CADTH Reimbursement Review
Selpercatinib (Retevmo)
Sponsor: Eli Lilly Canada
Therapeutic area: RET fusion–positive non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine amino transferase
AST
aspartate amino transferase
CI
confidence interval
CNS
central nervous system
CR
complete response
CrI
credible interval
DAC
Drug Advisory Committee
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EMA
European Medicines Agency
FISH
fluorescence in situ hybridization
GHS/QoL
global health status quality of life
HRQoL
health-related quality of life
IAS
integrated analysis set
IPD
individual patient-level data
IRC
independent radiographic committee
ITC
indirect treatment comparison
MID
minimally important difference
MTC
medullary thyroid cancer
MTD
maximum tolerable dose
NE
not estimable
NGS
next-generation sequencing
NMA
network meta-analysis
NOC/c
Notice of Compliance with Conditions
NSCLC
non–small cell lung cancer
ORR
objective response rate
OS
overall survival
OSAS
overall safety analysis set
PAS
primary analysis set
PCR
polymerase chain reaction
PD-1
programmed cell death protein 1
PD-L1
programmed cell death ligand 1
PFS
progression-free survival
PK
pharmacokinetics
PR
partial response
PSM
propensity score matching
PSW
propensity score weighting
RANO
Response Assessment in Neuro-Oncology
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumors Version 1.1
RET
rearranged during transfection
RP2D
recommended phase II dose
SAE
serious adverse event
SAS
supplemental analysis set
SD
standard deviation
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Selpercatinib (Retevmo), 40 mg and 80 mg, capsules, oral |
Indication | As monotherapy for the treatment of metastatic RET fusion–positive NSCLC in adult patients |
Reimbursement request | As monotherapy for the first-line treatment of adult patients with metastatic RET fusion–positive NSCLC and as monotherapy for the treatment of adult patients with metastatic RET fusion–positive NSCLC who have received prior systemic therapy |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC/c date | June 15, 2021 |
Sponsor | Eli Lilly Canada Inc. |
NOC/c = Notice of Compliance with conditions; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Introduction
Lung cancer is the most frequently diagnosed cancer in Canada and the leading cause of cancer-related deaths in males and females,1 with more than 29,600 new diagnoses (12.5% of new cases in males and 13.3% of new cases in females) and 21,000 disease-related deaths (24.2% of male cancer-related deaths and 25.8% of female cancer-related deaths) projected in 2021.1 The adjusted 5-year net survival estimate in Canada for all forms of lung cancers is 22%1 and the anticipated 5-year survival rate for patients with non–small cell lung cancer (NSCLC) is approximately 25% and 7% for patients with stage IV disease.2 Smoking, which is an established risk factor for developing lung cancer, accounts for more than 72% of newly diagnosed cases in Canada.1,3
Several treatments are available in practice for patients without prior testing for rearranged during transfection (RET) gene fusion. The drug plans and clinician input group highlighted the following treatment strategies: In patients who are treatment naive, first-line treatment combinations with platinum plus pemetrexed and pembrolizumab are preferred options for patients with programmed cell death ligand 1 (PD-L1) expression of less than 50%, and possibly in those with PD-L1 expression levels below 50% who are non-smokers, female, have increased disease, or symptom burdens. Pembrolizumab alone is preferred for those with PD-L1 expression below 50%. For patients who progressed on pembrolizumab as a first-line systemic therapy, treatment options involving platinum plus pemetrexed are preferred. Anti–PD-L1 therapies, including pembrolizumab, nivolumab, and atezolizumab, are available for patients who received platinum plus pemetrexed in the first-line setting, and docetaxel for those who progressed on platinum plus pemetrexed and pembrolizumab. These treatments were consistent with those highlighted by the clinical experts consulted by CADTH. The experts highlighted that the most preferred therapy used in the first-line setting for patients with RET fusion mutations across jurisdictions in Canada (except Prince Edward Island, where pembrolizumab is not funded) is the triple-therapy combination of platinum plus pemetrexed and pembrolizumab regardless of the PD-L1 tumour proportion score because of the limited activity reported in the literature for single-drug immunotherapy in the RET fusion population.
Selpercatinib (Retevmo) is a highly selective, adenosine triphosphate–competitive small-molecule inhibitor of the RET receptor tyrosine kinase, which is available in 2 oral formulations of 40 mg and 80 mg capsules. It received market authorization following the issuance of a Notice of Compliance with conditions (NOC/c) from Health Canada on June 16, 2021, for 3 indications: as a monotherapy in the treatment of metastatic RET fusion–positive NSCLC in adult patients, RET-mutant medullary thyroid cancer (MTC) in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease, and RET fusion–positive differentiated thyroid carcinoma in adult patients with advanced or metastatic disease (not amenable to surgery or radioactive iodine therapy) following prior treatment with sorafenib and/or lenvatinib. Initiation of treatment with selpercatinib is recommended only after testing for and confirmation of the RET gene mutation in patients. No past reviews have been submitted to CADTH for the RET fusion–positive NSCLC population.
The dosage recommended in the product monograph is 120 mg orally twice daily for patients who weigh less than 50 kg and 160 mg orally twice daily for patients who weigh 50 kg or more.
The objective of this CADTH review is to perform a systematic review of the efficacy and safety of selpercatinib as monotherapy for the first-line treatment of adult patients with metastatic RET fusion–positive NSCLC and as monotherapy for the treatment of adult patients with metastatic RET fusion–positive NSCLC who have received prior systemic therapy.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
This section was prepared by CADTH based on the input provided by patient groups. The full patient group input is included in the Stakeholder Input section at the end of this report.
Three patient groups submitted input for the review. The Canadian Lung Cancer Advocacy Group Breathe Hope, the CanCertainty Coalition, and Lung Cancer Canada (LCC). A single respondent from the Canadian Lung Cancer Advocacy Group Breathe Hope. highlighted symptom burden management due to disease progression and treatment toxicity from chemotherapy as major drawbacks associated with the disease and available treatment options. Access to selpercatinib was considered valuable to the patient, who was willing to accept side effects from the treatment as a trade-off for reduced tumour growth.
Input provided by the CanCertainty Coalition highlighted potential limitations with access to treatments across jurisdictions in Canada, citing Ontario and the Atlantic provinces as jurisdictions where the level of access to oral cancer medications varies. The coalition recommended that CADTH examine equitable access to treatment across jurisdictions in Canada. They also cited potential issues associated with safety and the dispensing of take-home oral cancer treatments and recommended that these issues be considered during the review if the drug were to receive public funding.
In its input, LCC emphasized key concerns such as a lack of screening programs to detect disease in earlier stages. Lung Cancer Canada also noted the need for new treatments in the first and second line that improve patient-reported outcomes and overcome resistance to treatment, as well as the toxicity-related events, decreased functionality, and increased dependence of patients on caregivers associated with current chemotherapy and radiation therapy, which have provided less benefit to patients.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Two clinical experts provided expert knowledge regarding treatment strategies in Canada. The clinical experts reported that no therapy is currently available for patients with RET fusion–positive NSCLC. Treatment goals identified by experts were similar to those highlighted by the clinician group. The clinical experts indicated that the most important goals are to achieve overall survival (OS), reduce symptom burden, delay disease progression, prolong life with improved quality of life, and decrease or eliminate hospital admissions and hospital stays. All these were considered valuable in this patient population.
The experts noted that if selpercatinib is approved for funding, it will likely be used as first-line therapy for patients with metastatic RET fusion–positive NSCLC. The experts described platinum plus pemetrexed and pembrolizumab (triplet therapy) as the preferred treatment option in the first line across jurisdictions (except the province of Prince Edward Island, where pembrolizumab is not funded) regardless of a patient’s PD-L1 tumour proportion score. Beyond the first line, the experts noted that docetaxel is funded and can be administered depending on whether the patient received triplet therapy as first-line treatment. Patients may also receive single-drug immunotherapies (pembrolizumab, nivolumab, or atezolizumab) in the second line if they had received platinum and pemetrexed in the first line; however, as noted in the clinical experts’ input, patients with RET fusion are known to respond poorly to immunotherapy, and docetaxel may be administered in place of an immunotherapy in next-line settings. The clinical experts recommended that treatment be made available to all RET fusion–positive patients with advanced or metastatic NSCLC.
The clinician experts indicated that response to treatment in practice is usually assessed using the same methods implemented in the LIBRETTO-001 trial. However, the frequency of assessments differs from those of the trial setting. As described by the experts, the standard will be to perform radiographic assessments every 8 to 12 weeks or sooner if the patient reports new symptoms or if physical findings indicate disease progression. The experts also noted that, in practice, symptom severity and adverse events (AEs) are generally reported every 3 to 4 weeks in patients receiving oral targeted therapies.
The experts noted that several molecular testing techniques are available to test RET fusion mutations across jurisdictions in Canada. Next-generation sequencing (NGS) was cited as the most commonly used technique, while NGS with RNA sequencing was considered the best test because of its sensitivity (100%) and specificity (99% using MSK IMPACT testing).
Clinician Group Input
This section was prepared by CADTH based on the input provided by clinician groups. The full clinician group input is included in the Stakeholder Input section at the end of this report.
The clinician group input was submitted by 2 groups: LCC and the Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancers Drug Advisory Committee (DAC). Ontario Health drug advisory committees provide timely evidence-based clinical and health-system guidance on drug-related issues in support of Cancer Care Ontario’s mandate, the Provincial Drug Reimbursement Programs, and the Systemic Treatment Program. Twelve clinicians from LCC and 2 clinicians from the DAC provided input for this review. Both groups mentioned similar treatment goals for patients with advanced or metastatic NSCLC. Key goals noted by both clinician groups included: improvement in median OS in patients, rapid and prolonged improvement in symptoms, a median progression-free survival (PFS), and reduced toxicity-related AEs. Experts from LCC added that treatment goals include the prevention or treatment of brain metastases, reduction of resource utilization, and evaluation of the impact of COVID-19 on the safety of systemic therapy. Input from LCC emphasized that current treatments for patients with RET fusion–positive NSCLC have not improved OS in patients and are not associated with rapid and prolonged improvement in lung cancer symptoms as measured by median time to response, objective response rate (ORR), progressive disease rate, and median PFS.
Both groups mentioned that adding selpercatinib to the Canadian treatment paradigm will allow the drug to be administered as a first-line therapy in newly diagnosed patients with RET fusion–positive metastatic NSCLC. Clinicians in the LCC group noted that newly diagnosed patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 to 3 could benefit from selpercatinib if it is approved for funding, although they expressed uncertainty about the best therapy for the second line and suggested that subsequent therapy could include docetaxel and anti–PD-L1 therapy for those who have not received such drugs in prior lines of therapy.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. For the CADTH review of selpercatinib, the drug plans emphasized the different treatment strategies in place for patients with NSCLC and provided questions pertaining to the initiation of therapy, the prescribing of therapy, generalizability, funding algorithms, care provision, and system and economic issues. These questions were addressed by the clinician experts consulted for the CADTH review and their responses were based on the evidence presented by the sponsor in the LIBRETTO-001 trial. Clinician expert responses have been included in the Drug Program Input section (Table 4).
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
A single, ongoing, combined phase I and II, multi-centre, multi-cohort, open-label study met the criteria for the CADTH systematic review. The LIBRETTO-001 trial evaluated the safety and efficacy of selpercatinib in patients with advanced solid tumours, including RET fusion–positive solid tumours (e.g., NSCLC and thyroid, pancreatic, and colorectal cancers), RET-mutant MTC, and other tumours with RET activation (e.g., mutations in other tumour types or other evidence of RET activation). Patients recruited were 12 years or older (depending on the site and country).
The study was initiated in May of 2017 and has more than 84 participating centres across Australia, Canada, Denmark, France, Germany, Hong Kong, Israel, Italy, Japan, Singapore, Spain, South Korea, Switzerland, Taiwan, and the US. Three interim analyses were planned to support regulatory submissions in different jurisdictions. This review presents data obtained at the second and third interim data cut-offs of December 16, 2019, and March 30, 2020, respectively. Data obtained at interim 1 were updated at interim 2 and formed the basis of the Health Canada submission.
The study consisted of a dose-escalation phase (I) and a dose-expansion phase (II). The phase I portion was conducted initially as a 3 + 3 design (cohorts of 3 patients were assigned to increasing dose levels until 1 or more dose-limiting toxicities was observed) but was later updated to a Fibonacci dose-escalation design after the third escalation was implemented in patients in increments of approximately 67%, 50%, and 33%. The primary objective in phase I was to assess the maximum tolerable dose (MTD) and/or recommended phase II dose (RP2D) and any dose-limiting toxicities. The secondary objective at phase I was to evaluate the safety and tolerability of selpercatinib, characterize the pharmacokinetic (PK) properties, and assess the antitumour activity of selpercatinib.
The phase II portion, which is ongoing, has 5 cohorts, which include patients with a confirmed RET gene alteration in their tumours. Cohort 1 included patients with a RET fusion–positive solid tumour who progressed on or were intolerant to 1 or more prior standard first-line therapies. Cohort 2 was composed of patients with RET fusion–positive solid tumours without prior standard first-line therapy. The primary objective at phase II was to evaluate the antitumour activity of selpercatinib in patients recruited into the 5 cohorts. This was achieved by measuring the ORR using the Response Evaluation Criteria in Solid Tumors Version 1.1 (RECIST 1.1) or Response Assessment in Neuro-Oncology (RANO) guidelines, according to tumour type and as performed by an independent radiographic committee (IRC) and the study investigator. Other outcomes were assessed as secondary objectives in phase II. These included best change in tumour size from baseline, duration of response (DOR), central nervous system (CNS) ORR, CNS DOR, time to any and best response, clinical benefit rate, PFS, OS, safety and tolerability of selpercatinib, and the characterization of the PK properties. Health-related quality of life (HRQoL) was assessed as an exploratory outcome.
This CADTH review focuses on outcomes observed in patients with NSCLC with a confirmed RET fusion gene mutation enrolled in cohorts 1 and 2 at phase II of the LIBRETTO-001 trial. These patients were further subgrouped into 3 datasets based on clinically meaningful distinctions observed during the trial. These subgroups include the primary analysis set (PAS), which consists of the first consecutively enrolled patients previously treated with platinum-based chemotherapy; the integrated analysis set (IAS), which consists of patients treated with platinum-based chemotherapy; and the supplementary analysis sets (SASs), which consists of patient who are treatment naive (SAS1), patients treated with other systemic therapies that are not platinum-based (SAS2), and patients without measurable disease according to RECIST 1.1 (SAS3). These datasets supported the regulatory submission for marketing approval by Health Canada, the FDA, and the European Medicines Agency (EMA).
Efficacy Results
The key efficacy outcomes investigated in the LIBRETTO-001 trial are presented in Table 2. Data consist of findings obtained at interim analysis 2 (December 16, 2019) and interim analysis 3 (March 30, 2020).
Table 2: Summary of Key Results From the LIBRETTO-001 Trial (March 30, 2020, and December 16, 2019, Data Cut-Off Dates)
Result | PAS (prior platinum chemotherapy RET fusion–positive NSCLC) by IRC | IAS (prior platinum chemotherapy RET fusion–positive NSCLC) by IRC | Treatment-naive RET fusion–positive NSCLC (SAS1) by IRC | |||||
|---|---|---|---|---|---|---|---|---|
March 30, 2020 N = 105 | December 16, 2019 N = 105 | June 15, 2021 N = 247 | March 30, 2020 N = 218 | December 16, 2019 N = 184 | June 15, 2021 N = 69 | March 30, 2020 N = 48 | December 16, 2019 N = 39 | |
Overall survival | ||||||||
Duration of overall survival (months), median (95%CI) | NE (25.7 to NE) | ||||||||||||||||| | NE (33.5 to NE) | NE (25.7 to NE) | ||||||||||||||||| | NE (27.9 to NE) | NE (NE to NE) | ||||||||||||||||| |
Duration of follow-up (months), median | 19.94 | ||||||||||||||||| | 26.4 | 14.26 | ||||||||||||||||| | 25.2 | 12.58 | ||||||||||||||||| |
Progression-free survival | ||||||||
Duration of PFS, median (95% CI) | 19.3 (13.9 to NE) | 16.53 (13.7 to NE) | 24.94 (19.3 to NE) | 19.3 (16.5 to NE) | 19.32 (13.9, NE) | 21.95 (13.8 to NE) | NE (13.8 to NE) | NE (13.8 to NE) |
Duration of follow-up (months), median | 16.76 | 13.86 | 24.7 | 13.6 | 10.97 | 21.9 | 10.84 | 9.17 |
Objective response rate | ||||||||
ORR, n (%) | 67 (63.8) | 67 (63.8) | 61.1% | 124 (56.9) | 104 (56.5) | 84.1% | 41 (85.4) | 33 (84.6) |
95% CI | (53.9 to 73.0) | (53.9 to 73.0) | NR | 50.0 to 63.6 | (49.0 to 63.8) | NR | (72.2 to 93.9) | (69.5 to 94.1) |
Duration of response (months) | ||||||||
Median (95% CI) | 17.51 (12.1 to NE) | 17.51 (12.0 to NE) | 28.6 (20.4, NE) | 17.51 (12.1 to NE) | 17.51 (12.1 to NE) | 20.2 (13.0 to NE) | NE (12.0 to NE) | NE (12.0 to NE) |
Duration of response follow-up (months), median | 15.67 | 12.06 | 21.2 | 11.99 | 9.23 | 20.3 | 9.79 | 7.39 |
AE = adverse event; ALT = alanine transaminase; AST = aspartate transaminase; CI = confidence interval; IRC = independent radiographic committee; NE = not estimable; NR = not reported; NSCLC = non–small cell lung cancer; RET = rearranged during transfection; SAE = serious adverse event; SD = standard deviation.
Note: Data cut-off dates of December 16, 2019; March 30, 2020; and June 15, 2021.
Source: Minchom et al. (2021),7 Canadian product monograph, summary of product characteristics,4 Clinical Study Report,16 and sponsor’s submission package, Retevmo (selpercatinib).5
Overall Survival
Primary and integrated analysis sets (RET fusion–positive NSCLC with prior platinum chemotherapy): At the December 16, 2019, data cut-off, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
At the March 30, 2020, data cut-off, the median OS in the PAS was not estimable (NE) and the median follow-up was 19.94 months. In the IAS population, the median OS was NE, and the median follow-up was 14.26 months.
The sponsor conducted a follow-up analysis in the IAS population at a new cut-off date of June 15, 2021. The median OS was NE at this data cut-off. The median follow-up of survival was 26.4 months.
Treatment-naive RET fusion–positive NSCLC (SAS1): At the December 16, 2019, data cut-off, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
At the March 30, 2020, data cut-off, the median OS was NE and the median follow-up was 12.58 months.
The sponsor conducted a follow-up analysis in the treatment-naive population at a new cut-off date of June 15, 2021. The median OS was NE at this data cut-off. The median follow-up of survival was 21.9 months.
Prior other systemic therapy RET fusion–positive NSCLC (SAS2) and non-measurable disease RET fusion–positive NSCLC (SAS3): At the December 16, 2019, data cut-off, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
At the March 30, 2020, data cut-off, the median OS was 28.88 months (95% CI, 11.0 to NE) and the median follow-up was 17.05 months for prior other systemic therapy RET fusion–positive NSCLC (SAS2); the median OS was NE and the median follow-up was 10.48 months for non-measurable disease RET fusion–positive NSCLC.
Health-Related Quality of Life
The exploratory outcome of HRQoL was assessed in the entire NSCLC population (n = 253) using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) disease-specific instrument. Scores were collected at baseline (cycle 1, day 1), every 8 weeks (until cycle 13), and every 12 weeks after cycle 13 (until end of treatment). A change of 10 or more points from baseline scores in the different domains was considered clinically meaningful.
No EORTC QLQ-C30 data were available at the March 30, 2020, data cut-off.
At the December 16, 2019, data cut-off, 3 subgroups were created, including the treatment-naive group (n = 39), the 1 prior line of therapy group (n = 64), and a group with 2 or more prior lines of therapy (n = 136). Lower scores obtained in functional subscales compared to the defined thresholds of 83 (physical function), 71 (emotional function), 58 (role function, social function), or 75 (cognitive function) were considered clinically meaningful problems for patients. Higher scores obtained in symptom subscales compared to the thresholds of 8 (nausea or vomiting), 39 (fatigue), 25 (pain), 17 (diarrhea, dyspnea, and financial difficulties), or higher than 50 (appetite loss, insomnia, and constipation) were considered clinically meaningful problems.
The mean score for global health status quality of life (GHS/QoL) at baseline in the overall population (all patients with NSCLC, n = 253) was 61.5. In the treatment-naive group, 1 line of prior therapy group, and 2 or more prior lines of therapy group, the obtained GHS/QoL mean scores were 60.2, 65.2, and 60.4, respectively.
The baseline scores for physical function in the overall population (all patients with NSCLC, n = 253) was 75.9. In the individual groups, the baseline scores for physical function were 72.6 in the treatment-naive group, 79.8 in the 1 prior line of therapy group, and 76.1 in the 2 or more prior lines of therapy group). As these were lower than the threshold score of 83, they were considered clinically important impairments at baseline. Improvements (≥ 10-point increase) in physical function were reported at cycle 3 in all 3 groups (naive = 43.5%; 1 prior line of therapy = 28.1%; and ≥ 2 prior lines of therapy = 29.8%).
Baseline scores for dyspnea exceeded the clinically meaningful threshold of 17 points in the overall population (all patients with NSCLC, n = 253) and in each subgroup (overall = 31.3; treatment-naive = 28.4; 1 prior line of therapy = 23.1; ≥ 2 prior lines = 37.7; standard deviation [SD] = 28.3) and were therefore considered clinically meaningful impairments. The proportion of patients who experienced a change in dyspnea from baseline by cycle of study treatment was higher in patients who reported improved symptoms compared to patients who reported worsened symptoms across cycles 3 to 13.
Because baseline scores for fatigue and insomnia did not meet a clinically meaningful threshold in the overall population (all patients with NSCLC, n = 253), they were not considered clinically meaningful impairments. The threshold was exceeded in the treatment-naive group (baseline mean = 41.6) and the group with 2 or more prior lines of therapy (baseline mean fatigue = 41.8), and these impairments were also considered clinically meaningful. The threshold was not met in the 1 prior line of therapy group, and was not considered a clinically meaningful impairment. More patients experienced improved outcomes in the change in baseline by cycle in insomnia scores compared to those who reported worsened outcomes across cycles 3 to 13. However, due to the decrease in the number of patients completing the questionnaires from baseline to cycle 13, these findings are uncertain. Data for the change from baseline by cycle in fatigue scores were not available.
Baseline scores for pain met a clinically meaningful threshold of 25 points in the overall population (mean = 29.4) and in all subgroups, and was therefore considered a clinically meaningful impairment. All line of therapy subgroups for nausea and vomiting exceeded the clinically meaningful threshold of 8 points. Data for the change from baseline by cycle in pain scores was not available.
Progression-Free Survival
Primary and integrated analysis sets (RET fusion–positive NSCLC with prior platinum chemotherapy): At the December 16, 2019, data cut-off, the median PFS in the PAS as assessed by the IRC was 16.53 months (95% confidence interval [CI],13.7 to NE). In the IAS population, the median PFS was 19.32 months (95% CI, 13.9 to NE).
At the March 30, 2020, data cut-off, the median PFS in the PAS as assessed by the IRC was 19.3 months (95% CI,13.9 to NE). In the IAS population, the median PFS was 19.3 months (95% CI, 16.5 to NE).
The sponsor conducted a follow-up analysis at a new data cut-off of June 15, 2021. The median PFS estimated in the IAS population was 24.94 months (95% CI, 19.3 to NE).
Treatment-naive RET fusion–positive: At the December 16, 2019, data cut-off, the median PFS by IRC assessment was NE and the median follow-up estimated was 9.17 months.
At the March 30, 2020, data cut-off, the median PFS by IRC assessment was NE and the median follow-up estimated was 10.84 months.
The sponsor conducted a follow-up analysis at a new data cut-off of June 15, 2021. The median PFS estimated in the treatment-naive population was 21.95 months (95% CI, 13.8 to NE).
Prior other systemic therapy RET fusion–positive NSCLC (SAS2) and non-measurable disease RET fusion–positive NSCLC (SAS3): At the December 16, 2019, data cut-off, the median PFS ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
At the March 30, 2020, data cut-off, the median PFS by IRC assessment was NE in both groups.
Objective Response Rate
Primary and integrated analysis sets (RET fusion–positive NSCLC with prior platinum chemotherapy): At the December 16, 2019, data cut-off, the ORR estimated by the IRC was 64% (95% CI, 53.9 to 73.0) in the PAS population, and in the IAS population, the ORR was 57% (104 of 184; 95% CI, 49.0 to 63.8).
At the March 30, 2020, data cut-off, the ORR by IRC was 63.8% (95% CI, 53.9 to 73.0) and 56.9% (95% CI, 50.0 to 63.6) in the PAS and IAS, respectively.
The sponsor conducted a follow-up analysis at a new data cut-off of June 15, 2021. The ORR estimated in the IAS population was 61.1% (95% CI, 54.7 to 67.2), which was consistent with previous analysis.
Treatment-naive RET fusion–positive NSCLC (SAS1): At the December 16, 2019, data cut-off, the ORR estimated by the IRC for the treatment-naive RET fusion–positive NSCLC population was 84.6% (95% CI, 69.5 to 94.1).
At the March 30, 2020, data cut-off, the ORR by IRC assessment was 85.4% (95% CI, 72.2 to 93.9).
The sponsor conducted a follow-up analysis at a new data cut-off of June 15, 2021. The ORR estimated in the treatment-naive population was 84.1% (95% CI, 73.3 to 91.8), which was consistent with previous analysis.
Prior other systemic therapy RET fusion–positive NSCLC (SAS2) and non-measurable disease RET fusion–positive NSCLC (SAS3): The ORR obtained by the IRC assessment in the prior other systemic therapy RET fusion–positive NSCLC (SAS2) was |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| at the December 16, 2019, analysis date and 44.4% (8 of 18; 95% CI, 21.5 to 69.2) at the March 30, 2020, data cut-off.
The ORR obtained by the IRC assessment in the non-measurable disease RET fusion–positive NSCLC (SAS3) was |||||||||||||||||||||||||||||||||||||||| at the December 16, 2019, data cut-off and 33.3% (95% CI, 13.3 to 59.0) at the March 30, 2020, data cut-off.
Subgroup Analysis
Central Nervous System Metastasis at Baseline
At the December 16, 2019, data cut-off, the IRC identified 22 patients with measurable CNS disease out of the 80 patients with CNS metastasis at baseline. The CNS ORR in the 22 patients was 82% (18 of 22; 95% CI, 59.7 to 94.8). The CNS ORR in the 80 patients with measurable and non-measurable disease was 48% (38 of 80; 95% CI, 36.2 to 59.0).
At the March 30, 2020, data cut-off, 23 patients of 96 were assessed with measurable disease at baseline, and the CNS ORR was 87% (95% CI, 66.5 to 97.2). In the 96 patients with CNS disease at baseline (measurable and non-measurable disease), the CNS ORR was 46.9% (95% CI, 36.6 to 57.3).
Performance Status, Number of Prior Therapies, Prior Anti–Programmed Cell Death Protein 1 and Anti–PD-L1 Therapy, and Prior Multikinase Inhibitor Therapy
At the December 16, 2019, data cut-off, the ORRs in the following subgroups were:
ECOG PS of 0: ORR 74.2% (95% CI, 55.4 to 88.1); ECOG PS of 1 or 2: ORR 59.5% (95% CI, 7.4 to 70.7)
number of prior therapies: 1 to 2: ORR 58.7% (95% CI, 43.2 to 73.0); 3 or more: ORR 67.8% (95% CI, 54.4 to 79.4)
prior anti–programmed cell death protein 1 (PD-1) or anti–PD-L1 therapy: yes: ORR 65.5% (95% CI, 51.9 to 77.5); no: ORR 61.7% (95% CI, 46.4 to 75.5)
prior multikinase inhibitor therapy: yes: ORR 64.0% (95% CI, 49.2 to 77.1); no: ORR 63.6% (95% CI, 49.6 to 76.2).
No ORR subgroup data were available at the March 30, 2020, data cut-off.
Duration of Response
Primary and integrated analysis sets (RET fusion–positive NSCLC with prior platinum chemotherapy): At the December 16, 2019, data cut-off, a median DOR as assessed by the IRC of 17.5 months (95% CI, 12.0 to NE) was reported, with a median DOR follow-up of 12.1 months in the PAS population. In the IAS, a median DOR of 17.5 months (95% CI, 12.1 to NE) by IRC assessment, with an estimated median DOR follow-up of 9.2 months, was reported.
At the March 30, 2020, data cut-off, the median DOR as assessed by the IRC was 17.51 months (95% CI, 12.1 to NE) in the PAS and a median DOR by IRC of 17.51 months (95% CI, 12.1 to NE) in the IAS population.
The sponsor conducted a follow-up analysis at a new data cut-off date of June 15, 2021. The median DOR obtained in the IAS population was 28.6 months (95% CI, 20.4 to NE).
Treatment-naive RET fusion–positive NSCLC: At the December 16, 2019, data cut-off, the DOR was assessed by the IRC in 33 patients in the treatment-naive cohort. The median DOR was NE.
At the March 30, 2020, data cut-off, 65% of the responses were ongoing at 12 months by IRC assessment.
The sponsor conducted a follow-up analysis at a new data cut-off date of June 15, 2021. The median DOR estimated in the treatment-naive population was 20.2 months (95% CI, 13.0 to NE).
Prior other systemic therapy RET fusion–positive NSCLC (SAS2) and non-measurable disease RET fusion–positive NSCLC (SAS3): At the December 16, 2019, data cut-off, the median DOR was ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
At the March 30, 2020, data cut-off, the DOR was NE in both groups.
Harms Results
At the December 16, 2019 data cut-off, there were 329 patients in the NSCLC set and 702 patients in the overall safety set (OSAS). Overall, 98.8% of patients in the NSCLC set and 99.0% in the OSAS reported at least 1 adverse event (AE); 35.9% of patients in the NSCLC set and 33.3% in the OSAS reported at least 1 serious AE; and 6.4% patients in the NSCLC set versus 5.3% in the OSAS discontinued study due to an AE. At the March 30, 2020, cut off date, 746 patients were included in the OSAS, 99.2% reported at least 1 AE, 35.1% reported a serious AE, and 45 (6%), discontinued the study due to an AE.
At the December 16, 2019, data cut-off, the most common AEs reported in the patients with NSCLC population in the LIBRETTO-001 trial were dry mouth, diarrhea, hypertension, increased aspartate transaminase (AST), increased alanine transaminase (ALT), fatigue, constipation, peripheral edema, headache, and nausea. Serious events in the NSCLC population were commonly associated with pneumonia, increased ALT and AST, abdominal pain, pleural effusion, drug hypersensitivity, diarrhea, and acute kidney injury.
At the December 16, 2019, data cut-off, AEs leading to dose withdrawal, interruption, and dose reductions in the RET fusion–positive NSCLC population were consistent with those in the overall population. AEs commonly associated with treatment discontinuations in the NSCLC population were increased ALT, sepsis, increased AST, drug hypersensitivity, fatigue thrombocytopenia. Increases in ALT and AST were commonly associated with dose reductions and dose interruptions.
At the December 16, 2019, data cut-off, treatment was discontinued due to death in 6 patients, and 38 patients discontinued the study due to death. At the March 30, 2020, data cut-off, in the NSCLC population, treatment was discontinued due to death in 6 (1.7%) patients, and 55 (15.9%) patients discontinued the study due to death. In total, 36 patient deaths (10.4%) were attributed to disease progression, 13 deaths (3.9%) occurred due to AEs, and 6 deaths (1.7%) were attributed to other reasons. A single report of death (0.3%), which had occurred more than 28 days after the last selpercatinib dose, was identified in the NSCLC population. In the overall safety analysis set (OSAS) population, treatment was discontinued due to death in 11 patients (1.5%), and 103 patients (13.8%) discontinued the study due to death.
Notable harms reported in the NSCLC set were consistent with the OSAS at the March 30, 2020, and December 16, 2019, data cut-offs). At the December 2019 data cut-off, notable harms reported in the NSCLC set and the OSAS included electrocardiogram QT prolongation (16.7% versus 16.5%), increased AST (32.8% versus 29.9%), increased ALT (31.0% versus 28.6%), hypertension (31.9% versus 35.9%), and hypersensitivity (2.4% versus 4.3%), respectively. At the March 30, 2020, data cut-off, notable harms reported in the OSAS population included electrocardiogram QT prolongation (18.1%), increased AST (32.6%), increased ALT (32.6%), hypertension (37.4%), hypersensitivity (5.2%), and hemorrhage (2.4%).
Critical Appraisal
The open-label, non-comparative design of the LIBRETTO-001 trial, with no statistical testing, is the key limitation. In its statistical analysis plan, the sponsor did not provide hypothesis statements for statistical significance for the primary outcomes of the secondary and subgroup analyses.8 This design increases the risk of bias in estimating treatment effects because the potential for confounding effects related to variation in health status, and other unidentified prognostic factors could affect subjectively assessed outcomes (i.e., response, HRQoL, and AEs). The potential for bias was reduced by using an IRC assessment for key study outcomes such as ORR and DOR.
The lack of direct comparative data means there is uncertainty regarding the magnitude of effects obtained for the efficacy outcomes. Although the clinical experts consulted by CADTH emphasized that the safety profile of selpercatinib was favourable compared to the other therapies available as standard of care in Canada, in the absence of a comparative arm, the findings obtained from the safety analysis are uncertain, as the single-arm design does not allow for the differentiation of the symptoms of underlying NSCLC disease from treatment-related AEs.9 The sponsor agreed to provide results from the |||||||||||||||||||||||||||||||||||||||||||||| to confirm the clinical benefit of selpercatinib in patients with previously treated RET fusion–positive NSCLC according to the NOC/c issued by Health Canada. The sponsor had noted in its response that |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The sponsor submitted additional data with a new cut-off date of June 15, 2021, during the completion of this CADTH review. (Appendix 3 provides new data). Despite the results obtained from the updated (pre-specified or post hoc) analyses performed on June 15, 2021, whether the end points investigated are durable for the long-term in this patient population remains uncertain.
The primary objective investigated at the phase II portion of the LIBRETTO-001 study was the ORR as measured by RECIST 1.1. The FDA considers ORR alone a surrogate measurement when assessing treatment response in patients with advanced or metastatic NSCLC, and this may not correlate well with survival, unless the effect size of the ORR is large and the responses are durable. The sponsor hypothesized a true ORR of 50% or greater in the primary analysis of effectiveness, ruling out a lower limit of 30% for the ORR, which was considered clinically meaningful and consistent with the estimated response rates seen with approved targeted therapies in molecularly defined populations of patients who have failed prior therapies (e.g., osimertinib, crizotinib, alectinib). The ORR obtained by IRC in the PAS, IAS, and SAS1 sets were above the lower limit of 30% that the sponsor assumed in the sample size calculation for patients with RET fusion–positive NSCLC who progressed on or after receipt of platinum-based chemotherapy.5 Although the FDA review team noted that the magnitude of the ORR and DOR obtained in patients with RET fusion–positive NSCLC of the LIBRETTO-001 trial was large, and considered it sufficient to establish clinical benefit,10 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.9 The sponsor |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||to provide results from |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| to confirm the clinical benefit of selpercatinib in patients with previously treated RET fusion–positive NSCLC according to the NOC/c issued by Health Canada. The sponsor also noted that ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.9 In the LIBRETTO-001 trial, radiographic scans were performed by an accredited laboratory and assessed by an independent radiology committee, which reduced bias. Results obtained from both IRC and investigator assessments did not differ greatly, which increases the validity of the ORR-related outcomes.
The time-to-events analyses, particularly the OS and PFS results, were considered exploratory by |||||||||||||||||, the FDA,25,30 and CADTH due to the lack of a control arm. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||9 Due to immature data in the PAS, IAS, and SAS1 populations at the March 31, 2020, and December 16, 2019, cut-offs, the results were considered exploratory by CADTH. The sponsor submitted additional data to CADTH for a new cut-off date of June 15, 2021, later during the completion of the review. Although the sponsor reported a median PFS of 24.94 months (95% CI, 19.3 to NE) in the IAS and a median PFS of 21.95 months (95% CI, 13.8 to NE) in the SAS1 population, the information was considered insufficient to form concrete conclusions about PFS in this population because of the single-arm design of the LIBRETTO-001 trial and immature data. The median OS was NE in the IAS and SAS1 datasets at the June 15, 2021, cut-off, creating uncertainty about whether the observed magnitude of benefit related to tumour response with selpercatinib would be translated as OS in patients in the 2 groups.
The analysis sets — the PAS, IAS, and 3 SASs — were not predefined in the original statistical analysis plan; they were developed following consultation with the FDA and EMA. A key concern is that these were post hoc analyses and may have been susceptible to bias. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. CADTH reviewers agreed ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, these were unlikely to introduce bias because the investigators remained blinded to results until after the revisions were made.9
The 3 planned interim analyses were pre-specified. However, the analyses were carried out using observed data only, with no formal hypothesis testing and only descriptive statistics provided, further complicating assessments of the magnitude of the effect observed in the different groups.
The exploratory outcome of HRQoL was evaluated. The validity of the findings is uncertain because the number of patients who completed questionnaires decreased from baseline through to cycles 13, resulting in considerable missing data at later time points. In the absence of a comparator arm and given an open-label design that introduced reporting bias, the impact of selpercatinib on patient-reported outcomes relative to other therapies is unknown. Although CADTH recognizes that the rarity of RET fusion–positive mutations in NSCLC may have contributed to the small sample size in the datasets at baseline, and may have influenced the number of patients available to complete the questionnaires at later stages of the trial, no strong, definitive conclusions can be made from the findings obtained for HRQoL in the different population sets of patients with NSCLC.
The clinical experts consulted during this CADTH review indicated that the findings obtained for the ORR, DOR, CNS ORR, and HRQoL outcomes investigated in the LIBRETTO-001 study are clinically meaningful for patients in practice. The LIBRETTO-001 trial recruited patients with an ECOG PS of 0, 1, or 2. The clinician experts consulted considered these findings generalizable to patients with an ECOG PS of 0 to 3 (but not for patients with an ECOG PS 4). As the experts also considered the baseline findings obtained in the trial to be similar to those observed in practice, the findings are generalizable to patients in Canada. The RET fusion mutation in patients was identified in the LIBRETTO-001 trial using polymerase chain reaction (PCR) testing and NGS. The clinical experts noted that NGS is available across several jurisdictions in Canada for testing oncogenic driver mutations at initial diagnosis.
Indirect Comparisons
Description of Studies
Two sponsor-submitted indirect treatment comparisons (ITCs) were summarized and critically appraised. Both aimed to evaluate the clinical efficacy of selpercatinib relative to other active treatments for RET fusion–positive NSCLC in patients with11 or without prior systemic therapies.12 All included studies enrolled patients with unknown RET fusion status, with the exception of LIBRETTO-001. The 3 outcomes that were analyzed were OS, PFS, and ORR.
Efficacy Results
The sponsor-submitted ITCs conducted a systematic review to identify relevant individual studies and used Bayesian network meta-analysis to evaluate the clinical efficacy of selpercatinib relative to other treatments for NSCLC. In both ITCs, a pseudo-control arm was needed due to the lack of a comparison arm in the study of selpercatinib. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the ITC of a treatment-naive population, selpercatinib was favoured over other treatments for OS (||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||), PFS (|||||||||||||||||||||||||||||||||||||||||||||||||||) and ORR (||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||). Selpercatinib was compared to monotherapy or a combination of platinum-based chemotherapy and immunotherapy drugs.
In the ITC of a population with treatment experience, results suggested that selpercatinib was favoured over other treatments for OS (|||||||||||||||||||||||||||||||||||||||||||||||||||), PFS (||||||||||||||||||||||||||||||||||) and ORR (|||||||||||||||||||||||||||||||||||||||||||||||||||). Selpercatinib was compared to monotherapy or combination of chemotherapy drugs and immunotherapy drugs, such as docetaxel, cabozantinib, atezolizumab, and nivolumab.
Harms Results
Harms were not assessed in the sponsor-submitted ITCs.
Critical Appraisal
These ITCs have a number of limitations that affect their internal and external validity, such as not being able to comprehensively assess the clinical heterogeneities across the included individual studies and their influence on the study results. Due to the lack of reporting certain patient characteristics, the treatment effect of selpercatinib, despite various adjustments, remains uncertain, and the generalizability of the study findings to patients with RET fusion–positive could be limited. In addition, other important outcomes, such as DOR, HRQoL and safety, were not assessed.
Other Relevant Evidence
Description of Studies
LIBRETTO-431: The CADTH review team identified an ongoing phase III, randomized, open-label study (LIBRETTO-431) comparing selpercatinib to platinum-based (carboplatin or cisplatin) and pemetrexed therapy with or without pembrolizumab in patients who are treatment naive and have locally advanced and/or metastatic RET fusion–positive non-squamous NSCLC. No results are currently available, as this trial is actively recruiting patients. The estimated primary completion date (at which the last participant in a clinical study will be examined or receive an intervention to collect final data for the primary outcome measure) and study completion date (when the last participant in a clinical study will be examined or receive an intervention or treatment to collect final data for the primary outcome measures, secondary outcome measures, and AEs) are January 15, 2023, and August 18, 2025, respectively.
SIREN: The CADTH review team identified another study analyzing the safety and efficacy of selpercatinib in a real-world setting (SIREN), in which the data were retrospectively collected and analyzed from patients with RET fusion–positive NSCLC participating in a selpercatinib access program.
The ORR, defined as a complete response (CR) or partial response (PR), was 68% (95% CI, 53 to 81), and the median PFS was 15.6 months (95% CI, 8.8 to 22.4) after a median follow-up of 9.4 months among all patients. In patients with untreated or previously progressed and measurable brain metastases (n = 8), the intracranial ORR reached 100%. In terms of AEs, 43 (88%) of 50 patients experienced treatment-related AEs of any grade, a large majority of them grade 1 or 2. The most frequent treatment-related AEs reported were fatigue or asthenia (40%), increased liver enzyme levels (34%), hypertension (26%), dry mouth (26%), and peripheral edema (20%). Treatment-related AEs of grade 3 or higher were reported in 12 patients (24%), with the most common being increased liver enzyme levels (10%), abdominal pain (4%), prolonged corrected QT time (4%), hypertension (4%), and fatigue or asthenia (4%).13
The following limitations were identified. First, the retrospective study design is prone to bias (e.g., reporting bias and nondifferential biases) and the patient population recruited may not be similar to that of the LIBRETTO-001 trial due to differences in the eligibility and exclusion criteria applied in the study (potential selection bias). The ORR, although measured using RECIST 1.1, was assessed by an unblinded review of practising physicians. There is also a potential measurement bias due to differences in the frequency and conduct of disease assessments in clinical practice versus the trial setting, the follow-up time frame in the study (which differs from that of the trial), and the therapies administered beyond disease progression. The small sample size of the study also limits the generalizability of the findings. Although the SIREN study provides additional data on the effectiveness and safety of selpercatinib in the real-world setting, the limitations identified introduces uncertainty.
Conclusions
The evidence supporting the funding request of selpercatinib was derived from an ongoing phase I and II, open-label, non-randomized, multi-cohort, single-arm study (LIBRETTO-001). The ORR observed in the LIBRETTO-001 trial suggested favourable tumour response in both the treatment-naive and treatment-experienced groups and was consistent with further follow-up analyses. The ORR and DOR, including the CNS ORR, obtained in both patient populations were considered clinically meaningful by the clinical experts consulted during the review. Time-to-event end points such as OS were NE at the March 30, 2020, and December 16, 2019, data cut-offs in the PAS, IAS, and SAS1 populations due to data immaturity. The median PFS was NE in the treatment-naive group at the March 30, 2020, and December 16, 2019, data cut-offs. Combined with the single-arm trial design, the evidence was considered insufficient to interpret OS and PFS findings. The sponsor provided additional data to CADTH for a new data cut-off of June 15, 2021. Although estimates obtained at the June 15, 2021, data cut-off suggested an improvement in median PFS in the IAS and SAS1 populations, the median OS was NE. CADTH considered these findings insufficient to provide concrete conclusions on the comparative treatment effect (PFS and OS) due to the single-arm trial design and immature data. It is therefore uncertain whether the observed magnitude of benefit related to tumour response with selpercatinib would be translated to OS in patients in the treatment-naive and treatment-experienced groups. As well, the limitations related to the single-arm, non-randomized design of the LIBRETTO-001 trial precluded drawing strong, definitive conclusions on the effects of selpercatinib on HRQoL, although HRQoL findings were described by the clinical experts consulted by CADTH as clinically meaningful. Safety information was reported for all patients who received a single dose of selpercatinib in the LIBRETTO-001 trial at both data cut-offs. Selpercatinib was associated with corrected QT prolongation, increased AST and ALT, hypertension, and drug hypersensitivity. These events have been labelled under the warnings and precautions section of the Canadian approved product monograph for selpercatinib. However, these notable harms were considered by the clinical experts as manageable and favourable compared to current standard of care treatment options. Although the SIREN study provided additional data on both the effectiveness and safety of selpercatinib in the RET fusion–positive NSCLC population, several limitations were identified with the study, and concrete conclusions could not be drawn to support the primary data obtained from the LIBRETTO-001 trial. The ITCs submitted to provide information on the comparative effects of selpercatinib were also associated with limitations that prevented drawing conclusions. The comparative effectiveness and safety of selpercatinib are therefore uncertain.
Introduction
Disease Background
Lung cancer is the most frequently diagnosed cancer in Canada and the leading cause of cancer-related deaths in males and females,1 with more than 29,600 new diagnoses (12.5% of new cases in males and 13.3% of new cases in females) and 21,000 disease-related deaths (24.2% of male cases and 25.8% of female cases) projected in 2021.1 The adjusted 5-year net survival estimate in Canada for all forms of lung cancers is 22%1 and the anticipated 5-year survival for patients with NSCLC is approximately 25%, and 7% for patients showing stage IV disease.2 Smoking is an established risk factor for developing lung cancer, accounting for more than 72% of newly diagnosed cases in Canada.1,3
Lung cancers are classified into 2 types based on histology: small cell lung cancer and NSCLC. The latter are the most common, and are further categorized into 3 types based on cell types: adenocarcinomas, squamous cell carcinomas, and large-cell carcinomas. Adenocarcinomas are the most commonly diagnosed forms of NSCLC in Canada, accounting for 48% of new cases.1
Early diagnosis improves prognosis and patient responsiveness to therapy. Diagnosis is based on histology and symptom presentation.3,14 Patients may experience worsening coughs, chest pain, hemoptysis, malaise, weight loss, dyspnea, and hoarseness at clinical presentation or upon chest imaging.1,3 In advanced or metastatic disease, patients experience additional symptom burdens such as trouble breathing, chronic cough and chest pain, pain in bones or the spine, yellowing of the skin or eyes, weakness or numbness of arms or legs, fatigue and unexplained weight loss depression, insomnia, and pain.15,16 Staging at diagnosis is key in determining disease prognosis and facilitates treatment selection.3,16 Late diagnosis is a significant contributing factor to early mortality and also challenging for disease management in real-world practice. Unfortunately, almost 50% of NSCLC diagnoses in Canada are made at stage IV, with only 23.1% of cases diagnosed at stage I.1
The expression of oncogenic driver mutations on tumours plays a vital role in patient response to treatment.16 Several predictive drivers identified in recent years, including mutations of the EGFR (epidermal growth factor receptor), ROS1 (C-ROS oncogene 1), KRAS, and BRAF genes, ALK (anaplastic lymphoma kinase) fusions, and others have greatly influenced treatment strategies in practice, improved patient quality of life, and increased OS for patients.5,16-18 The RET protein, a transmembrane tyrosine kinase receptor encoded by the RET gene, is known to play a substantial role in the development and maintenance of many systems (including the enteric nervous and genitourinary systems in neonates).19 Abnormal RET receptor activation by rearrangement or mutation was recognized as an oncogenic driver for many cancers, including NSCLC. These alterations were commonly associated with patients with adenocarcinoma histology, younger patients (usually ≤ 60 years), and those with a non-smoking or light smoking status.5 Prevalence estimates from studies show that only about 1% to 2% of NSCLC cases are RET fusion–positive.5,20 Testing for driver mutations at initial diagnosis using molecular techniques such as NGS panel testing or PCR testing methods is available across jurisdictions in Canada.16,17
Standards of Therapy
The clinician experts and clinician groups consulted during the review outlined similar treatment goals for patients with advanced or metastatic disease, which include improvement in median OS, rapid and prolonged improvement in cancer-related symptoms and improvement in quality of life (given that patients with advanced and metastatic disease experience greater symptom burden), reduced treatment-related toxicity and prevention, and treatment of brain metastasis.
Expert opinion from the clinician groups and drug plans consulted during the CADTH review highlighted treatment combinations funded in practice for patients without confirmed RET fusion. For the naive-treatment population, first-line treatment combinations with platinum plus pemetrexed and pembrolizumab were identified as the most preferred in patients with PD-L1 expression below 50% — and possibly in those with PD-L1 expression above 50% who are non-smokers, female, have increased disease, or symptom burdens — and pembrolizumab alone for those with PD-L1 expression above 50%. Among patients who progressed on prior systemic therapy, treatment options with platinum plus pemetrexed are preferred for those who had received pembrolizumab in the first-line therapy. Anti–PD-L1 therapy, including pembrolizumab, nivolumab, and atezolizumab, is recommended for those who had received platinum plus pemetrexed as first-line therapy (a small number of patients), and docetaxel is advised for those who have progressed on platinum plus pemetrexed and pembrolizumab.
The drug plans consulted by CADTH identified several treatment options with the potential for funding for first-line treatment, including pembrolizumab and atezolizumab (depending on the patient’s PD-L1 status). In the second-line setting, the drug plans noted that funded options may include immune checkpoint inhibitors, if no prior PD-1 inhibitor (pembrolizumab, nivolumab, or atezolizumab, depending on patient’s PD-L1 status) was administered to the patient, or chemotherapy following treatment with a PD-1 inhibitor (docetaxel or pemetrexed). The LCC clinician group pointed out that evidence from some cohort studies indicates that patients with RET fusion NSCLC are sensitive to pemetrexed, and that, in the absence of any randomized data, pemetrexed plus platinum will likely be the most efficacious therapy in patients with RET fusion NSCLC who had received only pembrolizumab as first-line therapy.
The clinician experts consulted identified treatments similar to those outlined by the clinician group and drug plans. The experts mentioned in their report that the most preferred therapy used in the first-line setting across jurisdictions in Canada (except Prince Edward Island, were pembrolizumab is not funded) is a triplet therapy combination of platinum plus pemetrexed and pembrolizumab, regardless of the PD-L1 tumour proportion score. This choice of therapy was based on available evidence that reported similar outcomes (PFS and OS). While they acknowledged that platinum doublets and single-drug immunotherapies are approved and available in practice, they noted that some studies have reported poor response rates to immunotherapy in the RET fusion population. The experts indicated in their input that patients with RET fusion (most likely with adenocarcinoma histology) have shown to respond to a combination of platinum and pemetrexed, but other platinum doublets are of limited significance.
The clinical experts also added that, beyond the first line (after administration of a triple therapy), single drugs such as docetaxel are the typical standard of care, although there is limited evidence for outcomes specific to patients with RET fusion using docetaxel. If a patient received pembrolizumab in the first line, the doublet combination of platinum and pemetrexed may be administered and if they received platinum plus pemetrexed in the first line, they may likely receive immunotherapy (e.g., pembrolizumab, nivolumab, or atezolizumab) in the second line. However, patients tested for RET fusion may be placed on docetaxel in the second line rather than immunotherapy (based on evidence that reports low response rates to immunotherapy in patients who are RET fusion positive). The experts also added gemcitabine and vinorelbine as available therapies in the second line and beyond. Other nonsystemic options outlined included radiation and surgical interventions employed as aggressive modalities in patients with oligometastatic disease or as palliative interventions with the goal of alleviating symptoms.
Drug
Selpercatinib is a highly selective, adenosine triphosphate–competitive small-molecule inhibitor of the RET receptor tyrosine kinases available in 2 oral formulations of 40 mg and 80 mg capsules. It received market authorization following the issuance of an NOC/c from Health Canada on June 16, 2021, for 3 indications: as a monotherapy in the treatment of metastatic RET fusion–positive NSCLC in adult patients, RET-mutant MTC in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease, and RET fusion–positive differentiated thyroid carcinoma in adult patients with advanced or metastatic disease (not amenable to surgery or radioactive iodine therapy) following prior treatment with sorafenib and/or lenvatinib.4 The sponsor is requesting funding for the following indications:
as monotherapy for the first-line treatment of adult patients with metastatic RET fusion–positive NSCLC
as monotherapy for the treatment of adult patients with metastatic RET fusion–positive NSCLC who have received prior systemic therapy.
Treatment initiation with selpercatinib is recommended only after an initial testing and confirmation of the RET gene mutation in patients. Selpercatinib has obtained regulatory approval and is marketed by other regulatory agencies, including the FDA (May 08, 2020) and the EMA (February 11, 2021) for indications similar to those outlined in the Canadian product monograph. Market approval in Canada was granted based on evidence generated from the LIBRETTO-001 trial, a phase I and II trial conducted in patients 18 years and older (in some countries in patients as young as 12) with advanced solid tumours, including RET fusion–positive solid tumours (e.g., NSCLC and thyroid, pancreatic, and colorectal cancer), RET-mutant MTC, and other tumours with RET activation (e.g., mutations in other tumour types or other evidence of RET activation).19
Dosing recommendations of selpercatinib are based on body weight. Patients weighing less than 50 kg are recommended to take 120 mg twice a day and patients with a body weight of 50 kg and above are recommended to take 160 mg of capsules twice a day every 12 hours. Dose adjustments are recommended for patients with severe hepatic impairment (a Child-Pugh score with a severity in the C range) irrespective of body weight.
Mechanism of Action
Selpercatinib demonstrated potent in vitro and in vivo activity as a selective inhibitor of both wild-type and oncogenically activated RET, including RET fusions, “founder” mutations, and anticipated acquired resistance mutations. The nonclinical development program also showed that selpercatinib treatment resulted in significant cytotoxicity only in human cancer cell lines that harbour endogenous RET gene alterations (e.g., fusions and mutations), with minimal cytotoxicity in human cancer cell lines without an endogenous RET gene alteration, as expected for a highly specific inhibitor of RET.5
Selpercatinib was found to be more than 250-fold more selective for RET than 98% of 329 non-RET kinases tested in a large in vitro screen. This high degree of selectivity was maintained against both kinase and non-kinase off-targets when validated in additional enzyme, cell-based, radio-ligand binding, and in vivo assays.5
Table 3: Key Characteristics of Selpercatinib
Characteristic | Selpercatinib |
|---|---|
Mechanism of action | Orally available highly selective, adenosine triphosphate–competitive small-molecule inhibitor of the RET receptor tyrosine kinase |
Indicationa |
|
Route of administration | Oral |
Recommended dose |
|
Serious adverse effects or safety issues |
|
Other | Testing using a validated test to confirm the presence of the RET gene fusion is needed for patients with NSCLC or thyroid cancer, and a RET gene mutation (for patients with MTC) is required before selpercatinib treatment initiation |
MTC = medullary thyroid cancer; NSCLC = non–small cell lung cancer; RET = rearranged during transfection; RTK = receptor tyrosine kinase.
aHealth Canada–approved indication.
Source: Canadian product monograph for Retevmo and clinical summary of efficacy (submission package).4,19
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH based on input provided by patient groups. The full patient group input is included in the Stakeholder Input section at the end of this report.
Three patient groups submitted input for the review: the Canadian Lung Cancer Advocacy Group Breathe Hope, CanCertainty, and LCC.
The Canadian Lung Cancer Advocacy Group Breathe Hope is composed of Canadian lung cancer patients. The group is driven by the need to establish a Canadian lung cancer community of patients and caregivers; provide a supportive, confidential environment; raise awareness about lung cancer through personal contacts or events and connections with national, provincial, and local stakeholder individuals or organizations; share new, innovative lung cancer treatments and scientific research; and promote conference opportunities and web events. The input provided was based on a single patient’s experience with standard of care treatment options offered in Canada and selpercatinib.
The CanCertainty Coalition is a united voice of more than 30 Canadian patient groups, cancer health charities, and caregiver organizations from across the country working with oncologists and cancer care professionals to significantly improve the affordability and accessibility of cancer treatment.
Lung Cancer Canada is a registered national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research, and advocacy. A member of the Global Lung Cancer Coalition, LCC is the only organization in Canada focused exclusively on lung cancer. Its input was based on 5 patient experiences. Three respondents lived in Canada and 2 patients lived in the US. All patients had completed RET fusion gene testing and had received selpercatinib treatment either in the first- or second-line setting. Patient information was collected through interviews (n = 4), questionnaires, and previous discussions with LCC (n = 1).
Most patient respondents from LCC (3 of 5) had been treated with chemotherapy, immunotherapy, or radiation before receiving selpercatinib. Two patients had received selpercatinib in the first-line setting. Patients with prior experience with other lines of therapy emphasized key undesirable effects associated with these therapies, which included treatment-associated toxicities, decreased functionality, and increased dependence on caregivers. The respondents identified several expectations for selpercatinib, which included improved management of their symptoms and improved quality of life (described by 1 patient as “allowing patients to have a full and worthwhile quality of life”). Most patients reported being hopeful the use of selpercatinib would result in gains in independence and functionality (which would reduce caregiver burden), more manageable treatment-related toxicities, improvements in OS, delayed disease progression, and long-term remission for improved survivorship.
Respondents reported positive experiences following the use of selpercatinib. Most respondents expressed noticeable improvements in symptoms and some improvement in quality of life after using selpercatinib. One patient described having experienced tumour shrinkage 2 months after commencing therapy and another patient mentioned discontinuing oxygen 2 weeks after treatment initiation and recovery of the ability to walk 1 month into treatment. Another respondent reported achieving long-term remission with 4 years of stable disease after using selpercatinib and another described experiencing noticeable improvement in brain metastasis. Treatment toxicity events following the use of selpercatinib were described by some respondents as minimal and manageable, while others stated that these events had less impact on their daily life compared to other treatment options (chemotherapy and radiation therapy). The most frequently reported AEs were fatigue, dry mouth, and edema. Other events such as constipation, bloating, and occasional abdominal pain were described as minor. No respondent reported experiencing a severe-grade treatment-related AE while on selpercatinib. Respondents indicated that they could return to functionality similar to states before disease diagnosis because they had experienced great improvement in their quality of life. Respondents reported revival of hope and dreams, which allowed them to set meaningful goals for the future.
CanCertainty’s input emphasized the need for equity of access to oral cancer treatments across jurisdictions in Canada. The group recommended addressing the variability in access to treatment in Ontario and the Atlantic provinces if selpercatinib was to receive public funding. One patient described a potential issue related to access to gene testing for RET fusion mutations at diagnosis, while another brought to light issues related to the absence of screening programs for early lung cancer detection across jurisdictions in Canada. Another patient emphasized the need for new targeted therapies that could improve patient-reported outcomes for patients expressing driver mutations such as RET fusion gene mutations.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NSCLC.
Unmet Need
The clinical experts outlined similar treatment goals for patients with advanced or metastatic NSCLC disease. These included improved OS, reduced symptom burden, delayed disease progression, improved quality of life (ability to function independently and decreased caregiver burden), and a decrease in or elimination of hospital admissions and hospital lengths of stay, all of which would result in a reduction in health care utilization. As cited by the experts, patients with RET fusion tend to be younger than the average lung cancer patient, less likely to be retired, and more likely to have children as dependents. The experts also indicated a need for therapies that treat or prevent metastasis because of the high rate of metastasis in this population. The experts noted that approximately 40% of patients with advanced or metastatic disease will develop brain metastasis (the proportion may go as high as 60% in patients with the RET fusion mutation). They pointed out that brain metastasis has a devastating impact on patient survival, quality of life, and ability to function. The expert also emphasized the need for a treatment that will minimize risk of exposure to COVID-19 from in-person health care visits.
Place in Therapy
Both clinical experts indicated that selpercatinib is likely to be administered in the first-line setting and preferably as a single drug. The experts emphasized that platinum plus pemetrexed and pembrolizumab (triplet therapy) was the preferred treatment option in the first line across jurisdictions (except in the province of Prince Edward Island, where pembrolizumab is not funded). Beyond the first line, the experts noted that docetaxel is funded and can be administered depending on whether the patient received triplet therapy at the first line. Patients may also receive single-drug immunotherapies (e.g., pembrolizumab, nivolumab, or atezolizumab) in the second line if they had received platinum and pemetrexed in the first-line setting. However, as noted by the experts, patients with RET fusion are known to show low response rates to immunotherapy in practice, and docetaxel may be administered in place of an immunotherapy in next-line settings.
The clinical experts indicated that selpercatinib will address the underlying disease in patients because of its mechanism of action and its favourable safety profile. They added that selpercatinib should be prioritized in the first-line setting to ensure that all patients with the RET fusion mutation have access. The experts further explained that, in patients who had received prior therapy, selpercatinib may likely be used in the next line after progression, thereby shifting all other treatment options. The experts noted that it would not be appropriate to start patients with other therapies before considering selpercatinib if selpercatinib received public funding because other therapies are less effective, more toxic, and impose a larger burden on the health care system as a whole, and because IV therapies that have to be administered in a chemotherapy suite are more likely to require in-person (or in-hospital) supportive care for adverse effects.
Patient Population
Both experts consulted agreed that treatment should be made available to patients with metastatic RET fusion–positive mutations. The experts emphasized that patients with incurable disease due to RET fusion are likely to respond to selpercatinib. They added that, because patients are most likely to response well in first-line settings, therapy should be prioritized for patients in the first-line but also recommended to all patients as next-line options if they are currently on a different treatment.
However, the experts cautioned that patients with early-stage disease who are eligible for curative-intent therapy should not be offered selpercatinib. Patients are also ineligible to receive selpercatinib if they were previously treated with another selective RET inhibitor, have severely impaired performance status (e.g., an ECOG PS of 4), or have organ dysfunction that precludes safe administration of the drug; this included patients who are unable to take medications orally or absorb medications due to gastrointestinal tract complications.
The experts listed different molecular testing techniques that are available across jurisdictions in Canada to test RET fusion mutations in patients at initial diagnosis. The NGS technique was cited as the most commonly used technique, while NGS with RNA sequencing was considered the best test because of its 100% sensitivity and 99% specificity using the MSK IMPACT testing.
Assessing Response to Treatment
The clinical experts indicated that radiographic assessment methods used in practice (CT or MRI scans) are the same as those used in trials to assess response to treatment. However, the frequency of assessments differs in both settings (trial versus real-world). The standard frequency most likely to be implemented in practice for patients receiving selpercatinib involves conducting assessments every 8 to 12 weeks, or sooner if patients experience new symptoms or show physical findings that suggest progression. The experts added that the frequency of assessments for AEs, and the presence and severity of symptoms is every 3 to 4 weeks for patients receiving oral targeted therapy in clinical practice. Assessments may be carried out at shorter intervals at treatment initiation and subsequently spaced out after therapy has been established and patients are doing well in terms of tolerance and symptom control.
Discontinuing Treatment
Both clinical experts identified similar deciding factors for determining whether to discontinue treatment. These include disease progression (symptomatic disease progression — with the exception of oligoprogression amenable to a local intervention such as radiation or surgery to achieve disease control — or progression in the CNS that is only amenable to brain-targeted therapy such as radiation), the presence of unacceptable or unsafe adverse effects that cannot be managed using appropriate dose reductions and/or supportive care medications, and patient preference.
Prescribing Conditions
The clinical experts indicated that a medical oncologist would be best suited to oversee the administration of selpercatinib.
Clinician Group Input
This section was prepared by CADTH based on the input provided by clinician groups. The full clinician group input is included in the Stakeholder Input section at the end of this report.
Clinician input was submitted by 2 clinician groups: LCC and the Ontario Health (Cancer Care Ontario) DAC.
Ontario Health’s drug advisory committees provide timely evidence-based clinical and health-system guidance on drug-related issues in support of Cancer Care Ontario’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program.
Twelve clinicians associated with LCC and 2 from the DAC provided input.
Unmet Needs
Both clinician groups identified similar treatment goals for patients with advanced or metastatic disease. Improvement in median OS, rapidity of and prolonged improvement in lung cancer–related symptoms measured by median time to response, ORR, progressive disease rate and median PFS, toxicity, prevention or treatment of brain metastases, resource utilization, and impact of COVID-19 on the safety of systemic therapy were emphasized by clinicians. The LCC clinician group input noted that current treatments for patients with RET fusion–positive NSCLC have not improved OS in patients and are not associated with rapid and prolonged improvement in lung cancer symptoms as measured by median time to response, ORR, or progressive disease rate and median PFS. Input from the DAC stated that current treatments fail for all patients within months to a few years.
Clinicians at LCC reported a need for a treatment that improves HRQoL in patients, given that patients with advanced or metastatic disease usually experience greater symptom burden, and that achievement of rapid and prolonged improvement in related symptoms (measured by median time to response, ORR, or progressive disease rate and median PFS) will translate to improved quality of life. The clinicians also pointed out that treatment-related toxicities associated with new treatments are important since they influence adherence to therapy and are directly related to patient quality of life. The prevention or treatment of brain metastasis was also relevant as the group presented evidence that demonstrates almost 40% of patients with advanced or metastatic disease present with brain metastasis during treatment. As noted, brain metastasis influences quality of life and carries a poor prognosis.
Assessing Response to Treatment
The LCC group described documentation of lung cancer–related symptom stabilization or improvement by frequency and severity with or without radiological evidence of tumour shrinkage or radiographic reduction of documented sites of known disease at baseline as clinically meaningful responses to treatment. The group noted that all available systemic therapy for metastatic NSCLC, including chemotherapy, anti–PD-L1 therapeutics, and their combinations have yet to demonstrate superiors outcomes and toxicity profiles in patients with RET fusion metastatic NSCLC.
Patient Population
The most appropriate candidates to be treated with selpercatinib among patients with metastatic NSCLC are those whose tumours or blood have documented RET fusion as validated molecular diagnostics, including but not limited to NGS or fluorescence in situ hybridization (FISH). Clinicians at LCC stated that eligible patients will be identified based on RET fusion testing of tumours or blood by NGS or FISH. The clinician group mentioned that the majority of the provinces already have testing in place or will be implementing NGS testing for fusion mutations at initial diagnosis. At the time their input was supplied, they had identified 7 jurisdictions in Canada that had NGS testing in place (New Brunswick, Ontario, Manitoba, Alberta and Northwest Territories, and British Columbia and Yukon).
Place in Therapy
Both groups noted that adding selpercatinib to the Canadian treatment paradigm will allow the drug to be administered as first-line therapy in newly diagnosed patients with RET fusion metastatic NSCLC. Clinicians in the LCC group mentioned that newly diagnosed patients with an ECOG PS of 0, 1, 2, or 3 could benefit from selpercatinib if the drug is approved for funding, although they expressed uncertainty about the best therapy for second-line treatment and suggested that decisions regarding subsequent therapy should consider docetaxel and anti–PD-L1 therapy for those who have not received such drugs in prior lines of therapy. They added that, in patients previously treated for RET fusion metastatic NSCLC, selpercatinib could be administered based on evidence drawn from data updates from the LIBRETTO-001 trial.
Discontinuing Treatment
Treatment may be discontinued in the following situations: multiple toxicities despite multiple dose reductions, patient preference, concurrent medical condition(s) that could jeopardize the safety of selpercatinib, and symptomatic disease progression (with the exceptions previously identified).
Drug Program Input
The drug plans provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
The drug plans emphasized the different treatment strategies in place for patients with NSCLC. In patients with no test results for RET fusion–positive mutations, funded treatments may likely include pembrolizumab as a single drug (if PD-L1 levels are 50% or higher), platinum plus pembrolizumab and pemetrexed, or a platinum-based therapy based on a histology in patients who are treatment naive. In patients previously treated with systemic therapy, potential treatment options will include immune checkpoint inhibitors if patient with no prior experience with an PD-L1 inhibitor (pembrolizumab, nivolumab, or atezolizumab depending on PD-L1 status), or chemotherapy if the patient has experience with a PD-L1 inhibitor (docetaxel or pemetrexed). They also noted that patients being treated with selpercatinib may require different dosing schedules and dose intensity, as outlined in the Canadian product monograph.
According to the monograph, the recommended dose, to be administered approximately every 12 hours, is based on body weight. Patients weighing less than 50 kg should receive 120 mg twice a day and those weighing 50 kg or more should receive 160 mg twice a day. Patients with severe hepatic impairment (as indicated by a Child-Pugh score in the C range) should receive a reduced dose of 80 mg twice a day.
The drug plans also noted that if selpercatinib is approved for public funding, it may modify the treatment paradigm in practice and change treatments reimbursed for subsequent lines. The drug plans pointed out that access to companion testing is needed to identify eligible patients.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Additional implementation questions from the drug programs | Clinical expert response |
|---|---|
Relevant comparators | |
The trial did not have a comparator. If patients are not tested for RET fusion status, the funded treatments for patients who are treatment naive would be pembrolizumab single drug if PD-L1 ≥ 50%; platinum plus pembrolizumab and pemetrexed; or platinum-based chemotherapy based upon histology. For previously treated patients, the funded treatment options would be an immune checkpoint inhibitor in the absence of a prior PD-L1 inhibitor (pembrolizumab, nivolumab, or atezolizumab depending on the PD-L1 status), or chemotherapy if a PD-L1 inhibitor (docetaxel or pemetrexed) had been used. | No response. For pERC consideration. |
Considerations for initiation of therapy | |
The trial included several analysis sets, including patients who received 1 or more lines of prior platinum-based chemotherapy and patients who received prior systemic therapy other than platinum-based chemotherapy. Should eligible patients be required to receive a certain class of systemic therapy before selpercatinib? Should there be a limit on the number of lines of therapy a patient can receive before selpercatinib? | No to both questions. |
Considerations for continuation or renewal of therapy | |
In the trial, patients with documented disease progression could continue to receive selpercatinib if the patient was thought to still benefit from treatment. Can pERC clarify the discontinuation criteria for selpercatinib? | Discontinuation criteria include:
|
Considerations for prescribing of therapy | |
The recommended dose is approximately every 12 hours and is based on body weight:
Patients with severe hepatic impairment (Child-Pugh C) should receive a reduced dose of 80 mg orally twice daily. | No response. For pERC consideration. |
Generalizability | |
In the study, all patients in the treatment-naive population had an ECOG PS of 0 to 1. Only 2% of patients in the previously treated population had an ECOG of 2. Can all patients with an ECOG PS of 0 to 2 be considered eligible, whether treatment-naive or not? Can patients with an ECOG PS > 2 be considered eligible? |
|
Funding algorithm (oncology only) | |
This drug may change the place in therapy of drugs reimbursed in subsequent lines | No response. For pERC consideration. |
Care provision issues | |
RET testing needs to be in place to identify eligible patients. | No response. For pERC consideration. |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee; RET = rearranged during transfection.
Clinical Evidence
The clinical evidence included in the review of selpercatinib is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of selpercatinib capsules, 40 mg and 80 mg, for oral administration:
as monotherapy for the first-line treatment of adult patients with metastatic RET fusion–positive NSCLC
as monotherapy for the treatment of adult patients with metastatic RET fusion–positive NSCLC who have received prior systemic therapy.
Methods
Studies selected for inclusion in the systematic review will include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population |
Subgroups
|
Intervention | Selpercatinib capsules, 40 mg and 80 mg, orally administered, dosed: < 50 kg: 120 mg twice daily ≥ 50 kg: 160 mg twice daily |
Comparators | First line
Second line
|
Outcomes | Efficacy outcomes:
Harm outcomes:
|
(continued) | Notable harms:
|
Study design | Published and unpublished phase II, III and IV randomized controlled trials |
CNS = central nervous system; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
aComparators identified by the drug programs.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.21
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were selpercatinib (Retevmo/Retsevmo) and synonyms. Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register. No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides detailed search strategies. The initial search was completed on November 4, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on March 9, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature resource.22 Included in this search were the websites of regulatory agencies (FDA and EMA). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for indirect comparisons dealing with selpercatinib for NSCLC was run in MEDLINE All (1946–) on November 3, 2021. No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results.
Findings From the Literature
One study was identified from the literature for inclusion in the systematic review (Figure 1). The study is summarized in Table 6.
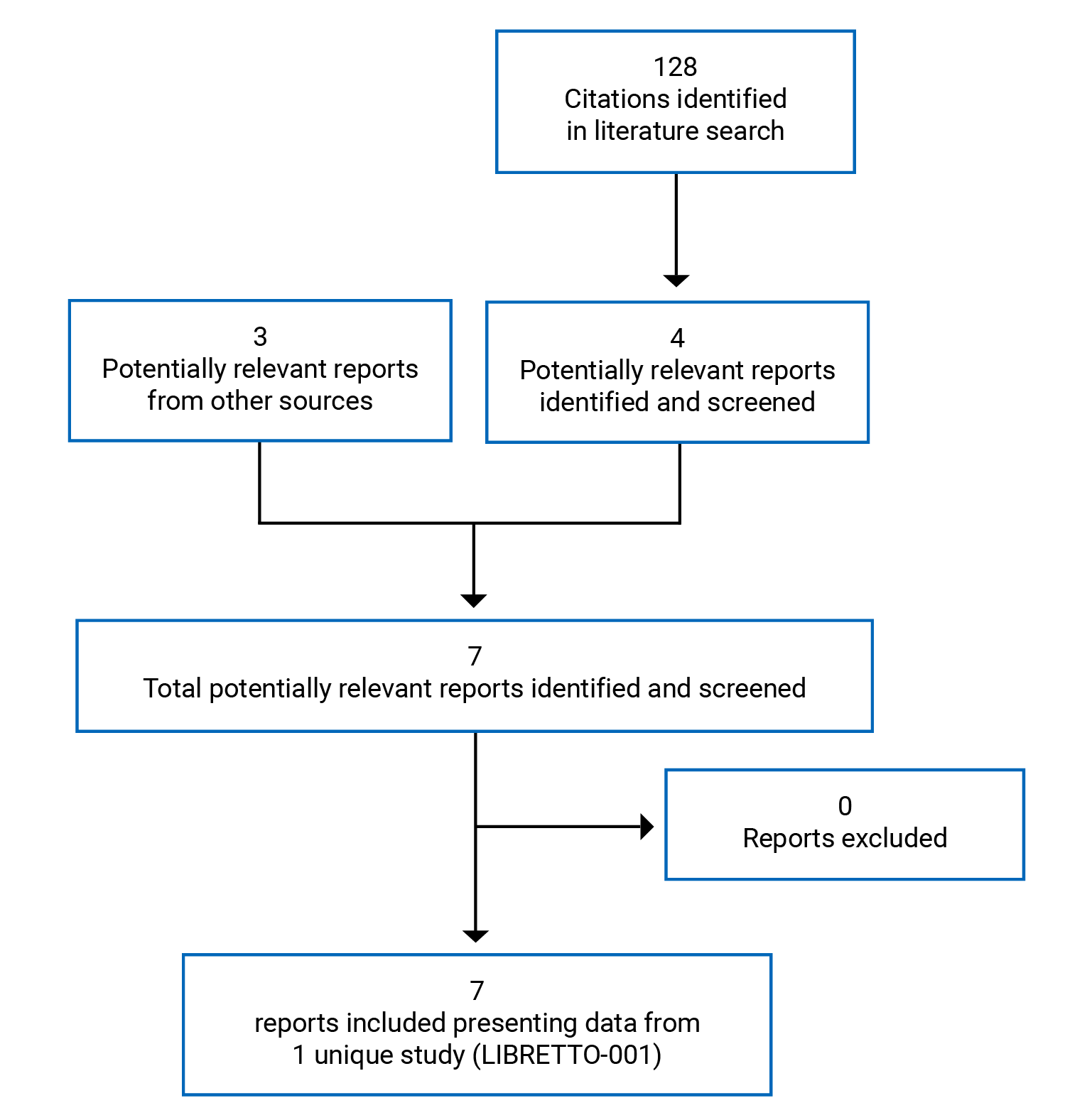
Table 6: Details of Included Studies
Item | Study detail |
|---|---|
Study design | Ongoing multi-centre, open-label, multi-cohort, phase I and II study |
Locations | Australia, Canada, Denmark, Germany, Japan, Hong Kong, Israel, Singapore, France, Italy, Spain, South Korea, Switzerland, Taiwan, and the US |
Patient enrolment dates | Trial start date: May 2017 Patient enrolment stop date for data cut-off: June 17, 2019 Data cut-off date for second interim analysis: December 16, 2019 Data cut-off third interim analysis: March 30, 2020 |
Number of patients | March 30, 2020, data cut-off:
December 16, 2019, data cut-off:
|
Inclusion criteria |
|
Exclusion criteria |
|
(continued) |
|
Intervention | Phase I:
Phase II:
|
Comparator(s) | None |
Phase | |
Phase I | Dose escalation |
Phase II | Dose expansion |
Follow-up | Ongoing |
Primary end point | Phase I: Identification of the maximum tolerable dose or recommended phase II dose of selpercatinib Phase II: ORR based on RECIST 1.1 or RANO |
Secondary and exploratory end points | Phase I:
Phase II: Primary outcome: ORR (RECIST 1.1 or RANO) Secondary outcomes:
|
(continued) |
|
Publications | Drilon et al. (2020)23 Subbiah et al. (2021)24 Solomon et al. (2021)25 Minchom et al. (2021)7 |
CNS = central nervous system; ECG = electrocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; LPS = Lansky Performance Status; MTD = maximum tolerable dose; NSCLC = non–small cell lung cancer; ORR = objective response rate; RANO = Response Assessment in Neuro-Oncology; RECIST = Response Evaluation Criteria in Solid Tumors Version 1.1; RET = rearranged during transfection.
Note: Three additional reports were included.6,9,10
Source: Clinical Study Report for the LIBRETTO-001 trial.19
Description of Studies
The LIBRETTO-001 trial is an ongoing phase I and II, multi-centre, multi-cohort, open-label study consisting of a dose-escalation phase and a dose-expansion phase.
The study was initiated in May of 2017 and has more than 84 participating centres, including centres in Canada and the US.
The median age of all patients enrolled in the LIBRETTO-001 trial as of December 16, 2019, who had received at least 1 dose of selpercatinib (safety analysis set, n = 702) was 59 years. More men (52.4%) than women (47.6%) participated in the study. Most patients recruited were White (69%), followed by patients of Asian descent (21.9%), patients who are Black (3.4%), and others (5.6%).19
Trial Design
Phase I: Dose Escalation and MTD Determination
The primary objective of phase I of the study was to use dose escalation to determine the MTD and RP2D of selpercatinib.
Secondary objectives for phase I included evaluation of the safety of selpercatinib, characterization of the pharmacokinetic (PK) properties, and assessment of the antitumour activity of selpercatinib (i.e., determining the ORR).
A “3 + 3” dose-escalation design with 3 or 6 patients enrolled in each dose cohort was used to assess the MTD and RP2D.
Phase II: Dose Expansion
The phase II portion of LIBRETTO-001 is ongoing and includes patients from phase I, enrolled into 1 of 5 pre-specified cohorts based on tumour type (Figure 2). Patients who were recruited into cohorts 1 through 4 required confirmed evidence of an RET gene alteration in a tumour before enrolment.
Cohort 1: RET fusion–positive solid tumour progressed on or intolerant to 1 or more prior standard first-line therapy
Cohort 2: RET fusion–positive solid tumour without prior standard first-line therapy
Cohort 3: RET-mutant MTC progressed on or intolerant to 1 or more prior standard first-line cabozantinib and/or vandetanib
Cohort 4: RET-mutant MTC without prior standard first-line cabozantinib or vandetanib or other kinase inhibitors(s) with anti-RET activity
A fifth cohort, cohort 5, included:
cohorts 1 through 4 without measurable disease
MTC not meeting the requirements for cohorts 3 or 4
MTC syndrome spectrum cancers (e.g., MTC or pheochromocytoma), or poorly differentiated thyroid cancers with other RET alteration/activation could be allowed with
prior sponsor approval
cfDNA positive for a RET gene alteration not known to be present in a tumour sample.
The primary objective of the phase II study was to evaluate the antitumour activity of selpercatinib in patients recruited into each of the 5 cohorts. Secondary objectives included evaluating outcomes related to DOR, CNS ORR, CNS DOR, time to any and best response, clinical benefit rate, PFS, OS, safety, and PK properties.19
Figure 2: Study Design of the LIBRETTO-001 Trial
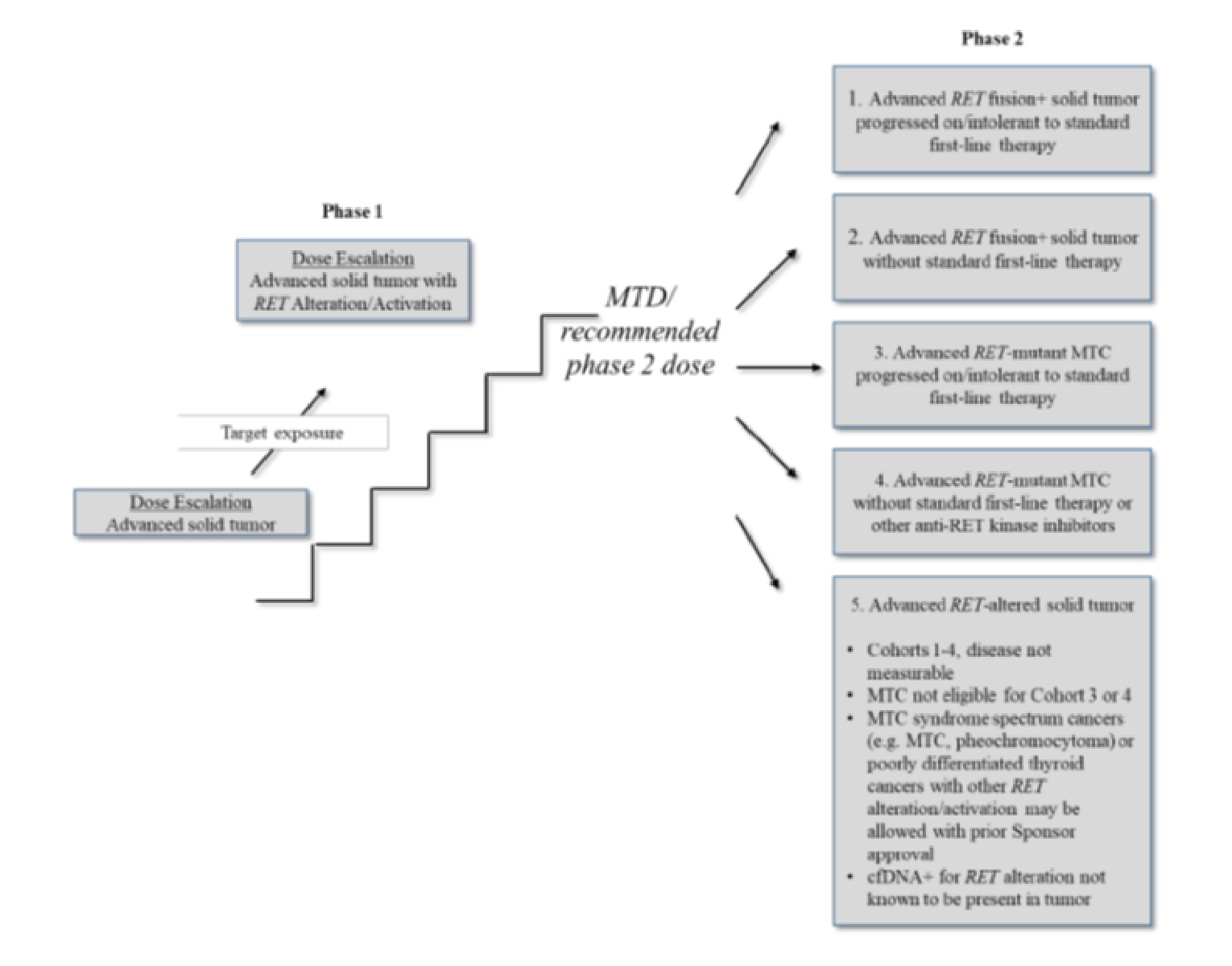
MTC = medullary thyroid cancer; MTD = maximum tolerable dose; RET = rearranged during transfection.
Source: Clinical Study Report (data cut-off of December 16, 2019).19
This CADTH review focuses on outcomes observed in patients with NSCLC and a confirmed RET fusion gene mutation enrolled into cohort 1 and 2 at phase II of the LIBRETTO-001 study. These patients were further subgrouped into 3 datasets to form the primary efficacy population for patients with NSCLC based on clinically meaningful distinctions observed during the trial. The primary efficacy population was initially negotiated by the sponsor and regulatory agencies (FDA and EMA) before the first data cut-off date of June 17, 2019,5 and supported the regulatory submission for new drugs at Health Canada.
Populations
Inclusion and Exclusion Criteria
Patients who were 18 years of age and older (12 years and older at some sites) with a locally advanced or metastatic solid tumour with progression or who were intolerant to standard therapy were included in phase I of the trial (Table 6). Patients were also included in cases where, in the investigator’s opinion, no standard therapy existed, the patients were not candidates for therapy or would be unlikely to tolerate or derive significant clinical benefit from standard therapy, or who declined standard therapy. The initial protocol for the phase I study did not focus on identifying specific genetic targets. However, patients with an RET alteration in a tumour (not just specific to detection in blood) confirmed by PCR or NGS testing were identified during phase I based on pre-clinical data of the inhibitory action of selpercatinib, and RET gene alteration was required for continued dose escalation once pre-specified PK criteria were met. Evidence of an RET gene alteration in a tumour was required for entry into phase II of the trial. Patients with an ECOG PS score of 0, 1, or 2 (age ≥ 16 years) or a Lansky Performance Status score of 40% or higher (age < 16 years) with no sudden deterioration 2 weeks before the first dose of study treatment were also enrolled.19
At the initial stages of the phase I study, patient enrolment did not require a confirmed diagnosis of an RET gene fusion or mutation in the solid tumour. New changes were made to the study protocol that incorporated the need for a confirmed RET fusion at screening for phase I and a confirmed RET fusion status before the patient was subsequently enrolled into phase II. These changes were proposed and implemented after the evaluation of clinical data for the first patients enrolled at phase I, in which selpercatinib exhibited favourable inhibitory properties in patients harbouring the RET mutation. Mandatory screening and confirmation of the RET mutation was implemented before enrolment in phase II.
Patients were excluded from phase II cohorts 1 to 4 if they had another validated oncogenic driver that could result in treatment resistance to selpercatinib. For both phases, those who had previously received RET inhibitor therapy, including investigational products, were ineligible. Patients were also ineligible if they had a clinically significant active cardiovascular disease or history of myocardial infarction within 6 months before the planned start of selpercatinib or prolongation of the QT interval corrected for heart rate.19
Baseline Characteristics in the RET Fusion–Positive NSCLC Population
At the data cut-off date of December 16, 2019, a total of 253 patients with NSCLC who met the eligibility criteria at phase I and II and had received at least 1 dose of selpercatinib at interim 1 (cut-off date of June 17, 2019), with at least 6 months of follow-up data, were included in the efficacy analysis. The NSCLC population consists of 3 subgroups (PAS, IAS, and SAS), which reflect the specified populations outlined in the reimbursement request. Table 7 presents the baseline characteristics observed in the NSCLC population at the December 16, 2019, data cut-off.5
The median age observed in the overall NSCLC population was 61 years (range = 23 to 83). More females were enrolled than males, and the majority of patients (51%) were White or of Asian descent (38%). The median body weight was 64.0 kg (range = 38.9 to 148). Most patients (61%) had a baseline ECOG PS score of 0 or 1, and 70% of patients had never smoked. Most patients had stage IV disease (67.2%) and 98% of patients had a history of metastasis. Overall, patients in the prior systemic therapy group had received platinum chemotherapy (100%) including other therapies (anti–PD-1 and anti–PD-L1 = 54.3%; multikinase therapy = 36.4%) in the first and second lines, and the median number of therapies observed was 3.5
Table 7: Summary of Baseline Characteristics for the RET Fusion–Positive NSCLC Population in the LIBRETTTO-001 Trial (December 16, 2019, Data Cut-Off Date)
Characteristic | PAS (subset of IAS) N = 105 | IAS Prior platinum chemotherapy N = 184 | SAS1 Treatment-naive N = 39 | SAS2 Prior other systemic therapy N = 16 | SAS3 Non-measurable disease N = 14 | Total N = 253 |
|---|---|---|---|---|---|---|
Age, years | ||||||
Median (range) | 61.0 (23 to 81) | 62.0 (23 to 81) | 61.0 (23 to 86) | 58.5 (47 to 71) | 60.0 (44 to 80) | 61.0 (23 to 86) |
Sex, n (%) | ||||||
Male | 43 (41.0) | 79 (42.9) | 17 (43.6) | 6 (37.5) | 6 (42.9) | 108 (42.7) |
Female | 62 (59.0) | 105 (57.1) | 22 (56.4) | 10 (62.5) | 8 (57.1) | 145 (57.3) |
Race, n (%) | ||||||
White | 55 (52.4) | 86 (46.7) | 28 (71.8) | 11 (68.8) | 5 (35.7) | 130 (51.4) |
Asian | 40 (38.1) | 82 (44.6) | 7 (17.9) | 5 (31.3) | 9 (64.3) | 103 (40.7) |
Black or African-American | 5 (4.8) | 9 (4.9) | 3 (7.7) | 0 | 0 | 12 (4.7) |
American Indian or Alaska Native | 0 | 1 (0.5) | 0 | 0 | 0 | 1 (0.4) |
Native Hawaiian or other Pacific Islander | 0 | 0 | 0 | 0 | 0 | 0 |
Other/missing | 5 (4.8) | 6 (3.3) | 1 (2.6) | 0 | 0 | 7 (2.8) |
Body weight | ||||||
n | 104 | 183 | 39 | 16 | 14 | 252 |
Median (range) | 64 (42.2 to 148) | 64 (38.9 to 148) | 72 (45.6 to 130.5) | 57.6 (48.6 to 109.5) | 62.1 (46.9 to 106.8) | 64 (38.9 to 148) |
ECOG PS, n (%) | ||||||
0 | 31 (29.5) | 66 (35.9) | 18 (46.2) | 3 (18.8) | 6 (42.9) | 93 (36.8) |
1 | 72 (68.6) | 114 (62.0) | 21 (53.8) | 12 (75.0) | 8 (57.1) | 155 (61.3) |
2 | 2 (1.9) | 4 (2.2) | 0 | 1 (6.3) | 0 | 5 (2.0) |
RET fusion type, n (%) | ||||||
KIF5B | 59 (56.2) | 113 (61.4) | 26 (66.7) | 13 (81.3) | 10 (71.4) | 162 (64.0) |
CCDC6 | 24 (22.9) | 42 (22.8) | 8 (20.5) | 1 (6.3) | 2 (14.3) | 53 (20.9) |
NCOA4 | 2 (1.9) | 4 (2.2) | 0 | 1 (6.3) | 1 (7.1) | 6 (2.4) |
Other | 8 (7.6) | 11 (6.0) | 1 (2.6) | 1 (6.3) | 0 | 13 (5.1) |
Unknown | 12 (11.4) | 14 (7.6) | 4 (10.3) | 0 | 1 (7.1) | 19 (7.5) |
Smoking history, n (%) | ||||||
Never smoked | 75 (71.4) | 125 (67.9) | 29 (74.4) | 11 (68.8) | 11 (78.6) | 176 (69.6) |
Former smoker | 29 (27.6) | 55 (29.9) | 9 (23.1) | 5 (31.3) | 3 (21.4) | 72 (28.5) |
Current smoker | 1 (1.0) | 4 (2.2) | 1 (2.6) | 0 | 0 | 5 (2.0) |
Missing | 0 | 0 | 0 | 0 | 0 | 0 |
Stage at diagnosis, n (%) | ||||||
I, IA, IB | 1 (1.0) | 2(1.1) | 0 | 1(6.3) | 1 (7.1) | 4 (1.6) |
II, IIA, IIB | 0 | 2 (1.1) | 1 (2.6) | 1 (6.3) | 2 (14.2) | 6 (2.4) |
IIIA, IIIB | 3 (2.9) | 10 (5.4) | 0 | 0 | 0 | 10 (4.0) |
IIIC | 0 | 0 | 1 (2.6) | 0 | 0 | 1 (0.4) |
IV | 84 (80.0) | 121 (65.8) | 31 (79.5) | 10 (62.5) | 8 (57.1) | 170 (67.2) |
IVA | 9 (8.6) | 18 (9.8) | 2 (5.1) | 1 (6.3) | 1 (7.1) | 22 (8.7) |
IVB | 4 (3.8) | 18 (9.8) | 2 (5.1) | 1 (6.3) | 2 (14.3) | 23 (9.1) |
IVC | 4 (3.8) | 13 (7.1) | 1 (2.6) | 2 (12.5) | 0 | 16 (6.3) |
Missing | 0 | 0 | 1 (2.6) | 0 | 0 | 1 (0.4) |
Time from diagnosis, months | ||||||
Median (range) | 30.10 (1.5 to 142.3) | 24.20 (1.5 to 164.8) | 2.00 (0.7 to 8.1) | 7.15 (2.0 to 112.5) | 19.50 (7.4 to 223.7) | 18.40 (0.7 to 223.7) |
History of metastatic disease, n (%) | ||||||
Yes | 103 (98.1) | 179 (97.3) | 39 (100) | 16 (100) | 14 (100) | 248 (98.0) |
No | 2 (1.9) | 5 (2.7) | 0 | 0 | 0 | 5 (2.0) |
At least 1 measurable lesion by investigator, n (%) | ||||||
Yes | 104 (99.0) | 183 (99.5) | 39 (100) | 16 (100) | 0 | 238 (94.1) |
No | 1 (1.0) | 1 (0.5) | 0 | 0 | 14 (100) | 15 (5.9) |
CNS metastases at baseline by investigator, n (%) | ||||||
Yes | 38 (36.2) | 61 (33.2) | 7 (17.9) | 10 (62.5) | 2 (14.3) | 80 (31.6) |
No | 67 (63.8) | 123 (66.8) | 32 (82.1) | 6 (37.5) | 12 (85.7) | 173 (68.4) |
Type of prior systemic therapy, n (%) | ||||||
Platinum chemotherapy | 105 (100) | 184 (100) | 0 | 0 | 13 (92.9) | 197 (77.9) |
Anti–PD-1/PDL1 therapy | 58 (55.2) | 100 (54.3) | 0 | 10 (62.5) | 6 (42.9) | 116 (45.8) |
MKI | 50 (47.6) | 67 (36.4) | 0 | 6 (37.5) | 3 (21.4) | 76 (30.0) |
Prior systemic regimens, n (%) | ||||||
0 | 0 | 0 | 39 (100) | 0 | 0 | 39 (15.4) |
1 to 2 | 46 (43.8) | 100 (54.3) | 0 | 14 (87.5) | 9 (64.3) | 123 (48.6) |
≥ 3 | 59 (56.2) | 84 (45.7) | 0 | 2 (12.5) | 5 (35.7) | 91 (36.0) |
Best response to last systemic treatment, n (%) | ||||||
Complete response | 0 | 1 (0.5) | 0 | 0 | 0 | 1 (0.4) |
Partial response | 15 (14.3) | 24 (13.0) | 0 | 0 | 0 | 24 (9.5) |
Stable disease | 37 (35.2) | 62 (33.7) | 0 | 2 (12.5) | 5 (35.7) | 69 (27.3) |
Progression | 32 (30.5) | 55 (29.9) | 0 | 10 (62.5) | 5 (35.7) | 70 (27.7) |
Not evaluated | 20 (19.0) | 41 (22.3 | 0 | 4 (25.0) | 4 (28.6) | 49 (19.4) |
Unknown | 1 (1.0) | 1 (0.5) | 39 (100) | 0 | 0 | 40 (15.8) |
Prior radiotherapy, n (%) | ||||||
Yes | 62 (59.0) | 103 (56.0) | 11 (28.2) | 9 (56.3) | 9 (64.3) | 132 (52.2) |
No | 43 (41.0) | 81 (44.0) | 28 (71.8) | 7 (43.8) | 5 (35.7) | 121 (47.8) |
Prior cancer-related surgery, n (%) | ||||||
Yes | 52 (49.5) | 87 (47.3) | 14 (35.9) | 9 (56.3) | 7 (50.0) | 117 (46.2) |
No | 53 (50.5) | 97 (52.7) | 25 (64.1) | 7 (43.8) | 7 (50.0) | 136 (53.8) |
Time on study,a months | ||||||
Median (range) | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IAS = integrated analysis set; MKI = multikinase inhibitor; NR = not reported; NSCLC = non–small cell lung cancer; PAS = primary analysis set; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1; RET = rearranged during transfection; SAS = supplemental analysis set.
Note: For the PAS, a subset analysis included the FDA breakthrough therapy designation population (n = 58) who received prior platinum-based chemotherapy and an anti–PD-1 or anti–PD-L1 antibody. The IAS included all patients previously treated with platinum-based chemotherapy. SAS1 comprised patients who were treatment naive . SAS2 included patients treated with other systemic therapies that are not platinum-based. SAS3 consisted of patients without measurable disease, according to Response Evaluation Criteria in Solid Tumors Version 1.1. For RET fusion–positive NSCLC, the PAS includes the first 105 patients of the IAS. The total column is the sum of the IAS, SAS1, SAS2, and SAS3.
aTime on study (months) = (study exit date − first dose date + 1)/30.4375 for patients who exited the study on or before the data cut-off date; time on study (months) = (data cut-off date − first dose date + 1)/30.4375 for patients who were still in the treatment phase as of the data cut-off date; time on study (months) = (last visit date − first dose date + 1)/30.4375 for patients who were in the long term follow-up as of the data cut-off date of December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Interventions
Treatment
Patients received selpercatinib as an oral capsule or suspension (introduced within study protocol version 5) once daily or twice daily, depending on the cohort assignment. The dosing regimen in the trial followed a fixed-milligram format and had a consistent timing in administration each day (approximately 12-hour intervals for the twice daily dosing schedule). A minimum period of 6 hours was required between administration of consecutive doses. Patients were required to skip doses that would have been administered more than 6 hours late and were expected to log them as missed in the patient diaries. Earlier versions of the study protocol (until version 7.0) discouraged patients from consuming any food at least 2 hours before and 1 hour after the administration of selpercatinib. However, the protocol was later amended to allow for the administration of selpercatinib with or without food based on new evidence from a food-effect study in healthy volunteers that showed minimal effects of food on the bioavailability of selpercatinib.19
Treatment Assignation
At phase I, patients received oral selpercatinib through a pre-specified dose-escalation plan, starting with 20 mg daily and progressing to 240 mg twice daily or until the safety review committee and sponsor determined that a suitable dose was achieved based on safety, PK exposure, and clinical activity. A dosage of 160 mg twice daily was selected at the end of phase I by the safety review committee as the RP2D.
All patients at phase II received selpercatinib 160 mg twice daily and continued treatment until disease progression, unacceptable toxicity, or other reasons for treatment discontinuation.19
Dose modifications, including reductions or schedule modifications, were approved at the investigator’s discretion for AEs in individual patients. Dose reductions were to be considered a dose-limiting toxicity if the dose was reduced during cycle 1 for a toxicity that could not be reasonably attributed to the patient’s underlying disease, other medical condition, or concomitant medications. Otherwise, no dose adjustments were to be made during the conduct of the trial. Re-escalation to a higher dose after a previous dose reduction was allowed; however, dose escalations above 160 mg twice daily were not authorized.19
Concomitant Medications
Concomitant medications were allowed only if patients had declared them at the screening phase and if they were considered acceptable before study enrolment. The most frequently reported therapeutic classes of concomitant medications were thyroid hormones (57.1%), natural opium alkaloids (37.3%), and anilides (35.2%). Standard supportive medications (e.g., hematopoietic growth factors [not for prophylaxis in cycle 1] and anti-emetics) were permitted.19
The sponsor also approved local treatment (palliative radiation therapy or surgery for bone metastases) while patients received selpercatinib but recommended holding selpercatinib for approximately 5 half-lives (approximately 2 to 3 days) before and after radiation therapy or surgery. Prohibited concomitant medications included systemic anticancer drugs, hematopoietic growth factors for prophylaxis in cycle 1, therapeutic monoclonal antibodies, drugs with immunosuppressant properties, or medications known to be strong inhibitors or inducers of CYP3A4 were prohibited as concomitant therapies. The use of proton pump inhibitors was also prohibited.19
Treatment Adherence
Treatment adherence was evaluated using patient diaries, visits to clinics, and medication counts from returned medication bottles. Administration of concomitant medications was also documented in diaries.19
Censoring
Patients could withdraw their consent to participate in the study whenever they regarded it best. Investigators received the sponsor’s approval to censor patients who showed disease progression from the RECIST 1.1 or RANO evaluations of tumours (except in cases of a demonstrated clinical benefit following drug use), demonstrated unaccepted toxicity, experienced intercurrent illness compromising their ability to fulfill protocol requirements, became pregnant, needed an alternative treatment (e.g., local radiation or surgery for disease that does not meet the definition of disease progression) unless treatment was temporary, showed significant protocol noncompliance, or withdrew consent, and in the event of patient loss to follow-up, death, study termination by the sponsor.19
Outcomes Investigated
A list of the efficacy end points assessed in the LIBRETTO-001 trial and included in this review is provided in Table 8.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | LIBRETTO-001 end point | Definition |
|---|---|---|
Overall survival | Secondary | The number of months elapsed between the date of the first dose of selpercatinib and the date of death (whatever the cause); patients who were alive or lost to follow-up as of the data cut-off date were right-censored |
Progression-free survival | Secondary | The number of months elapsed between the date of the first dose of selpercatinib and the earliest date of documented disease progression or death (whatever the cause) |
HRQoL using the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30 | Exploratory | A 36-item, generic, self-reported questionnaire with a recall period of 28 days consisting of 8 subscales and 2 component summary scores for physical and mental health; subscale and summary scores range from 0 to 100, with a higher score indicating better HRQoL
|
Objective response rate | Primary | The proportion of patients with best overall response of confirmed complete response or confirmed partial response based on RECIST 1.1 |
Duration of response | Secondary | The number of months from the start date of complete or partial response (whichever was observed first) and subsequently confirmed, to the first date that recurrent or progressive disease was objectively documented |
HRQoL = health-related quality of life; RECIST = Response Evaluation Criteria in Solid Tumors Version 1.1.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Efficacy Measurement for Primary and Secondary Outcomes
Tumour Measurements and Assessments of Disease Response Using RECIST 1.1
Given the open-label and non-randomized nature of the LIBRETTO-001 trial, tumour evaluation for the primary end point using the RECIST 1.1 guidelines was planned as a third-party blinded central review to improve the internal validity of the study. However, at the interim analysis, tumour size was evaluated by both the investigator and an IRC.
Tumours were assessed at screening, within 28 days of cycle 1 at day 1, by CT or MRI of the neck, chest, or abdomen and pelvis, as indicated. Head and neck CT scans were not required for malignancies other than those involving the head and neck. Post-baseline assessments were conducted every 8 weeks (± 1 week) from cycle 3 through cycle 13, and 12 weeks onward until an identifiable disease progression, withdrawal of patient consent, initiation of a new cancer therapy, or if any discontinuation criteria were met. The protocol also allowed investigators to conduct an initial tumour evaluation 4 weeks after treatment initiation and a confirmatory evaluation 4 weeks after the tumour evaluation showed a CR or PR by RECIST 1.1 (or RANO) if consistent with the local regulatory requirements. Patients with an identified RET fusion–positive gene mutation in a tumour or a history of CNS metastases, or those with a clinical indication were required to undergo brain imaging at baseline at phase II. Post-baseline CNS imaging was also completed for patients presenting with baseline metastasis. Assessments were performed at the end-of-treatment visit if they had not been performed within the previous 2 cycles. Subsequent assessments followed the same radiographic methods as used during screening. During screening, tumour lesions were categorized as measurable versus non-measurable and target versus non-target.
Measurable Versus Non-Measurable
Measurable: lesions that could accurately be measured in at least 1 dimension, the longest diameter in the plane of measurement to be recorded as:
tumour lesions: 10 mm or larger by CT scan
malignant lymph nodes: to be considered pathologically enlarged and measurable, the node must be 15 mm or greater on the short axis when assessed by CT scan. At baseline and in follow-up, only the short axis was measured and followed. Nodes that have a short axis shorter than 10 mm are considered nonpathological and should not be recorded or followed.
Non-measurable: All other lesions, including small lesions (longest diameter < 10 mm or pathological lymph nodes with ≥ 10 to < 15 mm short axis), and truly non-measurable lesions.
Target Versus Non-Target
Target: all measurable lesions up to a maximum of 2 lesions per organ and 5 lesions in total, representative of all involved organs, are to be identified as target lesions and measured and recorded at screening. Target lesions are to be selected based on their size (i.e., those with the longest diameter) and suitability for accurate repeated measurement. Lymph nodes may be selected as target lesions; they must be defined as measurable, and only the short axis of the node will contribute to the baseline sum. All other pathologic nodes with a short axis 10 mm or longer but shorter than 15 mm should be considered non-target lesions.
Non-target: all other lesions not classified as target lesions (or sites of disease) are to be identified as non-target lesions and are to be recorded in the electronic case report form. Measurement of non-target lesions is not required.
The sum of the diameters (the longest for non-nodal lesions and the short axis for nodal lesions) for all target lesions were calculated. Disease response in target and non-target lesions were assessed by the investigator using RECIST 1.1, according to the categories and criteria.
Response Assessment in Neuro-Oncology Criteria for Primary CNS Malignancies
The RANO criteria was used to assess lower-grade primary CNS malignancies.
A measurable lesion was evaluated by contrast-enhancing MRI using the following definition:
it has clearly defined margins
it is visible on 2 or more axial slices, preferably less than 5 mm thick
it is at least 10 mm in size if slice thickness is less than 5 mm (or twice the slice thickness if greater than 5 mm thick)
it does not measure a cystic cavity
non-measurable lesions are those that do not fit the criteria above, and specifically lesions that are cystic, necrotic, or include a surgical cavity should not be considered measurable
measurements were calculated by summing the products of perpendicular diameters of all measurable enhancing lesions.
Follow-up
At phase II, a short-term follow-up assessment was designed to occur 4 weeks (at least 28 days [plus 7 days room allowed for the follow-up assessment]) after the last dose of the study drug. Patients were allowed to continue selpercatinib at the discretion of the investigator in cases of a documented progression of disease. Long-term follow-up assessments were scheduled every 3 months and could be conducted by phone. Long-term could include subsequent anticancer therapy and survival status. Assessments included periodic radiologic evaluation and ongoing safety assessments.19
Statistical Analysis
The primary efficacy dataset to support regulatory submission was initially negotiated by the sponsor and regulatory agencies (FDA and EMA) before the first data cut-off date of June 17, 2019. At the December 16, 2019, and the March 30, 2020, data cut-offs, the datasets supporting the evidence for the funding request differed from the population cohorts defined at phase I and II.
As a rationale for modifying the population sets, the sponsors noted that the analysis sets defined in the LIBRETTO-001 protocol and statistical analysis plan for the Clinical Study Report were designed for a study conducted in all tumour types. Subsequently, analysis sets were defined for each of the 3 predominant histologies of patient who had enrolled in the LIBRETTO-001 trial to understand efficacy by tumour type, rather than taking a tumour-agnostic approach, and to support the initial submissions to the FDA and EMA.
Various datasets were created to facilitate a regulatory review of the LIBRETTO-001 data in support of the proposed indications for marketing authorization. Information was maximized through consolidation of data from both the phase I and phase II parts of the LIBRETTO-001 trial, and groupings were based on clinically meaningful distinctions, resulting in similarity of patients within a group and facilitating interpretation of results.
The inclusion criteria and statistical considerations for the primary datasets supporting the proposed indications were agreed to by the EMA (July 09, 2019) and FDA (MTC: December 19, 2018; NSCLC: January 16, 2019).5,9
Analysis Population
The second interim analysis on December 16, 2019, supported the FDA and Health Canada submissions. Patients included in this analysis had received at least 1 dose of selpercatinib at or before the first interim cut-off date of June 17, 2019. Data analyzed at a third interim data cut-off date of March 30, 2020, were also part of the submission request and this interim analysis was pre-planned to support the regulatory submission in Japan. Results obtained at the second and third cut-offs are presented in this report. The following datasets were defined for the efficacy and safety analysis of selpercatinib in the NSCLC population.5,19
Efficacy Analysis Sets
At the December 16, 2019, and March 30, 2020, data cut-offs, the following subgroups were included in the analysis:
The PAS (n = 105) is composed of the first consecutively enrolled patients previously treated with platinum-based chemotherapy (a subset of the IAS). This subset analysis includes the FDA breakthrough therapy designation population (n = 58) who received prior platinum-based chemotherapy and an anti–PD-1 and anti–PD-L1 antibody.
The IAS (n = 184 and n = 218 for December 16, 2019, and March 30, 2020, data cut-off, respectively) is composed of all patients treated with platinum-based chemotherapy.
The SASs include 3 subsets:
SAS1 (n = 39 and n = 48 for December 16, 2019, and March 30, 2020, data cut-off, respectively) is composed of patients who are treatment naive.
SAS2 (n = 16 and n = 18 for December 16, 2019, and March 30, 2020, data cut-off, respectively) is composed of patients treated with other systemic therapies that are not platinum-based.
SAS3 (n = 14 at the December 16, 2019, data cut-off, and n = 18 for at the March 30, 2020, data cut-off) consists of patients without measurable disease according to RECIST 1.1.
Central Nervous System Response Analysis Set
The CNS response analysis set included all treated RET fusion–positive NSCLC and other patients with a solid tumour who met the first criteria of PAS and had an investigator-assessed CNS metastases at baseline (reported as target or non-target lesion according to RECIST 1.1). The IRC reviewed all CNS scans and provided a CNS-only best overall response and DOR by RECIST 1.1 for each patient. The analysis was conducted by tumour type (NSCLC and other) as well as overall.
Health-Related Quality of Life Dataset
At the December 16, 2019, data cut-off, of the 253 patients enrolled in the NSCLC population, 239 were included in the HRQoL analysis. These patients were further subgrouped into 3 populations:7
treatment-naive (n = 39)
1 prior line of therapy (n = 64)
2 or more prior lines of therapy (n = 136).
Overall Safety Analysis Set
The RET fusion–positive NSCLC safety analysis set includes all patients with documented RET fusion who were enrolled in the LIBRETTO-001 study and received 1 or more doses of selpercatinib as of the cut-off date. The safety analysis set at the December 16, 2019, data cut-off was composed of 702 patients treated with selpercatinib irrespective of the cohort assignation. At the March 30, 2020, data cut-off, 746 patients who had received at least 1 dose of selpercatinib were included in the OSAS, while at the December 16, 2019, data cut-off, 702 patients who had received at least 1 dose of selpercatinib were included in the OSAS.
Figure 3: Selpercatinib Enrolment and Analysis Populations
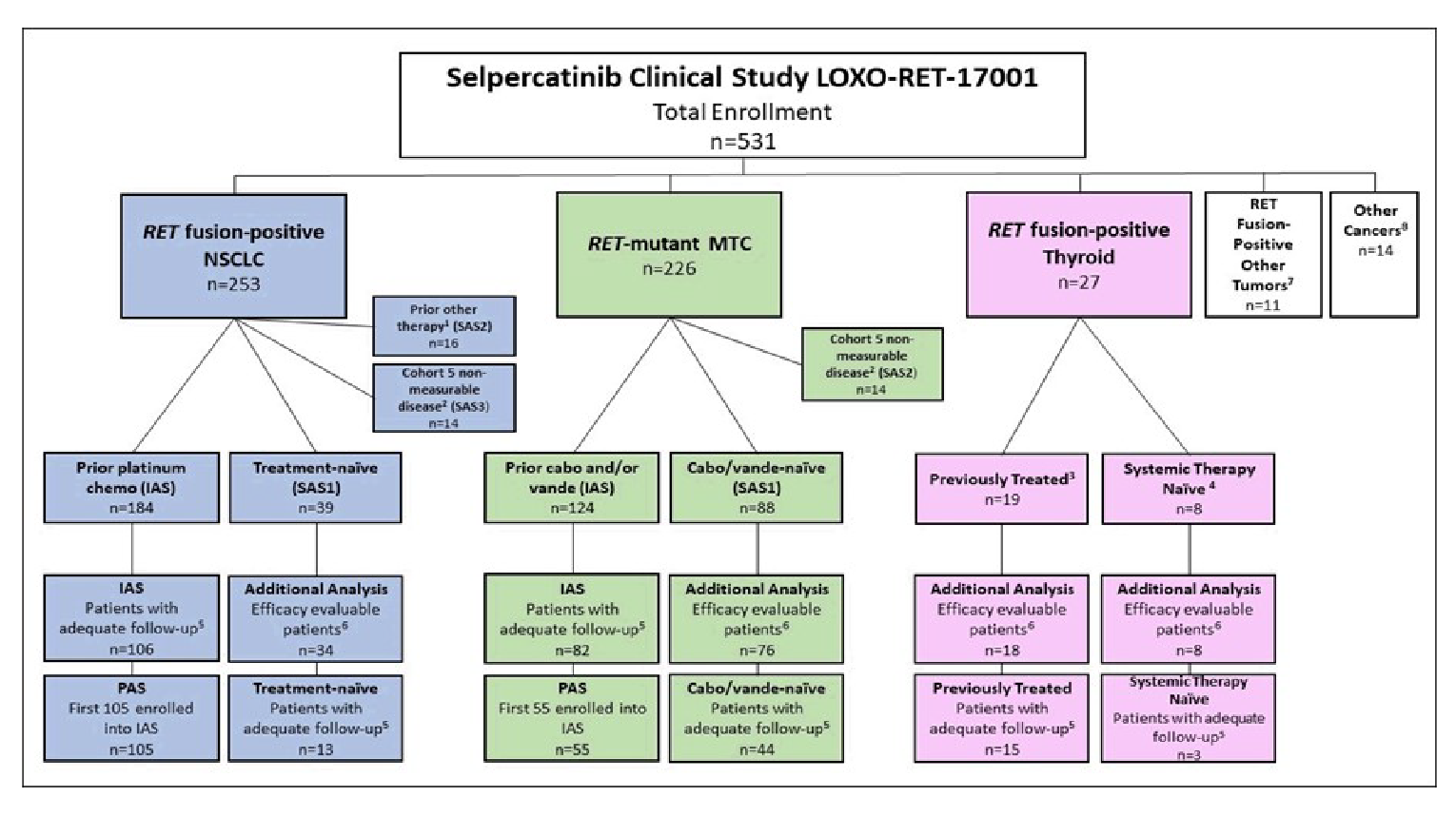
cabo = cabozantinib; CNS = central nervous system; IAS = integrated analysis set; MTC = medullary thyroid cancer; NSCLC = non–small cell lung cancer; PAS = primary analysis set; RET = rearranged during transfection; SAS = supplemental analysis set; vande = vandetanib.
Note: Three analysis subsets are not shown: CNS efficacy in the NSCLC PAS, CNS efficacy in all patients with RET fusion–positive NSCLC, and a subset of PAS patients with prior programmed cell death protein 1 or programmed cell death ligand 1 therapy. Enrolment date: June 17, 2019.
1 RET fusion–positive other tumours include pancreatic cancer, rectal neuroendocrine cancer, salivary gland cancer, carcinoid cancer, cancers of the colon and small intestine, and xanthogranuloma.
2 Other solid tumours that do not fit the other disease cohorts.
3 Prior systemic therapy other than platinum-based chemotherapy.
4 Patients without measurable disease who were enrolled in phase I dose-expansion cohort 5 (per-protocol version 4.0 or earlier) or phase II cohort 5 (per-protocol version 5.0 and later).
5 Previously treated RET fusion–positive thyroid cancer.
Source: Sponsor’s submission package, Retevmo (selpercatinib),5 LIBRETTO-001.26
Sample Size Definition
Primary Analysis Set
For the PAS, an ORR of 50% or more was hypothesized by the sponsor when selpercatinib is administered to patients with RET fusion–positive NSCLC who progressed on or after receipt of platinum-based chemotherapy. A sample size of 105 patients was estimated to provide more than 98% power to achieve a lower boundary of a 2-sided 95% exact binomial CI about an estimated ORR that exceeds 30%. Ruling out a lower limit of 30% for the ORR was considered clinically meaningful by the sponsor for the patient population. Under the primary analysis, the effectiveness of selpercatinib was established if the lower limit of the 95% CI will exceed 30% when the estimated ORR is 40% or greater (using the Clopper-Pearson method).5
The IAS included all patients with RET fusion–positive NSCLC enrolled in the LIBRETTO-001 study by the data cut-off date who met the PAS eligibility criteria.
Planned Analysis
There were 3 interim analyses planned to support regulatory submissions in different jurisdictions.
The first interim analysis at the data cut-off of June 17, 2019, supported the original New Drug Application at the FDA but was later updated with results from the Day 60 Efficacy and Safety Update with a data cut-off of December 16, 2019.
The second interim analysis at the data cut-off of December 16, 2019, provides an additional 6 months of follow-up information for patients who were enrolled and had received at least 1 dose of selpercatinib before or at the data cut-off date of June 17, 2019. This formed the basis of the Health Canada regulatory submission and FDA submission and therefore efficacy results related to the first analysis are not reported.
The third interim analysis at the March 30, 2020, data cut-off date, which was planned to support the regulatory submission in Japan, provides additional information for relevant outcomes (ORR, DOR, OS, PFS, and safety) investigated in the LIBRETTO-001 trial. Efficacy results are presented for 2 data cut-off dates (March 30, 2020, and December 16, 2019) in this report for relevant outcomes in specific patient populations related to the reimbursement populations (i.e., patients with RET fusion–positive NSCLC).
Primary Outcome Analysis
The ORR was determined by the IRC and calculated based on the maximum likelihood estimator (i.e., crude proportion of patients with best objective response of CR or PR), and a 2-sided 95% exact binomial CI using the Clopper-Pearson method was provided. The ORR represents the proportion of patients with a best objective response of confirmed CR or confirmed PR based on RECIST 1.1.
The point estimate of the ORR was calculated based on the maximum likelihood estimator (i.e., crude proportion of patients in the PAS with best overall response of confirmed CR or confirmed PR). The point estimate was accompanied by a 2-sided 95% exact binomial CI using the Clopper-Pearson method. The effectiveness of selpercatinib was demonstrated if the lower limit of the 2-sided 95% CI exceeded 30%.5
Sensitivity Analyses
The IAS was used to perform sensitivity analysis on the data. No further details of the sensitivity analysis were provided.
Subgroup Analyses
Supportive analyses were performed on selected subgroups and special populations. These analyses were conducted on the PAS population and selected analysis sets as appropriate. The point estimates of the ORR (and 95% CI) and the median DOR (and range) based on IRC was calculated for the subgroups and special populations defined by the following:
age at enrolment (< 65 years, ≥ 65 years)
sex (male, female)
race (White, Asian, other)
ECOG PS at baseline (0, 1, or 2)
smoking status (never smoked or smoker)
type of molecular assay (NGS on tumour or PCR, NGS on plasma, FISH)
RET fusion gene (KIF5B, non-KIF5B, unknown)
history of metastatic disease (yes, no)
CNS metastasis at baseline by investigator (yes, no)
number of prior systemic therapies (0, 1 or 2, ≥ 3)
Prior anti–PD-1 or anti–PD-L1 (yes, no)
Prior multikinase inhibitor (yes, no).
The CADTH review protocol identified 4 subgroups of interest for which data will be presented. These include performance status at baseline, prior class or type of therapy, number of prior therapies, and CNS metastases at baseline.
Analysis of Secondary Outcomes
Duration of Response
The DOR was defined as the number of months from start date of CR or PR (whichever came first) and subsequently confirmed, to the first date that recurrent or progressive disease was objectively documented. If a patient died, irrespective of cause, without prior documentation of recurrent or progressive disease, then the date of death was used to denote the response end date. Calculations were performed only in patients who achieved a CR and PR. Kaplan–Meier methods were used to summarize the DOR, and median follow-up was estimated based on the Kaplan–Meier estimate of potential follow-up.5
The DOR was summarized descriptively using the Kaplan–Meier method. The Kaplan–Meier estimate with a 95% CI was calculated using the Brookmeyer and Crowley method to provide for the median. The event-free rate with a 95% CI was calculated using Greenwood’s formula for selected time points. The median follow-up for DOR was estimated according to the Kaplan–Meier estimate of potential follow-up.
DOR (months) = (event or censoring date − response start date + 1)/30.4375
Progression-Free Survival
Progression-free survival was defined as the number of months that elapsed between the date of the first dose administration of selpercatinib and the earliest date of documented disease progression or death (whatever the cause).
Values for PFS were summarized descriptively using the Kaplan–Meier method and the median follow-up was estimated according to the Kaplan–Meier estimate of potential follow-up.
PFS (months) = (event or censoring date − first dose date + 1)/30.4375
Overall Survival
Overall survival was defined as the number of months that elapsed between the date of the first dose administration of selpercatinib and the date of death (whatever the cause). Patients who were alive or lost to follow-up as of the data cut-off date were right-censored. The censoring date was determined from the date the patient was last known to be alive.
Values for OS were summarized descriptively using the Kaplan–Meier method and the median follow-up was estimated according to the Kaplan–Meier estimate of potential follow-up.5
OS (months) = (death or censoring date − first dose date + 1)/30.4375
Central Nervous System Objective Response Rate
The CNS ORR was analyzed using the same method described for the analyses of ORR and DOR and summarized overall and by baseline disease measurability as assessed by IRC.5
Health-Related Quality of Life
Version 3 of the EORTC QLQ-C30 instrument was used to measure HRQoL in patients participating in the LIBRETTO-001 trial. This self-administered questionnaire is composed of 30 items, measuring patient health in 2 different domains, the functional subscales domain and the symptom subscale domain. It includes 9 items: nausea and vomiting (2 items), fatigue (3 items), pain (2 items), diarrhea (1 item), dyspnea (1 item), appetite loss (1 item), insomnia (1 item), constipation (1 item), and financial difficulties (1 item). The minimally important difference (MID) was defined as a “10-point difference from the baseline assessment value.”19 A definite change (improvement or worsening) was defined as an improvement or worsening, respectively, from baseline of 10 or more points without any further reduction or increase in score of 10 or more points, respectively.
Higher scores obtained in the EORTC QLQ-C30 signified better functioning. Scores were linearly transformed to a 0-to-100 scale. Missing values were handled based on the suggested techniques in the EORTC QLQ-C30 manual. Only raw scores with complete information on at least 50% of the items in the scale or subscale were computed. Scores values were not imputed. All subscales in the EORTC QLQ-C30 were scored from 0 to 100. Higher scores obtained in the quality of life and functional subscales represented improved functioning, while lower scores obtained in the symptom subscales represented fewer symptoms. Clinically important thresholds used in the assessment were obtained from published literature.7 Results were presented as descriptive statistics (median and quartile, mean and SD, and mean change and standard error from baseline) for each subscale at each study visit.
Lower scores obtained in functional subscales were compared to the following defined thresholds: 83 (physical function), 71 (emotional function), 58 (role function, social function), or 75 (cognitive function) and were considered a clinically meaningful problem for patients.
Higher scores obtained in symptom subscales were compared to the following thresholds: 8 (nausea or vomiting), 39 (fatigue), 25 (pain), 17 (diarrhea, dyspnea, financial difficulties), or higher than 50 (appetite loss, insomnia, constipation), and were considered clinically meaningful problems.
The MID considered was a change of at least 10 points from baseline. “Improvement” was defined as a change from baseline of 10 or more points without any further deterioration in score of 10 or more points. “Worsening” was defined as a change from baseline of at least 10 points without any further improvement in score of 10 points or more.
The Kaplan–Meier method was used to derive time to improvement and time to worsening. Patients with least 6 months of follow-up data and those who had experienced events before the 6-month time frame were also included in their analyses. Patients were censored at the last cycle for which they had completed the questionnaire and if their score did not vary by 10 points from baseline at any subsequent assessment.
Handling of Missing Data
No imputation was performed on missing data; all analyses were based on observed data only.
Protocol Amendments
Several updates to the protocol made during the study were identified and documented before data cut-off for the regulatory submission as presented in Table 9. Changes to the protocol did not affect the study’s efficacy and safety outcomes.19
Table 9: Protocol Versions and Dates
Version | Date | Major changes |
|---|---|---|
1.0 | NA |
|
2.0 | March 27, 2017 |
|
3.0 | July 20, 2017 |
|
4.0 | November 21, 2017 |
|
4.5 | April 11, 2018 |
|
5.0 | May 30, 2018 |
|
5.1 | June 15, 2018 |
|
6.0 | September 11, 2018 |
|
6.1 | September 11, 2018 |
|
7.0 | October 18, 2018 |
|
7.1 | October 18, 2018 |
|
7.2 | October 18, 2018 |
|
7.3 | December 26, 2018 |
|
8.0 | NA |
|
AE = adverse event; HRQoL = health-related quality of life; NA = not available; PK = pharmacokinetics; RET = rearranged during transfection; SAE = serious adverse event.
Source: Sponsor’s submission package, Retevmo (selpercatinib),5 LIBRETTO-001.19
Protocol Deviations
Important protocol deviations were reported in 40 patients (7.5%). The most frequently reported and important protocol deviations were those related to the investigational product in 17 patients, and inclusion criteria and serious adverse event (SAE) reporting, each in 8 patients.
Results
Patient disposition
Table 10 provides a summary of patient disposition in the NSCLC efficacy set as of December 16, 2019, data cut-off. A total of 253 patients with NSCLC were RET fusion–positive. Of the 105 patients included in the PAS, 40% of patients had discontinued treatment, with the most common reason for discontinuation being disease progression.5 Greater than 20% of patients in total and 31% of those in the PAS stayed on treatment post-progression at the investigator’s discretion.
Table 10: Patient Disposition (December 16, 2019, Data Cut-Off Date)
Disposition | PAS | IAS | SAS1 Treatment-naive | SAS2 Prior other systemic therapy | SAS3 Non-measurable disease | Total |
|---|---|---|---|---|---|---|
Treated, n | 105 | 184 | 39 | 16 | 14 | 253 |
Treatment discontinued, n (%) | 42 (40.0) | 59 (32.1) | 9 (23.1) | 8 (50.0) | 5 (35.7) | 81 (32.0) |
Disease progression | 25 (23.8) | 34 (18.5) | 6 (15.4) | 6 (37.5) | 4 (28.6) | 50 (19.8) |
Adverse event | 5 (4.8) | 11 (6.0) | 2 (5.1) | 0 | 1 (7.1) | 14 (5.5) |
Withdrawal of consent | 6 (5.7) | 7 (3.8) | 0 | 0 | 0 | 7 (2.8) |
Death | 2 (1.9) | 3 (1.6) | 1 (2.6) | 2 (12.5) | 0 | 6 (2.4) |
Other | 4 (3.8) | 4 (2.2) | 0 | 0 | 0 | 4 (1.6) |
Treatment continued post-progression, n (%) | 33 (31.4) | 42 (22.8) | 5 (12.8) | 5 (31.3) | 1 (7.1) | 53 (20.9) |
Study status continuing, n (%) | 70 (66.7) | 138 (75.0) | 37 (94.9) | 10 (62.5) | 10 (71.4) | 195 (77.1) |
Study discontinued, n (%) | 35 (33.3) | 46 (25.0) | 2 (5.1) | 6 (37.5) | 4 (28.6) | 58 (22.9) |
Withdrawal of consent | 12 (11.4) | 16 (8.7) | 1 (2.6) | 1 (6.3) | 2 (14.3) | 20 (7.9) |
Death | 23 (21.9) | 30 (16.3) | 1 (2.6) | 5 (31.3) | 2 (14.3) | 38 (15.0) |
IAS = integrated analysis set; NSCLC = non–small cell lung cancer; PAS = primary analysis set; RET = rearranged during transfection; SAS = supplemental analysis set.
Note: The PAS included a subset analysis of the FDA breakthrough therapy designation population (n = 58) who received prior platinum-based chemotherapy and an anti–programmed cell death protein 1 or anti–programmed cell death ligand 1 antibody. The IAS included all patients previously treated with platinum-based chemotherapy. SAS1 included patients who were treatment naive. SAS2 included patients previously treated with other systemic therapies that are not platinum-based. SAS3 consisted of patients without measurable disease according to the Response Evaluation Criteria in Solid Tumors Version 1.1. For patients with RET fusion–positive NSCLC, the PAS includes the first 105 patients of the IAS. The total column is the sum of the IAS, SAS1, SAS2, and SAS3 at the December 16, 2019, data cut-off.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Exposure to Study Treatments
At the December 16, 2019, data cut-off, most patients with RET fusion–positive NSCLC (93%) had received 160 mg of selpercatinib twice daily, either as the starting dose (82%), through protocol-allowed intra-patient dose escalation (10%), or through dose reductions from 240 mg twice daily (1%). Dosing was also consistent across the analysis sets.5 Table 11 presents information of starting doses, time on treatment, and time on study.
Table 11: Selpercatinib Starting Doses for Patients Who Received at Least 1 Dose of 160 mg of Selpercatinib Twice Daily, Time on Treatment, and Time on Study
Characteristic | RET FUSION–POSITIVE NSCLC | ||||||
|---|---|---|---|---|---|---|---|
PAS (subset of IAS) N = 105 | IAS Prior platinum chemo N = 184 | SAS1 Treatment-naive N = 39 | SAS2 Prior other systemic therapy N = 16 | SAS3 Non-measurable disease N = 14 | Total N = 253 | ||
Selpercatinib starting doses, n (%) | |||||||
20 mg q.d. | 4 (3.8) | 4 (2.2) | 0 | 0 | 0 | 4 (1.6) | |
20 mg b.i.d. | 5 (4.8) | 5 (2.7) | 0 | 1 (6.3) | 0 | 6 (2.4) | |
40 mg b.i.d. | 9 (8.6) | 9 (4.9) | 0 | 0 | 0 | 9 (3.6) | |
60 mg b.i.d. | 3 (2.9) | 3 (1.6) | 0 | 2 (12.5) | 0 | 5 (2.0) | |
80 mg b.i.d. | 3 (2.9) | 3 (1.6) | 2 (5.1) | 0 | 0 | 5 (2.0) | |
120 mg b.i.d. | 11(10.5) | 11 (6.0) | 0 | 2 (12.5) | 0 | 13 (5.1) | |
160 mg b.i.d.a | 69 (65.7) | 148 (80.4) | 36 (92.3) | 10 (62.5) | 14 (100) | 208 (82.2) | |
240 mg b.i.d. | 1 (1.0) | 1 (0.5) | 1 (2.6) | 1 (6.3) | 0 | 3 (1.2) | |
Patients who received at least 1 dose of 160 mg b.i.d. selpercatinib, time on treatment, and time on study, n (%) | |||||||
Received at least one dose of 160 mg b.i.d. | 92 (87.6) | 171 (92.9) | 39 (100) | 12 (75.0) | 14 (100) | 236 (93.3) | |
Starting dose of 160 mg b.i.d. | 69 (65.7) | 148 (80.4) | 36 (92.3) | 10 (62.5) | 14 (100) | 208 (82.2) | |
Intra-patient dose escalated to 160 mg b.i.d. | 22 (21.0) | 22 (12.0) | 2 (5.1) | 1 (6.3) | 0 (0) | 25 (9.9) | |
Dose reduced to 160 mg b.i.d. | 1 (1.0) | 1 (0.5) | 1 (2.6) | 1 (6.3) | 0 (0) | 3 (1.2) | |
Time on treatment, months | |||||||
Median (range) | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | |
Time on study,b months | |||||||
Median (range) | ||||||||||||||||| | ||||||||||||||||| | |||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | |
b.i.d. = twice daily; IAS = integrated analysis set; NSCLC = non–small cell lung cancer; PAS = primary analysis set; q.d. = once daily; RET = rearranged during transfection; SAS = supplemental analysis set.
Note: The PAS included a subset analysis of the FDA breakthrough therapy designation population (n = 58) who received prior platinum-based chemotherapy and an anti–programmed cell death protein 1 or anti–programmed cell death ligand 1 antibody. The IAS included all patients previously treated with platinum-based chemotherapy. SAS1 included patients who were treatment naive. SAS2 included patients previously treated with other systemic therapies that are not platinum-based. SAS3 consisted of patients without measurable disease according to Response Evaluation Criteria in Solid Tumors Version 1.1. For patients with RET fusion–positive NSCLC, the PAS includes the first 105 patients of the IAS. The total column is the sum of the IAS, SAS1, SAS2, and SAS3.
aThe recommended phase II dose at the December 16, 2019, data cut-off was 160 mg b.i.d.
bTime on study (months) = (study exit date − first dose date + 1)/30.4375 for patients who exited the study on or before the data cut-off date; time on study (months) = (data cut-off date − first dose date + 1)/30.4375 for patients who were still in the treatment phase as of the data cut-off date; time on study (months) = (last visit date − first dose date + 1)/30.4375 for patients who were in the long term follow-up as of the data cut-off date of December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Efficacy
Overall Survival
Primary and Integrated Analysis Sets (Patients with RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
Table 12 summarizes information on OS in the PAS and IAS populations for 2 cut-off dates. At the March 30, 2020, data cut-off, 73.3% of patients were still alive in the PAS population. The median OS was NE, and the median follow-up was estimated at 19.9 months. In the IAS population, 81.2% patients were still alive. The median OS was NE and the median follow-up obtained was 14.3 months.5 Figure 4 presents the Kaplan–Meier plot of OS in the PAS set (December 16, 2019, only).5
The sponsor conducted a follow-up analysis in the IAS population at a new cut-off date of June 15, 2021. The median OS was NE at this data cut-off. The median follow-up in months was 26.4.
Table 12: Overall Survival — PAS and IAS Sets (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
Survival status, n (%) | PAS | IAS | |||
|---|---|---|---|---|---|
March 30, 2020 N = 105 | December 16, 2019 N = 105 | June 15, 2021 N = 247 | March 30, 2020 N = 218 | December 16, 2019 N = 184 | |
Overall survival | |||||
Dead | NR | ||||||||||||||||| | NR | NR | ||||||||||||||||| |
Alive | NR | ||||||||||||||||| | NR | NR | ||||||||||||||||| |
Disease progression | 28 (26.7) | ||||||||||||||||| | NR | 41 (18.8) | ||||||||||||||||| |
censored | 77 (73.3) | ||||||||||||||||| | NR | 177 (81.2) | ||||||||||||||||| |
Duration of follow-up (months), median | 19.94 | ||||||||||||||||| | 26.4 | 14.26 | ||||||||||||||||| |
25th to 75th percentiles | 16.7 to 23.7 | ||||||||||||||||| | NR | 10.1 to 19.5 | ||||||||||||||||| |
Median OS, months (95% CI) | NE (25.7 to NE) | ||||||||||||||||| | NE (33.5 to NE) | NE (25.7 to NE) | ||||||||||||||||| |
Overall survival at 6-month time points, % (95% CI) | |||||
6 months or more | 96.2 (90.1 to 98.5) | ||||||||||||||||| | NR | 95.4 (91.6 to 97.5) | ||||||||||||||||| |
12 months or more | 88.3 (80.3 to 93.2) | ||||||||||||||||| | 88 | 88.1 (82.5 to 91.9) | ||||||||||||||||| |
18 months or more | 78.4 (68.8 to 85.4) | ||||||||||||||||| | NR | 77.6 (69.4 to 83.9) | ||||||||||||||||| |
24 months or more | 68.0 (55.3 to 77.8) | ||||||||||||||||| | 69 | 67.3 (55.4 to 76.7) | ||||||||||||||||| |
CI = confidence interval; IAS = integrated analysis set; NE = not estimable; NR = not reported; NSCLC = non–small cell lung cancer; OS = overall survival; PAS = primary analysis set; RET = rearranged during transfection.
Note: The PAS included a subset analysis of the FDA breakthrough therapy designation population (n = 58) who received prior platinum-based chemotherapy and an anti–programmed cell death protein 1 and anti–programmed cell death ligand 1 antibody. The IAS included all patients previously treated with platinum-based chemotherapy, at the December 16, 2019; March 30, 2020; and June 15, 2021, data cut-offs.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Figure 4: Kaplan–Meier Plot of Overall Survival — Primary Analysis Set (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
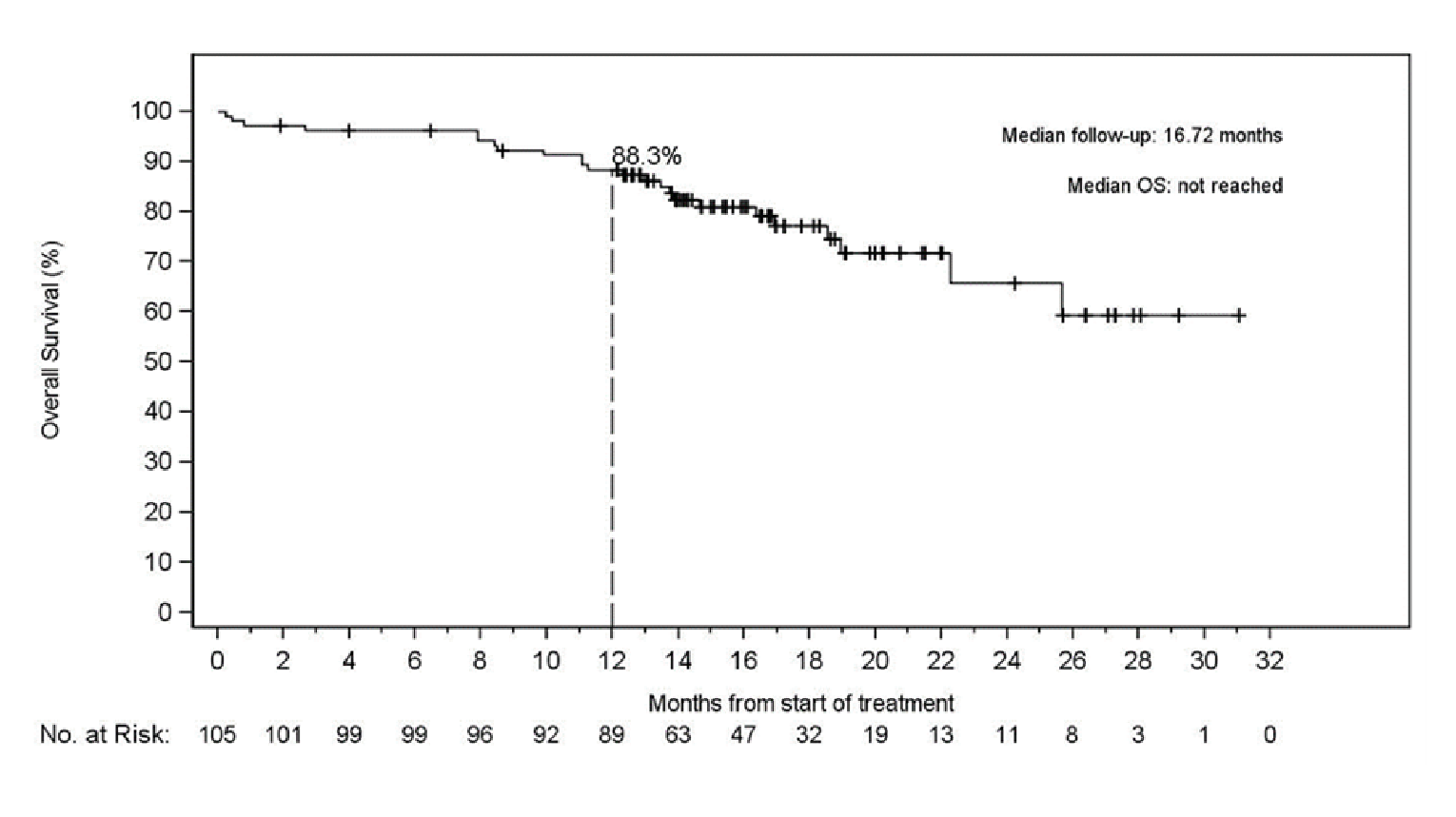
+ = censored; OS = overall survival; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note: Data cut-off: December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Treatment-Naive RET Fusion–Positive NSCLC Cohort (SAS1)
Table 13 presents information on OS at both data cut-offs. Given the small number of events, the median OS was NE at either analysis time point.5
The sponsor conducted a follow-up analysis in the treatment-naive population at a new data cut-off date of June 15, 2021. The median OS was NE at this data cut-off. The median follow-up was 21.9 months.
Table 13: Overall Survival — Patients With Treatment-Naive RET Fusion–Positive NSCLC
Outcome | Treatment-naive RET fusion–positive NSCLC (supplemental analysis set 1) | ||
|---|---|---|---|
June 15, 2021 N = 69 | March 30, 2020 N = 48 | December 16, 2019 N = 39a | |
Overall survival | |||
Survival status (n, %) | |||
Died | NR | NR | ||||||||||||||||| |
Alive | NR | NR | ||||||||||||||||| |
Disease progression | NR | 4 (8.3) | ||||||||||||||||| |
Censored | NR | 44 (91.7) | ||||||||||||||||| |
Duration of follow-up (months), median | 25.2 | 12.58 | ||||||||||||||||| |
25th to 75th percentiles | NR | 9.9 to 16.7 | ||||||||||||||||| |
Duration of overall survival, months | |||
Median (95% CI) | NE (27.9 to NE) | NE (NE to NE) | ||||||||||||||||| |
Overall survival at 6-month time points, % (95% CI) | |||
6 months or more | NR (NR, NR) | 95.8 (84.4 to 98.9) | ||||||||||||||||| |
12 months or more | 93 (NR, NR) | 93.2 (80.1 to 97.8) | ||||||||||||||||| |
18 months or more | NR (NR, NR) | 88.0 (68.6 to 95.8) | ||||||||||||||||| |
24 months or more | 69 (NR, NR) | 88.0 (68.6 to 95.8) | ||||||||||||||||| |
CI = confidence interval; NE = not estimable; NR = not reported; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note: Supplemental analysis set 1 included patients who were treatment naive with December 16, 2019; March 30, 2020; and June 15, 2021, data cut-offs.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Prior Other Systemic Therapy RET Fusion–Positive NSCLC Patients (Supplemental Analysis Set 2) and Non-Measurable Disease RET Fusion–Positive NSCLC Patients (Supplemental Analysis Set 3)
The OS results obtained in the SAS2 and SAS3 populations at both data cut-offs are presented in Table 14. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 14: OS — Prior Other Systemic Therapy for Patients With RET Fusion–Positive NSCLC Patients (Supplemental Analysis Set 2) and Non-Measurable Disease RET Fusion–Positive NSCLC Patients (Supplemental Analysis Set 3)
Outcome | Prior other systemic therapy for patients with RET fusion–positive NSCLC (SAS2) March 30, 2020 N = 18 | Prior other systemic therapy for patients with RET fusion–positive NSCLC (SAS2) December 16, 2019, N = 16 | Non-measurable disease in patients with RET fusion–positive NSCLC (SAS3) March 30, 2020 N = 18 | Non-measurable disease in patients with RET fusion–positive NSCLC (SAS3) December 16, 2019 N = 14 |
|---|---|---|---|---|
Overall survival | ||||
Patients with an event (n, %) | ||||
Disease progression | 6 (33.3) | ||||||||||||||||| | 3 (16.7) | ||||||||||||||||| |
Censored | 12 (66.7) | ||||||||||||||||| | 15 (83.3) | ||||||||||||||||| |
Duration of follow-up (months) | ||||
Median | 17.05 | ||||||||||||||||| | 10.48 | ||||||||||||||||| |
25th to 75 percentiles | 10.3 to 18.3 | ||||||||||||||||| | 8.6 to 12.9 | ||||||||||||||||| |
Duration of overall survival | ||||
Median | 28.88 | ||||||||||||||||| | NE | ||||||||||||||||| |
95%CI | 11.0 to NE | ||||||||||||||||| | NE, NE | ||||||||||||||||| |
NE = not estimable; NR = not reported; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note: December 16, 2019, March 30, 2020, data cut-off.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Subgroup Analysis
Data on subgroup analysis were not reported.
Health-Related Quality of Life
Patients recruited in the LIBRETTO-001 trial were asked to complete the EORTC QLQ-C30 questionnaire at baseline (cycle 1, day 1), every 8 weeks (until cycle 13), and every 12 weeks after cycle 13 (until end of treatment). Patients were evaluated at odd-numbered cycles. A descriptive analysis of results was presented, and assessments of change were made from baseline. Lower scores obtained in functional subscales were compared to the following defined thresholds: 83 (physical function), 71 (emotional function), 58 (role function, social function), or 75 (cognitive function) and were considered a clinically meaningful problems for patients. Higher scores obtained in symptom subscales were compared to the following thresholds: 8 (nausea or vomiting), 39 (fatigue), 25 (pain), 17 (diarrhea, dyspnea, and financial difficulties), or higher than 50 (appetite loss, insomnia, and constipation) and were considered clinically meaningful problems. Table 15 provides a summary of the HRQoL findings.
Table 15: Summary of Findings for Health-Related Quality of Life (December 16, 2019, Data Cut-Off)
Domain | Treatment-naive set (n = 39) | 1 prior line of therapy set (n = 64) | 2 or more prior lines of therapy set (n = 136) |
|---|---|---|---|
Global health status | |||
Overall baseline score, mean (SD) | 61.5 (23.6) | ||
Baseline, mean (SD) | 60.2 (23.4) | 65.2 (23.5) | 60.4 (22.6) |
Improvement, % | 66.7% | 64.1% | 61.1% |
Physical function | |||
Overall score at baseline, mean (SD) | 75.9 (22.2) | ||
Baseline, mean (SD) | 72.6 (24.1) | 79.8 (21.0) | 76.1 (18.8) |
Improvement, % | 55.6 | 41.0 | 48.2 |
Symptom scales | |||
Dyspnea, mean (SD) | |||
Overall, mean (SD) | 31.3 (30.3) | ||
Baseline, mean (SD) | 28.4 (33.0) | 23.1 (27.7) | 37.7 (28.3) |
Improvement, % | 48.1 | 33.3 | 61.1 |
Insomnia | |||
Improvement, % | 55.6 | 38.5 | 50.0 |
Fatigue | |||
Baseline overall score, mean (SD) | 37.9 (26.0) | ||
Baseline, mean (SD) | 41.6 (27.7) | Not met | 41.8 (26.3) |
Improvement, % | 77.8 | 56.4 | 66.7 |
Pain | |||
Overall baseline score, mean (SD) | 29.4 (28.5) | ||
Improvement, % | 63.0 | 46.2 | 50 |
SD = standard deviation.
Source: Minchom et al. (2021).7
Global Health Status
The mean GHS/QoL in the overall population was 61.5 (SD = 23.6). The mean GHS at baseline was 60.2 (SD = 23.4) in the treatment-naive population and 65.2 (SD = 23.5) in the patient population with 1 line of prior therapy. The mean GHS at baseline for patients with 2 or more lines of therapy was 60.4 (SD = 22.6). The proportion of patients who showed improved GHS/QoL from baseline was high across cycles 3 to cycle 13 in all 3 subgroups. However, the sample size of patients who completed the questionnaires decreased at every cycle. Because fewer patients (n = 28) had completed the questionnaire at cycle 13 in the overall population compared to the other cycles, the results are uncertain and cannot be fully interpreted. Findings from the time-to-event analysis showed improvements in GHS/QoL in all 3 subgroups: 66.7% (18 of 27) in the treatment-naive population, 64.1% (25 of 39) in patients with 1 prior line of therapy, and 61.1% (33 of 54) in patients who had received 2 or more prior lines of therapy at study enrolment).7 Figure 5 presents the GHS/QoL data (from the EORTC QLQ-C30) at different treatment cycles.
Figure 5: Global Health Status/QoL (EORTC QLQ-C30) — Patients With RET Fusion–Positive NSCLC
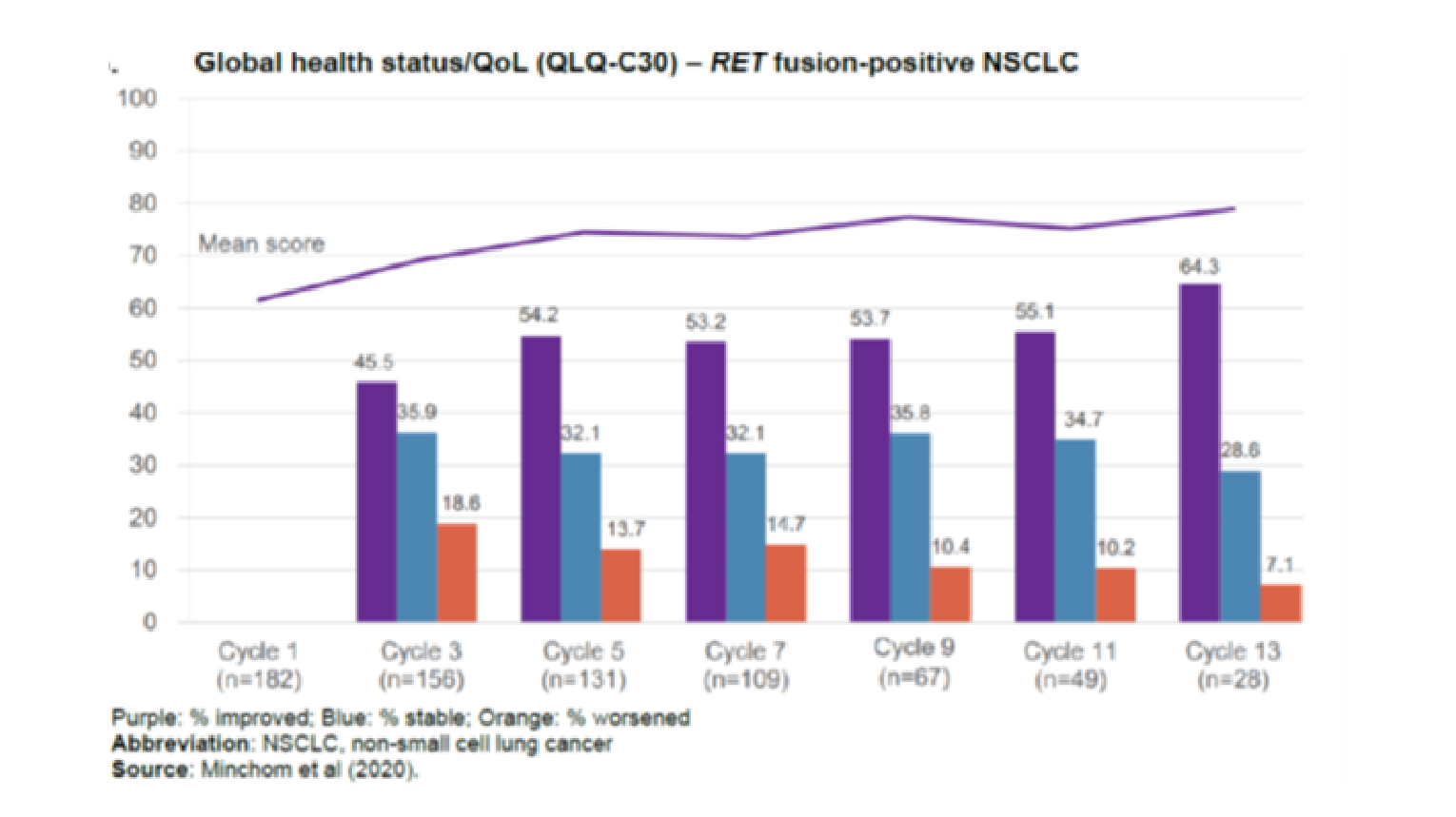
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NSCLC = non–small cell lung cancer; QoL = quality of life; RET = rearranged during transfection.
Note: Data cut-off or December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Physical Function
The mean baseline obtained in the physical function scale for the overall population was 75.9 (SD = 22.2). The mean baseline score for physical function was 72.6 (SD = 24.1) in the treatment-naive subgroup, 79.8 (SD = 21.0) in patients with 1 prior line of therapy, and 76.1 (SD = 18.8) in the group with 2 or more lines of therapy. Baseline scores in the physical function scale in all 3 subgroups were lower than the threshold score of 83, and were considered clinically important impairments. The proportions of patients reported to have experienced improvement in physical function scores were higher across the subgroups and in the overall population compared to those who experienced worsened symptoms across cycle 3 to cycle 13. The majority of patients reported stable outcomes in physical function scores across cycles. However, due to the small sample size observed at later cycles, the interpretability of these findings is uncertain. An “improvement” (≥ 10-point increase) in physical function was observed at the start of cycle 3 (43.5%, 28.1% and 29.8% in the treatment-naive, 1 prior line, and 2 or more lines, respectively). The time-to-event analysis showed improvements in physical function in 55.6% (15 of 27), 41.0% (16 of 39) and 48.2% (26 of 54) of patients who were treatment-naive, had 1 prior line of therapy, or 2 or more prior lines of therapy, respectively.7 Figure 6 presents scores obtained in the physical function scale at different treatment cycles.
Figure 6: Physical Function (EORTC QLQ-C30) — Patients With RET Fusion–Positive
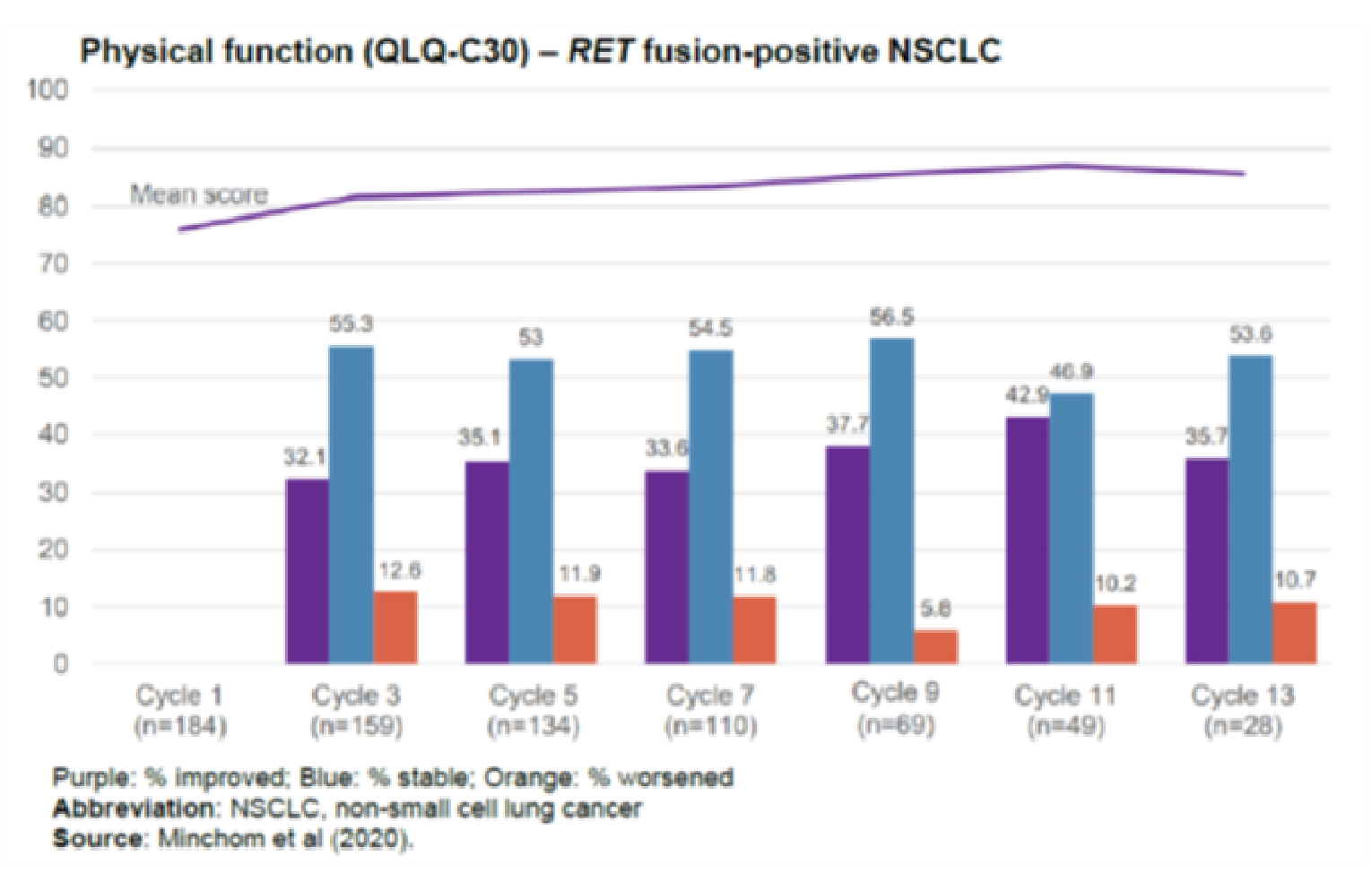
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note: Data cut-off: December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Symptom Subscales
Figure 7 presents the proportion of patients meeting a definite change in the RET fusion NSCLC population at the December 16, 2019, data cut-off.
Figure 7: Proportion of Patients Meeting “Definite” Change — RET Fusion–Positive NSCLC
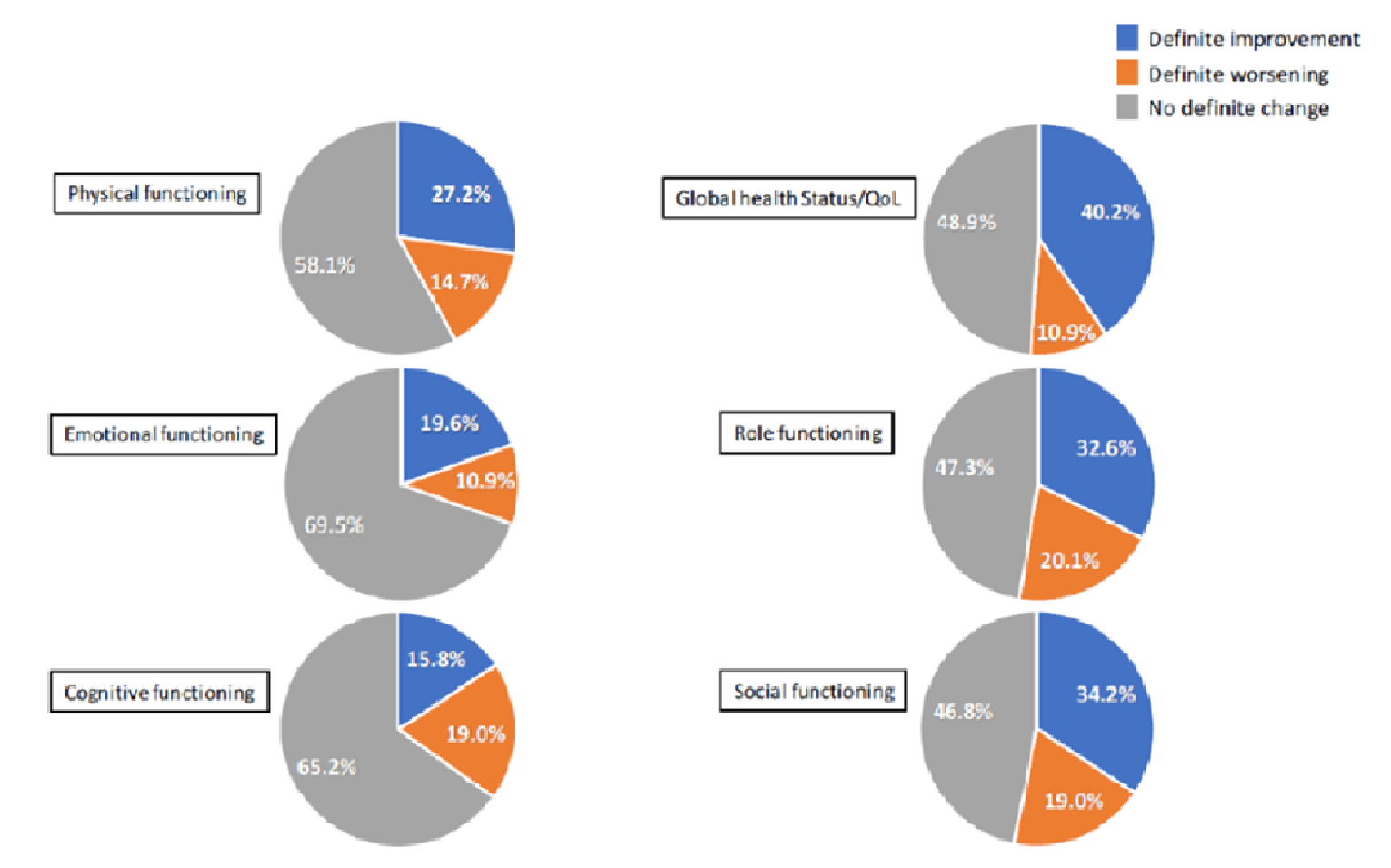
NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note: A definite change is defined as a ≥ 10 point change from their baseline score and no further change of ≥ 10 points in the score were observed at any subsequent assessment.
Data cut-off of December 16, 2019
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Dyspnea
The mean baseline scores obtained for dyspnea exceeded the clinically meaningful threshold of 17 points in the overall population and in each subgroup (overall = 31.3 [SD = 30.3]; treatment-naive = 28.4 [SD = 33.0]; 1 prior line of therapy = 23.1 [SD = 27.7]; ≥ 2 prior lines = 37.7 [SD = 28.3]) and were considered clinically meaningful impairments. The proportion of patients who experienced a change in dyspnea from baseline by cycle of study treatment was high in patients who reported improved symptoms compared to patients who reported worsened symptoms across cycles 3 to 13. The proportion of patients who reported stable outcomes was higher but constant across cycles assessed. Findings from the time-to-event analysis showed improvements in dyspnea (≥ 10-point decrease). In the treatment-naive group, 48.1% of patients (13 of 27) showed improvement, with 33.3% of patients in the 1 prior line of therapy group (13 of 39) and 61.1% in the 2 or more prior lines of therapy group (33 of 54) showing improvement.7
Insomnia
Baseline scores for insomnia did not meet a clinically meaningful threshold in any group and were not considered clinically meaningful impairments. The proportion of patients who reported stable symptoms in insomnia from baseline across cycles 3 to 13 was higher than that of patients who reported improved or worsened outcomes. More patients experienced improved outcomes compared to those who reported worsened outcomes across cycle 3 to 13. However, due to the decrease in number of patients completing the questionnaires from baseline to cycle 13, these findings are uncertain. The time-to-event analyses showed improvement (≥ 10-point decrease) in insomnia in 55.6% of the naive group (15 of 27), 38.5% of the 1 prior line of therapy group (15 of 39), and 50.0% in group 2 or more prior lines of therapy group (27 of 54). The median time to first improvement of insomnia was 4.1 months (95% CI, 1.9 to not reached) in the naive group, 13.8 months (95% CI, 3.7 to not reached) in the 1 prior line of therapy group, and 7.2 months (95% CI, 3.9 to not reached) in the 2 or more prior lines of therapy group.7
Fatigue
Baseline scores for fatigue did not meet a clinically meaningful threshold in the overall population (mean = 37.9; SD = 26.0) and so were not considered evidence of a clinically meaningful impairment. The 39-point threshold was exceeded in the naive group (baseline mean = 41.6; SD = 27.7) and the group with 2 or more prior lines of therapy (baseline mean fatigue = 41.8; SD = 26.3) and so was considered a clinically meaningful impairment. The threshold was not met in the 1 prior line of therapy group and so was not to be a clinically meaningful impairment. The time-to-event analyses showed improvements (≥ 10-point decrease) in fatigue in 77.8% of the naive group (21 of 27), 56.4% of the 1 prior line of therapy group (22 of 39), and 66.7% of the 2 or more prior lines of therapy group (36 of 54).
Pain
Baseline scores for pain met a clinically meaningful threshold of 25 points overall (mean = 29.4; SD = 28.5) and in all subgroups and was considered a meaningful impairment. Time-to-event analyses showed improvements (≥ 10-point decrease) in pain in 63.0% of the naive group (17 of 27), 46.2% of the 1 prior line of therapy group (18 of 39), and 50.0% of the 2 or more prior lines of therapy group (27 of 54). All line of therapy subgroups exceeded the clinically meaningful threshold of 8 points for nausea and vomiting; no other subscales met the threshold signifying a clinically meaningful problem.7
As fewer patients were available to complete questionnaires as cycles increased, the obtained findings should be interpreted with caution.
Progression-Free Survival
Primary and Integrated Analysis Sets (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
Table 16 summarizes information on PFS in the PAS and IAS populations. At the March 30, 2020, data cut-off, 52.4% of patients in the PAS population were alive and progression-free, with a median follow-up of 16.8 months by IRC. The median PFS in the PAS was estimated by the IRC to be 19.3 months (95% CI, 13.9 to NE). In the IAS population, 66.1% of patients were alive and progression-free, with a median follow-up of 13.6 months at the March 30, 2020, data cut-off. The median PFS was estimated as 19.3 months (95% CI, 16.5 to NE).
The sponsor conducted a follow-up analysis at a new data cut-off date of June 15, 2021. The median PFS estimated in the IAS population was 24.94 months (95% CI, 19.3 to NE).
Figure 8 and Figure 9 present the Kaplan–Meier plots of PFS based on IRC assessments of the PAS and IAS (December 16, 2019, data cut-off only).
Table 16: Progression-Free Survival — PAS and IAS (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
Outcome | PAS | IAS | |||
|---|---|---|---|---|---|
March 30, 2020 N = 105 | December 16, 2019 N = 105 | June 15, 2021 N = 247 | March 30, 2020 N = 218 | December 16, 2019 N = 184 | |
Progression-free survival by IRC | |||||
Patients with an event, n (%) | |||||
Disease progression | 50 (47.6) | 39 (37.1) | NR | 74 (33.9) | 47 (25.5) |
Died (no prior disease progression) | NR | 5 (4.8) | NR | NR | 9 (4.9) |
Censored | 55 (52.4) | 61 (58.1) | NR | 144 (66.1) | 128 (69.6) |
Duration of follow-up (months), median | 16.76 | 13.86 | 24.7 | 13.6 | 10.97 |
25th to 75th percentiles | 14.7 to 21.9 | 11.3 to 19.1 | NR | 9.0 to 16.6 | 7.4 to 16.3 |
Median PFS, months, (95% CI) | 19.3 (13.9 to NE) | 16.53 (13.7 to NE) | 24.94 (19.3 to NE) | 19.3 (16.5 to NE) | 19.32 (13.9 to NE) |
PFS at 6-month time points, % (95% CI) | |||||
6 months or more | 82.1 (73.1 to 88.3) | 82.1 (73.1 to 88.3) | NR | 84.4 (78.7 to 88.7) | 83.8 (77.4 to 88.5) |
12 months or more | 65.7 (55.5 to 74.2) | 65.7 (55.4 to 74.1) | 71 | 69.7 (62.2 to 75.9) | 69.1 (60.6 to 76.1) |
18 months or more | 52.0 (41.1 to 61.9) | NR | NR | 54.2 (44.4 to 63.1) | NR |
24 months or more | 42.0 (29.5 to 53.9) | NR | 51 | 43.7 (31.5 to 55.4) | NR |
CI = confidence interval; IAS = integrated analysis set; IRC = independent radiographic committee; NE = not estimable; NR = not reached; PAS = primary analysis set.
Note: The PAS included a subset analysis of the FDA breakthrough therapy designation population (n = 58) who received prior platinum-based chemotherapy and an anti–programmed cell death protein 1 or anti–programmed cell death ligand 1 antibody. The IAS included all patients previously treated with platinum-based chemotherapy. Data cut-off dates were December 16, 2019; March 30, 2020; and June 15, 2021.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Figure 8: Kaplan–Meier Plot of Progression-Free Survival Based on IRC Assessment — Primary Analysis Set (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
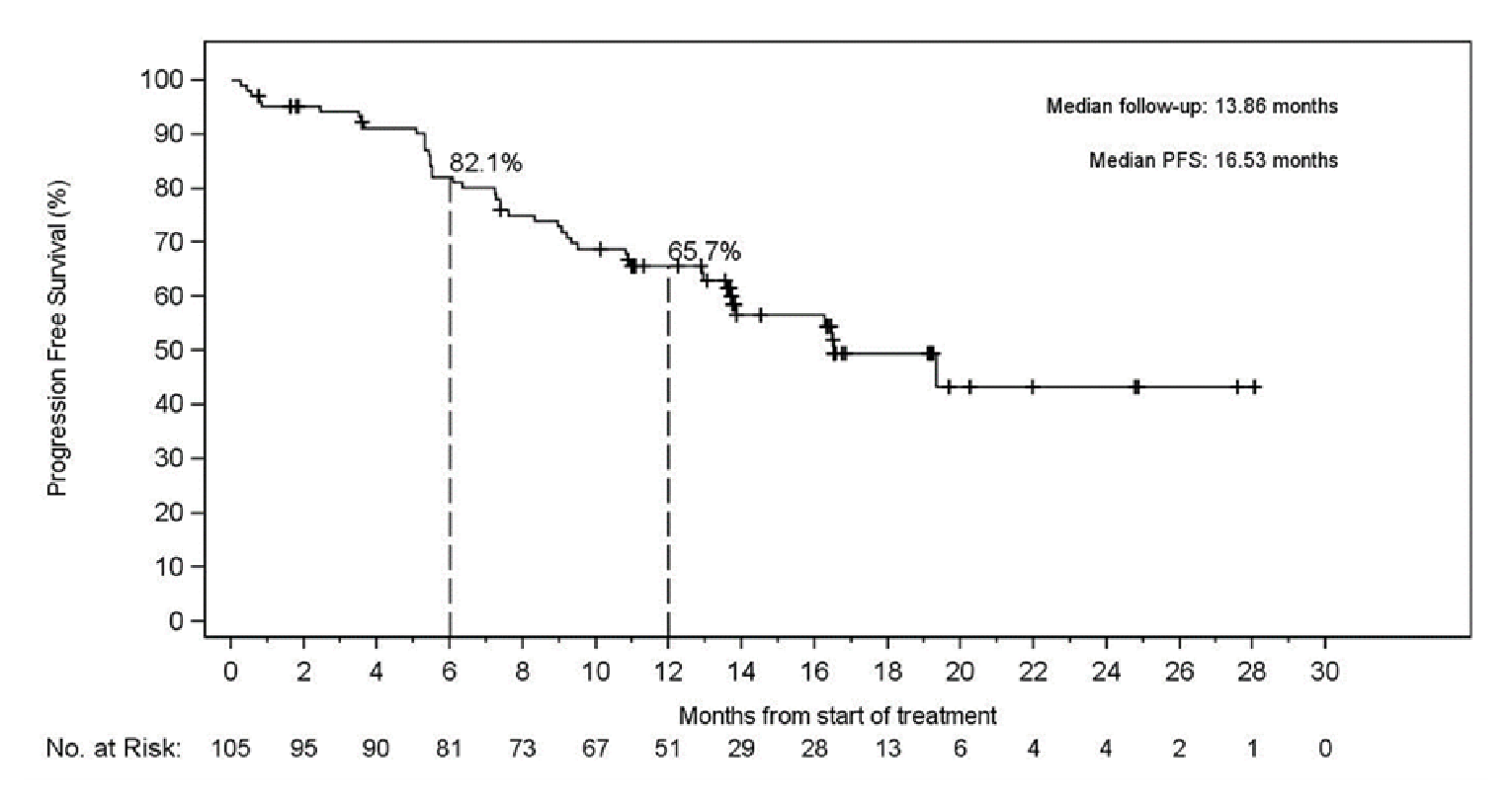
+ = censored; IRC = independent radiographic committee; NSCLC = non–small cell lung cancer; PFS = progression-free survival; RET = rearranged during transfection.
Note:. December 16, 2019, data cut-off.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Figure 9: Kaplan–Meier Plot of Progression-Free Survival Based on IRC Assessment — Integrated Analysis Set (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
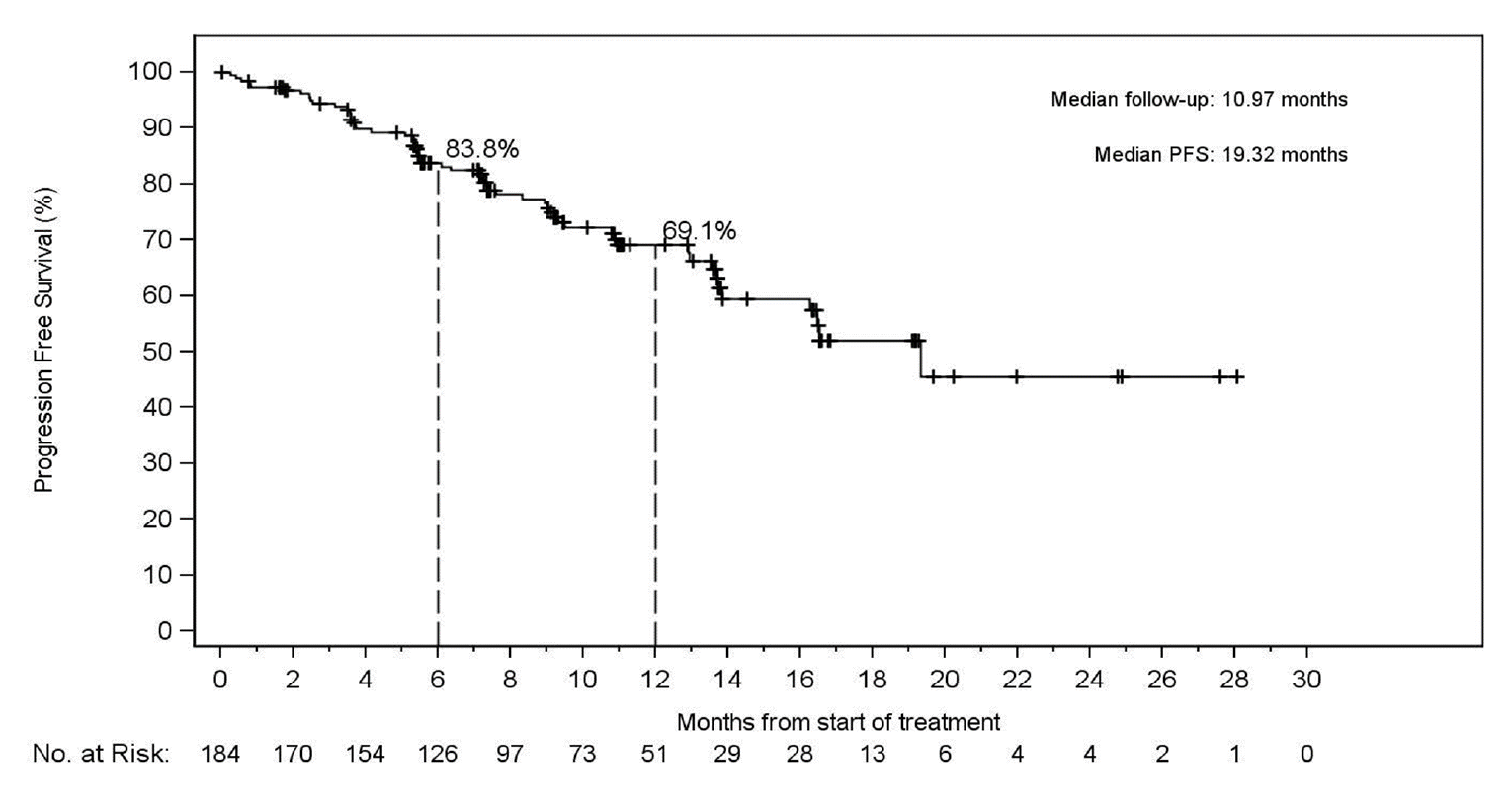
+ = censored; IRC = independent radiographic committee; NSCLC = non–small cell lung cancer; PFS = progression-free survival; RET = rearranged during transfection.
Note: December 16, 2019, data cut-off.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Treatment-Naive RET Fusion–Positive
Findings related to PFS in the treatment-naive population are presented in Table 17. At the March 30, 2020, data cut-off, 70.8% of patients were alive and progression-free at a median follow-up of 10.84 months. The median PFS by IRC assessment was NE.
At the December 16, 2019, data cut-off, 39 patients in the treatment-naive cohort had completed at least 6 months of follow-up from the first administered dose of selpercatinib. The median PFS was NE at the data cut-off date (95% CI, 13.8 to NE) according to the IRC assessment. Nine (23%) of 39 events had occurred, and a median follow-up of 9.2 months was reported. Figure 10 presents the Kaplan–Meier plot of PFS based on the IRC assessment.5
The sponsor conducted a follow-up analysis at a new data cut-off of June 15, 2021. The median PFS estimated in the treatment-naive population was 21.95 months (95% CI, 13.8 to NE).
Table 17: Progression-Free Survival — Treatment-Naive RET Fusion–Positive
Outcome | Treatment-naive RET fusion–positive NSCLC (SAS1) | ||
|---|---|---|---|
June 15, 2021 | March 30, 2020 N = 48 | December 16, 2019 N = 39 | |
Progression-free survival by IRC | |||
Responders | NR | 48 | 39 |
Patients with an event, n (%) | |||
Disease progression | NR | 14 (29.2) | 8 (20.5) |
Died (no prior disease progression) | NR | NR | 1 (2.6) |
Censored | NR | 34 (70.8) | 30 (76.9) |
Duration of follow-up (months), median (95% CI) | 21.9 | 10.84 | 9.17 |
25th to 75th percentiles | NR | 9.0 to 14.2 | 7.2 to 11.1 |
Duration of PFS, median (95% CI) | 21.95 (13.8 to NE) | NE (13.8 to NE) | NE (13.8 to NE) |
PFS at 6-month time points, % (95% CI) | |||
6 months or more | NR | 85.1 (71.2 to 92.6) | 86.4 (70.3 to 94.1) |
12 months or more | 71 | 67.6 (49.5 to 80.3) | 75.3 (56.0 to 87.0) |
18 months or more | NR | 61.4 (40.9 to 76.6) | NR |
24 months or more | 42 | NE (NE to NE) | NR |
IRC = independent radiographic committee; NE = not estimable; NR = not reported; NSCLC = non–small cell lung cancer; PFS = progression-free survival; RET = rearranged during transfection; SAS = supplemental analysis set.
Note: SAS1 included patients who were treatment naive. Data cut-off dates of December 16, 2019, March 30, 2020, and June 15, 2021.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Figure 10: Kaplan–Meier Plot of Progression-Free Survival Based on IRC Assessment — Treatment-Naive RET Fusion–Positive NSCLC
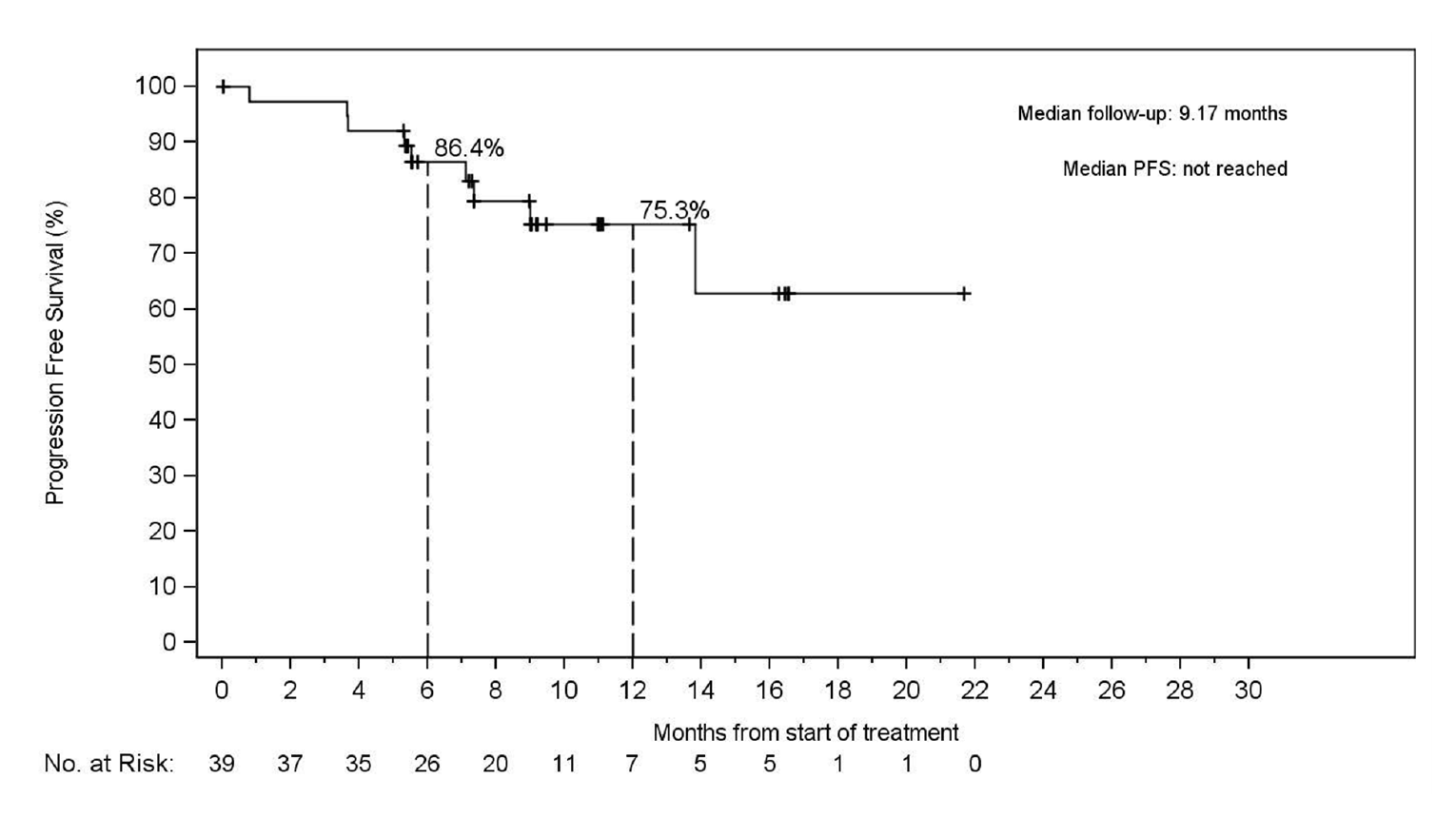
+ = censored; IRC = independent radiographic committee; NSCLC = non–small cell lung cancer; PFS = progression-free survival; RET = rearranged during transfection.
Note: Data cut-off date of December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Prior Other Systemic Therapy RET Fusion–positive NSCLC (Supplemental Analysis Set 2) and Non-Measurable Disease RET Fusion–Positive NSCLC (Supplemental Analysis Set 3)
PFS findings obtained in the SAS2 and SAS3 populations are presented in Table 18. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 18: PFS — Prior Other Systemic Therapy RET Fusion–Positive NSCLC (Supplemental Analysis Set 2) and Non-measurable Disease RET Fusion–Positive NSCLC (Supplemental Analysis Set 3)
Outcome | Prior other systemic therapy RET fusion–positive NSCLC (SAS2) March 30, 2020 N = 18 | Prior other systemic therapy RET fusion–positive NSCLC (SAS2) December 16, 2019 N = 16 | Non-measurable disease RET fusion–positive NSCLC (SAS3) March 30, 2020 N = 18 | Non-measurable disease RET fusion–positive NSCLC (SAS 3) December 16, 2019 N = 14 |
|---|---|---|---|---|
Progression-free survival | ||||
Status (n, %) | ||||
Disease progression | 6 (33.3) | ||||||||||||||||| | 6(33.3) | ||||||||||||||||| |
censored | 12 (66.7) | ||||||||||||||||| | 12 (66.7) | ||||||||||||||||| |
Duration of follow-up months | ||||
median | 11.53 | ||||||||||||||||| | 9.23 | ||||||||||||||||| |
25th to 75th percentiles | 7.6 to 16.1 | ||||||||||||||||| | 7.2 to 11.3 | ||||||||||||||||| |
Duration of progression-free survival (months) | ||||
median | NE | ||||||||||||||||| | NE | ||||||||||||||||| |
95% CI | 3.9 to NE | ||||||||||||||||| | 9.1 to NE | ||||||||||||||||| |
NE = not estimable; NSCLC = non–small cell lung cancer; RET = rearranged during transfection; SAS = supplemental analysis set.
Note: SAS2 included patients treated with other systemic therapies that are not platinum-based. SAS3 included patients with non-measurable RET fusion–positive NSCLC. Data cut-off dates of December 16, 2019, and March 30, 2020.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Subgroup Analysis
Data for the subgroup analyses were not provided.
Objective Response Rate
Primary and Integrated Analysis Sets (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
The ORR obtained at both cut-off dates (March 30, 2020, and December 16, 2019) in the PAS and IAS is summarized in Table 19.
At the December 16, 2019, data cut-off, an ORR of 64% (95% CI, 53.9 to 73.0) was estimated by the independent radiographic committee (IRC) in the PAS population, and in the IAS population, an ORR of 57% (104 of 184; 95% CI, 49.0 to 63.8) was estimated by the IRC.5
At the March 30, 2020, data cut-off, an ORR of 63.8% (53.9 to 73.0) and ORR of 56.9% (CI, 50.0 to 63.6) were reported by the IRC in the PAS and IAS, respectively. Of the patients with a confirmed best response of a CR or PR, 58.2% were ongoing in the PAS at a median follow-up of 15.67 months, and 69.4% of responses were ongoing in the IAS at a median follow-up of 11.99 months.
The sponsor conducted another analysis at a new data cut-off of June 15, 2021. The ORR estimated in the IAS population was 61.1% (95% CI, 54.7 to 67.2), which was consistent with previous analyses.
Table 19: Objective Response Rate in the PAS and IAS (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
Outcome | PAS | IAS | |||
|---|---|---|---|---|---|
March 30, 2020 N = 105 | December 16, 2019 N = 105 | June 15, 2021 N = 247 | March 30, 2020 N = 218 | December 16, 2019 N = 184 | |
Objective response rate | |||||
n (%) | 67 (63.8) | 67 (63.8) | 61.1% | 124 (56.9) | 104 (56.5) |
95% CI | 53.9 to 73.0 | 53.9 to 73.0 | 54.7 to 67.2 | 50.0 to 63.6 | 49.0 to 63.8 |
Best overall response, n (%) | |||||
Complete response | 3 (2.9) | 2 (1.9) | 18 (7.3) | 9 (4.1) | 6 (3.3) |
Partial response | 64 (61.0) | 65 (61.9) | 133 (53.8) | 115 (52.8) | 98 (53.3) |
Stable disease | 30 (28.6) | 30 (28.6) | 81 (32.7) | 81 (37.2) | 69 (37.5) |
Progressive disease | 4 (3.8) | 4 (3.8) | 7 (2.8) | 5 (2.3) | 4 (2.2) |
Not evaluable | 4 (3.8) | 4 (3.8) | 8 (3.2) | 8 (3.7) | 7 (3.8) |
CI = confidence interval; IAS = integrated analysis set; PAS = primary analysis set; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note: The PAS includes a subset analysis of the FDA breakthrough therapy designation population (n = 58) who received prior platinum-based chemotherapy and an anti–programmed cell death protein 1 or anti–programmed cell death ligand 1 antibody. It also includes 5 patients with non-measurable disease according to the investigator, and 4 patients with non-measurable disease according to the IRC. The IAS includes all patients previously treated with platinum-based chemotherapy. Data cut-off dates of December 16, 2019; March 30, 2020; and June 15, 2021.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Treatment-Naive RET Fusion–Positive NSCLC (SAS1)
Table 20 summarizes the ORR obtained in the treatment-naive RET fusion–positive NSCLC population. At the December 16, 2019, data cut-off, the IRC-assessed ORR for the treatment-naive RET fusion–positive NSCLC population was 85% (33 of 39, 95% CI, 69.5 to 94.1).5 At the March 30, 2020, data cut-off, the ORR by IRC assessment was 85.4% for the treatment-naive set and consisted of 2.1% CRs and 83.3% PRs.
The sponsor conducted follow-up analysis with a new data cut-off of June 15, 2021. The ORR estimated in the treatment-naive population was 84.1% (95% CI, 73.3 to 91.8), which was consistent with previous analyses.
Table 20: Objective Response Rate — Treatment-Naive RET Fusion–Positive NSCLC
Outcome | Treatment-naive RET fusion–positive NSCLC (SAS1) | ||
|---|---|---|---|
June 15, 2021 (N = 69) | March 30, 2020 (N = 48) | December 16, 2019 (N = 39)a | |
Objective response rate | |||
n (%) | 84.1% | 41 (85.4) | 33 (84.6) |
95% CI | 73.3 to 91.8 | 72.2 to 93.9 | 69.5 to 94.1 |
Best overall response, n (%) | |||
Complete response | 4 (5.8) | 1 (2.1) | 0 |
Partial response | 54 (78.3) | 40 (83.3) | 33 (84.6) |
Stable disease | 6 (8.7) | 4 (8.3) | 4 (10.3) |
Progressive disease | 3 (4.3) | 2 (4.2) | 1 (2.6) |
Not evaluable | 2 (2.9) | 1 (2.1) | 1 (2.6) |
CI = confidence interval; NSCLC = non–small cell lung cancer; RET = rearranged during transfection; SAS = supplemental analysis set.
Note: SAS1 included patients who were treatment naive.
aTwo partial responses were unconfirmed.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Prior Other Systemic Therapy RET Fusion–Positive NSCLC (Supplemental Analysis Set 2) and Non-Measurable Disease RET Fusion–Positive NSCLC (Supplemental Analysis Set 3)
The ORR obtained by the IRC assessment in the prior other systemic therapy RET fusion–positive NSCLC (SAS2) was |||||||||||||||||||||||||||||||||| at the December 16, 2019, analysis and 44.4% (8 of 18; 95% CI, 21.5 to 69.2) at the March 30, 2020, analysis in patients with RET fusion–positive NSCLC who had received a previous systemic therapy other than a platinum-based chemotherapy. Table 21 summarizes ORR data obtained at both cut-offs in this subset.
The ORR obtained by the IRC assessment in the non-measurable disease RET fusion–positive NSCLC (SAS3) was |||||||||||||||||||||||||||||||||| at the December 16, 2019, data cut-off and 33.3% (95% CI, 13.3 to 59.0) at the March 30, 2020, data cut-off.
Table 21: ORR – Prior Other Systemic Therapy RET Fusion–Positive NSCLC (Supplemental Analysis Set 2) and Non-Measurable Disease RET Fusion–Positive NSCLC (Supplemental Analysis Set 3)
Outcome | Prior other systemic therapy RET fusion–positive NSCLC (SAS2) March 30, 2020 N = 18 | Prior other systemic therapy RET fusion–positive NSCLC (SAS2) December 16, 2019 N = 16 | Non-measurable disease RET fusion–positive NSCLC (SAS3) March 30, 2020 N = 18 | Non-measurable disease RET fusion–positive NSCLC (SAS3) December 16, 2019 N = 14 |
|---|---|---|---|---|
Objective response rate | ||||
n (%) | 8 (44.4) | ||||||||||||||||| | 6 (33.3) | ||||||||||||||||| |
95% CI | 21.5 to 69.2 | ||||||||||||||||| | 13.3 to 59.0 | ||||||||||||||||| |
Best overall response, n (%) | ||||
Complete response | 0 | ||||||||||||||||| | 1 (5.6) | ||||||||||||||||| |
Partial response | 8 (44.4) | ||||||||||||||||| | 5 (27.8) | ||||||||||||||||| |
Stable disease | 9 (50) | ||||||||||||||||| | 9 (50) | ||||||||||||||||| |
Progressive disease | 1 (5.6) | ||||||||||||||||| | 0 | ||||||||||||||||| |
Not evaluable | 0 | ||||||||||||||||| | 3 (16.7) | ||||||||||||||||| |
CI = confidence interval; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Subgroup Analysis
CNS Metastasis at Baseline (Overall NSCLC Population)
At the December 16, 2019, data cut-off, a total of 80 patients in the overall RET fusion–positive NSCLC population (independent of analysis set, n = 253) had undergone an investigator-assessed CNS metastasis at baseline and had accumulated at least 6 months of follow-up from the first administered selpercatinib dose. Table 22 presents an overview of the CNS ORR in the overall population of RET fusion–positive NSCLC with measurable and non-measurable CNS lesions at baseline.
A CNS measurable lesion (by RANO criteria) was defined in the LIBRETTO-001 trial as: having clearly defined margins; visible on 2 or more axial slices, preferably less than 5 mm thick; at least 10 mm in size if slice thickness is less than 5 mm (or twice the slice thickness if more than 5 mm thick); and not measuring a cystic cavity. Non-measurable CNS lesions were defined as those that did not fit the criteria for measurable lesion; more specifically, lesions that are cystic or necrotic or include a surgical cavity should not be considered measurable.
At the December 16, 2019, data cut-off, the IRC identified 22 patients with measurable CNS disease out of the 80 with CNS metastasis at baseline. Among the 22 patients, a CNS ORR of 82% (18 of 22; 95% CI, 59.7 to 94.8) was reported, with 5 patients (23%) reportedly exhibiting CRs and 13 patients (59%) exhibiting PRs. The median response was 9.4 months (95% CI, 7.4 to NE). Stable disease was reported in 18% of patients.5,24 At the March 30, 2020, data cut-off, of the 23 patients assessed with measurable disease at baseline, the estimated CNS ORR was 87% (95% CI, 66.5 to 97.2) — 21.7% had a CR and 65.2% had a PR. The median CNS duration was 9.4 months (95% CI, 6.7 to 12.1).
Table 22: CNS ORR by IRC Assessment — CNS Analysis Set With a Measurable Lesion (RET Fusion–Positive NSCLC)
Response | Patients with measurable CNS disease | |
|---|---|---|
March 30, 2020 | December 16, 2019 | |
N | 23 | 22 |
CNS objective response rate (CR + PR) | ||
n (%) | 20 (87.0) | 18 (82) |
95% CI | 66.4 to 97.2 | 59.7 to 94.8 |
CNS best overall response, n (%) | ||
Complete response | 5 (21.7) | 5 (23) |
Partial response | 15 (65.2) | 13 (59) |
Stable disease | 3 (13.0) | 4 (18) |
Progressive disease | NR | 0 |
Not evaluable | NR | 0 |
CNS duration of response status (n, %) | ||
Died (no prior disease progression) | NR | 1 (5.6) |
Disease progression | NR | 9 (50.0) |
Censored | NR | 8 (44.4) |
CNS median duration of follow-up, months | 12.98 | 9.5 |
25th to 75th percentiles | 12.0 to 21.1 | 9.2 to 15.7 |
CNS duration of response, months | ||
Median (95% CI) | 9.36 (6.7 to 12.1) | 9.4 (7.4 to NE) |
CI = confidence interval; CNS = central nervous system; CR = complete response; IRC = independent radiographic committee; NSCLC = non–small cell lung cancer; NR = not reported; ORR = objective response rate; PR = partial response; RET = rearranged during transfection.
Note: % is calculated based on the number of patients with CNS best response of CR or PR as denominator.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Table 23 presents an overview of the CNS ORR obtained in the overall RET fusion–positive NSCLC population with measurable and non-measurable CNS lesions at baseline at the 2 data cut-offs (March 30, 2020, and December 16, 2019). At the December 16, 2019, data cut-off, of 80 patients with CNS disease at baseline, a CNS ORR of 48% (38 of 80; 95% CI, 36.2 to 59.0) was reported by the IRC. At the March 30, 2020, data cut-off, of the 96 patients with CNS at baseline, the estimated CNS ORR was 46.9% (95% CI, 36.6 to 57.3).
The median CNS duration of response at the March 30, 2020, data cut-off was 9.36 months (95% CI, 6.7 to 12.1), with a follow-up duration of 12.98 months. At the December 16, 2019, data cut-off, the median DOR was NE (95% CI, 9.3 to NE) at a median duration of follow-up of 9.5 months. Twenty-five patients (31%) had a CNS DOR of at least 6 months, and 5 patients (6%) had a CNS DOR of at least 12 months. The assessment identified 25 patients (31%) with a CNS DOR of at least 6 months, and 5 patients (6%) with a CNS DOR of at least 12 months.5
Table 23: CNS ORR by IRC Assessment — Analysis Set with Measurable and Non-Measurable CNS Lesions
Response | Patients with measurable or non-measurable CNS by IRC March 30, 2020 | Patients with measurable or non-measurable CNS by IRC December 16, 2019 |
|---|---|---|
n | 96 | 80 |
Patients with best response of confirmed CR or PR | 45 | 38 |
CNS ORR | ||
n (%) | 45 (46.9) | 38 (47.5) |
95% CI | 36.6 to 57.3 | 36.2 to 59.0 |
CNS best overall response, n (%) | ||
Complete response | 30 (31.3) | 25 (31.3) |
Partial response | 15 (15.6) | 13 (16.3) |
Stable disease | 3 (3.1) | 4 (5.0) |
CNS duration of response | — | — |
Duration of response status, n (%) | ||
Disease progression | NR | 9 (23.7) |
Died (no prior disease progression) | NR | 2 (5.3) |
Censored | NR | 27 (71.1) |
CNS duration of response follow-up, months | ||
Median | 11.99 | 9.5 |
25th to 75th Percentiles | 7.4 to 14.6 | 5.7 to 12.0 |
CNS duration of response, months | ||
Median | NE | NE |
95% CI | 9.3 to NE | 9.3 to NE |
CI = confidence interval; CNS = central nervous system; CR = complete response; IRC = independent radiographic committee; NE = not estimable; NR = not reported; ORR = objective response rate; PR = partial response.
Note: Data cut-off dates of December 16, 2019, and March 30, 2020.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Performance Status, Number of Prior Therapies, Prior Anti–PD-1 and Anti–PD-L1 Therapy, and Prior Multikinase Inhibitor Therapy Subgroup Analysis
The ORR and DOR obtained in the subgroups (performance status, number of prior therapies, prior anti–PD-1 and anti–PD-L1 therapy, and prior multikinase inhibitor therapy) at the December 16, 2019, data cut-off are presented in Table 24.
Table 24: ORR and DOR — ECOG PS, Number and type of Prior Therapy Based on IRC Assessment
Study characteristic | N | Responders | ORR% (95% CI) | DOR months, median (95% CI) |
|---|---|---|---|---|
Overall | 105 | 67 | 63.8 (53.9 to 73.0) | 17.51 (1.9+ to 26.2+) |
ECOG PS | ||||
0 | 31 | 23 | 74.2 (55.4 to 88.1) | NR (7.4+ to 26.2+) |
1 to 2 | 74 | 44 | 59.5 (47.4 to 70.7) | 12.12 (1.9+ to 24.0+) |
Number of prior therapies | ||||
1 to 2 | 46 | 27 | 58.7 (43.2 to 73.0) | 17.51 (1.9+ to 18.5+) |
3 or more | 59 | 40 | 67.8 (54.4 to 79.4) | NR (1.9+ to 26.2+) |
Prior anti–PD-1/PD-L1 therapy | ||||
Yes | 58 | 38 | 65.5 (51.9 to 77.5) | NR (1.9+ to 26.2+) |
No | 47 | 29 | 61.7 (46.4 to 75.5) | 17.51 (2.8 to 24.0+) |
Prior multikinase inhibitor therapy | ||||
Yes | 50 | 32 | 64.0 (49.2 to 77.1) | NR (1.9+ to 26.2+) |
No | 55 | 35 | 63.6 (49.6 to 76.2) | 17.51 (1.9+ to 18.5+) |
+= censored; CI = confidence interval; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IRC = independent radiographic committee; ORR = objective response rate; NR = not reached; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1.
Note: Data cut-off date of December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Duration of Response
Primary and Integrated Analysis Set (RET Fusion–Positive NSCLC with Prior Platinum Chemotherapy)
The DORs obtained at both cut-off dates (March 30, 2020, and December 16, 2019) in the PAS and IAS are summarized in Table 25. At the December 16, 2019, data cut-off, a median DOR of 17.5 months (95% CI, 12.0 to NE) was reported by IRC, 24 (34%) of 67 events had occurred, and a median DOR follow-up of 12.1 months was estimated in the PAS population. In the IAS, a median DOR of 17.5 months (95% CI, 12.1 to NE), with 25 (24%) of 104 events, and a median DOR follow-up of 9.2 months was reported in the IRC assessment.
At the March 30, 2020, data cut-off, the median DOR reported by the IRC was 17.51 months (95% CI, 12.1 to NE) in the PAS and the median DOR was 17.51 months (95% CI, 12.1 to NE) in the IAS population.
The sponsor conducted a follow-up analysis at a new data cut-off of June 15, 2021. The median DOR obtained in the IAS population was 28.6 months (95% CI, 20.4 to NE).
The Kaplan–Meier estimates (December 16, 2019, cut-off) for the PAS population and the IAS population are presented in Figure 11 and Figure 12, respectively.5
Table 25: Duration of Response — PAS and IAS (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
Response | PAS | IAS | |||
|---|---|---|---|---|---|
March 30, 2020 N = 105 | December 16, 2019 N = 105 | June 15, 2021 N = 247 | March 30, 2020 N = 218 | December 16, 2019 N = 184 | |
Duration of response by IRC | |||||
Patients with confirmed CR or PR, n | 67 | 67 | NR | 124 | 104 |
Patients with an event, n (%) | |||||
Disease progression | 26 (38.8) | 21(31.3) | NR | 34 (27.4) | 23 (22.1) |
Died (no prior disease progression) | 2 (3.0) | 2 (3.0) | NR | 4 (3.2) | 2 (1.9) |
Censored | 39 (58.2) | 44 (65.7) | NR | 86 (69.4) | 79 (76.0) |
Reason for being censored | |||||
Alive without documented disease progression | 37 (55.2) | 42 (62.7) | NR | 83 (66.9) | 77 (74.0) |
Subsequent anticancer therapy or cancer-related surgery without documented disease progression | 2 (3.0) | 2 (3.0) | NR | 3 (2.4) | 2 (1.9) |
Discontinued from study without documented disease progression | NR | 0 | NR | NR | 0 |
Duration of response follow-up (months), median | 15.67 | 12.06 | 21.2 | 11.99 | 9.23 |
25th to 75th percentiles | 12.1 to 18.2 | 9.2 to 14.8 | NR | 7.4 to 15.9 | 5.6 to 13.9 |
Duration of response (months), median (95% CI) | 17.51 (12.1 to NE) | 17.51 (12.0 to NE) | 28.6 (20.4 to NE) | 17.51 (12.1 to NE) | 17.51 (12.1 to NE) |
Observed duration of response, n (%)a | |||||
< 6 months | 10 (14.9) | 13 (19.4) | NR | 36 (29.0) | 39 (37.5) |
≥ 6 to 12 months | 21 (31.3) | 30 (44.8) | 73 | 51 (41.1) | 41 (39.4) |
≥ 12 to 18 months | 28 (41.8) | 20 (29.9) | NR | 29 (23.4) | 20 (19.2) |
≥ 18 to 24 months | 5 (7.5) | 3 (4.5) | NR | 5 (4.0) | 3 (2.9) |
≥ 24 months | 3 (4.5) | 1 (1.5) | 56 | 3 (2.4) | 1 (1.0) |
CI = confidence interval; CR = complete response; IAS = integrated analysis set; IRC = independent radiographic committee; NE = not estimable, NR = not reported; NSCLC = non–small cell lung cancer; PAS = primary analysis set; PR = partial response; RET = rearranged during transfection.
aIncludes censored patients whose disease has not yet progressed.
Note: The PAS includes the FDA breakthrough therapy designation population (n = 58) who received prior platinum-based chemotherapy and an anti–programmed cell death protein 1 or anti–programmed cell death ligand 1 antibody. The IAS included all patients previously treated with platinum-based chemotherapy. Data cut-off dates of December 16, 2019, March 30, 2020, and June 15, 2021.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Figure 11: Kaplan–Meier Plot of Duration of Response Based on IRC Assessment — Primary Analysis Set (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy
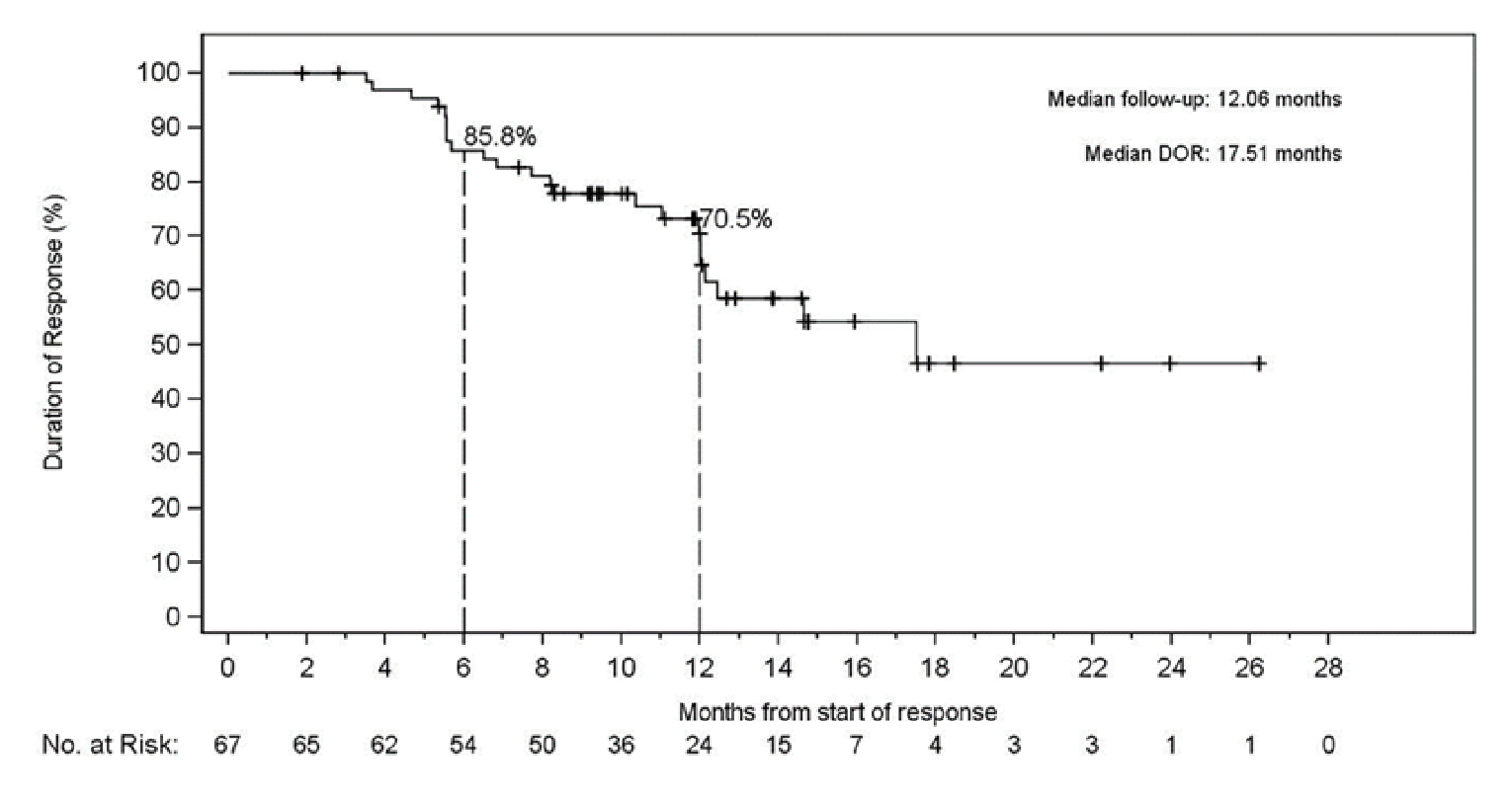
+ = censored; DOR = duration of response; IRC = independent radiographic committee; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note: Data cut-off date of December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Figure 12: Kaplan–Meier Plot of Duration of Response Based on IRC Assessment —Integrated Analysis Set (RET Fusion–Positive NSCLC With Prior Platinum Chemotherapy)
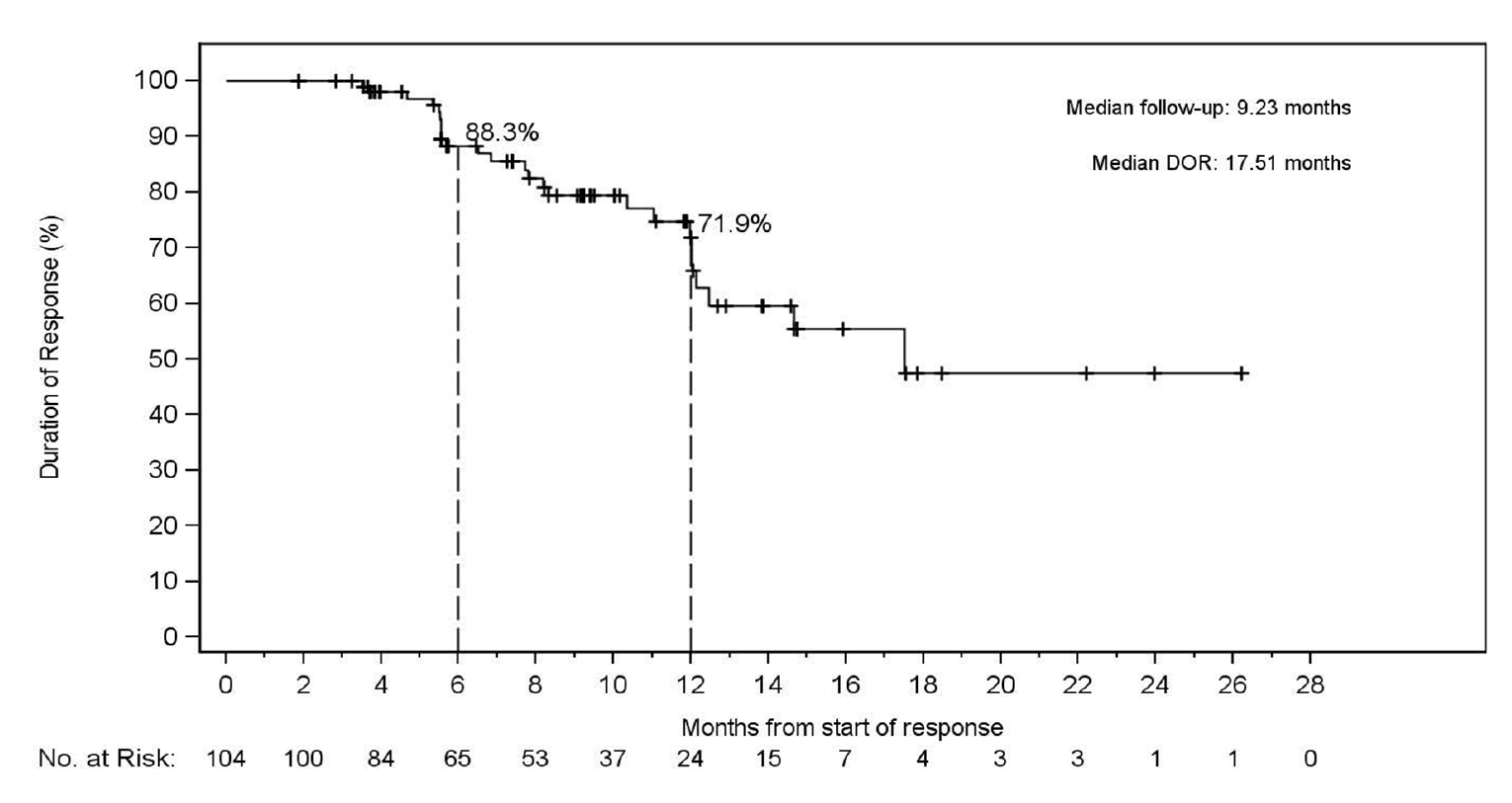
+ = censored; DOR = duration of response; IRC = independent radiographic committee; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note: Data cut-off date of December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Treatment-Naive RET Fusion–Positive NSCLC Population
Table 26 summarizes information on the DOR obtained in the treatment-naive RET fusion–positive NSCLC population. At the December 16, 2019, data cut-off, the DOR in 33 patients in the treatment-naive cohort was assessed by the IRC. The median DOR was NE. At the data cut-off date of March 30, 2020, 65% of the responses were ongoing at 12 months, according to the IRC assessment. Figure 13 presents the Kaplan–Meier plot of the DOR based on the IRC assessment.5
The sponsor conducted a follow-up analysis at a new data cut-off of June 15, 2021. The median DOR estimated in the treatment-naive population was 20.2 months (95% CI, 13.0 to NE).
Table 26: Duration of Response — Treatment-Naive RET Fusion–Positive NSCLC Population
Response | Treatment-naive RET fusion–positive NSCLC (SAS1) | ||
|---|---|---|---|
June 15, 2021 N = 69 | March 30, 2020 N = 48 | December 16, 2019 N = 39a | |
Duration of response (months) | |||
Responders with best response of confirmed CR or PR | NR | 41 | 33 |
Patients with an event (n, %) | |||
Disease progression | NR | 10 (24.4) | 7 (21.2) |
Died (no prior disease progression) | NR | 0 | NR |
Censored | NR | 31 (75.6) | 26 (78.8) |
Reason censored (n, %) | NR | ||
Alive without documented disease progression | NR | 30 (73.2) | 25 (75.8) |
Subsequent anticancer therapy or cancer-related surgery without documented disease progression | NR | 1 (2.4) | NR |
Duration of response follow-up (months), median | 20.3 | 9.79 | 7.39 |
25th to 75th percentiles | NR | 7.0 to 13.1 | 5.5 to 12.0 |
Duration of response (months) | |||
Median (95% CI) | 20.2 (13.0 to NE) | NE (12.0 to NE) | NE (12.0 to NE) |
Observed duration of response, n (%)a | |||
< 6 months | NR | 13 (31.7) | 14 (42.4) |
≥ 6 to 12 months | 66 | 17 (41.5) | 14 (42.4) |
≥ 12 to 18 months | NR | 9 (22.0) | 4 (12.1) |
≥ 18 to 24 months | NR | 2 (4.9) | 1 (3.0) |
≥ 24 months | 42 | 0 | 0 |
CI = confidence interval; CR = complete response; NE = not estimable; NR = not reached; NSCLC = non–small cell lung cancer; PR = partial response; RET = rearranged during transfection; SAS = supplemental analysis set.
Note: SAS1 includes patients who were treatment naive. Data cut-off dates of December 16, 2019; March 30, 2020; and June 15, 2021.
aIncludes censored patients whose disease has not yet progressed.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Prior Other Systemic Therapy RET Fusion–Positive NSCLC (Supplemental Analysis Set 2) and Non-Measurable Disease RET Fusion–Positive NSCLC (Supplemental Analysis Set 3)
The DOR obtained in the prior other systemic therapy RET fusion–positive NSCLC (SAS2) and non-measurable disease RET fusion–positive NSCLC (SAS 3) populations at both data cut-offs are presented in Table 27.
Figure 13: Kaplan–Meier Plot of Duration of Response Based on IRC Assessment — Treatment-Naive RET Fusion–Positive NSCLC Population
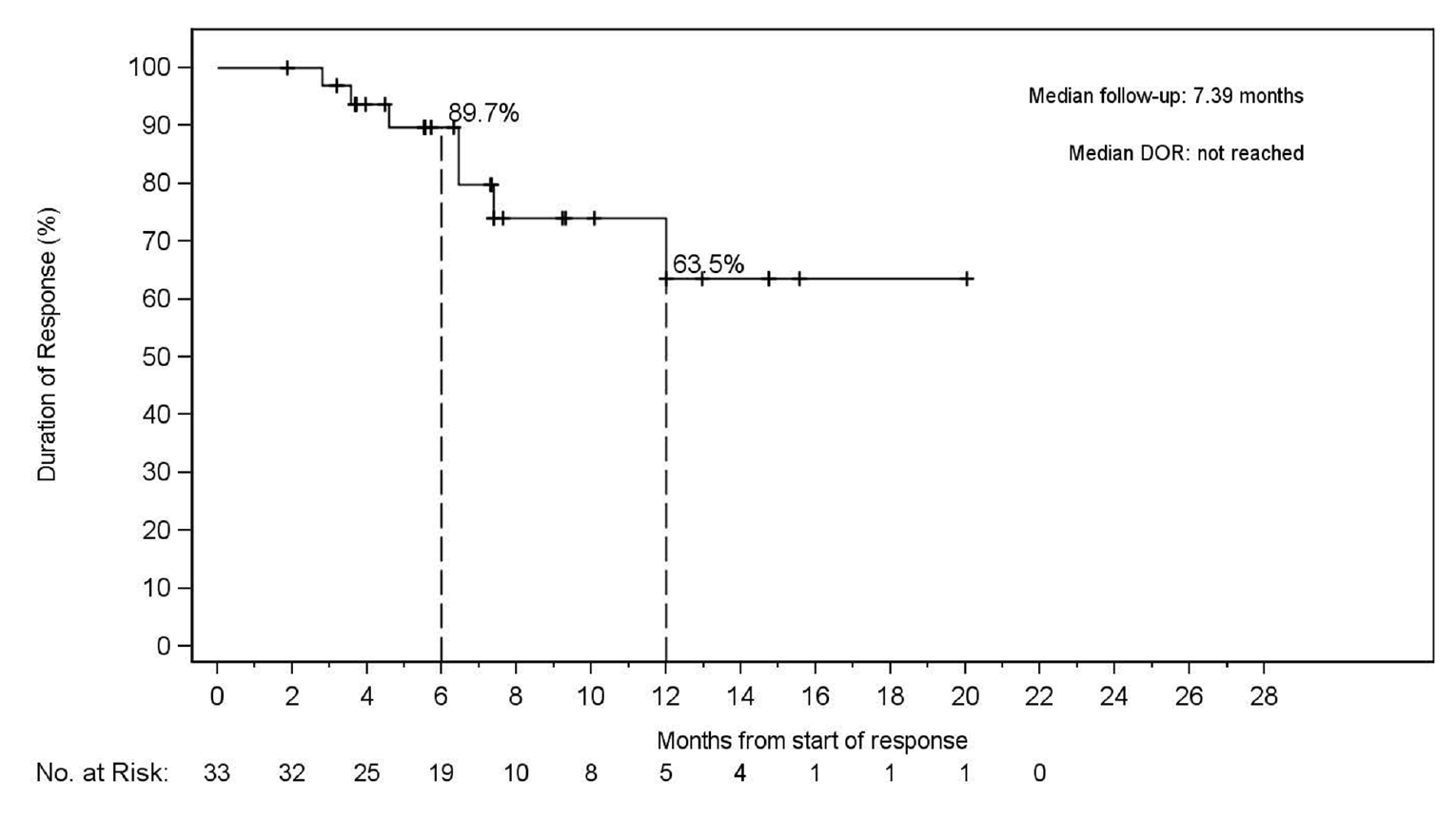
+ = censored; DOR = duration of response; IRC = independent radiographic committee; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Note:.Data cut-off date of December 16, 2019.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Table 27: DOR — Prior Other Systemic Therapy RET Fusion–Positive NSCLC (Supplemental Analysis Set 2) and Non-Measurable Disease RET Fusion–Positive NSCLC (Supplemental Analysis Set 3)
Duration of response | Prior other systemic therapy RET fusion–positive NSCLC (SAS2) March 30, 2020 N = 18 | Prior other systemic therapy RET fusion–positive NSCLC (SAS2) December 16, 2019 N = 16 | Non-measurable disease RET fusion–positive NSCLC (SAS3) March 30, 2020 N = 18 | Non-measurable disease RET fusion–positive NSCLC (SAS3) December 16, 2019 N = 14 |
|---|---|---|---|---|
Patients with an event (n, %) | ||||
Disease progression | 1 (12.5) | ||||||||||||||||| | 0 | ||||||||||||||||| |
Died (no prior disease progression) | 0 | ||||||||||||||||| | 0 | ||||||||||||||||| |
Censored | 7 (87.5) | ||||||||||||||||| | 6 (100) | ||||||||||||||||| |
Duration of response follow-up, months | ||||
Median | 10.43 | ||||||||||||||||| | 7.39 | ||||||||||||||||| |
25th to 75th percentiles | 9.2 to 14.4 | ||||||||||||||||| | 3.7 to 9.6 | ||||||||||||||||| |
Duration of response, months | ||||
median (95% CI) | NE (12 to NE) | ||||||||||||||||| | NE (NE to NE) | ||||||||||||||||| |
CI = confidence interval; DOR = duration of response; NE = not estimable; NR = not reported; NSCLC = non–small cell lung cancer; RET = rearranged during transfection; SAS = supplemental analysis set.
Note: SAS2 included patients treated with other systemic therapies that are not platinum-based. SAS3 included patients with non-measurable disease RET fusion–positive NSCLC. Data cut-off dates of December 16, 2019, and March 30, 2020.
Source: Sponsor’s submission package, Retevmo (selpercatinib).5
Subgroup Analysis
Performance Status, Number of Prior Therapies, Prior Anti–PD-1 and Anti–PD-L1 Therapy, and Prior Multikinase Inhibitor Therapy Subgroup Analysis
The DORs obtained in the subgroups of interest identified in the CADTH protocol are presented in Table 24.
Harms
Only harms identified in the CADTH review protocol are reported here.5 AEs are presented for the OSAS (March 30, 2020, and December 16, 2019, data cut-offs) and for the NSCLC population (December 16, 2019, data cut-off) in the LIBRETTO-001 trial (Table 28). The focus for the review is the frequency of AEs on the NSCLC population.
Adverse Events
At the December 16, 2019, data cut-off, the most common AEs in the NSCLC population were dry mouth, diarrhea, hypertension, increased AST and ALT, fatigue, constipation, peripheral edema, headache, and nausea.5
At the March 30, 2020, data cut-off, AEs specific to the NSCLC population were not presented. In total, 99.7% of patients (n = 345) in the NSCLC population had at least 1 treatment-emergent AE and 61.2% had grade 3 or 4 events. The AEs reported in the NSCLC population were consistent with the overall safety set at both data cut-offs.
Serious Adverse Events
At the December 16, 2019, data cut-off, the most common SAEs in this population were pneumonia, increased ALT and AST, abdominal pain, pleural effusion, drug hypersensitivity, diarrhea, and acute kidney injury.5 At the March 30, 2020, data cut-off, SAEs specific to the NSCLC population were not reported.6 Table 28 presents SAEs reported in the NSCLC population at the December 16, 2019, data cut-off and in the overall safety population at the 2 data cut-offs (March 30, 2020, and December 16, 2019).
Withdrawals
At the December 16, 2019, data cut-off, AEs leading to dose withdrawal, interruption, and dose reductions in the RET fusion–positive NSCLC population were consistent with those observed in the overall safety set at both data cut-offs (March 30, 2020, and December 16, 2019). AEs commonly associated with treatment discontinuations in the NSCLC population were increased ALT, sepsis, increased AST, drug hypersensitivity, fatigue thrombocytopenia. Increased ALT and AST were commonly associated with dose reductions and dose interruptions. Table 28 presents data on the AEs leading to withdrawals, reductions, and interruptions in the OSAS (at the March 30, 2020, and December 16, 2019, cut-offs) and NSCLC populations.
Mortality
At the December 16, 2019 data cut-off, treatment was discontinued owing to death in 6 patients and 38 patients discontinued the study due to death. At the March 30, 2020 data cut-off, in the NSCLC population, treatment was discontinued owing to death in 6 (1.7%) patients and 55 (15.9%) patients discontinued the study due to death. In total, 36 patient deaths (10.4%) were attributed to disease progression, 13 of deaths (3.9%) occurred due to AEs, and 6 deaths (1.7%) were attributed to other reasons. One report of death (0.3%) identified in the NSCLC population had occurred more than 28 days after the last selpercatinib dose. In the OSAS population, treatment was discontinued due to death in 11 patients (1.5%) and 103 patients (13.8%) discontinued the study due to death.
Notable Harms
Notable harms reported in the NSCLC set were consistent with those in the OSAS (at the March 30, 2020, and December 16, 2019, data cut-offs). The most common AEs were increased ALT (32.8%), increased AST (31%), hypertension (31.9%), drug hypersensitivity (2.4%), and electrocardiogram QT prolongation (16.7%). Table 28 presents a summary of notable harms in the OSAS (at the 2 data cut-offs) and in the NSCLC population.
Table 28: Summary of Harms in the LIBRETTO-001 Trial for the Overall Safety Analysis Set (March 30, 2020, and December 16, 2019, Data Cut-Offs) and the NSCLC Population (December 16, 2019, Data Cut-Off)
Harms | OSAS March 30, 2020 cut-off N = 746 | OSAS December 16, 2019 cut-off N = 702 | NSCLC December 16, 2019 cut-off N = 329 |
|---|---|---|---|
Adverse events, n (%) | 740 (99.2) | 695 (99) | 325 (98.8) |
Adverse events in ≥ 15% of patients, n (%) | |||
Dry mouth | 300 (40.2) | 272 (38.7) | 134 (40.7) |
Diarrhea | 289 (38.7) | 254 (36.2) | 133 (40.4) |
Hypertension | 273 (36.6) | 246 (35.0) | 105 (31.9) |
Increased AST | 243 (32.6) | 210 (29.9) | 108 (32.8) |
Increased ALT | 243 (32.6) | 201 (28.6) | 102 (31.0) |
Fatigue | 233 (31.2) | 197 (28.1) | 78 (23.7) |
Constipation | 202 (27.1) | 178 (25.4) | 66 (20.1) |
Edema | 192 (25.7) | 165 (23.5) | 81 (24.6) |
Headache | 176 (23.6) | 161 (22.9) | 65 (19.8) |
Nausea | 175 (23.5) | 159 (22.6) | 69 (21.0) |
Blood creatinine increased | 154 (20.6) | 136 (19.4) | 58 (17.6) |
Abdominal pain | 140 (18.8) | 124 (17.7) | 46 (14.0) |
Serious adverse events ( ≥ 1% of patients), n (%) | 262 (35.1) | 234 (33.3) | 118 (35.9) |
Pneumonia | 23 (3.1) | 21 (3.0) | 13 (4.0) |
Dyspnea | 14 (1.9) | 12 (1.7) | 8 (2.4) |
Hyponatremia | 14 (1.9) | 12 (1.7) | 7 (2.1) |
Increased ALT | 12 (1.6) | 12 (1.7) | 9 (2.7) |
Increased AST | 12 (1.6) | 12 (1.7) | 9 (2.7) |
Abdominal pain | 11 (1.5) | 10 (1.4) | 1 (0.3) |
Pleural effusion | 11 (1.5) | 7 (1.0) | 6 (1.8) |
Drug hypersensitivity | 10 (1.3) | 8 (1.1) | 8 (2.4) |
Diarrhea | 9 (1.2) | 8 (1.1) | 3 (0.9) |
Acute kidney injury | 8 (1.1) | 8 (1.1) | 4 (1.2) |
Patients who permanently discontinued study treatment due to AEs, n (%) | 45 (6) | 37 (5.3) | 21 (6.4) |
Increased ALT | 3 (0.4) | 3 (0.4) | 2 (0.6) |
Sepsis | 3 (0.4) | 3 (0.4) | 0 |
Increased AST | 2 (0.3) | 2 (0.3) | 2 (0.6) |
Drug hypersensitivity | 2 (0.3) | 2 (0.3) | 2 (0.6) |
Fatigue | 2 (0.3) | 2 (0.3) | 2 (0.6) |
Thrombocytopenia | 2 (0.3) | 2 (0.3) | 2 (0.6) |
Dose reductions due to AE (occurring in ≥ 1%), n (%) | 251 (33.6) | 219 (31.2) | 117 (35.6) |
Increased ALT | 53 (7.1) | 45 (6.4) | 25 (7.6) |
Increased AST | 48 (6.4) | 39 (5.6) | 20 (6.1) |
Electrocardiogram QT prolonged | 19 (2.5) | 16 (2.3) | 10 (3.0) |
Fatigue | 20 (2.7) | 15 (2.1) | 5 (1.5) |
Drug hypersensitivity | 17 (2.3) | 12 (1.7) | 11 (3.3) |
Thrombocytopenia | NR | 10 (1.4) | 8 (2.4) |
Diarrhea | NR | 9 (1.3) | 6 (1.8) |
Dose interruptions owing to AE ≥ 1%, n (%) | 334 (44.8) | 294 (41.9) | 143 (43.5) |
Increased ALT | 42 (5.6) | 36 (5.1) | 19 (5.8) |
Increased AST | 37 (5.0) | 34 (4.8) | 17 (5.2) |
Hypertension | 37 (5.0) | 32 (4.6) | 16 (4.9) |
Diarrhea | 24 (3.2) | 18 (2.6) | 7 (2.1) |
Pyrexia | 20 (2.7) | 17 (2.4) | 9 (2.7) |
Electrocardiogram QT prolonged | 16 (2.1) | 15 (2.1) | 7 (2.1) |
Notable harms, n (%) | |||
AST increased | 410 (55) | 210 (29.9) | 108 (32.8) |
ALT increased | 369 (49.5) | 201 (28.6) | 102 (31.0) |
Hypertension | 279 (37.4) | 252 (35.9) | 105 (31.9) |
Hypersensitivity | 39 (5.2) | 30 (4.3) | 8 (2.4) |
Electrocardiogram QT prolonged | 135 (18.1) | 116 (16.5) | 55 (16.7) |
Hemorrhage | 18 (2.4) | 104 (14.8) | NR |
Embryo-fetal toxicity | NR | NR | NR |
Tumour lysis syndrome | NR | NR | NR |
AE = adverse event; ALT = alanine transaminase; AST = aspartate transaminase; NR = not reported; NSCLC = non– small cell lung cancer; OSAS = overall safety analysis set; NR = not reported.
Source: Sponsor’s submission package, Retevmo (selpercatinib)5 and European Medicines Agency report.6
Critical Appraisal
Internal Validity
The phase I and II design of the LIBRETTO-001 trial was used to determine the target population and the optimal drug dosage(s) for phase III.27 The design was insufficient for evaluating long-term outcomes for new drugs because of potential biases (e.g., inflated type I error due to the small sample sizes and multiple comparison tests conducted).28 The Notice of Compliance issued by Health Canada for the regulatory approval of selpercatinib outlined several conditions in accordance with the NOC/c, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The sponsor has initiated a phase III trial (LIBRETTO-431) to assess the efficacy and safety of selpercatinib against active comparators currently used in clinical practice in the treatment-naive population (NCT04194944).29 The clinical experts consulted by CADTH noted that there is limited evidence that patients with metastatic RET fusion–positive NSCLC benefit from currently available single-drug immunotherapy in practice, and not all patients respond to chemotherapy plus immunotherapy, indicating an unmet need for this patient population.
The open-label, non-comparative design of the LIBRETTO-001 trial, with no statistical testing, is the key limitation. The sponsor did not provide any hypothesis statements for statistical significance for the primary outcome, including secondary and subgroup analyses.8 The design increases the risk of bias in estimating treatment effects because the potential for confounding effects related to variations in health status and other unidentified prognostic factors that could affect subjectively assessed outcomes (i.e., response, HRQoL, and AEs). The potential for bias was reduced by using IRC assessments for key study outcomes, such as ORR and DOR. However, the lack of direct comparative data means the magnitude of effects obtained for the efficacy outcomes is uncertain. Although the clinical experts emphasized that the safety profile of selpercatinib was favourable compared to the other therapies available as standard of care in Canada, in the absence of a comparative arm, the findings obtained from the safety analysis are uncertain as the single-arm design does not allow for the differentiation of the symptoms of underlying NSCLC disease from treatment-related AEs.9 The sponsor agreed to provide results from ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| to confirm the clinical benefit of selpercatinib in patients with previously treated RET fusion–positive NSCLC according to the NOC/c issued by Health Canada. The sponsor noted in its response that ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The sponsor submitted additional data with a new cut-off date of June 15, 2021, during the completion of this CADTH review. Despite the results obtained from the updated (pre-specified or post hoc) analyses performed on June 15, 2021, whether the end points investigated are durable for long-term in this patient population remains uncertain.
The primary objective investigated in the phase II portion of the LIBRETTO-001 study was the ORR measured by RECIST 1.1. The FDA considers ORR alone to be a surrogate measurement when assessing treatment response in patients with advanced or metastatic NSCLC, and it may not correlate well with survival, unless the effect size of the ORR is large and the responses are durable. The sponsor hypothesized a true ORR of 50% or higher in the primary analysis of effectiveness and ruled out a lower limit of 30% for the ORR, which was considered clinically meaningful and consistent with the estimated response rates seen with approved targeted therapies in molecularly defined patient populations who have failed prior therapies (e.g., osimertinib, crizotinib, and alectinib). The ORRs obtained by the IRC for the PAS, IAS, and SAS1 were above the lower limit of 30% that the sponsor assumed in the sample size calculation for patients with RET fusion–positive NSCLC who progressed on or after receipt of platinum-based chemotherapy.5 Although the FDA review team noted that the magnitude of the ORR and DOR obtained in patients with RET fusion–positive NSCLC in the LIBRETTO-001 trial was large and considered it sufficient to establish clinical benefit,10 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||9 The sponsor agreed to provide results from ||||||||||||||||||||||||||||||||||||||||||||||||||| to confirm the clinical benefit of selpercatinib in patients with previously treated RET fusion–positive NSCLC according to the NOC/c issued by Health Canada. The sponsor also noted that |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||9 In the LIBRETTO-001 trial, radiographic scans were performed by an accredited laboratory and assessed by an IRC, reducing bias. Results obtained from both the IRC and investigator assessments did not differ greatly, which increases the validity of the ORR-related outcomes.
The time-to-events analyses, particularly the OS and PFS results, were considered exploratory by |||||||||||||||||, the FDA,10,30 and CADTH due to the lack of a control arm. Health Canada ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||9 Due to immature data in the PAS, IAS, and SAS1 populations at the March 31, 2020, and December 16, 2019, cut-offs, CADTH considered the results exploratory. The sponsor submitted additional data to CADTH for a new cut-off date of June 15, 2021, later during the completion of the review. Although the sponsor reported a median PFS of 24.94 months (95% CI, 19.3 to NE) in the IAS and 21.95 months (95% CI, 13.8 to NE) in the SAS1 population, the information was considered insufficient to form concrete conclusions on PFS in this population because of the single-arm design of the LIBRETTO-001 trial and immature data. The median OS was NE in the IAS and SAS1 datasets at the June 15, 2021, cut-off. Whether the observed magnitude of benefit related to tumour response with selpercatinib would be translated as OS in patients in the 2 groups is therefore uncertain.
The analysis sets — the PAS, IAS, and 3 SASs — were not predefined in the original statistical analysis plan; they were developed following consultation with the FDA and EMA. A key concern therefore is that these were post hoc analyses and may have been susceptible to bias. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| CADTH reviewers agreed |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, these were unlikely to introduce bias because the investigators remained blinded to results until after the revisions were made.9
The 3 planned interim analyses were pre-specified. However, the analyses were performed on observed data only, with no formal hypothesis testing, and only descriptive statistics were provided, further complicating assessment of the magnitude of effects observed in the different groups investigated.
Many of the subgroup analyses that were identified as relevant for this review were pre-specified in the statistical analysis plan for LIBRETTO-001. However, the subgroups had limited sample sizes, resulting in imprecise results for many of the subgroups. There were no tests for statistical differences between subgroups.
HRQoL was evaluated using the EORTC QLQ-C30 questionnaire. This questionnaire has been validated in patients with NSCLC and is considered appropriate for advanced or metastatic forms of the disease. Although this was an exploratory outcome investigated in the LIBRETTO-001 trial, the clinical experts and clinician groups noted that findings for quality of life are clinically significant because patients with advanced disease usually experience greater symptom burdens due to disease progression. The experts consulted during the CADTH review noted that HRQoL findings were clinically meaningful to patients, particularly because available therapies have not been confirmed to improve HRQoL in patients. However, there is uncertainty regarding these findings because the number of patients who completed questionnaires decreased from baseline through to cycle 13, resulting in considerable missing data at later time points. The magnitude of effect may have been overestimated due to the small sample size in the overall population and in the subgroups investigated. In addition, whether these findings are generalizable to patients who underwent treatments beyond cycle 13 is uncertain. As indicated by the sponsor, fewer patients were available to complete questionnaires at later cycles. There is also a potential for selection bias over time given that long-term survivors in the trials tend to be healthier patients. In the absence of a comparator arm and given the possibility that the open-label design introduced reporting bias, the impact of selpercatinib on patient-reported outcomes in relation to other therapies is unknown. Although CADTH recognizes that the rarity of RET fusion–positive mutations in patients with NSCLC may have contributed to the small sample size in the datasets at baseline and may have influenced the number of patients available to complete the questionnaires at later stages of the trial, no strong, definitive conclusions can be made from the findings obtained for HRQoL in the different population sets of patients with NSCLC.
External Validity
The LIBRETTO-001 trial is a multi-centre study with more than 84 participating sites across different countries, including Canada and the US. The clinical experts consulted during the review acknowledged that the baseline characteristics observed in the trial were reflective of patients seen in Canadian practice settings, and the results are therefore generalizable to the Canadian population.
According to published literature, RET gene fusions are more common in patients with NSCLC and adenocarcinoma histology and are rare in patients with squamous cell carcinoma. The clinical experts noted that they would generally expect a patient who is RET fusion–positive to have adenocarcinoma, as driver mutations are rare in squamous cell carcinoma. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| The clinical experts indicated that, if a non-adenocarcinoma patient was to be found to harbour an RET fusion, they should still be offered selpercatinib, as the presence of the mutations far outweighs the histology in terms of biology and likely response to targeted therapy.
Most patients in the NSCLC population were between the ages of 45 and 74 years. The clinical experts consulted confirmed that the median age of patients in the NSCLC population of the LIBRETTO-001 trial is reflective of Canadian practice. The experts added that, among the patients with NSCLC seen in practice, those with RET fusion–positive status tended to be younger than average lung cancer patients. These patients are also likely to have had no beforebacco exposure. The population of the trial is therefore representative of the Canadian practice setting with respect to these characteristics.
The patients with RET fusion–positive NSCLC recruited in the trial had an ECOG PS of 0, 1, or 2; however, only approximately 2% of enrolled patients had an ECOG PS of 2. It is uncertain if the results are generalizable to patients with an ECOG PS of 2, 3 or 4 with worse performance status. The clinical experts consulted during the review stated that they would still use selpercatinib in patients with an ECOG PS of 2 or 3 because selpercatinib is well-tolerated and would improve symptom burden, and therefore may improve ECOG PS. The experts discouraged the use of selpercatinib in patients with an ECOG PS of 4 or organ dysfunction (e.g., liver failure), in patients lacking an RET fusion, or those who had previously received another selective RET inhibitor, including patients who are unable to take medications orally or absorb medications due to gastrointestinal complications.
Most patients had advanced or metastatic disease, most of which were stage IV. Few patents with stage I to III disease were enrolled in the group with prior systemic therapy. The clinical experts noted that the use of selpercatinib in the metastatic setting is not intended as a curative option for patients and advised against using selpercatinib in patients who are eligible to receive curative-intent therapies. The clinician experts emphasized that patients with early-stage disease may only be eligible to receive selpercatinib if they were confirmed as having incurable disease or were not eligible or refused potentially curative local therapies, such as surgery or radiation therapy.
The median number of therapies used in the prior systemic therapy group was 2 (half of the IAS population received at least 2 prior lines of therapy and a quarter had received more than 3 prior lines). Given that most evidence on the efficacy of selpercatinib was generated in the subset of patients who were RET fusion positive who had received prior systemic therapies (more patients in that subset compared to the treatment-naive subset), it was important to assess whether the number of prior lines of therapy administered to patients could influence patient response to selpercatinib. In addition, it is uncertain whether there will be differences in outcomes in the treatment-naive and the prior systemic therapy group in practice, given the study design and the small sample size of the group that was treatment naive. The clinical experts indicated that the number of lines of therapy a patient had received before receiving selpercatinib will not influence a patient’s response to selpercatinib based on the drug’s mechanism of action.
The clinical experts consulted during the CADTH review noted that most patients in the NSCLC population have comorbidities, some of which include cardiovascular disease, which is to be expected given that some patients are long-time smokers. The experts also emphasized that, in practice, patients with underlying cardiovascular disease will usually be referred to cardio-oncology subspecialists from cardiology who will treat the disease while the patient undergoes cancer treatments. As follow-up sessions will require electrocardiogram checks, the clinical experts concluded that that administering selpercatinib to these patients will not present an issue because they will be constantly followed throughout treatments.
Selpercatinib dosing and the drug administration interval in the trial align with Health Canada’s indication and are generalizable to the Canadian setting. Dose adjustments made in the trial for patients experiencing AEs and variation in body weight, including those using concomitant therapies, are explicitly described in the product monograph to ensure that patients receive adequate therapy throughout treatment.
In the trial, RET fusion mutations were identified by PCR or NGS techniques. The only approved molecular testing technique was FISH, which was considered an acceptable technique for detecting RET fusion tumours for the phase I dose-escalation portion of LIBRETTO-001 and for cohort 5, but not for cohorts 1 and 2 of phase II. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The sponsor recommended the NGS technique due to its accuracy in detecting oncogenic fusions and other alterations. The clinician group input and the clinical experts pointed out that NGS and PCR testing are available in Canadian practice, and testing for multiple oncogenic drivers is routinely conducted at initial diagnosis. According to the clinician experts consulted during the review, RET fusion will be included as part of the larger panel of targetable mutations for which testing is conducted upfront at diagnosis. As noted by the clinician, NGS is the most common molecular technique used for oncogenic testing among others available across jurisdictions in Canada (e.g., reverse-transcription PCR, FISH, immunohistochemistry, and NGS with DNA and RNA sequencing). Both reverse-transcription PCR and FISH were used in the trial.
Tumour assessments were conducted at screening within 28 days of cycle 1 at day 1 via CT or MRI. Post-baseline assessments were conducted every 8 weeks (± 1 week) from cycles 3 through 13. The clinician experts indicated that the frequency of assessments implemented in the trial was appropriate, but the frequency differed from real-world practice. The clinical experts consulted emphasized that it is standard practice to perform radiographic assessments every 8 to 12 weeks. However, this time frame may be accelerated if patients report new symptoms or their physical findings indicate progression. In addition, the clinical experts noted that, while patients receiving oral targeted therapies are assessed for the presence and severity of symptoms every 3 to 4 weeks, these timelines may be shortened at treatment initiation and spaced out after therapy has been established and patients are doing well in terms of tolerance and symptom control.
The majority of patients enrolled in the trial were evaluated for outcomes after completing 6 months of follow-up following the first administered dose of selpercatinib as of the first interim data cut-off date (June 17, 2019). |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| The clinical experts consulted by CADTH considered the duration of treatment implemented in the trial to be appropriate and the duration of follow-up sufficient to evaluate the tumour response in patients with RET fusion–positive NSCLC.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
As there was no direct evidence comparing selpercatinib to other active therapies for the treatment of RET fusion–positive NSCLC in adult patients, a review of indirect evidence was undertaken. CADTH conducted a literature search to identify potentially relevant ITCs in patients with RET fusion–positive NSCLC. A focused literature search for ITCs dealing with selpercatinib or NSCLC was run in MEDLINE All (1946–) on November 3, 2021. No filters were applied to limit retrieval by study type. Retrieval was not limited by publication date or by language. Titles, abstracts, and full-text articles were screened for inclusion by 1 reviewer based on the population, intervention, comparator, and outcome criteria outlined in Table 28.
No potentially relevant ITCs were identified in the literature search.
Two sponsor-submitted ITCs were summarized and critically appraised, 1 for treatment-naive NSCLC11 and the other for previously treated NSCLC.12 These ITCs were used to inform the pharmacoeconomic models.
Description of Indirect Comparisons
Both sponsor-submitted ITCs included a systematic review of the literature (to identify trials investigating selpercatinib or comparator interventions in patients with RET fusion NSCLC or papillary thyroid cancer or RET-mutant MTC) and a network meta-analysis (NMA) that compared selpercatinib to other active treatments in patients with NSCLC who were treatment-naive or who had received previous treatments. In the sponsor-submitted ITCs, selpercatinib was compared to various chemotherapies or immunotherapies.
Methods of ITCs of Patients With NSCLC Who Were Treatment Naive and Treatment Experienced
Objectives
The objective of the sponsor-submitted report for patients with NSCLC who are treatment naive was to identify evidence from clinical trials and, if possible, an NMA, to evaluate the relative efficacy of selpercatinib versus other active treatments for this population.
The objective of the sponsor-submitted report for patients with NSCLC who are treatment experienced was to identify evidence from clinical trials and if possible, an NMA, to evaluate the relative efficacy of selpercatinib versus other active treatments for this population.
Study Selection Methods
Patients Who Were Treatment Naive
The randomized controlled trials (RCTs) that were used to inform the ITC were identified through a systematic literature search conducted by the ITC authors. Multiple databases were searched to identify clinical trials that evaluated the efficacy of drug therapies for RET fusion–positive NSCLC. It is unclear if the studies were selected independently by 2 reviewers. Data extraction was performed by 1 reviewer and verified by a second reviewer. It was unknown if the quality of the included studies was assessed.
Patients Who Were Treatment Experienced
The RCTs and single-arm trials that were used to inform the ITC were identified through a systematic literature search conducted by the ITC authors. Multiple databases were searched to identify clinical trials that evaluated the efficacy of drug therapies for RET fusion–positive NSCLC. It is unclear if the studies were selected independently by 2 reviewers. Data extraction was performed by 1 reviewer and verified by a second reviewer. Quality of the included RCTs was assessed using the standard National Institute for Health and Care Excellence checklist. Quality of the included single-arm trials was assessed using the Critical Appraisal Skills Programme cohort study checklist.
Inclusion and exclusion criteria for the clinical studies for each ITC are presented in Table 29.
Table 29: Study Selection Criteria and Methods for Indirect Treatment Comparisons
Study criteria | ITC comparing selpercatinib with comparators as first-line therapy | ITC comparing selpercatinib with comparators as second-line or beyond therapy |
|---|---|---|
Population | Adult patients with locally advanced or metastatic NSCLC (stage IIIB or IV), no prior exposure to systemic therapy | Adult patients with advanced or metastatic NSCLC, required second- or subsequent-line therapy for NSCLC |
Intervention and comparators |
|
|
Outcome |
|
|
Study design | RCTs (RCTs with mixed histologic populations were included when results specifically for the non-squamous population were reported) | Randomized, controlled, prospective clinical trials (single-arm trials in patients with RET alterations were eligible) |
Exclusion criteria | Studies including only a mutation positive–specific population (EGFR positive, ALK positive) | Children (< 18 years); other types of cancer; studies that do not have an intervention or comparator of interest in at least 1 arm; nonpharmacological treatment; single-arm trials in patients without RET alterations; prospective observational studies; pre-clinical studies; prognostic studies; case reports; commentaries and letters; consensus reports; nonsystematic reviews; registry studies; case-control studies; cross-sectional surveys |
Databases searched |
| |
Selection process | Unclear whether 2 reviewers selected studies independently | |
Data extraction process | Data were extracted by 1 reviewer and checked by a second reviewer | |
Quality assessment | Unclear if quality of the included trials was assessed | Standards recommended by NICE for RCTs; Critical Appraisal Skills Programme cohort study checklist for single-arm trials |
ALK = anaplastic lymphoma kinase gene; EGFR = epidermal growth factor receptor; ESMO = European Society for Medical Oncology; IASLC = International Association for the Study of Lung Cancer; ITC = indirect treatment comparison; NICE = National Institute for Health and Care Excellence; NSCLC = non–small cell lung cancer; RCT = randomized controlled trial; RET = rearranged during transfection.
Source: ITCs for population of those who are treatment naive and those who have treatment experience.12
Indirect Treatment Comparison Analysis Methods
Patients Who Were Treatment Naive
As LIBRETTO-001 was a single-arm study, a pseudo-control arm was needed to connect the first-line treatment arm in the LIBRETTO-001 study (selpercatinib) to the other comparators in the network. The ITC authors used individual patient-level data (IPD) available for the pemetrexed plus platinum chemotherapy arm from the KEYNOTE-189 study to simulate this pseudo-control arm. The KEYNOTE-189 study was an RCT comparing pembrolizumab combined with pemetrexed and platinum chemotherapy versus pemetrexed plus platinum chemotherapy alone in patients with advanced or metastatic NSCLC who had not previously received systemic therapy. Real-world data from the Flatiron database were used to adjust the pemetrexed plus platinum arm from the KEYNOTE-189 study for the prognostic impact of an RET fusion–positive status, and an adjustment factor was estimated for the prognostic effect of the RET fusion status. Subsequently, adjustment was done to match other prognostic factors of the RET-adjusted pemetrexed plus platinum arm from the KEYNOTE-189 study to the selpercatinib arm in the LIBRETTO-001 study. These prognostic factors included: |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Three statistical methods were used: propensity score matching (PSM) using logistic regression, propensity score weighting (PSW) using generalized boosted models, and targeted minimum loss-based estimation. For OS and PFS, Cox regression and nonparametric model were applied to the generated pseudo-control arm and selpercatinib to estimate the treatment effect of selpercatinib. The hazard ratios estimated for selpercatinib were included in the NMA to estimate the relative treatment effects of selpercatinib and comparators.
Bayesian NMAs were conducted. These analyses formed the base-case results and allowed for comparisons between treatments in the included trials. Frequentist NMAs were conducted as sensitivity analyses. Subgroup analyses based on the level of PD-L1 expression (≥ 50%) were conducted using a Bayesian approach. All the analyses were performed for each of the end points (OS, PFS, and overall response rate), using both fixed-effect and random-effect models.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
When PSM by logistic regression was used, the results were more clinically plausible for pemetrexed plus platinum. This model was therefore chosen to match data from the pemetrexed plus platinum and selpercatinib arms.
Patients With Treatment Experience
For the patients who had received prior systemic therapies, a pseudo-control arm was also needed to connect the second- or later-line treatment cohort of the LIBRETTO-001 study to other active treatments. This pseudo-control arm was simulated for LIBRETTO-001 using IPD available for the docetaxel plus placebo arm from the REVEL study, which was an RCT assessing the effectiveness of docetaxel plus ramucirumab to docetaxel plus placebo in the treatment of patients with stage IV NSCLC in the second-line setting. To adjust the docetaxel plus placebo control arm for RET fusion–positive status, real-world data from the Flatiron database were used. Patients were selected from the Flatiron database if they had advanced or metastatic NSCLC, were RET fusion–positive, and had received prior systemic therapy. The size of the impact was estimated from Flatiron database information on both RET fusion–positive and –negative patients. A subsequent adjustment was done to match other prognostic factors of the RET-adjusted docetaxel control arm to the selpercatinib arm. These prognostic factors included ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Similar to the ITC of the treatment-naive population, 3 different methods were used: PSM with logistic regression, PSW with generalized boosted models, and targeted minimum loss-based estimation. For OS and PFS, Cox regression and nonparametric models were applied to the generated pseudo-control arm and selpercatinib arm to estimate the treatment effect of selpercatinib. The hazard ratios estimated for selpercatinib were included in the NMA to estimate the relative treatment effects of selpercatinib and relevant comparators. In the second-line setting, only survival data (OS or PFS) were adjusted for the REVEL study’s docetaxel plus placebo arm; ORR data were not adjusted for RET fusion–positive status and other prognostic factors because sufficient response data for the docetaxel plus placebo arm were not available in the Flatiron database.
Bayesian NMAs were conducted using both fixed-effect and random-effect models. A hierarchical exchangeable model was used to take into account PD-L1 expression as a class in the model, and subgroup analyses of patients by level of PD-L1 expression were therefore not performed. As the fixed-effect hierarchical exchangeable model can accommodate the outcomes by PD-L1 status — and based on model-fit statistics — it was considered the primary model. Sensitivity analyses were not performed in this study.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
When PSM by logistic regression was used, the PFS results were more clinically plausible for docetaxel. This model was therefore chosen to match data from the docetaxel plus placebo and selpercatinib arms.
Heterogeneity across included trials was examined by using standard pairwise meta-analysis or closed loops. A meta-regression method was also adopted to explore heterogeneity, including the covariates of ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
In both ITCs for treatment-naive and pre-treated populations, efficacy outcomes were presented as hazard ratios with corresponding 95% credible intervals (CrI) for OS and PFS, and as odds ratios with corresponding 95% CrIs for ORR.
Table 30 below presents a summary of the methods used for the ITCs.
Table 30: Indirect Treatment Comparison Analysis Methods
Analysis component | ITC comparing selpercatinib with comparators as first-line therapy | ITC comparing selpercatinib with comparators as second-line or beyond therapy |
|---|---|---|
ITC methods | Bayesian approach | |
Priors | Vague priors were set for model parameters: a mean of 0 and variance of 100; for the random-effect model, the prior distribution for the between-trial variance term was uniform (0 to 5) | Vague priors were given in the usual way (not specified) |
Assessment of model fit | Deviance information criterion Residual deviance No meaningful difference between the fixed-effect and random-effect models | A hierarchical exchangeable model was used to take into account PD-L1 expression as a class in the model Meta-regression was used to examine model fit; results showed that inclusion of covariates (|||||||||||||||||||||||||||||||||||||||||) improved model fit |
(continued) | Results showed that a fixed-effect hierarchical exchangeable model without covariates adjustments was likely to provide most robust estimates and was considered the primary model | |
Assessment of consistency | Unrelated mean effects model No statistically significant difference between the unified mean effects and consistency models | Inconsistency was monitored when a closed loop, not composed only by data from multi-arm trials, was formed within the network No statistically significant difference (P > 0.05) between the indirect and direct comparisons |
Assessment of convergence | Assessed by monitoring caterpillar, density, Brooks-Gelman-Rubin plots and autocorrelation plots | Through the use of Gelman and Rubin diagnostics, iteration plots and verification by fitting an equivalent frequentist model |
Outcomes | OS, PFS, ORR | |
Follow-up time points | NR | |
Construction of nodes | NR | |
Sensitivity analyses | Frequentist NMA | No |
Subgroup analysis | Based on level of PD-L1 expression | No |
Methods for pairwise meta-analysis | NR | |
ITC = indirect treatment comparison; NMA = network meta-analysis; NR = not reported; ORR = overall response rate; OS = overall survival; PD-L1 = programmed cell death ligand 1; PFS = progression-free survival.
Source: ITCs for treatment-naive population11 and treatment-experienced population.12
Results of ITCs of Patients With NSCLC Who Were Treatment Naive and Treatment Experienced
Summary of Included Studies
Treatment-Naive Population
A total of 29 studies were identified from the systematic literature review, and 19 of them were included in the ITC. The end points analyzed included OS (18 trials), PFS (18 trials) and ORR (17 trials).
Table 31 compares baseline characteristics before and after PSM. The pemetrexed plus platinum arm from the KEYNOTE-189 trial has been adjusted based on RET fusion–positive status and other prognostic factors, such as |||||||||||||||||||||||||||||||||||||||||||||||||||.
Characteristic | Before propensity score matching | After propensity score matching | |
|---|---|---|---|
Selpercatinib | Pemetrexed plus platinum | Pemetrexed plus platinum | |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
ECOG PS = Eastern Cooperative Oncology Group Performance Status.
aOne patient with histology that is not non-squamous has been excluded from further matching process.
bTwo patients with histology that is not non-squamous have been excluded from further matching process.
Source: Indirect treatment comparison for the treatment-naive population.11
Figure 14 to Figure 16 present |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Treatment-Experienced Population
A total of 29 studies were included for this ITC. The end points analyzed included OS (18 trials), PFS (18 trials) and ORR (17 trials).
Table 32 compares baseline characteristics before and after PSM. The docetaxel plus placebo arm from the REVEL study has been adjusted based on RET fusion–positive status and other prognostic factors such as |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 32: Baseline Characteristics of LIBRETTO-001 and REVEL Before and After Propensity Score Matching by Logistic Regression
Characteristic | Before propensity score matchinga | After propensity score matchinga | |
|---|---|---|---|
Selpercatinib | Docetaxel plus placebo | Docetaxel plus placebo | |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
ECOG PS = Eastern Cooperative Oncology Group Performance Status.
aThe analysis used greedy match as a matching algorithm.
Source: Indirect treatment comparison for the treatment-experienced population.12
Figure 17 to Figure 19 present ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Results
Treatment-Naive Population
Overall Survival
Eighteen studies reported OS data (Figure 14). The publication dates for these studies were between 2004 and 2019. Results of the fixed-effect model are presented for the base-case analysis for OS as the fixed-effect model was the best fit compared to the random-effect model.

Note: Figure 14 contained confidential information and was removed at the request of the sponsor.
The analysis suggested that selpercatinib was favoured for OS compared to other treatments for adult patients with NSCLC.
Progression-Free Survival
Eighteen studies reported PFS data (Figure 15). Results from a fixed-effect model are presented for the base-case analysis for PFS.
The analysis suggested that selpercatinib was favoured for PFS compared to other treatments for adult patients with NSCLC.

Note: Figure 15 contained confidential information and was removed at the request of the sponsor.
Overall Response Rate
Seventeen studies reported overall response rate data (Figure 16). A random-effect model was chosen for the base-case analysis of ORR as informative prior was not available. Overall response rates are presented as an odds ratio and associated 95% CrI. An odds ratio greater than 1 indicates of better response for the treatment of selpercatinib versus other treatments in the column.

Note: Figure 16 contained confidential information and was removed at the request of the sponsor.
Treatment with selpercatinib was favoured compared with other treatments for ORR in adult patients with NSCLC.
Details of the results in patients with NSCLC who were treatment naive are presented in Table 33.
Table 33: Base-Case Analysis for OS, PFS, ORR in the Treatment-Naive Population
SELc | OS (HR (95% CrI)) | PFS (HR (95% CrI)) | ORR (OR (95% CrI)) |
|---|---|---|---|
PEMc + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
BEVc + PEMc | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
BEVc + PEMc + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
BEVc + PACi + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
PACi + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
IPIc + NIVc | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
PEMc + PLATi + RAMc | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
ATEZc + BEVc + PACi + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
BEVi + PEMc + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
PEMc + PEMBROc + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
PEMBROc | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
(GEMi or PACi or PEMc) + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
PEMc | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
IPIc-concurrent + PACi + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
IPIc-phased + PACi + PLATi | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
ATEZ = atezolizumab; BEV = bevacizumab; c = continuous; GEM = gemcitabine; HR = hazard ratio; i = induction; IPI = ipilimumab; NA = not applicable; OR = odds ratio; ORR = overall response rate; OS = overall survival; PAC = paclitaxel (solvent-based); PEM = pemetrexed; PEMBRO = pembrolizumab; PFS = progression-free survival; PLAT = platinum; RAM = ramucirumab, Sel = selpercatinib.
Note: The comparisons are selpercatinib vs. comparators. Values for OS and PFS were obtained from fixed-effect models; an HR greater than 1 favours selpercatinib. The ORR was obtained from random-effect models; an OR greater than 1 indicates better response for selpercatinib vs. other treatments.
Source: Indirect treatment comparison for the treatment-naive population.11
Treatment-Experienced Population
Overall Survival
Eighteen studies reported OS data in this ITC (Figure 17). Results of the fixed-effect hierarchical exchangeable model are presented for the base-case analysis for OS.
The analysis suggested that selpercatinib was favoured for OS compared to other treatments for adult patients with NSCLC.

Note: Figure 17 contained confidential information and was removed at the request of the sponsor.
Progression-Free Survival
Eighteen studies reported PFS data in this ITC (Figure 18). Results of the fixed-effect hierarchical exchangeable model are presented for the base-case analysis for PFS.
The analysis suggested that selpercatinib was favoured for PFS compared to all other treatments for adult patients with NSCLC.

Note: Figure 18 contained confidential information and was removed at the request of the sponsor.
Overall Response Rate
Seventeen studies reported ORR data (Figure 19). A fixed-effect hierarchical exchangeable model was chosen for the base-case analysis of ORR. Results of ORR are presented as odds ratios and associated 95% CrI. An odds ratio greater than 1 indicates of better response for the treatment of selpercatinib versus other treatments.

Note: Figure 19 contained confidential information and was removed at the request of the sponsor.
Treatment with selpercatinib was favoured compared to docetaxel, docetaxel plus nintedanib, docetaxel plus ramucirumab, gefitinib, nivolumab, nivolumab (for PD-L1 < 1%), pemetrexed and pemetrexed plus nintedanib, but not to other treatments included in this ITC, for adult patients with NSCLC in the second-line setting.
Details of the results in patients with NSCLC who were treatment experienced are presented in Table 34.
Table 34: Base-Case Analysis for OS, PFS, ORR in the Treatment-Experienced Population
SELc | OS | PFS | ORR |
|---|---|---|---|
Docetaxel | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Cabozantinib | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Dacomitinib | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Atezolizumab | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Docetaxel (60 mg) + ramucirumab | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Docetaxel + nintedanib | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Docetaxel + ramucirumab | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Erlotinib | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Erlotinib + cabozantinib | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Erlotinib + pemetrexed | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Gefitinib | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Nivolumab | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Nivolumab < 1% | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Nivolumab > 1% | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Pembrolizumab (pooled) | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Pemetrexed | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Pemetrexed + carboplatin | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Pemetrexed + nintedanib | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Avelumab | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
HR = hazard ratio; NA = not applicable; OR = odds ratio; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; SELc = continuous selpercatinib.
Note: The comparisons are selpercatinib vs. comparators. Values for OS and PFS were obtained from fixed-effect hierarchical exchangeable models; an HR greater than 1 favours selpercatinib. The ORR was obtained from fixed-effect hierarchical exchangeable models; an OR greater than 1 indicates a superior response for selpercatinib vs. other treatments.
Source: Indirect treatment comparison for the treatment-experienced population.12
Critical Appraisal of Sponsor-Submitted Indirect Treatment Comparisons
The sponsor submitted 2 ITCs to provide indirect evidence for treatment with selpercatinib compared to other active treatments in treatment-naive and treatment-experienced populations. In the ITC for a treatment-naive population, selpercatinib was compared to monotherapy or a combination of platinum-based chemotherapy and immunotherapy drugs. In the ITC for a treatment-experienced population, selpercatinib was compared to monotherapy or a combination of chemotherapy drugs and immunotherapy drugs, such as docetaxel, cabozantinib, atezolizumab, or nivolumab. In both ITCs, studies were identified by searching multiple databases, based on pre-specified inclusion and exclusion criteria. It was unclear whether 2 independent reviewers selected the studies. Data extraction was conducted by 1 reviewer and verified by a second reviewer. In the ITC for patients who were treatment naive, it was unknown if quality assessment of the included individual studies was performed. In the ITC for patients who were treatment experienced, quality assessment of the included studies was performed using a validated tool. However, there was no discussion on how any potential biases in the trials could have affected data analyses in the ITC and the possible solutions. For example, it is not clear if sensitivity analyses were conducted to assess the impact of studies with poor quality. Efficacy outcomes relevant to patients with NSCLC (OS, PFS, and ORR) were analyzed in both ITCs. Other important outcomes, such as DOR, HRQoL, and safety, were not assessed.
In the ITC for a treatment-naive population, a pseudo-control arm was generated to assist in connecting selpercatinib with other active treatments in the study population in the first-line setting, as there was a lack of a comparator group in the LIBRETTO-001 study. All IPD for selpercatinib were drawn from the LIBRETTO-001 study and for pemetrexed plus platinum from the KEYNOTE-189 study. Data from the Flatiron database were used to adjust IPD for pemetrexed plus platinum using various statistical tests to create a pseudo-control arm reflecting RET fusion–positive status NSCLC. In the ITC for a treatment-experienced population, a pseudo-control arm was generated in the second- or later-line setting, as there was a lack of comparator group in the LIBRETTO-001 study. The IPD for selpercatinib were drawn from the LIBRETTO-001 study and for docetaxel plus placebo from the REVEL study. Data from the Flatiron database were used to adjust IPD for docetaxel using various statistical tests to create a pseudo-control arm reflecting RET fusion–positive status NSCLC.
In both ITCs, different matching approaches, including PSM and/or PSW, were used to adjust the comparator data (pemetrexed plus platinum from the KEYNOTE-189 study; docetaxel plus placebo from the REVEL study) to match the LIBRETTO-001 study for other prognostic factors, such as ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. According to the clinical experts consulted by CADTH, some important patient characteristics at baseline were not included in the matching process (e.g., brain metastasis or previous lines of therapy) and may be related to a substantial risk of bias in the result interpretation. Despite various statistical techniques employed to lessen the impact of potential clinical heterogeneity on the estimated treatment effect of selpercatinib, similar trends were observed, and there is still significant uncertainty in the ITC results.
In the ITC for a treatment-naive population, although some patient demographic and disease characteristics at baseline were provided from the LIBRETTO-001 and KEYNOTE-189 studies, trial characteristics and patient baseline characteristics of all the individual studies included in the systematic review and ITC were not reported. In the ITC for a treatment-experienced population, patient demographic and disease characteristics at baseline were not provided in sufficient details, either. Assessing heterogeneity across these trials (by examining, for example, study design, dosage administered, comorbidity, or CNS metastasis) was therefore not feasible.
As well, there were imbalances between the LIBRETTO-001 and KEYNOTE-189 studies and between the LIBRETTO-001 and REVEL studies in patient characteristics at baseline, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Similarity among all major confounders — both those included in the propensity score development itself and other potential confounders — must be achieved to obtain unbiased estimates with these types of analyses. Given the remaining imbalances, which are likely due to small patient numbers, the potential for bias cannot be ruled out and there is uncertainty in the results.
In addition, all patients in the LIBRETTO-001 study were RET fusion–positive, while patient RET fusion status was not examined in all the other included studies. In the Flatiron database, among patients with NSCLC who have not received prior treatments, only a small proportion are RET fusion–positive (||||||||||).11 These patients differ from those who have RET fusion–negative disease, in that patients with RET-positive status tend to be younger, are less likely to smoke and more likely to have non-squamous cell carcinoma, and have received different prior treatments. Therefore, patients with positive or negative RET fusion may respond differently to selpercatinib. In sum, it is unclear how similar the patient populations in the comparator studies were to those enrolled in the LIBRETTO-001 study despite the various adjustments.
The uncertainty in the results is further highlighted by the small hazard ratios and large odds ratios, along with wide CrIs for the point estimates for each of the comparisons.
In the LIBRETTO-001 study, the OS and PFS data were immature. The ITC reports did not specify the analysis time points for these outcomes for selpercatinib and the comparators.
The study populations in the ITCs were patients with NSCLC with unspecified RET fusion status, which is broader than the Health Canada–approved indication for selpercatinib (treatment for RET fusion–positive NSCLC only). In the ITC for a treatment-experienced population, it was not possible to adjust the RET status in the docetaxel control arm in the ORR analysis. As a result, the findings of this ITC may not be generalizable to patients with RET fusion–positive NSCLC.
Other Relevant Evidence
In addition to the pivotal LIBRETTO-001 phase I and II study with no comparator arm, the following studies were considered relevant: LIBRETTO-43125,31 and SIREN.13 The CADTH review team identified an ongoing phase III, randomized, open-label study (LIBRETTO-43125,31) that met systematic review inclusion criteria with the exception that no results are currently available, as this trial is actively recruiting patients, and for this reason, the study is summarized here. The CADTH review team identified another study analyzing the safety and efficacy of selpercatinib in a real-world setting (SIREN), in which the data were retrospectively collected from patients with RET fusion–positive NSCLC participating in a selpercatinib access program.13
LIBRETTO-431 Study25,31
The LIBRETTO-431 study is a phase III, randomized, multi-centre, open-label trial comparing selpercatinib to platinum-based (carboplatin or cisplatin) and pemetrexed therapy with or without pembrolizumab in patients with locally advanced and/or metastatic RET fusion–positive non-squamous NSCLC who were treatment naive. Patients will be enrolled in approximately 230 sites in 26 countries across the Americas (including Canada), Asia, Africa, Europe, and Oceania.25,31 Table 35 provides more details.
Table 35: Details of Other Relevant Studies — LIBRETTO-431 and SIREN
Criteria | LIBRETTO-431 | SIREN |
|---|---|---|
Designs and populations | ||
Study design | Phase III, multi-centre, randomized, open-label | Retrospective, noninterventional, international, multi-centre |
Locations | Approximately 230 sites in 26 countries across the Americas (including Canada), Asia, Africa, Europe, and Oceania | 27 centres in 12 countries, including Canada, Europe, and Australia |
Patient enrolment date | February 17, 2020 | August 2019 |
Estimated primary completion datea | January 15, 2023 | NA |
Estimated study completion date b | August 18, 2025 | January 2021 |
Randomized (N) | Planned: 250 Enrolled: NA (currently recruiting) | As retrospective data analysis/real-world evidence were involved, no randomization Data documented for 50 patients |
Inclusion criteria |
|
|
Exclusion criteria |
| NR |
(continued) |
| |
Drugs | ||
Intervention | Selpercatinib: 160 mg twice daily, oral, for 21-day cycles | Selpercatinib: 160 mg twice daily, oral, (two 80 mg capsules) |
Comparator(s) | Active comparator: Pemetrexed (500 mg/m2, IV) every 3 weeks plus investigator’s choice of carboplatin (area under the curve: 5, maximum dose 750 mg, IV) every 3 weeks for 4 cycles or cisplatin (75 mg/m2, IV) every 3 weeks for 4 cycles with or without pembrolizumab (200 mg IV) up to 35 cycles | Comparison between subgroups were made based on: previous lines of systemic anticancer therapy (platinum-based chemotherapy, anti–programmed cell death protein 1 or anti–programmed death ligand 1 therapy, a tyrosine kinase inhibitor), or pre-treated patients vs. treatment-naïve patients or different RET fusion partners (kinesin-1 heavy chain [KIF5B], coiled-coil domain-containing protein 6 [CCDC6]) |
Phase | ||
Run-in | Patient eligibility and baseline characteristics will be evaluated during the baseline phase. Prior to enrolment, the presence of RET fusion must be confirmed in the tumour or in the blood by a laboratory test; patients will be stratified by geographic region, presence of brain metastases and randomized treatment | NA |
Blinding | Open-label: patient, trial-site personnel, and the sponsor or designee will not be blinded to treatment, but the independent central review team will be | NA |
Follow-up | The post-treatment phase will consist of a short-term follow-up period and a long follow-up period: Short follow-up period is when the patient will no longer continue therapy, until completing a safety assessment (30 ± 7 days) after the last dose of treatment Long-term follow-up will begin after the completion of the short-term follow-up period and will continue until death, study withdrawal, the patient is lost to follow-up, or final study completion | NA |
Outcomes | ||
Primary end points | Progression-free survivalc | Systemic ORR, as per RECIST 1.1 |
Secondary end points |
|
|
Notes | Ongoing study, results not available at this time | Retrospective study |
Publications | Illini et al. (2021)13 | |
CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; NA = not applicable; NR = not reported; NSCLC = non–small cell lung cancer; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; RANO = Response Assessment in Neuro-Oncology; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; RET = rearranged during transfection.
aThe date on which the last participant in a clinical study was examined or received an intervention to collect final data for the primary outcome measure. Whether the clinical study ended according to the protocol or was terminated does not affect this date. For clinical studies with more than 1 primary outcome measure with different completion dates, this term refers to the date on which data collection is completed for all the primary outcome measures.
bThe date on which the last participant in a clinical study was examined or received an intervention/treatment to collect final data for the primary outcome measures, secondary outcome measures, and adverse events (i.e., the last participant's last visit).
cAssessed by blinded independent central review.
dAssessed by investigator.
Source: Solomon et al. (2021),25 LIBRETTO-431 trial,31 and Illini et al. (2021).13
This study is currently recruiting participants, with a planned enrolment of approximately 250 patients. The estimated primary completion date (on which the last participant in a clinical study is examined or receives an intervention to collect final data for the primary outcome measure) and study completion date (on which the last participant in a clinical study is examined or receives an intervention and/or treatment to collect final data for the primary outcome measures, secondary outcome measures, and AEs) are January 15, 2023, and August 18, 2025, respectively. Patients are to be randomized in a 2:1 ratio to receive selpercatinib (n = 167) for 21-day cycles or an active comparator, pemetrexed (n = 83), every 3 weeks plus 4 cycles of carboplatin or cisplatin every 3 weeks, with or without pembrolizumab for up to 35 cycles. The primary end point is PFS (according to RECIST 1.1) assessed by the blinded independent central review, whereas the secondary end points include OS, ORR and/or DOR assessed by both blinded independent central review and the investigator, intracranial ORR and/or DOR, PFS2 assessed by investigator, time to deterioration in pulmonary symptoms, progression after the next line of therapy, RET fusion status (local versus central), and safety and/or tolerability.25,31
SIREN Study13
The SIREN study (for Selpercatinib in RET fusion–positive NSCLC) is a retrospective cohort study, as well as non-interventional, international, multi-centre study, in which the investigators looked at patient charts retrospectively to evaluate the efficacy and safety of selpercatinib among 50 patients with RET fusion–positive advanced NSCLC at 27 centres in 12 countries, including Canada, Europe, and Australia. Data about patient demographics and clinical characteristics (e.g., age, gender, smoking habit, race, performance status, disease stage, histology, metastases, previous regimens, and RET fusion partners), selpercatinib treatment (e.g., dose, duration, best response, and the date, type, and location of progression), and safety information had been extracted retrospectively between August 2019 and January 2021. Among these 50 patients, 45 (90%) were not Asian, 30 (60%) were female, 37 (74%) were non-smokers, and 16 (32%) and 18 (34%) had brain and bone metastases, respectively. The median age was 65 years (range = 38 to 89). Regarding previous treatment, 13 patients (26%) were treatment-naive, whereas 37 patients (74%) were pre-treated with a median of 3 lines of therapy (range = 1 to 8).
The primary outcome of the SIREN study was the systemic ORR (as determined by RECIST 1.1), whereas the secondary outcomes included treatment-related AEs as determined by the treating physician; a disease control rate defined as the proportion of patients with a CR, PR, or stable response; the intracranial ORR; the median duration of treatment defined as the time between the start to end dose of selpercatinib; the median duration of response defined as the time between the initial response to therapy and subsequent disease progression or death due to any cause; and the median PFS measured as the time from first dose of selpercatinib to first progression event (as determined by RECIST 1.1).
Only results for ORR, intracranial ORR, and PFS are presented in accordance with the protocol for the CADTH review. The ORR (defined as a CR or PR) was 68% (95% CI, 53 to 81), and the median PFS was 15.6 months (95% CI, 8.8 to 22.4) after a median follow-up of 9.4 months among all patients. In patients with untreated or previously progressed and measurable brain metastases (n = 8), the intracranial ORR reached 100%. The ORRs for patients with NSCLC who were treatment naive and previously treated were 69% (95% CI, 39 to 91) and 68% (95% CI, 50 to 82), respectively, whereas the median PFS values for these 2 groups were 15.6 (95% CI, not reached) and 12.2 (95% CI, not reached), respectively.
In terms of AEs, 43 (88%) of 50 patients experienced treatment-related AEs of any grade, a large majority of them grade 1 or 2. The most frequently reported treatment-related AEs were fatigue or asthenia (40%), increased liver enzyme levels (34%), hypertension (26%), dry mouth (26%), and peripheral edema (20%). Treatment-related AEs of grade 3 or higher were reported in 12 patients (24%), with the most common being increased liver enzyme levels (10%), abdominal pain (4%), prolonged corrected QT time (4%), hypertension (4%), and fatigue or asthenia (4%).13
Several limitations were identified. The retrospective study design is prone to bias (e.g., reporting bias and nondifferential biases), the patient population recruited may not be similar to the LIBRETTO-001 trial due to differences in the eligibility, and exclusion criteria applied in the study (potential selection bias). The ORR, although measured using the RECIST 1.1 criteria, was assessed by an unblinded review of practising physicians. There is also a potential measurement bias due to differences in the frequency and conduct of disease assessments in clinical practice versus the trial setting. The follow-up time frame in the study differs from that of the LIBRETTO-001 trial, and the therapies administered beyond disease progression were different. The small sample size of the study also limits the generalizability of the findings. Although the SIREN study provides additional data on the effectiveness and safety of selpercatinib in the real-world setting, the limitations identified introduce uncertainty.
Discussion
Summary of Available Evidence
The systematic review of selpercatinib included a phase I and II, single-arm, multi-cohort, open-label, dose-escalation, and dose-expansion study. In addition, 2 ITCs and 1 retrospective study were summarized and appraised. The LIBRETTO-001 trial is still ongoing and patients are being recruited in more than 84 centres in different countries, including Canada. The study enrolled patients with metastatic RET fusion–positive NSCLC as well as patients with other solid tumours (thyroid, pancreatic, and colorectal).
The primary outcome in the dose-expansion phase II was ORR measured using RECIST 1.1 guidelines or the RANO tool, depending on tumour type (for the NSCLC cohort, it was exclusively RECIST 1.1). The secondary outcomes investigated that were relevant for this review were DOR, CNS ORR, PFS, OS, and AEs. In addition, HRQoL was evaluated as an exploratory outcome.
Interim analyses were planned to support regulatory submissions in different jurisdictions. There were 3 interim analyses in total. Data from the second interim analysis (the day 60 efficacy and safety update with a data cut-off date of December 16, 2019) and the third interim analysis (data cut-off of March 30, 2020) provide the evidence necessary to support this reimbursement submission. All interim analyses were pre-planned.
This CADTH review focused on outcomes observed in patients with NSCLC with a confirmed RET fusion gene mutation enrolled in cohort 1 and 2 at phase II of the LIBRETTO-001 trial. These patients were further subgrouped into 3 datasets based on clinically meaningful distinctions observed during the trial. These subgroups include the PAS (the first consecutively enrolled patients previously treated with platinum-based chemotherapy), the IAS (patients treated with platinum-based chemotherapy), and 3 SASs: SAS1 (patients who were treatment naive), SAS2 (patients treated with other systemic therapies that are not platinum-based) and SAS3 (patients without measurable disease according to RECIST 1.1).
The assessment of the primary outcome — ORR based on RECIST criteria — was carried out by an IRC, which reduces assessment bias. However, this objective is a surrogate measure for OS, which is highly dependent on effect size. It also does not provide the true clinical benefit of the treatment unless the treatment effect is large and responses are durable. The effect size defined for this objective was considered. The clinical experts consulted during this CADTH review noted that the findings obtained from the ORR, DOR, and CNS ORR, were clinically meaningful to patients and reflect improvement in overall quality of life.
The sponsor requested reimbursement for selpercatinib as monotherapy in treatment-naive (first-line) and treatment-experienced (those who have received prior systemic therapy) adult patients with metastatic RET fusion–positive NSCLC.
Interpretation of Results
Efficacy
The clinical experts consulted during the review identified several important goals of treatment of advanced NSCLC, which included prolonging a patient’s life, reducing symptom burden, delaying progression, improving HRQoL, and decreasing or eliminating hospital admissions and stays. They confirmed that the outcomes (ORR, OS, PFS, DOR, CNS ORR, and HRQoL) investigated in the LIBRETTO-001 trial were appropriate and align with the needs of patients, caregivers, and clinicians in practice.
The clinical experts consulted during the CADTH review considered the ORR responses obtained in both the treatment-naive and treatment-experienced populations to be clinically meaningful to patients in practice. They emphasized that, in their experience, the ORR and DOR obtained are larger and longer compared to other therapies offered as standard of care. The clinical experts noted that there is limited evidence that patients with metastatic RET fusion–positive NSCL benefit from currently available single-drug immunotherapy in practice, and not all patients respond to chemotherapy plus immunotherapy, indicating an unmet need for this patient population.
At the data cut-off date of March 30, 2020, the ORR observed by the IRC in the LIBRETTO-001 trial was 85% (33 of 39, 95% CI, 69.5 to 94.1) in the treatment-naive group and 64% (95% CI, 53.9 to 73.0; based on PAS) in the prior platinum therapy treatment-experienced group. The sponsor conducted a follow-up analysis for the IAS and treatment-naive population at a new cut-off date of June 15, 2021. The estimated ORR was consistent with that of previous analyses; in the IAS dataset, the estimated ORR was 61.1% (95% CI, 54.7 to 67.2) and in the treatment-naive dataset it was 84.1% (95% CI, 73.3 to 91.8). The median DOR was NE in the treatment-naive group, but it was estimated to be 17.5 months in the treatment-experienced primary analysis at the March 30, 2020, analysis point. The follow-up analysis conducted at the June 15, 2021, cut-off in the IAS and treatment-naive population showed a median DOR of 28.6 months (95% CI, 20.4 to NE) in the IAS and 20.2 months (95% CI,13.0 to NE) in the treatment-naive dataset. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| In the LIBRETTO-001 trial, radiographic images were assessed by an IRC, which reduces the potential bias of evaluation. Consistent with the approach used for other treatments that received early approval before phase III comparative studies being conducted, Health Canada issued an NOC/c for selpercatinib. As previously described, the sponsor is currently recruiting patients into LIBRETTO-431, a phase III, randomized, multi-centre, open-label study comparing selpercatinib to platinum-based (carboplatin or cisplatin) and pemetrexed therapy with or without pembrolizumab in patients with locally advanced and/or metastatic RET fusion–positive non-squamous NSCLC who are treatment naive. The treatment effects of selpercatinib observed in the LIBRETTO-001 study in patients with RET fusion–positive NSCLC have therefore yet to be confirmed.
The ORR was numerically larger in the treatment-naive population than in the treatment-experienced populations in LIBRETTO-001 at all data cut-off dates submitted by the sponsor. The clinical experts stated they would prioritize using selpercatinib in the treatment-naive population based on the mechanism of action, the natural history of disease, and the results described in this review. However, the study was not designed to make comparisons between analysis sets and no statistical comparisons were conducted. As a result, no concrete conclusions can be drawn regarding the treatment effects of selpercatinib based on treatment history, or on any of the subpopulations that were evaluated. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The clinical experts explained that selpercatinib acts on the driver mutation expressed by the tumour, and this pathway for activity is not necessarily directly involved with a patient’s immune system. The clinical experts indicated that the number of lines of therapy a patient had received before receiving selpercatinib will not influence the patient’s response to selpercatinib based on the drug’s mechanism of action. The experts noted in their input that selpercatinib should be prioritized for patients in the first-line setting because the patients are most likely to demonstrate a positive response. The clinical experts also encouraged its use in next-line settings if patients are currently placed on a different treatment.
The experts considered the safety profile of selpercatinib favourable, and described the harms reported in the trial as manageable in comparison to those associated with other drugs used by patients in practice. They also identified several concomitant medications that could have contributed to abnormal liver function tests and corrected QT prolongation in patients and other events of special interest listed in the trial. Patients with active cardiovascular disease, a history of myocardial infarction or prolongation of the QT interval corrected for heart rate using Fridericia’s formula greater than 470 ms on at least 2 of 3 consecutive electrocardiograms and a mean corrected hear rate greater than 470 ms on all 3 electrocardiograms during screening were excluded from the trial. The experts highlighted that patients will not be eligible to receive treatment in practice if they have active cardiovascular disease, although the strict values used by the sponsor in the trial will not be implemented in practice.
The experts also considered the findings from the subgroup analysis in patients with CNS metastasis at baseline, and CNS ORR in particular, to be clinically meaningful. According to the clinical experts, approximately 40% of patients with advanced and/or metastatic NSCLC develop brain metastasis (the literature indicates this proportion can reach 60% in patients with RET fusion mutations). As noted by the clinical experts, standard treatments such as chemotherapy are less effective on brain tumours because of limited penetration. These patients will usually be given radiation to treat brain metastases, with potentially serious treatment-related AEs and limited benefits.
The OS and PFS were NE in both populations at the March 30, 2020, and December 16, 2019, data cut-offs due to data immaturity and insufficient duration of follow-up. The FDA guidance document for designing clinical trials for NSCLC states that OS is the most appropriate outcome in patients with NSCLC in a well-conducted randomized trial because it provides direct evidence of a drug’s benefit to patients and its measurement in a clinical trial setting is generally considered accurate. The LIBRETTO-001 trial was not adequately designed to evaluate OS and PFS, in part due to the early phase nature of the studies, with the primary objective of determining the dosage of selpercatinib and tumour response.9,10 The CADTH reviewers agreed with ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| The sponsor provided additional data to CADTH for a new cut-off of June 15, 2021, which showed that a median PFS was obtained in the IAS and SAS1 populations (IAS dataset: 24.94 months [95% CI, 19.3 to NE]; SAS1 dataset: 21.95 months [95% CI, 13.8 to NE]). However, the median OS was still NE in each population. Despite the results estimated at the new cut-off (June 15, 2021), CADTH concluded that the findings are insufficient to form concrete conclusions on the comparative treatment effect (PFS and OS) for the PAS, IAS, and SAS1 populations due to the single-arm design of the trial and immature data. Health Canada’s NOC/c outlined several conditions to be fulfilled by the sponsor, including additional evidence of the drug’s benefit obtained ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.9
Health Canada pointed out that the median DOR obtained in the PAS and IAS was 17.5 months.9 The median duration of follow-up in months was 12.1 in the PAS and 9.1 in the IAS. In the treatment-naive group, the median DOR was not achieved, and the median duration of follow-up was 7.4 months. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| The clinical experts consulted during the CADTH review considered the duration of follow-up employed during the LIBRETTO-001 trial sufficient to evaluate the efficacy of selpercatinib in achieving tumour response in patients with RET fusion NSCLC.
In the LIBRETTO-001 trial, HRQoL was assessed as an exploratory outcome during the trial using the EORTC QLQ-C30 disease-specific questionnaire, and measurements were collected at baseline (cycle 1, day 1), every 8 weeks (until cycle 13), and every 12 weeks after cycle 13 (until end of treatment). A change of at least 10 points from baseline scores in the different domains was considered clinically meaningful. The EORTC QLQ-C30 has been validated in different patient populations, including patients with NSCLC. One study conducted in patients with NSCLC reported that a change of 10 points in any scale is clinically relevant,33 which aligns with the MID used in the LIBRETTO-001 trial. The mean scores for global health status in the treatment-naive group, 1 line of prior therapy group, and 2 or more prior lines of therapy group were 60.2, 65.2, and 60.4, respectively. The high patient-attrition rates at later cycles and the exploratory analysis introduce uncertainty to the reported findings.
In addition to these limitations, the key limitation of the LIBRETTO-001 trial was the open-label, non-randomized, single-arm design. As well, the absence of formal statistical testing, lack of multiplicity testing in subgroup analysis, and relatively small sample size (reflecting the phase I and II nature of the design), limits the interpretability of the results, particularly the time-to-event end points and HRQoL. Although the sponsor, clinical experts, and clinician groups consulted considered the RET fusion mutation to be rare (occurring in only 1% to 2% of the NSCLC population), the CADTH reviewers agreed that the rarity of the disease may have contributed to the small sample sizes obtained in the defined population set. ||||||||||||||||||||||||||||||||||||||||||||||||||| In the absence of a comparator arm typically used in standard of care, CADTH considers the findings uncertain with respect to the true treatment effect of selpercatinib on the 2 populations.
Given the lack of direct comparative evidence, the sponsor submitted 2 separate ITCs to compare selpercatinib to other active treatments in patients with NSCLC who had not been treated with prior systemic therapies, and in patients who had received prior systemic therapies. In both ITCs, a pseudo-control arm was needed due to the lack of a comparison arm in the study of selpercatinib. Adjustments on a number of prognostic factors for NSCLC, such ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, were made to match the comparator arm with the selpercatinib arm. The results of both ITCs suggest that treatment with selpercatinib was associated with improved OS and PFS, and a higher probability of achieving a treatment response, when compared to other active treatments in first-line or later-line settings. However, the ITCs have a number of limitations that affect their internal and external validity, including an inability to comprehensively assess the clinical heterogeneities across the included individual studies and their impact on the study results. Consequently, uncertainty remains regarding the treatment effect of selpercatinib despite various adjustments to make LIBRETTO-001 comparable to trials of comparators. Generalizability of the study findings to patients with RET fusion–positive NSCLC could be limited. The critical limitations mean that no conclusions can be drawn based on both analyses.
The retrospective SIREN study evaluated the efficacy and safety of selpercatinib in 50 patients with RET fusion–positive NSCLC, using a primary outcome of the ORR. The study estimated an ORR of 68% (95% CI, 53 to 81), a median PFS of 15.6 months (95% CI, 8.8 to 22.4), and a median follow-up of 9.4 months. The safety findings showed that 88% of patients experienced an AE of any grade. The most commonly reported AEs were fatigue or asthenia (40%), increased liver enzyme levels (34%), hypertension (26%), dry mouth (26%), and peripheral edema (20%). The most common AEs of grade 3 or higher were increased liver enzyme levels (10%), abdominal pain (4%), prolonged corrected QT time (4%), hypertension (4%), and fatigue or asthenia (4%).13 Several limitations to the SIREN study were identified, including the retrospective study design (which is prone to reporting and nondifferential biases) and the differences in patient population compared with the LIBRETTO-001 trial due to the eligibility and exclusion criteria applied in each study (selection bias). The ORR, although measured using RECIST 1.1, was assessed by an unblinded review of practising physicians. There is a potential for measurement bias due to differences between clinical practice and the trial with respect to the frequency and conduct of disease assessments, the follow-up time frame in the study, and the therapies administered beyond disease progression. The small sample size of the study also limits the generalizability of the findings. Although the SIREN study provides additional data on the effectiveness and safety of selpercatinib in the real-world setting, these limitations introduce uncertainty, and no conclusions were drawn from the findings.
Harms
A reduction in AEs and a decrease in symptom burden was emphasized by the clinical experts, patient groups, and clinician group as key goals for the treatment of advanced or metastatic NSCLC. The experts considered the safety profile of selpercatinib to be favourable because it showed reduced toxicity-related events in comparison to other therapies available in practice. The experts further revealed that current treatment options (chemotherapy alone and chemotherapy with immunotherapy) have significant potential adverse effects that may require intensive supportive care, including additional hospital stays. In addition, respondents in the patient group input who had received selpercatinib in either the first- or second-line settings also described reduced toxicity-related events, reductions in tumours, and relief in symptom burden following administration of the drug.
At the December 16, 2019, data cut-off, the most common AEs reported in the NSCLC population in LIBRETTO-001 trial were dry mouth, diarrhea, hypertension, increased AST and ALT, fatigue, constipation, peripheral edema, headache, and nausea. Serious AEs commonly reported in the NSCLC population were pneumonia, increased ALT and AST, abdominal pain, pleural effusion, drug hypersensitivity, diarrhea, and acute kidney injury.
At the December 16, 2019, data cut-off, AEs leading to dose withdrawal, interruption, and dose reductions in the RET fusion–positive NSCLC population were consistent with those in the overall population. The AEs commonly associated with treatment discontinuations in the NSCLC population were increased ALT, sepsis, increased AST, drug hypersensitivity, fatigue, and thrombocytopenia. Increased ALT and AST were commonly associated with dose reductions and dose interruptions.
At the December 16, 2019, data cut-off, treatment was discontinued due to death in 6 patients and 38 patients discontinued the study due to death. At the March 30, 2020, data cut-off, in the NSCLC population, treatment was discontinued due to death in 6 patients (1.7%), and 55 patients (15.9%) discontinued the study due to death. In total, 36 patient deaths (10.4%) were attributed to disease progression, 13 deaths (3.9%) occurred due to AEs, and 6 deaths (1.7%) were attributed to other reasons. One report of death (0.3%), which was identified in the NSCLC population, occurred more than 28 days after the last selpercatinib dose. In the OSAS population, treatment was discontinued due to death in 11 patients (1.5%) and 103 patients (13.8%) discontinued the study due to death.6
Notable harms reported in the NSCLC set were consistent with those in the OSAS (at the March 30, 2020, and December 16, 2019, data cut-offs). The most common AEs were increased ALT (32.8%), increased AST (31%), hypertension (31.9%), drug hypersensitivity (2.4%), and electrocardiogram QT prolongation (16.7%). All notable harms identified in the LIBRETTO-001 trial have been properly labelled under the warnings and precautions section of the Canadian product monograph. The clinician experts consulted indicated that the safety profile of selpercatinib was favourable compared to other therapies offered as standard of care in Canada. However, in the absence of a comparative arm, the findings obtained from the safety analysis are uncertain as the single-arm design does not allow for differentiation of the symptoms of underlying NSCLC disease from treatment-related AEs.9
Conclusions
The evidence supporting the funding request of selpercatinib was derived from an ongoing phase I and II, open-label, non-randomized, multi-cohort, single-arm study (LIBRETTO-001). The ORR observed in the LIBRETTO-001 trial suggested favourable tumour response in both the treatment-naive and treatment-experienced groups and was consistent with further follow-up analyses. The ORR and DOR, including the CNS ORR, obtained in both patient populations were considered clinically meaningful by the clinician experts consulted during the review. Time-to-event end points such as OS and PFS were NE at the March 30, 2020, and December 16, 2019, data cut-offs in the PAS, IAS, and SAS1 populations due to data immaturity. The median PFS was NE in the treatment-naive group at the March 30, 2020, and December 16, 2019, data cut-offs. Combined with the single-arm trial design, the evidence was not considered sufficient to interpret OS and PFS findings. The sponsor provided additional data to CADTH for a new data cut-off of June 15, 2021. Although estimates obtained at the June 15, 2021, data cut-off suggested an improvement in median PFS in the IAS and SAS1 populations, the median OS was NE. CADTH considered these findings insufficient to provide concrete conclusions on the comparative treatment effects (PFS and OS) due to the single-arm trial design and immature data. Whether the observed magnitude of benefit related to tumour response with selpercatinib would be translated to OS in patients in the treatment-naive and treatment-experienced groups is therefore uncertain. As well, the limitations stemming from the single-arm, non-randomized design of the LIBRETTO-001 trial precluded drawing strong, definitive conclusions on the effects of selpercatinib on HRQoL, although the HRQoL findings were described as clinically meaningful by the clinician experts consulted by CADTH. Safety information was reported for all patients who received a single dose of selpercatinib in the LIBRETTO-001 trial at both data cut-offs. Selpercatinib was associated with corrected QT prolongation, increased AST and ALT, hypertension, and drug hypersensitivity. These events have been labelled in the warnings and precautions section of the Canadian approved product monograph for selpercatinib. However, the clinical experts considered these notable harms to be manageable and favourable compared to current standard of care treatment options. Although the SIREN study provided additional data on both the effectiveness and safety of selpercatinib in the RET fusion–positive NSCLC population, several limitations were identified with the study, and concrete conclusions could not be drawn to support the primary data obtained from the LIBRETTO-001 trial. The ITCs submitted to inform the comparative effects of selpercatinib were associated with limitations that prevented drawing conclusions on the results, and the comparative effectiveness and safety of selpercatinib remain uncertain.
References
1.Canadian Cancer Cancer Advisory Committee. Canadian cancer statistics. 2021; https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2022 Jan 5.
2.Cancer.Net American Society of Clinical Oncology (ASCO). Lung cancer - non-small cell: statistics. 2021; https://www.cancer.net/cancer-types/lung-cancer-non-small-cell/statistics. Accessed 2022 Jan 12.
3.National Cancer Institute. Non-small cell lung cancer treatment (PDQ®) – health professional version. 2021; https://www.cancer.gov/types/lung/hp/non-small-cell-lung-treatment-pdq. Accessed 2021 Dec 4.
4.Retevmo (selpercatinib): capsules, 40 mg and 80 mg, oral [product monograph]. Toronto: Eli Lilly Canada Inc; 2021 Jun 11.
5.Drug Reimbursement Review sponsor submission: Retevmo (selpercatinib), capsules, 40 mg and 80 mg, oral [internal sponsor's package]. Toronto: Eli Lilly Canada Inc; 2021.
6.Committee For Medicinal Products For Human Use. Retsevmo (selpercatinib). Amsterdam (Netherlands): European Medicines Agency; 2021: https://www.ema.europa.eu/en/medicines/human/EPAR/retsevmo. Accessed 2021 Dec 5.
7.Minchom A, Tan AC, Massarelli E, et al. Patient-reported outcomes with selpercatinib among patients with RET fusion–positive non-small cell lung cancer in the phase I/II LIBRETTO-001 trial. Oncologist. 2021;15:15. PubMed
8.Oxnard GR, Wilcox KH, Gonen M, Polotsky M, Hirsch BR, Schwartz LH. Response rate as a regulatory end point in single-arm studies of advanced solid tumors. JAMA Oncology. 2016;2(6):772-779. PubMed
9.Health Canada reviewer's report: Retevmo (selpercatinib) [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Retevmo (selpercatinib), capsules, 40 mg and 80 mg, oral. Toronto: Eli Lilly Canada Inc; 2021.
10.Center for Drug Evaluation and Research. Multidiscipline review(s). Retevmo (selpercatinib) capsule. Company: Loxo Oncology, Inc. Application No.:213246. Approval date: 05/08/2020 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2020 May 8: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2020/213246Orig1s000MultidisciplineR.pdf. Accessed 2021 Oct 27.
11.Lenvima (lenvatinib capsules), 4 mg and 10 mg lenvatinib (as lenvatinib mesylate) [product monograph]. Mississauga (ON): Eisai Limited; 2021 May 3.
12.Drug Reimbursement Review sponsor submission: Lenvima (lenvatinib) in combination with pembrolizumab (Keytruda), 4 mg and 10 mg lenvatinib mesylate capsules [internal sponsor's package]. Mississauga (ON): Eisai Limited; 2021 Nov.
13.Illini O, Hochmair MJ, Fabikan H, et al. Selpercatinib in RET fusion–positive non-small-cell lung cancer (SIREN): a retrospective analysis of patients treated through an access program. Ther Adv Med Oncol. 2021;13:17588359211019675. PubMed
14.Lung Cancer Canada. Lung canacer staging in Canada. 2020; https://www.lungcancercanada.ca/Lung-Cancer/Staging.aspx. Accessed 2021 Dec 4.
15.Iyer S, Roughley A, Rider A, Taylor-Stokes G. The symptom burden of non-small cell lung cancer in the USA: a real-world cross-sectional study. Support Care Cancer. 2014;22(1):181-187. PubMed
16.National Comprehensive Cancer Network (NCCN). Non-small cell lung cancer. NCCN Clinical Practice Guidelines in Oncology. 2021; https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450 (free registration required). Accessed 2021 Dec 4.
17.Planchard D, Popat S, Kerr K, et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Lugano (Switzerland): European Society for Medical Oncology; 2020: https://www.esmo.org/content/download/347819/6934778/1/ESMO-CPG-mNSCLC-15SEPT2020.pdf. Accessed 2021 Dec 4.
18.Ellis PM, Vella ET, Ung YC. Systemic treatment for patients with advanced non-small cell lung cancer. (Guideline 7-10, version 3). Toronto: Cancer Care Ontario; 2016: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/31811 Accessed 2021 Dec 4.
19.Interim Clinical Study Report: LOXO-RET-17001 (LIBRETTO-001). A phase 1/2 study of oral LOXO-292 in patients with advanced solid tumors, including RET fusion–positive solid tumors, medullary thyroid cancer and other tumors with RET activation (LIBRETTO-001) [internal sponsor's report]. Toronto: Loxo Oncology, Inc; 2019.
20.Cascetta P, Sforza V, Manzo A, et al. RET inhibitors in non-small-cell lung cancer. Cancers (Basel). 2021;13(17):01.
21.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
22.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Oct 27.
23.Drilon A, Oxnard GR, Tan DSW, et al. Efficacy of selpercatinib in RET fusion–positive non-small-cell lung cancer. N Engl J Med. 2020;383(9):813-824. PubMed
24.Subbiah V, Gainor JF, Oxnard GR, et al. Intracranial efficacy of selpercatinib in RET fusion–positive non-small cell lung cancers on the LIBRETTO-001 trial. Clin Cancer Res. 2021;27(15):4160-4167. PubMed
25.Solomon BJ, Zhou CC, Drilon A, et al. Phase III study of selpercatinib versus chemotherapy +/− pembrolizumab in untreated RET positive non-small-cell lung cancer. Fut Oncol. 2021;17(7):763-773. PubMed
26.Clinical Study Report Addendum: LOXO-RET-17001 (LIBRETTO-001). A phase 1/2 study of oral LOXO-292 in patients with advanced solid tumors, including RET fusion–positive solid tumors, medullary thyroid cancer and other tumors with RET activation (LIBRETTO-001) [internal sponsor's report]. Toronto: Loxo Oncology, Inc; 2019.
27.Brown SR, Gregory WM, Twelves CJ, et al. Designing phase II trials in cancer: a systematic review and guidance. Br J Cancer. 2011;105(2):194-199. PubMed
28.Van Norman GA. Phase II trials in drug development and adaptive trial design. JACC Basic Transl Sci. 2019;4(3):428-437. PubMed
29.Solomon BJ, Zhou CC, Drilon A, et al. Phase III study of selpercatinib versus chemotherapy ± pembrolizumab in untreated RET positive non-small-cell lung cancer. Future Oncol. 2021;17(7):763-773. PubMed
30.Fleming TR, Rothmann MD, Lu HL. Issues in using progression-free survival when evaluating oncology products. J Clin Oncol. 2009;27(17):2874-2880. PubMed
31.Loxo Oncology Inc. NCT04194944: A Study of selpercatinib (LY3527723) in participants with advanced or metastatic RET fusion–positive non-small cell lung cancer (LIBRETTO-431). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2019: https://clinicaltrials.gov/ct2/show/NCT04194944?id=NCT04194944. Accessed 2021 Nov 15.
32.Clinical trial end points for the approval of non-small cell lung cancer drugs and biologics: guidance for industry. Rockville (MD): U.S. Food and Drug Administration; 2015: https://www.fda.gov/media/116860/download. Accessed 2021 Dec 14.
33.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
34.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
35.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
36.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-1028. PubMed
37.Fayers PM, Aaronson NK, Bjordal K, et al. The EORTC QLQ-C30 Scoring Manual. 3rd ed. Brussels: European Organisation for Research and Treatment of Cancer; 2001: https://qol.eortc.org/manuals/. Accessed 2022 Feb 11.
38.Osoba D, Zee B, Pater J, Warr D, Kaizer L, Latreille J. Psychometric properties and responsiveness of the EORTC quality of Life Questionnaire (QLQ-C30) in patients with breast, ovarian and lung cancer. Qual Life Res. 1994;3(5):353-364. PubMed
39.Bedard G, Zeng L, Zhang L, et al. Minimal important differences in the EORTC QLQ-C30 in patients with advanced cancer. Asia Pac J Clin Oncol. 2014;10(2):109-117. PubMed
40.Maringwa JT, Quinten C, King M, et al. Minimal important differences for interpreting health-related quality of life scores from the EORTC QLQ-C30 in lung cancer patients participating in randomized controlled trials. Support Care Cancer. 2011;19(11):1753-1760. PubMed
41.Revicki D, Hays RD, Cella D, Sloan J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J Clin Epidemiol. 2008;61(2):102-109. PubMed
42.Van Der Weijst L, Surmont V, Schrauwen W, Lievens Y. Real life data on Patient-Reported Outcomes and neuro-cognitive functioning of lung cancer patients: the PRO-Long study. Front Oncol. 2021;11:685605. PubMed
43.Smit EF, van Meerbeeck JP, Lianes P, et al. Three-arm randomized study of two cisplatin-based regimens and paclitaxel plus gemcitabine in advanced non-small-cell lung cancer: a phase III trial of the European Organization for Research and Treatment of Cancer Lung Cancer Group--EORTC 08975. J Clin Oncol. 2003;21(21):3909-3917. PubMed
44.Sarna L, Swann S, Langer C, et al. Clinically meaningful differences in patient-reported outcomes with amifostine in combination with chemoradiation for locally advanced non-small-cell lung cancer: an analysis of RTOG 9801. Int J Radiat Oncol Biol Phys. 2008;72(5):1378-1384. PubMed
45.Rutkowski J, Szymanik M, Blok M, Kozaka J, Zaucha R. Prospective evaluation of anxiety, depression and quality of life in medically inoperable early stage non-small cell lung cancer patients treated with stereotactic ablative radiotherapy. Rep Pract Oncol Radiother. 2017;22(3):217-222. PubMed
46.Rittmeyer A, Gorbunova V, Vikstrom A, et al. Health-related quality of life in patients with advanced nonsquamous non-small-cell lung cancer receiving bevacizumab or bevacizumab-plus-pemetrexed maintenance therapy in AVAPERL (MO22089). J Thorac Oncol. 2013;8(11):1409-1416. PubMed
47.Ponce Aix S, Talbot D, Govindan R, et al. Quality of life with second or third line nab-paclitaxel-based regimens in advanced non-small-cell lung cancer. Fut Oncol. 2020;16(12):749-762. PubMed
48.Movsas B, Scott C, Langer C, et al. Randomized trial of amifostine in locally advanced non-small-cell lung cancer patients receiving chemotherapy and hyperfractionated radiation: radiation therapy oncology group trial 98-01. J Clin Oncol. 2005;23(10):2145-2154. PubMed
49.Mathieu D, Campeau MP, Bahig H, et al. Long-term quality of life in early-stage non-small cell lung cancer patients treated with robotic stereotactic ablative radiation therapy. Pract Radiat Oncol. 2015;5(4):e365-373. PubMed
50.Larsson M, Ljung L, Johansson BB. Health-related quality of life in advanced non-small cell lung cancer: correlates and comparisons to normative data. Eur J Cancer Care. 2012;21(5):642-649. PubMed
51.Hui R, Ozguroglu M, Villegas A, et al. Patient-reported outcomes with durvalumab after chemoradiotherapy in stage III, unresectable non-small-cell lung cancer (PACIFIC): a randomised, controlled, phase 3 study. Lancet Oncol. 2019;20(12):1670-1680. PubMed
52.Hechtner M, Eichler M, Wehler B, et al. Quality of life in NSCLC survivors - a multicenter cross-sectional study. J Thorac Oncol. 2019;14(3):420-435. PubMed
53.Fiteni F, Anota A, Bonnetain F, et al. Health-related quality of life in elderly patients with advanced non-small cell lung cancer comparing carboplatin and weekly paclitaxel doublet chemotherapy with monotherapy. Eur Respir J. 2016;48(3):861-872. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid.
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: November 4, 2021.
Alerts: Biweekly search updates until project completion.
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits: Conference abstracts were excluded.
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ab | Abstract |
.dq | Candidate term word (Embase) |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE, Embase) |
.nm | Name of substance word (MEDLINE) |
.ot | Original title |
.pt | Publication type |
.rn | Registry number |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(selpercatinib* or Retevmo* or Retsevmo* or LOXO-292 or LOXO292 or ARRY-192 or ARRY192 or LY3527723 or LY-3527723 or WHO-10967 or WHO10967 or CEGM9YBNGD).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*selpercatinib/
(selpercatinib* or Retevmo* or Retsevmo* or LOXO-292 or LOXO292 or ARRY-192 or ARRY192 or LY3527723 or LY-3527723 or WHO-10967 or WHO10967).ti,ab,kf,dq.
3 or 4
5 use oemezd
6 not (conference abstract or conference review).pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search terms – selpercatinib OR Retevmo OR Retsevmo OR LOXO-292 OR LOXO292 OR ARRY-192 OR ARRY192 OR LY3527723 OR LY-3527723]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms – (selpercatinib* or Retevmo* or Retsevmo* or LOXO-292 or LOXO292 or ARRY-192 or ARRY192 or LY3527723 or LY-3527723) NOT NCT*]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms – selpercatinib, Retevmo, Retsevmo]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms – selpercatinib OR Retevmo OR Retsevmo OR LOXO-292 OR LOXO292 OR ARRY-192 OR ARRY192 OR LY3527723 OR LY-3527723]
Grey Literature
Search dates: October 27 and November 1, 2021
Keywords: selpercatinib, Retevmo, Retsevmo, non-small cell lung cancer, RET kinase inhibitors
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
European Organization for Research and Treatment of Cancer, 30 Item Core Quality of Life Questionnaire (EORTC QLQ C-30)
Findings
Table 37: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ C-30 | A 30-item, patient-reported, cancer-specific, quality of life questionnaire using 4- and 7-point Likert scales | Validity, Reliability, and Responsiveness: Evidence of validity, reliability, and responsiveness in populations with lung cancer | Patients with NSCLC, breast cancer and small-cell lung cancer (SCLC)
Patients with breast cancer, followed by lung, prostate, gastrointestinal, renal cell, and other advanced cancers
Patients with RET fusion–positive NSCLC For the submitted study, the sponsor defined increase or reduction of symptom severity as a ≥10-points change from the baseline. |
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
Description
The EORTC QLQ-C30, is one of the most commonly used patient-reported outcomes (PRO) measures in oncology clinical trials.34 It is a multi-dimensional, cancer-specific, evaluative measure of health-related quality of life (HRQoL). This standardized, patient self-administered questionnaire has been designed to evaluate the quality of life of patients with cancer participating in clinical trials.35
The EORTC QLQ-C30 is composed of both multi-item scales and single-item measures. These include 5 functional scales (physical, role, emotional, cognitive, and social functioning), 3 symptom scales (fatigue, nausea/vomiting, and pain), and 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). This instrument also includes a global health status and overall quality of life section.36
Scoring
The EORTC QLQ-C30 uses a 1-week recall period in assessing function and symptoms. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. For the 2 items from the global quality of life scale, however, the response format is a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent).
Raw scores for each scale are computed as the average of the items that contribute to a particular scale. This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of 1 unit). All scales and individual item measures range in score from 0 to 100. Higher scores for the functioning scales and global health status/QoL denote a better level of functioning (i.e., a better state of the patient), while higher scores on the symptom scales indicate a higher burden of symptoms (i.e., a worse state of the patient). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better quality of life (i.e., higher scores simply reflect higher levels of response on that scale).
According to the EORTC QLQ-C30’s scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.37
Assessment of Validity
In its initial development, the EORTC QLQ-C30 underwent an evaluation of its psychometric properties and demonstrated reliability and validity in lung cancer patients in an international field trial of 305 patients in 13 countries, including Canada. Aaronson et al.35 tested construct validity of EORTC QLQ-C30 in these patients with nonresectable lung cancer (of 287 patients with reported histologic types, 63.1% had NSCLC) undergoing either radiotherapy or chemotherapy.
The validity of the instrument was evaluated using the correlations among the EORTC QLQ-C30 scales and the known-groups comparison method. While assessing the correlations, a substantial correlation (Pearson’s r ≥ 0.40) was expected among the conceptually related scales, such as physical functioning and fatigues, whereas lower correlations (Pearson’s r < 0.40) were expected among the scales with less commonality with each other, such as, cognitive functioning and nausea/vomiting. In the known-groups comparison method, the ability of the questionnaire scores to differentiate between the patient subgroups with different clinical status was evaluated.
The strongest correlations were observed (before and during treatment) between physical functioning, role functioning, and fatigue scales, with an r ranging between 0.54 and 0.63. Based on the known-groups approach, patients with better ECOG PS scores at the pre-treatment stage reported significantly higher physical, cognitive, and role functioning and overall QoL scores, as well as significantly lower symptom scores (ANOVA: n = 295, P < 0.001 to P < 0.05), compared with patients with poorer PS scores. In addition, statistically significant group differences were observed as expected for all functional and symptom scores, according to the on-treatment ECOG PS grouping variable (ANOVA: n = 265, P < 0.001 to P < 0.05), and for 5 out of 6 functional scales and 5 out of 7 symptom measures, based on toxicity ratings as group variable (ANOVA: n = 244, P < 0.001 to P < 0.05). Similarly, statistically significant group differences were observed in pre-treatment when patients having less weight loss reported better QoL scores as expected (ANOVA: n = 295, P < 0.001 to P < 0.05).35
Nicklasson et al.36 conducted construct, criterion, and concurrent validity tests of EORTC QLQ-C30 with 112 Swedish patients diagnosed with advanced lung cancer or pleural mesothelioma, including 85 (76%) patients with NSCLC, not amenable to curative or life prolonging treatment. Construct validity was examined by multitrait analysis, based on the definition of item convergent validity as a correlation of ≥.4 between an item and its own hypothesized scale, and of scaling error as the case when an item correlated > 1 standard error better with another scale than its own hypothesized scale. Criterion validity/ clinical validity was assessed by variance and correlation with an array of clinical parameters, including performance status, 6-min walk test, spirometry, tumour stage, and blood tests. Concurrent validity was evaluated by established scales for emotional distress (Hospital Anxiety and Depression Scale or HADS) and pain (Brief Pain Inventory or BPI). Correlations were designated as strong (>0.60), substantial (>0.40) or moderate (>0.20).
While assessing the criterion validity/ clinical validity based on WHO PS, significant interaction effects were observed for global health status/QoL, and physical, role and social functions (P < 0.0001). For a standardized 6-minute walk test, strongest interaction effect was seen with physical, role, and social functioning, fatigue, and global QoL (P < 0.0001). In a correlation analysis employing walking distance (> 200m, n = 58) as a continuous variable, a strong correlation (r = 0.77) with physical functioning, and substantial correlation (r > 0.4) with role functioning, fatigues, and global health status/QoL was observed. With spirometry, a correlation (r = not reported) with global health status/QoL was observed such that patients with an FEV1 predicted value <50% (n = 27) scored worse than did patients with an FEV1 predicted value ≥50% (n = 61).
While assessing the concurrent validity, a strong correlation (- 0.75) was observed between emotional functioning and the HADS anxiety scale, along with a substantial correlation (- 0.47) with global QoL. In addition, the HADS depression scale correlated substantially (>0.40) with all functioning scales, appetite loss and fatigue. On the other hand, the BPI intensity subscale (BPI-I) correlated strongly (r = 0.72) with the QLQ-C30 pain scale, moderately but significantly (>0.40) with functioning scales (except physical and social functioning), global QoL, and the remaining symptom scales (except nausea/vomiting). The BPI function subscale (BPI-F) correlated substantially (>0.40) with all functioning scales, global QoL, dyspnea, and pain measures.
Assessment of Reliability
Aaronson et al.35 tested reliability/internal consistency in the same population as described above in the validity section. The reliability (Cronbach alpha) coefficients for global quality of life were 0.86 before treatment and 0.89 during treatment, which can be considered a good reliability.
Nicklasson et al.36 performed reliability testing in the same population as described in the validity section above. Reliability of the global health status/QoL scale showed an internal consistency of 0.70 or higher, which is an accepted threshold for group comparisons.
Responsiveness to Change
Aaronson et al.35 measured the responsiveness in the context of improvement or deterioration of health status, which was estimated based on at least one level upward or downward shift on the ECOG PS scale. Statistically significant changes in EORTC QLQ-C30 scores were tested using repeated-measures ANOVA, as a function of observed changes in PS. Using this repeated-measures ANOVA with divided patient samples based on ECOG PS, statistically significant between-group differences over time were observed for global quality of life (P < 0.01), physical functioning (P < 0.001), role functioning (P < 0.001), fatigue (P < 0.01), and nausea/vomiting (P < 0.05) scale. No changes were noted in QLQ-C30 scores among those patients whose performance status had remained unchanged.
Table 38: Responsiveness of EORTC QLQ-C30 Scores Over Timea
EORTC QLQ-C30 scale | Improved ECOG (n = 34) | Deteriorated ECOG (n = 79) | ||||||
|---|---|---|---|---|---|---|---|---|
Pre-treatment | On-treatment | Pre-treatment | On-treatment | |||||
Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
Global Health Status‡ | 53.3 | 21.8 | 62.9 | 19.4 | 56.2 | 25.5 | 50.5 | 25.0 |
Physical Functioning+ | 58.1 | 27.1 | 67.5 | 22.6 | 67.8 | 27.6 | 54.7 | 32.0 |
Role Functioning+ | 55.9 | 36.4 | 67.6 | 34.6 | 60.1 | 38.7 | 44.3 | 39.2 |
Fatigue‡ | 43.1 | 27.6 | 40.1 | 26.0 | 42.6 | 25.7 | 53.2 | 27.7 |
Nausea and Vomiting& | 11.8 | 20.7 | 14.7 | 20.8 | 9.9 | 18.4 | 26.4 | 29.2 |
ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire – Core 30; SD = standard deviation
a Based on repeated measures ANOVA. Statistical tests for group x time interaction with 3 groups (improved, deteriorated, and unchanged ECOG PS) and 2 assessment points (pre-treatment and on-treatment). N = 262 due to missing ECOG PS ratings. Mean for the unchanged ECOG group are not presented.
‡P < 0.01
+P < 0.001
&P < 0.05
Source: Aaronson et al.35
One study by Osoba et al.38 aimed to assess the responsiveness of the EORTC QLQ-C30 in 160 lung cancer patients who received chemotherapy. The QLQ-C30 showed responsiveness to changes in disease state and treatment to chemotherapy in the expected direction. Patients with metastatic disease and those who received chemotherapy had diminished scores in the domains of physical and social role functions, and global quality of life, and had greater fatigue and nausea and vomiting compared with before chemotherapy.38
Minimally Important Difference
For use in clinical trials, scores on the EORTC QLQ-C30 can be compared between groups of patients or within a group of patients over time. One study conducted in breast cancer and small-cell lung cancer patients in 1998 estimated a clinically relevant change in score on any scale of the EORTC QLQ-C30 to be 10 points.33 The estimate was based on a study that used an anchor-based approach to estimating the MID in which patients who reported “a little” change (for better or worse) on the subjective significance questionnaire had corresponding changes on a function or symptom scale of the EORTC QLQ-C30 of approximately 5 to 10 points. Participants who reported a “moderate” change had corresponding changes in the EORTC QLQ-C30 of about 10 to 20 points, and those who reported being “very much” changed had corresponding changes of more than 20 points.33
In 2014, a Canadian study estimated the MID for EORTC QLQ-C30 in 369 patients with advanced cancer who completed the questionnaire at baseline and 1-month post-radiation.39 The most common cancer type was breast cancer, followed by lung, prostate, gastrointestinal, renal cell, and other cancers. The MID was estimated using both anchor- and distribution-based methods for improvement and deterioration. Two anchors of overall health and overall QoL were used, both taken directly from the EORTC QLQ-C30 (questions 29 and 30) where patients rated their overall health and QoL themselves. Improvement and deterioration were categorized as an increase or decrease by 2 units to account for the natural fluctuation of patient scoring. With these 2 anchors, the estimated MIDs across all EORTC QLQ-C30 scales ranged from 9.1 units to 23.5 units for improvement, and from 7.2 units to 13.5 units for deterioration. Distribution-based estimates were closest to 0.5 SD.39
Maringwa et al.40 estimated MIDs based on anchor-based method by pooling data from 2 RCTs on EORTC. Total 812 patients with palliative, locally advanced, and/or metastatic NSCLC undergoing treatment were enrolled. As for anchors chosen, physician-rated WHO PS and weight change were used based on their relevance to patients with NSCLC. An effect size of 0.2 SD, 0.5 SD, and threshold of 1 standard error of mean (SEM) of HRQoL scores have been reported as distribution-based MIDs to compare with the anchor-based MIDs.
MID estimates for improvement (i.e., 1 category change in PS, 5 - <20% weight gain) were: 9 and 4 for physical functioning, 14 and 7 for role functioning, 5 and 7 for social functioning, 14 and 5 for fatigue, 16 and 2 for pain, and 9 and 4 for global health status. The respective MID estimates for deterioration (i.e., 1 category change in PS, 5 - <20% weight loss) were: 4 and 6 for physical functioning, 5 for role functioning, 7 and 9 for social functioning, 6 and 11 for fatigue, 3 and 7 for pain, and 4 for global health status. MID estimates based on anchor-based and distribution-based methods are shown in Table 39.
Table 39: Summary of MIDs for the EORTC QLQ-C30 Subscale
EORTC QLQ-C30 scales | MID for improvement (anchor-based) | MID for deterioration (anchor-based) | MID (distribution-based) | MID (distribution-based) | MID (distribution-based) |
|---|---|---|---|---|---|
PS, weight gain | PS, weight loss | SEM | 0.5SD | 0.25SD | |
Global Health Status | 9, 4 | 4, 4 | 9 | 11 | 4 |
Physical Functioning | 9, 5 | 4, 6 | 7 | 12 | 5 |
Role Functioning | 14, 7 | 5, 5 | 14 | 17 | 6 |
Social Functioning | 5, 7 | 7, 9 | 10 | 14 | 6 |
Fatigue | 14, 5 | 6, 11 | 11 | 13 | 5 |
Pain | 16, 2 | 3, 7 | 12 | 16 | 6 |
EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire – Core 30; MID = minimal important difference; PS = performance status; SD = standard deviation; SEM = standard error of mean.
Source: Maringwa et al.40
The limitation of MID estimation performed by Maringwa et al.40 is poor correlations between changes in either anchor (WHO PS or weight) and QLQ-C30. For example, for changes in global health status scores and changes in both anchors, the correlations coefficients range from 0.10 to 0.14 in absolute values. The Spearman rank correlation of at least 0.30 is suggested to be acceptable association.41
Meaningful clinical important differences (MCIDs) and/or clinically significant/relevant differences were also applied in other studies to assess changes in HRQoL among 50 patients with locally advanced and metastatic NSCLC in Belgium,42 480 patients with advanced NSCLC (stage IIIB and stage IV) in Europe, South Africa and Egypt,43 138 patients with NSCLC (stage IIA-IIIB) in the US and Canada,44 51 patients with medically inoperable, early NSCLC in Poland,45 376 patients with advanced non-squamous NSCLC in Europe, Russia, Turkey and United Arab Emirates,46 240 patients with NSCLC in US, Canada, UK, and Europe,47 120 patients with NSCLC in US and Canada,48 45 patients with early-stage NSCLC in US and Canada,49 334 patents with advanced NSCLC in Sweden,50 713 stage III, unresectable NSCLC in North and South America (including Canada), Asia, Australia, Europe, UK, and South Africa,51 717 NSCLC survivors in Germany,52 and 451 elderly patients with advanced NSCLC in France.53 A 10-point change in score within a patient over time was considered the threshold of MCIDs and/or clinically significant/relevant differences in all of these studies, except for Rutkowski et al.,45 where the clinically meaningful improvement/clinical relevance were considered to be less than 7%, for Larsson et al.,50 where clinically relevant differences were considered small for 5 to 10 points changes, moderate for 11 to 19 points changes, and large for changes greater than 20 points, based on the Osoba et al. study,33 and for Fiteni et al.,53 in which a 5-point decrease was used as the MCID.
For the submitted study, the sponsor defined increase or reduction of symptom severity as a ≥10-points change from the baseline. In the ongoing LIBRETTO-001 study, 253 patients with RET fusion–positive NSCLC were assigned to take selpercatinib. Among them, 61.1% to 66.7% reported clinically meaningful improvements for global health status, 33.3% to 61.1% for dyspnea, and 46.2% to 63.0% for pain. Among the patients with improved dyspnea, 61.1% had ≥2 prior lines of therapy, with a 3.4-month median time to first improvement.7
Appendix 3: Follow-Up Analysis
Note that this appendix has not been copy-edited.
Table 40: Follow-Up Analysis With June 15, 2021, Cut-Off Date
Outcome | June 15, 2021i IAS (n = 247) | SAS1 (n = 69) |
|---|---|---|
Progression-free survival | ||
Median, months (95% CI) | 24.94 (19.3 to NE) | 21.95 (13.8 to NE) |
1-year PFS (%) 2-year PFS (%) | 71 51 | 71 42 |
Median follow-up, months | 24.7 | 21.9 |
Censoring rate (%) | 55.9 | 53.6 |
Overall survival | ||
Median (95% CI) | NE (33.5 to NE) | NE (27.9 to NE) |
1-year OS (%) 2-year OS (%) | 88 69 | 93 69 |
Median follow-up, months | 26.4 | 25.2 |
Censoring rate, % | 68.4 | 71.0 |
ORR (%) | 61.1 | 84.1 |
95% CI | 54.7 to 67.2 | 73.3 to 91.8 |
BOR (%) CR PR SD PD Not evaluable | 18 (7.3) 133 (53.8) 81 (32.7) 7 (2.8) 8 (3.2) | 4 (5.8) 54 (78.3) 6 (8.7) 3 (4.3) 2 (2.9) |
DOR Median, months 95% CI Censoring rate (%) Median Follow-up (months) 1-year DOR (%) 2-year DOR (%) | 28.6 (20.4 to NE) 47.7 21.2 73 56 | 20.2 (13.0 to NE) 55.2 20.3 66 42 |
TTR | ||
Median (months) Range, months | 1.9 0.7 to 21.9 | 1.8 0.7 to 10.8 |
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
BIC
Bayesian information criteria
ICER
incremental cost-effectiveness ratio
NSCLC
non–small cell lung cancer
OS
overall survival
PD-L1
programmed death ligand 1
PFS
progression-free survival
QALY
quality-adjusted life-year
RET
rearranged during transfection
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Selpercatinib (Retevmo) |
Submitted price | Selpercatinib, 80 mg, $133 per oral capsule ($7,980 per 60-capsule bottle) Selpercatinib, 40 mg, $66.50 per oral capsule ($3,990 per 60-capsule bottle) |
Indication | As monotherapy for the treatment of metastatic RET fusion–positive NSCLC in adult patients |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC/c date | June 15, 2021 |
Reimbursement request | As monotherapy for the first-line treatment of adult patients with metastatic RET fusion–positive NSCLC As monotherapy for the treatment of adult patients with metastatic RET fusion–positive NSCLC and who have received prior systemic therapy |
Sponsor | Eli Lilly Canada Inc. |
Submission history | Currently under review Indications: RET-mutant medullary thyroid cancer for patients with unresectable advanced or metastatic disease; RET fusion–positive differentiated thyroid cancer following prior treatment with sorafenib and/or lenvatinib Recommendation: pending |
NOC/c = Notice of Compliance with Conditions; NSCLC = non–small cell lung cancer; RET = rearranged during transfection.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target populations | As monotherapy for the first-line treatment of adult patients with metastatic RET fusion–positive NSCLC As monotherapy for the treatment of adult patients with metastatic RET fusion–positive NSCLC who have received prior systemic therapy |
Treatment | Selpercatinib |
Comparators | Treatment naive: pembrolizumab + pemetrexed + carboplatin or cisplatin (triple therapy), pemetrexed + carboplatin or cisplatin (dual therapy) Treatment experienced: docetaxel, atezolizumab, nivolumab |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs, LYs |
Time horizon | 10 years |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; LY = life-year; NSCLC = non–small cell lung cancer; QALY = quality-adjusted life-year; RET = rearranged during transfusion.
Conclusions
The clinical evidence indicated that data from the pivotal trial were inadequate to interpret overall survival (OS) and progression-free survival (PFS) findings due to the single-arm trial design and immature data. Evidence generated from the indirect treatment comparison was insufficient to make comparisons across therapies due to a significant amount of uncertainty arising from patient heterogeneity between trials.
Given that OS and PFS are key components required to derive the health economic analysis, and no robust comparative evidence could be generated, CADTH was unable to derive a reliable base-case estimation of cost-effectiveness. To inform the exploratory reanalysis, CADTH revised the sponsor’s model to more accurately reflect how patients transition between the progression-free, post-progression, and dead states. CADTH also adopted appropriate estimates of treatment costs and subsequent therapy costs for those who progress beyond second-line therapy. Not all the concerns with the sponsor’s submission could be addressed and these outstanding limitations, such as no change in relative treatment effects and no vial sharing, biased the results in favour of selpercatinib.
Based on CADTH’s exploratory reanalysis, selpercatinib was not cost-effective at a $50,000 per quality-adjusted life-year (QALY) threshold, in either patients who are treatment naive or experienced. Results were largely driven by the drug acquisition cost for selpercatinib. In the treatment-naive setting, selpercatinib was associated with an incremental cost-effective ratio (ICER) of $418,720 ($495,313 including full testing costs) versus triple therapy. A price reduction of 70% (77% with inclusion of full testing costs) would be required to ensure selpercatinib was cost-effective at a $50,000 per QALY threshold in the treatment-naive setting. In the treatment-experienced setting, selpercatinib was associated with an ICER of $500,589 ($529,397 including testing) versus docetaxel. A price reduction of 87% (93% with inclusion of full testing costs) would be required to ensure selpercatinib was cost-effective at a $50,000 per QALY threshold in this setting.
While CADTH was able to make some corrections, given the uncertain comparative clinical evidence for selpercatinib and the lack of transparency and flexibility of the submitted model, the exploratory results and subsequent price reductions are likely biased in favour of selpercatinib.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received patient input from 3 groups in response to the call for patient input: Lung Cancer Canada, Canadian Lung Cancer Advocacy Group Breathe Hope, and CanCertainty. Information for this submission was captured through personal interviews and questionnaires. Five patients, 3 of whom lived in Canada, had experience with selpercatinib. The current standard of care for patients is chemotherapy and radiation, but their use over the long-term is limited due to unacceptable side effects. Patients on chemotherapy reported severe chest and back pain as well as nausea and extreme fatigue. The input noted that no curative therapy is currently available as first-line treatment, and new treatments are necessary to improve patient outcomes and overcome resistance to second-line treatment and beyond. Patients experienced with selpercatinib have reported improved disease control through a reduction in the number and size of both primary and metastasized tumours. Patients also reported increased energy levels, functionality, and independence, all while experiencing minimal side effects.
CADTH received 2 responses to the call for clinician input from Lung Cancer Canada and the Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancers Drug Advisory Committee. Clinicians indicated that the current standard of care for patients with treatment-naive advanced or metastatic non–small cell lung cancer (NSCLC) would be chemotherapy with platinum or pemetrexed with or without pembrolizumab, or pembrolizumab monotherapy. Second-line options include platinum or pemetrexed (for those who received pembrolizumab monotherapy in the first line), nivolumab, atezolizumab, or docetaxel. Clinicians indicated that selpercatinib should be offered as a first-line treatment in all patients with newly diagnosed metastatic NSCLC who test positive for a fusion mutation of the rearranged during transfection (RET) gene, as well as those identified as having the mutation after being previously treated (i.e., second-line and greater).
Feedback from the drug plans indicated that RET testing would need to be in place to identify patients eligible for selpercatinib.
One of these concerns was addressed in the sponsor’s mode:
The choice of comparators aligned with the input received.
In addition, CADTH addressed the following concern:
CADTH explored the impact of including testing costs in both the pharmacoeconomic and budget impact analysis (BIA).
Economic Review
The current review is for selpercatinib (Retevmo) as monotherapy for adult patients with metastatic RET fusion–positive NSCLC as both a first-line treatment and for those who have received prior systemic therapy.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The submitted analysis is a cost-utility analysis comparing selpercatinib to alternative therapeutic options both as a first-line treatment and as a subsequent treatment after prior systemic therapy for adult patients with metastatic RET fusion–positive NSCLC.1 According to the sponsor’s submission, selpercatinib is available as 40 mg and 80 mg oral capsules. It is to be used as a monotherapy with a recommended dosage of 160 mg twice daily for patients (weighing 50 kg or more) until loss of clinical benefit or unacceptable toxicity.
For use as a first-line therapy, 2 comparators were identified in the submission. Dual therapy with pemetrexed and carboplatin was assumed to be given at a dose of 500 mg/m2 for pemetrexed and 5 mg/mL for carboplatin every 3 weeks. Pemetrexed was assumed to be given once every 3 weeks until disease progression or unacceptable toxicity. Carboplatin was assumed to be given for 6 cycles. Triple therapy is a combination of pembrolizumab with pemetrexed and carboplatin given every 3 weeks. Pemetrexed and carboplatin were assumed to be given at the same dosages as dual therapy, although carboplatin was assumed to be given for only 4 cycles. Pembrolizumab was assumed to be given at a dose of 200 mg for up to 2 years or until loss of clinical benefit or unacceptable toxicity. All comparators were administered by IV.
For use as a second-line therapy, 3 comparators were identified in the submission. Atezolizumab would be given at a dose of 1,200 mg once every 3 weeks until loss of clinical benefit or unacceptable toxicity. Nivolumab would be given at 3 mg/kg of body weight once every 2 weeks until disease progression. Docetaxel would be given at a dose of 75 mg/m2 for up to 6 cycles until disease progression or unacceptable toxicity.
Selpercatinib is dispensed in a package of 60 oral capsules at a cost of $133 per 80 mg capsule and $66.50 for a 40 mg capsule. The daily cost of treatment is $532, for a cost per pack of $7,980. This would lead to an annual cost of $194,180.
The cost of dual therapy varies over time given the use of carboplatin for only the first 6 cycles. Based on the recommended dosing, the costs per cycle would be $827 for the first 6 cycles and $765 for subsequent cycles, assuming no wastage and 100% dose intensity and using the sponsor’s estimates for vial cost. Based on this, the annual costs (for 18 cycles) would be $14,142. The cost of triple therapy also varies over time given the use of carboplatin for only 6 cycles and pembrolizumab for a maximum of 2 years. Based on the recommended dosing, the costs per cycle would be $7,075 for the first 4 cycles, $7,073 for subsequent cycles up to 2 years, and $765 for subsequent cycles beyond 2 years, assuming no wastage and 100% dose intensity and using the sponsor’s estimates for vial costs. The annual costs in the first year (for 18 cycles) would be $126,484.
The cost per cycle for docetaxel would be $1,576. leading to a maximum cost per patient (6 cycles) of $9,459. The cost per cycle of nivolumab would be $4,165, leading to an annual cost for 26 cycles of $108,299. The cost per cycle of atezolizumab would be $6,776, leading to an annual cost for 18 cycles of $121,968.
As selpercatinib is orally administered, there are no administration costs, although the implications with respect to additional clinician visits are unclear. The costs of IV infusion were considered for all comparators. In the sponsor’s analysis, the costs of comparator therapies were adjusted upward by assuming drug wastage, and the costs of all therapies for subsequent cycles were reduced by ||||% by assuming reduced dose intensity. CADTH notes that the sponsor’s estimated costs for many comparator therapies are likely incorrect due to incorrect costs being applied to many of the vial sizes. This is detailed further in the section on CADTH’s appraisal of the sponsor’s economic evaluation.
Analysis takes the form of a health care system perspective with a 10-year time horizon and an equivalent annual discount rate of 1.5% for all outcomes.
Model Structure
The model takes the form of a partitioned survival model in which the patient population is assumed at each time point to be split between 3 health states: progression-free, post-progression, and dead. Within the model, the proportions are estimated on a weekly basis, and costs (relating to treatment, treatment-related adverse events [AEs], and disease state) and utilities (relating to AEs and disease states) are allocated.
Due to the nature of partitioned survival models, the transition of patients between health states is not taken into account. Instead, the proportion of patients who are progression-free and the proportion who are alive at each time point are estimated independently.
Model Inputs
Analysis is based on 2 patient cohorts: previously treated patients (treatment experienced) with RET fusion–positive NSCLC and patients with RET fusion–positive NSCLC who have not had treatment. The treatment-experienced cohort involves a comparison of second-line therapies and was assumed to have the same characteristics as a combination of the 105 patients within the primary analysis set of the LIBRETTO-001 study (phases I and II) who had previously been treated with platinum-based chemotherapy, as well as a further 79 patients who met the same criteria and were enrolled in the LIBRETTO-001 study by the data cut-off date.1,2 The treatment-naive cohort involves a comparison of first-line therapies and was assumed to have the same characteristics as the 39 patients who were part of a supplementary analysis set.
A partitioned survival model requires survival functions relating to PFS and OS for all comparators within the model. This is problematic given the lack of comparative data for selpercatinib and data for comparators specific to RET fusion–positive NSCLC.
Information on PFS and OS for RET fusion–positive NSCLC patients who were treatment naive or treatment experienced and were then treated with selpercatinib was obtained from a single-arm study encompassing both a phase I (dose-escalation) and a phase II (dose-expansion) trial. Analysis was based on 184 patients who had received previous systemic therapy and 39 patients who were treatment naive.
Given the lack of head-to-head comparisons with alternative treatment options, an assessment of the relative effects of selpercatinib on PFS and OS required a synthetic comparison.
For therapies in the treatment-experienced cohort, an unanchored indirect treatment comparison was conducted first to compare selpercatinib with docetaxel, with the intention of developing artificial PFS and OS functions for docetaxel. Individual patient-level data for selpercatinib (from the LIBRETTO study) and for docetaxel (from an arm of the REVEL study) were used.2,3 As the REVEL study did not involve RET fusion–positive patients, manipulation of the available data for docetaxel was required to create a pseudo-control arm. This required adjusting the survival curves for docetaxel using 2 methods:
adjusting data to reflect the improved outcomes with RET fusion–positive NSCLC patients based on data from the US Flatiron Clinico-Genomic Database
adjusting data by propensity score matching to adjust for further differences between the patients within the LIBRETTO and REVEL studies with respect to additional prognostic factors.2,3
This allowed for an artificial comparison of selpercatinib with docetaxel in RET fusion–positive NSCLC patients. No data source for the Flatiron database was provided.
Based on the raw data from LIBRETTO and the simulated data for docetaxel, parametric survival functions were estimated for both PFS and OS to allow for extrapolation beyond the limited time horizon of the relevant data. Seventeen parametric functions were fit to the data, with the choice of function for the analysis stated in the report to be based on statistical fit and clinical plausibility as assessed by a clinician from the UK. For PFS, a stratified Gompertz function was selected for both selpercatinib and docetaxel, and a spline/knot = 1 function was selected for OS. For PFS, the chosen functional form was ranked 12th in statistical fit as assessed by Bayesian information criteria (BIC) and the choose function for OS was ranked seventh. The report is unclear whether either of these functions was supported by the clinical expert.
The next step required estimation of parametric survival functions for atezolizumab and nivolumab. To obtain hazard ratios for PFS and OS for atezolizumab and nivolumab, a further network meta-analysis of clinical trial data was carried out to compare docetaxel to nivolumab and atezolizumab in terms of PFS and OS, although this was performed in patients regardless of RET status and the incidence of further prognostic factors.1 However, no relevant PFS data for atezolizumab could be identified and the analysis assumed the same relative effect on PFS from docetaxel and pembrolizumab. Finally, hazard ratios derived through this process were used to adjust the survival functions for docetaxel to obtain PFS and OS survival functions for atezolizumab and nivolumab.
For first-line therapies, a similar approach was adopted. First, an unanchored indirect treatment comparison was conducted to compare selpercatinib with pemetrexed plus platinum. Individual patient-level data for selpercatinib (from the LIBRETTO study) and for pemetrexed plus platinum (from the KEYNOTE-189 study) was used.2,4 As the KEYNOTE-189 study did not involve RET fusion–positive patients, manipulation of the available data for pemetrexed plus platinum was required to create a pseudo-control arm to allow for such comparisons. This required adjusting the survival curves for pemetrexed plus platinum using the methods described in the previous section: adjusting the data to reflect the improved outcomes with RET fusion–positive NSCLC and further adjusting the data by propensity score matching to account for further differences between the patients within the LIBRETTO and KEYNOTE-189 studies with respect to additional prognostic factors.2,4 This allowed for an artificial comparison of selpercatinib with pemetrexed plus platinum in RET fusion–positive NSCLC patients.
Parametric survival functions were estimated for both PFS and OS to allow for extrapolation beyond the limited time horizon of the relevant data. For PFS, 16 parametric functions were fit to the raw data from LIBRETTO and the simulated data for pemetrexed plus platinum, with the choice of function for the analysis stated in the report to be based on statistical fit and clinical plausibility as assessed by a Canadian clinician. For PFS, the Weibull function was selected for both selpercatinib and pemetrexed plus platinum. The Weibull function was ranked seventh in statistical fit using BIC. For OS, the sponsor did not apply the parametric models estimated from the obtained OS data for selpercatinib. The sponsor argued that the OS data were limited and therefore it used an approach in which post-progression survival was modelled using data from the US Flatiron Clinico-Genomic Database, assuming a constant rate of post-progression mortality. However, for pemetrexed plus platinum, this approach was not adopted. Instead, the artificial OS functions described previously were fit to a Weibull distribution, which incorporated an increasing rate of mortality over time. The Weibull function was ranked sixth in statistical fit using BIC.
The next step required estimation of parametric survival functions for pembrolizumab plus pemetrexed and platinum. To obtain hazard ratios for PFS and OS for pembrolizumab plus pemetrexed and platinum, a further network meta-analysis of clinical trial data was performed to compare pemetrexed plus platinum with pembrolizumab plus pemetrexed and platinum in terms of PFS and OS, although this was performed in patients regardless of RET status or the incidence of further prognostic factors.1 Finally, the derived hazard ratios were used to adjust the survival functions for pemetrexed plus platinum to obtain PFS and OS survival functions for pembrolizumab plus pemetrexed and platinum.
For both analyses, the relative effects of treatment were assumed to last for the time horizon of the model, including once treatment was curtailed.
AEs were incorporated at model onset as 1-off disutilities and costs. The probabilities of each type of AE for each therapeutic alternative were based on analysis of trial data.2,5,6 Analysis was limited to AEs of grade 3 or higher and for which there was at least a 2% difference in frequency between interventions. For selpercatinib, AE rates were based on 329 patients within the LIBRETTO trial.2 The numbers relating to initial therapy and subsequent therapy AE rates are derived from a wider patient population compared with the survival data used within the economic evaluation.
Quality of life data were collected in the LIBRETTO study through administration of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30.2 Health-state utility values based on the EQ-5D utility instrument were derived from this data for the progression-free and post-progression health states for both first-line and subsequent therapies based on a published mapping algorithm.7 Scenario analysis was based on alternative values obtained from a published study that did not involve RET fusion–positive patients.8 A 1-off disutility related to treatment-related AEs was obtained by weighting the proportion of patients who experience AEs of grade 3 or higher (as previously described) by the duration of the AEs and an associated utility decrement.9-16 The sources for utility decrements were provided but the basis for choosing between alternative sources was not provided. The duration of AEs was obtained through assumptions.
The analysis incorporated the costs of the following: drug acquisition, drug administration, AEs, management of patients with progression-free disease, management of patients with disease progression, subsequent therapy after disease progression, and death. Analysis did not include the cost of screening and identifying patients with RET fusion–positive NSCLC.
Costs of comparator therapies were derived as previously described, with the costs of IV therapy adjusted to be higher by assuming drug wastage, and the costs of all therapies for subsequent cycles were reduced by ||||% due to reduced dose intensity. Treatment discontinuation was based on disease progression and capped at the maximum number of treatment cycles as specified by the product monograph. In addition, patients treated with selpercatinib were assumed to incur costs for 7 electocardiograms.17
Drug administration costs related to IV fusion and prescription costs for selpercatinib were also applied.17
Adverse event costs were obtained from the Ontario Case Costing Initiative with the assumption that all identified AEs required hospitalization. A 1-off cost related to treatment-related AEs was applied at the onset of the model and was estimated by weighting the proportion of patients who experience each AE of grade 3 or higher (as previously described) by the associated cost.18
The cost of subsequent treatment after failing the first or second line of therapy is applied in the model as a 1-off cost at the time of disease progression. Costs of subsequent therapies were based on assumptions relating to cost and durations. The distribution of subsequent treatments based on comparator received was based on Canadian clinical expert opinion. The approach led to different distributions and costs for subsequent therapies by comparator.
For disease management, the frequency of resource use in the progression-free and post-progression states was based on Canadian clinical expert opinion and then weighted by appropriate unit costs.17 For the costs of death, a published estimate of end-of-life palliative care was used.19
Summary of Sponsor’s Economic Evaluation Results
The sponsor submitted probabilistic analyses for both treatment-naive and treatment-experienced populations based on 1,000 replications. The results of the probabilistic analyses were broadly in line with the deterministic analyses. However, multiple errors were identified in the probabilistic analysis, both in terms of the specification of uncertainty around input parameters and in the derivation of the probabilistic results. It was not possible to correct for all these limitations, and CADTH was therefore restricted to considering only the results of the deterministic analyses. A full discussion of these concerns is provided in Appendix 3.
Base-Case Results
The sponsor’s economic evaluation base case concluded that selpercatinib was not cost-effective at a $50,000 per QALY threshold, as first-line or subsequent therapy, for patients with RET fusion–positive NSCLC.
In the treatment-naive setting, average annual costs were $122,227 for dual therapy, $267,104 for triple therapy, and $536,882 for selpercatinib, while average QALYs were 1.64 for dual therapy, 2.73 for triple therapy and 4.19 for selpercatinib (Table 3). The ICER for selpercatinib was $162,972 versus dual therapy and $185,667 versus triple therapy. In a sequential analysis, the ICER for triple versus dual therapy was $132,755 and the ICER for selpercatinib versus triple therapy was $185,667. Incremental costs for selpercatinib were primarily due to higher drug costs, and incremental QALYs were due to assumptions of greater time in both the progression-free and post-progression states (Appendix 3). As the trial was single arm in design, 100% of the incremental QALYs are derived from extrapolation methods rather than direct trial evidence.
In the treatment-experienced setting, average annual costs were $60,644 for docetaxel, $119,412 for atezolizumab, $130,152 for nivolumab, and $356,403 for selpercatinib, while average QALYs were 1.71 for docetaxel, 2.21 for atezolizumab, 2.15 for nivolumab, and 3.35 for selpercatinib (Table 4). The ICER for selpercatinib was $180,583 versus docetaxel, $209,410 versus atezolizumab, and $189,620 versus nivolumab. In a sequential analysis, the ICER for atezolizumab versus docetaxel was $116,120, and the ICER for selpercatinib versus atezolizumab was $209,410; nivolumab was subject to dominance by atezolizumab. Incremental costs for selpercatinib were primarily due to higher drug costs, and incremental QALYs were due to assumptions of greater time in both the progression-free and post-progression states (Appendix 3). As the trial was single arm in design, 100% of the incremental QALYs are derived from extrapolation methods rather than direct trial evidence.
The submitted analysis is based on the publicly available prices of the comparator treatments, although these were incorrectly derived by the sponsor. Given the errors in the probabilistic analysis, more detailed descriptions of the CADTH appraisal of the economic evaluation and deterministic results are presented in the following section.
Table 3: Summary of the Sponsor’s Economic Evaluation — Deterministic Results for Patients Who Were Treatment Naive
Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
Dual therapy | 122,227 | 1.64 | Reference |
Triple therapy | 267,104 | 2.73 | 132,755 |
Selpercatinib | 536,882 | 4.19 | 185,667 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission, deterministic analysis.1
Table 4: Summary of the Sponsor’s Economic Evaluation — Deterministic Results for Patients Who Were Treatment Experienced
Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
Docetaxel | 60,644 | 1.71 | Reference |
Atezolizumab | 119,412 | 2.21 | 116,120 |
Selpercatinib | 356,403 | 3.35 | 209,410 |
Nivolumab | 130,152 | 2.15 | Dominated by atezolizumab |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission, deterministic analysis.1
Disaggregated results from the sponsor’s submitted probabilistic base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
Subgroup analyses were presented for both first-line and subsequent therapies for patients with RET fusion–positive, programmed cell death ligand 1 (PD-L1)-positive NSCLC. There are multiple serious limitations with this subgroup analysis: the analyses were not based on selpercatinib data specific to RET fusion–positive, PD-L1–positive NSCLC as PD-L1 status was not assessed in the LIBRETTO-001 trial; the method for interpolating the survival curves for selpercatinib compared with other therapies was based on RET fusion–positive NSCLC data regardless of PD-L1 status; the relative effectiveness of other therapies for PD-L1–positive NSCLC was based on a network meta-analysis anchored on docetaxel for all patients; and PFS and OS were modelled relative to the survival curves for docetaxel for all patients.
The sponsor presented several scenario and sensitivity analyses for patients who were treatment naive and treatment experienced relating to the choice of survival function for OS and PFS, inclusion of testing costs, and an alternative source of utility values. In all scenarios, results were similar to those of the base-case analysis in that selpercatinib was not cost-effective at a $50,000 per QALY threshold in either patient population.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Relative effect on PFS: There is considerable uncertainty with respect to the relative effect of selpercatinib on delaying progression given the absence of randomized controlled evidence, the small sample size of RET fusion–positive patients in both the LIBRETTO-001 trial (particularly for patients who were treatment naive) and the US Flatiron Clinico-Genomic Database used to interpolate a treatment effect, and the reliance on data for comparators not relating to RET fusion–positive patients for PFS. The sponsor used 5 alternative methods to estimate the relative effect of selpercatinib by adjusting the comparator data to match the population within the LIBRETTO study. The sponsor only provided relative effects derived from the propensity score matching method, which gave the most favourable estimate of relative effect. CADTH requested the sponsor provide analyses using alternative methods, but the sponsor declined to meet this request. The clinical experts consulted by CADTH for this review agreed that the true effect size was highly uncertain and could lie between the optimistic effect size estimated by the sponsor and the same effect size as the most effective comparator in the sponsor’s network meta-analysis.
CADTH was unable to address this limitation as the sponsor did not provide effect estimates based on a different methodology. Relative effect estimates may have been overestimated.
Long-term survival post-progression: The sponsor’s primary analysis assumed that OS is independent of whether individuals are on treatment and whether they are in the progression-free or post-progression state. Clinical expert opinion suggested that, as survival is linked to progression, the transition probability to death should vary for patients within the progression-free state and those in the post-progression state. The sponsor’s partition survival model framework, which assumes survival is independent of progression, is therefore inappropriate and an alternative model framework that allows for such transitions would be appropriate.
In its original model, the sponsor did provide the option of modelling post-progression survival. This was specifically incorporated into the base case only for selpercatinib as a first-line therapy, assuming a constant mortality rate. As the mortality rate for other comparators was assumed to increase with time, this led to a bias within the submitted results, leading to substantial gains in post-progression survival with selpercatinib, with the modelled implicit hazard ratio showing an increasing effect size for selpercatinib in the long-term. The sponsor’s model did allow the assumption of equal post-progression survival across all comparators for first-line therapy, and CADTH requested the same option be provided for the treatment-experienced setting.
Analysis adopting equal post-progression survival partially addresses this issue. However, the sponsor’s approach assumes that all patients survive to progression, while analysis of the LIBRETTO-001 study clearly demonstrates that a proportion of patients die before progression. CADTH assumed that, given the lack of evidence, the probability of dying in a cycle before progression will be independent of treatment. As the sponsor argues that selpercatinib will delay progression, a greater proportion of patients on selpercatinib will die before progression. To address this issue, the sponsor was asked to provide the mean time in post-progression state within the trial to allow for estimation of a mortality rate in the pre-progression state. The sponsor declined this request.
CADTH assumed that survival post-progression would be the same regardless of which therapy the patient received. CADTH also assumed patients could die pre-progression. This mortality rate was derived from the proportion of patients who died before progression in the LIBRETTO trial. The OS benefit derived from selpercatinib in CADTH’s exploratory reanalysis was therefore directly linked to delays in PFS.
Model transparency: The model lacks transparency and is programmed such that the validity of the model cannot be fully assessed. The coding of the model is highly inefficient, with simple calculations being spread over multiple sheets. CADTH identified serious errors regarding simple calculations. The model incorporates numerous uses of IFERROR and ISERROR functions, which generally should be unnecessary. These functions are problematic as they allow the model to run even in the presence of an error. The results of the model are also hard-coded — i.e., they are not directly linked to the input parameters within the model. Separate models are also not provided for each comparator, which precludes making direct comparisons simultaneously. User-created functions are employed, which limits transparency.
The sponsor was asked to provide a model that limited the use of IFERROR statements, removed hard coding of model results, provided separate models for each comparator, and did not include user-created functions. A revised model provided by the sponsor contained more than 3,000 IFERROR statements and the sponsor declined to remove hard coding, provide a separate model for each comparator, or exclude user-created functions.
The revised model from the sponsor still seriously restricts the ability to fully validate the model. Given that CADTH also had to make further changes to the model (as noted in the following section), the validity of both the sponsor’s model and the subsequent reanalyses should be considered with caution. Further discussion of these concerns is provided in Appendix 3.
Drug costs: The sponsor’s analysis underestimated the unit costs of carboplatin based on the most recent Delta PA costs obtained by CADTH, biasing the results against selpercatinib. CADTH also noted that the sponsor miscalculated the cost of pemetrexed by assuming that a 500 mg vial costs the same as a 100 mg vial. Given that the cost of a 100 mg vial is approximately 1-fifth that of a 500 mg vial, this meant that the sponsor drastically underestimated the costs associated with pemetrexed. This error biased the results against selpercatinib. CADTH noted this error may be due to treatment-cost calculations being made across multiple sheets with incorrect labelling.
The sponsor’s analysis assumed wastage with all comparator therapies, which increased the associated treatment costs. According to advice from drug plans, vial sharing is common for pembrolizumab and nivolumab, and this significantly reduces the amount of wastage. The sponsor’s assumptions therefore biased the results in favour of selpercatinib. As the model is programmed such that wastage can only be considered either for all comparator therapies or no comparators, there was a severe lack of flexibility to incorporate more appropriate cost estimates. A scenario analysis is provided that assumes no wastage for all therapies.
The sponsor’s analysis assumed less than 100% treatment intensity after the first cycle, based on data from the LIBRETTO-001 study, which was partially a dose-escalation study. However, as selpercatinib is an oral therapy, it is unclear how a reduced dose intensity would translate into drug costs if the full prescription was dispensed. Likewise, the model independently models treatment discontinuation and it is unclear how this could affect dose intensity. Given the higher treatment costs for selpercatinib, this biased the results in favour of selpercatinib.
o CADTH corrected the cost of carboplatin and pemetrexed and applied a 100% dose intensity to all comparators. CADTH was unable to address wastage assumptions due to inflexibility with the modelling approach and unnecessarily complex cost calculations. CADTH assumed no wastage for all comparators as a scenario analysis.
Subsequent therapy costs: The sponsor’s assumptions relating to subsequent therapies after second-line treatment appear to be biased in that there are lower costs for subsequent therapies after progression following treatment with selpercatinib. The sponsor’s assumptions (e.g., 56% of patients who received docetaxel as a second-line treatment would receive docetaxel as a third-line treatment), lacked validity.
Given the absence of evidence that subsequent therapy use after second-line therapy would be higher for current treatment options, CADTH assumed equal subsequent treatment costs for all comparators in the treatment-experienced setting.
Testing costs: The sponsor’s base case does not include the cost of testing for RET fusion–positive patients. The clinical experts expressed a lack of availability for RET fusion–positive testing in many jurisdictions. If selpercatinib were funded, increased testing may be required.
CADTH conducted 2 analyses, 1 in which no testing costs were included and 1 in which the full cost of panel testing would be included.
Probabilistic analyses: CADTH identified multiple issues relating to the specification of uncertainty within the model not meeting best practices and errors in the determination of the results of the probabilistic analysis. Given the multiple concerns identified in this review, and due to the sponsor’s failure to supply a model that provides both models for each comparator and an analysis that removes all hard coding, validation of the sponsor’s probabilistic analysis was not possible.
CADTH’s exploratory analysis was conducted deterministically as the probabilistic results could not be validated. Further details on issues with the probabilistic results are discussed in Appendix 3.
Subgroup analyses: There were multiple issues with respect to the subgroup analysis specific to patients with RET fusion–positive, PD-L1–positive NSCLC: analyses were not based on selpercatinib data specific to RET fusion–positive, PD-L1 positive NSCLC as PD-L1 status was not assessed in the LIBRETTO-001 trial; the method for interpolating the survival curves for selpercatinib compared with other therapies was based on RET fusion–positive NSCLC data regardless of PD-L1 status; the relative effectiveness of other therapies for PD-L1–positive NSCLC was based on a network meta-analysis anchored on docetaxel for all patients; and PFS and OS were modelled relative to the survival curves for docetaxel for all patients.
CADTH was unable to resolve these issues, and the cost-effectiveness of selpercatinib versus pembrolizumab as a monotherapy remains unknown.
Additionally, key assumptions made by the sponsor were appraised by CADTH (Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Adverse event rates for comparators based on studies not specific to RET fusion–positive NSCLC | Reasonable assumption not likely to affect results |
State-specific utility values derived from data from LIBRETTO-001 using published mapping algorithms | Uncertain, although not likely to substantially affect results |
NSCLC = non–small cell lung cancer; RET = rearranged during transfusion.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Given the uncertainty over costs of testing for RET fusion–positive status, CADTH can only provide an exploratory analysis for patients who were treatment naive and treatment experienced based on the inclusion and exclusion of testing costs. As these analyses are based on the sponsor’s optimistic estimate of treatment effectiveness and inclusion of drug wastage, the results are likely biased in favour of selpercatinib. Even the lowest ICER estimates are therefore likely biased in favour of selpercatinib.
The results of the CADTH exploratory analyses were derived by making changes in model parameter values and assumptions in consultation with clinical experts. These changes included: assuming equal post-progression survival for each comparator within each indication, assuming mortality before progression, revising drug costs to make them reflect true prices, assuming 100% treatment intensity, and assuming equal subsequent therapy costs after second-line therapies.
An additional scenario analysis excluding wastage for all therapies was conducted.
Table 6: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | None. | None. |
Changes to derive the CADTH reanalysis | ||
1a. Post-progression survival | Assumed improved post-progression survival with selpercatinib | Assumed patients who do not die before progression will have the same post-progression survival |
1b. Mortality before progression | Assumed no patients died before progression | Assumed a mortality rate before progression based on the mortality rate derived from the 12-month PFS estimate from the LIBRETTO-001 trial and the proportion of patients who die before progression |
2a. Unit costs of comparator drugs | Assumed a cost of:
| Assumed costs based on IQVIA Delta PA of:
|
2b. Dose intensity | Assumed a reduction in drug costs due to reduced dose intensity | Assumed no reduction in dose intensity |
3. Subsequent therapy costs (only applies to the analysis for patients who have received a prior line of therapy) | Assumed reduced subsequent therapy costs after selpercatinib as a second-line treatment compared to comparator therapies | Assumed equal subsequent therapy costs after second-line treatments |
4. Genetic testing | Excluded costs of testing for RET fusion status | Provided analysis including testing costs |
CADTH exploratory analyses (treatment naive) CADTH exploratory analyses (treatment experienced) | — | 1 + 2 ( + 4 to explore the upper limit of potential testing costs) 1 + 2 + 3 ( + 4 to explore the upper limit of potential testing costs) |
PFS = progression-free survival; RET = rearranged during transfection.
The CADTH exploratory analyses found that selpercatinib is not cost-effective in patients who were either treatment naive or treatment experienced at a $50,000 per QALY threshold.
For patients who are treatment naive, the ICER for selpercatinib was $408,722 versus dual therapy and $418,720 versus triple therapy if the costs of testing were excluded. Including the costs of testing increased the respective ICERs to $445,455 and $495,313. In a sequential analysis, the ICER for triple versus dual therapy was $399,509 (regardless of inclusion of testing) and the ICER for selpercatinib versus triple therapy was $418,720. Incremental costs for selpercatinib were primarily due to higher drug costs, and incremental QALYs were due to assumptions of longer periods of time in the progression-free state (Appendix 4).
In the treatment-experienced setting, the incremental cost per QALY gained (ICER) for selpercatinib was $500,589 versus docetaxel, $422,880 versus nivolumab, and $440,326 versus atezolizumab if the costs of testing were excluded. Including the costs of testing increased the respective ICERs to $529,397, $453,673, and $471,292. In a sequential analysis, nivolumab and atezolizumab were subject to extended dominance regardless of the inclusion of testing; with the ICER for docetaxel versus selpercatinib $500,589. Incremental costs for selpercatinib were primarily due to higher drug costs, and incremental QALYs were due to assumptions of greater time in the progression-free state (Appendix 4).
These analyses are based on publicly available prices of the comparator treatments and rely on optimistic assumptions about the relative effectiveness of selpercatinib and wastage of drugs with comparator therapies. The estimated ICERs, although speculative, are therefore likely optimistic and favour selpercatinib.
Given the serious limitations with the sponsor’s probabilistic analysis, no assessment of the probability of selpercatinib being cost-effective can be presented.
Table 7: Summary of the Stepped Analysis of the CADTH Reanalysis — Treatment Naive
Stepped analysis | ICER ($ per QALY): selpercatinib vs. comparator | Sequential analysis ($ per QALY) |
|---|---|---|
Sponsor’s base case | vs. dual therapy: $162,972 vs. triple therapy: $185,667 | Triple therapy vs. dual therapy: $132,755 |
CADTH reanalysis 1 | vs. dual therapy: $375,305 vs. triple therapy: $503,341 | Triple therapy vs. dual therapy: $257,317 |
CADTH reanalysis 2 | vs. dual therapy: $172,203 vs. triple therapy: $142,999 | Selpercatinib vs. dual therapy: $172,203 |
CADTH reanalysis 3 | NR as it only applies to the treatment experienced | NR as it only applies to the treatment experienced |
CADTH reanalysis 4 | vs. dual therapy: $178,474 vs. triple therapy: $212,812 | Triple therapy vs. dual therapy: $132,755 |
CADTH exploratory analysis (1 + 2) | vs. dual therapy: $408,722 vs. triple therapy: $418,720 | Triple therapy vs. dual therapy: $399,509 |
CADTH exploratory analysis (1 + 2 + 4) | vs. dual therapy: $445,455 vs. triple therapy: $495,313 | Triple therapy vs. dual therapy: $399,509 |
ICER = incremental cost-effectiveness ratio; NR = not reported; QALY = quality-adjusted life-year.
Note: Analysis based on deterministic analyses based on limitations of sponsor’s probabilistic analysis.
Table 8: Summary of the Stepped Analysis of the CADTH Reanalysis — Treatment Experienced
Stepped analysis | ICER ($ per QALY): selpercatinib vs. comparator | Sequential analysis ($ per QALY) |
|---|---|---|
Sponsor’s base case | vs. docetaxel: $180,583 vs. nivolumab: $189,620 vs. atezolizumab: $209,410 | Atezolizumab vs. docetaxel: $116,120 |
CADTH reanalysis 1 | vs. docetaxel: $398,807 vs. nivolumab: $327,641 vs. atezolizumab: $345,642 | Selpercatinib vs. docetaxel $398,807 |
CADTH reanalysis 2 | vs. docetaxel: $225,019 vs. nivolumab: $242,837 vs. atezolizumab: $264,862 | Atezolizumab vs. docetaxel: $135,924 |
CADTH reanalysis 3 | vs. docetaxel: $181,897 vs. nivolumab: $191.423 vs. atezolizumab: $211,312 | Atezolizumab vs. docetaxel: $116,120 |
CADTH reanalysis 4 | vs. docetaxel: $193,456 vs. nivolumab: $207,290 vs. atezolizumab: $228,040 | Atezolizumab vs. docetaxel: $116,120 |
CADTH exploratory analysis (1 + 2 + 3) | vs. docetaxel: $500,589 vs. nivolumab: $422,880 vs. atezolizumab: $440,326 | Selpercatinib vs. docetaxel $500,589 |
CADTH exploratory analysis (1 + 2 + 3 + 4) | vs. docetaxel: $529,397 vs. nivolumab: $453,673 vs. atezolizumab: $471,292 | Selpercatinib vs. docetaxel $529,397 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Analysis based on deterministic analyses based on limitations of sponsor’s probabilistic analysis. Bold text highlights the cost-effectiveness of selpercatinib as it appears on the cost-effectiveness frontier.
Scenario Analysis Results
CADTH conducted a scenario analysis excluding wastage for all therapies that led to reduced costs for comparator therapies and, therefore, higher estimated ICERs with respect to selpercatinib versus the comparators. For first-line therapies, the ICERs for selpercatinib versus dual therapy and triple therapy without testing were $430,843 and $580,120, respectively, and $467,576 and $656,714, respectively with testing. For subsequent therapies, the ICERs for selpercatinib versus docetaxel, atezolizumab, and nivolumab without testing were $501,374, $446,886, and $441,045, respectively, and $530,182, $477,632 and $472,058, respectively, with testing. These results were substantially higher than those in the CADTH exploratory analysis that assumed full wastage.
Based on the CADTH exploratory analysis, with full wastage included, a price reduction for selpercatinib of between 70% and 77% is required for the ICER to be reduced to $50,000 per QALY in the treatment-naive setting, depending on the extent of additional testing costs. Similarly, a price reduction for selpercatinib of between 87% and 93% is required for the ICER to be reduced to $50,000 per QALY in the treatment-experienced setting.
These analyses are based on publicly available prices of the comparator treatments and rely on optimistic assumptions about the relative effectiveness of selpercatinib and wastage of drugs compared with comparator therapies. The estimated required price reductions are therefore likely optimistic and in favour of selpercatinib and should be seen as the minimum price reduction required.
Table 9: CADTH Price Reduction Analyses — Treatment Naive
Reduction | Sequential ICERs for selpercatinib vs. relevant comparators on cost-effectiveness frontier | ||
|---|---|---|---|
Price reduction | Sponsor base case | CADTH exploratory analysis — excluding testing | CADTH exploratory analysis — including testing |
No price reduction | $185,667 vs. triple therapy | $418,720 vs. triple therapy | $495,313 vs. triple therapy |
10% | $156,112 vs. triple therapy | $357,367 vs. dual therapy | $394,099 vs. dual therapy |
20% | $129,216 vs. dual therapy | $306,011 vs. dual therapy | $342,744 vs. dual therapy |
30% | $112,338 vs. dual therapy | $254,655 vs. dual therapy | $291,388 vs. dual therapy |
40% | $95,459 vs. dual therapy | $203,299 vs. dual therapy | $240,032 vs. dual therapy |
50% | $78,581 vs. dual therapy | $151,944 vs. dual therapy | $188,676 vs. dual therapy |
60% | $61,703 vs. dual therapy | $100,588 vs. dual therapy | $137,321 vs. dual therapy |
67% | $50,000 vs. dual therapy | $64,639 vs. dual therapy | $101,372 vs. dual therapy |
69.9% | $44,994 vs. dual therapy | $50,000 vs. dual therapy | $86,479 vs. dual therapy |
70% | $44,825 vs. dual therapy | $49,232 vs. dual therapy | $85,965 vs. dual therapy |
77% | $40,943 vs. dual therapy | $13,282 vs. dual therapy | $50,000 vs. dual therapy |
ICER = incremental cost-effectiveness ratio; vs. = versus.
Table 10: CADTH Price Reduction Analyses — Treatment Experienced
Reduction | Sequential ICERs for selpercatinib vs. relevant comparators on cost-effectiveness frontier | ||
|---|---|---|---|
Price reduction | Sponsor base case | CADTH exploratory analysis — excluding testing | CADTH exploratory analysis —including testing |
No price reduction | $209,410 vs. atezolizumab | $500,589 vs. docetaxel | $529,397 vs. docetaxel |
10% | $182,608 vs. atezolizumab | $449,079 vs. docetaxel | $477,887 vs. docetaxel |
20% | $155,805 vs. atezolizumab | $397,568 vs. docetaxel | $426,376 vs. docetaxel |
30% | $129,002 vs. atezolizumab | $346,057 vs. docetaxel | $374,866 vs. docetaxel |
40% | $102,199 vs. atezolizumab | $294,547 vs. docetaxel | $323,355 vs. docetaxel |
50% | $93,541 vs. docetaxel | $243,036 vs. docetaxel | $271,844 vs. docetaxel |
60% | $76,181 vs. docetaxel | $191,526 vs. docetaxel | $220,334 vs. docetaxel |
70% | $58,821 vs. docetaxel | $140,015 vs. docetaxel | $168,823 vs. docetaxel |
75% | $50,000 vs. docetaxel | $114,264 vs. docetaxel | $143,072 vs. docetaxel |
80% | $41,461 vs. docetaxel | $88,505 vs. docetaxel | $117,313 vs. docetaxel |
87% | $29,309 vs. docetaxel | $50,000 vs. docetaxel | $81,260 vs. docetaxel |
90% | $24,101 vs. docetaxel | $36,999 vs. docetaxel | $65,802 vs. docetaxel |
93% | $18,893 vs. docetaxel | $21,546 vs. docetaxel | $50,000 vs. docetaxel |
ICER = incremental cost-effectiveness ratio; vs. = versus.
Issues for Consideration
Results are dependent on whether there will be additional costs of testing for RET fusion–positive status. The issue is whether the rate of testing will increase if selpercatinib is funded.
The CADTH analysis could not address the cost-effectiveness of selpercatinib versus pembrolizumab as a monotherapy.
Overall Conclusions
The clinical evidence indicated that data from the pivotal trial were inadequate to interpret OS and PFS finding, due to the single-arm trial design and immature data. Evidence generated from the indirect treatment comparison was insufficient to make comparisons across therapies due to a significant amount of uncertainty arising from patient heterogeneity between trials.
Given that OS and PFS were the key components to derive the health economic analysis and no robust comparative evidence could be generated, CADTH was unable to derive a reliable base-case estimation of cost-effectiveness. Selpercatinib may reduce disease progression as either a first-line or subsequent therapy; however, the extent to which it reduces disease progression compared to alternative therapeutic options is highly uncertain.
To inform the exploratory reanalysis, CADTH revised the sponsor’s model to more accurately reflect how patients transition between the progression-free, post-progression, and dead states while retaining the same estimates of relative treatment effect. CADTH also adopted appropriate estimates of treatment costs and costs for those who progress beyond second-line therapy. Not all the concerns with the sponsor’s submission could be addressed and these outstanding limitations likely bias the analysis in favour of selpercatinib. The probabilistic analysis within the sponsor’s model was not fit for purpose, and reanalysis focused solely on the deterministic analysis. The key area of uncertainty is the relative effect of selpercatinib on reducing disease-progression rates. Given the lack of clinical data on relative effects, CADTH reanalyses are likely an optimistic representation of the cost-effectiveness of selpercatinib.
Based on CADTH’s exploratory reanalysis, selpercatinib was not cost-effective at a $50,000 per QALY threshold, as either a first-line therapy or subsequent therapy following failure of at least 1 prior therapy. Results are largely driven by the drug acquisition cost for selpercatinib. In the first-line setting, selpercatinib was associated with an ICER of $418,720 ($495,313 including full testing costs) versus triple therapy. A price reduction of 70% (77% with inclusion of full testing costs) would be required to ensure selpercatinib was cost-effective at a $50,000 per QALY threshold in the treatment-naive setting. As a therapy for those who have failed 1 prior therapy, selpercatinib was associated with an ICER of $500,589 ($529,397 including testing) versus docetaxel. A price reduction of 87% (93% with inclusion of full testing costs) would be required to ensure selpercatinib was cost-effective at a $50,000 per QALY threshold in this setting.
While CADTH was able to make some corrections, given the uncertain comparative clinical evidence for selpercatinib and lack of transparency and flexibility with the submitted model, the exploratory results and subsequent price reductions are likely biased in favour of selpercatinib.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Retevmo (selpercatinib), capsules, 40 mg and 80 mg, oral. Toronto: Eli Lilly Canada Inc; 2021.
2.Drilon A, Oxnard GR, Tan DSW. Efficacy of selpercatinib in RET fusion-positive non-small cell lung cancer. N Engl J Med. 2020;383:9. PubMed
3.Garon E, Ciuleanu T, Arrieta O. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind randomised phase 3 trial. Lancet. 2014;384:9944. PubMed
4.Gadgeel S, Rodriguez-Abreu D, Speranza G. Updated analysis from KEYNOTE-189: pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metaststatic nonsquamous non-small-cell lung cancer. J Clin Oncol. 2020;38(14). PubMed
5.Reck M, Rodriguez-Abreu D, Robinson A. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19). PubMed
6.Gandhi L, Rodriguez-Abreu D, Gadgeel S. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22). PubMed
7.Young T, Mukuria C, Rowen D, Brazier J, Longworth L. Mapping functions in health related quality of life: mapping from two cancer-specific health-related quality-of-life instruments to EQ-5D-3L. Med Decis Mak. 2015;35:912-926. PubMed
8.Labbe C, Leung Y, Silva Lemes J. Real-world EQ5D health utility score for patients with metastatic lung cancer by molecular alteration and response to therapy. Clin Lung Cancer. 2017;18(4). PubMed
9.Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6(1):84. PubMed
10.Sullivan P, Slejko J, Sculpher M, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Mak. 2011;31(6):800-804. PubMed
11.Doyle S, Lloyd A, Walker M. Health state utility scores in advanced non-small cell lung cancer. Lung Cancer. 2008;62(3):374-380. PubMed
12.Westwood M, van Asselt T, Ramaekers B. KRAS mutation testing of tumours in adults with metastatic colorectal cancer: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2014;18(62):1-132. PubMed
13.Mangen M, Huijts S, Bonten M, de Wit G. The impact of community-acquired pneumonia on the health-related quality-of-life in elderly. BMC Infect Dis. 2017;17(1). PubMed
14.Tabberer M, Stamuli E, Walker M, Summerhayes M, Lees M. PCN74 Utilities associated with non-small cell lung cancer (NSCLC): a community study. Value Health. 2006;9(6).
15.National Institute for Health and Care Excellence (NICE). Nivolumab for previously treated non-squamous non-small-cell lung cancer. (Technology appraisal guidance TA484). 2019; https://www.nice.org.uk/guidance/ta484. Accessed 2021 Feb 10.
16.Economic evaluation of unfractionated heparin versus low-molecular-weight heparin to prevent venous thromboembolism in general medical and non-orthopedic surgical patients. Technology review issue 4. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/anticoagulants-vte-prevention-hospital-setting. Accessed 2021 Feb 10.
17.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto: Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2021 Dec 13.
18.Ontario Case Costing Initiative (OCCI). Toronto: Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2021 Dec 13.
19.Dumont S, Jacobs P, Turcotte V, Turcotte S, Johnston G. Palliative care costs in Canada: a descriptive comparison of studies of urban and rural patients near end of life. Palliat Med. 2015;29(10). PubMed
20.DeltaPA. Ottawa (ON): IQVIA; 2021: https://www.iqvia.com/. Accessed 2021 Dec 13.
21.Baracos V, Reiman T, Mourtzakis M, Gioulbasanis I, Antoun S. Body composition in patients with non-small cell lung cancer: a contemporary view of cancer cachexia with the use of computed tomography image analysis. Am J Clin Nutr. 2010;91:1133S-1137S. PubMed
22.Tecentriq, atezolizumab, concentrate for solution for infusion, 60 mg/mL [product monograph]. Mississauga (ON): Hoffman-La Roche Limited; 2019 Aug 8: https://pdf.hres.ca/dpd_pm/00052588.PDF. Accessed 2021 Dec 13.
23.Carboplatin injection bp (carboplatin injection), sterile solution, 10 mg/mL (50 mg, 150 mg, 450 mg, 600 mg of carboplatin per vial) [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2019 Dec 16: https://pdf.hres.ca/dpd_pm/00054389.PDF.
24.Opdivo, nivolumab for injection [product monograph]. Montreal: Bristol-Myers Squibb Canada Co.; 2019 Mar 13: https://pdf.hres.ca/dpd_pm/00050129.PDF. Accessed 2021 Dec 13.
25.Keytruda, pembrolizumab solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc.; 2021 Nov 24: https://www.merck.ca/static/pdf/KEYTRUDA-PM_E.pdf. Accessed 2021 Dec 13.
26.Pemetrexed, pemetrexed disodium for injection [product monograph]. Toronto: Apotex Inc.; 2016 Jun 1: https://pdf.hres.ca/dpd_pm/00035165.PDF. Accessed 2021 Dec 13.
27.GlobalRPh. Carboplatin AUC calculator. 2021; https://globalrph.com/medcalcs/carboplatin-auc-calculator/. Accessed 2021 Dec 13.
28.Canadian Cancer Society. Canadian Cancer Statistics: A 2020 special report on lung cancer. 2020; 10.24095/hpcdp.40.10.05. Accessed 2021 Dec 13.
29.Cong X, Yang L, Chen C, Liu Z. KIF5B-RET fusion gene and its correlation with clinicopathological and prognostic features in lung cancer: a meta-analysis. Onco Targets Ther. 2019;12:4533-4542. PubMed
30.Sacher A, Le L, Lau A, Earle C, Leighl N. Real-world chemotherapy treatment patterns in metastatic non-small cell lung cancer: are patients undertreated? Cancer. 2015;121:2562-2569. PubMed
31.pan-Canadian Oncology Drug Review final clinical guidance report: Pembrolizumab (Keytruda) for nonsquamous non-small cell lung cancer. Ottawa: CADTH; 2019: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10153PembroNSQ-NSCLC_fnCGR_REDACT_Post_31May2019_final.pdf. Accessed 2021 Feb 10.
32.Tajarernmuang P, Ofiara L, Beaudoin S, Wang H, Benedetti A, Gonzalez A. Real-world outcomes of patients with advanced non-small cell lung cancer treated with anti-PD1 therapy on the basis of PD-L1 results in EBUS-TBNA vs histological specimens. Chest. 2021. PubMed
33.Stock-Martineau S, Laurie K, McKinnon M, Zhang T, Wheatley-Price P. Evolution of systemic treatment uptake and survival in advanced non-small cell lung cancer. Current Oncology. 2020;28:60-68. PubMed
34.Seung S, Hurry M, Walton R, Evans W. Real-world treatment patterns and survival in stage IV non-small-cell lung cancer in Canada. Current Oncology. 2020;27(4):e361-e367. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 11: CADTH Cost Comparison Table for Metastatic Non–Small Cell Lung Cancer
Treatment | Strength / concentration | Form (vial size if single-use) | Price | Recommended dosagea | Average daily cost | 28-day cost |
|---|---|---|---|---|---|---|
Selpercatinib (Retevmo) | 40 mg 80 mg | Capsule | $66.5000 $133.0000 | <50 kg: 120 mg twice daily ≥50 kg: 160 mg twice daily | $399.00 to $532.00 | $11,172 to $14,896 |
First-line therapies | ||||||
Monotherapies | ||||||
Pembrolizumab | 25 mg/mL | 4 mL solution for IV injection | $4,400.0000 | 2 mg/kg to 200 mg per 3 weeks | $419.05 | $11,733 |
Combination regimens | ||||||
Carboplatin | 10 mg/mL | 5 mL 15 mL 45 mL 60 mL | $70.0000 $210.0000 $600.0000 $775.0000 | AUC 5 mg/mL per 3 weeksb | $31.90 | $893 |
Cisplatin | 1 mg/mL | 50 mL 100 mL Solution for IV injection | $323.0000 $646.0000 | 75 mg/m2 per 3 weeks | $46.14 | $1,292 |
Pemetrexed | 25 mg/mL | 100 mg 500 mg Powder for IV injection | $429.0000 $2,145.0000 | 500 mg/m2 per 3 weeks | $204.29 | $5,720 |
Carboplatin + pemetrexed + pembrolizumab | $655.24 | $18,347 | ||||
Cisplatin + pemetrexed + pembrolizumab | $669.48 | $18,745 | ||||
Carboplatin + pemetrexed | $236.19 | $6,613 | ||||
Cisplatin + pemetrexed | $250.43 | $7,012 | ||||
Second-line therapies | ||||||
Monotherapies | ||||||
Atezolizumab | 60 mg/mL | 20 mL solution for IV infusion | $6,776.0000 | 1,200 mg per 3 weeks | $322.67 | $9,035 |
Docetaxel | 10 mg/mL | Solution for IV injection | $115.6250 | 75 to 100 mg/m2 per 3 weeks | $75.98 to $101.31 | $2,128 to $2,837 |
Nivolumab | 10 mg/mL | 4 mL 10 mL Solution for IV infusion | $782.2200 $1,955.5600 | 3 mg/kg to 240 mg per 2 weeks | $335.24 | $9,387 |
Pembrolizumab | 25 mg/mL | 4 mL solution for IV injection | $4,400.0000 | 2 mg/kg to 200 mg per 3 weeks | $419.05 | $11,733 |
GFR = glomerular filtration rate.
Note: All prices are from the IQVIA Delta PA database (accessed December 13, 2021),20 unless otherwise indicated, and do not include dispensing fees. Costs are based on patient characteristics reported in the literature including a weight of 71 kg, body surface area of 1.84 m2, and glomerular filtration rate of 73 mL/minute.21 Vial sharing was not considered, and wastage was assumed to occur where applicable.
aRecommended dosages are per the respective product monographs.22-26
bDose is calculated as = target AUC × (GFR + 25).27
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | The model lacks transparency and is inefficiently programmed. The sponsor was asked to provide a revised model to address these concerns but declined to meet many of the requests made by CADTH. |
Model structure is adequate for decision problem | No | The states are appropriate but assumptions relating to the independence of the overall survival and progression-free survival lacks validity. A Markov model structure would more accurately reflect the disease pathway by explicitly modelling the relationship between PFS and OS. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | There are numerous errors in the propagation of uncertainty which leads the reviewer to conclude that the probabilistic analysis is not fit for purpose. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Parameter uncertainty could not be adequately considered. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The model lacked transparency. The provided user guide did not describe the flow of the model thus precluding any detailed validation testing. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of the Sponsor’s Base Case
Table 13: Sponsor’s Disaggregated Results — Treatment Naive
Parameter | Selpercatinib | Triple Therapy | Dual Therapy |
|---|---|---|---|
Discounted LYs | |||
Progression-free | 2.81 | 1.99 | 1.11 |
Post-progression | 2.31 | 1.36 | 0.89 |
Total | 5.12 | 3.35 | 2.01 |
Discounted QALYs | |||
Progression-free | 2.36 | 1.67 | 0.93 |
Post-progression | 1.76 | 1.04 | 0.68 |
Total | 4.12 | 2.71 | 1.62 |
Discounted costs of study treatment ($) | |||
Acquisition | 429,437 | 211,088 | 17,462 |
Administration | 104 | 2,439 | 1,220 |
Monitoring | 702 | 0 | 0 |
Adverse events | 8,450 | 7,626 | 6,627 |
Total | 438,692 | 221,153 | 25,308 |
General disease management costs ($) | |||
Progression-free | 3,996 | 2,832 | 1,585 |
Post-progression | 11,069 | 6,509 | 4,284 |
Total | 15,065 | 9,340 | 5,869 |
Other costs ($) | |||
Subsequent treatment | 59,166 | 9,847 | 61,941 |
End of life | 24,214 | 27,646 | 29,183 |
Total | 83,381 | 37,493 | 91,123 |
Total costs ($) | |||
Total | 537,138 | 267,987 | 122,300 |
Source: Sponsor’s pharmacoeconomic submission, probabilistic analysis.
Table 14: Sponsor’s Disaggregated Results — Treatment Experienced
Parameter | Selpercatinib | Nivolumab | Docetaxel | Atezolizumab |
|---|---|---|---|---|
Discounted LYs | ||||
Progression-free | 1.92 | 0.67 | 0.60 | 0.68 |
Post-progression | 2.25 | 2.07 | 1.57 | 2.14 |
Total | 4.17 | 2.74 | 2.17 | 2.82 |
Discounted QALYs | ||||
Progression-free | 1.61 | 0.56 | 0.50 | 0.57 |
Post-progression | 1.69 | 1.56 | 1.18 | 1.61 |
Total | 3.30 | 2.12 | 1.68 | 2.18 |
Discounted costs of study treatment ($) | ||||
Acquisition | 304,283 | 80,515 | 7,367 | 71,320 |
Administration | 72 | 958 | 367 | 661 |
Monitoring | 688 | 0 | 0 | 0 |
Adverse events | 8,781 | 2,549 | 8,707 | 1,381 |
Total | 313,824 | 84,022 | 16,440 | 73,362 |
General disease management costs ($) | ||||
Progression-free | 2,719 | 948 | 846 | 960 |
Post-progression | 10,794 | 9,950 | 7,527 | 10,255 |
Total | 13,513 | 10,898 | 8,373 | 11,215 |
Other costs ($) | ||||
Subsequent treatment | 4,730 | 7,025 | 7,009 | 7,024 |
End of Life | 25,330 | 28,272 | 28,929 | 28,198 |
Total | 30,060 | 35,297 | 35,939 | 35,222 |
Total costs ($) | ||||
Total | 357,397 | 130,218 | 60,751 | 119,800 |
Source: Sponsor’s pharmacoeconomic submission, probabilistic analysis.
Concerns With the Sponsor’s Model: Lack of Transparency
The submitted model suffers from a severe lack of transparency which limits the capacity to validate the model. Issues identified are as follows:
The model involves unnecessarily complex programming which CADTH identified as leading to numerous errors within the model with respect to specifying uncertainty, but with the potential for many further errors which may not have been identified. The model includes many redundant cells relating to options within the model that are not utilized and treatment comparators that are not considered.
The coding of the model is highly inefficient with simple calculations being spread over multiple sheets. The approach is unnecessary. This seriously impairs the assessment of the validity of the model. Likewise, this unnecessary level of complexity led to numerous errors. For example:
Data suggests for those who received selpercatinib 9 patients out of 329 had Diarrhea. The uncertainty around this parameter is correctly specified in one instance in the model as a Beta distribution: Beta (9,320). Thus, the probability should be 2.7%. The Beta distribution correctly specified is not used to generate results in the final analysis. Instead, a separate calculation is made, and the Beta distribution used in the model is incorrectly defined as Beta (8.973, 319.027). Thus, the unnecessary re-calculation of parameters leads to an error in the specification of the distribution, which is unnecessary, as the distribution was correctly specified already within the model. CADTH is concerned that there may be further inaccuracies that cannot be detected due to the unduly and unnecessary complexity of the model.
The original sponsor’s model contained 5,900 uses of IFERROR functions. IFERROR functions are designed to deal with errors in formulas by replacing an error message with a specific value. They should be unnecessary if a model is appropriately coded. The sponsor was asked to provide a model which limited the use of IFERROR statements. A revised model provided by the sponsor still contained over 3,000 IFERROR statements.
Concerns With the Sponsor’s Model: Inappropriate Probabilistic Analysis
CADTH found several concerns with the sponsor’s submitted probabilistic analysis and concluded that the probabilistic analysis was not appropriate for use. The following are examples of the concerns noted.
Assumptions concerning the uncertainty over relative effect sizes and parameters for survival functions are not truly reflective of their uncertainty and substantially underestimate the underlying uncertainties. Parametric survival functions for docetaxel and dual therapy and relative effects for selpercatinib are estimated using highly uncertain methodologies and assumptions. However, this additional uncertainty is not incorporated into the analysis.
Beta distributions for certain parameters (e.g., utilities) are characterized incorrectly through using standard error in the formula for deriving Alpha and Beta rather than variance. This leads to an over-estimate of the associated uncertainty.
For variables for which no uncertainty data are available, a 10% of the mean calculation for standard error is adopted. This is inappropriate for beta distributions which relate to probabilities as uncertainty must be equal for the corollary event. For example, the probability of being on docetaxel after immunotherapy is 56%. The standard error is assumed to be 0.056. Yet the probability for not being on docetaxel could equally have been specified and based on the sponsors methods would have a standard error of 0.044. This is incorrect. If uncertainties around parameters are not available a more nuanced approach for estimating uncertainty must be adopted.
The distribution of subsequent therapies is characterized by individual Beta distributions. This is incorrect as it can lead to simulations where more than 100% of patients are on subsequent therapies. When the distributions are multivariate, a Dirichlet distribution should have been adopted.
Drug administration costs which are derived from the Ontario schedule of benefits are assumed uncertain based on an arbitrary 10% standard error approach. This is inappropriate.
The sponsor’s probabilistic results lack face validity. For certain parameters estimated values do not vary by simulation.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Results of CADTH Exploratory Analyses
Table 15: CADTH Exploratory Analysis Disaggregated Results — Treatment Naive
Parameter | Selpercatinib | Triple therapy | Dual therapy |
|---|---|---|---|
Discounted LYs | |||
Progression-free | 2.81 | 1.97 | 1.11 |
Post-progression | 2.02 | 2.26 | 2.47 |
Total | 4.83 | 4.24 | 3.59 |
Discounted QALYs | |||
Progression-free | 2.37 | 1.66 | 0.94 |
Post-progression | 1.59 | 1.79 | 1.95 |
Total | 3.96 | 3.44 | 2.89 |
Discounted costs of study treatment ($) | |||
Acquisition | 551,433 | 375,913 | 103,523 |
Administration | 104 | 2,404 | 1,221 |
Monitoring | 701 | 0 | 0 |
Adverse events | 8,457 | 7,639 | 6,632 |
Total | 560,684 | 385,956 | 111,377 |
General disease management costs ($) | |||
Progression-free | 3,979 | 2,785 | 1,579 |
Post-progression | 9,656 | 10,869 | 11,840 |
Total | 13,635 | 13,654 | 13,419 |
Other costs ($) | |||
Subsequent treatment | 51,711 | 9,044 | 62,114 |
End of life | 24,079 | 25,836 | 27.012 |
Total | 75,791 | 34,881 | 89,126 |
Testing costs ($) | |||
Total | 39,442 | 0 | 0 |
Total costs ($) | |||
Total (excluding testing costs) | 650,100 | 434,491 | 211,244 |
Total (including testing costs) | 689,552 | 434,491 | 211,244 |
Table 16: CADTH Exploratory Analysis Disaggregated Results — Treatment Experienced
Parameter | Selpercatinib | Nivolumab | Docetaxel | Atezolizumab |
|---|---|---|---|---|
Discounted LYs | ||||
Progression-free | 1.91 | 0.67 | 0.60 | 0.68 |
Post-progression | 1.87 | 2.32 | 2.34 | 2.32 |
Total | 3.78 | 2.99 | 2.94 | 2.99 |
Discounted QALYs | ||||
Progression-free | 1.59 | 0.56 | 0.49 | 0.56 |
Post-progression | 1.44 | 1.79 | 1.81 | 1.79 |
Total | 3.03 | 2.35 | 2.30 | 2.35 |
Discounted costs of study treatment ($) | ||||
Acquisition | 376,983 | 90,705 | 8,241 | 81,937 |
Administration | 72 | 962 | 367 | 656 |
Monitoring | 687 | 0 | 0 | 0 |
Adverse events | 8,777 | 2,557 | 8,691 | 1,383 |
Total | 386,519 | 94,244 | 17,300 | 83,976 |
General disease management costs ($) | ||||
Progression-free | 2,708 | 949 | 846 | 958 |
Post-progression | 8,932 | 11,100 | 11,201 | 11,092 |
Total | 11,640 | 12,049 | 12,047 | 12,049 |
Other costs ($) | ||||
Subsequent treatment | 5,475 | 6,641 | 6,695 | 6.636 |
End of life | 26,580 | 27,759 | 27,814 | 27,754 |
Total | 32,056 | 34,399 | 34,509 | 34,390 |
Testing costs ($) | ||||
Total | 21,083 | 0 | 0 | 0 |
Total costs ($) | ||||
Total (excluding testing costs) | 430,215 | 140,673 | 63,856 | 130,415 |
Total (including testing costs) | 451,298 | 140,673 | 63,856 | 130,415 |
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 17: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted BIA assessed the introduction of selpercatinib for the treatment of adults with metastatic RET+ non- small cell lung cancer. Two separate populations were assessed, a treatment-naive population and one who had previously received systemic therapy. The analysis was taken from the perspective of the Canadian public drug plans using an epidemiology-based approach, with only drug acquisition costs included. A 3-year time horizon was used, from 2022 to 2024, with 2021 as a base year. The population size was derived using a series of attritions for patients with lung cancer and public drug coverage applied to the Canadian population.
In the treatment-naive population, the reference case scenario included the comparators pembrolizumab + pemetrexed + carboplatin, pemetrexed + carboplatin, and pembrolizumab monotherapy. In the second-line setting, the reference case scenario included the comparators pembrolizumab, nivolumab, atezolizumab, and docetaxel. The new drug scenarios included the same comparators with the addition of selpercatinib. Key inputs to the BIA are documented in Table 18.
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) | |
|---|---|---|
Target population | Treatment-naive | Previously treated (2L+) |
Incidence of lung cancer | 0.078%28 | 0.078%28 |
Proportion of cases with NSCLC | 88%28 | 88%28 |
Proportion with stage IIIB or IV cancer | 58%1 | 58%1 |
Proportion tested for RET fusion | 70% / 80% / 90%1 | 70% / 80% / 90%1 |
Proportion testing positive for RET fusion | 1.9%29 | 1.9%29 |
Proportion receiving first-line systemic therapy | 75%1 | 75%1 |
Proportion receiving second-line therapy | NA | 31.32%30 |
Proportion with public drug coverage | 65%1 | 65%1 |
Proportion PD-L1 ≥ 50% | 30%31 | NA |
Proportion PD-L1 < 50% | 70%31 | NA |
Proportion PD-L1 ≥ 1% | NA | 80%32 |
Proportion PD-L1 < 1% | NA | 20%32 |
Number of patients eligible for selpercatinib | 77 / 89 / 102 | 24 / 28 / 32 |
Market uptake (3 years) | ||
Uptake (reference scenario) | ||
PD-L1–positive | ||
Selpercatinib | 0% / 0% / 0% | 0% / 0% / 0% |
Pembrolizumab | 20% / 20% / 20% | 48% / 48% / 48% |
Pembrolizumab + pemetrexed + carboplatin | 80% / 80% / 80% | 0% / 0% / 0% |
Pemetrexed + carboplatin | 0% / 0% / 0% | 0% / 0% / 0% |
Nivolumab | 0% / 0% / 0% | 48% / 48% / 48% |
Atezolizumab | 0% / 0% / 0% | 5% / 5% / 5% |
Docetaxel | 0% / 0% / 0% | 0% / 0% / 0% |
PD-L1–negative | ||
Selpercatinib | 0% / 0% / 0% | 0% / 0% / 0% |
Pembrolizumab | 0% / 0% / 0% | 0% / 0% / 0% |
Pembrolizumab + pemetrexed + carboplatin | 95% / 95% / 95% | 0% / 0% / 0% |
Pemetrexed + carboplatin | 5% / 5% / 5% | 0% / 0% / 0% |
Nivolumab | 0% / 0% / 0% | 80% / 80% / 80% |
Atezolizumab | 0% / 0% / 0% | 0% / 0% / 0% |
Docetaxel | 0% / 0% / 0% | 20% / 20% / 20% |
Uptake (new drug scenario) | ||
PD-L1–positive | ||
Selpercatinib | 75% / 80% / 85% | 75% / 80% / 85% |
Pembrolizumab | 5% / 4% / 3% | 12% / 10% / 7% |
Pembrolizumab + pemetrexed + carboplatin | 20% / 16% / 12% | 0% / 0% / 0% |
Pemetrexed + carboplatin | 0% / 0% / 0% | 0% / 0% / 0% |
Nivolumab | 0% / 0% / 0% | 12% / 10% / 7% |
Atezolizumab | 0% / 0% / 0% | 1% / 1% / 1% |
Docetaxel | 0% / 0% / 0% | 0% / 0% / 0% |
PD-L1–negative | ||
Selpercatinib | 75% / 80% / 85% | 75% / 80% / 85% |
Pembrolizumab | 0% / 0% / 0% | 0% / 0% / 0% |
Pembrolizumab + pemetrexed + carboplatin | 24% / 19% / 14% | 0% / 0% / 0% |
Pemetrexed + carboplatin | 1% / 1% / 1% | 0% / 0% / 0% |
Nivolumab | 0% / 0% / 0% | 20% / 16% / 12% |
Atezolizumab | 0% / 0% / 0% | 0% / 0% / 0% |
Docetaxel | 0% / 0% / 0% | 5% / 4% / 3% |
Cost of treatment (per patient) | ||
Selpercatinib | $134,929 / $96,960 / $69,048 | $134,444 / $86,668 / $50,276 |
Pembrolizumab | $104,778 / $46,663 / $0 | $78,606 / $14,500 / $0 |
Pembrolizumab + pemetrexed + carboplatin | $128,742 / $74,234 / $4,410 | NA |
Pemetrexed + carboplatin | $11,254 / $4,028 / $1,527 | NA |
Nivolumab | NA | $66,374 / $13,185 / $1,566 |
Atezolizumab | NA | $59,318 / $10,855 / $1,359 |
Docetaxel | NA | $7,380 / $0 / $0 |
NA = not applicable; PD-L1 = programmed death ligand 1.
Summary of the Sponsor’s Budget Impact Analysis Results
The estimated budget impact of funding selpercatinib for the treatment of adults with metastatic RET+ non- small cell lung cancer was $1,872,676 in year 1, $5,196,037 in year 2, and $11,014,210 in year 3 for a 3-year total of $18,082,923.
Among patients who were treatment naive only, the budget impact was $677,764 in year 1, $2,387,693 in year 2, and $6,685,247 in year 3, for a 3-year total of $9,750,704. Among patients with treatment experience, the budget impact was $1,194,912 in year 1, $2,808,344 in year 2, and $4,328,963 in year 3, for a 3-year total of $8,332,219.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Sponsor did not differentiate between adenocarcinomas and squamous cell carcinomas: The population size for the BIA was derived using a series of attritions; however, the sponsor did not differentiate between adenocarcinomas and squamous cell carcinomas. The clinical experts consulted by CADTH highlighted that RET fusion mutations would likely only be relevant in the adenocarcinoma population, estimated to make up 70% of cases of metastatic NSCLC. This estimate aligns with a 2018 estimate from Ontario of 75% of patients with adenocarcinoma.33 The experts noted that patients with squamous cell cancer are not routinely tested for genetic mutations because of their rarity in this group and, as such, would likely not be eligible for selpercatinib.
As part of the base case, CADTH reduced the population size by an additional 30% in order to only consider patients with adenocarcinomas.
Proportion of patients receiving first-line systemic therapy overestimated: For both patient populations, the treatment naive and treatment experienced, the sponsor estimated that 75% of patients would receive first-line systemic therapy. Clinical experts indicated that, in current practice, this proportion was too high and would not be representative of a general patient population seen primarily by their family physician, and only referred to a specialist as needed. The sponsor used this estimate of 75% to reduce the population size, implying that those not currently receiving first-line therapy would not be eligible for selpercatinib. Data from the literature estimate that 15% of patients with stage IV non-squamous NSCLC received first-line chemotherapy, while others received chemoradiation or radiotherapy.34 However, selpercatinib is an agent specifically targeted for RET+ cases, and it seems more likely that any patient testing positive for this mutation would be eligible for selpercatinib. Currently it may be the case that only 15% of RET+ cases receive systemic therapy, however if a targeted agent for RET+ existed this would likely increase the proportion of individuals who receive systemic therapy. Moreover, clinical experts emphasized that the estimate of the proportion of patients receiving first-line chemotherapy is uncertain and dependent on how the population was sampled (e.g., all NSCLC patients or only those seen by a medical oncologist).
CADTH performed a scenario analysis in which 15% of RET+ patients were assumed to receive first-line systemic therapy in the reference scenario (no targeted therapies exist), as per the published literature. In the new drug scenario where selpercatinib is funded, however, the original assumption of 75% was retained. Market shares were not changed in this scenario analysis.
Frequency of immunotherapy use in second-line overestimated: The sponsor assumed that most patients in the second-line setting would receive mono-immunotherapy, either pembrolizumab, nivolumab, or atezolizumab. This assumption does not align with the feedback received from clinical experts, who noted that because most patients will be receiving pembrolizumab first-line as part of triple therapy, very few would be trialled again on immunotherapy second-line. Indeed, in the sponsor’s base case between 80%-95% were assumed to receive triple therapy based on PD-L1 status. Clinical experts estimated that 70% of patients in the second line would be receiving docetaxel instead, with the remainder receiving immunotherapy.
As part of the base case, CADTH assumed 70% of patients would receive docetaxel in the second line, regardless of PD-L1 status.
Updated drug acquisition costs to align with the pharmacoeconomic model: The sponsor included drug acquisition costs based on the pharmacoeconomic model, but these values were hard-coded and hard to validate. As CADTH included reanalyses pertaining to drug costs in the pharmacoeconomic model, these updated costs were also required to assess the budget impact.
As part of the base case, CADTH included the per year drug acquisition costs obtained from the updated pharmacoeconomic model. Of note, given the issues with pembrolizumab monotherapy outlined in the pharmacoeconomic section these costs could not be updated. The sponsor’s original cost estimates were retained in this case.
Exclusions of testing costs: The sponsor’s base case did not include the cost of testing for RET fusion–positive patients. The clinical experts expressed a lack of availability of testing for RET fusion–positive patients in many jurisdictions and if selpercatinib were funded increased testing may be required.
As part of a scenario analysis, CADTH included the costs of RET fusion testing.
CADTH Reanalyses of the Budget Impact Analysis
As part of the base case, CADTH only included adenocarcinoma cases of NSCLC, reduced the proportion of previously treated patients who had received first-line systemic therapy, reduced frequency of immunotherapy use in second-line, and updated drug acquisition costs based on the pharmacoeconomic model (Table 19).
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None. | None. | None. |
Changes to derive the CADTH base case | ||
1. NSCLC population | Included both adenocarcinomas and squamous cell carcinomas | Only included adenocarcinomas (70%) of NSCLC cases |
2. Frequency of docetaxel use in second-line | 0-20% depending on PD-L1 status | 70% |
3. Drug acquisition costs | From sponsor’s base case pharmacoeconomic model | From sponsors pharmacoeconomic model updated with CADTH’s changes: Treatment-naive (Year 1 / Year 2 / year 3)
Previously treated (Year 1 / Year 2 / year 3)
|
CADTH base case | Reanalysis 1 + 2 + 3 | |
NSCLC = non–small cell lung carcinoma.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21. Based on the CADTH base case, the budget impact of the reimbursement of selpercatinib for the treatment of metastatic RET+ NSCLC is expected to be $792,667 in year 1, $2,921,482 in year 2, and $7,031,748 in year 3, with a 3-year total of $10,745,897.
Among patients who were treatment naive only, the budget impact was -$938,174 in year 1, -$537,954 in year 2, and $2,013,086 in year 3, for a 3-year total of $536,959. Among patients on second-line and greater therapies, the budget impact was $1,730,841 in year 1, $3,459,436 in year 2, and $5,018,662 in year 3, for a 3-year total of $10,208,939.
The scenario in which testing costs were included resulted in a 3-year budget impact of $14,045,569. In the scenario where the presence of a mutation targeted systemic therapy increases systemic therapy uptake the budget impact increases to $52,634,584.
Table 20: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $18,082,923 |
CADTH reanalysis 1 – adenocarcinoma only | $12,658,046 |
CADTH reanalysis 2 – reduced immunotherapy in second-line | $21,293,755 |
CADTH reanalysis 3 – updated drug costs | $11,928,915 |
CADTH base case | $10,745,897 |
Table 21: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis (Treatment Naive)
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $9,354,817 | $14,810,637 | $16,699,191 | $19,295,775 | $50,805,604 |
New drug | $9,354,817 | $15,488,401 | $19,086,884 | $25,981,022 | $60,556,307 | |
Budget impact | $0 | $677,764 | $2,387,693 | $6,685,247 | $9,750,704 | |
CADTH base case | Reference | $10,331,962 | $16,313,895 | $19,314,198 | $21,980,865 | $57,608,959 |
New drug | $10,331,962 | $15,375,722 | $18,776,244 | $23,993,951 | $58,145,917 | |
Budget impact | $0 | -$938,174 | -$537,954 | $2,013,086 | $536,959 | |
CADTH scenario analysis 1: 15% systemic therapy use in first line in reference scenario, 75% in new drug scenario | Reference | $2,066,392 | $3,262,779 | $3,862,840 | $4,396,173 | $11,521,792 |
New drug | $2,066,392 | $10,705,893 | $17,772,807 | $23,993,951 | $52,472,652 | |
Budget impact | $0 | $7,443,114 | $13,909,968 | $19,597,778 | $40,950,860 | |
CADTH scenario analysis 2: included the costs of RET testing | Reference | $10,331,962 | $16,313,895 | $19,314,198 | $21,980,865 | $57,608,959 |
New drug | $10,331,962 | $16,048,583 | $19,607,978 | $25,002,051 | $60,658,612 | |
Budget impact | $0 | -$265,312 | $293,780 | $3,021,186 | $3,049,654 |
BIA = budget impact analysis; PE = pharmacoeconomic.
Table 22: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis (Treatment Experienced)
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $1,626,304 | $1,959,773 | $2,247,499 | $2,568,115 | $6,775,387 |
New drug | $1,626,304 | $3,154,685 | $5,055,843 | $6,897,079 | $15,107,607 | |
Budget impact | $0 | $1,194,912 | $2,808,344 | $4,328,963 | $8,332,219 | |
CADTH base case | Reference | $475,215 | $555,251 | $638,292 | $728,786 | $1,922,329 |
New drug | $475,215 | $2,286,092 | $4,097,728 | $5,747,448 | $12,131,268 | |
Budget impact | $0 | $1,730,841 | $3,459,436 | $5,018,662 | $10,208,939 | |
CADTH scenario analysis 1: 15% systemic therapy use in first line in reference scenario, 75% in new drug scenario | Reference | $95,043 | $111,050 | $127,658 | $145,757 | $384,466 |
New drug | $95,043 | $2,227,386 | $4,093,356 | $5,747,448 | $12,068,190 | |
Budget impact | $0 | $2,116,335 | $3,965,697 | $5,601,691 | $11,683,724 | |
CADTH scenario analysis 2: included the costs of RET testing | Reference | $475,215 | $555,251 | $638,292 | $728,786 | $1,922,329 |
New drug | $475,215 | $2,496,833 | $4,358,226 | $6,063,185 | $12,918,244 | |
Budget impact | $0 | $1,941,581 | $3,719,935 | $5,334,399 | $10,995,915 |
BIA = budget impact analysis; PE = pharmacoeconomic.
Stakeholder Input
Patient Group Input
Canadian Lung Cancer Advocacy Group Breathe Hope
About Canadian Lung Cancer Advocacy Group Breathe Hope
Describe the purpose of your organization. Include a link to your website.
Created by a group of Canadian lung cancer patients. At our core, we saw the value in having a supportive, collaborative and sharing community which would reach Canadian LC patients and care-givers from coast to coast.
#CanadianLCBreatheHope is driven by the following:
To establish a Canadian LC community made up of both patients and care-givers.
To provide a supportive, confidential environment for patients and care-givers to share their experiences.
To raise awareness about LC through personal contacts or events and through connections with national/provincial/ local stakeholder individuals or organizations.
Such as Lung Cancer Canada, Canadian Cancer Survivors Network, Lung Health Foundation
To share new, innovative LC treatments and scientific research.
To bring attention to conference opportunities and web events. https://www.facebook.com/groups/520424908293279
Information Gathering
CADTH is interested in hearing from a wide range of patients and caregivers in this patient input submission. Describe how you gathered the perspectives: for example, by interviews, focus groups, or survey; personal experience; or a combination of these. Where possible, include when the data were gathered; if data were gathered in Canada or elsewhere; demographics of the respondents; and how many patients, caregivers, and individuals with experience with the drug in review contributed insights. We will use this background to better understand the context of the perspectives shared.
The perspective gathered is one of my own personal experience. After a year and a half of being on the wrong treatment/standard of care, I developed rapid progression of my nsclc along with severe toxicity effects of treatment. During the summer of 2020, I was able to access comprehensive molecular testing via a blood biopsy. RET fusion (CCDC6) was discovered. After double platinum chemotherapy treatment failed during last summer, I was granted access to selpercatinib through Eli Lilly’s compassionate access program. I am the only patient in the above mentioned group that is on this targeted therapy drug and the first patient that my oncologist has ever treated with it.
However, I have joined a U.S. group called “RET Renegades”. From this group, I have learned about the tremendous success of this drug for treating this rarer oncogene as all of its members have the RET fusion and are on either selpercatinib or pralsetinib. Members are from all over the world that belong to this group.
I have researched the clinical trial data from the FDA to learn about the efficacy and response rate of this TKI. Along with direct patient sharing of information from the RET Renegades, I have learned much about this drug including direct positive benefits from the patient voices.
I am thrilled that Health Canada has just approved this drug in June of 2021.
Disease Experience
CADTH involves clinical experts in every review to explain disease progression and treatment goals. Here we are interested in understanding the illness from a patient’s perspective. Describe how the disease impacts patients’ and caregivers’ day-to-day life and quality of life. Are there any aspects of the illness that are more important to control than others?
I have Stage IV nsclc, adenocarcinoma, PDL-1 positive, 75% expression, RET fusion (CCDC6)
I had to immediately stop working as a full-time elementary SCIENCE/MATH teacher and part time horseback riding coach at my private facility. My disease progressed slowly over the next year and then very rapidly. I was in tremendous pain initially due to bone pain/cancer lesions on ribs, vertebrae, shoulder, hip. It took months for radiotherapy to be effective and reduce the bone pain.
My life basically stopped as I knew it. I suffered from depression as well as the physical pain of the disease. Fatigue and illness and pain and anxiety about progression were my new “normal”. I could not engage in any of the activities that kept me healthy and gave me a purpose for living in the first year and a half. I had to quit my job, I couldn’t ride my own horses or go hiking with my family and the dogs. I could barely get outside to do simple tasks such as gardening or anything that I use to do that gave me pleasure and contentment.
My oldest daughter had to move back home to help care for me and help on the farm. My husband was overloaded with worry and took on most of the physical aspects of caring for the home and farm.
Controlling the progression of the cancer was foremost although managing the intense pain was also paramount. Managing toxic side effects was becoming more and more difficult as my treatments changed from immunotherapy, to a clinical trial, and then double platinum chemotherapy. None of these three treatments worked to prevent rapid progression and new cardiac/gastric pain.
The burden on caregivers is huge! Handling the brunt of everyday tasks, rearranging job schedules to be available for driving for appts/treatments, trips to the ED becomes wearing. The emotional burden of staying positive for the cancer patient creates its own challenges with mental health.
During the months where my cancer continued to progress on every three-month scan took its toll on everyone. Getting ready to prepare for death when you feel there are no options left for treatment is devastating on many levels for the whole family and community of caregivers.
Experiences With Currently Available Treatments
CADTH examines the clinical benefit and cost-effectiveness of new drugs compared with currently available treatments. We can use this information to evaluate how well the drug under review might address gaps if current therapies fall short for patients and caregivers.
Describe how well patients and caregivers are managing their illnesses with currently available treatments (please specify treatments). Consider benefits seen, and side effects experienced and their management. Also consider any difficulties accessing treatment (cost, travel to clinic, time off work) and receiving treatment (swallowing pills, infusion lines).
Started pembrolizumab May 13, 2019. (PDL-1 of 75%) Scans showed continued progression all the way through to April 2021. Bone scan in Dec., 2019 showed some shrinkage of bone mets with sclerotic changes. Minor toxicity with drug.
Sept, 2019: 5 lung tumour lesions and several lymph node lesions progressing. Radiotherapy added for one left lobe large tumour and supraclavicular lymph node. Initial response and shrinkage but only for about 4 months.
Feb, 2020: started on DPX Survivac Clinical Trail.
March, 2020: 3 new lung tumours appeared and the same supraclavicular lymph grew again. Radiotherapy ordered again on the lymph node.
Increasing difficulties with managing dehydration and IV treatments every three weeks causing collapsing veins
April 2020: worsening symptoms of coughing, shortness of breath, general illness. Clinical trial was stopped.
May 4, 2020: Double platinum chemotherapy with Cisplatin was begun. Extreme toxicity in first cycle. Subsequent cycles were with Carboplatin and Pemetrexed. Toxicity continued. Appetite loss and home care required for IV hydration treatment. Inability to get out of bed of chair for more than 50% of the day. Lack of sleep due to increasing pain and general lack of wellbeing.
July 24th, 2020: First scan showed mixed results: some tumour shrinkage, some stable, some still progressing.
Severe pain began over the following three weeks in chest and back areas. Severe coughing with vomiting occurring multiple times daily.
Went to ED on Aug. 26, 2020: admitted into cardiac ward. New CT scan showed several tumours had tripled in size esp. in lungs and chest lymph nodes. Chemo was ended and narcotics were introduced again to manage the severe pain.
Aug. 31st: first dose of selpercatinib was ordered (during the summer, biopsy identified the RET fusion oncogene)
Four days later I asked to be released: pain was gone, appetite was resumed, coughing was gone, vomiting was gone
Travel for treatments, tests etc was about 130 km each trip. If I was not well enough to drive myself, a friend or my daughter or husband had to do it. My daughter often had to book time off work to make the trip for me. I often had to go in several times a month and when I had radiotherapy I had to go in daily for 20 days at a time. This happened several times over the course of my journey.
Improved Outcomes
CADTH is interested in patients’ views on what outcomes we should consider when evaluating new therapies. What improvements would patients and caregivers like to see in a new treatment that is not achieved in currently available treatments? How might daily life and quality of life for patients, caregivers, and families be different if the new treatment provided those desired improvements? What trade-offs do patients, families, and caregivers consider when choosing therapy?
Improvements:
Reduced side effects from treatment, better efficacy, PFS for longer periods.
Noticeable reduction of tumours and symptoms of disease (reduced coughing, better appetite, ability to function with more normal routines and activities)
Less impact on healthy cells with treatment, reduced need to use pain and other medications (and dealing with side effects of those drugs)
Results:
Greater chance of patient resuming a more normal life, perhaps even returning to work or feeling well enough to begin exercising again
Better mental health and overall well-being when not dealing with toxicity from treatments
Feeling that there is more of a future for living: being able to reach milestones with family: weddings, birth of children, etc.
Caregivers can assume more of a normal routine as well: less anxiety about the cancer patient, able to go back and work and feeling better about making an income to support the family
Trade offs: willing to accept some side effects of the treatment if evidence shows that cancer is regressing and disease effects are also lessened. The benefits of the treatment must outweigh the overall toxicity of the treatment. Families may want the patient to continue any and all treatments, regardless of side effects, whereas the patient may choose to refuse treatments if the side effects make them feel too ill to live their life.
Experience With Drug Under Review
CADTH will carefully review the relevant scientific literature and clinical studies. We would like to hear from patients about their individual experiences with the new drug. This can help reviewers better understand how the drug under review meets the needs and preferences of patients, caregivers, and families.
How did patients have access to the drug under review (for example, clinical trials, private insurance)?
Access to selpercatinib, not yet approved in Canada and only approved by the FDA on May 8, 2020, was achieved by my oncologist reaching out to Eli Lilly and gaining access for me based on compassionate reasons.
Compared to any previous therapies’ patients have used, what were the benefits experienced?
Almost immediate resolution of coughing/vomiting/lack of appetite/chest and back pain within a few days.
Feeling almost like my precancer self! No feelings of nausea or other general illness. Energy to resume my duties in the barn with the horses on a slowly increasing basis. Able to walk further distances. Better clarity of mind. Eating regularly. Complete weaning off of pain medication, anti-nausea meds, and anti-anxiety meds.
First scan two months after beginning selpercatinib: up to 75% reduction of the eight lung tumours with continuing shrinking of tumours to date. Complete resolution of the three chest lymph node tumours and supraclavicular node tumour: no new adenopathy and no new lesions appearing anywhere as of August 2021.
This is my “miracle” drug! I have hope now for a decent quality of life and can reinvent myself as I now have the physical and emotional ability to do so.
What were the disadvantages?
Ongoing fatigue but with no feelings of illness or nausea. No pain anywhere related to the disease. Some bloating, dry mouth, some constipation but all very manageable. Becoming tired more quickly than precancer. Some days really good and no feelings of having cancer or side effects from drug at all.
Need to pace myself carefully to avoid doing too much in a given time frame. Need to limit screen time on my computer and phone – get mentally tired if stay on longer than an hour or two.
Some risk of elevated liver enzymes or heart issues but I have had neither of these as evidenced by months tests and checkups.
How did the benefits and disadvantages impact the lives of patients, caregivers, and families?
My family, friends, and caregivers are elated that any immediate danger to my life has been staved off for the immediate future. My recently married daughter is moving forward to more out and start her life with her husband. My younger daughter has accepted a university program and is less worried about moving away from me. They both can see that I can look after myself far better than while on the previous three treatments. The disadvantages have not really affected them at all!
Consider side effects and if they were tolerated or how they were managed. Was the drug easier to use than previous therapies? If so, how?
There is NO question that selpercatinib have given me a new lease on life and more TIME! There is no comparison to the level of toxicity I suffered on the other “standards of care”. The disease was wining on the other treatments and now I feel that I am winning. The side effects are so minor compared to what I went through being on the wrong treatments for so long. Since this is an oral pill, I no longer need to travel to the cancer clinic for hours at a time to be hooked up to an IV. My veins are very relieved! I have been able to stay out of the hospital setting during Covid more often. There has been no need for trips to the ED. My body has tolerated this drug far, far, better than anything else! I am ever so grateful for all the hard work my oncologist has done on my behalf.
Are there subgroups of patients within this disease state for whom this drug is particularly helpful? In what ways?
I am not aware of subgroups. To my knowledge, selpercatinib is specific to RET positive nsclc and medullary thyroid cancers only.
If applicable, please provide the sequencing of therapies that patients would have used prior to and after in relation to the new drug under review.
Selpercatinib should be used as first line treatment if comprehensive molecular testing has been done and the RET oncogene discovered. Efficacy is round 86%.
For second line treatment, efficacy was found to be around 68%. Still an excellent response.
This is my FOURTH line of treatment, and my personal results are still astounding. I am alive today because of this drug.
I was unable to start this drug once we learned I had the RET fusion and had rapid progression as I had just started chemotherapy. I was told that until we knew whether or not the chemo worked, I could not ‘jump ship” and start the selpercatinib. The reason was should the new drug not work, OHIP would not cover the cost of going back to chemo. I had to have either progression or toxicity on the chemo to stop it. I had both. But I am resentful that I had to wait another three months to begin the selpercatinib while my cancer raged on, and I became sicker and sicker.
Please also include a summary statement of the key values that are important to patients and caregivers with respect to the drug under review.
That the correct safe dosage has been determined to reach maximum benefit for reducing the cancer load in the body.
That the potential side effects of the drug are monitored closely by the medical team and dosage adjustments made when warranted.
That the palliative care team be on standby to deal with easily managed medications that would assist with reduction of certain side effects from the disease and/or the drug.
That the patient is able to resume a better quality of life participating in activities that improve mental and physical well-being.
That pain related to the disease, or any other symptoms of the disease are well managed or even eliminated by selpercatinib.
Companion Diagnostic Test
If the drug in review has a companion diagnostic, please comment. Companion diagnostics are laboratory tests that provide information essential for the safe and effective use of particular therapeutic drugs. They work by detecting specific biomarkers that predict more favourable responses to certain drugs. In practice, companion diagnostics can identify patients who are likely to benefit or experience harms from particular therapies or monitor clinical responses to optimally guide treatment adjustments.
What are patient and caregiver experiences with the biomarker testing (companion diagnostic) associated with regarding the drug under review?
Consider:
Access to testing for example, proximity to testing facility, availability of appointment.
Initial desire (Nov. 2020) to have comprehensive molecular testing was not feasible due to the high cost of this testing ( >$6000). Testing was not done through cancer was progressing while on first treatment.
Testing: for example, how was the test done? Did testing delay the treatment from beginning? Were there any adverse effects associated with testing?
NGS testing was not offered at DX. Standard 4 biomarkers were done with the first tissue biopsy in March 2020. Only PDL-1 was found positive. It took 4 wks to get the results. I choose to wait until there were back before starting standard of care.
Waiting for the test results meant increasing anxiety thinking about the cancer growing and disease symptoms becoming worse in that time.
Cost of testing: Who paid for testing? If the cost was out of pocket, what was the impact of having to pay? Were there travel costs involved?
I would have had to pay for the comprehensive testing and I could not have afforded this. Eventually, in the spring of 2021, my oncologist advocated on my behalf and was able to get the testing covered by Foundation One. That is the only way that we found I have the rare RET fusion driving my cancer.
Travel was to my regular cancer clinic, about an hour away from home, for the blood biopsy.
How patients and caregivers feel about testing: for example, understanding why the test happened, coping with anxiety while waiting for the test result, uncertainty about making a decision given the test result.
We knew that the progression of the cancer was due to a mutation that was more that just the PDL-1 pathway driver as I was not responding to immunotherapy. We also knew that with the comprehensive molecular testing that we would find something but would that something have a treatment for it? That is precisely what happened. However, the good news was that selpercatinib had just been fast tracked by the FDA last year. The anxiety around would I be able to access this life saving drug was immense. Lung Cancer Canada was also waiting to help me get access to it should my oncologist be unsuccessful. It tool a huge strength of will on my part and my family’s to not worry about the outcome. In the meantime, I was becoming more and more ill.
Anything Else?
Is there anything else specifically related to this drug review that CADTH reviewers or the expert committee should know?
Perhaps keep in mind that the side effects/potential risks for me on this drug have been significantly less and even negligible compared to the degree of toxicity my body experienced on the first three treatments.
I cannot help but reflect how much better I would be now had I been given the RIGHT treatment at the RIGHT time when I was first diagnosed.
How much better would I feel now? Would I have been able to resume my career as a teacher and earn an income? How much less would the financial burden of my disease have been on me and my family? Would my cancer have been completely cured? (as is the case with some Stage IV patients that have had this as their first line treatment and have been NED for over 5 years and still going strong!)
Also, how much money would the health care system have saved by treating me correctly rather than spending all the money on ineffective treatments.
And all because we do not test for enough biomarkers at diagnosis!
At this time, I have one pre-existing tumour out of the many, which shrank significantly on selpercatinib, that is now progressing. Likely a new mutation. Would this have even happened if I had been able to access selpercatinib right from the start? Probably not. My cancer has had two years to learn how to escape treatment and mutate.
This just supports the huge need for NGS testing immediately in order to start the patient on targeted drugs, if available.
They say that the RET mutation/fusion is rare (1 – 2% in nsclc). But it is “rare” because it just doesn’t get tested for in Canadian patients? I propose that if this is part of standard testing, it will be found in more and more patients and more lives will be saved with selpercatinib and even pralsetinib.
Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No help was needed or given.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No help was given.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Not applicable.
Table 1: Conflict of Interest Declaration for Canadian Lung Cancer Advocacy Group Breathe Hope
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Position: Patient Advocate
Patient Group: Canadian Lung Cancer Advocacy Group “Breathe Hope”
Date: July 29, 2021
Lung Cancer Canada
About Lung Cancer Canada
Lung Cancer Canada is a registered national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research and advocacy. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only organization in Canada focused exclusively on lung cancer. https://www.lungcancercanada.ca/
Lung Cancer Canada is registered with CADTH.
Information Gathering
Data Collection: The information discussed throughout this submission consists of the thoughts and experiences of patients and caregivers. They were collected through interviews, questionnaires, and previous discussions Lung Cancer Canada had with the patient. All information was gathered and accessed between August-September 2021.
X’s experience was gathered through a questionnaire and previous interviews that Lung Cancer Canada had with her. She was unable to participate in an updated interview prior to submission.
Demographic Data: RET-fusion-positive NSCLC is a relatively rare mutation, and a common feature of RET-fusion patients include non-smoking status at diagnosis. All of the patients discussed are RET-positive and have experience with selpercatinib. Specific treatment experience can be found in the Experience With Drug Under Review section.
Table 2: Information About Patients Interviewed by Lung Cancer Canada
Gender | Patient/Caregiver | Source | Line of treatment with selpercatinib | Location |
|---|---|---|---|---|
Female | Patient | Questionnaire and previous interviews | 4th-line | Canada |
Female | Patient | Interview | 4th-line | USA |
Female | Patient | Interview | 4th-line | USA |
Male | Patient | Interview | 1st-line | Canada |
Male | Patient | Interview | 1st-line | Canada |
Disease Experience
For X, life as a new mom and full-time physician was very busy for her with her young daughter and another child on the way. However, being diagnosed with Stage 4 lung cancer in 2015 was essentially the last thing on her mind when she developed a dry cough that did not go away, as she had never smoked a day in her life. It was an extremely shocking discovery that drained her of all hope, and she was told she may only have a year left to live. Unfortunately, this is the reality of many lung cancer patients’ stories, as lung cancer is rarely detected in its early stages due to the lack of screening programs available. This leads to a majority of diagnoses occurring in advanced stages, where metastases may be widespread and the list of available treatment options dwindling down to few. However, the recent advancements that biomarker testing and targeted therapies for RET-fusion lung cancer has had recently has allowed patients like X to be living a full and meaningful life even 6 years later. There is still no cure for first-line treatment, and in second-line and beyond, new treatments are necessary to improve patient outcomes and overcome resistance to treatment. Selpercatinib has the potential to achieve this.
Genetic alterations in the RET proto-oncogene drive 1-2% of non-small-cell lung cancers (NSCLCs), with a global cancer burden of over 10,000 cases each year (Drilon et al., 2020). NSCLCs are the most common type of lung cancer, occurring on 80-85% of lung cancer cases, and is typically found in younger patients and never-smokers, with the use of chemotherapy or immunotherapy as the current standard of care in Canada for first line treatment for patients with RET-rearrangements and NSCLC (Stinchcombe, 2020). However, targeted therapy has since emerged as an important mean of disease management for NSCLC patients with a targetable mutation, including RET. This form of treatment has greatly improved patient outcomes and quality of life, and is now a treatment option that is some patients’ only hope. It has seen incredible success and has allowed patients survivorship, something that they may never had thought would be possible before. Patients like X, who has an ALK-positive mutation, has lived 12 years with stage 4 lung cancer, thanks to targeted therapies. She would never have imagined she’d still be alive today if she had not had the opportunities she got with targeted therapy. Selpercatinib has given patients such as X and X a new chance at life, and to live one that is meaningful.
Selpercatinib works as a highly selective RET kinase inhibitor and was approved by the FDA after the successful results of the LIBRETTO-001 study, where NSCLC patients saw an average of 17.5 months of progression-free survival and objective response rate of 64% (Drilon et al., 2020). After one year on selpercatinib, 66% of patients were still progression-free (Drilon et al., 2020). This is critical for lung cancer patients, as a majority of diagnoses occur in late stages when survival rates are low and disease progression occurs rapidly. The opportunity to have this progression-free survival time is critical for patients to maximize their quality of life and be able to continue with their daily lives with autonomy and dignity.
The development of selpercatinib represents a fundamental change in the treatment of RET-fusion and non-small cell lung cancer, as this agent has shown to be clinically beneficial, RET-specific, and is well tolerated by patients. Selpercatinib is the first of its kind in Canada for RET-fusion-positive targeted therapies, as the discovery of RET mutations in lung cancer is so new, where not much research or treatment has been publicly available. As a result, this is the first opportunity for Canada to have a publicly funded targeted therapy for RET-fusion, and there is an incredible amount of potential for selpercatinib to be able to drive the pathway for future lung cancer treatment for thousands of Canadians, and we strongly encourage CADTH to take this into consideration for selpercatinib to be reimbursed as it would lead the pathway to new developments, new treatments, improvements in accessibility, and affordability for lung cancer patients across the country.
Experiences With Currently Available Treatments
The current standard of care for RET-fusion-positive NSCLC patients is chemotherapy, radiation, and potentially, targeted therapy. Chemotherapy and radiation have been long-standing and well-documented standards of care for lung cancer patients and they have seen some benefits, though are limited as viable long-term treatment options due to their harsh side effects. In addition to not necessarily being successful with controlling the symptoms of lung cancer, they also created additional burdens on patients through harsh side effects, decreased functionality, and increased dependence on caregivers in their daily activities that have been documented time and time again without bringing much benefit. Thus, they are typically only used as a source of initial first-line treatment. Targeted therapy has since emerged as another important treatment option for those with targetable mutations, such as RET-fusion, particularly in second-line and beyond. Targeted therapies have been met with much greater success in lung cancer patients, that they essentially overcome the limited benefits that chemotherapy and radiation are able to provide, whist being able to also manage and treat the symptoms that patients experience with NSCLC. This has made them extremely valuable to patients.
For X, she started chemotherapy as a first-line treatment in 2016, which was met with improvements in her tumours for about a year, but eventually stopped working while also leaving her with an array of side effects such as nausea and extreme fatigue. She constantly needed help with routine activities and was unable to physically do much as she had to take naps throughout the day. Her husband, who was also her caregiver, needed to do most of the work around the house while also caring for her young children, which was extremely hard. Ultimately, she was moved off of chemotherapy and onto immunotherapy; however, it also did not work for her, and she was left fully oxygen-dependant when she started selpercatinib in late August 2017.
X’s experience with double platinum chemotherapy was also one that was met with mixed results, and extreme toxicities from side effects. She began treatment chemotherapy in May 2020 but had to stop 3.5 months later due to significant disease progression and severe side effects that ultimately led her to being admitted to the hospital. Severe chest and back pain, vomiting multiple times a day, loss of appetite, requirement of IV hydration treatment at home, and inability to get out of bed or chairs for more than 50% of the day were just some of the many effects that X had to experience while on chemotherapy. It left incredibly heavy burdens on her caregivers and family, and in 3 months’ time, her scans showed her lung and chest lymph nodes tumours had tripled in size, leaving her condition worse by the end of chemotherapy than when she had started.
Radiation is another common first-line treatment option, though is usually only met with mixed results in lung cancer patients due to the extent of metastases in many patients, in which a majority are diagnosed at late stages. X, for example, had a short experience with radiation as a first-line treatment between August to September 2019, as it was only used for the metastases in his brain. However, it left him with a variety of negative side effects, including short term memory loss, which he is only slowly regaining today about 2 years post-radiation, as well as extreme fatigue where he was unable to continue working or performing daily activities without assistance. It also was not targeted to the tumours in his lung or liver. He started selpercatinib right after and has been on it in the 22 months ever since.
X, a stage 3 patient at diagnosis, had 30 rounds of radiation to her lung, which improved her condition for a while up until December 2020, but was also tied with a negative impact on her home life and ultimately, did not give her the results her doctors were hoping for. It left her with some sun burns to her skin, fatigue, and unfortunately, she had to stop when the tumours had spread to her lymph nodes near the esophagus, making it extremely hard for her to swallow, eat, or drink. She was able to tolerate the side effects fairly well in comparison to other patients, but the biggest hurdle for her was that she had to move 8 hours away from home to a different state so she could start the treatment as soon as possible. This took her away from her family and added on more stressors of living alone for 6 weeks without any support from caregivers, family, or friends.
Improved Outcomes
There have been many incredible advancements in recent years for lung cancer treatment that have changed the paradigm for patients. With RET being a relatively new discovery in lung cancer research, there has not been many previous opportunities for the development and refinement of new targeted therapy treatments for RET-fusion, until now. It has been seen that RET-targeted therapies, including selpercatinib, have been met with incredible success that gives patients their livelihoods back, allows them to hope for a better tomorrow and plan further down the line for a possible future. These outcomes play a huge role in the goals that patients have in their treatment decisions, including:
Improved management of their symptoms of non-small cell lung cancer
Allowing patients to have a full and worthwhile quality of life
Having manageable side effects
Allowing patients to live longer and maintain their independence and functionality so minimize the burden on their caregivers and loved ones
Delaying disease progression and settling patients into long-term remission for improved survivorship
Experience With Drug Under Review
Selpercatinib was effective in shrinking tumours and maintaining stable disease.
When X was diagnosed in March 2019 with stage 4 NSCLC, her initial disease progression was slow for the first year, but then suddenly became very rapid. She was in tremendous pain from the metastases that were in her lymph nodes and bones, including her ribs, vertebrae, shoulder, and hip, in addition to the numerous lung tumours that had appeared over the course of her cancer journey up until she started selpercatinib in August 2020. Two months after starting selpercatinib, scans revealed a nearly 75% reduction of the eight tumours in her lungs, with continuous shrinking of her tumours to date. There has been a complete resolution of 3 tumours in her chest lymph nodes and one in her supraclavicular node, and no new lesions have appeared as of August 2021. After 1.5 years of being on the wrong treatments, she has finally been able to maintain stable disease ever since.
When the phase 1 trial for selpercatinib had opened up for X, she had very widespread disease and only had an initial prognosis of 6-12 months when she was on chemotherapy right before starting selpercatinib. She initially started selpercatinib at ¼ of the recommended dosage, but selpercatinib was so incredibly successful in her case that “she felt like she was magically healed”. X was completely off oxygen just 2 weeks after starting the drug, and in a month, she was able to walk around the block and trick-or-treat with her kids. With selpercatinib, her liver and bone metastases completely disappeared, and her brain metastases were completely resolved. The skin metastases she developed due to a rash from a drainage catheter completely disappeared after starting selpercatinib, and essentially gave her long-term remission with 4 years of stable disease.
With selpercatinib being a first-line treatment for X, the size of his original lung tumour was approximately 3cm x 4cm at diagnosis, along with other brain and liver metastases. However, with selpercatinib, his tumours had been reduced by 30% overall after six months of being on the treatment. His CT scans in June 2021 revealed there has been over 75% reduction in his lung tumour, in which his doctors actually told him if his tumour was this small two years ago at diagnosis, it would not have been detected at all. About 60% of his brain lesions are showing full encapsulation, and X has not seen any progression of disease ever since.
Selpercatinib was effective in improving symptoms experienced.
Prior to starting treatment with selpercatinib, X was admitted to the hospital with severe vomiting, coughing, and chest/back pain as a result of significant disease progression. Within a few days of starting selpercatinib, all of those symptoms were virtually gone, and she was asked to be released from the hospital as there was almost immediate resolution of her symptoms. Her appetite resumed, there were no feelings of nausea or general illness, energy levels were back up, she was able to walk further distances, and felt like she was transported back to her pre-cancer self. She was also completely weaned off of pain medication, anti-nausea meds, and anti-anxiety meds.
In X’s experience, she started selpercatinib in September 2017 as her 4th-line of treatment, and has been on it ever since. Prior to it, she was fully oxygen-dependant, extremely fatigued, had severe nausea that required management with an anti-nausea drug, Zofran, was immunocompromised, and had virtually no other treatment options left. She initially started the treatment at ¼ of the recommended dosage, but selpercatinib was so incredibly successful in her case that “she felt like she was magically healed”. X was completely off oxygen just 2 weeks after starting the drug, and in a month, she was able to walk around the block and trick-or-treat with her kids. She did not need constant naps throughout the day, and ultimately, it gave her the ability to be independent again.
For X, the delays that he experienced in waiting for the drug to be approved for him felt like they would never end. Between getting diagnosed in September 2020 and finally getting access to start selpercatinib in March 2021, his symptoms had kept multiplying throughout that period that he felt like he had no other choice. He was admitted into the hospital when diagnosed, and over the course of a week, he went from having a persistent cough to having sharp pains in his lower back, worsening shortness of breath, and he was unable to stand up whenever a cough came. He had to have radiation for his lower back pain and chemotherapy to help relieve some of his symptoms in the meantime but stopped after seeing disease progression. Once he was able to start selpercatinib as his true first line of treatment, it felt like he had won the lottery. His cough subsided and shortness of breath was no longer an issue. He could feel himself getting better a month into taking selpercatinib when it would previously take him 10 mins to walk from the 1st to 2nd floors of his home with stops needed to catch his breath. But a month into treatment, he was able to walk upstairs no problem. This felt like a miracle drug to him and his family.
Selpercatinib was effective at treating brain metastases.
Selpercatinib was also shown to be effective at treating brain metastases in patients. Before he knew he had lung cancer, X first noticed he was having some miscoordination in his left hand, which turned out to be a result of a tumour in his brain, which led to his diagnosis of NSCLC. He was first treated with radiation to his brain lesions for a month, which left him with fatigue and short-term memory loss, in which he is only slowly regaining to this day.
Radiation is the most common treatment for brain metastases in lung cancer patients, which has the risk of potential cognitive impairment, and in some cases, this impairment can be permanent. This carries significant burdens on not only the patient, but also their family and caregivers who have to care for them. Selpercatinib has seen to almost completely, if not fully, resolve these brain tumours, as seen with X and X’s case, without leaving any lingering effects from treatment other than minor side effects associated with the drug. This allows for a huge burden to be lifted off of patients and eliminates the risk for cognitive impairment that is seen with other treatments.
Selpercatinib has minimal and manageable side effects that had much less impact on daily life in comparison to other treatment options.
The list of side effects that have been attributed to selpercatinib include diarrhea, dry mouth, hypertension, fatigue, constipation, nausea, peripheral edema, headache, rash, and abdominal pain, amongst others that are much less common (Drilon et al., 2020). These are all relatively minor side effects that carry much less burden to the patient in comparison to other available treatments that are used to treat patients with RET-fusion-positive NSCLC, such as chemotherapy and radiation.
Amongst the patients that Lung Cancer Canada interviewed for this submission, fatigue and dry mouth were the main side effects experienced by most, though the levels of fatigue were collectively nowhere near the extent prior to starting selpercatinib. Edema was also experienced by two patients, one mainly around his eye pockets and occasionally, their legs, while the other patient experienced swelling around their legs, feet, and to a lesser extent, their face. Other minor effects such as constipation, bloating, and occasional abdominal pain were also mentioned by patients, though all patients said their side effects were extremely manageable in comparison to the effects experienced during other treatment regimens. None of the patients experienced any severe-grade adverse events that were related to the treatment.
Selpercatinib allowed patients to return to functionality and similar to that of pre-diagnosis.
Possibly one of the most important outcomes that lung cancer patients wish for since being diagnosed is to be able to return to a stable state in their journey that resembles what their life was like pre-diagnosis, and all the patients that were interviewed were able to achieve this with selpercatinib. In X’s case, she was able to help out around the house and was not as fatigue-ridden as she was prior to treatment, was able to interact with her children more, and return to her role as a mom and spend time with her kids. For X, most of her symptoms that she was experiencing right before starting selpercatinib were resolved within days of starting treatment, and this allowed her to be released from the hospital much sooner than anticipated. She was no longer bed-ridden or unable to sit up for more than 50% of the day, she regained her energy to walk around the house and long distances, and overall, had a better state and clarity of mind.
X didn’t even need to take much time off of work while on selpercatinib and continued to work as much as she could. Having this freedom and flexibility gave her the much-needed relief to be able to reunite with her husband and young daughter and spend as much time as she could with her family to make up for the time lost while she was away in another state during her previous radiation treatments. Being able to regain the functionality and sense of self that these patients once had before they were diagnosed with lung cancer really lifted their spirits and helped them regain the confidence they needed for their well-being.
For months, X felt like he was playing a waiting game just to have the approval from his oncologist that he was able to finally start taking selpercatinib. He was not able to cook, showering took up a lot of his energy, he was either on the sofa or in bed for most of the day, and he could barely walk up the stairs at home without needing to catch his breath. This really limited him in the relatively active lifestyle he used to have. However, 3 months into taking selpercatinib, he felt so rejuvenated and returned to functionality that was so similar to pre-diagnosis, in that he was even able to return to playing soccer and badminton with friends again and is able to enjoy himself and socialize at family gatherings. It made such a difference in his world, in that he would have ranked himself at a physical functionality level of 2 or 3 out of 10 prior to selpercatinib, though by September 2021, his feelings of returning to normal functionality were at a 7 out of 10.
Selpercatinib also helped patients regain their independence and relieve the burden on caregivers.
When X was diagnosed, her life as she knew it basically stopped, and she was no longer able to do many things herself and constantly required help from caregivers and family. She could no longer do any of the activities that she loved and kept her healthy for a long while, such as gardening, taking care of her barn, hiking with her family, or other simple tasks until selpercatinib came into play. The caregiver burden that is in place with lung cancer patients and their families is incredibly difficult and often times, caregivers find themselves with just as much anxiety as the patients themselves. X had to have a nanny to help take care of her kids and house while her husband was at work, and this was extremely difficult for them as X could not do much herself. The amount of stress on her husband as the sole caregiver of their 2 young children was very hard on him and having to come home after a long day of work to do handle everyday tasks around the house, rearranging work schedules to be available to drive to appointments, caring his wife while she was sick became very wearing. The emotional burden of staying positive for the cancer patient creates many of its own challenges with the caregiver’s mental health.
Being able to regain their independence with selpercatinib has been incredibly healing and almost “magical” for these patients. X knows that without selpercatinib, she would not be able to move back home with her family, take care of her daughter and send her to school, and continue to go to work regularly as she is now. Similar to X’s husband being the caregiver for the entire family, X’s husband also was the sole caregiver for their child when X moved away for radiation treatment. This was also extremely hard on him and took a toll on their emotional and mental health. Once selpercatinib was in play for them, X was able to regain her energy, functionality, and independence, and help out with taking care of her daughter once she moved back home and relieve that heavy burden off her husband’s shoulders.
X also did not require much help throughout his cancer journey while on selpercatinib, as his life now is comparable to that before diagnosis. He is able to walk long distances and even run a little, drive himself to appointments, listen to music, and cook dinner for his family on a regular basis. With this being his first line of treatment, he never lost much of his independence as a patient, which is a very stark contrast to other patients who may have gone through chemotherapy or radiation as their first-line treatments instead. As a cancer patient, being able to have this autonomy to be independent and take care of themselves without much help or burden on caregivers is tremendously rare in comparison to other treatments available.
Selpercatinib gave patients their lives back and allowed them to return to work.
X has continued to work for the most part throughout her cancer journey, though her experience with selpercatinib has allowed her to physically go to work almost every day, which is something she thought she would not have been able to do previously. In fact, as Lung Cancer Canada was interviewing X, she was driving herself home from work. Prior to selpercatinib, she was still able to regularly work from home while away for radiation treatment, which also coincided with the shutdown of in-person offices during the pandemic in 2020. X was also busy with her career as a physician before diagnosis, and when she went on selpercatinib in 2017, her disease progression had stabilized and she felt well enough to return to work; however, that got cut short due to the pandemic. She still occasionally works from home whenever she can, and also runs a lung cancer patient support group for RET-positive patients. She felt as if “she got her life back” with selpercatinib and felt a sense of normalcy of a life that is similar to her pre-cancer self. This shows the incredible autonomy and ability to return to work and return to an “almost normal” life that selpercatinib has given her and many other patients.
Being able to also have a social life and meet with friends and family is another aspect that patients have been able to return to with selpercatinib, as it gives them the freedom to take their oral pills as scheduled, and then be on their way. MM is able to keep his quality of life stable these last 2 years since diagnosis and has the independence to continue to do many activities himself without giving up much. He regularly goes grocery shopping himself, is well enough to even travel on a plane for vacations and is overall living a very similar life as before diagnosis. He never received any recommendations from his physicians to abstain from flying and travelling, pandemic aside, and regularly visits his family and friends to continue to build that social support network. He is currently out of work, however, and on long-term disability insurance, but has mentioned that if he was able to go back to work, he would do so as soon as he could. Selpercatinib has allowed patients to get their livelihoods back, which is ultimately one of the most important outcomes that patients wish for in a treatment option.
Selpercatinib revived hopes and dreams and allowed patients to set meaningful goals for the future.
Along with being able to return to work and regain their livelihoods, selpercatinib has also allowed patients to revive and fulfill their hopes and dreams, and plan further into the future, which had previously looked bleak prior to selpercatinib. The ease and freedom that the oral nature of selpercatinib has given patients such as has been incredibly rewarding, almost as if they have a second chance at life. It gives them more time to be with family, friends, themselves, work on self-development and self-healing, time for other commitments, activities, and overall enjoying the extra time that they now have thanks to selpercatinib. For example, X has been taking courses on topics that he enjoys and is passionate about, such as psychoneuroimmunology, and really feels fulfillment in studying and learning. He would not have imagined he would have the time or ability to do so at diagnosis, and he would not be where he is today without the “magical wonders” of selpercatinib.
The biggest wish that X had for herself when she was diagnosed with stage 4 lung cancer was to see her daughter go to school, and to live a life long enough for her kids to remember her by. Being pregnant with her second daughter when diagnosed, the initial feelings that X had at the time was one of shock and fear that set in and left her wondering if she’d be able to live long enough for her baby on-the-way to remember her by. The first few months were extremely hard and worrisome, and planning for a future was one of the last things on her list of concerns. However, when she started selpercatinib, it “genuinely gave her life back”, and worked wonders on her functionality, independence, and outlook on life that allowed her to start having hopes and dreams again and plans for the future. Compared to previous treatments, she needed almost no help when on selpercatinib, and was able to take care of the kids and the house, drive her daughter to piano lessons, and even get back to work. She was able to travel to Hawaii and Bora Bora on family vacations, start downhill skiing, and being active and exercising. These were all things that she had only imagined of doing prior to treatment with selpercatinib. She has been able to make long-lasting memories with her husband and children that they will remember for the rest of their lives, which was the ultimate wish AB had at diagnosis.
Many people tend to measure life by the accomplishments they had, meaningful milestones they were able to reach, and moments that made them feel like they had all the time in the world. Being diagnosed with lung cancer is such a shock to a patient’s mentality and perspectives on life, that unfortunately, drives many into a physical and mental state of mind that is not positive at all. However, as seen with all the patient experiences Lung Cancer Canada has discussed in this submission, this has not been the case for any of these patients at all once they had started selpercatinib. They were able to regain the functionality, independence, and lives that they had in a sense that was so incredibly similar to the ones they had before diagnosis, and this is the aspect that we hope CADTH takes into consideration. Selpercatinib has allowed for meaningful moments for these cancer patients that they had previously thought would be impossible, allows for them to return to placing these markers of milestones and meaningful moments in their lives, and shines a sense of hope on them for their future.
Companion Diagnostic Test
Companion diagnostic testing for RET-fusion is required and is currently covered by many provinces in Canada.
Anything Else?
“When I was initially diagnosed with lung cancer, I just wanted to live long enough for my children to remember me.”
A diagnosis of lung cancer shatters this wish that all parents have, but for RET-positive NSCLC patients, selpercatinib has helped put the pieces of patients’ lives and dreams back together. Four years later, AB’s children are old enough to have shared memories and there are plans for the future.
In evaluating this file, CADTH may question the certainty of the data. It is important to remember that selpercatinib is a targeted therapy. It is present in 1-2% of the lung cancer population. Its clinical efficacy is consistent to other targeted therapies, and due to the definition of targeted therapy, the population will remain small. All NSCLC targeted therapies that have been evaluated by CADTH have proven to exceed expectations on value in both follow-up data and real-world evidence. All this evidence indicates that threshold for certainty in targeted therapies differ from non-targeted therapies and we encourage CADTH to deliberate with that standard in mind. In the past year, CADTH has also lowered, without consultation, the QALY threshold for cost effectiveness to $50,000. This is consistent with non-cancer drugs. Lung Cancer Canada strongly disagrees with this threshold as it undermines the premise of separate deliberations for cancer vs non-cancer drugs. It is expected that cancer treatments will cost more than, for example, an antibiotic or a proton pump inhibitor. Lowering the threshold QALY devalues innovation in life-threatening or complex diseases and creates an unreasonable barrier in accessing life-saving treatments for cancer patients. This threshold QALY in combination of CADTH’s interpretation of uncertainty in the clinical efficacy of treatment may lead to CADTH using projections that clinicians believe to have a low probability of occurrence to calculate cost effectiveness. We ask CADTH to re-evaluate the threshold QALY for cancer treatments in recognition that cancer is a life-threatening disease with far reaching impact on society.
We ask CADTH to keep these principles in mind when evaluating the reimbursement submission for selpercatinib for RET-positive NSCLC.
References
Drilon, A., Oxnard, G.R., Tan, D.S., Loong, H.H., Johnson, M., Gainor, J., & Subbiah, V. (2020). Efficacy of selpercatinib in RET fusion–positive non–small-cell lung cancer. New England Journal of Medicine, 383(9):813-824. DOI: 10.1056/NEJMoa2005653
Stinchcombe T.E. (2020). Current management of RET rearranged non-small cell lung cancer. Therapeutic Advances in Medical Oncology, 12, 1758835920928634. DOI: 10.1177/1758835920928634
Patient Group Conflict of Interest Declaration
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No, Lung Cancer Canada did not receive any outside help to complete this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No, Lung Cancer Canada did not receive any outside help to collect/analyze the data used in this submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 3: Conflict of Interest Declaration for Lung Cancer Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Eli Lilly Canada Inc. | X | — | — | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Position: Director, Programs and Stakeholder Relations
Patient Group: Lung Cancer Canada
Date: September 13th, 2021
CanCertainty
About CanCertainty
The CanCertainty Coalition is the united voice of more than 30 Canadian patient groups, cancer health charities, and caregiver organizations from across the country, joining together with oncologists and cancer care professionals to significantly improve the affordability and accessibility of cancer treatment.
For more information about the CanCertainty Coalition, please visit: https://www.cancertaintyforall.ca/
Information Gathering
Selpercatinib is indicated for patients with non-small cell lung cancer (NSCLC) whose tumours have mutations that lead to the fusion of the RET gene with other nearby genes. As an orally administered oncology drug, selpercatinib is not automatically funded by certain provincial governments. In Ontario and the Atlantic provinces, only individuals over the age of 65 are automatically covered for oral oncology medication. For the small number of patients under 65 living in these provinces, their diagnosis could lead to severe economic hardships. However, if selpercatinib is fully funded by all provinces, these patients will instead be able to focus on their treatment and spending time with their family and friends.
Our data collection efforts aimed to estimate the number of patients who are at risk of severe financial burden as a result of their diagnosis. To do this, we calculated the number of RET fusion-positive NSCLC cases in Canada each year among the under 65 population who do not have private or automatic public prescription drug coverage. As selpercatinib is indicated as a monotherapy for first-line treatment, it was sufficient to calculate the RET fusion-positive NSCLC rate in Canada (calculating remission rates from first and second-line treatment was not required). Selpercatinib is a novel, highly selective inhibitor of RET kinase1. It is intended to supplant the use of multi-targeted kinase inhibitors that were affective against RET kinase. Selpercatinib can target diverse RET alterations and has been shown to have anti-tumor activity in the brain.
RET mutations are rare. We estimate that about 513 Canadians are diagnosed with RET fusion- positive NSCLC each year. Of these 513 cases, 128 will be under the age of 65. Depending on where these individuals live, their oral oncology medication may not be covered by their provincial government. For the 39 patients under 65 living in British Columbia, Alberta, Saskatchewan, and Manitoba, oral oncology medication is automatically covered. Residents of Ontario and the Atlantic provinces under the age of 65 are not automatically covered under public plans. Their route to treatment access is not simple. By our estimations, 7 of these Ontario cancer patients will not have private health insurance. Before they can receive their medication, these patients will have to navigate a complicated process of funding applications, approval delays, locating a pharmacy, and waiting for their medication in the mail. They will incur out-of-pocket costs and sizeable portion of their income will go towards their medication. This is a small number of patients to be impacted by such restrictive reimbursement policy.
Lung cancer incidence data was sourced from the Canadian Cancer Society (Statistics Canada)2 in collaboration with the provincial and territorial cancer registries. In their 2020 special report on lung cancer, the Canadian Cancer Society provided lung cancer data for all of Canada (excluding Quebec) broken down into age groups (Figure 1). We applied the age-specific lung cancer incidence rates to the 2016 population demographics3 of each province to arrive at the number of new lung cancer cases each year by age and province.
The RET mutation has only been identified in patients with NSCLC. We used lung cancer incidence from the Canadian Cancer Society data estimate the number of NSCLC cases each year by age and province. The RET mutation is present in approximately 2% of NSCLC4. With these percentages, we estimated the number of yearly lung cancer cases with the RET mutation by age and province. In other words, this is the estimated number of Canadian residents who will become eligible for selpercatinib each year.
We measured “potential financial toxicity” using data on lack of private drug coverage. The Canadian Life and Health Insurance Association5 provides data on “extended health coverage.” For each province, we extracted the percentage of individuals under the age of 65 without private drug coverage AND without automatic public drug coverage. These province specific percentages were applied to the RET fusion-positive NSCLC case rates to arrive at the final estimation: the number of yearly RET fusion- positive NSCLC cases among the under 65 population without private or automatic public prescription drug coverage.
Assuming selpercatinib is ultimately funded by the provinces and territories, the following chart details the number of patients in each province/territory that would face financial barriers in accessing this treatment.
Figure 1: Number of Patients in Each Province/Territory That Would Face Financial Barriers in Accessing Treatment
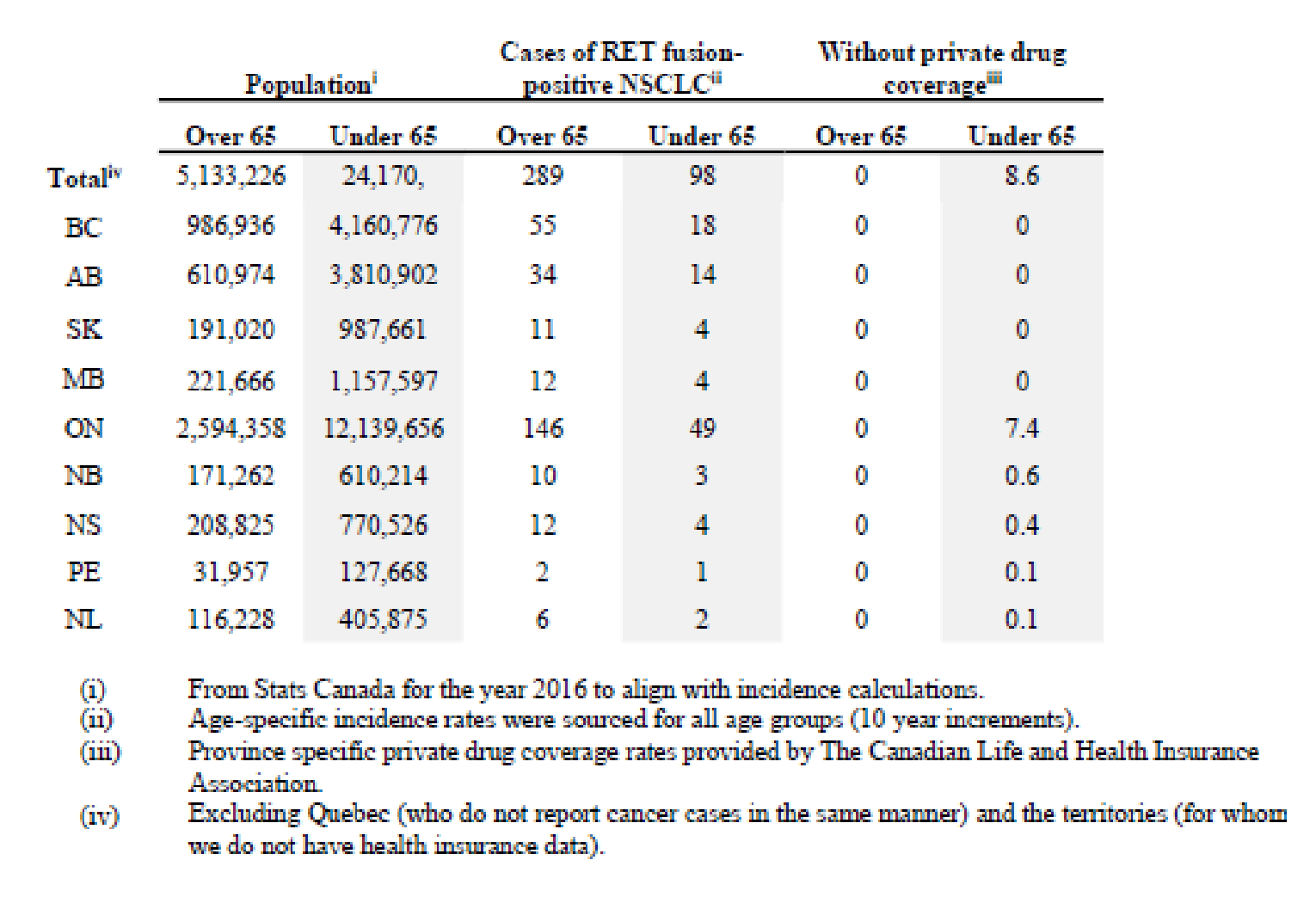
Limitations
We calculated these estimates to highlight an issue, not to be absolutely precise.
Just because someone younger than 65 does not have private insurance does not mean that they are without financial support for their oral oncology medication. In each province, multiple programs exist to support individuals with high drug costs. Based on our experience as a patient advocacy group, we made the assumption that individuals with private health insurance incur less cost when prescribed oral oncology drugs.
The RET mutation rates were not sourced from a Canadian population. Differing demographics across the provinces may skew the actual case counts.
Disease Experience
The access problems are so difficult that in many hospitals and cancer centres across Canada, such as those in Ontario, a new type of social worker known as a drug access navigator has been established (and funded) to assist patients and clinicians navigate the byzantine treatment access structures. In Ontario, the organization that supports these navigators is known as the Oncology Drug Access Navigators of Ontario (ODANO). They describe the problem that their association works to resolve as follows: Drugs are an important part of cancer treatment, yet patients often have difficulty accessing coverage for the most effective medicines. The complexity of cancer drug coverage in Canada can overwhelm patients and families.
and
For example, although cancer drugs administered in hospitals and clinics are often offered free of charge to patients, half of all new cancer drugs are taken at home and, therefore, many are not covered by the public health system. Unfortunately, many of our patients do not have any private insurance. If a patient is fortunate enough to have private coverage, many drug plans require a 20% co-payment, which can quickly become a financial burden to patients on expensive medications.
British Columbia, Alberta, Saskatchewan, Manitoba, Quebec, NWT, Yukon, and Nunavut cover the reimbursement of oral cancer drugs for all in need. Ontario and the Atlantic provinces do not.
In Ontario and Atlantic provinces, with respect to access to approved cancer treatments, there is institutional discrimination against those who are young, uninsured and who have cancer requiring take- home cancer treatment. With 60% of all new cancer drugs being developed with oral formulations, this issue urgently needs to be resolved through policy change. Traditionally, cancer treatments were administered to patients by an IV in the hospital. Over the past 15 or so years, an increasing number of effective cancer treatments can be taken at home by pill or injection. Take-home cancer medications are now a fundamental part of today’s cancer treatments and should be recognized equally within our health care systems. Patients requiring an intravenous treatment can start that medication as soon as needed and don’t face any financial or administrative burdens provided the drug is included on the provincial formulary.
However, when take-home cancer medications are prescribed, patients in Ontario and the Atlantic provinces, who are under 65, and lack adequate private insurance, have to apply to a variety of funding assistance programs and ultimately pay a significant deductible or co-pay from their personal savings. In some cases, the cost to the patient might be as high as $23,400 annually, based upon Nova Scotia’s Family Pharmacare Program. To qualify for assistance programs, patients and their families have to submit significant amounts of personal and financial information and often face weeks of stressful delay in starting their cancer treatment until the paperwork and approvals are resolved.
Even for patients with private drug insurance, the reality is that many face significant co-pays, deductibles or annual/lifetime caps. For example, some private insurance plans have a cap of $2,000 for prescription drugs for the entire year. The majority of take-home cancer drugs cost more than $20,000 per year. Two-tiered pharmacare in Ontario and the Atlantic Provinces discriminates on the basis of age, income, geography, cancer type, and cancer treatment, and is financially ruining many lives.
A survey6 of over 1,600 Nova Scotians, commissioned by the CanCertainty Coalition, demonstrates that drug coverage for cancer patients is a serious and growing problem.
More than half (57 percent) of Nova Scotians expect the provincial health care system will pay for take-home cancer medications. In reality, patients will ultimately pay a significant deductible or co-pay from their personal funds.
Three out of five people in Nova Scotia (60 percent) said they would consider leaving the province if faced with having to pay for their cancer drugs. Only seven percent could afford monthly drug costs of over $200.
Experiences With Currently Available Treatments
Take-home cancer drugs (THCD) are medications used for the active treatment of cancer and are usually dispensed for administration in the home (e.g., oral chemotherapy). These drugs have become a standard treatment for many cancers and present opportunities for patients, providers, and the health system. However, flaws in our current drug coverage system result in some patients not being able to access these treatments.
The term “financial toxicity” describes the distress and hardship arising from the financial burden of cancer treatment. Even in counties with government funded universal healthcare, financial toxicity is an issue for cancer patients and their families. Financial toxicity comes in many forms: out of pocket costs, lost income, travel expenses etc. Patients may deal with their financial burden by delaying or foregoing care. They may take less medication than prescribed, utilize over-the-counter drugs in place of prescribed medications, decline procedures, and skip appointments in an attempt to defray costs. The combination of high drug prices, particularly of oral targeted anticancer drugs, and increased cost sharing has made patients more vulnerable to medication non-adherence. Patients who are younger, have lower income, and are uninsured appear to be at greater risk of medication non-adherence. Although government funded public healthcare exists in many very high development index countries, financial toxicity is still common among cancer patients and caregivers. The evidence suggests that those with a shorter time since diagnosis, not currently working, and with more severe cancers have higher rates of financial toxicity, including stress and strain7.
An unfunded oral oncology drug is financially toxic compared to a funded IV oncology drug. The disease experience of cancer patients that require oral drugs is a dual track of disease and economic hardships. After receiving their diagnosis, deciding on a medication, and dealing with the side effects, patients in Ontario and the Atlantic provinces have to consider the financial side of their diagnosis. “Hearing that you have cancer is devastating. Finding out that you can’t pay for the medication that will make you well is catastrophic. It doesn’t have to be this way” (X Ontario).
The financial side of cancer treatment is unnecessarily burdensome. “When you are going through any kind of sickness, whatever the severity of it, the last thing you should have to worry about is your medication cost” (Ontario). In addition to dealing with cancer, and not being well enough to work, patients in Ontario and the Atlantic provinces spend days on end, sometimes months, wading through paperwork in order to get approval for coverage of the oral chemotherapy that has kept them alive.
Because some cancer treatments are not automatically funded, treatment is delayed for many patients. They wait weeks for government approval before dealing with insurance companies and pharmacies to receive their prescription. Patients often pay out of pocket for the first few weeks of their treatment, which they may not be reimbursed for. “My doctor prescribed a new drug that is not covered by the government therefore I had to find insurance to cover it which costs around $5000.00 a month, I came up with insurance to cover it but I had to pay the pharmacy first then the insurance would reimburse me some time later. My problem I do not have the $5000 to pay out let alone wait till they reimburse me” (Ontario).
“Cancer isn’t fair, but access to treatment should be!”
Experience With Drug Under Review
CanCertainty’s focus for this submission is on issues related the distress and hardship arising from the financial burdens associated with cancer treatment. If selpercatinib were to be reimbursed for patients with RET fusion-positive NSCLC who have progressed on previous treatments, there would be some patients under 65 in Ontario and Atlantic Canada that would face significant financial and administrative barriers in accessing treatment.
Companion Diagnostic Test
N/A
Anything Else?
Equitable Access
We recommend that pCODR, when assessing and reporting on implementation issues with respect to selpercatinib, examine the issues of equitable access across all Canadian jurisdictions.
Safety
With respect to implementation, we believe pCODR should also examine the issue of safety with respect to take-home cancer drugs. From 2006 to 2001, it is estimated that Ontario’s computerized provider entry system, the Oncology Patient Information System (OPIS) prevented 8,500 adverse drug events, 5,000 physician office visits, 750 hospitalizations, 57 deaths, and saved millions in annual healthcare costs. But, this system is only used for only IV Drugs8. As a result, patients requiring take- home cancer drugs (THCD) in Ontario are (currently) subject to significant safety challenges, and health systems are subject to significant annual costs (physician office visits, hospitalizations etc).
In Ontario, dispensing and delivery models for THCD have been documented to be inconsistent and pose serious safety concerns for patients and their families. Some patients receive their medication from hospital pharmacies, some from specialty pharmacies, and some from community pharmacies that lack specialization and training in the handling of toxic cancer medications. This contrasts with the robust guidelines and clear processes that have been developed for intravenous cancer drugs (IVCD) where delivery is more comprehensive, organized, safer and patient-centred than THCD. There are numerous known safety and quality deficits related to the current method of community dispensing of THCD including incorrect dosing and handling, limited monitoring and non-adherence (which can lead to under or overdosing), serious toxicity, morbidity, and mortality. Patient lives and well-being are at stake. Ontario urgently needs to reform its systems for THCD dispensing that embed high-quality, safe practices that recognize the unique aspects of these drugs.
In April 2017, Cancer Care Ontario organized the Oncology Pharmacy Task Force with the mandate to advise Cancer Care Ontario (CCO) on how to enhance the current system for THCD delivery to optimize quality and safety; and subsequently, to deliver a report to the Ministry of Health and Long- Term Care (MOHLTC) based on the findings of the Task Force. The Task Force included representatives from patient advocacy groups, pharmacy and pharmacist associations, regulatory and standard setting organizations, and subject matter experts. On March 25th, 2019 the report was completed and published on the CCO website, but there has been no follow up or action taken to the many important recommendations. The report Enhancing the Delivery of Take-Home Cancer Drugs in Ontario (March 2019) can be found at: https://www.cancercareontario.ca/sites/ccocancercare/files/guidelines/full/1_CCO_THCD_Report_25Apr2019.pdf
CanCertainty suggests that pCODR examine the issues of safety and dispensing when examining and reporting on issues concerning pan-Canadian implementation of selpercatinib.
References
1. Drilon, Alexander et al (2020). Efficacy of Selpercatinib in RET Fusion-Positive Non Small-Cell Lung Cancer. New England Journal of Medicine, 383(9), 813–824. doi:10.1056/NEJMoa2005653
2. Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Toronto, ON: Canadian Cancer Society; 2020. Available at: cancer.ca/Canadian-Cancer-Statistics-2020-EN
3. Statistics Canada. (2020) Annual Demographic Estimates: Canada, Provinces and Territories [Data Visualisation Tool]. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501
4. Drilon, Alexander et al (2020). Efficacy of Selpercatinib in RET Fusion-Positive Non Small-Cell Lung Cancer. New England Journal of Medicine, 383(9), 813–824. doi:10.1056/NEJMoa2005653
5. Sutherland, Greg, and Thy Dinh. Understanding the Gap: A Pan-Canadian Analysis of Prescription Drug Insurance Coverage. Published in Canada | All rights reserved | Agreement No. 40063028 | *Incorporated as AERIC Inc.
6. Strategic Directions. Cancertainty & Strategic Directions IVR Report. 2017. Available at: https://d3n8a8pro7vhmx.cloudfront.net/cancertainty/pages/119/attachments/original/1490212245/CanCertaintySurvey_October2016.pdf
7. Longo, C.J., Fitch, M.I., Banfield, L. et al. Financial toxicity associated with a cancer diagnosis in publicly funded healthcare countries: a systematic review. Support Care Cancer 28, 4645–4665 (2020). https://doi.org/10.1007/s00520-020-05620-9
8. eHealth Ontario. Cancer Care Ontario and eHealth Ontario Partner to Deliver Safer Chemotherapy Treatment. Toronto, ON: 2011. Available at: https://ehealthontario.on.ca/en/news/view/cancer-care-ontario-ehealth-ontario-partner-to-deliver-safer-chemotherapy

Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was completed exclusively using CanCertainty resources and personnel and contract personnel.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Data was collected and analyzed using CanCertainty personnel/contract personnel.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 4: Conflict of Interest Declaration for CanCertainty
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AstraZeneca | — | — | X | — |
Merck | — | — | X | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Name: Position: Co-Lead
Patient Group: CanCertainty
Date: Sept 12, 2021
Clinician Group Input
Lung Cancer Canada
Current treatments
Describe the current treatment paradigm for the disease.
The current standard of care in the treatment-naïve advanced or metastatic non-small cell lung cancer (NSCLC) based on reimbursement in all the provinces whose tumours harbour RET fusion includes:
platinum/pemetrexed doublet chemotherapy;
platinum/pemetrexed and pembrolizumab for those with PDL-1 expression <50%, and possibly those with PDL-1 expression > 50% who are non-smokers, female, high disease, or symptom burdens; and
pembrolizumab alone for those with PDL-1 expression > 50%.
Options 2 and 3 will be contraindicated in those who have active autoimmune disease or who have organ or bone marrow transplantation and are on active immunosuppressants.
In a retrospective analysis by Gautschi et al, the overall response rates (ORR) were 51% and 49%, median progression-free survival (mPFS) were 7.8 months and 6.4 months, and median overall survival were 24.8 months and 23.6 months in 84 mNSCLC who received either platinum-based chemotherapy or platinum/pemetrexed, respectively [Gautschi et al. J Clin Oncol 2017;35(13):1403-1410]. Drilon et al. [Ann Oncol 2016;27(7):1286-1291] also reported sensitivity of RET fusion NSCLC to pemetrexed-based chemotherapy with an ORR of 40%, and mPFS of 19 months.
Chemotherapy and pembrolizumab are preferred in PDL-1 > 50% patients who are non-smokers, high disease or symptom burden and female patients, where the combination is more likely to provide a higher ORR and mPFS. Sheng et al. [Ther Adv Med Oncol 2021 May 29;13:17588359211018537] performed a meta-analysis of 26 randomized trials demonstrated improved mPFS for chemotherapy + pembrolizumab (HR=0.70; 95% CI: 0.58-0.80) without improvement in median overall survival (mOS; HR=0.90; 95% CI 0.79-1.05). The meta-analysis of Keynote (KN) trials, 024, 042, 021, 189 and 407, also demonstrated an improvement in ORR for the chemotherapy and pembrolizumab combination (Relative Risk: 1.6; 95% CI 1.2-2.2) and mPFS (HR=0.55; 95% CI: 0.32-0.94) while there was no difference detected in mOS (HR=0.76; 95% CI: 0.51-1.14) [Zhou et al. J Immunother Cancer 2019;7(1):120.] Based on Offin et al. [J Clin Oncol Prec Oncol 2019;3: PO.18.00386], only 19% of RET fusion positive NSCLC patients will have PDL-1 expression > 50%, and more commonly these individuals will not have a smoking history; thus, in these patients, platinum/pemetrexed and pembrolizumab will be more likely to be used in the clinic than pembrolizumab alone.
There is still an ongoing debate as to whether the addition of pembrolizumab improves the outcome of platinum/pemetrexed in RET fusion NSCLC. Hess et al. [BMC Cancer2021;21(1):28] reported comparably similar ORR (75% versus 60.5%, p=0.15), mPFS (6.6 months versus 5.7 months, p=1.0) and mOS (p=0.36) for RET fusion (N=9) and non-RET fusion (N=605) NSCLC patients treated with platinum/pemetrexed/pembrolizumab. In a series from South Korea by Lee et al.[Jpn J Clin Oncol 2020;5(5):594-60], 46 RET fusion NSCLC treated with the pemetrexed-based combination, including only 36 of which received its as first-line therapy, reported the mPFS was 9 months while mOS was 24 months. Amongst the 13 patients who had prior immunotherapy, 4 of whom received nivolumab as first line therapy, the ORR was 0%.
For the RET fusion NSCLC who progressed on prior systemic therapy, the options include:
Platinum/pemetrexed for those who had received pembrolizumab as first-line therapy,
Anti-PD(L)1 therapy, including pembrolizumab, nivolumab and atezolizumab, for those who had received platinum/pemetrexed as first-line therapy (but with the adoption of platinum/pemetrexed and pembrolizumab as first-line therapy, this represents a very small number of patients), and
Docetaxel for those who have progressed on platinum/pemetrexed and pembrolizumab.
RET fusion NSCLC is very sensitive to pemetrexed as reported by both Drilon et al. and Gautschi et al. So pemetrexed/platinum is likely the most efficacious therapy in the RET fusion NSCLC patient who had received only pembrolizumab as first-line therapy, in the absence of any randomized data.
The efficacy of anti-PD(L)1 therapy is low. A majority of the retrospective series reported an ORR 0-20% and mPFS of 1.5-2.1 months [Mazieres et al. Ann Oncol 2019;30(8):1321-1328; Lee et al. Jpn J Clin Oncol 2020;5(5)”:594-560; Offin et al. J Clin Oncol Prec Oncol 2019;3: PO.18.00386] except for the outlier retrospective series by Guisier et al, where the ORR was 32.5%, mPFS was 7.6 months and 1-year OS was 89% among the 9 RET fusion NSCLC who received PD(L)1 therapy as second-line and beyond [Guisier et al. J Thorac Oncol 2020;15(6):628-636]. Furthermore, Tan et al. [J Thorac Oncol 2020;15(12):1928-1934] reported that RET fusion NSCLC patients who had or had not received immunotherapy at any time during their metastatic disease setting had similar mOS (37.7 months versus 49.3 months, p=0.53).
The clinical outcome of RET fusion NSCLC treated with single-agent docetaxel after prior systemic chemotherapy has not been reported. All in all, the ORR was 7%, mPFS of 10.6 weeks and mOS of 7.5 months for unselected, previously treated, advanced or metastatic NSCLC [Shepherd et al. J Clin Oncol 2000;18(10):2095-2103]. Based on the subgroup analysis of CM057, KN010, and OAK, patients with EGFR or ALK aberration derived similar benefit from docetaxel and PD(L)1 therapy [Horn et al. J Clin Oncol 2017;35(35):3924-3933; Herbst et al. Lancet 2016;387(10027):1540-1550; Ritt,eyer et al. Lancet 2017;389(10066):255-265]. Thus, it is believed that patients with RET fusion NSCLC will benefit from docetaxel in a manner similar to patients with EGFR, ALK or unselected, previously treated, advanced or metastatic NSCLC.
The final question is whether RET fusion is a driver mutation for NSCLC. Driver mutation is a genomic alteration that provides a cancer cell with a fundamental growth advantage for its neoplastic transformation. By targeting the driver mutation, the therapy will alter the disease outcome. RET fusion resected NSCLC has similar median recurrence-free survival and mOS when compared to RET fusion negative patients. But in the metastatic setting, RET fusion NSCLC who had received multi-kinase inhibitor to RET had better mOS than those who did not (49.3 months versus 15.3 months, p<0.001) [Tan et al. J Thorac Oncol 2020;15(12):1928-1934]. Despite the modest anti-tumour activity of multi-kinase inhibitor to RET, Hedge et al.[ESMO Open 2020;5(5):e000799] reported a trend towards better mPFS with multi-kinase inhibitors over immunotherapy (9.3 months versus 3.4 months, p=0.16). These findings resemble that of ALK positive NSCLC and thus RET fusion is a driver mutation.
Treatment Goals
What are the most important goals that an ideal treatment would address?
In the advanced or metastatic NSCLC setting, the goals of therapy are, in the order of priority,
Improvement in mOS: the holy grail for all anti-cancer systemic therapy. But in a randomized trial with a crossover design, especially if there is a high crossover rate from the standard of care arm to the experimental arm and the ORR and mPFS of the experimental arm are high, there will be a good chance that the mOS will not be significantly improved as in PROFILE 1014 and the recently updated J-ALEX study [Solomon et al. J Clin Oncol 2018;36(22):2251-2258 and Yoshioka et al. PASCO 2021;39(15_Suppl):A9022]. The mOS from any non-comparative trials can be used for benchmarking with randomized data for potential major difference in OS outcome.
Rapidity of and prolonged improvement in lung cancer related symptoms measured by median time-to-response, ORR, or progressive disease rate and mPFS: As majority of advanced or metastatic NSCLC are symptomatic at the time of initial diagnosis and at the time of progression from prior therapy, early and prolonged symptoms improvement without disease progression radiologically will provide clinically relevant improvement in health-related quality-of-life.
Toxicity: Incidences of Grade 2 toxicity experienced daily and Grade 3 or higher clinically important toxicity and dose reduction or dose discontinuation are especially important to consider for any systemic therapy. For one, constant grade 2 toxicity, such as nausea, vomiting, diarrhea, and so on, can negatively impact on the quality-of-life (QoL) of patients and oral medication adherence. The latter can further adversely affect the real life efficacy or effectiveness of an oral therapy. Second, as mentioned above, advanced, or metastatic NSCLC patients have high symptom burden, which can further impair patient well-being in the setting of frequent and clinically significant toxicity.
Prevention or treatment of brain metastases: Up to 40% of advanced or metastatic NSCLC can present with brain metastases during their treatment journey. As reported by Peters et al. [Cancer Treat Rev. 2016;45(2):139-162], brain metastases have a negative impact on QoL and carry a poor prognosis. Only a small number of mNSCLC patients will be candidates for surgical resection and stereotactic brain radiation/gammaknife (GK). The majority will be treated with whole brain radiation (WBRT), which carries significant short-term and long-term toxicity, such as immediate memory loss, loss of higher cortical function and fatigue, can negatively impair the functional status, independence and QoL of patients. Therefore, brain penetrating systemic therapy, not only treat but also prevent/delay brain metastases, will improve the QoL and preserve functional status of mNSCLC patients.
Resource utilization: Intravenous systemic therapy is given every 3-6 weeks, requiring resources for clinical assessment, laboratory investigation and drug administration for 1-3 hours, depending on the regimen used. But oral therapy can potentially reduce resources used, especially if there is a low incidence of grade 2 toxicity requiring clinical intervention and grade 3 or 4 toxicity. This is especially important in the Canadian setting due to clinic and chemotherapy daycare space constraints.
Impact of COVID on safety on systemic therapy: With ongoing issue with COVID, oral therapy will reduce the patient footprint in cancer centres, which can reduce the chance of outbreak and the exposure to potential COVID infection. Oral therapy can minimize disruption of therapy. Currently, chemotherapy, radiation and immunotherapy are considered to have increased risk for serious outcome from COVID due to their effect on the immune system, as compared to targeted agents.
Treatment Gaps (Unmet Needs)
Considering the treatment goals in the previous section, please describe goals (needs) that are not being met by currently available treatments.
Improvement in OS: At this time, there is no randomized data of selpercatinib versus standard therapy in the RET fusion mNSCLC setting. The updated LIBRETTO-1 data by Besse et al. in ASCO 2021 [PASCO 2021:A9065] reported 2-year OS rates for the 218 previously-treated patients and the 48 treatment naïve patients. In the treatment-naïve setting, the 2-year OS rate was 88% for selpercatinib. In comparison, the 2-year OS rate was only 43% with pembrolizumab and 30% with platinum/pemetrexed for patients with PDL-1 > 50% from the KN 024 trial [Reck et al. J Clin Oncol 2019;37(7):537-546]; this 2-year OS rate was 45.7% with chemotherapy/pembrolizumab and 27.3% for platinum/pemetrexed alone from the KN189 trial [Gray et al. WCLC Jan 2021]; in addition, the real world mOS was 23.6 months with platinum/pemetrexed as reported by Gautschi et al.[J Clin Oncol 2017;35(13):1403-1410]. In the setting of previously-treated patients, the 2-year OS rate for selpercatinib was 67% as compared to the real world mOS for chemotherapy +/- immunotherapy of 16.2-24 months.
Rapid and prolonged improvement in lung cancer related symptoms measured by median time-to-response, ORR, or progressive disease rate and mPFS: As previously discussed in the Current Treatments section, the real world mPFS for carboplatin/pemetrexed/pembrolizumab, the most common regimen used in the advanced or metastatic NSCLC setting regardless of PDL-1 status, was similar between those with or without RET fusion (5.7 months versus 6.6 months, p=1.0). This is similar with that reported in the randomized, phase 3 studies in the treatment-naïve setting for the PD(L)1 +/- chemotherapy arms. Besse et al reported the updated mPFS by central review for selpercatinib in the treatment-naïve setting as not reached.
In the pretreated setting, the mPFS in unselected patients receiving either PD(L)1 or docetaxel were 2-4.7 months and 4 months, respectively, as discussed in the Current Treatments section, respectively; in contrast, it was 19.3 months by central review for selpercatinib.
From the analysis of ORR with prior first-line therapy in the 218 previously treated RET fusion NSCLC patients from the LIBRETTO-1 trial, the ORRs for chemotherapy/PD(L)1, single agent PD(L)1, chemotherapy, or multi-kinase inhibitor to RET were 14%, 3%, 15% and 19%, respectively. In contrast, the corresponding ORRs to subsequent salpercatinib were 57%, 48%, 58%, and 64%, respectively. The primary progression rate for first-line therapy in this cohort was 28% while that of subsequent selpercatinib was only 6%. The ORR for selpercatinib in the treatment-naïve setting was 85% with primary progression rate of only 7%. [Drilon et al. PASCO 2021:A9032]
Toxicity (Table 5)
Criteria | LIBRETTO-1 | KN024 | KN189 | ||
|---|---|---|---|---|---|
Chemotherapy | Pembrolizumab | Chemotherapy | Chemotherapy + pembrolizumab | ||
Treatment-related grade 3-4 toxicity (%) | 32% | 53.3% | 26.6% | 42.1% | 52.1% |
Treatment-related discontinuation of therapy (%) | 6.7% | 10.7% | 7.1% | 10.9% | 29.4% |
All cause related death (%) | 3.9% | NA | NA | 5.9% | 6.7% |
Treatment-related death (%) | 0% | 2.0% | 1.3% | NA | NA |
Unique toxicities have been reported with selpercatinib: [Drilon et al. NJEM 2020;383(9):813-824]
There is a hypersensitivity reaction that usually occurs in 5% of patients (including 1.7% presented as grade 3) commonly during early treatment trajectory. It was commonly managed with dose reduction.
Prolongation of QT interval occurs in a total of 7% (any grade) and 4% (grade 3 or higher). Torsade de Pointe was not seen, and the asymptomatic prolongation of QT interval was managed with dose reduction.
Elevated AST/ALT occurred in 33% of patients, but <10% were of grade 3 or higher.
All the above toxicity will require frequent clinical, laboratory and ECG monitoring especially at the beginning of therapy. Clinician, pharmacist and ultimately patient education and communication of these unique toxicities, and in particular QT prolongation, will be necessary during clinical adoption.
As a comparison, the clinical adoption of immune-related toxicity from PD(L)1 alone or in combination with chemotherapy also required additional clinical, laboratory and imaging follow-up, until these toxicities were routinely assessed and managed. The same applies to hyperlipidemia with lorlatinib, and pneumonitis with EGFR inhibitors.
Patient education on drug related toxicity and outpatient monitoring and management protocols will reduce the probability of toxicity leading to dose interruption, dose reduction, dose termination and mortality and morbidity from any therapy as well as health care utilization.
Prevention or treatment of brain metastases: Based on the longitudinal CNS metastases data by Lee et al. [Jpn J Clin Oncol 2020;5(5):584-601], >60% of patients with metastatic RET fusion NSCLC developed CNS disease after 24 months of follow-up.
Selpercatinib is a CNS penetrating RET inhibitor. Subbiah et al. [Clin Cancer Res 2021;27:4160–167] reported that 80 RET fusion mNSCLC patients from the LIBRETTO-1 study presented with brain metastasis at baseline, of which 22 had measurable disease and 58 had non-measurable but evaluable disease. At the time of the report, 50 were censored and the intracranial mPFS by independent review was 13.5 months. Further, 46/80 (58%) had ongoing CNS response after a median follow-up of 9.5 months. Of the 22 patients with measurable disease, the intracranial ORR was 82% and disease-control rate of 100%, with a 12-month progression-free rate of 55%.
Four retrospective studies [Baerz et al. Lung Cancer 2010;68:264-268; Bailon et al. Neuro Oncol 2012;14(4):491-495; Yu et al. Medicine 2019;98(3):e14110; and Barlesi et al Ann Oncol 2011;22(11):2466-2470] reported the intracranial ORR of 40% (38.4%-41%) and median intracranial PFS of 7.4-9.5 months with pemetrexed-based therapy for those who have untreated or progressing brain metastases. Equren-Santamaria et al. [Clin Cancer Res 2020;26:4186-4192] performed a meta-analysis of PD(L)1-based therapy in unselected mNSCLC with either asymptomatic or progressing brain metastases, and reported an intracranial ORR of 0-27%. Specifically, the prospective study by Goldberg et al. [JCO 2018:35(15_Suppl:2009)] reported an intracranial ORR of almost 30% in the 34 highly selected patients with PDL-1 >1% mNSCLC who had CNS metastases that measured <2 cm, were asymptomatic, and who did not require steroid. The largest retrospective study of 73 patients reported an intracranial ORR of 35.7% and 11.1% for those with PDL-1 expression > 1% and <1%, respectively [Hendriks et al. J Thorac Oncol 2019;14:1244-1254].
Resource utilization: Selpercatinib is an orally administered agent that will utilize no chemotherapy daycare services. Although clinical assessments for toxicity and response are needed, follow-up of QT interval, AST/ALT and other laboratory related toxicity can occur with virtual or in-person clinic visits. But platinum/pemetrexed, PD(L)1, and their combinations will require more clinical and laboratory evaluation. Immune-related toxicity though more commonly occurs during the first 3-6 months of single agent PD(L)1, and later in platinum/pemetrexed/PD(L)1, can happen at any time. The majority of these toxicities will require ongoing and urgent clinically assessments in scheduled ambulatory, unscheduled acute care and inpatient settings.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Only 1-2% of all advanced or metastatic NSCLC patients harbour RET fusion. All advanced or metastatic RET fusion NSCLC patients with ECOG 0-3, including those with treated or untreated brain metastases and with or without prior systemic therapy, should be candidates for selpercatinib.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Newly diagnosed RET fusion mNSCLC: Based on the ORR, mPFS and intracranial ORR of selpercatinib relative to chemotherapy, immunotherapy, or their combinations, selpercatinib should be offered as first-line therapy in all newly diagnosed RET fusion mNSCLC with ECOG 0-3. As discussed in the Current Treatments section, it is unclear whether the most optimal second-line therapy should be platinum/pemetrexed or platinum/pemetrexed/pembrolizumab for RET fusion mNSCLC with PDL-1<50% and platinum/pemetrexed or pembrolizumab or platinum/pemetrexed/pembrolizumab for those with PDL-1> 50%. For subsequent therapy, docetaxel, and anti-PD(L)1 therapy for those who have not received such agents in prior lines of therapy can be considered.
Previously-treated RET fusion mNSCLC: Based on the updated efficacy, measured by ORR, mPFS and intracranial ORR, patients with prior therapy and patients who were identified to have RET fusion after receiving prior therapy should receive selpercatinib.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
Based on the treatment paradigm for mNSCLC that those with a driver mutation should be treated with the corresponding tyrosine kinase inhibitor based on higher ORR, longer mPFS and intracranial activity, RET fusion mNSCLC should be treated with a RET targeted agent, such as selpercatinib, once the driver mutation is documented. To date, all available systemic therapy for mNSCLC, including chemotherapy, anti-PD(L)1 therapeutics and their combinations have not demonstrated better outcome and toxicity profile.
How would this drug affect the sequencing of therapies for the target condition?
Newly diagnosed RET fusion mNSCLC: Based on the ORR, mPFS and intracranial ORR of selpercatinib relative to chemotherapy, immunotherapy, or their combinations, selpercatinib should be offered as first-line therapy in all newly diagnosed RET fusion mNSCLC with ECOG 0-3. As discussed in the Current Treatments section, it is unclear whether the most optimal second-line therapy should be platinum/pemetrexed or platinum/pemetrexed/pembrolizumab for RET fusion mNSCLC with PDL-1<50% and platinum/pemetrexed or pembrolizumab or platinum/pemetrexed/pembrolizumab for those with PDL-1> 50%. For subsequent therapy, docetaxel, and anti-PD(L)1 therapy for those who have not received these agents in prior lines of therapy can be considered.
Previously-treated RET fusion mNSCLC: Based on the updated efficacy, measured by ORR, mPFS and intracranial ORR, patients with prior therapy and patients who were identified to have RET fusion after receiving prior therapy should receive selpercatinib.
Which patients would be best suited for treatment with the drug under review?
The most appropriate mNSCLC patients to be treated with selpercatinib are those whose tumour or blood have documented RET fusion by validated molecular diagnostic, including but not limited to next generation sequencing (NGS) or FISH.
How would patients best suited for treatment with the drug under review be identified?
Ideally, all mNSCLC, regardless of histological subtypes, should have either tumour or blood tested for RET fusion by NGS or FISH. Scientific literature reports that RET fusion is a rare event in squamous histology. At the least, all non-squamous mNSCLC should have RET fusion tested using validated methods, not limited to NGS or FISH. Every province either has implemented or will be implementing NGS including RET due to cost effectiveness over gene-by-gene molecular diagnostics including EGFR, ALK, ROS1, BRAF V600E, KRAS, NTRK 1-3 and RET. Below is a table on the availability of RET testing in all the provinces.
Table 6: Availability of RET Testing in All Provinces
Province | Availability of RET Fusion Testing | Funding of RET Testing |
|---|---|---|
Newfoundland | Unknown | Unknown |
New Brunswick | Yes by NGS | Yes |
Nova Scotia | Yes by NGS | No |
Prince Edward Island | Unknown | Unknown |
Quebec | Limited to Montreal area by McGill University | No |
Ontario | Yes by NGS | Yes |
Manitoba | Yes by NGS | Yes |
Saskatchewan | Yes by NGS | No |
Alberta/Northwest Territories | Yes by NGS in November | Yes |
British Columbia/Yukon | Yes by NGS | Yes |
Which patients would be least suitable for treatment with the drug under review?
The benefit of selpercatinib is demonstrated in RET fusion NSCLC patients both in the treatment-naïve and previously treated setting regardless of the 5’ fusion partners. It is debatable whether ECOG 3-4, RET fusion NSCLC should be offered selpercatinib. Given less than 5% of RET fusion NSCLC has primary progression and the median time to response was < 2months from LIBRETTO-1, one can argue that those with ECOG 3 should be selpercatinib. Only RET fusion negative NSCLC patients and RET fusion NSCLC with ECOG 4 will not be candidate for selpercatinib.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
There is no other predictive biomarker for efficacy identified for salpercatinib in RET fusion NSCLC in LIBRETTO-1 study.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
In clinical practice, selpercatinib will continue until one or more of the following conditions is/are fulfilled:
Toxicity despite multiple dose reductions
Patient preference
Concurrent medical condition(s) that will jeopardize the safety of selpercatinib
Symptomatic disease progression except
those who have oligoprogression that are amendable to aggressive local therapy such as radiation or surgery. Based on study by Gomez et al. from MD Anderson Cancer Centre, patients who experienced oligoprogression had an improvement in both mPFS (14.2 months versus 4.4 months. P=0.022) and mOS (37.6 months versus 9.4 months, p=0.034) with aggressive local therapy over observation or continuation of systemic therapy. [Gomez et al. 2019;37(18):1558-1565.]
those who have newly diagnosed or progression of brain metastases who should continue with selpercatinib after receiving brain radiation.
those who have asymptomatic disease progression, also known as treatment beyond RECIST progression.
What would be considered a clinically meaningful response to treatment?
In clinical practice, the definition of a clinically meaningful response to selpercatinib is defined as:
documentation of lung cancer-related symptoms stabilization or improvement by frequency and severity with or without radiological evidence of tumour shrinkage, or
documentation of radiographic reduction of documented sites of known disease at baseline.
How often should treatment response be assessed?
Given the median time to response is <2 months, the first assessment for both toxicity and CXR response can occur by 1-2 months from initiation of selpercatinib. Like other oral tyrosine kinase inhibitors, imaging by CT/MRI for response the selpercatinib of known sites of primary and metastatic disease can be performed every 3 months. Based on the longitudinal CNS metastases data by Lee et al. [Jpn J Clin Oncol 2020;5(5):594-601], >60% of RET fusion mNSCLC patients developed CNS disease at 24 months, the implementation of MR brain at initiation of therapy and every 3 months thereafter probably until termination of selpercatinib will be necessary. Subbiah et al. [Clin Cancer Res 2021;27:4160–167] reported 80 RET fusion mNSCLC patients had brain metastasis at baseline, of which 22 had measurable disease and 58 had non-measurable but evaluable disease. At the time of the report, 50 were censored and the intracranial mPFS was 13.5 months and 46/80 (58%) had ongoing CNS response after a median follow-up of 9.5 months. Long-term follow-up data is needed to confirm the duration of MR brain required.
What factors should be considered when deciding to discontinue treatment?
In clinical practice, selpercatinib will continue until one or more of the following conditions is/are fulfilled:
Toxicity despite multiple dose reductions
Patient preference
Concurrent medical condition(s) that will jeopardize the safety of selpercatinib
Symptomatic disease progression except
those who have systemic oligoprogression that are amendable to aggressive local therapy such as radiation or surgery. Based on study by Gomez et al. from MD Anderson Cancer Centre, patients who experienced ologoprogression had an improvement in both mPFS (14.2 months versus 4.4 months. P=0.022) and mOS (37.6 months versus 9.4 months, p=0.034) with aggressive local therapy over observation or continuation of systemic therapy.
those who have newly diagnosed or progression of brain metastases who should continue with selpercatinib while receiving brain radiation.
those who have asymptomatic disease, also known as treatment beyond RECIST progression.
What settings are appropriate for treatment with the drug under review?
Treatment with selprecatinib can be delivered through both academic and community cancer settings, like other orally administered tyrosine kinase inhibitors.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
NA
Additional Information
Is there any additional information you feel is pertinent to this review?
No comments
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Quincy Chu
Position: Medical Oncologist, Cross Cancer Institute
Date: Sep 18 2021
Table 7: Declaration for Lung Cancer Canada Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Abbvie | X | — | — | — |
Amgen | X | — | — | — |
Astellas | X | — | — | — |
Astra Zeneca | — | X | — | — |
BI | X | — | — | — |
BMS | — | X | — | — |
Eli Lilly | X | — | — | — |
Eisai | X | — | — | — |
J and J | X | — | — | — |
Merck | X | — | — | — |
Novartis | — | X | — | — |
Pfizer | X | — | — | — |
Roche | X | — | — | — |
Takeda | X | — | — | — |
Merck KgaA- DSMB | — | — | — | — |
Astra Zeneca-research funding | — | — | — | — |
Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancers Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancers Drug Advisory Committee
Please describe the purpose of your organization. Include a link to your website (if applicable).
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Please describe how you gathered the information included in the submission.
This input was jointly discussed via email.
Current Treatments
Describe the current treatment paradigm for the disease
Currently chemotherapy and immunotherapy, palliative care, radiation.
Treatment Goals
What are the most important goals that an ideal treatment would address?
Prolong life, delay disease progression, improve health-related quality of life
Treatment Gaps (Unmet Needs)
Considering the treatment goals in the Treatment Goals section, please describe goals (needs) that are not being met by currently available treatments.
All patients have current treatments fail within months to short years.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Patients with a targetable RET fusion mutation
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Will be used as first or second line treatment depending on when fusion is identified. Given characteristics of this group, will mainly be used as first line treatment.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
No, it would not.
How would this drug affect the sequencing of therapies for the target condition?
After selpercatinib, other non-kinase targeted treatments would be used (immunotherapy, chemotherapy)
Which patients would be best suited for treatment with the drug under review?
No response.
How would patients best suited for treatment with the drug under review be identified?
Metastatic lung cancer with RET fusion.
Which patients would be least suitable for treatment with the drug under review?
No RET fusion.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
Yes, next generation sequencing including RNA.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Response on scans, symptoms. Yes.
What would be considered a clinically meaningful response to treatment?
Improvement in symptoms, stabilization (no deterioration) in symptoms. It is not likely to be physician dependent.
How often should treatment response be assessed?
Every clinic visit (4-8 wks) with history and physical, imaging at discretion of treating physician.
What factors should be considered when deciding to discontinue treatment?
Disease progression (unequivocal global disease progression on imaging or symptomatic worsening)
What settings are appropriate for treatment with the drug under review?
Outpatient specialty clinics
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
NA
Additional Information
Is there any additional information you feel is pertinent to this review?
None.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Gail Darling
Position: Cardiothoracic Surgeon/Ontario Cancer Lead
Date: 13 Sept 2021
Table 8: Declaration for Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancers Drug Advisory Committee Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Eli Lilly - No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Andrew Robinson
Position: Medical oncologist
Date: 10 Sep 2021
Table 9: Declaration for Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancers Drug Advisory Committee Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Eli Lilly - No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.