Drugs, Health Technologies, Health Systems
Peer-Reviewed Article
Mapping the Landscape of Infusion Care for People Prescribed IV Medicines in Canada
Quinn Grundy, Dana Hart, Sarah Elkhalifa, Joel Lexchin, Marc-André Gagnon, Navindra Persaud, Mina Tadrous
Abstract
Background: Historically, medically necessary infusion services were provided within publicly funded hospitals under the Canada Health Act. In the early 2000s, pharmaceutical manufacturers set up third-party private infusion clinics to facilitate patient access to new IV drugs. We aimed to document the extent of infusion-related care provided by private infusion clinics.
Methods: We conducted a descriptive, cross-sectional study between April 1 and June 14, 2024, to identify all infusion clinic locations in Canada and a structured content analysis of web-based sources to characterize their ownership, settings, amenities, and types of medicines infused.
Results: We identified 1,097 infusion clinics that provided outpatient care for people prescribed IV medications. Approximately half of the clinics were owned by private entities and funded through manufacturers’ patient support programs, private insurance, or out-of-pocket by patients (573 of 1,097; 52.2%); 4 for-profit companies owned and operated 39.6% of all infusion clinics (434 of 1,097). Private infusion clinics were clustered around existing publicly funded hospitals (distance from hospital: median = 2.4 km; interquartile range = 1 to 5 km). Of the clinics offering infusion services for biologics and cancer immunotherapy, more than 85% were private, for-profit companies, whereas 99% of clinics providing chemotherapy or blood products were in the publicly funded system.
Interpretation: Half of all infusion clinics are owned and operated by a small number of private, for-profit entities funded outside the public system. Further research into clinic operations and care outcomes would enhance governments’ abilities to adopt formal policies about infusion care, including decisions about the optimal degree of private sector involvement and strategies to ensure equitable and sustainable access to medically necessary care.
Introduction
Biologics, a class of drugs manufactured in living cells, were first available in Canada in the early 2000s. Many biologic medicines require regular (typically every 4 to 8 weeks) IV infusion by a registered nurse who monitors their infusion with a physician available on call.1 Historically, medically necessary infusion services were provided within hospitals under the terms of the Canada Health Act and funded through the publicly funded health system. Since the 2000s, with changes in the provision of supportive care, the availability of new medications, and a desire to optimize hospital capacity, health systems have shifted many infusion therapies from inpatient to outpatient settings; for example, cancer treatment is now largely on an outpatient basis.2 When high-cost biologic infusion therapies first entered the Canadian market, pharmaceutical manufacturers elected to set up networks of private clinics to provide access to their drugs.3 Currently, there are hundreds of private, for-profit infusion clinics operating across Canada.4-8
When patent protection for biologics began to expire, manufacturers sought market authorization for biosimilars, which are highly similar — but nonidentical — and are judged to have no clinically meaningful differences in efficacy and safety to their biologic counterparts.9 With the emergence of biosimilars as cost-effective alternatives for biologic originators,10 biosimilar manufacturers created equivalent, but distinct, networks of infusion services. As provinces and territories began to adopt a range of biosimilar switching policies for patients prescribed originator biologics,11-13 they largely relied on biosimilar manufacturers to ensure continuity in access to infusion services. However, the costs of delivering these programs are high, and although biosimilars are now listed on all provincial formularies, their sales relative to the biologic originator remains variable across the country and are low compared to other Organisation for Economic Co-operation and Development (OECD) nations.10
The reliance on drug manufacturers to fund infusion care raises important questions about access, oversight, accountability, continuity of care, and the extent to which the provision of private infusion care is incorporated into the cost of these drugs. Further, it is important to understand whether the publicly funded health system has capacity to provide infusion care in cases in which manufacturers do not elect to fund such services. In 2021, CADTH (now Canada’s Drug Agency) assessed the landscape of private infusion clinic locations in Canada, and identified 423 locations across the 10 provinces and Yukon run by 8 different private entities.14 Due to the rapidly changing landscape of private infusion care, we sought to extend this previous work by identifying both private and publicly funded clinics in Canada that provide infusion services for people prescribed IV medications on an outpatient basis. Using publicly available data sources, we describe the types of entities which own and operate infusion services, their funding models, settings, geographical distribution, amenities, and services for specific categories of medications.
Methods
Study Design
We conducted a cross-sectional study to identify all infusion clinic locations, including those operated by private providers and within the publicly funded health care system. We then conducted a structured content analysis of web-based sources to characterize their ownership, settings, geographic distribution, amenities, and specific medicines offered at each location. Our sampling and data collection began April 1, 2024, and our list of clinics was finalized June 14, 2024. We relied on publicly available data sources to identify and describe infusion clinics. We limited data collection to publicly available sources because these sources are currently available to referring clinicians, patients seeking care, researchers, and policy-makers.
We report the study according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines (Supplementary File 1).15
Infusion Clinic Sampling and Screening
Because there is no existing database of infusion clinics, we employed a systematic, purposeful sampling strategy, which entailed first sampling the most information-rich data sources in an iterative and additive way and continuing to sample until the search strategy yielded no new information.16,17 We purposefully sampled clinics based on a set of inclusion criteria informed by preliminary studies.3,14,18 We included any clinic setting that explicitly provided IV infusions for prescription medicines to patients on an outpatient basis. We excluded clinics that exclusively provide wellness infusions (e.g., nonprescription hydration and vitamin therapies), hemodialysis, or infusion therapies for off-label indications (i.e., lidocaine for pain management or ketamine therapies for mental health treatment), those that only offer non-infusion services to people prescribed IV medications (e.g., patient support programs that coordinate infusions), services that only administer IVs in home care settings, and clinics that had closed or had future opening dates.
We adopted a phased approach to purposefully and comprehensively identify all settings in Canada where patients can receive outpatient infusions for prescription medicines. First, we used the 2021 CADTH report14 to generate an initial sampling frame of companies providing infusion care. We searched each company’s website for a list of infusion clinics and extracted the clinic names and addresses verbatim.
Second, we downloaded the Statistics Canada Open Database of Healthcare Facilities (ODHF) Version 1.1.19 This database compiles the names, types, and addresses of health care facilities across Canada. We generated a list of included (i.e., likely to perform IV infusions) and excluded (i.e., unlikely to perform IV infusions) health care facility types (refer to Appendix 2, Table 4), which was reviewed and confirmed by team members. We then googled the name of each included facility and searched relevant websites for evidence of outpatient infusion services for prescription medicines. If the website indicated that infusion services were available, the clinic was included and we extracted the clinic’s name, address, provider name, and URL of the source. We also saved copies of web pages containing information about the clinic services (e.g., types of drugs infused) to Zotero (reference management software).
Next, based on previously developed search methods,18,20 we conducted structured Google searches to identify additional providers not identified in the previous steps. First, we tested a combination of relevant search terms in both English and French on 2 cities (Bathurst and Moncton) in New Brunswick because the province mandates use of both official languages, and selected the search structure that provided the highest return of relevant results. For each census metropolitan area in the 2021 Census,21 we conducted searches in English using “[name of city] [province/territory] intravenous” and French searches using “clinique de perfusion intraveineuse IV [nom de ville] [province/territoire].” We reviewed the results of each search until no new information was presented. We extracted the name and address of the clinics and saved web pages containing evidence of infusion to Zotero. We did not screen or sample clinics in duplicate due to feasibility, but anything ambiguous was reviewed by another team member.
Variables, Data Extraction, and Coding
For each clinic, we determined the entity responsible for delivering the infusion care and categorized the provider type (Appendix 2, Table 5). In some cases, multiple entities worked in partnership to deliver the infusion care.
We extracted province and postal code from the clinic addresses. Some of the private companies provided a clinic locator containing varying information about amenities, including parking, Wi-Fi, snacks, distance from a hospital, and hours of operation; we extracted this information if it was available. We extracted the same information from the other clinic web pages when available. For clinics that did not provide the distance to the nearest hospital, we used the Google Maps “search nearby” function to locate the closest hospital to each clinic and recorded the distance in kilometres.
For each clinic included, we used the clinic’s website or Google Maps (including street view) to identify the clinic setting (Appendix 2, Table 5). For clinics that reported hours of operation, we coded for evening (after 6 p.m.) or weekend (Saturday or Sunday) availability. Where indicated, we extracted the specific medications for which infusion services were provided verbatim, and coded these, iteratively and thematically, into therapeutic categories of medicines (Appendix 2, Table 5).
Analysis
We conducted a descriptive analysis on the full sample of clinics, generating crude descriptive statistics using frequencies and percentages for categorical characteristics using Excel. We conducted a directed content analysis22 to describe the characteristics of the major for-profit infusion providers operating across multiple provinces.
Results
We identified 1,097 infusion clinics across Canada that provided outpatient infusion care for at least 1 IV medication.
Providers and Funding
We identified 438 clinics (39.9%) from the websites of the 7 infusion providers identified in the 2021 CADTH report. We then identified 526 (48.0%) clinics associated with facilities in the ODHF that had evidence of outpatient infusion care. The remainder (n = 133; 12.1%), identified through structured Google searches, were companies that operated regional or local infusion clinics or clinic networks, including specialty pharmacies and professional medical, nursing, or naturopath practices as well as medical aesthetics spas.
Table 1 provides an overview of clinics by provider type and main source of funding. We classified clinics as “publicly funded” if they were operated by government health authorities or hospital organizations. Nearly half the clinics identified were operated by publicly funded health facilities or contracts (n = 524; 47.8%), including government health authorities, provincially coordinated cancer agencies (including networks of cancer centres and satellite oncology clinics), hospitals, and community health centres. Of these, 84 clinics were private home health agencies offering community nursing under provincial ministry contracts.
Table 1: Clinics by Provider Type and Source of Funding
Provider type | Clinics (N = 1,097), n (%) |
|---|---|
Privately funded (n = 573; 52.2%) | |
Company | 513 (46.8%) |
Privately held | 272 (24.8%) |
Publicly traded | 241 (22.0%) |
Professional practice | 60 (5.5%) |
Medical, naturopath | 1 (0.1%) |
Medical | 16 (1.5%) |
Naturopath | 25 (2.3%) |
Nursing | 14 (1.3%) |
Pharmacy, nursing | 2 (0.2%) |
Pharmacy | 2 (0.2%) |
Publicly funded (n = 524; 47.8%) | |
Government-contracted | 84 (7.7%) |
Hospital | 135 (12.3%) |
Hospital (alone) | 44 (4.0%) |
Hospital and cancer agency | 91 (8.3%) |
Cancer agency (alone) | 33 (3.0%) |
Health authority | 269 (24.5%) |
Provincial | 89 (8.1%) |
Provincial and cancer agency | 18 (1.6%) |
Regional | 138 (12.6%) |
Regional and cancer agency | 24 (2.2%) |
Territorial government | 2 (0.2%) |
Tribal council | 1 (0.1%) |
Approximately half the clinics identified were owned and operated by private entities and relied on private funding sources (573 of 1,097; 52.2%). Most of the privately owned and funded entities were for-profit companies (513 of 573; 89.5%). The remainder were professional practices (60 of 573; 10.5%), including medical practices, private nursing services, and naturopath practices (licensed in British Columbia to infuse iron23). In 1 case, a for-profit company operated both a privately funded national network of infusion clinics and, separately, operated infusion clinics under a provincial government contract.
Privately funded providers largely identified that services would be covered by drug manufacturers’ patient support programs, private payers, or out-of-pocket by patients; we did not find evidence that they bill public insurance for infusion services. For example, some clinics indicated that services were often covered through patient support programs or instructed patients to check with their insurers if they wished to claim reimbursement for their infusion. Clinics offering iron infusions advertised out-of-pocket costs of between $125 and $600 for the medication (e.g., Venofer or Monoferric, dosing varied), and between $100 and $350 for the infusion (noting that infusions could last between 40 minutes and 4 hours).
Geography and Setting
Figure 1 shows the distribution of infusion clinics across the provinces and territories. Only 8 clinics (0.73%) were located in the territories, 5 (62.5%) of which were publicly funded health facilities.
Figure 1: Number of Clinics by Jurisdiction and Funder Type
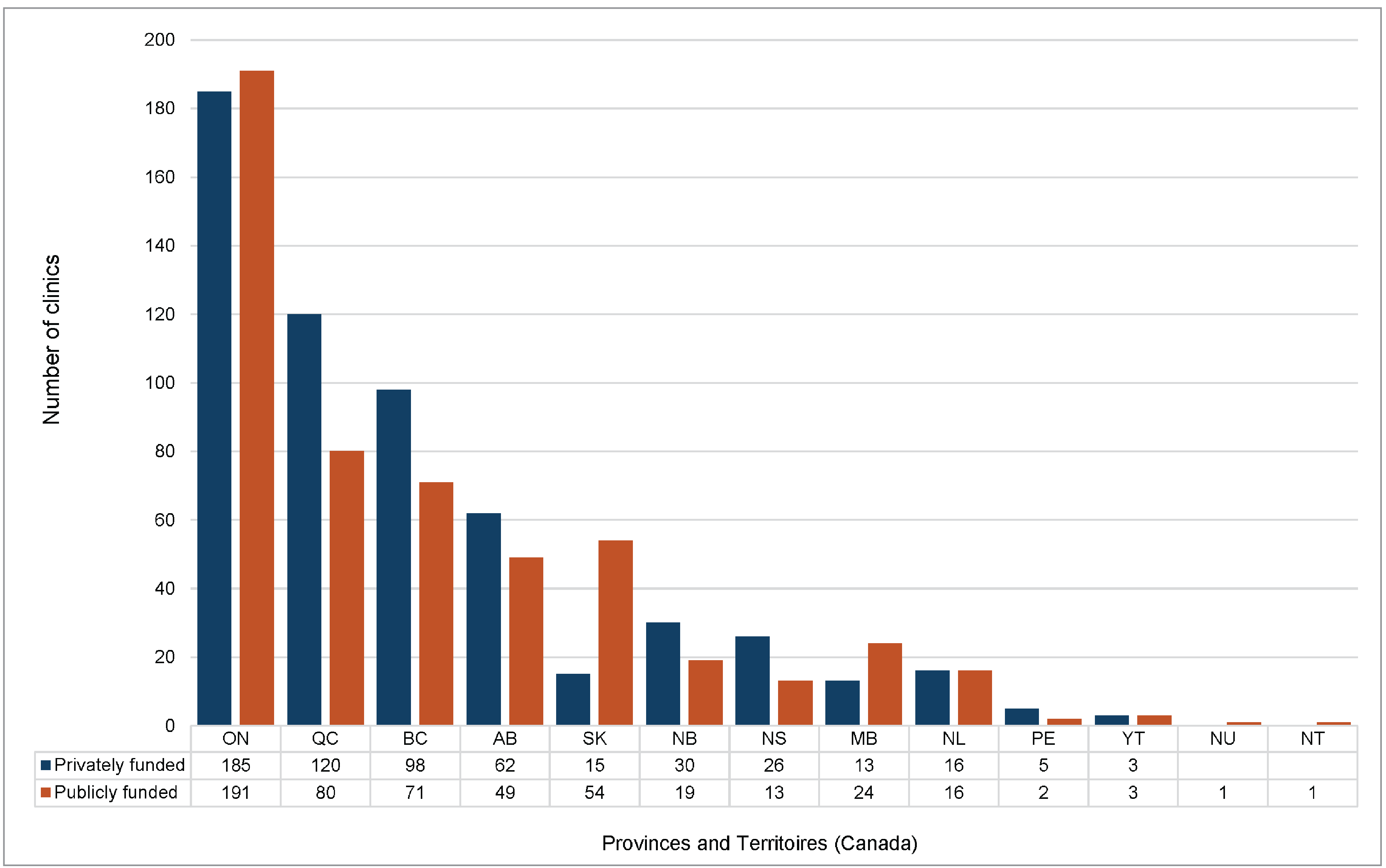
AB = Alberta; BC = British Columbia; MB = Manitoba; NB = New Brunswick; NL = Newfoundland and Labrador; NS = Nova Scotia; NT = Northwest Territories; NU = Nunavut; ON = Ontario; PE = Prince Edward Island; QC = Quebec; SK = Saskatchewan; YT = Yukon.
We identified 6 providers (Bayshore HealthCare, BioScript Solutions, Innomar Strategies, INVIVA, SRx Health, and Specialty Health Network by Shoppers) that operated clinics across multiple jurisdictions (Appendix 2, Table 6). Of these 6 providers, the 4 with the most clinics, Bayshore HealthCare, BioScript Solutions, Innomar Strategies, and INVIVA, accounted for roughly 40% of all infusion clinics in Canada (434 of 1,097; 39.6%). These 4 companies provide a suite of services across the life cycle of a medication that can include consulting on regulatory and commercialization strategies, wholesale drug distribution, and management of patient support programs.
A total of 449 of 1,097 infusion clinics (41%) were located within hospitals or cancer centres, usually medical day units, chemotherapy or systemic therapy clinics, transfusion clinics, ambulatory care clinics, or in a few cases, the emergency department. In 4 cases, a for-profit company operated an infusion clinic at a hospital address, suggesting that companies may be renting clinic spaces from the hospital. However, we found no information further specifying the nature of this relationship. Of these clinics, 42.2% (463 of 1,097) were located within a unit or suite in a medical or professional building; 12.9% (142 of 1,097) in a commercial or retail setting such as strip mall or shopping mall; and the remainder within a physician’s office, pharmacy, school, recreational centre, or a freestanding clinic building. Additionally, 88 of 1,097 clinics (8.0%) shared a street address with another infusion clinic, such as in the same building but different suites; the majority (86 of 88) of these different companies operated competing clinics within the same building.
Of the 573 clinics categorized as privately funded, 73.8% (n = 423) were located within 5 km of a hospital and 23.6% (n = 135) within 1 km. In terms of access to care, clinics were generally clustered around existing health facilities, located a median of 2.4 km from a hospital [interquartile range = 1 to 5 km), with a range of 0 km (in a hospital) to 238 km.
Amenities
All the sampled clinics offered infusion by appointment only. Only 24 clinics, all publicly funded, were oriented toward pediatric services or explicitly noted they provided pediatric infusion care. Table 2 details the amenities provided by privately funded infusion clinics that advertised on some of the companies’ clinic locator webpages (Bayshore HealthCare, BioScript Solutions, Innomar Strategies) or on individual clinic websites. Information on amenities was not fully available across the sample, with parking type and hours of operation being the most frequently detailed. Generally, publicly funded facilities provided information on amenities on a “visitor information” page that detailed parking, Wi-Fi, and food services.
Table 2: Privately Funded Clinic Amenities (N = 573)
Amenity | Amenity availability, n (%) | ||
|---|---|---|---|
Available | Not available | Missing data | |
Hours | NA | NA | 484 (84.47) |
Evening | 16 (2.8) | 73 (12.74) | NA |
Weekend | 22 (3.84) | 67 (11.69) | NA |
Parking | 332 (57.94) | 39 (6.81) | 202 (35.25) |
Free | 287 (50.17) | NA | NA |
Paid | 45 (7.69) | NA | NA |
Snacks | 212 (37.00) | 10 (1.75) | 351 (61.26) |
Wi-Fi | 192 (33.51) | 24 (4.19) | 357 (62.30) |
NA = not applicable.
Treatment Availability
Most clinics (1,033 of 1,097; 94.2%) provided some information about the types of medications for which they administered infusions; the remainder did not specify the types of infusion treatments offered (i.e., “IV therapy” or “infusion services”) (Table 3). The most frequently specified infusions were for biologics and biosimilars (566 of 1,033; 54.8%), cancer immunotherapies or hormonal therapies (512 of 1,033; 49.6%), and iron infusions (480 of 1,033; 46.5%). Infusion services for biologics and biosimilars (516 of 566; 91.2%), cancer immunotherapy (437 of 512; 85.4%), and iron infusions (265 of 480; 55.2%) were concentrated within the privately funded, for-profit infusion clinics. In contrast, publicly funded infusion clinics almost exclusively provided chemotherapy (284 of 285; 99.6%), blood and blood products (174 of 176; 98.9%), plasma-derived medicines (129 of 209; 61.7%), antibiotics (136 of 179; 76.0%), and iron infusions (215 of 480; 44.8%). Of the clinics that indicated biologic or biosimilar infusions, only 8.8% (50 of 566) were publicly funded.
Table 3: Availability of Treatments in Clinic by Therapeutic Category and Provider Type (N = 1,097)
Provider type | Clinics offering IV medication by therapeutic category, n (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Chemo-therapya | Bloodb | Plasmac | Antibiotic | Iron | Cancer therapyd | Biologice | Bonef | Steroid | Otherg | NSh | |
Privately funded | 1 | 2 | 80 | 43 | 265 | 437 | 516 | 35 | 2 | 31 | 19 |
Company | 1 | 0 | 80 | 42 | 225 | 432 | 503 | 24 | 0 | 22 | 8 |
Professional practice | 0 | 2 | 0 | 1 | 40 | 5 | 13 | 11 | 2 | 9 | 11 |
Publicly funded | 284 | 174 | 129 | 136 | 215 | 75 | 50 | 31 | 28 | 52 | 45 |
Government contractor | 0 | 0 | 3 | 82 | 83 | 3 | 3 | 0 | 0 | 2 | 1 |
Hospital | 104 | 56 | 32 | 24 | 41 | 14 | 10 | 4 | 3 | 13 | 9 |
Cancer agency | 33 | 1 | 0 | 0 | 0 | 18 | 0 | 0 | 0 | 0 | 0 |
Health authority | 146 | 116 | 93 | 29 | 90 | 40 | 37 | 27 | 25 | 36 | 35 |
Territorial government | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
Tribal Council | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
Clinics, n (%) | 285 (26.0) | 176 (16.0) | 209 (19.1) | 179 (16.3) | 480 (43.8) | 512 (46.7) | 566 (51.6) | 66 (6.02) | 30 (2.73) | 83 (7.57) | 64 (5.83) |
NS = not specified.
aChemotherapy or specific chemotherapy drug.
bWhole blood or blood components.
cImmunoglobulin or other plasma-derived medication.
dCancer therapies other than chemotherapy, such as hormonal therapies or immunotherapy.
eOriginator biologics and biosimilars for diseases other than cancer.
fBone health medicines for “osteoporosis” or “bone disorders” (e.g., bisphosphonates).
gIndicates they offer additional, unspecified medications for infusion beyond those specified.
hDoes not specify the types of infusion treatments offered.
Only 11% (124 of 1,097) of clinics identified a specific medication (product name or active pharmaceutical ingredient) for which they provided infusion services. Four patient support programs and 1 patient advocacy organization provided clinic locator tools on their websites that showed infusion services for specific brands of medications, but only for clinics operated by a few specific companies,24-28 suggesting that drug manufacturers may have exclusive agreements with particular for-profit infusion clinic networks.
Interpretation
More than half of all infusion clinics in Canada are owned and operated by private, for-profit entities with just 4 for-profit companies owning nearly 40% of infusion clinics nationally. Depending on the category of medication prescribed, a patient in Canada will receive infusion care in 1 of 2 parallel health systems; patients prescribed biologics for chronic conditions almost exclusively receive infusions in a private, for-profit health system funded by drug manufacturers through patient support programs or private payers or paid out-of-pocket by patients themselves. In contrast, publicly funded health facilities provide the majority of blood product, antibiotic, and chemotherapy infusions. We identified a similar number and geographic distribution of private infusion clinics to the 2021 CADTH report;14 however, the change in the number and variety of company owners and specific clinic addresses suggests that clinics frequently move locations or change ownership.
The largest proportion of infusion clinics in Canada are operated by 4 for-profit companies that are highly diversified in terms of the types of products and services they offer and vertically integrated in terms of owning multiple aspects of their own supply chain, providing services primarily to drug manufacturers across the life cycle of a drug. Functioning as intermediaries between patients, prescribers, payers, and drug manufacturers, these companies have created closed, and sometimes exclusive, service networks that include specialty pharmacies, patient support programs, and infusion clinics, raising concerns about anticompetitive practices and patient steering due to a lack of informed patient choice29,30 and whether, and to what extent, access to exclusive, proprietary services influences treatment decisions.31 Reliance on a small number of private companies to provide the majority of infusion care for people prescribed biologics and biosimilars poses a health system risk should companies decide to alter, scale back, or cease provision of these services, which currently have no standards requirements or public oversight.
The privately funded, for-profit infusion clinics largely cluster geographically around existing publicly funded health services and there remain critical issues with access to infusion care in the territories. Although proximity to hospitals may signal access to emergencies services in case of infusion reactions, it also suggests the need to closely examine the duplication of infusion services within the health system. Further, we identified clinics run by different providers that operated at the same address. Thus, these findings raise concerns about a duplication of services that risk straining scarce health human resources, especially related to nursing care. At the same time, there are critical gaps in access to infusion care; for example, for people living in the territories who must travel to access infusion care.32,33
Strengths and Limitations
Our 3-phased approach provides a comprehensive listing of infusion clinic locations that reflects the information available to patients, clinicians, and policy-makers. We relied on publicly available web sources to identify clinic and service information. We did not take additional steps to verify with providers whether this information was up-to-date or accurate, Thus, as a cross-sectional sample, our dataset may have missed clinic locations, and some clinics may have moved or changed their service offerings. Beyond the scope of this study, additional infusion services may be available through homecare from both publicly and privately funded providers.
Conclusion
Approximately half of all infusion clinics in Canada are owned by private, for-profit entities, funded outside the public system, with 4 companies dominating the landscape. Dependence on a small number of commercial interests for the provision of essential infusion therapy services poses health system risks should companies decide to alter, scale back, or cease provision of these services. Further research into clinic operations and care outcomes would enhance governments’ ability to adopt formal policies to ensure equitable and sustainable access to medically necessary infusion care and inform decisions about the optimal degree of private sector involvement.
References
1.Casey J. Effectiveness of scheduled vital signs assessment during infliximab infusions in detecting infusion reactions: A multi-centre retrospective data review. British Journal of Nursing. 2022;31(2):S16–S22. PubMed
2.Wu I, Lim F, Koh L. Outpatient care. In: Aljurf M, Majhail N, Koh M, Kharfan-Dabaja M, Chao N, eds. The comprehensive cancer center: Development, integration, and implementation: Springer; 2022.
3.Grant K. How a blockbuster drug tells the story of why Canada’s spending on prescriptions is sky high. The Globe and Mail 2018; https://www.theglobeandmail.com/canada/article-how-a-blockbuster-drug-tells-the-story-of-why-canadas-spending-on/.
4.Bayshore Healthcare. Infusions and injection services. 2022; https://www.bayshore.ca/services/patient-assistance-programs/infusion-and-injection/.
5.BioScript Solutions. Our services: Clinics and nursing. n.d.; https://bioscript.ca/en-CA/Our-Services/Clinics-Nursing. Accessed February 22, 2022.
6.Innomar Strategies. InnomarClinics and nursing. 2022; https://www.innomar-strategies.com/our-integrated-model/clinics-and-nursing.
7.Vincent G. Welcome to the Provis infusion clinic. n.d.; https://provisinfusion.com/.
8.McKesson CanadaF. INVIVA & Access to Care (A2C). 2022; https://www.mckesson.ca/inviva.
9.Health Canada. Biosimilar biologic drugs in Canada: Fact Sheet. 2019; https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/applications-submissions/guidance-documents/fact-sheet-biosimilars.html#a2.
10.McClean A, Law, MR, Harrison, M, Bansback, N, Gomes, T, Tadrous, M. Uptake of biosimilar drugs in Canada: Analysis of provincial policies and usage data. CMAJ. 2022;194(15):E556–E560. PubMed
11.Government of Alberta. Biosimilar drugs. 2022; https://www.alberta.ca/biosimilar-drugs.aspx.
12.Ministry of Health British Columbia. Biosimilars initiative for patients. 2021; https://www2.gov.bc.ca/gov/content/health/health-drug-coverage/pharmacare-for-bc-residents/what-we-cover/biosimilars-initiative-patients.
13.New Brunswick Department of Health. Biosimilars initiative: Information for patients. n.d.; https://www2.gnb.ca/content/gnb/en/departments/health/DrugPlans/NBDrugPlan/biosimilars/patients.html. Accessed February 22, 2022.
14.Baddeley A. Health system readiness report: The availability of privately funded IV infusion clinics in Canada. Canadian Journal of Health Technologies. 2022;2(6). PubMed
15.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke, JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLOS Medicine. 2007;4(10):e296. PubMed
16.Emmel N. Sampling and choosing cases in qualitative research: A realist approach. SAGE Publications Ltd.; 2013.
17.Patton M. Purposeful sampling and case selection: Overview of strategies and options. Qualitative research & evaluation methods: Integrating theory and practice (4th ed.): SAGE Publications; 2014.
18.Grundy Q QA, Hart D, Chaudhry S, Tavangar F, Lexchin J, Gagnon M-A, Tadrous M. Prevalence and nature of manufacturer-sponsored patient support programs for prescription drugs in Canada: A cross-sectional study. CMAJ. 2023;195(46):E1565–E1576. PubMed
19.Statistics Canada. The Open Database of Healthcare Facilities [Dataset]. 2020; https://www.statcan.gc.ca/en/lode/databases/odhf.
20.Grundy Q, Millington A, Robinson A, Held F, Fabbri A. Exposure, access and interaction: A global analysis of sponsorship of nursing professional associations. Journal of Advanced Nursing. 2022;78(4):1140–1153. Medline PubMed
21.Statistics Canada. Focus on geography series, 2021 census of population: Browse geography for New Brunswick. 2022; https://www12.statcan.gc.ca/census-recensement/2021/as-sa/fogs-spg/search-recherche.cfm?Lang=E&topic=1&GEOCODE=13.
22.Hsieh H-F, Shannon S. Three approaches to qualitative content analysis. Qualitative Health Research. 2005;15(9):1277–1288. PubMed
23.College of Naturopathic Physicians of British Columbia. Naturopathic doctors: Scope of practice standards, limits, conditions. 2024; https://cnpbc.bc.ca/wp-content/uploads/CNPBC-Restricted-Activities-Document.pdf.
24.Amgen Canada. Avsola infusion sites. https://www.avsola.ca. Accessed July 10, 2024.
25.Chron’s and Colitis Canada. Service finder: Support for you. 2019; https://crohnsandcolitis.ca/Support-for-You/Health-Service-Finder.
26.Organon Canada. Harmony by Organon infusion clinic locator: Renflexis. 2022; https://harmonyorganon.ca/en/renflexis/infusion/#infusion-clinics.
27.Pfizer Canada. Infusion clinic locator: Monoferric. 2023; https://www.monoferric.ca/clinic-locator.
28.Pfizer Canada. PfizerFlex clinic locator: Inflectra. 2024; https://www.inflectra.ca/locate-clinic.
29.Anti-competitive practices and abusive concentration in the distribution of specialty medications: Québec’s association of owner-pharmacists seeks class action lawsuit against some of its members [press release]. June 12, 2024.
30.Benchetrit J. Manulife-Loblaw deal raises questions over ties between insurance companies, big drug retailers. CBC News https://www.cbc.ca/news/business/manulife-loblaw-deal-deliver-specialty-drugs-1.7098861.
31.Prémont M-C, Gagnon, MA. Trois types de stratégies des fabricants pour la fidélisation aux médicaments de marque. Healthcare Policy. 2014;10(2):79–89. PubMed
32.Iqaluit woman has to fly south for Crohn’s disease drug. 2015; https://www.cbc.ca/news/canada/north/iqaluit-woman-has-to-fly-south-for-crohn-s-disease-drug-1.3092119.
33.MacIntyre C. Some chronic medical treatment no longer available in Dawson City, Yukon. 2023; https://www.cbc.ca/news/canada/north/chronic-medical-treatment-dawson-city-yukon-1.6975407.
Appendix 1: Author Information
Quinn Grundy, PhD, RN1; Dana Hart, MA1; Sarah Elkhalifa, BSc1; Joel Lexchin, MS, MD2,3; Marc-André Gagnon, PhD4; Navindra Persaud, MSc, MD3; Mina Tadrous, PharmD, PhD5
1Lawrence Bloomberg Faculty of Nursing, University of Toronto, Toronto, Ontario, Canada
2School of Health Policy and Management, York University, Toronto, Ontario, Canada
3Department of Family and Community Medicine, University of Toronto, Ontario, Canada
4School of Public Policy and Administration, Carleton University, Ottawa, Ontario, Canada
5Leslie Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada
Corresponding Author
Quinn Grundy
ORCID: 0000-0002-7640-8614
Address: 155 College St, Suite 130, Toronto, ON, Canada, M5T1P8
Email: quinn.grundy@utoronto.ca
Telephone: 416-978-2852
Conflicts of Interest
QG, DH, and SE declare no conflicts of interest. Joel Lexchin received payments for writing briefs about the role of promotion in generating prescriptions for 2 legal firms, is a member of the Boards of the Canadian Health Coalition and Canadian Doctors for Medicare, and he receives royalties from University of Toronto Press and James Lorimer & Company. MAG acted as an expert witness for Justice Canada on a case relating to patented drug prices. MAG was also hired as consultant for Association des Pharmaciens en Établissement de Santé du Québec (APES) and for Association Québécoise des Pharmaciens Propriétaires (AQPP). Mina Tadrous reports consulting fees from Canada’s Drug Agency, Health Canada, and Green Shield Canada.
Funding
This study was supported by the Canadian Institutes of Health Research (CIHR) Project Grant #186096 and a CIHR Undergraduate Student Research Award.
Role of Funding Source
The funders had no role in the study design; collection, analysis, and interpretation of data; or writing of the report; nor did the funder place any restrictions regarding the submission of the report for publication. The researchers were fully independent from the funders and all authors had full access to all the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Ethics Approval
This study did not include human subjects or their data and thus was exempt from ethics review per the University of Toronto Research Health Ethics Board.
Data Availability Statement
All data underlying the analysis is publicly available with no restrictions through the University of Toronto Borealis Dataverse (doi:10.5683/SP3/RXRJEK).
Contributors and Sources
Quinn Grundy conceived the idea. Quinn Grundy, Dana Hart, Joel Lexchin, Marc-André Gagnon, Navindra Persaud, and Mina Tadrous designed the study. Quinn Grundy, Dana Hart, and Sarah Elkhalifa contributed to data acquisition. Quinn Grundy and Dana Hart performed the analysis. All authors were involved in data interpretation. Quinn Grundy and Dana Hart drafted the manuscript. All authors revised it critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Appendix 2: Facility Types, Amenities, and Characteristics
Please note that this appendix has not been copy-edited.
Table 4: Included and Excluded Health Care Facility Types in ODHF
ODHF facility type | Open Database of Healthcare Facilities (ODHF) V1.1 |
|---|---|
Facility type included in search | |
Hospitals | Active acute hospital Cancer, cancer treatment centre, oncologie Cardiology Emergency Health centre Hospital, hospital – corporation, hospital site, hospital (emergency), hôpitaux, Centre hospitalier Centre hospitalier de soins généraux et spécialisés (CHSGS) General Pediatrics, children's treatment centre, pediatric Tertiary Blanks |
Ambulatory health care services | Centre local de services communautaires (CLSC) Clinic, ambulatory, outpatient community health, community health centre integrated outpatient clinic Family health team, primary care, primary care clinic, King's primary care network, nurse practitioner led clinic Medical centre, medical clinic Other Regional Blanks |
Facility type excluded from search | |
Hospitals (psychiatric) | Centre hospitalier de soins psychiatriques (CHPSY), Psychiatric, psychiatric hospital, psychiatrique |
Ambulatory health care services (diagnostic and laboratory services) | Diagnostic centre Medical laboratory |
Ambulatory health care services (episodic) | Walk-in clinic Street clinic |
Ambulatory health care services (mental health) | Mental health, mental health clinic, mental health and addiction organization, mental health and addictions |
Ambulatory health care services (public health and health systems administration) | Aids bureau Children services, nutrition Communicable disease control Environmental health Home care office Offices/Public Health, public health office, public health unit office, Health office |
Ambulatory health care services (rehabilitation) | Centre de réadaptation pour les personnes ayant des déficiences physiques auditives (CRDPA) Centre de réadaptation pour les personnes ayant des déficiences physiques langage (CRDPL) Centre de réadaptation pour les personnes ayant une déficience physique motrice (CRDPM) Centre de réadaptation pour les personnes ayant une déficience physique visuelle (CRDPV) |
Ambulatory health care services (reproductive health) | Midwifery clinic Women’s health |
Nursing and residential care facilities | Addictions services Assisted living Chronic care Centre d’hébergement et de soins de longue durée (CHSLD) Centre de réadaptation pour les personnes qui en raison de leur dépendance à l’alcool, aux drogues, aux jeux de hasard ou toute autre dépendance (CRD) Centre de réadaptation en déficience intellectuelle et en troubles envahissants du développement (CRDITED) Centre de réadaptation pour jeunes en difficulté d'adaptation (CRJDA) Centre de réadaptation pour jeunes mères en difficulté d'adaptation (CRMDA) Extended care Home care Licensed nursing home Long-term care Mental health Mental health and addiction Nursing home Private nursing home Psychiatric Psychiatrique Public care home Public nursing home Rehabilitation Residential care facility Retirement home Senior active living centre Senior’s home Shelter Soins aux malades chroniques Soins prolongés Special care Special care home |
Variable | Description | Examples |
|---|---|---|
AMENITIES | ||
Snacks | ||
Y | Any provision of food, beverages, or refreshments in the clinic (free or unspecified) | “The clinic provides coffee, tea, juice and cookies” “free refreshments and snacks” “We have drinks and snacks available for you” “our oncology department offers lunch and beverages as a courtesy” |
N | Food/beverages are not available or are paid only | If a clinic locator indicates whether snacks are provided, clinics that do not indicate snacks are recorded as not having snacks available |
No information | Information regarding food and beverages provided was unavailable. | — |
Wifi | ||
Y | WiFi available (any duration) | “wifi” “Free wifi” “1 hour free” |
N | No wifi | If a clinic locator indicates whether there is wifi, clinics that do not indicate wifi are recorded as not having wifi available |
No information | Information regarding wifi availability was unavailable. | — |
Parking | ||
Yes, free or unspecified | Free parking available (any duration) or parking available unspecified if free or paid | “Paid hourly or free parking” “Free on-site” “First 90 minutes free” |
Yes, paid | Paid parking available only | “discounted rate for cancer patients” “paid parking” |
No | No on-site parking available | “street parking” “none” |
No information | Information regarding parking availability was unavailable. | — |
Clinic hours | ||
Evening | Appointments available after 6pm | “M,W,F 8:00 a.m. to 5:00 p.m; Tu Thu 8:00 a.m. to 7:30 p.m” “Lundi, mercredi et vendredi 08:30-16:30” “Mardi 13:30-16:30 Jeudi 13:00-21:00” |
Weekends | Appointments available on Saturday and/or Sunday | “Lundi au vendredi 08:00-17:00” “Samedi, dimanche et jours fériés 08:00-12:00 et 13:00-16:00” “Mon-Sun 8am-8pm” |
No information | Information regarding was unavailable. | — |
Provider type | ||
Company Public Private | A private, for-profit entity that is either privately held or publicly traded. | Investor- or privately owned clinics Patient support program management companies Corporate pharmacy chains |
Professional practice Medical Nursing Naturopath Pharmacy | An entity primarily providing services performed by registered health professionals; typically, the services are provided through a professional corporation and/or the practice is owned by the health professional or a group of health professionals | Solo or group medical practice (primary care or specialty) Naturopath or integrated wellness practice Medical aesthetics practice or medical spa Pharmacist-owned independent pharmacy Nurse-owned private nursing service or clinic |
Health authority Provincial Regional Territorial Tribal Council | Government-established organizations responsible for health care services within a specific geographic region. | Alberta Health Services, Vitalité Health Authority, Centre intégré de santé et des services sociaux, File Hills Qu’Appelle Tribal Council, Government of Nunavut |
Provincial cancer agency | Government-established organizations coordinating cancer services within a province. | Comprehensive cancer centres Community satellite oncology clinics Regional Cancer programs |
Hospital | Health care facilities, largely with charitable organization status, that provide inpatient and/or emergency services, outpatient or ambulatory services, or long-term or residential care. | Hospitals operated by Catholic health services Academic teaching hospitals Community hospitals |
Government-contracted service provider organization | Private for-profit or not-for-profit nursing service and home care providers operating community nursing clinics under provincial ministry contracts. | Home care providers operating community nursing clinics |
Setting type | ||
Hospital | Acute care facility with inpatient beds | Hospital |
Cancer centre | Standalone facility treating people with cancer; including (but not limited to) cancer centres and community cancer clinics; may or may not have inpatient beds | BC Cancer – Centre for the North Cross Cancer Institute |
Hospital/cancer centre | The facility treats people with cancer through/with/by the provincial cancer agency but is housed within a larger hospital facility (with acute care inpatient beds) | Community oncology centres or clinics within a hospital |
Integrated facility | Long-term care or residential facility with acute care beds/inpatients | Extended care, integrated care, |
Pharmacy | Located within a pharmacy | Pharmacy |
Physician practice | Located within a physician practice/clinic/office (generalist or specialist) | Dr. X’s offices |
Medical/professional services building | An office, tower, strip containing primarily medical/professional services | Medical Arts building, medical services tower |
Commercial/retail | Located in an area that is primarily commercial or retail | Strip mall, shopping centre, shopping plaza, mall, commercial district |
Community health centre | Acute care facility with no inpatient beds | Regional health centres with no inpatient services |
Freestanding clinic | A clinic located on its own as a freestanding building, not attached to anything else | — |
Educational setting | Located with a primary or secondary school or postsecondary institution | University campus Secondary school |
Recreation centre | Located within a recreation centre | Recreation centre |
Unknown | Not enough information available to determine the setting | — |
Medication | ||
Antibiotics | IV antibiotics infused in an outpatient setting | The name of any specific antibiotics IV antibiotics, antimicrobial therapy |
Blood products | Transfusion of any whole blood or blood components | Transfusion; red blood cells; platelets; plasma; whole blood |
Plasma-derived medicines | Infusion of immunoglobulin or other plasma-derived medication | Immunoglobulin, IvIG, IG hemophilia treatments |
Iron | Provides iron infusion or iron therapy, or names a specific iron product | Iron, iron infusion Monoferric/iron isomaltoside, iron sucrose/Venofer, Ferrlecit/fer gluconate de sodium |
Bone health medicines | Provides infusions for “osteoporosis” or “bone health,” “bone disorders,” bisphosphonates | Zoledronate/zoledronic acid/Zometa/Aclasta, denosumab, teriparatide, bone health, osteoporosis, pamidronate/Aredia, bisphosphonates |
Chemotherapy | Provides chemotherapy or any specific chemotherapy drug | Chemotherapy cyclophosphamide, cytophosphane |
Cancer therapies | Cancer therapies other than chemotherapy such as hormonal therapies, monoclonal antibodies, or immunotherapy | “Cancer therapies” Firmagon/degarelix, fulvestrant, Adcetris, “immunotherapy,” “targeted therapy,” “hormonal therapy” |
Steroids | Infusion of IV steroids | methylprednisolone |
Biologics/biosimilars | Any evidence that biologics or biosimilars are infused in this setting | “biologic therapies for inflammatory autoimmune diseases such as Crohn’s Disease, Ulcerative Colitis, Rheumatoid Arthritis, Multiple Sclerosis and Psoriasis” infliximab, Tremya/guselkumab, Simponi/golimumab, Stelara/ustekinumab, Entyvio/vedolizumab |
More, unspecified | Indication that there are other meds available for infusion in addition to those listed | — |
Table 6: Characteristics of Private, For-Profit Infusion Providers Operating National Infusion Clinic Networks
Characteristic | Bayshore HealthCare | BioScript Solutions (Coverdale Clinics) | Innomar Strategies | INVIVA McKesson Canada | SRx Health Solutions | SHN by Shoppers |
|---|---|---|---|---|---|---|
Parent company | None | None | Cencora Inc. (formerly Amerisource Bergen) | McKesson Corporation | None | Loblaws, Shoppers Drug Mart |
Sibling companies/ divisions | Bayshore Home Health, Bayshore Home Care Solutions, Bayshore Specialty Rx | BioScript Pharmacy, NavieGo Patient Support Programs, A&D Wholesale, and BioScript Logistics | AvidityHealth, Cameron Stewart LifeScience (CSL) | Guardian/IDA/Remedy's Rx, Rexall Health, Medicine Shoppe Pharmacy, Uniprix, Proxim, Well.ca, Sivem, AMEGA Health | None | Wellwise by Shoppers Drug Mart, mediSystem by Shoppers Drug Mart, ACCURO Electronic Medical Records, the Health Clinic by Shoppers |
Company main activities | infusion clinic network patient support program management specialty pharmacy services wholesale drug distribution home health care and case management service provider | infusion clinic network patient support program management retail and specialty pharmacy network wholesale drug distribution | infusion clinic network patient support program management specialty pharmacy network wholesale drug distribution pharmaceutical commercialization and regulatory services and consulting pharmacovigilance solutions licensed drug importer | infusion clinic network specialty and franchise pharmacy services wholesale drug distribution drug procurement and sourcing | infusion clinic network patient support program management specialty and franchise pharmacy services wholesale drug distribution clinical trials services travel health clinics compounding services | infusion clinic network patient support program management retail and specialty pharmacy network wholesale drug distribution pharmacovigilance solutions |
Ownership structure | Privately held company | Privately held company | Publicly traded company | Publicly traded company | Privately held company (initial public offering scheduled in 2024) | Privately held company |
Clinics | Not specified | > 100 | > 165 | > 75 | 55 | Not specified |
Clinicians | Not specified | > 300 nurses | > 685 plus regional nurse educators and management team | > 300 nurses | Not specified | 3,000+ pharmacists |
Employeesa | 5,001 to 10,000 | 501 to 1,000 | 5,001 to 10,000 | 1,001 to 5,000 | 251 to 500 | 251 to 500 |
Infusion drugs | > 58 | Not specified | > 100 | Not specified | Not specified | Not specified |
Headquarters | Mississauga, ON | Moncton, NB | Oakville, ON; Conshohocken, PA, US | Saint-Laurent, QC Canada; Irving, TX, US | Toronto, ON | Mississauga, ON |
Service area | all provinces (no Labrador); no territories | all provinces (no Labrador); no territories | all provinces (incl. Labrador); Yukon territory | all provinces (no Labrador); no territories | AB, BC, ON, NS, SK | Not specified; “nationwide” |
Ownership of pharmacy networks | Yes, 11 | Yes, 13 | Yes, “in every province” | Yes, McKesson SPS Pharmacy | Yes, 35+ | 1,400+ (400+ trained on specialty medications) |
aEmployee range sourced from “Number of Employees” listed for each company on Crunchbase.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.