CADTH Health Technology Review
Emergency Department Overcrowding: An Environmental Scan of Contributing Factors and a Summary of Systematic Review Evidence on Interventions
Environmental Scan and Summary
Authors
Environmental scan of contributing factors: Robyn Haas, Francesca Brundisini
Summary of systematic review evidence on interventions: Angela Barbara, Nazia Darvesh, Lindsay Ritchie
Research Information Services: Danielle MacDougall, Carolyn Spry
Program development: Jeff Mason
Content expertise: Justin Hall, Warren Ma, Ivy Cheng
Acknowledgements
The authors would like to thank Grant Innes and Maggie Keresteci for reviewing the project protocol. The authors would like to acknowledge Allison Gates, Renata Axler, Ana Komparic, Sean Secord, Amil Reddy, Murray Maracle, David Kaunelis, Pierre Martinelli, Gino De Angelis, and Laura Weeks.
Reviewers
These individuals kindly provided comments on a draft version of this report:
Edward Xie, MD, MSc, CCFP(EM), DTM&H
Assistant Professor, University of Toronto
Toronto, Ontario
Peter Vanberkel, PEng, PhD
Professor, Dalhousie University
Halifax, Nova Scotia
Abbreviations
AMSTAR 2
A MeaSurement Tool to Assess systematic Reviews 2
ATP
advanced triage protocol
CFIR
Consolidated Framework for Implementation Research
ED
emergency department
HTERP
Health Technology Expert Review Panel
LOS
length of stay
NRS
nonrandomized study
RCT
randomized controlled trial
Key Messages
Emergency department (ED) overcrowding occurs when the demand for health services in the ED exceeds the capacity of the ED, hospital, or community to deliver quality care in a reasonable amount of time. Overcrowding is worsening in jurisdictions across Canada and there is a need to address its many causes and identify potential solutions.
This report uses a modified version of a conceptual model developed by Asplin et al. (2003) that organizes the emergency care system into 3 interdependent parts: input (arrival to the ED), throughput (flowing through the ED), and output (leaving the ED). We also examined an additional fourth part related to contextual factors and systems that affect overcrowding but lay outside of input, throughout, and output.
Examples of factors include, but are not limited to, increased complexity of needs (input), diagnostic testing and procedures (throughput), boarding (output), and limited resources for mental health and substance use (outside the ED).
Examples of interventions that were effective in some settings include, but are not limited to, prehospital decision-making by first responders, which reduced ED visits (input); short stay crisis units for people experiencing mental health challenges, which improved emergency department length of stay, wait times, boarding, and patient safety (throughput); ED-based discharge planning, which reduced ED return visits (output); and time-based policy reforms, which reduced ED length of stay (outside the ED).
Most of the factors we identified in the published literature existed either outside of the ED or at the interface of the ED and other health care services (input and output), whereas most of the interventions we identified existed within the ED (throughput).
We heard from participants (during multistakeholder dialogue sessions) and content experts that ED overcrowding is a complex health system issue for which the causes, impacts, and solutions extend beyond the ED. Specifically, the novel insights we heard included:
ED overcrowding is better viewed as a problem of hospital overcrowding and strained resources in the broader social and health care systems. Contributing factors both within and outside the ED influence and interact with each other and are affected by economic, cultural, and institutional realities.
Solving the issue requires addressing accountability and implementing multifaceted solutions in which several systems and voices work collaboratively.
Existing technologies and data use and collection are not being used to their full potential; they can be better leveraged to alleviate this issue.
In the identified literature, there was a lack of explicit reporting around equity and ethical considerations for factors contributing to, and interventions to alleviate, ED overcrowding. Future work should strive to deliberately and explicitly include ethical considerations inherent in research, planning, and policy-making; considerations of equity-deserving groups; and dedicate the time needed to consider the various facets of this issue.
This CADTH report and our series of reports on ED overcrowding are a starting point to bridge the literature, stakeholder discussion, and expert opinion to help decision-makers understand the various parts of the issue and consult the relevant updated evidence to inform their work.
What Is the Issue?
Recent evidence suggests that the problem of emergency department (ED) overcrowding, the situation where the demand for health services in the ED exceeds the ability to provide care in a reasonable amount of time, is worsening in jurisdictions across Canada.1,2
Between April 2021 and March 2022, approximately 14 million patients visited EDs in Canada.3
ED overcrowding puts patients’ lives and health at risk when health care monitoring and intervention needs within the ED exceed the resources required to address them.1
The causes and consequences of ED overcrowding are complex and varied and extend beyond the ED.1,4,5 Left unchecked, ED overcrowding contributes to a deteriorating standard of care as staff become overworked and burned out.4
What Did We Do?
The objectives of this report are to understand what has been published in the literature about factors contributing to overcrowding, and what has been published in the literature about the effectiveness of interventions:
To address these objectives, we conducted:
an environmental scan to identify literature about factors contributing to ED overcrowding internationally and in Canada
a summary of systematic review evidence on the effectiveness of different interventions to alleviate ED overcrowding.
Multistakeholder dialogue sessions6 were conducted in the summer of 2023 to discuss the interim results describing factors contributing to ED overcrowding and potential interventions that have been studied, in addition to hearing perspectives about local context and implementation issues, and to identify and discuss important concerns. Participants included clinical, patient, and community members and we heard perspectives from people who identified as emergency physicians, pediatric emergency physicians, emergency nurses, pediatric researchers, pharmacists, patient and family advisors, directors, geriatric psychiatrists, and emergency medicine residents.
For clarity and continuity across this health technology assessment, CADTH has adopted the following definitions:
ED: a hospital unit intended to provide timely evaluation, diagnosis, and treatment of people with injuries, illnesses, behavioural disorders, and mental health conditions who require expeditious care for potentially life-threatening conditions (e.g., severe chest pain, stroke, trauma) without a prior appointment.
ED overcrowding: an imbalance where the demand for health services in the ED exceeds the capacity of the ED, hospital, or community to deliver quality care in a reasonable amount of time1,7
Why Did We Do This?
Changes in the body of evidence and the collection and reporting of data about ED use in Canada since CADTH’s 2006 4-report series8-11 have contributed to jurisdictional needs for objective, impartial, and trusted guidance about causes and consequences, and which interventions are most effective for alleviating ED overcrowding in Canada.
This pan-Canadian issue calls for real solutions and CADTH is examining the evidence and expert-informed considerations about the causes and consequences of, and solutions to, ED overcrowding in health care systems across the country.
The information presented in this report will be used to inform and support policy- and decision-making related to an emerging administrative priority about ED wait times in a health care environment that is seeing ED visitations return to pre–COVID-19 pandemic levels.12
What Else Is CADTH Doing?
This report is part of a series of publications that CADTH produced on the topic of ED overcrowding in Canada as an update to our 2006 publications.8-11 Separate publications not described in this report will be published in the fall of 2023 to address:
the impact ED overcrowding has on quality of care and patient safety (i.e., the risks of overcrowding), and on health professional learner experiences and staff well-being
how ED overcrowding in Canada has changed since the last series of reports
the identification of new and emerging interventions to alleviate ED overcrowding (those not captured in this summary of systematic review evidence on intervention effectiveness)
a summary of CADTH’s multistakeholder dialogue sessions.
CADTH’s Health Technology Expert Review Panel (HTERP) will use the CADTH deliverables as inputs into deliberations that will result in the development of guidance to address the decision problem of what evidence-informed solutions should be considered to guide decision- and policy-making to effectively alleviate overcrowding of adult and pediatric ED services in urban, rural, and remote health care settings in Canada?
What Did We Find in Our Environmental Scan and Summary of Systematic Reviews?
ED overcrowding is an international, complex, and multifactorial issue. This project set out to identify as many factors contributing to, and interventions to alleviate, ED overcrowding as were available in the included literature. Some factors and interventions may not have been identified in this research, and some may be more relevant and applicable than others, depending on the context of the place where one lives, works, and receives health care.
Quantity of Research Available
Environmental Scan
We identified 1,542 articles and included 27 that described factors contributing to ED overcrowding.1,7,13-37
For causal factors contributing to ED overcrowding, 67% of the articles discussed input factors, 63% of the articles discussed throughput factors, and 85% of the articles discussed output factors. For contextual factors contributing to ED overcrowding, 7% of the articles discussed micro-level factors, 30% of the articles discussed meso-level factors, and 30% of the articles discussed macro-level factors.
The articles detailed public, private, and public-private EDs in urban locations, some of which had academic affiliations. Several articles described EDs as specialized or tertiary care centres. The EDs served pediatric, adult, and older adult populations. Of the 27 included articles, 48% did not specify setting details and 52% did not specify population age.
The types of literature included were primary studies, systematic reviews, narrative reviews, position statements, and technical and/or task force reports.
Four articles were specific to the Canadian context.1,17,18,37
In terms of equity characteristics, 15% of the articles reported on people with mental health conditions and 4% of the articles compared ED overcrowding in a high-income setting to ED overcrowding in a low-income setting.
Summary of Systematic Review Evidence on Interventions
We included 64 systematic reviews that reported on the effectiveness of interventions to alleviate ED overcrowding.29,38-100 Inclusion criteria are provided in the Supporting Information document.
Approximately 50% of the included systematic reviews included adult populations (those aged 18 years and older), 33% included pediatric patients (those aged up to 18 years), 33% included older adults (those aged 65 years and older), and 2 systematic reviews included adolescents (as defined by the systematic review authors). Twenty percent of the systematic reviews did not report which specific age groups were included.
Approximately 25% of the systematic reviews included primary studies that took place in urban settings. Nine percent of the systematic reviews40,58,63,70,75 included at least 1 primary study in a rural setting. Two systematic reviews63,81 included at least 1 primary study set in a remote area. Sixty-three percent of the systematic reviews did not specify the setting in which the interventions were assessed or the location of the ED.
Twenty-five percent of the systematic reviews reported input interventions, 67% of the systematic reviews included throughput interventions, 6% of the systematic reviews reported output interventions, 16% of the systematic reviews included postdischarge case management interventions, 2% of the systematic reviews included hospital-wide collaboration with ED interventions, 8% of the systematic reviews included policy reform interventions, and 14% of the systematic reviews included multicomponent interventions.
Equity Characteristics
Forty-seven percent of the systematic reviews included at least 1 primary study conducted in Canada.
Twenty percent of the systematic reviews reported the “sex” of the population, although it is unclear whether it was sex or gender identity as this was poorly defined and reported in the literature.40,42,46-48,52,59-61,68,82,89,96
Eight percent of the systematic reviews reported disability status (e.g., using activities of daily living) in people with specific medical conditions and/or older adults.44,66,82,84,98
Twenty percent of the systematic reviews reported on studies with people experiencing mental health challenges,40,44,47,53,63,72,82,84,85,94-96,100 and 5% of the systematic reviews focused on throughput interventions for people experiencing mental health challenges.41,58,80
Five percent of the systematic reviews included people experiencing substance use challenges.44,47,74
Five percent of the systematic reviews reported on studies that included people with lower incomes.81,82,84
Three percent of systematic reviews reported on studies with people who were experiencing houselessness.44,96
One and a half percent of systematic reviews reported on studies that included people whose first language was not English.81
Six percent of the systematic reviews reported on studies that identified the race or ethnicity of the included population.64,81,82,89
Nine percent of the systematic reviews reported on studies of people with lower socioeconomic status.51,54,81,82,84,91
None of the systematic reviews reported any information about gender identity, newcomer status, or sexual orientation.
The characteristics of the included systematic reviews are provided in the detailed findings tables in the Supporting Information document.
Confidence in the Results of the Included Systematic Reviews
The assessments of our confidence in the results of the 64 included systematic reviews, which we conducted with A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2),101 are presented in the Supporting Information document. Our confidence in the results of almost half of the systematic reviews (47%) was moderate. We had high confidence in the results of 8% of the systematic reviews, and low or critically low confidence in the results of 41% and 5% of the systematic reviews, respectively.
Summary of Findings
Environmental Scan
The objective of this environmental scan was to identify and describe the causal and contextual factors contributing to ED overcrowding, as described in the literature. We included 27 articles from the published and grey literature.
Setting and Population Age
We collected information about the setting and population served as it was described in each of the articles. We did not identify any notable trends in the relationship between the causes of ED overcrowding and the ED setting and/or populations served. We extracted data related to geographic location (e.g., country, jurisdiction), ED location (i.e., urban, rural, remote), and ED type (e.g., community, academic). For the population, we extracted data related to the age group served (e.g., pediatric, adult). Articles that examined EDs in individual countries included those in Australia, Canada, China, Ireland, Italy, Japan, the Netherlands, Nigeria, Pakistan, South Africa, South Korea, Turkey, the UK, and the US.1,13-20,22,23,25-27,30-33,35-37 Additionally, 3 articles reported information and data from multiple countries, including Australia, Canada, Denmark, Germany, Ghana, Hong Kong, Japan, India, Italy, New Zealand, Saudi Arabia, Singapore, the Netherlands, Thailand, Turkey, the UK, and the US.7,21,29 Eight articles reported information on EDs in an urban location, while no articles reported information on rural or remote EDs.15,17,18,22,25,30,36,37 Six articles focused on EDs that were classified as either academic, university-affiliated, or teaching.16,22,25,27,30,36 Three articles reported information on public EDs,13,26,27 3 articles reported information on private EDs,13,26,35 and 1 article reported on a public-private ED.26 The public and private status refers to the ownership and funding of a hospital (e.g., a public hospital receives government funding). Four articles reported information on tertiary care centres, level I EDs, or level II EDs, meaning that they had some degree of specialization and handle more complicated cases.15,26,35,37 One article reported information on a general ED, meaning that it was not specialized.26 Finally, 1 article reported information on an ED dedicated to veterans.15 Thirteen articles did not report setting details aside from country.1,7,14,19-21,23,24,28,29,31-34 Two articles included information relevant to pediatric populations only,19,37 6 articles included information relevant to adult and older adult populations,16-18,27,30,36 and 5 articles included information relevant to populations of all ages.15,22,29,33,35 Fourteen articles did not report information on population age.1,7,13,14,20,21,23-26,28,31,32,34
Equity Characteristics
In addition to collecting details about the setting and population age groups included in the articles, we also sought to extract data about additional equity-deserving group characteristics (e.g., 2SLGBTQ+ identity, racial and ethnic identity), if they were described in the literature. Few of the included articles reported any additional information on equity-deserving group characteristics. Two articles noted that patients living with mental health conditions were at greater risk of harm due to ED overcrowding.19,23 Two articles also noted that the number of individuals who are seeking care for mental health conditions in the ED is increasing and that these patients are spending longer in the ED than those who are not seeking care for mental health conditions.14,19 These articles also discussed the factors of boarding and access block in relation to people with mental health conditions, noting that these individuals are especially susceptible to being boarded in the ED for long periods of time as a result of the limited services for mental health and addictions.14,23 Another article specifically discussed how children with mental health conditions were negatively impacted, noting that mental and behavioural emergencies were increasing among children, yet specialists in pediatric mental health services were in short supply.19 They also noted that the limited number of specialists delayed consult times for children experiencing mental health emergencies in the ED.19
One article compared overcrowding in 2 EDs; 1 ED was in a high-income country and the other was in a low-income country.35 This article found both similarities and differences in the causes of ED overcrowding in these settings. ED visits in the low-income setting were often a last resort option; when patients still needed a specialist after seeing other doctors first. In the high-income setting, ED use was primarily a result of complex conditions associated with older age.35 Throughput factors were similar in both EDs.35
We also identified literature that discussed insurance coverage. The articles examined whether disparities in insurance coverage contributed to the volume of overcrowding. Yet, they did not investigate equity implications of what it means to have different insurance coverages (e.g., insured, underinsured, uninsured) for those who may access, use, and benefit from health care services in the ED, and whether inequities related to different insurance coverages contribute to ED overcrowding. We present further details about these disparities in a later section of this report.
Equity-related details were not reported in any of the identified Canadian literature.
Figure 1 and Figure 2 present how the results of this environmental scan, and factors contributing to ED overcrowding, are categorized in this report.
Causal Factors Contributing to ED Overcrowding
We identified 25 articles that discussed the causal factors contributing to ED overcrowding. In this report, we use the term causal factors to indicate the factors contributing to ED overcrowding that could be targeted by interventions specifically aimed to alleviate ED overcrowding. We categorized these factors into 3 interdependent components as described by the conceptual model developed by Asplin et al. (2003):102 input, throughput, and output. In the following sections we present and describe these factors and provide details on how and why they contribute to ED overcrowding as discussed in the literature. Though not all identified articles provided this level of detail for each factor, the information from those who did is discussed in the following sections. The information about which factors, and how and why factors contribute to ED overcrowding, is from both international and Canadian literature. Of note, this review does not intend to measure the impact of these factors and the findings are not presented in order of magnitude of their impact.
Figure 1: Categorization of Causal Factors Contributing to ED Overcrowding
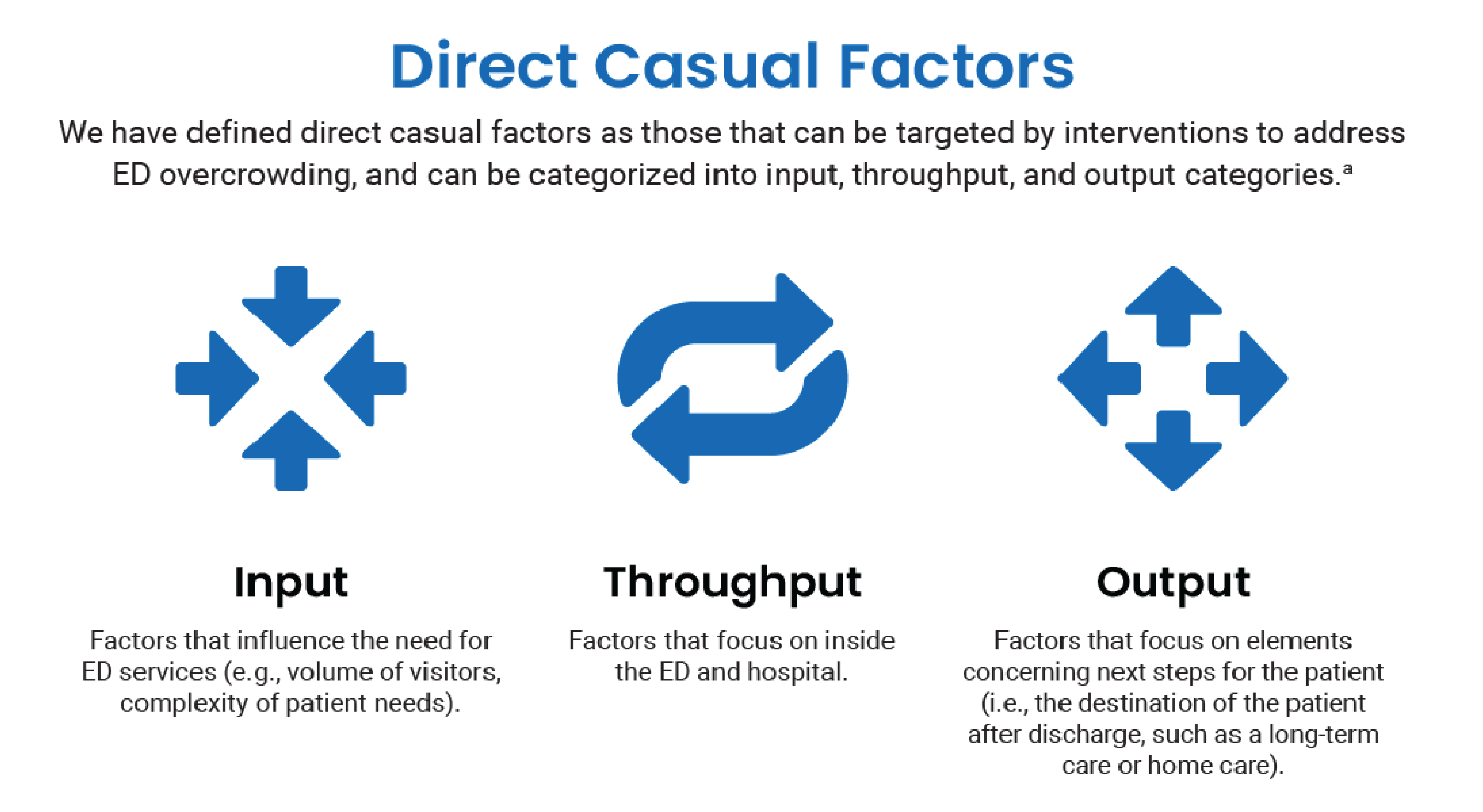
ED = emergency department.
a Input, throughput, and output are defined based on the conceptual model developed by Asplin et al. (2003).
Input Factors
Input factors are those that influence the need for ED services and relate to patient access to the ED.102 They have been described as factors that cannot be controlled by the ED.7 We identified 18 articles that discussed input factors that contribute to ED overcrowding internationally and in Canada.7,15,17,19-26,29,32-37 We categorized the identified factors into the following themes: primary care and community health services, repeated and low-acuity visits to the ED, growing patient volume and complexity of needs, and access via multiple avenues.
Primary Care and Community Health Services
The specific factors related to this theme include:
Community and outpatient care service issues: limited availability and difficulty accessing health care services (e.g., diagnostic testing) outside of the ED (4 articles).19,25,29,33
Primary care issues: limited availability of primary care providers and/or accessing their services in a timely manner (5 articles).19,21,23,29,33
Repeated Visits and Low-Acuity Visits to the ED
The specific factors related to this theme include:
Low-acuity visits: visits to the ED that could potentially be addressed in another setting (i.e., visits that would not be classified as urgent, emergent, or needing resuscitation when triaged in the ED) (7 articles).7,21,24,29,33,34,36 While we identified this factor in the literature, we acknowledge that there is also evidence that patients with low-acuity presentations have minimal impact on overcrowding and that their reasons for ED use are valid and varied.103 We have provided additional discussion in the section about the impact of input, throughput, and output factors.
People who access the ED frequently: individuals who seek care in the ED repeatedly and recurrently (2 articles).32,33
Growing Patient Volume and Complexity of Needs
The specific factors related to this theme include:
Complexity of needs: the increasingly severe or complicated care needs of people attending the ED (10 articles).7,15,20,21,23,24,29,33,35,36
Increase in older adults: the increasing proportion of older adults visiting the ED (7 articles).21,22,26,29,33,35,36
Volume of visitors: the quantity of patients, attendees, visits, and/or admissions to the ED (11 articles).7,15,18,20-23,26,33,34,37
Access Via Multiple Avenues
The specific factors related to this theme include:
Ambulance arrival: presentation to the ED via an ambulance (3 articles).7,22,24
Referral by a health care provider: presentation to the ED based on the direction of a provider outside the ED (e.g., a specialist or primary care provider) (3 articles).15,23,34
Self-referral: the presentation to the ED on one’s own (3 articles).19,22,33
These factors were included in the literature; however, the articles provided minimal description about the connections between the factors and ED overcrowding. Consequently, we were unable to comment on impact beyond what is provided in the following section.
How and Why Input Factors Contribute to ED Overcrowding
Literature that focused on issues around access to primary and community care services predominantly examined this factor in relation to the probability of ED visits for low-acuity matters, and thus, how it affects overcrowding. One study predicted that general practitioner care practices that had better access for patients could result in a decrease of self-referred ED visits by of approximately 10% and another concluded that having access to a primary care provider had the potential to reduce low-acuity ED visits by 40%.29 Finally, many primary care providers are choosing to work part-time hours, which exacerbates physician shortages, and the limited availability of primary care services.19 Of note, as mentioned earlier, we acknowledge that while the included literature identified low-acuity visits as a factor, further evidence shows that patients with low-acuity presentations have minimal impact on overcrowding and that their reasons for ED use are valid and varied.103
When considering the increasing complexity of patient needs and the volume of older adults, the literature reported that EDs were designed to serve the type of population and patients presenting to hospitals when they were established decades ago.36 Over time, the population and the needs of the populations have changed and the present set-up of the ED no longer matches these needs.36 Additionally, more complex patients require increased time and resources from providers and services.23 Consequently, this places a greater strain on ED services.23 Generally, when referring to complexity of needs, articles made reference to complexities associated with older patients and chronic conditions; however, it is likely that complexities arise in other ways that were not discussed in the literature. Two articles noted that patients who are older and/or have high acuity and complex needs are also more likely to be those who visit the ED more frequently, which can cause strain on time and resources in EDs.18,26 Another noted that people who access the ED frequently represented the patients who were the most sick, had the greatest rates of admission, had the highest mortality rates, and consumed a disproportionate number of resources, all of which can add to the burden of the health care system and therefore contribute to ED overcrowding.32 In addition to the type of patients, the volume of patients was also described as a contributor to ED overcrowding. One observational study from a Canadian ED noted a 35% increase in pediatric visits over the course of 9 years and stated that this increase was likely the reason for the deterioration of patient flow.37
While a small number of articles identified in this report described ambulance arrival, self-referral, and health care provider referral as contributing factors, the included literature does not provide a detailed understanding of why they might contribute to ED overcrowding. Arrival by ambulance is a factor that can act as both a cause and consequence of ED overcrowding. Ambulance diversion from 1 hospital, which is the result of overcrowded EDs, can lead to the arrival of ambulances at other nearby hospitals, compounding other presentations to the ED.7,24 Additionally, as 1 of our experts noted, health care standards and regulations may also play a role accessing the ED via ambulance. For example, in some Canadian jurisdictions, paramedics are mandated to bring all people who call 911 to a hospital for assessment.104,105 One article reported that the majority of people who come to the ED were those who self-referred.33 Self-referrals are connected to limited access to primary, outpatient, and community care. People may choose to self-refer to the ED for a multitude of reasons. For many, primary care providers can act as the gatekeepers to specialist and secondary care (e.g., some diagnostic testing), which can make secondary care more difficult to access when primary care is not available or accessible. Unlike primary care providers and specialists, the ED does not require appointments or referrals, offers secondary care, and might be the only way people can access secondary care. Finally, 1 study also described health care providers referring patients to the ED as contributing to overcrowding. Primary care providers and specialists may send patients to the ED because services such as imaging, laboratory tests, and consults can be provided within a matter of hours compared to days or weeks outside of the ED;23 and the same study highlights how this places additional demand on the system and services.23
Throughput Factors
Throughput factors are those that are focused within the ED.102 We identified 17 articles that discussed throughput factors that contribute to ED overcrowding internationally and in Canada.7,15-26,29,33-35 We categorized identified factors into the following themes: consultation, testing, and decision delays; staffing considerations; and operational inefficiencies.
Consultation, Testing, and Decision Delays
The specific factors related to this theme include:
Consultations for people visiting the ED: the availability and timeliness of consult services from other specialist health care providers in the hospital outside of the ED (e.g., neurology, gastroenterology) (9 articles).7,16,19,20,23-25,33,34
Diagnostic testing and procedures: the time spent waiting to receiving diagnostic testing and imaging (e.g., X-rays, blood work) in the context of limited diagnostic and imaging devices and technology capacity, as well as the time spent waiting for the results (12 articles).7,17,18,21-25,29,33-35
Disposition decision delays: the time a patient spends waiting for health care providers’ disposition decisions and recommendations (5 articles).19,21,29,33,35
Staffing Considerations
The specific factors related to this theme include:
Staff skill mix: the characteristics and make-up of staff and their experience level (e.g., learners, junior staff, experienced staff) (6 articles).7,19,24,26,29,34
Staff ratios: low staff-to-patient ratios, resulting from a shortage of numerous types of staff, including nurses, physicians, lab technicians, and so forth (10 articles).7,15,19-21,23,24,26,29,33
Barriers to Optimal Operational Efficiency
The specific factors related to this theme include:
Patient processing: the administrative processes for admitting patients to the hospital (2 articles).7,34
Patient triaging: the assessment and determination of the severity of the presentation, which can be susceptible to inadvertent change during periods of overcrowding (5 articles).7,24,33-35
Infrastructure: considerations around items such as bed availability, bed placement, and number of consultation rooms (6 articles).7,19,20,24,25,33
Simultaneous duties of staff: multiple ongoing commitments and distractions that health care providers must attend to at the same time (e.g., referral calls, electronic medical record documentation) (2 articles).23,34
How and Why Throughput Factors Contribute to ED Overcrowding
Literature focusing on throughput factors described how the need for diagnostic tests and imaging (e.g., ultrasound, CT, MRI) contribute to an increased patient length of stay (LOS), both through wait time for, and the performance of, these tests.17,18,22,23 The lengthened wait and evaluation time of patients delays assessment of new patients, ultimately contributing to overcrowding.17,18,22,23 Furthermore, in some cases, the literature quantified diagnostic testing as the largest contributing factor to patient LOS compared to all other factors identified.17,22 The articles also discuss details around staffing issues in the ED as an important factor in overcrowding. One article examined EDs in South Korea and noted that the most crowded EDs had higher overall numbers of staff but lower staff-to-patient ratios.15 Nursing shortages were noted as particularly problematic. There is a high level of burnout associated with shortages among ED nurses, which, in turn, can lead to bed closures and inefficiencies in the ED.23 This shortage and subsequent turnover of nurses can result in the hiring of less experienced nurses.23 An article discussed the consequences of less experienced staff, stating that the addition of 1 junior doctor to a shift resulted in an increased ED LOS of discharged patients by 1 minute.29 In a similar vein, consultations from physicians outside of the ED also contribute to ED overcrowding. The involvement of specialist consultations can both complicate patient throughput processes and prolong ED LOS.16,35 The reasons for this were cited as being twofold. First, because of difficulty reaching the consult physician or a delay in concluding the consultations, and second, because of waiting for the completion of consultations with patients with numerous consultation requirements.16 One article pointed out that mental health consultation services are especially limited for children, which increases their ED LOS.19 EDs are, by nature, complex environments intended to handle busy and chaotic operations.106 The size and scale of ED operations may contribute to difficulty achieving optimal operational efficiency. Specific aspects of this identified in the literature included patient processing, patient triaging, infrastructure, and the simultaneous duties of staff.
Output Factors
Output factors are those that concern patient disposition; that is, a patient’s next steps and venue of care after the ED visit (e.g., to inpatient or outpatient care).102 We identified 23 articles that discussed output factors that contribute to ED overcrowding internationally and in Canada.1,7,14,15,17-30,32-36 We categorized the identified factors into the following themes: boarding and access block, strained hospital-wide resources, and impediments to exiting the ED.
Access Block and Boarding
The specific factors related to this theme include:
Access block: a situation where patients are unable to gain access to appropriate hospital resources (e.g., inpatient beds) due to limited capacity. This is sometimes called “exit block,” depending on the geographic region (10 articles).1,14,20,21,23,29,30,33,35,36
Boarding: the practice of holding patients in the ED after they have been admitted to the hospital because inpatient beds are not available (12 articles).7,14,17-19,24,27,28,30,32,33,35
Of note, these 2 concepts are closely related to each other, and the terms may sometimes be used interchangeably. Access block may also be considered an impediment to exiting the ED; however, it is highlighted separately here due to its relation to boarding and its prominence in the literature.
Demand on Hospital Resources Outside the ED
The specific factors related to this theme include:
Inpatient volume and bed availability: the number of patients admitted to the hospital and the proportion of beds occupied by these patients (11 articles).7,15,17,19,22,24,25,29,33,34,36
Gravity of inpatient care needs: the severity and complexity of the condition(s) of those who are being treated in the hospital wards (3 articles).7,19,24
Staffing resources outside of the ED: the number and ratio of hospital staff (3 articles).7,19,24
Impediments to Exiting the ED
The specific factors related to this theme include:
Transport delays and inefficient care transfer processes: logistical and coordination issues with moving patients from within the ED to outside the ED (e.g., to an inpatient service, to long-term care, to home) (8 articles).7,23-26,30,33,34
Inpatient capping and/or blocking: a rationing strategy that uses the practice of reserving or holding inpatient beds for a specific type of patient (e.g., patients who have had surgery), typically implemented to cope with scarce resources (2 articles).23,24
Follow-up and alternate level of care resources: the availability and capacity of health and social care services to accept those leaving the ED and/or the hospital (e.g., long-term care facilities, rehab, dedicated end-of-life care) (4 articles).7,23,24,36
How and Why Output Factors Contribute to ED Overcrowding
Generally, literature focusing on output factors identified boarding and access block as major contributors to ED overcrowding. One study examined the ED LOS for input, throughput, and output phases and found that patients spent the most time in the output phase.27 Six studies noted that boarding and access block result from hospitals operating close to, or over, capacity, as well as hospital-wide inefficiencies.1,14,15,23,28,32 While other patients wait to leave or be transferred to another facility, incoming patients admitted to inpatient care cannot leave the ED to get into the hospital.35 Output factors as a whole intensify the burden on the availability of beds and physical space.7,24,33 Moreover, they also intensify the burden on other health care resources such as equipment, diagnostic tests, and the attention of staff.24 For example, health care providers may need to spend time attending to patients who have already received medical attention but cannot leave the ED due to access block.7,24 Additionally, patients who board in the ED for prolonged periods of time can then have a longer hospital admission LOS, ultimately perpetuating the cycle of limited inpatient capacity and constrained output.24 People with severe and complex needs in inpatient hospital wards often require more intensive treatment and remain in the hospital for longer periods of time than those with less severe or complex conditions. Prolonged stays in hospital wards can contribute to access block and boarding in the ED.7,19,24 Strained staffing resources outside of the ED can further compound this issue as a lack of staff in inpatient settings can mean that patients wait longer to receive care and be discharged.7,19,24 In addition to the role that lack of hospital beds plays in overcrowding, the lack of alternate levels of care in the community (e.g., home care, long-term care, and palliative care) are also important factors. When end-of-life care is unavailable, patients with palliative care needs may be directed to intensive care units and other inpatient beds, which further compounds the bed availability issue.23 Additionally, some of the literature reported that, when it came to transferring people out of the ED, the highest number of patients were those who requested publicly funded long-term care beds.30
Impact of Identified Input, Throughput, and Output Factors
Across all of the identified factors, the authors of the included studies emphasized the shared understanding that output factors, particularly boarding and access block, were the leading contributors to ED overcrowding compared to input and throughput factors. In particular, 6 articles noted that out of all the factors, boarding was the most important one when it came to ED overcrowding.1,7,20,21,28,32 In contrast, however, 2 articles published in Canada and 1 article published in Japan found that throughput factors related to medical testing and diagnostic scans had as great or greater effect on ED overcrowding compared to boarding.15,17,22 One article stated that while input factors contributed to ED overcrowding, they were less important than throughput and output factors.7 However, it should be noted that this article did not document a lack of primary or community care as types of input factors.
We found discrepancies in the literature related to other factors, as well. For instance, while 7 studies noted that low-acuity visits to the ED was a contributing factor to ED overcrowding,7,21,24,29,33,34,36 5 articles noted that a high number of patients with low-acuity conditions was not the most important cause of crowding, had only a small effect on measures related to crowding (such as LOS), and that these visits may be the result of an inability to access care in another setting first.7,21,24,25,32 Similarly, while 3 studies noted that ambulance arrival was a factor contributing to ED overcrowding, another study stated that they did not find an association between the number of patients transferred by ambulance and ED overcrowding.15 These discrepancies may be a reflection of differences in settings and contexts (e.g., geographic location, hospital type, and health care system) across the studies included in this environmental scan and the relative impact of these factors may be context dependent.
Contextual Factors Impacting ED Overcrowding
Factors contributing to ED overcrowding are also present at the broader system level. We have defined contextual factors as those that exist outside of the input-throughput-output categories. Drawing upon the constructs outlined in the Consolidated Framework for Implementation Research (CFIR) and the descriptions of contextual factors identified in the literature, we have categorized these factors into micro level, meso level, and macro level.107 The CFIR is designed to guide the selection of implementation strategies tailored to best address contextual factors. While this review does not focus on specific innovations or implementation strategies, it uses the constructs of the CFIR to help capture relevant contextual determinants that contribute to ED overcrowding and that may be considered in the context of potential future innovations.107 Further elaboration on how these levels were created and informed by the CFIR is included in each of the following subsections.
Figure 2: Categorization of Contextual Factors Contributing to ED Overcrowding
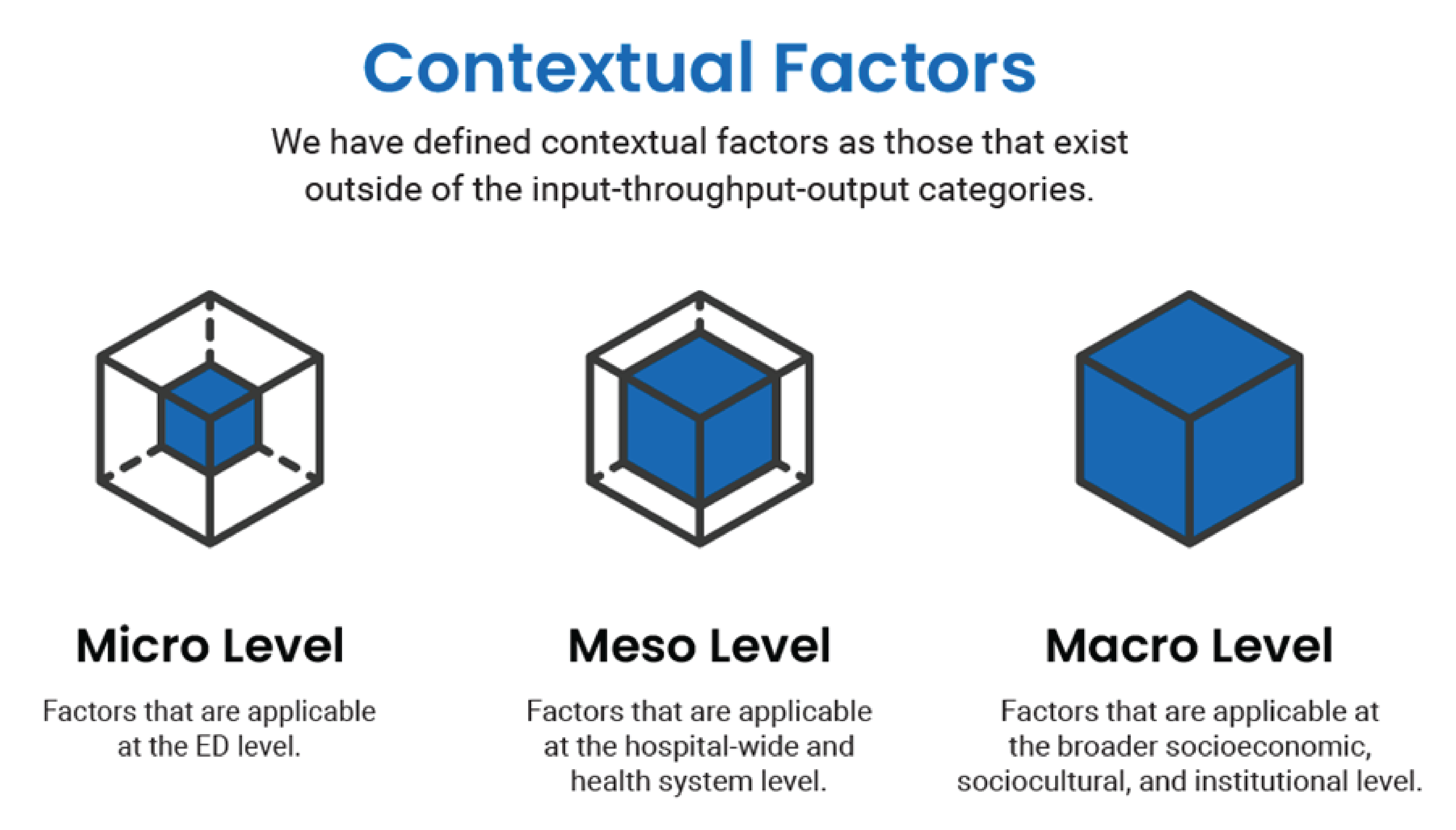
ED = emergency department.
We identified 11 articles that discussed contextual factors contributing to ED overcrowding.13,14,20,23,29-34,36 Importantly, the contextual factors identified did not come from the Canadian literature. Rather, we identified relevant literature from China, Australia, the US, the UK, Ireland, and Italy. As a result, not all of the listed contextual factors will be applicable and relevant in a Canadian setting. Nevertheless, we included them to provide a fulsome picture of the factors contributing to ED overcrowding. Additionally, several of these factors were identified and discussed by participants of CADTH’s multistakeholder dialogue sessions, all of whom were working and/or living in Canada.6 In the What Did We Learn section of this report, we offer further insights from the participants’ regarding the relevance of these international findings to the Canadian context.
In the following sections we present and describe the contextual factors as discussed in the literature. Of note, the identified literature did not discuss or describe the impact of contextual factors in terms of the magnitude or extent to which they influence ED overcrowding. However, further discussion on how and why these factors contribute to ED overcrowding is included in the subsequent section. Though not all identified articles provided detailed accounts for each factor, the information from those that did is discussed in the following sections. The information about which contextual factors, and how and why these factors contribute to ED overcrowding, was identified from the international literature only.
Micro-Level Factors
We have defined micro-level contextual factors as those that are applicable at the ED level. We used the CFIR’s “Inner Setting” domain to help inform this category and identify contextual factors specifically related to the ED setting. The Inner Setting refers to “the setting in which the innovation is implemented.”107 Though we are not focused on interventions, these factors may be useful to consider for future work related to specific innovations or implementation strategies relevant to this domain. We identified 2 articles23,33 that discussed micro-level contextual factors, which include:
ED closures: closures of EDs related to growing staffing shortages and difficult working conditions.
Crisis fatigue: prolonged exposure to stressful events within the ED that result in a burnout response among staff, which can affect performance and lead to turnover.
How and Why Micro-Level Factors Contribute to ED Overcrowding
Some of the literature described that ED closures resulted in the rerouting of patients to other, often geographically farther, functioning EDs, which increased the volume of visits and demand on resources.33 Working in the ED inevitably entails exposure to stressful events by staff and frequent ED crowding is 1 of them.23 Exposure to this stress was described as a tolerated reality and ED staff observed that solutions are not routinely implemented, which ultimately contributes to burnout and loss of staff.23
Meso-Level Factors
We have defined meso-level contextual factors as those that are applicable at the hospital-wide and health system level. We used the CFIR’s “Outer Setting” domain to help inform this category. The Outer Setting is “the setting in which the inner setting exists, and that there can be more than one level within the Outer Setting.”107 In this case, we have identified 2 levels belonging to the Outer Setting: the hospital and health system. The ED exists within both of these settings. We identified 8 articles14,20,23,29-31,34,36 that discussed meso-level contextual factors, which include:14,20,23,29-31,34,36
Limited postacute care and alternate level of care resources: the lack of care capacity outside of the acute hospital setting, including facilities and services such as primary care, hospice care, community services, nursing homes, home care, and so forth.
Elective surgeries: nonemergency surgeries that can be scheduled in advance.
Limited health resources: when resources in the health system, including funding, staffing, hospital capacity, and inpatient capacity do not keep up with demand, resulting in delayed or reduced care for patients and poor working conditions for staff.
Hospital culture: ingrained values, beliefs, attitudes, and behaviours that exist within the hospital, which can act as barriers to enacting change and shifting approaches.
Limited resources for mental health and substance use: decreasing services related to mental health and addiction conditions both within the hospital and outside of the community, including a decrease in available beds.
Community hospital closures: the closure of local hospitals, particularly in areas with smaller populations.
Limited inpatient workforce: loss of staff, including nurses, physicians, lab technicians, and others, across inpatient services, which can result in a diminished number of patient beds.
Limited care hours: primary care, community services, and some non-ED hospital services operate primarily during business hours, with limited after-hours care (e.g., fewer staff, reduced services), making the ED 1 of the only options outside of business hours.
Misalignment of leadership and priorities: disagreement among hospital administrations over the importance of, and order in which, hospital-wide issues (including ED overcrowding) need to be addressed, leading to difficulty implementing change.
How and Why Meso-Level Factors Impact ED Overcrowding
The literature discussing the limited postacute care and alternate level of care resources described how inpatient beds become occupied while patients are waiting for a placement in another facility and discharges are delayed.23,30,34,36 Notably, a strong association between delayed discharges and ED boarding has been found, suggesting that delayed discharges due to limited postacute capacity plays a role in boarding.30 One small observational study from Australia examined the difference in access block delays when elective surgeries were being performed compared to when they were not being performed.29 During the period when there were not any elective surgeries, there was a reduction in access block delays and ED LOS.29 Mental health and substance use resources can facilitate the timely disposition of patients experiencing mental health concerns from the ED.14,23 A lack of these services, however, hinders this and patients who are in need of these services may be boarded for days awaiting access and placement.14 Trends show that patients in the ED with mental health needs are increasing in number and that they spend longer in the ED compared to patients who do not have mental health needs.14 Limited and reduced beds for these patients can exacerbate the issue of crowding.14,23 Similar to the closure of EDs, community hospital closures lead to the diversion of patients to other hospitals, which increases the volume of visits and decreasing hospital capacity.34 The included literature further outlines how various aspects concerning the constraints on health care resources contribute to ED overcrowding. Within hospitals, a lack of inpatient nurses results in a diminished number of patient beds which, in turn, further decreases hospital capacity and functional ability.23 Limited care hours among primary care providers, community services, and non-ED hospital services reduces access to services at the time they are needed.20,23 In the hospital setting, there is a 24 hour a day, 7 day a week demand for care, yet operations are most intensive and functional during standard business hours. This results in a misalignment in needs versus available services. In the primary care setting, limited hours of care can lead to the potential deterioration or exacerbation of acute and chronic conditions, ultimately increasing ED visits and hospitalizations.20,23 Finally, misaligned leadership and priorities at all levels of hospital administration and services were reported to undermine and lessen the likelihood of success of proposed solutions.23 The authors of the included articles described that while there may be agreement that ED overcrowding is an issue that needs to be addressed, each unit of the hospital must also attend to its own priorities.23 In a survey of directors of emergency medicine in Australia, participants noted that a lack of engagement from both inpatient specialties and executives is a barrier to addressing crowding.31 Furthermore, a lack of agreement over the way in which to proceed to address this issue can act as a barrier to change.23 In the same survey of directors, 44 participants reported that they believed a lack of resources, including funding, staffing, and hospital capacity, was a barrier to alleviating ED overcrowding and access block. Additionally, 19 participants reported that they believed an entrenched culture within the hospital was a barrier to alleviating overcrowding and therefore a factor in sustaining this problem.31
Macro-Level Factors
We have defined macro-level contextual factors as those that are applicable at the broader socioeconomic, sociocultural, and institutional level. We used the CFIR’s “Outer Setting” domain to help inform this category. Similar to the meso level, this is another level within the Outer Setting. In this case, it is the broadest level as it refers to socioeconomic, sociocultural, and institutional characteristics. The health system, hospital, and ED all exist within this setting. We identified 8 articles13,19,20,23,31-33,36 that discussed macro-level contextual factors, which include:
Insurance policies: the altering or expansion of insurance schemes (e.g., Medicaid), resulting in changed access to insurance and medical care coverage. We note that this factor will not be relevant in a Canadian setting.
Political will: uncertainty over agreed-upon courses of action to effectively address issues at a political level, leading to difficulty implementing changes.
Population growth and shift: the increase and change in populations over time.
Seasonality and temporal patterns: the spike in ED visits related to time of year, seasonality (e.g., flu season), weekends, and/or holidays.
How and Why Macro-Level Factors Impact ED Overcrowding
Literature from countries that have privately funded, or a mix of private and publicly funded, health care systems described insurance status and changes to insurance policies as affecting patterns of ED use and, consequently, ED overcrowding. This factor does not apply to the Canadian setting but can help provide insight into the phenomena of ED overcrowding as a whole. While some literature suggested that underinsurance can result in “preventable ED visits and hospital admissions” related to chronic conditions,23 other literature noted that there is evidence to refute the idea that individuals who are uninsured or underinsured use the ED more than people who are insured.24,32 Population growth and shift provides broader context around the input factor of volume of visitors and complexity of needs. As populations grow, the overall number of people who may need ED services also grows.20 Furthermore, aging populations that are associated with population growth increase the likelihood of the presentation to EDs for chronic, complex conditions (another input factor).20 While the included literature provides insights regarding population growth and shifts, specifically as it relates to aging populations, this factor may also result from changes other than birth rate and aging population (e.g., immigration), and should be considered when applying this factor to a Canadian context. In terms of seasonality and temporal pattens, while patients present to the ED at all times of day and throughout the year, some of the literature described how EDs often experience peak arrivals times.33 Some of these peaks are weekday evening arrivals due to daytime referrals from primary care providers, and arrivals after weekends and bank holidays.33 EDs and hospitals will fill up during these times due, in part, to lack of access to senior decision-makers, diagnostics, treatments, and discharge enablers.33 In a survey of directors of emergency medicine in Australia, 16 participants reported that they believed political will was a barrier to alleviating ED crowding and access block and was therefore a factor in sustaining this problem.31 Another study highlighted that to effectively address overcrowding, it is key that governments are involved and that they make this issue a priority.108
Summary of Systematic Review Evidence on the Effectiveness of Interventions
Figure 3 describes the 7 intervention categories we found in systematic reviews, and may not include all interventions that have been used to alleviate ED overcrowding. We included categories outside of the input-throughput-output model to highlight that there are interventions that can affect ED overcrowding that fall outside of our model. These categories were validated by our content experts. We recognize that several interventions could fit into multiple categories and several categories are overlapping; however, for simplicity of reporting, we selected 1 category for each intervention-comparison. We considered interventions to be multicomponent if the systematic review authors identified them as such. If the interventions had additional components but the systematic review authors only focused on the 1 component for the synthesis, they were not included in the multicomponent category.
The interventions found in the literature were categorized according to an adaptation of the conceptual model developed by Asplin et al. (2003) (please refer to Figure 3).
The Supporting Information document contains the selection of systematic reviews we included (via a flow chart), the list of studies we excluded with reasons, detailed findings tables with the data we extracted from the systematic reviews, and our confidence in the results of the included systematic reviews using AMSTAR 2101 criteria.
We included 64 systematic reviews 29,38-100 with 667 unique primary studies. Of those primary studies, 117 were included in 2 or more systematic reviews (i.e., overlapped). Of the 64 systematic reviews, 45 had at least 1 overlapping primary study. The overlap in primary studies across systematic reviews is presented in the Supporting Information document. The interventions for which we identified conclusive evidence relative to any comparator are briefly presented in the following, and the findings for all conclusive and inconclusive evidence we identified are in the detailed findings tables in the Supporting Information document.
Interventions With Evidence of Favourable Effect
An intervention was effective versus a comparator based on 2 criteria:
The outcomes data were both favourable and certain (refer to the Methods section and Table 1).
We had moderate to high confidence about the methodological quality of the systematic review (refer to the Methods section).
The intervention comparisons with moderate- to high-quality evidence of favourable effect(s) are presented in Table 1.
Figure 3: Categorization of Findings on the Effectiveness of Interventions
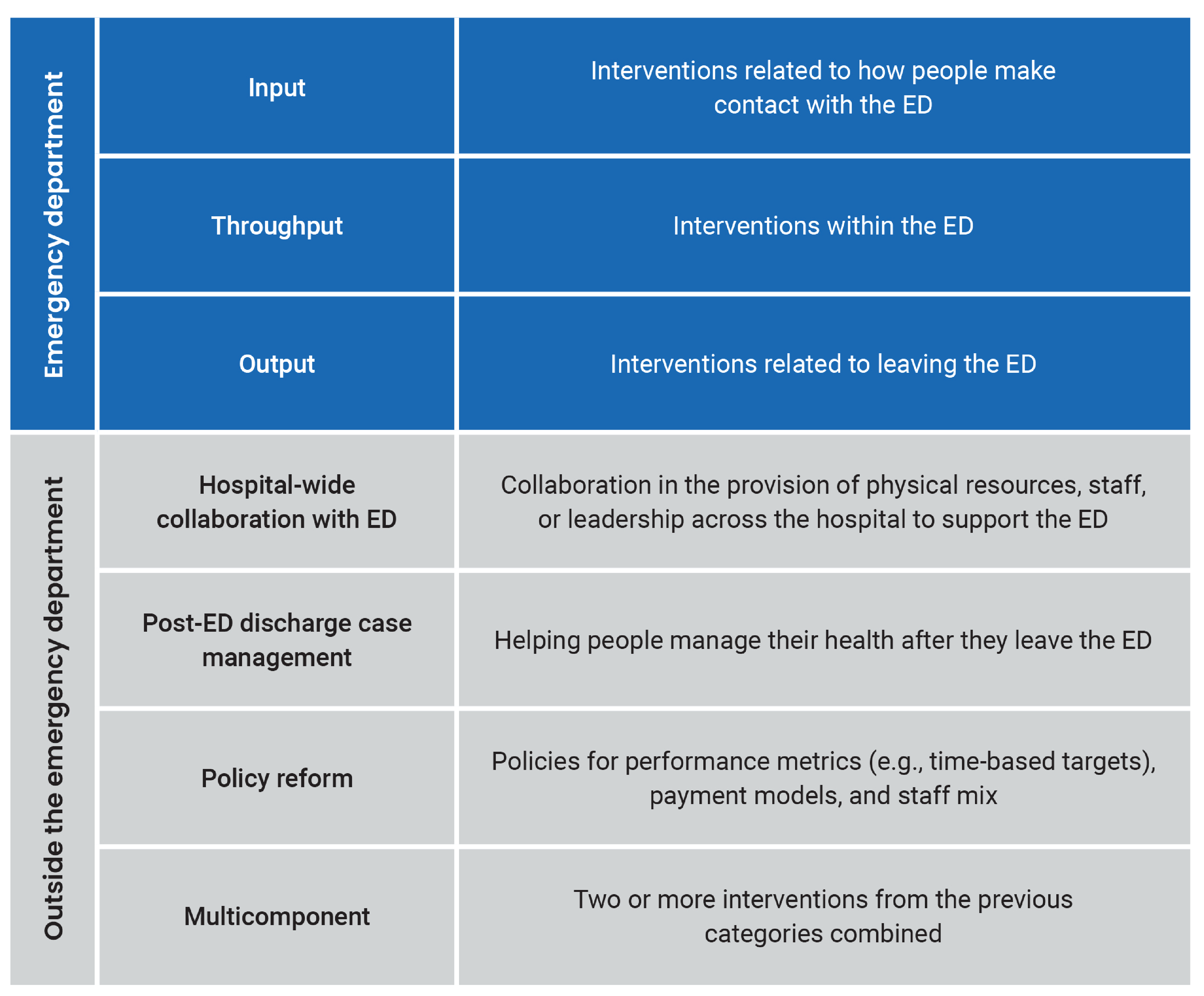
ED = emergency department.
Note: The definitions of input, throughput, and output were adapted from the conceptual model developed by Asplin et al. (2003).102 Although some of our other categories may be traditionally considered “input” according to this model, we have separated the more upstream categories to highlight the various interventions that can take place outside the ED.
Table 1: Evidence of Favourablea Effect by Outcome
Category | Intervention | Comparator | Population |
|---|---|---|---|
ED LOS | |||
Throughput | Short stay crisis unit for mental health | Usual care41 | Adults experiencing mental health challenges |
Throughput | Advanced triage protocols (with or without OAR) | Conventional triage, CTAS, or MTS92 | Adults and children |
Policy reform | Time-based targets | No intervention71 | Admitted patients |
ED-related wait times | |||
Input | Paramedic practitioner service | Inactive paramedic service68 | Older adults |
Throughput | Short stay crisis unit for mental health | Usual care41 | Adults |
Boarding | |||
Throughput | Short stay crisis unit for mental health | Usual care41 | Adults |
ED visits | |||
Input | EMS prehospital decision-making | Direct transport to ED68 | Older adults |
Input | Paramedic practitioner service | Inactive paramedic service68 | Older adults |
Postdischarge case management | Hospital moderate- to high-intensity transitional care | Usual care99 | Older adults with CHF |
Postdischarge case management | Care coordination strategies | Usual care96 | Older adults who access the ED often |
ED return visits | |||
Output | Discharge planning and coordination of services in the ED | Usual care97 | Older adults and those of all ages who access the ED often |
Patients who left prematurely | |||
Policy reform | Time-based targets | No intervention71 | NR |
Patient satisfaction | |||
Input | Paramedic practitioner service | Inactive paramedic service68 | Older adults |
Throughput | Advanced triage protocols (with or without OAR) | Conventional triage, CTAS, or MTS92 | Adults and pediatrics |
Safety | |||
Throughput | Short stay crisis unit for mental health | Usual care41 | Adults |
CHF = congestive heart failure; CTAS = Canada Triage and Acuity Scale; ED = emergency department; EMS = emergency medical services; LOS = length of stay; NR = not reported; MTS = Manchester Triage System; OAR = Ottawa Ankle Rules.
aFavourable means there is certain evidence or evidence with some uncertainty of better effectiveness of the intervention versus a comparator, or that the systematic review authors reported a high or moderate level of certainty of better effectiveness of the intervention versus a comparator.
ED LOS
Two throughput interventions were effective for reducing ED LOS:
Short stay mental health crisis units are hospital-based units that allow patients to stay overnight for a time-limited period and provide assessment and referral in an environment that facilitates stabilization. The short stay crisis units included in the meta-analysis by Anderson et al. (2022)41 were named 24-hour behavioural or psychiatric assessment unit; 48-hour psychiatric assessment and planning unit emergency psychiatric, assessment, treatment, and health unit (or EmPATH); 48-hour crisis assessment linkage and management (or CALM) service; and short-term psychiatric decisions unit.41 The meta-analysis41 found a reduction in ED LOS by 164 minutes (95% confidence interval, 261 to 67 minutes reduction) with short stay crisis units for mental health.
Advanced triage protocols (ATPs) are standard face-to-face approaches whereby the nurse or physician in triage initiates diagnostic or therapeutic actions in a specific group of patients before they are seen by a physician. The meta-analysis by Soster et al. (2022)92 found a 36-minute reduction in ED LOS (95% confidence interval, 55 to 17 minutes reduction) with the implementation of ATPs. The meta-analysis92 also found that ATPs that used the Ottawa Ankle Rules for imaging exams were as effective at reducing ED LOS as were ATPs that did not use the Ottawa Ankle Rules, compared to other triage interventions.92
One policy reform intervention was effective for reducing ED LOS — timed patient disposition targets to improve the timeliness of ED care. One systematic review71 reported moderate certainty evidence that national and provincial time-based targets in Australia and New Zealand (but not in England) reduced ED LOS in patients who were admitted after their introduction (magnitude not reported). ED LOS for all patients and for patients who were discharged was also favourable, but with low and very low certainty, respectively. Another systematic review29 also reported favourable but inconclusive evidence for all patients. A third systematic review87 reported mixed results of time-based targets on ED LOS, based on data that the 4-Hour Rule in England resulted in increased ED LOS following its implementation.
ED-Related Wait Times
Two interventions were effective for reducing measures of waiting time related to the ED, 1 input intervention and 1 throughput intervention:
In a cluster randomized controlled trial (RCT) in the systematic review by Huntley et al. (2017),68 paramedic practitioners received additional training to “assess and treat” or to refer older patients with a range of conditions, as part of prehospital care (i.e., input). This intervention reduced the time from receiving the emergency 999 call to ED discharge by 42 hours (95% confidence interval, 59.5 to 25 hours reduction).41
The introduction of short stay mental health crisis units resulted in less wait time to be seen by a clinician (from a median of 68 minutes in the control group to 40 minutes in the intervention group), less wait time for a mental health review (from 139 minutes to 117 minutes), and fewer patients who waited in the ED for longer than 24 hours (i.e., throughput).41
Boarding Outcomes
One nonrandomized study (NRS) found that psychiatric boarding (i.e., the time waiting in the ED for a bed or transfer) was decreased by a mean of 189 minutes (95% confidence interval, 228 to 50 minute decrease) with short stay mental health crisis units (i.e., throughput).41
ED Visits
Two input interventions were described in the systematic review by Huntley et al. (2017):68
In 1 RCT,68 older participants were randomized to emergency medical services in which ambulance personnel had training in and access to the prehospital decision system and associated decision support tool and could triage eligible individuals to alternative health care (intervention). After assessing the individual’s medical situation and care needs, the ambulance nurse was able to decide whether the individual required full ED services or would benefit more from being transported to an assessment at the community hospital instead. In the comparison group, ambulance personnel (at a different emergency medical services company) had no training in the system and tool, and transported all individuals to a full-service ED at a tertiary hospital. The intervention resulted in less subsequent transfers to the ED.68
The paramedic practitioner service also reduced ED attendance.68
Two other interventions were effective for reducing ED visits:
In the narrative synthesis by Vedel et al. (2015),99 moderate- to high-intensity transitional care interventions consisted of telephone follow-up combined with home visits, clinic follow-up, and/or video visits with older patients with congenital heart failure who were discharged from hospital inpatient departments to home.
In the meta-analysis by Tricco et al. (2014),96 the intervention (care coordination strategy) was defined as “the deliberate organization of patient care activities between 2 or more participants (including the patient) involved in a patient’s care to facilitate the appropriate delivery of health care services.” The proportion of all patients who visited the ED did not different significantly between the intervention and usual care group, although this finding was inconclusive. However, there was a favourable (conclusive) effect among older patients. There was also a reduction in the mean number of ED visits per month in all patients with care coordination compared to usual care.96
ED Return Visits
The narrative synthesis by van den Broek (2023)97 found that discharge planning and coordination of services in the ED reduced the number of ED return visits compared to usual care. In 2 NRSs, a nurse liaison made a personalized ED discharge plan and arranged referrals to community services. In an RCT, a patient navigator in the ED (i.e., nurse trained in hospital case management) reviewed the patients’ medical diagnosis and medication prescriptions, arranged transportation, and found community resources for follow-up for patients of all ages who used the ED more than 5 times in the past year.97
Patients Who Left Prematurely
Time-based targets in Australia and New Zealand reduced the number of patients who did not wait in the ED to complete assessment or care.71 Two other systematic reviews29,87 also reported fewer patients who left before being seen or who did not wait following the introduction of time-based targets, but the evidence was uncertain.
Patient Satisfaction
There was increased patient satisfaction, as measured on the EQ-5D survey, with active paramedic practitioner services as compared to inactive paramedic services.92 ATPs were effective for increasing patient satisfaction, as measured on various instruments, in those who received the interventions compared to other triage instruments.92
Safety
Code grey event rates (ED security responses) and the use of restraints in patients (e.g., physical or mechanical restraints, therapeutic sedation) were reduced with short stay mental health crisis units.41
Interventions With Evidence of Neutral Effect
An intervention had no effect versus a comparator based on 2 criteria:
The outcomes data were both neutral and certain (refer to the Methods section and Table 1).
We had moderate to high confidence about the methodological quality of the SR (refer to the Methods section).
Intervention comparisons with moderate- to high-quality evidence of neutral effect are presented in Table 2.
Table 2: Evidence of Neutrala Effect by Outcome
Category | Intervention | Comparator | Population |
|---|---|---|---|
ED LOS | |||
Throughput | Rapid influenza testing | Usual care55 | Pediatrics |
ED-related wait times | |||
Throughput | Nurse-initiated X-rays in ED | Physician-initiated X-rays49 | Adults and children with distal limb injuries |
ED visits | |||
Input | Remote triage | Usual care89 | Adults |
Postdischarge case management | Hospital low-intensity transitional care intervention | Usual care99 | Older adults with CHF |
ED return visits | |||
Throughput | Nurse-initiated X-rays in ED | Physician-initiated X-rays49 | Adults with minor distal limb injuries |
People who left prematurely | |||
Throughput | Short stay crisis unit for people experiencing mental health challenges | Usual care41 | Adults |
CHF = congestive heart failure; ED = emergency department; LOS = length of stay; NR = not reported; SR = systematic review.
aNeutral means there is certain evidence (high certainty) or evidence with some uncertainty (moderate certainty) that neither the intervention nor comparator was favoured.
ED LOS
A narrative synthesis55 reported that rapid viral testing in the ED had no effect on ED LOS in pediatric EDs.
ED-Related Wait Times
One RCT in a systematic review49 found that nurse-initiated X-rays in adults with distal limb injuries compared to physician-initiated X-rays in the ED had no effect on time from triage to medical assessment.
ED Visits
A narrative synthesis89 found no effect on ED use with the implementation of remote triage (input intervention), defined as triage from a distance, including telephone, video, web, or short message service.
In the narrative synthesis by Vedel et al. (2015),99 a low-intensity transitional care intervention that involved structured telephone follow-up found no effect on ED visits in older adults with congenital heart failure discharged from hospital inpatient departments to home.
ED Return Visits
One RCT in a systematic review49 found that nurse-initiated X-rays in adults with minor injuries compared to physician-initiated X-rays in the ED had no effect on unplanned ED reattendance.
People Who Left Prematurely
There was no effect on the number of patients leaving the ED without being seen or leaving against medical advice or authorization after the introduction of a short stay mental health crisis unit.41
Interventions With Evidence of Unfavourable Effect
An intervention had an unfavourable effect versus a comparator based on 2 criteria:
The outcomes data were both unfavourable and certain (refer to the Methods section and Table 1).
We had moderate to high confidence about the methodological quality of the systematic review (refer to the Methods section).
We did not identify any intervention comparisons with moderate- to high-quality evidence of unfavourable effect on any outcomes.
Other Evidence
We did not find any evidence for the effect of interventions on the number or proportion of patients in the ED waiting room.
There were 7 intervention comparisons for which the evidence was categorized as favourable, but our confidence in the results of the systematic review was low due to methodological limitations. These included 3 interventions in the input category (e.g., positive effect of telemedicine and home care visits on ED visits) and 4 interventions in the throughput category (e.g., positive effect of physician in triage, team triage, and patient streaming on ED LOS).
There were 11 intervention comparisons for which the evidence was categorized as neutral, but our confidence in the results of the systematic review was low due to methodological limitations. These included 6 interventions in the input category (e.g., no effect of asthma pathway of urgent care in children or direct mailing intervention in older adults on ED visits), 2 interventions in the throughput category (e.g., no effect of medical scribes on ED LOS), 1 in the output category (e.g., no effect of identification of seniors at risk assessment and referral to ED services upon discharge in older adults on ED return visits), 1 in the postdischarge case management category (e.g., no effect of home-based intervention in older adults on ED visits), and 1 in the multicomponent intervention category (e.g., no effect of ED community multicomponent care transition interventions on ED return visits).
We found an abundance of evidence on a wide array of interventions to alleviate ED overcrowding. Although many interventions have been applied to address the problem, most of the evidence on effectiveness was inconclusive due to moderate or high uncertainty (e.g., low or very low certainty of evidence).
We identified 208 intervention comparisons across 47 systematic reviews for which the evidence was deemed favourable, but inconclusive. These included intervention comparisons in all intervention categories, mostly compared with no intervention or usual care, as detailed in the findings tables of the Supporting Information document. We found 25 intervention comparisons in the input category (e.g., positive effect of general practitioner cooperation, primary care-based care coordination, written educational materials, and long-term care interventions on ED visits), 131 in the throughput category (e.g., positive effects of triage, additional health care provider roles in the ED, patient streaming, separative physical spaces for observation and assessment, testing strategies, and technology in the ED on various outcomes), 4 in the output category (e.g., positive effect of active bed management on ED wait times), 3 in the postdischarge case management category (positive effect of 30-day health care provider follow-up on ED return visits), 7 in the hospital-wide collaboration with ED category (e.g., positive effect of hospital leadership support on boarding time), 21 in the policy reform category (e.g., positive effect of time-based targets on ED occupancy), and 12 in the multicomponent category (e.g., positive effect of integrated approaches in the ED on ED LOS and number of patients who left prematurely).
We identified 96 intervention comparisons across 38 systematic reviews for which the evidence was neutral, but inconclusive. These included input interventions (e.g., no effect of home-based care and primary care-based case management on ED visits), throughput interventions (e.g., no effect of physical therapy, early assessment by a care coordination team, or the addition of an advance practice nurse in the ED on return visits), output interventions (e.g., no effect of enhanced care or discharge planning on ED return visits), postdischarge case management interventions (e.g., no effect of postdischarge telemedicine on ED visits), hospital-wide collaboration with ED interventions (e.g., effect of full capacity protocols on patients who left prematurely), policy reform (e.g., no effect of fee-for-service on ED LOS), and multicomponent interventions (e.g., no effect on ED-based care transitions), mostly compared with no intervention or usual care.
We found 14 intervention comparisons in 10 systematic reviews for which the evidence was unfavourable, but inconclusive. These included input interventions (negative effect of hospital-at-home on ED LOS), throughput interventions (e.g., negative effect of pharmacist on ED return visits, and negative effect of pediatric ED versus general ED on ED visits), policy reform interventions (negative effect on time-based targets on boarding time), and multicomponent interventions (e.g., negative effect of postdischarge management on ED LOS), mostly compared with usual care.
We identified 16 intervention comparisons across 11 systematic reviews for which the evidence was mixed. These included input interventions (e.g., effect of primary care models and walk-in centres on ED visits), throughput interventions (e.g., effect of nurse-initiated protocols on ED LOS), output interventions (e.g., effect of caseworker-assigned discharge plans on ED visits), hospital-wide collaboration with ED interventions (e.g., effect of full capacity protocols on ED LOS), policy reform interventions (e.g., effect on time-based targets on ED LOS and ED return visits), and multicomponent interventions (e.g., ED-based care transitions on patient satisfaction), mostly compared with usual care.
The detailed findings for these interventions are presented in the tables in the Supporting Information document. We could not draw any conclusions as to the effectiveness of these interventions relative to the comparator studied in the systematic reviews because of the low level of certainty and/or low confidence in the methodological quality. As such, we have not described their results here in detail.
Interventions and Contributing Factor Themes
While we conducted the reviews on factors and interventions separately and simultaneously, the 2 topics are related. Table 3 presents intervention comparisons, for which we identified conclusive evidence, organized by the factor themes reported in the environmental scan. For simplicity, we have listed each intervention that maps to the input, throughput, and output categories beside a single theme of factors. However, some interventions listed may target factors themes outside the ED and some interventions listed may target multiple themes or multiple individual factors within the themes.
Table 3: Interventions With Favourablea or Neutralb Outcomes, Organized by Contributing Factors
Factor theme | Intervention | Comparator | Population | Setting | Outcome(s) | Effectiveness |
|---|---|---|---|---|---|---|
Input | ||||||
Primary care and community health services | No intervention comparison for which we found conclusive evidence of effectiveness | — | — | — | — | — |
Repeated visits and low-acuity visits to the ED | Remote triage | Usual care89 | Adults | NR | ED visits | Neutrala |
Growing patient volume and complexity of needs | No intervention comparison for which we found conclusive evidence of effectiveness | — | — | — | — | — |
Access via multiple avenues | Paramedic practitioner service | Inactive paramedic service68 | Older adults | NR | ED wait times, ED visits, patient satisfaction | Favourableb |
EMS prehospital decision-making | Direct transport to ED68 | Older adults | NR | ED visits | Favourable | |
Throughput | ||||||
Consultation, testing, and decision delays | Rapid influenza testing | Usual care55 | Pediatrics | Urban | ED LOS | Neutral |
Staffing considerations | Nurse-initiated X-rays in ED | Physician-initiated X-rays49 | Adults and children with distal limb injuries | NR | ED wait times, ED return visits | Neutral |
Barriers to optimal operational efficiency | Short stay crisis units for mental health (therapeutic spaces for stabilization, assessment, and appropriate referral; with the aim of reducing ED mental health presentations and wait times, and/or psychiatric admissions) | Usual care41 | Adults experiencing mental health challenges | NR | ED LOS, ED wait times, boarding, patient safety | Favourable |
Short stay crisis units for mental health (therapeutic spaces for stabilization, assessment, and appropriate referral; with the aim of reducing ED mental health presentations and wait times, and/or psychiatric admissions) | Usual care41 | Adults experiencing mental health challenges | NR | Patients who left prematurely | Neutral | |
Advanced triage protocols (with or without OAR) | Conventional triage, CTAS, or MTS92 | Adult and pediatric patents | NR | ED LOS, patient satisfaction | Favourablec | |
Output | ||||||
Access block and boarding | Time-based targets | No intervention71 | Patients who were admitted | Urban | ED LOS | Favourable |
Time-based targets | No intervention71 | NR | Urban | Patients who left prematurely | Favourable | |
Demand on hospital resources outside the ED | No intervention comparison for which we found conclusive evidence of effectiveness | — | — | — | — | — |
Impediments to exiting the ED | Hospital moderate- to high-intensity transitional care | Usual care99 | Older adults with CHF | NR | ED visits | Favourablec |
Care coordination strategies | Usual care96 | Older adults who access the ED often | Urban | ED visits | Favourablec | |
Discharge planning and coordination of services in the ED | Usual care97 | Older adults, and those of all ages who access the ED often | NR | ED return visits | Favourable | |
Hospital low-intensity transitional care intervention | Usual care99 | Older adults with CHF | NR | ED visits | Neutralc | |
ED-community multicomponent care transition strategies | Usual care76 | Older adults | NR | ED return visits | Neutralc | |
CHF = congestive heart failure; CTAS = Canada Triage and Acuity Scale; ED = emergency department; EMS = emergency medical services; LOS = length of stay; MTS = Manchester Triage System; NR = not reported; OAR = Ottawa Ankle Rules.
aNeutral means there is certain evidence or evidence with some uncertainty that neither the intervention nor comparator was favoured.
bFavourable means there is certain evidence (high certainty) or evidence with some uncertainty (moderate certainty) of better effectiveness of the intervention versus the comparator.
cAt least 1 primary study was conducted in Canada.
What Did We Learn?
The factors contributing to ED overcrowding that we identified in the literature exist both within and outside of the ED and fall into input, throughput, and output categories, as well as micro-level, meso-level, and macro-level categories. Out of all these categories, it is only the throughput category that includes factors focused within the ED. Other categories, like input and output, include factors that interface with health care services outside of the ED (e.g., availability and accessibility of primary care and/or long-term care). These findings align with the current body of literature, suggesting that ED overcrowding is not restricted to the 4 walls of an ED.
Upon reviewing and describing the factors contributing to overcrowding, it became clear that many of them are interconnected and influence each other. For example, difficulty finding and accessing a primary care provider and frequent visits to the ED are related, as repeated visits to the ED might stem from limited access to primary care. Similarly, contextual factors can influence and help explain some causal factors. For instance, a limited inpatient workforce would affect demand on hospital resources outside of the ED such as inpatient volume and bed availability. This interconnectedness demonstrates the importance of viewing ED overcrowding as a system-wide matter.
There was variation in the degree of importance of factors that were identified in the literature. Some factors, such as boarding, were clearly described as major causes for ED overcrowding.1,14,15,23,28,32 Other factors, such as low-acuity visits, were described as having a relatively minor impact on ED overcrowding.7,21,24,25,32 This reflects the idea that while the identified factors could all potentially have an influence on overcrowding, not all factors are equally influential. Furthermore, the influence and applicability of factors can vary depending on context. The literature broadly identifies population growth and shift as a factor contributing to ED overcrowding; though, the nature of this growth and shift will vary depending on where it is taking place. The literature broadly discusses this factor in relation to overall volume of people as well as aging populations. However, in Canada, population growth can also be attributed to the number of new immigrants and nonpermanent residents.109 This context is important in understanding how population changes may then influence who visits the ED, the reasons for which they present to the ED, and how their interactions in the ED may be affected. For instance, a shift in population composition related to new immigrants and nonpermanent residents can contribute to changing health and social needs around language accommodations and health care system navigation assistance. Therefore, contextualizing factors is critical when trying to fully understand and address them.
Overall, the findings from the environmental scan on factors contributing to ED overcrowding illustrate how overcrowding is an international, complex, and multifactorial issue.
Interventions that were effective in alleviating ED overcrowding also existed both within and outside of the ED. In the summary of systematic review evidence on interventions, we considered interventions to be effective based on moderate to high certainty of the systematic review evidence and moderate to high confidence in the systematic review quality.
Examples of factors include, but are not limited to, increased complexity of needs (input), diagnostic testing and procedures (throughput), boarding (output), and limited resources for mental health and substance use (outside the ED).
Examples of interventions that were effective in some settings include, but are not limited to, prehospital decision-making by first responders, which reduced ED visits (input); short stay crisis units for people experiencing mental health challenges, which improved ED LOS, wait times, boarding, and patient safety (throughput); ED-based discharge planning, which reduced ED return visits (output); and time-based policy reforms, which reduced ED LOS (outside the ED).
Most of the factors we identified existed either outside of the ED or at the interface of the ED and other health care services, whereas most of the interventions we identified existed within the ED.
How Has the Evidence Changed Since the 2006 CADTH Report?
This document is an update of CADTH’s 2006 4-part series entitled Emergency department overcrowding in Canada: What are the issues and what can be done?8-11 For this update, we used different approaches and methodologies to inform recommendations about how the problem of ED overcrowding may be addressed in Canada.
The 2006 reports relied on a survey from Canadian ED directors to highlight important factors and measures of overcrowding, whereas the current environmental scan identified factors from the literature.11 Despite this difference, some of the factors in both reports are similar (e.g., a lack of admitting beds in the hospital).11
The summary of systematic review evidence on interventions further strengthened the systematic review findings in the 2006 CADTH report Interventions to Reduce Overcrowding in Emergency Department.13 We also found that fast track systems can reduce ED LOS; however, their effect on waiting times was neutral but inconclusive, and favourable but inconclusive for patients who left without being seen. While the 2006 report recommended that ambulance diversion strategies and short stay units had limited evidence and should be further explored, we found conclusive evidence for the effectiveness of these interventions. Like the 2006 report, we also found inconclusive evidence for many triage interventions that we identified, apart from physician in triage and team triage, which we found to be effective for reducing ED LOS. While the 2006 systematic review found limited evidence for staffing change and system-wide interventions, we identified new evidence, but all was inconclusive. The 2006 systematic review reported that primary studies did not compare active interventions to each other.
Strengths and Limitations
The conduct of our work has strengths and limitations that should be noted when interpreting the findings. In terms of strengths, we conducted a comprehensive search for the environmental scan, and we selected literature with a broad scope and from a variety of literature (e.g., primary studies, reviews, position statements) to allow us to explore and comprehensively describe the wide range of factors that have been identified in the literature as contributing to ED overcrowding. Our findings can help inform future research by supporting the identification and selection of key interventions that consider the complexity of ED overcrowding and address factors both within and outside of the control of the ED. For the summary of systematic review evidence on interventions, we conducted a comprehensive search, used rigorous methods to select and appraise systematic reviews, and appraised the certainty of evidence considering study limitations, inconsistency in effects across studies, imprecision of effects, and publication bias. Another strength is that both the environmental scan and the summary of systematic review evidence on interventions were supplemented with insights from other sources; we engaged with various stakeholders through our multistakeholder dialogue of lived experiences, and our content experts who reviewed our protocol110 and the conduct of our work throughout the process. We believe this approach provides an enriched and nuanced perspective of this complex issue as we were able to add a “real-world” perspective and context to the research literature. By engaging with people who live and work in Canada, we were able to contextualize our findings from the literature and emphasize aspects particularly relevant to the Canadian context.
In terms of limitations, while the environmental scan aimed to provide a summary of factors contributing to ED overcrowding internationally and in Canada, and we strove to ensure this scan identified as many factors as we were able, there is the potential that certain factors may not have been captured in the identified literature. Because our scope was broad, as is typical in an environmental scan, we included a wide range of study designs and therefore did not apply quality appraisal criteria intended for traditional knowledge syntheses. We also only included literature written in English, so we may not have captured relevant studies written in another language, and we identified few articles in the Canadian literature that met our selection criteria, limiting the relevance and transferability of the results to a Canadian context. Additionally, even within Canada, where health care is administered at the provincial, territorial, and federal levels, there can be variation in the factors and concerns across jurisdictions. Variation may also exist across urban, rural, or remote locations. Each of these settings can face their own unique set of challenges. To help mitigate issues around comprehensiveness and contextualization in Canada, we were able to compare the content from the multistakeholder dialogue sessions with the results from the literature. We noted gaps, differences, and similarities. Additionally, because we included literature from any country, we identified literature from a range of countries with varying types of health care systems that were both similar to and different from Canada. The findings across studies were relatively consistent, suggesting that factors contributing to ED overcrowding exist among many types of health care systems.
Furthermore, when we embarked on this review, our intent was to comprehensively identify factors and explore why they contributed to ED overcrowding (e.g., why do people choose to use the ED for low-acuity visits?). Yet, due to rapid project timelines, we narrowed the scope of work to centre our efforts on identifying these factors and capturing the associated descriptions for why they contributed to ED overcrowding within the same pool of studies. This approach, while effective in meeting our research objectives, did necessitate the exclusion of additional studies that might have offered further insights.
The environmental scan was also intended to be descriptive in nature, reporting only the details described in the literature. As such, there was a limit to our ability to interpret the findings from the identified studies. This meant that we had to rely on the study authors’ descriptions and terminology to clearly define and report the factors that contributed to ED overcrowding. If the reporting was unclear in describing a factor, or the link between the factor and ED overcrowding, then the study was excluded. Furthermore, the differences in terminology used across the literature also limited our ability to interpret findings. Finally, we may have missed studies that discussed equity-related matters or would contribute to understanding how equity-deserving groups may experience or be subject to contributing factors differently. This is because we aimed to include literature that reported equity-related findings if they were discussed in a study that explicitly reported factors contributing to ED overcrowding. It is important that equity-related findings and considerations are intentionally and explicitly included in future research and decision-making.
As noted, it is possible that not all factors contributing to ED overcrowding were reported in the identified literature. Based on feedback from content experts, other relevant factors that were not reported in the included literature are the roles of insurance policies in the Canadian setting (e.g., limited publicly funded insurance for dental care, prescriptions, drugs, mental health services, long-term care), climate change,111,112 agency nursing (e.g., private versus public nurses), health policies (e.g., wage caps), and social context (e.g., poverty). Some of these factors were discussed in the multistakeholder dialogues.6 While this is not an exhaustive list, these areas can serve as a starting point for opportunities to focus future work. Generally, future work may also benefit from further examining the explanations and reasons behind the factors in this report. Some examples of this include understanding why consultations can add to ED LOS, examining efficiency around the use of diagnostic tests,113,114 and investigating potential delays related to inadequate, inappropriate, or resource-intensive technology infrastructures in the ED. This can ultimately help provide a deeper understanding and more fulsome picture of overcrowding.
The findings from the summary of systematic review evidence on interventions also have some limitations. We only included systematic reviews written in English, and thus may have missed important systematic reviews written in other languages. As we were interested in any intervention aimed at alleviating ED overcrowding, we relied on the systematic review authors’ reporting that the interventions investigated were aimed at alleviating ED overcrowding (or that the focus of the review was to investigate interventions that alleviate ED overcrowding). If they did not mention this concept, the systematic review was excluded, even if the intervention could be aimed at alleviating ED overcrowding. This meant that certain systematic reviews about the same intervention may have been included or excluded depending on how the systematic review authors reported the connection to ED overcrowding. Similarly, we relied on the systematic review authors’ conclusions and level of detail of their results as we did not consult their included primary studies; the results we present are therefore also limited to information provided by systematic review authors. Given the rapidly evolving nature of this research area, some of the systematic reviews may be considered to be out of date and new information may have been made available since the time of their publication that would change the conclusions and/or the certainty of the evidence.
We did not formally rate the directness (i.e., generalizability) of the observed effects when rating our certainty in the evidence for the comparison-outcomes presented in the included systematic reviews. Instead, we made informal judgments about the potential generalizability to the Canadian context. However, given that health care services can vary across Canada and that the effectiveness of any intervention and feasibility of its implementation are likely to vary by context, the applicability of the findings of the systematic reviews will need to be carefully considered when making recommendations.
Due in part to the rapid nature of the work, amendments were made to the planned methods throughout the review process. We included evidence from systematic reviews with overlapping primary studies rather than selecting the most suitable systematic review per intervention-comparison outcome. As such, individual studies contribute more than once to the findings, but we were unable to assess the impact of the primary study overlap on the results per intervention-comparison outcome. We were unable to investigate discrepancies (e.g., in reported results, risk of bias, or methodological quality appraisals) across overlapping systematic reviews, or to reconcile conflicting conclusions across systematic reviews reporting results for the same intervention-comparison outcome. One reviewer completed the data extraction and while a second reviewer independently verified 11% of the systematic review evidence (i.e., 7 of the 64 systematic reviews), there is in increased risk of error and bias in the reported results that were not verified. We were unable to extract individual systematic review results; as such, the size and precision of effects for all intervention-comparison outcomes are not reported. However, we did report the magnitude of effects on select outcomes (e.g., LOS, waiting times, boarding time) for interventions with evidence of effectiveness (when provided by the systematic review). We were unable to extract and report on the risk of bias of the individual primary studies contained within each SR; however, these were considered when drawing conclusions about the conclusiveness of each systematic review’s results. Due to the volume of available literature and limited and inconsistent reporting by the systematic review authors, we were unable to provide detailed descriptions of the characteristics of the systematic reviews and their included studies, nor of the interventions and comparators investigated. As a result, decision-makers may need to consult the systematic reviews and their included primary studies for additional context.115
As our summary of systematic review evidence on interventions is limited to findings in systematic reviews, we may have missed interventions that have not yet been incorporated into systematic reviews, including novel and emerging interventions and/or interventions that have been tried but not formally studied; to address this we supplemented our work with an additional CADTH report to identify new and emerging interventions to alleviate ED overcrowding.116
Finally, we conducted the environmental scan of contributing factors and summary of systematic review evidence on interventions simultaneously. A staged approach to conducting these 2 reviews (i.e., conducting the environmental scan first, followed by the summary of systematic review evidence) may have helped refine the scope of the problem. It also may have facilitated a better understanding of the relationship between the factors and interventions as the findings from the environmental scan could have informed which interventions to examine.
Insights From the Multistakeholder Dialogue
As part of the series of publications that CADTH is producing on the topic of ED overcrowding in Canada, CADTH engaged people with personal and/or professional experience with ED care. We gathered participants’ perspectives on the factors and interventions found in the literature and sought to understand if they believed that any factors or interventions were missing. For each session, 8 to 10 people participated and had the following backgrounds: emergency physician, pediatric emergency physician, emergency nurse, pediatric researcher, pharmacist, patient and family advisor, director, geriatric psychiatrist, and emergency medicine resident. A summary of the multistakeholder dialogue sessions will be published as part of CADTH’s series of work on this topic.6
The multistakeholder dialogue sessions provided valuable comments and insights that were subsequently used to contextualize the factors identified in the international literature included in the environmental scan to the Canadian setting. They provided nuanced details as to why specific factors might contribute to ED overcrowding in Canada. For example, some participants indicated that despite Canada’s rapidly aging population, safeguards and resources to adequately meet the needs of this population have not been established (e.g., long-term care).
Furthermore, while a few participants disagreed with some of the factors presented from the literature, most of the participants provided additional insights to consider when thinking about the factors. For example, some participants acknowledged a lack of primary care options, yet they did not identify this factor as a driving force of ED overcrowding. Additionally, some participants described how efficiency in the ED (i.e., throughput factors) has already been maximized and that factors related to efficiency were not particularly relevant. When discussing the factor of low-acuity visits to the ED, 1 participant noted a disconnect between patient expectations and the services the ED can provide, which can ultimately lead to tensions and frustrations. Participants also emphasized the importance of factors like staffing issues and boarding and access block as major driving forces behind ED overcrowding, which aligns with the findings from the literature.
Notably, participants introduced and discussed factors that aligned with the contextual factors we identified in the literature. These include hospital culture, lack of postacute care resources, and issues around care hours (e.g., the ED is open 24h hours a day, 7 days a week, but other services are not), among others. At the time of the multistakeholder dialogue sessions we had not yet identified, and thus had not presented, the contextual factors to the participants. Moreover, once identified, no contextual factor was from the Canadian literature. As such, the fact that the multistakeholder dialogue participants independently brought up such factors highlights how the contextual factors identified in the international literature may be relevant to the Canadian setting despite their absence in the included literature.
Though there weren’t any instances where all participants fully disagreed with a specific factor found in the literature, their discussions did emphasize the importance of reframing the idea of ED overcrowding and its causes. In particular, they noted the need to think of the issue as a hospital overcrowding problem and broader systems issue instead of solely an ED issue (e.g., systems such as housing, poverty, and health care as a whole). The participants also discussed the need to view ED overcrowding through a lens of the social determinants of health to help understand the complexity of the problem and the reasons that individuals may seek out ED services. Finally, the participants discussed the effect that culture and human nature have on health care and use of ED services. Specifically, they mentioned that patients tend to prefer to receive care through what is perceived to be the easiest (or safest, most appropriate, or most effective) route possible, which can help explain why ED services are so heavily used as many patients and non-ED health care providers view the ED as an accessible path to receiving care. Additionally, participants noted that Canada has a diverse population and that frustrations can increase when there is a difference of culture, language, social status, needs, or expectations (e.g., providers may need to spend additional time on cases where there are communication barriers). All of these points can help us examine factors contributing to ED overcrowding from new, different, and more equitable perspectives.
The multistakeholder dialogue sessions also provided important insights into the interventions found in the summary of systematic review evidence on interventions and key considerations for what these interventions mean for the people who are most directly impacted by them. For example, the participants thought that postdischarge follow-up interventions could be a way to prevent revisits. While the systematic review evidence was inconclusive for the effect of postdischarge case management on revisits, we did find that ED-based discharge planning and coordination of services by a nurse liaison or nurse navigator reduced ED return visits in older adults. The participants elaborated that patients may need additional details about diagnostic tests or their treatment following their visit, and sometimes the hospitals have closed their case and their primary care provider has not yet caught up on this most recent ED visit. The idea of more longitudinal care and follow-up was also part of discussions about urgent or walk-in centres for which we found uncertain evidence within systematic reviews and mixed evidence across systematic reviews for the effect on ED visits, and neutral but inconclusive evidence for the effect on the workload of clinicians in the ED; 1 participant mentioned that they felt these clinics may not actually provide patient-focused long-term care and could be seen as a “pseudo-access” solution where care is actually disconnected.
Several of the interventions found in the literature were ways to gain efficiencies in the ED (i.e., throughput interventions); however, the participants mentioned that efficiency interventions have been tried for decades with the overcrowding issue persisting. For example, we identified systematic reviews on lean health care interventions to increase efficiencies, based on lean manufacturing,94 that provided uncertain evidence for ED LOS, ED-related wait times, left-without-been-seen, patient satisfaction, and boarding time. Participants mentioned that efficiency interventions could be useful but that it was important not to misinterpret these interventions as aiming to achieve 100% capacity in the ED because the ideal capacity in an ED should be 85% to provide safety and accommodate for a potential surge; however, EDs in Canada often reach and exceed 100% capacity.117
We identified several interventions in the literature where clinicians were given new roles and responsibilities (to address staff make-up, ratios, and shortages), which the participants also discussed these during the dialogues. The participants said that nurse-led interventions could improve efficiencies but that all health care workers would need to agree on nurses taking on new tasks such as initiating X-rays. In the literature, we found that interventions where nurses initiated X-rays were inconclusive for ED LOS, time to X-rays, time from triage to medical assessment, missed injuries, and patient satisfaction, and were neutral for unplanned ED reattendance (i.e., there was moderate or highly certain evidence that neither nurse-initiated X-rays nor physician-initiated X-rays were favoured on unplanned ED reattendance). The participants also mentioned that social workers, geriatricians, paramedics, and pharmacists with extended scopes of practice could also help address the overcrowding issue. In the literature, we found no interventions where social worker care was assessed on its own outside of an interdisciplinary team, and we found inconclusive evidence for interventions led by geriatrics-trained staff for nursing home residents, structured needs assessments by geriatric ED nurses, or specialist geriatric EDs. One participant mentioned that psychiatry is important for those experiencing mental health conditions but they felt there is a lack of care when people who need these services present to the ED in the evenings or weekends because psychiatry services are only available on Monday to Friday during business hours. In the literature we found that weekday rounds by attending psychiatrists for patients in the ED with mental health challenges and liaison psychiatry services in the ED for adults had uncertain evidence of effectiveness. Furthermore, the experts consulted on this review also pointed out that conducting research investigating changes in nurse or physician staffing could be challenging as they could be influenced by unions, hospital employment contracts, and government payment formulas.
Another intervention we identified in the literature was increasing resources for the ED, such as beds and staff, as part of policy reform. The participants agreed that increased resources were needed; however, they also mentioned that staff burnout needed to be addressed, especially as they felt that most of the interventions discussed put more pressure on staff who are already overworked. One participant suggested that giving staff breaks, putting them on easier rotations to recover, or giving nurses more focused roles could help with this concern; we did not find evidence on these specific types of interventions. Another participant mentioned that if adding staff included adding external staff, this could reduce morale and create resentment if the roles or salaries differed from the original staff.
Home care, community care, and long-term care interventions were also found in the literature and considered valuable by participants. There was disparate evidence for the effectiveness of these interventions in the literature. One participant mentioned that opening the lines of communication between long-term care providers and ED physicians with patients’ needs in mind was necessary, as well as coordination of primary care providers, pharmacists, physiotherapists, occupational therapists, and home care nurses, especially for an aging population. Although interventions in long-term care homes were found, 1 participant mentioned that there was actually a need to first increase the number of spots in care homes, as many cannot find long-term care beds to begin with; however, our summary of systematic reviews of interventions did not seek to specifically identify studies of long-term care bed availability.
In addition to the discussion among participants on the interventions found in the literature, there were also ideas mentioned during the dialogues that were not found in the summary of systematic review evidence on interventions. For example, there was no systematic review that focused solely on interventions for rural populations and few primary studies within systematic reviews looked at rural communities. Participants in the multistakeholder dialogues suggested that solutions were required for long-term care access for rural communities, health care provider training on rural care, application of unique solutions for rural EDs that were not just reapplications of urban ED solutions, access to alternate health care in rural and remote areas for those not wishing to go to an ED (e.g., older adults), and using technology for rural and remote populations. Although the literature contained some interventions on using technology, such as remote triage (e.g., virtual communication) and electronic health records in EDs, participants mentioned the need for broader technology adoption that could reduce barriers, leverage data, and increase integration. In the literature we found the remote triage evidence was uncertain for patient satisfaction and did not appear better than usual care for ED use. One participant mentioned that a new technology that they used personally that was supposed to indicate patient wait times was not reliable in practice, so having accurate and reliable information when implementing these kinds of interventions was important. Other participants mentioned how senior hospital leadership could be resistant to change with digital solutions, while others mentioned that implementing technology would need careful consideration of cost, bandwidth, health information security, and hospital reputation.
As most of the literature we found based on our eligibility criteria focused on specific interventions that changed 1 or a few aspects to address ED overcrowding, the participants discussed that the solution to this issue is much larger and multifaceted; they expressed that it includes a complete system redesign involving collaboration and integration between the government, education systems, social services, the public, and the health care system. Participants notes that, ideally, such multifaceted solutions would target root causes, address accountability, and provide early access to quality care by multidisciplinary teams. One participant mentioned that implementing good ideas from what has worked in other publicly funded health care systems would be ideal. Another participant mentioned that the rate limiting factor for overcrowding is always changing so solutions may need to adjust to demands, further reiterating that ED overcrowding is a complex problem with many moving parts; as a result, there may not be specific interventions that work to solve the issue but a multitude of interventions that work in harmony.
Ethical and Equity Considerations
Our research incorporated several equity and ethical considerations both in the way we conducted the work and the information we discovered from the literature. The ethical considerations raised here may apply across populations or groups. Through the following discussion we aim to demonstrate the relationship between ethics and equity considerations. Attention to equity within an ethical analysis can help identify the ways that certain groups differentially and/or disproportionately experience harm.
As outlined in our protocol,110 we used the equity checklist for HTA118 to guide us during each step of the work, and PROGRESS-Plus119 to help us identify the populations reported in the literature that may experience inequities. We also included outcomes such as patient satisfaction and health care provider capacity (e.g., burnout, staffing insufficiencies) to address measures of intervention effectiveness from these important perspectives.
Although some systematic reviews reported on equity-deserving groups and PROGRESS-Plus criteria,119 most of the evidence we found discussed neither equity nor how various individuals and groups are differentially impacted by factors contributing to ED overcrowding.120 It is possible that, due to the rapid nature of our work or our methodological limitations, we were unable to find literature that speaks to equity-deserving groups. There may also be a lack of research on how ED overcrowding factors and interventions affect different populations. Notably, limited understanding of how ED overcrowding factors and interventions affect different populations has ethical and equity implications for decision-making about potential interventions, including whether and how certain interventions, including those that aim to improve efficiency, might address, or exacerbate, existing inequities in EDs and broader health care.
There was an overall lack of explicit reporting around equity and ethical considerations for both factors and interventions using the methodology and approaches outlined in our protocol.110 For the summary of systematic review evidence on interventions, less than one-third of the systematic reviews reported on sex, disability status, populations experiencing mental health concerns, socioeconomic status, populations experiencing houselessness, populations speaking languages other than English, race (e.g., IBPOC), or ethnicity. No systematic reviews reported information about gender identity, religion, newcomer status, or 2SLGBTQ+ communities. For the environmental scan, 1 article compared ED overcrowding in a “high-income” setting to ED overcrowding in a “low-income” setting, and 2 articles discussed ED overcrowding specifically in relation to populations experiencing mental health concerns; other equity-related considerations were not reported. In addition, for both the factors and interventions literature, if sex was mentioned, it was not defined, so it is unclear whether the studies measured sex or gender identity, if any assumptions were made, or if the terms were used interchangeably. This is because sex and gender identity were poorly defined and reported in the literature that we found. Furthermore, beyond reporting on these dimensions of diversity, there were limited findings related to the impacts or implications of interventions on these different population groups. We understand that researchers may not have set out to study ED overcrowding in equity-deserving groups specifically. As outlined in our protocol,110 we used the PROGRESS-Plus criteria119 to present literature results by equity dimensions if available. While this criteria offers a wide range of equity dimensions to consider, and perhaps not all are relevant to ED overcrowding to a similar degree, it was a way for us to capture what is and what is not reported in the current scientific literature.
An important consideration for ED overcrowding is the setting where ED services or those seeking ED services are located. Yet, few studies reported on populations in Canada, and only 1 primary study discussed factors related to geographic differences in ED use or resource disparities across regions. For the environmental scan, all literature that reported where EDs were located (e.g., whether they were urban, rural, remote) examined factors contributing to ED overcrowding in urban EDs only. For the summary of systematic review evidence on interventions, one-quarter of the systematic reviews included primary studies that identified urban settings and 7 systematic reviews identified primary studies in either rural or remote mountainous areas. Over 60% of the systematic reviews did not report the setting where the interventions took place or where the ED was located. The content experts engaged for this review also mentioned that there may be a lack of research infrastructure in rural areas, which could be due to limited health resources that may favour clinical infrastructure over research infrastructure. This emphasis on urban settings in the literature may result in a gap in our understanding of how factors contributing to ED overcrowding differ between urban EDs and rural or remote EDs and the implications for those who work in or attempt to access these services. It can also mean that experiences unique to individuals living in, working in, and accessing ED services in rural and remote locations may not have been represented in the literature that we identified and included. For interventions, it is also unclear whether there is a lack of information or research in rural or remote settings because there are fewer EDs there or they have fewer resources to conduct and report on novel or trial interventions, whether interventions have been conducted in rural or remote settings at all, or if research has just not been captured in systematic reviews. We heard from our multistakeholder dialogue sessions that older adults in rural areas may experience inequitable access to primary care and long-term care and that this can affect experiences in the ED. Understanding the unique situation in rural and remote settings is a crucial part of identifying potential inequities and underserved settings in Canada. Urban EDs also likely face unique challenges related to the diversity of populations that might access these services, as well as larger populations of equity-deserving groups, such as those experiencing houselessness.
Other important considerations relate to how specific populations may experience or be impacted by ED overcrowding differentially. For the summary of systematic review evidence on interventions, there were several systematic reviews that focused on older adults, people who experience mental health challenges, and people who use the ED frequently. It is possible that these populations may visit the ED if their needs are not being served in other ways, such as through primary care, long-term care, home care, or follow-up appointments. For example, 1 of the ED overcrowding interventions we found in the literature was services for nursing home residents provided onsite, which was inconclusive; some older adults may not be able to afford long-term care and would therefore not have access to this type of intervention at all. Another example is that those seeking mental health services may not be able to access or afford appropriate mental health care, which is not provided universally in Canada. The multistakeholder dialogue participants mentioned that psychiatry services in the ED are not available in the evenings and on weekends, which can create barriers for those who seek care during these times. People who access the ED frequently were also a group that some systematic reviews focused on. We found that some systematic reviews referred to this group as “frequent users,” which may not be appropriate language as it may stigmatize or villainize a group of people who access the ED frequently because they may not have anywhere else to go. The more appropriate focus is on the root needs of various groups visiting the ED instead, and the systemic social and health care factors that may lead these groups to visit EDs in Canada. For example, we heard from content experts that there are groups of people who access the ED due to unmet social needs such as inadequate housing, social isolation, frailty, or poverty.
The multistakeholder engagement sessions aimed to capture different perspectives of those impacted by ED overcrowding, including people receiving care and their caregivers, staff who provide care to patients but may also struggle with issues around workplace resources and supports, trainees who are learning how to provide care in a new setting, and hospital administrators who are considering where and how to allocate funding and resources. We acknowledge, however, that there may be voices that were not captured in the multistakeholder engagement processes or literature reviewed for the series of reports for this project. As well, our engagement strategy did not target certain groups that we later learned through the dialogues may have key perspectives to the overcrowding issue; these include primary care physicians, long-term care professionals, and pharmacists, among others. We are aware of the potential for response bias in this case, where those most directly affected by and entrenched within the challenges of ED overcrowding may have the fewest resources to participate in engagement sessions such as this one, thus biasing engagement to those who have more resources.
A topic that emerged from the literature and our multistakeholder dialogues was how technologies aimed at addressing ED overcrowding may entail unintended harms or consequences or affect different groups differentially or inequitably. An important consideration as new digital tools are developed, such as electronic health records and ED wait time applications, is which groups may or may not end up using these resources due to variables such as socioeconomic status (e.g., affordability), geographic region (e.g., working Wi-Fi or data, “digital deserts” with limited access to the internet), accessibility (e.g., tool having accessible features), or language considerations (e.g., ability to understand the tool), and how this “digital divide” may further entrench existing health and social disparities. Furthermore, new technologies and data collection can also introduce bias, discrimination, and issues of privacy and confidentiality. For example, tools may present information in a way that is catered to some groups of people and not others (e.g., instructions on how to use a tool may have assumptions about how knowledgeable people are about using that specific technology), or people using the tool may not feel comfortable with sharing information and may not trust data holders due to a history of past harms (e.g., how much information a tool shares about how long a person has been waiting, any identifying information about them). While these digital tools may be beneficial in managing ED throughput factors, who benefits from these tools and who may lack access, as well as issues related to privacy and data stewardship for data storage, retention, and use, should be considered.120,121 When equity-deserving groups and characteristics are not discussed in research literature, it may lead to the assumption that all individuals experience a phenomenon (i.e., ED overcrowding) or interventions to address that phenomenon in the same way. However, this is typically not the case, as members of equity-deserving groups are often disproportionately negatively affected by these issues and may experience discrimination, racism, or harm.122 Interventions meant to address these issues can also exacerbate inequities for these groups. It is also important to understand how these identities can intersect (e.g., a person who is Black and also identifies as nonbinary, a person experiencing mental health challenges who also has an injury and may visit different specialists for each condition) and how these intersecting factors further influence the ways individuals experience disparities in access to and delivery of health care.
In systematic reviews identified in the summary of systematic review evidence on interventions, we were unable to find evidence on whether equity-deserving groups had access to interventions and how they may have been affected by them (e.g., based on where they live, and their race, ethnicity, religion, languages spoken, access to housing, mobility, health conditions, education, occupation, socioeconomic status, and/or gender identity). Even when the literature may show a certain intervention to be favourable, different groups may have different levels of access to and uptake of those interventions, understand and experience health care in unique ways, benefit or not benefit from the interventions, or be treated differently in EDs. For example, as indicated by some of the experts that are part of HTERP, some people may not be able to arrive at the ED in an ambulance and arrive by foot or public transit, or ambulance arrival may also be related to socioeconomic status rather than just severity of condition. One of the emergency medicine clinicians who we consulted on this project noted that when considering the effectiveness of interventions, what helps 1 group may harm another, depending on what outcomes are measured; for instance, reducing emergency medical services workload could lead to an increase in ED nurse workload. This concept is also highlighted in recent health care approaches, such as the quintuple aim for health care improvement, where health equity is an important component alongside improving population health, enhancing the care experience, reducing costs, and staff experiences (e.g., burnout).123
Future research by both CADTH and other research groups can start with understanding who may be at risk of experiencing heightened and disproportionate negative effects of ED overcrowding, and then better refine search and selection of the evidence to ensure that data related to equity-deserving groups are captured or point to gaps in the research where these groups have not been considered but should be. Future work should strive to deliberately and explicitly include ethical considerations inherent in research, planning, and policy-making; include considerations of equity-deserving groups; and dedicate the time needed to consider the various facets of this issue.
The Complexity of ED Overcrowding
ED overcrowding is a complex, multifaceted issue, and 1 that has persisted for years. Since CADTH’s 4-report series on ED overcrowding in Canada in 2006, the problem has only worsened.1,2,8-11 This persistence and worsening speaks to the complicated nature of this issue and how difficult it is to implement effective, equitable, and sustainable solutions. This is likely because it is not a problem only of ED overcrowding, but a problem of hospital overcrowding and more than that, of scarce and strained resources throughout broader social and health care systems. ED overcrowding has been referred to as a complex adaptive system because of the many interconnected and dynamic variables that are involved and where solutions are not simple.124 Table 16 highlights that even when factors for ED overcrowding are identified, there is not necessarily a singular intervention that can specifically and effectively target each factor. Rather, there exists a range of interventions that can potentially address 1 or more factors both within and outside of the ED. Because there could be multiple interventions implemented at the same time, they may influence the effectiveness of each other (e.g., the effectiveness of “input intervention X” could be strengthened, weakened, or remain the same if “throughput intervention Y” is also implemented). The potential for these interactions further highlights the complexity of overcrowding and reinforces the need for a system-wide approach to solving this issue. When examining these issues in silos, there is a risk that unintended side effects can go unnoticed.
By drawing from our findings and the multistakeholder dialogue sessions, we can discern how ED’s place in the health care system and the jurisdictional administration of health care in Canada contribute to the complexity of this matter.6 Unlike other health care services, most EDs are always open, available to anyone, and do not require any type of appointment. Primary care providers, on the other hand, often work during typical business hours with limited after-hour services and are often only accessible to those who are on their care roster.23 As participants from the multistakeholder dialogues pointed out, people may view the ED as a reliable, trustworthy, and easily accessible option for receiving care and use it even when their concerns could potentially be adequately addressed by another service. This is often a consequence of not having access to these services.19,21,33 Canada also has a unique challenge because of how health care is administered and funded across the country. Funding of health care in Canada may come from different sources such as the federal government, provincial and territorial taxation, and fiscal transfers,125,126 while health care is administered at the federal, provincial, and territorial levels with different organizational structures and processes across and within these regions.127 There are likely to be differences in the issues faced by jurisdictions as well as the solutions that can feasibly be implemented, and specific considerations for how funding investment and resources should be distributed equitably within each specific region. Geographic differences between and within jurisdictions (e.g., urban versus rural) also contribute to these differences. Consequently, there is not a one-size-fits-all approach to alleviate ED overcrowding within Canada. All of these aspects reinforce that ED overcrowding is not an issue limited to the ED.
Conceptualizing ED overcrowding as a health system–wide problem aligns with the findings from the environmental scan on factors contributing to ED overcrowding. When we examine these results, it is evident that most of the identified factors lie outside of the ED. From input factors like volume of patient visits, to output factors such as boarding and access block, to contextual factors such as population growth and hospital culture, most contributing factors to ED overcrowding are those outside the control of the ED and relate to hospital-wide and health system–wide capacity. A smaller number of throughput factors, which can potentially be controlled by the ED, were identified, while most of interventions we identified in the summary of systematic review evidence on interventions targeted throughput issues with a particular emphasis on maximizing efficiencies within the ED. Despite decades of work in this area, overcrowding continues to be an issue. The discrepancy between the distribution of input, throughput, and output factors that contribute to overcrowding and evidence to support input, throughput, and output interventions to alleviate overcrowding suggests a mismatch and a need for focused research and evaluations of input and output interventions. As noted in the multistakeholder dialogue sessions, a substantial amount of time and effort has been put into making EDs as efficient as possible; however, the persistence of overcrowding indicates that it has not been enough to solve the issue2,6 and we do not have a clear understanding of whether efficiency-promoting interventions differentially benefit or harm certain populations. As Morley et al. (2018) point out in their review, there is general agreement that because so many of the causes of crowding lay outside of the ED, so too must the answers.29 Findings from qualitative literature have shown that when considering issues of patient flow, focusing on only 1 part of a patient’s journey (for example, when they are in the ED) can represent a decentralized way of thinking that fragments responsibility and misses an opportunity to introduce a cohesive strategy to alleviate overcrowding.128
In addition, because ED overcrowding is not merely an ED issue, true solutions cannot exist only at the ED level. In fact, solutions may not even exist solely within the health care sector because the health of people and populations is affected by the social determinants of health. Complex issues require creative and innovative approaches and we heard from the participants in the multistakeholder dialogues that possible approaches to target overcrowding at both the ED and hospital level might include the involvement of industries and systems outside of health care, such as housing and community services, engineering, and infrastructure, among others. Other industries can provide novel perspectives that can address aspects of overcrowding from a new point of view. Similarly, as technology continues to advance, we can look to leverage new and emerging digital tools to come up with innovative solutions. The content experts also indicated that complex problems may require approaches beyond typical medical research methodologies, which alone may not be sufficient to evaluate the effectiveness of interventions . For example, in quality improvement programs, the intervention(s) are dynamic and improved on an ongoing basis to adapt to changing needs. This can help address broad and complex phenomena like ED overcrowding, where the interconnectedness of variables in unknown or unclear. This speaks to how solutions may not solely lay in traditional medical research methods (e.g., RCTs) as it can be difficult to measure or study more “real-world” scenarios. The content experts indicated that a more sophisticated framework to assess interventions in a complex open system with multiple interconnected variables may ultimately be the most useful approach.
This report along with the other series of reports on ED overcrowding are a way to bridge knowledge and insights from research literature, stakeholder dialogues, and expert feedback to address this complicated issue. Our work can be used as a starting point to understand what we’ve learned from these different knowledge sources (e.g., which factors are relevant, which interventions are effective) and begin to find solutions that are multifaceted (e.g., what do people who work in and use the ED think and feel about these factors and interventions) as previous ways of framing the issue that focus on the ED only, or only used knowledge from a single source, have not captured a wider scope of understanding. We also need to ensure that solutions consider a range of representative voices to fully inform any decisions made moving forward (e.g., for equity-deserving groups) and to carefully consider where some interventions may affect some groups differently or be beneficial on some outcomes and harmful on others. Multiple systems and voices need to work in collaboration with each other rather than in silos, with constant reevaluation, to appropriately address the dynamic nature of this important issue.124
Methods
Research Questions
Environmental scan of contributing factors:
What are the input, throughput, and output factors that contribute to ED overcrowding internationally and in Canada? How does the literature describe the impact of input, throughput, and output factors on ED overcrowding?
What are the contextual factors (at the micro, meso, and macro levels) that have an impact on ED overcrowding internationally and in Canada? How does the literature describe their impact on ED overcrowding?
What are the explanations provided by the literature about how and why the identified input, throughput, output, and contextual factors contribute to ED overcrowding internationally and in Canada?
Summary of systematic review evidence on interventions:
For individuals of any age who may need to access ED services, what is the effectiveness and safety of interventions to alleviate ED overcrowding?
To address the objectives of this report, we conducted an environmental scan of contributing factors to ED overcrowding and a summary of systematic review evidence of the effectiveness of interventions to alleviate ED overcrowding. We followed a protocol that was written a priori.110 We prospectively registered the protocol for the summary of systematic review evidence on interventions in the international repository PROSPERO (registration number: CRD42023428073). The literature search methods for the environmental scan and summary of systematic review evidence on interventions are available in the Supporting Information document. Due to time and resource constraints that arose during the review process, we made changes to the methods identified in our protocol110 to expedite work. As such, we were unable to adhere to all methodological and reporting standards as originally planned.115 All protocol deviations for the summary of systematic review evidence on interventions are listed in the Protocol Amendments table in the Supporting Information document.
This report uses a conceptual model developed by Asplin et al. (2003),102 which divides the emergency care system into 3 interdependent parts: input, throughput, and output. The input component focuses on aspects that influence the need for ED services, the throughput component focuses on aspects and processes inside of the ED and hospital, and the output component focuses on elements concerning patient disposition (e.g., to inpatient care, to outpatient care, to home).
The environmental scan of contributing factors and the summary of systematic review evidence on interventions were conducted concurrently by 2 separate teams of researchers using different research questions, methods, and selection criteria. Once the results for both were prepared, we examined and highlighted how the factors and interventions related to each other. We organized the effectiveness findings of the interventions by the factors being targeted by their implementation.
We conducted an environmental scan to identify literature about factors contributing to ED overcrowding internationally and in Canada. This study design is suited to the broad, exploratory nature of the research questions and allowed us to investigate the breadth of information available on the topic. The findings of this environmental scan are based on a limited search of the published and grey literature. Furthermore, we collaborated and communicated with the lead author and the broader project team to identify causal and contextual factors relevant to the summary of systematic review evidence on interventions. The environmental scan also drew on the insights shared and discussed by people with extensive personal and/or professional experience with ED care within the Canadian health system.
Due to the rapid nature of the work, the environmental scan of contributing factors only included literature that explicitly stated that factors caused or contributed to overcrowding. Detailed inclusion criteria are available in the Supporting Information document. We only included articles that explored and discussed these factors in more detail if they were clearly linked to overcrowding (e.g., we excluded articles only focused on reasons for frequent visits to the ED). We also only included articles that discussed ED visits among specific populations if it was specifically described in the context of causes of overcrowding. After completion of our protocol,110 and based on input from content experts, we also screened additional literature that focused on research stemming from the fields of engineering management and operations.
We conducted a summary of systematic review evidence on interventions to summarize evidence from systematic reviews on the effectiveness of different interventions to alleviate ED overcrowding. We selected this study design because of the overwhelming number of primary studies that were identified during our scoping search of interventions evaluating the effectiveness and safety of interventions to alleviate ED overcrowding. We planned our methods with consideration of those suggested within the Cochrane Handbook Overviews of Reviews129 chapter and we aimed to report the conduct of our work in accordance with the Preferred Reporting Items for Overviews of Reviews (PRIOR) as much as possible.115
The methods for the summary of systematic review evidence on interventions are detailed in our protocol.110 An information specialist conducted a peer-reviewed literature search, using MeSH and keywords related to overcrowding and emergency medicine, in MEDLINE, Embase, CINAHL, and Cochrane Database of Systematic Reviews. The search was conducted on March 27, 2023, and limited to English- and French-language documents published since January 1, 2013. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, overviews of reviews, or indirect treatment comparisons. A grey literature search was also conducted. To be considered systematic reviews, reports had to include a research question, sources searched with a reproducible search strategy, eligibility criteria, selection methods, reporting of methodological quality and/or risk of bias of the included studies, and information about data analysis and synthesis that would allow the results to be reproduced. Systematic reviews also had to be focused on ED overcrowding; use risk of bias methods that assessed allocation concealment and blinding for RCTs, and confounding and selection bias for NRSs; and provide numerical results for most of their primary studies. Detailed inclusion criteria are available in the Supporting Information document. After completion of our protocol,110 and based on input from content experts, we ran additional customized searches in Scopus and PsycINFO, as well as a focused internet search for literature in the engineering, management, and operations fields related to both the environmental scan and summary of systematic review evidence on interventions. These searches were conducted between June 20 and 23, 2023. Two independent reviewers completed title-abstract and full-text screening and agreed on the final list of included systematic reviews. We included all eligible systematic reviews and mapped the overlap in primary studies across those included.
One reviewer extracted data from included systematic reviews such as first author and date of publication, years searched, number of primary studies and whether they were randomized, countries where the primary studies were conducted, type of synthesis, intervention and comparator, population details, and author conclusions. A second reviewer independently verified all extracted data elements from a subset (approximately 10%) of the included systematic reviews. Two independent reviewers assessed their confidence in the results of the included systematic reviews using AMSTAR 2101 and agreed on the final judgments. According to ASMTAR 2101 criteria, we classified our confidence in the results of the included systematic reviews as critically low, low, moderate, or high.
Table 4: Intervention Effectiveness Definitions
Effectiveness | Definition |
|---|---|
Favourable | There is certain evidence or evidence with some uncertainty of better effectiveness of the intervention vs. a comparator, or the SR authors reported a high or moderate level of certainty on other scales, such as GRADE or ECP, of better effectiveness of the intervention vs. a comparator. |
Favourable, inconclusive | There is evidence of better effectiveness of an intervention vs. a comparator, yet we rated the evidence as very uncertain or the SR authors reported a low or very low level of certainty. |
Neutral | There is certain evidence or evidence with some uncertainty (moderate or high certainty) that neither the intervention nor the comparator was favoured. |
Neutral, inconclusive | There is evidence that the neither the intervention nor the comparator was favoured, yet the evidence is very uncertain (low or very low certainty). |
Mixed, inconclusive | There are heterogeneous results for effectiveness of an intervention vs. a comparator, and the heterogeneity is too serious to draw a conclusion. |
Unfavourable | There is certain evidence or evidence with some uncertainty (moderate or high certainty) of worse effectiveness of the intervention vs. a comparator. |
Unfavourable, inconclusive | There is evidence of worse effectiveness of the intervention vs. a comparator, yet the evidence is very uncertain (low or very low certainty). |
No evidence | There is no evidence from primary studies.a |
ECP = Evidence-based Practice Center program of the Agency of Healthcare Research and Quality; GRADE = Grading of Recommendation, Assessment, Development and Evaluation; SR = systematic review; vs. = versus.
aThis was assigned only to outcomes reported by the SR authors as the primary outcome of interest47 or included in the primary objective of the SR.93
We revised existing classification scales for summarizing evidence for systematic reviews130-132 and categorized the effectiveness of each intervention-comparison outcome based on:
the direction of the effects — whether the findings were favourable (effect in favour of the intervention), neutral (neither intervention was favoured), unfavourable (effect in favour of the comparator), or mixed (evidence for both directions of effect), were categorized by 1 reviewer per the definitions in Table 1.
the certainty of evidence — we drew on the evidence assessments as reported in the systematic reviews. When the certainty of evidence was not reported, 1 reviewer assessed the certainty of evidence for each comparison-outcome by considering the following aspects, as reported in the systematic reviews: study design, risk of bias in the primary studies, inconsistency in effects across included studies, imprecision of effects, and publication bias. We assigned following levels: certain (i.e., no uncertainty or high level of certainty), some uncertainty (i.e., moderate uncertainty), and very uncertain (i.e., inconclusive). When outcomes data were based on solely nonrandomized primary studies, we set the baseline at some uncertainty due to concerns for selection bias and residual confounding. We did not assess certainty based on indirectness (i.e., generalizability to the Canadian context). However, we did point out when findings were potentially not applicable to Canada because the primary studies were not conducted in Organization for Economic Cooperation and Development countries with high income and universal health care.133
Clinical, Patient, and Community Engagement
To enhance the quality and relevance of this work, CADTH engaged people with extensive personal and/or professional experience with ED care within a Canadian health system. Specifically, CADTH engaged with health care professionals who are providing or supporting care in the ED (e.g., ED physicians, primary care physicians, nurses, social workers, paramedics, administrators, leadership) and people with experience receiving care in the ED (e.g., patients, family members, caregivers).
Through an open call on CADTH’s website, CADTH invited people to complete a statement of interest outlining their connection to the topic of ED overcrowding, and how their experiences and views might add to the diversity of perspectives. Interested individuals were engaged as expert consultants to ensure the relevance and accuracy of the clinical context; as peer reviewers to provide feedback on appropriate language, scope, and definitions and help ensure relevance to the Canadian context; and as expert HTERP members to support deliberations and the development of recommendations.
Stakeholders were also given the opportunity to participate in a multistakeholder dialogue, consisting of a series of consultations led by CADTH’s Engagement team in the summer of 2023. We aimed to engage a wide range of stakeholders and ensure that the perspectives of interested and affected families, clinicians, and community member were heard and reflected in our work — with a focus on diversity and to ensure representation from underserved populations. The purpose of the multistakeholder dialogue was to support the development of recommendations by HTERP by sharing interim results of CADTH literature reviews that identify the factors contributing to ED overcrowding in Canada and interventions to alleviate ED overcrowding, and to highlight areas where no literature was found. A further objective was to understand and discuss these results, hear perspectives about local context and implementation issues, and identify and discuss important concerns for patients, families, ED staff and trainees, and communities emerging from the project.
Guiding Principles
Cocreation: We began by assembling a small working group of 3 patient and clinician partners (Frank Scheuermeyer, Maggie Keresteci, Sameer Sharif) and CADTH staff members (Gino De Angelis, Nazia Darvesh, Francesca Brundisini, Tamara Rader).
Transparency: A call for statements of interest was launched and shared widely via CADTH networks with the goal of assembling a diverse group of interested and affected people. Participants completed a conflict of interest form and are acknowledged in the summary of the multistakeholder dialogue sessions.
Inclusion: Participants were selected from a pool of those who responded to an open call. An emotional support person was engaged to help ensure a safe and welcoming discussion. All stakeholders were included equally in each multistakeholder dialogue session. CADTH staff acted as notetakers, observers, and facilitator.
Recruitment
The open call was shared with subscribers to CADTH E-Alerts. CADTH E-Alerts are time-sensitive alerts about CADTH, feedback opportunities, corporate news. About 150 Canadian clinician groups and patient groups are subscribed.
In addition to E-Alerts, invitations to complete or share the open call for statements of interest was shared with the following stakeholder groups:
Canadian Association of Emergency Physicians
National Emergency Nurses Association
Paramedic Chiefs of Canada
Society of Rural Physicians of Canada
Black Physicians of Canada
Patient and Family Advisors Network
Patient Advisors Network
Shepherds of Good Hope
Ottawa Inner City Health Inc.
Canadian Coalition for Seniors’ Mental Health
Canadian Alliance to End Homelessness
Carers Canada.
A full summary of CADTH’s multistakeholder dialogue is published separately.6
References
1.Affleck A, Parks P, Drummond A, Rowe BH, Ovens HJ. Emergency department overcrowding and access block. CJEM. 2013;15(6):359-384. PubMed
2.Rowe BH, McRae A, Rosychuk RJ. Temporal trends in emergency department volumes and crowding metrics in a western Canadian province: a population-based, administrative data study. BMC Health Serv Res. 2020;20(1):356. PubMed
3.Canadian Institute for Health Information. NACRS emergency department visits and lengths of stay. 2023; https://www.cihi.ca/en/nacrs-emergency-department-visits-and-lengths-of-stay. Accessed 2023 Apr 06.
4.Position statement on over-crowded emergency departments. West Melbourne (AU): International Federation for Emergency Medicine; 2022: https://assets.nationbuilder.com/ifem/pages/546/attachments/original/1670806966/IFEM_Position_Statement_on_Emergency_Department_Overcrowding_December_2022.pdf?1670806966. Accessed 2023 Apr 06.
5.Canadian emergency care is being crushed - and why that matters for all of us. Ottawa (ON): Canadian Association of Emergency Physicians; 2023: https://caep.ca/wp-content/uploads/2023/01/Letter-Canadian-Emergency-Care-is-Being-Crushed-Jan-2023.pdf. Accessed 2023 Apr 06.
6.Rader T, Ritchie L. Multi-stakeholder dialogue: emergency department overcrowding in Canada. (CADTH health technology review). Can J Health Technol. 2023;3(10). https://canjhealthtechnol.ca/index.php/cjht/article/view/OP0553/OP0553. Accessed 2023 Oct 25.
7.Savioli G, Ceresa IF, Gri N, et al. Emergency department overcrowding: understanding the factors to find corresponding solutions. J Pers Med. 2022;12(2):279. PubMed
8.Bond K, Opsina M, Blitz S, et al. Interventions to reduce overcrowding in emergency departments. (CADTH Technology report no. 67.4). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320d_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Mar 28.
9.Ospina MB, Bond K, Schull M, et al. Measuring overcrowding in emergency departments: a call for standardization. (CADTH Technology report no. 67.1). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320a_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Mar 28.
10.Rowe B, Bond K, Opsina M, et al. Data collection on patients in emergency departments in Canada. (CADTH Technology report no. 67.2). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320b_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Mar 28.
11.Rowe B, Bond K, Opsina M, et al. Frequency, determinants, and impact of overcrowding in emergency departments in Canada: a national survey of emergency department directors. (CADTH Technology report no. 67.3). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320c_Overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Mar 28.
12.Canadian Institute for Health Information. COVID-19’s impact on emergency departments. Ottawa (ON): CIHI; 2021: https://www.cihi.ca/en/covid-19-resources/impact-of-covid-19-on-canadas-health-care-systems/emergency-departments. Accessed 2023 Apr 28.
13.Allen L, Gian CT, Simon K. The impact of Medicaid expansion on emergency department wait times. Health Serv Res. 2022;57(2):294-299. PubMed
14.Crowding, boarding, and patient throughput. J Emerg Nurs. 2018;44(2):176-183. PubMed
15.Cha WC, Ahn KO, Shin SD, Park JH, Cho JS. Emergency department crowding disparity: a nationwide cross-sectional study. J Korean Med Sci. 2016;31(8):1331-1336. PubMed
16.Demircan C, Gürsoy V, Akköse Ş. The problems related to internal medicine consultations in the emergency department. Eur Res J. 2022;8(3):368-374.
17.Doupe M, Chateau D, Derksen S, et al. Factors affecting emergency department waiting room times in Winnipeg. Winnipeg (MB): Manitoba Centre for Health Policy; 2017: http://mchp-appserv.cpe.umanitoba.ca/reference/ER2011_report_Web.pdf. Accessed 2023 May 04.
18.Doupe MB, Chateau D, Chochinov A, et al. Comparing the effect of throughput and output factors on emergency department crowding: a retrospective observational cohort study. Ann Emerg Med. 2018;72(4):410-419. PubMed
19.Gross TK, Lane NE, Timm NL, Committee on Pediatric Emergency Medicine. Crowding in the emergency department: challenges and recommendations for the care of children. Pediatrics. 2023;151(3):e2022060971. PubMed
20.Higginson I, Boyle A. What should we do about crowding in emergency departments? Br J Hosp Med (Lond). 2018;79(9):500-503. PubMed
21.Javidan AP, Hansen K, Higginson I, et al. Report from the Emergency Department Crowding and Access Block Task Force. West Melbourne (AU): International Federation for Emergency Medicine; 2020: https://assets.nationbuilder.com/ifem/pages/270/attachments/original/1650595379/ED-Crowding-and-Access-Block-Report-Final-June-30-2020.pdf?1650595379. Accessed 2023 May 04.
22.Kawano T, Nishiyama K, Hayashi H. Execution of diagnostic testing has a stronger effect on emergency department crowding than other common factors: a cross-sectional study. PLoS One. 2014;9(10):e108447. PubMed
23.Kelen GD, Wolfe R, D’Onofrio G, et al. Emergency department crowding: the canary in the health care system. NEJM Catalyst. 2021. https://catalyst.nejm.org/doi/abs/10.1056/CAT.21.0217. Accessed 2023 Jun 30.
24.Kenny JF, Chang BC, Hemmert KC. Factors affecting emergency department crowding. Emerg Med Clin North Am. 2020;38(3):573-587. PubMed
25.Makama JG, Iribhogbe P, Ameh EA. Overcrowding of accident & emergency units: is it a growing concern in Nigeria? Afr Health Sci. 2015;15(2):457-465. PubMed
26.Marsilio M, Roldan ET, Salmasi L, Villa S. Operations management solutions to improve ED patient flows: evidence from the Italian NHS. BMC Health Serv Res. 2022;22(1):974. PubMed
27.Mashao K, Heyns T, White Z. Areas of delay related to prolonged length of stay in an emergency department of an academic hospital in South Africa. Afr J Emerg Med. 2021;11(2):237-241. PubMed
28.McKenna P, Heslin SM, Viccellio P, Mallon WK, Hernandez C, Morley EJ. Emergency department and hospital crowding: causes, consequences, and cures. Clin Exp Emerg Med. 2019;6(3):189-195. PubMed
29.Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316. PubMed
30.Mustafa F, Gilligan P, Obu D, et al. 'Delayed discharges and boarders': a 2-year study of the relationship between patients experiencing delayed discharges from an acute hospital and boarding of admitted patients in a crowded ED. Emerg Med J. 2016;33(9):636-640. PubMed
31.Rixon A, Wilson S, Hussain S, Terziovski M, Judkins S, White P. Leadership challenges of directors of emergency medicine: an Australasian Delphi study. Emerg Med Australas. 2020;32(2):258-266. PubMed
32.Salway RJ, Valenzuela R, Shoenberger JM, Mallon WK, Viccellio A. Emergency department (ED) overcrowding: evidence-based answers to frequently asked questions. Rev Med Clin Las Condes. 2017;28(2):213-219.
33.Sartini M, Carbone A, Demartini A, et al. Overcrowding in Emergency Department: causes, consequences, and solutions-a narrative review. Healthcare (Basel). 2022;10(9):1625. PubMed
34.Silvester K, Harriman P, Walley P, Burley G. Does process flow make a difference to mortality and cost? An observational study. Int J Health Care Qual Assur. 2014;27(7):616-632. PubMed
35.Van Der Linden MC, Khursheed M, Hooda K, Pines JM, Van Der Linden N. Two emergency departments, 6000km apart: Differences in patient flow and staff perceptions about crowding. Int Emerg Nurs. 2017;35:30-36. PubMed
36.Wang Z, Xiong X, Wang S, Yan J, Springer M, Dellinger RP. Causes of Emergency Department Overcrowding and Blockage of Access to Critical Services in Beijing: A 2-Year Study. J Emerg Med. 2018;54(5):665-673. PubMed
37.Doan Q, Genuis ED, Yu A. Trends in use in a Canadian pediatric emergency department. CJEM. 2014;16(5):405-410. PubMed
38.Abdulwahid MA, Booth A, Kuczawski M, Mason SM. The impact of senior doctor assessment at triage on emergency department performance measures: systematic review and meta-analysis of comparative studies. Emerg Med J. 2016;33(7):504-513. PubMed
39.Abraham J, Kannampallil T, Caskey RN, Kitsiou S. Emergency department-based care transitions for pediatric patients: a systematic review. Pediatrics. 2016;138(2):e20160969. PubMed
40.Aghajafari F, Sayed S, Emami N, Lang E, Abraham J. Optimizing emergency department care transitions to outpatient settings: a systematic review and meta-analysis. Am J Emerg Med. 2020;38(12):2667-2680. PubMed
41.Anderson K, Goldsmith LP, Lomani J, et al. Short-stay crisis units for mental health patients on crisis care pathways: systematic review and meta-analysis. BJPsych Open. 2022;8(4):e144. PubMed
42.Beals T, Naraghi L, Grossestreuer A, Schafer J, Balk D, Hoffmann B. Point of care ultrasound is associated with decreased ED length of stay for symptomatic early pregnancy. Am J Emerg Med. 2019;37(6):1165-1168. PubMed
43.Benabbas R, Shah R, Zonnoor B, Mehta N, Sinert R. Impact of triage liaison provider on emergency department throughput: a systematic review and meta-analysis. Am J Emerg Med. 2020;38(8):1662-1670. PubMed
44.Berkman ND, Chang E, Seibert J, et al. Management of high-need, high-cost patients: a “best fit” framework synthesis, realist review, and systematic review. (Comparative effectiveness review no. 246). Rockville (MD): Agency for Healthcare Research and Quality; 2022: https://www.ncbi.nlm.nih.gov/books/NBK575200/pdf/Bookshelf_NBK575200.pdf. Accessed 2023 Mar 27.
45.Burgess L, Kynoch K, Theobald K, Keogh S. The effectiveness of nurse-initiated interventions in the Emergency Department: a systematic review. Australas Emerg Care. 2021;24(4):248-254. PubMed
46.Cabilan CJ, Boyde M. A systematic review of the impact of nurse-initiated medications in the emergency department. Australas Emerg Nurs J. 2017;20(2):53-62. PubMed
47.Cassarino M, Robinson K, Quinn R, et al. Impact of early assessment and intervention by teams involving health and social care professionals in the emergency department: a systematic review. PLoS One. 2019;14(7):e0220709. PubMed
48.Cicolo EA, Nishi FA, Peres HHC, Cruz D. Effectiveness of the Manchester Triage System on time to treatment in the emergency department: a systematic review. JBI Evid Synth. 2020;18(1):56-73. PubMed
49.Considine J, Shaban RZ, Curtis K, Fry M. Effectiveness of nurse-initiated X-ray for emergency department patients with distal limb injuries: a systematic review. Eur J Emerg Med. 2019;26(5):314-322. PubMed
50.Crawford J, Cooper S, Cant R, DeSouza R. The impact of walk-in centres and GP co-operatives on emergency department presentations: a systematic review of the literature. Int Emerg Nurs. 2017;34:36-42. PubMed
51.Crede SH, O'Keeffe C, Mason S, et al. What is the evidence for the management of patients along the pathway from the emergency department to acute admission to reduce unplanned attendance and admission? An evidence synthesis. BMC Health Serv Res. 2017;17(1):355. PubMed
52.Curr S, Xyrichis A. Does nurse-led initiation of Ottawa ankle rules reduce ED length of stay? Int Emerg Nurs. 2015;23(4):317-322. PubMed
53.Detollenaere J, Van de Voorde C, Van den Heede K. Organisational models at the emergency department to reduce hospital admissions among paediatric patients: a systematic literature review. Eur J Emerg Med. 2022;29(5):329-340. PubMed
54.Dick S, MacRae C, McFaul C, Wilson P, Turner SW. Interventions in primary and community care to reduce urgent paediatric hospital admissions: systematic review. Arch Dis Child. 2023;108(6):486-491. PubMed
55.Doan Q, Enarson P, Kissoon N, Klassen TP, Johnson DW. Rapid viral diagnosis for acute febrile respiratory illness in children in the Emergency Department. Cochrane Database Syst Rev. 2014;9:CD006452. PubMed
56.Dobson I, Doan Q, Hung G. A systematic review of patient tracking systems for use in the pediatric emergency department. J Emerg Med. 2013;44(1):242-248. PubMed
57.Eustache J, El-Kefraoui C, Ekmekjian T, Latimer E, Lee L. Do postoperative telemedicine interventions with a communication feature reduce emergency department visits and readmissions?-A systematic review and meta-analysis. Surg Endosc. 2021;35(11):5889-5904. PubMed
58.Evans R, Connell J, Ablard S, Rimmer M, O'Keeffe C, Mason S. The impact of different liaison psychiatry models on the emergency department: a systematic review of the international evidence. J Psychosom Res. 2019;119:53-64. PubMed
59.Galipeau J, Pussegoda K, Stevens A, et al. Effectiveness and safety of short-stay units in the emergency department: a systematic review. Acad Emerg Med. 2015;22(8):893-907. PubMed
60.Godard-Sebillotte C, Le Berre M, Schuster T, Trottier M, Vedel I. Impact of health service interventions on acute hospital use in community-dwelling persons with dementia: a systematic literature review and meta-analysis. PLoS One. 2019;14(6):e0218426. PubMed
61.Goncalves-Bradley D, Khangura JK, Flodgren G, Perera R, Rowe BH, Shepperd S. Primary care professionals providing non-urgent care in hospital emergency departments. Cochrane Database Syst Rev. 2018;2:CD002097. PubMed
62.Gottlieb M, Palter J, Westrick J, Peksa GD. Effect of medical scribes on throughput, revenue, and patient and provider satisfaction: a systematic review and meta-analysis. Ann Emerg Med. 2021;77(2):180-189. PubMed
63.Grant KL, Bayley CJ, Premji Z, Lang E, Innes G. Throughput interventions to reduce emergency department crowding: a systematic review. CJEM. 2020;22(6):864-874. PubMed
64.Hall KK, Petsky HL, Chang AB, O'Grady KF. Caseworker-assigned discharge plans to prevent hospital readmission for acute exacerbations in children with chronic respiratory illness. Cochrane Database Syst Rev. 2018;11:CD012315. PubMed
65.Health Quality Ontario. Effect of early follow-up after hospital discharge on outcomes in patients with heart failure or chronic obstructive pulmonary disease: a systematic review. Ont Health Technol Assess Ser. 2017;17(8):1-37. https://www.hqontario.ca/Portals/0/Documents/evidence/reports/recommendation-follow-up-discharge-copd-en-1705.pdf. Accessed 2023 Aug 21. PubMed
66.Hesselink G, Sir O, Schoon Y. Effectiveness of interventions to alleviate emergency department crowding by older adults: a systematic review. BMC Emerg Med. 2019;19(1):69. PubMed
67.Ho JK, Chau JP, Cheung NM. Effectiveness of emergency nurses' use of the Ottawa Ankle Rules to initiate radiographic tests on improving healthcare outcomes for patients with ankle injuries: a systematic review. Int J Nurs Stud. 2016;63:37-47. PubMed
68.Huntley AL, Chalder M, Shaw ARG, et al. A systematic review to identify and assess the effectiveness of alternatives for people over the age of 65 who are at risk of potentially avoidable hospital admission. BMJ Open. 2017;7(7):e016236. PubMed
69.Jennings N, Clifford S, Fox AR, O'Connell J, Gardner G. The impact of nurse practitioner services on cost, quality of care, satisfaction and waiting times in the emergency department: a systematic review. Int J Nurs Stud. 2015;52(1):421-435. PubMed
70.Jeyaraman MM, Alder RN, Copstein L, et al. Impact of employing primary healthcare professionals in emergency department triage on patient flow outcomes: a systematic review and meta-analysis. BMJ Open. 2022;12(4):e052850. PubMed
71.Jones P, Haustead D, Walker K, et al. Review article: has the implementation of time-based targets for emergency department length of stay influenced the quality of care for patients? A systematic review of quantitative literature. Emerg Med Australas. 2021;33(3):398-408. PubMed
72.Kimmel HJ, Brice YN, Trikalinos TA, Sarkar IN, Ranney ML. Real-time emergency department electronic notifications regarding high-risk patients: a systematic review. Telemed J E Health. 2019;25(7):604-618. PubMed
73.Kinnear N, Herath M, Barnett D, et al. A systematic review of dedicated models of care for emergency urological patients. Asian J Urol. 2021;8(3):315-323. PubMed
74.Kirkland SW, Soleimani A, Rowe BH, Newton AS. A systematic review examining the impact of redirecting low-acuity patients seeking emergency department care: is the juice worth the squeeze? Emerg Med J. 2019;36(2):97-106. PubMed
75.Leduc S, Cantor Z, Kelly P, Thiruganasambandamoorthy V, Wells G, Vaillancourt C. The safety and effectiveness of on-site paramedic and allied health treatment interventions targeting the reduction of emergency department visits by long-term care patients: systematic review. Prehosp Emerg Care. 2021;25(4):556-565. PubMed
76.Lowthian JA, McGinnes RA, Brand CA, Barker AL, Cameron PA. Discharging older patients from the emergency department effectively: a systematic review and meta-analysis. Age Ageing. 2015;44(5):761-770. PubMed
77.Matifat E, Mequignon M, Cunningham C, Blake C, Fennelly O, Desmeules F. Benefits of musculoskeletal physical therapy in emergency departments: a systematic review. Phys Ther. 2019;99(9):1150-1166. PubMed
78.Ming T, Lai A, Lau PM. Can team triage improve patient flow in the emergency department? A systematic review and meta-analysis. Adv Emerg Nurs J. 2016;38(3):233-250. PubMed
79.Mullins A, O'Donnell R, Mousa M, et al. Health outcomes and healthcare efficiencies associated with the use of electronic health records in hospital emergency departments: a systematic review. J Med Syst. 2020;44(12):200. PubMed
80.Newton AS, Hartling L, Soleimani A, Kirkland S, Dyson MP, Cappelli M. A systematic review of management strategies for children's mental health care in the emergency department: update on evidence and recommendations for clinical practice and research. Emerg Med J. 2017;34(6):376-384. PubMed
81.O'Cathain A, Foster A, Carroll C, et al. Health literacy interventions for reducing the use of primary and emergency services for minor health problems: a systematic review. Health Soc Care Deliv Res. 2022;10(38). https://www.ncbi.nlm.nih.gov/books/NBK587674/pdf/Bookshelf_NBK587674.pdf. Accessed 2023 Mar 27. PubMed
82.Peterson K, Helfand M, Humphrey L, Christensen V, Carson S. Evidence brief: effectiveness of intensive primary care programs. (Evidence-based Synthesis Program project #09-199). Washington (DC): U.S. Department of Veterans Affairs; 2013: https://www.ncbi.nlm.nih.gov/books/NBK384618/pdf/Bookshelf_NBK384618.pdf. Accessed 2023 Mar 27.
83.Poku BA, Hemingway P. Reducing repeat paediatric emergency department attendance for non-urgent care: a systematic review of the effectiveness of interventions. Emerg Med J. 2019;36(7):435-442. PubMed
84.Pritchard C, Ness A, Symonds N, et al. Effectiveness of hospital avoidance interventions among elderly patients: a systematic review. CJEM. 2020;22(4):504-513. PubMed
85.Pulcini CD, Coller RJ, Houtrow AJ, Belardo Z, Zorc JJ. Preventing emergency department visits for children with medical complexity through ambulatory care: a systematic review. Acad Pediatr. 2021;21(4):605-616. PubMed
86.Ratsimbazafy C, Schwab C, Dechartres A, Fernandez C, Hindlet P. Readmissions of elder patients presenting to hospital for a fall (RELIEF): a systematic review. J Am Med Dir Assoc. 2020;21(10):1451-1457.e1456. PubMed
87.Reddy S, Jones P, Shanthanna H, Damarell R, Wakerman J. A systematic review of the impact of healthcare reforms on access to emergency department and elective surgery services: 1994-2014. Int J Health Serv. 2018;48(1):81-105. PubMed
88.Rennke S, Nguyen OK, Shoeb MH, Magan Y, Wachter RM, Ranji SR. Hospital-initiated transitional care interventions as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 Pt 2):433-440. PubMed
89.Rushton S, Boggan JC, Lewinski AA, et al. Effectiveness of remote triage: a systematic review. (Evidence Synthesis Program project #09-010). Washington (DC): U.S. Department of Veterans Affairs; 2019: https://www.ncbi.nlm.nih.gov/books/NBK553039/pdf/Bookshelf_NBK553039.pdf. Accessed 2023 Mar 27.
90.Santosaputri E, Laver K, To T. Efficacy of interventions led by staff with geriatrics expertise in reducing hospitalisation in nursing home residents: a systematic review. Australas J Ageing. 2019;38(1):5-14. PubMed
91.Sharma S, Rafferty AM, Boiko O. The role and contribution of nurses to patient flow management in acute hospitals: a systematic review of mixed methods studies. Int J Nurs Stud. 2020;110:103709. PubMed
92.Soster CB, Anschau F, Rodrigues NH, Silva L, Klafke A. Advanced triage protocols in the emergency department: a systematic review and meta-analysis. Rev Lat Am Enfermagem. 2022;30:e3511. PubMed
93.Thamm C, Teleni L, Chan RJ, Stone L, McCarthy AL. Nurse-led interventions for cancer patients in emergency departments: systematic review. Collegian. 2019;26(2):311-319.
94.Tlapa D, Tortorella G, Fogliatto F, et al. Effects of lean interventions supported by digital technologies on healthcare services: a systematic review. Int J Environ Res Public Health. 2022;19(15):9018. PubMed
95.Tlapa D, Zepeda-Lugo CA, Tortorella GL, et al. Effects of lean healthcare on patient flow: a systematic review. Value Health. 2020;23(2):260-273. PubMed
96.Tricco AC, Antony J, Ivers NM, et al. Effectiveness of quality improvement strategies for coordination of care to reduce use of health care services: a systematic review and meta-analysis. CMAJ. 2014;186(15):E568-578. PubMed
97.van den Broek S, Westert GP, Hesselink G, Schoon Y. Effect of ED-based transitional care interventions by healthcare professionals providing transitional care in the emergency department on clinical, process and service use outcomes: a systematic review. BMJ Open. 2023;13(3):e066030. PubMed
98.van Galen LS, Lammers EM, Schoonmade LJ, Alam N, Kramer MH, Nanayakkara PW. Acute medical units: the way to go? A literature review. Eur J Intern Med. 2017;39:24-31. PubMed
99.Vedel I, Khanassov V. Transitional care for patients with congestive heart failure: a systematic review and meta-analysis. Ann Fam Med. 2015;13(6):562-571. PubMed
100.Voaklander B, Gaudet LA, Kirkland SW, Keto-Lambert D, Villa-Roel C, Rowe BH. Interventions to improve consultations in the emergency department: a systematic review. Acad Emerg Med. 2022;29(12):1475-1495. PubMed
101.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
102.Asplin BR, Magid DJ, Rhodes KV, Solberg LI, Lurie N, Camargo CA, Jr. A conceptual model of emergency department crowding. Ann Emerg Med. 2003;42(2):173-180. PubMed
103.Schull MJ, Kiss A, Szalai JP. The effect of low-complexity patients on emergency department waiting times. Ann Emerg Med. 2007;49(3):257-264, 264.e251.
104.Emergency Health Services: Patient Care Models. Toronto (ON): Ontario Ministry of Health and Ministry of Long-Term Care; 2022: https://health.gov.on.ca/en/pro/programs/emergency_health/patient_care_models/default.aspx. Accessed 2023 Sep 18.
105.Emergency Health Services: paramedic practice documents. Toronto (ON): Ontario Ministry of Health and Ministry of Long-Term Care; 2023: https://www.health.gov.on.ca/en/pro/programs/emergency_health/edu/practice_documents.aspx. Accessed 2023 Sep 18.
106.Seow E. Leading and managing an emergency department—a personal view. J Acute Med. 2013;3(3):61-66.
107.Consolidated Framework for Implementation Research. Ann Arbor (MI): CFIR Research Team-Center for Clinical Management Research; 2022: https://cfirguide.org/. Accessed 2023 Apr 06.
108.The health care safety net is ripping: Canadians should know how the next federal government will ensure timely access to emergency care in their time of need. Ottawa (ON): Canadian Association of Emergency Physicians; 2021: https://caep.ca/wp-content/uploads/2021/09/SafetyNet-Ripping-1.pdf. Accessed 2023 Sep 05.
109.Census profile, 2021 census of population. (Statistics Canada Catalogue no. 98-316-X2021001). Ottawa (ON): Statistics Canada; 2023: https://www12.statcan.gc.ca/census-recensement/2021/dp-pd/prof/details/page.cfm?LANG=E&GENDERlist=1,2,3&STATISTIClist=1&HEADERlist=23&SearchText=Canada&DGUIDlist=2021A000011124. Accessed 2023 Aug 31.
110.Emergency department overcrowding: an environmental scan of contributing factors and an overview of reviews of effectiveness of interventions - project protocol. (CADTH health technology review). Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/pdf/htis/2023/OP0553-Emergency-Department-Overcrowding-Project-Protocol.pdf. Accessed 2023 Aug 15.
111.Douglas-Vail M, Jiang A, Erdelyi S, Brubacher JR, Abu-Laban RB. Association of air quality during forest fire season with respiratory emergency department visits in Vancouver, British Columbia. J Clim Chang Health. 2023;13:100255.
112.Fischer JW. Climate change and Canadian emergency medicine: exploring alternative futures. CJEM. 2020;22(2):137-138. PubMed
113.Bouck Z, Calzavara AJ, Ivers NM, et al. Association of low-value testing with subsequent health care use and clinical outcomes among low-risk primary care outpatients undergoing an annual health examination. JAMA Intern Med. 2020;180(7):973-983. PubMed
114.Cheng I, Zwarenstein M, Kiss A, Castren M, Brommels M, Schull M. Factors associated with failure of emergency wait-time targets for high acuity discharges and intensive care unit admissions. CJEM. 2018;20(1):112-124. PubMed
115.Gates M, Gates A, Pieper D, et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022;378:e070849. PubMed
116.Mason J, Secord S, MacDougall D. New and emerging interventions to alleviate emergency department overcrowding: a compilation of new and emerging health technologies and interventions from around the world. (CADTH horizon scan). Can J Health Technol. 2023;3(10). https://canjhealthtechnol.ca/index.php/cjht/article/view/EN0051/EN0051. Accessed 2023 Oct 25.
117.Surge capacity and the Canadian emergency department. Ottawa (ON): Canadian Association of Emergency Physicians; 2020: https://caep.ca/wp-content/uploads/2020/03/Surge-Capacity-and-the-Canadian-Emergency-Department-CLEAN-March23PP.pdf. Accessed 2023 Sep 14.
118.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37:e17. PubMed
119.Cochrane Methods Equity. PROGRESS-Plus. 2023; https://methods.cochrane.org/equity/projects/evidence-equity/progress-plus. Accessed 2023 Aug 30.
120.Walter LA, Schoenfeld EM, Smith CH, et al. Emergency department-based interventions affecting social determinants of health in the United States: a scoping review. Acad Emerg Med. 2021;28(6):666-674. PubMed
121.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. PubMed
122.Bartels SA, MacKenzie M, Douglas SL, et al. Emergency department care experiences among members of equity-deserving groups: quantitative results from a cross-sectional mixed methods study. BMC Emerg Med. 2023;23(1):21. PubMed
123.Nundy S, Cooper LA, Mate KS. The quintuple aim for health care improvement: a new imperative to advance health equity. JAMA. 2022;327(6):521-522. PubMed
124.Petrie DA, Comber S. Emergency Department access and flow: complex systems need complex approaches. J Eval Clin Pract. 2020;26(5):1552-1558. PubMed
125.Canada's health care system. (Reports and publications - health care system). Ottawa (ON): Health Canada; 2019: https://www.canada.ca/en/health-canada/services/health-care-system/reports-publications/health-care-system/canada.html. Accessed 2023 Sep 01.
126.Canada's health care system: learn about Canada's health care system, including Medicare, funding, accessing health care services and delivery. (Health system and services). Ottawa (ON): Health Canada; 2023: https://www.canada.ca/en/health-canada/services/canada-health-care-system.html. Accessed 2023 Sep 01.
127.Leatt P, Pink GH, Guerriere M. Towards a Canadian model of integrated healthcare. Healthc Pap. 2000;1(2):13-35. PubMed
128.Kreindler SA. Six ways not to improve patient flow: a qualitative study. BMJ Qual Saf. 2017;26(5):388-394. PubMed
129.Pollock M, Fernandes RM, Becker LA, Pieper D, Hartling L. Chapter V: overviews of reviews. In: Higgins JPT, Thomas J, Chandler J, et al., eds. Cochrane handbook for systematic reviews of interventions version 6.3 (updated February 2022). London (UK): Cochrane; 2022: www.training.cochrane.org/handbook. Accessed 2023 Mar 28.
130.Tricco AC, Tetzlaff J, Pham B, Brehaut J, Moher D. Non-Cochrane vs. Cochrane reviews were twice as likely to have positive conclusion statements: cross-sectional study. J Clin Epidemiol. 2009;62(4):380-386.e381. PubMed
131.Dosenovic S, Jelicic Kadic A, Miljanovic M, et al. Interventions for neuropathic pain: an overview of systematic reviews. Anesth Analg. 2017;125(2):643-652. PubMed
132.Brett K, Wells C, Sinclair A, Tenenbaum H, Freeman B, Spry C. Interventions for temporomandibular joint disorder: an overview of systematic reviews. (CADTH rapid response report: overview of systematic reviews). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/attachments/2022-01/re0035-temporomandibular-joint-disorder.pdf. Accessed 2023 Aug 30.
133.Moir M, Barua B. Comparing performance of universal health care countries, 2022. Vancouver (BC): Fraser Institute; 2022: https://www.fraserinstitute.org/studies/comparing-performance-of-universal-health-care-countries-2022. Accessed 2023 Aug 21.
134.Glossary of IDEA terms: a reference tool for inclusion, diversity, equity, and accessibility terminology. Toronto (ON): Canadian Centre for Diversity and Inclusion; 2023: https://ccdi.ca/media/4005/20230509-glossary-of-idea-terms-en.pdf. Accessed 2023 Aug 30.
135.EUnetHTA Joint Action 2, Work Package 8. HTA Core Model version 3.0. Diemen (NL): EUnetHTA; 2016: https://www.eunethta.eu/wp-content/uploads/2018/03/HTACoreModel3.0-1.pdf. Accessed 2023 Aug 20.
136.Rainbow Health Ontario, Sherbourne Health. Glossary. 2022; https://www.rainbowhealthontario.ca/news-publications/glossary/. Accessed 2023 Aug 30.
137.The 519. The 519 glossary of terms. 2020; https://www.the519.org/education-training/glossary/#S. Accessed 2023 Aug 20.
138.Kerman S. Homeless, houseless, and unhoused: a glossary of terms used to talk about homelessness. Carlton (OR): Blanchet House; 2023: https://blanchethouse.org/homeless-houseless-unhoused-glossary-about-homelessness/. Accessed 2023 Aug 30.
139.World Health Organization. Social determinants of health. https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1. Accessed 2023 Aug 30.
Appendix 1: Glossary of Ethics and Equity Terms
Note that this appendix has not been copy-edited.
Please note that the terms and definitions in this glossary will change over time as work around equity-related language and vocabulary continues to develop. The terms and definitions included in this list are not standardized and their use may vary between individuals, groups, and regions.
Table 5: Glossary of Ethics and Equity Terms
Terms | Definitions |
|---|---|
Bias | A conscious (explicit) or unconscious (implicit) opinion, preference, prejudice, or inclination, formed without reasonable justification, that prevents a balanced or even-handed judgement.134 |
Ethics | ‘Ethics’ is broadly used to describe activities relating to the understanding and study of ‘the moral life.’ The term ‘morality’ encompasses beliefs, standards of conduct, principles and rules which may guide personal and professional behaviour and the behaviour of institutions. Ethics analysis considers prevalent social and moral norms and values relevant to the technology in question. It involves an understanding of the consequences of implementing or not implementing a health care technology.135 |
Ethnicity | A socially defined category or membership of people who may share a nationality, heritage, language, culture, and/or religion.136 |
Equity | Where everyone is treated according to their diverse needs in a way that enables all people to participate, perform, and engage to the same extent.137 |
Equity-deserving/Equity-seeking | Groups of people who have been historically disadvantaged and under-represented. These groups include but are not limited to the 4 designated groups in Canada – women, racialized groups, Indigenous Peoples, and people with disabilities – and people in the 2SLGTBQ+ community/people with diverse gender identities and sexual orientations. Equity-deserving groups often identify barriers and unequal access and deserve social justice.134 |
Gender identity | A person’s internal and individual experience of gender. It refers to one’s sense of being a woman, man, both, neither, or anywhere along the gender spectrum. A person’s gender identity may be the same or different from their sex assigned at birth. A person’s gender identity is fundamentally different from and not related to their sexual orientation.136,137 |
Houseless/unhoused/person experiencing houselessness | More frequently, the terms houseless/unhoused/person experiencing houselessness are used in place of “homeless/homelessness.” The reason is the important distinction between a house and a home and/or to emphasizes the humans at the centre of this crisis rather than the houses. People described as “homeless” are not necessarily without a home, but are precariously housed, unhoused, or without a permanent residence.138 |
IBPOC | An acronym for Indigenous, Black, and People of Colour. In Canada, IBPOC may be used (BIPOC is an acronym originating in the US around 2010 and may be more familiar) in efforts to recognize ‘First Peoples first’ because of the unique history and context of colonization, displacement, and cultural genocide enacted upon Indigenous Peoples in Canada, and the ongoing national conversation about reconciliation. |
Nonbinary | Individuals who do not follow gender stereotypes based on the sex they were assigned at birth. They might identify and express themselves as “feminine men” or “masculine women,” or as androgynous, outside of the categories of “boy/man” and “girl/woman.” People who are gender nonbinary may or may not identify as trans.137 |
PROGRESS-Plus | An acronym used to identify characteristics that stratify health opportunities and outcomes. PROGRESS refers to: place of residence, race/ethnicity/culture/language, occupation, gender/sex, religion, education, socioeconomic status, social capital. Plus refers to: (1) personal characteristics associated with discrimination (e.g., age, disability). (2): features of relationships (e.g., smoking parents, excluded from school), (3) time-dependent relationships (e.g., leaving the hospital, respite care, other instances where a person may be temporarily at a disadvantage).119 |
Race | Culturally or socially constructed divisions of humankind, based on distinct characteristics that can be based on: physicality, culture, history, beliefs, practices, language, origin, and so forth.136,137 |
Sex | The classification of people as male, female, or intersex. Sex is typically assigned at birth and is based on an assessment of one’s reproductive systems, hormones, chromosomes, and other physical characteristics.136,137 |
Sexual orientation | The direction of one’s sexual, emotional, and/or romantic interest or attraction. People may use the terms gay, straight, lesbian, bi, or pan to describe their experience.136,137 |
Social determinants of health | Nonmedical factors that influence a person’s ability to be physically, mentally, and socially healthy. They are the conditions in which people are born, grow, work, live, and age, as well as the broader systems that influence the conditions of daily life. Examples include education, employment and job security, social inclusion, food insecurity, structural conflict, among others.139 |
Socioeconomic status | Socioeconomic status (otherwise known as SES) refers to an individual’s level of income, wealth, education, and prestige. |
2SLGBTQ+ | An acronym that stands for: Two-Spirit, Lesbian, Gay, Bisexual, Trans, Queer. The plus sign represents other sexual and gender identities that fall under the queer umbrella. |
Disability | Under the medical model, this term refers to a limitation or loss of physiological abilities, whether apparent or not. These can be physical, cognitive, learning, and visual disabilities. Under the social model, disability is identified as a disadvantage or restriction of activity caused by systemic barriers, negative attitudes, and exclusion by society.137 |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.