CADTH Reimbursement Review
Asciminib (Scemblix)
Sponsor: Novartis Pharmaceuticals Canada Inc.
Therapeutic area: Philadelphia chromosome-positive chronic myeloid leukemia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AP
accelerated phase
ATP
adenosine triphosphate
BC
blast crisis
BM
bone marrow
BMA
bone marrow aspirate
CCyR
complete cytogenetic response
CHR
complete hematological response
CI
confidence interval
CML
chronic myeloid leukemia
CP
chronic phase
CRF
case report form
ECOG
European Cooperative Oncology Group
ELN
European LeukemiaNet
EQ-5D-5L
EQ-5D 5-Levels
ESS
effective sample size
FAS
full analysis set
HR
hematological response
HRQoL
health-related quality of life
IPD
individual patient data
IS
International Standard
LLSC
Lymphoma and Leukemia Society of Canada
MAIC
matching adjusted indirect comparison
MCyR
major cytogenetic response
MDASI
MD Anderson Symptom Inventory
MID
minimally important difference
MMR
major molecular response
OS
overall survival
PCyR
partial cytogenetic response
PGIC
patients’ global impression of change
Ph
Philadelphia chromosome
PFS
progression-free survival
PS
performance score
RCT
randomized controlled trial
RT-PCR
reverse transcription polymerase chain reaction
SAE
serious adverse event
SD
standard deviation
SLR
systematic literature review
STAMP
specifically targeting the ABL myristoyl pocket
TKI
tyrosine kinase inhibitor
TTD
time to treatment discontinuation
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Asciminib (Scemblix), 80 mg q.d. or 40 mg b.i.d. oral tablets |
Indication | For the treatment of adult patients with Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase previously treated with 2 or more tyrosine kinase inhibitors |
Reimbursement request | As per the indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | June 22, 2022 |
Sponsor | Novartis Pharmaceuticals Canada Inc. |
b.i.d. = twice daily; NOC = Notice of Compliance; q.d. = once daily.
Introduction
Chronic myeloid leukemia (CML) is a clonal bone marrow (BM) stem cell disorder resulting in the unregulated growth of myeloid precursor cells and production of excessive neutrophils, eosinophils, and basophils in the BM.1 Blood and BM cells in patients with CML usually contain a characteristic chromosomal abnormality known as the Philadelphia chromosome (Ph), the result of a balanced translocation between chromosomes 9 and 22.2 The incidence rate of CML across all ages and sexes in Canada, excluding Quebec, ranged from 510 cases in 2011 to 585 cases in 2018. This corresponds to an incidence rate of 2.0 per 100,000 population in 2018.3
The majority of patients (greater than 95%) with CML are in chronic phase (CP) at diagnosis.4 The use of oral tyrosine kinase inhibitors (TKIs) targeting the BCR-ABL kinase represents the standard of care for patients with newly diagnosed CP-CML. Imatinib was the first drug in this class to be approved, and reports of improvements in population-based CML outcomes can largely be attributed to the use of this drug.5 Roughly one-third of patients treated with imatinib will discontinue therapy, either because of intolerance from side effects or loss of response due to drug resistance. The second-generation TKIs, dasatinib, nilotinib, and bosutinib have a much smaller spectrum of resistance mutations, but none are able to overcome the T315I mutation. These drugs have similar efficacy when used as second-line therapies.6,7 Ponatinib is a third-generation TKI with activity against wild-type and mutant BCR-ABL, though it is associated with serious toxicity, including cardiovascular, cerebrovascular, and peripheral vascular events.6,7
Asciminib is a potent inhibitor of ABL/BCR-ABL1 tyrosine kinase with a novel mode of action. It inhibits the ABL1 kinase activity of the BCR-ABL1 fusion oncoprotein, by specifically targeting the ABL myristoyl pocket (STAMP). Asciminib is administered as an oral tablet at a dosage of 80 mg daily and has received a Notice of Compliance (NOC) from Health Canada for the treatment of adult patients with Ph positive (Ph+) CP-CML previously treated with 2 or more TKIs.
The objective of this review is to perform a systematic review of the beneficial and harmful effects of asciminib 40 mg oral tablets for the treatment of adult patients with Ph+ CP-CML previously treated with 2 or more TKIs.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from the clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient group submissions were received: 1 from the Chronic Myelogenous Leukemia Society of Canada and 1 from the Lymphoma and Leukemia Society of Canada (LLSC) and the Canadian CML Network. The Chronic Myelogenous Leukemia Society of Canada gathered information from 10 patients with CML and their caregivers through remote surveys and interviews between January and February 2022. The LLSC and the Canadian CML Network conducted an anonymous online survey collaboratively for patients with CML between November 30, 2021, and January 3, 2022. Overall, 16 participants responded to this survey, of which 11 were patients with CML and 5 were a caregiver, friend, or family member of a patient with CML.
According to the submission from the Chronic Myelogenous Leukemia Society of Canada, most patients do not feel sick at the time they are diagnosed with CML in CP, but patients are overwhelmed and physically and emotionally drained due to the financial stress associated with the cost of treatment and frequent appointments and testing. Family members also suffer as the family routine changes significantly and caregivers and/or spouses become more responsible for household management. In both submissions, patients described numerous side effects to the various TKIs, such as fatigue, muscle cramps or pain, rash, joint pain, headaches, fluid retention, and serious cardiovascular problems. It was clear that side effects can seriously impact patients’ quality of life. Those who responded to the LLSC and Canadian CML Network survey indicated that daily life was impacted through moderate impacts on ability to exercise, ability to work, mental health, ability to concentrate, ability to travel, personal image, and ability to continue daily activities. Similarly, respondent indicated moderate impacts of stress, anxiety and/or worry, difficulty sleeping, loss of sexual desire, financial impacts, interruption of life goals and/or accomplishments, and depression.
Patients identified extended survival, improved quality of life, minimization of side effects, and a return to normal life as being important. The majority of patients treated with asciminib rated a positive impact of this treatment on their ability to perform daily activities. All of respondents who had experience with asciminib treatment agreed (11%) or strongly agreed (89%) that asciminib improved health-related quality of life (HRQoL), and all would recommend this treatment to other patients diagnosed with CML.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
Two clinical experts with experience in the diagnosis and management of CML highlighted the need for more treatment options to be made available for patients that have received 2 or more prior TKIs. Ponatinib has been shown to be effective in this setting but has serious safety concerns and patients with cardiovascular risk factors will be contraindicated and have limited options available. Asciminib would likely become the preferred treatment used in the third line. The clinical experts noted that the end point of major molecular response (MMR) is a clinically useful measure of response, and that treatment discontinuation should be assessed according to European LeukemiaNet (ELN) guidelines for treatment failure or the inability of the patient to tolerate treatment.
Clinician Group Input
Clinician group input on the review of asciminib for the treatment of adult patients with Ph+ CML in CP previously treated with 2 or more TKIs was received from 2 groups: Ontario Health – Cancer Care Ontario Hematology Drug Advisory Committee (2 clinicians) and a peer group of hematologists across Canada who are involved in treating patients with CML (14 clinicians). The clinician groups both highlighted that the least suitable patients for asciminib would be those in accelerated phase (AP) or blast crisis (BC), and the second group emphasized that tolerance is important for treatment adherence, which affects suppression of the leukemic clone.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The drug plans identified implementation issues related to relevant comparators; considerations for initiation, prescribing, and discontinuation of therapy; generalizability; funding algorithm; care provision; system issues; and economic considerations. The clinical experts consulted by CADTH for this review weighed evidence from the included study and other clinical considerations to provide responses to the drug plan’s implementation questions.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
ASCEMBL (N = 233) is a phase III, open-label, randomized study of asciminib compared to bosutinib in patients with CP-CML who had received 2 or more TKIs and experienced treatment failure or intolerance to the most recent TKI. The primary objective of ASCEMBL was to determine the efficacy of asciminib (40 mg twice daily) as compared to bosutinib (500 mg daily) in achieving MMR at the 24-week time point. HRQoL, overall survival (OS), progression-free survival (PFS), and complete cytogenetic response (CCyR) were secondary end points in the trial. Patients were treated until treatment failure or intolerance. Patients in the bosutinib group were permitted to switch to asciminib if they experienced treatment failure. The end of study was defined as 96 weeks after the last patient received their first dose or up to 48 weeks after the last patient switched from bosutinib to asciminib. The mean age in both groups was 51.0 years with a slightly higher proportion of males in the asciminib group (52.2%) compared to the bosutinib group (40.8%). The proportion of patients who identified as Hispanic or Latino was higher in the bosutinib group (22.4%) compared to the asciminib group (9.6%). There were differences in baseline characteristics of important prognostic factors, such as number of prior TKIs and reason for prior TKI discontinuation.
Efficacy Results
Key efficacy outcomes are summarized in Table 2.
Health-Related Quality of Life
Baseline mean EQ visual analogue scale (VAS) (higher scores indicate better HRQoL) was 71.3 (standard deviation [SD] = 21.71) in the asciminib group and 74.2 (SD = 18.79) in the bosutinib group. Mean change from baseline at week 24 was 7.5 (SD = 23.36) in the asciminib group (N = 106) and 0.5 (SD = 17.87) in the bosutinib group (N = 38); this outcome was not tested statistically.
OS and PFS
OS and PFS outcomes were immature at the time of primary analysis (May 25, 2020; mean duration of follow-up = 15.6 months) and at the updated data cut-off (January 1, 2021; mean duration of follow-up = 23.0 months). At the primary analysis, 2.5% of patients in the asciminib group and 1.3% of patients in the bosutinib group experienced a survival event and 4.5% of patients in the asciminib group and 6.6% of patients in the bosutinib group experienced a progression event.
Major Molecular Response
MMR at the 24-week time point was the primary end point of ASCEMBL. At the primary analysis, the MMR rate at 24 weeks in the asciminib group was 25.48% (95% confidence interval [CI], 18.87% to 33.04%) and in the bosutinib group it was 13.16% (95% CI, 6.49% to 22.87%). The primary end point was based on a common risk stratification of major cytogenetic response (MCyR) versus no MCyR at baseline and the difference in MMR rate based on common risk difference was 12.24% (95% CI, 2.19% to 22.30%) with a P value of 0.029. At the updated data cut-off at 48 weeks, the MMR rate was 26.11% (95% CI, 19.44% to 33.72%) in the asciminib group and 11.84% (95% CI, 5.56% to 21.29%) in the bosutinib group; the difference in response rate based on common risk difference was 16.09% (95% CI, 5.69% to 26.49%; not tested statistically).
Complete Cytogenetic Response
The CCyR at 24 weeks in the asciminib group was 40.78% (95% CI, 31.20% to 50.90%) and in the bosutinib group was 24.19% (95% CI, 14.22% to 36.74%). Assessed by common risk stratification of MCyR versus no MCyR at baseline, the difference in response rate based on common risk difference was 17.30% (95% CI, 3.62% to 30.99%). At the updated data cut-off, the difference in response rate at 48 weeks based on common risk difference was 19.05% (95% CI, 4.87 to 33.24). This analysis was not adjusted for multiplicity.
Duration of Response
At the time of primary analysis, 5.6% of the 54 patients receiving asciminib who had gained an MMR at any time had gone on to lose their response, compared to 0% of the 14 patients receiving bosutinib who had gained a response at any time. At the updated data cut-off, these values were 3.2% and 5.6%, respectively.
At the time of primary analysis, 2.3% of the 44 patients receiving asciminib who had gained a CCyR at any time had gone on to lose their response, compared to 5.3% of the 19 patients receiving bosutinib who had gained a response at any time. At the updated data cut-off, these values were 2.0% and 4.5%, respectively.
Time to Response
At the time of primary analysis, the mean time to first MMR in the 54 patients receiving asciminib who had achieved an MMR at any time was 19.0 weeks (SD = 14.40) and 22.8 weeks (SD = 18.37) for the 14 patients receiving bosutinib that had gained a response at any time. At the updated data cut-off, these values were 24.7 weeks (SD = 21.71) and 31.1 weeks (SD = 25.81), respectively.
At the time of primary analysis, the mean time to first CCyR in the 44 patients receiving asciminib who had achieved an MMR at any time was 25.4 weeks (SD = 5.09) and 29.0 weeks (SD = 11.50) for the 19 patients receiving bosutinib who had gained a response at any time. At the updated data cut-off, these values were 29.1 weeks (SD = 13.47) and 31.6 weeks (SD = 12.60), respectively.
Harms Results
A summary of harms is included in Table 2. At the time of primary analysis almost all patients in both treatment groups had experienced at least 1 treatment-emergent adverse event; 89.7% in the asciminib group and 96.1% in the bosutinib group. The most common adverse events (AEs) in the asciminib group were thrombocytopenia (22.4% versus 13.2% in the bosutinib group), neutropenia (17.9% versus 17.1% in the bosutinib group), and headache (16.0% versus 13.2% in the bosutinib group). The most common AEs in the bosutinib group were diarrhea (71.1% versus 11.5% in the asciminib group), nausea (46.1% versus 11.5% in the asciminib group), and increased alanine aminotransferase (27.6% versus 3.8% in the asciminib group). Serious adverse events (SAEs) occurred in 13.5% of patients in the asciminib group and 18.4% of patients in the bosutinib group, with none, other than pyrexia, occurring in more than 1 patient. Deaths occurred in 2.6% of patients in the asciminib group and 1.3% of patients in the bosutinib group. The largest differences between the study treatments were in hepatotoxicity, in which 8.3% of patients in the asciminib group reported AEs compared to 30.3% of patients in the bosutinib group, and in gastrointestinal toxicity, in which 31.4% of patients in the asciminib group reported AEs compared to 78.9% of patients in the bosutinib group. Pancreatic toxicity was similar between the treatment groups, with 8.3% of patients in the asciminib group reporting AEs compared to 9.2% of patients in the bosutinib group.
Table 2: Summary of Key Results From Pivotal and Protocol Selected Studies
Outcome | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | Asciminib N = 157 | Bosutinib N = 76 | |
HRQoL: EQ VAS | ||||
Baseline, mean (SD) [N] | 71.3 (21.71) [149] | 74.2 (18.79) [69] | NR | NR |
Week 24, mean (SD) [N] | 77.4 (20.91) [108] | 73.5 (21.65) [41] | NR | NR |
Mean change from baseline (SD) [N] | 7.5 (23.36) [106] | 0.5 (17.87) [38] | NR | NR |
OS | ||||
Number of patients with an event, n (%) | 4 (2.5) | 1 (1.3) | 4 (2.5) | 1 (1.3) |
KM % event free, 1 year (95% CI) | 97.5 (92.4 to 99.2) | 98.6 (90.2 to 99.8) | 98.0 (93.8 to 99.3) | 98.6 (90.2 to 99.8) |
PFS | ||||
Number of patients with an event, n (%) | 7 (4.5) | 5 (6.6) | 7 (4.5) | 5 (6.6) |
KM % event free, 1 year (95% CI) | 95.1 (89.2 to 97.8) | 88.6 (72.8 to 95.5) | 96.3 (91.3 to 98.5) | 91.1 (79.5 to 96.3) |
MMR | ||||
Response, n (%) | 40 (25.48) | 10 (13.16) | 41 (26.11) | 9 (11.84) |
95% CIa | (18.87 to 33.04) | (6.49 to 22.87) | (19.44 to 33.72) | (5.56 to 21.29) |
Common risk difference, %b (95% CI)c | 12.24 (2.19 to 22.30) | Reference | 16.09 (5.69 to 26.49) | Reference |
P valued | 0.029 | Reference | NA | NA |
CCyR | ||||
Response, n (%) [N] | 42 (40.78) [103] | 15 (24.19) [62] | 41 (39.81) [103] | 13 (20.97) [62] |
95% CIa | (31.20 to 50.90) | (14.22 to 36.74) | (30.29 to 49.92) | (11.66 to 33.18) |
Common risk difference, %b (95% CI)c | 17.30 (3.62 to 30.99) | Reference | 19.05 (4.87 to 33.24) | Reference |
P valued | 0.019e | Reference | NR | NR |
Harms, n (%) | ||||
AEs | 140 (89.7) | 73 (96.1) | NR | NR |
SAEs | 21 (13.5) | 14 (18.4) | NR | NR |
WDAEs (from study treatment) | 9 (5.8) | 16 (21.1) | NR | NR |
Deaths | 4 (2.6) | 1 (1.3) | NR | NR |
Notable harms, n (%) | ||||
Myelosuppression | 58 (37.2) | 27 (35.5) | NR | NR |
Pancreatic toxicity | 13 (8.3) | 7 (9.2) | NR | NR |
Hepatotoxicity | 13 (8.3) | 23 (30.3) | NR | NR |
Gastrointestinal toxicity | 49 (31.4) | 60 (78.9) | NR | NR |
Cardiac failure | 2 (1.3) | 1 (1.3) | NR | NR |
AE = adverse event; CCyR = complete cytogenetic response; CI = confidence interval; HRQoL = health-related quality of life; KM = Kaplan–Meier; MCyR = major cytogenetic response; MMR = major molecular response; NA = not applicable; NR = not reported; OS = overall survival; PFS = progression-free survival; SAE = serious adverse event; SD = standard deviation; VAS = visual analogue scale; WDAE = withdrawal due to adverse event.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off, updated data cut-off was January 1, 2021.
aClopper-Pearson 95% 2-sided CI.
bWald 95% 2-sided CI.
cThe common risk difference after adjusting for stratum: baseline MCyR status (based on randomization data) and its 95% CI were estimated using the Mantel-Haenszel method.
dCochrane-Mantel-Haenszel 2-sided test was stratified by baseline MCyR status (based on randomization data).
eNot adjusted for multiplicity.
Source: Asciminib Clinical Study Report.8
Critical Appraisal
The primary end point of the ASCEMBL trial was stratified based on MCyR at baseline; however, there was an imbalance within the patients in MCyR at baseline and proportionally more patients in the asciminib group were in CCyR than in the bosutinib group, which may have biased the study results in favour of asciminib. Additionally, there was a substantial number of patients with missing MCyR data at baseline, resulting in 15.9% of patients receiving asciminib and 14.5% of patients receiving bosutinib assigned to the incorrect stratum. A sensitivity analysis was conducted to correct for this using BCR-ABL1 ratio as a proxy for cytogenetic response, the results of which are consistent with the primary analysis. Formal statistical testing was only conducted on the primary end point and none of the other analyses, aside from the primary end point analysis, were controlled for multiplicity (including MMR at 48 weeks). There were slight differences in baseline characteristics of important prognostic factors with proportionally more patients in the bosutinib group having received higher numbers of prior TKIs and having discontinued their prior TKI due to resistance, suggesting bias in favour of asciminib. However, logistic regression adjusting for these factors found similar results with the primary analysis.
According to clinical experts consulted by CADTH, the demographic and disease characteristics of the ASCEMBL population were reflective of the Canadian population with CP-CML after 2 or more prior TKIs; however, it should be noted that patients with the T315I or V299L mutations were excluded from the trial population, which impacted the generalizability to this group of patients. The dosage of asciminib in the ASCEMBL trial (40 mg twice daily) represents only one of the Health Canada–approved dosages (40 mg twice daily and 80 mg once daily). It is unclear if the ASCEMBL evidence is generalizable to an 80 mg once daily dose. All outcomes evaluated in the trial and considered in this review (i.e., MMR, CCyR, OS, PFS, HRQoL) were clinically relevant, important to patients, and are used in clinical practice. The duration of follow-up was sufficient for assessment of the primary outcome of MMR at 24 weeks, CCyR, and HRQoL; however, conclusions regarding longer-term outcomes of PFS and OS cannot be drawn given the immaturity of the data. Subgroup analysis was not powered to detect treatment differences in patients who experienced treatment failure on their most recent TKI compared to treatment intolerance, line of therapy, disease severity at baseline, or mutational status, and there was no test for subgroup differences. Nevertheless, the clinical experts consulted for this review felt that the results were generalizable across strata for all these subgroups.
Indirect Comparisons
Description of Studies
One matching adjusted indirect comparison (MAIC) report was submitted by the sponsor and included in this report. In the absence of direct comparative evidence from trials, the aim of each MAIC was to compare the efficacy (response rate [MMR and CCyR] and time to treatment discontinuation [TTD]) of asciminib versus ponatinib, nilotinib, and dasatinib in patients with CP-CML who have received at least 2 prior TKIs. To identify evidence for relevant comparators a systematic literature review (SLR) was conducted to identify evidence from interventional and observational studies. Given the availability of individual patient data from the ASCEMBL index trial, the sponsor aimed to adjust for between-study differences in the distribution of prognostic factors and treatment effect modifiers. The sponsor consulted with an expert clinician to identify which characteristics should be adjusted for in the analysis and their relative importance. For response comparisons, the ponatinib single-arm phase II study PACE9 (N = 203), nilotinib and dasatinib single-centre prospective cohort study10 (N = 26; 6 of whom received nilotinib), and dasatinib single-centre retrospective chart review11 (N = 24) were used.
Efficacy Results
In the comparison of MMR rate and CCyR rate at both 6 and 12 months in the weighted sample of patients from the ASCEMBL trial compared with the PACE trial (ponatinib), ||||||||| ||| |||||||| |||| ||||||| || ||| || ||| | ||| || ||||| ||||||||||| |||| || |||| ||||| |||| || |||| |||| ||| |||| || ||||| ||| |||| |||| ||| |||| || |||||| ||||||||||||| ||| || |||| ||| ||| |||| || ||| ||||||| ||||||||| ||| |||| ||||| || ||||| ||| |||| ||||| || ||||| || ||| |||||||| |||||||||.
The comparison of efficacy end points was only available for CCyR at both 6 and 12 months in the weighted sample of patients from the ASCEMBL trial compared with patients treated with dasatinib or nilotinib. ||||||||| ||| |||||||| |||| ||||||| || |||| || ||| | ||| |||||||| ||||||||||| |||| || || || |||| |||| ||| |||| || |||||| ||| |||| |||| ||| |||| || |||||| ||||||||||||.
The comparison of efficacy end points was only available for MMR at 6 months in the weighted sample of patients from the ASCEMBL trial compared with patients treated with dasatinib. ||| || ||| ||| || |||||||| ||| |||| |||| ||| |||| || |||||.
Critical Appraisal
The sponsor submitted 1 MAIC report that included comparisons of interest for asciminib against ponatinib, dasatinib, and nilotinib. The choice to conduct an unanchored MAIC was justified considering the lack of a common comparator. There were important differences in the design of the comparator studies that limit the ability to draw conclusions about the efficacy of asciminib compared with the other treatments. ASCEMBL was a randomized phase III interventional trial, while comparator trials included observational trials. These are prone to unique biases (e.g., selection bias, confounding) compared with those collected from prospective interventional studies (like randomized controlled trials [RCTs] and single-arm trials) that cannot be controlled for using MAIC methods.
An important limitation, inherent to all MAIC analyses, is that all prognostic factors should ideally be adjusted between index and comparator trials to eliminate as much bias from the comparison as possible. This includes both measured and unmeasured characteristics and thus can never be fully accounted for. The list of characteristics provided by the sponsor that were adjusted for were not informed by a systematic review of literature or clinical expert identification; rather, they were chosen because they were included in the comparator trials and could be reliably calculated for patients in the ASCEMBL trial. This limitation was in addition to the fact that all identified prognostic factors could not be matched due to non-convergence and concerns for effective sample size (ESS).
The ESS for most comparisons was very small, resulting in very wide CIs that precluded the ability to draw conclusions from the data. For the comparison of nilotinib specifically, the only available trial that included response data was a retrospective trial of 26 patients, of whom only 6 received nilotinib while the other 20 received dasatinib, though the issue of small ESS is present in all comparisons. As such, there is very little that can be said regarding the comparative efficacy of asciminib versus the chosen comparators with regards to response.
Other Relevant Evidence
Description of Studies
The sponsor submitted a phase I, multicentre, open-label study. The primary objective was to determine the maximum tolerated dose and/or recommended dose for expansion of asciminib single drug or in combination with other drugs. Among the 317 enrolled patients, 30 patients without the T315I mutation were treated with the 40 mg twice daily dosage and 17 were treated with the 80 mg once daily dosage.
Efficacy Results
MMR results were consistent with the pivotal trial. Patients receiving asciminib 40 mg twice daily had an MMR rate of 16% at 24 weeks, while patients receiving asciminib at 80 mg daily had an MMR rate of 28.6% at 24 weeks.
Harms Results
All patients in the 40 mg twice daily group (n = 30) and 80 mg daily group (n = 17) had AEs. SAEs were found among 11 (36.7%) and 8 (47.1%) patients taking 40 mg twice daily and 80 mg daily, respectively. AEs leading to dose adjustment or interruption were observed among 14 (46.7%) and 10 (58.8%) patients taking 40 mg daily and 80 mg daily dosages, respectively. Among the notable harms were myelosuppression (36.7% and 41.2%), pancreatic toxicity (53.3% and 29.4%), hepatotoxicity (including laboratory terms) (16.7% and 17.6%), gastrointestinal AEs (70.0% and 52.9%), and cardiac failure (6.7% and 17.6%) for all grades in asciminib 40 mg twice daily and 80 mg once daily groups, respectively. The safety profile seen was similar to that in the pivotal trial.
Critical Appraisal
There are several internal validity concerns that limit the certainty of conclusions that can be drawn from this trial. The primary concern is that there was no control group and no adjustment for known prognostic factors or effect modifiers; thus, causal conclusions cannot be established, and the findings are at high risk of confounding. Since the trial was open label, there is a risk that common subjective harms may have been overreported. Though the inclusion and exclusion criteria are clear, some details of the participant disposition are limited (i.e., number screened versus randomized). There was no hypothesis testing in the trial. The small sample size may negatively impact the reliability of the findings. The patients were not randomized, and there is a possibility of selection bias because it is not clear whether the patients were consecutively enrolled.
Conclusions
The ASCEMBL trial showed a statistically significant benefit with asciminib 80 mg daily over bosutinib 500 mg daily in MMR at 24 weeks in patients who had received 2 or more TKIs and experienced treatment failure on or intolerance to the most recent TKI. In the opinion of the clinical experts consulted by CADTH, the MMR rate at 24 weeks represents a clinically significant benefit for asciminib over bosutinib. Secondary end points such as HRQoL, duration of response, and time to response favoured asciminib but were not statistically tested; therefore, few conclusions can be drawn. CCyR results were supportive of the MMR results, though the analysis was not adjusted for multiplicity. Data on OS and PFS were immature at the time of analysis. The submitted MAIC provided indirect evidence for relative efficacy for asciminib compared to ponatinib, dasatinib, and nilotinib, but the significant limitations with the analysis prohibit any conclusions from being drawn. Asciminib appears to be more tolerable than bosutinib, though comparative safety evidence against other relevant comparators is lacking.
Introduction
Disease Background
CML is a clonal BM stem cell disorder resulting in the unregulated growth of myeloid precursor cells and production of excessive neutrophils, eosinophils, and basophils in the BM.1 Although up to 50% of patients are asymptomatic at diagnosis, common signs and symptoms (e.g., fatigue, weight loss, malaise, easy satiety, left lower quadrant fullness or pain) result from anemia and splenic enlargement. Blood and BM cells in patients with CML usually contain a characteristic chromosomal abnormality resulting from a balanced translocation between chromosomes 9 and 22 (Ph).2 The gene product of this BCR-ABL translocation is a tyrosine kinase that is constitutively active, resulting in the continuous activation of other cell cycle regulatory proteins and unrestrained BM proliferation. This kinase is now the key therapeutic target in the treatment of CML, and the presence of cells bearing the t(9;22) translocation in the blood and BM form the basis of response monitoring in this disorder.2 Initial signs of CML are identified through typical findings in the blood and BM and confirmed by identification of the Ph chromosome, BCR-ABL1 fusion gene, or BCR-ABL1 fusion mRNA using conventional cytogenetics, fluorescence in situ hybridization analysis, or reverse transcription polymerase chain reaction (RT-PCR).12
The incidence rate of CML across all ages and sexes in Canada, excluding Quebec, ranged from 510 cases in 2011 to 585 cases in 2018. This corresponds to an incidence rate of 2.0 per 100,000 population in 2018.3 The 20-year prevalence rate in 2015 was higher in males in Canada (15.8 per 100,000) than in females in Canada (11.7 per 100,000).3 The 20-year prevalence of CML across all ages and sexes in Canada, excluding Quebec, ranged from 3,110 cases in 2012 to 3,760 cases in 2015. This corresponds to a 20-year prevalence rate of 13.7 per 100,000 population in 2015.3 The 20-year prevalence rate in 2015 was higher in males in Canada (15.8 per 100,000) than in females in Canada(11.7 per 100,000).3 The average age at diagnosis is 64 years of age, as CML is rarely diagnosed in children.13
The majority of patients (greater than 95%) with CML are in CP at diagnosis.4 In the distant past, without treatment or with chemotherapy using busulfan or hydroxyurea, this was followed by progression to accelerated and blast phases, which was invariably fatal. OS before the use of modern treatments was approximately 3 to 5 years.14 Allogeneic stem cell transplant from a sibling or matched unrelated donor resulted in cure of 70% to 80% of patients treated in CP, but was limited to younger patients and those with available donors, representing less than 25% of the patient population. Hence, CML was previously fatal for 80% to 90% of patients before the introduction of specific inhibitors of the BCR-ABL kinase. For those who were not candidates for allogeneic stem cell transplant, or for whom a donor could not be found, interferon alpha was effective in producing hematologic and occasional cytogenetic responses, but side effects limited its use to those younger than 50 years of age.14 Following the development of the first TKIs in 2001, 10-year survival rates have improved from approximately 20% to approximately 80% to 90% today.2
Standards of Therapy
The use of oral TKIs targeting the BCR-ABL kinase represents the standard of care for patients with newly diagnosed CP-CML. Imatinib was the first drug in this class to be approved, and reports of improvements in population-based CML outcomes can largely be attributed to the use of this drug.5 Long-term follow-up of patients in the original phase III randomized trial comparing imatinib to interferon alpha plus cytarabine therapy showed that at 5 years, 87% of patients had a CCyR (no evidence of the Ph chromosome in the BM) and only 6% had progressed to AP or BP.15
Roughly one-third of patients treated with imatinib will discontinue therapy, due either to intolerance from side effects (e.g., diarrhea, fatigue, edema) or loss of previous molecular, cytogenetic, or hematologic response because of drug resistance. Mutations to the adenosine triphosphate (ATP) binding site of BCR-ABL, which is the site of contact of TKIs active in these diseases, are associated with drug resistance and a high risk of progression. While some binding site mutations may preserve the activity of alternative TKIs, the T315I mutation is associated with universal resistance to first- and second-generation drugs. The second-generation TKIs dasatinib, nilotinib, and bosutinib have a much smaller spectrum of resistance mutations, but none can overcome the T315I mutation. These drugs produce similar rates of MMR and have similar PFS and OS when used as second-line therapies.6,7
Ponatinib is a third-generation TKI with activity against wild-type and mutant BCR-ABL. It was designed to fit into the ATP binding domain of mutant forms of BCR-ABL and is known to bind firmly even in the presence of mutations such as T315I that are associated with resistance to first and second-generation TKIs. Ponatinib is associated with serious toxicity including cardiovascular, cerebrovascular, and peripheral vascular as well as the elevation of pancreatic enzymes, pancreatitis, dermatitis and fatigue.6,7
Patients with Ph+ CML whose disease becomes resistant or who become intolerant to imatinib in the first-line setting may receive second-line second-generation TKIs such as bosutinib, dasatinib, or nilotinib. Patients who received a second-generation TKI in the first line may receive an alternative second-generation TKI in the second-line setting. Rarely, they may be stepped back onto imatinib in the second line if the change is being made for intolerance. Treatment options for patients whose disease becomes resistant or who become intolerant to 2 prior lines of TKI therapy are ponatinib, hematopoietic stem cell transplant, or any second-generation TKI that has not already been used in a prior line of therapy.6,7
As patients with CP-CML who have failed on 2 or more previous TKI therapies have an advanced disease, achievement of an MMR as soon as possible reduces the risk of disease progression and is an important treatment goal. Durability of this response is another important goal for continuous suppression of the leukemic clone. Patients who have failed on 2 or more previous TKI therapies have few options for treatment; therefore, tolerability of therapy is an important treatment goal as well.
Drug
Asciminib is a potent inhibitor of ABL/BCR-ABL1 tyrosine kinase with a novel mode of action. It inhibits the ABL1 kinase activity of the BCR-ABL1 fusion oncoprotein, by the mechanism known as STAMP. Asciminib received an NOC from Health Canada, indicated for the treatment of adult patients with Ph+ CP-CML who have been previously treated with 2 or more TKIs and has not previously been reviewed by CADTH for any indication. The sponsor is requesting reimbursement for the indication as reviewed by Health Canada. On October 29, 2021, asciminib was approved by the FDA for patients with Ph+ CP-CLM who have been previously treated with 2 or more prior TKIs.16 The FDA also gave approval for patients with Ph+ CP-CLM with the T315I with a recommended dosage of 200 mg twice daily. This dose is specifically for patients with the T315I mutation, a patient population that is not part of the requested reimbursement population.
Asciminib is administered as an oral tablet at a dosage of 80 mg daily. Key characteristics of asciminib and relevant comparators are shown in Table 3.
Table 3: Key Characteristics of Asciminib, Bosutinib, Nilotinib, Dasatinib, and Ponatinib
Characteristic | Asciminib | Bosutinib | Nilotinib | Dasatinib | Ponatinib |
|---|---|---|---|---|---|
Mechanism of action | Asciminib is a potent inhibitor of ABL/BCR-ABL1 tyrosine kinase and inhibits the ABL1 kinase activity of the BCR-ABL1 fusion protein, by specifically targeting the ABL myristoyl pocket. | Bosutinib inhibits the activity of the oncogenic BCR-ABL kinase that promotes CML, through binding of the ATP binding site of the BCR-ABL oncoprotein. | Nilotinib inhibits the activity of the oncogenic BCR-ABL kinase that promotes CML, through binding of the ATP binding site of the BCR-ABL oncoprotein. | Dasatinib inhibits the activity of the oncogenic BCR-ABL kinase that promotes CML, binding both the inactive and active conformations of the enzyme. | Ponatinib is a potent pan–BCR-ABL inhibitor with structural elements, including a carbon-carbon triple-bond that enables high-affinity binding to native BCR-ABL and mutant forms of the ABL kinase. |
Indicationa | For the treatment of adult patients with Ph+ CP-CML previously treated with 2 or more TKIs. | For the treatment of adult patients with chronic, accelerated, or blast phase Ph+ CML with resistance or intolerance to prior TKI therapy. | For the treatment of adult patients with chronic phase and accelerated phase Ph+ CML resistant to or intolerant of at least 1 prior therapy, including imatinib. | For the treatment of adult patients with Ph+ chronic, accelerated, or blast phase CML with resistance or intolerance to prior therapy including imatinib. | For the treatment of adult patients with chronic, accelerated, or blast phase CML or Ph+ ALL for whom other TKI therapy is not appropriate, including CML or Ph+ ALL that is T315I mutation positive or where there is prior TKI resistance or intolerance. |
Route of administration | Oral | Oral | Oral | Oral | Oral |
Recommended dose | Either 80 mg once daily or 40 mg twice daily at approximately 12-hour intervals | The recommended dosage is 500 mg daily with food | The recommended dosage is 400 mg twice daily | The recommended dosage is 100 mg once daily | The recommended starting dosage is 45 mg once daily |
Serious adverse effects or safety issues | Warnings and/or precautions for QT interval prolongation, hypertension, embryo-fetal toxicity, myelosuppression, pancreatic toxicity, and hepatitis B reactivation | Serious warnings and precautions for gastrointestinal toxicity, hepatic toxicity, cardiac toxicity, pancreatic toxicity, fluid retention, hemorrhage, QT interval prolongation, myelosuppression, tumour lysis syndrome, hepatitis B reactivation, and second primary malignancies | Serious warnings and precautions for cardiac deaths, QT interval prolongation, ischemic heart disease, ischemic cerebrovascular events, peripheral arterial occlusive disease, hepatoxicity, pancreatitis, and myelosuppression | Serious warnings and precautions for myelosuppression, hemorrhage, fluid retention, congestive heart failure, and pulmonary arterial hypertension | Serious warnings and precautions for arterial occlusions, venous thromboembolism, heart failure, hemorrhage events, hepatotoxicity, myelosuppression, and pancreatitis |
Other | NA | NA | NA | NA | Ponatinib should only be prescribed and monitored by a physician who has completed the certification with the ICLUSIG Controlled Distribution Program. |
ALL = acute lymphoblastic leukemia; ATP = adenosine triphosphate; CML = chronic myeloid leukemia; CP = chronic phase; NA = not applicable; Ph+ = Philadelphia chromosome positive; TKI = tyrosine kinase inhibitor.
aHealth Canada–approved indication.
Source: Asciminib draft product monograph,17 Bosutinib product monograph,18 Nilotinib product monograph,19 Dasatinib product monograph,20 Ponatinib product monograph.21
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full patient group submissions can be found at the end of this report in the Stakeholder Feedback section.
Two patient group submissions were received: 1 from the Chronic Myelogenous Leukemia Society of Canada and 1 from the LLSC and the Canadian CML Network. The Chronic Myelogenous Leukemia Society of Canada gathered information from 10 patients with CML and their caregivers through remote surveys and interviews between January and February 2022. The LLSC and the Canadian CML Network conducted an anonymous online survey collaboratively for patients with CML between November 30, 2021, and January 3, 2022. Overall, 16 participants responded to this survey, of which 11 were patients with CML and 5 were a caregiver, friend, or family member of a patient with CML.
According to the submission from the Chronic Myelogenous Leukemia Society of Canada, most patients do not feel sick at the time they are diagnosed with CP-CML, but patients are overwhelmed and physically and emotionally drained due to the financial stress associated with the cost of treatment and frequent appointments and testing. Family members also suffer as the family routine changes significantly and caregivers and/or spouses become more responsible for household management. In both submissions, patients described numerous side effects to the various TKIs, such as fatigue, muscle cramps or pain, rash, joint pain, headaches, fluid retention, and serious cardiovascular problems. It was clear that side effects can seriously impact patients’ quality of life. Those who responded to the LLSC and Canadian CML Network survey indicated that daily life was impacted through moderate impacts on ability to exercise, ability to work, mental health, ability to concentrate, ability to travel, personal image, and ability to continue daily activities. Similarly, respondent indicated moderate impacts of stress, anxiety and/or worry, difficulty sleeping, loss of sexual desire, financial impacts, interruption of life goals and/or accomplishments, and depression.
Patients identified extended survival, improved quality of life, minimization of side effects, and a return to normal life as being important. The majority of patients treated with asciminib rated a positive impact of this treatment on their ability to perform daily activities. All of respondents who had experience with asciminib treatment agreed (11%) or strongly agreed (89%) that asciminib improved HRQoL, and all would recommend this treatment to other patients diagnosed with CML.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of CML.
Unmet Needs
The clinical experts commented that some patients do not respond to, lose response to, or experience intolerance to first- and second-line TKI therapy and have few options remaining for them in the third line and beyond setting. At this stage of treatment, intolerance and safety become strong considerations for selecting treatment for a patient. The third-generation therapy, ponatinib, has been shown to be effective but is associated with elevated cardiovascular complications. Patients with cardiovascular risk factors are contraindicated for ponatinib and have limited options available to them. Patients who have failed on the second- and/or third-generation TKIs are left with very low chance of long-term survival and their treatment options include allogeneic stem cell transplant or management with hydroxyurea and/or interferon and cytarabine.
Place in Therapy
The clinical experts highlighted that asciminib has a novel mechanism of action known as STAMP. As such, asciminib has been shown to maintain clinical activity even in patients whose disease has become resistant to other TKIs. Therefore, asciminib would likely be the preferred treatment in the third line for patients who have failed on or become intolerant to 2 or more previous TKIs.
Patient Population
The clinical experts confirmed that patients with CP-CML who have failed on or become intolerant to 2 or more TKIs are best suited for the drug under review. Diagnostic investigations to diagnose and monitor CML are now standard of care and readily available. Given that pregnant patients, as well as patients under 18 years of age, were not included in the trial, these patients would be less suitable for treatment with asciminib. One of the 2 experts consulted suggested that patients with AP-CML or BC-CML would not be suitable for treatment with asciminib, given that they were not included in the trial. It is also expected that patients who are intolerant (rather than resistant) to their previous TKI would have a better response because their disease is not yet resistant.
Assessing Response to Treatment
The clinical experts commented that patient response would be measured by the depth of molecular response, as measured by RT-PCR performed every 3 months, as was done in the clinical trial. Other blood tests are conducted as part of disease and side effect monitoring. BM aspiration is only conducted as needed in the case of investigation of disease resistance or progression. The primary end point of the trial, MMR at 24 weeks, is considered a clinically meaningful response indicative of successful CML treatment because of its association with superior long-term outcomes, including survival. Patients would also be monitored for how well they tolerate the therapy.
Discontinuing Treatment
The clinical experts commented that patients should discontinue therapy upon disease progression, as defined by the ELN guideline for failure to meet milestones, or the inability of the patient to tolerate asciminib.
Prescribing Conditions
The clinical experts commented that CML can be appropriately managed in both community and academic settings, with the majority of patients being managed as outpatients. Patients with CML should be managed by a practitioner with experience treating CML, commonly a hematologist or occasionally a medical oncologist.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full clinician group submissions can be found at the end of this report in the Stakeholder Feedback section.
Clinician group input on the review of asciminib for the treatment of adult patients with Ph+ CP-CML previously treated with 2 or more TKIs was received from 2 groups: Ontario Health – Cancer Care Ontario Hematology Drug Advisory Committee (2 clinicians) and a peer group of hematologists across Canada who are involved in treating patients with CML (14 clinicians). The clinician groups both highlighted that the least suitable patients for asciminib would be those in AP or BC, the second group emphasized that tolerance is important for treatment adherence, which affects suppression of the leukemic clone.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The ASCEMBL trial compared asciminib with bosutinib, which is an appropriate comparator. Other potential comparators include ponatinib, dasatinib, and nilotinib. In one jurisdiction, bosutinib is not funded in the fourth-line setting. | For consideration by pERC. |
Considerations for initiation of therapy | |
Should patients in AP or BC be eligible? | There is a phase I trial where these patients were included; however, these were dose-finding trials and these patients were not included in the ASCEMBL trial. Patients in AP and BC represent a small percentage of overall patients that is unlikely to be studied in a randomized trial. Although the sponsor has not submitted for this population, 1 of the 2 clinical experts indicated that when considering the lack of options for this patient population, asciminib should be made available. |
Should patients with T315I or V299L mutations be eligible for asciminib and if so, would treatment with 2 prior TKIs be required? | The sponsor did not submit for this specific patient population. The FDA has approved treatment of these patients with a higher dose. If asciminib were to be made available for patients with T315I or V299L mutations, it would be reasonable to require 2 prior TKIs with an exception made for patients with risk factors for vascular complications (i.e., not fit for ponatinib). |
It is noted that the FDA-approved dosing for asciminib in patients with the T315I mutation and CML is 200 mg twice daily. | For consideration by pERC. |
The funding request for asciminib is specifically for patients with CP-CML. Bosutinib and ponatinib received reimbursement recommendations for CML in CP, AP, or BC. | For consideration by pERC. |
Considerations for discontinuation of therapy | |
Should treatment failure and therefore discontinuation be informed by ELN 2020 recommendations for treatment of CML? | The ELN 2020 recommendations are appropriate for this patient population. |
Consideration for prescribing of therapy | |
Asciminib 40 mg twice daily by mouth. Tablets will be available in 20 mg and 40 mg strength in blister packs of 10 blisters per card (6 cards per carton). Pricing is nonlinear with dose. | For consideration by pERC. |
Generalizability | |
In the event of a positive funding recommendation, should patients receiving alternative TKI (third line or later) be eligible to switch to asciminib when funding becomes available? | In order for patients to be switched from 1 therapy to another, either treatment intolerance or treatment failure must be met. |
Funding algorithm | |
Drug may change the place in therapy of comparator drugs | For consideration by pERC. |
What is the place in therapy for asciminib relative to the other TKIs (e.g., bosutinib, ponatinib)? | Asciminib should be used in the same manner that it was used in the ASCEMBL trial, which is consistent with the submitted indication (i.e., patients with CP-CML that have received at least 2 prior TKIs). Note that this includes patients who have received bosutinib as 1 of the 2 prior TKIs. |
The ASCEMBL trial allowed patients who failed on bosutinib to switch to asciminib but the efficacy data on the switch was not included in the trial publication. Should sequencing between asciminib and bosutinib be funded? | Patients who have failed on bosutinib were not included in the ASCEMBL trial, which limits the ability of the clinical experts to conclude with certainty that asciminib is effective in these patients. However, the clinical experts feel that, given the similarities in mechanism of action between bosutinib and the other, non-asciminib TKIs, asciminib should be effective in patients who have failed on or who are intolerant to 2 or more TKIs, including bosutinib. As such, the clinical experts feel that sequencing between asciminib and bosutinib should be funded. |
Care provision issues | |
Asciminib is associated with potential drug-drug, drug-food, and drug-herb interactions requiring assessment and management; this will increase use of pharmacy resources. | For consideration by pERC. |
System and economic issues | |
There is confidential pricing for bosutinib, ponatinib, and nilotinib. Imatinib and dasatinib are available as generics. | For consideration by pERC. |
AP = accelerated phase; BC = blast crisis; CML = chronic myeloid leukemia; CP = chronic phase; ECLN = European LeukemiaNet; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; TKI = tyrosine kinase inhibitor.
Clinical Evidence
The clinical evidence included in the review of asciminib is presented in 3 sections. The first section, Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of asciminib 40 mg oral tablets for the treatment of adult patients with Ph+ CML in CP previously treated with 2 or more TKIs.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with Ph+ CML in CP previously treated with 2 or more TKIs. Subgroups:
|
Intervention | Asciminib (80 mg daily or 40 mg twice daily), oral tablets |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; CP = chronic phase; CML = chronic myeloid leukemia; CyR = cytogenetic response; DOR = duration of response; HR = hematological response; HRQoL = health-related quality of life; MMR = major molecular response; MR = molecular response; OS = overall survival; Ph+ = Philadelphia chromosome positive; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; TKI = tyrosine kinase inhibitor; TTR = time to response; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.22
Published literature was identified by searching the following bibliographic databases: Medline All (1946–) via Ovid and Embase (1974–) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Scemblix and asciminib. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on February 17, 2022. Regular alerts updated the search until the CADTH pERC meeting on June 8, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature resource.23 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy. Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 3 reports8,24,25 of 1 study were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 2.
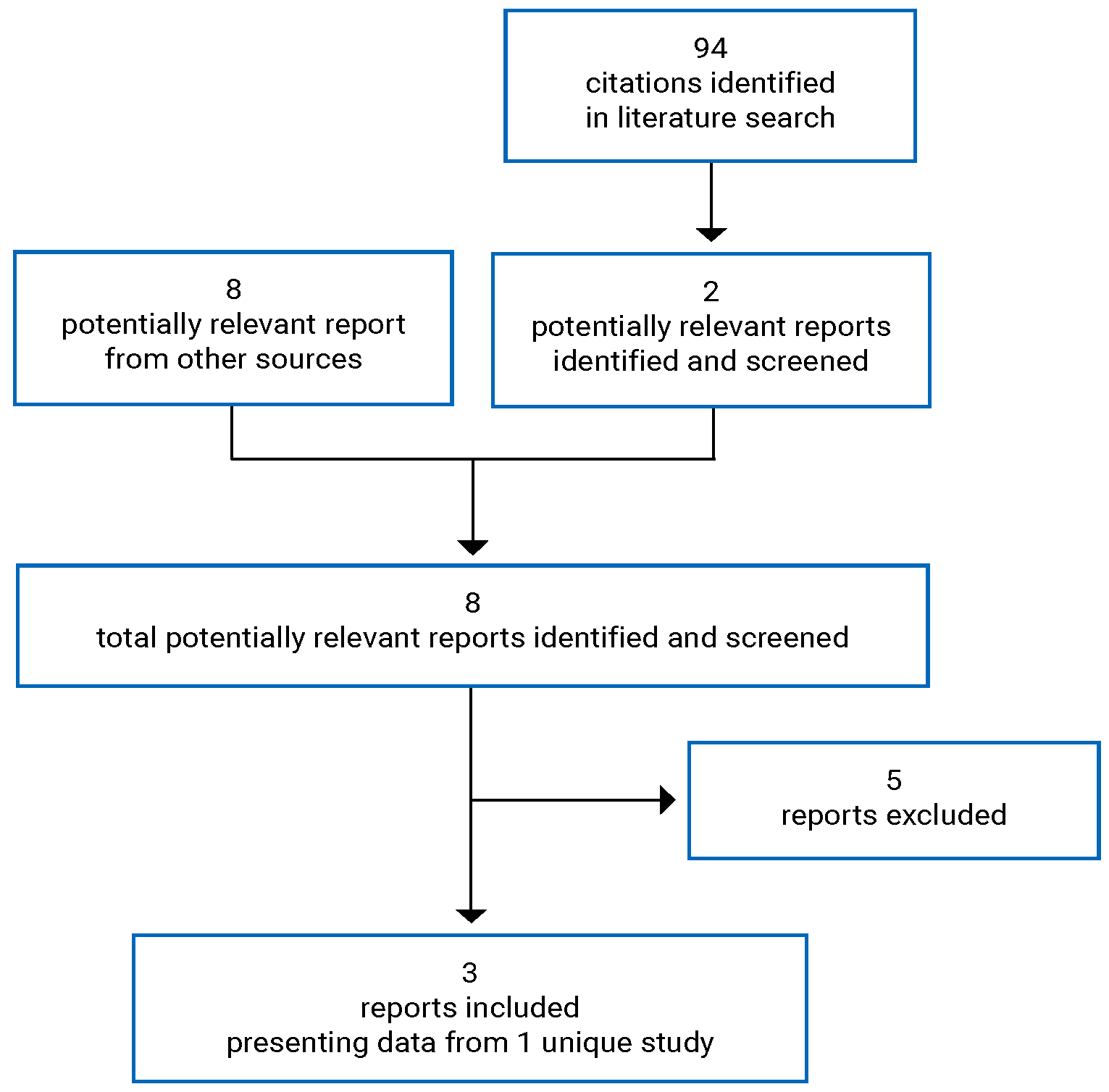
Table 6: Details of Included Study
Detail | ASCEMBL |
|---|---|
Designs and populations | |
Study design | Phase III, OL, randomized, multicentre RCT |
Locations | 87 sites from Canada, US, Mexico, South America, Europe, Asia, Australia |
Patient enrolment dates | October 26, 2017 |
Randomized (N) | 233 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | 40 mg asciminib twice daily, oralb |
Comparator | 500 mg bosutinib once daily, oral |
Duration | |
Phase | |
Screening | 56 days |
OL treatment | Patients treated until treatment failure or intolerance. Patients planned to received treatment up to 96 weeks after the last patient received their first dose or up to 48 weeks after the last patient switched to asciminib. |
Survival follow-up | Patients that discontinued treatment at any time were followed for survival and disease progression for up to 5 years from the date that the last patient randomized received their first dose. |
Outcomes | |
Primary end point | MMR (BCR-ABL1 ratio IS ≤ 0.1%) achieved at 24 weeks while on study treatment without meeting treatment failure criteria |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Notes | |
Publications | Rea et al. (2021)25 |
AP = accelerated phase; ATP = adenosine triphosphate; BC = blast crisis; CCyR = complete cytogenetic response; CML = chronic myeloid leukemia; CP = chronic phase; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ELN = European LeukemiaNet; GI = gastrointestinal; IS = International Standard; MDASI = MD Anderson Symptom Inventory; MMR = major molecular response; OL = open-label; OS = overall survival; PD = pharmacodynamic; PFS = progression-free survival; PGIC = patient global impression of change; PK = pharmacokinetic; RCT = randomized controlled trial; TKI = tyrosine kinase inhibitor.
aChanged from ≥ 1.0% BCR-ABL1 according to the November 2018 protocol amendment, with 87 patients already randomized. No more than 66 patients (33% of the overall population), with < 1% BCR-ABL1 were to be recruited.
bHealth Canada indication allows for either 40 mg twice daily or 80 mg once daily dosing.
Source: Asciminib Clinical Study Report.8
Description of Study
ASCEMBL is a phase III, open-label, randomized study of asciminib compared to bosutinib in patients with CP-CML who had received 2 or more TKIs and experienced treatment failure on or intolerance to the most recent TKI. Novartis funded the study. The primary objective of the ASCEMBL trial was to determine the efficacy of asciminib (40 mg twice daily) as compared to bosutinib (500 mg daily) in achieving MMR at the 24-week time point. Beginning October 26, 2017, a total of 233 patients with CP-CML who had previously received 2 or more TKIs were enrolled in ASCEMBL at 87 sites across North America (n = 5 patients from 1 site in Canada), South America, Europe, Australia, and Asia. Patients were randomized 2:1 to either asciminib or bosutinib; randomization was stratified by cytogenic response status at screening (i.e., yes or no).
Patients were screened for a period of up to 56 days before beginning study treatment. Patients were treated until treatment failure or intolerance. Patients in the bosutinib group were permitted to switch to asciminib if they experienced treatment failure. The end of study was defined as 96 weeks after the last patient received their first dose or up to 48 weeks after the last patient switched from bosutinib to asciminib. Patients who discontinued study treatment at any time were followed for survival and disease progression for up to 5 years from the date that the last patient randomized received their first dose. Study visits were conducted every 4 weeks during the treatment phase up to 96 weeks and every 12 weeks during survival follow-up.
The primary analysis was conducted based on the May 25, 2020, data cut-off date, when all patients randomized had been on study treatment for 24 weeks or discontinued earlier. A future planned updated analysis to conduct testing on the 96-week secondary end points was not presented. An unplanned updated data cut-off was provided based on a January 1, 2021, data cut, when all patients randomized had been on study treatment for 48 weeks or discontinued earlier.
There were 3 amendments made to the trial protocol, 2 of which were made after patients had been randomized. A July 2018 amendment was made to align the frequency of BM aspirate collection in patients having achieved MMR with the recommendations from ELN26 and National Comprehensive Cancer Network.27 The December 2018 amendment was made after 86 patients had been randomized, changing the inclusion requirement for baseline BCR-ABL1 ratio (International Standard [IS] percentage) from 1% or more to more than 0.1% specifically for patients who were intolerant to their most recent TKI. The reasoning given was that physicians would not wait for transcript level to increase before switching an intolerant patient to their next treatment option.26 No more than 66 patients fitting these characteristics were to be enrolled in the study. Patients who failed on their most recent TKI were still required to meet the criteria defined by ELN.26
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria are summarized in Table 6. Adult patients (age 18 years or older) with CML-CP that had received prior treatment with 2 or more ATP binding site TKIs and had experienced treatment failure or intolerance to their most recent TKI were eligible for inclusion. Treatment failure was defined according to the 2013 ELN guidelines. Intolerance was defined as patients with grade 3 or 4 nonhematological toxicity while on therapy, or with persistent grade 2 toxicity, unresponsive to optimal management, including dose adjustments (unless dose reduction was not considered in the best interest of the patient if response is already suboptimal). The definition of intolerance also included patients with grade 3 or 4 hematological toxicity (absolute neutrophil count or platelets) while on therapy that was recurrent after dose reduction to the lowest doses recommended by the manufacturer. Evidence of BCR-ABL1 transcript was required at time of screening. Patients who were intolerant to their most recent TKI were required to have a BRC-ABL1 ratio of greater than 0.1%, in accordance with the protocol amendment. Eligible patients were required to have an European Cooperative Oncology Group (ECOG) Performance Status (PS) of 0 to 2.
Patients were considered ineligible for inclusion in the ASCEMBL trial if there was known presence of a T315I or V299L mutation at any point before study entry as these mutations confer resistance to the efficacy of bosutinib. Excluded from the study population were patients for which this was their second-known CP of CML after previous progression to AP or BC, previous treatment with hematopoietic stem cell transplant, cardiac or cardiac repolarization abnormality, or previous treatment with or hypersensitivity to asciminib or bosutinib.
Baseline Characteristics
The baseline characteristics of patients randomized (i.e., full analysis set [FAS]) in the ASCEMBL trial are shown in Table 7. The mean age in both groups was 51.0 years with a slightly higher proportion of males in the asciminib group (52.2%) compared to the bosutinib group (40.8%). The proportion of patients who identified as Hispanic or Latino was higher in the bosutinib group (22.4%) than in the asciminib group (9.6%). All other baseline characteristics were broadly similar between the groups.
Table 7: Summary of Baseline Characteristics — FAS
Characteristic | ASCEMBL | |
|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | |
Age | ||
Mean (SD) | 51.0 (13.49) | 51.0 (13.95) |
Median (Range) | 52.0 (24 to 83) | 52.0 (19 to 77) |
< 65, n (%) | 128 (81.5) | 61 (80.3) |
≥ 65, n (%) | 29 (18.5) | 15 (19.7) |
Sex, n (%) | ||
Female | 75 (47.8) | 45 (59.2) |
Male | 82 (52.2) | 31 (40.8) |
Race, n (%) | ||
White | 118 (75.2) | 56 (73.7) |
Asian | 22 (14.0) | 11 (14.5) |
Black or African American | 8 (5.1) | 2 (2.6) |
American Indian or Alaska Native | 1 (0.6) | 0 |
Other | 5 (3.2) | 7 (9.2) |
Unknown | 3 (1.9) | 0 |
Ethnicity, n (%) | ||
Hispanic or Latino | 15 (9.6) | 17 (22.4) |
Not Hispanic or Latino | 102 (65.0) | 43 (56.6) |
Not Reported | 23 (14.6) | 11 (14.5) |
Unknown | 17 (10.8) | 5 (6.6) |
Body mass index (kg/m2) | ||
N | 152 | 76 |
Mean (SD) | 27.9 (6.52) | 27.4 (7.16) |
Median (Range) | 26.7 (18 to 74) | 25.8 (18 to 68) |
ECOG PS, n (%) | ||
0 | 126 (80.3) | 62 (81.6) |
1 | 28 (17.8) | 14 (18.4) |
2 | 2 (1.3) | 0 |
Missing | 1 (0.6) | 0 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; SD = standard deviation.
Source: Asciminib Clinical Study Report.8
A summary of baseline disease characteristics for patients randomized is shown in Table 8. The mean time in years since initial diagnosis of CML was 6.2 (SD = 5.75) in the asciminib group and 7.0 (SD = 5.63) in the bosutinib group. There were 28.0% and 27.6% of patients in MCyR at baseline according to bone marrow aspirate (BMA) measurements in the asciminib and bosutinib groups, respectively. Of note, there were 22.3% and 11.8% of patients with missing BMA measurements at baseline in the asciminib and bosutinib groups, respectively. MCyR is classified as 0% to 35%, inclusive Ph+ metaphases in BM. In the asciminib group there was 12.1% of patients at 0% Ph+ metaphases in the BM and 15.9% at greater than 0% to 35% or less, while in the bosutinib group, these values were 6.6% and 21.1%, respectively. Patients with any mutation were balanced at baseline with 12.7% in the asciminib group and 13.2% in the bosutinib group. Patients were identified as T315I positive (1.9% in the asciminib group and 1.3% in the bosutinib group) and V299L positive (0% in the asciminib group and 1.3% in the bosutinib group) despite this being an exclusion criterion for the study. In the asciminib group, 1.9% of patients had multiple mutations while there were no patients with multiple mutations in the bosutinib group.
Table 8: Summary of Disease Characteristics — FAS
Characteristic | ASCEMBL | |
|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | |
Time since initial diagnosis of CML (years) | ||
Mean (SD) | 6.2 (5.75) | 7.0 (5.63) |
Median (Range) | 3.8 (1, 28) | 5.1 (1, 21) |
Extramedullary involvement, n (%) | ||
No | 149 (94.9) | 72 (94.7) |
Yes | 8 (5.1) | 4 (5.3) |
Location of extramedullary involvement, n (%) | ||
Spleen | 8 (5.1) | 4 (5.3) |
Liver | 1 (0.6) | 1 (1.3) |
Major cytogenic response according to baseline BMA,a n (%) | ||
Yes | 44 (28.0) | 21 (27.6) |
No | 78 (49.7) | 46 (60.5) |
Missing | 35 (22.3) | 9 (11.8) |
Ph+ metaphases in BM | ||
Mean (SD) | 61.63 (39.481) | 64.37 (38.754) |
Median (Range) | 75.00 (0 to 100) | 85.00 (0 to 100) |
> 95% | 41 (26.1) | 25 (32.9) |
> 65% to ≤ 95% | 26 (16.6) | 13 (17.1) |
> 35% to ≤ 65% | 11 (7.0) | 8 (10.5) |
> 0% to ≤ 35% | 25 (15.9) | 16 (21.1) |
0% | 19 (12.1) | 5 (6.6) |
Missing | 35 (22.3) | 9 (11.8) |
Blasts in BM | ||
Mean (SD) | 1.42 (1.698) | 1.76 (2.192) |
Median (Range) | 1.00 (0.0 to 11.0) | 1.00 (0.0 to 14.8) |
Promyelocytes in BM | ||
Mean (SD) | 3.55 (4.175) | 2.81 (2.989) |
Median (Range) | 2.00 (0.0 to 26.0) | 2.00 (0.0 to 11.0) |
BCR-ABL1 mutational status, n (%) | ||
Patients with any mutation | 20 (12.7) | 10 (13.2) |
Patients with multiple mutations | 3 (1.9) | 0 |
F317L | 3 (1.9) | 2 (2.6) |
T315I | 3 (1.9) | 1 (1.3) |
Y253H | 3 (1.9) | 0 |
F359V | 3 (1.9) | 0 |
G250E | 2 (1.3) | 0 |
E255K | 2 (1.3) | 0 |
E255V | 1 (0.6) | 1 (1.3) |
M244V | 0 | 2 (2.6) |
E459K | 1 (0.6) | 0 |
E462K | 1 (0.6) | 0 |
F359C | 1 (0.6) | 0 |
F359I | 0 | 1 (1.3) |
F486S | 1 (0.6) | 0 |
L248V | 1 (0.6) | 0 |
Q252H | 0 | 1 (1.3) |
R473Q | 0 | 1 (1.3) |
V299L | 0 | 1 (1.3) |
BM = bone marrow; BMA = bone marrow aspirate; CML = chronic myeloid leukemia; Ph+ = Philadelphia chromosome positive; SD = standard deviation
aBased on BM aspirate results; results based on the randomization data collected in the Interactive Response Technology system were similar.
Source: Asciminib Clinical Study Report.8
Table 9 summarizes the prior antineoplastic therapy received by patients randomized in each treatment group. The most commonly received TKIs were dasatinib, imatinib, and nilotinib, all received by more than 65% of patients in each treatment group. Ponatinib had been received by 14.6% of patients in the asciminib group and 23.7% of patients in the bosutinib group. A similar number of patients had received between 2 and 3 lines of prior TKI therapy in each treatment group, though there was a higher proportion of patients who had received only 2 prior TKI therapies in the asciminib group (52.2%) compared to in the bosutinib group (39.5%). There was a higher number of patients who had discontinued their most recent TKI due to lack of efficacy (60.5% in the asciminib group and 71.1% in the bosutinib group) compared to patients who discontinued due to intolerance (37.5% in the asciminib group and 28.9% in the bosutinib group). The reasons for discontinuation of the previous TKI were imbalanced across the treatment groups.
Table 9: Summary of Prior Antineoplastic Therapy
Characteristic | ASCEMBL | |
|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | |
Prior TKIs, n (%) | ||
Dasatinib | 131 (83.4) | 65 (85.5) |
Imatinib | 130 (82.8) | 63 (82.9) |
Nilotinib | 104 (66.2) | 56 (73.7) |
Ponatinib | 23 (14.6) | 18 (23.7) |
Other | 5 (3.2) | 4 (5.3) |
Radotinib | 4 (2.5) | 2 (2.6) |
Number of prior TKIs, n (%) | ||
2 | 89 (56.7) | 33 (43.4) |
3 | 53 (33.8) | 33 (43.4) |
4 | 14 (8.9) | 7 (9.2) |
≥ 5 | 1 (0.6) | 3 (3.9) |
Number of lines of prior TKI therapy, n (%) | ||
2 | 82 (52.2) | 30 (39.5) |
3 | 44 (28.0) | 29 (38.2) |
4 | 24 (15.3) | 10 (13.2) |
≥ 5 | 7 (4.5) | 7 (9.2) |
Reason to discontinue last TKI, n (%) | ||
Lack of efficacy | 95 (60.5) | 54 (71.1) |
Lack of tolerability | 59 (37.6) | 22 (28.9) |
Other | 3 (1.9) | 0 |
Prior non-TKI therapy, n (%) | ||
No | 101 (64.3) | 51 (67.1) |
Yes | 56 (35.7) | 25 (32.9) |
TKI = tyrosine kinase inhibitor.
Source: Asciminib Clinical Study Report.8
Baseline BCR-ABL1 ratio (IS percentage) by reason for discontinuation of prior TKI for patients who were randomized is summarized in Table 10. There was 1 patient in the asciminib group with a BCR-ABL1 ratio greater than 0.1% to less than or equal to 1% who had entered the study after treatment failure of most recent TKI therapy, while 22.0% and 18.2% of the patients who were intolerant to their prior TKI therapy had a BCR-ABL1 ratio greater than 0.1% to less than or equal to 1% in the asciminib and bosutinib groups, respectively. Distribution among BCR-ABL1 ratio categories were broadly similar in both groups.
Table 10: Baseline BCR-ABL1 Ratio (IS Percentage) By Reason for Discontinuation of Prior TKI
Characteristic | ASCEMBL | |
|---|---|---|
Failure | Intolerance | |
Asciminib | 95 | 59 |
> 0.1% to ≤ 1% | 1 (1.1) | 13 (22.0) |
> 1% to ≤ 10% | 27 (28.4) | 17 (28.8) |
> 10% | 67 (70.5) | 29 (49.2) |
Bosutinib | 54 | 22 |
> 0.1% to ≤ 1% | 0 | 4 (18.2) |
> 1% to ≤ 10% | 15 (27.8) | 8 (36.4) |
> 10% | 39 (72.2) | 10 (45.5) |
TKI = tyrosine kinase inhibitor.
Source: Asciminib Clinical Study Report.8
Interventions
Patients in the ASCEMBL trial were administered asciminib or bosutinib as oral tablets in accordance with 40 mg twice daily and 500 mg daily dosing regimens, respectively. Asciminib was to be taken in a fasted state, that is, food was to be avoided for 2 hours before dose administration and for 1 hour after, only water was permitted. Bosutinib was to be taken with food. Asciminib tablets were given in 20 mg and 40 mg forms, while bosutinib tablets were given in 100 mg and 500 mg forms. For patients who were unable to tolerate the protocol-specified dosing schedule, dose modifications and/or reductions were to follow the provided step-down rules. Asciminib, from the starting dose of 40 mg twice daily, was reduced to 20 mg twice daily at the first dose-reduction level and no further dose reductions were permitted. Bosutinib, from the starting dose of 500 mg daily, was reduced to 400 mg daily at the first dose-reduction level, and further to 300 mg daily at the second dose-reduction level. Dose escalation beyond the standard 40 mg twice daily dosage of asciminib was not permitted, but dose escalation to 600 mg daily bosutinib was allowed for patients who were taking 500 mg daily, did not have grade 3 or higher AEs, and who either did not reach complete hematological response by week 8 or did not reach CCyR by week 12. Any concomitant medication or therapies deemed necessary for the supportive care of the patient were permitted unless specifically prohibited. Prohibited concomitant therapies for asciminib included other anticancer drugs; strong CYP3A4, 5 inhibitors, inducers and strong UGT1A/2B inducers; drugs with known, possible, or conductional risk of Torsades de Pointes; and herbal medications. For bosutinib prohibited concomitant therapies included other anticancer drugs, strong or moderate CYP3A inhibitors or inducers, or pH altering medications. Patients could voluntarily withdraw for any reason at any time. A patient was considered withdrawn if they stated an intention to withdraw, failed to return for visits, or became lost for follow-up for any reason.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trial included in this review is provided in Table 11. These end points are further summarized in the following. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 11: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | ASCEMBL |
|---|---|
HRQoL | Exploratory |
OS | Secondary |
PFS | Secondary |
MMR | Primary |
MR | Not reported |
HR | Not reported |
CyR | Secondary |
DOR | Secondary |
TTR | Secondary |
AEs, SAEs, WDAEs, mortality, and notable harms | Safety |
AE = adverse event; CyR = cytogenetic response; DOR = duration of response; HR = hematological response; HRQoL = health-related quality of life; MMR = major molecular response; MR = molecular response; OS = overall survival; PFS = progression-free survival; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
HRQoL was measured using the EQ-5D 5-Levels (EQ-5D-5L) and indirectly measured using the MD Anderson Symptom Inventory (MDASI) and patients’ global impression of change (PGIC). All patient-reported outcome questionnaires were completed at scheduled visits before clinical assessments. The EQ-5D is a generic HRQoL instrument that may be applied to a wide range of health conditions and treatments.28,29 The first of 2 parts of the EQ-5D is a descriptive system that classifies respondents (aged 12 years and older) based on the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D-5L has 5 possible levels for each domain representing “no problems,” “slight problems,” “moderate problems,” “severe problems,” and “extreme problems.” Respondents are asked to choose the level that reflects their health state for each of the 5 dimensions. The second part is a 20 cm VAS that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state.” No assessments of minimally important difference (MID) were identified in patients with CML for the EQ-5D-5L.
The MDASI is a brief measure used to assess the severity and impact of cancer-related symptoms and its treatment. The MDASI-CML is a modified 26 item self-administered questionnaire suitable for adult patients with CML.30 Twenty of the items in the MDASI-CML measure the severity of disease-related symptoms and are scored from 0 (not present) to 10 (as bad as you can imagine), whereas 6 items measure symptom interference with daily life scored from 0 (did not interfere) to 10 (interfered completely). Higher scores represent worse HRQoL. No assessments of MID were identified in patients with CML for the MDASI. The PGIC uses a 7-point scale where 1 indicates very much improved and 7 indicates very much worse. No assessments of MID were identified in patients with CML for the PGIC.
OS was defined as the time from the date of randomization to the date of death due to any cause, including the survival follow-up period. PFS was defined as the time from the date of randomization to the earliest occurrence of documented disease progression to AP or BC or the date of death from any cause, including progressions and deaths observed during the survival follow-up period.
MMR was defined as at least a 3.0 log reduction in BCR-ABL1 transcript compared to standardized baseline, which is equivalent to 0.1% or less BCR-ABL1/ABL percentage by IS as measured by RT-PCR. Treatment discontinuation for any reason (intolerance, treatment failure, death) within the first 24 weeks of treatment was considered a nonresponse. Molecular response is similar in that it is equivalent to 1% or less BCR-ABL1/ABL percentage by IS percentage. Molecular response was not a specific end point in the ASCEMBL trial. Hematological response (HR) was also not a reported end point in ASCEMBL.
Treatment failure events were based on the ELN criteria,26 including:
no complete hematologic response (CHR) or greater than 95% Ph+ metaphases at 3 months after randomization or thereafter
BCR-ABL1 ratio greater than 10% IS and/or greater than 65% Ph+ metaphases at 6 months after randomization or thereafter
BCR-ABL1 ratio greater than 10% IS and/or greater than 35% Ph+ metaphases at 12 months after randomization or thereafter
loss of CHR, CCyR, or partial cytogenetic response (PCyR) at any time after randomization
detection of new BCR-ABL1 mutations that potentially cause resistance to study treatment at any time after randomization
confirmed loss of MMR in 2 consecutive tests
new clonal chromosome abnormalities in Ph+ cells at any time after randomization
discontinuation from randomized treatment for any reason.
Cytogenetic response was assessed locally as the percentage of Ph+ metaphases in BM according to the following categories:
CCyR — 0% Ph+ metaphases
PCyR — greater than 0 to 35% Ph+ metaphases
MCyR — 0 to 35% Ph+ metaphases
minor cytogenetic response — greater than 35% to 65% Ph+ metaphases
minimal cytogenetic response — greater than 65% to 95% Ph+ metaphases
no cytogenetic response — greater than 95% to 100% Ph+ metaphases.
Duration of response (MMR and CCyR) was defined as the time from the date of first documented MMR or CCyR to the earliest date of loss of MMR or CCyR, progression to AP or BC, or CML-related death. Time to response (MMR and CCyR) was defined as the time from the date of randomization to the date of the first documented MMR or CCyR.
Safety outcomes were assessed and graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. Grades 1 to 5 were used to characterize severity of AEs.
Statistical Analysis
To test the null hypothesis that the primary end point of MMR rate at 24 weeks is equal in the 2 treatment groups, based on a 2-sided 5% level of significance and with 90% power, 222 patients were estimated to be needed in total (i.e., 148 patients in the asciminib group and 74 patients in the bosutinib group based on 2:1 randomization allocation).
The key secondary end point of MMR rate at 96 weeks was only to be tested if statistical significance was found in the primary end point of MMR rate at 24weeks. The data for this end point will be available in the future. The overall alpha is therefore controlled at the 5% 2-sided level using a gatekeeping strategy. This is the only secondary end point that was to be formally tested, and data were not analyzed at the latest available data cut-offs. No confirmatory statistical testing was undertaken for other end points, including secondary end points, patient-reported outcomes, and harms; however, nominal P values were presented in some cases.
Only patients with MMR at the 24-week visit were considered responders for the primary end point. In other words, any patient who achieved MMR before 24 weeks, but was no longer in MMR at 24 weeks, was considered a nonresponder in the primary analysis. Patients who discontinued the randomized treatment before 24 weeks due to any reason were considered nonresponders. One exception was if the 24-week PCR evaluation was missing, but both a PCR evaluation at 16 weeks and a PCR evaluation at 36 weeks indicated MMR, in which case the 24-week assessment was imputed as a “response.” If PCR evaluations were performed at unscheduled visits closer to the week 24 visit (before or after), these were used to impute the 24-week value.
Statistical analysis of the efficacy end points is summarized in Table 12. The primary analysis was conducted according to randomization stratum (MCyR versus no MCyR at baseline). Patients with missing BMA data at baseline were inferred to be in MCyR if baseline BCR-ABL1 ratio (IS%) was 10% or lower. The primary analysis included 46 patients receiving asciminib and 22 patients receiving bosutinib in MCyR at baseline. However, based upon the previously stated assumption, 15.9% of patients receiving asciminib and 14.5% of patients receiving bosutinib were assigned to the incorrect stratum. A sensitivity analysis was conducted to explore the impact of this. Concordance between randomization strata and strata as per the baseline case report form (CRF) data was 84.5%. The model used to test between-treatment group differences was the Cochran-Mantel-Haenszel chi-square test, stratified by cytogenetic response status (MCyR versus no MCyR) at screening, at a 2-sided 5% level of significance. Response rates were presented along with 95% CI based on the Clopper-Pearson method and treatment differences between groups were presented along with 95% CI based on the Wald method. Preplanned exploratory subgroup analyses for the primary efficacy end point that were relevant according to the CADTH protocol were those based on baseline MCyR status, baseline or week 1 on day 1 BCR-ABL1 ATP binding site mutation status, failure versus intolerance to prior TKIs, and line of therapy. P values for the subgroup analyses were not produced or presented.
Table 12: Statistical Analysis of Efficacy End Points
End point | Statistical model | Sensitivity analyses |
|---|---|---|
Primary end point | ||
MMR rate at 24 weeks |
|
|
Secondary end points | ||
CCyR rate | No confirmatory statistical testing was performed; nominal P values presented according to the same model used to the primary end point | NA |
Time to response (MMR and CCyR) | Time to response presented descriptively and using a KM approach. Time to MMR was censored at the last PCR test date on treatment before or at the cut-off date, if no events or competing risk occurred before or at the cut-off date or the end of treatment. | NA |
Duration of response | Duration of response presented using a KM approach. For patients in the responder set who had not yet experienced any event, the duration was censored at the last PCR test indicating MMR or the last cytogenic assessment date on treatment. | NA |
TTF, PFS, OS | Analysis was stratified by randomization stratification factor (MCyR vs. no MCyR at screening) | NA |
Patient-reported outcomes | ||
HRQoL (EQ-5D-5L and EQ VAS) | Repeated measures model was used to estimate differences between treatment groups | NA |
Subjective symptoms (MDASI-CML and PGIC) | Repeated measures model was used to estimate differences between treatment groups | NA |
Safety outcomes | ||
AEs, SAEs, WDAEs, mortality, and notable harms | Safety outcomes were analyzed descriptively | NA |
AE – adverse event; CCyR = complete cytogenetic response; CI = confidence interval; CML = chronic myeloid leukemia; CRF = case report form; EQ-5D-5L = EQ-5D 5-Levels; EQ VAS = EQ Visual Analogue scale; HRQoL = health-related quality of life; KM = Kaplan–Meier; MCyR = major cytogenetic response; MDASI = MD Anderson Symptom Inventory; MMR = major molecular response; NA = not applicable; OS = overall survival; PCR = polymerase chain reaction; PFS = progression-free survival; PGIC = patient global impression of change; SAE = serious adverse event; TTF = time to treatment failure; vs. = versus; WDAE = withdrawal due to adverse event.
Analysis Populations
The FAS included all patients who were randomized, analyzed according to the treatment and stratum assigned at randomization. Unless otherwise specified, this analysis set was used for the primary and all secondary end points. The FAS was also used for the patient disposition, demographics, and baseline characteristics.
The safety set included all patients who received at least 1 dose of study treatment. Patients were analyzed according to their treatment and stratum assigned at randomization. This analysis set was used for the analysis of safety outcomes.
The MMR responder set was a subset of the FAS and included any patient that achieved an MMR at any time on treatment. This subset was used in the analysis of time to MMR and duration of MMR.
The CCyR analysis set was a subset of the FAS, and included patients who were not already in CCyR at baseline. This subset was used in the analysis of time to CCyR and duration of CCyR.
The CCyR responder set included all patients from the CCyR analysis set who achieved CCyR at any time on treatment. This subset was used in the analysis of time to CCyR and duration of CCyR.
The switch analysis set was a subset of the FAS and included patients from the bosutinib treatment group who received asciminib following discontinuation of bosutinib.
Results
Patient Disposition
In the ASCEMBL trial, a total of 319 patients were screened, of which 233 (73%) were enrolled. Full patient disposition is summarized in Table 13. Of the 157 patients who were randomized to receive asciminib, 29.3% were placed in the MCyR stratum and 70.7% were placed in the no MCyR stratum. Of the 76 patients randomized to receive bosutinib, these values were 28.9% and 71.1%, respectively. At the time of primary analysis, 61.8% of patients in the asciminib group and 28.9% of patients in the bosutinib group were receiving ongoing treatment. The most common reason for treatment discontinuation in both treatment groups was lack of efficacy (21.0% in the asciminib group and 31.6% in the bosutinib group). A lower proportion of patients in the asciminib group discontinued treatment due to AEs compared to the bosutinib group (5.1% versus 21.2%). Patient disposition was similar based on the updated January 1, 2021, data cut-off. The FAS included all 157 patients randomized to asciminib and 76 patients randomized to bosutinib. One patient randomized to asciminib developed cytopenia, did not receive any study treatment, and was therefore excluded from the safety analysis set. The mean duration of follow-up for all patients randomized at the primary analysis was 15.6 months and 23.0 months at the updated data cut-off.
Patient disposition | ASCEMBL | |
|---|---|---|
Asciminib | Bosutinib | |
Screened, N | 319 | |
Randomized, N | 157 | 76 |
Randomization stratum, MCyR, N (%) | 46 (29.3) | 22 (28.9) |
Randomization stratum, no MCyR, N (%) | 111 (70.7) | 54 (71.1) |
Treatment ongoing at the May 25, 2020, data cut-off, N (%) | 97 (61.8) | 22 (28.9) |
Discontinued from study, N (%) | 59 (37.6) | 54 (71.1) |
< week 24 | 26 (16.6) | 25 (32.9) |
≥ week 24 and < week 48 | 22 (14.0) | 28 (36.8) |
≥ week 48 and < week 96 | 11 (7.0) | 1 (1.3) |
Reason for discontinuation, N (%) | ||
Lack of efficacy | 33 (21.0) | 24 (31.6) |
Physician decision | 10 (6.4) | 6 (7.9) |
Adverse event | 8 (5.1) | 16 (21.1) |
Patient or guardian decision | 4 (2.5) | 3 (3.9) |
Death | 1 (0.6) | 0 |
Lost to follow-up | 1 (0.6) | 2 (2.6) |
Progressive disease | 1 (0.6) | 3 (3.9) |
Protocol deviation | 1 (0.6) | 0 |
Switched to receive asciminib | NA | 22 (28.9) |
Treatment ongoing at the January 1, 2021, data cut-off, N (%) | 89 (56.7) | 17 (22.4) |
Discontinued from study,a N (%) | 67 (42.7) | 59 (77.6) |
< week 24 | 26 (16.6) | 25 (32.9) |
≥ week 24 and < week 48 | 25 (15.9) | 29 (38.2) |
≥ week 48 and < week 96 | 15 (9.6) | 3 (3.9) |
≥ week 96 | 1 (0.6) | 2 (2.6) |
Reason for discontinuation,a N (%) | ||
Lack of efficacy | 37 (23.6) | 27 (35.5) |
Physician decision | 13 (8.3) | 6 (7.9) |
Adverse event | 9 (5.7) | 18 (23.7) |
Patient or guardian decision | 4 (2.5) | 3 (3.9) |
Death | 1 (0.6) | 0 |
Lost to follow-up | 1 (0.6) | 2 (2.6) |
Progressive disease | 1 (0.6) | 3 (3.9) |
Protocol deviation | 1 (0.6) | 0 |
Switched to receive asciminiba | NA | 24 (31.6) |
FAS, N (%) | 157 (100) | 76 (100) |
MMR responder set, N (%) | 54 (34.4) | 14 (18.4) |
CCyR analysis set, N (%) | 103 (65.6) | 62 (81.6) |
CCyR responder set, N (%) | 44 (28.0) | 19 (25.0) |
Safety, N (%) | 156 (99.4) | 76 (100) |
Mean duration of follow-up at May 25, 2020, data cut-off, months (SD) | 15.6 (6.45) | |
Mean duration of follow-up at January 1, 2021, data cut-off, months (SD) | 23.0 (6.45) | |
CCyR = complete cytogenetic response; FAS = full analysis set; MCyR = major cytogenetic response; MMR = major molecular response; NA = not applicable; SD = standard deviation.
aData from the January 1, 2021, data cut-off.
Source: Asciminib Clinical Study Report.8
Protocol deviations at the time of the primary analysis are summarized in Table 14. Overall, deviations were more common in the asciminib group, speculated by the sponsor to be possibly due to the longer duration of treatment exposure (median = 43.4 weeks in the asciminib group versus 29.2 weeks in the bosutinib group). The most common deviations were reported within the “other” category, including visits done outside of study site due to COVID-19 (20.4% in the asciminib group versus 14.5% in the bosutinib group), stratification to the wrong randomization stratum (15.3% in the asciminib group versus 13.2% in the bosutinib group), and study procedure noncompliance (15.3% in the asciminib group versus 9.2% in the bosutinib group). Study procedure noncompliance included BMA performed despite patient being in MMR (a stipulation added in a protocol amendment after patients had been randomized), key procedures to assess eligibility assessed on the basis of local laboratory instead of central laboratory, and routine pregnancy test not performed as per protocol. A larger proportion of patients in the asciminib than the bosutinib group were enrolled despite being ineligible (15.9% versus 5.3%, respectively). A respective 8.3% versus 2.6% did not meet the exclusion criteria and 7.6% versus 2.6% did not meet the inclusion criteria.
Table 14: Summary of Protocol Deviations — FAS
Deviation | ASCEMBL | |
|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | |
Any protocol deviation, n (%) | 111 (70.7) | 43 (56.6) |
Other deviation | 90 (57.3) | 29 (38.2) |
Treatment deviation | 48 (30.6) | 25 (32.9) |
Prohibited concomitant medication | 22 (14.0) | 8 (10.5) |
Exclusion criteria not met | 13 (8.3) | 2 (2.6) |
Inclusion criteria not met | 12 (7.6) | 2 (2.6) |
Patient not withdrawn as per protocol | 7 (4.5) | 3 (3.9) |
FAS = full analysis set.
Source: Asciminib Clinical Study Report.8
Exposure to Study Treatments
Treatment exposure in the ASCEMBL trial is shown in Table 15. At the time of primary analysis, the mean duration of exposure for patients in the asciminib group was 49.38 (SD = 31.49) weeks and 33.66 (SD = 26.41) weeks for patients in the bosutinib group. Patients received a mean relative dose intensity of 89.1% (SD = 18.17%) in the asciminib group and 85.9% (SD = 17.61%) in the bosutinib group. At the time of the updated data cut-off. The mean duration of exposure was 68.33 (SD = 42.49) weeks in the asciminib group and 42.02 (SD = 36.52) weeks in the bosutinib group. The relative dose intensity was similar to the primary analysis.
Table 15: Exposure to Study Treatment — Safety Analysis Set
Exposure | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 156 | Bosutinib N = 76 | Asciminib N = 156 | Bosutinib N = 76 | |
Duration of exposure (weeks) | ||||
Mean (SD) | 49.38 (31.49) | 33.66 (26.41) | 68.33 (42.49) | 42.02 (36.52) |
Median (Range) | 43.36 (0.1 to 129.9) | 29.21 (1.0 to 117.0) | 67.14 (0.1 to 162.1) | 29.71 (1.0 to 149.3) |
Duration of exposure categories, n (%) | ||||
Less than 24 weeks | 28 (17.9) | 27 (35.5) | 27 (17.3) | 27 (35.5) |
At least 24 weeks | 128 (82.1) | 49 (64.5) | 129 (82.7) | 49 (64.5) |
At least 48 weeks | 71 (45.5) | 13 (17.1) | 105 (67.3) | 22 (28.9) |
At least 96 weeks | 16 (10.3) | 5 (6.6) | 38 (24.4) | 8 (10.5) |
Patient treatment time (patient-years)a | 147.6 | 49.0 | 204.3 | 61.2 |
Average daily dose (mg) | ||||
Mean (SD) | 74.2 (11.87) | 466.5 (58.44) | 73.7 (12.52) | 463.7 (59.99) |
Median (Range) | 80.0 (39 to 80) | 500.0 (312 to 568) | 80.0 (39 to 80) | 500.0 (312 to 568) |
Relative dose intensity, % | ||||
Mean (SD) | 89.1 (18.17) | 85.9 (17.61) | 88.8 (18.38) | 85.2 (17.56) |
Median (Range) | 99.7 (41 to 100) | 95.4 (36, 100) | 99.8 (41 to 100) | 92.8 (36 to 100) |
SD = standard deviation.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
aPatient treatment time is the sum of each patient’s treatment exposure in patient-years.
Source: Asciminib Clinical Study Report.8
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported in the following. See Appendix 3 for detailed efficacy data.
Health-Related Quality of Life
Results for HRQoL measured using the EQ-5D-5L at baseline and up to week 48. EQ VAS results are shown in Table 16. Completion of the EQ-5D-5L questionnaire at week 24 was 83.1% in the asciminib group and 82.0% in the bosutinib group. Baseline mean EQ VAS was 71.3 (SD = 21.71) in the asciminib group and 74.2 (SD = 18.79) in the bosutinib group. Mean change from baseline at week 24 was 7.5 (SD = 23.36) in the asciminib group and 0.5 (SD = 17.87) in the bosutinib group. Between-treatment differences for asciminib versus bosutinib for the EQ VAS was 2.50 (95% CI, –2.31 to 7.30). The proportion of patients reporting no problems within EQ-5D-5L domains at 24 weeks in the asciminib versus the bosutinib group, respectively, was 55.4% versus 48.0% for mobility, 74.6% versus 68.0% for self-care, 56.2% versus 48.0% for usual activities, 48.5% versus 32.0% for pain/discomfort, and 51.5% versus 44.0% for anxiety/depression.
Table 16: EQ VAS Over Time — FAS
Time point | Asciminib (N = 157) | Bosutinib (N = 76) | ||||||
|---|---|---|---|---|---|---|---|---|
Score | Change from baseline | Score | Change from baseline | |||||
n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |
Baseline | 149 | 71.3 (21.71) | NA | NA | 69 | 74.2 (18.79) | NA | NA |
Week 12 | 125 | 76.4 (18.69) | 123 | 6.1 (22.77) | 54 | 76.1 (18.22) | 50 | 1.8 (16.46) |
Week 24 | 108 | 77.4 (20.91) | 106 | 7.5 (23.36) | 41 | 73.5 (21.65) | 38 | 0.5 (17.87) |
Week 48 | 60 | 78.0 (19.60) | 59 | 8.3 (23.63) | 12 | 78.7 (19.03) | 12 | 4.8 (11.91) |
NA = not applicable; FAS = full analysis set; SD = standard deviation.
Source: Asciminib Clinical Study Report.8
Other indirect measures of HRQoL (including the MDASI-CML and PGIC) are presented in Appendix 3. Compliance for completing the MCASI-CML at 24 weeks was 83.1% in the asciminib group and 82.0% in the bosutinib group. Between-treatment differences for the change in severity and interference scores were –0.65 (95% CI, –1.01 to –0.29) and –0.16 (95% CI, –0.67 to 0.36), respectively. Compliance for completing the PGIC at 24 weeks was 82.3% in the asciminib group and 82.0% in the bosutinib group. Seventeen percent of patients in the asciminib group and 8.0% of those in the bosutinib group rated their overall health as very much improved.
Overall Survival
The results for OS are summarized in Table 17. At the time of primary analysis, death had occurred in 2.5% of patients in the asciminib group and 1.3% of patients in the bosutinib group. The median OS had not been reached. The 1-year Kaplan–Meier (KM) estimate of OS was 97.5% (95% CI, 92.4% to 99.2%) in the asciminib group and 98.6% (95% CI, 90.2% to 99.8%) in the bosutinib group. The OS results at the updated data cut-off were consistent with the primary analysis.
Table 17: Overall Survival at 24 Weeks and 48 Weeks — FAS
Outcome | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | Asciminib N = 157 | Bosutinib N = 76 | |
Number of patients with an event, n (%) | 4 (2.5) | 1 (1.3) | 4 (2.5) | 1 (1.3) |
Maximum follow-up (years) | 2.3 | 2.5 | 3.0 | 3.0 |
Median follow-up (years) | 1.1 | 1.0 | 1.6 | 1.6 |
KM % event free (95% CI)a | ||||
1 year | 97.5 (92.4 to 99.2) | 98.6 (90.2 to 99.8) | 98.0 (93.8 to 99.3) | 98.6 (90.2 to 99.8) |
2 years | NE | NE | 97.2 (92.8 to 99.0) | 98.6 (90.2 to 99.8) |
CI = confidence interval; KM = Kaplan–Meier; NE = not estimable.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
aKM estimates of percent event free are based on the Greenwood formula.
Source: Asciminib Clinical Study Report.8
Progression-Free Survival
The results for PFS are summarized in Table 18. At the time of primary analysis, a PFS event had occurred in 4.5% of patients in the asciminib group and 6.6% of patients in the bosutinib group. The median PFS had not been reached. The 1-year KM estimate of PFS was 95.1% (95% CI, 89.2% to 97.8%) in the asciminib group and 88.6% (95% CI, 72.8% to 95.5%) in the bosutinib group. The PFS results at the updated data cut-off were consistent with the primary analysis.
Table 18: Progression-Free Survival at 24 Weeks and 48 Weeks — FAS
Outcome | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | Asciminib N = 157 | Bosutinib N = 76 | |
Number of patients with an event, n (%) | 7 (4.5) | 5 (6.6) | 7 (4.5) | 5 (6.6) |
Maximum follow-up (years) | 2.3 | 2.1 | 3.0 | 2.8 |
Median follow-up (years) | 0.8 | 0.7 | 1.2 | 1.1 |
KM % event free (95% CI)a | ||||
1 year | 95.1 (89.2 to 97.8) | 88.6 (72.8 to 95.5) | 96.3 (91.3 to 98.5) | 91.1 (79.5 to 96.3) |
2 years | NE | NE | 94.2 (87.9 to 97.2) | 91.1 (79.5 to 96.3) |
CI = confidence interval; KM = Kaplan–Meier; NE = not estimable.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
aKM estimates of percent event free are based on the Greenwood formula.
Source: Asciminib Clinical Study Report.8
MMR and Molecular Response
The results for MMR at 24 and 48 weeks are presented in Table 19. At the primary analysis, the MMR rate at 24 weeks in the asciminib group was 25.48% (95% CI, 18.87% to 33.04%) and in the bosutinib group it was 13.16% (95% CI, 6.49% to 22.87%). The unstratified difference in response rate was 12.32% (95% CI, 2.11% to 22.53%). Based on a common risk stratification of MCyR versus no MCyR at baseline, the difference in response rate based on common risk difference was 12.24% (95% CI, 2.19% to 22.30; P = 0.029). At the updated data cut-off, the MMR rate at 48 weeks was 26.11% (95% CI, 19.44% to 33.72%) in the asciminib group and 11.84% (95% CI, 5.56%, 21.29%) in the bosutinib group. The unstratified difference in response rate was 16.14% (95% CI, 5.73% to 26.55%). The common risk difference in response rate based on MCyR stratification was 16.09% (95% CI, 5.69% to 26.49%). The difference was not tested statistically.
Sensitivity analyses were consistent with the primary analysis. The common risk difference when BMA data were stratified as reported in the CRF was 11.54% (95% CI, 1.73% to 21.34%); when dealing with missing PCR evaluations without the imputation rule, the common risk difference was 12.24% (95% CI, 2.19% to 22.30%); when removing patients with a planned 24-week visit after the start of the COVID-19 pandemic, the common risk difference was 16.1% (95% CI, 4.91% to 27.36%); and when excluding patients with T315I or V299L mutation at week 1, day 1, the common risk difference was 12.43% (95% CI, 2.15% to 22.71%). These results are presented in Appendix 3. The OR of the treatment effect adjusted for MCyR at randomization only (2.35; 95% CI, 1.08 to 5.12) was consistent with the treatment effect adjusted by sex, line of therapy, and reason for discontinuation from the last TKI in addition to MCyR at randomization (2.38; 95% CI, 1.06 to 5.35) or CRF data (2.37; 95% CI, 1.04 to 5.37).
Table 19: MMR Rate at 24 Weeks (Primary End Point) and 48 weeks (Updated Data Cut-off) — FAS
Outcome | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | Asciminib N = 157 | Bosutinib N = 76 | |
Response, n (%) | 40 (25.48) | 10 (13.16) | 41 (26.11) | 9 (11.84) |
95% CI for response,a % | (18.87 to 33.04) | (6.49 to 22.87) | (19.44 to 33.72) | (5.56 to 21.29) |
Unstratified difference in response rate (vs. bosutinib), % | 12.32 | Reference | 16.14 | Reference |
95% CI for difference,b % | (2.11 to 22.53) | Reference | (5.73 to 26.55) | Reference |
Common risk difference,c % | 12.24 | Reference | 16.09 | Reference |
95% CI for difference, % | (2.19 to 22.30) | Reference | (5.69 to 26.49) | Reference |
P valued | 0.029 | Reference | NA | NA |
CI = confidence interval; FAS = full analysis set; MMR = major molecular response; NA = not applicable; vs. = versus.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
aClopper-Pearson 95% 2-sided CI.
bWald 95% 2-sided CI.
cThe common risk difference after adjusting for stratum: baseline MCyR status (based on randomization data) and its 95% CI were estimated using the Mantel-Haenszel method.
dCochrane-Mantel-Haenszel 2-sided test was stratified by baseline MCyR status (based on randomization data).
Source: Asciminib Clinical Study Report.8
Shown in Table 20 is the distribution of patients across BCR-ABL1 ratios (IS percentage) at 24 weeks at the primary analysis and at 48 weeks at the updated data cut-off. MMR is considered as a BCR-ABL1 ratio of 0.01% or less. Within this range, at 24 weeks 8.9% of patients in the asciminib group had a BCR-ABL1 ratio of 0.0032% or lower while 1.9% had a BCR-ABL1 ratio greater than 0.0032% to 0.01% or less. The corresponding values for patients in the bosutinib group were 1.3% and 3.9%, respectively. With regards to the patients with missing data, 2.5% in the asciminib group and 5.3% in the bosutinib group were receiving treatment without treatment failure. All other patients with missing data had either failed on treatment or discontinued. The proportions of patients with MMR in each treatment group at the time of the updated data cut-off were similar to those of the primary analysis.
Table 20: BCR-ABL1 Ratio (IS) at 24 Weeks (Primary Analysis) and 48 Weeks (Updated Data Cut-Off) — FAS
Outcome | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | Asciminib N = 157 | Bosutinib N = 76 | |
≤ 0.0032% | 14 (8.9) | 1 (1.3) | 12 (7.6) | 1 (1.3) |
> 0.0032% to ≤ 0.01% | 3 (1.9) | 3 (3.9) | 5 (3.2) | 2 (2.6) |
> 0.01% to ≤ 0.1% | 23 (14.6) | 6 (7.9) | 29 (18.5) | 7 (9.2) |
> 0.1% to ≤ 1% | 37 (23.6) | 8 (10.5) | 27 (17.2) | 6 (7.9) |
> 1% to ≤ 10% | 21 (13.4) | 12 (15.8) | 13 (8.3) | 4 (5.3) |
> 10% | 23 (14.6) | 17 (22.4) | 0 | 1 (1.3) |
Missing | 36 (22.9) | 29 (38.2) | 71 (45.2) | 55 (72.4) |
Ongoing without treatment failure | 4 (2.5) | 4 (5.3) | 8 (5.1) | 1 (1.3) |
Ongoing with treatment failure | 9 (5.7) | 3 (3.9) | 13 (8.3) | 2 (2.6) |
Discontinued due to lack of efficacy, PD, death | 7 (4.5) | 7 (9.2) | 29 (18.5) | 27 (35.5) |
Discontinued due to other reasons | 16 (10.2) | 15 (19.7) | 21 (13.4) | 25 (32.9) |
FAS = full analysis set; IS = International Standard; PD = progressive disease.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off, updated data cut-off was January 1, 2021.
Source: Asciminib Clinical Study Report.,8
Preplanned exploratory subgroup analyses were conducted on the primary end point of MMR at 24 weeks, and these are summarized in Table 21. For patients in with and without MCyR at baseline, the risk differences were 27.5% (95% CI, 5.9% to 49.1%) and 6.0% (95% CI, –4.9% to 16.9%), respectively. For patients with BCR-ABL1 transcript levels of 1% or greater and less than 1% at baseline, the risk differences were 12.8% (95% CI, 2.7% to 22.9%) and –10.0% (95% CI, –64.9% to 44.9%), respectively. For patients who discontinued their prior TKI due to failure and due to intolerance, the risk differences were 15.5% (95% CI, 5.3% to 25.7%) and 2.1% (–20.8% to 25.0%), respectively. For patients who had been treated with 2, 3, or 4 or more previous TKIs, the risk differences were 12.2% (95% CI, –4.1% to 28.4%), 10.5% (95% CI, –5.3% to 26.4%), and 6.7% (95% CI, –6.0% to 19.3%), respectively. For patients with and without a BCR-ABL1 mutation at baseline, the risk differences were 10.3% (95% CI, –27.3% to 47.9%) and 13.7% (85% CI, 2.8% to 24.5%), respectively.
Table 21: MMR Rate at 24 Weeks; Subgroup Analyses — FAS
Outcome | ASCEMBL primary analysis | |
|---|---|---|
Asciminib | Bosutinib | |
Strata based on randomization | ||
Major cytogenetic response, n/N (%) | 21/46 (45.7) | 4/22 (18.2) |
Risk difference,a % (95% CI) | 27.5 (5.9 to 49.1) | Reference |
No major cytogenetic response, n/N (%) | 19/111 (17.1) | 6/54 (11.1) |
Risk difference,a % (95% CI) | 6.0 (—4.9 to 16.9) | Reference |
BCR-ABL1 transcript level (IS) at baseline | ||
≥ 1%, n/N (%) | 34/142 (23.9) | 8/72 (11.1) |
Risk difference,a % (95% CI) | 12.8 (2.7 to 22.9) | Reference |
< 1%, n/N (%) | 6/15 (40.0) | 2/4 (50.0) |
Risk difference,a % (95% CI) | —10.0 (—64.9 to 44.9) | Reference |
Reason for discontinuation of prior TKI | ||
Failure, n/N (%) | 20/95 (21.1) | 3/54 (5.6) |
Risk difference,a % (95% CI) | 15.5 (5.3 to 25.7) | Reference |
Intolerance, n/N (%) | 20/59 (33.9) | 7/22 (31.8) |
Risk difference,a % (95% CI) | 2.1 (—20.8 to 25.0) | Reference |
Number of prior TKIs | ||
2, n/N (%) | 27/89 (30.3) | 6/33 (18.2) |
Risk difference,a % (95% CI) | 12.2 (—4.1 to 28.4) | Reference |
3, n/N (%) | 12/53 (22.6) | 4/33 (12.1) |
Risk difference,a % (95% CI) | 10.5 (—5.3 to 26.4) | Reference |
≥ 4, n/N (%) | 1/15 (6.7) | 0/10 (0) |
Risk difference,a % (95% CI) | 6.7 (—6.0 to 19.3) | Reference |
BCR-ABL1 mutation at day 1 of week 1 | ||
Unmutated, n/N (%) | 31/125 (24.8) | 7/63 (11.1) |
Risk difference,a % (95% CI) | 13.7 (2.8 to 24.5) | Reference |
Mutated, n/N (%) | 6/17 (35.3) | 2/8 (25.0) |
Risk difference,a % (95% CI) | 10.3 (—27.3 to 47.9) | Reference |
CI = confidence interval; FAS = full analysis set; IS = International Standard; MMR = major molecular response; TKI = tyrosine kinase inhibitor.
Note: n represents the number of patients with response and N represents the total number of patients in the subgroup and treatment group. Risk difference is asciminib versus bosutinib.
aWald 95% 2-sided CI.
Source: Asciminib Clinical Study Report.8
Hematologic Response
Hematologic response was not reported in the ASCEMBL trial.
Cytogenic Response
CcyR among patients who were not already in CcyR at baseline is summarized in Table 22. At the primary analysis, the CcyR at 24 weeks in the asciminib group was 40.78% (95% CI, 31.20% to 50.90%) and in the bosutinib group it was 24.19% (95% CI, 14.22% to 36.74%). The unstratified difference in response rate was 16.58% (95% CI, 2.31% to 30.86%). Assessed by common risk stratification of McyR versus no McyR at baseline, the common risk difference was 17.30% (95% CI, 3.62% to 30.99%). At the updated data cut-off, the CcyR rate at 48 weeks was 39.81% (95% CI, 30.29% to 49.92%) in the asciminib group and 20.97% (95% CI, 11.66% to 33.18%) in the bosutinib group. The unstratified difference in response rate was 18.84% (95% CI, 4.98% to 32.70%). The common risk difference based on McyR stratification was 19.05% (95% CI, 4.87% to 33.24%).
Table 22: CcyR Rate (Among Patients Who Were Not Already in CcyR at Baseline) at 24 Weeks and 48 Weeks — CcyR Analysis Set
Outcome | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 103 | Bosutinib N = 62 | Asciminib N = 103 | Bosutinib N = 62 | |
Response, n (%) | 42 (40.78) | 15 (24.19) | 41 (39.81) | 13 (20.97) |
95% CI for responsea | (31.20 to 50.90) | (14.22 to 36.74) | (30.29 to 49.92) | (11.66 to 33.18) |
Unstratified difference in response rate (vs. bosutinib), % | 16.58 | Reference | 18.84 | Reference |
95% CI for differenceb | (2.31 to 30.86) | Reference | (4.98 to 32.70) | Reference |
Common risk difference,c % | 17.30 | Reference | 19.05 | Reference |
95% CI for difference | (3.62 to 30.99) | Reference | (4.87 to 33.24) | Reference |
P valued | 0.019 | Reference | NA | NA |
CI = confidence interval; CcyR = complete cytogenetic response; MMR = major molecular response; NA = not applicable; vs. = versus.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
aClopper-Pearson 95% 2-sided CI.
bWald 95% 2-sided CI.
cThe common risk difference after adjusting for stratum: baseline McyR status (based on randomization data) and its 95% CI were estimated using the Mantel-Haenszel method.
dNominal P value, not adjusted for multiplicity.
Duration of Response
Duration of response among patients who achieved an MMR is summarized in Table 23. At the primary analysis, loss of response occurred in 5.6% patients of the 54 patients who had achieved MMR in the asciminib group, and no patient who achieved MMR in the bosutinib group lost response. At the updated data cut-off, loss of response had occurred in 3.2% of patients achieving response while receiving asciminib and 5.6% of patients achieving response while receiving bosutinib.
Table 23: Duration of First MMR Among Patients Who Achieved MMR at 24 Weeks and 48 Weeks — MMR Responder Set
Outcome | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 54 | Bosutinib N = 14 | Asciminib N = 62 | Bosutinib N = 18 | |
Loss of response, n (%) | 3 (5.6) | 0 | 2 (3.2) | 1 (5.6) |
KM % in response (95% CI) | ||||
24 weeks | 95.4 (82.8 to 98.8) | 100.0 (NE to NE) | 98.1 (87.6 to 99.7) | 100.0 (NE to NE) |
48 weeks | 92.6 (78.6, 97.6) | 100.0 (NE to NE) | 96.1 (85.4 to 99.0) | 90.0 (47.3 to 98.5) |
CI = confidence interval; CcyR = complete cytogenetic response; KM = Kaplan–Meier; NE = not estimable; SD = standard deviation.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
Source: Asciminib Clinical Study Report.8
Duration of response among patients who achieved a CcyR is summarized in Table 24. At the primary analysis, loss of response occurred in 2.3% patients of the 44 patients who had achieved CcyR in the asciminib group, and 5.3% of the 19 patients who achieved CcyR in the bosutinib group lost response. At the updated data cut-off, loss of response had occurred in 2.0% of patients achieving response while receiving asciminib and 4.5% of patients achieving response while receiving bosutinib.
Table 24: Duration of CcyR Among Patients Who Achieved CcyR — CcyR Responder Set
Outcome | ASCEMBL Primary Analysis | ASCEMBL Updated Data Cut-off | ||
|---|---|---|---|---|
Asciminib N = 44 | Bosutinib N = 19 | Asciminib N = 49 | Bosutinib N = 22 | |
Loss of response, n (%) | 1 (2.3) | 1 (5.3) | 1 (2.0) | 1 (4.5) |
KM % in response (95% CI) | ||||
24 weeks | 96.7 (78.6 to 99.5) | 85.7 (33.4 to 97.9) | 97.6 (84.3 to 99.7) | 91.7 (53.9 to 98.8) |
48 weeks | 96.7 (78.6 to 99.5) | 85.7 (33.4 to 97.9) | 97.6 (84.3 to 99.7) | 91.7 (53.9 to 98.8) |
CcyR = complete cytogenetic response; CI = confidence interval; KM = Kaplan–Meier
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
Source: Asciminib Clinical Study Report.8
Time to Response
Time to first MMR among patients who achieved an MMR is summarized in Table 25. At the primary analysis the mean time to MMR was 19.0 (SD = 14.40) weeks in the asciminib group and 22.8 (SD = 18.37) weeks in the bosutinib group. At the updated data cut-off, the corresponding mean time to MMR values were 24.7 (SD = 21.71) weeks in the asciminib group and 31.1 (SD = 25.81) weeks in the bosutinib group.
Table 25: Time to First MMR Among Patients Who Achieved MMR — MMR Responder Set
Outcome | ASCEMBL primary analysis | ASCEMBL updated data cut-off | ||
|---|---|---|---|---|
Asciminib N = 54 | Bosutinib N = 14 | Asciminib N = 62 | Bosutinib N = 18 | |
Time to MMR (weeks) | ||||
Mean (SD) | 19.0 (14.40) | 22.8 (18.37) | 24.7 (21.71) | 31.1 (25.81) |
Median (Range) | 12.7 (4 to 76) | 14.3 (7 to 66) | 15.6 (4 to 121) | 24.0 (7 to 96) |
MMR = major molecular response; SD = standard deviation.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
Source: Asciminib Clinical Study Report.8
Time to first CcyR among patients who achieved a CcyR is summarized in Table 26. At the primary analysis the mean time to CcyR was 25.4 (SD = 5.09) weeks in the asciminib group and 29.0 (SD = 11.50) weeks in the bosutinib group. At the updated data cut-off, the corresponding mean time to CcyR values were 29.1 (SD = 13.47) weeks in the asciminib group and 31.6 (SD = 12.60) weeks in the bosutinib group.
Table 26: Time to First CcyR Among Patients Who Achieved CcyR — CcyR Responder Set
Outcome | ASCEMBL Primary Analysis | ASCEMBL Updated Data Cut-off | ||
|---|---|---|---|---|
Asciminib N = 44 | Bosutinib N = 19 | Asciminib N = 49 | Bosutinib N = 22 | |
Time to CcyR (weeks) | ||||
Mean (SD) | 25.4 (5.09) | 29.0 (11.50) | 29.1 (13.47) | 31.6 (12.60) |
Median (Range) | 24.2 (23.1 to 48.7) | 24.1 (12.1 to 53.3) | 24.3 (23.1 to 92.7) | 24.2 (12.1 to 53.3) |
CcyR = complete cytogenetic response; SD = standard deviation.
Note: Primary analysis was conducted according to the May 25, 2020, data cut-off; the updated data cut-off was January 1, 2021.
Source: Asciminib Clinical Study Report.8
Harms
Only those harms identified in the review protocol are reported in the following. See Table 27 for detailed harms data.
Adverse Events
At the time of primary analysis almost all patients in both treatment groups experienced treatment-emergent AEs, 89.7% in the asciminib group and 96.1% in the bosutinib group. The most common AEs in the asciminib group were thrombocytopenia (22.4% versus 13.2% in the bosutinib group), neutropenia (17.9% versus 17.1% in the bosutinib group), and headache (16.0% versus 13.2% in the bosutinib group). The most common AEs in the bosutinib group were diarrhea (71.1% versus 11.5% in the asciminib group), nausea (46.1% versus 11.5% in the asciminib group), and increased alanine aminotransferase (27.6% versus 3.8% in the asciminib group).
Serious Adverse Events
SAEs occurred in 13.5% of patients in the asciminib group and 18.4% of patients in the bosutinib group. The only SAE that occurred in more than 1 patient was pyrexia, which occurred in 1.3% of patients in the asciminib group.
Withdrawals Due to AEs
Withdrawal from study treatment due to AEs occurred in 5.8% of patients in the asciminib group and 21.1% of patients in the bosutinib group. The AE that most commonly resulted in withdrawal in the asciminib group was thrombocytopenia (5.8% of patients) and in the bosutinib group it was increased alanine aminotransferase (5.3% of patients).
Mortality
Deaths occurred in 2.6% of patients in the asciminib group and 1.3% of patients in the bosutinib group. The causes of death were arterial embolism and ischemic stroke in the asciminib group and septic shock in the bosutinib group. Two of the 4 deaths reported in the asciminib group occurred during survival follow-up and were due to underlying disease.
Notable Harms
Notable harms specified in the CADTH review protocol are included in the Table 27 summary. The largest differences between the study treatments were in hepatotoxicity, in which 8.3% of patients in the asciminib group reported AEs compared to 30.3% of patients in the bosutinib group; and in gastrointestinal toxicity, in which 31.4% of patients in the asciminib group reported AEs compared to 78.9% of patients in the bosutinib group. Pancreatic toxicity was similar between the treatment groups with 8.3% of patients in the asciminib group reporting AEs compared to 9.2% of patients in the bosutinib group.
Table 27: Summary of Harms — Safety Analysis Set
Harms | ASCEMBL | |
|---|---|---|
Asciminib N = 156 | Bosutinib N = 76 | |
Patients with ≥ 1 adverse event | ||
n (%) | 140 (89.7) | 73 (96.1) |
Most common events,a n (%) | ||
Thrombocytopenia | 35 (22.4) | 10 (13.2) |
Neutropenia | 28 (17.9) | 13 (17.1) |
Headache | 25 (16.0) | 10 (13.2) |
Diarrhea | 18 (11.5) | 54 (71.1) |
Hypertension | 18 (11.5) | 3 (3.9) |
Nausea | 18 (11.5) | 35 (46.1) |
Fatigue | 16 (10.3) | 7 (9.2) |
Rash | 11 (7.1) | 18 (23.7) |
Vomiting | 11 (7.1) | 20 (26.3) |
Abdominal pain | 7 (4.5) | 11 (14.5) |
Increased alanine aminotransferase | 6 (3.8) | 21 (27.6) |
Increased aspartate aminotransferase | 6 (3.8) | 16 (21.1) |
Patients with ≥ 1 SAE | ||
n (%) | 21 (13.5) | 14 (18.4) |
Most common events,b n (%) | ||
Pyrexia | 2 (1.3) | 0 |
Patients who stopped treatment due to AEs | ||
n (%) | 9 (5.8) | 16 (21.1) |
Most common events,b n (%) | ||
Thrombocytopenia | 3 (1.9) | 1 (1.3) |
Neutropenia | 2 (1.3) | 3 (3.9) |
Decreased neutrophil count | 2 (1.3) | 0 |
Decreased platelet count | 2 (1.3) | 0 |
Increased alanine aminotransferase | 0 | 4 (5.3) |
Increased aspartate aminotransferase | 0 | 2 (2.6) |
Diarrhea | 0 | 2 (2.6) |
Deaths | ||
n (%) | 4 (2.6) | 1 (1.3) |
Embolism arterial, n (%) | 1 (0.6) | 0 |
Ischemic stroke, n (%) | 1 (0.6) | 0 |
Septic shock, n (%) | 0 | 1 (1.3) |
Notable harms | ||
Myelosuppression, n (%) | 58 (37.2) | 27 (35.5) |
Grade 3 | 17 (10.9) | 14 (18.4) |
Grade 4 | 24 (15.4) | 4 (5.3) |
SAE | 2 (1.3) | 1 (1.3) |
AE resulting in treatment discontinuation | 6 (3.8) | 4 (5.3) |
AE resulting in dose reduction | 8 (5.1) | 3 (3.9) |
AE resulting in treatment interruption | 36 (23.1) | 13 (17.1) |
Pancreatic toxicity, n (%) | 13 (8.3) | 7 (9.2) |
Grade 3 | 5 (3.2) | 3 (3.9) |
Grade 4 | 1 (0.6) | 0 |
SAE | 0 | 0 |
AE resulting in treatment discontinuation | 1 (0.6) | 0 |
AE resulting in dose reduction | 0 | 0 |
AE resulting in treatment interruption | 6 (3.8) | 2 (2.6) |
Hepatotoxicity, n (%) | 13 (8.3) | 23 (30.3) |
Grade 3 | 1 (0.6) | 13 (17.1) |
Grade 4 | 0 | 0 |
SAE | 0 | 0 |
AE resulting in treatment discontinuation | 0 | 4 (5.3) |
AE resulting in dose reduction | 0 | 3 (3.9) |
AE resulting in treatment interruption | 4 (2.6) | 11 (14.5) |
Gastrointestinal toxicity, n (%) | 49 (31.4) | 60 (78.9) |
Grade 3 | 3 (1.9) | 9 (11.8) |
Grade 4 | 0 | 0 |
SAE | 2 (1.3) | 1 (1.3) |
AE resulting in treatment discontinuation | 0 | 2 (2.6) |
AE resulting in dose reduction | 0 | 10 (13.2) |
AE resulting in treatment interruption | 7 (4.5) | 10 (13.2) |
Cardiac failure, n (%) | 2 (1.3) | 1 (1.3) |
Grade 3 | 2 (1.3) | 1 (1.3) |
Grade 4 | 0 | 0 |
SAE | 2 (1.3) | 1 (1.3) |
AE resulting in treatment discontinuation | 1 (0.6) | 0 |
AE resulting in dose reduction | 0 | 0 |
AE resulting in treatment interruption | 0 | 1 (1.3) |
QTc prolongation | 4 (2.6) | 1 (1.3) |
Grade 3 | 2 (1.3) | 0 |
Grade 4 | 0 | 0 |
SAE | 0 | 0 |
AE resulting in treatment discontinuation | 0 | 0 |
AE resulting in dose reduction | 0 | 0 |
AE resulting in treatment interruption | 1 (0.6) | 0 |
Ischemic heart and CNS conditions | 6 (3.8) | 4 (5.3) |
Grade 3 | 1 (0.6) | 2 (2.6) |
Grade 4 | 1 (0.6) | 0 |
SAE | 2 (1.3) | 1 (1.3) |
AE resulting in treatment discontinuation | 1 (0.6) | 0 |
AE resulting in dose reduction | 0 | 0 |
AE resulting in treatment interruption | 3 (1.9) | 1 (1.3) |
AE = adverse event; CNS = central nervous system; QTc = corrected QT; SAE = serious adverse event.
NOTE: Numbers for patients with a Grade 3 or 4 AE are based on the maximum grade experienced.
aAEs only presented if occurring in greater than 10% of patients in either treatment group.
bAEs only presented if occurring in more than 1 patient in either treatment group.
Source: Asciminib Clinical Study Report.8
Critical Appraisal
Internal Validity
ASCEMBL was a phase III, open-label RCT that evaluated asciminib in comparison to bosutinib in patients with CP-CML who had failed on or become intolerant to 2 or more prior TKI therapies. The outcomes assessed in the ASCEMBL trial (MMR, CcyR, PFS, OS, HRQoL) are standard in CML and are considered clinically meaningful. Given that ASCEMBL is an open-label trial, there is possibility for bias in favour of asciminib in the patient-reported outcomes of HRQoL, AE reporting, and general discontinuation rates between the treatment groups. However, the primary end point of MMR and key secondary end point of CCyR are objective measures and are therefore less likely to be subject to bias. There were slight differences in baseline characteristics of important prognostic factors with proportionally more patients in the bosutinib group having received higher numbers of prior TKIs and having discontinued their prior TKI due to resistance, suggesting bias in favour of asciminib; however, the sponsor did provide a logistic regression adjusting for these factors and found similar results with the primary analysis.
The statistical analysis was appropriate, although given that only the primary end point was formally tested for statistical significance there are few conclusions beyond the primary end point that can be draw. For the HRQoL and related outcomes, the lack of responsiveness and MID studies conducted in patients with CML for the EQ-5D-5L and PGIC further impacts the certainty of the conclusions. Further, none of the analyses aside from the primary end point analysis were controlled for multiplicity, so there is an increased risk of false-positive conclusions. Of the 2 data cut-offs presented, both are interim analyses, only 1 of which was preplanned. Also, survival data are immature given that so few patients had progressed or died, impacting the conclusions that can be drawn for these OS and PFS. According to the clinical experts consulted, an important predictor of treatment success is the severity of disease upon study entry. The statistical plan for the ASCEMBL trial accounted for this fact through stratification of patients based on whether they were in MCyR at baseline to ensure a common risk difference when analyzing the primary end point of the trial. Although the binary categorization of in MCyR versus not in MCyR at baseline is a rough proxy for disease severity and patient risk, MCyR can further be classified into CCyR and PCyR and an imbalanced distribution within these 2 categories could indicate an imbalanced disease severity between treatment groups even with stratification. In the asciminib group, of the patients in MCyR at baseline, 43% were in CCyR, while in the bosutinib group, of the patients in MCyR at baseline, 24% were in CCyR. This imbalance introduces bias in favour of asciminib for all outcomes that use MCyR stratification to account for common risk difference.
Furthermore, there were 22.3% of patients in the asciminib group and 11.8% of patients in the bosutinib group who had missing MCyR data at baseline, leading to 15.9% of patient receiving asciminib and 14.5% of patients receiving bosutinib assigned to the incorrect stratum. Sensitivity analysis was conducted to correct for this using BCR-ABL1 ratio as a proxy for cytogenetic response, the results of which were consistent with the primary analysis. It should be noted, however, that additional testing is not adjusted for multiplicity and should be interpreted with caution.
Patients positive for T315I and V299L mutations were excluded from the ASCEMBL trial due those mutations conferring resistance to the comparator drug bosutinib. There were, however, 3 patients in the asciminib group and 2 patients in the bosutinib group who were identified as being positive for those mutations at the first study visit post-screening. Although these are a small number of patients in each group, there would be slight bias toward asciminib given the lack of efficacy of bosutinib in these patients, although the asciminib dose received by these patients is lower than the FDA-approved dose for patients with the T315I mutation. The sponsor provided a scenario analysis excluding these patients from the analysis and showed results consistent with the primary analysis. Predefined subgroup analyses were also provided; however, these end points were exploratory and the estimates were very imprecise due to small sample sizes leading to an inability to draw conclusions.
There were protocol amendments implemented after patients had been randomized and began treatment in the ASCEMBL trial. One specifically of note was an adjustment of inclusion criteria to allow patients who were intolerant of their most recent TKI to enrol if their BCR-ABL1 ratio was greater than 0.1%. While an amendment to inclusion criteria after patients have been randomized is always a concern for internal validity, the clinical experts consulted by CADTH agreed with the provided rationale that it was important to capture the third-line intolerant population and the study was unlikely to adequately enroll patients who were intolerant with a requirement for BCR-ABL1 ratio greater than 1%.
External Validity
According to clinical experts consulted by CADTH, the demographic and disease characteristics of the ASCEMBL trial population were reflective of the Canadian population with CP-CML after 2 or more prior TKIs. According to the clinical experts, and as in most oncology trials, the enrolment criteria likely selected for a healthier cross-section of the overall patient population who were most likely to benefit from and more able to tolerate protocol therapies. This is further evidenced from the proportion of screening failures (27%), indicating the patient population was indeed a select group. Patients with the T315I or V299L mutation were excluded from the trial given that they would be unlikely to respond to bosutinib treatment; therefore, there is an evidence gap for the efficacy of asciminib in patients with these mutations.
The dosage of asciminib in the ASCEMBL trial (40 mg twice daily) represents only one of the Health Canada–approved dosages (40 mg twice daily and 80 mg once daily).17 The FDA has approved both 40 mg twice daily and 80 mg once daily dosages for the corresponding indication.16 It is unclear if the ASCEMBL trial evidence is generalizable to an 80 mg once daily dosage. The study allowed for patients to receive treatment for up to 96 weeks after the last patient received their dose or up to 48 weeks after the last patient receiving bosutinib switched to asciminib. The mean duration of follow-up at the primary analysis was 15.6 months, and at the updated data cut-off it was 23.0 months. While this does represent a reasonably long follow-up, CML is a chronic disease and patients in the third-line setting are expected to be on treatment indefinitely so long as they are experiencing treatment benefit. Therefore, the trial may not be generalizable beyond the follow-up time reported; however, the clinical experts consulted for this review do not anticipate issues with extending treatment beyond the follow-up times in the trial.
All outcomes evaluated in the trial and considered in this review (i.e., MMR, CCyR, OS, PFS, time to response, duration of response, and HRQoL) were clinically relevant, important to patients, and are used in clinical practice. The duration of follow-up was sufficient for assessment of the primary outcome of MMR at 24 weeks, CCyR, and HRQoL; however, longer-term outcomes of PFS and OS are difficult to interpret given the immaturity of the data. Subgroup analysis was not powered to detect treatment differences in patients who experienced treatment failure on their most recent TKI compared to treatment intolerance, line of therapy, disease severity at baseline, or mutational status. Nevertheless, the clinical experts consulted for this review felt that the results were generalizable across strata for all these subgroups.
Since administration of asciminib would occur mainly in the outpatient setting, background care (e.g., hematologist or oncologist visits, monitoring) would be expected to be similar for patients in Canada compared with those participating in the ASCEMBL trial.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to provide a summary and appraisal of the indirect evidence submitted by the sponsor, which included MAICs,31 comparing asciminib to other treatments used for patients with CP-CML who have received at least 2 prior TKI therapies.
A focused literature search for network meta-analyses that included asciminib as a comparator was run in Medline All (1946-) on February 15, 2022. No limits were applied. The literature search identified a total of 29 citations, none of which met the eligibility criteria.
Description of MAICs
The sponsor submitted a MAIC report aiming to demonstrate the efficacy of asciminib compared to relevant treatments for CP-CML following the use of at least 2 prior TKIs. The analysis used individual patient data (IPD) from the phase III trial ASCEMBL and aggregate data from published interventional and observational studies to compare efficacy outcomes for asciminib, ponatinib, nilotinib, dasatinib, and omacetaxine. Note that omacetaxine was not a comparator of interest for the current review.
Methods of the MAIC
Objectives
In the absence of direct comparative evidence from trials, the aim of each analysis was to compare the efficacy (response rate [MMR and CCyR] and TTD) of asciminib in patients with CP-CML who have received at least 2 prior TKIs versus ponatinib, nilotinib, dasatinib, and omacetaxine.
Study Selection Methods
The index trial was based on the asciminib group’s IPD from the phase III ASCEMBL trial (n = 157). To identify evidence for relevant comparators a SLR was conducted to identify evidence from interventional and observational studies. The studies identified from the SLR were further refined to fit the purposes. The refined selection criteria for inclusion in the indirect treatment comparison are summarized in Table 28. Of note, the selection criteria included interventions imatinib, omacetaxine, and hydroxycarbamide, which are not of interest to the current review and will not be commented on. Furthermore, the efficacy outcome of TTD was not of interest to the current review and will not be commented on.
Table 28: Study Selection Criteria and Methods for SLR Informing the MAIC
Criteria | ITC1 |
|---|---|
Population | Studies reporting outcomes for adult (≥ 18 years) patients with CML in CP where ≥ 75% of patients had prior experience with ≥ 2 TKIs and did not harbour the T315I mutation |
Intervention |
|
Comparator |
|
Outcome |
|
Study design |
|
Publication characteristics | Required to report > 20 patients in the target population and to report patient characteristics for the interventions of interest |
Databases searched | EMBASE, Medline, CENTRAL up to May 13, 2021 |
Selection process | Articles screened independently by 2 researchers |
Data extraction process | 2 independent reviewers extracted data with a third reviewer to resolve discrepancies |
Quality assessment | Cochrane Collaboration’s Risk of Bias assessment was used for RCT studies32 Newcastle-Ottawa quality assessment tool was used for cohort studies33 |
CCyR = complete cytogenetic response; CML = chronic myeloid leukemia; CP = chronic phase; MAIC = matching adjusted indirect comparison; MMR = major molecule response; RCT = randomized controlled trial; SLR = systematic literature review; TKI = tyrosine kinase inhibitor.
Source: Sponsor-submitted MAIC report.3.1
A total of 2,728 citations were screened and 7 studies of interest were included for analysis in the MAIC. Presented in Table 29 are the 4 studies that were available for response rate analysis (MMR and CCyR at 6 and 12 months) along with key population characteristics.
The ASCEMBL trial was rated as having high risk for detection bias and unclear risk for performance bias according to the Cochrane Collaboration’s Risk of Bias assessment. According to the Newcastle-Ottawa quality assessment tool, the PACE trial scored a 6-star rating, Ibrahim et al. (2010) scored a 3-star rating, and Tan et al. (2019) scored a 4-star rating. Higher scores indicate lower risk of bias.
Table 29: Characteristics of Included Studies Used for Response Rate Analysis
Characteristics | Asciminib | Ponatinib | Nilotinib or dasatinib | Dasatinib | ||
|---|---|---|---|---|---|---|
Study | ASCEMBL8
| PACE9
| Ibrahim et al. (2010)10
| Tan et al. (2019)11
| ||
Study location | International | International | UK | China | ||
Inclusion criteria |
|
|
|
| ||
Patients, n | 157 (all patients) | 103 (PACE scenario 1)a | 138 (PACE scenario 2)a | 203 (With the exclusion of patients enrolled in PACE who were T315I positive) | 26 (20 patients received dasatinib; 6 patients received nilotinib) | 24 |
2 prior TKIs (%) | 52% | 53% | 57% | 34% | 100% | NR |
No mutation (%) | 87% | 86% | 86% | 67% | 54% | 54% |
ECOG PS = 0 (%) | 80% | 77% | 79% | 69% | NR | NR |
Median age (years) | 52 | 51.5 | 52 | 61 | 64 | 50 |
Male (%) | 52% | 44% | 49% | 47% | 54% | 63% |
White (%) | 75% | 72% | 74% | 86% | NR | NR |
CCyR = complete cytogenic response; ECOG PS = European Cooperative Oncology Group Performance Status; NR = not reported; TKI = tyrosine kinase inhibitor.
aFor a comparison against PACE, the ASCEMBL trial population was adjusted to account for the fact that patients in CCyR were permitted in the ASCEMBL trial. Scenario 1 removes all patients in the ASCEMBL trial who were in CCyR at baseline or for whom CCyR data was missing at baseline. Scenario 2 removes only the patients who were in CCyR at baseline.
Source: Sponsor-submitted matching adjusted indirect comparison report.31
MAIC Analysis Methods
In the absence of direct trial evidence for relevant comparators or RCTs to form a connected network, an unanchored MAIC was deemed to be the only means by which to estimate relative treatment effects between asciminib and the identified relevant comparators.
Given the availability of IPD from the index trial ASCEMBL, the sponsor aimed to adjust for between-study differences in the distribution of prognostic factors and treatment effect modifiers. The sponsor extracted all characteristics reported in the included studies and consulted with an expert clinician who ranked these in priority order based on their impact on the outcomes.
Specifically for the comparison between asciminib and ponatinib, patients needed to be removed from ASCEMBL to address the difference in inclusion criteria between the studies. In ASCEMBL patients in CCyR at baseline were permitted to enrol in the study whereas in PACE, these patients were excluded. To account for this, the sponsor created 3 scenarios. Scenario 1 removed all 54 patients from ASCEMBL that were either in CCyR at baseline, or for whom CCyR data was not available at baseline. Scenario 2 removed only the 19 patients from ASCEMBL that were in CCyR at baseline. Scenario 3 removed the 24 patients from ASCEMBL that were either in CCyR at baseline or had BCR-ABL1 ratio ≤ 1% (a proxy for CCyR) at baseline. Additionally, due to PACE including patients with the T315I mutation, only the subgroup of 203 patients that were not positive for T315I were included in the analyses.
The list of factors is presented in Table 30. Of note, data on best cytogenetic response to the last TKI were not available within the ASCEMBL IPD. Furthermore, patients harbouring the T315I mutation were excluded from ASCEMBL and, therefore, adjustments were not possible for this prognostic factor. Logistic propensity score models were used to estimate weights for the IPD from ASCEMBL so that the weighted mean baseline characteristics would match those observed for the comparator trials. The remaining variables were examined to ensure that there was sufficient overlap between the populations, and to ensure that the propensity score models were numerically stable. Patient weights were analyzed to ensure that no patients were too heavily weighted, for example, although number of mutations factor was originally categorized into 0, 1, and ≥ 2, due to extreme weights in the model, this was reduced to 0 and ≥ 1. Finally, if the propensity score model did not converge using the full set of characteristics, characteristics were removed from the model in a stepwise fashion until convergence was achieved. Characteristics that were least clinically relevant or that were already well balanced between studies were removed first. Once the model had achieved convergence a further reduction of characteristics from the model was possible to achieve a balance between a large ESS and the highest number of characteristics that could be balanced in the model.
Table 30: Baseline Characteristics and Disease Characteristics Used in Matching Procedure
Relative importance | Characteristic |
|---|---|
1 | Number of prior TKIs received before study entry |
2 | Resistance to prior TKIs
|
3 | Intolerance to prior TKIs
If data not available on the previous criteria, then, intolerance of last TKI |
4 | Cytogenetic response to the last TKI |
5 | Cytogenetic response status of patients at study entry |
6 | T315I mutation status |
7 | Number of mutations (0, 1, ≥ 2) |
8 | ECOG Performance Status at study entry |
9 | Age at study entry |
10 | Gender |
11 | Race |
ECOG = European Cooperative Oncology Group; TKI = tyrosine kinase inhibitor.
Source: Sponsor-submitted matching adjusted indirect comparison report.31
Results of MAIC
Asciminib Versus Ponatinib
The model could not converge when all prognostic factors and effect modifiers were included. To balance the largest number of matched factors, the model that was selected included age, ECOG PS, no mutation, PCyR, and 2 prior TKIs. The ESS of this selected model was 53.
Patient characteristics from the PACE trial and the ASCEMBL trial before and after applying the matching methodology are summarized in Table 31. As the characteristics of race and sex were not included in the propensity scoring model, there remained imbalances in these characteristics. The other characteristics included in the propensity score model were well matched post-weighting.
Table 31: Patient Characteristics Before and After MAIC With PACE
Characteristic | Ponatinib PACE | Asciminib | |
|---|---|---|---|
ASCEMBL: Pre-matching | ASCEMBL: Post-matching | ||
Number of patients (ESS) | N = 203 | N = 103 | ||||||| |
Race — White | 85.7% | 71.8% | ||||||| |
Sex — male | 46.8% | 43.7% | ||||||| |
Median age | 61 | 53 | ||||||| |
ECOG PS — 0 | 68.5% | 76.7% | ||||||| |
No mutation | 67.0% | 86.4% | ||||||| |
PCyR at baseline | 19.2% | 24.3% | ||||||| |
2 prior TKIs | 31.5% | 53.4% | ||||||| |
ECOG = European Cooperative Oncology Group; ESS = effective sample size; MAIC = matching adjusted indirect comparison; PCyR = partial cytogenetic response; TKI = tyrosine kinase inhibitor.
Source: Sponsor-submitted MAIC report.31
The comparison of efficacy end points MMR and CCyR at both 6 and 12 months in the patients post-MAIC from the ASCEMBL trial compared with the PACE trial is shown in Table 32. Following the MAIC, ||||||||| ||| |||||||| |||| ||||||| || ||| || ||| | ||| |||||||| ||||||||||| |||| || |||| ||| || |||| |||||| ||||| ||| |||| |||||| |||||| ||||||||||||| ||| || |||| ||| ||| |||| || ||| ||||||| ||||||||| ||| |||| |||||| ||||| ||| |||| |||||| ||||| || ||| |||||||| |||||||||.
Table 32: Efficacy End Points Before and After MAIC With PACE
End point | Asciminib | Ponatinib N = 203 | |
|---|---|---|---|
ASCEMBL: Pre-matching N = 103 | ASCEMBL: Post-matching ||| | || | ||
MMR by 6 months (95% CI) | 28% (20% to 38%) | ||| ||||| |||| | 19% (NR) |
OR (95% CI) | NA | |||| |||||| ||||| | Reference |
MMR by 12 months (95% CI) | 35% (26% to 45%) | ||| ||||| |||| | 23% (NR) |
OR (95% CI) | NA | |||| |||||| ||||| | Reference |
CCyR by 6 months (95% CI) | 41% (31% to 51%) | ||| ||||| |||| | 34% (NR) |
OR (95% CI) | NA | |||| |||||| ||||| | Reference |
CCyR by 12 months (95% CI) | 46% (36% to 56%) | ||| ||||| |||| | 43% (NR) |
OR (95% CI) | NA | |||| |||||| ||||| | Reference |
CCyR = complete cytogenetic response; CI = confidence interval; MAIC = matching adjusted indirect comparison; MMR = major molecular response; NA = not applicable; NR = not reported; OR = odds ratio.
Source: Sponsor-submitted MAIC report.31
Asciminib Versus Nilotinib and Dasatinib
For this comparison, the comparator trial Ibrahim et al. (2010) was a cohort trial of 26 patients, 20 of whom received dasatinib, 6 of whom received nilotinib. Analysis was conducted on the full cohort of combined patients. The model could not converge when all prognostic factors and effect modifiers were included. To balance the largest number of matched factors, the model that was selected included prior intolerance, prior resistance, and 2 prior TKIs. The ESS of this selected model was 35.
Patient characteristics from the Ibrahim et al. (2010) prospective cohort and the ASCEMBL trial before and after applying the matching methodology are summarized in Table 33. As the characteristics of race, sex, and proportion of patients with no mutation were not included in the propensity scoring model, there remained imbalanced in these characteristics. The other characteristics included in the propensity score model were well matched post-weighting.
Table 33: Patient Characteristics Before and After MAIC With Ibrahim et al. (2010)
End point | Nilotinib and dasatinib Ibrahim et al. (2010) | Asciminib ASCEMBL: Pre-matching | ASCEMBL: Post-matching |
|---|---|---|---|
Number of patients (ESS) | N = 26 | N = 103 | |||||| |
Sex — male | 54% | 44% | |||||| |
Median age | 64 | 53 | ||||| |
No mutation | 54% | 86% | ||||| |
Nilotinib or dasatinib resistance | 27% | 70% | ||||| |
Nilotinib or dasatinib intolerance | 65% | 40% | ||||| |
2 prior TKIs | 100% | 53% | ||||| |
ESS = effective sample size; MAIC = matching adjusted indirect comparison; TKI = tyrosine kinase inhibitor.
Source: Sponsor-submitted MAIC report.31
The comparison of efficacy end points was only available for CCyR at both 6 and 12 months in patients post-MAIC from the ASCEMBL trial compared with the Ibrahim et al. (2010) trial. The results are shown in Table 34. Following the MAIC, ||||||||| ||| |||||||| |||| ||||||| || |||| || ||| | ||| || ||||| ||||||||||| |||| || |||| ||| || |||| |||||| |||||| ||| |||| |||||| |||||| ||||||||||||.
Table 34: Efficacy End Points Before and After MAIC With Ibrahim et al. (2010)
End point | Asciminib | Nilotinib and dasatinib N = 26 | |
|---|---|---|---|
ASCEMBL: Pre-matching N = 103 | ASCEMBL: Post-matching ||| | || | ||
CCyR by 6 months (95% CI) | 41% (31% to 51%) | ||| ||||| |||| | 15% (NR) |
OR (95% CI) | NA | |||| |||||| |||||| | Reference |
CCyR by 12 months (95% CI) | 46% (36% to 56%) | ||| ||||| |||| | 31% (NR) |
OR (95% CI) | NA | |||| |||||| ||||| | Reference |
CCyR = complete cytogenetic response; CI = confidence interval; MAIC = matching adjusted indirect comparison; NA = not applicable; NR = not reported; OR = odds ratio
Source: Sponsor-submitted MAIC report.31
Asciminib Versus Dasatinib
The model could not converge when all prognostic factors and effect modifiers were included. To balance the largest number of matched factors, the model that was selected included sex, age, no mutation, nilotinib resistance, nilotinib intolerance, and 2 prior TKIs. The ESS of this selected model was 23.
Patient characteristics from the Tan et al. (2010) retrospective chart review and the ASCEMBL trial before and after applying the matching methodology are summarized in Table 35. The presented characteristics are the factors that were matched in the model; factors that could not be matched due to lack of reporting in the comparator trial are not shown. The characteristics that changed the most from pre-MAIC to post-MAIC in patients in the ASCEMBL trial ||| ||||| ||| ||||| || | |||| || |||||.
Table 35: Patient Characteristics Before and After MAIC With Tan et al. (2019)
Characteristic | Dasatinib Tan et al. (2019) | Asciminib | |
|---|---|---|---|
ASCEMBL: Pre-matching | ASCEMBL: Post-matching | ||
Number of patients (ESS) | N = 24 | N = 157 | |||||| |
Sex — Male | 63% | 52% | ||||| |
Median age | 50 | 52 | ||||| |
No mutation | 54% | 87% | ||||| |
Nilotinib intolerant | 50% | 23% | ||||| |
Nilotinib resistance | 59% | 38% | ||||| |
2 prior TKIs | 100% | 43% | |||||| |
ESS = effective sample size; MAIC = matching adjusted indirect comparison; TKI = tyrosine kinase inhibitor.
Source: Sponsor-submitted MAIC report.31
The comparison of efficacy end points was only available for MMR at 6 months in patients post-MAIC from the ASCEMBL trial compared with the Tan et al. (2019) retrospective chart review. The results are shown in Table 36. Following the MAIC, the OR for MMR at the 6-month time point was 1.40 (95% CI, 0.49 to 3.98).
Table 36: Patient Characteristics Before and After MAIC With Tan et al. (2019)
Characteristic | Asciminib | Dasatinib N = 24 | |
|---|---|---|---|
ASCEMBL: Pre-matching N = 157 | ASCEMBL: Post-matching ||| | || | ||
MMR by 6 months (95% CI) | 27% (21% to 35%) | ||| ||||| |||| | 21% (NR) |
OR (95% CI) | NA | |||| |||||| ||||| | Reference |
CI = confidence interval; MAIC = matching adjusted indirect comparison; MMR = major molecular response; NA = not applicable; NR = not reported; OR = odds ratio.
Source: Sponsor-submitted MAIC report.31
Critical Appraisal of the Sponsor-Submitted MAICs
The sponsor submitted 1 MAIC report that included comparisons of interest for asciminib against ponatinib, dasatinib, and nilotinib. The choice to conduct an unanchored MAIC was justified considering the lack of a common comparator. In all cases, the ASCEMBL trial was used as the index trial. The comparator trials were identified via an SLR that identified publications that were further refined for the purposes of the MAIC analysis. Given the use of a systematic approach to identify publications, there is a low risk of selection bias.
There were important differences in the design of the comparator studies that limit the ability to draw strong conclusions about the efficacy of asciminib compared with the other treatments. ASCEMBL was a randomized phase III interventional trial, while comparator trials included observational trials such as Ibrahim et al. (2010) and Tan et al. (2019). Data analyzed in an observational fashion are prone to unique biases (e.g., selection bias, confounding) compared with those collected from prospective interventional studies (like RCTs and single-arm trials) that cannot be controlled for using MAIC methods.
The data collection period and setting of the included studies varied, with enrolment as far back as 2005, whereas the ASCEMBL trial began in 2017. Some studies recruited internationally, whereas others recruited from single nations (UK or China). There may be differences in clinical practice by region at varying time points, though the direction of potential bias is unclear.
An important limitation, inherent to all MAIC analyses, is that all prognostic factors should ideally be matched between index and comparator trials to eliminate as much bias from the comparison as possible. This includes both measured and unmeasured characteristics and thus can never be fully accounted for. The list of characteristics provided by the sponsor that were adjusted for were not informed by a systematic review of literature or clinical expert identification, rather they were chosen because they were included in the comparator trials and could be reliably calculated for patients in the ASCEMBL trial. The consulted clinical expert provided input on the ranking of the relative importance of the chosen clinical characteristics. This introduces bias and uncertainty into the results due to the potential for important prognostic factors that went unadjusted in the analysis. Furthermore, due to the instability in the propensity score model for some comparisons, as well as a lack of reporting in the comparator trials, clinical characteristics were either removed from the model to achieve convergence or could not be included in the model. Notably, these factors that could not be adjusted included the proportion of patients with T315I mutation, prior resistance or intolerance, and baseline cytogenetic response, introducing uncertainty given the lack of adjustment of these important prognostic factors. The results of the propensity score model resulted in ESS in the index trial that were significantly reduced compared to the original sample size of the ASCEMBL trial and included some patients with a weighting greater than 5, further introducing uncertainty into the reliability of the results.
There were differences in the trial inclusion criteria specifically for the asciminib versus ponatinib comparison. Because the ASCEMBL trial enrolled patients who were already in CCyR at baseline and the PACE trial did not, the ASCEMBL population was adjusted to account for difference through the removal of patients that were in CCyR at baseline as well as patients who had missing CCyR data at baseline. The sponsor provided a scenario analysis with the removal of only patients who were in CCyR at baseline; however, this analysis was conducted on the full PACE population, including patients positive for the T315I mutation, which has been acknowledged as an important prognostic factor. No scenario analysis was provided for the third scenario that excluded the patients in CCyR at baseline as well as the patients with missing CCyR data provided they showed BCR-ABL1 ratio less than1%. Given the strength of the relationship between BCR-ABL1 ratio and CCyR, this was potentially a very informative scenario analysis that was not provided, further increasing the uncertainty of the MAIC results.
The ESS for most comparisons was very small, resulted in very wide CIs and precluding the ability to draw conclusions from the data. For the comparison of nilotinib specifically, the only available trial that included response data was a retrospective trial of 26 patients, of which only 6 received nilotinib while the other 20 received dasatinib, though the issue of small ESS is present in all comparisons. As such, there is very little that can be said regarding the comparative efficacy of asciminib versus the chosen comparators with regards to response. Reporting bias may have further impacted the results given that Giles et al. (2010) does report CCyR data at the 12-month time point according to the sponsor-submitted SLR. It is unclear why this data was not considered in the submitted MAIC. Given that MAIC methodology adjusts the index trial to be more similar to the comparator trials, consideration must be given to the external validity with the target population of the index trial for which the reimbursement request is based on. Additionally, there are various outcomes such as HRQoL, PFS, and OS that could not be analyzed despite being important to patients.
Other Relevant Evidence
This section includes 2 reports of 1 submitted phase I, multicentre, open-label study provided within the sponsor’s submission to CADTH that wase considered to supplement evidence included in the systematic review. The multi-arm, dose-finding phase I trial provides long-term evidence on the safety and tolerability of asciminib as well as some preliminary evidence of long-term efficacy of asciminib in patients with CML or Ph+ acute lymphoblastic leukemia, given as single drug or in combination with either nilotinib, imatinib, or dasatinib. Though it is a multi-arm trial, CADTH will only review patients with CP-CML without the T315I mutation who received asciminib as a single drug (40 mg twice daily and 80 mg daily dosages) for the purpose of this report.34
Sponsor-Submitted Phase I, Multicentre, Open-Label Study34,35
Description of Study
The primary objective of the study was to determine the maximum tolerated dose and/or recommended dose for expansion of asciminib as a single drug or in combination with other drugs. There were 5 arms; however, for the present review CADTH will only include patients with CP-CML without the T315I mutation who received asciminib as a single drug (40 mg twice daily and 80 mg once daily dosages). Patients needed an ECOG PS of 2 or greater to be enrolled.
Patients had to be adults with CP-CML and an ECOG PS of 2 or greater and had to be previously treated with 2 or more TKIs and have relapsed, been refractory to, or intolerant of TKIs to be enrolled in the study. Among the 317 enrolled patients, 115 patients with CP-CML without the T315I mutation were treated with asciminib as a single drug. Of these, 30 patients were treated with the 40 mg twice daily dosage and 17 were treated with the 80 mg once daily dosage. Patients were treated until progression or unacceptable toxicity. The median ages of patients taking 40 mg twice daily and 80 mg once daily were 53.0 (range = 27 to 75) and 59.0 (range = 30 to 86) years, respectively. Table 37 shows the baseline characteristics and Table 38 presents the patient disposition and exposure to study treatment for these patients. The study enrolled patients who received at least 2 prior TKIs. Full details of prior treatment with TKIs and BCR-ABL1 ratio (IS percentage) categories for patients with CP-CML without the T315I mutation treated with asciminib single drug are also shown in Table 37 along with the baseline characteristics.
Outcomes of interest to this review included MMR and AEs, SAEs, withdrawals due to AEs, mortality, and notable harms up to 30 days after the last dose of asciminib. The definition of MMR was the same as in the pivotal trial.
Table 37: Baseline Characteristics of Patients in Phase I Study for Single-Drug Asciminib in CP-CML Without the T315I Mutation at Screening (FAS)
Characteristic | Asciminib 40 mg b.i.d. N = 30 | Asciminib 80 mg q.d. N = 17 |
|---|---|---|
Age | ||
Mean (SD) | 51.8 (14.29) | 58.9 (14.02) |
Median (Range) | 53.0 (27 to 75) | 59.0 (30 to 86) |
< 65, n (%) | 24 (80.0) | 11 (64.7) |
≥ 65, n (%) | 6 (20.0) | 6 (35.3) |
Sex, n (%) | ||
Female | 13 (43.3) | 10 (58.8) |
Male | 17 (56.7) | 7 (41.2) |
Race, n (%) | ||
White | 23 (76.7) | 14 (82.4) |
Asian | 5 (16.7) | 2 (11.8) |
Black or African American | 2 (6.7) | 1 (5.9) |
Other | 0 | 0 |
Unknown | 0 | 0 |
Ethnicity, n (%) | ||
Hispanic or Latino | 0 | 1 (5.9) |
East Asian | 4 (13.3) | 1 (5.9) |
Southeast Asian | 1 (3.3) | 0 |
Other | 18 (60.0) | 8 (47.1) |
Not reported | 4 (13.3) | 5 (29.4) |
Unknown | 3 (10.0) | 2 (11.8) |
ECOG PS, n (%) | ||
0 | 20 (66.7) | 13 (76.5) |
1 | 8 (26.7) | 4 (23.5) |
2 | 2 (6.7) | 0 |
Number of prior TKIs, n (%) | ||
1 | 0 | 0 |
2 | 7 (23.3) | 1 (5.9) |
3 | 15 (50.0) | 7 (41.2) |
4 | 6 (20.0) | 8 (47.1) |
≥ 5 | 2 (6.7) | 1 (5.9) |
Individual prior TKIs, n (%) | ||
Bosutinib | 11 (36.7) | 8 (47.1) |
Dasatinib | 28 (93.3) | 17 (100) |
Imatinib | 19 (63.3) | 14 (82.4) |
Nilotinib | 24 (80.0) | 15 (88.2) |
Ponatinib | 9 (30.0) | 5 (29.4) |
Radotinib | 2 (6.7) | 1 (5.9) |
BCR-ABL1 ratio (% IS) categories, n (%) | ||
≤ 0.0032% | 0 | 0 |
> 0.0032% to ≤ 0.01% | 1 (3.3) | 0 |
> 0.01% to ≤ 0.1% | 4 (13.3) | 2 (11.8) |
> 0.1% to ≤ 1% | 6 (20.0) | 4 (23.5) |
> 1% to ≤ 10% | 6 (20.0) | 2 (11.8) |
> 10% | 13 (43.3) | 8 (47.1) |
Atypical, p190, unknown transcripts | 0 | 1 (5.9) |
b.i.d. = twice daily; CML = chronic myeloid leukemia CP = chronic phase; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FAS = full analysis set; q.d. = once daily; SD = standard deviation; TKI = tyrosine kinase inhibitor.
Source: CABL001X2101 Clinical Study Report.34
Table 38: Patient Disposition in Phase I Study for Single-Drug Asciminib in CP-CML Without the T315I Mutation at Screening (FAS)
Disposition | Asciminib 40 mg b.i.d. N = 30 | Asciminib 80 mg q.d. N = 17 |
|---|---|---|
Patients treated, n (%) | ||
Treatment ongoinga | 19 (63.3) | 12 (70.6) |
End of treatment | 11 (36.7) | 5 (29.4) |
Primary reason for end of treatment, n (%) | ||
Adverse event | 4 (13.3) | 2 (11.8) |
Death | 0 | 1 (5.9) |
Physician decision | 2 (6.7) | 2 (11.8) |
Progressive disease | 3 (10.0) | 0 |
Patient or guardian decision | 2 (6.7) | 0 |
b.i.d. = twice daily; CML = chronic myeloid leukemia CP = chronic phase; FAS = full analysis set; q.d. = once daily.
aPatients ongoing at the time of the cut-off April 2, 2020.
Source: CABL001X2101 Clinical Study Report.34
Results
Details of MMR by time point are shown in Table 40. In the 40 mg twice daily and 80 mg once daily groups, 60% and 50% patients achieved MMR, respectively. Clinically meaningful MMR rates were achieved by patients with CP-CML without the T315I mutation across all lines of therapy. The results were similar to those observed in the pivotal trial. An overview of AEs is presented in Table 49. All patients in the 40 mg twice daily (n = 30) and 80 mg once daily (n = 17) groups had AEs. SAEs were experienced among 11 (36.7%) and 8 (47.1%) patients taking 40 mg twice daily and 80 mg once daily dosages, respectively. AEs leading to dose adjustments or interruptions were observed among 14 (46.7%) and 10 (58.8%) patients taking 40 mg twice daily and 80 mg daily dosages, respectively.
Table 41 shows a summary of harms. The most common AEs observed in 40 mg twice daily dosage group were increased lipase (46.7%), fatigue (43.3%), abdominal pain (33.3%), diarrhea (30.0%), rash (30.0%), headache (26.7%), hypertension (26.7%), and arthralgia (26.7%). In 80 mg daily dosage group the most common AEs were upper respiratory tract infection (47.1%), fatigue (41.2%), headache (29.4%), hypertension (29.4%), and thrombocytopenia (29.4%). Four patients in each group (13.3% in the 40 mg twice daily dosage group and 23.5% in the 80 mg daily dosage group) stopped treatment due to AEs. Increase of lipase and amylase, pancreatitis and pancreatitis acute (1 each for asciminib 40 mg twice daily group), acute kidney injury, cardiac arrest, leukocytosis, and thrombocytosis (1 each for asciminib 80 mg daily group) were the 8 AEs for which patients stopped treatment. There was 1 death in the 80 mg daily dosage group due to cardiac arrest. Among the notable harms were myelosuppression (36.7% and 41.2%), pancreatic toxicity (53.3% and 29.4%), hepatotoxicity (including laboratory terms) (16.7% and 17.6%), gastrointestinal issues (70.0% and 52.9%), and cardiac failure (6.7% and 17.6%) for all grades in the asciminib 40 mg twice daily and 80 mg once daily groups, respectively.34
Table 39: Exposure to Study Treatment — Single-Drug Asciminib in CP-CML Without the T315I Mutation at Screening (SS)
Exposure | Asciminib 40 mg b.i.d. N = 30 | Asciminib 80 mg q.d. N = 17 |
|---|---|---|
Duration of exposure (weeks) | ||
Mean (SD) | 169.6 (97.06) | 158.0 (49.65) |
Duration of exposure categories, n (%) | ||
Less than 4 weeks | 1 (3.3) | 0 |
At least 4 weeks | 29 (96.7) | 17 (100) |
At least 8 weeks | 28 (93.3) | 17 (100) |
At least 12 weeks | 28 (93.3) | 17 (100) |
At least 24 weeks | 26 (86.7) | 16 (94.1) |
At least 48 weeks | 24 (80.0) | 16 (94.1) |
At least 96 weeks | 21 (70.0) | 16 (94.1) |
At least 144 weeks | 20 (66.7) | 12 (70.6) |
b.i.d. = twice daily; CML = chronic myeloid leukemia CP = chronic phase; q.d. = once daily; SD = standard deviation; SS = safety set.
Source: CABL001X2101 Clinical Study Report.34
Table 40: MMR by Time Point — Single-Drug Asciminib in CP-CML Without the T315I Mutation and Not in MMR at Screening, MMR Evaluable (FAS)
Response category | Asciminib 40 mg b.i.d. N = 25 | Asciminib 80 mg q.d. N = 14 |
|---|---|---|
Overall MMR | 15 (60.0) | 7 (50.0) |
MMR by week 24 | 4 (16.0) | 4 (28.6) |
MMR by week 48 | 6 (24.0) | 5 (35.7) |
MMR by week 72 | 8 (32.0) | 6 (42.9) |
MMR by week 96 | 11 (44.0) | 6 (42.9) |
b.i.d. = twice daily; CML = chronic myeloid leukemia CP = chronic phase; FAS = full analysis set; MMR = major molecular response; q.d. = once daily.
Source: CABL001X2101 Clinical Study Report.34
Harms | Asciminib 40 mg b.i.d. N = 30 | Asciminib 80 mg q.d. N = 17 |
|---|---|---|
Patients with ≥ 1 adverse event (all grades) | ||
n (%) | 30 (100) | 17 (100) |
Most common events,a n (%) | ||
Increased lipase | 14 (46.7) | 4 (23.5) |
Fatigue | 13 (43.3) | 7 (41.2) |
Abdominal pain | 10 (33.3) | 4 (23.5) |
Diarrhea | 9 (30.0) | 3 (17.6) |
Rash | 9 (30.0) | 3 (17.6) |
Headache | 8 (26.7) | 5 (29.4) |
Hypertension | 8 (26.7) | 5 (29.4) |
Arthralgia | 8 (26.7) | 4 (23.5) |
Vomiting | 7 (23.3) | 3 (17.6) |
Increased amylase | 7 (23.3) | 2 (11.8) |
Cough | 7 (23.3) | 2 (11.8) |
Nausea | 6 (20.0) | 4 (23.5) |
Pain in extremity | 6 (20.0) | 2 (11.8) |
Edema peripheral | 6 (20.0) | 1 (5.9) |
Anemia | 6 (20.0) | 3 (17.6) |
Increased weight | 6 (20.0) | 2 (11.8) |
Upper respiratory tract infection | 6 (20.0) | 8 (47.1) |
Thrombocytopenia | 5 (16.7) | 5 (29.4) |
Constipation | 5 (16.7) | 3 (17.6) |
Dizziness | 5 (16.7) | 4 (23.5) |
Back pain | 5 (16.7) | 3 (17.6) |
Bone pain | 5 (16.7) | 2 (11.8) |
Dyspnea | 5 (16.7) | 3 (17.6) |
Neutropenia | 4 (13.3) | 4 (23.5) |
Hypertriglyceridemia | 4 (13.3) | 3 (17.6) |
Nasopharyngitis | 4 (13.3) | 0 |
Myalgia | 4 (13.3) | 1 (5.9) |
Pruritus | 4 (13.3) | 2 (11.8) |
Abdominal pain upper | 3 (10.0) | 2 (11.8) |
Dry eye | 3 (10.0) | 1 (5.9) |
Hyperglycemia | 3 (10.0) | 2 (11.8) |
Hyperhidrosis | 1 (3.3) | 3 (17.6) |
Patients with ≥ 1 SAE (all grades) | ||
n (%) | 11 (36.7) | 8 (47.1) |
Most common events, n (%) | ||
Pneumonia | 2 (6.7) | 1 (5.9) |
Pleural effusion | 1 (3.3) | 0 |
Cardiac failure congestive | 1 (3.3) | 1 (5.9) |
Cataract | 1 (3.3) | 1 (5.9) |
Atrial fibrillation | 1 (3.3) | 0 |
Acute kidney injury | 0 | 1 (5.9) |
Bronchospasm | 1 (3.3) | 0 |
Pancreatitis acute | 1 (3.3) | 0 |
Hematuria | 0 | 1 (5.9) |
Patients who stopped treatment due to AEs | ||
n (%) | 4 (13.3) | 4 (23.5) |
Most common events, n (%) | ||
Increased lipase | 1 (3.3) | 0 |
Increased amylase | 1 (3.3) | 0 |
Acute kidney injury | 0 | 1 (5.9) |
Cardiac arrest | 0 | 1 (5.9) |
Leukocytosis | 0 | 1 (5.9) |
Pancreatitis | 1 (3.3) | 0 |
Pancreatitis acute | 1 (3.3) | 0 |
Thrombocytosis | 0 | 1 (5.9) |
Deaths | ||
n (%) | 0 | 1 (5.9) |
Cardiac arrest | 0 | 1 (5.9) |
Notable harms | ||
Myelosuppression,b n (%) | ||
All grades | 11 (36.7) | 7 (41.2) |
Grade ≥ 3 | 7 (23.3) | 3 (17.6) |
Pancreatic toxicity, n (%) | ||
All grades | 16 (53.3) | 5 (29.4) |
Grade ≥ 3 | 10 (33.3) | 3 (17.6) |
Hepatotoxicity (including laboratory terms), n (%) | ||
All grades | 5 (16.7) | 3 (17.6) |
Grade ≥ 3 | 0 | 1 (5.9) |
Gastrointestinal toxicity, n (%) | ||
All grades | 21 (70.0) | 9 (52.9) |
Grade ≥ 3 | 1 (3.3) | 1 (5.9) |
Cardiac failure, n (%) | ||
All grades | 2 (6.7) | 3 (17.6) |
Grade ≥ 3 | 1 (3.3) | 3 (17.6) |
AE = adverse event; b.i.d. = twice daily; q.d. = once daily; SAE = serious adverse event.
aReported in ≥ 10% in at least one group.
bMyelosuppression includes erythropenia, leucopenia, thrombocytopenia, and cytopenias affecting more than 1 lineage.
Source: CABL001X2101 Clinical Study Report.34
Critical Appraisal
There are several internal validity concerns that limit the certainty of conclusions that can be drawn. The primary concern is that there was no control group and no adjustment for known prognostic factors or effect modifiers; thus, causal conclusions cannot be established, and the findings are at high risk of confounding. Since the trial was open label, there is a risk that common subjective harms may have been overreported. Though the inclusion and exclusion criteria are clear, some details of the participant disposition are limited (i.e., number screened versus randomized). There was no hypothesis testing in the trial. The small sample size may negatively impact the reliability of the findings. The patients were not randomized, and there is a possibility of selection bias since it is not clear whether the patients were consecutively enrolled.
Despite some differences in setting (study sites were located in the US, Europe, Australia, Asia) than would be seen in clinical practice, the clinical experts consulted by CADTH did not express concern in generalizing the evidence to patients with CP-CML living in Canada.
Discussion
Summary of Available Evidence
The pivotal trial submitted for this review, ASCEMBL (N = 233), is a phase III, open-label, randomized study of asciminib compared to bosutinib in patients with CP-CML who had received 2 or more TKIs and experienced treatment failure on or intolerance to the most recent TKI. The primary objective of the ASCEMBL trial was to determine the efficacy of asciminib (80 mg daily) as compared to bosutinib (500 mg daily) in achieving MMR at the 24-week time point. The average age was 51 years, with 28% of patients in MCyR at baseline. Patients with the T315I and V299L mutations were excluded given the inactivity of bosutinib in that population.
The sponsor submitted a MAIC report aiming to demonstrate the efficacy of asciminib compared to relevant treatments for CP-CML following the use of 2 or more prior TKIs. The report compared IPD from the phase III ASCEMBL trial to published interventional and observational studies reporting efficacy outcomes for ponatinib, nilotinib, dasatinib, and omacetaxine. Note that omacetaxine was not a comparator of interest for the current review. To identify evidence for relevant comparators an SLR was conducted. In the absence of identified head-to-head trial evidence for relevant comparators or RCTs to form a connected network, an unanchored indirect comparison was justified as the only means by which to estimate relative treatment effects between asciminib and the identified relevant comparators. The MAICs evaluated MMR and CCyR at 6 and 12 months. The ponatinib single-arm phase II study PACE9 (N = 203), a nilotinib or dasatinib single-centre prospective cohort study10 (N = 26; 6 of which received nilotinib), and a dasatinib single-centre retrospective chart review11 (N = 24) were used for comparisons.
The sponsor submitted a phase I, multicentre, open-label study, which provided additional evidence for the long-term safety and efficacy of asciminib in patients with CP-CML without the T315I mutation. The primary objective was to determine the maximum tolerated dose and/or recommended dose for expansion of asciminib as a single drug or in combination with other drugs.
Interpretation of Results
Efficacy
In the pivotal trial ASCEMBL, the primary end point was MMR at 24 weeks. Patients receiving asciminib had an MMR rate of 25.48%, while patients receiving bosutinib had a 13.16% response rate. This corresponds to an unstratified difference in response rate of 12.32% (95% CI, 2.11% to 33.04%). In accordance with the statistical analysis plan, the primary end point was tested with patients stratified according to baseline MCyR to account for common risk difference. The stratified difference in response was 12.24% (95% CI, 2.19% to 22.30%) with a P value of 0.029. This represents a statistically significant improvement in MMR compared to bosutinib and was noted by the clinical experts to be a clinically meaningful response. The depth of response also favoured asciminib with patients who achieved MMR in general achieving a deeper response than patients who received bosutinib. Preplanned subgroup analyses across key groups were exploratory and conclusions could not be drawn from these data. Secondary end points such as HRQoL, duration of response, and time to response favoured asciminib but were not statistically tested. CCyR results were supportive of the MMR results, though the analysis was not adjusted for multiplicity and conclusions cannot be drawn. Furthermore, we are unable to draw conclusions from immature outcomes such as OS and PFS that are nonetheless important to patients.
While there were internal validity concerns with potential bias in favour of asciminib, namely the number of patients at baseline with missing stratification data, imbalance of patients within the MCyR category across treatment groups, number of prior TKIs, and reason for discontinuation of a prior TKI, it should be noted that multiple scenario analyses were presented to address most of the internal validity concerns. These scenario analyses were not adjusted for multiplicity so conclusions should be drawn with caution; however, they do suggest that the clinically significant benefit seen with asciminib is consistent across various scenarios.
Although the pivotal trial provided a head-to-head comparison against bosutinib, to determine relative efficacy compared to other relevant comparators, indirect comparisons by way of MAICs were submitted. The uncertainty in efficacy of asciminib versus these comparators is much higher relative to the head-to-head evidence against bosutinib. There were differences in study design and differences in inclusion criteria that lead to the removal of patients from the ASCEMBL index trial, potentially introducing bias as well as reducing the generalizability of the results. An uncertain method of selecting prognostic factors to adjust for and inability to match on all factors suggests that important characteristics between trials may have impacted results, while a very small ESS introduced further uncertainty into the results through very wide CIs. Asciminib was favoured with regards to response rates against ponatinib and a population that received nilotinib or dasatinib; however, there is very high uncertainty associated with these results given the small ESS, wide CIs, and between-study differences that could not be adjusted for.
Given the stated need from clinician groups and patient groups for additional treatment options in the third line and onward for patients with CMP-CP whose disease has become resistant or who have become intolerant to previous TKI therapies, particularly with respect to the varying safety profiles of the available therapies, asciminib appears to provide a more effective option compared to bosutinib. The efficacy of asciminib versus ponatinib, dasatinib, and nilotinib, the other relevant comparators in this setting, is unclear.
Harms
In the ASCEMBL trial, asciminib appeared to be more tolerable than bosutinib. A greater proportion of patients receiving bosutinib discontinued due to an AE (21.1%) than those receiving asciminib (5.8%). Thrombocytopenia was elevated with asciminib compared to bosutinib (22% versus 13%) and gastrointestinal toxicity and hepatotoxicity were less common with asciminib versus bosutinib. The longer-term safety results from the phase I trial were consistent with the reported harms in the ASCEMBL trial. The heterogeneity in safety profiles among the TKIs used in this disease space highlight the need for options, given that certain patients may be intolerant to certain TKIs or contraindicated based on risk factors. However, there is no comparative safety evidence for asciminib against comparators other than bosutinib. The clinical experts consulted for this review felt the safety profile of asciminib in patients with CP-CML is acceptable and could be managed with appropriate supportive care, and this aligned with the perspectives of patients gathered from patient groups, which felt the side effects of asciminib were manageable and worth the potential benefit.
Conclusions
The ASCEMBL trial showed a statistically significant benefit with asciminib 80 mg daily over bosutinib 500 mg daily in MMR at 24 weeks in patients who had received 2 or more TKIs and experienced treatment failure or intolerance to the most recent TKI. In the opinion of the clinical experts consulted by CADTH, the MMR rate at 24 weeks represents a clinically significant benefit for asciminib over bosutinib. Secondary end points, such as HRQoL, duration of response, and time to response, favoured asciminib but were not statistically tested; therefore, few conclusions can be drawn. CCyR results were supportive of the MMR results, though the analysis was not adjusted for multiplicity. Data on OS and PFS were immature at the time of analysis. The submitted MAIC provided indirect evidence for relative efficacy for asciminib compared to ponatinib, dasatinib, and nilotinib, but the significant limitations with the analysis prohibit any conclusions from being drawn. Asciminib appears to be more tolerable than bosutinib, though comparative safety evidence against other relevant comparators is lacking.
References
1.Perrotti D, Jamieson C, Goldman J, Skorski T. Chronic myeloid leukemia: mechanisms of blastic transformation. J Clin Invest. 2010;120(7):2254-2264. PubMed
2.Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2018 update on diagnosis, therapy and monitoring. Am J Hematol. 2018;93(3):442-459. PubMed
3.Table 13-10-0751-01. Number of prevalent cases and prevalence proportions of primary cancer by prevalence duration, cancer type, attained group and sex. Ottawa (ON): Statistics Canada; 2021: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310075101&pickMembers%5B0%5D=2.1&pickMembers%5B1%5D=3.1&pickMembers%5B2%5D=4.53&pickMembers%5B3%5D=5.1&cubeTimeFrame.startYear=2011&cubeTimeFrame.endYear=2015&referencePeriods=20110101%2C20150101. Accessed 2022 Mar 24.
4.Faderl S, Talpaz M, Estrov Z, Kantarjian HM. Chronic myelogenous leukemia: biology and therapy. Ann Intern Med. 1999;131(3):207-219. PubMed
5.Höglund M, Sandin F, Hellström K, et al. Tyrosine kinase inhibitor usage, treatment outcome, and prognostic scores in CML: report from the population-based Swedish CML registry. Blood. 2013;122(7):1284-1292. PubMed
6.Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34(4):966-984. PubMed
7.Hochhaus A, Breccia M, Saglio G, et al. Expert opinion-management of chronic myeloid leukemia after resistance to second-generation tyrosine kinase inhibitors. Leukemia. 2020;34(6):1495-1502. PubMed
8.Clinical Study Report: CABL001A2301. A phase III, multi-center, open-label, randomized study of oral ABL001 (asciminib) versus bosutinib in patients with chronic myelogenous leukemia in chronic phase (CML-CP), previously treated with 2 or more tyrosine kinase inhibitors [internal sponsor's report]. 2021.
9.Cortes JE, Kim DW, Pinilla-Ibarz J, et al. Ponatinib efficacy and safety in Philadelphia chromosome-positive leukemia: final 5-year results of the phase 2 PACE trial. Blood. 2018;132(4):393-404. PubMed
10.Ibrahim AR, Paliompeis C, Bua M, et al. Efficacy of tyrosine kinase inhibitors (TKIs) as third-line therapy in patients with chronic myeloid leukemia in chronic phase who have failed 2 prior lines of TKI therapy. Blood. 2010;116(25):5497-5500. PubMed
11.Tan J, Xue M, Pan J, et al. Responses to dasatinib as a second- and third-line tyrosine kinase inhibitor in chronic phase chronic myeloid leukaemia patients. Acta Haematol. 2019;142(2):79-86. PubMed
12.Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. PubMed
13.Key statistics for chronic myeloid leukemia. Atlanta (GA): American Cancer Society; 2021: https://www.cancer.org/content/dam/CRC/PDF/Public/8684.00.pdf. Accessed 2022 Apr 14.
14.Kiladjian JJ, Mesa RA, Hoffman R. The renaissance of interferon therapy for the treatment of myeloid malignancies. Blood. 2011;117(18):4706-4715. PubMed
15.Hochhaus A, O'Brien SG, Guilhot F, et al. Six-year follow-up of patients receiving imatinib for the first-line treatment of chronic myeloid leukemia. Leukemia. 2009;23(6):1054-1061. PubMed
16.Scemblix (asciminib) tablets, for oral use: prescribing information. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2021: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/215358s000Orig2lbl.pdf. Accessed 2022 Mar 29.
17.PrScemblix® (asciminib): 20 mg and 40 mg, oral tablets [product monograph]. 2021 Jul 22.
18.PrBosulif® (bosutinib): 100 mg, 400 mg, 500 mg, oral tablets [product monograph]. Kirkland (QC): Pfizer Canada; 2021.
19.PrTasinga® (nilotinib): 150 mg, 200 mg, oral capsules [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada; 2015.
20.PrSprycel® (dasatinib): 20 mg, 50 mg, 70 mg, 80 mg, 100 mg, 140 mg, oral tablets [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2021.
21.PrIclusig® (ponatinib): 15 mg, 45 mg, oral tablets [product monograph]. Saint-Laurent (QC): ARIAD Pharmaceuticals; 2019.
22.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
23.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Feb 4.
24.Center for Drug Evaluation Research. Multi-discipline review. Scemblix (asciminib) oral tablets. Company: Novartis. Application No.: 215358. Approval dae: 10/292021 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2020: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2021/215358Orig1s000,Orig2s000MultidisciplineR.pdf. Accessed 2022 Apr 14.
25.Rea D, Mauro MJ, Boquimpani C, et al. A phase 3, open-label, randomized study of asciminib, a STAMP inhibitor, vs bosutinib in CML after 2 or more prior TKIs. Blood. 2021;138(21):2031-2041. PubMed
26.Baccarani M, Deininger MW, Rosti G, et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood. 2013;122(6):872-884. PubMed
27.Deininger MW, Shah NP, Altman JK, et al. Chronic Myeloid Leukemia, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2020;18(10):1385-1415. PubMed
28.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
29.EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
30.Cleeland CS, Mendoza TR, Wang XS, et al. Assessing symptom distress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer. 2000;89(7):1634-1646. PubMed
31.Compare time to treatment discontinuation (TTD) and responses for asciminib vs ponatinib, nilotinib, dasatinib and omacetaxine through MAIC for CML CP patients who were treated with 2 or more TKIs [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Scemblix (asciminib) 20 mg and 40 mg oral tablets. Dorval (QC): Novartis Pharmaceuticals Canada; 2022 Jan 19.
32.Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. PubMed
33.Wells G, Shea B, O'Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa (ON): Ottawa Hospital; 2000: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 2022 Apr 15.
34.Clinical Study Report: A phase I, multicenter, open-label study of oral ABL001 in patients with chronic myelogenous leukemia or Philadelphia Chromosome-positive acute lymphoblastic leukemia [internal sponsor's report]. 2021.
35.Hughes TP, Mauro MJ, Cortes JE, et al. Asciminib in chronic myeloid leukemia after ABL kinase inhibitor failure. N Engl J Med. 2019;381(24):2315-2326. PubMed
36.Williams LA, Garcia Gonzalez AG, Ault P, et al. Measuring the symptom burden associated with the treatment of chronic myeloid leukemia. Blood. 2013;122(5):641-647. PubMed
37.Yu H, Zeng X, Sui M, et al. A head-to-head comparison of measurement properties of the EQ-5D-3L and EQ-5D-5L in acute myeloid leukemia patients. Qual Life Res. 2021;30(3):855-866. PubMed
38.Nunnally JC, Bernstein IH. Psychometric theory. New York (NY): McGraw-Hill; 1994.
39.Harman HH. Modern factor analysis. Chicago (IL): University of Chicago Press; 1967.
40.Sinnott PL, Joyce VR, Barnett PG. Guidebook: preference measurement in economic analysis. Menlo Park (CA): Health Economics Research Center; 2007: https://www.herc.research.va.gov/files/BOOK_419.pdf. Accessed 2022 Mar 31.
41.Yu CL, Fielding R, Chan CL, et al. Measuring quality of life of Chinese cancer patients: a validation of the Chinese version of the Functional Assessment of Cancer Therapy-General (FACT-G) scale. Cancer. 2000;88(7):1715-1727. PubMed
42.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. PubMed
43.Rajmil L. Health measurement scales. A practical guide to their development and use, 3rd ed. J Epidemiol Community Health. 2005;59(3):250-251.
44.Cohen J. Statistical power analysis for the behavioral sciences. Abingdon (UK): Routledge; 2013.
45.Yfantopoulos JN, Chantzaras AE. Validation and comparison of the psychometric properties of the EQ-5D-3L and EQ-5D-5L instruments in Greece. Eur J Health Econ. 2017;18(4):519-531. PubMed
46.Janssen MF, Bonsel GJ, Luo N. Is EQ-5D-5L better than EQ-5D-3L? A head-to-head comparison of descriptive systems and value sets from seven countries. Pharmacoeconomics. 2018;36(6):675-697. PubMed
47.Vickrey BG, Hays RD, Genovese BJ, Myers LW, Ellison GW. Comparison of a generic to disease-targeted health-related quality-of-life measures for multiple sclerosis. J Clin Epidemiol. 1997;50(5):557-569. PubMed
48.Petrou S, Morrell J, Spiby H. Assessing the empirical validity of alternative multi-attribute utility measures in the maternity context. Health Qual LIfe Outcomes. 2009;7(1):40. PubMed
49.Petrou S, Hockley C. An investigation into the empirical validity of the EQ-5D and SF-6D based on hypothetical preferences in a general population. Health Econ. 2005;14(11):1169-1189. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: February 17, 2022
Alerts: Biweekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits: Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(asciminib* or Scemblix* or ABL001* or ABL-001* or L1F3R18W77 or C5U34S9XFV).ti,ab,ot,kf,hw,nm,rn.
1 use medall
*asciminib/
(asciminib* or Scemblix* or ABL001* or ABL-001*).ti,ab,kf,dq.
3 or 4
5 use oemezd
6 not (conference abstract or conference review).pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
Search -- Studies with results | asciminib
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
Search terms -- asciminib
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search terms -- asciminib
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Search terms – asciminib
Grey Literature
Search dates: Feb 7 to 11, 2022
Keywords: Scemblix, asciminib, chronic myeloid leukemia
Limits: none
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Study | Reason |
|---|---|
Mauro MJ, Minami Y, Réa D, et al., Efficacy and safety results from ASCEMBL, a multicenter, open-label, phase 3 study of asciminib, a first-in-class STAMP inhibitor, vs bosutinib in patients with chronic myeloid leukemia in chronic phase after ≥ 2 prior tyrosine kinase inhibitors: update after 48 weeks. Presented at the 2021 American Society of Hematology (ASH) Annual Meeting, December 11 to 14, 2021. | Publication type |
Hochhaus, A, Boquimpani, B, Rea, D, et al., Efficacy and safety results from ASCEMBL, a multicenter, open-label, phase 3 study of asciminib, a first-in-class STAMP inhibitor, vs bosutinib in patients with chronic myeloid leukemia in chronic phase previously treated with ≥ 2 tyrosine kinase inhibitors. Presented at the 2020 American Society of Hematology (ASH) September 2020. Annual Meeting (Virtual), December 5 to 8, 2020. | Publication type |
Mauro, MJ, Hochhaus, A, Boquimpani, C, et al., A multicenter, randomized, phase3 study of asciminib (ABL001) vs bosutinib in patients with chronic myeloid leukemia in chronic phase previously treated with ≥ 2 tyrosine kinase inhibitors. Presented at the 7th Annual Meeting of the Society of Hematologic Oncology (SOHO), Houston, TX, September 11 to 14, 2019. | Publication type |
Hughes TP, Mauro MJ, Cortes JE, et al. Asciminib in chronic myeloid leukemia after ABL kinase inhibitor failure. N Engl J Med 2019;381:2315 to 26. | Study design |
Clinical Study Report: A phase I, multicenter, open-label study of oral ABL001 in patients with chronic myelogenous leukemia or Philadelphia Chromosome-positive acute lymphoblastic leukemia [internal sponsor's report]. Novartis; 2021. | Study design |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Primary End Point Sensitivity Analyses
Table 44: MMR Rate at 24 Weeks, Excluding Patients With T315I or V299L Mutations at Week 1, Day 1 — FAS
Outcome | ASCEMBL Primary Analysis | |
|---|---|---|
Asciminib N = 154 | Bosutinib N = 74 | |
Response, n (%) | 40 (25.97) | 10 (13.51) |
95% CI for responsea | (19.25, 33.65) | (6.68, 23.45) |
Unstratified difference in response rate (vs. bosutinib), % | 12.46 | Reference |
95% CI for differenceb | (2.04, 22.88) | Reference |
Common risk differencec, % | 12.43 | Reference |
95% CI for difference | (2.15, 22.71) | Reference |
P valued | 0.030 | Reference |
CI = confidence interval; MMR = major molecular response.
aClopper-Pearson 95% 2-sided CI.
bWald 95% 2-sided CI.
cThe common risk difference after adjusting for stratum: baseline major cytogenetic response status (based on randomization data) and its 95% CI were estimated using the Mantel-Haenszel method.
dCochrane-Mantel-Haenszel 2-sided test was stratified by baseline major cytogenetic response status (based on randomization data).Analysis was not adjusted for multiplicity
Source: Asciminib Clinical Study Report.8
Table 45: MMR Rate at 24 Weeks Stratified According to MCyR as Recorded in the CRF — FAS
Outcome | ASCEMBL Primary Analysis | |
|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | |
Response, n (%) | 40 (25.48) | 10 (13.16) |
95% CI for responsea | (18.87, 33.04) | (6.49, 22.87) |
Unstratified difference in response rate (vs. bosutinib), % | 12.32 | Reference |
95% CI for differenceb | (2.11, 22.53) | Reference |
Common risk differencec, % | 11.54 | Reference |
95% CI for difference | (1.73, 21.34) | Reference |
P valued | 0.037 | Reference |
CI = confidence interval; CRF = case report form; MMR = major molecular response.
aClopper-Pearson 95% 2-sided CI.
bWald 95% 2-sided CI.
cThe common risk difference after adjusting for stratum: baseline major cytogenetic response status (based on CRF data) and its 95% CI were estimated using the Mantel-Haenszel method.
dCochrane-Mantel-Haenszel 2-sided test was stratified by baseline major cytogenetic response status (based on CRF data).Analysis was not adjusted for multiplicity
Source: Asciminib Clinical Study Report.8
Table 46: MMR Rate at 24 Weeks Without Imputation Rule for Missing PCR Evaluations — FAS
Outcome | ASCEMBL Primary Analysis | |
|---|---|---|
Asciminib N = 157 | Bosutinib N = 76 | |
Response, n (%) | 40 (25.48) | 10 (13.16) |
95% CI for responsea | (18.87, 33.04) | (6.49, 22.87) |
Unstratified difference in response rate (vs. bosutinib), % | 12.32 | Reference |
95% CI for differenceb | (2.11, 22.53) | Reference |
Common risk differencec, % | 12.24 | Reference |
95% CI for difference | (2.19, 22.30) | Reference |
P valued | 0.029 | Reference |
CI = confidence interval; MMR = major molecular response.
aClopper-Pearson 95% 2-sided CI.
bWald 95% 2-sided CI.
cThe common risk difference after adjusting for stratum: baseline major cytogenetic response status (based on randomization data) and its 95% CI were estimated using the Mantel-Haenszel method.
dCochrane-Mantel-Haenszel 2-sided test was stratified by baseline major cytogenetic response status (based on randomization data). Analysis was not adjusted for multiplicity
Source: Asciminib Clinical Study Report.8
Asciminib Switch Analysis Set Safety
Table 47: Exposure to Study Treatment — Switch Analysis Set
Exposure | Bosutinib to Asciminib N = 22 |
|---|---|
Duration of exposure (weeks) | |
Mean (SD) | 24.1 (15.97) |
Median (Min, Max) | 20.9 (1, 57) |
Duration of exposure categories, n (%) | |
Less than 24 weeks | 12 (54.5) |
At least 24 weeks | 10 (45.5) |
At least 48 weeks | 3 (13.6) |
Patient treatment time (years) | 10.2 |
Average daily dose (mg) | |
Mean (SD) | 74.9 (8.91) |
Median (Min, Max) | 80.0 (57, 80) |
Relative dose intensity, % | |
Mean (SD) | 86.9 (21.22) |
Median (Min, Max) | 100.0 (34, 100) |
SD = standard deviation.
Note: The switch analysis set was a subset of the full analysis set and included patients from the bosutinib treatment group that received asciminib following discontinuation of bosutinib.
Source: Asciminib Clinical Study Report.8
Table 48: Summary of Harms — Switch Analysis Set
Harms | Bosutinib to Asciminib N = 22 |
|---|---|
Patients with ≥ 1 adverse event | |
n (%) | 13 (59.1) |
Most common eventsa, n (%) | |
Thrombocytopenia | 8 (36.4) |
Neutropenia | 8 (36.4) |
Alopecia | 2 (9.1) |
Nausea | 2 (9.1) |
Patients with ≥ 1 SAE | |
n (%) | 1 (4.5) |
Most common events, n (%) | |
AML (Ph-negative) | 1 (4.5) |
Patients who stopped treatment due to adverse events | |
n (%) | 2 (9.1) |
Most common events, n (%) | |
Thrombocytopenia | 1 (4.5) |
AML (Ph-negative) | 1 (4.5) |
Deaths | |
n (%) | 0 |
Notable harms | |
Myelosuppression, n (%) | 9 (40.9) |
Hepatotoxicity, n (%) | 1 (4.5) |
Gastrointestinal toxicity, n (%) | 2 (9.1) |
AML = acute myeloid leukemia; Ph = Philadelphia chromosome; SAE = serious adverse event.
aFrequency > 5%
Note: The switch analysis set was a subset of the full analysis set and included patients from the bosutinib treatment group that received asciminib following discontinuation of bosutinib.
Source: Asciminib Clinical Study Report.8
Indirect Measures of HRQoL
MDASI-CML
Between-treatment differences for the change in severity and interference scores for asciminib versus bosutinib evaluated using a linear mixed effect model was −0.65 (95% CI, −1.01, −0.29) and −0.16 (95% CI, −0.67, 0.36), respectively.
Table 49: MDASI-CML Over Time — FAS
Outcomes measure | Asciminib (N = 157) | Bosutinib (N = 76) | ||||||
|---|---|---|---|---|---|---|---|---|
Scorea | Change from baseline | Scorea | Change from baseline | |||||
n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |
Total Severity | ||||||||
Baseline | 151 | 2.0 (1.77) | 70 | 1.9 (1.71) | ||||
Week 12 | 126 | 1.6 (1.67) | 124 | —0.5 (1.33) | 55 | 1.6 (1.79) | 52 | —0.0 (1.33) |
Week 24 | 108 | 1.5 (1.66) | 106 | —0.6 (1.53) | 41 | 1.9 (2.08) | 39 | —0.0 (1.48) |
Week 48 | 60 | 1.4 (1.33) | 59 | —0.7 (1.51) | 12 | 1.8 (2.38) | 12 | 0.1 (1.26) |
Total Interference | ||||||||
Baseline | 151 | 2.2 (2.58) | 70 | 2.5 (2.70) | ||||
Week 12 | 126 | 1.8 (2.37) | 124 | —0.5 (1.96) | 55 | 1.9 (2.26) | 52 | —0.5 (2.25) |
Week 24 | 108 | 1.6 (2.28) | 106 | —0.6 (2.06) | 41 | 2.2 (2.60) | 39 | —0.7 (2.08) |
Week 48 | 60 | 1.8 (2.10) | 59 | —0.4 (2.65) | 12 | 1.9 (2.76) | 12 | —0.5 (1.05) |
MDASI-CML = MD Anderson Symptom Inventory – Chronic Myeloid Leukemia; SD = standard deviation.
Source: Asciminib Clinical Study Report.8
Table 50: Distribution of PGIC CML Symptoms Over Time — FAS
Outcome | Asciminib N = 157 | Bosutinib N = 76 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Level 1 | Level 2 | Level 3 | Level 4 | Level 5 | Level 6 | Level 7 | Missing | Level 1 | Level 2 | Level 3 | Level 4 | Level 5 | Level 6 | Level 7 | Missing | |
Week 4, n (%) | 13 (8.6) | 38 (25.0) | 23 (15.1) | 46 (30.3) | 6 (3.9) | 3 (2.0) | 0 | 23 (15.1) | 3 (4.2) | 12 (16.7) | 12 (16.7) | 30 (41.7) | 4 (5.6) | 2 (2.8) | 1 (1.4) | 8 (11.1) |
Week 12, n (%) | 16 (11.2) | 49 (34.3) | 25 (17.5) | 31 (21.7) | 3 (2.1) | 1 (0.7) | 0 | 18 (12.6) | 9 (13.8) | 9 (13.8) | 13 (20.0) | 21 (32.3) | 1 (1.5) | 1 (1.5) | 0 | 11 (16.9) |
Week 24, n (%) | 22 (16.9) | 42 (32.3) | 11 (8.5) | 26 (20.0) | 5 (3.8) | 1 (0.8) | 0 | 23 (17.7) | 4 (8.0) | 9 (18.0) | 8 (16.0) | 17 (34.0) | 3 (6.0) | 0 | 0 | 9 (18.0) |
Week 48, n (%) | 19 (27.1) | 31 (44.3) | 1 (1.4) | 8 (11.4) | 1 (1.4) | 0 | 0 | 10 (14.3) | 6 (46.2) | 2 15.4) | 1 (7.7) | 3 (23.1) | 0 | 0 | 0 | 1 (7.7) |
Source: Asciminib Clinical Study Report.8
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
M. D. Anderson Symptom Inventory – Chronic Myeloid Leukemia (MDASI-CML)
EQ-5D-5L
No relevant studies were found for the Patient’s Global Impression of Change for patients with CML.
Findings
Table 51: Summary of Outcome Measures and Their Measurement Properties
Outcome Measure | Type | Conclusions about Measurement Properties | MID |
|---|---|---|---|
M. D. Anderson Symptom Inventory – Chronic Myeloid Leukemia (MDASI-CML)36 | A 26-item self-administered questionnaire suitable for adult CML patients36 | Validity: Content validity was established by patient input into item generation and selection and confirmed by cognitive debriefing. For patients with CML, the developers reported Spearman correlations between symptom and interference scores, and HRQoL scores between −0.269 and −0.436 (P < 0.01), demonstrating concurrent validity. The developers reported moderate to large effect size differences between imatinib and 2 other TKIs (nilotinib and dasatinib) for some mean individual symptom scores and the mean score for the CML-specific symptom subscale, demonstrating known-group validity. Moderate effect sizes were also reported for distress, vomiting, and headache between nilotinib and dasatinib. The developers reported that principal axis factoring for construct validity showed an acceptable fit with a 3-factor solution with a smaller SD of the residuals (0.045) than the reciprocal of the square root of the sample size (0.081).36 Reliability: The developers reported that all symptom and interference scales and subscales showed good internal consistency (Alpha > 0.7) with values ranging from 0.80 to 0.95. The intraclass correlations showed good test-retest reliability with values ≥ 0.89 for all symptom and interference scales and subscales administered 2 weeks apart.36 Responsiveness: No relevant studies found | No relevant studies found for patients with CML. |
Patient-reported, generic quality of life instrument | Validity: No relevant studies were found for patients with CML. Among patients with acute myeloid leukemia (AML), moderate to strong correlations were found based on Spearman’s rank correlation coefficient between similar dimensions of EQ-5D-5L and the subscales of FACT-G: between all dimensions and physical well-being (r = − 0.39 to − 0.55); between all dimensions and functional well-being (r = − 0.43 to − 0.56); between ‘anxiety/depression’ and emotional well-being (r = − 0.56), assessing convergent validity. The AUROC value ranged from 0.81 to 0.94 demonstrating a good distinction between all dichotomous configurations.37 Reliability: No relevant studies were found for patients with CML. Among patients with AML, the test-retest reliability (for responses provided 2 to 3 days apart) based on the weighted kappa coefficient ranged from 0.69 to 0.79, indicating substantial agreement. The ICCs for the total index score was 0.89, indicating goodreproducibility.37 Responsiveness: No relevant studies found. | No relevant studies found for patients with CML. |
AML = Acute Myeloid Leukemia; AUROC = area under the receiver operating characteristics curve; CML = Chronic Myeloid Leukemia; ECOG-PS = Eastern Cooperative Oncology Group performance status; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30; EQ VAS = EuroQol Visual Analogue Scale; ES = effect size; FACT-G = Functional Assessment of Cancer Therapy-General; MDASI = MD Anderson Symptom Inventory; MID = minimal important difference; SD = standard deviation; TKI = Tyrosine kinase inhibitors.
M. D. Anderson Symptom Inventory – Chronic Myeloid Leukemia (MDASI-CML)
Description
The MD Anderson Symptom Inventory (MDASI) is a brief measure used to assess the severity and impact of cancer-related symptoms and its treatment. The MD Anderson Symptom Inventory – Chronic Myeloid Leukemia (MDASI-CML) is a modified 26 item self-administered questionnaire suitable for adult patients with CML.30
Scoring
Twenty of the items in the MDASI-CML measure the severity of disease-related symptoms and are scored from 0 (not present) to 10 (as bad as you can imagine), whereas 6 items measure symptom interference with daily life scored from 0 (did not interfere) to 10 (interfered completely). The MDASI is used to evaluate both the severity of cancer-related symptoms and the level of symptom interference with functioning in patients.30
Psychometric Properties
Reliability
Williams et al. (2013) conducted a study using 3 cohorts of patients or content experts to develop and validate the MDASI-CML for patients with CML.36 Cohort 1 was a group of English-speaking Ph+ CML patients of at least 18 years of age (n = 35) and who were under treatment in the Leukemia Center at MD Anderson Cancer Center in the US during November to December 2009. Cohort 2 were a panel of content experts (n = 15) containing physicians, nurses, CML patients, and family caregivers. Cohort 3 was a group of English-speaking CML patients aged 18 years and older (n = 152) not receiving active treatment for another malignancy who were seen in the MD Anderson’s Leukemia Center. Cohort 1 was used to generate a list of potential symptom items; cohort 2 was used to reduce the list to the most relevant symptom items; and cohort 3 was used to evaluate the validity and reliability of the refined and final MDASI-CML.
Internal consistency reliability for each of 3 MDASI-CML subscales was calculated using Cronbach’s Alpha value – the core subscale containing 13 core MDASI symptom items, the CML-specific subscale containing 7 CML-specific symptom items, and lastly the interference subscale containing 6 interference items. All MDASI-CML symptom and interference scales and subscales showed good internal consistency (Alpha > 0.7)38 with values ranging from 0.80 to 0.95. Test-retest reliability was calculated using intraclass correlations for the 3 MDASI-CML subscales assessed from cohort 3 administered 2 weeks apart. The intraclass correlation values showed good test-retest reliability with values ≥ 0.89 for all MDASI-CML symptom and interference scales and subscales administered 2 weeks apart.36
Validity
Williams et al. (2013) established the validity of the MDASI-CML. Content validity of the MDASI-CML was established by using patient input into item generation and selection.36 Results of cognitive debriefing during the final validation confirmed the evidence of content validity. Concurrent validity was evaluated using Spearman correlations of mean MDASI-CML symptoms, interference scores and mean HRQoL scores for the same patients. For this study, Spearman correlations were between −0.269 and −0.436 (P < 0.01), demonstrating concurrent validity.
Known-group validity was evaluated by testing the MDASI-CML’s sensitivity to different TKIs. The magnitude of differences in the symptom severity scores reported by CML patients were established using effect sizes (ESs). Differences in symptom scores between different TKI treatment groups (imatinib, nilotinib, dasatinib) were found nonsignificant. Some moderate to large ES differences between imatinib and each of the other 2 TKIs (nilotinib and dasatinib) were found for some mean individual symptom scores and the mean score for the CML-specific symptom subscale, suggesting known-group validity. The moderate effects were observed particularly from the reference in mean severity of headache (1.19 vs 0.56, ES = 0.48), distress (1.86 vs 1.03, ES = 0.45), and vomiting (0.50 vs 0.09, ES = 0.45) between nilotinib and dasatinib, respectively.
Construct validity was examined using factor analysis with direct oblimin rotation. A 3-factor solution for the MDASI-CML symptom items was observed from the principal axis factoring, instead of the hypothesized 2-factor structure (a general severity factor and a CML-specific factor) in this study. A generalized symptom factor, an organ-specific symptom factor, and a gastrointestinal symptom factor were the 3-factor solution found from the analysis. The adequacy of these 3-factor solution was tested using Harman criteria.39 An acceptable fit with the 3-factor solution was established from the results, where a smaller SD of the residuals (0.045) was found than the reciprocal of the square root of the sample size (0.081).36
Responsiveness
There were not relevant studies reporting on the responsiveness of the MDASI-CML among patients with CML.
MID
There were no relevant studies reporting the MID among patients with CML.
EQ-5D-5L
Description
The EQ-5D-5L is a generic HRQoL instrument that may be applied to a wide range of health conditions and treatments.28,29 The first of 2 parts of the EQ-5D-5L is a descriptive system that classifies respondents (aged ≥ 12 years) based on the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D-5L has 5 possible levels for each domain representing ‘no problems’, ‘slight problems’, ‘moderate problems’, ‘severe problems’, and ‘extreme problems’. Respondents are asked to choose the level that reflects their health state for each of the 5 dimensions, corresponding to 3,125 different health states.
Scoring
A scoring function can be used to assign a value (EQ-5D-5L index score) to self-reported health states from a set of population-based preference weights.28,29 The second part is a 20 cm visual analogue scale (EQ-VAS) that has end points labelled 0 and 100, with respective anchors of ‘worst imaginable health state’ and ‘best imaginable health state’. Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ-VAS which best represents their health on that day. Hence, the EQ-5D-5L produces 3 types of data for each respondent:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor (e.g., 11121, 33211),
A population preference-weighted health index score based on the descriptive system,
A self-reported assessment of health status based on the EQ-VAS.
The EQ-5D-5L index score is generated by applying a multi-attribute utility function to the descriptive system. Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK).40
Psychometric Properties
No relevant studies on the psychometric properties of the EQ-5D-5L were found for patients with CML.
Reliability
Among 168 acute myeloid leukemia (AML) patients in China, test-retest reliability (for responses provided 2 to 3 days apart) of the EQ-5D-5L was calculated in 2 ways in 1 study41– using intraclass correlation coefficient (ICC) for the index scores and using the weighted Cohen’s Kappa coefficient for the 5-dimensional responses. The strength of agreement for the Kappa values were based on the guidelines of Landis and Koch.42 The weighted kappa coefficient ranged from 0.69 to 0.79, indicating substantial agreement. The ICC was 0.89, indicating good (≥ 0.70) reproducibility.43
Validity
Among 168 patients with AML, convergent validity was assessed in 1 study by comparing with FACT-G, which is a widely used and validated instrument for assessing HRQoL in cancer patients, including leukemia patients.41 The strength of association between dimensions of EQ-5D-5L and subscales of FACT-G was tested using Spearman’s rank correlation coefficient.44 Moderate to strong correlations were found between similar dimensions of the EQ-5D-5L and the subscales of FACT-G: correlation between all dimensions and physical well-being (r = − 0.39 to − 0.55); correlation between all dimensions and functional well-being (r = − 0.43 to − 0.56); ‘anxiety/depression’ and emotional well-being (r = − 0.56).
Known-groups validity was also evaluated using ECOG status, self-reported health status, number of complications, risk category, depression, anxiety, and levels of social support. The expectation was to observe a higher EQ-5D-5L index score for patients with lower ECOG PS, lower risk category, less anxiety and milder depression, higher self-reported health status and social support, and no complication. The linear trend in ordered alternative variables with 3 or more groups was assessed using the Jonckheere trend test.45 Moreover, the differences between 2 independent groups were evaluated using non-parametric Mann–Whitney test. The relative efficiency of instruments measuring patient-reported outcome was evaluated using analysis of variance (ANOVA),46,47 where a higher F statistic value implies a higher relative efficiency. The discriminatory ability was also assessed using the area under the receiver operating characteristics curve (AUROC),46 where AUROC scores of 1.0 and 0.5 were considered as the perfect and no discrimination of utility measure, respectively.45,48,49 In this analysis, self-reported health status, ECOG status, and risk category were dichotomized in all possible ways. The AUROC value ranged from 0.81 to 0.94, demonstrating a good distinction between all dichotomous configurations.
Responsiveness
There were no relevant studies reporting on responsiveness among patients with CML.
MID
There were no relevant studies reporting the MID among patients with CML.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
Allo-SCT
allogeneic stem cell transplant
AP
accelerated phase
BIA
budget impact analysis
BC
blast crisis
CML
chronic myeloid leukemia
CP
chronic phase
ICER
incremental cost-effectiveness ratio
KM
Kaplan-Meier
LY
life-year
MAIC
matched-adjusted indirect treatment comparison
MMR
major molecular response
OS
overall survival
PFS
progression-free survival
Ph+
Philadelphia chromosome positive
RDI
relative dose intensity
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
TKI
tyrosine kinase inhibitor
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Asciminib (Scemblix), oral tablets |
Submitted price | Asciminib 40 mg: $85.00 per tablet Asciminib 20 mg: $63.00 per tablet |
Indication | Proposed: For the treatment of adult patients with Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase previously treated with 2 or more tyrosine kinase inhibitors. |
Health Canada approval status | Under review (pre-NOC) |
Health Canada review pathway | Standard |
NOC date | Anticipated: June 24, 2022 |
Reimbursement request | As per indication |
Sponsor | Novartis Pharmaceuticals Canada Inc. |
Submission history | Not previously reviewed |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adult patients (≥ 18 years) with CP-CML with prior experience with 2 or more TKIs. (Aligns with reimbursement request.) |
Treatment | Asciminib |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (40 years) |
Key data source | ASCEMBL trial |
Submitted results | Asciminib dominated (i.e., more effective, less costly) bosutinib, ponatinib, nilotinib, and dasatinib. The ICER for asciminib was $86,436 per QALY when compared to Allo-SCT (incremental cost = $303,529; incremental QALYs = 3.51). |
Key limitations | The comparative effectiveness of asciminib is uncertain for all comparators. The CADTH Clinical review found insufficient evidence to draw conclusions about comparative OS for asciminib compared to bosutinib in the ASCEMBL trial. The comparative efficacy evidence for all other comparators was derived from highly uncertain indirect evidence, and no conclusions could be drawn. The sponsor’s base case relied heavily on long-term extrapolations of benefit and a lack of treatment waning that were not supported by trial evidence and that clinical experts felt to be overly optimistic. The sponsor estimated OS based on MMR, the ASCEMBL trial’s primary outcome, using a method that lacked face validity and was also highly uncertain. While clinical experts agreed that MMR is correlated to OS, the data that were used to establish the surrogacy relationship appeared to violate the proportional hazard assumption and did not fit well to the parametric survival function that was used to estimate long-term OS. The cost of subsequent treatments was likely overestimated. The sponsor assumed a full dose for all subsequent therapies. The clinical experts consulted by CADTH suggested that this assumption was unrealistic and does not match clinical practice or guidelines published in the literature. Other methodological limitations were identified by the CADTH review: lack of time-to-discontinuation and OS data for some comparator treatments; the sponsor’s choice of a partitioned survival model contributed additional uncertainty due to a lack of mature OS and PFS data; the model produced inconsistent estimates of asciminib effectiveness depending on the choice of comparator therapy; and the choice of subsequent treatment was independent of third-line treatment, which lacked face validity. |
CADTH reanalysis results | CADTH made the following revisions to address the identified limitations: corrected public listed price for dasatinib; and reduced dosing intensity for dasatinib, nilotinib, and ponatinib as subsequent treatments. In the CADTH base case, asciminib was associated with an ICER of $207,406 (incremental costs = $121,148; incremental QALYs = 0.58) compared to bosutinib. CADTH was not able to estimate a base-case ICER for asciminib vs. other comparators due to uncertain comparative efficacy evidence. A price reduction of at least 26% would be needed for asciminib to be cost-effective compared to bosutinib at a willingness-to-pay threshold of $50,000 per QALY. |
Allo-SCT = allogenic stem cell transplant; CML = chronic myeloid leukemia; CP = chronic phase; ICER = incremental cost-effectiveness ratio; LY = life-year; MMR = major molecular response; OS = overall survival; QALY = quality-adjusted life-year; TKI = tyrosine kinase inhibitor; vs. = versus.
Conclusions
The CADTH clinical review found that evidence from the ASCEMBL trial indicated that asciminib (80 mg daily), as compared to bosutinib (500 mg daily), showed a clinically meaningful and statistically significant benefit in achieving major molecular response (MMR) at the 24-week time point in patients with chronic phase (CP) chronic myeloid leukemia (CML) who had received 2 or more tyrosine kinase inhibitors (TKIs) and experienced treatment failure or intolerance to the most recent TKI. The comparative overall survival (OS) and progression-free survival (PFS) between asciminib and bosutinib was uncertain due to the immaturity of the ASCEMBL trial data. As the study is ongoing, additional long-term efficacy and safety information are anticipated. Results from the sponsor’s submitted matching-adjusted indirect comparison (MAIC) were uncertain for MMR; thus, conclusions on comparative efficacy could not be drawn.
CADTH identified several key limitations with the sponsor’s economic analysis, specifically, the uncertainty associated with the long-term efficacy of asciminib; lack of survival data for some comparators; overly optimistic relative dose intensities (RDIs) for subsequent treatments; and an uncertain relationship between MMR and OS. CADTH undertook reanalysis by removing comparators with inadequate survival data, correcting public listed price for dasatinib, and aligning the dosing for subsequent therapies with clinical practice. CADTH’s base case resulted in an incremental cost-effectiveness ratio (ICER) of $207,406 per quality-adjusted life-year (QALY) compared to bosutinib. A price reduction of at least 26% would be required for asciminib to be cost-effective at a willingness-to-pay threshold of $50,000 per QALY. The ICER was sensitive to assumptions around the dosing and costs of subsequent therapy, particularly for ponatinib.
Due to a lack of mature data from the ASCEMBL trial, the cost-effectiveness model was heavily influenced by the assumed relationship between MMR (the trial end point) and OS, which itself was highly uncertain. This assumption was used to estimate long-term incremental effectiveness, nearly 90% of which was gained through extrapolation. The incremental cost was estimated based on assumptions about subsequent treatment that did not match clinical experience with treating CP-CML and appeared to meaningfully overestimate the cost of current practice. Consequently, while the cost of treatment with asciminib is higher than currently available alternatives, the benefit to patients and overall impact on health care system costs are highly uncertain. An additional price reduction may be warranted.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received 2 patient input submissions for the review of asciminib for adults with Philadelphia chromosome positive (Ph+) CML-CP: 1 from the CML Society of Canada and a joint submission from the Lymphoma and Leukemia Society of Canada and the Canadian CML Network. Both submissions conducted online surveys in late 2021 or early 2022 and received responses from 10 patients (from the CML Society, and including an unspecified “few” patients from the US) and 16 patients and caregivers (joint submission, all in Canada). Most patients had experience with asciminib. Both submissions noted the specific and potentially debilitating side effects associated with each available TKI, which may not be immediately apparent, notably neuro- and cardiovascular toxicities associated with ponatinib, another later-line option. Key values important to patients included improving quality of life, improved side effects, ease and confidence in disease management, and improved length of survival. In total, 89% of patients with asciminib experience responding to the joint submission’s survey indicated that they strongly agreed with the statement that asciminib improved their quality of life compared to other treatments they’d received for CML, though side effects such as gastrointestinal issues, headaches, fatigue, and arthralgia. Most patients had received asciminib through clinical trials, compassionate programs, or private insurance (if in the US), and both submissions included at least 1 patient who was using asciminib to treat a T315I mutation.
Two clinician group submissions were received from the Ontario Health Cancer Care Ontario Hematology Drug Advisory Committee and a peer group of hematologists across Canada involved in treating patients with CML. Both clinician groups agreed that resistance and intolerance to previous TKIs due to toxicities are the main issues with current treatments for Ph+ CML. Both groups indicated that asciminib would be a preferred third-line therapy option given its differing mechanism of actions and favourable toxicity profile, which would make it potentially well suited to patients who have had significant intolerance to TKIs or those for whom ponatinib may not be suitable due to cardiovascular toxicity. Ponatinib was still seen as the preferred therapy for patients with the T315I mutation, but patients with accelerated or blastic phase CML, or those who have already achieved molecular milestones with other treatments were not seen as suitable for treatment with asciminib. Outcomes used to determine whether a patient’s disease responds to treatment were molecular response, blood counts, and improvement in symptoms, while disease progression and significant intolerance were seen as factors important to discontinuing treatment. The Ontario Health Cancer Care Ontario Hematology Drug Advisory Committee noted that in some jurisdictions, the current funding paradigm for patients who had relapsed, been refractory, or were intolerant to 2 or more TKIs limited the use of some comparators at later lines of therapy. Should asciminib be used in the third line, the current funding criteria may not allow the use of bosutinib in the fourth line, and should asciminib be used as fourth line, potentially neither bosutinib nor ponatinib would be accessible in the fifth line.
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review process. Issues identified by the drug plans regarding asciminib included bosutinib not being reimbursed in a fourth-line setting in all jurisdictions; the appropriateness of other comparators beyond bosutinib (ponatinib, dasatinib, nilotinib); the potential use of asciminib in patients with accelerated phase (AP) or blastic crisis (BC) CML and those with T315I or V299L mutations; whether it was appropriate for patients to switch from their current treatments to asciminib once funded; concerns that the potential drug-drug, drug-food, and drug-herm interactions of asciminib might increase use of pharmacy resources; and that confidential pricing agreements exist for bosutinib, ponatinib, and nilotinib, while imatinib and dasatinib are available as generic products. Further information can be found in Table 4 of the CADTH Clinical Review Report.
CADTH addressed some of these concerns as follows:
The known toxicities associated with available TKIs were assumed to impact RDIs in the model.
CADTH explored a lower long-term dose of ponatinib, and using asciminib as a subsequent treatment for those who fail on third-line bosutinib in scenario analyses.
CADTH was unable to address the following concerns raised from stakeholder input:
Subgroup analysis for the patients with the T315I mutation was not included due to lack of data.
Economic Review
The current review is for asciminib (Scemblix) for third-line treatment of patients with CML-CP patients who were already treated with at least 2 TKIs.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing costs and outcomes for asciminib for the third-line treatment of adult patients with Ph+ CML in CP previously treated with 2 or more TKIs.1 Comparators included bosutinib, ponatinib, nilotinib, dasatinib, and allogeneic stem cell (Allo-SCT) therapy. The modelled population was in line with the reimbursement request and the pending Health Canada–approved indication.2
Asciminib is available as an oral tablet (40 mg or 20 mg). The recommended dosage is 40 mg twice daily. At the submitted price of $85 per 40 mg tablet, the average annual cost is $62,092.50. The average annual cost was $55,602 for bosutinib, $128,213 for ponatinib, $60,569 for nilotinib, and $48,313 for dasatinib.
The clinical outcome was QALYs and life-years (LYs). The economic analysis was undertaken over a time horizon of 40 years from the perspective of a Canadian publicly funded health care system. Costs and QALYs were discounted at a rate of 1.5% per annum.
Model Structure
The sponsor submitted a nonhomogeneous partitioned survival model with states defined on treatment, progression, and death. Specifically, model health states included CP-CML (on third-line treatment), CP-CML (discontinued third-line treatment), AP-CML, BC-CML, Allo-SCT in the CP (relapse free or relapsed), Allo-SCT in the progressed phase (relapse free or relapsed), and death (refer to Appendix 3, Figure 1). The proportion of patients who were progression free, who experienced progressive disease, or who were dead at any time over the model horizon was derived from non-mutually exclusive survival curves. All patients entered the model with non-progressed disease and were assumed to receive treatments until disease progression and/or the development of treatment-limiting or treatment-related adverse events (AEs).
All patients who received a third-line TKI entered the analysis in the “CP-CML: On 3L treatment” health state. Upon discontinuing third-line treatment, patients transitioned to the “CP-CML: Off 3L treatment” health state. Patients received subsequent fourth-line or higher therapy in this health state until disease progression. Progressed disease was modelled using 2 health states specific to AP-CML and BC-CML.
Allo-SCT was included in the model as both a comparator and a subsequent treatment. The health state structure contained 2 submodels for patients who receive an Allo-SCT in CP and progressed phases of disease, respectively. The Allo-SCT submodels included relapse-free and relapsed health states.
Model Inputs
The modelled population reflected the baseline characteristics of with the enrolment population in the ASCEMBL trial,3,4 a phase III, multicenter, open-label, randomized study of oral asciminib versus bosutinib in patients with CML-CP previously treated with 2 or more TKIs. Based on the ASCEMBL enrolment, the submitted model assumed female sex for 47.8% of the population and a mean age of 51.0 (standard error = 13.5) years.
Time to treatment discontinuation (TTD) curves for asciminib and bosutinib were generated using patient-level data from the ASCEMBL trial (30-day safety cut-off, maximum follow-up of 48 weeks). The sponsor used parametric models to extrapolate TTD beyond trial follow-up. Kaplan-Meier (KM) data from the trial was used to fit an independent log-logistic parametric survival model for TTD in the asciminib and bosutinib arms. This distribution was selected based on visual inspection, clinical plausibility, and model fit statistics. The sponsor did not have access to TTD survival curves for ponatinib, nilotinib, and dasatinib. As such, the sponsor used MAIC to estimate the TTD survival curve based on previously published mean TTDs for each of the comparators.
As OS and PFS data from the ASCEMBL trial had yet not matured, the sponsor used MMR as a surrogate to estimate long-term survival. To establish the surrogacy relationship, the sponsor used data from ||| || |||||||||||||| |||||||||| |||||||| ||||||| |||||| that compared OS among patients who achieved MMR by 6 or 12 months to those who did not achieve MMR by those time points. ||| || |||| |||| ||| | ||||||| |||||| || || ||||||||||||| ||| ||||||| The sponsor used exponential curves to extrapolate observed || || |||| |||| to 40 years. The sponsor did not justify the choice of the model to extrapolate data.
Having established the surrogacy relationship, the sponsor used ASCEMBL trial data to estimate OS for the proportion of patients on asciminib and bosutinib who achieved MMR. Similarly, the sponsor used available MMR rates for ponatinib and dasatinib to estimate OS. MMR rates for nilotinib were not available. The sponsor assumed a 6-month MMR rate for nilotinib to be equal to that of dasatinib. Importantly, for ponatinib, nilotinib, and dasatinib, the patient subgroup from which mean TTD was sourced was different from the patient subgroup used for MMR rates. PFS to AP CML, PFS to BC CML, and OS were estimated using MMR-specific OS curves.
Health utility values were based on descriptive analysis of the (EQ-5D Five-Levels [EQ-5D-5L]) patient responses collected in the ASCEMBL trial and other published sources. In the ASCEMBL trial, utility values by health state were estimated from a mixed-effect model for repeated measures, accounting for multiple assessments per patients and including baseline EQ-5D-5L as a covariate. The analysis assumed the same utility values for each health state, irrespective of the treatment arm. Incidence rates for AEs were estimated using clinical trials of CML-CP or other publications. Health utilities were adjusted for age and sex. The model included utility decrements to account for the impact of AEs. Disutility values for each AE were based on the literature.
Costs included drug (acquisition, monitoring), disease management, AEs, subsequent treatments, and terminal care. Cost inputs from previous years were inflated to 2021 values the health care component of the consumer price index. Drug acquisition costs were sourced from IQVIA DeltaPA. An RDI, defined as the ratio between the administered doses and the prescribed doses within a year, was applied to account for situations where patients do not take the correct dose or AEs prevent tolerance of the correct dose. Assumed dose intensities for asciminib and bosutinib were set to 88.8% and 85.2%, respectively, based on the ASCEMBL trial. For all other comparators, the sponsor did not have data to support dosing and therefore assumed a dose intensity of 100%. Administration cost for oral drugs were assumed to be 0. Allo-SCT costs were based on the Ontario Case Costing Index. Disease monitoring costs included blood counts and testing for liver function, serum lipase, vascular occlusion, electrocardiogram, renal function, blood lipids, glucose, and electrolytes, and were based on Ontario Health Insurance Plan’s Schedule of Benefits for Laboratory Services and Physician Services. The model also considered disease management costs, including imaging, tests, transfusions, and medical consultations. Disease management costs were sourced from Ontario Health Insurance Plan’s Schedule of Benefits and Répertoire québécois et système de mesure des procédures de biologie médicale. The sponsor assumed that 100% of patients received subsequent treatment and that the distribution across treatments was the same regardless of the third-line treatment received. Terminal care costs were applied to patients who transitioned to the death health state; the cost estimate was obtained from an economic evaluation study by Walker et al. (2011).5
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically with 1,000 iterations for the base-case analysis and 300 iterations for scenario analyses. The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following.
Base-Case Results
Asciminib was cost saving (incremental costs = –$63,895) and more effective (incremental QALYs = 0.59) compared to bosutinib. When compared to Allo-SCT, asciminib was associated with an ICER of $86,436 over a 40-year time horizon (refer to Table 3). All other available TKIs, ponatinib, nilotinib, and dasatinib were also dominated by asciminib as they were more costly and generated fewer QALYs. At a willingness-to-pay threshold of $50,000 per QALY, the probability of asciminib being cost-effective was 94.7% when compared with bosutinib and 1.8% when compared with Allo-SCT.
The main cost driver was subsequent treatment cost, followed by drug acquisition cost and disease management cost. Asciminib was associated with 0.52 additional LYs when compared with bosutinib and 2.38 additional LYs when compared with Allo-SCT. At the end of the model time horizon (i.e., 40 years), the model estimated that around 9% of the patients are alive in the asciminib arm. The sponsor’s base case estimated 0.59 incremental QALYs for asciminib (11.55 QALYs) compared to bosutinib (10.96 QALYs). Of these, 89.8% of incremental QALYs (0.06) for asciminib (2.37 QALYs) compared to bosutinib (2.31 QALYs) were estimated during the observation period of the trial (approximately 37 months).
Table 3: Summary of the Sponsor’s Economic Evaluation Results (Bosutinib and allo-SCT)
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Allo-SCT | 721,350 | Reference | 7.52 | Reference | Reference |
Asciminib | 1,024,878 | 303,529 | 11.03 | 3.51 | 86,436 |
Bosutinib | 1,142,281 | Reference | 10.96 | Ref. | Reference |
Asciminib | 1,078,386 | –63,895 | 11.55 | 0.59 | –108,948 |
Allo-SCT = allogeneic stem cell transplant; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; MAIC = matched-adjusted indirect treatment comparison’ vs. = versus.
Notes: Bosutinib, ponatinib, nilotinib, and dasatinib were dominated by asciminib. Estimates for ponatinib, nilotinib, and dasatinib are presented in Appendix 4.
The sponsor’s model used a MAIC to estimate the relative effectiveness of asciminib vs. other comparators. As a result, the QALYs estimated for asciminib differ depending on the chosen comparator. CADTH was not able to resolve this issue.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor performed scenario analyses by considering a societal perspective for the study, alternative assumptions for discount rates, time horizon of 20 years, alternative parametric survival and treatment duration models, alternative mean time of survival in AP and BC, and alternative utility values. Base-case results remained valid across different scenario analysis. One exception was the comparison between asciminib and ponatinib, where ponatinib was dominated in base-case analysis, but became the more cost-effective option when either higher discounting (3% as opposed to 1.5% in the base case) or a shorter time horizon (20 years as opposed to 40 years in the base case) was considered.
Asciminib drug costs, utility values, and disease management costs had the greatest impact on the results of the sensitivity analysis.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The comparative effectiveness of asciminib is uncertain for all comparators: The CADTH clinical review of the ASCEMBL trial was not able to draw any conclusions about comparative OS or PFS between asciminib and bosutinib from the available trial data. CADTH’s appraisal of the sponsor’s indirect evidence was similarly unable to draw conclusions about comparative OS and PFS for any comparator treatments. The clinical experts consulted by CADTH agreed that asciminib resulted in a clinically meaningful benefit for patients with Ph+ CML compared to bosutinib, but indicated that the long-term efficacy of both asciminib and bosutinib are highly uncertain. The time horizon of the economic analysis (i.e., 40 years) far exceeds the duration of the trial (i.e., approximately 37 months). Extrapolated QALYs, representing nearly 90% of the estimated incremental benefit, are therefore highly uncertain. The clinical experts further noted the lack of long-term safety data for asciminib, which adds additional uncertainty to estimated incremental QALYs. Additionally, the sponsor’s base case produced survival estimates that suggested that patients would experience better long-term survival than the general population, and applied background mortality rates to correct for this effect. Despite this correction, the results suggest that the base-case results are unrealistically optimistic.
Due to a lack of long-term data, CADTH was unable to address this issue in reanalysis. An alternative curve assumption was explored in a scenario analysis.
Uncertain surrogate data for deriving OS and PFS from MMR: Although the clinical experts agreed that an improvement in MMR was likely to lead to an improvement in OS, the method used by the sponsor to establish the surrogacy relationship lacked face validity. Observed KM curves ||| ||||| ||||||||| ||| || | |||||| |||||||| || ||||| ||| ||| |||| ||| ||| || ||||||| |||||||| || ||||||| ||| |||||||||||| |||||| |||||||||| ||||| |||||||| |||||| ||||||| ||| did not appear to fit well to the parametric exponential curves that were used to extrapolate for long-term survival (refer to Figure 2). Additionally, for ponatinib, nilotinib, and dasatinib, the subpopulation from which median TTD was obtained was different from the subgroup from which MMR rates were obtained, which adds additional uncertainty.
CADTH was unable to address this limitation in reanalysis, and the relationship between MMR and OS remains highly uncertain.
Dosing for subsequent therapies does not match expected clinical practice: The sponsor estimated the dosing for asciminib and bosutinib based on the RDI received by patients within the ASCEMBL trial. The sponsor assumed, in the absence of data, that patients would receive 100% of the dose for all other treatments, whether they were received in third line or as subsequent therapy. The clinical experts consulted by CADTH indicated that this assumption did not reflect clinical practice, and that patients would likely instead receive a dose reduction over time. Sources in the literature supported the idea of a dose reduction strategy for ponatinib, which was both the most frequent and most costly subsequent therapy.6-8 Given that patients are expected to remain on subsequent therapy for the remainder of their lives, the results of the economic evaluation are highly sensitive to the cost of subsequent therapies. In the sponsor’s base case, subsequent treatment costs represented the majority of total costs for patients treated with asciminib (55%) and bosutinib (83%). As such, a reduction in dose intensities of subsequent therapies had a large impact on the estimated incremental cost that disproportionately affected asciminib.
Dosing for subsequent therapies was adjusted in the CADTH reanalysis. Based on input from the clinical experts, dose intensities were set to 60% for nilotinib, 60% for dasatinib, 33% for ponatinib, and 100% for imatinib. CADTH performed this adjustment by setting all RDIs to 100% in the model, and then reweighting drug prices by multiplying them by a factor equivalent to the desired RDI. For example, for dasatinib, the RDI in the sponsor’s model was set to 100% and the drug price was multiplied by 0.6. Due to a nonlinear dosing strategy for ponatinib, the cost for this drug was set to be the equivalent of the 15 mg dose (i.e., 33% of the 45 mg default); an effective price adjustment of 44.7%.
Lack of survival or TTD data for most comparators: The sponsor did not submit TTD data for dasatinib, nilotinib, and ponatinib. Instead, the sponsor used a MAIC to estimate KM curves for TTD using a single summary statistic value (median TTD) from published literature. The estimated KM curves were in turn used to fit a parametric survival function to extrapolate TTD to 40 years. This approach was subject to the same limitations highlighted in CADTH’s review of the sponsor’s MAIC: a small effective sample size resulting in wide confidence intervals, and an inability to match the index and comparator trials on all important prognostic factors. This methodology used to estimate TTD curves in the absence of TTD data is associated with a high degree of uncertainty, and does not allow for robust estimation of time on treatment.
CADTH was unable to address this limitation in reanalysis. Cost-effectiveness estimates for these comparators was estimated in exploratory analysis.
Model structure introduces uncertainty around comparative effectiveness: CADTH also noted additional uncertainty associated with the estimated survival benefits of asciminib due to the sponsor’s use of a partitioned survival model. This modelling approach introduces structural assumptions about the relationship between PFS and OS (i.e., non-mutually exclusive curves).9 The propensity score matching in this analysis was additionally uncertain given that PFS and OS were not directly observed from the ASCEMBL trial data, but estimated through a proxy measure. This uncertainty could not be adjusted for in CADTH’s reanalysis due to limitations within the submitted model structure.
CADTH was not able to address this issue through reanalysis.
Estimated QALYs for asciminib are inconsistently estimated: The sponsor’s pharmacoeconomic model incorporates clinical inputs like TTD from a MAIC, and uses these inputs to estimate the comparative effectiveness of asciminib. As a consequence of this methodological approach, the model produces notably different estimates of asciminib effectiveness depending on which comparator is chosen. For example, the sponsor’s base-case estimate of total QALYs for patients receiving asciminib is 11.55 when bosutinib is chosen as a comparator. When Allo-SCT is chosen as a comparator, the base-case estimate of total QALYs for patients receiving asciminib is 11.03. The difference between these 2 estimates (0.52 QALYs) is comparable to the estimated comparative effectiveness of asciminib versus bosutinib (0.58 QALYs), despite ostensibly representing an identical population of patients receiving the identical treatment. This output lacks face validity and suggests that all estimates of asciminib effectiveness are highly uncertain.
CADTH was not able to address this issue in reanalysis. CADTH’s base-case results for asciminib versus bosutinib are presented in this report. Other CADTH estimates are presented in Appendix 4 as exploratory analysis.
Additional limitations were identified, but were not considered to be key limitations. These limitations are:
The sponsor has assumed that 33% of patients on third-line bosutinib will receive bosutinib as a subsequent fourth-line therapy, which lacks face validity and was not supported by the clinical experts consulted by CADTH. Subsequent treatment allocation from third-line bosutinib to fourth-line bosutinib was set to 0% in CADTH reanalysis, with the 33% of remaining patients redistributed proportionally across nilotinib, dasatinib, ponatinib, and imatinib.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patient characteristics (i.e., age, sex, weight, body surface area) based on patients participated in the ASCEMBL trial. | The clinical experts consulted by CADTH found this assumption acceptable. |
The sponsor has used MMR as a proxy for overall survival. | The clinical experts consulted by CADTH found this assumption acceptable. |
The sponsor has excluded omacetaxine and interferon alpha as potential comparators. | The clinical experts consulted by CADTH found this assumption acceptable. |
The sponsor has assumed that in the absence of data, MMR by 6 months for nilotinib will be same as that of dasatinib. | The clinical experts consulted by CADTH did not find this assumption acceptable but agreed it was unlikely to substantively impact the results. |
The same utility values were assumed for each health state, irrespective of the treatment arm. | The clinical experts consulted by CADTH found this assumption acceptable. |
The sponsor assumed an RDI of 85.2% for bosutinib based on the results of the trial. | The clinical experts consulted by CADTH considered the assumed RDI to be an overestimate; however, the assumption did not substantively impact the results. |
MMR = major molecular response; RDI = relative dose intensity.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Due to a lack of robust evidence for several comparators and issues created by the methodological approach chosen by the sponsor, cost-effectiveness results are presented only for the comparison of asciminib and bosutinib. CADTH corrected the sponsor’s model by updating drug prices based on publicly available prices of the comparator and subsequent treatments and adjusted the dosing assumptions for subsequent treatments. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. CADTH’s base case assumed that patients who fail on third-line bosutinib will not receive bosutinib as a subsequent treatment, and adjusted dosing assumptions for subsequent therapy to match expected clinical practice.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Listed price (cost per mg) for dasatinib | $1.3227 | $0.389 |
2. Apply RDIs to subsequent treatments | Sponsor’s model had implicitly assumed a 100% RDI for all subsequent treatments. | Corrected the model to apply RDIs to subsequent treatments, as well as 3L treatments. |
Changes to derive the CADTH base case | ||
1. Subsequent treatment allocation after 3L bosutinib | Nilotinib: ||| Dasatinib: ||| Ponatinib: ||| Imatinib: ||| Bosutinib: ||| | Nilotinib: 17% Dasatinib: 16% Ponatinib: 59% Imatinib: 7% Bosutinib: 0% |
2. Subsequent treatment dosing intensity | Nilotinib: 100% Dasatinib: 100% Ponatinib: 100% Imatinib: 100% | Nilotinib: 60% Dasatinib: 60% Ponatinib: 33% Imatinib: 100% |
CADTH base case | — | 1+ 2 |
3L = third line; 4L = fourth line; RDI = relative dose intensity.
NOTE: RDI adjustments were made by setting the RDIs in the model to 100% and adjusting drug prices instead, due to a lack of flexibility in the sponsor’s pharmacoeconomic model to adjust the RDI for subsequent therapies. For example, for dasatinib, the RDI in the sponsor’s model was set to 100% and the drug price was multiplied by 0.6. Due to a nonlinear dosing strategy for ponatinib, the cost for this drug was set to be the equivalent of the 15 mg dose (i.e., 33% of the 45 mg default); an effective price adjustment of 44.7%.
Results from CADTH’s base case suggest that asciminib was associated with higher costs ($121,148) and improved QALYs (0.58 QALYs) with an ICER of $207,406 per QALY compared to bosutinib. The results of the CADTH reanalysis were notably different from the sponsor’s base case, which suggested that asciminib would be cost saving compared to bosutinib. This difference in results is primarily due to the change in assumed dosing for subsequent treatments. The probability that asciminib is cost-effective compared to bosutinib was 4.5% at a willingness-to-pay threshold of $50,000 per QALY.
Of the 11.58 QALYs estimated for asciminib when compared to bosutinib in the CADTH base case, approximately 2.43 (21%) were estimated to occur during the pivotal trial time frame (approximately 37 months). Similar to the sponsor’s base case, 89% of incremental QALYs for asciminib versus bosutinib were estimated through extrapolation. Of the $804,503 total cost for patients receiving asciminib, $356,246 (44%) were treatment acquisition costs and $318,304 (40%) were subsequent treatments costs.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Bosutinib | 1,142,281 | 10.96 | Reference |
Asciminib | 1,078,386 | 11.55 | –108,948 | |
Sponsor’s corrected base case | Bosutinib | 1,067,630 | 10.96 | Reference |
Asciminib | 1,032,745 | 11.54 | –60,354 | |
CADTH reanalysis 1 (subsequent treatment allocation fixed) | Bosutinib | 1,221,444 | 10.96 | Reference |
Asciminib | 1,032,800 | 11.55 | –319,707 | |
CADTH reanalysis 2 (subsequent treatment dosing) | Bosutinib | 703,176 | 10.97 | Reference |
Asciminib | 804,669 | 11.49 | 194,756 | |
CADTH base case (deterministic) | Bosutinib | 683,387 | 10.96 | Reference |
Asciminib | 804,668 | 11.54 | 209,824 | |
CADTH base case | Bosutinib | 683,354 | 11.00 | Reference |
Asciminib | 804,503 | 11.58 | 207,406 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
Based on CADTH's base case, a series of scenario analyses were conducted. These analyses explored the impact of the following model parameters and assumptions: limiting analysis time horizon to 10 and 5 years, using alternative parametric survival models for extrapolation beyond trial follow-up, and allowing asciminib to be a subsequent therapy for 33% of patients who fail on bosutinib assuming equal efficacy in the third line and fourth line. A scenario analysis was considered where the price of ponatinib was reduced by an arbitrary value of 10% to investigate the sensitivity of the ICER to that parameter. An additional scenario analysis considered 100% dosing for dasatinib and nilotinib. The list price of dasatinib varies between jurisdictions, and so a scenario analysis was performed using a higher value ($1.3227 per mg), per the sponsor’s base case.
Results from a scenario analysis (Appendix 4) demonstrated that cost-effectiveness was driven by the cost of subsequent treatments (especially ponatinib) and extrapolation of the results of the trial to a 40-year time horizon were the key drivers of the cost-effectiveness findings.
Repeating the analysis with time horizons of 10 and 5 years resulted in an ICER of $299,673 and $371,375 per QALY, respectively, when comparing asciminib with bosutinib. In the 5-year follow-up scenario, of the 3.58 QALYs estimated for asciminib, 2.37 (66%) were estimated during the period of the pivotal trial (approximately 37 months). In the same scenario, of the $250,826 total cost, $144,927 (58%) were treatment acquisition costs and $71,283 (28%) were subsequent treatments costs for asciminib. Using an alternative parametric survival model (a Weibull accelerated time failure model) for extrapolating treatment duration beyond trial follow-up resulted in an ICER of $193,190 per QALY. Allowing asciminib to be used in subsequent therapies for patients who failed on third-line bosutinib improved the ICER to $90,354 per QALY. A scenario in which the price of ponatinib was discounted by 10% found an increased ICER of $265,962. A scenario in which RDIs for asciminib and bosutinib were set to 100% increased the ICER to $297,489 per QALY. As shown in the CADTH base case, the ICER was also sensitive to the cost of comparators — the scenario using the higher price for dasatinib returned an ICER of $81,171. Exploratory analyses of the cost-effectiveness of asciminib versus ponatinib, dasatinib, and imatinib are presented in Appendix 4.
Price reduction analysis was conducted based on the sponsor’s base case and CADTH’s reanalysis (refer to Table 7). The results indicate that a price reduction of at least 26% (based on CADTH’s base case) is required for asciminib to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY. In CADTH’s base case, asciminib was estimated to be cost saving at a price reduction of 35%. When an RDI of 100% was assumed for asciminib and bosutinib (refer to Appendix 4, Scenario Analysis 7), a price reduction of at least 36% was needed to make asciminib cost-effective at a willingness-to-pay threshold of $50,000. In this key scenario, asciminib was estimated to be cost saving at a price reduction of 43%. This estimate is highly uncertain due to the other sources of uncertainty identified within this review, including the use of a proxy measure to estimate OS and the lack of long-term efficacy and safety data for asciminib.
Table 7: CADTH Price Reduction Analyses
Price reduction analysis | ICERs for asciminib vs. bosutinib ($/QALY) | |
|---|---|---|
Sponsor base case (deterministic) | CADTH reanalysis (deterministic) | |
No price reduction | –108,414 | 209,824 |
10% | –170,047 | 148,190 |
20% | –231,681 | 86,557 |
24% | –256,334 | 61,904 |
26% | –268,660 | 49,557 |
ICER = incremental cost-effectiveness ratio; vs. = versus.
Issues for Consideration
Some comparators have patents that are expected to expire in the near future. While generic versions are already available for imatinib and dasatinib,10 the other TKI comparators have patents expiring between 2023 and 2033.11 The potential impact of patent expiration on drug acquisition costs was not considered in the analysis.
Overall Conclusions
Evidence from the ASCEMBL trial indicated that asciminib (80 mg daily), as compared to bosutinib (500 mg daily), showed a clinically meaningful and statistically significant benefit in achieving MMR at the 24-week time point in patients with CP-CMP who had received 2 or more TKIs and experienced treatment failure or intolerance to the most recent TKI. Results from the sponsor’s MAIC were uncertain for MMR, and conclusions about comparative efficacy could not be drawn between asciminib and ponatinib, dasatinib, and nilotinib.
CADTH identified several limitations within the sponsor’s economic analysis, specifically the uncertainty associated with the long-term efficacy of asciminib, lack of survival data for some comparators, overly optimistic RDIs for subsequent treatments, inadequate surrogate data for estimating OS and PFS, and the inability to conduct sequential comparisons between multiple comparators due to MAIC. CADTH was unable to address all the limitations identified, but made several corrections and revisions to derive the CADTH base case: reducing dosing intensity for subsequent treatments (based on published literature and clinical expert opinion), and reallocating the frequency at which subsequent therapies were prescribed. In the CADTH base case, the ICER for asciminib was $207,406 per QALY compared to bosutinib. Asciminib was not cost-effective at a $50,000 per QALY willingness-to-pay threshold at the submitted price. A price reduction of at least 26% would be required for asciminib to be cost-effective at this threshold. CADTH analyses were driven by the assumptions regarding the use and costs of subsequent line therapy, particularly the cost of ponatinib. Given the lack of robust OS and PFS data and the long extrapolation period, CADTH’s price reductions are highly uncertain.
CADTH conducted a scenario analysis where the time horizon was reduced to 5 years and an alternative treatment duration curve that allows for a waning treatment effect was chosen. The ICER in this scenario analysis was $335,401 per QALY for asciminib compared to bosutinib, with 33% of incremental QALYs with asciminib occurring in the extrapolation period (compared to 89% in the base case). This finding suggests that the long-term cost-effectiveness of asciminib relies heavily on extrapolation of treatment benefit over a 40-year time horizon, despite the lack of long-term efficacy or safety data.
Due to a lack of mature data from the ASCEMBL trial, the cost-effectiveness model was heavily influenced by the assumed relationship between MMR (the trial end point) and OS, which itself was highly uncertain. This assumption was used to estimate long-term incremental effectiveness, nearly 90% of which was gained through extrapolation. The incremental cost was estimated based on an assumption about subsequent treatment dosing that did not match clinical experience with treating CP-CML, did not match guidelines in the published literature, and appeared to meaningfully overestimate the cost of current practice. Consequently, while the cost of treatment with asciminib is higher than currently available approaches, the benefit to patients is highly uncertain. An additional price reduction may be warranted.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Scemblix (asciminib) 20 mg and 40 mg oral tablets. Dorval (QC): Novartis Pharmaceuticals Canada; 2022 Jan 19.
2.PrScemblix® (asciminib): 20 mg and 40 mg, oral tablets [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada; 2021 Jul 22.
3.Rea D, Mauro MJ, Boquimpani C, et al. A phase 3, open-label, randomized study of asciminib, a STAMP inhibitor, vs bosutinib in CML after 2 or more prior TKIs. Blood. 2021;138(21):2031-2041. PubMed
4.Clinical Study Report: CABL001A2301. A phase III, multi-center, open-label, randomized study of oral ABL001 (asciminib) versus bosutinib in patients with chronic myelogenous leukemia in chronic phase (CML-CP), previously treated with 2 or more tyrosine kinase inhibitors [internal sponsor's report]. 2021.
5.Walker H, Anderson M, Farahati F, et al. Resource use and costs of end-of-Life/palliative care: Ontario adult cancer patients dying during 2002 and 2003. J Palliat Care. 2011;27(2):79-88. PubMed
6.Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34(4):966-984. PubMed
7.Jabbour EJ, Deininger MW, Abruzzese E, et al. Dose modification dynamics of ponatinib in patients with chronic-phase chronic myeloid leukemia (CP-CML) from the PACE and Optic trials. Blood. 2021;138(Suppl 1):2550-2550.
8.Cortes J, Apperley J, Lomaia E, et al. Ponatinib dose-ranging study in chronic-phase chronic myeloid leukemia: a randomized, open-label phase 2 clinical trial. Blood. 2021;138(21):2042-2050. PubMed
9.Woods B, Sideris E, Palmer S, Latimer N, Soares M. Partitioned survival analysis for decision modelling in health care: a critical review. (NICE DSU Technical Support Document 19).
10.Health Canada Drug Product Database.
11.Health Canada Patent Register.
12.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index.
13.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2022: Accessed 2022 Feb 24.
14.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: Accessed 2022 Feb 16.
15.Table 17-10-0005-01 Population estimates on July 1st, by age and sex.
16.Table 13-10-0751-01 Number of prevalent cases and prevalence proportions of primary cancer, by prevalence duration, cancer type, attained age group and sex.
17.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Scemblix (asciminib) 20 mg and 40 mg oral tablets. Dorval (QC): Novartis Pharmaceuticals Canada; 2022 Jan 19.
18.Prescribed drug spending in Canada 2019: a focus on public drug programs.
19.Dinh T, Sutherland G. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage.
20.Cortes JE, Kim DW, Pinilla-Ibarz J, et al. Ponatinib efficacy and safety in Philadelphia chromosome-positive leukemia: final 5-year results of the phase 2 PACE trial. Blood. 2018;132(4):393-404. PubMed
21.Giles FJ, Abruzzese E, Rosti G, et al. Nilotinib is active in chronic and accelerated phase chronic myeloid leukemia following failure of imatinib and dasatinib therapy. Leukemia. 2010;24(7):1299-1301. PubMed
22.Jain NA, Ito S, Tian X, et al. Clinical and biological predictors of outcome following relapse of CML post-allo-SCT. Bone Marrow Transplant. 2015;50(2):189-196. PubMed
23.Russo Rossi A, Breccia M, Abruzzese E, et al. Outcome of 82 chronic myeloid leukemia patients treated with nilotinib or dasatinib after failure of two prior tyrosine kinase inhibitors. Haematologica. 2013;98(3):399-403. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Adults With Ph+CML-CP
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual costa |
|---|---|---|---|---|---|---|
Asciminib (Scemblix) | 20 mg 40 mg | Tablet | $63.0000a $85.0000a | 80 mg daily, either as 80 mg once daily or 40 mg twice daily | $170.00 | $62,092 |
Protein-tyrosine kinase inhibitors | ||||||
Bosutinib (Bosulif) | 100 mg 500 mg | Tablet | $38.9787b $152.2403b | 500 mg once daily | $152.24 | $55,602 |
Dasatinib (generics) | 20 mg 50 mg 70 mg 80 mg 100 mg | Tablet | $9.6713c $19.4643c $21.4510c $34.5077c $38.9020c | 100 mg once daily | $38.90 | $14,209 |
Imatinib mesylate (generics) | 100 mg 400 mg | Tablet | $5.2079b $20.8314b | 400 mg once daily | $20.83 | $7,609 |
Nilotinib (Tasigna) | 150 mg 200 mg | Capsule | $29.7800b $41.4575b | 400 mg twice daily | $165.83 | $60,569 |
Ponatinib (Iclusig) | 15 mg 45 mg | Tablet | $157.0815b $351.0267b | 45 mg once daily | $351.03 | $128,213 |
Procedure | ||||||
Allo-SCT | — | — | $62,577d | — | — | — |
Allo-SCT = allogenic stem cell transplant; Ph+CML-CP = Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase.
Note: Prices do not include dispensing fees. Assumes a 365.25-day year.
aSponsor’s submitted price.1
bOntario Drug Benefit or Ontario Drug Benefit Exceptional Access Program list price (accessed Feb 2022).12,13
cIQVIA Delta PA wholesale price (accessed Feb 2022).14
dCited as OCCI 2017 to 2018, inflated to 2021 dollars.1
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | See CADTH appraisal section. |
Model has been adequately programmed and has sufficient face validity | No | RDIs were not being taken into account for subsequent treatments. In addition, 33% of the patients who fail 3L bosutinib had been assumed to receive 4L bosutinib which does not have face validity. |
Model structure is adequate for decision problem | No | See CADTH appraisal section. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
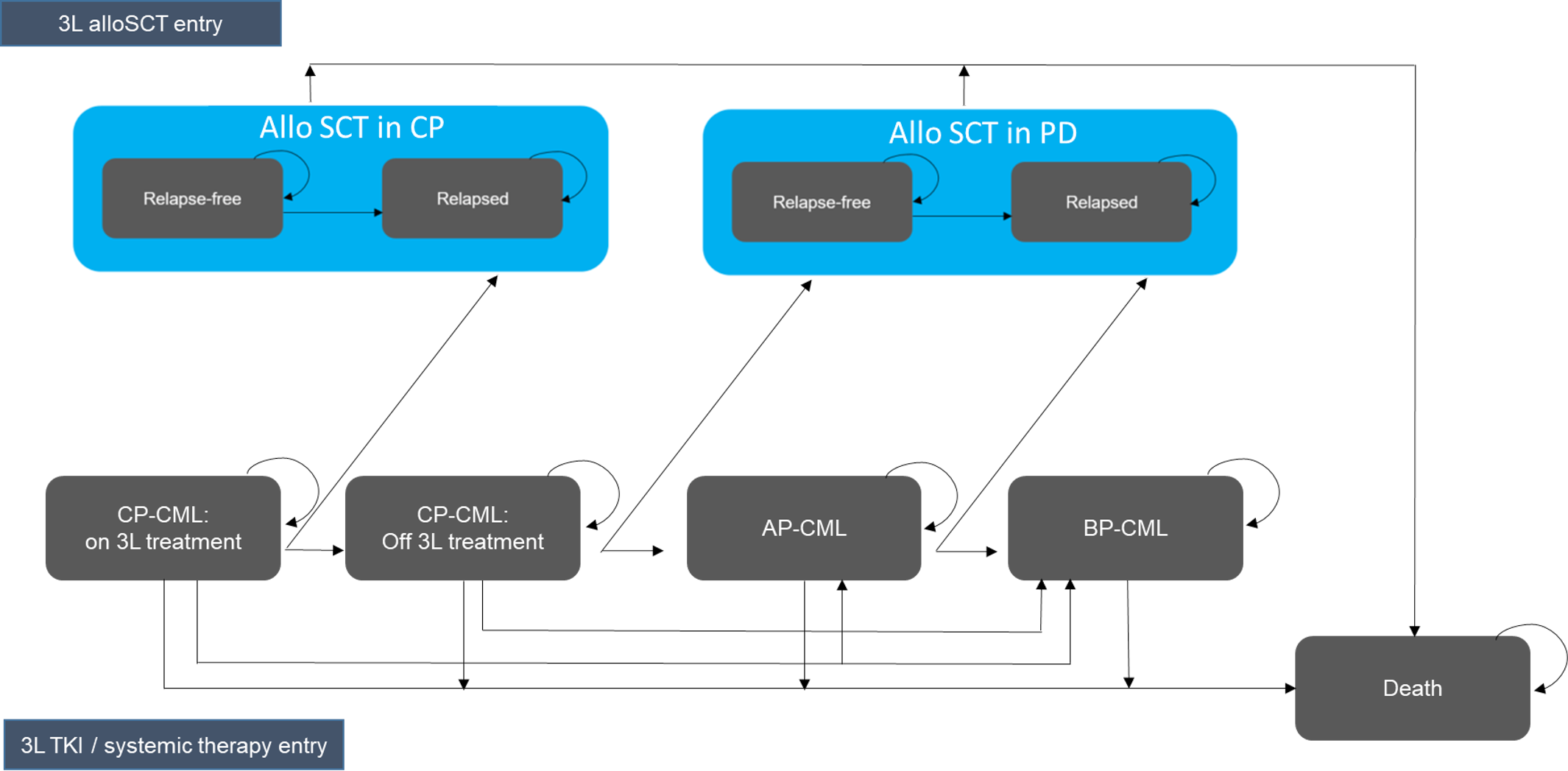
Figure 2: Sponsor’s Base Case — Relationship Between MMR and Overall Survival (Redacted)

Note: This figure has been redacted at the request of the sponsor.
Source: Sponsor’s submission.1
Figure 3: Sponsor’s Base Case — Long-Term Overall Survival Extrapolation (Redacted)

Note: This figure has been redacted at the request of the sponsor.
Source: Sponsor’s submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Cost-Effectiveness of Asciminib vs. Bosutinib
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Bosutinib | 1,141,857 | Ref. | 10.96 | Ref. | Ref. |
Asciminib | 1,079,192 | −62,665 | 11.54 | 0.58 | −108,414 |
Ref. = reference; vs. = versus.
Table 11: Cost-Effectiveness of Asciminib vs. allo-SCT
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Allo-SCT | 721,350 | Ref. | 7.52 | Ref. | Ref. |
Asciminib | 1,024,878 | 303,529 | 11.03 | 3.51 | 86,436 |
Ref. = reference; vs. = versus.
Table 12: Cost-Effectiveness of Asciminib vs. Ponatinib
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Ponatinib | 1,375,137 | Ref. | 11.04 | Ref. | Ref. |
Asciminib | 1,146,962 | −228,175 | 11.10 | 0.07 | −3,383,184 |
Ref. = reference; vs. = versus.
Table 13: Cost-Effectiveness of Asciminib vs. Nilotinib
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Nilotinib | 1,180,759 | Ref. | 11.03 | Ref. | Ref. |
Asciminib | 1,135,917 | −44,841 | 11.35 | 0.32 | −140,203 |
Ref. = reference; vs. = versus.
Table 14: Cost-Effectiveness of Asciminib vs. Dasatinib
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Dasatinib | 1,152,958 | Ref. | 11.26 | Ref. | Ref. |
Asciminib | 1,148,257 | −4,702 | 11.47 | 0.21 | −22,648 |
Ref. = reference; vs. = versus.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 15: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Asciminib | Bosutinib | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 14.00 | 13.48 | 0.52 |
Discounted QALYs | |||
Total | 11.58 | 11.00 | 0.58 |
By health state or data source | |||
CP On Treatment | 5.65 | 1.36 | 4.29 |
CP Off Treatment | 4.87 | 8.55 | −3.68 |
Allo-SCT Relapse Free | 0.27 | 0.32 | −0.04 |
Allo-SCT Relapsed | 0.16 | 0.18 | −0.03 |
AP | 0.27 | 0.28 | −0.01 |
BC | 0.32 | 0.30 | 0.02 |
Allo-SCT Relapse Free | 0.02 | 0.02 | 0.00 |
Allo-SCT Relapsed | 0.01 | 0.01 | 0.00 |
Adverse Events | −0.03 | −0.06 | 0.03 |
Discounted costs ($) | |||
Total | 804,503 | 683,354 | 121,148 |
Acquisition | 356,246 | 74,821 | 281,425 |
Monitoring | 12,660 | 3,254 | 9,405 |
SCT Costs | 4,052 | 4,521 | −469 |
Subsequent Treatment | 318,304 | 488,493 | −170,189 |
Disease Management | 79,702 | 75,386 | 4,316 |
Terminal Care | 27,899 | 28,461 | −563 |
Adverse Events | 5,640 | 8,417 | −2,777 |
ICER ($/QALY) | 207,406 | ||
Allo-SCT: Allogeneic Stem Cell Therapy; AP: Accelerated phase; BC = blast crisis; CP: Chronic phase; ICER = incremental cost-effectiveness ratio; LY = life-year; SCT: Stem Cell Therapy, QALY = quality-adjusted life-year.
Scenario Analyses
Table 16: Summary of CADTH Scenario Analyses
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
Sponsor's corrected base case | |||
Bosutinib | 1,067,630 | 10.96 | Reference |
Asciminib | 1,032,745 | 11.54 | −60,354 |
CADTH's base case | |||
Bosutinib | 683,354 | 11.00 | Reference |
Asciminib | 804,503 | 11.58 | 207,406 |
CADTH's scenario analysis 1: Reducing time horizon to 10 years | |||
Bosutinib | 360,286 | 5.90 | Reference |
Asciminib | 416,666 | 6.09 | 299,673 |
CADTH's scenario analysis 2: Reducing time horizon to 5 years | |||
Bosutinib | 218,455 | 3.49 | Reference |
Asciminib | 250,826 | 3.58 | 371,375 |
CADTH's scenario analysis 3: Using a Weibull survival model for extrapolating treatment duration | |||
Bosutinib | 683,418 | 10.95 | Reference |
Asciminib | 769,578 | 11.40 | 193,190 |
CADTH's scenario analysis 4: Using asciminib as a subsequent treatment for 33% of patients who fail on 3rd line Bosutinib | |||
Bosutinib | 730,594 | 10.97 | Reference |
Asciminib | 769,546 | 11.40 | 90,354 |
CADTH's scenario analysis 5: Assuming a 10% discount on ponatinib list price | |||
Bosutinib | 644,976 | 10.99 | Reference |
Asciminib | 788,496 | 11.53 | 265,962 |
CADTH's scenario analysis 6: Assuming 100% RDIs for dasatinib and nilotinib | |||
Bosutinib | 744,147 | 10.90 | Reference |
Asciminib | 831,365 | 11.55 | 134,639 |
CADTH's scenario analysis 7: Assuming 100% RDIs for asciminib and bosutinib | |||
Bosutinib | 696,748 | 10.96 | Reference |
Asciminib | 868,701 | 11.54 | 297,489 |
CADTH's scenario analysis 8: using higher list price for dasatinib | |||
Bosutinib | 748,942 | 11.00 | Reference |
Asciminib | 830,114 | 11.58 | 81,171 |
Note: Under CADTH's scenario analysis 7: Assuming 100% RDIs for asciminib and bosutinib, a price reduction of at least 36% would be required to make asciminib cost-effective at a willingness-to-pay of $50,000 per QALY. Under CADTH’s scenario analysis 8: using higher list price for dasatinib, the $50,000 per QALY threshold was reached at a 9% reduction in the price of asciminib.
Table 17: Cost-Effectiveness of Asciminib vs. allo-SCT in CADTH Exploratory Analysis
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Allo-SCT | 516,387 | Ref. | 7.56 | Ref. | Ref. |
Asciminib | 773,051 | 256,664 | 11.06 | 3.50 | 73,297 |
Ref. = reference
Table 18: Cost-Effectiveness of Asciminib vs. Ponatinib in CADTH Exploratory Analysis
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Ponatinib | 716,029 | Ref. | 11.05 | Ref. | Ref. |
Asciminib | 739,504 | −23,475 | 11.15 | 0.10 | Dominates ponatinib |
Ref. = reference
Table 19: Cost-Effectiveness of Asciminib vs. Nilotinib in CADTH Exploratory Analysis
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Nilotinib | 677,464 | Ref. | 11.05 | Ref. | Ref. |
Asciminib | 748,709 | 71,245 | 11.34 | 0.29 | 243,101 |
Ref. = reference
Table 20: Cost-Effectiveness of Asciminib vs. Dasatinib in CADTH Exploratory Analysis
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Dasatinib | 624,509 | Ref. | 11.28 | Ref. | Ref. |
Asciminib | 751,172 | 126,663 | 11.48 | 0.20 | 640,729 |
Ref. = reference
Appendix 5: Submitted BIA and CADTH Appraisal
Table 21: Summary of Key Take-Aways
Key Take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of asciminib for the treatment of adults with Ph+CML-CP without the T315i mutation who have previously been treated with 2 or more TKIs. The BIA was conducted from the perspective of a Canadian public drug payer over a 3-year time horizon (2022 to 2024) using an epidemiological approach and included only drug acquisition costs, including markups and dispensing fees. Subsequent treatment costs were not considered in the base case.
Data for the model were obtained from: Statistics Canada,15,16 physician surveys conducted by the sponsor,17 CIHI18 and the Conference Board of Canada,19 formulary12 and wholesale list prices.14 Key inputs to the BIA are documented in Table 22.
Key assumptions included:
Patients with the T315i mutation will not be treated with asciminib.
Due to the use of prevalence data to calculate the target patient population, duration of therapy only impacts costs for comparators with durations less than 1 year. Otherwise, a full 12 months of treatment is assumed for each comparator per year in the base case.
The market share of comparators is not changing over time, nor will that of asciminib after its initial introduction.
Wholesale list price variation between jurisdictions can be generalized to variation in costs paid by jurisdictional public cancer drug payers.
Table 22: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target Population | |
Total Canadian population excluding Quebec | 30,743,667 / 31,081,712 / 31,423,891a |
Proportion covered by public drug plans | 80.27%b |
Prevalence of CML per 100,000 | 17 / 18 / 19c |
Proportion of CML patients who are CML-Ph+ | ||||||| |
Proportion of CML-Ph+ patients who are in chronic phase | ||||||| |
Proportion of CML-CP Ph+ patients who are treated | ||||||| |
Proportion of treated CML-CP Ph+ patients in 3L+ treatment | 11.00%e |
Proportion of 3L+ patients without T315I mutation | 95.43%d |
Number of patients eligible for drug under review | 400 / 420 / 440 |
Market Uptake (reference scenario - > new drug scenario, all 3 years)d | |
Asciminib | || || ||||| |
Imatinib | |||| || |||| |
Nilotinib | ||||| || ||||| |
Dasatinib | ||||| || ||||| |
Bosutinib | ||||| || ||||| |
Ponatinib | ||||| || ||||| |
Allo-SCT | |||| || |||| |
Cost of treatment (per patient per year)g | |
Asciminib (MTD = 25 months, RDI = 89%)h | $55,138 |
Imatinib (MTD = 32 months, RDI = 100%)ik | $7,609 to $29,886 |
Nilotinib (MTD = 11 months, RDI = 100%)jk | $47,199 to $55,522 |
Dasatinib (MTD = 14 months, RDI = 100%)jk | $14,209 to $48,311 |
Bosutinib (MTD = 6.9 months, RDI = 85%)h | $26,034 to $27,083 |
Ponatinib (MTD = 32.1 months,RDI = 100%)jk | $128,213 |
Allo-SCT (one time treatment)j | $62,577 |
3L = third line; allo-SCT = allogenic stem cell transplant; CML = chronic myeloid leukemia; CP = chronic phase; MTD = median time to discontinuation; Ph+ = Philadelphia chromosome positive; RDI = relative dose intensity.
aStatistics Canada, Population Estimates15
bWeighted average for Canada (excluding Quebec) derived from CIHI18 and Conference Board of Canada19 reports.
cWeighted average prevalence by jurisdiction from Statistics Canada,16 presumably linearly extrapolated. NIHB was assumed to be the same as the weighted average of Canada excluding QC.
d||||| || | |||||| ||||||||| || ||| ||||||| || |||| |||| || || |||||||| |||||||||| ||| ||||| |||||||| |||| |||.17
e||||| || | |||||| ||||||||| || ||| ||||||| || |||| || || |||||||| |||||||||| ||| ||||| |||||||| |||| |||.17
f||||| || | |||||| ||||||||| || ||| ||||||| || |||| || || |||||||| |||||||||| ||| ||||| |||||||| |||| |||.17
gBased on formulary and wholesale list prices in each jurisdiction as reported by IQVIA Delta PA and ODB12,14 excluding markups and dispensing fees. List prices are substantially higher for imatinib in Alberta, British Columbia, and Saskatchewan than other jurisdictions, while list prices for dasatinib are substantially higher in Alberta, British Columbia, Ontario, Saskatchewan, and NIHB than other jurisdictions.
hDerived from the ASCEMBL trial, Jan 6 2021 data cutoff.4
iDerived from an analysis agreed upon by the sponsor and the Groupe québécois de recherche en leucémie myéloïde chronique (LMC) et néoplasies myéloprolifératives (NMP).17
jDerived from the literature.20-23
kAssumption.
Summary of the Sponsor’s BIA Results
Results for the sponsor’s base case indicated that reimbursement of asciminib for the treatment of Ph+CML-CP in patients who have used at least 2 previous TKIs is associated with a budgetary impact of $1,291,142 in Year 1, $1,353,905 in Year 2, and $1,419,897 in Year 3, for a 3-year total incremental cost of $4,064,943 including markups and dispensing fees. The 3-year total incremental cost without markups and dispensing fees was $3,691,993.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Model lacked flexibility and transparency: The sponsor’s methodology was poorly reported in the submitted BIA report which in some instances appeared contradictory (e.g., the methods section describes the implementation of subsequent treatment costs. These costs were excluded in the analysis, which was not mentioned until the results section), while the model contained many hardcoded inputs making it difficult to test alternate market share and displacement assumptions.
CADTH was unable to fully account for this limitation. Decreased transparency provided to the review increases uncertainty in any resulting analyses, while decreased flexibility limits the ability to explore different assumptions, also increasing uncertainty.
Relative dose intensities were inconsistent: The sponsor incorporated dose intensities from the ASCEMBL trial for asciminib and bosutinib and assumed all other comparators would be used at 100% of the indicated dose. The clinical experts consulted by CADTH did not support this assumption, stating that nilotinib and dasatinib would be used at approximately a 60% dose intensity, and that ponatinib especially tends to be used at lower doses than stipulated in the product monograph, generally 15 mg for long-term patients rather than 45 mg, due to cardiac toxicities. These toxicities were highlighted by patient and clinician input received by CADTH. The use of a 15 mg dose for ponatinib was also supported by sources within the published literature.6-8
After consultation with clinical experts, CADTH reduced the dose intensities of dasatinib and nilotinib to 60%, while that of ponatinib was reduced to 44.75% to reflect the cost difference between the 15 mg and 45 mg tablet strengths.. A scenario analysis was conducted increasing the RDI of asciminib and bosutinib to 100%..
Market share and market capture is uncertain: The clinical experts consulted by CADTH did not agree with the sponsor’s market share assumptions in the reference scenario, believing the sponsor underestimated the proportion of patients in the 3L+ setting who would receive ponatinib and bosutinib. While the experts considered the sponsor’s estimate that asciminib would capture ||||% of the market share in Year 1 to be reasonable, they indicated that asciminib’s market capture, if funded, would continue to grow throughout the time horizon, to a maximum of 60% in Year 3.
CADTH altered the market share distribution in the reference scenario as outlined in Table 23, and increased the market uptake of asciminib to 50% and 60% in Years 2 and 3, respectively. The proportion of asciminib market share displaced from each comparator was kept approximately the same as assumed by the sponsor, though exact proportions could not be maintained due to the hard-coded market share entries submitted.
Subsequent treatments were improperly modelled and excluded from the base case: The sponsor’s model took a non-standard approach to treatment duration due to its reliance on prevalence data rather than incidence data to inform the size of the patient population. While each treatment was assigned a duration of therapy derived from a naïve comparison of median treatment durations in individual clinical trials or registries, only those with a duration of less than 12 months (i.e., bosutinib and nilotinib) impacted the model. This effect was due to the sponsor’s assumption that all therapies would reset every year. Thus asciminib, imatinib, dasatinib, and ponatinib accrue costs across all 36 months of the time horizon, with Allo-SCT also assumed to occur for the proportion of the population assigned to it every 12 months (presumably to different patients), while bosutinib and nilotinib only accrue drug acquisition costs for 7 out of 12 and 11 out of 12 months of each year, respectively. While the sponsor appears to be attempting to model general proportions of TKI use within the entire population eligible for asciminib, the approach does not appropriately reflect clinical prescribing, or how changes in usage patterns in 1 year would affect the subsequent years’ usage. While the sponsor’s model did have the option to incorporate a “subsequent therapy costs” function, this function only applied subsequent therapy costs to the bosutinib and dasatinib treatment arms. The results of this analysis option were not reported by the sponsor. Additionally, this function was non-transparently modelled, requiring input tracing across multiple sheets and inadequately labelled cells while producing non-intuitive results.
CADTH was unable to appropriately adjust for this limitation due to inflexibility in the model’s structure. A scenario analysis was conducted altering the “duration of therapy” for all comparators to 12 months to reconceptualize the model’s market share assumptions to represent the proportion of prevalent patients on each TKI therapy at any given time, with some patients starting nilotinib or bosutinib mid-year as others discontinue them, however this scenario should be considered strictly exploratory.
The NIHB population was doubled counted: The sponsor’s model included the total population of each province in Canada extrapolated from Statistics Canada data (excluding Quebec) as well as the total client population of the NIHB, extrapolated from NIHB annual reports. However, clients of NIHB are included in Statistics Canada population data. Furthermore, oncology products are covered for all residents within the boundaries of Alberta and Saskatchewan, including those who are clients of NIHB, and NIHB clients residing within the boundaries of Ontario who are under 25 or over 65 years of age are also reimbursed by the provincial plan for pharmaceutical products.
CADTH removed the population reimbursed for oncology products by NIHB from each provincial jurisdiction. NIHB clients residing within Alberta and Saskatchewan, as well as those under 25 or over 65 years of age in Ontario, were instead removed from the NIHB population.
Comparator costs based on wholesale list prices which varied across jurisdictions: The sponsor’s drug acquisition costs for comparator products were based on list prices as reported by IQVIA’s Delta PA database as proxies for confidential prices paid by public plans. However, the list prices of imatinib and dasatinib varied across jurisidictions, with some provinces having prices for all versions of the product in line with the originator brand list price, while others had pricing in line with generic versions. It is likely that the costs paid by the provincial plans are less than these publicly available list prices, especially for products with generics versions available.
CADTH conducted a scenario analysis where the list prices of imatinib and dasatinib as reported in the least expensive jurisdictions were applied to all jurisdictions.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analysis by: updating relative dose intensities, altering the initial market shares of the comparators and increasing uptake of asciminib in Years 2 and 3, and removing NIHB clients who were double counted in the sponsor’s analysis. These changes are outlined in Table 23.
Table 23: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption | ||
|---|---|---|---|---|
Corrections to sponsor’s base case | ||||
None. | — | — | ||
Changes to derive the CADTH base case | ||||
1. RDIs corrected to match CUA assumptions | Nilotinib: 100% Dasatinib: 100% Ponatinib: 100% Imatinib: 100% Asciminib: 88.8% Bosutinib: 85.2% | Nilotinib: 60% Dasatinib: 60% Ponatinib: 44.75%a Imatinib: 100% Asciminib: 88.8% Bosutinib: 85.2% | ||
2. Market Share | Reference Scenario Asciminib: 0% Imatinib: ||||% Nilotinib: ||||% Dasatinib: ||||% Bosutinib: ||||% Ponatinib: ||||% Allo-SCT: ||||% New Drug Scenario Asciminib: ||||% Imatinib: ||||% Nilotinib: ||||% Dasatinib: ||||% Bosutinib: ||||% Ponatinib: ||||% Allo-SCT: ||||% | Reference Scenario Asciminib: 0% Imatinib: 4% Nilotinib: 13% Dasatinib: 12% Bosutinib: 37% Ponatinib: 28% Allo-SCT: 5% New Drug Scenario Asciminib: 42% / 50% / 60% Imatinib: 2% / 2% / 2% Nilotinib: 7% / 6% / 5% Dasatinib: 7% / 6% / 5% Bosutinib: 17% / 14% / 11% Ponatinib: 20% / 18% / 15% Allo-SCT: 4.5% / 3.9% / 3.5% | ||
3. NIHB double counting correction | Base Year (2021) Provinces, excluding Quebec: 29,513,720 NIHB: 895,982 Total: 30,409,702 | Base Year (2021) Provinces, excluding Quebec: 29,148,897 NIHB: 513,108 Total: 29,662,005 | ||
CADTH base case | 1 + 2 + 3 | |||
BIA = budget impact analysis; NIHB = Non-Insured Health Benefits; RDI = relative dose intensity; SCT = stem cell transplant.
Note: Changes to RDI and market share assumptions were derived with input from the clinical experts consulted by CADTH.
aWhile the intended RDI of ponatinib was 33% of the monograph-recommended dosing (i.e., 15 mg daily rather than 45 mg daily), ponatinib was modelled at an RDI of 44.7% to better reflect the cost difference between the 45 mg and 15 mg tablets
The results of the CADTH step-wise re-analysis are presented in summary format in Table 24 and a more detailed breakdown is presented in Table 25. Applying these changes resulted in a 3-year budget impact of $13,266,975.
Table 24: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $4,064,943 |
CADTH reanalysis 1: Dose intensity | $4,401,363 |
CADTH reanalysis 2: Market share and displacement | $640,449 |
CADTH reanalysis 3: NIHB double counting correction | $3,953,785 |
CADTH base case, reanalyses 1 thru 3 | $13,266,975 |
BIA = budget impact analysis; NIHB = Non-Insured Health Benefits; RDI = relative dose intensity.
CADTH also conducted scenarios assuming that dasatinib and imatinib would be available throughout Canada at prices consistent with their price in the least expensive jurisdiction, assuming durations of therapy of 12 months to explore the impact of considering the market share to represent the proportion of patients on each therapy at any given time, increasing the RDI of asciminib and bosutinib to 100%, removing markups and dispensing fees from the analysis, and considering a 26% price reduction in the price of asciminib, consistent with that required for the CADTH base case to be cost-effective at a willingness to pay of $50,000 per QALY.
Table 25: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $22,719,047 | $23,833,168 | $25,004,637 | $26,236,523 | $75,074,328 |
New drug | $22,719,047 | $25,124,310 | $26,358,542 | $27,656,420 | $79,139,272 | |
Budget impact | $0 | $1,291,142 | $1,353,905 | $1,419,897 | $4,064,943 | |
CADTH base case | Reference | $15,307,582 | $16,059,062 | $16,921,049 | $17,909,297 | $50,889,408 |
New drug | $15,307,582 | $19,656,337 | $21,248,571 | $23,251,475 | $64,156,383 | |
Budget impact | $0 | $3,597,276 | $4,327,522 | $5,342,178 | $13,266,975 | |
CADTH scenario A: dasatinib and imatinib at lowest price | Reference | $14,236,589 | $14,934,912 | $15,736,109 | $16,654,858 | $47,325,878 |
New drug | $14,236,589 | $19,006,719 | $20,657,390 | $22,768,102 | $62,432,211 | |
Budget impact | $0 | $4,071,807 | $4,921,281 | $6,113,244 | $15,106,332 | |
CADTH scenario B: 12-month duration for all therapies | Reference | $18,445,116 | $19,350,400 | $20,388,809 | $21,579,320 | $61,318,529 |
New drug | $18,445,116 | $21,162,502 | $22,579,777 | $24,319,350 | $68,061,629 | |
Budget impact | $0 | $1,812,101 | $2,190,968 | $2,740,030 | $6,743,100 | |
CADTH scenario C: asciminib and bosutinib RDI is 100% | Reference | $15,951,581 | $16,734,535 | $17,632,619 | $18,662,249 | $53,029,403 |
New drug | $15,951,581 | $21,100,481 | $22,946,104 | $25,280,293 | $69,326,878 | |
Budget impact | $0 | $4,365,946 | $5,313,485 | $6,618,044 | $16,297,475 | |
CADTH scenario D: markups and dispensing fees removed | Reference | $13,982,263 | $14,666,129 | $15,450,228 | $16,348,847 | $46,465,204 |
New drug | $13,982,263 | $18,187,585 | $19,694,720 | $21,603,439 | $59,485,744 | |
Budget impact | $0 | $3,521,456 | $4,244,493 | $5,254,593 | $13,020,541 | |
CADTH scenario E: 26% price reduction per CADTH CUA base case | Reference | $15,307,582 | $16,059,062 | $16,921,049 | $17,909,297 | $50,889,408 |
New drug | $15,307,582 | $17,173,415 | $18,134,320 | $19,296,357 | $54,604,092 | |
Budget impact | $0 | $1,114,353 | $1,213,271 | $1,387,060 | $3,714,685 |
BIA = budget impact analysis; CUA = cost-utility analysis; RDI = relative dose intensity.
Stakeholder Input
Patient Input
The Lymphoma & Leukemia Society of Canada and The Canadian Chronic Myelogenous Leukemia Network
About the Lymphoma & Leukemia Society of Canada and the Canadian Chronic Myelogenous Leukemia Network
The organizations involved in this submission are Canadian registered charities that provide support, education, and advocacy for their patient constituents. To learn more about the organizations involved in this submission, you can visit their respective websites:
The Lymphoma and Leukemia Society of Canada (LLSC) - https://bloodcancers.ca
The Canadian CML Network - https://cmlnetwork.ca/
Information Gathering
The patient organizations in collaboration conducted an anonymous online survey for patients with CML between November 30, 2021 – January 3, 2022. The survey was made available via social media outlets, including Twitter, Instagram and Facebook accounts, and was further sent to physicians to share with their patients. The survey had a combination of multiple choice, rating and open-ended questions. Skipping logic was built into the survey so that respondents were asked questions only relevant to them. Open- ended responses to surveys that reflected the sentiment of a majority are included verbatim to provide a deeper understanding of patient perspectives.
There were 16 respondents to the survey, of which 11 were people with CML and 5 were a caregiver, friend or family member answering on behalf of someone with CML. 11 patients received treatment with Asciminib. The remainder of the patients without treatment experience were able to provide their experience with CML. All of the patients that responded to this survey, (see Tables 1 and 2), live in Canada, 56% are female and 69% are ≥ 55 years- old.
Table 1: Country of Survey Respondents (16 Respondents)
Respondents | BC | NS | NWT | ON | QC | Total |
|---|---|---|---|---|---|---|
Patients WITHOUT Ascminib experience | 1 | 1 | 1 | 2 | 5 | |
Patients WITH Asciminib experience | 9 | 2 | 11 |
Table 2: Gender and Age of Survey Respondents (16 Respondents)
Respondents | Age Range | Gender | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
<18 | 18- 24 | 25- 34 | 35- 44 | 45- 54 | 55- 64 | 65- 74 | 75+ | Female | Male | Total | |
Patients WITHOUT Asciminib experience | 1 | 1 | 1 | 1 | 1 | 3 | 2 | 5 | |||
Patients WITH Asciminib experience | 1 | 1 | 2 | 5 | 2 | 4 | 7 | 11 | |||
Of the respondents, 10 were (at the time of the survey) in the chronic phase of CML, 2 were in remission, and 4 did not know which phase of CML they were in.
Disease Experience
The majority of the respondents (69%) have been living with CML for 5 or more years (13 respondents). Patients without asciminib experience have received an average of 2.6 lines of treatment for their CML and patients with ascimnib experience have received an average of 4 lines of treatment for their CML (see Table 3).
Table 3: Number of Years Living With CML and Number of Lines of Treatment
Respondents | Number of years living with CML | Total # of lines of treatment received for CML | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
<1 mo | 1-6 mos | 6-12 mos | 1-3 yrs | 3-5 yrs | 5+ yrs | Total | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Total | |
Patients WITHOUT Asciminib experience | 1 | 1 | 2 | 1 | 1 | 2 | 1 | 5 | |||||||
Patients WITH Asciminib experience | 1 | 1 | 9 | 11 | 1 | 3 | 3 | 2 | 1 | 10 | |||||
CML can have a lasting impact on a patient’s life, as symptoms can continue for years. On a scale of 1 (no impact)to 5 (extremely large impact) 14 respondents rated how symptoms of CML have impacted their day-to-day lives: ability to exercise (2.21), mental health (2.15), ability to work (2.15), ability to travel (2.08), ability to concentrate(2.08), personal image (2.00), and ability to continue daily activities (2.00).
CML can also have a psychological/social impact on a patient’s life as shown in Table 4:
Table 4: Quality of Life Impacts Related to CML
Psychological/Social Impact | Weighted Average | Significant Impact (4-5) |
|---|---|---|
Stress/anxiety/worry | 2.43 | 14% |
Difficulty sleeping | 2.31 | 15% |
Loss of sexual desire | 2.25 | 25% |
Financial impacts (cost of travel, inability to work, etc.) | 2.23 | 15% |
Interruption of life goals/accomplishments (career, schooling, etc.) | 2.08 | 15% |
Depression | 2.00 | 8% |
Experiences With Currently Available Treatments
One respondent indicated that they have received Tyrosine Kinase Inhibitors (TKIs) for their CML after diagnosis. 3 respondents have also had chemotherapy and 1 respondent has had biological therapy.
Experience with TKIs: Table 5 illustrates the number of different TKIs patients have taken.
Table 5: Number of Different TKIs Taken (10 Respondents)
Respondents | 1 | 2 | 3 | 4 + | Total |
|---|---|---|---|---|---|
Patients WITHOUT Ascminib experience | 1 | 1 | |||
Patients WITH Asciminib experience | 2 | 4 | 3 | 9 |
Of the 10 patients that have received TKIs, 6, at one point or another, have had to discontinue therapy due to intolerance or toxicity. When asked to explain why, they provided the following responses:
“I was initially on Gleevac, but the CML mutated to 315TI, and Gleevac is ineffective. I was put on Ponatinib with high risk for heart issues, which occurred after two years and I had to discontinue. I was put on Asciminib three years ago, as last resort.”
“side effects and have to stay in hospital for treatment.”
“One tki bad headache next one felt like I had the flu last one did something to my liver “
“The Whole-body Rash”
“Elevated liver enzymes on Bosulif. Pleural effusion with Sprycel, Tasigna. Required thoracentesis.”
Impact of Side Effects of TKIs: Patients were asked to describe how the side effects experienced with TKIs have impacted their quality of life. Rated on a scale from (1=did not experience side effect, to 5=extremely significantimpact). Fatigue was reported as most prominent with an average rating of 3.1 (moderate) with 50% of respondents scoring it either a 4 (significant impact) or 5 (extremely significant impact). See Table 6.
Table 6: TKI Side Effect Impact on Quality of Life
Side Effect | Weighted Average | Significant Impact (4-5) |
|---|---|---|
Fatigue/Tiredness | 3.1 | 50% |
Rash | 2.7 | 30% |
Muscle Cramps or Pain | 2.6 | 40% |
Joint Pain | 2.4 | 20% |
Headaches | 2.3 | 20% |
Diarrhea | 2.3 | 10% |
Low white blood counts (infections) | 2.2 | 20% |
Low platelet count (bruising, bleeding) | 2.1 | 10% |
Abdominal Pain | 2.1 | 10% |
Fluid Retention | 2.1 | 20% |
Dizziness | 2.0 | 10% |
Some respondents provided additional feedback about their experience with CML and its treatment:
“Both TKI treatments that I've taken did not effectively reduce my BCR/ABL levels to achieve a Major Molecular Response”
“Generally I was able to cope with very mild side effects. I took ibuprofin for pain and magnesium supplement for control of problems.”
“They all have significant side effects, which are always minimized by the physicians. Ponatinib had the least day-to-day side effects, but it has a high risk of heart issues. Asciminib to date does not seem to have any serious side effects. Personally it has caused me significant GI issues (i.e. colitis), but I believe it is partly due to the fact that I have had a history of colitis on and off. Headaches and arthralgia/myalgia are an issue for me, along with fatigue and poor sleep. That being said, my CML molecular count is currently not detectable at a dosage of 160 mg. per day.”
“Hope I have this correct the tki"s that I tried my body didn't like but the asciminib is working great “
“I experienced a significant fluid retention that limited my ability to walk (shortness of breath, pleuritis with large amount of fluid that required additional diagnostic tests and treatment). Fatigue that limited my activity. Rash with pruritis the interfered with my quality of life and sleep.”
“Need to spend a lot of energy on drug control”
“Muscle and bone/joint pain. Pain constant but can be distracted from by my working or taking part in other activities.”
“Physicians/specialists should be more forthcoming about the side effects. Their main goal is to keep you alive and this philosophy is shared by most patients, but not all. In my case, quality of life is more important than longevity. Also, when the physicians start these KTI treatments, they should be administered on a gradual basis rather than instantly taking the maximum dose required. The body needs to adjust to these medications and a slower approach will be easier on the patient and may result in a more successful outcome. An exercise routine is really important to maintain. Proper diet is vital as well.”
Improved Outcomes
When making a decision about taking a new CML treatment, patients rated the impact on quality of life as themost important factor on a scale from 1-5 (1= not important at all, and 5 =extremely important) (Table 7).
Table 7: Important Considerations Related to New CML Treatments (11 Respondents)
Consideration | Rating (4-5) | Consideration | Rating (4-5) |
|---|---|---|---|
That the treatment Improves Quality of Life | 100% | Outpatient treatment (no overnight hospital stay required) | 83.3% |
Severity of side effects | 91.66% | Covered by insurance/drug plan | 83.33% |
Recommended by healthcare team | 83.3% | The impact to caregiver/partner/family | 75% |
Least amount of travel required for treatment | 83.3% | Improved length of survival | 75% |
Degree of certainty that it will improve my condition | 83.3% |
Some respondents provided additional feedback about what they would like to see in new treatments for CML:
“A treatment that is 100% effective in eliminating the detectable cancer cells in the blood. Basically a cure for this disease.”
“minimal side effects, improvement of the length of survival, and improvement of quality of life”
“More convenient, live longer”
“Once daily dose whenever possible.”
Experience With Drug Under Review
Two patients were treated with asciminib and shared their experience with the drug. Patients received this treatment for 1-3 years (64%), 1-6 months (18%), 6-12 months (9%), or less than 1 month (9%). 10 patients were still receiving this treatment while completing the survey and one patient indicated that they had to stop/reduce the dose for approximately 2 weeks because of problems with the delivery of the drug.
Patients were able to access this treatment through a compassionate use program (45.5%), clinical trial (45.5%) or having it paid for by a cancer board/agency or government (9%). Patients were questioned about the difficulty in obtaining the drug, and on a scale of 1 to 5 (1=not difficult, 5=extremely difficult), 1 patient found it extremely difficult to get a prescription from a physician and 1 patient found it extremely difficult to get the drug delivered to them.
Side Effects of Treatment: Patients were asked to describe the side effects they experienced with Asciminib treatment. Rated on a scale from (1=did not experience side effect, to 5=very serious side effect), most patients rated their side effects at 3 or below, indicating that the side effect was either not experienced, or it was minor or manageable. Side effects that were rated 4 (Serious) are: Fatigue (1), Nausea (1), and Vomiting (1). The side effects that were rated 5 (Very serious) include: Musculoskeletal Pain (1), Arthralgia (1), Rash (1), and Itchy Skin (1).
Quality of Life: To understand the impacts of Asciminib on patients’ quality of life, on a weighted scale from 1-5 (1=strongly negative impact, 3= no impact, 5=strongly positive impact), the majority of patients rated a positive impact of this treatment on their ability to perform daily activities (Table 8).
Table 8: Quality of Life Impacts with Asciminib Treatment (11 Respondents)
Impact | Weighted Average |
|---|---|
Perform daily activities | 4.09 |
Relationships with family/friends | 3.82 |
Mental health | 3.82 |
Ability to work/go to school/volunteer | 3.73 |
Personal image | 3.64 |
Travel | 3.45 |
Intimate relationships | 3.40 |
Patients were asked how much they agree with the following statement “Asciminib improved my quality of life compared to other treatments I have received for CML.” On a scale of 1 – 5 (1=strongly disagree, 3=neither agree nor disagree, 5=strongly agree), 89% of patients strongly agreed with the statement and 11% agreed with the statement. (9 respondents)
Overall Experience: Based on their experience with Asciminib, all 11 patients would recommend this treatment toother patients diagnosed with CML. They provided the following comments on their overall experience with Asciminib:
“Asciminib has been paramount for me to live the best life possible while having CML.”
“I just started 2 weeks ago and everything is good.”
“I was one of the first patients in Canada to take it. The initial recommended dosage was too much for me to tolerate, but luckily it has worked at lower doses than initially recommended to T315I mutation. It has produced excellent results for the CML (now not detectable), but it does have side effects that impact quality of life (in my case pre-existing conditions are part of the problem).”
“Excellent experience”
“Great medicine. Got back my normal life”
“I'm really impressed .the first few treatments with other drugs gave me headaches. Felt sick one made my liver start to fail.”
“The best CML treatment that has no side effects on me, improved not only my quality of life but the quality of life of my family members ( they are less worry and not anxious as I do not have any side effects). I have good energy level and do not feel fatigued , able to perform all of my activities of daily leaving. Easy to take pill.”
“The effect that can be felt makes me feel more and more relaxed in my life.”
“I find it tolerable but really do not know how well it is controlling the leukaemia. I had BCR abl blood work today so will know in a few weeks. The delivery delay and being off a drug was unsettling and stressful for me. How might this have contributed to progression of the CML.”
“Best thing that happened to me, new lease to life, since Glyvec and Bosulif were no longer an option for me”
“Good”
Companion Diagnostic Test
There is no companion diagnostic testing required for this treatment.
Patient Group Conflict of Interest Declaration — The Leukemia & Lymphoma Society of Canada and Canadian Chronic Myelogenous Leukemia Network
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Response: No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Response: No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 9: Conflict of Interest Declaration for The Leukemia & Lymphoma Society of Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | — | — | — | X |
Table 10: Conflict of Interest Declaration for Canadian Chronic Myelogenous Leukemia Network
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | — | X | — | — |
Chronic Myelogenous Leukemia Society of Canada
About the Chronic Myelogenous Leukemia Society of Canada
Describe the purpose of your organization. Include a link to your website.
Response: Established in 2006, the CML (chronic myelogenous leukemia) Society of Canada provides support, education, and information on CML, current and emerging treatments and research initiatives for people living with CML and their families. The mission of the CML Society is to help reduce suffering and improve care and the quality of life of CML patients.
Treatment of CML has drastically extended survival with the advent of targeted tyrosine kinase inhibitors (TKI). The CML Society of Canada, acts as the eyes, ears, and voice of its CML community, working to change the treatment paradigm as well as the course of this disease while supporting its constituents.
Information Gathering
CADTH is interested in hearing from a wide range of patients and caregivers in this patient input submission. Describe how you gathered the perspectives: for example, by interviews, focus groups, or survey; personal experience; or a combination of these. Where possible, include when the data were gathered; if data were gathered in Canada or elsewhere; demographics of the respondents; and how many patients, caregivers, and individuals with experience with the drug in review contributed insights. We will use this background to better understand the context of the perspectives shared.
Response: The patient input covered in this submission was gathered using Survey’s, and interviews. The data was gathered during the month of January and February 2022. The information was gathered in Canada, by the internet and includes the responses given to us by ten (10) patients and caregivers with CML. An even mix of male to female and an age group of 40 – 70 years of age. Note: we only used remote/internet due to the constraints of the pandemic.
Disease Experience
CADTH involves clinical experts in every review to explain disease progression and treatment goals. Here we are interested in understanding the illness from a patient’s perspective. Describe how the disease impacts patients’ and caregivers’ day-to-day life and quality of life. Are there any aspects of the illness that are more important to control than others?
Response: Most patients are diagnosed with CML during a routine blood test. However, once it is diagnosed, treatment must be started quickly. These patients are usually diagnosed in the more treatable, chronic phase of the disease. If the disease progresses or has a chance to develop mutations, treatments options can be very limited and much more invasive. In most cases the patients didn’t really ‘feel’ sick, so starting treatment with Tyrosine Kinase Inhibitors can cause some unpleasant side effects at the beginning of treatment. The main side effects of treatment are fatigue, muscle cramps and spasms, as well as severe water retention in some cases. These side effects might sound rather benign, but their impact on a patient’s quality of life can be such that it makes it difficult for patients to be compliant in taking their treatment. To confirm the diagnoses of CML, the healthcare team needs to do a bone marrow aspiration (biopsy). Some patients do not experience too much discomfort during this procedure, but for others it can be quite painful. Patients will also need to have PCR diagnostic test done at the time of diagnoses as this helps to understand the phase of the disease and may also provide guidance as to which treatment to start (there are currently 4 different TKI’s available). The biggest impact for newly diagnosed patients is the financial aspect regarding the cost of the treatment as well as determining drug coverage issues with insurance. CML is usually considered a disease that occurs later in life, but there are many patients who are diagnosed in their 30’s and 40’s. This is obviously a very critical point in a person’s life. These patients are trying to continue with their jobs, raise families, pay mortgages and other living expenses. A diagnose of CML in this age group is very difficult to manage for these patients as they very often feel overwhelmed, extremely fatigued, and emotionally drained. It takes a toll on every member of the family as the family routine changes significantly. During the first year of treatment the patient needs to have closely scheduled regular checkups along with PCR diagnostic tests to make sure that the patient is responding to treatment. Monthly, and quarterly doctor visits can be very stressful. Very often caregivers/spouses must take on more burdens of running/managing the family household which causes additional stresses.
Experiences With Currently Available Treatments
CADTH examines the clinical benefit and cost-effectiveness of new drugs compared with currently available treatments. We can use this information to evaluate how well the drug under review might address gaps if current therapies fall short for patients and caregivers.
Describe how well patients and caregivers are managing their illnesses with currently available treatments (please specify treatments). Consider benefits seen, and side effects experienced and their management. Also consider any difficulties accessing treatment (cost, travel to clinic, time off work) and receiving treatment (swallowing pills, infusion lines).
Response: Because Ascinimib is only being offered to CML patients who have failed at least 2 other TKI treatments, we describe the issues with the patients interviewed which led them to being offered Ascinimib. Patients interviewed reported 1.) side effects from previous TKI treatments were so severe that quality of life was seriously impacted. Imatinib caused severe digestive issues and swelling, Dasatinib caused severe pulmonary hypertension or serious levels of pleural effusion, bosutinib caused severe chronic diarrhea, nilotinib cause ischemic attacks, and serious cardiovascular problems. Some patients seem to be doing well on their TKI treatment but suddenly were found to develop a severe almost fatal mutation or disease progression. One patient was put on Ascinimib after having a bone marrow transplant and relapsing within 100 days post-transplant. In this patient Ascinimib has been a life extending/lifesaving drug. These patients needed to be managed with closer follow ups increasing clinic/hospital visits, extended time off work, quality of life issues, and various medical insurance expenses. These patients were able to access Ascinimib either through a clinical trial or compassionate use.
Improved Outcomes
CADTH is interested in patients’ views on what outcomes we should consider when evaluating new therapies. What improvements would patients and caregivers like to see in a new treatment that is not achieved in currently available treatments? How might daily life and quality of life for patients, caregivers, and families be different if the new treatment provided those desired improvements? What trade-offs do patients, families, and caregivers consider when choosing therapy?
Response: As mentioned above, each TKI has a certain set of potential debilitating side effects. In the patients we surveyed/interviewed, reported a reduction in serious side effects with Ascinimib as well as having the benefit of their ‘difficult to treat’ CML being better clinically managed. Since there are generic equivalents of both Gleevec (imatinib) and Sprycel (dasatinib) a big tradeoff is that Ascinimib costs more than these generic versions of TKI’s
Experience With Drug Under Review
CADTH will carefully review the relevant scientific literature and clinical studies. We would like to hear from patients about their individual experiences with the new drug. This can help reviewers better understand how the drug under review meets the needs and preferences of patients, caregivers, and families.
How did patients have access to the drug under review (for example, clinical trials, private insurance)? Compared to any previous therapies patients have used, what were the benefits experienced? What were the disadvantages? How did the benefits and disadvantages impact the lives of patients, caregivers, and families? Consider side effects and if they were tolerated or how they were managed. Was the drug easier to use than previous therapies? If so, how? Are there subgroups of patients within this disease state for whom this drug is particularly helpful? In what ways? If applicable, please provide the sequencing of therapies that patients would have used prior to and after in relation to the new drug under review. Please also include a summary statement of the key values that are important to patients and caregivers with respect to the drug under review.
Response: These patients’ access Ascinimib through clinical trials, compassionate use, and in the case of the few patients located in the U.S. (where Ascinimib is FDA approved) through their private insurance. For these patients, there really are not other viable options for treatments other than Ascinimib for the reasons that we stated above. All the patients interviewed noted that their side effects on Ascinimib were better tolerated than with the prior TKI’s. Ascinimib will be an important drug for patients for whom currently available TKIs do not offer them a reasonably good quality of life, or if they have the T315I mutations, or other mutations that may reduce the ability of currently available TKI’s in disease management. Usually, CML patients are offered imatinib at diagnosis if their CML is in the chronic early stage. If the patient doesn’t respond well or if the patient cannot tolerate imatinib, the healthcare team may switch the patient to either Nilotinib or Dasatinib. If the patient’s disease does not respond to these drugs, or if they are associated with self-limiting side effects the patient might be switched to Ascinimib (if it gains market approval). The key values important to patients and caregivers are - improving quality of life, better disease management, life extending, a return to a ‘normal’ life with better managed side effects.
Companion Diagnostic Test
If the drug in review has a companion diagnostic, please comment. Companion diagnostics are laboratory tests that provide information essential for the safe and effective use of particular therapeutic drugs. They work by detecting specific biomarkers that predict more favourable responses to certain drugs. In practice, companion diagnostics can identify patients who are likely to benefit or experience harms from particular therapies, or monitor clinical responses to optimally guide treatment adjustments.What are patient and caregiver experiences with the biomarker testing (companion diagnostic) associated with regarding the drug under review?
Consider: Access to testing: for example, proximity to testing facility, availability of appointment; Testing: for example, how was the test done? Did testing delay the treatment from beginning? Were there any adverse effects associated with testing?; Cost of testing: Who paid for testing? If the cost was out of pocket, what was the impact of having to pay? Were there travel costs involved?; How patients and caregivers feel about testing: for example, understanding why the test happened, coping with anxiety while waiting for the test result, uncertainty about making a decision given the test result.
Response: All CML patients, regardless of treatment must have access to a PCR test. This test determines the level of the oncogene transcripts (BCR ABL) in the patients’ blood and is the most important tool available to clinicians in determining the response to the treatment. PCR tests are done at the hospital lab at the time of the healthcare team visit by having a blood draw. In Canada the PCR testing is paid by the hospital. In general, CML patients understand the need for PCR testing and understand what the test is looking for.
Anything Else?
Is there anything else specifically related to this drug review that CADTH reviewers or the expert committee should know?
Response: In time, with more use/experience with this drug we may find that this drug offers additional benefits for patients who have a T315I mutation. Currently there is a drug on the market, Ponatinib, that is specifically used to treat CML patients with hard to manage disease or who have the T315I disease.
However, for some patients, Ponatinib can cause serious cerebral neurovascular side effects. Ascinimib might be a better choice for those patients and help some patients avoid a bone marrow transplant.
Patient Group Conflict of Interest Declaration — Chronic Myelogenous Leukemia Society of Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Response: No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Response: No
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 11: Conflict of Interest Declaration — Chronic Myelogenous Leukemia Society of Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
None declared | — | — | — | — |
Since 2015, The CML Society of Canada has not received any funding from either pharmaceutical companies or any other business or government grant. We are volunteers and are self-funding.
Clinician Input
OH-CCO Hematology Cancer Drug Advisory Committee
About the OH-CCO Hematology Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
This input was jointly discussed via Drug Advisory Committee meeting and email.
Current Treatments
Regarding relapsed/refractory CP-CML or with intolerance to previous two TKIs, bosutinib is available, but not after third line therapy. Ponatinib is available for T315 mutations and as third line therapy. Allogeneic stem cell transplant is available for eligible patients who have shown progression on multiple TKIs or severe intolerance and typically would be considered after 3 lines of therapy. In very palliative cases, Cytarabine, Interferon or hydroxyurea or busulfan could be used.
Treatment Goals
Major molecular responses are the primary goals as they result in improved quality of life, improved blood counts and/or organomegaly and avoidance or delay in the need for allogeneic stem cell transplant. Major molecular responses are a standard primary outcome measure in CML trials and have been associated with improved survival, decreased blastic transformation and improved outcomes in studies.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Response: Some patients will have intolerance or progression on prior TKIs and will need a third line therapy. Asciminib would be a preferred option instead of bosutinib as third line therapy given its favourable efficacy and toxicity profile. Different mechanism of action may be well suited to those patients who have had significant intolerance to prior TKIs. Ponatinib is also available as third line therapy but does have some cardiovascular toxicity that may not be well suited for certain patients.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Response: Those with significant intolerance or progression on at least two prior TKIs.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Response: Asciminib may be the preferred third line therapy for third line CP-CML. This would still allow access in Ontario to Ponatinib as fourth line therapy, but not Bosutinib with current funding criteria. This would delay the need for allogeneic stem cell transplant.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Response: As the study has shows better tolerability and efficacity than bosutinib, asciminib would be a better choice as third line therapy.
How would this drug affect the sequencing of therapies for the target condition?
Response: First line treatment with a first or second line TKI would not be affected. Asciminib may be the preferred third line agent, and still preserve access to ponatinib as 4th line. In the event that asciminib is used as 4th line therapy, current funding does not allow ponatinib or bosutinib as 5th line therapy.
Which patients would be best suited for treatment with the drug under review?
Response: As per submission, CP-CML after at least two lines of TKI therapy.
How would patients best suited for treatment with the drug under review be identified?
Response: Hematologist’s current practices.
Which patients would be least suitable for treatment with the drug under review?
Response: Those with accelerated/blastic phase CML. Those with the T315i mutation would also be better suited for treatment with ponatinib.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Response: No.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Response: Standard CML laboratory values (molecular response), as well as blood counts and improvement in symptoms.
What would be considered a clinically meaningful response to treatment?
Response: Major molecular response at 6 months. If a lesser response but clinically improved, can also continue on asciminib, as long as there is no progression or intolerance.
How often should treatment response be assessed?
Response: As per standard CML practice, monthly CBCs and other labs and molecular monitoring every 3 months.
What factors should be considered when deciding to discontinue treatment?
Response: Disease progression and/or significant intolerance.
What settings are appropriate for treatment with the drug under review?
Response: Oral therapy taken at home.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Response: N/A
Additional Information
In another small study, there is some evidence to suggest this drug is helpful for T315I mutation. See attached link - https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-asciminib-philadelphia-chromosome-positive- chronic-myeloid-leukemia
Conflict of Interest Declarations — OH-CCO Hematology Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Response: OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
Response: No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Tom Kouroukis
Position: OH-CCO Hematology Cancer Drug Advisory Committee Lead
Date: 25/01/2022
Table 12: Conflict of Interest Declaration for OH-CCO Hematology Cancer Drug Advisory Committee — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
None declared | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Pierre Villeneuve
Position: OH-CCO Hematology Cancer Drug Advisory Committee Member
Date: 25/01/2022
Table 13: Conflict of Interest Declaration for OH-CCO Hematology Cancer Drug Advisory Committee — Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
None declared | — | — | — | — |
Clinician Group of Hematologists Across Canada
About the Clinician Group of Hematologists Across Canada
Please describe the purpose of your organization. Include a link to your website (if applicable).
Response: The Clinician Group is a peer group of hematologists across Canada involved in the care of patients with Chronic Myeloid Leukemia (CML). Our group represents the diversity of hematology practice in Canada. Many of the authors are members of the Canadian Leukemia Study Group, the Canadian MPN Group and the Canadian Hematology Society.
Information Gathering
Please describe how you gathered the information included in the submission.
Response: This submission was co-authored by those listed at the end of the document. Clinical trial data were obtained from published manuscripts of the clinical trials leading to asciminib’s registration and abstracts presented at the American Society of Hematology meetings. Real world data were obtained from colleagues across the country who have had direct experience in the prescription and monitoring of asciminib through an access program.
Current Treatments
Describe the current treatment paradigm for the disease.
Response: There is currently an unmet need in the management of patients with both relapsed/refractory Philadelphia chromosome-positive chronic myeloid leukemia as well as those currently experiencing dose-limiting toxicities related to currently funded tyrosine kinase inhibitors (TKIs).
Currently, therapeutic options are limited in the third line and beyond setting. Clinicians have the option of further pursuing one of four different TKIs, including Nilotinib, Dasatinib, Bosutinib and Ponatinib. Non-TKI therapies include allogeneic stem cell transplantation or consider other novel agents like, Omacetaxine (not Health Canada approved).
When trying to determine the best TKI therapy, there are important patient, disease and therapy-related factors that must be taken into consideration, as each TKI has its own unique side effect profile. As an example, Dasatinib, a second generation TKI often used in early lines of therapy, is associated with the development of pleural effusions, necessitating hospitalizations, dose reductions and treatment discontinuation. Nilotinib, another second generation TKI and Ponatinib, a third generation TKI, have both been associated with the development of arterial occlusive events, with the latter drug also being associated with the development of heart failure—making these agents less ideal therapeutic options for patients with significant cardiovascular risk factors. Finally, Bosutinib, a second generation TKI, currently approved in second line, can be associated with significant GI toxicities and transaminitis, whose side effect profiles increases risk of dose reductions or discontinuation.
Amongst those patients with treatment failure, or those who are not achieving critical treatment milestones, the currently approved TKIs have disappointing rates of success of disease control. Moreover, the use of sequential treatments with different TKIs can lead to the emergence of new mutations that cause resistance to TKI therapy. The T315I mutation, which confers resistance to all approved therapies apart from ponatinib and allogeneic stem cell transplantations. In this setting, where a lack of efficacy can have significant life-limiting potential, achieving disease control with an efficacious and safe agent, with novel mechanism of action is important.
Treatment Goals
What are the most important goals that an ideal treatment would address?
Response: The goal of CML therapy varies depending on its clinical situation. After failing 2 lines of therapy, the primary goal of CML therapy is achievement of a molecular response quickly which would reduce the risk of disease progression significantly. When CML patients achieve major molecular response (defined as ≥ 0.1% or 3 log reduction or deeper level of BCR-ABL transcript level), the risk of disease progression is less than 2%. In comparison, this risk of disease progression is estimated as 10% when only complete cytogenetic response or MR2 response (defined as ≥ 1% or 2 log reduction or deeper level of BCR-ABL transcript level) is achieved, while this risk goes above 30-50% if patient fails to achieve cytogenetic response quickly within 12 months. Thus, the primary goal of CML therapy in patients treated for 3rd line therapy or beyond should be rapid achievement of major molecular response.
In addition, durability of molecular response is another important goal of CML therapy in this setting. Failure to at least 2 lines of CML therapy implies that the patients have advanced disease. Without any effective treatment to suppress leukemic clone, the leukemic clone easily acquires additional genomic/genetic changes. . Thus, durable molecular response is a very important surrogate for continuous suppression of the leukemic clone.
Also, tolerability and safety of treatment is critical during CML therapy in this setting of 3rd line therapy and beyond. If a patient cannot tolerate the medication, it will reduce compliance significantly and interrupt appropriate drug delivery, thus losing the chance to suppress the leukemic clone effectively. Also, because the patients have already failed 2 lines of TKI drugs, they have very limited options of other TKI drugs. Furthermore, due to other comorbidities or medical conditions they could be further precluded from the use of other TKI options. Accordingly, tolerability and reduction of adverse event resulting in discontinuation is a very important goal of CML treatment in this situation of CML patients having limited options of future lines of therapy.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Response: There are treatment gaps for two reasons: one resistance, and the other intolerance. Treatment failure to tyrosine kinase inhibitors occur in one third of CML patients, among which 2/3 are due to resistance while 1/3 is from intolerance. After failing 2 or more lines of therapy, the risk of progression to advanced disease becomes higher with more frequent clonal evolution in their CML clone. The molecular response of 3rd line therapy or beyond with currently available 2nd generation TKI drugs are somewhat unsatisfactory either by a lower response rate with a higher failure rate or by increasing the risk of intolerance with increasing risk of cardiovascular toxicity.
Another gap is intolerance to TKI therapy. Each TKI drug has its own toxicity profile, which limits the use of certain TKI drugs in the patients with certain comorbidities. For example, patients that have a past history of clinical vascular events such as myocardial infarction or stroke, or those having significant cardiovascular risk factors would be contraindicated to certain TKIs known to increase the risk of cardiovascular toxicity. In that case, remaining treatment options are very tight because they have already failed two TKIs or more, with restriction to other TKIs.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Response: Those patients having the following features/history would have the greatest unmet need: 1) failure to more than 2 TKI drugs including previous 2nd generation TKI with resistance/intolerance, and 2) past history of clinical cardiovascular events such as myocardial infarction or stroke or significant cardiovascular risks which precludes the use of other 2nd generation TKI drugs with potential to increase cardiovascular toxicity.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
1. Is there a mechanism of action that would complement other available treatments, and would it be added to other treatments?
Response: Asciminib has a unique mechanism of action to prevent the activity of the fusion oncogene BCR-ABL that is the founding event as a result of a chromosomal translocation between chromosomes 9 and 22 in chronic myeloid leukemia. The ABL gene is located on chromosome 9 and its product functions as a tyrosine kinase, an enzyme that has a binding pocket for ATP and separate binding pockets for the substrate that would contain the amino acid tyrosine that is to be phosphorylated by the enzymatic activity of the ABL protein, which hydrolyzes the terminal phosphate of ATP and transfer it to tyrosine. There are many potential targets of ABL for this tyrosine phosphorylation activity and the biological effect of which is to increase cell division, migration, and resistance to cell death (apoptosis). In the fusion oncogene BCR-ABL as a result of the chromosomal translocation, ABL is placed behind the gene BCR on chromosome 22. This BCR gene is normally transcribed in hematopoietic cells but in the case of cells containing the chromosomal translocation a fusion transcript arises containing the 5” (front end) of BCR attached to the whole of ABL which follows it. However, because the first exon of ABL does not contain a splice acceptor site, it is always spliced out in the final transcript of the fusion product. It is this fusion transcript lacking the first exon of ABL that causes it to act as an oncogene. This occurs because the tyrosine kinase activity of ABL is no longer regulated. In physiological circumstances where Exon-1 of ABL is expressed the amino terminal contains a site that can be modified by the addition of a fatty acid moiety called myrstoyl. This myrstoyl can bind to a pocket near the back end of ABL, and in this compressed “head to tail” configuration the binding pocket for ATP is “covered up” in a functional sense and the catalytic activity of ABL is inhibited. In normal circumstances the myrstoylation of the amino terminal of ABL is under physiological control to allow the tyrosine kinase activity to be appropriately turned on and off when the cell is required to divide, migrate, and continue to survive in a harsh environment. However, in BCR ABL the myrstoyl binding pocket is still present but there is no myrstoyl to bind to it as the Exon-1 part of ABL is not present.
In the treatment of CML the many orthostatic tyrosine kinase inhibitors that started the “targeted cancer drug” revolution in oncology all function as “decoy” ATP that bind to the ATP binding pocket and prevent the catalytic activity of tyrosine kinase. Resistance to these various tyrosine kinases occurs when point mutations occur around this region in CML that occurs as a frequent resistance mechanism in advanced stages of the disease. By contrast Asciminib functions as a myrstoyl decoy that supplies the missing inhibitory signal in BCR ABL. The catalytic activity of BCR ABL is exquisitely sensitive to these allosteric conformational change that shuts down the ability to bind ATP indirectly; therefore Asciminib is extremely potent at low nanomolar doses in preventing the catalytic activity of BCR ABL in vitro including variants that contain mutations that prevent binding of the ATP competitive inhibitors (imatinib, dasatinib, bosutinib, etc.) which translates into clinical activity in patients whose CML harbours these mutations conferring resistance to “standard” tyrosine kinase inhibitors. Moreover, because Asciminib is extremely active at low doses it is also clinically effective at preventing the catalytic activity of BCR ABL in patients who have resistance to standard tyrosine kinase inhibitors without identifiable mutations in the oncogene. It is this important potent biological activity that is the basis for the clinical efficacy of Asciminib as a monotherapy in producing clinical cytogenetic and molecular responses of patients resistant to two prior lines of tyrosine kinase inhibitors in the ASCEMBL trial. Therefore, because of this unique mechanism of action, Asciminib clearly complements other available activities as a single agent therapy.
2. Is the drug under review the first treatment approved that will address the underlying disease process rather than being a symptomatic management therapy?
Response: Asciminib allosterically inhibits the catalytic activity of the BCR ABL oncogene as described above. This is the founding mutation of CML and therefore prevention of this catalytic activity addresses the core underlying disease process. Asciminib inhibits this by a unique mechanism comparted to the other previously developed and clinically available tyrosine kinase inhibitors that affect BCR ABL such as imatinib, dasatinib, nilotinib, bosutinib, and ponatinib. These other orthostatic tyrosine kinase inhibitors also affect the underlying disease process but by a different mechanism of action and the allosteric inhibition affected by Asciminib is complimentary to this. Long-lasting effective inhibition of BCR ABL activity is now recognized to lead to functional cure of chronic myeloid leukemia in a substantial proportion of patients confirming the notion that addition of BCR ABL truly affects the underlying disease process.
3. Would the drug under review be used as a first-line treatment, in combination with other treatments, or as a later (or last) line of treatment.
Response: The ASCEMBL trial under review compares Asciminib with bosutinib in third-line treatment, i.e. after patients are resistant and/or intolerant to two previous other orthostatic tyrosine kinase inhibitors. In the ASCEMBL trial Asciminib is used as a monotherapy. However, because of its unique mechanism of action and potential synergistic inhibitory activity against BCR ABL there are other ongoing trials using Asciminib in combination in later lines therapy and third line and in first-line therapy as a monotherapy that will be the subject of future drug development not relevant to the current application.
4. Is the drug under review expected to cause a shift in the current treatment paradigm?
Response: For patients who experience resistance and/or intolerance to first- and second-line tyrosine kinase inhibitor therapy the current treatment paradigm is represented by the control arm where patients would be treated with bosutinib which is less commonly used in first- or second-line therapy. Because of the notable increase in the efficacy of Asciminib compared to bosutinib and its greater tolerability as shown by treatment discontinuation differences, it has been widely acknowledged in the Canadian community of hematologists as a significant improvement for treatment of patients at this stage in their disease course, and would therefore represent a shift in current treatment paradigm.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
If so, please describe which treatments should be tried, in what order, and include a brief rationale.
Response: Asciminib represents the best option for treatment in third line in chronic myeloid leukemia based on the results of the ASCEMBL trial and comparison and clinical experience with other available alternatives. The ASCEMBL trial shows that in direct comparison with bosutinib it is more effective and better tolerated. The other option that has been tested in this setting is the third-generation orthostatic tyrosine kinase inhibitor ponatinib that has been investigated in the PACE and OPTIC trials. In these trials the efficacy in terms of obtaining a complete cytogenetic response was comparable to what was seen with Asciminib at about 40% as well as a comparable number of patients achieving a major molecular response (26% in Asciminib ASCEMBL and 34% in the PACE ponatinib trial). However, in both ponatinib trials there was a significant higher rate of discontinuation, more than 50% compared to 37% in the Asciminib trial and it is well recognized by clinicians in Canada that ponatinib is a much more difficult drug to use because of its very high association with cardiovascular side effects and the requirement for concomitant medications to prevent hypertension and hypercholesterolemia that are recommended in most patients taking this medication. Because of different mechanism of action of ponatinib, and the fact that it is the most potent orthostatic tyrosine kinase inhibitor of BCR ABL, it would be very reasonable to reserve this medication for fourth-line treatment in those patients that do not respond to or tolerate Asciminib. For patients who are young enough and who have an available donor, stem cell transplantation is an option for patients who are resistant to at least three lines of therapy but because of the toxicity of this procedure the vast majority of clinicians would use this as an option only when the more convenient and safer ABL inhibitors have been tested, which (once funding is approved) would definitely include Asciminib in third line.
How would this drug affect the sequencing of therapies for the target condition?
If appropriate for this condition, please indicate which treatments would be given after the therapy has failed and specify whether this is a significant departure from the sequence employed in current practice. Would there be opportunity to treat patients with this same drug in a subsequent line of therapy? If so, according to what parameters?
Response: Tyrosine kinase inhibitors (TKIs) are the mainstay for the treatment of chronic myeloid leukemia in chronic phase (CML). Initial TKI therapy is usually with imatinib mesylate (IM) or a second generation TKI (dasatinib or nilotinib). Subsequent sequencing of TKI therapies for second or third line and beyond is largely guided by the choice of the front-line agent, whether the switch is for intolerance or resistance, BCR-ABL mutation analysis in the case of resistance and patient comorbidities. For patients that have previously been treated with IM and a second generation TKI (nilotinib and dasatinib), the next TKI option (3rd line and beyond) would be bosutinib or ponatinib. Asciminib offers a potentially new therapy in the 3rd line and beyond scenario. In the recent phase III ASCEMBEL trial, asciminib was found to be superior to bosutinib in patients with CML in chronic phase receiving > 2 lines of TKI therapy. Therefore for patients in 3rd line (having previously received a second generation TKI), the options would be ponatinib or asciminib. The choice between the two drugs would be dependent on patient comorbidities, and whether a T315I mutation is present (may favour ponatinib). Since asciminib is a novel BCR-ABL targeting the myristoyl pocket of ABL, unlike the tyrosine kinase inhibitors, it provides a different inhibitory site distinct from all the other TKI drugs.
With regards to therapies after asciminib failure in 3rd line and beyond, the options become limited to ponatinib (if not utilized previously) or allogeneic stem cell transplantation (SCT). Currently SCT is considered for patients in 3rd line or beyond. Asciminib could be utilized as a bridge to allogeneic stem cell transplantation or as an alternative to SCT if longer term data shows durability of response to asciminib in this heavily pre-treated population.
Which patients would be best suited for treatment with the drug under review?
Response: In line with the ASCEMBL study population, patients who are CP-CML resistant or intolerant to two or more prior TKI's. T315I patients are not part of the CADTH submission so we should not specify that though it is a US indication.
Which patients are most likely to respond to treatment with the drug under review?
Response: The ASCEMBL data demonstrates that benefit (with regards to MMR at 6 months) comes from the TKI resistant group and TKI intolerant group. Both resistant and intolerant group will respond to the new treatment.
Which patients are most in need of an intervention?
Response: Those with resistance (resistant to 2 prior TKI therapies or beyond) and those with serious or potentially life-threatening intolerance. Those with grade 2 or higher intolerance and cardiovascular risk factors. Those with a history of recurrent effusions.
Would this differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease)?
Response: Patients with serious cardiovascular comorbidities might be more in need of a switch than say those with grade 2 nuisance intolerance but I don't think we should specify that. In the ASCEMBL study, intolerance was defined as nonhematologic grade 3 or 4 toxicity while on therapy, persistent grade 2 toxicity, that is unresponsive to optimal management, including dose adjustments; or hematologic grade 3 or 4 toxicity while on therapy, that recurs after dose reduction to the lowest recommended dose. Protocol amendment 3, on December 14, 2018, allowed the inclusion of patients intolerant to their most recent tyrosine kinase inhibitor (TKI) and BCR-ABL1 transcript levels on the international scale (BCR-ABL1IS) >0.1%
How would patients best suited for treatment with the drug under review be identified?
Examples: Clinician examination or judgement, laboratory tests (specify), diagnostic tools (specify)
Response: Identified by the treating physician based on patient history (intolerance) and molecular test results indicating response to therapy (resistance).
Is the condition challenging to diagnose in routine clinical practice?
Response: No
Are there any issues related to diagnosis? (e.g., tests may not be widely available, tests may be available at a cost, uncertainty in testing, unclear whether a scale is accurate or the scale may be subjective, variability in expert opinion.)
Response: No, all CML treaters have access to the testing that is required.
Is it likely that misdiagnosis occurs in clinical practice (e.g., underdiagnosis)?
Response: Perhaps underreporting of grade 2 toxicities occurs, and once we have an option of a non-TKI drug, additional prevalent cases may be identified.
Should patients who are pre-symptomatic be treated considering the mechanism of action of the drug under review?
Response: Not applicable to the current drug / indication.
Which patients would be least suitable for treatment with the drug under review?
Response: Patients with CML in accelerated phase or blast crisis. Patients with CML who have met molecular milestones and are tolerating their current treatment.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
If so, how would these patients be identified?
Response: Patients who would match the inclusion and exclusion criteria for the clinical trials of Asciminib are post positioned to respond. It is likely that those who are intolerant to their current TKI would be more likely to respond to treatment with Asciminib both related to disease biology and increased chance of compliance with treatment.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response: Yes.
What would be considered a clinically meaningful response to treatment?
Examples: Reduction in the frequency or severity of symptoms (provide specifics regarding changes in frequency, severity, and so forth), Attainment of major motor milestones, Ability to perform activities of daily living, Improvement in symptoms, Stabilization (no deterioration) of symptoms. Consider the magnitude of the response to treatment. Is this likely to vary across physicians?
Response: Improvement in symptoms (disease related- constitutional symptoms, early satiety and toxicity-related to prior therapy- bowel changes, muscle cramps, rash etc.) in patients with active disease (e.g. no response) at the time of starting treatment. Attainment of complete hematologic response and ultimately major molecular response while tolerating drug treatment is the main goal of treatment.
How often should treatment response be assessed?
Response: As per standard practice for CML patients- CBC, liver enzyme, creatinine, and QT-PCR of BCR-ABL are done every 3 months for monitoring. Bone marrow aspiration, biopsy and mutational analysis are done as indicated clinically.
What factors should be considered when deciding to discontinue treatment?
Examples: Disease progression (specify; e.g., loss of lower limb mobility), Certain adverse events occur (specify type, frequency, and severity), Additional treatment becomes necessary (specify)
Response: Patients who fail to meet the treatment milestones set out by the European Leukemia Network or those who have severe toxicity or intolerances to Asciminib.
What settings are appropriate for treatment with the drug under review?
Response: Outpatient clinics with experience in treating patients with CML. Clinics require timely access to molecular testing (QT-PCR) for treatment response.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Response: N/A
Conflict of Interest Declarations — Clinician Group of Hematologists Across Canada
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Response: Novartis Canada provided us with notification that the Asciminib was submitted to CADTH and the dates the clinician input is due.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
Response: No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Matthew Kang
Position: Hematologist, Joseph Brant Hospital Oncology Clinic Assistant Clinical Professor (Adjunct), McMaster University
Date: 13-12-2021
Table 14: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
BMS | X | — | — | — |
Janssen | — | — | X | — |
KiTE | X | — | — | — |
Medison | X | — | — | — |
Novartis | X | — | — | — |
Sobi | X | — | — | — |
Declaration for Clinician 2
Name: Dennis Kim
Position: Did not provide
Date: 15-12-2021
Table 15: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | — | — | X | — |
Pfizer | — | X | — | — |
Paladin | — | X | — | — |
Jazz | — | X | — | — |
Declaration for Clinician 3
Name: Brian Leber
Position: Hematologist, Juravinski Hospital and Cancer Centre
Date: 13-12-2021
Table 16: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | — | X | — | — |
Pfizer | — | X | — | — |
Paladin | X | — | — | — |
Declaration for Clinician 4
Name: Donna Forrest
Position: Did not provide
Date: 18-01-2022
Table 17: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | X | — | — | — |
Paladin | X | — | — | — |
Declaration for Clinician 5
Name: Isabelle Bence-Bruckler
Position: Did not provide
Date: 19-01-2022
Table 18: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | X | — | — | — |
Pfizer | X | — | — | — |
Paladin | X | — | — | — |
Declaration for Clinician 6
Name: Selay Lam
Position: Hematologist, Associate Professor
Date: 19-01--2022
Table 19: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Abbvie | — | — | X | — |
Amgen | — | X | — | — |
AstraZeneca | — | X | — | — |
BieGene | X | — | — | — |
Bristol-Myers Squibb | X | — | — | — |
Hoffman-La Roche | — | X | — | — |
Janssen | — | — | X | — |
Novartis | X | — | — | — |
Sanofi | X | — | — | — |
SeaGen | X | — | — | — |
Declaration for Clinician 7
Name: Kuljit Grewal
Position: Did not provide
Date: 14-12-2021
Table 20: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | X | — | — | — |
Pfizer | X | — | — | — |
BMS | X | — | — | — |
Declaration for Clinician 8
Name: Philip Kuruvilla
Position: Did not provide
Date: 14-12-2021
Table 21: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 8
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Janssen | — | — | X | — |
Novartis | X | — | — | — |
Amgen | X | — | — | — |
AstraZeneca | X | — | — | — |
Abbvie | X | — | — | — |
Pfizer | — | X | — | — |
Declaration for Clinician 9
Name: Mitchell Sabloff
Position: Associate Professor, University of Ottawa
Date: 15-12-2021
Table 22: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 9
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Pfizer | X | — | — | — |
BMS | — | — | X | — |
Novartis | X | — | — | — |
Declaration for Clinician 10
Name: Carolyn Faught
Position: Did not provide
Date: 13-12-2021
Table 23: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 10
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 11
Name: Mohamed Elemary
Position: Did not provide
Date: 13-12-2021
Table 24: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 11
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BMS | X | — | — | — |
AbbVie | X | — | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 12
Name: Christopher Hillis
Position: Assistant Professor, Department of Oncology
Date: 01-25-2022
Table 25: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 12
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | — | X | — | — |
Pfizer | X | — | — | — |
Paladin | X | — | — | — |
Bristol-Myers Squibb | X | — | — | — |
Janssen | X | — | — | — |
Sierra Oncology | X | — | — | — |
AstraZeneca | X | — | — | — |
Declaration for Clinician 13
Name: Ismail Sharif
Position: Did not provide
Date: 26-01-2022
Table 26: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 13
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Abbvie | X | — | — | — |
Amgen | — | X | — | — |
J&J | X | — | — | — |
Declaration for Clinician 14
Name: Lalit Saini
Position: Did not provide
Date: 26-01-2022
Table 27: Conflict of Interest Declaration for Clinician Group of Hematologists Across Canada — Clinician 14
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astellas | X | — | — | — |
Roche | X | — | — | — |
Amgen | X | — | — | — |
Jazz | X | — | — | — |
BMS | X | — | — | — |
Abbvie | X | — | — | — |
Novartis | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.