Drugs, Health Technologies, Health Systems
Peer-Reviewed Article
Coverage With Evidence Development: An Environmental Scan of Funding Programs Leveraging Real-World Evidence to Support Funding Decisions
Authors: Caroline Muñoz, Jessica Arias, Alayna Brown, Mitali Garg, Scott Gavura
Abstract
Background: New cancer drugs with increasing costs and uncertainties in clinical trial evidence are being approved and funded faster. Coverage with evidence development (CED), using real-world evidence (RWE), has the potential to help manage drug costs and address uncertainties in evidence. A national CED program in Canada may facilitate patient access to new drugs while assessing clinical performance and value for money to support final funding decisions. Descriptions of Canadian and international CED policies using RWE to support final funding decisions are limited.
Objectives: This Environmental Scan aimed to identify the use of CED for drug funding in Canadian and international jurisdictions, describe the components of various CED programs in which RWE is generated to support decision-making, and report on the limitations of CED.
Methods: To complete the Environmental Scan, we identified CED programs where RWE was used to support decision-making. We searched Embase and various health-related websites, from 2007 to 2024. Search terms related to CED, funding, decision-making, and RWE were applied. Data were extracted on article information, jurisdiction, CED policies, RWD collection, and RWE generation. We reported on which jurisdictions have applied CED, the processes for drug funding and RWE generation during the CED period, and the limitations of CED experiences.
Results: We identified the use of CED agreements in 13 jurisdictions. Variation in the CED components and processes were observed between jurisdictions with limited transparency in the details of CED agreements. Performance-based or outcome-based agreements and/or financial agreements are used as part of CED agreements to support risk-sharing between payers and manufacturers. Limitations of CED include a lack of defined outcomes to support final funding decision-making, entry and exit criteria, project timelines, and feasibility of data collection and evidence generation to address uncertainties.
Conclusion: This Environmental Scan highlights the variation in how CEDs are applied between jurisdictions as well as the limitations of using RWE to inform drug funding decisions. CED supports risk-sharing and evidence development, but challenges related to implementation, transparency, and decision-making criteria have been documented. Lessons learned from international experiences can be leveraged to explore the development of a robust Canadian CED model.
Background
Health technology assessment (HTA) committees play an important role in helping payers manage access to expensive new drugs, particularly when evidence of clinical effectiveness and cost-effectiveness is minimal and the pressure to accelerate funding is high. In Canada, provincial drug coverage and reimbursement policies are established following HTAs by the Institut national d'excellence en santé et en services sociaux (INESSS) in Quebec and Canada’s Drug Agency (CDA-AMC) in the remaining provinces and territories.1,2 During HTAs, a drug’s clinical effectiveness and cost-effectiveness are assessed based on a review of the submitted evidence, which is summarized to support informed decision-making by policy-makers.3 In cases where the clinical evidence or cost-effectiveness is uncertain, CDA-AMC may issue a recommendation to reimburse with conditions (e.g., price reduction required to make the therapy cost-effective).
Reimbursement recommendations with conditions are common across many jurisdictions and are similarly based on uncertainties in the clinical effectiveness and cost-effectiveness data submitted. Uncertainties in clinical trial data can be a consequence of suboptimal trial design, limited follow-up time for clinical and cost-effectiveness outcomes, and the inclusion of patients that are not comparable to real-world populations.3 Public funding agencies have sought to facilitate patient access to these drugs by funding them through managed entry agreements (MEAs).4,5
“MEA” is an umbrella term that encompasses a variety of agreements between manufacturers and payers aimed at increasing and accelerating patient access to novel therapies while meeting conditions specific to each agreement.5 MEAs can be financial agreements or performance-based agreements.4,5 Financial agreements, such as rebates, price caps, and price-volume agreements, aim to address uncertainties around the financial impact of a drug by reducing its cost.4,5 Performance-based agreements aim to address uncertainties around the performance or clinical benefit of a drug and can include outcomes-based agreements (OBAs), coverage with evidence development (CED), and payment by result. Payers agree to reimburse the cost of a drug when evidence is submitted demonstrating the drug has achieved clinical end points set out in the terms of the agreement.4,5 Performance-based agreements often include a financial agreement component to support risk-sharing of high drug costs between manufacturers and payers.4,5
In the case of CED, an interim funding period is the set time during which a drug receives temporary public funding, allowing patients to access the drug while clinical effectiveness and/or cost-effectiveness data are collected on patients receiving the drug.4,5 Data collected during the interim funding period are used to generate clinical trial evidence or real-world evidence (RWE) to support assessments of the drug’s performance at a later date. RWE, generated with real-world data (RWD), may be described as “evidence generated from multiple types of data, collected from multiple sources, aggregated, shared, and often reaggregated in multiple sectors of the health care system.”6,7
In recent years, Canada has made advancements in accelerating access to cancer drugs through various initiatives. Most relevant to CED is the introduction of CDA-AMC’s Time-Limited Recommendations and the pan-Canadian Pharmaceutical Alliance (pCPA)’s Temporary Access Process (pTAP).8,9 These programs launched in 2023 to expedite the listing of drugs, fulfilling an unmet need. In these cases of CED, the manufacturer is expected to submit updated phase III trial data to CDA-AMC to obtain a final funding recommendation. Both programs are meant to be evaluated with the potential to expand this recommendation category and negotiation process to additional drugs, potentially where phase III data will not be available or where phase III data still have uncertainties. Additionally, bilateral agreements between the federal and provincial governments in Canada are facilitating access to drugs for rare diseases (DRD) with the expectation that RWE is used to support further decision-making about DRD.10,11
Developing a national approach could be strengthened by examining existing CED programs both within Canada and in countries around the world where RWE is used to support funding decisions. There is limited literature describing jurisdictional CED polices and the use of RWE to support final funding decisions. Consequently, the objectives of this Environmental Scan were to identify the use of CED for drug funding in Canadian and international jurisdictions, describe the components of various CED programs in which RWE is generated to support decision-making, and report on the limitations of CED.
Methods
An Environmental Scan was conducted to identify and describe CED programs implemented in Canada and in international jurisdictions. To ensure a comprehensive search was undertaken, multiple evidence sources were searched. Table 1 presents a list of all evidence sources and key websites.
In consultation with a research librarian, a database-specific search strategy was designed for Embase using a combination of the following terms with the Boolean operators (“and” and “or”): evidence building, evidence development, coverage with evidence, managed entry, managed access, agreement, and outcome. Searches were limited to the English language and to results published within the past 17 years (from 2007 to November 2024). The scan started in 2022, and a 15-year look-back period for sources was established based on expert input. The scan was updated in November 2024, resulting in a period of 2007 to November 2024 to capture relevant sources. The database search was not limited to any specific jurisdiction but was limited to articles in English. To ensure a comprehensive search strategy was developed, the inclusion of terms related to RWE, drug funding, and decision-making concepts was too restrictive, and thus these concepts were omitted from the final search strategy. The Embase search strategy is presented in Appendix 1.
To locate grey literature and white papers, we also conducted a web-based search using the Google search engine and reviewed key organizational websites (e.g., for the National Institute for Health and Care Excellence [NICE]) for potentially relevant literature. Google searches and organizational website searches were conducted using a combination of the key search terms presented in Table 2 and the jurisdictions of interest. Seven jurisdictions of interest were selected through consultation with HTA experts. RWE, drug funding, and decision-making concept terms were included in the grey literature searches as they increased the accuracy of the searches.
Study Selection
Articles were identified using a 2-phase screening approach: phase 1 for title and abstract screening, and phase 2 for full-text screening. All articles identified from the electronic database search were imported into Microsoft Excel for the removal of duplicate articles and screening.
Title and abstract screening was conducted by 3 reviewers: CM, AB, and MG. Articles were classified as potentially relevant based on the study selection criteria outlined in Table 3. All 3 reviewers independently reviewed the same randomly selected 12 abstracts to ensure accuracy and transparency in the selection of relevant abstracts. Discussions were held to achieve consensus on the 12 trial abstracts, and the final inclusion decision was documented in the Excel abstract screening document.
A full-text review of the articles selected for inclusion from title and abstract screening was conducted by CM. CM reviewed the reference lists of articles to identify additional potentially relevant articles for inclusion.
CM reviewed the first 5 pages of the Web-based search results from Google and key organization websites for relevant grey literature. The search terms used to identify relevant grey literature were documented in a Microsoft Excel spreadsheet. Grey literature was included if it met the study selection criteria outlined in Table 3.
Data Extraction
A single reviewer extracted data from included studies with respect to general study information, program characteristics, and program structures and operations. Appendix 2 presents a sample data extraction form for articles, reports, and web pages included in the scan.
Data Synthesis
Extracted data were summarized by jurisdiction to provide a description of the structure and operations of jurisdictional CED programs. The results presented are organized by CED program structural and operational themes. The intent with this organization is to demonstrate high-level trends and variation in CED program structures and operations among jurisdictions.
Results
This scan identified 70 articles describing the structure and operations of CED programs in 12 countries (13 jurisdictions), including Australia, Belgium, Canada (2 jurisdictions: Alberta and Ontario), France, Germany, Ireland, Italy, the Netherlands, Scotland, Sweden, the UK, and the US (Figure 1). The search strategy in Embase produced 852 relevant abstracts, of which 121 articles (14%) underwent full-text review, and data were extracted from 37 articles (4%). The grey literature scan resulted in full-text review for 105 articles and data extraction for 33 (31%) of 105 articles.
Figure 1: Study Selection Process (PRISMA Diagram)
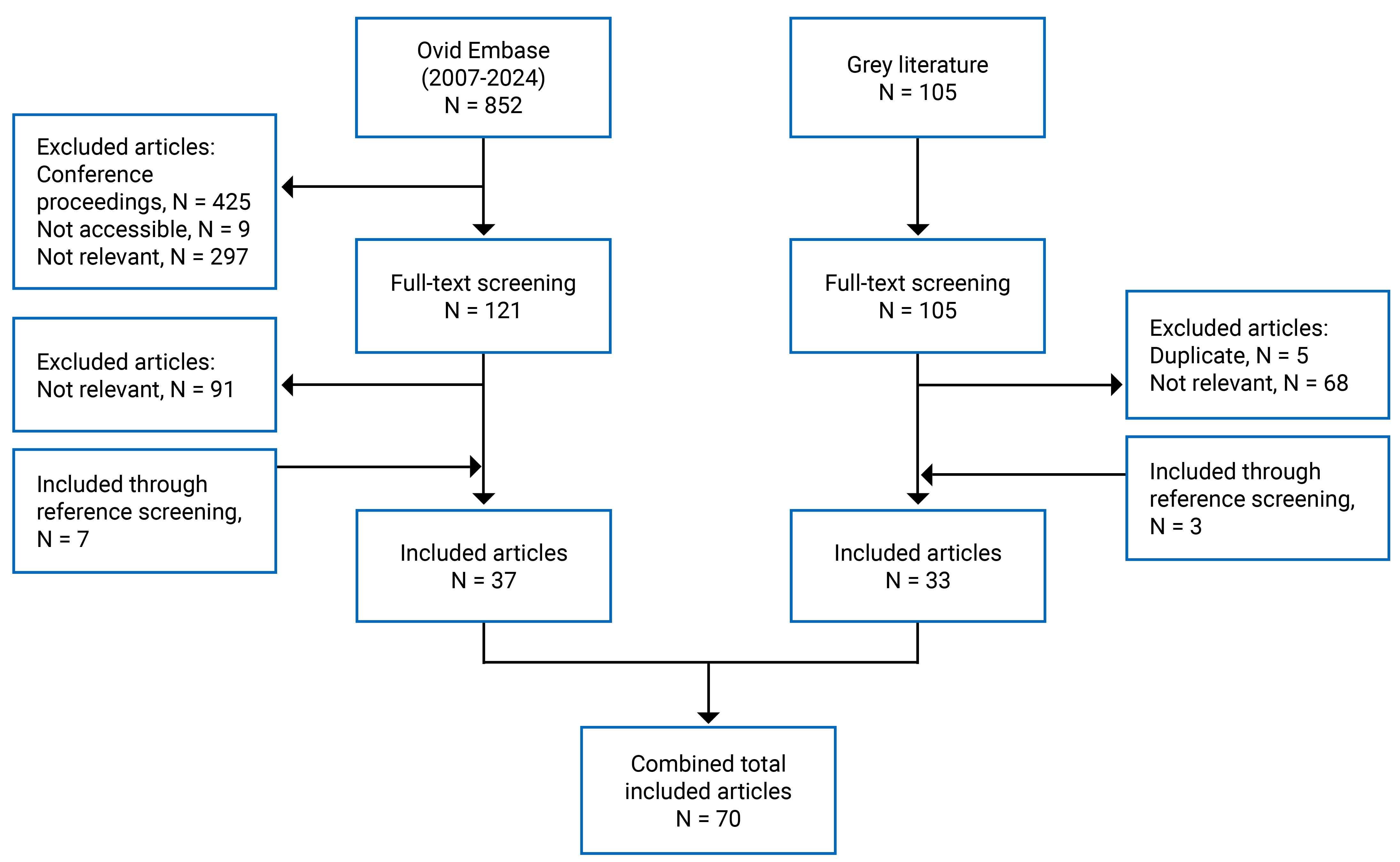
PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
CED Common Terms
The MEA nomenclature varies between jurisdictions. Literature on agreements from Belgium, Canadian jurisdictions, France, Germany, the Netherlands, Scotland, Sweden, the UK, and the US refer specifically to CED or evidence-building agreements.12-38 Literature on agreements from Australia, Ireland, and Italy use the term MEAs while describing CED agreements as funding agreements with conditions to provide additional evidence to support final funding statuses.12,17,19,39-43
CED Objectives
The objective for CEDs is common across all jurisdictions: enable patient access to new drugs and indications while generating clinical and/or cost-effectiveness evidence to address uncertainties and support final funding recommendations.4,12-15,19,20,22-24,26,31,44-52 In Belgium, France, and Italy, an additional objective of CED agreements is to improve forecasting and limit the budget impact of high-cost drugs.4,31,49
CED Framework
Across jurisdictions, there appears to be a common framework for funding drugs with CED agreements. Common elements within the framework include having processes for health system partner engagement, drug selection, RWD collection, RWE generation, establishing financial terms and duration of interim funding, and making a final funding decision. (Figure 2). Each jurisdiction may approach these aspects differently. The various approaches are discussed in further detail in the next sections. Table 4 details CED characteristics and frameworks by jurisdiction.
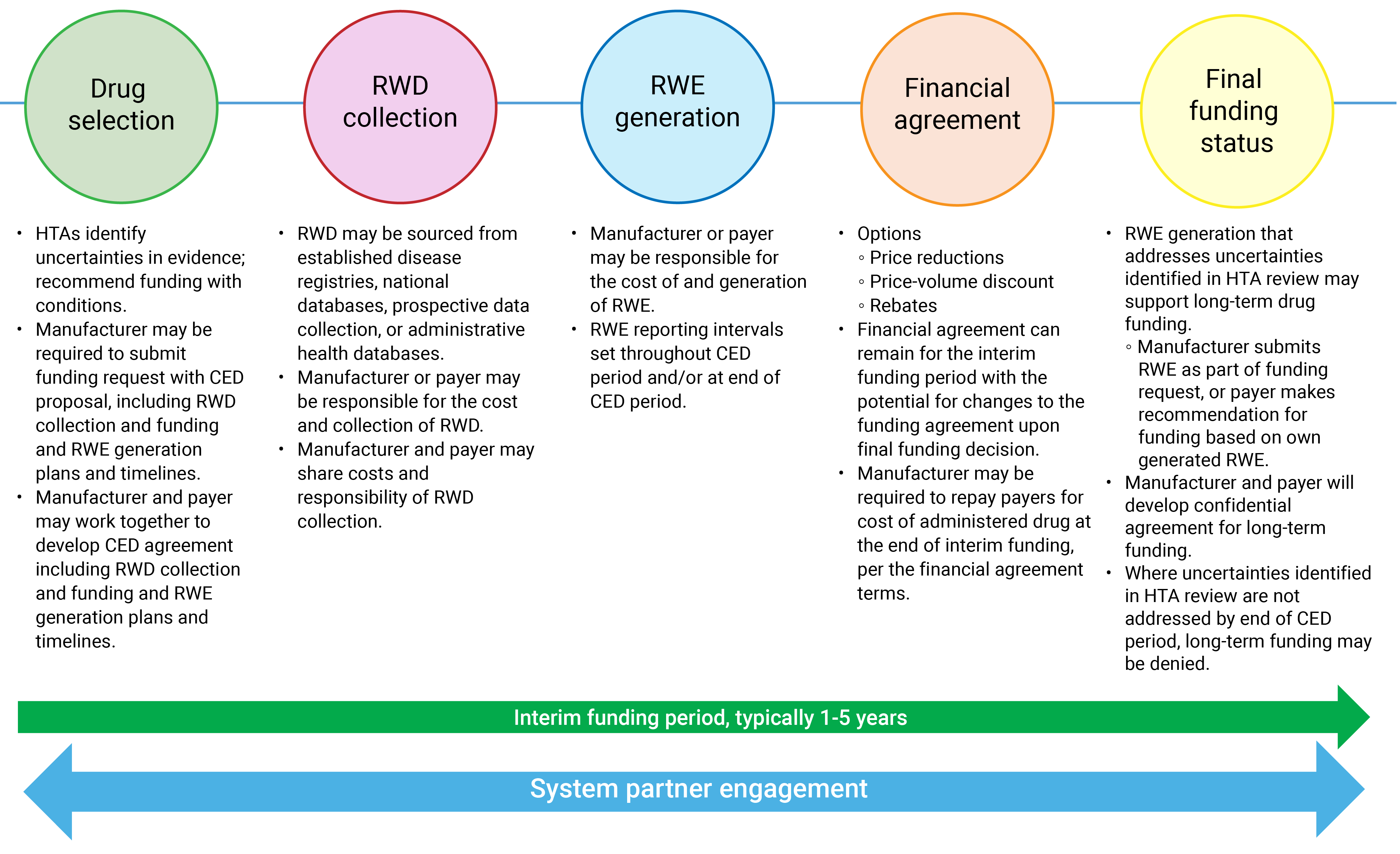
CED = coverage with evidence development; HTA = health technology assessment; RWD = real-world data; RWE = real-world evidence.
Drug Selection
Funding agreements with CED components are most common when a drug receives a conditional funding recommendation by regional or national HTA agencies and/or ministries of health (Figure 2). Uncertainties in initial evidence identified through HTAs can be addressed with additional data collection and evidence generation. Such evidence generation can be completed during interim funding periods as part of a CED agreement.12,14,17-27,31,32,34-37,40,41,43,44,46,49,51,53-57
A drug with a conditional funding recommendation requiring additional evidence generation has to meet defined inclusion criteria to be considered for CED in most jurisdictions. Common themes of criteria include uncertainties in clinical-effectiveness and/or cost-effectiveness evidence; addressing a disease with high, unmet clinical need; feasibility of collecting additional data; and ability of collected data to generate evidence to address uncertainties during a prespecified period.4,15,21,49,58,59 In Ontario (Canada), France, Germany, and Sweden, 1 CED program inclusion criterion is the use of RWD collection during interim funding to generate additional evidence.15,18-21,31,49,53,60 CED agreements have been established for oncology drugs,46,52 CAR T-cell therapies,12,17,19 orphan drugs,12,43 and DRD.4,18 In the UK, separate CED programs have been established: the Cancer Drug Fund (CDF) for oncology drugs and the Innovative Medicines Funds (IMF) for non-oncology drugs.23,37,61 Drugs considered for funding with CED agreements must meet medical technology designations including “innovative status” in Italy, “ultra orphan drug” in Scotland, or “reasonable and necessary” in the US.12,17-19,26,27,43
Drug Funding
We identified national and regional governments that are responsible for paying for drugs funded with CED agreements. In Australia, Ontario (Canada), Ireland, Italy, Scotland, and the UK, national departments or ministries of health provide funding to national or regional drug funding programs that are responsible for organizing and providing reimbursements of drug costs to hospitals that administer treatments.12,15,17-21,13,26,28,31,32,34-37,39-41,43-45,48,54,56,57,62-65 Countries including Belgium, France, the Netherlands, and Sweden have statutory national health insurance programs that receive funding from national health service departments and are responsible for organizing and distributing drug cost reimbursements to hospitals.4,13,18,21,28,48,59 In Germany and the US, health insurance organizations determine which drugs will be funded with CED agreements. Only patients with health insurance organized by these organizations are eligible to receive CED-funded drugs.18,21,40,50,60 In the US, these health insurance organizations include the Centers for Medicare & Medicaid Services (CMS) and private insurance companies.40,50,66,67
RWD Collection for RWE Generation
Processes for and funding related to RWD collection and RWE generation for CED programs vary across jurisdictions and may differ across drugs and indications. When it comes to RWD, the 2 primary sources appear to be prospective data and health care administrative databases. Prospective data collection starts when a patient is approved to receive a funded drug, and it can continue throughout the interim funding period.49 Registries and observational studies were the most frequently identified tools for prospective data collection.40,58 Web-based registries can be created specifically for CED-funded drugs, as is the case with Italy’s Italian Medicine Agency (Agenzia Italiana del Farmaco [AIFA]) registries.12,18,21,43 Alternatively, existing registries collecting data on the patient population of interest may be used, as is the case with the UK’s Systemic Anti-Cancer Therapy (SACT) datasets. SACT datasets capture data on patients with a particular disease or receiving a specific therapy and are organized and maintained by the National Cancer Registry Analysis Service at Public Health England.4,12,17-19,21,38,40,54,68,69 Administrative health databases are another source for RWD and can be the sole source for data or combined with prospective data collection. In Ontario (Canada), data from administrative databases are combined with prospective data collection to generate supporting evidence.15 CMS guidance notes that RWD can come from patients enrolled in prospective clinical studies or through disease registries that can be linked with claims data.67,69-71
In France, new clinical trial data must be accompanied by RWD from disease registries, electronic medical records, or claims databases.4,12,20,59 Germany’s Federal Joint Committee (Gemeinsamer Bundesausschuss [G-BA]), requires that data be collected to produce comparative evidence resubmitted at the end of interim funding.18,21 In Ontario (Canada), the Netherlands, and the UK, CED programs set out the source and method of data collection to generate additional evidence.4,15,23,25,32,54 The UK’s CDF and IMF programs require data collection agreements and commercial access agreements. The data collection agreement details the end points that must be reported to address identified uncertainties in clinical effectiveness and/or cost-effectiveness, and the commercial access agreement details the cost of drugs and any risk-sharing conditions.26-30,68,72,73 In the UK, drugs funded through the CDF must demonstrate whether data collected in the SACT datasets can be used for evidence generation.4,32,54,56,61,68 Data for evidence generation may also come from Blueteq data, Public Health England data, established disease registries, market share data, or chart review.4,12,17,19,35,37,38,54,57,72
Across jurisdictions, it is common for the manufacturer to be responsible for setting up and carrying out the data collection methods.4,12,18,19,21,22,25,28,30,40,44,53,58,60,63,67 In Australia, France, Germany, Italy, the Netherlands, Scotland, and Sweden, the manufacturer is responsible for funding data collection through real-world studies. In Belgium, the UK, and the US, the funding source and organization of data collection vary by each funded drug and may be the responsibility of the manufacturer, the payer, or both partners.4,12,13,18,21,28,35-37,40,48,56 In Italy, manufacturers are responsible for providing financial support for AIFA registry data collection with help from the Italian Ministry of Health and National Health Service.12,18,20,21,43,45,46 In Belgium, the manufacturer provides funding for data analysis processes.12 Ontario (Canada) was the only jurisdiction identified where RWD collection through the Ontario Health Provincial Drug Reimbursement Programs, is consistently paid for by the payer (i.e., Ontario Ministry of Health).15
Financial Agreements
Following the announcement of a conditional funding agreement with a CED requirement, the manufacturer, market authorization holder, funder, and payers will typically collaborate to develop the funding agreement. Risk-sharing may be used in addition to the CED requirements, as identified in Australia, Belgium, France, Ireland, Italy, the UK, and the US.12,13,19-21,28,30,35,37,40-43,45,46 We identified common requirements as part of agreement schemes across jurisdictions. For example, Australia, Belgium, France, Italy, and the US require manufacturers to provide full or partial refunds for patients who do not achieve outcomes specified before funding, regardless of approval for long-term funding at the end of interim funding.4,13,23,28,39,45,49,58,59
During interim funding periods, CED agreements may have a set price per volume or maximum budgetary amount, both of which can be reviewed at the end of interim funding. After final HTA review, the long-term price or budget cap can be altered along with the eligibility criteria of the drug, depending on the generated evidence. We identified price alterations in Australia, France, Germany, Italy, and the UK.18,20,21,40,46,49,58,59,63 In Germany, the manufacturer can be penalized with a price reduction for not generating agreed-upon evidence by the end of the set interim funding period.19,21,48 In Italy, drug payments are provided at set intervals, with the final interval payment being withheld until the manufacturer provides the additionally generated evidence.4,21,45,48
Final Funding Status
At the end of the interim funding period, the generated RWE is usually reviewed by the HTA agency and funder to determine if the uncertainties identified in the initial HTA are addressed and whether the terms of the CED agreement are met.18,19,21 The manufacturer is typically the group required to submit evidence generated to address clinical and cost-effectiveness uncertainties identified by the HTA agency during the initial funding review.15,17,25,32,35,37,49,50,53,54,58,62 In Belgium, preliminary evidence reviews are conducted 6 months before the end of the interim funding period to determine whether the CED agreement should be terminated or prolonged for a maximum of 1 year.13,31 In the US, the CMS requires evidence generated during CED to be publicly available in peer-reviewed journals or in online registries of clinical studies as part of their final review for funding.67,71,74 Based on the outcome of the HTA reassessment, the drug may be recommended for long-term drug funding through standard reimbursement processes or an end to funding altogether, with the final funding decision determined by the national or regional ministry or department of health.4,12,15,17,18,20,21,23,25,31,37,41,45,48,49,53,54,59,71,75 Long-term funding for the drug may not be agreed upon if the terms of the CED agreement have not been met or if the generated evidence does not address clinical and/or cost-effectiveness uncertainties.
System Partners Involvement
Parties involved in CED agreements include the manufacturer, payer, funder, HTA advisory committees, clinicians, pharmacists, patients, patient organizations, health professionals, health economists, and consumer representatives. HTA advisory committees responsible for reviewing and summarizing clinical and cost-effectiveness evidence at initial assessments and reassessments may consist of clinicians, health professionals, pharmacists, and health economists.18,58 Advisory committees of clinicians with expertise on rare diseases are involved in evidence review during HTAs of highly specialized technologies in the Netherlands and the UK.18 In France, Germany, Sweden, and the UK, patients and patient organizations are involved during CED negotiation and final decision-making.12,17-19,21,23,31,32,34-37,41,42,51,54,56,57,60,76 Representatives — including clinicians, nurses, pharmacists, hospitals, universities, and disease registry organizations — may be involved in the CED agreement, depending on data collection processes.19,35,39,58
In the UK, CED agreement oversight committees include NICE employees, NHS England employees, clinicians, patient organization representatives, manufacturer company representatives, and NHS data custodian representatives.35,72 Oversight committees and task forces have the following responsibilities: to support determination of appropriate outcome measurements for evidence generation during initial CED negotiations; during interim funding periods, to regularly review submitted evidence to ensure the data collection is progressing on track; and to support issues related to analysis planning, access to treatment service issues, clinical assessment issues, and safety issues as signalled by patients and/or clinicians.31,35,72
Interim Funding Period Duration
The length of interim drug funding periods varies between CEDs. We noted that most CED interim funding periods range from 1 to 5 years (Table 4).4,12,17-20,22,23,32,34,35,44,45,54,66, Some jurisdictions set the same length of funding for all drugs or set drug-specific periods of funding based on the length of time needed to collect data and generate additional evidence. The length of interim funding to support sufficient data collection and evidence generation is estimated by the partners involved in arranging the CED agreement.12,15,20,21,40,46,49,71
CED Limitations
Common limitations were identified among jurisdictions with experience conducting CED. CED programs lacked clearly defined entry and exit criteria, exit plans, deliverables, and project timelines. Such issues were noted to have an impact on programs’ abilities to successfully make decisions about funding by the end of interim funding periods, leading to overspending.4,22,23,25,29,66,70,76,77 We identified limited transparency in the details of CED agreements and the accompanying financial terms. Specifically, there was limited information available related to evidence-generation plans, how evidence was used at the end of interim funding to support a final funding decision, how drugs were priced in the interim, and drug eligibility criteria.4,13,18,49
CED agreements that rely on RWD collection and RWE generation are faced with high resource demand to set up and maintain data collection platforms or access existing data. Where data are prospectively collected, health care providers must devote additional time and resources to RWD collection.4,13 The use of RWD captured from administrative health data sources or registries may result in limited length of follow-up of patients, resulting in immature data that do not address uncertainties in clinical benefit and cost-effectiveness. The use of existing data sources and registries can limit the cohort identification, comparator populations, and study end points.25,54 Additionally, RWE limitations of CED were identified as contributing to overspending and uncertainties persisting at the end of interim funding periods.4,13,18,21-23,49,51,58
Discussion
This paper identified and described CED agreements applied in 13 jurisdictions that leverage RWE to address uncertainties in evidence submitted as part of HTAs. We reported on the processes of drug selection for CED agreements, RWD collection and RWE generation, financial agreements tied to CED, determination of final funding status, health system partner engagement, and limitations of these CED agreements. The findings of our scan demonstrate variation in the structure of CED agreements and limited transparency on the eventual outcomes of whether and how RWE supports a final funding decision.
CED Agreement Variation
Variation between CED agreements may be driven by several factors, including types of drugs selected, RWD availability, financial agreements, health care delivery structure, and information sharing. Drug selection results in a particular treatment population, and this can impact CED terms. Drugs targeting rare diseases with low annual patient volumes may require extended length of interim funding to allow for appropriate data collection and evidence-generation timelines. Patient population sizes can also impact RWE generation plans, including the end points that can be assessed and whether comparative evidence assessments can be conducted.
RWD availability and accessibility may also be a source of variation between CED agreements. Depending on the required data, prospective data collection and/or administrative health data sources may be leveraged. Where the use of RWD is not possible due to availability and accessibility limitations, CED agreements may have to rely on phase IV clinical trial data, which are out of scope for this Environmental Scan.
Variation in the type of financial agreements applied during CED was identified. We noted the use of refunds, interval payments, price alterations and reductions, price per volume agreements, and budget caps applied with CED agreements. However, the availability of agreement details in the literature and sources included in our scan were limited, likely due to the confidential nature of financial agreements.
Additional variability was identified among different health care system structures, and this impacted both the CED terms and financial agreements. For example, decentralized health care systems may require support from all regions to engage in CED and collaborate on RWD collection and RWE generation, whereas centralized systems may have more direct access to and consistency across data elements within jurisdictions. With regard to funding RWD collection and RWE generation, the responsibility may shift between the payer and drug manufacturer, depending on a jurisdiction’s health care system. Single-payer systems and universal health care payers may have more straightforward access to administrative health data, which could increase their involvement in data collection plans, funding, and RWE generation as compared to systems with private health care coverage options. Single-payer systems and universal health care payers should also have access to claims data for their entire jurisdiction’s population, increasing the generalizability of evidence generated with the data.
Finally, restricted availability of and access to information on how CED agreements are established and structured may lead to further variation. CED agreements may be similar between jurisdictions, but details on patient eligibility, RWD sources, clinical-effectiveness and cost-effectiveness end points, financial agreements, and CED outcomes are limited. This limits what other countries can learn about CED and how to apply it in their own jurisdictions.
CED Agreement Transparency
This Environmental Scan also revealed the extent of missing information related to the outcomes of CED agreements using RWE (i.e., the eventual funding decisions). This limits the ability to evaluate the benefit of CED and determine whether future applications of CED are appropriate. Kang et al. and Morel et al. conducted reviews of the UK’s CDF final appraisal documents and reported limited use of RWE to support final funding decisions.48,54 RWE from SACT databases was reviewed as part of the final funding review for 15 CDF drugs, of which only 5 reviews used RWD for parametric purposes and 2 of the 5 reviews used RWD for primary end points.54 The CDF program provides annual activity reports detailing the number of MEAs under the program and reappraisals following interim funding by NICE. As of January 2025, NICE had conducted reappraisals of 39 drugs funded through the CDF program, of which 34 received recommendations for long-term funding, 2 were not approved for long-term funding, 2 did not proceed due to lack of evidence submitted by the drug manufacturers, and 1 had a withdrawn product licence.78 Reappraisal meeting documents for 1 of the 2 drugs not approved for long-term funding — pembrolizumab — are available online and describe the RWE included in the reassessment.79 However, the details that went into these final funding recommendations remain limited. RWE to support CED may remain infrequently used for final decision-making if limited transparency into CED agreements and their outcomes persists. Knowledge-sharing among jurisdictions may increase the likelihood of using RWE for CED, as it can save time when selecting drugs, establishing financial terms, developing analysis plans, and evaluating evidence.
An exception to the noted transparency around CED agreements was the CMS in the US. The CMS makes several CED guidance documents, reviews of CMS processes, and final funding decisions following CED available, intended for use by all system partners. Further, the CMS website lists therapies funded with CED and includes details of clinical trials and RWE studies planned and under way to support final funding decisions. Final decisions are posted online with descriptions of evidence used to inform the final funding decisions.67,71,74 The weight of RWE in contributing to a final funding decision remains unclear; however, the degree of transparency of the CMS’s CED processes and final reviews provides a fine example for other jurisdictions.
Overcoming Limitations
The high variation in and limited transparency of jurisdictional CED programs do not negate the potential benefits of CED and opportunities for using RWE to support accelerating access to drugs where there is a high unmet need and/or limited evidence. Still, criticisms of CED and strategies to address these criticisms must be discussed.
A drawback of CED from the payer perspective is its potential to encourage manufacturers to present preliminary evidence with uncertainties to HTA organizations, thereby securing interim funding, shifting the risk to payers and patients. A further criticism is that manufacturers may not feel committed to providing data for evidence generation that is required per the agreement if they are receiving funding upfront.13,17,18 CED, however, may enable HTA agencies and payers to have more oversight into the quality and robustness of data collection and evidence generation.30 For example, CED agreements can stipulate regular data review or evidence-sharing during interim funding periods, with interval payments paid to the manufacturer upon receipt of data or evidence.4 Outcome-based or performance-based agreements may help ensure continued evidence generation and promote risk-sharing if manufacturers are required to provide repayments or discounts for not achieving agreed-upon outcomes.21,25
Another limitation of CEDs is the lack of clear entry and exit criteria, as was the case with the UK’s original MEA process, which led to its reorganization and introduction as the CDF in 2016.54 Clearly defined entry criteria, deliverables, exit plans, reporting intervals, data sources, and project timelines should be set to ensure programs achieve their goals, maintain transparency, and avoid overspending.4,22,23,25,29,66,70,77 Research questions, objectives, and end points needed to address uncertainties must also be clearly identified to avoid resource wastage and meet evidence-generation goals.4,22,25,26,29,49,54
A limitation of CED specific to countries with decentralized health care systems — such as Canada, Italy, and Spain — is the potential for inequitable access to drugs funded with CED agreements between regions, provinces, and/or territories. Maintaining national organization of drugs funded with CED agreements supports patients and clinicians by ensuring patients in all jurisdictions have equitable access to the same therapies.34 National organization of funded drugs should include data collection plans that allow for data sharing and comparison across jurisdictions to increase the generalizability and potential validity of study outcomes. National disease registries have been implemented in Italy (AIFA registries) and Spain (Valtermed registries), despite their decentralized health care systems, to support MEAs. In Italy, AIFA registries have been established for a number of years to support OBAs and CED.12,18,21,43 Spain’s Valtermed registries were more recently established (in 2019) and, to our knowledge, have only supported OBAs.80,81 The existence of these registries not only allows for generated RWE to be more representative of patients across a country but for national funding decisions to be applied across all jurisdictions and to ensure equitable access to publicly funded drugs.
Early planning and partner engagement during the development of CED agreements can improve their success and mitigate the previously noted limitations. An appropriate mix of system partners — such as HTA representatives, clinicians, payers, patients, patient representatives, methodologists, and manufacturer representatives — should be included throughout the entire CED process. CED member roles should be clearly defined to ensure system partners achieve and are accountable for their responsibilities.13,30,66,76
CED is often viewed as costly due to the resource use and population-level data collection processes.4,13 The cost to set up and maintain data collection platforms and the time required to collect data, often by clinicians, may be barriers to implementing CED. Exploring the use of routinely collected data that can support CED may eliminate costly prospective data collection. While time- and resource-intensive, CED agreements to expand patient access to and confirm value of costly therapies is justified if the added resource demands can be minimized or well placed. System partners must collaborate to identify the specific circumstances in which CEDs may be cost-beneficial. For example, establishing drug-selection criteria and a clear mechanism to renegotiate or delist a drug can provide added assurances that the health system and patients may benefit. The cost may prove to be a worthwhile investment if generated evidence demonstrates clear clinical benefit; identifies safety concerns; leads to price renegotiations; or, in cases where clinical benefit is not identified, leads to delisting of drugs.
Opportunities for Canada
In the last several years, Canada has made advancements in accelerating access to cancer drugs through various initiatives. Health Canada joined Project Orbis in 2019, led the by FDA in the US, with the goal of accelerating access to promising new treatments through streamlining regulatory reviews.82 In 2025, the pCPA implemented the Early Negotiation Process (ENP) to support Canadian provinces and territories in expediting public listing of Project Orbis drugs after negotiation.83 Ontario also implemented the Funding Accelerated for Specific Treatments (FAST) pilot program to expedite the listing of Project Orbis drugs.84 Most relevant to CED was the establishment of the TLR pathway by CDA-AMC8 and pTAP by the pCPA.8,9
Faster regulatory pathways may result in submissions that lack mature outcomes data or long-term evidence of a drug’s benefit and financial impact. The development of novel access pathways given evidence limitations provides an opportunity in Canada to incorporate RWE into drug funding decisions. Ontario (Canada) has already demonstrated success using RWE to facilitate CED through the Ontario Health (Cancer Care Ontario) Evidence Building Program. The Evidence Building Program has used RWD and RWE to support final funding decisions for 2 drugs. Cheung et al. explored the feasibility of using RWD from administrative health data sources in Alberta (Canada) to support OBAs for oncology drugs.85 The findings demonstrated that it is feasible to leverage OBAs using Alberta (Canada) RWD with little additional data outside of what is available in administrative health data sources.85 There is an opportunity to learn from current and past experiences with the goal of implementing a CED program that uses RWD and RWE to facilitate expedited access to promising new therapies.
Limitations
This Environmental Scan had limitations. The approach was pragmatic and, as such, relevant literature may have been missed and thus not included in this scan. Details about jurisdictional CED agreements may have been missed or not presented if jurisdictions limited the availability or accessibility of information about their CED agreements, or if information was not provided in English.
Conclusion
This Environmental Scan sought to identify CED programs globally, specifically where RWE is generated to support decision-making. Programs were identified in Canadian and international jurisdictions, and we described the various components and discussed the limitations of these CED programs. Many countries use CED agreements to fund drugs where there are uncertainties in submitted evidence. Variation exists in the CED components and processes between jurisdictions, and limited transparency into CED details has an impact on what can be learned from jurisdictions that have already applied CED. Increased CED policy-planning within jurisdictions and sharing between jurisdictions can contribute to improved efficiencies and sustainability in health care systems.
Jurisdictional experiences with and lessons learned from their CED programs can be leveraged to explore the development of a robust Canadian CED model. Given the increasing pressure to accelerate funding, CED may provide an opportunity to enable earlier patient access to promising, expensive therapies while assessing value and benefit to support long-term funding decisions.
Acknowledgements
The authors would like to acknowledge Sadaf Ullah, who provided support as a medical librarian for Ontario Health (Cancer Care Ontario) at the time that this scan was conducted and who is currently employed with Unity Health Toronto. The authors would also like to acknowledge Senior Research Associates Pam Takhar and Jaemin Kim, from Ontario Health’s Evidence Search and Review Synthesis team, for their support on this Environmental Scan and in the review of this manuscript. The authors would like to acknowledge Nany Guo, Gabriella Sgrignuoli, and Laureen Rance from the Ontario Ministry of Health for their review of this manuscript.
Author Information
Caroline Muñoz, Jessica Arias, Alayna Brown, Mitali Garg, Scott Gavura
Ontario Health, 525 University Avenue, Toronto, Ontario
Corresponding Author
Caroline Muñoz, MSc
Senior Analyst, Provincial Drug Reimbursement Programs, Acute and Hospital-Based Care, Ontario Health
525 University Avenue, Toronto, Ontario, Canada
Telephone: (647) 953-1618
caroline.munoz@ontariohealth.ca
Authorship confirmation: All authors certify that they meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship.
Funding or support: The authors received no financial support for this research.
References
1.Battista RN, Côté B, Hodge MJ, Husereau D. Health technology assessment in Canada. Int J Technol Assess Health Care. 2009;25(SUPPL.S1). doi:10.1017/S0266462309090424 PubMed
2.Quay T, Dulong C, Lachance CC, Topfer LA. Collaboration in Health Technology Assessment in Canada.; 2019. https://www.cadth.ca/sites/default/files/es/es0329-hta-collaboration.pdf
3.CADTH. Procedures for CADTH Reimbursement Reviews.; 2023. https://www.cadth.ca/sites/default/files/Drug_Review_Process/CADTH_Drug_Reimbursement_Review_Procedures.pdf
4.Wenzl M, Chapman S. Performance-based managed entry agreements for new medicines in OECD countries and EU member states: How they work and possible improvements going forward. OECD Heal Work Pap. 2019;(115):102. https://dx.doi.org/10.1787/6e5e4c0f-en
5.Pauwels K, Huys I, Vogler S, Casteels M, Simoens S. Managed entry agreements for oncology drugs: Lessons from the European experience to inform the future. Front Pharmacol. 2017;8(APR). doi:10.3389/fphar.2017.00171 PubMed
6.Malone DC, Brown M, Hurwitz JT, Peters L, Graff JS. Real-World Evidence: Useful in the Real World of US Payer Decision Making? How? When? And What Studies? Value Heal. 2018;21(3). doi:10.1016/j.jval.2017.08.3013 Medline PubMed
7.Hurwitz JT, Brown M, Graff JS, Peters L, Malone DC. Is real-world evidence used in P&T monographs and therapeutic class reviews? J Manag Care Spec Pharm. 2017;23(6). doi:10.18553/jmcp.2017.16368 Medline PubMed
8.Canada’s Drug Agency. Our Time-Limited Recommendation Category Aims to Support Earlier Access to Promising Drugs. 2023. Accessed January 15, 2025. https://www.cda-amc.ca/news/our-time-limited-recommendation-category-aims-support-earlier-access-promising-drugs
9.pan-Canadian Pharmaceutical Alliance. pCPA Temporary Access Process (pTAP). 2025. Accessed January 15, 2025. https://www.pcpacanada.ca/ptap
10.CADTH. Drugs for Rare Diseases: A Review of National and International Health Technology Assessment Agencies and Public Payers’ Decision-Making Processes.; 2021. https://www.cadth.ca/sites/default/files/es/es0355-drugs-for-rare-diseases-pw.pdf
11.Government of Canada. The National Strategy for Drugs for Rare Diseases. 2024. Accessed December 29, 2025. https://www.canada.ca/en/health-canada/services/health-care-systems/national-pharmacare/strategy-drugs-rare-diseases.html
12.Facey KM, Espin J, Kent E, et al. Implementing Outcomes-Based Managed Entry Agreements for Rare Disease Treatments: Nusinersen and Tisagenlecleucel. Pharmacoeconomics. 2021;39(9):1021-1044. doi:https://dx.doi.org/10.1007/s40273-021-01050-5 PubMed
13.Gerkens S, Neyt M, San Miguel L, Vinck I, Thiry N, Cleemput I. How to improve the Belgian process for managed entry agreements? An analysis of the Belgian and international experience. Heal Serv Res Brussels Belgian Heal Care Knowl Cent. 2017;KCE report:75. https://kce.fgov.be/sites/default/files/2021-11/KCE_288_Improve_Belgian_process_managed_entry_agreements_Report.pdf
14.Alberta Health. Alberta Health -Alberta Health Product Listing Agreement Policy.; 2022.
15.Cancer Care Ontario. Evidence Building Program (EBP). Accessed March 13, 2022. https://www.cancercareontario.ca/en/Funding/Evidence_Building_Program
16.Cancer Care Ontario. Provincial Drug Reimbursement Programs. https://www.cancercareontario.ca/en/cancer-care-ontario/programs/provincial-drug-reimbursement
17.Jørgensen J, Hanna E, Kefalas P. Outcomes-based reimbursement for gene therapies in practice: the experience of recently launched CAR-T cell therapies in major European countries. J Mark Access Heal Policy. 2020;8(1):1715536. doi:10.1080/20016689.2020.1715536 PubMed
18.Stafinski T, Glennie J, Young A, Menon D. HTA decision-making for drugs for rare diseases: comparison of processes across countries. Orphanet J Rare Dis. 2022;17(1):258. doi:https://dx.doi.org/10.1186/s13023-022-02397-4 PubMed
19.Jørgensen J, Kefalas P. The use of innovative payment mechanisms for gene therapies in Europe and the USA. Regen Med. 2021;16(4):405-421. doi:10.2217/rme-2020-0169 PubMed
20.Jarosawski S, Toumi M. Market Access Agreements for pharmaceuticals in Europe: Diversity of approaches and underlying concepts. BMC Health Serv Res. 2011;11. doi:10.1186/1472-6963-11-259 PubMed
21.Grubert N. Lessons Learned from Europe, the United States, Canada and Australia Pharmaceutical Managed Entry Agreements. 2018;(December).
22.Van Harten WH. Innovations that reach the patient: Early health technology assessment and improving the chances of coverage and implementation. Ecancermedicalscience. 2016;10:683. doi:https://dx.doi.org/10.3332/ecancer.2016.683 PubMed
23.Faulkner SD, Lee M, Qin D, et al. Pricing and reimbursement experiences and insights in the European Union and the United States: Lessons learned to approach adaptive payer pathways. Clin Pharmacol Ther. 2016;100(6). doi:10.1002/cpt.508 PubMed
24.Niezen M, de Bont A, Stolk E, Eyck A, Niessen L, Stoevelaar H. Conditional reimbursement within the Dutch drug policy. Health Policy (New York). 2007;84(1). doi:10.1016/j.healthpol.2006.11.005 PubMed
25.Makady A, van Veelen A, Hillege H, Klungel OH. Implementing managed entry agreements in practice: The Dutch reality check. Health Policy (New York). 2019;123(3):267-274. doi:https://dx.doi.org/10.1016/j.healthpol.2018.09.016 PubMed
26.Lewis JRR, Kerridge I. Coverage with evidence development and managed entry in the funding of personalized medicine: Practical and ethical challenges for oncology. J Clin Oncol. 2015;33(34):4112-4117. doi:https://dx.doi.org/10.1200/JCO.2015.61.2838 PubMed
27.Relyea-Chew A. Ethical considerations in CMS’s coverage with evidence development. J Am Coll Radiol. 2011;8(12):838-841. doi:https://dx.doi.org/10.1016/j.jacr.2011.08.011 PubMed
28.Stafinski T, McCabe C. Funding the unfundable: Mechanisms for managing uncertainty in decisions on the introduction of new and innovative technologies into healthcare systems. Pharmacoeconomics. 2010;28(2):113-142. doi:https://dx.doi.org/10.2165/11530820-000000000-00000 PubMed
29.Mohr PE. Access with evidence development: The US experience. Pharmacoeconomics. 2010;28(2):153-162. doi:https://dx.doi.org/10.2165/11531050-000000000-00000 PubMed
30.Trueman P, Grainger DL. Coverage with evidence development: Applications and issues. Int J Technol Assess Health Care. 2010;26(1):79-85. doi:https://dx.doi.org/10.1017/S0266462309990882 PubMed
31.Ferrario A. Dealing with uncertainty and high prices of new medicines: A comparative analysis of the use of managed entry agreements in Belgium, England, the Netherlands and Sweden. Soc Sci Med. 2015;124:39-47. doi:https://dx.doi.org/10.1016/j.socscimed.2014.11.003 PubMed
32.Shengnan D, Zixuan L, Na Z, Weikai Z, Yuanyuan Y, Jiasu L. Using 5 consecutive years of NICE guidance to describe the characteristics and influencing factors on the economic evaluation of orphan oncology drugs. Front public Heal. 2022;10:964040. doi:https://dx.doi.org/10.3389/fpubh.2022.964040 PubMed
33.Kang J, Cairns J. “Don’t Think Twice, It’s All Right”: Using Additional Data to Reduce Uncertainty Regarding Oncologic Drugs Provided Through Managed Access Agreements in England. PharmacoEconomics - Open. 2023;7(1). doi:10.1007/s41669-022-00369-9 PubMed
34.Mayor S. New “managed access” process for Cancer Drugs Fund to go ahead, NHS England confirms. BMJ. 2016;352. doi:10.1136/bmj.i1208 PubMed
35.NICE. Managed Access. 2023. https://www.nice.org.uk/about/what-we-do/our-programmes/managed-access
36.NHS England. Cancer Drugs Fund. https://www.england.nhs.uk/cancer/cdf/
37.NHS England. Innovative Medicines Fund. https://www.england.nhs.uk/medicines-2/innovative-medicines-fund/
38.Simoens S, De Groote K. Critical Reflections on Reimbursement and Access of Advanced Therapies. Front Pharmacol. 2022;13:771966. doi:https://dx.doi.org/10.3389/fphar.2022.771966 PubMed
39.Kim H, Comey S, Hausler K. A real world example of coverage with evidence development in Australia - ipilimumab for the treatment of metastatic melanoma. J Pharm Policy Pract. 2018;11(1):4. doi:https://dx.doi.org/10.1186/s40545-018-0131-4 PubMed
40.Lexchin J. Coverage with evidence development for pharmaceuticals: A policy in evolution? Int J Heal Serv. 2011;41(2):337-354. doi:https://dx.doi.org/10.2190/HS.41.2.h PubMed
41.Health Service Executive. Managed Access Protocols. 2023. https://www.hse.ie/eng/about/who/cspd/ncps/medicines-management/managed-access-protocols/
42.Gorry C, Daly M, Barrett R, et al. Utilising Health Technology Assessment to Develop Managed Access Protocols to Facilitate Drug Reimbursement in Ireland. Appl Health Econ Health Policy. Published online November 1, 2024. doi:10.1007/s40258-024-00904-1 PubMed
43.Xoxi E, Facey KM, Cicchetti A. The Evolution of AIFA Registries to Support Managed Entry Agreements for Orphan Medicinal Products in Italy. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.699466 PubMed
44.Australian Government Department of Health and Aged Care. Framework for the introduction of a Managed Entry Scheme for submissions to the Pharmaceutical Benefits Advisory Committee. 2011. https://www.pbs.gov.au/info/publication/factsheets/shared/framework-for-introduction-of-managed-entry-scheme-for-PBAC-submissions
45.Montilla S, Xoxi E, Russo P, Cicchetti A, Pani L. Monitoring registries at Italian medicines agency: Fostering access, guaranteeing sustainability. Int J Technol Assess Health Care. 2015;31(4). doi:10.1017/S0266462315000446 PubMed
46.Adamski J, Godman B, Ofierska-Sujkowska G, et al. Risk sharing arrangements for pharmaceuticals: Potential considerations and recommendations for European payers. BMC Health Serv Res. 2010;10. doi:10.1186/1472-6963-10-153 PubMed
47.Mohseninejad L, Van Gils C, Uyl-De Groot CA, Buskens E. Evaluation of patient registries supporting reimbursement decisions: The case of oxaliplatin for treatment of stage III colon cancer. Value Heal. 2015;18(1):84-90. doi:https://dx.doi.org/10.1016/j.jval.2014.10.008 PubMed
48.Morel T, Arickx F, Befrits G, et al. Reconciling uncertainty of costs and outcomes with the need for access to orphan medicinal products: A comparative study of managed entry agreements across seven European countries. Orphanet J Rare Dis. 2013;8(1). doi:10.1186/1750-1172-8-198 PubMed
49.Ferrario A, Kanavos P, Dabbous O, et al. Managed entry agreements for pharmaceuticals: the European experience. Ecancermedicalscience. 2013;12(2):1-151. https://doi.org/10.1016/j.jval.2018.11.010%0Ahttp://www.oecd.org/health/health-systems/Pharmaceutical-Innovation-and-Access-to-Medicines-Executive-Summary-ENGLISH.pdf%0Ahttps://www.duo.uio.no/bitstream/handle/10852/58667/Peters_Marjolein_Master_Thesis_EuH
50.CMS. Guidance for the Public, Industry, and CMS Staff National Coverage Determinations with Data Collection as a Condition of Coverage: Coverage with Evidence Development. 2006;(410). http://www.cms.hhs.gov/center/coverage.asp%5Cnhttp://www.cms.hhs.gov/InfoExchange/06_contactus.asp#TopOfPage.
51.World Health Organization Regional Office for Europe. Access to New Medicines in Europe: Technical Review of Policy Initiatives and Opportunities for Collaboration and Research.; 2015. https://ppri.goeg.at/sites/ppri.goeg.at/files/inline-files/WHO_AccessNewMedicines_Report_FINAL2015_1.pdf
52.Cancer Care Ontario. Evidence Building Program Policy. 2011;(October). https://www.cancercareontario.ca/sites/ccocancercare/files/assets/CCOEvidenceBuildingPolicy.pdf
53.Willis M, Persson U, Zoellner Y. Reducing uncertainty in value-based pricing using evidence development agreements: The case of continuous intraduodenal infusion of levodopacarbidopa (Duodopa) in Sweden. Appl Health Econ Health Policy. 2010;8(6):377-386. doi:https://dx.doi.org/10.2165/11531160-000000000-00000 PubMed
54.Kang J, Cairns J. “Don’t Think Twice, It’s All Right”: Using Additional Data to Reduce Uncertainty Regarding Oncologic Drugs Provided Through Managed Access Agreements in England. PharmacoEconomics - Open. 2023;7(1). doi:https://dx.doi.org/10.1007/s41669-022-00369-9 PubMed
55.Pouwels X, Grutters J, J. B, Ramaekers B. Uncertainty and Coverage With Evidence Development: Does Practice Meet Theory? Value Heal. 2019;22(7):799-807. doi:https://dx.doi.org/10.1016/j.jval.2018.11.010 PubMed
56.Lee J, Trevor N, Adedokun L, Lilley C. Optimizing Managed Access: Lessons From the Cancer Drugs Fund. ISPOR. 2021;7(2).
57.National Audit Office C and AG. Investigation into the Cancer Drugs Fund.; 2015. https://www.nao.org.uk/wp-content/uploads/2015/09/Investigation-into-the-Cancer-Drugs-Fund1.pdf
58.Tuffaha HW, Scuffham PA. The Australian Managed Entry Scheme: Are We Getting it Right? Pharmacoeconomics. 2018;36(5). doi:10.1007/s40273-018-0633-6 PubMed
59.HAS. Innovative medicines assessment action plan. 2020;(January):1-6. https://www.has-sante.fr/upload/docs/application/pdf/2020-03/innovative_medicine_action_plan_27.01.20.pdf
60.IGES Institute. Reimbursement of Pharmaceuticals in Germany 2020/2021 - Finding Your Way into the German Pharmaceutical Market. Published online 2021. https://www.iges.com/e15094/e15095/e15096/e17469/IGES_Reimbursement_Pharmaceuticals_Germany_2020_2021_WEB_ger.pdf
61.NHS England. NHS commercial framework for new medicines.
62.Robinson MF. Characteristics of managed access agreements for medicines in Australia. Value Heal. 2017;20(5):A65. https://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed18&NEWS=N&AN=617600325
63.Vitry A. Managed entry agreements for pharmaceuticals in Australia. Health Policy (New York). 2014;117(3):345-352. doi:https://dx.doi.org/10.1016/j.healthpol.2014.05.005 PubMed
64.Australian Government Department of Health and Aged Care. PBAC Minutes for the Managed Access Program Framework - March 2015. 2015. https://www.pbs.gov.au/info/news/2015/07/pbac-minutes-for-the-managed-access-program-framework
65.Wonder M, Backhouse ME, Sullivan SD. Australian Managed Entry Scheme: A New Manageable Process for the Reimbursement of New Medicines? Value Heal. 2012;15(3):586-590. doi:10.1016/j.jval.2012.02.004 PubMed
66.Zeitler EP, Gilstrap LG, Coylewright M, Slotwiner DJ, Colla CH. Coverage with Evidence Development: Where Are We Now? Am J Manag Care. 2022;28(8):382-389. doi:https://dx.doi.org/10.37765/ajmc.2022.88870 PubMed
67.Centers for Medicare & Medicaid Services. Coverage with Evidence Development.; 2024. https://www.cms.gov/files/document/ced-guidance2024pdf.pdf
68.Farmer C, Barnish MS, Trigg LA, et al. An evaluation of managed access agreements in England based on stakeholder experience. Int J Technol Assess Health Care. 2023;39(1). doi:10.1017/S0266462323000478 PubMed
69.McPhail M, Bubela T. Can Managed Access Agreements Mitigate Evidentiary, Economic and Ethical Issues with Access to Expensive Drugs for Rare Diseases in the Canadian Context? Healthc Pap. 2023;21(1). doi:10.12927/hcpap.2023.26994 PubMed
70.Lakdawalla D, Tunis S, Neumann P, Whicher D, Zeitler E, Liden B. A Roadmap for Improving Medicare’s Application of Coverage With Evidence Development. Value Heal. 2024;27(9):1191-1195. doi:10.1016/j.jval.2024.05.008 PubMed
71.Centers for Medicare & Medicaid Services. Guidance for the Public, Industry, and CMS Staff: Coverage with Evidence Development. 2014. https://www.cms.gov/medicare-coverage-database/view/medicare-coverage-document.aspx?MCDId=27
72.National Institute for Health and Care Excellence. Data collection agreement. 2024. https://www.nice.org.uk/what-nice-does/our-guidance/about-technology-appraisal-guidance/data-collection-agreement
73.Trigg LA, Barnish MS, Hayward S, et al. An Analysis of Uncertainties and Data Collection Agreements in the Cancer Drugs Fund. PharmacoEconomics - Open. 2024;8(2). doi:10.1007/s41669-023-00460-9 PubMed
74.Segal J, Levy J, DiStefano M, et al. Analysis of Requirements for Coverage With Evidence Development (CED) – Topic Refinement.; 2022. https://www.cms.gov/files/document/id110ta.pdf
75.Medicines Australia. Finding common ground for accelerating access. 2023. https://www.health.gov.au/sites/default/files/2023-12/attachment_a_-_meeting_26_medicine_australia_slides_deep_dive_accelerated_access.pdf
76.Bishop D. Politics and its intersection with coverage with evidence development: a qualitative analysis from expert interviews. BMC Health Serv Res. 2013;13:88. doi:https://dx.doi.org/10.1186/1472-6963-13-88 PubMed
77.Hutton J, Trueman P, Henshall C. Coverage with evidence development: an examination of conceptual and policy issues. Int J Technol Assess Heal Care. 2007;23(4):452-32. doi:10.1017/S0266462307070651 PubMed
78.NHS England. Cancer Drugs Fund activity update Q2 2024-25. 2025. Accessed December 29, 2025. https://www.england.nhs.uk/long-read/cancer-drugs-fund-activity-update-q2-2024-25/
79.National Institute for Health and Care Excellence. Pembrolizumab for untreated PD-L1-positive, locally advanced or metastatic urothelial cancer when cisplatin is unsuitable (terminated appraisal). 2021. Accessed December 29, 2025. https://www.nice.org.uk/guidance/ta674
80.Tomassy J, Caban A, Hammes F. PNS225 CURRENT STATUS OF OUTCOMES-BASED AGREEMENTS IN SELECTED EUROPEAN COUNTRIES AND CANADA. Value Heal. 2019;22(Supplement 3):S799. doi:https://dx.doi.org/10.1016/j.jval.2019.09.2125
81.Angulo-Pueyo E, Bernal-Delgado E. A new information system to assess the therapeutic value of drugs in real practice. European Observatory on Health Systems and Policies. 2019. Accessed December 27, 2025. https://eurohealthobservatory.who.int/monitors/health-systems-monitor/updates/hspm/spain-2018/a-new-information-system-to-assess-the-therapeutic-value-of-drugs-in-real-practice
82.Government of Canada. Project Orbis. 2022. Accessed January 15, 2025. https://www.canada.ca/en/health-canada/services/drugs-health-products/international-activities/project-orbis.html
83.pan-Canadian Pharmaceutical Alliance. Early Negotiation Process (ENP). 2025. Accessed November 29, 2025. https://www.pcpacanada.ca/enp-pathway
84.Government of Ontario. Funding Accelerated for Specific Treatments (FAST) pilot program. 2025. Accessed December 29, 2025. https://www.ontario.ca/page/funding-accelerated-specific-treatments-fast-pilot-program
85.Cheung WY, Cameron C, Mitha A, Wills A. Building infrastructure for outcomes-based agreements in Canada: can administrative health data be used to support an outcomes-based agreement in oncology? Support Care Cancer. 2023;31(1). doi:10.1007/s00520-022-07486-5 PubMed
86.Haute Autorité de Santé. Real-World Studies for the Assessment of Medicinal Products and Medical Devices.; 2021. https://www.has-sante.fr/upload/docs/application/pdf/2021-06/real-world_studies_for_the_assessment_of_medicinal_products_and_medical_devices.pdf
87.Dabbous M, Chachoua L, Caban A. Managed Entry Agreements: Policy Analysis From the European Perspective. Value Heal. 2020;23(4):425-433. doi:https://dx.doi.org/10.1016/j.jval.2019.12.008 PubMed
88.Koleva-Kolarova R, Buchanan J, Vellekoop H, et al. Financing and Reimbursement Models for Personalised Medicine: A Systematic Review to Identify Current Models and Future Options. Appl Health Econ Health Policy. 2022;20(4):501-524. doi:https://dx.doi.org/10.1007/s40258-021-00714-9 PubMed
89.Phillips KA. CMS Coverage with Evidence Development - Challenges and Opportunities for Improvement. JAMA Heal Forum. 2022;3(9). doi:10.1001/jamahealthforum.2022.3061
Appendix 1: Tables
Please note that this appendix has not been copy-edited.
Table 1: Sources of Research Evidence
Source of research evidence | Source |
|---|---|
Electronic databases | Embase |
Grey literature, organizations | Google Search Engine Australian Government website – Australia Canada’s Drug and Health Technology Agency, now Canada’s Drug Agency – Canada Canadian Provincial Government websites Centers for Medicare & Medicaid Services – US Gemeinsamer Bundesausschuss – Germany Health Services Executive – Ireland National Health Care Institute – Netherlands National Institute for Health and Care Excellence – UK |
Additional sources | Reference lists of included articles |
Table 2: Web-Based Concepts and Search Terms, and Jurisdictions of Interest
Concepts | Search terms |
|---|---|
Coverage with evidence development | Coverage with evidence Coverage with evidence building Coverage with evidence development Access with evidence development Managed access Managed entry agreement Evidence-based agreement Outcomes-based agreement |
Jurisdiction of interest | Australia Canada Germany Ireland Netherlands UK US |
Note: Singular and plural forms of terms searched.
Table 3: Study Selection Criteria
Item | Response options |
|---|---|
Is the article written in the English language? | Yes No |
Is the program exclusive to human patients receiving drugs as part of CED programs? | Yes No |
Is the program for medical drugs that have been approved for use by national department of health and health policy? | Yes No |
Is the program currently active or was active and has been retired? | Yes No |
Are drugs funded under CED program publicly funded during evidence generation? | Yes No |
Does the program require evidence generation to address uncertainties in effectiveness, safety, and cost-effectiveness of funded drugs? | Yes No |
Does the evidence process generated require the use of RWE studies? | Yes No |
Is the RWE used for evidence generation to support policy and practice? | Yes No |
CED = coverage with evidence development. RWE = real-world evidence.
Table 4: Jurisdictional CED Agreement Characteristics and Processes
CED feature | Jurisdiction |
|---|---|
Australia | |
Program name | MAP, originally referred to as Managed Entry Scheme |
Year of first drug funded with CED | 2004, MAP officially started in 201139 |
Type of therapy funded with CED | |
Determination of CED agreement and terms | MAP may be recommended by Australian HTA agency or Australian government of health or may be initiated by manufacturer after being denied funding with initial evidence submitted. The conditions set in the MAP funding agreement are discussed between the PBAC, Australian Government Department of Health and Aging Care, and manufacturers. PBAC may provide support to the manufacturer in terms of clearly defining areas of uncertainty within their submitted evidence, and specific requirements to address the uncertainties.39,44,58,65 |
Length of interim funding | Approximately 4 years44 |
Drug funding source | Public funding administered through PBS.26,28,39,40,44,62,63,65,75 |
RWD sources and responsible party or parties | The manufacturer is responsible for real-world data collection via CED specific registry. Administrative health service data sources may also be used. Nontrial data may only be used to support economic evaluations.21,28,30,40,44,58,63,65 |
RWE sharing at end of interim funding | Additional evidence will be shared with PBAC for their review at time points specified in the prefunding MAP deed of agreement. At the end of the MAP funding period the manufacturer will prepare a resubmission package with evidence generated during the funding period to address initial uncertainties.58,62 |
Financial agreements applied with CED | The manufacturer may be required to provide a refunds or rebates due to differences in an observed and predicted outcome.39,58 |
End of CED period outcomes | Change in PBS listing price is dependent on outcomes submitted at the end of the MAP funding period. PBAC reviews the additional evidence and makes a funding recommendation regarding the permanent funding of a drug through the PBS. The funding recommendation may include a change to the policy eligibility criteria or drug list price.21,44,63 |
Belgium | |
Program name | Not available |
Year of first drug funded with CED | 201031 |
Type of therapy funded with CED | CAR T-cell therapies, orphan drugs, drugs for rare diseases, oncology therapies4,12,31 |
Determination of CED agreement and terms | The INAMI CTG/CGM may determine that the reimbursement requested by the manufacturer does not align with their requirements for agreeing to fund a drug and/or identify uncertainties in the submitted evidence and provide a recommendation to fund with conditions. The manufacturer or INAMI – CTG/CGM can suggest funding with CED and work together with the Minister of Social Affairs and the Minister of Budget to define the terms of the CED agreement. The manufacturer must submit proposed CED to the INAMI – CTG/CGM and Minister of Social Affairs and the Minister of Budget for their approval and acceptance of the CED agreement.12,13 |
Length of interim funding | 1 to 3 years, exceptions can be made to length of interim funding by drug12,13,48 |
Drug funding source | |
RWD sources and responsible party or parties | Manufacturer or INAMI is responsible for funding and the organization and maintenance registries to collect data on patients receiving drugs in CED program. If observational studies are conducted for RWE generation the funding and conduct of the studies is the responsibility of the manufacturer.4,12,13,48 |
RWE sharing at end of interim funding | The manufacturer is responsible for funding data analysis regardless of which system partner was responsible for funding and organized the data collection.12 |
Financial agreements applied with CED | During interim funding the financial agreement details the price and reimbursement terms for the drug. Risk-sharing models can include refunds on a prespecified amount of the manufacturer’s turnover for the drug, refunds on all or part of the difference between the estimated and observed drug expenditures, price reductions on other drugs from the manufacturer that are already receiving reimbursement, or refunds on the difference between the proposed price of the drug and its value corresponding to the value determined through cost-effectiveness evaluation as part of the CED agreement.13 |
End of CED period outcomes | The manufacturer prepares and submits the generated evidence to the INAMI – CTG/CGM at the end of the interim funding period. Six months before the end of the interim funding period the INAMI – CTG/CGM reviews the available evidence to determine whether the CED agreement can be met or if further evidence is required to meet the agreement terms, in which case interim funding may be extended up to 1 year. In cases where the evidence generated through additional data collection does not address uncertainties identified before a drug being funded through CED, reimbursement for a drug can be withdrawn. In cases where the additional evidence addresses initial uncertainties, the drug may be reimbursed through standard reimbursement processes with potential changes to the eligibility criteria for patients able to receive the drug. Final funding decision is made by the Minister of Social Affairs and the Minister of Budget.13,31 |
Alberta (Canada) | |
Program name | Coverage with Evidence Development Agreement |
Year of first drug funded with CED | Not available |
Type of therapy funded with CED | Not available |
Determination of CED agreement and terms | After reviewing a manufacturer’s submission for reimbursement, the Alberta Ministry of Health can invite the manufacturers to submit an RFPLA through a CED agreement. The request will be reviewed, and a recommendation made to the Ministry of Health by an expert committee tasked with evaluating drugs. The CED agreement includes a conceptual or clinical framework and propose study design must be developed including a plan for evidence dissemination at the end of the funding period.14 |
Length of interim funding | Not available |
Drug funding source | Public funding through Alberta Health14 |
RWD sources and responsible party or parties | Prospective data collection as part of cohort study40 |
RWE sharing at end of interim funding | Not available |
Financial agreements applied with CED | Not available |
End of CED period outcomes | Not available |
Ontario (Canada) | |
Program name | EBP |
Year of first drug funded with CED | |
Types of therapy funded with CED | |
Determination of CED agreement and terms | The oncology DAC is responsible for putting together a submission for a drug to be funded through the EBP with help from EBP representatives. The submission details the rationale for funding the drug through the EBP, adherence to the EBP criteria, and a proposal for data collection and analysis of end points. The submission is reviewed by the Ontario Provincial Drug Program, Ontario Health - Cancer Care Ontario, and an expert advisory committee. If the submission satisfies the inclusion criteria and demonstrates high priority, it will be provided to the Executive Officer for their review. Submissions will be accepted for the EBP or rejected and returned to the oncology DAC with details of the submission’s limitations.15,52 |
Length of interim funding | Not available |
Drug funding source | Public funding through Ministry of Health Ontario Public Drug Programs - EBP15,16,52 |
RWD sources and responsible party or parties | RWD from administrative health data sources is used. Prospectively collected data of patients enrolled in the EBP is captured at enrolment and set intervals during the interim funding period by health care providers. Data collection is drug specific. The collection of real-world data is funded by the Ontario Ministry of Health as administered by the EBP.15,52 |
RWE sharing at end of interim funding | The EBP a submits a report to the Executive Officer of the Ontario Public Drug Programs to facilitate a final funding decision.15,52 |
Financial agreements applied with CED | Not available. |
End of CED period outcomes | Drugs may receive continued funding through the New Drug Funding Program following interim funding through the EBP or be delisted.15,52 |
France | |
Program name | Innovative Medicines Action Plan59 |
Year of first drug funded with CED | 201518 |
Types of therapy funded with CED | CAR T-cell therapies, orphan drugs, drugs for rare diseases, cancer therapies12,17,19 |
Determination of CED agreement and terms | HAS Agency Transparency Committee reviews initial reimbursement requests and requests that the manufacturer provides additional evidence in the form of real-world comparative studies that rely on the collection of RWD. The data must be collected over a predefined long period of time to address uncertainties in a drug’s effectiveness, safety, and utilization. A protocol must be drafted with support from HAS. The HAS Agency Transparency Committee upon making this request will recommend the drug be funded through a CED agreement to meet the requirements of their request. The Ministry of Health is responsible for the final decision to interim funding with a CED agreement. Depending on the agreement, the manufacturer may be requested to agree to cover the cost of the funded drug in patients who do not demonstrate predefined outcome responses.17-20,86,87 |
Length of interim funding | |
Drug funding source | Public funding through the French National Health Insurance System28 |
RWD sources and responsible party or parties | Additional data are collected through established or newly created disease registries. Registry data collection is typically facilitated through disease registry organizers. Clinical trial data can also be used to generate additional evidence but should be complimented with real-world data. Real-world data are used in observational studies to address uncertainties. The manufacturer is responsible for funding additional data collection.12,17-20,59,86 |
RWE sharing at end of interim funding | The manufacturer is responsible for creating a submission to inform the HAS Agency Transparency Committee review of the additional data and reimbursement recommendation.17 |
Financial agreements applied with CED | Most agreements include a price-volumes agreement which are monitored by CEPS. Interval payment may be applied with patient outcomes achieved. Manufacturers supply drug up to a maximum budgetary amount and repay the national health insurer for additional revenue above the maximum.21,28,49,88 |
End of CED period outcomes | The price of the drug may remain the same if the generated evidence is able to demonstrate the claims effectiveness of the drug. Funds may be held in escrow until evidence generated during interim funding is provided for final review. In the case were the claimed benefits were not demonstrated, the price of the drug may be reduced and the manufacturer required to pay for the cost of the drug for patients that did not demonstrate predefined outcomes or pay back the difference between the cost of the drug during the interim funding period and the new lower price.28,49,59,87 |
Germany | |
Program name | Not available |
Year of first drug funded with CED | Not available |
Types of therapy funded with CED | CAR T-cell therapies, drugs for rare diseases, cancer therapies18,19 |
Determination of CED agreement and terms | The IQWiG reviews the evidence submitted by the manufacturer at the time they are seeking reimbursement for a drug. The IQWiG summarizes and provides the evidence to the G-BA, joint public health agencies, which reviews the summarized evidence and may recommend CED due to uncertainty in the evidence of the drug’s benefit.19,21 |
Length of interim funding | Up to 7 years21 |
Determination of CED agreement and terms | Public funding through the German Health insurance (public GKV insurance or private PKV insurance). Drugs funded with CED agreements are reimbursed through health insurance organizations. Thus, only patients with health insurance organized by companies that participate in the CED agreement will be able to receive the drug. Participating PKVs must agree to the collection of data for evidence generation. The health insurers will reimburse the manufacturer for the cost of the drug during the CED interim funding period. In the agreement, the G-BA sets the time period for data collection which may vary between drugs. G-BA requires that only comparative evidence be submitted for review at the end of the interim funding period.18,19,21,60 |
RWD sources and responsible party or parties | The manufacturer is responsible for setting up a registry to collect data to address uncertainties as identified in the GBA’s review and recommendation. Data from new registries created per CED agreement or established disease registries is used for prospective observational studies. The manufacturer is responsible for funding and organization of data collection.18,19,60 |
RWE sharing at end of interim funding | The manufacturer is required to submit generated RWE at prespecified time points as outlined in the CED agreement.18,21,49 |
Financial agreements applied with CED | Drugs are freely priced for 1 year until national pricing agreements have been negotiated. The manufacturer and participating health insurers negotiate the price of the drug during the interim funding period, the price of the drug may be influenced by G-BA review of the initially submitted evidence. Financial agreements can include interval payments, rebates, price-volumes agreement, or payment caps.19,21,48,88 |
End of CED period outcomes | The manufacturer may be penalized, such as the price of the drug being reduced, if they are not able to generate evidence by the end of the interim funding period or the evidence does not demonstrate added value. Evidence may be submitted at prespecified intervals during the funding period for G-BA to review and potentially apply price changes.18,21 |
Ireland | |
Program name | Managed Access Protocols through Medicines Management Programme41 |
Year of first drug funded with CED | Not available |
Types of therapy funded with CED | Expensive drugs, orphan drugs, CAR T-cell therapies, cancer therapies.41,42 |
Determination of CED agreement and terms | The HSE makes a reimbursement recommendation to the HSE Executive Management Team with the help of the National Centre for Pharmacoeconomics. The HSE Executive Management Team makes a final reimbursement to apply a health technology management strategy of funding with conditions to address uncertainty in the manufacturer’s submitted evidence. HSE and the manufacturer establish CED agreement protocols and outcomes to support reimbursement.42 |
Length of interim funding | Not available |
Drug funding source | Public funding through HSE, national publicly funded health care provider administered by the National Cancer Control Programme.12,41 |
RWD sources and responsible party or parties | Routinely collected administrative health data may be used for evidence generation. Prospective data collected by health care providers for patient enrolled to receive drug funded with CED agreement12,42 |
RWE sharing at end of interim funding | Not available |
Financial agreements applied with CED | Not available |
End of CED period outcomes | HSE uses generated evidence generated to confirm long-term funding.42 |
Italy | |
Program name | Italian conditional reimbursement scheme |
Year of first drug funded with CED | 200517 |
Types of therapy funded with CED | CAR T-cell therapies, orphan drugs, drugs for rare diseases, cancer therapies12,17,19,43 |
Determination of CED agreement and terms | AIFA is responsible for reviewing the initial evidence submitted by the manufacturers and identifying and describing any uncertainties in a drug’s effectiveness and/or safety. Based on the review, AIFA may recommend a drug be funded with conditions, possibly including a performance and/or financial-based agreement. Payment-by-results financial agreements may be applied where reimbursements are only provided of patients whose disease responds to treatment and the manufacturer may be required to partially or fully refund the drug costs in patients whose disease does not respond to treatment. Additionally, the manufacturer may receive interval-based payments based on evidence submitted which demonstratives clinical improvement in patients.4,12,17,19-21,28,43,45,46,48 |
Length of interim funding | Varies by drug |
Drug funding source | Public funding through Italian National Health Service, funds allocated to which are responsible for directly reimbursing hospitals which use the drug.17,18,20,21,28,43,45,48 |
RWD sources and responsible party or parties | Data are collected through the national AIFA registries that can be already established or can be created for a newly funded drug. The data collected through the AIFA registries is used for prospective observational studies. Data in the AIFA registries come from administrative clinical data collected by physicians at participating hospitals. The MFR may be responsible for providing funding to support the collection of data for their evidence generation through the AIFA registries. The Ministry of Health and National Health Service may also support the AIFA registries. The AIFA registries are data custodians for data collected and housed in AIFA registries.12,17,18-21,23,43,45,46,48 |
RWE sharing at end of interim funding | Not available |
Financial agreements applied with CED | The manufacturer may be required to repay the payer at internals or at the end of interim funding.4,21,45,48 |
End of CED period outcomes | AIFA reviews the submitted additionally generated evidence and makes a long-term funding recommendation to the NHS. For cases of financial uncertainty, the manufacturer may need to demonstrate they have met a specified financial target by the end of the interim funding period. After the end of interim funding, AIFA may decide to fully fund the drug at the same price during the interim funding period, or the price of the drug may be altered for example to bring it down to a comparable cost to similar types of drugs.12,20,21,23,43,45 |
Netherlands | |
Program name | Dutch Coverage with Evidence Development program |
Year of first drug funded with CED | 200631 |
Type of therapy funded with CED | Orphan drugs, drugs for rare diseases, expensive drugs, oncology therapies12,22,24,31,47,48 |
Determination of CED agreement and terms | An initial reimbursement submission package is provided to the ZIN and NZa, which comprise the Dutch Health care Insurance Board, appraisal committee which reviews the clinical, safety, and cost-effective evidence. ZIN provides recommendations for reimbursement to conditions to the Dutch Ministry of Health. The manufacturer must submit a proposal for how additional evidence would be generated during the interim CED funding period as part of meeting the criteria for a CED agreement. ZiN may provide methodological guidance to the manufacturer to support CED planning. During review of the drug for funding through a CED agreement, the Dutch Health care Insurance Board will provide input on the feasibility of completing and appraising the additional evidence within the 4-year funding period. The Dutch Ministry of Health is responsible for the final reimbursement decisions. Payment-by-performance may be applied as part of the agreement.12,22-25 |
Length of interim funding | 4 years22 |
Drug funding source | Public funding from Dutch Ministry of Health. Reimbursement to hospitals for cost of drug is provided by Dutch Health care Insurance Board.22 |
RWD sources and responsible party or parties | Data can be collected through the use of national disease or treatment registries and through prospective cohort studies. The manufacturer is responsible for funding data collection during the 4-year CED period. The manufacturer is responsible for the organization of data collection which can include coordination of collection through pharmacies, academic hospitals, and universities4,12,23-25,47 |
RWE sharing at end of interim funding | At 6-month intervals, progress meetings are held to review collected data and ensure the study is progressing to meet the 4-year funding end date. At the end of the funding period the manufacturer submits a package to ZiN with the additional clinical and/or cost-effectiveness evidence required to address initial unceratinties.12,22-25 |
Financial agreements applied with CED | Adaptive pricing may be applied.25 |
End of CED period outcomes | At the end of the 4-year interim funding period, the Dutch Health care Insurance Board reviews the generated evidence and provides a recommendation to the Ministry of Health for its future funding. The Ministry of Health may accept a drug for funding without conditions and move it to the national statutory funding package. If funded, the funding indication may be updated per the Dutch Health care Insurance Board’s recommendation. Alternatively, if the drug does not provide evidence to address initial uncertainties funding can be withdrawn.12,22-25,51 |
Scotland | |
Program name | Not available |
Year of first drug funded with CED | Not available |
Type of therapy funded with CED | |
Determination of CED agreement and terms | The manufacturer submits their initial evidence to the SMC who is responsible for a HTA of the clinical, safety, and cost-effectiveness evidence. Drugs that meet the criteria for drugs for rare diseases or orphan drugs may be recommended for a CED agreement (sometimes referred to as the Patient Access Scheme) per the SMC’s recommendation.18 |
Length of interim funding | |
Drug funding source | Public funding through the Scottish National Health System.17,18 |
RWD sources and responsible party or parties | The manufacturer is responsible for the cost of data collection through disease registries.18 |
RWE sharing at end of interim funding | Not available |
Financial agreements applied with CED | Not available |
End of CED period outcomes | The outcome of SMC’s re-review is to make a funding recommendation for the drug funded with a CED agreement. The outcome of the review can be to accept the drug for routine public funding, to accept the drug for routine public funding but with restricted use of the drug (detailed in the final reimbursement acceptance documents), or to not routinely fund the drug.17,18 |
Sweden | |
Program name | Not available |
Year of first drug funded with CED | Not available |
Type of therapy funded with CED | Oncology drugs, orphan drugs, and drugs for rare diseases18,46 |
Determination of CED agreement and terms | The national TLV conducts a review of the initial evidence submitted and may suggest a CED agreement to address uncertainties in the clinical or cost-effectiveness of a drug. TLV typically makes a recommendation based on the cost-effectiveness of a drug. The manufacturer must agree to collect real-world data on the drug during the interim funding and submitted generated evidence for review by TLV at the end of the interim funding period. The TLV may work with regional councils and manufacturers to negotiate the terms of the CED, or the regional councils may work directly with the manufacturer to negotiate terms. If regional councils work directly with the manufacturer, their government funding from the national Department of Health will be reduced the following year in an effort for the Department of Health to maintain uniform national pricing policies. TLV may aid the manufacturer in developing the data collection protocol if assistance is requested. The Swedish central Department of Health and TLV negotiate with the manufacturer a price for the drug during the temporary funding period. Payment-by-results may be applied tying payment to the manufacturer submitting evidence of patients achieving prespecified outcomes.4,20,21,31,48,49,53 |
Length of interim funding | Not available |
Drug funding source | National health insurance is provided by the Department of Health to all citizens. Regional and municipal governments are responsible for financing and delivering care.4 |
RWD sources and responsible party or parties | Data for evidence generation may come from claims data, disease/patient registries, or as part of prospective observational studies. The manufacturer is responsible for funding data collection and obtaining data access.4,31,49,53 |
RWE sharing at end of interim funding | The manufacturer provides a resubmission package for the TLV, including a new economic model.49,53 |
Financial agreements applied with CED | Pricing may be set for the interim funding period with possibility to renegotiate at the end of interim funding.20,31,46,49,53 |
End of CED period outcomes | The TLV may recommend stopping funding for a drug that does not demonstrate anticipated clinical or cost-effectiveness outcomes or recommend funding for a drug that demonstrates cost-effectiveness.20,31,49,53,87 |
UK | |
Program name | CDF, IMF |
Year of first drug funded with CED | Cancer Drug Fund began in 2010 with an update in 2016. Innovative Medicines Fund first introduced in 2022.23,37 |
Type of therapy funded with CED | Cancer Drug Fund: oncology drugs, CAR T-cell therapies, orphan drugs. Innovative Medicines Fund: noncancer drugs.23,37 |
Determination of CED agreement and terms | NICE is responsible for reviewing the initially submitted request for funding and making a recommendation for funding the drug with conditions if the identified uncertainties can be addressed through additional evidence generation. NICE must review the submission and provide their support for funding through the CDF/IMF. The Department of Health, through National Health Service (NHS) England, provides a final decision whether or not to fund the drug through the CDF/IMF. The manufacturer and payer agreements have 2 components, a DCA and CAA. The DCA details the end points that must be reported on with additional evidence to address identified uncertainties in clinical or cost-effectiveness areas. The CAA details the cost of the drug and any risk-sharing conditions. As part of the DCA and CCA, funding for the drug may be conditional on the ability of the generated evidence to demonstrate specific end points or provide a discount on the price of the drug if the end point is not met. The DCA may specify that additional data collection is accomplished through SACT datasets. The CAA will provide an outline for the evidence sharing during the interim funding period at regular intervals. The CDF/IMF oversight group will regularly meet to review submitted evidence to ensure the data collection is progressing on track, and to support in issues of analysis planning, access to treatment service issues, clinical assessment issues, and safety issues as signalled by patients and/or clinicians21,32,35-38,54,57,72,73 |
Length of interim funding | |
Drug funding source | |
RWD sources and responsible party or parties | Data for additional evidence generation may come from SACT datasets, Bluteq dataset, Public Health England datasets, established disease registries, market share data, or chart review. NHS Digital is responsible for the data collection, compiling, quality review, and analyses using SACT datasets. SACT datasets are funded through NHS England. Additional funding and organization for data collection may be provided by the manufacturer, or the price of the drug as set by the manufacturer may take into consideration resources requirements for data collection if outside manufacturer funded clinical trials.4,12,17,19,35,37,38,54,57,68,69,72 |
RWE sharing at end of interim funding | At the end of the interim funding period the manufacturer is responsible for providing NICE with a submission package summarizing the additional evidence generated through data collection.35,36,54,72 |
Financial agreements applied with CED | The CAA details the cost of the drug and any risk-sharing conditions. The price of drug will be submitted by the manufacturer and should take into consideration the uncertainties of the drug and the NHS England resources that will be required for additional data collection. Discounts, interval payments, and rebates may be applied as part of the financial agreement.32,35,36,88 |
End of CED period outcomes | NICE reviews the additionally generated evidence and can recommend the drug to be funded through routine NHS England funding pathways or may recommend not to continue funding. NICE may recommend continued funding if the end points related to original uncertainties have been provided and the level of cost-effectiveness of the drug is acceptable. The cost of the drug may be adjusted based on the cost-effectiveness analysis outcomes. NHS England provides a final say on whether they will provide routine funding for a drug and at what price.4,17,20,35-37,54 |
US | |
Program name | Coverage with evidence development |
Year of first drug funded with CED | |
Type of therapy funded with CED | Drugs covered through The CMS or private insurer.26,27,40,50,66 |
Determination of CED agreement and terms | CMS and the Agency for Health care Research and Quality conduct health technology assessments of cancer drugs to determine what drugs should be funded through CMS and could be included in private insurance plans. CMS makes the recommendation to fund a drug with conditions through a CED agreement. CMS provides 2 types of funding agreements for CED drugs: 1) Coverage under study protocol, where the initial submitted evidence does not provide adequate information to confidently accept the drug for full funding without the incorporation of additional data collection, and (2) Coverage with appropriateness determinations, where a drug meets the definition of “reasonable and necessary” but there are uncertainties in its safety and/or effectiveness among use at the population level or within a clinic setting, or if inclusion of the drug would significantly alter patient management. For CAD funding additional data collection is also needed to ensure the drug is appropriately administered in setting outlined in the National Coverage Determination (set by CMS). Funding is only available for patients who agree to data collection. An outcomes-guarantee agreement may be added to the CED agreement conditions whereby the manufacturer would be responsible for refunding all or a portion of the cost of the drug for patients that do not demonstrate benefit by a set period of time.26-30 |
Length of interim funding | Specific per drug, usually determined by amount of time to collect necessary data40,50 |
Drug funding source | |
RWD sources and responsible party or parties | Additional evidence can be generated through the collection of data from prospective clinical studies or disease registries. Funding for data collection may be shared by the manufacturer and CMS. CMS may provide support to disease registries for which data are required to address uncertainties The registry data will be linked with Medicare claims data to support cost-effectiveness evidence generation. At the end of the funding period, CMS is the data owner and custodian.4,26,28,40,69-71,77 |
RWE sharing at end of interim funding | Even if the study does not produce evidence for its primary outcome, the data collection must be completed and available data be submitted for HTA review by CMS.50 |
Financial agreements applied with CED | |
End of CED period outcomes | As part of CMS considering ending the interim funding, generated evidence should be published in a peer-reviewed journal or available in online registries of clinical studies. CMS will consider the following factors when determining whether to end data collection:
Continued funding may be provided for the drug or denied at the end of the data collection period after CMS conducts a review of the generated evidence.71 |
AIFA = Agenzia Italiana del Farmaco; CAA = commercial access agreement; CAR = chimeric antigen receptor; CED = coverage with evidence development; CEPS = Comité Economique Des Produits De Santé; CDF = Cancer Drug Fund; CTG/CGM = Commission for Reimbursement of Medicines; CMS = Centers for Medicare & Medicaid Services; DAC = Drug Advisory Committee; DCA = data collection agreement; EBP = evidence building program; G-BA = Gemeinsamer Bundesausschuss; GKV = Gesetzliche Krankenversicherung; HAS = Haute Autorité de santé; HSE = Health Service Executive; HTA = health technology assessment; IMF = Innovative Medicines Fund; INAMI = National Institute for Health and Disability Insurance; IQWiG = Institute for Quality and Efficiency in Health Care; MAP = managed access program; NHS = National Health Service; NICE = National Institute for Health and Care Excellence; NZa = Nederlandse Zorgautoriteit; PBAC = Pharmaceutical Benefits Advisory Committee; PBS = Pharmaceutical Benefits Scheme; PKV = Private Krankenversicherung; RFPLA = Request for Product Listing Agreement; RWD = real-world data; RWE = real-world evidence; SACT = systemic anti-cancer therapy; SMC = Scottish Medicines Consortium; TLV = Tandvårds-och Läkemedelsförmånsverket; ZIN = Zorginstituut Nederland.
Appendix 2: Search Strategy — Embase, 2007 to November 6, 2024
Please note that this appendix has not been copy-edited.
((coverage adj3 evidence adj3 (development or building)).ti,ab,kw.
((coverage or access) adj3 evidence adj3 (development or building)).ti,ab,kw.
(managed adj1 access).ti,ab,kw.
(managed adj3 entry adj3 (access or agreement)).ti,ab,kw.
((evidence or outcome*) adj3 based adj3 agreement)).ti,ab,kw.
1 or 2 or 3 or 4 or 5
Limit 6 to (English language and yr=”2007-Current”)
Appendix 3: Sample Data Extraction Form
Please note that this appendix has not been copy-edited.
Table 5: Sample Data Extraction Form
Category | Subcategory | Data item |
|---|---|---|
General study information | Author/Organization | |
Publication year/Year of last update | ||
Title | ||
Publication type | ||
Source | ||
Program characteristics | Program characteristics | Jurisdiction |
Program name | ||
Program types | ||
Program objectives | ||
Number of years active | ||
Key program components | ||
Participant/Health technology characteristics | Patient population, if applicable | |
Type of health technology, if applicable | ||
Results | Program structure | Criteria for inclusion of drug in program |
Source of funding for drugs | ||
Funding decision-making process | ||
Length of funding period | ||
Program system partner roles | ||
System partner engagement process | ||
Program operations | Manufacturer agreement structure pre‑evidence generation | |
Type of RWD | ||
Source of RWD | ||
Collection of RWD | ||
Party responsible for conducting RWE analyses | ||
Party responsible for funding data collection | ||
Evidence sharing process | ||
Manufacturer agreement structure after evidence generation | ||
Program objective achievement | ||
Limitations of program and lessons learned | ||
Any other relevant information relating to the program structure and operations | ||
HTA = health technology assessment; RWD = real-world data; RWE = real-world evidence.
Appendix 4: Supplemental Material
Please note that this appendix has not been copy-edited.
Table 6: Sources Included in Environmental Scan, Identified Through Web-Based Searches and Embase Database
In-text citation | Title | First author | Publication year | Article type or online source | Jurisdictions where CED discussed |
|---|---|---|---|---|---|
4 | Performance-based managed entry agreements for new medicines in OECD countries and EU member states: How they work and possible improvements going forward | Wenzl M. | 2019 | Online report | Belgium, Italy, Sweden, the Netherlands, France, Australia, UK, US |
12 | Implementing Outcomes-Based Managed Entry Agreements for Rare Disease Treatments: Nusinersen and Tisagenlecleucel | Facey K. | 2021 | Review | Belgium, UK, Scotland, the Netherlands, Ireland, Italy, Australia, France |
13 | How to Improve the Belgian Process for Managed Entry Agreements? An Analysis of the Belgian and International Experience | Gerkens S. | 2017 | Online report | Belgium |
22 | Innovations that reach the patient: Early health technology assessment and improving the chances of coverage and implementation. | Van Harten W. | 2016 | Discussion | The Netherlands |
23 | Pricing and Reimbursement Experiences and Insights in the European Union and the United States: Lessons Learned to Approach Adaptive Payer Pathways | Faulkner S. | 2016 | Discussion | US |
24 | Conditional reimbursement within the Dutch drug policy | Niezen M. | 2007 | Review, qualitative study | The Netherlands |
25 | Conditional Financing of Drugs in the Netherlands: Past, Present, and Future—Results From Stakeholder Interviews | Makady A. | 2016 | Qualitive study | The Netherlands |
26 | Coverage with evidence development and managed entry in the funding of personalized medicine: Practical and ethical challenges for oncology | Lewis J. | 2015 | Discussion | US, Australia |
27 | Ethical considerations in CMS's coverage with evidence development | Relyea-Chew et al. | 2011 | Policy review | US |
28 | Funding the unfundable: Mechanisms for managing uncertainty in decisions on the introduction of new and innovative technologies into health care systems | Stafinski T. | 2010 | Comparative review | Italy, US, Canada, Australia, France, UK |
29 | Access with evidence development: The US experience | Mohr P. | 2010 | Commentary | US |
30 | Coverage with evidence development: Applications and issues | Trueman P. | 2010 | Descriptive study | US, UK, Australia |
31 | Dealing with uncertainty and high prices of new medicines: A comparative analysis of the use of managed entry agreements in Belgium, England, the Netherlands and Sweden | Ferrario A. | 2015 | Comparative review | Belgium, UK, the Netherlands, Sweden |
14 | Alberta Health Product List Agreement Policy | — | 2022 | Government of Alberta institutional document | Canada (Alberta) |
32 | Using 5 consecutive years of NICE guidance to describe the characteristics and influencing factors on the economic evaluation of orphan oncology drugs | Shengnan D. | 2022 | Policy analysis | UK, Scotland |
34 | New “managed access” process for Cancer Drugs Fund to go ahead, NHS England confirms | Mayor S. | 2016 | News article | UK |
35 | Managed access | — | 2023 | NICE institutional website | UK |
36 | Cancer Drugs Fund | — | — | NHS England institutional website | UK |
37 | Innovative Medicines Fund | — | — | NHS England institutional website | UK |
38 | Critical Reflections on Reimbursement and Access of Advanced Therapies | Simoens S. | 2022 | Narrative review | Italy, UK |
15 | Evidence Building Program | — | 2011 | Ontario Health (Cancer Care) institutional website | Canada (Ontario) |
16 | Provincial Drug Reimbursement Programs | — | 2011 | Ontario Health (Cancer Care) institutional website | Canada (Ontario) |
17 | Outcomes-based reimbursement for gene therapies in practice: the experience of recently launched CAR-T-cell therapies in major European countries | Jørgensen J. | 2020 | Discussion | France, Italy, UK, Scotland |
18 | HTA decision-making for drugs for rare diseases: comparison of processes across countries | Stafinski T. | 2022 | Scoping review | France, Italy, Scotland, Australia, UK, the Netherlands, Germany, Sweden |
19 | The use of innovative payment mechanisms for gene therapies in Europe and the US | Jørgensen J. | 2018 | Discussion | France, Germany, Italy, UK |
20 | Market Access Agreements for pharmaceuticals in Europe: diversity of approaches and underlying concepts. | Jaroslawski S. | 2011 | Comparative review | Sweden, France, Italy |
21 | Pharmaceuticals managed entry agreements: Lessons Learned from Europe, the United States, Canada and Australia | Grubert, N and Morse | 2018 | Online report | Italy, UK, France, Germany, the Netherlands, Sweden, Australia, Canada, US |
39 | A real world example of coverage with evidence development in Australia - ipilimumab for the treatment of metastatic melanoma | Kim H. | 2018 | Retrospective observational study | Australia |
40 | Coverage with evidence development for pharmaceuticals: A policy in evolution?. | Lexchin J. | 2011 | Comparative study | Australia, Canada (Alberta), US, UK |
41 | Managed Access Protocols | — | 2023 | HSE Scotland institutional website | Scotland |
42 | Utilizing Health Technology Assessment to Develop Managed Access Protocols to Facilitate Drug Reimbursement in Ireland | Gorry C. | 2024 | Discussion | Ireland |
43 | The Evolution of AIFA Registries to Support Managed Entry Agreements for Orphan Medicinal Products in Italy | Xoxi E. | 2021 | Policy analysis | Italy |
44 | Framework for the introduction of a Managed Entry Scheme for submissions to the Pharmaceutical Benefits Advisory Committee | — | 2015 | Australian Government – Pharmaceutical Benefits Scheme institutional website | Australia |
45 | Monitoring Registries at Italian Medicines Agency: Fostering Access, Guaranteeing Sustainability | Montilla S. | 2015 | Discussion | Italy |
46 | Risk sharing arrangements for pharmaceuticals: potential considerations and recommendations for European payers | Adamski J. | 2010 | Literature review | Italy |
47 | Evaluation of patient registries supporting reimbursement decisions: The case of oxaliplatin for treatment of stage III colon cancer. | Mohseninejad L. | 2015 | Policy analysis | The Netherlands |
48 | Reconciling uncertainty of costs and outcomes with the need for access to orphan medicinal products: a comparative study of managed entry agreements across 7 European countries | Morel T. | 2013 | Review | Belgium, Italy, the Netherlands, Sweden |
49 | Managed entry agreements for pharmaceuticals: the European experience | Ferrario M. | 2013 | Discussion | UK, France, the Netherlands, Sweden |
50 | National Coverage Determinations with Data Collection as a Condition of Coverage: Coverage with Evidence Development | — | 2006 | CMS institutional website | US |
51 | Access to new medicines in Europe: technical review of policy initiatives and opportunities for collaboration and research | — | 2015 | WHO Regional Office for Europe | Belgium, Sweden, UK, The Netherlands |
52 | Evidence Building Program Policy | — | 2011 | Ontario Health (Cancer Care) institutional website | US |
53 | Reducing uncertainty in value-based pricing using evidence development agreements: The case of continuous intraduodenal infusion of levodopacarbidopa (Duodopa) in Sweden | Willis M. | 2010 | Review of case study | Sweden |
54 | “Don't Think Twice, It's All Right”: Using Additional Data to Reduce Uncertainty Regarding Oncologic Drugs Provided Through Managed Access Agreements in England | Kang C. | 2023 | Review | UK, Scotland |
55 | Uncertainty and Coverage With Evidence Development: Does Practice Meet Theory? | Pouwels X. | 2019 | Qualitative study | The Netherlands |
56 | Optimizing Managed Access: Lessons From the Cancer Drugs Fund | Lee J. | 2021 | ISPOR report | UK |
57 | Investigation into the Cancer Drugs Fund | — | 2015 | Department of Health and NHS England, National Audit report | UK |
58 | The Australian Managed Entry Scheme: Are We Getting it Right? | Tuffaha H. | 2018 | Policy review | Australia |
59 | Innovative medicines assessment action plan | 2020 | — | Haute Autorité de Santé report | France |
60 | Reimbursement of Pharmaceuticals in Germany | — | 2020 | IGES Institute report | Germany |
61 | NHS commercial framework for new medicines | — | 2021 | NICE institutional website | UK |
62 | Characteristics of managed access agreements for medicines in Australia | Robinson M. | 2017 | Policy analysis | Australia |
63 | Managed entry agreements for pharmaceuticals in Australia. | Vitry A. | 2014 | Discussion | Australia |
65 | Australian Managed Entry Scheme: A New Manageable Process for the Reimbursement of New Medicines? | Wonder M. | 2012 | Discussion | Australia |
66 | Coverage with Evidence Development: Where Are We Now? | Zeitler E. | 2022 | Systematic review | US |
67 | Coverage with Evidence Development | — | 2024 | CMS institutional website | US |
69 | Can Managed Access Agreements Mitigate Evidentiary, Economic and Ethical Issues with Access to Expensive Drugs for Rare Diseases in the Canadian Context? | McPhail M. | 2023 | Commentary | US, Canada |
68 | An evaluation of managed access agreements in England based on stakeholder experience | Farmer C. | 2023 | Qualitative study | UK |
70 | A Roadmap for Improving Medicare's Application of Coverage With Evidence Development | Lakdawalla D. | 2024 | Discussion | US |
71 | Guidance for the Public, Industry, and CMS Staff: Coverage with Evidence Development | — | 2014 | CMS institutional website | US |
72 | Data collection agreement | — | 2024 | NICE institutional website | UK |
73 | An Analysis of Uncertainties and Data Collection Agreements in the Cancer Drugs Fund | Trigg L. | 2024 | Policy analysis | UK |
74 | Analysis of CED Criteria | Segal L. | 2022 | CMS institutional website | US |
75 | Finding common ground for accelerating access | — | 2023 | Australian Government – Pharmaceutical Benefits Scheme institutional website | Australia |
76 | Politics and its intersection with coverage with evidence development: a qualitative analysis from expert interviews | Bishop D. | 2013 | Qualitive study | Australia, Canada, US, UK |
77 | Coverage with evidence development: An examination of conceptual and policy issues. | Hutton J. | 2007 | Discussion | US |
86 | Real-world studies for the assessment of medicinal products and medical devices | — | 2021 | Haute Autorité de Santé institutional website | France |
87 | Managed Entry Agreements: Policy Analysis From the European Perspective | Dabbous M. | — | Policy analysis | UK, Sweden, The Netherlands, Germany, France |
88 | Financing and Reimbursement Models for Personalised Medicine: A Systematic Review to Identify Current Models and Future Options | Koleva-Kolarova R. | 2022 | Literature | France, Germany, UK |
89 | CMS Coverage With Evidence Development-Challenges and Opportunities for Improvement | Philips K. | 2022 | Discussion | US |
AIFA = Agenzia Italiana del Farmaco; CAR = chimeric antigen receptor; CED = coverage with evidence development; CMS = Centers for Medicare & Medicaid Services; EU = Europe; HTA = health technology assessment; HSE = Health Service Executive; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NHS = National Health Service; NICE = National Institute for Health and Care Excellence; OCED = Organization for Economic Co-operation and Development.
Note: References to the term “stakeholder” are included from original sources.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.