In fact, most second line treatments are ineffective.
How would this drug affect the sequencing of therapies for the target condition?
Treatment after failure of first line therapy for ES SCLC must be individualized. Progression after atezolizumab would be treated with systemic chemotherapy as per the current treatment paradigm. Only patients of good performance status would be offered second line chemotherapy, and selection of drugs would depend on the extent of the chemotherapy free interval. Radiation might be given to localized symptomatic lesions for palliation of symptoms, but with no expectation of prolongation of survival. Many patients receive no second line treatment and receive only best supportive care.
In IMpower133, there was a significant difference in progression free survival. This would mean that there would be a larger number of patients who remained progression free at the key timepoint of 6 months after completion of EP. This group is considered to be platinum sensitive, and in clinical practice, rechallenge with EP at the time of progression is standard of care for patients who are clinically well enough. Thus, the administration of atezolizumab would have the downstream impact of making a larger number of patients eligible for the benefit of a second course of EP chemotherapy.
There is no data at this time to support atezolizumab use, or the use any other immunotherapy checkpoint inhibitor, in the second line setting for ES SCLC, and thus there would be no opportunity to treat patients with this same drug in a subsequent line of therapy.
Which patients would be best suited for treatment with the drug under review?
There are no specific biomarkers or patient/disease characteristics that are predictive of a higher likelihood of response to A+EP, and hence there are no specific patient groups with ES SCLC who are more likely to respond and derive benefit.
An analysis of long-term survivors treated on the IMpower133 trial (defined as patients who lived ≥18 months post randomization) reported at ESMO 2020 by Liu et al showed that all subgroups as defined by patient and disease characteristics stood to benefit from the addition to atezolizumab to EP chemotherapy, with no predictive characteristic identified in multivariate Cox regression analysis.
ALL patients with ES SCLC are in need of better treatment options. Thus A+EP should be offered to all patients who have an ECOG performance status of 0-2 at the time of initiation of first line systemic therapy, assuming they have no contraindications to immunotherapy (e.g., active severe autoimmune disease). Given the propensity of patients with a worse performance status at the time of initiating the first cycle of chemotherapy to respond rapidly and have an associated improvement in symptom burden and performance status, we feel that the introduction of atezolizumab for patients who have achieved a performance status of 0-2 before the second cycle of chemotherapy would be reasonable at that time.
How would patients best suited for treatment with the drug under review be identified?
All pathologists and pathology departments have the capability to diagnose SCLC.
All hospitals in Canada can undertake the pathologic, hematologic, biochemical and radiologic tests necessary to diagnose and treat SCLC. Advanced molecular profiling is not necessary.
In selection of ES SCLC patients for the addition to atezolizumab to EP chemotherapy, no special testing is required.
Misdiagnosis is unlikely. In the case of uncertainty, most local pathology departments would request external review, usually at an academic centre.
Underdiagnosis is not an issue with ES SCLC. Virtually all patients with SCLC are symptomatic. They present with rapidly progressive disease at an advanced stage and early treatment is essential.
Which patients would be least suitable for treatment with the drug under review?
Patient with severe or symptomatic auto-immune disorders are generally not suitable for treatment with atezolizumab.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
There have been no biomarkers identified to date to identify those patients who are most likely to exhibit a response to treatment with atezolizumab, or any other immunotherapy checkpoint inhibitor, in SCLC. This includes biomarkers that have predictive utility in other tumour types, including PD-L1 and tumour mutational burden (TMB). Specifically, in the IMpower133 trial, Liu et al reported an exploratory biomarker analysis at the American Academy for Cancer Research (AACR) Virtual Meeting II in June 2020 (Abstract 9759) that concluded that TMB and PD-L1 status were not predictive of outcomes with A+EP and should not be used for patient selection for this regimen.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
In clinical practice, patients are evaluated for response (and toxicity) before each cycle of therapy by history, physical examination, bloodwork, and/or chest radiographs. CT scans and/or MRIs are performed every 2-3 months, and always at the completion of chemotherapy.
These assessments to determine clinical outcomes are aligned with those investigated in clinical trails of ES SCLC, including IMpower133.
What would be considered a clinically meaningful response to treatment?
ASCO guidelines have evaluated “Clinically Meaningful” responses for non-small cell lung cancer. For SCLC this has been less clearly defined owing to the lack of success of studied agents. A two-month overall survival benefit compared to EP chemotherapy for this aggressive disease has been considered clinically meaningful.
Further, durability of the survival benefit as measured by survival rates at key landmark time points, including 12 months, 18 months and 24 months would be key in this disease where the majority of patients do not live longer than 8-10 months with chemotherapy alone.
The magnitude and duration of survival benefit from durvalumab has already been determined to be of significance by CADTH with the recommendation to fund D+EP. The results from IMpower133 are highly comparable, and thus should also be considered equally meaningful and worthy of funding. As illustrated in the table below, the magnitude of survival benefit is essentially identical in terms of median OS and OS measured at key landmark timepoints. Any differences in OS HR are attributable to the fact that the control EP arms had larger variability in OS outcomes between the two trials, while the outcomes of D+EP and A+EP are remarkably similar.
Table 6: Comparative Survival Outcomes CASPIAN and IMpower133 Trials
Trials | Median OS | Improvement in median OS compared to EP | 12-month OS | 18-month OS | 24-month OS |
|---|---|---|---|---|---|
CAPSIAN D+EP1 | 12.9 months | 2.4 months | 52.8% | 32% | 22.9% |
IMpower133 A+EP2 | 12.3 months | 2.0 months | 51.9% | 34% | 22% |
1PazAres et al ASCO 2020; 2Liu et al ESMO 2020
As discussed in section 5.1, the development of brain metastasis is a common event for patients with ES SCLC. In recent report presented at ASTRO in 2020 by Higgins et al, they reported the patterns of disease progression in patients receiving A+EP for ES SCLC. While similar numbers of patients in both the A+EP and EP trial arms ultimately developed new brain lesions, the time to intra-cranial progression (ICP) was significantly longer in those patients who had received A+EP with a median time to ICP of 20.2 months compared to 10.5 months in those patients receiving EP alone (HR 0.66(0.44, 1.00), p=0.046). These data suggest CNS efficacy of atezolizumab in ES SCLC. This is very clinically relevant for patients with ES SCLC, as living with longer without brain metastases translates into longer preservation of QoL and functional status while delaying the time of heavier caregiver burden.
For all patients receiving treatment in IMpower133, there was an improvement in patient reported function and health-related quality of life (HRQoL) in both the A+EP and EP arms, however, as reported by Mansfield et al (Annals of Oncology, January 2020) those improvements in HRQoL were both more pronounced and persistent in the A+EP arm.
The translation of the meaningful survival benefit seen with A+EP to the real world (RW) setting has been shown in two studies. First, in the US, where A+EP has been in widespread use since its approval by the US Food and Drug Administration in 2019, a study reported by Tsui et al at ESMO 2021 (poster 1650P) investigated outcomes of the A+EP regimen in a RW community oncology setting using data from the US nationwide Flatiron Health electronic health record-derived deidentified US database. They found that in patient characteristics and clinical outcomes, their RW cohort aligned with outcomes from the IMpower133 trial. Specifically, the real-world progression free survival (rwPFS) was identical at 5.2 months in their full RW cohort as was reported in the IMpower133 trial for patients receiving A+EP. Moreover, the subset of their RW cohort who were defined as being “IMpower133 trial eligible like” had a higher rwPFS of 5.8 months than that reported in the trial.
There is comparable data that published by Elegbede et al (JTO Clinical and Research Reports 2021; 2:100249) that reported on a real-world evaluation of A+EP in patients with ES SCLC in Canada who received A+EP in the province of Alberta via a special access program. When they compared patients who had receive A+EP vs EP there was an improved median PFS of 6.0 months vs 4.3 months (HR 0.53 (0.28-1.02)) and median OS of 12.8 months vs 7.1 months (HR 0.42 (0.20-0.88)).
How often should treatment response be assessed?
As per previous section, clinical reassessments with or without a chest radiograph should be done before each cycle, and more extensive radiographic reassessments with CT or MRI should be done every 2-3 months.
What factors should be considered when deciding to discontinue treatment?
Treatment should be discontinued in the setting of unequivocal disease progression, intolerable treatment related adverse effect or patient choice to stop treatment for other reasons.
What settings are appropriate for treatment with the drug under review?
Chemotherapy and atezolizumab can be administered as an outpatient in a systemic therapy treatment unit. Treatment most often would be given in a specialized cancer hospital with chemotherapy and immunotherapy experience. This is standard in most regions of Canada.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
This is not applicable, as the A+EP regimen is only intended to treat patients with cancer.
Additional Information
The updated results from the IMpower133 trial clearly show that this is a regimen that has a clinically meaningful net benefit in a patient population of significant unmet need, that of ES SCLC. Longer term follow up data has shown that these clinically meaningful benefits have translated into durable long term survival benefits for those patients who respond. Of specific note, the long-term OS results in terms of median OS, and OS at key landmark timepoints are strikingly similar to those reported by the CASPIAN trial for D+EP, which has already been determined by CADTH to represent a benefit worthy of public funding for this indication. A comparable recommendation would hence be appropriate for A+EP, which would represent an ALTERNATIVE as opposed to an ADDITIONAL option for the current treatment algorithm, and hence not be expected to add extra cost to health care budgets.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Stephanie Snow
Position: President, Lung Cancer Canada; Medical Oncologist, The QEII Health Sciences Center
Date: Feb 17, 2022
Table 7: Conflict of Interest Declaration for Lung Cancer Canada Clinician 1
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Amgen | Advisory Role | X | — | — | — |
Astra Zeneca | Advisory Role | — | — | X | — |
Bayer | Advisory Role | — | X | — | — |
Boehringer Ingeiheim | Advisory Role | X | — | — | — |
Bristol-Myers Squibb | Advisory Role | — | — | X | — |
Eisai | Advisory Role | X | — | — | — |
Merck | Advisory Role | — | — | X | — |
Novartis | Advisory Role | X | — | — | — |
Pfizer | Advisory Role | X | — | — | — |
Purdue | Advisory Role | X | — | — | — |
Roche | Advisory Role | — | — | X | — |
Taiho | Advisory Role | X | — | — | — |
Takeda | Advisory Role | — | X | — | — |
Declaration for Clinician 2
Name: Dr. Paul Wheatley-Price
Position: Medical Oncologist, The Ottawa Hospital. Associate Professor, Department of Medicine, University of Ottawa
Date: 09-02-2022
Table 8: Conflict of Interest Declaration for Lung Cancer Canada Clinician 2
Company | Check appropriate dollar range* | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
Sanofi | X | — | — | — |
Astra Zeneca | X | — | — | — |
Jazz Pharmaceuticals | X | — | — | — |
Amgen | X | — | — | — |
Janssen | X | — | — | — |
Novartis | X | — | — | — |
Merck | X | — | — | — |
BMS | X | — | — | — |
Roche | X | — | — | — |
EMD Serono | X | — | — | — |
Pfizer | X | — | — | — |
Bayer | X | — | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 3
Name: Dr. Rosalyn Juergens
Position: Chair, LCC Medical Advisory Committee; Medical Oncologist, Juravinski Cancer Center
Date: Feb 17, 2022
Table 9: Conflict of Interest Declaration for Lung Cancer Canada Clinician 3
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
Bristol Myers Squibb | X | — | — | — |
Astra Zeneca | — | X | — | — |
Merck Sharp and Dohme | X | — | — | — |
Roche | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Geoffrey Liu
Position: Medical Oncologist, Princess Margaret Cancer Centre
Date: Feb 17, 2022
Table 10: Conflict of Interest Declaration for Lung Cancer Canada Clinician 4
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Takeda Canada | Advisory Board, Health Technology Assessment Submission Advice, Speaker’s Bureau, past 10 years | — | — | X | — |
Takeda Canada | (To institution, not individual) Observational Study funding, past 10 years | — | — | — | X |
Hoffman La Roche | Advisory Board, Health Technology Assessment Submission Advice, past 10 years | — | — | X | — |
Pfizer | Advisory Board, Health Technology Assessment Submission Advice, part 10 years | — | — | X | — |
AstraZeneca | Advisory Board, Health Technology Assessment Submission Advice, Speaker’s Bureau, past 10 years, | — | — | X | — |
AstraZeneca | (To institution, not individual) Observational Study funding, past 10 years | — | — | — | X |
Bristol Myers Squibb | Advisory Board | X | — | — | — |
Boehringer Ingerheim | (To institution, not individual) Observational Study funding, past 10 years | — | — | X | — |
Abbvie | Advisory Board, past 10 years | — | X | — | — |
Merck | Advisory Board, Health Technology Assessment Submission Advice, past 10 years | — | X | — | — |
EMD Serono | Speaker’s Bureau, past 10 years | X | — | — | — |
Novartis | Advisory Board, past 10 years | — | — | X | — |
Glaxo Smith Kline | Advisory Board, past 10 years | — | X | — | — |
Declaration for Clinician 5
Name: Dr Jeffrey Rothenstein
Position: Medical Oncologist, Lakeridge Health
Date: Feb 17, 2022
Table 11: Conflict of Interest Declaration for Lung Cancer Canada Clinician 5
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
Roche | X | — | — | — |
Declaration for Clinician 6
Name: Dr Nicole Bouchard
Position: Respirologist, Sherbrooke University Hospital
Date: Feb 17, 2022
Table 12: Conflict of Interest Declaration for Lung Cancer Canada Clinician 6
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Astra Zeneca | Advisory Role/Conference | X | — | — | — |
Bristol-Myers Squibb | Advisory Role/Research | X | — | — | — |
Merck | Advisory Role/Research/Conference | X | — | — | — |
Bayer | Advisory Role | X | — | — | — |
Pfizer | Conference/Research | X | — | — | — |
Roche | Advisory Role | X | — | — | — |
Declaration for Clinician 7
Name: Dr Normand Blais
Position: Medical Oncologist, Hôpital Notre Dame du CHUM
Date: Feb 17, 2022
Table 13: Conflict of Interest Declaration for Lung Cancer Canada Clinician 7
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
Novartis | X | — | — | — |
Declaration for Clinician 8
Name: Dr. David Dawe
Position: Medical Oncologist, CancerCare Manitoba
Date: Feb 17, 2022
Table 14: Conflict of Interest Declaration for Lung Cancer Canada Clinician 8
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
AstraZeneca | Advisory boards | X | — | — | — |
Merck | Advisory Boards | X | — | — | — |
AstraZeneca | Research Grant | — | — | X | — |
Boehringer-Ingelheim | Honoraria | X | — | — | — |
Declaration for Clinician 9
Name: Dr Randeep Sangha
Position: Medical Oncologist, Cross Cancer Institute
Date: Feb 17, 2022
Table 15: Conflict of Interest Declaration for Lung Cancer Canada Clinician 9
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
N/A | — | — | — | — |
Declaration for Clinician 10
Name: Dr Catherine Labbé
Position: Head of Respiratory Medicine Service, Université de Laval
Date: Feb 17, 2022
Table 16: Conflict of Interest Declaration for Lung Cancer Canada Clinician 10
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
Astra Zeneca | — | X | — | — |
Brystol-Myers Squibb | X | — | — | — |
Jazz Pharmaceuticals | X | — | — | — |
LEO Pharma | X | — | — | — |
Merck | X | — | — | — |
Pfizer | X | — | — | — |
Roche | X | — | — | — |
Sanofi Genzyme | X | — | — | — |
Declaration for Clinician 11
Name: Dr. Donna Maziak
Position: Thoracic Surgeon, The Ottawa Hospital
Date: Feb 17, 2022
Table 17: Conflict of Interest Declaration for Lung Cancer Canada Clinician 11
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
N/A | — | — | — | — |
Declaration for Clinician 12
Name: Dr Sunil Yadav
Position: Medical Oncologist, Saskatoon Cancer Centre
Date: Feb 17, 2022
Table 18: Conflict of Interest Declaration for Lung Cancer Canada Clinician 12
Bristol-Myers Squibb | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Bristol-Myers Squibb | Advisory Board | X | — | — | — |
Astra Zeneca | Advisory Board and Speaking | X | — | — | — |
Merck | Advisory Board and Speaking | — | — | X | — |
Roche | Advisory Board and Speaking | — | X | — | — |
Takeda | Advisory Board and Speaking | X | — | — | |
Declaration for Clinician 13
Name: Dr. Quincy Chu
Position: Medical Oncologist, Cross Cancer Institute
Date: Feb 17, 2022
Table 19: Conflict of Interest Declaration for Lung Cancer Canada Clinician 13
Bristol-Myers Squibb | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Abbvie | Advisory Board and Honoraria | X | — | — | — |
Amgen | Advisory Board and Honoraria | X | — | — | — |
Astra Zeneca | Advisory Board and Honoraria | — | — | X | — |
Boehringer Ingeiheim | Advisory Board and Honoraria | — | X | — | — |
Bristol-Myers Squibb | Advisory Board and Honoraria | — | X | — | — |
Eisai | Advisory Board and Honoraria | X | — | — | — |
Merck | Advisory Board and Honoraria | — | — | X | — |
Novartis | Advisory Board and Honoraria | — | X | — | — |
Pfizer | Advisory Board and Honoraria | — | X | — | — |
Roche | Advisory Board and Honoraria | — | X | — | — |
Astra Zeneca | Research Funding | — | — | — | X |
Bristol-Myers Squibb | Educational Grant | X | — | — | — |
Declaration for Clinician 14
Name: Dr. Ronald Burkes
Position: Medical oncologist, Mount Sinai Health
Date: Feb 17, 2022
Table 20: Conflict of Interest Declaration for Lung Cancer Canada Clinician 14
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
N/A | — | — | — | — |
Declaration for Clinician 15
Name: Dr. Shaqil Kassam
Position: Medical Oncologist, Southlake Regional Hospital
Date: Feb 17, 2022
Table 21: Conflict of Interest Declaration for Lung Cancer Canada Clinician 15
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 | |
Roche | X | — | — | — |
Merck | X | — | — | — |
BMS | X | — | — | — |
Takeda | X | — | — | — |
Novartis | X | — | — | — |
Ipsen | X | — | — | — |
Sanofi | X | — | — | — |
Pfizer | X | — | — | — |
Declaration for Clinician 16
Name: Dr. Kevin Jao
Position: Medical Oncologist, Hôpital Sacré-Cœur, Montreal
Date: Feb 17, 2022
Table 22: Conflict of Interest Declaration for Lung Cancer Canada Clinician 16
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Bristol-Myers Squibb | Advisory Role | X | — | — | — |
Declaration for Clinician 17
Name: Dr. Barb Melosky
Position: Medical Oncologist, BC Cancer
Date: Feb 17, 2022
Table 23: Conflict of Interest Declaration for Lung Cancer Canada Clinician 17
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Novartis | Advisory Board | X | — | — | — |
Roche | Advisory Board | X | — | — | — |
Merck | Advisory Board | X | — | — | — |
Declaration for Clinician 18
Name: Dr. Parneet Cheema
Position: Medical Director of Cancer Care, William Osler Health System
Date: Feb 17, 2022
Table 24: Conflict of Interest Declaration for Lung Cancer Canada Clinician 18
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Bristol Myers Squibb | Advisory board/Honoraria | X | — | — | — |
Merck | Advisory board/Honoraria | X | — | — | — |
AstraZeneca | Advisory board/Honoraria | X | — | — | — |
Roche | Advisory board/Honoraria | X | — | — | — |
Novartis | Advisory board/Honoraria | X | — | — | — |
Declaration for Clinician 19
Name: Dr. Mahmoud Abdelsalam
Position: Medical Oncologist, Horizon Health Network
Date: Feb 17, 2022
Table 25: Conflict of Interest Declaration for Lung Cancer Canada Clinician 19
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
BMS | Advisory role, Honoraria and travel grants | — | X | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.