Drugs, Health Technologies, Health Systems
Peer-Reviewed Article
Severity Weighting of Quality-Adjusted Life-Years for Economic Evaluation: What, How, and Where Next?
Shehzad Ali, Alexander Haines, Karen Lee
Abstract
Some health technology assessment (HTA) agencies have implemented methods to incorporate severity weighting into their health economic evaluations. This process involves 2 steps: defining severity (to help identify disease areas we may value interventions in more), and valuing severity (so health gains can be given more weight in populations with “severe” disease). This paper reviews evidence on societal preferences for prioritizing severity, the methods used by HTA agencies to implement severity weighting, and the gaps requiring attention for effective implementation.
A case for severity weighting has been made based on societal concern for health-related suffering and the preference to reduce “unfair” variations in lifetime health among individuals. Our umbrella review identified 2 systematic reviews on societal concern for disease severity in decision-making, each including 19 studies. There was notable heterogeneity in the definitions of severity and the methods for eliciting preferences. Most studies indicated a willingness to sacrifice some level of aggregate health to prioritize the severely ill. Few studies were conducted within Canada.
HTA agencies commonly use the absolute shortfall (AS) and proportional shortfall (PS) measures to quantify disease severity. These measures differ in their impact on reimbursement decisions related to younger and older patients, chronic conditions, and the end-of-life period. The shortfall measures are used in conjunction with “decision modifiers” that increase the value of quality-adjusted life-year (QALY) gains for conditions that qualify for a severity premium. In the UK, the modifier value ranges from 1 to 1.7, while in the Netherlands and Sweden, it ranges from 1 to 4.
Further research is needed to better understand societal values regarding severity and the appropriate weighting of disease severity in economic evaluations. Current approaches are jurisdiction-specific and may require validation before being applied to other HTA settings.
For author information, refer to Appendix 1.
Introduction
Economic evaluations are used to inform decision-making in many publicly funded health systems, including Canada.1,2 Health Technology Assessment (HTA) agencies, including Canada’s Drug Agency (CDA-AMC) and the National Institute for Health and Care Excellence (NICE), have produced guidelines for best practices in conducting economic evaluations to inform decision-making.1,3 HTA agencies recommend using cost-utility analysis (CUA), a type of cost-effectiveness analysis, to inform HTA decisions. In a CUA, the health effects are quantified using quality-adjusted life-years (QALYs), which incorporate both the length of life (survival) and the quality of life (QoL), with the latter valued between 0 (death) and 1 (full health).4,5 In this framework, health gains and losses are weighted equally across individuals, disease types, and severity. One proposed objective is to maximize total population health (measured in QALYs) given available resources (health maximization). When it comes to health gains, the approach assumes that “a QALY is a QALY,” irrespective of who receives the health gains.6 This distributive neutrality implies that all QALYs have equal value to the decision-maker (i.e., social value), which has been argued to be impartial as the decision-maker is indifferent between health conditions and situational factors.7,8
A Case for Severity Weighting
The health maximization approach of the CUA framework focuses on the absolute health gains attributable to technologies under investigation. As such, this approach is agnostic to the pre-intervention level of QoL (i.e., disease severity). For example, if a treatment improved an individual’s QoL from 0.7 to 0.9 (a return to near-perfect health), this would be valued the same as a treatment that improved QoL from 0.1 to 0.3 (very low to low QoL).
In the HTA literature, a moral case is sometimes made for prioritizing treatments for severe conditions by valuing the health gains higher than those of treatments for less severe conditions.9,10 Often, the most common argument is that society places a higher value on health gains in patients experiencing a greater level of suffering. Consequently, prioritizing resources based on disease severity represents a “compassion premium” for individuals enduring severe and progressively worsening illnesses that impose substantial burden of morbidity, mortality, or both.11
Another argument is based on societal concern for reducing “unfair” variation in lifetime health between individuals, insofar as it is considered unfair for people to lead relatively short and unhealthy lives due to the premature onset of severe illness, in relation to the average lifetime health expectancy of the population in the jurisdiction.12 Finally, in many cases, individuals experiencing severe health conditions — such as those receiving palliative care — may have a relatively low capacity to benefit from treatment in terms of health improvements, which may make it less likely for treatments for severe conditions to be cost-effective.
Objectives
The overall aim of this paper is to introduce and critically appraise the concepts and methods used for severity weighting of QALYs in economic evaluations. Specific objectives are to thoroughly examine the following: the existing evidence on societal preferences for severity weighting of health outcomes; the common approaches used by HTA agencies to quantity disease severity; the approaches used to operationalize severity weighting for decision-making and their impact on the cost-effectiveness thresholds; and current knowledge gaps and recommendations for future research. The first objective was implemented by conducting a targeted literature search of Canadian studies, while the other objectives were informed by HTA guidelines of the countries that have implemented severity weighting in practice.
Evidence on Societal Preference for Severity Weighting of QALYs
For a value principle to be incorporated into economic evaluation, it must demonstrate “social legitimacy” (i.e., it should be supported by empirical evidence on societal value judgments). Several studies have investigated societal preferences to consider disease severity in decision-making. We conducted a targeted umbrella review (i.e., a review of reviews) to identify key studies that evaluated societal preferences for severity weighting. The search strategy was based on Gu et al. (2015)13 and included the following terms: resource allocation, health system rationing, health priorities, technology assessment, drug approval, reimbursement decision, preferences, trade-offs, societal values, and distributional weight. The search was conducted in Ovid MEDLINE on June 12, 2024, with no date restriction. The complete search strategy can be found in the supplementary appendix of Gu et al. (2015). We further limited the search to systematic reviews. Reviews were included if they met the following inclusion criteria: they were systematic reviews and/or meta-analyses, they investigated societal preferences for considering disease severity in resource allocation decisions, and they included studies using quantitative methods involving trade-offs. Reviews were excluded if they were not in English or French, or if they did not sample from the general population. Data extraction was conducted by the first author and included information on the study design, setting, severity definition, and findings of societal preferences. The initial search yielded 199 studies. Titles and abstracts of these studies were screened, and relevant articles received full-text screening (n = 10). Only 2 systematic reviews met the inclusion criteria: Gu et al. (2015) and Shah et al. (2009). Both reviews identified 19 studies each, with significant overlap. In general, these studies evaluate willingness to trade larger health gains in less severe conditions with smaller gains in more severe conditions. While there is significant heterogeneity among studies in the definition of severity and methodological design, the results broadly support giving greater weight to health gains in more severe conditions than less severe ones.13-15
Gu et al. (2015)13 identified 19 studies, the majority of which used a discrete choice experiment (DCE) or a person trade-off design. Severity was defined as QoL (loss) if untreated (52.2%), life expectancy if untreated (17.4%), and pre-treatment health problems (30.4%). The majority of studies (16 of 19) found that the general public was inclined to assign higher priority to patients with more severe diseases; 2 of these studies (Dolan and Shaw [2003]16 and Diederich et al. [2012]17) reported that participants ranked disease severity as the most important attribute for health care priority setting. The remaining studies (3 of 19) found either a small preference or no preference at all for severity, including Lancsar et al. (2011),18 which reported preference for health maximization over severity weighting. Gu et al.13 also investigated distributional weights for disease severity as reported in the literature. Four of 19 studies reported severity weights, but their relevance and utility are questionable due to heterogeneity in the definition of severity.
Shah et al. (2009) included 19 studies in their systematic review, with many also included in Gu et al. (2015). Shah et al. also found that, on the whole, participants in the majority of studies were willing to sacrifice at least some level of aggregate health to prioritize resources for the severely ill; however, the level of sacrifice varied across studies. Two studies — Dolan (1998)19 and Dolan and Cookson (2000)20 — found evidence for a threshold effect (i.e., participants were willing to favour the severely ill up to a certain point, beyond which they switched to health maximization). Shah et al. (2009) also noted that the definition of severity varied across studies. Most studies described it in terms of the pretreatment health state, while some defined it based on the level of need for health care.
Gu et al. (2015)13 did not identify any studies conducted in Canada addressing the valuation of disease severity for priority setting; however, Shah et al. (2009)21 identified a study by Abelson et al. (1995)22 that employed a ranking exercise to compare decision-making criteria for resource allocation in Canada. This study found that severity, defined as health care need, was ranked the most important criterion by the general population, health care workers, and policy-makers.
Further studies were identified through forward citation searching of the included systematic reviews. One study conducted in recent years in Canada was identified. Skedgel et al. (2015)23 conducted a DCE to investigate the welfare effects of prioritizing resources for severe health states. They found that respondents did not prioritize resource allocation based on baseline disease severity. Additionally, they reported negative preference for prioritizing older patients and those with short life expectancy (i.e., those close to the end of life). This contrasts with a small study (N = 32) conducted in Alberta by Stafinski et al. (2017)24 using 2 citizens’ juries that deliberated on priority setting for cancer treatments. They found general support for funding technologies benefiting the most severely ill patients (defined as those who are unable to perform daily activities or who are experiencing extreme pain or depression) and those facing imminent death.
A recent study by Lancsar et al. (2020)14 identified nuances of severity-related prioritization. In their DCE study of 1,000 Australian participants, they investigated societal values in relation to QALY gains produced purely by gains in survival, improvements in QoL, or changes in both. They found that, all else being equal, when a treatment improves only QoL without improving survival, the same QoL improvement is valued more in patients with severe health problems (defined as those with a QoL of 30% of full health) than in patients with nonsevere health conditions (where moderate health problems were defined as 60% of full health or mild health problems at 90% of full health). However, in cases where a treatment extends life or extends life while also improving QoL, the QALY improvement is valued most in patients with moderate health problems. Lancsar et al. (2020) suggest that this may relate to the idea of thresholds such that health gains above certain thresholds can significantly impact individuals’ lives, such as enabling them to return to work. For example, an individual who has moderate health problems may not be able to work due to health concerns, meaning a small improvement in their health could have a substantial impact on their life. However, this threshold effect needs further investigation.
One of the largest Canadian studies, conducted by Rizzardo et al. (2019),15 included an online sample of 2,539 adults who were tasked with ranking 13 values to prioritize drug funding. Disease severity, defined as “how severe or serious the disease is and its effect on quality and quantity of life,” was ranked as the fourth-highest priority by respondents. The ranking placed severity after treatment safety, impact on ability to work, and potential effect on QoL. Interestingly, severity was ranked higher than the impact of intervention on life extension, which was placed fifth in the rankings.
In summary, there is notable heterogeneity in the evidence regarding the prioritization of disease severity. In the Canadian context, while the literature is limited, more studies support considering disease severity for resource allocation than those that do not. However, there has been limited work done to quantify the magnitude of severity weight which is crucial to determine the size of a modifier to prioritize severe diseases. Recently, NICE has recommended further research to quantify severity trade-off weights for the UK population. Similar research is needed in Canada to determine country-specific values for prioritizing disease severity in resource allocation decisions. Such studies will go beyond simple ranking exercises to explicitly quantify trade-offs, which can then be used in economic models.
Quantifying Disease Severity in Practice: The Shortfall Approach
There are various methods to conceptualize and quantify severity of illness,25 but the most common conceptualization relates to the expected loss of future health due to the disease, with higher losses indicating greater severity. This approach integrates both life expectancy and QoL (captured using QALYs) and adjusts for age and sex. In practice, 2 approaches — the AS and PS — are being considered or used by HTA agencies to measure severity.26,27
The Shortfall Approach: Definitions
The AS approach: The AS approach represents the total quantity of future health expected to be lost due to the health condition. The AS value is calculated as the absolute difference between the expected QALYs without the condition, given the age and sex of the individual (A in Figure 1), and the QALYs experienced with the condition under the standard of care (B in Figure 1). For example, consider an individual who has experienced 40 QALYs thus far and would have experienced another 20 QALYs if they did not have the disease under consideration. Because of the disease, their remaining QALY expectancy is reduced from 20 to 5. The AS attributable to the disease is 15 QALYs (i.e., 20 minus 5). The minimum value of AS is zero, representing a person whose expected QALYs with the disease equal the expected QALYs without the disease in the general population (i.e., no loss of QoL or length of life). The maximum value of AS applies to a patient who faces imminent death and equals the expected number of QALYs in the general population without the disease.
Figure 1: Diagrammatic Representation of Absolute and Proportional Shortfall
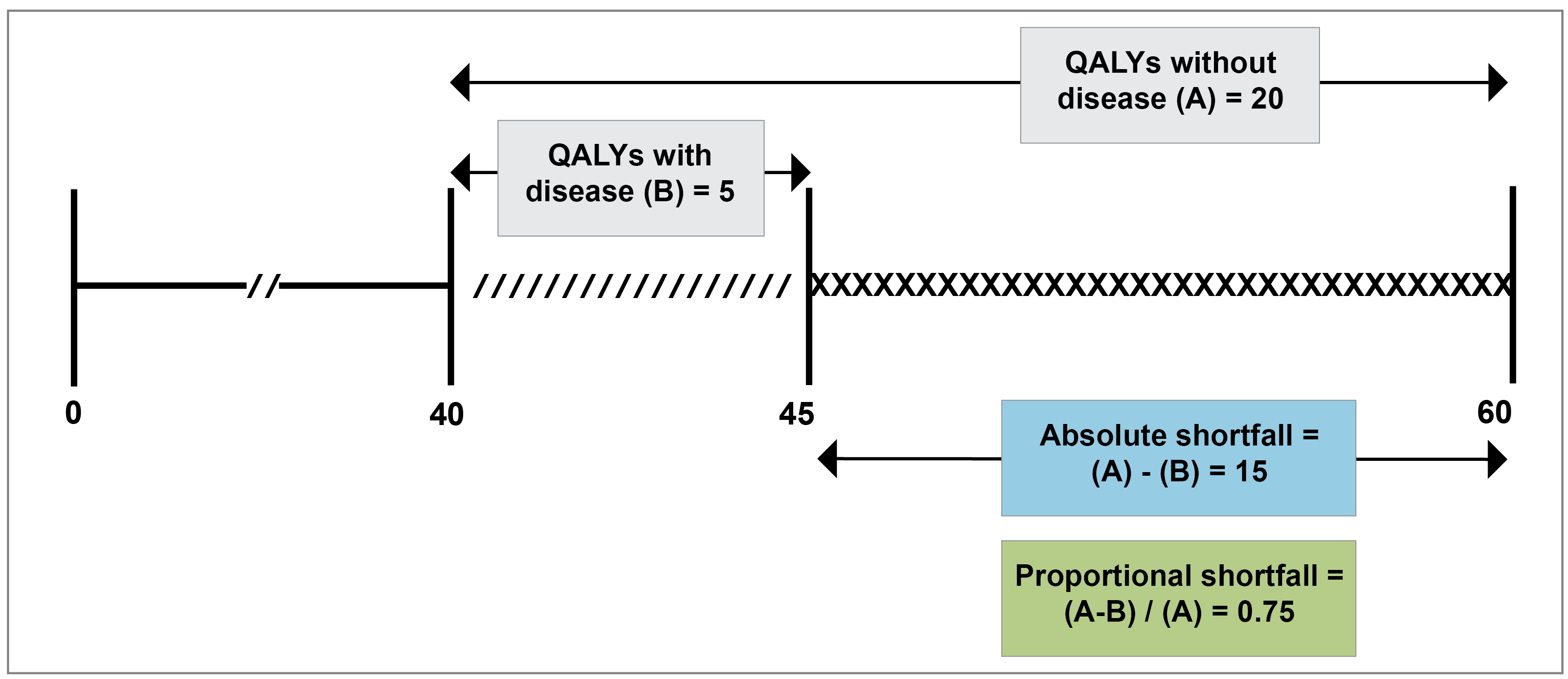
QALY = quality-adjusted life-year.
The PS approach: The PS measure represents relative future health loss and is computed as a ratio of the AS and the expected QALYs without the disease (Figure 1): PS = (A-B)/A. Following the example in Figure 1, the PS attributable to the disease is 0.75 (i.e., 15 QALYs [AS] divided by 20 QALYs [expected QALY without the disease]). The minimum value of PS is zero, which applies to a person with no AS (i.e., their expected QALYs are the same as the general population without disease). The maximum value of PS is 1, which would apply to a patient who faces imminent death (i.e., AS is equal to QALYs without the disease). Table 1 presents a summary of the calculation, interpretation, and limitations of the shortfall measures.
Implications of the Shortfall Approach
The use of severity weighting will benefit some patient groups more than others. The AS measure is based on the expected QALYs without the disease, and as such gives priority to diseases that occur in younger patients. Diseases that occur later in life have a smaller AS and therefore receive a lower weight, because patients have less future health to lose. This can put older patients at a disadvantage.28 The PS measure overcomes this by using relative health loss in relation to the remaining QALYs without the disease. However, critics of the PS approach point out that it unduly favours older patients even when they experience the same illness and prognosis as younger patients.
The shortfall approach also has implications for HTA decisions related to end-of-life interventions.29,30 The PS measure gives a greater weight to terminal illnesses; this is because PS increases as patients approach death, reaching the maximum value of 1 when death is imminent. Another point of discussion relates to how the shortfall approach treats chronic health conditions. The PS measure assigns a lower value to chronic conditions compared to life-threatening conditions. As a result, chronic conditions, such as asthma and rheumatoid arthritis, would receive a lower PS value in an HTA analysis, compared to most cancers.31 On the other hand, the AS measure may assign a higher value to a chronic condition in a younger patient than a life-threatening condition in an older patient. The ethical implications of employing these measures to inform resource allocation needs further investigation.
Table 1: Summary of the Calculation, Interpretation, and Some Considerations of Using the AS and PS Measures for QALY Weighting
Item | Absolute shortfall | Proportional shortfall |
|---|---|---|
Calculation | The absolute difference between the expected QALYs without the condition and the QALYs experienced with the condition under standard of care. | Ratio of the expected QALY loss due to the disease and the expected QALYs without the disease. |
Interpretation | Presented as an absolute number with higher values indicating a larger impact of the condition. | Presented as a value between 0 and 1, with 0 implying no impact of the condition and 1 implying imminent death from the condition. |
Implications |
|
|
AS = absolute shortfall; PS = proportional shortfall; QALY = quality-adjusted life-year.
Alternative conceptualizations of severity have been investigated in the literature, including pretreatment QoL, QoL if untreated, and life expectancy if untreated.13,21 These measures of severity are limited, as they do not consider both the duration of life and QoL; this has resulted in convergence across HTA bodies on the use of the shortfall approach.26
Operationalizing Severity Weighting: The Decision Modifier
Considerations for disease severity can be incorporated into decision-making using an explicit approach or an implicit, deliberative process. The latter allows for contextual flexibility but can affect consistency and transparency of decision-making and can create opportunities to influence decisions.26 The explicit approach, considered by HTA agencies such as NICE and Zorginstituut Nederland (ZIN) for example, can — at least in principle — overcome some of these challenges.
In 2022, NICE replaced the end-of-life weights with severity weights. The approach for severity weighting is based on explicit categories of weights, called the “decision modifiers,” based on shortfall values associated with the health condition under evaluation (Table 2).32 The decision modifier is applied to the cost-effectiveness threshold to reflect a higher value (or willingness to pay) for incremental QALYs in patients with severe health conditions. Table 2 shows the AS and PS value ranges and the corresponding QALY modifier used in the UK. A modifier greater than 1 would be applied to the willingness-to-pay threshold if either the AS is greater than or equal to 12 QALYs or the PS is greater than or equal to 0.85. The weighting approach uses either the AS or PS value for the condition, whichever is higher, to determine the relevant modifier to be applied. For instance, if the PS value is less than 0.85 (with a corresponding QALY weight of 1) and the AS value is 14 (with a QALY weight of 1.2), then a modifier of 1.2 will be used. If either the AS or PS value is at the cut-off mark of the range (e.g., a PS value of 0.95), then the higher of the 2 modifier values would be applied.
Table 2: Decision Modifier Based on the Proportional and Absolute Shortfall Values in the UK
Proportional shortfall | Absolute shortfall (QALYs) | QALY weights or decision modifier (and the resulting effective threshold)b |
|---|---|---|
< 0.85 | < 12 | 1 (£30,000/QALY) |
0.85 to 0.95 | ≥ 12 and < 18 | × 1.2 (£36,000/QALY)a |
≥ 0.95 | ≥ 18 | × 1.7 (£51,000/QALY)a |
QALY = quality-adjusted life-year.
aThese modifiers apply if either the proportional shortfall criteria or absolute shortfall criteria are met.
Source: https://www.nice.org.uk/process/pmg36/chapter/committee-recommendations.
HTA jurisdictions use different numbers of ranges and weights for decision modifiers. There is a trade-off between using large severity weights applied to a small set of severe conditions versus small weights applied to a larger set. In the UK, NICE determined the severity weights by taking an “opportunity cost neutral” approach in relation to the end-of-life criterion (i.e., the weights previously applied to incremental QALYs for end-of-life treatments were reallocated to those for severe diseases such that the overall expected impact on reimbursement is cost neutral.)33
In the Netherlands, Zorginstituut Nederland (ZIN)34 adjusts the cost-effectiveness threshold based on PS to give greater weight to more severe conditions (Table 3). Three categories of PS are used: 0.1 to 0.4, 0.41 to 0.70, and greater than or equal to 0.71, with cost-effectiveness thresholds of €20,000 per QALY, €50,000 per QALY, and €80,000 per QALY, respectively. The lower threshold value of €20,000 per QALY was based on the cut-off value established for vaccines in the Netherlands' National Vaccination Program and used to assess preventive interventions. The higher threshold value of €80,000 per QALY was derived from life insurance estimates provided by the Council for Public Health and Health Care (RVZ).
In Norway, the Ministry of Health uses the AS approach to define 6 classes of severity, ranging from a shortfall of 0 to 3.9 QALYs to 20 or more QALYs (approximately 4 QALYs in each class, except for the final or open class). The corresponding cost-effectiveness threshold ranges from NOK 275,000 to NOK 825,000, and relative weights increase by 0.4 in each successive class.35 The lowest threshold value (NOK 275,000) was determined based on the estimated cost per QALY of interventions displaced in the lowest severity group. The highest value, set at 3 times the lowest (NOK 825,000), was recommended by the committee as consistent with standard practice in Norway. Relative weights were then assigned incrementally across severity groups, ranging from 1 for the lowest class to 3 for the highest class.
Sweden defines 4 categories of disease severity and the relevant cost-effectiveness thresholds: most severe (threshold of SEK 1,000,000), severe (threshold of SEK 750,000), moderate (threshold of SEK 500,000), and least severe (threshold of SEK 250,000).36 These categories then attract relative weights (multiplied by 2, 3, and 4 for the moderate, severe, and most severe categories, respectively) in relation to the least severe level. Explicit criteria used to define classes of severity were not available.
Table 3: Cost-Effectiveness Threshold Modifiers Used in the Netherlands and Norway
Proportional shortfall | Absolute shortfall (QALYs) | Cost-effectiveness threshold | Implied weight |
|---|---|---|---|
Netherlands: the Dutch National Health Care Institute (Zorginstituut Nederland) | |||
0.1 to 0.40 | Not used | €20,000 | 1 |
0.41 to 0.70 | €50,000 | × 2.5 | |
≥ 0.71 | €80,000 | × 4.0 | |
Norway Ministry of Health | |||
Not used | 0 to 3.9 | NOK 275,000 | 1 |
4 to 7.9 | NOK 385,000 | × 1.4 | |
8 to 11.9 | NOK 495,000 | × 1.8 | |
12 to 15.9 | NOK 605,000 | × 2.2 | |
16 to 19.9 | NOK 715,000 | × 2.6 | |
≥ 20 | NOK 825,000 | × 3 | |
NOK = Norwegian krone; QALY = quality-adjusted life-year.
Source: Rapport fra arbeidsgruppe nedsatt av Helse- og omsorgsdepartementet;35 Barra et al. 2020.36
Where Do We Go From Here?
To develop further understanding of severity weighting and its implications for the Canadian HTA context, we recommend the following next steps.
Consultation With Parties of Interest
An important early step would be to conduct formal consultations with parties of interest, including (but not limited to) the industry, drug plans, patient and citizen groups, and academic experts. NICE conducted such consultations by first developing an initial proposal discussing the scope of severity weights and potential changes to the Methods Guide. Parties of interest were asked to provide written feedback on this proposal, which was used to revise the scope and strategies for severity weighting. A similar iterative process can be considered in Canada to inform how severity is operationalized in HTA decision-making and to understand potential concerns over the impact of decision modifiers. Another aspect involves assessing the readiness of the HTA system to implement severity weighting. Parties of interest must be well informed about the implications of this change. Having the necessary data, such as utility values, is also crucial for effectively applying severity weighting.
Eliciting Societal Preferences on Severity Weighting
As discussed, there is limited Canadian evidence on societal values regarding severity weighting. This research is critical to understanding the degree to which society favours allocating resources to severe diseases and the willingness to accept displacement of health benefits when trade-offs are involved. This work will produce quantitative weights to be considered as decision modifiers. In the absence of this evidence, it might not be appropriate to base a severity premium on arbitrary values (or the weights used in other HTA jurisdictions).
Societal values are typically elicited using choice experiments involving the general public. One potential challenge relates to the methodology of value elicitation. Previous research has found significant heterogeneity in elicited values, which is explained (among other factors) by differences in the design of valuation exercises, framing effects, cognitive bias, and sampling approaches.13,37-39 Innovative designs should be considered to overcome these challenges.
Understanding the Opportunity Cost of Severity Weighting
An opportunity cost analysis is important to understand the potential impact of introducing a decision modifier. Such analysis would explicitly examine the trade-offs involved in prioritizing treatments for severe conditions (i.e., how funding new technologies and services based on a severity modifier might displace health care across the system). This reallocation entails opportunity costs in terms of health foregone due to displaced services. NICE conducted the opportunity cost analysis to evaluate a range of options for severity weights with the intention of keeping the weight allocation ”opportunity cost neutral” in relation to the end-of-life criterion being used at the time.40
The opportunity cost analysis would help identify conditions and technologies that might qualify for a severity premium, quantify the budget impact on the health system, and identify the interventions or conditions that might be displaced or down-weighted by the introduction of severity weights. This analysis can be undertaken by using previous technology appraisals conducted by CDA-AMC to understand the expected distribution of conditions or treatments that might qualify for a severity premium based on different decision modifiers.
Discussion
Severity weighting has gained significant momentum in the last decade. This is primarily motivated by ethical arguments of compassion for people who are unwell with a severe illness, and the societal concern for reducing “unfair” variation in lifetime health between individuals. This paper has laid out the main approaches for severity weighting that are currently being used, their implications and key considerations to inform the way forward.
A common mechanism to quantitatively incorporate severity weighting in HTA analysis is the shortfall approach. Three approaches are currently used in practice: the Norway model, based on AS only; the Netherlands model, based on PS only; and the NICE approach in the UK, which considers both AS and PS measures and uses the higher of the 2 values. Several considerations should be made when using shortfall measures, as they may prioritize 1 group over another. Compared to PS, the AS measure tends to prioritize allocation to early-life health conditions, when patients have more health stock to lose. This measure can, however, disadvantage older people. The PS measure reduces dependence on age of onset by using relative health loss, but may unduly favour older patients even when they experience the same illness and prognosis as a younger patient. PS is also relatively insensitive to the magnitude of health loss. However, PS allows for the inclusion of end-of-life considerations. The NICE approach can safeguard against the challenges of using AS or PS measures alone but has a high opportunity cost, as it widens the net and will allow more technologies to qualify for the severity premium.
Another consideration relates to how decision modifiers (i.e., the explicit categories of weights) are defined to implement the shortfall approach. HTA jurisdictions vary in terms of the categories of decision modifiers and the magnitude of severity weights. The number of categories varies between 3 (used by Norway and the UK) and 6 (used by the Netherlands). The range of weights from the lowest to highest varies from 0.7 (1 to 1.7 in the UK) to 3 (1 to 4.0 in Norway). NICE’s approach requires an expected health loss of at least 12 QALYs to qualify for AS-based weighting; for Norway, the minimum expected loss is 4. For PS, NICE’s modifier requires a value of at least 0.85 compared to the Netherlands value of 0.41. However, these categories and weights are not informed by societal preferences but by pragmatic resource allocation decisions; for instance, NICE’s decision is based on an opportunity cost neutral approach, relative to the previously used end-of-life criterion. This shows that any approach is tailored to the jurisdiction to which the severity weight is being applied. If another country’s approach to severity weighting is copied, this may make implementation and uptake of severity weighting challenging as it may not meet the needs or preferences of patients and decision-makers in Canada. Of note, the pan-Canadian Pharmaceutical Alliance (pCPA) has mentioned disease severity in discussing the pricing of products eligible through their Temporary Access Process program.41 This shows there is an appetite to use severity weighting within the Canadian landscape.
In conclusion, to consider severity weighting for HTA decision-making in Canada, further groundwork is needed to better understand societal values on distributional trade-offs between severe and nonsevere conditions, considerations for parties of interest in relation to decision modifiers, and the opportunity cost of interventions that might be displaced by severity weights. This work will require collaboration with decision-makers and patients within Canada to ensure the approach is fit for purpose and is implementable.
References
1.Sharma D, Aggarwal AK, Downey LE, Prinja S. National healthcare economic evaluation guidelines: a cross-country comparison. PharmacoEconomics-Open 2021; 5: 349-64. PubMed
2.Torbica A. HTA around the world: broadening our understanding of cross-country differences. Value in Health 2020; 23(1): 1-2. PubMed
3.CADTH. Guidelines for the Economic Evaluation of Health Technologies: Canada. Canada: CADTH, 2021.
4.Weinstein MC, Torrance G, McGuire A. QALYs: the basics. Value in health 2009. PubMed
5.Whitehead SJ, Ali S. Health outcomes in economic evaluation: the QALY and utilities. British medical bulletin 2010; 96(1): 5-21. PubMed
6.Weinstein MC. A QALY is a QALY is a QALY—or is it?: North-Holland; 1988. p. 289-90.
7.Schwappach DL. Resource allocation, social values and the QALY: a review of the debate and empirical evidence. Health Expectations 2002; 5(3): 210-22. PubMed
8.Bobinac A, van Exel NJA, Rutten FF, Brouwer WB. Inquiry into the relationship between equity weights and the value of the QALY. Value in Health 2012; 15(8): 1119-26. PubMed
9.Nord E. Concerns for the worse off: fair innings versus severity. Social science & medicine 2005; 60(2): 257-63. PubMed
10.Cookson R, McCabe C, Tsuchiya A. Public healthcare resource allocation and the Rule of Rescue. Journal of medical ethics 2008; 34(7): 540-4. PubMed
11.NICE. Responses to TA Methods Addendum Public Consultation, 2014.
12.Ottersen T, Mæstad O, Norheim OF. Lifetime QALY prioritarianism in priority setting: quantification of the inherent trade-off. Cost Effectiveness and Resource Allocation 2014; 12(1): 1-10. PubMed
13.Gu Y, Lancsar E, Ghijben P, Butler JR, Donaldson C. Attributes and weights in health care priority setting: a systematic review of what counts and to what extent. Social Science & Medicine 2015; 146: 41-52. PubMed
14.Lancsar E, Gu Y, Gyrd-Hansen D, et al. The relative value of different QALY types. Journal of Health Economics 2020; 70: 102303. PubMed
15.Rizzardo S, Bansback N, Dragojlovic N, et al. Evaluating Canadians’ values for drug coverage decision making. Value in Health 2019; 22(3): 362-9. PubMed
16.Dolan P, Shaw R. A note on the relative importance that people attach to different factors when setting priorities in health care. Health expectations 2003; 6(1): 53-9. PubMed
17.Diederich A, Swait J, Wirsik N. Citizen participation in patient prioritization policy decisions: An empirical and experimental study on patients' characteristics. PLoS One 2012; 7(5): e36824. PubMed
18.Lancsar E, Wildman J, Donaldson C, Ryan M, Baker R. Deriving distributional weights for QALYs through discrete choice experiments. Journal of health economics 2011; 30(2): 466-78. PubMed
19.Dolan P. The measurement of individual utility and social welfare. Journal of health economics 1998; 17(1): 39-52. PubMed
20.Dolan P, Cookson R. A qualitative study of the extent to which health gain matters when choosing between groups of patients. Health Policy 2000; 51(1): 19-30. PubMed
21.Shah KK. Severity of illness and priority setting in healthcare: a review of the literature. Health policy 2009; 93(2-3): 77-84. PubMed
22.Abelson J, Lomas J, Eyles J, Birch S, Veenstra G. Does the community want devolved authority? Results of deliberative polling in Ontario. CMAJ. 1995; 153(4): 403. PubMed
23.Skedgel C, Wailoo A, Akehurst R. Societal preferences for distributive justice in the allocation of health care resources: a latent class discrete choice experiment. Medical Decision Making 2015; 35(1): 94-105. PubMed
24.Stafinski T, Menon D. Explicating social values for resource allocation decisions on new cancer technologies: We, the jury, find⋯. Journal of Cancer Policy 2017; 14: 5-10.
25.Johansson KA, Coates MM, Økland J-M, et al. Health by disease categories. Distributional cost-effectiveness analysis: Quantifying health equity impacts and trade-offs 2020: 105.
26.Skedgel C, Henderson N, Towse A, Mott D, Green C. Considering Severity in Health Technology Assessment: Can We Do Better? Value in Health 2022; 25(8): 1399-403. PubMed
27.Tranvåg EJ, Haaland ØA, Robberstad B, Norheim OF. Appraising Drugs Based on Cost-effectiveness and Severity of Disease in Norwegian Drug Coverage Decisions. JAMA Network Open 2022; 5(6): e2219503-e.
28.Stolk EA, van Donselaar G, Brouwer WB, Busschbach JJ. Reconciliation of economic concerns and health policy: illustration of an equity adjustment procedure using proportional shortfall. Pharmacoeconomics 2004; 22: 1097-107. PubMed
29.Altmann S. Against proportional shortfall as a priority-setting principle. Journal of Medical Ethics 2018; 44(5): 305-9. PubMed
30.Shield A, Oshin L, Heer S, Maruszczak M. EE117 Understanding the Expected Severity Modifiers Across Diseases Following Changes to NICE Methodology. Value in Health 2022; 25(12): S76.
31.Sinha A, Howard D, Thurgar E. HTA37 The NICE Disease Severity Modifier: A Retrospective Analysis on Its Potential Impact on Previous Reimbursement Decisions in England. Value in Health 2022; 25(12): S303.
32.NICE. NICE health technology evaluations: the manual. 2022. https://www.nice.org.uk/process/pmg36/chapter/committee-recommendations (accessed 2023.
33.NICE. Review of methods for health technology evaluation programmes: proposals for change. 2021. https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/chte-methods-and-processes-consultation.
34.nederland Z. Cost-effectiveness in practice, 2015.
35.prioritering PraAo. Rapport fra arbeidsgruppe nedsatt av Helse- og omsorgsdepartementet, 2015.
36.Barra M, Broqvist M, Gustavsson E, et al. Severity as a priority setting criterion: setting a challenging research agenda. Health Care Analysis 2020; 28(1): 25-44. PubMed
37.Ali S, Tsuchiya A, Asaria M, Cookson R. How robust are value judgments of health inequality aversion? Testing for framing and cognitive effects. Medical Decision Making 2017; 37(6): 635-46. PubMed
38.Morrell L, Wordsworth S, Rees S, Barker R. Does the public prefer health gain for cancer patients? A systematic review of public views on cancer and its characteristics. Pharmacoeconomics 2017; 35: 793-804. PubMed
39.Whitty JA, Lancsar E, Rixon K, Golenko X, Ratcliffe J. A systematic review of stated preference studies reporting public preferences for healthcare priority setting. The Patient-Patient-Centered Outcomes Research 2014; 7: 365-86. PubMed
40.Njoroge MW, Walton M, Hodgson R. Understanding the National Institute for Health and Care Excellence Severity Premium: Exploring Its Implementation and the Implications for Decision Making and Patient Access. Value in Health 2024. PubMed
41.CDA. pCPA Temporary Access Process (pTAP). 2024. https://www.pcpacanada.ca/pTAP (accessed November 22 2024).
Appendix 1: Author Information
Shehzad Ali,1 Alexander Haines,2 Karen Lee2
1 Department of Epidemiology and Biostatistics, Western University, London, Ontario; Department of Health Sciences, University of York, UK; WHO Collaborating Centre for Knowledge Translation and Health Technology Assessment in Health Equity, Canada
2 Canada’s Drug Agency, Ottawa, Ontario
Funding
This work was funded by Canada’s Drug Agency.
Corresponding Author
Shehzad Ali MBBS, MPH, MSc, PhD
Canada Research Chair, Public Health Economics
Department of Epidemiology and Biostatistics
Schulich School of Medicine & Dentistry, Western University, London, Ontario
w: https://www.schulich.uwo.ca/epibio/people/faculty/core_appointees/dr_shehzad_ali.html
e: shehzad.ali@uwo.ca
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.