CADTH Health Technology Review
Internet-Delivered Cognitive Behavioural Therapy for the Management of Chronic Non-Cancer Pain
PROSPERO Registration Number: CRD42021283994
Health Technology Assessment
Abbreviations
ACT
acceptance and commitment therapy
ANOVA
analysis of variance
CBT
cognitive behavioural therapy
CPAQ-R
Chronic Pain Acceptance Questionnaire-Revised
FIQ
Fibromyalgia Impact Questionnaire
GRADE
Grading of Recommendations, Assessment, Development and Evaluation
HADS
Hospital Anxiety and Depression Scale
HRQoL
health-related quality of life
HTA
Health Technology Assessment
iCBT
internet-delivered cognitive behavioural therapy
nRCT
non-randomized controlled trial
PASS-20
Pain Anxiety Symptoms Scale-Short Form 20-Item
PCCL
Pain Coping and Cognition List
PHQ-9
Patient Health Questionnaire-9
PTSD
posttraumatic stress disorder
RCT
randomized controlled trial
RoB 2
Risk of Bias 2
RoBANS
Risk of Bias Assessment tool for Non-randomized Studies
SF12-MCS
Short Form-12 Mental Component Summary
SF12-PCS
Short Form-12 Physical Component Summary
SD
standard deviation
SR
systematic review
VAS
Visual Analogue Scale
Authorship
Clinical Review
Calvin Young assisted with the protocol development for the Clinical Review; screened and selected studies; extracted, tabulated, critically appraised, and interpreted data; verified calculations to standardize outcome measures; co-wrote the Clinical Review; contributed to revisions per reviewers’ feedback; and provided final approval of the version of the report submitted for publication.
Yan Li led the protocol development for the Clinical Review; screened and selected studies; extracted, tabulated, critically appraised, and interpreted data; performed calculations to standardize outcome measures; co-wrote the Clinical Review; contributed to revisions per reviewers’ feedback; and provided final approval of the version of the report submitted for publication.
Michelle Gates provided methodological oversight, assisted in interpretation of the results, revised the report for important intellectual content, and approved the final version.
Patients’ Perspectives
Elijah Herington developed, in collaboration with Tamara Rader and Francesca Brundisini, the protocol for the Patients’ Perspectives study; developed the interview guide and conducted interviews with patient contributors in collaboration with Tamara Rader and Francesca Brundisini; conducted analysis and wrote the Patients’ Perspectives study in collaboration with Jamie Bentz, Francesca Brundisini, and Tamara Radar; and revised the protocol and reports based on internal review, external peer review, and stakeholder feedback; and provided final approval of the version of the report submitted for publication.
Jamie Bentz contributed to the analysis and write-up of the Patients’ Perspectives study in collaboration with Elijah Herington, wrote summaries of interviews with patient contributors and responded to their feedback before disseminating summaries to the larger project team, contributed to the development and write-up of the Discussion section in collaboration with project leads, and provided final approval of the version of the report submitted for publication.
Francesca Brundisini contributed to the study design during protocol development; provided methodological oversight and support throughout the conduct of the study, including the development of the interview guide; attended interviews with patient contributors; conducted the analysis of 2 transcripts; participated in the discussions for the analysis of the Patients’ Perspectives study; provided critical review of the contents of the report; and provided final approval of the version of the report submitted for publication.
Patient Engagement
Tamara Rader led patient engagement activities and wrote the summary of those activities included in the report. She also reviewed the protocol and drafts of the Patients’ Perspectives study and provided final approval of the version of the report submitted for publication.
Operational Aspects
Keeley Farrell led the protocol development for the Operational Aspects section, screened and selected publications, developed and distributed the survey, analyzed survey responses, extracted data from the survey and selected publications, wrote the Operational Aspects section, revised the section based on reviewers’ feedback, and provided final approval of the version of the report submitted for publication.
Research Information Services
Danielle MacDougall designed the database search strategies for all sections of the report, executed the search strategies, completed grey literature searches, maintained search alerts, prepared the search methods and appendix, and provided final approval to the version of the report submitted for publication.
David Kaunelis peer-reviewed the search strategies, assisted with report referencing, and approved the final version of the report submitted for publication.
Program Development
Bert Dolcine led the development of the project plan; authored the Introduction, Conclusions, and Implications for Decision- or Policy-Making sections; reviewed the Discussion section; and provided final approval of the version of the report submitted for publication.
Knowledge Mobilization
Colleen Donder collaborated with project team members to formulate the key messages, reviewed and contributed to the drafting of the protocol and report, and provided final approval of the version of the report submitted for publication.
Contributors
The authors would like to acknowledge Joanne Kim for project oversight and coordination throughout the planning, conduct, and reporting of the Clinical Review, including providing methodological input and critically reviewing drafts of the protocol and final report; Gino De Angelis for providing oversight and coordination throughout the planning, conduct, and reporting of the Operational Aspects analysis and for critically reviewing drafts of the protocol and final report; Patricia Poulin for reviewing drafts of the protocol and final report of the Clinical Review and for assisting with interpretation of the clinical data; Christa Bergquist for providing input on the protocol and final report and for supporting alignment of the project with jurisdictional needs; and Pierre Martinelli for providing project management support. The authors would also like to thank the external stakeholders who submitted feedback on the draft report. Finally, the authors would like to thank the patient contributors who offered feedback on the review protocol and gave their insights into and experiences of living with chronic pain and commented on the suitability of iCBT for various pain conditions and for people experiencing chronic pain, as well as other factors to support decision-making.
External Reviewers
These individuals kindly provided comments on a draft version of this report.
Kathryn Birnie, PhD, RPsych
Assistant Professor, University of Calgary
Assistant Scientific Director, Solutions for Kids in Pain (SKIP)
Psychologist, Alberta Children’s Hospital
Calgary, AB
Lori Montgomery, MD, CCFP, FCFP, CHE
Clinical Associate Professor
University of Calgary
Calgary, AB
Swati Mehta, PhD
Scientist
Lawson Health Institute
London, ON
Conflicts of Interest
Dr. Birnie serves in a leadership role at Solutions for Kids in Pain (SKIP), a Networks of Centres of Excellence (NCE) Knowledge Mobilization network.
Dr. Montgomery received honorariums for teaching and committee work from the College of Family Physicians of Canada, the Alberta College of Family Physicians, University of Calgary, and CBT Canada; received funding from the Hotchkiss Brain Institute at the University of Calgary to conduct a pilot clinical trial of a medication for opioid withdrawal; and is in a medical leadership role within Alberta Health Services.
Protocol Amendments
Section | Amendment | Page number in protocol | Rationale |
|---|---|---|---|
Study selection in the Clinical Review | We did not screen records retrieved by the electronic literature searches from clinical trials registries. | 16 | Literature searches conducted in clinical trials registries yielded a high number of results. Due to feasibility constraints, these were not screened using the methods outlined for the database and grey literature searches. |
Data extraction in the Clinical Review | We used both Microsoft Word and Microsoft Excel for the data extraction process. | 16 | Due to the complexity of the detailed results data from the included trials, we conducted some of the data extraction using Microsoft Excel as we expected it would be easier to manage and interpret compared to data extracted in Microsoft Word. |
Critical appraisal in the Clinical Review | We edited the RoBANS domain ‘measurement of exposure’ to instead address risk of bias due to deviations from the intended interventions. | 17 to 18 | Since our included study pertained to an intervention rather than an exposure, the domain in the original tool was not relevant. The addition ensured that all relevant key domains of risk of bias were assessed. |
Data analysis and synthesis in the Clinical Review | As part of the data analysis and synthesis, we combined the results from the nRCT with the RCTs. Specifically, the presentation of data in the Summary of Findings tables was not separated by study design, and GRADE assessments for these study designs were conducted together. Outcome comparisons that included data from the nRCT and RCTs started as high-certainty evidence (i.e., before any rating down for concerns related to risk of bias, inconsistency across studies, indirectness, imprecision of effects, and/or publication bias following the GRADE approach). | 18 to 20 | We considered the RCTs alongside the 1 nRCT as this approach seemed to be more informative than presenting findings separately by design. |
Key Messages
This Health Technology Assessment (HTA) was conducted to inform decision-makers about whether internet-delivered cognitive behavioural therapy (iCBT) should be offered as a treatment option for chronic non-cancer pain as part of a multidisciplinary approach when in-person cognitive behavioural therapy (CBT) would otherwise be offered. This HTA consists of a systematic review of clinical effectiveness and safety, an interview study, and an Environmental Scan.
In this HTA, iCBT is defined as psychotherapy based on CBT principles delivered through the internet, including self-directed app-based programs (with or without therapist support) and CBT delivered through the internet in real time by a therapist (e.g., videoconference).
The Clinical Review found there was little to no difference between iCBT and in-person CBT for most outcomes, but the evidence was very uncertain because of risk of bias, inconsistency, indirectness, and imprecision. The uncertain clinical evidence prevents a strong conclusion about the safety and effectiveness of iCBT as a treatment option when in-person CBT would otherwise be offered for chronic non-cancer pain.
Five women living with chronic non-cancer pain were interviewed regarding their experiences with, or perspectives on, the use of iCBT for chronic pain. All the women interviewed felt iCBT has the potential to be a supportive treatment option if offered as part of comprehensive, multidisciplinary pain care. Based on their experiences, the women interviewed reported that multidisciplinary pain care does not always happen in practice, and they described potential concerns of offering iCBT in the absence of other treatments. They also indicated that determining a patient’s readiness for iCBT is important. If iCBT is determined to be appropriate, the women emphasized that a tailored treatment approach and a strong therapeutic relationship between the patient and iCBT provider might improve the success of iCBT treatment for chronic pain.
The Environmental Scan identified 16 iCBT programs for chronic pain that are available in Canada. Many potential facilitators (e.g., improving access, improving treatment experience, efficiency, and convenience) and barriers (preference for in-person treatment, privacy concerns, technology issues, and no access to a device or internet connection) for iCBT programs in Canada were identified.
If decision-makers decide to implement an iCBT program for chronic pain as part of their multidisciplinary pain care approach, they may wish to consider offering programs that:
are guided by therapists specifically trained in chronic pain
foster strong therapeutic relationships, encourage shared decision-making practices, and can be tailored to the needs of the person living with chronic pain
consider the readiness and suitability of the person living with chronic pain before offering iCBT
consider privacy and technological concerns or challenges.
Abstract
Context and Decision Problems
The aim of cognitive behavioural therapy (CBT) in pain management is to provide people with increased coping ability and self-efficacy by helping them identify and reshape their thoughts, emotions, and behaviours that can be detrimental to effective pain management or inhibit treatment progress. In this Health Technology Assessment (HTA), internet-delivered CBT (iCBT) is defined as psychotherapy based on CBT principles delivered exclusively through the internet via an app or a website using a computer or mobile device or delivered through the internet in real time by a therapist (e.g., via videoconference). The scope of this HTA includes guided and unguided iCBT (i.e., with or without therapeutic support by a trained professional) delivered via a computer or mobile device either synchronously or asynchronously (i.e., there is a delayed exchange of therapeutic communication between a trained professional and a client).
The importance of multidisciplinary care approaches in the treatment of chronic pain is broadly recognized and emphasized in current recommendations and guidelines for chronic pain. Psychological interventions, such as CBT, are increasingly integrated in care approaches for pain; however, the availability of these therapies in their traditional, in-person format is limited. Canadian jurisdictions have indicated interest in exploring and using iCBT as an option for the management of chronic pain to improve access to psychological care. However, jurisdictions note there is a need for reliable evidence and information to guide decisions about the integration of this intervention in care delivery for people living with chronic pain. Previous research1-4 has suggested that both in-person CBT and iCBT may provide benefits with small effect sizes for adults with chronic pain compared with wait-list or various active controls; however, little is known about the effectiveness of iCBT when directly compared with in-person CBT.
This HTA informs the following decision problems:
With a view to increase access to CBT-based therapy, the purpose of this HTA is to inform decisions about whether iCBT should be offered as a treatment option, as part of a multidisciplinary approach, in the delivery of care for chronic non-cancer pain when CBT would otherwise be provided.
Additionally, if evidence demonstrates that iCBT should be offered, the HTA could also inform whether there are criteria to guide decision-making regarding the suitability of iCBT for various pain conditions and people experiencing chronic pain, or other factors that should guide its implementation.
Patient Engagement
CADTH involves patients, families, and patient groups to improve the quality and relevance of our assessments. Our patient engagement activities are guided by the belief that patients have knowledge, perspectives, and experiences that are unique and contribute to essential evidence for this HTA.
Patients’ perspectives gained through CADTH’s engagement processes were used to ensure the relevance of the outcomes of interest for the Clinical Review, to identify and learn from other patients with experience of iCBT, and to discuss other considerations to inform the Discussion section of this report. The questions and subsequent discussion with the patient contributors helped to clarify the technology under review and comment on the relevance of the findings of this report to people living in Canada who are living with chronic pain due to a range of conditions. Furthermore, the patient contributors suggested other people with lived experience to participate in the Patients’ Perspectives study.
Involving patients allowed the research team to consider the evidence with an understanding of the wider experiences of people living with chronic pain and their families and comment on the suitability of iCBT for various pain conditions and people experiencing chronic pain or other factors that could support decision-making.
Clinical Effectiveness and Safety Evidence
We conducted a systematic review of primary studies that examined the comparative clinical effectiveness and safety of iCBT versus in-person CBT for the management of chronic non-cancer pain. Eligible outcome domains were pain control (e.g., intensity, severity, frequency, duration), changes in use of pharmacotherapy, health-related quality of life or overall well-being, psychological or psychosocial function or symptoms, sleep, physical function, participant acceptability or satisfaction with care, individual participation, and any measures of harms (e.g., emergency department visits, hospitalizations, any adverse event). We selected eligible outcomes following patient consultation and engaged with a clinical expert.
In total, we identified 3 randomized controlled trials and 1 non-randomized controlled clinical trial for the Clinical Review. These clinical studies analyzed data from a total of 354 participants. We assessed all outcomes evaluated in the included clinical studies as having at least some concerns with risk of bias, with a majority judged as having a high risk of bias. The evidence for all outcomes was considered very uncertain as judged using the GRADE approach. This high level of uncertainty is primarily due to concerns related to risk of bias and imprecision, but there were also inconsistency and indirectness concerns for many outcome comparisons. Based on the uncertainty of the evidence, there is a very high likelihood that the true effect of iCBT versus in-person CBT will be substantially different than what was observed in these trials. We identified no relevant studies regarding the comparative safety of iCBT versus in-person CBT. Additionally, there were no data on the comparative effectiveness of iCBT versus in-person CBT for children and for people with pain conditions that were not represented in the included studies. The generalizability of findings from the studies summarized in the Clinical Review to other populations may be limited.
Patients’ Perspectives
We conducted an interview study exploring people’s expectations or experiences with iCBT for chronic pain. Five women in Canada living with chronic non-cancer pain participated in semi-structured interviews. Interview transcripts were analyzed with a modified framework analysis approach using the thematic categories identified in CADTH’s previous 2 qualitative reviews on iCBT.
The women interviewed considered iCBT as a potentially beneficial intervention, but only when offered within the context of comprehensive chronic pain care. Access to such care was difficult for the women to obtain, with nearly all reporting experiences of being dismissed or neglected by various health care providers when seeking diagnoses or treatments related to their pain. Even after their health care providers acknowledged their pain, most of the women had trouble accessing affordable multidisciplinary pain care and relied strongly on self-advocacy and, in some cases, significant out-of-pocket expenses to obtain treatment.
For this HTA, it was assumed iCBT programming would only be offered in the context of broader multidisciplinary care; however, the women we spoke with nonetheless felt it was important to emphasize some potential harms of offering iCBT as a first-line or stand-alone treatment option for people living with chronic pain. They described how health care providers who offer iCBT as a first-line treatment might cause harm by potentially missing or failing to treat the root causes of pain, thus prolonging the pain experience. They also noted that people in severe, untreated pain would be unlikely to benefit from the intervention.
Findings of the Patients’ Perspectives interview study also indicated that offering iCBT in the appropriate context and at the right time is dependent on the concept of readiness. The women reflected on how readiness — understood as an assemblage of treatment history, available current care practices, material realities, and individual needs or desires — is best assessed within the context of a trusting therapeutic relationship. The women also considered a strong therapeutic relationship, wherein a provider assesses and actively tailors content to an individual’s needs, as a vital component of successful engagement with the therapy. For this reason, the women interviewed noted that people living with chronic pain may benefit most from provider-guided and, at least partially, synchronous programs. The women also emphasized the importance of these iCBT providers having specialized knowledge in managing and responding to the unique needs of people living with chronic pain. The women believed such providers would have the knowledge and skills necessary to help them live better with pain, which they understood to be the ultimate objective of the therapy.
Operational Aspects
An Environmental Scan was conducted to identify iCBT programs for the management of chronic non-cancer pain available or in development in Canada and describe their characteristics and related operational aspects. The Environmental Scan was informed by a limited literature search and survey. According to the results of the literature search and survey, there are at least 16 iCBT programs available or in development in various jurisdictions in Canada that support people living with chronic non-cancer pain. The characteristics of these programs vary in terms of the level of therapist involvement, overall program length, number and length of modules, and topics covered. Survey respondents identified a variety of patient-related, clinician-related, and organizational factors that act as facilitators or barriers to the implementation of iCBT. Commonly identified facilitators to iCBT implementation included reaching people who would otherwise be unreachable, improvement in patients’ experiences, efficiency (in clinical practice and use of resources), and convenience for patients. Commonly identified barriers to iCBT implementation included privacy concerns, preference for in-person or other treatment options (of both patients and clinicians), patients’ lack of familiarity with technology, and patients’ lack of available or appropriate devices or adequate internet connection.
Conclusions and Implications for Decision- or Policy-Making
This HTA sought to analyze the available evidence to help determine whether iCBT should be offered as part of a multidisciplinary care approach for the treatment of chronic non-cancer pain when in-person CBT would have otherwise been provided. The results of the Clinical Review suggest the available evidence that compares the benefits of the virtual and in-person forms of CBT is very uncertain because of serious concerns about risk of bias, inconsistency, indirectness, and imprecision. Therefore, the effect estimates are not likely to provide a reliable indication of the true effect of iCBT versus in-person CBT, and we could not draw any conclusions on whether iCBT was better or worse based on the uncertain evidence. Additionally, we identified no relevant studies that provided outcome data regarding the comparative safety of iCBT versus in-person CBT (e.g., proportion of participants who experienced pain worsening, hospitalizations, rates of adverse events). Based on these findings, we were unable to draw an evidence-based conclusion regarding whether iCBT represents a comparable alternative to in-person CBT that should be offered when CBT would be otherwise provided to address the psychological care needs of individuals with chronic non-cancer pain.
The Environmental Scan conducted as part of this review identified 16 iCBT programs that currently exist in various Canadian jurisdictions and there is information to suggest that more of these programs may be implemented in the future. Working to improve access to psychological treatment for pain by leveraging virtual forms of CBT seems to be a promising avenue that is worth exploring. At the same time, the findings of the review suggest that more research is needed to be able to understand if iCBT programs are responding to the psychological care needs of people with chronic pain and are achieving the same desired outcomes as CBT delivered in person. Although our HTA aimed to describe the potential role of iCBT when CBT would otherwise be provided, decision-makers considering the implementation of iCBT programs as a method of increasing access to psychological care for those who otherwise may not receive any form of CBT should consider the broader iCBT literature.3,5-9
This HTA also sought to identify and examine criteria that can help guide decisions about who and what pain conditions iCBT is suitable for, and other factors that should be considered as iCBT programs are implemented in the context of the very uncertain evidence regarding comparative clinical benefits. As is commonly the case with internet-delivered psychological interventions, aspects such as the person’s readiness, a provider with adequate training in care for the condition (i.e., chronic pain, in this case), the strength of the therapeutic relationship between the person receiving iCBT and the provider, and tailoring the treatment to the individual person’s needs were identified in this review as notable factors that may impact the usefulness of iCBT programs. Additionally, iCBT programs may not be suitable for people experiencing severe, untreated chronic pain or active suicidal ideation.
Introduction
Background and Rationale
Chronic pain affects approximately 19% of adults in Canada.10 Prevalence estimates among children and adolescents range from 11% to 38%.11 Available evidence suggests that the prevalence of chronic pain increases with age and is higher among women compared with men.10-12 For people with employment, the type of occupation also correlates with prevalence rates; people who are involved in manual work, deal with difficult job requirements, or have low job autonomy and satisfaction, for example, are more likely to report experiencing chronic pain than those who perform non-manual work or who perceive their job situation as more satisfactory.12 Studies also report that socioeconomic factors have an impact on the prevalence of chronic pain and rates tend to be higher among some populations due to socioeconomic inequalities.11,12 Individuals living with chronic pain can experience substantial physical and psychological morbidity, which can contribute to reduced quality of life and increased socioeconomic difficulties.11,13 In addition, chronic pain is associated with a significant economic impact. In Canada, on an annual basis, more than $6 billion is spent on direct health care costs to address chronic pain, while the indirect costs to the overall economy are estimated at more than $37 billion dollars.13 In the US, annual societal costs associated with chronic pain are estimated at between $560 and $600 billion.14
Chronic pain is defined by WHO as pain that lasts or recurs for more than 3 months and is recognized as a disease in its own right by.15 The condition can be further classified as chronic primary pain and chronic secondary pain. Chronic primary pain is pain that affects 1 or more anatomical regions, persists or recurs for more than 3 months, is associated with significant emotional distress and/or significant functional disability, and for which symptoms are not better accounted for by another diagnosis.15 Conditions considered as chronic primary pain include chronic widespread pain, complex regional pain syndrome, chronic primary headache or orofacial pain, chronic primary visceral pain, and chronic primary musculoskeletal pain.15 Chronic secondary pain is defined as pain that originates as a symptom of another condition but the pain problem may persist and become a condition in its own right after the underlying condition has been treated.16 Examples of chronic secondary pain syndromes include chronic cancer-related pain, chronic postsurgical or post-traumatic pain, chronic neuropathic pain, chronic secondary headache or orofacial pain, chronic secondary visceral pain, and chronic secondary musculoskeletal pain.15 Chronic non-cancer pain, the focus of this Health Technology Assessment (HTA), is a broad category that includes chronic primary pain and chronic secondary pain conditions other than cancer-related pain. The management of cancer-related pain is commonly based on separate and different guidelines and protocols from those for non-cancer pain and is therefore beyond the scope of this HTA.
Pain is recognized as a complex, multi-dimensional condition characterized by an interplay of biological, psychological, and social factors.11 People living with pain often experience comorbid mental health issues, such as depression and anxiety, which highlights the broad psychological component of chronic pain as a disease.17,18 Current recommendations and strategies to address pain emphasize the need for multidisciplinary care approaches to target the different dimensions of pain and improve treatment outcomes.11,13,19 Multidisciplinary care strategies draw from a range of potential interventions like pharmacotherapy, physical and rehabilitative therapies, psychological therapy, medical devices, manual therapy, and self-management.11 There are indications that availability of multidisciplinary care for chronic pain is limited in Canada. For example, a 2020 report of the Canadian Pain Task Force that examined current gaps and challenges in chronic pain care in Canada observed that while the importance of the multidisciplinary approach to chronic pain care is broadly recognized, there are considerable gaps in its application in practice, both at the clinical level and in devising policies to address the care needs of individuals with chronic pain.20
Cognitive behavioural therapy (CBT) is one of the most frequently used psychological interventions for the management of chronic pain.21-23 The aim of CBT is to increase the coping ability and self-efficacy of people living with chronic pain by helping them identify and reshape their thoughts, emotions, and behaviours that can be detrimental to effective pain management or inhibit treatment progress.7,22,24 In a 2019 CADTH Rapid Review Report (Summary With Critical Appraisal)25 on the clinical effectiveness of CBT for the management of chronic non-cancer pain, 1 of the 5 identified systematic reviews (SRs) was a 2018 Cochrane SR1 that investigated the effectiveness of in-person psychological therapies including CBT in the management of children living with chronic pain. Findings from this Cochrane SR1 suggested that psychological therapies including CBT may be associated with decreased pain intensity, anxiety, and disability post-treatment in children living with mixed pain conditions (e.g., recurrent abdominal pain, musculoskeletal pain) compared with usual care and wait-list controls. The authors of the Cochrane SR2 that assessed the effectiveness of in-person CBT for the management of chronic pain (excluding headache) in adults concluded that there is strong evidence for CBT having very small benefits at the treatment end for pain and disability compared with an active control and small benefits for pain, disability, and distress compared with treatment as usual. The authors of the review2 stated they were unable to make any meaningful translation of these effect sizes into clinically interpretable changes due to variability of outcome metrics within each domain and considerable heterogeneity at baseline (i.e., the clinical significance of these results was unclear). Although the benefits of in-person CBT were characterized as small or very small for individuals with chronic pain, there may be a large population benefit. The authors of this Cochrane SR2 concluded that the body of evidence was sufficient (i.e., large and of moderate quality) to support the benefits of in-person CBT and was not likely to change with additional studies. Of note, in a previous edition26 of this Cochrane SR, the authors stated that psychologically informed subgroup analyses may be helpful in identifying which individuals can benefit most from CBT, an important consideration given the therapeutic effect of CBT is likely to vary by individual.27-29 The authors also evaluated the risk for adverse events related to CBT; however, the evidence was of very low certainty due to inconsistency and indirectness.
Although psychological interventions, such as CBT, are increasingly integrated in care approaches for pain, a notable challenge stems from limited availability of these therapies in their traditional, in-person format. Financial barriers and the ability to pay, stigma, and long wait times are among factors that can deter those who need care from seeking and engaging in traditional psychotherapy.30-35 Amid these various challenges, internet-based delivery of psychological treatments, such as CBT, is increasingly considered an option that may help improve access to psychological care for chronic pain.36-40 In this HTA, access is defined broadly, capturing factors related to the demand and supply sides of a health care service, such as the needs and desire for care or the availability of care, and the barriers and enablers that may impede or facilitate the use of, and ability to benefit from, that service, such as issues related to the affordability, physical accessibility, or acceptability of that service.41,42
Internet-delivered CBT (iCBT) is psychotherapy based on CBT principles delivered exclusively through the internet via an app or a website on a computer or mobile device. Available iCBT programs vary in terms of content, quality, and adherence to the principles of CBT. In the context of this HTA, the term internet-delivered cognitive behavioural therapy is used to encompass the various forms of CBT-based therapies that are provided over the internet. The delivery of iCBT programs may be self-guided or therapist-assisted. The latter, which is also referred to as guided iCBT, includes therapeutic support provided by a trained therapist who may be a social worker, a psychologist, a psychotherapist, or other health professional. The support commonly consists of planned or ad hoc guidance and feedback to the person seeking care as they go through the internet-based treatment. Communication between the therapist and person seeking care is typically asynchronous but iCBT programs may also include synchronous interaction that occurs on an as-needed basis or at predefined steps in the therapy process.38,40 In this HTA, iCBT also includes CBT that is delivered through the internet in real time by a therapist (e.g., via videoconference). In short, the scope of this HTA includes guided and unguided iCBT delivered via a computer or mobile device, either synchronously or asynchronously.
The clinical effectiveness of iCBT for the management of chronic non-cancer pain has been examined in previous research. For example, a 2019 Cochrane review4 investigated the effectiveness of remotely delivered psychological therapies for children and adolescents with chronic or recurrent pain. The authors of the review concluded that there was insufficient evidence to confidently say whether psychological therapies delivered via technology (e.g., the internet, computer programs, smartphone applications) can reduce symptoms associated with chronic pain due to the very low quality of available literature.4 Findings from a 2022 systematic review and meta-analysis3 of randomized controlled trials (RCTs) suggested that iCBT may provide benefits of small effect sizes for interference or disability, depression, anxiety, pain intensity, self-efficacy, and pain catastrophizing compared with wait-list or active controls (i.e., participation in online discussion forums, expressive pain writing, or psychoeducation) in adults with chronic pain. Despite this previous research, the effectiveness of iCBT relative to in-person CBT for the management of people with chronic non-cancer pain is unclear.
To improve access to psychological care for chronic pain, including times when public health measures require physical distancing, medical and mental health care services may need to be delivered virtually via internet, videoconference, or apps. The COVID-19 pandemic, particularly the unprecedented constraints that it has imposed on in-person care delivery, has highlighted the need for comprehensive integration of virtual care options in the health care system. Early assessments of the impact of the pandemic on the delivery of health services indicate that the situation may have spurred a significant increase in interest in, acceptability of, and adoption of virtual care in Canada and globally.43,44 In May 2021, the Canadian Pain Task Force published an action plan that includes a number of recommended actions for integrating and scaling up virtual care programs and resources in the delivery of pain care in Canada.45 Further, according to a 2021 report46 published by the Canadian Institutes of Health Research (CIHR), high-quality evidence-based virtual care modalities for children living with chronic pain should be promoted. The CIHR report46 also suggested that engagement with children and their families would help facilitate the selection and implementation of virtual care for the management of chronic pain. Internet-delivered CBT (iCBT) programs for pain management are emerging in Canada and the number of providers offering this type of service appears to be limited at the moment.43-45,47-49 This suggests that in the current context it is timely for CADTH to conduct an HTA to help inform discussions and decisions regarding the use of iCBT in treatment of chronic pain, with a view to increase access to CBT-based therapy.
Canadian jurisdictions have indicated an interest in exploring and using iCBT as an option for the management of chronic pain to improve access to psychological care. However, jurisdictions note there is a need for reliable evidence and information to guide decisions regarding the integration of this intervention in care delivery for people living with chronic pain. The 2020 Canadian Pain Task Force Report notes that outcomes are improved when multiple professionals and caretakers are involved in addressing chronic pain.20 A key question that prevails about iCBT is whether this therapy should be offered as part of a multidisciplinary (pharmacological and non-pharmacological) strategy for chronic pain management and care when CBT-based therapies are being considered. There is also interest in determining who this therapy should be offered to and if there are individuals with chronic pain for whom iCBT is not appropriate, such as due to co-occurring conditions, cognitive problems, goals, preferences, readiness, and unstable housing or lack of a reliable internet connection. A related question pertains to the circumstances in which iCBT should or should not be considered in the broader context of provision of care services for chronic pain. Finally, there is an interest in understanding the factors that could affect the implementation and uptake of iCBT and what conditions could promote or hinder achievement of the objective of improving access to psychological treatment.
Decision Problems
This HTA informs the following decision problems:
With a view to increasing access to CBT-based therapy, the purpose of this HTA is to inform decisions as to whether iCBT should be offered as a treatment option, as part of a multidisciplinary approach, in the delivery of care for chronic non-cancer pain when CBT would otherwise be provided.
Additionally, if evidence demonstrates that iCBT should be offered, the HTA could also inform whether there are criteria to guide decision-making regarding the suitability of iCBT for various pain conditions and people experiencing chronic pain, or other factors that should guide its implementation.
Objective
The objective of this HTA is to inform the decision problems with an assessment of the clinical effectiveness and safety of iCBT, the perspectives and experiences of patients and caregivers, and the operational aspects associated with the use of iCBT in the management of chronic non-cancer pain when CBT-based therapies would otherwise be provided.
Research Questions
This HTA informs the decision problems by exploring the following research questions. Details on the specific interventions and outcomes are included in Table 2.
Clinical effectiveness and safety
What is the comparative clinical effectiveness of internet-delivered cognitive behavioural therapy versus in-person cognitive behavioural therapy for the management of chronic non-cancer pain?
What is the comparative safety of internet-delivered cognitive behavioural therapy versus in-person cognitive behavioural therapy for the management of chronic non-cancer pain?
Patients’ perspectives
How do the experiences of people living with chronic non-cancer pain, and their caregivers, resonate (or not) with known experiences of iCBT for depression, anxiety, or post-traumatic stress disorder (PTSD), when CBT would otherwise be provided?
What do people living with chronic non-cancer pain and their caregivers expect to access or experience accessing (or not) with regard to iCBT for the management of chronic non-cancer pain, when CBT would otherwise be offered?
Operational aspects
Which iCBT programs for the management chronic non-cancer pain are currently available or are in development in Canada, and what are their characteristics?
What operational considerations contribute to the establishment and provision, or lack, of iCBT programs, specifically for the management of chronic non-cancer pain, at the system or site level in Canada and internationally?
Methods
To inform the conduct of this HTA, a preliminary scoping review of the existing literature — including HTAs and systematic reviews — was conducted. A protocol was written a priori, using appropriate reporting guidelines (e.g., the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols [PRISMA-P]) for guidance on clarity and completeness and they were followed throughout the HTA process. Any deviations from the protocol were disclosed in this final report and updates were made to the PROSPERO submission accordingly (Clinical Review: CRD42021283994).
The Clinical Review conducted a systematic review of the clinical literature looking at primary studies comparing iCBT to in-person CBT for the management of chronic non-cancer pain. For the Patients’ Perspectives study, we conducted an interview study exploring people's expectations of, or experiences with, iCBT as a component of care in the management of their chronic non-cancer pain. The Environmental Scan consisted of a limited literature search and a survey distributed to stakeholders involved in iCBT for chronic non-cancer pain.
Opportunities for Stakeholder Feedback
Stakeholders were given the opportunity to provide feedback on the draft-included studies list and the draft report. All feedback provided by stakeholders was considered, and as appropriate, edits to the draft report were made in response and are reflected in this final report.
Clinical Review
Overview
Research Questions
What is the comparative clinical effectiveness of internet-delivered cognitive behavioural therapy versus in-person cognitive behavioural therapy for the management of chronic non-cancer pain?
What is the comparative safety of internet-delivered cognitive behavioural therapy versus in-person cognitive behavioural therapy for the management of chronic non-cancer pain?
Key Messages
We identified 3 randomized controlled trials and 1 non-randomized controlled clinical trial that examined the comparative clinical effectiveness of internet-delivered versus in-person cognitive behavioural therapy for the management of chronic non-cancer pain.
The clinical evidence on the balance of comparative benefits and harms of internet-delivered versus in-person cognitive behavioural therapy is very uncertain due to concerns related to risk of bias, inconsistency across studies, indirectness, and imprecision of effects, meaning it is not a reliable indication of how effective internet-delivered cognitive behavioural therapy is compared to in-person cognitive behavioural therapy. The available evidence was from only a few internet-delivered cognitive behavioural therapy programs and none of the relevant studies included children.
Higher quality research on the effectiveness of internet-delivered cognitive behavioural therapy programs compared to in-person cognitive behavioural therapy programs for chronic pain is needed. The certainty of the evidence could be improved through future clinical studies that use more rigorous methodological approaches, collect safety data, and to strive to lower participant drop out rate.
The clinical data did not provide insight into how internet-delivered cognitive behavioural therapy may potentially reduce or widen existing inequities, as compared to providing in-person CBT as the only form of CBT.
Study Design
To inform the design of this Clinical Review, we conducted detailed scoping activities that included an informal scoping review of existing literature and CADTH Rapid Review Reports regarding the clinical effectiveness of iCBT for the management of chronic pain in adults published in December 202050 and CBT for chronic non-cancer pain in adults published in September 2019.25 Details on the complete methodology for the Rapid Review Reports are available in their publications.25,50
We identified a considerable body of evidence pertaining to the clinical effectiveness of iCBT for chronic pain in the 2020 CADTH Rapid Review Report (Reference List).50 Specifically, we identified 9 SRs (6 with meta-analyses), 28 RCTs, and 5 non-randomized trials.50 Five5,7,23,51,52 of the 9 identified SRs included only RCTs. However, the available evidence was characterized by a notable degree of clinical heterogeneity, arising from grouping together different types of treatments (e.g., iCBT, in-person CBT, other psychological therapies, computer-based interventions), different underlying pain conditions (e.g., mixed chronic pain, back pain, recurrent pain, fibromyalgia, headache), and various comparator groups (e.g., wait-list, usual care, pharmacotherapy, internet-delivered education, in-person CBT). None of the available SRs fully addressed our current scope. For example, although findings from 1 SR5 suggested that iCBT was superior to controls (i.e., wait-list, attention control, usual care) in improving mood and disability among people with fibromyalgia, there were no comparisons between iCBT and in-person CBT. Authors of another SR23 found beneficial effects in internet-delivered psychological therapies, including iCBT, for pediatric populations with chronic headache and mixed pain conditions (e.g., musculoskeletal pain, neuropathic pain) compared to controls; however, the authors did not categorize the included studies by treatment or control type (e.g., active, wait-list), making it difficult to draw meaningful conclusions that addressed our research questions. The existing literature provided limited discussion on the potential impact of iCBT on access to equitable health care, which was an important consideration for informing our decision problems.
Since there was a lack of up-to-date SRs addressing the comparison of interest for this review (i.e., iCBT versus in-person CBT) or matching the scope of the current research questions, we conducted a SR of primary studies comparing the effectiveness and safety of iCBT to in-person CBT to help provide Canadian decision-makers with evidence regarding the role of iCBT in the management of chronic non-cancer pain.
Methods
Review Conduct
We followed a protocol for this Clinical Review that was written a priori. We prospectively registered the protocol for the Clinical Review in the international repository PROSPERO (registration number: CRD42021283994). We have disclosed any deviations from the prospectively registered protocol in this final report (Table 1). We have reported the Clinical Review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses 2020 Statement (PRISMA 2020).53
Literature Search Strategy
An information specialist performed a literature search for clinical studies using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies tool.54 The complete search strategy is presented in Appendix 1.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid, Embase (1974–) via Ovid, APA PsycINFO (1806–) via Ovid, and the Cochrane Central Register of Controlled Trials (CENTRAL) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote, was used to remove duplicate search results. Controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings) and keywords, were used in the search strategy. The main search concepts were iCBT and chronic pain. Searches for clinical trials used the following registries: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
CADTH-developed search filters were applied to limit retrieval to any types of clinical trials or observational studies, health technology assessments, SRs, meta-analyses, or network meta-analyses. Retrieval was limited to English- or French-language results that were published from January 01, 2001, onward. Search results excluded conference abstracts.
An information specialist performed the initial literature search on September 27, 2021. Regular alerts updated the database literature searches until the publication of the final report. The clinical trials registries search was updated before the completion of the final stakeholder feedback period.
Relevant sections of the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature tool,55 which includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, systematic review repositories, patient-related groups, and professional associations, were searched to identify grey literature (literature that is not commercially published). Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of the included studies and SRs closely associated with the topic of interest, and through contacts with experts, as appropriate. The grey literature search was updated before the completion of the final stakeholder feedback period. Refer to Appendix 1 for more information on the grey literature search strategy.
Study Eligibility Criteria
Table 2 presents the study eligibility criteria for the clinical research questions.
Inclusion Criteria
Studies meeting the eligibility criteria outlined in Table 2 were included.
There were no restrictions placed on age, sex or gender, ethnicity, comorbidities, cause of chronic non-cancer pain, or severity of symptoms. We planned to conduct subgroup analyses based on underlying causes of chronic non-cancer pain, severity of chronic non-cancer pain, population age, sex or gender, race and/or ethnicity, comorbidities (e.g., depression, anxiety), and place of residence.
Participants could receive CBT or iCBT in conjunction with other interventions (e.g., pharmacological and non-pharmacological options) as part of a multidisciplinary approach. Usual care could vary between the CBT and iCBT arms within each study. Explicit reporting and a description of the multidisciplinary approach was not required for study inclusion.
Traditional iCBT or CBT or psychotherapies firmly grounded in CBT approaches or based on “third-wave” CBTs59-62 were eligible for inclusion (e.g., acceptance and commitment therapy (ACT),63 compassionate mind training, dialectical behavioural therapy, behavioural activation, metacognitive therapy, exposure-based CBT, mindfulness-based cognitive therapy, mindfulness-based stress reduction, or mindfulness-based CBT).64
Table 2: Study Eligibility Criteria for Clinical Research Questions
Criteria | Description |
|---|---|
Population | People (any age) with chronic non-cancer paina |
Interventions | Guided and unguidedb iCBT delivered via a computer or mobile device, either synchronously or asynchronouslyc and in either individual or group settings, in combination with other interventions for the management of chronic non-cancer paina |
Comparators | In-person CBT, in combination with other interventions, for the management of chronic non-cancer paina |
Outcomesd | Question 1:
Question 2:
All instruments and all time points were eligible for inclusion |
Setting | Any setting |
Study design | Randomized and non-randomized comparative study designs, including:
Exclusions:
|
Time frame | 2001 to presente |
CBT = cognitive behavioural therapy; iCBT = internet-delivered cognitive behavioural therapy; RCT = randomized controlled trial.
aChronic non-cancer pain associated with health conditions such as (but not limited to) fibromyalgia, headache, migraine, rheumatoid arthritis, osteoarthritis, multiple sclerosis, surgical procedures, chronic primary pain, or injuries to muscle, nerve, or ligament. Chronic pain is commonly defined as lasting or recurring for at least 3 months15; however, explicit reporting of the pain duration was not required for study inclusion.
bGuided iCBT programs involve support from a clinician or technician (e.g., via email or phone call), whereas unguided iCBT programs are delivered entirely by computer and driven by participants.56
cAsynchronous counselling refers to a delayed exchange of therapeutic communication between a licensed mental health care professional and the client.57
dWe selected eligible outcomes based on our detailed scoping activities in consideration for the core outcome domains identified as clinically important.58 Two patient contributors and a clinical expert reviewed our list of eligible outcomes and provided feedback during protocol development.
eAs part of the detailed scoping process, a 2020 Rapid Review Report (Reference List)50 identified SRs, which included primary studies dating back to the early 2000s. Therefore, studies published in 2001 or later were eligible because it should capture all relevant literature of interest.
Exclusion Criteria
The following are the reasons for exclusion:
Studies that included participants using iCBT or CBT primarily for indications other than chronic non-cancer pain (e.g., primary diagnosis of major depressive disorder, anxiety disorder, PTSD) were not included.
Any psychological interventions not based on CBT were excluded (e.g., interventions based on online psychoeducation or exposure alone, psychodynamic therapy, humanistic approaches [e.g., emotion-focused therapy, internal family systems-based interventions]).
Comparisons between interventions that differ in treatment protocols (e.g., dialectical behavioural therapy versus CBT) in addition to delivery method (i.e., in-person versus internet-delivered) were excluded.
Studies that did not measure outcomes of interest were excluded.
We limited the eligible study designs to RCTs and non-randomized comparative studies. Although RCTs offer the highest internal validity for measuring efficacy and safety, we included non-randomized comparative studies to help capture populations that may not have been included in RCTs and could provide additional context (e.g., geographical, social, economic, cultural, political) pertaining to equity in access to iCBT.
We limited eligibility to studies published in English and French. Although there is evidence65,66 that suggests excluding non-English publications from evidence synthesis on medical topics does not alter review conclusions, publications in French were also eligible because CADTH has the capacity for reviewing in both languages.
Study Selection
We used the SR management software DistillerSR (Evidence Partners, Ottawa, ON) to facilitate study selection. Two reviewers independently screened titles and abstracts of all retrieved citations for relevance to the clinical research questions; due to feasibility constraints, we did not screen records retrieved from clinical trial registries. A single reviewer scanned the reference lists of the included studies and relevant SRs to locate additional studies of potential interest. We retrieved full-text articles that at least 1 reviewer judged to be potentially relevant and independently assessed these for possible inclusion based on the pre-determined selection criteria outlined in Table 2 (i.e., if 1 reviewer believed the citation should be screened at the full-text level, it was moved forward to the next level of screening without conflict resolution). The 2 reviewers then independently examined all full-text articles and compared their decisions. The reviewers discussed discrepancies and reached consensus on the included studies. A third reviewer was consulted to resolve discrepancies for 4 studies. No attempts were made to contact study authors because no information needed to assess study eligibility was deemed unclear or missing. We posted a list of studies selected for inclusion in the Clinical Review to the CADTH website for stakeholder review for 10 business days for feedback and planned to review any additional studies identified for potential inclusion; however, no additional studies were identified.
We screened studies identified through search alerts using the previously mentioned process and incorporated those studies that met the selection criteria of the review into the analysis if they were identified before the end of the final stakeholder feedback period. We describe studies identified after the final stakeholder feedback period in the Discussion section, and compare the results of their feedback with those obtained from the synthesis of earlier reports included in the review.
We generated lists of included studies and excluded studies (with reasons) and have presented these in Appendix 3 and Appendix 4.
Data Extraction
A single reviewer performed data extraction with independent verification for accuracy and completeness by a second reviewer. The reviewers resolved disagreements through discussion until consensus was reached. Reviewers extracted data directly into tables created in Microsoft Word and Microsoft Excel, which were piloted using data from 1 included study. As a result of the piloting exercises, we made some modifications to data extraction tables, and we decided Microsoft Excel would be primarily used for extracting detailed results data. The information extracted included characteristics of the study (e.g., design, setting, funding source), population (number of participants, types of chronic non-cancer pain conditions, duration of pain, sex and/or gender, race and/or ethnicity, comorbidities, and place of residence), intervention and comparators (e.g., type of iCBT and in-person CBT, features of the iCBT and in-person CBT programs, treatment duration, types of concurrent interventions), outcomes and their ascertainment (e.g., instruments used for measurement), and results data regarding the outcomes and the subgroups of interest:
underlying causes of chronic non-cancer pain (as defined by the International Association for the Study of Pain classification of chronic pain system)
severity of chronic non-cancer pain
population age (e.g., children, adolescents, adults, older adults)
sex and/or gender
race and/or ethnicity
type of iCBT (e.g., self-guided or therapist-assisted, synchronous or asynchronous, face-to-face traditional CBT via videoconference versus online modules and without face-to-face contact, individual or group)
components of iCBT (e.g., number of sessions, type of modules)
length of follow-up after completion of iCBT
presence and type of concurrent interventions
presence of comorbidities (e.g., depression, anxiety)
participants’ place of residence (e.g., urban, rural).
We extracted all data that were compatible with each relevant outcome domain at any duration of follow-up, including measures of treatment effects (e.g., mean changes in outcome scores from baseline to follow-up), and any results of statistical tests reported on those measures. Outcome measures, such as the Pain Catastrophizing Scale and Pain Coping and Cognition List (PCCL), are used in the literature related to chronic pain. These scales include terminology (e.g., “catastrophizing”) that has negative connotations to some patient and clinician groups and may perpetuate pain shaming.67 In this report, when possible, we have attempted to avoid such terminology with negative connotations, and we refer to “pain catastrophizing” as “pain-related worrying.” Although we acknowledge “pain-related worrying” is not universally accepted as a substitution for “pain catastrophizing” due to the multicomponent nature of catastrophizing as a construct, this term has been proposed as an appropriate alternative.68,69 However, when citing published literature related to data extracted from the Pain Catastrophizing Scale and PCCL scale, we used such terms for clarity and consistency with the cited literature. We made no assumptions about the presence or absence of an outcome if it was not reported in the study. For example, we did not assume that no adverse events occurred only because the authors did not report on any. No attempts were made to contact study authors because no relevant data were deemed unclear or missing or needed for data synthesis.
Critical Appraisal
Two independent reviewers assessed outcome-level risk of bias (or for groups of outcomes believed to be at similar risk of bias, for feasibility reasons) of RCTs from the intention-to-treat perspective using the revised Cochrane risk-of-bias tool for randomized trials, Risk of Bias 2 (RoB 2).70 The RoB 2 assessment tool is structured into 5 domains to assist in evaluating biases arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. For each domain, we assigned a judgment of low risk of bias, high risk of bias, or some concerns. We then judged the overall risk of bias of each trial as low risk of bias, some concerns, or high risk of bias based on the domain-level determinations. We predicted the direction of the potential risk of bias when possible and provide a rationale for decisions about the risk of bias for both the domain-level and overall assessments.
We assessed the outcome-level risk of bias in non-randomized studies using the Risk of Bias Assessment tool for Non-randomized Studies (RoBANS).71 RoBANS contains 8 domains that may be used to evaluate the risk of biases in a study based on participant selection, confirmation and consideration of confounding variables, measurement of exposure, blinding of outcome assessment, methods of measuring outcomes, incomplete outcome data, and selective reporting of outcomes. We selected this tool for its reliability, promising validity, and user-friendly design.71 We assigned a judgment of low risk of bias, high risk of bias, or unclear risk of bias for each domain using the criteria provided in the instrument.71 Because our included study was an intervention rather than an exposure, instead of “measurement of exposure” we assessed the risk of bias due to deviations from the intended interventions for this domain. We then classified the overall risk of bias for each study as low, some concerns, or high, based on the domain-level judgments about the risk of bias, following the RoB 2 guidance,70 because RoBANS does not provide a specific approach for making study-level judgments. We predicted the direction of the potential risk of bias when possible and provided a rationale for decisions about the risk of bias for both the domain-level and overall assessments. No attempts were made to contact study authors to obtain or confirm information for the critical appraisals.
Reviewers resolved disagreements in the risk of bias for the domain-level and overall assessments through discussion. In evaluating the included studies, we considered other methodological weaknesses beyond the risk of bias. We did not exclude studies from the review based on the results of the critical appraisal. However, we incorporated the critical appraisal results into assessments of the certainty in the body of evidence for each outcome comparison.
Data Analysis and Synthesis
We considered all trials reporting any data related to the outcome domains of interest to be eligible for synthesis within their respective domains. Data were available for multiple heterogeneous time points across the included trials, and we chose to synthesize data at the 2 time points: directly post-program (i.e., post-treatment) and at the longest follow-up point. We considered other lengths of follow-up if the findings appeared to differ substantially compared with the longest follow-up point, but this was not the case for any of the trials. The included trials reported outcomes continuously; if possible, we standardized the outcome measure used across studies to facilitate interpretation (if possible, using mean difference in change from baseline), using standard formulas.72 This included calculating standard deviations (SDs) when standard errors were reported (1 RCT73), and computing mean change from baseline when only baseline and follow-up measures were reported (3 RCTs73-75). We assumed a correlation coefficient of 0.5 between measurements in calculating the SD when the correlation coefficients were not presented in the included trials.72
We considered clinical and methodological heterogeneity across the included trials, as well as the reported outcome measures, in our decision about whether to pool findings statistically via meta-analysis. We did not perform a statistical synthesis because it was rare that more than 2 trials reported on a single outcome and measures of effect were presented heterogeneously across the trials (e.g., different tools). Instead, we performed a narrative synthesis of the results reported in the trials considering available guidance.76,77 This included the presentation of study characteristics and findings by outcome within summary tables, together with descriptions in the main text. To synthesize study findings, we first grouped trials by outcome domain and time point of interest for the main comparison (iCBT versus in-person CBT). We considered the RCTs together with the 1 non-randomized controlled trial (nRCT) because this approach seemed to be more informative than presenting findings separately by design, and inclusion of the nRCT did not negatively affect the certainty of the evidence for any outcome comparison. We then developed a preliminary synthesis by organizing the findings and identifying patterns in the size and direction of reported effects. We considered the sample size of the included trials and their risk of bias in determining the relative weight of each study’s findings in the overall conclusion. Reviewers then came to consensus on a single overall conclusion across trials for each outcome comparison (i.e., favouring either treatment, little to no difference).
If findings across the trials were heterogeneous (especially in terms of direction of observed effects), we had planned to explore the heterogeneity using within- and between-study subgroup analyses. No within-study subgroup analyses were reported in the included trials, and the small number of trials representing various subgroups precluded drawing credible conclusions about the potential sources of heterogeneity. Therefore, we drew conclusions based on the main comparison (iCBT versus in-person CBT) and do not present separate conclusions by subgroups of the population or intervention. Instead, we considered this unexplained heterogeneity in our assessments of the certainty of the evidence. Additionally, we had planned to use within- and between-study subgroup analyses to explore how offering iCBT may reduce or widen existing health inequities compared with providing in-person CBT as the only form of CBT; however, these investigations were not possible as these subgroup analyses were not available.
We had planned to assess the risk of small study bias for meta-analyses containing at least 8 studies of variable size, but since we only included 4 trials and performed no meta-analysis, we were unable to complete this assessment.
Certainty of the Evidence
Two independent reviewers rated the certainty of the body of evidence for each outcome comparison using the methods of the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group.78,79 Reviewers discussed discrepancies until consensus was reached. No attempts were made to contact study authors to obtain or confirm information for the GRADE assessments.
Following the GRADE approach, RCTs started as high-certainty evidence79,80; as noted previously, the syntheses for some outcome comparisons included a single nRCT among the RCTs because we considered this to be the most informative way to present the findings. These comparisons started as high-certainty evidence despite the inclusion of the non-randomized trial. Outcome comparisons including only the non-randomized trial started as low-certainty evidence. Certainty in treatment effect estimates were then rated down for concerns related to risk of bias, inconsistency across studies, indirectness, imprecision of effects, and/or publication bias.79,80 The possibility of rating up the certainty of evidence was considered, but was not appropriate for any outcome comparison.79,80 Ultimately, the GRADE approach resulted in an assessment of the certainty of a body of evidence in 1 of 4 grades81:
High: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.
Very low: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
The results of GRADE assessments are reported in the Summary of Findings tables, which include explanations for all decisions to rate down the certainty of the evidence for any given outcome comparison. Within the text, we use the word “may” for low-certainty evidence and “probably” or “likely” for moderate-certainty evidence.82 We describe very low–certainty evidence as “very uncertain.”82
Results
Quantity of Research Available
We identified a total of 1,889 unique citations via the electronic literature search and excluded 1,770 records by title and abstract. We retrieved 2 additional records from the grey literature search or search alerts. From full-text review of the 121 potentially relevant articles, we excluded 117 and included 4 unique studies. No additional unique studies were identified during the stakeholder review of the included studies. The study selection process is outlined in Appendix 2 (Figure 1) using a Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA)83 flow chart. Lists of included and excluded studies, with details describing the rationale for those excluded, are presented in Appendix 3 and Appendix 4, respectively.
Trial and Participant Characteristics
Table 3 provides a high-level overview of trial and participant characteristics. Full details regarding the characteristics of included trials are presented in Table 13 in Appendix 2. Two trials included participants with a specific pain condition (i.e., fibromyalgia75) or pain location (i.e., chronic back pain84), while 2 trials included participants with a wide range of chronic pain conditions.73,74 Participant race was reported in 2 trials conducted in the US, with the predominant races being Caucasian, African American, and Hispanic.73,84 None of the trials reported participants’ place of residence (beyond the country in which the trial was conducted). Outcomes of interest included pain interference, pain control, health-related quality of life (HRQoL) or overall well-being, psychological or psychosocial function or symptoms (i.e., pain acceptance; anxiety, depression, or general psychological distress; self-efficacy; pain-related worrying and pain coping; fatigue), sleep, physical activity level, physical function, prescription opioid use, satisfaction with care, and participation.73-75,84 Various self-reported outcome scales were used such as Brief Pain Inventory Interference and Severity Subscale, and Chronic Pain Acceptance Questionnaire-Revised (CPAQ-R). Detailed descriptions of all outcome measures are available in Table 14 of Appendix 2. No relevant studies were identified regarding the comparative safety of iCBT versus in-person CBT.
Table 3: Overview of Trial Characteristics of the Included Primary Clinical Trials
Trial citation,a country, trial design | Participant characteristics | Relevant intervention and comparator | Length of follow-up |
|---|---|---|---|
Randomized controlled trials | |||
Herbert et al. (2017)73 US Multi-centre, open-label, non-inferiority parallel-group RCT | Veterans (older than 18 years) with a chronic, nonterminal pain condition and average pain severity and interference (BPI) rated > 4 of 10 N = 129 randomized % female: 17.8% Mean age: 52 (SD = 13.3) years | Manualized ACT intervention for chronic pain with the help of at-home assignments. Intervention: Therapist-delivered individual videoconference sessions (led by therapists with at least master’s level training in psychology) Comparator: Therapist-delivered individual in-person sessions (led by therapists with at least master’s level training in psychology) Sessions: 8 weekly sessions | Baseline, mid-, and post-treatment, and 3 and 6 months after completion |
Vallejo et al. (2015)75 Spain Single-centre, open-label, parallel-group RCT | Adults (aged 18 years and older) with FM N = 60 randomized % female: 100% Mean age: 49.8 (SD = 11.0) years | CBT with components such as psychoeducation about FM Intervention: Self-directed online application (junior therapist under the supervision of a senior clinical psychologist) Comparator: Therapist-delivered in-person group sessions (led by a PhD-level clinical psychologist) Sessions: 10 weekly sessions | Baseline, post-treatment, and 3, 6, and 12 months after completion |
de Boer et al. (2014)74 The Netherlands Single-centre, unblinded, non-inferiority parallel-group RCT | Adults (aged 18 years and older) with nonspecific chronic pain N = 72 randomized % female: 68.2% (intervention) and 60.7% (comparator) Mean age: 50.6 (SD = 10.7) years (intervention) and 53.2 (SD = 11.7) years (comparator) | The course is focused on the cognitive behavioural model of pain circle. Intervention: Self-directed internet course with intermittent psychologist contact/feedback by email Comparator: Psychologist-delivered in-person group sessions Sessions: 7 weekly sessions plus a booster session | Baseline, immediately after the 7-week course (i.e., treatment completion), and immediately after the booster session 2 months after completion |
Non-randomized controlled clinical trial | |||
Mariano et al. (2021)84 US Single-centre, open-label, parallel-group nRCT | Adults (aged 18 to 90 years) with daily back pain for more than 3 months, pain intensity rated ≥ 4 on a 0 to 10 scale (higher score = worse pain) N = 93 participants self-selected their treatment % female: 70.2% (intervention group) and 57.8% (comparator group) Mean age: 54.5 (SD = 14.3) years (intervention group) and 59.7 (SD = 13.0) years (comparator group) | CBT intervention for chronic pain that included goal setting, skills training, relaxation exercises, group discussion, and practice assignments. Intervention: Group WebEx videoconference sessions accessed at home (MD- or PhD-level licensed facilitator) Comparator: Group in-person sessions (PhD-level licensed facilitator) Sessions: 8 weekly sessions | Baseline and at 2 (intervention group) or 3 (comparator group) months after completion |
ACT = acceptance and commitment therapy; BPI = Brief Pain Inventory; CBT = cognitive behavioural therapy; FM = fibromyalgia; n = number of participants; nRCT = non-randomized controlled trial; RCT = randomized controlled trial; SD = standard deviation; years = years.
aPublications are organized according to trial design and in reverse chronological order.
Critical Appraisal
Table 4 and Table 5 show a summary of the risk of bias assessments for the 3 RCTs and the 1 nRCT. Full details are in Table 15 and Table 16 of Appendix 2. Overall, all outcome domains from each of the included trials exhibited some concerns for risk of bias, with most outcome domains having a high risk of bias. A summary of the risk of bias assessments is provided subsequently.
Risk of Bias in the Randomized Controlled Trials
The risk of bias for each outcome domain within the 3 included RCTs73-75 was assessed using the RoB 2 tool.70
All RCTs73-75 were judged to be at high overall risk of bias for most outcomes (all outcomes except for individual participation in 2 RCTs73,74), primarily due to bias arising from the randomization process (2 RCTs74,75), bias due to missing outcome data (2 RCTs74,75), bias in the measurement of the outcomes (3 RCTs73-75), and bias in the selection of the reported results (3 RCTs73-75). There was concern about at least some risk of bias arising from the randomization process for 2 of the RCTs74,75 because of limited detail on methods of randomization provided by study authors and/or baseline imbalances in important prognostic factors suggesting failure of the randomization process. All outcomes reported in 2 RCTs (except for individual participation) were at a high risk of bias due to missing outcome data because data were unavailable for a substantial number of participants in the trials, there were imbalances in missing data between intervention groups, and it was likely that the reason for the missing outcome data depended on their true values. All outcomes measured in the 3 RCTs73-75 except those for individual participation were at a high risk of bias in their measurement because outcomes were self-reported by participants who were aware of their treatment allocation and it was likely that assessment of outcomes was influenced by this knowledge. There were some concerns with bias in the selection of reported results in 3 RCTs73-75 because it was unclear if data that produced the results for all outcomes were analyzed in accordance with a pre-specified analysis plan that was finalized before unblinding of outcome data. The overall predicted direction of bias for all outcomes was unclear. A summary of the results of the risk-of-bias assessments of the RCTs73-75 is provided in Table 4.
Risk of Bias in Non-Randomized Studies
The risk of bias for each outcome domain within the included non-randomized study84 was assessed using the RoBANS tool.71
All outcomes assessed in the nRCT84 were judged to be at high overall risk of bias, primarily due to bias arising from the selection of target group comparisons, the consideration of confounders, outcome assessment, incomplete outcome data, and selective outcome reporting. The risk of selection bias due to the selection of an inappropriate comparison target group was judged to be high because the iCBT and in-person CBT groups differed in several important prognostic factors, such as severity of pain. Similarly, there was a high risk of selection bias due to inappropriate confounder confirmation and consideration because the authors did not adjust their analyses for potential confounders. The risk of confirmation bias due to inappropriate blinding of outcome assessors was high for all outcomes except for individual participation, which was judged to have a low risk of bias due to its objectivity. There was a high risk of attrition bias due to inappropriate handling of incomplete data for all outcomes except for individual participation due to the amount of missing data, the imbalance in missing data between intervention groups, and the lack of reporting on reasons for missing data. All outcomes were at an unclear risk of reporting bias due to selective outcome because there was no reference to a published protocol that could be used to verify whether outcomes were reported according to a pre-specified plan. The overall predicted direction of bias for all outcomes was unclear. A summary of the results of the risk-of-bias assessments of the non-randomized study is provided in Table 5.
Table 4: Risk of Bias Summary — RCTs (RoB 2)
Study citation | Bias arising from the randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of the outcome | Bias in selection of the reported result | Overall risk of bias |
|---|---|---|---|---|---|---|
Herbert et al. (2017)73 | All outcomes: Low risk | All outcomes: Low risk | Individual participation: Low risk All other outcomes: High risk (ND) | Individual participation: Low risk All other outcomes: High risk (?) | All outcomes: Some concerns (ND) | Individual participation: Some concerns (?) All other outcomes: High risk (?) |
Vallejo et al. (2015)75 | All outcomes: High risk (+) | All outcomes: Low risk (?) | All outcomes: Low risk | Individual participation: Low risk All other outcomes: High risk (?) | All outcomes: Some concerns (?) | All outcomes: High risk (?) |
de Boer et al. (2014)74 | All outcomes: Some concerns (?) | All outcomes: Low risk (?) | Individual participation: Low risk All other outcomes: High risk (ND) | Individual participation: Low risk All other outcomes: High risk (?) | All outcomes: Some concerns (ND) | Individual participation: Some concerns (?) All other outcomes: High risk (?) |
RCT = randomized controlled trial; RoB 2 = Risk of Bias 2.
Note: The predicted direction of bias arising from each domain and the overall risk of bias is indicated in brackets: (+) suggests the bias may favour the intervention (i.e., iCBT), (−) suggests the bias may favour the comparator (i.e., in-person CBT), (ND) suggests the bias may influence the result toward the null, and (?) suggests the predicted direction is unclear.
Table 5: Risk of Bias Summary — Non-Randomized Controlled Clinical Trial (RoBANS)
Study citation | Bias in target group comparisons | Bias in target group selection | Bias in considerations of confounders | Bias due to deviations from intended interventions | Bias in outcome assessment (assessors) | Bias in outcome measurement (tools) | Bias due to incomplete outcome data | Bias due to selective outcome reporting | Overall risk of bias |
|---|---|---|---|---|---|---|---|---|---|
Mariano et al. (2021)84 | All outcomes: High risk (?) | All outcomes: Low risk | All outcomes: High risk (?) | All outcomes: Low risk | Individual participation: Low risk All other outcomes: High risk (?) | All outcomes: Low risk | Individual participation: Low risk All other outcomes: High risk (ND) | All outcomes: Unclear (?) | All outcomes: High risk (?) |
RoBANS = Risk of Bias Assessment tool for Non-randomized Studies.
Note: The predicted direction of bias arising from each domain and the overall risk of bias is indicated in square brackets: (+) suggests the bias may favour the intervention (i.e., iCBT), (−) suggests the bias may favour the comparator (i.e., in-person CBT), (ND) suggests the bias may influence the result toward the null, and (?) suggests the predicted direction is unclear.
Additional Limitations
Both RCTs73,74 that were conducted as non-inferiority trials provided a seemingly arbitrary statistical basis for deciding on their non-inferiority margins or did not justify their selected non-inferiority margins, which decreases credibility in the non-inferiority conclusions made in these trials. Additionally, neither of the non-inferiority trials73,74 provided a comparison of the effect of treatment with in-person CBT observed in the trials with the effect observed in historical clinical studies that compared in-person CBT versus no treatment or standard care alone. Therefore, it was possible that the constancy assumption was violated. Thus, the conclusions made in this report were not based on the 2 trials’ non-inferiority findings. We did not incorporate the non-inferiority conclusions made by the authors of these RCTs73,74 into our interpretation of the evidence synthesized in our Clinical Review because of their lack of credibility. In 1 trial,73 the authors concluded that non-inferiority of individual videoconference-based ACT versus in-person ACT was supported for pain interference, HRQoL, pain acceptance, depression, sleep, and physical activity at post-treatment as well as pain interference, pain control, HRQoL, depression, and sleep at 6 months after treatment completion. Non-inferiority of individual videoconference-based ACT versus in-person ACT was not supported at post-treatment or 6 months for anxiety.73 In another trial,74 the authors indicated that non-inferiority of iCBT versus in-person CBT was supported for pain-related worrying at post-treatment and at 2 months.
Findings for iCBT Versus In-Person CBT
Table 6 presents a high-level overview of the findings and certainty of evidence assessments for each outcome comparison on the comparative clinical effectiveness of iCBT versus in-person CBT for the management of chronic non-cancer pain (refer to Table 17 to Table 26 in Appendix 2 for detailed GRADE Summary of Findings tables which include an explanation of reasons for rating down the certainty of the evidence). We judged the evidence regarding the comparative clinical effectiveness of iCBT versus in-person CBT on all reported outcomes to be very uncertain. We identified no relevant trials regarding the comparative safety of iCBT versus in-person CBT.
Question 1: Clinical Effectiveness
Table 6: High-Level Overview of Trial Findings and GRADE Assessments
Outcome | Time point | Number of participants (trials) | Certainty of the evidence (reasons) | Conclusion |
|---|---|---|---|---|
Pain interference | Post-treatment | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on pain interference at post-treatment, but the evidence is very uncertain. | |
Longest follow-up (2 to 6 months) | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on pain interference at the longest follow-up, but the evidence is very uncertain. | ||
Pain control | Post-treatment | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on pain interference at post-treatment, but the evidence is very uncertain. | |
Longest follow-up (2 to 6 months) | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on pain interference at the longest follow-up, but the evidence is very uncertain. | ||
HRQoL or overall well-being | Post-treatment | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on HRQoL and overall well-being at post-treatment, but the evidence is very uncertain. | |
Longest follow-up (2 to 12 months) | Very low (a, c, d) | The findings for the effect of iCBT vs. in-person CBT on HRQoL and overall well-being at the longest follow-up are heterogeneous, and the evidence is very uncertain. | ||
Pain acceptance | Post-treatment | 128 (1 RCT)73 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on pain acceptance at post-treatment, but the evidence is very uncertain. |
Longest follow-up (6 months) | 128 (1 RCT)73 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on pain acceptance at the longest follow-up, but the evidence is very uncertain. | |
Anxiety, depression, or general psychological distress | Post-treatment | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on anxiety, depression, and general psychological distress at post-treatment, but the evidence is very uncertain. | |
Longest follow-up (3 to 12 months) | Very low (a, c, d) | The findings for the effect of iCBT vs. in-person CBT on anxiety, depression, and general psychological distress at the longest follow-up are heterogeneous, and the evidence is very uncertain. | ||
Self-efficacy | Post-treatment | 40 (1 RCT)75 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on self-efficacy at post-treatment, but the evidence is very uncertain. |
Longest follow-up (12 months) | 40 (1 RCT)75 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on self-efficacy at the longest follow-up, but the evidence is very uncertain. | |
Pain-related worrying | Post-treatment | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on pain-related worrying at post-treatment, but the evidence is very uncertain. | |
Longest follow-up (2 to 12 months) | Very low (a, b, c, d) | The findings for the effect of iCBT vs. in-person CBT on pain-related worrying at the longest follow-up are heterogeneous, and the evidence is very uncertain. | ||
Coping with pain | Post-treatment | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on coping with pain at post-treatment, but the evidence is very uncertain. | |
Longest follow-up (2 to 12 months) | Very low (a, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on coping with pain at the longest follow-up, but the evidence is very uncertain. | ||
Fatigue | Post-treatment | 72 (1 RCT)74 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on fatigue at post-treatment, but the evidence is very uncertain. |
Longest follow-up (2 months) | 72 (1 RCT)74 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on fatigue at the longest follow-up, but the evidence is very uncertain. | |
Sleep | Post-treatment | 128 (1 RCT)73 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on sleep at post-treatment, but the evidence is very uncertain. |
Longest follow-up (6 months) | 128 (1 RCT)73 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on sleep at the longest follow-up, but the evidence is very uncertain. | |
Physical activity level | Post-treatment | 128 (1 RCT)73 | Very low (a, b, c, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on physical activity level at post-treatment, but the evidence is very uncertain. |
Longest follow-up (6 months) | 128 (1 RCT)73 | Very low (a, b, c) | In-person CBT may be favoured vs. iCBT with respects to physical activity level at the longest follow-up, but the evidence is very uncertain. | |
Physical function | Post-treatment | No trials identified | Not applicable | No trials were identified containing data on physical function at post-treatment. |
Longest follow-up (3 months) | 93 (1 nRCT)84 | Very low (a, b, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on physical function at the longest follow-up, but the evidence is very uncertain. | |
Prescription opioid use | Post-treatment | No trials identified | Not applicable | No trials were identified containing data on prescription opioid use at post-treatment. |
Longest follow-up (3 months) | 93 (1 nRCT)84 | Very low (a, b, d) | There may be little to no difference in the effect of iCBT vs. in-person CBT on prescription opioid use at the longest follow-up, but the evidence is very uncertain. | |
Satisfaction with care | Post-treatment | Very low (a, c) | There may be little to no difference in the effect of iCBT vs. in-person CBT on satisfaction with care, but the evidence is very uncertain. | |
Longest follow-up | No trials identified | Not applicable | No trials were identified containing data on satisfaction with care at time points other than post-treatment. | |
Individual participation | Post-treatment | Very low (a, c, d) | The findings for effect of iCBT vs. in-person CBT on individual participation are heterogeneous, and the evidence is very uncertain. | |
Longest follow-up | No trials identified | Not applicable | No trials were identified containing data on individual participation at time points other than post-treatment. |
CBT = cognitive behavioural therapy; HRQoL = health-related quality of life; iCBT = internet-delivered cognitive behavioural therapy; nRCT = non-randomized controlled trial; RCT = randomized controlled trial.
Note: “Very uncertain” means that the estimates of effect from the body of evidence may be very different from the true effect.
a = risk of bias; b = inconsistency; c = indirectness; d = imprecision.
Pain Interference
Three trials (2 RCTs,73,74 1 nRCT84; N = 293), all with high risk of bias (unclear direction), reported on pain interference measured by the Brief Pain Inventory Interference Subscale73,84 or Visual Analogue Scale (VAS) Interference Scale.74 The trials involved adult participants (mean ages were 50 to 59 years; primarily females in 2 trials74,84; veterans only, primarily male in 1 trial73) with various chronic pain conditions73,74 or chronic back pain.84 The CBT programs were highly variable; 2 trials compared therapist-delivered videoconference-based ACT73 or CBT84 to content-matched in-person ACT (individual-based) or CBT (group-based), respectively, and the third trial compared individual self-directed iCBT (psychologist-guided) to content-matched psychologist-delivered group in-person CBT.74
The results from these studies indicated that there may be little to no difference in the effect of iCBT versus in-person CBT on pain interference post-treatment73,74 and at the longest follow-up point (2 months,74 3 months,84 or 6 months73), but the evidence was very uncertain because of very serious concerns about risk of bias and serious concerns about indirectness and imprecision (Table 17). All trials were judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition) and self-reported subjective outcomes that may have been affected by the open-label nature of the trials.73,74,84 We considered the comparison of iCBT to in-person CBT to be indirect in 1 trial because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison.74 Finally, imprecision was difficult to judge because there were no formal between-group comparisons; however, within-group SDs were wide in all 3 trials.73,74,84
Pain Control
Three trials (2 RCTs,73,74 1 nRCT84; N = 293), all with high risk of bias (direction unclear), reported on pain control measured by the Brief Pain Inventory Severity Subscale73,84 or VAS Pain Intensity Scale.74 The trials involved adult participants (mean ages were 50 to 59 years; primarily females in 2 trials74,84; veterans only, primarily males in 1 trial73) with various chronic pain conditions73,74 or chronic back pain.84 The CBT programs were highly variable; 2 trials compared therapist-delivered videoconference-based ACT73 or CBT84 to content-matched in-person ACT (individual-based) or CBT (group-based) and the third trial compared individual self-directed iCBT (psychologist-guided) to content-matched psychologist-delivered group in-person CBT.74
The results from the trials showed there may be little to no difference in the effect of iCBT versus in-person CBT on pain control post-treatment73,74 and at the longest follow-up point (2 months,74 3 months,84 or 6 months73), but the evidence is very uncertain because of very serious concerns about risk of bias and serious concerns about indirectness and imprecision (Table 18). All trials were judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition) and self-reported subjective outcomes that may have been affected by the open-label nature of the trials.73,74,84 We considered the comparison of iCBT to in-person CBT to be indirect in 1 trial because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison.74 Finally, imprecision was difficult to judge because there were no formal between-group comparisons; however, within-group SDs were wide in all 3 trials.73,74,84
HRQoL or Overall Well-Being
Three RCTs (N = 240),73-75 all with high risk of bias (direction unclear), reported on HRQoL or overall well-being measured by the 12-Item Short Form (SF-12) Mental Component Summary (MCS) and SF-12 Physical Component Summary (PCS),73 Fibromyalgia Impact Questionnaire (FIQ) (0 = no impairment to 100 = maximum impairment),75 or Research and Development 36-Item Health Survey (RAND-36) (0 = worse health to 100 = better health).74 The trials included adult participants (mean ages were 49 to 53 years; primarily females in 2 trials74,75; veterans only, primarily males in 1 trial73) with various chronic pain conditions73 or fibromyalgia.75 The CBT programs were highly variable; 2 RCTs compared content-matched individual self-directed iCBT to group in-person CBT (with guidance from a therapist75 or psychologist74), and the third RCT compared content-matched individual videoconference-based ACT to individual in-person ACT.73
The results across the trials showed there may be little to no difference in the effect of iCBT versus in-person CBT on HRQoL or overall well-being post-treatment73-75; results at the longest follow-up point (2 months,74 6 months,73 or 12 months75) were heterogeneous. At both time points (i.e., post-treatment and the longest follow-up point), the evidence was very uncertain because of very serious concerns about risk of bias and serious concerns about indirectness and imprecision (Table 19). All trials were judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition)73,74 and self-reported subjective outcomes that may have been affected by the open-label nature of the trials.73-75 We considered the comparison of iCBT to in-person CBT to be indirect in 2 trials because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison.74,75 Finally, imprecision was difficult to judge because there were no formal between-group comparisons; however, within-group SDs were wide in all 3 trials.73-75
At the longest follow-up point, 1 trial showed little to no difference in SF-12 MCS and SF-12 PCS,73 1 trial showed little to no difference for all but 1 of the 9 RAND-36 subscales (individual iCBT was favoured in perceived health change; calculated mean changes for individual iCBT and group in-person CBT were 22.50 [SD = 24.17] and 0 [SD = 32.67], respectively; P < 0.05),74 and 1 trial showed individual iCBT was favoured in mean change in FIQ score from post-treatment to the longest follow-up point (analysis of variance [ANOVA] P < 0.001; calculated mean changes for individual iCBT and group in-person CBT were −5.12 [SD = 17.98] and −3.29 [SD = 18.76], respectively).75 Calculation methods for mean changes are described in the Data Analysis and Synthesis section of this report.
Psychological or Psychosocial Function or Symptoms
Pain Acceptance
One RCT (N = 128),73 with high risk of bias (direction unclear), reported pain acceptance measured by the CPAQ-R. The aim of this RCT was to change participants’ expectations from living pain-free to living as well as possible with pain. In this RCT, individual videoconference-based ACT was compared with individual in-person ACT (content-matched) in veterans (17.8% female; mean age = 52 years) with a chronic, nonterminal pain condition.73
The results of the trial showed there may be little to no difference in the effect of individual videoconference-based ACT versus in-person ACT on pain acceptance post-treatment and at the longest follow-up point (6 months),73 but the evidence is very uncertain because of very serious concerns for risk of bias and serious concerns for inconsistency, indirectness, and imprecision (Table 20). This trial was judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition) and self-reported subjective outcomes that may have been affected by the open-label nature of the trial. There was limited evidence of consistency because only 1 trial was available that reported on the outcome. We considered the comparison of iCBT to in-person CBT to be indirect because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison. Furthermore, this trial only included veterans and examined ACT; therefore, it is unclear if findings from this trial are generalizable to other populations and types of CBT. Finally, there was a concern about imprecision because of the wide between-group SDs.
Anxiety, Depression, or General Psychological Distress
Three trials (2 RCTs,73,75 1 nRCT84; N = 261), all with high risk of bias (direction unclear), reported on anxiety, depression, or general psychological distress measured by the Patient Health Questionnaire-9 (PHQ-9),73 Pain Anxiety Symptoms Scale-Short Form 20-Item (PASS-20),73 Hospital Anxiety and Depression Scale (HADS),75,84 or the Beck Depression Inventory (0 = no depression to 63 = maximum depression).75 The trials included adult participants (mean ages were 49 to 59 years; primarily females in 2 trials75,84; veterans only, primarily males in the third trial73) with various chronic pain conditions,73 chronic back pain,84 or fibromyalgia.75 The CBT programs were highly variable with 1 trial comparing individual videoconference-based ACT to individual in-person ACT,73 1 trial comparing group videoconference-based CBT to group in-person CBT,84 and the third trial comparing individual self-directed iCBT to group in-person CBT (therapist-guided) (all content-matched between groups).75
The results from the trials showed there may be little to no difference in the effect of iCBT versus in-person CBT on anxiety, depression, or general psychological distress post-treatment73,75; results were heterogeneous at the longest follow-up point (3 months,84 6 months,73 or 12 months75). The evidence overall was very uncertain because of very serious concerns about risk of bias and serious concerns about indirectness and imprecision (Table 20). All trials were judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition)73,84 and self-reported subjective outcomes that may have been affected by the open-label nature of the trials.73,75,84 We considered the comparison of iCBT to in-person CBT to be indirect in 1 trial because there were differences in delivery format (individual versus group) across arms that may have confounded the comparison.75 Finally, imprecision was difficult to judge because there were no formal between-group comparisons; however, within-group SDs were wide in all 3 trials.73,75,84
At the longest follow-up point, 1 trial showed little to no difference in PHQ-9 and PASS-20 scores,73 1 trial showed little to no difference in HADS scores,84 and 1 trial showed little to no difference in HADS scores and individual iCBT to be favoured in mean change in the Beck Depression Inventory score from post-treatment to the longest follow-up point (ANOVA P = 0.004; calculated mean change for individual iCBT and group in-person CBT = −6.90 [SD = 3.91] and −2.54 [SD = 6.22], respectively).75 Calculation methods for mean changes are described in the Data Analysis and Synthesis section of this report.
Self-Efficacy
One RCT (N = 40),75 with high risk of bias (direction unclear), reported on self-efficacy measured by the Chronic Pain Self-Efficacy scale. This RCT included progressive relaxation training and cognitive restructuring, and compared content-matched individual self-directed iCBT to group in-person CBT in adults (100% female; individual iCBT: mean age = 49.82 years; group in-person CBT: mean age = 53.50 years) with fibromyalgia.75
The findings of the trial showed that there may be little to no difference in the effect of iCBT versus in-person CBT on self-efficacy post-treatment and at the longest follow-up point (i.e., 12 months),75 but the evidence was very uncertain because of serious concerns for risk of bias, inconsistency, indirectness, and imprecision (Table 20). This trial was judged to be at high risk of bias because of self-reported subjective outcomes that may have been affected by the open-label nature of the trial. There was limited evidence of consistency because only 1 trial was available that reported on self-efficacy. We considered the comparison of iCBT to in-person CBT to be indirect because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison. Furthermore, this trial only included female participants; therefore, it is unclear if findings from this trial can be generalized to other populations. Finally, there was a concern about imprecision because there were no between-group comparisons and within-group SDs were wide.
Pain-Related Worrying
Two RCTs (N = 112),74,75 both with high risk of bias (direction unclear), reported on pain-related worrying measured by the Pain Catastrophizing Scale (global pain catastrophizing: 0 = no pain catastrophizing to 52 = maximum pain catastrophizing; rumination: 0 to 16; magnification: 0 to 12; helplessness: 0 to 24). The trials included adult participants (mean ages were 49 to 53 years; only females in 1 trial75; the second trial consisted of primarily female participants74) with various chronic pain conditions74 or fibromyalgia.75 The RCTs compared content-matched individual self-directed iCBT to group in-person CBT with guidance from a therapist75 or psychologist,74 and included variable CBT program content.74,75
The results from the trials showed there may be little to no difference in the effect of iCBT versus in-person CBT on pain-related worrying post-treatment74,75; results were heterogeneous at the longest follow-up point (2 months74 or 12 months75), but the evidence was very uncertain because of very serious concerns for risk of bias and serious concerns for indirectness and imprecision at post-treatment and the longest follow-up point (Table 20). The trials were judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition)74 and self-reported subjective outcomes that may have been affected by the open-label nature of the trials.74,75 We considered the comparison of iCBT to in-person CBT to be indirect in both trials because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison.74,75 Imprecision was difficult to judge because there were no formal between-group comparisons and there were wide within-group SDs in both trials, although based on available data (completers analysis) at least some imprecision may exist.74,75 Additionally, there were serious concerns for inconsistency at the longest follow-up point because the findings of both trials differed,74,75 and it was not possible to credibly explain the differences in subgroup analyses due to the small number of included trials.
In 1 trial, ANOVA group × time analyses were not statistically significant on the Pain Catastrophizing Scale global score for the change from baseline to 2 months post-treatment between groups.74 Meanwhile, ANOVA group × time analyses for 12 months post-treatment compared with post-treatment in the second trial were statistically significant (favoured iCBT) for the Pain Catastrophizing Scale global score (P < 0.001) and 2 subscales (helplessness: P = 0.009; magnification: P < 0.001) but were not statistically significant for the rumination subscale (P > 0.05).75 Mean change scores for individual iCBT were −10.68 (SD = 4.97) for pain catastrophizing, −4.10 (SD = 2.54) for rumination, −4.53 (SD = 4.18) for helplessness, and −2.06 (SD = 1.98) for magnification. Mean change scores for group in-person CBT were −0.52 (SD = 12.47) for pain catastrophizing, −1.33 (SD = 3.93) for rumination, −0.76 (SD = 5.97) for helplessness, and 1.58 (SD = 3.86) for magnification. Findings showed maintenance or improvement in the Pain Catastrophizing Scale global score and 3 subscales (rumination, helplessness, magnification) in the iCBT group. However, scores were maintained or worsened (i.e., magnification subscale) in the in-person CBT group at 12 months post-treatment.75
Coping With Pain
Two RCTs (N = 112),74,75 both with high risk of bias (direction unclear), reported on coping with pain measured by the Chronic Pain Coping Inventory75 or PCCL.74 The trials included adult participants (mean ages were 49 to 53 years; only females in 1 trial75; and the second trial consisted of primarily female participants74) with various chronic pain conditions74 or fibromyalgia.75 The RCTs compared content-matched individual self-directed iCBT with group in-person CBT with guidance from a therapist75 or psychologist,74 with variable CBT program content.75
The results from the trials showed there may be little to no difference in the effect of iCBT versus in-person CBT on coping with pain post-treatment and at the longest follow-up point (274 or 12 months,75) but the evidence was very uncertain because of very serious concerns for risk of bias and serious concerns for indirectness and imprecision (Table 20). The trials were judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition)74 and self-reported subjective outcomes that may have been affected by the open-label nature of the trials.74,75 We considered the comparison of iCBT to in-person CBT to be indirect in both trials because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison.74,75 Imprecision was difficult to judge because there were no formal between-group comparisons and there were wide within-group SDs in both trials.74,75
Fatigue
One RCT (N = 72),74 with high risk of bias (direction unclear), reported on fatigue measured by VAS Fatigue Scale (0 = not at all to 10 = extremely). This RCT focused on the cognitive behavioural model of pain circle and compared content-matched individual iCBT with group in-person CBT in adults (individual iCBT: 68.2% female, mean age = 50.6 years; group in-person CBT: 60.7% female, mean age = 53.2 years) with nonspecific chronic pain and/or chronic pain for which no somatic treatment could be offered.74
The results of the trial showed there may be little to no difference in the effect of iCBT versus in-person CBT on fatigue post-treatment and at the longest follow-up point (2 months),74 but the evidence was very uncertain because of very serious concerns for risk of bias and serious concerns for inconsistency, indirectness, and imprecision (Table 20). This trial was judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition) and self-reported subjective outcomes that may have been affected by the open-label nature of the trial. There was limited evidence of consistency because only 1 trial was available that reported on fatigue. We considered the comparison of iCBT to in-person CBT to be indirect because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison. Finally, there was a concern about imprecision because there were no formal between-group comparisons and there were wide within-group SDs.
Sleep
One RCT (N = 128),73 with high risk of bias (direction unclear), reported on sleep measured by the Pittsburgh Sleep Quality Index. The aim of the RCT was to change participants’ expectations from living pain-free to living as well as possible with pain. It compared individual videoconference-based ACT to individual in-person ACT (content-matched) in veterans (17.8% female; mean age = 52 years) with a chronic, nonterminal pain condition.73
The findings of the trial showed there may be little to no difference in the effect of individual videoconference-based ACT versus in-person ACT on sleep post-treatment and at the longest follow-up point (6 months),73 but the evidence was very uncertain because of very serious concerns for risk of bias and serious concerns for inconsistency, indirectness, and imprecision (Table 21). This trial was judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition) and self-reported subjective outcomes that may have been affected by the open-label nature of the trial. There was limited of evidence of consistency because only 1 trial was available that reported on sleep. We considered the comparison of iCBT to in-person CBT to be indirect because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison. Furthermore, this trial only included veterans and examined ACT; therefore, it is unclear if findings from this trial can be generalized to other populations and types of CBT. Finally, there was a concern about imprecision because there were no formal between-group comparisons and there were wide within-group SDs.
Physical Activity Level
One RCT (N = 128),73 with high risk of bias (direction unclear), reported on physical activity level measured by the West Haven-Yale Multidimensional Pain Inventory Activity Subscale (0 to 6 with higher scores indicating greater levels of general activity). This RCT aimed to change participants’ expectations from living pain-free to living as well as possible with pain; it compared individual videoconference-based ACT to individual in-person ACT (content-matched) in veterans (17.8% female; mean age = 52 years) with a chronic, nonterminal pain condition.73
The findings of the trial showed there may be little to no difference in the effect of individual videoconference-based ACT versus in-person ACT on physical activity level post-treatment,73 but the evidence was very uncertain because of very serious concerns for risk of bias and serious concerns for inconsistency, indirectness, and imprecision (Table 22). In-person ACT may be favoured; there were higher levels of general activity (between-group difference in change rates: 0.31; 95% CI, 0.02 to 0.60; P = 0.03) at the longest follow-up point (6 months), but the evidence was very uncertain because of very serious concerns for risk of bias and serious concerns for inconsistency and indirectness.73 This trial was judged to be at high risk of bias at post-treatment and the longest follow-up point because of incomplete outcome data (large and unbalanced attrition) and self-reported subjective outcomes that could have been affected by the open-label nature of the trial. There was limited evidence of consistency because only 1 trial was available that reported on physical activity level. We considered the comparison of iCBT to in-person CBT to be indirect because there were differences in delivery format (individual versus group) across arms that may have confounded the comparison. Furthermore, this trial only included veterans and examined ACT; therefore, it is unclear if findings from this trial can be generalizable to other populations and types of CBT. At post-treatment, there was concern about imprecision because there were no formal between-group comparisons and there were wide within-group SDs.
Physical Function
One nRCT (N = 93),84 with high risk of bias (direction unclear), reported on physical function as measured by Oswestry Disability Index. With topics such as stress management, social support, and relapse management, this nRCT compared content-matched group videoconference-based CBT to group in-person CBT in adults (group videoconference-based CBT: 70.2% female, mean age 54.5 years; group in-person CBT: 57.8% female, mean age = 59.7 years) with chronic back pain.84
The findings of the trial showed there may be little to no difference in the effect of group videoconference-based CBT versus in-person CBT on physical activity level at the longest follow-up point (videoconference-based CBT: 2 months; in-person CBT: 3 months),84 but the evidence is very uncertain because of very serious concerns for risk of bias and serious concerns for inconsistency and imprecision (Table 23). Post-treatment data were not reported in this trial. The trial was judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition) and lack of consideration of confounders. There was limited of evidence of consistency because only 1 trial was available that reported on physical function. Finally, there was a concern about imprecision because there were no formal between-group comparisons and there were wide within-group SDs.
Prescription Opioid Use
One nRCT (N = 93),84 with high risk of bias (direction unclear), reported on prescription opioid use measured by the Current Opioid Misuse Measure. This nRCT included stress management, social support, and relapse management, and compared content-matched group videoconference-based CBT with group in-person CBT in adults (group videoconference-based CBT: 70.2% female, mean age = 54.5 years; group in-person CBT: 57.8% female, mean age = 59.7 years) with chronic back pain.84
The findings of the trial showed there may be little to no difference in the effect of group videoconference-based CBT versus in-person CBT on prescription opioid use at the longest follow-up point (videoconference-based CBT: 2 months; in-person CBT: 3 months),84 but the evidence was very uncertain (Table 24). Post-treatment data were not reported in this trial. The trial was judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition) and lack of consideration of confounders. There was limited evidence of consistency because only 1 trial was available that reported on prescription opioid use. Finally, there was a concern about imprecision because there were no formal between-group comparisons and there were wide within-group SDs.
Satisfaction With Care
Two RCTs (N = 200),73,74 both with high risk of bias (direction unclear), reported on satisfaction with care. The trials involved adult participants (mean ages were 50 to 53 years; primarily females in 1 trial74; veterans only, primarily males in the second trial73) with various chronic pain conditions. The CBT programs were highly variable; 1 RCT74 compared content-matched individual self-directed iCBT to group in-person CBT (psychologist-guided) and the second RCT compared content-matched individual videoconference-based ACT to individual in-person ACT.73
The evidence from the trials showed there may be little to no difference in the effect of iCBT versus in-person CBT on satisfaction with care,73,74 but the evidence was very uncertain because of very serious concerns for risk of bias and serious concerns for indirectness (Table 25). The trials were judged to be at high risk of bias because of incomplete outcome data (large and unbalanced attrition) and self-reported subjective outcomes which could have been affected by the open-label nature of the trials.73,74 We considered the comparison of iCBT to in-person CBT to be indirect in 1 trial because there were differences in delivery format (individual versus group) across arms that may have confounded the comparison.74
Individual Participation
Two RCTs,73,74 with some risk of bias, and 1 RCT75 and 1 nRCT,84 with high risk of bias (direction unclear), reported on individual participation in the interventions (N = 333). The trials involved adult participants (mean ages were 49 to 59 years; primarily or all females in 3 trials74,75,84; veterans only, primarily males in the fourth trial73) with various chronic pain conditions,73,74 chronic back pain,84 or fibromyalgia.75 The CBT programs were highly variable; 2 trials compared content-matched videoconference-based ACT73 or CBT84 with in-person ACT or CBT (the ACT was individual whereas the CBT was group-based), and 2 trials compared content-matched individual self-directed iCBT with group in-person CBT (with guidance from a therapist75 or psychologist74).
The results were heterogeneous for the effect of iCBT versus in-person CBT on individual participation,73-75,84 and the evidence was judged to be very uncertain because of serious concerns for risk of bias, indirectness, and imprecision (Table 26). Specifically, the certainty of the evidence was rated down because of concerns for risk of bias from the randomization processes.73-75 We considered the comparison of iCBT to in-person CBT to be indirect in 2 trials because there were differences in delivery format (individual versus group) across arms that could have confounded the comparison.74,75 Finally, there was concern about imprecision because the number of events did not meet the optimal information size (< 300 events).73-75,84 Compared with in-person CBT groups, participants in iCBT groups exhibited higher withdrawal rates in 3 RCTs (20% to 46%),73-75 and lower withdrawal rates in the nRCT (14.9%).84 The lower withdrawal rates in the iCBT group of the nRCT84 may be attributed to participants’ ability to self-select into their preferred group. Meanwhile, results on attendance rates (when reported) were heterogeneous with higher attendance rates (95.2% attended all modules) in the iCBT group in 1 RCT74 and little to no difference in attendance rates (mean sessions attended) in the nRCT.84
Question 2: Safety
We identified no relevant studies that provided outcome data about the comparative safety of iCBT versus in-person CBT.
Limitations
Due to feasibility constraints, we did not screen the search results from trial registries. There is a small risk that some relevant data may have been missed using this approach, and we cannot comment on ongoing studies of relevance.
We chose to synthesize data directly post-program (i.e., post-treatment) and at the longest follow-up point reported in the included clinical trials. Although we believe this approach is most informative, data were available for multiple heterogenous time points across trials. For example, the longest follow-up point ranged between 2 and 12 months after treatment completion in the included trials. However, we did not encounter any outcome comparison in which heterogeneity across studies could be explained by differences in the length of the longest follow-up point.
Another potential limitation to consider is the generalizability of the findings from the 4 included trials to all people with different forms of chronic non-cancer pain and various types and modes of delivery of iCBT.73-75,84 Chronic non-cancer pain is a heterogenous condition that affects many different types of people and can be associated with various health conditions, such as fibromyalgia, headache, migraine, rheumatoid arthritis, osteoarthritis, multiple sclerosis, surgical procedures, chronic primary pain, or injuries to a muscle, nerve, or ligament.85 The trials included in the Clinical Review were specific to a small subset of chronic non-cancer pain populations, including veterans with nonterminal pain conditions,73 adult females with fibromyalgia,75 and adults with daily back pain84 or nonspecific chronic pain.74 None of the included trials had pediatric participants. Furthermore, pain acceptance, sleep, and physical activity level were reported in only 1 trial,73 which included only veterans and examined ACT. It is unclear if these outcomes can be generalizable to non-veteran populations and other types of CBT.73 Self-efficacy was reported in only 1 trial,75 which included only female participants with fibromyalgia. Physical function and prescription opioid use was reported in only 1 trial,84 which included participants with chronic back pain. In all cases, the 4 trials73-75,84 excluded people with various comorbidities, such as those with unstable medical conditions, mental health conditions (e.g., bipolar disorder, substance use disorder), or suicidal ideation. It is unclear if the findings from the included trials are generalizable to other chronic pain populations (e.g., adolescents, people who have comorbidities that would have prohibited them from participating in the clinical trials). Similarly, iCBT and in-person CBT programs can vary in their program content, number of modules, duration of sessions, number of sessions, format (i.e., individual versus group-based), types of support (e.g., phone, email, videoconference, in-person), and frequency of support. It is unclear whether the results of the 4 included trials,73-75,84 which examined 4 iCBT and in-person CBT interventions, are generalizable to other contexts. None of the trials reported on participants’ place of residence; thus, it is unclear if the results would differ for participants living in urban versus rural settings. Additionally, none of the included primary trials73-75,84 were conducted in Canada. Although there was no strong indication that the findings from the included trials, which were conducted in Spain,75 the Netherlands,74 and the US,73,84 would not apply to Canadian settings, there may be some differences (e.g., due to variations in health systems in these countries). In summary, there appeared to be little to no difference in the effect of iCBT versus in-person CBT on most reported outcomes post-treatment and at the longest follow-up point; however, because of the very low certainty of the evidence across all outcomes, the true effect of iCBT versus in-person CBT may differ from the findings described in this Clinical Review. Furthermore, because of the lack of reporting on safety data, the overall findings in this report should be interpreted with caution.
Summary of Results
Three RCTs73-75 and 1 nRCT84 were identified about the comparative clinical effectiveness of iCBT versus in-person CBT for the management of chronic non-cancer pain. No relevant studies were identified about the comparative safety of iCBT versus in-person CBT for the management of chronic non-cancer pain. These trials included a small subset of chronic non-cancer pain populations, including veterans with nonterminal pain conditions,73 adult females with fibromyalgia,75 or adults with daily back pain84 or nonspecific chronic pain.74 The CBT programs were highly variable; 2 trials compared content-matched videoconference-based ACT73 or CBT84 with in-person ACT (individual-based) or CBT (group-based), respectively, and 2 trials compared content-matched individual self-directed iCBT to group in-person CBT.74,75 The relevant outcomes reported included pain interference,73,74,84 pain control,73,74,84 HRQoL or overall well-being,73-75 psychological or psychosocial function or symptoms (i.e., pain acceptance; anxiety, depression, or general psychological distress; self-efficacy; pain-related worrying; coping with pain; fatigue),73-75,84 sleep,73 physical activity level,73 physical function,84 prescription opioid use,84 satisfaction with care,73,74 and individual participation.73-75,84
The certainty of evidence for all outcomes post-treatment and at longest follow-up point was very low, primarily because of very serious concerns about risk of bias and large imprecision across most outcome comparisons. Additionally, many comparisons were affected by serious indirectness (i.e., there were differences across study arms that may have confounded the main comparison of interest) and inconsistency. The very low certainty suggests the evidence does not provide a reliable indication of the likely treatment effect and that there is a very high likelihood that the true effect of iCBT versus in-person CBT could be substantially different than what was indicated in the 4 included trials.
Patients’ Perspectives
Overview
Research Questions
How do the experiences of people living with chronic non-cancer pain, and their caregivers, resonate (or not) with known experiences of iCBT for depression, anxiety, or PTSD when CBT would otherwise be provided?
What do people living with chronic non-cancer pain and their caregivers expect to access or experience accessing (or not) with regard to iCBT for the management of chronic non-cancer pain when CBT would otherwise be offered?
Key Messages
The 5 women we spoke with suggested that iCBT could become a supportive component of comprehensive chronic pain care when CBT would otherwise be provided; however, this potential benefit comes with some caveats:
Although iCBT for chronic pain is ideally part of an existing comprehensive and multidisciplinary chronic pain care strategy, the women noted that access to this kind of care was not currently a reality for many people living with chronic pain in Canada.
If jurisdictions were to pursue iCBT without also improving the availability of other components of chronic pain care, the women were concerned that iCBT would become a “quick fix” in the absence of broader multidisciplinary care options. Therefore, jurisdictions could consider the suite of multidisciplinary services available in their locales before determining whether iCBT programming would meet their needs relating to gaps in access.
The women suggested that referring people to iCBT too early could risk causing harm by potentially missing the root causes of their pain and failing to treat them accordingly. The women described how being referred to iCBT too early could also further validate feelings of worthlessness for people who have already been subjected to experiences of disbelief, dismissal, and neglect when seeking care for their pain. There is the potential that some people living with pain would appreciate early engagement with iCBT, particularly those with secondary chronic pain. The women felt that determining the appropriate candidates should on a case-by-case basis rather than as a standardized approach.
Considerations about for whom and at what points iCBT might be considered an appropriate intervention pivot around the concept of readiness. Readiness can be understood as an assemblage of treatment history, available current care practices, material realities of one’s condition, and individual needs or desires. The women we spoke with suggested that policies around iCBT that take these into account could help limit or prevent reinforcing experiences of dismissal, neglect, and untreated pain in people living with chronic pain.
As in previous reviews of iCBT for major depressive disorder (MDD), anxiety, and PTSD, a strong therapeutic relationship, and tailored approaches to iCBT programming were seen as vital components of successful engagement with iCBT for chronic non-cancer pain. This suggests that iCBT would ideally be provider-guided with enough space to develop and maintain a strong relationship. Our study further highlighted the importance to women we spoke with of engaging with providers who have adequate training in dealing with chronic pain.
Study Design
We conducted an interview study that explored people’s expectations of, or experiences with, iCBT as a component of care in the management of their chronic non-cancer pain. Further details on study design have been published in the full HTA protocol.86
Invitation to Participate and Consent
Patient collaborators meeting the following criteria were identified through connections to advocacy groups and organizations that had previously engaged with CADTH on other projects:
adults (18 years of age or older) living with chronic non-cancer pain or involved in the care of a person living with chronic non-cancer pain
individuals who had experienced (or had been offered) either CBT or iCBT as part of their pain management strategy in Canada.
Although not an eligibility criterion, we worked to include a diversity of people who could speak to whether iCBT (or in-person CBT) for chronic pain accounts for (or not) how the presence of and care for chronic pain is gendered, racialized, and differently distributed across socioeconomic dynamics.11,20 Similarly, because CBT can offer treatment for the management of chronic non-cancer pain from anywhere, we also worked to identify and engage with people who lived in geographically and demographically diverse areas (i.e., urban, rural, and remote).
To do this, the CADTH Patient Engagement team contacted Pain BC, the Patients of Eastern Ontario Pain Lifestyle Education (PEOPLE) Centre, Canadian Arthritis Patient Alliance, MindBeacon (a developer of iCBT), the YouthNet Chronic Pain Support Group at the Children’s Hospital of Eastern Ontario, the Canadian Pain Task Force, the Strategy for Patient-Oriented Research (SPOR)-funded Chronic Pain Network, and the Women’s College Hospital Institute for Health System Solutions and Virtual Care to share the opportunity to participate as a patient collaborator.
The Patient Engagement team obtained participants’ informed consent to share their information and summarized comments with CADTH staff. An additional consent form described how the information provided would be used in the report. Before or at the beginning of each interview, participants were reminded that they might be asked to share personal or sensitive information and that they could raise their concerns or end the interview at any time. Collaborators were also offered an honorarium for their time and participation.
Participants
Five adults living with chronic non-cancer pain responded to our invitation to participate. Two were engaged during protocol development as remained as patient contributors for the entirety of the project and also participated in the interview study. The other 3 participants were engaged and interviewed specifically for the interview study.
Although we actively worked to engage a diverse group of people, we were ultimately unsuccessful. When asked to describe how they would identify themselves (open-ended), all 5 participants described themselves as White or Jewish women. Furthermore, 4 of the 5 women interviewed reported having experience working in health care. Similarly, despite efforts to recruit participants from geographically diverse areas, all 5 women lived in metropolitan areas: 3 in Ontario, 1 in Quebec, and 1 in British Columbia. Of note, 1 participant moved from a rural to a metropolitan area to access specialized pain care.
Two of the women lived with a form of chronic primary pain and the remaining 3 lived with various forms of chronic secondary pain. Participants ranged from approximately 20 to 60 years of age and had been living with chronic pain between 6 and 30 years at the time of interview.
Interviews
We used semi-structured interviews guided by the research questions and thematic categories identified in CADTH’s previous 2 iCBT qualitative reviews.87,88 Although these thematic categories were foundational to our work, we kept the opportunity open in our interviews for participants to highlight differences in their experiences and respond in ways that might not map onto these pre-established categories.
The interviews were conducted by the primary qualitative researcher, and all were done as videoconference calls. Interviews were recorded, and notes were taken throughout the interview with the consent of the people being interviewed. Audio files, transcripts, and summaries of these interviews were shared with project team members working on other components of the HTA.
Analysis Methods
We used a modified framework analysis approach89 to describe and summarize the perspectives and experiences of using iCBT for people living with chronic non-cancer pain. Using this approach allowed us to reflect on and explore the meaning of findings identified in our previous reports on iCBT for MDD or anxiety87 and PTSD88 in the context of iCBT for chronic non-cancer pain. To do so, our analysis developed around thematic categories identified in our previous iCBT reviews87,88 while remaining open to new and emergent ideas. These thematic categories included expectations and experiences related to:
Context: Involves experiences with the ways in which both personal (e.g., severity of condition) and structural (e.g., availability of intervention) situations influence engagement with iCBT.
Relationality: Involves perceptions of and experiences with a provider or supporter throughout the use of iCBT.
Process: Involves experiences with the accessibility, convenience, flexibility, anonymity, and privacy (or not) of iCBT. It also involves participants’ perceptions on what is required for them to successfully engage with iCBT (or not), and experiences with completing these requirements in the given time frame.
Content: Involves experiences with iCBT modules and how these are designed to facilitate knowledge transfer (or not) to the participant. It also involves experiences regarding modes of communication within the intervention, the adaptability of the intervention to the participant, and the navigation skills necessary to use the intervention.
The analysis followed a stepped approach adapted to accommodate both deductive and inductive thinking. The primary and secondary qualitative researchers first read and familiarized themselves with 2 interview transcripts and notes taken throughout interviews, while memoing any analytical thoughts or impressions defined by the thematic categories identified in the 2 previous iCBT reviews. A third qualitative researcher concurrently read the 2 transcripts and independently noted key ideas informed by the same predefined categories. All researchers then met to critically reflect on and discuss emergent ideas, define the framework, and agree on a set of key ideas to apply to subsequent transcripts.
The primary and secondary qualitative researchers then read and applied the framework to all the transcripts, continuing to take notes and beginning to summarize the identified characteristics of and differences within and across ideas and thematic categories, interrogating predefined concepts and drawing out connections to explore their relationships. When potentially new thematic categories emerged, the framework was adapted to accommodate these emergent ideas after discussion with the team.
The findings described in the following section result from a process that included explicit considerations of researchers’ theoretical and methodological backgrounds (e.g., training, expertise, and knowledge) to address, modify, and hone their understanding of the data. To enhance the credibility of these findings, the primary and secondary qualitative researchers positioned themselves in relation to the emergent analysis by engaging in critical reflection, memoing, and regular discussions with the study teams. They refined their analysis as appropriate based on these activities to ensure that the findings were grounded in what the study participants said. To further contribute to the credibility of the findings, the Patient Engagement Officer referred the patient contributors and other study participants toward the final synthesized report for review during stakeholder feedback.
Results
Analysis
Of the 5 women who participated in this study, only 1 had experience with some form of iCBT. Although technically meeting the definition of iCBT used in this report, it was only at the onset of the COVID-19 pandemic that she moved to online, synchronous videoconference with a provider she had already been working with in person for years. The other 4 women were either offered, or had undergone, some other form of CBT. Of note, none of the women we interviewed had experienced unguided or asynchronous courses delivered entirely online.
Context 3
Previous qualitative CADTH reviews of iCBT have used the thematic heading of “context” to categorize peoples’ descriptions of various structural and personal elements that had affected (or might affect) their engagement with iCBT. The following provides an exploration of the resonance of this category for people living with chronic pain and identifies where their expectations or experiences might diverge from those living with MDD, anxiety, or PTSD.
Structural Contextual Elements
CADTH reviews of iCBT for MDD or anxiety87 and PTSD88 describe how persistent stigma around these conditions, the limited treatment opportunities for people living with these conditions, and experienced discrimination (e.g., sexism, racism, colonialism) toward some people living with these conditions were all common structural elements that affect the value of iCBT. For example, the persistence of stigma around MDD or anxiety was described by some people as contributing to their concern that being offered iCBT too soon could feel like they were not taken seriously by their providers.87 This could be particularly challenging in situations in which the limited availability of alternative interventions made iCBT 1 of the only treatment options they were offered. Although people might have been willing to accept, at times, iCBT over wait-listing for other treatments (or no treatment at all), many described wishing they had the opportunity to explore other options before engaging with iCBT.87,88 Further compounding these condition-specific concerns, people also described how social determinants of health (e.g., age, race, gender, socioeconomic status, geographic location)87 and colonialism88 affect life with and potential treatment of these conditions with iCBT.87,88
The women included in this study validated what we learned from previous reviews as relevant for people with chronic pain and reiterated the importance of carefully considering how these structural elements might affect the utility of iCBT. Without this consideration, they felt it is unlikely that introducing iCBT will address concerns about accessible and equitable comprehensive pain care. Although the nuances of these elements might look different in the space of chronic pain care, the women we spoke with described a similar series of structural concerns associated with iCBT becoming a supportive component of their care. Nearly all the women had struggled with being recognized as living with chronic pain or having that pain cared for by their providers. Even after their pain was recognized as chronic, many described their own, or other people’s, challenges in accessing CBT or iCBT specifically and comprehensive multidisciplinary chronic pain care broadly. Although none of the women were explicit about how race or colonialism affected chronic pain care in their lives or their expectations about iCBT, the women periodically reminded us of how being a woman could affect how they respond or act around care providers to be seen as a legitimate patient.
The Challenge of Being Heard
The movement from acute to chronic pain involves a period of uncertainty in which people must experience ongoing pain but they have not lived long enough with that ongoing pain for it to be considered chronic. During this period, people living with not-yet-chronic pain may continue to receive care for pain that may eventually be identified as chronic. However, according to the women we spoke with, this period of uncertainty can also be distressing and is often filled with experiences of disbelief, dismissal, and neglect.
One reason suggested for why these are such common early experiences was that family doctors (or other providers with specialties outside of pain) receive limited training in how to care for people living with pain. This limited training, paired with what 1 woman described as “bad publicity” about opioids that continues to stigmatize people living with pain, can mean “we’re at a crossroads and the patient is caught in the middle.” Caught between the limited training of their providers and this “bad publicity,” the women described how challenging it was to find providers who are open (or able) to hear their concerns as more than a “complaint” or “drug-seeking.” Based on their own experiences, they described how this is particularly concerning given these providers’ roles as both evaluators of whether someone has moved from acute to chronic pain and as gatekeepers to broader pain-specific services.
Therefore, a primary challenge is being heard. For 1 woman (who lives with chronic primary pain), this meant modifying her behaviour so she would not be seen as helpless or over-the-top by her providers. She noted that her experience as a health care professional allowed her to see from the “other side of the table” and helped to pitch herself in a language that her providers could hear. But people do not always have previous experience working in health care or the bandwidth to both manage their pain and advocate for themselves in languages that their providers can hear. Instead, they may be pushed into defensive positions of self-advocacy that can be demoralizing and exhausting.
One woman described returning to her orthopedic surgeon every 2 weeks wondering why it felt like “someone literally soaked my arm in gasoline and lit it on fire.” Although she was ultimately diagnosed with a severe form of chronic primary pain, it took months of being brushed off with comments such as “you’re older now — pain hurts” and “stop exaggerating” before receiving this diagnosis. The problem was not necessarily in the length of time it took to be diagnosed with a chronic form of pain (technically this happened within a clinically acceptable time frame), but rather the need to undergo such dismissive behaviour to reach this stage. And although it may seem far removed from the opportunity to engage with iCBT (or not), she repeatedly described how this early experience has affected every treatment decision made since then.
This is discussed more in the Readiness section; note that harms that may happen along the diagnostic pathway to chronic pain can have longstanding effects for people living with chronic pain and can affect the impact of future treatment opportunities — particularly those like iCBT that are not primarily focused on the physicality of chronic pain.
iCBT Needs to Be Situated Within a Comprehensive and Multidisciplinary Care Approach
Upon diagnosis, people with chronic pain ideally would be referred to a series of multidisciplinary pain services that could approach and address their pain in a comprehensive way. As stated in the decision problem for this HTA, it is assumed that iCBT programming would only ever be offered as part of this multidisciplinary care. However, the women we spoke with were concerned that, in practice, this was not a current reality. Instead, accessing the right treatment at the right time (if at all) was described as challenging given how fragmented, difficult to navigate, and expensive chronic pain care can be in Canada.
To this point, 1 woman described how family doctors may “refus[e] to take patients back” once they have been diagnosed with chronic pain given the challenges associated with caring for that chronic pain. If there are no pain clinics that can take them on, the person living with chronic pain might then be caught in a holding pattern in which their pain can worsen before specialized care becomes available (if it ever does). Although she felt that iCBT might be able to serve as a stopgap for people stuck in this holding pattern, she was clear that it should only be understood as a bare minimum that is meant to support people who might otherwise be presenting to the emergency department because “they just can’t handle [the pain] and they’re losing their cookies.”
What was troubling for some of the women we spoke with, however, was just how easily iCBT could be offered outside of comprehensive, multidisciplinary care approaches. Because iCBT can be delivered online and remotely, there is an assumption that iCBT is more accessible than in-person CBT and that the decreased time commitments from providers may free them to support more patients. Although this is an appealing feature of iCBT, the women were concerned that this may also foster a slippage in which iCBT becomes a “quick fix” solution and permanent stopgap rather than a small component of a broader multidisciplinary approach. In the short term, iCBT may seem like a solution that helps patients, but in the long term, as 1 woman worried, “They may be really harming the patient by taking the easier route and not investigating what the cause of that pain is.”
With this in mind, the women we spoke with clearly felt iCBT could become a useful and supportive tool when situated within a broader multidisciplinary approach. Although it is possible that offering iCBT early on may help keep some people out of the emergency department, they felt that using iCBT as a stopgap for everyone waiting for multidisciplinary care could risk missing underlying causes of their chronic pain and reinforcing experiences of dismissal, disbelief, and neglect. In light of these considerations, it may help to consider the broader chronic pain care practices, programming, and treatment options already publicly available (or not) when considering funding and providing iCBT for chronic pain.
Personal Contextual Elements
In our previous reviews of iCBT,87,88 personal factors included concerns about how the severity of one’s condition, or the presence of comorbidities, might interfere with the potential therapeutic impact of iCBT. Without additional supports in place, or other interventions at the ready, people worried that those living through severe episodes of pain might be discouraged, or even harmed, by iCBT given the demands of this form of “self-help” intervention (p. 32).87 Similarly, those living with comorbidities might be better served by treating the comorbidities first or, potentially, by deliberately including them within iCBT programming. In iCBT for MDD or anxiety, personal factors were also described as “physical and experiential barriers, such as illness challenge, concentration difficulty, apathy, mood, lack of motivation, discomfort writing, fatigue and pain” (p. 32).87
This is consistent with how the women we spoke with described the use of iCBT for chronic pain. Although the women felt iCBT may be a valuable addition to chronic pain care strategies, they agreed that challenges with other comorbidities or the severity of the pain might interfere with the ability of iCBT to be a supportive intervention.
For example, the type of pain — primary or secondary — may relate to the appropriateness of offering, or timing of when to offer, iCBT. They felt that, for those living with chronic primary pain, it would be important to exhaust every possible physical intervention before suggesting or engaging with iCBT because people would not be able to focus on the work required to benefit from iCBT if the pain was too severe. But for those living with chronic secondary pain, there seemed to be more of a willingness to engage early on. Given the chronic pain coincides with other chronic or degenerative illnesses, it is possible there is less of a need to explore exactly what is causing the pain because it is already known.
Chronic pain looks different for everyone, and what this pain is related to can, at times, be difficult to identify. This complexity around identifying an underlying cause or understanding how pain presents in different people’s lives demonstrates how challenging it can be to know when to suggest iCBT.
Readiness
Regarding what makes someone ready for iCBT, previous CADTH reviews87,88 have primarily focused on understanding the responsibility that people with PTSD, MDD, or anxiety have when determining readiness. As an individualized responsibility, the person living with 1 of these conditions is required to both understand their own care needs (or desires) and how iCBT might have a role in meeting those needs (or desires).
Although this understanding of the individualized responsibility of readiness does correspond with much of what the women living with chronic pain told us, the women also drew on earlier conversations of structural and personal contexts (as described previously) to articulate how they might expect iCBT to become a viable option for them. As such, based on our conversations with women living with chronic pain, we understand the concept of readiness as describing a process under constant negotiation. Navigating this process is a collective effort with providers that draws from an assemblage of treatment histories, available care practices, material realities of one’s condition, and individual needs or desires.
As a process under constant negotiation, women felt that readiness for an intervention like iCBT would be best supported by repeat engagement with, and guidance from, care providers who have adequate training in chronic pain. This is challenging given, as discussed previously, how few people living with chronic pain have access to publicly funded specialists or specialized pain care in Canada. Similarly, building toward readiness becomes even more challenging when we consider what the women described as the repeated, and potentially ongoing, dismissals people with chronic pain can experience across their interactions with some aspects of the health care system.
Negotiation of readiness for iCBT is present in those initial interactions between the general practitioner and the person presenting with pain and is still present after years of specialist care. Therefore, readiness is as much about ongoing practice of things like trauma-informed care as it is about earlier experiences where choices are made to offer and pursue iCBT.
Readiness is also about how these experiences with the health care system and the supportive practices of health care providers might crystallize at particular moments into specific choices and actions. As a facilitator of a peer-support group for people living with chronic pain, 1 woman in our study worked with people at different stages in their journey with chronic pain. This work, paired with her own experience living with chronic pain, led her to believe that 1 of the more consistent differences between someone who might be “ready” for iCBT (or CBT) and someone who is not ready often comes down to how long they have been living with pain. Some people are “really interested in their patterns and their thinking. And examining those things. And other people [are] not ready for something like this yet because they’re still looking for ‘what’s the medical fix?’”
Having struggled for so long “against” the pain, becoming ready for iCBT programming that is organized around coping with chronic pain requires an openness to seeing one’s pain as something to be “liv[ed] with.” Following years of specialist care and treatments through her pain management unit, 1 woman described how she knew she was ready to visit a psychologist after a trial infusion of ketamine. Following her third infusion she decided “it’s not worth it because I feel the pain goes away 100 percent, but then it comes back. And when it comes back it’s worse because now I remember what it is to have no pain. And I needed, actually, to see a psychologist after that to deal with this pain now coming back.”
With all other treatment options exhausted or already in play, the dissonance between her “almost out-of-body” experience with ketamine and the lived-in-body with pain was unbearable. Although it was at this moment that her “readiness” to visit a psychologist seemed to crystallize into a particular decision or action, she described this as unthinkable without the years of trying that preceded this experience. Readiness came once it was proven that her being, and her pain, mattered and were cared for “because, if you realize you’ve gotten to the end of the line for what they can do to help your pain and this is what most of your life is likely going to be like, it’s not just acceptance therapy, it’s what else can you do.”
Readiness, however, does not require an out-of-body experience or that all physical interventions are attempted first. Although this woman’s path toward psychological help (in this case, face-to-face group-based ACT) played out in this way, this moment also represents an assemblage of her treatment history, current care practices, the material realities of her condition, and her individual needs or desires. This would also typically include some sort of directed work on the physicality of pain so that one can tolerate reflecting on their thoughts or behaviours around pain; however, how complete this physical pain management is might vary by person and the type of pain or other condition(s) they are living with.
The women we spoke seemed to think that iCBT could be a supportive addition to a larger suite of care practices and interventions around chronic pain, yet it was also seen as something that could not work in isolation from a more comprehensive approach. Policy about iCBT that reflects readiness as an assemblage of treatment history, current care practices, material realities of one’s condition, and individual needs or desires could help to limit or prevent reinforcing experiences of dismissal, neglect, and uncared for pain in people living with chronic pain.
Relationships
In the Context section, we examined a variety of ways in which people described how their engagement with (or interest in) iCBT, or traditional CBT broadly, could be affected by each person’s structural and personal circumstances. Using the concept of “readiness” we demonstrated how these contexts might weave together to create space for iCBT programming to become a realistic and supportive option (or not) for people living with chronic pain.
The Relationships section expands on this and marks out both what is at stake in iCBT and how fundamental a strong therapeutic alliance is to holding (and working on) these stakes. When thinking of self and others, we are interested in further clarifying expectations of how iCBT may be supportive. We identify how a strong therapeutic relationship with a particular provider can be supportive to an effective engagement with iCBT.
Although none of the women we spoke with had experienced asynchronous, modular iCBT — 1 woman had moved from traditional CBT to videoconference at the onset of COVID-19 — all were able to tie their experiences with CBT or their expectations to iCBT.
Relationship With Self and Others
Shifting capacities of people living with chronic pain can make it challenging to fit within normalized, able-bodied standards of functional life. Women we spoke with described needing to step back from their careers or missing out on social and family life due to their chronic pain. Some people, as was the case for 1 woman we spoke with, may be faced with the impossible decision to move away from family to a larger city with more readily available supports for life with chronic pain. For others, there is a gradual isolation or separation from friends and family because “if for the 14th time you’re supposed to be going out with your friends and you say ‘Oh, I have to cancel, I don’t know, I’m in too much pain,’ a lot of your friends disappear.”
Women described that not being able to be a part of life around them in the ways they used to be could lead to an overwhelming sense of guilt for people living with chronic pain. One of the women indicated that “there’s a huge amount of guilt — especially if you’re a parent and can’t play with your kids. Or lift your kids. Or brush your daughter’s hair. Or, you know, there’s a huge amount of guilt involved in that. And if you can’t work, it’s worse.” So much of living with chronic pain is self-protection or, as 1 participant put it, “wanting to cover and just seem capable.”
But “cover[ing] and just seem[ing] capable” is not always possible, and that can be devastating. The impossibility of always looking and behaving the same as before chronic pain can lead to thoughts of worthlessness or, potentially, suicide. Women described times when they felt their life was “a write-off” or that they were no longer “worth anything because I was no longer a professional.” Although her thoughts were not driven by depression, 1 woman described moments when she contemplated the value of her life and whether it was worth living. Another woman we spoke with suggested that life with chronic pain is “all about managing expectations — as much other people’s as your own.” Although higher doses of medications might help for a while, “eventually you break.” For some women we spoke with, this is how iCBT (or in-person CBT) may be able to provide some support for people with chronic pain — as a way of protecting themselves from the ongoing threat of loss or “from one day wanting to kill yourself.”
Importantly, iCBT is not so much about working on pain as it is working on how someone relates to and manages living with that pain. As 1 participant put it, “it was about how can you make things better for those around you so they’re not constantly worrying about you. And at the same time, what can you do to ask for support when you need support without feeling guilty about it — or without feeling like you’re ruining their lives because [there’s] a lot of guilt involved in chronic pain.” Within this understanding of iCBT (or in-person CBT) programming, we might also recognize it as supporting a form of empowerment among people living with chronic pain.
One of the ways iCBT might support relating to and managing living with pain is by introducing and teaching techniques like pacing (described further in the Utility of Content section). Pacing is about slowing down and tending to both your present and future self. A person living with chronic pain might learn that it is okay to say “no” or to delay some action. But the difficult reality is that they are also always going to be outside of the norm. Although they may learn to occupy that space and make it work for them, the challenge is that much of the world around them is still ableist.
One way of supporting people through losses associated with chronic pain can be through a strong relationship with the person delivering iCBT (or traditional CBT).
Relationships With Provider
As described in previous reviews of iCBT,87,88 the women we spoke with consistently identified that developing and maintaining strong relationships with providers are pivotal components of successful iCBT programs. In the review of iCBT for PTSD,88 strong therapeutic relationships were described as ones that are less focused on the provider’s expertise by way of unilateral knowledge sharing but are more focused on a shared sense of humanity or ensuring people feel heard in those clinical encounters. This does not mean that there is no exchange of “knowledge” in these clinical encounters, but rather that for this “knowledge” to mean, or do, anything it requires work, consistency, patience, and care.
Engaging with iCBT for chronic pain requires the same careful attention to the space shared between providers and the person receiving care. One participant used the language of “trust” to describe this shared space and emphasized how challenging this can be to build in the context of iCBT for chronic pain. One of the goals of iCBT is to challenge assumptions or negative thought patterns people have toward their experience with pain in a way that the person does not feel blamed or that it is all in their head, which requires delicacy and tact. Given that some people living with chronic pain experience dismissal and neglect, a challenge would be acknowledging that providers hold the realities of a person’s pain while also attending to the moments or places where beliefs or actions might be harmful.
The women discussed that a way trust could be fostered was through providers who are specifically trained in how to work with chronic pain. Without this expertise, the women we spoke with were concerned that providers might stick too strictly to a script that was not aligned with their actual needs. Because some people with chronic pain have experiences feeling as if they are low to no priority, 1 woman we spoke with felt “if you throw a junior [physician] in the room, they’ll chew them up and spit them out.” In a way, strong relationships are built before the encounters actually happen.
Trust was described as being fostered through reassurance that providers had pain-specific knowledge and experience, but ideally providers would focus on the individual during the encounter. As 1 participant put it, “There’s not just sort of 1 blanket approach that we are going to take. Like, there’s a curiosity and an interest in who you are as a person and how you live with pain and what is important to you in the quality of life.” Instead of “talking down to a person,” she believed iCBT providers should inquire about what a person already knows about and does for their pain. The other participants all echoed this sentiment. Working with the uniqueness of chronic pain in one’s life and taking one’s whole being into consideration during iCBT (or traditional CBT) is fundamental to building a successful relationship with a provider. This increases confidence in the person’s ability to manage their condition: “It’s building that trust that you are a smart, capable, high-functioning individual [and] that you understand what’s happening.”
Another way strong therapeutic relationships could be fostered in iCBT is through what 1 participant called “voice consistency.” Even though people might be comfortable with asynchronous communication from their provider, people wanted to make sure they were developing a relationship with 1 provider. One participant described wanting to “be seeing the same person…[because] it’s a vulnerable situation, being in therapy.” As someone who provides psychotherapy herself, this participant emphasized that a single provider is better able to track someone’s progress and offer consistent approaches because “two therapists can have very different understandings and [ways] they progress in their therapy.” Another woman voiced concern that having inconsistent providers during iCBT might hinder the development of rapport and require a person to unnecessarily repeat vulnerable aspects of their story, which people living with chronic pain may need to do often when seeking health care.
Process
In previous CADTH reports on iCBT,87,88 process was intricately related to the themes of context and relationships. People living with MDD, anxiety, and PTSD found iCBT particularly convenient, given their ability to access the therapy from the comfort of their own home on a schedule that suited them.87,88 This flexibility alleviated contextual challenges associated with accessing face-to-face therapy (e.g., the inability to physically commute to treatment or take time off work for therapy).87,88 Accessing therapy from home also eliminated the need to obtain treatment in health care settings that users sometimes associated with unpleasant experiences.87,88 However, these previous reports also emphasized that engaging with iCBT required time, effort, and energy on behalf of participants.87,88 For this reason, successful continued engagement depended on buy-in, which, as detailed in the report on PTSD,88 could be fostered within the context of a trusting, empathetic therapeutic relationship.
These findings resonated with the women we spoke with who reflected on how iCBT may be particularly convenient for people living with chronic pain because it could help to alleviate some of the challenges related to geographic proximity to chronic pain treatment. However, all the women we spoke with emphasized that a therapeutic relationship, in which a provider can assess the appropriateness of the therapy to the individual and foster buy-in by tailoring that therapy to their personal needs, could facilitate successful engagement with iCBT.
Physical Accessibility and Convenience
As detailed in the Context section, to successfully engage with iCBT, a person living with chronic pain will first need to navigate challenges influencing their ability to access treatment that acknowledges and physically addresses their condition. These challenges include experienced dismissal, a perception that general health care providers lack of knowledge about chronic pain and its treatment, the need for self-advocacy, health literacy (which is often influenced by gendered, racial, and socioeconomic inequities), the monetary burden of out-of-pocket pain care, and geographic proximity (or lack thereof) to available treatments.
Some participants envisioned that pain care delivered over the internet might at least address contextual barriers related to one’s geographic proximity to treatment options. One woman, for example, noted that having virtual access to pain services may have circumvented the need for her to move to a metropolitan area to gain treatment. Another anticipated that therapies accessible online might eliminate the need to physically commute to treatment when in pain, noting that when she has a flare-up, “I’m not going anywhere. I want to be home.” One participant similarly remarked how people living with chronic pain might find commuting to in-person treatments physically exhausting.
The women we spoke with highlighted how reducing geographic and physical barriers to therapy can support engagement with iCBT. However, access to iCBT does not necessarily mean that a person can engage with it successfully or safely. These women emphasized the importance of developing strong, consistent, and trusting therapeutic relationships built on a shared and empathetic understanding within the context of iCBT for chronic pain. These therapeutic relationships become vital to the effective engagement, or anticipated engagement, with the intervention.
Assessment
Ongoing, consistent engagement in a therapeutic relationship with a provider invested in a person’s needs may be helpful even before an individual is offered iCBT. Continuous engagement can help ensure that providers develop a therapeutic judgment that responds to and understands the needs and desires of people living with chronic non-cancer pain. Before offering iCBT to a person living with chronic pain, 1 participant noted an “actual living, breathing psychologist” should conduct a phone or video-based psychological assessment to ensure that the person will benefit from it. In her case, this assessment was not a series of predefined questions to clearly categorize her as someone who would benefit from the therapy. Instead, it was a therapeutic judgment formed by 2 psychologists who developed personal, ongoing relationships with her over the course of 10 to 11 individual sessions ranging from 1 to 1.5 hours each. She also noted that CBT might not be appropriate for some individuals living with chronic pain. Had she been offered the therapy while in severe, untreated pain, she described that she may have been more likely to contemplate suicide because she would have thought “is this [treatment] all there is?”
The depth of the initial assessment process may not be required in every instance in which a provider considers offering iCBT to a person living with chronic pain. However, this participant’s statements emphasize the importance people can place on iCBT providers’ attention toward the needs of the individual before therapy begins. People living with chronic pain may be more likely to uncover nuanced information relevant to this initial assessment within the context of a trusting therapeutic relationship. In this way, assessment, and the process of beginning iCBT, relates to readiness, as detailed in our discussion in the Context section.
This initial assessment of an individual’s experience of pain may not only allow a provider to decide whether it is appropriate to offer iCBT and may also help identify what needs to be worked on and when. One participant, for example, suggested that providers might consider where in their pain journey a person is situated before offering a particular program. She noted that a recently injured person might benefit from an introductory course, while someone with more experience managing their pain may benefit from a program with more advanced content. Furthermore, the participant suggested that people have the option to revisit course concepts after completion because what is relevant to, and therefore retained by, a person evolves over time.
Tailoring and Buy-In
The concept of tailoring exists at the intersection of process and content. CADTH’s report on iCBT for MDD or anxiety87 emphasized the importance of programs adopting a malleable, rather than prescriptive, approach to fit each user’s learning style and mental health engagement needs. The therapeutic relationship was a foundation for this tailoring. In the review, study participants’ perspectives varied about what designs, content, and levels of provider engagement were most beneficial to them; however, the participants felt that provider guidance could better align the intervention to the individual. Specifically, providers could critically think about the relevance of an iCBT program to the person accessing it; offer ongoing support, monitoring, and personalized responses to their progress; and tailor the program’s content and level of support offered based on their unique needs.
In the current study, participants believed that considering and responding to individual needs should occur throughout iCBT programming rather than being a 1-time event at the outset of treatment. One woman stated that because no 2 people have the same experience with chronic pain, “the assumption that [the experience of pain is] a little, like, interchangeable can be really problematic.” Therefore, when reflecting upon what she would expect from an iCBT program, she emphasized that content would need to flexibly adapt to an individual’s needs throughout the therapy rather than following a machine-like algorithm. Flexibly adapting a program to a person’s needs would require a provider to conduct an ongoing assessment of those needs throughout the iCBT process. Ideally, the content of an iCBT program might be as diverse as the experiences of the people accessing it.
A thorough assessment and understanding of who might engage with an iCBT program is an important component of process. As evidenced across previous reviews,87,88 dropout is a concern in iCBT programs. One participant’s experience illustrated how a provider may foster “buy-in” by considering and incorporating an individual’s assets and needs into treatment. As detailed in our discussion in the Relationships section, she described how her CBT provider moved beyond a “blanket approach” to tailor her therapy effectively because of the provider’s genuine attention toward her personal pain experience, including what she already knew and did about her pain. This allowed the provider to offer content built upon the participant’s strengths and knowledge, and ensured that she could conceptualize the content as benefiting her specifically and that therapy was “not just another make-work project,” which motivated her to continue engaging with the treatment.
This participant emphasized that CBT providers should understand that people living with chronic pain continuously calculate how much energy and resources they can expend to engage in new tasks: “You’re always kind of negotiating if you’re going to make space for a new activity…it’s got to be realistic.” To be motivated to engage with program content, including assigned homework (e.g., journaling, thought tracking activities, and practising mindfulness), participants need reassurance that assigned activities are both attainable and useful to them personally.
For this reason, 2 of the women were insistent that the duty of care could not be satisfied by providing impersonal educational material alone or using apps run by artificial intelligence. They were concerned with how easily unguided iCBT might slot into what they described as the increased industrialization of health care which was perceived to deemphasize caring relationships with providers and lead to a loss of knowledge and history developed through these relationships. As 1 of them put it, “We’re not machines here…we’re talking about very personal things.” Therefore, having a real person who could actively tailor content throughout the iCBT program was described as helpful to foster a feeling they are being cared for and encourage them to continue with iCBT programming.
To support the process of tailoring, people living with chronic pain are typically required to share intimate details about their lived experience with their provider. As outlined in our discussion in the Relationships section, women described how important it is that providers of CBT or iCBT consider past traumas that people may have experienced when disclosing their pain to others. For some people living with chronic pain, sharing their experiences may have resulted in being disbelieved, dismissed, neglected, or perceived as being less “able” or, as 1 woman we spoke with described, less likeable. For this reason, engaging in therapy demands vulnerability from those living with chronic pain. It follows that the process of engaging in therapy, and the information collected through it, would be private and protected.
When deciding whether to implement iCBT programs, health care decision-makers could help ensure that processes are in place to protect the experiences and information of those receiving the care. One participant emphasized that it should be clear how personal information collected online will be accessed and stored and by whom. Additionally, she stated that, given the relative novelty of iCBT for chronic pain, people should be informed if they are participating in a program that is under development or being researched (i.e., to make an informed decision to engage in iCBT over traditional CBT) and whether their information (anonymized or not) will be shared with others. She also emphasized that, when receiving iCBT in the home, a person must have access to a private place where others cannot hear them. Finally, although we previously discussed the potential benefits of obtaining group-based CBTs for chronic pain, another participant emphasized the need to carefully vet people accessing virtual group therapy to reduce the risk of having an attendee collect personal information from those receiving treatment.
Content
Of the 5 participants in the current study, only 1 had experienced iCBT; she received iCBT via videoconference synchronously guided by a neuropsychologist with whom she already had a therapeutic relationship. Of note, none of the women interviewed had experienced asynchronous, non-guided iCBT courses delivered entirely online. Therefore, this discussion of “content” is grounded primarily in the value participants attributed to the experienced or expected content and design of CBT for chronic pain, rather than iCBT specifically. The women we interviewed emphasized that iCBT content should be pain-specific, practical, focused on living better with chronic pain, and ideally delivered synchronously with careful use of language through a medium that allows the provider and user to visualize each other.
Necessity of Pain-Specific Content
In our discussion in the Process section, participants described that the content of iCBT programs ideally would be tailored to, and therefore useful for, the individual receiving it. To ensure that content is useful for people living with chronic pain, it could specifically address the needs of those living with pain as opposed to the needs of people living with mental health or substance use disorders, for example. Two participants who participated in group-based, in-person CBT programs emphasized that chronic pain (unlike MDD, anxiety, or PTSD) is a physical health issue that is exacerbated, rather than driven, by emotional and behavioural issues. Although she acknowledged that mental health disorders may occur concurrently with chronic pain, 1 participant reflected on how there is a “misunderstanding that chronic pain is a mental health condition.” She noted that CBT for anxiety or depression seeks to address the “root cause” of a person’s symptoms, but “CBT [for pain] will be helping you deal with it better, but it’s not going to…solve the underlying physical problem.” It follows that the content of iCBT programs for chronic pain would ideally differ from that for programs treating mental health disorders. Two women we spoke with noted that because their CBT programs could not address the physical causes of their pain, the content instead focused on the teaching skills required to live better with the condition.
For this reason, and as presented in in the Relationships section, both women stressed that providers specializing in chronic pain are best suited to develop and deliver relatable, relevant, and appropriate content for people living with chronic pain. Comparing CBT for pain and CBT for substance use disorders, 1 woman said, “There are some parallels, but it should be, in my opinion, black and white. It can’t be the same course. It can’t be the same people who deliver it.” She noted that although a provider specializing in substance use disorders might appropriately include content prioritizing independence from substances, a program specializing in chronic pain would more appropriately acknowledge medications as 1 of many tools used to relieve symptoms and enhance functioning. She also discussed how providers with pain-specific knowledge and experience could be better able to provide practical and memorable information specific to chronic pain management (e.g., ways to reflect upon and manage how emotions and breathing patterns influenced, and are influenced by, pain). She raised the potential value of forming relationships with a patient provider who has “lived experience” of chronic pain to gain additional support while navigating treatments, including iCBT. She described these people as other potential providers who could better contextualize the concepts taught by pain specialists. This emphasizes the importance that our participants placed on the providers who create and provide iCBT programs for chronic pain having adequate training in pain management.
Utility of Content
All the participants who had received CBT for chronic pain noted that content focused on “living better with” the condition; however, the meaning and utility that the women ascribed to this content varied. Although 1 participant did not provide specific details about her 12-week program, she noted that the skills gained through it allowed her to obtain a higher level of functioning on lower dosages of medications. She conceptualized these skills as a source of protection against being left without a way to manage pain when unable to access immediate medical care (e.g., during holiday periods when hospitals have fewer pain services or when in-between care providers). Another participant, in contrast, reflected on how the content of her 8-week program, which included teachings about positive thinking techniques, mindful meditation, and visualization exercises, allowed her to accept and cope with the fact that she had already explored all available treatment options to manage her physical pain symptoms.
Another participant provided perhaps the most clear reflections on how CBT content allowed her to live better with pain. Through the therapy, she learned how to challenge negative thoughts related to pain and focus on the “whole big picture” of where she found quality in life rather than ruminating on the adverse experience of her symptoms and their consequences. Learning to challenge negative automatic thoughts also encouraged an improved self-concept because she could now “reality test” beliefs such as “I’m not worth anything because I am no longer a professional” or the perception that her pain negatively impacted her likeability. Finally, learning the skill she referred to as “pacing” allowed her to avoid all-or-nothing thinking and behaviours to engage more fully in activities she otherwise would have avoided. To describe the technique, she said, “I’m not going to walk around the whole block. I’m going to walk half of the block if that’s what I can do that day…so with pacing, you’re slowly kind of extending your endurance, for example, and you’re sort of teaching your body and your nervous system to find kind of credible safety in movement.” The principles of pacing and thought challenging also allowed her to set manageable goals in social settings.
Effectively Delivering Content
In the CADTH report on iCBT for PTSD,88 the participants emphasized the importance of interventions that deliver content in a manner that considers and responds to the individual. For example, people living with PTSD valued therapy content that provided them with skills to gain control over their affective responses. Homework helped consolidate these skills but was sometimes challenging to engage with because of unrelatable language used to present the information. It was proposed in the CADTH report that providers consider each person’s ability to relate to the language used in a program before deciding whether they would benefit from it.
Participants in the current study also considered how modes and methods of communication might influence their experience engaging with CBT or iCBT for chronic pain. They described that the language used to deliver content matters. As detailed in our discussion in the Relationships section, most participants interviewed had interactions with health care providers who had in their experience not believed in their pain. For this reason, 1 participant emphasized that when teaching how thoughts influence pain, providers should explain concepts in a way that does not imply that a person is at fault for their symptoms.
The women we interviewed also expressed a desire to communicate with their iCBT providers synchronously. One participant anticipated that this method of communication would allow a provider to exercise clinical judgment to adapt program content in real time to respond to the immediate needs of a person living with chronic pain. She raised that this immediate tailoring may be especially important if a person living with severe pain were, for example, to disclose that they had considered suicide to relieve their symptoms. In situations like these, she hoped that real-time conversations with an experienced therapist trained in chronic pain care could help navigate the gravity of a comparison between being better off dead versus life with chronic pain without automatically pivoting to iCBT programming focused specifically on suicide prevention. She expressed, “I’m very much afraid that the rest of the iCBT program would throw the patient into purely suicide prevention, which is not a place you want to send a chronic pain patient who is not suicidal because then you’re potentially putting ideas in their head that aren’t there.”
Because pain is a phenomenon that originates in the body, some participants reflected on the importance of visual cues when delivering content. For example, 1 woman questioned whether a provider could effectively teach soft tissue manipulation or breathing techniques without viewing the entire body of a person receiving therapy while the person receiving therapy viewed them. Reflecting on her experience of CBT for trauma, 1 participant also noted the importance of non-verbal communication in establishing rapport with her provider. It follows that iCBT programs may benefit from incorporating videoconference technologies that allow the provider and person receiving care to interact with each other.
Finally, participants reflected upon other requisites for the effective delivery of iCBT content. Two participants commented that navigating an iCBT program would require, at minimum, basic computer skills. Another woman similarly anticipated that people receiving iCBT would need access to resources such as a reliable internet connection (a potential issue in rural and remote communities) and appropriate software. Notably, she commented that some conditions causing pain (e.g., severe arthritis in the hands) might prevent a person from operating a computer, a concern previously identified in the CADTH report on iCBT for MDD and anxiety.87,88 These reflections are important to consider because they emphasize the potential benefit of keeping the option of obtaining traditional, in-person CBT available and accessible to those who may not benefit from accessing content online.
Summary of Results
The study participants reported that iCBT could become a supportive component of comprehensive chronic pain care when CBT would otherwise be provided. However, this potential benefit came with some expressed caveats. Although these particular caveats represent the nuance distinguishing iCBT for chronic pain from CADTH’s previous reviews of iCBT for MDD or anxiety87 and iCBT for PTSD,88 findings were largely similar across all 3 reports. Taking into consideration these particularities we have identified for chronic pain could support decisions about whether iCBT could be a useful component of chronic pain care.
One particularity is consideration of the availability of comprehensive, multidisciplinary chronic pain care. We have assumed that, if implemented, iCBT for chronic pain would be integrated into pre-existing comprehensive multidisciplinary chronic pain care networks; however, the women we spoke with noted concern with this assumption given their experiences with and observations of the limited availability of multidisciplinary pain care across Canada. They worried that without a broad investment in comprehensive pain care, iCBT programming might become seen as a “quick fix” because of its assumed accessibility and low cost. Although it is possible that iCBT could be a supportive component of comprehensive multidisciplinary chronic pain care for some people, without broad availability of multidisciplinary pain care, iCBT may not achieve the intended objectives. This corresponds with the literature about chronic pain that emphasizes the importance of people having access to comprehensive, multidisciplinary care approaches that can target the multiple dimensions of pain and hopefully improve treatment outcomes.11,13,19,45
The women we spoke with were also concerned that early offers of iCBT might risk causing further harm by missing an opportunity to identify the root causes of the pain and treating it accordingly. Further, as people who described experiencing disbelief and dismissal within the health care system, the women felt that referring someone to iCBT too early in their treatment pathway could validate their feelings that they do not matter. Paired with understandings that many family physicians have limited training in pain, the women were concerned that the apparent simplicity of referring to iCBT could interfere with determining the root causes of pain.90-92 As family physicians are often people’s primary point-of-contact with the health care system, receiving a suggestion for iCBT too soon may exacerbate patients’ frustrations if patients believed iCBT was the only option available. Some people living with pain may appreciate earlier engagement with iCBT, particularly those with chronic secondary pain, although the women we spoke with suggested that determining appropriate candidates should be done on a case-by-case basis rather than as a standardized approach.
The concept of readiness relates to whom and at what time points iCBT might be considered an appropriate intervention. Readiness can be understood as an assemblage of treatment history, available current care practices, material realities of 1’s condition, and individual needs or desires. The women we spoke with suggested that policies about iCBT that take this assemblage into account could help limit or prevent reinforcing experiences of dismissal, neglect, and untreated pain in people living with chronic pain.
As in previous CADTH reviews of iCBT for MDD, anxiety, and PTSD, a strong therapeutic relationship and tailored approaches to iCBT programming were seen as vital components of successful engagement with iCBT.87,88 This suggests that iCBT would ideally be provider-guided with enough space and time for the development and maintenance of a strong therapeutic relationship. The current study further highlights the importance of people engaging with iCBT through providers who are specifically trained in dealing with chronic pain. Without this expertise in pain, the women we spoke with felt that providers might struggle to be attentive to and understand the challenges of living with chronic pain, which could impact the development of a strong and trusting therapeutic relationship and ultimately the ability of that provider to tailor the programming to the needs of the person living with pain.
This Patients’ Perspectives study has several limitations that may affect the transferability of our findings across Canadian jurisdictions and to the diversity of people living with chronic pain. First, none of the women we interviewed had experienced asynchronous or unguided iCBT for chronic non-cancer pain. Furthermore, despite our efforts to include a diverse sample, all people interviewed described themselves as White or Jewish, when asked to describe how they would identify themselves in an open-ended question. We relied on our connections to advocacy groups and organizations that had previously engaged with CADTH on other projects, which may have limited our ability to reach a more diverse population. Furthermore, 4 of the 5 women interviewed reported having experience working in health care. Although most of the women reported having had distressing experiences with health care providers and had difficulty accessing multidisciplinary pain care, it is possible the experiences of other individuals, particularly individuals who experience marginalization or racism attempting to access the same care would be different. Future qualitative research is needed on the experiences of people who have used iCBT for chronic pain, including those who have used non-synchronous and unguided iCBT programs. This research should include the voices of those who identify as male; are different races and ethnicities; and people who experience marginalization for other reasons, and may be less likely to have access multidisciplinary pain care.11,20
Patient Engagement
Overview
CADTH involves patients, families, and patient groups to improve the quality and relevance of our assessments while ensuring that those affected by the assessments also have an opportunity to contribute to them. CADTH has adopted a Framework for Patient Engagement in HTA93 that includes Standards for Patient Involvement in Individual HTAs which is used to support and guide our activities involving patients. For this HTA, our patient engagement activities have been guided by the belief that patients have knowledge, perspectives, and experiences that are unique and contribute to the essential evidence for HTA. CADTH engaged 2 people living with chronic pain who had previously offered feedback on CADTH projects related to chronic pain to offer insights on the current project.
Methods
Invitation to Participate and Consent
A CADTH Patient Engagement Officer contacted potential contributors by email to explore their interest in becoming involved with this HTA. The preliminary request included the purpose and scope of this project, the purpose of engagement, and the nature of engagement activities. The Patient Engagement Officer obtained the person’s informed consent to share their lived experiences with CADTH staff. Compensation in the form of an honorarium was offered to the participants.
Engagement Activities
A person with experience of chronic pain reflected on their own personal experiences at several time points during assessment including:
before protocol finalization
during drafting of the initial reviews
after completion of the draft final report during the feedback period.
Results
Patients’ perspectives gained through the engagement processes were used to ensure the relevance of the outcomes of interest for the clinical assessment, to identify other patients with experience of iCBT, and to discuss other considerations to inform the Discussion section. The questions and subsequent discussion with the patient contributors helped to clarify the technology under review and comment on the relevance of the findings to people living in Canada living with chronic pain due to a range of conditions. Furthermore, the patient contributors suggested other people with lived experience who might be available and willing to participate in the Patients’ Perspectives section.
Involving patients enabled the research team to consider the evidence together with the wider experiences of people living with chronic pain and their families and comment on the suitability of iCBT for various pain conditions and people experiencing chronic pain, or other factors that could support decision-making.
The patient collaborators and the wider community were invited to provide feedback on the report during the final stakeholder feedback period. Patient engagement activities and results are reported using the Guidance for Reporting Involvement of Patients and the Public (GRIPP2) Short Form checklist (Table 7)94 to provide reflections and critical perspectives on the experience of the patients, other members of the chronic pain community, and the research team.
Table 7: Patient and Public Involvement in Internet-Delivered Cognitive Behavioural Therapy in the Treatment of Chronic Non-Cancer Pain
Section and topic | Item | Report section |
|---|---|---|
Aim | Two people with lived experience of chronic pain and CBT were involved in developing the protocol and commenting on outcomes important to people living with chronic pain. | Patient Engagement |
Methods | We engaged 2 people who met the following criteria:
After giving informed consent, the people we engaged discussed their experience of chronic pain and their perspectives about the important aspects of CBT and multidisciplinary care in the context of CADTH’s plans for this report. The conversation took place via video teleconference and email communication. An honorarium was offered for participating in teleconferences and reviewing a summary of the discussion. These people and other community members were invited to provide stakeholder feedback on the draft of the full Health Technology Assessment. | Patient Engagement Methods Opportunities for Stakeholder Feedback |
Results of patient engagement | The researchers were made aware of the importance of several considerations about the interventions and outcomes, which allowed the research team to consider the evidence in the context of the wider experiences of patients and caregivers when preparing the assessment. Quality: The quality of the iCBT program matters to people living with chronic pain. We heard that a good quality program is delivered by a therapist knowledgeable about chronic pain and can be customized so people can focus on the most relevant modules. The iCBT program should be relevant to a person’s condition and their goals, not something generic. Timing: Behavioural interventions such as iCBT should be offered after a full clinical examination and after efforts have been made to address the source of the pain. Ongoing support and “booster” sessions should be made available to practice and maintain what was learned in the iCBT program. Privacy: People participating in an iCBT program need to be aware and informed of how their information will be stored and shared. If any information will be used for research or evaluation of the iCBT program, this also needs to be explained clearly and this information needs to be managed with care. There may be privacy risks for people receiving care in their home because they may not have adequate personal space or they may use a shared device for accessing treatment. The importance of trauma-informed care: One patient contributor shared that a trauma-informed approach should be considered. Clinicians delivering CBT should be aware of the possibility that they may hold perceptions and assumptions that stigmatize patients. Trauma-informed care is a way of approaching patients that emphasizes safety and trust for patients. We heard that some groups of people, particularly women, may have experienced trauma at the hands of the health care system by having their concerns dismissed or their pain minimized, which delayed treatment while their symptoms worsened. Equity issues: Fairness is an important value. We heard that if iCBT was to be offered to patients, it would be important to also continue to offer in-person CBT for the people who are unable to access it, so people are not left behind. People who are physically disabled, lack transportation, or reside in a rural or remote area may welcome an online option instead of having to travel to access a program. | Key Messages Clinical Review: Outcomes in Table 2 Discussion: Risk 3 |
Discussion and conclusions | The 2 patient collaborators were highly engaged in the conversation with researchers. They had clear opinions and concerns during the teleconference. They shared that multidisciplinary care delivered by clinicians who are knowledgeable about chronic pain is not always available. The burden of coordinating their own appointments with multiple practitioners, in addition to significant self-management tasks of chronic pain, can be substantial for some people. Ethical and equity issues are sometimes revealed when patients tell of their experiences. Examples of factors that put some people at a disadvantage for accessing iCBT are lack of adequate technology or a high-quality internet connection; lack of ability or a lack of confidence in using technology; lack of support or instruction; lack of space at home for private, uninterrupted conversations with a therapist; disability; cognitive impairment; low literacy; speaking a language other than English or French; and cultural or religious taboos about pain treatment. | Patient Experiences Results |
Reflections and critical perspective | Patient involvement in this report was successful based on several factors, including:
There were also limitations, including:
| Patient Engagement Methods |
CBT = cognitive behavioural therapy; iCBT = internet-delivered cognitive behavioural therapy.
Operational Aspects
Overview
The objectives of this Environmental Scan were to identify iCBT programs in Canada that are established or in development, their characteristics, and the related operational aspects associated iCBT programs for the management of chronic non-cancer pain.
Research Question(s)
The following questions related to identifying operational aspects of iCBT implementation and delivery were addressed:
Which iCBT programs for the management of chronic non-cancer pain are currently available or are in development in Canada and what are their characteristics?
What operational considerations contribute to the establishment and provision, or lack, of iCBT programs, specifically for the management of chronic non-cancer pain, at the system or site level in Canada?
Key Messages
Sixteen iCBT programs that support people living with chronic non-cancer pain were identified that are available or in development in Canada. Seven of the identified iCBT programs are available across Canada and 8 of the programs are available in specific provinces. One of the iCBT programs is in development.
The majority of the iCBT programs identified provide care to people living with different types of chronic pain. The characteristics of the iCBT programs vary in terms of the level of therapist involvement, overall program length, number and length of modules, topics covered, funding model, and patient reimbursement eligibility.
Commonly identified facilitators to iCBT included reaching patients that would otherwise be unreachable, improvement in patients’ experiences, efficiency (in clinical practice and use of resources), and convenience for patients.
Commonly identified barriers to iCBT included privacy concerns, preference for in-person or other treatment options (for both patients and clinicians), patients’ lack of familiarity with technology, and patients’ lack of available and appropriate devices or an adequate internet connection.
Methods
Study Design
An Environmental Scan was conducted to identify iCBT programs in Canada that are established or in development, their characteristics, and the related operational aspects associated with iCBT programs for the management of chronic non-cancer pain. The findings of this Environmental Scan are based on a limited literature search, online survey, and stakeholder feedback. We used an iterative process to obtain feedback on the Environmental Scan draft report. We first sought feedback from stakeholders who responded to the survey and then from those involved with programs identified through the literature search and feedback to verify the reported information and address information gaps.
Literature Search Methods
A literature search was conducted by an information specialist on key grey literature (literature that is not commercially published) resources. Grey literature was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature tool,55 which includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, systematic review repositories, patient-related groups, and professional associations. Google was used to search for additional internet-based materials. The main search concepts were iCBT and chronic pain. The search was also limited to English-language documents published between January 1, 2000, and September 21, 2021. Refer to Appendix 1 for more information on the grey literature search strategy.
Selection Criteria
Screening and Selecting Publications for Inclusion
One author screened publications from the literature search for inclusion based on the criteria outlined in Table 8. Publications eligible for inclusion were those that described iCBT programs and/or provided insights on the operational aspects associated with iCBT programs for the management of chronic non-cancer pain from the perspectives of patients, health professionals, and decision-makers in Canada. Programs that included patients using iCBT primarily for indications other than chronic non-cancer pain (e.g., primary diagnosis of MDD, anxiety disorder, PTSD), and programs unavailable in Canada or that are in development outside of Canada, were excluded for research question 1. For research question 2, publications eligible for inclusion were those that identified operational aspects of iCBT programs in Canada. Publications that described experimental studies (e.g., RCTs) and those that did not provide a summary or describe Canadian iCBT programs for the management of pain were excluded.
Table 8: Components for Literature Screening and Information Gathering
Criteria | Description |
|---|---|
Population | Patients (any age) with chronic non-cancer pain, regulated health professionals, and decision-makers |
Intervention | Guided and unguided iCBT delivered via a computer or mobile device, either synchronously or asynchronously, in combination with other interventions for the management of chronic non-cancer pain |
Settings | Settings of care (e.g., primary, home, tertiary, community, long-term care) in rural, remote, and urban areas in Canada |
Outcomes |
|
iCBT = internet-delivered cognitive behavioural therapy.
Survey Methods
A 31-question online survey (Appendix 5) was developed to address the research questions of the Environmental Scan. The survey questions were developed based on a previous survey used in the 2018 CADTH Environmental Scan on iCBT for Major Depressive Disorder and Anxiety Disorders.95 The survey included sections on demographic information and iCBT program characteristics as well as 3 sections on implementation considerations (facilitators, barriers, and access). Both open-ended and closed-ended questions were included in the survey. The questionnaire was distributed by email on October 14, 2021, and administered electronically using SurveyMonkey.96 The questionnaire was only available in English. Respondents were identified through CADTH’s Implementation Support and Knowledge Mobilization team networks, and other available networks via stakeholder and expert suggestions. Contacts were also identified by referral through other survey respondents. The goal of survey recruitment was to capture information relevant to each province or territory and from a wide range of stakeholders involved in iCBT for chronic non-cancer pain. These included regulated health professionals (e.g., physicians, nurses, psychotherapists, psychologists, occupational therapists, social workers, other mental health professionals, program managers), policy-makers, decision-makers involved in program or practice development, information management professionals, employee assistance program providers, online CBT platform developers, and staff at community organizations that support people living with chronic non-cancer pain. Stakeholders from the following jurisdictions received the survey from CADTH: Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and Labrador, Nova Scotia, Ontario, Quebec, and Saskatchewan. Responses to the survey were gathered from October 14 to October 29, 2021. A response was considered partially completed if 1 or more questions were not filled out by the respondent. If a respondent indicated they were not involved in the development, delivery, funding, or regulation of an iCBT program that supports people living with chronic non-cancer pain, they were not eligible for the survey and were not asked to respond to further questions. Partial responses from those eligible to complete the survey were included. All respondents gave explicit written permission to use the provided information for the purpose of this report.
Synthesis Approach
One reviewer analyzed the data collected from each of the data sources (i.e., literature search, survey). A descriptive analysis was conducted to respond directly to the research questions and produce a narrative summary that reflected the included data. Details on patient eligibility and program characteristics were extracted from publicly available information on iCBT program websites. For the survey data, descriptive statistics are provided for responses to closed-ended questions and narrative summaries are provided to summarize responses to open-ended questions. The demographic information about respondents who indicated they were not involved in the development, delivery, funding, or regulation of an iCBT program that supports people living with chronic non-cancer pain was excluded.
Results
The results are based on the literature search, survey, and stakeholder feedback and are presented for each research question in this report. The literature search identified 3 websites that provided information on iCBT programs available in Canada that support people living with chronic non-cancer pain. The literature search did not yield any publications that provided information about the operational considerations of iCBT programs for the management of chronic non-cancer pain.
Thirty individuals received the survey directly from CADTH. A total of 13 survey responses were retrieved after responses from respondents who indicated they were not involved with an iCBT program that supports people living with chronic non-cancer pain (6 responses) and respondents who only answered the demographic questions (2 responses) were excluded. The survey responses included 11 complete responses and 2 partial responses. The respondents were from the following provinces: Alberta (4 responses), British Columbia (1 response), Newfoundland and Labrador (1 response), Nova Scotia (1 response), Ontario (4 responses), Quebec (1 response), and Saskatchewan (1 response). Additional characteristics of survey respondents are presented in Appendix 6.The 11 complete responses represented stakeholders from all the previously mentioned provinces. The most common settings where respondents indicated they worked were pain clinics (6 responses) and hospital or specialist clinics (6 responses). The most common professions or roles of the respondents were health care provider (6 responses) and researcher (5 responses). All the respondents indicated they were involved in either the development or delivery of 1 or more iCBT programs.
Question 1: Which iCBT Programs for the Management of Chronic Non-Cancer Pain Are Currently Available or Are in Development in Canada and What Are Their Characteristics?
Overview of iCBT Programs in Canada
Ten iCBT programs were identified through the survey, and 3 programs (AbilitiCBT, Cognitive Behavior Therapy Institute of Manitoba, iCBT Program for Chronic Pain) were identified through the literature search.97-99 Three additional programs (LivePlanBe, LivePlanBe+, and MyCarepath) were suggested through stakeholder feedback on the Environmental Scan.100-102 These 3 programs are self-directed and provide access to a variety of articles, videos, and other resources, some of which are based on CBT strategies. Thirteen survey respondents provided information on the iCBT programs available or in development in their respective jurisdiction. An overview of the iCBT programs that were identified is provided in Table 9. Note that the programs included in the table vary in structure; some programs are completely self-guided with access to a variety of resources and other programs consist of structured modules with therapist support.
Table 9: Description of iCBT Programs in Canada
Program name | Patient age | Program access and use | Program characteristics | |||
|---|---|---|---|---|---|---|
Level of therapist involvement | Length | Number of modules | Patient reimbursement | |||
National (across Canada) | ||||||
16 years and older | Unknown | Therapist-assisted | Access to therapist for 12 weeks, access to program for 1 year | 10 | No cost for Ontario and Manitoba, reimbursed through insurance elsewhere | |
All ages | Unknown | Self-guided | Self-paced, access for 1 year | 8 | There is a cost to access the program, unknown if patients can be reimbursed | |
18 to 100 years | Self-referral by patients | Self-guided, therapist-assisted | 8 to 12 weeks | 9 | Publicly funded | |
Adults | Self-referral by patients | Self-guided | Self-paced | Self-directed articles and videos | No cost | |
Adults | Self-referral by patients | Self-guided | Self-paced | Self-directed articles and videos | No cost | |
16 years and older | Self-referral by patients, referral by a clinician, as 1 component of a broader program, as a complement to standard care, as a stand-alone treatment, stay at work and return to work, disability management | Therapist-assisted | 12 weeks | 10 to 12 with additional modules available | No upfront cost if publicly funded (Ontario), reimbursed if through insurance | |
Youth and adolescents | Self-referral by patients | Self-guided | Self-paced | Self-directed articles and videos | No cost | |
Alberta and Ontario | ||||||
10 to 17 years | Referral by a clinician, as 1 component of a broader program, as a stand-alone treatment | Therapist-directed | 3 weeks | 3 | Publicly funded | |
Alberta | ||||||
18 years and older | Referral by a clinician, as 1 component of a broader program | Therapist-directed | 4 to 8 weeks | 4 to 8 | Publicly funded | |
Manitoba | ||||||
Unknown | Unknown | Therapist-directed | Unknown | Unknown | Patients can seek reimbursement through insurance | |
Newfoundland and Labrador | ||||||
18 to 65 years | As part of a clinical trial103 | Therapist-assisted | 8 weeks | 7 | No cost | |
Nova Scotia | ||||||
18 years and older | Self-referral by patients, referral by a clinician, as 1 component of a broader program, as a complement to standard care, as a stand-alone treatment | Therapist-assisted | 5 weeks | 10 | Publicly funded | |
Psychological Skills for Coping with Pain and Distressc | 8 weeks | 8 | ||||
Quebec | ||||||
Traiter la douleur chez soi (treat your pain at home)c | 18 to 99 years | As a stand-alone treatment | Therapist-assisted | 9 weeks | 8 | Unknown |
Saskatchewan | ||||||
18 years and older | Self-referral by patients, referral by a clinician, as a stand-alone treatment | Therapist-assisted | 8 weeks of support, 5 months of access to program | 5 core modules with additional modules available | Publicly funded | |
In development | ||||||
11 to 25 years | Research study (participants can enrol through self-referral or referral by a clinician) | Self-guided | 8 weeks (chronic pain and JIA) to 20 weeks (post-operative pain) | App uses short self-directed articles rather than modules | Unknown | |
iCBT = internet-delivered cognitive behavioural therapy; JIA = juvenile idiopathic arthritis.
Note: provincial and territorial availability was determined by information available on the program’s website or survey responses in the case of programs without a website.
aWebsite provides access to a variety of articles, videos, and other resources, some of which are based on CBT strategies.
bWebsite states that sessions are available virtually due to the pandemic.
cWebsite not provided.
These results indicate that iCBT programs that support people living with chronic non-cancer pain are currently available in all 13 provinces and territories. Seven of the identified iCBT programs are available across Canada and the others are only available in specific provinces. To gain a better understanding of the characteristics of these iCBT programs, survey participants were asked several questions; their responses are summarized in the following sections.
Patient Eligibility
Survey participants were asked to provide information about the characteristics of the patients receiving iCBT, including questions about the geographical settings and health conditions of the patients eligible for the program. All 13 survey respondents provided an answer to the question about geographical settings, and 11 respondents answered the question about health conditions. The results of these questions are summarized in Table 10. The age range of eligible participants for each of the programs are summarized in Table 9. The age range for most of the programs is aged 16 or 18 years and older. People with a variety of health conditions associated with chronic non-cancer pain are eligible for all the iCBT programs. One respondent indicated that in addition to several of the indications listed in Table 10, people with juvenile idiopathic arthritis and postsurgical pain are eligible for the iCanCope program.
Table 10: Characteristics of Patients Eligible for iCBT Programs
Survey question | Response | Number of responses (%) |
|---|---|---|
Does the iCBT program you are involved with provide care to patients in 1 or more of these geographical settings? (13 total responses, multiple answers accepted)a | Urban | 13 (100) |
Rural | 12 (92.3) | |
Remote | 8 (61.5) | |
Are patients with chronic non-cancer pain associated with the following health conditions eligible for the iCBT program? (11 total responses, multiple answers accepted) | Fibromyalgia | 11 (100) |
Headache or migraine | 11 (100) | |
Muscle and ligament injuries | 10 (90.1) | |
Neuropathic pain | 11 (100) | |
Rheumatoid arthritis | 10 (90.1) | |
Osteoarthritis | 10 (90.1) | |
Multiple sclerosis | 10 (90.1) | |
Pelvic pain | 11 (100) | |
Lower back pain | 11 (100) | |
Abdominal pain | 11 (100) | |
Otherb | 3 (27.3) |
iCBT = internet-delivered cognitive behavioural therapy.
aUrban: area with a population of at least 1,000 and a population density of at least 400 persons per square kilometre.104 Rural: an area that does not fit the definition of “urban” or “remote.” Remote: Health Canada defines various levels of remote, ranging from “remote isolated” (i.e., no scheduled flights or road access and minimal telephone or radio service) to “non-isolated remote” (i.e., road access and less than 90 km away from physician service).105 Self-identified based on the respondent’s local understanding of the criteria for remote.
bResponses included any type of pain, pediatric patient with chronic pain followed at the hospital, juvenile idiopathic arthritis, and postsurgical pain.
Access to and Use of iCBT Programs
Survey participants were asked how the iCBT program they are involved with is currently being used. Eleven respondents answered this question, and the results are summarized in Appendix 7. Respondents indicated that patients most commonly use iCBT through referral by a clinician (7 responses, 63.6%). Five respondents (45.4%) indicated that iCBT is used through self-referral by patients. Approximately half (6 responses, 54.5%) of respondents indicated that iCBT is used as a component of a broader program, and 3 respondents (27.3%) indicated that iCBT is used as a complement to standard care. Six respondents (54.5%) indicated that iCBT is used as a stand-alone treatment.
Characteristics of iCBT Programs
Survey respondents provided information on therapist characteristics (i.e., the level of therapist involvement and required therapist credentials and training) as well as how long it takes to complete the iCBT program, the number of modules, the topics covered, and the technology requirements. Eleven respondents answered all the questions related to the characteristics of the iCBT programs. The responses to the closed-ended questions related to the characteristics of iCBT programs are summarized in Appendix 7. Responses indicated that therapists were involved through pre-scheduled phone calls or emails, as-needed support through asynchronous messaging or phone calls, facilitation and delivery of the iCBT program, and interaction with a case manager (in cases of return to work) or referring clinician as-needed. One respondent indicated that therapists developed and reviewed the content but are not directly involved in the program. Additionally, survey participants indicated that the credentials of the therapists included psychologists, psychotherapists, mental health clinicians, registered nurses, social workers, occupational therapists, certified counsellors, and graduate students under supervision of a registered professional. One of the respondents specified that the graduate students must be enrolled in a clinical psychology program and be supervised by a clinical psychologist with experience in chronic pain management. Another respondent specified that the course content was developed by psychologists, physiotherapists, registered nurses, and physicians. Regarding training, 1 respondent indicated that therapists receive 6 weeks of onboarding training.
Survey participants were also asked to specify the total length of time it takes to complete the iCBT program. Most responses ranged from 3 to 12 weeks. One respondent indicated that the program takes up to 20 weeks for people with post-operative pain. When asked about the number of modules included in the iCBT program, respondents indicated a range from 3 to 12 modules. Three respondents indicated that additional supplemental modules can be added by the patient or therapist. One respondent indicated that the program uses short self-directed articles rather than modules. Participants were asked what topics are covered in the modules and the approximate time it takes to complete each module. Of the 11 respondents, 10 provided information on the topics covered and 6 provided information on the time required to complete each module. Common topics included general information about chronic pain, relaxation, mindfulness, values, goal setting, pacing, communication, sleep, thoughts, emotions and mood, beliefs, and problem-solving. Responses on the time required to complete each module ranged from 5 minutes to 3 hours.
Respondents were also asked about the technology requirements for the iCBT program. All 11 respondents indicated that an internet connection is required for the iCBT program. One respondent indicated that the program requires the use of a smartphone, and 4 respondents indicated that either a phone, tablet, or computer can be used. Three respondents indicated that a device with video and audio capability is required.
Question 2: What Operational Considerations Contribute to the Establishment and Provision, or Lack, of iCBT Programs, Specifically for the Management of Chronic Non-Cancer Pain, at the System or Site Level in Canada?
Facilitators
Eleven survey respondents provided information on the patient-related, clinician-related, and organizational factors that have facilitated or would facilitate the use of iCBT. These results are summarized in Appendix 7.
Commonly identified patient-related facilitators to the use of iCBT were convenience (10 responses, 90.9%), preference (9 responses, 81.8%), satisfaction with care (9 responses, 81.8%), and access (9 responses, 81.8%). The most commonly identified clinician-related facilitators were reaching people who would otherwise be unreachable (11 responses, 100%), efficiency in clinical practice (10 responses, 90.9%), and training, knowledge, or experience with iCBT (9 responses, 81.8%). Commonly identified organizational facilitators included improvement in people’s experiences (11 responses, 100%), more efficient use of resources (10 responses, 90.9%), and reaching more people or serving a broader population (9 responses, 81.8%).
Participants were also asked if they had any additional comments about factors that facilitated or would facilitate iCBT in their facility or jurisdiction, and 6 responses were received. Additional facilitators identified included resources such as information technology support, clerical support (for patient registration and maintenance of participation), and funding (to support outcome tracking). Personalized care, triage to appropriate care, assignment of a single therapist, health equity outreach, and consistent access to technology (for both provider and patient) were also mentioned as potential facilitators. One participant mentioned that the intervention being available in French in Quebec was a facilitator. One participant identified having a self-referral option as a potential facilitator to iCBT because centralized intake and physician referral creates a barrier to treatment access.
Barriers
Eleven survey respondents provided information on the patient-related, clinician-related, and organizational factors they have identified as barriers to the use of iCBT. These results are summarized in Appendix 7.
Commonly identified patient-related barriers to iCBT included privacy concerns (9 responses, 81.8%), lack of familiarity with technology (8 responses, 72.7%), and lack of available devices or adequate internet connection (8 responses, 72.7%). Preference for in-person or other treatment options was identified as a common patient-related (8 responses, 72.7%) and clinician-related (9 responses, 81.8%) barrier. Another commonly identified clinician-related barrier was lack of education or training on iCBT and delivering services via distance (7 responses, 63.6%). Organizational culture (5 responses, 45.4%) and resources (e.g., personnel, technology, funding) (5 responses, 45.4%) were the most commonly identified organizational barriers.
Survey participants were asked if they had any additional comments about barriers to iCBT, and 1 response was received. The respondent mentioned several potential barriers including reduced capacity for change management due to the COVID-19 pandemic, reluctance of provinces to be the first to implement a program, and lack of coverage for mental health under the Canada Health Act.
Access
Survey participants were asked whether any patient groups required specific considerations when considering access to iCBT. Participants were asked to specify the patient groups and whether there were any specific barriers or facilitators to accessing iCBT for these patients. Eleven respondents answered these questions, and the results are summarized in Table 11. Two respondents did not specify a patient group, but did mention additional facilitators and barriers. Several respondents indicated that people living in rural or remote settings and people unfamiliar with or without access to technology are groups that require specific considerations. Access to adequate internet and technology was highlighted as a barrier to iCBT for these people. Potential facilitators that were identified for these groups were enabling content to be available offline, providing funding for technology resources, and providing learning sessions on the use of technology. People in crisis were also identified as a group that requires specific considerations. One survey respondent indicated that iCBT may not be suitable for people who are actively suicidal.
Table 11: Facilitators and Barriers to Accessing iCBT for Specific Patient Groups
Patient group | Facilitator | Barrier |
|---|---|---|
People in rural areas without reliable internet | Do not need to drive to a health centre; reduced cost of gas and parking | Lack of internet access |
People who live in remote areas where internet access is not reliable | Tools and resources are available even when offline | None identified |
People in remote areas; people without access to privacy or an appropriate device | Finances for technology resources | Lack of finances |
People in rural or remote areas; people living in homes with many other people (i.e., lack of privacy); people who aged 16 to 25 years; people who belong to 1 of the following groups: people of different races and ethnicities, LGBTQ+, first responders and health care workers, and students | Targeted outreach with associations and community organizations who can help develop content, culturally sensitive content, integration with traditional Indigenous healing | Lack of awareness, stigma, lack of integration with traditional Indigenous healing |
People who do not speak English; people who are not able to read at a grade 8 level | Phone calls to support patients who struggle with email | Lack of knowledge of the service |
People with financial challenges; people requiring interpretation services | Language Line which can be used over phone or video conference | Lack of data or minutes to use iCBT; some people and providers are not familiar with how to use the technology available for interpretation |
People unfamiliar with technology; people with learning disabilities; people with autism spectrum disorder | Learning sessions on use of technology, 1:1 support | No access to technology |
People who are actively suicidal | Presence of a satisfactory, mutually agreed upon safety plan | None identified |
People in crisis; people unfamiliar with technology | Easy and/or free access | Lack of motivation, lack of appropriate technology |
No specific subgroup identified | Opportunities for shared decision-making of in-person vs. virtual | Lack of access to internet or devices; decreased ability for participants to engage with one another; lack of time to attend program |
No specific subgroup identified | Population-specific content and voice; self-referral vs. centralized intake | Lack of knowledge that programs exist; centralized intake vs. self-referral |
iCBT = internet-delivered cognitive behavioural therapy; LGBTQ+ = lesbian, gay, bisexual, transgender, and queer; NA = not applicable.
Summary of Results
This Environmental Scan was informed by a literature search, survey, and stakeholder feedback. The literature search identified 3 websites that provided descriptions of iCBT programs available in Canada; however, no publications were identified that provided information on the operational considerations of iCBT programs that support people living with chronic non-cancer pain. A total of 13 survey responses (11 complete responses and 2 partial responses) that represented stakeholders involved in the funding, regulation, development, or delivery of iCBT were included in the analyses. Survey respondents were from Alberta, British Columbia, Newfoundland and Labrador, Nova Scotia, Ontario, Quebec, and Saskatchewan. Three iCBT programs were identified through stakeholder feedback.
Regarding decision problems, the characteristics of the iCBT programs that were identified through this Environmental Scan could help inform decisions about whether iCBT should be offered. Additionally, the barriers and facilitators identified may be factors that should guide the implementation of iCBT.
From the results of the literature search, survey, and stakeholder feedback, there are at least 16 iCBT programs available or in development in various jurisdictions in Canada that support people living with chronic non-cancer pain. The characteristics of these programs vary in terms of the level of therapist involvement, overall program length, number and length of modules, and topics covered. All the programs require internet access. Most programs are therapist-assisted or therapist-directed with the level of therapist involvement ranging from as-needed support to facilitation and/or delivery of the program.
The results of the survey highlighted some of the operational considerations of iCBT programs for the management of chronic non-cancer pain in Canada. Survey respondents identified a variety of patient-related, clinician-related, and organizational factors that are facilitators or barriers to iCBT. Commonly identified facilitators to iCBT included reaching people who would otherwise be unreachable, improvement in patients’ experiences, efficiency (in clinical practice and use of resources), and convenience for patients. Commonly identified barriers to iCBT included privacy concerns, preference for in-person or other treatment options (of both patients and clinicians), lack of familiarity with technology, and lack of available devices or adequate internet connection.
Additionally, survey respondents identified patient groups that may require specific considerations when considering access to iCBT, such as people living in rural or remote settings and people unfamiliar with or without access to technology. Lack of access to adequate internet or technology was highlighted as a barrier to iCBT for these patients. Potential facilitators that were identified for these groups were enabling content to be available offline, providing funding for technology resources and learning sessions on the use of technology.
The findings of this Environmental Scan were informed by the results of a limited literature search and survey distributed to stakeholders involved with iCBT programs that support people living with chronic non-cancer pain in Canada. Alternative research methods such as a systematic review or broader stakeholder engagement approach would provide a more comprehensive understanding about the operational considerations for the implementation of iCBT for the management of chronic non-cancer pain in Canada.
Limitations
This Environmental Scan presents an overview of iCBT programs for the management of chronic non-cancer pain in Canada and the characteristics and related operational aspects of these programs. The findings are based on a survey and a limited literature search. A comprehensive systematic review was not conducted as part of this Environmental Scan.
The survey was distributed directly to 30 stakeholders identified by CADTH. However, because the survey was distributed through our targeted efforts as well as referrals, the exact number of stakeholders who received the survey was not quantifiable. A total of 13 responses were received and included in the analysis (2 partial responses and 11 complete responses). Because the survey was sent to stakeholders identified by CADTH, it is likely that not all relevant stakeholders were identified and contacted. CADTH was not able to identify stakeholders from the following jurisdictions: Prince Edward Island, Northwest Territories, Nunavut, or Yukon. The survey results are based on a small sample of respondents that is not representative of all stakeholders across Canadian jurisdictions. Additionally, respondents were only able to answer the survey questions based on personal experiences with the iCBT program they are involved with. The responses may not reflect all iCBT programs available in Canada. The survey was not sent to people with lived experience with chronic pain; therefore, the perspectives of people with lived experience with chronic pain were not captured in the survey results. However, insights on iCBT from the perspective of people with lived experience with chronic pain were explored in the Patients’ Perspectives component of this HTA. Information on the clinical evidence supporting the iCBT programs was not collected as part of this Environmental Scan. The clinical evidence supporting iCBT programs for people living with chronic non-cancer pain was evaluated in the Clinical Review component of this HTA.
The literature search identified 3 websites that provided descriptions of iCBT programs available in Canada; however, no publications were identified that provided information on the operational considerations of iCBT programs that support people living with chronic non-cancer pain.
Considering these limitations, it is likely this Environmental Scan did not identify all iCBT programs that support people living with chronic non-cancer pain that are available in Canada.
Discussion
Overview
The evidence assessed in this HTA is intended to support Canadian jurisdictions regarding the following decision problems:
With a view to increasing access to CBT-based therapy, the purpose of this HTA is to inform decisions as to whether iCBT should be offered as a treatment option, as part of a multidisciplinary approach, in the delivery of care for chronic non-cancer pain when CBT would otherwise be provided.
Additionally, if evidence demonstrates that iCBT should be offered, the HTA could also inform whether there are criteria to guide decision-making regarding the suitability of iCBT for various pain conditions and people experiencing chronic pain, or other factors that should guide its implementation.
To address these decision problems using the evidence presented in this HTA, we discuss some points for decision-makers to consider when deciding whether to offer iCBT as a treatment option in the context of multidisciplinary chronic pain care. We also detail factors that might guide the implementation of this intervention in Canadian jurisdictions and suggest potential strategies that may address the issues discussed.
Should iCBT Be a Treatment Option in Multidisciplinary Chronic Pain Care When In-Person CBT Would Otherwise Be Offered?
The findings from the Clinical Review suggest that the available evidence on the balance of comparative benefits of iCBT versus in-person CBT is very uncertain, meaning it does not provide a reliable indication of how these treatments may compare. Across all outcomes, the certainty of the clinical evidence is insufficient to determine if iCBT is clinically better, worse, or equivalent to in-person CBT. However, when imagined within the contexts of multidisciplinary care, people living with chronic pain who participated in the Patients’ Perspectives study could appreciate how iCBT might become a helpful tool as people worked to “live better” with their pain. Previous systematic reviews1-4 have suggested that both in-person CBT and iCBT may provide benefits of small effect sizes for people with chronic pain compared with wait-list or various active controls. While the evidence evaluated in this HTA suggests there may be potential for the use of iCBT for the management of chronic non-cancer pain, limitations of the clinical evidence make it challenging to provide an answer to the question of whether iCBT should (or should not) be offered as a treatment option when in-person CBT would otherwise be offered.
Paired with an absence of any high-quality clinical data about the comparative effectiveness of iCBT and in-person CBT for chronic pain, we found no safety data on the potential comparative harms of iCBT versus in-person CBT. Jurisdictions considering iCBT should be aware that there is little empirical evidence about the safety of iCBT relative to in-person CBT for people living with chronic pain. In addition, very little empirical evidence is available about the safety of in-person CBT itself20; therefore, indirect inferences from that treatment modality to iCBT are not possible.
Considerations and Factors to Guide Implementation of iCBT
Although the evidence assessed in this review is insufficient to conclude whether iCBT should be offered when CBT would otherwise be provided, we understand the ongoing challenges to meet the psychological care and treatment needs of people living with chronic pain and the potential of virtual care to be part of the solution. Based on the evidence reviewed in this HTA and the previous CADTH assessments of iCBT as a treatment for depression and anxiety88,106 and for PTSD,88 we propose some key points to consider in implementing iCBT for chronic pain in circumstances in which in-person CBT would otherwise be offered. Prioritizing the careful examination of these considerations, and how they might be mitigated in practice, should support implementing iCBT programs that have the best chance of supporting people living with chronic pain. We cannot provide a thorough and succinct list of what this mitigation will look like for each jurisdiction because mitigation will be contextualized based on local circumstances, and we highlight areas for consideration based on the evidence throughout this HTA.
Population Considerations
Dropout and How it Could Be Mitigated
In the 3 included RCTs,73-75 participants treated with iCBT were more likely to withdraw before study completion than those who received in-person CBT. This is similar to findings from CADTH’s Optimal Use of iCBT for PTSD in which it was found that participants treated with iCBT were at a higher risk of dropout than those allocated to comparators (i.e., wait-list or usual care).88 In that review, qualitative data suggested the higher dropout rates could potentially be connected to poorly developed therapeutic relationships and divergent, or untailored, treatment goals.88 Evidence from the Patients’ Perspectives section of this HTA suggests that, in some cases, dropout from iCBT (or in-person CBT) might be exacerbated if providers are not specifically trained in chronic pain care or people are referred to iCBT (or CBT) before a sense of “readiness” has been reached.
Attending to the biopsychosocial nature of chronic pain through comprehensive multidisciplinary care is vital to providing good care for people living with chronic pain. However, people involved in the Patients’ Perspectives study worried that providers without any expertise — or at least specific training — in chronic pain would struggle to be attentive to and understand the challenges of living with chronic pain. The participants felt this could negatively impact the development of a strong and trusting therapeutic relationship and ultimately the ability of that provider to tailor the programming to the needs of the person living with pain. One way to address this potential challenge is by developing (or implementing) iCBT programs that are guided by therapists specifically trained in chronic pain (rather than unguided programs without therapist support).
Fostering a sense of “readiness” might be a bit more challenging and require work beyond the implementation of a new iCBT program. In the Patients’ Perspectives study, we describe readiness as an assemblage of treatment history, current care practices, material realities of 1’s condition, and individual needs or desires. This implies that the building toward readiness for an intervention such as iCBT occurs from the moment someone presents with pain and will continue throughout subsequent treatment (or lack thereof) experiences with the health care system. As such, developing a sense of readiness not only involves having access to comprehensive multidisciplinary care, but also a demonstration that one’s pain is believed and truly cared for by providers.
We will discuss the importance of comprehensive, multidisciplinary chronic pain care subsequently, and here we suggest the importance of building pain care strategies that incorporate principles of trauma-informed care. There is a growing understanding of the pervasiveness of trauma in people’s lives; therefore, the principles of trauma-informed care are meant to be applied throughout both clinical and organizational practice to support people seeking care regardless of whether there is a known history of traumatic experience.107 This general application of trauma-informed care practices was also identified in the ethics review of CADTH’s Optimal Use on iCBT for PTSD in which the author noted that “fulfilling the ethical obligations of nonmaleficence in the context of PTSD therapy requires an approach that is trauma informed” (p.89).88 People living with chronic pain, including most of the women we spoke with for the Patients’ Perspectives study, may have had past experiences of dismissal or neglect by health care providers and those in their social spheres,108 and childhood trauma is a possible risk factor for developing chronic pain109,110; therefore, trauma may be just as important in the context of chronic pain as PTSD. Although approaches to and conceptualizations of trauma-informed care may vary,107,111,112 finding ways to incorporate these principles throughout chronic pain care regimens may help mitigate iCBT dropout.
Suitability
Survey respondents to CADTH’s Environmental Scan for this HTA suggested that people in crisis may require specific considerations and that iCBT may not be suitable for people who are actively suicidal. This corresponds with findings from the Patients’ Perspectives section in which women described being unlikely to benefit from iCBT when in severe physical pain. Interestingly, findings from CADTH’s previous reviews of iCBT88,106 suggested that it may be more challenging for clinicians to adequately monitor and respond to changes in users’ suicide risk with iCBT compared with in-person CBT. However, more research is necessary to provide specific suggestions about who might be most likely to benefit from iCBT, including considerations other than pain severity.
Program Design Considerations
Therapeutic Relationship, Shared Decision-Making, Assessment and Program Length, and Tailoring
In the absence of evidence clearly supporting the comparative clinical effectiveness and safety of iCBT versus in-person CBT for chronic pain, some proactive measures may help to limit the possibility of causing unforeseen harm if iCBT is to be implemented. Evidence from the Patients’ Perspectives study suggests this goal could be supported with iCBT programs that help foster strong therapeutic relationships, encourage shared decision-making practices, and have the flexibility to be tailored to a person’s specific needs.
Not only does the importance of therapeutic relationships resonate with findings from CADTH’s previous reviews of iCBT88,106 but it also sets the ground work for attending to the ideals of shared decision-making113 that were important to the women we spoke with for the Patients’ Perspectives study. In our conversations with these women, they emphasized the value of knowing specifics about the content of iCBT programs, the expected effort required, and how this effort might benefit them in the long run before engaging with iCBT. This process takes time and cannot be rushed. Optimizing care with iCBT for people living with chronic pain might involve creating programming that accounts for this slower pace.
A slower pace may involve including longer assessment periods during which a provider and person living with chronic pain can get to know each other before diving into the full iCBT programming. All the women we spoke with for the Patients’ Perspectives study noted an appreciation for synchronous and in-depth assessments; 1 in particular described an appreciation for her assessment period that took place over a series of weeks and involved more than 10 hours with a therapist. Although this may not be attainable (or necessary) for some programs or participants’ iCBT programming, it does indicate the importance of an assessment that is tailored, synchronous, and thorough. Similarly, there may not be clinical data indicating when study participants may begin to notice benefits (if they do at all), but the women participating in the Patients’ Perspectives study described that it may be helpful to reengage with iCBT programming multiple times before all the modules can begin to make sense with their lived realities. As the Environmental Scan indicates that the current programming available in Canada lasts anywhere from 3 to 20 weeks, it may be beneficial to consider implementing programming that is on the longer end of that range or includes the opportunity to revisit specific modules, at least for some people.
In addition to pace of assessment and programming, it would seem important to also consider how flexible and responsive the available iCBT programming is before implementing a particular program. The women we spoke with for the Patients’ Perspectives study emphasized that iCBT program content must be tailored to the needs and desires of the individual, which is consistent with what we found in previous CADTH reviews of iCBT.88,106 Active tailoring might involve the ongoing availability of a provider who is able to assess and respond to their client’s needs. To allow for this real-time tailoring, the women anticipated guided, and at least partially synchronous, iCBT programs would most benefit them.
The Environmental Scan found that level of provider involvement in the identified iCBT programs could be wide-ranging and included “as-needed” support, asynchronous messaging, periodic phone calls, and videoconference delivery of the iCBT program. When considering the implementation of iCBT, it could be beneficial to consider programs that incorporate elements such as close monitoring, consistent guidance from a therapist, and coordination with a person’s primary health care provider.
Access Considerations
Importance of Multidisciplinary Chronic Pain Care
Although this HTA assumes that iCBT for chronic pain is offered as part of a more comprehensive multidisciplinary care strategy, the women interviewed in the Patients’ Perspectives study repeatedly described how challenging it was to access multidisciplinary care in their experience. This concern is consistent with the published literature which has similarly acknowledged that timely access to comprehensive multidisciplinary chronic pain care is not the norm across Canada.11,20,45 With this in mind, the women we spoke with were concerned about a slippage between iCBT being available as a component of multidisciplinary care iCBT as a “quick fix” solution in the absence of other treatment options.
Improving the availability of multidisciplinary services may help iCBT become a supportive component of care for those living with chronic pain. As such, the Canadian Pain Tasks Force’s final report, An Action Plan for Pain in Canada,45 may be a useful starting point. Goal 2 in this report may be particularly relevant in relation to iCBT because it includes specific recommendations for virtual care within the context of broader system reform.45 CADTH’s recent Environmental Scan on Models of Care for Chronic Pain114 may be another useful resource for understanding how other jurisdictions are approaching the challenges of comprehensive chronic pain care.
Privacy Concerns, Technological Challenges, and Equity
The information collected in our interviews and our Environmental Scan identified privacy as another area of concern for people engaging with iCBT. It follows that offering iCBT may not be appropriate if a person cannot engage with the content in a private location or in contexts in which the programs do not have methods of collecting and storing personal information in a secure way. The women we interviewed noted that privacy concerns could be addressed through carefully considering how information is collected and stored, and vetting participants of group iCBT programs.
There may be other contexts in which iCBT is not appropriate. In our Patients’ Perspectives study, the women interviewed suggested that iCBT would not be appropriate in cases in which an intended user has limited computer skills or limited access to required hardware, software, or a stable internet connection. The Environmental Scan identified similar barriers to engaging with iCBT (i.e., a lack of familiarity with technology, a lack of access to devices required for engagement, and a lack of a stable internet connection, especially in rural and remote locations).
Respondents to the Environmental Scan offered some suggestions for potential ways to mitigate barriers to engaging with iCBT, including providing funding for personal devices, enabling content to be available offline, and providing learning sessions on the use of technology. Personal factors identified in our Patients’ Perspectives study and Environmental Scan, including preferences for in-person treatment options for pain conditions limiting the use of the hands, may also limit someone’s ability or willingness to engage with iCBT. For these reasons, if offering iCBT, it may be helpful to ensure the option to receive in-person CBT also remains available and accessible in some cases.
The common assumption that increased availability of iCBT will improve access to CBT-based therapy has not been explored in this review, and the available evidence did not enable an improved understanding of how the availability of iCBT could narrow or widen existing inequities in access to care. Without this information, it still seems important to ensure that available iCBT programs have an inclusive and accessible design, and are relevant for people from a variety of sociocultural backgrounds.115 This may help to improve access for underserved groups and people who would otherwise have difficulty accessing iCBT programs.115
Limitations and Sources of Uncertainty
In our Clinical Review of the available evidence comparing iCBT to in-person CBT we located 4 small trials that enrolled adults with chronic pain. In these trials, the certainty of evidence for all outcomes at post-treatment and at longest follow-up point was very low due to very serious concerns related to risk of bias and large imprecision across most outcome comparisons. Some comparisons were also affected by serious indirectness (i.e., there were differences across study arms that may have confounded the main comparison of interest) and unexplained heterogeneity. The very low certainty suggests that the evidence does not provide a reliable indication of the true comparative treatment effect, and that there is a very high likelihood that the true effect of iCBT versus in-person CBT could be substantially different than what was presented in the 4 included studies. The generalizability of our findings to all people with chronic pain and all types and modes of delivery of iCBT also is uncertain because the included clinical trials were specific to a small subset of chronic non-cancer pain populations (i.e., veterans with nonterminal pain conditions, adult females with fibromyalgia, and adults with daily back pain or nonspecific chronic pain). We also did not locate any evidence about the comparative effectiveness of iCBT versus in-person CBT among children, people living in rural or remote areas, or people who experience marginalization for whom the effect of iCBT compared with in-person CBT could differ. As such, this lack of evidence precluded any examination of how the availability of iCBT might affect access to psychological pain care for different groups or affect existing inequities.
The Patients’ Perspectives study had several limitations that potentially affect the transferability of our findings across Canadian jurisdictions and to the diversity of people living with chronic pain. First, none of the women we interviewed had experienced asynchronous or non-guided iCBT for chronic pain. Despite our efforts to include a diverse sample of participants, all the people interviewed identified as women and as White or Jewish when asked to describe how they would identify themselves in an open-ended question. Furthermore, 4 of the 5 women interviewed reported having experience working in health care. Although most of the women reported distressing experiences with health care providers and difficulty accessing multidisciplinary pain care, it is possible the experiences of others attempting to access the same care would be different.
Directions for Future Research
The limited and uncertain nature of the available clinical evidence suggests that further research is needed on the comparative clinical effectiveness of iCBT versus in-person CBT. We encourage future clinical studies to use more rigorous methodological approaches (e.g., robust participant allocation methods and a priori protocols), deliberately collect safety data, make direct comparisons of iCBT and in-person CBT without other differences across treatment groups (e.g., the use of group and individual CBT across different study arms), and to strive to lower participant dropout rates. The first decision problem considered for this HTA focused on whether iCBT could be an alternative to in-person CBT; therefore, future non-inferiority studies should use clinically meaningful and justified non-inferiority margins as well as adequate sample sizes when testing the non-inferiority of iCBT versus in-person CBT. We also encourage investigators of future trials to use consistent outcome measures, particularly those from core outcome domains that have been identified as clinically important.58 This would facilitate comparisons across clinical studies and quantitative synthesis in SRs. Finally, additional studies across heterogeneous populations, including children and underrepresented populations, are needed because the current clinical evidence cannot be used to draw inferences about the effect of iCBT versus in-person CBT by pain condition or population and does not provide insight on how iCBT could affect potential health inequities.
Conclusions and Implications for Decision- or Policy-Making
This aim of this HTA was to analyze the available evidence to help determine whether iCBT should be offered as part of a multidisciplinary care approach for the treatment of chronic non-cancer pain when in-person CBT would otherwise be provided. The Clinical Review suggests the available evidence that compares the benefits of the virtual and in-person forms of CBT is very uncertain because of numerous limitations across the body of evidence. Additionally, we identified no relevant clinical studies that provided outcome data regarding the comparative safety of iCBT versus in-person CBT. These findings do not allow for drawing an evidence-based conclusion regarding whether iCBT represents a comparable alternative to in-person CBT that should be offered when CBT would be otherwise provided to address the psychological care needs of individuals with chronic non-cancer pain.
The Environmental Scan conducted as part of this review identified 16 iCBT programs that currently exist in various Canadian jurisdictions, and there is information to suggest that more of these programs may be implemented in the future. Working to improve access to psychological treatment for pain by leveraging virtual forms of CBT seems to be a promising avenue worth exploring. At the same time, the findings of our review suggest that more research is needed to understand if iCBT programs are responding to the psychological care needs of people with chronic pain and are achieving the desired outcomes when compared to CBT delivered in person. While our HTA aimed to describe the potential role of iCBT when CBT would otherwise be provided, decision-makers considering the implementation of iCBT programs as a method of increasing access to psychological care for those who otherwise may not receive any form of CBT should consider the broader iCBT literature.3,5-9
The review also aimed to identify and examine criteria that can help guide decisions about who and what pain conditions iCBT is suitable for and other factors that should be considered as iCBT programs are implemented in the context of the very uncertain evidence about comparative clinical benefits. As is commonly the case with internet-delivered psychological interventions, aspects such as the person’s readiness, a provider with adequate training in care for the condition (i.e., chronic pain, in this case), the strength of the therapeutic relationship between the person receiving CBT and the provider, and tailoring the treatment to individual needs were identified in this review as notable factors that may impact the usefulness of iCBT programs. Additionally, iCBT programs may not be suitable for people experiencing severe, untreated chronic pain or who have active suicidal ideation.
References
1.Fisher E, Law E, Dudeney J, Palermo TM, Stewart G, Eccleston C. Psychological therapies for the management of chronic and recurrent pain in children and adolescents. Cochrane Database Syst Rev. 2018;9:CD003968. PubMed
2.Williams ACC, Fisher E, Hearn L, Eccleston C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2020;8:CD007407. PubMed
3.Gandy M, Pang STY, Scott AJ, et al. Internet-delivered cognitive and behavioural based interventions for adults with chronic pain: a systematic review and meta-analysis of randomized controlled trials. Pain. 2022. PubMed
4.Fisher E, Law E, Dudeney J, Eccleston C, Palermo TM. Psychological therapies (remotely delivered) for the management of chronic and recurrent pain in children and adolescents. Cochrane Database Syst Rev. 2019;4:CD011118. PubMed
5.Bernardy K, Klose P, Welsch P, Hauser W. Efficacy, acceptability and safety of Internet-delivered psychological therapies for fibromyalgia syndrome: a systematic review and meta-analysis of randomized controlled trials. Eur J Pain. 2019;23(1):3-14. PubMed
6.Mariano TY, Wan L, Edwards RR, Jamison RN. Online teletherapy for chronic pain: A systematic review. J Telemed Telecare. 2021;27(4):195-208. PubMed
7.Tang WX, Zhang LF, Ai YQ, Li ZS. Efficacy of Internet-delivered cognitive-behavioral therapy for the management of chronic pain in children and adolescents: A systematic review and meta-analysis. Medicine (Baltimore). 2018;97(36):e12061. PubMed
8.Vugts MAP, Joosen MCW, van der Geer JE, Zedlitz A, Vrijhoef HJM. The effectiveness of various computer-based interventions for patients with chronic pain or functional somatic syndromes: A systematic review and meta-analysis. PLoS One. 2018;13(5):e0196467. PubMed
9.Vigerland S, Lenhard F, Bonnert M, et al. Internet-delivered cognitive behavior therapy for children and adolescents: A systematic review and meta-analysis. Clin Psychol Rev. 2016;50:1-10. PubMed
10.Schopflocher D, Taenzer P, Jovey R. The prevalence of chronic pain in Canada. Pain Res Manag. 2011;16(6):445-450. PubMed
11.The Canadian Pain Task Force. Chronic pain in Canada: laying a foundation for action. (Canadian Pain Task Force report: June 2019). Ottawa (ON): Health Canada; 2019: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2019.html. Accessed 2021 Mar 18.
12.Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273-e283. PubMed
13.Fashler SR, Cooper LK, Oosenbrug ED, et al. Systematic Review of Multidisciplinary Chronic Pain Treatment Facilities. Pain Res Manag. 2016;2016:5960987. PubMed
14.Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715-724. PubMed
15.Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003-1007. PubMed
16.Nicholas M, Vlaeyen JWS, Rief W, et al. The IASP classification of chronic pain for ICD-11: chronic primary pain. Pain. 2019;160(1):28-37. PubMed
17.Buhrman M, Syk M, Burvall O, Hartig T, Gordh T, Andersson G. Individualized Guided Internet-delivered Cognitive-Behavior Therapy for Chronic Pain Patients With Comorbid Depression and Anxiety: A Randomized Controlled Trial. Clin J Pain. 2015;31(6):504-516. PubMed
18.Doan L, Manders T, Wang J. Neuroplasticity underlying the comorbidity of pain and depression. Neural Plast. 2015;2015:504691. PubMed
19.National Pain Strategy: pain management for all Australians. Deakin (AU): Pain Australia; 2011: https://www.painaustralia.org.au/static/uploads/files/national-pain-strategy-2011-wfvjawttsanq.pdf. Accessed 2020 Jun 22.
20.The Canadian Pain Task Force. Working together to better understand, prevent and, manage chronic pain: What We Heard. (Canadian Pain Task Force report: October 2020). Ottawa (ON): Health Canada; 2020: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2020.html. Accessed 2021 Feb 02.
21.Dear BF, Gandy M, Karin E, et al. The Pain Course: a randomised controlled trial examining an internet-delivered pain management program when provided with different levels of clinician support. Pain. 2015;156(10):1920-1935. PubMed
22.Ehde DM, Dillworth TM, Turner JA. Cognitive-behavioral therapy for individuals with chronic pain: efficacy, innovations, and directions for research. Am Psychol. 2014;69(2):153-166. PubMed
23.Fisher E, Law E, Palermo TM, Eccleston C. Psychological therapies (remotely delivered) for the management of chronic and recurrent pain in children and adolescents. Cochrane Database Syst Rev. 2015;3:CD011118. PubMed
24.Monticone M, Cedraschi C, Ambrosini E, et al. Cognitive-behavioural treatment for subacute and chronic neck pain. Cochrane Database Syst Rev. 2015;5:CD010664. PubMed
25.Cognitive behavioural therapy for chronic non-cancer pain: a review of clinical effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1181%20CBT%20for%20pain%20Final.pdf. Accessed 2021 Aug 18.
26.Williams AC, Eccleston C, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2012;11:CD007407. PubMed
27.Kowal J, McWilliams LA, Péloquin K, Wilson KG, Henderson PR, Fergusson DA. Attachment insecurity predicts responses to an interdisciplinary chronic pain rehabilitation program. J Behav Med. 2015;38(3):518-526. PubMed
28.Kowal J, Wilson KG, Geck CM, Henderson PR, D'Eon JL. Changes in perceived pain severity following interdisciplinary treatment for chronic pain. Pain Res Manag. 2011;16(6):451-456. PubMed
29.Pfeifer A-C, Penedo JMG, Ehrenthal JC, et al. Impact of attachment behavior on the treatment process of chronic pain patients. J Pain Res. 2018;11:2653-2662. PubMed
30.Bekker MJ, Griffiths KM, Barrett PM. Improving accessibility of cognitive behavioural therapy for children and adolescents: review of evidence and future directions. Clin Psychol. 2020;21(3):157-164.
31.Collins KA, Westra HA, Dozois DJ, Burns DD. Gaps in accessing treatment for anxiety and depression: challenges for the delivery of care. Clin Psychol Rev. 2004;24(5):583-616. PubMed
32.Hundt NE, Mott JM, Cully JA, Beason-Smith M, Grady RH, Teng E. Factors associated with low and high use of psychotherapy in veterans with PTSD. Psychol Trauma. 2014;6(6):731-738.
33.Mohr DC, Ho J, Duffecy J, et al. Perceived barriers to psychological treatments and their relationship to depression. J Clin Psychol. 2010;66(4):394-409. PubMed
34.Ndegwa S, Dolcine B, Frey F, Quay T. Access to and availability of non-pharmacological treatments for chronic non-cancer pain in Canada: an environmental scan. (Environmental scan no. 81). Ottawa (ON): CADTH; 2018: https://cadth.ca/sites/default/files/pdf/es0313_access-to-non-pharmacological-treatment-of-pain.pdf. Accessed 2021 Mar 18.
35.Ringle VA, Read KL, Edmunds JM, et al. Barriers to and facilitators in the implementation of cognitive-behavioral therapy for youth anxiety in the community. Psychiatr Serv. 2015;66(9):938-945. PubMed
36.E-mental health in Canada: transforming the mental health system using technology. Briefing document. Ottawa (ON): Mental Health Commission of Canada; 2014: https://www.mentalhealthcommission.ca/sites/default/files/MHCC_E-Mental_Health-Briefing_Document_ENG_0.pdf. Accessed 2019 Sep 06.
37.Ascribe Marketing Communications Inc. Addressing the access gap: leveraging the potential of e-mental health in Canada. Summary report. Ottawa (ON): Mental Health Commission of Canada; 2017: https://www.mentalhealthcommission.ca/sites/default/files/2017-07/MHCC%20January%20Roundtable_FINAL%20EN.pdf. Accessed 2019 Apr 18.
38.Kuester A, Niemeyer H, Knaevelsrud C. Internet-based interventions for posttraumatic stress: a meta-analysis of randomized controlled trials. Clin Psychol Rev. 2016;43:1-16. PubMed
39.McGrath P, Newton A, Hartling L, et al. Advancing the evolution: insights into the state of e-mental health services in Canada. Ottawa (ON): Mental Health Commission of Canada; 2017: https://www.mentalhealthcommission.ca/sites/default/files/2017-08/eMH%20Environmental%20Scan_FINAL%20EN.pdf. Accessed 2019 Apr 18.
40.Simblett S, Birch J, Matcham F, Yaguez L, Morris R. A Systematic Review and Meta-Analysis of e-Mental Health Interventions to Treat Symptoms of Posttraumatic Stress. JMIR Ment Health. 2017;4(2):e14. PubMed
41.Gulliford M, Figueroa-Munoz J, Morgan M, et al. What does 'access to health care' mean? J Health Serv Res Policy. 2002;7(3):186-188. PubMed
42.Levesque JF, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12(1):18. PubMed
43.King A. How COVID-19 has pushed health care into the virtual world, helping patients get treated at home. Toronto (ON): CBC; 2020: https://www.cbc.ca/news/canada/toronto/covid-19-transformed-healthcare-virtual-world-1.5572650. Accessed 2020 Jun 16.
44.Webster P. Virtual health care in the era of COVID-19. Lancet. 2020;395(10231):1180-1181. PubMed
45.The Canadian Pain Task Force. An Action Plan for Pain in Canada. (Canadian Pain Task Force Report: March 2021). Ottawa (ON): Health Canada; 2021: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2021.html. Accessed 2022 Apr 19.
46.Knowledge Synthesis: COVID-19 in Mental Health and Substance Use. Ottawa (ON): Canadian Institutes of Health Research (CIHR); 2021: https://covid19mentalhealthresearch.ca/wp-content/uploads/2021/01/BIRNIE_CMH-KS-Executive-Lay-Summary-Report-November23.pdf. Accessed 2021 Aug 18.
47.AbilitiCBT. AbilitiCBT Programs. 2020; https://myicbt.com/programs. Accessed 2020 Jun 23.
48.Online Therapy Unit. Chronic Health Conditions including Chronic Pain Course. https://www.onlinetherapyuser.ca/chronic-conditions. Accessed 2020 Jun 25.
49.Therapist Assistance Online (TAO). Welcome to TAO. https://taoconnect.org/what_is_tao/ns/. Accessed 2020 Jun 25.
50.Internet-delivered cognitive behavioural therapy for chronic pain: clinical effectiveness. (CADTH reference list). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RA1155%20iCBT%20for%20Chronic%20Pain%20Final.pdf. Accessed 2021 Aug 18.
51.Sharpe L, Dudeney J, Williams ACC, et al. Psychological therapies for the prevention of migraine in adults. Cochrane Database Syst Rev. 2019;7:CD012295. PubMed
52.Buhrman M, Gordh T, Andersson G. Internet interventions for chronic pain including headache: a systematic review. Internet Interv. 2016;4:17-34. PubMed
53.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. PubMed
54.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
55.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Aug 17.
56.Morgan C, Mason E, Newby JM, et al. The effectiveness of unguided internet cognitive behavioural therapy for mixed anxiety and depression. Internet Interv. 2017;10:47-53. PubMed
57.Frye-Cox N, O’Neal CW, Wendling S, Nichols LR, Lucier-Greer M. Understanding asynchronous counseling: a review of effectiveness and implementation considerations. Auburn (AL): Military REACH; 2020: https://militaryreach.auburn.edu/dr?id=bfeb5522-8d83-43ec-b348-846607589444&rt=rs. Accessed 2021 Sep 27.
58.Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. 2003;106(3):337-345. PubMed
59.Hayes SC. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav Ther. 2004;35(4):639-665. PubMed
60.Hayes SC, Hofmann SG. The third wave of cognitive behavioral therapy and the rise of process-based care. World Psychiatry. 2017;16(3):245-246. PubMed
61.Hunot V, Moore TH, Caldwell DM, et al. 'Third wave' cognitive and behavioural therapies versus other psychological therapies for depression. Cochrane Database Syst Rev. 2013;10:CD008704. PubMed
62.Hofmann SG, Sawyer AT, Fang A. The Empirical Status of the “New Wave” of Cognitive Behavioral Therapy. Psychiatr Clin North Am. 2010;33(3):701-710. PubMed
63.Bendelin N, Bjorkdahl P, Risell M, et al. Patients' experiences of internet-based Acceptance and commitment therapy for chronic pain: a qualitative study. BMC Musculoskelet Disord. 2020;21(1):212. PubMed
64.Ehde DM, Alschuler KN, Day MA, et al. Mindfulness-based cognitive therapy and cognitive behavioral therapy for chronic pain in multiple sclerosis: a randomized controlled trial protocol. Trials. 2019;20(1):774. PubMed
65.Morrison A, Polisena J, Husereau D, et al. The effect of English-language restriction on systematic review-based meta-analyses: a systematic review of empirical studies. Int J Technol Assess Health Care. 2012;28(2):138-144. PubMed
66.Nussbaumer-Streit B, Klerings I, Dobrescu AI, et al. Excluding non-English publications from evidence-syntheses did not change conclusions: a meta-epidemiological study. J Clin Epidemiol. 2020;118:42-54. PubMed
67.Herman G. “Catastrophizing”: a form of pain shaming. West Hartford (CT): US Pain Foundation; 2020: https://uspainfoundation.org/blog/catastrophizing-a-form-of-pain-shaming/. Accessed 2022 Apr 12.
68.Petrini L, Arendt-Nielsen L. Understanding Pain Catastrophizing: Putting Pieces Together. Front Psychol. 2020;11:603420. PubMed
69.Crombez G, De Paepe AL, Veirman E, Eccleston C, Verleysen G, Van Ryckeghem DML. Let's talk about pain catastrophizing measures: an item content analysis. PeerJ. 2020;8:e8643. PubMed
70.Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. PubMed
71.Kim SY, Park JE, Lee YJ, et al. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J Clin Epidemiol. 2013;66(4):408-414. PubMed
72.Higgins JPT, Li T, Deeks JJ, (editors). Chapter 6: Choosing effect measures and computing estimates of effect. In: Higgins JPT, Thomas J, Chandler J, et al., eds. Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). London (UK): Cochrane; 2021: www.training.cochrane.org/handbook. Accessed 2021 Dec 16.
73.Herbert MS, Afari N, Liu L, et al. Telehealth versus in-person acceptance and commitment therapy for chronic pain: a randomized noninferiority trial. J Pain. 2017;18(2):200-211. PubMed
74.de Boer MJ, Versteegen GJ, Vermeulen KM, Sanderman R, Struys MM. A randomized controlled trial of an Internet-based cognitive-behavioural intervention for non-specific chronic pain: an effectiveness and cost-effectiveness study. Eur J Pain. 2014;18(10):1440-1451. PubMed
75.Vallejo MA, Ortega J, Rivera J, Comeche MI, Vallejo-Slocker L. Internet versus face-to-face group cognitive-behavioral therapy for fibromyalgia: A randomized control trial. J Psychiatr Res. 2015;68:106-113. PubMed
76.Popay J, Roberts H, Sowden A, et al. Guidance on the conduct of narrative synthesis in systematic reviews. Swindon (UK): ESRC Methods Programme; 2006: https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf. Accessed 2022 Apr 20.
77.McKenzie JE, Brennan SE. Chapter 12: Synthesizing and presenting findings using other methods. In: Higgins JPT, Thomas J, eds. Cochrane Handbook for Systematic Reviews of Interventions, version 6.3. London (UK): Cochrane; 2022: https://training.cochrane.org/handbook/current/chapter-12. Accessed 2022 Mar 28.
78.Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328(7454):1490. PubMed
79.Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383-394. PubMed
80.Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-926. PubMed
81.GRADE Handbook. In: Schunemann H, Brozek J, Guyatt G, Oxman A, eds. Hamilton (ON): Grading of Recommendations Assessment, Development and Evaluation (GRADE); 2013: https://gdt.gradepro.org/app/handbook/handbook.html. Accessed 2021 Sep 27.
82.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
83.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. PubMed
84.Mariano TY, Wan L, Edwards RR, Lazaridou A, Ross EL, Jamison RN. Online group pain management for chronic pain: preliminary results of a novel treatment approach to teletherapy. J Telemed Telecare. 2021;27(4):209-216. PubMed
85.Vellucci R. Heterogeneity of chronic pain. Clin Drug Investig. 2012;32(Suppl 1):3-10.
86.Internet-delivered cognitive behavioural therapy in the treatment of chronic non-cancer pain: project protocol. (CADTH health technology review - project protocol). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/hta-he/HT0037-OP0550_iCBT%20for%20Chronic%20Pain-protocol-Final.pdf. Accessed 2022 Apr 20.
87.Internet-delivered cognitive behavioural therapy for major depressive disorder and anxiety disorders: patients' perspectives and experiences, implementation, and ethical issues. (CADTH Optimal use report vol. 8, no. 2b). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/ou-tr/OP0534%20iCBT%20for%20MDD%20and%20Anxiety%20Disorders%20Final%20Report.pdf. Accessed 2022 Apr 19.
88.Internet-delivered cognitive behavioural therapy for post-traumatic stress disorder: a health technology assessment. (CADTH Optimal use report vol. 9, no. 3b). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/internet-based-cognitive-behavioural-therapy-post-traumatic-stress-disorder. Accessed 2019 Nov 15.
89.Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117. PubMed
90.Johnson M, Collett B, Castro-Lopes JM. The challenges of pain management in primary care: a pan-European survey. J Pain Res. 2013;6:393-401. PubMed
91.Mezei L, Murinson BB, Johns Hopkins Pain Curriculum Development Team. Pain education in North American medical schools. J Pain. 2011;12(12):1199-1208. PubMed
92.Watt-Watson J, McGillion M, Hunter J, et al. A survey of prelicensure pain curricula in health science faculties in Canadian universities. Pain Res Manag. 2009;14(6):439-444. PubMed
93.CADTH framework for patient engagement in health technology assessment. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2021 May 31.
94.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res Involv Engagem. 2017;3:13. PubMed
95.Young C, Helis E, Williams D. Internet-delivered cognitive behavioural therapy for major depressive disorder and anxiety disorders. (Environmental scan; no. 78). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pdf/ES0331%20iCBT%20for%20Major%20Depression%20and%20Anxiety_Final%20formatted%20BA_JH.pdf. Accessed 2022 Feb 16.
96.SurveyMonkey. 2022; https://www.surveymonkey.com/. Accessed 2022 Jan 19.
97.AbilitiCBT. 2021; https://myicbt.com/home?gclid=Cj0KCQjwtMCKBhDAARIsAG-2Eu8ZJTgQlhvnrjmsMPkxMspBtD2Cj2tqZ6AdWPUSC-Bl-s-Q3TWRhOwaApreEALw_wcB. Accessed 2022 Jan 06.
98.Cognitive Behavior Therapy Institute of Manitoba. 2021; https://cbtmanitoba.com/. Accessed 2022 Jan 06.
99.Wilderman Medical Clinic. iCBT Program for Chronic Pain. 2020; https://cbt.drwilderman.com/icbt. Accessed 2022 Jan 06.
100.Pain BC, Live Plan Be. Pain Education. 2020; https://www.liveplanbe.ca/pain-education. Accessed 2022 Feb 25.
101.MyCarePath. Learn. Plan. Take Charge of Pain. 2022; https://mycarepath.ca/. Accessed 2022 Feb 25.
102.UBC Department of Pediatrics. LivePlanBe+. 2022; https://liveplanbeplus.ca/. Accessed 2022 May 12.
103.Memorial University of Newfoundland. NCT04009135: The Internet Therapy for Depression Trial (INTEREST). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT04009135. Accessed 2022 Jan 06.
104.Statistics Canada. Definitions: Urban area (UA). Ottawa (ON): Government of Canada; 2007: https://www12.statcan.gc.ca/census-recensement/2006/ref/dict/geo049-eng.cfm. Accessed 2022 Jan 19.
105.Health Canada. Closing the Gaps in Aboriginal Health. (Health Policy Research, iss. 5). Ottawa (ON): Government of Canada; 2003: https://www.canada.ca/en/health-canada/services/science-research/reports-publications/health-policy-research/closing-gaps-aboriginal-health.html. Accessed 2022 Jan 19.
106.Internet-delivered cognitive behavioural therapy for major depressive disorder and anxiety disorders: recommendations. (CADTH Optimal use report vol. 8, no. 2c). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/ou-tr/op0534-iCBT-recommendations.pdf. Accessed 2019 Apr 18.
107.Substance Abuse and Mental Health Services Administration. SAMHSA's Concept of Trauma and Guidance for a Trauma-Informed Approach. (HHS Publication No. (SMA) 14-4884). Rockville (MD): Substance Abuse and Mental Health Services Administration; 2014: https://ncsacw.acf.hhs.gov/userfiles/files/SAMHSA_Trauma.pdf. Accessed 2022 Mar 03.
108.Nicola M, Correia H, Ditchburn G, Drummond P. Invalidation of chronic pain: a thematic analysis of pain narratives. Disabil Rehabil. 2021;43(6):861-869. PubMed
109.Burke NN, Finn DP, McGuire BE, Roche M. Psychological stress in early life as a predisposing factor for the development of chronic pain: Clinical and preclinical evidence and neurobiological mechanisms. J Neurosci Res. 2017;95(6):1257-1270. PubMed
110.Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J Pain. 2016;17(9 Suppl):T70-92. PubMed
111.Goddard A, Jones R, Etcher L. Trauma informed care in nursing: A concept analysis. Nurs Outlook. 2022;70(3):429-439. PubMed
112.Hanson RF, Lang J. A Critical Look At Trauma-Informed Care Among Agencies and Systems Serving Maltreated Youth and Their Families. Child Maltreat. 2016;21(2):95-100. PubMed
113.Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361-1367. PubMed
114.Brett K, MacDougall D. Models of Chronic Pain Care. (CADTH Environmental scan). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/es/ES0350%20_to%20Publishing%20Final.pdf. Accessed 2022 Apr 19.
115.Budhwani S, Fujioka J, Thomas-Jacques T, et al. Challenges and strategies for promoting health equity in virtual care: findings and policy directions from a scoping review of reviews. J Am Med Inform Assoc. 2022;29(5):990-999. PubMed
116.Cleeland CS. Brief Pain Inventory (Short Form). New York (NY): National Palliative Care Research Center; 1991: http://www.npcrc.org/files/news/briefpain_short.pdf. Accessed 2022 Jan 07.
117.36-Item Short Form Survey (SF-36) Scoring Instructions. Santa Monica (CA): RAND Corporation; 2022: https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form/scoring.html. Accessed 2022 Jan 07.
118.McCracken L, Vowles KE, Eccleston C. Chronic Pain Acceptance Questionnaire – Revised (CPAQ-R). Atlanta (GA): Division 12 of the American Psychological Association; 2006: https://www.div12.org/wp-content/uploads/2015/06/Chronic-Pain-Acceptance-Questionniare-Revised.pdf. Accessed 2022 Jan 07.
119.West Haven-Yale Multidimensional Pain Inventory. Chicago (IL): Shirley Ryan Ability Lab; 2017: https://www.sralab.org/rehabilitation-measures/west-haven-yale-multidimensional-pain-inventory. Accessed 2022 Jan 07.
120.Kroenke K, Spitzer RL, Williams JB. Patient Health Questionnaire (PHQ-9). Victoria (BC): Government of BC; 2001: https://www2.gov.bc.ca/assets/gov/health/practitioner-pro/bc-guidelines/depression_patient_health_questionnaire.pdf. Accessed 2022 Jan 07.
121.McCracken LM, Dhingra L. A short version of the Pain Anxiety Symptoms Scale (PASS-20): preliminary development and validity. Pain Res Manag. 2002;7(1):45-50. PubMed
122.Pittsburgh Sleep Quality Index (PSQI). Bloomfield Hills (MI): Oakland Psychiatric Associates PC: http://www.opapc.com/uploads/documents/PSQI.pdf. Accessed 2022 Jan 07.
123.Larsen DL, Attkisson CC, Hargreaves WA, Nguyen TD. Client Satisfaction Questionnaire (CSQ-8). Hamilton (ON): McMaster Univsersity; 1979: http://apntoolkit.mcmaster.ca/index.php?view=article&id=94%3Aclient-satisfaction-questionnaire-csq-8&format=pdf&option=com_content. Accessed 2022 Jan 07.
124.Burckhardt CS, Clark SR, Bennett RM. Fibromyalgia Impact Questionnaire (FIQ). Leawood (KS): American Academy of Family Physicians; 1991: https://www.aafp.org/afp/2007/0715/afp20070715p247-of1.pdf. Accessed 2022 Jan 07.
125.Zeltzer L, Kloda L. Hospital Anxiety and Depression Scale (HADS). (Stroke Engine Assessments). Montreal (QC): Stroke Engine; 2008: https://strokengine.ca/en/assessments/hospital-anxiety-and-depression-scale-hads/. Accessed 2022 Jan 07.
126.Beck's Depression Inventory. Indianapolis (IN): Indiana State Medical Association: https://www.ismanet.org/doctoryourspirit/pdfs/Beck-Depression-Inventory-BDI.pdf. Accessed 2022 Jan 07.
127.Sullivan M. The Pain Catastrophizing Scale. Montreal (QC): McGill University; 2009: https://aspecthealth.ca/wp-content/uploads/2017/03/PCSManual_English1.pdf. Accessed 2022 Jan 07.
128.Cheng ST, Chen PP, Chow YF, et al. Developing a Short Multidimensional Measure of Pain Self-efficacy: The Chronic Pain Self-efficacy Scale-Short Form. Gerontologist. 2020;60(3):e127-e136. PubMed
129.Jensen MP, Turner JA, Romano JM, Nielson WR. Chronic Pain Coping Inventory. Lutz (FL): PAR Psychological Assessment Resources, Inc.; 2008: https://www.parinc.com/WebUploads/samplerpts/CPCI_Score.pdf. Accessed 2022 Jan 07.
130.Fairbank JCT, Pynsent PB. Oswestry Low Back Pain Disability Questionnaire. East Lansing (MI): Michigan State University; 2000: https://www.rehab.msu.edu/_files/_docs/Oswestry_Low_Back_Disability.pdf. Accessed 2022 Jan 07.
131.Current Opioid Misuse Measure (COMM). Newton (MA): Pain EDU, Inflexxion, Inc; 2008: https://www.womenscollegehospital.ca/assets/pdf/TAPMI/Current%20Opioid%20Misuse%20Measures.pdf. Accessed 2022 Jan 07.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Cochrane Central Register of Controlled Trials (CCTR)
APA PsycINFO (1806-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: September 27, 2021
Alerts: Monthly search updates until project completion
Search filters applied: Systematic reviews; meta-analyses; network meta-analyses; health technology assessments; randomized controlled trials; controlled clinical trials; and observational studies.
Limits:
Publication date limit: 2001-present
Humans
Language limit: English and French language
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
? | Truncation symbol for 1 or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ab | Abstract |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase); keyword (CCTR) |
.dq | Candidate term word (Embase) |
.id | Key concept (PyscINFO) |
.yr | Publication year |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
psyh | Ovid database code; APA PyscINFO, 1806 to present, updated weekly |
Multi-Database Strategy
exp Cognitive Behavioral Therapy/ or Psychotherapy/ or Desensitization, Psychologic/ or Implosive Therapy/ or Dialectical Behavior Therapy/
(((cognitive or behavio* or facilitate* or guided or saturat* or unguided or dialectical* or acceptance* or commitment* or metacognitive or meta cognitive or exposure*) adj2 (therap* or psychotherap* or psycho-therap*)) or cognitive behavio* or cognition therap* or CBT* or mindfullness* or behavioural activation* or behavioral activation*).ti,ab,kf,kw.
(self-manag* or selfmanag* or self-help* or selfhelp*).ti,ab,kf,kw.
((psycholog* adj3 desensiti*) or imaginal flooding* or (imager* adj3 exposure*)).ti,ab,kf,kw.
((exposure or flooding* or implosive or saturation) adj3 therap*).ti,ab,kf,kw.
or/1-5
Internet/ or internet-based intervention/ or exp Computers/ or Therapy, Computer-Assisted/ or Computer-Assisted Instruction/ or Distance Counseling/ or exp Cell Phone/ or Mobile Applications/ or telemedicine/ or remote consultation/ or exp Videoconferencing/ or Medical Informatics Applications/
(internet* or digital* or app or apps or computer* or cyber-therap* or cybertherap* or e mail* or email* or electronic mail* or "Information and communication technology" or "Information and communication technologies" or emedicine or e medicine or ehealth* or e health* or emental health* or e mental health* or etherap* or e therap* or epsychiatr* or e psychiatr* or epsychol* or e psychol* or media deliver* or mobile* or phone* or online* or telephone* or tele phone* or cell phone* or cellphone* or smartphone* or smart phone* or smart watch* or smartwatch* or telemedicine or tele medicine or telehealth* or tele health* or telemental health* or tele mental health* or telecare or tele care or teletherap* or tele therap* or telepsychiatr* or tele psychiatr* or telepsychol* or tele psychol* or telepsycho-therap* or tele-psycho-therap* or telepsychotherap* or tele-psychotherap* or tele-coach* or telecoach* or m health* or mhealth* or virtual or virtualist? or webbased or web based or web deliver* or webdeliver*).ti,ab,kf,kw.
or/7-8
(iCBT* or cCBT* or eCBT* or dCBT*).ti,ab,kf,kw.
((internet* or computer* or cyber* or digital* or digital* or web*) adj6 (CBT* or CPT*)).ti,ab,kf,kw.
((internet* or computer* or cyber* or digital* or digital* or web* or technolog*) adj6 (cognitive behavior* or cognitive behaviour* or cognitive process*) adj6 (coach* or deliver* or intervention* or psychiatr* or psycho-dynamic or psychodynamic or psycholog* or psycho-therap* or psychotherap* or therap* or technique* or training or treatment*)).ti,ab,kf,kw.
(MoodGym* or Mood Gym* or Big White Wall* or Togetherall* or Together All* or "Beating the Blues*" or Fear Fighter* or FearFighter* or E compass* or Ecompass* or mycompass* or my compass* or Deprexis* or Moodkit* or Mood kit* or "Living Life to the Full*" or Woebot* or AbilitiCBT* or ALAViDA* or TruReach* or Tru Reach* or Beacon* or MindBeacon* or Mind Beacon* or i-Volve* or iVolve* or Interapy* or CBT-I Coach* or CBTi Coach* or CPT Coach* or Life Armor* or "T2 Mood Tracker*" or SilverCloud* or Silver Cloud* or "What’s Up*" or MindShift* or Mind Shift* or MoodMission* or Mood Mission* or Depression CBT* or Brave Online* or "Camp Code A Lot*" or BounceBack* or Bounce Back* or Pacifica* or iCANCOPE* or "i can cope*" or WebMap* or ManageMyPain or "Manage My Pain*" or ABC-Schema* or ABCSchema* or Aventurine Mood Improver* or "Catch It*" or CBT Diary* or CBT Journal* or CBT Thought Record* or Cgoni or Cognitive Diary or Cognitive Styles* or End Anxiety Hypnosis or Good Blocks* or Happify* or Happy Habits* or Jitters CBT* or Joyable* or Lantern* or Merrier* or Mindbliss* or Moodpath* or MoodTools* or See Betty* or TF-CBT* OT TFCBT* or Wysa* or Youper*).ti,ab,kf,kw.
or/10-13
Chronic Pain/ or exp Neuralgia/ or Nociceptive Pain/ or Pain, Intractable/ or Pain, Referred/ or exp Myofascial Pain Syndromes/ or exp Pain, Postoperative/ or Fibromyalgia/ or exp Arthritis/ or exp Inflammatory Bowel Diseases/ or Endometriosis/
exp Chronic Disease/ and (Back Pain/ or Musculoskeletal Pain/ or exp Headache Disorders/ or exp Headache/ or exp Cumulative Trauma Disorders/)
((pain or pains or paining or painful or ache or aches or aching) adj5 (chronic* or subacute* or sub-acute* or recurr* or re-curr* or unresolv* or persist* or intractable or refract* or severe* or debilitat* or nociceptive* or neuropathic* or superficial* or visceral or burning or crushing or migratory or radiat* or splitting or somatic* or constant* or continu* or widespread or non malignant* or nonmalignan* or non-cancer* or noncancer* or myofascial* or prolong* or sustain*)).ti,ab,kf,kw.
((chronic* or recurr* or re-curr* or unresolv* or persist*) adj5 (headache* or head ache* or back* or carpal tunnel* or cubital tunnel* or cephalalgia* or hemicrania* or cephalodynia* or cephalgia*)).ti,ab,kf,kw.
((pain or pains or paining or painful or ache or aches or aching) adj5 (migraine* or arthriti* or osteoarthriti* or polyarthriti* or endometrioma* or endometrioses or endometriosis or colitis* or crohn* or fibromyalgia* or post operat* or postoperat* or post surg* or postsurg* or phantom*)).ti,ab,kf,kw.
((repetitive stress* or repetitive strain* or repetition stress* or repetition strain* or overuse cumulativ*) adj5 (injur* or syndrome* or trauma*)).ti,ab,kf,kw.
((pain or pains or paining or painful or ache or aches or aching or compress* or entrap*) adj5 nerve*).ti,ab,kf,kw.
or/15-21
6 and 9 and 22
14 and 22
or/23-24
use medall
25 use cctr
limit 27 to yr=2001-current
exp Cognitive Behavior Therapy/ or Cognitive Therapy/ or psychotherapy/ or implosive therapy/ or exp exposure therapy/ or Dialectical Behavior Therapy/ or Mindfulness/ or Mindfulness-Based Interventions/
(((cognitive or behavio* or facilitate* or guided or saturat* or unguided or dialectical* or acceptance* or commitment* or metacognitive or meta cognitive or exposure*) adj2 (therap* or psychotherap* or psycho-therap*)) or cognitive behavio* or cognition therap* or CBT* or mindfullness* or behavioural activation* or behavioral activation*).ti,ab,id.
(self-manag* or selfmanag* or self-help* or selfhelp*).ti,ab,id.
((psycholog* adj3 desensiti*) or imaginal flooding* or (imager* adj3 exposure*)).ti,ab,id.
((exposure or flooding* or implosive or saturation) adj3 therap*).ti,ab,id.
or/29-33
exp internet/ or digital interventions/ or exp computers/ or exp Computer Assisted Therapy/ or exp Computer Assisted Instruction/ or Computer Assisted Instruction/ or exp Mobile Phones/ or exp mobile phones/ or mobile applications/ or exp Telemedicine/
(internet* or digital* or app or apps or computer* or cyber-therap* or cybertherap* or e mail* or email* or electronic mail* or "Information and communication technology" or "Information and communication technologies" or emedicine or e medicine or ehealth* or e health* or emental health* or e mental health* or etherap* or e therap* or epsychiatr* or e psychiatr* or epsychol* or e psychol* or media deliver* or mobile* or phone* or online* or telephone* or tele phone* or cell phone* or cellphone* or smartphone* or smart phone* or smart watch* or smartwatch* or telemedicine or tele medicine or telehealth* or tele health* or telemental health* or tele mental health* or telecare or tele care or teletherap* or tele therap* or telepsychiatr* or tele psychiatr* or telepsychol* or tele psychol* or telepsycho-therap* or tele-psycho-therap* or telepsychotherap* or tele-psychotherap* or tele-coach* or telecoach* or m health* or mhealth* or virtual or virtualist? or webbased or web based or web deliver* or webdeliver*).ti,ab,id.
or/35-36
(iCBT* or cCBT* or eCBT* or dCBT*).ti,ab,id.
((internet* or computer* or cyber* or digital* or digital* or web*) adj6 (CBT* or CPT*)).ti,ab,id.
((internet* or computer* or cyber* or digital* or digital* or web* or technolog*) adj6 (cognitive behavior* or cognitive behaviour* or cognitive process*) adj6 (coach* or deliver* or intervention* or psychiatr* or psycho-dynamic or psychodynamic or psycholog* or psycho-therap* or psychotherap* or therap* or technique* or training or treatment*)).ti,ab,id.
(MoodGym* or Mood Gym* or Big White Wall* or Togetherall* or Together All* or "Beating the Blues*" or Fear Fighter* or FearFighter* or E compass* or Ecompass* or mycompass* or my compass* or Deprexis* or Moodkit* or Mood kit* or "Living Life to the Full*" or Woebot* or AbilitiCBT* or ALAViDA* or TruReach* or Tru Reach* or Beacon* or MindBeacon* or Mind Beacon* or i-Volve* or iVolve* or Interapy* or CBT-I Coach* or CBTi Coach* or CPT Coach* or Life Armor* or "T2 Mood Tracker*" or SilverCloud* or Silver Cloud* or "What’s Up*" or MindShift* or Mind Shift* or MoodMission* or Mood Mission* or Depression CBT* or Brave Online* or "Camp Code A Lot*" or BounceBack* or Bounce Back* or Pacifica* or iCANCOPE* or "i can cope*" or WebMap* or ManageMyPain or "Manage My Pain*" or ABC-Schema* or ABCSchema* or Aventurine Mood Improver* or "Catch It*" or CBT Diary* or CBT Journal* or CBT Thought Record* or Cgoni or Cognitive Diary or Cognitive Styles* or End Anxiety Hypnosis or Good Blocks* or Happify* or Happy Habits* or Jitters CBT* or Joyable* or Lantern* or Merrier* or Mindbliss* or Moodpath* or MoodTools* or See Betty* or TF-CBT* OT TFCBT* or Wysa* or Youper*).ti,ab,id.
or/38-41
chronic pain/ or exp neuralgia/ or exp Neuropathic Pain/ or exp Myofascial Pain/ or exp Fibromyalgia/ or exp arthritis/ or exp colitis/ or irritable bowel syndrome/
chronic illness/ and (back pain/ or exp headache/ or somatoform pain disorder/ or exp musculoskeletal disorders/)
((pain or pains or paining or painful or ache or aches or aching) adj5 (chronic* or subacute* or sub-acute* or recurr* or re-curr* or unresolv* or persist* or intractable or refract* or severe* or debilitat* or nociceptive* or neuropathic* or superficial* or visceral or burning or crushing or migratory or radiat* or splitting or somatic* or constant* or continu* or widespread or non malignant* or nonmalignan* or non-cancer* or noncancer* or myofascial* or prolong* or sustain*)).ti,ab,id.
((chronic* or recurr* or re-curr* or unresolv* or persist*) adj5 (headache* or head ache* or back* or carpal tunnel* or cubital tunnel* or cephalalgia* or hemicrania* or cephalodynia* or cephalgia*)).ti,ab,id.
((pain or pains or paining or painful or ache or aches or aching) adj5 (migraine* or arthriti* or osteoarthriti* or polyarthriti* or endometrioma* or endometrioses or endometriosis or colitis* or crohn* or fibromyalgia* or post operat* or postoperat* or post surg* or postsurg* or phantom*)).ti,ab,id.
((repetitive stress* or repetitive strain* or repetition stress* or repetition strain* or overuse cumulativ*) adj5 (injur* or syndrome* or trauma*)).ti,ab,id.
((pain or pains or paining or painful or ache or aches or aching or compress* or entrap*) adj5 nerve*).ti,ab,id.
or/43-49
34 and 37 and 50
42 and 50
or/51-52
use psyh
exp cognitive behavioral therapy/ or "acceptance and commitment therapy"/ or exp mindfulness/ or psychotherapy/ or exp exposure therapy/
behavior therapy/ and cognitive therapy/
(((cognitive or behavio* or facilitate* or guided or saturat* or unguided or dialectical* or acceptance* or commitment* or metacognitive or meta cognitive or exposure*) adj2 (therap* or psychotherap* or psycho-therap*)) or cognitive behavio* or cognition therap* or CBT* or mindfullness* or behavioural activation* or behavioral activation*).ti,ab,kw,dq.
(self-manag* or selfmanag* or self-help* or selfhelp*).ti,ab,kw,dq.
((psycholog* adj3 desensiti*) or imaginal flooding* or (imager* adj3 exposure*)).ti,ab,kw,dq.
((exposure or flooding* or implosive or saturation) adj3 therap*).ti,ab,kw,dq.
or/55-60
internet/ or web-based intervention/ or exp computer/ or computer assisted therapy/ or e-counseling/ or exp mobile phone/ or exp mobile application/ or telemedicine/ or teleconsultation/ or telediagnosis/ or telemonitoring/ or telepsychiatry/ or teletherapy/ or videoconferencing/ or webcast/
(internet* or digital* or app or apps or computer* or cyber-therap* or cybertherap* or e mail* or email* or electronic mail* or "Information and communication technology" or "Information and communication technologies" or emedicine or e medicine or ehealth* or e health* or emental health* or e mental health* or etherap* or e therap* or epsychiatr* or e psychiatr* or epsychol* or e psychol* or media deliver* or mobile* or phone* or online* or telephone* or tele phone* or cell phone* or cellphone* or smartphone* or smart phone* or smart watch* or smartwatch* or telemedicine or tele medicine or telehealth* or tele health* or telemental health* or tele mental health* or telecare or tele care or teletherap* or tele therap* or telepsychiatr* or tele psychiatr* or telepsychol* or tele psychol* or telepsycho-therap* or tele-psycho-therap* or telepsychotherap* or tele-psychotherap* or tele-coach* or telecoach* or m health* or mhealth* or virtual or virtualist? or webbased or web based or web deliver* or webdeliver*).ti,ab,kw,dq.
or/62-63
(iCBT* or cCBT* or eCBT* or dCBT*).ti,ab,kw,dq.
((internet* or computer* or cyber* or digital* or digital* or web*) adj6 (CBT* or CPT*)).ti,ab,kw,dq.
((internet* or computer* or cyber* or digital* or digital* or web* or technolog*) adj6 (cognitive behavior* or cognitive behaviour* or cognitive process*) adj6 (coach* or deliver* or intervention* or psychiatr* or psycho-dynamic or psychodynamic or psycholog* or psycho-therap* or psychotherap* or therap* or technique* or training or treatment*)).ti,ab,kw,dq.
(MoodGym* or Mood Gym* or Big White Wall* or Togetherall* or Together All* or "Beating the Blues*" or Fear Fighter* or FearFighter* or E compass* or Ecompass* or mycompass* or my compass* or Deprexis* or Moodkit* or Mood kit* or "Living Life to the Full*" or Woebot* or AbilitiCBT* or ALAViDA* or TruReach* or Tru Reach* or Beacon* or MindBeacon* or Mind Beacon* or i-Volve* or iVolve* or Interapy* or CBT-I Coach* or CBTi Coach* or CPT Coach* or Life Armor* or "T2 Mood Tracker*" or SilverCloud* or Silver Cloud* or "What’s Up*" or MindShift* or Mind Shift* or MoodMission* or Mood Mission* or Depression CBT* or Brave Online* or "Camp Code A Lot*" or BounceBack* or Bounce Back* or Pacifica* or iCANCOPE* or "i can cope*" or WebMap* or ManageMyPain or "Manage My Pain*" or ABC-Schema* or ABCSchema* or Aventurine Mood Improver* or "Catch It*" or CBT Diary* or CBT Journal* or CBT Thought Record* or Cgoni or Cognitive Diary or Cognitive Styles* or End Anxiety Hypnosis or Good Blocks* or Happify* or Happy Habits* or Jitters CBT* or Joyable* or Lantern* or Merrier* or Mindbliss* or Moodpath* or MoodTools* or See Betty* or TF-CBT* OT TFCBT* or Wysa* or Youper*).ti,ab,kw,dq.
or/65-68
chronic pain/ or exp neuralgia/ or nociceptive pain/ or intractable pain/ or referred pain/ or myofascial pain/ or postoperative pain/ or fibromyalgia/ or exp arthritis/ or exp colitis/ or exp inflammatory bowel disease/ or endometriosis/
chronic disease/ and (exp backache/ or musculoskeletal pain/ or exp "headache and facial pain"/ or exp cumulative trauma disorder/)
((pain or pains or paining or painful or ache or aches or aching) adj5 (chronic* or subacute* or sub-acute* or recurr* or re-curr* or unresolv* or persist* or intractable or refract* or severe* or debilitat* or nociceptive* or neuropathic* or superficial* or visceral or burning or crushing or migratory or radiat* or splitting or somatic* or constant* or continu* or widespread or non malignant* or nonmalignan* or non-cancer* or noncancer* or myofascial* or prolong* or sustain*)).ti,ab,kw,dq.
((chronic* or recurr* or re-curr* or unresolv* or persist*) adj5 (headache* or head ache* or back* or carpal tunnel* or cubital tunnel* or cephalalgia* or hemicrania* or cephalodynia* or cephalgia*)).ti,ab,kw,dq.
((pain or pains or paining or painful or ache or aches or aching) adj5 (migraine* or arthriti* or osteoarthriti* or polyarthriti* or endometrioma* or endometrioses or endometriosis or colitis* or crohn* or fibromyalgia* or post operat* or postoperat* or post surg* or postsurg* or phantom*)).ti,ab,kw,dq.
((repetitive stress* or repetitive strain* or repetition stress* or repetition strain* or overuse cumulativ*) adj5 (injur* or syndrome* or trauma*)).ti,ab,kw,dq.
((pain or pains or paining or painful or ache or aches or aching or compress* or entrap*) adj5 nerve*).ti,ab,kw,dq.
or/70-76
61 and 64 and 77
69 and 77
or/78-79
use oemezd
not conference abstract.pt.
26 or 54 or 82
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Clinical Study or Adaptive Clinical Trial or Equivalence Trial).pt.
(Clinical Trial or Clinical Trial, Phase I or Clinical Trial, Phase II or Clinical Trial, Phase III or Clinical Trial, Phase IV or Clinical Trial Protocol).pt.
Multicenter Study.pt.
Clinical Studies as Topic/
exp Clinical Trial/ or exp Clinical Trials as Topic/ or Clinical Trial Protocol/ or Clinical Trial Protocols as Topic/ or exp "Clinical Trial (topic)"/
Multicenter Study/ or Multicenter Studies as Topic/ or "Multicenter Study (topic)"/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
Cross-Over Studies/ or Crossover Procedure/
(random* or sham or placebo*).ti,ab,hw,kf,kw.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
(control* adj3 (study or studies or trial* or group*)).ti,ab,hw,kf,kw.
(clinical adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf,kw.
(phase adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
((crossover or cross-over) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
((multicent* or multi-cent*) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf,kw.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(pragmatic study or pragmatic studies).ti,ab,hw,kf,kw.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf,kw.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
trial.ti,kf,kw.
or/84-118
exp animals/
exp animal experimentation/
exp models animal/
exp animal experiment/
nonhuman/
exp vertebrate/
animal.po.
or/120-126
exp humans/
exp human experiment/
human.po.
or/128-130
127 not 131
119 not 132
epidemiologic methods.sh.
epidemiologic studies.sh.
observational study/
observational studies as topic/
clinical studies as topic/
controlled before-after studies/
cross-sectional studies/
historically controlled study/
interrupted time series analysis/
exp seroepidemiologic studies/
national longitudinal study of adolescent health/
cohort studies/
cohort analysis/
longitudinal studies/
longitudinal study/
prospective studies/
prospective study/
follow-up studies/
follow up/
followup studies/
retrospective studies/
retrospective study/
case-control studies/
exp case control study/
cross-sectional study/
observational study/
quasi experimental methods/
quasi experimental study/
single-case studies as topic/
(observational study or validation studies or clinical study).pt.
(observational adj3 (study or studies or design or analysis or analyses)).ti,ab,kf,kw.
cohort*.ti,ab,kf,kw.
(prospective adj7 (study or studies or design or analysis or analyses)).ti,ab,kf,kw.
((follow up or followup) adj7 (study or studies or design or analysis or analyses)).ti,ab,kf,kw.
((longitudinal or longterm or (long adj term)) adj7 (study or studies or design or analysis or analyses or data)).ti,ab,kf,kw.
(retrospective adj7 (study or studies or design or analysis or analyses or data or review)).ti,ab,kf,kw.
((case adj control) or (case adj comparison) or (case adj controlled)).ti,ab,kf,kw.
(case-referent adj3 (study or studies or design or analysis or analyses)).ti,ab,kf,kw.
(population adj3 (study or studies or analysis or analyses)).ti,ab,kf,kw.
(descriptive adj3 (study or studies or design or analysis or analyses)).ti,ab,kf,kw.
((multidimensional or (multi adj dimensional)) adj3 (study or studies or design or analysis or analyses)).ti,ab,kf,kw.
(cross adj sectional adj7 (study or studies or design or research or analysis or analyses or survey or findings)).ti,ab,kf,kw.
((natural adj experiment) or (natural adj experiments)).ti,ab,kf,kw.
(quasi adj (experiment or experiments or experimental)).ti,ab,kf,kw.
((non experiment or nonexperiment or non experimental or nonexperimental) adj3 (study or studies or design or analysis or analyses)).ti,ab,kf,kw.
(prevalence adj3 (study or studies or analysis or analyses)).ti,ab,kf,kw.
case series.ti,ab,kf,kw.
case reports.pt.
case report/
case study/
(case adj3 (report or reports or study or studies or histories)).ti,ab,kf,kw.
organizational case studies.sh.
or/134-185
(systematic review or meta-analysis).pt.
meta-analysis/ or systematic review/ or systematic reviews as topic/ or meta-analysis as topic/ or "meta analysis (topic)"/ or "systematic review (topic)"/ or exp technology assessment, biomedical/ or network meta-analysis/
((systematic* adj3 (review* or overview*)) or (methodologic* adj3 (review* or overview*))).ti,ab,kf,kw.
((quantitative adj3 (review* or overview* or synthes*)) or (research adj3 (integrati* or overview*))).ti,ab,kf,kw.
((integrative adj3 (review* or overview*)) or (collaborative adj3 (review* or overview*)) or (pool* adj3 analy*)).ti,ab,kf,kw.
(data synthes* or data extraction* or data abstraction*).ti,ab,kf,kw.
(handsearch* or hand search*).ti,ab,kf,kw.
(mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab,kf,kw.
(met analy* or metanaly* or technology assessment* or HTA or HTAs or technology overview* or technology appraisal*).ti,ab,kf,kw.
(meta regression* or metaregression*).ti,ab,kf,kw.
(meta-analy* or metaanaly* or systematic review* or biomedical technology assessment* or bio-medical technology assessment*).mp,hw.
(medline or cochrane or pubmed or medlars or embase or cinahl).ti,ab,hw.
(cochrane or (health adj2 technology assessment) or evidence report).jw.
(comparative adj3 (efficacy or effectiveness)).ti,ab,kf,kw.
(outcomes research or relative effectiveness).ti,ab,kf,kw.
((indirect or indirect treatment or mixed-treatment or bayesian) adj3 comparison*).ti,ab,kf,kw.
(meta-analysis or systematic review).md.
(multi* adj3 treatment adj3 comparison*).ti,ab,kf,kw.
(mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf,kw.
umbrella review*.ti,ab,kf,kw.
(multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kw,kf.
(multiparamet* adj2 evidence adj2 synthesis).ti,ab,kw,kf.
(multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kw,kf.
or/187-209
83 and 133
83 and 186
83 and 210
or/211-213
limit 214 to (english or french)
limit 215 to yr=2001-current
28 or 216
remove duplicates from 217
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | iCBT OR cognitive therapy OR cognitive behavior OR cognitive behaviour OR behavior therapy OR acceptance therapy OR commitment therapy OR dialectical behavior OR dialectical therapy OR behavioral activation OR metacognitive therapy OR exposure-based | Recruiting, Not yet recruiting, Active, not recruiting, Completed, Enrolling by invitation, Unknown status Studies | pain OR headache OR migraine OR fibromyalgia OR arthritis OR osteoarthritis OR endometriosis]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- (iCBT OR cognitive therapy OR cognitive behavior OR cognitive behaviour OR behavior therapy OR acceptance therapy OR commitment therapy OR dialectical behavior OR dialectical therapy OR behavioral activation OR metacognitive therapy OR exposure-based cognitive OR exposure therapy OR mindfulness) AND (pain OR headache OR migraine OR fibromyalgia OR arthritis OR osteoarthritis OR endometriosis)]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms – iCBT AND pain]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- (iCBT OR "cognitive therapy" OR "cognitive behavior" OR "cognitive behaviour" OR "behavior therapy" OR "acceptance therapy" OR "commitment therapy" OR "dialectical behavior" OR "dialectical therapy" OR "behavioral activation" OR "metacognitive therapy" OR "exposure-based cognitive" OR "exposure therapy" OR mindfulness) AND (pain OR headache OR migraine OR fibromyalgia OR arthritis OR osteoarthritis OR endometriosis)]
Grey Literature
Search dates: October 12, 2021 to November 3, 2021
Keywords: (iCBT OR cognitive therapy OR cognitive behavior OR cognitive behaviour OR behavior therapy OR acceptance therapy OR commitment therapy OR dialectical behavior OR dialectical therapy OR behavioral activation OR metacognitive therapy OR exposure-based cognitive OR exposure therapy OR mindfulness) AND (pain OR headache OR migraine OR fibromyalgia OR arthritis OR osteoarthritis OR endometriosis)
Limits: Publication years: 2001-present
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Clinical Practice Guidelines
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Ethics
Patient Involvement
Open Access Journals
Appendix 2: Tables and Figures
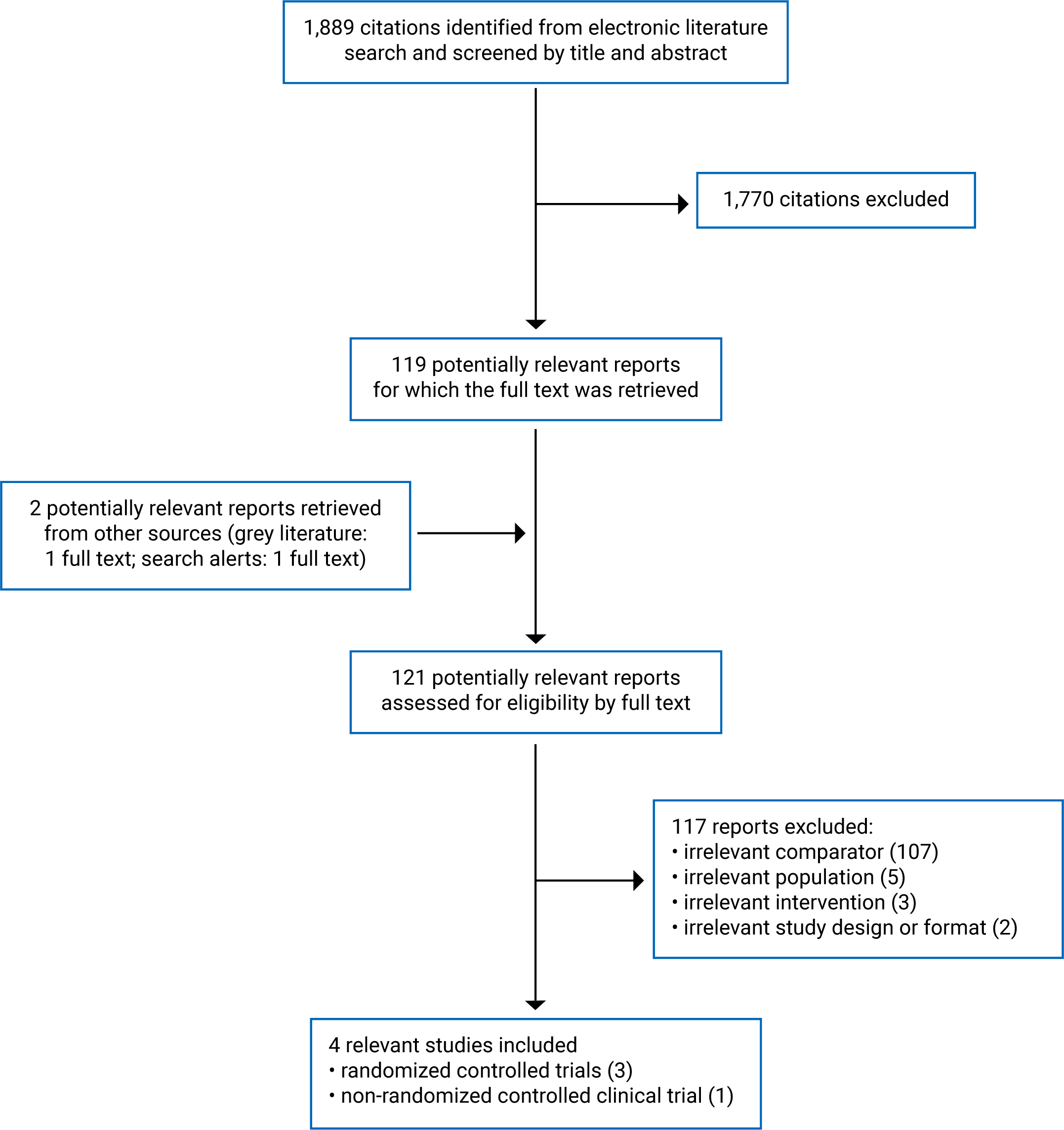
Table 13: Study and Participant Characteristics of Included Primary Clinical Trials — Clinical Review
Trial citation,a country, funding source | Trial design and setting | Participant characteristics | Relevant intervention and comparator | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Randomized controlled trials | ||||
Herbert et al. (2017)73 US Funding source: US Department of Veterans Affairs | Trial design: Multi-centre, open-label, non-inferiority parallel-group RCT Setting: VA San Diego Healthcare System facilities (California, US). Participants were recruited between April 2010 and April 2013 using flyers, clinician referral, and word of mouth. | Inclusion criteria: Veterans (aged over 18 years) diagnosed with a chronic, nonterminal pain condition and exhibiting average pain severity and interference rated > 4 of 10 over the past week (as measured using BPI) Excluded: Those with a serious or unstable medical or psychiatric condition or psychosocial instability that could impact trial participation; suicidal ideation; current participation in group psychotherapy for pain or individual psychotherapy of any type; previous ACT; or unwillingness to agree not to alter pain or mood treatments unless medically indicated Number of participants: 129 randomized and 128 analyzed; 17.8% female; mean (SD) age 52 (13.3) years Most common pain conditions: degenerative disc disease (43%), OA (20%), musculoskeletal pain (12%) Common pain locations: back (78%), upper extremity (48%), knee (45%), neck (38%), lower extremity (38%) (participants could report > 1 pain location) Duration of pain: NR Race: White (47%), Black or African American (28%), Hispanic/Latino (14%), other (11%) Medication usage: psychotropic medications (55%), NSAIDs (53%), opioids (41%), muscle relaxants (20%) Presence of comorbidities: NR Place of residence: NR Demographic variables, pain conditions, and medication usage NR for each group. | Manualized ACT intervention for chronic pain with the help of at-home assignments. The ACT aimed to change participants’ expectations from eliminating pain entirely to living as well as possible with chronic pain. Mindfulness exercises were designed to increase awareness of experiences other than pain. Metaphors and experiential exercises were used to encourage psychological and behavioral flexibility. Participants were encouraged to identify personal values, establish goals to improve quality of life and functioning, and live as well as possible with chronic pain. Delivery method: Individual videoconference sessions at a self-chosen VA site (intervention group [n = 63]) or individual in-person sessions at the La Jolla Medical Centre (comparator group [n = 65]) Guidance: Therapist-delivered ACT. Number of sessions: 8 weekly sessions Treatment duration: 60 minutes per week Presence and type of concurrent interventions: Both groups continued receiving usual care including medical treatment for pain (additional details for usual care NR) | Clinical Effectiveness Outcomes: Primary outcome: Pain interference (BPI Short Form Interference Subscale) Secondary outcomes:
Safety Outcomes: NR
mid-treatment, post-treatment, and 3 and 6 months after treatment completion |
Vallejo et al. (2015)75 Spain Funding source: Government of Spain | Trial design: Single-centre, open-label, parallel-group RCT Setting: Rheumatology Unit of the Institute of Rehabilitation at the Hospital Universitario “Gregorio Maranon” (Madrid, Spain). Methods used to recruit participants and the time period in which the trial was conducted were NR. | Inclusion criteria: Adults (aged 18 years and over) diagnosed with FM, exhibiting adequate reading comprehension, and with access and ability to use a computer Excluded: Those with a diagnosis of any mental health disorder, exhibiting suicidal ideation, prior or current psychological treatment for FM or other chronic pain syndromes, or surgery scheduled in the next 3 months Number of participants: 60 randomized and analyzed; 100% female; mean (SD) age 49.82 (11.01) years (intervention group) and 53.50 (8.56) years (comparator group) Duration of FM diagnosis: mean (SD) 8.6 (7.85) years (intervention group) and 8.8 (6.94) years (comparator group) Duration of generalized pain: mean (SD) 13.82 (9.89) years (intervention group) and 14.9 (11.07) years (comparator group) Race: NR Medication usage: NR Presence of comorbidities: NR Place of residence: NR | The main components of the CBT treatment protocol included psychoeducation about FM and pain, progressive relaxation training, emotional training, cognitive restructuring, and managing negative thoughts. Each session contained content, activities, and homework according to the multi-dimensional model of pain and multicomponent pain programs, with some adaptations for people with FM. Delivery method: Online application accessed individually (physical location of application access NR) (intervention group [n = 20]) or in-person group sessions at the Rheumatology Unit of the Institute of Rehabilitation (comparator group [n = 20]) Guidance: Therapist available for feedback and to respond to participants’ online messages (synchronicity NR) (intervention group) or therapist-delivered CBT (comparator group) Number of sessions: 10 weekly sessions Treatment duration: Online modules made available in the appropriate week and remained available during the trial duration (time commitment for each module NR) (intervention group) or 120 minutes per week (comparator group) Presence and type of concurrent interventions: Both groups received standard care including conventional pharmacological treatments (additional details for standard care NR) | Clinical Effectiveness Outcomes: Primary outcome: Global impact of FM (FIQ) Secondary outcomes:
Safety Outcomes: NR Follow-up: Participants were assessed at baseline, post-treatment, and 3, 6 and 12 months after treatment completion |
de Boer et al. (2014)74 The Netherlands Funding source: None | Trial design: Single-centre, unblinded, non-inferiority parallel-group RCT Setting: Pain Centre of the University Medical Centre Groningen (Groningen, The Netherlands). Participants were recruited using clinician referral between October 2008 and September 2012. | Inclusion criteria: Adults (aged 18 years and over) with access to the internet and nonspecific chronic pain and/or chronic pain for which no somatic treatment could be offered Excluded: Those with severe psychopathology (as measured by the Symptom Checklist 90 [cut-off score of 224] and a psychodiagnostic interview) or those that have not achieved primary education (since the course requires adequate reading and writing abilities and computer skills) Number of participants: 72 randomized and analyzed (50 completers also analyzed separately); 68.2% female (intervention group) and 60.7% female (comparator group); mean (SD) age 50.6 (10.7) years (intervention group) and 53.2 (11.7) years (comparator group) Pain conditions: NR Common pain locations: throughout the body (48.0%), head/neck (16.0%), back (10.0%), leg/hip/knee (10.0%), others (< 10% each) Origins of pain: unknown (40.0%), strain (18.0%), accident (2.0%), pregnancy (2.0%), and other (38.0%) Duration of pain: mean (SD) 118.2 (121.7) months (intervention group) and 90.0 (77.1) months (comparator group) Race: NR Medication usage: NR Presence of comorbidities: NR Place of residence: NR Demographic variables, characteristics of pain, and pain duration data for 50 completers. | The “Learning to live with pain” course is described in a protocol and is focused on the cognitive behavioural model of pain circle, which consists of various aspects of the pain experience (e.g., pain sensations, feelings, behaviour). Each session contained content, activities, and homework regarding various approaches used to escape this circle. Delivery method: Internet course accessed individually (physical location of internet access NR) (intervention group [n = 22]) or in-person group sessions in a meeting room at the hospital (comparator group [n = 28]) Guidance: Psychologist available by email or telephone (intervention group) or psychologist-delivered CBT (comparator group) Number of sessions: 7 weekly sessions plus a booster session occurring 2 months after the last session Treatment duration: Online modules made available in the appropriate week (time commitment for each module and for how long each module is made available NR) (intervention group) or 120 minutes per week (comparator group) Presence and type of concurrent interventions: NR | Clinical Effectiveness Outcomes: Primary outcome: Pain-related worrying (PCS) Secondary outcomes:
Safety Outcomes: NR Follow-up: Participants were assessed at baseline, immediately after the 7-week course (i.e., treatment completion), and immediately after the booster session 2 months after treatment completion |
Non-randomized controlled clinical trial | ||||
Mariano et al. (2021)84 US Funding source: None | Trial design: Single-centre, open-label, parallel-group nRCT Setting: People attending Partners HealthCare hospital system (Boston, Massachusetts) who were interested in group CBT pain management were invited to participate in either arm of the trial. The time period in which the trial was conducted was NR. | Inclusion criteria: Adults (aged 18 to 90 years) with daily back pain for more than 3 months, pain intensity rated ≥ 4 on a 0 to 10 scale (details of scale NR), and ability to speak and understand English Excluded: Those with a current diagnosis of substance use disorder; diagnosis of bipolar disorder, schizophrenia, or other chronic psychotic condition that may impact trial participation; recent or scheduled back surgery in the next 4 months; current malignancy, infection, autoimmune disorder, or amyotrophic lateral sclerosis; visual or motor impairment that may impact computer usage; or any condition deemed by the investigators which may impact trial participation Number of participants: 93 participants self-selected their treatment condition and analyzed; 70.2% female (intervention group) and 57.8% female (comparator group); mean (SD) age 54.5 (14.3) years (intervention group) and 59.7 (13.0) years (comparator group) Duration of pain: mean (SD) 13.0 (10.6) years (intervention group) and NR (comparator group) Race: Caucasian (71.7%), Hispanic (17.4%), African American (6.5%) (intervention group) and Caucasian (73.3%), Hispanic (4.3%), African American (20.0%) (comparator group) Medication usage: NR Presence of comorbidities: NR Place of residence: NR | CBT intervention for chronic pain that included goal setting, skills training, relaxation exercises, group discussion, and practice assignments. Main topics discussed included Gate Control Theory, stress management, problem-solving, social support, sleep and weight management, and relapse prevention. Delivery method: Group WebEx videoconference sessions accessed at home (intervention group [n = 47]) or group in-person sessions (specific location NR) (comparator group [n = 46]) Guidance: MD- or PhD-level licensed facilitator (intervention group) or PhD-level licensed facilitator (comparator group) Number of sessions: 8 weekly sessions Treatment duration: 120 minutes per week Presence and type of concurrent interventions: NR | Clinical Effectiveness Outcomes: Primary outcomes:
Secondary outcomes:
Safety Outcomes: NR Follow-up: Participants were assessed at baseline and at 2 (intervention group) or 3 (comparator group) months after treatment completion |
ACT = acceptance and commitment therapy; BDI = Beck Depression Inventory; BPI = Brief Pain Inventory; cognitive behavioural therapy; COMM = Current Opioid Misuse Measure; CPAQ = Chronic Pain Acceptance Questionnaire-Revised; CPCI = Chronic Pain Coping Inventory; CPSS = Chronic Pain Self-efficacy Scale; CSQ = Client Satisfaction Questionnaire; FIQ = Fibromyalgia Impact Questionnaire; FM = fibromyalgia; HADS = Hospital Anxiety and Depression Scale; iCBT = internet-delivered cognitive behavioural therapy; MPI = West Haven-Yale Multidimensional Pain Inventory; n = number of participants; NR = not reported; nRCT = non-randomized controlled trial; NSAID = nonsteroidal anti-inflammatory drug; OA = osteoarthritis; ODI = Oswestry Disability Index; PASS-20 = 20-item Pain Anxiety Symptoms Scale-Short Form; PCCL = Pain Coping and Cognition List; PCS = Pain Catastrophizing Scale; PHQ-9 = Patient Health Questionnaire-9; PSQI = 19-item Pittsburgh Sleep Quality Index; RAND-36 = RAND 36-Item Health Survey; RCT = randomized controlled trial; SD = standard deviation; SF12-MCS = 12-Item Short Form Mental Component Summary; SF12-PCS = 12-Item Short Form Physical Component Summary; VA = Veteran Affairs; ; VAS = visual analogue scale.
aPublications are organized according to trial design and in reverse chronological order.
Table 14: Detailed Descriptions of Outcome Measurement Tools — Clinical Review
Measurement tool | Description |
|---|---|
BPI Short Form Pain Interference Subscale116 | The BPI Short Form Interference Subscale consists of 7 items that evaluate the extent to which pain interferes with different aspects of life. A 0 (does not interfere) to 10 (completely interferes) scale was used to rate the degree of interference to general activity, mood, walking ability, normal work, relations with other people, sleep, and enjoyment of life. |
BPI Pain Severity Subscale116 | The BPI Pain Severity Subscale consists of 4 items that evaluate the severity of pain using a 0 (no pain) to 10 (pain as bad as you can imagine) scale. The 4 items include pain at its worst in the last 24 hours, pain at its least in the last 24 hours, pain on average, and pain right now. |
SF12-MCS117 | The Medical Outcomes Study SF12-MCS evaluates mental health-related quality of life outcomes (e.g., emotional well-being, social functioning). Scores for each item are recoded to a corresponding 0 to 100 scale with a higher score indicating a more favourable health state. |
SF12-PCS117 | The Medical Outcomes Study SF12-PCS evaluates physical health-related quality of life outcomes (e.g., physical functioning, role limitations due to physical health). Scores for each item are recoded to a corresponding 0 to 100 scale with a higher score indicating a more favourable health state. |
CPAQ-R118 | The CPAQ-R consists of 20 items that assess the degree to which respondents have accepted and adjusted to their pain in relation to their identity and lifestyle. Each item is scored on a 7-point Likert scale ranging from 0 (never true) to 6 (always true). The total score from all 20 items ranges from 0 to 120. Higher scores indicate higher levels of pain acceptance and predict better responses to rehabilitation programs. |
MPI119 | The MPI consists of 52 items forming 12 subscales, which evaluates pain interference, negative mood, pain intensity, life control, perceived support, responses of significant others, and activity level. MPI-Activity is a single measure that combines 4 subscales that assess different types of activities (i.e., household chores, outdoor work, activities away from home, social activities). Each item is scored from 0 to 6 and a general activity score is obtained by taking an average of all the scores. A higher score indicates a greater level of general activity. |
PHQ-9120 | Used to evaluate depressive symptoms, the PHQ-9 is based on Diagnostic and Statistical Manual of Mental Disorders Fourth Revision criteria for depressive disorders. Each item is scored from 0 (not at all) to 3 (nearly every day) with a total score ranging from 0 (none) to 27 (severe). A higher score indicates more severe depressive symptoms. |
PASS-20121 | Used to evaluate pain-related anxiety symptoms, the PASS-20 measures cognitive anxiety responses, escape and avoidance, fearful, thinking and physiological anxiety responses. Scores range from 0 (never) to 5 (always) for each item with total score ranging from 0 to 100. A higher score represents more severe anxiety symptoms. |
PSQI122 | The PSQI consists of 19 items and evaluates sleep quality to help distinguish good and poor sleepers. Each item is scored from 0 (no difficulty) to 3 (severe difficulty), which is added to yield a global score range of 0 to 21. A higher global score indicates more difficulty with sleep. |
CSQ123 | The CSQ consists of 8 items and measures treatment satisfaction. Each item is scored from 0 to 4, which is added to yield a total score ranging from 9 to 32. A higher total score indicates greater treatment satisfaction. |
FIQ124 | The FIQ consists of 10 items that evaluate the global impact of fibromyalgia on physical functioning, work status, depression, anxiety, sleep, pain, stiffness, fatigue, and well-being. Since raw scores for the 10 items have different ranges, each of the 10 scores is normalized to range from 0 (no impairment) to 10 (maximum impairment). The total score ranges from 0 to 100, with a higher score indicating more impairment. |
HADS125 | The HADS consists of 2 subscales: anxiety (7 items) and depression (7 items). Scores for some items range from 0 (no not at all) to 3 (yes definitely), while other items are reverse scored ranging from 0 (yes definitely) to 3 (no not at all). The global HADS score is obtained by adding the anxiety and depression scales resulting in a range of 0 (no distress) to 42 (maximum distress). |
BDI126 | The BDI consists of 21 items used to evaluate the level of depression. Each item is scored from 0 to 3, with a total score ranging from 0 (no depression) to 63 (maximum depression). |
PCS127 | The PCS consists of 13 items across 3 subscales: rumination (4 items), magnification (3 items), and helplessness (6 items). The total score of the 3 subscales represents the global score of catastrophizing. Each item is scored from 0 (not at all) to 4 (all the time). Score ranges for rumination is 0 to 16, magnification is 0 to 12, helplessness is 0 to 24, and global score of catastrophizing is 0 (no pain catastrophizing) to 52 (maximum pain catastrophizing). |
CPSS128 | The CPSS consists of 22 items across 3 subscales: self-efficacy for pain management (5 items), self-efficacy for physical function (9 items), and self-efficacy for coping with symptoms (8 items). Scores for each subscale range from 10 (very uncertain) to 100 (very certain). A higher score indicates greater self-efficacy. |
CPCI129 | The CPCI 64-item scale (Jensen et al. 1995) uses 8 subscales to assess coping strategies. Scores ranged from 0 to 7, which indicates the total number of days that each coping strategy was used in the past week. These 8 subscales fall under 2 broad categories: illness-focused coping and wellness-focused coping. Responses to the illness-focused coping subscales (i.e., guarding, resting, asking for assistance) are considered maladaptive, where a lower score would indicate an improvement. Responses to the wellness-focused coping subscales (i.e., exercise/stretch, relaxation, task persistence, coping self-statements, and seeking social support) are considered adaptive, where a higher score would indicate an improvement. |
VAS74 | VAS scores ranged from 0 (not at all) to 10 (extremely). Three items were measured using VAS: pain intensity (How much pain did you experience during the last 2 days?); pain interference (To what extent did you experience interference in your daily activities because of your pain during the last 2 days?); and fatigue (How much fatigue did you experience during the last 2 days?). |
PCCL74 | The PCCL consists of 42 items that evaluate pain coping, locus of control, and pain cognitions. The PCCL contains 4 subscales: catastrophizing (higher score indicates more catastrophic thinking), pain coping (higher score indicates better coping), internal pain management (higher score indicates greater internal pain control), and external pain management (higher score indicates greater external pain control). Each item is scored from 1 to 6 and an average score is calculated to yield the subscale scores. |
RAND-3674 | Used to assess global health-related quality of life, RAND-36 consists of 9 domains: physical functioning, social functioning, role impairment due to physical problems, role impairment due to emotional problems, mental health, vitality, pain, general health appraisal and perceived health change. Scores are recoded to a corresponding 0 to 100 scale for each domain with a higher score indicating better health. |
ODI130 | The ODI consists of 10 sections and is used to evaluate physical function and disability. Each section contains 6 statements with the first statement scored as 0 (no impairment) and the last statement scored as 5 (highest impairment). The total score ranges from 0 to 100. |
COMM131 | The COMM consists of 17 items and is used to identify people living with chronic pain currently on opioid therapy who may be misusing prescription opioids. Each item is scored from 0 (never) to 4 (very often) based on the respondent’s behaviour in the past 30 days. The total score ranges from 0 to 68 with a cut-off score of ≥9 indicating a positive result (i.e., respondent may be misusing their opioid medication). |
BDI = Beck Depression Inventory; BPI = Brief Pain Inventory; COMM = Current Opioid Misuse Measure; CPAQ-R = Chronic Pain Acceptance Questionnaire-Revised; CPCI = Chronic Pain Coping Inventory; CPSS = Chronic Pain Self-efficacy Scale; CSQ = Client Satisfaction Questionnaire; FIQ = Fibromyalgia Impact Questionnaire; HADS = Hospital Anxiety and Depression Scale; MPI = West Haven-Yale Multidimensional Pain Inventory; ODI = Oswestry Disability Index; PASS-20 = 20-item Pain Anxiety Symptoms Scale-Short Form; PCCL = Pain Coping and Cognition List; PCS = Pain Catastrophizing Scale; PHQ-9 = Patient Health Questionnaire-9; PSQI = 19-item Pittsburgh Sleep Quality Index; RAND-36 = Research and Development 36-Item Health Survey; SF12-MCS = Short Form 12-Item Mental Component Summary; SF12-PCS = Short Form 12-Item Physical Component Summary; VAS = visual analogue scale.
Table 15: Critical Appraisal of Included Primary Studies (Clinical Review) — Risk of Bias in the Included Randomized Controlled Trials Assessed Using RoB 2
Study citation | Bias arising from the randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of the outcome | Bias in selection of the reported result | Overall risk of bias |
|---|---|---|---|---|---|---|
Herbert et al. (2017)73 | All outcomes: Low risk 1.1 (Y). Allocation sequence was random (participants were assigned via random permuted blocks) 1.2 (Y). Allocation sequence was concealed until participants were enrolled and assigned to intervention 1.3 (PN). Probably no baseline differences between intervention groups did not suggest a problem with the randomization process | All outcomes: Low risk 2.1 (Y). Participants were aware of their assigned intervention during the trial (open-label) 2.2 (Y). Carers and people delivering the intervention were aware of the participants’ assigned intervention during the trial (open-label) 2.3 (N). There were no reported deviations from the intended intervention that arose because of the trial context 2.6 (Y). Appropriate analysis was used to estimate the effect of assignment to intervention (ITT analysis) | PI: High risk (ND) PC: High risk (ND) HRQoL: High risk (ND) PPFS: High risk (ND) Sleep: High risk (ND) PAL: High risk (ND) SC: High risk (ND) P: Low risk 3.1 (N; Y for P). Across most outcomes (all except P), data were not available at 6 months for 35/64 (54.7%) and 18/65 (27.7%) participants assigned to iCBT and in-person CBT, respectively. Individual participation data were available for all enrolled participants 3.2 (N). There was no evidence (e.g., sensitivity analyses) to indicate that the results were not biased by missing outcome data 3.3 (Y). It is possible that missingness in the outcome depended on its true value 3.4 (PY). It is likely that missingness in the outcome depended on its true value. | PI: High risk (?) PC: High risk (?) HRQoL: High risk (?) PPFS: High risk (?) Sleep: High risk (?) PAL: High risk (?) SC: High risk (?) P: Low risk 4.1 (PN). Across all outcomes, the methods of measurement were probably appropriate (PI using BPI Interference; PC using BPI Pain Severity; HRQoL using SF12-MCS and SF12-PCS; PPFS using CPAQ-R, PHQ-9, and PASS-20; sleep using PSQI; PAL using MPI-Activity; SC using CSQ; PP using withdrawal rates) 4.2 (PN). It is not likely that the measurement or ascertainment of the outcome differed between intervention groups 4.3 (Y). Outcome assessors were aware of the intervention received by study participants. Most outcomes (all except for P) were self-reported. 4.4 (Y; N for P). The assessment of the outcome could have been influenced by knowledge of the intervention received (there is a high level of subjectivity for all outcomes assessed, excluding P) 4.5 (PY; N for P). Across most outcomes, it is likely that assessment of outcomes was influenced by knowledge of the intervention received | All outcomes: Some concerns (ND) 5.1 (NI). While a protocol for the trial was registered on ClinicalTrials.gov (NCT01055639), there was no information on whether the analysis plan was finalized before unblinded outcome data were available for analysis 5.2 (N). The numerical results being assessed were not likely to have been selected on the basis of results from multiple eligible outcome measurements within the outcome domain as the outcome measurements were pre-specified in the trial registry 5.3 (NI). There was no information available to judge if the numerical results being assessed were likely to have been selected on the basis of the results from multiple eligible analyses of the data | Pain: Some concerns (?) All other outcomes: High risk (?) |
Vallejo et al. (2015)75 | All outcomes: High risk (+) 1.1 (Y). Allocation sequence was random (participants were assigned using a computer-generated randomization schedule) 1.2 (NI). No information about whether the allocation sequence was concealed until participants were enrolled and assigned to interventions 1.3 (PY). The baseline differences between groups may suggest a problem with the randomization process (iCBT group seemed to have improved clinical status at baseline, such as decreased fibromyalgia-related impairment and less severe depressive symptoms) | All outcomes: Low risk 2.1 (Y). Participants were aware of their assigned intervention during the trial (open-label) 2.2 (Y). Carers and people delivering the intervention were aware of the participants’ assigned intervention during the trial (open-label) 2.3 (N). There were no reported deviations from the intended intervention that arose because of the trial context 2.6 (Y). Appropriate analysis was used to estimate the effect of assignment to intervention (ITT analysis) | HRQoL: Low risk PPFS: Low risk P: Low risk 3.1 (Y). Across all outcomes, data were available for all, or nearly all participants randomized | HRQoL: High risk (?) PPFS: High risk (?) P: Low risk 4.1 (PN). Across all outcomes, the methods of measurement were probably not inappropriate (HRQoL using FIQ; PPFS using HADS, BDI, CPSS, PCS, and CPCI; P using lost to follow-up) 4.2 (PN). It is not likely that the measurement or ascertainment of the outcome differed between intervention groups 4.3 (Y). Outcome assessors were aware of the intervention received by study participants. Most outcomes (all except for P) were self-reported. 4.4 (Y; N for P). The assessment of the outcome could have been influenced by knowledge of the intervention received (there is a high level of subjectivity for all outcomes assessed, excluding P) 4.5 (PY; N for P). Across most outcomes, it is likely that assessment of outcomes was influenced by knowledge of the intervention received | All outcomes: Some concerns (?) 5.1 (NI). There was no information available to judge whether the data that produced the results were analyzed in accordance with a pre-specified analysis plan that was finalized before unblinding of outcome data (i.e., there was no mention of a trial protocol) 5.2 (NI). There was no information available to judge if the numerical results being assessed were likely to have been selected on the basis of results from multiple eligible outcome measurements within the outcome domains 5.3 (NI). There was no information available to judge if the numerical results being assessed were likely to have been selected on the basis of the results from multiple eligible analyses of the data | All outcomes: High risk (?) |
de Boer et al. (2014)74 | All outcomes: Some concerns (?) 1.1 (Y). Allocation sequence was random (participants were assigned using computer-generated permuted block randomization, with block sizes of 14) 1.2 (PY). Allocation sequence was likely concealed until participants were enrolled and assigned to intervention using sequential numbered, opaque, sealed envelopes (i.e., the block size was not likely deducible by trial personnel) 1.3 (PY). The baseline differences between groups may suggest a problem with the randomization process (there were baseline imbalances in some characteristics, such as employment, length of pain, and origin of pain) | All outcomes: Low risk 2.1 (Y). Participants were aware of their assigned intervention during the trial (open-label) 2.2 (Y). Carers and people delivering the intervention were aware of the participants’ assigned intervention during the trial (open-label) 2.3 (N). There were no reported deviations from the intended intervention that arose because of the trial context 2.6 (Y). Appropriate analysis was used to estimate the effect of assignment to intervention (ITT analysis) | PI: High risk (ND) PC: High risk (ND) HRQoL: High risk (ND) PPFS: High risk (ND) SC: High risk (ND) P: Low risk 3.1 (N; Y for P). Across most outcomes (all except PP), data were not available at 14 weeks for 16/38 (42.1%) and 10/34 (29.4%) participants assigned to iCBT and in-person CBT, respectively. Individual participation data were available for all enrolled participants 3.2 (N). There was no evidence (e.g., sensitivity analyses) to indicate that the results were not biased by missing outcome data 3.3 (Y). It is possible that missingness in the outcome depended on its true value 3.4 (PY). It is likely that missingness in the outcome depended on its true value. | PI: High risk (?) PC: High risk (?) HRQoL: High risk (?) PPFS: High risk (?) SC: High risk (?) P: Low risk 4.1 (PN). Across all outcomes, the methods of measurement were probably appropriate (PI using VAS Interference; PC using VAS Pain; HRQoL using RAND-36; PPFS using PCS and PCCL; SC using an unnamed 10-point scale; P using attendance rates) 4.2 (PN). It is not likely that the measurement or ascertainment of the outcome differed between intervention groups 4.3 (Y). Outcome assessors were aware of the intervention received by study participants. Most outcomes (all except for P) were self-reported. 4.4 (Y; N for P). The assessment of the outcome could have been influenced by knowledge of the intervention received (there is a high level of subjectivity for all outcomes assessed, excluding P) 4.5 (PY; N for P). Across most outcomes, it is likely that assessment of outcomes was influenced by knowledge of the intervention received | All outcomes: Some concerns (ND) 5.1 (NI). There was no information available to judge whether the data that produced the results were analyzed in accordance with a pre-specified analysis plan that was finalized before unblinding of outcome data (i.e., there was no mention of a trial protocol) 5.2 (NI). There was no information available to judge if the numerical results being assessed were likely to have been selected on the basis of results from multiple eligible outcome measurements within the outcome domains 5.3 (NI). There was no information available to judge if the numerical results being assessed were likely to have been selected on the basis of the results from multiple eligible analyses of the data | Pain: Some concerns (?) All other outcomes: High risk (?) |
BDI = Beck Depression Inventory; BPI = Brief Pain Inventory; CBT = cognitive behavioural therapy; CPAQ = Chronic Pain Acceptance Questionnaire-Revised; CPCI = Chronic Pain Coping Inventory; CPSS = Chronic Pain Self-efficacy Scale; CSQ = Client Satisfaction Questionnaire; FIQ = Fibromyalgia Impact Questionnaire; HADS = Hospital Anxiety and Depression Scale; HRQoL = health-related quality of life; iCBT= internet-delivered cognitive behavioural therapy; MPI = West Haven-Yale Multidimensional Pain Inventory; N = no; NI = no information; NR = not reported; IP = individual participation; PAL = physical activity level; PASS-20 = 20-item Pain Anxiety Symptoms Scale-Short Form; PC = pain control; PCCL = Pain Coping and Cognition List; PCS = Pain Catastrophizing Scale; PF = physical function; PHQ-9 = Patient Health Questionnaire-9; PI = pain interference; PPFS = psychological or psychosocial function or symptoms; PSQI = 19-item Pittsburgh Sleep Quality Index; PY = probably yes; RAND-36 = RAND 36-Item Health Survey; RoB 2 = Risk of Bias 2; SC = satisfaction with care; SF12-MCS = 12-Item Short Form Mental Component Summary; SF12-PCS = 12-Item Short Form Physical Component Summary; UoM = use of medication; VAS = visual analogue scale; Y = yes.
Note: the predicted direction of bias arising from each domain and the overall risk of bias is indicated in square brackets. (+) suggests the bias may favour the intervention (i.e., iCBT); (−) suggests the bias may favour the comparator (i.e., in-person CBT); (ND) suggests the bias may influence the result toward no difference between groups (i.e., favour the null hypothesis, or toward non-inferiority in non-inferiority trials); (?) suggests the predicted direction is unclear.
Table 16: Risk of Bias in the Included Non-Randomized Study Assessed Using RoBANS
Study citation | Bias in target group comparisons | Bias in target group selection | Bias in consideration of confounders | Bias due to deviations from intended interventions | Bias in outcome assessment (assessors) | Bias in outcome measurement (tools) | Bias due to incomplete outcome data | Bias due to selective outcome reporting | Overall risk of bias |
|---|---|---|---|---|---|---|---|---|---|
Mariano et al. (2021)84 | All outcomes: High risk (?) Intervention groups differed in several baseline characteristics (e.g., pain, disability) | All outcomes: Low risk Participant recruitment strategy was consistent for both intervention groups (e.g., standar‑dized inclusion and exclusion criteria were applied) | All outcomes: High risk (?) There was no adjustment in the analyses for potential confounders (e.g., age, body mass index, medication usage). | All outcomes: Low risk Participants and investigators were aware of the interventions, but it is unlikely that deviations from the intended intervention arose because of the trial context, and appropriate analysis was used. | PI: High risk (?) PC: High risk (?) PPFS: High risk (?) PF: High risk (?) UoM: High risk (?) SC: High risk (?) P: Low risk Outcome assessors were aware of the intervention received by study participants. For subjective outcomes (i.e., all except P), this is judged as potentially affecting outcomes | PI: Low risk PC: Low risk PPFS: Low risk PF: Low risk UoM: Low risk SC: Low risk P: Low risk Across all outcomes, the methods of measurement were probably appropriate (PI using BPI Interference; PC using BPI Pain; PPFS using HADS; PF using ODI; UoM using COMM; SC using an unnamed 7-item helpfulness questionnaire; P using attendance rates) | PI: High risk (ND) PC: High risk (ND) PPFS: High risk (ND) PF: High risk (ND) UoM: High risk (ND) SC: High risk (ND) P: Low risk Across most outcomes (all except PP), data were not available at 2 or 3 months for 15/47 (31.9%) and 24/46 (52.2%) participants assigned to iCBT and in-person CBT, respectively. Individual participation data were available for all enrolled participants | All outcomes: Unclear (?) Although the study reported on most of the expected main outcomes, there was no reference to a published protocol to confirm whether outcomes were selectively reported | All outcomes: High risk (?) |
BPI = Brief Pain Inventory; CBT = cognitive behavioural therapy; COMM = Current Opioid Misuse Measure; HADS = Hospital Anxiety and Depression Scale; iCBT= internet-delivered cognitive behavioural therapy; ODI = Oswestry Disability Index; P = individual participation; PC = pain control; PF = physical function; PI = pain interference; PPFS = psychological or psychosocial function or symptoms; RoBANS = Risk of Bias Assessment tool for Non-randomized Studies; SC = satisfaction with care; UoM = use of medication.
Note: the predicted direction of bias arising from each domain and the overall risk of bias is indicated in square brackets. (+) suggests the bias may favour the intervention (i.e., iCBT); (−) suggests the bias may favour the comparator (i.e., in-person CBT); (ND) suggests the bias may influence the result toward no difference between groups (i.e., favour the null hypothesis, or toward non-inferiority in non-inferiority trials); (?) suggests the predicted direction is unclear.
Table 17: GRADE Summary of Findings for Pain Interference — Clinical Review
Outcome, follow-up, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Pain interference Follow-up: post-treatment73,74 and 2 months,74,84 3 months,84 and 6 months73 after treatment completion 293 (2 RCTs, 1 nRCT) | Three trials (2 RCTs,73,74 1 nRCT84; N = 293), all with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on pain interference at post-treatment and longest follow-up (274 to 6 months73). The trials included people with heterogeneous chronic pain conditions. Participants had a mean age of 50 to 59 years across trials, and in 2 trials the participants were primarily females (60% to 70%)74,84; the third trial included only veterans who were primarily males (82%).73 The CBT programs were highly variable; 2 trials compared content-matched videoconference-based ACT73 or CBT84 to IP ACT or CBT (the ACT was individual while the CBT was group-based). A third trial compared individual self-directed iCBT to content-matched group IP CBT.74 Across the 3 trials, there may be little to no difference in change in pain interference from baseline to post-treatment and the longest follow-up in pain interference, as measured by the BPI Interference Subscale (0 = does not interfere to 10 = completely interferes)73,84 or VAS Interference Scale (0 = not at all to 10 = extremely).74 Mean differences in change scores (reported or calculatedb) were in the range of less than 1 point on these scales, with SDs indicating that neither treatment was favoured over the other. | Very low Due to very serious concerns for risk of bias, serious concerns for indirectness and imprecision.a | There may be little to no difference in the effect of iCBT vs. IP CBT on pain interference at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on pain interference at the longest follow-up, but the evidence is very uncertain. |
ACT = acceptance and commitment therapy; BPI = Brief Pain Inventory; CBT = cognitive behavioural therapy; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; nRCT = non-randomized controlled trial; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale; vs. = versus.
aPain interference: rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns for inconsistency; rated down once due to serious concerns for indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) in 1 trial; rated down once due to serious concerns about imprecision, which was difficult to judge due to a lack of between-group comparisons, but findings across groups had wide within-group SDs; publication bias was not detected.
bCalculation methods for mean changes are described in the Data Analysis and Synthesis section of this report.
Table 18: GRADE Summary of Findings for Pain Control
Outcome, follow-up, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Pain control Follow-up: post-treatment73,74 and 2 months,74,84 3 months,84 and 6 months73 after treatment completion 293 (2 RCTs, 1 nRCT) | Three trials (2 RCTs,73,74 1 nRCT84; N = 293), all with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on pain control at post-treatment and longest follow-up (274 to 6 months73). The trials included participants with heterogeneous chronic pain conditions. Participants had a mean age of 50 to 59 years across trials, and in 2 trials the participants were primarily females (60% to 70%)74,84; the third trial included only veterans who were primarily males (82%).73 The CBT programs were highly variable; 2 trials compared content-matched videoconference-based ACT73 or CBT84 to IP ACT or CBT (the ACT was individual while the CBT was group-based). A third trial compared individual self-directed iCBT to content-matched group IP CBT.74 Across the 3 trials, there may be little to no difference in change in pain control from baseline to post-treatment and the longest follow-up in pain control, as measured by the BPI Severity Subscale (0 = no pain to 10 = pain as bad as you can imagine)73,84 or VAS Pain Intensity Scale (0 = not at all to 10 = extremely).74 Mean differences in change scores (reported or calculatedb) were in the range of less than 1 point on these scales, with SDs indicating that neither treatment was favoured over the other. | Very low Due to very serious concerns for risk of bias, serious concerns for indirectness and imprecision.a | There may be little to no difference in the effect of iCBT vs. IP CBT on pain control at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on pain control at the longest follow-up, but the evidence is very uncertain. |
ACT = acceptance and commitment therapy; BPI = Brief Pain Inventory; CBT = cognitive behavioural therapy; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; nRCT = non-randomized controlled trial; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale; vs. = versus.
aPain Control: rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns for inconsistency; rated down once due to serious concerns for indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) in 1 trial; rated down once due to serious concerns about imprecision, which was difficult to judge due to a lack of between-group comparisons, but findings across groups had wide within-group SDs; publication bias was not detected.
bCalculation methods for mean changes are described in the Data Analysis and Synthesis section of this report.
Table 19: GRADE Summary of Findings for Health-Related Quality of Life or Overall Well-Being
Outcome, follow-up, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
HRQoL or overall well-being (change from baseline to post-treatment) Follow-up: post-treatment73-75 and 2 months,74 3 months,75 6 months,73,75 and 12 months75 after treatment completion 240 (3 RCTs) | Three RCTs (N = 240),73-75 all with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on HRQoL or overall well-being at post-treatment. The trials included participants with heterogeneous chronic pain conditions. Participants had a mean age of 49 to 53 years across trials, and in 2 trials the participants were primarily females (60% to 100%)74,75; the third trial included only veterans who were primarily males (82%).73 The CBT programs were highly variable; 2 RCTs74,75 compared content-matched individual self-directed iCBT to group IP CBT, while the third RCT compared content-matched individual videoconference-based ACT to individual IP ACT.73 Across the 3 trials, there may be little to no difference in change in HRQoL or overall well-being from baseline to post-treatment, as measured by SF12-MCS and SF12-PCS (0 = less favourable to 100 more favourable health state),73 FIQ (0 = no impairment to 100 = maximum impairment),75 or RAND-36 (0 = worse to 100 = better health).74 In 2 trials73,74 there was no significant difference between groups in the change from baseline to post-program, with wide variation. In the last trial, there were no between-group comparisons, but within-group SDs suggested wide variation in scores across participants, and an overlap in the distribution of change scores across groups.75 | Very low Due to very serious concerns for risk of bias, serious concerns for indirectness and imprecision.a | There may be little to no difference in the effect of iCBT vs. IP CBT on HRQoL or overall well-being at post-treatment, but the evidence is very uncertain. |
HRQoL or overall well-being (change from baseline to longest follow-up) Follow-up: post-treatment73-75 and 2 months,74 3 months,75 6 months,73,75 and 12 months75 after treatment completion 240 (3 RCTs) | Three RCTs (N = 240),73-75 all with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on HRQoL or overall well-being at longest follow-up (274 to 12 months75). The trials included participants with heterogeneous chronic pain conditions. Participants had a mean age of 49 to 53 years across trials, and in 2 trials the participants were primarily females (60% to 100%)74,75; the third trial included only veterans who were primarily males (82%).73 The CBT programs were highly variable; 2 RCTs74,75 compared content-matched individual self-directed iCBT to group IP CBT, while the third RCT compared content-matched individual videoconference-based ACT to individual IP ACT.73 The results were heterogeneous with little to no difference in change in HRQoL or overall well-being from baseline to longest follow-up, as measured by SF12-MCS and SF12-PCS (0 = less favourable to 100 more favourable health state),73 FIQ (0 = no impairment to 100 = maximum impairment),75 or RAND-36 (0 = worse to 100 = better health),74 in all trials with 2 exceptions. In 1 RCT, individual iCBT was favoured in 1 of the 9 RAND-36 subscales (perceived health change) at longest follow-up (calculated* mean change [SD] for individual iCBT and group IP CBT, completer analyses [ITT NR]: 22.50 [24.17] and 0 [32.67]).74 In another RCT, individual iCBT was favoured in mean FIQ change from post-treatment to the longest follow-up (ANOVA analysis P < 0.001).75 In the final study, the calculatedb mean changes (SD) in the RAND-36 role impairment physical domain were 21.45 (37.19) and 6.56 (30.97) for iCBT and IP CBT, respectively. No significant difference was found due to wide SDs (mean difference = 14.89; P = 0.218). | Very low Due to very serious concerns for risk of bias, serious concerns for indirectness and imprecision.c | The findings for the effect of iCBT vs. IP CBT on HRQoL or overall well-being at the longest follow-up are heterogeneous, and the evidence is very uncertain. |
ACT = acceptance and commitment therapy; ANOVA = analysis of variance; CBT = cognitive behavioural therapy; FIQ = Fibromyalgia Impact Questionnaire; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; RAND-36 = Research and Development 36-Item Health Survey; RCT = randomized controlled trial; SD = standard deviation; SF12-MCS = Short Form 12-Item Mental Component Summary; SF12-PCS = Short Form 12-Item Physical Component Summary; vs. = versus.
aHRQoL or Overall Well-Being (change from baseline to post-treatment): rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns for inconsistency; rated down once due to serious concerns for indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) in 2 trials; rated down once due to serious concerns about imprecision, as between and within-group findings (when between-group were unavailable) were associated with wide variation; publication bias was not detected.
bCalculation methods for mean changes are described in the Data Analysis and Synthesis section of this report.
cHRQoL or Overall Well-Being (change from baseline to longest follow-up): rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns for inconsistency; rated down once due to serious concerns for indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) in 2 trials; rated down once due to serious concerns about imprecision, as between and within-group findings (when between-group were unavailable) were associated with wide variation;; publication bias was not detected.
Table 20: GRADE Summary of Findings for Psychological or Psychosocial Function or Symptoms
Outcome, follow-up, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Pain acceptance Follow-up: post-treatment73 and 6 months73 after treatment completion 128 (1 RCT) | One RCT (N = 128),73 with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on pain acceptance at post-treatment and longest follow-up (i.e., 6 months). With an aim to change participants’ expectations from living pain-free to living as well as possible with pain, this RCT compared individual videoconference-based ACT to individual IP ACT (content-matched) in veterans (17.8% female; mean age 52 years) with a chronic, nonterminal pain condition.73 There may be little to no difference in change in pain acceptance from baseline to post-treatment and longest follow-up, as measured by CPAQ-R (0 to 120 with higher scores indicating higher levels of pain acceptance).73 Mean differences in calculateda change scores were −1.84 (95% CI, −7.84 to 4.16) at post-treatment and 3.45 (95% CI, −3.13 to 10.03) at longest follow-up, with SDs indicating that neither treatment was favoured over the other. | Very low Due to very serious concerns for risk of bias, serious concerns for inconsistency, indirectness and imprecision.b | There may be little to no difference in the effect of iCBT vs. IP CBT on pain acceptance at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on pain acceptance at the longest follow-up, but the evidence is very uncertain. |
Anxiety, depression, or general psychological distress (baseline to post-treatment) Follow-up: post-treatment73,75 and 3 months,75 6 months,73,75 and 12 months75 after treatment completion 168 (2 RCTs) | Two RCTs (N = 168),73,75 both with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on anxiety, depression, or general psychological distress at post-treatment. The trials included participants with heterogeneous chronic pain conditions, and participants had a mean age of 49 to 53 years across trials. One trial included only veterans who were primarily males (82%),73 while participants in the second trial were all female.75 The CBT programs were highly variable; 1 trial compared individual videoconference-based ACT to individual IP ACT,73 while the second trial compared individual self-directed iCBT to group IP CBT (all content-matched between groups).75 Across the 2 trials, there may be little to no difference in change in anxiety, depression, or general psychological distress from baseline to post-treatment, as measured by PHQ-9 (0 to 27 with higher scores indicating more severe depressive symptoms),73 PASS-20 (0 to 100 with higher scores representing more severe anxiety symptoms),73 HADS (0 = no distress to 42 = maximum distress),75 or BDI (0 = no depression to 63 = maximum depression).75 Mean differences in change scores in 1 trial were −0.51 (95% CI, −2.42 to 1.40) on the PHQ-9 and −4.20 (95% CI, −10.58 to 2.17) on the PASS-20. In the second trial, calculateda the mean (SD) changes scores for iCBT and in-person CBT were −5.10 (3.22) and −1.51 (5.07) respectively for the HADS, and −6.52 (4.03) and −5.11 (6.06) respectively for the BDI. | Very low Due to very serious concerns for risk of bias, serious concerns for indirectness and imprecision.c | There may be little to no difference in the effect of iCBT vs. IP CBT on anxiety, depression, or general psychological distress at post-treatment, but the evidence is very uncertain. |
Anxiety, depression, or general psychological distress (baseline to longest follow-up) Follow-up: post-treatment73,75 and 2 months,84 3 months,75,84 6 months,73,75 and 12 months75 after treatment completion 261 (2 RCTs, 1 nRCT) | Three trials (2 RCTs,73,75 1 nRCT84; N = 261), all with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on anxiety, depression, or general psychological distress at longest follow-up (384 to 12 months75). The trials included participants with heterogeneous chronic pain conditions. Participants had a mean age of 49 to 59 years across trials, and in 2 trials the participants were primarily females (57% to 100%)75,84; the third trial included only veterans who were primarily males (82%).73 The CBT programs were highly variable; 1 trial compared individual videoconference-based ACT to individual IP ACT,73 1 trial compared group videoconference-based CBT to group IP CBT,84 and 1 trial compared individual self-directed iCBT to group IP CBT (all content-matched between groups).75 The results were heterogeneous with little to no difference in change in anxiety, depression, or general psychological distress from baseline to longest follow-up, as measured by PHQ-9 (0 to 27 with higher scores indicating more severe depressive symptoms),73 PASS-20 (0 to 100 with higher scores representing more severe anxiety symptoms),73 HADS (0 = no distress to 42 = maximum distress),75,84 or BDI (0 = no depression to 63 = maximum depression),75 in 2 trials.73,84 In 1 RCT, individual iCBT was favoured in mean BDI change from post-treatment to the longest follow-up (ANOVA analysis P=0.004).75 In the other 2 trials, no significant between-group differences were reported. Mean differences in change scores (reported or calculated*) were 1.07 (PHQ-9), 4.01 (PASS-20), 5.41 (HADS), and 4.36 (BDI), with SDs indicating that neither treatment was favoured over the other. | Very low Due to very serious concerns for risk of bias, serious concerns for indirectness and imprecision.d | There were heterogeneous results for the effect of iCBT vs. IP CBT on anxiety, depression, or general psychological distress at the longest follow-up, and the evidence is very uncertain. |
Self-efficacy Follow-up: post-treatment75 and 3 months,75 6 months,75 and 12 months75 after treatment completion 40 (1 RCT) | One RCT (N = 40),75 with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on self-efficacy at post-treatment and longest follow-up (i.e., 12 months). With topics such as progressive relaxation training and cognitive restructuring, this RCT compared individual iCBT to group IP CBT (content-matched) in adults (individual iCBT: 100% female, mean age 49.82 years; group IP CBT: 100% female, mean age 53.50 years) with FM.75 There may be little to no difference in change in self-efficacy from baseline to post-treatment and longest follow-up, as measured by CPSS (10 to 100 with higher scores indicating greater self-efficacy).75 At post-treatment, mean change scores (SD) in global self-efficacy were calculateda to be 6.54 (13.96) and 3.55 (17.99) for individual iCBT and group IP CBT, respectively. At the longest follow-up, mean change scores (SD) in global self-efficacy were calculateda to be 7.65 (11.80) and −1.11 (17.21) for individual iCBT and group IP CBT, respectively. | Very low Due to serious concerns for risk of bias, inconsistency, indirectness, and imprecision.e | There may be little to no difference in the effect of iCBT vs. IP CBT on self-efficacy at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on self-efficacy at the longest follow-up, but the evidence is very uncertain. |
Pain-related worrying (change from baseline to post-treatment) | Two RCTs (N = 112),74,75 both at high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on pain-related worrying at post-treatment. One trial included people with nonspecific chronic pain or chronic pain for which somatic treatment could not be offered,74 and the other included people affected by fibromyalgia.75 Participants had a mean age of 49 to 53 years across trials; 1 trial enrolled only females,75 and the other was a mixed population (60% female).74 The RCTs compared content-matched individual self-directed iCBT to group IP CBT, with CBT program content being variable.74,75 Across the 2 RCTs, there may be little to no difference in the change from baseline to post-treatment in pain-related worrying as measured by pain catastrophizing scales. In the trial by de Boer et al., ANOVA group × time analyses were not statistically significant on the PCS global pain catastrophizing scale.74 Vallejo et al. did not statistically compare the change in PCS scores across groups, but changes in the global score and well as subscales of the PCS did not appear to differ substantially between groups, given wide variability (SDs) in change scores.74,75 | Very low Due to very serious concerns for risk of bias, serious concerns for indirectness and imprecision.f | There may be little to no difference in the effect of iCBT vs. IP CBT on pain-related worrying at post-treatment, but the evidence is very uncertain. |
Pain-related worrying (change from baseline to longest follow-up) Follow-up: 274 to 1275 months after treatment completion | Two RCTs (N = 112),74,75 both at high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on pain-related worrying at longest follow-up (274 to 12 months75). One trial included people with nonspecific chronic pain or chronic pain for which somatic treatment could not be offered,74 and the other included people affected by fibromyalgia.75 Participants had a mean age of 49 to 53 years across trials; 1 trial enrolled only females,75 and the other was a mixed population (60% female).74 The RCTs compared content-matched individual self-directed iCBT to group IP CBT, with CBT program content being variable.74,75 Across the 2 RCTs, the findings relating to change from baseline to longest follow-up in pain-related worrying as measured by pain catastrophizing scales were heterogeneous. In the trial by de Boer et al., ANOVA group × time analyses were not statistically significant on the PCS global pain catastrophizing scale when comparing the change from baseline to 2 months post-treatment across groups.74 Meanwhile, ANOVA group × time analyses for 12 months post-treatment relative to post-treatment in the Vallejo et al. trial were statistically significant (favoured iCBT) for global catastrophizing and 2 subscales (i.e., helplessness, magnification) (not statistically significant for the rumination subscales).75 Findings showed maintenance or improvement in global catastrophizing as well as subscales of the PCS (rumination, helplessness, magnification) in the iCBT group. Meanwhile, in the IP CBT group, scores were maintained or worsened (magnification subscale) at 12 months post-treatment.75 | Very low Due to very serious concerns for risk of bias, serious concerns for inconsistency, indirectness and imprecision.g | The results were heterogeneous for the effect of iCBT vs. IP CBT on pain-related worrying at the longest follow-up, and the evidence is very uncertain. |
Coping with pain Follow-up: post-treatment74,75 and 2 months,74 3 months,75 6 months,75 and 12 months75 after treatment completion 112 (2 RCTs) | Two RCTs (N = 112),74,75 both at high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on coping with pain at post-treatment. One trial included people with nonspecific chronic pain or chronic pain for which somatic treatment could not be offered,74 and the other included people affected by fibromyalgia.75 Participants had a mean age of 49 to 53 years across trials; 1 trial enrolled only females,75 and the other was a mixed population (60% female).74 The RCTs compared content-matched individual self-directed iCBT to group IP CBT, with CBT program content being variable.74,75 Across the 2 RCTs, there may be little to no difference in the change in coping with pain from baseline to post-treatment and longest follow-up (274 to 12 months75), as measured by various coping scales. In the trial by de Boer et al., ANOVA group × time analyses were not statistically significant (P > 0.05) for the PCCL subscales related to coping with pain.74 Vallejo et al. did not statistically compare the change in CPCI scores across groups, but changes in the global score and well as subscales of the CPCI did not appear to differ substantially between groups, given small within-group changes and some variation (SDs) in change scores.75 Furthermore, ANOVA group × time analyses for 12 months post-treatment relative to post-treatment were not statistically significant (P > 0.05) for any of the CPCI subscales.75 | Very low Due to very serious concerns for risk of bias, serious concerns imprecision and indirectness.h | There may to be little to no difference in the effect of iCBT vs. IP CBT on coping with pain at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on coping with pain at the longest follow-up, but the evidence is very uncertain. |
Fatigue Follow-up: post-treatment74 and 2 months after treatment completion74 72 (1 RCT) | One RCT (N = 72),74 with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on fatigue at post-treatment and longest follow-up (i.e., 2 months). With a focus on the cognitive behavioural model of pain circle, this RCT compared individual iCBT to group IP CBT (content-matched) in adults (individual iCBT: 68.2% female, mean age 50.6 years; group IP CBT: 60.7% female, mean age 53.2 years) with nonspecific chronic pain and/or chronic pain for which no somatic treatment could be offered.74 There may be little to no difference in change in fatigue from baseline to post-treatment and longest follow-up, as measured by VAS Fatigue Scale (0 = not at all to 10 = extremely).74 The calculateda mean change (SD) for individual iCBT and group IP CBT were −0.35 (2.44) and 0.02 (2.15) at post-treatment; and −0.43 (2.36) and 0.25 (2.28) at longest follow-up (completer analyses; ITT NR).74 | Very low Due to very serious concerns for risk of bias, serious concerns for inconsistency, indirectness and imprecision.i | There maybe little to no difference in the effect of iCBT vs. IP CBT on fatigue at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on fatigue at the longest follow-up, but the evidence is very uncertain. |
ACT = acceptance and commitment therapy; ANOVA = analysis of variance; BDI = Beck's Depression Inventory; CBT = cognitive behavioural therapy; CPAQ-R = Chronic Pain Acceptance Questionnaire-Revised; CPCI = Chronic Pain Coping Inventory; CPSS = Chronic Pain Self-efficacy Scale; HADS = Hospital Anxiety and Depression Scale; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; nRCT = non-randomized controlled trial; PASS-20 = Pain Anxiety Symptoms Scale-Short Form 20-Item; PCS = Pain Catastrophizing Scale; PCCL = Pain Coping and Cognition List; PHQ-9 = Patient Health Questionnaire-9; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale; vs. = versus.
aCalculation methods for mean changes are described in the Data Analysis and Synthesis section of this report.
bPain acceptance: rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcome (participant reported subjective outcome); rated down once due to serious concerns for inconsistency because of limited of evidence of consistency as only 1 trial was available that reported on the outcome; rated down once due to serious concerns for indirectness because the trial involved only veterans and examined ACT (unclear generalizability); rated down once due to serious concerns about imprecision, because of wide between-group SDs; publication bias was not detected.
cAnxiety, depression, or general psychological distress (change from baseline to post-treatment): rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns for inconsistency; rated down once due to serious concerns for indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) in 1 trial; rated down once due to serious concerns about imprecision, as between and within-group findings (when between-group were unavailable) were associated with wide variation; publication bias was not detected.
dAnxiety, depression, or general psychological distress (change from baseline to longest follow-up): rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns for inconsistency; rated down once due to serious concerns for indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) in 1 trial; rated down once due to serious concerns about imprecision, as between-group comparisons were associated with wide variation; publication bias was not detected.
eSelf-efficacy: rated down once for risk of bias due to serious concerns about the potential for bias in measurement of the outcome (participant reported subjective outcome); rated down once due to serious concerns for inconsistency because of limited of evidence of consistency as only 1 trial was available that reported on the outcome; rated down once due to serious concerns for indirectness, because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) and all participants being female (generalizability concern); rated down once due to serious concerns about imprecision, which was difficult to judge due to a lack of between-group comparisons, but findings across groups had wide within-group SDs; publication bias was not detected.
fPain-related worrying (change from baseline to post-treatment): rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns about inconsistency; rated down once due to serious concerns about indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group); rated down once due to serious concerns about imprecision, which was difficult to judge due to a lack of presentation of data for between-group findings in the 2 trials, but findings across groups had wide within-group SDs; publication bias not detected.
gPain-related worrying (change from baseline to longest follow-up): rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); rated down once due to serious concerns about inconsistency, as the findings of both trials differed, and it was not possible to credibly explain the differences in subgroup analysis due to the small number of included trials; rated down once due to serious concerns about indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group); rated down once due to serious concerns about imprecision, which was difficult to judge due to a lack of presentation of data for between-group findings in the 2 trials, but findings across groups had wide within-group SDs, though it is suspected based on available data (completers analysis) that at least some imprecision exists; publication bias not detected.
hPain coping: rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns about inconsistency; rated down once due to serious concerns about indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group); rated down once due to serious concerns about imprecision, which was difficult to judge due to a lack of presentation of data for between-group findings in the 2 trials, but findings across groups had wide within-group SDs; publication bias not detected.
iFatigue: rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcome (participant reported subjective outcome); rated down once due to serious concerns for inconsistency because of limited of evidence of consistency as only 1 trial was available that reported on the outcome; rated down once due to serious concerns for indirectness, because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group); rated down once due to serious concerns about imprecision, difficult to judge due to a lack of presentation of data for between-group findings but within-group SDs were wide; publication bias was not detected.
Table 21: GRADE Summary of Findings for Sleep
Outcome, follow-up, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Sleep Follow-up: post-treatment73 and 6 months73 after treatment completion 128 (1 RCT) | One RCT (N = 128),73 with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on sleep at post-treatment and longest follow-up (i.e., 6 months). With an aim to change participants’ expectations from living pain-free to living as well as possible with pain, this RCT compared individual videoconference-based ACT to individual IP ACT (content-matched) in veterans (17.8% female; mean age 52 years) with a chronic, nonterminal pain condition.73 There may be little to no difference in change in sleep from baseline to post-treatment and longest follow-up, as measured by PSQI (0 to 21 with higher scores indicating more difficulty with sleep).73 At post-treatment, mean PSQI change scores (SD) were calculateda to be −0.69 (4.47) and −0.90 (4.08) for individual videoconference-based ACT and individual IP ACT, respectively. At the longest follow-up, mean PSQI change scores (SD) were calculateda to be −0.57 (4.79) and −0.70 (4.21) for individual videoconference-based ACT and individual IP ACT, respectively. | Very low Due to very serious concerns for risk of bias, serious concerns for inconsistency, indirectness and imprecision.b | There may be little to no difference in the effect of iCBT vs. IP CBT on sleep at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on sleep at the longest follow-up, but the evidence is very uncertain. |
ACT = acceptance and commitment therapy; CBT = cognitive behavioural therapy; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; PSQI = Pittsburgh Sleep Quality Index; RCT = randomized controlled trial; SD = standard deviation; vs. = versus.
aCalculation methods for mean changes are described in the Data Analysis and Synthesis section of this report.
bSleep: rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcome (participant reported subjective outcome); rated down once due to serious concerns for inconsistency because of limited of evidence of consistency as only 1 trial was available that reported on the outcome; rated down once due to serious concerns for indirectness because the trial involved veterans and examined ACT (unclear generalizability); rated down once due to serious concerns about imprecision, which was difficult to judge due to a lack of between-group comparisons, but within-group SDs were wide; publication bias was not detected.
Table 22: GRADE Summary of Findings for Physical Activity Level
Outcome, follow-up, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Physical activity level (change from baseline to post-treatment) Follow-up: post-treatment73 and 6 months73 after treatment completion 128 (1 RCT) | One RCT (N = 128),73 with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on physical activity level at post-treatment. With an aim to change participants’ expectations from living pain-free to living as well as possible with pain, this RCT compared individual videoconference-based ACT to individual IP ACT (content-matched) in veterans (17.8% female; mean age 52 years) with a chronic, nonterminal pain condition.73 There may be little to no difference in change in MPI-Activity from baseline to post-treatment, as measured by MPI-Activity (0 to 6 with higher scores indicating greater levels of general activity).73 At post-treatment, mean MPI-Activity change scores (SD) were calculatedb to be 0.33 (0.96) and 0.18 (0.89) for individual videoconference-based ACT and individual IP ACT, respectively (mean difference=0.15). | Very low Due to very serious concerns for risk of bias, serious concerns for inconsistency, indirectness and imprecision.a | There may be little to no difference in the effect of iCBT vs. IP CBT on physical activity level at post-treatment, but the evidence is very uncertain. |
Physical activity level (change from baseline to longest follow-up) Follow-up: post-treatment73 and 6 months73 after treatment completion 128 (1 RCT) | One RCT (N = 128),73 with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on physical activity level at longest follow-up (i.e., 6 months). With an aim to change participants’ expectations from living pain-free to living as well as possible with pain, this RCT compared individual videoconference-based ACT to individual IP ACT (content-matched) in veterans (17.8% female; mean age 52 years) with a chronic, nonterminal pain condition.73 Individual IP ACT was favoured (P=0.03) in physical activity level at longest follow-up relative to baseline.73 The calculatedb mean change (SD) in MPI-Activity (0 to 6 with higher scores indicating greater levels of general activity) for individual videoconference-based ACT and individual IP ACT were −0.05 (1.01) and 0.26 (0.93), respectively (mean difference 0.31 [95% CI, 0.02 to 0.60]). | Very low Due to very serious concerns for risk of bias, serious concerns for inconsistency, and indirectness.c | IP ACT may be favoured vs. IP ACT with respects to physical activity level at the longest follow-up, but the evidence is very uncertain. |
ACT = acceptance and commitment therapy; CBT = cognitive behavioural therapy; CI = confidence interval; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; MPI = West Haven-Yale Multidimensional Pain Inventory; RCT = randomized controlled trial; SD = standard deviation; vs. = versus.
aPhysical Activity Level (change from baseline to post-treatment): rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcome (participant reported subjective outcome); rated down once due to serious concerns for inconsistency because of limited of evidence of consistency as only 1 trial was available that reported on the outcome; rated down once due to serious concerns for indirectness because the trial involved veterans and examined ACT (unclear generalizability); rated down once due to serious concerns about imprecision which was difficult to judge due to a lack of between-group comparisons, but within-group SDs were wide; publication bias was not detected.
bCalculation methods for mean changes are described in the Data Analysis and Synthesis section of this report.
cPhysical Activity Level (change from baseline to longest follow-up): rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcome (participant reported subjective outcome); rated down once due to serious concerns for inconsistency because of limited of evidence of consistency as only 1 trial was available that reported on the outcome; rated down once due to serious concerns for indirectness because the trial involved veterans and examined ACT (unclear generalizability); no serious concerns about imprecision; publication bias was not detected.
Table 23: GRADE Summary of Findings for Physical Function
Outcome, follow-up, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Physical function Follow-up: 2 and 3 months after treatment completion84 93 (1 nRCT) | One nRCT (N = 93),84 with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on physical function at longest follow-up (i.e., 2 and 3 months). With topics such as stress management, social support, and relapse management, this nRCT compared group videoconference-based CBT to group IP CBT (content-matched) in adults (group videoconference-based CBT: 70.2% female, mean age 54.5 years; group IP CBT: 57.8% female, mean age 59.7 years) with chronic back pain.84 There may be little to no difference in change in physical function from baseline to the longest follow-up, as measured by ODI (0 to 100 with higher scores indicating more impairment).84 The mean ODI change scores (SD) were 0.1 (3.9) and 3.0 (5.8) for group videoconference-based CBT and group IP CBT, respectively. | Very low Due to serious concerns for risk of bias, inconsistency, and imprecision.a | There may be little to no difference in the effect of iCBT vs. IP CBT on physical function at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on physical function at the longest follow-up, but the evidence is very uncertain. |
CBT = cognitive behavioural therapy; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; nRCT = non-randomized controlled trial; ODI = Oswestry Disability Index; SD = standard deviation; vs. = versus.
aPhysical Function: rated down once for risk of bias due to very serious concerns about the potential for bias arising from incomplete outcome data and lack of consideration of confounders adjustment rated down once due to serious concerns for inconsistency because of limited evidence of consistency as only 1 trial reported the outcome; no serious concerns for indirectness; rated down once due to serious concerns about imprecision, which was difficult to judge due to a lack of between-group comparisons, but within-group SDs were wide; publication bias was not detected.
Table 24: GRADE Summary of Findings for Changes in Use of Pharmacotherapy
Outcome, follow-up, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Prescription opioid use Follow-up: 2 and 3 months after treatment completion84 93 (1 nRCT) | One nRCT (N = 93),84 with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on prescription opioid use at longest follow-up (i.e., 2 and 3 months). With topics such as stress management, social support, and relapse management, this nRCT compared group videoconference-based CBT to group IP CBT (content-matched) in adults (group videoconference-based CBT: 70.2% female, mean age 54.5 y; group IP CBT: 57.8% female, mean age 59.7 years) with chronic back pain.84 There may be little to no difference in prescription opioid use at longest follow-up, as measured by COMM (0 to 68 with a cut-off score of ≥ 9 indicating that the respondent may be misusing their opioid medication).84 The mean COMM change scores (SD) were 1.4 (5.4) and 3.1 (5.0) for group videoconference-based CBT and group IP CBT, respectively. | Very low Due to serious concerns for risk of bias, inconsistency, and imprecision.a | There may be little to no difference in the effect of iCBT vs. IP CBT on prescription opioid use at post-treatment, but the evidence is very uncertain. There may be little to no difference in the effect of iCBT vs. IP CBT on prescription opioid use at the longest follow-up, but the evidence is very uncertain. |
CBT = cognitive behavioural therapy; COMM = Current Opioid Misuse Measure; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; nRCT = non-randomized controlled trial; SD = standard deviation; vs. = versus.
aPrescription Opioid Use: rated down once for risk of bias due to very serious concerns about the potential for bias arising from incomplete outcome data and lack of consideration of confounders; rated down once due to serious concerns for inconsistency because of limited of evidence of consistency because only 1 trial reported the outcome; no serious concerns for indirectness; rated down once due to serious concerns about imprecision which was difficult to judge due to a lack of between-group comparisons, but within-group SDs were wide ; publication bias was not detected.
Table 25: GRADE Summary of Findings for Satisfaction With Care
Outcome, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Satisfaction with care | Two RCTs (n = 200),73,74 both with high risk of bias (predicted direction of bias unclear), reported on the impact of iCBT vs. IP CBT on satisfaction with care. The trials included participants with heterogeneous chronic pain conditions, and participants had a mean age of 50 to 53 years across trials. One trial included only veterans who were primarily males (82%),73 while participants in the second trial were primarily females (60% to 68%).74 The CBT programs were highly variable; 1 trial compared individual videoconference-based ACT to individual IP ACT,73 while the second trial compared individual self-directed iCBT to group IP CBT (all content-matched between groups).74 There may be little to no difference between groups in satisfaction with care.73,74 In 1 trial, mean (SD) in CSQ for individual videoconference-based ACT and individual IP ACT were 4.40 (0.57) and 4.47 (0.41), respectively (P = 0.53).73 In the second trial, mean (SD) in overall course rating (1 = very bad to 10 = excellent) for individual iCBT and group IP CBT were 7.37 (1.50) and 7.46 (0.78), respectively (P = 0.800).74 Furthermore, participants rated the degree (very well to very bad) to which they were able to proceed independently with the course instructions (statistical comparison NC); 0% of participants responded “very well,” 55% responded “well,” 40% responded “reasonably well,” 0% responded “badly,” and 5% responded “very badly” in the individual iCBT group, while 12.5% responded “very well,” 37.5% responded “well,” 41.7% responded “reasonably well,” 8.3% responded “badly,” and 0% responded “very badly” in the group IP CBT group.74 | Very low Due to very serious concerns for risk of bias, serious concerns for indirectness.a | There may be little to no difference in the effect of iCBT vs. IP CBT on satisfaction with care, but the evidence is very uncertain. |
CBT = cognitive behavioural therapy; CI = confidence interval; CSQ = Client Satisfaction Questionnaire; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; RCT = randomized controlled trial; SD = standard deviation; vs. = versus.
aSatisfaction with Care: rated down twice for risk of bias due to very serious concerns about the potential for bias arising from a large quantity of missing outcome data and bias in measurement of the outcomes (participant reported subjective outcomes); no serious concerns for inconsistency; rated down once due to serious concerns for indirectness because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) in 1 trial; no serious concerns about imprecision; publication bias was not detected.
Table 26: GRADE Summary of Findings for Individual Participation
Outcome, no. participants (trials) | Findings | Certainty of the evidence (GRADE) | What happens? |
|---|---|---|---|
Individual participation | Two RCTs73,74 with some risk of bias, and 1 RCT75 and 1 nRCT84 with high risk of bias, all with unclear predicted direction of bias, reported on individual participation (N = 333). The trials included people with heterogeneous chronic pain conditions, and participants had a mean age of 49 to 59 years across trials. In 3 trials the participants were primarily females (57% to 100%)74,75,84; the fourth trial included only veterans who were primarily males (82%).73 The CBT programs were highly variable; 2 trials compared content-matched videoconference-based ACT73 or CBT84 to IP ACT or CBT (the ACT was individual while the CBT was group-based), while 2 trials compared individual self-directed iCBT to content-matched group IP CBT.74,75 The results on individual participation were heterogeneous with higher withdrawal rates in the iCBT vs. IP CBT group in 3 RCTs (46% vs. 23%,73 20% vs. 15%,75 and 33.3% vs. 6.7%74), and lower withdrawal rates in the iCBT vs. IP CBT group in the 1 nRCT (14.9% vs. 34.8%).84 Furthermore, results on attendance rates (when reported) were heterogeneous with higher attendance rates (i.e., 95.2% vs. 46.4% attended all modules) in the iCBT vs. IP CBT group in 1 RCT,74 and little to no difference in attendance rates (i.e., mean sessions attended [SD] iCBT 5.2 [2.9] vs. IP CBT 4.1 [3.4], P = 0.09) in the 1 nRCT.84 | Very low Due to serious concerns for risk of bias, indirectness, and imprecision.a | The results were heterogenous about the effect of iCBT vs. IP CBT on individual participation, but the evidence is very uncertain. |
ACT = acceptance and commitment therapy; CBT = cognitive behavioural therapy; CI = confidence interval; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; nRCT = non-randomized controlled trial; RCT = randomized controlled trial; SD = standard deviation; vs. = versus.
aIndividual Participation: rated down once for risk of bias due to serious concerns about the potential for bias arising from the randomization process; no serious concerns for inconsistency; rated down once due to serious concerns for indirectness, because the effect of the intervention (iCBT vs. IP CBT) cannot be isolated due to differences in the delivery format (individual vs. group) in 2 trials; rated down once due to serious concerns about imprecision as the number of events did not meet the optimal information size (< 300 events); publication bias was not detected.
Table 27: Summary of Detailed Findings for Pain Interference
Outcome, follow-up, no. participants (trials) | Detailed findings |
|---|---|
Pain interference Follow-up: post-treatment73,74 and 2 months,74,84 3 months,84 and 6 months73 after treatment completion 293 (2 RCTs, 1 nRCT) | Three trials (2 RCTs,73,74 1 nRCT84) provided evidence for pain interference as measured by the BPI Interference Subscale73,84 or VAS Interference Scale.74 |
Mariano et al. (2021)84 Between-group comparisons in average interference change scores (calculated as baseline score minus follow-up score) NC. However, change scores (SD) as measured by the BPI Interference Subscale (ITT: n = 93) were reported: Group videoconference-based CBT (2 months after treatment completion): 0.6 (1.3) Group IP CBT (3 months after treatment completion): 0.6 (1.7) | |
Herbert et al. (2017)73 Between-group differences in change rates in BPI Interference (ITT: n = 128): Post-treatment: 0.32 (95% CI, −0.34 to 0.98) 6 months after treatment completion: 0.70 (95% CI, −0.07 to 1.48) | |
de Boer et al. (2014)74 Mean changes (SD) in VAS Interference Scale NR for ITT analyses. ANOVA effects (group × time interaction) (ITT: n = 72) were reported: Post-treatment: ANOVA effects (group × time interaction) P > 0.05 2 months after treatment completion: ANOVA effects (group × time interaction) P > 0.05 |
ANOVA = analysis of variance; BPI = Brief Pain Inventory; CBT = cognitive behavioural therapy; CI = confidence interval; IP = in-person; ITT = intent to treat; NC = not conducted; NR = not reported; nRCT = non-randomized controlled trial; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale.
Table 28: Summary of Detailed Findings for Pain Control
Outcome, follow-up, no. participants (trials) | Detailed findings |
|---|---|
Pain control Follow-up: post-treatment73,74 and 2 months,74,84 3 months,84 and 6 months73 after treatment completion 293 (2 RCTs, 1 nRCT) | Three trials (2 RCTs,73,74 1 nRCT84) provided evidence for pain severity as measured by the BPI Severity Subscale73,84 or VAS Pain Intensity Scale.74 |
Mariano et al. (2021)84 Between-group comparisons in change scores (calculated as baseline score minus follow-up score) NC. However, change scores (SD) as measured by the BPI Pain Severity Subscale (ITT n = 93) were reported: Group videoconference-based CBT (2 months after treatment completion): worst 0.7 (1.4), least −0.1 (1.4), average 0.1 (1.1), right now −0.4 (1.7) Group IP CBT (3 months after treatment completion): worst 1.4 (2.5), least 0.1 (2.1), average 0.4 (1.9), right now 0.1 (2.5) | |
Herbert et al. (2017)73 Between-group differences in change rates in BPI Interference (ITT n = 128): Post-treatment: −0.38 (95% CI, −0.99 to 0.22) 6 months after treatment completion: −0.06 (95% CI, −0.72 to 0.60) | |
de Boer et al. (2014)74 Mean changes (SD) in VAS Interference Scale NR for ITT analyses. ANOVA effects (group × time interaction) (ITT n=72) were reported: Post-treatment: ANOVA effects (group × time interaction) P > 0.05 2 months after treatment completion: ANOVA effects (group × time interaction) P=0.070 |
ANOVA = analysis of variance; BPI = Brief Pain Inventory; CBT = cognitive behavioural therapy; CI = confidence interval; IP = in-person; ITT = intent to treat; NC = not conducted; NR = not reported; nRCT = non-randomized controlled trial; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale.
Table 29: Summary of Detailed Findings for Health-Related Quality of Life or Overall Well-Being
Outcome, follow-up, no. participants (trials) | Detailed findings |
|---|---|
HRQoL or overall well-being Follow-up: post-treatment73-75 and 2 months,74 3 months,75 6 months,73,75 and 12 months75 after treatment completion 240 (3 RCTs) | Three RCTs73-75 provided evidence for HRQoL or overall well-being as measured by SF12-MCS and SF12-PCS,73 FIQ,75 or RAND-36.74 |
Herbert et al. (2017)73 Between-group differences in change rates (ITT n = 128): SF12-MCS Post-treatment: 0.46 (95% CI, −3.59 to 4.50) 6 months after treatment completion: −1.72 (95% CI, −6.13 to 2.70) SF12-PCS Post-treatment: −1.56 (95% CI, −4.54 to 1.42) 6 months after treatment completion: −2.20 (95% CI, −5.46 to 1.07) | |
Vallejo et al. (2015)75 Between-group comparisons in change scores NC. However, mean change scores (SD) as measured by FIQ (ITT n=40) were calculated:a Post-treatment: Individual iCBT: 0.35 (19.05) Group IP CBT: −10.23 (19.06) 12 months after treatment completion: Individual iCBT: −5.12 (17.98) Group IP CBT: −3.29 (18.76) ANOVA effects (time × group interaction) at 12 months relative to post-treatment: P < 0.001 (favoured individual iCBT) | |
de Boer et al., 201474 Mean changes (SD) in VAS Interference Scale NR for ITT analyses. ANOVA effects (group × time interaction) (ITT n = 72) were reported: Post-treatment: P > 0.05 for all subscales (i.e., physical functioning, social functioning, role impairment physical, role impairment emotional, mental health, vitality, pain, general health appraisal, perceived health change) 2 months after treatment completion: P > 0.05 for all subscales except perceived health change P < 0.05 (specific P value NR) (favoured iCBT) |
ANOVA = analysis of variance; CBT = cognitive behavioural therapy; CI = confidence interval; FIQ = Fibromyalgia Impact Questionnaire; HRQoL = health-related quality of life; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; ITT = intent to treat; NC = not conducted; NR = not reported; RAND-36 = Research and Development 36-Item Health Survey; RCT = randomized controlled trial; SD = standard deviation; SF12-MCS = Short Form 12-Item Mental Component Summary; SF12-PCS = Short Form 12-Item Physical Component Summary.
aCalculation methods for mean changes are described in the Data Manipulation section of this report.
Table 30: Summary of Detailed Findings for Psychological or Psychosocial Function or Symptoms
Outcome, follow-up, no. participants (trials) | Detailed findings |
|---|---|
Pain acceptance Follow-up: post-treatment73 and 6 months73 after treatment completion 128 (1 RCT) | One RCT73 provided evidence for pain acceptance as measured by CPAQ-R.73 |
Herbert et al. (2017)73 Between-group differences in change rates (ITT n = 128): Post-treatment: −1.84 (95% CI, −7.84 to 4.16) 6 months after treatment completion: 3.45 (95% CI, −3.13 to 10.03) | |
Anxiety, depression, or general psychological distress Follow-up: post-treatment73,75 and 2 months,84 3 months,75,84 6 months,73,75 and 12 months75 after treatment completion 261 (2 RCTs and 1 nRCT) | Three trials (2 RCTs,73,75 1 nRCT84) provided evidence for anxiety, depression, or general psychological distress as measured by PHQ-9,73 PASS-20,73 HADS,75,84 or BDI.75 |
Mariano et al. (2021)84 Between-group comparisons in change scores (calculated as baseline score minus follow-up score) NC. However, change scores (SD) as measured by HADS (ITT n=93) were reported: Group videoconference-based CBT (2 months after treatment completion): Anxiety 0.5 (2.6), depression 0.2 (2.4) Group IP CBT (3 months after treatment completion): Anxiety −0.5 (5.5), depression −0.3 (5.2) | |
Herbert et al. (2017)73 Between-group differences in change rates in BPI Interference (ITT n = 128) were reported: PHQ-9 Post-treatment: −0.51 (95% CI, −2.42 to 1.40) 6 months after treatment completion: 1.22 (95% CI, −0.88 to 3.32) PASS-20 Post-treatment: −4.20 (95% CI, −10.58 to 2.17) 6 months after treatment completion: −4.01 (95% CI, −11.01 to 3.00) | |
Vallejo et al. (2015)75 Between-group comparisons in change scores NC. However, mean change scores (SD) as measured by HADS and BDI (ITT n = 40) were calculated:a HADS Post-treatment: Individual iCBT: −5.10 (3.22) Group IP CBT: −1.51 (5.07) 12 months after treatment completion: Individual iCBT: −5.36 (3.05) Group IP CBT: 0.05 (4.67) ANOVA effects (time × group interaction) at 12 months relative to post-treatment: P > 0.05 BDI Post-treatment: Individual iCBT: −6.52 (4.03) Group IP CBT: −5.11 (6.06) 12 months after treatment completion: Individual iCBT: −6.90 (3.91) Group IP CBT: −2.54 (6.22) ANOVA effects (time × group interaction) at 12 months relative to post-treatment: P = 0.004 (favoured individual iCBT) | |
Self-efficacy Follow-up: post-treatment75 and 3 months,75 6 months,75 and 12 months75 after treatment completion 40 (1 RCT) | One RCT75 provided evidence for self-efficacy as measured by CPSS. |
Vallejo et al. (2015)75 Between-group comparisons in change scores NC. However, mean change scores (SD) as measured by CPSS (ITT n = 40) were calculated:a Post-treatment: Individual iCBT: pain self-efficacy 5.52 (15.36), coping symptoms 7.63 (16.11), physical function 4.86 (17.47), and global self-efficacy 6.54 (13.96) Group IP CBT: pain self-efficacy −0.47 (17.25), coping symptoms 5.77 (20.51), physical function 4.50 (20.91), and global self-efficacy 3.55 (17.99) 12 months after treatment completion: Individual iCBT: pain self-efficacy 7.31 (11.81), coping symptoms 7.37 (15.67), physical function 6.60 (16.88), and global self-efficacy 7.65 (11.80) Group IP CBT: pain self-efficacy −4.00 (16.23), coping symptoms 0.95 (18.66), physical function −10.64 (20.44), and global self-efficacy −1.11 (17.21) ANOVA effects (time × group interaction) at 12 months relative to post-treatment: P > 0.05 (all subscales) | |
Pain-related worrying and pain coping Follow-up: post-treatment74,75 and 2 months,74 3 months,75 6 months,75 and 12 months75 after treatment completion 112 (2 RCTs) | Two RCTs74,75 provided evidence for pain-related worrying as measured by PCS,74,75 CPCI,75 or PCCL.74 |
Vallejo et al. (2015)75 Between-group comparisons in change scores NC. However, mean change scores (SD) as measured by PCS and CPCI (ITT n = 40) were calculated:a PCS Post-treatment: Individual iCBT: pain catastrophizing −3.84 (5.25), rumination −1.79 (2.50), helplessness −1.06 (4.21), and magnification −1.00 (2.34) Group IP CBT: pain catastrophizing −6.95 (10.26), rumination −2.57 (3.37), helplessness −3.14 (5.25), and magnification −1.24 (2.91) 12 months after treatment completion: Individual iCBT: pain catastrophizing −10.68 (4.97), rumination −4.10 (2.54), helplessness −4.53 (4.18), and magnification −2.06 (1.98) Group IP CBT: pain catastrophizing −0.52 (12.47), rumination −1.33 (3.93), helplessness −0.76 (5.97), and magnification 1.58 (3.86) ANOVA effects (time × group interaction) at 12 months relative to post-treatment: pain catastrophizing (P < 0.001), helplessness (P = 0.009), and magnification (P < 0.001) all favoured individual iCBT; rumination (P > 0.05) CPCI Post-treatment: Individual iCBT: guarding 0.16 (1.20), resting 0.03 (1.41), asking for assistance 0.06 (1.37), seeking social support 0.05 (1.44), relaxation 0.74 (1.28), task persistence 0.16 (1.51), exercise/stretch 0.21 (1.79), coping self-statements −0.26 (1.55) Group IP CBT: guarding −0.29 (1.20), resting −0.40 (1.22), asking for assistance 0.05 (1.50), seeking social support 0.19 (1.53), relaxation 1.24 (1.74), task persistence −0.15 (1.35), exercise/stretch 0.29 (1.67), coping self-statements −0.09 (1.67) 12 months after treatment completion: Individual iCBT: guarding 0.24 (1.18), resting 0.70 (1.44), asking for assistance −0.05 (1.39), seeking social support −1.00 (1.50), relaxation 0.37 (1.16), task persistence −0.15 (1.38), exercise/stretch 0 (1.80), coping self-statements −1.31 (1.52) Group IP CBT: guarding 1.01 (1.38), resting 0.61 (1.23), asking for assistance 0.38 (1.46), seeking social support 0.05 (1.51), relaxation 0.86 (1.81), task persistence −0.24 (1.32), exercise/stretch 0.10 (1.59), coping self-statements −0.90 (1.60) ANOVA effects (time × group interaction) at 12 months relative to post-treatment: P > 0.05 (all subscales) | |
de Boer et al. (2014)74 Mean changes (SD) in PCS and PCCL NR for ITT analyses. ANOVA effects (group × time interaction) (ITT n = 72) were reported: PCS Post-treatment: ANOVA effects (group × time interaction) P > 0.05 2 months after treatment completion: ANOVA effects (group × time interaction) P = 0.315 PCCL Post-treatment: ANOVA effects (group × time interaction): pain catastrophizing P > 0.05, pain coping P > 0.05, internal pain management P > 0.05, external pain management P > 0.05 2 months after treatment completion: ANOVA effects (group × time interaction): pain catastrophizing P > 0.05, pain coping P = 0.121, internal pain management P > 0.05, external pain management P > 0.05 | |
Fatigue Follow-up: post-treatment74 and 2 months after treatment completion74 72 (1 RCT) | One RCT74 provided evidence for fatigue as measured by VAS Fatigue Scale.74 |
de Boer et al. (2014)74 Mean changes (SD) in VAS Fatigue Scale NR for ITT analyses. ANOVA effects (group × time interaction) (ITT n = 72) were reported: Post-treatment: ANOVA effects (group × time interaction) P > 0.05 2 months after treatment completion: ANOVA effects (group × time interaction) P > 0.05 |
ANOVA = analysis of variance; BDI = Beck's Depression Inventory; CBT = cognitive behavioural therapy; CI = confidence interval; CPAQ-R = Chronic Pain Acceptance Questionnaire-Revised; CPCI = Chronic Pain Coping Inventory; CPSS = Chronic Pain Self-efficacy Scale; iCBT = internet-delivered cognitive behavioural therapy; HADS = Hospital Anxiety and Depression Scale; IP = in-person; ITT = intent to treat; NC = not conducted; NR = not reported; nRCT = non-randomized controlled trial; PASS-20 = Pain Anxiety Symptoms Scale-Short Form 20-Item; PCCL = Pain Coping and Cognition List; PCS = Pain Catastrophizing Scale; PHQ-9 = Patient Health Questionnaire-9; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale.
aCalculation methods for mean changes are described in Data Manipulation section of this report.
Table 31: Summary of Detailed Findings for Sleep
Outcome, follow-up, no. participants (trials) | Detailed findings |
|---|---|
Sleep Follow-up: post-treatment73 and 6 months73 after treatment completion 128 (1 RCT) | One RCT73 provided evidence for sleep as measured by PSQI. |
Herbert et al. (2017)73 Between-group differences in change rates in BPI Interference (ITT n = 128): Post-treatment: −0.21 (95% CI, −1.63 to 1.20) 6 months after treatment completion: −0.14 (95% CI, −1.69 to 1.42) |
CI = confidence interval; ITT = intent to treat; PSQI = Pittsburgh Sleep Quality Index; RCT = randomized controlled clinical trial.
Table 32: Summary of Detailed Findings for Physical Activity Level
Outcome, follow-up, no. participants (trials) | Detailed findings |
|---|---|
Physical activity level Follow-up: post-treatment73 and 6 months73 after treatment completion 128 (1 RCT) | One RCT73 provided evidence for physical activity level as measured by MPI-Activity. |
Herbert et al. (2017)73 Between-group differences in change rates in BPI Interference (ITT n = 128): Post-treatment: −0.15 (95% CI, −0.41 to 0.11) 6 months after treatment completion: 0.31 (95% CI, 0.02 to 0.60, P = 0.03, favoured IP ACT) |
CI = confidence interval; ITT = intent to treat; MPI = The West Haven-Yale Multidimensional Pain Inventory; RCT = randomized controlled clinical trial.
Table 33: Summary of Detailed Findings for Physical Function
Outcome, follow-up, no. participants (trials) | Detailed findings |
|---|---|
Physical function Follow-up: 2 and 3 months after treatment completion84 93 (1 nRCT) | One nRCT84 provided evidence for physical function as measured by ODI. |
Mariano et al. (2021)84 Between-group comparisons in change scores (calculated as baseline score minus follow-up score) NC. However, change scores (SD) as measured by ODI (ITT: n = 93) were reported: Group videoconference-based CBT (2 months after treatment completion): 0.1 (3.9) Group IP CBT (3 months after treatment completion): 3.0 (5.8) |
CBT = cognitive behavioural therapy; IP = in-person; ITT = intent to treat; NC = not conducted; nRCT = non-randomized controlled trial; ODI = Oswestry Disability Index; SD = standard deviation.
Table 34: Summary of Detailed Findings for Changes in Use of Pharmacotherapy
Outcome, follow-up, no. participants (trials) | Detailed findings |
|---|---|
Prescription opioid use Follow-up: 2 and 3 months after treatment completion84 93 (1 nRCT) | One nRCT84 provided evidence for prescription opioid use as measured by COMM. |
Mariano et al. (2021)84 Between-group comparisons in change scores (calculated as baseline score minus follow-up score) NC. However, change scores (SD) as measured by COMM (ITT: n = 93) were reported: Group videoconference-based CBT (2 months after treatment completion): 1.4 (5.4) Group IP CBT (3 months after treatment completion): 3.1 (5.0) |
CBT = cognitive behavioural therapy; COMM = Current Opioid Misuse Measure; IP = in-person; ITT = intent to treat; NC = not conducted; nRCT = non-randomized controlled trial; SD = standard deviation.
Table 35: Summary of Detailed Findings for Satisfaction With Care
Outcome and no. participants (trials) | Detailed findings |
|---|---|
Satisfaction with care | Two RCTs73,74 provided evidence for data on satisfaction with care. |
Herbert et al. (2017)73 Mean (SD) in CSQ for each group (P = 0.53): Individual videoconference-based ACT: 4.40 (0.57) Individual IP ACT: 4.47 (0.41) | |
de Boer et al. (2014)74 Participants rated the course as a whole from 1 (very bad) to 10 (excellent) (P = 0.800): Individual iCBT: 7.37 (1.50) Group IP CBT: 7.46 (0.78) Participants rated the degree to which they were able to proceed independently with course instructions (statistical comparison NC). Individual iCBT: 0 (0%) participants responded “very well,” 11 (55%) responded “well,” 8 (40%) responded “reasonably well,” 0 (0%) responded “badly,” and 1 (5%) responded “very badly” Group IP CBT: 3 participants (12.5%) responded “very well,” 9 (37.5%) responded “well,” 10 (41.7%) responded “reasonably well,” 2 (8.3%) responded “badly,” and 0 (0%) responded “very badly” |
ACT = acceptance and commitment therapy; CBT = cognitive behavioural therapy; CSQ = Client Satisfaction Questionnaire; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; RCT = randomized controlled trial; SD = standard deviation.
Table 36: Detailed Findings for Individual Participation
Outcome, no. participants (trials) | Individual participation |
|---|---|
Individual participation | Three RCTs73-75 and 1 nRCT84 provided data on individual participation. |
Mariano et al. (2021)84 Withdrawal rates for each group (statistical comparison NC): Group videoconference-based CBT: Seven (14.9%) participants completed baseline assessment, but withdrew from trial without attending any sessions (reason NR) Three (6.4%) withdrew after attending a few sessions due to scheduling conflicts (specific number of sessions NR) Four (8.5%) were unresponsive to repeated requests to complete the follow-up questionnaire Group IP CBT: Sixteen (34.8%) participants completed baseline assessment, but withdrew from trial without attending any sessions (reason NR) Two (4.3%) withdrew after attending a few sessions (specific number of sessions and reason NR) Six (13.0%) were unresponsive to repeated requests to complete the follow-up questionnaire Mean (SD) sessions attended (counting those who consented that did not attend any sessions) for each group were reported (P = 0.09). Group videoconference-based CBT: 5.2 (2.9) Group IP CBT: 4.1 (3.4) Age-related participation comparison: Older participants tended to select the videoconference-based CBT intervention more often than younger participants (P < 0.05) (additional details NR) | |
Herbert et al. (2017)73 Withdrawal rates for each group (P = 0.01): Individual videoconference-based ACT: 29 of 63 (46%) Reasons: Time demands of trial (6), transportation (2), time and transportation (5), protocol violation (4), conflict with employment (1), development of a serious medical illness (3), therapy not effective (1), adverse life event (1), lost interest or illness (5), no specific reason (2) Individual IP ACT: 15 of 65 (23%) Reasons: Time demands of trial (2), transportation (2), time and transportation (3), conflict with employment (1), lost interest (2), protocol violation (4), development of a serious medical illness (1) | |
Vallejo et al. (2015)75 Loss to follow-up rates (reasons NR) for each group were reported (statistical comparison NC). Individual iCBT: 4 of 20 (20%) Group IP CBT: 3 of 20 (15%) | |
de Boer et al. (2014)74 Withdrawal rates (i.e., started but did not complete treatment) for each group were reported (statistical comparison NC). Individual iCBT: 11 of 33 (33.3%) Group IP CBT: 2 of 30 (6.7%) Full attendance rates (i.e., attended all modules or session) for each group were reported (P < 0.001). Individual iCBT: 95.2% Group IP CBT: 46.4% |
ACT = acceptance and commitment therapy; CBT = cognitive behavioural therapy; iCBT = internet-delivered cognitive behavioural therapy; IP = in-person; NC = not conducted; NR = not reported; nRCT = nonrandomized controlled trial; RCT = randomized controlled trial; SD = standard deviation.
Appendix 3: List of Included Publications — Clinical Review
Note that this appendix has not been copy-edited.
The citations provided in this list are the publications that were included in this Clinical Review (in reverse chronological order):
Mariano TY, Wan L, Edwards RR, Lazaridou A, Ross EL, Jamison RN. Online group pain management for chronic pain: preliminary results of a novel treatment approach to teletherapy. J Telemed Telecare. 2021;27(4):209-216.
Herbert MS, Afari N, Liu L, et al. Telehealth versus in-person acceptance and commitment therapy for chronic pain: a randomized noninferiority trial. J Pain. 2017;18(2):200-211.
Vallejo MA, Ortega J, Rivera J, Comeche MI, Vallejo-Slocker L. Internet versus face-to-face group cognitive-behavioral therapy for fibromyalgia: a randomized control trial. J Psychiatr Res. 2015;68:106-113.
de Boer MJ, Versteegen GJ, Vermeulen KM, Sanderman R, Struys MM. A randomized controlled trial of an Internet-based cognitive-behavioural intervention for non-specific chronic pain: an effectiveness and cost-effectiveness study. Eur J Pain. 2014;18(10):1440-1451.
Appendix 4: List of Excluded Publications and Reasons for Exclusion — Clinical Review
Note that this appendix has not been copy-edited.
The citations provided in this list are studies that were excluded after full-text review by 2 independent reviewers as part of the Clinical Review (in reverse chronological and alphabetical order).
Irrelevant Population (n = 5)
Hoefnagels JW, Fischer K, Bos RAT, et al. A feasibility study on two tailored interventions to improve adherence in adults with haemophilia. Pilot and Feasibility Studies. 2020;6(1).
Chadi N, Weisbaum E, Malboeuf-Hurtubise C, et al. In-person vs. Ehealth mindfulness-based intervention for adolescents with chronic illnesses: A pilot randomized trial. Adolesc Psychiatry. 2019;9(1):11-23.
Levy RL, Langer SL, van Tilburg MA, et al. Brief telephone-delivered cognitive behavioral therapy targeted to parents of children with functional abdominal pain: A randomized controlled trial. Pain. 2017;158(4):618-628.
Mikocka-Walus A, Bampton P, Hetzel D, Hughes P, Esterman A, Andrews JM. Cognitive-behavioural therapy has no effect on disease activity but improves quality of life in subgroups of patients with inflammatory bowel disease: a pilot randomised controlled trial. BMC Gastroenterol. 2015;15:54.
Ammerlaan J, van Os-Medendorp H, Scholtus L, et al. Feasibility of an online and a face-to-face version of a self-management program for young adults with a rheumatic disease: experiences of young adults and peer leaders. Pediatr Rheumatol Online J. 2014;12:10.
Irrelevant Intervention (n = 3)
Gomez-Perez MC, Garcia-Palacios A, Castilla D, Zaragoza I, Suso-Ribera C. Brief Acceptance and Commitment Therapy for Fibromyalgia: Feasibility and Effectiveness of a Replicated Single-Case Design. Pain Res Manag. 2020;2020:7897268.
Heapy AA, Higgins DM, Goulet JL, et al. Interactive Voice Response-Based Self-management for Chronic Back Pain: The COPES Noninferiority Randomized Trial. JAMA Intern Med. 2017;177(6):765-773.
Igna R, Stefan S, Onac I, Onac I, Ungur R-A, Szentagotai Tatar A. Mindfulness-based cognitive-behavior therapy (MCBT versus virtual reality (VR) enhanced CBT, versus treatment as usual for chronic back pain. A clinical trial. Journal of Evidence-Based Psychotherapies. 2014;14(2):229-247.
Irrelevant Comparator (n = 107)
Sitges C, Terrasa JL, Garcia-Dopico N, et al. An Educational and Exercise Mobile Phone-Based Intervention to Elicit Electrophysiological Changes and to Improve Psychological Functioning in Adults With Nonspecific Chronic Low Back Pain (BackFit App): Nonrandomized Clinical Trial. JMIR Mhealth Uhealth. 2022;10(3):e29171.
Baumeister H, Paganini S, Sander LB, et al. Effectiveness of a Guided Internet- and Mobile-Based Intervention for Patients with Chronic Back Pain and Depression (WARD-BP): A Multicenter, Pragmatic Randomized Controlled Trial. Psychother Psychosom. 2021;90(4):255-268.
Bendelin N, Gerdle B, Blom M, Södermark M, Andersson G. Internet-Delivered Acceptance and Commitment Therapy Added to Multimodal Pain Rehabilitation: A Cluster Randomized Controlled Trial. J Clin Med. 2021;10(24).
Carvalho SA, Trindade IA, Duarte J, et al. Efficacy of an ACT and Compassion-Based eHealth Program for Self-Management of Chronic Pain (iACTwithPain): Study Protocol for a Randomized Controlled Trial. Front Psychol. 2021;12:630766.
Colomina J, Drudis R, Torra M, et al. Implementing mhealth-enabled integrated care for complex chronic patients with osteoarthritis undergoing primary hip or knee arthroplasty: Prospective, two-arm, parallel trial. J Med Internet Res. 2021;23(9).
Friesen LN. A randomized controlled trial of internet-delivered cognitive behaviour therapy for individuals with fibromyalgia. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2021;82(9-B).
Gohir SA, Eek F, Kelly A, Abhishek A, Valdes AM. Effectiveness of Internet-Based Exercises Aimed at Treating Knee Osteoarthritis: The iBEAT-OA Randomized Clinical Trial. JAMA netw. 2021;4(2):e210012.
Goren G, Schwartz D, Friger M, et al. Randomized Controlled Trial of Cognitive-Behavioral and Mindfulness-Based Stress Reduction on the Quality of Life of Patients With Crohn Disease. Inflammatory bowel diseases. 2021;13.
Macfarlane GJ, Beasley M, Scott N, et al. Maintaining musculoskeletal health using a behavioural therapy approach: a population-based randomised controlled trial (the MAmMOTH Study). Ann Rheum Dis. 2021;80(7):903-911.
Palermo TM, Law EF, Topazian MD, et al. Internet Cognitive-Behavioral Therapy for Painful Chronic Pancreatitis: A Pilot Feasibility Randomized Controlled Trial. Clin Transl Gastroenterol. 2021;12(6):e00373.
Rini C, Katz AWK, Nwadugbo A, Porter LS, Somers TJ, Keefe FJ. Changes in Identification of Possible Pain Coping Strategies by People with Osteoarthritis who Complete Web-based Pain Coping Skills Training. Int J Behav Med. 2021;28(4):488-498.
Wicksell R. Make friends with your pain monster: Internet-delivered acceptance- and value-based exposure in chronic pain: Model and treatment. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2021;82(9-B).
Winhusen T, Wilson M, Dolor RJ, et al. Design considerations for a remote randomized multi-site clinical trial evaluating an e-health self-management program for chronic pain patients receiving opioid therapy. Contemp Clin Trials. 2021;101:106245.
van Hooff ML, Vriezekolk JE, Kroeze RJ, O'Dowd JK, van Limbeek J, Spruit M. Targeting self-efficacy more important than dysfunctional behavioral cognitions in patients with longstanding chronic low back pain; a longitudinal study. BMC Musculoskelet Disord. 2021;22(1):824.
Xie H, Guarino H, Moore SK, et al. Web-based cognitive behavior therapy for chronic pain patients with aberrant drug-related behavior: How did it work and for whom? Journal of behavioral medicine. 2021;12.
Carleton RN, Asmundson GJG, Korol SL, et al. Evaluating the efficacy of an attention modification program for patients with fibromyalgia: a randomized controlled trial. Pain. 2020;161(3):584-594.
Curtis ME. Evaluating a mindfulness meditation smartphone app among chronic pain patients. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2020;81(7-B).
Dharmasri CJ, Griesemer I, Arbeeva L, et al. Acceptability of telephone-based pain coping skills training among African Americans with osteoarthritis enrolled in a randomized controlled trial: a mixed methods analysis. BMC Musculoskelet Disord. 2020;21(1):545.
Ezenwa MO, Yao Y, Nguyen MT, et al. Randomized Pilot Study: a Mobile Technology-based Self-management Intervention for Sickle Cell Pain. West J Nurs Res. 2020;42(8):629-639.
Forbes G, Newton S, Cantalapiedra Calvete C, et al. MEMPHIS: a smartphone app using psychological approaches for women with chronic pelvic pain presenting to gynaecology clinics: a randomised feasibility trial. BMJ Open. 2020;10(3):e030164.
Gentili C, Zetterqvist V, Rickardsson J, Holmstrom L, Simons LE, Wicksell RK. ACTsmart - development and feasibility of digital Acceptance and Commitment Therapy for adults with chronic pain. npj digit. 2020;3:20.
Jonassaint CR, Kang C, Prussien KV, et al. Feasibility of implementing mobile technology-delivered mental health treatment in routine adult sickle cell disease care. Transl Behav Med. 2020;10(1):58-67.
Moman RN, Hooten WM. The Major Barrier Facing Patients and Clinicians Who Are Interested in Utilization of Electronic and Mobile Health Technologies. Pain Medicine (United States). 2020;21(2):E243-E246.
Palermo TM, de la Vega R, Murray C, Law E, Zhou C. A digital health psychological intervention (WebMAP Mobile) for children and adolescents with chronic pain: results of a hybrid effectiveness-implementation stepped-wedge cluster randomized trial. Pain. 2020;161(12):2763-2774.
Sander LB, Paganini S, Terhorst Y, et al. Effectiveness of a Guided Web-Based Self-help Intervention to Prevent Depression in Patients With Persistent Back Pain: The PROD-BP Randomized Clinical Trial. JAMA Psychiatry. 2020;77(10):1001-1011.
Sodermark M, Linton SJ, Hesser H, Flink I, Gerdle B, Boersma K. What Works? Processes of Change in a Transdiagnostic Exposure Treatment for Patients With Chronic Pain and Emotional Problems. Clin J Pain. 2020;36(9):648-657.
Taylor PC. Adopting PROs in virtual and outpatient management of RA. Nature Reviews Rheumatology. 2020;16(9):477-478.
Berube M, Gelinas C, Feeley N, et al. Feasibility of a Hybrid Web-Based and In-Person Self-management Intervention Aimed at Preventing Acute to Chronic Pain Transition After Major Lower Extremity Trauma (iPACT-E-Trauma): A Pilot Randomized Controlled Trial. Pain Med. 2019;20(10):2018-2032.
Boersma K, Sodermark M, Hesser H, Flink IK, Gerdle B, Linton SJ. Efficacy of a transdiagnostic emotion-focused exposure treatment for chronic pain patients with comorbid anxiety and depression: a randomized controlled trial. Pain. 2019;160(8):1708-1718.
Burke D, Lennon O, Blake C, et al. An internet-delivered cognitive behavioural therapy pain management programme for spinal cord injury pain: A randomized controlled trial. European Journal of Pain. 2019;23(7):1264-1282.
Goel A. Internet-delivered exposure therapy was cost-effective for increasing treatment response in fibromyalgia. Ann Intern Med. 2019;170(2):JC11.
Moore AA, Lake JE, Glasner S, et al. Establishing the feasibility, acceptability and preliminary efficacy of a multi-component behavioral intervention to reduce pain and substance use and improve physical performance in older persons living with HIV. J Subst Abuse Treat. 2019;100:29-38.
Boston Children's Hospital. NCT04093921: Ready for Change: a Telehealth, Motivational Enhancement Pre-habilitation Training to Increase Engagement in Children and Families Entering Intensive Interdisciplinary Pain Rehabilitation. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/show/NCT04093921.
Petrozzi MJ, Leaver A, Ferreira PH, Rubinstein SM, Jones MK, Mackey MG. Addition of MoodGYM to physical treatments for chronic low back pain: A randomized controlled trial. Chiropr Man Therap. 2019;27:54.
Rosen MI, Becker WC, Black AC, Martino S, Edens EL, Kerns RD. Brief counseling for veterans with musculoskeletal disorder, risky substance use, and service connection claims. Pain Medicine (United States). 2019;20(3):528-542.
Smith J, Faux SG, Gardner T, et al. Reboot Online: A Randomized Controlled Trial Comparing an Online Multidisciplinary Pain Management Program with Usual Care for Chronic Pain. Pain Med. 2019;20(12):2385-2396.
Zuidema R, van Dulmen S, Nijhuis-van der Sanden M, et al. Efficacy of a Web-Based Self-Management Enhancing Program for Patients with Rheumatoid Arthritis: Explorative Randomized Controlled Trial. J Med Internet Res. 2019;21(4):e12463.
Alberts NM, Law EF, Chen AT, Ritterband LM, Palermo TM. Treatment engagement in an internet-delivered cognitive behavioral program for pediatric chronic pain. Internet Interv. 2018;13:67-72.
Berube M, Gelinas C, Feeley N, et al. A pilot randomised controlled trial of a hybrid webbased and in-person self-management intervention aimed at preventing acute to chronic pain transition after major lower extremity trauma (ipact-e-trauma). Orthopaedic world congress. 2018.
Dear BF, Gandy M, Karin E, et al. The Pain Course: 12- and 24-Month Outcomes From a Randomized Controlled Trial of an Internet-Delivered Pain Management Program Provided With Different Levels of Clinician Support. J Pain. 2018;19(12):1491-1503.
Ferwerda M, van Beugen S, van Middendorp H, et al. Tailored, Therapist-Guided Internet-Based Cognitive Behavioral Therapy Compared to Care as Usual for Patients With Rheumatoid Arthritis: Economic Evaluation of a Randomized Controlled Trial. J Med Internet Res. 2018;20(10):e260.
Guarino H, Fong C, Marsch LA, et al. Web-Based Cognitive Behavior Therapy for Chronic Pain Patients with Aberrant Drug-Related Behavior: Outcomes from a Randomized Controlled Trial. Pain Med. 2018;19(12):2423-2437.
Knoerl R, Barton DL, Holden JE, Krauss JC, LaVasseur B, Smith EML. Potential mediators of improvement in painful chemotherapy-induced peripheral neuropathy via a web-based cognitive behavioural intervention. Can Oncol Nurs J. 2018;28(3):178-183.
Knoerl R, Smith EML, Barton DL, et al. Self-Guided Online Cognitive Behavioral Strategies for Chemotherapy-Induced Peripheral Neuropathy: A Multicenter, Pilot, Randomized, Wait-List Controlled Trial. J Pain. 2018;19(4):382-394.
Mecklenburg G, Smittenaar P, Erhart-Hledik JC, Perez DA, Hunter S. Effects of a 12-Week Digital Care Program for Chronic Knee Pain on Pain, Mobility, and Surgery Risk: Randomized Controlled Trial. J Med Internet Res. 2018;20(4):e156.
Murphy SL, Janevic MR, Lee P, Williams DA. Occupational Therapist-Delivered Cognitive-Behavioral Therapy for Knee Osteoarthritis: A Randomized Pilot Study. The American journal of occupational therapy : official publication of the American Occupational Therapy Association. 2018;72(5):7205205040p7205205041-7205205040p7205205049.
Olason M, Andrason RH, Jonsdottir IH, Kristbergsdottir H, Jensen MP. Cognitive Behavioral Therapy for Depression and Anxiety in an Interdisciplinary Rehabilitation Program for Chronic Pain: a Randomized Controlled Trial with a 3-Year Follow-up. Int J Behav Med. 2018;25(1):55-66.
O'Moore K A, Newby JM, Andrews G, et al. Internet Cognitive-Behavioral Therapy for Depression in Older Adults With Knee Osteoarthritis: A Randomized Controlled Trial. Arthritis Care Res (Hoboken). 2018;70(1):61-70.
Rutledge T, Atkinson JH, Chircop-Rollick T, et al. Randomized Controlled Trial of Telephone-delivered Cognitive Behavioral Therapy Versus Supportive Care for Chronic Back Pain. Clin J Pain. 2018;34(4):322-327.
Scott W, Chilcot J, Guildford B, Daly-Eichenhardt A, McCracken LM. Feasibility randomized-controlled trial of online Acceptance and Commitment Therapy for patients with complex chronic pain in the United Kingdom. European Journal of Pain. 2018;28:28.
Simister HD, Tkachuk GA, Shay BL, Vincent N, Pear JJ, Skrabek RQ. Randomized Controlled Trial of Online Acceptance and Commitment Therapy for Fibromyalgia. J Pain. 2018;19(7):741-753.
Sullivan M, Langford DJ, Davies PS, et al. A Controlled Pilot Trial of PainTracker Self-Manager, a Web-Based Platform Combined With Patient Coaching, to Support Patients' Self-Management of Chronic Pain. J Pain. 2018;19(9):996-1005.
Taylor SS, Oddone EZ, Coffman CJ, Jeffreys AS, Bosworth HB, Allen KD. Cognitive Mediators of Change in Physical Functioning in Response to a Multifaceted Intervention for Managing Osteoarthritis. Int J Behav Med. 2018;25(2):162-170.
Wang Y, Lombard C, Hussain SM, et al. Effect of a low-intensity, self-management lifestyle intervention on knee pain in community-based young to middle-aged rural women: a cluster randomised controlled trial. Arthritis Res Ther. 2018;20(1):74.
An Internet-based intervention for chronic pain - A three-arm randomized controlled study of the effectiveness of guided and unguided acceptance and commitment therapy. Dtsch. 2017;114(41):681-688.
Ammerlaan J, van Os-Medendorp H, de Boer-Nijhof N, et al. Short term effectiveness and experiences of a peer guided web-based self-management intervention for young adults with juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2017;15(1):75.
Dear BF, Gandy M, Karin E, et al. The pain course: a randomised controlled trial comparing a remote-delivered chronic pain management program when provided in online and workbook formats. Pain. 2017;158(7):1289-1301.
Ferwerda M, van Beugen S, van Middendorp H, et al. A tailored-guided internet-based cognitive-behavioral intervention for patients with rheumatoid arthritis as an adjunct to standard rheumatological care: results of a randomized controlled trial. Pain. 2017;158(5):868-878.
Goldthorpe J, Lovell K, Peters S, et al. A Pilot Randomized Controlled Trial of a Guided Self-Help Intervention to Manage Chronic Orofacial Pain. J Oral Facial Pain Headache. 2017;31(1):61-71.
Lombardero A. Smoking cessation for patients in multidisciplinary pain treatment settings: A preliminary test of acceptance and commitment therapy. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2017;77(11-B(E)).
Mikocka-Walus A, Bampton P, Hetzel D, Hughes P, Esterman A, Andrews JM. Cognitive-Behavioural Therapy for Inflammatory Bowel Disease: 24-Month Data from a Randomised Controlled Trial. Int J Behav Med. 2017;24(1):127-135.
Uppsala University. NCT03316846: Internet-delivered Cognitive Behavioral Therapy for Patients With Chronic Pain and Psychiatric Distress. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/show/NCT03316846.
Yang SY, Moss-Morris R, McCracken LM. iACT-CEL: A Feasibility Trial of a Face-to-Face and Internet-Based Acceptance and Commitment Therapy Intervention for Chronic Pain in Singapore. Pain Res Treat. 2017;2017:6916915.
Ferwerda M, Van Beugen S, Van Riel PCLM, et al. Measuring the Therapeutic Relationship in Internet-Based Interventions. Psychother Psychosom. 2016;85(1):47-49.
McCombie A, Gearry R, Andrews J, Mulder R, Mikocka-Walus A. Does Computerized Cognitive Behavioral Therapy Help People with Inflammatory Bowel Disease? A Randomized Controlled Trial. Inflamm Bowel Dis. 2016;22(1):171-181.
Muller R, Gertz KJ, Molton IR, et al. Effects of a Tailored Positive Psychology Intervention on Well-Being and Pain in Individuals With Chronic Pain and a Physical Disability: A Feasibility Trial. Clin J Pain. 2016;32(1):32-44.
Noel M, Alberts N, Langer SL, Levy RL, Walker LS, Palermo TM. The Sensitivity to Change and Responsiveness of the Adult Responses to Children's Symptoms in Children and Adolescents With Chronic Pain. J Pediatr Psychol. 2016;41(3):350-362.
Palermo TM, Law EF, Fales J, Bromberg MH, Jessen-Fiddick T, Tai G. Internet-delivered cognitive-behavioral treatment for adolescents with chronic pain and their parents: a randomized controlled multicenter trial. Pain. 2016;157(1):174-185.
Beasley M, Prescott GJ, Scotland G, et al. Patient-reported improvements in health are maintained 2 years after completing a short course of cognitive behaviour therapy, exercise or both treatments for chronic widespread pain: long-term results from the MUSICIAN randomised controlled trial. RMD Open. 2015;1(1):e000026.
Buhrman M, Syk M, Burvall O, Hartig T, Gordh T, Andersson G. Individualized Guided Internet-delivered Cognitive-Behavior Therapy for Chronic Pain Patients With Comorbid Depression and Anxiety: A Randomized Controlled Trial. Clin J Pain. 2015;31(6):504-516.
Cuperus N, Hoogeboom TJ, Kersten CC, den Broeder AA, Vlieland TP, van den Ende CH. Randomized trial of the effectiveness of a non-pharmacological multidisciplinary face-to-face treatment program on daily function compared to a telephone-based treatment program in patients with generalized osteoarthritis. Osteoarthritis Cartilage. 2015;23(8):1267-1275.
DasMahapatra P, Chiauzzi E, Pujol LM, Los C, Trudeau KJ. Mediators and moderators of chronic pain outcomes in an online self-management program. Clin J Pain. 2015;31(5):404-413.
Dear BF, Gandy M, Karin E, et al. The Pain Course: a randomised controlled trial examining an internet-delivered pain management program when provided with different levels of clinician support. Pain. 2015;156(10):1920-1935.
Fales J, Palermo TM, Law EF, Wilson AC. Sleep outcomes in youth with chronic pain participating in a randomized controlled trial of online cognitive-behavioral therapy for pain management. Behav Sleep Med. 2015;13(2):107-123.
Garcia-Palacios A, Herrero R, Vizcaino Y, et al. Integrating virtual reality with activity management for the treatment of fibromyalgia: acceptability and preliminary efficacy. Clin J Pain. 2015;31(6):564-572.
Hutting N, Staal JB, Engels JA, Heerkens YF, Detaille SI, Nijhuis-van der Sanden MW. Effect evaluation of a self-management programme for employees with complaints of the arm, neck or shoulder: a randomised controlled trial. Occup Environ Med. 2015;72(12):852-861.
Law EF, Beals-Erickson SE, Noel M, Claar R, Palermo TM. Pilot Randomized Controlled Trial of Internet-Delivered Cognitive-Behavioral Treatment for Pediatric Headache. Headache. 2015;55(10):1410-1425.
Trompetter HR, Bohlmeijer ET, Fox JP, Schreurs KM. Psychological flexibility and catastrophizing as associated change mechanisms during online Acceptance & Commitment Therapy for chronic pain. Behav Res Ther. 2015;74:50-59.
Evers AWM, Gieler U, Hasenbring MI, Van Middendorp H. Incorporating biopsychosocial characteristics into personalized healthcare: A clinical approach. Psychother Psychosom. 2014;83(3):148-157.
Tierce-Hazard S, Sadarangani T. Optimizing the primary care management of chronic pain through telecare. J Clin Outcomes Manag. 2014;21(11):493-495.
Carmody TP, Duncan CL, Huggins J, et al. Telephone-delivered cognitive-behavioral therapy for pain management among older military veterans: a randomized trial. Psychol Serv. 2013;10(3):265-275.
Ammerlaan JW, Scholtus LW, Bijlsma HJ, Prakken BJ, Kruize AA. An urge for change: Transitional care for young adults with juvenile idiopathic arthritis. Patient Educ Couns. 2013;92(1):127-129.
Anonymous. The Cochrane Database of Systematic Reviews - Issue 10 2013. J Evid Based Med. 2013;6(4):305-306.
Kristjansdottir OB, Fors EA, Eide E, et al. A smartphone-based intervention with diaries and therapist feedback to reduce catastrophizing and increase functioning in women with chronic widespread pain. part 2: 11-month follow-up results of a randomized trial. J Med Internet Res. 2013;15(3):e72.
Kristjansdottir OB, Fors EA, Eide E, et al. A smartphone-based intervention with diaries and therapist-feedback to reduce catastrophizing and increase functioning in women with chronic widespread pain: randomized controlled trial. J Med Internet Res. 2013;15(1):e5.
Kroenke K. Telephone-based cognitive-behavioural therapy and a structured exercise programme are effective for chronic widespread pain (fibromyalgia). Evid Based Med. 2013;18(1):23-24.
McBeth J, Prescott G, Scotland G, et al. Cognitive behavior therapy, exercise, or both for treating chronic widespread pain. Arch Intern Med. 2012;172(1):48-57.
Ruehlman LS, Karoly P, Enders C. A randomized controlled evaluation of an online chronic pain self management program. Pain. 2012;153(2):319-330.
Buhrman M, Nilsson-Ihrfeldt E, Jannert M, Strom L, Andersson G. Guided internet-based cognitive behavioural treatment for chronic back pain reduces pain catastrophizing: a randomized controlled trial. J Rehabil Med. 2011;43(6):500-505.
Linkoeping University. NCT01329861: Internet-based Cognitive Behavioural Treatment for Chronic Back Pain. ClinicalTrials.gov. Bethesda (MD): US National Library of Medicine; 2011: https://clinicaltrials.gov/show/NCT01329861.
Oerlemans S, van Cranenburgh O, Herremans P-J, Spreeuwenberg P, van Dulmen S. Intervening on cognitions and behavior in irritable bowel syndrome: A feasibility trial using PDAs. J Psychosom Res. 2011;70(3):267-277.
Ang DC, Chakr R, Mazzuca S, France CR, Steiner J, Stump T. Cognitive-behavioral therapy attenuates nociceptive responding in patients with fibromyalgia: a pilot study. Arthritis Care Res (Hoboken). 2010;62(5):618-623.
Landy SH. A randomized controlled trial of Internet-based self-help training for recurrent headache in children and adolescents: comments. Headache. 2010;50(7):1227-1228.
Moss-Morris R, McAlpine L, Didsbury L, Spence M. A randomized controlled trial of a cognitive behavioural therapy-based self-management intervention for irritable bowel syndrome in primary care. Psychol Med. 2010;40(1):85-94.
Naylor MR, Naud S, Keefe FJ, Helzer JE. Therapeutic Interactive Voice Response (TIVR) to reduce analgesic medication use for chronic pain management. J Pain. 2010;11(12):1410-1419.
Stinson JN, McGrath PJ, Hodnett ED, et al. An internet-based self-management program with telephone support for adolescents with arthritis: a pilot randomized controlled trial. J Rheumatol. 2010;37(9):1944-1952.
Trautmann E, Kroner-Herwig B. A randomized controlled trial of Internet-based self-help training for recurrent headache in childhood and adolescence. Behav Res Ther. 2010;48(1):28-37.
Williams DA, Kuper D, Segar M, Mohan N, Sheth M, Clauw DJ. Internet-enhanced management of fibromyalgia: a randomized controlled trial. Pain. 2010;151(3):694-702.
Palermo TM, Wilson AC, Peters M, Lewandowski A, Somhegyi H. Randomized controlled trial of an Internet-delivered family cognitive-behavioral therapy intervention for children and adolescents with chronic pain. Pain. 2009;146(1-2):205-213.
Jerant A, Moore M, Lorig K, Franks P. Perceived control moderated the self-efficacy-enhancing effects of a chronic illness self-management intervention. Chronic Illn. 2008;4(3):173-182.
Lorig KR, Ritter PL, Laurent DD, Plant K. The internet-based arthritis self-management program: a one-year randomized trial for patients with arthritis or fibromyalgia. Arthritis Rheum. 2008;59(7):1009-1017.
Nguyen HQ, Donesky-Cuenco D, Wolpin S, et al. Randomized controlled trial of an internet-based versus face-to-face dyspnea self-management program for patients with chronic obstructive pulmonary disease: pilot study. J Med Internet Res. 2008;10(2):e9.
Trautmann E, Kroner-Herwig B. Internet-based self-help training for children and adolescents with recurrent headache: A pilot study. Behav Cogn Psychother. 2008;36(2):241-245.
Schulz PJ, Rubinell S, Hartung U. An internet-based approach to enhance self-management of chronic low back pain in the italian-speaking population of Switzerland: results from a pilot study. Int J Public Health. 2007;52(5):286-294.
Connelly MA. 'Headstrong': A computer-based cognitive-behavioral intervention for recurrent pediatric headache. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2005;65(11-B):6040.
Ehde DM, Jensen MP. Feasibility of a cognitive restructuring intervention for treatment of chronic pain in persons with disabilities. Rehabil Psychol. 2004;49(3):254-258.
Ahles TA, Seville J, Wasson J, Johnson D, Callahan E, Stukel TA. Panel-based pain management in primary care. a pilot study. J Pain Symptom Manage. 2001;22(1):584-590.
Irrelevant Study Design or Format (n = 2)
Heapy AA, Driscoll MA, Buta E, et al. Co-Operative Pain Education and Self-management (COPES) Expanding Treatment for Real-World Access (ExTRA): Pragmatic Trial Protocol. Pain Med. 2020;21(12 Suppl 2):S21-S28.
Domenech J, Banos R, Penalver L, et al. Design considerations of a randomized clinical trial on a cognitive behavioural intervention using communication and information technologies for managing chronic low back pain. BMC Musculoskelet Disord. 2013;14:142.
Appendix 5: Survey Questions
Note that this appendix has not been copy-edited.
iCBT for Chronic Pain Survey
General
In which jurisdiction do you primarily work?
Alberta
British Columbia
Manitoba
New Brunswick
Newfoundland and Labrador
Northwest Territories
Nova Scotia
Nunavut
Ontario
Prince Edward Island
Quebec
Saskatchewan
Yukon
Federal
Other (please specify):
Do you work in 1 or more of these settings? (Please select all that apply)
Pain clinic
Primary care clinic
Hospital or specialist clinic
Long-term care facility
Health authority
Provincial ministry of health
Other (please specify):
What is your profession or role? (Please select all that apply)
Health care provider (e.g., nurse, therapist, physician)
Hospital or health facility administrator (e.g., director or manager)
Software or online platform developer
Technical services personnel (e.g., technician or information technologist)
Researcher
Policy-maker
Public funder
Private insurance or Employee Assistance Program (EAP) representative
Other (please specify):
What level of involvement do you have with iCBT programs that support people living with chronic non-cancer pain? (Please select all that apply)
Involved in the delivery of 1 or more iCBT program(s)
Involved in the development of 1 or more iCBT program(s)
Involved in the funding or regulation of 1 or more iCBT program(s)
None of the above
Please specify the name of the iCBT program you are involved with and if possible, a URL to the website:
Does the iCBT program you are involved with provide care to patients in 1 or more of these geographical settings? (Please select all that apply)
Note: Health Canada defines various levels of remote, ranging from remote isolated (i.e., no scheduled flights or road access and minimal telephone or radio service) through to non-isolated remote (i.e., road access and less than 90 km away from physician service).
Urban (i.e., area with a population of at least 1,000 and a population density of at least 400 persons per square kilometre)
Rural (i.e., not fitting the definition of “urban” or “remote”)
Remote (please self-identify based on your local understanding of the aforementioned criteria)
iCBT Program Characteristics
The following questions pertain to the iCBT program for the management of chronic non-cancer pain that you are involved with (through development, delivery, funding, or regulation).
Are patients with chronic non-cancer pain associated with the following health conditions eligible for the iCBT program? (Please select all that apply)
Fibromyalgia
Headache or migraine
Muscle and ligament injuries
Neuropathic pain
Rheumatoid arthritis
Osteoarthritis
Multiple sclerosis
Pelvic pain
Low back pain
Abdominal pain
Other (please specify):
Please specify the age range of participants who are eligible for the iCBT program.
How is the iCBT program currently being utilized? (Please select all that apply)
Self-referral by patients
Referral by a clinician
As 1 component of a broader program
As a complement to standard care
As a stand-alone treatment
Other (please specify):
Not applicable
Is the iCBT program self-guided or therapist assisted?
Self-guided
Therapist assisted
Therapist directed
Other (please specify):
Not applicable
Please specify the level of therapist involvement. (e.g., pre-scheduled calls, as-needed support, delivery of the iCBT program, etc.)
What are the required credentials and/or training for the therapists?
Was the iCBT program co-developed with people with lived experience with chronic non-cancer pain?
Yes
No
Not applicable
How many weeks does it take to complete the iCBT program?
How many modules are included in the iCBT program?
Please list the modules, topics covered, and approximate time it takes to complete each module.
What are the technology requirements for the iCBT program (e.g., internet connection, device requirements, etc.)?
What is the funding model of the iCBT program?
Public
Not-for-profit
Private/for-profit
Other (please specify):
Not applicable
How is the iCBT program reimbursed for patients?
Patients pay out-of-pocket
Publicly funded
Privately funded (i.e., through private insurance)
Other (please specify):
Not applicable
Implementation Considerations – Facilitators
What patient-related factors have facilitated or would facilitate the implementation of iCBT in your facility or jurisdiction? (Please select all that apply)
Privacy (compared with face-to-face CBT)
Insurance coverage and reimbursement
Other financial benefits (e.g., transportation cost savings, not missing work)
Preference (over face-to-face CBT)
Clinical effectiveness
Satisfaction with care (including educational materials and follow-up support)
Recommended by a health care provider
Access (e.g., 24-hour availability of care, access from any place with internet connectivity including rural or remote settings)
Convenience (e.g., does not require taking time off work or school and can access outside of regular business hours)
Involves greater self-management
Option for choice of language of instruction
Absence of feasible alternatives (have not benefited from other types of services)
Other (please specify):
Do not know
What clinician-related factors have facilitated or would facilitate the implementation of iCBT in your facility or jurisdiction? (Please select all that apply)
Efficiency in clinical practice (e.g., allows clinician to care for more patients)
Financial benefits (e.g., additional income if reimbursed)
Preference for this treatment option over other forms of therapy
Reaching patients that would otherwise be unreachable
Therapy fits into patient’s routine schedule
Desire to improve skills
Training, knowledge, or experience with iCBT
Other (please specify):
Do not know
What organizational factors have facilitated or would facilitate the implementation of iCBT in your facility or jurisdiction? (Please select all that apply)
Within mandate or policy
Allows more efficient use of resources
Improvement in patients’ experiences
Improvement in clinicians’ experiences
Financial benefit (e.g., return on investment if reimbursed)
Reaching more patients or serving a broader population (including patients in rural and remote areas)
Commitment to improving services
Easier option to track outcomes
Interest of funders in technology-based solutions
Other (please specify):
Do not know
Do you have any additional comments about factors that facilitated or would facilitate the implementation of iCBT?
Implementation Considerations – Barriers
What patient-related factors have you or your organization identified as barriers to the implementation of iCBT? (Please select all that apply)
Privacy concerns (e.g., unable to access iCBT in a private location)
Preference for in-person or other treatment options
Negative perceptions about effectiveness
Financial issues (e.g., lack of coverage/reimbursement, cost of internet access)
Lack of knowledge about iCBT
Unfamiliar with technology
Lack of available devices or adequate connection to the internet
Difficulty understanding the program (because of limited reading and writing skills)
Limited availability in options for language instruction
Higher severity and complexity of diagnosis
Other (please specify):
Do not know
What clinician-related factors have you or your organization identified as barriers to the implementation of iCBT? (Please select all that apply)
Professional liability
Preference for in-person treatment or other treatment options
Lack of education or training on iCBT and delivering services via distance
Financial losses (e.g., inadequate compensation)
Lack of available devices or adequate connection to the internet
Difficulty using the program (because of limited computer skills)
Other (please specify):
Do not know
What organizational factors have you or your organization identified as barriers to the implementation of iCBT? (Please indicate relevant examples, e.g., time, funds, devices, personnel, internet connectivity in the text box below)
Not within mandate or lack of relevant policies and procedures on how to deliver iCBT
Legal issues/liability
Organizational culture
Resources (please indicate relevant examples, e.g., time, funds, devices, personnel, internet connectivity)
Other (please specify):
Do not know
Do you have any additional comments about barriers to the implementation of iCBT?
Implementation Considerations – Access
When considering access to iCBT programs, are there any patient groups that require specific considerations (e.g., patients living in rural or remote settings, patients that belong to a marginalized group)? If yes, please specify the patient group(s).
Are there any specific facilitators to accessing iCBT for these patients?
Are there any specific barriers to accessing iCBT for these patients?
General
Can you suggest any other individuals who (or organizations that) would be willing to be consulted further on this topic, and/or complete this survey?
Appendix 6: Information on Survey Respondents
Note that this appendix has not been copy-edited.
Table 37: Characteristics of Survey Respondents
Survey question | Response | Number of responses (% of total) |
|---|---|---|
In which jurisdiction do you primarily work? (13 total responses) | Alberta | 4 (30.8%) |
British Columbia | 1 (7.7%) | |
Manitoba | 0 | |
New Brunswick | 0 | |
Newfoundland and Labrador | 1 (7.7%) | |
Northwest Territories | 0 | |
Nova Scotia | 1 (7.7%) | |
Nunavut | 0 | |
Ontario | 4 (30.8%) | |
Prince Edward Island | 0 | |
Quebec | 1 (7.7%) | |
Saskatchewan | 1 (7.7%) | |
Yukon | 0 | |
Other | 0 | |
Do you work in 1 or more of these settings? (13 total responses, multiple answers accepted) | Pain clinic | 6 (46.1%) |
Primary care clinic | 0 | |
Hospital or specialist clinic | 6 (46.1%) | |
Long-term care facility | 0 | |
Health authority | 1 (7.7%) | |
Provincial ministry of health | 0 | |
Othera | 7 (53.8%) | |
What is your profession or role? (13 total responses, multiple answers accepted) | Hospital or health facility administrator (e.g., director or manager) | 2 (15.4%) |
Health care provider (e.g., nurse, therapist, physician) | 6 (46.1%) | |
Software or online platform developer | 1 (7.7%) | |
Technical services personnel (e.g., technician or information technologist) | 0 | |
Researcher | 5 (38.5%) | |
Policy-maker | 0 | |
Public funder | 0 | |
Private insurance or Employee Assistance Program (EAP) representative | 0 | |
Otherb | 5 (38.5%) | |
What level of involvement do you have with iCBT programs that support people living with chronic non-cancer pain? (Please select all that apply) (13 total responses, multiple answers accepted) | Involved in the delivery of 1 or more iCBT program(s) | 9 (69.2%) |
Involved in the development of 1 or more iCBT program(s) | 9 (69.2%) | |
Involved in the funding or regulation of 1 or more iCBT program(s) | 0 | |
None of the above | 0 |
aResponses included: research lab affiliated with pain clinic, Online Therapy Unit clinic, private clinic, academic/research/private practice, university, digital mental health provider.
bResponses included: completing survey on behalf of clinician/scientist, psychologist, professor/psychologist/researcher, public sector business development.
Appendix 7: Survey Results
Note that this appendix has not been copy-edited.
Table 38: Use of iCBT Programs for Chronic Non-Cancer Pain in Canada
Response | Number of responses (% of total)a |
|---|---|
Self-referral by patients | 5 (45.4%) |
Referral by a clinician | 7 (63.6%) |
As 1 component of a broader program | 6 (54.5%) |
As a complement to standard care | 3 (27.3%) |
As a stand-alone treatment | 6 (54.5%) |
Otherb | 3 (27.3%) |
Not applicable | 0 |
iCBT = internet-delivered cognitive behavioural therapy.
a11 total responses, multiple answers accepted.
bResponses included: stay at/return to work; disability management; clinical trial/research study.
Table 39: Characteristics of iCBT Programs for Chronic Pain Available or in Development in Canada
Survey question | Response | Number of responses (% of total) |
|---|---|---|
Is the iCBT program self-guided or therapist assisted? (11 total responsesa) | Self-guided | 2 (18.2%) |
Therapist assisted | 7 (63.6%) | |
Therapist directed | 3 (27.3%) | |
Other | 0 | |
Not applicable | 0 | |
Was the iCBT program co-developed with people with lived experience with chronic non-cancer pain? (11 total responses) | Yes | 6 (54.5%) |
No | 5 (45.4%) | |
Not applicable | 0 | |
What is the funding model of the iCBT program? (11 total responses) | Public | 6 (54.5%) |
Not-for-profit | 2 (18.2%) | |
Private/for-profit | 0 | |
Otherb | 3 (27.3%) | |
Not applicable | 0 | |
How is the iCBT program reimbursed for patients? (11 total responses) | Patients pay out-of-pocket | 0 |
Publicly funded | 6 (54.5%) | |
Privately funded (i.e., through private insurance) | 0 | |
Otherc | 3 (27.3%) | |
Not applicable | 2 (18.2%) |
iCBT = internet-delivered cognitive behavioural therapy.
aOne respondent indicated that the program was both self-guided and therapist assisted.
bResponses included: combination of public and private; research grant; publicly funded in Ontario and privately funded elsewhere.
cResponses included: no cost; no upfront cost if publicly funded and reimbursed if covered by insurance; publicly funded in Ontario and privately funded through extended health benefits and employers elsewhere.
Table 40: Facilitators to the Implementation of iCBT for Chronic Pain in Canada
Survey question | Response | Number of responses (% of total) |
|---|---|---|
What patient-related factors have facilitated or would facilitate the implementation of iCBT in your facility or jurisdiction? (11 total responses, multiple answers accepted) | Privacy (compared with face-to-face CBT) | 5 (45.4%) |
Insurance coverage and reimbursement | 2 (18.2%) | |
Other financial benefits (e.g., transportation cost savings, not missing work) | 8 (72.7%) | |
Preference (over face-to-face CBT) | 9 (81.8%) | |
Clinical effectiveness | 8 (72.7%) | |
Satisfaction with care (including educational materials and follow-up support) | 9 (81.8%) | |
Recommended by a health care provider | 6 (54.5%) | |
Access (e.g., 24-hour availability of care, access from any place with internet connectivity including rural or remote settings) | 9 (81.8%) | |
Convenience (e.g., does not require taking time off work or school and can access outside of regular business hours) | 10 (90.9%) | |
Involves greater self-management | 7 (63.6%) | |
Option for choice of language of instruction | 3 (27.3%) | |
Absence of feasible alternatives (have not benefited from other types of services) | 5 (45.4%) | |
Othera | 3 (27.3%) | |
Do not know | 0 | |
What clinician-related factors have facilitated or would facilitate the implementation of iCBT in your facility or jurisdiction? (11 total responses, multiple answers accepted) | Efficiency in clinical practice (e.g., allows clinician to care for more patients) | 10 (90.9%) |
Financial benefits (e.g., additional income if reimbursed) | 3 (27.3%) | |
Preference for this treatment option over other forms of therapy | 6 (54.5%) | |
Reaching patients that would otherwise be unreachable | 11 (100%) | |
Therapy fits into patient’s routine schedule | 8 (72.7%) | |
Desire to improve skills | 7 (63.6%) | |
Training, knowledge, or experience with iCBT | 9 (81.8%) | |
Otherb | 1 (9.1%) | |
Do not know | 0 | |
What organizational factors have facilitated or would facilitate the implementation of iCBT in your facility or jurisdiction? (11 total responses, multiple answers accepted) | Within mandate or policy | 8 (72.7%) |
Allows more efficient use of resources | 10 (90.9%) | |
Improvement in patients’ experiences | 11 (100%) | |
Improvement in clinicians’ experiences | 8 (72.7%) | |
Financial benefit (e.g., return on investment if reimbursed) | 2 (18.2%) | |
Reaching more patients or serving a broader population (including patients in rural and remote areas) | 9 (81.8%) | |
Commitment to improving services | 8 (72.7%) | |
Easier option to track outcomes | 6 (54.5%) | |
Interest of funders in technology-based solutions | 6 (54.5%) | |
Otherc | 1 (9.1%) | |
Do not know | 0 |
iCBT = internet-delivered cognitive behavioural therapy.
aResponses included: all the listed facilitators exist to varying degrees; COVID risk; difficulty accessing platform.
bResponse: interoperability; comorbidity with other mental health conditions; stepped care integration.
cResponse: billing code; centralized intake; collection of outcome measures.
Table 41: Barriers to the Implementation of iCBT for Chronic Pain in Canada
Survey question | Response | Number of responses (% of total) |
|---|---|---|
What patient-related factors have you or your organization identified as barriers to the implementation of iCBT? (11 total responses, multiple answers accepted) | Privacy concerns (e.g., unable to access iCBT in a private location) | 9 (81.8%) |
Preference for in-person or other treatment options | 8 (72.7%) | |
Negative perceptions about effectiveness | 5 (45.4%) | |
Financial issues (e.g., lack of coverage/reimbursement, cost of internet access) | 4 (36.4%) | |
Lack of knowledge about iCBT | 5 (45.4%) | |
Unfamiliar with technology | 8 (72.7%) | |
Lack of available devices or adequate connection to the internet | 8 (72.7%) | |
Difficulty understanding the program (because of limited reading and writing skills) | 4 (36.4%) | |
Limited availability in options for language instruction | 5 (45.4%) | |
Higher severity and complexity of diagnosis | 5 (45.4%) | |
Othera | 2 (18.2%) | |
Do not know | 0 | |
What clinician-related factors have you or your organization identified as barriers to the implementation of iCBT? (11 total responses, multiple answers accepted) | Professional liability | 2 (18.2%) |
Preference for in-person treatment or other treatment options | 9 (81.8%) | |
Lack of education or training on iCBT and delivering services via distance | 7 (63.6%) | |
Financial losses (e.g., inadequate compensation) | 2 (18.2%) | |
Lack of available devices or adequate connection to the internet | 3 (27.3%) | |
Difficulty using the program (because of limited computer skills) | 3 (27.3%) | |
Otherb | 4 (36.4%) | |
Do not know | 1 (9.1%) | |
What organizational factors have you or your organization identified as barriers to the implementation of iCBT? (11 total responses, multiple answers accepted) | Not within mandate or lack of relevant policies and procedures on how to deliver iCBT | 3 (27.3%) |
Legal issues/liability | 2 (18.2%) | |
Organizational culture | 5 (45.4%) | |
Resources (please indicate relevant examples, e.g., time, funds, devices, personnel, internet connectivity) | 5 (45.4%) | |
Otherc | 6 (54.5%) | |
Do not know | 1 (9.1%) |
iCBT = internet-delivered cognitive behavioural therapy.
aResponses included: patient hesitation due to virtual mental health care being a relatively new modality; employers may think employee assistance programs are sufficient; confusion with other virtual services that are not as rigorous; centralized intake.
bResponses included: patient hesitation given relatively new modality; threat to livelihood; dissonance of multiple platforms that have emerged; patients not as engaged and/or distracted; learning curve to use new virtual technology; clinicians do not face barriers to using iCBT due to convenience as well as compensation and resources provided.
cResponses included: shortage of psychologists/assessors; restrictive policies for fee for service/hourly and do not recognize added value of platform; COVID policies; resource for technology; centralized intake versus self-referral; providers do not have computers with cameras/microphones; lack of funds to advertise and increase uptake.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca