CADTH Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Renal cell carcinoma, adjuvant treatment
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
BICR
blinded independent central review
CI
confidence interval
cLDA
constrained longitudinal data analysis
DFS
disease-free survival
DRSS
disease recurrence–specific survival
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EFS
event-free survival
EORTC QLQ-C30
European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EQ-5D-5L
5-Level EQ-5D
FKSI-DRS
Functional Assessment of Cancer Therapy Kidney Symptom Index–Disease-Related Symptoms
HR
hazard ratio
HRQoL
health-related quality of life
IKCC
International Kidney Cancer Coalition
irAE
immune-related adverse event
ITT
intention to treat
KCC
Kidney Cancer Canada
KCRNC
Kidney Cancer Research Network of Canada
KM
Kaplan-Meier
M0
no distant metastasis
M1
distant metastasis
M1 NED
M1 with no evidence of disease
MID
minimally important difference
OS
overall survival
PD-1
programmed cell death
PD-L1
programmed cell death ligand-1
PRO
patient-reported outcome
RCC
renal cell carcinoma
SAE
serious adverse event
SD
standard deviation
SE
standard error
SSIGN
stage, size, grade, and necrosis
TNM
tumour, node, metastasis
TKI
tyrosine kinase inhibitors
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), supplied as:
|
Indication | Adjuvant treatment of adult patients with RCC at intermediate-high or high risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions |
Reimbursement request | Per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | August 18, 2022 |
Sponsor | Merck Canada Inc. |
NOC = Notice of Compliance; RCC = renal cell carcinoma.
Introduction
Renal cell carcinoma (RCC) accounts for more than 80% of all cases of kidney cancer across the globe.1,2 Histologically, clear cell RCC is the most common form of RCC, accounting for 80% of all cases observed in clinical practice.1,3 In 2021, kidney and renal pelvis cancers were reported to be the seventh most common cancers in Canada among males (5,200 new cases; 2.8% disease-related deaths) and the 12th most common among females (2,600 new cases; 1.7% disease-related deaths).4 Approximately 65% of individuals are typically diagnosed when their tumour is confined to a primary site (local disease), whereas a smaller proportion of patients is diagnosed when the tumour has spread to regional lymph nodes or metastatic sites (16% at regional and 16% at distant stages).5 Because of the widespread use of noninvasive abdominal imaging, approximately 50% of kidney tumours are detected incidentally, and many are asymptomatic.2,3,6 Classic symptoms (flank pain, visible hematuria, and palpable abdominal mass) are usually associated with more advanced disease stages and poorer prognoses.2,6 Survival rates among patients with RCC largely depend on clinical factors, such as tumour stage, grade, RCC subtype, presence of sarcomatoid features, local extent of the tumour, presence of regional nodal metastasis, and evidence of metastatic disease at presentation.2 Scoring systems — such as stage, size, grade, and necrosis (SSIGN) scoring and the University of California Los Angeles Integrated Staging System — classify patients as low, intermediate, or high risk following nephrectomy.3,7 Estimated rates of 5-year metastasis-free survival among individuals at low, intermediate, and high SSIGN risk are more than 95%, approximately 80%, and less than 40%, respectively.3,8
In Canada, the current standard of care for nonmetastatic RCC is nephrectomy.9 Adjuvant treatment is not recommended in patients with nonmetastatic RCC after nephrectomy, according to the Kidney Cancer Research Network of Canada (KCRNC).10 Moreover, there were no Health Canada–approved adjuvant treatment options for patients with RCC following nephrectomy at the time of this CADTH review. The current oncologic standard of care for these patients is “observation.”
Pembrolizumab is a high-affinity humanized monoclonal antibody that exerts dual ligand blockade of the programmed cell death receptor 1 (PD-1) pathway, enhances immune system detection of tumours, and facilitates tumour regression. Pembrolizumab is available as a solution for IV infusion in a 100 mg per 4 mL vial and as a 50 mg powder for reconstitution in a single-use vial. Recommended dosing for patients at intermediate-high or high risk of recurrence following nephrectomy or following nephrectomy and resection of metastatic lesions is 200 mg every 3 weeks or 400 mg every 6 weeks until disease recurrence, unacceptable toxicity or up to 1 year (12 months) or 17 doses for 200 mg or 9 doses for 400 mg, whichever is longer, in patients without disease progression.11
Pembrolizumab received Health Canada approval on August 18, 2022, for the adjuvant treatment of adult patients with RCC at intermediate-high or high risk of recurrence following nephrectomy or following nephrectomy and resection of metastatic lesions.
The objective of this review is to perform a systematic review of the beneficial and harmful effects of pembrolizumab for the adjuvant treatment of RCC in patients with intermediate-high or high risk of recurrence following nephrectomy or following nephrectomy and resection of metastatic lesions.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups that responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
One response to CADTH’s call for patient input was received from Kidney Cancer Canada (KCC), which is a national community that provides support and education for patients living with kidney cancer and advocates for their care. The submission was based on 2 online surveys conducted by KCC in 2018 and March 2022, 1 online survey conducted by KCC in collaboration with the International Kidney Cancer Coalition (IKCC) in 2020, and 1 online survey conducted by IKCC in May 2021. Moreover, direct input was collected in March 2022 from 1 American patient with RCC who had experience with pembrolizumab. The 2018 survey supported a previous submission reviewed by CADTH by reporting on the challenges met by patients and caregivers living with kidney cancer. Among the 2,012 respondents to the 2020 international survey, 241 were from Canada; of these, 205 (85%) were patients with kidney cancer, 34 (14%) were caregivers, and the status of the other 2 (0.8%) was undisclosed. A total of 141 patients with RCC responded to the 2021 survey. Of the 106 respondents to the 2022 survey, 65 (61%) were patients or caregivers from Canada.
KCC reported that a large proportion of patients with RCC may eventually experience disease recurrence after nephrectomy, leading to a substantially shortened life expectancy. The patient group input indicated that in the absence of adjuvant therapy options, patients at intermediate to high risk of recurrence experience anxiety and emotional distress from the expectation of recurrence and progression of disease. Nearly half (49%) of survey respondents indicated they would accept adjuvant immunotherapy if it reduced the risk of disease recurrence by 40% to 50%. Approximately 50% of respondents indicated they would accept the risk of side effects associated with steroid use, in the range of 20% to 25%, to manage the side effects of adjuvant immunotherapy.
According to the 1 patient who had experience with pembrolizumab in the adjuvant setting, the side effects of the treatment, including slight occasional rash, slight fatigue, and hyperkalemia, are manageable.
KCC emphasized that there is currently an unmet need for an effective adjuvant therapy for kidney cancer that reduces the risk of disease recurrence and improves patient outcomes by, for example, reducing the number of patients who develop metastatic disease and the costs associated with RCC care.
A copy of the patient input from KCC is presented in the Stakeholder section of this review.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH emphasized that there is an unmet need among patients with a higher risk of recurrent disease after surgery for kidney cancer. Currently, there is no approved adjuvant treatment in this setting. The experts reported that pembrolizumab would be offered as monotherapy in the adjuvant setting after resection of kidney cancer in patients at intermediate-high or high risk of recurrence. In the opinion of the clinical experts consulted, patients with clear cell carcinoma with M1 (distant metastasis) resected metastases would benefit most from adjuvant treatment, followed by patients with the pathological T3 (pT3) to pathological T4 (pT4) tumours (those at high risk of recurrence), and patients with T2 grade 3 to 4 tumours (those at intermediate risk of recurrence). The experts identified patients with autoimmune diseases requiring steroids as those who should not receive adjuvant pembrolizumab. The clinical experts noted that overall survival (OS) and disease-free survival (DFS) are important outcome measures for the assessment of patient’s response to treatment. Discontinuation of treatment was recommended by the clinical experts in the case of disease recurrence or intolerable treatment toxicities. The experts reported that treatment administration and monitoring should be undertaken by a medical oncologist in an outpatient or community cancer setting.
Clinician Group Input
Two clinician groups provided input for this review: the Kidney Cancer Research Network of Canada and the Ontario Health Genitourinary Cancer Drug Advisory Committee. Two clinicians affiliated with the Kidney Cancer Research Network of Canada and 1 clinician on behalf of Ontario Health Genitourinary Cancer Drug Advisory Committee contributed to this submission. The clinician groups agreed that there is an unmet need for adjuvant therapy to lower the risk of disease recurrence in patients with localized RCC following nephrectomy in Canada. The clinician groups indicated that, if funded, pembrolizumab would be the first adjuvant therapy option for patients with RCC in Canada.
A copy of the clinician input from the Kidney Cancer Research Network of Canada and Ontario Health Genitourinary Cancer Drug Advisory Committee is presented in the Stakeholder section of this review.
Drug Program Input
Drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The drug plans anticipated that adjuvant pembrolizumab might cause a shift in subsequent therapy lines that are reimbursed in the Canadian setting. The drug plans anticipated changes to the dosing modality in practice, with changes toward weight-based dosing schedule for pembrolizumab. Implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Clinical Evidence
Pivotal and Protocol-Selected Study
Description of Study
The KEYNOTE-564 trial is an ongoing multicentre, randomized, double-blind, phase III study with a primary objective to compare the efficacy and safety of pembrolizumab versus placebo as an adjuvant treatment for adult patients with RCC postnephrectomy or post nephrectomy and resection of metastatic lesions. The trial was conducted at 212 sites in 21 countries, including Canada. The study enrolled patients aged 18 years and older with a histologically confirmed diagnosis of RCC with a clear cell component with or without sarcomatoid features. The study included patients at intermediate-high or high risk of recurrence, based on pathological tumour, node, metastasis (TNM) staging, Fuhrman grade, and the presence of sarcomatoid features, and patients following metastatic disease who had undergone complete resection of primary and metastatic lesions. Patients were also required to be tumour-free, have an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 or 1, and have no prior systemic treatment for RCC.12 The primary outcome investigated in the KEYNOTE-564 trial was DFS, assessed by the investigator. The key secondary outcome was OS, and other secondary outcomes included disease recurrence–specific survival (DRSS), event-free survival (EFS) assessed by blinded independent radiology review, safety, and health-related quality of life (HRQoL).12
Patients were randomized in 1:1 ratio to receive either pembrolizumab (200 mg IV infusion every 3 weeks) or placebo (saline solution IV every 3 weeks) for up to a maximum of 17 infusions or (approximately) 1 year, until confirmation of recurrence, treatment discontinuation, or study termination. Randomization was based on metastasis status variable (M0 [no distant metastasis] versus M1 NED [distant metastasis with no evidence of disease] defined as primary kidney tumour plus solid, isolated, soft tissue metastases that were completely resected at nephrectomy [synchronous] or no more than 1 year after nephrectomy [metachronous]), and within the M0 group on following stratification factors: ECOG PS (0 or 1) and US participant (yes or no). By the first interim analysis (December 14, 2020), 1,406 patients were screened and 994 were randomized into the trial (496 to pembrolizumab and 488 to placebo arms). One additional analysis (efficacy update report) was implemented after 6 additional months of follow-up, with a cut-off date of June 14, 2021.
The median age of patients enrolled in the KEYNOTE-564 study was 60 years, and the majority of participants were White men. Most patients had tumours without sarcomatoid features and with intermediate-high risk for recurrence. Baseline characteristics were equally balanced in the 2 study arms. More patients discontinued treatment in the pembrolizumab arm (38.9%) than in the placebo arm (26.2%), primarily due to adverse events (AEs). More patients in the placebo arm (22.5%) received subsequent systemic anti-cancer treatment compared with the pembrolizumab arm (15.3%).12
Efficacy Results
The key efficacy findings of the KEYNOTE-564 study are summarized in Table 2.
Overall Survival
At the first interim analysis data cut-off (December 14, 2020), the median follow-up durations were 24 months (range = 2.5 to 41.5 months) and 23.8 months (range = 3.5 to 41.4 months) for patients in pembrolizumab and placebo arms, respectively. Median OS was not reached in either treatment arm. A hazard ratio (HR) of 0.54 (95% CI, 0.30 to 0.96; P = 0.0164) was estimated for the comparison between pembrolizumab and placebo. Additional 6-month follow-up data from the efficacy update report analysis (June 14, 2021, data cut-off) showed that median OS was not reached in either groups, with an observed HR of 0.52 (95% CI, 0.31 to 0.86; P = 0.005).
DFS Assessed by Investigator
Similarly, median DFS was not reached in either treatment group at the time of the first interim analysis (December 14, 2020). The HR obtained for pembrolizumab versus placebo was 0.68 (95% CI, 0.53 to 0.87; P = 0.001). In the efficacy update report analysis, with a data cut-off date of June 14, 2021, the HR was 0.63 (95% CI, 0.50 to 0.80; P < 0.0001). Median DFS was not reached in either group at the time of the efficacy update report analysis.
According to the pre-specified subgroup analysis, HRs for DFS in the metastatic staging groups was 0.74 (95% CI, 0.57 to 0.96) for the M0 group and 0.29 (95% CI, 0.12 to 0.69) for the M1 NED group. Similar findings were observed in the efficacy update report analysis, which had 6 additional months of follow-up; for the M0 subgroup, the HR was 0.68 (95% CI, 0.53 to 0.88), and for the M1 NED subgroup, the HR was 0.28 (95% CI, 0.12 to 0.66). The efficacy update report results for the post hoc subgroup analysis of recurrence risk showed the following estimates: HR = 0.68 (95% CI, 0.52 to 0.89) for intermediate-high risk, HR = 0.60 (95% CI, 0.33 to 1.10) for high risk, and HR = 0.28 (95% CI, 0.12 to 0.66) for M1 NED risk.
Health-Related Quality of Life
HRQoL assessments included the overall least squares mean difference estimated for the pembrolizumab and placebo arms. Among patients completing the health-related quality of life measures, patients in both arms appeared to experience a slight deterioration in HRQoL and symptom worsening assessed at week 52. The overall least squares mean difference in Functional Assessment of Cancer Therapy Kidney Symptom Index–Disease-Related Symptoms (FKSI-DRS) score was –0.67 (95% CI, –1.23 to –0.12). The least squares mean difference in the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) questionnaire was –2.57 (95% CI, –5.22 to 0.08) for global health status/quality of life (QoL) scale and –0.91 (95% CI, –2.79 to 0.97) for the physical functioning scale.
Harms Results
The proportion of patients with at least 1 treatment-emergent adverse event appeared higher in the pembrolizumab arm (96.3%) than in the placebo group (91.1%). Serious adverse events (SAEs) were reported in 20.5% of individuals who received pembrolizumab treatment compared with 11.3% of individuals receiving placebo. There were more AEs leading to drug discontinuations (pembrolizumab versus placebo: 20.7% versus 2.0%) and more treatment interruptions in the pembrolizumab group (25.8% versus 14.9%). Overall, 2 deaths were reported in the pembrolizumab arm (0.4%) and 1 death was reported in the placebo arm (0.2%).
Notable harms were higher in the pembrolizumab group than in the placebo group, including hyperthyroidism (21.1% versus 6.9%) hypothyroidism (11.9% versus 0.2%), pneumonitis (2.3% versus 1%), adrenal insufficiency (2% versus 0.2%), type 1 diabetes mellitus (1.8% versus 0%), colitis (1.6% versus 0.2%), severe skin reactions (1.6% versus 0.4%), infusion reactions (1.4% versus 1%), thyroiditis (1.2% versus 0.2%), and hepatitis (1% versus 0%).
Table 2: Summary of Key Results From the Pivotal and Protocol-Selected Study (KEYNOTE-564)
Result | Pembrolizumab arm N = 496 | Placebo arm N = 498 |
|---|---|---|
OS (ITT population) | ||
Patients with events, n (%) | 18 (3.6) | 33 (6.6) |
Median OS (95% CI), monthsa | NR (NR to NR) | NR (NR to NR) |
HR (95% CI)b | 0.54 (0.30 to 0.96) | |
Log-rank test P valuec | 0.0164037 | |
24-month OS rate, % (95% CI) | 96.6 (94.3 to 98.0) | 93.5 (90.5 to 95.6) |
DFS (ITT population) | ||
Patients with events, n (%) | 109 (22.0) | 151 (30.3) |
Median DFS (95% CI), monthsa | NR (NR to NR) | NR (NR to NR) |
HR (95% CI)b | 0.68 (0.53 to 0.87) | |
Log-rank test P valuec | 0.0010 | |
24-month DFS rate, % (95% CI) | 77.3 (72.8 to 81.1) | 68.1 (63.5 to 72.2) |
FKSI-DRS (FAS population) | ||
Baseline | ||
n | 435 | 447 |
Mean (SD) | 32.86 (3.50) | 32.79 (3.53) |
At week 52 | ||
n | 300 | 328 |
Mean (SD) | 31.85 (4.69) | 32.51 (4.13) |
CFB to week 52 | ||
n | 483 | 492 |
LSM (95% CI)d | –1.12 (–1.53 to –0.71) | –0.45 (–0.84 to –0.05) |
LSM difference (95% CI; P value)d | –0.67 (–1.23 to –0.12; P = 0.0170) | |
EORTC QLQ-C30 global health status/QoL (FAS population) | ||
Baseline | ||
n | 438 | 450 |
Mean (SD) | 79.22 (18.46) | 77.04 (17.61) |
At week 52 | ||
n | 301 | 325 |
Mean (SD) | 74.92 (18.26) | 76.82 (19.56) |
CFB to week 52 | ||
n | 484 | 492 |
LSM (95% CI)d | –4.25 (–6.32 to –2.19) | –1.68 (–3.69 to 0.32) |
LSM difference (95% CI; P value)d | –2.57 (–5.22 to 0.08; P = 0.0571) | |
EORTC QLQ-C30 physical functioning (FAS population) | ||
Baseline | ||
n | 438 | 450 |
Mean (SD) | 88.58 (14.95) | 88.61 (14.26) |
At week 52 | ||
n | 301 | 325 |
Mean (SD) | 86.60 (17.33) | 88.96 (15.89) |
CFB to week 52 | ||
n | 484 | 492 |
LSM (95% CI)d | –1.81 (–3.19 to –0.43) | –0.90 (–2.23 to 0.44) |
LSM difference (95% CI; P value)d | –0.91 (–2.79 to 0.97; P = 0.3410) | |
Harms, APaT population, n (%) | ||
N | 488 | 496 |
≥ 1 AE | 470 (96.3) | 452 (91.1) |
Toxicity, grade 3 to 5 AEs | 158 (32.4) | 88 (17.7) |
≥ 1 SAE | 100 (20.5) | 56 (11.3) |
AE leading to drug discontinuation | 101 (20.7) | 10 (2.0) |
AE leading to treatment interruption | 126 (25.8) | 74 (14.9) |
SAE leading to drug discontinuation | 49 (10.0) | 5 (1.0) |
Death | 2 (0.4) | 1 (0.2) |
Notable harms | ||
Hypothyroidism | 103 (21.1) | 18 (3.6) |
Hyperthyroidism | 58 (11.9) | 1 (0.2) |
Pneumonitis | 11 (2.3) | 5 (1.0) |
Adrenal insufficiency | 10 (2.0) | 1 (0.2) |
Type 1 diabetes mellitus | 9 (1.8) | 0 (0.0) |
Colitis | 8 (1.6) | 1 (0.2) |
Severe skin reactions | 8 (1.6) | 2 (0.4) |
Infusion reactions | 7 (1.4) | 5 (1.0) |
Thyroiditis | 6 (1.2) | 1 (0.2) |
Hepatitis | 5 (1.0) | 0 (0.0) |
Sarcoidosis | 4 (0.8) | 0 (0.0) |
Nephritis | 3 (0.6) | 0 (0.0) |
Myasthenic syndrome | 3 (0.6) | 0 (0.0) |
Hypophysitis | 2 (0.4) | 0 (0.0) |
Myositis | 2 (0.4) | 1 (0.2) |
Vasculitis | 2 (0.4) | 0 (0.0) |
Encephalitis | 1 (0.2) | 0 (0.0) |
Myocarditis | 1 (0.2) | 0 (0.0) |
Uveitis | 0 (0.0) | 1 (0.2) |
AE = adverse event; APaT = all participants as treated; CFB = change from baseline; CI = confidence interval; DFS = disease-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; FKSI-DRS = Functional Assessment of Cancer Therapy Kidney Symptom Index–Disease-Related Symptoms; HR = hazard ratio; ITT = intention to treat; LSM = least squares mean; NR = not reached; OS = overall survival; SAE = serious adverse events; SD = standard deviation.
Notes: For PROs at baseline and week 52, n is the number of participants in each treatment group with no missing assessments at the specific time point; for change from baseline, n is the number of participants in the analysis population in each treatment group.
Data cut-off: December 14, 2020.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (yes vs. no) within M0 group by investigator.
cOne-sided P value based on log-rank test stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (yes vs. no) within M0 group by investigator.
dBased on a cLDA model with the PRO scores as the response variable with covariates for treatment by study visit interaction, stratification factors metastasis status (M0 vs. M1 NED), and within M0 group further stratified by ECOG PS (0 vs. 1) and US participant (yes vs. no) as covariates.
Source: Clinical Study Report.12
Critical Appraisal
The KEYNOTE-564 trial is an ongoing multicentre, randomized, placebo-controlled, double-blind study. The randomization scheme implemented in the trial minimized the risk of bias due to unknown confounders. Because of the placebo-controlled design, unblinding might potentially have occurred due to higher frequencies of immune-related AEs in the pembrolizumab compared with the placebo arm. Baseline and demographic characteristics were balanced in the 2 study arms, suggesting successful randomization. Concomitant medications permitted in the trial, as well as subsequent anti-cancer therapies administered, were considered appropriate by the clinical experts consulted by CADTH and were reflective of treatments used in Canadian practice.
OS, DFS, and HRQoL, which were investigated in the KEYNOTE-564 trial, were considered clinically meaningful outcomes by the clinical experts and reflective of outcomes assessed in clinical practice. Other surrogate end points, such as DRSS and EFS, were considered to be of lower clinical relevance, according to the clinical experts.
The primary outcome (DFS) was assessed by local investigators, and blinded independent central review (BICR) assessments were introduced to evaluate the robustness of the DFS findings. Findings of DFS by BICR were consistent with the primary analysis, suggesting a low possibility of evaluation bias. Multiplicity adjustments were implemented adequately for the analysis of DFS and OS, and sensitivity analyses were also pre-specified and conducted for DFS. The findings from the sensitivity analyses were consistent with the primary intention-to-treat (ITT) analyses. Median DFS and OS were not reached at the time of the interim analyses, suggesting data immaturity. More patients in the placebo arm received post-treatment anti-cancer therapies compared with the pembrolizumab arm, which might have produced biased estimates of OS (favouring the placebo group). Of note, surgery in patients with RCC is performed with curative intent, and rates of 5-year disease-specific survival are high in patients at intermediate (about 80%) and high risk of recurrence (from 40% to 55%) postnephrectomy. Hence, longer follow-up is needed to observe the effects of adjuvant pembrolizumab on survival outcomes. Findings from the analysis of secondary and exploratory outcomes (EFS, DRSS, HRQoL), as well as defined subgroups, were considered exploratory, as no multiplicity adjustments were performed. The magnitude of effect of pembrolizumab on the HRQoL of patients in the adjuvant setting is uncertain because of the lack of formal hypothesis testing, possible violation of missing data assumptions in the model applied, and high attrition rates.
There were several interim analyses pre-specified in the protocol before the first interim analysis (December 14, 2020), which was used as the base for this CADTH report. Another interim analysis (i.e., efficacy update report) with 6 months of additional follow-up data was added between the first and the second interim analysis to respond to potential requests from regulatory agencies. The final OS analysis will take place after approximately 200 deaths are observed between the pembrolizumab and placebo groups. Adjustments were made to account for alpha spending in the interim analyses.
The clinical experts consulted by CADTH for this review reported that baseline characteristics and findings from KEYNOTE-564 can be generalized to adults with RCC living in Canada who are at intermediate-high or high risk of recurrence following nephrectomy or following nephrectomy and resection of metastatic lesions. The administered dosage of pembrolizumab was 200 mg every 3 weeks for up to 17 doses, which is aligned with the approved Health Canada indication. The clinical experts noted that dosing of 400 mg every 6 weeks for up to 9 doses is more commonly applied in real clinical practice. The appropriateness of placebo as the comparator was confirmed by the clinical experts because there are no Health Canada–approved adjuvant treatment options available in Canada. According to the clinical experts, patients recruited in the pivotal trial had more frequent disease assessments and follow-up procedures compared with what would be applied in patients in real-world practice.
Conclusions
One sponsor-submitted, multicentre, randomized, double-blind, phase III trial (KEYNOTE-564) comparing adjuvant pembrolizumab with placebo in patients with RCC was included in this CADTH systematic review.
Overall, pembrolizumab improved DFS outcome, compared with placebo, as an adjuvant treatment for patients with RCC who are at intermediate-high or high risk of recurrence after nephrectomy or following nephrectomy and resection of metastatic lesions. However, the effects of adjuvant pembrolizumab relative to placebo on OS could not be determined because of the immature survival data, uncertain influence of subsequent treatments, and uncertainty about the correlation between DFS and OS in the adjuvant treatment of RCC. Likewise, limitations with the HRQoL analyses in the single randomized controlled trial precluded the ability to draw conclusions about the effects of pembrolizumab on this outcome. The safety profile of pembrolizumab was similar to that observed in other trials of this drug, including effects on the thyroid and adrenal glands. The clinical experts indicated that baseline characteristics and findings from the KEYNOTE-564 trial could be generalized to patients with RCC in the adjuvant setting in Canada.
Introduction
Disease Background
RCC is the most common form of kidney cancer, accounting for more than 80% of all cases in the world.1,2 Histologically, RCCs are further classified into different subtypes: clear cell, papillary, chromophobe, clear cell papillary, collecting duct, medullary, and unclassified.1,3 Almost all types of RCC can have or develop sarcomatoid features, but they are reported most often in chromophobe histological subtypes.13 Clear cell RCC is the most common form, accounting for approximately 80% of all RCC cases in clinical practice.3,5 The estimated proportions of individuals diagnosed at the local (confined to primary site), regional (spread to regional lymph nodes), and distant (metastasized cancer) stages are 65%, 16%, and 16%, respectively.5
With the widespread use of noninvasive abdominal imaging, almost half of all kidney tumours are detected incidentally, many of which are asymptomatic.2,3,6 The classic symptoms of flank pain, visible hematuria, and palpable abdominal mass are associated with more advanced disease stages and poorer prognosis.2,6 Common diagnostic methods for identifying and characterizing tumours and assessing disease progression include CT scans, MRI, X-rays, and bone scans.3,5 Known risk factors for RCC include smoking, hypertension, obesity, medications (over-the-counter pain killers, phenacetin-containing compounds, and diuretics), family history of RCC, genetic conditions (von Hippel-Lindau disease), and hereditary papillary RCC.5,14
The Canadian epidemiological estimates from 2021 showed that kidney and renal pelvis cancers were the seventh most common cancers in males (accounting for 5,200 new cases and 2.8% of disease-related deaths) and the 12th most common in females (2,600 new cases and 1.7% of disease-related deaths). The predicted 5-year age-standardized survival was 73% for both sexes. The predicted net survival was higher for patients within the age group of 15 to 44 years (92%) compared with patients aged 85 years and older (33%).4 The 5-year survival rate depends on clinical, anatomic, and histological factors, such as tumour stage, grade, RCC subtype, presence of sarcomatoid features, local extent of tumour, presence of regional nodal metastasis, and evidence of metastatic disease at presentation.2 The 5-year relative survival rates for patients with localized, regional, or distant kidney or renal pelvis cancer was 92.7%, 71%, and 13.9%, respectively.5
Different scoring systems that assess the probability of survival in patients postnephrectomy, based on histological and clinical features, have been proposed.3 SSIGN scoring is based on TNM stage and different pathologic features (size, nuclear grade, and presence of necrosis). The estimated 5-year metastasis-free survival among individuals at low, intermediate, and high risk is estimated to be more than 95%, approximately 80%, and less than 40%, respectively.3,8 Another scoring model, the University of California Los Angeles Integrated Staging System, incorporates TNM staging, ECOG PS, and Fuhrman pathological grading to classify individuals with localized and metastatic disease into low-, intermediate-, and high-risk subgroups following nephrectomy.3,7 The 5-year disease-specific survival for individuals with localized disease is estimated to be 91.1% for patients at low risk, 80.4% for patients at intermediate risk, and 54.7% for patients at high risk.3 For patients with metastatic disease, survival probabilities are worse, at 32%, 19.5% and 0% in the low-, intermediate-, and high-risk subgroups, respectively).3
Standards of Therapy
In the Canadian clinical context, the current standard of care for nonmetastatic RCC is nephrectomy.9 The most recent consensus statement from the KCRNC does not recommend adjuvant therapy in patients with nonmetastatic RCC following nephrectomy, but encourages patient participation in clinical trials whenever possible.10 At the time of this CADTH review, there were no Health Canada–approved adjuvant treatment options for patients with RCC following nephrectomy. The current oncologic standard of care for these patients is observation.
According to the clinical experts consulted by CADTH, important treatment goals for patients on adjuvant treatment include prolonging survival and reducing the risk of recurrence with no negative impact on quality of life.
Drug
Pembrolizumab is a high-affinity humanized monoclonal antibody that blocks the PD-1 pathway (Table 3).
Health Canada has issued market authorization for pembrolizumab for the treatment of various types of tumours.11
Pembrolizumab received Health Canada approval for the following indication: adjuvant treatment of adult patients with RCC at intermediate-high or high risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions. The CADTH reimbursement request aligns with the approved Health Canada indication.
Table 3: Key Characteristics of Pembrolizumab
Characteristic | Pembrolizumab |
|---|---|
Mechanism of action | A high-affinity antibody with dual ligand blockade of the PD-1 pathway, including PD-L1 and PD-L2, on antigen-presenting or tumour cells. Pembrolizumab reactivates tumour-specific cytotoxic T-lymphocytes in the tumour microenvironment. |
Indicationa | Adjuvant treatment of adults with RCC at intermediate-high or high risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions. |
Route of administration | IV |
Recommended dose | 200 mg every 3 weeks or 400 mg every 6 weeks until disease recurrence, unacceptable toxicity, or up to 1 year (12 months) or 17 doses for 200 mg or 9 doses for 400 mg, whichever is longer, in patients without disease recurrence. |
Serious adverse effects or safety issues | Immune-mediated adverse reactions (such as immune-mediated pneumonitis, immune-mediated colitis, immune-mediated hepatitis, immune-mediated nephritis and renal dysfunction, and immune-mediated endocrinopathies), adrenal insufficiency, hypophysitis, type 1 diabetes mellitus, thyroid disorders, severe skin reactions, and infusion-related reactions. |
PD-1 = programmed cell death; PD-L1 = programmed cell death ligand-1; PD-L2 = programmed cell death ligand-2; RCC = renal cell carcinoma.
aHealth Canada proposed indication.
Source: Health Canada product monograph.11
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full patient group input is included in the Stakeholder Input section of this review.
One response to CADTH’s call for patient input was received for this review: a submission from KCC. KCC is a national community that provides support and education to individuals living with kidney cancer and advocates for their care.
The information in the submission was based on 4 online surveys: 2 conducted by KCC in 2018 and in March 2022, 1 conducted in collaboration with the IKCC in 2020, and 1 conducted by IKCC in May 2021. Additionally, direct input was collected in March 2022 from 1 American patient with RCC who had experience with pembrolizumab. The 2018 survey supported a previous submission reviewed by CADTH by reporting on the challenges faced by patients and caregivers living with kidney cancer. Among the 2,012 respondents of the 2020 international survey, 241 were from Canada; of these, 205 (85%) were patients with kidney cancer, 34 (14%) were caregivers, and the status of the other 2 (0.8%) was undisclosed. A total of 141 patients with RCC responded to the 2021 survey. Among the 106 respondents to the 2022 survey, 65 (61%) patients and caregivers were from Canada.
KCC described the experience of patients with kidney cancer as they navigate the health care system. Notably, KCC stated that a large proportion of patients with RCC may eventually experience disease recurrence after nephrectomy, leading to a substantially shortened life expectancy. KCC also noted that there are currently no available treatment options funded in Canada for adjuvant therapy to reduce the risk of disease recurrence, and in the absence of adjuvant therapy options, patients at intermediate to high risk of recurrence experience anxiety and emotional distress related to concerns about recurrence and progression of disease following nephrectomy. Nearly half (49%) of survey respondents indicated that they would accept adjuvant immunotherapy postsurgery if the therapy reduced the risk of disease recurrence by 40% to 50%. Approximately 50% of respondents indicated that they would accept the risk of side effects associated with steroid use to manage the side effects of adjuvant immunotherapy if that level of risk is in the range of 20% to 25%. Approximately 51% of respondents equated DFS with a “longer period of time that I remain cancer free on surveillance scans.” More than half (56%) of respondents equated OS with “longer survival – living a longer life, even if my kidney cancer eventually does return.”
According to the 1 patient who had experience with pembrolizumab for the indication under review, the side effects of treatment, which included slight occasional rash, slight fatigue, and hyperkalemia, were manageable. KCC emphasized that there is currently an unmet need for an effective adjuvant therapy for kidney cancer to reduce the risk of disease recurrence and improve patient outcomes by, for example, reducing the number of patients who develop metastatic disease and the costs associated with RCC care.
A copy of the patient input from KCC is presented in the Stakeholder Input section of this review.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of RCC.
Unmet Needs
In Canada, there are currently no approved adjuvant treatments following surgery for kidney cancer. Clinical experts highlighted that there is an unmet need among patients at a higher risk of recurrent disease after nephrectomy. Important treatment goals would include lengthening survival of these patients and reducing the risk of recurrence, without negatively influencing patients’ quality of life.
Place in Therapy
The clinical experts consulted by CADTH reported that pembrolizumab would be considered monotherapy in the adjuvant setting in patients who have undergone resection of kidney cancer who are at intermediate-high or high risk of recurrence. The experts believed that adjuvant pembrolizumab would cause a shift in treatment paradigm for a couple of reasons. First, clinicians are not currently offering adjuvant treatment in this setting. Medical oncologists would be required to offer balanced and informed discussions about adjuvant pembrolizumab. Second, downstream treatment options may be affected in cases in which a patient develops metastatic disease. For instance, if a patient experiences relapse while on adjuvant treatment, the clinical experts suggested using tyrosine kinase inhibitors (TKIs)-based agents (e.g., sunitinib, cabozantinib, pazopanib, and axitinib) instead of ipilimumab plus nivolumab or axitinib plus pembrolizumab. In the case of disease recurrence after at least 6 months of adjuvant treatment, the experts suggested re-treatment with a PD-1 combination (e.g., ipilimumab plus nivolumab or axitinib plus pembrolizumab).
Patient Population
In the opinion of the clinical experts consulted, patients with M1 resected metastases would benefit the most from adjuvant pembrolizumab, followed by pT3 to pT4 patient population (who are at high risk of recurrence) and T2, grade 3 to 4 patient population (who are at intermediate risk of recurrence). There is no sufficient evidence to support adjuvant treatment with pembrolizumab in patients with kidney cancer histologies other than clear cell. Moreover, patients at low risk of recurrence would not require adjuvant treatment. One of the clinical experts noted that patients with autoimmune disease who require steroids should not receive adjuvant pembrolizumab, whereas patients with mild autoimmune diseases (not requiring steroids > 10 mg prednisone equivalent) would require a thorough risk-benefit discussion before considering adjuvant pembrolizumab treatment. The clinical experts noted that identification of patients eligible for adjuvant treatment would be done by urologists following surgery, and referral to a medical oncologist would be required. Both experts indicated that misdiagnosis or underdiagnosis is very unlikely because of tangible pathological reporting and the fact that these patients undergo definitive surgery. The experts highlighted the lack of diagnostic biomarkers that would identify the patients most likely to respond to adjuvant treatment.
Assessing Response to Treatment
In terms of patients’ response to treatment, the clinical experts reported that both OS and DFS are important outcomes. When assessing treatment response, the clinical experts consulted by CADTH reported that the frequency of treatment assessments should be aligned with the pivotal clinical trial (i.e., CT scans of the chest, abdomen, and pelvis every 12 weeks during the first year, every 16 weeks in years 2 to 4, and every 24 weeks after 5 years). However, the experts also noted that, in clinical practice, tumour assessments might be conducted less frequently.
Discontinuing Treatment
According to the clinical experts, treatment with pembrolizumab in adjuvant setting should be discontinued in the case of disease recurrence or intolerable treatment toxicities (e.g., myocarditis, encephalitis, severe colitis requiring steroids). One clinical expert noted that discontinuation of treatment would not be required if patients experienced thyroid or hormonal dysfunction, mild rash, or mild colitis.
Prescribing Conditions
The clinical experts consulted by CADTH indicated that treatment administration and the monitoring of patients on adjuvant pembrolizumab should be undertaken by a qualified medical oncologist experienced in immuno-oncologic treatment and capable of identifying and handling immune-related adverse events (irAEs). The experts advised that adjuvant pembrolizumab be administered in an outpatient cancer centre or community cancer centre, and that an on-call service be available to manage irAEs that occur after hours.
Additional Considerations
Both clinical experts highlighted the unmet need for patients at highest risk for recurrence (M1 resected NED, T3 to T4 high grade 3 to 4/4). One expert noted that the previously conducted clinical trials in the adjuvant setting demonstrated limited efficacy of a TKI-based agent, sunitinib, that is currently in use only in the US.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full clinician group input is included in the Stakeholder Input section of this review.
Two clinician groups provided input for this review: the KCRNC and the Ontario Health Genitourinary Cancer Drug Advisory Committee. Two clinicians affiliated with the KCRNC and 1 clinician on behalf of Ontario Health Genitourinary Cancer Drug Advisory Committee contributed to this submission. The clinician groups agreed that there is an unmet need for adjuvant therapy to lower the risk of disease recurrence in patients with localized RCC following nephrectomy in Canada. The clinician groups indicated that, if funded, pembrolizumab would be the first adjuvant therapy option for patients with RCC in Canada.
A copy of the clinician input from the KCRNC and the Ontario Health Genitourinary Cancer Drug Advisory Committee is presented in the Stakeholder Input section of this review.
Drug Program Input
Drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
There are no publicly funded comparators for the adjuvant treatment of intermediate-high to high-risk RCC following nephrectomy, or following nephrectomy and resection of metastatic lesions. It is the understanding of PAG members that observation or enrolment in a clinical trial would be the usual practice in this setting. At the time of disease recurrence or evidence of metastatic disease, several drugs are publicly funded, including pembrolizumab plus axitinib, ipilimumab plus nivolumab, nivolumab, sunitinib, pazopanib, sorafenib, axitinib, cabozantinib, and everolimus. | Clinical experts consulted by CADTH reported that there is currently no approved adjuvant treatment for patients at intermediate-high to high risk of RCC following nephrectomy, or following nephrectomy and resection of metastatic lesions in Canada. The current oncologic standard of care in Canada is observation or enrolment in a clinical trial. |
Considerations for initiation of therapy | |
What stages and grades of RCC are eligible? What are the eligibility criteria or definitions for intermediate-high to high risk of recurrence? | In the opinion of the clinical experts, eligibility of patients with RCC for adjuvant pembrolizumab treatment should be aligned with the inclusion criteria in the pivotal clinical trial (KEYNOTE-564). Specifically, following criteria should be applied:
|
The KEYNOTE-564 study required treatment with pembrolizumab to be initiated within 12 weeks following surgery. What is the appropriate time frame following surgery for initiation of adjuvant pembrolizumab treatment in clinical practice? | The clinical experts consulted by CADTH noted that, in the Canadian clinical setting, adjuvant pembrolizumab would be offered about 12 weeks postnephrectomy to reduce patient’s risk of recurrence. Of note, the sponsor provided some additional information in the sponsor’s comments template provided to CADTH. Specifically, fewer than 50 patients initiated study treatments > 90 days after their prestudy surgery. Moreover, the sponsor emphasized the limited interpretability of a possible subgroup analysis according to the < 90 days and > 90 days postsurgery subgroups because of the small sample size and exploratory nature of subgroup analysis. |
Can immune checkpoint inhibitor therapy be given again to patients who relapse following completion of adjuvant pembrolizumab? What is the progression-free interval that would be appropriate to reuse immune checkpoint inhibitor therapy? (Note: Previous pERC recommendations followed by PAG members typically use a 6-month interval.) | The clinical experts reported that TKI-based drugs (e.g., sunitinib, cabozantinib, pazopanib, and axitinib) should be offered to patients who experience relapse while on adjuvant pembrolizumab treatment. The clinical experts believed that ipilimumab plus nivolumab and axitinib plus pembrolizumab combinations should be discouraged. If disease relapse occurs after at least 6 months of adjuvant treatment, re-treatment with a PD-1 combination could be considered (e.g., ipilimumab plus nivolumab or axitinib plus pembrolizumab). |
The KEYNOTE-564 trial enrolled patients with clear cell RCC histology. Would patients with non-clear cell histology who otherwise meet the eligibility criteria benefit from adjuvant pembrolizumab? | The eligibility criteria from the KEYNOTE-564 trial covered a histologically confirmed diagnosis of RCC with a clear cell component with or without sarcomatoid features assessed by local reviewers.12 The clinical experts noted that there is no sufficient evidence to support adjuvant treatment with pembrolizumab in patients with kidney cancers with histology other than clear cell. The experts also reported that sarcomatoid features can occur in almost all types of RCCs, and that sarcomatoid differentiation is not considered a unique histological subtype of RCC. Notably, the presence of sarcomatoid features was considered a predictor of poor prognosis in patients with RCC, which suggests a need for adjuvant therapy, according to the experts. |
Considerations for discontinuation of therapy | |
What criteria should be used to discontinue therapy? | The experts noted that treatment with adjuvant pembrolizumab should be discontinued in the case of disease recurrence or intolerable treatment toxicities (e.g., myocarditis, encephalitis, severe colitis requiring steroids). |
Pembrolizumab was administered in the KEYNOTE-564 study every 3 weeks for up to 17 cycles (approximately 1 year). If there are dose interruptions, should treatment be stopped at 1 year regardless of the number of doses administered, or could any missed doses be administered after the 1-year time period provided no disease progression has occurred? If so, what is the appropriate time period to complete the 17 doses (every 3-week cycle)? | The clinical experts suggested that treatment with adjuvant pembrolizumab can be administered for up to 17 doses, regardless of the time interval. The remaining cycles of treatment could be continued in the case of any practical interruptions or upon resolution of AEs related to the treatment. |
Considerations for prescribing of therapy | |
In the KEYNOTE-564 study, pembrolizumab was administered every 3 weeks. However, the product monograph indicates that administration either every 3 weeks or every 6 weeks is acceptable for other adjuvant use even if clinical trials used a 3-week frequency (e.g., melanoma). Is it appropriate to implement a dosing regimen choice of every 3 weeks or every 6 weeks? PAG would like to inform pERC they plan to implement weight-based dosing up to the fixed dose for pembrolizumab — 2 mg/kg (up to 200 mg) every 3 weeks — and if the every-6-week regimen is recommended by pERC or approved by Health Canada, 4 mg/kg (up to 400 mg) every 6 weeks. (Note: At the time of PAG input, the product monograph and dosing information was not available.) | The experts believed that both 3-week and 6-week dosing schedules are appropriate. However, they noted that 400 mg every 6 weeks is more commonly used in clinical practice. Usually, patients would start with dosing of every 3 weeks and then switch to every 6 weeks once comfortable. Moreover, 1 of the experts stated that some provinces offer weight-based pembrolizumab dosing for patients with metastatic RCC, leading to a dose lower than the 200 mg threshold based on body weight. |
Generalizability | |
In the KEYNOTE-564 study, patients with an ECOG PS of 0 or 1 were eligible. Can patients with an ECOG PS > 1 also be considered eligible? | The clinical experts consulted by CADTH expressed uncertainty regarding adjuvant pembrolizumab in patients with an ECOG PS > 1. However, the experts reported that this judgment can be left for consideration of the treating physician. |
Funding algorithm | |
Drug may change place in therapy of drugs reimbursed in subsequent lines. | For pERC consideration. The clinical experts consulted provided information regarding drug sequencing after adjuvant treatment. In case of a disease relapse that occurs more than 6 months after adjuvant treatment, the clinicians noted that available therapies would include: 1) ipilimumab plus nivolumab combination, followed by sunitinib or pazopanib, and cabozantinib; and 2) axitinib plus pembrolizumab combination, followed by cabozantinib. Clinical experts also noted that in patients who experience relapse less than 6 months after adjuvant therapy, available options would not include immunotherapy (i.e., sunitinib or pazopanib, followed by cabozantinib or axitinib). |
System and economic issues | |
The projected number of patients in Canada (excluding Quebec) starting pembrolizumab as a monotherapy in the adjuvant setting is 108 in the first year, increasing to 331 in year 2, and 456 patients in year 3, for a total of 895 patients over 3 years. At list price, this represents a total 3-year cost of $83,187,113 for pembrolizumab and an incremental cost of $5,080,096 in the first year, $25,018,568 in the second year and $40,774,291 in the third year, for a 3-year net incremental cost of $70,872,955. PAG is unsure if the market share assumptions for eligible patients (15% in year 1, 45% in year 2, 60% in year 3) are appropriate, and therefore if patient estimates in the BIA model are accurate. If the market share assumptions are low, the patient numbers and subsequent BIA could be underestimates, resulting in affordability concerns. Additionally, if the manufacturer opens a compassionate patient support program, sometimes there is a bolus of prevalent patients added on to the incident patients in year 1 at the time of public funding, which may result in a further underestimate of the BIA for the first year. | For pERC consideration. |
AE = adverse event; BIA = budget impact analysis; ECOG PS = Eastern Cooperative Oncology Group Performance Status; M0 = no distant metastasis; N0 = no regional lymph node metastasis; PAG = Provincial Advisory Group; PD-1 = programmed cell death; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee; pT3 = pathological T3; RCC = renal cell carcinoma; TKI = tyrosine kinase inhibitor.
Clinical Evidence
The clinical evidence included in the review of pembrolizumab is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada and studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor (if submitted) and indirect evidence selected from the literature that met the selection criteria specified in the review. For this submission, the sponsor did not provide indirect evidence. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of pembrolizumab (200 mg, IV, once every 3 weeks; or 400 mg, IV, once every 6 weeks) for the adjuvant treatment of RCC in patients at intermediate-high or high risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada and studies meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Of note, the systematic review protocol presented in this section was established before the granting of a Notice of Compliance from Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults with RCC at intermediate-high or high risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions Subgroups
|
Intervention | Pembrolizumab for IV infusion: 200 mg every 3 weeks or 400 mg every 6 weeks until unacceptable toxicity, disease recurrence, or for up to 1 year or 17 doses for 200 mg or 9 doses for 400 mg, whichever is longer. |
Comparator | No adjuvant treatment |
Outcomesa | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; DFS = disease-free survival; EFS = event-free survival; HRQoL = health-related quality of life; M0 = no distant metastases; M1 = distant metastasis; M1 NED = M1 with no evidence of disease; OS = overall survival; RCC = renal cell carcinoma; RCT = randomized controlled trial; SAE = serious adverse event; SSIGN = stage, size, grade, and necrosis scoring; UISS = University of California Los Angeles Integrated Staging System; WDAE = withdrawal due to adverse event.
aThese outcomes were identified as being of particular importance to patients in the input received by CADTH from patient groups.
The literature search was performed by an information specialist using a peer-reviewed search strategy.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy, according to the PRESS Peer Review of Electronic Search Strategies checklist.15
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946—) via Ovid and Embase (1974—) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Keytruda (pembrolizumab) and RCC. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on April 1, 2022. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee (CDEC) on August 10, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature reference.16 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
The manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
One study was identified for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6. A list of excluded studies is presented in Appendix 2.
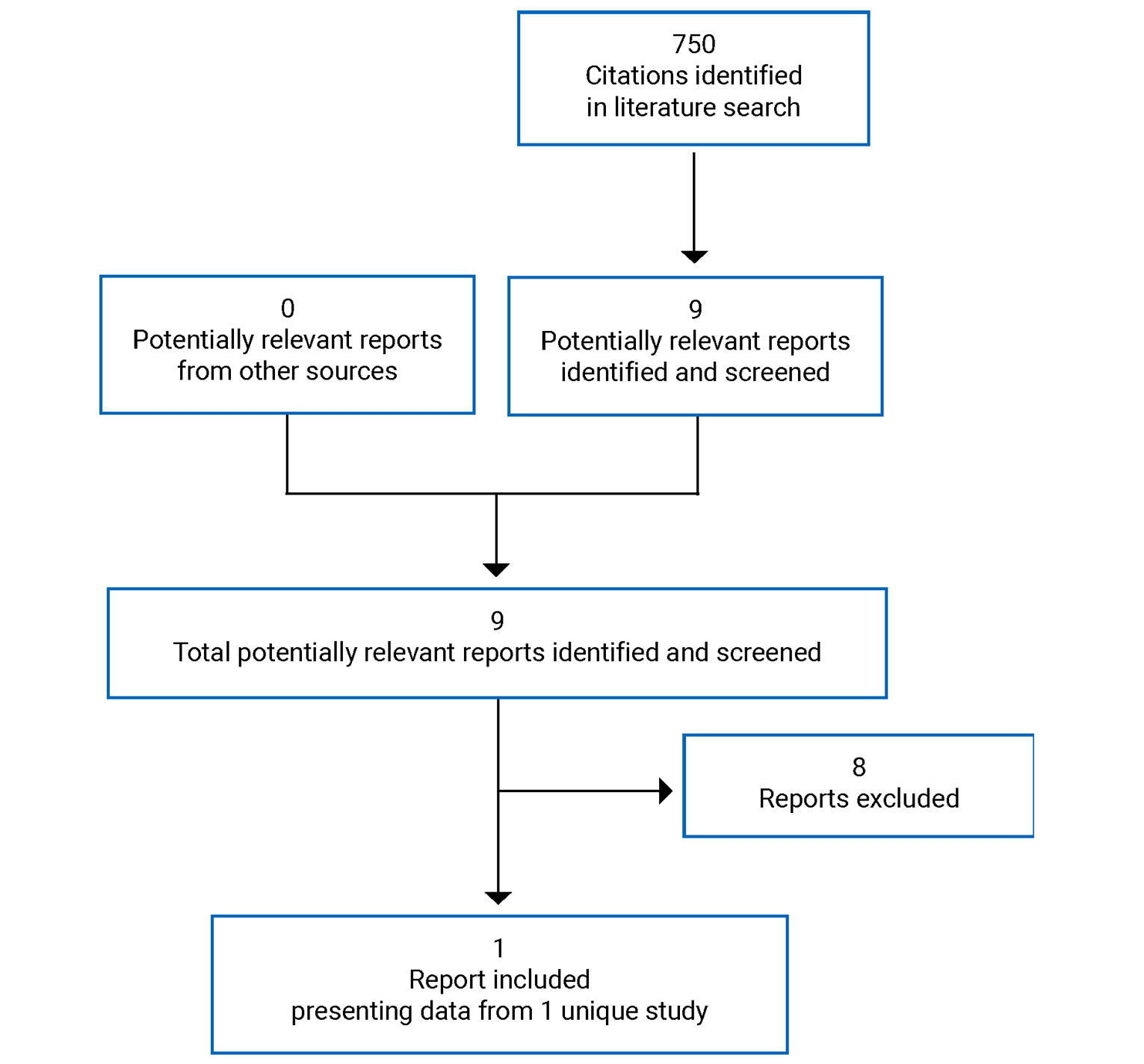
Table 6: Details of Included Studies
Study detail | KEYNOTE-564 |
|---|---|
Designs and populations | |
Study design | Multicentre, randomized, placebo-controlled, double-blind, phase III study |
Locations | 212 study sites in 21 countries: Canada (10), US (47), South America (35), Europe (73), Russia (11), Asia (29), Australia (7) |
Study duration |
|
Data cut-off date |
|
Patient enrolment dates | June 30, 2017, to September 20, 2019 |
Randomized (n) | 994 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Pembrolizumab 200 mg IV every 3 weeks |
Comparator | Placebo: saline solution 0 mg IV every 3 weeks |
Duration | |
Phase | |
Screening | 42 days; first participant was screened on June 9, 2017 |
Treatment | Participants were randomized from June 30, 2017, to September 20, 2019 (approximately 27 months) |
Follow-upa | Safety follow-up: for AEs, 30 days after last dose of the treatment or before the initiation of a new anti-cancer treatment, whichever comes first; for SAEs, 90 days after last dose of the treatment or 30 days after cessation of treatment if the participant initiates a new anti-cancer therapy Efficacy follow-up: every 12 weeks in year 1, every 16 weeks in years 2 to 4, and every 24 weeks in year 5 for the assessment of DFS (all participants who complete 17 cycles or discontinue treatment for reasons other than disease recurrence) Survival follow-up: every 12 weeks for the assessment of survival status until death, withdrawal of consent, or the end of the study, whichever occurs first Quality-of-life follow-up: once a year after last dose of the treatment, until disease recurrence or initiating a new anti-cancer treatment |
Outcomes | |
Primary end point | DFS assessed by investigator |
Secondary and exploratory end points | Secondary:
Exploratory:
Safety end points:
|
Notes | |
Publications | Choueiri et al. (2021)17 |
AE = adverse event; BICR = blinded independent central review; DFS = disease-free survival; DRSS = disease recurrence–specific survival; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = 5-Level EQ-5D; FKSI-DRS = Functional Assessment of Cancer Therapy Kidney Symptom Index–Disease-Related Symptoms; IA1 = first interim analysis; IV = intravenously; M0 = patients with no distant metastases; M1 NED = patients with a primary kidney tumour plus solid, isolated, soft tissue metastases that were completely resected at nephrectomy (synchronous) or ≤ 1 year after nephrectomy (metachronous); MRI = MRI; OS = overall survival; PD-1 = programmed cell; PD-L1 = programmed cell death ligand-1; PD-L2 = programmed cell death ligand-2; PRO = patient-reported outcome; RCC = renal cell carcinoma; SAE = serious adverse event; TMN = tumour, node, and metastasis staging; VAS = visual analogue scale.
aFor participants who discontinue treatment intervention and who will not enter the efficacy follow-up phase, the first survival follow-up contact will be scheduled 12 weeks after discontinuation visit and/or the safety follow-up visit (whichever is last). For participants who completed assessments in the efficacy follow-up phase, the first survival follow-up contact will be scheduled 12 weeks after the last efficacy follow-up visit had been performed.
Source: Clinical Study Report.12
Description of Studies
KEYNOTE-564 is an ongoing multicentre, randomized, double-blind, phase III study with a primary objective to compare the efficacy and safety of pembrolizumab versus placebo (saline solution) as an adjuvant treatment for adult patients with RCC postnephrectomy or postnephrectomy and resection of metastatic lesions.
The trial was conducted at 212 global sites in 21 countries (including Canada). The key characteristics of the study design are summarized in Table 6 and Figure 2.
Stratified randomization using central Interactive Voice Response Systems and Interactive Web Response Systems was implemented at participating trial sites. Patients were stratified by metastasis status (M0 versus M1 NED), which was predefined. Moreover, in the M0 group, 2 additional stratification factors were pre-specified: ECOG PS (0 versus 1) and US participant (yes versus no).
The first patient was randomized on June 30, 2017, and the last patient was enrolled September 20, 2019. The cut-off date for first interim analysis was December 14, 2020, and database lock date was January 26, 2021. One additional analysis (efficacy update report) was implemented after 6 additional months of follow-up, with a cut-off date of June 14, 2021.
Figure 2: KEYNOTE-564 Study Design
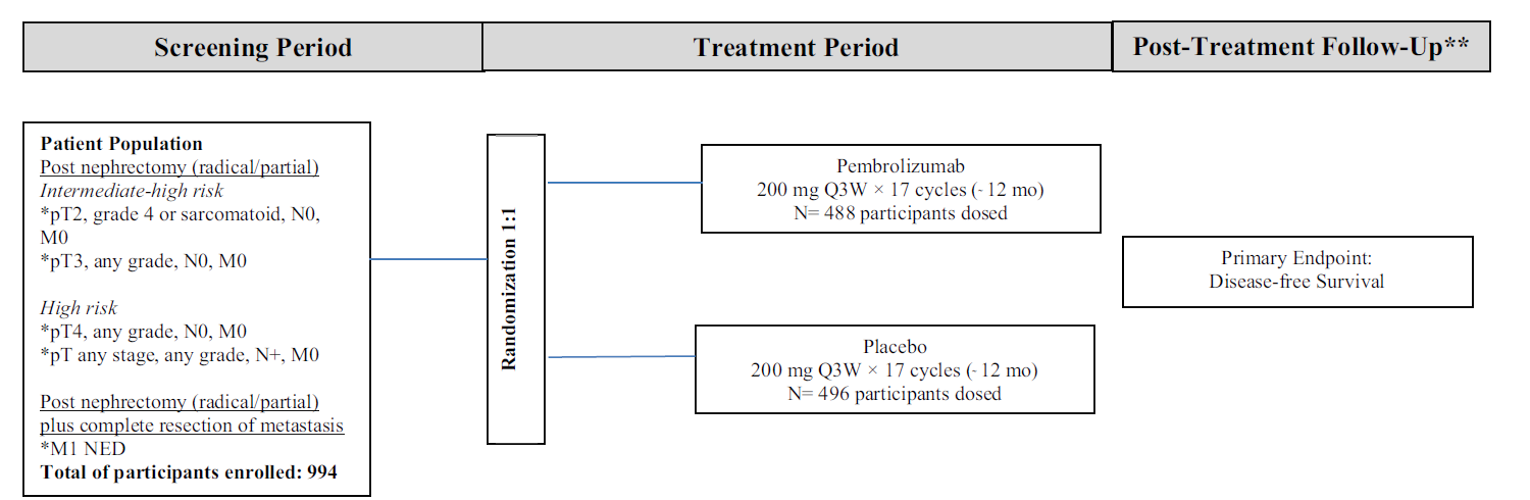
mo = month; NED = no evidence of disease; Q3W = every 3 weeks.
** Safety follow-up: 30 days after last dose; efficacy follow-up: every 12, 16, or 24 weeks; survival follow-up: every 12 weeks. Survival follow-up status is assessed approximately every 12 weeks until death, withdrawal of consent, or the end of the study, whichever occurs first. For participants who discontinue treatment intervention and who will not enter the efficacy follow-up phase, the first survival follow-up contact will be scheduled 12 weeks after the discontinuation visit and/or the safety follow-up visit (whichever is last). For participants who completed assessments in the efficacy follow-up phase, the first survival follow-up contact will be scheduled 12 weeks after the last efficacy follow-up visit had been performed.
Source: Clinical Study Report.12
Populations
Inclusion and Exclusion Criteria
Eligible patients included individuals aged 18 years and older with histologically confirmed clear cell RCC, with or without sarcomatoid features, and with intermediate-high or high risk of recurrence following nephrectomy or following nephrectomy and resection of metastatic lesions. Recurrence risk categories were defined by pathological TNM staging, Fuhrman grade, and presence of sarcomatoid features (Table 6). Patients could not have received prior systemic treatment for RCC. Patients with prior major surgery other than nephrectomy and/or resection of pre-existing metastases for M1 NED disease, and those with residual thrombus postnephrectomy in the renal vein or vena cava were excluded from the trial. Moreover, patients who had received prior systemic treatment or radiotherapy for RCC or who had pre-existing brain or bone metastasis were not eligible.
Baseline Characteristics
As of the first interim analysis data cut-off (December 14, 2020), the median age of patients randomized in the KEYNOTE-564 study was 60 years (range for pembrolizumab group = 27 to 81 years; range for placebo group = 25 to 84 years), more males than females were enrolled (70.0% and 72% in pembrolizumab and placebo arms, respectively), and the majority of patients were White (75.0% and 75.7% in pembrolizumab and placebo arms, respectively). Most patients had tumours with an absence of sarcomatoid features and were at intermediate-high risk of recurrence. Overall, baseline characteristics were balanced in the 2 study arms. Table 7 presents the baseline summary characteristics of the ITT population.
Regarding prior treatment, 1 participant had received prior anti-cancer drug therapy (pazopanib hydrochloride), and 95% of participants in both the pembrolizumab and placebo arms had at least 1 concomitant medical condition. The most frequently reported medical conditions in participants receiving pembrolizumab were hypertension (53%) and type 2 diabetes mellitus (12%), and in participants receiving placebo were hypertension (50%), gastroesophageal reflux disease (12%), back pain (12%), benign prostatic hyperplasia (12%), and hyperlipidemia (11%).
Table 7: Summary of Patient Baseline Characteristics (ITT Population) in the KEYNOTE-564 Trial
Characteristic | Pembrolizumab arm (N = 496) | Placebo arm (N = 498) |
|---|---|---|
Age, years | ||
Median (range) | 60.0 (27 to 81) | 60.0 (25 to 84) |
< 65 years, n (%) | 338 (68.1) | 326 (65.5) |
≥ 65 years, n (%) | 158 (31.9) | 172 (34.5) |
Sex, n (%) | ||
Male | 347 (70.0) | 359 (72.1) |
Female | 149 (30.0) | 139 (27.9) |
Race, n (%) | ||
White | 372 (75.0) | 377 (75.7) |
Asian | 63 (12.7) | 75 (15.1) |
American Indian or Alaska Native | 10 (2.0) | 2 (0.4) |
Black or African American | 7 (1.4) | 5 (1.0) |
Multiple | 8 (1.6) | 5 (1.0) |
Missing | 36 (7.3) | 34 (6.8) |
Geographic region of enrolling site, n (%) | ||
North America | 133 (26.8) | 125 (25.1) |
European Union | 188 (37.9) | 187 (37.6) |
Rest of the world | 175 (35.3) | 186 (37.3) |
ECOG PS, n (%) | ||
0 | 421 (84.9) | 426 (85.5) |
1 | 75 (15.1) | 72 (14.5) |
Type of nephrectomy, n (%) | ||
Partial | 37 (7.5) | 38 (7.6) |
Radical | 459 (92.5) | 460 (92.4) |
PD-L1 status, n (%) | ||
CPS < 1 | 124 (25.0) | 113 (22.7) |
CPS ≥ 1 | 365 (73.6) | 383 (76.9) |
Missing | 7 (1.4) | 2 (0.4) |
Primary tumour stage, n (%) | ||
T1 | 11 (2.2) | 15 (3.0) |
T2 | 27 (5.4) | 33 (6.6) |
T3 | 444 (89.5) | 437 (87.8) |
T4 | 14 (2.8) | 13 (2.6) |
Tumour grade, n (%) | ||
Grade 1 | 19 (3.8) | 16 (3.2) |
Grade 2 | 153 (30.8) | 150 (30.1) |
Grade 3 | 219 (44.2) | 213 (42.8) |
Grade 4 | 103 (20.8) | 119 (23.9) |
Missing | 2 (0.4) | 0 (0.0) |
Sarcomatoid feature, n (%) | ||
Presence | 52 (10.5) | 59 (11.8) |
Absence | 417 (84.1) | 415 (83.3) |
Unknown | 27 (5.4) | 24 (4.8) |
Lymph nodes stage, n (%) | ||
N0 | 465 (93.8) | 467 (93.8) |
N1 | 31 (6.3) | 31 (6.2) |
Metastatic staging, n (%) | ||
M0 | 467 (94.2) | 469 (94.2) |
M1 NED | 29 (5.8) | 29 (5.8) |
RCC risk category, n (%) | ||
M0-intermediate-high risk | 422 (85.1) | 433 (86.9) |
M0-high risk | 40 (8.1) | 36 (7.2) |
M0-other | 5 (1.0) | 0 (0.0) |
M1 NED | 29 (5.8) | 29 (5.8) |
CPS = combined positive score; ECOG PS = Eastern Cooperative Oncology Group Performance Statis; ITT = intention to treat; M0 = patients with no distant metastases; M1 NED = patients with a primary kidney tumour plus solid, isolated, soft tissue metastases that were completely resected at nephrectomy (synchronous) or ≤ 1 year after nephrectomy (metachronous); PD-L1 = programmed cell death ligand-1.
Notes: Participants in the M0-intermediate-high risk category have pT2 (grade 4 or sarcomatoid), N0, M0 disease; or pT3 (any grade), N0, M0 disease. Participants in the M0-high-risk category have pT4 (any grade), N0, M0 disease; or pT any (any grade), N1 or greater, M0 disease. Participants in the M1 NED category present not only with the primary kidney tumour, but also with solid, isolated, soft tissue metastases that were completely resected at the time of nephrectomy (synchronous) or 1 year from nephrectomy (metachronous). Participants in the M0-other category have T2 (grade ≤ 3) N0, M0 disease; or T1, N0, M0 disease.
Data cut-off: December 14, 2020.
Source: Clinical Study Report.12
Interventions
Patients were randomized to receive 1 of the following treatments:
pembrolizumab (200 mg as a 30-minute IV infusion every 3 weeks)
placebo (saline solution IV every 3 weeks).
Study treatments were administered to a maximum of 17 infusions (or up to approximately 1 year) on an outpatient basis or until confirmation of disease recurrence or the criteria for treatment discontinuation are met.
Concomitant Medication
Patients were prohibited from receiving the following therapies during the trial: antineoplastic systemic chemotherapy or biologic therapy, immunotherapy or chemotherapy not specified in the trial protocol, investigational drugs other than pembrolizumab, radiation therapy, live vaccines in the 30 days before the first dose of the study treatment (e.g., measles, mumps, rubella, varicella-zoster, yellow fever, rabies, Bacillus Calmette-Guérin, typhoid vaccine), systemic glucocorticoids for any purpose other than to modulate symptoms from an AE suspected to have an immunologic etiology. Details of treatment with other, permitted concomitant medications are presented in the Table 14.
Treatment Discontinuation Criteria
Discontinuation of the study treatment was considered for patients who received 17 cycles of study treatment, experienced progression or recurrence of the malignancy under study, experienced a new malignancy requiring active treatment or any other intercurrent illness that prevents administration of the study treatment. Patients were also discontinued from study treatment in case of the development of unacceptable toxicity, development of recurrent grade 2 pneumonitis, positive serum pregnancy test, patients’ request, investigator’s decision, or study termination due to a withdrawal of consent. Discontinuation from the study treatment was considered permanent and patients were not allowed to restart study treatment after their discontinuation.
Outcomes
The primary objective was to assess whether pembrolizumab prolongs DFS, assessed by the investigator, compared with placebo. The key secondary objective was to assess whether pembrolizumab prolongs OS, compared with placebo. Other secondary objectives included a comparison of safety and tolerability, DRSS, EFS by blinded independent radiology review, DFS and OS according to programmed death ligand-1 (PD-L1) expression, EORTC QLQ-C30 (global health status/QoL and physical functioning scales) and FKSI-DRS scores in the pembrolizumab and placebo arms. Exploratory objectives included pharmacokinetic parameters, the presence of antidrug antibodies, biomarker analyses, EORTC QLQ-C30 symptom subscale scores, 5-Level EQ-5D (EQ-5D-5L) visual analogue scale (VAS) scores, and the proportion of patients experiencing deterioration, stability, improvement, and stability and improvement, as indicated by EORTC QLQ-C30 and FKSI-DRS scores.
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 8, and detailed summaries of the end points follow. A detailed discussion and critical appraisal of outcome measures are provided in Appendix 4.
Table 8: Summary of Outcomes of Interest in the KEYNOTE-564 Trial Identified in the CADTH Review Protocol
Outcome measure | Outcome level | Description | Inclusion in multiple testing procedure |
|---|---|---|---|
DFS | Primary | DFS, assessed by the investigator, is defined as the time from randomization to the first documented local recurrence, the occurrence of distant kidney cancer metastasis(es), or death due to any cause, whichever occurs first | Yes |
OS | Secondary | OS is defined as the time from randomization to death due to any cause | Yes |
DRSS | Secondary | DRSS1 is defined as the time from randomization to the first documented local recurrence of RCC as assessed by the investigator. DRSS2 is defined as the time from randomization to the first documented local recurrence with visceral lesion or the occurrence of distant kidney cancer metastasis(es) with visceral lesion, whichever occurs first, as assessed by the investigator. | No |
EFS | Secondary | EFS, assessed by BICR, is defined as the time from randomization to the first documented local recurrence or occurrence of distant kidney cancer metastasis(es) in participants considered by BICR to be disease-free at baseline (M0/M1 NED); or disease progression in participants considered by BICR to have baseline disease (M1), or death due to any cause, whichever occurs first | No |
HRQoL | Secondary | EORTC QLQ-C30 global health status/quality of life and physical functioning subscales | No |
Secondary | FKSI-DRS | No | |
Exploratory | EQ-5D-5L VAS | No | |
Safety | Secondary | Safety parameters included, but were not limited to, the incidence, causality, and outcome of AEs and SAEs, and changes in laboratory values | No |
AE = adverse event; BICR = blinded independent central review; DFS = disease-free survival; DRSS = disease recurrence–specific survival; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = 5-Level EQ-5D; FKSI-DRS = Functional Assessment of Cancer Therapy Kidney Symptom Index–Disease-Related Symptoms; HRQoL = health-related quality of life; M0 = patients with no distant metastases; M1 = distant metastasis; M1 NED = M1 with no evidence of disease; OS = overall survival; RCC = renal cell carcinoma; SAE = serious adverse event; VAS = visual analogue scale.
Efficacy Measurement for Primary and Secondary Outcomes
Tumour assessments (consisting of CT or MRI scans of the brain, chest, abdomen, and pelvis and a bone scan) were performed within 28 days before randomization. For each patient, the same imaging modality and image-acquisition protocol was used consistently across all time points.
During the treatment period, patients who discontinued the study treatment for a reason other than disease recurrence were considered to be on study and continued with scheduled assessments. During treatment, imaging assessments of the chest, abdomen, and pelvis were performed every 12 weeks from randomization. On-treatment bone and brain scans were performed only as clinically indicated during the postrandomization period.
Safety follow-up visits were conducted 30 days (± 7 days) after the last dose of the study treatment or before the initiation of new anti-cancer treatment, whichever occurred first.
All individuals who completed 17 cycles of the study treatment or discontinued treatment for reasons other than disease recurrence entered the efficacy follow-up and were monitored for disease status on the following schedule: every 12 weeks in year 1, every 16 weeks in years 2 to 4, and every 24 weeks in year 5 and beyond. Disease imaging continued until disease recurrence, pregnancy, the start of a new anti-cancer treatment, withdrawal of consent, death, or the end of the trial, whichever occurred first.
For the assessment of DFS, radiographic evidence of disease recurrence was required and biopsy or cytology confirmation was strongly encouraged. The date of disease recurrence was the date the first radiographic image was obtained, regardless of the timing of additional confirmatory procedures (e.g., repeat imaging, biopsy, and/or cytology). Disease progression was assessed in participants considered to have baseline disease by BICR and was defined as the unequivocal progression of baseline disease or the appearance of new lesions, assessed by BICR.
Patients who completed all efficacy assessments and/or patients who did not have further efficacy assessments (including patients who discontinued treatment and did not enter efficacy follow-up phase) entered the survival follow-up phase. Assessment of survival occurred approximately every 12 weeks until death, withdrawal of consent, or the end of the trial, whichever occurred first.
Health-Related Quality of Life
HRQoL measures were assessed using the generic cancer HRQoL instrument (EORTC QLQ-C30), the RCC-specific HRQoL instrument (FKSI-DRS), and the generic HRQoL instrument (EQ 5D-5L). The HRQoL instruments were completed electronically by study participants at various time points: during treatment (cycles 1, 5, 9, 13, and 17), at treatment discontinuation, at 30-day follow-up, and annually during the post-treatment period until disease recurrence or the start of a new anti-cancer treatment. A detailed discussion and critical appraisal of these outcomes are available in Appendix 4.
EORTC QLQ-C30
EORTC QLQ-C30 is a self-reported cancer-specific, multidimensional questionnaire that assesses HRQoL associated with treatment in patients with cancer.18 This 30-item questionnaire incorporates 5 multi-item functional scales (physical, role, cognitive, emotional, and social), 3 multi-item symptom scales (fatigue, pain, nausea and vomiting), 6 single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial impact) and a 2-item quality-of-life scale (global QoL).19 Higher scores on the functional scale, the symptom scale and items, and the global health status/QoL scale indicate a higher level of functioning, a higher level of symptomatology, and a higher level of quality of life, respectively.19 The validity, reliability, responsiveness, and minimally important differences (MIDs) of the EORTC QLQ-C30 questionnaire have not been documented in patients with RCC in the adjuvant setting (Appendix 4).
FKSI-DRS
FKSI-DRS is a kidney-cancer-specific, self-reported instrument that evaluates disease-related symptoms. The 9-item questionnaire assesses symptoms of kidney cancer deemed to be important to patients with and clinicians treating advanced kidney cancer (lack of energy, pain, weight loss, bone pain, fatigue, shortness of breath, cough, fever, blood in urine).20 Total scores for FKSI-DRS range from 0 (severely symptomatic) to 36 (asymptomatic).21 Validity, reliability, and responsiveness to change has been demonstrated in patients with advanced RCC, but not in the adjuvant setting. The MID estimated using different anchors ranged from 0.62 to 3 points for patients with advanced RCC.
EQ-5D-5L VAS
The EQ-5D-5L is a generic, utility-based measure of HRQoL comprising a descriptive system and the VAS. Only the VAS was assessed in the trial. The EQ VAS is a vertical VAS with values between 100 (best imaginable health) and 0 (worst imaginable health) on which patients provide a global assessment of their health.22 The validity, reliability, and responsiveness of the EQ-5D-5L questionnaire and its VAS have not been evaluated in patients with RCC in the adjuvant setting.
HRQoL thresholds defined in the KEYNOTE-564 study were as follows:
EORTC QLQ-C30 functional and the global health status/QoL score: a change of 10 points or more was considered to be clinically meaningful23
FKSI-DRS score: a change of 3 points or more was considered to be clinically meaningful).20,24
Statistical Analysis
Sample Size and Power Calculation
Sample size calculations were based on the primary end point (DFS) and the main secondary end point (OS). The study plan was to randomize 950 patients in a 1:1 ratio to pembrolizumab or placebo, but the power calculations by the sponsor were performed on 990 participants, which aligned with the actual number of randomized participants.
The study was designed to achieve 95% power at the 1-sided alpha level of 2.5% to detect a statistically significant difference in DFS between pembrolizumab and placebo (HR = 0.67). A total of 332 DFS events were expected to occur, with 1 interim analysis reaching about 80% of the targeted events.
The power to detect a HR of 0.67 and 0.635 at an overall alpha level of 2.5% in OS between the pembrolizumab and placebo arms was 79% and 88%, respectively. This was conditional upon the rejection of the null hypothesis for DFS, targeted 200 OS events and 3 interim analyses reaching about 47%, 66%, and 86% of the target events.
In the calculation of power for the DFS and OS analyses, the sponsor assumed the following: DFS following a Poisson mixture cure rate model with assumed cure rate of 0.3, based on historical data25; a median DFS of 45 months for individuals not cured in the placebo arm; OS following an exponential distribution and a median of 145 months for the placebo arm; 27-month enrolment with monthly accrual of 20 participants, 30 participants, and 1 participant during the first 5 months, from month 6 to month 21, and for the last month, respectively; and a yearly dropout rate of 2% for DFS and 1% for OS.
Multiplicity
Multiplicity testing adjustments included an overall type I error control at 2.5% (1-sided) for the primary end point (DFS) and key secondary end point (OS). The trial incorporated a fixed testing sequence: DFS at alpha level of 2.5% (1-sided) was tested first, and the alpha was passed to OS if the hypothesis test for DFS is declared successful. A group sequential approach (Maurer and Bretz) was implemented to allocate the alpha between the interim and final analyses.
For DFS and OS, the information fraction at each analysis was based on 332 and 200 final planned events, respectively. Lan-DeMets O’Brien-Fleming alpha spending function was used to set the efficacy bounds. Nonbinding futility spending was implemented by controlling the probability of crossing the futility bound under the null hypothesis (total of 1-alpha = 97.5%); a Hwang-Shih-DeCani spending function, with γ = –6 used to set testing boundaries at each analysis. All the bounds were adjusted in line with the actual number of events accrued at each analysis.
Multiplicity adjustments were not made for other secondary or exploratory analyses.
Planned Analysis
There were 3 planned interim analyses and 1 planned final analysis in the KEYNOTE-564 trial (Table 9). The interim efficacy analyses were conducted by an external unblinded statistician and scientific programmer who had no other responsibilities in the study and were reviewed by an external data monitoring committee. Periodic safety monitoring was conducted by the committee, the frequency of which was defined in the committee charter (about every 6 months in the first year and every 12 months after the first year).
Table 9: Summary of Interim and Final Efficacy Analyses
Analysis identifier | End point | Timing |
|---|---|---|
IA1 | DFS, OS | Enrolment complete, at least 265 DFS events (assessed by investigator) have occurred, and a minimum follow-up time (from last participant randomized to IA1) of 12 months is achieved (approximately 94 OS events are expected at this time) |
Efficacy update report | DFS, OS | Additional 6 months of follow-up after the IA1 data cut-off date |
IA2 | DFS, OS | 332 DFS events; if DFS was rejected before IA2, timing was driven by 132 OS events |
IA3 | OS | 172 OS events |
Final analysis | OS | 200 OS events |
IA1 = first interim analysis; IA2 = second interim analysis; IA3 = third interim analysis; DFS = disease-free survival; OS = overall survival.
Source: Clinical Study Report.12,26
Of note, additional amendments to the supplemental statistical plan were implemented to incorporate potential requests from regulatory agencies. Specifically, an efficacy update report was added between 2 planned interim analyses (first and second interim analysis). The efficacy update report incorporated 6 additional months of follow-up from the first interim analysis (approximately 66 OS events), with June 14, 2021, as the data cut-off date. Median follow-up duration was 29.9 months (range = 2.5 to 47.5 months) for individuals in pembrolizumab group and 29.2 months (range = 3.5 to 47.4 months) for individuals in the placebo group. All the amendments were made before the data cut-off date, and the results were reviewed by an external data monitoring committee.
The sponsor indicated that the alpha levels would be spent on the efficacy update based on the observed number of events at the efficacy update report analysis, in line with the alpha spending function initially specified in the protocol, and that the alpha spending and interim analysis-final analysis boundary properties at subsequent interim and final analyses would be updated accordingly. Similar to the initial power calculations, the power to detect a HR of 0.67 and 0.635 at an overall alpha level of 2.5% in OS between the pembrolizumab and placebo arms was 79% and 88%, respectively. The amendment reported the following conditions for this power calculation: rejection of the null hypothesis for DFS; 200 OS events targeted; and 3 interim analyses and a possible efficacy update report analysis reaching about 26%, 33%, 66%, and 86% of the target events.
Primary Outcome: DFS
Median DFS for the pembrolizumab and placebo treatment arms were estimated and plotted using the nonparametric Kaplan-Meier (KM) method (Table 10). The primary hypothesis (i.e., treatment difference in DFS) was evaluated by comparing DFS using a stratified log-rank test. The HRs were estimated using a stratified Cox regression model with Efron’s method of tie handling, with a single-treatment covariate. The stratification factors implemented for both the stratified log-rank test and the stratified Cox model included stratification factors used in randomization (metastasis status [M0 versus M1 NED] and, in the M0 group, ECOG PS [0 versus 1] and US participant [yes versus no]). The analysis of DFS was based on the ITT population.
Subgroup Analyses
Pre-specified subgroups analysis was performed for the primary end point (DFS).
Subgroup analyses did not account for multiplicity. This CADTH review identified 3 subgroups of interest in the protocol, 1 of which was included in the pre-specified subgroup analysis (patients with different metastatic status [M0 or M1 NED] at baseline). Moreover, the efficacy update report analysis presented findings of an additional subgroup analysis of interest for this CADTH review (DFS, according to recurrence risk groups), which was not pre-specified in the analysis plan for the trial.
Sensitivity Analyses
A sensitivity analysis was performed to account for the different time-to-event distribution in individuals enrolled with baseline disease, assessed by BICR, compared to those who were disease-free at baseline. The stratified Cox model and stratified log-rank test was implemented with baseline disease status assessed by BICR as an additional stratum. In particular, 6 strata were used (M0 + ECOG PS 0 + US participant versus M0 + ECOG PS 0 + non-US participant versus M0 + ECOG PS 1 + US participant versus M0 + ECOG PS 1 + non-US participant versus M1 NED versus M1 by BICR). Another sensitivity analysis included the assessment of DFS by BICR and the censoring of individuals with baseline disease, assessed by BICR at the randomization date. The robustness of the DFS end point was assessed in a third pre-specified sensitivity analysis with a different set of censoring rules. This sensitivity analysis took into account new anti-cancer treatment or missed disease assessments. Specifically, the sensitivity analysis followed the same principles as the primary analysis, except in the case of events that occurred after 2 consecutive missed disease assessments or after new anti-cancer therapy, in which case censoring was done at the last disease assessment before the missed assessments and the initiation of new anti-cancer therapy. Censoring rules for primary and sensitivity analysis are described in Table 11.
Secondary Outcome: OS
The analytical approach for the main secondary outcome (OS) was similar to the 1 adopted for the primary outcome of the study. Median OS in both treatment arms was estimated and plotted using the nonparametric KM method. A stratified log-rank test was used to assess the treatment difference in survival. HRs were estimated using a stratified Cox regression model with Efron’s method of tie handling, with a single-treatment covariate. The stratification factors implemented for both the stratified log-rank test and the stratified Cox model included stratification factors used in randomization (metastasis status [M0 versus M1 NED] and, in the M0 group, ECOG PS [0 versus 1], and US participant [yes versus no]). The analysis of OS was based on the ITT population.
Other Secondary Outcomes
Details of the statistical approaches used to assess DRSS and EFS are outlined in the Table 10. Briefly, a nonparametric cumulative incidence estimator was used to estimate DRSS curves in the pembrolizumab and placebo treatment groups. The analyses included DRSS1, for which only local recurrence was considered an event, and DRSS2, for which only local disease recurrence with visceral lesion or occurrence of distant kidney cancer metastasis(es) with visceral lesion were considered as events. Censoring rules for DRSS1 and DRSS1 are described in Table 10.
For EFS, the nonparametric KM method was used to estimate the curve in each treatment arm. No formal hypothesis testing was performed, and nominal P values from the stratified log-rank test were provided. The stratified Cox regression model with Efron’s method of tie handling, with a single-treatment covariate, was used for estimation of HRs. The stratification factors implemented for the stratified Cox model included stratification factors used in randomization, with baseline disease status assessed by BICR as an additional stratum.
HRQoL measures included the EORTC QLQ-C30 (global health status/QoL and physical functioning scales) and FKSI-DRS. These were assessed as secondary outcomes through a constrained longitudinal data analysis (cLDA) model, with the scores as the response variable, and the treatment-by-time interaction and stratification factors used for randomization as covariates. Model-based treatment differences in terms of the least squares mean change from baseline and least squares mean values by treatment arm at the baseline and postbaseline time points (52 weeks) were reported. The full analysis set was used to assess patient-reported outcomes (PROs), defined as all randomized patients with at least 1 HRQoL assessment available for the specific end point and who have received at least 1 dose of the study intervention.
Exploratory Outcomes
Exploratory outcomes included mean change from baseline on the EORTC QLQ-C30 symptom subscales (nausea and vomiting, diarrhea symptoms) and EQ-5D-5L VAS scores, using the methodology described for other secondary outcomes.
Furthermore, an assessment of improvement and improvement plus stability rates in patient-reported end points for the 2 treatment groups was assessed (EORTC QLQ-C30 global health status/QoL and physical functioning scales and FKSI-DRS), in line with the definitions presented in the Appendix 3. The stratified Miettinen and Nurminen method was implemented to compute the difference in the overall improvement (or improvement plus stability) rate between the pembrolizumab and placebo groups and its corresponding 95% CI, with strata weighting by sample size and stratification factors used for randomization. Moreover, the exact binomial method of Clopper and Pearson was adopted to calculate point estimates and the corresponding 95% CI by treatment group.
Safety Outcomes
Safety analyses were considered secondary outcomes in the KEYNOTE-564 trial and followed a tiered approach (refer to Table 10 for description). Tier 1 safety end points (subject to inferential testing for statistical significance) were not evaluated in the study, as no enhanced safety signals were expected. Tier 2 parameters were assessed with descriptive statistics and point estimates with 95% CIs for between-group comparisons, whereas tier 3 safety parameters were only evaluated using descriptive statistics.
Table 10: Statistical Analysis of Efficacy End Points in the KEYNOTE-564 Study
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
DFS | The nonparametric KM method (for estimation of the DFS curves) Stratified log-rank test (for testing the hypothesis of treatment difference in DFS). Stratified Cox proportional hazard model with Efron’s method of tie handling (for estimation of HR). | Stratification factors applied to both the stratified log-rank test and the stratified Cox model included metastasis status (M0 vs. M1 NED), ECOG PS (0 vs. 1), and US participant (yes vs. no) |
|
OS | The nonparametric KM method (for estimation of the DFS curves) Stratified log-rank test (for testing the hypothesis of treatment difference in DFS). Stratified Cox proportional hazard model with Efron's method of tie handling (for estimation of HR). | Stratification factors applied to both the stratified log-rank test and the stratified Cox model included metastasis status (M0 vs. M1 NED), ECOG PS (0 vs. 1), and US participant (yes vs. no) | No |
DRSS | The nonparametric cumulative incidence estimator (for estimation of the DRSS1 and DRSS2 curves) For DRSS1, death or occurrence of distant kidney cancer metastasis(es) was censored at the documented date of disease metastasis or death, whichever occurred first. For DRSS2, death, local recurrence without visceral lesion, or distant metastasis without visceral lesion was censored at the documented date of disease recurrence or death, whichever occurred first. | No | No |
EFS | The nonparametric KM method (to estimate EFS curves) A stratified Cox proportional hazards model with Efron's method of tie handling (to estimate HR) Stratification factors for both log-rank test and Cox model included stratification factors used for randomization and additional baseline disease status assessed by BICR. | Stratification factors applied to the stratified Cox model included metastasis status (M0 vs. M1 NED), ECOG PS (0 vs. 1) and US participant (yes vs. no), with baseline disease status assessed by BICR as an additional stratum | No |
HRQoL | cLDA model with the PRO score as the response variable, and treatment-by-time interaction and stratification factors used for randomization as covariates The treatment difference in terms of LS mean change and 95% CI from baseline was estimated from the model Model-based LS mean and 95% CI were provided by treatment group for PRO scores at baseline and at the postbaseline time point. | cLDA model included the stratification factors used for randomization as covariates | No |
Safety | A tiered approach was followed Tier 1 parameters (AEs of special interest) were not analyzed Tier 2 parameters (specific SAEs with an incidence of ≥ 5% of patients in 1 treatment group; specific grade 3 to 5 AEs with an incidence of ≥ 5% of patients in 1 treatment group; specific AEs or system organ class with an incidence of ≥ 10% of patients in 1 treatment group) were assessed using point estimates, with 95% CIs provided for between-group comparisons (Miettinen and Nurminen method, an unconditional, asymptotic method) Tier 3 parameters (any AEs; any SAEs; any grade 3 to 5 AEs; any drug-related AEs; any serious and drug-related AEs; any grade 3 to 5 and drug-related AEs; dose interruption due to AE; discontinuation due to AE; death; specific AEs or SOCs with an incidence of < 10% of patients in all of the treatment groups); change from baseline results (labs, ECGs, vital signs) were assessed with only point estimates by treatment group. | No | No |
AE = adverse events; BICR = blinded independent central review; CI = confidence interval; cLDA = constrained longitudinal data analysis; DFS = disease-free survival; DRSS = disease recurrence–specific survival; ECG = electrocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EFS = event-free survival; HR = hazard ratio; HRQoL = health-related quality of life; KM = Kaplan-Meier; LS = least squares; M0 = patients with no distant metastases; M1 NED = patients with a primary kidney tumour plus solid, isolated, soft tissue metastases that were completely resected at nephrectomy (synchronous) or ≤ 1 year after nephrectomy (metachronous); OS = overall survival; PRO = patient-reported outcome; SAE = serious adverse event; SOC = system organ class; vs. = versus.
Note: Tier 1 safety end points were subject to inferential testing for statistical significance with P values and 95% CI provided for between-group comparisons. Because of the known safety signals of pembrolizumab from previous studies, as well as the lack of expectation of an enhanced safety signal in the adjuvant setting (i.e., participants do not have a tumour burden and their existing safety profile might be less intensive), the sponsor did not analyze tier 1 safety end points.
Table 11: Censoring Rules for Derivation of DFS
Censor rule number | Situation | Primary analysis outcome | Sensitivity analysis outcome |
|---|---|---|---|
1 | No recurrence and no death; new anti-cancer treatment not initiated | Censored at last disease assessment | Censored at last disease assessment |
2 | No recurrence and no death; new anti-cancer treatment is initiated | Censored at last disease assessment | Censored at last disease assessment before new anti-cancer treatment |
3 | Recurrence or death documented after ≤ 1 missed disease assessment and before new anti-cancer treatment, if any | Event at date of documented recurrence or death | Event at date of documented recurrence or death |
4 | Recurrence or death documented immediately after ≥ 2 consecutive missed disease assessments, or after new anti-cancer treatment, if any | Event at date of documented recurrence or death | Censored at the last disease assessment before the earlier date of ≥ 2 consecutive missed disease assessments and new anti-cancer treatment, if any |
DFS = disease-free survival.
Source: Clinical Study Report.12
Analysis Populations
The efficacy analysis set (ITT population) was used for the primary and key secondary efficacy analyses, and consisted of all randomized patients, regardless of the treatment received.
The safety analysis set (all participants as treated population) consisted of randomized patients who had received at least 1 dose of any study drug, and analysis was based on the as-treated principle.
The HRQoL analysis set (PRO full analysis set population) consisted of all patients who had at least 1 PRO assessment available and received at least 1 dose of the study treatment. Participants were analyzed in the treatment group to which they were randomized.
Protocol Amendments
The original protocol (v1.0) was issued on February 24, 2017. There were 4 protocol amendments made by the first interim analysis data cut-off date of December 14, 2020 (Table 29).
Amendment 1 (November 2, 2017): At study inception, the inclusion of metachronous and synchronous M1 NED patients was intended; however, during protocol finalization, metachronous was accidentally removed. This amendment corrected the mistake and added minor adjustments to improve protocol clarity, address real-time feedback from investigators, and adjust language inconsistencies.
Amendment 2 (September 4, 2019): The second interim analysis was retooled as the first interim analysis, where the trigger is 80% DFS events accrued. This would represent roughly a minimum follow-up of 12 months after enrolment is finished.
Amendment 3 (May 11, 2020): The trigger for the first interim analysis timing was changed; the total number of targeted events for the final analysis of DFS by investigator review (second interim analysis) was changed; a secondary end point (EFS assessed by blinded independent radiology review) was added.
Amendment 4 (October 13, 2020): The censoring rules were updated, per the most recent oncology standard for an adjuvant study, to follow the ITT rule and remove the pharmacokinetic and antidrug antibodies sample collection.
All protocol amendments were submitted to the appropriate health authorities and institutional review boards and/or independent ethics committees for information and approval, in accordance with local requirements and/or national regulations.
An additional amendment to the supplemental statistical plan was implemented to incorporate additional months of follow-up and potential agency requests. This amendment specified that the alpha would be spent on the efficacy update, based on the observed number of events at the analysis, per the alpha spending function specified in the initial protocol, whereas the alpha spending and interim analysis-final analysis boundary properties at subsequent interim and final analyses would be updated accordingly.
Results
Patient Disposition
Patient disposition in the KEYNOTE-564 study is presented in Table 12. Screening evaluation was conducted to determine whether participants met the entry requirements (inclusion and exclusion criteria) for the trial. In total, 1,406 patients were screened and 994 were randomized in a 1:1 ratio to receive either pembrolizumab or placebo. A total of 412 patients were screened out of the study, and the reported reason for nonrandomization of these participants was screening failure. Specifically, the most frequently reported reasons for screening failure involved a failure to meet the study inclusion criteria, and included the presence of baseline disease (n = 156; 37.9%), failure to meet criteria for intermediate-high risk, high risk, or M1 NED RCC (n = 66; 16.0%), withdrawal of patient consent (n = 65; 15.8%), absence of prior nephrectomy and/or metastasectomy (n = 42; 10.2%), absence of prior partial or radical nephrectomy or metastasectomy with negative surgical margins (n = 25; 6.1%), inadequate organ function (n = 26; 6.3%), and lack of histologically confirmed RCC diagnosis with clear cell component (n = 21; 5.1%).
A total of 496 patients were randomized to receive adjuvant pembrolizumab and 498 were randomized to receive placebo. Of the 994 randomized patients, 8 (1.6%) in the pembrolizumab arm and 2 (0.4%) in placebo arm did not receive their assigned treatment. No reasons were provided for failure to take the assigned medication.
At the time of the data cut-off date of December 14, 2020, 190 (38.9%) patients had discontinued pembrolizumab and 130 (26.2%) had discontinued placebo. The main reasons for discontinuation of pembrolizumab were AEs (n = 104; 21.3%), disease relapse (n = 51; 10.5%), and withdrawal by patient (n = 21; 4.3%), and for discontinuation of placebo were disease relapse (n = 101; 20.4%), AEs (n = 11; 2.2%), and withdrawal by patient (n = 10; 2.0%).
There were no patients receiving pembrolizumab treatment at the time of the first IA, while 1 patient was reported to be still ongoing placebo treatment. The sponsor clarified that the 1 patient for whom study treatment was reported as ongoing in the placebo arm had received the last dose of study treatment but had not completed the study treatment discontinuation visit at the time of the first interim analysis.
Table 12: Patient Disposition in the KEYNOTE-564 Trial (ITT Population)
Disposition | Pembrolizumab | Placebo |
|---|---|---|
Screened, N | 1,406 | |
Randomized, N (%) | 496 (100.0) | 498 (100.0) |
Patients treated, N (%) | 488 (98.4) | 496 (99.6) |
Status for trial | ||
Discontinued, n (%) | 33 (6.7) | 44 (8.8) |
Death | 18 (3.6) | 33 (6.6) |
Withdrawal by patient | 15 (3.0) | 11 (2.2) |
With COVID-19, no further information | 1 (0.2) | 0 (0.0) |
Association with COVID-19 unspecified, no further information | 14 (2.8) | 11 (2.2) |
Status for study medication in the trial | ||
Started, N | 488 | 496 |
Completed, n (%) | 298 (61.1) | 365 (73.6) |
Discontinued, n (%) | 190 (38.9) | 130 (26.2) |
AE | 104 (21.3) | 11 (2.2) |
Disease relapse | 51 (10.5) | 101 (20.4) |
Nonadherence with protocol | 3 (0.6) | 2 (0.4) |
Physician decision | 10 (2.0) | 6 (1.2) |
Associated with COVID-19 | 0 (0.0) | 2 (0.4) |
Protocol violation | 1 (0.2) | 0 (0.0) |
Withdrawal by patient | 21 (4.3) | 10 (2.0) |
Associated with COVID-19 | 2 (0.4) | 4 (0.8) |
Continuing treatment, n (%) | 0 (0.0) | 1 (0.2) |
ITT population, N | 496 | 498 |
Safety (APaT) population, N | 488 | 496 |
AE = adverse event; APaT = all participants as treated; ITT = intention to treat.
Notes: If the overall number of participants is displayed in the first row of a section (status in trial and status of study medication in the trial), then that is used as the denominator for the percentage calculation; otherwise, the number of participants in the population is used as the denominator for the percentage calculation.
Database cut-off date: December 14, 2020
Source: Clinical Study Report.12
Major Protocol Deviations
Major protocol deviations considered to be clinically important (i.e., with the potential to compromise critical data analyses pertaining to primary efficacy and/or safety end points or participants’ safety) occurred in 2 participants receiving pembrolizumab and 3 participants receiving placebo. The major protocol deviations deemed clinically important were:
Inclusion and exclusion criteria (4 patients: 2 in the pembrolizumab arm; 2 in placebo arm): 1 participant in the pembrolizumab group and 1 participant in placebo group were randomized with pre-existing brain or bone metastatic lesion(s); 1 participant in the pembrolizumab group and 1 participant in placebo group were randomized with residual thrombus postnephrectomy in the renal vein or vena cava.
Safety reporting (1 patient in placebo arm): 1 participant receiving placebo had a reportable safety event and/or follow-up safety event information that was not reported per the timelines outlined in the protocol.
Exposure to Study Treatments
At the first data cut-off (December 14, 2020), the median duration on treatment observed was 11.1 months in both the pembrolizumab and placebo arms (range = 0.0 to 14.3 and 0.0 to 15.4, respectively). Treatment exposure in the KEYNOTE-564 study is presented in the Table 13. The median follow-up duration at the first interim analysis for patients in the pembrolizumab arm was 24 months (range = 2.5 to 41.5 months) and for patients in the placebo arm was 23.8 months (range = 3.5 to 41.4 months).
Concomitant Medications
Overall, 94.7% of patients in the pembrolizumab arm and 93.8% in the placebo arm received at least 1 concomitant medication during the study.
The most frequently administered concomitant medications in the pembrolizumab arm were drugs in the Anatomic Therapeutic Chemical pharmacologic subclasses of analgesics (53.9%), drugs that act on the renin-angiotensin system (41.4%), drugs for acid-related disorders (33.8%), and systemic antibacterial drugs (36.7%), and in the placebo arm were analgesics (50.8%), drugs that act on the renin-angiotensin system (35.9%), and lipid-modifying drugs (31.7%). Table 14 outlines the list of antineoplastic drugs reported in any frequency and other concomitant medications reported in at least 15% of patients in either arm.
Anti-Cancer Medications Received by Patients During the Follow-Up Phase
The proportion of patients receiving subsequent anti-cancer treatment was higher in the placebo arm (22.5%) compared to the pembrolizumab arm (15.3%). Subsequent anti-cancer therapies included drug therapy, radiation, and surgery. Anti–vascular endothelial growth factor treatment (n = 56 [11.3%] in pembrolizumab and n = 76 [15.3%] in the placebo arm) and anti-PD-1/PD-L1 checkpoint inhibitor therapies (n = 14 [2.8%] in pembrolizumab and n = 46 [9.2%] in the placebo arm) were the most commonly reported drug therapies. An overview of subsequent anti-cancer therapies received by patients in both study arms is presented in Table 15.
Table 13: Exposure to Study Treatments (APaT Population; IA1)
Category | Pembrolizumab arm N = 488 | Placebo arm N = 496 |
|---|---|---|
Duration of treatment, monthsa | ||
Mean (SD) | 9.0 (3.7) | 9.8 (3.1) |
Median (range) | 11.1 (0.0 to 14.3) | 11.1 (0.0 to 15.4) |
Number of administrations | ||
Mean (SD) | 13.5 (5.2) | 14.7 (4.4) |
Median (range) | 17.0 (1.0 to 17.0) | 17.0 (1.0 to 17.0) |
APaT = all participants as treated; IA1 = first interim analysis; SD = standard deviation.
Note: Database cut-off date: December 14, 2020.
aDuration of treatment (months) = (date of last dose of study drug – date of first dose of study drug + 1) / 30.4375.
Source: Clinical Study Report.12
Table 14: Concomitant Medications (APaT Population, IA1)
Concomitant medication | Pembrolizumab arm, n (%) N = 488 | Placebo arm, n (%) N = 496 |
|---|---|---|
Patients with 1 or more concomitant medication | 462 (94.7) | 465 (93.8) |
Patients with no concomitant medication | 26 (5.3) | 31 (6.3) |
Alimentary tract and metabolism therapies | ||
Drugs for acid-related disorders | 165 (33.8) | 143 (28.8) |
Drugs for constipation | 75 (15.4) | 58 (11.7) |
Drugs for diabetes | 105 (21.5) | 75 (15.1) |
Vitamins | 80 (16.4) | 78 (15.7) |
Anti-infective therapies for systemic use | ||
Antibacterials for systemic use | 179 (36.7) | 136 (27.4) |
Antineoplastic and immunomodulating therapies | ||
Antineoplastic drugs | 7 (1.4) | 3 (0.6) |
Aflibercept | 1 (0.2) | 1 (0.2) |
Fluorouracil | 0 (0.0) | 1 (0.2) |
Methotrexate | 2 (0.4) | 0 (0.0) |
Oxaliplatin | 0 (0.0) | 1 (0.2) |
Pazopanib | 1 (0.2) | 0 (0.0) |
Sunitinib malate | 3 (0.6) | 1 (0.2) |
Endocrine therapy | 3 (0.6) | 0 (0.0) |
Immunostimulants | 1 (0.2) | 1 (0.2) |
Immunosuppressants | 5 (1.0) | 1 (0.2) |
Therapies for blood and blood-forming organs | ||
Antithrombotic drugs | 84 (17.2) | 67 (13.5) |
Blood substitutes and perfusion solutions | 73 (15.0) | 49 (9.9) |
Therapies for the cardiovascular system | ||
Drugs acting on the renin-angiotensin system | 202 (41.4) | 178 (35.9) |
Beta-blocking drugs | 101 (20.7) | 104 (21.0) |
Calcium channel blockers | 110 (22.5) | 111 (22.4) |
Diuretics | 68 (13.9) | 73 (14.7) |
Lipid-modifying agents | 135 (27.7) | 157 (31.7) |
Dermatologic therapies | ||
Corticosteroids, dermatologic preparations | 98 (20.1) | 46 (9.3) |
Musculoskeletal system drugs | — | — |
Anti-inflammatory and antirheumatic products | 113 (23.2) | 102 (20.6) |
Nervous system therapies | ||
Analgesics | 263 (53.9) | 252 (50.8) |
Acetaminophen | 155 (31.8) | 153 (30.8) |
Aspirin | 79 (16.2) | 78 (15.7) |
Psycholeptic drugs | 114 (23.4) | 92 (18.5) |
Respiratory system therapies | ||
Antihistamines for systemic use | 146 (29.9) | 114 (23.0) |
Drugs for obstructive airway diseases | 74 (15.2) | 65 (13.1) |
Systemic hormonal preparations, excluding sex hormones and insulins | ||
Corticosteroids for systemic use | 188 (38.5) | 65 (13.1) |
Thyroid therapy | 136 (27.9) | 49 (9.9) |
APaT = all participants as treated; IA1 = first interim analysis.
Notes: Every participant is counted a single time for each applicable specific concomitant medication. A participant with multiple concomitant medications within a medication category is counted a single time for that category.
Database cut-off date: December 14, 2020
Source: Clinical Study Report.12
Table 15: Subsequent Anti-Cancer Therapy (ITT Population, IA1)
Category | Pembrolizumab arm N = 496 | Placebo arm N = 498 |
|---|---|---|
Participants who had any subsequent anti-cancer therapy for RCC, n (%) | 76 (15.3) | 112 (22.5) |
Subsequent radiation | 14 (2.8) | 17 (3.4) |
Subsequent surgery | 19 (3.8) | 32 (6.4) |
Subsequent anti-cancer drug medication | 63 (12.7) | 86 (17.3) |
Anti-PD1 and anti-PD-L1 therapiesa | 14 (2.8) | 46 (9.2) |
VEGF and VEGFR targeted therapiesb | 56 (11.3) | 76 (15.3) |
Otherc | 12 (2.4) | 26 (5.2) |
IA1 = first interim analysis; ITT = intention to treat; PD-1 = programmed cell death; PD-L1 = programmed cell death ligand-1; RCC = renal cell carcinoma; VEGF = vascular endothelial growth factor; VEGFR = vascular endothelial growth factor receptor.
Notes: The total number of patients in the subcategories under any subsequent anti-cancer drug therapy can exceed the total number of patients with any subsequent anti-cancer drug therapy because a patient can receive multiple types of subsequent anti-cancer drug therapy.
Database cut-off date: December 14, 2020.
aIncluded pembrolizumab, avelumab, nivolumab, atezolizumab, and durvalumab.
bIncluded axitinib, pazopanib, sunitinib, sorafenib, cabozantinib, lenvatinib, tivozanib, and bevacizumab.
cIncluded all anti-cancer drugs other than anti-PD1 and anti-PDL1 therapies and VEGF and VEGFR targeted therapies.
Source: Clinical Study Report.12
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported here (refer to Appendix 3 for detailed efficacy data). Findings presented in this review were obtained from the first interim analysis (December 14, 2020). Results from the efficacy update report analysis with additional 6 months of follow-up are presented for the primary (DFS) and main secondary (OS) outcomes.
Overall Survival
At the first interim analysis, median OS was not reached. A total of 51 OS events occurred (18 in the pembrolizumab group and 33 in the placebo group). A HR of 0.54 (95% CI, 0.30 to 0.96; P = 0.0164) was estimated for the comparison between pembrolizumab and placebo. Table 16 presents a summary of efficacy findings, and Figure 3 presents the KM plot for OS.
Additional 6-month follow-up data from the efficacy update report analysis showed similar findings. There was a total of 66 events as of June 14, 2021, data cut-off (23 in the pembrolizumab group and 43 in the placebo group). Median OS was not reached, and a HR of 0.52 was reported (95% CI, 0.31 to 0.86; P = 0.005) (Table 30, Figure 8).
Table 16: Overall Survival at IA1 — Efficacy Analysis Set (ITT Population)
OS event | Pembrolizumab arm N = 496 | Placebo arm N = 498 |
|---|---|---|
Patients with events, n (%) | ||
Total | 18 (3.6) | 33 (6.6) |
OS, months | ||
Median (95% CI)a | NR (NR to NR) | NR (NR to NR) |
Q1 to Q3 | NR to NR | NR to NR |
HR (95% CI)b | 0.54 (0.30 to 0.96) | |
P valuec | 0.0164037 | |
OS rate, % (95% CI) | ||
12 months | 98.6 (97.0 to 99.3) | 98.0 (96.3 to 98.9) |
18 months | 97.9 (96.1 to 98.9) | 96.8 (94.8 to 98.0) |
24 months | 96.6 (94.3 to 98.0) | 93.5 (90.5 to 95.6) |
CI = confidence interval; HR = hazard ratio; IA1 = first interim analysis; ITT = intention to treat; NR = not reached; OS = overall survival; Q1 = first quartile; Q3 = third quartile.
Database cut-off date: December 14, 2020.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by metastasis status (M0 vs. M1 NED assessed by investigator) and ECOG PS (0 vs. 1), US participant (yes vs. no) within M0 group by investigator.
cOne-sided P value based on log-rank test stratified by metastasis status (M0 vs. M1 NED assessed by investigator) and ECOG PS (0 vs. 1), US participant (yes vs. no) within M0 group by investigator.
Source: Clinical Study Report.12
Figure 3: Kaplan-Meier Plot of OS at IA1 — Full Analysis Set
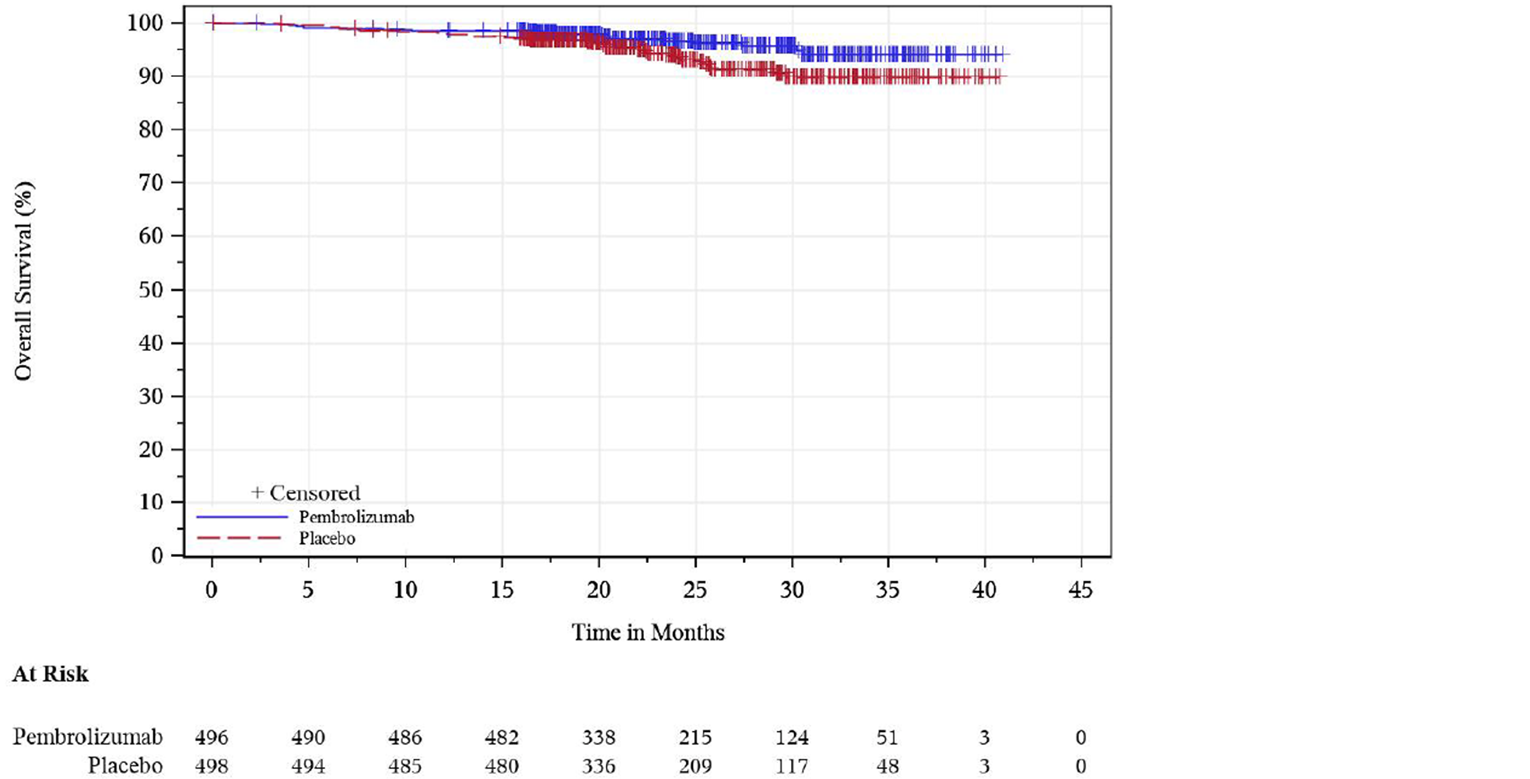
+ Censored = censored observations; IA1 = first interim analysis; KM = Kaplan-Meier; OS = overall survival.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
DFS, Assessed by Investigator
At the preplanned first interim analysis, 260 DFS events had occurred (109 [22.0%] in pembrolizumab arm and 151 [30.3%] in placebo arm). Median DFS was not reached in either group. The HR between pembrolizumab and placebo was 0.68 (95% CI, 053 to 0.87; P = 0.001) (Table 17, Figure 4)
At the efficacy update report analysis (data cut-off date of June 14, 2021), 114, and 169 DFS events had occurred in the pembrolizumab and placebo arms, respectively. Median DFS was not reached, and a HR of 0.63 (95% CI, 0.50 to 0.80; P < 0.0001) was reported (Table 31, Figure 9).
Table 17: Disease-Free Survival at IA1 — Efficacy Analysis Set (ITT Population)
DFS event | Pembrolizumab arm N = 496 | Placebo arm N = 498 |
|---|---|---|
Patients with events, n (%) | ||
Total | 109 (22.0) | 151 (30.3) |
Death | 6 (1.2) | 2 (0.4) |
Disease recurrence | 103 (20.8) | 149 (29.9) |
Censored | 387 (78.0) | 347 (69.7) |
Last tumour assessment showing no disease recurrence | 375 (75.6) | 344 (69.1) |
No postbaseline disease status assessment | 12 (2.4) | 3 (0.6) |
DFS, months | ||
Median (95% CI)a | NR (NR to NR) | NR (NR to NR) |
Q1 to Q3 | 25.8 to NR | 13.8 to NR |
HR (95% CI)b | 0.68 (0.53 to 0.87) | |
P valuec | 0.0010 | |
DFS rate, % (95% CI) | ||
12 months | 85.7 (82.2 to 88.5) | 76.2 (72.2 to 79.7) |
18 months | 81.5 (77.7 to 84.8) | 71.9 (67.7 to 75.7) |
24 months | 77.3 (72.8 to 81.1) | 68.1 (63.5 to 72.2) |
CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; IA1 = first interim analysis; ITT = intention to treat; NR = not reached; Q1 = first quartile; Q3 = third quartile.
Note: Database cut-off date: December 14, 2020.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by metastasis status (M0 vs. M1 NED assessed by investigator) and ECOG PS (0 vs. 1) and US participant (yes vs. no) within M0 group by investigator.
cOne-sided P value based on log-rank test stratified by metastasis status (M0 vs. M1 NED assessed by investigator) and ECOG PS (0 vs. 1), US participant (yes vs. no) within M0 group by investigator.
Source: Clinical Study Report.12
Figure 4: Kaplan-Meier Plot of DFS at IA1 — Full Analysis Set
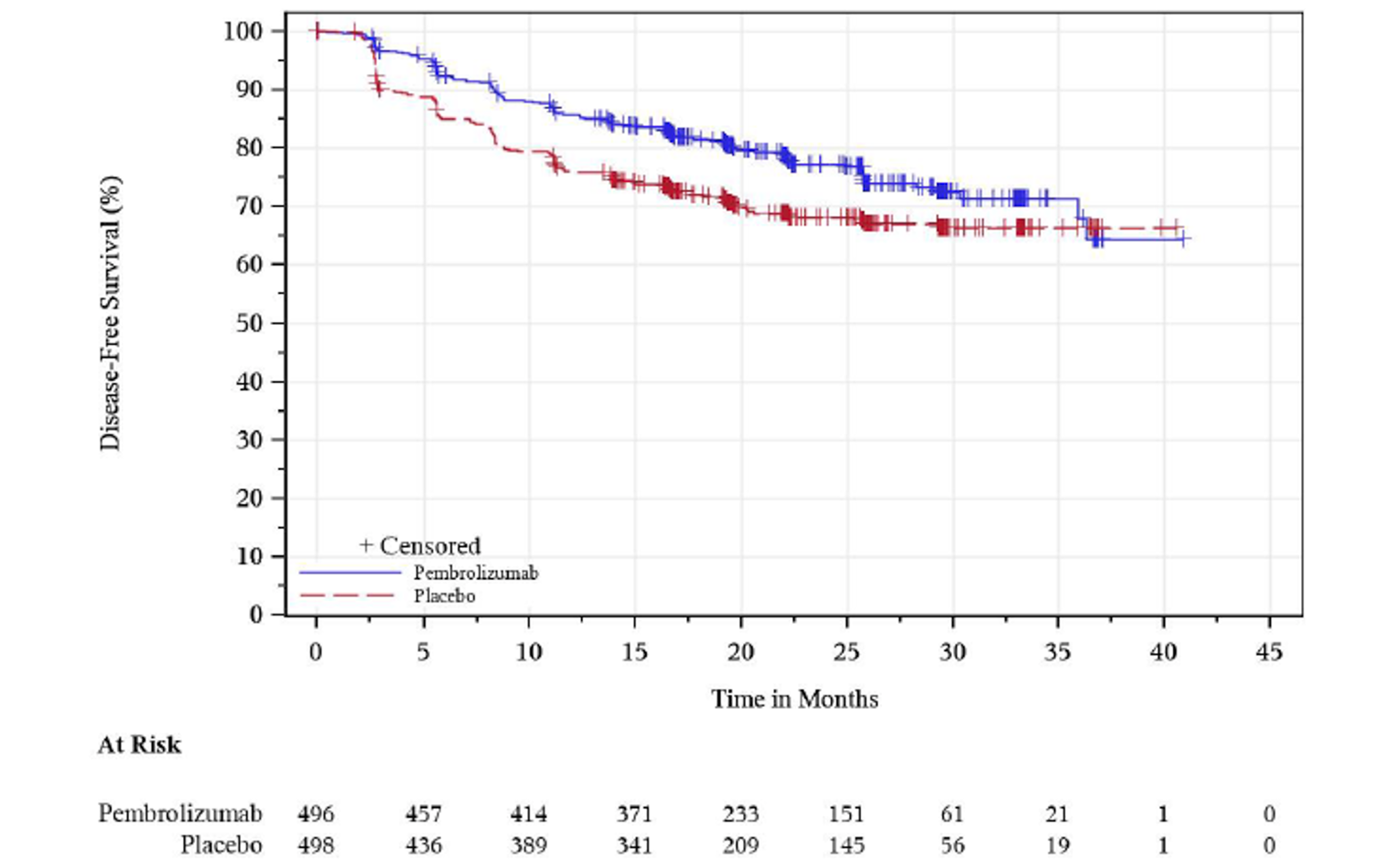
+ Censored = censored observations; DFS = disease-free survival; IA1 = first interim analysis; KM = Kaplan-Meier.
Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Subgroup Analysis: DFS
The pre-specified subgroup analysis for DFS, according to the metastatic staging of patients and assessed by the investigator at baseline, is presented in the Table 32.
The following results were observed at the time of the first interim analysis:
M0 group: A total of 102 patients out of 467 and 132 patients out of 469 had events in the pembrolizumab and placebo arms, respectively. The HR for DFS obtained from an unstratified Cox model for the pembrolizumab versus placebo was 0.74 (95% CI, 0.57 to 0.96).
M1 NED group: A total of 7 patients out of 29 and 19 patients out of 29 had events in the pembrolizumab and placebo arms, respectively. The HR for DFS obtained between the pembrolizumab and placebo groups was 0.29 (95% CI, 0.12 to 0.69).
Similar findings were observed in the efficacy update report analysis, which had 6 additional months of follow-up, for the M0 subgroup (HR = 0.68; 95% CI, 0.53 to 0.88) and for the M1 NED subgroup (HR = 0.28; 95% CI, 0.12 to 0.66).
Post hoc analyses from efficacy update report, which reported DFS results according to recurrence risk subgroups, showed the following estimates:
Intermediate-high risk group: A total of 87 patients out of 422 and 127 patients out of 433 had events in the pembrolizumab and placebo arms, respectively. The HR for DFS obtained for the pembrolizumab versus placebo was 0.68 (95% CI, 0.52 to 0.89).27
High-risk group: A total of 20 patients out of 40 and 23 patients out of 36 had events in the pembrolizumab and placebo arms, respectively. The HR for DFS obtained between the pembrolizumab and placebo groups was 0.60 (95% CI, 0.33 to 1.10).27
M1 NED risk group: A total of 7 patients out of 29 and 19 patients out of 29 had events in the pembrolizumab and placebo arms, respectively. The HR for DFS obtained between the pembrolizumab and placebo groups was 0.28 (95% CI, 0.12 to 0.66).27
Sensitivity Analyses: DFS
Three pre-specified sensitivity analyses for DFS were reported, as per first interim analysis. In the sensitivity analysis in which disease recurrence or death documented immediately after more than 2 consecutive missed disease assessments or after initiation of new anti-cancer treatment was censored, the HR for pembrolizumab versus placebo was 0.67 (95% CI, 0.52 to 0.86; P = 0.0007) (Table 33).
Another sensitivity analysis included additional stratum for baseline disease status, based on BICR review of baseline scans, in the stratified Cox model for DFS assessment. The HR obtained for pembrolizumab versus placebo was 0.70 (95% CI, 0.54 to 0.89; P = 0.0021) (Table 34).
Participants with baseline disease, assessed by BICR, were censored in the final sensitivity analysis of DFS (presented in the Table 35). A total of 101 (20.4%) and 129 (25.9%) DFS events occurred in the pembrolizumab and placebo groups, respectively. The HR for DFS for pembrolizumab versus placebo was 0.74 (95% CI, 0.56 to 0.95; P = 0.0097).
Overall, the sensitivity analyses were consistent with the findings observed in the primary analysis of DFS and showed that the benefit of using pembrolizumab was maintained over placebo.
Disease Recurrence–Specific Survival
At the time of the first interim analysis, a total of 17 events (3.4%) of local recurrence occurred in the pembrolizumab arm and 32 events (6.4%) of local recurrence occurred in placebo arm. Distant recurrence was reported in 94 (19%) and 134 (26.9%) patients in the pembrolizumab and placebo groups, respectively. The cumulative incidence of local (DRSS1) and distant (DRSS2) recurrence, estimated with a nonparametric method adjusted for competing risks, was consistently lower in the pembrolizumab arm than in the placebo arm (Table 18, Figure 5, Figure 6).
Table 18: Disease Recurrence–Specific Survival at IA1 — Efficacy Analysis Set (ITT Population)
DRSS event | Pembrolizumab arm N = 496 | Placebo arm N = 498 |
|---|---|---|
DRSS1 | ||
Patients with events, n (%) | ||
Eventsa | 17 (3.4) | 32 (6.4) |
Competing eventsb | 92 (18.5) | 119 (23.9) |
Censored | 387 (78.0) | 347 (69.7) |
Cumulative incidence of events, % (95% CI) | ||
12 months | 1.9 (0.9 to 3.4) | 5.5 (3.7 to 7.8) |
18 months | 2.8 (1.6 to 4.6) | 5.9 (4.1 to 8.3) |
24 months | 3.4 (2.0 to 5.4) | 6.6 (4.6 to 9.2) |
DRSS2 | ||
Patients with events, n (%) | ||
Eventsc | 94 (19.0) | 134 (26.9) |
Competing eventsd | 15 (3.0) | 17 (3.4) |
Censored | 387 (78.0) | 347 (69.7) |
Cumulative incidence of events, % (95% CI) | ||
12 months | 12.8 (10.0 to 16.0) | 21.2 (17.7 to 24.9) |
18 months | 16.3 (13.1 to 19.8) | 25.0 (21.2 to 28.9) |
24 months | 19.8 (16.1 to 23.9) | 28.2 (24.1 to 32.5) |
CI = confidence interval; DRSS = disease recurrence–specific survival; IA1 = first interim analysis; ITT = intention to treat.
Notes: Cumulative incidence estimates at specified time points are based on nonparametric estimations of cumulative incidence of the event of interest, accounting for competing risk events.
Database cut-off date: December 14, 2020.
aLocal recurrence of RCC is counted as an event.
bDistant kidney cancer metastasis(es) or death are counted as competing events.
cLocal recurrence with visceral lesion or distant kidney cancer metastasis(es) with visceral lesion are counted as events.
dDeath, local recurrence without visceral lesion, and distant metastasis without visceral lesion are counted as competing events.
Source: Clinical Study Report.12
Figure 5: Cumulative Incidence Plot of DRSS1 at IA1 Based on Investigator Assessment — Full Analysis Set
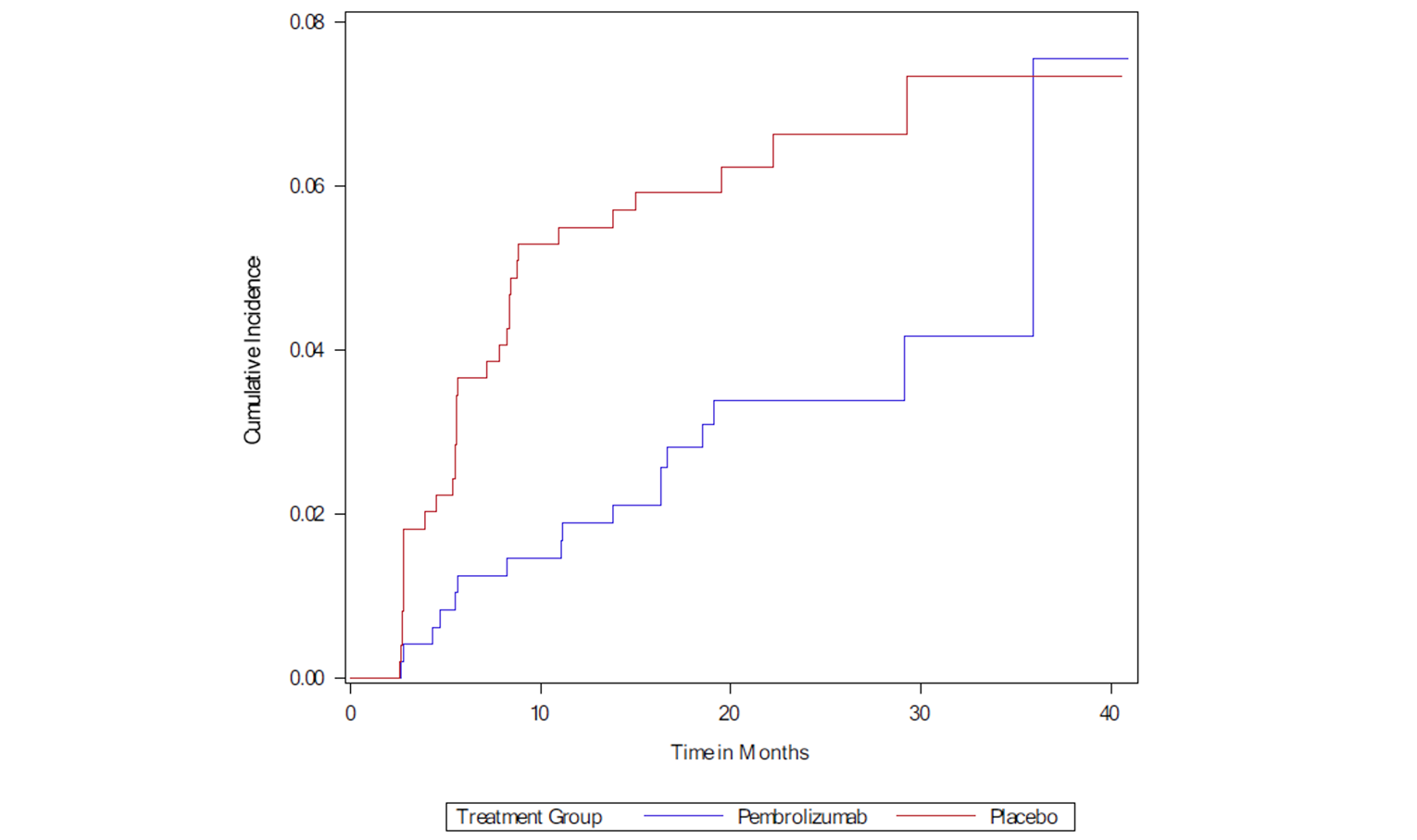
DRSS = disease recurrence–specific survival; IA1 = first interim analysis; RCC = renal cell carcinoma.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Figure 6: Cumulative Incidence Plot of DRSS2 at IA1 Based on Investigator Assessment — Full Analysis Set
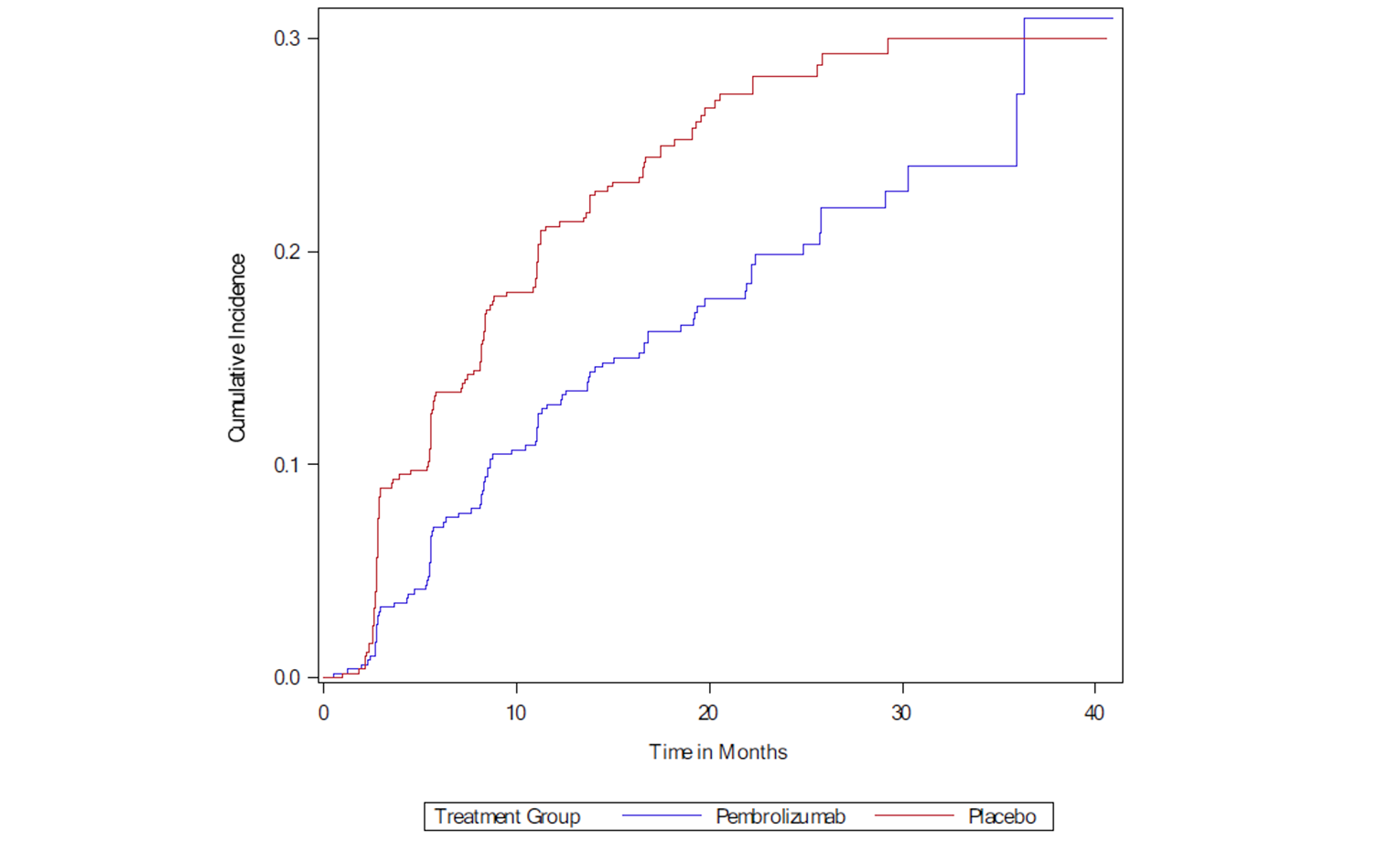
DRSS = disease recurrence–specific survival.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Event-Free Survival
According to the findings at the first interim analysis, 116 events (23.4%) occurred in pembrolizumab arm, of which 95 were disease recurrence, 14 were disease progression, and 7 were deaths. In the placebo arm, 155 events (31.1%) occurred, of which 128 were disease recurrence, 25 were disease progression, and 2 were deaths. Median EFS was not reached in either group. HR for the comparison of EFS by BICR, with baseline disease status based only on baseline scans, in the pembrolizumab versus placebo groups was 0.72 (95% CI, 0.56 to 0.91; P = 0.0035) (Table 19, Figure 7).
Table 19: Event-Free Survival at IA1 Based on BICR (Baseline Disease Status Based on BICR Review of Baseline Scan Only) — Efficacy Analysis Set (ITT Population)
EFS event | Pembrolizumab arm N = 496 | Placebo arm N = 498 |
|---|---|---|
Patients with events, n (%) | ||
Total | 116 (23.4) | 155 (31.1) |
Death | 7 (1.4) | 2 (0.4) |
Disease progression | 14 (2.8) | 25 (5.0) |
Disease recurrence | 95 (19.2) | 128 (25.7) |
Censored | 380 (76.6) | 343 (68.9) |
Last tumour assessment showing no disease recurrence or progression | 368 (74.2) | 340 (68.3) |
No postbaseline disease status assessment | 12 (2.4) | 3 (0.6) |
EFS, months | ||
Median (95% CI)a | NR (NR to NR) | NR (NR to NR) |
Q1 to Q3 | 25.7 to NR | 10.9 to NR |
HR (95% CI)b | 0.72 (0.56 to 0.91) | |
P valuec | 0.0035 | |
EFS rate, % (95% CI) | ||
12 months | 81.6 (77.8 to 84.8) | 73.0 (68.9 to 76.8) |
18 months | 77.7 (73.5 to 81.2) | 70.9 (66.7 to 74.8) |
24 months | 75.6 (71.3 to 79.4) | 66.5 (61.8 to 70.8) |
BICR = blinded independent central review; CI = confidence interval; EFS = event-free survival; HR = hazard ratio; IA1 = first interim analysis; ITT = intention to treat; NR = not reached; Q1 = first quartile; Q3 = third quartile.
Notes: For participants who were assessed as baseline NED by BICR of baseline scan only, but who had a postbaseline scan that triggered retrospective assessment of the baseline disease, the date of that scan is used as the event date.
Database cut-off date: December 14, 2020.
aFrom product-limit (KM) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by baseline disease status by BICR (NED by BICR vs. non-NED by BICR), then within the NED by BICR group, further stratified by randomization strata: M0 vs. M1 NED by investigator and ECOG PS (0 vs. 1), US participant (yes vs. no) within M0 group by investigator.
cOne-sided P value based on log-rank test stratified by baseline disease status by BICR (NED by BICR vs. non-NED by BICR), then within the NED by BICR group, further stratified by randomization strata: M0 vs. M1 NED by investigator and ECOG PS (0 vs. 1), US participant (yes vs. no) within M0 group by investigator.
Source: Clinical Study Report.12
Figure 7: Kaplan-Meier Plot of EFS at IA1 — Full Analysis Set
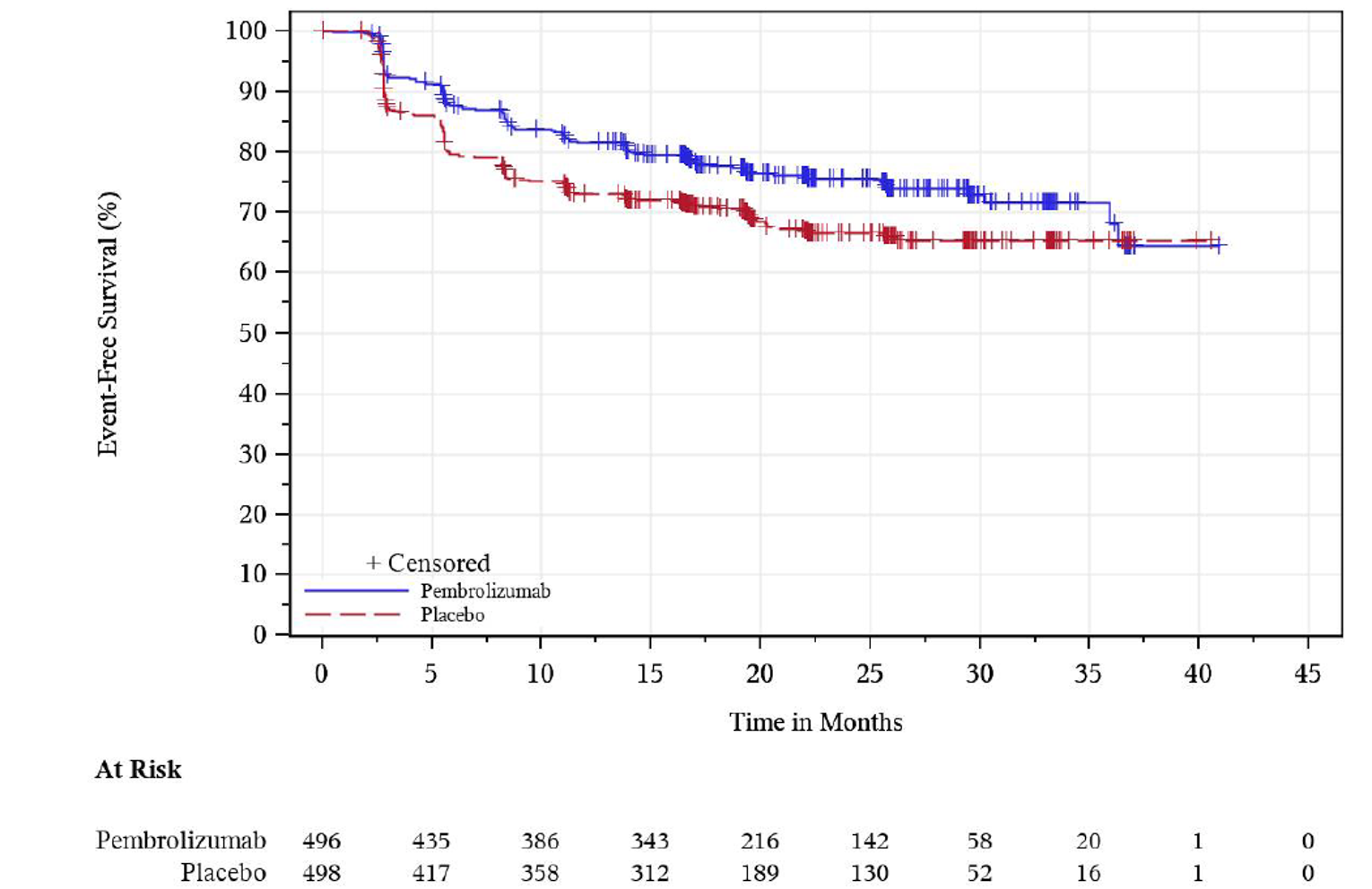
+ Censored = censored observations; EFS = event-free survival; IA1 = first interim analysis; KM = Kaplan-Meier
Notes: For participants who were assessed as baseline NED by BICR of baseline scan only, but who had a postbaseline scan that triggered retrospective assessment of the baseline disease, the date of that scan is used as the event date.
Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Results of the assessment of EFS based on baseline and postbaseline scans are presented in the Appendix 3.
Health-Related Quality of Life
HRQoL outcomes (FKSI-DRS, EORTC QLQ-C30 global health status/QoL and physical functioning) of the first interim analysis, presented as the overall least squares mean difference estimated for pembrolizumab versus placebo, are reported in Table 20. Scores on HRQoL measures decreased from baseline for patients in both treatment arms at week 52 (Table 20). The between-group least squares mean differences were –0.67 points (95% CI, –1.23 to –0.12; P = 0.0170) for FKSI-DRS, –2.57 points (95% CI, –5.22 to 0.08; P = 0.0571) for global health status/QoL of the EORTC QLQ-C30, and –0.91 points (95% CI, –2.79 to 0.97; P = 0.3410) for physical functioning of the EORTC QLQ-C30.
Overall least squares mean differences for the exploratory HRQoL outcomes were as follows: –0.10 points (95% CI, –1.57 to 1.37) for the nausea and vomiting symptoms of the EORTC QLQ-C30, 1.11 points (95% CI, –1.26 to 3.49) for the diarrhea symptoms of the EORTC QLQ-C30, and –1.58 points (95% CI, –3.59 to 0.42) for the EQ-5D-5L VAS (Table 39).
Appendix 3 contains the model-based least squares mean changes in EORTC QLQ-C30 global health status/QoL, functioning, and symptom scales from baseline to 52 weeks postbaseline.
The percentage of participants with improvement and improvement plus stability in FKSI-DRS and EORTC QLQ-C30 (global health status and physical functioning) scores were, overall, lower in the pembrolizumab group than in the placebo group, whereas the percentage of participants experiencing deterioration was higher in the pembrolizumab group than in the placebo group (Table 41). Differences in the percentage of participants with improvement plus stability was –9.2 (95% CI, –15.2 to –3.1) for the FKSI-DRS score, –13.6 (95% CI, –19.7 to –7.5) for the EORTC QLQ-C30 global health status, and –4.5 (95% CI, –10.3 to 1.4) for EORTC QLQ-C30 physical functioning.
Table 20: Analysis of Change From Baseline to Week 52 in PROs, Defined as Secondary End Points in the KEYNOTE-564 Trial (FKSI-DRS and EORTC QLQ-C30) — PRO FAS Population (IA1)
Treatment | Baseline | Week 52 | CFB to week 52 | Difference in CFB, pembrolizumab vs. placebo | |||
|---|---|---|---|---|---|---|---|
N | Mean (SD) | N | Mean (SD) | N | LS mean (95% CI)a | LSM CFB (95% CI),a P valuea | |
FKSI-DRS | |||||||
Pembrolizumab | 435 | 32.86 (3.50) | 300 | 31.85 (4.69) | 483 | –1.12 (–1.53 to –0.71) | –0.67 (–1.23 to –0.12) P = 0.0170 |
Placebo | 447 | 32.79 (3.53) | 328 | 32.51 (4.13) | 492 | –0.45 (–0.84 to –0.05) | |
EORTC QLQ-C30 global health status/QoL | |||||||
Pembrolizumab | 438 | 79.22 (18.46) | 301 | 74.92 (18.26) | 484 | –4.25 (–6.32 to −2.19) | –2.57 (–5.22 to 0.08) P = 0.0571 |
Placebo | 450 | 77.04 (17.61) | 325 | 76.82 (19.56) | 492 | –1.68 (–3.69 to 0.32) | |
EORTC QLQ-C30 physical functioning | |||||||
Pembrolizumab | 438 | 88.58 (14.95) | 301 | 86.60 (17.33) | 484 | –1.81 (–3.19 to −0.43) | –0.91 (–2.79 to 0.97) P = 0.3410 |
Placebo | 450 | 88.61 (14.26) | 325 | 88.96 (15.89) | 492 | –0.90 (–2.23 to 0.44) | |
CFB = change from baseline; CI = confidence interval; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FKSI-DRS = Functional Assessment of Cancer Therapy Kidney Symptom Index–Disease-Related Symptoms; IA1 = first interim analysis; LS = least squares; LSM = least squares mean; QoL = quality of life; SD = standard deviation; vs. = versus.
Notes: For baseline and week 52, N is the number of patients in each treatment group with non-missing assessments at the specific time point; for change from baseline, N is the number of patients in the analysis population in each treatment group.
Database cut-off date: December 14, 2020.
aBased on a cLDA model with PRO scores as the response variable with treatment by study visit interaction, stratification factors of metastasis status (M0 vs. M1 NED), and within the M0 group further stratified by ECOG PS (0 vs. 1) and US participant (yes vs. no) as covariates.
Source: Clinical Study Report.12
Harms
Only those harms identified in the review protocol are reported here. Refer to Table 21, Table 22, Table 23, Table 24, and Table 25. for detailed harms data.
Adverse Events
A total of 96.3% of patients in the pembrolizumab group and 91.1% of patients in the placebo group experienced at least 1 AE (Table 21). The most common AEs were fatigue (29.7% in pembrolizumab versus 24.2% in placebo arm), diarrhea (25.4% in pembrolizumab versus 22.4% in placebo arm), pruritus (22.7% in pembrolizumab versus 13.1% in placebo arm), arthralgia (22.1% in pembrolizumab versus 18.8% in placebo arm), hypothyroidism (21.1% in pembrolizumab versus 3.6% in placebo arm), and rash (20.1% in pembrolizumab versus 10.7% in placebo arm). Table 22 summarizes the AEs occurring in at least 10% of patients receiving pembrolizumab or placebo in the KEYNOTE-564 trial. Figure 16 provides risk differences and 95% CIs for between-group comparisons of events occurring in at least 10% of patients in either arm.
Table 21: Summary of AEs in the KEYNOTE-564 Trial (APaT Population; IA1)
Category | Pembrolizumab arm, n (%) N = 488 | Placebo arm, n (%) N = 496 |
|---|---|---|
≥ 1 AE | 470 (96.3) | 452 (91.1) |
Toxicity, grade 3 to 5 AEs | 158 (32.4) | 88 (17.7) |
≥ 1 SAE | 100 (20.5) | 56 (11.3) |
AE leading to drug discontinuation | 101 (20.7) | 10 (2.0) |
AE leading to treatment interruption | 126 (25.8) | 74 (14.9) |
SAE leading to drug discontinuation | 49 (10.0) | 5 (1.0) |
Death | 2 (0.4) | 1 (0.2) |
Notable harms | 173 (35.5) | 34 (6.9) |
AE = adverse event; APaT = all participants as treated; IA1 = first interim analysis; SAE = serious adverse event.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Table 22: Summary of AEs in the KEYNOTE-564 Trial (Incidence ≥ 10% in 1 or More Treatment Groups; APaT Population) — IA1
Category | Pembrolizumab arm, n (%) N = 488 | Placebo arm, n (%) N = 496 |
|---|---|---|
≥ 1 AE | 470 (96.3) | 452 (91.1) |
Fatigue | 145 (29.7) | 120 (24.2) |
Diarrhea | 124 (25.4) | 111 (22.4) |
Pruritus | 111 (22.7) | 65 (13.1) |
Arthralgia | 108 (22.1) | 93 (18.8) |
Hypothyroidism | 103 (21.1) | 18 (3.6) |
Rash | 98 (20.1) | 53 (10.7) |
Nausea | 80 (16.4) | 48 (9.7) |
Cough | 76 (15.6) | 50 (10.1) |
Headache | 69 (14.1) | 62 (12.5) |
Hyperthyroidism | 58 (11.9) | 1 (0.2) |
Asthenia | 50 (10.2) | 36 (7.3) |
Blood creatinine increase | 50 (10.2) | 42 (8.5) |
Back pain | 49 (10.0) | 64 (12.9) |
AE = adverse event; APaT = all participants as treated; IA1 = first interim analysis.
Notes: Every participant is counted a single time for each applicable row and column. A specific AE appears only if its incidence in at least 1 column meets the incidence criterion in the title, after rounding.
Non-SAEs up to 30 days and SAEs up to 90 days following the last dose in the initial treatment phase are included. The following MedDRA preferred terms not related to the drug have been excluded: neoplasm progression, malignant neoplasm progression, and disease progression.
Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Serious Adverse Events
A total of 20.5% and 11.3% of individuals experienced at least 1 SAE in the pembrolizumab and placebo arms, respectively (Table 23). The most reported SAEs (occurring in ≥ 1% of patients in 1 or more treatment arm) were acute kidney injury, adrenal insufficiency, pneumonia, colitis, and diabetic ketoacidosis. SAEs of grade 3 or higher were more frequently reported in the pembrolizumab arm compared with the placebo arm (32.4% versus 17.7%) (Table 23).
Table 23: Summary of Grade 3 to 5 AEs and SAEs up to 90 Days From Last Dose of Treatment (Incidence ≥ 1% in 1 or More Treatment Groups; APaT Population) — IA1
Category | Pembrolizumab, n (%) (N = 488) | Placebo, n (%) (N = 496) |
|---|---|---|
Grade 3 to 5 AEsa | ||
≥ 1 AE | 158 (32.4) | 88 (17.7) |
Hypertension | 14 (2.9) | 13 (2.6) |
Alanine aminotransferase increase | 11 (2.3) | 1 (0.2) |
Aspartate aminotransferase increase | 8 (1.6) | 1 (0.2) |
Diarrhea | 8 (1.6) | 1 (0.2) |
Hyperglycemia | 7 (1.4) | 3 (0.6) |
Pneumonia | 7 (1.4) | 1 (0.2) |
Adrenal insufficiency | 6 (1.2) | 1 (0.2) |
Lipase increase | 6 (1.2) | 0 (0.0) |
Acute kidney injury | 5 (1.0) | 0 (0.0) |
Diabetic ketoacidosis | 5 (1.0) | 0 (0.0) |
Fatigue | 5 (1.0) | 0 (0.0) |
Hyponatremia | 2 (0.4) | 6 (1.2) |
SAEsb | ||
≥ 1 AE | 100 (20.5) | 56 (11.3) |
Acute kidney injury | 6 (1.2) | 0 (0.0) |
Adrenal insufficiency | 6 (1.2) | 0 (0.0) |
Pneumonia | 6 (1.2) | 1 (0.2) |
Colitis | 5 (1.0) | 1 (0.2) |
Diabetic ketoacidosis | 5 (1.0) | 0 (0.0) |
AE = adverse event; APaT = all participants as treated; IA1 = first interim analysis; SAE = serious adverse event.
Notes: Every participant is counted a single time for each applicable row and column. A specific AE appears only if its incidence in 1 or more of the columns meets the incidence criterion in the report title, after rounding. The following MedDRA preferred terms not related to the drug have been excluded: neoplasm progression, malignant neoplasm progression, and disease progression.
Database cut-off date: December 14, 2020.
aNon-SAEs up to 30 days and SAEs up to 90 days following the last dose in the initial treatment phase are included.
bSAEs up to 90 days after last dose of the initial treatment phase are included.
Source: Clinical Study Report.12
Withdrawals Due to AEs
Discontinuations Due to AEs
All-cause AEs leading to study discontinuation were reported in 20.7% of patients receiving pembrolizumab and 2.0% receiving placebo. The most common AEs resulting in treatment discontinuation included increased levels of alanine aminotransferase (1.6%), adrenal insufficiency (1.0%) and colitis (1.0%) in pembrolizumab arm.
Treatment Interruption Due to AEs
More patients (25.8%) receiving pembrolizumab experienced AEs leading to treatment interruption compared with those receiving placebo (14.9%). The most common AEs leading to the interruption of pembrolizumab were increased aspartate aminotransferase (2.3%), increased alanine aminotransferase (1.4%), hypothyroidism (1.6%), diarrhea (1.4%), fatigue (1.4%), arthralgia (1.6%), vomiting (1.0%), decreased appetite (1.0%), and rash (1.0%) in the pembrolizumab group. In the placebo group, the most frequent AEs resulting in interruption included nasopharyngitis (1.2%), diarrhea (1.0%), increased alanine aminotransferase (1.0%), and increased blood creatinine (1.0%) in the placebo group.
Mortality
At the time of the first interim analysis, 2 patients in pembrolizumab arm (0.4%) and 1 patient in placebo arm (0.2%) died due to an AE, none of which were considered treatment-related by the investigator (Table 24). In the pembrolizumab arm, 1 death was due to multiple organ dysfunction syndrome and the other was due to pneumonia; in the placebo arm, the 1 death was due to intracranial hemorrhage.
Table 24: Summary of AEs Resulting in Death up to 90 Days From Last Dose of Treatment (Incidence > 0% in 1 or More Treatment Groups; APaT Population) — IA1
Category | Pembrolizumab, n (%) N = 488 | Placebo, n (%) N = 496 |
|---|---|---|
≥ 1 AE | 2 (0.4) | 1 (0.2) |
General disorders and administration-site conditions | 1 (0.2) | 0 (0.0) |
Multiple organ dysfunction syndrome | 1 (0.2) | 0 (0.0) |
Infections and infestations | 1 (0.2) | 0 (0.0) |
Pneumonia | 1 (0.2) | 0 (0.0) |
Nervous system disorders | 0 (0.0) | 1 (0.2) |
Intracranial hemorrhage | 0 (0.0) | 1 (0.2) |
AE = adverse event; APaT = all participants as treated; IA1 = first interim analysis.
Notes: Every participant is counted a single time for each applicable row and column. A specific AE appears only if its incidence in 1 or more columns meets the incidence criterion in the report title, after rounding. Non-SAEs up to 30 days and SAEs up to 90 days after the last dose in the initial treatment phase are included. The following MedDRA preferred terms not related to the drug have been excluded: neoplasm progression, malignant neoplasm progression, and disease progression.
Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Notable Harms
Hyperthyroidism occurred in 21.1% of patients treated with pembrolizumab and 6.9% of patients treated with placebo, and hypothyroidism occurred in 11.9% of patients treated with pembrolizumab and 0.2% of patients treated with placebo (Table 25). Other notable harms reported in at least 1% of patients in either treatment arm were pneumonitis (2.3% versus 1%), adrenal insufficiency (2% versus 0.2%), type 1 diabetes mellitus (1.8% versus 0%), colitis (1.6% versus 0.2%), severe skin reactions (1.6% versus 0.4%), infusion reactions (1.4% versus 1%), thyroiditis (1.2% versus 0.2%), and hepatitis (1% versus 0%).
Table 25: Summary of Notable Harms in the KEYNOTE-564 Trial (Incidence > 0% in 1 or More Treatment Groups; APaT Population) — IA1
Category | Pembrolizumab arm, n (%) N = 488 | Placebo arm, n (%) N = 496 |
|---|---|---|
≥ 1 AE | 173 (35.5) | 34 (6.9) |
Hypothyroidism | 103 (21.1) | 18 (3.6) |
Hyperthyroidism | 58 (11.9) | 1 (0.2) |
Pneumonitis | 11 (2.3) | 5 (1.0) |
Adrenal Insufficiency | 10 (2.0) | 1 (0.2) |
Type 1 diabetes mellitus | 9 (1.8) | 0 (0.0) |
Colitis | 8 (1.6) | 1 (0.2) |
Severe skin reactions | 8 (1.6) | 2 (0.4) |
Infusion reactions | 7 (1.4) | 5 (1.0) |
Thyroiditis | 6 (1.2) | 1 (0.2) |
Hepatitis | 5 (1.0) | 0 (0.0) |
Sarcoidosis | 4 (0.8) | 0 (0.0) |
Nephritis | 3 (0.6) | 0 (0.0) |
Myasthenic syndrome | 3 (0.6) | 0 (0.0) |
Hypophysitis | 2 (0.4) | 0 (0.0) |
Myositis | 2 (0.4) | 1 (0.2) |
Vasculitis | 2 (0.4) | 0 (0.0) |
Encephalitis | 1 (0.2) | 0 (0.0) |
Myocarditis | 1 (0.2) | 0 (0.0) |
Uveitis | 0 (0.0) | 1 (0.2) |
AE = adverse event; APaT = all participants as treated; IA1 = first interim analysis.
Notes: Every participant is counted a single time for each applicable row and column. Non-SAEs up to 30 days and SAEs up to 90 days after the last dose in the initial treatment phase are included. The following MedDRA preferred terms not related to the drug have been excluded: neoplasm progression, malignant neoplasm progression, and disease progression.
Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Critical Appraisal
Internal Validity
The KEYNOTE-564 trial is an ongoing, multicentre, randomized, placebo-controlled, double-blind study. Treatment allocation was performed centrally through an Interactive Voice Response Systems and Interactive Web Response Systems. The study randomization was stratified first by patients’ metastasis status (M0 versus M1 NED). In the M0 group, ECOG PS (0 or 1) and US participant (yes or no) were additional stratification factors.
Overall, the baseline and demographic characteristics were balanced in the 2 study arms, suggesting that randomization was successfully implemented. A relatively small proportion of patients did not receive their assigned treatment (1.6% in the pembrolizumab arm and 0.4% in placebo arm), which is unlikely to have a significant impact on the comparative efficacy assessment in the ITT analysis.
Based on the study protocol, patients in the KEYNOTE-564 trial were prohibited from receiving antineoplastic systemic chemotherapy or biologic therapy, and immunotherapy during the treatment phase. However, 10 individuals (7 in the pembrolizumab arm and 3 in the placebo arm) received antineoplastic agents as concomitant medications during the trial. A small number of patients received concomitant aflibercept and fluorouracil. The clinical experts consulted by CADTH noted that these drugs are not commonly used in practice for the treatment of RCC but suggested that these patients might have experienced another type of malignancy for which they would have required chemotherapy. Even though the reasoning for concomitant anti-cancer therapy was not clearly described in the Clinical Study Report for KEYNOTE-564, it was unlikely that these concomitant therapies modified the treatment effects of pembrolizumab or had an impact on outcomes, given that they are not expected to be efficacious in the adjuvant treatment of RCC. The clinical experts consulted by CADTH agreed that the differential use of these concomitant therapies was not likely to have a meaningful effect on outcomes.
DFS and OS were the primary and the main secondary outcomes in the KEYNOTE-564 trial, respectively. Both outcomes were considered clinically relevant for patients with RCC in the adjuvant setting, according to the clinical experts consulted and the patient input provided. DFS, assessed by the investigator, was defined as the time from randomization to the first documented local recurrence, occurrence of distant kidney cancer metastasis(es), or death due to any cause, whichever occurs first. Assessment of DFS required radiologic evidence of disease recurrence, and pathologic assessment was strongly encouraged. To evaluate the robustness of the DFS findings, the sponsor introduced BICR assessments in the pivotal trial. Results showed that there was a discrepancy in the level of concordance between the investigators and BICR when it came to disease recurrence assessments. Among participants with disease recurrence, BICR agreed with investigator assessment in 81.6% of cases in the pembrolizumab group and in 86.6% in the placebo group. Conversely, among the participants without disease recurrence, BICR agreed with investigator assessment in 92.6% of cases in the pembrolizumab group and in 92.2% in the placebo group (Table 37). Furthermore, the pivotal trial provided evidence of early and late discrepancy rates, which allowed assessment of the frequency in which local investigators declared recurrence earlier or later than the BICR in each treatment group. Early and late discrepancy rates did not cross the threshold values identified in the literature that would indicate the presence of evaluation bias in favour of pembrolizumab (Table 37).28 As described by the sponsor, discrepancies in disease recurrence assessments observed might have been related to the fact that disease recurrence assessed by investigators required radiographic evidence, with strong encouragement for pathology assessments, whereas BICR assessed recurrence based on radiographic evidence only. Among the 39 individuals (19 in the pembrolizumab group and 20 in the placebo group) for whom disease recurrence was declared by investigator but not by BICR, 17.9% of disease recurrences (pembrolizumab versus placebo: 15.8% versus 20.0%) were declared by the investigators based on both radiographic and pathological evidence. Moreover, among the 55 patients (28 in the pembrolizumab group and 27 in the placebo group) in whom there was no disease recurrence according to the investigators but not BICR, lack of recurrence was declared by investigators on the basis of both radiographic and pathologic evidence in 9.1% of individuals (pembrolizumab versus placebo: 14.3% versus 3.7%) (Table 38). To minimize the risk of differential measurement error, a sensitivity analysis of DFS assessment by BICR, in which participants enrolled with baseline disease assessed by BICR were censored at their randomization date, was pre-specified and conducted in the pivotal trial (Appendix 3). The sensitivity analysis suggested consistent findings with the primary DFS analysis. The clinical experts consulted by CADTH acknowledged that discrepancies in disease assessments are common in large clinical trials and noted that discrepancies in the KEYNOTE-564 trial might have been related to the fact that BICR only had radiographic information, with no other clinical information, for the trial participants. There was no clear evidence that DFS assessment by the investigator introduced bias in the results of the primary outcome evaluation.
OS was defined as the time from randomization to death due to any cause. It is important to note that surgery in patients with RCC is performed with curative intent, and that the disease-specific survival period postnephrectomy is rather long in patients with intermediate- or high-risk disease (i.e., 5-year rates are about 80% for individuals at intermediate risk and 40% to 55% for individuals at high risk).3 Thus, a longer follow-up is likely required to observe the effect of treatment on survival outcomes in the adjuvant setting, which was evidenced by the fact that median DFS and OS were not reached in the pivotal study, and was further validated by the clinical experts consulted for this CADTH review. In the KEYNOTE-564 study, treatment was limited to 17 doses (or approximately 1 year of treatment), and patients could receive subsequent systemic anti-cancer regimens (e.g., radiation, surgery, medication) after discontinuing their study treatment. Specifically, more patients in the placebo arm (22.5%) received post-treatment anti-cancer therapies compared to the pembrolizumab arm (15.3%). An increased use of anti-cancer therapies among patients in the placebo group would introduce bias in the comparative assessment of OS and would make it harder to demonstrate between-group differences in OS during the trial period (i.e., the direction of bias would likely go against pembrolizumab). Furthermore, subsequent treatments also make it difficult to determine the longer-term benefits of adjuvant pembrolizumab on OS. CADTH reviewers therefore deemed that it is difficult to determine the benefits of pembrolizumab on improving survival in the adjuvant setting, based on the current trial evidence.
Sample size and power calculations were based on DFS and OS. When calculating sample size and power of the KEYNOTE-564 trial, the sponsor assumed that DFS would follow a Poisson mixture cure rate model with a cure rate of 0.3 in the long term, based on previously published data.25 However, the study protocol did not specify which recurrence risk groups this estimate applied to (intermediate-high, high, or both) or the time frame the estimate was applied to. The clinical experts consulted by CADTH agreed with the reviewers that these strata would affect the cure rate used. Nevertheless, the clinical experts acknowledged that the assumptions are consistent with a cure rate averaged across the recurrence risk strata and noted that it seemed reasonable for the a priori estimation of sample size for a trial.
The Cox proportional hazards model, used for the assessment of primary and secondary study outcomes, assumes that the hazards are proportional in the 2 treatment arms. Because a violation of this assumption may lead to biased estimates in the regression model, the sponsor’s statistical analysis plan pre-specified that proportional hazards assumptions related to DFS and OS would be assessed visually and analytically, if warranted. If that visual inspection yielded evidence of nonproportional hazards, the sponsor pre-specified possible supportive analyses using restricted mean survival time and parametric methods.29,30 Survival curves were estimated using the KM model. CADTH’s visual assessment of the DFS curve did not provide evidence suggestive of any violation in proportional hazards.
The amounts of censored data across the efficacy outcomes were fairly balanced between the pembrolizumab and placebo study groups. However, censoring in the study might have been affected by imbalances in treatment discontinuation due to AEs (38.9% in the pembrolizumab arm; 26.2% in the placebo arm), as well as by potential unblinding of the study due to irAEs (35.5% in the pembrolizumab arm; 6.9% in the placebo arm). The sponsor did not pre-specify a sensitivity analysis that would consider censoring related to AEs. Still, a conservative approach was adopted to handle treatment discontinuation (i.e., patients who completed the study treatment or discontinued treatment due to a reason other than disease recurrence were considered to be on study and followed scheduled efficacy assessments). In addition, the outcomes of DFS and EFS analyses by BICR showed findings consistent with the primary analysis. CADTH reviewers considered that the potential for informative censoring due to treatment discontinuation related to AEs and the potential for unblinding in the KEYNOTE-564 trial were minimal.
HRQoL was assessed as a secondary outcome in the KEYNOTE-564 trial using the FKSI-DRS and EORTC QLQ-C30 (global health status/QoL and physical functioning) questionnaires. The EQ-5D-5L VAS was assessed as an exploratory outcome in the trial. None of the HRQoL outcomes were controlled for multiplicity. The clinical experts consulted by CADTH noted that the questionnaires used in the KEYNOTE-564 trial were appropriate for assessing PROs in patients with RCC in the adjuvant setting. The validity of the FKSI-DRS questionnaire has been documented in patients with advanced and metastatic RCC, with evidence of reliability and responsiveness, but no evidence was found for patients in the adjuvant setting. Both EORTC QLQ-C30 and EQ-5D-5L have been widely used in oncologic trials in different cancer populations, but the validity of these questionnaires has not been documented in patients with RCC in the adjuvant setting. Similarly, no MID was established for EORTC QLQ-C30 and EQ-5D-5L measures in the population of interest for this review. Statistical analysis of PROs included a cLDA model, which is best suited for data that are missing at random or missing completely at random. In the current analysis, estimates from this model might have been biased, as there is a high likelihood that data in the KEYNOTE-564 trial are not missing at random. It was not reported whether the sensitivity analysis was performed to investigate the impact of the missing data or whether the missing-at-random assumption was met. Interpretation of the HRQoL results is more difficult with missing outcome data at later time points, as evidenced by the decline in rates of completed questionnaires to approximately 60% at week 52. According to the study protocol, the handling of missing data was model-based. However, the exact structure of the model was not specified, and the appropriateness of the model could not be determined.
Regarding the multiplicity adjustments, the type I error rate was controlled with a fixed testing sequence (DFS at a 1-sided alpha level of 2.5% first, and if DFS was successful, the alpha was then passed to OS). Sensitivity analyses and adjustments of covariates were conducted for DFS, and the findings were consistent with the primary analysis in the ITT set. Multiplicity adjustments were not conducted for other secondary or exploratory end points (DRSS, EFS, and HRQoL), including the analysis of subgroups.
A set of subgroup analyses was pre-specified in the protocol. There was no evidence of formal statistical tests of interaction being performed to test whether treatment effects differed among subgroups for the primary end point. The subgroup analysis of interest in this CADTH report (metastasis status) was based on a randomization stratification variable and was not adjusted for multiplicity. The small sample size in the M1 NED group suggests that this analysis might be underpowered to detect a meaningful difference between the study arms. Moreover, an additional subgroup analysis of DFS according to the recurrence risk groups was provided at the efficacy update report analysis but was not pre-specified in the protocol. Therefore, the study was not adequately designed to evaluate the effects of adjuvant pembrolizumab across all relevant subgroups.
The results reported in the Clinical Study Report for KEYNOTE-564 were based on the first interim analysis, with a data cut-off date of December 14, 2020. The study protocol specified 3 interim and 1 final analyses, with stopping rules defined a priori. Moreover, the sponsor implemented an additional amendment to the supplemental statistical plan to accommodate potential requests from regulatory agencies (efficacy update report analysis). The efficacy update report analysis, with an additional 6 months of follow-up and a data cut-off of June 14, 2021, was added between the first and second interim analysis. The group sequential approach that was used to allocate alpha between the interim and final analyses was considered appropriate by the CADTH reviewers.
The analysis for the primary and main secondary outcomes (DFS and OS) was conducted based on the ITT principle. Overall, clinically important protocol deviations were reported for 2 participants receiving pembrolizumab and 3 participants receiving placebo at the first interim analysis. In the study analyses, no data points were excluded because of an important protocol deviation. No per protocol analysis was conducted to check for consistency with the ITT analysis, but the number of patients with important deviations was low and balanced in the 2 study groups. Hence, CADTH deemed the risk of bias owing to protocol deviations to be low, and to likely have a negligible influence on comparative efficacy findings.
External Validity
The KEYNOTE-564 study was a multinational, multicentre trial. Of the 212 sites in 21 countries that participated, there were 10 sites in Canada. The population for the requested reimbursement aligns with the approved Health Canada indication.
The clinical experts consulted by CADTH agreed that the inclusion and exclusion criteria of the trial were appropriate for the RCC population in the adjuvant setting (Table 26). The experts also noted that the baseline characteristics of patients in the KEYNOTE-564 trial could be generalized to patients in the Canadian setting. According to the experts, the proportion of patients in the different risk-of-recurrence groups was deemed to be reflective of the population they would consider for adjuvant pembrolizumab treatment in real-world practice. It is uncertain whether the findings can be generalized to patients with a histology other than clear cell and with an ECOG PS of at least 2, as no such patients were included in the study.
In terms of the frequency of disease assessment, the clinical experts anticipated that disease assessments would be conducted less frequently in real-world practice than they were in the trial. Concomitant medications administered during the trial and subsequent anti-cancer therapies administered during follow-up were considered appropriate by the clinical experts consulted and reflective of medications administered in the Canadian setting.
In the KEYNOTE-564 trial, the only administered dosage of pembrolizumab was 200 mg every 3 weeks for up to 17 doses. The clinical experts indicated that physicians would prefer a dosing of 400 mg every 6 weeks for up to 9 doses in real-world clinical practice. Furthermore, the experts reported that weight-based dosing has been introduced in some Canadian provinces to optimize the costs and decrease drug wastage.
Placebo was considered an appropriate comparator because there are no Health Canada–approved adjuvant treatment options available in the Canadian setting.
The clinical experts consulted during this CADTH review highlighted that OS, DFS, HRQoL, and safety are appropriate outcomes to consider for patients with RCC in the adjuvant setting.
Table 26: Assessment of the Generalizability of Evidence for Pembrolizumab
Domain | Factor | Evidence | CADTH's assessment of generalizability |
|---|---|---|---|
Population | Risk of recurrence | Patients eligible for the KEYNOTE-564 study included individuals with RCC postnephrectomy, who needed to be of intermediate-high risk (pT2, grade 4 or sarcomatoid, N0, M0; or pT3, any grade, N0, M0), high risk (pT4, any grade, N0, M0; or pT any stage, any grade, N+, M0), or M1 NED (to have a primary kidney tumour and a solid, isolated, soft tissue metastasis, completely resected either at the time of [synchronous] or ≤ 1 year after nephrectomy [metachronous]). | The magnitude of benefit of adjuvant pembrolizumab in a population at low risk of recurrence is uncertain. However, this population is outside the proposed indication submitted to Health Canada. The clinical experts noted that patients were eligible for inclusion in the KEYNOTE-564 trial if they were at intermediate-high to high risk of recurrence or had M1 NED. Therefore, patients in clinical practice could benefit from therapy if they fall within the categories identified in the KEYNOTE-564 trial. The clinical experts noted that the distribution of patients across the different risk categories was expected and was reflective of a patient population that would be considered for adjuvant treatment, given the eligibility criteria of the trial. |
Histology | Patients were expected to have a clear cell component in tumour histology with or without sarcomatoid features to be eligible for the KEYNOTE-564 trial. | The magnitude of benefit of adjuvant pembrolizumab is uncertain for patients with RCC and a histology other than clear cell. In line with the inclusion criteria of the KEYNOTE-564 trial, the clinical experts noted that patients in clinical practice would benefit from adjuvant pembrolizumab therapy if they had an identified clear cell histology with or without sarcomatoid features. | |
ECOG PS | Patients were expected to have an ECOG PS of 0 or 1. | It is uncertain whether the finding can be generalized to patients with an ECOG PS of 2 or higher, because no such patients were included in the trial. Even though the clinical experts consulted by CADTH expressed doubts about whether adjuvant pembrolizumab should be considered for patients with an ECOG PS higher than 1, they reported that this judgment can be left for consideration of the treating physician. | |
Frequency of disease assessments and follow-up duration | During the treatment period, patients in the KEYNOTE-564 trial underwent frequent assessments for tumour and safety outcomes (every 12 weeks). In the trial, patients were followed when they went off treatment. Efficacy assessments were conducted every 12 weeks in year 1, every 16 weeks in years 2 to 4, and every 24 weeks in year 5 until a documented disease recurrence, new anti-cancer therapy, pregnancy, withdrawal of consent, end of trial, or death. Patients were followed every 12 weeks for OS until death, withdrawal of consent, or the end of the trial. | The clinical experts indicated that the frequency and follow-up duration of the trial assessments were appropriate to investigate the outcomes in the adjuvant setting. In the real-world setting, the clinical experts would expect the tumour assessments are conducted less frequently, although patients are constantly monitored for treatment-related AEs. | |
Subsequent anti-cancer medications and concomitant noncancer medications | Concomitant noncancer medications were allowed in the trial. Subsequent anti-cancer therapies (surgery, radiation, or medication) were administered to patients in both groups. | Overall, the clinical experts considered the concomitant medications allowed during the trial and the subsequent anti-cancer therapies administered to patients in the follow-up phase appropriate and reflective of medications administered in the Canadian setting. Concomitant antineoplastic therapy was reported in a small proportion of individuals in the trial, and the experts suggested this would not influence the overall study findings. The clinical experts acknowledged that patients are likely to require subsequent anti-cancer therapies in the case of disease recurrence or receive concomitant therapies as part of postnephrectomy care, to treat any underlying conditions, or treat AEs related to adjuvant therapy, which is consistent with the therapies outlined in the study protocol. The clinical experts did not identify any medications that may confound the results obtained in both study groups. | |
Intervention | Pembrolizumab | The trial intervention was administered as a 200 mg IV infusion every 3 weeks for up to 17 doses (approximately 1 year), or until disease recurrence or unacceptable toxicity. | In line with the dosing schedule applied in the KEYNOTE-564 trial, clinical experts noted that the dosing regimen of adjuvant pembrolizumab is appropriate. In the real-world setting, the clinical experts reported that adjuvant pembrolizumab as a 400 mg IV infusion each 6 weeks is more common in Canada. Of note, both the 200 mg (every 3 weeks for up to 17 doses) and 400 mg (every 6 weeks for up to 9 doses) dosing are reported in the product monograph submitted to Health Canada. Moreover, the experts noted that weight-based dosing has been introduced in some provinces of Canada to optimize the costs and decrease drug waste. |
Comparator | Placebo | Saline solution IV every 3 weeks. | The clinical experts consulted by CADTH for this review noted that there are currently no effective adjuvant treatments for RCC available in Canada. They noted that the current oncologic standard of care for these patients is observation, which supports the appropriateness of a placebo comparator group in the trial. |
Outcomes | DFS, OS, DRSS, EFS, HRQoL, safety | DFS was the primary outcome, and OS was the main secondary outcome. Additional secondary outcomes included DRSS, EFS, HRQoL, and safety. Only the DFS and OS outcomes had a formal hypothesis testing performed and type I error rate accounted for. The ITT set was used to assess DFS, OS, DRSS, and EFS; the FAS set was used to assess HRQoL; and the APaT set was used to assess safety. | The clinical experts consulted during the CADTH review highlighted that OS, DFS, HRQoL, and safety are appropriate outcomes to consider in RCC patients within the adjuvant setting. The experts noted that the DFS findings were clinically meaningful, as patients want to prevent disease recurrence and subsequent metastatic treatment. Ideally, OS benefits would have been observed, but the experts expressed optimism and noted that evidence from the KEYNOTE-564 trial can be considered suggestive. Regarding HRQoL, the experts observed that there was not a large decrease in quality-of-life outcomes among patients in the pembrolizumab and placebo groups. The clinical experts deemed other surrogate outcomes (DRSS and EFS) to be of lower clinical relevance but noted that these end points are often captured in large clinical trials. The experts highlighted that the observed safety profile of pembrolizumab is expected for immunotherapy. Also, the clinical experts indicated that immune-related AEs, even if rarely reported, should not be underestimated, as some of them are irreversible conditions that can be life-altering for patients (e.g., type 1 diabetes, pneumonitis). |
Setting | Multinational, multicentre study | 212 sites across 21 countries (Canada, US, and 19 other countries in Europe, South America, Asia, and Oceania), including 10 sites in Canada. | There were 10 sites in Canada. The clinical experts acknowledged that the findings are generalizable to Canadian patients. |
AE = adverse event; APat = all participants as treated; DFS = disease-free survival; DRSS = disease recurrence–specific survival; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EFS = event-free survival; FAS = full analysis set; HRQoL = health-related quality of life; ITT = intention to treat; IV = IV; M0 = no distant metastases; M1 NED = solid, isolated, soft tissue metastases that are either synchronous (i.e., completely resected at the time of nephrectomy) or metachronous (i.e., completely resected ≤ 1 year from nephrectomy); OS = overall survival; RCC = renal cell carcinoma.
Indirect Evidence
Through screening the articles yielded by the literature search, CADTH reviewers identified a systematic review and a network meta-analysis of safety and efficacy outcomes that compared adjuvant pembrolizumab with adjuvant TKIs in patients with nonmetastatic RCC postnephrectomy.31 This publication was ultimately excluded from the current review because the comparators were deemed irrelevant for the Canadian context.
Other Relevant Evidence
No other relevant study was identified in this review.
Discussion
Summary of Available Evidence
This CADTH systematic review included evidence from 1 pivotal study (KEYNOTE-564) and considered additional input from patient groups, clinical experts, clinician groups, and drug plans.
The KEYNOTE-564 trial is an ongoing multicentre, randomized, double-blind, phase III study comparing the efficacy and safety of pembrolizumab with placebo as an adjuvant treatment for adult patients with RCC postnephrectomy or postnephrectomy and resection of metastatic lesions. The study enrolled patients aged 18 years and older with a histologically confirmed diagnosis of RCC with a clear cell component, with or without sarcomatoid features. The study included patients at intermediate-high risk (pT2, grade 4 or sarcomatoid, N0, M0; or pT3, any grade, N0, M0), or high risk (pT4, any grade, N0, M0; or pT any stage, any grade, N+, M0) of recurrence, and M1 NED patients (patients with a primary kidney tumour and solid, isolated, soft tissue metastases completely resected either at the time of [synchronous] or 1 year or less after nephrectomy [metachronous]).
Patients were randomized in a 1:1 ratio to 1 of 2 treatment arms (pembrolizumab or placebo) based on following stratification factors: metastasis status variable (M0 versus M1 NED) and, in the M0 group, ECOG PS (0 or 1) and US participant (yes or no). The primary outcome of the KEYNOTE-564 trial was DFS, assessed by the investigator, and the main secondary outcome was OS. Other secondary and exploratory outcomes investigated included EFS, DRSS, HRQoL, and safety.12
Patients in the KEYNOTE-564 trial received either pembrolizumab (200 mg IV infusion every 3 weeks) or placebo (saline solution IV every 3 weeks) for up to a maximum of 17 infusions (or approximately 1 year), or until confirmation of recurrence, treatment discontinuation, or study termination. At the first interim analysis (December 14, 2020), 994 patients were randomized into the trial (496 in the pembrolizumab arm and 488 in the placebo arm; 10 patients did not receive their assigned treatment). The median age of the patients enrolled in the study was 60 years, and majority of participants were male and White. Most patients had tumours with an absence of sarcomatoid features and were at intermediate-high risk of recurrence. Baseline characteristics were balanced in the 2 study arms.
No indirect treatment comparisons or other relevant studies were identified for this review.
Interpretation of Results
Efficacy
Both the clinical experts and clinician groups consulted during the CADTH review highlighted that lengthening survival (OS) and reducing the risk of recurrence (DFS), without negatively influencing patients’ HRQoL are considered important treatment goals for patients with RCC in the adjuvant setting. Patient group input highlighted the need for adjuvant treatment options that would reduce the risk of disease recurrence after nephrectomy. Specifically, the input collected from patient groups by CADTH revealed that patients experience distress from the expectation of recurrence, and that almost half of the patients would be willing to accept adjuvant immunotherapy postsurgery if the therapy reduced the risk of disease recurrence by 40% to 50%.
The CADTH review protocol identified OS, DFS, EFS, DRSS, HRQoL, and safety as important outcomes for patients. All these outcomes were pre-specified in the KEYNOTE-564 trial before the first interim data cut-off (December 14, 2020), and the type I error rate was adequately controlled for OS and DFS. The CADTH review identified 3 subgroups of interest (histology, recurrence risk, and metastatic staging). The KEYNOTE-564 trial pre-specified metastatic staging as a subgroup analysis for DFS, which was also a stratification variable used in the randomization. Other subgroup analysis of DFS by recurrence risk groups was provided at the efficacy update report analysis, which had an additional 6 months of follow-up but was not pre-specified in the protocol. None of the subgroup analyses accounted for multiplicity. Sensitivity analyses were conducted for DFS, and the findings obtained were consistent with the primary DFS findings. Analyses of other outcomes, such as the EFS, DRSS, HRQoL, and safety, were not adjusted for multiplicity in the analysis.
The primary outcome was statistically significant at the first interim analysis data cut-off. Median DFS was not reached in either study group. The HR for DFS for pembrolizumab versus placebo was 0.68 (95% CI, 0.53 to 0.87; P = 0.001). The DFS rates at 24 months were 77.3% (95% Cl, 72.8% to 81.1%) in the pembrolizumab arm and 68.1% (95% Cl, 63.5% to 72.2%) in the placebo arm, suggesting a 9.2% relative difference. Findings from the efficacy update report analysis were consistent with results presented at first interim analysis. The clinical experts acknowledged that the DFS results were clinically meaningful.
The pre-specified DFS subgroup analysis according to the metastatic staging revealed a more pronounced effect in the M1 group (HR = 0.29; 95% CI, 0.12 to 0.69) than in the M0 group (HR = 0.74; 95% CI, 0.57 to 0.96) at the first interim analysis. These findings were consistent with data from the additional 6-months of follow-up presented in the efficacy update report analysis. The efficacy update report post hoc analysis of DFS by recurrence risk group showed a HR of 0.68 (95% CI, 0.52 to 0.89), 0.60 (95% CI, 0.33 to 1.10), and 0.28 (95% CI, 0.12 to 0.66) for the intermediate-high, high, and M1 NED risk groups, respectively. The findings from the analysis of subgroups were considered exploratory, as sample sizes were relatively small in certain subgroups and no multiplicity adjustments were used in these analyses.
Median OS had not been reached at the time of first interim analysis (December 14, 2020) or efficacy update report (June 14, 2021) analyses. The HR estimates for pembrolizumab versus placebo were 0.54 (95% CI, 0.30 to 0.96; P = 0.0164) at the first interim analysis and 0.52 (95% CI, 0.31 to 0.86; P = 0.005) at the efficacy update report analysis. Surgery in patients with RCC is performed with curative intent, and 5-year disease-specific survival is relatively long in patients at intermediate (about 80%) and high risk (from 40% to 55%) of recurrence postnephrectomy.3 The median duration of follow-up at the first interim analysis was approximately 24 months in the 2 treatment groups. In consultation with the clinical experts for CADTH, OS data from the pivotal KEYNOTE-564 trial were considered immature, owing to the shorter follow-up time relative to the natural history of patients in the adjuvant setting with RCC. Moreover, the fixed treatment duration recommended for pembrolizumab (median on-treatment exposure in the study was slightly longer than 11 months), with the opportunity for patients in either group to receive subsequent anti-cancer treatments, makes it difficult to determine the true effect of pembrolizumab on OS. Of note, there was a higher proportion of individuals receiving post-treatment anti-cancer therapies in the placebo than in the pembrolizumab group, which might have introduced bias against pembrolizumab in the assessment of OS. Because of these issues, the benefit of adjuvant pembrolizumab for OS in patients with RCC postnephrectomy or postnephrectomy and resection of metastatic lesions remains uncertain. Longer follow-up is likely required to observe the effects of adjuvant treatment on survival. Interim analyses 2 and 3 as well as the final OS analysis are planned when a pre-specified number of events have accrued in the pivotal trial (N = 132; N = 172, and N = 200, respectively).
Through the discussions with the clinical experts consulted for this review, the CADTH team collected feedback on the importance of OS as an outcome for patients with RCC in the adjuvant setting. It is important to note that evidence of the relationship between OS and its surrogate end point (DFS) is uncertain and is moderate, according to the limited data published in the literature (correlations ranging from 0.44 to 0.7).32,33
The results of EFS and the EFS sensitivity analysis described in the KEYNOTE-564 trial were, overall, aligned with results from the DFS primary ITT analysis. Cumulative incidence rates of disease recurrence were consistently lower in the pembrolizumab arm compared with the placebo arm for both local (DRSS1) and distant (DRSS2) recurrence events. However, these outcomes were not adjusted for multiplicity and were considered to be of lower clinical importance as described by the clinical experts consulted for this CADTH review.
The clinician and patient groups consulted during the CADTH review identified patient-reported and HRQoL outcomes as important treatment goals. In the KEYNOTE-564 trial, HRQoL was assessed using 3 questionnaires. The FKSI-DRS has been validated in patients with advanced and metastatic RCC, with MIDs ranging from 0.62 to 3 points, depending on the different anchors. No studies assessing validity and MIDs were found for the adjuvant setting. No studies assessing the validity, reliability, and responsiveness of EORTC QLQ-C30 (secondary outcome) and EQ-5D-5L (exploratory outcome) in patients with RCC in the adjuvant setting have been identified in published literature. The clinical experts highlighted the absence of HRQoL literature in the adjuvant setting and noted that the questionnaires in the KEYNOTE-564 trial may be considered appropriate for this RCC patient population. The clinical experts emphasized the importance of a patient’s quality of life not deteriorating during adjuvant treatment and reported that differences in HRQoL measures between the pembrolizumab and placebo arms did not seem substantial. Despite the higher proportion of irAEs in the pembrolizumab group, the clinicians noted that changes in functioning in the pembrolizumab group were comparable to those observed in the placebo group. The rates of completed questionnaires declined to about 60% at week 52 in both treatment arms. It was unclear whether the cLDA model used for the analysis of HRQoL outcomes adequately accounted for missing data, given the limited information provided. Moreover, HRQoL analyses were exploratory and did not adjust for multiplicity, so the results presented in the pivotal trial were considered descriptive by CADTH. The impact of adjuvant pembrolizumab on HRQoL, compared with placebo, is uncertain, given the lack of formally established MIDs and the limitations identified in the analyses.
According to the clinical experts consulted by CADTH, patients recruited in the trial were considered to be representative of patients in Canadian clinical practice. The distribution of patients in the different risk-of-recurrence groups was considered to be reflective of the population that might be considered for adjuvant pembrolizumab treatment in clinical practice, according to the experts. There were no major concerns about the generalizability of the findings to Canadian practice. The clinical experts acknowledged that it is uncertain whether the findings can be generalized to patients with histologies other than clear cell or to patients with an ECOG PS of 2 or higher, as no such patients were included in the pivotal trial.
Harms
Overall, the proportion of patients with at least 1 AE was higher in the pembrolizumab group (96.3%) than in the placebo group (91.1%). The frequency of SAEs was also higher in the pembrolizumab arm (20.5%) than in the placebo arm (11.3%) in the KEYNOTE-564 study. There were more AEs leading to drug discontinuations (pembrolizumab versus placebo: 20.7% versus 2.0%) and treatment interruptions (25.8% versus 14.9%) in the pembrolizumab arm compared to placebo. Two deaths were reported in the pembrolizumab arm (0.4%), and 1 death was reported in the placebo arm (0.2%), none of which were considered to be related to treatment by the investigator. Notable harms were more frequently reported in the pembrolizumab group compared with the placebo group. The higher incidence of notable harms in the pembrolizumab group than in the placebo group was driven by hyperthyroidism (pembrolizumab versus placebo: 21.1% versus 6.9%), hypothyroidism (11.9% versus 0.2%), pneumonitis (2.3% versus 1.0%), adrenal insufficiency (2.0% versus 0.2%), type 1 diabetes mellitus (1.8% versus 0.0%), colitis (1.6% versus 0.2%), severe skin reactions (1.6% versus 0.4%), infusion reactions (1.4% versus 1.0%), thyroiditis (1.2% versus 0.2%), and hepatitis (1.0% versus 0.0%).
Input from patient groups received for this review reported that approximately half of patients would be willing to accept the risk of side effects associated with steroid use to manage the side effects of adjuvant immunotherapy, if that level of risk was in the range of 20% to 25%.
Overall, the clinical experts consulted by CADTH for this review reported that the safety profile of pembrolizumab observed in this study appeared to be consistent with the known safety profile of immune-oncologic therapy, and no additional safety signals were identified. Moreover, the clinical experts indicated that irAEs should not be underestimated, as some of them are irreversible conditions that can be life-altering for the patients (e.g., type 1 diabetes, pneumonitis). Finally, the experts highlighted the importance of frequent and close monitoring for treatment-related AEs.
Conclusions
One sponsor-submitted, multicentre, randomized, double-blind, phase III trial (KEYNOTE-564) was included in this CADTH systematic review.
Overall, pembrolizumab improved DFS outcome, compared with placebo, as an adjuvant treatment for patients with RCC who are at intermediate-high or high risk of recurrence after nephrectomy or following nephrectomy and resection of metastatic lesions. However, the effects of adjuvant pembrolizumab relative to placebo on OS could not be determined because of the immature survival data, uncertain influence of subsequent treatments, and uncertainty about the correlation between DFS and OS in the adjuvant treatment of RCC. Likewise, limitations in the HRQoL analyses in the single randomized controlled trial precluded the drawing of conclusions about the effects of pembrolizumab on this outcome. The safety profile of pembrolizumab was similar to that observed in other trials of this drug, including effects on the thyroid and adrenal glands. The clinical experts considered the baseline characteristics and the findings from the KEYNOTE-564 trial to be generalizable to patients with RCC in the adjuvant setting in Canada.
References
1.NCCN guidelines for patients: kidney cancer. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2022: https://www.nccn.org/patients/guidelines/content/PDF/kidney-patient.pdf. Accessed 2022 May 11.
2.EAU guidelines on renal cell carcinoma. Arnhem (NL): European Association of Urology; 2022: https://uroweb.org/guidelines/renal-cell-carcinoma. Accessed 2022 May 11.
3.Renal cell carcinoma: ESMO clinical practice guidelines. Lugano (CH): European Society for Medical Oncology; 2019: https://www.esmo.org/guidelines/genitourinary-cancers/renal-cell-carcinoma Accessed 2022 May 11.
4.Canadian cancer statistics. 2021. Toronto (ON): Canadian Cancer Society; 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2022 May 11.
5.National Cancer Institute. Kidney (renal cell) cancer—health professional version 2022; https://www.cancer.gov/types/kidney/hp. Accessed 2022 May 11.
6.Rini BI, Campbell SC, Escudier B. Renal cell carcinoma. Lancet. 2009;373(9669):1119-1132. PubMed
7.Patard JJ, Kim HL, Lam JS, et al. Use of the University of California Los Angeles integrated staging system to predict survival in renal cell carcinoma: an international multicenter study. J Clin Oncol. 2004;22(16):3316-3322. PubMed
8.Zigeuner R, Hutterer G, Chromecki T, et al. External validation of the Mayo Clinic stage, size, grade, and necrosis (SSIGN) score for clear-cell renal cell carcinoma in a single European centre applying routine pathology. Eur Urol. 2010;57(1):102-109. PubMed
9.Renal cell carcinoma. Edmonton (AL): Cancer Care Alberta; 2021: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gu003-renal-cell.pdf. Accessed 2022 May 11.
10.Canil C, Kapoor A, Basappa NS, et al. Management of advanced kidney cancer: Kidney Cancer Research Network of Canada (KCRNC) consensus update 2021. Can Urol Assoc J. 2021;15(4):84-97. PubMed
11.Keytruda (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada; 2021 Aug 13.
12.Clinical Study Report: P564V01MK3475. A phase 3, randomized, double-blind, placebo- controlled clinical trial of pembrolizumab (MK-3475) as monotherapy in the adjuvant treatment of renal cell carcinoma post nephrectomy (KEYNOTE-564) [internal sponsor's report]. Rahway (NJ): Merck Sharp & Dohme Corp; 2021 Jun 7.
13.Leibovich BC, Lohse CM, Crispen PL, et al. Histological subtype is an independent predictor of outcome for patients with renal cell carcinoma. J Urol. 2010;183(4):1309-1315. PubMed
14.BC Cancer. Kidney. 2021; http://www.bccancer.bc.ca/health-info/types-of-cancer/urinary/kidney Accessed 2022 May 11.
15.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
16.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Mar 21.
17.Choueiri TK, Tomczak P, Park SH, et al. Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. N Engl J Med. 2021;385(8):683-694. PubMed
18.EORTC Quality of Life Group. EORTC QLQ-C30 - FAQ. 2021; https://qol.eortc.org/faq. Accessed 2021 Dec 23.
19.EORTC Quality of Life Group, Fayers P, Aaronson N, et al. The EORTC QLQ-C30 scoring manual, 3rd ed. Brussels (BE): European Organisation for Research and Treatment of Cancer; 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2021 Dec 23.
20.Cella D, Yount S, Brucker PS, et al. Development and validation of a scale to measure disease-related symptoms of kidney cancer. Value Health. 2007;10(4):285-293. PubMed
21.FACIT Group. FKSI-DRS Scoring Menu. Functional Assessment of Cancer Therapy – Kidney Symptom Index – Disease Related Symptoms (FKSI-DRS). Scoring guidelines (version 4). 2021; https://www.facit.org/measures-scoring-downloads/fksi-drs-scoring-downloads. Accessed 2021 Dec 23.
22.EuroQol Research Foundation. EQ-5D-5L user guide: basic information on how to use the EQ-5D-5L instrument. 2019; https://euroqol.org/publications/user-guides/. Accessed 2022 May 11.
23.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
24.Cella D, Li JZ, Cappelleri JC, et al. Quality of life in patients with metastatic renal cell carcinoma treated with sunitinib or interferon alfa: results from a phase III randomized trial. J Clin Oncol. 2008;26(22):3763-3769. PubMed
25.Leibovich BC, Blute ML, Cheville JC, et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: a stratification tool for prospective clinical trials. Cancer. 2003;97(7):1663-1671. PubMed
26.Clinical Study Report (efficacy update report): P564V01MK3475. 2.7.3 summary of clicnical efficacy [internal sponsor's report]. Rahway (NJ): Merck Sharp & Dohme Corp;.
27.Choueiri TK, Tomczak P, Park SE, et al. Pembrolizumab as post nephrectomy adjuvant therapy for patients with renal cell carcinoma: results from 30-month follow-up of KEYNOTE-564. J Clin Oncol. 2022;40(6 suppl):290.
28.Mannino FV, Amit O, Lahiri S. Evaluation of discordance measures in oncology studies with blinded independent central review of progression-free survival using an observational error model. J Biopharm Stat. 2013;23(5):971-985. PubMed
29.Uno H, Claggett B, Tian L, et al. Moving beyond the hazard ratio in quantifying the between-group difference in survival analysis. J Clin Oncol. 2014;32(22):2380-2385. PubMed
30.Anderson KM. A nonproportional hazards Weibull accelerated failure time regression model. Biometrics. 1991;47(1):281-288. PubMed
31.Laukhtina E, Quhal F, Mori K, et al. Pembrolizumab outperforms tyrosine kinase inhibitors as adjuvant treatment in patients with high-risk renal cell carcinoma after nephrectomy. Eur Urol Oncol. 2022;5(1):120-124. PubMed
32.Haas NB, Song Y, Willemann Rogerio J, et al. Disease-free survival as a predictor of overall survival in localized renal cell carcinoma (RCC) following first nephrectomy. J Clin Oncol. 2021;39(15 suppl):4581.
33.Harshman LC, Xie W, Moreira RB, et al. Evaluation of disease-free survival as an intermediate metric of overall survival in patients with localized renal cell carcinoma: a trial-level meta-analysis. Cancer. 2018;124(5):925-933. PubMed
34.Capitanio U, Larcher A, Montorsi F. Re: Toni K. Choueiri, Piotr Tomczak, Se Hoon Park, et al. Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. N Engl J Med 2021;385:683-94: Adjuvant pembrolizumab after nephrectomy: a plea to reconsider the need for lymph node dissection. Eur Urol. 2022;81(1):e28. PubMed
35.Khene ZE, Bex A, Bensalah K. Adjuvant therapy after surgical resection of nonmetastatic renal cell carcinoma: one size does not fit all. Eur Urol. 2022;81(4):432-433. PubMed
36.Magee DE, Kutikov A. Re: adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. Eur Urol. 2022;81(3):317-318. PubMed
37.Saleh K, Kordahi M, Felefly T, Kourie HR, Khalife N. Pembrolizumab: first adjuvant immunotherapy in renal cell carcinoma? Future Oncol. 2022;18(5):519-522. PubMed
38.Msaouel P, Grivas P, Zhang T. Adjuvant systemic therapies for patients with renal cell carcinoma: choosing treatment based on patient-level characteristics. Eur Urol Oncol. 2021. PubMed
39.Nierengarten MB. Pembrolizumab may be a new adjuvant treatment following renal cell carcinoma surgery. Cancer. 2021;127(20):3713. PubMed
40.Sharma A, Sahoo RK, Batra A. Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. N Engl J Med. 2021;385(20):1919. PubMed
41.Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 200mg, intravenous infusion [internal sponsor's package]. Kirkland (QC): Merck Canada; 2022 Mar 3.
42.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
43.FACIT Group. FKSI-DRS: Overview. 2021; https://www.facit.org/measures/FKSI-DRS. Accessed 2021 Dec 23.
44.Cella D, Motzer RJ, Rini BI, et al. Important group differences on the Functional Assessment of Cancer Therapy-Kidney Symptom Index Disease-Related Symptoms in patients with metastatic renal cell carcinoma. Value Health. 2018;21(12):1413-1418. PubMed
45.EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
46.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
47.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644-650. PubMed
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: April 1, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475 or DPT0O3T46P).ti,ab,kf,ot,hw,rn,nm.
Kidney Neoplasms/ or Carcinoma, Renal Cell/
((kidney* or renal or hypernephroid or hyper-nephroid* or collecting duct* or Grawitz* or nephroid) adj3 (cancer* or carcinoma* or neoplas* or tumor* or tumour* or adenocarcinoma* or adeno-carcinoma* or pyelocarcinoma* or metast* or malignan* or sarcoma*)).ti,ab,kf.
(hypernephroma* or nephroma* or reninoma* or RCC or mRCC).ti,ab,kf.
or/2-4
1 and 5
6 use medall
*pembrolizumab/
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475).ti,ab,kf,dq
8 or 9
exp Kidney cancer/
((kidney* or renal or hypernephroid or hyper-nephroid* or collecting duct* or Grawitz* or nephroid) adj3 (cancer* or carcinoma* or neoplas* or tumor* or tumour* or adenocarcinoma* or adeno-carcinoma* or pyelocarcinoma* or metast* or malignan* or sarcoma*)).ti,ab,kf,dq.
(hypernephroma* or nephroma* or reninoma* or RCC or mRCC).ti,ab,kf,dq.
or/11-13
10 and 14
15 use oemezd
16 not (conference review or conference abstract).pt.
7 or 17
remove duplicates from 18
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | pembrolizumab or Keytruda and renal cell carcinoma]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- pembrolizumab or Keytruda and renal cell carcinoma]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- pembrolizumab or Keytruda and renal cell carcinoma]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- pembrolizumab or Keytruda and renal cell carcinoma]
Grey Literature
Search dates: March 21 to March 28, 2022
Keywords: pembrolizumab, Keytruda, renal cell carcinoma
Limits: None
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Capitanio, U., et al. Re: Toni K. Choueiri, Piotr Tomczak, Se Hoon Park, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med 2021;385:683-94: Adjuvant Pembrolizumab After Nephrectomy: A Plea to Reconsider the Need for Lymph Node Dissection. European Urology. 2022. 81(1):e28.34 | Study design |
Khene, Z. E., et al. Adjuvant Therapy After Surgical Resection of Nonmetastatic Renal Cell Carcinoma: One Size Does Not Fit All. European Urology. 2022. 81(4)(432-433.35 | Study design |
Laukhtina, E., et al. Pembrolizumab outperforms tyrosine kinase inhibitors as adjuvant treatment in patients with high-risk renal cell carcinoma after nephrectomy. European Urology Oncology. 2022. 5(1):120-124.31 | Study design |
Magee, D. E., et al. Re: Adjuvant Pembrolizumab After Nephrectomy in Renal-cell Carcinoma. European Urology. 2022. 81(3):317-318.36 | Study design |
Saleh, K., et al. Pembrolizumab: first adjuvant immunotherapy in renal cell carcinoma? Future Oncology. 2022. 18(5):519-522.37 | Study design |
Msaouel, P., et al. Adjuvant Systemic Therapies for Patients with Renal Cell Carcinoma: Choosing Treatment Based on Patient-level Characteristics. European Urology Oncology. 2021. S2588-9311(21)00155-3.38 | Study design |
Nierengarten, M. B. Pembrolizumab may be a new adjuvant treatment following renal cell carcinoma surgery. Cancer. 2021. 127(20):3713.39 | Study design |
Sharma, A., et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. New England Journal of Medicine. 2021. 385(20):1919.40 | Study design |
Appendix 3: Detailed Outcome Data
Note this appendix has not been copy-edited.
Document | Date of issue | Overall rationale |
|---|---|---|
3475-564-00 | February 24, 2017 | Not applicable |
3475-564-01 | November 2, 2017 | In the global implementation of protocol approved on February 24, 2017, deficiencies were noted. The initial intent was to include metachronous and synchronous M1 NED post-operative nephrectomy ≤ 1 year. Since study inception, the inclusion of metachronous and synchronous M1 NED patients was intended; however, during protocol finalization metachronous was inadvertently removed. Additionally, minor adjustments were incorporated to enhance the clarity of the protocol intent, reflect real-time feedback from investigators, and address language inconsistencies. |
3475-564-02 | September 04, 2019 | Because of the extension of study enrolment from 18 months to 25 months, there was not sufficient minimum follow-up time if IA1 was triggered based on the originally desired number of DFS events projected at 3 months after last participant randomized. Thus, IA2 has been retooled as IA1 where the trigger is 80% DFS events accrued. This would represent roughly a minimum follow-up of 12 months after enrolment is finished. |
3475-564-03 | May 11, 2020 | Changed the trigger for IA1 timing and total number of targeted events for final analysis of DFS by investigator review (IA2) and added secondary end point to compare EFS as assessed by the blinded independent radiology review for participants treated with pembrolizumab vs. those receiving placebo. |
3475-564-04 | October 13, 2020 | To update the censoring rules and remove the PK/ADA sample collection. |
DFS = disease-free survival; EFS = event-free survival; IA = interim analysis; M1 NED = patients who present not only with the primary kidney tumour but also solid, isolated, soft tissue metastases that were completely resected at the time of nephrectomy (synchronous) or ≤ 1 year from nephrectomy (metachronous).
Source: Clinical Study Report.12
Table 30: Analysis of Overall Survival in the Efficacy Update Report (Primary Censoring Rule; ITT Population)
Survival | Pembrolizumab arm (n = 496) | Placebo arm (n = 498) |
|---|---|---|
Patients with events, n (%) | ||
Total | 23 (4.6) | 43 (8.6) |
OS (months) | ||
Median (95% CI)a | NR (NR, NR) | NR (NR, NR) |
Q1, Q3 | NR, NR | NR, NR |
Hazard ratio (95% CI)b | 0.52 (0.31 to 0.86) | |
P valuec | 0.0047677 | |
OS rate (%) (95% CI) | ||
12 months | 98.6 (97.0 to 99.3) | 98.0 (96.3 to 98.9) |
18 months | 97.8 (96.0 to 98.8) | 96.8 (94.8 to 98.0) |
24 months | 96.2 (94.1 to 97.6) | 93.8 (91.3 to 95.6) |
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; NR = not reached; OS = overall survival.
Note: Database cut-off date was June 14, 2021.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
cOne-sided p value based on log-rank test stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
Source: Clinical Study Report efficacy update report.26
Figure 8: Kaplan-Meier Plot of Overall Survival in the Efficacy Update Report (ITT Population)
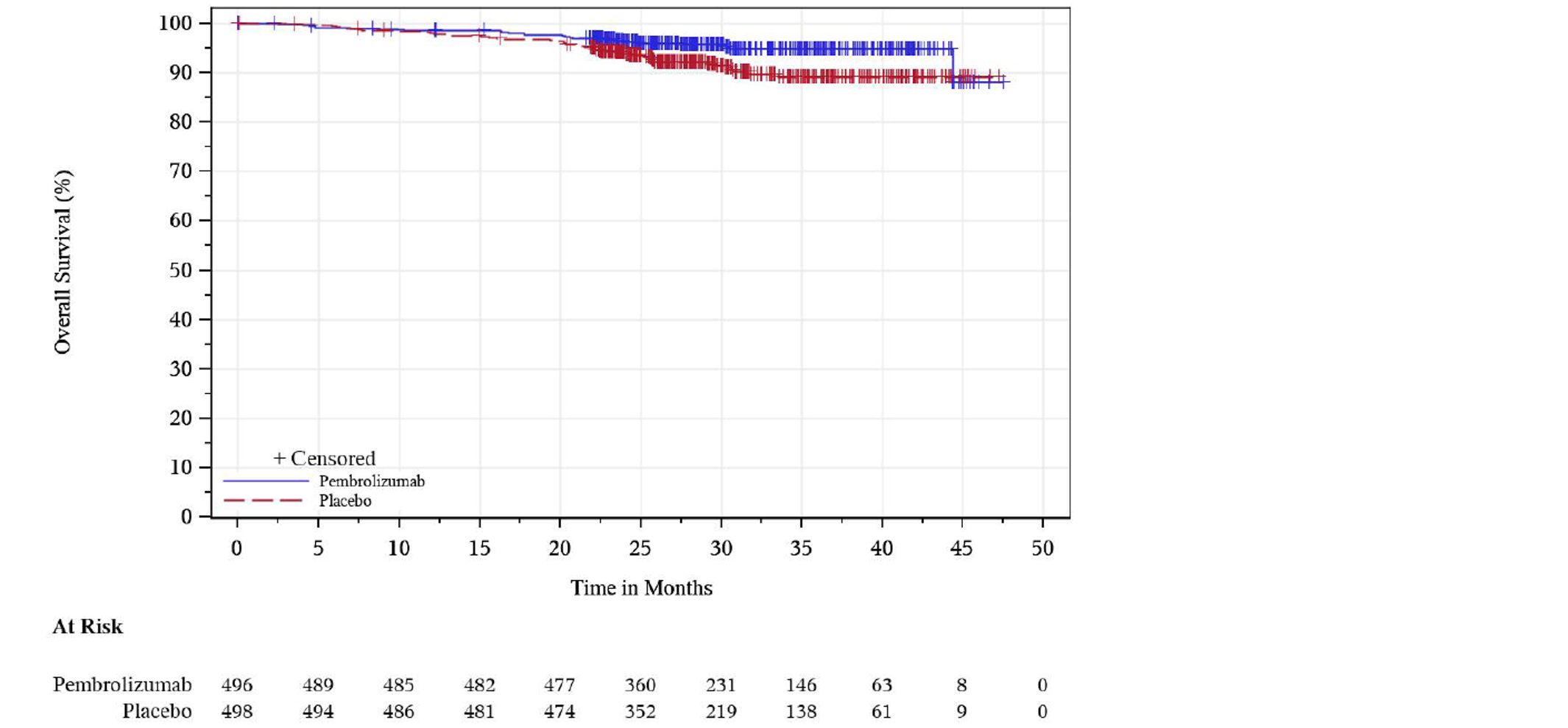
+ = censored observations; ITT = intention to treat.
Note: Database cut-off date: June 14, 2021.
Source: Clinical Study Report efficacy update report.26
Table 31: Analysis of Disease-Free Survival at Efficacy Update Report (Primary Censoring rule; ITT Population)
Disease-free survival | Pembrolizumab arm (n = 496) | Placebo arm (n = 498) |
|---|---|---|
Patients with events, n (%) | ||
Total | 114 (23.0) | 169 (33.9) |
Death | 6 (1.2) | 3 (0.6) |
Disease recurrence | 108 (21.8) | 166 (33.3) |
Censored, n (%) | 382 (77.0) | 329 (66.1) |
Last tumour assessment showing no disease recurrence | 370 (74.6) | 326 (65.5) |
No postbaseline disease status assessment | 12 (2.4) | 3 (0.6) |
DFS (months) | ||
Median (95% CI)a | NR (NR, NR) | NR (40.5, NR) |
Q1, Q3 | 30.2, NR | 13.8, NR |
Hazard ratio (95% CI)b | 0.63 (0.50 to 0.80) | |
P valuec | < 0.0001 | |
DFS rate (%) (95% CI) | ||
12 months | 85.5 (82.0 to 88.4) | 76.0 (72.0 to 79.5) |
18 months | 82.1 (78.3 to 85.3) | 71.3 (67.0 to 75.1) |
24 months | 78.3 (74.3 to 81.8) | 67.3 (62.9 to 71.3) |
CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; ITT = intention to treat; NR = not reached.
Note: Database cut-off date: June 14, 2021.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
cOne-sided p value based on log-rank test stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
Source: Clinical Study Report efficacy update report.26
Figure 9: Kaplan-Meier Plot of Disease-Free Survival Based on the Investigator Assessment in the Efficacy Update Report (Primary Censoring Rule; ITT Population)
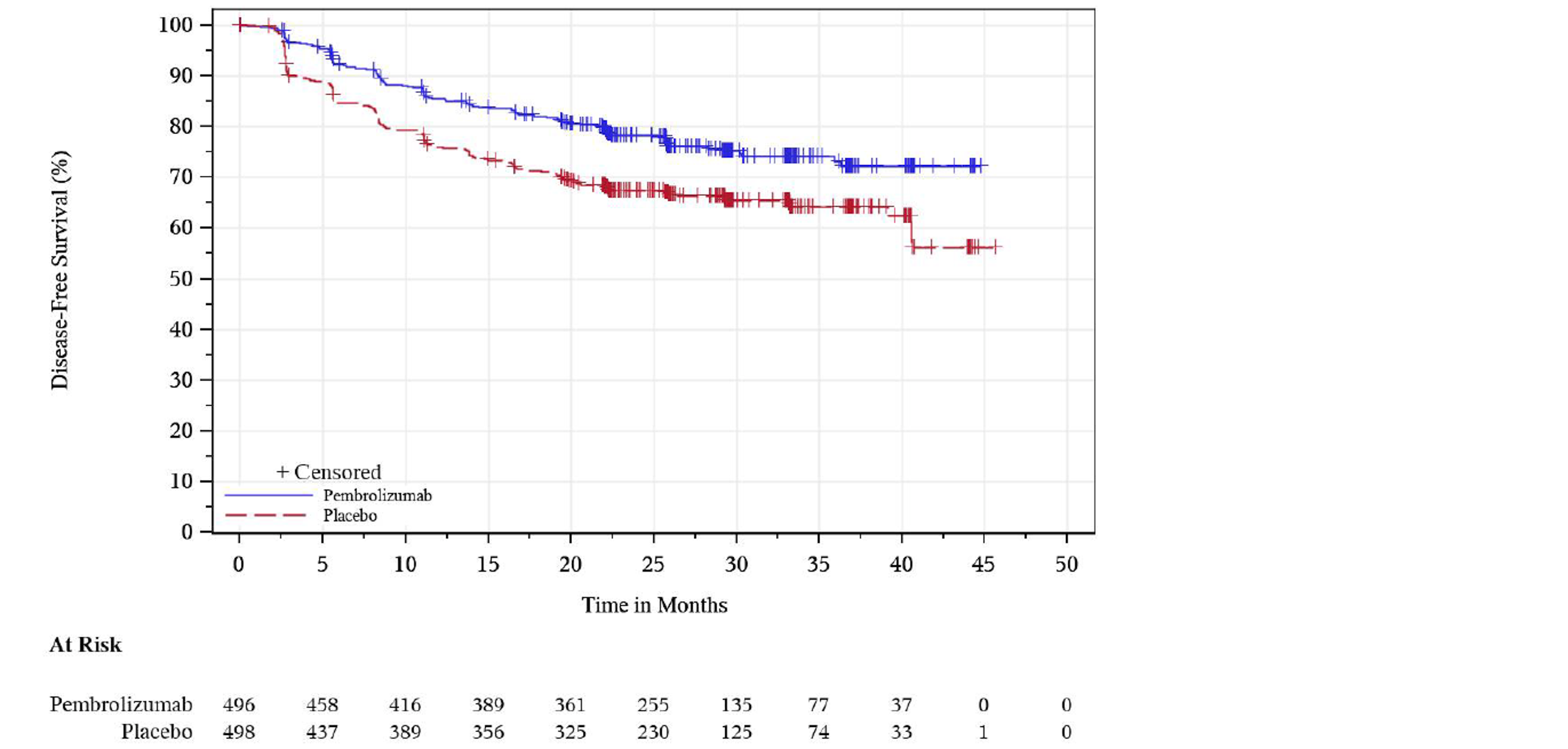
+ = censored observations; ITT = intention to treat.
Note: Database cut-off date was June 14, 2021.
Source: Clinical Study Report efficacy update report.26
Table 32: Prespecified Subgroup Analysis of DFS at IA1
Subgroup | Pembrolizumab | Placebo | Pembrolizumab vs. placebo | ||||||
|---|---|---|---|---|---|---|---|---|---|
N | Number of events | N | Number of events | HR (95% CI) | |||||
Death | Recurrence | Death | Recurrence | ||||||
Overall primary analysis | 496 | 6 | 103 | 498 | 2 | 149 | 0.68 (0.53 to 0.87) | ||
Subgroup analysis | |||||||||
M0 | 467 | 5 | 97 | 469 | 1 | 131 | 0.74 (0.57 to 0.96) | ||
M1 NED | 29 | 1 | 6 | 29 | 1 | 18 | 0.29 (0.12 to 0.69) | ||
CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; IA1 = first interim analysis; M0 = patients with no distant metastases; M1 NED = patients who present not only with the primary kidney tumour but also solid, isolated, soft tissue metastases that were completely resected at the time of nephrectomy (synchronous) or ≤ 1 year from nephrectomy (metachronous).
Source: Clinical Study Report.12
Figure 10: Post Hoc Subgroup Analysis of DFS According to the Recurrence Risk Subgroups in the Efficacy Update Report — (ITT Population)
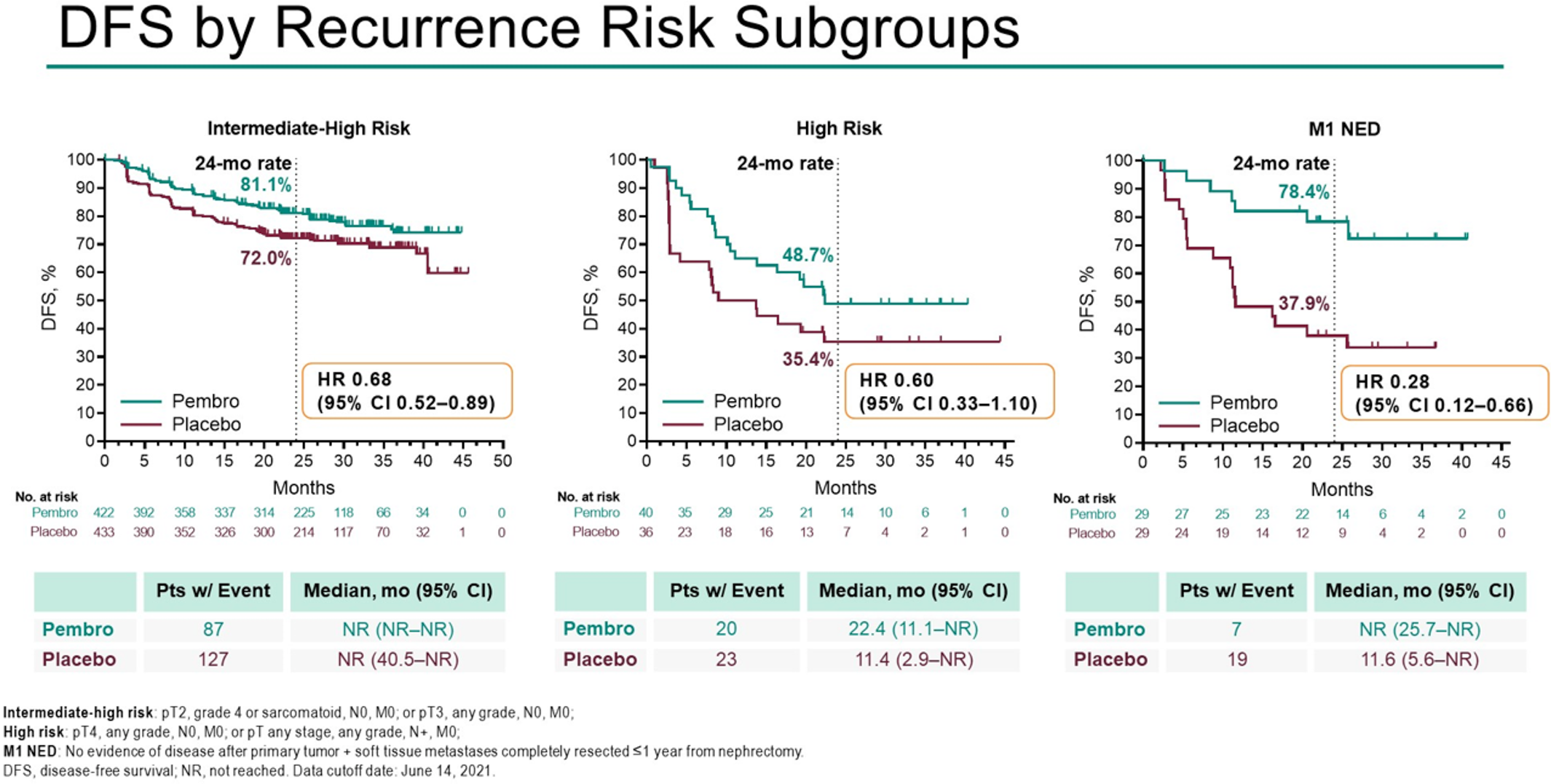
DFS = disease-free survival; ITT = intention to treat.
Source: Sponsor submission41
Table 33: Sensitivity Analysis of Disease-Free Survival at IA1 (Sensitivity Censoring Rule; ITT Population)
Disease-free survival | Pembrolizumab arm (n = 496) | Placebo arm (n = 498) |
|---|---|---|
Patients with events, n (%) | ||
Total | 107 (21.6) | 151 (30.3) |
Death | 5 (1.0) | 2 (0.4) |
Disease recurrence | 102 (20.6) | 149 (29.9) |
Censored, n (%) | 389 (78.4) | 347 (69.7) |
Last tumour assessment showing no disease recurrence | 375 (75.6) | 344 (69.1) |
Last tumour status assessment before new anti-cancer therapy showing no disease recurrence | 1 (0.2) | 0 (0) |
No postbaseline disease status assessment | 13 (2.6) | 3 (0.6) |
DFS (months) | ||
Median (95% CI) a | NR (NR, NR) | NR (NR, NR) |
Q1, Q3 | 25.8, NR | 13.8, NR |
Hazard ratio (95% CI) b | 0.67 (0.52 to 0.86) | |
P value c | 0.0007 | |
DFS rate (%) (95% CI) | ||
12 months | 85.7 (82.2 to 88.5) | 76.2 (72.2 to 79.7) |
18 months | 81.7 (77.8 to 84.9) | 71.9 (67.7 to 75.7) |
24 months | 77.7 (73.3 to 81.5) | 68.1 (63.5 to 72.2) |
CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; IA1 = first interim analysis; NR = not reached.
Note: Database cut-off date: December 14, 2020.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
cOne-sided P value based on log-rank test stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
Source: Clinical Study Report.12
Figure 11: Kaplan-Meier Plot of Disease-Free Survival (Sensitivity Censoring Rule; ITT Population)
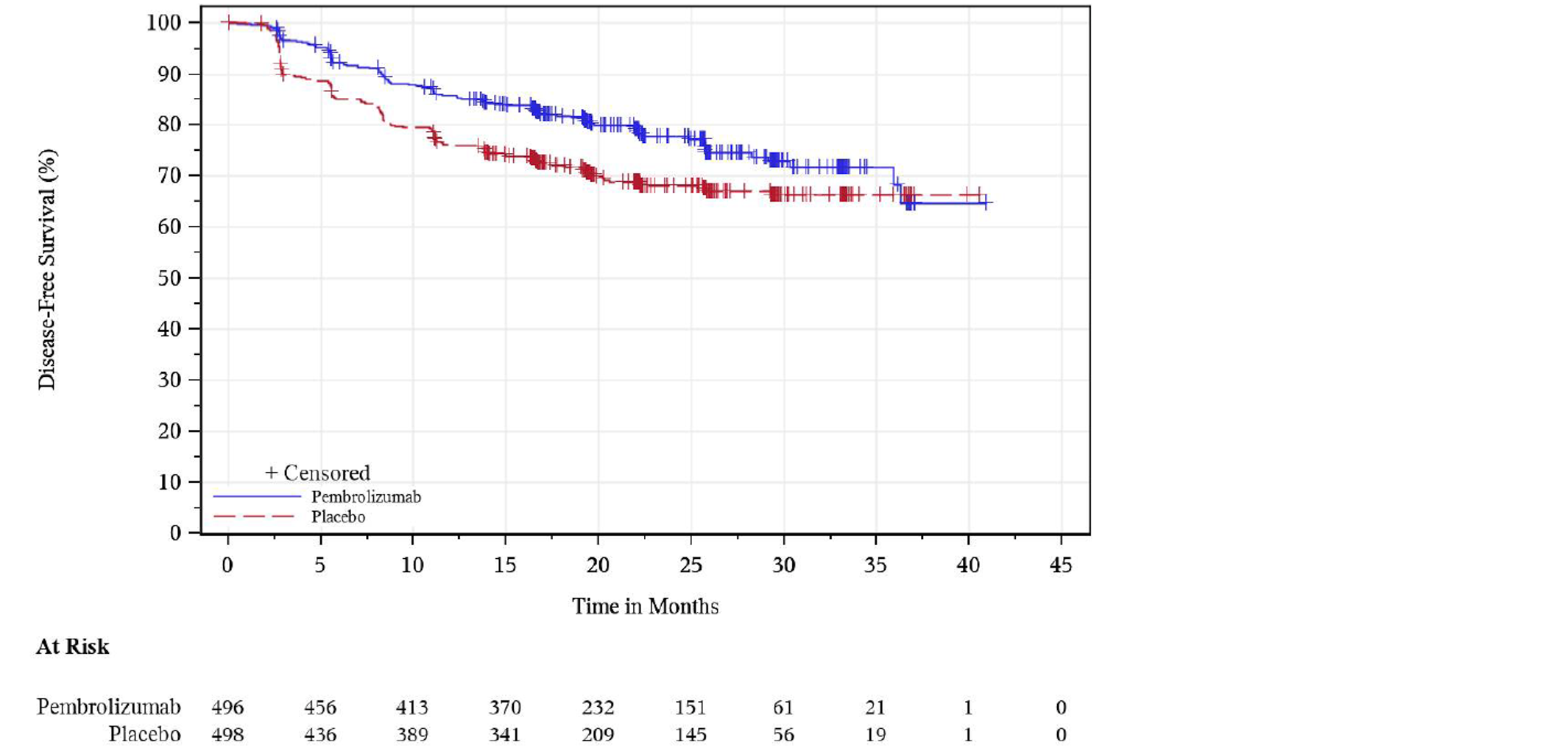
+ = censored observations; ITT = intention to treat.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Table 34: Sensitivity Analysis of Disease-Free Survival at IA1 (Sensitivity Analysis with Additional Stratum for Baseline Disease Status Based on BICR Review of Baseline Scan Only; ITT Population)
Disease-free survival | Pembrolizumab arm (n = 496) | Placebo arm (n = 498) |
|---|---|---|
Patients with events, n (%) | ||
Total | 109 (22.0) | 151 (30.3) |
Death | 6 (1.2) | 2 (0.4) |
Disease recurrence | 103 (20.8) | 149 (29.9) |
Censored, n (%) | 387 (78.0) | 347 (69.7) |
Last tumour assessment showing no disease recurrence | 375 (75.6) | 344 (69.1) |
No postbaseline disease status assessment | 12 (2.4) | 3 (0.6) |
DFS (months) | ||
Median (95% CI)a | NR (NR, NR) | NR (NR, NR) |
Q1, Q3 | 25.8, NR | 13.8, NR |
Hazard ratio (95% CI)b | 0.70 (0.54 to 0.89) | |
P valuec | 0.0021 | |
DFS rate (%) (95% CI) | ||
12 months | 85.7 (82.2 to 88.5) | 76.2 (72.2 to 79.7) |
18 months | 81.5 (77.7 to 84.8) | 71.9 (67.7 to 75.7) |
24 months | 77.3 (72.8 to 81.1) | 68.1 (63.5 to 72.2) |
BICR = blinded independent central review; CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; IA1 = first interim analysis; ITT = intention to treat; NR = not reached.
Notes: Analyses are based on primary censoring rule.
Database cut-off date: December 14, 2020.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by baseline disease status by BICR (NED by BICR vs. Non-NED by BICR), then within NED by BICR further stratified by randomization strata: M0 vs. M1 NED by investigator and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
cOne-sided P value based on log-rank test stratified by baseline disease status by BICR (NED by BICR vs. Non-NED by BICR), then within NED by BICR further stratified by randomization strata: M0 vs. M1 NED by investigator and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
Source: Clinical Study Report.12
Table 35: Sensitivity Analysis of Disease-Free Survival by BICR at IA1 (Sensitivity Analysis in Participants With Baseline Evidence of Disease [Non-NED] Based on BICR of Baseline Scan Only and Censored at Baseline; ITT Population)
Disease-free survival | Pembrolizumab arm (n = 496) | Placebo arm (n = 498) |
|---|---|---|
Patients with events, n (%) | ||
Total | 101 (20.4) | 129 (25.9) |
Death | 6 (1.2) | 1 (0.2) |
Disease Recurrence | 95 (19.2) | 128 (25.7) |
Censored, n (%) | 395 (79.6) | 369 (74.1) |
Censored at baseline | 19 (3.8) | 29 (5.8) |
Last tumour assessment showing no disease recurrence | 376 (75.8) | 340 (68.3) |
DFS (months) | ||
Median (95% CI)a | NR (NR, NR) | NR (NR, NR) |
Q1, Q3 | 30.2, NR | 16.6, NR |
Hazard ratio (95% CI)b | 0.73 (0.56 to 0.95) | |
P valuec | 0.0097 | |
DFS rate (%) (95% CI) | ||
12 months | 83.5 (79.8 to 86.6) | 76.5 (72.3 to 80.1) |
18 months | 80.0 (75.9 to 83.4) | 74.8 (70.5 to 78.5) |
24 months | 78.2 (74.0 to 81.9) | 70.4 (65.7 to 74.6) |
BICR = blinded independent central review; CI = confidence interval; DFS = disease-free survival; IA1 = first interim analysis; ITT = intention to treat; HR = hazard ratio; NR = not reached.
Notes: Baseline non-NED was assessed by BICR review of baseline scan only.
Database cut-off date was December 14, 2020.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
cOne-sided P value based on log-rank test stratified by metastasis status (M0 vs. M1 NED by investigator) and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
Source: Clinical Study Report.12
Figure 12: Kaplan-Meier Plot of Disease-Free Survival (Sensitivity Analysis in Participants With Baseline Evidence of Disease [Non-NED] Based on BICR of Baseline Scan Only and Censored at Baseline; ITT Population)
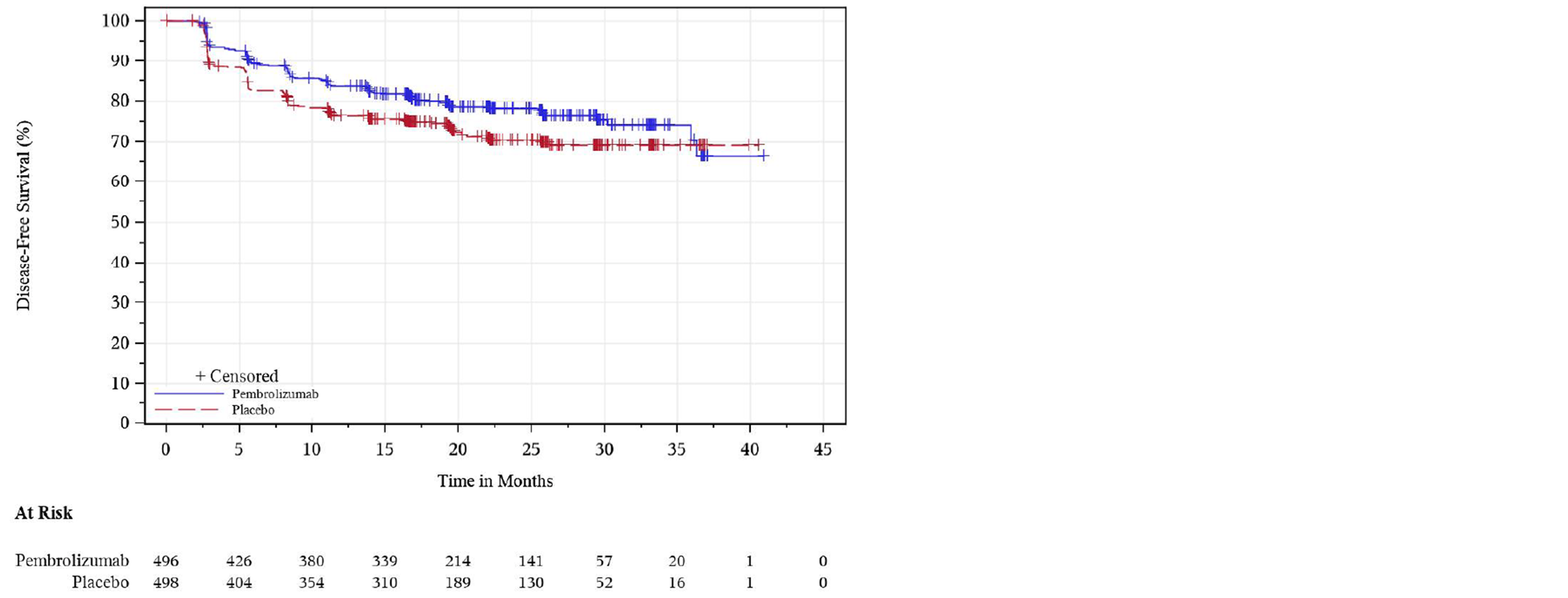
+ = censored observations; BICR = blinded independent central review; ITT = intention to treat.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Figure 13: Kaplan-Meier Plot of Event-Free Survival Based on BICR (Baseline Disease Status Based on BICR Review of Both Baseline and Postbaseline Scans) at IA1 — Full Analysis Set
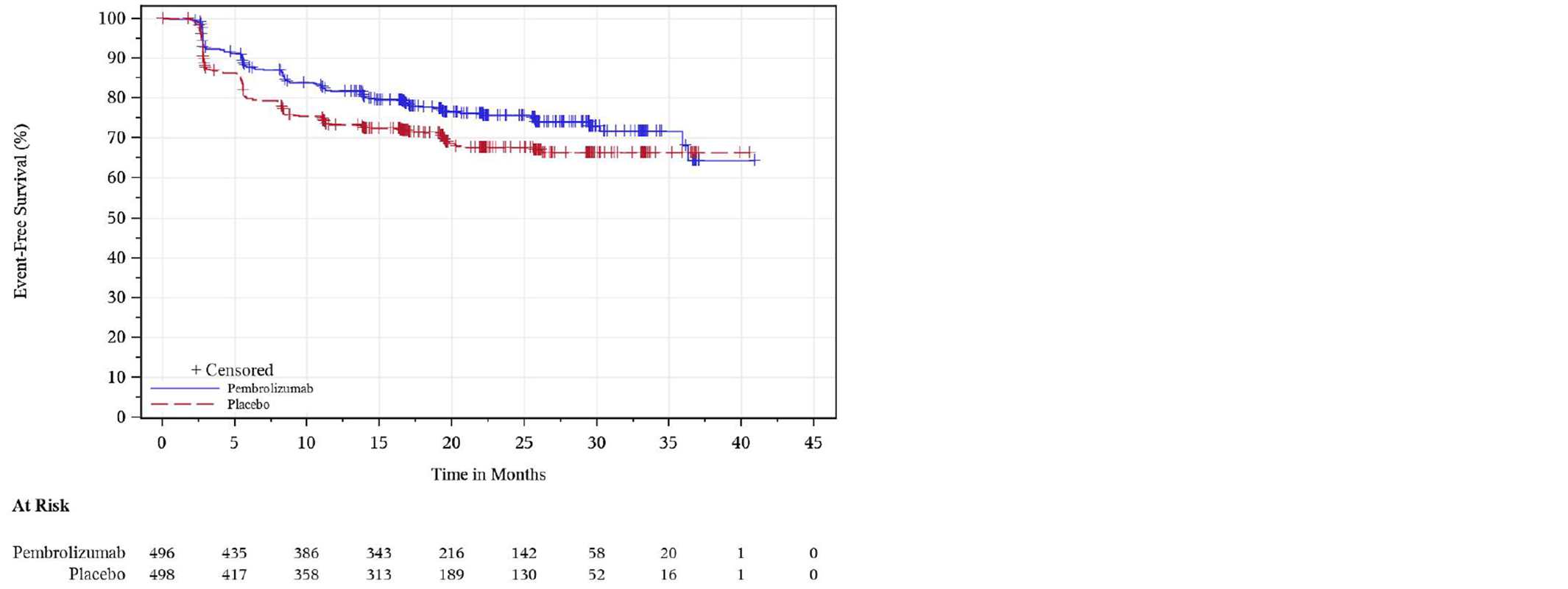
+ = censored observations; IA1 = first interim analysis.
Notes: For participants who were assessed to have baseline disease based on BICR review of both baseline and postbaseline scans, the date of disease progression is used as event date if it occurs.
Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Table 36: Event-Free Survival at IA1 Based on BICR (Baseline Disease Status Based on BICR Review of Both Baseline and Postbaseline Scans) — Efficacy Analysis Set (ITT Population)
Event-free survival | Pembrolizumab arm (n = 496) | Placebo arm (n = 498) |
|---|---|---|
Patients with events, n (%) | ||
Total | 116 (23.4) | 151 (30.3) |
Death | 7 (1.4) | 2 (0.4) |
Disease progression | 47 (9.5) | 74 (14.9) |
Disease recurrence | 62 (12.5) | 75 (15.1) |
Censored, n (%) | 380 (76.6) | 347 (69.7) |
Last tumour assessment showing no disease recurrence/progression | 368 (74.2) | 344 (69.1) |
No postbaseline disease status assessment | 12 (2.4) | 3 (0.6) |
EFS (months) | ||
Median (95% CI)a | NR (NR, NR) | NR (NR, NR) |
Q1, Q3 | 25.7, NR | 11.0, NR |
Hazard Ratio (95% CI)b | 0.83 (0.65 to 1.06) | |
P valuec | 0.0717 | |
EFS rate (%) (95% CI) | ||
12 months | 81.6 (77.8 to 84.8) | 73.2 (69.0 to 76.9) |
18 months | 77.7 (73.5 to 81.2) | 71.6 (67.3 to 75.4) |
24 months | 75.6 (71.3 to 79.4) | 67.6 (62.9 to 71.8) |
BICR = blinded independent central review; CI = confidence interval; EFS = event-free survival; HR = hazard ratio; IA1 = first interim analysis; ITT = intention to treat; NR = not reached.
Notes: For participants who were assessed to have baseline disease based on BICR review of both baseline and postbaseline scans, the date of disease progression is used as event date if it occurs.
Database cut-off date was December 14, 2020.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by baseline disease status by BICR (NED by BICR vs. Non-NED by BICR), then within NED by BICR further stratified by randomization strata: M0 vs. M1 NED by investigator and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
cOne-sided P value based on log-rank test stratified by baseline disease status by BICR (NED by BICR vs. Non-NED by BICR), then within NED by BICR further stratified by randomization strata: M0 vs. M1 NED by investigator and ECOG PS (0 vs. 1), US participant (Yes vs. No) within M0 group by investigator.
Source: Clinical Study Report.12
Table 37: Concordance of Disease Recurrence Assessments at IA1 (ITT Population)
Disease recurrence | Pembrolizumab arm (n = 496) | Placebo arm (n = 498) |
|---|---|---|
Investigator Assessment – Disease Recurred | 103 | 149 |
BICR Agreed | 84 (81.6) | 129 (86.6) |
BICR And Investigator Agreed on Time | 52 (50.5) | 86 (57.7) |
BICR Declared at Earlier Time | 32 (31.1) | 43 (28.9) |
BICR Disagreed | 19 (18.4) | 20 (13.4) |
Investigator Assessment – No Disease Recurred | 379 | 346 |
BICR Agreed | 351 (92.6) | 319 (92.2) |
BICR Disagreed | 28 (7.4) | 27 (7.8) |
No postbaseline assessment by investigator | 14 | 3 |
No BICR Assessment | 14 (100.0) | 3 (100.0) |
EDR | 0.184 | 0.134 |
LDR | 0.627 | 0.683 |
Difference in EDR (Pembrolizumab – Placebo) | 0.050 | |
Difference in LDR (Pembrolizumab – Placebo) | –0.056 | |
BICR = blinded independent central review; EDR = early discrepancy rate, calculated as BICR disagreed / (BICR agreed + BICR disagreed); IA1 = first interim analysis; ITT = intention to treat; LDR = late discrepancy rate, calculated as BICR declared at earlier time / (BICR declared at earlier time + BICR disagreed).
Notes: Number of participants with disease recurred, not recurred and no postbaseline assessments by investigator are used as the denominators for the percentage calculation for the corresponding block of rows.
Discrepancy on disease recurrence time is counted when more than 1 imaging assessment time point difference is observed.
A difference in EDR ≤ −0.05 or a difference in LDR > = 0.075 are suggestive of a systematic bias in the investigator assessment favouring the pembrolizumab arm.28
Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Table 38: Summary of Pathological Assessments for Disease Recurrence at IA1 (ITT Population)
Disease recurrence, n (%) | Pembrolizumab arm (n = 496) | Placebo arm (n = 498) | Total (n = 994) |
|---|---|---|---|
Disease recurrence by INV, with BICR agreed | 84 | 129 | 213 |
Determined by imaging without pathological confirmation | 68 (81.0) | 105 (81.4) | 173 (81.2) |
Determined by imaging first with subsequent pathological confirmation | 16 (19.0) | 20 (15.5) | 36 (16.9) |
Determined by pathological assessment first with subsequent imaging confirmation | 4 (3.1) | 4 (1.9) | |
Disease recurrence by INV, with BICR disagreed | 19 | 20 | 39 |
Determined by imaging without pathological confirmation | 16 (84.2) | 15 (75.0) | 31 (79.5) |
Determined by imaging first with subsequent pathological confirmation | 3 (15.8) | 4 (20.0) | 7 (17.9) |
Determined by pathological assessment without imaging confirmation | 1 (5.0) | 1 (2.6) | |
No disease recurrence by INV, with BICR disagreed | 28 | 27 | 55 |
Pathological assessment was taken with negative results by INV | 4 (14.3) | 1 (3.7) | 5 (9.1) |
BICR = blinded independent central review; IA1 = first interim analysis; ITT = intention to treat; INV = investigator assessment.
Notes: Pathological assessment of radiographic disease recurrence by investigator’s review is optional. Disease recurrence by BICR is determined by BICR of imaging alone, regardless of pathological assessment results.
Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Table 39: Analysis of Change From Baseline to Week 52 in PROs Defined as Exploratory End Points in KEYNOTE-564 Trial (EORTC QLQ-C30) — PRO FAS Population (IA1)
Treatment | Baseline | Week 52 | CFB to week 52 | Difference of CFB (pembrolizumab vs. placebo) | |||
|---|---|---|---|---|---|---|---|
N | Mean (SD) | N | Mean (SD) | N | LS Mean (95% CI)a | LSM CFB (95% CI)a P valuea | |
EORTC QLQ-C30- Nausea and Vomiting Symptom | |||||||
Pembrolizumab | 438 | 2.05 (7.54) | 301 | 3.10 (10.35) | 484 | 0.96 (–0.16 to 2.08) | –0.10 (–1.57 to 1.37) P = 0.8963 |
Placebo | 450 | 2.26 (8.99) | 325 | 3.18 (9.98) | 492 | 1.06 (–0.03 to 2.14) | |
EORTC QLQ-C30- Diarrhea Symptom | |||||||
Pembrolizumab | 438 | 4.34 (11.89) | 301 | 6 0.87 (16.24) | 484 | 3.38 (1.58 to 5.18) | 1.11 (–1.26 to 3.49) P = 0.3573 |
Placebo | 450 | 4.07 (11.37) | 325 | 6 0.56 (15.65) | 492 | 2.27 (0.52 to 4.01) | |
EQ-5D-5L VAS | |||||||
Pembrolizumab | 446 | 84.02 (13.97) | 301 | 80.75 (15.76) | 484 | –3.36 (–4.90 to –1.82) | –1.58 (–3.59 to 0.42) P = 0.1220 |
Placebo | 460 | 83.12 (14.63) | 327 | 82.52 (14.87) | 493 | –1.78 (–3.27 to –0.29) | |
CFB = change from baseline; CI = confidence interval; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; IA1 = first interim analysis; LSM = least squares mean; PRO = patient-reported outcome; SD = standard deviation; VAS = visual analogue scale.
Notes: For baseline and week 52, N is the number of patients in each treatment group with non-missing assessments at the specific time point; for change from baseline, N is the number of patients in the analysis population in each treatment group.
Database cut-off date: December 14, 2020.
aBased on a cLDA model with the PRO scores as the response variable with covariates for treatment by study visit interaction, stratification factors metastasis status (M0 vs. M1 NED), and within M0 group further stratified by ECOG PS (0 vs. 1) and US participant (Yes vs. No) as covariates.
Source: Clinical Study Report.12
Figure 14: LS Mean Change From Baseline to Week 52 and 95% CI in EORTC QLQ-C30 Global Health Status/QoL and Functional Scales (PRO FAS Population)
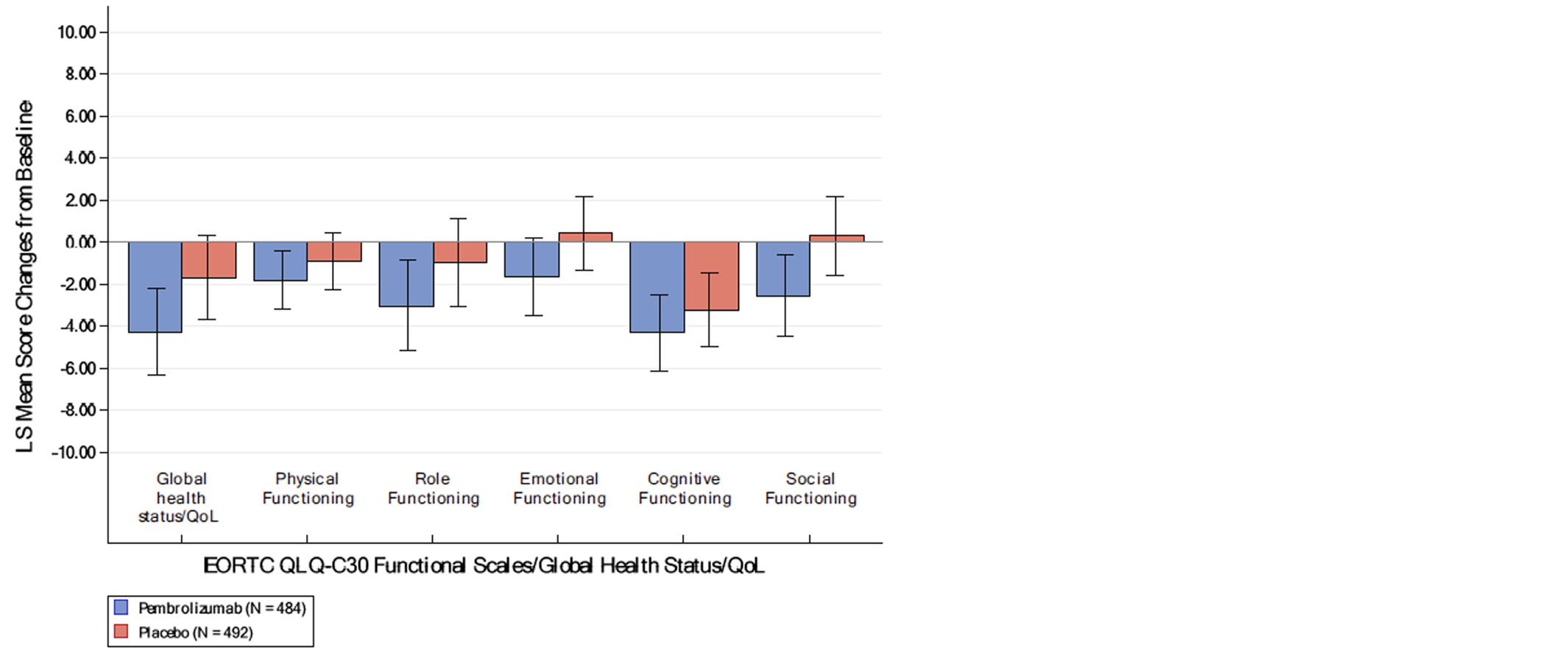
CI = confidence interval; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; PRO = patient-reported outcome; QoL = quality of life.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Figure 15: LS Mean Change From Baseline to Week 52 and 95% CI in EORTC QLQ-C30 Symptom Scales (PRO FAS Population)
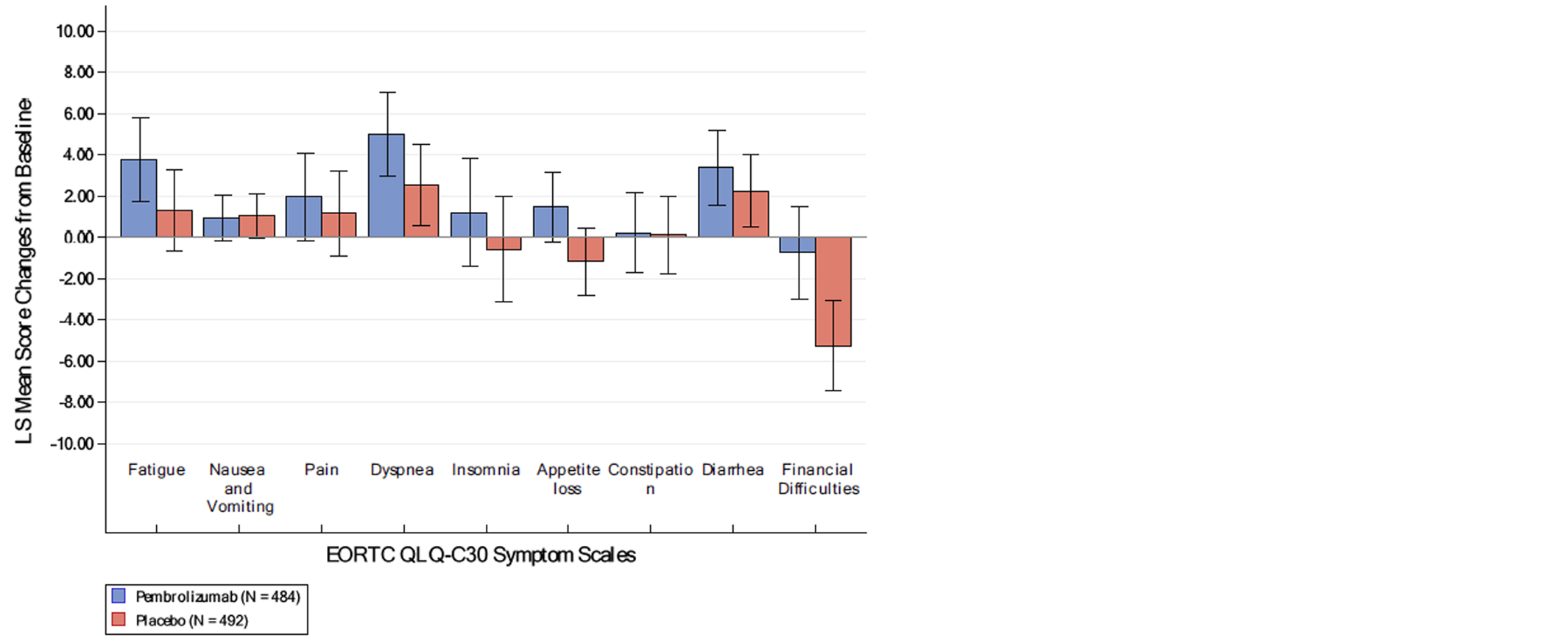
CI = confidence interval; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; PRO = patient-reported outcome; QoL = quality of life.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Table 40: Definition of Deterioration, Stability, Improvement, Stability Plus Improvement for the Analyses of PROs — EORTC QLQ-C30 Global Health Status/QoL, and Functional (Physical Functioning) Scale and FKSI-DRS
Parameter | EORTC QLQ-C30 global health status / QoL, and functional (physical functioning) scale definition | FKSI-DRS score definition |
|---|---|---|
Improvement | 10 points or more increase in score (in the positive direction) from baseline at any time during the study and confirmed by 10 points or more improvement at the next consecutive visit | A 3-points or more increase in score (in the positive direction) from baseline at any time during the study and confirmed by a 3- points or more improvement at the next consecutive visit |
Stability | When the criteria for improvement are not met, a less than 10 points worsening in score from baseline at any time during the study and confirmed by a less than 10 points worsening at the next consecutive visit | When the criteria for improvement are not met, a less than 3 points worsening in score from baseline at any time during the study and confirmed by a less than 3 points worsening at the next consecutive visit |
Stability + improvement | An improvement or less than 10 points worsening in score from baseline at any time during the trial and confirmed by an improvement or less than 10 points worsening in score at the next consecutive visit | An improvement or less than 3 points worsening in score from baseline at any time during the trial and confirmed by an improvement or less than 3 points worsening in score at the next consecutive visit |
Deterioration | When the criteria for improvement or stability are not met, a 10 points or greater worsening from baseline at any time during the study | When the criteria for improvement or stability are not met, a 3 points or greater worsening from baseline at any time during the study |
EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FKSI-DRS = Functional Assessment of Cancer Therapy Kidney Symptom Index - Disease-Related Symptoms; PRO = patient-reported outcome; QoL = quality of life.
Source: Clinical Study Report.12
Table 41: Overall Improvement and Stability Rate for PROs at IA1 (FKSI-DRS Score, EORTC QLQ-C30 Global Health Status, EORTC QLQ-C30 Physical Functioning) — PRO FAS Population
Summary | Pembrolizumab | Placebo | Pembrolizumab vs. placebo | |||||
|---|---|---|---|---|---|---|---|---|
N | % | 95% CIa | N | % | 95% CIa | Difference in % Improved (estimate, 95% CIb; P valuec) | Difference in % improved + stable (estimate, 95% CIb; P valuec) | |
FKSI-DRS Score | 483 | 100 | NA | 493 | 100 | NA | NA | NA |
Improved | 37 | 7.7 | 5.5 to 10.4 | 60 | 12.2 | 9.4 to 15.4 | –4.4 (–8.3 to –0.7) P = 0.0203c | –9.2 (–15.2 to –3.1) P = 0.0031 |
Stable | 238 | 49.3 | 44.7 to 53.8 | 266 | 54.0 | 49.4 to 58.4 | ||
Improved+ Stable | 275 | 56.9 | 52.4 to 61.4 | 326 | 66.1 | 61.8 to 70.3 | ||
Deteriorated | 148 | 30.6 | 26.6 to 35.0 | 114 | 23.1 | 19.5 to 27.1 | ||
No Assessment | 60 | 12.4 | 9.6 to 15.7 | 53 | 10.8 | 8.2 to 13.8 | ||
EORTC QLQ-C30 Global Health Status/QoL | 484 | 100 | NA | 493 | 100 | NA | NA | NA |
Improved | 51 | 10.5 | 7.9 to 13. 6 | 71 | 14.4 | 11.4 to 17.8 | –3.8 (–8.0 to 0.3) P = 0.0706 | –13.6 (–19.7 to –7.5) P < 0.0001 |
Stable | 206 | 42.6 | 38.1 to 47.1 | 258 | 52.3 | 47.8 to 56.8 | ||
Improved+ Stable | 257 | 53.1 | 48.5 to 57.6 | 329 | 66.7 | 62.4 to 70.9 | ||
Deteriorated | 169 | 34.9 | 30.7 to 39.3 | 114 | 23.1 | 19.5 to 27.1 | ||
No Assessment | 58 | 12.0 | 9.2 to 15.2 | 50 | 10.1 | 7.6 to 13.2 | ||
EORTC QLQ-C30 Physical Functioning | 484 | 100 | NA | 493 | 100 | NA | NA | NA |
Improved | 47 | 9.7 | 7.2 to 12.7 | 51 | 10.3 | 7.8 to 13.4 | –0.6 (–4.4 to 3.2) P = 0.7669 | –4.5 (–10.3 to 1.4) P = 0.1377 |
Stable | 263 | 54.3 | 49.8 to 58.8 | 287 | 58.2 | 53.7 to 62.6 | ||
Improved+ Stable | 310 | 64.0 | 59.6 to 68.3 | 338 | 68.6 | 64.3 to 72.6 | ||
Deteriorated | 116 | 24.0 | 20.2 to 28.0 | 105 | 21.3 | 17.8 to 25.2 | ||
No Assessment | 58 | 12.0 | 9.2 to 15.2 | 50 | 10.1 | 7.6 to 13.2 | ||
CI = confidence interval; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FKSI-DRS = Functional Assessment of Cancer Therapy Kidney Symptom Index–Disease-Related Symptoms; IA1 = first interim analysis; NA = not applicable.
Note: Database cut-off date: December 14, 2020.
aBased on binomial exact confidence interval method.
bBased on Miettinen and Nurminen method with population-based weighting stratified by metastasis status (M0 vs. M1 NED), and within M0 group further stratified by ECOG PS (0 vs. 1) and US participant (Yes vs. No).
cTwo-sided P value for testing. H0: difference in % = 0 vs. H1: difference in % does not equal 0.
Source: Clinical Study Report.12
Figure 16: Between-Treatment Comparisons in Adverse Events (≥ 10% Incidence) at IA1 (APaT Population)
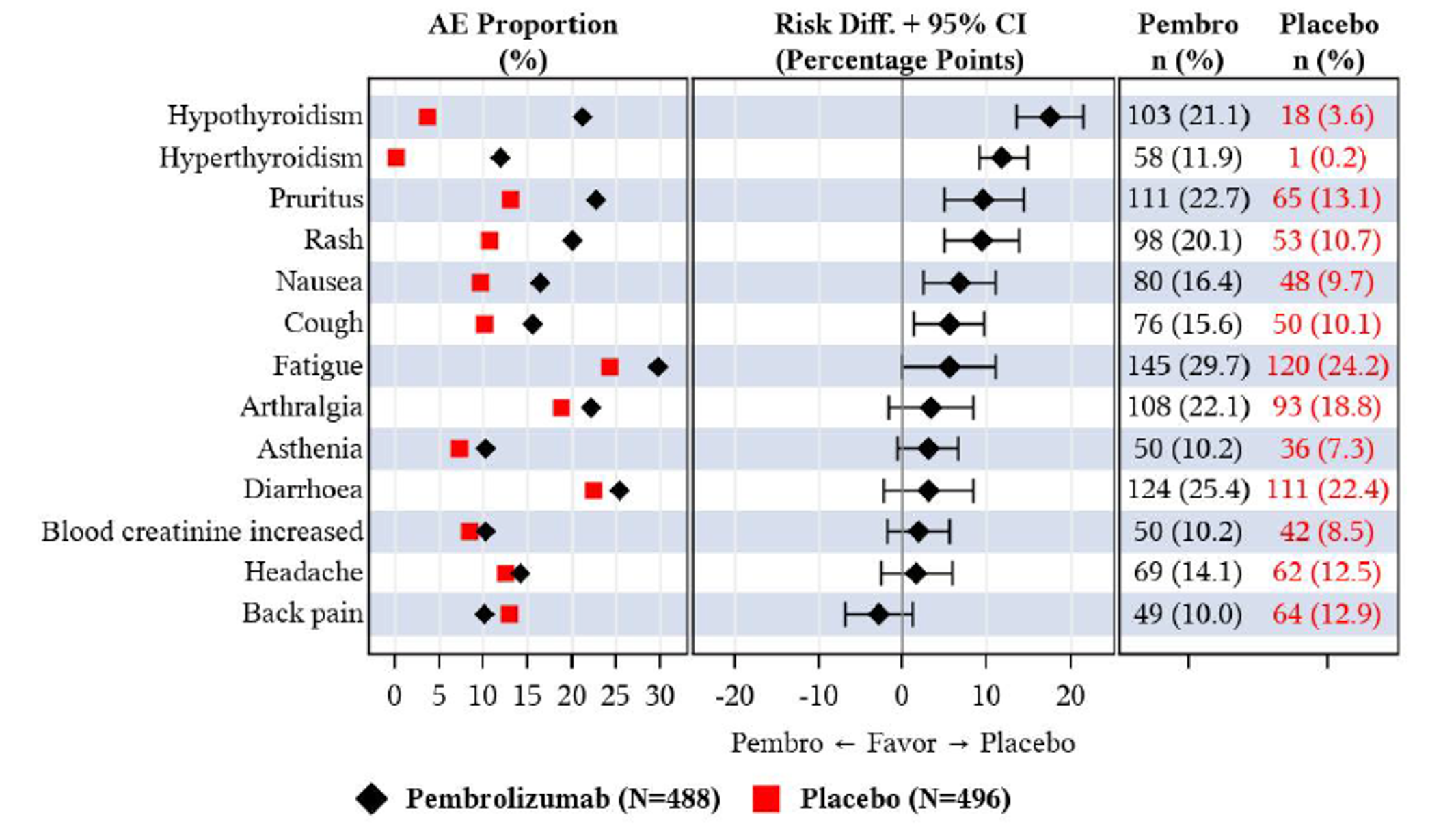
APaT = All Participants as Treated; IA1 = first interim analysis.
Note: Database cut-off date: December 14, 2020.
Source: Clinical Study Report.12
Appendix 4: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties including validity, reliability, responsiveness to change, and minimally important difference:
European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – Core 30 (EORTC QLQ-C30)
Functional Assessment of Cancer Therapy Kidney Cancer Symptom Index – Disease-Related Symptoms (FKSI-DRS)
5-Level EQ-5D 5 (EQ-5D-5L)
Findings
Table 42: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A 30-item, patient-reported, cancer-specific questionnaire used to assess change in HRQoL in response to treatment. The recall period is 1 week. Items are rated on a 4- or 7-point Likert scale. Raw scores are transformed onto a 0 to 100 scale. A higher score on the functional scale, the symptom scale and items, and the global health status/quality of life scale indicates a higher level of functioning, a higher level of symptomatology, and a higher level of quality of life, respectively.18,19,42 | Validity: Not identified for patients with RCC in the adjuvant setting. Reliability: Not identified for patients with RCC in the adjuvant setting. Responsiveness: Not identified for patients with RCC in the adjuvant setting. | Not identified for patients with RCC in the adjuvant setting. |
FKSI-DRS | A 9-item, kidney cancer-specific, patient-reported outcome measure used to assess disease-related symptoms. The recall period is 1 week. Items have 5 response options: “not at all,” “a little bit,” “somewhat,” “quite a bit,” “very much,” which correspond to scores ranging from 0 to 4. Total scores range from 0 (severely symptomatic) to 36 (asymptomatic).20,21,43,44 | The following psychometric properties are summarized for patients with RCC only and have not been identified for patients with RCC in the adjuvant setting. Validity: Evidence for convergent and discriminative validity was demonstrated by its strong correlations with FACT-G functional (r = 0.69 to 0.71) and physical (r = 0.84 to 0.85) domains and the ability to differentiate between patients categorized by known groups based on their ECOG PSR (P < 0.0001).20 Reliability: Evidence for internal consistency and test-retest reliability was demonstrated by the Cronbach alpha of 0.75 to 0.78 and intraclass correlation coefficient of 0.85, respectively.20 Responsiveness: Patients who self-rated as worsened, improved, or no change on the GRCS had worsened, improved, or no change scores on the FKSI-DRS, respectively (effect size was 0.60 to 1.40).20 | Estimated MIDs are reported for patients with (advanced and metastatic) RCC only and have not been identified for patients with RCC in the adjuvant setting. Estimated between-group MID: A more recent study estimated it to be a 0.62- or 1-point difference but given the weak correlations with the anchors used, the MID should be interpreted with caution (i.e., underestimated).44 An earlier study estimated the MID to be a 2- to 3-point difference. It was not explicitly stated whether the MID was in reference to between- or within-group.20 Studies determining the true MID were not identified. |
EQ-5D-5L | A generic instrument used to assess health status. It consists of a descriptive system and a VAS. Patients respond to each of the 5 dimensions in the descriptive system using 5 levels that best reflect their health state which are then converted into a single, country-specific index score. The VAS records the patient’s self-rated health on that day on a vertical VAS labelled with 0 (the worst health imaginable) and 100 (the best health imaginable).22,45,46 | Validity: Not identified for patients with RCC in the adjuvant setting. Reliability: Not identified for patients with RCC in the adjuvant setting. Responsiveness: Not identified for patients with RCC in the adjuvant setting. | Not identified for patients with RCC in the adjuvant setting. |
ECOG PSR = Eastern Cooperative Oncology Group Performance Status rating; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – Core 30; EQ-5D-5L = 5-Level EQ-5D; FACT-G = Functional Assessment of Cancer Therapy-General; FKSI-DRS = Functional Assessment of Cancer Therapy Kidney Cancer Symptom Index – Disease-Related Symptoms; GRCS = Global Rating of Change Scale; HRQoL = health-related quality of life; MID = minimally important difference; RCC = renal cell carcinoma; VAS = visual analogue scale.
European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – Core 30 (EORTC QLQ-C30)
The EORTC QLQ-C30 is 1 of the most commonly used instruments in oncology clinical trials.42 The questionnaire is a cancer-specific, multidimensional, patient-reported outcome measure used to assess change in HRQoL in response to treatment.18 The core questionnaire of the EORTC QLQ-C30 consists of 30 items (questions) that are scored to create 5 multi-item functional scales (physical, role, cognitive, emotional, and social), 3 multi-item symptom scales (fatigue, pain, nausea and vomiting), 6 single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial impact [these are symptoms commonly reported by patients with cancer]), and a global health status/quality of life scale.19 The recall period is 1 week.19 Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. For the 2 items that form the global health status/quality of life scale, the response format is a 7-point Likert-type scale, with anchors of 1 (very poor) to 7 (excellent).19 Raw scores for each scale are computed as the average of the items that contribute to a particular scale.19 Each raw scale score is converted to a standardized score that ranges from 0 to 100. A higher score on the functional scale, the symptom scale and items, and the global health status/quality of life scale indicates a higher level of functioning, a higher level of symptomatology, and a higher level of quality of life, respectively.19
No literature that assessed the validity, reliability, responsiveness to change, or the minimally important difference (MID) of EORTC QLQ-C30 in patients with RCC and in the adjuvant setting was identified.
Functional Assessment of Cancer Therapy Kidney Cancer Symptom Index–Disease-Related Symptoms (FKSI-DRS)
The FKSI-DRS is a kidney cancer-specific, patient-reported outcome measure used to assess disease-related symptoms.20 The questionnaire consists of 9 items (questions) that evaluate the symptoms of kidney cancer deemed to be the most important to monitor by patients and clinicians (lack of energy, pain, weight loss, bone pain, fatigue, shortness of breath, cough, fever, blood in urine), when treating advanced kidney cancer.20 The recall period is 1 week.43 All items on the questionnaire have 5 response options: “not at all,” “a little bit,” “somewhat,” “quite a bit,” “very much,” which correspond to scores ranging from 0 to 4.21 To compute the scale score, each item response first undergoes score reversal (i.e., a score of 0 indicates the most symptoms and 4 indicates the absence of symptoms). The sum of the reversed scores is then multiplied by 9 and divided by the number of items answered to give the total score, which can range from 0 (severely symptomatic) to 36 (asymptomatic).21,44
The following psychometric properties are summarized for patients with RCC only and have not been identified for patients with RCC in the adjuvant setting.
Cella et al. (2007)20 evaluated the psychometric properties of FKSI-DRS in 141 patients with advanced kidney cancer, of which 82.1% had a patient-rated Eastern Cooperative Oncology Group (ECOG) performance status rating of 0 to 1 at baseline and 34.0% were currently receiving therapy (not further specified by the authors). The mean age was 59.6 years (SD = 9.8), and the majority were male (67.4%) and White (98.6%). It should be noted that the data on the items that make up the FKSI-DRS were extracted from the validation study of the original Functional Assessment of Cancer Therapy Kidney Symptom Index-15 (FKSI-15) to assess the validity of FKSI-DRS.
Convergent validity of FKSI-DRS was assessed by measuring the strength of Spearman correlations with the Functional Assessment of Cancer Therapy-General (FACT-G) (a validated HRQoL instrument) subscales (Physical Well-Being, Social/family Well-Being, Emotional Well-Being, and Functional Well-Being).20 Strong correlations were observed between the FKSI-DRS and the functional (r = 0.69 to 0.71) and physical (r = 0.84 to 0.85) domains, while low-to-moderate correlations (r = 0.30 to 0.52) were observed between the FKSI-DRS and the emotional and social domains. These correlations were expected because the FKSI-DRS captures the physical symptoms of the disease. Based on cross-sectional analyses, the FKSI-DRS was able to differentiate between patients categorized by known groups based on their ECOG performance status rating (P < 0.0001), supporting the discriminant validity of FSKI-DRS.20
The Cronbach alpha was 0.75 to 0.78 and the intraclass correlation coefficient was 0.85, indicating the FKSI-DRS has an acceptable level of internal consistency and test-retest reliability between baseline and 3 to 7 days postbaseline, respectively.20
Evidence for responsiveness to change in clinical status (i.e., worse, same, or better) was assessed using the Global Rating of Change Scale (GRCS) as an anchor between baseline and 2 to 3 months postbaseline.20 The results supported its responsiveness to change; patients who self-rated as worsened, improved, or no change on the GRCS had worsened, improved, or no change scores on the FKSI-DRS, respectively. Further, the effect size was moderate-to-large (0.60 to 1.40).
Cella et al.20 estimated the MID to range from 4 to 5 points and 2 to 3 points using an anchor-based approach with the performance status rating and GRCS, respectively. A distribution-based approach was also used which estimated a broader range of MID between 1 to 3 points, with most estimates falling in the 2-to-3-point range. Based on these estimates, the investigators concluded that the most reasonable MID range was estimated to be 2 to 3 points but did not explicitly indicate if this is for between- or within-group difference.
Cella et al. (2018)44 further estimated the between-group MID using multiple anchor-based analyses with data from 2 separate phase III clinical studies that compared sunitinib with interferon alfa and axitinib with sorafenib in patients with clear cell metastatic RCC (n = 750 and n = 723, respectively). A 1-category difference in the FKSI item (“I am bothered by side effects of treatment”) score corresponded to a 1.20- or 1.26-point change in the FKSI-DRS (Pearson correlation coefficient [r] = 0.28 and 0.31, respectively); the item was thought to reflect a patient’s perception of their feelings and functioning. A 0.10-point decrease in the EQ-5D utility score corresponded to a 0.62- and 0.63-point decrease in the FKSI-DRS (r = 0.44 and 0.49, respectively). A 1-grade increase in the severity of the adverse event fatigue and asthenia corresponded to a 0.62- and 0.74-point decrease in the FKSI-DRS, respectively (r < 0.3). The investigators concluded that since a 0.1-point change in the EQ-5D utility score was considered clinically relevant, the estimated MID of FKSI-DRS was suggested to be 0.63 points. Further, a 1-point difference in the FKSI-DRS score between treatment groups was suggested to be potentially important when considering both the anchor- and distribution-based results.44 However, the results should be interpreted with caution due to the weak correlations which can underestimate the MID. Finally, the investigators suggested that the within-group MID will likely require a greater magnitude of change but was not assessed in the study. No studies determining the true within-group and between-group MID of FKSI-DRS were identified.
5-Level EQ-5D
The EQ-5D-5L is a generic, patient-reported outcome measure that is applicable to a wide range of health conditions and treatments used to assess health status.22,45,46 The instrument consists of a descriptive system questionnaire and the EQ VAS.22 The descriptive system comprises of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Patients respond to each dimension using 5 levels where 1 = no problems, 2 = slight problems, 3 = moderate problems, 4 = severe problems, and 5 = extreme problems or unable to perform. Respondents are asked to choose the level that reflects their health state. In terms of measurement properties, these are ordinal data; they do not have interval properties and therefore, are not used to produce an individual dimension score. Results from the EQ-5D-5L descriptive system can be converted into a single, country-specific index value using a scoring algorithm taking the local patient and population preferences into account.22 A health state index score of 0 represents the health state dead and 1.0 reflects perfect health. Negative scores are also possible for health states that society, not the patient, considers to be worse than dead. The EQ VAS records the respondent’s self-rated health on a vertical VAS where the end points are labelled 0 (the worst health imaginable) and 100 (the best health imaginable). Respondents are asked to mark an “X” on the scale that best represents their health on that day.22
No literature that assessed the validity, reliability, or responsiveness to change of EQ-5D-5L in patients with RCC and in the adjuvant setting was identified.
A Canadian-specific estimate of a MID for the EQ-5D-5L (descriptive system only) was generated by simulating the effects of single-level transitions in each dimension.47 The results yielded MIDs with a summarized mean of 0.056 (SD = 0.011), and a summarized median of 0.056 (interquartile range = 0.049 to 0.063). After exclusion of the maximum-valued scoring parameter (a single-level transition that results in a change in the index score that is larger than the estimate MID), the results yielded MIDs with a summarized mean of 0.037 (SD = 0.001), and a summarized median of 0.037 (interquartile range = 0.037 to 0.038). No literature that assessed the MID in patients with RCC and in the adjuvant setting was identified.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
DF
disease-free
DFS
disease-free survival
DM
distant metastasis
ICER
incremental cost-effectiveness ratio
IO
immunotherapy
LRR
locoregional recurrence
LY
life-year
OS
overall survival
QALY
quality-adjusted life-year
RCC
renal cell carcinoma
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), IV infusion, 100 mg/4 mL |
Submitted price | $4,400.00 per 100 mg/4 mL vial |
Indication | Adjuvant treatment of adult patients with RCC at intermediate-high or high risk of recurrence after nephrectomy or after nephrectomy and resection of metastatic lesions |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | August 18, 2022 |
Reimbursement request | Per indication |
Sponsor | Merck |
Submission history | Previously reviewed: Yes Pembrolizumab (Keytruda) has been reviewed by CADTH for multiple indications. The following indications were reviewed in 2020 and 2021: Indication: Esophageal carcinoma, gastroesophageal junction adenocarcinoma
Indication: Classical Hodgkin lymphoma
Indication: Metastatic or unresectable recurrent head and neck squamous cell carcinoma
Indication: Advanced RCC
|
NOC = Notice of Compliance; RCC = renal cell carcinoma.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult patients with RCC at intermediate-high or high risk of recurrence after nephrectomy or after nephrectomy and resection of metastatic lesions |
Treatment | Pembrolizumab |
Comparator | Routine surveillance alone |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (41.6 years) |
Key data source | KEYNOTE-564 trial |
Submitted results | ICER = $52,746 per QALY (incremental QALYs = 1.13; incremental costs = $59,526) |
Key limitations | DFS and OS data were not mature in both groups by the data cut-off date of June 14, 2021. The sponsor assumed a relationship between DFS and OS, based on a retrospective data study, but other studies in the literature did not find strong correlation between the 2 outcomes. Because the association between the 2 outcomes has not been established, it is uncertain whether benefits in DFS would translate into benefits in OS in actual practice. The sponsor assumed the benefit of pembrolizumab would be sustained indefinitely after 1 year of treatment in terms of DFS and OS. According to the clinical experts consulted by CADTH for this review and the sponsor’s analysis of the Kaplan–Meier curves, the effect of adjuvant pembrolizumab on long-term DFS or OS (especially after the 1-year treatment period) is uncertain for patients with intermediate-high or high-risk RCC. The submitted model did not consider the possibility of cure after nephrectomy, which is not aligned with the disease pathway, according to the clinical experts. The submitted model overestimated the survival of patients who experience distant metastasis. The sponsor applied RDI in the derivation of the costs for pembrolizumab and subsequent therapies, which is inappropriate because RDI can be influenced by many different factors. |
CADTH reanalysis results | CADTH undertook reanalyses to address limitations related to uncertainty about the persistence of treatment effect, lack of the possibility of cure after nephrectomy, underestimation of survival in patients who develop metastatic recurrence, and use of RDI. In the CADTH base case for the proposed Health Canada–indicated population, pembrolizumab was associated with an ICER of $93,053 compared with routine surveillance (incremental costs = $79,750; incremental QALYs = 0.86). For pembrolizumab to be cost-effective compared with routine surveillance at a willingness-to-pay threshold of $50,000 per QALY, a price reduction of 26% is required. |
DFS = disease-free survival; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year; RDI = relative dose intensity; RCC = renal cell carcinoma.
Conclusions
Based on an appraisal of the KEYNOTE-564 trial, treatment with adjuvant pembrolizumab may be associated with improved disease-free survival (DFS) in adult patients with intermediate-high or high-risk renal cell carcinoma (RCC) after nephrectomy or after nephrectomy and resection of metastatic lesions. Because of the relatively short duration of follow-up in this adjuvant setting study, neither DFS nor overall survival (OS) data were mature at the time of the data cut-off. Notable harms were higher in the pembrolizumab group than in the placebo group. Health-related quality of life assessments in the KEYNOTE-564 trial were considered uncertain in the CADTH clinical appraisal.
The cost-effectiveness of adjuvant pembrolizumab is contingent on long-term DFS and whether this translates into OS benefits. Although the sponsor provided data from a retrospective study to support the relationship between DFS and OS, other published studies suggest no strong correlation between the 2 outcome measures. The CADTH clinical review concluded that inferences regarding the efficacy of pembrolizumab on improved OS could not be made because of data immaturity at the time of the planned interim analysis. Another consideration is that OS benefit is intrinsically connected with eligibility for subsequent treatment options. Patients who develop distant metastasis (DM) within 18 months of starting adjuvant therapy with pembrolizumab will likely be ineligible for treatment with pembrolizumab and other immunotherapies in the metastatic setting. The impact of this ineligibility among patients with metastatic RCC is uncertain. Therefore, the uncertainty in the relationship between DFS and OS in the adjuvant setting is deemed highly relevant and needs to be considered in the context of its long-term implication in the metastatic setting.
CADTH identified several additional limitations in the economic analyses submitted by the sponsor. The key limitations addressed in CADTH’s reanalysis included incorporation of the treatment-effect waning assumption, a change in transition probability from the disease-free (DF) state to locoregional recurrence (LRR) and DMs to 0.0 after 10 years to reflect the possibility of a cure, adjustment of survival after the development of DM, and elimination of the use of relative dose intensity (RDI). These changes resulted in an incremental cost-effectiveness ratio (ICER) of $93,053 per quality-adjusted life-year (QALY) for adjuvant treatment with pembrolizumab, compared with routine surveillance (pembrolizumab is $79,750 more costly and yielded 0.86 more QALYs). Of note, the CADTH reanalysis still resulted in a survival benefit for adjuvant treatment with pembrolizumab (incremental life-years [LYs] = 0.95), which is uncertain given the current available evidence. A price reduction of 26% would be necessary to achieve an ICER of $50,000 per QALY. The cost-effectiveness of pembrolizumab was highly sensitive to different assumptions about treatment waning, as well as to the use of fixed versus weight-based dosing.
Additionally, feedback from clinical experts suggested that a sizable number of patients may not derive any survival benefit from adjuvant treatment at all, either because it is not effective or because it is not necessary. These patients will nevertheless incur the costs and adverse effects of pembrolizumab treatment, which could not be accurately estimated with the sponsor’s pharmacoeconomic model. Uncertainty about the long-term effectiveness of pembrolizumab may be resolved as data become available from the continued follow-up of patients in KEYNOTE-564.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from Kidney Cancer Canada, a national, nonprofit organization dedicated to helping patients with kidney cancer. Input from this group was based on responses to online surveys from 306 patients or caregivers in Canada and an interview with 1 patient. Patient input highlighted that most patients with localized RCC undergo either nephrectomy or partial nephrectomy. Patients noted that there are no currently available funded adjuvant therapy options in Canada for patients with RCC who undergo nephrectomy. Patient input indicated that a key concern after surgery was disease recurrence that would lead to a substantially shortened life expectancy. Most patients were seeking new treatments that would reduce the risk of recurrence by 40% to 50%. One patient had experience with pembrolizumab in the adjuvant setting and reported minor side effects (e.g., occasional rash, fatigue, hyperkalemia) that were easily manageable.
Clinician input was received from 2 groups: the Ontario Health Genitourinary Cancer Drug Advisory Committee and the Kidney Cancer Research Network of Canada. Clinician feedback highlighted the lack of adjuvant treatment options for RCC and that patients at the highest risk for disease recurrence have the greatest unmet needs for adjuvant therapy. Clinician input indicated that a clinically meaningful response includes improvement in DFS and/or improvement in OS. The ideal treatment would maintain a patient’s DF status and provide patients with normal life expectancy. Clinician input also highlighted that therapy administered in the adjuvant setting has a curative intent, with the objective of preventing disease recurrence to a more advanced stage. However, it was recognized that a significant proportion of patients with local or locoregional disease are cured with surgery alone, and that the use of pembrolizumab in patients at intermediate or high risk of recurrence after nephrectomy will likely result in unnecessary treatment of some patients. Finally, the use of pembrolizumab in the adjuvant setting could limit the use of other immunotherapies in subsequent treatment lines because patients who were treated with adjuvant pembrolizumab and then experience metastatic recurrence during treatment or within 6 months of treatment initiation would not likely be treated with pembrolizumab for metastatic disease as is current standard practice.
No drug plan input was received for this review.
Several of these concerns were addressed in the sponsor’s model:
DFS and OS outcomes were included in the model.
The model structure allowed for analysis of distinct eligibility criteria for pembrolizumab as a subsequent therapy, which was dependent on the time of disease progression.
In addition, CADTH addressed some of these concerns as follows:
CADTH modified the structure of the economic evaluation to reflect the curative intent of the adjuvant therapy.
Economic Review
The current review is for pembrolizumab (Keytruda) for treatment of adult patients with RCC at intermediate-high or high risk of recurrence after nephrectomy or after nephrectomy and resection of metastatic lesions.1
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of adjuvant pembrolizumab therapy after nephrectomy or after nephrectomy and resection of metastatic lesions in patients with RCC who have intermediate-high or high risk of recurrence or soft tissue metastases compared with routine surveillance alone (i.e., no adjuvant treatment). The model population comprised adult patients aged 18 years and older who had undergone nephrectomy or nephrectomy and resection of metastatic lesions for RCC and had intermediate-high or high risk of recurrence or soft tissue metastases, including both clear cell and non–clear cell subtypes, which is aligned with the Health Canada indication.
Pembrolizumab is available as a solution for infusion 100 mg/4 mL in a single-use vial. Pembrolizumab is administered intravenously for 30 minutes. The recommended dosage for pembrolizumab is 200 mg every 3 weeks or 400 mg every 6 weeks until unacceptable toxicity, disease progression, or for up to 12 months (17 doses for 200 mg or 9 doses for 400 mg).
At the submitted price of $4,400 per 4 mL vial, the standard cycle (28 days) cost of pembrolizumab was estimated to be $11,733, assuming 100% dose intensity. In the base case, the sponsor considered routine surveillance alone (i.e., no adjuvant treatment) as the comparator because there were no other treatments approved by Health Canada for adjuvant treatment of RCC.
Outcomes of the model included QALYs and LYs over a time horizon of 41.6 years. The base-case analysis was conducted from the perspective of the Canadian public health care system, with an annual discount rate of 1.5% applied to both costs and outcomes.
Model Structure
The sponsor submitted a Markov model with 4 mutually exclusive health states — DF, LRR, DM, and death — to track the disease course over time, with a weekly cycle length. A figure of the sponsor’s model structure is available in Appendix 3 (Figure 1).
All patients began in the DF health state, where they could remain or transition to the LRR or DM states. Patients in the LRR state could remain in this health state or transition to the DM state. Patients in the DM state could only transition to death. Patients in any health state could transition to death starting in the first cycle.
First-line therapy in the DM state for patients who received pembrolizumab was defined based on the time the transition to the DM state occurred. If patients transitioned before 18 months from adjuvant treatment initiation, they would be considered ineligible to receive the following immunotherapies (IOs): pembrolizumab plus axitinib or nivolumab plus ipilimumab. A second-line of systemic therapy for patients with DM was considered in the costs, but the transition probability from DM to death was assumed to be dependent on the first-line therapy.
Half-cycle correction was applied to costs and effectiveness, with the exception of costs and effectiveness parameters that occurred in the beginning of a cycle, including drug acquisition, administration costs, and adverse event costs, and adverse events disutility.
Model Inputs
The model’s baseline population characteristics and clinical efficacy parameters were characterized by the KEYNOTE-564 trial, a randomized, double-blind, placebo-controlled, multicentre phase III study designed to evaluate the efficacy of pembrolizumab as adjuvant therapy after nephrectomy compared with routine surveillance alone. The sponsor assumed that the KEYNOTE-564 population (baseline characteristics: mean age = 58.4 years; 29% female) reflected the Canadian population.
Transition probabilities were derived from a variety of data sources, including the KEYNOTE-564 trial, real-world retrospective data analysis, a network meta-analysis, Canadian life tables, and other studies in the literature. Data from the KEYNOTE-564 trial were used to model transitions from the DF health state to the LRR and DM health states. Mortality among those in the DF state was assumed to be equal to that of the general Canadian population.
A real-world retrospective database analysis was used to calculate transition probabilities from LRR to DM health states. For those in the LRR state, the probability of mortality was assumed to be the same as the probability of transition from DM to death observed in the KEYNOTE-564 trial.
The first-line therapy for patients who developed DM consisted in 2 distinct weighted “baskets” of therapies — eligible to receive the immunotherapies pembrolizumab plus axitinib or nivolumab plus ipilimumab (IO-eligible) and ineligible to receive pembrolizumab plus axitinib or nivolumab plus ipilimumab (IO-ineligible) — with the weights representing their market shares. The estimation of OS for each bucket was calculated as weighted average of expected OS associated with different first-line treatments. For first-line sunitinib, the estimates were based on results from a clinical trial, whereas hazard ratios for OS of other treatments versus sunitinib were estimated using a network meta-analysis.2 The market shares were estimated using Canada-specific market research data and clinician input.
Parametric survival modelling was used to derive the health state case-specific hazards of each transition, with survival distributions separately fitted to KEYNOTE-564 trial data for each treatment arm. The base-case parametric functions were selected based on visual inspection of fit, fit based on mean squared error, external validity, and clinical plausibility of long-term projections. A competing-risks approach was used to model transitions from the DF state. In the sponsor’s model, for each specific type of DF failure, the 2 competing failure types were treated as censored events. Survival distributions were then transformed into transition probabilities.
In the base-case analysis, pembrolizumab was assumed to have a persistent treatment effect, without waning in efficacy. In a scenario analysis, the model incorporated the possibility of a linear treatment-waning effect starting at year 7 after treatment initiation, assuming that the hazard of transitions from the DF state would be the same for the pembrolizumab and routine surveillance groups by year 10.
Adverse events (AEs) of grade 3 or higher that occurred in the KEYNOTE-564 trial at a frequency of more than 5% (all grades) were incorporated into the model with an associated cost and disutility. These were applied as a 1-time utility decrement in the first model cycle. The AEs observed in the metastatic setting were not included in the model.
Health state utility values for the base-case DF, LRR, and DM health states were derived from the KEYNOTE-564 trial, and other sources from the literature were used in the scenario analysis. In the base-case analysis, the utility for DM was not differentiated between the pre- versus post-progression substates because disease progression after DM is not identifiable within the KEYNOTE-564 trial data. All utility values are described in Table 11. Utility decrement for AEs were also sourced from the KEYNOTE-564 trial and incorporated as a single disutility in the first cycle.
Costs in the model included treatment-acquisition costs for adjuvant pembrolizumab and subsequent therapies, state-specific disease management, AE management, and terminal care costs. Dosing for adjuvant pembrolizumab therapy was derived from the IQVIA Delta PA database and was incorporated by multiplying the price per 200 mg per cycle ($8,800 per 200 mg) by the RDI of 98.9% (as reflected in the pembrolizumab arm of KEYNOTE-564) to account for any delays or interruptions in administration (e.g., those due to AEs).3 The proportion of patients remaining on adjuvant pembrolizumab at each scheduled infusion was based on the observed Kaplan–Meier curve for time to treatment discontinuation in the KEYNOTE-564 trial. The base-case analysis also incorporated the cost of administration of IV pembrolizumab, which was derived from the literature.4
Treatment costs for subsequent therapies were sourced from IQVIA Delta PA and the CADTH pan-Canadian Oncology Drug Review report for nivolumab plus ipilimumab in advanced RCC.3 Patients who had not progressed 18 months after the initiation of adjuvant pembrolizumab therapy could be re-treated with pembrolizumab upon progression (i.e., IO-eligible), whereas those who progressed less than 18 months after initiation could not (I.e., IO-ineligible). Costs of first- and second-line therapy after progression were included in the model, although OS was determined depending on the first-line therapy weighted basket used (i.e., IO-eligible or IO-ineligible). Drug acquisition and administration costs associated with subsequent therapies (including both first-line and second-line subsequent therapies) were applied as a 1-time cost upon entry into the DM state and were calculated in the model as a function of the unit drug cost, defined dosing schedule, and RDI for each drug.
Disease-management costs included those for routine monitoring and were based on published literature for the LRR and DM health states. Management costs in the DF state were based on a study by the sponsor using the frequencies of services from the Canadian Urological Association guidelines for the follow-up of patients after treatment of nonmetastatic RCC and the clinical expert’s input. Unit costs for these resource-use elements were obtained from the Ontario Schedule of Benefits and other studies in the literature.
The unit costs of AE management per episode were obtained from the Ontario Case Costing Initiative and a cost-of-illness study by Dranitsaris et al. (2005).5 Finally, patients who transitioned to death were assumed to incur a 1-time cost associated with palliative or terminal care, which was derived from the literature.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base case and 1,000 for scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented here.
Base-Case Results
In the sponsor’s base-case analysis, adjuvant treatment with pembrolizumab was associated with an ICER of $52,746 per QALY gained compared with routine surveillance. Almost all (97%) the incremental QALYs were estimated through extrapolation beyond the trial period (median = 29.7 months). The probability of pembrolizumab being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained was 49.5%.
The submitted analysis is based on the publicly available prices of all treatments, including subsequent therapies.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. routine surveillance ($/QALY) |
|---|---|---|---|---|---|
Routine surveillance | 225,549 | Reference | 11.91 | Reference | Reference |
Pembrolizumab | 285,075 | 59,526 | 13.04 | 1.13 | 52,746 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.
Sensitivity and Scenario Analysis Results
The sponsor conducted several sensitivity and scenario analyses. The scenario analysis included a shorter time horizon (30 years), considering a societal perspective, using alternate assumptions for efficacy and transition probabilities, assuming treatment efficacy waning, and alternate scenarios for subsequent treatment lines (i.e., limit costs to first-line therapy only and assume equal market shares for both treatment arms). Of note, the change in ICER was greatest when a treatment efficacy waning assumption (a linear treatment-waning effect starting at year 7 from adjuvant treatment initiation) was used (ICER = $91,569 per QALY).
In addition, the sponsor included a univariate sensitivity analysis with various discount rates (0%, 3%), efficacy and transition probabilities (± 20%), drug acquisition and administration costs (± 20%), disease-management costs (± 20%), AE-related costs (± 20%), and utilities. The drivers of change in ICER based on the sensitivity analysis were the variation in discount rate (3% resulted in an ICER of $70,112 per QALY) and variation in the exponential rates of transition probabilities from LRR to DM and from LRR to death states (low input value of –20% resulted in an ICER of $55,594 per QALY).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
Relationship between DFS and OS is uncertain: Neither the median DFS nor the median OS was reached in any of the groups by the data cut-off date (June 14, 2021). According to the CADTH clinical review, the hazard ratios estimated for comparing OS between pembrolizumab and placebo arms were considered interim when both analyses were presented. As information on OS in the trial was immature, the sponsor used a Markov model to predict long-term outcomes based on progression from the DF state. In the submitted model, patients treated with pembrolizumab accumulated an additional 2.59 LYs in the DF state, 70% of which were accrued between 10 and 30 years after adjuvant treatment. The sponsor-submitted model using DFS estimates as an intermediate outcome to predict OS, based on results from a retrospective analysis of 643 patients from the Surveillance, Epidemiology, and End Results (SEER) Medicare database (2007 to 2016), showed that each additional year of DFS was associated with 0.73 years of OS. This study was only available as a conference abstract. However, a meta-analysis assessing the 5-year relationship between DFS and OS in 13 trials that included patients with localized RCC showed only a modest correlation between the 2 estimates (R-square = 0.48; 95% CI, 0.14 to 0.67).6 Therefore, it is uncertain whether benefits in DFS translate into benefits in OS, or whether they merely delay the time to recurrence.
The OS benefit is also intrinsically connected to eligibility for subsequent treatment options. Patients who develop DM within 18 months of starting adjuvant therapy with pembrolizumab will likely to be ineligible for treatment with pembrolizumab and other immunotherapies in the metastatic setting, potentially leading to shorter survival. Therefore, the uncertainty in the relationship between DFS and OS in the adjuvant setting is deemed highly relevant and needs to be considered in the context of the long-term implications of pembrolizumab in the metastatic setting.
CADTH could not address this limitation because it is related to the immaturity of the data.
Waning of treatment effect: The sponsor’s DFS and OS extrapolations assume that the DFS and OS benefit of pembrolizumab is sustained up to 18 years after pembrolizumab is discontinued. According to the clinical experts consulted by CADTH for this review, the impact of adjuvant pembrolizumab on long-term DFS or OS, especially after the 1-year treatment period is completed, is unknown in patients with intermediate-high and high risk RCC. If the impact of pembrolizumab is not sustained after discontinuation, the separation in the DFS curves that is assumed within the sponsor’s base case (Figure 2) after adjuvant therapy initiation, may not be maintained up to 18 years after the completion of adjuvant therapy. This makes long-term extrapolation from the trial data challenging because the trial data do not capture long-term impacts for those who discontinue pembrolizumab (i.e., 100% of patients after 12 months). According to the clinical experts consulted by CADTH for this review, the trial findings appear favourable and clinically important, but the impact of adjuvant pembrolizumab on DFS and OS is uncertain. Although the experts felt that a benefit with pembrolizumab was plausible, the magnitude of such a benefit was uncertain in the absence of more robust evidence.
Given the above, assumptions related to continued treatment effects may have a substantial impact on the pharmacoeconomic results. An analysis of the sponsor’s submitted data for time to an event was performed by CADTH and is presented in Figure 3 (Appendix 3). In this figure, the line represents the relative risk of an event with pembrolizumab versus routine surveillance over 5-month periods based on the raw data from the clinical trial. Data shown in the figure are simply “1 – survival at time t + 1/survival at time t.” The data suggested a lower relative risk of events up to 20 months; after 20 months, the data showed limited relative effects. This suggests that pembrolizumab prevented disease progression in the first 20 months after treatment initiation; there was no evidence of a reduction in DFS beyond this period.
CADTH performed a reanalysis of the pharmacoeconomic model that considered these limitations and clinical expert opinion to address the uncertainty in long-term treatment effect. This reanalysis incorporated an assumption that the treatment effect of pembrolizumab would start to decrease after 2 years and be limited in time as of the first 4 years, as the submitted only allow changes using full-year increments.
CADTH conducted 2 scenario analyses that tested alternative waning-effect assumptions on the CADTH base case: the first assumed no long-term benefit with pembrolizumab, with waning effect starting at 1 year and completed at 3 years and the second assumed treatment effect with pembrolizumab would last longer, with waning starting only after 7 years and completed at 10 years.
The model structure does not appropriately capture the disease pathway: The Markov model assumes that patients will continuously progress to either LRR or DM health states. This assumption is not aligned with the disease pathway. Nephrotomy in patients with this stage of RCC has curative intent, and approximately 40% to 50% of patients never experience subsequent LRR or metastatic disease, according to the clinical experts consulted for this review and the literature.7
In addition, according to the clinical experts consulted by CADTH for this review, the probability of transition to the LRR and DM health states decreases as patients spend more time in the DF state, with very few patients (less than 1%) presenting with DM 10 years after surgery. The submitted pharmacoeconomic model did not reflect the curative intent of adjuvant treatment, as the probability of transitioning to another state is not dependent on how long the patient has spent in a given health state.
CADTH addressed this limitation by changing the probability of transition from DF to LRR and from DF to DM to 0 after 10 years. Consequently, after 10 years, patients in the DF state could only transition to death. These changes were intended to represent the possibility of cure, which is in line with the expected disease pathway, according to feedback from the clinical experts.
The probability of survival in DM state was overestimated: CADTH noted concerns about the model over the long-term survival of patients experiencing DM. In the sponsor’s model, survival at 2, 5, and 10 years after the development of DM was 66.5%, 36.2%, and 13.1%, respectively, for IO-ineligible patients, and 72.8%, 45.5%, and 20.7% for IO-eligible patients. CADTH noted that the literature suggests that OS is approximately 15% for patients with intermediate-risk metastatic RCC and 0% for patients with poor-risk metastatic RCC.8
CADTH weighted the probability of death from DM so that it replicated a conservative assumption of 5-year OS for 15% of IO-ineligible patients. The same weight was applied to the probability of death from DM in IO-eligible patients.
RDI: The sponsor’s base case incorporated reduced dose intensities for all therapies (i.e., for adjuvant and subsequent therapies). As with previous reviews, given the inability to link reduced dose intensity to outcomes, the CADTH base case does not incorporate reduced dose intensity. A reduction in RDI can be derived from a delayed dose, a missed dose, or a reduction in dose. When considering wastage, each component can have a very different influence on drug costs. Likewise, it is unclear how treatment discontinuation influences RDI.
CADTH used the functionality in the sponsor’s model to exclude RDI.
Weight-based dosing for pembrolizumab: Pembrolizumab dosing in KEYNOTE-564 was a fixed dose of 200 mg intravenously every 21 days. Input from participating public drug plans indicated that jurisdictions would likely implement a weight-based dose for pembrolizumab of 2 mg/kg (up to a cap of 200 mg) every 3 weeks, with the possibility of extended dosing intervals to every 6 weeks (4 mg/kg up to a 400 mg cap). The clinical experts agreed that this approach seemed reasonable, given the clear interchangeable use in dosing for other cancer sites. CADTH notes that weight-based dosing will reduce the ICER associated with pembrolizumab and give greater flexibility in dosing. However, CADTH noted that it is not possible to make the direct assumption that the use of weight-based dosing will lead to the same outcomes as a fixed dose, as exposure to a lower dose this may improve the AE profile, reducing the rate of discontinuation. This may, in turn, affect treatment efficacy. In the absence of any data on these outcomes, a scenario analysis was conducted that assumed equivalent efficacy but a lower treatment cost.
CADTH conducted a scenario analysis using weight-based dosing based on an average weight of 83.9 kg.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (see Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The sponsor assumed the exponential rate of transition between LRR and death was equal to the rate of transition between DF and death in the placebo arm of KEYNOTE-564. | Inappropriate. Patients who develop LRR have a better survival rate than patients who develop DM. The sponsor justified the assumption based on the low number of events observed during the KEYNOTE-564 trial. However, given the probabilities of transition from the LRR to DM state and from the LRR to death state were assumed to be the same in both groups, and that the costs incurred in each state were a 1-time cost, it is unlikely that this assumption would have greater implications for the incremental costs and QALYs. |
Health utility scores were assumed to be the same value for pre- and post-progression after disease metastases. | Acceptable as a simplifying assumption. |
Costs and disutilities related to AEs of grade 3 or higher with an incidence of at least 5% in the KEYNOTE-564 trial were included in the model. | Inappropriate. The sponsor selected an arbitrary threshold to capture the impact of treatment-related AEs, rather than selecting the most clinically meaningful AEs to include in the model. CADTH’s guidelines recommend that all AEs that have clinical or cost significance be included in the model. As noted in the CADTH clinical review, hyperthyroidism and hypothyroidism (all grades) were more common in patients who received pembrolizumab than routine surveillance (hyperthyroidism: 21.1% vs. 6.9% and hypothyroidism: 11.9% vs. 0.2%, respectively). The inclusion of only grade 3 or higher hyperthyroidism and hypothyroidism in the pharmacoeconomic model may underestimate the cost of treatment associated with these AEs, as additional visits to a health care provider and drug treatments may be required. Additionally, the AEs included in the sponsor’s model do not capture the range of AEs deemed to be of special interest to clinicians (i.e., type 1 diabetes mellitus) based on clinical expert input received by CADTH for this review. Although type 1 diabetes mellitus occurred in approximately 2% of patients in the pembrolizumab group, its consequences to both HRQoL and the cost of treatment are significant and lifelong. |
AE = adverse event; DF = disease-free; DM = distant metastasis; HRQoL = health-related quality of life; LRR = locoregional recurrence; QALY = quality-adjusted life-year; vs. = versus.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH’s reanalysis addressed several limitations within the economic model. The CADTH base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts. Table 5 details each change made to derive the CADTH-revised base case, which was conducted in a step-wise approach to highlight the impact of each change. The summary of results from the stepped reanalysis are presented in Table 6 and Table 13.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Treatment-waning effect | Persistent over time | Treatment waning starts at year 2 and was completed at year 4 |
2. Change in the probability of transition from DF to LRR and from DF to DM after 10 years | Used data from the model probabilities | Assumption the transition probabilities from DF to LRR and DF to DM were set to 0 after 10 years |
3. Change in the probability of survival within DM state | Used data from the KEYNOTE-564 trial to model probabilities | Given concerns about the overestimation of life expectancy assumed in DM states, CADTH adopted revised probabilities to reflect the current literature |
4. Change in RDI | Assumed reduced dose intensity with all therapies | Assumed full dose intensity with all therapies |
CADTH base case | — | 1 + 2 + 3 + 4 |
DF = disease-free; DM = distant metastasis; LRR = locoregional recurrence; RDI = relative dose intensity.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Routine surveillance | 225,571 | 11.89 | Reference |
Pembrolizumab | 286,456 | 13.08 | 51,522 | |
CADTH reanalysis 1: Waning of treatment effect | Routine surveillance | 225,571 | 11.89 | Reference |
Pembrolizumab | 312,571 | 12.50 | 142,363 | |
CADTH reanalysis 2: Probabilities of transition between DF to LRR and DF to DM | Routine surveillance | 185,073 | 12.45 | Reference |
Pembrolizumab | 246,103 | 13.65 | 50,781 | |
CADTH reanalysis 3: Survival in the DM state | Routine surveillance | 206,786 | 10.56 | Reference |
Pembrolizumab | 271,792 | 12.04 | 44,139 | |
CADTH reanalysis 4: RDI | Routine surveillance | 241,045 | 11.89 | Reference |
Pembrolizumab | 300,212 | 13.08 | 50,067 | |
CADTH base case: 1 + 2 + 3 + 4 | Routine surveillance | 182,912 | 11.34 | Ref. |
Pembrolizumab | 262,661 | 12.20 | 93,053 |
DF = disease-free; DM = distant metastasis; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; RDI = relative dose intensity.
Results of CADTH’s stepped analysis are presented in Table 7. CADTH’s base-case reanalysis demonstrated that, compared with routine surveillance, pembrolizumab was $79,750 more costly and yielded 0.86 more QALYs, resulting in an ICER of $93,053 per QALY (Table 7).
A treatment-waning effect starting 2 years after adjuvant treatment initiation led to 0.77 fewer QALYs for pembrolizumab and increased the total costs for pembrolizumab in comparison with sponsor’s submitted base case. All (100%) of the 0.72 incremental QALYs for pembrolizumab compared with routine surveillance occurred in the DF state. In the LRR and DM health state, 1.90 QALYs were accrued for pembrolizumab compared with 2.23 for routine surveillance (Table 11). At a $50,000 per QALY threshold, there is a 16.4% chance that pembrolizumab is cost-effective. In the CADTH base case, 92% of predicted QALYs were generated through extrapolation beyond the period of the available KEYNOTE-564 trial data (29.7 months).
Scenario Analysis Results
CADTH conducted price-reduction analyses based on the CADTH base case. These analyses demonstrated that a price reduction of 25.7% would be necessary to achieve cost-effectiveness at a willingness-to-pay threshold of $50,000 per QALY.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for pembrolizumab vs. routine surveillance | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 52,678 | 93,053 |
2.3% | 50,000 | 88,910 |
10% | 41,019 | 76,117 |
20% | 29,359 | 59,503 |
25.7% | 21,548 | 50,000 |
30% | 17,700 | 42,890 |
40% | 6,041 | 26,276 |
50% | Pembrolizumab dominates | 9,662 |
60% | Pembrolizumab dominates | Pembrolizumab dominates |
70% | Pembrolizumab dominates | Pembrolizumab dominates |
ICER = incremental cost-effectiveness ratio; vs. = versus.
In addition, CADTH conducted a series of exploratory analyses to determine the impact of alternative assumptions on the cost-effectiveness of adjuvant pembrolizumab, as follows:
treatment effect of pembrolizumab starts to wane at year 1 and ends at year 3
treatment effect of pembrolizumab starts to wane at year 7 and ends at year 10
weight-based dosing for pembrolizumab (100% vial sharing)
weight-based dosing for pembrolizumab (50% vial sharing).
CADTH considered 2 scenarios to address uncertainty regarding the duration of the marginal treatment effect beyond the trial’s observation period. In the first scenario, the ICER increased to $115,775 per QALY. In the second scenario, the ICER was $48,834 per QALY. These findings illustrate the centrality of the treatment-waning assumption to the estimated cost-effectiveness of adjuvant pembrolizumab in patients with RCC.
CADTH also considered 2 scenarios to address changes in the pembrolizumab dose: fixed dosing and weight-based dosing. In the first scenario, vial sharing was assumed to be 100%, resulting in an ICER of $74,168 per QALY, which reflected the reduction in incremental costs between strategies. When vial sharing was assumed to be 50%, the ICER was $83,869 per QALY.
Issues for Consideration
Assessment of time spent away from work for pembrolizumab infusion (administered every 3 or 6 weeks) was not included in the sponsor’s base case, although the perspective is required for submissions to CADTH. These costs were considered in a scenario analysis in the economic submission. In addition to productivity loss, travel costs are relevant for patients (and their families) who do not live near an infusion centre. Disparities in funding and treatment access may vary, depending on the province or territory, and the requirement for access to a centre where infusions can be performed may have equity-of-access implications that were not substantively considered in the economic submission.
It was noted by clinical experts that the prescription of pembrolizumab might require an assessment by an oncologist. Patients living in areas where there are no oncologists would incur substantive out-of-pocket cost to travel to specialist appointments.
Overall Conclusions
Based on an appraisal of the KEYNOTE-564 trial, CADTH’s clinical review found that adjuvant pembrolizumab may be associated with DFS benefits in adult patients with intermediate-high or high-risk RCC after nephrectomy or after nephrectomy and resection of metastatic lesions. However, it is important to note that, because of the relatively short duration of follow-up in this adjuvant setting study, neither DFS nor OS data were mature at the trial data cut-off date. This represents a limitation of this study, and CADTH considered the benefit of adjuvant pembrolizumab in improving OS in patients with RCC at intermediate-high or high risk of recurrence after nephrectomy or after nephrectomy and resection of metastatic lesions uncertain owing to data immaturity. Despite these limitations, the clinical experts consulted by CADTH noted that the findings appeared favourable and clinically important, while the CADTH clinical review found the KEYNOTE-564 study to be generalizable. Notable harms were higher in the pembrolizumab group than in the placebo group. However, the magnitude of effect of pembrolizumab on health-related quality of life of patients in the adjuvant setting is uncertain because of the lack of formal hypothesis testing, a possible violation of assumptions in the model applied to assess the data, and low attrition rates.
The cost-effectiveness of adjuvant pembrolizumab is contingent on long-term DFS, and whether this translates into OS benefits. Although the sponsor provided data from a retrospective study to indicate a link between DFS and OS, other studies in the literature indicated no strong correlation between the 2 outcome measures. The CADTH clinical review concluded that inferences regarding the efficacy of pembrolizumab on improved OS could not be made because of data immaturity at the time of the planned interim analysis. Therefore, longer-term evidence is required to validate OS for patients receiving pembrolizumab as adjuvant therapy. Another consideration is that OS benefit is intrinsically connected to eligibility for subsequent treatment options. Patients who develop DM within 18 months of starting adjuvant therapy with pembrolizumab will likely to be ineligible for treatment with pembrolizumab and other immunotherapies in the metastatic setting, potentially leading to shorter survival. Therefore, uncertainty about the relationship between DFS and OS in the adjuvant setting is deemed to be highly relevant and needs to be considered in the context of long-term implications in the metastatic setting. This lack of long-term evidence is particularly of note, given that 92% of estimated QALYs were generated in the post-trial period, for which there is no direct comparative evidence, and where different assumptions about the pattern of long-term efficacy exert a notable influence on incremental effectiveness.
CADTH identified several limitations in the economic analyses submitted by the sponsor, beyond uncertainty about the impact of pembrolizumab on long-term DFS and OS. These key limitations included uncertainty regarding persistence of treatment effect, lack of the possibility of cure after nephrotomy, underestimation of the survival of patients who develop metastatic recurrence, and use of RDI. CADTH conducted a reanalysis that incorporated a treatment-effect waning assumption, changed transition probabilities from the DF state to the LRR and DM state to 0 after 10 years to reflect the possibility of cure, adjusted survival after the development of DM, and eliminated the use of RDI. Based on the CADTH reanalysis, adjuvant treatment with pembrolizumab was $79,750 more costly and yielded 0.86 more QALYS, resulting in an ICER of $93,053 per QALY. A price reduction of 26% would be necessary to achieve an ICER of $50,000 per QALY.
Considering the limitations identified, and in alignment with clinical expert opinion, the reanalysis conducted by CADTH assumed that pembrolizumab would confer modest long-term DFS and corresponding OS benefits relative to active surveillance. As such, relative to the sponsor’s base case, the CADTH reanalysis resulted in a reduction in LY gains in patients in the DF state (2.56 versus 1.35 LY gains in DF state for the sponsor’s base case vs CADTH reanalysis, respectively). The cost-effectiveness of pembrolizumab varied significantly when more optimistic and more pessimistic treatment-effect waning assumptions were considered. In addition, results from additional scenario analyses indicated that the cost-effectiveness of pembrolizumab is sensitive when administration is changed from fixed to weight-based dosing.
The cost-effectiveness of adjuvant pembrolizumab compared with routine surveillance is heavily dependent on the assumption that immediate-term improvements in DFS are associated with long-term improvements in OS, and that the treatment effect of pembrolizumab persists for years after discontinuation. Neither of these assumptions was supported by evidence from the KEYNOTE-564 trial, adding considerable uncertainty to the cost-effectiveness results. Additionally, feedback from clinical experts suggested that a sizable number of patients may not derive any survival benefit at all from adjuvant treatment, either because it is not effective or because it is not necessary. These patients will nevertheless incur the costs and adverse effects of pembrolizumab treatment, which could not be accurately estimated from the sponsor’s pharmacoeconomic model. The uncertainty in the long term effectiveness of pembrolizumab may be resolved as data become available from continued follow-up of patients in the KEYNOTE-564 trial.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 200mg, intravenous infusion Kirkland (QC): Merck Canada; 2022 Mar 3.
2.Riaz IB, He H, Ryu AJ, et al. A living, interactive systematic review and network meta-analysis of first-line treatment of metastatic renal cell carcinoma. Eur Urol. 2021;80(6):712-723. PubMed
3.DeltaPA. Ottawa (ON): IQVIA; 2021: https://www.iqvia.com/. Accessed 2022 Mar 3.
4.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
5.Dranitsaris G, Maroun J, Shah A. Severe chemotherapy-induced diarrhea in patients with colorectal cancer: a cost of illness analysis. Support Care Cancer. 2005;13(5):318-324. PubMed
6.Harshman LC, Xie W, Moreira RB, et al. Evaluation of disease-free survival as an intermediate metric of overall survival in patients with localized renal cell carcinoma: a trial-level meta-analysis. Cancer. 2018;124(5):925-933. PubMed
7.Motzer RJ, Jonasch E, Agarwal N, et al. Kidney cancer, version 2.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2017;15(6):804-834. PubMed
8.Heng DY, Xie W, Regan MM, et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013;14(2):141-148. PubMed
9.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 200mg, intravenous infusion. Kirkland (QC): Merck Canada; 2022 Mar 3.
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Renal Cell Carcinoma at Intermediate-High or High Risk of Recurrence
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Cost per 28-day cyclea ($) |
|---|---|---|---|---|---|---|
Pembrolizumab (Keytruda) | 100 mg/4 mL | 100 mg | 4,400.0000b | 200 mg, every 3 weeks 400 mg, every 6 weeks | 419.05 | 11,733 |
aCost standardized to 28-day cycles to allow for comparison among regimens of different cycle lengths.
bSponsor’s submitted price.
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | See CADTH appraisal. The submitted model did not consider the possibility of cure, and the probability of survival within DM state was overestimated. |
Model structure is adequate for decision problem | No | See CADTH appraisal. The Markov model assumes that all patients will continuously progress to either LRR or DM states. This assumption is not aligned with the disease pathway, as nephrotomy at this stage of RCC has curative intent. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
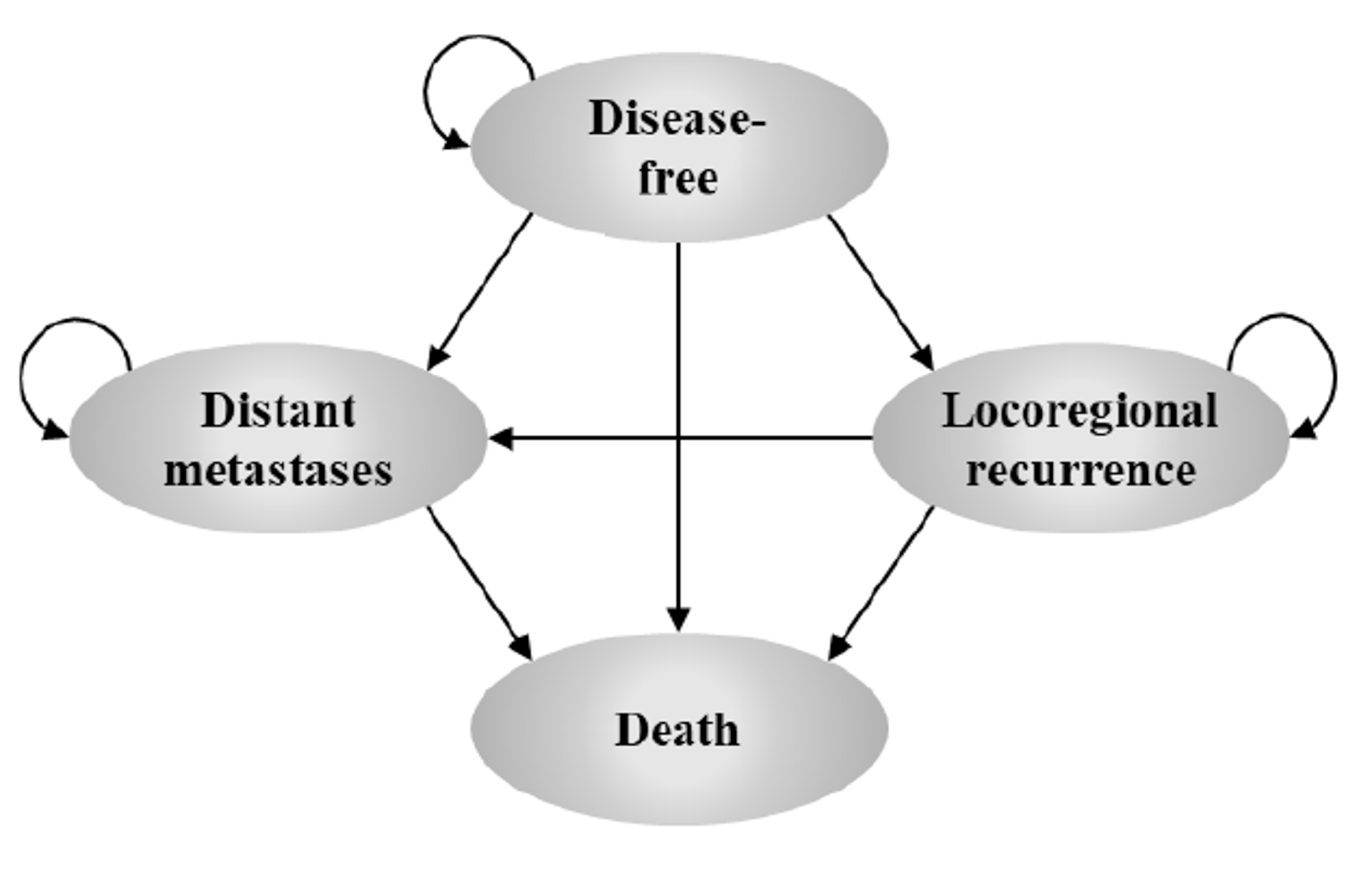
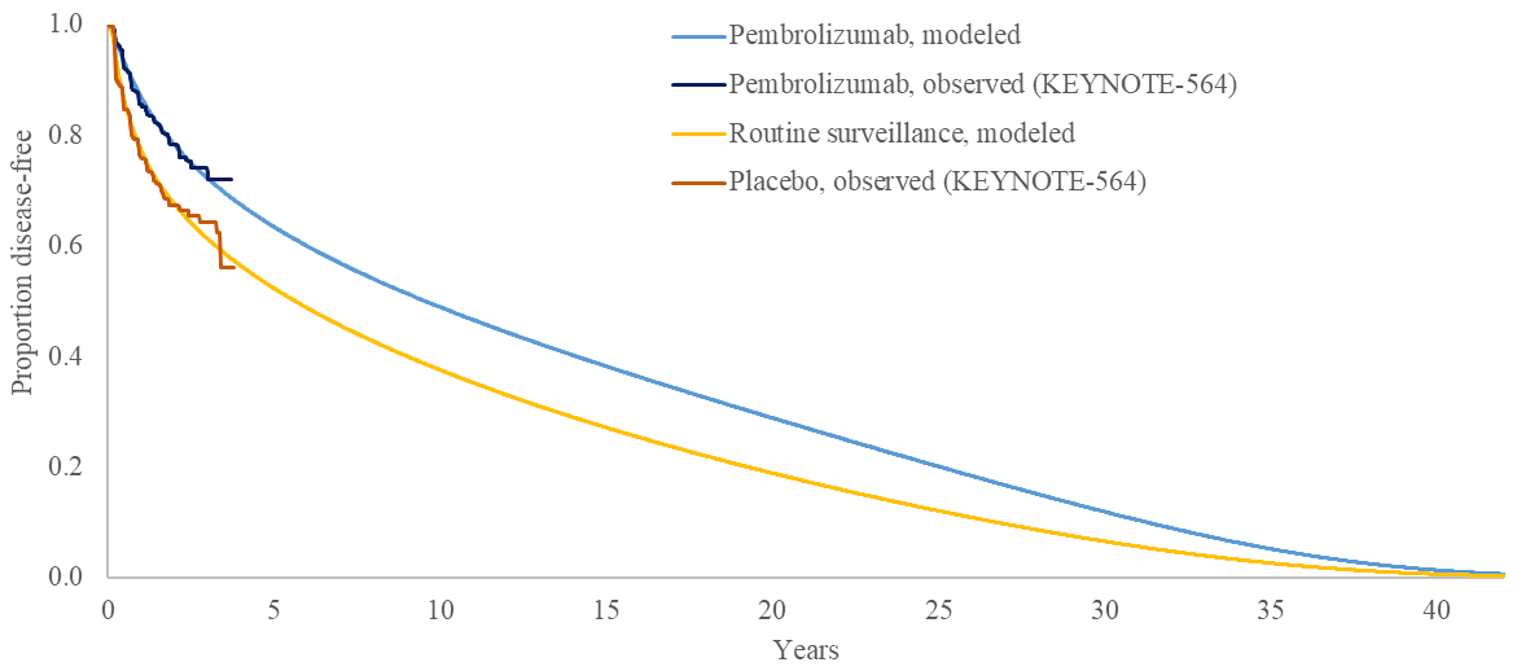
Figure 3: Relative Risk of Having an Event for Pembrolizumab in Comparison With Routine Surveillance
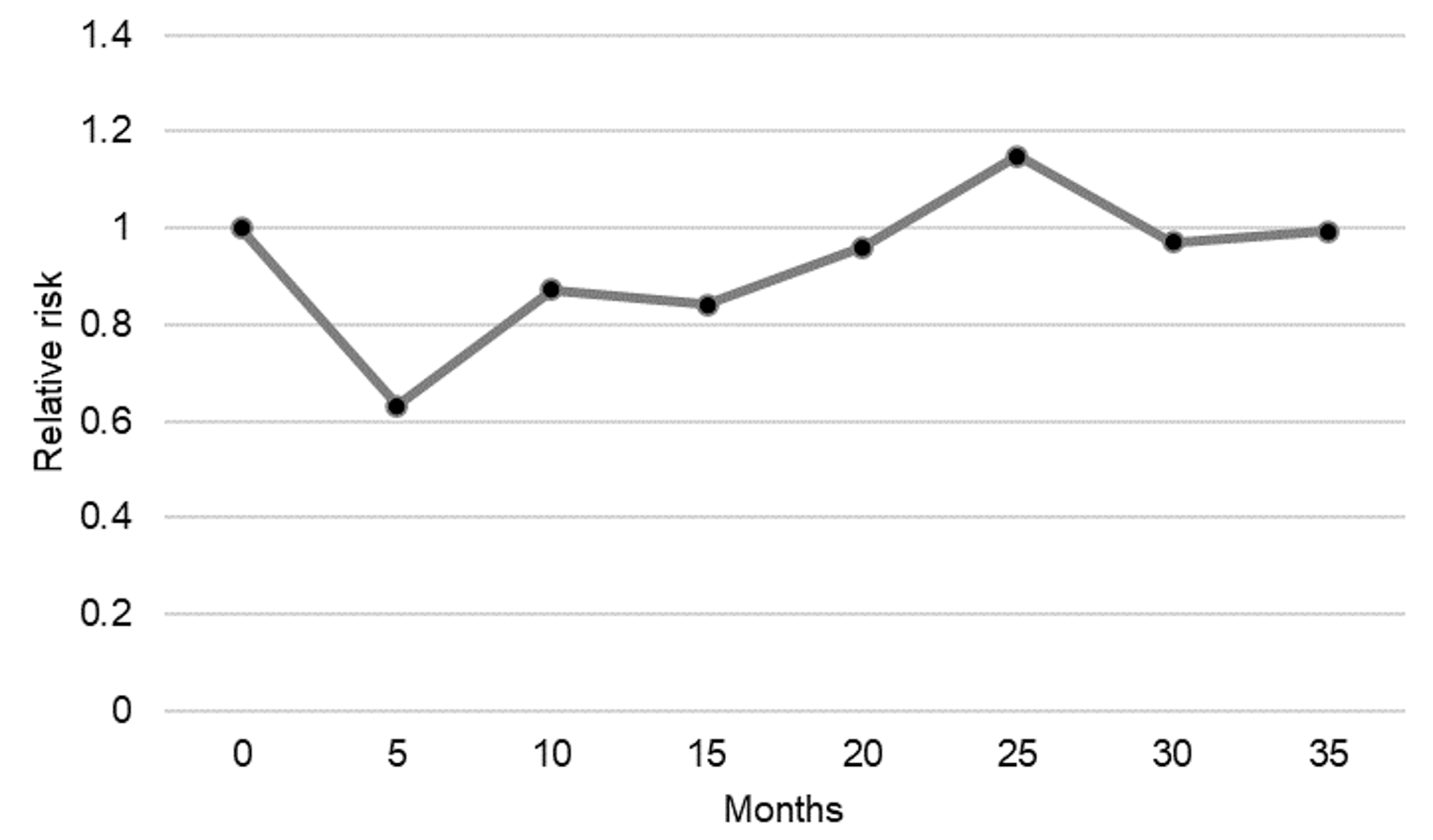
Note: An event was defined as experiencing one of the following: locoregional recurrence, distant metastatic recurrence, or death from any cause.
Source: CADTH calculation based on the KEYNOTE-564 trial.
Detailed Results of the Sponsor’s Base Case
Table 10: Data Sources and Sponsor’s Distribution Choices for Health State Transitions
TP | Transition | Data source | Sponsor’s selected survival distribution |
|---|---|---|---|
TP1 | DF to LRR | KEYNOTE-564 | Exponential |
TP2 | DF to DM | KEYNOTE-564 | Generalized gamma |
TP3 | DF to death | Canadian life tables | NA |
TP4 | LRR to DM | Patient-level analysis of SEER-Medicare database | Exponential |
TP5 | LRR to death | KEYNOTE-564 | Exponential |
TP6 | DM to death | KEYNOTE-426 + NMA | Exponential |
DM = distant metastatic; DF = disease-free; LRR = locoregional recurrence; NMA = network meta-analysis; NA = not applicable.
Source: Sponsor’s pharmacoeconomic submission.1
Table 11: Health State Utility Values
Health state | Sponsor’s base case utility value |
|---|---|
Disease-free | 0.887 (KEYNOTE-564) |
Local/regional recurrence | 0.868 (KEYNOTE-564) |
Distant metastatic (pre-progression) | 0.840 (KEYNOTE-564) |
Distant metastatic (post-progression) |
Source: Sponsor’s pharmacoeconomic submission.1
Table 12: Disaggregated Summary of Sponsor’s Economic Evaluation Results (Probabilistic)
Parameter | Pembrolizumab | Routine surveillance | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 14.88 | 13.66 | 1.22 |
By health state | |||
DF | 11.12 | 8.56 | 2.56 |
LRR | 0.81 | 1.29 | –0.49 |
DM | 2.96 | 3.81 | –0.85 |
Discounted QALYs | |||
Total | 13.04 | 11.91 | 1.13 |
By health state | |||
DF | 9.86 | 7.59 | 2.27 |
LRR | 0.70 | 1.12 | –0.42 |
DM | 2.48 | 3.20 | –0.71 |
By time period | |||
During trial period (up to 4 years) | 3.27 | 3.23 | 0.04 |
Beyond trial period (after 4 years) | 9.77 | 8.68 | 1.09 |
Discounted costs ($) | |||
Total | 285,075 | 225,549 | 59,526.28 |
DF | 125,358 | 3,745 | 121,612.65 |
LRR | 702 | 1,122 | –420.28 |
DM | 146,885 | 206,100 | –59,215.10 |
Death | 12,130 | 14,581 | –2,450.99 |
Adjuvant treatment costs | 120,382 | 0 | 120,382 |
Drug acquisition cost | 117,462 | 0 | 117,462 |
Drug administration cost | 2,920 | 0 | 2,920 |
Subsequent treatment costs | 110,639 | 159,432 | 110,639 |
Drug acquisition cost | 109,220 | 157,054 | 109,220 |
Drug administration cost | 1,420 | 2,378 | 1,420 |
AEs costs | 634 | 303 | 634 |
Disease-management costs | 41,290 | 51,232 | 41,290 |
DF | 4,342 | 3,442 | 4,342 |
LRR | 702 | 1,122 | 702 |
DM | 36,246 | 46,668 | 36,246 |
Terminal care costs | 12,130 | 14,581 | 12,130 |
ICER ($/QALY) | 52,746 | ||
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results (Probabilistic)
Parameter | Pembrolizumab | Routine surveillance | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 13.86 | 12.90 | 0.95 |
By health state | |||
DF | 11.58 | 10.23 | 1.35 |
LRR | 0.76 | 0.85 | –0.09 |
DM | 1.51 | 1.83 | –0.31 |
Discounted QALYs | |||
Total | 12.20 | 11.34 | 0.86 |
By health state | |||
DF | 10.27 | 9.07 | 1.20 |
LRR | 0.66 | 0.74 | –0.08 |
DM | 1.27 | 1.53 | –0.26 |
By time period | |||
During trial period (up to 4 years) | 3.19 | 3.13 | 0.06 |
Beyond trial period (after 4 years) | 9.01 | 8.21 | 0.79 |
Discounted costs ($) | |||
Total | 262,661 | 182,912 | 79,750 |
DF | 126,898 | 4,279 | 122,619 |
LRR | 651 | 725 | –74 |
DM | 123,998 | 165,452 | –41,453 |
Death | 11,114 | 12,456 | –1,343 |
Adjuvant treatment costs | 121,774 | 0 | 121,774 |
Drug acquisition cost | 118,854 | 0 | 118,854 |
Drug administration cost | 2,920 | 0 | 2,920 |
Subsequent treatment costs | 105,454 | 143,038 | –37,583 |
Drug acquisition cost | 104,275 | 141,093 | –36,818 |
Drug administration cost | 1,180 | 1,945 | –765 |
AEs costs | 634 | 303 | 331 |
Disease-management costs | 23,685 | 27,115 | –3,430 |
DF | 4,490 | 3,976 | 514 |
LRR | 651 | 725 | –74 |
DM | 18,544 | 22,414 | –3,870 |
Terminal care costs | 11,114 | 12,456 | –1,343 |
ICER ($/QALY) | 93,053 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Stepped analysis | Comparator | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH’s base case | Routine surveillance | 182,912 | 11.34 | Reference |
Pembrolizumab | 262,661 | 12.20 | 93,053 | |
CADTH scenario 1: Treatment effect of pembrolizumab starts to wane at year 1 | Routine surveillance | 182,912 | 11.34 | Reference |
Pembrolizumab | 265,825 | 12.06 | 115,775 | |
CADTH scenario 2: Treatment effect of pembrolizumab starts to wane at year 7 | Routine surveillance | 182,912 | 11.34 | Reference |
Pembrolizumab | 248,513 | 12.69 | 48,834 | |
CADTH scenario 3: Weight-based dosing for pembrolizumab (100% vial sharing) | Routine surveillance | 175,410 | 11.34 | Reference |
Pembrolizumab | 238,974 | 12.20 | 74,168 | |
CADTH scenario 4: Weight-based dosing for pembrolizumab (50% vial sharing) | Routine surveillance | 178,599 | 11.34 | Reference |
Pembrolizumab | 250,477 | 12.20 | 83,869 |
Appendix 5: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) estimating the budget impact of introducing pembrolizumab as adjuvant treatment of adult patients with RCC at intermediate-high or high risk of recurrence following nephrectomy or following nephrectomy and resection of metastatic lesions.9 The BIA base case was undertaken from a publicly funded drug plan perspective considering only drug costs over a 3-year time horizon. Costs included that of adjuvant therapy and first-line treatments used among patients who progress. Pembrolizumab costs were calculated by incorporating a RDI of 0.99 and were based on the duration of pembrolizumab therapy, and increase in DFS, estimated data from KEYNOTE-564 trial. Costs of first-line subsequent therapies were included as all patients who entered this state were assumed to receive a systemic treatment for metastatic RCC. The market shares for subsequent treatments were dependent on whether patients received pembrolizumab adjuvant or routine surveillance alone, and, whether they recurred within 18 months after starting adjuvant therapy. Patients who had received pembrolizumab and had a recurrence within 18 months, could not receive it as first-line therapy in the distant metastatic setting; those who had recurrence after 18 months or were in the routine surveillance alone group could. The sponsor estimates that pembrolizumab will reach a market share of ||||% after 3 years. The sponsor also assumed that 10% of patients would be participating on clinical trials.
The analytic framework, which used an epidemiology-based approach, leveraged data from multiple sources in the literature and assumptions based on clinical expert input to determine the estimated population size (Figure 4). The sponsor compared a reference scenario where pembrolizumab is not reimbursed as adjuvant therapy, with a new drug scenario, where pembrolizumab is funded as adjuvant therapy as per the Health Canada indication. Treatments available in the reference included routine surveillance alone, which was assumed to consist of no active treatment, and treatments for recurrence. Key inputs to the BIA are documented in Table 16.
Figure 4: Sponsor’s Estimation of the Size of the Eligible Population
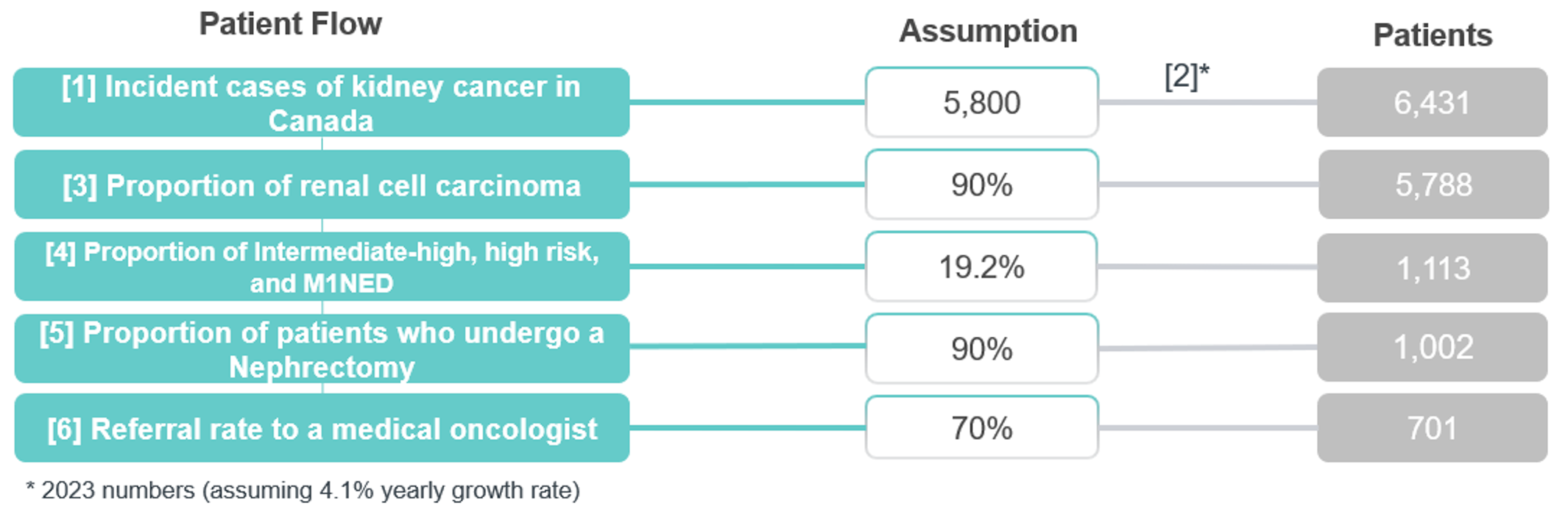
Source: Sponsor’s budget impact submission.8
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 701 / 730 / 760 |
Market uptake (3 years) | |
Uptake (reference scenario) Routine surveillance Clinical trials | 90% / 90% / 90% 10% / 10% / 10% |
Uptake (new drug scenario) Pembrolizumab Routine surveillance Clinical trials | ||||% / ||||% / ||||% ||||% / ||||% / ||||% ||||% / ||||% / ||||% |
Cost of treatment (per patient) | |
Cost of treatment over 21-days cycle Pembrolizumab Routine surveillance Clinical trials | $8,703.20 $0 $0 |
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding pembrolizumab as for adjuvant treatment of adult patients with RCC at intermediate-high or high risk of recurrence following nephrectomy or following nephrectomy and resection of metastatic lesions was $5,080,096, $25,018,568, $40,774,291 for Year 1, 2, and 3, respectively. The 3-year total was $70,872,955.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The sponsor’s assumption regarding patient enrolment in clinical trials as a comparator is uncertain: The sponsor assumed that 10% of patients were enrolled in clinical trials and as a result received trial medications – not incurring treatment/ drug costs. This artificially decreases the estimated market size, omitting treatment costs incurred by patients in clinical trials and underestimating the budget impact. Likewise, if pembrolizumab was approved this may decrease clinical trial use as patients may forego an effective therapy to be placed on the trial. Clinical experts consulted for this review noted that patient enrolment in clinical trials can vary significantly by province.
In CADTH reanalysis, clinical trials were removed from the market mix; the market share of clinical trials was re-distributed over other comparators.
The sponsor’s assumption regarding referral rate to medical oncologist may be underestimated: The sponsor assumed that 70% of patients would be referred to a medical oncologist. According with clinical experts consulted for this review, if pembrolizumab is funded, it would be expected that the vast majority of patients would be referred to a medical oncologist to discuss the option of adjuvant treatment with pembrolizumab.
In CADTH reanalysis, the referral rate was changed to 90% based on clinical expert opinion.
The market uptake for pembrolizumab is uncertain: In their BIA, the sponsor estimated that 15% of patients would have pembrolizumab prescribed in the first year, and ||||% in the third year. According to the clinical experts consulted for this review, there is some uncertainty regarding final uptake percentages among all clinicians in Canada, given that oncologists have experience prescribing pembrolizumab.
CADTH performed a scenario analysis to explore the uncertainty in market uptake, with market uptake rates starting from 30% in the first year, reaching 60% in year 2.
Weight-based dosing for pembrolizumab: Pembrolizumab dosing in KEYNOTE-564 was a fixed dose of 200 mg intravenously every 21 days. After consultation, CADTH notes that in line with other indications for pembrolizumab, jurisdictions would likely implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks with the possibility of extended dosing intervals of every 6 weeks (4 mg/kg up to a 400 mg cap). The clinical experts agreed that this approach seemed reasonable, given the interchangeable use in dosing for other cancer sites.
CADTH assumed pembrolizumab would be provided using a weight-based dosing based on an average weight of 83.9 kg. A scenario analysis was conducted using a fixed dose as per the KEYNOTE-564 trial.
Use of RDI is inappropriate: The sponsor’s base case incorporates reduced dose intensities for all therapies (i.e., adjuvant and subsequent therapies). Consistent with previous reviews, given the inability to link reduced dose intensity with outcomes, the CADTH base case does not incorporate reduced dose intensity. CADTH notes RDI estimates derived from the trial apply to a fixed based dose and therefore would not be applicable to a weight-based dose.
CADTH uses the functionality within the sponsor’s model to exclude reduced dose intensity.
Budget impact of patients diagnosed in years 1 to 3 not fully captured: To provide a more exact estimate over 3 years the sponsor assumed those diagnosed with intermediate-high and high risk RCC would be spread evenly over the year. Although CADTH’s base case noted that 977 patients are diagnosed in the final year of the analysis, full adjuvant costs will only be captured for those diagnosed in the first week (as costs are incurred over a year). Although this approach potentially provides a more accurate estimate of costs that are incurred in a 3-year period the analysis omits a substantial impact on the budget that will be incurred in year 4. Likewise, this approach makes the BIA more complex and difficult to validate.
Given complexities in the sponsor’s modelling approach CADTH conducted a scenario analysis which estimated the full neoadjuvant/adjuvant costs for all incident patients diagnosed in years 1 to 3. To calculate this budget impact CADTH assumed in the new drug scenario: 902, 938 and 977 patients would be diagnosed in years 1 to 3, respectively. In year 1, 15% (135 patients) would receive pembrolizumab, in year 2 45% (422 patients) would receive pembrolizumab and in year 3 60% (586 patients) would receive pembrolizumab. The rest would remain in routine surveillance. In the reference scenario, CADTH assumes 100% of patients in all years were under routine surveillance.
The total cost of adjuvant therapy, using a fixed dose, was taken from the sponsor’s cost-utility analysis,1 and was estimated to be $118,854 for those receiving pembrolizumab. The cost of routine surveillance was considered to be 0.
For simplicity, CADTH considered that subsequent therapy costs would remain the same as in the CADTH’s base-case analysis.
Additional limitations were identified but were not considered to be key limitations. These limitations include:
NIHB population was not submitted although subsequent treatment includes drugs funded by NIHB: Subsequent treatments include drugs funded by NIHB. Therefore, the NIHB population should have been submitted to demonstrate the expected budget impact introduced by funding the drug under review.
CADTH Reanalyses of the BIA
CADTH’s base case revised the proportion of patients on clinical trials, market uptake, RDI, and assumed a weight-based dosing for pembrolizumab.
Table 17: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Proportion of patients on clinical trials | 10% | 0% |
2. Referral rate | 70% | 90% |
3. Use of RDI | Yes | No |
4. Weight base dosage | Fixed dose of 200 mg every 3 weeks or 400 every 6 weeks | Dosage of 2 mg/kg every 3 weeks (or 4 mg/kg every 6 weeks) considering mean weight of 83.9 kg based on KEYNOTE-564 trial, with no wastage |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 | |
RDI = relative dose intensity.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19.
Based on the BIA base case, the expected budget impact for funding pembrolizumab for the treatment of pembrolizumab for adjuvant intermediate-high and high risk RCC is expected to be in $5,473,403 in Year 1, $26,671,665 in Year 2, and $42,802,218 in Year 3, with a 3-year budget impact of $74,947,286.
Table 18: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $70,872,955 |
CADTH reanalysis 1 | $70,555,248 |
CADTH reanalysis 2 | $91,122,371 |
CADTH reanalysis 3 | $70,773,653 |
CADTH reanalysis 4 | $58,170,221 |
CADTH base case | $74,947,286 |
BIA = budget impact analysis.
Table 19: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Routine surveillance | $3,424,848 | $17,548,841 | $32,936,025 | $45,914,368 | $96,399,234 |
Pembrolizumab | $3,424,848 | $22,606,164 | $57,842,441 | $86,505,878 | $166,954,482 | |
Budget impact | $0 | $5,080,096 | $25,018,568 | $40,774,291 | $70,872,955 | |
CADTH reanalysis 1 | Routine surveillance | $3,424,848 | $17,548,841 | $32,936,025 | $45,914,368 | $96,399,234 |
Pembrolizumab | $3,424,848 | $22,606,164 | $57,842,441 | $86,505,878 | $166,954,482 | |
Budget impact | $0 | $5,057,323 | $24,906,416 | $40,591,509 | $70,555,248 | |
CADTH reanalysis 2 | Routine surveillance | $4,403,376 | $22,562,795 | $42,346,318 | $59,032,759 | $123,941,872 |
Pembrolizumab | $4,403,376 | $29,065,068 | $74,368,852 | $111,221,843 | $214,655,763 | |
Budget impact | $0 | $6,502,273 | $32,022,535 | $52,189,083 | $90,713,891 | |
CADTH reanalysis 3 | Routine surveillance | $3,756,466 | $19,274,310 | $36,199,438 | $50,538,174 | $106,011,923 |
Pembrolizumab | $3,756,466 | $24,376,467 | $61,245,012 | $91,164,097 | $176,785,575 | |
Budget impact | $0 | $5,102,157 | $25,045,574 | $40,625,922 | $70,773,653 | |
CADTH reanalysis 4 | Routine surveillance | $3,224,631 | $16,417,827 | $30,765,556 | $42,990,950 | $90,174,333 |
Pembrolizumab | $3,224,631 | $20,638,700 | $51,408,946 | $76,296,908 | $148,344,554 | |
Budget impact | $0 | $4,220,874 | $20,643,390 | $33,305,958 | $58,170,221 | |
CADTH base case (1 + 2 + 3 + 4) | Routine surveillance | $4,558,199 | $23,247,331 | $43,598,461 | $61,012,799 | $127,858,591 |
Pembrolizumab | $4,558,199 | $28,720,734 | $70,270,126 | $103,815,017 | $202,805,877 | |
Budget impact | $0 | $5,473,403 | $26,671,665 | $42,802,218 | $74,947,286 |
BIA = budget impact analysis.
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 20:
Alternative market uptake (30% / 60% / 60%).
Consider wastage at 50%.
Fixed pembrolizumab dose of 200 mg every 3 weeks (400 mg every 6 weeks) using the sponsor provided option to do so.
Incidence of RCC to occur at the beginning of each year using CADTH calculations.
Results of CADTH’s scenario analyses demonstrate that the estimated budget impact is highly sensitive to the changes in dosing and wastage. CADTH notes that scenario analysis 4 indicates that the current analysis does not account for a substantial amount of budget impact that will occur in year 4. It was unclear whether this increase was due entirely to the timing of when individuals were diagnosed due to the complexity in the sponsor’s model.
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
CADTH’s base case | Routine surveillance | $4,558,199 | $23,247,331 | $43,598,461 | $61,012,799 | $127,858,591 |
Pembrolizumab | $4,558,199 | $28,720,734 | $70,270,126 | $103,815,017 | $202,805,877 | |
Budget impact | $0 | $5,473,403 | $26,671,665 | $42,802,218 | $74,947,286 | |
CADTH scenario 1: alternative market uptake (30% / 60% / 60%) | Routine surveillance | $4,558,199 | $23,247,331 | $43,598,461 | $61,012,799 | $127,858,591 |
Pembrolizumab | $4,558,199 | $33,927,142 | $85,252,333 | $103,055,766 | $222,235,241 | |
Budget impact | $0 | $10,679,811 | $41,653,871 | $42,042,966 | $94,376,649 | |
CADTH scenario 2: wastage 50% | Routine surveillance | $4,693,970 | $24,014,293 | $45,070,298 | $62,995,226 | $136,079,817 |
Pembrolizumab | $4,693,970 | $30,030,953 | $74,506,857 | $110,512,999 | $215,050,809 | |
Budget impact | $0 | $6,016,660 | $29,436,559 | $47,517,773 | $82,970,991 | |
CADTH scenario 3: fixed pembrolizumab dose | Routine surveillance | $4,829,742 | $24,781,256 | $46,542,135 | $64,977,653 | $136,301,043 |
Pembrolizumab | $4,829,742 | $31,341,172 | $78,743,587 | $117,210,981 | $227,295,740 | |
Budget impact | $0 | $6,559,916 | $32,201,452 | $52,233,329 | $90,994,697 | |
CADTH scenario 4: incidence of cases to occur at start of each year | Routine surveillance | $4,829,742 | $24,781,256 | $46,542,135 | $64,977,653 | $136,301,043 |
Pembrolizumab | $4,829,742 | $46,450,410 | $123,415,922 | $176,963,086 | $346,829,418 | |
Budget impact | $0 | $21,557,566 | $76,664,211 | $111,692,842 | $210,528,375 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Kidney Cancer Canada
About Kidney Cancer Canada
Kidney Cancer Canada is a national community of patients, caregivers and health professionals who work to provide every Canadian touched by kidney cancer with support, education and advocacy for their care pathways and treatment options.
Information Gathering
In 2020 Kidney Cancer Canada, helped design and promote an international online survey of patients and caregivers in affiliation with the International Kidney Cancer Coalition (IKCC). This survey included 2,012 respondents (patients and caregivers) from 41 countries sharing their experiences and insights. Canada had 241 respondents of which 205 (86%) were patients diagnosed with kidney cancer, and 24 (10%) were caregivers to someone who has been diagnosed with kidney cancer, and 2 (0.8%) were undisclosed. The survey was designed to explore and benchmark worldwide patient experience in:
Patient knowledge, expectations of treatment and shared decision making
Clinical trials, research awareness and sources of information
Quality of life and overall health status of respondents
The IKCC 2020 Patient Survey Global Report and the Canada report is available here. here:
Further, Kidney Cancer Canada attempted to identify patients who had experience with pembrolizumab for the adjuvant treatment of renal cell carcinoma by i) appealing to Canadian physician investigators who had patients enrolled in the Keynote 564 trial to connect these patients with KCC ii) including an appeal to Keynote 564 enrollees within a survey to participate in qualitative interviews. Only one patient with experience with pembrolizumab for the adjuvant treatment of RCC was identified through these efforts.
Further, in May 2021 the International Kidney Cancer Coalition (IKCC) conducted a survey of 141 RCC patients to gather their perspectives on adjuvant immunotherapy for renal cell carcinoma. Kidney Cancer Canada, in March 2022, relaunched a survey including the same questions regarding perspectives on adjuvant immunotherapy for RCC. 106 patients and caregivers responded to the survey, 65 of whom reside in Canada.
Also, in support of a previous patient submission for a treatment being reviewed by CADTH in 2018, Kidney Cancer Canada conducted an online survey of patients and caregivers in 2018 to assess the challenges kidney cancer patients and caregivers face. Some results from that survey are presented herein.
This report reflects the results of the IKCC survey, KCC’s various surveys of patients and caregivers, and our one-on-one interview with a patient with experience with the treatment under review. This submission is also informed by intelligence and insights Kidney Cancer Canada has garnered from more than 15 years of experience in patient support, research and advocacy in Canada related to kidney cancer.
Disease Experience
The Canadian Cancer Society (CCS) estimates that (in 2017) there were 6,600 new cases of kidney cancer diagnosed in Canada. It is the sixth most common cancer in men and the eleventh most common cancer in women. Of the 6,600 Canadians diagnosed annually with kidney cancer, approximately 25% will be diagnosed as stage IV. Metastatic renal cell carcinoma (mRCC) is a fatal disease with no known cure. For patients with stage IV disease, the survival rate is poor with less than 10% of these patients surviving for 5 years or longer.
The majority of patients (65%) with RCC have localized disease when they receive their diagnosis. When the disease is confined to the kidney, surgery to remove the cancer, either through nephrectomy or partial nephrectomy is the standard of care. While variations in retrospective data collection complicate the ability to accurately estimate the number of patients who may experience disease recurrence after surgery, most models put the risk of recurrence at between 40% and 50%. Nonetheless, a very large proportion of patients will eventually have disease recurrence leading to a substantially shortened life expectancy. For patients with renal-cell carcinoma who undergo nephrectomy there are no currently available funded options in Canada for adjuvant therapy to reduce the risk of recurrence.
While kidney cancer survival has significantly improved over the last dozen years because of new innovative treatments and improved access to those treatments, there remain unmet treatment needs in both the adjuvant and metastatic setting.
Experiences With Currently Available Treatments
There are no currently available funded options in Canada for adjuvant therapy to reduce the risk of recurrence of disease. Prior to pembrolizumab, randomized controlled trials of adjuvant therapy with TKI therapy demonstrated no survival (OS) benefit and uncertain disease-free survival (DFS) benefit. In other jurisdictions (most notably the U.S., South Korea, Brazil), sunitinib was approved for intermediate and high- risk patients based upon DFS benefit given the lack of any other treatment option in the adjuvant setting.
Kidney Cancer Canada took the position at that time that the potential benefits of adjuvant sunitinib did not outweigh the toxicities and did not support its use in Canada.
Improved Outcomes
In our March 2022 survey re: perspectives on adjuvant immunotherapy for RCC we asked:
Q: Imagine, you (or your loved one) have had surgery to remove your kidney cancer, but you still have a high risk that your kidney cancer will come back later on. Your doctor offers you one year of systemic/intravenous immunotherapy treatment (immunotherapy). What would you, as a patient in that situation, consider the necessary reduction of risk of your kidney cancer coming back to accept immunotherapy after your surgery?
Table 1: Necessary Reduction of Risk of Your Kidney Cancer Coming Back to Accept Immunotherapy
Survey | 10% of Risk Reduction Required | 20% of Risk Reduction Required | 30% of Risk Reduction Required | 40% of Risk Reduction Required | 50% of Risk Reduction Required | I would not accept immunotherapy after surgery at all | Total |
|---|---|---|---|---|---|---|---|
2022 KCC survey | 9.64% N=8 | 21.69% N=18 | 16.87% N=14 | 9.64% N=8 | 39.76% N=33 | 2.41% N=2 | N=83 |
2021 IKCC survey | 10.7% N=15 | 14.3% N=20 | 16.4% N=23 | 9.3% N=13 | 40% N=56 | 9.3% N=13 | N=140 |
Combined | 10.31% N=23 | 17.04% N=38 | 16.59% N=37 | 9.42% N=21 | 39.91% N=89 | 6.73% N=15 | N=223 |
These data illustrate patient goals and perspectives regarding adjuvant immunotherapy. Less than 7% would not accept immunotherapy in this setting. Of those who would accept this adjuvant immunotherapy, 50% would require an estimated risk reduction of 40-50% in their individual case. Kidney Cancer Canada expects to work with medical experts on evidence-based patient decision aids for adjuvant treatment that will assist with patient selection and shared decision making.
Q: Immunotherapy treatment often causes side effects, which can usually be managed by taking steroids so that you can finish the therapy. Steroids, in turn, can also have side effects, such as water retention (puffiness), weight gain, and even permanent side effects like diabetes, or fibrosis (tissue scarring). Knowing that there is a risk you may need high dose steroid treatment in addition to the immunotherapy, what level of risk for steroid use would be acceptable for you?
Table 2: Acceptable Level of Risk for Steroid Use
Survey | 5% risk of steroid side effects | 10% risk of steroid side effects | 15% risk of steroid side effects | 20% risk of steroid side effects | 25% risk of steroid side effects | I would not accept any risk of steroid use | Total |
|---|---|---|---|---|---|---|---|
2022 KCC survey | 9.3% N=8 | 13.95% N=12 | 15.12% N=13 | 17.44% N=15 | 38.37% N=33 | 5.81% N=5 | N=86 |
2021 IKCC survey | 7.9% N=11 | 21.4% N=30 | 11.4 N=16 | 20.7% N=29 | 26.4% N=37 | 12.1% N=17 | N=140 |
Combined | 8.4% N=19 | 18.58% N=42 | 12.83% N=29 | 19.47% N=44 | 30.97% N=70 | 9.74% N=22 | N=226 |
These data address patient perspectives of potential toxicities. Less than 10% of patients would decline adjuvant immunotherapy to avoid these treatment-related risks altogether. Of those who would be prepared to proceed with an understanding of treatment-related risks, approximately 50% would accept the risk of any steroid use if that risk fell in the range of 20-25%.
Experience With Drug Under Review
In March 2022, KCC Canada attempted to contact patients who had experience with pembrolizumab for the adjuvant treatment of adult patients with RCC at intermediate-high or high risk of recurrence following nephrectomy. The Keynote 564 study did have Canadian participants and KCC asked Canadian Keynote 564 investigators to connect the patients enrolled in this study with KCC for one-on-one interviews.
Additionally, KCC put out a survey that was distributed through both Canadian and international channels with a request that any patients who were part of Keynote 564 schedule an interview with us. While various patients volunteered to be interviewed, most of those patients turned out to have been treated with pembrolizumab in the metastatic setting (with axitinib). Finding patients with experience with pembrolizumab monotherapy for adjuvant treatment of RCC proved to be extremely difficult. As a result, we were only able to interview one patient that had experience with pembrolizumab in the Keynote 564 trial.
Patient: Male, 72 years old residing in New York State, USA
On March 21, 2022, a representative of Kidney Cancer Canada interviewed a 72-year-old patient living in New York “DM”.
In February 2020, during the COVID19 outbreak, DM went for his yearly physical, which included a urine test. Blood was subsequently discovered in his urine. A blood test and CT scan followed, where they discovered a 10cm tumour in his left kidney.
DM required a nephrectomy, but New York Presbyterian Hospital had canceled all surgeries due to the pandemic. However, DM’s surgeon made a special appeal for surgery to take place, and on March 23 DM had a complete nephrectomy. Two subsequent follow-up scans showed no evidence of tumors.
Then in November 2020 DM experienced mobility issues with his left hand, so scheduled an appointment with a neurologist. An MRI was ordered, where a 5cm tumor was found in his brain, which, upon testing was identified as metastatic renal cell carcinoma. Subsequently he had surgery (craniotomy) to remove the tumor, plus two rounds of gamma knife radiosurgery for remaining lesions.
DM was doing some personal research regarding the adjuvant treatment of kidney cancer following surgery and viewed an online video describing Keynote 564 from Dr. Sumanta Kumar Pal. Then, in Spring 2021 at an appointment with his oncologist, DM advocated to be enrolled in Keynote 564.
Upon confirming his eligibility for the trial, he began adjuvant treatment with pembrolizumab in July 2021.
DM remains on treatment (20mg every three weeks. Here is a summary of his experience.
DM is very happy with his experience thus far. He reports that that the side effects are easily manageable. The side effects he reports are:
slight occasional rash
slight fatigue
hyperkalemia (treated with sodium zirconium cyclosilicate)
He reports “keeping a close eye on creatine and eGFR” and “drinking lots of water:
All of his scans since starting treatment show “M0” (no distant cancer spread has been found).
DM noted in the interview scheduling instrument: “I am a current patient of Keytruda, and it is doing a great job without and significant side-effects. I strongly recommend this immunotherapy.”
His next scan is May 28, 2022.
In many cancers, such as breast cancer, colon cancer and lung cancer, patients can take additional “insurance policy” treatments to reduce the chance of the cancer coming back, including chemotherapy, hormone therapy, radiation therapy, immunotherapy, and targeted therapy. Past studies indicated that adjuvant treatments did not seem to work for patients with kidney cancer. Effective adjuvant therapy for kidney cancer is an urgent unmet need to reduce recurrence risk and improve outcomes. Without any adjuvant therapy options, patients with intermediate and high risk of recurrence face tremendous stress and anxiety and the very real expectation of recurrence within the first two years of surgery, knowing that with recurrence and a stage iv diagnosis, their disease is incurable, and the treatment options are limited.
Finally, with Keynote 564, pembrolizumab treatment has demonstrated significant improvement in disease- free survival (DFS) as compared with placebo after surgery among patients with kidney cancer who were at high risk for recurrence. While we await confirmation of overall survival benefit (OS) that may take several more years to mature, we appreciate the very real patient needs today, in clinics across Canada, by those patients whose pathology, staging and grading indicates a very high likelihood of recurrence before that data arrives. Those patients cannot afford the luxury of waiting for more data. Currently oncologists have nothing whatsoever to offer these patients beyond surveillance and support for their emotional distress.
In the long term, this new adjuvant treatment may dramatically improve outcomes for patients, and by reducing the number of patients who incur metastatic disease, may also reduce costs for the treatment of RCC overall. In the short term, in the Canadian context we have the opportunity to collect real world evidence in the Canadian Kidney Cancer Information System (CKCis) to inform long-term reimbursement strategy.
Companion Diagnostic Test
Current approaches to predicting recurrence risk in the adjuvant setting are based on various scoring methods that stratify patients based on features of the primary tumour, presence or absence of nodal and distant metastases, and Eastern Cooperative Oncology Group (ECOG) performance status. While these approaches are effective in predicting recurrence risk in the adjuvant setting for ccRCC, development of novel biomarkers is needed to improve and unify existing prognostic models.
Anything Else?
To better understand kidney cancer patients’ understanding of clinical trial endpoints, we also asked in our March 2022 survey:
What does the term “Disease-Free Survival” mean to you personally? (check answer that best fits your understanding)
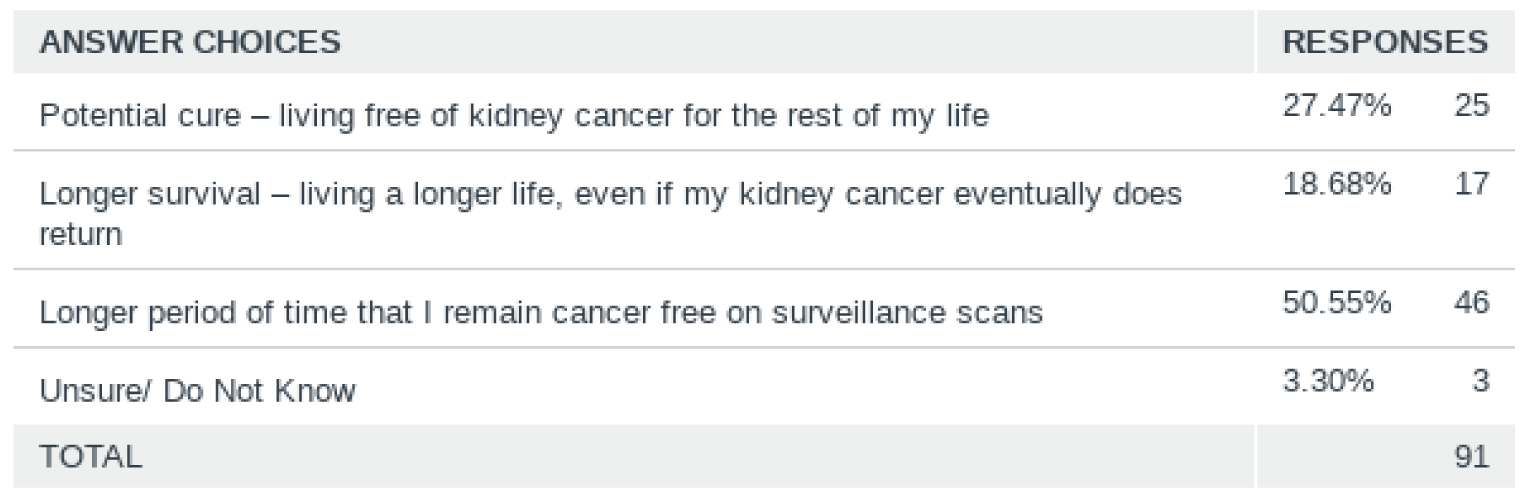
And we asked: What does the term “Overall Survival” mean to you personally? (check answer that best fits your understanding)
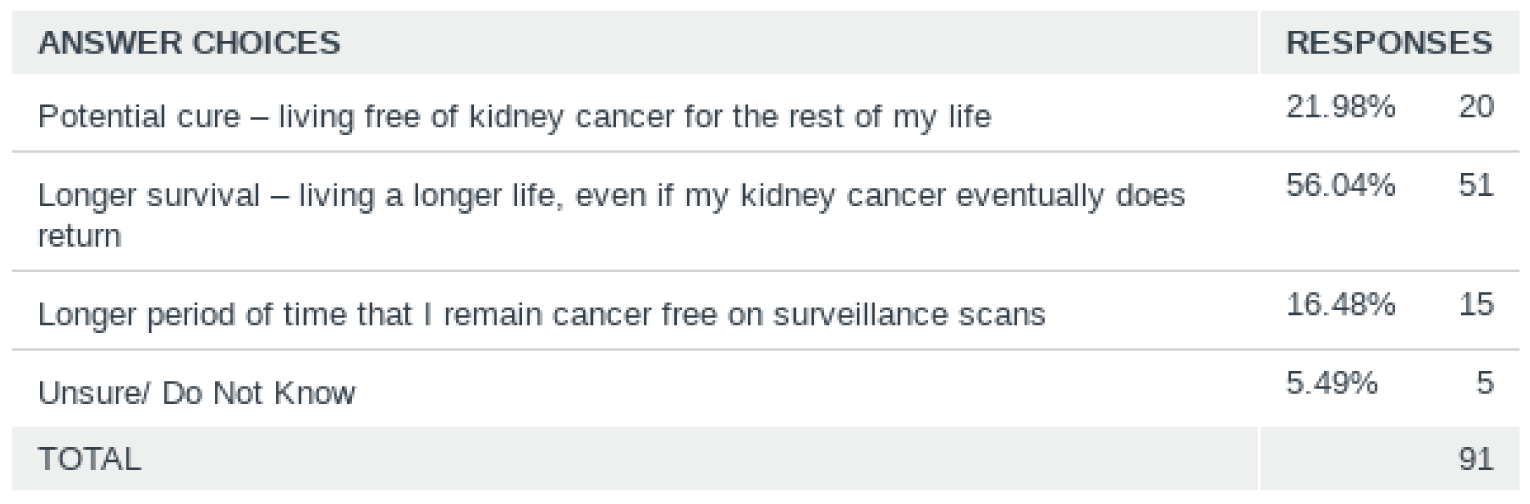
We asked these questions to get a better understanding of how patients value and comprehend the different endpoints used to demonstrate efficacy of new treatments. Recognizing that most of the respondents to these questions have likely never received any focused counseling or education on the meaning of various end points used in clinical trials, we expected that there would be variance in how people defined these terms. However, most patients seem to understand the meaning of Disease-Free Survival (DFS) and Overall Survival (OS) with 50.55% of patients correctly selecting the definition for DFS and 56.04% of patients selecting the definition of OS.
Nonetheless, Kidney Cancer Canada recognizes that an adjuvant treatment approved with data that relies significantly on a surrogate endpoint such as DFS will require patient groups to provide valuable information to assist patients with treatment decision-making. Further, treating physicians should be prepared to provide careful patient counselling with respect to the current state of evidence of therapy in the adjuvant setting.
While we understand that DFS is not a surrogate for OS, we believe that DFS in the context of intermediate and high-risk RCC has significant and immediate value to patients and their families.
Kidney Cancer Canada recognizes also that adjuvant use of pembrolizumab (or any other future adjuvant therapy) should always be presented as “optional” for patients deemed to be at intermediate-risk or high-risk of cancer recurrence following surgery.
Conflict of Interest Declaration for Kidney Cancer Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
The patient group submission was completed exclusively with Kidney Cancer Canada resources. No external help was used to complete this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 3: Financial Disclosures for Kidney Cancer Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
BMS | — | — | X | — |
Eisai | — | — | X | — |
Ipsen | — | — | X | — |
Merck | — | — | X | — |
Novartis | — | X | — | — |
Pfizer | — | — | — | X |
Clinician Input
Ontario Health (CCO) Genitourinary Cancer Drug Advisory Committee
About the Ontario Health (CCO) Genitourinary Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Discussed jointly via email
Current Treatments
Patients who are diagnosed with localized renal cell carcinoma (RCC) and who undergo a nephrectomy are generally followed with standard of care surveillance. Collectively, the previously conducted clinical trials evaluating adjuvant therapy with targeted agents (VEGF-TKIs, mTOR inhibitors) have not shown a significant clinical benefit (ie significant DFS benefit) in the overall populations studied. One study, the S-TRAC trial using adjuvant sunitinib for 1-year, showed a DFS improvement from 5.6 years (placebo) to 6.8 years (sunitinib); however, this came at a significant cost of toxicity (N Engl J Med 2016; 375:2246-2254) and therefore has not been accepted as a standard of care for adjuvant therapy in most global jurisdictions, including Canada. There is currently no accepted standard adjuvant therapy for this RCC patient population.
Treatment Goals
In the adjuvant setting, delaying time to disease recurrence or death (ie definition of DFS in Keynote-564) would be a meaningful endpoint in this disease, given that metastatic RCC is not curable and patients die from their disease. An improvement in overall survival (OS) would also be a meaningful clinical endpoint – although in a phase III trial this would require longer follow up and contextualize the international locations where said trial took place, as well as standard options available (post trial) in those jurisdictions. Given the widely evolving therapies for metastatic RCC, it has been accepted by global approval agencies that DFS (a composite of recurrence or death) would be acceptable for a drug in this localized RCC indication. Importantly, this definition of DFS has also been an acceptable endpoint by patient advocacy groups and their surveys of patients with RCC (https://kccure.org/category/patient-stories).
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There is currently no accepted standard adjuvant therapy for this RCC patient population. Therefore, this drug would fill a significant unmet need not currently addressed by any oncology drug in this disease setting. A significant proportion of patients with localized RCC will still recur post surgery, particularly those studied in the Keynote-564 trial of adjuvant pembrolizumab. Given that treatment in the recurrent/metastatic setting is generally palliative in nature, there remains a need to improve outcomes for patients who are diagnosed in the localized setting.
Which patients have the greatest unmet need for an intervention such as the drug under review?
The Keynote-564 study evaluated adjuvant pembrolizumab for 1-year and included patients with intermediate-high risk, high risk, or M1 NED (no evaluable disease after resection of oligometastic sites up to 1 year from nephrectomy). The recent update of Keynote-564 (30 month follow up), showed a significantly improved HR for DFS (0.63) for the entire population studied. The DFS benefits were seen irrespective of risk status (intermediate-high risk, HR 0.68; high risk HR 0.60; M1 NED HR 0.28). Therefore, this drug intervention would be applied to the overall studied trial population in totality.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Given there is no standard systemic treatment for this adjuvant RCC setting, this drug would provide the first acceptable adjuvant therapy for all applicable patients. Importantly, this drug already has efficacy and safety data in the metastatic RCC setting (either combination or monotherapy), therefore, this is a drug well known to the patient and physician community who treat these patients.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
It would not be appropriate to recommend another adjuvant drug therapy in this setting. There are no other accepted standard of care systemic treatments in this space.
How would this drug affect the sequencing of therapies for the target condition?
This drug therapy (pembrolizumab, an anti-PD-1 therapy) would be the first acceptable standard therapy for adjuvant RCC. There are no other standard adjuvant therapies. In the metastatic RCC setting, the standard of care includes combination anti-PD-1 therapy with either anti-CTLA-4 therapy (combination nivolumab plus ipilimumab) or with a VEGF-TKI (combination pembrolizumab plus axitinib, or pembrolizumab plus lenvatinib).
For patients treated with adjuvant pembrolizumab who were then to recur with metastatic disease AT or AFTER 6 months of completing adjuvant therapy, that standard combination treatments for metastatic RCC should still be offered.
For patients treated with adjuvant pembrolizumab who were then to recur with metastatic disease while ON or WITHIN 6 months of completing adjuvant therapy, these patients would be treated with standard therapies in the “post anti-PD-1 therapy” metastatic RCC setting. These standard options include available VEGF-TKIs.
Which patients would be best suited for treatment with the drug under review?
The Keynote-564 study evaluated adjuvant pembrolizumab for 1-year and included patients with intermediate-high risk, high risk, or M1 NED (no evaluable disease after resection of oligometastic sites up to 1 year from nephrectomy). The recent update of Keynote-564 (30 month follow up), showed a significantly improved HR for DFS (0.63) for the entire population studied. The DFS benefits were seen irrespective of risk status (intermediate-high risk, HR 0.68; high risk HR 0.60; M1 NED HR 0.28). Therefore, this drug intervention would be applied to the overall studied trial population in totality.
How would patients best suited for treatment with the drug under review be identified?
Eligibility for adjuvant therapy would require pathology results post-surgery. Therefore, these patients would be identified based on standard synoptic reporting of their nephrectomy. These patients would be initially identified by their surgeon (urologist, uro-oncologist). These patients would then be referred to Centres or teams within Centres who have expertise to provide systemic IV anti-PD-1 therapy as in pembrolizumab.
Which patients would be least suitable for treatment with the drug under review?
Patient with RCC treated with nephrectomy who do not meet eligibility per the Keynote-564 study would be least suitable for consideration of therapy – assuming patient is otherwise clinically suitable.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Beyond eligibility for treatment based on Keynote-564, there is no additional biomarker to select patients most likely to benefit to this therapy.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Patients would be clinically assessed during therapy to ensure safety and suitability to continue to receive therapy (ie toxicity assessment). During treatment, patients would be assessed by CT imaging (generally every 3 months while on therapy) to assess for disease recurrence.
What would be considered a clinically meaningful response to treatment?
Overall, delaying time to disease recurrence or death would be meaningful for patients at a high level. At an individual level, benefit would be determined by physician-patient interaction to ensure tolerability of drug treatment, balancing toxicity and continued performance status that would be applicable in the adjuvant setting.
How often should treatment response be assessed?
Patients would be clinically assessed during therapy to ensure safety and suitability to continue to receive therapy (ie toxicity assessment). During treatment, patients would be assessed by CT imaging (generally every 3 months while on therapy) to assess for disease recurrence.
What factors should be considered when deciding to discontinue treatment?
As is standard of care for physicians experienced with this drug (pembrolizumab), clinical assessment will take into account toxicity of drug (immune related adverse events) and patient performance status and in total assess suitability to continue or discontinue therapy. This drug is well known across Cancer programs in Canada and is not a novel drug in the RCC space. Physicians who use this drug would have expected clinical experience to assess suitability of treatment.
What settings are appropriate for treatment with the drug under review?
This drug is widely used in Canada in the outpatient clinical setting. This is a standard IV treatment that would require infusion at a Cancer Centre setting.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
This is an oncology drug. This may vary by Centre but would generally be within the purview of medical oncology to date. Eligible patients identified post nephrectomy would thus be expected to be referred to medical oncology, or the appropriate Centres/teams, to discuss the indications, side effects, and logistics of this therapy.
Additional Information
Please note that while most patients will be identified within 12-weeks post nephrectomy, there are patients potentially designated M1 NED (ie oligometastatic disease resected within 1 year post nephrectomy), who would be eligible for this therapy in the adjuvant setting. Therefore, the occurrence of metastatic disease per se in a patient’s chart will not be suitable to withhold this treatment from RCC patients – so long as they meet the M1 NED definition, they should still be afforded this therapy per criteria within Keynote-564.
Conflict of Interest Declarations for the Ontario Health (CCO) Genitourinary Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Aly-Khan Lalani
Position: Genitourinary Drug Advisory Committee Member
Date: 3/16/2022
Table 4: Conflict of Interest Declaration for Ontario Health (CCO) Genitourinary Cancer Drug Advisory Committee — Clinician 1
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
Kidney Cancer Research Network of Canada
About the Kidney Cancer Research Network of Canada
The Kidney Cancer Research Network of Canada (KCRNC) is a virtual and inclusive national network of researchers committed to the facilitation of kidney cancer research to enhance the knowledge of kidney cancer and its treatment.
https://www.kcrnc.ca/
Information Gathering
Information used to inform this submission was from clinical experience treating patients with metastatic renal cell carcinoma (mRCC), from reading the published data on relevant clinical trials, and from participating in research. One clinician that participated in preparation of this submission was a Canadian investigator in the Keynote 564 trial: Safety and Efficacy Study of Pembrolizumab (MK-3475) as Monotherapy in the Adjuvant Treatment of Renal Cell Carcinoma Post Nephrectomy. (ClinicalTrials.gov Identifier: NCT03142334).
Current Treatments
The standard of care for non-metastatic renal cell carcinoma (nmRCC) remains nephrectomy, however, despite complete resection and negative margins, up to 50 percent of patients may experience disease recurrence putting them at risk of significant morbidity and death from RCC. For patients with renal-cell carcinoma who undergo nephrectomy there are no currently available funded options in Canada for adjuvant therapy to reduce the risk of recurrence.
Prior to Keynote 564 study, randomized controlled trials of adjuvant therapy with TKI therapy after nephrectomy for nmRCC showed no OS benefit and equivocal DFS benefit. These findings were confirmed by a meta-analysis (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5994982/ conducted by The Kidney Cancer Research Network of Canada (KCRNC) in 2018 where we reviewed the published data and performed of studies that focused on vascular endothelial growth factor receptor (VEGFR) tyrosine kinase inhibitors (TKIs) resulting in the KCRNC, in its 2018 consensus statement on the role of adjuvant therapy after nephrectomy for high-risk, non-metastatic renal cell carcinoma to recommend: adjuvant TKI-based adjuvant therapy is not recommended for routine use after nephrectomy for high-risk nmRCC.
Treatment Goals
Recognizing that many patients may experience disease recurrence following nephrectomy that put them at risk of death from RCC, and ideal treatment would maintain a patient’s disease-free status and provide patients with normal life expectancy.
However, in recognition that there are no existing pharmacological treatments that are curative for all populations of patients with renal cell carcinoma or metastatic renal cell carcinoma in any setting, therapies in the adjuvant setting that offer significant and clinically meaningful improvement in disease-free survival are important breakthroughs.
Therapy administered in the adjuvant setting is with curative intent, with the objective of preventing disease recurrence to a more advanced stage.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
The standard-of-care treatment for non-metastatic renal-cell carcinoma remains nephrectomy, however, nearly half of patients undergoing nephrectomy will experience disease recurrence after surgery. This demonstrates a significant unmet need for therapy in the post-surgical setting.
There are no currently available funded options in Canada for adjuvant therapy to reduce the risk of recurrence.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Patients at the highest risk for disease recurrence have the greatest unmet need for adjuvant therapy. As defined by the Keynote 564 study, adjuvant pembrolizumab should be considered for patients with intermediate- or high-risk operable ccRCC.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
There are no currently available funded options in Canada for adjuvant therapy to reduce the risk of recurrence for patients with renal-cell carcinoma who undergo surgery. Therefore, the availability of pembrolizumab in this setting would cause no shifts in the current treatment paradigm.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
There are no other treatment options in this setting.
How would this drug affect the sequencing of therapies for the target condition?
There are no currently available funded options in Canada for adjuvant therapy to reduce the risk of recurrence for patients with renal-cell carcinoma who undergo surgery. If funded/available, pembrolizumab would represent the only available therapy with no other sequencing opportunities in the non-metastatic setting.
If a non-metastatic patient were to experience disease recurrence/metastasis while on, or after treatment with adjuvant pembrolizumab, the selection of 1st line metastatic treatment for these patients may be different than for patients who have not received adjuvant therapy. There is currently no data to recommend the best 1st line treatment option for patients who develop metastatic disease while on, or after, treatment with adjuvant pembrolizumab. However, in general if a patient develops disease recurrence after adjuvant pembrolizumab, this patient would not likely be treated with 1st line pembrolizumab for metastatic disease.
Most likely, this patient would be treated with a 1st line TKI, but more data is needed to recommend this.
Which patients would be best suited for treatment with the drug under review?
As defined by the Keynote 564 study, adjuvant pembrolizumab should be considered for patients with intermediate- or high-risk operable ccRCC post-surgery.
How would patients best suited for treatment with the drug under review be identified?
KCRNC recognizes that a significant proportion of patients with local/locoregional disease are cured by surgery alone, and that the use of pembrolizumab for patients at intermediate- or high-risk of recurrence following nephrectomy will result in unnecessary treatment of some patients. This is yet another instance that points to the need for clinical and molecular biomarkers to guide treatment decision-making for renal cell carcinoma.
Given the heterogeneity of renal mass biology, developing reliable means of determining diagnosis, optimal therapy, and prognosis is the focus of much current research. However, the opportunity to provide patients with effective therapies in the adjuvant setting should not be impeded by the absence of biomarkers at this time.
KCRNC recognizes that adjuvant use of pembrolizumab should always be presented as “optional” for patients at intermediate- or high-risk of recurrence following nephrectomy, and that discussion of therapy in this setting needs to be complemented with careful patient counselling with respect to the current state of evidence and potential long-term adverse events.
The KCRNC annually produces a disease management consensus statement in the management of renal cell cancer (published in the Canadian Urological Association Journal) based on the deliberations and conclusions of key Canadian opinion leaders at the annual Canadian Kidney Cancer Forum (CKCF). At the Forum experts review previous disease management consensus statements and recent relevant evidence.
In October 2022 physicians from across Canada who treat RCC/mRCC will be convening to update treatment recommendations at the annual CKCF. At this time, we will be developing recommendations for the adjuvant use of pembrolizumab. Included in our deliberations will be the matters of patient selection, patient counseling and patient monitoring.
The KCRNC welcomes attendance by member(s) of the CADTH team working on the review of pembrolizumab for the adjuvant treatment of patients with RCC at intermediate-high or high risk of recurrence following nephrectomy.
Which patients would be least suitable for treatment with the drug under review?
Low risk patients post-surgery would not be suitable for adjuvant pembrolizumab.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
See previous section.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
In clinical practice, intermediate and high-risk patients with or without adjuvant pembrolizumab are monitored every 3-6 months with cross-sectional imaging to assess for disease recurrence in the first year, then every 6 months for 5-10 years.
What would be considered a clinically meaningful response to treatment?
Clinically significant response would be the absence of disease recurrence while on adjuvant pembrolizumab and afterwards during routine follow-up post-surgery.
How often should treatment response be assessed?
Cross-sectional imaging every 3-6 months for the first year and then every 6 months for up to 5-10 years post-surgery, regardless if on adjuvant pembrolizumab or not (no additional imaging is recommended for patients on adjuvant pembrolizumab).
What factors should be considered when deciding to discontinue treatment?
Treatment with adjuvant pembrolizumab would be discontinued in cases of 1) disease recurrence on routine cross sectional imaging on follow-up, or 2) significant toxicity from pembrolizumab treatment.
What settings are appropriate for treatment with the drug under review?
As pembrolizumab is administered intravenously this should be done in an approved oncology infusion clinic in an outpatient hospital setting.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
N/A
Additional Information
While Keynote 564 demonstrates a promising OS signal with the use of pembrolizumab (along with an acceptable tolerability profile) in the adjuvant setting, KCRNC acknowledge that there remains uncertainty with the correlation between DFS and OS for operable ccRCC, and that maturing RCT evidence along with real world evidence can reduce this uncertainty.
Of critical importance however is that this new adjuvant treatment has tremendous potential to dramatically improve outcomes for patients, along with strong potential to reduce costs for the treatment of RCC overall.
The KCRNC is uniquely positioned to provide real world evidence through use of the Canadian Kidney Cancer information system (CKCis). The KCRNC, in 2009 established a centralized Canadian kidney cancer database called the Canadian Kidney Cancer information system (CKCis) to collect data from medical centres across the country. CKCis is a web-based national registry supporting the development of clinical and basic research in kidney cancer across Canada. It contains pertinent retrospective, as well as prospective de-identified patient data collected from consented patients who have been diagnosed and treated for renal cell carcinoma.
CKCis is a flexible database platform that can integrate different data needs to accommodate creative innovations considered for research, including those to inform reimbursement decision-making. Data fields are updated as new information emerges regarding the treatment of renal cell carcinoma.
CKCis has now been in operation for over 10 years. Sixteen Canadian centres actively accrue kidney cancer patients into the CKCis registry, and as of March 2021 over 19,000 patients are enrolled with their data being collected. CKCis is now central to the activities of the KCRNC and the data has matured enough resulting in the publication of many manuscripts and abstracts. The network continues to bring together interested clinicians and researchers in kidney cancer and supports the development of active kidney cancer research programs in Canada.
As proof of concept of the ability for the KCRNC to generate high-quality RWE, in April 2017 CKCis was used to inform the very first pCODR Request for Advice (RFA) seeking advice on funding axitinib as an alternative to everolimus for the 2nd line treatmen of mRC. Details here: www.cadth.ca/sites/default/files/pcodr/pcodr_rfa_axitinib_inlyta_mrcc_rfa_cgr.pdf.
The Kidney Cancer Research Network of Canada is prepared to work with the pan Canadian Pharmaceutical Alliance and the pan Canadian Oncology Drug Review to support evidence-building on an ongoing basis to determine the real word effectiveness of new and existing drugs approved for use in Canada for RCC.
Conflict of Interest Declarations for the Kidney Cancer Research Network of Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Anil Kapoor
Position: Professor of Surgery (Urology), McMaster University
Date: 07-03-2022
Table 5: Conflict of Interest Declaration for Kidney Cancer Research Network of Canada — Clinician 1
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
Eisai | X | — | — | — |
Ipsen | X | — | — | — |
Merck | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Nawar Hanna
Position: Urologist, University of Montreal
Date: 23-03-2022
Table 6: Conflict of Interest Declaration for Kidney Cancer Research Network of Canada — Clinician 2
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
Sanofi | X | — | — | — |
Bayer | X | — | — | — |
Abbvie | X | — | — | — |
Tolmar | X | — | — | — |
Astellas | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines.
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.