Peer-Reviewed Article
Oncology Drug Approvals Under Health Canada’s Notice of Compliance With Conditions Policy: A Retrospective Cohort Analysis
Anna Martin, Melissa Hunt, Scott Blommaert, Suji Udayakumar, Brandon Lu, Shreya Chatterjee, Gaaya Sathiyabalan, Jan Brun, Melissa Kampman, Laurie Lambert, Nicole Mittmann, Kelly Robinson, Kelvin KW Chan
Abstract
Objectives: Health Canada’s Notice of Compliance with conditions (NOC/c) policy provides expedited access to promising new therapies for serious conditions. We sought to examine the use of the NOC/c policy for oncology drugs, to determine whether confirmatory studies are aligned with the approved indication, and to assess the impact of the NOC/c policy by quantifying the number of oncology drugs approved under this policy that become the standard of care treatment for their respective indications.
Methods: This retrospective cohort analysis used data gathered from Health Canada databases for all brand name oncology drugs issued an NOC/c from the introduction of the policy in 1998 to December 1, 2021. The Kaplan-Meier method was used to determine median time from NOC/c issuance to fulfillment of conditions. Treatment settings of initial and confirmatory trials associated with each NOC/c were gathered from study publications and ClinicalTrials.gov, and were compared to determine whether they were aligned with each other and with the approved indication. National Comprehensive Cancer Network (NCCN) guidelines were searched for any NOC/c issued between 2018 and 2021 to determine whether NOC/c-approved indications were incorporated into standard of care guidelines.
Results: In total, 149 drug indications received an NOC/c, of which 70% were for oncology indications. There was an increasing trend of NOC/c issued for oncology drugs (11% from 1998 to 2001 versus 94% from 2018 to 2021). The median time to fulfillment of conditions for NOC/c was 53 months, without a significant difference between oncology and non-oncology indications (P = 0.36). Among fulfilled NOC/c (n = 57), most had all conditions met, with only 12% (n = 7) of authorizations under the NOC/c policy being revoked. Of the 91 indications with enough information to determine treatment settings, 61 (67.0%) of the confirmatory trials associated with NOC/c were deemed aligned with regard to treatment setting, 17 (18.7%) were partially aligned, and 13 (14.3%) were not aligned. Irrespective of alignment, 29 of 34 NOC/c issued between 2018 and 2021 had been incorporated into NCCN guidelines, with 47.1% being preferred treatment options for their respective indications.
Conclusions: Our findings suggest that Health Canada’s NOC/c policy has been successful in providing expedited access to promising new therapies. However, ensuring that confirmatory trials are under way at the time of NOC/c issuance may provide assurance that studies addressing the uncertainty associated with NOC/c will not be unnecessarily prolonged. The inclusion of real-world evidence (RWE) as part of confirmatory evidence may help fill gaps.
Introduction
Health Canada’s Notice of Compliance with conditions (NOC/c) policy was introduced in 1998 in an effort to provide people in Canada with timely access to new therapies while ensuring that marketing authorizations are issued based on adequate evidence of safety and clinical benefit. Under the policy, Health Canada can issue market authorizations with associated conditions on the basis of promising evidence of efficacy — including, but not limited to surrogate end points — for drugs indicated for serious, life-threatening, or severely debilitating diseases or conditions.1 Eligible drugs must either demonstrate a significant increase in efficacy and/or a significant decrease in risk such that the overall benefit-risk profile is improved over existing therapies, or address a significant unmet need for conditions with no existing therapy available in Canada.1 When an NOC/c is issued, Health Canada stipulates the conditions that must be fulfilled, which include confirmatory studies intended to verify the clinical benefit of the drug and safety monitoring.
It is important that confirmatory studies intended to lift the conditions of an NOC/c are designed to demonstrate efficacy, are consistently monitored to ensure maintenance of a favourable benefit-risk profile and are completed in a timely manner. Drugs eligible for consideration for authorization under the NOC/c policy are often indicated for rare conditions — frequently rare cancer indications — which have a limited number of patients eligible for participation in clinical trials. Small eligible populations make it difficult and time-consuming to conduct the large clinical trials typically submitted to support authorization through the standard drug approval pathway, making the NOC/c pathway a good option for providing timely access to these therapies while clinical trials to demonstrate efficacy are brought to completion. In tandem with the increasingly rapid pace of research on oncological therapies, this contributes to an increasing number of NOC/c issued for drugs with oncology indications.1,2 Although the confirmatory studies associated with NOC/c have long been a major point of interest for researchers in Canada, how well these studies reflect the initial trials that led to the product approval has not yet been investigated. Moreover, few studies have addressed the policy as it relates specifically to oncology drugs and the impact of these NOC/c drugs on the treatment landscape.
In this study, we looked at the number of NOC/c issued by Health Canada overall and for oncology drugs over time, and examined the timelines associated with the fulfillment of conditions relative to the corresponding patent protection periods. We also sought to compare the initial studies that led to each NOC/c issuance and the Health Canada–approved indication with the confirmatory studies requested as conditions of the NOC/c to determine whether these studies were designed to demonstrate efficacy in the authorized indication. Finally, to understand whether providing early access to promising new drugs for cancer patients via the NOC/c pathway results in a meaningful impact on the treatment landscape, we sought to determine the proportion of these drugs that become the standard of care for their respective indications per evidence-based cancer guidelines.
Methods
Study Design and Data Sources
In this retrospective cohort study, a list of all NOC/c issued by Health Canada from the introduction of the policy in May 1998 to December 1, 2021 was gathered from the Health Canada NOC/c website and verified with the NOC database. Different indications for the same drug submitted individually to Health Canada were considered separately. Each NOC/c for an oncology indication submitted as a New Drug Submission (NDS) or a Supplement to a New Drug Submission (SNDS) was selected, thereby excluding any NOC/c for a generic version of a previously approved product. NDSs (including biosimilars) are typically filed for drug products by the company that created the product, while generic drugs are filed as Abbreviated New Drug Submissions (ANDSs). SNDSs and, similarly, Supplements to an Abbreviated New Drug Submission (SANDSs) are filed by the manufacturer when changes (such as the addition of an indication) need to be made to a previously authorized product.3
The name of the drug, active ingredient, indication, submission type, date of NOC/c issuance and date of fulfillment of conditions were recorded for each NOC/c. In any case of discrepancy between the NOC/c website and the NOC database, where no definitive reason for the discrepancy was available, the NOC database was used as the preferred data source because it was more often congruent with other Health Canada sources. Details of the initial and confirmatory studies associated with each NOC/c were extracted from Qualifying Notices and Dear Health Care Professional letters available on the NOC/c website, product monographs, and the Drug and Health Product Register. A search was then conducted using ClinicalTrials.gov for each NOC/c using the information provided by Health Canada, which was also used to identify study publications. Studies were matched by study ID, name, number and type of participants, and study details, depending on the information made available by Health Canada for each study. Since Health Canada receives reports about study findings separately from those that are published, publications with results and timelines most closely matching information provided by Health Canada were chosen. Details of study populations, drug combinations, and study designs were first extracted from Health Canada documentation, then study publications, and finally ClinicalTrials.gov if no publications were available. Initial and confirmatory trial treatment settings and dates of confirmatory study activations were extracted from study publications first, then ClinicalTrials.gov if no publications were available, and then Health Canada documentation if no publications or ClinicalTrials.gov pages could be identified. Patent numbers and dates of first patent expiry were recorded for each included drug from the Patent Register. If a patent was removed before the official patent expiry date, the original date of patent expiration was recorded alongside the date of removal.
All extractions were conducted independently by 2 reviewers and any disagreements were settled by consensus. If an agreement could not be reached, a third reviewer was consulted.
The percentage of NOC/c issued for an oncology drug indication was calculated for each 4-year period from the date of introduction of the NOC/c policy to December 1, 2021. As this dataset included every NOC/c from the introduction of the policy that met the study specifications, statistical analysis methods characterizing uncertainty from sampling bias were not needed.
The data for our analyses were aggregated from several Health Canada sources, which may have been outdated at the time of extraction, resulting in some uncertainty when databases were incongruent. These uncertainties were minimized by consulting Health Canada personnel directly about incongruencies and missing data, who verified information and assumptions using Health Canada documentation.
Timeline Analysis
The Kaplan-Meier method was used to generate failure plots for the analysis of time from NOC/c issuance to the fulfillment of conditions, time from NOC/c issuance to the date of first patent expiry, and to publication of confirmatory trial results. Any NOC/c that remained active without a date of fulfillment as of December 1, 2022, was censored. In the first time to publication analysis, each confirmatory trial without a publication as of December 1, 2022, was censored. In the second time to publication analysis, which grouped together all confirmatory trials associated with each NOC/c, any NOC/c without a publication for all associated confirmatory trials as of December 1, 2022, was censored. Patent expiry analysis was used to provide a comparison of the time taken to fulfill conditions relative to the “life cycle” of the drug. The time to fulfillment of conditions was compared between brand name oncology and non-oncology drugs using the log-rank test. Failure plots were generated using R Statistical Software (version 4.1.3)4,5 and their respective summary statistics were calculated using SAS Studio 3.8 (Enterprise Edition).
The date of confirmatory study activation was compared with the date of NOC/c issuance for all confirmatory trials that differed from initial trials to determine whether confirmatory trials were initiated before or after NOC/c issuance.
Comparison of Treatment Settings
“Treatment setting” is defined here as the drug combination and study population including cancer type, biomarker, previous treatment, and treatment line. Treatment settings of confirmatory and initial trials were assessed and compared with each other and with the Health Canada–approved NOC/c indications to evaluate whether confirmatory studies were consistently designed to assess efficacy in the treatment settings for which they were originally tested and approved. Treatment settings of initial trials were compared to the NOC/c authorized indications, and confirmatory trials were compared to their respective initial trials and NOC/c authorized indications.
In the comparison of initial trials with the NOC/c indication, treatment settings were deemed “aligned” if the drug combination and population evaluated in the initial trials collectively covered the population authorized under the NOC/c indication. A “partial alignment” categorization was given if part of the population eligible under the NOC/c indication was not evaluated in the initial trials, and an NOC/c was considered “not aligned” when the population or drug combination assessed in the initial trial excluded the population eligible under the NOC/c. The same method was followed for the comparison of confirmatory trials with the NOC/c authorized indication. In the comparison of confirmatory trials with initial trials, an NOC/c was considered aligned if the confirmatory trials collectively assessed the same population evaluated in the initial trials. An NOC/c was considered partially aligned if the confirmatory trials evaluated a smaller population than the initial trials. A nonaligned designation was given when the confirmatory trials evaluated a different drug combination or treatment line than the initial trials. Where multiple initial or confirmatory studies were associated with a single NOC/c, the scope covered by all confirmatory studies and all initial studies were evaluated collectively.
Comparison of Study Designs
Details of initial and confirmatory trial designs, including study phase, randomization, sample size, and primary end points, were extracted for each NOC/c. Summary statistics were used to compare study designs of the initial trials with the confirmatory trials.
Assessment of Standard of Care Status
To examine whether NOC/c drugs eventually become the standard of care for their respective indications in Canada, we looked at the proportion of these drugs that are included in National Comprehensive Cancer Network (NCCN) guidelines. The NCCN is a US alliance of cancer centres that issues comprehensive evidence-based cancer guidelines that are recognized as a standard for clinical decision-making.7 Although these guidelines are developed in the US, the trials upon which they are based often include international populations and/or populations in Canada, and are followed in the Canadian context. We searched the NCCN guidelines for brand name oncology drugs issued an NOC/c between January 1, 2018, and the study cut-off date (December 1, 2021). Drugs issued an NOC/c before 2018 were excluded to minimize the effect of new therapies that may replace older drugs in the standard of care guidelines. Drugs were grouped by NCCN categorizations into “preferred,” “other recommended,” “useful under certain circumstances,” and “not stated.” Where the NCCN guidelines did not divide recommendations into categories, drugs were given a nonspecified positive or negative categorization.4,6
Results
Use of the NOC/c Policy in Oncology
From the introduction of the NOC/c policy in May 1998 to December 1, 2021, Health Canada issued 149 NOC/c for new brand name drugs, generic drugs, or new indications for previously approved drugs. Seventy percent (104 of 149) of these were issued for oncology indications. Of the 104 NOC/c issued for oncology indications, 92 (88.5%) were filed for new brand name drugs or new indications for brand name drugs previously approved under a different indication, and the remaining 12 (11.5%) were filed for generic drugs submitted as an ANDS or SANDS (Figure 1). Within the same time frame, 45 NOC/c were issued for non-oncology drugs, 38 of which were issued an NDS or SNDS. The final list of each included NOC/c is reported in the Supplementary Appendix. Unless otherwise stated, all further results will focus on any NOC/c issued for brand name oncology drugs.
Figure 1: Flow Chart of Dataset Creation
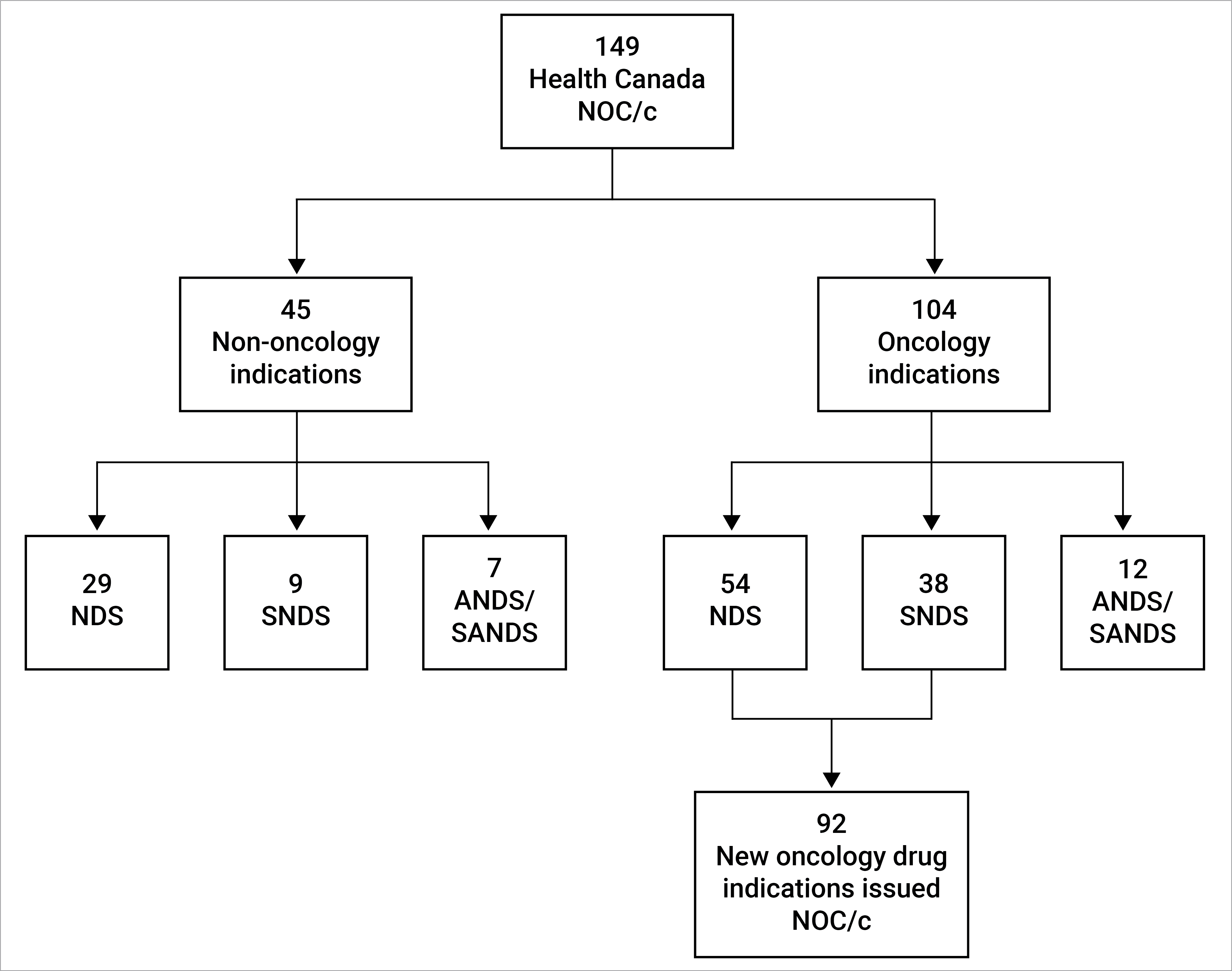
ANDS = Abbreviated New Drug Submission; NDS = New Drug Submission; NOC/c = Notice of Compliance with conditions; SANDS = Supplement to an Abbreviated New Drug Submission; SNDS = Supplement to a New Drug Submission.18
Over time, an upward trend was observed in the proportion of all NOC/c issued for oncology drug indications (Figure 2 and Figure 3). Between 1998 and 2001, 2010 and 2013, and 2018 and 2021, 11.1%, 66.7%, and 94.4% of all NOC/c for brand name drugs were for cancer indications, respectively. In both 2019 and 2021, all NOC/c issued by Health Canada were for oncology indications.
Figure 2: Percentage of NOC/c for Oncology Indications in 4-Year Intervals From Policy Introduction to December 1, 2021

NOC/c = Notice of Compliance with conditions; vs = versus.
Figure 3: Percentage of NOC/c for Brand Name Oncology Drugs in 4-Year Intervals From Policy Introduction to December 1, 2021

NOC/c = Notice of Compliance with conditions; vs = versus.
To date, 4 (4.3%) of the NOC/c issued for brand name oncology drugs have been suspended or discontinued due to clinical trial results that indicate increased risk or lack of efficacy. Three additional NOC/c were withdrawn by the manufacturers before their conditions were fulfilled.2 These findings are described in more detail in the Supplementary Appendix.
Timeline Analysis
Kaplan-Meier analysis of NOC/c for brand name oncology drugs — shown in Figure 4 — revealed that the median time to fulfillment of the NOC/c conditions for brand name oncology drugs was 53 months (interquartile range [IQR], 35 to 82). One year after NOC/c issuance, conditions for 97.8% of brand name oncology drugs remained unfulfilled. This number decreased to 45.1% by 5 years after initial authorization. The longest time to NOC/c fulfillment as of December 1, 2021, was 148 months (> 12 years).2,7 The shortest time to fulfillment was 8 months.2,8 There was no statistically significant difference between time to fulfillment of brand name oncology drugs and non-oncology drugs (P = 0.36 using log-rank test).
Figure 4: Kaplan-Meier Failure Plot Representing Time to Fulfillment of Conditions of NOC/c Issued for Brand Name Oncology Drugs vs. Brand Name Non-Oncology Drugs
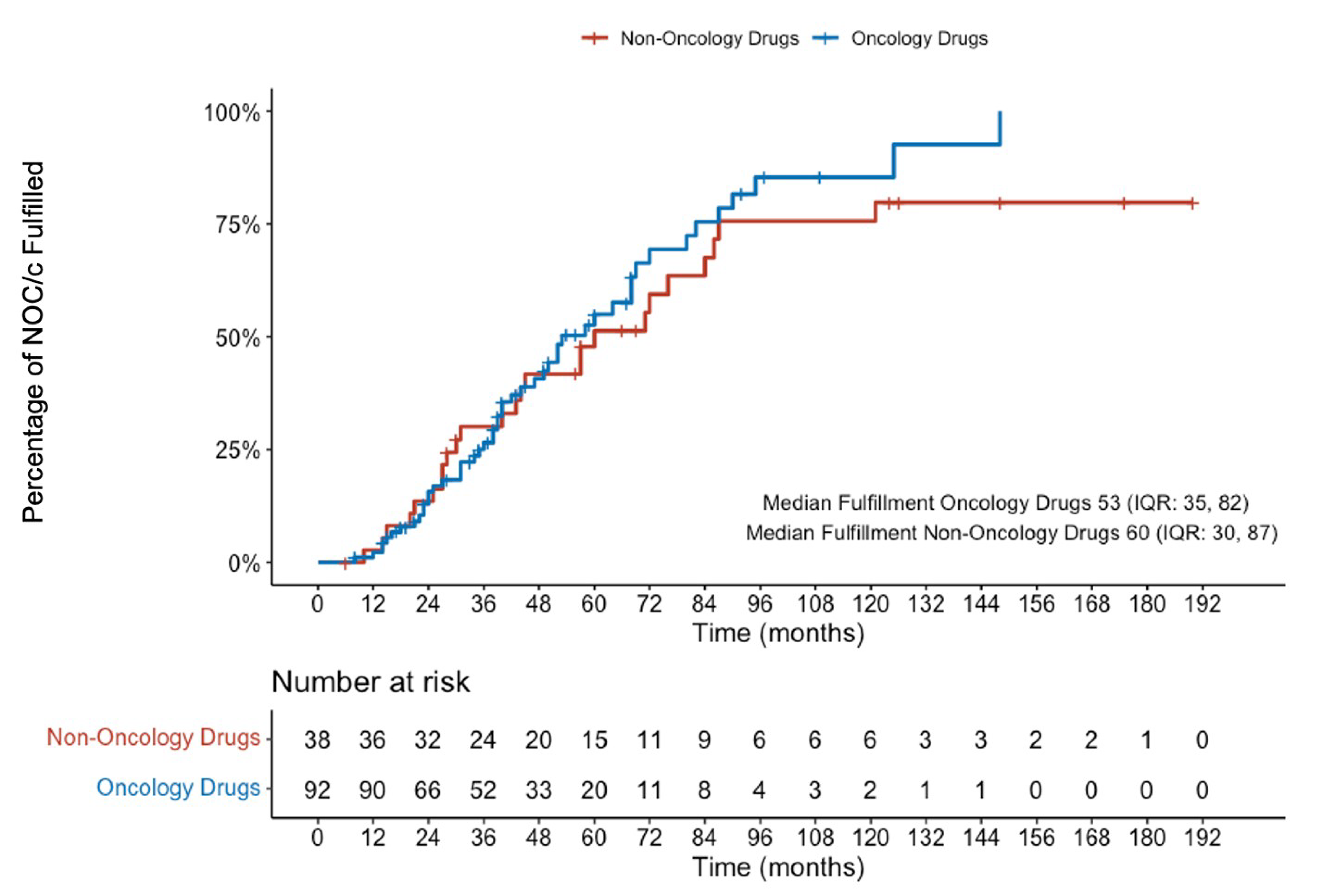
IQR = interquartile range; NOC/c = Notice of Compliance with conditions; vs. = versus.
The median time from NOC/c issuance to patent expiry was 114 months (IQR, 72 to 147) (Figure 5). Using the 20-year patent protection period as a measure of a drug’s life cycle, comparison of the median time to patent expiry with the median time from NOC/c issuance to the fulfillment of conditions revealed that drugs issued an NOC/c spend a median of 46.5% (53 of 114 months) of their life cycle under the NOC/c policy.
Figure 5: Kaplan-Meier Failure Plot Representing Time to Fulfillment of Conditions of NOC/c Issued for Brand Name Oncology Drugs vs. Time From NOC/c Issuance to Date of First Patent Expirya
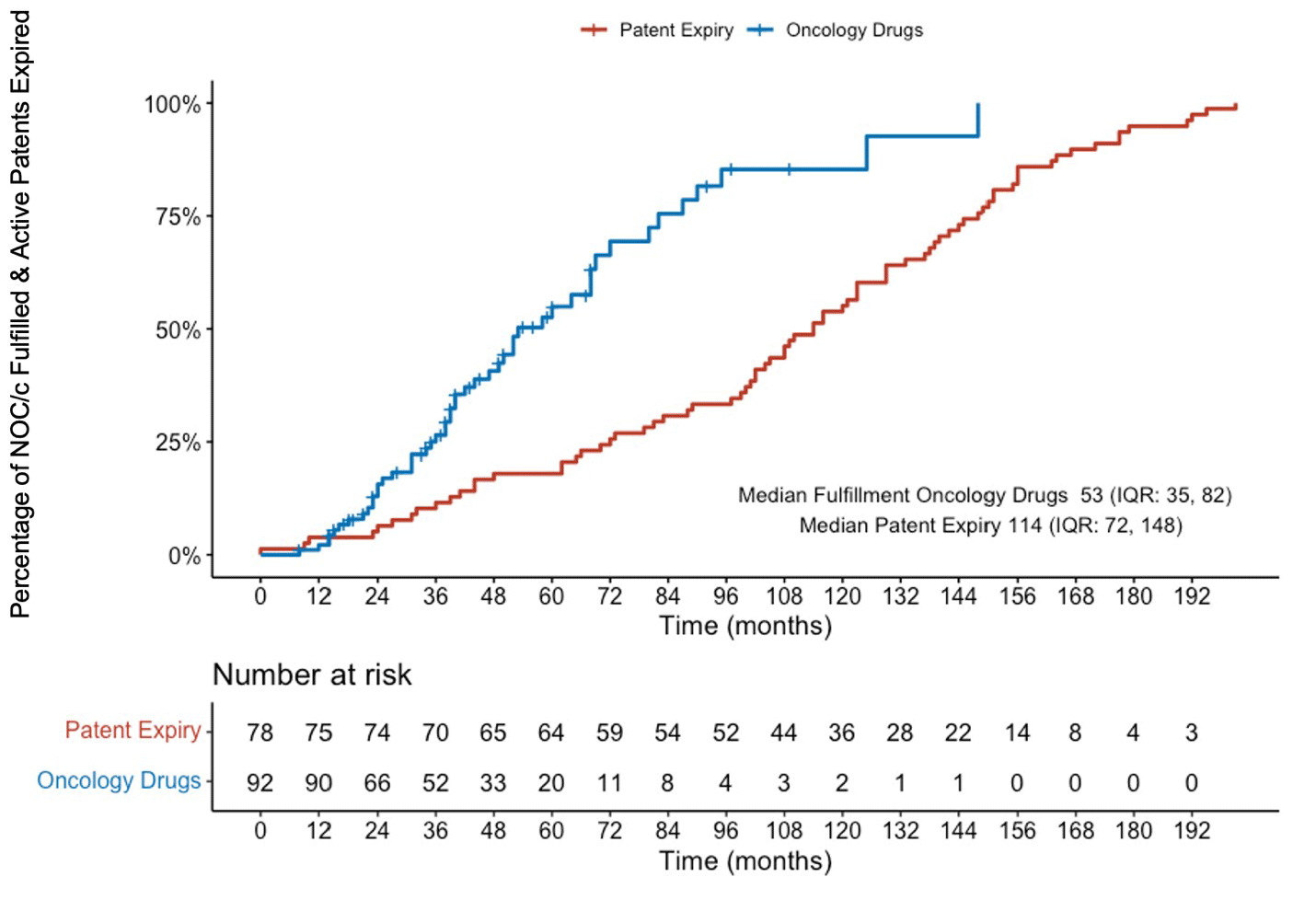
IQR = interquartile range; NOC/c = Notice of Compliance with conditions; vs. = versus.
a First patent expiry is used as a proxy for the “life cycle” of the drug.
Results of individual confirmatory trials were published a median of 43 months after NOC/c issuance (Figure 6). Publication of all confirmatory trials associated with an NOC/c occurred a median of 50 months after NOC/c issuance (Figure 7). Compared to the median time to NOC/c fulfillment, the confirmatory study findings used to evaluate whether conditions have been fulfilled were all published a median of 8 months before the NOC/c was marked as fulfilled.
Figure 6: Kaplan-Meier Failure Plot Representing Time to Fulfillment of Conditions of NOC/c Issued for Brand Name Oncology Drugs vs. Time From NOC/c Issuance to Date of Publication of Results of Each Confirmatory Trial
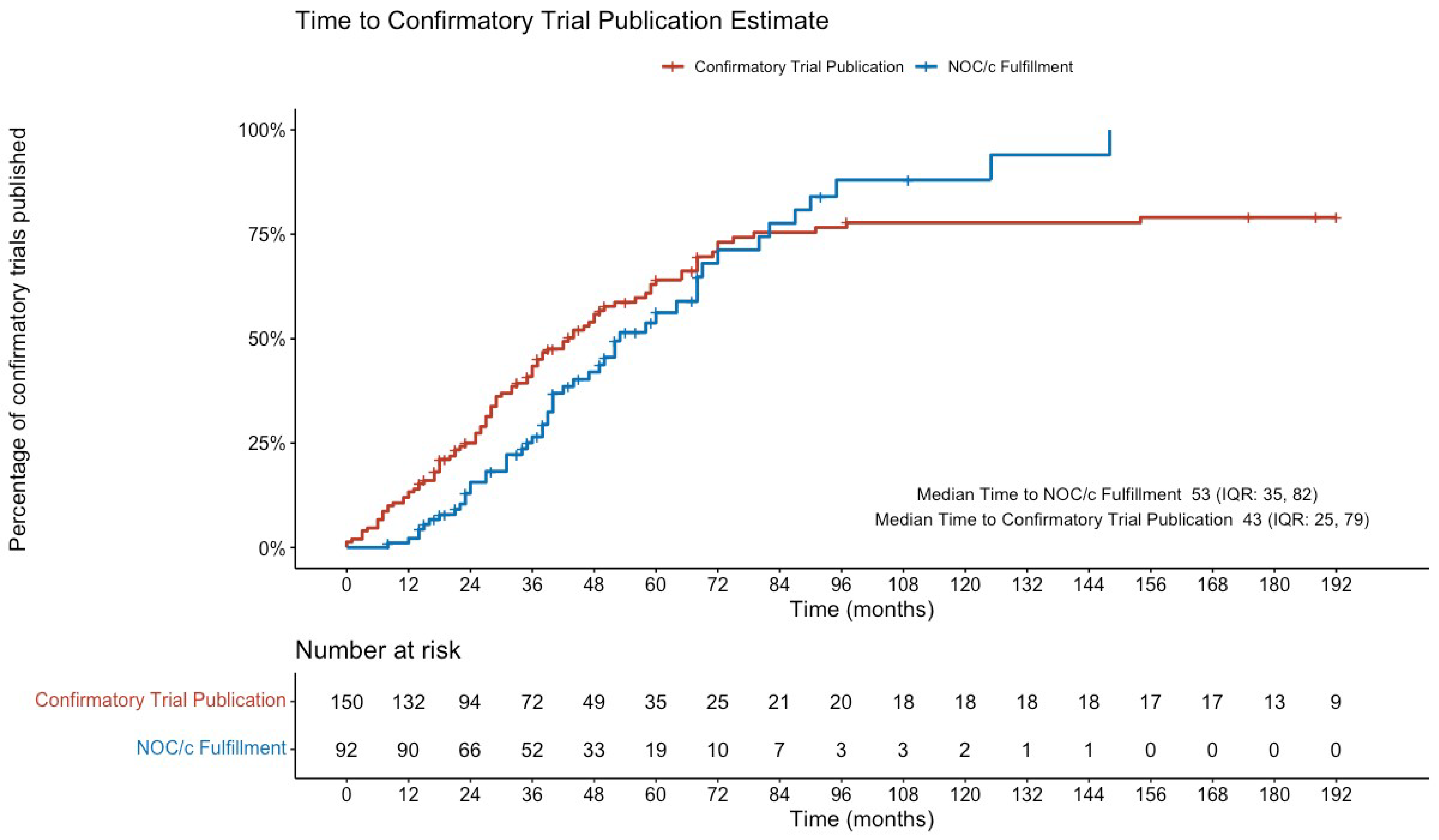
IQR = interquartile range; NOC/c = Notice of Compliance with conditions; vs. = versus.
Figure 7: Kaplan-Meier Failure Plot Representing Time to Fulfillment of Conditions of NOC/c Issued for Brand Name Oncology Drugs vs. Time From NOC/c Issuance to Date of Publication of All Confirmatory Trials Associated With Each NOC/c
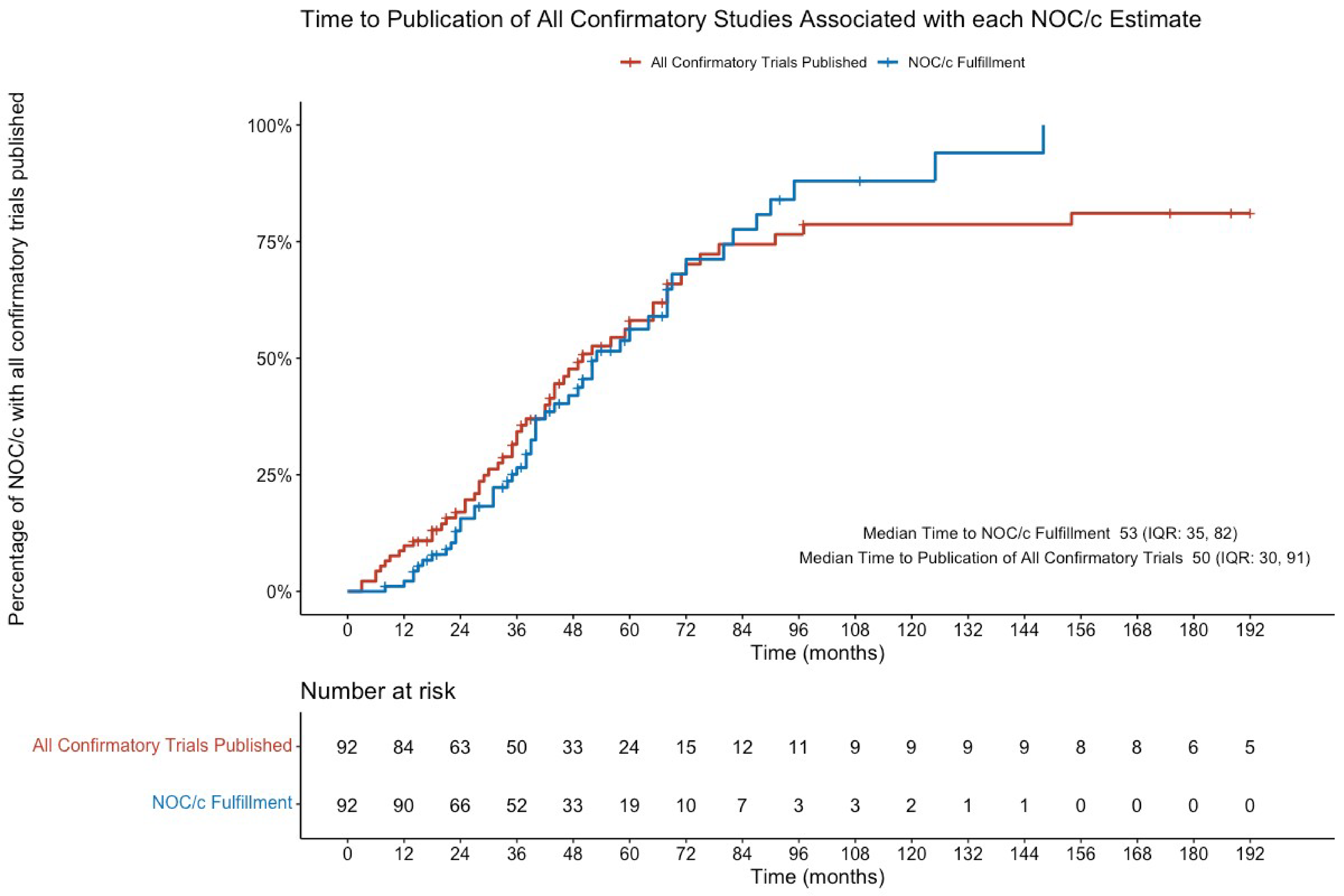
IQR = interquartile range; NOC/c = Notice of Compliance with conditions; vs. = versus.
Confirmatory studies that were not a continuation of the initial study (or studies) on which the NOC/c was based began participant recruitment a median of 24.5 months before NOC/c issuance (IQR, −33 to −15). Confirmatory studies associated with a total of 5 (5.4%) NOC/c began recruitment after NOC/c issuance. These studies were activated 2, 9, 15, 18, and 24 months after NOC/c issuance, respectively.
Comparison of Treatment Settings
Figure 8 shows a summary of the comparison of treatment settings between the NOC/c authorized indication, initial studies, and confirmatory studies associated with each NOC/c. There was not enough information available to determine and compare treatment settings of the confirmatory trial associated with 1 of the 92 authorizations because the confirmatory trial had not yet been registered. Of the remaining 91 authorizations, the NOC/c indication, initial trials, and confirmatory trials of 61 NOC/c (67.0%) were aligned. Seventeen NOC/c (18.7%) were deemed partially aligned with respect to treatment setting. These had confirmatory trials that evaluated a subset of the population included within the NOC/c indication and/or that evaluated in the initial trial. Treatment settings of these NOC/c were partially aligned in relation to previous treatment (n = 9), cancer type (n = 5), and/or biomarker (n = 4). A total of 13 NOC/c (14.3%) — described in more detail in the Supplementary Appendix — were deemed not aligned with respect to treatment setting of the NOC/c indication and the treatment setting evaluated in the initial and confirmatory trials. Twelve of these were associated with a confirmatory trial that evaluated a different treatment line than the NOC/c indication and initial trial, and 1 evaluated the drug of interest in a different combination than that specified in the NOC/c indication and initial trial. Details of these NOC/c are reported in the Supplementary Appendix.
Figure 8: Flow Chart Comparing Treatment Settings of Approved Indication, Initial Studies, and Confirmatory Studies Associated With NOC/c for Brand Name Oncology Drugs
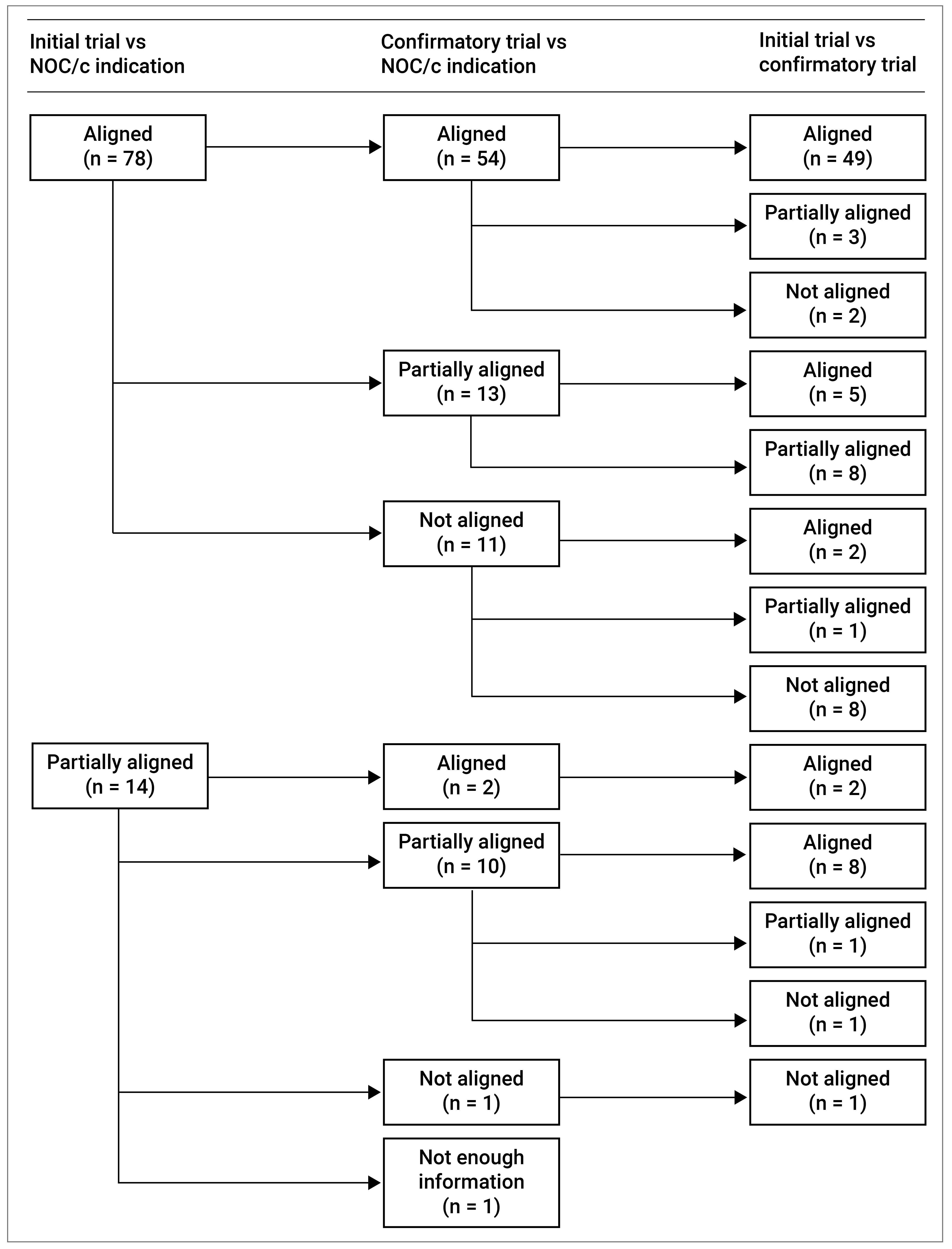
NOC/c = Notice of Compliance with conditions; vs = versus.
Comparison of Study Designs
Initial Studies
Study design comparisons have been summarized in Figure 9. Together, phase I and phase II studies represented the highest level of initial evidence supporting NOC/c issuance for 72.8% (67 of 92) of oncology drugs. Surrogate measures accepted as evidence supporting NOC/c issuance included overall and objective response rates (ORRs), progression-free survival (PFS), and disease-free survival (DFS). Twenty-three NOC/c (25.0%) included an initial trial with a randomized design comparing the drug of interest with an active comparator (typically a therapeutic drug authorized for the same treatment setting and/or considered the standard of care). Eleven of 92 initial studies (12.0%) included at least 1 initial trial with overall survival (OS) as a primary end point. The median total sample size of all initial trials supporting each NOC/c was 247 (IQR, 138 to 520).
Figure 9: Study Design of Initial and Confirmatory Trials
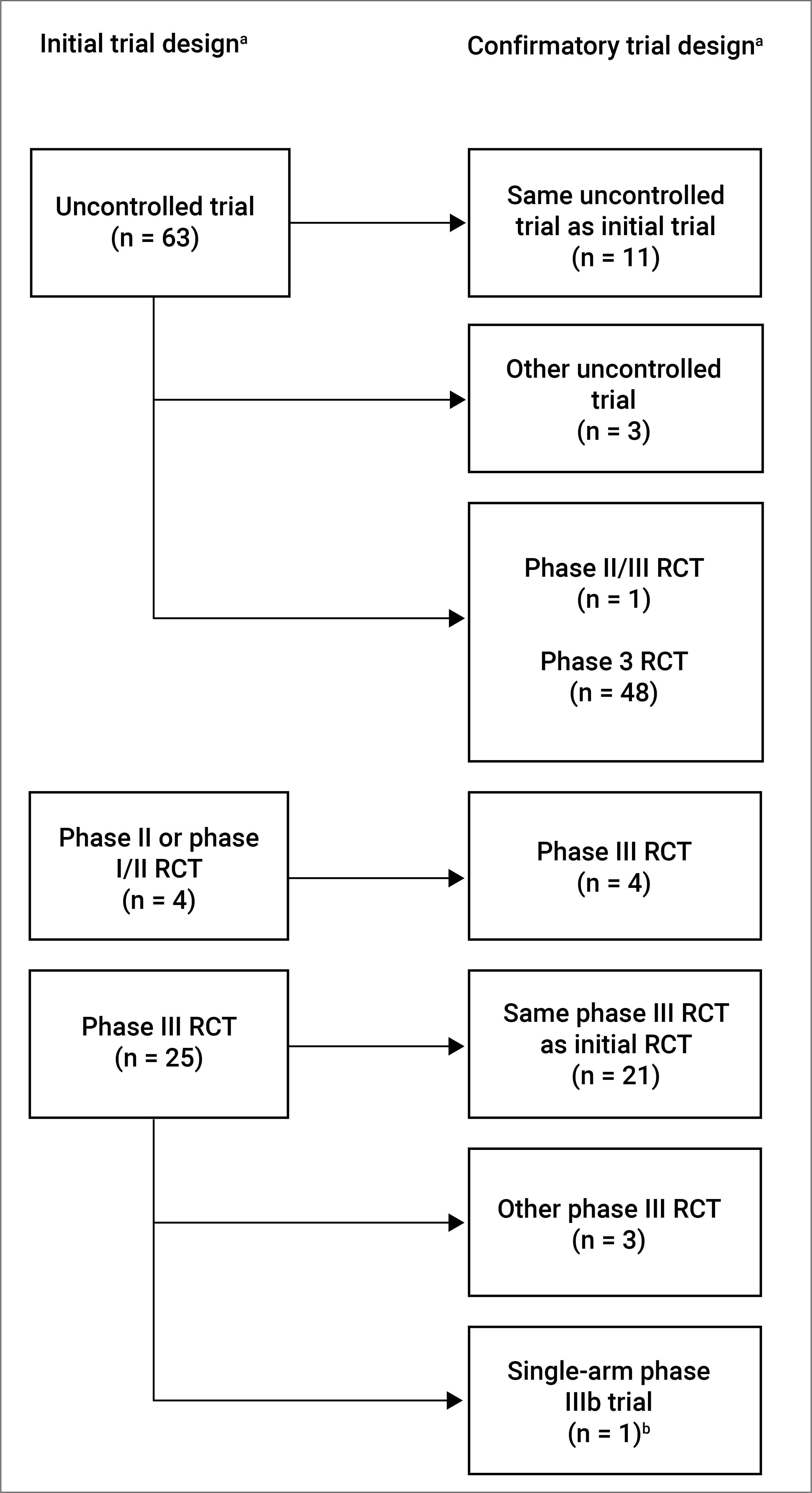
NOC/c = Notice of Compliance with conditions; RCT = randomized controlled trial.
a Where a single NOC/c was associated with more than 1 trial, the study offering the highest level of evidence was used.
b One NOC/c that was issued based on results from an initial phase III RCT was associated with a phase IIIb single-arm confirmatory trial.32,33
Confirmatory Studies
Conversely, phase III confirmatory studies represented the highest level of evidence requested by Health Canada as a condition for 83.7% (77 of 92) of the NOC/c. One NOC/c was associated with a condition of generating real-world evidence (RWE). Sixty-two of the 92 NOC/c (67.3%) included at least 1 randomized confirmatory trial with an active comparator. Thirty of 92 NOC/c (32.6%) had at least 1 confirmatory trial that included OS as a primary end point, and 44 (47.8%) included at least 1 confirmatory trial with PFS as a primary end point. The sample size of confirmatory trials was comparatively larger than the initial trials with a median of 702 (IQR, 429 to 1,077) participants.
Assessment of Standard of Care Status
NCCN standard of care recommendations are summarized in Table 1. Of 34 NOC/c issued between January 1, 2018, and December 1, 2021, 29 (82.4%) were recommended by the NCCN in their respective indications. Sixteen (47.1%) of these were listed as “preferred” regimens, 1 (2.9%) was listed as an “other recommended option,” and 2 (5.9%) were listed as “useful in certain circumstances.” Ten drug indications (26.5%) were recommended within the NCCN guidelines but were not specifically categorized as preferred, other recommended, or useful in certain circumstances. Five of 34 NOC/c drugs (14.7%) were not listed in the NCCN recommendations.
Table 1: NCCN Recommendations for Brand Name Oncology Drugs Issued NOC/c Between January 1, 2018, and December 1, 2021
NCCN Standard of Care (2018 to 2022) | Number (%) |
|---|---|
Recommended | 29 (82.4) |
Preferred | 16 (47.1) |
Other recommended option | 1 (2.9) |
Useful in certain circumstances | 2 (5.9) |
Recommended (no preferred option stated) | 10 (26.5) |
Not included in NCCN recommendations | 5 (14.7) |
NCCN = National Comprehensive Cancer Network; NOC/c = Notice of Compliance with conditions.
Discussion
In recent years, many oncology drugs have received marketing approval under the NOC/c policy. The policy aims to provide more timely access to new therapeutics that offer the potential to considerably improve treatment options for serious, life-threatening, or severely debilitating diseases. To do so, Health Canada grants authorization under the NOC/c policy to drugs that have demonstrated an acceptable safety profile and promising evidence of efficacy (in the context of a positive benefit-risk assessment) and stipulates conditions that must be fulfilled to ensure that a favourable benefit-risk profile is maintained. Drugs approved under the NOC/c policy have full market approval while further evidence to confirm early promise of clinical benefit is generated. Through the analysis of approval timelines, study designs, and treatment settings, we characterized trends related to initial and confirmatory studies associated with NOC/c issued for oncology drugs. We found that drugs approved for early market authorization via the NOC/c policy are more frequently for oncology indications than non-oncology indications. Once approved, they remained under the NOC/c policy for a median of 53 months (4.4 years) or 42.3% of their life cycle before the conditions of the NOC/c were met. Seven out of a total of 92 NOC/c issued for brand name oncology drugs between 1998 and December 1, 2021, had been removed, withdrawn, or suspended. Most confirmatory trials were under way before NOC/c issuance; however, 14.3% (n = 13) of these confirmatory trials were not aligned with the treatment settings of the Health Canada–approved indications and/or the initial trials that led to the authorizations. A further 18.7% (n = 17) of NOC/c were found to have partial alignment between the NOC/c indications, the initial trials, and the confirmatory trials. Regardless of alignment, most drugs approved through the NOC/c policy (82.4% of drugs issued NOC/c between 2018 and 2021) eventually became integrated into standard of care practices, based on NCCN guidelines.
Drugs that meet the criteria for approval under the NOC/c policy are most often indicated for rare cancers, making clinical trials designed to demonstrate clinical efficacy challenging, time-consuming, and costly to complete.1 This — coupled with a lack of formal incentive for the market authorization holder to complete confirmatory trials in a timely manner, and the potential for a lack in clinical equipoise when a therapy is quickly adopted into clinical practice — has led to growing concern that approval under the NOC/c policy may have the unintended consequence of the drug remaining under the NOC/c policy for extended periods of time.9-11 Our finding that the median time to fulfillment of NOC/c conditions for brand name oncology drugs was 53 months and that drugs spend a median of 46.5% of their life cycle (patent life) under the NOC/c policy supports that assertion. While a drug remains on the market based on promising evidence of efficacy, there is risk that patients might be receiving a less effective treatment. As such, faster NOC/c fulfillment reduces the amount of time drugs remain on the market with the risk that they may not be as effective as existing standard of care therapies. Regulatory bodies in the US and the European Union (EU) — both of which have policies analogous to Health Canada’s NOC/c policy — have measures in place intended to address this concern in their respective markets. However, the degree to which these measures have been successful remains unclear, given that both the US and EU have experienced similar challenges to Health Canada with respect to the timely completion of confirmatory trials.12-16 The European Medicines Agency’s Conditional Marketing Authorisation (CMA) program sets out timelines for the fulfillment of conditions and requires conditional authorizations to be renewed each year.17 Financial penalties can also be imposed if manufacturers fail to fulfill conditions within the stipulated time period.11 Although rarely enforced in the US, the FDA can seek to withdraw drugs from the market if they fail to fulfill the postmarket requirements of an accelerated approval, which includes the timely completion of confirmatory trials with “due diligence.”18,19 Health Canada can similarly consider using various regulatory tools (such as invoking section C.01.013 of the Food and Drug Regulations) should they suspect that a product is unsafe or ineffective. Additionally, through the NOC/c policy, Health Canada requires sponsors to submit annual status updates related to ongoing confirmatory trials to enable tracking and follow-up of the commitments made. Within the NOC/c policy, there is no regulatory measure to specifically compel the timely submission of confirmatory data.11 In addition to incentivizing manufacturers to complete confirmatory trials in a timely manner, ensuring that whenever feasible, confirmatory trials are already under way at the time of authorization under the NOC/c policy may help prevent an extended time to completion of confirmatory trials. Although our analysis showed that the majority of confirmatory trials commence before the NOC/c is issued, no NOC/c with a confirmatory trial activation date after NOC/c issuance has been fulfilled to date, limiting our ability to draw conclusions as to whether this affects time to NOC/c fulfillment. Even if having confirmatory trials under way at the time of NOC/c issuance may not decrease the time to NOC/c fulfillment, it would provide some assurance that the studies addressing the uncertainty associated with authorization under the NOC/c policy will not be unnecessarily prolonged.
Ensuring that confirmatory trials are of appropriate design to assess and confirm efficacy is central to the NOC/c policy. Previous studies have used sample size, study phase, randomization, and end points of NOC/c confirmatory studies to assess whether they have been appropriately designed.20,21 Our analysis of treatment settings demonstrates that there are situations where a confirmatory study has been accepted that does not align with the indicated population (e.g., different treatment setting). This may lead to challenges related to a clear understanding of benefit in the indicated population and assessment of value in the real-world setting by health care decision-making partners, such as health technology assessment (HTA) bodies. While this approach may be appropriate when considering a number of factors — including the need for product access, the feasibility of a study in the indicated population, and the global context — it nonetheless introduces challenges and uncertainties. Confirmatory studies are often already under way at the time of submission, and due to the relatively small size of the Canadian market, it would be difficult for Health Canada to insist on confirmatory trials that differ from those requested and accepted by foreign regulatory agencies.20,21 Doing so could have the unintended result of confirmatory trials that take much longer to be completed or corporate decisions not to bring a medication to Canada.
Use of RWE to contribute to the totality of the evidence available to regulatory agencies is increasingly being considered as an option to help fill evidence gaps.22-24 Although generation of RWE in the context of an NOC/c may lead to longer times to fulfillment of all of the conditions associated with an NOC/c, drugs maintain market access while under the NOC/c policy, and monitoring procedures to ensure timeliness of clinical confirmatory trial completion can continue while RWE is gathered. Successful inclusion of RWE within submissions put forth under the NOC/c policy would require a willingness on the part of the submission sponsor to integrate RWE into their overall evidence generation and submission planning, particularly in relation to proposed confirmatory trials that are not wholly aligned with the initial trials. RWE could provide data on the effectiveness of the drug in real-life clinical settings, and fill gaps in efficacy outcomes. Ensuring timely access in Canada to promising new therapies is extremely important. Thus, employing strategies to reduce the time to completion of confirmatory trials as well as greater consideration of RWE to fill evidence gaps, where appropriate, could enable better (and possibly faster) decisions around the confirmation of benefit for therapies, which is of particular importance given that many of these therapies are in the domain of rare disease.
Conclusions
Health Canada’s NOC/c policy has been effective in providing Canadians expedited access to innovative new oncological therapies based on promising data. More than half (54.9%) of the NOC/c for these drugs had all of their associated conditions lifted within 5 years of NOC/c issuance, and 85.7% of drugs issued NOC/c between 2018 and 2021 have become integrated into standard of care guidelines for their respective indications in Canada, demonstrating the success and clinical importance of this regulatory pathway. Some drugs, however, do remain under the NOC/c policy for long periods of time. Although not confirmed in our analysis, ensuring that confirmatory trials are already under way at the time of regulatory submission may decrease the time to confirmation of clinical benefit. It may also promote confidence for regulators and health system partners that the trial will be completed in a timely manner. While Health Canada does not currently have the regulatory authority to levy financial penalties or compel the submission of confirmatory data, they have posted a proposal for the introduction of terms and conditions that could be imposed when there is a need to manage risk or address uncertainties.25 CADTH has also recently proposed an HTA framework for time-limited recommendations to further address the evidentiary uncertainties reflected in regulatory approvals with conditions.26 Greater consideration by sponsors and other stakeholders as to the role RWE could play in the confirmation of benefit and risk should be further explored, particularly when the proposed confirmatory trials are not fully aligned with the approved indication. It is expected that the integration of these various approaches will increase the confidence in approvals granted under the NOC/c policy and help to inform future reforms and initiatives by various stakeholders.27
References
1.Health Canada. Guidance document: Notice of Compliance with conditions (NOC/c). Government of Canada. Published September 14, 2016. Accessed April 21, 2022. https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/applications-submissions/guidance-documents/notice-compliance-conditions.html
2.Health Canada. Notice of Compliance with conditions (NOC/c). Government of Canada. Published October 19, 2021. Accessed May 3, 2022. https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/notice-compliance/conditions.html
3.Health Products and Food Branch. Access to Therapeutic Products: The Regulatory Process in Canada.; 2006. Accessed April 21, 2022. https://publications.gc.ca/collections/collection_2007/hc-sc/H164-9-2006E.pdf
4.R Core Team. R: A language and environment for statistical computing. . R Foundation for Statistical Computing. Published online 2021. Accessed May 3, 2022. https://www.r-project.org./
5.Kassambara A, Kosinski M, Bieek P, Fabian S. Survminer: Drawing Survival Curves using “ggplot2.” Published online 2021.
6.Allaire JJ, Ellis P, Gandrud C, et al. D3 JavaScript Network Graphs from R. Published online March 18, 2017. Accessed July 4, 2023. https://cran.r-project.org/package=networkD3
7.About Clinical Practice Guidelines. National Comprehensive Cancer Network. Accessed August 7, 2023. https://www.nccn.org/guidelines/guidelines-process/about-nccn-clinical-practice-guidelines
8.Health Canada. Summary Basis of Decision for Ibrance. Published January 6, 20212019. Accessed February 25, 2023. https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?linkID=SBD00287
9.Andersen SK, Penner N, Chambers A, Trudeau ME, Chan KKW, Cheung MC. Conditional approval of cancer drugs in Canada: Accountability and impact on public funding. Current Oncology. 2019;26(1). doi:10.3747/co.26.4397 PubMed
10.Lexchin J. Notice of Compliance with Conditions: A Policy in Limbo. Healthcare Policy. 2007;2(4):114-122. doi:10.12927/HCPOL.2007.18862 PubMed
11.Law MR. The characteristics and fulfillment of conditional prescription drug approvals in Canada. Health Policy (New York). 2014;116(2-3):154-161. doi:10.1016/J.HEALTHPOL.2014.03.003 PubMed
12.Naci H, Smalley KR, Kesselheim AS. Characteristics of Preapproval and Postapproval Studies for Drugs Granted Accelerated Approval by the US Food and Drug Administration. JAMA. 2017;318(7):626-636. doi:10.1001/JAMA.2017.9415 PubMed
13.Gyawali B, Hey SP, Kesselheim AS. Assessment of the Clinical Benefit of Cancer Drugs Receiving Accelerated Approval. JAMA Intern Med. 2019;179(7):906-913. doi:10.1001/JAMAINTERNMED.2019.0462 PubMed
14.Bloem LT, Mantel-Teeuwisse AK, Leufkens HGM, De Bruin ML, Klungel OH, Hoekman J. Postauthorization Changes to Specific Obligations of Conditionally Authorized Medicines in the European Union: A Retrospective Cohort Study. Clin Pharmacol Ther. 2019;105(2):426-435. doi:10.1002/CPT.1169 PubMed
15.Hoekman J, Klamer TT, Mantel-Teeuwisse AK, Leufkens HGM, De Bruin ML. Characteristics and follow-up of postmarketing studies of conditionally authorized medicines in the EU. Br J Clin Pharmacol. 2016;82(1):213-226. doi:10.1111/bcp.12940 PubMed
16.Salcher-Konrad M, Naci H, Davis C. Approval of Cancer Drugs With Uncertain Therapeutic Value: A Comparison of Regulatory Decisions in Europe and the United States. Milbank Q. 2020;98(4):1219-1256. doi:10.1111/1468-0009.12476 PubMed
17.European Medicines Agency. Conditional marketing authorisation. Accessed May 3, 2022. https://www.ema.europa.eu/en/human-regulatory/marketing-authorisation/conditional-marketing-authorisation
18.U.S. Food & Drug Administration. Accelerated Approval Program. Published October 26, 2020. Accessed May 3, 2022. https://www.fda.gov/drugs/information-health-care-professionals-drugs/accelerated-approval-program
19.Fashoyin-Aje LA, Mehta GU, Beaver JA, Pazdur R. The On- and Off-Ramps of Oncology Accelerated Approval. New England Journal of Medicine. 2022;387(16):1439-1442. doi:10.1056/NEJMP2208954/SUPPL_FILE/NEJMP2208954_DISCLOSURES.PDF PubMed
20.Lexchin J. Quality of evidence considered by Health Canada in granting full market authorisation to new drugs with a conditional approval: a retrospective cohort study. BMJ Open. 2018;8:e020377. doi:10.1136/BMJOPEN-2017-020377 PubMed
21.Mcphail M, Bubela T. Legal and Regulatory Enablers and Barriers to Conditional Regulatory and Reimbursement Alternatives in Canadian Health Systems White Paper. CLEO. Published online 2022.
22.Council for International Organizations of Medical Sciences (CIOMS). Real-World Data and Real-World Evidence in Regulatory Decision Making. CIOMS Working Group Report.; 2023. Accessed July 25, 2023. https://cioms.ch/publications/.
23.Murphy G, de Léséleuc L, Kaunelis D, Adcock L. Use of Real-World Evidence in Single-Drug Assessments.; 2018. Accessed May 22, 2023. https://www.cadth.ca/sites/default/files/pdf/es0323-rwe-in-single-drug-appraisal.pdf
24.Lau CY, Jamali F, Loebenberg R, Lau C. Health Canada Usage of Real World Evidence (RWE) in Regulatory Decision Making Compared with FDA/EMA Usage Based on Publicly Available Information. Vol 25.; 2022. www.cspsCanada.org
25.Health Canada. Consultation on proposed agile regulations and guidance for licensing drugs and medical devices. Published March 6, 2023. Accessed April 16, 2023. https://www.canada.ca/en/health-canada/programs/consultation-proposed-agile-regulations-guidance-licensing-drugs-medical-devices.html
26.CADTH. CADTH Consultation: Proposed Process for Time-Limited Reimbursement Recommendations.; 2023. Accessed April 20, 2023. https://www.cadth.ca/sites/default/files/Drug_Review_Process/CADTH_TLR_Consultation.pdf
27.Teixeira T, Kweder SL, Saint-Raymond A. Are the European Medicines Agency, US Food and Drug Administration, and Other International Regulators Talking to Each Other? Clin Pharmacol Ther. 2020;107(3):507. doi:10.1002/CPT.1617 PubMed
28.Leslie Kux. Final Decision on Withdrawal of Breast Cancer Indication for AVASTIN (Bevacizumab) Following Public Hearing.; 2021. Accessed May 12, 2022. https://www.federalregister.gov/documents/2012/02/27/2012-4424/final-decision-on-withdrawal-of-breast-cancer-indication-for-avastin-bevacizumab-following-public
29.Government of Canada. Avastin (bevacizumab) - Health Canada has Suspended Approval for Use in Metastatic Breast Cancer. Recalls and Safety Alerts. Published November 29, 2011. Accessed May 3, 2022. https://recalls-rappels.canada.ca/en/alert-recall/avastin-bevacizumab-health-canada-has-suspended-approval-use-metastatic-breast-cancer
30.Tap WD, Wagner AJ, Schöffski P, et al. Effect of Doxorubicin Plus Olaratumab vs Doxorubicin Plus Placebo on Survival in Patients With Advanced Soft Tissue Sarcomas: The ANNOUNCE Randomized Clinical Trial. JAMA. 2020;323(13):1266-1276. doi:10.1001/JAMA.2020.1707 PubMed
31.Government of Canada. LARTRUVO (olaratumab) - New clinical trial information important to prescribing decisions. Recalls and Safety Alerts. Published January 30, 2019. Accessed May 12, 2022. https://recalls-rappels.canada.ca/en/alert-recall/lartruvo-olaratumab-new-clinical-trial-information-important-prescribing-decisions
32.Poveda AM, Davidson R, Blakeley C, Milner A. Olaparib maintenance monotherapy in platinum-sensitive, relapsed ovarian cancer without germline BRCA mutations: OPINION Phase IIIb study design. Future Oncology. 2019;15(32):3651-3663. doi:10.2217/fon-2019-0343 PubMed
33.Health Canada. Regulatory Decision Summary for Lynparza. Published July 14, 2017. Accessed June 28, 2023. https://hpr-rps.hres.ca/reg-content/regulatory-decision-summary-detail.php?linkID=RDS00398
Appendix 1: Author Information
Anna Martin,1 Melissa Hunt,2 Scott Blommaert,1 Suji Udayakumar,1 Brandon Lu,1 Shreya Chatterjee,1 Gaaya Sathiyabalan,2 Jan Brun,2 Melissa Kampman,2 Laurie Lambert,3 Nicole Mittmann,3 Kelly Robinson,2 Kelvin KW Chan1,4-6
Author Affiliations
1 Evaluative Clinical Sciences, Odette Cancer Centre Research Program, Sunnybrook Research Institute, Toronto, Ontario, Canada.
2 Health Canada, Ottawa, ON, Canada.
3 CADTH, Ottawa, ON, Canada.
4 Odette Cancer Centre, Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada.
5 Department of Medicine, University of Toronto, Toronto, Ontario, Canada.
6 Canadian Centre for Applied Research in Cancer Control, Toronto, Ontario, Canada.
Notes:
Preliminary results of this study were presented at the 2022 Canadian Centre for Applied Research in Cancer Control (ARCC) conference.
Portions of this material are based on work developed with financial support from CADTH. The analyses, conclusions, opinions, and statements expressed in this material are those of the authors and do not necessarily reflect the views of CADTH.
The analyses, conclusions, opinions, and statements expressed in this material are those of the authors and do not necessarily reflect the views of Health Canada.
Appendix 2: Supplementary Tables
Table 2: NOC/c for Brand Name Oncology Drugs Issued From the Introduction of the NOC/c Policy in May 1998 to December 1, 2021 (n = 92)
Drug | Indicationa | Date of NOC/c issuance | Date of NOC/c fulfillment | Time to NOC/c fulfillment in months |
|---|---|---|---|---|
Abecma (idecabtagene vicleucel) | Treatment of adult patients with multiple myeloma who have received at least three prior therapies, including an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 antibody and who are refractory to their last treatment. | May 26, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Adcetris (brentuximab vedotin) |
| February 1, 2013 | May 12, 2020 | 87 |
Alecensaro (alectinib) | Monotherapy for the treatment of patients with anaplastic lymphoma kinase (ALK)-positive, locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer (NSCLC) who have progressed on or are intolerant to crizotinib. | September 29, 2016 | September 26, 2018 | 23 |
Alunbrig (brigatinib) | Monotherapy for the treatment of adult patients with anaplastic lymphoma kinase (ALK)-positive metastatic non–small cell lung cancer (NSCLC) who have progressed on, or who were intolerant to an ALK inhibitor (crizotinib). | July 26, 2018 | July 20, 2022 | 47 |
Arimidex (anastrozole) | The adjuvant treatment of postmenopausal women with hormone receptor positive early breast cancer. | June 30, 2004 | December 2, 2008 | 53 |
Aromasin (exemestane) | Adjuvant treatment of early breast cancer. | May 12, 2006 | June 6, 2008 | 24 |
Arzerra (ofatumumab) | Treatment of patients with CLL refractory to fludarabine and alemtuzumab. | March 9, 2012 | January 17, 2017 | 58 |
Arzerra (ofatumumab) | In combination with chloramucil, for the treatment of patients with chronic lymphocytic leukemia (CLL) who have not received prior therapy and for whom fludarabine-based therapy is considered inappropriate. | October 2, 2014 | Cancelledb,c March 1, 2019 | NA |
Atriance (nelarabine) | Treatment of patients with T-cell acute lymphoblastic leukemia and T-cell lymphoblastic lymphoma whose disease has not responded to or has relapsed following treatment with at least two chemotherapy regimens. | September 22, 2007 | January 22, 2020 | 148 |
Avastin (bevacizumab) | As a single agent for the treatment of patients with glioblastoma after relapse or disease progression, following prior therapy. | March 24, 2010 | Withdrawna,c May 26, 2014 | NA |
Avastin (bevacizumab) | In combination with paclitaxel for the treatment of patients with metastatic HER2-negative breast cancer and who are ECOG class 0 to 1. | February 6, 2009 | Suspendede November 25, 2011 | NA |
Balversa (erdafitinib) | Treatment of adult patients with locally advanced or metastatic urothelial carcinoma whose tumours have susceptible fibroblast growth factor receptor (FGFR) 2 or FGFR3 genetic alterations and who have disease progression during or following at least one line of prior chemotherapy, including within 12 months of neoadjuvant or adjuvant chemotherapy. | October 25, 2019 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Bavencio (avelumab) | Treatment of metastatic Merkel cell carcinoma in previously treated adults. | December 18, 2017 | January 13, 2021 | 36 |
Bavencio (avelumab) | Treatment of adult patients with metastatic Merkel cell carcinoma (MCC). | November 6, 2019 | January 13, 2021 | 14 |
Bavencio (avelumab) | Treatment of patients with locally advanced or metastatic urothelial carcinoma who have received prior platinum-based chemotherapy. | May 4, 2018 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Blincyto (blinatumomab) | New indication: Treatment of patients with Philadelphia chromosome-negative CD19 positive B-precursor acute lymphoblastic leukemia (ALL) in first or second hematologic complete remission with minimal residual disease (MRD) greater than or equal to 0.1%. | December 19, 2019 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Blincyto (blinatumomab) | The treatment of pediatric patients with Philadelphia chromosome-negative relapsed or refractory B-cell precursor acute lymphatic leukemia (ALL). | April 28, 2017 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Blincyto (blinatumomab) | Treatment of adults with Philadelphia chromosome-negative relapsed or refractory B precursor acute lymphoblastic leukemia (ALL). | December 22, 2015 | November 16, 2017 | 22 |
Bosulif (bosutinib) | Treatment of chronic, accelerated, or blast phase Ph+ CML in adult patients with resistance or intolerance to prior tyrosine kinase inhibitor therapy, and for whom subsequent treatment with imatinib, nilotinib, and dasatinib is not clinically appropriate. | March 7, 2014 | August 2, 2017 | 40 |
Casodex (bicalutamide) | For immediate therapy in some patients with localized (T1-T2) prostate cancer who are inappropriate for surgery or radiotherapy. | November 25, 2002 | Suspendedf August 13, 2003 | NA |
Darzalex (daratumumab) | Treatment of patients with multiple myeloma who have received at least three prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory agent (IMiD), or who are refractory to both a PI and an IMiD. | June 29, 2016 | October 10, 2018 | 27 |
Enhertu (trastuzumab deruxtecan) | Treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received prior treatment with trastuzumab emtansine (T-DM1). | April 15, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Femara (letrozole) | Adjuvant treatment of postmenopausal women with hormone receptor positive early breast cancer. | October 6, 2006 | December 17, 2010 | 50 |
Femara (Letrozole) | Extended adjuvant treatment of early breast cancer in post menopausal women who have received prior standard adjuvant tamoxifen therapy. | April 1, 2005 | December 17, 2010 | 68 |
Folotyn (pralatrexate) | Treatment of patients with relapsed or refractory peripheral T-cell lymphoma (PTCL). | October 26, 2018 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Gavreto (pralsetinib) | Treatment of adult patients with rearranged during transfection (RET) fusion-positive locally advanced unresectable or metastatic non–small cell lung cancer (NSCLC). | June 30, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Gleevec (imatinib mesylate) | Treatment of patients with Kit- (CD 117) positive unresectable and/or metastatic gastrointestinal stromal tumours (GISTs). | August 7, 2002 | February 1, 2013 | 125 |
Gleevec (imatinib mesylate) | Adjuvant treatment of adult patients who are at intermediate to high risk of relapse following complete resection of Kit (CD117) positive GIST. | December 22, 2009 | November 24, 2017 | 95 |
Gleevec (imatinib mesylate) | Treatment of pediatric patients with newly diagnosed Philadelphia chromosome-positive, chronic myeloid leukemia (CML) in chronic phase. | May 24, 2007 | February 21, 2013 | 68 |
Gleevec (imatinib mesylate) | Newly diagnosed chronic myeloid leukemia (CML). | October 8, 2003 | June 17, 2010 | 80 |
Gleevec (imatinib mesylate) | Chronic myeloid leukemia (CML) in blast crisis, accelerated phase, or in chronic phase after failure of interferon-alpha therapy. | September 20, 2001 | December 29, 2004 | 39 |
Ibrance (palbociclib) | Use in combination with letrozole for the treatment of postmenopausal women with estrogen receptor (ER)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer as initial endocrine-based therapy for their metastatic disease. | March 16, 2016 | November 17, 2016 | 8 |
Iclusig (ponatinib hydrochloride) | Treatment of adult patients with chronic phase, accelerated phase, or blast phase chronic myeloid leukemia (CML) or Philadelphia chromosome positive acute lymphoblastic leukemia (Ph+ ALL) for whom other tyrosine kinase inhibitor (TKI) therapy is not appropriate, including CML or Ph+ ALL that is T315I mutation positive or where there is prior TKI resistance or intolerance. | April 2, 2015 | October 3, 2022 | 90 |
Idhifa (enasidenib) | Treatment of adult patients with relapsed or refractory Acute Myeloid Leukemia (AML) with an isocitrate dehydrogenase-2 (IDH2) mutation. | February 6, 2019 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Imbruvica (ibrutinib) | Treatment of patients with previously treated mantle cell lymphoma (MCL). | July 28, 2015 | September 12, 2017 | 25 |
Imfinzi (durvalumab) | Treatment of patients with locally advanced or metastatic urothelial carcinoma who:
| November 3, 2017 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Imfinzi (durvalumab) | Treatment of patients with locally advanced, unresectable non–small cell lung cancer (NSCLC) whose disease has not progressed following platinum-based chemoradiation therapy (CRT). | May 4, 2018 | August 23, 2019 | 15 |
Iressa (gefitinib) | Third line treatment of patients with locally advanced or metastatic non–small cell lung cancer after failure of two prior chemotherapy regimens (platinum-based and docetaxel). | December 17, 2003 | December 18, 2009 | 72 |
Istodax (romidepsin) | Treatment of patients with relapsed/refractory peripheral T-cell lymphoma (PTCL) who are not eligible for transplant and have received at least one prior systemic therapy. | October 16, 2013 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Keytruda (pembrolizumab) | Treatment of adult and pediatric patients with refractory or relapsed classical Hodgkin Lymphoma (cHL) who have failed autologous stem cell transplant (ASCT), or who are not candidates for multi-agent salvage chemotherapy and ASCT. | February 5, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Keytruda (pembrolizumab) | Refractory or relapsed classical Hodgkin lymphoma (cHL) as monotherapy in adults who have failed autologous stem cell transplant (ASCT) and brentuximab vedotin (BV) or who are not ASCT candidates and have failed BV. | September 8, 2017 | Withdrawnb,c February 3, 2021 | NA |
Keytruda (pembrolizumab) | Treatment of adult patients with bacillus Calmette-Guérin (BCG)-unresponsive, high-risk, non-muscle invasive bladder cancer (NMIBC) with carcinoma in situ (CIS) with or without papillary tumours who are (in)eligible for or have elected not to undergo cystectomy. | December 14, 2020 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Keytruda (pembrolizumab) | Treatment of patients with locally advanced unresectable or metastatic urothelial carcinoma, as monotherapy, in adults who are not eligible for cisplatin-containing chemotherapy and whose tumours express PD-L1 [Combined Positive Score (CPS) ≥ 10] as determined by a validated test, or in adults who are not eligible for any platinum-containing chemotherapy regardless of PD-L1 status. | April 11, 2019 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Keytruda (pembrolizumab) | Monotherapy for the treatment of adult patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair deficient (DMMR) colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin and irinotecan or endometrial cancer that has progressed following prior therapy and who have no satisfactory alternative treatment options. | April 18, 2019 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Keytruda (pembrolizumab) | Treatment of patients with metastatic non–small cell lung cancer (NSCLC) whose tumours express programmed death ligand 1 (PD-L1) (as determined by a validated test, see Dosage and Administration) and who have disease progression on or after platinum-containing chemotherapy. Patients with epithelial growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumour aberrations should have disease progression on authorized therapy for these aberrations before receiving Keytruda. | April 15, 2016 | September 10, 2019 | 40 |
Keytruda (pembrolizumab) | Treatment of patients with unresectable or metastatic melanoma and disease progression following ipilimumab therapy and, if BRAF V600 mutation positive, following a BRAF or MEK inhibitor. | May 19, 2015 | December 22, 2017 | 31 |
Keytruda (pembrolizumab) | Treatment of adult and pediatric patients with refractory primary mediastinal B-cell lymphoma (PMBCL) or who have relapsed after 2 or more lines of therapy, as monotherapy. | September 21, 2018 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Lartruvo (olaratumab) | In combination with doxorubicin for the treatment of adult patients with advanced soft tissue sarcoma (STS) not amenable to curative treatment with radiotherapy or surgery and for whom treatment with an anthracycline-containing regimen is appropriate. | November 23, 2017 | Discontinuedf October 8, 2020 | NA |
Lenvima and Keytruda (lenvatinib mesylate and pembrolizumab) | Lenvima in combination with pembrolizumab, for the treatment of adult patients with advanced endometrial carcinoma that is not microsatellite instability high (MSI-H) or mismatch repair deficient (dMMR), who have disease progression following prior platinum-based systemic therapy, and are not candidates for curative surgery or radiation. | September 20, 2019 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Libtayo (cemiplimab) | Treatment of adult patients with metastatic or locally advanced cutaneous squamous cell carcinoma (CSCC) who are not candidates for curative surgery or curative radiation. | April 10, 2019 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Lorbrena (lorlatinib) | Monotherapy for the treatment of adult patients with anaplastic lymphoma kinase (ALK)-positive metastatic non–small cell lung cancer (NSCLC) who have progressed on:
| February 22, 2019 | May 20, 2022 | 38 |
Lumakras (sotorasib) | Treatment of adult patients with Kirsten rat sarcoma viral oncogene homologue (KRAS) G12C-mutated locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer (NSCLC) who have received at least one prior systemic therapy. | September 10, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Lynparza (olaparib) | Monotherapy for the maintenance treatment of adult patients with platinum-sensitive relapsed BRCA-mutated (germline or somatic) high grade serous epithelial ovarian, fallopian tube or primary peritoneal cancer who are in response (complete response or partial response) to platinum-based chemotherapy. | April 29, 2016 | May 2, 2018 | 24 |
Lynparza (olaparib) | Monotherapy for the maintenance treatment of adult patients with platinum-sensitive relapsed (PSR) BRCA wild type high-grade epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response (complete response or partial response) to platinum-based chemotherapy. | May 4, 2018 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Minjuvi (tafasitamab) | In combination with lenalidomide for the treatment of adult patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) not otherwise specified, including DLBCL arising from low grade lymphoma, who are not eligible for autologous stem cell transplant (ASCT). | August 19, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Nexavar (sorafenib) | Treatment of locally advanced/metastatic renal cell (clear cell) carcinoma (RCC) in patients who failed prior cytokine therapy or are considered unsuitable for such therapy. | July 28, 2006 | June 28, 2009 | 35 |
Opdivo (nivolumab) | In combination with ipilimumab for the treatment of adult patients with microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) metastatic colorectal cancer after prior fluoropyrimidine-based therapy in combination with oxaliplatin or irinotecan. | February 11, 2021 | NA | 9 |
Opdivo (nivolumab) | New indication: Monotherapy for the treatment of adult patients with advanced (not amenable to curative therapy or local therapeutic measures) or metastatic hepatocellular carcinoma (HCC) who are intolerant to or have progressed on sorafenib therapy. | March 23, 2018 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Opdivo (nivolumab) | New indication: Monotherapy, for the treatment of adult patients with classical Hodgkin Lymphoma (cHL) that has relapsed or progressed after:
| November 10, 2017 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Opdivo (nivolumab) | Treatment of patients with unresectable or metastatic melanoma and disease progression following ipilimumab and, if BRAF V600 mutation positive, a BRAF inhibitor. | April 29, 2016 | February 21, 2018 | 21 |
Opdivo (nivolumab) | Treatment of patients with unresectable or metastatic melanoma in previously untreated adults when used in combination with ipilimumab. | October 26, 2016 | March 1, 2021 | 52 |
Pemazyre (pemigatinib) | Treatment of adults with previously treated, unresectable locally advanced or metastatic cholangiocarcinoma with a fibroblast growth factor receptor 2 (FGFR2) fusion or other rearrangement. | September 17, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Polivy (polatuzumab vedotin) | Treatment of adult patients with relapsed or refractory diffuse large B-cell lymphoma, not otherwise specified, who are not eligible for autologous stem cell transplant and have received at least one prior therapy. | July 9, 2020 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Retevmo (selpercatinib) | Treatment of metastatic RET fusion-positive non–small cell lung cancer (NSCLC) in adult patients, RET-mutant medullary thyroid cancer (MTC) in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease, RET fusion-positive differentiated thyroid carcinoma in adult patients with advanced or metastatic disease (not amenable to surgery or radioactive iodine therapy) following prior treatment with sorafenib and/or lenvatinib. | June 15, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Revlimid (lenalidomide) | Treatment of patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes (MDS) associated with a deletion 5q cytogenetic abnormality with or without additional cytogenetic abnormalities. | January 17, 2008 | June 6, 2013 | 64 |
Rozlytrek (entrectinib) | Treatment of adult patients with unresectable locally advanced or metastatic extracranial solid tumours, including brain metastases, that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion without a known acquired resistance mutation, and with no satisfactory treatment options. | February 10, 2020 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Sprycel (dasatinib) | Treatment of adults with chronic, accelerated, or blast phase chronic myeloid leukemia (CML) with resistance or intolerance to prior therapy including imatinib mesylate. | March 26, 2007 | November 19, 2009 | 31 |
Sprycel (dasatinib) | Treatment of adults with newly diagnosed Philadelphia chromosome positive (Ph+) chronic myeloid leukemia (CML) in chronic phase. | July 19, 2011 | November 26, 2015 | 52 |
Sutent (sunitinib malate) | Treatment of metastatic renal cell carcinoma (MRCC) of clear cell histology | May 1, 2008 | April 23, 2010 | 23 |
Sutent (sunitinib malate) | Treatment of metastatic renal cell carcinoma of clear cell histology after failure of cytokine-based therapy or in patients who are considered likely to be intolerant of such therapy. | August 17, 2006 | April 23, 2010 | 44 |
Tafinlar and Mekinist (dabrafenib and trametinib) | Dabrafenib in combination with trametinib for the treatment of patients with unresectable or metastatic melanoma with a BRAF V600 mutation. | March 6, 2015 | May 13, 2016 | 14 |
Tagrisso (osimertinib) | Treatment of patients with locally advanced or metastatic EGFR T790M mutation-positive non–small cell lung cancer (NSCLC) who have progressed on or after EGFR tyrosine kinase inhibitor (TKI) therapy. | July 5, 2016 | January 19, 2018 | 18 |
Tasigna (nilotinib hydrochloride monohydrate) | Treatment of adult patients with newly diagnosed Philadelphia chromosome positive chronic myeloid leukemia (Ph+ CML) in chronic phase. | June 22, 2011 | August 19, 2015 | 49 |
Tasigna (nilotinib hydrochloride monohydrate) | Treatment of chronic phase Philadelphia chromosome positive chronic myeloid leukemia (CML) in adult patients resistant to or intolerant of at least one prior therapy including imatinib. | July 22, 2010 | August 18, 2011 | 12 |
Tasigna (nilotinib hydrochloride monohydrate) | Treatment of accelerated phase (AP) Philadelphia chromosome-positive chronic myeloid leukemia (CML) in adult patients resistant to or intolerant of at least one prior therapy including imatinib. | September 9, 2008 | November 30, 2011 | 38 |
Taxotere (docetaxel) | In combination with doxorubicin and cyclophosphamide for the adjuvant treatment of patients with operable node-positive breast cancer. | December 14, 2006 | September 26, 2012 | 69 |
Tecentriq (atezolizumab) | In combination with nab-paclitaxel, for the treatment of adult patients with unresectable, locally advanced or metastatic triple-negative breast cancer (TNBC) whose tumours have PD-L1 expression ≥ 1%, and who have not received prior chemotherapy for metastatic disease. | September 21, 2019 | December 21, 2022 | 39 |
Tecentriq (atezolizumab) | Treatment of patients with locally advanced or metastatic urothelial carcinoma who:
| April 12, 2017 | Withdrawnb,c March 29, 2022 | NA |
Tepadina (thiotepa) | in combination with other chemotherapeutic products as part of a high-dose chemotherapy (HDCT) consolidation regimen followed by autologous stem cell transplantation (ASCT) for adult patients with central nervous system (CNS) lymphoma. | March 29, 2017 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Tepmetko (tepotinib) | The treatment of adult patients with locally advanced unresectable or metastatic non–small cell lung cancer (NSCLC) harbouring mesenchymal-epithelial transition (MET) tyrosine kinase receptor exon 14 skipping alterations. | May 27, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Truseltiq (infigratinib) | Treatment of adults with previously treated, unresectable locally advanced or metastatic cholangiocarcinoma with a fibroblast growth factor receptor 2 fusion or other rearrangement. | September 27, 2021 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Vectibix (panitumumab) | Monotherapy for the treatment of patients with EGFR expressing metastatic colorectal carcinoma (mCRC) with non-mutated (wild-type) KRAS after failure of fluoropyrimidine-, oxaliplatin-, and irinotecan-containing chemotherapy regimens. | April 3, 2008 | February 19, 2015 | 82 |
Velcade (bortezomib) | Treatment of multiple myeloma patients who have relapsed following front-line therapy and are refractory to their most recent therapy. | January 27, 2005 | September 11, 2007 | 31 |
Velcade (bortezomib) | Treatment of progressive multiple myeloma in patients who have received at least one prior therapy and who have already undergone or are unsuitable for stem cell transplantation. | April 24, 2006 | September 11, 2007 | 16 |
Venclexta (venetoclax) | Monotherapy for the treatment of patients with chronic lymphocytic leukemia (CLL) with 17p deletion who have received at least one prior therapy, or patients with CLL without 17p deletion who have received at least one prior therapy and for whom there are no other available treatment options. | September 30, 2016 | January 13, 2020 | 39 |
Verity-BCG (bacillus Calmette-Guérin [BCG]: strain Russian BCG-1) | Adjuvant therapy after transurethral resection (TUR) of a primary or relapsing superficial papillary urothelial cell carcinoma of the bladder stage Ta (grade 2 or 3) or T1 (grade 1, 2, or 3), without concomitant carcinoma in situ. | December 24, 2020 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Vitrakvi (larotrectinib) | Treatment of adult and pediatric patients with solid tumours that have a Neurotrophic Tyrosine Receptor Kinase (NTRK) gene fusion without a known acquired resistance mutation:
| July 10, 2019 | NA | Not yet fulfilled as of cut-off date of December 1, 2022 |
Xalkori (crizotinib) | Monotherapy for use in patients with ALK-positive advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer (NSCLC). | April 25, 2012 | November 18, 2015 | 42 |
Xeloda (capecitabine) | Adjuvant treatment of patients with stage III (Dukes' stage C) colon cancer. | December 7, 2005 | October 23, 2008 | 34 |
Zepzelca (lurbinectedin) | Treatment of adults with stage III or metastatic small cell lung cancer (SCLC) who have progressed on or after platinum-containing therapy. | September 29, 2021 | NA | 2 |
Zydelig (idelalisib) | Monotherapy for the treatment of patients with follicular lymphoma who have received at least two prior systemic regimens and are refractory to both rituximab and an alkylating agent. | March 27, 2015 | April 21, 2020 | 60 |
Zykadia (ceritinib) | Monotherapy for use in patients with anaplastic lymphoma kinase (ALK)-positive locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer (NSCLC) who have progressed on or who were intolerant to crizotinib. | March 27, 2015 | NA | 80 |
ALK = anaplastic lymphoma kinase; ALL = acute lymphoblastic leukemia; AML = acute myeloid leukemia; AP = accelerated phase; ASCT = autologous stem cell transplant; BCG = bacillus Calmette-Guérin; BV = brentuximab vedotin; cHL = classical Hodgkin lymphoma; CIS = carcinoma in situ; CLL = chronic lymphocytic leukemia; CML = chronic myeloid leukemia; CNS = central nervous system; CPS = combined positive score; CRT = chemoradiation therapy; CSCC = cutaneous squamous cell carcinoma; DLBCL = diffuse large B-cell lymphoma; dMMR = deficient mismatch repair; ECOG = Eastern Cooperative Oncology Group; EGFR = epithelial growth factor; ER = estrogen receptor; FGFR = fibroblast growth factor receptor; GIST = gastrointestinal stromal tumour; HCC = hepatocellular carcinoma; HDCT = high-dose chemotherapy; HER2 = human epidermal growth factor receptor 2; HL = Hodgkin lymphoma; IDH2 = isocitrate dehydrogenase 2; IMiD = immunomodulatory drug; KRAS = Kirsten rat sarcoma viral oncogene homologue; MCC = Merkel cell carcinoma; MCL = mantle cell lymphoma; mCRC = metastatic colorectal carcinoma; MDS = myelodysplastic syndrome; MEK = mitogen-activated extracellular signal-regulated kinase; MET = mesenchymal-epithelial transition; MRCC = metastatic renal cell carcinoma; MRD = minimal residual disease; MSI-H = microsatellite instability high; MTC = medullary thyroid cancer; NA = not applicable; NMIBC = non-muscle invasive bladder cancer; NOC/c = Notice of Compliance with conditions; NSCLC = non–small-cell lung cancer; NTRK = neurotrophic tyrosine receptor kinase; PD-L1 = programmed cell death 1 ligand 1; Ph+ = Philadelphia chromosome positive; PI = proteosome inhibitor; PMBCL = primary mediastinal B-cell lymphoma; PSR = platinum-sensitive relapsed; PTCL = peripheral T-cell lymphoma; RCC = renal cell carcinoma; RET = rearranged during transfection; sALCL = systemic anaplastic large cell lymphoma; SCLC = small cell lung cancer; STS = soft tissue sarcoma; T-DM1 = trastuzumab emtansine; TKI = tyrosine kinase inhibitor; TNBC = triple-negative breast cancer; TUR = transurethral resection.
aIndications at the time of NOC/c were extracted from qualifying notices, letters of undertaking, summary basis of decision documents, regulatory decision summaries, or product monographs, depending on availability.
bCompanies are not required to publicly state a reason for withdrawal. Withdrawal may be due to factors outside of clinical benefit or risk.
cReason for removal not listed.
dStudy findings did not confirm clinical benefit.1
eStudy findings indicated no significant reduction in tumour size or extension of life and potentially life-threatening risks.2
fResults of clinical trials indicate increased mortality.3
gStudy findings did not confirm clinical benefit.4,5
Table 3: NOC/c Oncology Drugs With Nonaligned Trials
Drug | Reason for nonalignment | NOC/c indication | Initial trial(s) | Confirmatory trial(s) |
|---|---|---|---|---|
Alunbrig (brigatinib) | Previous treatment | Patients must have received previous treatment with an ALK inhibitor. | Patients must have received previous treatment.6,7 | Patients must not have received previous treatment with an ALK inhibitor.8 |
Avastin (bevacizumab) | Drug combination | Avastin is to be used as a single agent. | Avastin is evaluated as a monotherapy.9 | Avastin is evaluated in combination with lomustine.10 |
Bavencio (avelumab) | Previous treatment | Patients must have received previous treatment. | Patients must have received previous treatment.11,12 | Patients must be treatment-naive.13 |
Imfinzi (durvalumab) | Previous treatment | Patients must have received prior platinum-containing chemotherapy. | Patients must have received previous treatment.14 | Patients must be previously untreated.15 |
Istodax (romidepsin) | Previous treatment | Patients must have received at least 1 prior systemic therapy. | Patients must have received at least 1 prior systemic therapy.16 | Patients must be previously untreated.17 |
Keytruda (pembrolizumab) | Previous treatment | Patients must have experienced failure of prior brentuximab vedotin. | Patients must have progressed following prior brentuximab vedotin.18,19 | Patients must be naive to brentuximab vedotin or have responded to previous brentuximab vedotin.20 |
Lorbrena (lorlatinib) | Previous treatment | Patients must have progressed on an ALK inhibitor. | Patients must be treatment-naive in the advanced setting or have progressed on a TKI. 21,22 | Patients must not have received previous systemic treatment.23 |
Minjuvi (tafasitamab) | Previous treatment | Patients must have relapsed or refractory disease. | Patients must be relapsed after or refractory to at least 1 but no more than 3 systemic regimens.24 | Patients must be previously untreated.25 |
Opdivo (nivolumab) | Previous treatment | Patients must be intolerant to or have progressed on sorafenib. | Patients must have received at least 1 prior line of systemic therapy including sorafenib or be intolerant to or have refused sorafenib.26 | Patients must not have received prior systemic therapy.27 |
Opdivo (nivolumab) | Previous treatment | Patients must have relapsed or progressed following prior autologous stem cell transplantation and brentuximab vedotin or 3 or more lines of systemic therapy. | Patients must have relapsed or refractory disease.28,29 | Patients must be previously untreated.30,31 |
Pemazyre (pemigatinib) | Previous treatment | Patients must have received previous treatment. | Patients must have progressed following at least 1 previous systemic therapy.32 | Patients must be previously untreated.33 |
Polivy (polatuzumab) | Previous treatment | Patients must have received at least 1 prior therapy. | Patients may be previously untreated or may have received previous treatment.34-38 | Patients must be previously untreated.39 |
Truseltiq (infigratinib) | Previous treatment | Patients must have received previous treatment. | Patients must have received previous gemcitabine.40 | Patients must not have received prior systemic anticancer therapy.41 |
ALK = anaplastic lymphoma kinase; NOC/c = Notice of Compliance with conditions; TKI = tyrosine kinase inhibitor.
Leslie Kux. Final Decision on Withdrawal of Breast Cancer Indication for AVASTIN (Bevacizumab) Following Public Hearing.; 2021. Accessed May 12, 2022. https://www.federalregister.gov/documents/2012/02/27/2012-4424/final-decision-on-withdrawal-of-breast-cancer-indication-for-avastin-bevacizumab-following-public
Government of Canada. Avastin (bevacizumab) - Health Canada has Suspended Approval for Use in Metastatic Breast Cancer. Recalls and Safety Alerts. Published November 29, 2011. Accessed May 3, 2022. https://recalls-rappels.canada.ca/en/alert-recall/avastin-bevacizumab-health-canada-has-suspended-approval-use-metastatic-breast-cancer
Health Canada. Notice of Compliance with conditions (NOC/c). Government of Canada. Published October 19, 2021. Accessed May 3, 2022. https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/notice-compliance/conditions.html
Tap WD, Wagner AJ, Schöffski P, et al. Effect of Doxorubicin Plus Olaratumab vs Doxorubicin Plus Placebo on Survival in Patients With Advanced Soft Tissue Sarcomas: The ANNOUNCE Randomized Clinical Trial. JAMA. 2020;323(13):1266-1276. doi:10.1001/JAMA.2020.1707
Government of Canada. LARTRUVO (olaratumab) - New clinical trial information important to prescribing decisions. Recalls and Safety Alerts. Published January 30, 2019. Accessed May 12, 2022. https://recalls-rappels.canada.ca/en/alert-recall/lartruvo-olaratumab-new-clinical-trial-information-important-prescribing-decisions
Kim DW, Tiseo M, Ahn MJ, et al. Brigatinib in Patients With Crizotinib-Refractory Anaplastic Lymphoma Kinase-Positive Non-Small-Cell Lung Cancer: A Randomized, Multicenter Phase II Trial. J Clin Oncol. 2017;35:2490-2498. doi:10.1200/JCO
Gettinger SN, Bazhenova LA, Langer CJ, et al. Activity and safety of brigatinib in ALK-rearranged non-small-cell lung cancer and other malignancies: a single-arm, open-label, phase 1/2 trial. Lancet Oncol. 2016;17(12):1683-1696. doi:10.1016/S1470-2045(16)30392-8
Camidge DR, Kim HR, Ahn MJ, et al. Brigatinib versus Crizotinib in ALK-positive non-small cell lung cancer. New England Journal of Medicine. 2018;379(21):2027-2039.
Raizer J. Bevacizumab in Treating Patients With Recurrent or Progressive Glioma. Published February 7, 2020. Accessed June 29, 2023. https://classic.clinicaltrials.gov/ct2/show/NCT00337207
Wick W, Gorlia T, Bendszus M, et al. Lomustine and Bevacizumab in Progressive Glioblastoma. New England Journal of Medicine. 2017;377(20):1954-1963. doi:10.1056/nejmoa1707358
Kaufman HL, Russell J, Hamid O, et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016;17(10):1374-1385. doi:10.1016/S1470-2045(16)30364-3
Kaufman HL, Russell JS, Hamid O, et al. Updated efficacy of avelumab in patients with previously treated metastatic Merkel cell carcinoma after ≥1 year of follow-up: JAVELIN Merkel 200, a phase 2 clinical trial. J Immunother Cancer. 2018;6(1). doi:10.1186/s40425-017-0310-x
D’Angelo SP, Lebbé C, Mortier L, et al. First-line avelumab in a cohort of 116 patients with metastatic Merkel cell carcinoma (JAVELIN Merkel 200): Primary and biomarker analyses of a phase II study. J Immunother Cancer. 2021;9(7). doi:10.1136/jitc-2021-002646
Health Canada. Summary Basis of Decision for Imfinzi. Published July 14, 2021. Accessed June 29, 2023. https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?linkID=SBD00384
Powles T, van der Heijden MS, Castellano D, et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2020;21(12):1574-1588. doi:10.1016/S1470-2045(20)30541-6
Coiffier B, Pro B, Prince HM, et al. Results from a pivotal, open-label, phase II study of romidepsin in relapsed or refractory peripheral T-cell lymphoma after prior systemic therapy. Journal of Clinical Oncology. 2012;30(6):631-636. doi:10.1200/JCO.2011.37.4223
Bachy E, Camus V, Thieblemont C, et al. Romidepsin Plus CHOP Versus CHOP in Patients With Previously Untreated Peripheral T-Cell Lymphoma: Results of the Ro-CHOP Phase III Study (Conducted by LYSA). J Clin Oncol. 2021;40:242-251. doi:10.1200/JCO.21
Chen R, Zinzani PL, Fanale MA, et al. Phase II Study of the Efficacy and Safety of Pembrolizumab for Relapsed/Refractory Classic Hodgkin Lymphoma. J Clin Oncol. 2017;35:2125-2132. doi:10.1200/JCO
Armand P, Shipp MA, Ribrag V, et al. Programmed death-1 blockade with pembrolizumab in patients with classical hodgkin lymphoma after brentuximab vedotin failure. In: Journal of Clinical Oncology. Vol 34. American Society of Clinical Oncology; 2016:3733-3739. doi:10.1200/JCO.2016.67.3467
Kuruvilla J, Ramchandren R, Santoro A, et al. Pembrolizumab versus brentuximab vedotin in relapsed or refractory classical Hodgkin lymphoma (KEYNOTE-204): an interim analysis of a multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 2021;22(4):512-524. doi:10.1016/S1470-2045(21)00005-X
Shaw AT, Felip E, Bauer TM, et al. Lorlatinib in non-small-cell lung cancer with ALK or ROS1 rearrangement: an international, multicentre, open-label, single-arm first-in-man phase 1 trial. Lancet Oncol. 2017;18(12):1590-1599. doi:10.1016/S1470-2045(17)30680-0
Solomon BJ, Besse B, Bauer TM, et al. Lorlatinib in patients with ALK-positive non-small-cell lung cancer: results from a global phase 2 study. Lancet Oncol. 2018;19(12):1654-1667. doi:10.1016/S1470-2045(18)30649-1
Shaw AT, Bauer TM, de Marinis F, et al. First-Line Lorlatinib or Crizotinib in Advanced ALK -Positive Lung Cancer. New England Journal of Medicine. 2020;383(21):2018-2029. doi:10.1056/nejmoa2027187
Salles G, Duell J, González Barca E, et al. Tafasitamab plus lenalidomide in relapsed or refractory diffuse large B-cell lymphoma (L-MIND): a multicentre, prospective, single-arm, phase 2 study. Lancet Oncol. 2020;21(7):978-988. doi:10.1016/S1470-2045(20)30225-4
MorphoSys AG. Tafasitamab + Lenalidomide + R-CHOP Versus R-CHOP in Newly Diagnosed High-intermediate and High Risk DLBCL Patients (frontMIND). Published April 6, 2023. Accessed June 29, 2023. https://classic.clinicaltrials.gov/ct2/show/NCT04824092
El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. The Lancet. 2017;389(10088):2492-2502. doi:10.1016/S0140-6736(17)31046-2
Yau T, Park JW, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022;23(1):77-90. doi:10.1016/S1470-2045(21)00604-5
Armand P, Engert A, Younes A, et al. Nivolumab for Relapsed/Refractory Classic Hodgkin Lymphoma After Failure of Autologous Hematopoietic Cell Transplantation: Extended Follow-Up of the Multicohort Single-Arm Phase II CheckMate 205 Trial. J Clin Oncol. 2018;36:1428-1439. doi:10.1200/JCO
Lesokhin AM, Ansell SM, Armand P, et al. Nivolumab in patients with relapsed or refractory hematologic malignancy: Preliminary results of a phase ib study. Journal of Clinical Oncology. 2016;34(23):2698-2704. doi:10.1200/JCO.2015.65.9789
Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. New England Journal of Medicine. 2017;377(14):1345-1356. doi:10.1056/nejmoa1709684
Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Long-Term Outcomes With Nivolumab Plus Ipilimumab or Nivolumab Alone Versus Ipilimumab in Patients With Advanced Melanoma. J Clin Oncol. 2021;40:127-137. doi:10.1200/JCO.21
Abou-Alfa GK, Sahai V, Hollebecque A, et al. Pemigatinib for previously treated, locally advanced or metastatic cholangiocarcinoma: a multicentre, open-label, phase 2 study. Lancet Oncol. 2020;21(5):671-684. doi:10.1016/S1470-2045(20)30109-1
Bekaii-Saab TS, Valle JW, Van Cutsem E, et al. FIGHT-302: First-line pemigatinib vs gemcitabine plus cisplatin for advanced cholangiocarcinoma with FGFR2 rearrangements. Future Oncology. 2020;16(30):2385-2399. doi:10.2217/fon-2020-0429
Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. New England Journal of Medicine. 2022;386(4):351-363. doi:10.1056/nejmoa2115304
Tilly H, Morschhauser F, Bartlett NL, et al. Polatuzumab vedotin in combination with immunochemotherapy in patients with previously untreated diffuse large B-cell lymphoma: an open-label, non-randomised, phase 1b–2 study. Lancet Oncol. 2019;20(7):998-1010. doi:10.1016/S1470-2045(19)30091-9
Sehn LH, Herrera AF, Flowers CR, et al. Polatuzumab Vedotin in Relapsed or Refractory Diffuse Large B-Cell Lymphoma. J Clin Oncol. 2019;38:155-165. doi:10.1200/JCO.19
Palanca-Wessels MCA, Czuczman M, Salles G, et al. Safety and activity of the anti-CD79B antibody-drug conjugate polatuzumab vedotin in relapsed or refractory B-cell non-Hodgkin lymphoma and chronic lymphocytic leukaemia: A phase 1 study. Lancet Oncol. 2015;16(6):704-715. doi:10.1016/S1470-2045(15)70128-2
Morschhauser F, Flinn IW, Advani R, et al. Polatuzumab vedotin or pinatuzumab vedotin plus rituximab in patients with relapsed or refractory non-Hodgkin lymphoma: final results from a phase 2 randomised study (ROMULUS). Lancet Haematol. 2019;6(5):e254-e265. doi:10.1016/S2352-3026(19)30026-2
Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. New England Journal of Medicine. 2022;386(4):351-363. doi:10.1056/nejmoa2115304
Javle M, Roychowdhury S, Kelley RK, et al. Infigratinib (BGJ398) in previously treated patients with advanced or metastatic cholangiocarcinoma with FGFR2 fusions or rearrangements: mature results from a multicentre, open-label, single-arm, phase 2 study. Lancet Gastroenterol Hepatol. 2021;6(10):803-815. doi:10.1016/S2468-1253(21)00196-5
Makawita S, K Abou-Alfa G, Roychowdhury S, et al. Infigratinib in patients with advanced cholangiocarcinoma with FGFR2 gene fusions/translocations: The PROOF 301 trial. Future Oncology. 2020;16(30):2375-2384. doi:10.2217/fon-2020-0299