CADTH Reimbursement Review
Atezolizumab (Tecentriq)
Sponsor: Hoffman-La Roche Ltd.
Therapeutic area: Non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
ALK
anaplastic lymphoma kinase
BSC
best supportive care
CCO
Cancer Care Ontario
CI
confidence interval
CNS
central nervous system
DAC
Drug Advisory Committee
DFS
disease-free survival
ECOG
Eastern Cooperative Oncology Group
EGFR
epidermal growth factor receptor
HR
hazard ratio
IC
immune cell
IHC
immunohistochemistry
ITT
intention to treat
KM
Kaplan-Meier
LCC
Lung Cancer Canada
LHF
Lung Health Foundation
NOC
Notice of Compliance
NSCLC
non–small cell lung cancer
OH
Ontario Health
OS
overall survival
PD-1
programmed death-1
PD-L1
programmed death-ligand 1
SAE
serious adverse event
TC
tumour cell
TNM
tumour, node, metastasis
UICC
Union for International Cancer Control
ULN
upper limit of normal
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Atezolizumab (Tecentriq), 1,200 mg/mL and 840 mg/14 mL, IV infusion |
Indication | As monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adult patients with stage II to IIIA (according to AJCC/UICC 7th edition1) NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs. |
Reimbursement request | As monotherapy for adjuvant treatment following complete resection and platinum-based chemotherapy for patients with stage II to IIIA (according to AJCC or UICC 7th edition1) NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs and do not have EGFR or ALK genomic tumour aberrations. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review + Project Orbis |
NOC date | January 14, 2022 |
Sponsor | Hoffmann-La Roche Ltd. |
AJCC = American Joint Committee on Cancer; ALK = anaplastic lymphoma kinase; EGFR = epidermal growth factor receptor; NOC = Notice of Compliance; NSCLC = non–small cell lung cancer; PD-L1 programmed death-ligand 1; TC = tumour cell; UICC = Union for International Cancer Control.
Introduction
Lung cancer is one of the most commonly diagnosed cancers and is the leading cause of cancer deaths in Canada,2 with non–small cell lung cancer (NSCLC) accounting for approximately 88% of lung cancer cases.2,3 Approximately half of all NSCLC cases in Canada are stage I to III at diagnosis,2 and 1-third of patients with NSCLC have operable disease.4 The 5-year net survival for lung cancer is 22%.5 The high mortality rate associated with lung cancer reflects both its high incidence rate and its low survival rate.
The primary goal of treatment for patients with stage IB to IIIA (per the AJCC Cancer Staging Manual, 7th edition1; the equivalent stages according to the AJCC Cancer Staging Manual, 8th edition6 are stages IIA to IIIB) NSCLC is to cure and prolong life. The secondary goal of treatment is to delay disease relapse, thereby allowing patients a longer period of time living disease-free. Attaining these treatment goals primarily involves surgical resection of the tumour,4,7 followed by adjuvant cisplatin-based doublet chemotherapy.
Atezolizumab is an Fc-engineered humanized IgG1 monoclonal antibody that directly binds to programmed death-ligand 1 (PD-L1) and blocks interactions with the programmed death-1 (PD-1) and B7.1 receptors, releasing PD-L1 and PD-1 pathway–mediated inhibition of the immune response, including reactivating the antitumour immune response. Atezolizumab is administered as an IV infusion at a dosage of 840 mg every 2 weeks, 1,200 mg every 3 weeks, or 1,680 mg every 4 weeks.
Atezolizumab received Notice of Compliance (NOC) from Health Canada on January 14, 2022, as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to the AJCC Cancer Staging Manual, 7th edition1) NSCLC whose tumours have PD-L1 expression on at least 50% of tumour cells (TCs). Although the original indication proposed to Health Canada was for patients with NSCLC whose tumours had PD-L1 expression on at least 1% of TCs, the approved Health Canada indication was limited to patients with stage II to IIIA disease with PD-L1 expression on at least 50% of TCs because of uncertainty about the clinical benefit of atezolizumab in the population with stage II to IIIA NSCLC and PD-L1 expression on 1% to 49% of TCs; Health Canada noted that the improvement in disease-free survival (DFS) was mainly driven by the subgroup of patients with PD-L1 expression on at least 50% of TCs.8
Although the reimbursement request for the current review was for atezolizumab as monotherapy for adjuvant treatment after complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to the AJCC Cancer Staging Manual, 7th edition1) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs and no epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumour aberrations, the review will focus on the Health Canada indication described previously, which is boarder in scope. Therefore, the objective of this report is to perform a systematic review of the beneficial and harmful effects of atezolizumab as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to UICC and AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs.
Table 2: Summary of Key Results From IMpower010 Study for Patients With Stage II to IIIA Disease and PD-L1 Expression on at Least 50% of TCs (Clinical Data Cut-Off Date of January 21, 2021)
Outcome | BSC group N = 114 | Atezolizumab group N = 115 |
|---|---|---|
OS | ||
Death event, n (%) | ||
Patients with event | 26 (22.8) | 11 (9.6) |
Patients without event | 88 (77.2) | 104 (90.4) |
Time to event, monthsa | ||
Median (range) | NE (0.2b to 57.5b) | NE (0.2b to 54.2b) |
95% CI | NE | NE |
25th to 75th percentiles | 36.4 to NE | NE |
Stratified analysisc | ||
HRd (95% CI) | 0.40 (0.20 to 0.81) | |
P value, log-ranke | 0.0089 | |
Unstratified analysis | ||
HRd (95% CI) | 0.37 (0.18 to 0.74) | |
P value, log-ranke | 0.0036 | |
Time point analysis | ||
3 years | ||
Patients remaining at risk | 43 | 56 |
Event-free rate (%) | 76.67 | 90.94 |
95% CI | 68.38 to 84.97 | 85.21 to 96.67 |
Difference in event-free rate (95% CI) | 14.27 (4.19 to 24.35) | |
P value (z-test)e | 0.0055 | |
DFS | ||
Recurrence event, n (%) | ||
Patients with event | 52 (45.6) | 28 (24.3) |
Death | 2 (1.8) | 3 (2.6) |
Disease recurrence | 50 (43.9) | 25 (21.7) |
Patients without event | 62 (54.4) | 87 (75.7) |
Time to event, monthsa | ||
Median (range) | 35.7 (0.0b to 54.9b) | NE (0.0b to 54.2b) |
95% CI | 29.7 to NE | 42.3 to NE |
25th to 75th percentiles | 12.0 to NE | 35.3 to NE |
Stratified analysisc | ||
HRd (95% CI) | 0.47 (0.29 to 0.75) | |
P value, log-ranke | 0.0012 | |
Unstratified analysis | ||
HRd (95% CI) | 0.43 (0.27 to 0.68) | |
P value (log-rank)e | 0.0002 | |
Time point analysis | ||
3 years | ||
Patients remaining at risk | 19 | 30 |
Event-free rate, % | 48.61 | 73.79 |
95% CI | 38.03 to 59.18 | 64.35 to 83.23 |
Difference in event-free rate (95% CI) | 25.18 (11.01 to 39.36) | |
P value (z-test)e | 0.0005 | |
Site of disease recurrence, n (%) | ||
nf | 50 | 25 |
Locoregional only | 17 (34.0) | 15 (60.0) |
Distant only | 21 (42.0) | 6 (24.0) |
Site of distant recurrenceg | ||
Bone or bone marrow | 5 (10.0) | 1 (4.0) |
CNS | 8 (16.0) | 1 (4.0) |
Contralateral lung | 1 (2.0) | 2 (8.0) |
Ipsilateral lung | 1 (2.0) | 0 (0.0) |
Liver | 2 (4.0) | 1 (4.0) |
Lymph node | 2 (4.0) | 0 (0.0) |
Other | 6 (12.0) | 1 (4.0) |
CNS onlyh | 7 (14.0) | 1 (4.0) |
Locoregional + distant | 9 (18.0) | 4 (16.0) |
Site of distant recurrence | ||
Bone or bone marrow | 0 (0.0) | 2 (8.0) |
CNS | 3 (6.0) | 1 (4.0) |
Contralateral lung | 1 (2.0) | 0 (0.0) |
Liver | 0 (0.0) | 2 (8.0) |
Lymph node | 4 (8.0) | 1 (4.0) |
Other | 2 (4.0) | 3 (12.0) |
Secondary primary lung | 3 (6.0) | 0 (0.0) |
Secondary primary lung only | 3 (6.0) | 0 (0.0) |
Harms, n (%) | ||
n | 112 | 113 |
Patients with ≥ 1 AE | 78 (69.6) | 107 (94.7) |
Patients with ≥ 1 grade 3 or 4 AE | 13 (11.6) | 23 (20.4) |
Patients with ≥ 1 grade 5 AE | 0 (0.0) | 0 (0.0) |
Patients with ≥ 1 SAE | 6 (5.4) | 17 (15.0) |
Patients with ≥ 1 does interruption due to AE | NA | 33 (29.2) |
Patients who stopped treatment due to AE | NA | 21 (18.6) |
Treatment-related deaths | 0 (0.0) | 0 (0.0) |
Notable harms | ||
Immune-mediated reactions | ||
Hypothyroidism | 0 (0.0) | 16 (14.2) |
Hyperthyroidism | 2 (1.8) | 5 (4.4) |
Rash | 2 (1.8) | 21 (18.6) |
Grade 3 or 4 rash | 0 (0.0) | 1 (0.9) |
Severe cutaneous reactions | 0 (0.0) | 2 (1.8) |
Colitis, grade 3 or 4 | 0 (0.0) | 1 (0.9) |
Pneumonitis | 0 (0.0) | 6 (5.3) |
Grade 3 or 4 pneumonitis | 0 (0.0) | 1 (0.9) |
Immune-mediated hepatitis | 5 (4.5) | 15 (13.3) |
Grade 3 or 4 immune-mediated hepatitis | 0 (0.0) | 6 (5.3) |
Infusion-related reaction | NR | NR |
AE = adverse event; BSC = best supportive care; CI = confidence interval; CNS = central nervous system; DFS = disease-free survival; HR = hazard ratio; NA = not applicable; NE = not estimable; NR = not reported; OS = overall survival; PD-L1 = programmed death-ligand 1; SAE = serious adverse events; TC = tumour cell.
aSummaries of durations (median and percentiles) are Kaplan-Meier estimates. 95% CIs for the medians are computed using the methods of Brookmeyer and Crowley.42
bCensored.
cStratification factors for patients with stage II to IIIA NSCLC and PD-L1 expression on ≥ 50% of TCs: stage from electronic case report form (eCRF) (IB or II vs. IIIA), sex from eCRF (female vs. male), histology from eCRF (squamous vs. nonsquamous).
dHRs were estimated with Cox regression.
eStatistical testing for these end points was not adjusted for multiple comparisons, resulting in an increased risk of false-positive conclusions.
fFor the site of disease recurrence only, there were 50 patients in the BSC group 25 in the atezolizumab group.
gA patient could have more than 1 distant site.
hPatients who had CNS distant site only were included. Patients who had any other recurrent site (i.e., locoregional, other distant site, secondary primary lung, or secondary primary non-lung) in addition to CNS distant site were not included in the CNS-only category.
Source: Clinical Study Report for IMpower010.9
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Patient input was provided by 2 groups: Lung Cancer Canada (LCC) and the Ontario Lung Association (OLA). LCC is a national charity and a member of the Global Lung Cancer Coalition, and serves as a resource for lung cancer education, patient support, research, and advocacy. The OLA, also known as the Lung Health Foundation (LHF), is a charity that provides education, programs, and services for patients and health care providers, and invests in research and policy improvement in lung health. LCC collected the thoughts and experiences from 9 patients with NSCLC or small cell lung cancer and 1 caregiver (from Canada, the US, the UK, and Australia) in December 2021 via phone interviews and environmental scans. LHF conducted phone interviews with 3 patients (Ontario, Manitoba, and Quebec) in September and October 2021 and a registered nurse and certified respiratory educator.
Patients who responded to the 2 surveys reported difficulty coping with their diagnosis and noted that they felt like there was “no hope, no light, and [were] less human” because of the poor prognosis of lung cancer. These feeling were amplified when the cancer was detected late. Patient respondents also reported that cancer-related symptoms were hard to manage. Although the physical symptoms of shortness of breath, cough, and fatigue were reported to be mild, the psychosocial effects (such as anxiety, distress, depression) and some of the harsh side effects of chemotherapy, radiation, and surgery (e.g., nausea, vomiting, neuropathy, lung injury) were harder to manage. Similarly, the psychosocial burden placed on family members and caregivers affected their emotional well-being, ability to travel and socialize, and work life.
Patient respondents deemed the following outcomes as important: delayed disease progression and increased long-term remission that ultimately improved survivorship; minimal side effects from treatments; maintenance of independence and functionality (to minimize burden on caregivers and loved ones); and full and worthwhile quality of life. The survey respondents emphasized a lack of treatment options for patients with PD-L1-positive, driver-mutation-negative lung cancer to reduce a risk of recurrence after post-surgery chemotherapy. Patients emphasized the desire for a choice of therapies that work in the early stages of disease (as opposed to the metastatic stage) with durable efficacy to maintain stable disease and increase chance of cure.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Based on input from the clinical experts consulted by CADTH, despite the current standard of care with adjuvant chemotherapy, many patients who have undergone surgical resection and adjuvant chemotherapy experience disease relapse. In the majority of these cases, the disease is often incurable. The survival benefit that accompanies adjuvant chemotherapy is modest; there is an unmet need for other effective treatments for this patient population. If adopted, atezolizumab would be an additional therapy, not a replacement for pre-existing therapy (i.e., atezolizumab would be given in addition to, not instead of, adjuvant chemotherapy). Also, if adopted, atezolizumab would be offered to patients with resected NSCLC and tumours larger than 5 cm and to patients with node-positive tumours, regardless of the size of the primary tumour, and a PD-L1 tumour score of at least 50%. According to the clinical experts, the only way to know if adjuvant therapy is successful in NSCLC is to follow a patient who has completed all curative-intent therapy to disease relapse. The majority of cases of disease relapse, according to the clinical experts, occur in the 5 years after completion of therapy. The clinical experts recommended that treatment with atezolizumab be discontinued in the event of dangerous or intolerable adverse events (AEs), disease relapse, or patient choice to stop therapy. Atezolizumab may be administered at any outpatient cancer systemic therapy infusion unit where immunotherapy checkpoint inhibitors are already administered.
Clinician Group Input
Input was received from 3 clinicians on behalf of the Cancer Care Ontario (OH-CCO) Drug Advisory Committee (DAC) and 17 physicians who treat lung cancer in Canada on behalf of LCC.
The OH-CCO Lung and Thoracic DAC indicated the need for therapy that increased cure and overall survival (OS) rates. Both clinician input groups stated that patients with stage II to III (according to UICC and AJCC [8th edition]6 staging criteria) lung cancer have the greatest unmet need. Both clinician groups also indicated that atezolizumab would supplement and/or be added to the current post-operative management of resected NSCLC after at least 1 dose of adjuvant (platinum-doublet) chemotherapy, and not be a replacement for current therapies. The OH-CCO Lung and Thoracic DAC indicated that patients with PD-L1 tumour scores of at least 50% and all PD-L1-positive patients are suited for atezolizumab. LCC suggested that patients with stage II to IIIA (UICC and AJCC [7th edition]1 staging criteria) resected lung cancer with a PD-L1–positive tumour (≥ 1%) determined by immunohistochemistry (IHC) after at least 1 cycle of adjuvant therapy, regardless stage or nodal status, are suitable for atezolizumab.
The OH-CCO Lung and Thoracic DAC considered DFS a clinically meaningful outcome measure. LCC emphasized that recurrent disease (DFS) should be considered a critical outcome on its own (besides OS, which is the gold standard), given the high patient, health care, and social-level ramifications associated with recurrence. Both groups indicated that therapy should be discontinued at disease progression or unacceptable toxicity. As for the treatment settings, hospital (outpatient clinic) and any oncology settings where infusions are performed were considered appropriate prescribing settings for atezolizumab by the OH-CCO Lung and Thoracic DAC and LCC, respectively. The OH-CCO Lung and Thoracic DAC agreed that the end points reported in the trial can reasonably be expected to correlate with OS. Also, both clinical groups believed other strategies (e.g., a short course with only 3 doses of neoadjuvant immunotherapy plus chemotherapy) are expected to be less expensive than a full-year course of adjuvant immunotherapy.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for atezolizumab:
consideration for initiation of therapy
generalizability
care provision.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
One ongoing phase III, global, multi-centre, open-label, randomized study was included in the review. The IMpower010 trial compared the efficacy and safety of atezolizumab versus best supportive care (BSC) in patients with stage IB to stage IIIA (per UICC and AJCC [7th edition]1 staging system) NSCLC after complete resection and adjuvant cisplatin-based chemotherapy. A total of 1,005 patients were randomized across 204 sites in 21 countries in North America (including 2 sites in Canada), Europe, Asia, and Australia.
The primary efficacy outcome was DFS, assessed by the investigator. Secondary efficacy outcomes included OS, 3-year and 5-year DFS, and DFS in subpopulations with PD-L1 expression on at least 50% of TCs, assessed with SP263 IHC assay, in patients with stage II to IIIA NSCLC as defined by the UICC and AJCC (7th edition) staging criteria.1 The IMpower010 study consisted of 2 phases: an enrolment phase and a randomized phase. In the enrolment phase, patients who had undergone completed resection of their NSCLC were screened and, if eligible, received 1 of 4 cisplatin-based chemotherapy regimens (cisplatin plus vinorelbine, docetaxel, gemcitabine, or pemetrexed), based on investigator choice. Patients who were still deemed eligible to continue with the study after up to 4 cycles of cisplatin-based chemotherapy proceeded to the randomization phase, in which patients were randomized in a 1:1 ratio to receive atezolizumab or BSC. The clinical report provided to CADTH presented a protocol-specified interim analysis for DFS of study data collected from the date of the first patient randomized (February 26, 2016) to the clinical data cut-off date of January 21, 2021.
At baseline, there were 229 patients with stage II to IIIA NSCLS and PD-L1 expression on at least 50% of TCs. The indication population had a median age of 62 (range = 36 to 84) years, was predominantly male (72.9%) and White (70.3%), had high functional performance (57.2% with an Eastern Cooperative Oncology Group [ECOG] performance status score of 0), and most reported previous tobacco use (69.9%). At diagnosis, most patients were diagnosed with stage IIIA (48.0%) disease and with nonsquamous histology (59.8%). Of the 137 patients with nonsquamous histology, 94.2% were identified as having adenocarcinoma subtype. EGFR or ALK mutation was detected in 8.7% of patients. Most patients had undergone prior lobectomy (74.2%) and mediastinal lymph node dissection (81.7%)
Efficacy Results
Efficacy results are presented for the subpopulation of patients who had stage II to IIIA NSCLC with PD-L1 expression on at least 50% of TCs (per the indication under review), unless otherwise specified.
Overall Survival
Among the subpopulation of patients with stage II to IIIA disease and PD-L1 expression on at least 50% of TCs, the observed deaths at the time of the interim analysis (median follow-up = 32.2 [range = 0 to 58.8] months) were 22.8% and 9.6% in the BSC and atezolizumab treatment groups, respectively. The stratified hazard ratio (HR) was 0.40 (95% CI, 0.20 to 0.81) in favour of atezolizumab. The median OS could not be estimated in either treatment arm because of the low rate of death events at the time of the planned interim analysis. At year 3, 90.85% of patients in the atezolizumab treatment group were event-free compared with 76.67% of the BSC treatment group, for a difference in proportion of 14.27% (95% CI, 4.19% to 24.35%).
Disease-Free Survival
In the subpopulation of patients with stage II to IIIA disease and PD-L1 expression on at least 50% of TCs, 45.6% in the BSC treatment arm experienced a disease recurrence or death compared with 24.3% in the atezolizumab arm. The stratified HR for DFS was 0.47 (95% CI, 0.29 to 0.75). At year 3, 73.79% of patients in the atezolizumab group were event-free compared with 48.61% in the BSC group, representing a difference in event-free rate of 25.18% (95% CI, 11.01% to 39.36%).
Type of Recurrence
Of patients with stage II to IIIA NSCLC and PD-L1 expression on at least 50% of TCs who experienced a protocol-defined disease recurrence (n = 50 for BSC; n = 25 for atezolizumab), locoregional disease recurrence was experienced by 60% of patients in the atezolizumab treatment arm and by 34% in the BSC arm. Distant-only disease recurrence was experienced by 42% of patients in the BSC arm and 24% in the atezolizumab arm. Central nervous system (CNS)-only disease recurrence was experienced by 14% of patients in the BSC arm and 4% in the atezolizumab arm. Combined locoregional plus distant disease recurrence was similar in the 2 treatment arms (BSC = 18%; atezolizumab = 16%).
Harms Results
Adverse Events
Among patients with stage II to IIIA NSCLC and PD-L1 expression on at least 50% of TCs, 94.7% of patients who received atezolizumab and 69.6% who received BSC reported at least 1 AE. The top 5 reported AEs (BSC versus atezolizumab) were cough (10.7% versus 14.2%), nasopharyngitis (12.5% versus 8.8%), arthralgia (5.4% versus 13.3%), pruritis (2.7% versus 11.5%), and anemia (8.0% versus 7.1%). The following AEs had a difference of at least 5% between the 2 treatment arms, with a greater proportion of affected patients in the atezolizumab arm: arthralgia, asthenia, increased blood creatine, diarrhea, rash, pruritus, and pyrexia.
Adverse Events by Grade
Among patients with stage II to IIIA NSCLC and PD-L1 expression on at least 50% of TCs, at least 1 grade 3 or 4 AE was reported in 11.6% and 20.4% of patients randomized to BSC and atezolizumab, respectively. The most commonly reported grade 3 or 4 AEs in patients who received BSC were decreased neutrophil count (1.8%); in patients who received atezolizumab, the most common AEs were increased alanine aminotransferase (1.8%) and abnormal hepatic function (2.7%). No grade 5 AEs were reported.
Serious Adverse Events
Among patients with stage II to IIIA NSCLC and PD-L1 expression on at least 50% of TCs, 15% of patients who received atezolizumab reported at least 1 serious adverse event (SAE) compared with 5.4% who received BSC. The most commonly reported SAE was pyrexia (1.8%).
Dose Interruptions Due to Adverse Events
Among patients with stage II to IIIA NSCLC and PD-L1 expression on at least 50% of TCs, 29.2% of patients who received atezolizumab had at least 1 dose interruption due to an AE. Reasons for the dose interruptions included hyperthyroidism (3.5%), pneumonia (2.7%), upper respiratory tract infection (1.8%), pyrexia (1.8%), rash (1.8%), and oropharyngeal pain (1.8%).
Discontinuation of Treatment Due to Adverse Events
Among patients with stage II to IIIA NSCLC and PD-L1 expression on at least 50% of TCs, 18.6% of patients who received atezolizumab stopped treatment due to an AE. Reasons for the discontinuation were not available for this subpopulation.
Among the overall safety population, 18.2% of patients who received atezolizumab stopped treatment due to an AE. The most common events leading to treatment discontinuation were pneumonitis (1.4%), hypothyroidism (1.4%), and aspartate aminotransferase increase (1.4%).
Mortality
There were no treatment-related death data in the subpopulation of patients with stage II to IIIA NSCLS and PD-L1 expression on at least 50% of TCs.
Among the overall safety population, the proportion of patients who died was similar in the BSC (18.2%) and atezolizumab (19.2%) treatment groups. Of these deaths, 95.1% occurred more than 30 days after the last study treatment or safety visit. Treatment-related deaths due to AEs occurred in 0.6% and 1.6% of patients in the BSC and atezolizumab arms, respectively. The majority of deaths were due to disease progression.
Notable Harms
Among the subpopulation of patients with stage II to IIIA NSCLC and PD-L1 expression on at least 50% of TCs, reported immune-mediated reactions related to endocrinopathies included hypothyroidism (atezolizumab = 14.2%; BSC = 0%) and hyperthyroidism (atezolizumab = 4.4%; BSC = 1.8%). Overall immune-mediated rashes were reported by 1.8% and 18.6% of patients who received BSC and atezolizumab, respectively. One person who received atezolizumab experienced a grade 3 or 4 rash. Immune-mediated colitis (grade 3 or 4) was reported by 1 person who received atezolizumab. Immune-related pneumonitis was reported by 5.3% of patients who received atezolizumab, 1 case of which was grade 3 or 4. Immune-mediated hepatitis was reported by 4.5% and 13.3% of patients who received BSC and atezolizumab, respectively. Among patients who received atezolizumab, 5.3% experienced grade 3 or 4 immune-mediated hepatitis.
Data related to infusion-related reactions were not reported for the subpopulation of patients with stage II to IIIA NSCLS and PD-L1 expression on at least 50% of TCs.
Critical Appraisal
The critical appraisal of the IMpower010 study by CADTH was limited by a decision made by Health Canada to amend the NOC from the original indication population to only the subset of patients with stage II to IIIA NSCLC whose tumour had PD-L1 expression on at least 50% of TCs. Randomization was stratified by sex (female versus male), tumour histology (squamous versus nonsquamous), extent of disease (stage IB versus stage II versus stage IIIA based on the UICC and AJCC [7th edition] staging criteria) and PD-L1 expression status (TC2/3 and any immune cells [ICs] versus TC0/1 and IC2/3 versus TC0/1 and IC0/1, using the SP142 IHC assay). The choice of stratification factors was considered to be reasonable and, as noted in the Health Canada report, stage of disease is a known prognostic factor for NSCLC and PD-L1 tumour performance status is a predictive factor for immunotherapy efficacy in the setting of incurable NSCLC.8 The enrolled subpopulation of patients that met the Health Canada indication only accounted for 22.8% of the total randomized population, and was not a defined subpopulation for the primary end points in the analysis in the IMpower010 trial design. As such, the IMpower010 trial was not powered for the Health Canada indication under review. Of note, Health Canada’s decision to amend the indication to PD-L1 expression on at least 50% of TCs at the time of the interim analysis was due to uncertainty about the clinical benefit of atezolizumab for patients with stage II to IIIA NSCLC and PD-L1 expression on 1% to 49% of TCs; Health Canada noted that the improvement in DFS was mainly driven by the subgroup of patients with PD-L1 expression on at least 50% of TCs.8 Likewise, the European Medicines Agency also considered the subgroup with PD-L1 expression on at least 50% of TCs to be the most relevant for labelling at the time of the interim analysis.10
Although DFS in patients with PD-L1 expression on at least 50% of TCs was a pre-specified secondary end point, it was absent from the statistical testing hierarchy. Thus, the statistical analyses of the efficacy outcomes were conducted with no control for multiplicity, which increases the risk of false-positive conclusions. Several subgroup analyses were performed to examine the consistency of the treatment effect observed for the primary and key secondary efficacy end points. However, proper interpretation of all subgroups was not possible because of the lack of sample size considerations and their absence from the statistical testing hierarchy. Moreover, data for OS were immature, and although clinical experts believe it is plausible that the findings for DFS will translate into OS, there remains uncertainty about this.11,12
Among the subgroup of patients with PD-L1 expression on at least 50% of TCs and stage II to IIIA disease, there were some minor imbalances across groups but these did not universally favour either group and may be considered reasonable, given the small sample size.8 Additionally, minor differences in characteristics between this subgroup and the intention-to-treat (ITT) population were not expected to confound the efficacy analyses.8
The demographic characteristics of the study population were considered by the clinical experts to be generally reflective of the relevant population with NSCLC in Canada. The clinical experts considered the results of the IMpower010 multi-national, multi-centre study to be generalizable to the Canadian setting. The clinical experts did highlight a few notable differences in disease characteristics (i.e., the larger proportion of patients with squamous lung cancer) and treatment regimen (i.e., cisplatin doublets containing gemcitabine and docetaxel are not commonly used in Canadian lung cancer practice in the adjuvant setting) between the trial population and the Canadian NSCLC population. Outcomes important to patients, such as health-related quality of life, were not reported.
Indirect Comparisons
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH or identified in the literature search.
Conclusions
Based on the IMpower010 trial, uncertainty remains about the efficacy of adjuvant atezolizumab in increasing DFS in adults with stage II or IIIA (per the UICC and AJCC [7th edition] staging criteria) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs following complete resection and no progression after platinum-based adjuvant chemotherapy at the time of the planned interim analysis, because the analysis was absent from the statistical hierarchy and not controlled for multiplicity. Although based on clinical expert opinion, the findings appeared favourable and are considered clinically important. Conclusions regarding the efficacy of atezolizumab on improved OS cannot be made because of the immature nature of the data at the time of the planned interim analysis. Despite these limitations, the findings from the IMpower010 trial appeared to be generalizable to the real-world setting.
Introduction
Disease Background
Lung cancer is one of the most commonly diagnosed cancers, and the leading cause of cancer deaths in Canada.2 Survival after lung cancer across all stages and histologies is poor. Indeed, more Canadians die of lung cancer than colorectal, pancreatic, and breast cancer combined.2 Moreover, the 5-year net survival rate for lung cancer is 22%.5 The high mortality rate associated with lung cancer reflects both its high incidence rate and its low survival rate. There are 2 types of lung cancer that are classified by the type of cell in which the cancer started: small cell lung cancer and NSCLC.13 NSCLC accounts for approximately 80% to 88% of all lung cancer diagnoses in Canada.2,3 NSCLC is further classified into histologic subtypes, with the most common being adenocarcinoma and squamous cell carcinoma. Squamous cell cancer is a subtype of NSCLC that usually starts in the cells that lie the bronchi in the centre of the lungs. The most common subtype of NSCLC is adenocarcinoma, which usually starts in the glandular cells on the outer part of the lung. Approximately 15% of Canadians with NSCLC also have an EGFR-activating mutation in the region encoding the tyrosine kinase domain.14-16 A further 2% to 6% have an ALK fusion.17 The majority of patients with an EGFR or ALK driver mutation are in the adenocarcinoma subset and are less likely to have a history of significant tobacco use.
To determine a patient’s prognosis and treatment, NSCLC is staged using the Union for International Cancer Control (UICC) and American Joint Committee on Cancer (AJCC) staging criteria, which involves tumour, node, metastasis (TNM) classification of the disease based on the size and spread of the primary tumour (T), lymph node involvement (N), and the occurrence of metastasis (M).18 For invasive NSCLC there are 4 stages: I to IV. The International Association for the Study of Lung Cancer Lung Cancer Project, which collected survival data on more than 81,000 patients with lung cancer from 19 countries, including Canada, found that 5-year OS for NSCLC decreased with increasing stage.5 Indeed, the 5-year OS of 92% at diagnosis at stage IA1 declined with each stage to less than 40% at stage IIIA and higher.
Approximately half of all lung cancer cases in Canada are stage I to III at diagnosis,2 and approximately 1-third of patients with NSCLC have operable disease.4 Early-stage (i.e., stages I to IIIA per the AJCC [7th edition]1 staging criteria) NSCLC is often asymptomic.18,19 When patients do present with symptoms, these are usually nonspecific and difficult to directly attribute to lung cancer.19 The most common symptoms include fatigue, cough, chest or shoulder pain, hemoptysis, weight loss, dyspnea, hoarseness, bone pain, and fever.19 Diagnostic procedures include CT, PET, and/or MRI scans, bronchoscopy with or without endobronchial ultrasound or tissue biopsy.4 Pathologic testing of biomarkers on lung biopsy specimens assists in decisions about treatment options and risk stratification.
Standards of Therapy
The primary goal of treatment for patients with stage IB to IIIA (per the UICC and AJCC [7th edition]1 staging criteria; the equivalent stages using the AJCC [8th edition]6 staging criteria are stages IIA to IIIB) NSCLC is to cure and prolong life. The secondary goal of treatment is to delay disease relapse, thereby allowing patients a longer period of time living disease-free. These treatment goals are primarily attained via surgical resection of the tumour and, for some groups, adjuvant therapy is recommended.4,7
The clinical experts consulted by CADTH noted that although surgery is the gold standard of care for patients with NSCLC that is anatomically amenable to resection, some patients with stage I disease may not be good operative candidates (e.g., those who have significant comorbidities for which general anesthetic is contraindicated), and others may refuse surgery. Those with an appropriate disease location and adequate lung function can be treated with curative intent with stereotactic ablative radiation. Likewise, some patients who are not surgical candidates or who refuse surgery for stage II disease that is too anatomically extensive for stereotactic ablative radiation may receive curative-intent combined chemo-radiation. Patients who undergo curative-intent resection of a NSCLC where the primary tumour is 4 cm or larger, or with involved lymph nodes, are then considered for 4 cycles of adjuvant cisplatin-based doublet chemotherapy, usually with vinorelbine or pemetrexed. This is based on the Lung Adjuvant Cisplatin Evaluation (LACE) meta-analysis, which showed an absolute benefit of 5% in 5-year OS (HR = 0.89; 95% CI, 0.82 to 0.96; I2 = 6%; P = 0.005).20 The LACE meta-analysis also demonstrated an absolute benefit of chemotherapy on DFS of 5.8% and 5.8% at 3 years and 5 years, respectively (HR = 0.84; 95% CI, 0.78 to 0.91; I2 = 0.27; P < 0.001).
If a resected tumour is known to harbour 1 of the common EGFR mutations (e.g., exon 19 deletion or L858R), evidence from the ADAURA trial21 supports 3 years of osimertinib after adjuvant chemotherapy, if it was given, based on a DFS benefit of 24 months (HR = 0.17, 99% CI, 0.11 to 0.26; P < 0.0001) for those with stage II to IIIA (per the AJCC [7th edition] staging criteria) disease.
Meta-analyses have estimated a 5-year OS benefit of approximately 4% to 5% with adjuvant platinum-based chemotherapy.20,22,23 Adjuvant chemotherapy is recommended for patients with stage II to IIIA (AJCC [7th edition]1 staging criteria) disease and stage IB (AJCC [7th edition]1 staging criteria) patients considered to be at high risk of relapse (e.g., those with tumours > 4 cm in diameter, nodal involvement, perineural or lymphovascular invasion, or spread through airspaces).4,24 However, not all patients receive post-operative adjuvant chemotherapy. A retrospective cohort study conducted in Europe, which included 831 patients with stage IB to IIIA (AJCC [7th edition] staging criteria)1 NSCLC, showed that 48% of patients received adjuvant chemotherapy (15.1% with stage IB, 55.1% with stage II, and 71.4% with stage IIIA).25 The most common reasons for not receiving adjuvant chemotherapy were that it was declined by the patient (12.6%), comorbidities (11.9%), complication or delay in surgery recovery (8.4%), and poor performance status (7.0%).25 Additionally, approximately 1-third of patients who received chemotherapy did not finish the planned number of cycles.25
In Canada, cisplatin-based adjuvant chemotherapy is the standard of care. According to the clinical experts consulted by CADTH, the most common chemotherapy combinations are cisplatin plus vinorelbine and cisplatin plus pemetrexed. Carboplatin-based chemotherapy is used by some physicians for patients who are ineligible for cisplatin adjuvant chemotherapy, although its use is controversial.4,24 Adjuvant radiotherapy is generally only considered in the setting of positive surgical margins; after complete surgical resection, radiation is not routinely recommended.4,24 After adjuvant chemotherapy is complete, patients receive active surveillance, which most commonly involves CT scans every 3 to 6 months for 2 to 3 years, and annually thereafter until year 5.7,24
Since January 2021, osimertinib has been approved in Canada as adjuvant therapy after tumour resection and completion of adjuvant chemotherapy for patients with stage IB to IIIA (per the UICC and AJCC [7th edition]1 staging criteria) NSCLC with EGFR exon 19 deletions or exon 21 (L858R) substitution driver mutations.
Drug
Atezolizumab is an Fc-engineered humanized immunoglobulin G1 monoclonal antibody that directly binds to PD-L1 and blocks interactions with the PD-1 and B7.1 receptors, releasing PD-L1- and PD-1-pathway–mediated inhibition of the immune response, including reactivation of the antitumour immune response. Atezolizumab leaves the PD-L1 and PD-1 interaction intact.
Atezolizumab received an NOC from Health Canada on January 14, 2022 as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to the AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs. Although the original indication proposed to Health Canada was for the patients with NSCLC whose tumours had PD-L1 expression on at least 1% of TCs, the approved Health Canada indication was limited to patients with stage II to IIIA disease with PD-L1 expression on at least 50% because of uncertainty about the clinical benefit of atezolizumab in the population with PD-L1 expression on 1% to 49% of TCs; Health Canada noted that the improvement in DFS was mainly driven by improvement in the subgroup with PD-L1 expression on at least 50% of TCs.8 Although the reimbursement request from the sponsor was for atezolizumab as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to the AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs and no EGFR or ALK genomic tumour aberrations, the current review is focused on Health Canada indication described previously, which is boarder in scope.
Atezolizumab is also indicated:
in combination with carboplatin and etoposide for the first-line treatment of adults with extensive-stage small cell lung cancer
as monotherapy for the first-line treatment of patients with metastatic NSCLC whose tumours have high PD-L1 expression (PD-L1 stained ≥ 50% of TCs or PD-L1 stained tumour-infiltrating ICs covering ≥ 10% of the tumour area), determined by a validated test, and with no EGFR or ALK genomic tumour aberrations
in combination with bevacizumab, paclitaxel, and carboplatin for the first-line treatment of adults with metastatic nonsquamous NSCLC, no EGFR or ALK genomic tumour aberrations, and no prior systemic chemotherapy treatment for metastatic nonsquamous NSCLC
in combination with nanoparticle albumin-bound paclitaxel and carboplatin for the first-line treatment of adults with metastatic nonsquamous NSCLC and no EGFR or ALK genomic tumour aberrations
for the treatment of adults with locally advanced or metastatic NSCLC with progression on or after platinum-based chemotherapy
in combination with bevacizumab for the first-line treatment of adults with unresectable or metastatic hepatocellular carcinoma who require systemic therapy.
Health Canada has also issued a NOC with conditions for the use of atezolizumab in combination with nanoparticle albumin-bound paclitaxel for the treatment of adults with unresectable, locally advanced, or metastatic triple-negative breast cancer whose tumours have PD-L1 expression on at least 1% of TCs and who have not received prior chemotherapy for metastatic disease.
Atezolizumab has received approval as adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA disease (according to the AJCC [7th edition] staging criteria)1 whose tumours have PD-L1 expression on at least 50% of TCs in Switzerland (Swissmedic)26 and the UK (Medicine and Healthcare products Regulatory Agency).27 The FDA has approved atezolizumab as adjuvant treatment after resection and platinum-based chemotherapy in patients with PD-L1 expression on at least 1% of TCs in patients with stage II to IIIA (AJCC [7th edition] staging criteria)1 NSCLC.28 Atezolizumab was approved by Australia’s Therapeutic Goods Administration on September 7, 2022, and by the European Medicines Agency on April 25, 2022.
Atezolizumab was previously reviewed by CADTH in combination with bevacizumab for the first-line treatment of adults with unresectable or metastatic hepatocellular carcinoma who require system therapy.
Atezolizumab is administered as an IV infusion at a dosage of 840 mg every 2 weeks, 1,200 mg every 3 weeks, or 1,680 mg every 4 weeks.
Key characteristics of medical treatments for resected NSCLC are presented in Table 3.
Table 3: Key Characteristics of Medications for the Treatment of Resected NSCLC
Characteristic | Atezolizumab | Osimertinib |
|---|---|---|
Mechanism of action | An Fc-engineered humanized IgG1 monoclonal antibody that directly binds to PD-L1 and blocks interactions with PD-1 and B7.1 receptors, releasing PD-L1- and PD-1-pathway–mediated inhibition of the immune response, including reactivation of the antitumour immune response. Atezolizumab leaves the PD-L1 and PD-1 interaction intact. | Selective irreversible inhibitor of EGFR sensitizing mutations and T790M resistance mutation that has limited activity against wild-type EGFR. |
Indicationa | As monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to UICC and AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs.b | As adjuvant therapy after tumour resection in patients with stage IB to IIIA (per the AJCC [7th edition]1 staging criteria) NSCLC whose tumours have EGFR exon 19 deletions or exon 21 (L858R) substitution mutations. |
Route of administration | IV infusion | Oral |
Recommended dose | 840 mg every 2 weeks, 1,200 mg every 3 weeks, or 1,680 mg every 4 weeks | 80 mg once a day |
SAEs or safety issues | Warnings and precautions Immune-mediated adverse reactions:
Infusion-related reactions:
Complications of allogeneic HSCT:
Embryo-fetal toxicity:
Adverse reactions
| Warnings and precautions
Adverse reactions
|
Other | — | A validated test is required to identify PD-L1 and EGFR-mutation-positive status in tumour tissue before treatment |
AJCC = American Joint Committee on Cancer; EGFR = epidermal growth factor receptor; HSCT = hematopoietic stem cell transplantation; IgG1 = immunoglobulin G1; NSCLC = non–small cell lung cancer; PD-1 = programmed death-1; PD-L1 programmed death-ligand 1; TC = tumour cell; UICC = Union for International Cancer Control.
aHealth Canada–approved indication
bAtezolizumab is also indicated for use in adults with small cell lung cancer, NSCLC, and hepatocellular carcinoma in the metastatic setting.
Source: Product monograph for atezolizumab (Tecentriq),29 product monograph for osimertinib (Tagrisso).30
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Patient input was provided by 2 groups: LCC and) LHF. LCC is a national charity and a member of the Global Lung Cancer Coalition and serves as a resource for lung cancer education, patient support, research, and advocacy. LHF is a charity that provides education, programs, and services for patients and health care providers, and invests in research and policy improvement in lung health. LCC collected the thoughts and experiences from 9 patients with NSCLC or small cell lung cancer and from 1 caregiver (from Canada, the US, the UK, and Australia) in December 2021 with phone interviews and environmental scans. LCC conducted phone interviews with 3 patients (from Ontario, Manitoba, and Quebec) in September and October 2021.
Patients who responded to the 2 surveys reported difficulty coping with their diagnosis and noted that they felt like there was “no hope, no light, and [that they were] less human” because of the poor prognosis of lung cancer. These feelings were amplified when the cancer was detected late. Patients also reported that cancer-related symptoms were hard to manage. Although the physical symptoms of shortness of breath, cough, and fatigue were reported to be mild, the psychosocial effects (such as anxiety, distress, depression) and some of the harsh side effects from chemotherapy, radiation, and surgery (e.g., nausea, vomiting, neuropathy, and lung injury) were harder to manage. Similarly, the psychosocial burden placed on family members and caregivers affected their emotional well-being, ability to travel and socialize, and work life.
Patient respondents deemed the following outcomes as important: delayed disease progression and increased long-term remission that ultimately improved survivorship, minimal side effects from treatments, maintenance of independence and functionality (to minimize burden on caregivers and loved ones), and full and worthwhile quality of life. The survey respondents emphasized a lack of treatment options for patients with PD-L1–positive, driver mutation–negative lung cancer to reduce a risk of recurrence after post-surgery chemotherapy. Patients emphasized wanting a choice in therapy that works in the early stages of disease (as opposed to the metastatic stage) with durable efficacy to maintain stable disease and increase chance of cure.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NSCLC.
Unmet Needs
Based on input from the clinical experts consulted by CADTH, despite the current standard of care with adjuvant chemotherapy, many patients who have undergone surgical resection and adjuvant chemotherapy experience disease relapse. In these cases, the disease is most often incurable. The survival benefit that accompanies adjuvant chemotherapy is modest, so there is an unmet need in this patient population. As noted by the clinical experts, modern population-based survival data from a time when adjuvant chemotherapy was in widespread use mirrors these outcomes.31 A 2016 report from the US Surveillance, Epidemiology, and End Results database reported 5-year OS rates ranging from 30% to 55% for patients with stage I to III NSCLC.31 The 8th edition of cancer staging from the AJCC,6 which is the current staging system being used, reports 5-year survival rates as 60%, 53%, and 36% for stage IIA, stage IIB, and stage IIIA NSCLC, respectively.
Place in Therapy
The clinical experts consulted by CADTH suggested that if adopted, atezolizumab would be an additional therapy, and not a replacement for pre-existing therapy (i.e., atezolizumab would be given in addition to, not instead of, adjuvant chemotherapy). The clinical experts agreed that atezolizumab would be only for use in the curative-intent setting after surgery, with the goal of increasing time before disease recurrence and, presumably, reducing the overall number of patients who experience disease recurrence.
The clinical experts noted that in the IMpower010 study,32 the subset of patients that received cisplatin plus gemcitabine as their adjuvant chemotherapy regimen before atezolizumab did not seem to derive benefit from adjuvant atezolizumab. The clinical experts also noted that there is mounting evidence across multiple tumour types that treatment with gemcitabine chemotherapy may attenuate the efficacy of immunotherapy checkpoint inhibitors.33,34 Although the use of cisplatin plus gemcitabine is not common in Canada in the adjuvant setting for NSCLC, the clinical experts recommended that the combination not be used at all if there are any other available options if adjuvant atezolizumab is being considered. Specifically, cisplatin plus vinorelbine or cisplatin plus pemetrexed should be recommended, in keeping with the majority of adjuvant chemotherapy currently used in Canada.
According to the clinical experts, there could a potential shift the treatment paradigm for patients who experience disease recurrence while receiving adjuvant atezolizumab, or within 6 months of completion, because standard first-line therapy for this patient population, when diagnosed with incurable disease, is single-agent pembrolizumab or platinum-doublet chemotherapy combined with pembrolizumab; however, that may not be appropriate if their disease is likely to be resistant to PD-L1 inhibition. The clinical experts noted that, currently, there are no data on which to base recommendations for the use of checkpoint inhibitors in the advanced setting if a patient progressed on, or shortly, after adjuvant atezolizumab. The clinical experts did note that 12.2% of patients in the IMpower010 study who experienced disease relapse after receiving adjuvant atezolizumab went on to receive immunotherapy checkpoint inhibitors at the time of relapse32,35; however, the details of the interval time between completion of atezolizumab and the subsequent immunotherapy is unknown. Also unknown are the specific immunotherapy checkpoint inhibitors used after relapse and the outcomes in this population. Once these data become available, we may be able to clarify this issue.
Patient Population
The clinical experts consulted by CADTH suggested that if adopted, atezolizumab would be offered to patients with resected NSCLC with a PD-L1 tumour proportion score of at least 50% and tumours larger than 5 cm, and to patients with node-positive tumours, regardless of the size of the primary tumour. Accordingly, companion IHC diagnostic testing of PD-L1 would be required. Although the IMpower010 study used the SP263 IHC assay, the clinical experts verified that, according to the Blueprint phase 2 project,36 the SP263 assay has a high concordance with the 22C3 assay, which is currently in use in most pathology laboratories in Canada. Given the high concordance between the 2 IHC procedures, PD-L1 testing with the SP263 assay would not need to be implemented. The clinical experts did acknowledge, however, that there is wide variation in Canadian pathology labs in the current use of PD-L1 testing for patients with stage I to III NSCLC treated for cure. In jurisdictions where PD-L1 testing is currently limited to those with advanced, incurable NSCLC, this indication would expand the need for PD-L1 IHC testing in the broader population.
Eligible patients would be identified by thoracic surgeons, who would then refer patients to a medical oncologist for consideration for systemic adjuvant therapy after resection. Misdiagnosis is not an issue in this setting; however, with lung cancer screening across Canada currently limited to recently launched programs in selected jurisdictions, underdiagnosis of patients with early-stage asymptomatic disease is still an issue. As lung cancer screening programs gain momentum and become more widespread across Canada, more people will be diagnosed at an earlier stage, when still asymptomatic, and may then be eligible for curative-intent surgery and adjuvant therapy; otherwise, they may not be diagnosed until after they develop incurable metastatic disease.
The clinical experts noted that patients who were solid organ transplant recipients, who had severe active autoimmune disease, or who were considered unsuitable for immunotherapy checkpoint therapy, in general, would not be good candidates for adjuvant atezolizumab. In addition, the clinical experts recommended that patients with common EGFR mutations (exon 19 deletion and exon 21 L858R), although included in the IMpower010 trial, not be offered adjuvant atezolizumab instead of adjuvant osimertinib if they were considered to be candidate and had access to both. The clinical experts also noted that the other driver-mutation-defined population in the IMpower010 trial, patients with ALK fusion, is a population in which immunotherapy checkpoint inhibitors do not have significant activity in the advanced setting. Accordingly, it would not be unreasonable to presume limited, if any, benefit from adjuvant immunotherapy for a resected ALK-positive patient.
Assessing Response to Treatment
According to the clinical experts, the only way to know if adjuvant therapy is successful is to follow a patient with NSCLC from completion of all curative-intent therapy to disease relapse. The majority of disease relapse, as noted by the clinical experts, occurs in the 5 years after completion of therapy. Therefore, the clinical experts recommended that 5-year OS and DFS are the gold-standard metrics for success; patients who are alive and disease-free at this key landmark time point are generally considered to be “cured.”
The clinical experts noted that prolongation of DFS, even for patients who ultimately have disease recurrence, is important. When lung cancer recurs, it is usually incurable and generally carries with it significant physical and psychologic impacts that translate into decreased quality of life, decreased functioning and ability to contribute to society, and increased caregiver burden. Further, current standard-of-care therapy in the setting of incurable NSCLC has a significant burden on health care resources. From the point of view of the clinical experts, delaying the time of relapse has value from patient, health care, and societal perspectives.
The clinical experts recommended that patients receiving adjuvant atezolizumab undergo clinical and laboratory monitoring before each treatment (i.e., every 3 weeks). Radiographic reassessments should be done every 3 to 6 months during therapy. The clinical experts did note that follow-up after completion of curative-intent therapy is not standardized, given the lack of definitive literature suggesting the most appropriate timing for serial radiography. However, most commonly, patients are followed for 5 years with CT scans, which are sometimes done more frequently in the first 2 years after surgery, when relapses are most common. Individual practices will vary, however, depending on which guidelines are being followed, but intervals between CT scans of 6 months for the first 2 years and then 12 months out to year 5 are common. This follow-up regimen would not be affected by adjuvant atezolizumab and is already in place for patients who have received adjuvant chemotherapy after surgery. Finally, an initial diagnosis of NSCLC increases a patient’s risk of developing a second primary NSCLC, so lung cancer screening with low-dose, unenhanced chest CT scans may be appropriate after 5 years of surveillance.
Discontinuing Treatment
The clinical experts recommended that treatment with atezolizumab be discontinued in the event of dangerous or intolerable AEs, disease relapse, or a patient's decision to stop therapy.
Prescribing Conditions
The clinical experts recommended that any outpatient cancer systemic therapy infusion unit where immunotherapy checkpoint inhibitors are already administered would be appropriate for the administration of adjuvant atezolizumab. The clinical experts also noted that atezolizumab should be prescribed and supervised by a cancer specialist, generally a medical oncologist, with experience in the treatment of lung cancer and the use of immunotherapy checkpoint inhibitors.
Additional Considerations
The clinical experts noted that data for the subgroup of IMpower010 that includes the stage IB (AJCC [7th edition]1 staging criteria; primary tumour 4 to 5 cm and node-negative) patient population remain immature; the analysis has yet to be formally completed. If results of the trial are positive for this patient population, the indication may need to be modified. The clinical experts noted that although the Health Canada NOC indication, and hence CADTH, is concerned with patients with PD-L1 expression on at least 50% of TCs, which is the group that derived the most benefit on based on post hoc analysis,32,35 the entire stage II to III (AJCC [7th edition]1 staging criteria) population, regardless of PD-L1 status, benefited from atezolizumab. The clinical experts further noted that another positive adjuvant immunotherapy trial, KEYNOTE091 (PEARLS), was presented at the European Society for Medical Oncology virtual plenary in March 2022.37 Using a very similar trial design, the anti-PD-1 inhibitor pembrolizumab was delivered to patients with stage IB to IIIA (UICC and AJCC [7th edition]1 staging criteria) NSCLC; however, this trial did not mandate adjuvant chemotherapy, but rather stated it should be considered in stage IB and was strongly recommended in stage II to III (AJCC [7th edition]1 staging criteria). In the KEYNOTE091 trial, the HR for DFS of 0.76 (95% CI, 0.63 to 0.91; P = 0.0014) was similar to that seen in the IMpower010 study (DFS HR = 0.79; 95% CI, 0.64 to 0.96; P = 0.0205 in the stage II to III any PD-L1 analysis).32,36 Interestingly, although the data from KEYNOTE091 were not mature for the other primary end point of DFS in the group with a PD-L1 tumour proportion score of at least 50%, the HR at the time of reporting was 0.82 (95% CI, 0.57 to 1.18; P = 0.14).
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Input was received by the following clinician groups: OH-CCO DAC and LCC. OH-CCO DAC provides clinical and health system guidance on drug-related issues in support of CCO’s mandate, including provincial drug-reimbursement programs and the Systemic Treatment Program. Three clinicians provided input on behalf of OH-CCO Lung and Thoracic DAC via email. As described previously, LCC is a national charity and resource for lung cancer education, patient support, research, and advocacy with both regional (Ontario) and pan-Canadian initiatives. LCC gathered expert opinions from 17 physicians who treat lung cancer in Canada and summarized data from published manuscripts and recent presentations.
Unmet Needs
The OH-CCO Lung and Thoracic DAC indicated the need for therapy with better cure and OS rates. According to LCC, currently available therapies provide inadequate 5-year OS (which is far below that of other cancer sites) and DFS (which is associated with OS in early-stage NSCLC). Both groups stated that patients with stage II to III (UICC and AJCC [8th edition]6 staging criteria) lung cancer have the greatest unmet need. The OH-CCO Lung and Thoracic DAC added that patients with resected stage II to III (UICC and AJCC [8th edition]6 staging criteria) NSCLC and no EGFR mutations who have not received neoadjuvant immunotherapy have the greatest unmet need. LCC emphasized that there has not been a new adjuvant therapy for stage IB to III resected NSCLC in the last 2 decades since adjuvant chemotherapy was introduced. In the meantime, however, there has been significant progress in therapies for metastatic disease.
Place in Therapy
Both clinician groups indicated that atezolizumab would supplement and/or be added to the current post-operative management of resected NSCLC after at least 1 dose of adjuvant (platinum-doublet) chemotherapy, and not be a replacement for current therapies. LCC added that there is currently no alternative PD-L1 inhibitor to atezolizumab. Moreover, LCC suggested that re-treatment with immunotherapy such as atezolizumab after relapse with locoregional disease and/or more than 6 months after completion of prior treatment should be considered.
Patient Population
The OH-CCO Lung and Thoracic DAC indicated that patients with a PD-L1 tumour proportion score of at least 50% and all PD-L1-positive patients are suited for atezolizumab. LCC suggested that patients with stage II to IIIA (UICC and AJCC [7th edition]1 staging criteria) resected lung cancer with a PD-L1 tumour proportion score of at least 1%, determined with IHC after at least 1 cycle of adjuvant therapy, regardless of stage or nodal status, are suitable for atezolizumab. LCC explained that as long as a test is validated, the results are acceptable, regardless of whether the SP263, 22C3, or 28 to 8 assay is from a commercial vendor or is an institution in-house option. Also, LCC specified the following patient characteristics that are least suitable for atezolizumab: contraindication to immunotherapy (organ transplant), PD-L1–negative disease, and prior gemcitabine treatment (based on results from the POSEIDON trial).38 According to LCC, for patients with a resected lung cancer with a sensitizing EGFR mutation and PD-L1 expression, clinicians should choose the better option (i.e., atezolizumab or osimertinib, based on an assessment of risks and benefits for each individual patient). As for NSCLC with ALK translocation, LCC recommended that atezolizumab not be used unless other treatment options have been exhausted. Last, because active autoimmune disease is considered a relative contraindication, LCC recommended that the risks and benefits of atezolizumab be discussed with patients with prior or active autoimmune disease.
Assessing Response to Treatment
The OH-CCO Lung and Thoracic DAC considered DFS a clinically meaningful outcome measure. LCC suggested that “response to therapy” is not an appropriate outcome in the early-stage resected-cancer setting as it is in the advanced or metastatic setting. LCC added that, based on the standard set by adjuvant chemotherapy in NSCLC, a DFS benefit with a HR of 0.84 or lower may be considered a clinically meaningful response, as demonstrated in the trial by Pignon et al. (2008).20 Both groups agreed that outcome measures (e.g., recurrence rates via DFS) and cure rates (represented by 5-year OS and KM curves for OS) in clinical trials are aligned with clinical practice. LCC emphasized that even though treatment response cannot be determined in the adjuvant setting, radiographic imaging initially performed at 3 to 4 months, and then at intervals of more than 6 months, should be considered. Further, with laboratory and clinical assessments conducted at 3-week intervals (before each cycle of atezolizumab, for toxicity), physical signs or symptoms suggestive of recurrent disease could be identified. However, LCC acknowledged that there is a wide range of follow-up intervals across Canada, and globally, with no consensus. In most settings, LCC indicated that patients with resected stage IB to IIIA (AJCC [7th edition]1 staging criteria) NSCLC are generally followed for at least 5 years post-operatively by at least 1 (surgical or medical) oncologist. Last, LCC emphasized that recurrent disease (DFS) should be considered a critical outcome on its own (besides OS, which is the gold standard), given the high patient, health care, and social-level ramifications associated with recurrence.
Discontinuing Treatment
Both groups indicated that therapy should be discontinued at disease progression or in the case of unacceptable toxicity.
Prescribing Conditions
As for the treatment settings, hospital (outpatient clinic) and any oncology setting where infusions are performed are considered appropriate prescribing settings for atezolizumab by the OH-CCO Lung and Thoracic DAC and LCC.
Additional Considerations
The OH-CCO Lung and Thoracic DAC agreed that the end points reported in the trial can reasonably be expected to correlate with OS. Also, both clinical groups believed that other strategies (e.g., a short course with only 3 doses of neoadjuvant immunotherapy plus chemotherapy) are expected to be less expensive than a full-year course of adjuvant immunotherapy.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Responses
Drug program implementation questions | Clinical expert response |
|---|---|
Consideration for initiation of therapy | |
Atezolizumab is indicated as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to AJCC [7th edition] staging criteria) NSCLC whose tumours have PD-L1 expression on > 50% of TCs. PAG noted that the AJCC (8th edition) staging system is available.
| The eligible population would include fully resected patients who had a primary tumour > 5 cm, regardless of nodal status, and patients who are node-positive, regardless of primary tumour size.
|
Are patients who received chemotherapy with a non-cisplatin-containing doublet eligible for atezolizumab? | Guidelines and mature trial data do not support the use of non-cisplatin doublet chemotherapy as adjuvant chemotherapy. Moreover, there were no non-cisplatin-based regimens studied in IMpower010. |
Is there a minimum number of cycles of chemotherapy required to be eligible for atezolizumab? | Given the propensity for adjuvant cisplatin-based chemotherapy to be toxic (and those toxicities can be permanent and serious in some patients), any amount of chemotherapy would be acceptable. This is also reflective of the trial design. There is a group of patients that became ineligible for cisplatin after 1 cycle due to toxicities (such as renal toxicity and ototoxicity). This group of patients should be eligible to receive atezolizumab. Further, given that the mechanism of action of atezolizumab is independent of chemotherapy, it can be argued that patients who are not candidates for adjuvant chemotherapy, but are eligible for immunotherapy, should be able to receive atezolizumab. According to the OH-CCO DAC and LCC, atezolizumab would supplement and/or be added to the current post-operative management of resected NSCLC after at least 1 dose of adjuvant (platinum-doublet) chemotherapy, and not be a replacement for current therapies. |
Can patients be re-treated with downstream PD-1 or PD-L1 inhibitors if disease recurrence occurs more than 6 months after the last dose of adjuvant atezolizumab? | Yes. Further, if the final data from IMpower010 on re-treatment with immunotherapy at relapse after adjuvant atezolizumab suggest there is a benefit, even if relapse occurs on or within 6 months of therapy, that should be taken into consideration and the recommendation revisited, as the recommendation to not rechallenge within 6 months is not evidence-based, but rather based on the pharmacokinetics of immunotherapy drugs. |
In clinical practice, when should chemotherapy be initiated after surgical resection? When should atezolizumab be initiated after chemotherapy? | Chemotherapy should be initiated within 12 weeks of surgical resection. Starting atezolizumab 3 to 8 weeks after the completion of chemotherapy is reasonable in the real world. |
Would alternate dosing (i.e., 1,680 mg IV every 4 weeks) be reasonable to offer? | Although alternative dosing is reasonable, supportive pharmacokinetic data would be advisable before an alternative dosing recommendation in the curative-intent setting can be made. |
Generalizability | |
Can the trial results be extended to patients with an ECOG performance status > 1? | Yes. The clinical experts explained that if a patient were robust enough to receive chemotherapy and had an ECOG performance status of 2, they would be robust enough to receive atezolizumab. The clinical experts further noted, with an extrapolation from the metastatic setting, that patients with an ECOG performance status of 2 can benefit from immunotherapy. Last, the clinical experts added that they would not offer atezolizumab to patients with an ECOG performance status of 3 or 4. |
Should atezolizumab be offered to patients who received platinum-chemotherapy in a setting in which atezolizumab was not accessible, provided all other trial criteria are met? | The clinical experts recommended that atezolizumab be initiated within 12 weeks. Patients must have access to the program to make use of atezolizumab. |
Care provision issues | |
Is PD-L1 testing needed to confirm patient eligibility? | The companion diagnostic test of PD-L1 IHC would be required; however, the testing does not specifically have to be completed using the SP263 antibody. |
AJCC = American Joint Committee on Cancer; DAC = Drug Advisory Committee; ECOG = Eastern Cooperative Oncology Group; IHC = immunohistochemistry; LCC = Lung Cancer Canada; NSCLC = non–small cell lung cancer; OH-CCC = Ontario Health-Cancer Care Ontario; PAG = Provincial Advisory Group; PD-1 = programmed death-1; PD-L1 = programmed death-ligand 1; TC = tumour cell; UICC = Union for International Cancer Control.
Clinical Evidence
The clinical evidence included in the review of atezolizumab is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as studies that were selected in accordance with an a priori protocol. The second section includes indirect evidence from the sponsor, if submitted, and indirect evidence selected from the literature that met the selection criteria specified in the protocol. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of atezolizumab 840 mg every 2 weeks, 1,200 mg every 3 weeks, or 1,680 mg every 4 weeks delivered by IV infusion as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy of adults with stage II to IIIA (according to AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults with stage II or IIIA (according to AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs following complete resection and no progression after platinum-based adjuvant chemotherapy. Subgroups:
|
Intervention | Atezolizumab 840 mg every 2 weeks, 1,200 mg every 3 weeks, or 1,680 mg every 4 weeks delivered by IV infusion for 1 year, unless there is disease recurrence or unacceptable toxicity. Initial dose is administered over 60 minutes, with subsequent doses administered over 30 minutes. |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, TEAEs, SAEs, WDAEs, mortality, and notable harms
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; AJCC = American Joint Committee on Cancer; ALK = anaplastic lymphoma kinase; ALT = alanine aminotransaminase; AST = aspartate aminotransaminase; BSC = best supportive care; DFS = disease-free survival; ECOG = Eastern Cooperative Oncology Group; EGFR = epidermal growth factor receptor; NSCLC = non–small cell lung cancer; OS = overall survival; PD-1 = programmed death-1; PD-L1 = programmed death-ligand 1; RCT = randomized controlled trial; SAE = serious adverse event; TEAE = treatment-emergent adverse event; WDAE = withdrawal due to adverse event.
aAn important outcome to patients.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.39
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Tecentriq (atezolizumab) and NSCLC. The following clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
CADTH-developed search filters were applied to limit retrieval to randomized controlled trials or controlled clinical trials. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on March 23, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on July 13, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist.40 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 389 studies were identified from the literature for inclusion in the systematic review (Figure 1). One single study (IMpower010) was selected for inclusion.32 The included study is summarized in Table 6. A list of excluded studies is presented in Appendix 2.
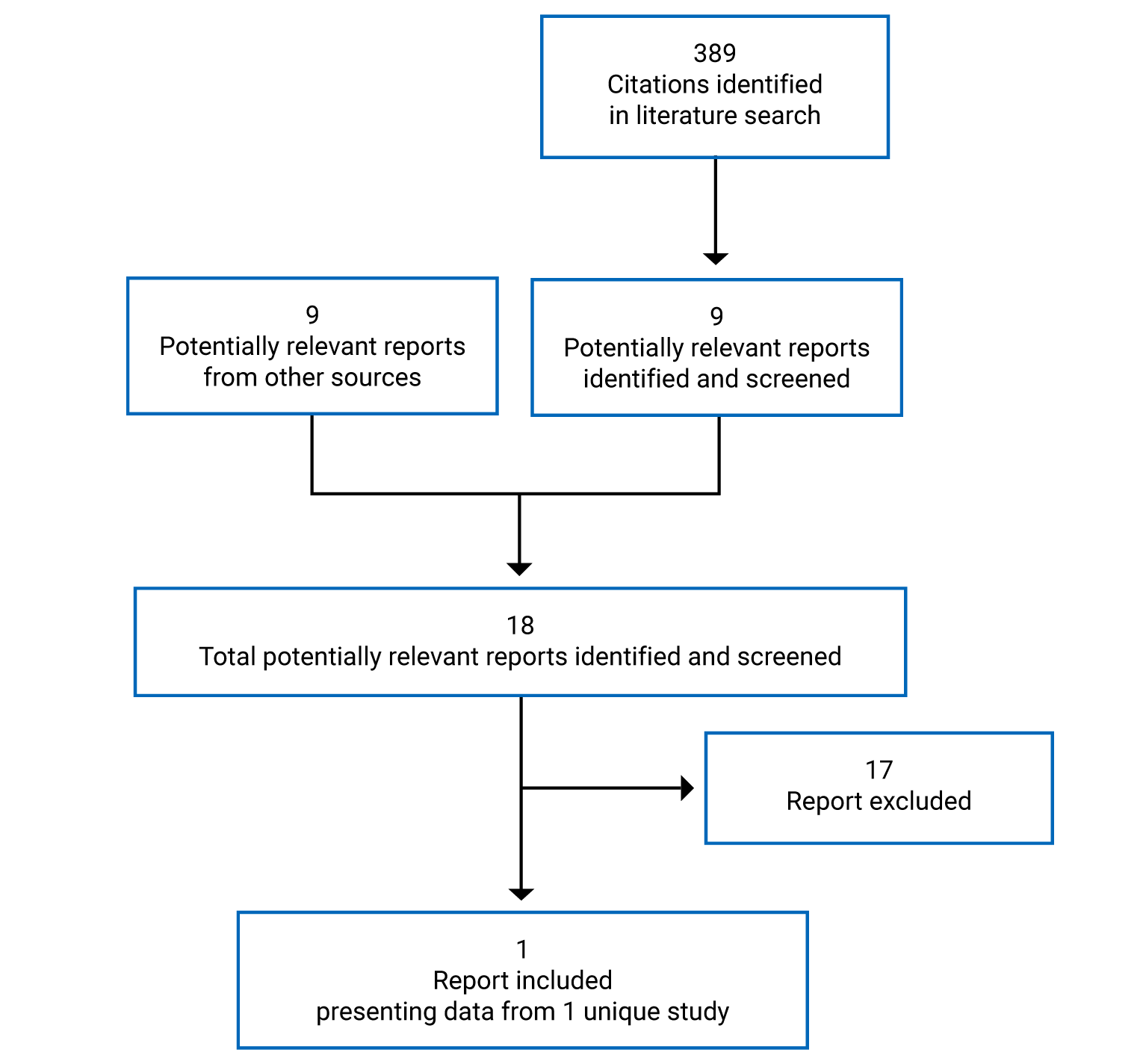
Table 6: Details of the Impower010 Study
Study characteristics | IMpower010 study |
|---|---|
Design and population | |
Study design | Phase III, multi-centre, open-label RCT |
Locations | The study was conducted at 204 centres across 21 countries within North America, Europe, Asia, and Australia(of which 2 sites were in Canada) |
Patient enrolment dates |
|
Randomized (N) | 1,005 |
Inclusion criteria | Main inclusion criteria for enrolment phase
Main inclusion criteria for randomization phase: Adequate hematologic and end-organ function |
Exclusion criteria | Exclusion from the enrolment phase
Exclusion from the randomization phase
|
Drugs | |
Intervention | Enrolment phase Up to 4 cycles (21 days) of cisplatin 75 mg/m2 IV day 1, plus 1 of the following, based on investigator choice:
Randomization phase: Atezolizumab 1,200 mg by IV infusion on day 1 of every 21-day cycle for 16 cycles |
Comparator(s) | Enrolment phase Up to 4 cycles (21 days) of cisplatin 75 mg/m2 IV day 1, plus 1 of the following, based on investigator choice:
Randomization phase
|
Duration | |
Phase | |
Enrolment | Up to 12 weeks |
Open-label treatment | 48 weeks |
Follow-up | 5 years (ongoing)a |
Outcomes | |
Primary end point | DFS assessed by the investigator in the PD-L1 subpopulation defined as > 1% TC expression by SP263 IHC assay, in the stage II to IIIA population, in all randomized patients with stage II to IIIA, and in the ITT population |
Secondary and exploratory end points | Secondary:
Exploratory:
Safety:
Pharmacokinetic:
|
Notes | |
Publications | Felip et al. (2021)32 |
AE = adverse event; AJCC = American Joint Committee on Cancer; ALT = alanine aminotransaminase; AST = aspartate aminotransferase; BSC = best supportive care; DFS = disease-free survival; ECOG = Eastern Cooperative Oncology Group; EGFR = epidermal growth factor receptor; FFPE = formalin-fixed paraffin-embedded; IC = immune cell; IHC = immunohistochemistry; ITT = intention to treat; NGS = next-generation sequencing; NSCLC = non–small cell lung cancer; OS = overall survival; PD-1 = programmed death-1; PD-L1 = programmed death-ligand 1; qRT-PCR = quantitative reverse transcriptase-polymerase chain reaction; RCT = randomized controlled trial; SAE = serious adverse event; TC = tumour cell; UICC = Union for International Cancer Control.
Notes: Two additional reports were included.8,28
Staging was defined using the AJCC (7th edition) staging criteria.1
aPatients who have not experienced recurrence of disease will undergo tumour assessments every 6 months in years 3 to 5 with CT and X-ray after randomization (starting with CT scan, alternating with X-ray), and annually thereafter by X-ray until disease recurrence, death, loss to follow-up, consent withdrawal, or study termination by the sponsor, whichever occurs first.
Source: Clinical Study Report for IMpower010.9
Description of the Study
The IMpower010 is an ongoing phase III, global, multi-centre, open-label, randomized study comparing the efficacy and safety of atezolizumab with BSC in patients with stage IB to IIIA (per the UICC and AJCC [7th edition] staging system)1 NSCLC after complete resection and adjuvant cisplatin-based chemotherapy. A total of 1,280 patients were enrolled across 227 sites in 22 countries within North America (including 2 sites in Canada), Europe, Asia, and Australia. The primary efficacy outcome was DFS, assessed by the investigator. Secondary efficacy outcomes included OS, 3-year and 5-year DFS rates, and DFS in the PD-L1 subpopulations defined as 50% or higher TC expression by detected SP263 immunohistochemistry (IHC) assay in patients with stage II to IIIA NSCLC as defined by the UICC and AJCC (7th edition) staging criteria.1
To measure PD-L1 expression status, sections from tumour specimens from eligible patients were stained and evaluated by external central laboratories using the VENTANA PD-L1 (SP263) assay. Tumour specimens were scored in accordance with the assay’s instruction for use, and the findings were used to define the primary analysis population.
A schematic of the IMpower010 study is presented in Figure 2. The IMpower010 study consisted of 2 phases: an enrolment phase and a randomized phase. In the enrolment phase, patients who had undergone complete resection of their NSCLC were screened, and if eligible (n = 1,280), were enrolled to receive 1 of 4 cisplatin-based chemotherapy regimens (cisplatin plus vinorelbine, docetaxel, gemcitabine, or pemetrexed) based on investigator choice. The 1,005 patients (from 204 centres in 21 countries, including 2 sites in Canada) deemed eligible to continue with the study after up to 4 cycles of cisplatin-based chemotherapy proceeded to the randomization phase. In the randomization phase, patients were randomized in a 1:1 ratio to receive atezolizumab or BSC. The randomization sequence was generated using a permuted-block randomization method in interactive Voice/Web Response System (IxRS) and was stratified by the following factors: sex (female versus male), tumour histology (squamous versus nonsquamous), extent of disease (stage IB versus stage II versus stage IIIA based on the UICC and AJCC [7th edition]1 staging criteria), and PD-L1 expression status (TC2 or TC3 and any IC versus TC0 or TC1 and IC2 or IC3 versus TC0 or TC1 and IC0 or IC1, detected with the SP142 IHC assay).
All patients underwent tumour assessment by the investigator every 4 months in the first year, and every 6 months in the second year after randomization through year 5, and annually from year 6 until disease recurrence, death, loss to follow-up, consent withdrawal, or study termination by the sponsor, whichever occurs first. In addition, at the first evidence of radiographic disease recurrence, patients from both treatment arms underwent a mandatory tumour biopsy sample collection.
All patients were monitored for safety and tolerability throughout the study.
The clinical report provided to CADTH presented the analysis of study data collected from the date of the first patient randomized (February 26, 2016) to the clinical data cut-off date of January 21, 2021, for the protocol-specific interim analysis on DFS.
Figure 2: Schematic of the IMpower010 Study
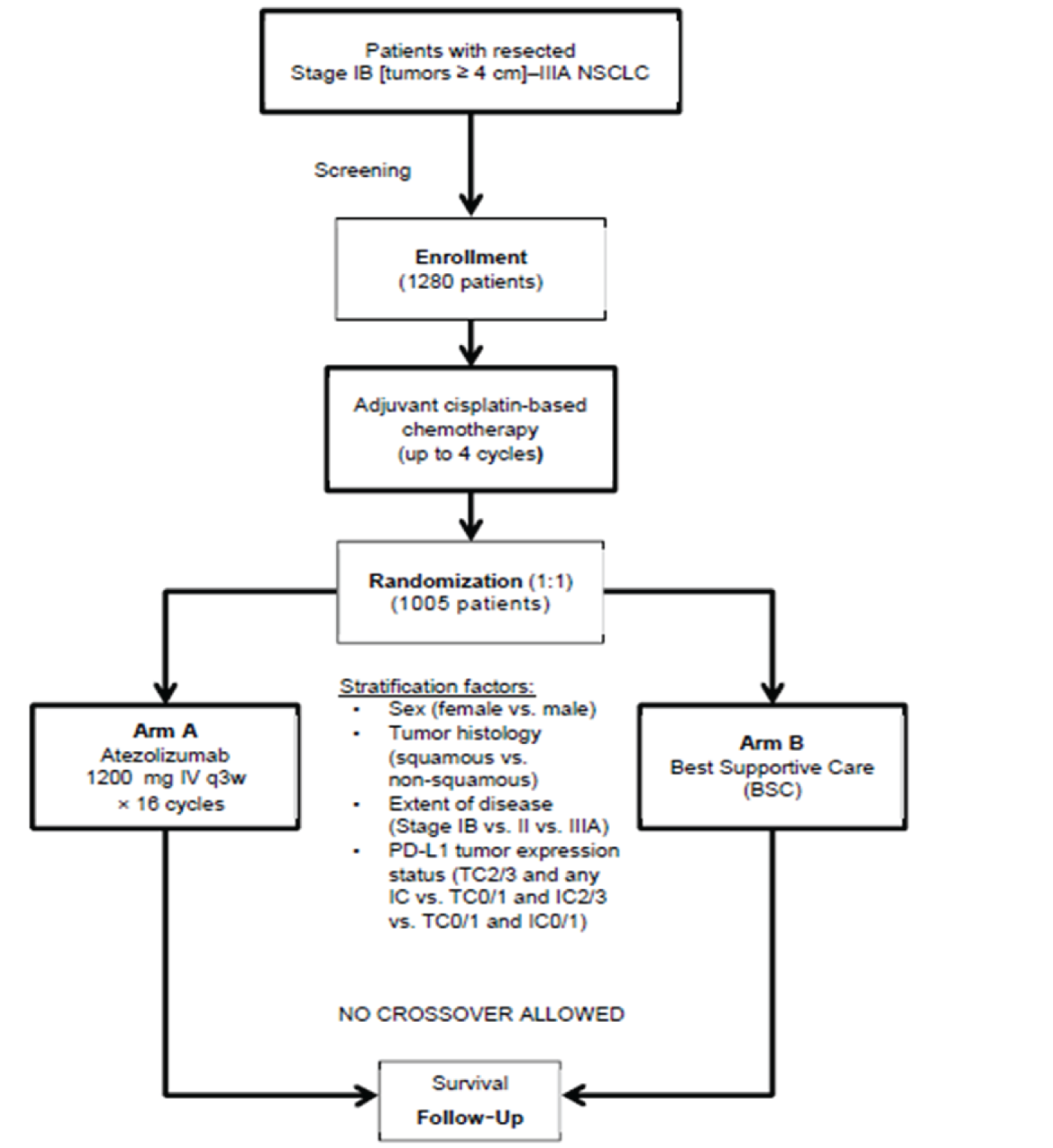
IC = tumour-infiltrating immune cell; NSCLC = non–small cell lung cancer; PD-L1 = programmed death-ligand 1; q3w = every 3 weeks; TC = tumour cell.
Notes: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Patients received up to 4 cycles of cisplatin-based chemotherapy unless unacceptable toxicity or disease relapse occurred, or a patient decided to discontinue therapy.
Source: Clinical Study Report for IMpower010.9
Protocol Amendments
Key protocol amendments for the IMpower010 study are detailed in Appendix 3. The first version of the study protocol was issued on April 1, 2015. The protocol was globally amended 7 times. The key protocol amendments are listed in Appendix 3. The 2 most notable amendments were the inclusion of a PD-L1 subpopulation, defined as TC2 or TC3 or IC2 or IC3 with the SP142 IHC assay and stage II to IIIA disease (protocol version 5 and 6), from the initial enrolment population, defined as only TC3 or IC3 with the SP142 IHC assay (protocol versions 1 to 4); and the introduction of the SP263 IHC assay to defined the primary biomarker analysis population in protocol version 8, which replaced the SP142 IHC assay used in previous versions of the protocol.
Populations
Inclusion and Exclusion Criteria
The key inclusion and exclusion criteria applied in the IMpower010 study are summarized in Table 6.
Briefly, patients who had a complete surgical resection of stage IB (tumours ≥ 4 cm) to IIIA (T2 to 2, N0, T1N1 to T3N1, T1N2 to T3N2, T2N0) per the UICC and AJCC (7th edition)1 staging system NSCLC were eligible for the enrolment phase of the study. A complete resection of NSCLC was required 4 to 12 weeks before enrolment by any of the following procedures: lobectomy, sleeve lobectomy, bilobectomy, or pneumonectomy. Patients were required to have adequately recovered from surgery, to be eligible to receive a cisplatin-based chemotherapy regimen, and to have adequate hematologic and end-organ functioning. Patients with malignancies other than NSCLC in the 5 years before enrolment, except those with a negligible risk of metastasis or death (e.g., expected 5-year OS > 90%) treated with expected curative outcomes, were excluded from enrolment. Patients who had completed the enrolment phase and up to 4 cycles of cisplatin-based therapy and continued to meet eligibility criteria were eligible for the randomization phase of the study. Patients were required to continue to present with adequate hematologic and end-organ function. Patients who presented with signs or symptoms of infection, who received therapeutic oral or IV antibiotics, or who were treated with systemic corticosteroids or other immunosuppressive medications in the 14 days before randomization were excluded from the randomization phase.
Baseline Characteristics
The baseline characteristics of patients with stage II to IIIA disease and PD-L1 expression on at least 50% of TCs are summarized in Table 7 Baseline characteristics of the overall ITT population are presented in Appendix 5.
The indication population had a median age of 62 (range = 36 to 84) years, was predominantly male (72.9%) and White (70.3%), had high functional performance (57.2% had an ECOG performance status score of 0), and most reported previous tobacco use (69.9%).
At diagnosis, most patients had stage IIIA disease (48.0%) with nonsquamous histology (59.8%). Among the 137 patients with nonsquamous histology, 94.2% were identified as having the adenocarcinoma subtype. EGFR or ALK mutations were detected in 8.7% of patients. The majority of patients had undergone prior lobectomy (74.2%) and mediastinal lymph node dissection (81.7%).
Table 7: Summary of Baseline Characteristics in the Impower010 Study of Patients With Stage II to IIIA Disease With PD-L1 Expression on at Least 50% of TCs
Characteristic | BSC group (N = 114) | Atezolizumab group (N = 115) |
|---|---|---|
Demographic characteristics | ||
Age at randomization,a years | ||
Mean (SD) | 61.3 (9.2) | 61.1 (8.5) |
Median (range) | 62.0 (36 to 84) | 62.0 (34 to 77) |
Age group at randomizationa, years, n (%) | ||
< 65 | 68 (59.6) | 70 (60.9) |
65 to 74 | 40 (35.1) | 43 (37.4) |
75 to 84 | 6 (5.3) | 2 (1.7) |
Sex per eCFR, n (%) | ||
Male | 78 (68.4) | 89 (77.4) |
Female | 36 (31.6) | 26 (22.6) |
Race, n (%) | ||
Asian | 26 (22.8) | 36 (31.3) |
Black or African American | 0 (0.0) | 1 (0.9) |
Native Hawaiian or other Pacific Islander | 0 (0.0) | 1 (0.9) |
White | 86 (75.4) | 75 (65.2) |
Multiple | 0 (0.0) | 0 (0.0) |
Unknown | 2 (1.8) | 2 (1.7) |
ECOG performance status at randomization,a n (%) | ||
0 | 60 (52.6) | 71 (61.7) |
1 | 53 (46.5) | 44 (38.3) |
2 | 1 (0.9) | 0 (0.0) |
Tobacco use history, n (%) | ||
Never | 15 (13.2) | 16 (13.9) |
Current | 22 (19.3) | 16 (13.9) |
Previous | 77 (67.5) | 83 (72.2) |
Disease characteristics | ||
Stage of initial diagnosis eCRF, n (%) | ||
Stage IIA | 41 (36.0) | 35 (30.4) |
Stage IIB | 16 (14.0) | 27 (23.5) |
Stage IIIA | 57 (50.0) | 53 (46.1) |
Histology per eCRF, n (%) | ||
Squamous | 45 (39.5) | 47 (40.9) |
Nonsquamous | 69 (60.5) | 68 (59.1) |
Histology subtype in nonsquamous disease, n (%) | ||
nb | 69 | 68 |
Adenocarcinoma | 64 (92.8) | 65 (95.6) |
Adenosquamous | 1 (1.4) | 0 (0.0) |
Large cell | 2 (2.9) | 3 (4.4) |
Undifferentiated | 2 (2.9) | 0 (0.0) |
EGFR mutation status, n (%) | ||
Detected | 8 (7.0) | 6 (5.2) |
Not detected | 64 (56.1) | 60 (52.2) |
Unknown | 42 (36.8) | 49 (42.6) |
ALK mutation status, n (%) | ||
Yes | 3 (2.6) | 3 (2.6) |
No | 62 (54.4) | 62 (53.9) |
Unknown | 49 (43.0) | 50 (43.5) |
Prior surgery | ||
Surgical procedures, n (%) | ||
Lobectomy | 85 (74.6) | 85 (73.9) |
Bilobectomy | 7 (6.1) | 7 (6.1) |
Pneumonectomy | 20 (17.5) | 20 (17.4) |
Sleeve lobectomy | 1 (0.9) | 2 (1.7) |
Other | 2 (1.8) | 3 (2.6) |
Mediastinal lymph node dissection, n (%) | ||
Yes | 92 (80.7) | 95 (82.6) |
No | 22 (19.3) | 20 (17.4) |
Lymph node sampling conduction, n (%) | ||
Yes | 23 (20.2) | 19 (16.5) |
No | 2 (1.8) | 3 (2.6) |
ALK = anaplastic lymphoma kinase; BSC = best supportive care; ECOG = Eastern Cooperative Oncology Group; eCRF = electronic case report form; EGFR = epidermal growth factor receptor; max = maximum; min = minimum; PD-L1 = programmed death-ligand 1; SD = standard deviation; TCs = tumour cells.
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
aAt randomization is defined as the last assessment value before the start of treatment in the randomization period.
bFor the histology subtype in nonsquamous disease, there were 69 patients in the BSC group and 68 in the atezolizumab group.
Source: Clinical Study Report for IMpower010.9
Interventions
Cisplatin Chemotherapy (Enrolment Phase)
All eligible, surgically resected patients received cisplatin 75 mg/m2 on day 1, plus 1 of the following 4 options:
vinorelbine 30 mg/m2 IV push (days 1 and 8)
docetaxel 75 mg/m2 IV (day 1)
gemcitabine 1,250 mg/m2 IV (days 1 and 8)
pemetrexed 500 mg/m2 day 1; nonsquamous NSCLC only).
The investigator selected the chemotherapy regimen (cisplatin plus either vinorelbine, docetaxel, gemcitabine, or pemetrexed) for each patient before enrolment. Each enrolled patient received up to 4 cycles of cisplatin-based chemotherapy, with each cycle being 3 weeks (21 days) in length. The use of antiemetics and hydration modifications were permitted during cisplatin-based chemotherapy.
Atezolizumab (Randomization Phase)
In the randomization phase, patients were assigned to either atezolizumab or BSC. Subsequent cancer therapies were permitted. Patients who were randomized to the atezolizumab arm received 1,200 mg atezolizumab by IV infusion on day 1 of every 21-day cycle for up to 16 cycles. Atezolizumab was infused over 60 (± 15) minutes for the first administration and, if tolerated, subsequent infusions were administered over 30 (± 10) minutes. Dose modifications to atezolizumab were not permitted. However, interruptions or discontinuation due to AEs were allowed.
Best Supportive Care (Randomization Phase)
Patients randomized to the BSC arm received no treatment during the randomized phase of the study other than 16 cycles of BSC. Patients were followed starting on day 1 of each 21-day cycle, for 1 year, and then entered the survival follow-up period. Crossover to the atezolizumab arm was not permitted, but subsequent cancer therapies were permitted.
To maintain a similar frequency of study assessment in the study arms, including assessments of disease recurrence, safety, symptoms, and AEs, patients in the BSC arm had medical contact every 3 weeks during the first year.
Concomitant Medications
The following medications were permitted during the study:
oral contraceptives
hormone-replacement therapy
prophylactic or therapeutic anticoagulation therapy, including low-molecular-weight heparin or warfarin at a stable dose level
inactive influenza vaccinations (during influenza season only)
megestrol administered as an appetite stimulant
corticosteroids (≤ 10 mg oral prednisone or equivalent) for chronic obstructive pulmonary disease
mineralocorticoid (e.g., fludrocortisone)
low-dose corticosteroids for patients with orthostatic hypotension or adrenocortical insufficiency.
Pre-medication with antihistamines was permitted for any atezolizumab infusion after cycle 1.
The following medications were prohibited during the study period:
any live, attenuated vaccine (e.g., FluMist) in the 4 weeks before initiation of study treatment, during atezolizumab treatment, or in the 5 months after the final dose of atezolizumab (for patients randomized to atezolizumab)
steroids to pre-medicate patients in whom CT scans with contrasts are contraindicated (i.e., patients with contrast allergy or impaired renal clearance); instead, noncontrast CT of the chest and noncontrast CT or MRI of another location (if needed) was recommended.
Although the concomitant use of herbal therapies was not recommended because of unknown pharmacokinetics, safety profiles, and potential drug-drug interactions, their use was allowed at the discretion of the investigator. However, herbal therapies intended for the treatment of cancer were prohibited.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 8. These end points are further summarized below.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | IMpower010 study |
|---|---|
OS in ITT population | Secondary |
OS in patients with stage II to IIA disease and PD-L1 expression on ≥ 50% of TCs | Exploratory |
DFS in ITT population | Primary |
DFS in patients with stage II to IIA disease and PD-L1 expression on ≥ 50% of TCs | Secondary |
Site of disease recurrence in patients with stage II to IIA disease and PD-L1 expression on ≥ 50% of TCs | Not specified |
3-year and 5-year DFS in patients with stage II to IIA disease and PD-L1 expression on ≥ 50% of TCs | Secondary |
DFS and OS rate every year from randomization in patients with stage II to IIA disease and PD-L1 expression on ≥ 50% of TCs | Exploratory |
AE, SAE, treatment or study discontinuation due to AE, deaths due to AE, non-SAE of special interest | Safety |
AE = adverse event; DFS = disease-free survival; ITT = intention to treat; OS = overall survival; PD-L1 = programmed death-ligand 1; SAE = serious adverse event; TC = tumour cell.
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Protocol for IMpower010.41
Overall Survival
OS was a secondary efficacy end point in the IMpower010 study. OS was defined as the time from the date of randomization to death from any cause. Data for patients who were not reported as having died at the date of analysis were censored at the date they were last known to be alive. If no post-baseline data were available, then OS was censored at the date of randomization.
Survival follow-up information was collected from telephone calls, patient medical records, and/or clinic visits approximately every 3 months until death, loss to follow-up, withdrawal of consent, or termination of study by the sponsor, whichever occurred first. All patients were followed for survival and new anti-cancer therapy information, unless the patient asked to be withdrawn from follow-up, was lost to follow-up, died, or the study was terminated by the sponsor, whichever occurred first. For patients who withdrew from the study, the use of public data (e.g., county records) to obtain information about survival status only was permitted.
Disease-Free Survival
DFS, as assessed by the investigator, was a primary efficacy end point in the IMpower010 study. DFS was defined as the time from the date of randomization to the date of the first documented, investigator-assessed recurrence of disease, new primary NSCLC, or death from any cause, whichever occurred first. Data for patients who were not reported as experiencing disease recurrence, a new primary NSCLC, or death were censored at the date of the last tumour assessment. If no post-baseline data were available, DFS was censored at the time of randomization.
Patients underwent scheduled tumour assessment via CT scan at baseline, every 4 months in the first year, and every 6 months in the second year after randomization. Patients who did not experience disease recurrence underwent tumour assessment every 6 months with CT scan and X-ray at year 3 and year 5 after randomization, and annually thereafter with X-ray. In the absence of disease recurrence, tumour assessments continued, regardless of whether patients started new anti-cancer therapy, until disease recurrence, withdrawal of consent, death, loss to follow-up, or study termination by the sponsor, whichever occurred first. Patients who discontinued treatment before completing the 16 cycles of atezolizumab for reasons other than disease recurrence (e.g., toxicity) continued with their scheduled tumour assessments at the same frequency as they would have if they had remained on the study treatment until disease recurrence, death, withdrawal of consent, loss to follow-up, or study end, whichever occurred first. In addition, patients in either treatment arm who started a new anti-cancer therapy in the absence of disease recurrence were followed according to the protocol schedule, unless they withdrew consent, died, experienced disease recurrence, were lost to follow-up, or the study ended, whichever occurred first.
At the first evidence of radiologic disease recurrence or confirmation of a new primary NSCLC, patients from either treatment arm underwent mandatory tumour biopsy sample collection (within 40 days of disease recurrence or before the start of the next anti-cancer therapy, which was sooner), unless it was not clinically feasible. Acceptable samples included core needle biopsies for deep tumour tissue (at least 3 cores) embedded into a single paraffin block; excisional, incisional, punch, or forceps biopsy specimens for cutaneous, subcutaneous, or mucosal lesions; and tumour tissue resection.
Safety
The following safety outcomes were assessed during the enrolment phase and the randomization phase of the study, and for 90 days after the last dose of the study treatment (last study assessment for patients in the BSC treatment arm) or initiation of a new anti-cancer therapy, which ever occurred first:
AEs
SAEs
Treatment or study discontinuation due to AEs
Death
Non-SAEs of special interest, such as:
drug-induced liver injury that includes elevated aspartate aminotransferase or alanine aminotransferase levels in combination with either elevated bilirubin or clinical jaundice
suspected transmission of an infectious agent by the study drug
treatment-emergent autoimmune conditions (including pneumonitis and grade ≥ 3 hypoxia or dyspnea); colitis; endocrinopathies (including diabetes mellitus, pancreatitis, and adrenal insufficiency); vasculitis; hepatitis; transaminitis: grade 2 or higher (AST or ALT > 3 × upper limit of normal [ULN] and bilirubin > 2 ULN or AST/ALT > 10 × ULN); systemic lupus erythematosus; Guillain-Barré syndrome; and skin reactions (including vitiligo and pemphigoid)
events suggestive of hypersensitivity, cytokine-release syndrome, influenza-like illness, systemic inflammatory response system, or infusion-reaction syndromes.
The toxicity profile of the study treatments for all patients were classified according to the National Cancer Institute Common Toxicity Criteria for Adverse Events version 4.0 (NCI CTCAE v4.0).
Statistical Analysis
The statistical analysis for efficacy end points conducted in the IMpower010 trial is summarized in Table 9.
Efficacy Analysis
Sample Size Determination
Approximately 1,280 patients were expected to be accrued during the enrolment phase of the study. With an expected dropout rate of 21% during the adjuvant cisplatin-based chemotherapy, approximately 1,005 patients were expected to enter the randomization phase, including approximately 882 patients in the stage II to IIIA population; of these, approximately 474 were in the subpopulation with PD-L1 expression on at least 1% of TCs (detected with the SP263 IHC assay).
Of note, the trial was not powered for the Health Canada–recommended NOC indication. Moreover, the planned sample size did not consider significant efficacy findings for the Health Canada–indicated population.
For the final DFS analysis to occur, approximately |||||||||||||||| in the subpopulation with PD-L1 expression on at least 1% of TCs (detected with the SP263 assay) of the stage II to IIIA population are required. The number of events is expected to correspond to a minimum detectable difference in HR of approximately |||||||||| in the PD-L1 subpopulation with TC expression of at least 1% (detected with the SP263 assay) in the stage II to IIIA population.
For the final OS analysis to occur, given a sample size of 1,005, approximately ||||||||| OS events in all randomized stage IB to IIIA patients are required.
Primary Efficacy Analysis
The HR for duration of DFS was estimated in the ITT population using a stratified Cox regression model, which included a 2-sided 95% CI (Table 10). The KM methodology was used to estimate median DFS for each treatment arm, with KM curves constructed to illustrate potential differences between atezolizumab and BSC. The 2-sided 95% CI for median DFS for each treatment arm was constructed using the methodology of Brookmeyer and Crowley.42
Type and site of disease recurrence were summarized as counts and frequencies.
To control for the overall level of significance at a 1-sided error of 0.025, comparisons between the treatment arms were conducted hierarchically for the PD-L1 subpopulation defined by SP263 TC of at least 1% within the stage II to IIIA population, the entire randomized stage II to IIIA population, and the ITT population (Figure 3)
Of note, the analysis of the indicated population under review was not controlled for multiplicity.
Secondary Efficacy Analysis
The secondary efficacy of OS was assessed in the ITT population using a stratified Cox regression model, which included a 2-sided 95% CI. The KM methodology was used to estimate the median OS for each treatment arm, with KM curves constructed to illustrate the differences between atezolizumab and BSC. The 2-sided 95% CI for median OS for each treatment arm was constructed using the methodology of Brookmeyer and Crowley.42 The OS testing schema, as described for the DFS analysis, is illustrated in Figure 3.
The DFS rate at 3 years and at 5 years was analyzed for the subpopulation with PD-L1 expression on at least 50% of TCs (detected with the SP263 assay). These DFS rates were estimated using the KM methodology for each treatment arm, with 2-sided 95% CI using the Greenwood formula.43
DFS in the subpopulation with PD-L1 expression on at least 50% of TCs (detected with the SP263 assay) in all randomized patients with stage II to IIIA NSCLC was assessed using stratified Cox regression model, including a 2-sided 95% CI) (Table 9). The analysis methodology used was the same as described for the primary efficacy analysis. Of note, the analysis of the indicated population under review was not controlled for multiplicity.
Interim Analyses
One interim analysis for DFS was planned for the date when approximately 190 DFS events (approximately |||||||||| of expected observations) occurred in the subpopulation with PD-L1 expression on at least 1% of TCs (detected with the SP263 assay) of the stage II to IIIA population. This was expected to occur approximately |||||||||| after the first patients was randomized. To control for type I error DFS at a 1-sided alpha of 0.025, the stopping boundaries for the DFS interim analysis were computed using the Hwang-Shih-Decani alpha-spending function with gamma parameters of –0.9.44
|||||||||||||||||||||||||||||||||||||||| for OS were planned. The first OS interim analysis was planned for the time of the DFS interim analysis if DFS was positive, as shown in Figure 3. The results presented for OS in this report are based on this interim analysis. Further interim analyses are planned at |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Analysis timing and stopping boundaries for DFS and OS are summarized in Appendix 4.
Figure 3: Overview of the Alpha Control
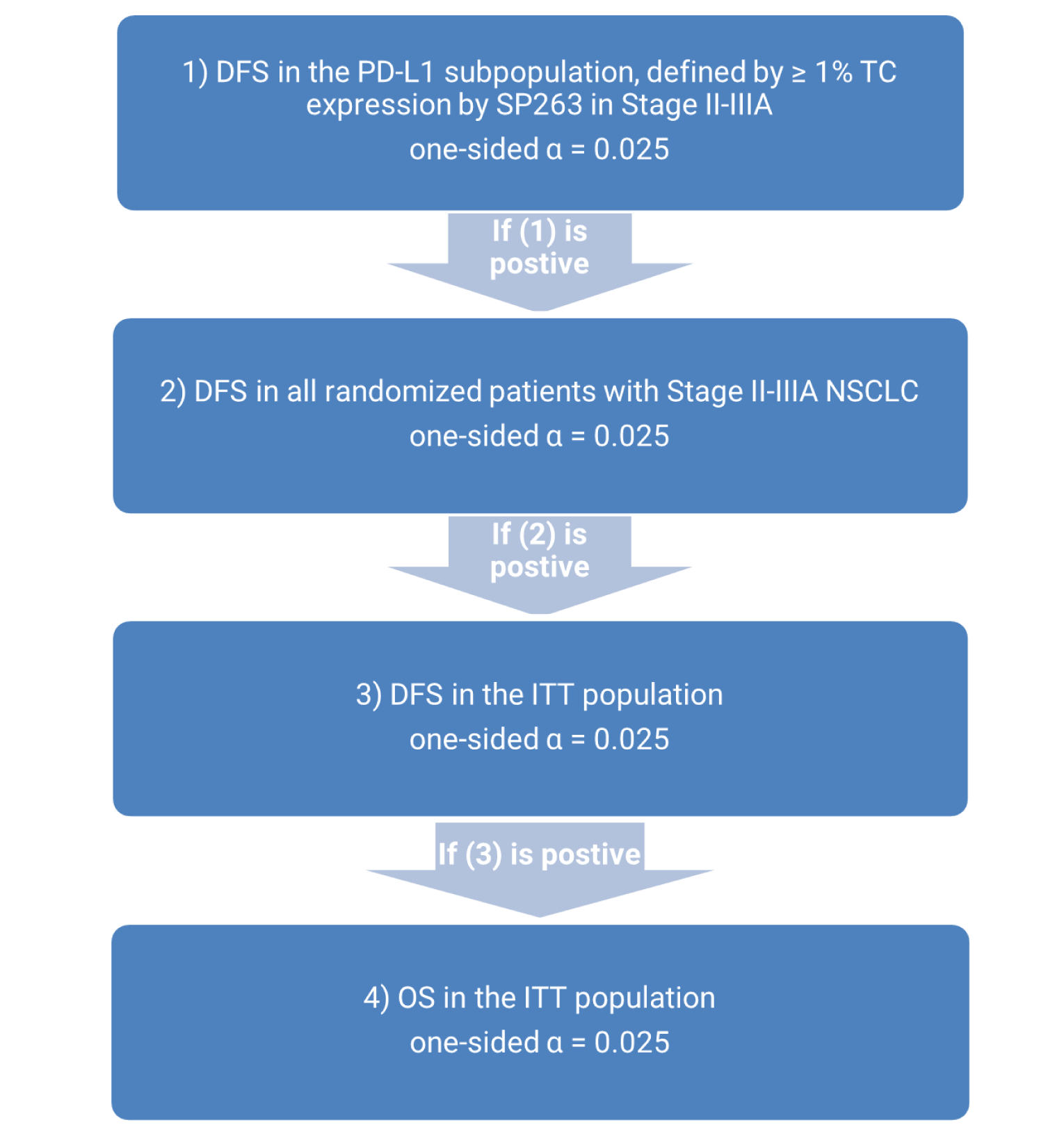
DFS = disease-free survival; ITT = intention to treat; NSCLC = non–small cell lung cancer; OS = overall survival; PD-L1 = programmed death-ligand 1; TC = tumour cell.
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Protocol for IMpower010.41
Sensitivity Analysis
To evaluate the impact of loss to follow-up, a sensitivity analysis (“worst-case” analysis) was planned if more than 5% of patients were lost to follow-up for DFS in either treatment arm; patients who were lost to follow-up were considered to have recurrent disease at the date of their last tumour assessment.
To evaluate the impact of missed visits, sensitivity analyses with different censoring rules were performed for the primary end point of DFS. Data for patients with a DFS event who missed 2 or more schedule assessments immediately before the event were censored at the most recent date with adequate radiological assessment before the missed visit.
Subgroup Analysis
The following subgroup analyses for duration of DFS and OS were conducted in the ITT population: demographic variables (e.g., age), and baseline prognostic characteristics (e.g., tumour stage, chemotherapy regimen before randomization, histology, smoking history, and ECOG performance status). Results were also presented for the population with PD-L1 expression on at least 50% of TCs and stage II to IIA disease, which is of direct interest as it reflects the indicated population under review. Summaries of DFS and OS were constructed for each level of categorical variable using unstratified HR estimates from Cox proportional hazards models and KM estimates of median survival time.
Exploratory Analysis
DFS and OS rates every year from randomization were estimated using KM methodology for each treatment arm with the Greenwood formulas for exploratory purposes.
DFS rates in other PD-L1 subpopulations were estimated for exploratory purposes, including the stage II to IIA population with PD-L1 expression on at least 50% of TCs, which is of direct interest as it reflects the indicated population under review. Data were analyzed using the same methods used in the primary analysis of DFS.
OS in other subpopulations was estimated for exploratory purposes and analyzed using the same methods as in the secondary analysis of OS. Subpopulations of interest included the stage II to IIIA subpopulation with PD-L1 expression on at least 50% of TCs (detected with the SP263 assay), which reflects the indicated population under review.
Safety Analysis
Safety analyses were performed on all randomized patients who received any amount of study treatment and had at least 1 post-baseline assessment. All AEs that occurred during or after the first study drug dose were summarized using counts and frequencies by treatment arm and NCI CTCAE grade.
Table 9: Statistical Analysis of Efficacy End Points in the IMpower010 Study
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
|
| ITT population:
For PD-L1 subpopulation defined by SP263 as TCs ≥ 50% in all randomized patients with stage II to IIIA NSCLC
|
|
DFS at 3 years and 5 years | Median estimated via KM methodology with 2-sided 95% CIs constructed using Greenwood’s formula | NA | None performed |
CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; IC = immune cell; IHC = immunohistochemistry; ITT = intention to treat; KM = Kaplan-Meier; NA = not applicable; NSCLC = non–small cell lung cancer; OS = overall survival; PD-L1 = programmed death-ligand 1; TC = tumour cell; vs. = versus.
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Protocol for IMpower010.41
Analysis Populations
ITT Population
The ITT population was defined as all randomized patients with resected stage IB (tumours ≥ 4 cm) to IIIA NSCLC, regardless of whether or not the patient received their assigned treatment. Patients were grouped by their assigned treatment at randomization by IxRS. The population of interest to the CADTH review was a subset of the randomized patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs.
Safety-Evaluable Population
The safety-evaluable population was defined as all randomized patients who received at least 1 dose of atezolizumab and all randomized patients who were randomized to the receive BSC and no atezolizumab, but who had at least 1 post-baseline safety assessment (e.g., AEs, laboratory tests, vital signs), regardless of their assigned treatment at randomization (i.e., patient data were analyzed according to the treatment received). The population of interest to the CADTH review was a subset of safety-evaluable patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs.
Results
Patient Disposition
Details of patient disposition are summarized in Table 10.
A total of 1,600 patients were screened for entry into enter the IMpower010 study. Of those, 1,280 entered the enrolment phase of the study and received adjuvant chemotherapy. From those, 1,070 were screened to enter the randomization phase of the study, in which 498 patients were randomized to treatment with BSC and 507 to treatment with atezolizumab. Treatment is ongoing for 371 (74.5%) and 386 (76.1%) patients randomized to receive BSC and atezolizumab, respectively.
Among patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, 144 and 155 patients were randomized to receive BSC or atezolizumab, respectively. In this subpopulation, treatment is ongoing for a greater proportion of patients randomized to receive atezolizumab versus BSC (86.1% versus 71.1%), primarily because of a higher number of deaths in the BSC group (22.8%) than in the atezolizumab group (9.6%).
The most common reason for discontinuation from the study was death, followed by withdrawal by the patient.
Duration of Follow-Up
Duration of follow-up to date is summarized in Table 11. Duration of follow-up of the overall ITT population is presented in Appendix 5.
Among all patients randomized into the trial, the median length of follow-up was approximately 32 months (interquartile range = 27.60 to 36.64). Among the subpopulation of patients with stage II to IIIA disease and PD-L1 expression on at least 50% of TCs, the median duration of follow-up was slightly longer in those randomized to atezolizumab (35.98 months; interquartile range [IQR], 29.7 to 40.67) than BSC (33.2 months; IQR, 26.61 to 39.75).
Protocol Deviations
Major protocol deviations related to the inclusion criteria, exclusion criteria, medication, and procedures are summarized in Appendix 5.
Major protocol deviations among the subpopulation of patients with stage II to IIIA and PD-L1 expression on at least 50% of TCs was unavailable.
In the ITT population, at least 1 major protocol deviation was recorded for 24.7% and 29.0% of patients randomized to BSC and atezolizumab, respectively. The most common deviations (BSC versus atezolizumab) were related to study procedures (21.5% versus 22.9%), followed by deviations related to inclusion criteria (4.0% versus 2.6%), exclusion criteria (1.0% versus 1.2%), and medication (0.4% versus 4.1%).
Exposure to Study Treatments
Exposure to atezolizumab is summarized in Table 12. Exposure to atezolizumab in the overall ITT population is presented in Appendix 5.
The median treatment duration with atezolizumab was 10.4 (range = 0 to 16) months, at a median dose intensity of 100% (range = 40% to 100%). The median total cumulative dose of atezolizumab received was 19,200 mg (range = 1,200 mg to 19,200 mg), with most patients receiving 16 doses per cycle.
Concomitant Medications and Nonprotocol Anti-Cancer Therapies
The use of concomitant medications and nonprotocol anti-cancer therapies during the trial is summarized in Table 13. Additional data on the use of concomitant medication and nonprotocol anti-cancer therapies in the overall ITT population are presented in Appendix 5.
Use of concomitant medication among the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs was unavailable.
Among the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, the proportion of patients who reported treatment with at least 1 nonprotocol anti-cancer therapy was 26.3% and 17.4% among those randomized to BSC and atezolizumab, respectively. The most common nonprotocol antineoplastic drug used was carboplatin (7.0% in the BSC group versus 7.8% in the atezolizumab group), followed by pembrolizumab and cisplatin.
Table 10: Patient Disposition in the Impower010 Study (Clinical Data Cut-Off Date of January 21, 2021)
Disposition | All patients (ITT population) | Patients with stage II to IIIA disease with PD-L1 expression on ≥ 50% of TCs | ||
|---|---|---|---|---|
BSC group | Atezolizumab group | BSC group | Atezolizumab group | |
Screened, n | 1,600 | NR | NR | |
Enrolled in study and received adjuvant chemotherapy, n | 1,280 | NR | NR | |
Screened for randomization, n | 1,070 | NR | NR | |
Randomized, n | 498 | 507 | 114 | 115 |
Received treatment, n (%) | 495 (99.4) | 495 (97.6) | 112 (98.2) | 113 (98.3) |
Ongoing treatment, n (%) | 371 (74.5) | 386 (76.1) | 81 (71.1) | 99 (86.1) |
Discontinued from study, n (%) | 127 (25.5) | 121 (23.9) | 33 (28.9) | 16 (13.9) |
Reason for discontinuation, n (%) | ||||
Death | 88 (17.7) | 91 (17.9) | 26 (22.8) | 11 (9.6) |
Disease relapse | 0 (0.0) | 1 (0.2) | 0 (0.0) | 0 (0.0) |
Lost to follow-up | 4 (0.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Physician decision | 3 (0.6) | 0 (0.0) | 2 (1.8) | 0 (0.0) |
Protocol deviation | 0 (0.0) | 2 (0.4) | 0 (0.0) | 0 (0.0) |
Withdrawal by patient | 32 (6.4) | 27 (5.3) | 5 (4.4) | 5 (4.3) |
ITT, n | 498 | 507 | 114 | 115 |
Safety-evaluable patients, n | 495 | 495 | 112 | 113 |
BSC = best supportive care; ITT = intention to treat; NR = not reported; PD-L1 = programmed death-ligand 1; TC = tumour cell.
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Clinical Study Report for IMpower010.9
Table 11: Duration of Follow-Up in the Impower010 Study for Patients With Stage II to IIIA Disease With PD-L1 Expression on at Least 50% of TCs (Clinical Data Cut-Off Date of January 21, 2021)
Duration of follow-up in months | BSC group N = 114) | Atezolizumab group N = 115 |
|---|---|---|
n | 114 | 115 |
Median (IQR) | 33.2 (26.61 to 39.75) | 35.98 (29.70 to 40.67) |
Range (months) | 0.2 to 57.5 | 0.2 to 54.2 |
BSC = best supportive care; ITT = intention to treat; PD-L1 = programmed death-ligand 1; TC = tumour cell.
Source: Clinical Study Report for IMpower010.9
Table 12: Exposure to Atezolizumab in the Impower010 Study (Safety Population; Clinical Data Cut-Off Date of January 21, 2021)
Exposure | Patients with stage II to IIIA disease with PD-L1 expression on ≥ 50% of TCs (N = 113) |
|---|---|
Treatment duration, months | |
Median (range) | 10.4 (0 to 16) |
Dose intensity (%) | |
Median (range) | 100.0 (67 to 100) |
Total cumulative dose, mg | |
n | 113 |
Median (range) | 19,200.0 (1,200 to 19,200) |
Number of doses or cycles received | |
n | 113 |
Median (range) | 16 (1 to 16) |
Number of doses per cycles, n (%) | |
0 to < 8 | 20 (17.7) |
≥ 8 to < 16 | 8 (7.1) |
≥ 16 | 85 (75.2) |
BSC = best supportive care; PD-L1 = programmed death-ligand 1; TC = tumour cell.
Source: Clinical Study Report for IMpower010.9
Table 13: Concomitant Medication and Nonprotocol Anti-Cancer Therapy in the IMpower010 Study for Patients With Stage II to IIIA Disease With PD-L1 Expression on at Least 50% of TCs (Clinical Data Cut-Off Date of January 21, 2021)
Concomitant medications | BSC group (N = 114) | Atezolizumab group (N = 115) |
|---|---|---|
Concomitant medications | ||
Total number of patients with at least 1 treatment | NR | NR |
Total number of treatments | NR | NR |
Class of concomitant medicationa | ||
Ophthalmological | NR | NR |
Analgesics | NR | NR |
Stomatological preparations | NR | NR |
Topical products for joint and muscular pain | NR | NR |
Otologicals | NR | NR |
Nonprotocol anti-cancer therapy | ||
At least 1 treatment, n (%) | 30 (26.3) | 20 (17.4) |
Total number of treatments, n | 66 | 48 |
Antineoplastic drugs,b n (%) | ||
Patients with at least 1 treatment | 30 (26.3) | 20 (17.4) |
Carboplatin | 8 (7.0) | 9 (7.8) |
Pembrolizumab | 14 (12.3) | 3 (2.6) |
Cisplatin | 6 (5.3) | 4 (3.5) |
Docetaxel | 6 (5.3) | 4 (3.5) |
Gemcitabine | 4 (3.5) | 5 (4.3) |
Pemetrexed | 5 (4.4) | 3 (2.6) |
Paclitaxel | 2 (1.8) | 3 (2.6) |
BSC = best supportive care; NR = not reported; PD-L1 = programmed death-ligand 1; TC = tumour cell.
aThe most frequently used (by Anatomical Therapeutic Chemical class level 2, > 40% incidence in any treatment group).
bOnly treatments reported to be used in at least 2% in any treatment group are listed.
Source: Clinical Study Report for IMpower010.9
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported here. Refer to Appendix 5 for additional efficacy data related to the overall ITT population and subgroup analyses of the ITT population.
Overall Survival
OS data are summarized in Table 14. A KM plot of median OS for the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs is illustrated in ||||||||||. The OS results presented here are descriptive only, given that data were based on subgroup analysis.
Among the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, the observed deaths at the time of the interim analysis were 22.8% and 9.6% in the BSC and atezolizumab treatment groups, respectively. The stratified HR was 0.40 (95% CI, 0.20 to 0.81) in favour of atezolizumab. The median OS could not be estimated in either treatment arms because of the low rate of death events at the time of the planned interim analysis. At year 3, a greater proportion of patients in the atezolizumab treatment group (90.85%) were event-free than in the BSC group (76.67%), for a difference in proportion of 14.27% (95% CI, 4.19% to 24.35%). The corresponding year 5 event-free rates were not estimated and require longer follow-up.
Because of the low number of events, the KM estimated median OS could not be calculated.
Disease-Free Survival
DFS data are summarized in Table 15.
A greater proportion of patients in the BSC treatment arm (45.6%) experienced a disease recurrence or death than in the atezolizumab arm (24.3%). The stratified HR of 0.47 (95% CI, 0.29 to 0.75) favoured atezolizumab. At year 3, 73.79% of patients in the atezolizumab group were event-free compared with 48.61% of those in the BSC group, for a difference in the event-free rate of 25.18% (95% CI, 11.01% to 39.36%). Corresponding year 5 event-free rates were not estimated and require longer follow-up.
The findings for DFS with atezolizumab and BSC were consistent across most subgroups in exploratory subgroup analyses (refer to Appendix 3).
Table 14: Overall Survival in the Impower010 Study for Patients With Stage II to IIIA Disease With PD-L1 Expression on at Least 50% of TCs (Clinical Data Cut-Off Date of January 21, 2021)
Outcome | BSC group (N = 114) | Atezolizumab group (N = 115) |
|---|---|---|
Death event, n (%) | ||
Patients with event | 26 (22.8) | 11 (9.6) |
Patients without event | 88 (77.2) | 104 (90.4) |
Time to event, monthsa | ||
Median (range) | NE (0.2b to 57.5b) | NE (0.2b to 54.2b) |
95% CI | NE | NE |
25th, 75th percentiles | 36.4, NE | NE |
Stratified analysisc | ||
HRd (95% CI) | 0.40 (0.20 to 0.81) | |
P value, log-rank | 0.0089e | |
Unstratified analysis | ||
HRd (95% CI) | 0.37 (0.18 to 0.74) | |
P value, log-rank | 0.0036e | |
Time point analysis | ||
3 years | ||
Patients remaining at risk | |||||||||| | |||||||||| |
Event-free rate (%) | |||||||||| | |||||||||| |
95% CI | |||||||||| | |||||||||| |
Difference in event-free rate (95% CI) | |||||||||| | |
P value, z-test | |||||||||| | |
5 years | |||||||||| | |||||||||| |
BSC = best supported care; CI = confidence interval; HR = hazard ratio; NE = not estimable; OS = overall survival; PD-L1 = programmed death-ligand 1; TC = tumour cell.
aSummaries of durations (median and percentiles) are Kaplan-Meier estimates. 95% CIs for the medians are computed using the methods of Brookmeyer and Crowley.
bCensored.
cStratification factors: stage from eCRF (IB or II vs. IIIA), sex from eCRF (female vs. male), histology from eCRF (squamous vs. nonsquamous).
dHRs were estimated by Cox regression.
eP values were not adjusted for multiple comparisons; therefore, there is an increased risk of false-positive conclusions.
Source: Clinical Study Report for IMpower010.9
Table 15: Disease-Free Survival in the Impower010 Study for Patients With Stage II to IIIA Disease With PD-L1 Expression on at Least 50% of TCs (Clinical Data Cut-Off Date of January 21, 2021)
Outcome | BSC group (N = 114) | Atezolizumab group (N = 115) |
|---|---|---|
Recurrence event | ||
Patients with event, n (%) | 52 (45.6) | 28 (24.3) |
Death, n | 2 | 3 |
Disease recurrence, n | 50 | 25 |
Patients without event, n (%) | 62 (54.4) | 87 (75.7) |
Time to event, monthsa | ||
Median (range) | 35.7 (0.0b to 54.9b) | NE (0.0b to 54.2b) |
95% CI | 29.7 to NE | 42.3 to NE |
25th, 75th percentiles | 12.0, NE | 35.3, NE |
Stratified analysisc | ||
HRd (95% CI) | 0.47 (0.29 to 0.75) | |
P value, log-rank | 0.0012e | |
Unstratified analysis | ||
HRd (95% CI) | 0.43 (0.27 to 0.68) | |
P value, log-rank | 0.0002e | |
Time point analysis | ||
3 years | ||
Patients remaining at risk, n | 19 | 30 |
Event-free rate, % | 48.61 | 73.79 |
95% CI | 38.03 to 59.18 | 64.35 to 83.23 |
Difference in event-free rate (95% CI) | 25.18 (11.01 to 39.36) | |
P value, z-test | 0.0005e | |
5 years | NE | NE |
BSC = best supportive care; CI = confidence interval; DFS = disease-free survival; HR = hazard ratio; NE = not estimable; PD-L1 = programmed death-ligand 1; TC = tumour cell.
aSummaries of durations (median and percentiles) are Kaplan-Meier estimates. 95% CIs for the medians are computed using the methods of Brookmeyer and Crowley.42
bCensored.
cStratification factors: stage from eCRF (IB or II vs. IIIA), sex from eCRF (female vs. male), histology from eCRF (squamous vs. nonsquamous).
dHRs were estimated by Cox regression.
eP values were not adjusted for multiple comparisons, resulting in an increased risk of false-positive conclusions.
Source: Clinical Study Report for IMpower010.9
KM plots of estimated median DFS among patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs (detected with the SP263 assay), including and excluding EGFR- or ALK-positive mutation, are illustrated in Figure 4. The results presented for the subgroup of patients without EGFR- or ALK-positive mutation are based on a post hoc subgroup analysis provided by the sponsor.
Because of the low number of events in the atezolizumab arm, the KM median DFS for all patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs could not be estimated. The KM median DFS was 35.7 months (lower bound of 95% CI, 29.7 months) in the BSC treatment arm. The KM curve began to separate in favour of atezolizumab approximately 4 to 5 months after randomization, and the separation was maintained.
Because of the low number of events in the atezolizumab arm, the KM estimated median DFS could not be calculated for patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs and without EGFR- or ALK-positive mutation. In the BSC treatment arm, the KM median DFS for patients without an EGFR- or ALK-positive mutation was similar to that for patients with the mutation at 37.5 months and 35.7 months, respectively. The unstratified HR for DFS between the treatment arms was similar for patients with and without an EGFR or ALK mutation (HR = 0.43; 95% CI, 0.26 to 0.71).
The clinical benefit of atezolizumab, compared with BSC, seemed consistent across most subgroups (i.e., age, sex, ECOG performance status score) in exploratory subgroup analyses in the reimbursement indication (Appendix 5).
Figure 4: KM Plot of DFS Among Patients With Stage II to IIIA NSCLC and PD-L1 (SP263) in at Least 50% of TCs by EGFR- or ALK-Positive Mutation Status (Clinical Data Cut-Off Date of January 21, 2021)
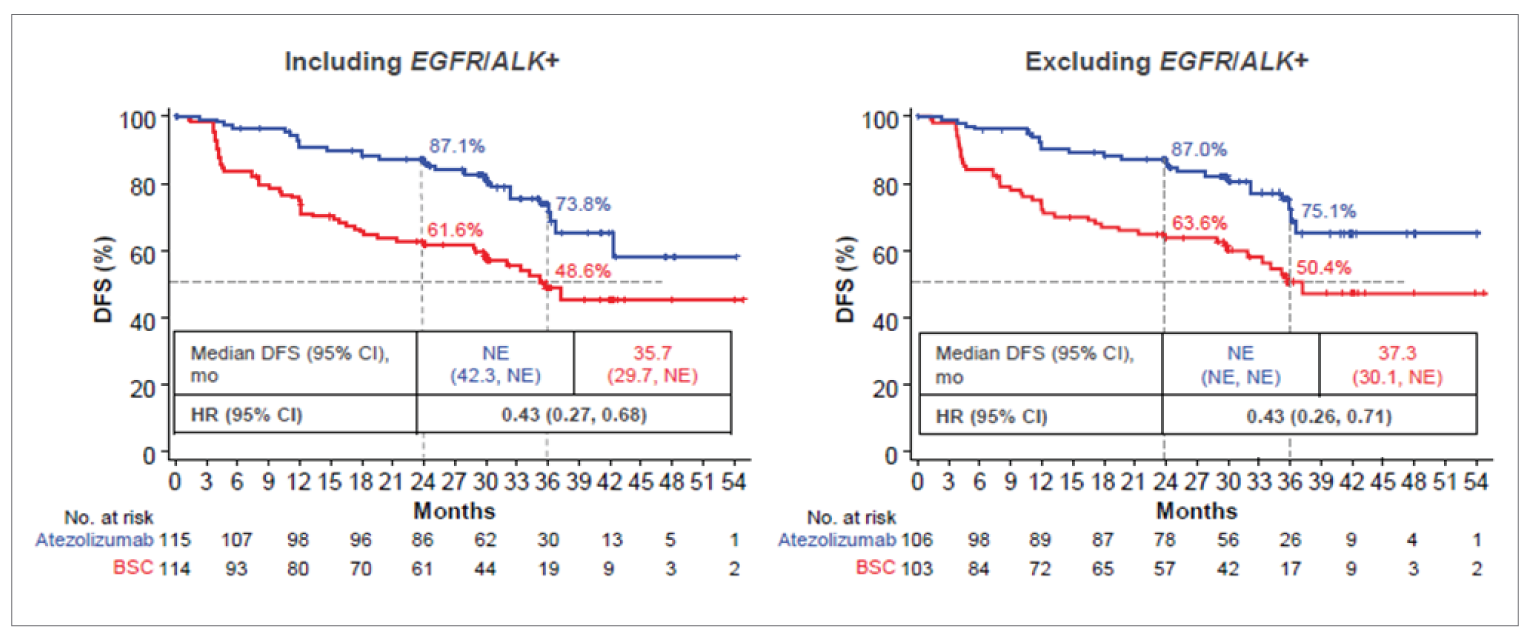
ALK = anaplastic lymphoma kinase; BSC = best supportive care; CI = confidence interval; DFS = disease-free survival; EGFR = epidermal growth factor receptor; EGFR/ALK+ = EGFR- or ALK-positive mutations; HR = hazard ratio; KM = Kaplan-Meier; NE = not estimable; PD-L1 = programmed death-ligand 1; TC = tumour cell.
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Clinical Study Report for IMpower010.9
Type of Recurrence
The sites of disease recurrence for patients with protocol-defined disease relapse among patients with stage II to IIIA disease and PD-L1 expression on at least 50% of TCs, including and excluding EGFR and ALK mutations, are summarized in Table 16.
At the time of the planned interim analysis, disease recurrence was observed in 50 and 25 patients who had stage II to IIIA disease with PD-L1 at least 50% of TCs randomized to the BSC and atezolizumab treatment groups, respectively. Of those patients, locoregional disease recurrence was experienced by 60% of patients in the atezolizumab treatment arm and 34% in the BSC arm. Distant-only disease recurrence occurred in 42% of patients in the BSC arm and 24% in the atezolizumab arm. CNS-only disease recurrence occurred in 14% of patients in the BSC arm and 4% in the atezolizumab arm. The rate of combined locoregional plus distant disease recurrence was 18% in the BSC arm and 16% in the atezolizumab arm.
In patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs and without an EGFR or ALK mutation, disease recurrence was observed in 43 and 21 patients randomized to the BSC and atezolizumab treatment groups, respectively. Of those patients, locoregional disease recurrence was experienced by 61.9% of patients in the atezolizumab treatment arm and 32.6% in the BSC arm. Distant-only disease recurrence was experienced by 41.9% of patients in the BSC arm and 23.8% in the atezolizumab arm. CNS-only disease recurrence occurred in 16.3% of patients in the BSC arm and 0% in the atezolizumab arm. Locoregional plus distant disease recurrence occurred in 18.6% of patients in the BSC arm and 14.3% in the atezolizumab arm.
Table 16: Site of Disease Recurrence in the Impower010 Study (Clinical Data Cut-Off Date of January 21, 2021)
Site of disease recurrence, n (%) | Patients with stage II to IIIA disease with PD-L1 expression on ≥ 50% of TCs | Patients with stage II to IIIA disease with PD-L1 expression on ≥ 50% of TCs and without EGFR- or ALK-positive mutations | ||
|---|---|---|---|---|
BSC group N = 50 | Atezolizumab group N = 25 | BSC group N = 43 | Atezolizumab group N = 21 | |
Locoregional only | 17 (34.0) | 15 (60.0) | 14 (32.6) | 13 (61.9) |
Distant only | 21 (42.0) | 6 (24.0) | 18 (41.9) | 5 (23.8) |
Site of distant recurrencea | ||||
Bone or bone marrow | 5 (10.0) | 1 (4.0) | 5 (11.6) | 1 (4.8) |
CNS | 8 (16.0) | 1 (4.0) | 8 (18.6) | 0 (0.0) |
Contralateral lung | 1 (2.0) | 2 (8.0) | 0 (0.0) | 2 (9.5) |
Ipsilateral lung | 1 (2.0) | 0 (0.0) | 0 (0) | 0 (0) |
Liver | 2 (4.0) | 1 (4.0) | 1 (2.3) | 1 (4.8) |
Lymph node | 2 (4.0) | 0 (0.0) | 2 (4.7) | 0 (0.0) |
Other | 6 (12.0) | 1 (4.0) | 4 (9.3) | 1 (4.8) |
CNS onlyb | 7 (14.0) | 1 (4.0) | 7 (16.3) | 0 (0.0) |
Locoregional + distant | 9 (18.0) | 4 (16.0) | 8 (18.6) | 3 (14.3) |
Site of distant recurrence | ||||
Bone or bone marrow | 0 (0.0) | 2 (8.0) | 0 (0.0) | 1 (4.8) |
CNS | 3 (6.0) | 1 (4.0) | 3 (7.0) | 0 (0.0) |
Contralateral lung | 1 (2.0) | 0 (0.0) | 1 (2.3) | 0 (0.0) |
Liver | 0 (0.0) | 2 (8.0) | 0 (0.0) | 2 (9.5) |
Lymph node | 4 (8.0) | 1 (4.0) | 3 (7.0) | 1 (4.8) |
Other | 2 (4.0) | 3 (12.0) | 2 (4.7) | 2 (9.5) |
Secondary primary lung | 3 (6.0) | 0 (0.0) | 3 (7.0) | 0 (0.0) |
Secondary primary lung only | 3 (6.0) | 0 (0.0) | 3 (7.0) | 0 (0.0) |
ALK = anaplastic lymphoma kinase; BSC = best supportive care; CNS = central nervous system; EGFR = epidermal growth factor receptor; PD-L1 = programmed death-ligand 1; TC = tumour cell.
aA patient could have more than 1 distant site.
bPatients who had CNS distant site only were included. Patients who had any other recurrent site (i.e., locoregional, other distant site, secondary primary lung, or secondary primary non-lung) in addition to CNS distant site were not included in the CNS-only category.
Source: Clinical Study Report for IMpower010.9
Health-Related Quality of Life
Health-related quality of life was not measured in the IMpower010 study.
Harms
Only those harms identified in the review protocol are reported here. Refer to Table 17 for detailed harms data. Harms related to the overall safety population are summarized in Appendix 5.
Table 17: Summary of Harms in the Impower010 Study for Patients With Stage II to IIIA Disease and PD-L1 Expression on at Least 50% of TCs (Safety Population; Clinical Data Cut-Off Date of January 21, 2021)
Harms | BSC group N = 112 | Atezolizumab group N = 113 |
|---|---|---|
Patients with ≥ 1 AE | ||
n (%) | 78 (69.6) | 107 (94.7) |
Most common events, with ≥ 5% in any treatment group, n (%) | ||
Nasopharyngitis | 14 (12.5) | 10 (8.8) |
Cough | 12 (10.7) | 16 (14.2) |
Anemia | 9 (8.0) | 8 (7.1) |
Headache | 8 (7.1) | 5 (4.4) |
Arthralgia | 6 (5.4) | 15 (13.3) |
Pruritis | 3 (2.7) | 13 (11.5) |
Pyrexia | 3 (2.7) | 11 (9.7) |
Asthenia | 3 (2.7) | 9 (8.0) |
ALT increase | 3 (2.7) | 8 (7.1) |
Nausea | 3 (2.7) | 6 (5.3) |
Dizziness | 3 (2.7) | 6 (5.3) |
Constipation | 2 (1.8) | 6 (5.3) |
Blood creatine increase | 1 (0.9) | 10 (8.8) |
Rash | 0 (0.0) | 9 (8.0) |
Diarrhea | 0 (0.0) | 7 (6.2) |
Patients with ≥ 1 grade 3 or 4 AE | ||
n (%) | 13 (11.6) | 23 (20.4) |
Most common events, with ≥ 1% in any treatment group, n (%) | ||
ALT increase | 0 (0.0) | 2 (1.8) |
Abnormal hepatic function | 0 (0.0) | 3 (2.7) |
Neutrophil count decrease | 2 (1.8) | 0 (0.0) |
Patients with ≥ 1 grade 5 AE | ||
n (%) | 0 (0.0) | 0 (0.0) |
Patients with ≥ 1 SAE | ||
n (%) | 6 (5.4) | 17 (15.0) |
Most common events, with ≥ 1% in any treatment arm, n (%) | ||
Pyrexia | 0 (0.0) | 2 (1.8) |
Patients with ≥ 1 does interruption due to AE | ||
n (%) | NA | 33 (29.2) |
Most common events, with ≥ 1% of patients in any treatment group, n (%) | ||
Hyperthyroidism | NA | 4 (3.5) |
Pneumonia | NA | 3 (2.7) |
Upper respiratory tract infection | NA | 2 (1.8) |
Pyrexia | NA | 2 (1.8) |
Rash | NA | 2 (1.8) |
Oropharyngeal pain | NA | 2 (1.8) |
Arthralgia | NA | 2 (1.8) |
Patients who stopped treatment due to AE | ||
n (%) | NA | 21 (18.6) |
Most common events, with ≥ 1% of patients in any treatment group, n (%) | ||
Pneumonitis | NA | NR |
Hypothyroidism | NA | NR |
AST increase | NA | NR |
Deaths | ||
n (%) | 0 (0.0) | 0 (0.0) |
Notable harms, n (%) | ||
Immune-mediated reactions | ||
Cardiotoxicity | ||
Myocarditis | 0 (0.0) | 0 (0.0) |
Vasculitis | 0 (0.0) | 0 (0.0) |
Endocrinopathies | ||
Hypothyroidism | 0 (0.0) | 16 (14.2) |
Hyperthyroidism | 2 (1.8) | 5 (4.4) |
Adrenal insufficiency | 0 (0.0) | 0 (0.0) |
Diabetes mellitus | 0 (0.0) | 0 (0.0) |
Hypophysitis | 0 (0.0) | 0 (0.0) |
Immune-mediated rash | ||
Rash | 2 (1.8) | 21 (18.6) |
Grade 3 or 4 rash | 0 (0.0) | 1 (0.9) |
Severe cutaneous reactions | 0 (0.0) | 2 (1.8) |
Gastrointestinal toxicity | ||
Grade 3 or 4 colitis | 0 (0.0) | 1 (0.9) |
Pancreatitis | 0 (0.0) | 0 (0.0) |
Pulmonary toxicity | ||
Pneumonitis | 0 (0.0) | 6 (5.3) |
Grade 3 to 4 pneumonitis | 0 (0.0) | 1 (0.9) |
Nephrotoxicity | ||
Nephritis | 0 (0.0) | 0 (0.0) |
Immune-mediated hepatitis (diagnosis and lab abnormalities) | 5 (4.5) | 15 (13.3) |
Grade 3 or 4 immune-mediated hepatitis | 0 (0.0) | 6 (5.3) |
Infusion-related reaction | 0 (0.0) | 0 (0.0) |
AE = adverse event; ALT = alanine aminotransaminase; AST = aspartate aminotransferase; BSC = best supported care; NA = not applicable; NR = not reported; PD-L1 = programmed death-ligand 1; SAE = serious adverse event; TCs = tumour cells
Source: Clinical Study Report for IMpower010.9
Adverse Events
Among patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, a greater proportion of patients who received atezolizumab (94.7%) than BSC (69.6%) reported at least 1 AE. The top 5 reported AEs (BSC versus atezolizumab) were cough (10.7% versus 14.2%); nasopharyngitis (12.5% versus 8.8%), arthralgia (5.4% versus 13.3%), pruritis (2.7% versus 11.5%), and anemia (8.0% versus 7.1%). The following AEs had a difference of at least 5% between treatment arms, with a greater proportion in the atezolizumab arm: arthralgia, asthenia, increased blood creatine; diarrhea, rash, pruritus, and pyrexia.
Adverse Events by Grade
Among patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, at least 1 grade 3 or 4 AE was reported in 11.6% and 20.4% of patients randomized to BSC and atezolizumab, respectively. The most commonly reported grade 3 or 4 AEs were decreased neutrophil count (1.8%) in patients who received BSC, and increased alanine aminotransferase (1.8%) and abnormal hepatic function (2.7%) in patients who received atezolizumab. No grade 5 AEs were reported.
Serious Adverse Events
Among patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, a greater proportion of patients who received atezolizumab reported at least 1 SAEs compared with BSC (15.0% versus 5.4%). The most commonly reported SAE (BSC versus atezolizumab) for the subpopulation of patients with PD-L1 expression on at least 50% of TCs was pyrexia (0.0% versus 1.8%).
Dose Interruptions Due to Adverse Events
Among patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, 29.2% of patients who received atezolizumab had at least 1 dose interruption due to an AE. Reasons for the dose interruptions included hyperthyroidism (3.5%), pneumonia (2.7%), upper respiratory tract infection (1.8%), pyrexia (1.8%), rash (1.8%), and oropharyngeal pain (1.8%).
Discontinuation of Treatment Due to Adverse Events
Among patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, 18.6% of patients who received atezolizumab stopped treatment due to an AE. Data on specific AEs leading to discontinuation were not available for this subpopulation.
In the overall safety population, 18.2% of patients who received atezolizumab stopped treatment due to an AE. The most common events leading to treatment discontinuation were pneumonitis (1.4%), hypothyroidism (1.4%), and aspartate aminotransferase increased (1.4%).
Mortality
There were no data on deaths due to AEs in the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs.
In the overall safety population, the proportion of patients who died was similar in the BSC (18.2%) and atezolizumab (19.2%) treatment groups. Of these deaths, 95.1% occurred more than 30 days after last study treatment or safety visit. Deaths due to AEs occurred in 0.6% and 1.6% of patients in the BSC and atezolizumab arms, respectively. The majority of deaths were due to disease progression.
Notable Harms
The number of patients who experienced each notable harm event are presented. Among the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, reported immune-mediated reactions related to endocrinopathies (BSC versus atezolizumab) included hypothyroidism (0% versus 14.2%) and hyperthyroidism (1.8% versus 4.4%). Overall immune-mediated rash was reported by 1.8% and 18.6% of patients who received BSC and atezolizumab, respectively. One person who received atezolizumab experienced a grade 3 or 4 rash. Immune-mediated colitis (grade 3 or 4) was reported by 1 person who received atezolizumab. Immune-related pneumonitis was reported by 5.3% of patients who received atezolizumab; 1 of these patients experienced graded 3 or 4 pneumonitis. Immune-mediated hepatitis was reported by 4.5% and 13.3% of patients who received BSC and atezolizumab, respectively. Among patients who received atezolizumab, 5.3% had at least 1 grade 3 or 4 immune-mediated hepatitis event.
Infusion-related reactions were not reported for the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs.
Critical Appraisal
Internal Validity
The IMpower010 trial used appropriate methods for randomization and allocation concealment (i.e., central randomization by a computerized system). Randomization was stratified by sex (female versus male), tumour histology (squamous versus nonsquamous), extent of disease (stage IB versus stage II versus stage IIIA based on the UICC and AJCC [7th edition]1 staging criteria) and PD-L1 expression status (TC2/3 and any IC versus TC0/1 and IC2/3 versus TC0/1 and IC0/1, detected with the SP142 IHC assay). The choice of stratification factors was considered to be reasonable and, as noted in the Health Canada report, disease stage is a known prognostic factor for NSCLC and PD-L1 tumour performance status is a predictive factor for immunotherapy efficacy in the setting of incurable NSCLC.8 Baseline characteristics of the ITT population appeared to be relatively similar across groups, indicating that randomization was likely successful. However, the Health Canada–indicated population was a subgroup of the main ITT population, so cannot truly be considered randomized. Among the subgroup of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, there were some minor imbalances across groups, but these did not universally favour either group and may be considered reasonable, given the small sample size.8 Additionally, minor differences in characteristics between this subgroup and the ITT population are not expected to confound the efficacy analyses.8
Despite being an open-label study, the investigators remained blinded to treatment assignment information — including treatment assignment at randomization and patient-level PD-L1 status with a link to patient indication — until the boundary for statistical significance of the planned DFS interim analysis was crossed, as reviewed by the Independent Data Monitoring Committee. The interim analysis that the clinical report was based on was conducted, as specified, by the statistical analysis plan (i.e., when approximately 190 DFS events occurred in the subpopulation with PD-L1 expression on at least 1% of TCs, detected with the SP263 assay, in the stage II to IIIA population). However, at the time of the data cut-off, the pre-specified interim analysis alpha boundary (2-sided alpha = 0.0368) for DFS was not crossed in the ITT population, and OS data were immature. As such, OS was presented as descriptive only, precluding definitive conclusions.
The IMpower010 efficacy end points were well described and employed appropriate censoring criteria. Although OS is the gold standard for demonstrating clinical benefit in cancer treatment trials, the time required to observe a clinically meaningful effect can be long. Accordingly, DFS was the primary outcome and OS was the key secondary outcome in the IMpower010 trial. The European Medicines Agency recommends that when DFS is the primary end point, OS should be the secondary end point, which was done in the IMpower010 trial.45 The use of DFS as an surrogate end point for OS is accepted by the FDA for both accelerated and regular approval.46 To minimize any bias of the open-label study design on investigator-determined tumour assessment for treatment response, American Society of Clinical Oncology, National Comprehensive Cancer Network, and European Society for Medical Oncology guidelines were adhered to by ensuring standard of care in both treatment arms. In response to the Health Canada review report,8 it was noted that recurrence events in the ITT population were confirmed by radiologic evidence in 99.4% and 98% of patients in the atezolizumab and BSC arms, respectively. The remaining recurrence events were determined with biopsy. Furthermore, a retrospective audit demonstrated a concordance rate of 92% between the blinded independent central review and investigator assessment of DFS in a subset of the ITT population. Therefore, the risk of bias related to the open-label investigator-determined tumour assessments is low.
As described earlier, the study protocol underwent several amendments in response to emerging evidence from the POPLAR study,47 which demonstrated increasing improvement in OS with increasing PD-L1 expression, and from the KEYNOTE-024 and KEYNOTE-042 studies and the PACIFIC study that supported the use of the SP263 IHC assay to define the primary biomarker analysis population.48-51 The protocol amendments were well addressed and unlikely to affect the end results or introduce bias related to end point evaluation or patient selection.
A greater proportion of patients in the BSC arm than in the atezolizumab arm discontinued the study (29% versus 14%). The primary reason for study discontinuation was death (23% versus 9.6%). Patients for whom the outcome was not known would have been censored in the efficacy analyses. Although the direction of any bias is unclear, it did not appear to favour atezolizumab.8
The analysis of the IMpower010 study presented here was limited by design issues that were affected by the decision of Health Canada to amend the indicated population to include only a subset of the enrolled population at the time of the interim analysis, which had an impact on the ability to draw definitive conclusions about efficacy in the subgroup of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs. The IMpower010 study population included patients who had a complete surgical resection of stage IB (tumours > 4 cm) to IIIA (T2 to 2, N0, T1 to 3 N1, T1 to 3 N2, T2 N0) NSCLC per the UICC and AJCC (7th edition)1 staging system. The Health Canada–indicated population, however, was a more narrow population, consisting of patients with stage II or IIIA (per the UICC and AJCC [7th edition]1 staging system) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs following complete resection and no progression after platinum-based adjuvant chemotherapy. The enrolled subpopulation of patients with PD-L1 expression on at least 50% of TCs only accounted for 22.8% of the total randomized population. As such, the IMpower010 trial was not powered for the Health Canada indication under review. Moreover, according to the statistical analysis plan, alpha control was achieved with hierarchical testing of DFS in the population with PD-L1 expression on at least 1% of TCs (detected with the SP263 assay) and stage II to IIIA disease; DFS in the stage II to IIIA population; DFS in the ITT population; and OS in the ITT population. Although DFS in the stage II to IIIA population with PD-L1 expression on at least 50% of TCs was a pre-specified secondary end point, it was absent from the statistical testing hierarchy. Thus, the statistical analyses of the efficacy outcomes were conducted with no control for multiplicity, which resulted in the inability to draw definitive conclusions because of the increased risk of false-positive findings. Moreover, as the reported results were based on an interim analysis, there is some risk that the efficacy findings are overestimated.52 Analyses related to the reimbursement request population (i.e., stage II to IIIA population with PD-L1 expression on at least 50% of TCs and no EGFR or ALK mutations) included a small number of patients and were available only as post hoc analyses provided by the sponsor; these are therefore affected by uncertainty related to the underpowered sample and potential bias because the analysis was not pre-specified nor adjusted for multiple testing, which increases the risk of false-positive conclusions.53
Several subgroup analyses were performed to examine the consistency of the treatment effect observed for the primary and key secondary efficacy end points. However, drawing conclusions about these subgroups was not possible because of a lack of sample size considerations for these subgroups and their absence from the statistical testing hierarchy.
External Validity
Table 18 summarizes the generalizability of the evidence.
The demographic characteristics of the study population were considered by the clinical experts to be generally reflective of the relevant population with NSCLC in Canada. The clinical experts considered the results of the IMpower010 multi-national, multi-centre study to be generalizable to the Canadian setting. The clinical experts did highlight a few notable differences in disease characteristics and treatment regimens between the trial population and the Canadian NSCLC population, as follows.
Disease Characteristics
Approximately 50% of patients in the study population were diagnosed with stage IIIA NSCLC. According to the clinical experts consulted, it is not typical to have such a high proportion of resected patients with stage IIIA disease in the adjuvant setting. Moreover, the clinical experts noted that the trial population had a higher proportion of patients with squamous lung cancer compared with the Canadian lung cancer population. The clinical experts noted that squamous lung cancer is associated with smoking history, and that the proportion of patients with squamous lung cancer in the trial is reflective of patients enrolled from countries with higher rates of tobacco use.
EGFR and/or ALK Mutations
Patients with an EGFR and/or ALK mutation account for less than 10% of the randomized patient population. As the proportion of patients with EGFR or ALK mutations was small, the results were likely not affected by their inclusion, so the results can be generalized to those without the mutations. The clinical experts highlighted that although the study results are generalizable to patients with EGFR or ALK mutations, given that these patients were included in the IMpower010 study, they would not use atezolizumab for patients with an EGFR or ALK mutation. The clinical experts explained that there are better treatment options for these patients (i.e., adjuvant osimertinib), as immunotherapy tends to be ineffective in metastatic ALK-mutated NSCLC. The clinical experts noted that it would be less complicated to analyze the benefits of adjuvant atezolizumab in patients who are EGFR- or ALK-negative, as that obviates the need to make a comparison with adjuvant osimertinib in the population with a classic exon 19 deletion or exon 21 L858R EGFR mutation.
PD-L1 Expression Assessment
In the IMpower010 study, the VENTANA PD-L1 SP142 assay was used to recruit and stratify patients, whereas the VENTANA PD-L1 SP263 assay was used to determine PD-L1 expression for the evaluation of efficacy outcomes. Although the VENTANA PD-L1 SP263 assay is authorized for use in Canada, it is the 22C3 assay that is currently in use in most Canadian pathology laboratories. Based on the Blueprint study,36 the SP263 IHC assay is comparable to the 22C3 assay in its analytical performance of assessing PD-L1 expression on TCs. Thus, the current IHC assay used in Canada is adequate, and the IMpower010 efficacy results may be applied to the Canadian system of PD-L1 expression testing. As described in the Health Canada product monograph, patients who should be selected for treatment have PD-L1 expression on at least 50% of TCs, determined by an experienced laboratory using a validated test equivalent to that used in the IMpower010 trial.29
AJCC/UICC Staging
Disease staging in the IMpower010 study was based on the UICC and AJCC (7th edition) staging system.1 Currently, the 8th edition of the AJCC staging system6 is used in clinical practice. The clinical experts consulted by CADTH stressed that the 7th edition staging system1 should be used to interpret and apply to the trial results in clinical practice. This is because under the current 8th edition staging system,6 eligibility criteria would change because of shifts between editions. For example, some patients diagnosed as stage IB according to the 7th edition1 would be stage II according to the 8th edition.6 Given that even more changes in stage definition are expected in the future, with the advent of the 9th edition and beyond, eligibility criteria for adjuvant atezolizumab in this setting should be defined by the specific disease characteristics used to define stage II and III disease in the 7th edition,1 as opposed to disease stage determined using the 8th edition definition.6 Doing so would mean that for the current Health Canada indication, any patient with completely resected NSCLC with a PD-L1 score of at least 50% and either a primary tumour 5 cm or larger or a primary tumour of any size completely resected with associated lymph node involvement would be eligible for adjuvant atezolizumab.
Table 18: Assessment of Generalizability of Evidence for Atezolizumab
Domain | Factor | Evidence | CADTH's assessment of generalizability |
|---|---|---|---|
Population | Patients with EGFR and ALK tumours | Less than 10% of patients randomized to the IMpower010 trial were EGFR- or ALK-positive | Trial results are generalizable to the EGFR- and ALK-positive population; however, clinicians would not use atezolizumab for most EGFR patients with exon 19 deletion or exon 21 L858R mutations in favour of recommending adjuvant osimertinib for patients eligible for both. Further, given the lack of significant benefit for ALK-positive patients in the metastatic setting who are treated with immunotherapy checkpoint inhibitors, the risk-benefit profile for this group will likely lead many clinicians to not recommend adjuvant atezolizumab in this population. |
PD-L1 testing | In the IMpower010 trial, patients were recruited and stratified based on the SP142 assay, but efficacy analysis was based on the SP263 assay | Based on the Blueprint study,36 the SP263 IHC assay is comparable to the 22C3 assay used in most pathology labs in Canada in its analytical performance of the assessment of PD-L1 expression on TCs in NSCLC. Thus, the current IHC assay used in Canada is adequate, and the IMpower010 study efficacy results may be applied to the Canadian system of PD-L1 expression testing. | |
UICC and AJCC staging | The 7th edition of the AJCC Cancer Staging Manual and UICC staging was used at the time of the IMpower010 study period, but the most current staging system used in clinical practice is the 8th edition of the AJCC Cancer Staging Manual | Based on the clinical expert input, the 7th edition of AJCC Cancer Staging Manual and UICC staging was used throughout the review, as it was used to define eligibility in IMpower010. Given the stage shifts that occurred with the introduction of the currently used 8th edition, when making reimbursement recommendations, the disease characteristics that correlated to stage II or III in the 7th edition should be used, the clinical experts stated that patients with complete resection of either a primary tumour 5 cm or larger or a primary tumour of any size with associated lymph node involvement would be eligible for adjuvant atezolizumab. | |
Intervention | Cisplatin therapy | All patients received cisplatin 75 mg/m2 day 1) plus 1 the following 4 options:
| Of the 4 options, only 2 represent the current majority practice in Canada (i.e., cisplatin + vinorelbine or pemetrexed) and are considered adequate in the Canadian clinical setting. On subset analysis, IMpower010 patients who received the cisplatin + gemcitabine adjuvant chemotherapy regimen did not appear to derive benefit from adjuvant atezolizumab, so maintenance of current practice, which favours the use of cisplatin + vinorelbine or cisplatin + pemetrexed, is advised, and cisplatin + gemcitabine should be used only when there are no other available options, (e.g., a chemotherapy shortage). |
Requirement of adjuvant therapy | All patients in IMpower010 received at least 1 cycle of adjuvant cisplatin chemotherapy | According to the clinical experts, atezolizumab would be considered off-label in practice without prior adjuvant chemotherapy. Those who cannot complete all 4 cycles should not be excluded from eligibility for adjuvant atezolizumab, however, as a relatively large number of patients cannot tolerate a full course of cisplatin-based chemotherapy because of toxicity. | |
Outcomes | DFS | DFS used as a surrogate for OS | According to the clinical experts, DFS is clinically meaningful on its own because recurrence has effects at the individual, health care system, and societal levels. DFS is also considered a meaningful end point for patients.54 |
Setting | Multi-national, multi-centre study | Trial included 2 Canadian sites, consisting of 7 patients | Clinical experts felt the trial results were generalizable to the Canadian setting. |
AJCC = American Joint Committee on Cancer; ALK = anaplastic lymphoma kinase; DFS = disease-free survival; EGFR = epidermal growth factor receptor; IHC = immunohistochemistry; NSCLC = non–small cell lung cancer; OS = overall survival; PD-L1 = programmed death-ligand 1; TC = tumour cell; UICC = Union for International Cancer Control.
Cisplatin Therapy
In the IMpower010 trial, all patients received cisplatin 75 mg/m2 on day 1 plus 1 the following 4 options: vinorelbine 30 mg/m2 IV push (days 1 and 8), docetaxel 75 mg/m2 IV (day 1), gemcitabine 1,250 mg/m2 (days 1 and 8), or pemetrexed 500 mg/m2 (day 1; nonsquamous cell NSCLC only). Although all the 4 options used in the IMpower010 trial are available in Canada, gemcitabine and docetaxel are not commonly used in practice. Further, on subset analysis, the patients in IMpower010 who received the cisplatin and gemcitabine adjuvant chemotherapy regimen did not derive benefit from adjuvant atezolizumab. Thus, of the 4 options, the clinical experts consulted by CADTH encourage maintaining current practice, which favours the use of cisplatin plus vinorelbine or cisplatin plus pemetrexed, and only using cisplatin plus gemcitabine when there are no other available options (e.g., a chemotherapy shortage).
Requirement of Adjuvant Chemotherapy
The IMpower010 study required patients to undergo at least 1 cycle of adjuvant chemotherapy before the initiation of anti-PD-L1 therapy. The clinical experts noted that atezolizumab would be considered off-label in practice without any prior adjuvant chemotherapy. However, it should be made available to patients who have received any adjuvant chemotherapy. Specifically, there is a relatively large group of patients who cannot tolerate all recommended cycles of a cisplatin doublet because of toxicity, but even having received 1 cycle should be enough to be considered for adjuvant atezolizumab.
Outcome
The primary efficacy end point in the IMpower010 trial was DFS. According to the clinical experts, it is plausible that improved DFS will translate into OS benefit. Moreover, the clinical experts noted that DFS is a clinically meaningful outcome on its own, as the impact of recurrence is felt at the individual, personal, and health care system levels. From the perspective of patients with lung cancer, DFS is also considered a meaningful end point.54 Of note, outcomes important to patients, such as health-related quality of life, were not measured in the IMpower010 trial. Although the clinical experts acknowledged that it is biologically plausible that improvement in DFS will translate into OS benefit, uncertainty remains given that there is not yet empirical evidence to support this.11,12
Indirect Evidence
A focused literature search for network meta-analyses dealing with NSCLC was run in MEDLINE All (1946–) on March 23, 2022. No limits were applied to the search.
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH or identified in the literature search.
Discussion
Summary of Available Evidence
The current CADTH systematic review included 1 phase III, global, multi-centre, open-label, randomized study: the IMpower010 trial. The IMpower010 trial evaluated the efficacy and safety of atezolizumab, compared with BSC, in patients with stage IB to IIIA (per the UICC and AJCC [7th edition]1 staging system) NSCLC after complete resection and adjuvant cisplatin-based chemotherapy. The IMpower010 study consisted of 2 phases: an enrolment phase, and a randomized phase. In the enrolment phase, patients who had undergone complete resection of their NSCLC were screened and, if eligible, received 1 of 4 cisplatin-based chemotherapy regimens (cisplatin plus vinorelbine, docetaxel, gemcitabine, or pemetrexed), based on investigator choice. Patients who were deemed eligible to continue the study after up to 4 cycles of cisplatin-based chemotherapy proceeded to the randomization phase of the study and were randomized to receive atezolizumab or BSC. The primary efficacy outcome was DFS assessed by the investigator. Secondary efficacy outcomes included OS, 3-year and 5-year DFS rates, and DFS in the subpopulation with PD-L1 expression on at least 50% of TCs (detected with SP263 IHC assay) and with stage II to IIIA (per UICC and AJCC [7th edition]1 staging criteria) NSCLC (i.e., the Health Canada–indicated population). The clinical report provided to CADTH presented the analysis of study data collected from the date of the first patient randomized (February 26, 2016) to the clinical data cut-off date of January 21, 2021, for the protocol-specific interim analysis on DFS.
Although the reimbursement request for the current review was for atezolizumab as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to the AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs and who do not have EGFR or ALK genomic tumour aberrations, the systematic review was focused on the Health Canada indication. Therefore, the objective of this review was to perform a systematic review of the beneficial and harmful effects of atezolizumab as monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA (according to UICC and AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs. Of note, the number of patients with EGFR or ALK mutations made up a small proportion of population (< 10%). Moreover, the Clinical Study Report did not include data specific to the reimbursement population, but was received post hoc from the sponsor.
Among patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs, 144 and 155 patients were randomized to receive BSC or atezolizumab, respectively. In this subpopulation, follow-up is ongoing for a greater proportion of patients who were randomized to receive atezolizumab versus BSC (86.1% versus 71.1%). The indication population had a median age of 62 (range = 36 to 84) years, was predominantly male (72.9%) and White (70.3%), had high functional performance (57.2% had an ECOG performance status score of 0), and most reported previous tobacco use (69.9%). At diagnosis, 48.0% of patients were diagnosed with stage IIIA (per AJCC [7th edition] staging criteria1) disease and 59.8% had nonsquamous histology. Among the 137 patients with nonsquamous histology, 94.2% were identified as having adenocarcinoma subtype. EGFR or ALK mutations were detected in 8.7% of patients.
No indirect treatment comparisons or other evidence were included in the sponsor’s submission to CADTH or identified in the literature search. However, indirect treatment comparisons were not expected, as there are no relevant comparators to atezolizumab, except for a subset of EGFR- or ALK-positive patients for whom osimertinib may be comparator.
The IMpower010 study was limited by design issues that were affected by the Health Canada decision to amend the indication population to include only a subset of the enrolment population. The enrolled subpopulation of patients who made up the indication population (stage II to IIIA disease with PD-L1 expression on at least 50% of TCs) only accounted for 22.8% of the total randomized population. As such, the IMpower010 trial was not powered for the indication under review. In addition, all relevant outcomes in the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs were absent from the statistical testing hierarchy. This precluded definitive conclusions about efficacy in this population, given the increased risk of false-positive results. Despite these limitations, the study results were found to be generalizable to the clinical setting.
Interpretation of Results
Efficacy
The results from the IMpower010 trial were from a planned interim analysis, in which the median length of follow-up was 32.2 (range = 0 to 58.8) months in the ITT population and similar between groups. In the IMpower010 trial, the proportion of deaths observed in patients who were randomized to receive BSC was 23%, compared with 10% in patients who received atezolizumab in the subpopulation of patients who had stage II to IIIA disease with PD-L1 expression on at least 50% of TCs. At year 3, the difference in the proportion of patients in the atezolizumab group who were event-free compared with the BSC group, was 14.27% (95% CI, 4.19% to 24.35%). Similarly, 46% of patients in the BSC treatment arm experienced a disease recurrence or death compared with 24% in the atezolizumab arm at the time of the planned interim analysis. At year 3, the difference in the proportion of patients in the atezolizumab group who were event-free compared with the BSC arm was 25.18% (95% CI, 11.01% to 39.36%).
DFS was considered an important outcome by the clinical experts consulted by CADTH, clinician groups, and the patient-advocacy groups that provided input for this review. The clinical experts consulted by CADTH remarked that the protective effects of atezolizumab against death and/or disease recurrence (DFS) (HR = 0.47; 95% CI, 0.29 to 0.75) was impressive. It should be noted, however, that the relative importance of DFS compared with OS is controversial among clinicians who treat NSCLC,11,12 and it is unclear whether benefits in DFS translate into benefits in OS or just delay the time to recurrence in this particular trial. Regardless, the clinical experts consulted by CADTH for this review found the protective effects of atezolizumab against death at the time of the interim analysis to be equally notable (OS) (HR = 0.40; 95% CI, 0.20 to 0.81). Although the available data for OS were immature at the time of analysis, the clinical experts agreed that improved DFS is likely to translate to improved OS and a higher proportion of patients who are cured. The clinical experts specifically cited the example of the PACIFIC trial, in which 1 year of anti-PD-L1 Immunotherapy checkpoint inhibition delivered in the curative-intent setting in NSCLC with durvalumab was approved for funding in Canada before mature OS results were available, a decision that was confirmed to have been the correct choice, as the 5-year updated data from PACIFIC showed significant OS benefit (HR = 0.72; 95% CI, 0.59 to 0.89; median = 47.5 versus 29.1 months), and an ongoing approximate 10% difference in OS rates at the 5-year mark, illustrating that consolidation durvalumab has led to improved OS by achieving more cures, not just by delaying relapse. The durability of immunotherapy’s survival benefit has also been demonstrated in patients with metastatic NSCLC55 and advanced melanoma.56 Additionally, the clinical experts noted that DFS is a clinically meaningful outcome on its own because the impact of recurrence is felt at the individual, personal, and health care system level.
According to the clinical experts consulted by CADTH, patients with 1 of the 2 common EGFR mutations (exon 19 deletion or L858R) should be considered for adjuvant osimertinib or adjuvant atezolizumab, and the superior efficacy of osimertinib in this setting will mean that osimertinib is the best choice for most patients eligible for both. Patients in this group should not receive both adjuvant osimertinib and adjuvant atezolizumab.
Interpretability of the efficacy end points may be limited because the subpopulation of patients who have stage II to IIIA disease with PD-L1 expression on at least 50% of TCs only accounted for 23% of the total randomized population. Any minor differences in characteristics between this subgroup and the ITT population, however, were not expected to confound the efficacy analyses. The decision by Health Canada to amend the indication population to only include patients who had stage II to IIIA disease with a PD-L1 expression on at least 50% of TCs underpowered the trial to detect a meaningful statistical difference. The Health Canada indication limited to patients with stage II to IIIA disease with PD-L1 expression on at least 50% of TCs because of uncertainty about the clinical benefit of atezolizumab in patients with stage II to IIIA disease with PD-L1 expression on 1% to 49% of TCs; Health Canada noted that the improvement in DFS was mainly driven by the subgroup with PD-L1 expression on at least 50% of TCs.8 Likewise, the European Medicines Agency considered the subgroup with PD-L1 expression on at least 50% of TCs the most relevant for labelling at the time of the interim analysis.10 It should be noted that findings for DFS in patients who had stage II to IIIA with PD-L1 expression on at least 1% of TCs (stratified HR = 0.66; 95% CI, 0.50 to 0.88; P = 0.0039) and in all patients with stage II to IIIA disease (stratified HR = 0.79; 95% CI, 0.64 to 0.96; P = 0.0205) also favoured atezolizumab, although the CIs in those groups (especially the all-stage II to IIIA group) included the potential that the benefit was small. Findings in the ITT population did not cross the pre-specified interim analysis alpha boundary. However, given that the statistical analyses of the efficacy outcomes were conducted with no control for multiplicity, which increases the risk of false-positive findings, precludes the ability to draw definitive conclusions. Moreover, there is some risk that the effect has been overestimated because it is derived from an interim analysis.
Regarding type of recurrence site, it appeared that distant relapse was lower and locoregional relapse was higher in the atezolizumab arm. According to the clinical experts, locoregional relapse increases the likelihood of definitive management with surgery, radiation, or combined chemotherapy-radiation on relapse. Moreover, fewer patients had CNS relapses and rates of new primary lung cancers seemed lower in patients treated with atezolizumab. Based on clinical expert opinion, atezolizumab may be protective against future NSCLC or more widespread, incurable relapse, both of which would derive significant ancillary benefits from adjuvant atezolizumab. However, such statements must be tempered with caution, as there are limited data to support the hypothesis.
Finally, the patient-advocacy groups that provided input for this review emphasized the importance of treatments maintaining health-related quality of life. In the IMpower010 study, health-related quality of life was not assessed. As such, the impact of adjuvant atezolizumab on health-related quality of life in patients with NSCLC is unknown. In other tumour sites, however, PD-1 and PD-L1 have not been shown to negatively affect patients’ quality of life or symptom scores.57-60
Harms
Atezolizumab appeared to be well tolerated, with no concerning safety signals identified. According to the clinical experts consulted by CADTH, the overall safety profile of atezolizumab in IMpower010 appeared consistent with its well-established safety profile in the monotherapy setting across other indications. Of note, there were no AEs with fatal outcomes reported in the atezolizumab treatment arm.
The product monographs for atezolizumab contains warnings and precautions for immune-mediated adverse reactions, including immune-mediated pneumonitis, immune-mediated colitis, immune-mediated hepatitis, immune-mediated endocrinopathies, immune-mediated dermatologic adverse reactions, immune-mediated nephritis and renal dysfunction, and solid organ transplant rejection. The most common adverse reactions (≥ 20%) as a single agent were fatigue and asthenia, decreased appetite, nausea, cough, and dyspnea. The most common adverse reactions (≥ 20%) related to atezolizumab used in combination with other antineoplastic drugs in patients with NSCLC were fatigue and asthenia, nausea, alopecia, constipation, diarrhea, and decreased appetite.
Conclusions
Based on the IMpower010 trial, uncertainty remains about the efficacy of adjuvant atezolizumab in increasing DFS in adults with stage II or IIIA (per the UICC and AJCC [7th edition]1 staging criteria) NSCLC whose tumours have PD-L1 expression on at least 50% of TCs following completed resection and no progression after platinum-based adjuvant chemotherapy at the time of the planned interim analysis, because the analysis was absent from the statistical hierarchy and not controlled for multiplicity. Based on clinical expert opinion, the findings appeared favourable and are considered clinically important. Conclusions regarding the efficacy of atezolizumab on improved OS cannot be made because of the immature nature of the data at the time of the planned interim analysis. Despite these limitations, the findings from the IMpower010 trial appeared to be generalizable to the real-world setting.
References
1.Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. AJCC cancer staging manual. 7th ed. New York (NY): Springer; 2010.
2.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. 2020; https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf. Accessed 2022 Mar 23.
3.Dela Cruz CS, Tanoue LT, Matthay RA. Lung cancer: epidemiology, etiology, and prevention. Clin Chest Med. 2011;32(4):605-644. PubMed
4.BC Cancer. Lung. 2013; http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/lung/lung. Accessed 2021 Jun 3.
5.Canadian Cancer Society. Survival statistics for non-small cell lung cancer. 2020; https://cancer.ca/en/cancer-information/cancer-types/lung/prognosis-and-survival/non-small-cell-lung-cancer-survival-statistics. Accessed 2022 Apr 21.
6.Amin MB, Edge S, Greene F, et al., eds. AJCC cancer staging manual. 8th ed. Chicago (IL): American College of Surgeons and Springer Nature; 2017.
7.National Comprehensive Cancer Network. Non-small cell lung cancer. Version 4.2021. (NCCN Clinical practice guidelines in oncology). Plymouth Meeting (PA): National Comprehensive Cancer Network; 2021.
8.Health Canada reviewer's report: Tecentriq (atezolizumab) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tecentriq (atezolizumab), concentrate for solution for infusion, 60mg/mL; 1200 mg/20mL and 840 mg/14mL single use vials Ottawa (ON): Hoffmann-La Roche Limited; 2022 Jan 31.
9.Clinical Study Report: Study GO29527 (IMpower010). A phase III, open-label, randomized study to investigate the efficacy and safety of atezolizumab (anti-PD-L1 antibody) compared with best supportive care following adjuvant cisplatin-based chemotherapy in patients with completely resected stage IB-IIIA non-small cell lung cancer. Report No. 1106726 [internal sponsor's report]. Standford (CA): F. Hoffman-La Roche Ltd.; 2021 May.
10.Araujo-Fernandez I, Delgado J, Moscetti L, et al. The European Medicines Agency review of the initial application of atezolizumab and the role of PD-L1 expression as biomarker for checkpoint inhibitors. ESMO Open. 2021;6(1):100008. PubMed
11.Gyawali B, Prasad V. Making adjuvant therapy decisions with uncertain data. Ann Oncol. 2019;30(3):361-364. PubMed
12.Prasad V, Kim C, Burotto M, Vandross A. The strength of association between surrogate end points and survival in oncology: a systematic review of trial-level meta-analyses. JAMA Intern Med. 2015;175(8):1389-1398. PubMed
13.Canadian Cancer Society. What is lung cancer? 2020: https://cancer.ca/en/cancer-information/cancer-types/lung/what-is-lung-cancer. Accessed 2022 Mar 23.
14.Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9):2892-2911. PubMed
15.Graham RP, Treece AL, Lindeman NI, et al. Worldwide frequency of commonly detected EGFR mutations. Arch Pathol Lab Med. 2018;142(2):163-167. PubMed
16.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. PubMed
17.Williams AS, Greer W, Bethune D, Craddock KJ, Flowerdew G, Xu Z. ALK+ lung adenocarcinoma in never smokers and long-term ex-smokers: prevalence and detection by immunohistochemistry and fluorescence in situ hybridization. Virchows Arch. 2016;469(5):533-540. PubMed
18.Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The Eighth Edition Lung Cancer Stage Classification. Chest. 2017;151(1):193-203.
19.Birring SS, Peake MD. Symptoms and the early diagnosis of lung cancer. Thorax. 2005;60(4):268-269. PubMed
20.Pignon J-P, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26(21):3552-3559. PubMed
21.Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N Engl J Med. 2020;383(18):1711-1723. PubMed
22.Arriagada R, Auperin A, Burdett S, et al. Adjuvant chemotherapy, with or without postoperative radiotherapy, in operable non-small-cell lung cancer: two meta-analyses of individual patient data. Lancet. 2010;375(9722):1267-1277. PubMed
23.Artal Cortes A, Calera Urquizu L, Hernando Cubero J. Adjuvant chemotherapy in non-small cell lung cancer: state-of-the-art. Transl Lung Cancer Res. 2015;4(2):191-197. PubMed
24.Non-small cell lung cancer stage III. (Clinical practice guideline LU-003). Edmonton (AB): Alberta Health Services; 2012: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lu003-nlscs-stage3.pdf. Accessed 2021 Jun 3.
25.Chouaid C, Danson S, Andreas S, et al. Adjuvant treatment patterns and outcomes in patients with stage IB-IIIA non-small cell lung cancer in France, Germany, and the United Kingdom based on the LuCaBIS burden of illness study. Lung Cancer. 2018;124:310-316. PubMed
26.Swissmedic. Tecentriq®. Refdata 2022; https://www.refdata.ch/fr/. Accessed 2022 Apr 11.
27.Tecentriq (atezolizumab). Annex 1: Summary of product characteristics. Amsterdam (NL): European Medicines Agency; 2022 May 11: https://www.ema.europa.eu/en/documents/product-information/tecentriq-epar-product-information_en.pdf. Accessed 2022 Apr 11.
28.Center for Drug Evaluation and Research. Summary Review. Application number: 76104Orig1s000. Silver Spring (MD): U.S. Food and Drug Administration; 2016: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2016/761041Orig1s000SumR.pdf. Accessed 2022 Apr 11.
29.Tecentriq (atezolizumab): concentrate for solution for infusion, 60mg/mL; 1200 mg/20mL and 840 mg/14mL single use vials [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; 2022 Jan 14.
30.Tagrisso (osimertinib as osimertinib mesylate): 40 mg and 80 mg tablets [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Mar 1: https://pdf.hres.ca/dpd_pm/00064905.PDF. Accessed 2022 Jun 24.
31.Loder N. Treating cancer: Progress on many fronts. The Economist Technology Quarterly. 2017 Sep 16. https://www.economist.com/technology-quarterly/2017-09-16/treating-cancer. Accessed 2022 May 19.
32.Felip E, Altorki N, Zhou C, et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet. 2021;398(10308):1344-1357. PubMed
33.Johnson ML, Cho BC, Luft A, et al. PL02.01 Durvalumab ± tremelimumab + chemotherapy as first-line treatment for mNSCLC: results from the phase 3 POSEIDON study. J Thorac Oncol. 2021;16(Suppl 10):S844.
34.Galluzzi L, Humeau J, Buqué A, Zitvogel L, Kroemer G. Immunostimulation with chemotherapy in the era of immune checkpoint inhibitors. Nat Rev Clin Oncol. 2020;17(12):725-741. PubMed
35.Felip E, Vallieres E, Zhou C, et al. LBA9 - IMpower010: Sites of relapse and subsequent therapy from a phase III study of atezolizumab vs best supportive care after adjuvant chemotherapy in stage IB-IIIA NSCLC. Ann Oncol. 2021;32(Suppl 5):S1283-S1346.
36.Tsao MS, Kerr KM, Kockx M, et al. PD-L1 immunohistochemistry comparability study in real-life clinical samples: results of Blueprint phase 2 project. J Thorac Oncol. 2018;13(9):1302-1311. PubMed
37.Paz-Ares L, O'Brien MER, Mauer M, et al. VP3-2022: Pembrolizumab (pembro) versus placebo for early-stage non-small cell lung cancer (NSCLC) following complete resection and adjuvant chemotherapy (chemo) when indicated: Randomized, triple-blind, phase III EORTC-1416-LCG/ETOP 8-15 – PEARLS/KEYNOTE-091 study. Ann Oncol. 2022;33(4):451-453.
38.AstraZeneca. Imfinzi and Imfinzi plus tremelimumab delayed disease progression in Phase III POSEIDON trial for 1st-line treatment of stage IV non-small cell lung cancer. 2019; www.astrazeneca.com/media-centre/press-releases/2019/imfinzi-and-imfinzi-plus-tremelimumab-delayed-disease-progression-in-phase-iii-poseidon-trial-for-1st-line-treatment-of-stage-iv-non-small-cell-lung-cancer.html. Accessed 2022 Apr 11.
39.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
40.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Mar 11.
41.Protocol GO29527. A phase III, open-label, randomized study to investigate the efficacy and safety of atezolizumab (anti-PD-L1 antibody) compared with best supportive care following adjuvant cisplatin-based chemotherapy in patients with completely resected stage IB-IIIA non-small cell lung cancer [internal sponsor's report]. Basel (CH): F. Hoffmann-La Roche Ltd; 2020 Feb 11.
42.Brookmeyer R, Crowley J. A confidence interval for the median survival time. Biometrics. 1982;38:12.
43.Greenwood M. The natural duration of cancer. (Reports on Public Health and Medical Subjects no. 33). London (GB): His Majesty's Stationery Office; 1926.
44.Hwang IK, Shih WJ, De Cani JS. Group sequential designs using a family of type I error probability spending functions. Stat Med. 1990;9(12):1439-1445. PubMed
45.Guideline on the clinical evaluation of anticancer medicinal products. London (GB): European Medicines Agency; 2019: https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-evaluation-anticancer-medicinal-products-man-revision-6_en.pdf. Accessed 2021 Apr 26.
46.Guidance for industry: clinical trial endpoints for the approval of cancer drugs and biologics. Rockville (MD): U.S. Food and Drug Administration; 2007 May.
47.Fehrenbacher L, Spira A, Ballinger M, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet. 2016;387(10030):1837-1846. PubMed
48.Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819-1830. PubMed
49.Reck M. Pembrolizumab as first-line therapy for metastatic non-small-cell lung cancer. Immunotherapy. 2018;10(2):93-105. PubMed
50.Antonia SJ, Villegas A, Daniel D, et al. Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N Engl J Med. 2018;379(24):2342-2350. PubMed
51.Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2017;377(20):1919-1929. PubMed
52.Guyatt GH, Briel M, Glasziou P, Bassler D, Montori VM. Problems of stopping trials early. BMJ. 2012;344:e3863. PubMed
53.Schandelmaier S, Briel M, Varadhan R, et al. Development of the Instrument to assess the Credibility of Effect Modification Analyses (ICEMAN) in randomized controlled trials and meta-analyses. CMAJ. 2020;192(32):E901-E906. PubMed
54.Bever A, Manthorne J, Rahim T, Moumin L, Szabo SM. The importance of disease-free survival as a clinical trial endpoint: a qualitative study among Canadian survivors of lung cancer. Patient. 2022;15(3):307-316. PubMed
55.Reck M, Rodriguez-Abreu D, Robinson AG, et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score >/= 50. J Clin Oncol. 2021;39(21):2339-2349. PubMed
56.Schadendorf D, Wolchok JD, Hodi FS, et al. Efficacy and safety outcomes in patients with advanced melanoma who discontinued treatment with nivolumab and ipilimumab because of adverse events: a pooled analysis of randomized phase II and III trials. J Clin Oncol. 2017;35(34):3807-3814. PubMed
57.Choueiri TK, Tomczak P, Park SH, et al. Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. N Engl J Med. 2021;385(8):683-694. PubMed
58.Indini A, Grossi F. Adjuvant pembrolizumab for melanoma: update from the EORTC 1325-MG/KEYNOTE-054 trial. Lancet Oncol. 2021;22(5):573-575. PubMed
59.Weber J, Mandala M, Del Vecchio M, et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. N Engl J Med. 2017;377(19):1824-1835. PubMed
60.Kelly RJ, Ajani JA, Kuzdzal J, et al. Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer. N Engl J Med. 2021;384(13):1191-1203. PubMed
61.Anonymous. Atezolizumab extends DFS after NSCLC relapse. Cancer Discov. 2021;11(11):OF3. PubMed
62.Department of Error. Lancet. 2021;398(10312):1686.
63.Akinboro O, Larkins E, Pai-Scherf LH, et al. FDA Approval Summary: Pembrolizumab, Atezolizumab, and Cemiplimab-rwlc as single agents for first-line treatment of advanced/metastatic PD-L1 high NSCLC. Clin Cancer Res. 2022;31:31. PubMed
64.Altorki N, Felip E, Zhou C. PL02.05 - IMpower010: Characterization of stage IBIIIA NSCLC patients by type and extent of therapy prior to adjuvant atezolizumab. Paper presented at: 2021 World Conference on Lung Cancer; 2021 Sep 8-14.
65.Bossageon M, Swalduz A, Chouaid C, Bylicki O. First-line treatment of advanced non-small-cell lung cancer with immune-checkpoint inhibitors: new combinations and long-term data. Biodrugs. 2022;36(2):137-151. PubMed
66.Gadgeel S, Hirsch FR, Kerr K, et al. Comparison of SP142 and 22C3 immunohistochemistry PD-L1 assays for clinical efficacy of atezolizumab in non-small cell lung cancer: results from the randomized OAK trial. Clin Lung Cancer. 2022;23(1):21-33. PubMed
67.Majem M, Cobo M, Isla D, et al. PD-(L)1 inhibitors as monotherapy for the first-line treatment of non-small-cell lung cancer patients with high PD-L1 expression: a network meta-analysis. J Clin Med. 2021;10(7). PubMed
68.Nogami N, Barlesi F, Socinski MA, et al. IMpower150 final exploratory analyses for atezolizumab plus bevacizumab and chemotherapy in key NSCLC patient subgroups with EGFR mutations or metastases in the liver or brain. J Thorac Oncol. 2022;17(2):309-323. PubMed
69.Shibaki R, Akamatsu H, Kato T. A phase II study of cisplatin plus vinorelbine combined with atezolizumab as adjuvant therapy for completely resected non-smallcell lung cancer with EGFR mutation (west japan oncology group 1719L/ADJUST study). Ther Adv Med Oncol. 2021;13. PubMed
70.Teng MM, Chen SY, Yang B, et al. Determining the optimal PD-1/PD-L1 inhibitors for the first-line treatment of non-small-cell lung cancer with high-level PD-L1 expression in China. Cancer Med. 2021;10(18):6344-6353. PubMed
71.Wakelee H, Altorki N, Zhou C, et al. IMpower010: primary results of a phase III global study of atezolizumab vs best supportive care after adjuvant chemotherapy in resected stage IB-IIIA non-small cell lung cancer (NSCLC). J Clin Oncol. 2021;39(Suppl 15):8500-8500.
72.Wang L, Yang Y, Yu J, et al. Efficacy and safety of anti-PD-1/PD-L1 in combination with chemotherapy or not as first-line treatment for advanced non-small cell lung cancer: A systematic review and network meta-analysis. Thoracic Cancer. 2022;13(3):322-337. PubMed
73.Yan M, Durm G, Jalal S, et al. FP01.04 BTCRC LUN19-396: Adjuvant chemotherapy plus atezolizumab in stage IB-IIIA resected NSCLC and clearance of ctDNA. J Thorac Oncol. 2021;16(3):S187-S188.
74.Zhou C, Thakur M, Srivastava M, et al. 20 - IMpower010: biomarkers of disease-free survival (DFS) in a Phase 3 study of atezolizumab (atezo) vs best supportive care (BSC) after adjuvant chemotherapy in stage IB-IIIA NSCLC. Ann Oncol.32(Suppl 7):S1373-S1391.
75.Hoffmann-La Roche response to April 1, 2022 DRR request for additional information regarding Tecentriq (atezolizumab) DRR review [internal additional sponsor's information]. Mississauga (ON): Hoffmann-La Roche Limited; 2022.
Appendix 1: Literature Search Strategy
Note that this appendix is not copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: March 23, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: randomized controlled trials; controlled clinical trials
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(atezolizumab* or Tecentriq* or tecntriq or MPDL3280A or MPDL-3280A or RG7446 or RG-7446 or L01FF05 or 52CMI0WC3Y).ti,ab,kf,ot,hw,rn,nm.
((Carcinoma, Non-Small-Cell Lung/ or exp LUNG/) and Carcinoma, Large Cell/) or exp Adenocarcinoma of Lung/
(exp Lung/ or exp Lung neoplasms/) and (Carcinoma, Large Cell/ or Adenocarcinoma/)
(NSCLC* or LCLC* or mNSCLC* or mLCLC*).ti,ab,kf.
((non small cell* or nonsmall cell* or large cell or undifferentiated) adj5 (lung* or bronch* or pulmonar*) adj5 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kf.
((bronchial or pulmonary or lung) adj3 (adenocarcinoma* or adeno-carcinoma*)).ti,ab,kf.
((bronchioloalveolar or bronchiolo alveolar) adj3 (carcinoma* or cancer* or neoplas* or tumor* or tumour*)).ti,ab,kf.
or/2-7
1 and 8
9 use medall
*atezolizumab/
(atezolizumab* or Tecentriq* or tecntriq or MPDL3280A or MPDL-3280A or RG7446 or RG-7446 or L01FF05).ti,ab,kf,dq.
11 or 12
non small cell lung cancer/ or large cell lung carcinoma/ or lung adenocarcinoma/
(NSCLC* or LCLC* or mNSCLC* or mLCLC*).ti,ab,kf,dq.
((non small* cell or nonsmall cell* or large cell or undifferentiated) adj5 (lung* or bronch* or pulmonary*) adj5 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kf,dq.
((bronchial or pulmonary or lung) adj3 (adenocarcinoma* or adeno-carcinoma*)).ti,ab,kf,dq
((bronchioloalveolar or bronchiolo alveolar) adj3 (carcinoma* or cancer* or neoplas* or tumor* or tumour*)).ti,ab,kf,dq.
or/14-18
13 and 19
20 use oemezd
21 not (conference review or conference abstract).pt.
23.10 or 22
remove duplicates from 23
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
"Randomized Controlled Trial (topic)"/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
"Controlled Clinical Trial (topic)"/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf.
pragmatic study or pragmatic studies).ti,ab,hw,kf
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf
(phase adj3 (III or "3") adj3 (study or studies or trial*)).ti,hw,kf.
or/25-55
23 and 56
remove duplicates from 57
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | atezolizumab or Tecentriq and non-small cell lung cancer]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- atezolizumab or Tecentriq and non-small cell lung cancer]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- atezolizumab or Tecentriq and non-small cell lung cancer]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- atezolizumab or Tecentriq and non-small cell lung cancer]
Grey Literature
Search dates: March 11 to March 23, 2022
Keywords: atezolizumab or Tecentriq, non-small cell lung cancer
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note that this appendix is not copy-edited.
Reference | Reason for exclusion |
|---|---|
Anonymous et al.61 | Not relevant study population |
Anonymous et al. 202162 | Not RCT |
Akinboro et al. 202263 | Not RCT |
Altorki et al. 202164 | No added information |
Bossageon et al. 202265 | Not RCT |
Felip et al. 202135 | No added information |
Gadgeel et al. 202266 | Not RCT |
Majem et al. 202167 | Not relevant study population |
Nagami et al. 202268 | Not relevant study population |
Shibaki et al. 202169 | Not relevant study design |
Teng et al. 202170 | Not RCT |
Wakelee et al.71 | No added information |
Wang et al. 202272 | Not RCT |
Yan et al.73 | Not relevant study design |
Zhou et al. 202174 | No added information |
RCT = randomized controlled trial
Appendix 3: Protocol Amendments
Note that this appendix is not copy-edited.
Table 21: Key Protocol Amendments for the IMpower010 Study
Protocol sections | Protocol versions 1 to 4 | Protocol versions 5 and 6 | Protocol version 7 | Protocol version 8 |
|---|---|---|---|---|
Date | April 1 ,2015; June 8, 2015; September 5, 2015; October 5, 2015 | June 20, 2016; March 2, 2018 | October 30, 2018 | February 11, 2020 |
Number of randomized patients planned | 760 | 1,014 | 990 | 1,005 |
Population for enrolment | TC3 or IC3 by SP142 | All comers | No change from previous version | No change from previous version |
Primary end point | INV-assessed DFS | No change from previous version | No change from previous version | No change from previous version |
First hypothesis to be tested | DFS for all randomized Stage II-IIIA patients | DFS for the PD-L1 subpopulation defined as TC2/3 or IC2/3 by SP142 in Stage II-IIIA patients | No change from previous version | DFS for the PD-L1 subpopulation defined s TC ≥ 1% by SP263 in Stage II-IIIA patients |
Interim analysis for DFS | No interim analysis for DFS | No change from previous version | One interim analysis for DFS | No change from previous version |
Alpha-spending function | Lan-DeMets O'Brien-Fleming approximation spending function for OS | No change from previous version | Lan-DeMets O'Brien-Fleming approximation spending function for DFS and OS | Hwang-Shih-DeCani alpha-spending function with the gamma parameter of -0.9 for DFS and the alpha-spending function with the cumulative one-sided alpha of 0.001, 0.012, 0.022, 0.024, and 0.025 for 4 interim analyses and 1 final analysis for OS |
Trigger for first analysis | The number of DFS events in Stage II-IIIA patients, DFS events in ITT, and the last patient being randomized | The number of DFS events in PD-L1 subpopulations (defined as TC2/3 or IC2/3 and TC1/2/3 or IC1/2/3 by SP142) in Stage II-IIIA patients, DFS events in all randomized Stage II-IIIA patients, DFS events in PD-L1 subpopulations (defined as TC2/3 or IC2/3 and TC1/2/3 or IC1/2/3 by SP142) in ITT, DFS events in ITT, and the last patient being randomized | The number of DFS events in PD-L1 subpopulations (defined as TC2/3 or IC2/3 and TC1/2/3 or IC1/2/3 by SP142) in Stage II-IIIA patients, DFS events in all randomized Stage II-IIIA patients, DFS events in ITT | The number of DFS events in PD-L1 subpopulation (defined as TC ≥ 1% by SP263) in Stage II-IIIA |
Secondary efficacy end points | OS in all randomized Stage II-IIIA patients and OS in ITT | OS in the PD-L1 subpopulations (defined as TC2/3 or IC2/3 and TC1/2/3 or IC1/2/3 by SP142) in both Stage II-IIIA patients and ITT; OS in all randomized Stage II-IIIA patients, OS in ITT; 3-year DFS and 5-year DFS in PD-L1 subpopulations (defined as TC2/3 or IC2/3 and TC1/2/3 or IC1/2/3 by SP142) in both Stage II-IIIA patients and ITT; 3-year DFS and 5-year DFS in all randomized Stage II-IIIA patients; and 3-year DFS and 5-year DFS in ITT | OS in ITT; DFS in PD-L1 Subpopulations defined by SP263 in both Stage II-IIIA patients and ITT; 3-year DFS and 5-year DFS in PD-L1 subpopulations (defined as TC2/3 or IC2/3 and TC1/2/3 or IC1/2/3 by SP142) in both Stage II-IIIA patients and ITT; 3-year DFS and 5-year DFS in both Stage II-IIIA randomized patients and in ITT | OS in ITT; DFS in the PD-L1 subpopulation defined as TC ≥ 50% by SP263 in Stage II-IIIA patients; 3-year DFS and 5-year DFS in PD-L1 subpopulations (defined as TC ≥ 1% and TC ≥ 50% by SP263) in both Stage II-IIIA patients and ITT; 3-year DFS and 5-year DFS in both Stage II-IIIA patients and ITT |
Stratification factors |
|
| No change from previous version | No change from previous version |
DFS = disease-free survival; IC = tumour-infiltrating immune cell; INV = investigator; ITT = intention to treat; OS = overall survival; PD-L1 = programmed death-ligand 1; TC = tumour cell
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Clinical Study Report for IMpower0109
Appendix 4: Statistical Analysis
Note that this appendix has not been copy-edited.
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|---|---|---|---|---|---|
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
|||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Note: This table has been redacted as per the sponsor’s request.
Appendix 5: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 23: Summary of Baseline Characteristics of Patients in the IMpower010 Study
Characteristic | All patients (ITT Population) | Patients with PD-L1 expression on ≥ 50% of TC (ITT population) | ||
|---|---|---|---|---|
BSC group (N = 498) | Atezolizumab group (N = 507) | BSC group (N = 114) | Atezolizumab group (N = 115) | |
Demographic characteristics | ||||
Age at randomizationa, years | ||||
Mean (SD) | 61.1 (9.2) | 61.2 (8.4) | 61.3 (9.2) | 61.1 (8.5) |
Median (range) | 62.0 (26 to 84) | 62.0 (26 to 84) | 62.0 (36 to 84) | 62.0 (34 to 77) |
Age group at randomizationa, years n (%) | ||||
< 65 years | 300 (60.2) | 323 (63.7) | 68 (59.6) | 70 (60.9) |
≥ 65 years | 198 (39.8) | 184 (36.3) | 46 (40.4) | 45 (39.1) |
Age group at randomizationa, years n (%) | ||||
< 65 | 300 (60.2) | 323 (63.7) | 68 (59.6) | 70 (60.9) |
65 to 74 | 173 (34.7) | 164 (32.2) | 40 (35.1) | 43 (37.4) |
75 to 84 | 25 (5.0) | 20 (3.9) | 6 (5.3) | 2 (1.7) |
Sex per eCFR | ||||
Male | 335 (67.3) | 337 (66.5) | 78 (68.4) | 89 (77.4) |
Female | 163 (32.7) | 170 (33.5) | 36 (31.6) | 26 (22.6) |
Race, n (%) | ||||
Asian | 112 (22.5) | 130 (25.6) | 26 (22.8) | 36 (31.3) |
Black or African American | 1 (0.2) | 5 (1.0) | 0 | 1 (0.9) |
Native Hawaiian or other Pacific Islander | 1 (0.2) | 1 (0.2) | 0 | 1 (0.9) |
White | 376 (75.5) | 362 (71.4) | 86 (75.4) | 75 (65.2) |
Multiple | 1 (0.2) | 0 | NA | NA |
Unknown | 07 (1.4) | 09 (1.8) | 2 (1.8) | 2 (1.7) |
Weight (kg) at randomizationa | ||||
n | 495 | 495 | 112 | 113 |
Mean (SD) | 74.45 (15.8) | 73.62 (16.53) | 76.15 (18.08) | 74.54 (17.39) |
Median (range) | 73.0 (43.1 to 140.0) | 71.5 (39.6 to 132.5) | 74.0 (43.5 to 126.3) | 71.5 (46.6 to 132.5) |
ECOG performance status at randomizationa | ||||
0 | 283 (56.8) | 273 (53.8) | 60 (52.6) | 71 (61.7) |
1 | 214 (43.0) | 232 (45.8) | 53 (46.5) | 44 (38.3) |
2 | 1 (0.2) | 2 (0.4) | 1 (0.9) | 0 |
Tobacco use history | ||||
Never | 108 (21.7) | 114 (22.5) | 15 (13.2) | 16 (13.9) |
Current | 86 (17.3) | 76 (15.0) | 22 (19.3) | 16 (13.9) |
Previous | 304 (61.0) | 317 (62.5) | 77 (67.5) | 83 (72.2) |
Disease characteristics | ||||
Stage per eCRF, n (%) | ||||
Stage IB | 58 (11.6) | 65 (12.8) | 0 | 0 |
Stage IIA | 148 (29.7) | 147 (29) | 41 (36.0) | 35 (30.4) |
Stage IIB | 84 (16.9) | 90 (17.8) | 16 (14.0) | 27 (23.5) |
Stage IIIA | 208 (41.8) | 205 (40.4) | 57 (50.0) | 53 (46.1) |
Histology per eCRF | ||||
Squamous | 167 (33.5) | 179 (35.3%) | 45 (39.5) | 47 (40.9) |
Nonsquamous | 331 (66.5) | 328 (64.7) | 69 (60.5) | 68 (59.1) |
Histology subtypes in nonsquamous, n (%) | ||||
n | 331 | 328 | 69 | 68 |
Adenocarcinoma | 308 (93.1) | 300 (91.5) | 64 (92.8) | 65 (95.6) |
Adenocarcinoma with neuroendocrine features | 2 (0.6) | 4 (1.2) | 0 | 0 |
Adenosquamous | 5 (1.5) | 7 (2.1) | 1 (1.4) | 0 |
Bronchioloalveolar carcinoma | 2 (0.6) | 4 (1.2) | 0 | 0 |
Large cell | 11 (3.3) | 8 (2.4) | 2 (2.9) | 3 (4.4) |
Not applicable | 0 | 3 (0.9) | 0 | 0 |
Sarcomatoid | 1 (0.3) | 0 | 0 | 0 |
Undifferentiated | 2 (0.6) | 1 (0.3) | 2 (2.9) | 0 |
Unknown | 0 | 1 (0.3) | 0 | 0 |
Time since initial NSCLC diagnosis to first treatment in randomization (months) | ||||
n | 493 | 491 | 112 | 112 |
Mean (SD) | 5.43 (1.27) | 5.47 (1.13) | 5.3 (1.27) | 5.59 (1.09) |
Median (range) | 5.19 (2.3 to 13.2) | 5.29 (2.4 to 10.0) | 5.24 (2.6 to 10.1) | 5.36 (3.7 to 8.9) |
EGFR mutation status, n (%) | ||||
Detected | 64 (12.9) | 53 (10.5) | 8 (7.0) | 6 (5.2) |
Not detected | 266 (53.4) | 261 (51.5) | 64 (56.1) | 60 (52.2) |
Unknown | 168 (33.7) | 193 (38.1) | 42 (36.8) | 49 (42.6) |
ALK mutation status, n (%) | ||||
Yes | 18 (3.6) | 15 (3.0) | 3 (2.6) | 2 (2.6) |
No | 294 (59.0) | 280 (55.2) | 62 (54.4) | 62 (53.9) |
Unknown | 186 (37.3%) | 212 (41.8) | 49 (43.0) | 50 (43.5) |
EGFR mutation or ALK mutation, n (%) | ||||
Yes | 82 (16.5) | 67 (13.2) | 11 (9.6) | 9 (7.8) |
No | 230 (46.2) | 221 (43.6) | 54 (47.4) | 52 (45.2) |
Unknown | 186 (37.3) | 219 (43.2) | 49 (43.0) | 54 (47.0) |
KRAS mutation, n (%) | ||||
Detected | 17 (3.4) | 21 (4.1) | 4 (3.5) | 7 (6.1) |
Not detected | 35 (7.0) | 45 (8.9) | 6 (5.3) | 7 (6.1) |
Unknown | 446 (89.6%) | 441 (87.0) | 104 (91.2) | 101 (87.8) |
Largest tumour diameter (cm) | ||||
Mean | 4.46 (2.25) | 4.42 (2.14) | 4.67 (2.48) | 4.41 (2.37) |
Median (range) | 4.20 (0.6 to 16.0) | 4.00 (0.6 to 14.2) | 4.05 (1.0 to 12.5) | 4 (1.0 to 13.5) |
Site of primary tumour, n (%) | ||||
Bilateral | 1 (0.2) | 0 | NA | NA |
Left | 239 (48.0) | 227 (44.8) | 48 (42.1) | 50 (43.5) |
Right | 258 (51.8) | 280 (55.2) | 66 (57.9) | 65 (56.5) |
Primary tumour stage, n (%) | ||||
T1A | 46 (9.2) | 36 (7.1) | 11 (9.6) | 13 (11.3) |
T1B | 37 (7.4) | 51 (10.1) | 6 (5.3) | 18 (15.7) |
T2A | 191 (38.4) | 206 (40.6) | 44 (38.6) | 28 (24.3) |
T2B | 81 (16.3) | 72 (14.2) | 20 (17.5) | 16 (13.9) |
T3 | 116 (23.3) | 120 (23.7) | 26 (22.8) | 36 (31.3) |
T4 | 26 (5.2) | 22 (4.3) | 6 (5.3) | 4 (3.5) |
Tx | 1 (0.2) | 0 | 1 (0.9) | 0 |
Regional lymph node stage (N), n (%) | ||||
N0 | 169 (33.9) | 183 (36.1) | 21 (18.4) | 30 (26.1) |
N1 | 178 (35.7) | 170 (33.5) | 52 (45.6) | 43 (37.4) |
N2 | 151 (30.3) | 154 (30.4) | 41 (36.0) | 42 (36.5) |
Regional lymph node-positive, n (%) | ||||
Yes | 329 (66.1) | 324 (63.9) | 93 (81.6) | 85 (73.9) |
No | 169 (33.9) | 183 (36.1) | 21 (18.4) | 30 (26.1) |
PD-L1 expression status | ||||
PD-L1 status by SP263 cut-off 1, n (%) | ||||
n | 486 | 493 | 114 | 115 |
≥ 1% | 252 (51.9) | 282 (57.4) | 114 (100) | 115 (100) |
< 1% | 234 (48.1) | 210 (42.6) | 0 | 0 |
PD-L1 status by SP263 cut-off 3, n (%) | ||||
n | 486 | 493 | 114 | 115 |
≥ 50% | 127 (26.1) | 131 (26.6) | 114 (100) | 115 (100) |
< 50% | 359 (73.9) | 362 (73.4) | 0 | 0 |
Prior medicationb, n (%) | ||||
Ophthalmologicals | 463 (93.0) | 456 (89.9) | NR | NR |
Antiemetics and antinauseants | 459 (92.2) | 457 (90.1) | NR | NR |
Systemic corticosteroids | 452 (90.8) | 447 (88.2) | NR | NR |
Topical corticosteroids | 451 (90.6) | 442 (87.2) | NR | NR |
Anti-acne preparations | 448 (90.0) | 438 (86.4) | NR | NR |
Otologicals | 444 (89.2) | 440 (86.8) | NR | NR |
Stomatological preparations | 443 (89.0) | 436 (86.0) | NR | NR |
Nasal preparations | 439 (88.2) | 432 (85.2) | NR | NR |
Ophthalmological ontological preparations | 429 (86.1) | 419 (82.6) | NR | NR |
Vasoprotectives | 422 (84.7) | 414 (81.7) | NR | NR |
Drugs for obstructive airway disease | 411 (82.5) | 395 (77.9) | NR | NR |
Prior surgery, n (%) | ||||
Lung cancer surgery | ||||
At least 1 surgery, n (%) | 498 (100) | 507 (100) | 114 (100) | 115 (100) |
Total number of surgeries, n | 507 | 514 | 116 | 117 |
Surgical procedures, n (%) | ||||
Lobectomy | 391 (78.5) | 394 (77.7) | 85 (74.6) | 85 (73.9) |
Bilobectomy | 19 (3.8) | 31 (6.1) | 7 (6.1) | 7 (6.1) |
Pneumonectomy | 83 (16.7) | 77 (15.2) | 20 (17.5) | 20 (17.4) |
Sleeve lobectomy | 4 (0.8) | 4 (0.8) | 1 (0.9) | 2 (1.7) |
Other | 6 (1.2) | 6 (1.2) | 2 (1.8) | 3 (2.6) |
Time since last surgery to first treatment in enrolment period (months) | ||||
Mean (SD) | 1.83 (0.52) | 1.87 (0.51) | 1.76 (0.48) | 1.87 (0.55) |
Median | 1.74 | 1.84 | 1.68 | 1.81 |
Min – Max | 0.8 to 5.2 | 0.9 to 5.3 | 0.8 to 3.0 | 1.0 to 4.0 |
Time since last surgery to first treatment in randomization period (months) | ||||
n | 495 | 495 | 112 | 113 |
Mean (SD) | 5.14 (0.88) | 5.20 (0.76) | 4.99 (0.90) | 5.24 (0.78) |
Median (range) | 5.13 (2.3 to 8.0) | 5.16 (2.4 to 7.7) | 5.06 (2.3 to 7.2) | 5.19 (3.4 to 7.7) |
Time since diagnosis to last surgery (months) | ||||
n | 496 | 503 | 114 | 114 |
Mean (SD) | 0.33 (0.83) | 0.31 (0.76) | 0.41 (0.85) | 0.38 (0.70) |
Median (range) | 0.03 (-1.7 to 5.6) | 0.03 (-1.5 to 3.9) | 0.03 (-0.9 to 4.1) | 0.03 (-0.9 to 3.3) |
Mediastinal lymph node dissection, n (%) | ||||
Yes | 409 (82.1) | 402 (79.3) | 92 (80.7%) | 95 (82.6%) |
No | 89 (17.9) | 105 (20.7) | 22 (19.3%) | 20 (17.4%) |
Lymph node sampling conduction, n (%) | ||||
Yes | 88 (17.7) | 93 (18.3) | 23 (20.2%) | 19 (16.5%) |
No | 12 (2.4) | 21 (4.1) | 2 (1.8%) | 3 (2.6%) |
Location of lung surgery, n (%) | ||||
Right | 262 (52.6) | 285 (56.2) | 67 (58.8%) | 65 (56.5%) |
Left | 243 (48.8) | 227 (44.8) | 49 (43.0%) | 51 (44.3%) |
Bilateral | 0 | 1 (0.2) | 0 | 1 (0.9%) |
Final microscopic margin | ||||
Negative | 498 (100) | 507 (100) | 114 (100) | 115 (100) |
ALK = anaplastic lymphoma kinase; ECOG = Eastern Cooperative Oncology Group; eCRF = electronic Case Report Form; EGFR = epidermal growth factor receptor; ITT = intention to treat; NA = no applicable; NR = not reported; PD-L1 = programmed death-ligand 1; SD = standard deviation; IxRS = Interactive Web/Voice Response System
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.
aAt randomization is defined as the last assessment value before the start of treatment date in the randomization period.
bThe most frequently used (by ATC Class Level 2, > 80% incidence in any treatment group)
Source: Clinical Study Report for IMpower0109
Table 24: Major Protocol Deviations in the IMpower010 Study (Clinical Data Cut-Off Date: January 21, 2021)
Protocol deviations | All patients | Patients with PD-L1 expression on ≥ 50% of TC | ||
|---|---|---|---|---|
BSC group (N = 498) | Atezolizumab group (N = 507) | BSC group (N = 114) | Atezolizumab group (N = 115) | |
Patients with ≥ 1 deviation, n (%) | 123 (24.7) | 147 (29.0) | NR | NR |
Total number of deviations | 195 | 203 | NR | NR |
Inclusion criteria, n (%) | ||||
Patients with ≥ 1 deviation | 20 (4.0) | 12 (2.6) | NR | NR |
Total number of deviation event | 23 | 15 | NR | NR |
ICF – other (e.g., procedural issues) | 4 (0.8) | 1 (0.2) | NR | NR |
Inclusion criteria procedural issue (e.g., out of window) | 7 (1.4) | 2 (0.4) | NR | NR |
Inclusion criteria related test not done | 5 (1.0) | 5 (1.0) | NR | NR |
Inclusion lab values outside allowed limits | 3 (0.6) | 3 (0.6) | NR | NR |
Non-Stage IB (> 4 cm) – IIIA NSCLC | 2 (0.4) | 1 (0.2) | NR | NR |
Other inclusion criteria | 0 (0.0) | 1 (0.2) | NR | NR |
Exclusion criteria, n (%) | ||||
Patients with ≥ 1 deviation | 5 (1.0) | 6 (1.2) | NR | NR |
Total number of deviation events | 5 | 6 | NR | NR |
Exclusion criteria procedural issue (e.g., out of window) | 1 (0.2) | 3 (0.6) | NR | NR |
History of excluded conditions | 1 (0.2) | 0 | NR | NR |
Other randomization exclusion criteria | 1 (0.2) | 1 (0.2) | NR | NR |
Severe infection within 4 wees of antibiotics within 2 weeks | 2 (0.4) | 2 (0.4) | NR | NR |
Medication, (%) | ||||
Patients with ≥ 1 deviation | 2 (0.4) | 21 (4.1) | NR | NR |
Total number of deviation events | 2 | 22 | NR | NR |
Continuation with study treatment in conflict with protocol | 0 (0.0) | 5 (1.0) | NR | NR |
Dose missed or significantly out of window | 0 (0.0) | 10 (2.0) | NR | NR |
Received incorrect study medication | 1 (0.2) | 2 (0.4) | NR | NR |
Received prohibited concomitant therapy/medication | 1 (0.2) | 3 (0.6) | NR | NR |
Significant deviation from planned chemotherapy dose | 0 (0.0) | 1 (0.2) | NR | NR |
Procedural, n (%) | ||||
Patients with ≥ 1 deviation | 107 (21.5) | 116 (22.9) | NR | NR |
Total number of deviation events | 165 | 160 | NR | NR |
Error with stratification or randomization | 14 (2.8) | 28 (5.5) | NR | NR |
Fail to report SAE or pregnancy according to protocol | 6 (1.2) | 7 (1.4) | NR | NR |
ICF – Other (e.g., procedural) | 39 (7.8) | 61 (12.0) | NR | NR |
Omission of any tumour assessment | 9 (1.8) | 14 (2.8) | NR | NR |
Omission of non-tumour study assessment | 50 (10.0) | 25 (4.9) | NR | NR |
On study disease assessment outside of window during treatment | 4 (0.8) | 2 (0.4) | NR | NR |
BSC = Best supported care; ICF = informed consent form; ITT = intention to treat; NR = not reported; PD-L1 = programmed death-ligand 1; SAE = severe adverse event
Notes: Includes protocol deviations occurring on or after the randomization date.
Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Clinical Study Report for IMpower0109
Table 25: Duration of Follow-Up in the Impower010 Study (Clinical Data Cut-Off Date: January 21, 2021)
Duration of follow-up (months) | All patients | Stage II to IIIA disease with PD-L1 expression on ≥ 50% of TC | ||
|---|---|---|---|---|
BSC group (N = 498) | Atezolizumab group (N = 507) | BSC group (N = 114) | Atezolizumab group (N = 115) | |
n | 498 | 507 | 114 | 115 |
Median (range) | 32.31 (0.2 to 58.5) | 32.00 (0.0 to 58.8) | 33.2 (0.2 to 57.5) | 35.98 (0.2 to 54.2) |
25th and 75th percentile | 27.60, 38.64 | 27.40, 38.24 | 26.61, 39.75 | 29.70, 40.67 |
BSC = best supportive care; ITT = intention to treat; PD-L1 = programmed death-ligand 1
Source: Clinical Study Report for IMpower0109
Table 26: Exposure to Atezolizumab in the IMpower010 study (Safety Population; Clinical Data Cut-Off Date: January 21, 2021)
Exposure to atezolizumab | All patients (N = 495) | Patients with stage II to IIIA disease with PD-L1 expression on ≥ 50% of TC (N = 113) |
|---|---|---|
Treatment duration (months) | ||
Median (range) | 10.4 (0 to 16) | 10.4 (0 to 16) |
Dose intensity (%) | ||
Median (range) | 100.0 (40 to 100) | 100.0 (67 to 100) |
Total cumulative dose (mg) | ||
n | 495 | 113 |
Median (range) | 19,200.0 (1,200 to 19,200) | 19,200.0 (1,200 to 19,200) |
Number of doses/cycles received | ||
n | 495 | 113 |
Median (range) | 16.0 (1 to 16) | 16 (1 to 16) |
Number of doses/cycles, n (%) | ||
0 to < 8 | 125 (25.3) | 20 (17.7) |
≥ 8 to < 16 | 47 (9.5) | 8 (7.1) |
≥ 16 | 323 (65.3) | 85 (75.2) |
BSC = best supportive care; NA = not applicable; NA = non-applicable; PD-L1 = programmed death-ligand 1
Source: Clinical Study Report for IMpower0109
Table 27: Concomitant Medication and Nonprotocol Anti-Cancer Therapy in the IMpower010 Study (Clinical Data Cut-Off Date: January 21, 2021)
Medication or therapy | All patients | Patients with stage II to IIIA disease with PD-L1 expression on ≥ 50% of TC | ||
|---|---|---|---|---|
Best supported care group (N = 498) | Atezolizumab group (N = 507) | Best supported care group (N = 114) | Atezolizumab group (N = 115) | |
Concomitant medications | ||||
Total number of patients with at least 1 treatment | 444 (89.2) | 464 (91.5) | NR | NR |
Total number of treatments | 3,521 | 5,438 | NR | NR |
Class of concomitant medicationa | ||||
Ophthalmological | 213 (42.8) | 319 (62.9) | 1 (0.9) | 0 |
Analgesics | 215 (43.2) | 268 (52.9) | NR | NR |
Stomatological preparations | 173 (34.7) | 257 (50.7) | NR | NR |
Topical products for joint and muscular pain | 196 (39.4) | 221 (43.6) | NR | NR |
Otologicals | 130 (26.1) | 213 (42.0) | NR | NR |
Nonprotocol anti-cancer therapy | ||||
At least 1 treatment, n (%) | 135 (27.1) | 107 (21.1) | 30 (26.3) | 20 (17.4) |
Total number of treatments, n | 350 | 265 | 66 | 48 |
Antineoplastic agentsb, n (%) | ||||
Patients with at least 1 treatment | 133 (26.7) | 105 (20.7) | 30 (26.3) | 20 (17.4) |
Carboplatin | 59 (11.8) | 46 (9.1) | 8 (7.0) | 9 (7.8) |
Pembrolizumab | 31 (6.2) | 12 (2.4) | 14 (12.3) | 3 (2.6) |
Cisplatin | 21 (4.2) | 20 (3.9) | 6 (5.3%) | 4 (3.5) |
Docetaxel | 24 (4.8) | 17 (3.4) | 6 (3.5) | 4 (3.5) |
Gemcitabine | 15 (3.0) | 10 (2.0) | 4 (3.5) | 5 (4.3) |
Pemetrexed | 26 (5.2) | 18 (3.6) | 5 (4.4) | 3 (2.6) |
Paclitaxel | 30 (6.0) | 19 (3.7) | 2 (1.8) | 3 (2.6) |
Etoposide | 7 (1.4) | 12 (2.4) | 2 (1.8) | 2 (1.7) |
Nivolumab | 18 (3.6) | 4 (0.8) | 1 (0.9) | 0 |
Bevacizumab | 12 (2.4) | 9 (1.8) | 0 | 1 (0.9) |
Atezolizumab | 12 (2.4) | 1 (0.2) | 0 | 0 |
ITT = intention to treat; NR = not reported; PD-L1 = programmed death-ligand 1
aThe most frequently used (by ATC Class Level 2, > 40% incidence in any treatment group)
bOnly treatments reported to be used in at least 2% in any treatment group are listed
Source: Clinical Study Report for IMpower0109
Table 28: Overall Survival in the Overall ITT Population and Subpopulation of Patients With Stage II to IIIA Disease With PD-L1 in at Least 50% of TCs (Clinical Data Cut-Off Date: January 21, 2021)
Overall survival | All patients | Stage II to IIIA disease with PD-L1 expression on ≥ 50% of TC | ||
|---|---|---|---|---|
BSC group (N = 498) | Atezolizumab group (N = 507) | BSC group (N = 114) | Atezolizumab group (N = 115) | |
Death event, n (%) | ||||
Patients with death event | 90 (18.1) | 97 (19.1) | 26 (22.8) | 11 (9.6) |
Patients without event | 408 (81.9) | 410 (80.9) | 88 (77.2) | 104 (90.4) |
Time to event (months)a | ||||
Median (range) | NE (0.2b to 58.5b) | NE (0.0b to 58.8b) | NE (0.2b to 57.5b) | NE (0.2b to 54.2b) |
95% CI | NE | NE | NE | NE |
25th and 75th percentile | 46.4, NE | NE | 36.4, NE | NE |
Stratified analysisc | ||||
Hazard ratiod (95% CI) | 1.07 (0.80 to 1.42) | 0.40 (0.20 to 0.81) | ||
P value (log-rank) | 0.6651e | 0.0089e | ||
Unstratified analysis | ||||
Hazard ratiod (95% CI) | 1.06 (0.79 to 1.41) | 0.37 (0.18 to 0.74) | ||
P value (log-rank) | 0.6983e | 0.0036e | ||
Time-point analysis | ||||
3 years | ||||
Patients remaining at risk | 169 | 170 | 43 | 56 |
Event-free rate (%) | 81.18 | 78.63 | 76.67 | 90.94 |
95% CI | 77.37 to 84.99 | 74.61 to 82.65 | 68.38 to 84.97 | 85.21 to 96.67 |
Difference in event-free rate (95% CI) | –2.55 (–8.09 to 2.99) | 14.27 (4.19 to 24.35) | ||
P value, z-test | 0.3666e | 0.0055 | ||
5 years | NE | NE | NE | NE |
BSC = best supported care; CI = confidence interval; DFS = disease-free survival; ITT = intention to treat; NE = not estimable; PD-L1 = programmed death-ligand 1
aSummaries of durations (median and percentiles) are Kaplan-Meier estimates. 95% Cis for the medians are computed using the methods of Brookmeyer and Crowley.42
bCensored
cStratification factors: For all patients: Stage from eCRF (IB/II vs. IIIA), sex from eCRF (female vs. male), histology from eCRF (squamous vs. nonsquamous) and PD-L1 tumour expression status by SP142 IHC assay from IxRS (TC2/3 or IC2/3 vs. TC0/1 and IC0/1). For patient group with PD-L1 expression on > 50% of TC: Stage from eCRF (IB/II vs. IIIA), sex from eCRF (female vs. male), histology from eCRF (squamous vs. nonsquamous)
dHazard ratios were estimated by Cox regression
eP values are based on a pre-specified interim analysis alpha boundary for DFS was not crossed in the ITT population and they were not adjusted for multiplicity, resulting in an increased risk of false-positive conclusions.
Source: Clinical Study Report for IMpower0109
Table 29: Disease-Free Survival in Overall ITT Population and Subpopulation of Patients With Stage II to IIIA Disease With PD-L1 in at Least 50% of TCs (Clinical Data Cut-Off Date: January 21, 2021)
Disease-free survival | All patients | Patients with PD-L1 expression on ≥ 50% of TC | ||
|---|---|---|---|---|
BSC group (N = 498) | Atezolizumab group (N = 507) | BSC group (N = 114) | Atezolizumab group (N = 115) | |
Recurrence event, n (%) | ||||
Patients with event | 212 (42.6) | 187 (36.9) | 52 (45.6) | 28 (24.3) |
Death | 9 | 31 | 2 | 3 |
Disease recurrence | 203 | 156 | 50 | 25 |
Patients without event | 286 (57.4) | 320 (63.1) | 62 (54.4) | 87 (75.7) |
Time to event (months)a | ||||
Median (range) | 37.2 (0.0 b to 55.3b) | NE (0.0b to 54.3b) | 35.7 (0.0b to 54.9b) | NE (0.0b to 54.2b) |
95% CI | 31.6 to NE | 36.1 to NE | 29.7 to NE | 42.3 to NE |
25th and 75th percentile | 12.7, NE | 18.1, NE | 12.0, NE | 35.3, NE |
Stratified analysisc | ||||
Hazard ratiod (95% CI) | 0.81 (0.67 to 0.99) | 0.47 (0.29 to 0.75) | ||
P value (log-rank) | 0.0395 | 0.0012e | ||
Unstratified analysis | ||||
Hazard ratiod (95% CI) | 0.80 (0.66 to 0.98) | 0.43 (0.27 to 0.68) | ||
P value (log-rank) | 0.0271 | 0.0002e | ||
Time-point analysis | ||||
3 years | ||||
Patients remaining at risk | 90 | 97 | 19 | 30 |
Event-free rate (%) | 52.57 | 57.94 | 48.61 | 73.79 |
95% CI | 47.51 to 57.64 | 52.89 to 62.99 | 38.03 to 59.18 | 64.35 to 83.23 |
Difference in event-free rate (%; 95% CI) | 5.37 (-1.79 to 12.52) | 25.18 (11.01 to 39.36) | ||
P value, z-test | 0.1416e | 0.0005e | ||
5 years | NE | NE | NE | NE |
BSC = best supported care; CI = confidence interval; DFS = disease-free survival; ITT = intention to treat; NE = not estimable; TC = tumour cell; PD-L1 = programmed death-ligand 1
aSummaries of durations (median and percentiles) are Kaplan-Meier estimates. 95% Cis for the medians are computed using the methods of Brookmeyer and Crowley.42
bCensored
cStratification factors: For all patients: Stage from eCRF (IB/II vs. IIIA), sex from eCRF (female vs. male), histology from eCRF (squamous vs. nonsquamous) and PD-L1 tumour expression status by SP142 IHC assay from IxRS (TC2/3 or IC2/3 vs. TC0/1 and IC0/1). For patient group with PD-L1 expression on > 50% of TC: Stage from eCRF (IB/II vs. IIIA), sex from eCRF (female vs. male), histology from eCRF (squamous vs. nonsquamous)
dHazard ratios were estimated by Cox regression
eP values are nominal only as they were not adjusted for multiplicity
Source: Clinical Study Report for IMpower0109
Figure 5: Forest Plot for Subgroup Analysis of DFS For Patients With Stage II to IIIA Disease and PD-L1 SP263 in at Least 50% of TCs (Part 1; Clinical Data Cut-Off Date: January 21, 2021)
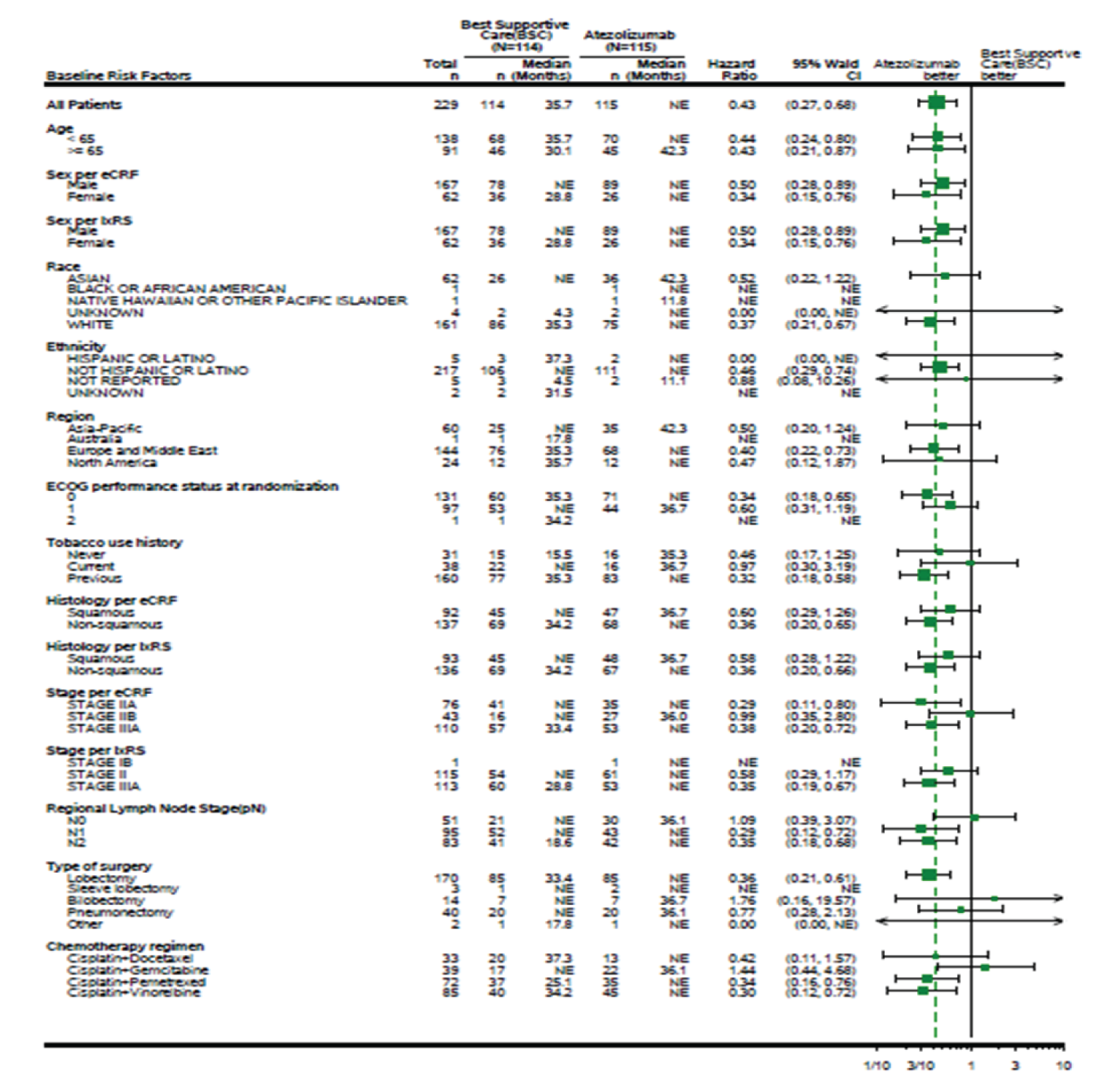
ALK = anaplastic lymphoma kinase; ECOG = Eastern Cooperative Oncology Group; eCRF = electronic Case Report Form; EGFR = epidermal growth factor receptor; DFS = disease-free survival; PD-L1 = programmed death-ligand 1; IxRS = Interactive Web/Voice Response System; PD-L1 = programmed death-ligand 1; TC = tumour cell
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Clinical Study Report for IMpower0109
Figure 6: Forest Plot for Subgroup Analysis of DFS For Patients With Stage II to IIIA Disease and PD-L1 SP263 in at Least 50% of TCs (Part 2; Clinical Data Cut-Off Date: January 21, 2021)
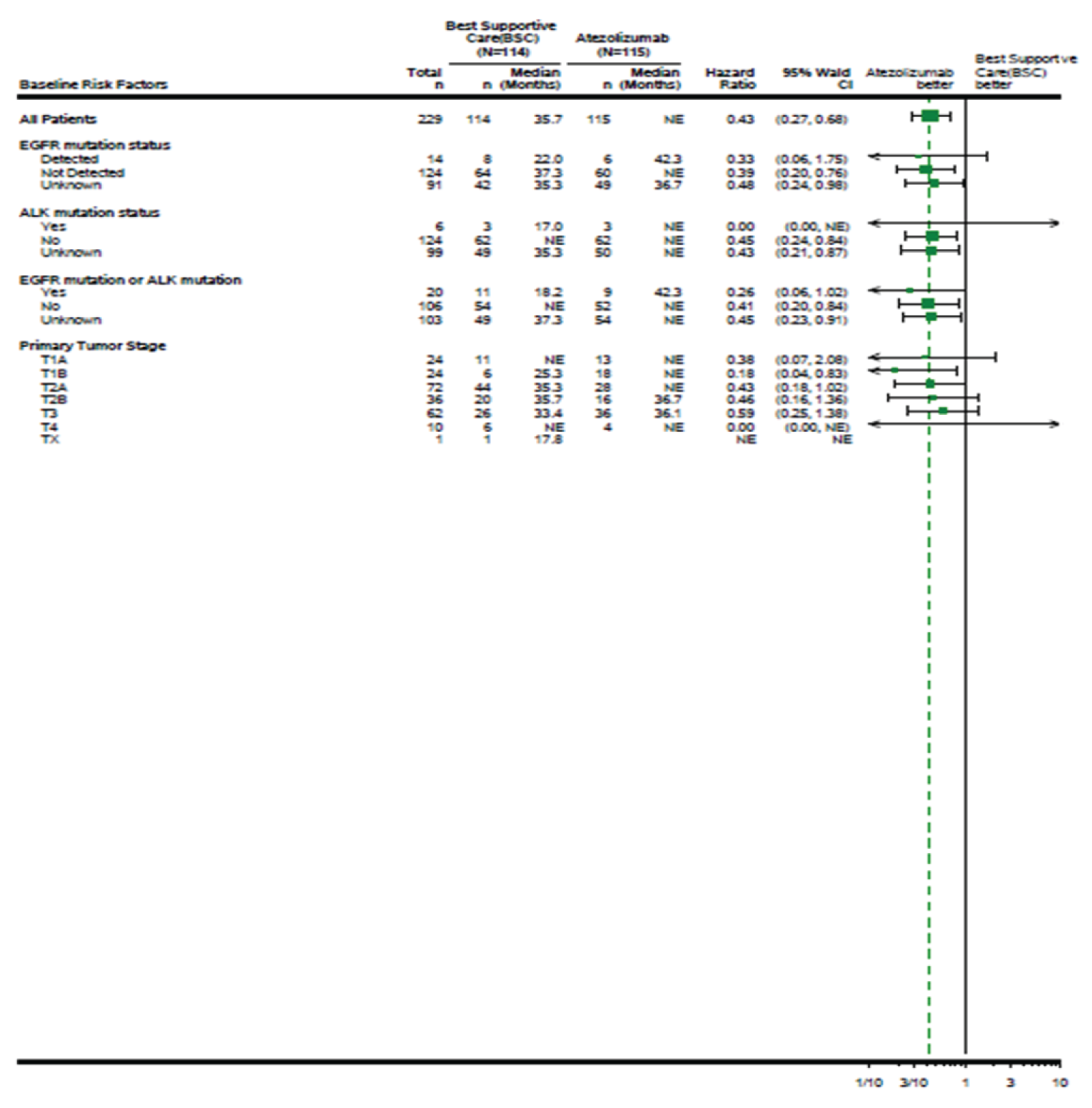
ALK = anaplastic lymphoma kinase; ECOG = Eastern Cooperative Oncology Group; eCRF = electronic Case Report Form; EGFR = epidermal growth factor receptor; DFS = disease-free survival; PD-L1 = programmed death-ligand 1; IxRS = Interactive Web/Voice Response System; PD-L1 = programmed death-ligand 1; TC = tumour cell
Note: Staging defined using the American Joint Committee on Cancer 7th edition.1
Source: Clinical Study Report for IMpower0109
Figure 7: Forest Plots in Key Subgroups in Patients With Stage II to IIIA Disease and PD-L1 SP263 in More Than 50% of TCs Stage II to IIIA, Excluding Those With EGFR and ALK+ (Clinical Data Cut-Off Date: January 21, 2021)
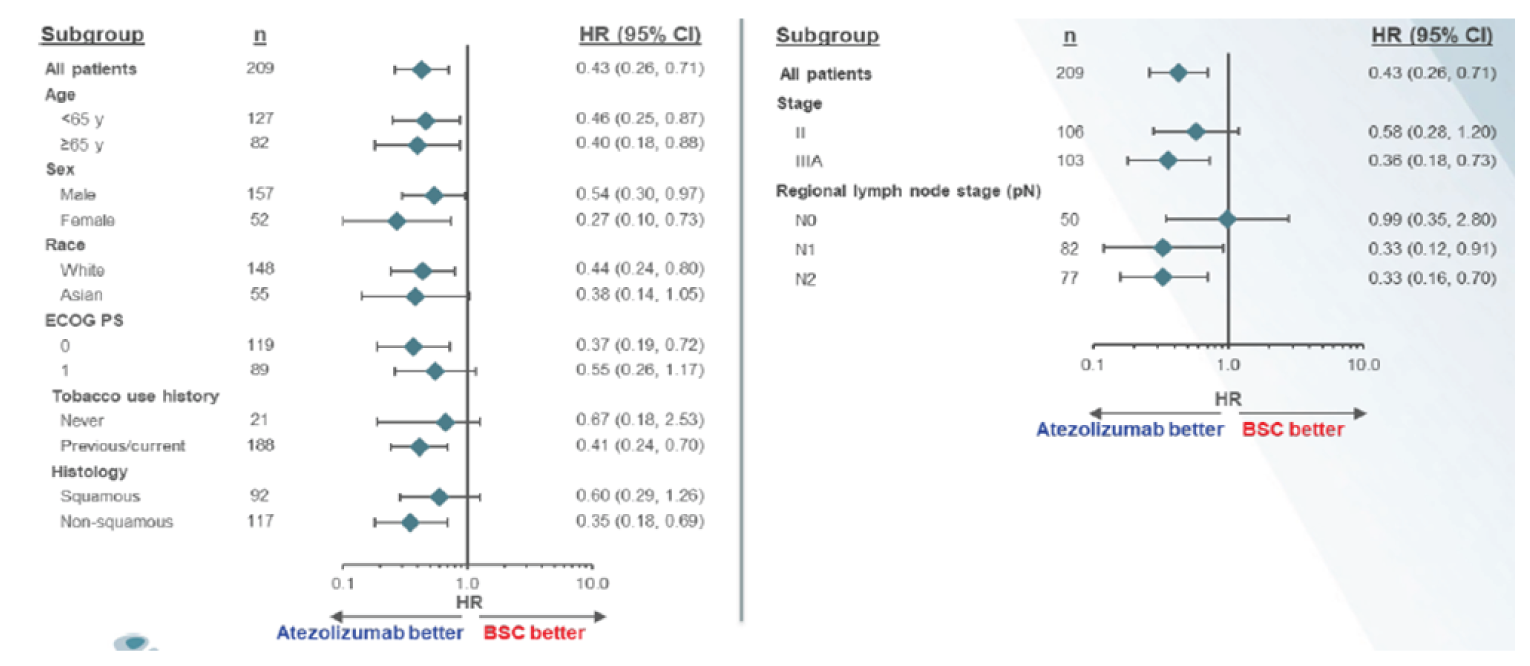
ALK = anaplastic lymphoma kinase; ECOG = Eastern Cooperative Oncology Group; EGFR = epidermal growth factor receptor; DFS = disease-free survival; PD-L1 = programmed death-ligand 1; PS = performance score; TC = tumour cell
Note: Staging defined using the American Joint Committee on Cancer (7th edition) staging criteria.1
Source: Additional sponsor-provided information75
Table 30: Summary of Harms in All Patients in the IMpower010 Study (Safety Population; Clinical Data Cut-Off Date: January 21, 2021)
Harms | BSC group (N = 495) | Atezolizumab group (N = 495) |
|---|---|---|
Patients with ≥ 1 AE | ||
n (%) | 350 (70.7) | 459 (92.7) |
Most common events (≥ 5% in any treatment group), n (%) | ||
Nasopharyngitis | 50 (10.1) | 33 (6.7) |
Upper respiratory tract infection | 12 (2.4) | 35 (7.1) |
Cough | 46 (9.3) | 66 (13.3) |
Dyspnea | 32 (6.5) | 31 (6.3) |
Pyrexia | 11 (2.2) | 65 (13.1) |
Asthenia | 14 (2.8) | 37 (7.5) |
Fatigue | 11 (2.2) | 33 (6.7) |
Alanine aminotransferase increased | 16 (3.2) | 53 (10.7) |
Aspartate aminotransferase increase | 16 (3.2) | 53 (10.7) |
Blood creatine increased | 15 (3.0) | 29 (5.9) |
Diarrhea | 9 (1.8) | 37 (7.5) |
Nausea | 16 (3.2) | 30 (6.1) |
Arthralgia | 26 (5.3) | 52 (10.5) |
Headache | 20 (4.0) | 28 (5.7) |
Pruritis | 3 (0.6) | 51 (10.3) |
Rash | 5 (1.0) | 48 (9.7) |
Anemia | 30 (6.1) | 38 (7.7) |
Hypothyroidism | 3 (0.6) | 55 (11.1) |
Hyperthyroidism | 3 (0.6) | 32 (6.5) |
Patients with ≥ 1 grade 3-4 AE | ||
n (%) | 57 (11.5) | 108 (21.8) |
Most common events (> 1% in any treatment group), n (%) | ||
Pneumonia | 3 (0.6) | 7 (1.4) |
Alanine aminotransferase increased | 1 (0.2) | 6 (1.6) |
Aspartate aminotransferase increase | 0 (0.0) | 7 (1.4) |
Rash | 0 (0.0) | 5 (1.0) |
Hypertension | 2 (0.4) | 5 (1.0) |
Patients with ≥ 1 grade 5 AE | ||
n (%) | 3 (0.6) | 8 (1.6) |
Grade 5 events, n (%) | ||
Pneumonia | 1 (0.2) | 0 (0.0) |
Septic shock | 1 (0.2) | 0 (0.0) |
Interstitial lung disease | 0 (0.0) | 1 (0.2) |
Pulmonary embolism | 1 (0.2) | 0 (0.0) |
Pneumothorax | 0 (0.0) | 1 (0.2) |
Multiple organ dysfunction | 0 (0.0) | 1 (0.2) |
Cerebrovascular accident | 0 (0.0) | 1 (0.2) |
Arrhythmia | 0 (0.0) | 1 (0.2) |
Cardiac failure acute | 0 (0.0) | 1 (0.2) |
Cardia tamponade | 1 (0.2) | 0 (0.0) |
Myocarditis | 0 (0.0) | 1 (0.2) |
Acute myeloid leukemia | 0 (0.0) | 1 (0.2) |
Patients with ≥ 1 SAE | ||
n (%) | 42 (8.5) | 87 (17.6) |
Most common events (≥1% in any treatment arm), n (%) | ||
Pneumonia | 5 (1.0) | 8 (1.6) |
Pyrexia | 1 (0.2) | 6 (1.2) |
Patients with ≥ 1 dose interruptions due to AE | ||
n (%) | 0 (0.0) | 142 (28.7) |
Most common events (> 1% of patients in any treatment group), n (%) | ||
Upper respiratory tract infection | 0 (0.0) | 7 (1.4) |
Pneumonia | 0 (0.0) | 5 (1.0) |
Aspartate aminotransferase increased | 0 (0.0) | 8 (1.6) |
Alanine aminotransferase increased | 0 (0.0) | 7 (1.4) |
Pyrexia | 0 (0.0) | 8 (1.6) |
Hyperthyroidism | 0 (0.0) | 14 (2.8) |
Hypothyroidism | 0 (0.0) | 6 (1.2) |
Rash | 0 (0.0) | 7 (1.4) |
Headache | 0 (0.0) | 6 (1.2) |
Patients who stopped treatment due to AE | ||
n (%) | 0 (0.0) | 90 (18.2) |
Most common events (≥ 1% of patients in any treatment group), n (%) | ||
Pneumonitis | 0 (0.0) | 7 (1.4) |
Hypothyroidism | 0 (0.0) | 7 (1.4) |
Aspartate aminotransferase increased | 0 (0.0) | 7 (1.4) |
Deaths | ||
n (%) | 90 (18.2) | 95 (19.2) |
< 30 days from last study treatment / safety visit | 5 (1.0) | 4 (0.8) |
< 30 days from last study treatment / safety visit | 85 (17.2) | 91 (18.4) |
Primary cause of death, n (%) | ||
Adverse event (Grade 5 AEs) | 3 (0.6) | 8 (1.6) |
Disease relapse | 77 (15.6) | 63 (12.7) |
Other | 10 (2.0) | 24 (4.8) |
Notable harms, n (%) | ||
Immune-mediated reactions | ||
Cardiotoxicity | ||
Myocarditis | 0 (0.0) | 2 (0.4) |
Vasculitis | 1 (0.2) | 0 (0.0) |
Endocrinopathies | ||
Hypothyroidism | 3 (0.6) | 86 (17.4) |
Hyperthyroidism | 4 (0.8) | 32 (6.5) |
Adrenal insufficiency | 0 (0.0) | 6 (1.2) |
Diabetes mellitus | 1 (0.2) | 4 (0.8) |
Hypophysitis | 0 (0.0) | 1 (0.2) |
Dermatological toxicity | ||
Rash | 11 (2.2) | 91 (18.4) |
Severe cutaneous reactions | 0 (0.0) | 2 (0.4) |
GI toxicity | ||
Colitis | 1 (0.2) | 4 (0.8) |
Pancreatitis | 1 (0.2) | 2 (0.4) |
Pulmonary toxicity | ||
Pneumonitis | 3 (0.6) | 19 (3.8) |
Nephrotoxicity | ||
Nephritis | 0 (0.0) | 1 (0.2) |
Hepatic toxicity | ||
Hepatitis (diagnosis and lab abnormalities) | 22 (4.4) | 86 (17.4) |
Infusion-related reaction | 0 (0.0) | 7 (1.4) |
AE = adverse event; BSC = best supportive care; CI = confidence interval; CNS = central nervous system; NA = not applicable; NE = not estimable; NR = not reported; PD-L1 = programmed death-ligand 1; SAE = serious adverse events; TC = tumour cells.
aThe most common AEs, defined as a frequency of ≥ 5% in any treatment arm are listed.
Source: Clinical Study Report for IMpower0109
Pharmacoeconomic Review
Abbreviations
1L MR
first-line metastatic recurrence
2L MR
second-line metastatic recurrence
AJCC
American Joint Committee on Cancer
ALK
anaplastic lymphoma kinase
DFS
disease-free survival
EGFR
epidermal growth factor receptor
ICER
incremental cost-effectiveness ratio
KM
Kaplan-Meier
LR
locoregional recurrence
NSCLC
non–small cell lung cancer
OS
overall survival
PD-L1
programmed death ligand-1
QALY
quality-adjusted life-year
TC
tumour cells
UICC
Union for International Cancer Control
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Atezolizumab (Tecentriq), solution for IV infusion, 1,200 mg/20 mL |
Submitted price | Atezolizumab, 1,200 mg/20 mL (60 mg/mL): $6,776.00 per 1,200 mg vial |
Indication | As monotherapy for adjuvant treatment following complete resection and no progression after platinum-based adjuvant chemotherapy for adults with stage II to IIIA NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | January 14, 2022 |
Reimbursement request | As monotherapy for adjuvant treatment following complete resection and platinum-based chemotherapy for patients with stage II to IIIA (according to AJCC/UICC, 7th edition) NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs and do not have EGFR or ALK genomic tumour aberrations |
Sponsor | Hoffmann-La Roche Ltd. |
Submission history | Previously reviewed: Yes Indication: Hepatocellular carcinoma
Indication: Small cell lung cancer
Indication: NSCLC
Indication: Advanced or metastatic triple-negative breast cancer
|
AJCC = American Joint Committee on Cancer; ALK = anaplastic lymphoma kinase; EGFR = epidermal growth factor receptor; NOC = Notice of Compliance; NSCLC = non–small cell lung cancer; PD-L1 = programmed death ligand-1; TC = tumour cell; UICC = Union for International Cancer Control.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target populations |
|
Treatment | Atezolizumab |
Comparator | Active surveillance, consisting of no active treatment |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (39 years) |
Key data source | IMpower010, a global, randomized, phase III trial comparing atezolizumab with active surveillance after complete resection and adjuvant platinum-based chemotherapy in stage IB to IIIA NSCLC |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
ALK = anaplastic lymphoma kinase; DFS = disease-free survival; EGFR = epidermal growth factor receptor; ICER = incremental cost-effectiveness ratio; LR = locoregional recurrence; LY = life-year; NSCLC = non–small cell lung cancer; OS = overall survival; PD-L1 = programmed death ligand-1; QALY = quality-adjusted life-year; TC = tumour cell.
Conclusions
Based on the IMpower010 trial, uncertainty remains about the efficacy of adjuvant atezolizumab in increasing disease-free survival (DFS) in adults with stage II to IIIA (according to UICC and AJCC [7th edition] staging criteria) non–small cell lung cancer (NSCLC), whose tumours have programmed death ligand-1 (PD-L1) expression on at least 50% of tumour cells (TCs) following complete resection and no progression after platinum-based adjuvant chemotherapy at the time of the planned interim analysis. It remains uncertain because the analysis was absent from the statistical hierarchy and it did not control for multiplicity. Finally, the interim nature of the analyses also increases the risk that efficacy may be overestimated, which is of concern because these data were used to extrapolate DFS over the entire lifetime time horizon in the submitted pharmacoeconomic model. No conclusions could be drawn on the effect of atezolizumab on overall survival (OS) because of data immaturity. Despite these limitations, the clinical experts consulted by CADTH noted that the findings appeared favourable and may be clinically important.
Based on the CADTH base case and the reimbursement request population deemed most reflective of the anticipated place in therapy — which included changes to DFS extrapolations, distribution of recurrence type, and time to establish cure to address identified key limitations — adjuvant treatment with atezolizumab is $76,019 more costly than active surveillance and yields 1.10 more quality-adjusted life-years (QALYs), resulting in an incremental cost-effectiveness ratio (ICER) of $68,858 per QALY. A price reduction of 24% would be necessary to achieve an ICER of $50,000 per QALY.
The results are contingent on DFS extrapolation from the observed trial data and whether that translates into OS gains. Although the sponsor’s approach to modelling the relationship between DFS and OS is evidence-based and appropriate, longer-term evidence is required to validate OS for patients receiving atezolizumab as adjuvant therapy. In light of these limitations, and in alignment with clinical expert opinion, the reanalyses conducted by CADTH assumed that atezolizumab would confer modest long-term DFS and corresponding OS benefits relative to active surveillance. The parametric extrapolations used in the CADTH base case to model transition probabilities from DFS were deemed more plausible than the sponsor’s base case, given that the vast majority (95%) of QALY gains conferred by atezolizumab in the submitted model were derived from the period beyond the median follow-up of the trial. As such, relative to the sponsor’s base case, the CADTH reanalysis resulted in a reduction in life-year gains in this patient population (from 3.2 to 1.5). The cost-effectiveness of atezolizumab varied significantly when more optimistic and pessimistic DFS extrapolations were considered.
CADTH was unable to address the following limitations: the model did not incorporate a possibility of cure for some patients with locoregional recurrence (LR) and it limited adverse events (AEs) to just the first month of treatment with atezolizumab. Addressing these limitations would likely increase the ICER (i.e., atezolizumab would be less cost-effective). Results from additional scenario analyses indicated that the cost-effectiveness of atezolizumab is also sensitive to changes in treatment duration and to the distribution of LR versus metastatic recurrence.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Two patient groups provided input: Lung Cancer Canada, a national charity and member of the Global Lung Cancer Coalition that serves as a resource for lung cancer education, patient support, research, and advocacy; and the Lung Health Foundation (LHF), a charity that offers education, programs, and services for patients and health care providers and invests in lung health research and policy advocacy. Lung Cancer Canada collected experiences from 5 patients with NSCLC, 4 patients with small cell lung cancer, and 1 caregiver (from Canada, the US, the UK, and Australia) in December 2021 via phone interviews and environmental scans. LHF conducted phone interviews with 3 patients living with lung cancer (from Ontario, Manitoba, and Quebec) in September and October 2021, and gathered input from a registered nurse and a certified respiratory educator. Overall, patients’ disease experience was influenced by the physical symptoms associated with lung cancer (e.g., fatigue, shortness of breath, cough), the psychosocial effect associated with fear of death and poor disease prognosis (e.g., anxiety, distress, depression), and the AEs related to treatment with chemotherapy and radiation (e.g., nausea, vomiting, neuropathy, lung injury). The most important outcomes for patients included delaying disease progression and achieving long-term remission, with the ultimate objectives of improving survival, minimizing side effects from treatments, preserving independence to minimizing the burden on caregivers, and maintaining an optimal quality of life. Patients emphasized the lack of adjuvant therapeutic options available to reduce the risk of recurrence after surgical resection and chemotherapy for PD-L1-positive and driver mutation-negative types of lung cancer. Patients valued having a choice of therapies with durable efficacy that target early-stage disease, with the aim of delaying recurrence and increasing the chance of cure.
Registered-clinician input was received from 2 groups: Lung Cancer Canada and the Ontario Health-Cancer Care Ontario (OH-CCO) Drug Advisory Committee. According to clinician input, patients with stage II to III (UICC, 8th edition) lung cancer have the greatest unmet need, so this review is especially relevant because it focuses on patients with resected NSCLC without EGFR mutations. Clinician input highlighted the lack of advancement in new adjuvant therapy for stage IB to III (UICC, 8th edition) resected NSCLC since the introduction of adjuvant chemotherapy 2 decades ago. This is in stark contrast to the significant progress made in metastatic disease. Clinicians noted that atezolizumab would supplement, not replace, the current management of resected NSCLC after at least 1 dose of adjuvant chemotherapy. In addition, clinicians indicated that re-treatment with atezolizumab after LR would be considered a viable therapeutic pathway in this patient population.
The input from drug programs regarding implementation issues questioned whether patients who receive atezolizumab in the adjuvant setting would be eligible for re-treatment with PD-L1 inhibitors in the locoregional and metastatic settings. Drug programs also considered whether eligibility for atezolizumab adjuvant immunotherapy would depend on the number of cycles or the type of chemotherapy (i.e., cisplatin-based doublet) received by candidate patients. Finally, drug programs noted that EGFR mutation testing would need to be expanded across jurisdictions to confirm patient eligibility for adjuvant atezolizumab in the reimbursement request population.
Several of these concerns were addressed in the sponsor’s model:
DFS and health state utilities that captured lung cancer symptoms and quality of life were included.
AEs associated with atezolizumab adjuvant therapy were included.
However, some of these concerns were not or could not be addressed by CADTH:
costs associated with expanded EGFR testing were not considered.
Economic Review
The current review is for atezolizumab (Tecentriq) for the treatment of adults with completely resected stage II to IIIA NSCLC who received platinum-based chemotherapy and whose tumours have PD-L1 expression on at least 50% of TCs, per the Health Canada indication. The sponsor also submitted a scenario analysis that assessed a requested reimbursement population that, in addition to the previously mentioned criteria, did not have epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) mutations.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of atezolizumab adjuvant immunotherapy after tumour resection and platinum-based chemotherapy in adults (≥ 18 years) with stage II to IIIA NSCLC whose tumours have PD-L1 expression on at least 50% of TCs, per the Health Canada indication. The sponsor also submitted a scenario analysis, aligned with their reimbursement request, in patients who, in addition to the above criteria, do not have an EGFR or ALK mutation. Atezolizumab was compared with active surveillance in all of the sponsor’s analyses.1 In the adjuvant setting, atezolizumab is expected to be used as monotherapy; as such, combination with other regimens need not be considered.
Atezolizumab is available as a 1,200 mg concentrate in 20 mL single-use vials (60 mg/mL) for infusion.2 The recommended dose of atezolizumab adjuvant therapy is 1,200 mg administered by IV infusion every 3 weeks.2 The initial dose should be administered over 60 minutes and, if tolerated, subsequent infusions may be administered over 30 minutes.2 Patients are expected to receive atezolizumab adjuvant therapy for up to 1 year unless there is disease recurrence or unacceptable toxicity. At the sponsor’s submitted price of $6,776.00 per 20 mL vial, the 28-cycle cost of atezolizumab adjuvant therapy would be $9,035, and the annual cost would be $98,673 (18 cycles).1 No drug-acquisition costs were modelled for active surveillance, which was assumed to consist of no active treatment.
The analysis was performed from the perspective of the Canadian publicly funded health care system. Costs and clinical outcomes (life-years and QALYs) were simulated over a lifetime time horizon of 39 years and discounted at an annual rate of 1.5% per annum.1
Model Structure
The sponsor submitted a Markov model with 9 mutually exclusive health states; transitions between states occurred on a monthly cycle length (Figure 1, Appendix 3).1 The same model structure was used for both the Health Canada–indicated population and the reimbursement request population. Patients entered the model in the disease-free health state. Patients treated with the intervention strategy received atezolizumab for 16 cycles and subsequently received follow-up care that consisted of active surveillance for a maximum of 5 years, whereas patients in the comparator arm received active surveillance alone. Patients could remain disease-free, transition to LR, or transition to first-line metastatic recurrence (1L MR). Patients with LR could be treated with curative or palliative intent or forgo treatment entirely. When treated with curative intent, patients with LR can remain in the LR health state or transition to the 1L MR state. However, patients with LR who receive palliative or no treatment can only transition to death. Once in 1L MR, patients could choose to be treated or not. Treated patients in 1L MR may remain in that health state or transition to second-line metastatic recurrence (2L MR), whereas those who forgoed treatment could only transition to death. Patients in 2L MR could also choose to either be treated or not, although they could only transition to death. Patients could transition to death from any health state at any time.
Model Inputs
Baseline patient characteristics were derived from IMpower010, a global, randomized, open-label, phase III clinical trial comparing atezolizumab with active surveillance after complete resection and adjuvant platinum-based chemotherapy in stage IB to IIIA (according to UICC and AJCC [7th edition] staging criteria) NSCLC. The average patient in the modelled cohort, which the sponsor assumed reflected the Canadian patient population, was aged 61 years, weighed 74 kg, and was more likely to be male than female (66.80%). These characteristics were used to inform the drug-dosage regimens, the age- and sex-specific distribution of the general population mortality risk, and the length of the lifetime horizon.1,3
Clinical efficacy parameters, including modelling of DFS and treatment duration, were derived from the IMpower010 clinical trial, using the January 21, 2021, data cut-off date. For the reimbursement request criteria, the sponsor used Kaplan–Meier (KM) data specific to the subgroup of patients in the IMpower010 trial without EGFR or ALK mutations to model DFS. Because the median follow-up of the trial was 32 months at the data cut-off, parametric survival modelling was used to extrapolate health state transition probabilities from DFS beyond time points available in the trial. Independent survival distributions were selected for the atezolizumab and active surveillance strategies based on clinical plausibility of long-term projections, visual inspection of fit, as well as Akaike and Bayesian information criterion.1 These were subsequently transformed into transition probabilities from the disease-free health state to the LR and 1L MR states. The model used data from the IMpower010 clinical trial to calculate the proportion of patients who had either LR or metastatic recurrence as a first DFS event across the atezolizumab and active surveillance arms.3 Citing data immaturity, the sponsor assumed that the ratio of disease-free patients who transitioned to the LR and 1L MR states across treatment arms would remain the same until the end of the model’s time horizon.
The sponsor applied cure and mortality to the extrapolated DFS curves in an attempt to realistically reflect the proportion of patients expected to be disease-free across the modelled lifetime time horizon.1 First, the model assumed that, among those receiving adjuvant atezolizumab and active surveillance, the proportion of patients not at risk of a DFS event increases linearly from the start of year 2, thereby reaching a maximum of 91.5% at year 5 based on estimates of cure rates from the literature.4 Such patients were assumed to experience the same long-term health outcomes as the general population. Second, irrespective of health state, the model shifted to the use of age-adjusted probabilities of death in the general population to calculate the proportion of patients that transition to death, although age-adjusted probabilities are greater than the probabilities estimated from literature and trial data. This mortality adjustment is meant to account for the higher probability of death that patients with lung cancer confront compared with the general population. Finally, although the model incorporated a functionality to explore treatment waning, the sponsor’s base case assumed that atezolizumab’s treatment effect is maintained over time.
Information used to inform clinical parameters in the model related to later disease stages, including LR and metastatic recurrence, was sourced from metastatic studies and from the scientific literature. Evidence from Nakamichi et al. (2017)5 was used to estimate progression-free survival in the LR health state and the probability that patients in LR who received curative treatment would transition to 1L MR and death. The study analyzed progression-free survival in 74 patients who experienced LR after surgery for stage I to III NSCLC and who were treated with chemoradiotherapy and/or radiotherapy. The model used evidence from Kruser et al. (2014)6 to calculate the probability that patients in the LR health state who received either palliative or no treatment would transition to death. The study analyzed OS in 37 patients who had LR after radiotherapy for stage I to IV NSCLC and who were re-treated with either palliative or curative radiotherapy.
Data from the IMpower150 and IMpower110 clinical trials were used to calculate the probability that patients in the 1L MR health state would transition to 2L MR and death.1 IMpower150 compared atezolizumab used in combination with carboplatin plus paclitaxel with or without bevacizumab with atezolizumab used in combination with carboplatin, paclitaxel, and bevacizumab in patients with stage IV nonsquamous NSCLC, whereas IMpower110 compared atezolizumab monotherapy with cisplatin or carboplatin plus pemetrexed or gemcitabine in patients with stage IV nonsquamous or squamous NSCLC. For patients in the 1L MR health state who choose not to receive treatment, the model used evidence from Wong et al. (2016),7 which analyzed OS in patients with metastatic recurrence after surgery for stage I to III NSCLC, to calculate the probability of transitioning to death. Although the sponsor relied on clinical expert opinion to determine the proportion of patients in the 2L MR state who underwent treatment, evidence from the OAK trial8 was used to calculate the monthly probability that patients with progression of metastatic recurrence would transition to death. The trial compared the effect of atezolizumab with docetaxel in patients with locally advanced or metastatic NSCLC who had failed platinum-containing therapy. The sponsor used the same trial data to model OS in patients in the 2L MR health state who did not undergo treatment and in patients in the 1L MR health state. The sponsor assumed these data were applicable to subsequent lines of therapy throughout the model.
Patients accrued health state-specific QALYs and treatment-related and health state-specific costs as they transitioned through disease progression. The model used utility values for the DFS health state from Jang et al. (2010),9 which derived utility scores from prospective quality-of-life data using the EQ-5D questionnaire in outpatients with stage I to IV NSCLC who attended a major Canadian cancer centre. AEs that qualified as at least grade 3 were incorporated in the sponsor’s model, as observed in the IMpower010 trial, with an associated cost and disutility.1,3 These were only applied to patients receiving atezolizumab adjuvant therapy in the disease-free state during the first month of treatment, after which no additional AE-related costs or disutilities were used. The model applied utility values from Chouiad et al. (2013),10 a prospective multi-centre study that compared patients with locally advanced and metastatic NSCLC with patients in the LR health state receiving treatment with curative intent. Moreover, utility values from van den Hout et al. (2006),11 a study that examined radiotherapy schedules in poor-prognosis patients with stage IIIA to IV NSCLC, were applied to patients receiving palliative treatment in the LR health state. For patients in the 1L MR and 2L MR states, the model applied utility values from the IMpower150 trial to patients on treatment and applied utility values from van den Hout et al. (2006)11 to patients who chose to forgo treatment.1 Because utility values are time-invariant, the model shifted to the use of age-adjusted general population utility estimates from Ara and Brazier (2011)12 when estimates were lower than values derived from the literature and trial data.
Drug-acquisition costs for atezolizumab were based on the sponsor’s submitted price.1 The model used information on treatment discontinuation from the IMpower010 trial to derive the proportion of patients who completed each cycle of atezolizumab adjuvant therapy during the 1-year duration of treatment, per the trial protocol. The proportion of patients on treatment, dose size, treatment schedule, and associated acquisition and administration costs were used to calculate the monthly and annual costs of atezolizumab for the Health Canada–indicated modelled cohort, which were $8,403.53 and $92,439, respectively.1 As observed in the IMpower010 trial, the proportion of patients on treatment by the 16th cycle of adjuvant atezolizumab (10.3 months) was 75.2% and 67.9% in the Health Canada–indication and reimbursement request populations, respectively. Costs associated with the management of treatment-emergent AEs of at least grade 3 were allocated to patients receiving atezolizumab adjuvant therapy and applied as a 1-time cost in cycle 1 of the model. These were calculated using information that pertained to their prevalence in the IMpower010 trial, and their respective cost of treatment was based on the Ontario Schedule of Benefits. Resource use related to follow-up care was allocated equally to patients receiving atezolizumab adjuvant therapy and to those receiving active surveillance alone, which consisted of biannual CT chest scans for 3 years, followed by annual CT scans until year 5. The model allows separate treatment options for the curative and palliative treatment of LR, whereas cisplatin in combination with vinorelbine is the only chemotherapy option available for both. For patients in the 1L MR health state, the likelihood of receiving a given subsequent treatment option was dependent on whether they received atezolizumab or active surveillance. First-line metastatic treatment was separated into 3 categories: pembrolizumab, pembrolizumab plus chemotherapy (pemetrexed), and chemotherapy (cisplatin plus vinorelbine) alone. Second-line metastatic treatment consisted exclusively of docetaxel. The sponsor did not incorporate costs associated with EGFR or ALK diagnostic testing in their assessment of eligibility for atezolizumab adjuvant therapy. Finally, the model considered a one-off end-of-life cost, valued at $33,205.18, per Walker et al. (2011).13
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted the reference case for the Health Canada and reimbursement request populations using a probabilistic sensitivity analysis with 1,000 simulations.1 The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently.
Base-Case Results
In the Health Canada–indicated population, atezolizumab adjuvant immunotherapy was associated with a QALY gain of 2.35 at an additional cost of $54,524, resulting in an ICER of $23,235 per QALY, compared with to active surveillance (Table 3). In the sponsor’s requested reimbursement population, atezolizumab was associated with a QALY gain of 2.42 at an additional cost of $48,844, resulting in an ICER of $20,179 per QALY, compared with active surveillance (Table 4). In both populations, the vast majority of the QALY benefit was derived in the disease-free health state, through life extension that occurred after the trial period, whereas 95% of the QALY benefit was derived from the extrapolated period in both the Health Canada–indication and the reimbursement request population. Atezolizumab was cost-effective at a willingness-to-pay threshold of $50,000 per QALY in more than 85% of the iterations.
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results — Health Canada Indication
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER vs. active surveillance ($/QALY) |
|---|---|---|---|---|---|---|---|
Active surveillance | $105,286 | Reference | 10.32 | Reference | 7.50 | Reference | Reference |
Atezolizumab | $159,809 | $54,524 | 13.52 | 3.20 | 9.84 | 2.35 | $23,235 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Table 4: Summary of the Sponsor’s Economic Evaluation Results — Reimbursement Request
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER vs. active surveillance ($/QALY) |
|---|---|---|---|---|---|---|---|
Active surveillance | $103,004 | Reference | 10.63 | Reference | 7.76 | Reference | Reference |
Atezolizumab | $151,848 | $48,844 | 13.92 | 3.29 | 10.18 | 2.42 | $20,179 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted sensitivity and scenario analyses. One-way sensitivity analyses were conducted to assess the impact of single parameters on the ICER, incremental QALYs, and incremental costs for the Health Canada–indicated and the reimbursement request populations. In general, the sponsor’s findings related to changes in single parameters were robust. The variables that had the largest impact on the ICER were the transition probabilities associated with DFS.
In addition, the sponsor assessed several model parameters in probabilistic scenario analyses. When a shorter time horizon was selected (i.e., 15 years), the ICER increased to $32,869 per QALY in the Health Canada–indicated population, and to $29,418 per QALY in the reimbursement request population. All other scenarios resulted in ICERs below $40,000 per QALY.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations in the sponsor’s analysis that have notable implications on the economic analysis:
Impact of atezolizumab on long-term DFS and OS is uncertain: The median follow-up in the IMpower010 trial was only 32 months at the most recent data cut-off (January 21, 2021). The sponsor relied on parametric survival modelling to extrapolate progression from DFS beyond the observable time points in the trial. The sponsor fitted separate log-logistic distributions to the observed KM curves, deemed best fit, to determine the DFS benefit of atezolizumab relative to active surveillance over the 39-year lifetime time horizon of the model. Along with a cure assumption, discussed in detail later in this section, the adjusted DFS extrapolations resulted in patients who received atezolizumab gaining an additional 3.63 disease-free years, compared with those who received active surveillance alone. This translated into a predicted survival benefit of 3.29 years for atezolizumab. On closer inspection, the adjusted extrapolation resulted in a persistent 20 percentage-point difference in DFS between atezolizumab and active surveillance (Figure 2), as well as prolonged survival benefits (Figure 3) for patients receiving atezolizumab. These benefits were sustained from the time of discontinuation up to 10 years after treatment initiation. Several limitations in the available evidence call into question the plausibility of the resulting DFS curves used by the sponsor.
In the absence of mature OS data, OS gains in the model were driven by differences in DFS and differences in the distribution of type of recurrence (discussed later in this section). Therefore, the sponsor’s model assumed that when patients remain disease-free, the probability of death is lower and patients live longer. Although there is some evidence to support this association, the absence of robust OS data leads to uncertainty. As per the evidence reviewed for this submission, there are no statistically significant findings that suggest that atezolizumab conferred an OS benefit relative to active surveillance alone.
Based on the IMpower010 trial, the ability of adjuvant atezolizumab to increase DFS in the indicated patient population remains uncertain. Although DFS in the subgroup of patients with PD-L1 expression on at least 50% of TCs was a pre-specified secondary end point, it was absent from the statistical testing hierarchy. As such, statistical analyses of the efficacy outcomes were conducted without controlling for multiplicity. Although several subgroup analyses were performed to examine the consistency of the treatment effect observed for the primary and secondary efficacy end points, proper interpretation of all subgroups was not be possible because of a lack of sample-size considerations and their absence from statistical testing hierarchy. Moreover, the interim nature of the analyses increases the risk that efficacy may be overestimated, which is of concern, given these data were used to extrapolate DFS for the entire lifetime time horizon in the submitted pharmacoeconomic model.
According to the clinical experts consulted by CADTH for this review, although the trial findings appeared favourable and clinically important, the impact of atezolizumab adjuvant therapy on DFS and OS is uncertain. A benefit with atezolizumab was deemed plausible, but the magnitude of such a benefit was uncertain in the absence of more robust evidence. Alternative parametric distributions for DFS, along with assumptions about treatment waning with atezolizumab, produced DFS and OS curves that were deemed more plausible.
In light of these limitations, and in line with clinical expert opinion, to address the uncertainty in long-term DFS, the reanalyses conducted by CADTH incorporated changes to derive more plausible DFS curves and resulting OS. Changes included the selection of KM trial data with exponential parametric tails to extrapolate transitions from DFS to the LR and 1L MR health states for patients receiving adjuvant atezolizumab or active surveillance. This was coupled with the assumption that the treatment effect of atezolizumab would be limited as of month 11 (i.e., the time at which patients stopped receiving treatment in the IMpower010 trial) and would gradually decrease and then disappear by month 32 (i.e., median follow-up in the IMpower010 trial). These changes achieved more plausible DFS and OS curves in the absence of long-term evidence, but still confer a benefit with atezolizumab.
CADTH conducted 2 scenario analyses to test alternative DFS assumptions on the CADTH base case: the first assumed no long-term benefit with atezolizumab, with the DFS curves merging at 5 years, and the second assumed that the treatment effect with atezolizumab would last longer, with waning occurring only after 5 years.
The distribution of patients with a disease recurrence who have LR and metastatic recurrence is uncertain: The model calculated the probability of a DFS event in each cycle by accounting for the patients who died and then assigning the remainder of the event probability as LR and 1L MR. The sponsor used data from the IMpower010 trial to calculate the proportion of patients with LR or metastatic recurrence as a first DFS event across the atezolizumab and active surveillance arms. This distribution was used for the entire lifetime time horizon. In so doing, the model assumed that the majority of patients who received atezolizumab adjuvant therapy would develop LR as the first DFS event (61.9%), whereas the majority of patients on active surveillance would develop metastatic recurrence as the first DFS event (65%) during their lives. This assumption is associated with uncertainty for 2 reasons. First, the sponsor’s analyses regarding sites of disease recurrence for patients with protocol-defined disease recurrence in both the Health Canada–indicated and reimbursement request populations had an insufficient number of events to determine whether the observed differences across the atezolizumab and active surveillance arms are statistically significant. Second, there is no evidence to inform how the proportions of recurrences evolve during patients’ lifetimes, particular beyond the median follow-up of 32 months. As a result, the potential that a greater proportion of recurrences would be locoregional with atezolizumab than with active surveillance is associated with significant uncertainty.
To address this limitation, the reanalyses conducted by CADTH pooled the proportions of first DFS event occurrence by type (i.e., LR versus 1L MR) across the atezolizumab and active surveillance arms. Pooled proportions were assumed to remain constant over the model’s lifetime time horizon.
CADTH conducted a scenario analysis that assumed that the ratio of patients who develop LR and 1L MR differs between the adjuvant atezolizumab and active surveillance groups, as per the sponsor’s base case.
Time to establish cure used is underestimated: The model assumed that, among those receiving adjuvant atezolizumab and active surveillance, the proportion of patients cured and considered not at risk of a DFS event increased linearly from year 2 onward, reaching a maximum of 91.5% of those remaining in a disease-free state at year 5. This cure adjustment resulted in the key underlying assumption that a non-negligible proportion of patients who are disease-free for more than 2 years may be considered cured (31% at year 3 and 61% at year 4), and would thus have the same long-term health outcomes as the general population. The clinical experts consulted by CADTH for this review confirmed that the assumption of cure in a proportion of disease-free patients is appropriate in the context of NSCLC, given that the therapeutic target after surgical resection is cure. However, the experts also noted that, in Canadian clinical practice, the time to establish cure typically starts 5 years after adjuvant chemotherapy. This would suggest that the time to establish cure in the sponsor’s base case, which monotonically increases after year 2, is faster than could be reasonably expected in clinical practice. Moreover, evidence points to the magnitude of late-recurrence risk in patients who remain recurrence-free 5 years after resection, which demonstrates that the recurrence-free probability 5 years after complete primary tumour resection may vary from 65% to 93%.14
In addition to a proportion of disease-free patients transitioning to cure, the clinical experts consulted by CADTH reported that some patients with LR could receive curative-intent treatment, meaning that cure may be possible for a proportion of patients in the LR state. Cure for patients in the LR state was not explicitly modelled in the sponsor’s base case, despite the sponsor stating that 80% of patients who recur locoregionally accessed subsequent treatment with curative intent. Instead, patients in the LR state remained at risk of progression to 1L MR.
Given the degree of uncertainty surrounding the risk of late recurrence that NSLSC patients may harbour beyond the 5-year landmark, CADTH conducted reanalyses that assumed that the proportion of patients not at risk of a DFS event, and who therefore could be considered cured, would linearly increase from year 5 and reach a maximum of 91.5% at year 7. This is aligned with CADTH’s recent review of osimertinib for NSCLC.15
CADTH conducted a scenario analysis that assumed that the maximum proportion of patients considered cured is reached at 120 months.
CADTH was unable to address the lack of incorporation of cure for LR patients treated with curative intent.
AEs were only assumed to occur in the first month of treatment: AEs qualified as grade 3 or higher were incorporated into the model, as they were in the IMpower010 trial, with an associated cost and disutility. AEs were only applied to patients receiving atezolizumab adjuvant therapy during the first cycle of the model. This approach would be appropriate if every treatment-emergent AE occurred in the first month of treatment with atezolizumab and if the experience of AEs caused all patients to discontinue treatment and, thus, no longer experience the AE. In the first model cycle, 4.4% of patients receiving atezolizumab discontinued treatment in the Health Canada–indicated population and 4.7% discontinued in the reimbursement request population, which is less than the overall proportion of patients who discontinued treatment due to AEs in the IMpower010 trial (18.2%). Moreover, patients in the IMpower010 trial discontinued treatment due to AEs well after the first month of therapy.
CADTH was unable to account for ongoing AEs because of difficulty determining the appropriate time frame during which AEs were experienced, as the trial is ongoing. If AEs are expected to occur after the first month of treatment, and AEs occurred with greater frequency in the atezolizumab than in the active surveillance arm, this limitation biases results favours atezolizumab.
Subsequent treatments in the LR setting were not aligned with Canadian clinical practice: The sponsor set chemoradiation therapy, consisting of cisplatin (80 mg/m2), vinorelbine (60 mg/m2), and radiotherapy, as the only possible curative treatment option available to patients who have a LR, although chemotherapy alone, consisting of cisplatin (80 mg/m2) and vinorelbine (60 mg/m2), was the only treatment option for patients with LR treated with palliative intent. The clinical experts consulted by CADTH noted that these therapeutic options were misaligned with current Canadian clinical practice. Indeed, the clinical experts indicated that patients in Canada being treated with curative or palliative intent would receive immunotherapy as the first-line therapeutic option after LR, consisting of either durvalumab or pembrolizumab. Moreover, the clinical experts specified that although chemotherapy would be the appropriate treatment course for patients who receive adjuvant atezolizumab and progress on or in the 6 months after therapy, rechallenge with durvalumab (curative intent) and pembrolizumab (palliative intent) would be the foreseeable appropriate course of treatment. The model submitted by the sponsor had several therapeutic options technically available in the locoregional setting for both curative and palliative intent, which included pembrolizumab. However, it was not possible to effectively run the model with any option other than cisplatin and vinorelbine, as other options were disabled. Moreover, although the sponsor’s model had a functionality that allowed rechallenge with immunotherapy after adjuvant atezolizumab for first-line metastatic recurrence, it did not allow rechallenge in the locoregional setting.
CADTH was unable to address this limitation because it was not possible to effectively run the model with any option other than cisplatin and vinorelbine in the locoregional setting, and the model did not allow rechallenge for patients in LR. As such, CADTH could not explore the effect that rechallenge with either durvalumab or pembrolizumab after adjuvant atezolizumab in the LR setting would have on the cost-effectiveness of atezolizumab relative to active surveillance. This limitation favoured the drug under review, considering that a greater proportion of patients who received atezolizumab would have transitioned to LR, thus incurring the costs of comparatively less-expensive subsequent therapies in the sponsor’s base case.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients with LR who are treated with palliative intent or not treated, and patients with metastatic recurrence who are not treated, can only transition to death. | Acceptable as a simplifying assumption. It is likely that the transition probabilities that the model uses, and the utility values that patients obtain in these health states, already account for the effect of disease progression. Furthermore, were the model to allow these patients to transition, it is unlikely that costs would change, as patients who choose to forgo treatment would not be treated with first-line or second-line metastatic therapies. |
Second recurrence after LR is metastatic recurrence. | Acceptable as a simplifying assumption. Although it is clinically plausible for patients to have a second LR, the clinical experts consulted by CADTH noted that the majority of second recurrences in NSCLC tend to be metastatic. |
Patients do not continue with subsequent lines of metastatic treatment after progression while on 2L MR. | Acceptable as a simplifying assumption. Although some patients may continue onto subsequent lines after 2L MR, the clinical experts consulted by CADTH indicated that this would be uncommon in clinical practice. However, this assumption may lead to a slight underestimation of the overall cost of treatment for metastatic recurrence. |
Transition probabilities are the same for patients being treated for metastatic recurrence with immunotherapy irrespective of specific immunotherapy, which also applies to chemotherapy. | Acceptable as a simplifying assumption. Although the model uses 2 separate transition probabilities for patients being treated for metastatic recurrence with immunotherapy and chemotherapy, it does not allow them to differ across types of immunotherapies and chemotherapies. With this assumption, the sponsor limits the use of digitized data from the literature to model the PFS or OS of other therapies. |
Atezolizumab was assumed to be prescribed and administered for 16 cycles (10.3 months), per the trial protocol. | It is acceptable for treatment duration to be aligned with trial protocol. However, the clinical experts consulted by CADTH noted that because the product monograph specifies the duration of treatment to be up to 1 year or until unacceptable toxicity, clinicians are likely to prescribe atezolizumab for 1 full year. As such, we have incorporated a scenario analysis that explores atezolizumab’s cost-effectiveness when duration of treatment is assumed to be 1 full year (18 cycles). |
LR = locoregional recurrence; 1L MR = first-line metastatic recurrence; 2L MR = second-line metastatic recurrence; NSCLC = non–small cell lung cancer; PFS = progression-free survival; OS = overall survival.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH’s reanalysis addressed several limitations of the economic model. The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. The following changes were applied: adjusting the parametric survival extrapolations with DFS to achieve a more plausible and stable difference in DFS beyond trial follow-up; using pooled trial data to inform the type of first-event recurrence, thereby assuming no differential proportions of LR and metastatic recurrence between patients receiving atezolizumab and those receiving active surveillance; and adjusting the time to establish cure so that the proportion of patients who may be considered cured starts to increase at month 60, attaining its maximum at month 84. Table 6 details each change made to derive the CADTH-revised base case, which was conducted with a stepwise approach to highlight the impact of each change. The summary of results from the stepped reanalysis are presented in Table 7 and Table 8.
In the Health Canada–indicated population, CADTH’s base-case reanalysis demonstrates that, compared with active surveillance, adjuvant treatment with atezolizumab is $78,826 more expensive and yields 1.14 greater QALYS, resulting in an ICER of $69,477 (Table 7). Likewise, in the reimbursement request population, CADTH’s base-case reanalysis demonstrates that, compared with active surveillance, adjuvant treatment with atezolizumab is $76,019 more expensive and yields 1.10 greater QALYS, resulting in an ICER of $68,858 (Table 8).
Assuming the treatment effect of atezolizumab is limited in time and incorporating KM trial data with exponential parametric tails to extrapolate DFS resulted in the largest change to the sponsor’s base case for both the Health Canada and the reimbursement request populations. The majority (87%) of the total costs for atezolizumab are treatment-acquisition costs. All the QALY gain with atezolizumab, compared with active surveillance, occurs in the DFS health state. In fact, 90% of the QALY benefit was derived from the extrapolated period in both the Health Canada–indication and the reimbursement request populations.
The probability that atezolizumab was cost-effective at a willingness-to-pay threshold of $50,000 per QALY for either population was 0%.
A detailed breakdown of the disaggregated results is available in Table 13 and Table 14.
Scenario Analysis Results
CADTH undertook price reduction analyses based on the CADTH base case. These analyses demonstrated that a price reduction of 21.8% would be necessary to achieve cost-effectiveness at a willingness-to-pay threshold of $50,000 per QALY in the Health Canada–indicated population (Table 9), whereas a price reduction of 24% would be required in the reimbursement request population (Table 10).
Table 6: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH’s value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Impact of atezolizumab on long-term DFS and OS is uncertain | Treatment effect
Parametric distribution of DFS
| Treatment effect
Parametric distribution of DFS
|
2. Assumption underlying the distribution of patients who have LR and metastatic recurrence is uncertain | First event occurrence split by type
| First event occurrence split by type
|
3. Time to establish cure may be underestimated |
|
|
CADTH base case | — | Reanalysis 1 + 2 + 3 |
1L MR = first-line metastatic recurrence; DFS = disease-free survival; KM = Kaplan–Meier; LR = locoregional recurrence; OS = overall survival.
Table 7: Summary of the Stepped Analysis of the CADTH Reanalysis Results — Health Canada Indication
Stepped analysis | Treatment | Total cost ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | Active surveillance | $105,286 | 7.50 | Reference |
Atezolizumab | $159,809 | 9.84 | $23,235 | |
CADTH reanalysis 1 | Active surveillance | $119,707 | 7.19 | Reference |
Atezolizumab | $183,790 | 9.07 | $34,146 | |
CADTH reanalysis 2 | Active surveillance | $105,182 | 7.63 | Reference |
Atezolizumab | $163,099 | 9.81 | $26,542 | |
CADTH reanalysis 3 | Active surveillance | $127,345 | 6.54 | Reference |
Atezolizumab | $186,154 | 8.67 | $27,592 | |
CADTH base case 1 + 2 + 3 (deterministic) | Active surveillance | $140,640 | 6.06 | Reference |
Atezolizumab | $219,241 | 7.21 | $68,340 | |
CADTH base case 1 + 2 + 3 (probabilistic) | Active surveillance | $138,491 | 6.01 | Reference |
Atezolizumab | $217,317 | 7.15 | $69,477 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 8: Summary of the Stepped Analysis of the CADTH Reanalysis Results — Reimbursement Request
Stepped analysis | Treatment | Total cost ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Active surveillance | $103,004 | 7.76 | Reference |
Atezolizumab | $151,848 | 10.18 | $20,179 | |
CADTH reanalysis 1 | Active surveillance | $115,092 | 7.45 | Reference |
Atezolizumab | $176,423 | 9.27 | $33,690 | |
CADTH reanalysis 2 | Active surveillance | $100,573 | 7.88 | Reference |
Atezolizumab | $154,969 | 10.05 | $25,138 | |
CADTH reanalysis 3 | Active surveillance | $122,623 | 6.80 | Reference |
Atezolizumab | $174,991 | 9.05 | $23,265 | |
CADTH base case 1 + 2 + 3 (deterministic) | Active surveillance | $136,324 | 6.31 | Reference |
Atezolizumab | $212,142 | 7.43 | $68,007 | |
CADTH base case 1 + 2 + 3 (probabilistic) | Active surveillance | $134,041 | 6.26 | Reference |
Atezolizumab | $210,060 | 7.36 | $68,858 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 9: CADTH Price Reduction Analyses — Health Canada Indication
Analysis | ICERs for atezolizumab vs. active surveillance | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $23,235 | $69,477 |
10% | $19,419 | $60,360 |
20% | $15,596 | $51,574 |
30% | $11,774 | $42,788 |
40% | $7,952 | $34,002 |
50% | $4,130 | $25,216 |
60% | $307 | $16,430 |
70% | Dominant | $7,644 |
80% | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; vs. = versus.
Table 10: CADTH Price Reduction Analyses — Reimbursement Request
Analysis | ICERs for atezolizumab vs. active surveillance | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $20,179 | $68,858 |
10% | $16,549 | $61,147 |
20% | $12,914 | $53,186 |
30% | $9,279 | $45,225 |
40% | $5,645 | $37,265 |
50% | $2,010 | $29,304 |
60% | Dominant | $21,343 |
70% | Dominant | $13,382 |
80% | Dominant | $5,421 |
90% | Dominant | Dominant |
ICER = incremental cost-effectiveness ratio; vs. = versus.
In addition, CADTH conducted a series of exploratory analyses to determine the impact of alternative assumptions on the cost-effectiveness of adjuvant atezolizumab, which are outlined as follows:
treatment duration assumed to be 1 full year (18 cycles rather than 16 cycles)
cure proportion assumed to reach maximum at 120 months
ratio of patients who develop LR and 1L MR differs between the adjuvant atezolizumab and active surveillance arms
DFS curves of atezolizumab and active surveillance merge at 60 months
treatment effect of atezolizumab starts to decrease at 60 months.
First, the sponsor’s base case considered that patients in the intervention arm would receive adjuvant atezolizumab for 16 cycles, which effectively equates to a 10.3-month treatment duration, per the IMpower010 trial protocol. However, the expected treatment duration, as stated in the product monograph, is up to 1 year unless there is disease recurrence or unacceptable toxicity. Moreover, the clinical experts consulted by CADTH concurred that clinicians would potentially prescribe up to a full year of adjuvant atezolizumab to eligible patients, per the product monograph. As such, CADTH considered it appropriate to explore a scenario in which treatment duration is aligned with foreseeable clinical practice. In this scenario, the ICER increased to $78,431 and $77,282 in the Health Canada–indication and reimbursement request populations, respectively. Second, CADTH conducted a scenario analysis assuming that the maximum proportion of patients that may be considered cured is reached at 120 months. This is a conservative assumption aligned with evidence pointing to the magnitude of late-recurrence risk in patients who remain recurrence-free 5 years after complete resection, which demonstrates that patients with NSCLC harbour a significant risk of late recurrence beyond the 5-year mark.14 In this scenario, the ICER increased to $80,743 and $80,052 in the Health Canada–indication and reimbursement request populations, respectively.
Third, CADTH conducted a scenario analysis assuming that the ratio of patients who develop LR and 1L MR differs between those who receive adjuvant atezolizumab and those who receive active surveillance. In this scenario, the ICER decreased to $46,946 and $44,366 in the Health Canada–indication and reimbursement request populations, respectively. Fourth, CADTH considered a scenario that assumed that the DFS curves of atezolizumab and active surveillance would merge at year 5 to address uncertainty regarding duration of the marginal treatment effect beyond the time points available in the trial. In this scenario, the ICER increased to $239,273 and $249,822 in the Health Canada–indication and reimbursement request populations, respectively. Finally, CADTH considered a scenario assuming that the treatment effect of atezolizumab would start to wane at year 5. In this scenario, the ICER decreased to $24,846 and $23,379 in the Health Canada–indication and the reimbursement request populations, respectively.
The results of these analyses are presented in Table 15 and Table 16 in Appendix 4.
Issues for Consideration
In compliance with CADTH submission requirements, the sponsor-submitted base case pertains to the population of adults with completely resected stage II to IIIA NSCLC who received platinum-based chemotherapy and whose tumours have PD-L1 expression on at least 50% of TCs, per the Health Canada indication. The sponsor also submitted a scenario analysis assessing a requested reimbursement population, which, in addition to the previous criteria, did not have EGFR or ALK mutations. The reimbursement request population is most reflective of adjuvant atezolizumab’s anticipated place in therapy and is aligned with guidance received from the clinical experts consulted by CADTH on the patient population most likely to benefit from treatment with atezolizumab. Moreover, clinical experts emphasized that the expectation in clinical practice is that osimertinib will become the standard of care among stage II to IIIA NSLSC patients with EGFR mutations in the adjuvant setting. Thus, although the population that meets the full indication criteria and the reimbursement request population are included in the CADTH reanalyses, CADTH advises that conclusions regarding the cost-effectiveness of adjuvant atezolizumab relative to active surveillance should be made on the basis of the analyses that concern the reimbursement request population.
Overall Conclusions
Based on the IMpower010 trial, uncertainty remains about the efficacy of adjuvant atezolizumab in increasing DFS in adults with stage II to IIIA (according to the UICC and AJCC [7th edition] staging criteria) NSCLC, whose tumours have PD-L1 expression on at least 50% of TCs following complete resection and no progression after platinum-based adjuvant chemotherapy at the time of the planned interim analysis because the analysis was absent from the statistical hierarchy and did not control for multiplicity. Finally, the interim nature of the analyses increases the risk that efficacy may be overestimated, which is of concern, given that these data were used to extrapolate DFS over the entire lifetime time horizon in the submitted pharmacoeconomic model. No conclusions could be drawn about the effect of atezolizumab on OS because of data immaturity. Despite these limitations, the clinical experts consulted by CADTH noted that the findings appear favourable and may be clinically important.
CADTH identified several limitations in the economic analyses submitted by the sponsor, beyond the uncertainty regarding the impact of atezolizumab on DFS and OS. These key limitations included uncertainty about the distribution of patients who have LR and metastatic recurrence when a recurrence occurs, underestimation of the time to establish cure, oversimplification of the assumption that AEs occur only in the first month of treatment with atezolizumab, and misalignment between the modelled subsequent treatments for LR and Canadian clinical practice. Based on the CADTH base case and considering the reimbursement request population is deemed most reflective of the anticipated place in therapy — which included changes to DFS extrapolations, distribution of recurrence type, and time to establish cure —adjuvant treatment with atezolizumab, compared with active surveillance, is $76,019 more costly and yields 1.10 more QALYS, resulting in an ICER of $68,858 per QALY. A price reduction of 24% would be necessary to achieve an ICER of $50,000 per QALY.
The results are contingent on DFS extrapolation from the observed trial data and whether this translates into OS gains. Although the sponsor’s approach of modelling the relationship between DFS and OS is evidence-based and appropriately modelled, longer-term evidence is required to validate OS for patients receiving atezolizumab as adjuvant therapy. In light of these limitations, and in alignment with clinical expert opinion, the reanalyses conducted by CADTH assumed that atezolizumab would confer modest long-term DFS and corresponding OS benefits relative to active surveillance. The parametric extrapolations used in the CADTH base case to model transition probabilities from DFS were deemed to be more plausible than the sponsor’s base case, given that the vast majority of the QALY gains (95%) conferred by atezolizumab in the submitted model were derived from the period beyond the median follow-up of the trial. As such, relative to the sponsor’s base case, the CADTH reanalysis resulted in a reduction of life-year gains in this patient population (from 3.2 to 1.5). The cost-effectiveness of atezolizumab varied significantly when more optimistic and pessimistic DFS extrapolations were considered.
CADTH was unable to address limitations related to the model not incorporating a possibility of cure for some patients with LR and limiting AEs only to the first month of treatment with atezolizumab. Addressing these limitations would likely increase the ICER (i.e., atezolizumab would be less cost-effective). Results from additional scenario analyses indicated that the cost-effectiveness of atezolizumab is sensitive to changes in treatment duration and to changes in the distribution of LR and metastatic recurrence.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tecentriq (atezolizumab), concentrate for solution for infusion, 60mg/mL; 1200 mg/20mL and 840 mg/14mL single use vials. Mississauga (ON): Hoffmann-La Roche Limited; 2022 Feb 24.
2.Tecentriq (atezolizumab): concentrate for solution for infusion, 60mg/mL; 1200 mg/20mL and 840 mg/14mL single use vials [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; 2022 Jan 14.
3.Felip E, Altorki N, Zhou C, et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet. 2021;398(10308):1344-1357. PubMed
4.Sonoda D, Matsuura Y, Ichinose J, et al. Ultra-late recurrence of non-small cell lung cancer over 10 years after curative resection. Cancer Manag Res. 2019;11:6765-6774. PubMed
5.Nakamichi S, Horinouchi H, Asao T, et al. Comparison of radiotherapy and chemoradiotherapy for locoregional recurrence of non-small-cell lung cancer developing after surgery. Clin Lung Cancer. 2017;18(6):e441-e448. PubMed
6.Kruser TJ, McCabe BP, Mehta MP, et al. Reirradiation for locoregionally recurrent lung cancer: outcomes in small cell and non-small cell lung carcinoma. Am J Clin Oncol. 2014;37(1):70-76. PubMed
7.Wong mL, McMurry TL, Stukenborg GJ, et al. Impact of age and comorbidity on treatment of non-small cell lung cancer recurrence following complete resection: A nationally representative cohort study. Lung Cancer. 2016;102:108-117.
8.Simeone JC, Nordstrom BL, Patel K, Klein AB. Treatment patterns and overall survival in metastatic non-small-cell lung cancer in a real-world, US setting. Future Oncol. 2019;15(30):3491-3502. PubMed
9.Jang RW, Isogai PK, Mittmann N, et al. Derivation of utility values from European Organization for Research and Treatment of Cancer Quality of Life-Core 30 questionnaire values in lung cancer. J Thorac Oncol. 2010;5(12):1953-1957. PubMed
10.Chouaid C, Danson S, Andreas S, et al. Adjuvant treatment patterns and outcomes in patients with stage IB-IIIA non-small cell lung cancer in France, Germany, and the United Kingdom based on the LuCaBIS burden of illness study. Lung Cancer. 2018;124:310-316. PubMed
11.van den Hout WB, Kramer GW, Noordijk EM, Leer JW. Cost-utility analysis of short- versus long-course palliative radiotherapy in patients with non-small-cell lung cancer. J Natl Cancer Inst. 2006;98(24):1786-1794. PubMed
12.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
13.Walker H, Anderson M, Farahati F, et al. Resource use and costs of end-of-Life/palliative care: Ontario adult cancer patients dying during 2002 and 2003. J Palliat Care. 2011;27(2):79-88. PubMed
14.Maeda R, Yoshida J, Hishida T, et al. Late recurrence of non-small cell lung cancer more than 5 years after complete resection: incidence and clinical implications in patient follow-up. Chest. 2010;138(1):145-150. PubMed
15.CADTH Reimbursement Review: osimertinib (Tagrisso). Can J Health Technol. 2022 Mar;2(3). https://www.cadth.ca/sites/default/files/DRR/2022/PC0246-Tagrisso.pdf. Accessed 2022 Jun 1.
16.Budget impact analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tecentriq (atezolizumab), concentrate for solution for infusion, 60mg/mL; 1200 mg/20mL and 840 mg/14mL single use vials. Mississauga (ON): Hoffmann-La Roche Limited; 2022 Feb 24.
Appendix 1: Cost Comparison Table
Note that this appendix is not copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 11: CADTH Cost Comparison Table for Adjuvant Therapies After Tumour Resection in Patients With Stage II to IIIA Non–Small Cell Lung Cancer Whose Tumours Have PD-L1 Expression on at Least 50% of Tumour Cells
Treatment | Strength or concentration | Form | Price ($) | Recommended dosage | Daily cost | 28-day cycle cost ($) |
|---|---|---|---|---|---|---|
Atezolizumab (Tecentriq) | 60 mg/mL | 14 mL 20 mL Single-use vial for IV infusion | 4,743.2000a 6,776.0000a | 1,200 mg every 3 weeks | 322.67 | 9,035 |
aSponsor’s submitted price. Assumes a 70 kg patient with a body surface area of 1.8 m2.
Appendix 2: Submission Quality
Note that this appendix is not copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | Yes | CADTH agrees with the appropriateness of choosing a Markov model structure rather than a partition survival model. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The reporting in the pharmacoeconomic and budget impact submissions is consistent with the respective Excel models. However, reporting of the pharmacoeconomic model relied heavily on the use of footnotes that offer sparse, partial, and at times insufficient, justification for substantial choices made throughout the model. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix is not copy-edited.
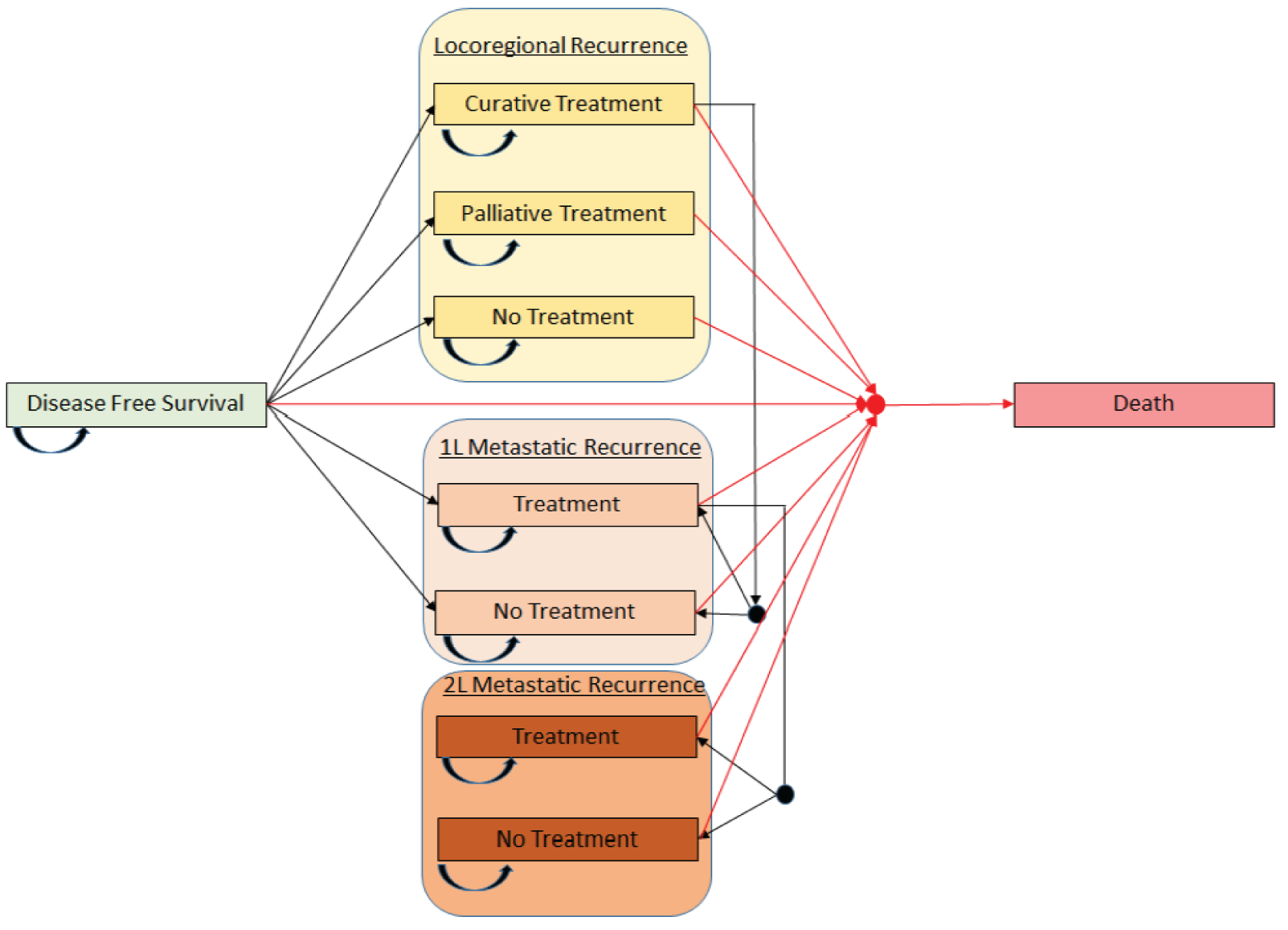
Detailed Results of the Sponsor’s Base Case
Figure 2: Predicted Disease-Free Survival Outcomes Based on Sponsor’s Parametric Survival Extrapolation Choices (Log-Logistic)
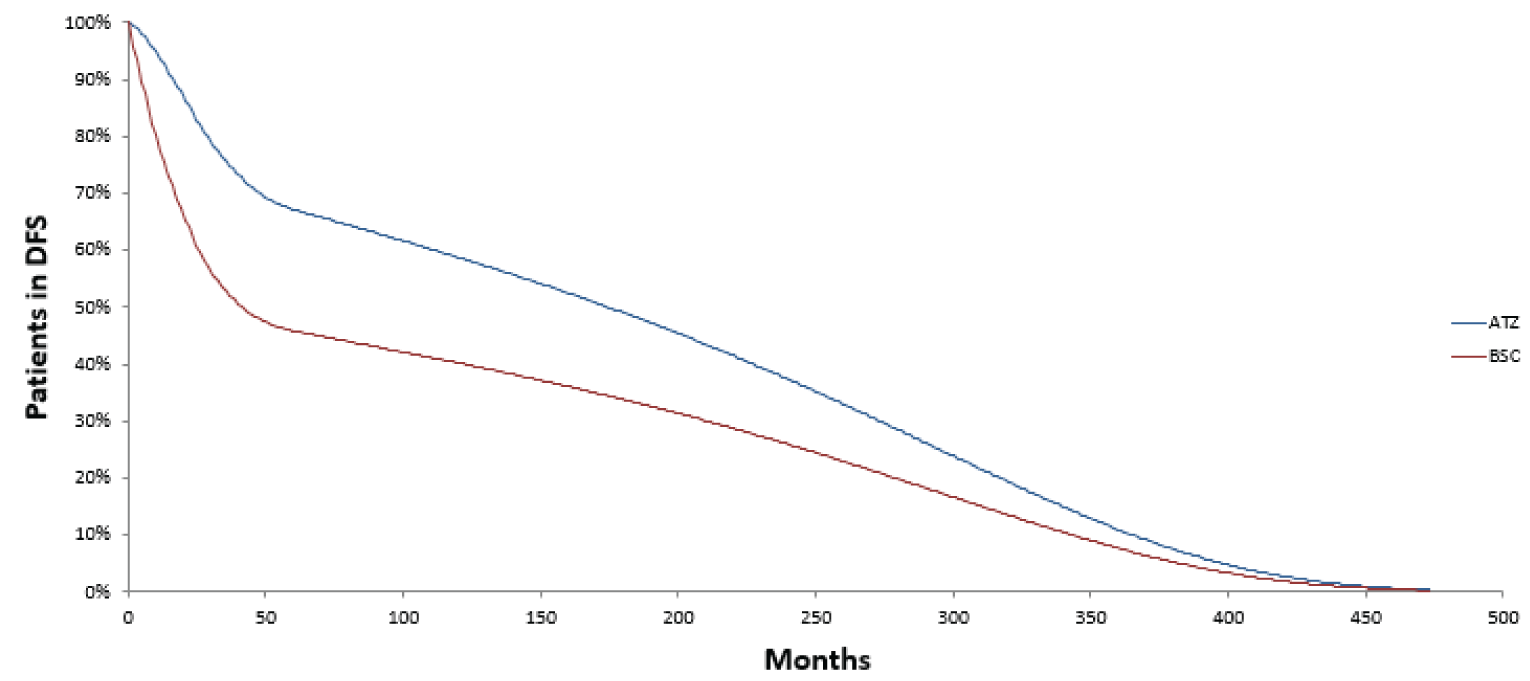
DFS = disease-free survival; ATZ = atezolizumab; BSC = best supportive care (i.e., active surveillance).
Source: Sponsor’s pharmacoeconomic submission.1
Figure 3: Predicted Overall Survival Outcomes Based on Sponsor’s Parametric Survival Extrapolation Choices
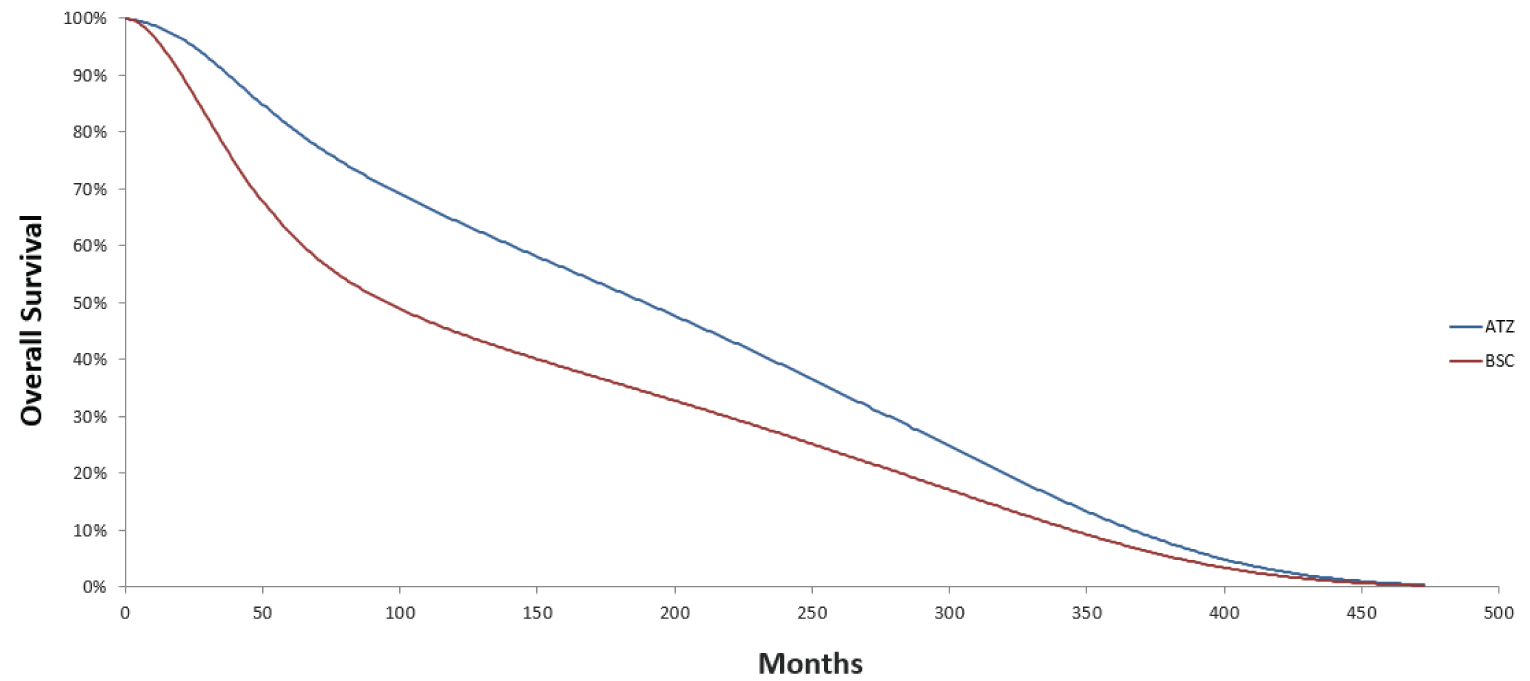
ATZ = atezolizumab; BSC = best supportive care (i.e., active surveillance).
Source: Sponsor’s pharmacoeconomic submission1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix is not copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results — Health Canada Indication
Parameter | Atezolizumab | Active surveillance | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 9.82 | 8.28 | 1.54 |
DFS | 7.65 | 5.84 | 1.81 |
LR - Curative treatment | 1.03 | 1.16 | –0.13 |
LR - Palliative treatment | 0.07 | 0.08 | –0.01 |
1L MR - On treatment | 0.63 | 0.73 | –0.10 |
1L MR - No treatment | 0.10 | 0.11 | –0.01 |
2L MR - On treatment | 0.19 | 0.22 | –0.03 |
2L MR - No treatment | 0.13 | 0.14 | –0.02 |
Discounted QALYs | |||
Total | 7.14 | 6.01 | 1.13 |
DFS | 5.63 | 4.31 | 1.33 |
LR - Curative treatment | 0.74 | 0.84 | –0.10 |
LR - Palliative treatment | 0.04 | 0.05 | –0.01 |
1L MR - On treatment | 0.46 | 0.51 | –0.06 |
1L MR - No treatment | 0.06 | 0.07 | –0.01 |
2L MR - On treatment | 0.13 | 0.15 | –0.02 |
2L MR - No treatment | 0.08 | 0.09 | –0.01 |
Discounted costs ($) | |||
Total | $217,317 | $138,491 | $78,826 |
DFS | $94,542 | $1,363 | $93,180 |
LR - Curative treatment | $8,582 | $9,648 | –$1,065 |
LR - Palliative treatment | $1,232 | $1,382 | –$151 |
1L MR - On treatment | $80,625 | $89,756 | –$9,131 |
1L MR - No treatment | $94 | $104 | –$10 |
2L MR - On treatment | $10,948 | $12,333 | –$1,385 |
2L MR - No treatment | $124 | $137 | –$13 |
End of life | $21,170 | $23,768 | –$2,598 |
ICER ($/QALY) | $69,477 | ||
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results — Reimbursement Request
Parameter | Atezolizumab | Active surveillance | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 10.12 | 8.62 | 1.50 |
DFS | 8.04 | 6.28 | 1.76 |
LR - Curative treatment | 0.98 | 1.11 | –0.13 |
LR - Palliative treatment | 0.07 | 0.08 | –0.01 |
1L MR - On treatment | 0.60 | 0.70 | –0.10 |
1L MR - No treatment | 0.09 | 0.11 | –0.01 |
2L MR - On treatment | 0.18 | 0.21 | –0.03 |
2L MR - No treatment | 0.12 | 0.14 | –0.02 |
Discounted QALYs | |||
Total | 7.36 | 6.26 | 1.10 |
DFS | 5.92 | 4.62 | 1.29 |
LR - Curative treatment | 0.70 | 0.80 | –0.09 |
LR - Palliative treatment | 0.04 | 0.05 | –0.01 |
1L MR - On treatment | 0.44 | 0.50 | –0.06 |
1L MR - No treatment | 0.06 | 0.07 | –0.01 |
2L MR - On treatment | 0.13 | 0.14 | –0.02 |
2L MR - No treatment | 0.08 | 0.09 | –0.01 |
Discounted costs ($) | |||
Total | $210,060 | $134,041 | $76,018 |
DFS | $91,485 | $1,400 | $90,084 |
LR - Curative treatment | $8,210 | $9,253 | –$1,043 |
LR - Palliative treatment | $1,201 | $1,352 | –$151 |
1L MR - On treatment | $77,902 | $86,816 | –$8,914 |
1L MR - No treatment | $89 | $99 | –$10 |
2L MR - On treatment | $10,506 | $11,863 | –$1,357 |
2L MR - No treatment | $120 | $133 | –$13 |
End of life | $20,547 | $23,126 | –$2,579 |
ICER ($/QALY) | $68,858 | ||
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analyses
Table 15: Summary of Scenario Analyses Conducted on CADTH Base Case — Health Canada Indication
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | Active surveillance | $138,491 | 6.01 | Ref. |
Atezolizumab | $217,317 | 7.15 | $69,477 | |
Scenario 1: Treatment duration assumed to be 1 full year | Active surveillance | $138,199 | 6.01 | Ref. |
Atezolizumab | $227,357 | 7.15 | $78,431 | |
Scenario 2: Cure proportion assumed to reach maximum at 120 months | Active surveillance | $146,354 | 5.64 | Ref. |
Atezolizumab | $227,915 | 6.65 | $80,743 | |
Scenario 3: Ratio of patients who have LR and 1L MR differs across arms | Active surveillance | $141,248 | 5.85 | Ref. |
Atezolizumab | $211,976 | 7.36 | $46,946 | |
Scenario 4: DFS curves of atezolizumab and active surveillance merge at 60 months | Active surveillance | $138,120 | 6.02 | Ref. |
Atezolizumab | $210,266 | 6.32 | $239,273 | |
Scenario 5: Treatment effect of atezolizumab starts to decrease at 60 months | Active surveillance | $137,833 | 6.00 | Ref. |
Atezolizumab | $196,378 | 8.36 | $24,846 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; LR = locoregional recurrence; 1L MR = first-line metastatic recurrence; Ref. = reference.
Table 16: Summary of Scenario Analyses Conducted on CADTH Base Case — Reimbursement Request
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | Active surveillance | $134,041 | 6.26 | Ref. |
Atezolizumab | $210,060 | 7.36 | $68,858 | |
Scenario 1: Treatment duration assumed to be 1 full year | Active surveillance | $133,651 | 6.26 | Ref. |
Atezolizumab | $219,038 | 7.36 | $77,282 | |
Scenario 2: Cure proportion assumed to reach maximum at 120 months | Active surveillance | $142,007 | 5.86 | Ref. |
Atezolizumab | $220,679 | 6.85 | $80,052 | |
Scenario 3: Ratio of patients who have LR and 1L MR differs across arms | Active surveillance | $136,455 | 6.10 | Ref. |
Atezolizumab | $203,470 | 7.61 | $44,366 | |
Scenario 4: DFS curves of atezolizumab and active surveillance merge at 60 months | Active surveillance | $133,300 | 6.27 | Ref. |
Atezolizumab | $203,344 | 6.55 | $249,822 | |
Scenario 5: Treatment effect of atezolizumab starts to decrease at 60 months | Active surveillance | $134,185 | 6.28 | Ref. |
Atezolizumab | $189,060 | 8.62 | $23,379 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; LR = locoregional recurrence; 1L MR = first-line metastatic recurrence; Ref. = reference.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix is not copy-edited.
Table 17: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor sought to determine the incremental budget impact of reimbursing atezolizumab adjuvant immunotherapy following tumour resection and platinum-based chemotherapy in patients with stage II to IIIA NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs, as well as in patients who, in addition to that, do not have EGFR/ALK mutations. The former eligible population is aligned with the Health Canada–indicated population (i.e., base case 1), while the latter with the sponsor’s requested reimbursement criteria (i.e., base case 2). Both base cases were undertaken from the perspective of the pan-Canadian cancer drug budget. The sponsor estimated the budget impact via an incremental comparison of 2 scenarios: a reference scenario where atezolizumab is not reimbursed as adjuvant therapy, with a new drug scenario, where atezolizumab is funded as adjuvant therapy as per the Health Canada indication, as well as per the reimbursement request. Since the current standard of care for patients after complete surgical resection and platinum-based chemotherapy is active surveillance, market share capture for atezolizumab in the new drug scenario was derived from patients who would have otherwise received active surveillance.
The analytic framework, which used an epidemiology-based approach, leveraged data from multiple sources in the scientific literature and assumptions based on clinical expert input to determine the eligible population size aligned with the Health Canada indication (Figure 4) and the reimbursement request (Figure 5). Given that the treatment duration of atezolizumab is up to 1 year (i.e., 16 cycles every 3 weeks), the model considers only incident cases of NSCLC in a given calendar year to determine patient eligibility. Drug and testing costs (i.e., SP263 PD-L1 test) were included in the analysis, costs associated with subsequent therapies were not. Atezolizumab costs were compared to active surveillance costs, which were assumed to be zero. The dosing regimen modelled for atezolizumab was 1,200 mg every 3 weeks for 16 cycles or 1 year, as per the IMpower010 trial. The total costs in the reference and new drug scenarios were estimated by multiplying the total number of patients by the cost of their respective treatment regimens according to the anticipated market distribution, as well as including testing costs. Costs associated with the cohort of eligible patients were forecasted over a 3-year time horizon, with an additional base year. Key inputs are documented in Table 19.
Figure 4: Sponsor’s Estimation of the Eligible Population Size — Health Canada Indication
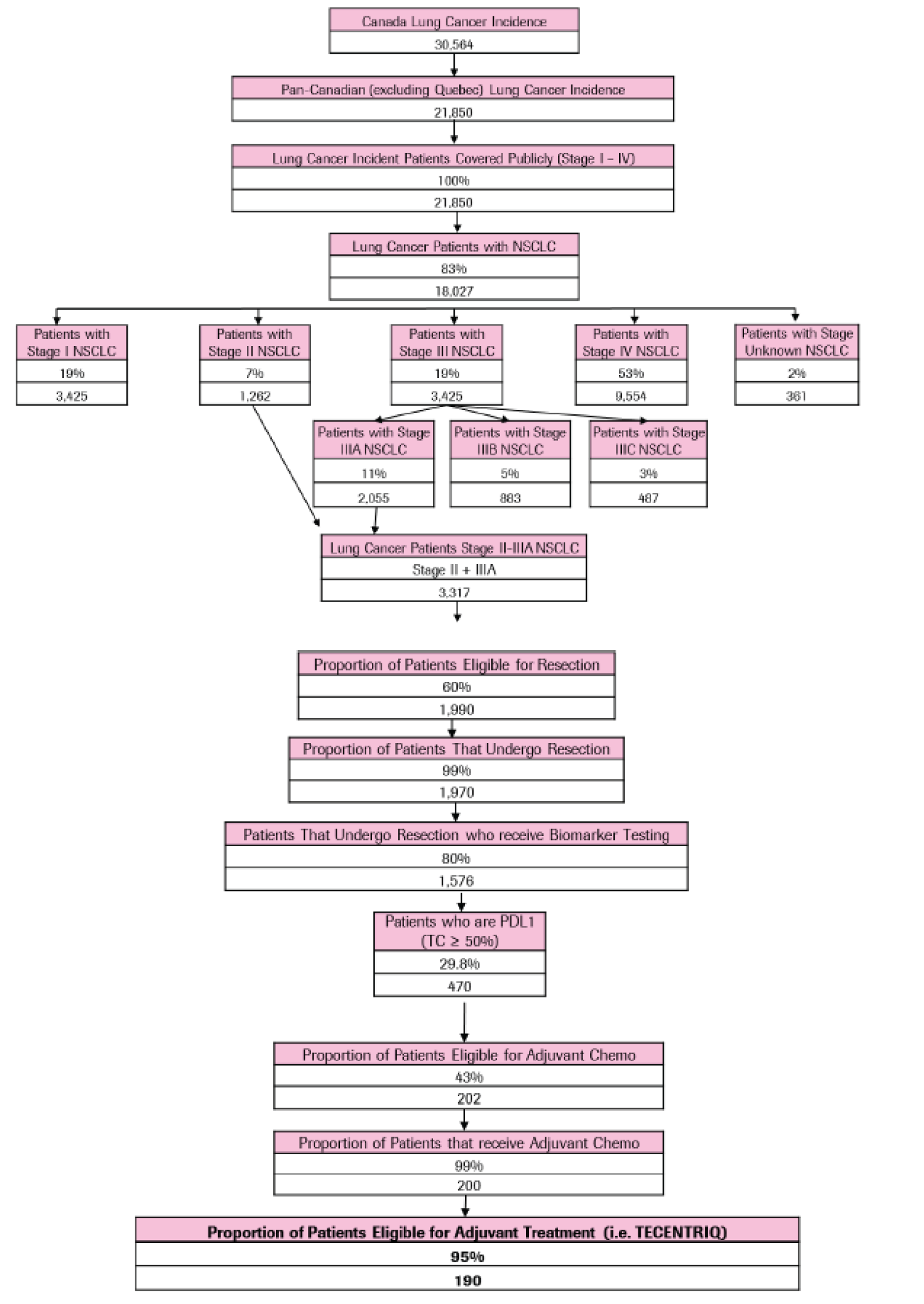
Source: Sponsor’s budget impact analysis submission.16
Figure 5: Sponsor’s Estimation of the Eligible Population Size — Reimbursement Request
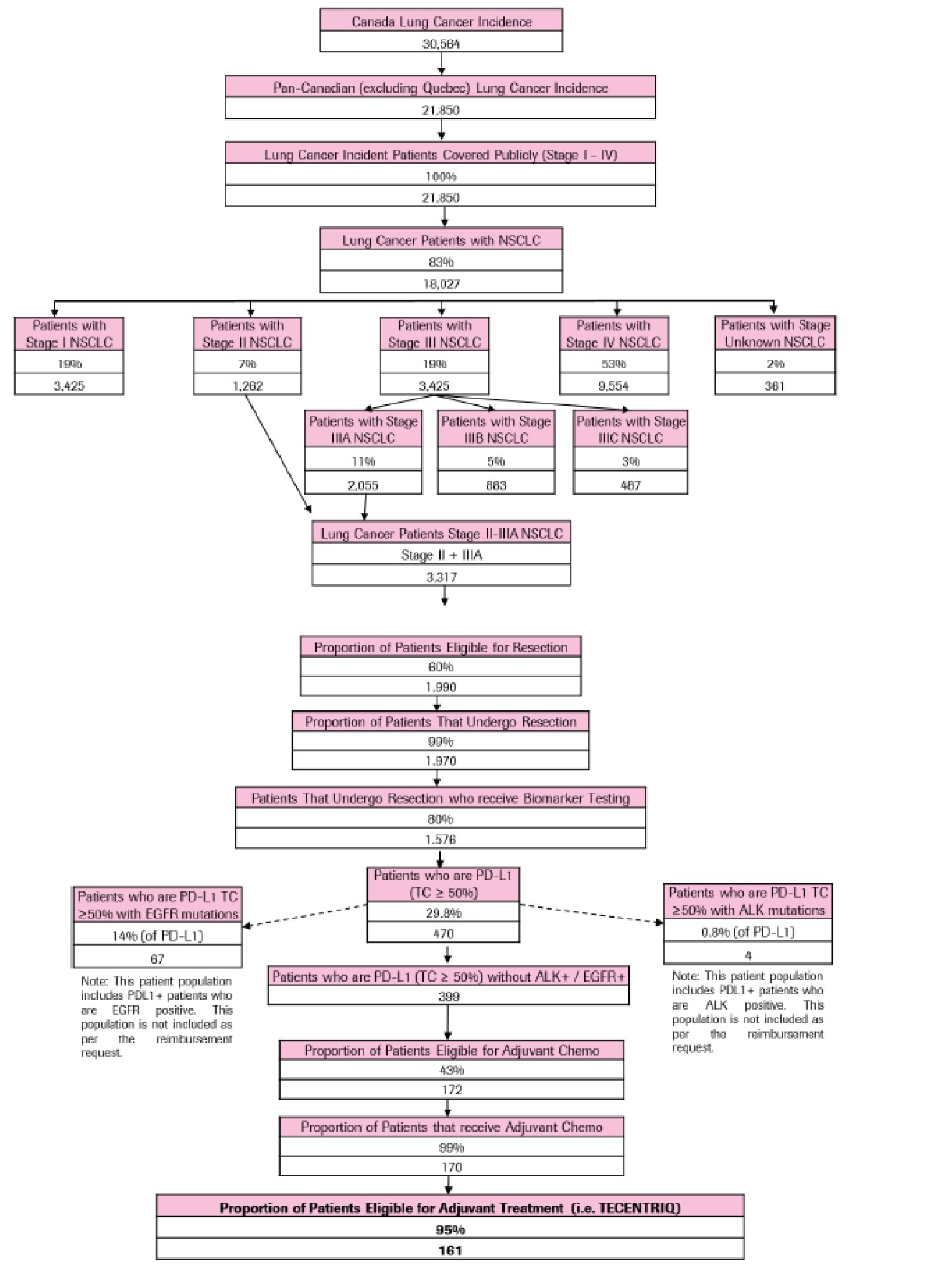
Source: Sponsor’s budget impact analysis submission.16
Key model assumptions included:
The model assumed that 60% of patients with stage II to IIIA NSCLC are eligible for tumour resection.
The model assumed a PD-L1 biomarker testing rate of 80% in the NSCLC adjuvant setting.
The model assumed that 99% of stage II to IIIA NSCLC patients who are eligible for adjuvant chemotherapy following surgical resection undergo adjuvant treatment.
The model assumed 95% eligibility for adjuvant immunotherapy.
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | |
Health Canada indication | 190 / 192 / 194 |
Reimbursement request | 161 / 163 / 165 |
Market uptake (3 years) | |
Uptake (reference scenario) | |
Atezolizumab | 0% / 0% / 0% |
Active surveillance | 100% / 100% / 100% |
Uptake (new drug scenario) | |
Atezolizumab | |||||||||||||||||||||||||||||| |
Active surveillance | |||||||||||||||||||||||||||||| |
Cost of treatment (per patient) | |
Cost of treatment per 21-day cycle | |
Atezolizumab | $6,776.00 |
Active surveillance | $0.00 |
Cost of treatment per regimen (1 year) | |
Atezolizumab | $108,416.00 |
Active surveillance | $0.00 |
Summary of the Sponsor’s BIA Results
Aligned with the Health Canada indication, the sponsor’ base case 1 estimated the net budget impact of introducing atezolizumab adjuvant immunotherapy following tumour resection and platinum-based chemotherapy in patients with stage II to IIIA NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs to be $10,454,733 in year 1, $12,655,910 in year 2, and $14,903,097 in year 3, for a total budget impact over 3 years of $38,013,740.
Aligned with the reimbursement request, the sponsor’ base case 2 estimated the net budget impact of introducing atezolizumab adjuvant immunotherapy following tumour resection and platinum-based chemotherapy in patients with stage II to IIIA NSCLC whose tumours have PD-L1 expression on ≥ 50% of TCs and do not have EGFR/ALK mutations to be $8,910,166 in year 1, $10,781,434 in year 2, and $12,691,810 in year 3 for a total budget impact over 3 years of $32,383,410.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Proportion of patients that would undergo PD-L1 biomarker testing is underestimated. The sponsor assumed that, once a therapy such as adjuvant atezolizumab is funded, a PD-L1 biomarker testing rate of 80% could be expected in the NSCLC adjuvant setting. While there is substantial variability as to whether PD-L1 assessment is currently available for all patients with early-stage disease, the clinical experts consulted by CADTH agreed that clinical practice in adjuvant NSLSC has rapidly adapted to provide the diagnostic assessment required to access new and evolving therapies. As such, there is high expectation among clinicians that once a therapy like adjuvant atezolizumab is funded in Canada, the vast majority of patients who undergo surgical resection would receive PD-L1 biomarker testing. Moreover, the clinical experts consulted by CADTH noted that since atezolizumab’s Health Canada indication includes the surgical resection criterion, there would be ample tissue available to ensure that biomarker testing is performed.
CADTH performed reanalyses, in line with clinician expert opinion, by assuming that 99% of patients who undergo surgical resection receive PD-L1 biomarker testing.
Projected market share of adjuvant atezolizumab is underestimated. The sponsor assumed that adjuvant atezolizumab would have a market share of |||||||||||||||| in years 1, 2, and 3, respectively. Market shares were applied to incident patients each year and were taken directly from active surveillance. The clinical experts consulted by CADTH emphasized that the sponsor’s market share projections were substantially lower than they would anticipate observing in practice once a therapy like adjuvant atezolizumab is funded. Indeed, adjuvant atezolizumab’s expected place in therapy would allow it to potentially capture the totality of the market in a space that currently has no other active treatments available for eligible patients.
CADTH performed reanalyses by adjusting the projected market share of atezolizumab to 80%, 90% and 100% in years 1, 2, and 3, respectively.
CADTH performed a scenario analysis assuming atezolizumab’s market shares to be 75%, 80% and 85% in years 1, 2, and 3, respectively in order to show how a more conservative projection may impact the budget.
Estimation of atezolizumab’s treatment duration may not be reflective of product monograph. The sponsor considered that patients in the new drug scenario would receive adjuvant atezolizumab for 16 cycles, which effectively equates to a 10.3-month treatment duration, as per the IMpower010 trial protocol. However, the expectation of treatment duration as stated in the product monograph is “up to 1 year unless there is disease recurrence or unacceptable toxicity” (i.e., 18 cycles).2 Moreover, the clinical experts consulted by CADTH noted it was possible clinicians might prescribe a full year of adjuvant atezolizumab to eligible patients. Thus, the number of cycles in the sponsor’s BIA is potentially underestimated.
CADTH performed a scenario analysis whereby patients in the new drug scenario received 18 cycles of adjuvant atezolizumab to reflect the anticipated full year treatment duration, as per atezolizumab’s product monograph and clinical expert opinion regarding foreseeable clinical practice in Canada.
CADTH Reanalyses of the BIA
CADTH conducted reanalyses of the BIA, for the Health Canada indication and the reimbursement request population, by revising the proportion of patients that would undergo PD-L1 biomarker testing, and adjusting the projected market share of atezolizumab.
The results of the CADTH stepwise reanalyses are presented in summary format in Table 20 and Table 21. Based on the CADTH base case, the budget impact associated with atezolizumab’s reimbursement in the Health Canada–indicated population is expected to be $20,583,339 in year 1, $23,393,902 in year 2, and $26,261,061 in year 3, with a 3-year total of $70,238,302. Moreover, the budget impact in the reimbursement request population is expected to be $17,525,096 in year 1, $19,914,406 in year 2, and $22,351,822 in year 3, with a 3-year total of $59,791,324.
CADTH conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results for the Health Canada indication and the reimbursement request population are provided in Table 22 and Table 23, respectively. Assuming treatment duration of atezolizumab is 1 full year (18 cycles).
Assuming a 21.8% price reduction in the Health Canada–indicated population and a 24% price reduction in the reimbursement request population.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Proportion of patients that would undergo PD-L1 biomarker testing is underestimated | 80% | 99% |
2. Projected market share of adjuvant atezolizumab is underestimated | Year 1: |||| Year 2: |||| Year 3: |||| | Year 1: 80% Year 2: 90% Year 3: 100% |
CADTH base case | Combined revisions 1 + 2 | |
Table 20: Summary of the CADTH Reanalyses of the BIA — Health Canada Indication
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $38,013,740 |
CADTH reanalysis 1 | $47,042,003 |
CADTH reanalysis 2 | $56,758,224 |
Submitted base case | $70,238,302 |
BIA = budget impact analysis.
Table 21: Summary of the CADTH Reanalyses of the BIA — Reimbursement Request
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $32,383,410 |
CADTH reanalysis 1 | $40,074,470 |
CADTH reanalysis 2 | $48,316,221 |
CADTH base case | $59,791,324 |
BIA = budget impact analysis.
Table 22: Detailed Breakdown of the CADTH Reanalyses of the BIA — Health Canada Indication
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $10,454,733 | $12,655,910 | $14,903,097 | $38,013,740 | |
Budget impact | $0 | $10,454,733 | $12,655,910 | $14,903,097 | $38,013,740 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $20,583,339 | $23,393,902 | $26,261,061 | $70,238,302 | |
Budget impact | $0 | $20,583,339 | $23,393,902 | $26,261,061 | $70,238,302 | |
CADTH scenario analysis 1: Treatment duration assumed to be 1 full year | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $23,131,875 | $26,293,481 | $29,518,761 | $78,944,117 | |
Budget impact | $0 | $23,131,875 | $26,293,481 | $29,518,761 | $78,944,117 | |
CADTH scenario analysis 2: 21.8% price reduction in the Health Canada–indicated population | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $16,138,693 | $18,337,034 | $20,579,633 | $55,055,360 | |
Budget impact | $0 | $16,138,693 | $18,337,034 | $20,579,633 | $55,055,360 | |
CADTH scenario analysis 3: Market share assumed to be 75%, 80% and 85% in years 1, 2 and 3, respectively. | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $19,309,071 | $20,816,497 | $22,351,822 | $62,477,390 | |
Budget impact | $0 | $19,309,071 | $20,816,497 | $22,351,822 | $62,477,390 |
BIA = budget impact analysis.
Table 23: Detailed Breakdown of the CADTH Reanalyses of the BIA — Reimbursement Request
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $8,910,166 | $10,781,434 | $12,691,810 | $32,383,410 | |
Budget impact | $0 | $8,910,166 | $10,781,434 | $12,691,810 | $32,383,410 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $17,525,096 | $19,914,406 | $22,351,822 | $59,791,324 | |
Budget impact | $0 | $17,525,096 | $19,914,406 | $22,351,822 | $59,791,324 | |
CADTH scenario analysis 1: Treatment duration assumed to be 1 full year | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $19,691,352 | $22,379,049 | $25,120,867 | $67,191,267 | |
Budget impact | $0 | $19,691,352 | $22,379,049 | $25,120,867 | $67,191,267 | |
CADTH scenario analysis 2: 24% price reduction in the reimbursement request population | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $13,365,886 | $15,182,291 | $17,035,256 | $45,583,434 | |
Budget impact | $0 | $13,365,886 | $15,182,291 | $17,035,256 | $45,583,434 | |
CADTH scenario analysis 3: Market share assumed to be 75%, 80% and 85% in years 1, 2 and 3, respectively. | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $16,441,969 | $17,723,612 | $19,028,968 | $53,194,549 | |
Budget impact | $0 | $16,441,969 | $17,723,612 | $19,028,968 | $53,194,549 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Lung Cancer Canada
About Lung Cancer Canada
Lung Cancer Canada is a registered national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research, and advocacy. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only organization in Canada focused exclusively on lung cancer.
https://www.lungcancercanada.ca/
Lung Cancer Canada is registered with CADTH.
Information Gathering
Lung Cancer Canada was unable to source patients on this specific treatment for the drug as indicated. This form of treatment is currently not yet available in Canada. However, LCC was able to source and document the experiences of some patients and caregivers on the same form of treatment. Please see chart below for details.
Data Collection
The information discussed throughout this submission consists of the thoughts and experiences of lung cancer patients and caregivers. Lung Cancer Canada collected these experiences through phone interviews and environmental scans. All information was gathered in December 2021.
Table 1: Experiences of Patients and Caregivers
Name | Patient/ Caregiver | Gender | Stage | Type of Lung Cancer | Location | Source |
|---|---|---|---|---|---|---|
||||||||| | ||||||||| | ||||||||| | ||||||||| | |||||||||| |||||||||| |||||||||| |||||||||| |||||||||| | |||||||||||| | |||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||| | | |||||||||| | |||||||||||| | |||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||| || | |||||||||| | ||||||||||||| | |||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||||||||| | |||||||||| | |||||| | |||||||||||||||| |||||||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||| || | |||||||||||||||||| |||||||||||||||||| ||||||||||||||| | |||||| | |||||||||||||||| |||||||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||| || | |||||| | |||||| | |||||||||||||||| |||||||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||| | | |||||| |||||||||||||||| | |||||||||||||||| | |||||||||||||||| |||||||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||| || | |||||||||||| | |||||| ||||||| | |||||||||||||||| |||||||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||| || | |||||||||||| | |||||| ||||||| | |||||||||||||||| |||||||||||||||| |
|||||| | ||||||||| | ||||||||| | |||||||||||| | |||||||||||| | |||| | |||||||||||||||| |||||||||||||||| |
Disease Experience
|| ||||||| ||||| || | ||||||||||| ||||||| felt pain in her chest. She was a long-distance runner in excellent shape, busy in the classroom – and wasn’t too concerned at first. Tests later revealed tumours in her right lung, with metastases to her pancreas and lymph nodes, and she was diagnosed with extensive stage small cell lung cancer (SCLC). “My mind went straight into a tailspin as I waited for the next appointment, waited for a biopsy, waited to know what was happening.” ||| || it was like entering a black hole where there is no hope, no light. “I couldn’t help then to feel more like a statistic and less like a human, a mother, in need of hope.” Once she started chemotherapy treatments, | ||||| || ||| ||||||| || |||| ||| |||||||||||| || ||| |||| |||| ||| ||||||| || |||||||||||| | | ||||||||| ||||||||||||| ||||||||| |||| ||||| |||| |||||| ||| ||||| With a 14-year-old son, her life was worth fighting for. “This diagnosis was devastating to me and my family – and when you know there is something out there that could help, you want to be able to at least try.” Soon after starting atezolizumab, she was astonished by the “night and day” difference it made in her quality of life, and she was back up and running again.
||||||||| |||| |||| |||||| ||||||| || ||| |||| |||||| |||| || |||| |||||| ||| |||||| || |||||| || ||| |||| |||||| |||||| ||| ||||| ||||| |||| |||||| ||||| |||| || ||||| |||||||| |||| |||||| ||||||||||| || ||||||| |||||||| ||||||| ||||||| | || ||||| || ||||| ||||||||| |||||||| ||||| ||||||| |||| ||| || ||||| | || ||| || ||||| | ||||||| |||||| || |||| |||||| |||| ||| |||||| |||||||||||| || |||| |||||| ||||||||| ||| ||||||||| ||||||| |||| |||||| ||||||||| || |||| |||||||| |||| |||||| ||| ||||||| ||| ||||||| |||||||| || |||| ||| |||||||| |||| ||||| ||||||||||| |||| ||||||||||| ||||| || |||||||| ||||||||| |||||||| || |||||||| ||||||||||||| |||||||| ||||| || |||| | |||||| |||| ||||||||||| || ||||||||||| ||||||| ||||| ||||||||||| ||||| ||| ||||||| |||||||| ||||||||| ||||||| |||| ||| |||||| |||||||||| || ||| |||||||| || |||||||||||| || |||| |||| |||| ||||||| ||| ||||||||| |||||||| ||| ||||| ||||||||| || ||||||||| || |||| |||||| || ||||| |||||||||||| ||| |||| |||||| |||||||||||| || |||||||| ||| ||||||||||| ||| |||||||||| |||| |||||||||||| ||| ||| |||||||||| ||| |||| ||| |||| ||| |||||||||| ||| |||||| ||||||||| |||| ||||| ||| |||||||||| |||||||| ||| |||| || |||| ||||||| || |||| || ||||| || |||||||||||| ||||| |||| |||| |||||| ||| ||||| ||||| ||| |||| | |||| ||||||| || ||||| |||||||||||| || | |||| || ||||||||| |||| ||| |||| |||||||| |||| ||||||||| |||| |||| |||||| ||||||| ||||| ||||||| |||| ||||| |||||||||| | |||||| || | |||||| ||||||||||
Experiences With Currently Available Treatments
||| ||||||| |||||||| || ||||||||| ||| ||||| |||||||| |||| ||||||| |||| ||||| ||||||||||| || ||||||| ||| |||||||||| ||||||||||||| |||||||||| ||| ||||||||||| ||||| |||||| |||||||||| ||||||||||| ||||||||| ||||||||||| ||| |||||||||||||| ||||| || ||||||||| || ||||| |||| || ||||||||| ||| |||| ||||| || ||||||||| |||| |||| ||||||||| || |||| |||||| ||||||||| || | |||| |||||| || || ||||||||| || ||||||| |||||||| |||| ||||||||| ||||||| ||||| || |||||| ||| |||| || ||||||||||| |||||||| ||||||| ||| ||||| |||| |||||||| ||||||||| |||||||||||||| ||| ||||||||| |||||||||| || |||||||||| || ||||| ||||| |||||||||| |||| |||| |||| |||||||||| || |||||||| ||| |||||||||||||||| |||||| |||||||| ||||||| ||||||||| |||| ||| | |||||| || |||||||||||| |||||||| || |||||||||||||| |||||||| ||| ||| |||| |||| || |||||||| | |||||| || |||||||||||| |||||| ||||||| || ||||||||| ||||||||| ||||||| ||| ||||||||||| |||| ||||| |||| ||||||| |||| |||| ||||||||||| ||| |||| ||||||||| |||| || ||| ||| ||||| ||||| ||| ||| ||||||||||| || ||| ||||||||| || ||||| |||| ||| ||| | ||||||| |||||| || |||||||||||| |||||||| || ||||||||||| |||||||||||| ||| || ||||||| |||| |||| || |||||||||||| ||||||||| |||||||| |||| ||| ||||||| ||||||||| ||| |||| ||| ||||||| |||||| ||||| || ||||||||||| ||||||| ||| |||||| || |||||| ||||||| ||||||||| ||| |||| ||| |||| ||||||||| |||| || ||||| ||| |||||||||| ||||||||||| ||||||||||||| |||| ||||||||||||| |||||||| ||| |||||||||| ||, a 67-year-old patient with small cell lung cancer, was diagnosed in May 2020 after a trip to the hospital due to a cough that would not subside. She had shortness of breath and fatigue along with her cough, which soon developed into pneumonia. She was in the hospital for 9 days, during which a CT scan revealed a mass in her lung. She endured 5 rounds of chemotherapy and had a PICC line replaced regularly by an ||| |||||| ||| ||||| ||| ||||| || |||| | ||||| |||||||||| ||| ||| || |||| ||||||||||||| ||| |||| ||| || |||||| || ||||||||| |||||||| || ||| |||||||||| || ||| |||||| ||||| ||||| ||||| ||| |||||| ||||| ||| |||| ||||||| ||| ||| ||| || ||||| ||||||| |||| |||||| |||||||||||| || |||||||||| || ||| ||| |||||||||| ||||||||||| ||||| |||| |||||| |||||| |||||||| ||| ||||||| ||||| ||| ||||| ||||||||| ||||||||| || ||||| |||||||| ||||| ||| ||||||| |||||||||||| ||| ||| |||| || || |||| |||||| ||| |||||||| || ||| ||||||||| || ||||| |||| ||||| ||||| |||||||| | |||| || ||| |||| || |||| || || ||| |||||| || ||| ||||||| || |||||||| ||| |||||||||||| ||| |||||||||||||| ||| |||||| ||| || |||||||| ||||||||| |||||| | ||||||| ||||| ||| ||||| |||| |||| ||||||| ||||| |||||||| ||||||||| || ||| ||||||| |||| || |||||||| | ||||||| ||||| || ||||||||||||| || |||||| |||||||||| |||| ||||||| |||| |||||||| ||| |||||| |||| |||| |||| |||||| |||| ||||| | ||||| ||| | ||||| ||| ||| |||| |||||| |||||||||||| || ||||| ||| ||||||| || |||| ||| |||| |||| ||||| |||||| ||| |||||| |||| ||||||||| |||||| |||| ||| |||||||||| ||||||||| || |||||||||| || ||||||| ||||| ||||||||| |||||| |||||||||||| ||||||| ||||||||| ||| ||||| ||||||||| ||| || |||||| |||| ||| |||| | |||| | |||||||| |||||||| ||||||||||| |||| ||||||| |||||||| |||||||| |||| |||| |||||||||| ||||| |||| ||||||||| |||||| || |||||||||||||||| ||| ||||| ||||| |||||| ||||||||| ||| |||||||| |||| ||||| || ||||| ||| |||||| |||||||||| ||| ||||||||||||| ||||| | |||||| |||||| || ||||||| ||| |||| || ||||| |||||||||||| ||||| |||| ||||| |
Improved Outcomes
There have been many incredible advancements in lung cancer research in recent years that have changed the treatment paradigm for patients in Canada. With immunotherapy, the treatment options for patients are limited in comparison to targeted therapies, as there’s no specific targetable mutation that can guide their treatments. In the case of locally advanced NSCLC patients with PD-L1 expression, the limited treatment options they have include chemotherapy and immunotherapy, in which both come with their benefits and disadvantages. For non-small cell lung cancer patients, they value being able to have additional treatment options in the market as an alternative, as it gives them a sense of ease and flexibility to fall back on if their current treatment is not proving to be effective. In a new therapy, patients most value:
Improvements in managing their NSCLC symptoms while having manageable side effects
Being able to have a full and worthwhile quality of life
Being able to maintain their independence and functionality to minimize the burden on their caregivers and loved ones
Delaying disease progression and settling patients into long-term remission for improved survivorship
In this case, as there is a comparable funded immunotherapy, patients expect atezolizumab to be as equally effective as the current standard of care
Experience With Drug Under Review
As discussed, there are gaps in the current treatment paradigm for lung cancer patients where those with early-stage disease need treatment options that can treat their symptoms, are durable, have manageable side effects and prolong survival. The ultimate treatment goal for those with early-stage disease is curative and with 49% of newly diagnosed lung cancer patients with stage I to III disease, atezolizumab, which is discussed below, has shown very promising results even for advanced stage patients; as such, it is a viable treatment option for these group of patients. As mentioned earlier, Lung Cancer Canada was unable to source early-stage NSCLC patient or caregiver experiences with the PDL-1 expression on the requested treatment, but was able to source and document the experiences of other lung cancer patients and caregivers treated with atezolizumab. We believe this will help highlight the efficacy of this form of treatment and help provide real world evidence (RWE).
Atezolizumab treats the cancer, is a durable form of treatment and has shown to be effective in maintaining stable disease.
||||| | was diagnosed in August 2016, she had metastases to her adrenal glands in addition to the primary lung cancer. She had chemotherapy and radiation, but only for a short time as her cancer always found a way around them. She then started her treatment with atezolizumab in May 2018 only two days after it was approved in the United Kingdom. 4 months later, she received good news, the primary tumour in her lung had shrunk from 5 centimeters to 4.2 centimeters, although she did have some growth in her adrenal glands. She was pleased to see that it is working after her previous experience with chemotherapy did not work well for her.
For |||||| |, her scans at diagnosis showed extensive metastases to her pancreas and lymph nodes, in addition to the significant number of tumours in her right lung. She was confined to her bed and wheelchair, her appetite was gone, she was eating very little, and her energy was fading. She felt as if there was no hope and no light at the end of the very dark tunnel; however, this all changed once she was treated with atezolizumab. Soon after starting three-week cycles each of chemotherapy and atezolizumab, her appetite returned, she abandoned her wheelchair, and was even running again. Her CT scans in mid 2020 revealed that the cancerous nodes in her lungs and pelvis had reduced by nearly half and the tumors in her breast and pancreas had nearly cleared. She could breathe better too, the tumor in her lung was no longer pressing on a pulmonary artery. It was a clear “night and day” difference that made her quality-of-life skyrocket, thanks to atezolizumab.
|||||| | has been on atezolizumab for several months now since July 2021, His oncologist noted he is responding extremely well to the drug, and his most recent scan in December 2021 showed his lung tumour has shrunk by almost 80%, which is incredible.
| ||| ||||||||| |||| ||||| | ||||| || ||| |||| || ||| |||| |||| ||| ||| ||||||| || |||||| ||| ||| |||| || ||| ||||| || ||| |||| ||||||| |||| | |||||| || |||||||||||| ||| ||| || |||||| |||| || ||||||||| |||||| |||||||||| ||||||||||| || ||| ||||| |||||| ||||||| || ||| ||||||| ||| |||| |||||| ||||| |||||||| |||||||||||| || |||| ||||| ||| |||| ||||| || ||||| |||| |||||| |||| ||| ||||||| || ||||||| ||| |||||| |||||| ||| |||||||||| || |||| |||| ||| ||||||| |||| ||| ||||| ||| || ||||| |||||||| ||||||||| ||| || || | |||||| |||||| |||||| ||||||| ||||||| ||||||||||| || ||| || ||| ||| |||||||| ||| |||||||||| ||||| ||||||||| || ||||||||| |||||||| ||| || || |||| |||||||||| || |||| |||| |||||||| |||| || ||| || || ||| |||||||||| ||| ||||||| |||| ||| |||| |||| |||||||||| ||||||||||||| |||||| |||||||| || || ||||||||||| ||| ||||||||||| ||| ||| ||| || ||| |||| ||| |||| || ||||| ||| ||||||||| || ||||| ||||| ||| ||| | ||||||| ||| |||||| |||||| || ||||||||||||||||| ||| ||||| |||||||||| ||||||| |||||| |||| ||| |||| |||| |||||| |||||| || |||| |||||| |||||| |||||||| |||||| ||| ||||| |||||||||||| ||||||| ||| ||| |||| |||||| |||| |||||| ||||||||| |||||| |||| |||||||| ||| |||||| |||||||||| ||||| ||| ||||| ||||| |||| |||| ||||||| ||| ||||||||| | ||||||||||| || |||| ||||||| |||| ||| ||||||||| |||| |||||||||||| ||||| |||| |||||||||| |||||||| ||| ||| |||| |||| || |||||| || | |||| |||||| ||||| ||| ||||||| ||||||||||| |||| ||||| ||| |||||| ||| |||||| ||| ||||| ||||| ||| |||| |||||||||||| ||||||||||| ||| |||| ||||||||||| |||||| |||| |||| || ||| ||||| ||||| ||| |||| |||| |||||| | ||| ||||| ||| ||||||||| ||| || ||||| |||| |||||||| ||| ||||||| ||||||||| ||||||||| |||| |||| ||||||||| ||||| |||| |||| |||||| |||| ||||||||| ||||||||| |||| |||||||||||| ||||||||| ||||||||| |||| ||||| ||| ||||||||||| ||||||||| || |||| ||||||| ||||| |||| ||||||||||||| | For ||||, aside from fatigue, dry mouth, and diarrhea, she did not experience too many major side effects from the treatment. |||| did not experience any major side effects from other than phlegm and |||| has not experienced any side effects from treatment aside from fatigue, which is a huge improvement from when he had chemotherapy as it took a toll on his well-being.
Companion Diagnostic Test
|||||||||||| |||| ||| ||||||| ||| ||||||||| |||||||| ||||| ||||||| || ||||||||| ||||||| |||||| ||| ||||||| ||| || ||||||||| |||| ||||||||||| ||| ||| |||||| ||| |||||||||| |||||||| || ||||||||| |||| |||| ||||||| |
Anything Else?
||||||||| |||| |||||||| |||||||||||| |||||||||||| ||| |||||||| |||||||||||| |||||| ||||||| |||| ||||||||||| ||||| |||||||| |||| ||| ||||| |||||||||| | |||||| ||||||||| ||||||| ||| |||| |||||||| |||| |||| ||||||||| |||| ||||| ||||||||| |||||||||||| ||||||||||||| ||||| || | |||| |||||||||| || ||| ||||||| |||| ||| |||||||| || |||||||||||| |||| ||||| |||| ||| |||| |||| ||| | |||||| || ||||||| | |||||||||| || ||||| ||||||| ||| ||||||| || ||| ||||| | ||||| ||||||||| ||||||| ||| ||||| |||||| |||| ||||||||| ||||||| ||| |||||||||||| | ||||||| |||| |||||||||||| ||| |||||||| |||| ||||||||||| |||||| ||| || |||||||| || ||| |||||||||||| ||||| ||| |||||||||||| |||||||| |||||| |||| | |||||| ||||| || ||||| ||| |||||| |||||||||||| |||||||| |||| ||| ||| || ||| |||||||||||| ||||| |||||||| || ||| ||| ||||| || |||| |||||||||| ||||| |||| || |||||||||| ||| ||||||| || ||| |||| |||||||||||| ||| ||||| || || |||| |||||||| |||| | |||||| |||||||||||| |||||||| |||||| || |||| |||||| |||||| || |||| |||||| ||| |||||||||| ||||| ||| ||| ||||| || |||||| ||||||||||| ||| |||||||||| |||||||||||| || |||||||||||| |||||||| || |||| |||||||| ||||||||| ||||||| ||| |||||||| |||| ||||| ||| ||||||| ||| ||||||||||||||| ||| ||||||||| ||| ||||| || ||| ||||||| ||| ||||||||| ||| |||||| ||| ||| ||| ||| ||| ||||| ||| |||||||||| ||| |||||||| ||| |||||||| ||| | |||||||||| ||||||||||||| ||||||| |||||||| |||||||||||| ||||| |||||||| |||||||||||| || |||||||| ||||| ||||||| |||||||||||||| |||| |||||| ||||||||||||| | ||||||||||| |||||||||||| ||||||||||| ||||| | |||||| ||| |||||| |||||||| ||||||||| ||||||||||| |||||||||| |||| ||||||||||||||||||||||||||||| |
Patient Group Conflict of Interest Declaration — Lung Cancer Canada
|||||| ||| ||||||| |||| |||| ||||||| |||| ||||||| ||||| || ||||||| || ||||||| |||| |||| || |||| ||||||||||| || |||| |||||| |||||| ||| |||| ||| ||| |||||||| ||||||||||| ||| ||||||||| || ||||||||||||| |||| |||| |||||||| |||| ||||| |||| ||||||||| ||||||| |||| ||| |||| | ||||| ||| ||| ||| |||| |||||| || |||||||| |||||||| || ||| |||| ||||| |||||||
Table 2: Conflict of Interest Declaration for Lung Cancer Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Roche | X | — | — | — |
Lung Health Foundation / The Ontario Lung Association
About the Lung Health Foundation / The Ontario Lung Association
The Ontario Lung Association (now named Lung Health Foundation) is registered with the CADTH and pCODR (www.lunghealth.ca). The Lung Health Foundation (Ontario Lung Association) is a registered charity that assists and empowers people living with or caring for others with lung disease. It is a recognized leader, voice and primary resource in the prevention and control of respiratory illness, tobacco cessation and prevention, and its effects on lung health. The Foundation provides programs and services to patients and health-care providers, invests in lung research and advocates for improved policies in lung health. It is run by a board of directors and has approximately 46 employees, supported by thousands of dedicated volunteers.
Information Gathering
The information provided from the Lung Health Foundation in this submission was obtained from three phone interviews that were conducted in September and October 2021 with two female patients and one male patient living with lung cancer. All the patients interviewed were over the age of 50. One of the female patients is based in Ontario and the other patient is based in Manitoba. The male patient was from Quebec. Input from a Registered Nurse is also included based on information gathered from monthly support groups attended by patients and their caregivers. Input from a certified respiratory educator was also obtained for this submission. The individual reviewed sections related to disease experience, experiences with available treatments and outcomes.
Disease Experience
Patients interviewed expressed that they found it difficult to cope with a lung cancer diagnosis. Lung cancer is associated with a poor prognosis and is the leading cause of cancer related deaths (Canadian Cancer Statistics, 2021). The patients interviewed report that the symptoms they experience with lung cancer were, in most cases, mild and are often associated with other conditions which led to a late diagnosis. One patient interviewed reported that she had a lingering cough for over 6 months before she was screened for lung cancer. She had been considered low risk because she did not have a smoking history. Another patient interviewed reported that she received her diagnosis during the peak of the COVID pandemic. There were delays in getting diagnostic tests and starting treatment which was a great source of distress for her.
The general consensus from the patients interviewed is that the symptoms of the disease itself are physically manageable. The challenge is the psychosocial effects of having a disease with a poor prognosis as well as the side effects associated with some treatments.
Some of the psychosocial effects reported were anxiety (66%), distress (100%) and depression (66%). One of the patients reports being depressed because she was advised that she had 6-18months left to live. Because she had children, this was devastating to her. She reports having lung cancer was also particularly isolating because of the stigma associated with lung cancer. She withdrew from all activities because she did not want people to know that she was diagnosed with lung cancer. She said, “I did not want anyone to know I had lung cancer, I wanted people to still have empathy for my children.”
Other patients interviewed described having a challenging time maintaining relationships with families and friends. They felt short tempered and impatient. Physical and emotional intimacy were also reported to be a challenge.
The side effects related to some treatments severely impact day to day and quality of life. One of the patients interviewed reported that he struggled with the side effects of chemotherapy. He reported having hair loss, loss of appetite, weight loss, poor sleep, difficulty breathing and this severely impacted his quality of life. Prior to starting treatment he was active and played sports, but once he started chemotherapy, he was unable to participate in his usual activities. This was very challenging for him. He also reported that the hair loss impacted his self-esteem because he looked visibly ill.
Another patient interviewed reported that she experienced neuropathy, difficulty swallowing, fatigue and scarring in her lungs resulting in breathing difficulties. This negatively impacted her quality of life and ability to work and care for her family.
Family members and caregivers of those living with lung cancer share the same psychosocial burdens as the patients. They also have the added responsibility of providing care. Being a caregiver affects their ability to work, their relationships with family and friends and their emotional well-being. Their independence and ability to travel and socialize are often impacted as well. Having to take time off work to drive those they are caring for to get groceries, run errands or attend medical appointments can be problematic for caregivers. Feelings of fatigue and emotional exhaustion are not uncommon
Experiences With Currently Available Treatments
The treatments tried by the respondents included surgery, radiation, chemotherapy, targeted therapy and immunotherapy. The medications tried included Cisplatin, Docetaxel, Gefitinib, Entrectnib, Alectinib, Brigatinib, Opdivo+Yervoy and Tagrisso.
The benefits experienced with the treatments were prolonged life, delayed disease progression and a reduction in the severity of disease-related symptoms. Although these benefits were noted, most patients struggled with lingering side effects. Respondents who received surgery, reported deconditioning and chronic fatigue. Some of the side effects reported from radiation were fatigue, skin changes, hair loss and tissue scarring. One patient reported that they now have COPD related to lung tissue scarring from radiation.
With oral and subcutaneous medications, the side effects reported included fatigue, nausea, vomiting, mood changes, diminished appetite, weight loss, hair loss, anemia, and neuropathy. Side effects from chemotherapy severely impacted the patients’ quality of life, ability to work and in some cases, the ability to perform activities of daily living.
When asked about challenges with access to treatment, the respondents reported that they struggled to navigate the healthcare system. In some cases, they were not clear where to go for information and support. Patients also found delays in treatment and diagnostic testing to be a great source of distress because lung cancer progresses quickly and advanced disease is associated with poorer outcomes.
Respondents would not only like to see biomarker testing done earlier, but also done for all biomarkers. This would allow patients to receive targeted therapy. Some patients felt that taking treatments before biomarker testing led them to suffer unnecessarily with side effects from medications that provided no therapeutic benefit. In addition, patients value having treatment options when they are deciding on their best course of action. Research has shown that lung cancer patient preferences for treatments can vary widely dependent on clinical and demographic attributes and that providing patients with an active role in decision-making can work to improve health outcomes (Janse et al., 2021).
Improved Outcomes
Key treatment outcomes for this group of lung cancer patients include stopping or slowing the progression of the disease with minimal side effects. Patients would also like to see medications that are effective for advanced disease. Due to the poor outcomes associated with advanced disease, patients describe feeling very anxious about any sign or prospect of disease progression.
Patients state that if treatments were more effective in treating lung cancer at any stage, then a diagnosis would not feel like a “death sentence”. One of the respondents reported that after she was given a prognosis of 6-18months, she was withdrawn and struggled to cope. She stated, “I did not want to go anywhere or do anything, I just wanted to spend every last second with my children". This isolation negatively impacted her quality of life and mental wellbeing.
Side effects are also a great source of distress for patients. Some reported that they had no symptoms from the actual cancer but struggled with the side effects from treatment more.
Patients would like treatments with minimal side effects so that they can carry on with regular activities while on treatment. The importance of maintaining some quality of life cannot be overstated.
When choosing therapy, patients are most interested in the efficacy of the medication.
One respondent commented that they would be more receptive to side effects if there was a guarantee that the medication would stop or slow down the progression of lung cancer.
Experience With Drug Under Review
No patients within this evidence group submission had experience with the medication under review. It is worth noting that fear of recurrence is a great source of distress from patients who had early stage disease and received surgery. One of the patients interviewed reported that she is always on high alert and anytime she has any ailment, she worries that her cancer has returned. New adjuvant strategies are needed to improve outcomes after complete surgical resection in patients with early-stage non-small-cell lung cancer and Atezolizumab offers a promising treatment option for patients (Felip et al, 2021).
Companion Diagnostic Test
Although patients in this submission group did not have experience with the drug under review, they did receive biomarker tests for other treatments. The majority of the respondents who went through the testing indicated they wished it had been done sooner. Depending on the stage of the cancer diagnosis, biomarker testing was not always an option at diagnosis. Delays in biomarker testing also resulted in patients delaying targeted therapies that would have produced better outcomes with less side effects.
Anything Else?
Not applicable
References
Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada and the Public Health Agency of Canada. Canadian Cancer Statistics 2021. Toronto, ON: Canadian Cancer Society; 2021.
Felip E, Altorki N, Zhou C, Csőszi T, Vynnychenko I, Goloborodko O, Luft A, Akopov A, Martinez-Marti A, Kenmotsu H, Chen YM, Chella A, Sugawara S, Voong D, Wu F, Yi J, Deng Y, McCleland M, Bennett E, Gitlitz B, Wakelee H; IMpower010 Investigators. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet. 2021 Oct 9;398(10308):1344-1357. doi: 10.1016/S0140-6736(21)02098-5. Epub 2021 Sep 20. Erratum in: Lancet. 2021 Sep 23;: PMID: 34555333.
Janse, S., Janssen, E., Huwig, T., Basu Roy, U., Ferris, A., Presley, C. J., & Bridges, J. F. (2021). Line of therapy and patient preferences regarding lung cancer treatment: a discrete- choice experiment. Current Medical Research and Opinion, 37(4), 643-653.
Patient Group Conflict of Interest Declaration — Lung Health Foundation / The Ontario Lung Association
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation.
Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 3: Conflict of Interest Declaration for the Lung Health Foundation / The Ontario Lung Association
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Hoffman-La Roche | X | — | — | — |
Clinician Input
Lung Cancer Canada – Clinician Group
About Lung Cancer Canada – Clinician Group
Lung Cancer Canada is a national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research and advocacy. Based in Toronto, Ontario, Lung Cancer Canada has a wide reach that includes both regional and pan-Canadian initiatives. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only organization in Canada focused exclusively on lung cancer.
Information Gathering
Information gathered for this submission was based on relevant published clinical data and expert evidence-based review amongst lung cancer medical oncologists across Canada.
The key sources of data relevant to this new indication are below.
Manuscript: Felip E, Altorki N, Zhou C, Csőszi T, Vynnychenko I, Goloborodko O, Luft A, Akopov A, Martinez-Marti A, Kenmotsu H, Chen YM, Chella A, Sugawara S, Voong D, Wu F, Yi J, Deng Y, McCleland M, Bennett E, Gitlitz B, Wakelee H; IMpower010 Investigators. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet. 2021 Oct 9;398(10308):1344-1357. doi: 10.1016/S0140-6736(21)02098-5. Epub 2021 Sep 20. Erratum in: Lancet. 2021 Sep 23;: PMID: 34555333.
ASCO 2021 Presentation: Heather A. Wakelee, Nasser K. Altorki, Caicun Zhou, Tibor Csőszi, Ihor O. Vynnychenko, Oleksandr Goloborodko, Alexander Luft, Andrey Akopov, Alex Martinez-Marti, Hirotsugu Kenmotsu, Yuh-Min Chen, Antonio Chella, Shunichi Sugawara, Barbara J. Gitlitz, Elizabeth Bennett, Fan Wu, Jing Yi, Yu Deng, Mark McCleland, and Enriqueta Felip. IMpower010: Primary results of a phase III global study of atezolizumab versus best supportive care after adjuvant chemotherapy in resected stage IB-IIIA non-small cell lung cancer (NSCLC). Journal of Clinical Oncology 2021 39:15_suppl, 8500-8500.
WCLC 2021 Presentation: N. Altorki, E. Felip, C. Zhou, E. Vallieres, V. Moiseyenko, A. Smolin, A. Rittmeyer, R. Vereshchako, M. Perol, W. Schutte, J. Fang, M. Tao, E. Teixeira, Y. Kim, B. Gitlitz, E. Bennett, V. Mcnally, F. Wu, Y. Deng, H. Wakelee. IMpower010: Characterization of Stage IB-IIIA NSCLC Patients by Type and Extent of Therapy Prior to Adjuvant Atezolizumab. Journal of Thoracic Oncology, 2021 Volume 16, Issue 10, S845 - S846.
ESMO 2021 Presentation: E. Felip, E. Vallieres, C. Zhou, H. Wakelee, I. Bondarenko, H. Sakai, H. Saito, G. Ursol, K. Kawaguchi, Y. Liu, E. Levchenko, N. Kislov, M. Reck, R. Liersch, V.A. McNally, Q. Zhu, B. Ding, E. Bennett, B. Gitlitz, N.K. Altorki. Annals of Oncology (2021) 32 (suppl_5): S1283-S1346. 10.1016/annonc/annonc741.
Current Treatments
In Canada, the treatment for Stages IB-IIIA non-small cell lung cancer (NSCLC) is stage dependent. Canadian practice is aligned with practices from around the world, as evidenced from data from both the IASLC Dataset and North American-based National Cancer Database.
For stage IB NSCLC, the primary goal is cure (i.e., to improve 5-year overall survival). To achieve this goal, the standard treatment is complete surgical resection (R0). Thereafter, a minority of fit patients are offered adjuvant platinum-doublet chemotherapy, particularly those with pathological findings consistent with high risk of relapse such as larger T-sizes and nodal disease. In a small fraction of cases, surgical resection leads to an incomplete resection, and adjuvant radiation is potentially offered in this context. In medically inoperable patients, sometimes localized radiation (external beam or stereotactic body radiation) is given in lieu of an operation.
For stage II NSCLC, the primary goal is cure (i.e., to improve 5-year overall survival). To achieve this goal the standard treatment is complete surgical resection (R0). Thereafter, fit patients are offered adjuvant platinum-doublet chemotherapy. In a small fraction of cases, surgical resection leads to an incomplete resection, and adjuvant radiation is potentially offered in this context, which would be given sequentially to adjuvant chemotherapy.
For stage IIIA NSCLC, the primary goal is cure (i.e., to improve 5-year overall survival). To achieve this goal, the standard treatment depends on whether the primary tumour is considered resectable or not, balancing benefits and risks, including peri-operative risks, the ultimate chance of cure, the number of lobes that will be resected (e.g. lobectomy vs pneumonectomy), and the long-term residual effects of the operation (e.g. expected residual pulmonary reserve and function after a resection). If surgery is considered reasonable, the next step would depend on whether mediastinal lymph nodes are known to be involved with cancer. If not (T4N0 or T3 or T4N1), medically eligible patients will start with surgery and then proceed to adjuvant platinum based chemotherapy. For those patients with N2 mediastinal lymph nodes involved, neoadjuvant chemotherapy concurrent with radiation, followed by complete surgical resection is typically offered if the nodal disease is non-bulky and limited in extent. If surgery is not considered reasonable, definitive chemotherapy concurrent with radiation is given, followed by consideration of a year of durvalumab. In a small fraction of cases, surgical resection leads to an incomplete resection, and adjuvant radiation is potentially offered in this context, but sequentially (and not concurrent) with any adjuvant chemotherapy.
Adjuvant platinum-doublet chemotherapy given after resection of stage IB-IIIA NSCLC patients typically consists of four cycles of treatment, with each cycle lasting 21-28 days, for a total of 12 -16 weeks of therapy. Specific platinum-doublet chemotherapy with the best evidence of efficacy has been with the combination of cisplatin and vinorelbine, but other platinum-doublet combinations such as cisplatin and pemetrexed have been increasingly used over the recent years.
The current staging system we use globally is the 8th edition of the Union of International Cancer Control (UICC) staging system. This trial was conducted using the 7th edition of the UICC staging system. Discussion above referenced the standard practice for the 7th edition which was used in the trial. Relevant differences include: stage IB cancers that are considered high risk for relapse (tumour size 4-5 cm) are now considered stage II tumours. Adjuvant chemotherapy is not required for patients with stage I cancers in the 8th edition system (< 4 cm, node negative). Stage III has now been divided into stage IIIA, IIIB and IIIC. Stage IIIC by definition are unresectable. A subset of patients with stage IIIA and B will be resected and offered adjuvant platinum based chemotherapy as described above. These patients previously were all typed as IIIA in the 7th edition staging.
Another treatment that has become recently available in the post resection setting is adjuvant osimertinib. Osimertinib is approved by Health Canada after tumour resection in patients with stage IB-IIIA non-small cell lung cancer (NSCLC) whose tumours have epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations. This population is a specific subgroup of NSCLC with a sensitizing mutation in the tyrosine kinase domain of EGFR and comprises 10-15% of adenocarcinomas. The ADAURA trial results identified a reduction in the recurrence rate with a hazard ratio (HR) of 0.17 (99% CI, 0.11-0.26); p<0.001 for resected Stages II-IIIA, and HR 0.20 resected for Stages IB-IIIA. This treatment is currently available to Canadian patients either through private insurance or through a compassionate access program.
References
Chansky K, Detterbeck FC, Nicholson AG, Rusch VW, Vallières E, Groome P, Kennedy C, Krasnik M, Peake M, Shemanski L, Bolejack V, Crowley JJ, Asamura H, Rami-Porta R; IASLC Staging and Prognostic Factors Committee, Advisory Boards, and Participating Institutions. The IASLC Lung Cancer Staging Project: External Validation of the Revision of the TNM Stage Groupings in the Eighth Edition of the TNM Classification of Lung Cancer. J Thorac Oncol. 2017 Jul;12(7):1109-1121. doi: 10.1016/j.jtho.2017.04.011. Epub 2017 Apr 28. PMID: 28461257.
Pignon JP, Tribodet H, Scagliotti GV, Douillard JY, Shepherd FA, Stephens RJ, Dunant A, Torri V, Rosell R, Seymour L, Spiro SG, Rolland E, Fossati R, Aubert D, Ding K, Waller D, Le Chevalier T; LACE Collaborative Group. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008 Jul 20;26(21):3552-9.
Yi-Long Wu, M.D., Masahiro Tsuboi, M.D., Jie He, M.D., Thomas John, Ph.D., Christian Grohe, M.D., Margarita Majem, M.D., Jonathan W. Goldman, M.D., Konstantin Laktionov, Ph.D., Sang-We Kim, M.D., Ph.D., Terufumi Kato, M.D., Huu-Vinh Vu, M.D., Ph.D., Shun Lu, M.D., et al., for the ADAURA Investigators* Osimertinib in Resected EGFR-Mutated Non–Small-Cell Lung Cancer. N Engl J Med 2020; 383:1711-1723.
Treatment Goals
The most important goal that an ideal treatment would have for any adjuvant therapy in early stage non-small cell lung cancer is to prolong cancer-free life and life itself (i.e., recurrence-free survival and overall survival).
Treatment Gaps (Unmet Needs)
UNMET NEED 1: Current therapies are inadequate to achieve high rates of cure in early stage resected IB-IIIA NSCLC patients, based on 5-year overall survival rates.
The outcomes of such patients remain poor even with the best current treatments, falling far below the outcomes of other cancer disease sites. Unlike metastatic disease (where there has been significant progress), the clinical impact of improving outcomes in early stage NSCLC is far greater, with patients having longer cancer-free intervals and being considered true cancer survivors (i.e. cured).
Lung cancer five-year survival, even amongst the early stages, has significantly worse outcomes than in other common cancers. Figure 1 below illustrates how much of a gap there is between lung cancer and other common cancers, such as breast, colon and prostate cancers. In Figure 1, for the localized and extended (i.e. non-metastatic) stages of common cancers, such as breast, colorectal, and prostate cancer, the five-year survival times sit above 75%. In contrast, the results are significantly worse in lung cancer (30-55% five-year survival for Stages I-III lung cancer). Similar results are echoed in Figure 2, which demonstrate that regardless of whether one uses the 7th or 8th edition of the AJCC/UICC lung cancer staging system, the 5-year overall survival rates are between 36% (Stage IIIA) and 66-68% (Stage IB). All of these results presented are in the contemporary era where adjuvant chemotherapy has been widely adopted.
The last time there had been improvements in NSCLC adjuvant therapy was through the incorporation of adjuvant chemotherapy in Stages IB-III resected NSCLC. Following an earlier large meta-analysis, the publication of the LACE collaborative pooled analysis of multiple trials (IALT, NCIC CTG BR.10, BLT, ALPI, ANITA), showed absolute survival improvements ranging from 8.8-15%. However, it has been almost two decades since the large-scale introduction of adjuvant chemotherapy into clinical practice across in Canada. There is a dire need to improve survival outcomes in our Stage IA-IIIB patients further, especially in the setting where long-term cancer-free survival and potential cure rates are involved.
UNMET NEED 2: Current therapies are inadequate to prevent recurrences in early stage resected IB-IIIA NSCLC patients, based on disease-free survival rates.
Improving lung cancer disease-free survival is an equally important unmet need, as it has biologic and clinical association with overall survival in early stage NSCLC patients. Further, in “Place in Therapy,” recurrences and disease-free survival are discussed in detail as to why these are legitimate and key clinical outcomes in their own right, with significant patient, healthcare and societal impacts.
Recurrences after resection of an initial early-stage NSCLC are primarily through distant spread or metastases. This metastatic disease is generally incurable (there are only rare instances of regional or oligometastatic recurrences where treatment may yield long term survival); looking at the survival curves of de novo stage IV cancers (see Figure 2 below) is evidence of the poor outcomes that occur once metastatic disease has been diagnosed. Clinically, these findings demonstrate that, to impact on NSCLC overall survival, one needs to reduce disease recurrence substantially in early-stage NSCLCs.
Further, disease-free and overall survival mirrored each other the last time there was an effective adjuvant therapy for stage IB-IIIA resected NSCLC: in the LACE collaborative, the overall survival benefit of adjuvant chemotherapy was HR = 0.89 (95% CI, 0.82 to 0.96; P = .005) whilst for recurrence-free survival, the results were similar, HR = 0.84 (95% CI, 0.78 to 0.91; P < .001).
Please also see “Place in Therapy,” which details the rationale for why disease-free survival should be its own clinically relevant critical outcome measure
References
Non-Small Cell Lung Cancer Collaborative Group: Chemotherapy in non-small cell lung cancer: A meta-analysis using updated data on individual patients from 52 randomized clinical trials. BMJ 311::899,1995-909
Figure 1: Gap Between Lung Cancer and Other Common Cancers
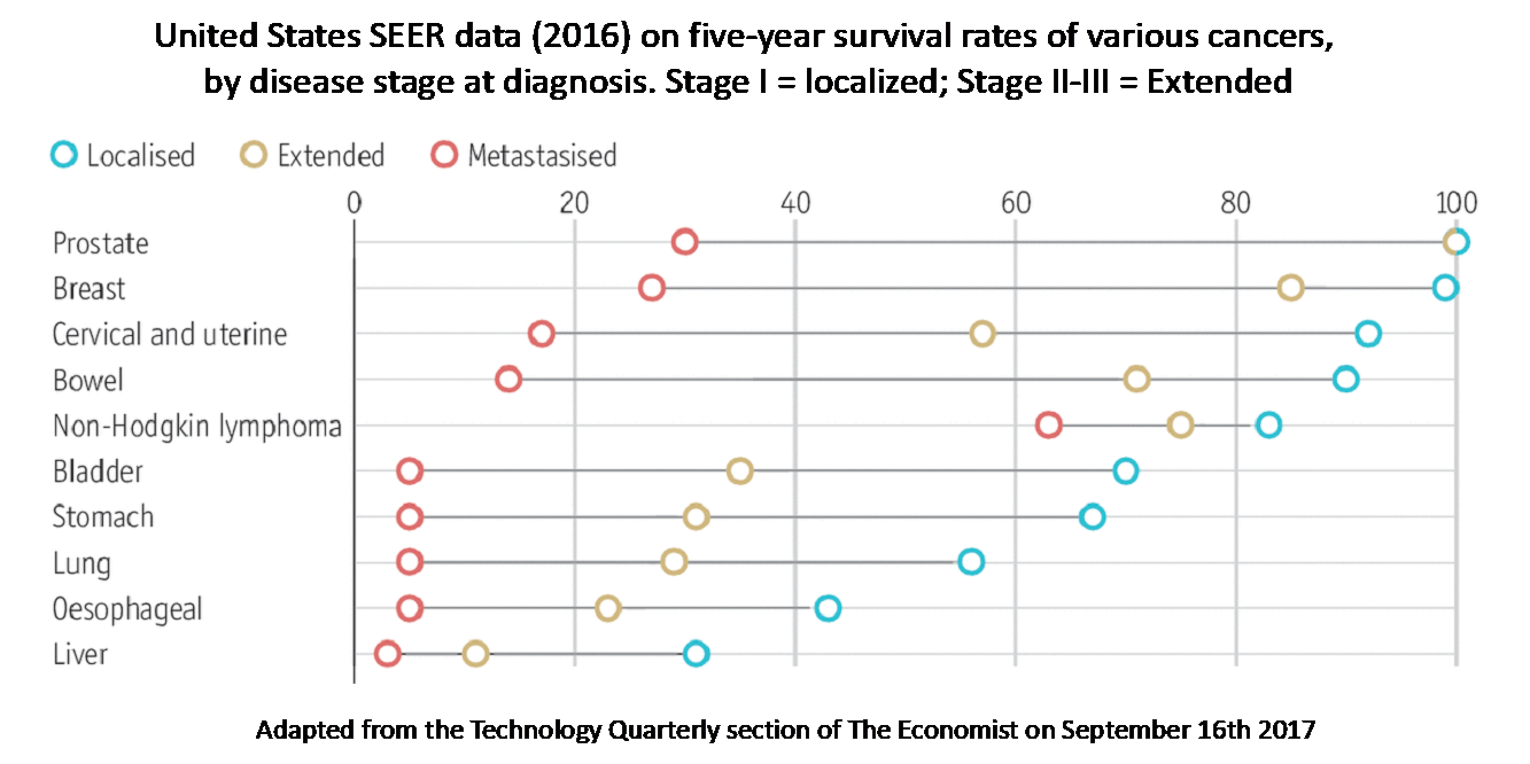
The relative poor outcomes, shown as 5-year overall survival rates, as demonstrated in Stage IB-IIIA lung cancer patients (represented by localized [blue, Stage I] and extended [yellow, stage II-III] open circles), when compared to other common cancers, such as prostate, breast, and colorectal cancer.
Figure 2: Five-Year Survival Rates for Lung Cancer
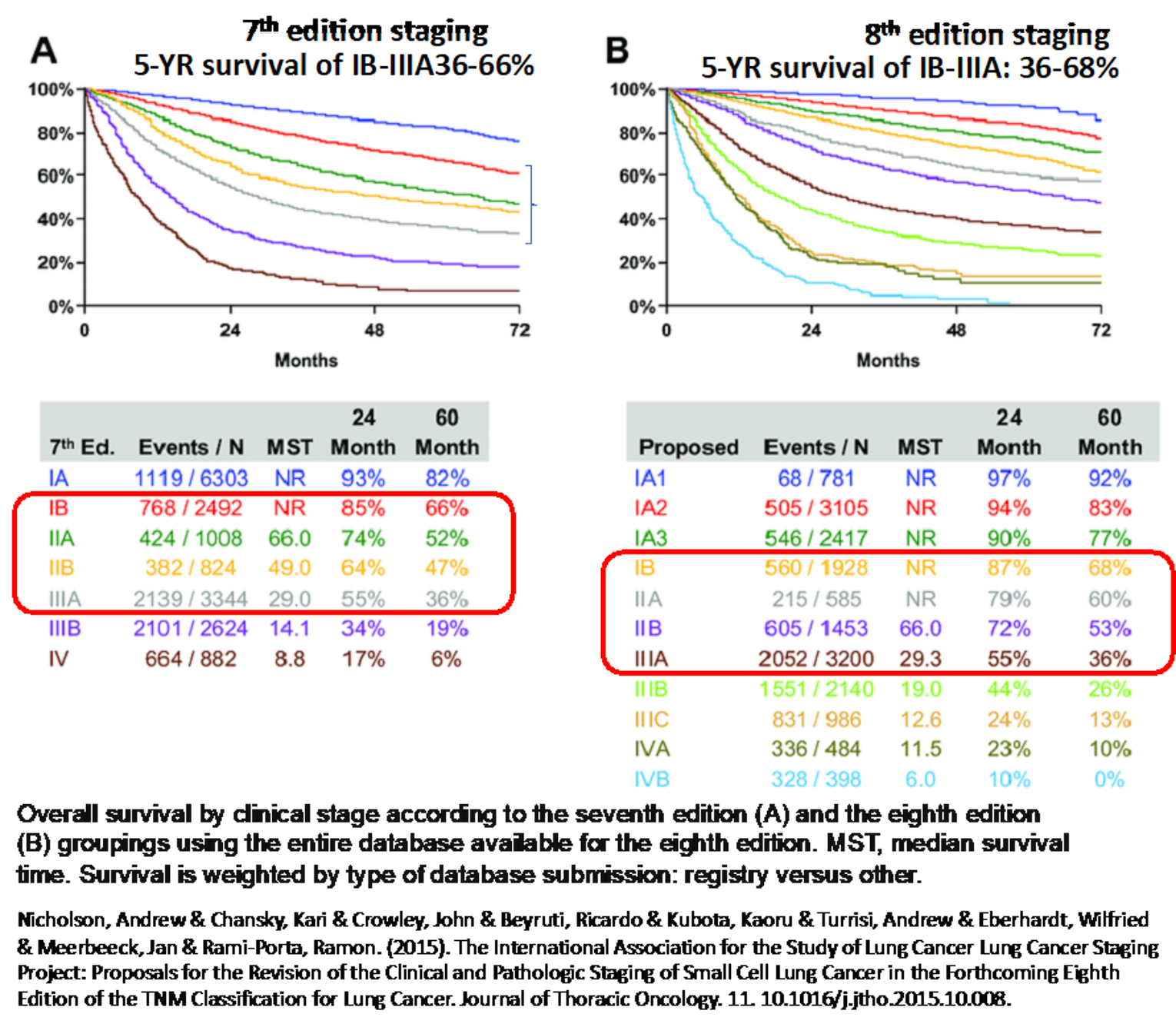
Overall survival is poor in Stage IB (red), IIA (green), IIB (yellow), and IIIA (grey) NSCLC patients, regardless of whether one is using the seventh or eighth edition of non-small cell lung cancer staging, ranging from 36% through 68%.
Which patients have the greatest unmet need for an intervention such as the drug under review? Would these patients be considered a subpopulation or niche population? Describe characteristics of this patient population. Would the drug under review address the unmet need in this patient population?
Response: Patients with NSCLC as mentioned above carry a worse prognosis stage for stage when compared to other curatively treated solid tumours. The risk of relapse jumps dramatically with each increase in stage. Currently, the only group where we recommend surgery alone are those patients with tumours less than 4 cm based on the data of platinum doublet chemotherapy. Once you reach stage II in the 8th edition of staging (4 cm or greater in size OR any lymph node involvement), the survival plummets to 60%. If you have a larger tumour or ipsilateral regional lymph node involvement which defines stage III the 5-year survival only ranges from 26-36%. Therapies that improve the outcomes in this group are a huge unmet need.
This is not a niche population. According to the Canadian Cancer Society’s 2020 special report on lung cancer, 29,800 people are estimated to be diagnosed with lung cancer this year. 49% of newly diagnosed lung cancer patients have stage I-III disease, 21% stage 1, 8% stage II and 20% stage III. Even if only one third of these patients are resected and of high enough stage to qualify for adjuvant chemotherapy that is still over 5000 Canadians who may benefit from this additional treatment.
Based on the data from other trials of immunotherapy in lung cancer and this new IMpower010 data, we agree that Atezolizumab does address an unmet need.
Reference: Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Toronto, ON: Canadian Cancer Society; 2020. Available at: cancer.ca/Canadian-Cancer-Statistics-2020-EN.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Response: Atezolizumab is the first immunotherapy that has been shown in a randomized clinical trial to improve outcomes in the post surgical setting. Based on the IMpower010 results, atezolizumab should be added to the current post-operative management of resected Stage II-IIIA (7th ed.) as a second adjuvant treatment. Patients in this trial must have received at least 1 cycle of platinum doublet chemotherapy for randomization on this trial. Adjuvant platinum doublet chemotherapy should remain as the first post-operative treatment initiated. Atezolizumab should not be considered a replacement for chemotherapy.
Immunotherapy, including atezolizumab, has been studied extensively in the metastatic lung cancer space both as monotherapy and in combination with chemotherapy. This treatment approach is highly effective. PD-1/L1 inhibitors are the first class of drugs that has led to a dramatic improvement in overall survival in the metastatic setting. Immunotherapy is now considered a new pillar of cancer treatment based on these trials. One of the benefits of immunotherapy is the durability of its benefit. These drugs work to block self tolerance allowing a patients own immune system an opportunity to eliminate any identified cancer cells. The other benefit of this class is the tolerability. In the process of blocking self tolerance, patients can manifest autoimmune phenomena that might have previously been suppressed. Fortunately, most autoimmune side effects can be readily managed with steroids or other immunosuppressants. The management of these side effects is now part of the expertise of oncologists as these agents are being used across many tumour types.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Response: This question is not designed for the current submission. Adjuvant chemotherapy should be administered independently of consideration of atezolizumab, where appropriate, as explained in Section 6.1. If the question is whether there is an alternative PD-1/L1 inhibitor to atezolizumab that could be used in place of atezolizumab, the answer at this time is no. Three more trials are still maturing with similar questions to the Impower010 trial using other PD-1/L1 inhibitors. Those trials and their results would need to be adjudicated once the results become available.
How would this drug affect the sequencing of therapies for the target condition?
Response: Re-using a drug in the metastatic setting after use in the adjuvant setting is a consideration.
Data is not available as to when and if to reuse immunotherapy in the recurrent/advanced/metastatic setting, when atezolizumab was used in the adjuvant setting. IMpower010 did not mandate how patients should be treated at disease recurrence. From the presentation by E. Felip at ESMO 2021, we do know that 12.2% of patients did receive immunotherapy as a subsequent treatment after atezolizumab on this trial. We do not have the data on the effectiveness of this strategy.
The presentation by E. Felip at ESMO 2021 also reported on sites of relapse. More patients on the atezolizumab arm relapsed with locoregional disease (47.9 vs 41.2%) which is generally treated differently than metastatic disease and might allow another attempt at cure. When patients relapsed with metastatic disease or the combination of both locoregional and metastatic disease, the relapses were on average later (17.3 vs 10.4 and 24 vs 5.3 months respectively). When relapses are historically more than 6 months after completion of prior treatment, we generally allow rechallenge with the same class of drug presuming there is no contraindication. As relapses on the atezolizumab arm were generally much later, first line metastatic treatments including immunotherapy should be allowed. A similar paradigm has been followed for unresectable stage III patients treated with consolidation durvalumab.
Which patients would be best suited for treatment with the drug under review?
Response: The primary outcome for this study was disease free survival of patients with stage II-IIIA resected lung cancer (UICC 7th edition) with a tumour that is determined to be PD-L1 positive (≥1%) by immunohistochemistry, after at least 1 cycle of adjuvant therapy. In this scenario, the stratified HR is 0.66 (95% CI: 0.50, 0.88). When reviewing the forest plot, nearly all subgroups benefited based on with point estimates for the HR below one with benefits identified regardless of stage or nodal status.
The trial was also analyzed reviewing the benefit in PD-L1 all comers. The disease free survival drops to 0.79 (95% CI: 0.64, 0.96). When you review the forest plot of this larger population, the patients who are PD-L1 positive are the ones that stand out as garnering the benefit. While the PD-L1 negative population is a subgroup, it is a large subgroup comprising over 40% of the study population and the lack of benefit in disease free survival gives this group pause. With the data currently in hand, we cannot recommend with confidence that there is a benefit in the PD-L1 negative patients and recommend awaiting further analysis including overall survival before making a determination on use of atezolizumab in this group.
The trial also includeincludeed patients with stage IB tumours. The analysis of this full ITT population has also been presented. In the full ITT population, the HR is 0.81 (95% CI: 0.67, 0.99) which has not yet met statistical significance. At this time, we cannot make a commentary on the benefit in the stage IB group. We do not have data available to us looking at the breakdown of benefit by different clinical characteristics in the ITT population as a forest plot for this group has not yet been presented. Stage IB in the 7th edition of the staging system is comprised of a mixed group of patients based on size as well as other pathological features of their tumour (visceral pleural invasion). Historical literature including that from the LACE meta-analysis have noted that patients with larger tumours (≥4 cm) have a worse prognosis and have now been included in stage II with the 8th edition update. We look forward to future updates evaluating the stage IB patients, especially those with tumours between 4-5 cm.
How would patients best suited for treatment with the drug under review be identified?
Response: Patients will be identified based on a combination of stage and PD-L1 status. Stage is the simple component. As these tumours are all resected, accurate staging will be determined by the pathologist and reported as part of the histologic description on the pathology report.
Determining PD-L1 status is slightly more complex. PD-L1 testing is routinely offered across the country and is generally done reflexively for all stages and histologic subtypes of NSCLC. In this study, the PD-L1 testing was done with the SP263 assay. Historically, specific companion diagnostics have not been required by provincial funders. Generally, a validated test is required. Extensive work has already been undertaken to validate PD-L1 testing across the country. Individual institutions have been allowed to choose to use a commercial test or to create a local test that would be validated. The International Association for the Study of Lung Cancer alongside the American Society of Clinical Oncology and the American Association for Cancer Research conducted a project comparing and contrasting the commercially developed assays for determination of PD-L1. The results of this work have shown that the SP263 assay is similar to the 22C3 and 28-8 assays that are generally used for clinical determination of PD-L1. One of the leaders of the Blueprint project is Dr. Ming Tsao, a highly respected Canadian pathologist who was instrumental in the validation of PD-L1 testing across Canada when PD-L1 testing was first being refined. Based on the Blueprint data, we do not feel a new assay needs to be created to identify patients for this treatment. The previously validated test used by the local lab will be sufficient.
References
Hirsch FR, McElhinny A, Stanforth D, Ranger-Moore J, Jansson M, Kulangara K, Richardson W, Towne P, Hanks D, Vennapusa B, Mistry A, Kalamegham R, Averbuch S, Novotny J, Rubin E, Emancipator K, McCaffery I, Williams JA, Walker J, Longshore J, Tsao MS, Kerr KM. PD-L1 Immunohistochemistry Assays for Lung Cancer: Results from Phase 1 of the Blueprint PD-L1 IHC Assay Comparison Project. J Thorac Oncol. 2017 Feb;12(2):208-222. doi: 10.1016/j.jtho.2016.11.2228. Epub 2016 Nov 29. PMID: 27913228.
Tsao MS, Kerr KM, Kockx M, Beasley MB, Borczuk AC, Botling J, Bubendorf L, Chirieac L, Chen G, Chou TY, Chung JH, Dacic S, Lantuejoul S, Mino-Kenudson M, Moreira AL, Nicholson AG, Noguchi M, Pelosi G, Poleri C, Russell PA, Sauter J, Thunnissen E, Wistuba I, Yu H, Wynes MW, Pintilie M, Yatabe Y, Hirsch FR. PD-L1 Immunohistochemistry Comparability Study in Real-Life Clinical Samples: Results of Blueprint Phase 2 Project. J Thorac Oncol. 2018 Sep;13(9):1302-1311. doi: 10.1016/j.jtho.2018.05.013. Epub 2018 May 22. PMID: 29800747; PMCID: PMC8386299.
Which patients would be least suitable for treatment with the drug under review?
Response: Patients least suitable for treatment are those patients who have a contraindication to immunotherapy treatment, such as organ transplant. Risks and benefits would need to be discussed with patients who have prior or active autoimmune disease as their risk of side effects is generally higher than for those patients without that history. Active autoimmune disease would be considered a relative contraindication. The primary outcome of this study was evaluation of patients who were determined to be PD-L1 positive. The enrolled population included patients of any PD-L1 status. Based on the information we have currently, patients whose PD-L1 score is 0, do not seem to benefit from this treatment. The PD-L1 negative group comprised 43% of the stage II-IIIA study population (383 pts) and the HR was 0.97 (95% CI:0.72, 1.31). With our current level of knowledge, this group is unlikely to benefit from atezolizumab treatment.
Patients with PD-L1 positive, EGFR mutated lung cancers were included in the IMpower010 trial as well (11.6% of the study population). The hazard ratio in the forest plot was 0.57 in favour of the use of atezolizumab but the confidence interval crossed 1 (0.26, 1.24). Given this is a small subgroup of the overall population, the lack of statistical significance is expected as the trial was not powered to look at this particular subgroup. When the data is expanded to include EGFR mutated cancers with any PD-L1 expression – the benefit disappears suggesting lack of benefit in the PD-L1 negative group. In the situation of a patient with a resected lung cancer with a sensitizing EGFR mutation and has PD-L1 expression identified, clinicians would have to choose one or the other as these agents cannot be safely administered concurrently. We recommend that risks and benefits of each of these therapies be reviewed with the patient and a choice be made for the best treatment for that individual patient.
The other group that may not benefit are patients with ALK translocations. Even in the metastatic setting, the data on the benefits of immunotherapy in ALK+ NSCLC is sparse and most clinicians do not recommend its use unless other treatment options have been exhausted.
One last bit of data to consider is the choice of adjuvant chemotherapy. In the presentation by Dr. Altorki at the World Congress of Lung Cancer in 2021, one of the patient groups that benefited less from adjuvant atezolizumab were those who were treated with adjuvant gemcitabine and platinum. Further data supporting concern over lack of benefit of immunotherapy when associated with gemcitabine was presented as part of the POSEIDON trial where patients who received chemotherapy that included gemcitabine and platinum with an PD-L1 inhibitor, durvalumab, did not benefit from combination chemotherapy and immunotherapy. Gemcitabine is not commonly used in this scenario in Canada. We would recommend that our current practice of use of vinorelbine or pemetrexed with platinum continue.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Response: We anticipate that this question was designed for submissions related to the advanced/metastatic setting, and not relevant for this submission involving adjuvant therapy.
“Response to therapy” is not an appropriate outcome in this population. If the purpose of this question is to address which patients are most likely to benefit, this has already been covered in Section 5.2.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Response: It should be noted that this question is framed in the context of advanced/metastatic setting, as responses to treatment are not a primary focus of early stage resected cancer.
We have re-framed this question to read “What outcomes are used to determine whether a patient is benefiting from this treatment in clinical practice”.
The primary outcome in this trial to determine whether atezolizumab has worked is whether disease recurrence has occurred, (disease-free survival) and ultimately, cure rates, as measured by 5-year OS and Kaplan Meier curves for OS. Typically, most recurrences of Stage IB-IIIA NSCLC patients occur within 2-3 years while OS typically requires a greater number of years of follow-up.
In the setting of early-stage NSCLC, there has been growing clinician recognition of the enormous negative impact of recurrent disease on patients, independent of overall survival. Recurrent disease can occur across a multitude of organ systems. For example, bone metastases and CNS metastases are often symptomatic, requiring local therapies such as radiation to manage symptoms. Lung metastases and pleural disease can lead to shortness of breath and requiring such procedures as thoracenteses. Reducing the rate of recurrence or delaying recurrences impacts patients greatly, independent of the treatment’s ultimate impact on overall survival.
The costs to patient health, quality of life, utilization of health care resources, economic loss of productivity, and overall costs to the society are substantial when a patient relapses especially those with metastatic disease. Delaying or reducing disease recurrence thus has enormous benefit from each of these perspectives.
One main feature of immunotherapy as noted in the metastatic setting is that the benefits are durable. For example, in the Keynote 24 trial, we now know that 33% of patients with highly PD-L1 positive NSCLCs (TPS ≥50%) treated with immunotherapy will be 5 year survivors). This type of statistic is unheard of from either chemotherapy or targeted therapy. We have also seen from the PACIFIC trial that the outcome of disease free survival translated into a clear overall survival benefit of 10% at 5 years. Based on the durability of response in the metastatic setting as well as the clear relationship between disease free survival and overall survival in the curative intent unresectable stage III setting, we anticipate a similar durability to the benefit in the adjuvant setting and overall survival benefit in the post-surgical setting.
Thus, in summary, outcomes used in current practice (recurrences or disease-free survival, and overall survival) are aligned with the IMpower010 primary and secondary clinical outcomes. In an older era, disease-free survival may only have been seen as a surrogate for overall survival; however, in our contemporary era, our clinician group sees recurrent disease as its own critical outcome, with substantial patient-level, health-care level, and societal-level ramifications. Disease free survival is already an acceptable outcome in other disease sites (e.g. breast, melanoma), partly because of such impact. The same standard should be applied to adjuvant NSCLC therapy.
References
Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, Gottfried M, Peled N, Tafreshi A, Cuffe S, O'Brien M, Rao S, Hotta K, Leal TA, Riess JW, Jensen E, Zhao B, Pietanza MC, Brahmer JR. Five-Year Outcomes With Pembrolizumab Versus Chemotherapy for Metastatic Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score ≥ 50. J Clin Oncol. 2021 Jul 20;39(21):2339-2349. doi: 10.1200/JCO.21.00174. Epub 2021 Apr 19. PMID: 33872070; PMCID: PMC8280089.
David R. Spigel, Corinne Faivre-Finn, Jhanelle Elaine Gray, David Vicente, David Planchard, Luis G. Paz-Ares, Johan F. Vansteenkiste, Marina Chiara Garassino, Rina Hui, Xavier Quantin, Andreas Rimner, Yi-Long Wu, Mustafa Ozguroglu, Ki Hyeong Lee, Terufumi Kato, Maike de Wit, Euan Macpherson, Michael Newton, Piruntha Thiyagarajah, and Scott Joseph Antonia. Five-year survival outcomes with durvalumab after chemoradiotherapy in unresectable stage III NSCLC: An update from the PACIFIC trial. Journal of Clinical Oncology 2021 39:15_suppl, 8511-8511.
What would be considered a clinically meaningful response to treatment?
Response: Again, this question is worded for the metastatic setting as response cannot be determined in a completely resected patient.
We will re-frame this question as “What would be considered a clinical meaningful improvement in outcome?”
The only comparison for adjuvant therapy in NSCLC is adjuvant chemotherapy, which has been accepted and funded in Canada and globally. Based on this standard, novel therapeutic strategies with a disease-free survival benefit of a hazard ratio of 0.84 or lower (Pignon et al) would be considered a clinical meaningful improvement in outcome. IMpower010’s disease-free-survival benefit has a HR of 0.66, a rate that is significantly better.
The gold standard is overall survival. The overall survival data from this trial are not mature but the current HR is 0.77 which is shows that the data is trending toward a benefit in this additional outcome.
How often should treatment response be assessed?
Again, this question is phrased for the advanced/metastatic NSCLC setting. In the adjuvant setting, treatment response cannot be determined.
We will re-frame this question to “How often should follow-up of patients with early stage lung cancer take place when atezolizumab is administered adjuvantly?”
Given that adjuvant atezolizumab is administered over a one-year period, there will need to be periodic follow-up for toxicity of the drug and periodic follow-up for recurrent disease.
Follow-up intervals for assessment of atezolizumab are generally each cycle (every 3 weeks) with laboratory and clinical assessments.
Time intervals between imaging will also vary. Initially, imaging scans at 3-4 month intervals would be common-place, but, imaging as sparse as 6+ months intervals may occur especially in the lower stage patients.
These follow-up and imaging time intervals, in part, reflect the wide range of follow-up practices across Canada and globally, where there has been no consensus. However, resected Stage IB-IIIA NSCLC patients generally are followed-up for at least 5-years post-operatively by at least one oncologist (typically surgical or medical oncologist) in most settings.
What factors should be considered when deciding to discontinue treatment?
Response: Treatment should continue for 16 cycles (1 year) or until side effects dictate that treatment should be discontinued or disease progression is detected. In the IMpower010 study, 65% of patients completed the full course of treatment,18% of participants discontinued drug due to adverse events and 11% discontinued due to disease progression.
What settings are appropriate for treatment with the drug under review?
Response: Atezolizumab can be given in any oncology setting where infusions are performed. Atezolizumab is a well-known drug to oncologists.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Response: Not applicable. This is an oncology drug.
Additional Information
N/A
Conflict of Interest Declarations — Lung Cancer Canada – Clinician Group
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Rosalyn Juergens
Position: Chair, LCC Medical Advisory Committee; Medical Oncologist, Juravinski Cancer Center
Date: December 22, 2021
Table 4: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Bristol Myers Squibb | X | — | — | — |
Astra Zeneca | — | X | — | — |
Merck Sharp and Dohme | X | — | — | — |
Roche | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Geoffrey Liu
Position: Medical Oncologist, Princess Margaret Cancer Centre
Date: Dec 22, 2021
Table 5: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 2
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Takeda Canada | Advisory Board, Health Technology Assessment Submission Advice, Speaker’s Bureau, past 10 years | — | — | X | — |
Takeda Canada | (To institution, not individual) Observational Study funding, past 10 years | — | — | — | X |
Hoffman La Roche | Advisory Board, Health Technology Assessment Submission Advice, past 10 years | — | — | X | — |
Pfizer | Advisory Board, Health Technology Assessment Submission Advice, part 10 years | — | — | X | — |
AstraZeneca | Advisory Board, Health Technology Assessment Submission Advice, Speaker’s Bureau, past 10 years, | — | — | X | — |
AstraZeneca | (To institution, not individual) Observational Study funding, past 10 years | — | — | — | X |
Bristol Myers Squibb | Advisory Board | X | — | — | — |
Boehringer Ingerheim | (To institution, not individual) Observational Study funding, past 10 years | — | — | X | — |
Abbvie | Advisory Board, past 10 years | — | X | — | — |
Merck | Advisory Board, Health Technology Assessment Submission Advice, past 10 years | — | X | — | — |
EMD Serono | Speaker’s Bureau, past 10 years | X | — | — | — |
Novartis | Advisory Board, past 10 years | — | — | X | — |
Glaxo Smith Kline | Advisory Board, past 10 years | — | X | — | — |
Declaration for Clinician 3
Name: Dr Jeffrey Rothenstein
Position: Medical Oncologist, Lakeridge Health
Date: Dec 22, 2021
Table 6: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Roche | X | — | — | — |
Declaration for Clinician 4
Name: Dr Nicole Bouchard
Position: Respirologist, Sherbrooke University Hospital
Date: Dec 22, 2021
Table 7: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 4
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Astra Zeneca | Advisory Role/Conference | X | — | — | — |
Bristol-Myers Squibb | Advisory Role/Research | X | — | — | — |
Merck | Advisory Role /Research/Conference | X | — | — | — |
Bayer | Advisory Role | X | — | — | — |
Pfizer | Conference/Research | X | — | — | — |
Roche | Advisory Role | X | — | — | — |
Declaration for Clinician 5
Name: Dr Normand Blais
Position: Medical Oncologist, Hôpital Notre Dame du CHUM
Date: Dec 22, 2021
Table 8: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | X | — | — | — |
Declaration for Clinician 6
Name: Dr. David Dawe
Position: Medical Oncologist, CancerCare Manitoba
Date: Dec 22, 2021
Table 9: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 6
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Astra Zeneca | Advisory boards | X | — | — | — |
Merck | Advisory Boards | X | — | — | — |
AstraZeneca | Research Grant | — | — | X | — |
Boehringer-Ingelheim | Honoraria | X | — | — | — |
Declaration for Clinician 7
Name: Dr Mahmoud Abdelsalam
Position: Medical Oncologist, The Moncton Hospital
Date: Dec 22, 2021
Table 10: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BMS | — | X | — | — |
Declaration for Clinician 8
Name: Dr Randeep Sangha
Position: Associate Professor, University of Alberta; Medical Oncologist, Cross Cancer Institute
Date: December 22, 2021
Table 11: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 8
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 9
Name: Dr Catherine Labbé
Position: Head of Respiratory Medicine Service, Université de Laval
Date: Dec 22, 2021
Table 12: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 9
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 10
Name: Dr. Parneet Cheema
Position: Medical Director, William Osler Health System
Date: Dec 22, 2021
Table 13: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 10
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Bristol Myers Squibb | Advisory board/Honoraria | X | — | — | — |
Merck | Advisory board/Honoraria | X | — | — | — |
AstraZeneca | Advisory board/Honoraria | X | — | — | — |
Roche | Advisory board/Honoraria | X | — | — | — |
Novartis | Advisory board/Honoraria | X | — | — | — |
Declaration for Clinician 11
Name: Dr. Donna Maziak
Position: Thoracic Surgeon, The Ottawa Hospital
Date: Dec 22, 2021
Table 14: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 11
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 12
Name: Dr Sunil Yadav
Position: Medical Oncologist, Saskatoon Cancer Centre
Date: Dec 22, 2021
Table 15: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 12
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Bristol-Myers Squibb | Advisory Board | X | — | — | — |
Astra Zeneca | Advisory Board and Speaking | X | — | — | — |
Merck | Advisory Board and Speaking | — | — | X | — |
Roche | Advisory Board and Speaking | — | X | — | — |
Takeda | Advisory Board and Speaking | X | — | — | — |
Declaration for Clinician 13
Name: Dr. Quincy Chu
Position: Medical Oncologist, Cross Cancer Institute
Date: Dec 22, 2021
Table 16: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 13
Company | Nature or description of activities or interests | Check Appropriate Dollar Range | |||
|---|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | ||
Abbvie | Advisory Board and Honoraria | X | — | — | — |
Amgen | Advisory Board and Honoraria | X | — | — | — |
Astra Zeneca | Advisory Board and Honoraria | — | — | X | — |
Boehringer Ingeiheim | Advisory Board and Honoraria | — | X | — | — |
Bristol-Myers Squibb | Advisory Board and Honoraria | — | X | — | — |
Eisai | Advisory Board and Honoraria | X | — | — | — |
Merck | Advisory Board and Honoraria | — | — | X | — |
Novartis | Advisory Board and Honoraria | — | X | — | — |
Pfizer | Advisory Board and Honoraria | — | X | — | — |
Roche | Advisory Board and Honoraria | — | X | — | — |
Astra Zeneca | Research Funding | — | — | — | X |
Bristol-Myers Squibb | Educational Grant | X | — | — | — |
Declaration for Clinician 14
Name: Dr. Ronald Burkes
Position: Medical oncologist, Mount Sinai Health
Date: Dec 22, 2021
Table 17: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 14
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 15
Name: Dr. Zhaolin Xu
Position: Pathologist, QEII Health Sciences Centre
Date: Sept 12, 2020
Table 18: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 15
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AstraZeneca | X | — | — | — |
Declaration for Clinician 16
Name: Dr. Shaqil Kassam
Position: Medical Oncologist, Southlake Regional Hospital
Date: December 22, 2021
Table 19: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 16
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 17
Name: Dr. Silvana Spadafora
Position: Medical Oncologist, Sault Area Hospital
Date: Dec 22, 2021
Table 20: Conflict of Interest Declaration for Lung Cancer Canada Clinician Group Clinician 17
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
The comments contained in this input were collected via emails.
Current treatments
Describe the current treatment paradigm for the disease
Response: The current treatment paradigm for the disease would be curative therapy for NSCLC and adjuvant platinum-based chemotherapy.
Treatment Goals
What are the most important goals that an ideal treatment would address?
Response: The most important goals that an ideal treatment would address are improve cure rates, improve overall survival, and improve quality of life.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Response: There is a need for an effective therapy to further increase cure and overall survival. Despite optimal surgical and adjuvant treatment, over 50% of stage 3 and over 30% of stage 2 will die of disease progression.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Response: Patients with resected NSCLC without EGFR mutations who did not receive neoadjuvant immunotherapy and have 8th edition stage 2 or stage 3 disease resected
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Response: The drug under review would fit after curative local therapy for NSCLC and at least one dose of adjuvant chemotherapy. This treatment would supplement current treatments.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Response: It would be appropriate to recommend that patients try curative local therapy and at least one dose of adjuvant chemotherapy before initiating treatment with the drug under review.
How would this drug affect the sequencing of therapies for the target condition?
Response: This treatment would supplement current treatments. The adoption of atezolizumab would be an additional treatment and not replace current treatment regimens.
Which patients would be best suited for treatment with the drug under review?
Response: Patients with higher PDL1 scores (over 50) will be better suited for atezolizumab, but all PDL1 positive are suited.
How would patients best suited for treatment with the drug under review be identified?
Response: The criteria from the trial are reasonable and aligns with the need in clinical practice.
Which patients would be least suitable for treatment with the drug under review?
Response: N/A
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review? If so, how would these patients be identified?
Response: No, it is not possible to identify those patients who are most likely to exhibit a response to treatment. A CT scan can be done to know if the treatment is not working.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response: The outcomes are aligned with the outcomes used in the clinical trial.
What would be considered a clinically meaningful response to treatment?
Response: Disease-free survival benefit.
How often should treatment response be assessed?
Response: Align with clinical trial.
What factors should be considered when deciding to discontinue treatment?
Response: Disease progression and toxicity.
What settings are appropriate for treatment with the drug under review?
Response: Hospital (outpatient clinic)
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review? If so, which specialties would be relevant?
Response: N/A
Additional information
Is there any additional information you feel is pertinent to this review?
Response: Currently, we do not know if the endpoints reported correlate with overall survival, but it can be reasonably expected to. In addition, other strategies such as short course neoadjuvant immunotherapy with chemotherapy using only 3 doses of immunotherapy are expected to be much cheaper than a full year.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee (DAC)
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the Lung DAC in completing this input submission.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Gail Darling
Position: Ontario Cancer Lead; Thoracic Surgeon
Date: 23 December 2021
Table 21: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Andrew Robinson
Position: OH-CCO Thoracic and Lung Drug Advisory Committee Member
Date: 22/12/2021
Table 22: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AstraZeneca – coinvestigator on other AZ trials but no direct financial payment disclosed | — | — | — | — |
Declaration for Clinician 3
Name: Dr Mohammad Rassouli
Position: OH-CCO Thoracic and Lung Drug Advisory Committee Member
Date: 22/12/2021
Table 23: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.