CADTH Reimbursement Review
Selpercatinib (Retevmo)
Sponsor: Eli Lilly Canada Inc.
Therapeutic area: Thyroid cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine aminotransferase
AST
aspartate aminotransferase
AUC
area under the concentration-time curve
BICR
blinded independent committee review
BSC
best supportive care
CCS
Canadian Cancer Society
CEA
carcinoembryonic antigen
CI
confidence interval
CNS
central nervous system
CR
complete response
DLT
dose-limiting toxicity
DOR
duration of response
DTC
differentiated thyroid cancer
ECG
electrocardiogram
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC
European Organisation for Research and Treatment of Cancer
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
HR
hazard ratio
HRQoL
health-related quality of life
IAS
integrated analysis set
IRC
independent review committee
ITC
indirect treatment comparison
LOXO-292
investigational product (selpercatinib)
MAIC
matching-adjusted indirect comparison
MID
minimally important difference
MKI
multikinase inhibitor
MTC
medullary thyroid cancer
mSTIDAT
modified Systemic Therapy Induced Diarrhea Assessment Tool
MTD
maximum tolerated dose
NSCLC
non–small cell lung cancer
OH-CCO
Ontario Health (Cancer Care Ontario)
ORR
objective response rate
OS
overall survival
PAS
primary analysis set
PD
progressive disease
PFS
progression-free survival
PK
pharmacokinetic(s)
POGO
Pediatric Oncology Group of Ontario
PR
partial response
PTC
papillary thyroid cancer
QTc
corrected QT
RANO
Response Assessment in Neuro-Oncology Criteria
RECIST 1.1
Response Evaluation Criteria in Solid Tumors version 1.1
RET
rearranged during transfection proto-oncogene
RP2D
recommended phase II dose
SAE
serious adverse event
SAS
supplemental analysis set
SD
standard deviation
SRC
safety review committee
STIDAT
Systemic Therapy Induced Diarrhea Assessment Tool
TEAE
treatment-emergent adverse event
TKI
tyrosine kinase inhibitor
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Selpercatinib (Retevmo), 40 mg and 80 mg capsules, oral |
Indication | For the treatment of RET-mutant medullary thyroid cancer in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease |
Reimbursement request | As per indication |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC date | June 15, 2021 |
Sponsor | Eli Lilly Canada Inc. |
NOC = Notice of Compliance; NOC/c = Notice of Compliance with Conditions; RET = rearranged during transfection.
Introduction
Thyroid cancer is 1 of the most commonly diagnosed cancers in Canada and the world. It is considered the most common endocrine malignancy and the fifth most common cancer in women.1,2 In 2020, the incidence of thyroid cancer in Canada was estimated to be 23 per 100,000 or about 8,600 new cases.3 Women are 3 times more at risk of having thyroid cancer than men.
Medullary thyroid cancer (MTC) is a less common type (1% to 2%) of thyroid cancer that originates from the parafollicular neuroendocrine cells of the thyroid (c cells) and is usually detected as a solitary thyroid nodule in patients in the fourth or sixth decade of life. Metastases to cervical lymph nodes is a common initial presentation; distant metastases can also occur. A common initial presentation is diarrhea, redness of the trunk and face skin (flushing), and an accompanying thyroid nodule. Of all MTC cases, approximately 75% are sporadic and 25% are hereditary. Of the sporadic cases, 50% will present somatic mutations in the rearranged during transfection (RET) proto-oncogene.4 Of the hereditary cases, almost all (98%) will present a germline RET mutation (inherited as autosomal dominant).5 Hereditary cases occur mostly in patients who have an inherited multiple endocrine neoplasia syndrome.5,6 RET genetic analysis is recommended when the diagnosis of MTC has been established because it allows defining the sporadic or hereditary nature of MTC and thus can guide future diagnostic and therapeutic options and strategies. The prognosis of MTC is unfavourable, with a 10-year survival rate of approximately 50%4 and a 5-year survival rate varying from 62% to 87%, according to different epidemiological studies series.7-10
Early diagnosis and total thyroidectomy with resection of local and regional metastases is the basis for initial treatment, plus subsequent hormone replacement with L-thyroxine.4,6 The treatment goals in patients with MTC are aimed at improving survival, delaying disease progression, and improving health-related quality of life (HRQoL).11 For patients with unresectable advanced or metastatic RET-mutant MTC — a condition with a very low cure rate — several targeted therapies have been used as first-line treatments,4,11,12 such as cabozantinib13 and vandetanib,14 which have both shown improvement in progression-free survival (PFS).13,14 Only vandetanib is approved and funded in Canada. After first-line treatments, patients can only continue using best supportive care (BSC) and, optionally, enter clinical trials.11
Selpercatinib (Retevmo or LOXO-292), 40 mg and 80 mg oral, is a new, highly selective inhibitor of the RET receptor that is indicated as monotherapy for the treatment of RET-mutant MTC in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease. Other indications include RET fusion–positive differentiated thyroid cancer (DTC) in adult patients with advanced or metastatic disease (not amenable to surgery or radioactive iodine therapy) following prior treatment with sorafenib and/or lenvatinib, and metastatic RET fusion–positive non–small cell lung cancer (NSCLC).15 The product monograph recommends confirming the presence of a RET gene mutation before starting treatment. The recommended dosage of selpercatinib is based on body weight as (< 50 kg) 120 mg twice daily or (≥ 50 kg) 160 mg twice daily. Selpercatinib received a Notice of Compliance with Conditions on June 15, 2021. It is the first Health Canada–approved therapy for patients with advanced RET-driven lung and thyroid cancers and it has not been previously reviewed by CADTH for MTC. Warnings in the product monograph include corrected QT (QTc) interval prolongation on electrocardiogram (ECG), hypertension, hypersensitivity, hepatotoxicity, hemorrhage, and embryo-fetal toxicity. These situations warrant caution and it is recommended that dosages be adjusted for these adverse events (AEs).15
The objective of this report is to perform a systematic review of the beneficial and harmful effects of selpercatinib (Retevmo) 40 mg and 80 mg capsules for the treatment of RET-mutant MTC in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and the from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Input was obtained from 2 patient groups: the CanCertainty Coalition and Canadian Cancer Society (CCS) together with Thyroid Cancer Canada. Raw patient input is presented in Appendix 1.
The CanCertainty Coalition, which is composed of more than 30 Canadian patient groups, caregiver organizations, and charities as well as oncologists and cancer care professionals, strives to improve the accessibility of cancer treatment. The group used the thyroid cancer incidence from Statistics Canada to estimate the number of RET-mutated thyroid cancer cases (both medullary and papillary) each year by age and province (i.e., the estimated number of Canadian residents who will become eligible for selpercatinib each year) and provided input on estimates of financial hardships for cancer patients from their database of surveys of 1,600 Nova Scotians. The group states that a cancer diagnosis could lead to financial hardships, especially when patients do not have private health insurance. Even though multiple programs support individuals who have high drug costs, there are administrative barriers in many provinces and territories. Patients often face weeks of delay in starting cancer treatments.
The CCS does research and provides advocacy and support to patients living with cancer. CCS’s patient panels and networks provided survey results from patients with thyroid cancer. In addition, Thyroid Cancer Canada’s patient networks submitted survey results and 2 testimonials from staff or board members who have had thyroid cancer. A total of 17 survey responses were collected across Canada between October 22 and November 10, 2021. None of the respondents had any direct or indirect experience with selpercatinib. Patients living with MTC referred to issues that impacted daily work and life, such as fatigue; brain fog; issues with mental health, body image, and cognitive ability; concerns about cancer returning; and concerns about the regulation of thyroid medications. Overall, 71% reported a financial barrier related to treatments, especially loss of income due to absence from work, parking costs, drug costs, and blood tests. Patients responded that they would like to see new treatments with improvements regarding cost, access, and support to improve their quality of life.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH agreed there is an unmet need for drugs that are better tolerated and with better safety profiles that can be used in patients with RET-mutant, advanced or metastatic MTC who, after surgery, have very few options. Treatment goals are improving overall survival (OS), PFS, and HRQoL by controlling symptoms such as diarrhea, flushing, minimizing adverse effects of treatments, and increasing work–life productivity. The experts indicated that selpercatinib would be an appropriate therapy for RET-driven thyroid malignancies, including using it as first-line therapy. At this stage, there is only 1 approved and/or funded therapy (vandetanib) in Canada, and the experts expect that selpercatinib will cause a shift in the current treatment paradigm.
The clinical experts consider that patients with RET-driven MTC whose disease cannot be managed or cured by locoregional (surgical) interventions and who are experiencing or are expected to experience symptomatic disease progression within the near future are the most likely to benefit from the use of selpercatinib. The experts did not find specific baseline characteristics or variables of prognostic value and indicated that patients’ responses will not differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease). They suggested that patients with progressive metastatic MTC need to be screened for RET mutations and rearrangements using locally available comprehensive molecular tests, which should be available in institutions treating patients with progressive metastatic MTC.
Patients should be assessed to measure evidence of response or stabilization of the disease, based on clinical grounds and radiological examination such as Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1) criteria, number and severity of symptoms, PFS, serum calcitonin, and carcinoembryonic antigen (CEA). All of these measurements are mostly aligned with clinical trial end points. Improvement in survival, PFS, and reduction in frequency and severity of symptoms (e.g., diarrhea) will be used to measure an adequate response, approximately every 3 to 6 months. Deterioration of symptoms, functional status, radiological evidence of disease progression (together with other clinical criteria), and unacceptable toxicity from treatment are among the issues that could be used to decide on a case-by-case basis whether to discontinue treatment.
Targeted therapies can have significant toxicity and related harms; the experts concluded that patients should only receive selpercatinib in a specialty outpatient clinic setting from clinicians with experience in the treatment of thyroid cancer.
Clinician Group Input
This section was prepared by CADTH based on the input provided by clinician groups.
Two clinician group summaries were received: 1 from the Pediatric Oncology Group of Ontario (POGO) and the other from the Ontario Health (Cancer Care Ontario) (OH-CCO) Head and Neck and Thyroid Cancer Drug Advisory Committee (DAC), gathering input from a total of 5 clinicians.
Overall, the clinician groups agreed with the input provided by the clinical experts consulted by CADTH.
These groups explained that for RET-mutant MTC, the only currently approved and funded option is vandetanib, which requires special training and monitoring (e.g., for QTc prolongation). Hence, an important goal of an ideal treatment would be reducing treatment-related toxicities. Once patients have progressed on currently available therapies, there is no other option.
In the treatment-naive adult setting, OH-CCO noted that some clinicians may want to use selpercatinib in the first-line setting. Although selpercatinib appears more active and less toxic, a phase III trial (LIBRETTO-531 comparing selpercatinib with a physician’s choice of cabozantinib or vandetanib) in the first-line setting is still ongoing.16 Given the broader receptor profile of vandetanib, OH-CCO also expressed that clinicians would also like to be able to use vandetanib in patients progressing on (or intolerant of) selpercatinib. OH-CCO highlighted that some clinicians may reserve selpercatinib for patients with RET-mutant MTC who are intolerant or unsuitable for vandetanib. In the previously treated population, OH-CCO expressed that selpercatinib offers a treatment option to those who have exhausted currently available treatments
In the pediatric setting, POGO highlighted that for children with MTC, the best chance of cure is comprehensive initial surgery, and that POGO continues to advocate comprehensive initial surgery as first-line therapy. For the rare child with residual disease, however, existing therapies (cabozantinib and vandetanib) are associated with inferior response rates and higher toxicities; thus, POGO would recommend selpercatinib as the initial second-line therapy. POGO also highlighted that a rare subset of pediatric patients with unresectable tumours may be considered for first-line therapy with selpercatinib in a neoadjuvant context to facilitate eventual surgical control.
The groups state that to identify eligible patients, RET testing is available in Ontario as part of reflex testing on all metastatic thyroid cancer. Patients whose disease does not have a RET mutation or those with a performance status that would not allow selpercatinib treatment would be the least suitable population.
Response to selpercatinib would be measured primarily by response rates while addressing other key outcomes such as PFS and toxicity. Clinically meaningful response to treatment can be determined by a reduction in tumour burden based on clinical assessment and/or imaging, cancer-related symptoms, and tumour marker levels. Treatment with selpercatinib should be reassessed every 8 to 12 weeks for the first 6 months to 1 year, then every 12 to 16 weeks thereafter, especially in patients who had initial responses, feel well, and have reduced CEA and/or calcitonin levels. However, specific intervals should not be mandated. In cases of a lack of response and/or the emergence of treatment-related toxicities, selpercatinib should be discontinued. As an oral, take-home cancer drug, selpercatinib is suitable for the community setting.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
One clinical study, LIBRETTO-001, is included in this report. This is an ongoing, multi-centre, open-label, phase I and II, single-arm study of oral selpercatinib (LOXO-292) in patients with advanced solid tumours, including RET fusion–positive solid tumours, MTC, and other tumours with RET activation. This CADTH report focuses on the population with MTC. The sponsor used different cut-off dates: first, a June 17, 2019 cut-off date was used for the initial submissions to the FDA and European Medicines Agency. Then, a December 16, 2019 data cut-off served as the basis of the summary of clinical efficacy in LIBRETTO-001, which was used in the submissions to the FDA, Health Canada, and the European Medicines Agency. The pre-planned analysis at the December 16, 2019 data cut-off was conducted to support the submission of the day 60 efficacy and safety update for the FDA, which provided at least 6 months of follow-up information for all patients enrolled as of the initial data cut-off of June 17, 2019. Furthermore, data for a cut-off of March 30, 2020, submitted by the sponsor, is described in this report. The main analyses of efficacy are presented in this report, with a data December 16, 2019 cut-off date, where the pre-planned primary analysis set (PAS) is described
There are 2 main phases in the LIBRETTO-001 study. The dose-escalation phase (phase I) and the dose-expansion phase (phase II). For both phases, patients were to be enrolled into 1 of 5 phase II cohorts to characterize the safety and efficacy of selpercatinib in specific RET abnormalities. Cohort 1 includes patients with a RET fusion–positive solid tumour who have progressed on or were intolerant to 1 or more prior standard first-line therapies. Cohort 2 includes patients with a RET fusion–positive solid tumour who have not had any prior standard first-line therapy. Cohort 3 includes patients with RET-mutant MTC who progressed on or were intolerant to 1 prior standard first-line therapy (cabozantinib and/or vandetanib). Cohort 4 includes patients with RET-mutant MTC who have not received a prior standard first-line therapy (cabozantinib or vandetanib or another kinase inhibitors) with anti-RET activity, and cohort 5 includes patients from cohorts 1 through 4:
without measurable disease
with MTC not meeting the requirements for cohorts 3 or 4
with MTC syndrome-spectrum cancers (e.g., MTC, pheochromocytoma)
with DTCs that are poorly differentiated and have other RET alterations or activations
with circulating cell-free DNA that is positive for a RET gene alteration not known to be present in a tumour sample.
This CADTH review focuses on the MTC population that was included in cohorts 3 and 4.
For phase I, the primary objective of the study was to determine the maximum tolerated dose (MTD) (recommended phase II dose [RP2D]) of selpercatinib. The secondary objectives for phase I included determining the safety and tolerability of selpercatinib, characterization of the pharmacokinetic (PK) properties, and assessment of the antitumour activity of selpercatinib. For phase II, the primary objective was to assess, for each expansion cohort, the antitumour activity of selpercatinib by determining the objective response rate (ORR) using RECIST 1.1 or Response Assessment in Neuro-Oncology (RANO), as appropriate to tumour type. Secondary objectives for phase II included other efficacy parameters including best change in tumour size from baseline, duration of response (DOR), central nervous system (CNS) ORR, CNS DOR, time to any and best response, clinical benefit rate, PFS, OS, and determination of the safety and tolerability of selpercatinib, and characterization of the PK properties. The exploratory objectives were PK and the collection of patient-reported outcomes data to explore disease-related symptoms and HRQoL. After MTD was defined, a dose-expansion assessment was conducted to obtain the recommended RP2D of 160 mg twice a day, selected by the safety review committee (SRC).
ORR was calculated based on the maximum likelihood estimator (i.e., crude proportion of patients with a best overall response of complete response [CR] or partial response [PR]) with 95% confidence intervals (CIs). DOR was defined, using Kaplan-Meier estimates for the median, as the number of months from the start date of the CR or PR for: right-censored patients with subsequent anti-cancer therapy or cancer-related surgery in the absence of documented disease progression, patients who died or experienced documented disease progression after missing 2 or more consecutively scheduled disease assessment visits, and patients alive and without documented disease progression on or before the data cut-off date. OS and PFS were assessed with methods similar to those used for DOR. All efficacy results presented were evaluated by an independent review committee (IRC).
For the December 16, 2019 data cut-off (n = 226), the mean age of patients with RET-mutant MTC was | | ||||| |||| |||| | |||||||| ||||| |||| |||| || ||||| || |||| ||| ||| |||||| ||||||| || ||| || ||||| || |||| || ||||| || ||||| || |||||||||||| || |||| ||||| |||| || ||| |||| ||| |||||| |||| |||||||| |||| |||| || |||||| || | || || |||| |||| || |||||| |||||||||| || |||| || || |||| || ||||||| || || |||||| ||||| |||||||||| ||| ||| ||| |||||||| ||| ||||||| || |||||||||| |||||||| |||| |||||||| ||||||||| |||||||| || |||||||| |||||||.
Efficacy Results
In the population of patients from LIBRETTO-001 with RET-mutant MTC (cut-off date December 16, 2019), for OS, with | |||||| |||||||| || |||||| || || |||| |||||| |||||||||||||| ||||| ||||| |||| || ||||| ||| |||||| ||| |||||||| ||| ||| ||||||| |||||||| ||| |||| | ||||| || |||||||| |||||||||| ||||||| |||| |||||||||||| || ||||||||||| |||||||||| ||| ||| ||||||| |||||| |||||| ||| |||||| || ||||| |||| |||| ||| || ||| |||||||||| ||| ||||| |||||||||| || |||||||| ||| ||| ||||| |||| |||| ||| || |||| |||||||. The rate of survival at 12 months or more was ||||| || ||| |||||||||| |||| || |||| || |||||. For the March 30, 2020 cut-off date, the group of patients in the PAS (n = 55) reached a median OS of 33.2 months (range 1.1+ to 33.3+) (+ indicates censored observation); values were similar in the integrated analysis set (IAS) group. The supplemental analysis set (SAS) did not reach the median of survival (Table 2).
For PFS (cut-off date December 16, 2019) with a median duration of follow-up of 16.7 months (||| |||| || ||||), the median for PFS for the PAS population was not reached and the range went from | || |||| ||||||. The rate of PFS at 12 months or more was ||||| of the population. For the March 30, 2020 cut-off date, no patients among the groups evaluated (PAS, IAS, SAS) reached a median for PFS (range 0.0+ to 32.2+).
The percentage of patients reaching an ORR (December 16, 2019 cut-off date) was 69.1% (95% CI, 55.2 to 80.9); overall, it was similar across the different sets. For the March 30, 2020, cut-off date, the results for the ORR were similar (69.1% for the PAS and similar across other sets).
With a median follow-up of 14.06 months ( | | | | | ||), the median DOR (December 16, 2019 cut-off date) was not reached in any analysis set except for SAS 1 (DOR of 21.9 months, ||||| ||| || ||). For the March 30, 2020 cut-off date, the results were similar, except for SAS 1, where the DOR reached a median of 21.9 months (range, 1.5 to 24.1), but with a median follow-up of 9.2 months. The percentage of patients who reached a DOR (December 16, 2019 cut-off date) of more than 12 months was 55.2% in the PAS. For the March 30, 2020 cut-off date, the percentage of patients reaching a DOR of more than 12 months was 68.4% in the PAS.
Published HRQoL data that included patients from the December 16, 2019 cut-off date was obtained from 1 sponsor publication.17 Of the 226 patients included, 88 (41.5%) were treatment-naive and 124 (58.5%) had previously received multikinase inhibitors (MKIs) at study entry. Of all patients evaluated, 18.7% (36 out of 193) met the criteria for a definite improvement and 13.0% (25 out of 193) met the criteria for a definite worsening in physical function in the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30). Among the patients in the treatment-naive and previously treated subgroups, respectively, 10.5% and 22.5% met the criteria for definite improvement and 14.5% and 11.3% met the criteria for a definite worsening in physical function in the EORTC QLQ-C30. Most patients improved or remained stable on the global health status/QoL (quality of life) subscale at each cycle (cycles of 28 days) during study treatment with selpercatinib. Of all patients, 29.0% (56 out of 193) met the criteria for a definite improvement in global health status and 13.0% (25 out of 193) met the criteria for a definite worsening in global health status. Among the treatment-naive and previous treatment subgroups, respectively, 26.3% and 31.3% met the criteria for definite improvement and 17.1% and 12.5% met the criteria for a definite worsening in the global health status/QoL subscale. Most patients’ diarrhea improved or remained stable at each cycle during study treatment with selpercatinib. Of all patients, 43.5% (84 out of 193) met the criteria for definite improvement in diarrhea and 9.8% (19 out of 193) met the criteria for a definite worsening in diarrhea.
Harms Results
AEs were reported in all but 2 patients taking selpercatinib. Among the 299 patients with RET-mutant MTC included in the safety population, ||| ||||||| ||||||||| || ||||| ||| ||| |||| ||||| ||| || |||| ||||| ||| ||| | ||| ||||||||||||| | ||||| || || |||||||| |||||| ||| ||| ||| |||||||||||| ||| ||||. The most commonly reported AEs (> 20% of patients with at least 1 of these) included hypertension, diarrhea, constipation, fatigue, headache, peripheral edema, nausea, and abdominal pain.
Serious AEs occurred in || ||||||| || ||| ||| |||||||| || ||| |||||| ||||||||||| |||| || |||||| ||||||||||| || ||||| ||||||| || |||||||||||||| ||||| |||||| | |||| |||||||| ||| | ||||| ||. The most common serious adverse events (SAEs) were |||||||||| ||||||||||||| ||| ||||||||||||| ||||| |||| ||||||| || ||||| ||||| ||| || || |||||||| ||||||||||||.
Among the 299 patients in the safety population with RET-mutant MTC, | |||||| |||||| |||||||| |||||| || |||| || |||| |||| || ||||||||||||| || ||| || ||||||| |||||||||||| | ||| || ||||||| |||||||| ||| || |||||| |||||||| |||| |||| || |||| ||||| ||| |||| ||||| || ||||| || |||||| ||| || ||||||| |||||||||||| | ||| || ||||||| ||||||| | ||| || ||||| |||||| |||||||||.
For harms of special interest, elevations of liver enzymes occurred frequently, with || ||||||| ||| || ||||||| |||||||| alanine aminotransferase (ALT) and aspartate aminotransferase (AST) elevations, respectively, although most were of low grade (Table 13). Hypertension was reported (reported as an AE by preferred term) in ||| ||||||| of patients. Diarrhea was present in || ||||||| of patients at any point, and hypersensitivity was rare (3 patients). A common concern among clinicians was QTc prolongation, which was reported in ||| ||||||| of patients with values that had increased by more than 30 msec from baseline, and || |||||||| ||||||| with values that had increased more than 60 msec.
For the March 30, 2020 cut-off date, the harm events were similar to the ones presented in the cut-off of December 16, 2019 with a total of 313 patients (99.4%) experiencing AEs and 97 patients (30.8%) experiencing at least 1 SAE. At this cut-off, 28 out of 315 deaths (8.9%) occurred within 28 days of the last dose of selpercatinib (18 due to disease progression, 8 due to AEs, and 2 due to other), and no death occurred more than 28 days after the last dose. The most common AEs (> 5%) included dry mouth ||||||, diarrhea ||||||, hypertension (|||), fatigue (|||), constipation (|||), increased AST (|||), increased ALT (|||), peripheral edema (|||), nausea (|||), increased blood creatinine level (|||), abdominal pain (|||), QT interval prolonged on ECG ( | |), arthralgia ( | |), cough ( | |), and rash ( | ||||). The safety data were analyzed by grade and SAEs.
Table 2: Summary of Key Results From LIBRETTO-001, December 16, 2019 and March 30, 2020 Cut-Off Dates
Variable | Cut-off date December 16, 2019 | Cut-off date March 30, 2020 | ||||||
|---|---|---|---|---|---|---|---|---|
PAS N = 55 | IAS N = 124 | SAS 1 N = 88 | SAS 2 N = 14 | PAS N = 55 | IAS N = 143 | SAS 1 N = 112 | SAS 2 N = 19 | |
Overall survivala | ||||||||
Median duration of overall survival, months (range)a | |||||||| |||||| | || |||||| |||||| | || |||||| |||||| | |||||| | 33.25 (1.1 to 33.3+) | 33.25 (0.4 to 33.3+) | NE (2.2+ to 29.8+) | NE (6.8+ to 19.9+) |
Median duration of follow-up, months (IQR) | |||||||||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | |||||| | 22.08 (19.9 to 28.3) | 15.70 (11.3 to 21.1) | 13.83 (9.6 to 18.4) | 14.19 (9.4 to 17.4) |
Rate of overall survival of 12 months or more, % (95% CI)b | 86.9 |||||| ||||| | |||| |||||| |||||| | ||||||||||| |||||| | |||||| | 86.9 (74.4 to 93.5) | 86.9 (79.7 to 91.6) | 100 (100.0 to 100.0) | 100 (100.0 to 100.0) |
Progression-free survival | ||||||||
Median duration of progression-free survival, months (range)a | NE |||| |||||| | ||||||||| |||||| | 23.56 |||||| |||||| | ||||||||| |||||| | NE (0.0+ to 32.2+) | NE (0.0+ to 32.2+) | NE (0.0+ to 25.8+) | NE (5.0+ to 19.1+) |
Median duration of follow-up, months (IQR) | 16.69 |||||| ||||| | |||||||||| |||| | 11.07 |||| |||| | |||||||||| |||| | 20.27 (19.1 to 27.6) | 13.90 (9.3 to 19.3) | 11.10 7.6 to 16.6 | 11.73 7.4 to 14.1 |
Duration of progression-free survival, n (%) | ||||||||
< 6 months | | |||||| | || |||||| | || |||||| | | ||||| | NR | NR | NR | NR |
≥ 6 to 12 months | | |||||| | || |||||| | || |||||| | | |||||| | NR | NR | NR | NR |
≥ 12 to 18 months | || |||||| | || |||||| | || |||||| | | |||||| | NR | NR | NR | NR |
≥ 18 to 24 months | | |||||| | | ||||| | | ||||| | | ||||| | NR | NR | NR | NR |
≥ 24 months | || |||||| | || ||||| | | ||||| | | ||||| | NR | NR | NR | NR |
Rate of progression-free survival, % (95% CI)b | ||||||||
≥ 6 months | NR | NR | NR | NR | 92.4 (81.0 to 97.1) | 89.5 (82.9 to 93.7) | 98.2 (92.9 to 99.5) | 94.1 (65.0 to 99.1) |
≥ 12 months | NR | NR | NR | NR | 82.3 (68.7 to 90.4) | 76.9 (67.9 to 83.7) | 92.9 (84.5 to 96.8) | 94.1 (65.0 to 99.1) |
≥ 18 months | NR | NR | NR | NR | 73.8 (59.1 to 83.9) | 67.9 (57.0 to 76.6) | 88.7 (78.0 to 94.4) | 94.1 (65.0 to 99.1) |
≥ 24 months | NR | NR | NR | NR | 66.8 (50.1 to 79.0) | 61.4 (48.0 to 72.4) | 59.2 (8.8 to 89.3) | NE (NE to NE) |
Objective response rate (CR plus PR)a,b | ||||||||
Patients, N (%) | 38 (69.1) | || |||||| | 64 (72.7) | | |||||| | 38 (69.1) | 99 (69.2) | 80 (71.4) | 5 (26.3) |
95% CIb | 55.2 to 80.9 | ||||| |||| | 62.2 to 81.7 | |||| |||| | 55.2 to 80.9 | 61.0 to 76.7 | 62.1 to 79.6 | 9.1 to 51.2 |
Duration of response | ||||||||
Median duration of response, months (range) | NE |||||| |||||| | NE |||||| |||||| | 21.95 |||||| ||||| | ||||||||| ||||| | NE (2.8+ to 26.7+) | NE (1.7+ to 26.7+) | 21.95 (1.5+ to 24.1) | NE (3.5+ to 10.3+) |
Median follow-up, months (IQR) | 14.06 |||||| ||||| | 8.31 ||||| ||||| | 7.79 ||||| ||||| | |||||||||| |||| | 17.45 (12.9 to 22.0) | 10.05 (5.9 to 15.9) | 9.26 (5.6 to 14.7) | 9.23 (3.7 to 9.3) |
Duration of response, n (%) < 6 months ≥ 6 to 12 months ≥ 12 to 18 months ≥ 18 to 24 months ≥ 24 months | ||||||||||| ||||||||| |||||||| |||||||| ||||| | ||||||||||||| ||||||||| |||||||| ||||||| ||||| | |||| |||||| ||| |||||| ||| |||||| || ||||||| ||||| | ||| |||||||| |||||||| ||||||| ||||| || ||||| | 6 (15.8) 6 (15.8) 14 (36.8) 8 (21.1) 4 (10.5) | 32 (32.3) 31 (31.3) 24 (24.2) 8 (8.1) 4 (4.0) | 30 (35.7) 25 (31.3) 17 (21.3) 7 (8.8) 1 (1.3) | 2 (40.0) 3 (60.0) 0 0 0 |
CI = confidence interval; CR = complete response; FAS = full analysis set; IAS = integrated analysis set; IQR = interquartile range; ITT = intention to treat; LS = least squares; NE = not estimable; NR = not reported; PAS = primary analysis set; + = censored observation; PR = partial response; SD = standard deviation; SAS = supplemental analysis set.
Note: Patients enrolled by March 30, 2020, with 6 months of potential follow-up.
All end points were based on independent review committee assessments.
aObjective response rate (%) is defined as the proportion of patients with a best overall response of confirmed CR or PR. Response was confirmed by a repeat assessment no less than 28 days later.
b95% CI was calculated using Clopper-Pearson method.
Source: LIBRETTO-001 Clinical Study Report.18
RET-mutant MTC, December 16, 2019 cut-off date | N = 299 |
|---|---|
Adverse events, N (%) | |
|||||||| |||| | | ||| | ||| |||||| |
||||| ||| | ||| |||||| |
||||| | | | ||||| |
||||||| ||||||| ||||||| | ||| | |
|||||||| |||| | | ||||||| ||| | || |||||| |
|||| |||||| ||||||| ||| |||||||||||||||||||||||| | || ||||||| ||||| |
||||||| ||| ||| ||||||| || ||||||||||||| | || ||||| |
|||||||| |||| ||||| ||| | | ||||| |
||||||| |||||| | | ||||| |
||||| |||||||||| | | ||||| |
||||||| ||||||| | | ||||| |
||||||| |||||||| |||||| ||||||||||||| | | ||||| |
|||||||||| | | ||||| |
|||| |||||||||| |||||||||| | | ||||| |
|||||||| |||| ||| ||| ||||||||||| |||||||||||| ||||| |||| | || ||||| |
|||| |||||| |||| | ||| | | |
|||||||||||| | ||| |||||| |
||| ||||| | ||| |||||| |
|||||||| | || |||||| |
|||||||||||| | || |||||| |
||||||| | || |||||| |
|||||||| | || |||||| |
|||||| |||||||||| | || |||||| |
|||||| | || |||||| |
||||||||| |||| | || |||||| |
||||||| |||||| || ||||||| ||||||||| | ||| | |
||| |||||||||| ||| ||||| | || |||||| |
||| ||||||||| ||| ||||| | || |||||| |
|||||||||||| | ||| |||||| |
|||| | ||||||| ||||||||||||| |||||| ||||||||| | || |||| |||| |||||||| | ||| |||||| |
|||| | ||||||| ||||||||||||| |||||| ||||||||| | || |||| |||| |||||||| | || |||||| |
|||||||| | || |||||| |
|||||||||||||||| | | ||||| |
||||||||||||| ||||||| |||| | || ||| |
AEs, N (%) | |
Patients with ≥ 1 AEs | 313 (99.4) |
Grade 3 or 4 | 188 (59.7) |
||||| | | | ||||| |
Serious AEs, N (%) | |
Patients with ≥ 1 serious AEs | 97 (30.8) |
Serious AEs and related to selpercatinib | 20 (6.3) |
Patients with fatal AEs | 8 (2.5) |
Patients with fatal AEs and related to selpercatinib | 0 (0) |
Patients with AEs and permanently discontinued study drug | 15 (4.8) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; MTC = medullary thyroid cancer; QTcF = QT interval corrected for heart rate using Fridericia formula.
Note: Cut-off date of December 16, 2019 = safety analysis set.
aFrequency > 2%.
bFrequency > 5%.
Source: LIBRETTO-001 Clinical Study Report.18
Critical Appraisal
The LIBRETTO-001 study is a single-arm, open-label, phase I and phase II study. As such, the study is descriptive in nature, as it does not formally evaluate the primary or secondary end points (e.g., ORR, DOR, OS, or PFS) with adjustment for multiple comparisons. These limitations stem from its single-arm design and lack of comparator groups and constrain the estimation of the relative effects of treatment with selpercatinib. The open-label design may also increase uncertainty in patient-reported outcomes (HRQoL), introducing bias due to the inherent subjectivity of the outcome in an unblinded assessor. This bias would be less likely in more objective outcomes such as ORR, OS, and PFS if evaluated against a properly a priori set hypothesis. Furthermore, HRQoL outcomes were evaluated as exploratory end points with no adjustments for multiplicity.
As of the December 16, 2019 cut-off date, ||||| of patients discontinued the study drug and ||||| discontinued from the study within the efficacy population, mostly due to disease progression and death, respectively. At the March 30, 2020 cut-off date, the discontinuation rates remained consistent (17.1% of patients discontinued treatment and 12.7% discontinued from the study, with 7.9% and 4.4% of patients discontinuing treatment due to progressive disease [PD] and AEs, respectively). The sponsor evaluates all 226 patients in the efficacy population and 299 patients in the safety population for primary and secondary end points.
There were fewer concerns about the generalizability of the population included and about the effects on survival and response. According to the clinical experts consulted by CADTH, except for the proportion of females, the baseline characteristics of the population included in the LIBRETTO-001 study were, overall, representative of the population of patients with RET-mutant MTC that is seen in Canadian clinical practice. The inverse ratio of female to male patients being lower than expected was noted by the clinical experts, although they did not consider it to be a concern for applicability. Most patients had good baseline performance status (i.e., low number of patients with an ECOG PS of 2 or higher), suggesting that the included population might be healthier when compared with Canadian clinical practice; however, the clinical experts did not consider it highly different from what would be expected. All outcomes measured in the LIBRETTO-001 study are of clinical relevance and, according to the clinical experts, important for patients and well known and used by clinicians in Canada. A main concern was the limitation of the follow-up, i.e., that it might be considered too short for assessing longer periods of observations for those patients continuing the study and for assessing OS.
Indirect Comparisons
Description of Studies
The sponsor submitted an indirect treatment comparison (ITC) that involved a systematic review and used an unanchored matching-adjusted indirect comparison (MAIC) to evaluate the relative clinical efficacy of selpercatinib versus cabozantinib, vandetanib, lenvatinib, sorafenib, and placebo for the treatment of advanced RET mutation–positive MTC. Of these comparators, cabozantinib, vandetanib, and placebo are considered relevant for this review. Three outcomes were analyzed: OS, PFS, and ORR. As part of the MAIC that compares selpercatinib and cabozantinib, weights were generated using propensity score matching with logistic regression. The same weights were reused for the comparison of selpercatinib with placebo.
Efficacy Results
The sponsor-submitted ITC reported that, after weighting, there was a statistically significant improvement in PFS for selpercatinib versus placebo ||| ||||| ||| ||| ||||| ||||| ||||||||, and a statistically significant improvement in OS for selpercatinib versus placebo ||| ||||| ||| ||| ||||| ||||| |||||||||. Sources of heterogeneity between the studies include differences in patient characteristics such as age, ECOG PS, RET M918T mutation status, and difference in trial design (single- versus multi-arm trials). The variables included in the weighting model were |||| ||||||| |||| ||||||||||| ||||||| |||| ||||||| ||||||| ||| ||| ||||| |||||||| ||||||. The effective sample size after matching was |||||.
Critical Appraisal
The sponsor-submitted ITC had several limitations, including the lack of inclusion of all prognostic factors and effect modifiers in the MAIC weighting process, which leads to a high risk of residual confounding; use of MAIC weights calculated for 1 comparison that involves a different patient population than another comparison; heterogeneity between the patient populations used in different components of the ITC; and lack of consideration and inclusion of outcomes from the CADTH systematic review protocol, including DOR, HRQoL, and safety outcomes. Given these limitations, there is uncertainty around the relative treatment effects estimated by the MAIC, which undermines the internal and external validity of the ITC.
Other Relevant Evidence
CADTH identified 3 ongoing studies relevant to this submission. LIBRETTO-531 (phase III randomized controlled trial of selpercatinib versus cabozantinib or vandetanib), LIBRETTO-321 (phase II conducted in China), and LIBRETTO-121 (phase I and II study in a pediatric population), none of which have peer-reviewed published data available at this time (except for LIBRETTO-121, the results for which are presented from a conference abstract); the studies are expected to be completed by 2026, 2025, and 2024, respectively.
New Data for Request for Reconsideration
New data as of a June 15, 2021 cut-off date, were submitted by the sponsor as part of a request to CADTH for reconsideration, requesting to include only adults (18 years of age and older) with unresectable advanced or metastatic RET-mutant MTC in the first-line setting. This represents an extension of the follow-up (now with a median of 26.3 months for OS and 24.5 months for PFS), supplementing the immature data observed in the analyses of the data from the initial cut-off dates, with agreement between the reported results from the base case and the later cut-off analyses. In this update, of 142 patients in SAS 1, 115 (81%) were treatment-naive and 27 (19%) had been treated with a prior systemic therapy other than cabozantinib and vandetanib. At the time of data cut-off, the ORR by IRC assessment in SAS 1 was 81.0% (95% CI; 73.6 to 87.1), which is similar to but numerically higher than the ORR observed at the previous data cut-off. With a median follow-up of 20.3 months, the median DOR by IRC assessment was not evaluable (|||||| ||||| ||||| ||||||). However, 81.7% of responders were still on treatment with no documented disease progression by IRC assessment at the time of data cut-off. For OS, the median by IRC assessment was not reached, with a median duration of follow-up of 26.3 months (||||||||||||| ||||| ||||| |||| || ||||) (Table 12). ||| ||||||| ||||| ||| || ||| |||| |||||| ||| ||||||||||. The rates of survival at 12 months or more and 24 months or more were 99.3% and 95.0%, respectively. Within the total MTC safety analysis set (N = 319), harm events at the June 15, 2021 data cut-off were similar to the ones presented from the March 30, 2020, data cut-off.
Conclusions
The evidence from a single-arm, open-label, unblinded study (LIBRETTO-001) suggests that treatment with selpercatinib is associated with survival and response end points that were considered relevant to both patients and clinicians (OS, PFS, ORR, DOR, HRQoL) when compared with the typical effects and clinical evolution observed by clinical experts among patients with RET-mutant, advanced and/or metastatic MTC after surgery.
Overall, the clinical experts deemed the harms and safety profile of selpercatinib better than the undesirable effects usually seen in clinical practice with vandetanib or cabozantinib. However, major limitations generate uncertainty around any effect estimates due to immature data, lack of comparative evidence, a high risk of bias (no blinding, attrition), no adjustment for multiple comparisons, and imprecision in time-to-event outcomes.
Evidence from a sponsor-submitted ITC is also associated with major limitations for the comparison between selpercatinib and BSC due to residual confounding (i.e., incomplete inclusion of prognostic factors and effect modifiers), surrogate use of weights for comparisons, and heterogeneity among included populations.
Overall, there is uncertain evidence that suggests that selpercatinib provides clinical benefits with similar or lower risks of harms (i.e., toxicity) when compared with what is expected with relevant comparators.
Introduction
Disease Background
Thyroid cancer is 1 of the most commonly diagnosed cancers in Canada and the world. Although it embodies less than 1% of all tumours, it is considered the most common endocrine malignancy and the fifth most common cancer in women.1,2 It is estimated that 8,200 new cases of thyroid cancer will be diagnosed in people living in Canada in 2019 and about 230 will die from it.19 For 2020, the incidence of thyroid cancer in Canada was estimated to be 23 per 100,000 patients or about 8,600 new cases.3
Thyroid cancer can originate from either thyroid follicular cells or parafollicular cells (c cells). Thyroid cancers arising from follicular cells include DTC, which groups papillary thyroid cancer (PTC), follicular thyroid cancer, Hurthle cell cancer. Among all types of thyroid cancer, DTC is the most common, accounting for more than 95% of cases.5,6
MTC originates from the parafollicular neuroendocrine cells of the thyroid (c cells). It is a less common condition, accounting for 1% to 2% of all thyroid cancers, and it is usually detected as a solitary thyroid nodule in patients in the fourth or sixth decade of life. Lymphadenopathy is also a common initial presentation due to frequent metastases to cervical lymph nodes, with up to 15% of sporadic cases presenting distant metastases in the mediastinum, liver, lungs, and bones. A common initial presentation is the presence of diarrhea with an accompanying thyroid nodule.
Of all MTC cases, approximately 75% are sporadic and 25% are hereditary. Of the sporadic cases, 50% will present somatic mutations in the RET proto-oncogene (of which the most common is the M918T), a small proportion (about 20% to 25%) will present a rat sarcoma (RAS) mutation, and about 20% to 25% will be defined as orphan mutations (yet to be identified).4 Of the hereditary cases, almost all (98%) will present a germline RET mutation (inherited as autosomal dominant).5 Hereditary cases occur mostly in patients who have an inherited multiple endocrine neoplasia syndrome.5,6
Diagnosis is based on physical examination, neck ultrasound, and ultrasound-guided fine-needle aspiration cytology. Levels of calcitonin are helpful, as they are usually diagnostic of MTC, especially with levels above 100 pg/mL.4 Other biomarkers can also be helpful, such as the serum CEA, which is usually elevated in advanced cases when distant metastases are present. RET germline mutation analysis is recommended when the diagnosis of MTC has been established because it allows defining the sporadic or hereditary nature of MTC, which can guide future diagnostic and therapeutic options and strategies.
The prognosis of MTC not cured by surgery is unfavourable, with a 10-year survival rate of approximately 50%,4 and a 5-year survival rate varying from 62% to 87%, according to different series.7-10 Early diagnosis and early appropriate surgical treatment are considered to positively affect the prognosis of these patients.
Standards of Therapy
In patients with both sporadic and hereditary MTC, early diagnosis and surgical therapy with total thyroidectomy and resection of local and regional metastases is the basis for initial treatment and the possibility of cure.6 Hereditary cases must also be investigated for the presence of pheochromocytoma and/or hyperparathyroidism, regardless of age and presenting symptoms; hence, serum calcitonin and CEA are part of the initial biochemical testing.4 After surgery, hormone replacement therapy with L-thyroxine (LT4) should be started to keep thyrotropin values within the normal range.
The treatment goals in patients with MTC are aimed at cure, improving survival, delaying disease progression, and improving HRQoL by controlling symptoms such as diarrhea, minimizing adverse effects of treatments, and increasing work–life productivity.11
For patients who have unresectable advanced or metastatic RET-mutant MTC — a condition with a very low cure rate — several targeted therapies have been used as first-line treatments.4,11,12 These include several multi-targeted tyrosine kinase inhibitors (TKIs), cabozantinib13 and vandetanib14 among them and which have both shown improvement in PFS in phase III randomized controlled trials.13,14 However, among these, only vandetanib has been approved and funded in Canada and can be prescribed regardless of RET mutational status. Cabozantinib is approved in Canada only for the treatment of renal and hepatocellular carcinoma; it is neither funded nor approved for use in patients with MTC.
Once patients progress on currently available therapies, or if vandetanib has to be discontinued due to side effects, there are no further best options. Presently, after first-line treatment, patients with RET-mutant advanced or metastatic MTC can only continue using BSC and, optionally, enter clinical trials.11
Vandetanib is prone to frequent AEs (as are other TKIs), and its administration requires special training and monitoring (for example, for QTc prolongation). An ideal treatment for patients with MTC should reduce treatment-related toxicities while increasing survival and improving HRQoL.
Drug
Selpercatinib (Retevmo or LOXO-292) as 40 mg and 80 mg capsules (oral), is a new chemical entity: a highly selective, adenosine triphosphate–competitive small-molecule inhibitor of the RET receptor. Selpercatinib is indicated as monotherapy for the treatment of RET-mutant MTC in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease. Other indications include RET fusion–positive DTC in adult patients with advanced or metastatic disease (not amenable to surgery or radioactive iodine therapy) following prior treatment with sorafenib and/or lenvatinib, and metastatic RET fusion–positive NSCLC.15
To start treatment with selpercatinib, the product monograph recommends that physicians confirm the presence of a RET gene fusion (for patients with NSCLC or thyroid cancer) or a RET gene mutation (for patients with MTC) using a validated test before starting treatment. The recommended dosage of selpercatinib is based on body weight:
less than 50 kg: 120 mg twice daily
50 kg or greater: 160 mg twice daily
It should be administered approximately every 12 hours until disease progression or unacceptable toxicity. Health Canada has not authorized its use in children younger than 12 years of age. The product monograph also recommends dose modifications for QT interval prolongation, increased AST or ALT, hypersensitivity, hypertension, hemorrhagic events, and other grade 3 or 4 adverse reactions.
Selpercatinib (Retevmo) received a Notice of Compliance with Conditions on June 15, 2021, pending the submission of new data from phase II and III studies (LIBRETTO-001 and LIBRETTO-531). It is the first Health Canada–approved therapy for patients with advanced RET-driven lung and thyroid cancers.
Several warnings and precautions are stated in the product monograph, such as QTc interval prolongation on ECG, hypertension, hypersensitivity, hepatotoxicity, hemorrhage, and embryo-fetal toxicity. These situations warrant caution and it is recommended that doses be adjusted for these AEs.15
Selpercatinib has not been previously reviewed by CADTH. However, at the time of this submission, 1 CADTH review for the treatment of RET fusion–positive DTC in adult patients with advanced or metastatic disease (not amenable to surgery or radioactive iodine therapy) following prior treatment with sorafenib and/or lenvatinib, and 1 for metastatic RET fusion–positive NSCLC were under way.
The characteristics of selpercatinib and vandetanib are presented in Table 4.
Table 4: Key Characteristics of Selpercatinib and Vandetanib
Characteristic | Selpercatinib | Vandetanib |
|---|---|---|
Mechanism of action | Small-molecule kinase inhibitor aimed at inhibiting the RET receptor tyrosine kinase. | Selective inhibitor of vascular endothelial growth factor receptor 2 (VEGFR-2, KDR), epidermal growth factor receptor (EGFR), RET receptor tyrosine kinases. |
Indicationa | Indicated as monotherapy for the treatment of:
| For the treatment of symptomatic or progressive MTC in adult patients with unresectable locally advanced or metastatic disease. Caprelsa use should be carefully considered based on a harm-benefit assessment in patients with indolent, asymptomatic, or slowly progressive disease because of the significant treatment-related harms. |
Route of administration | Oral capsules | Oral tablets |
Recommended dose |
| 300 mg once daily |
Serious adverse effects or safety issues | Diarrhea, bleeding, hepatotoxicity (AST or ALT increase), QTc prolongation, hypertension, photosensitivity. | QTcF interval prolongation, Torsade de Pointes, sudden death, fatal heart failure, hypertension, or hypertensive crisis. |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; DTC = differentiated thyroid carcinoma; KDR = kinase insert domain receptor; MTC = medullary thyroid cancer; NSCLC = non–small cell lung cancer; QTc = corrected QT interval; RET = rearranged during transfection.
aHealth Canada–approved indication.
Source: Selpercatinib (Retevmo)15 and vandetanib (Caprelsa)20 product monographs.
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. Input was obtained from 2 patient groups and is summarized subsequently. At the time of the open call to patient groups, input for both MTC and DTC was obtained; therefore, the input from the patient groups for these 2 conditions has been combined for this report.
CanCertainty Coalition
The CanCertainty Coalition, which is composed of more than 30 Canadian patient groups, caregiver organizations, and charities as well as oncologists and cancer care professionals, strives to improve the accessibility of cancer treatment. CanCertainty’s submission focused on financial burdens and safety issues associated with oral cancer medication.
For patients with cancer under the age of 65 living in British Columbia, Alberta, Saskatchewan, Manitoba, Quebec, Northwest Territories, Yukon, and Nunavut, oral oncology medication is covered. In Ontario and the Atlantic provinces, only medications for people over the age of 65 are covered. For the small number of patients under the age of 65 with RET-mutant MTC living in these provinces, a cancer diagnosis could lead to financial hardship, especially when they do not have private health insurance. Even though multiple programs support individuals who have high drug costs, there are administrative barriers. To qualify for assistance programs, patients and their families must submit a significant amount of personal and financial information. Therefore, the patients often face weeks of delay in starting cancer treatments until the issues with paperwork and approvals are resolved. Alternatively, they often pay out of pocket for the first few weeks of treatment, which may not be reimbursed. The access to cancer treatments is difficult in many hospitals and cancer centres across Canada. As a result, in Ontario, a new type of social worker known as a drug access navigator and an organization that supports these navigators, the Oncology Drug Access Navigators of Ontario, were established. Even for patients with private insurance, many face significant co-pays, deductibles, or annual or lifetime caps. For example, some private insurance plans have a cap of $2,000 per year for prescription drugs, even though many take-home cancer drugs cost more than $20,000 per year. A survey of more than 1,600 Nova Scotians commissioned by the CanCertainty Coalition, demonstrated that 3 out 5 people (60%) in Nova Scotia would consider leaving the province if faced with cancer therapy costs. Only 7% could afford monthly drug costs of more than $200. Patients deal with their financial burden by delaying or foregoing care. They may take less medication than prescribed, use over-the-counter drugs in place of prescribed medications, decline procedures, and skip appointments to reduce costs. Patients who are younger, uninsured, and earning a lower income appear to be at greater risk of medication nonadherence. Moreover, the evidence suggests that those with a shorter time since diagnosis, more severe cancers, and unemployed, have higher rates of financial burden.
There is also a safety issue with take-home cancer drugs. Some patients receive their medication from hospital pharmacies, specialty pharmacies, and community pharmacies that lack specialization and training to handle cancer medications. Safety and quality deficits have been reported related to the current method of dispensing take-home cancer drugs in the community, including incorrect handling and dosing, limited monitoring, nonadherence (leading to under- or over-dosing), SAEs, morbidity, and mortality. Thus, take-home cancer drugs require processes similar to those that have been developed for IV cancer drugs, where delivery is comprehensive, organized, safe, and patient-centred.
Canadian Cancer Society and Thyroid Cancer Canada
The CCS aims to improve the lives of all those affected by cancers through research, advocacy, and support, with the purpose of taking control of cancer. The CCS’s patient panels and networks provided survey results from patients with thyroid cancer. In addition, Thyroid Cancer Canada’s patient networks submitted survey results and 2 testimonials from staff or board members who have had thyroid cancer. A total of 17 survey responses were collected across Canada between October 22 and November 10, 2021. None of the respondents had any direct or indirect experience with selpercatinib.
The ability to concentrate (65%), exercise (59%), and work (41%) were the top 3 day-to-day activities that respondents said have been impacted in moderate or significant degrees by thyroid cancer. Seven respondents added that fatigue; brain fog; issues related to mental health, body image, and cognitive ability; concerns about their cancer returning, and concerns about the regulation of thyroid medications were the areas that have been affected by thyroid cancer. Overall, 71% reported a financial barrier related to treatments. The most significant financial barriers were loss of income due to absence from work (24%), parking costs (23%), and drug costs (12%). There was 1 patient (6%) who responded that blood test monitoring (thyroid-stimulating hormone, T3, T4) was the greatest financial barrier. Seven patients (29%) were being treated with surgery, 6 patients (25%) were not actively treated, and 4 patients (17%) were on hormone therapy. Of note, 9 out of 17 patients were on thyroid hormone replacement or suppression therapy, e.g., levothyroxine (Synthroid, Eltroxin). The treatment-related side effects that had a moderate or significant impact on patients were fatigue (71%), concentration and focus (64%), and weight changes (58.5%). Three respondents indicated that mental health issues (mood swings, suicidal thoughts, and feelings of loneliness and fear) were of concern. One patient said, “Synthroid is very difficult to adjust and regulate which leads to emotional ups and downs. I’ve been suicidal through this due to being over medicated and an emotional mess when under medicated.” For patients with experience with radioactive iodine or radiation therapy, there were additional concerns, such as the impact on salivary glands (dry mouth and increased risk of dental problems), long-term impacts of treatment, and isolation associated with radiation. One patient said, “Isolation of radiation, no one tells you how long to stay away from pets. How lonely it is because no support groups or info given on how to live afterwards with the fear of relapse or clear stages of the cancer.” From the submitted testimonials, fertility issues were raised as another significant concern along with difficulties with body temperature, weight, mood, energy, and regulating heart rate. Seven patients responded that they would like a new treatment with improvements regarding the cost of drugs, difficulty regulating drugs, low levels of access to information, long treatment wait times, and the lower level of support that thyroid cancer gets compared with other types of cancer, as thyroid cancer is treated outside of cancer clinics. One patient said, “I would like to be seen in a cancer clinic rather than be followed outside of the clinic. There is not enough support for thyroid cancer patients.”
Clinician Input
Input From the Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of thyroid cancer.
Unmet Needs
Treatment goals are improving OS, PFS, and HRQoL by controlling symptoms such as diarrhea, flushing, minimizing the adverse effects of treatments, and increasing work–life productivity. Both clinical experts agree there is an unmet need for better treatments that are available for patients who do not respond to or progress after first-line therapy, or for whom treatment with vandetanib or cabozantinib has to be discontinued or the dose reduced due to side effects; also, ideally, these treatments should have fewer harms.
Place in Therapy
According to the clinical experts consulted by CADTH, selpercatinib would be an appropriate therapy for RET-driven thyroid malignancies, including as first-line therapy rarely used in combination with local treatments. The mechanism of action would not lend itself to combination therapy with the other active drugs available at this time.
Since there is only 1 approved and funded systemic therapy option (vandetanib) in Canada, and patients usually do not have further options after first-line therapies, there is a place in therapy for selpercatinib, which is expected to cause a shift in the current treatment paradigm. Both clinical experts agree it would be more appropriate if selpercatinib were used as first-line therapy due to reports of better efficacy and tolerance compared with other options.
Patient Population
The clinical experts consider that patients with RET-driven MTC whose disease cannot be managed or cured by locoregional (surgical) interventions and who are experiencing or expected to experience symptomatic disease progression in the near future are the most likely to benefit from the use of selpercatinib, and it should be offered in every case. The experts did not find specific baseline characteristics or variables of prognostic value and consider that patients’ responses will not differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease).
Patients with progressive metastatic MTC need to be screened for RET mutations and rearrangements using locally available comprehensive molecular tests, which should be available in institutions treating patients with progressive metastatic MTC.
Assessing Response to Treatment
Patients are assessed with clinical examinations and evaluations of symptoms to measure evidence of response or stabilization of the disease, based on clinical grounds and radiological examination, such as RECIST criteria, number and/or severity of symptoms, PFS, serum calcitonin, and CEA. All of these measurements are mostly aligned with the clinical trial end points.
Improvement in survival, PFS, and a reduction in the frequency and severity of symptoms (e.g., diarrhea) will be used to measure an adequate response approximately every 3 to 6 months.
Discontinuing Treatment
Deterioration of symptoms, functional status, radiological evidence of disease progression (together with other clinical criteria), and unacceptable toxicity from treatment are among the issues commonly used in clinical practice to decide on a case-by-case basis whether to discontinue treatment.
Prescribing Conditions
Targeted therapies can have significant toxicity and related harms; patients should only receive selpercatinib from clinicians with experience in the treatment of thyroid cancer in a specialty outpatient clinic setting. A specialized team should be available to provide care in diagnosis, treatment, monitoring, and palliative care. The physicians involved will mostly be medical or surgical oncologists and endocrinologists.
According to the clinical experts, with the availability of selpercatinib, it must become standard practice to test patients with MTC for somatic RET fusions or mutations. Institutions treating patients with MTC must have a stepwise molecular testing strategy in place.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Two clinician group summaries were received: 1 from the POGO and the other from the OH-CCO Head and Neck and Thyroid Cancer DAC, gathering input from a total of 5 clinicians.
POGO
This group represents 5 pediatric cancer centres and advises the Ministry of Health and Long-Term Care on pediatric cancer care. POGO’s Therapeutic and Technology Advisory Committee members with clinical experience and insight into the use of selpercatinib contributed to the survey.
Pediatric MTC is a rare disease with approximately 75% of children carrying germline RET mutations and the majority of the remaining 25% carrying somatic RET mutations. Children with a family history get prophylactic thyroidectomy to avoid malignant transformation. Those without a family history often present with advanced diseases not amenable to complete resection.
Treatment options for metastatic disease, which has a very low cure rate, include multi-targeted TKIs, such as cabozantinib and vandetanib. Since these multi-targeted TKIs have limited impact on PFS and substantial DLTs, improved PFS and minimized off-target effects are desirable goals for the treatment of metastatic MTC. As the first-line treatment for the best chance of cure, children with MTC should undergo comprehensive initial surgery. For a rare population with residual disease, selpercatinib should be used as the preferred second-line therapy over existing therapies (i.e., cabozantinib or vandetanib), due to reduced toxicities and more favourable response rates to RET-driven MTC. For another rare population with unresectable tumours, selpercatinib may be considered as the first-line therapy in a neoadjuvant setting to facilitate eventual surgical control.
For children with progressive, metastatic MTC requiring systemic therapy, selpercatinib would replace existing MKIs as first-line treatment. Children with high-volume residual disease following surgery, residual disease threatening vital structures, PD (either structural or biochemical) that is not surgically resectable, or those with a post-operative serum calcitonin level greater than 150 pg/mL are best suited for selpercatinib if their disease is driven by a RET mutation. These children can be identified at a specialized tertiary centre and reviewed at tumour boards. Patients without structurally persistent disease, i.e., negative imaging following initial surgery, should not be considered for selpercatinib. Those with MTC with a germline or somatic RET mutation confirmed by tumour analysis are most likely to respond to selpercatinib. Responses to treatment can be assessed radiologically and biochemically in the known residual disease sites.
Clinically meaningful responses would be a reduction and/or resolution of known residual disease based on cross-sectional imaging and tumour markers, i.e., calcitonin and CEA. Those with miliary lung disease can be monitored for an objective improvement of respiratory status. Treatment response should be assessed every 3 to 6 months. In case of disease progression despite properly dosed and administered therapy or significant hypersensitivity not responsive to steroids and/or dose reduction, selpercatinib should be discontinued. Selpercatinib can be administered in an outpatient setting with a multidisciplinary team experienced in the care of pediatric MTC; however, diagnosis and monitoring should involve pediatric endocrinologists and head and neck pediatric surgeons.
OH-CCO Head and Neck and Thyroid Cancer DAC
The OH-CCO Head and Neck and Thyroid Cancer DAC, which provides evidence-based clinical and health system guidance, submitted input collected via email and teleconferences.
This group explained that for adult RET-mutant MTC, the only currently approved and funded option is vandetanib, which is prescribed regardless of RET mutational status. Cabozantinib is neither funded nor approved for MTC in Canada. Administering vandetanib requires special training and monitoring, e.g., blood tests and ECGs, since it has a black box warning for QTc prolongation that can lead to arrhythmia, which is caused by combined epidermal growth factor receptor, vascular endothelial growth factor, and RET TKI activities. Hence, an important goal of an ideal treatment would be reducing treatment-related toxicities. Once disease has progressed on currently available therapies, there is no other option; therefore, adult patients with metastatic, unresectable RET-mutant MTC would be the population with the greatest unmet need for selpercatinib.
If patients have been previously treated, selpercatinib would be the next line of therapy. In treatment-naive patients, selpercatinib would be an alternate treatment option based on its favourable toxicity profile. Some clinicians may want to use selpercatinib in the first-line setting due to its multiple advantages over existing therapies. Given the broader effect of vandetanib on other receptors, vandetanib would be used if patients progressed on or are intolerant to selpercatinib. Even though selpercatinib appears to be more active and less toxic, phase III trial data in the first-line setting are still ongoing. Thus, some clinicians may reserve selpercatinib for patients with RET-mutant MTC who are intolerant to or unsuitable for vandetanib.
To identify eligible patients, RET testing is available in Ontario as part of reflex testing on all metastatic thyroid cancer. Patients without a RET mutation or those with a performance status that would not allow selpercatinib treatment would be the least suitable population.
Response to selpercatinib would be measured primarily by response rate, and secondary outcomes of interest would be PFS and toxicity. A clinically meaningful response to treatment can be determined by a reduction in tumour burden based on clinical assessment and/or imaging, cancer-related symptoms, and tumour marker levels. Treatment with selpercatinib should be reassessed every 8 to 12 weeks for the first 6 months to 1 year then every 12 to 16 weeks thereafter, especially in patients who had initial responses, feel well, and have reduced CEA and/or calcitonin levels. However, specific intervals should not be mandated. In case of a lack of response and/or if treatment-related toxicities emerge, selpercatinib should be discontinued. As an oral take-home cancer drug, selpercatinib is suitable for the community setting.
Drug Program Input
Drug Program Input
The drug programs identified relevant implementation issues to be addressed through the CADTH’s reimbursement review process. Refer to Table 5 for more details.
In terms of considerations for the initiation of therapy, there were 2 main concerns. First, the uncertainty of selpercatinib use in the pediatric population since, in the LIBRETTO-001 trial, only 3 adolescent patients with MTC are included. The clinical experts acknowledged the scarcity of evidence, although they did not expect significant variations in outcomes for pediatric patients.
Regarding concerns about the discontinuation of therapy, the experts expressed that it would be difficult to state specific criteria, since different metastatic locations could respond differently in the same patient but, overall, they considered that patients with no signs of toxicity with selpercatinib would be able to continue treatment.
In terms of considerations for generalizability, there were issues with the low number of pediatric patients, very few of whom had an ECOG PS above 2. Experts considered that patients with an ECOG PS of 2 or greater should be judged to be able to receive treatment with selpercatinib on a case-by-case basis. The same applies for pediatric cases, as indicated earlier.
In general, the experts considered that selpercatinib will have a major impact on the current treatment paradigm in Canada.
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The LIBRETTO-001 trial was an open-label, non-randomized, non-comparative phase I and II trial evaluating selpercatinib in patients with RET-mutant MTC with or without prior vandetanib or cabozantinib treatment. The relevant funded comparator for first-line treatment would be vandetanib (for adult patients). Patients aged between 12 and 17 years currently do not have a funded comparator. In the second-line setting, the relevant comparator is best supportive care or clinical trial. | For pERC consideration. |
Considerations for initiation of therapy | |
In the LIBRETTO-001 trial, there were only 3 adolescent patients (aged 15, 16, and 17 years) with advanced or metastatic RET-mutant MTC; however, the requested indication is for patients 12 and older. Vandetanib, the current funded comparator for MTC, is funded only for adult patients. What is the relative safety and/or efficacy of selpercatinib for patients between 12 and17 years old with RET-mutant MTC? Patients of childbearing potential will require additional counselling and support due to the potential impact of selpercatinib on reproduction and fertility. | The clinical experts mentioned how little evidence exists regarding pediatric patients with RET-mutant MTC. This precludes the experts from giving specific numbers on the safety or efficacy for this group of patients. Due to the scarcity of evidence, the CADTH report will include data from a conference abstract for the LIBRETTO-121 study (pediatric patients) as presented in the Other Relevant Evidence section of this report. In this trial, 12 patients were enrolled (median age 14 years), with 8 patients diagnosed with RET-mutant MTC, and there were 8 patients still on treatment at the time of the analysis (ORR of 50%; 95% CI, 16% to 84%). The clinical experts noted that the balance between benefits and harms should always be considered, since this is a rare disease with a poor prognosis. |
Is the efficacy of selpercatinib expected to be similar across the various RET mutations? Is the efficacy of selpercatinib expected to be similar in patients with sporadic MTC vs. hereditary MTC? | The clinical experts consulted by CADTH do not expect to see variations in response based on any of the characteristics of these subgroups or populations. |
Considerations for continuation, renewal, and/or discontinuation of therapy | |
The LIBRETTO-001 trial evaluated patients through radiologic assessments every 8 weeks for 1 year and then every 12 weeks thereafter. Calcitonin and CEA levels were measured. In clinical practice, how will treatment response to selpercatinib be assessed? | Patients are assessed approximately every 3 to 6 months during follow-up visits, and clinicians will evaluate different measures of response (besides OS and PFS), such as the RECIST criteria, CEA, calcitonin, general symptoms, and HRQoL. |
In the LIBRETTO-001 trial, patients with documented disease progression could continue selpercatinib if they were deriving clinical benefit. What are the discontinuation criteria for selpercatinib? | Both clinical experts agreed that deterioration of symptoms, functional status, radiological evidence of disease progression (together with other clinical criteria), and unacceptable toxicity from treatment are among the issues commonly used in clinical practice to decide to discontinue treatment on a case-by-case basis. |
Considerations for prescribing of therapy | |
The selpercatinib 40 mg and 80 mg capsule dosage is based on weight:
It is administered at home by the patient or caregiver. | For pERC consideration. |
Generalizability | |
Patients with an ECOG PS greater than 2 were excluded from the trial. Can patients with an ECOG PS > 2 be considered eligible for treatment? Only patients 12 years and older were eligible for the trial. Can the results of the trial be applied to children under 12 years of age with unresectable or metastatic RET-mutant MTC? | For both situations, the clinical experts recognize that the evidence is very uncertain and scarce. Considering this, their input is that selpercatinib could be offered in the pediatric population on a case-by-case basis. The same would apply to patients with an ECOG PS above 2. |
Funding algorithm | |
| Both experts agreed that selpercatinib will have an impact on the treatment paradigm for patients with RET-mutant MTC. |
Care provision issues | |
Selpercatinib is supplied as 40 mg capsules (60 capsules per bottle) and 80 mg capsules (60 or 120 capsules per bottle). There are multiple dosing schedules and the potential for dose adjustments with selpercatinib. Current sponsor packaging and storage requirements allow for flexible dispensing options (e.g., blister packaging of doses, using capsules from 1 bottle for multiple prescriptions, if necessary). | For pERC consideration. |
RET testing needs to be in place to identify eligible patients. | For pERC consideration. |
CEA = carcinoembryonic antigen; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HRQoL = health-related quality of life; MTC = medullary thyroid cancer; OS = overall survival; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors; RET = rearranged during transfection.
Clinical Evidence
The clinical evidence included in the review of selpercatinib (Retevmo) is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as studies selected according to an a priori protocol. The second section covers indirect evidence from the sponsor and indirect evidence selected from the literature that meet the selection criteria specified in the review. The third section includes sponsor-submitted, long-term extension studies and additional relevant studies that are considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of selpercatinib (Retevmo) 40 mg and 80 mg capsules for the treatment of RET-mutant MTC in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. The outcomes included in the CADTH review protocol reflect the outcomes considered important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Patients 12 years of age and older with RET-mutant medullary thyroid cancer and unresectable advanced or metastatic disease Subgroups:
|
Intervention | Selpercatinib (Retevmo) 40 mg and 80 mg oral capsules. Dosage:
|
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
Notable harms and harms of special interest: diarrhea, bleeding, hepatotoxicity (AST or ALT increase), QTc prolongation, hypertension, photosensitivity. |
Study designs | Published and unpublished phase II, III, or IV RCTs. |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; DOR = duration of response; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = 5-level EQ-5D; HRQoL = quality of life; ORR = objective response rate; OS = overall survival; PedsQL = Pediatric Quality of Life Inventory; PFS = progression-free survival; QTc = corrected QT interval; RET = rearranged during transfection; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.21
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) through Ovid and Embase (1974–) through Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was selpercatinib. Clinical trial registries were searched: the US National Institutes of Health’s clinicaltrials.gov, the WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on November 24, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on April 13, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.22 Included in this search were the websites of regulatory agencies (the FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing the bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
A focused literature search for network meta-analyses dealing with thyroid cancer was run in MEDLINE All (1946–) on November 24, 2021. No limits were applied to the search.
Findings From the Literature
One study was identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
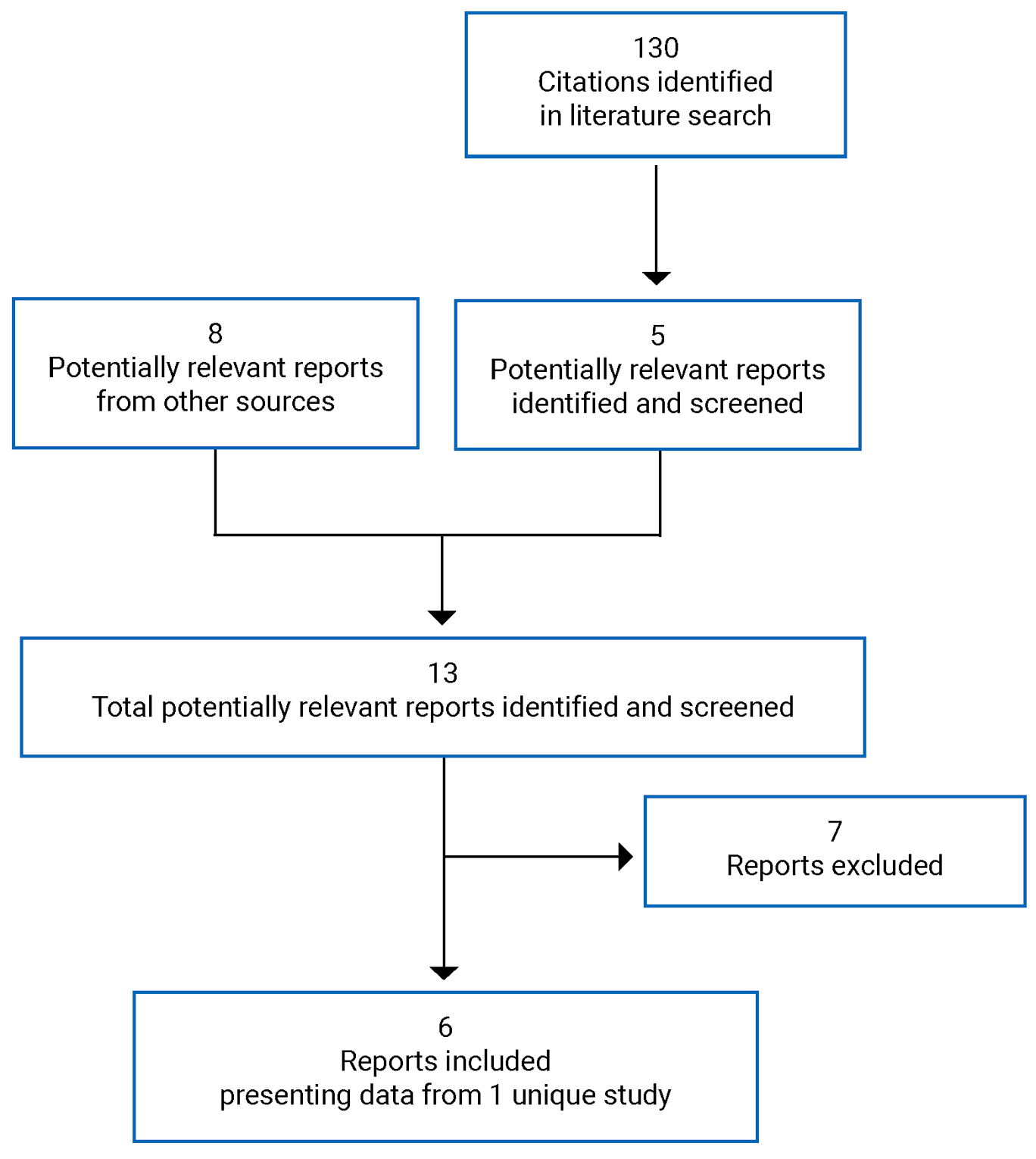
Table 7: Details of Included Studies
Criteria | LIBRETTO-001 |
|---|---|
Design and population | |
Study design | Open-label, multi-centre, phase I and II study |
Locations | 84 participating study sites in Australia, Canada, Denmark, Germany, Japan, Hong Kong, Israel, Singapore, France, Italy, Spain, South Korea, Switzerland, Taiwan, and the US as of June 17, 2019 |
Patient enrolment dates: |
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Selpercatinib for oral dosing was provided in the study as follows:
In the dose-escalation phase (phase I), the starting dose was 20 mg/day, given once daily. Dose escalation continued to 240 mg b.i.d. The RP2D of selpercatinib is 160 mg, b.i.d.; this dose was selected by the sponsor in conjunction with the SRC for the study. The RP2D is used in the phase II portion of the study (currently ongoing). |
Comparator(s) | No comparator (single-arm study) |
Duration | |
Phase | |
Phase I |
|
Phase II | Dose expansion with enrolment of patients into 1 of 5 cohorts |
Follow-up | Safety follow-up starting 28 days after the last dose of the study drug, with assessment every 3 months; study still ongoing |
Outcomes | |
Primary end point |
|
Secondary and exploratory end points | Phase I:
Phase II:
Exploratory end points:
|
Notes | |
Publications | Wirth (2020),23 Wirth (2021),17 Subbiah (2021),24 Minchom (2021),25 Drilon (2020).26 |
ACTH = adrenocorticotropic hormone; b.i.d. = twice daily; CAP = College of American Pathologists; CBR = clinical benefit rate; CEA = carcinoembryonic antigen; CLIA = Clinical Laboratory Improvement Amendments; CNS = central nervous system; CYP3A4 = cytochrome P450 3A4; DB = double blind; DLT = dose-limiting toxicity; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; IEC = independent ethics committee; ISO = International Organization for Standardization; MTC = medullary thyroid cancer; MTD = maximum tolerated dose; ORR = objective response rate; PD = progressive disease; PedsQL = Pediatric Quality of Life Inventory; PFS = progression-free survival; PK = pharmacokinetic; QTc = corrected QT interval; RANO = Response Assessment in Neuro-Oncology Criteria; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors version 1.1; RET = rearranged during transfection; RP2D = recommended phase II dose; SAE = serious adverse event; SRC = safety review committee; TEAE = treatment-emergent adverse event.
Source: LIBRETTO-001 Clinical Study Report18 and its main publications.17,23-26
Description of Studies
The LIBRETTO-001 study is a multi-centre, open-label, phase I and II, single-arm study of oral selpercatinib (LOXO-292) in patients with advanced solid tumours, including RET fusion–positive solid tumours, MTC, and other tumours with RET activation. The main focus for this CADTH review is the population of patients with RET-mutant MTC.
This study is still ongoing and is being conducted in 84 investigational sites among several countries and regions, including Canada, the US, Australia, Japan, Hong Kong, Taiwan, Israel, Singapore, and Europe.
Description of the phases and Cohorts of the LIBRETTO-001 Study
The study consisted of 2 main phases, the dose-escalation phase (phase I), and the dose-expansion phase (phase II), depicted in Figure 2. In these 2 phases, the sponsor generated 5 cohorts with the intention of better characterizing the safety and efficacy of the study drug in patients with specific anomalies in the RET gene. Cohort 1 included patients with a RET fusion–positive solid tumour who progressed on or were intolerant to 1 or more standard first-line therapies, while cohort 2 included patients with a RET fusion–positive solid tumour not previously treated with a standard first-line therapy. The population of interest for this CADTH report is cohort 3, which comprises patients with mutant RET MTC who progressed on or were intolerant to standard first-line treatments; however, cohort 4, comprising patients whose disease was not treated with standard first-line treatment (cabozantinib or vandetanib or other kinase inhibitors with anti-RET activity), will be described.
Cohort 5 includes patients from cohorts 1 to 4 without measurable disease, with MTC not meeting the requirements for cohorts 3 or 4, with other RET-altered solid tumours or other RET alterations or activations, or with circulating cell-free DNA that is positive for a RET gene alteration not known to be present in a tumour sample.
For phase I, the primary objective of the study was to determine the MTD (RP2D) for selpercatinib. Secondary objectives for phase I included the determination of the safety and tolerability of selpercatinib, characterization of the PK properties, and assessment of the antitumour activity of selpercatinib.
For phase II, the primary objective was to assess, for each expansion cohort, the antitumour activity of selpercatinib by determining the ORR using RECIST 1.1 or RANO criteria, as appropriate to tumour type. Secondary objectives for phase II included other efficacy parameters, including best change in tumour size from baseline, DOR, CNS ORR, CNS DOR, time to any and best response, clinical benefit rate, PFS, OS, determination of the safety and tolerability of selpercatinib, and the characterization of the PK properties.
Figure 2: Phase I and II of the LIBRETTO-001 Study
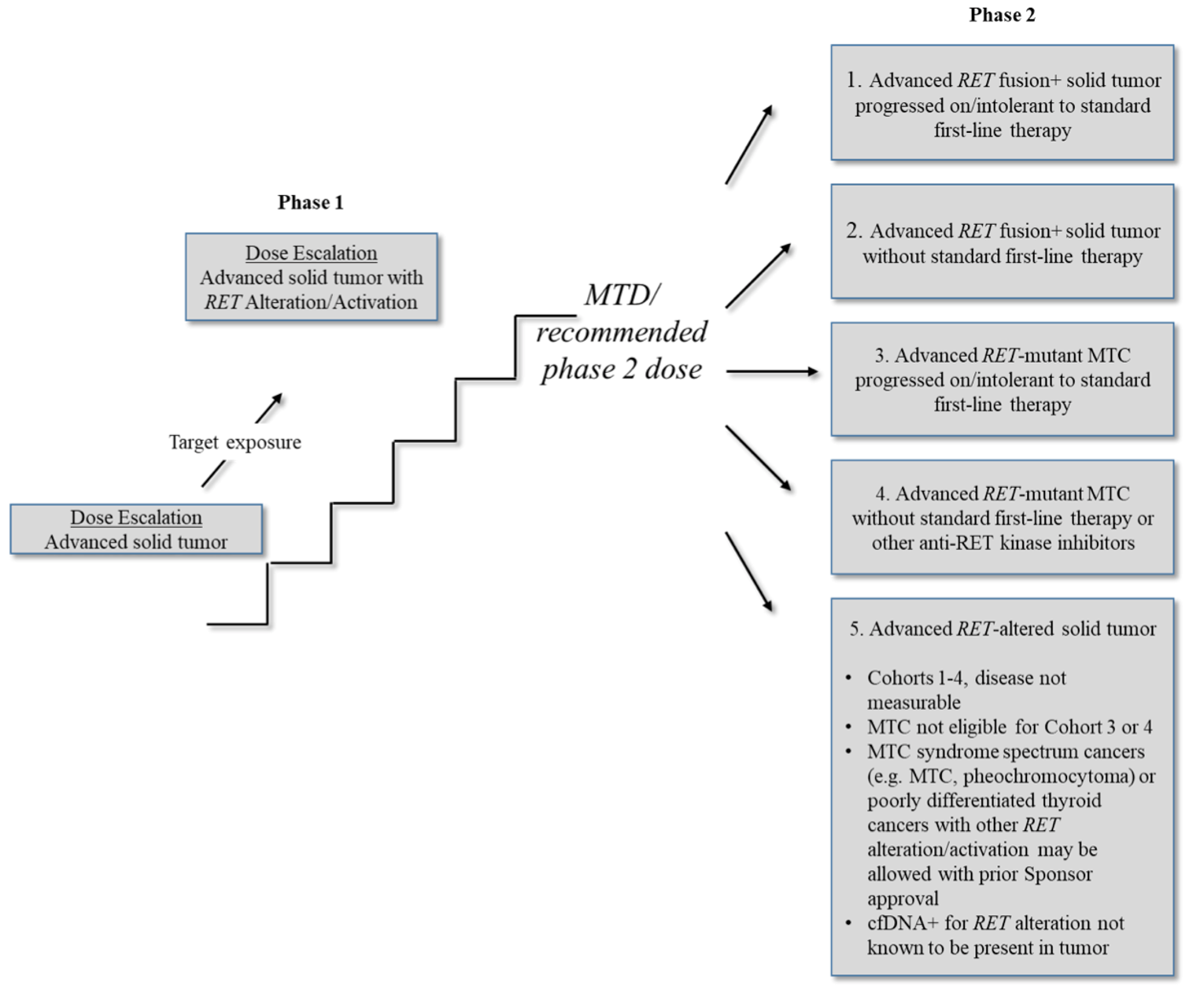
cfDNA = circulating cell-free DNA; MTC = medullary thyroid cancer; MTD = maximum tolerated dose; RET = rearranged during transfection.
Source: LIBRETTO-001 Clinical Study Report.18
The exploratory objectives of phase I and II included determination of the relationship between PK and drug effects, evaluation of serum tumour markers, CEA and calcitonin, and adrenocorticotropic hormone or cortisol (for patients with Cushing disease related to their cancer). Additional exploratory objectives include characterization of RET gene fusions and mutations and concurrently activated oncogenic pathways by molecular assays, and collection of patient-reported outcome data to explore disease-related symptoms and HRQoL.
During phase I, a dose-escalation strategy was conducted, starting the dose of selpercatinib at 20 mg/day and then proceeding through all dose levels or until the SRC and sponsor determined that a suitable dose was achieved based on available data (safety, PK exposure, clinical activity) using a modified Fibonacci dose escalation.27 The SRC evaluated whether the cohort at the prior dose level was considered to be receiving the MTD. Dose escalation was to proceed through the planned dose-escalation cohort levels or until the MTD was reached.
During phase II, a dose expansion was evaluated to obtain the RP2D of selpercatinib. An RP2D of 160 mg twice a day was selected by the SRC during phase I of the study. The LIBRETTO-001 study is currently ongoing and continuing to enrol up to approximately 750 patients with advanced solid tumours with evidence of a RET gene alteration in a tumour and/or blood.
Amendments to the Protocol of the Study
A detailed description of the major changes made to the protocol of the LIBRETTO-001 study is presented in Appendix 5. Of note was amendment 5.0 (May 2018) which updated the trial design from a 2-part phase I (dose escalation and dose expansion) study to a phase I and II study due to “promising early evidence” of durable antitumour activity in patients with RET-altered cancers (e.g., RET fusion–positive cancers and RET-mutant MTC), including those with resistance to prior MKIs and those with brain metastases.
Cut-Off Dates
The sponsor used different cut-off dates data based on regulatory submissions, which also had an effect on how the population sets were created and reported through interactions with regulators. An overview is presented in Figure 3.
Figure 3: Cut-Off Dates and Accrual of Patients With RET-Mutant MTC Included in the LIBRETTO-001 Study
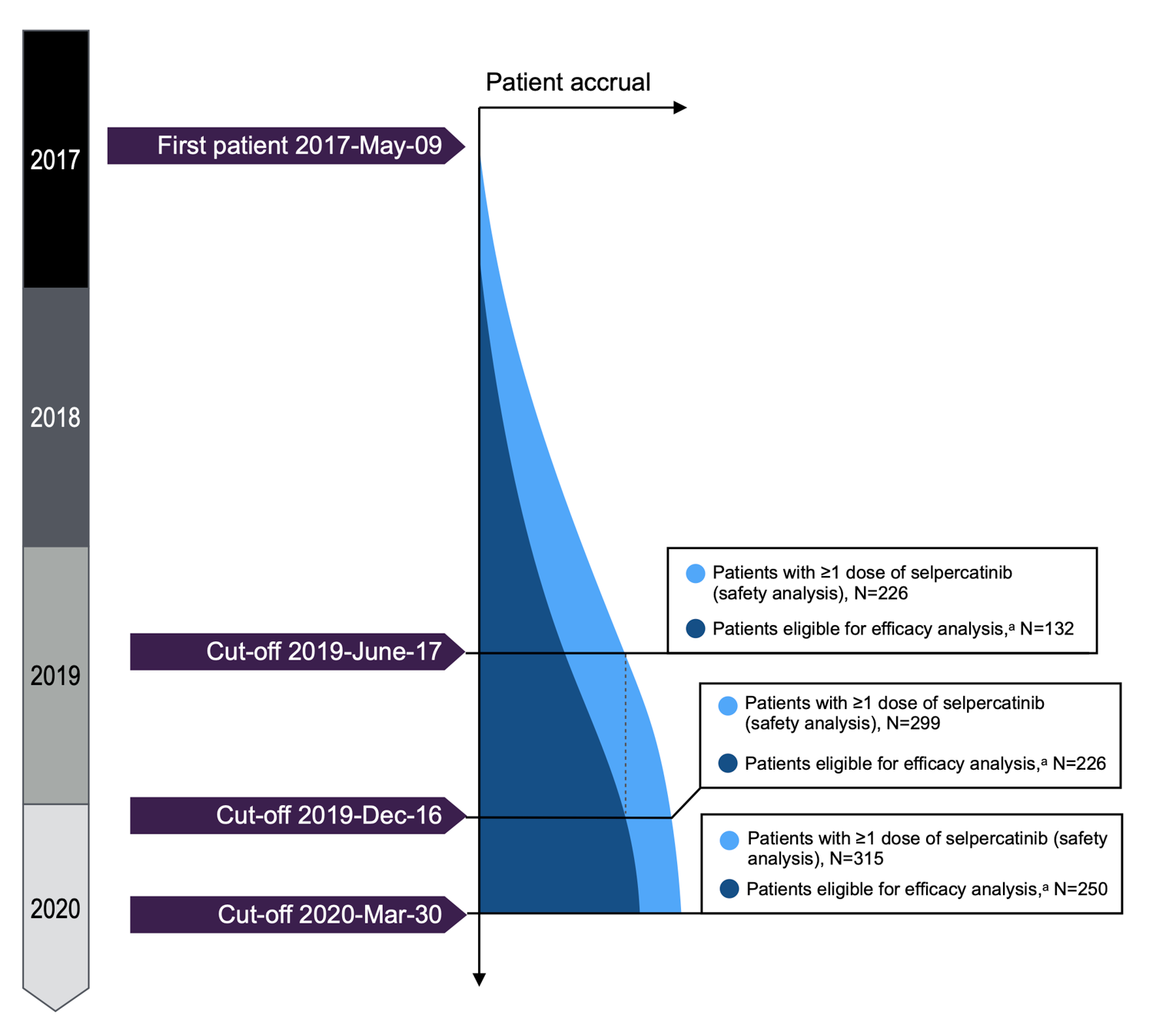
MTC = medullary thyroid cancer; RET = rearranged during transfection.
a Defined as those with at least 1 dose of selpercatinib and 6 months of follow-up.
Source: LIBRETTO-001 Clinical Study Report.18
The first planned cut-off date was on June 17, 2019 for FDA and European Medicines Agency submissions. This date was chosen so that the MTC efficacy-evaluable patients for ORR assessment had an opportunity to be followed for at least 6 months. At this cut-off date, the number of patients available for the safety analysis (i.e., those who had received at least 1 dose of selpercatinib) was 226, with 132 of these patients (58%) eligible for the efficacy analysis (those who received at least 1 dose of selpercatinib and were followed-up for at least 6 months).
An analysis using the December 16, 2019 cut-off date was conducted to support the FDA submission request to assess at least the day 60 efficacy and safety of selpercatinib for all patients initially enrolled (i.e., 6 months after the initial data cut-off of June 17, 2019). This pre-planned analysis at this cut-off point evaluated 299 patients for safety and 226 of these for efficacy using different analysis sets described in the next section. This cut-off date was also used for the submission to Health Canada and the pre-planned analysis and includes the 55 patients with MTC in the PAS for the primary end points assessed (defined subsequently).
Sponsor-submitted data for the March 30, 2020 cut-off date were also included and assessed by CADTH and are described in the tables addressing efficacy and harms in this report.
Derivation of New Analysis Sets Supporting Regulation Applications
Interactions with the FDA prompted the sponsor to create a different set of efficacy and safety analysis sets designed to support the indications sought. These agreed-upon analysis sets were not the same as those specified in the study protocol and are distinct from those described in the full Clinical Study Report. First, the efficacy datasets were categorized into broad groupings of patients with RET fusion–positive NSCLC, RET-mutant MTC, and RET fusion–positive thyroid cancer — of which MTC is the main focus for this CADTH review.
These grouping formed the basis for defining the PAS in patients with RET-mutant MTC who received prior cabozantinib or vandetanib, as shown in Figure 4. The MTC PAS was defined as the first 55 patients with RET-mutant MTC enrolled in LIBRETTO-001 who had been previously treated with cabozantinib or vandetanib. The PAS is a subset of the IAS, which includes all patients with RET-mutant MTC enrolled in LIBRETTO-001 who met the same eligibility criteria as the PAS by the June 17, 2019 data cut-off for the initial US submission (N = 124). SASs include SAS 1, comprising treatment-naive patients (n = 88), and SAS 2 (n = 14), comprising the patients in cohort 5 (defined earlier).
Figure 4: Overview of the LIBRETTO-001 Study Design and Populations Included
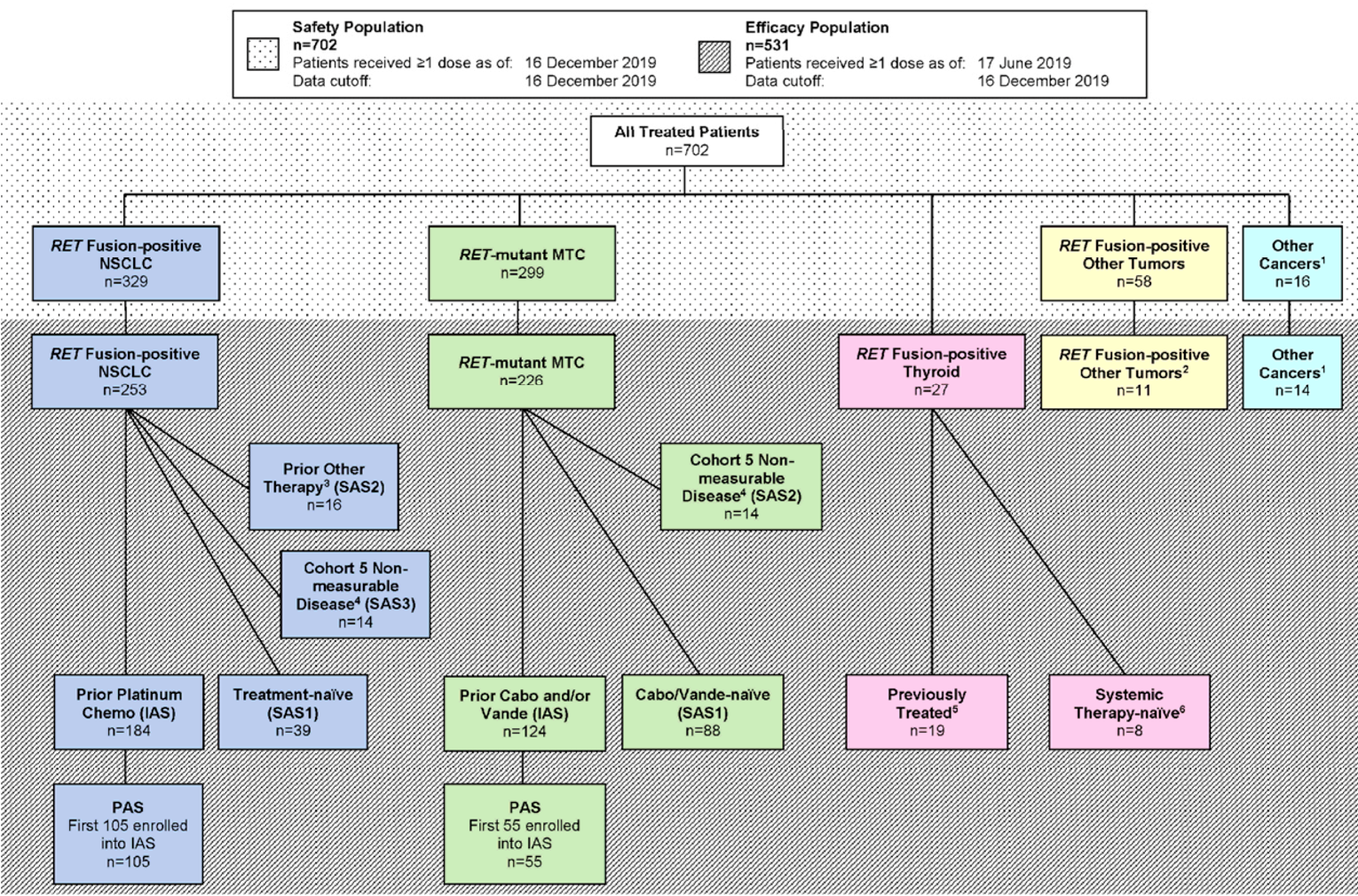
Cabo = cabozantinib; chemo = chemotherapy; IAS = integrated analysis set; MTC = medullary thyroid cancer; NSCLC = non–small cell lung cancer; PAS = primary analysis set; RET = rearranged during transfection; SAS = supplemental analysis set; Vande = vandetanib.
1Other tumours that do not fit the other disease cohorts.
Source: LIBRETTO-001 Clinical Study Report.18
Populations
Inclusion and Exclusion Criteria
As described in Table 7, patient inclusion criteria included those with a locally advanced or metastatic solid tumour whose disease has progressed on or who are intolerant to standard therapy, or no standard therapy exists or, in the opinion of the investigator, are not candidates for or would be unlikely to tolerate or derive significant clinical benefit from standard therapy, or who decline standard therapy.
Patients should have been at least 18 years of age. However, for countries and sites where approved, patients as young as 12 years of age could be enrolled. An ECOG PS score of 0, 1, or 2 (age ≥ 16 years) or a Lansky Performance Score of 40% or greater (age < 16 years) with no sudden deterioration 2 weeks before the first dose of the study treatment was used for inclusion. For patients being enrolled into a specific phase II dose expansion, evidence of a RET gene alteration in a tumour (i.e., not just blood), was required (a positive germline test for a RET mutation was acceptable for patients with MTC). Adequate hematologic, renal, and hepatic status was necessary to enter the study.
When considering previous treatment failure with standard of care, cabozantinib and vandetanib were both considered standard-of-care therapies for patients with RET-mutant MTC (cohort 3 of the entire LIBRETTO-001 study).
Patients were excluded if they had a specific oncogenic driver that could cause resistance to selpercatinib treatment. Also, they could be excluded if they had received prior treatment with RET inhibitors, an investigational drug, or an anti-cancer therapy within 5 half-lives or 2 weeks (whichever is shorter) before the planned start of selpercatinib. In addition, no concurrent investigational anti-cancer therapy was permitted. Major surgery, radiotherapy, unresolved toxicities from prior therapies, and symptomatic CNS tumour and metastases were considered exclusion criteria.
Baseline Characteristics
Baseline demographic information, disease characteristics, and prior medications are described in Table 8. This table reports on the subpopulation with RET-mutant MTC for the 3 cut-off dates.
The median age of the group was |||| ||||| |||| |||| | |||||||| ||||| |||| |||| || ||||| || |||| ||| |||||| ||||||| || ||| || ||||| || |||| || ||||| || ||||| || |||||||||||| || |||| ||||| |||| || ||| |||| ||| |||||. Most patients had an ECOG PS status of 0 or 1, with only || |||||| presenting with an ECOG PS of 2, and the majority were stage IV or above at diagnosis, |||| || ||||||| || || |||||| ||||| |||||||||. All but ||| patients had a history of metastatic disease. The majority of patients ( | |) had the M918T RET mutation type. |||| |||||||| ||||||||| |||||||| || |||||||| ||||||||.
In terms of previous therapies, the majority ||||||| had received prior systemic therapies at baseline, mostly consisting of vandetanib ||||||| and cabozantinib ||||||||. Only ||||| had not received any prior systemic regimen. Prior cancer-related therapy was reported in ||||| of patients.
Table 8: Summary of Baseline Characteristics, RET-Mutant MTC
Variable | December 16, 2019 cut-off date N = 226 | ||||
|---|---|---|---|---|---|
PAS N = 55 | IAS N = 124 | SAS 1 N = 88 | SAS 2 N = 14 | ||
Baseline demographic | |||||
Age in years, median (range) | 57 (17 to 84) | |||| |||| ||| | 58 (15 to 82) | |||| |||| ||| | |
||| |||||| | ||| | |||||
||| ||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|| || ||| ||||| | | |||||| | || |||||| | || |||||| | | |||||| | |
|| || ||| ||||| | || |||||| | || |||||| | || |||||| | | |||||| | |
|| || ||| ||||| | || |||||| | || |||||| | || |||||| | | |||||| | |
| || ||||| | | |||||| | || ||||| | | |||||| | | ||||| | |
Sex, n (%) | |||||
Male | 36 (65.5) | || |||||| | 58 (65.9) | | |||||| | |
Female | 19 (34.5) | || |||||| | 30 (34.1) | | |||||| | |
Race, n (%) | |||||
American Indian or Alaska Native | 0 (0.0) | | ||||| | 0 (0.0) | | ||||| | |
Asian | 0 (0.0) | | ||||| | 4 (4.5) | | ||||| | |
Black or African American | 1 (1.8) | | ||||| | 1 (1.1) | | ||||| | |
Native Hawaiian or Other Pacific Islander | 0 (0.0) | | ||||| | 1 (1.1) | | ||||| | |
Other | 5 (9.1) | | ||||| | 7 (8.0) | | ||||| | |
White | 49 (89.1) | 111 (89.5) | 75 (85.2) | 13 (92.9) | |
BMI (kg/m2), mean (SD) | ||||| |||||||| | ||||| |||||| | ||||| |||||| | ||||| |||||| | |
Weight (kg), mean (SD) | ||||| ||||||| | ||||| ||||||| | ||||| ||||||| | ||||| ||||||| | |
ECOG PS at screening, n (%) | |||||
0 | 11 (20.0) | || | ||||| | 43 (48.9) | | | ||||| | |
1 | 41 (74.5) | || | ||||| | 42 (47.7) | | | ||||| | |
2 | 3 (5.5) | | ||||| | 3 (3.4) | | ||||| | |
Calcitonin (pg/mL), mean (SD) | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||||||| | |
CEA (ng/mL), mean (SD) | ||||||||||||||| | ||||||||||||||| | |||||||||||||| | ||||||||||||| | |
Cancer history | |||||
Stage at initial diagnosis (n, %) | |||||
|||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|||| | | ||||| | | ||||| | | ||||| | | ||||| | |
||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|| | || |||||| | || |||||| | || |||||| | | |||||| | |
||| | | |||||| | || ||||| | | ||||| | | |||||| | |
||| | | ||||| | | ||||| | | ||||| | | ||||| | |
||| | || |||||| | || |||||| | || |||||| | | |||||| | |
||||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|||||| ||||| ||||||| |||||||||| |||| |||| | ||||||||||| | ||||||||||| | |||||||||||| | |||||||||||| | |
||||||| || |||||||||| ||||||| ||| || | || |||||| | ||| |||||| | || ||||| | || |||||| | |
|||||| ||||| ||||||| ||||||||| || |||||||||| |||||||| |||| |||| | |||||||||||| | |||||||||||| | ||||| |||||| | |||||||||||| | |
Disease characteristics | |||||
RET mutation type, n (%) | |||||
M918T | 33 (60.0) | ||||||||| | 49 (55.7) | |||||||| | |
Extracellular cysteine mutation | 7 (12.7) | ||||||||| | 20 (22.7) | |||||||| | |
V804 M/L | 5 (9.1) | ||||||| | 6 (6.8) | ||||||| | |
Other | 10 (18.2) | ||||||||| | 13 (14.8) | ||||||| | |
Molecular assay type, n (%) | |||||
NGS on tumour | || |||||| | ||||||||| | ||||||||| | || |||||| | |
PCR | 9 |||||| | || |||||| | || |||||| | | ||||| | |
||| || |||||||||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|||||||| || |||||||| || |||||||| ||| || | || | ||||| | || | ||||| | || | ||||| | | | ||||| | |
|| ||||| ||| |||||||||| |||||| ||| |||||||||||| ||| || | || |||||| | ||| |||||| | || |||||| | | ||||| | |
Prior cancer treatment | |||||
Received prior systemic therapy, n (%) | || ||||||| | ||| ||||||| | || ||||||| | | ||||||| | |
Type of prior systemic therapy, n (%) | |||||
MKI | |||||||||| | ||||||||||| | ||||||| | |||||||| | |
|||||||||||| | || |||||| | || |||||| | | ||||| | | |||||| | |
|||||||||| | || |||||| | || |||||| | | ||||| | | |||||| | |
||||||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|||||||||| | | |||||| | || ||||| | | ||||| | | ||||| | |
||||| |||| | || |||||| | || |||||| | | ||||| | | ||||| | |
|||||||||||| | | |||||| | || |||||| | | ||||| | | ||||| | |
|||||||| |||||||||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
||||||||||| |||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|||||||||||||| ||||||| | | |||||| | || ||||| | | ||||| | | ||||| | |
||||||||| ||| ||||||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
|||||| |||||||||||| | | ||||| | | ||||| | | ||||| | | ||||| | |
||||| |||||||| ||||||| | | |||||| | || |||||| | | ||||| | | ||||| | |
|||| | | ||||| | | ||||| | || |||||| | | |||||| | |
|||| | || |||||| | || |||||| | || |||||| | | |||||| | |
| || |||| | || |||||| | || |||||| | | ||||| | | ||||| | |
Number of prior systemic regimens, mean (SD)d | 2.2 |||||| | |||||||||| | 0.2 |||||| | ||| ||||||| | |
Partial response | | ||||| | || |||||| | | ||||| | | ||||| | |
|||||| ||||||| | || |||||| | || |||||| | | ||||| | | |||||| | |
||||||||||| ||||||| | || |||||| | || |||||| | | ||||| | | ||||| | |
||| ||||||||| | || |||||| | || |||||| | | ||||| | | |||||| | |
||||||| | | ||||| | | ||||| | || |||||| | | |||||| | |
||||| |||||||||||| ||| || | || |||||| | || |||||| | || |||||| | | |||||| | |
||||| |||||||||||||| ||||||| ||| || | || |||||| | ||| |||||| | || |||||| | || |||||| | |
BMI = body mass index; CEA = carcinoembryonic antigen; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IAS = integrated analysis set; MKI = multikinase inhibitor; MTC = medullary thyroid cancer; NGS = next-generation sequencing; NR = not reported; PAS = primary analysis set; PCR = polymerase chain reaction; RET = rearranged during transfection; SAS = supplemental analysis set; SD = standard deviation.
aSafety analysis set.
bPrior treatment with cabozantinib and/or vandetanib.
cIncludes all stage II and III.
dFor the March 30, 2020 data cut-off, the median and range are reported.
Source: LIBRETTO-001 Clinical Study Report.18
Interventions
Selpercatinib was to be administered as either oral capsule or suspension, once or twice daily, depending on cohort assignment. Dosing followed a fixed milligram format (as opposed to being based on weight or on body surface area).
In the dose-escalation phase (phase I) of the study, patients were to be assigned in a sequential (non-randomized) fashion to the planned dose levels. The starting dose of selpercatinib used was 20 mg, given once daily. Selpercatinib was provided in various forms for oral dosing as capsules (powder) containing 20 mg of the drug. These were provided to the sites in bottles of 25 capsules. Selpercatinib was also provided in a simple blend with excipients in a capsule in dose strengths of 10 mg, 20 mg, and 80 mg. A third option was the use of liquid suspension (from protocol version 5.0). Dose escalation continued to 240 mg twice a day.
The RP2D of selpercatinib was set at 160 mg twice a day; this dose was selected by the sponsor in conjunction with the SRC for the LIBRETTO-001 study. The RP2D is used in the phase II portion of the study, in which all patients began dosing at the recommended dose that was determined to be safe in the escalation portion.
Distribution of all patients from the LIBRETTO-001 study to the cohorts established (Figure 2) was made by the sites according to tumour type and was reviewed by the sponsor during screening. Patients in all cohorts received the same study drug in a non-randomized, non-blinded fashion.
Allowed concomitant medications included standard supportive medications used in accordance with institutional guidelines and investigator discretion. Examples include hematopoietic growth factors to treat neutropenia, anemia, or thrombocytopenia; anti-emetic, analgesics, and antidiarrheal medications; glucocorticoids, including short courses to treat asthma, chronic obstructive pulmonary disease, and so forth; thyroid replacement therapy for hypothyroidism, bisphosphonates, denosumab, and other medications for the treatment of osteoporosis and the prevention of skeletal-related events from bone metastases; and/or hypoparathyroidism. Local treatment while receiving selpercatinib (e.g., palliative radiation therapy or surgery for bone metastases) was permitted with sponsor approval.
Concomitant systemic anti-cancer drugs, hematopoietic growth factors for prophylaxis in cycle 1, therapeutic monoclonal antibodies, drugs with immunosuppressant properties, or medications known to be strong inhibitors or inducers of CYP3A4 were not allowed during the study, nor were other investigational drugs and proton pump inhibitors.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized subsequently. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | LIBRETTO-001 study end point |
|---|---|
Overall survival | Key secondary |
Progression-free survival | Key secondary |
Objective response rate | Primary |
Duration of response | Key secondary |
HRQoL
| Exploratory |
Harms (adverse events, serious adverse events, adverse events of special interest) | Key secondary |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life.
Source: LIBRETTO-001 Clinical Study Report.18
OS was derived for each patient as the number of months from the date of the first dose of the study drug to the date of death, irrespective of cause. Patients who were alive or lost to follow-up as of a data analysis cut-off date were right-censored. The censoring date was determined from the last date the patient was known to be alive or the data analysis cut-off date, whichever occurred first.
PFS was derived for each patient as the number of months from the date of the first dose of the study drug to the earlier of documented PD or death due to any cause. Patients who were alive and without documented PD as of a data analysis cut-off date were right-censored according to the censoring methods of the OS and DOR. PFS was right-censored for patients who met 1 or more of the following conditions:
no post-baseline disease assessments unless death occurred before the first planned assessment (in which case death will be considered a PFS event)
subsequent anti-cancer therapy or cancer-related surgery in the absence of documented disease progression
died or documented disease progression after missing 2 or more consecutively scheduled disease assessment visits
alive and without documented disease progression on or before the data cut-off date.
If a patient met more than 1 of these conditions, then the scenario that occurs first was used for analysis.
ORR was assessed in the LIBRETTO-001 study using RECIST 1.1 or RANO criteria as appropriate to tumour type. The analysis of ORR was conducted both by the responses determined by each investigator and responses as determined by IRC.
DOR was calculated for patients who achieved a CR or PR. For such patients, DOR was defined as the number of months from the start date of CR or PR (whichever response status is observed first) and subsequently confirmed, to the first date that PD was objectively documented. If a patient died, irrespective of cause, without documentation of PD beforehand, then the patient’s date of death was used to denote the response end date. DOR will be right-censored for patients who meet 1 or more of the following conditions:
subsequent anti-cancer therapy or cancer-related surgery in the absence of documented disease progression
died or experienced documented disease progression after missing 2 or more consecutively scheduled disease assessment visits
alive and without documented disease progression on or before the data cut-off date.
HRQoL end points were measured with the EORTC QLQ-C30, a commonly used patient-reported outcome measure in oncology clinical trials28 that consists of 30 questions. The questions are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item QoL scale. The tool uses a 1-week recall period for assessing function and symptoms. Most questions have 4 response options (not at all, a little, quite a bit, very much), with scores on these items ranging from 1 to 4.29. For the 2 items that form the global QoL scale, however, the response format is a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better QoL (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and QoL scales would reflect an improvement. Although this scale has been validated in different settings and clinical entities, no studies have assessed the validity and reliability in patients with RET-mutant MTC or other thyroid cancers. A clinically meaningful difference was defined by the sponsor as a 10-point difference (of the standardized 0 to 100 overall scale) from baseline for each patient based on a single study.29
Another HRQoL instrument used in the LIBRETTO-001 trial was the use of diarrhea or bowel diaries. The bowel diary used was a questionnaire-modified version of the Systemic Therapy Induced Diarrhea Assessment Tool (STIDAT), a standardized patient-reported questionnaire used to assess diarrhea in patients with cancer actively treated with chemotherapy or systemic therapies (with or without radiation) that are considered to have a high risk of causing diarrhea. The modified STIDAT (mSTIDAT) contains 11 questions and assesses all the dimensions in the original STIDAT except for use of antidiarrheal medication, which can reduce bowel movement frequency. In the mSTIDAT, the QoL subscale asks patients to rank the impact of bowel habits (questions 7 to 9) and diarrhea (questions 10 to 11) on their daily living from 0 (no impact) to 10 (extreme impact). The psychometric properties of STIDAT have not been validated in patients with thyroid cancer and/or those on targeted therapy. Also, no minimally important difference (MID) has been estimated for the STIDAT in either a general population or patients with thyroid cancer. Based on the ranges of scores for each severity, clinicians may categorize scores from 0 to 1.1 as no diarrhea, greater than 1.1 to 2 as mild diarrhea, greater than 2 to 3 as moderate diarrhea, and greater than 3 as severe diarrhea.
Statistical Analysis
Phase I of the study was aimed at evaluating the MTD and the RP2D (optimal dose) based on the dose-escalation process previously described. The primary end point of phase II of the LIBRETTO-001 study was to determine the antitumour activity of selpercatinib by determining the ORR using RECIST 1.1 with DOR, OS, and PFS stated as secondary end points. The frequency, severity, and relatedness of treatment-emergent adverse events (TEAEs) and SAEs, changes in hematology and blood chemistry values, assessments of physical examinations, vital signs, and ECGs were considered in both phases.
The primary analysis for the interim analysis of this study was based on data available at a cut-off of June 17, 2019. Additional 6-month follow-up data were assessed based on a December 16, 2019 cut-off date and used by the sponsor at the request of Health Canada. For the primary analysis, the PAS is presented in both cut-off dates; hence, the results from the December 16, 2019 cut-off point is the focus of this CADTH review.
Power and Sample Size
A total of approximately 120 patients was estimated to be enrolled in phase I.
For phase II of the study, in cohort 3 (patients with RET-mutant MTC who progressed on or were intolerant to vandetanib and/or cabozantinib), a true ORR of 35% or greater was hypothesized when selpercatinib was administered to such patients. A sample size of 83 patients was estimated to provide 85% power to achieve a lower boundary of a 2-sided 95% exact binomial CI for the estimated ORR that exceeds 20%. Ruling out a lower limit of 20% was considered clinically meaningful in patients who have failed prior MKI therapy (e.g., cabozantinib) and currently have limited treatment options for their advancing disease.
For cohort 4 (patients with RET-mutant MTC who are MKI-naive), a true ORR of ≥ 50% was hypothesized when selpercatinib was administered to such patients. A sample size of 55 patients was estimated to provide 85% power to achieve a lower boundary of a 2-sided 95% exact binomial CI for the estimated ORR that exceeds 30%.
Statistical Tests and Models for Efficacy End Points
The previously described safety analysis set was used for studying the primary end points of antitumour activity of selpercatinib. The sponsor presents efficacy analyses by each phase II cohort of the LIBRETTO-001 study. Patients treated during the phase I portion of the study who met the phase II eligibility criteria for 1 of the phase II cohorts were included as part of the evaluable patients for that cohort for the efficacy analyses. The analysis of response for the interim Clinical Study Report (June 6, 2019) was based on the responses determined by the investigator.
The estimate of ORR was calculated based on the maximum likelihood estimator (i.e., crude proportion of patients with a best overall response of CR or PR). The estimate of the ORR was accompanied by a 2-sided 95% exact binomial CI. Best overall response for each patient (CR, PR, stable disease, PD, or non-evaluable) occurring between the first dose of selpercatinib and the date of documented disease progression or the date of subsequent anti-cancer therapy or cancer-related surgery was determined based on the RECIST 1.1 criteria for primary solid tumours.
OS, PFS, and DOR were summarized descriptively using the Kaplan-Meier method. The Kaplan-Meier estimate with 95% CI calculated using the Brookmeyer and Crowley method was provided for the median. The event-free rate with the 95% CI calculated using the Greenwood formula was provided for selected time points. The median follow-up for each of these end points was estimated according to the Kaplan-Meier estimate of potential follow-up.30
EORTC QLQ-C30 (version 3.0) was assessed using descriptive analyses reporting the median or quartile, mean (SD), and mean change (standard deviation [SD]) from baseline for each subscale at each study visit for the study cohort. The sponsor reported the number and percentage of patients whose conditions were improving, stable, or worsening at each visit time point for all patients, and the number and proportion of patients experiencing definite improvement and time to definite improvement (defined as an improvement from baseline by 10 or more points without any further deterioration in score by 10 or more points). Similarly, the number and proportion of patients experiencing definite worsening and time to definite worsening (defined as time until the first worsening from baseline, i.e., a decrease of 10 or more points without any further improvement of 10 or more points) were also reported.
The results of the Pediatric Quality of Life Inventory 4.0 core module were also reported descriptively to report HRQoL in patients aged 13 to 17 years (using the teen version) and in patients aged 12 years (using the version for children).
The bowel diary questionnaire was used with a modified version of the STIDAT, a standardized patient-reported questionnaire used to assess systemic therapy–induced diarrhea in oncology patients. For this end point, the Kaplan-Meier method was used to evaluate time to first improvement (among those with diarrhea at baseline) and time to first worsening (for the entire MTC cohort), respectively, for which worsening is defined as any stepwise categorical decline in the diarrhea item 1 (e.g., no diarrhea to mild, moderate, or severe; mild to moderate or severe; moderate to severe), and improvement is defined as any stepwise improvement (e.g., mild to no diarrhea; moderate to mild or no diarrhea; severe to moderate, mild, or no diarrhea). For patients with improvement, the duration of improvement (defined as the time from the first improvement until any stepwise categorical decline) was reported as median with 95% CI, mean (SD) days.
Subgroup analyses were not determined a priori in the protocol stage or the main interim analysis (June 17, 2019); however, subgroups are presented in a latter cut-off date report (December 16, 2019) for ORR based on age at enrolment, sex, race, ECOG PS, RET mutation type, metastatic disease, and prior systemic therapies.
For these end points and analyses, an approach accounting for multiple testing was not described.
Sensitivity and Subgroup Analyses
Sensitivity analyses were described for an interim analysis as using report data based on IRC or based on investigator assessments. No specific sensitivity analyses are described in the protocol.
Similarly, subgroups were not defined in the protocol. However, a section of efficacy outcomes is presented descriptively without subgroup effects analyses for the December 16, 2019 cut-off date, based on age, sex, race, ECOG PS, RET mutation type, metastatic disease, prior systemic therapies, and RET molecular assay; all of these were described only for the outcome of ORR.
Analysis Populations
Analysis sets in all the LIBRETTO-001 populations are described in the Description of Studies and Populations sections of this report. The analysis sets created for the main analysis were the following:
Safety analysis set. The safety analysis set included all enrolled patients who received 1 or more doses of selpercatinib. The safety analysis was conducted on the SAS. A baseline measurement of at least 1 laboratory or other safety-related measurement obtained after treatment with the study drug may have been required for a specific safety parameter to be included in the analysis.
Dose-limiting toxicity (DLT) analysis set. The DLT analysis set included all patients enrolled in the phase I dose-escalation phase who had a DLT within the first 28 days on study, or those without a DLT but who completed safety assessments through the first 28 days of treatment in cycle 1 and received at least 75% of the planned total dose during cycle 1. Patients who were replaced for the determination of MTD were not included in this analysis set. Each patient who received less than 75% of planned doses during cycle 1 was reviewed by the SRC. If the SRC determined that the reason or reasons for treatment discontinuation were not related to the patient’s underlying disease, other medical condition, or concomitant medications, the treatment discontinuation was considered a DLT. The DLT summary was conducted on the DLT analysis set for the phase I dose escalation for each dose level.
Patient-reported outcome analysis set. These analysis sets were defined separately for each patient-reported outcome instrument and included all treated patients who had a baseline and at least 1 post-baseline patient-reported outcome assessment.
Efficacy analysis set. For the interim Clinical Study Report (cut-off date June 17, 2019), the efficacy analysis was conducted on the SAS by phase II cohort, unless otherwise specified. Patients enrolled during dose escalation and dose expansion (phase I) were to be included in the appropriate phase II cohort dataset if they met the enrolment criteria for that cohort.
For the population including patients with RET-mutant MTC, the analysis sets included the following:
PAS. This includes the first 55 patients with RET-mutant MTC enrolled in the phase I and phase II portions of LIBRETTO-001 as of June 17, 2019, who had been previously treated with cabozantinib or vandetanib.
IAS. This includes all patients with RET-mutant MTC enrolled in LIBRETTO-001 who met the same eligibility criteria as the PAS by the June 17, 2019 data cut-off for the initial US submission (N = 124). The PAS is a subset of patients in the IAS who had been previously treated with cabozantinib or vandetanib. This IAS provides further information on the efficacy of selpercatinib in a larger number of patients, providing increased information in the PAS results. The efficacy data presented in the Canadian submission is based on a December 16, 2019 cut-off date.
SAS 1. This includes all cabozantinib or vandetanib treatment-naive patients with RET-mutant MTC.
SAS 2. This includes patients without measurable disease by RECIST 1.1.
Results
Patient Disposition
The LIBRETTO-001 study screened a total of ||| patients of all populations for the initial inclusion criteria, of which || ||||||| did not meet the eligibility criteria, as shown in Table 10. The study included 531 patients in the efficacy population (i.e., those who received ≥ 1 dose of selpercatinib as of the June 17, 2019 and December 16, 2019 cut-off dates).
The study focus for this review is the population with RET-mutant MTC, which consisted of 226 patients in the efficacy population and 299 in the safety population. Of the patients in the efficacy population, ||||| |||||||||||| ||| ||||| ||||| |||||| ||| || ||||||| ||||||||||| || ||||||| |||||| ||| | |||||||| |||||||||||| ||||| |||| ||| || |||||.
Criteria | MTC population |
|---|---|
||||||||| | | ||| |
|||||| |||||||| | ||| | || |||||| |
|||||||| || ||| ||| ||||||||||| | ||| | ||| |
|||||||| ||| |||||||| || ||||| ||| |||| || ||||||||||||| ||| ||| | ||| | ||| |||||| |
|||||||||||| ||||| ||||| | ||| | || |||||| |
|||||| ||| ||||||||||||||| || ||||| ||||| | ||| | |
||||||| ||||||||||| | || ||||| |
||||||| |||||| | || ||||| |
||||| | | ||||| |
|||||||||| || ||||||| | | ||||| |
|||| || ||||||||| | |||| |
|||||||| ||||||||| | | ||||| |
||||| | | ||||| |
||||||||||||||| |||| |||||| | ||| | || |||||| |
|||||| ||| ||||||||||||||| |||| |||||| | ||| | |
|||||||||| || ||||||| | | ||||| |
|||| || ||||||||| | | ||||| |
||||| | || ||||| |
|||| | | |||| |
||| | | |||| |
Safety, Na | 299 |
ITT = intention to treat; MTC = medullary thyroid cancer; PP = per protocol.
Note: Cut-off date of December 16, 2019.
aSafety population (safety analysis set) included all enrolled patients who received 1 or more doses of selpercatinib.
Source: LIBRETTO-001 Clinical Study Report.18
As shown in Figure 3 and Figure 4, of the 226 patients within the MTC efficacy population, 88 were included in the treatment-naive (not treated with cabozantinib or vandetanib) patient group (SAS 1), 124 were among those previously treated with cabozantinib or vandetanib (IAS), and 14 were in cohort 5 with non-measurable disease (SAS 2). The first 55 patients previously treated with cabozantinib or vandetanib were included in the PAS, which is a subset of the IAS.
Exposure to Study Treatments
At the time of the December 16, 2019 interim analysis, of the 531 patients (all populations from the LIBRETTO-001 study) who received selpercatinib, the majority || | |||| were started at a phase II dose of 160 mg twice daily. Of the 439 patients who started at the phase II dose of 160 mg twice daily, ||| ||||||| patients were continuing treatment. The median actual dose intensity (milligrams of selpercatinib per day) was influenced by the fact that the patients underwent intra-patient dose escalation and, therefore, although actual dose intensity increased with increasing doses, many patients ultimately received higher doses than their starting dose, most often 160 mg twice a day. The median relative dose intensity (actual dose intensity divided by the planned dose intensity) ranged from |||||| || |||||| for all dose levels.
The 226 patients with RET-mutant MTC had a mean || |||| ||||||||| ||||||||| |||| || || |||||| || ||||||||| ||| | |||||| || |||| |||||| |||||||| |||| ||| || |||| |||||||.
Among the 299 patients in the safety analysis set, the most common concomitant medications used (in more than 20% of patients) included thyroid hormones in | | | |||||| | |||| | ||| | ||||||| | |||| | |||||||| | | | | |||||| | ||||||||| | | | |||||| | ||||||||| | ||||||||| | |||| | ||||||||| | | | |||||| | ||||||||||||| | | | |||||| | ||||||||||| | ||||||||||||||| | |||| | ||||| | | | |||||| | | | ||||||||||||| | | ||||||||.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported subsequently, and the primary analysis is focused on the PAS for the December 16, 2019 cut-off date. When available, the results of the previous data cut-offs of June 17, 2019 and March 30, 2020 are also presented. All of the efficacy results presented were evaluated by IRC.
Survival
Overall Survival
OS in the efficacy population with MTC (December 16, 2019 data cut-off date) had a median duration of follow-up of |||| |||||| |||||||||||||| ||||| ||||| |||| || ||||| ||| ||| |||||| ||| |||||||| ||| ||| ||| |||||||||| ||| ||| ||||||| |||||| |||||| ||| |||||| || ||||| |||| |||| ||| || ||| |||||||||| ||| ||||| |||||||||| || |||||||| ||| ||| ||||| |||| |||| ||| || |||| |||||| (Table 11 and Figure 5). The rate of survival at 12 months or more was ||||| || ||| |||||||||| |||| || |||| || ||||||.
For the March 30, 2020 cut-off date, the group of patients in the PAS (n = 55) reached a median OS of 33.2 months (range, 1.1+ to 33.3+) with similar values in the treatment-naive IAS group. The SAS group did not reach the median of survival (Table 11).
Table 11: Efficacy Outcomes of Survival — LIBRETTO-001 December 16, 2019 and March 30, 2020 Cut-Off Dates
Variable | December 16, 2019 cut-off date | March 30, 2020 cut-off date | ||||||
|---|---|---|---|---|---|---|---|---|
PAS N = 55 | IAS N = 124 | SAS 1 N = 88 | SAS 2 N = 14 | PAS N = 55 | IAS N = 143 | SAS 1 N = 112 | SAS 2 N = 19 | |
Overall survivala | ||||||||
Median duration of overall survival, months (range)a | NE ||||| |||||| | ||||| | ||||| | ||||| | 33.25 (1.1 to 33.3+) | 33.25 (0.4 to 33.3+) | NE (2.2+ to 29.8+) | NE (6.8+ to 19.9+) |
Median duration of follow-up, months (IQR) | |||||||||||| ||||| | ||||| | ||||| | ||||| | 22.08 (19.9 to 28.3) | 15.70 (11.3 to 21.1) | 13.83 (9.6 to 18.4) | 14.19 (9.4 to 17.4) |
Rate of overall survival of 12 months or more, % (95% CI) | |||| |||||| ||||| | ||||| | ||||| | ||||| | 86.9 (74.4 to 93.5) | 86.9 (79.7 to 91.6) | 100 (100.0 to 100.0) | 100 (100.0 to 100.0) |
Progression-free survival | ||||||||
Median duration of progression-free survival, months (range)a | NE |||| |||||| | ||||||||| |||||| | 23.56 |||||| |||||| | ||||||||| |||||| | NE (0.0+ to 32.2+) | NE (0.0+ to 32.2+) | NE (0.0+ to 25.8+) | NE (5.0+ to 19.1+) |
Median duration of follow-up, months (IQR) | 16.69 |||||| ||||| | |||||||||| |||| | 11.07 |||| |||| | |||||||||| |||| | 20.27 (19.1 to 27.6) | 13.90 (9.3 to 19.3) | 11.10 7.6 to 16.6 | 11.73 7.4 to 14.1 |
Duration of progression-free survival, n (%) | ||||||||
< 6 months | | |||||| | || |||||| | || |||||| | | ||||| | NR | NR | NR | NR |
≥ 6 to 12 months | | |||||| | || |||||| | || |||||| | | |||||| | NR | NR | NR | NR |
≥ 12 to 18 months | || |||||| | || |||||| | || |||||| | | |||||| | NR | NR | NR | NR |
≥ 18 to 24 months | | |||||| | | ||||| | | ||||| | | ||||| | NR | NR | NR | NR |
≥ 24 months | || |||||| | || ||||| | | ||||| | | ||||| | NR | NR | NR | NR |
Rate of progression-free survival, % (95% CI) | ||||||||
≥ 6 months | NR | NR | NR | NR | 92.4 (81.0 to 97.1) | 89.5 (82.9 to 93.7) | 98.2 (92.9 to 99.5) | 94.1 (65.0 to 99.1) |
≥ 12 months | NR | NR | NR | NR | 82.3 (68.7 to 90.4) | 76.9 (67.9 to 83.7) | 92.9 (84.5 to 96.8) | 94.1 (65.0 to 99.1) |
≥ 18 months | NR | NR | NR | NR | 73.8 (59.1 to 83.9) | 67.9 (57.0 to 76.6) | 88.7 (78.0 to 94.4) | 94.1 (65.0 to 99.1) |
≥ 24 months | NR | NR | NR | NR | 66.8 (50.1 to 79.0) | 61.4 (48.0 to 72.4) | 59.2 (8.8 to 89.3) | NE to (NE to NE) |
CI = confidence interval; FAS = full analysis set; IAS = integrated analysis set; IQR = interquartile range; IRC = independent review committee; ITT = intention to treat; LS = least squares; NE = not estimable; NR = not reported; PAS = primary analysis set; + = censored observation; SAS = supplemental analysis set; SD = standard deviation.
Note: All end points were based on IRC assessments with a December 16, 2019 cut-off date.
aEstimate based on Kaplan-Meier method.
Source: LIBRETTO-001 Clinical Study Report.18

+ = censored observation.
Figure contained confidential information and was removed at the request of the sponsor.
Source: LIBRETTO-001 Clinical Study Report.18
Progression-Free Survival
PFS in patients with MTC in the PAS at the December 16, 2019 cut-off date had a median duration of follow-up of 16.7 months |||| |||| || ||||||. The median for PFS for the PAS population was not reached and the range went from | || |||| |||||| (Table 11 and Figure 6, Figure 7, and Figure 8). The rate of PFS at 12 months or more was ||||| of the population.
For the March 30, 2020 cut-off date, no patients in the groups evaluated (PAS, IAS, SAS) reached the median for PFS (range 0.0+ to 32.2+).
Figure 6: Kaplan-Meier Plot of PFS Based on IRC Assessments (Primary Analysis Set, N = 55)
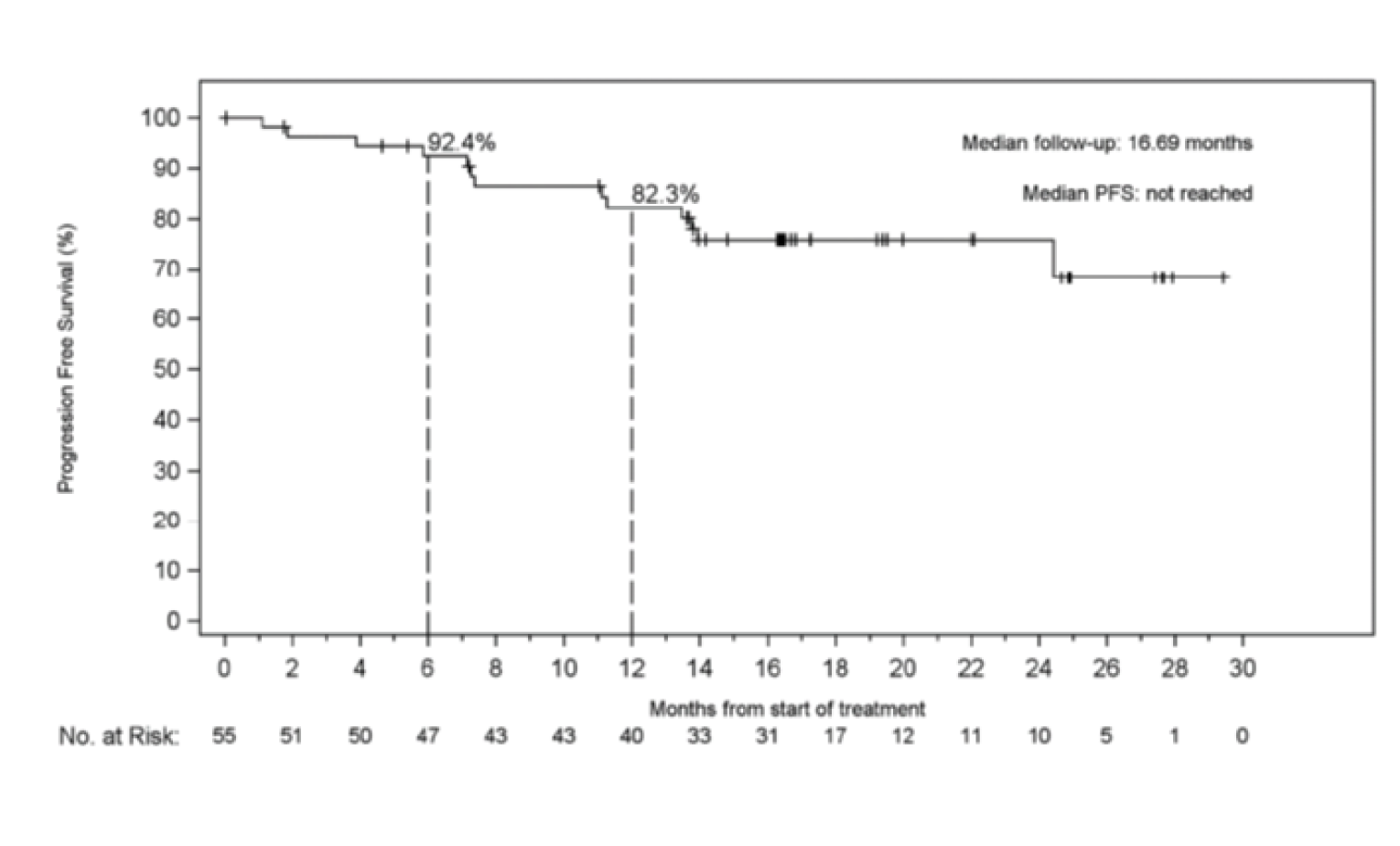
IRC = independent review committee; PFS = progression-free survival; + = censored observation.
Source: LIBRETTO-001 Clinical Study Report.18

+ = censored observation.
The figure contained confidential information and was removed at the request of the sponsor.
Source: LIBRETTO-001 Clinical Study Report.18

+ = censored observation.
Figure contained confidential information and was removed at the request of the sponsor.
Source: LIBRETTO-001 Clinical Study Report,18
Response and Remission
Objective Response Rate
The percentage of patients reaching an ORR for the PAS population was 69.1% (95% CI, 55.2 to 80.9) as of the December 16, 2019 cut-off date and, overall, it was similar across the different sets. Similarly, for the March 30, 2020 cut-off date, results for ORR were 69.1% for the PAS population and similar across other sets (Table 12).
Duration of Response
At the cut-off date of December 16, 2019, the DOR had a median follow-up of 14.06 months (||| || || ||||) in the PAS, and the median DOR was not reached in any analysis set, except for SAS 1 (21.9 months, ||||| ||| || ||). For the March 30, 2020 cut-off date, the results were similar, except for the SAS 1 group, where the DOR reached a median of 21.9 months (range, 1.5 to 24.1) but with a median follow-up of 9.26 months (Table 12, Figure 9).
The total percentage of patients reaching a DOR for more than 12 months was || ||||| || ||| |||| ||||| || ||| |||| ||||| || ||||| ||| || || |||| for the December 16, 2019 cut-off date. For the March 30, 2020 cut-off date, the percentage of patients reaching a DOR for more than 12 months was 68.4% in the PAS group (Table 12).
Table 12: Efficacy Outcomes of Response or Remission — LIBRETTO-001 MTC, December 16, 2019 and March 30, 2020 Cut-Off Dates
Variable | December 16, 2019 cut-off date | March 30, 2020 cut-off date | ||||||
|---|---|---|---|---|---|---|---|---|
PAS N = 55 | IAS N = 124 | SAS 1 N = 88 | SAS 2 N = 14 | PAS N = 55 | IAS N = 143 | SAS 1 N = 112 | SAS 2 N = 19 | |
Objective response rate (CR plus PR) a,b | ||||||||
Patients, N (%) | 38 (69.1) | || |||||| | 64 (72.7) | | |||||| | 38 (69.1) | 99 (69.2) | 80 (71.4) | 5 (26.3) |
95% CI | 55.2 to 80.9 | ||||| |||| | 62.2 to 81.7 | |||| |||| | 55.2 to 80.9 | 61.0 to 76.7 | 62.1 to 79.6 | 9.1 to 51.2 |
Duration of response | ||||||||
Median duration of response, months (range) | NE |||||| |||||| | ||||||||| |||||| | 21.95 (1.8+ to 21.9) | ||||||||| ||||| | NE (2.8+ to 26.7+) | NE (1.7+ to 26.7+) | 21.95 (1.5+ to 24.1) | NE (3.5+ to 10.3+) |
Median follow-up, months (IQR) | 14.06 |||||| ||||| | |||| |||||| ||||| | 7.79 ||||| ||||| | |||||||||| |||| | 17.45 (12.9 to 22.0) | 10.05 (5.9 to 15.9) | 9.26 (5.6, 14.7) | 9.23 (3.7 to 9.3) |
Duration of response, n (%) < 6 months ≥ 6 to 12 months ≥ 12 to 18 months ≥ 18 to 24 months ≥ 24 months | ||| |||||||| ||||||||| |||||||| |||||||| ||||| | |||| ||||||||| ||||||||| |||||||| ||||||| ||||| | |||| |||||| ||| |||||| ||| |||||| || ||||||| ||||| | ||| |||||||| |||||||| ||||||| ||||| || ||||| | 6 (15.8) 6 (15.8) 14 (36.8) 8 (21.1) 4 (10.5) | 32 (32.3) 31 (31.3) 24 (24.2) 8 (8.1) 4 (4.0) | 30 (35.7) 25 (31.3) 17 (21.3) 7 (8.8) 1 (1.3) | 2 (40.0) 3 (60.0) 0 0 0 |
CI = confidence interval; CR = complete response; FAS = full analysis set; IAS = integrated analysis set; IQR = interquartile range; ITT = intention to treat; LS = least squares; MTC = medullary thyroid cancer; NE = not estimable; PAS = primary analysis set; + = censored observation; PR = partial response; SAS = supplemental analysis set; SD = standard deviation; SE = standard error.
Note: All end points were based on independent review committee assessments.
aObjective response rate (%) is defined as the proportion of patients with a best overall response of confirmed CR or PR. Response was confirmed by a repeat assessment no less than 28 days later.
bThe 95% CI was calculated using the Clopper-Pearson method.
cEstimate based on Kaplan-Meier method.
Source: LIBRETTO-001 Clinical Study Report.18
Figure 9: Kaplan-Meier Plot of DOR Based on IRC Assessments (Primary Analysis Set)
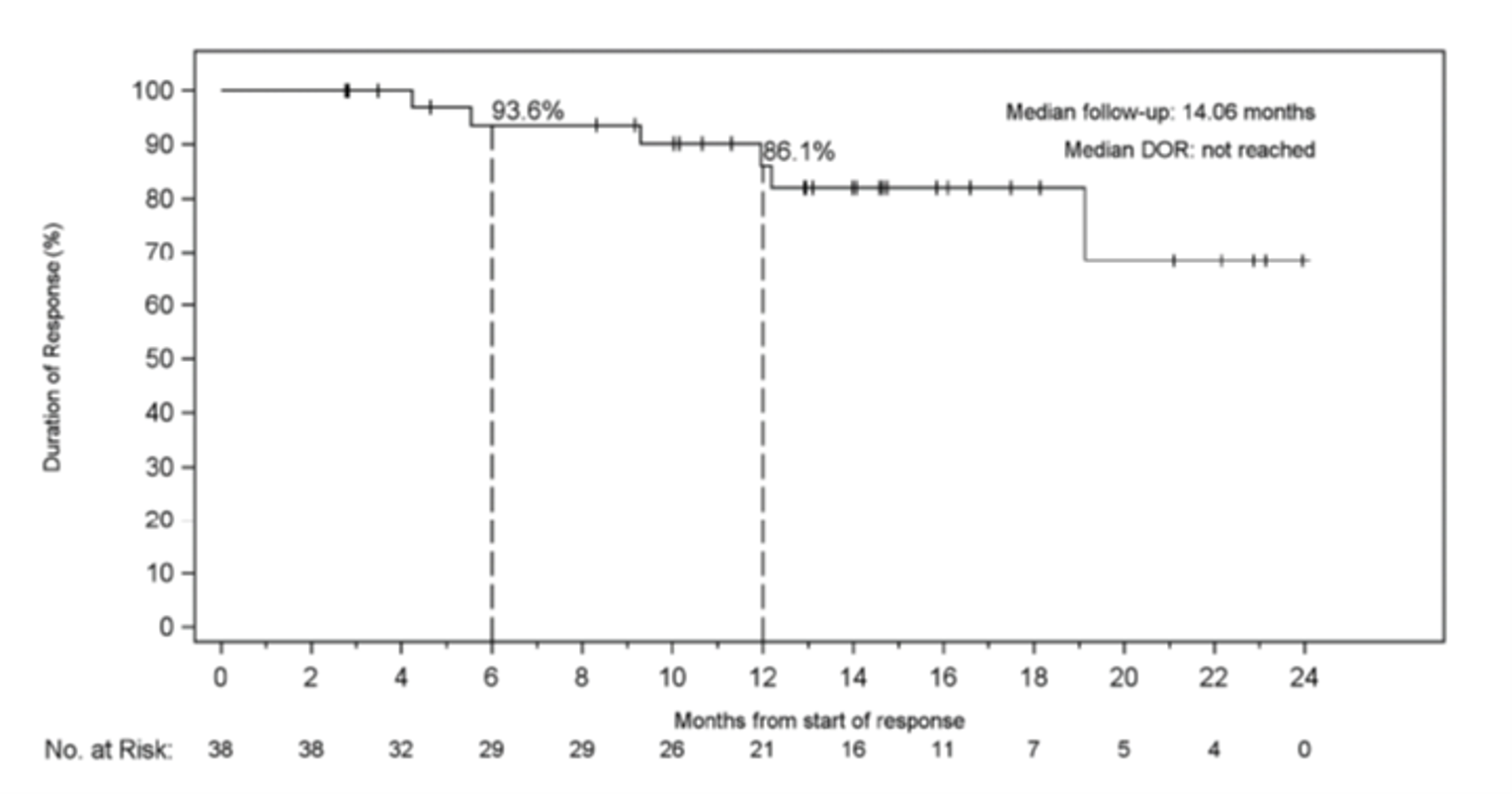
DOR = duration of response; IRC = independent review committee.
Source: LIBRETTO-001 Clinical Study Report.18
Health-Related Quality of Life
EORTC QLQ-C30
EORTC QLQ-C30 was measured as an exploratory end point in a specific analysis set of the MTC population (Table 13). No patients were able to complete the pediatric questionnaire for HRQoL; hence, no results are provided on this measurement. Patients completed the EORTC QLQ-C30 version 3.0 at baseline (cycle 1, day 1, before study treatment) and approximately every 8 weeks thereafter, corresponding to imaging assessments (approximately every other cycle) until cycle 13.
Data from the December 16, 2019 cut-off date was obtained from a publication by the sponsor,17 where a change in global health status/QoL or functional subscale score was considered an improvement if it increased from baseline by 10 or more points and considered a worsening if it decreased from baseline by 10 or more points. Conversely, a decrease from baseline of 10 or more points in symptom subscale score was considered an improvement, and an increase from baseline of 10 or more points in symptom subscale score was considered a worsening. Patients who met the threshold for either improvement or worsening in change from baseline subscale score, without further changes of 10 or more points reversing that change, were considered to have a definite improvement or definite worsening, respectively. Functional subscale values lower than the established thresholds were considered clinically meaningful: physical function scores less than 83, emotional function less than 71, role function less than 58, cognitive function less than 75, and social function less than 58. Conversely, symptom subscale values higher than the established thresholds were considered clinically meaningful: fatigue score greater than 39, pain greater than 25, diarrhea greater than 17, dyspnea greater than 17, appetite loss greater than 50, insomnia greater than 50, constipation greater than 50, and financial difficulties greater than 1.
Data from the publication17 included 88 patients (41.5%) who were treatment-naive (with either vandetanib or cabozantinib) and 124 patients (58.5%) who had previously received these MKIs at study entry. Baseline physical function subscale scores were 80.9 (SD = 20.0) overall, 85.2 (SD = 18.2) for patients who were treatment-naive, and 75.4 (SD = 21.9) for patients with previous treatment. All of these baseline values met a clinically meaningful threshold for reduced physical function (score below 83). Most patients improved or remained stable on the physical function subscale at each cycle during study treatment with selpercatinib. Of all patients, 18.7% (36 out of 193) met the criteria for a definite improvement and 13.0% (25 out of 193) met the criteria for a definite worsening in physical function. Baseline physical function subscale scores were 80.9 (SD = 20.0) overall, 85.2 (SD = 18.2) for patients who were treatment-naive, and 75.4 (SD = 21.9) for patients with previous treatment. Most patients improved or remained stable on the physical function subscale at each cycle during study treatment with selpercatinib. Of all patients, 18.7% (36 out of 193) met the criteria for a definite improvement and 13.0% (25 out of 193) met the criteria for a definite worsening in physical function. Among the treatment-naive and previous treatment subgroups, respectively, 10.5% and 22.5% met the criteria for a definite improvement and 14.5% and 11.3% met the criteria for a definite worsening in physical function.
For global health status, the mean baseline global health status/QoL subscale scores were 65.1 (SD = 23.8) overall, and 68.5 (SD = 23.7) and 60.6 (SD = 23.5) for patients who were treatment-naive or previously treated, respectively. Most patients improved or remained stable on the global health status/QoL subscale at each cycle. Of all patients, 29.0% (56 out of 193) met the criteria for a definite improvement in global health status/QoL and 13.0% (25 out of 193) met the criteria for a definite worsening in global health status/QoL. Among the treatment-naive and previously treated subgroups, respectively, 26.3% and 31.3% met the criteria for definite improvement and 17.1% and 12.5% met the criteria for a definite worsening in global health status (QoL). The median time to first improvement was 5.6 months (95% CI, 3.7 to not reached) for those in the treatment-naive subgroup and 3.6 months (95% CI, 2.0 to 7.4) for patients with previous treatment exposure.
Bowel Diaries
In the same published study, of the 123 English-speaking patients who completed the mSTIDAT at baseline (cycle 1), 99 (80.4%) reported experiencing diarrhea at study entry. The patient-reported severity of diarrhea at baseline was minimal among 22 patients (22.2%), moderate among 48 patients (48.5%), and severe among 25 (25.3%) patients reporting diarrhea. Less than half of all patients reported diarrhea at each assessment after cycle 2 (range, 33.3% to 48.3%) of treatment, with fewer patients than at baseline (range, 0% to 17.2%) reporting the severity to be severe. The impact of diarrhea reported on the mSTIDAT ranges from 0 (no impact) to 10 (extreme impact on family life, social life, and overall QoL). At baseline, the mean impact of diarrhea was 2.7 (SD = 3.0) for family life, 3.6 (SD = 3.2) for social life, and 3.5 (SD = 2.8) for overall QoL. Patients reported little impact of diarrhea on any of these aspects of daily living during study treatment with selpercatinib.
Table 13: Efficacy Outcomes: Health-Related Quality of Life
Criteria | Total | Treatment-naive | Previously treated |
|---|---|---|---|
EORTC QLQ-C30 | |||
Global health status | |||
Cycle 1 (baseline) | |||
N | 192 | 76 | 79 |
Mean (SD) | 65.10 (23.79) | 68.53 (23.71) | 62.94 (25.09) |
Cycle 7a | |||
N | 128 | 47 | 55 |
Mean (SD) | 74.54 (19.85) | 76.77 (20.40) | 71.21 (19.43) |
CFB mean (SD) | 7.55 (22.342) | 8.33 (25.948) | 9.70 (21.502) |
Worsened, % | 17.2 | 19.1 | 12.7 |
Improved, % | 42.2 | 48.9 | 45.5 |
Physical functioning | |||
Cycle 1 (baseline) | |||
N | 193 | 76 | 80 |
Mean (SD) | 80.71 (20.01) | 85.22 (18.19) | 75.42 (21.90) |
Cycle 7 | |||
N | 129 | 47 | 56 |
Mean (SD) | 87.60 (16.33) | 88.72 (14.03) | 84.46 (19.36) |
CFB mean (SD) | 4.13 (15.09) | 1.35 (15.01) | 7.08 (17.38) |
Worsened, % | 9.3 | 10.6 | 10.7 |
Improved, % | 25.6 | 19.1 | 33.9 |
CFB = change from baseline; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; SD = standard deviation.
aEach cycle of 28 days.
Source: LIBRETTO-001 Clinical Study Report.18
Sensitivity analyses based on IRC and investigator-evaluated end points were similar overall and robust between assessments. Subgroups described in the Clinical Study Report for the PAS were small in sample size (n = 55) and not determined to be examined a priori. In a visual assessment, no meaningful differences were noted between the subgroups presented (age, sex, race, ECOG PS, RET mutation type, metastatic disease, prior systemic therapies, and RET molecular assay).
Harms
Harms are summarized from the safety population of the LIBRETTO-001 study (cut-off date December 16, 2019), and only those harms of interest identified in the review protocol are reported subsequently. AEs in the LIBRETTO-001 study were defined as any unfavourable medical occurrence in a patient who had been administered the drug under investigation, i.e., selpercatinib, with the occurrence not necessarily related to the intervention. An SRC was in charge of overseeing the safety aspects from phase I to complete the dose-escalation assessments.
Adverse Events
The AEs are summarized in Table 14. Investigators graded the severity of AEs from grade 1 (mild), to grade 5 (fatal) according to the Common Terminology Criteria for Adverse Events version 4.03.31
Among the 299 patients with RET-mutant MTC included in the safety population, ||| ||||||| ||||||||| || ||||| ||| ||| |||| ||||| ||| || with grade 3 or 4 and grade 5 AEs, respectively. A total of || |||||||| |||||| had AEs and discontinued the drug.
The most commonly reported AEs (> 20% of patients with at least 1 of these) included hypertension, diarrhea, constipation, fatigue, headache, peripheral edema, nausea, and abdominal pain.
Serious Adverse Events
SAEs occurred in || ||||||| of the 299 patients in the safety population, with || |||||| categorized as being related to selpercatinib. Among these, |||| patients had a fatal AE. The most common SAEs were |||||||||| ||||||||||||| ||| ||||||||||||| ||||| |||| ||||||| || ||||| ||||| ||| || of patients, respectively (Table 14).
Mortality
As of the December 16, 2019 cut-off date, among the 299 patients in the safety population with RET-mutant MTC, | |||||| |||||| |||||||| |||||| || |||| || |||| |||| || ||||||||||||| || ||| || ||||||| |||||||||||| | ||| || ||||||| |||||||| ||| || |||||| |||||||| |||| |||| || |||| ||||| ||| |||| ||||| || |||||| ||| || ||||||| |||||||||||| | ||| || ||||||| ||||||| | ||| || ||||| |||||| ||||||||||.
AEs were reported at the March 30, 2020 cut-off date, although not broken down by diagnosis populations but rather as the totality of patients included in the LIBRETTO-001 trial (MTC, NSCLC, DTC; N = 746). Of these, the most frequently reported drug-related TEAEs (reported in at least 20% of participants) were similar to the previous cut-off date in the MTC, i.e., dry mouth (35.5%) ALT increased (26.4%), AST increased (26.3%), hypertension (25.5%), and diarrhea (21.8%). Most AEs related to the study intervention were grade 1 (||||||||||||||| ||||||| grade 2 |||| ||||||||||||| ||||||| and grade 3 |||| ||||||||||||| |||||). For these cut-off dates, there were | | ||||||||| | |||| | || | || | |||||||| | | || | |||||| | |||||| | ||| | | | |||| | | || | | || | || | | ||| | ||||||||||||.
Notable Harms
Harms of special interest stated in the protocol for this review included diarrhea, bleeding, hepatotoxicity (AST or ALT increase), QTc prolongation, hypertension, and photosensitivity.
Elevations of liver enzymes occurred frequently, with || ||||||| ||| || ||||||| patients with ALT and AST elevations, respectively, although most were low grade (Table 14). Hypertension was reported (as TEAE by preferred term) in ||| ||||||| of patients. Diarrhea was present in || ||||||| of patients at any point, and hypersensitivity was rare (| ||||||||).
A common concern among clinicians was QTc prolongation, which was reported in ||| ||||||| of patients, with values that had increased by more than 30 ms from baseline, and || |||||||| ||||||| with values that had increased by more than 60 ms.
Variable | Safety population, December 16, 2019 cut-off date (N = 299) |
|---|---|
AEs | |
Patients with ≥ 1 AEs | ||| |||||| |
||||| ||| | ||| |||||| |
||||| | | | ||||| |
|||| |||||| ||| | | |
|||||||| |||| | | ||||||| ||| | || |||||| |
|||| |||||| ||||||| ||| |||||||||||||||||||||||| | || ||||||| ||||| |
Patients with fatal AEs | | ||||| |
||||||| |||||| | | ||||| |
||||| |||||||||| | | ||||| |
|||| |||||| ||| | | |
|||||||||||| | ||| |||||| |
||| ||||| | ||| |||||| |
AEs of special interest | |
||| |||||||||| ||| ||||| | || |||||| |
||||| | | || |||||| |
||||| | | || ||||| |
March 30, 2020 cut-off date (N = 315) | |
AEs, N (%) | |
Patients with ≥ 1 AEs | 313 (99.4) |
Grade 3 or 4 | 188 (59.7) |
||||| | | | ||||| |
Patients with ≥ 1 serious AEs | 97 (30.8) |
Serious AEs and related to selpercatinib | 20 (6.3) |
Patients with fatal AEs | 8 (2.5) |
Patients with fatal AEs and related to selpercatinib | 0 (0) |
Patients with AEs and permanently discontinued study drug | 15 (4.8) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; MTC = medullary thyroid cancer; QTcF = QT interval corrected for heart rate using Fridericia formula.
aFrequency > 2%.
bFrequency > 5%.
Note: Redacted rows have been deleted.
Source: LIBRETTO-001 Clinical Study Report.18
The harms events for the March 30 2020 cut-off date were similar to the harms events for the December 16, 2019 cut-off date, with a total of 313 (99.4%) AEs, and 97 patients (30.8%) with at least 1 SAE. At this cut-off, 28 out of 315 (8.9%) deaths occurred within 28 days of the last dose of selpercatinib (18 due to disease progression, 8 due to AEs, and 2 due to other), and no death occurred more than 28 days after the last dose. The most common AEs (> 5%) included dry mouth |||||, diarrhea |||||, hypertension |||||, fatigue ||||||, constipation (|||), increased AST (|||), increase ALT (|||), peripheral edema (|||), nausea (|||), increased blood creatinine level (|||), abdominal pain (|||), QT interval prolonged on ECG (|||), arthralgia (|||), cough (|||), and rash (|||). Safety data were analyzed by grade and SAEs.
Critical Appraisal
Internal Validity
The LIBRETTO-001 study is a single-arm, open-label, phase I and phase II study. As such, the study is descriptive in nature, as it did not evaluate the primary or secondary end points (e.g., ORR, DOR, OS, PFS) formally with adjustments for multiple comparisons. These limitations stem from the single-arm design and lack of comparator groups and constrain the estimation of the relative effects of treatment with selpercatinib.
An open-label design may also increase uncertainty in patient-reported outcomes (HRQoL) introducing bias due to the inherent subjectivity of the outcome in an unblinded assessor. This bias would be less likely in more objective outcomes, such as ORR, OS, or PFS if evaluated against a properly a priori set hypothesis. Furthermore, HRQoL outcomes were evaluated as exploratory end points and with no adjustment for multiplicity.
Anti-cancer treatments and prior cancer-related surgery were commonly observed at baseline (which occurred in 85% to 90% of the included patients). Any magnitude of effect that these interventions could have on the outcomes evaluated in patients who received selpercatinib is uncertain, given the lack of comparators.
Sensitivity analyses based on IRC versus investigator assessments were similar overall in their results. The sponsor provides information on different subgroups (for age, sex, race, ECOG PS, RET mutation type, metastatic disease, prior systemic therapies, and RET molecular assay) in the ORR end point; however, the sample size was small, and the end point was evaluated as an exploratory outcome. Hence, evidence is limited for identifying potential subgroup effects in this population.
As of the December 16, 2019 cut-off date, ||||| of patients discontinued the study drug and ||||| discontinued from the study, mostly due to disease progression and death, respectively. At the March 30, 2020 cut-off date, the discontinuation rates remained consistent (17.1% of patients discontinued treatment and 12.7% discontinued from the study, with 7.9% and 4.4% of patients discontinuing treatment due to PD and AEs, respectively). The sponsor evaluated all 226 patients in the efficacy population and all 299 patients in the safety population for the primary and secondary end points.
External Validity
There were fewer concerns about the generalizability of the population included and about the effects on survival and response. According to the clinical experts consulted by CADTH, except for the proportion of females, the baseline characteristics of the population included in the LIBRETTO-001 study were representative overall of the population of patients with RET-mutant MTC seen in Canadian clinical practice. Age, ECOG PS, initial disease stage, cancer history, RET mutation types, and prior therapies were similar to those expected in clinical practice. The inverse ratio of female to male patients being lower than expected was noted by the clinical experts, although they did not consider it to be a concern for applicability.
Most patients had good baseline performance status (e.g., low number of patients with an ECOG PS of 2 or higher), suggesting that the included population might be healthier when compared with Canadian clinical practice; however, the clinical experts did not consider it highly different from what is expected.
All outcomes measured in the LIBRETTO-001 study are of clinical relevance and, according to the clinical experts, important for patients and well known and used by clinicians in Canada. The only concern was the limitation of the follow-up, i.e., that it might be considered too short for assessing longer periods of observations for those patients continuing the study and for assessing OS.
Table 15 summarizes the generalizability of the evidence.
Table 15: Assessment of Generalizability of Evidence for Selpercatinib
Domain | Factor | Evidence | CADTH’s assessment of generalizability |
|---|---|---|---|
Population | Patients with RET-mutant MTC, unresectable advanced or metastatic | Trial inclusion and exclusion criteria, and baseline and demographic characteristics | The inclusion and exclusion criteria in the LIBRETTO-001 study resulted in the recruiting of a population similar to what is observed in clinical practice and similar to the reimbursement criteria for this review. Children (although a rare presentation) are underrepresented. |
Intervention | Selpercatinib 160 mg twice daily (> 50 kg) or 120 mg (< 50 kg) twice daily | LIBRETTO trial phase II, protocol and study reports | The dosages seem to be the most appropriate according to the clinical expert consulted by CADTH, since this was obtained from a phase I and II study. There might still be uncertainty about the use in children, given the low number of pediatric patients included in the body of evidence. |
Comparator |
| Comparator tables for the CADTH submission from the sponsor and feedback from drug programs | Vandetanib is the only drug currently funded and approved by Health Canada. It is commonly used as first-line therapy. |
Outcomes | Survival (OS, PFS), Response or remission rate (ORR, DOR), HRQoL (EORTC QLQ-C30, PedsQL, bowel diaries) | Trial protocol and study reports | The outcomes are relevant to patients and clinicians and applicable to real clinical practice. There are some issues with the short-term duration of the evaluation of outcomes, as the study is still ongoing. |
Setting | Outpatient setting | Trial sites in protocol and study reports | The administration of selpercatinib does not require a special inpatient setting; however, it requires monitoring by a specialized health team. |
DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; MTC = medullary thyroid cancer; ORR = objective response rate; OS = overall survival; PedsQL = Pediatric Quality of Life Inventory; PFS = progression-free survival; RET = rearranged during transfection.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
Selpercatinib has been previously assessed in a single-arm randomized controlled trial. However, no head-to-head evidence of selpercatinib compared against other relevant treatments for advanced RET mutation–positive MTC was available for this review. Due to this gap in evidence, the sponsor submitted an ITC for CADTH to review. Electronic databases including MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL), were searched using a combination of MeSH and keywords. Websites of professional organizations, including the European Society for Medical Oncology, International Association for the Study of Lung Cancer, ClinicalTrials.gov, and the International Clinical Trials Registry Platform, were searched to identify relevant conference abstracts. Retrieval was not limited by publication date or by language. Titles, abstracts, and full-text articles were screened for inclusion by 1 reviewer based on population and disease condition, interventions, comparators, outcomes, and study types (PICOS criteria). CADTH also conducted a literature search to identify other potentially relevant ITCs.
One sponsor-submitted ITC was summarized and critically appraised. This ITC was used to inform the pharmacoeconomic model.
Description of Indirect Comparison(s)
The overall objective of the sponsor-submitted ITC was to estimate the treatment effect for selpercatinib versus cabozantinib, vandetanib, and BSC (including placebo) in all lines of treatment for RET-mutation MTC. The outcomes analyzed were OS, PFS, and ORR. The population, intervention, comparators, outcomes, and design of studies included in the sponsor’s ITC are provided in Table 16.
Table 16: Study Selection Criteria and Methods for ITCs
Detail | Sponsor-submitted ITC |
|---|---|
Population | Adult and pediatric patients with RET tumours |
Intervention | Selpercatinib, vandetanib, BSC (including placebo) |
Comparator | Any active systemic therapy, placebo, BSC, or no treatment |
Outcome | Overall survival, progression-free survival, objective response rate |
Study design | Randomized, controlled, prospective clinical trials, systematic reviews (including meta-analyses), single-arm trials or RCTs in RET-altered tumours (any tumour site, any intervention, any line of therapy) |
Publication characteristics | Language of publication was not restricted |
Exclusion criteria |
|
Databases searched | MEDLINE, Embase, CENTRAL |
Selection process | Articles screened independently by 2 researchers |
Data extraction process | Data extraction was performed by pairs of reviewers and compared for discrepancies |
Quality assessment | National Institute for Health and Care Excellence, Critical Appraisal Skills Programme |
BSC = best supportive care; CENTRAL = Cochrane Central Register of Controlled Trials; ITC = indirect treatment comparison; RCT = randomized controlled trial; RET = rearranged during transfection.
Source: Sponsor-submitted ITC.32
Methods of ITC 1
Objectives
The efficacy of selpercatinib was evaluated in a single-arm trial, LIBRETTO-001. Indirect comparisons were conducted for selpercatinib versus relevant comparators for the treatment of advanced RET mutation–positive MTC as head-to-head trials did not exist.
Study Selection Methods
The sponsor conducted a systematic literature review of published clinical studies to identify comparators for selpercatinib for the treatment of patients with MTC or PTC. The literature search was conducted on September 30, 2019. In total, 44 publications were identified that included patients with thyroid cancer, of which 16 were primary studies. Of the 16 studies, 11 were trials that included patients with MTC, 3 included patients with PTC, and 2 included patients with both MTC and PTC. Among these 16 primary studies, 2 were for advanced RET mutation–positive MTC and 2 for advanced RET fusion–positive thyroid cancer. The outcomes analyzed were OS, PFS, and ORR.
The trial characteristics, patient demographics, treatment history, treatment outcomes, and interventions found in the included clinical trials were extracted from the full-text publications. Resources retrieved from websites were printed to preserve a record of information in the event that the information on the websites changes or becomes unavailable. References to other publications within a trial were backtracked to the original sources, where appropriate.
Data were extracted by 1 researcher using Microsoft Excel and all data were quality-validated by an independent reviewer, who performed a verification of the data from the original source. Data were quality-checked before their use in the ITC.
For each eligible trial, a quality assessment was performed to the standards recommended by the National Institute of Health and Care Excellence (NICE). At the time of the review, no validated tool to assess the quality of single-arm trials existed; thus, the Critical Appraisal Skills Programme cohort study checklist was used to assess the quality of all single-arm trials.
ITC Analysis Methods
Because the LIBRETTO-001 trial is a single-arm trial and does not have a control arm, it was not possible to perform a network meta-analysis or an anchored ITC to estimate the relative efficacy of selpercatinib versus relevant comparators. As such, an unanchored matching-adjusted ITC (an unanchored MAIC) comparing LIBRETTO-001 with the EXAM trial was conducted to estimate the relative efficacy of selpercatinib versus cabozantinib and placebo.
The sponsor compared selpercatinib in the LIBRETTO-001 trial (including all patients previously treated with cabozantinib, vandetanib, or both, and all cabozantinib and vandetanib treatment-naive patients) against placebo from the intention-to-treat population of the EXAM trial, and against patients treated with cabozantinib in the RET mutation–positive and RET M918T subgroups from the EXAM trial.
An unanchored adjusted ITC was conducted using individual patient-level data from the LIBRETTO-001 trial and summary statistics from the EXAM trial. MAICs were conducted for PFS and OS in which outcomes in the LIBRETTO-001 trial using propensity score weighting.
Kaplan-Meier curves were not available for OS for the RET mutation–positive subgroup treated with cabozantinib or placebo from the EXAM trial. Therefore, the unweighted curves for the RET M918T–positive patients receiving cabozantinib or placebo in the EXAM trial were digitized from Schlumberger 201733 and compared with the weighted curve for the any-line LIBRETTO-001 population. Propensity score matching was performed using the LIBRETTO-001 data and the EXAM trial data such that the LIBRETTO-001 outcomes were adjusted to reflect the EXAM trial population characteristics for the RET mutation–positive subgroup treated with cabozantinib.
For PFS, the unweighted curves for the RET mutation–positive population receiving cabozantinib or placebo in the EXAM trial were digitized from Sherman 201634 and compared with the weighted curve for the LIBRETTO-001 population. Propensity score matching was performed using LIBRETTO-001 data and data from the EXAM RET mutation–positive subgroup treated with cabozantinib.
The MAIC was adjusted for baseline characteristics; known or potential associations with the efficacy outcomes were reported in both the LIBRETTO-001 trial and EXAM trial publication. Re-weighting of selpercatinib data (LIBRETTO-001 trial) was based on baseline characteristics of the cabozantinib arm (EXAM trial, RET mutation–positive subgroup only). However, a comparison of adjusted selpercatinib outcomes data was conducted for both the placebo and cabozantinib arms independently. Baseline characteristics between LIBRETTO-001 and EXAM before and post matching were obtained from a logistic regression model. Only baseline characteristics with complete data were adjusted and they included |||| ||||||| |||| ||||||||||| ||||||| |||| ||||||| ||||||| ||||| ||| |||||||| ||| ||| ||||| |||||||| |||||||
To balance the baseline characteristics between LIBRETTO-001 and EXAM, data from LIBRETTO-001 patients were assigned weights such that:
weighted mean baseline characteristics of LIBRETTO-001 patients exactly matched those reported for patients in the RET mutation–positive subgroup treated with cabozantinib in the EXAM trial
the weight for each patient was equal to the patient’s estimated propensity weight of being in LIBRETTO-001 versus EXAM (RET mutation–positive subgroup treated with cabozantinib), and
weights satisfying these conditions were obtained from a logistic regression model for the propensity of inclusion in the LIBRETTO-001 trial versus the EXAM study (RET mutation–positive subgroup treated with cabozantinib), with all matched-on baseline characteristics included as predictor variables in the model.
The logistic regression model was estimated using the method of moments because only summary statistics for baseline characteristics were available from the EXAM study. Using the method of moments estimates, the baseline means were exactly matched after weighting. The distribution of weights was investigated for potential extreme values, which can indicate poor overlap in the distributions of patient characteristics across trial populations.
Results of ITC 1
Summary of Included Studies
The process of study selection was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The searches identified a total of 7,142 records of which 3,390 met the eligibility criteria. Of these, 44 publications from 16 trials were identified that included patients with thyroid cancer. Of the 16 unique studies, 11 were trials including patients with MTC, 3 included patients with PTC, and 2 included patients with both MTC and DTC.
Three trials investigating selpercatinib, cabozantinib, and vandetanib at their recommended doses in patients with MTC were identified by the systematic literature review and deemed evaluable in the feasibility assessment. The 3 trials are LIBRETTO-001, EXAM, and ZETA. The key differences between trial design and reported outcomes are presented subsequently:
Crossover from placebo to vandetanib was permitted in the ZETA trial at disease progression. This is anticipated to improve the OS of the placebo arm and to bias the estimates of relative efficacy. In the EXAM trial, crossover was not permitted. As a result, there is uncertainty in the comparability of the placebo arms between ZETA and EXAM.
Outcomes available in EXAM:
PFS: Hazard ratio (HR) and Kaplan-Meier curve in ITT population, RET mutation–positive, RET M918T
OS: HR, Kaplan-Meier curve in ITT population, RET mutation–positive, RET M918T
ORR: ITT population, RET mutation–positive
Outcomes available in ZETA:
PFS: HR in ITT population
OS: HR and Kaplan-Meier curve in ITT population
ORR: RET mutation–positive, ITT population, and RET M918T
The EXAM trial reported hazard ratios for both PFS and OS in the RET mutation–positive subgroup and included Kaplan-Meier curves for PFS in the RET mutation–positive and for both PFS and OS in M918T subgroups. These data are comparable to LIBRETTO-001, which included patients with RET mutation–positive MTC. In the ZETA trial, the only outcome reported for the RET mutation–positive subgroup is ORR.
Key differences in the patient population characteristics across the 3 trials include:
The LIBRETTO-001 trial population is slightly older than the EXAM and ZETA trial populations.
The percentage of male patients in LIBRETTO-001 is slightly lower than in EXAM and higher than in ZETA.
A higher proportion of patients had an ECOG PS of 1 or 2 in the LIBRETTO-001 trial than in the EXAM and ZETA trial populations.
The proportion of patients in the LIBRETTO-001 trial with prior anti-cancer therapy was substantially higher than in the EXAM trial and slightly higher than in the ZETA trial.
The proportion of patients in the LIBRETTO-001 trial with prior TKI therapy was significantly higher than in the EXAM trial (data not reported for the ZETA trial).
The proportion of patients in the LIBRETTO-001 trial who never smoked was higher than in the EXAM trial (data not reported for the ZETA trial).
Due to these issues with patient heterogeneity, it was deemed infeasible to include the ZETA trial in the comparison.
Results
MAIC Comparison of Baseline Characteristics Between the LIBRETTO-001 and EXAM Trials
Only results for the comparison of selpercatinib and placebo from the MAIC were presented, since cabozantinib was not identified as a comparator of interest in our protocol.
Table 16 presents the comparison of baseline characteristics before and post matching for the datasets from LIBRETTO-001 and the RET mutation–positive subgroup treated with cabozantinib in EXAM. The MAIC adjusted for |||| ||||||| |||| ||||||||||| ||||||| |||| ||||||| ||||||| ||| ||| ||||| |||||||| ||||||. The effective sample size for LIBRETTO-001 after weighting was ||||| |||||| || ||| |||||||| |||||| |||| |||| ||||||||||||||. Distribution of weights in the MAIC indicate no evidence of extreme weights.
Characteristic | Before matching | After matching and weighting | |
|---|---|---|---|
LIBRETTO-001 selpercatinib (N = 212) | EXAM RET mutation–positive group treated with cabozantinib (N = 107) | LIBRETTO-001 selpercatinib (ESS = 166.8) | |
|||| |||| |||| | |||| |||||| | ||||| ||||||| | ||||| ||||||| |
|||||| ||||| |||| |||| | |||| ||||||| | ||||| ||||||| | ||||| ||||||| |
||||||| |||| | |||| | |||| | |||| |
|||| |||| | |||| | |||| | |||| |
|||||||| ||||||||||| | |||| | |||| | |||| |
||| ||||| |||||||| ||||||| |||| | |||| | |||| | |||| |
||||| |||| |||| | |||| | |||| | |||| |
|||| ||| ||||||| ||||||||||| |||||||| ||||| ||||||||||| ||||||| ESS = effective sample size; RET = rearranged during transfection; SD = standard deviation.
Source: Sponsor-submitted indirect treatment comparison.
The weighted comparisons of efficacy outcomes between selpercatinib in the LIBRETTO-001 trial and placebo in EXAM are presented in Table 18. For PFS, the HRs and corresponding 95% CIs were estimated from a weighted Cox proportional hazards model with ||||||||| ||||||||| as to the only covariate. For OS, the HRs and corresponding 95% CIs were estimated from a weighted Cox proportional hazards model with ||||||||| ||||||||| ||| ||| ||||| |||||| as covariates. After weighting, there was a statistically significant improvement in PFS for selpercatinib versus placebo ||| ||||| ||| ||| ||||| ||||| |||||||||. There was also a statistically significant improvement in OS for selpercatinib versus placebo ||| ||||| ||| ||| ||||| ||||| |||||||||.
Table 18: Comparison of PFS and OS for Selpercatinib Versus Placebo Before and After Propensity Score Matching
Detail | HR (95% CI) for PFS | HR (95% CI) for OS |
|---|---|---|
Selpercatinib vs. placebo | ||
Number of studies (patients), model | LIBRETTO-001 and EXAM | LIBRETTO-001 and EXAM |
Weighted | |||| |||||| ||||| | |||| |||||| ||||| |
CI = confidence interval; HR = hazard ratio; OS = overall survival; PFS = progression-free survival.
Source: Sponsor-submitted indirect treatment comparison.
Critical Appraisal of ITC 1
The sponsor’s rationale for conducting the ITC and the objectives of the ITC were clearly reported. A comprehensive systematic review was performed with a 2-stage dual-selection process, which was considered appropriate. The language of publication was not restricted, thereby minimizing publication bias. The clinical efficacy outcomes assessed were OS, PFS, and ORR.
The key limitation of the sponsor-submitted ITC was that no randomized clinical trial evidence was available for selpercatinib versus any comparator due to the LIBRETTO-001 trial being a single-arm design.
According to the clinical expert consulted by CADTH for this review, cabozantinib is not a relevant comparator for this evaluation but is included in the ITC. The estimation of the relative treatment effect of selpercatinib is based on the comparison between selpercatinib and cabozantinib for the survival outcomes.
In the weighting process of the MAIC used to estimate the relative treatment efficacy on the survival outcomes, only the baseline prognostic factors that were reported in LIBRETTO-001 and EXAM were included. Consequently, other potential prognostic factors and effect modifiers were not accounted for in the MAIC. As such, the MAIC and its treatment effect estimates are subject to potential bias due to latent or unmeasurable confounding. It is unlikely for an unanchored MAIC to account for all prognostic factors and effect modifiers.
Heterogeneity across the prognostic factors, effect modifiers, and other baseline characteristics was assumed, but specific baseline characteristics where excess heterogeneity was of concern were not identified, described, or addressed. The potential effect of such heterogeneity on the quality and reliability of the MAIC was not discussed. The risk of bias on the estimated relative treatment effects due to the exclusion of key factors in the weighting process was not discussed. Due to the absence of a reported assessment of residual bias, the sponsor-submitted unanchored MAIC is considered to have a high risk of residual bias.35
OS Kaplan-Meier data were not available from the EXAM trial for the RET mutation–positive subgroup to allow for evaluation of the data. The Kaplan-Meier curves for patients in the EXAM trial with RET M918T–positive MTC who received placebo were used instead. These data were compared using a propensity score-weighted approach for the LIBRETTO-001 population. The assumption was made that the OS rates for these different groups were sufficiently similar, but this is unknown.
Baseline characteristics were not reported for the ||| ||||| |||||||| |||||||| so, notwithstanding comparing with the outcomes of this subgroup, the LIBRETTO-001 trial data were matched and weighted to the broader RET mutation–positive cabozantinib arm in the EXAM trial. The assumption was made that the baseline characteristics of these patient groups were equivalent, but this is unknown.
Some relevant outcomes identified in the CADTH systematic review protocol were not assessed in the ITC, including DOR, HRQoL, and safety, so the comparative efficacy and safety of relevant treatments included remain unknown.
As part of the unanchored MAIC, the weights that were used to match patients in the LIBRETTO-001 and EXAM trials for the selpercatinib versus cabozantinib comparison were also used for the selpercatinib versus placebo comparison. The recommended methodological approach is to generate separate weights for these comparisons since they involve different patient subgroups. Although these randomized studies generally have a good balance in baseline characteristics between the 2 study arms, the cabozantinib group consists only of patients who are RET mutation–positive, whereas the placebo group consists of the entire ITT sample, which includes patients with RET mutation–positive and RET mutation–negative disease. As such, there may be important differences between these 2 patient groups that were not accounted for by the weights used in the MAIC, in addition to the other differences observed. Some of the characteristics used by the MAIC were not reported for the placebo arm. The inclusion of patients with RET mutation–positive and those with RET mutation–negative disease in the placebo comparison is another source of heterogeneity that was not accounted for in the MAIC.
Summary
The sponsor-submitted ITC included a systematic review and used a matching-adjusted, unanchored, ITC to evaluate the relative clinical efficacy of selpercatinib versus other comparators for the treatment of advanced RET mutation–positive MTC. Three outcomes were analyzed, including OS, PFS, and ORR.
The sponsor-submitted ITC reported that, after weighting, there was a statistically significant improvement in PFS for selpercatinib versus placebo ||| ||||| ||| ||| ||||| ||||| |||||||| and a statistically significant improvement in OS for selpercatinib versus placebo ||| ||||| ||| ||| ||||| ||||| ||||||||.
The sponsor-submitted ITC had several limitations, including that the following:
not all prognostic factors and effect modifiers were included in the MAIC weighting process, which leads to a high risk of residual confounding
the MAIC weights calculated for 1 comparison were used for another comparison that involves a different patient population
there was heterogeneity between the patient populations used in different components of the ITC.
Given these limitations, there is uncertainty around the relative treatment effects estimated by the MAIC, which undermines the internal and external validity of the ITC. However, given the magnitude of the difference in the results between selpercatinib and placebo, selpercatinib is likely more effective than BSC on patient survival, but there is no reliable estimate of how much more effective it is.
Other Relevant Evidence
This section includes submitted long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
In addition to the pivotal trial LIBRETTO-001, 3 ongoing studies were considered relevant for this report: LIBRETTO-531,16 LIBRETTO-321,36 and LIBRETTO-121.37 No complete results are currently available; rather, details of each trial are presented, as they provide additional context for the decision-making process.
LIBRETTO-531
LIBRETTO-53116 is a phase III, randomized, multi-centre, open-label study comparing selpercatinib with a physician’s choice of cabozantinib or vandetanib in adult and pediatric patients with progressive, advanced, kinase inhibitor–naive, RET-mutant MTC. Patients will be enrolled in approximately 158 sites in 21 countries across the Americas (including Canada) and in Asia, Europe, and Oceania. Refer to Table 19 for more details.
This study is currently recruiting participants, with a planned enrolment of approximately 400 patients. The estimated primary completion date (the date on which the last participant in a clinical study was examined or received an intervention so as to collect final data for all the primary outcome measures) and study completion date (the date on which the last participant in a clinical study was examined or received an intervention or treatment so as to collect final data for the primary and secondary outcome measures, as well as final data on AEs at the last participant’s last visit) are May 20, 2024, and November 13, 2026, respectively. Patients will be randomized 2:1 to selpercatinib (160 mg twice a day) versus the physician’s choice of cabozantinib (140 mg daily) or vandetanib (300 mg daily). Stratification factors are mutation (M918T versus other) and Intended treatment If randomized to active comparators (cabozantinib versus vandetanib).38 For patients in the active comparator arms, crossover to selpercatinib is allowed at progression. The primary end point is treatment failure–free survival by blinded independent committee review (BICR). The secondary end points include PFS by BICR, ORR by BICR, DOR by BICR, OS, PFS2 (second disease progression or death) by investigator, Functional Assessment of Cancer Therapy–General item GP5 (side effects), and concordance between the local laboratory and the central laboratory RET results.
LIBRETTO-321
LIBRETTO-32136 is a phase II, single group assignment, open-label study in China to assess the efficacy and safety of selpercatinib in participants with RET fusion–positive solid tumours, MTC, and other tumours with RET activation. Patients will be enrolled from multiple sites in China. Refer to Table 19 for more details.
The study is active but not currently recruiting, with a planned enrolment of approximately 75 patients. The actual primary completion date (the date on which the last participant in a clinical study was examined or received an intervention to collect final data for all the primary outcome measures) and the estimated study completion date (the date on which the last participant in a clinical study was examined or received an intervention or treatment to collect final data for the primary and secondary outcome measures as well as final data on AEs at the last participant’s last visit) are March 25, 2021, and November 20, 2025, respectively. All patients enrolled were given selpercatinib 160 mg orally twice daily in a 28-day cycle. Cohort 1 (n = 30) comprised patients with advanced RET fusion–positive solid tumours who had progressed on or were intolerant to 1 or more prior standard first-line therapies or those who had declined or were not suitable to receive standard frontline therapy. Cohort 2 (n = 26) enrolled patients with advanced RET-mutant MTC who either had or had not received previous systemic therapy. Lastly, those enrolled in cohort 3 (n = 21) had advanced RET-altered solid tumours that met the requirements for cohorts 1 or 2 but who did not have measurable disease, those with a RET-altered solid tumours or a RET alteration or activation that did not meet the criteria for cohorts 1 or 2, and those with circulating tumour DNA that is positive for a RET alteration that was not known to be present in their tumour.39 The primary end point is ORR by IRC. The secondary end points include DOR by IRC, time to response by IRC, clinical benefit rate, PFS by IRC, OS, and area under the concentration versus time curve (AUC).
LIBRETTO-121
LIBRETTO-12137 is a phase I and II, single group assignment, multi-centre, open-label study to find the appropriate dose of, as well as to assess safety and efficacy of selpercatinib in pediatric participants with an activating RET alteration and an advanced solid or primary CNS tumour. Patients will be enrolled in approximately 25 study locations in 10 countries across North America, Europe, Asia, and Oceania. Refer to Table 19 for more details.
This study is currently recruiting participants, with a planned enrolment of approximately 100 patients. The estimated primary completion date (the date on which the last participant in a clinical study was examined or received an intervention to collect final data for all the primary outcome measures) and study completion date (the date on which the last participant in a clinical study was examined or received an intervention or treatment to collect final data for the primary and secondary outcome measures, as well as final data on AEs at the last participant’s last visit) are March 26, 2023, and March 26, 2024, respectively. All patients enrolled were given selpercatinib orally (capsule or liquid suspension) twice daily continuously. Dosing started at the adult RP2D equivalent, 92 mg/m2 twice daily, to confirm RP2D in patients aged 2 years and older and older than 2 years.40 The primary end points in phase I are DLTs in pediatric participants with advanced solid tumours and those with primary CNS tumours. For phase II, the primary end points are ORR per RECIST 1.1 and RANO by IRC. Secondary end points for phase I include plasma concentration, AUC0 to 24 (from 0 to 24 hours), Cmax (maximum concentration),Tmax (time to maximum concentration), MTD, preliminary antitumour activity of selpercatinib in pediatric participants with tumours harbouring an activating RET alteration, as determined by ORR per RECIST 1.1, change from baseline in pain (Wong-Baker FACES Scale), and change from baseline HRQoL (Pediatric Quality of Life Inventory core module). The phase II secondary end points are AUC0 to 24 (AUC from 0 to 24 hours), Cmax, Tmax, ORR per RECIST 1.1 and RANO by investigator, DOR by investigator and IRC, PFS by investigator and IRC, OS, clinical benefit rate by investigator and IRC, frequency of AEs, concordance between a prior molecular test that detected a RET alteration within the participant’s tumour and the diagnostic tests by the sponsor, post-operative stage, surgical margin status, and descriptive analyses of pre-treatment surgical and post-treatment plans.
The sponsor submitted preliminary results for this study as a conference abstract.40 As of October 2, 2020, 11 patients (6 male) aged 2 to 20 years (MTC, n = 8; PTC, n = 2; osteosarcoma, n = 1) had been treated (phase I, n = 4; phase II, n = 7). At baseline, 7 patients had measurable disease. Prior therapies included surgery (n = 8), chemotherapy (n = 1), vandetanib (n = 1), and radiotherapy (n = 3), while 3 patients were previously untreated. Time on selpercatinib ranged from 0.9 to13.4 months and 9 patients remain on treatment. One patient experienced a dose reduction and 2 experienced dose interruptions due to TEAEs (elevated ALT and bilirubin). There were no TEAEs that led to the discontinuation of selpercatinib. TEAEs in greater than 15% of patients included elevated alkaline phosphatase, constipation, headache, elevated AST, diarrhea, hyperphosphatemia, hypoalbuminemia, hypothyroidism, nausea, pyrexia, urinary tract infection, vomiting, and weight gain. Best response was unconfirmed PRs in 4 patients, stable disease in 6 patients (2 lasting ≥ 16 weeks) and PD in 1 patient.
Table 19: Details of Other Relevant Studies — LIBRETTO-531, -321, and -121
Detail | LIBRETTO-531 | LIBRETTO-321 | LIBRETTO-121 |
|---|---|---|---|
Study design | Phase III, randomized (parallel assignment), multi-centre, open-label study | Phase II, single group assignment, open-label study | Phase I and II, single group assignment, multi-centre, open-label study |
Designs and populations | |||
Study design | Phase III, randomized (parallel assignment), multi-centre, open-label study | Phase II, single group assignment, open-label study | Phase I and II, single group assignment, multi-centre, open-label study |
Locations | 158 locations (US, Canada, EU, Australia, Brazil, Russia, Asia, Israel) | China | 25 locations (US, Canada, EU, Australia, Asia) |
Populations | Children and adults (12 years and older) with unresectable, locally advanced and/or metastatic MTC and no prior history of treatment with kinase inhibitors for advanced or metastatic disease | Adult participants (18 years and older) in China with RET fusion–positive solid tumours, MTC, and other tumours with RET activation | Pediatric participants (6 months to 21 years; 12 years of age or greater in Canada) with an activating RET alteration and an advanced solid or primary CNS tumour |
Enrolment dates | |||
Actual study start date | February 11, 2020 | March 16, 2020 | June 13, 2019 |
Primary completion date | Estimated: May 20, 2024 | Actual: March 25, 2021 | Estimated: March 26, 2023 |
Estimated study completion date | November 13, 2026 | November 20, 2025 | March 26, 2024 |
Participants | |||
Estimated enrolment (N) | 400 participants | 75 participants | 100 participants |
Inclusion criteria |
|
Cohorts 1 and 2:
|
|
Exclusion criteria |
|
|
|
Drugs | |||
Intervention | Selpercatinib 160 mg orally twice a day | Selpercatinib 160 mg orally twice a day | Selpercatinib:
|
Comparator(s) | Cabozantinib 140 mg daily or vandetanib 300 mg daily | None | None |
Outcomes | |||
Primary end points | Treatment failure–free survival by BICR | ORR (CR or PR) by IRC | Phase I:
Phase II:
|
Secondary end points |
|
| Phase I:
Phase II:
|
Publications | |||
Articles and presentations | Hernando J., Tarasova V., Hu M.I., et al.38 | Lu S., Cheng Y., Huang D., et al.39 | Morgenstern D.A., Mascarenhas L., Campbell, et al.40 |
AE = adverse event; AUC = area under the concentration-time curve; BICR = blinded independent central review; CBR = clinical benefit rate; Cmax = maximum concentration; CNS = central nervous system; CR = complete response; CTCAE = Common Terminology Criteria for Adverse Events; CVD = cardiovascular disease; DOR = duration of response; ECG = electrocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FACT-G = Functional Assessment of Cancer Therapy–General; FACT-GP5 = Functional Assessment of Cancer Therapy–General item GP5 (side effects); GI = gastrointestinal; HRQoL = health-related quality of life; IRC = independent review committee; MEN2 = multiple endocrine neoplasia type 2; MI = myocardial infarction; MTC = medullary thyroid cancer; MTD = maximum tolerated dose; ORR = objective response rate; OS = overall survival; PedsQL = Pediatric Quality of Life Inventory; PFS = progression-free survival; PR = partial response; QTcF = QT interval corrected for heart rate using Fridericia formula; RANO = Response Assessment in Neuro-Oncology; RECIST = Response Evaluation Criteria in Solid Tumors; RET = rearranged during transfection; RP2D = recommended phase II dose; SD = stable disease; TdP = Torsades de pointes; Tmax = time to maximum concentration.
aFACT-G is a validated instrument used to measure quality of life in participants with cancer. The single FACT-G item GP5, “I am bothered by side effects of treatment,” is a summary measure of the overall impact of treatment toxicity, based on its association with the number and degree of AEs in clinical trials. It uses a 5-point rating scale (0 = not at all and 4 = very much). Higher GP5 scores indicate more bother from side effects.
bThe Wong-Baker FACES pain scale includes pictures of facial expressions with correlating scores of 0 being “no hurt” and 10 being hurts worst.”
cPedsQL includes a list of problems with scores of 0 being “never a problem” and 4 being “almost always a problem.”
New Data for Request for Reconsideration
The sponsor requested an expansion of the initiation condition for selpercatinib to include only adults (18 years of age and older) with unresectable advanced or metastatic RET-mutant MTC in the first-line setting and has provided submitted data from a new cut-off date of June 15, 2021, as part of a request for reconsideration to CADTH on May 19, 2022.
Figure 10: Cut-Off Dates and Accrual of Patients With RET-Mutant MTC Included in the LIBRETTO-001 Study Up to the June 15, 2021 Cut-Off Date
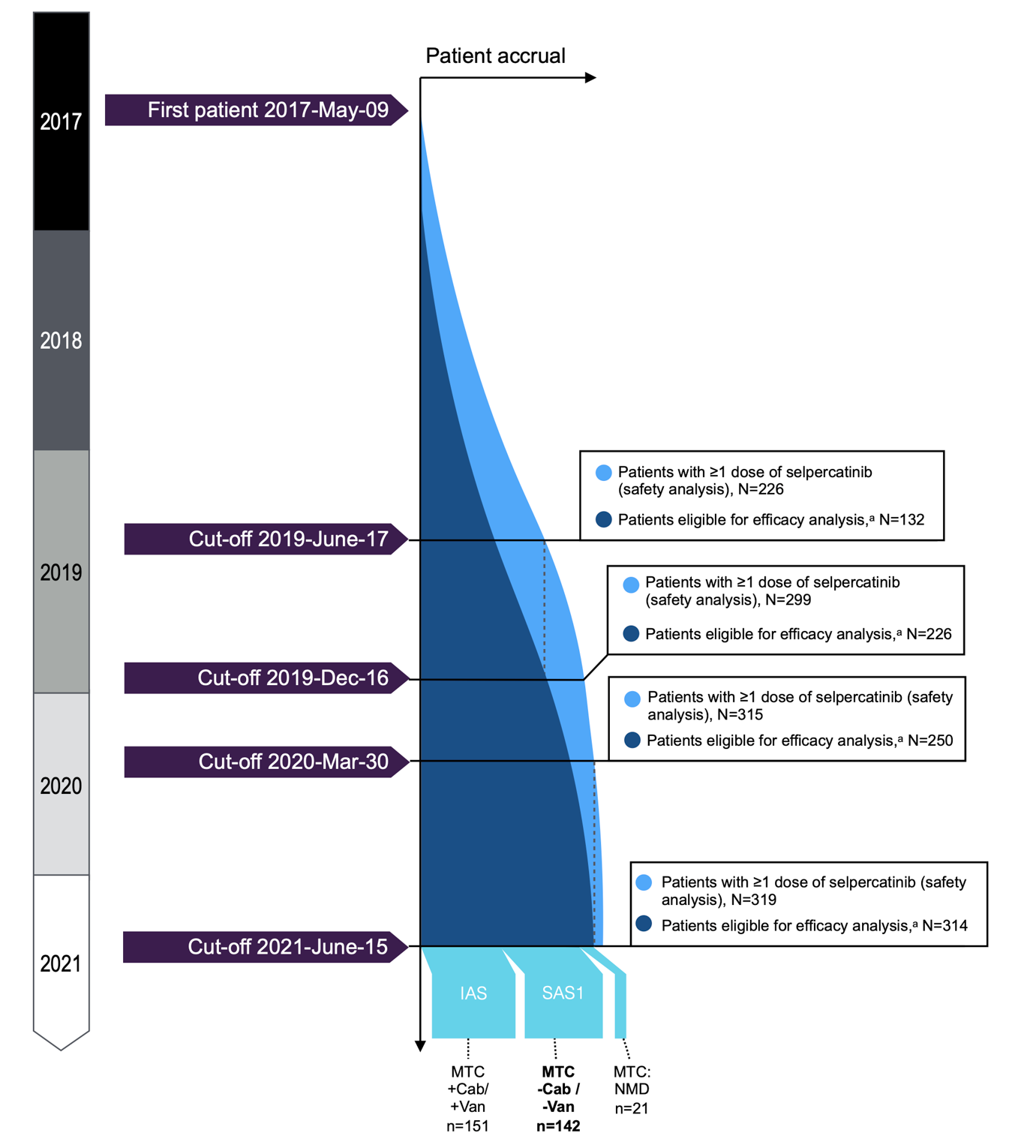
Cab = cabozantinib; IAS = integrated analysis set; MTC = medullary thyroid cancer; NMD = non-measurable disease; RET = rearranged during transfection; SAS1 = supplemental analysis set 1; Van = vandetanib.
a Defined as those with at least 1 dose of selpercatinib and 6 months of follow-up.
Source: LIBRETTO-001 Clinical Study Report.18
The new data submitted focus on the SAS 1 population (n = 142), i.e., in patients with treatment-naive RET-mutant MTC (Figure 10).
The data from a new cut-off were derived from cohorts of patients with RET-mutant MTC in LIBRETTO-001. The June 15, 2021 data cut-off consisted of the latest analyses and the interim Clinical Study Report and provides additional evidence with a focus on the cabozantinib- and vandetanib-naive (SAS 1) population, since that is the population of interest in the reconsideration request.
As of June 15, 2021, the median age of patients with RET-mutant MTC in all efficacy-eligible patients was 58.0 years, and in the overall safety population, 59.0 years (range, 15 years to 92 years). In addition, 140 patients (98.6%) were 18 years of age or older. The majority of the patients were male (60.5% in the efficacy set; 51.0% in the safety set), White (88.2% in the efficacy set; 68.5% in the safety set) and had an ECOG PS score of 1 (56.4% in the efficacy set; 56.4%; 58.3% in the safety set). At the time of enrolment, 97.5% of patients had a history of metastatic disease. For patients with MTC not previously treated with cabozantinib and/or vandetanib, the median time between initial diagnosis and metastatic disease was 54.4 months and 43.3 months, respectively; for patients with MTC previously treated with cabozantinib and/or vandetanib, the median was 70.9 months and 53.9 months, respectively.
Efficacy
Of the 142 patients in SAS 1, 115 (81%) were treatment-naive and 27 (19%) had been treated with a prior systemic therapy other than cabozantinib and vandetanib. At the time of data cut-off, the ORR by IRC assessment in SAS 1 was 81.0% (95% CI, 73.6 to 87.1), which is similar to but numerically higher than the ORR observed at the previous data cut-off (Table 20). With a median follow-up of 20.3 months, the median DOR by IRC assessment was not evaluable ( | |||| | ||| | |||). However, | ||| of responders were still on treatment with no documented disease progression by IRC assessment at the time of data cut-off.
Table 20: Efficacy Outcomes of Response or Remission by IRC Assessment — LIBRETTO-001 March 30, 2020 and June 15, 2021 MTC Cut-Off Dates
Variable | March 30, 2020 cut-off date | June 15, 2021 cut-off date |
|---|---|---|
SAS 1 (N = 112) | SAS 1 (N = 142) | |
ORR | ||
N (%) | 80 (71.4) | 115 (81.0) |
95% CI | 62.1 to 79.6 | 73.6 to 87.1 |
DOR | ||
Median DOR, months (range) | 21.95 (1.5+ to 24.1+) | NE | |||||||||| |
Median duration of follow-up (IQR) | 9.26 (5.6 to 14.7) | 20.27 |||||| ||||| |
DOR, n (%) < 6 months ≥ 6 to 12 months ≥ 12 to 18 months ≥ 18 to 24 months ≥ 24 months | 30 (35.7) 25 (31.3) 17 (21.3) 7 (8.8) 1 (1.3) | || |||||||| || ||||||| |||||| ||| ||||||||| |||||||| |||||||||| |
CI = confidence interval; DOR = duration of response; IRC = independent review committee; IQR = interquartile range; MTC = medullary thyroid cancer; NE = not evaluable; ORR = objective response rate; + = censored observation; SAS = supplemental analysis set.
Source: LIBRETTO-001 interim Clinical Study Report (2022).
For OS, the median by IRC assessment was not reached, with a median duration of follow-up of 26.3 months (interquartile range ||||| |||| || ||||| (Table 21). The maximum range for OS was |||| |||||| ||| ||||||||||. The rate of survival at 12 months or more and 24 months or more were ||||| and 95.0%, respectively.
Table 21: OS Outcomes by IRC Assessment — LIBRETTO-001 March 30, 2020 and June 15, 2021 MTC Cut-Off Dates
Variable | March 30, 2020 cut-off date | June 15, 2021 cut-off date |
|---|---|---|
SAS 1 (N = 112) | SAS 1 (N = 142) | |
OS | ||
Survival status, N (%) Died Censored | 2 (1.8) 110 (98.2) | || ||||||||| |||||| |
Median duration of overall survival, months (range) | NE (2.2+ to 29.8+) | NE ||||||| |||||| |
Median duration of follow-up, months (IQR) | 13.8 (9.6 to 18.4) | 26.3 ||||||| ||||| |
Rate of overall survival, % (95% CI) ≥ 12 months ≥ 24 months ≥ 36 months | 100.0 (100.0 to 100.0) 82.1 (29.6 to 96.9) — | ||||| |||||| |||||| 95.0 (89.0 to 97.7) |||| |||||| ||||| |
CI = confidence interval; IRC = independent review committee; IQR = interquartile range; MTC = medullary thyroid cancer; NE = not evaluable; OS = overall survival; SAS = supplemental analysis set.
Source: LIBRETTO-001 interim Clinical Study Report (2022).
For PFS, 83.1% of the patients remained alive and progression-free at the time of data cut-off, with a median duration of follow-up of 24.8 months (|||| |||| || ||||). The median PFS by IRC assessment was not reached at the time of data cut-off, and the maximum range for PFS was |||| |||||| ||| |||||||||| (Table 22). The rate of PFS at 12 months or more and 24 months or more were ||||| ||| ||||||, respectively (Figure 11 in Appendix 7). With the additional follow-up, the majority of the patients continue to remain alive and progression-free.
Table 22: PFS Outcomes by IRC Assessment — LIBRETTO-001 March 30, 2020 and June 15, 2021 MTC Cut-Off Dates
Variable | March 30, 2020 cut-off date | June 15, 2021 cut-off date |
|---|---|---|
SAS 1 (N = 112) | SAS 1 (N = 142) | |
Progression status, N (%) Disease progression Died (no disease progression beforehand) Censored | 9 (8.0) NE 103 (92.0) | ||||||||||| |
Median duration of PFS, months (range) | NE (0.0+ to 25.8+) | NE ||||||| |||||| |
Median duration of follow-up, months (IQR) | 11.1 (7.6 to 16.6) | 24.8 |||||| ||||| |
Rate of PFS, % (95% CI) ≥ 6 months ≥ 12 months ≥ 18 months ≥ 24 months | 98.2 (92.9 to 99.5) 92.9 (84.5 to 96.8) 88.7 (78.0 to 94.4) 59.2 (8.8 to 89.3) | ||||| |||||| || |||||||| ||| ||| |||||||||| ||| ||| | | | | |
CI = confidence interval; IRC = Independent Review Committee; MTC = medullary thyroid cancer; NE = not evaluable; PFS = progression-free survival; + = censored observation; SAS = supplemental analysis set.
Source: LIBRETTO-001 interim Clinical Study Report (2022).
Harms
Within the total MTC safety analysis set (N = 319), harm events at the June 15, 2021 data cut-off were similar to the events presented at the March 30, 2020 data cut-off (Table 30). Of the AEs, only |||| of patients had a serious TEAE related to selpercatinib. At the time of data cut-off, |||||| |||||| |||||| |||||||| |||||| || |||| || |||| |||| || ||||||||||||| || ||| || ||||||| |||||||||||| || ||| || ||||||| ||||||| ||| | ||| || ||||||| ||| |||||| |||||| |||||||| |||| |||| || |||| ||||| ||| |||| |||| ||| ||| || ||||||| |||||||||||| | ||| || ||||||| ||||||| ||| | ||| || ||||||. Similar to the March 30, 2020 data cut-off, AEs with a frequency of 20% or greater, in decreasing order, include diarrhea, hypertension, dry mouth, fatigue, constipation, AST increased, peripheral edema, nausea, headache, ALT increased, blood creatine increased, abdominal pain, arthralgia, hypocalcemia, vomiting, QT prolonged on ECG, cough, back pain, rash.
This new cut-off date information provides more data to supplement the immature evidence seen in the initial cut-off dates. The results from this later cut-off date were consistent for each end point (OS, PFS, ORR, harms) with the results from the initial cut-off date. There is still an unmet need for patients with MTC who have PD despite initial treatments as well as patients who are treatment-naive. The population assessed in this new cut-off date can be considered generalizable to the Canadian clinical landscape, since this group is mostly treatment-naive and would be similar to the population indicated in the reimbursement conditions discussed in this reconsideration (i.e., selpercatinib as first-line therapy). Overall, this is considered an improvement in terms of applicability.
Despite the new information, there is still uncertainty in the evidence supporting the use of selpercatinib due to the single-arm unblinded design of the LIBRETTO-001 study and imprecision due to the small number of patients and events, as stated in the critical appraisal section of this report.
Discussion
Summary of Available Evidence
One clinical study was included in this report evaluating the use of selpercatinib in patients with RET-mutant advanced (unresectable) or metastatic MTC.
The LIBRETTO-001 trial is a single-arm, open-label, phase I and II study being conducted in several countries (including Canada). The population integrated in the study consists of patients with RET-mutant advanced MTC who were eligible from a broader population, including those with DTC and NSCLC. The population as of the December 16, 2019 cut-off date was the main population used for the analyses and this report since it was the pre-planned analysis. This analysis provides 6 months of additional follow-up information for patients enrolled as of the initial data cut-off of June 17, 2019, and was the information used for the Health Canada submission. Further information was provided by the sponsor for safety and efficacy end points with a March 30, 2020 cut-off date. Patients were eligible if they presented with metastatic or locally advanced disease; had an ECOG PS of 0, 1, or 2; and were aged 12 years and older. The primary objective of phase I of the study was to find the MTD and RP2D. The recommended dose from the dose-escalation process from phase I was reached at 160 mg. At phase II, the primary end point was to evaluate the ORR based on RECIST criteria, with DOR, PFS, OS, safety, PK, and change in tumour size as secondary end points. Biomarker changes and HRQoL assessments were exploratory end points. CADTH identified 3 ongoing studies relevant to this submission. LIBRETTO-531 (phase III RCT of selpercatinib versus cabozantinib or vandetanib), LIBRETTO-321 (phase II conducted in China), and LIBRETTO-121 (phase I and II study in a pediatric population), none of which (except for LIBRETTO-121 presented as a conference abstract) have data available at this time. All are expected to be completed by 2026, 2025, and 2024, respectively.
New data were submitted by the sponsor for a June 15, 2021 cut-off date, as part of a request for reconsideration to CADTH, requesting to include only adults (18 years of age and older) with unresectable advanced or metastatic RET-mutant MTC in the first-line setting.
One sponsor-submitted ITC used a matching-adjusted, unanchored ITC to evaluate the relative clinical efficacy of selpercatinib compared with placebo (BSC) and against vandetanib for the treatment of advanced RET mutation–positive MTC. Three outcomes were analyzed: OS, PFS, and ORR.
Interpretation of Results
Efficacy
The LIBRETTO-001 study evaluated end points for efficacy (such as ORR and DOR), survival (such as PFS and OS), and HRQoL. All of these end points were considered by the clinical experts consulted by CADTH to be critical for clinical decision-making and relevant to the Canadian landscape according to other stakeholders, such as patient groups and the drug programs. The primary (ORR) and secondary and exploratory end points (including OS, PFS, DOR, and HRQoL measures) in LIBRETTO-001 were evaluated but not formally adjusted for multiple comparisons.
The results from the LIBRETTO-001 trial on its primary end point of ORR reached a value of 69.1% in its PAS, which was considered by the clinical experts of clinical significance and better than expected for patients with metastatic or unresectable MTC. These values were similar when evaluating the later cut-off dates of the study. Similarly, the DOR was of particular clinical significance since, at a median follow-up of 14 months, the patients in the PAS had not reached the median DOR.
In terms of survival, || ||| ||||| ||||| ||| || ||| |||||||||| |||||| ||| |||||||| || ||| ||| |||||| ||| || || ||||||| at the December 16, 2019 data cut-off. At a later cut-off date (March 30, 2020), OS reached 33.2 months (range, 0.4 months to 33.3 months) in patients previously treated with vandetanib or cabozantinib and “not reached” in treatment-naive patients. An OS of 12 months or more was reassuring for the clinical experts consulted by CADTH, observing that ||||| of patients survived 12 months or more at the December16 2019 cut-off date, and more than 88% survived 12 months or more at the March 30 2020 cut-off date.
These numbers were considered by the clinical experts to indicate an improvement and meaningful effects above the expected level, based on their experience. When comparing selpercatinib with best standard of care and/or with vandetanib (the only funded intervention in Canada), the experts considered the value that patients put on HRQoL outcomes and indicated that selpercatinib has the potential to fulfill an unmet need, as available treatment options are currently limited. Although the estimates of HRQoL, as with the rest of the outcomes, have the same methodological limitations associated with a single-arm trial plus the limitations associated with an open-label design, these estimates were still considered relevant by the clinical experts when considering issues commonly cited by patients such as diarrhea and the need for further treatment options, as both issues were brought up frequently in the patient group input.
An update on the data that extended the follow-up, now with a median of 26.3 months for OS and 24.5 months for PFS (previous cut-off medians for both end points were not reached), denotes an improvement in the immature data observed in the analyses at the initial cut-off dates, and there is agreement between the base case and subsequent analyses.
One sponsor-submitted ITC reported 3 end points (OS, ORR, PFS) considered important by the experts and patient groups. After weighting, there was a statistically significant improvement in PFS for selpercatinib versus placebo and a statistically significant improvement in OS for selpercatinib versus placebo. Similarly, the ITC reported improvements in the ORR when compared with vandetanib. However, the ITC has serious limitations since it considers single-arm evidence against aggregated data in a MAIC with a high possibility of residual confounding and clinical and/or population heterogeneity, as well as limitations in the assumptions of similar OS among populations and use of surrogate weights from 1 comparison to another.
Overall, the uncertainty in this body of evidence in the context of the scarcity of comparative (randomized) evidence reflects the challenges for conducting phase III studies in rare and indolent conditions such as MTC.
Harms
AEs were reported in all but 2 patients taking selpercatinib. The most common AEs (i.e., > 20% of patients with at least 1 of these) were hypertension, diarrhea, constipation, fatigue, headache, peripheral edema, nausea, and abdominal pain.
Overall, there were no major concerns from the LIBRETTO-001 study related to harms at either the evaluated cut-off points or at the later cut-off point (June 15, 2021). While SAEs occurred in | | of the safety population |||||||||| ||| ||||||||||||| ||||| |||| ||||||| || |||| ||| || || |||||||| ||||||||||||), all AEs of concern, such as hypertension, diarrhea, QTc prolongation, and elevations of liver enzymes, were considered by the experts consulted by CADTH to be manageable in the clinical setting and would not impact the use of the drug, as many of the precautions taken during the administration of selpercatinib are familiar and in common use among physicians and other health professionals.
Conclusions
Evidence from a single-arm, open-label, unblinded study (LIBRETTO-001) suggests that treatment with selpercatinib is associated with survival and response end points (OS, PFS, ORR, DOR, HRQoL) that were considered relevant to both patients and clinicians when compared with the typical effects and clinical evolution observed by clinical experts among patients with RET-mutant, advanced and/or metastatic MTC after surgery. Overall, the clinical experts deemed the harms and safety profile of selpercatinib to be better than the undesirable effects usually seen in clinical practice with vandetanib or cabozantinib.
However, major limitations generate uncertainty around any effect estimates due to immature data, lack of comparative evidence, a high risk of bias (no blinding, attrition), no adjustment for multiple comparisons, and imprecision in time-to-event outcomes.
Evidence from a sponsor-submitted ITC is also associated with major limitations for the comparison between selpercatinib and BSC due to residual confounding (i.e., incomplete inclusion of prognostic factors and effect modifiers), surrogate use of weights for comparisons, and heterogeneity among the included populations.
Overall, there is uncertain evidence that selpercatinib provides clinical benefits with similar or lower risks of harms (i.e., toxicity) when compared with what is expected with relevant comparators.
References
1.Pacini F, Castagna MG, Brilli L, Pentheroudakis G, ESMO Guidelines Working Group. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21 Suppl 5:v214-219. PubMed
2.Filetti S, Durante C, Hartl D, et al. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(12):1856-1883. PubMed
3.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-E205. PubMed
4.Viola D, Elisei R. Management of medullary thyroid cancer. Endocrinol Metab Clin North Am. 2019;48(1):285-301. PubMed
5.Cabanillas ME, McFadden DG, Durante C. Thyroid cancer. Lancet. 2016;388(10061):2783-2795. PubMed
6.Lee K, Anastasopoulou C, Chandran C, Cassaro S. Thyroid cancer. StatPearls. Treasure Island (FL): StatPearls Publishing; 2021: https://www.ncbi.nlm.nih.gov/pubmed/29083690. Accessed 2022 Mar 1.
7.Mathiesen JS, Kroustrup JP, Vestergaard P, et al. Survival and long-term biochemical cure in medullary thyroid carcinoma in Denmark 1997-2014: a nationwide study. Thyroid. 2019;29(3):368-377. PubMed
8.Torresan F, Cavedon E, Mian C, Iacobone M. Long-term outcome after surgery for medullary thyroid carcinoma: a single-center experience. World J Surg. 2018;42(2):367-375. PubMed
9.Torresan F, Mian C, Cavedon E, Iacobone M. Cure and survival of sporadic medullary thyroid carcinoma following systematic preoperative calcitonin screening. Langenbecks Arch Surg. 2019;404(4):411-419. PubMed
10.Brierley J, Tsang R, Simpson WJ, Gospodarowicz M, Sutcliffe S, Panzarella T. Medullary thyroid cancer: analyses of survival and prognostic factors and the role of radiation therapy in local control. Thyroid. 1996;6(4):305-310. PubMed
11.Wells SA, Jr., Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015;25(6):567-610. PubMed
12.Tappenden P, Carroll C, Hamilton J, et al. Cabozantinib and vandetanib for unresectable locally advanced or metastatic medullary thyroid cancer: a systematic review and economic model. Health Technol Assess. 2019;23(8):1-144. PubMed
13.Elisei R, Schlumberger MJ, Muller SP, et al. Cabozantinib in progressive medullary thyroid cancer. J Clin Oncol. 2013;31(29):3639-3646. PubMed
14.Wells SA, Jr., Robinson BG, Gagel RF, et al. Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol. 2012;30(2):134-141. PubMed
15.Retevmo™ (selpercatinib): capsules, 40 mg and 80 mg, oral [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2021 Jun 11.
16.Loxo Oncology Inc. NCT04211337: A study of selpercatinib (LY3527723) in participants with RET-mutant medullary thyroid cancer (LIBRETTO-531). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT04211337. Accessed 2022 Mar 1.
17.Wirth LJ, Robinson B, Boni V, et al. Patient-reported outcomes with selpercatinib treatment among patients with RET-mutant medullary thyroid cancer in the phase I/II LIBRETTO-001 trial. Oncologist. 2021;13:13. PubMed
18.Interim Clinical Study Report: LOXO-RET-17001. Phase 1/2 study of oral LOXO-292 in patients with advanced solid tumors, including RET fusion-positive solid tumors, medullary thyroid cancer and other tumors with RET activation (LIBRETTO-001) [internal sponsor's report]. Stamford (CT): Loxo Oncology, Inc.; 2019 Nov 28.
19.Public Health Agency of Canada. Thyroid cancer. 2017; https://www.canada.ca/en/public-health/services/chronic-diseases/cancer/thyroid-cancer.html. Accessed 2022 Jan 12.
20.Caprelsa (vandetanib): tablets, 100 and 300 mg, oral [product monograph]. Mississauga (ON): Sanofi Genzyme; 2020: https://pdf.hres.ca/dpd_pm/00055721.PDF. Accessed 2022 Jan 12.
21.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
22.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Nov 24.
23.Wirth LJ, Sherman E, Robinson B, et al. Efficacy of selpercatinib in RET-altered thyroid cancers. N Engl J Med. 2020;383(9):825-835. PubMed
24.Subbiah V, Gainor JF, Oxnard GR, et al. Intracranial efficacy of selpercatinib in RET fusion-positive non-small cell lung cancers on the LIBRETTO-001 trial. Clin Cancer Res. 2021;27(15):4160-4167. PubMed
25.Minchom A, Tan AC, Massarelli E, et al. Patient-reported outcomes with selpercatinib among patients with RET fusion-positive non-small cell lung cancer in the phase I/II LIBRETTO-001 trial. Oncologist. 2021;15:15. PubMed
26.Drilon A, Oxnard GR, Tan DSW, et al. Efficacy of selpercatinib in RET fusion-positive non-small-cell lung cancer. N Engl J Med. 2020;383(9):813-824. PubMed
27.Penel N, Kramar A. What does a modified-Fibonacci dose-escalation actually correspond to? BMC Med Res Methodol. 2012;12:103. PubMed
28.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
29.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
30.Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials. 1996;17(4):343-346. PubMed
31.Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. Washington (DC): US Department of Health and Human Services; 2010: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf. Accessed 2022 Jan 23.
32.A systematic literature review and indirect treatment comparison of selpercatinib for the treatment of advanced RET-mutant medullary thyroid cancer and advanced RET-fusion positive thyroid cancer [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Retevmo (selpercatinib), 40 and 80 mg capsules. Toronto (ON): Eli Lilly Canada Inc.; 2021 Feb.
33.Schlumberger M, Elisei R, Muller S, et al. Overall survival analysis of EXAM, a phase III trial of cabozantinib in patients with radiographically progressive medullary thyroid carcinoma. Ann Oncol. 2017;28(11):2813-2819. PubMed
34.Sherman SI, Clary DO, Elisei R, et al. Correlative analyses of RET and RAS mutations in a phase 3 trial of cabozantinib in patients with progressive, metastatic medullary thyroid cancer. Cancer. 2016;122(24):3856-3864. PubMed
35.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submission to NICE. Sheffield (GB): Decision Support Unit, ScHARR, University of Sheffield; 2016: https://nicedsu.sites.sheffield.ac.uk/tsds/population-adjusted-indirect-comparisons-maic-and-stc. Accessed 2022 Jan 12.
36.Loxo Oncology Inc. NCT04280081: A study of selpercatinib (LY3527723) in participants with advanced solid tumors including RET fusion-positive solid tumors, medullary thyroid cancer and other tumors with RET activation (LIBRETTO-321). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT04280081. Accessed 2022 Mar 1.
37.Loxo Oncology Inc. NCT03899792: A study of oral LOXO-292 (selpercatinib) in pediatric participants with advanced solid or primary central nervous system (CNS) tumors (LIBRETTO-121). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT03899792. Accessed 2022 Mar 1.
38.Hernando J, Tarasova V, Hu MI, et al. 1927TiP LIBRETTO-531: Selpercatinib in patients with treatment (Tx)-naïve RET-mutant medullary thyroid cancer (MTC). Ann Oncol. 2020;31:S1091.
39.Lu S CY, Huang D, et al. MA02.01 Efficacy and safety of selpercatinib in Chinese patients with RET fusion-positive non-small cell lung cancer: a phase 2 trial. J Thorac Oncol. 2021;16(10 Suppl):S888-S889.
40.Morgenstern DA, Mascarenhas L, Campbell M, et al. Oral selpercatinib in pediatric patients (pts) with advanced RET-altered solid or primary CNS tumors: Preliminary results from the phase 1/2 LIBRETTO-121 trial. J Clin Oncol. 2021;39(15_suppl):10009-10009.
41.Gao Q, Su J, Xiao F, Lin X, Yang J. Advances in the treatment of RET fusion-positive advanced non-small cell lung cancer. Zhongguo Fei Ai Za Zhi. 2021;24(12):853-861. PubMed
42.National Cancer Institute (NCI). NCT04320888: Selpercatinib for the treatment of advanced solid tumors, lymphomas, or histiocytic disorders with activating RET gene alterations, a pediatric MATCH treatment trial. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/ct2/show/NCT04320888. Accessed 2022 Mar 1.
43.National Cancer Institute (NCI). NCT03155620: Targeted therapy directed by genetic testing in treating pediatric patients with relapsed or refractory advanced solid tumors, non-Hodgkin lymphomas, or histiocytic disorders (The Pediatric MATCH Screening Trial). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/ct2/show/NCT03155620. Accessed 2022 Mar 1.
44.Lui M, Gallo-Hershberg D, DeAngelis C. Development and validation of a patient-reported questionnaire assessing systemic therapy induced diarrhea in oncology patients. Health Qual Life Outcomes. 2017;15(1):249. PubMed
45.Cocks K, King MT, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. PubMed
46.Donadio MVF, Vendrusculo FM, Campos NE, et al. The modified shuttle test as a predictor of risk for hospitalization in youths with cystic fibrosis: A two-year follow-up study. J Cyst Fibros. 2021;20(4):648-654. PubMed
47.Staubes BA, Metzger NL, Walker SD, Peasah SK. Evaluation of a once/day tobramycin regimen to achieve target concentrations in adult patients with cystic fibrosis. Pharmacotherapy. 2016;36(6):623-630. PubMed
48.Singer S, Jordan S, Locati LD, et al. The EORTC module for quality of life in patients with thyroid cancer: phase III. Endocr Relat Cancer. 2017;24(4):197-207. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: November 24, 2021
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(selpercatinib* or Retevmo* or Retsevmo* or LOXO-292 or LOXO292 or ARRY-192 or ARRY192 or LY3527723 or LY-3527723 or WHO-10967 or WHO10967 or CEGM9YBNGD).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*selpercatinib/
(selpercatinib* or Retevmo* or Retsevmo* or LOXO-292 or LOXO292 or ARRY-192 or ARRY192 or LY3527723 or LY-3527723 or WHO-10967 or WHO10967).ti,ab,kf,dq.
3 or 4
5 use oemezd
6 not (conference abstract or conference review).pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- (selpercatinib OR retevmo OR retsevmo OR LOXO-292 OR LOXO292)]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- selpercatinib OR retevmo OR retsevmo OR LOXO292 OR LOXO-292]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- selpercatinib, retevmo, retsevmo, LOXO-292, LOXO292]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms selpercatinib, retsevmo OR retevmo OR LOXO-292 OR LOXO292]
Grey Literature
Search dates: November 17 to 24, 2021
Keywords: selpercatinib, retevmo, retsevmo, LOXO-292, LOXO292, thyroid cancer
Limits: None
Updated: Search updated before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
(EMA) Retsevmo: early public assessment report. European Medicine Agency (EMA) Assessment report: EMA/9037/2021. 2021; https://www.ema.europa.eu/en/documents/assessment-report/retsevmo-epar-public-assessment-report_en.pdf.41 | Report submitted for regulatory purposes |
LIBRETTO-53116 | Ongoing study, no data available |
LIBRETTO-32136 | Ongoing study, no data available |
LIBRETTO-12137 | Ongoing study, no data available |
NCT0475991139 | Ongoing study, no data available |
NCT0432088842 | Ongoing study, no data available |
NCT0315562043 | Ongoing study, no data available |
Appendix 3: Changes to the Protocol
Note that this appendix has not been copy-edited.
Table 25: Summary of Major Changes to the Protocol
Version number and date | Major changes to the protocol |
|---|---|
1.0 (not implemented) | NA |
2.0 27 March 2017 | The following revisions were made based on FDA IND review:
|
3.0 20 July 2017 |
|
4.0 21 November 2017 |
|
4.5 11 April 2018 | Initial Japan-specific protocol. |
5.0 30 May 2018 |
Clarified the types of radiographic imaging to be performed at baseline and with each subsequent treatment. This includes baseline brain imaging in all patients with RET fusion–positive cancers as well as all patients with a history of CNS metastases and other patients if clinically indicated, including subsequent brain imaging in all patients with detectable brain metastases at baseline.
|
5.1 15 June 2018 | All revisions were made to align with v.5.0 (with the exception of the addition of the oral solution as with v.5.0; this version [5.1] did not include the oral solution). |
6.0 11 September 2018 |
|
6.1 11 September 2018 |
|
7.0 18 October 2018 |
|
7.1 18 October 2018 |
|
7.2 18 October 2018 |
|
7.3 26 December 2018 |
|
7.4 26 December 2018 |
|
8.0 |
|
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
The bowel diary questionnaire, a modified version of the STIDAT was used in the LOXO-RET-17001 / LBRETTO-001 trial as an exploratory outcome.
The EORTC QLQ-C30 version 3 was used in LOXO-RET-17001 / LIBRETTO-001 trial as an exploratory outcome.
Findings
A focused literature search was conducted to identify the psychometric properties and MID of each of the stated outcome measures.
The findings about validity, reliability, responsiveness, and MID of each outcome measure are summarized in Table 26.
Interpretation of the reliability and validity metrics were based on the following criteria:
Inter-rater reliability, kappa statistics (level of agreement):
< 0 = poor agreement
0.00—0.21 = slight agreement
0.21—0.40 = fair agreement
0.41—0.60 = moderate agreement
0.61—0.8 = substantial
0.81—1.00 = almost perfect agreement
Internal consistency (Cronbach alpha) and test–retest reliability: ≥ 0.7 is considered acceptable.
Validity, i.e., between-scale comparison (correlation coefficient, r):
≤ 0.3 = weak
0.3 to ≤ 0.5 = moderate
> 0.5 = strong
Table 26: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
The Bowel Diary (a modified STIDAT) | A self-completed, patient-reported outcome scale that assesses (presence and severity of) diarrhea and its impact on QoL. Consists of 12 questions clustered into 4 factors: patient’s perception of diarrhea, bowel movement frequency, fecal incontinence, and abdominal symptoms. Higher scores (greater than cut-off 1.35) represents increasing severity of diarrhea. | Validity, reliability, and responsiveness have not been tested in patients with thyroid cancer. | Unknown A cut-off score of 1.35 indicates occurrence of diarrhea.44 |
EORTC QLQ-C30 | A standardized, patient self-administered questionnaire for evaluating the QoL of patients with cancer. Consists of 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item QoL scale. Higher scores represent better function and QoL in the functional and QoL scales, respectively. Higher score indicates higher symptom burden on symptoms scale. | Validity, reliability, and responsiveness have not been tested in patients with thyroid cancer. | For improvement and deterioration in patients with various types of cancers including head and neck cancers45:
|
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; MID = minimal important difference; QoL = quality of life; STIDAT = Systemic Therapy Induced Diarrhea Assessment Tool.
The Bowel Diary Modified Systemic Therapy Induced Diarrhea Assessment Tool
Description
The bowel diary questionnaire is a modified version of the STIDAT, a standardized patient-reported questionnaire used to assess diarrhea in patients with cancer actively treated with chemotherapy or systemic therapies (with or without radiation) that are considered high-risk to cause diarrhea.
The original STIDAT was developed using the FDA Iterative Process for patient-reported outcome instrument to overcome a number of limitations of National Cancer Institute Common Terminology Criteria for Adverse Events scale and other algorithms in evaluating severity of STID in clinical trials. STIDAT defines diarrhea based on presence of watery stool and assesses patient’s perception of having diarrhea, daily number of bowel movements, daily number of diarrhea episodes, antidiarrheal medication use, the presence of urgency, abdominal pain, abdominal spasms, or fecal incontinence, patient’s perception of diarrhea severity, and QoL. QoL was evaluated based on the impact of diarrhea on the social life, mood, family life, ability to perform daily activities of living and energy level. STIDAT consists of 12 questions covering 5 dimensions: 1) Onset and duration (Question 1); 2) Stool frequency (Questions 2 to 3); 3) Diarrhea-associated symptoms (Questions 4 to 6); 4) Self-Treatment of Diarrhea (Question 7); 5) Impact on QoL (Questions 8 to 12). Questions 1 and 4 to 7 are answered yes or no. Questions 2 to 3 and 7 are answered with an integer greater than 0. Questions 8 to 12 are answered from 0 (no impact) to 10 (extreme impact). These dimensions are classified into 4 factors – patient’s perception of diarrhea, frequency of diarrhea, fecal incontinence, and abdominal symptoms for calculation of total score (Table 27). Patient is asked to recall in the last 7 days to self-complete the questionnaire.
The bowel diary or modified STIDAT questionnaire (mSTIDAT) used in the sponsor’s study contains 11 questions and assesses all the dimensions in the original STIDAT except for antidiarrheal medication use, which can reduce bowel movement frequency. Also, abdominal pain and abdominal spasms or fecal incontinence dimensions have been changed to abdominal discomfort (since patients may not understand spasms or confuse spasms with discomfort) and fecal incontinence (which may occur independent of diarrhea) dimensions. In the mSTIDAT, the QoL subscale asks patients to rank the impact of bowel habits (Questions 7 to 9) and diarrhea (Questions 10 to 11) on their daily living from 0 (no impact) to 10 (extreme impact). In the case of missing items in the QoL subscale, the sponsor excluded the scale from the analysis and no imputation was made.
The psychometric properties of STIDAT have not been validated in patients with thyroid cancer and/or those on targeted therapy. Also, no MID has been estimated for the STIDAT in either general population or patients with thyroid cancer.
Scoring
STIDAT uses the weighted scoring system based on how much each component contributes toward the incidence and severity of diarrhea. Scores of binary variables (yes/no questions) would be either 0 (no) or 1 (yes), scores for diarrhea severity vary from 0 (no diarrhea) to 3 (severe diarrhea) and scores of questions pertaining to episode frequency would be an integer starting from 0. The QoL score is the average of the 5 dimensions of QoL in the STIDAT. The negative sign in the component of QoL is because its questions are ranked in reverse. The score of each question corresponding to its component would be multiplied by its component weight. The total STIDAT score is the sum of all component scores and the adjustment factor (0.48), which offsets the minimum QoL score that a patient may reach to prevent a negative STIDAT score (Table 28).
Patients without diarrhea had a mean score of 0.72 (SD = 0.21), while patients with diarrhea had a score of 2.25 (SD = 0.73) (Welch’s t-test: t = 15.04; 95% CI, 1.33 to 1.73). Patients with a STIDAT score of 1.35 or higher are identified to have diarrhea.44
Table 27: Scoring System of STIDAT
Components | Proportion explaining diarrhea | Score calculation |
|---|---|---|
Factor 1: Patient’s perception of diarrhea | ||
Presence of diarrhea | 0.193 | N1 × 0.193 |
Severity of diarrhea | 0.529 | N2 × 0.529 |
Presence of urgency | 0.048 | N1 × 0.048 |
Factor 2: Bowel movement frequency | ||
Number of bowel movements | 0.050 | N3 × 0.050 |
Number of diarrhea episodes | 0.161 | N3 × 0.161 |
Medication use | 0.060 | N1 × 0.060 |
Quality of life | −0.048 | Average N1–5 × (−0.048) |
Factor 3: Fecal incontinence | ||
Presence of fecal incontinence | 0.016 | N1 × 0.016 |
Factor 4: Abdominal symptoms | ||
Presence of abdominal spasms | 0.032 | N1 × 0.032 |
Presence of abdominal discomfort | 0.031 | N1 × 0.031 |
TOTAL | — | Sum of component scores plus 0.48a |
N1: yes = 1, no = 0 (questions 1, 4 to 7).
N2: no = 0, mild = 1, moderate = 2, severe = 3 (question 1a).
N3: an integer of n ≥ 0 (questions 2 to 3, 7 to 12).
aAdjustment factor.
Source: Lui 2017; 15:249 (Copyright 2017 by the authors. Reprinted in accordance with CC BY 4.0).17
In Table 28, the STIDAT scores stratified by diarrhea severity are shown. Median scores of no, mild, moderate, and severe diarrhea cohorts were 0.64, 1.54, 2.38 and 3.63, respectively. Based on the ranges of scores for each severity, clinicians may categorize scores from 0 to 1.1 as no diarrhea, greater than 1.1 to 2 as mild diarrhea, greater than 2 to 3 as moderate diarrhea and greater than 3 as severe diarrhea.
Table 28: STIDAT Scores by Diarrhea Severity
Detail | Median | Interquartile range | Minimum | Maximum |
|---|---|---|---|---|
No diarrhea | 0.643984 | 0.726803 to 0.618736 = 0.108067 | 0.57867 | 1.095777 |
Mild diarrhea | 1.540987 | 1.774623 to 1.483602 = 0.291021 | 1.107415 | 2.076253 |
Moderate diarrhea | 2.375934 | 2.388316 to 2.363551 = 0.024764 | 1.909746 | 3.674208 |
Severe diarrhea | 3.630018 | 3.670862 to 3.475936 = 0.194926 | 2.899779 | 4.605079 |
Source: Lui 2017; 15:249. (Copyright 2017 by the authors. Reprinted in accordance with CC BY 4.0).44
The mean overall QoL scores (calculated as the average of the 5 QoL dimensions measured in the STIDAT) were 8.95 (95% CI, 8.50 to 9.40) in the no diarrhea group, 8.12 (95% CI, 7.38 to 8.87, P = 0.6164) in the mild diarrhea group, 7.1 (95% CI, 6.18 to 8.02) in the moderate diarrhea group and 4.44 (95% CI, 1.53 to 7.35) in the severe diarrhea group.
Based on the Dunnett-Tukey-Kramer test, there were significant decreases in QoL experienced by patients with moderate diarrhea (−1.86; 95% CI, −3.05 to −0.67; P < 0.001) and severe diarrhea (−3.64; 95% CI, −5.91 to −1.38; P < 0.001) compared with patients with no diarrhea. There was a trend toward a decrease in QoL in patients with severe diarrhea compared with those with mild diarrhea (−2.82; 95% CI, −5.3 to −0.37; P = 0.017). There was no difference in QoL between mild and no diarrhea, mild and moderate diarrhea, and moderate and severe diarrhea.
EORTC QLQ-C30
Description
The EORTC QLQ-C30, is 1 of the most commonly used patient-reported outcome measures in oncology clinical trials.28 It is a multi-dimensional, cancer-specific, evaluative measure of HRQoL. It was designed specifically for the purpose of assessing changes in participants’ HRQoL in clinical trials, in response to treatment.46 The core questionnaire of the EORTC QLQ-C30 consists of 30 questions that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item QoL scale, as outlined in Table 29. Version 3.0 of the questionnaire, used in the LIBRETTO-001 trial included in this report, is the most current version and has been in use since December 1997.47 It is available in 90 different languages and is intended for use in adult populations only. The questionnaire was answered by the subject to the best of his/her ability, before receiving drug on C1D1 (the baseline assessment) and before learning the results of the radiologic disease assessment for subsequent cycles. Paper QoL instruments were administered pre-dose on cycle 1 day 1 (baseline assessment for patient-reported outcome instruments). Only patients who had completed questionnaires at baseline were to complete subsequent questionnaires at the specified follow-up periods.
Table 29: Scales of EORTC QLQ-C30
Functional scales (15 questions) | Symptom scales (7 questions) | Single-item symptom scales (6 questions) | Global quality of life (2 questions) |
|---|---|---|---|
Physical function (5) | Fatigue (3) | Dyspnea (1) | Global quality of life (2) |
Role function (2) | Pain (2) | Insomnia (1) | — |
Cognitive function (2) | Nausea and vomiting (2) | Appetite loss (1) | — |
Emotional function (4) | — | Constipation (1) | — |
Social function (2) | — | Diarrhea (1) | — |
— | — | Financial impact (1) | — |
Scoring
The EORTC QLQ-C30 uses a 1-week recall period in assessing function and symptoms. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4.47 For the 2 items that form the global QoL scale, however, the response format is a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent).47
Raw scores for each scale are computed as the average of the items that contribute to a particular scale. This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of 1 unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better QoL (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and QoL scale would reflect an improvement. According to the EORTC QLQ-C30s scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least 1-half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.47
No studies assessing the validity and reliability of the questionnaire in the context of thyroid cancer were found. A preliminary EORTC QoL module for thyroid cancer (EORTC QLQ-THY34) was published in April 2017 before the first patient in the LIBRETTO-001 trial was treated (May 2017) but its validation is still ongoing.48
Minimal Important Difference
A study by Cocks, et al.45 used a systematic review of the literature and experts’ opinion to evaluate meaningful differences and magnitude of change in the QLQ-C30 scores. In a meta-analysis of 118 relevant papers (13.6% from US/Canada, 13.6% patients with head and neck cancers) with timescales ranging from 4 days to 5 years, authors estimated trivial, small, medium, and large size classes for meaningful change in the scales. Since medium and large changes could not be estimated for all scales due to insufficient data and response shift (i.e., psychological adaption of patients to their changing health status), small differences, as defined by subtle but nevertheless clinically meaningful changes, have been taken to represent the MIDs. For example, MID ranges (improvement and deterioration, respectively) are as follows: physical function (2 to 7, −10 to −5), role function (6 to 12, −14 to −7), cognitive function (3 to 7, −7 to −1), emotional function (6 to 9, −12 to −3), social function (3 to 8, −11 to −6), fatigue (−9 to −4, 5 to 10), pain (−9 to −5, 3 to 11), nausea/vomiting (−9 to −3, 5 to 11), single-item symptom scales (−11 to −2, 2 to 15) and global QoL score (5 to 8, −10 to −5) Cocks, 2012. The sponsor has taken a score of 10 to be an MID for both improvement and deterioration on a single study.29 To be more specific, patients with “improvement” demonstrated a ≥ 10 point change from their baseline score. Patients with “worsening” decreased by ≥ 10 points from their baseline score. A definite change (improvement or worsening) was defined as an improvement or worsening, respectively, from baseline ≥ 10 points without any further reduction or increase in score ≥ 10 points, respectively.
Appendix 5: New Data for the Request for Reconsideration
Note that this appendix has not been copy-edited.
The following tables and figures are to describe the new sponsor-submitted data for the request for reconsideration of 19 May 2022. The request for a major reconsideration of the draft recommendation is to expand the initiation condition for selpercatinib to include adult (18 years of age and older) with unresectable advanced or metastatic RET-mutant MTC in the first-line setting. New information is provided with the June 15, 2021 cut-off date.
Figure 11: Kaplan-Meier for PFS Based on IRC Assessments RET-Mutant MTC — SAS 1 (Cabozantinib- and/or Vandetanib-Naive, Primary Efficacy Analysis Set); June 15, 2021 Data Cut-Off
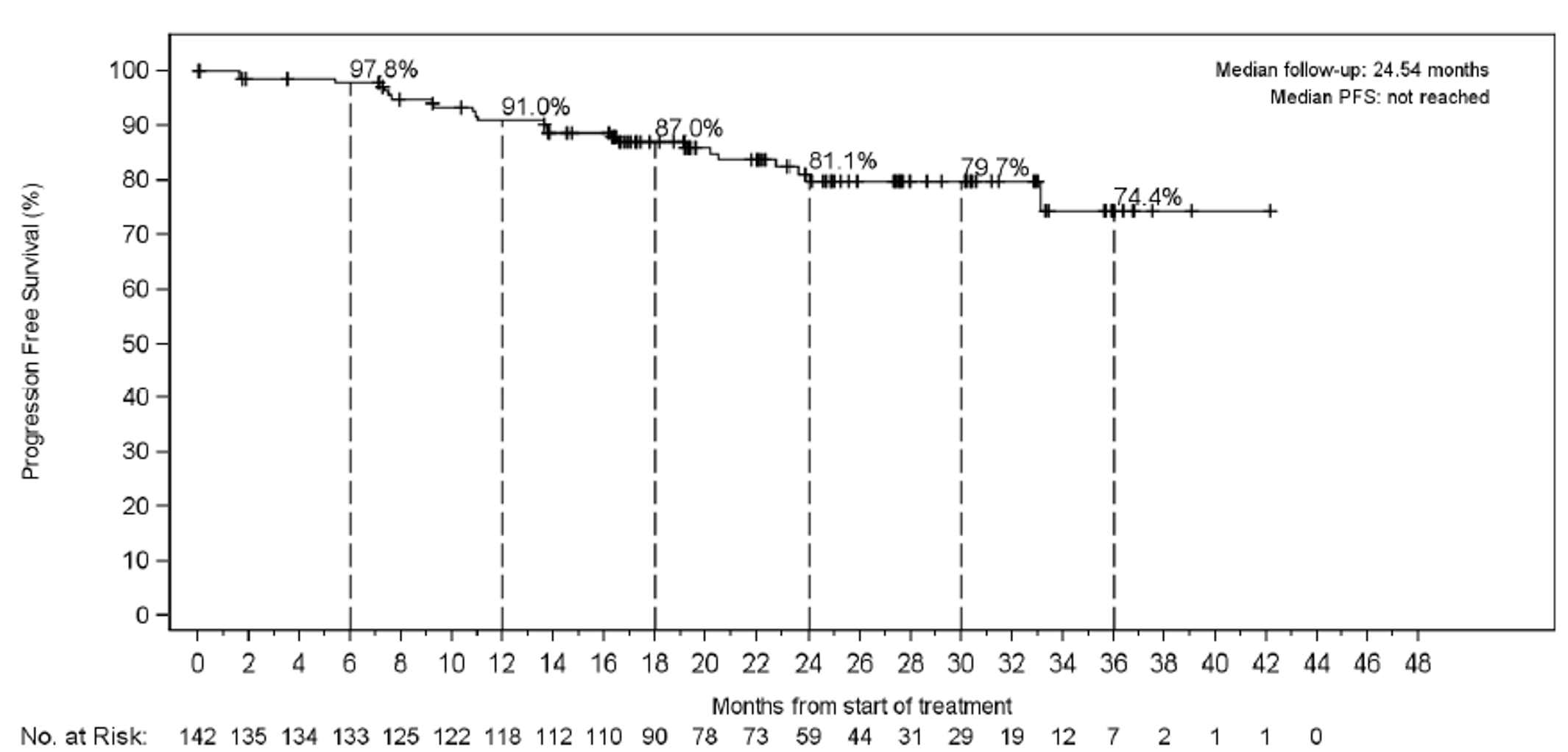
Source: LIBRETTO-001 interim Clinical Study Report (2022).
Table 30: Summary of Harms — LIBRETTO-001 Safety Analysis Sets, March 30, 2020 and June 15, 2021 Cut-Off Dates
Variable | Cut-off date | Cut-off date | |
|---|---|---|---|
Total MTC (N = 315) | Total MTC (N = 319) | Overall safety analysis set (N = 796) | |
Adverse events, N (%)a | |||
Patients with ≥ 1 AEs | 313 (99.4) | ||| |||||| | ||| |||||| |
Maximum severity = grade 3 or 4 | 188 (59.7) | ||| |||||| | ||| |||||| |
Maximum severity = grade 5 | | ||||| | || ||||| | || ||||| |
Serious adverse events, N (%) | |||
Patients with ≥ 1 serious AEs | 97 (30.8) | ||| |||||| | ||| |||||| |
Serious AEs and related to selpercatinib | 20 (6.3) | || ||||| | || |||||| |
Patients with fatal AEs | 8 (2.5) | || ||||| | || ||||| |
Patients with fatal AEs and related to selpercatinib | 0 (0) | | ||||| | | ||||| |
Patients with AEs and permanently discontinued study drug | 15 (4.8) | || ||||| | || ||||| |
Patients with AEs and permanently discontinued study drug and related to selpercatinib | 6 (1.9) | || ||||| | || ||||| |
AE = adverse event.
aAEs included treatment-emergent AEs not related to selpercatinib.
Source: LIBRETTO-001 interim Clinical Study Report (2022).
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
BSC
best supportive care
CUA
cost-utility analysis
ICER
incremental cost-effectiveness ratio
LY
life-year
MAIC
matched-adjusted indirect comparison
MTC
medullary thyroid cancer
OS
overall survival
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
RET
rearranged during transfection proto-oncogene
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Selpercatinib (Retevmo) |
Submitted price |
|
Indication | RET-mutant medullary thyroid cancer in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC date | June 15, 2021 |
Reimbursement request | As per indication |
Sponsor | Eli Lilly Canada Inc. |
Submission history |
|
NOC/c = Notice of Compliance with Conditions; RET = rearranged during transfection.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation |
|
Target populations | Patients aged 12 years and older with RET-mutant MTC, including treatment-naive RET-mutant MTC (i.e., first-line treatment) and previously treated RET-mutant MTC (i.e., second- and later-line treatment). |
Treatment | Selpercatinib |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 10 years |
Key data source |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; MAIC = matching-adjusted indirect comparison; MTC = medullary thyroid cancer; PFS = progression-free survival; PSM = partitioned survival model; RET = rearranged during transfection; QALY = quality-adjusted life-year.
Conclusions
The CADTH Clinical Review concluded the data from the LIBRETTO trial were insufficient to quantify the magnitude of overall survival (OS) and progression-free survival (PFS) benefit, due to the single-arm trial design and immature data. As noted in the CADTH Clinical Review, the sponsor’s indirect treatment comparison of selpercatinib to placebo (as a proxy for BSC) was subject to important limitations, including a high risk of residual confounding despite matching and heterogeneity in patient populations across trials. This uncertainty was further compounded by the sponsor’s use of a naive comparison between BSC and vandetanib to inform the pharmacoeconomic model. As a result, the comparative effectiveness of selpercatinib versus vandetanib and versus BSC is highly uncertain.
The sponsor submitted a model comparing the cost-effectiveness of selpercatinib with vandetanib and with BSC and reported results by first- and second-line treatment for rearranged during transfection proto-oncogene (RET)-mutant medullary thyroid cancer (MTC). The effectiveness data used to populate these analyses were not specific to a line of therapy, and the sponsor’s results cannot be interpreted as such. Further, given the lack of robust comparative data and critical limitations within the sponsor’s model, CADTH was unable to derive a reliable base-case estimation of the cost-effectiveness of selpercatinib. Notably, the choice of a partitioned survival model (PSM) was inappropriate, given that the OS and PFS data are highly uncertain. CADTH conducted exploratory reanalysis, revising the sponsor’s model to more accurately reflect the risk of death by disease stage and the drug acquisition cost of selpercatinib. CADTH was unable to address critical limitations related to the quality of the comparative clinical data, the lack of clinical data pertaining to the use of selpercatinib in the first- or second-line setting, and the structure sponsor’s model (i.e., choice of a PSM), as well as critical limitations with the transparency and programming of the economic model. Treatment of RET-mutant MTC with selpercatinib is more costly than treatment with vandetanib. Due to the highly uncertain comparative effectiveness data and the methodological limitations identified within the model, the cost-effectiveness of selpercatinib is unknown. Based on the CADTH exploratory analysis, price reductions of 78% and 87% would be required for selpercatinib to be considered cost-effective compared with vandetanib and BSC, respectively, at a willingness-to-pay (WTP) threshold of $50,000 per QALY. There is insufficient evidence to suggest that selpercatinib should be priced higher than vandetanib. While CADTH was able to make some corrections, given the uncertain comparative clinical evidence for selpercatinib and the lack of transparency and flexibility with the submitted model, the exploratory results and subsequent price reductions are likely biased in favour of selpercatinib. An additional price reduction may be warranted.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process (specifically, information that pertains to the economic submission).
Patient input was received from the Canadian Cancer Society and CanCertainty. The Canadian Cancer Society collected perspectives through a survey of patients with current or prior thyroid cancer (17 respondents) and patient testimonials (2 respondents) in Canada. CanCertainty described the financial impact of take-home cancer drugs on patients and their families. Input from the Canadian Cancer Society described the impact of thyroid cancer on patients’ ability to concentrate, exercise, work, travel, and spend time with family and friends. Survey respondents described fatigue; brain fog; issues with mental health, body image, and cognitive ability; high number of appointments; and concerns about the cancer returning as impacting their quality of life. Respondents noted financial barriers, including drug costs, lost income due to absence from work, and parking costs for medical appointments. Patients noted that they had experienced fatigue, problems with concentration and focus, weight and/or appetite changes, peripheral neuropathy, diarrhea, constipation, hair loss, pain, and mental health problems (e.g., mood swings, suicidal thoughts, feelings of loneliness and fear) with currently available treatments. None of the patients surveyed had experience with selpercatinib.
The clinician input received from the Ontario Health (Cancer Care Ontario) Head and Neck and Thyroid Cancer Drug Advisory Committee noted that vandetanib is the only currently approved and funded option for RET-mutant MTC in adults. Clinicians indicated that, for patients whose disease has progressed on currently available treatments, there are no other treatment options and that, for such patients, selpercatinib would represent an additional line of treatment. For treatment-naive patients, selpercatinib may be considered before vandetanib owing to a potentially more favourable toxicity profile. Clinicians noted that PFS and a reduction in treatment-related toxicity are key goals of treatment. The clinicians indicated that a clinically meaningful response to treatment would include a reduction in tumour burden, ascertained by clinical assessment and/or imaging, and the avoidance, improvement, or resolution of cancer-related symptoms, which may be associated with improvement in tumour marker levels.
CADTH-participating drug plans noted considerations related to clinical evidence, the relevant comparators, and potential implementation factors. The plans noted that, while vandetanib is the most relevant funded comparator for first-line treatment of MTC in adult patients, there is currently no funded treatment for MTC among patients aged 12 to 18 years. The plans further noted that patients with documented disease progression could continue selpercatinib in the LIBRETTO trial if they were deriving clinical benefit. Plans noted that the availability of selpercatinib may affect the place in therapy of vandetanib, and that there is currently an ongoing phase III trial for treatment-naive MTC patients comparing selpercatinib with physician’s choice (i.e., vandetanib or cabozantinib). Plans highlighted the potential for drug–drug interactions with selpercatinib and noted that additional assessment, monitoring, and/or intervention may be required to manage such interactions. Finally, the drug plans noted that prior RET testing is required to determine eligibility for selpercatinib use.
Several of these concerns were addressed in the sponsor’s model:
Selpercatinib was compared with vandetanib and BSC; however, the data used to inform the model were not specific to the line of therapy. As such, the cost-effectiveness of selpercatinib in specific lines of therapy is unknown.
The use of a cost-utility approach accounts for some issues related to quality of life; however, preferences for health states were not obtained from patients with MTC.
In addition, CADTH addressed some of these concerns, as follows:
CADTH explored the impact of including genetic testing costs in both the pharmacoeconomic and budget impact analyses.
CADTH was unable to address the following concerns raised from the stakeholder input:
The cost-effectiveness of selpercatinib in specific lines of therapy and among patients aged 12 to 17 years could not be addressed owing to a lack of clinical data.
Patients were assumed to discontinue treatment at the time of disease progression. This may underestimate drug costs.
Economic Review
The current review is for selpercatinib (Retevmo) for the treatment of advanced or metastatic RET-mutant MTC in patients aged 12 years and older.1
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Selpercatinib is indicated for the treatment of unresectable advanced or metastatic RET-mutant MTC in patients aged 12 years of age and older.2 The sponsor submitted a cost-utility analysis (CUA) to assess the cost-effectiveness of selpercatinib as first-line therapy among treatment-naive patients (i.e., those without prior exposure to systemic treatment for advanced or metastatic MTC) and treatment-experienced patients (i.e., patients who have previously received systemic treatment and require subsequent treatment in second and later lines, hereafter referred to as second-line therapy). The modelled population is consistent with the reimbursement request (i.e., consists of treatment-naive and -experienced patients). In the first-line setting, selpercatinib was compared with vandetanib, while selpercatinib was compared with BSC in the second-line setting, which the sponsor assumed would comprise monitoring and palliative care.
Selpercatinib is available as 40 mg or 80 mg capsules at a submitted price of $66.50 per 40 mg capsule or $133.00 per 80 mg capsule.1 The recommended dose for selpercatinib is 120 mg twice daily for patients who weigh less than 50 kg or 160 mg twice daily for those who weigh at least 50 kg, administered until disease progression or unacceptable toxicity.2 In the pharmacoeconomic model for the first 4 weeks of selpercatinib treatment, the sponsor assumed that |||||% patients would receive 160 mg twice daily and that |||||% would receive 80 mg twice daily ($13,364 for the first 4-week cycle). In subsequent cycles, the sponsor assumed that |||||% would receive 160 mg twice daily, while ||||||||||||||||||||||||||||||% of patients were assumed to receive 120 mg, 80 mg, or 40 mg twice daily, respectively ($11,340 per 4-week cycle). Vandetanib was assumed to cost $5,460 for the first 4-week cycle and $5,182 in subsequent cycles.
The clinical outcomes of interest were quality-adjusted life-years (QALYs) and life-years. The economic analysis was undertaken from the perspective of the publicly funded health care payer over a 10-year horizon. Discounting (1.5% per annum) was applied to both costs and outcomes.
Model Structure
The sponsor submitted a PSM that included 3 health states: progression-free, progressed disease, and death (Appendix 3). The modelled time cycle was 1 week. The proportion of patients who were progression-free, experienced disease progression, or dead at any time over the model’s time horizon was derived from non-mutually exclusive survival curves. All patients entered the model in the progression-free state; patients in this state were assumed to be stable or responding to therapy, as defined by the PFS measure assessed in the LIBRETTO trial (Response Evaluation Criteria in Solid Tumors version 1.1 criteria). The proportion of patients in the progressed disease state was calculated as the proportion alive (based on the OS curve) minus the proportion of patients alive and progression-free (based on the PFS curve). Treatment discontinuation was based on the modelled PFS curve such that patients were assumed to discontinue treatment at the time of disease progression. Patients were assumed to receive no subsequent treatment after disease progression. OS was capped in the model using general population mortality rates. Adverse events were assumed to occur during the first treatment cycle and were assumed to last for 1 month.
Model Inputs
The modelled cohort’s characteristics were based on the LIBRETTO trial (mean age 57 years; 35% female). For selpercatinib, PFS and OS data were obtained from the LIBRETTO trial from the pooled integrated analysis set (IAS) (includes patients with prior cabozantinib or vandetanib exposure) and supplementary analysis set (SAS) (SAS 1 includes patients with no prior cabozantinib or vandetanib exposure). A data cut-off of December 16, 2019, was used to inform the pharmacoeconomic model. For OS and PFS, an unanchored matched-adjusted indirect comparison (MAIC) was conducted using pooled data from the IAS and SAS 1 datasets, representing the “any line of treatment” data from LIBRETTO and the placebo arm of the EXAM trial (RET mutation–positive subgroup). In the model, the adjusted OS and PFS Kaplan–Meier data for selpercatinib and the placebo Kaplan–Meier data from the EXAM trial (as a proxy for BSC) were extrapolated over the 10-year model horizon. For vandetanib, the sponsor applied the observed hazard ratio between vandetanib and placebo from the ZETA trial to the extrapolated BSC survival function. For OS, the sponsor adopted the log-logistic distribution for selpercatinib and the Gompertz distribution for BSC. For PFS, the sponsor adopted the stratified log-logistic distribution for selpercatinib and the stratified Weibull distribution for BSC.
Health state utility values were obtained for the progression-free and progressed disease states from the literature,3 based on vignettes representing differentiated thyroid cancer, with preferences obtained from members of the UK general population. The sponsor assumed that utilities for patients with MTC would be equivalent to those for differentiated thyroid cancer and the same regardless of the line of therapy. Utilities were adjusted for age.4 The sponsor’s model included grade 3 or greater adverse events that had at least a 2% difference in frequency between interventions, as reported in the source trials (LIBRETTO, ZETA, EXAM), with disutility values obtained from the literature.
The model included costs related to drug acquisition and dispensing, monitoring, adverse events, and health care resource use in the progression-free and progressed health states, and terminal care costs. Drug acquisition costs for selpercatinib were based on the sponsor’s submitted price,1 while the price of vandetanib was based on the submitted price in the 2017 CADTH pan-Canadian Oncology Drug Review (pCODR) review.5 Drug costs were adjusted based on doses received in the LIBRETTO trial for selpercatinib and on the relative dose intensity for vandetanib (94.9%) from a National Institute of Health and Care Excellence (NICE) report pertaining to cabozantinib (TA516).6 BSC was assumed to comprise monitoring and palliative care (i.e., no drug costs). The cost of dispensing for selpercatinib and vandetanib was assumed to be incurred every 3 months and was based on the Ontario Drug Benefit dispensing fee for non-remote areas.7 Costs related to the treatment of grade 3 or higher adverse events were included in the model.8,9 Resource use in the progression-free and progressed health states was assumed to comprise oncologist visits, blood tests, and CT scans, with the frequency of each based on clinical expert opinion, and unit costs based on the Ontario Schedule of Benefits.10 Patients receiving selpercatinib were assumed to receive 7 electrocardiograms (ECGs) in the first 6 months of treatment, while patients receiving vandetanib were assumed to receive an ECG every 3 months. A 1-time end-of-life cost was obtained from the literature.11 The cost of diagnostic testing for RET mutations was excluded from the sponsor’s base case.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Base-Case Results
In the first-line setting, selpercatinib was associated with an incremental cost of $372,869 and 1.66 additional QALYs compared with vandetanib over a 10-year horizon, resulting in an incremental cost-effectiveness ratio (ICER) of $224,435 per QALY (Table 3). In the sponsor’s base case, selpercatinib had an 0% probability of being cost-effective compared with vandetanib at a WTP threshold of $50,000 per QALY.
Results were driven by the predicted differences in total life-years between selpercatinib and vandetanib (incremental life-years: 2.12) and the increased drug acquisition costs associated with selpercatinib (incremental costs = $368,498) (Appendix 3). The sponsor’s model estimated 0.63 incremental QALYs with selpercatinib treatment in the first 2 years, indicating that roughly 62% of the incremental benefits were accrued in the post-trial period (the model structure did not allow the evaluation of a 30-month time horizon to match the observation period of the submitted survival data from LIBRETTO). At the end of the 10-year time horizon, the percentage of patients estimated to remain alive was 5.9% in both groups.
Table 3: Summary of the Sponsor’s Economic Evaluation Results — First Line
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. vandetanib ($/QALY) |
|---|---|---|---|---|---|
Vandetanib | 98,912 | Reference | 1.71 | Reference | Reference |
Selpercatinib | 471,781 | 372,869 | 3.37 | 1.66 | 224,435 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission, probabilistic analysis.1
In the second-line setting, selpercatinib was associated with an incremental cost of $430,822 and 1.88 additional QALYs compared with BSC over a 10-year horizon, resulting in an ICER of $228,825 per QALY (Table 4). In the sponsor’s base case, selpercatinib had a 0% probability of being cost-effective compared with BSC at a WTP threshold of $50,000 per QALY.
Results were driven by the predicted differences in total life-years between selpercatinib and BSC (incremental life-years = 2.47) and the drug acquisition costs associated with selpercatinib (incremental costs = $423,252) (Appendix 3). The sponsor’s model estimated 0.73 incremental QALYs with selpercatinib treatment in the first 2 years, indicating that roughly 61% of the incremental benefits were accrued in the post-trial period. At the end of the 10-year time horizon, the percentage of patients estimated to remain alive was 4.2% in both groups.
Table 4: Summary of the Sponsor’s Economic Evaluation Results — Second-Line
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. BSC ($/QALY) |
|---|---|---|---|---|---|
BSC | 40,237 | Reference | 1.49 | Reference | Reference |
Selpercatinib | 471,059 | 430,822 | 3.37 | 1.88 | 228,825 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission, probabilistic analysis.1
Sensitivity and Scenario Analysis Results
The sponsor provided scenario analyses exploring the impact of an alternative time horizon (7 years) and including the cost of diagnostic testing, neither of which had an important impact on the ICER.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The comparative clinical efficacy of selpercatinib versus relevant comparators is highly uncertain. There have been no head-to-head trials of selpercatinib and vandetanib in the first-line setting or of selpercatinib and BSC in the second-line setting, and a key limitation of the clinical efficacy (i.e., OS and PFS) data informing selpercatinib in the economic model is that it is based on the LIBRETTO study. Given the non-randomized, open-label, single-arm design of the LIBRETTO trial, the interpretation of all outcomes is hampered by the lack of a control group, which makes the relative magnitude of any benefits highly uncertain. In the absence of comparative evidence from clinical trials, the sponsor undertook an unanchored MAIC of selpercatinib relative to BSC, followed by a naive comparison of vandetanib with BSC, to inform the pharmacoeconomic model. The CADTH Clinical Report raised several concerns regarding the interpretation of the findings of the sponsor’s MAIC, including the small number of included studies and the limited or missing data for matching and adjustment of clinically important baseline characteristics. Additional uncertainty was introduced by the use of a naive comparison of vandetanib versus BSC. As noted in the CADTH Clinical Review, selpercatinib is likely better than BSC; however, there is no reliable estimate for how much better it is. Based on the evidence submitted by the sponsor, it is highly uncertain whether selpercatinib improves PFS and/or OS compared with vandetanib. As such, there is substantial and unresolvable uncertainty with the interpretation of the clinical findings for the comparison of selpercatinib with vandetanib and with BSC.
Given the lack of direct evidence and limitations of the sponsor’s approach to indirect treatment comparisons, the cost-effectiveness of selpercatinib relative to vandetanib and BSC is highly uncertain.
The sponsor’s pharmacoeconomic analysis does not reflect cost-effectiveness by line of therapy. Although the sponsor’s pharmacoeconomic model purports to provide cost-effectiveness estimates for selpercatinib in the first- and second-line setting relative to vandetanib and BSC, respectively, the sponsor’s model uses effectiveness data for selpercatinib received at any line of treatment. The sponsor pooled effectiveness data from the LIBRETTO trial for patients who had received 1 or more prior lines of treatment with vandetanib or cabozantinib or who were naive to vandetanib and cabozantinib. Implicit in this is the assumption that the OS and PFS data from “any line of treatment” applies equally to patients receiving treatment in the first- and second-line setting. Given that the OS and PFS data pertaining to these subgroups is immature, it is highly uncertain whether this assumption is valid. Further, the OS and PFS data from the EXAM trial (used in the sponsor’s MAIC) were available only for “any line of treatment.” While prior use of tyrosine kinase inhibitors was included as a matching variable in the sponsor’s MAIC, there remains important uncertainty as to whether similar results would have been obtained had specific line-of-therapy data been analyzed. CADTH requested that the sponsor provide a revised pharmacoeconomic analysis in which the model was populated using effectiveness data by line of therapy, which the sponsor declined to address owing to a lack of effectiveness data for the comparators by line of therapy. As such, the outcomes associated with selpercatinib when used in specific lines of therapy are unknown.
As noted in the CADTH economic guidelines, stratified analyses require the use of parameter estimates pertinent to each subgroup under consideration.12 Given that the effectiveness data for the selpercatinib and comparators are not specific to the first or second line of therapy and that both the QALYs and cost estimates would be affected by this lack of data, the cost-effectiveness of selpercatinib in either the first- or second-line setting is unknown. CADTH notes that the Health Canada indication and the reimbursement request are not specific to a line of therapy. As such, in exploratory reanalyses, CADTH has explored the cost-effectiveness of selpercatinib when used in any line of therapy.
Limitations associated with the sponsor’s chosen modelling approach. The sponsor submitted a PSM, in which treatment efficacy is represented by PFS and OS curves. As noted in the CADTH Clinical Review, the median PFS and OS had not been reached in the LIBRETTO trial at the time of the data cut-off used in the pharmacoeconomic submission (December 16, 2019). Owing to the structure of PSMs, disease progression and OS are assumed to be independent; that is, any predicted gain in life-years is on the basis of OS, not PFS. The sponsor’s predicted incremental gain of 2.12 life-years with selpercatinib compared with vandetanib and 2.47 life-years compared with BSC are therefore highly questionable, given the high degree of uncertainty associated with the PFS and OS data from the LIBRETTO trial. Further, there are many uncertainties with the survival data used in the model. As noted earlier, there are important limitations with the sponsor’s MAIC and naive comparisons, which introduce substantial and unresolvable uncertainty into the analyses. Further, additional uncertainty was introduced into the long-term extrapolation through the use of immature efficacy data. The clinical experts consulted by CADTH for this review considered the incremental gains in PFS predicted for selpercatinib relative to vandetanib to be optimistic. The estimated ICER was highly sensitive to the parametric function chosen to extrapolate PFS and OS.
The sponsor’s original pharmacoeconomic submission suggested that a proportion of the incremental benefits with selpercatinib treatment (21% to 23%) would be accrued in the progressed disease health state, which implied that a considerable proportion of the incremental benefit would be realized after patients have discontinued selpercatinib. CADTH requested that the sponsor provide justification for this apparent post-progression benefit. In response, the sponsor provided an updated submission in which post-progression survival was assumed to be equal across treatments. However, in this model, all patients were assumed to survive to disease progression, which is inconsistent with data from the LIBRETTO study, which shows that a proportion of patients die before disease progression. If selpercatinib delays disease progression, a greater proportion of patients on selpercatinib would be expected to die before disease progression. To address this issue, CADTH requested that the sponsor provide the mean time of patients within the trial in the post-progression state to allow the estimation of a mortality rate for patients in that state. The sponsor declined this request.
All CADTH exploratory reanalyses used the sponsor’s revised model (i.e., assuming equal post-progression survival regardless of which treatment was received before disease progression). In exploratory reanalyses, CADTH assumed that patients were at risk of death before disease progression, which is supported by data from the LIBRETTO trial. The mortality rate adopted in CADTH reanalysis was derived from the proportion of patients who died before progression in the LIBRETTO trial.
Drug cost of selpercatinib is underestimated. In the calculation of selpercatinib drug costs, the sponsor incorporated the dose intensity observed in the LIBRETTO trial.1 The sponsor adjusted the dose of selpercatinib in the pharmacoeconomic submission such that, in the first treatment cycle, approximately |||||||% of patients initiated treatment on 160 mg of selpercatinib twice daily, while |||||||% patients initiated treatment on 80 mg selpercatinib daily, which is well below the recommended starting dose (< 50 kg: 120 mg twice daily3; ≥ 50 kg: 160 mg twice daily).2 In subsequent treatment cycles, patients were assumed to receive between 160 mg and 40 mg of selpercatinib, with the frequency of each based on the LIBRETTO trial, which may not reflect clinical practice. This adjustment of the dose received based on trial data is associated with substantial uncertainty, especially when viewed independently from treatment discontinuation. Given the higher treatment costs for selpercatinib, this biased the results in favour of selpercatinib.
An important factor for total drug acquisition costs is time on treatment. In the pharmacoeconomic model, the sponsor assumed that all patients would discontinue treatment at the time of disease progression (i.e., time on treatment was assumed to be equal to PFS). This is in contrast to the LIBRETTO trial, where patients could continue treatment after disease progression, with a mean lag of |||||||| days between disease progression and treatment discontinuation.1 The clinical experts consulted by CADTH for this review noted that the assumption that all patients discontinue treatment at the time of disease progression lacks face validity, as some patients may remain on treatment past disease progression, depending on patient preference and the lack of alternative therapies, while some patients may discontinue treatment before progression owing to adverse events.
In the CADTH reanalyses, 100% dose intensity was adopted for all treatments. CADTH explored the impact of treatment duration in exploratory scenario analyses.
Cost-effectiveness of selpercatinib among adolescent patients is unknown. Selpercatinib is indicated for patients aged 12 years and older, with weight-based dosing (< 50 kg: 120 mg twice daily3; ≥ 50 kg: 160 mg twice daily). The LIBRETTO trial enrolled ||||||| patients younger than 18 years, and the mean age of included patients at baseline was ||||||| years (IAS and SAS). In the pharmacoeconomic model, the sponsor assumed a cohort starting age of 57 years, and the 160 mg dosage of selpercatinib was adopted, reflecting an average patient weight above 50 kg. As noted in the CADTH Clinical Review, no subgroup analyses were provided pertaining to patients younger than 18 years of age. Further, the LIBRETTO trial did not collect quality of life data for adolescent patients, and the health state utility values incorporated in the sponsor’s pharmacoeconomic model reflect the preferences of an adult population. Finally, the relevant comparators for assessing the cost-effectiveness of selpercatinib in an adolescent population differ from the adult population, as there is no currently funded treatment for MTC among patients aged less than 18 years.
CADTH was unable to address this limitation owing to a lack of clinical data. As noted in the CADTH Clinical Review, preliminary data from the LIBRETTO-121 trial (12 patients, median age 14 years) are available; however, these data were not incorporated by the sponsor in the pharmacoeconomic model. The cost-effectiveness of selpercatinib among adolescents remains unknown.
Poor modelling practices were employed. The submitted pharmacoeconomic model was found to be lacking in transparency, highly inefficient, and had multiple issues related to the specification of uncertainty. The coding of the model is highly inefficient with simple calculations being spread over multiple sheets. The model incorporates numerous uses of IFERROR and ISERROR functions, which generally should be unnecessary, and includes 93 macros. The results of the model are hard coded; that is, the results are not directly linked to the input parameters within the model. Separate models are not provided for each comparator, which precludes direct simultaneous comparisons. Finally, user-created functions are employed in the model (i.e., for parametric extrapolation), which limits transparency. The sponsor was asked to provide a model that limited the use of IFERROR statements, removed all hard coding of model results, provided separate models for each comparator, and did not include user-created functions. A revised model provided by the sponsor contained more than 2,000 IFERROR statements and the sponsor declined to remove hard coding, provide a separate model for each comparator, or exclude user-created functions.
Additionally, CADTH identified multiple issues relating to the specification of uncertainty within the model not meeting best practices, as well as errors in the determination of the results of the probabilistic analysis. Given these errors and the lack of transparency described earlier, and due to the sponsor not providing a model that provides separate models for each comparator and an analysis that removes all hard coding, validation of the sponsor’s probabilistic analysis was not possible.
CADTH’s exploratory analysis was conducted deterministically, given that the probabilistic results could not be validated owing to the multiple issues with the model transparency and coding.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Clinical effectiveness data from the LIBRETTO trial as of December 16, 2019, were used to inform THE pharmacoeconomic submission | CADTH notes that more recent data cut points are available. The use of the December 16, 2019, cut point rather than more recent data to inform the pharmacoeconomic model was not justified by the sponsor. In response to a clarification request from CADTH, the sponsor noted that the December 2019 data were used to align the pharmacoeconomic submission with submissions to Health Canada, the FDA, and the European Medicines Agency. Data from a subsequent interim analysis (March 2020) were not provided. Given that the PFS and OS data were immature as of the December 2019 cut-off, and given the high degree of uncertainty associated with the extrapolations based on these estimates, the use of updated data may reduce this uncertainty. |
The sponsor adopted a 10-year analysis horizon | Inappropriate. As noted in the CADTH economic guidelines,12 the horizon should be sufficiently long to capture all the costs and outcomes associated with treatment. In the sponsor’s submission, approximately 5% of the people in each treatment group remained alive at the end of the 10-year horizon, indicating that not all costs and outcomes associated with treatment were captured within the results. CADTH adopted a lifetime horizon in exploratory scenario analyses. |
In the pharmacoeconomic submission, BSC was assumed by the sponsor to have no associated drug costs | Uncertain. The assumption of no drug costs associated with BSC in the sponsor’s CUA is in contrast to its submitted budget impact assessment, in which they assumed a 1-time per-patient cost of $1,561. In the BIA, the sponsor notes that BSC was assumed to consist of “different medications used to manage symptoms of late-stage disease.” The clinical experts consulted by CADTH for this review indicated that drug treatments may be used for symptom management by patients receiving BSC. The exclusion of palliative care drug costs as part of BSC is not expected to have an important impact on the ICER. |
Grade 3 AEs with at least a 2% difference in frequency between interventions were included in the pharmacoeconomic model | Uncertain. The incidence of AEs was based on a naive comparison between treatments. It is unclear how differences in the study populations may have affected AEs. The sponsor assumed that AEs could occur only once during treatment, which is additionally uncertain. Costs related to the treatment of AEs may be overestimated, as the cost of treating AEs was based on the Ontario Case Costing Initiative such that all AEs were assumed to be treated in hospital. CADTH further notes that utility decrements associated with all AEs were assumed to last for 1 week; the validity of this assumption is unclear. CADTH could not address these limitations owing to the structure of the sponsor’s model, and the impact on the ICER is uncertain. |
Health state utility values were adopted from the literature and were assumed to be equal for treatment-naive and -experienced patients | Uncertain. To inform the pharmacoeconomic model, the sponsor adopted health state utility values from the literature,3 with utility values elicited from adult members of the UK general population by use of vignettes representing DTC. The sponsor assumed that these utilities for DTC would be applicable to patients with MTC, which is uncertain. It is additionally uncertain whether the preferences of adults from the UK general population are aligned with those of Canadian patients with MTC. The preferences of patients younger than 18 years were not considered. CADTH explored the impact of alternative health state utility values on the ICER, provided by the sponsor from the ZETA trial for patients who received vandetanib. The use of these alternative utilities had little meaningful impact on the ICER. |
RET mutation testing costs were not considered | The sponsor excluded the cost of RET testing from the model. Given that treatment with selpercatinib should be initiated only following confirmation of a RET gene fusion or mutation using a validated test,2 but is not required for treatment with vandetanib or BSC, the exclusion of RET testing costs underestimates the incremental cost of selpercatinib treatment. The current proportion of patients with MTC screened for RET mutations is uncertain. The clinical experts indicated that the proportion of patients currently screened for RET mutations is low and that the availability of testing varies by jurisdiction. The experts additionally indicated that RET testing is expected to increase in 2022 in some jurisdictions. CADTH conducted 2 analyses, 1 where no testing costs were included and 1 where the full cost of panel testing would be included. These analyses used the cost of testing supplied by the sponsor, which may not reflect the true cost of RET testing. |
Health care resource use was based on the opinion of clinical experts consulted by the sponsor | Uncertain. The clinical experts consulted by CADTH for this review indicated that health care resource by patients with RET-positive MTC is variable and may depend on the treatment received as well as whether the patient is experiencing adverse events. CADTH was unable to address this owing to the structure of the sponsor’s model and a lack of data. |
AE = adverse event; BIA = budget impact analysis; BSC = best supportive care; CUA = cost-utility analysis; DTC = differentiated thyroid cancer; ICER = incremental cost-effectiveness ratio; MTC = medullary thyroid cancer; RET = rearranged during transfection.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
As noted earlier, there are key limitations associated with the available clinical data for selpercatinib and the sponsor’s model. Several limitations with the sponsor’s submission could not be adequately addressed due to data or structural limitations, including the notable limitations associated with the lack of comparative clinical data as well as the limitations associated with the sponsor’s modelling approach (i.e., PSM) and practices (i.e., lack of transparency, issues with the probabilistic analyses). The use of a PSM structure in the current review is inappropriate, given that PSMs rely on mature PFS and OS data to produce reliable cost-effectiveness estimates. Further, although the sponsor’s pharmacoeconomic model purports to assess the cost-effectiveness of selpercatinib by line of therapy, the data used to populate the economic model from the LIBRETTO trial and the sponsor’s MAIC pertain to “any line of therapy,” and it is inappropriate to ascribe the findings to a particular line of therapy. CADTH was unable to address these limitations with the sponsor’s model, which represent fundamental problems for interpreting the results of the sponsor’s economic evaluation (since the costs and QALYs used to calculate the ICER are derived from an inappropriate model type and based on highly uncertain evidence). CADTH was unable to conduct any base-case reanalysis of the sponsor’s model, given that any estimates of the incremental costs and incremental effectiveness would be misleading.
Scenario Analysis Results
Although CADTH did not conduct any formal reanalyses of the sponsor’s model, an exploratory analysis was undertaken to explore the impact that changes to model assumptions had on the ICER. CADTH notes that the key limitations of the sponsor’s base-case analysis — noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation — apply to this exploratory analysis, including the fundamental limitation that there is no direct evidence to support the comparative efficacy of selpercatinib versus vandetanib or BSC. As such, this exploratory analysis should not be interpreted as a CADTH base case, as there remains uncertainty regarding the true effect of selpercatinib.
As per the sponsor’s analysis, the CADTH exploratory analyses found that selpercatinib is not cost-effective at a $50,000 per QALY threshold. In the CADTH exploratory reanalyses, selpercatinib was associated with an ICER of $350,341 compared with vandetanib and an ICER of $347,785 compared with BSC over a 10-year horizon (genetic testing costs excluded). The inclusion of costs associated with genetic testing for RET mutation status had little impact on the ICER. Based on the CADTH exploratory analysis, which is subject to the key limitations of the sponsor’s model, as noted earlier, a price reduction for selpercatinib of 78% and 87% would be required for selpercatinib to be considered cost-effective compared with vandetanib and BSC, respectively, at a WTP threshold of $50,000 per QALY. CADTH notes that, when the least optimistic PFS extrapolation curve (of those provided by the sponsor) was chosen, the proportion of incremental QALYs accrued during the extrapolation period was reduced (44% versus 62%). Given that the estimates of incremental life-years (and hence QALYs) are highly uncertain and may not be representative of the true incremental effect of selpercatinib, the true price reduction required for selpercatinib to be cost-effective is unknown. Details of this exploratory analysis are provided in Appendix 4.
Issues for Consideration
A phase III RCT comparing selpercatinib to physician’s choice (vandetanib or cabozantinib) in patients with RET-mutant MTC is currently ongoing (NCT04211337). Direct comparative evidence may reduce the uncertainty associated with the cost-effectiveness estimate.
Pralsetinib, an oral kinase inhibitor, is currently under review by Health Canada. Pralsetinib is indicated in some countries for the treatment of RET-mutated advanced or metastatic MTC. The cost-effectiveness of selpercatinib compared with pralsetinib is unknown.
Genetic testing for RET mutation status is not routinely performed for all patients with MTC in all Canadian jurisdictions. The clinical experts consulted by CADTH for this review indicated that such testing is expected to become part of the standard of care in the near future. Different jurisdictions may choose to fund RET testing from different budgets or under different circumstances (i.e., at the point of diagnosis versus after progression following first-line treatment). As such, CADTH explored the impact of including genetic testing costs on the ICER as well as on the expected budget impact of reimbursing selpercatinib. Regardless of whether genetic testing costs were included, selpercatinib is not a cost-effective option at the submitted price at a WTP threshold of $50,000 per QALY.
Overall Conclusions
The CADTH Clinical Review concluded that data from the LIBRETTO pivotal trial was inadequate to interpret the OS and PFS findings, due to the single-arm trial design and immature data. As noted in the CADTH Clinical Review, the sponsor’s indirect treatment comparison of selpercatinib to placebo (as a proxy for BSC) was subject to important limitations, including a high risk of residual confounding despite matching and heterogeneity in patient populations across trials. This uncertainty was further compounded by the sponsor’s use of a naive comparison between BSC and vandetanib to inform the pharmacoeconomic model. As a result, the comparative effectiveness of selpercatinib versus vandetanib and BSC is highly uncertain.
The sponsor submitted a model comparing the cost-effectiveness of selpercatinib with vandetanib and with BSC and reported results by first- and second-line treatment for RET-mutant MTC. While the sponsor stratified the presentation of results by line of therapy, this is inappropriate, as the clinical data underlying this analysis pertain to the use of selpercatinib in any line of therapy (i.e., the predicted costs and QALYs are not specific to treatment-naive or -experienced patients), and the sponsor’s results cannot be interpreted as such.
CADTH was not able to conduct a reanalysis due to foundational limitations within the submitted evidence and the sponsor’s model. Notably, the choice of a PSM was inappropriate, given that the PFS and OS data are highly uncertain. CADTH conducted exploratory reanalyses, revising the sponsor’s model to more accurately reflect the risk of death by disease stage and drug acquisition costs. CADTH was unable to address critical limitations related to the submitted evidence (including the quality of the comparative clinical data and the lack of clinical data pertaining to the use of selpercatinib in the first or second line) and inappropriate model structure.
The limitations identified within the submitted evidence interact with each other. The uncertainty associated with the immature PFS and OS data from the LIBRETTO trial contributed structural uncertainty to the PSM approach chosen by the sponsor. The comparative effectiveness of selpercatinib versus vandetanib or BSC is confounded by issues related to the lack of head-to-head evidence and issues within the sponsor’s MAIC and the use of naive companions. Consequently, while the costs associated with selpercatinib are higher than those for vandetanib or BSC, the cost-effectiveness of selpercatinib relative to these comparators is unknown. While CADTH was able to make some corrections, given the highly uncertain comparative clinical evidence for selpercatinib and lack of transparency and flexibility with the submitted model, the exploratory results and subsequent price reductions are likely biased in favour of selpercatinib. Based on CADTH’s exploratory reanalysis, selpercatinib is not cost-effective at a $50,000 per QALY threshold when compared with either vandetanib or BSC, and price reductions of 78% and 87% would be required for selpercatinib to be considered cost-effective compared with vandetanib and BSC, respectively, at a WTP threshold of $50,000 per QALY. There is insufficient evidence to suggest that selpercatinib should be priced higher than vandetanib. An additional price reduction may be warranted.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Retevmo (selpercatinib), 40 and 80 mg capsules. Toronto (ON): Eli Lilly Canada Inc.; 2021 Feb.
2.Retevmo™ (selpercatinib): capsules, 40 mg and 80 mg, oral [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2021 Jun 11.
3.Fordham BA, Kerr C, de Freitas HM, et al. Health state utility valuation in radioactive iodine-refractory differentiated thyroid cancer. Patient Prefer Adherence. 2015;9:1561-1572. PubMed
4.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
5.Drug Reimbursement Review pharmacoeconomic report: vandetanib (Caprelsa) for medullary thyroid cancer. Ottawa (ON): CADTH; 2017 Mar 30: https://www.cadth.ca/sites/default/files/pcodr/pcodr_vandetanib_caprelsa_mtc_fn_egr.pdf. Accessed 2022 Jan 25.
6.National Institute for Health and Care Excellence. Cabozantinib for treating medullary thyroid cancer (Technology appraisal guidance TA516) 2018; https://www.nice.org.uk/guidance/ta516. Accessed 2022 Jan 25.
7.Ontario Ministry of Health and Ontario Ministry of Long-Term Care. Ontario Drug Benefit Program: dispensing fees. 2014; https://www.health.gov.on.ca/en/public/programs/drugs/programs/odb/opdp_dispensing_fees.aspx. Accessed 2022 Jan 25.
8.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Jan 25.
9.Meyers BM, Vogel A, Marotta P, et al. The cost-effectiveness of lenvatinib in the treatment of advanced or unresectable hepatocellular carcinoma from a Canadian perspective. Can J Gastroenterol Hepatol. 2021;2021:8811018. PubMed
10.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2022 Jan 25.
11.Dumont S, Jacobs P, Turcotte V, Turcotte S, Johnston G. Palliative care costs in Canada: A descriptive comparison of studies of urban and rural patients near end of life. Palliat Med. 2015;29(10):908-917. PubMed
12.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/dv/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2022 Jan 25.
13.Cancer Care Ontario. Vandetanib - provider monograph. 2020; https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/44261. Accessed 2021 Dec 15.
14.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2022 Jan 25.
15.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Retevmo (selpercatinib), 40 and 80 mg capsules. Toronto (ON): Eli Lilly Canada Inc.; 2021 Feb.
16.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-e205. PubMed
17.Shaw A, Semenciw R, Mery L. Cancer in Canada fact sheet series #1 - thyroid cancer in Canada. Chronic Dis Inj Can. 2014;34(1):64-68. PubMed
18.Geller G, Laskin J, Cheung WY, Ho C. A retrospective review of the multidisciplinary management of medullary thyroid cancer: eligibility for systemic therapy. Thyroid Res. 2017;10:6. PubMed
19.Wells SA, Jr., Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015;25(6):567-610. PubMed
20.Taccaliti A, Silvetti F, Palmonella G, Boscaro M. Genetic alterations in medullary thyroid cancer: diagnostic and prognostic markers. Curr Genomics. 2011;12(8):618-625. PubMed
21.Romei C, Ciampi R, Casella F, et al. RET mutation heterogeneity in primary advanced medullary thyroid cancers and their metastases. Oncotarget. 2018;9(11):9875-9884. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from the clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 6: CADTH Cost Comparison Table for RET-Altered Medullary Thyroid Cancer
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Selpercatinib (Retevmo)a | 40 mg 80 mg | Capsule | 66.5000 133.0000 | < 50 kg: 120 mg twice daily ≥ 50 kg: 160 mg twice daily | 399 532 | 11,172 14,896 |
aSelpercatinib price based on the sponsor’s submission;1 dosage based on the draft product monograph.2
Table 7: CADTH Cost Comparison Table for Medullary Thyroid Cancer
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Vandetanib (Caprelsa)a | 100 mg 300 mg | Tablet | 99.1573b 198.3150b | 300 mg daily | 198 | 5,553 |
aIndicated for the treatment of symptomatic or progressive medullary thyroid cancer in adult patients with unresectable locally advanced or metastatic disease.13
bOntario Exceptional Access Program, accessed January 21, 2022.14
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The sponsor conducted analyses purported to correspond to the use of selpercatinib in the first and second line; however, the effectiveness data used to populate the model were not specific to line of therapy. While selpercatinib is indicated for patients aged 12 years and older, the sponsor’s model considered the cost-effectiveness of selpercatinib among adults. The cost-effectiveness of selpercatinib among patients aged 12 to 17 years is unknown. |
Model has been adequately programmed and has sufficient face validity | No | The model lacks transparency and is inefficiently programmed. The sponsor was asked to provide a revised model to address these concerns but declined to meet many of the requests made by CADTH. |
Model structure is adequate for decision problem | No | The states are appropriate but assumptions relating to the independence of the overall survival and progression-free survival lack validity. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | There are numerous errors in the propagation of uncertainty which led CADTH to conclude that the probabilistic analysis is not fit for purpose. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Parameter uncertainty was not adequately considered. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The model lacked transparency. The provided user guide did not describe the flow of the model thus precluding any detailed validation testing. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of the Sponsor’s Base Case
Table 9: Disaggregated Summary of the Sponsor’s Economic Evaluation Results — First Line
Parameter | Selpercatinib | Vandetanib | Incremental (vs. vandetanib) |
|---|---|---|---|
Discounted LYs | |||
Progression-free | 2.83 | 0.78 | 2.04 |
Progressed disease | 2.33 | 2.24 | 0.08 |
Total | 5.15 | 3.03 | 2.12 |
Discounted QALYs | |||
Progression-free | 2.25 | 0.63 | 1.62 |
Progressed disease | 1.12 | 1.08 | 0.04 |
Total | 3.37 | 1.71 | 1.66 |
Discounted costs ($) | |||
Drug acquisition | 423,847 | 55,349 | 368,498 |
Administration | 104 | 32 | 72 |
Monitoringa | 741 | 0 | 741 |
Adverse events | 6,017 | 3,898 | 2,119 |
Diagnostic testing | 0 | 0 | 0 |
Disease management | 14,829 | 12,897 | 1,932 |
Progression-free | 3,960 | 1,447 | 5,513 |
Progressed disease | 10,869 | 11,450 | –581 |
Subsequent treatment | 0 | 0 | 0 |
End-of-life care | 26,242 | 26,736 | –494 |
Total | 471,781 | 98,912 | 372,869 |
ICER ($/QALY) | 224,435 | ||
ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year.
aIncludes electrocardiograms administered during the first 6 months of selpercatinib treatment.1 Monitoring of patients taking vandetanib was captured in the model as part of “Disease management.”
Source: Sponsor’s pharmacoeconomic submission, probabilistic analysis.1
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results — Second Line
Parameter | Selpercatinib | BSC | Incremental (vs. BSC) |
|---|---|---|---|
Discounted LYs | |||
Progression-free | 2.83 | 0.51 | 2.31 |
Progressed disease | 2.34 | 2.18 | 0.16 |
Total | 5.17 | 2.69 | 2.47 |
Discounted QALYs | |||
Progression-free | 2.21 | 0.40 | 1.81 |
Progressed disease | 1.16 | 1.09 | 0.08 |
Total | 3.37 | 1.49 | 1.88 |
Discounted costs ($) | |||
Drug acquisition | 423,252 | 0 | 423,252 |
Administration | 104 | 0 | 104 |
Monitoringa | 740 | 0 | 740 |
Adverse events | 5,976 | 1,748 | 4,228 |
Diagnostic testing | 0 | 0 | 0 |
Disease management | 14,885 | 10,922 | 3,963 |
Progression-free | 3,933 | 712 | 3,221 |
Progressed disease | 10,952 | 10,210 | 742 |
Subsequent treatment | 0 | 0 | 0 |
End-of-life care | 26,102 | 27,566 | –1,464 |
Total | 471,059 | 40,237 | 430,822 |
ICER ($/QALY) | 228,825 | ||
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY= life-year; QALY = quality-adjusted life-year.
aIncludes electrocardiograms administered during the first 6 months of selpercatinib treatment.1 Monitoring of patients taking vandetanib was captured in the model as part of “Disease management.”
Source: Sponsor’s pharmacoeconomic submission, probabilistic analysis.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Scenario Analyses
While CADTH did not conduct any formal reanalyses of the sponsor’s model, the economic review team performed an exploratory analysis to explore the impact of several key limitations on the ICER. These included assuming mortality prior to progression, assuming 100% dose intensity, and including the cost of genetic testing. These results of these analyses are presented as pairwise comparisons for selpercatinib versus vandetanib and versus BSC and reflect the use of selpercatinib in any line of treatment. Given limitations with the sponsor’s probabilistic analysis, no assessment of the probability of selpercatinib being cost-effective can be presented.
Of note, the fundamental limitations in the sponsor’s model persist within this exploratory analysis. There is no direct evidence to support the comparative efficacy of selpercatinib to vandetanib or to BSC. Therefore, this exploratory analysis should not be interpreted as a formal CADTH reanalysis to which credence should be given to the results; in particular, the incremental QALY benefit estimated as part of this exploratory analysis remains unlikely to be representative of the true effect of selpercatinib, such that the corresponding ICER is unlikely to be reflective of the true cost-effectiveness of selpercatinib.
CADTH was additionally unable to address the cost-effectiveness of selpercatinib in patients aged 12–17 years owing to a lack of clinical data. All CADTH exploratory reanalyses pertain to an adult cohort, and the cost-effectiveness of selpercatinib in patients aged 12–17 years is unknown.
Table 11: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Post-progression survival | The option to assume equal post-progression survival had not been properly implemented in the sponsor’s model (i.e., incremental LYs in the Post-Progression health state remained higher with selpercatinib than comparators). | The model option to assume equal post-progression survival was implemented for all comparators. Additional errors in the sponsor’s model were corrected (i.e., post-progression LYs and QALYs for cabozantinib were inappropriately attributed to selpercatinib). |
Changes to derive the CADTH exploratory case | ||
1. Mortality prior to progression | Assumed no patients died prior to progression | Assume a mortality rate prior to progression based on the mortality rate derived from the PFS estimate from the LIBRETTO trial and the proportion of patients who die before progression |
2. Drug costs | Assumed a reduction in drug costs due to reduced dose intensity | Assumed no reduction in dose intensity |
3. Genetic testing costs | Excluded | Included |
CADTH exploratory reanalysis | Reanalysis 1 + 2 Reanalysis 1 + 2 + 3 (to explore the potential impact of testing costs) | |
PFS = progression-free survival.
CADTH undertook a stepped analysis, incorporating each change proposed in Table 11 to sponsor’s base case to highlight the impact of each change. As per the sponsor’s analysis, the CADTH exploratory analyses found that selpercatinib is not cost-effective at a $50,000 per QALY threshold compared with vandetanib or BSC. The inclusion of genetic testing costs had little impact on the estimated ICER (Table 12, Table 13).
Table 12: Summary of the Stepped Analysis of the CADTH Exploratory Analysis Results Compared With Vandetanib
Stepped analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | Vandetanib | 98,641 | 1.71 | Reference |
Selpercatinib | 472,026 | 3.37 | 224,259 | |
Sponsor’s corrected base case | Vandetanib | 96,961 | 1.38 | Reference |
Selpercatinib | 470,742 | 2.94 | 240,814 | |
CADTH reanalysis 1 | Vandetanib | 96,414 | 1.33 | Reference |
Selpercatinib | 468,883 | 2.76 | 261,425 | |
CADTH reanalysis 2 | Vandetanib | 100,591 | 1.38 | Reference |
Selpercatinib | 601,057 | 2.94 | 322,433 | |
CADTH reanalysis 3 | Vandetanib | 96,961 | 1.38 | Reference |
Selpercatinib | 471,259 | 2.94 | 241,147 | |
CADTH exploratory analysis (1+2) | Vandetanib | 100,043 | 1.33 | Reference |
Selpercatinib | 599,198 | 2.76 | 350,341 | |
CADTH exploratory analysis (1+2+3) | Vandetanib | 99,407 | 1.32 | Reference |
Selpercatinib | 599,714 | 2.76 | 350,703 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aDeterministic analysis.
Table 13: Summary of the Stepped Analysis of the CADTH Exploratory Analysis Results Compared With BSC
Stepped analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | BSC | 40,370 | 1.49 | Reference |
Selpercatinib | 472,026 | 3.37 | 229,070 | |
Sponsor’s corrected base case | BSC | 38,670 | 1.18 | Reference |
Selpercatinib | 470,742 | 2.94 | 245,751 | |
CADTH reanalysis 1 | BSC | 38,340 | 1.14 | Reference |
Selpercatinib | 468,883 | 2.76 | 266,977 | |
CADTH reanalysis 2 | BSC | 38,670 | 1.18 | Reference |
Selpercatinib | 601,057 | 2.94 | 319,870 | |
CADTH reanalysis 3 | BSC | 38,670 | 1.18 | Reference |
Selpercatinib | 471,259 | 2.94 | 246,045 | |
CADTH exploratory analysis (1+2) | BSC | 38,340 | 1.14 | Reference |
Selpercatinib | 599,198 | 2.76 | 347,785 | |
CADTH exploratory analysis (1+2+3) | BSC | 38,340 | 1.14 | Reference |
Selpercatinib | 599,714 | 2.76 | 348,105 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aDeterministic analysis.
Several scenario and sensitivity analyses were conducted on the CADTH exploratory reanalysis. These scenario analyses explored the impact of the following model parameters and assumptions:
Adopting Gompertz distribution for PFS (least optimistic distribution provided by the sponsor)
Assuming patients discontinue selpercatinib 3 weeks after disease progression (based on submitted data from the LIBRETTO trial)1
Adopting a lifetime horizon (25 years)
Table 14: Summary of CADTH Exploratory Analysis — Selpercatinib Compared With Vandetanib
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER versus vandetanib ($/QALY) |
|---|---|---|---|---|---|
CADTH exploratory base case | |||||
Vandetanib | 100,043 | Reference | 1.33 | Reference | Reference |
Selpercatinib | 599,198 | — | 2.76 | 1.42 | 350,341 |
CADTH scenario 1: Progression-free survival: Gompertz distributiona | |||||
Vandetanib | 99,775 | Reference | 1.30 | Reference | Reference |
Selpercatinib | 423,563 | 323,788 | 2.09 | 0.78 | 414,327 |
CADTH scenario 2: Treatment duration | |||||
Vandetanib | 100,043 | Reference | 1.33 | Reference | Reference |
Selpercatinib | 609,610 | 509,566 | 2.76 | 1.42 | 357,649 |
CADTH scenario 3: Lifetime horizon | |||||
Vandetanib | 100,178 | Reference | 1.34 | Reference | Reference |
Selpercatinib | 624,348 | 524,170 | 2.88 | 1.54 | 340,093 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: all analyses deterministic. Cost of genetic testing for RET mutations not included.
aThe least optimistic distribution for selpercatinib progression-free survival was chosen for this analysis to explore the impact of progression-free survival on the ICER.
Table 15: Summary of CADTH Exploratory Analysis — Selpercatinib Compared With BSC
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER versus BSC ($/QALY) |
|---|---|---|---|---|---|
CADTH exploratory base case | |||||
BSC | 38,340 | Reference | 1.14 | Reference | Reference |
Selpercatinib | 599,198 | 560,858 | 2.76 | 1.61 | 347,785 |
CADTH scenario 1: Progression-free survival: Gompertz distributiona | |||||
BSC | 38,178 | Reference | 1.13 | Reference | Reference |
Selpercatinib | 423,563 | 385,385 | 2.09 | 0.96 | 401,241 |
CADTH scenario 2: Treatment duration | |||||
BSC | 38,340 | Reference | 1.14 | Reference | Reference |
Selpercatinib | 609,610 | 571,270 | 2.76 | 1.60 | 354,241 |
CADTH scenario 3: Lifetime horizon | |||||
BSC | 38,443 | Reference | 1.15 | Reference | Reference |
Selpercatinib | 624,348 | 585,904 | 2.88 | 1.73 | 338,598 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: all analyses deterministic. Cost of genetic testing for RET mutations not included.
aThe least optimistic distribution for selpercatinib progression-free survival was chosen for this analysis to explore the impact of progression-free survival on the ICER.
Price Reduction Analysis
Based on the CADTH exploratory analysis, a reduction in the price of selpercatinib by 78% would be required for selpercatinib to be cost-effective at a WTP threshold of $50,000 per QALY compared with vandetanib. An 87% reduction in the price of selpercatinib would be required for it to be considered cost-effective compared with BSC at this threshold. The inclusion of costs related to genetic testing had little impact on the price reduction required.
This deterministic analysis was subject to the key limitations of the sponsor’s model as noted in the CADTH Appraisal of the Sponsor’s Economic Evaluation section. It is important to note that this price reduction estimate is based on estimates of incremental life-years (and hence QALYs) that are highly uncertain and may not be representative of the true incremental effect of selpercatinib. Consequently, the price reduction required for selpercatinib to be cost-effective remains unknown.
Table 16: CADTH Price Reduction Analyses
Analysis | ICERs for selpercatinib versus comparator ($)a | ||
|---|---|---|---|
Price reduction | Sponsor base case | CADTH exploratory reanalysis | |
Analysis excluding testing | Analysis including testing | ||
No price reduction | 224,259 versus vandetanib 229,070 versus BSC | 350,341 versus vandetanib 347,785 versus BSC | 350,703 versus vandetanib 348,105 versus BSC |
10% | 199,866 versus vandetanib 207,517 versus BSC | 311,432 versus vandetanib 313,410 versus BSC | 311,795 versus vandetanib 313,729 versus BSC |
20% | 175,472 versus vandetanib 185,964 versus BSC | 272,524 versus vandetanib 279,034 versus BSC | 272,886 versus vandetanib 279,354 versus BSC |
30% | 151,079 versus vandetanib 164,411 versus BSC | 233, 615 versus vandetanib 244,659 versus BSC | 233,978 versus vandetanib 244,979 versus BSC |
40% | 126,685 versus vandetanib 142,858 versus BSC | 194,707 versus vandetanib 210, 284 versus BSC | 195,069 versus vandetanib 210,604 versus BSC |
50% | 102,292 versus vandetanib 121,304 versus BSC | 155,798 versus vandetanib 175, 908 versus BSC | 156,161 versus vandetanib 176,289 versus BSC |
60% | 77,898 versus vandetanib 99,751 versus BSC | 116,890 versus vandetanib 141, 533 versus BSC | 117,252 versus vandetanib 141,853 versus BSC |
70% | 53,505 versus vandetanib 78,198 versus BSC | 77,981 versus vandetanib 107,158 versus BSC | 78,344 versus vandetanib 107,478 versus BSC |
72% | 48,026 versus vandetanib | 70,199 versus vandetanib 100,283 versus BSC | 70,562 versus vandetanib 100,603 versus BSC |
78% | 60,562 versus BSC | 46,854 versus vandetanib 79,658 versus BSC | 47,217 versus vandetanib 79,978 versus BSC |
80% | 56,645 versus BSC | 72,782 versus BSC | 73,103 versus BSC |
84% | 48,023 versus BSC | 59,032 versus BSC | 59,353 versus BSC |
87% | NA | 48,720 versus BSC | 49,040 versus BSC |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio.
aPairwise comparison; deterministic analyses.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 17: Summary of Key Takeaways
Key takeaways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) estimating the incremental budget impact of reimbursing selpercatinib for use by patients aged 12 years and older with treatment-naive RET-mutant MTC (first line) and previously treated RET-mutant MTC (second line).15 The budgetary impact of reimbursing selpercatinib was estimated separately for first- and second-line use. The BIA was undertaken from the perspective of the Canadian public drug plans over a 3-year time horizon, and the sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec). Key inputs to the BIA are documented in Table 18.
The sponsor estimated the eligible population using an epidemiologic approach, assuming an incidence of 23 per 100,000 population per year for thyroid cancer.16 Of newly diagnosed thyroid cancers, 2% were estimated to be MTC.17 The sponsor assumed that 65% of patients would be eligible for public drug coverage based on internal estimates.15 In the sponsor’s submission, the reference scenario assumed that all patients would receive vandetanib in the first line and BSC in the second line. In the new-drug scenario, uptake of first-line selpercatinib was assumed by the sponsor to be 75% in year 1, 80% in year 2, and 85% in year 3. uptake of second-line selpercatinib was assumed to be 100% in each year.
In the sponsor’s base case, costs related to drug acquisition were captured. The duration of treatment was obtained from the sponsor’s pharmacoeconomic model, with patients assumed to discontinue treatment at the time of disease progression.1 The cost of selpercatinib was based on a planned dosage of 160 mg twice daily per 28-day cycle and the sponsor’s submitted price ($66.50 per 40 mg capsule, $133.00 per 80 mg capsule),1 adjusted by the dosages received in the LIBRETTO trial (first 28-day cycle: $13,364; subsequent cycles: $11,340). The drug cost of vandetanib was based on a dosage of 300 mg once daily per 28-day cycle and the submitted price as reported in the 2017 pCODR review of vandetanib5 and was adjusted by relative dose intensity (94.9%) adopted from the NICE review of cabozantinib for the treatment of MTC.6 BSC was assumed to be associated with a 1-time drug cost of $1,561. Costs related to screening for RET mutations were not included in the sponsor’s base case.
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate |
|---|---|
Target population | |
Population growth | 1.4% per yeara |
Incidence of thyroid cancer | 0.023%16 |
Covered by public drug plans | 65%b |
Medullary thyroid cancer | 2%17 |
Receive systemic therapy for unresectable or metastatic disease | 26%18 |
Received first-line treatment | 19%18 |
Tested for RET mutation (year 1 / year 2 / year 3) | 70% / 80% / 90%b |
RET mutation | |
Number of patients eligible for drug under review | |
Treatment-naive patients (1L) | 10 / 12 / 14 |
Treatment-experienced patients (2L+) | 2 / 2 / 3 |
Market uptake (3 years) (Year 1 / Year 2 / Year 3) | |
Uptake (reference scenario) | |
Treatment-naive (1L) | |
Selpercatinib | 0% / 0% / 0% |
Vandetanib | 100% / 100% / 100% |
Treatment-experienced (2L+) | |
Selpercatinib | 0% / 0% / 0% |
BSC | 100% / 100% / 100% |
Uptake (new-drug scenario) | |
Treatment-naive (1L) | |
Selpercatinib | 75% / 80% / 85% |
Vandetanib | 25% / 20% / 15% |
Treatment-experienced (2L+) | |
Selpercatinib | 100% / 100% / 100% |
BSC | 0% / 0% / 0% |
Mean cost of treatment (per patient)c | |
Treatment-naive patients (1L) | |
Selpercatinib | 321,861 |
Vandetanib | 55,258 |
Treatment-experienced patients (2L+) | |
Selpercatinib | 321,861 |
BSC | 1,561 |
1L = first line; 2L+ = second line or later; BSC = best supportive care.
a1.6% per year for Non-Insured Health Benefits population.
bBased on internal company data.
cBased on mean treatment duration in the sponsor’s pharmacoeconomic base case and incorporates relative dose intensity.
Summary of the Sponsor’s BIA Results
The sponsor estimated the net 3-year budget impact of introducing first-line selpercatinib for the treatment-naive RET-mutant MTC to be $5,040,772 (year 1: $739,822; year 2: $1,698,843; year 3: $2,602,107). For previously treated RET-mutant MTC, the sponsor estimated the 3-year budget impact of introducing second-line selpercatinib to be $1,559,402 (year 1: $277,945; year 2: $534,765; year 3: $746,693). The estimated 3-year impact of introducing selpercatinib for the treatment of all patients with RET-mutant MTC was $6,600,175 (year 1: $1,017,767; year 2: $2,233,607; year 3: $3,348,801).
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of eligible patients is uncertain: The sponsor estimated the number of patients eligible for selpercatinib treatment using an epidemiologic approach, with inputs based on assumptions and data from published literature, which are associated with some uncertainty. First, there is uncertainty regarding the proportion of thyroid cancer patients with MTC. The sponsor based their estimate on information from the published literature;17 however, CADTH was unable to appraise the methods used to calculate this value in the original source because the methodology was not reported. Clinical experts consulted for this review by CADTH noted that the percentage of thyroid cancer patients who have MTC may be closer to 10%. The sponsor assumed that 26% of MTC patients receive systemic therapy for unresectable or metastatic disease based on published literature.18 The context in which the sponsor used this parameter in the submission does not match the description of the population in the original source. In the source, 26% of MTC patients receiving systemic therapy developed unresectable recurrence or metastatic disease, which is not the same as the proportion of MTC patients receiving systemic therapy as used by the sponsor in deriving the eligible population size. As such, there is notable uncertainty associated with this parameter.
The sponsor assumed that the proportion of patients tested for RET mutation will be 70% in year 1, 80% in year 2 and 90% in year 3. the clinical experts consulted for this review by CADTH noted there is uncertainty in the proportion of patients who currently undergo RET screening owing to the lack of availability of RET screening in all jurisdictions. However, the clinical experts anticipate RET testing to be implemented across Canada in the near future, which may lead to an influx of patients undergoing RET mutation testing, especially in the first year that testing becomes available. Further, the clinical experts opined that all MTC patients receiving systemic therapy should be tested.
The sponsor derived the percentage of MTC patients with a RET mutation from the published literature.19,20 However, a more recent study found that the proportion of patients positive for a RET somatic mutation among metastatic MTC cases is 90%, which concurs with the opinion of clinical experts consulted by CADTH for this review. The clinical experts also noted that the percentage of patients with a RET mutation is likely higher among advanced cases.
Given the uncertainty in multiple parameters used to derive the population size, the number of patients eligible for selpercatinib treatment, and hence the budget impact of reimbursing selpercatinib, is uncertain. In CADTH reanalysis, the proportion of MTC patients positive for a RET mutation was assumed to be 90% based on published literature21 and feedback from clinical experts. CADTH explored the impact of uncertainty in other input parameters related to the number of eligible patients in scenario analyses.
Drug cost of selpercatinib was underestimated: The sponsor included drug acquisition costs based on the pharmacoeconomic model, which had several limitations that carried over into the BIA. In the pharmacoeconomic model, the sponsor adjusted drug acquisition costs by dose intensity observed in the LIBRETTO trial, which underestimated the cost of selpercatinib treatment. Given the higher treatment costs for selpercatinib, this biased the results in favour of selpercatinib. Further, the duration of treatment in the BIA was similarly based on data from the pharmacoeconomic model, where patients were assumed to discontinue treatment at the time of disease progression. This approach does not consider patients who remain on treatment past disease progression or who discontinue prior to progression (e.g., because of adverse events), as noted by the clinical experts consulted by CADTH for this review. The sponsor also assumed equal treatment duration for patients receiving first-line and subsequent-line therapy, which lacks face validity. Since the drug acquisition costs included in the BIA are based on the pharmacoeconomic model, which is not specific to line of therapy, treatment costs and the estimated budget impact may not be reflective of the costs accrued by line of therapy.
In CADTH reanalysis, 100% dose intensity was adopted for all treatments.
Misalignment of model inputs between the sponsor-submitted pharmacoeconomic and budget impact analyses: In the pharmacoeconomic model, the sponsor assumed that there is no drug cost associated with BSC, which is inconsistent with the submitted BIA. In the BIA, the sponsor adopted a 1-time per-patient drug cost of $1,561 for patients receiving BSC, which was noted to include “different medications used to manage symptom of late-stage disease.”15 The sponsor was not explicit as to what drugs were included as part of this cost. The clinical experts consulted by CADTH for this review indicated that drug treatments may be used for symptom management by patients receiving BSC. The BIA and CUA should be aligned and reflect clinical practice.
CADTH was unable to verify whether the drug cost associated with BSC in the sponsor’s BIA is representative of costs accrued in clinical practice. CADTH explored the impact of excluding drug costs associated with BSC in scenario analysis.
There is uncertainty in the market share of selpercatinib treatment in first-line setting: The sponsor estimated that selpercatinib would obtain a market share of 75% in Year 1, 80% in Year 2, and 85% in Year 3 among the eligible treatment-naive patient population. The clinical experts consulted for this review by CADTH anticipate a higher uptake of selpercatinib among the treatment-naive population, expressing a potential preference for clinicians to use selpercatinib as first-line therapy. Should market uptake of selpercatinib be higher than estimated, the budget impact may be underestimated in the sponsor’s analysis.
CADTH explored the impact of higher first-line selpercatinib uptake in a scenario analysis.
An additional limitation not considered to be key limitation was poor modelling practices (such as hard coding costs), which made it hard to validate model inputs. A scenario analysis was also conducted to estimate the impact of the inclusion of genetic testing costs.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by increasing the proportion of patients with RET mutation and updating drug acquisition costs (Table 18).
Table 19: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Percentage of MTC patients with a RET mutation | 61.2% | 90%21 |
2. Drug acquisition costs | Based on the pharmacoeconomic model (assumed a reduction in drug costs due to reduced dose intensity) | Assumed no reduction in dose intensity (selpercatinib: $14,896 per cycle; vandetanib: $5,553 per cycle) |
CADTH base case | Reanalysis 1 + 2 | |
BIA = budget impact analysis; MTC = medullary thyroid cancer.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 19 and a more detailed breakdown is presented in Table 20. Based on the CADTH base case, the budget impact of the reimbursement of selpercatinib for the treatment of RET-mutant MTC is expected to be $2,073,323 in year 1, $4,467,281 in year 2, and $6,654,738 in year 3, with a 3-year total of $13,195,342.
When approved for first line, the budget impact of reimbursing selpercatinib was $1,540,537 in year 1, $1,540,537 in year 2, and $1,540,537 in year 3, for a 3-year total of $10,197,357. In the second line, the budget impact was $532,786 in year 1, $1,028,241 in year 2, and $1,436,958 in year 3, for a 3-year total of $2,997,985.
In the scenario where the proportion of MTC increases, the 3-year budget impact for the RET-mutation population increases to $65,976,710.
Table 20: Summary of the CADTH Reanalyses of the BIA — RET-Mutant MTC
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 6,600,175 |
First-line setting | 5,040,772 |
Second-line setting | 1,559,402 |
CADTH reanalysis 1 | 9,706,140 |
First-line setting | 7,412,901 |
Second-line setting | 2,293,239 |
CADTH reanalysis 2 | 8,972,833 |
First-line setting | 6,934,203 |
Second-line setting | 2,038,630 |
CADTH base case | 13,195,342 |
First-line setting | 10,197,357 |
Second-line setting | 2,997,985 |
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 21. The scenario analysis involved:
Assuming 100% of patients undergo RET mutation testing in years 2 and 3.
Assuming 10% of patients with thyroid cancer have MTC.
Assuming a 25% increase in the proportion of MTC patients receiving systemic therapy.
Assuming higher uptake of selpercatinib in the first line (100% in all years).
Excluding BSC drug costs.
Including RET mutation testing costs.
Price of selpercatinib reduced by 78%.
Table 21: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 ($) (current situation) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year totala ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 488,620 | 567,960 | 647,806 | 740,300 | 1,956,065 |
New drug | 488,620 | 1,585,727 | 2,881,413 | 4,089,100 | 8,556,240 | |
Budget impact | 0 | 1,017,767 | 2,233,607 | 3,348,801 | 6,600,175 | |
CADTH base case | Reference | 767,323 | 892,315 | 1,017,711 | 1,163,027 | 3,073,052 |
New drug | 767,323 | 2,965,638 | 5,484,992 | 7,817,764 | 16,268,394 | |
Budget impact | 0 | 2,073,323 | 4,467,281 | 6,654,738 | 13,195,342 | |
CADTH scenario analysis: 100% of patients undergo RET mutation testing | Reference | 767,323 | 892,315 | 1,243,128 | 1,310,876 | 3,446,319 |
New drug | 767,323 | 2,965,638 | 6,340,834 | 8,893,630 | 18,200,102 | |
Budget impact | 0 | 2,073,323 | 5,097,707 | 7,582,754 | 14,753,784 | |
CADTH scenario analysis: MTC assumed to comprise 10% of TC cases | Reference | 3,836,617 | 4,461,576 | 5,088,554 | 5,815,133 | 15,365,262 |
New drug | 3,836,617 | 14,828,191 | 27,424,960 | 39,088,822 | 81,341,972 | |
Budget impact | 0 | 10,366,615 | 22,336,406 | 33,273,689 | 65,976,710 | |
CADTH scenario analysis: 25% increase in MTC patients receiving systemic therapy | Reference | 959,154 | 1,115,394 | 1,272,138 | 1,453,783 | 3,841,315 |
New drug | 959,154 | 3,707,048 | 6,856,240 | 9,772,205 | 20,335,493 | |
Budget impact | 0 | 2,591,654 | 5,584,102 | 8,318,422 | 16,494,178 | |
CADTH scenario analysis: 100% market share of selpercatinib | Reference | 767,323 | 892,315 | 1,017,711 | 1,163,027 | 3,073,052 |
New drug | 767,323 | 3,479,150 | 6,472,649 | 9,036,878 | 18,988,677 | |
Budget impact | 0 | 2,586,835 | 5,454,938 | 7,873,852 | 15,915,625 | |
CADTH scenario analysis: Excluding BSC drug costs | Reference | 762,918 | 887,848 | 1,012,534 | 1,157,122 | 3,057,504 |
New drug | 762,918 | 2,965,638 | 5,484,992 | 7,817,764 | 16,268,394 | |
Budget impact | 0 | 2,077,790 | 4,472,458 | 6,660,643 | 13,210,890 | |
CADTH scenario analysis: Including RET mutation testing costs | Reference | 767,323 | 892,315 | 1,017,711 | 1,163,027 | 3,073,052 |
New drug | 767,323 | 2,972,956 | 5,493,923 | 7,828,467 | 16,295,346 | |
Budget impact | 0 | 2,080,641 | 4,476,212 | 6,665,441 | 13,222,293 | |
CADTH scenario analysis: Price reduction by 78% | Reference | 767,323 | 892,315 | 1,017,711 | 1,163,027 | 3,073,052 |
New drug | 767,323 | 892,407 | 1,369,293 | 1,860,543 | 4,122,242 | |
Budget impact | 0 | 91 | 351,583 | 697,516 | 1,049,190 |
BIA = budget impact analysis; BSC = best supportive care; MTC = medullary thyroid cancer, TC = thyroid cancer.
aCombined first-line and second-line subgroups.
Stakeholder Input
Patient Input
CanCertainty
About CanCertainty
The CanCertainty Coalition is the united voice of more than 30 Canadian patient groups, cancer health charities, and caregiver organizations from across the country, joining together with oncologists and cancer care professionals to significantly improve the affordability and accessibility of cancer treatment.
For more information about the CanCertainty Coalition, please visit: https://www.cancertaintyforall.ca/
Information Gathering
Selpercatinib is indicated for patients with thyroid cancer whose tumours have mutations that lead to the fusion of the RET gene with other nearby genes. As an orally administered oncology drug, selpercatinib would not automatically be funded by certain provincial governments. In Ontario and the Atlantic provinces, only individuals over the age of 65 are automatically covered for oral oncology medication. For the small number of patients under 65 (with RET-mutant medullary thyroid cancer) living in these provinces, their diagnosis could lead to severe economic hardships. However, if selpercatinib were to be fully funded for all age groups, patients would instead be able to focus on their treatment and spending time with their family and friends instead of dealing with the added burden of financial hardship and difficulties in accessing treatment.
Our data collection efforts aimed to estimate the number of patients who are at risk of severe financial burden as a result of their diagnosis. To do this, we calculated the number of RET mutant thyroid cancer cases in Canada each year among the under 65 population who do not have private or automatic public prescription drug coverage. Selpercatinib is a novel, highly selective inhibitor of RET kinase1. It is intended to supplant the use of multi-targeted kinase inhibitors that were only marginally affective against RET kinase. Selpercatinib can target diverse RET alterations and has been shown to have anti-tumor activity in the brain.
RET mutations are rare. We estimate that about 495 Canadians are diagnosed with RET fusion-positive thyroid cancer each year (100 with RET mutant medullary thyroid cancer and 395 with RET fusion-positive papillary thyroid cancer). Of these 495 cases, 381 will be under the age of 65. Thyroid cancer disproportionately affects younger individuals. Depending on where these individuals live, their oral oncology medication may not be covered by their provincial government. For the 158 patients under 65 living in British Columbia, Alberta, Saskatchewan, and Manitoba, oral oncology medication is automatically covered. Residents of Ontario and the Atlantic provinces under the age of 65 are not automatically covered for orally administered treatments under public plans. Their route to treatment access is not simple. By our estimations, 29 of these Ontario cancer patients will not have private health insurance. Before they can receive their medication these patients will have to navigate a complicated process of funding applications, approval delays, locating a pharmacy, and waiting for their prescription. They will incur out-of-pocket costs and sizeable portion of their income may go towards their medication. This small number of patients would be unduly impacted by such restrictive treatment funding policies.
RET positive thyroid cancer is a disease that exemplifies the injustice of not providing oral oncology coverage for Canadians under 65. RET mutations are present in a higher proportion of pediatric thyroid cancer cases than among the adult population. These younger patients (and their families) are at risk of financial toxicity if they live in Ontario or the Atlantic provinces. Furthermore, patients who are prescribed selpercatinib will have already been prescribed sorafenib and/or lenvatinib, two oral oncology medications that are also not automatically covered in Ontario and the Atlantic provinces. Throughout the course of their treatment, younger patients and their families could suffer the financial toxicity of paying for three oral oncology medications.
Data Collection
The RET mutation is present in medullary thyroid cancer and differentiated thyroid cancer. Selpercatinib is indicated for both medullary and differentiated thyroid cancers. Papillary thyroid cancer is a type of differentiated thyroid cancer and represents about 85% of thyroid cancers2. The RET mutation is present in about 10% of papillary thyroid cancer cases3. Medullary thyroid cancer represents about 4% of thyroid cancers. It come in two forms, hereditary (25%) and sporadic (75%). RET mutation are present in 95% hereditary medullary thyroid cancer cases and in 40% of sporadic medullary thyroid cancer cases. With these percentages, we estimated the number of yearly thyroid cancer cases with the RET mutation by age and province. We used the thyroid cancer incidence from Statistics Canada to estimate the number of RET mutated thyroid cancer cases (both medullary and papillary) each year by age and province. In other words, this is the estimated number of Canadian residents who will become eligible for selpercatinib each year.
Selpercatinib is indicated for patients who have progressed on a previous treatment. We do not have data on remission rates for patients who have been previously prescribed sorafenib or lenvatinib. We calculated the number of at risk patients based on cancer incidence data alone. Therefore, our calculations are an overestimation of the number of Canadians who will become eligible for selpercatinib. Some patients will have success with their first-line treatment.
Thyroid cancer incidence data was sourced from Statistics Canada in collaboration with the provincial and territorial cancer registries. They provide thyroid cancer data for all of Canada (excluding Quebec) broken down into age groups. We applied the age-specific thyroid cancer incidence rates to the 2018 population demographics of each province to arrive at the number of thyroid cancer cases each year by age and province. From there, we separately applied the percentages of medullary and papillary thyroid cancers to the overall thyroid cancer case numbers. We then applied the specific RET mutation rates to the respective types of thyroid cancer.
We measured “potential financial toxicity” using data on lack of private drug coverage. The Canadian Life and Health Insurance Association provides data on “extended health coverage.” For each province, we extracted the percentage of individuals under the age of 65 without private drug coverage AND without automatic public drug coverage. These province specific percentages were applied to the RET fusion-positive thyroid cancer case rates to arrive at the final estimation: the number of yearly RET fusion-positive thyroid cases among the under 65 population without private or automatic public prescription drug coverage.
Disease Experience
The access problems are so difficult that in many hospitals and cancer centres across Canada, such as those in Ontario, a new type of social worker known as a drug access navigator has been established (and funded) to assist patients and clinicians navigate the byzantine treatment access structures. In Ontario, the organization that supports these navigators is known as the Oncology Drug Access Navigators of Ontario (ODANO). They describe the problem that their association works to resolve as follows: Drugs are an important part of cancer treatment, yet patients often have difficulty accessing coverage for the most effective medicines. The complexity of cancer drug coverage in Canada can overwhelm patients and families. And For example, although cancer drugs administered in hospitals and clinics are often offered free of charge to patients, half of all new cancer drugs are taken at home and, therefore, many are not covered by the public health system. Unfortunately, many of our patients do not have any private insurance. If a patient is fortunate enough to have private coverage, many drug plans require a 20% co-payment, which can quickly become a financial burden to patients on expensive medications.
British Columbia, Alberta, Saskatchewan, Manitoba, Quebec, NWT, Yukon, and Nunavut cover the reimbursement of oral cancer drugs for all in need. Ontario and the Atlantic provinces do not.
In Ontario and Atlantic provinces, with respect to access to approved cancer treatments, there is institutional discrimination against those who are young, uninsured and who have cancer requiring take-home cancer treatment. With 60% of all new cancer drugs being developed with oral formulations, this issue urgently needs to be resolved through policy change. Traditionally, cancer treatments were administered to patients by an IV in the hospital. Over the past 15 or so years, an increasing number of effective cancer treatments can be taken at home by pill or injection. Take-home cancer medications are now a fundamental part of today’s cancer treatments and should be recognized equally within our health care systems. Patients requiring an intravenous treatment can start that medication as soon as needed and don’t face any financial or administrative burdens provided the drug is included on the provincial formulary.
However, when take-home cancer medications are prescribed, patients in Ontario and the Atlantic provinces, who are under 65, and lack adequate private insurance, have to apply to a variety of funding assistance programs and ultimately pay a significant deductible or co-pay from their personal savings. In some cases, the cost to the patient might be as high as $23,400 annually, based upon Nova Scotia’s Family Pharmacare Program. To qualify for assistance programs, patients and their families have to submit significant amounts of personal and financial information and often face weeks of stressful delay in starting their cancer treatment until the paperwork and approvals are resolved.
Even for patients with private drug insurance, the reality is that many face significant co-pays, deductibles or annual/lifetime caps. For example, some private insurance plans have a cap of $2,000 for prescription drugs for the entire year. The majority of take-home cancer drugs cost more than $20,000 per year. Two-tiered pharmacare in Ontario and the Atlantic Provinces discriminates on the basis of age, income, geography, cancer type, and cancer treatment, and is financially ruining many lives.
A survey7 of over 1,600 Nova Scotians, commissioned by the CanCertainty Coalition, demonstrates that drug coverage for cancer patients is a serious and growing problem.
More than half (57 percent) of Nova Scotians expect the provincial health care system will pay for take-home cancer medications. In reality, patients will ultimately pay a significant deductible or co-pay from their personal funds.
Three out of five people in Nova Scotia (60 percent) said they would consider leaving the province if faced with having to pay for their cancer drugs. Only seven percent could afford monthly drug costs of over $200.
Experiences with Currently Available Treatments
Take-home cancer drugs (THCD) are medications used for the active treatment of cancer and are usually dispensed for administration in the home (e.g., oral chemotherapy). These drugs have become a standard treatment for many cancers and present opportunities for patients, providers, and the health system. However, flaws in our current drug coverage system result in some patients not being able to access these treatments.
The term “financial toxicity” describes the distress and hardship arising from the financial burden of cancer treatment. Even in counties with government funded universal healthcare, financial toxicity is an issue for cancer patients and their families. Financial toxicity comes in many forms: out of pocket costs, lost income, travel expenses etc. Patients may deal with their financial burden by delaying or foregoing care. They may take less medication than prescribed, utilize over-the-counter drugs in place of prescribed medications, decline procedures, and skip appointments in an attempt to defray costs. The combination of high drug prices, particularly of oral targeted anticancer drugs, and increased cost sharing has made patients more vulnerable to medication non-adherence. Patients who are younger, have lower income, and are uninsured appear to be at greater risk of medication non-adherence. Although government funded public healthcare exists in many very high development index countries, financial toxicity is still common among cancer patients and caregivers. The evidence suggests that those with a shorter time since diagnosis, not currently working, and with more severe cancers have higher rates of financial toxicity, including stress and strain.
An unfunded oral oncology drug is financially toxic compared to a funded IV oncology drug. The disease experience of cancer patients that require oral drugs is a dual track of disease and economic hardships. After receiving their diagnosis, deciding on a medication, and dealing with the side effects, patients in Ontario and the Atlantic provinces have to consider the financial side of their diagnosis. “Hearing that you have cancer is devastating. Finding out that you can’t pay for the medication that will make you well is catastrophic. It doesn’t have to be this way”.
The financial side of cancer treatment is unnecessarily burdensome. “When you are going through any kind of sickness, whatever the severity of it, the last thing you should have to worry about is your medication cost” (Ed, Ontario). In addition to dealing with cancer, and not being well enough to work, patients in Ontario and the Atlantic provinces spend days on end, sometimes months, wading through paperwork in order to get approval for coverage of the oral chemotherapy that has kept them alive. Because some cancer treatments are not automatically funded, treatment is delayed for many patients. They wait weeks for government approval before dealing with insurance companies and pharmacies to receive their prescription. Patients often pay out of pocket for the first few weeks of their treatment, which they may not be reimbursed for. “My doctor prescribed a new drug that is not covered by the government therefore I had to find insurance to cover it which costs around $5000.00 a month, I came up with insurance to cover it but I had to pay the pharmacy first then the insurance would reimburse me some time later. My problem I do not have the $5000 to pay out let alone wait till they reimburse me”. “Cancer isn’t fair, but access to treatment should be!”.
Experience with Drug Under Review
CanCertainty’s focus for this submission is on issues related the distress and hardship arising from the financial burdens associated with cancer treatment. If selpercatinib were to be reimbursed for patients with RET fusion-positive thyroid cancer who have progressed on previous treatments, there would be some patients under 65 in Ontario and Atlantic Canada that would face significant financial and administrative barriers in accessing treatment.
Companion Diagnostic Test
N/A
Anything Else?
Equitable Access
We recommend that pCODR, when assessing and reporting on implementation issues with respect to selpercatinib, examine the issues of equitable access across all Canadian jurisdictions.
Safety
With respect to implementation, we believe pCODR should also examine the issue of safety with respect to take-home cancer drugs. From 2006 to 2001, it is estimated that Ontario’s computerized provider entry system, the Oncology Patient Information System (OPIS) prevented 8,500 adverse drug events, 5,000 physician office visits, 750 hospitalizations, 57 deaths, and saved millions in annual healthcare costs. But, this system is only used for only IV Drugs9. As a result, patients requiring take-home cancer drugs (THCD) in Ontario are (currently) subject to significant safety challenges, and health systems are subject to significant annual costs (physician office visits, hospitalizations etc).
In Ontario, dispensing and delivery models for THCD have been documented to be inconsistent and pose serious safety concerns for patients and their families. Some patients receive their medication from hospital pharmacies, some from specialty pharmacies, and some from community pharmacies that lack specialization and training in the handling of toxic cancer medications. This contrasts with the robust guidelines and clear processes that have been developed for intravenous cancer drugs (IVCD) where delivery is more comprehensive, organized, safer and patient-centred than THCD. There are numerous known safety and quality deficits related to the current method of community dispensing of THCD including incorrect dosing and handling, limited monitoring and non-adherence (which can lead to under or overdosing), serious toxicity, morbidity, and mortality. Patient lives and well-being are at stake. Ontario urgently needs to reform its systems for THCD dispensing that embed high-quality, safe practices that recognize the unique aspects of these drugs.
In April 2017, Cancer Care Ontario organized the Oncology Pharmacy Task Force with the mandate to advise Cancer Care Ontario (CCO) on how to enhance the current system for THCD delivery to optimize quality and safety; and subsequently, to deliver a report to the Ministry of Health and Long-Term Care (MOHLTC) based on the findings of the Task Force. The Task Force included representatives from patient advocacy groups, pharmacy and pharmacist associations, regulatory and standard setting organizations, and subject matter experts. On March 25th, 2019 the report was completed and published on the CCO website, but there has been no follow up or action taken to the many important recommendations. The report Enhancing the Delivery of Take-Home Cancer Drugs in Ontario (March 2019) can be found at:
CanCertainty suggests that pCODR examine the issues of safety and dispensing when examining and reporting on issues concerning pan-Canadian implementation of selpercatinib.
Conflict of Interest Declaration for CanCertainty
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was completed exclusively using CanCertainty resources and personnel and contract personnel.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Data was collected and analyzed using CanCertainty personnel/contract personnel.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
No conflicts declared
Canadian Cancer Society and Thyroid Cancer Canada
About the Canadian Cancer Society and Thyroid Cancer Canada
Website Link: https://cancer.ca/en
Our purpose: To unite and inspire all Canadians to take control of cancer.
Our mission: In trusted partnership with donors and volunteers, we improve the lives of all those affected by cancer through world-class research, transformative advocacy, and compassionate support.
We set ourselves apart from other cancer charities by taking a comprehensive approach against cancer. We are also the only national charity that supports all Canadians living with all cancers across the country. We shared our survey to thyroid cancer patients and caregivers through our http://CancerConnection.ca forums as well as through patient panels.
Information Gathering
The Canadian Cancer Society gathered perspectives through distributing a survey to patients and caregivers. We also received two testimonials from staff/board members of Thyroid Cancer Canada who have had thyroid cancer but did not have experience with Retevmo. We received a total of 17 survey responses. Of the 17 survey respondents, none had taken or cared for someone who had taken Retevmo. The data was gathered within the time frame of October 22 – November 10.
Demographic Information for Survey Respondents
Demographic information collected from the survey is displayed below. Please note that not all survey options that were offered are shown within the charts as they are limited to the options respondents actually selected to optimize space in the figures. Responders had the opportunity to select various options for geographic location, age ranges, genders etc., as well as prefer not to answer.
1) Which of the following best describes you?
All 17 survey respondents identified as patients who currently have or previously had thyroid cancer. No caregivers completed the survey.
2) What Province or Territory do you currently reside in?
The majority of respondents resided in Alberta (35%) and Ontario (29%). The other 36% resided in British Columbia, Quebec, Nova Scotia or preferred not to say.
3) How old are you?
The majority of survey respondents were between 40 – 49 years of age (41%). The second largest cohort was 50 -59 years of age (17%). Age brackets 20 -29, 30 – 39, 60 – 69 and 70 -79 made up the rest of the 42% of participants.
4) What is your gender?
The large majority of responders (82%) self-identified as women, while 18% self-identified as men.
Disease Experience
1) How much of an impact do symptoms associated with thyroid cancer have on your day-to-day activities and quality of life? (select all that apply)
The ability to concentrate scored highest as a day-to-day activity where patients experienced difficulty, with eleven responses in the moderate to significant impact range. The ability to exercise was not far behind, with ten moderate to significant impact responses. The ability to work had the next most substantial impact, with seven responses in the moderate to significant range. There were 53 moderate to significant impact options selected across the 17 participants, which indicates that 39% of all responses were in the moderate to significant impact range.
Seven respondents provided further details and answered the question “Specify any other areas of your life that have been impacted and how significant the impact is”. Responders indicated that fatigue, brain fog, mental health, body image, cognitive ability, concerns about the cancer returning, and the regulation of thyroid medications are other issues related to thyroid cancer that are being experienced that impact quality of life. The section titled “Experiences With Currently Available Treatments” in this report delves deeper into impacts and side effects of treatment.
Responses from patients
“The fatigue and number of appointments I have to attend have the most impact”.
“I have brain fog some days and some days my heart races and I don’t feel well”.
“After the surgery I couldn't work for 6 months. I'm not cured, but I don't have any problems working now.” – This quote was translated from French to English.
“Some days after working 8 hours, I'm really tired and just have no energy to do much...those days prevent me from household chores or evening activities”.
“Mental health, body image, cognitive ability. I am extremely exhausted all the time”.
“My mental health”.
“Time I spend worrying of return. It takes my energy away to regulate thyroid meds. It varies daily”.
Experiences With Currently Available Treatments
1) What is the greatest financial barrier related to your treatment(s)?
The most significant financial barriers identified included loss of income due to absence from work (24%) and parking costs (23%). Overall, 71% of all responders reported a financial barrier related to their treatment. One responder selected “other” and further specified that a blood test monitor (testing TSH, T3, T4) was their greatest financial barrier.
2) How is your cancer currently being treated? (Select all that apply)
The majority of responders indicated surgery (29%) was their current line of therapy. The next most common treatment selected was hormone therapy (17%).
3) How much of an impact do the following cancer treatment side effects have on your daily life?
Table 3 below depicts how impactful prevalent cancer treatment side effects were to surveyed thyroid cancer patients. Please note that respondents could indicate “not applicable” if they did not have a specific side effect so “no impact” could indicate the side effect was present at some point, but to such a small degree it did not impact the person’s life. It is also pertinent to note that even if the individual indicated they are currently not receiving treatment (see figure 5), they still experienced side effects from prior cancer treatments.
To measure the side effects that were the most impactful to patients, we combined the total number of responses in the moderate to significant impact range for each side effect. The side effects that impacted this patient group the most included fatigue with twelve (71%) of responses, concentration and focus with eleven (64%) of responses and weight changes with ten (58.5%) of responses in the moderate to significant range.
Other side effects that held over 25% of responses in the moderate to significant range included peripheral neuropathy (41%), diarrhea (36%), hair loss (35.5%), appetite changes (35%), constipation (30%) and pain (29%).
There were a total of 94 responses in the moderate to significant range (32.5% of all responses).
Six respondents noted additional side effects not present in Table 3. and answered the question “If there are any other side effects caused by your current cancer treatment(s), please specify what they are and how significant their impact is on your life”. An important impact of note expressed by half of respondents was related to mental health (mood swings, suicidal thoughts, and feelings of loneliness and fear).
Responses from patients
“Heart palpitations - small impact.”
“Can't seem to lose weight...small impact.”
“I have had my salivary glands affected and now have scar tissue that prevents saliva from excreting properly. As a result I suffer from dry mouth which makes me more susceptible to dental problems.”
“Synthroid Is very difficult to adjust and regulate which leads to emotional ups and downs. I’ve been suicidal through this due to being over medicated and an emotional mess when under medicated.”
“Palpitations, mood swings”
“Isolation of radiation, no one tells you how long to stay away from pets. How lonely it is because no support groups or info given on how to live afterwards with the fear of relapse or clear stages of the cancer.”
4) What improvements would you like to see in new treatments that are not achieved in currently available treatments? For example: effectiveness for relieving certain symptoms or side effects, affordability, ease of use etc.
Seven patients responded to this question. Several issues were highlighted such as the cost of drugs, difficulty regulating drugs, low levels of access to information, long treatment wait times and the experience that their cancer receives less support than other cancers (i.e. lack of attention from physicians as it pertains to thyroid hormone regulation and being seen outside of cancer clinics).
Responses from patients
“I think that if you’ve had a full thyroidectomy due to thyroid cancer, then thyroid meds should be free as well as Thyrogen, if needed for scans.”
“Less wait times for treatments.”
“More information available about what the long term effects of treatment can do.”
“Ease of use, easier to know your levels and adjust medication as needed would be a huge benefit!”
“Easy access to information, easy access to reports from scans, etc.”
“Regulation, I’m so tired constantly at a hyperthyroid amount. Care of doctors this is still cancer. I lost an important organ and I’m just supposed to cope. Be more realistic that this is impacting every day activities and won’t return to normal.”
“I would like to be seen in a cancer clinic rather than be followed outside of the clinic. There is not enough support for thyroid cancer patients.
Anything Else?
Across survey responses, patients frequently echoed similar sentiments. From this patient group, 65% reported having at least one or more moderate to severe impacts on their life due to thyroid cancer. Additionally, 88% of responders reported at least one or more side effects that impact their lives in a moderate to severe way. Side effects of both cancer and its treatment were significant for this group. Furthermore, for patients with experience with RAI/radiation therapy, there were additional concerns such as the impact on salivary glands (and therefore dry mouth and increased risk of dental problems), long term impacts of treatment and isolation associated with radiation.
The regulation of medication was expressed several times as an area of difficulty. This is important as patients who undergo surgery are most often required to take thyroid regulating medications for the rest of their lives.
Patient Testimonials
“In the December of 2017 I was diagnosed with papillary thyroid cancer - the “good” kind with a positive prognosis and a high cure rate. In January 2018 I underwent a full thyroidectomy. After a few months of recovery I was referred to an Endocrinologist and was prescribed both Synthroid and Dessicated medication for thyroid function replacement. It’s been a challenge to find the right combination and maintain the delicate balance of keeping my TSH suppressed (and T3/T4 in check) and the rest of my thyroid (or lack thereof) symptoms at bay. Too much and I’m buzzing like a neon light. I can’t focus. I feel anxious. Too little and I can’t regulate my body temperature properly. I’m lethargic and depressed.
Any adjustments take time and an increase (or decrease) has to be introduced slowly. I wait a few months and I go for more blood work to see what the impact is. I take stock of how I feel. I record my results. But I don’t know what any of it means. When TSH is low but T3 and T4 are normal. Or when nothing has changed but levels start to climb. So I turn to Dr. Google and I’m overwhelmed and I’m lost. There are no definitive answers. No common path to take.
I’ve gained almost 25 lbs since my surgery and even though my thyroid levels are “normal” it is incredibly difficult to lose the weight. At no point did anyone say “this” is how you will feel or that it would be this hard.
We need answers. We need consistency. Thyroid cancer needs to be seen and our stories need to be heard”
“Your scans are clear.
This is what you hear when you’ve had Cancer and go for annual ultrasounds. They scan the part of your body that had cancer along with routine bloodwork to ensure all markers are looking healthy, and there isn’t a chance of re-occurrence. They look for tumour re-growth and scan abnormalities.
I book my scans annually with my doctor and monitor my thyroid levels throughout the year with routine bloodwork. Needles have become routine. I no longer have a thyroid - a vital organ that regulates your temperature, metabolism, energy levels and hormones. It’s what people refer to as your internal furnace or regulator. I had mine removed 7 years ago now and as a result take hormone replacement daily. Without this vital organ it can make things like regulating your weight, your energy levels, your body temperature, your heart rate, and your mood challenging.
In 2014 I was diagnosed with Thyroid Cancer. I was in great physical shape but felt terrible. As someone who was in-tune with my body, I knew something was off. Fast forward 6 years and I get scanned and monitored regularly. Thanks to Canadian healthcare and living in one of the largest cities with the best hospitals in the country - Toronto, this is something very accessible to me. This isn’t always the journey for some. I am also seen by a top endocrinologist as I sought out a team that had a specialization in fertility because yes - a challenge with thyroid function can also mean trouble conceiving.
I work with some of the best doctors in their fields, I sought them out and did my research. Thyroid issues can often mean infertility issues. I was 30 when I got my news. Surely not something I expected so early in life. Seven years ago I got connected with Thyroid Cancer Canada. It’s an organization that helped me get informed and find a new tribe of people going through what I was. Fast forward a few years I am now Board President and help steer the organization. We are growing the small non-profit and turning up the volume on a cause still not mainstream to most.
Take aways? Appreciate good health, honour your body, and listen to it. If something feels off rally a team of experts that might help you. If you’re privileged enough to have those options, recognize that too. Tough times make strong people, and this was just one of the things in my life that gave me more grace, voice and perspective.”
Conflict of Interest Declaration for the Canadian Cancer Society and Thyroid Cancer Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Patients within the network of Thyroid Cancer Canada participated in the survey along with patients within the CCS network. They also provided two testimonials from their staff/board members.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
The network of Thyroid Cancer Canada shared the survey amongst their network of patients. They also provided two testimonials from staff/board members.
No one assisted CCS with the analysis of the survey. CCS was the sole author of this submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Eli Lilly: $5,015
Clinician Input
Pediatric Oncology Group of Ontario
About the Pediatric Oncology Group of Ontario
POGO is a collaboration of Ontario’s 5 specialized childhood cancer centres and the official advisor to the Ministry of Health and Long-Term Care on pediatric cancer care and control. This submission represents a collaboration of pediatric cancer clinicians from across the province with membership informed by POGO’s Therapeutic and Technology Advisory Committee (TAC). For more information on POGO, please visit www.pogo.ca
Information Gathering
POGO surveyed the TAC members to identify those with clinical experience and insight into the use of selpercatinib. In turn, interested parties were engaged to collaborate, edit and approve the feedback presented here.
Current Treatments
Describe the current treatment paradigm for the disease
Response: Pediatric thyroid carcinoma is a rare entity. Older adolescents (15 and above) are much more likely to be impacted. Pediatric Differentiated Thyroid Cancers (DTC) carry substantially different clinical, pathologic and molecular characteristics compared to DTC in adults.
Papillary Thyroid Carcinoma (PTC) is by far the most dominant form of DTC in pediatrics. Compared to adult patients with PTC, the rate of regional lymph node involvement and pulmonary metastases is higher. Furthermore, unlike in adult patients, the presence of BRAF mutations is relatively rare in pediatric PTC, whereas RET/PTC rearrangements are more common, particularly in patients under 10 years of age. It is this younger group that most commonly develops distally metastatic disease.
Pediatric DTC is treated by multidisciplinary collaborations that include surgeons, endocrinologists and nuclear medicine professionals. In contrast to most other pediatric malignancies, pediatric oncologists are only rarely involved in the care of these patients.
Following the diagnosis of PTC, the first therapeutic step is surgical resection, usually a total thyroidectomy and potentially central and/or lateral neck dissection. Post-operative staging aims to identify residual disease.
Pediatric patients with iodine avid and unresectable localized or metastatic lesions will normally receive therapy with radioactive iodine (131I) with goal of achieving cure and long-term survival. Repeated administration of radioactive iodine, however, is associated with compromised lung function.
Pediatric MTC is far rarer than DTC. In children ~75% of those with MTC carry an inherited (germline)
RET mutation. The majority of the remaining 25% have tumours driven by somatic RET mutations. Children with a family history undergo prophylactic thyroidectomy and thus avoid malignant transformation. For those without family history, however, disease is often advanced at the time of presentation and may not be amenable to complete resection. Treatment options for metastatic disease include multi-tyrosine kinase inhibitors such as vandetanib and cabozantinib. Both are associated with substantial dose-limiting toxicities in children and have defined, but limited impact on progression-free survival.
Treatment Goals
What are the most important goals that an ideal treatment would address?
Response: DTC in children generally carries a favourable prognosis with death from disease very uncommon. Importantly though, careful attention must be paid to minimizing late effects of therapy, including second malignancy, salivary dysfunction and pulmonary fibrosis.
MTC, once metastatic, has a very low rate of cure. Improved progression-free survival and minimizing off- target effects are priorities for the rare child who merits systemic therapy.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Response: For children with 131I refractory RET-associated disease, current second line therapies such as lenvatinib and sorafenib impact multiple off-target pathways and not surprisingly more toxicity and intolerance.
Response rates are also inferior. The need therefore is to provide effective, well tolerated targeted therapy while minimizing toxicity.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Response: Younger patients with PTC are far more likely to harbour a RET fusion positive tumour and also more likely to have distally-metastatic disease. These young patients are in most need of access to selpercatinib. We are concerned the indication as submitted excludes patients younger than 12 and all children with PTC. This extremely small group of patients is unlikely to be studied specifically, and therefore we strongly suggest they not be excluded from therapy.
For children with metastatic MTC requiring systemic therapy, selpercatinib demonstrates a superior side- effect profile to existing therapies and has equal or superior efficacy.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Response: Prior to the advent of selpercatinib, patients that have 131I refractory disease were treated with multikinase inhibitors such as lenvatinib or sorafenib. The non-specific nature of these medications lead to multiple off target toxicities. Selpercatinib represents a more focused and less toxic option and therefore should in our opinion be considered second line after 131I.
Moreover, even among those with 131I-avid disease, multiple rounds of therapy may be required to clear disease. Repeated exposure to radioactive iodine places children at risk for acute and chronic toxicities, including secondary malignancy.
For children with MTC who merit systemic therapy, selpercatinib would replace existing multikinase inhibitors as first-line treatment for progressive, metastatic disease.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Response: 131I is the historical first line therapy following surgery. We support its continued use due to its efficacy and known long term toxicities. We do not feel, however that less specific multikinase agents such as sorafenib and lenvatinib should be offered prior to using selpercatinib, a more targeted agent for those patients with known RET fusions.
For children with MTC, the best chance of cure is comprehensive initial surgery. We continue to advocate this as first-line therapy. For the rare child with residual disease, however, existing therapies (cabozantinib and vandetanib) are associated with inferior response rates and higher toxicities, thus we would advocate selpercatinib as the initial second-line therapy.
A rare but important subset of patients with unresectable tumours may be considered for first line therapy with selpercatinib in a neoadjuvant context to facilitate eventual surgical control.
How would this drug affect the sequencing of therapies for the target condition?
Response: The current stated indication favours use of sorafenib and lenvatinib for children with DTC who have failed RAI. However, in patients with known RET fusions, we feel these therapies should be reserved for those not responding to selpercatinib.
We feel selpercatinib is preferable to other kinase inhibitors (cabozantinib and vandetanib) due to reduced toxicities and favourable response rates for RET-driven MTC.
Which patients would be best suited for treatment with the drug under review?
Response: Young patients with DTC, including those under the age of 12 are more likely to harbour RET fusions and metastatic disease. These patients are likely to be best suited for access to selpercatinib.
Children with MTC with high-volume residual disease following surgery, those with residual disease threatening vital structures or those with progressive disease (either structural or biochemical) that is not surgically resectable, where the tumour is driven by RET mutation, are best suited for access to selpercatinib.
How would patients best suited for treatment with the drug under review be identified?
Response: Pediatric patients with DTC routinely are referred to specialized pediatric care. Pathologic review of tumour samples will include routine molecular analysis including assessment for RET fusions. This testing is routinely available in Ontario. Patients with disease not responsive to 131I should be considered for selpercatinib therapy.
Children with MTC and a post-operative serum calcitonin >150 pg/mL, those with progressive disease and those with residual disease threatening a vital structure would be best suited for treatment. Such patients are typically seen in consultation at a specialized tertiary center and reviewed at tumour boards.
Which patients would be least suitable for treatment with the drug under review?
Response: DTC patients without residual disease, those that have not undergone initial post-operative therapy with 131-I or those without a known RET fusion should not be considered candidates for selpercatinib.
MTC patients without structurally persistent disease (i.e., those with negative imaging) following initial surgery should not be considered candidates for selpercatinib.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Response: Routine molecular tumour analysis for RET fusions identifies patients likely to respond to selpercatinib. For children with MTC, presence of either a germline RET mutation will be predictive or for those with normal germline, tumour analysis confirming a somatic RET mutation
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response: Radiologic and biochemical assessment of known residual disease sites allows for the assessment of disease stability or potential improvement.
What would be considered a clinically meaningful response to treatment?
Response: Clinically meaningful response is the reduction and/or resolution of known residual disease based on cross-sectional imaging and tumour markers (thyroglobulin for DTC, calcitonin and CEA for MTC). For patients with milliary lung disease, an objective improvement of respiratory status would also represent clinically meaningful response.
How often should treatment response be assessed?
Response: At minimum, treatment response should be assessed every 3-6 months.
What factors should be considered when deciding to discontinue treatment?
Response: Disease progression in the setting of properly dosed and administered therapy should result in discontinuation of selpercatinib. Significant hypersensitivity not responsive to steroid and dose reduction should also lead to cessation of therapy.
What settings are appropriate for treatment with the drug under review?
Response: Selpercatinib should be administered as an outpatient under the care of a multidisciplinary team experienced in the care of pediatric DTC or MTC.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review? If so, which specialties would be relevant?
Response: Pediatric endocrinology and Head & Neck/Pediatric surgery should be involved in the diagnosis and monitoring of all children with thyroid carcinoma.
Additional Information
Is there any additional information you feel is pertinent to this review?
Response: We are very mindful that the current submitted request (and the recent Health Canada approval) use a lower age cut-off of 12 years old. We are very concerned that this age cut-off does not reflect the burden of disease in young children who are at higher risk of experiencing high burdens of distant metastases. We strongly urge PERC to not limit their considerations to 12 and above, but rather consider younger patients with the same underlying disease and fusion. We think this is crucial to ensure equitable access to all patients who require this therapy. We are concerned that otherwise, this group will be left unaddressed given the relatively low incentive for a pharma submission for this small subset of patients.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict-of-interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No. This document reflects feedback and writing by the group of listed clinicians only.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No. This document reflects feedback and writing by the group of listed clinicians only.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Paul Gibson
Position: Pediatric Oncologist, McMaster Children’s Hospital; Associate Medical Director, Pediatric Oncology Group of Ontario
Date: 05-11-2021
Table 1: Conflict of Interest Declaration for Pediatric Oncology Group of Ontario Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
Bayer Canada | X | — | — | — |
Declaration for Clinician 2
Name: Daniel Morgenstern
Position: Staff Oncologist, Hosptial for Sick Children
Date: 03/11/2021
Table 2: Conflict of Interest Declaration for Pediatric Oncology Group of Ontario Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
Lilly (reimbursement of expenses) | X | — | — | — |
EUSA Pharma | X | — | — | — |
ymAbs Therapeutics | X | — | — | — |
Clarity Pharmaceuticals | X | — | — | — |
Boehringer Ingelheim | X | — | — | — |
Declaration for Clinician 3
Name: Jonathan D. Wasserman
Position: Staff Endocrinologist
Date: 04/11/2021
Table 3: Conflict of Interest Declaration for Pediatric Oncology Group of Ontario Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
Bayer Canada | X | — | — | — |
Ipsen Pharmaceuticals | X | — | — | — |
Declaration for Clinician 4
Name: Sarah Cohen-Gogo
Position: Clinical research fellow, Haematology/Oncology, The Hospital for Sick Children, Toronto
Date: 04-Nov-2021
Table 4: Conflict of Interest Declaration for Pediatric Oncology Group of Ontario Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
Ontario Health (Cancer Care Ontario) Head and Neck and Thyroid Cancer Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Head and Neck and Thyroid Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Please describe how you gathered the information included in the submission.
This input was jointly discussed via email and teleconference.
Current Treatments
Describe the current treatment paradigm for the disease
Response
RET-mutant medullary thyroid cancer (adult):
For MTC, the only currently approved/funded option is vandetanib (prescribed agnostic to RET status).
RET fusion-positive differentiated thyroid carcinoma in adult patients:
For radioactive iodine-refractory differentiated thyroid cancer (RAIR-DTC), lenvatinib is the only option currently funded and approved. There are no other therapies upon progression.
Treatment Goals
What are the most important goals that an ideal treatment would address?
Response
RET-mutant MTC; RET fusion-positive DTC in adult patients:
For both populations, progression free survival is the most important treatment goal.
For MTC patients, reduction in treatment-related toxicities is also important
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Response
RET-mutant MTC (adult):
Vandetanib requires special training and monitoring including blood tests and ECGs to prescribe.
It has a black box warning due to QT prolongation causing arrhythmia from combined EGFR, VEGR and RET TKI activity.
Selpercatinib would be a safer and more effective option for MTC patients with RET-mutated tumors. Cabozantinib is neither funded nor approved for MTC in Canada but does have randomized data supporting its use (also agnostic to RET status).
RET fusion-positive DTC in adult patients
Cabozantinib has good 2nd-line RCT data but the ORR is only 15% and it is toxic, and not funded/approved.
Selpercatinib would be a preferred option for the small subset of RAIR DTC patients with RET fusion mutations progressing despite lenvatinib.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Response
RET-mutant medullary thyroid cancer (adult):
Metastatic, unresectable RET-mutant MTC is a fairly common clinical scenario
RET fusion-positive differentiated thyroid carcinoma in adult patients:
RET fusion-positive DTC represents a minority of patients
For both groups of patients, once they progressed on currently available treatments, there are no other treatment options.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Response
RET-mutant medullary thyroid cancer (adult):
Previously treated – selpercatinib will be an additional line of treatment
Not previously treated – selpercatinib represents an alternate treatment option based on a more favourable toxicity profile
RET fusion-positive differentiated thyroid carcinoma in adult patients:
Previously treated – selpercatinib will be an additional line of treatment
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Response
RET-mutant medullary thyroid cancer (adult):
No. Selpercatinib has multiple advantages over the existing therapies.
RET fusion-positive differentiated thyroid carcinoma in adult patients:
Patients should undergo first-line treatment before using selpercatinib based on existing data.
How would this drug affect the sequencing of therapies for the target condition?
Response
RET-mutant medullary thyroid cancer (adult):
Not previously treated population – Some clinicians may want to use selpercatinib in the first-line setting. Although selpercatinib appears more active and less toxic, phase 3 trial assessing selpercatinib 1st-line is ongoing. Given the broader receptor profile of vandetanib, they would also like to be able to use vandetanib in patients progressing on (or intolerant of) selpercatinib.
Some clinicians may reserve selpercatinib for RET-mutant MTC patients who are intolerant or unsuitable for vandetanib.
Vandetanib remains the standard (currently only) option in RET-negative MTC.
Previously treated population – selpercatinib offers a treatment option to those who have exhausted currently available treatments
RET fusion-positive differentiated thyroid carcinoma in adult patients:
Previously treated – selpercatinib offers a treatment option to those who have exhausted currently available treatments
Which patients would be best suited for treatment with the drug under review?
Response: Adults with RET-mutant medullary thyroid cancer or RET fusion-positive differentiated thyroid carcinoma
How would patients best suited for treatment with the drug under review be identified?
Response: In Ontario, RET testing is available. It is included as part of reflex testing on all metastatic thyroid cancer, including sporadic medullary and radio-iodine refractory well differentiated thyroid cancer
Which patients would be least suitable for treatment with the drug under review?
Response: Patients who don’t have RET-mutant MTC or RET-fusion DTC. Patients whose performance status would not allow treatment with selpercatinib.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review? If so, how would these patients be identified?
Response: Reflex testing is available in Ontario.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Response: Primary outcome measure included response rate. Secondary outcome measures were PFS and toxicity.
What would be considered a clinically meaningful response to treatment?
Response: Clinically meaningful response to treatment (for both diseases) include reduction in tumor burden (ascertained by clinical assessment and/or imaging) associated with the avoidance, improvement, or resolution of cancer-related symptoms. Often this is also associated with improvement in tumor marker levels for these cancers.
How often should treatment response be assessed?
Response: Every 8-12 weeks for the first 6 months – 1 year is reasonable, then q12 to 16 weeks thereafter, especially in patients who have had an initial response, feel well and have CEA and/or calcitonin decrease; however, specific intervals should not be mandated.
What factors should be considered when deciding to discontinue treatment?
Response: RET-mutant medullary thyroid cancer (adult); RET fusion-positive differentiated thyroid carcinoma in adult patients
Lack of response/ongoing response
Treatment-related toxicities
What settings are appropriate for treatment with the drug under review?
Response: Community setting (selpercatinib is an oral take-home cancer drug)
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
Response: NA
Additional Information
Is there any additional information you feel is pertinent to this review?
Response: Although LIBRETTO-001 trial was a phase 1/2 trial, the outcome data is compelling and selpercatinib would be a meaningful treatment option for MTC and DTC patients.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Michael Odell
Position: Ontario Cancer Lead; Assistant Professor of Otolaryngology-Head and Neck Surgery
Date: 2-Nov-2021
Table 5: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Head and Neck and Thyroid Cancer Drug Advisory Committee Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
Eli Lilly – no COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Eric Winquist
Position: Medical oncologist
Date: 29-Oct-2021
Table 6: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Head and Neck and Thyroid Cancer Drug Advisory Committee Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
Local PI on LIBRETTO trial testing selpercatinib in MTC | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Sebastien Hotte
Position: Medical oncologist
Date: 29-Oct-2021
Table 7: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Head and Neck and Thyroid Cancer Drug Advisory Committee Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
Eli Lilly – no COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Stephanie Brule
Position: Medical oncologist
Date: 05-Nov-2021
Table 8: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Head and Neck and Thyroid Cancer Drug Advisory Committee Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In excess of $50,000 | |
Eli Lilly – no COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.