CADTH Health Technology Review
Cost-Effectiveness of Conjugate Pneumococcal Vaccines in At-Risk Adults Aged 18 to 64 Years
Technology Review
Abbreviations
CDC
US Centers for Disease Control and Prevention
CKD
chronic kidney disease
COPD
chronic obstructive pulmonary disease
CSF
cerebrospinal fluid
ICER
incremental cost-effectiveness ratio
IPD
invasive pneumococcal disease
JBI
Joanna Briggs Institute
NBP
nonbacteremic pneumonia
NPP
nonbacteremic pneumococcal pneumonia
OECD
Organisation for Economic Co-operation and Development
PCV9
pneumococcal 9-valent conjugate vaccine
PCV13
pneumococcal 13-valent conjugate vaccine
PCV15
pneumococcal 15-valent conjugate vaccine
PCV20
pneumococcal 20-valent conjugate vaccine
PCV21
pneumococcal 21-valent conjugate vaccine
PPSV23
pneumococcal polysaccharide 23-valent vaccine
QALY
quality-adjusted life-year
WTP
willingness to pay
Key Messages
Eight economic evaluations (6 peer-reviewed, 2 summarized in a single grey literature source) assessing the cost-effectiveness of pneumococcal conjugate vaccines in adults aged 18 to 64 years at high risk of invasive pneumococcal disease (IPD) in high-income countries were identified.
The 2 economic evaluations summarized in the single grey literature source were industry-sponsored analyses. A version of the results was previously summarized by the Public Health Agency of Canada. As such, the methods and results of the industry-funded models are only summarized in Appendix 3 for this review.
None of the peer-reviewed studies identified assessed the cost-effectiveness of pneumococcal 15-valent conjugate vaccine (PCV15), pneumococcal 20-valent conjugate vaccine (PCV20), or pneumococcal 21-valent conjugate vaccine (PCV21).
Of the peer-reviewed studies, 2 were conducted in the US, 2 in South Korea, 1 in Spain, and 1 in Hong Kong. All results were presented in terms of incremental cost-effectiveness ratios (ICERs) (i.e., incremental cost per quality-adjusted life-years gained).
Four studies concluded that 1 dose of pneumococcal 13-valent conjugate vaccine (PCV13) was cost-effective relative to either no vaccination, 2 doses of PCV13, PCV13 plus 2 doses of pneumococcal polysaccharide 23-valent vaccine (PPSV23), or 2 doses of PPSV23.
Two studies concluded that PCV13 plus PPSV23 was cost-effective relative to either no vaccination or 1 dose of PPSV23, but the studies did not evaluate the cost-effectiveness of PCV13 alone.
The studies did not all consider the same vaccination strategies.
The sources used to parameterize vaccine effectiveness in the peer-reviewed studies are highly uncertain, as the clinical evidence was either not representative of the target population or heavily reliant on expert input and assumptions.
The generalizability of the economic evaluations may be limited because the study settings were notably different from Canada. To estimate the potential cost-effectiveness of pneumococcal conjugate vaccines in Canada, a de novo economic evaluation conducted from a setting is Canada is required.
Introduction and Rationale
Background and Rationale
Pneumococcal conjugate vaccines are used to prevent complications from infection with the bacterium Streptococcus pneumoniae, which occurs most frequently among young children aged younger than 5 years, particularly those younger than 2, adults aged 65 years and older, and others who are considered to be at high risk of IPD.1,2 Individuals at high risk of IPD, as defined by the Public Health Agency of Canada in Appendix 1, Table 2, include those with certain nonimmunocompromising conditions, immunocompromising conditions, and/or other risk factors.1 Pneumococcal infections most commonly occur in the spring and winter and are a large contributor to morbidity and mortality, as infections can lead to pneumonia, meningitis, and bloodstream infections.3,4 Infections with antibiotic-resistant Streptococcus pneumoniae can increase the complexity and costs of treatment compared with infections caused by nonresistant pneumococcus, and pneumococcal vaccination is an effective tool for slowing the development of pneumococcal resistance.5 Therefore, using vaccines as a preventive measure is important not only from a public health perspective, but also from a health system perspective, as the use of the vaccines may aid in reducing future use of health care resources.
Currently, 3 pneumococcal conjugate vaccines and 1 pneumococcal polysaccharide vaccine available in Canada are indicated for use in adults:
pneumococcal 13-valent conjugate vaccine (PCV13) (Prevnar 13)
pneumococcal 15-valent conjugate vaccine (PCV15) (Vaxneuvance)
pneumococcal 20-valent conjugate vaccine (PCV20) (Prevnar 20)
pneumococcal polysaccharide 23-valent vaccine (PPSV23) (Pneumovax 23).
Appendix 1, Table 3 and Table 4 provide a comparison of the respective vaccine manufacturers, dates of initial authorization in Canada, vaccine type, adult dosage, indicated age, Health Canada indication, price per dose, and serotypes included in the respective vaccines. At the time of this review, a new pneumococcal conjugate vaccine, PCV21, is under review by Health Canada.6
At the time of this review, the National Advisory Committee on Immunization recommended adults at higher risk of IPD receive a single dose of PCV20, or, if PCV20 is unavailable, a single dose of PCV15 followed by a single dose of PPSV23.7
This review of literature was requested by the Public Health Agency of Canada to support a National Advisory Committee on Immunization statement on the use of pneumococcal vaccines in adults.
Research Question
What is the cost-effectiveness of pneumococcal conjugate vaccination in adults aged 18 to 64 years at high risk of IPD?
Methods
A review of the economic literature was undertaken to identify published economic evidence on the cost-effectiveness of the use of pneumococcal conjugate vaccination (i.e., PCV13, PCV15, PCV20, and PCV21) relative to no vaccination or other pneumococcal vaccination in adults aged 18 to 64 years at high-risk of IPD in high-income countries.
Literature Search Methods
An information specialist conducted a literature search on key databases, including MEDLINE, Embase, and the Cochrane Database of Systematic Reviews. Grey literature was also searched, including the International HTA Database, the websites of Canadian and major international health technology agencies, websites from the health economics section of CADTH’s Grey Matters: A Practical Tool for Searching Health-Related Grey Literature, as well as a focused internet search, including the websites of National Immunization Technical Advisory Groups. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were pneumococcal vaccines, adults, and high-income countries. CADTH-developed search filters were applied to limit retrieval to economic studies and, for background, health technology assessments, systematic reviews, meta-analyses, and indirect treatment comparisons. The search was completed on February 22, 2024, and limited to English- or French-language documents published since January 1, 2011. Retrieval was limited to the human population. Regular alerts updated the search until May 13, 2024.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults aged 18 to 64 years at high riska of invasive pneumococcal disease |
Intervention | Pneumococcal conjugate vaccination (i.e., PCV13, PCV15, PCV20, and PCV21) or a pneumococcal conjugate vaccine plus a pneumococcal polysaccharide vaccination (i.e., PPSV23) |
Comparators | No vaccination (i.e., placebo, no intervention) or other pneumococcal vaccination |
Outcomes | QALYs, disability-adjusted life-years, incremental costs and incremental cost-effectiveness ratio (e.g., cost per QALY gained or incremental cost per event or event avoided), net monetary benefit, net health benefit |
Study designs | Full economic evaluations (e.g., cost-minimization analysis, cost-consequence analyses, cost-effectiveness analyses, cost-utility analyses), health technology assessments, and systematic reviews |
PCV13 = pneumococcal conjugate 13-valent; PCV15 = pneumococcal 15-valent conjugate vaccine; PCV20 = pneumococcal 20-valent conjugate vaccine; PCV21 = 21-valent pneumococcal conjugate vaccine; PPSV23 = pneumococcal polysaccharide 23-valent; QALY = quality-adjusted life-year.
aRefer to Appendix 1, Table 2, for a list of high-risk factors, as defined by the Public Health Agency of Canada.
Exclusion Criteria
Studies were excluded if they:
did not meet the inclusion criteria outlined in Table 1
were duplicate publications
were published in languages other than English or French
were not conducted in countries identified as high income by the World Bank8
were systematic reviews whose primary cost-effectiveness studies were otherwise captured or excluded
were published before 2011
had insufficient information to include and did not have full-text available.
Data Extraction and Critical Appraisal
During data extraction, the following were collected: author, publication year, country, currency, source of funding, study design, modelling approach, study perspective, discounting, time horizon, outcomes, source of clinical efficacy, study population characteristics, and results. The quality of the included studies was critically appraised by 1 reviewer using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Economic Evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Cost-effectiveness outcomes were reported as unadjusted and adjusted. Where adjusted, outcomes were adjusted to 2024 Canadian dollars using Organisation for Economic Co-operation and Development (OECD)9 purchasing power parity rates and inflation rates from the Bank of Canada.10 Appendix 1, Table 5 details the purchasing power parity rates and inflation rates used to adjust monetary amounts to 2024 Canadian dollars.
Summary of Evidence
Quantity of Research Available
A total of 1,917 citations were identified in the literature search. Following the screening of titles and abstracts, 1,794 citations were excluded and 123 potentially relevant publications from the electronic search were retrieved for full-text review. In addition, 10 potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant publications, 126 were excluded for various reasons, leading to 7 publications that met the inclusion criteria and were included in this review. Eight economic evaluations that met the inclusion criteria were identified: 6 were original peer-reviewed economic evaluations,11-16 and 2 were summarized in a single grey literature source.17 Appendix 4, (Figure 1) presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow chart of the publication selection and reasons for exclusions.
The grey literature source (Kobayashi et al.) was a report published by the US Centers for Disease Control and Prevention (CDC), which included a summary of 3 economic models.17 The report compared 2 industry-funded models (1 produced by Merck and 1 produced by Pfizer) and a third economic model, termed the Tulane-CDC model.17 The Tulane-CDC model did not meet the inclusion criteria for this review and was thus not summarized.17 The 2 industry-funded economic evaluations described in Kobayashi et al.17 met the inclusion criteria and are only summarized in Appendix 3 of this review, as a version of the aforementioned economic evaluations were summarized previously by the Public Health Agency of Canada.7,18 Therefore, only the 6 peer-reviewed studies are summarized in the main text of this review.11-16
Of the modeling types used in the 6 peer-reviewed studies summarized in this review, there were 5 Markov models11-14,16 and 1 did not state the model structure, only that a sequential deterministic model was used.15 Two studies were conducted in the US,13,16 2 in South Korea,11,12 1 in Spain,14 and 1 in Hong Kong.15 All of the peer-reviewed studies included either PCV13 alone or 1 dose of PCV13 used in series with PPSV23 (i.e., PCV13 plus PPSV23) as the intervention.11-16 None of the peer-reviewed studies included PCV15, PCV20, or PCV21 as an intervention or comparator. Table 6 in Appendix 2 provides an overview of the characteristics of the 6 peer-reviewed studies.
Summary of Critical Appraisal
The 6 peer-reviewed studies included in this review ranged from meeting 3 to 6 out of 11 of the JBI Critical Appraisal Checklist criteria (Appendix 2, Table 7) regarding study quality and applicability to adults aged 18 to 64 years at high-risk of IPD. None of the publications included all issues of concern to users (e.g., none considered the cost-effectiveness of all the interventions of interest). It was unclear whether the economic evaluations were generalizable to the population in Canada because they were conducted in health care settings or countries dissimilar from Canada. Moreover, in 4 studies,12-15 PCV13 efficacy was primarily informed by the CAPiTA trial for the populations relevant to this review. Notably, the CAPiTA trial was restricted to adults aged 65 years and older who did not have an immune deficiency or suppression at time of enrolment.19 As the clinical evidence was not representative of the target population, clinical effectiveness in the population of interest for this review was not established. There is also uncertainty as to whether outcomes were measured accurately and valued credibly. No studies were excluded on the basis of these appraisals.
Funding Sources of Examined Literature
Among the 6 peer-reviewed studies, 3 did not receive any industry funding12,13,16 and the remaining 3 studies reported receiving funding from Pfizer.11,14,15 Notably, 2 authors from 1 study14 were employees of Pfizer, and authors from 2 studies15,16 reported previously receiving research funding for work unrelated to the published study.
Summary of Findings
As stated previously, as the results included in Kobayashi et al.17 were previously summarized,7,18 this section describes only the 6 peer-reviewed studies.11-16 The inputs for the peer-reviewed studies discussed in this section are also summarized in a series of tables in Appendix 2.11-16 Study characteristics and results for the 2 economic evaluations included in Kobayashi et al. are summarized in Appendix 3, Table 14 and Table 15.17
Methods
Population
The population risk factors included across the studies varied widely and are summarized in Appendix 2, Table 6. As studies may have included multiple target populations, only those relevant to this review are summarized.
Four studies had broader risk definitions and included multiple risk factors.11,12,15,16 Shami et al. included individuals with a history of IPD, which was not identified as a risk factor by the Public Health Agency of Canada (Table 2).7 This study was not excluded on this basis, as a history of IPD was not deemed to represent a significant source of heterogeneity in the target population.7,15 Two studies were specific to single chronic conditions (i.e., chronic kidney disease [CKD]13 and chronic obstructive pulmonary disease [COPD]).14 Smith et al. included a secondary analysis that was specific to individuals living with HIV.16
The age of the target population differed across studies. Four studies (Heo et al., Ishigami et al., Rodriguez Gonzalez-Moro et al., and Shami et al.) reported results for adults aged 50 to 64 years.12-15 Choi et al. reported results for adults aged 18 to 64 years,11 Smith et al. reported results for adults aged 19 to 64 years,16 and Shami et al. also reported results for a broader age range, consisting of adults aged 20 to 64 years.15
Perspective, Time Horizon, Discounting, and Reported Outcomes
Perspective, time horizon, and discounting inputs are summarized in Appendix 2, Table 6. Three studies (Choi et al., Ishigami et al., and Rodriguez Gonzalez-Moro et al.) were conducted from a health care payer perspective,11,13,14 and 3 studies (Heo et al., Shami et al., Smith et al.) were conducted from a societal perspective.12,15,16 Heo et al. and Smith et al. considered a 15-year time horizon,12,16 while the remaining studies considered a lifetime horizon (reported as 82 years in Rodriguez Gonzalez-Moro et al.;14 unreported by all other studies).11,13-15 There were slight differences in choice of discount rates: 5% in Heo et al.,12 4% in Shami et al.,15 and 3% in the remaining studies.11,13,14,16 All studies reported cost-effectiveness as ICERs using cost per quality-adjusted life-year (QALY) gained.11-16
Vaccination Strategies
While all of the peer-reviewed studies included either 1 dose of PCV13 or 1 dose of PCV13 sequentially with 1 dose of PPSV23 (PCV13 plus PPSV23) as the intervention of interest, the vaccination strategies that were compared varied across studies, and some studies compared multiple vaccination strategies. Unless otherwise stated, vaccination strategies assume 1 dose per vaccine. Strategies that were reported by multiple studies included:
PCV13 relative to no vaccination (Heo et al., Ishigami et al., and Smith et al.)12,13,16
PCV13 relative to PPSV23 (Heo et al. and Rodriguez Gonzalez-Moro et al.).12,14
Strategies that were reported only by 1 study included:
PCV13 plus PPSV23 relative to no vaccination (Choi et al.)11
PCV13 plus PPSV23 relative to PPSV23 (Shami et al.)15
PCV13 plus 2 doses of PPSV23 relative to PCV13 (Smith et al.)16
2 doses of PCV13 relative to PCV13 plus 2 doses of PPSV23 (Smith et al.).16
None of the peer-reviewed studies included PCV15, PCV20, or PCV21 as an intervention or comparator.
Vaccine Effectiveness
The sources for information on vaccine effectiveness were similar across studies. Appendix 2, Table 8 and Table 9 summarize the key clinical parameters of the peer-reviewed studies. With the exception of Choi et al.11 and Smith et al.,16 studies drew vaccine effectiveness for PCV13 from the CAPiTA clinical trial for the relevant populations included in this review.20
Estimates from an expert panel informed PCV13 vaccine effectiveness in Smith et al. and vaccine effectiveness in the moderate-risk population in Choi et al.11,16 Vaccine effectiveness estimates for PCV13 in Choi et al.11 and Heo et al.12 were also informed by a randomized controlled trial investigating the effectiveness of pneumococcal 9-valent conjugate vaccine (PCV9) in infants.21 Point estimates for initial PCV13 effectiveness against IPD and pneumonia ranged from 50% to 82% and 3.5% to 52.0%, respectively.11-16 A wider range was reported for vaccine effectiveness against pneumonia, as 1 study reported vaccine effectiveness against all-cause pneumonia,11 1 study reported vaccine effectiveness against all-cause nonbacteremic pneumonia (NBP),14 1 study reported vaccine effectiveness against all-cause NBP for PPSV23 but against NBP for PCV13,15 1 study reported vaccine effectiveness against noninvasive pneumococcal pneumonia,13 and 2 studies reported vaccine effectiveness against nonbacteremic pneumococcal pneumonia (NPP).12,16
Vaccine effectiveness for PPSV23 was informed by a Cochrane meta-analysis22 for the relevant populations included in this review in 2 studies (Heo et al. and Rodriguez Gonzalez-Moro et al.).12,14 The efficacy of PPSV23 in 1 study (Rodriguez Gonzalez-Moro et al.) was also informed by an observational study conducted in adults aged 65 years and older in addition to the Cochrane meta-analysis.23 All 5 studies (Choi et al., Heo et al., Rodriguez Gonzalez-Moro et al., Shami et al., and Smith et al.) that modelled PPSV23 relied on at least 1 assumption,11,12,14-16 but 2 of the studies (Choi et al. and Heo et al.) also relied on input from an expert panel to inform PPSV23 vaccine effectiveness.11,12 Point estimates for initial PPSV23 effectiveness against IPD ranged from 25% to 95.3%.11,12,14-16 In base-case analyses, Smith et al., assumed that vaccine effectiveness for PPSV23 was 50% of the base efficacy value for PCV13 against IPD.16 The 5 studies that considered PPSV23 in their economic evaluation assumed that PPSV23 did not protect against pneumonia.11,12,14-16
Vaccine Serotype Coverage
Apart from Ishigami et al., all studies reported vaccine serotype coverage (i.e., the proportion of disease due to the serotypes covered by the vaccine) (Appendix 2, Table 8).11,12,14-16 Three studies (Choi et al., Heo et al., and Rodriguez Gonzalez-Moro et al.) reported values specific to IPD and pneumonia,11,12,14 and 2 studies (Shami et al. and Smith et al.) reported age-specific values.15,16
Choi et al. and Heo et al. reported the same serotype coverage for PCV13 (IPD = 35.1% and NPP = 35.2%) and PPSV23 (IPD = 59.5% and NPP = 49.8%).11,12 Heo et al. was the only study that reported serotype coverage for PCV13 plus PPSV23 (IPD = 60.8% and NPP = 53.4%).12 Rodriguez Gonzalez-Moro et al. reported PCV13 and PPSV23 coverage for IPD serotypes as 70.0% and 76.5%, respectively.14 Additionally, Rodriguez Gonzalez-Moro et al. reported PCV13 coverage for any-cause NBP serotypes as 19.4% but did not report the coverage for PPSV23.14 Shami et al. reported PCV13 and PPSV23 serotype coverage as 65% and 76%, respectively.15 Smith et al. reported PCV13 and PPSV23 serotype coverage for adults aged 19 to 49 years as 51.9% and 78.0%, respectively.16
Vaccination Uptake and Indirect Effects
Vaccination uptake ranged from 0% to 100% across the 6 peer-reviewed studies (Appendix 2, Table 8).11-16 Shami et al. assumed 0% uptake of PPSV23 in adults 20 to 64 years, as PPSV23 is not indicated for this age cohort.15 Indirect effects of vaccination were considered in 4 studies.11,12,14,16
Utility Values
Utility values were reported by 5 studies.11-14,16 Shami et al. did not report the sources or utility values utilized in their economic evaluation.15
Choi et al.11 and Heo et al.12 derived their utility values from the same source.24 For moderate- and high-risk adults, Choi et al. reported utility values of 0.843 and 0.792 for adults aged 18 to 49 years and adults aged 50 to 64 years, respectively.11 For moderate-risk adults, Heo et al. reported utility values of 0.972 and 0.948 for adults aged 18 to 49 years and adults aged 50 to 64, respectively.12 Similarly, for high-risk adults, Heo et al. reported utility values of 0.843 and 0.792 for adults aged 18 to 19 years and adults aged 50 to 64 years, respectively.12 Heo et al. also applied utility values, stratified by age and risk, for acute events of IPD and NPP.12
Smith et al.16 used utility values from published literature and applied age-specific utility values for individuals with immunocompromising conditions ranging from 0.51 to 0.72.25,26 Smith et al.16 applied a utility value of 0.4 for individuals who developed a disability and 0.9 for vaccine adverse events.26 No details were provided for how adverse event utility values were applied in Smith et al.16
Three studies (Choi et al., Ishigami et al., and Smith et al.)11,13,16 used a utility weight of 0.2 for IPD and for NBP requiring hospitalization.24,25 It is unclear whether these values were applied as disutilities or health state utility values in the 3 studies.11,13,16
Health state utility values for studies focusing on a population with a specific health condition (i.e., CKD and COPD) in Rodriguez Gonzalez-Moro et al.14 and Ishigami et al.13 ranged from 0.53 to 0.83 and were drawn from published literature.25,27,28 Rodriguez Gonzalez-Moro et al. applied a disutility value of 0.1 for IPD and NBP in inpatients.29,30
Cost Inputs
All monetary amounts are reported in 2024 Canadian dollars in this review, unless stated otherwise. Vaccine costs were reported by all studies, apart from Shami et al.15 Five studies (Choi et al., Heo et al., Ishigami et al., Rodriguez Gonzalez-Moro et al., and Smith et al.) reported a cost for PCV13 that ranged from $80 to $227 per dose.11-14,16 Four studies (Choi et al., Heo et al., Rodriguez Gonzalez-Moro et al., and Smith et al.) reported PPSV23 costs that ranged from $21 to $76 per dose.11,12,14,16 The costs per dose from 2 studies (Smith et al. and Ishigami et al.) included administration costs.13,16
Three studies were conducted from a health care payer perspective.11,13,14 Choi et al. included direct health care costs associated with managing IPD, all-cause pneumonia, as well as vaccination costs associated with drug management, injection, and diagnoses.11 Ishigami et al. included acute hospitalization costs, baseline medical costs associated with the management of different stages of CKD, and vaccination costs.13 Rodriguez Gonzalez-Moro et al. included management costs for IPD and inpatient and outpatient management costs for all-cause NBP.14 This study also assumed vaccine administration costs were $0 under the assumption that because pneumococcal vaccinations would be administered alongside the influenza vaccine.14
The remaining 3 studies were conducted from a societal perspective.12,15,16 Heo et al. included hospitalization costs for NPP and IPD, vaccine administration costs, and societal costs such as transportation costs and caregiver time.12 Shami et al. included direct costs for hospitalization, inpatient care, outpatient consultation, and vaccination administration costs as well as indirect costs associated with productivity losses attributed to all-cause pneumonia and IPD.15 Smith et al. included hospitalization costs for IPD and NBP, stratified by whether a patient was discharged alive or died, and vaccine administration costs.16 Limited details were provided by Smith et al. regarding the methodology used to obtain costs from the Healthcare Cost and Utilization Project.16 While Smith et al. stated that the analysis was conducted from a societal perspective, the authors did not report on the indirect costs considered in their economic evaluation.16
Results
Population Intended for Vaccination: At-Risk Adults Aged 18 to 64 Years
Three studies (Choi et al., Shami et al., and Smith et al.) reported results for adults at least 18 years to 64 years.11,15,16 Unadjusted and adjusted results are reported in Appendix 2, Table 10 and Table 12, respectively.
Choi et al. reported the results of 2 vaccination strategies for at-risk adults aged 18 to 64.11 For this population, Choi et al. reported an ICER of $10,499 per QALY gained for PCV13 plus PPSV23 relative to no vaccination and $5,735 per QALY gained for PCV13 plus PPSV23 relative to PPSV23.11
Shami et al. also reported the results for PCV13 plus PPSV23 relative to PPSV23, but in adults aged 20 to 49 years (results were also presented for adults aged 50 to 64 years, discussed in the subsequent section).15 While Shami et al. assert that the sequential strategy was being compared with PPSV23, since uptake of PPSV23 is 0% among adults aged younger than 65 years, it is likely more appropriate to state that the sequential strategy was being compared with no vaccination in adults aged 20 to 49 years.15 However, this report maintains the author’s description, as it was unclear whether the sequential strategy was being compared with no vaccination. Shami et al. reported ICERs of $39,597 per QALY gained and $24,788 per QALY gained for PCV13 plus PPSV23 relative to PPSV23, respectively, for adults aged 20 to 49 years with selected chronic conditions (chronic cardiac, pulmonary, liver or renal disease; diabetes mellitus; or cerebrospinal fluid [CSF] leakage) and are at high risk (defined as having a history of IPDs, immunocompromising conditions [asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to use of immunosuppressive drugs/systemic steroids], chronic conditions, or cochlear implants).15 PCV13 plus PPSV23 was dominant (i.e., less costly and more effective) compared with PPSV23 in adults aged 20 to 49 years with immunocompromising conditions.15
Smith et al. reported ICERs for 3 vaccination strategies that were not reported by the other studies assessing pneumococcal vaccines in adults aged at least 18 years to 64 years: PCV13 relative to no vaccination, PCV13 plus 2 doses of PPSV23 relative to PCV13, and 2 doses of PCV13 relative to PCV13 plus 2 doses of PPSV23.16 The results for each vaccination strategy were reported separately for adults aged 19 to 64 years with immunocompromising conditions (defined as “HIV infection, Hodgkin disease, leukemia, lymphoma, myeloma, generalized malignancy, chronic renal failure, nephrotic syndrome, solid organ or bone marrow transplant, immunoglobulin deficiency, asplenia, sickle cell disease, or current immunosuppressive therapy [including radiation, systemic steroids, or chemotherapy]”) and those with HIV infection only.16 Smith et al. estimated ICERs of $125,724 per QALY gained and $78,543 per QALY gained for people who are immunocompromised and HIV-positive, respectively, for PCV13 relative to no vaccination.16 For PCV13 plus 2 doses of PPSV23 relative to PCV13, Smith et al. reported ICERs of $242,320 per QALY gained and $158,431 per QALY gained for people who are immunocompromised and HIV-positive, respectively.16 Last, in both people who are immunocompromised and HIV-positive, 2 doses of PCV13 was dominated by PCV13 plus 2 doses of PPSV23.16 Additionally, both 1 dose of PPSV23 and 2 doses of PPSV23 were subject to extended dominance through no vaccination and PCV13.16
Results of sensitivity analyses were reported by all 3 studies.11,15,16 However, 1 study (Choi et al.) conducted a sensitivity analysis only for adults aged 65 years and older; thus, this report does not discuss the results, as the population is not relevant to this review.11
One-way sensitivity analyses were conducted by Shami et al. and Smith et al.15,16 The studies identified vaccine effectiveness,15,16 incidence of inpatient pneumonia,15 and life expectancy16 as influential parameters. Shami et al. found that PCV13 plus PPSV23 was still considered cost-effective relative to PPSV23 at the regional willingness-to-pay (WTP) threshold of $68,564 (US$46,193) per QALY gained.15 Smith et al. found that PCV13 and PCV13 plus 2 doses of PPSV23 exceeded the regional WTP threshold of $177,233 (US$100,000) per QALY gained when life expectancy was 8 years or less and were less than the WTP threshold when life expectancy exceeded 19 years.16 The average life expectancy in the base case for people who are immunocompromised was 11.7 years.16
In 2-way sensitivity analyses, Smith et al. found that, when varying parameters associated with greater uncertainty, such as PPSV23 effectiveness against IPD relative to PCV13 and PCV13 effectiveness against NPP relative to effectiveness against IPD, PPSV23 was favoured for people who are immunocompromised at a WTP of $177,233 (US$100,000) per QALY gained.16 This finding assumed that the relative effectiveness of PPSV23 was high and PCV13 effectiveness against NPP was low.16 Smith et al. also found that, when vaccine effectiveness against NPP was high for PCV13 and PPSV23 vaccine effectiveness was low, a single dose of PCV13 was favoured for people who are immunocompromised.16 Among people who are in the immunocompromised population, PCV13 plus 2 doses of PPSV23 was favoured only if vaccine effectiveness was high for both vaccines.16 Similar results were presented for people who are HIV-positive, such that PCV13 plus 2 doses of PPSV23 was the preferred vaccination strategy if the relative vaccine effectiveness of PCV13 against NPP was more than 52% and the effectiveness of PPSV23 relative to PCV13 was greater than 49%.16
In probabilistic sensitivity analyses, Smith et al. found that no vaccination was likely to be considered the optimal strategy among the immunocompromised population if the WTP threshold was $177,233 (US$100,000).16 If the WTP threshold was increased to $119,072 (US$110,000), PCV13 was likely the optimal strategy among people who are immunocompromised.16 If the WTP threshold was increased to $248,127 (US$140,000), PCV13 plus 2 doses of PPSV23 was likely the optimal strategy among people who are immunocompromised.16 Among those who are HIV-positive, PCV13 plus 2 doses of PPSV23 was considered the optimal strategy if the WTP threshold was $177,233 (US$100,000) or greater.16
Choi et al. concluded that, at a regional WTP threshold of $43,673 (US$27,633), PCV13 plus PPSV23 was cost-effective relative to no vaccination and PPSV23 among at-risk individuals aged 18 to 64 years.11 Shami et al. concluded that PCV13 plus PPSV23 is dominant compared with PPSV23 among individuals with immunocompromising and chronic conditions aged 20 to 64 years.15 Smith et al. concluded that, among people who are immunocompromised aged 18 to 64 years, PCV13 is more cost-effective than 2 doses of PPSV23 and may be more cost-effective than PCV13 plus 2 doses of PPSV23 (the recommendation at the time of the analysis), depending on the cohort life expectancy. As well, the efficacy of PPSV23 was higher than predicted by the expert panel consulted for the study.16
Population Intended for Vaccination: At-Risk Adults Aged 50 to 64 Years
Four studies (Heo et al., Ishigami et al., Rodriguez Gonzalez-Moro et al., and Shami et al.) presented results for adults aged 50 to 64 years.12-15 Two studies (Heo et al. and Shami et al.) reported the results for a broader population in which multiple risk factors were considered.12,15 Unadjusted and adjusted results are reported in Appendix 2, Table 11 and Table 13, respectively.
Heo et al. reported the results for PCV13 relative to no vaccination and for PCV13 relative to PPSV23.12 In the moderate-risk population (individuals must have at least 1 of the following: diabetes mellitus, chronic liver disease, chronic pulmonary disease, or chronic cardiovascular or other chronic conditions affecting cardiac function), Heo et al. reported that, relative to no vaccination, PCV13 was associated with an ICER of $26,523 per QALY gained. In the high-risk population (individuals must have at least 1 of the following: splenic dysfunction including postsplenectomy status, hematologic malignancy, a condition affecting the bone marrow or lymphatic system, solid organ or stem cell transplant, CKD, HIV infection, high-dose corticosteroid use lasting 2 or more weeks, or treatment with a recombinant human immunomodulator), PCV13 was associated with an ICER of $11,360 per QALY gained relative to no vaccination.12 Relative to PPSV23, Heo et al. reported that PCV13 was associated with ICERs of $16,666 and $5,944 per QALY gained among the moderate-risk population and high-risk population, respectively.12
Shami et al. reported the results for PCV13 plus PPSV23 relative to PPSV23.15 However, as stated previously, as uptake of 1 dose of PPSV23 was 0% among adults aged younger than 65 years, it appears that the sequential strategy was compared with no vaccination in adults aged 20 to 49 years.15 Shami et al. reported that PCV13 plus PPSV23 was dominant relative to PPSV23 in all risk populations examined (chronic conditions, immunocompromised, and high-risk).15
Two studies presented the results for populations in which only 1 health condition was considered.13,14 Ishigami et al. reported ICERs of $36,150, $24,582, and $1,446 per QALY gained for people with moderate-risk CKD, high-risk CKD, and kidney failure or the nephrotic range of the urinary albumin-creatinine ratio, respectively, for PCV13 relative to no vaccination.13 Rodriguez Gonzalez-Moro et al. reported an ICER of $23,300 per QALY gained for PCV13 relative to PPSV23 among adults aged 50 to 64 years with COPD.14
Sensitivity analysis results were reported by all 4 studies.12-15 However, Heo et al. conducted sensitivity analyses only for adults aged 65 years and older; thus, this report does not discuss the results, as the population is not relevant to this review.12 Additionally, the sensitivity analyses and conclusions by Shami et al. are summarized in the previous section of the report (At-Risk Adults Aged 18 to 64 Years) and thus are not discussed further in this section.15
In sensitivity analyses, vaccine effectiveness,13,14 price per dose,13,14 and time horizon14 were identified as influential parameters. Although the analyses were sensitive to selected parameters, Ishigami et al. and Rodriguez Gonzalez-Moro et al. concluded that PCV13 is cost-effective relative to either no vaccination13 or a single dose of PPSV23,14 with all reported ICERs being less than the specified regional WTP thresholds.13,14
Discussion
The review identified 8 economic evaluations conducted in high-income countries that assessed the cost-effectiveness of pneumococcal conjugate vaccines in adults aged 18 to 64 years at high-risk of IPD. Six of the economic evaluations11-16 were peer reviewed and summarized in-depth in this review, and 2 economic evaluations17 were retrieved from a single grey literature source and are summarized in Appendix 3. Of the 6 peer-reviewed studies, 3 studies presented findings spanning from individuals aged at least 18 years to 64 years.11,15,16 Four studies reported results specific to adults aged 50 to 64 years.12-15 All 6 peer-reviewed studies assessed and reported the cost-effectiveness associated with PCV13, either alone or sequentially with PPSV23, in terms of an ICER.11-16
Four studies concluded that PCV13 was cost-effective relative to no vaccination;12,13,16 PPSV23;12,14,16 2 doses of PCV13;16 PCV13 plus 2 doses of PPSV23;16 or 2 doses of PPSV23.16 Two studies concluded that PCV13 plus PPSV23 was cost-effective relative to either no vaccination11 or PPSV23,11,15 but the studies did not evaluate the cost-effectiveness of PCV13 alone.11,15 The studies did not all consider the same vaccination strategies. Reported ICERs were not significantly influenced in scenario analyses, apart from the analyses conducted by Smith et al., which found that values for vaccine effectiveness and life expectancy influenced which vaccine strategy was considered optimal.16
Limitations
None of the 6 peer-reviewed studies included in this review assessed the cost-effectiveness of PCV15, PCV20, or PCV21 or included individuals who use illicit drugs, who are experiencing homelessness, or who live in communities or settings experiencing sustained high IPD rates. Based on the critical appraisal using the JBI criteria, the studies are of poor quality, as pertinent details (e.g., cost per dose, costs considered, utility values or utility value sources, and epidemiologic and incidence rates) were frequently lacking and methods were often vague and unclear. One study (Shami et al.) reported that results were presented for PCV13 plus PPSV23 relative to PPSV23.15 However, as uptake of PPSV23 was assumed to be 0% among adults aged younger than 65 years, it is likely more appropriate to state that the sequential strategy was being compared with no vaccination in adults aged 20 to 49 years.15 As stated previously, this report maintains the author’s description, as it was unclear whether the sequential strategy was being compared with no vaccination. Additionally, 2 studies did not conduct sensitivity analyses on the population of interest for this review (i.e., sensitivity analyses were conducted only on adults aged 65 years and older).11,12
Importantly, the sources used to parameterize vaccine effectiveness in all studies were highly uncertain, as the clinical evidence was either not representative of the target population or heavily reliant on expert input and assumption. Four studies relied on the CAPiTA trial to inform PCV13’s efficacy for the relevant populations included in this review.12-15 The CAPiTA trial was conducted in the Netherlands and assessed the efficacy of PCV13 relative to placebo in adults aged 65 years and older who did not have an immune deficiency or suppression at time of enrolment.19 The trial was also restricted to individuals who had not previously received a pneumococcal vaccination and did not reside in a nursing home, long-term care home, or similar facility.19 Hence, the CAPiTA trial failed to establish clinical efficacy in the target population of the economic evaluations because it excluded the population of interest. Results from the CAPiTA trial had not yet been published at the time of Smith et al.’s study, and efficacy estimates informing that evaluation are, in general, considerably lower than those reported by the other peer-reviewed studies that relied on the CAPiTA trial to inform PCV13 efficacy.16 Thus, it follows that the estimated ICERs from Smith et al. were higher than those from the other studies included in this review. Additionally, while several studies compared PCV13 or PCV13 plus PPSV23 to PPSV23, neither direct nor indirect evidence assessing the relative treatment effect among the interventions informed the analyses. As a result, a direct comparison of the cost-effectiveness of these vaccines should not be made.
The price per dose for PCV13 and PPSV23 varied widely across studies, with costs ranging from $80 to $227 per dose for PCV1311-14,16 and $21 to $76 per dose for PPSV23.11,12,14,16 Based on wholesale prices obtained from IQVIA DeltaPA, the cost per dose for PCV13 and PPSV23 is $99.91 and $35.24, respectively, in Canada (Appendix 1, Table 3).31 Thus, the range of vaccine prices considered by the peer-reviewed studies may not reflect Canadian prices. However, the price per dose, while identified as an influential parameter by 2 studies,13,14 did not result in the ICERs exceeding the regional WTP thresholds used in the studies. Additionally, 2 studies did not conduct a sensitivity analysis on adults aged younger than 65 years. Thus, it is unclear whether the conclusions drawn apply to adults aged younger than 65 years.11,12
Three studies reported receiving funding from industry, which should be considered when assessing the results.11,14,15
Generalizability
None of the included economic evaluations are broadly applicable to the health care systems in Canada, despite being conducted in high-income countries, as defined by the World Bank.8 The review did not identify any economic evaluations from a setting in Canada. Two peer-reviewed studies were set in the US,13,16 2 in South Korea,11,12 1 in Spain,14 and 1 in Hong Kong.15 These studies may not be generalizable to the health care setting in Canada, given differences in the structure of the health care systems, culture, access to health care services, mortality rates, and health care costs.32-34 Specifically, unit cost parameters for health care resource use were specific to the study settings and may not reflect clinical practice or health care costs in Canada. As a result, the model structures may be adaptable to the context in Canada, but the results reported by the publications may not be generalizable to the setting in Canada.
Conclusions
Eight economic evaluations (6 peer-reviewed, 2 from grey literature) assessing the cost-effectiveness of pneumococcal conjugate vaccines in adults aged 18 to 64 years at high-risk of IPD were identified. The 2 economic evaluations summarized in a single grey literature source were industry-sponsored analyses and have been summarized previously by the Public Health Agency of Canada. The methods and results of the industry-funded models are summarized in Appendix 3 for this review.
Of the 6 peer-reviewed studies summarized in this report, 4 concluded that PCV13 was cost-effective relative to no vaccination, 2 doses of PCV13, PCV13 plus 2 doses of PPSV23, or 2 doses of PPSV23. Two studies concluded that PCV13 plus PPSV23 was cost-effective relative to either no vaccination or PPSV23, but the studies did not evaluate the cost-effectiveness of PCV13 alone. Vaccination strategies considered in the included studies varied. After adjusting for currency and inflation, more than 75% of the reported ICERs were cost-saving or less than $50,000 per QALY. Smith et al. was the only study that reported ICERs exceeding $50,000 per QALY.16 The Smith et al. study based PCV13 efficacy on estimates sourced from an expert panel.16 By contrast, the other studies relied on the CAPiTA trial results, which were not yet available at the time of the Smith et al. study. Furthermore, the CAPiTA trial excluded high-risk adults aged younger than 65 years. Therefore, clinical efficacy in the population of interest for this review was not established in any of the peer-reviewed studies.
Clinical efficacy in the target population and the generalizability of the economic evaluations to the health care setting in Canada are unknown. To understand the potential cost-effectiveness of pneumococcal conjugate vaccination, a de novo economic evaluation conducted from a setting in Canada is required.
References
1.Canadian Immunization Guide: Part 4. Immunizing agents. Pneumococcal vaccines. Ottawa (ON): Public Health Agency of Canada; 2024: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines/page-16-pneumococcal-vaccine.html#a10. Accessed 2024 Mar 14.
2.Public Health Agency of Canada. Invasive Pneumococcal Disease: Risks. 2023; https://www.canada.ca/en/public-health/services/immunization/vaccine-preventable-diseases/invasive-pneumococcal-disease/risks.html. Accessed 2024 May 17.
3.Public Health Agency of Canada. Invasive Pneumococcal Disease: For Health Professionals. 2023; https://www.canada.ca/en/public-health/services/immunization/vaccine-preventable-diseases/invasive-pneumococcal-disease/health-professionals.html. Accessed 2024 Mar 18.
4.Public Health Agency of Canada. Invasive Pneumococcal Disease. 2023; https://www.canada.ca/en/public-health/services/immunization/vaccine-preventable-diseases/invasive-pneumococcal-disease.html. Accessed 2024 Mar 18.
5.U.S. Centers for Disease Control and Prevention (CDC). Antibiotic-resistant Streptococcus pneumoniae. 2024; https://www.cdc.gov/pneumococcal/php/drug-resistance/?CDC_AAref_Val=https://www.cdc.gov/pneumococcal/clinicians/drug-resistance.html. Accessed 2024 May 17.
6.Government of Canada. Drug and Health Product Submissions Under Review (SUR): New drug submissions under review. https://www.canada.ca/en/health-canada/services/drug-health-product-review-approval/submissions-under-review/new-drug-submissions-under-review.html. Accessed 2024 May 16.
7.National Advisory Committee on Immunization (NACI). Public health level recommendations on the use of pneumococcal vaccines in adults, including the use of 15-valent and 20-valent conjugate vaccines. An Advisory Committee Statement (ACS). Ottawa (ON): Public Health Agency of Canada; 2023: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/public-health-level-recommendations-use-pneumococcal-vaccines-adults-including-use-15-valent-20-valent-conjugate-vaccines.html#t1. Accessed 2024 Mar 14.
8.The World Bank. The world by income and region. 2022; https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html. Accessed 2023 Nov 8.
9.Organisation for Economic Co-operation and Development (OECD). OECD Data Explorer. Annual Purchasing Power Parities and exchange rates. 2024; https://data-explorer.oecd.org/vis?pg=0&bp=true&snb=47&tm=PPP&df[ds]=dsDisseminateFinalDMZ&df[id]=DSD_NAMAIN10%40DF_TABLE4&df[ag]=OECD.SDD.NAD&df[vs]=1.0&pd=2000%2C2023&dq=A.AUS%2BAUT%2BCRI%2BEA19%2BEU27_2020%2BALB%2BARG%2BBRA%2BBGR%2BCPV%2BCMR%2BCHN%2BHRV%2BCYP%2BGEO%2BHKG%2BIND%2BIDN%2BMDG%2BMLT%2BMAR%2BMKD%2BROU%2BRUS%2BSAU%2BSEN%2BSRB%2BSGP%2BZAF%2BZMB%2BBEL%2BCAN%2BCHL%2BCOL%2BCZE%2BDNK%2BEST%2BFIN%2BFRA%2BDEU%2BGRC%2BHUN%2BISL%2BIRL%2BISR%2BITA%2BJPN%2BKOR%2BLVA%2BLTU%2BLUX%2BMEX%2BNLD%2BNZL%2BNOR%2BPOL%2BPRT%2BSVK%2BSVN%2BESP%2BSWE%2BCHE%2BTUR%2BGBR%2BUSA...PPP_B1GQ.......&ly[rw]=REF_AREA&ly[cl]=TIME_PERIOD&to[TIME_PERIOD]=false&vw=tb. Accessed 2024 Mar 27.
10.Bank of Canada. Inflation calculator. 2024; https://www.bankofcanada.ca/rates/related/inflation-calculator/. Accessed 2024 Apr 3.
11.Choi MJ, Kang SO, Oh JJ, Park SB, Kim MJ, Cheong HJ. Cost-effectiveness analysis of 13-valent pneumococcal conjugate vaccine versus 23-valent pneumococcal polysaccharide vaccine in an adult population in South Korea. Hum Vaccin Immunother. 2018;14(8):1914-1922. PubMed
12.Heo JY, Seo YB, Choi WS, et al. Cost-effectiveness of pneumococcal vaccination strategies for the elderly in Korea. PLoS One. 2017;12(5):e0177342. PubMed
13.Ishigami J, Padula WV, Grams ME, et al. Cost-effectiveness of Pneumococcal Vaccination Among Patients With CKD in the United States. Am J Kidney Dis. 2019;74(1):23-35. PubMed
14.Rodriguez Gonzalez-Moro JM, Menendez R, Campins M, et al. Cost Effectiveness of the 13-Valent Pneumococcal Conjugate Vaccination Program in Chronic Obstructive Pulmonary Disease Patients Aged 50+ Years in Spain. Clin Drug Investig. 2016;36(1):41-53. PubMed
15.Shami JJP, Pathadka S, Chan EW, et al. Evaluating the cost-effectiveness of a sequential pneumococcal vaccination compared to single-dose vaccination strategy for adults in Hong Kong. Hum Vaccin Immunother. 2020;16(8):1937-1944. PubMed
16.Smith KJ, Nowalk MP, Raymund M, Zimmerman RK. Cost-effectiveness of pneumococcal conjugate vaccination in immunocompromised adults. Vaccine. 2013;31(37):3950-3956. PubMed
17.Kobayashi M, Pilishvili T, Farrar JL, et al. Pneumococcal Vaccine for Adults Aged ≥19 Years: Recommendations of the Advisory Committee on Immunization Practices, United States, 2023. MMWR Recomm Rep. 2023;72(3):1-39. PubMed
18.Leidner AJ. Summary of three economic models assessing pneumococcal vaccines in US adults [presentation slides]. Atlanta (GA): U.S. Centers for Disease Control and Prevention; 2021: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-09-29/02-Pneumococcal-Leidner-508.pdf. Accessed 2024 Apr 1.
19.Pfizer. NCT00744263: Study Evaluating the Efficacy of a 13-Valent Pneumococcal Conjugate Vaccine (13vPnC) in Adults (CAPITA). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2014: https://www.clinicaltrials.gov/study/NCT00744263. Accessed 2024 Apr 8.
20.Bonten MJ, Huijts SM, Bolkenbaas M, et al. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med. 2015;372(12):1114-1125. PubMed
21.Klugman KP, Madhi SA, Huebner RE, Kohberger R, Mbelle N, Pierce N. A trial of a 9-valent pneumococcal conjugate vaccine in children with and those without HIV infection. N Engl J Med. 2003;349(14):1341-1348. PubMed
22.Moberley S, Holden J, Tatham DP, Andrews RM. Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev. 2013;2013(1):CD000422. PubMed
23.Andrews NJ, Waight PA, George RC, Slack MP, Miller E. Impact and effectiveness of 23-valent pneumococcal polysaccharide vaccine against invasive pneumococcal disease in the elderly in England and Wales. Vaccine. 2012;30(48):6802-6808. PubMed
24.Smith KJ, Wateska AR, Nowalk MP, Raymund M, Nuorti JP, Zimmerman RK. Cost-effectiveness of adult vaccination strategies using pneumococcal conjugate vaccine compared with pneumococcal polysaccharide vaccine. JAMA. 2012;307(8):804-812. PubMed
25.Sisk JE, Whang W, Butler JC, Sneller VP, Whitney CG. Cost-effectiveness of vaccination against invasive pneumococcal disease among people 50 through 64 years of age: role of comorbid conditions and race. Ann Intern Med. 2003;138(12):960-968. PubMed
26.Gold MR, Franks P, McCoy KI, Fryback DG. Toward Consistency in Cost - Utility Analyses Using National Measures to Create Condition-Specific Values. Med Care. 1998;36(6):778-792. PubMed
27.Ara R, Brazier JE. Using health state utility values from the general population to approximate baselines in decision analytic models when condition-specific data are not available. Value Health. 2011;14(4):539-545. PubMed
28.Liem YS, Bosch JL, Hunink MG. Preference-based quality of life of patients on renal replacement therapy: a systematic review and meta-analysis. Value Health. 2008;11(4):733-741. PubMed
29.Melegaro A, Edmunds WJ. Cost-effectiveness analysis of pneumococcal conjugate vaccination in England and Wales. Vaccine. 2004;22(31-32):4203-4214. PubMed
30.Bennett JE, Sumner W, 2nd, Downs SM, Jaffe DM. Parents' utilities for outcomes of occult bacteremia. Arch Pediatr Adolesc Med. 2000;154(1):43-48. PubMed
31.DeltaPA. Ottawa (ON): IQVIA; 2022: https://www.iqvia.com/. Accessed 2024 May 6.
32.Moir M, Barua B. Comparing Performance of Universal Health Care Countries, 2021. Vancouver (BC): Fraser Institute; 2021: https://www.fraserinstitute.org/sites/default/files/comparing-performance-universal-health-care-countries-2021.pdf. Accessed 2024 Apr 15.
33.Kong X, Yang Y, Gao J, et al. Overview of the health care system in Hong Kong and its referential significance to mainland China. J Chin Med Assoc. 2015;78(10):569-573. PubMed
34.Papanicolas I, Woskie LR, Jha AK. Health Care Spending in the United States and Other High-Income Countries. JAMA. 2018;319(10):1024-1039. PubMed
35.Prevnar 13, Pneumococcal 13-valent conjugate vaccine (Diphtheria CRM197 protein), suspension for intramuscular injection [product monograph]. Kirkland (QC): T.M. Wyeth LLC, Pfizer Canada ULC, Licensee; 2019: https://pdf.hres.ca/dpd_pm/00052583.PDF. Accessed 2024 Mar 14.
36.VAXNEUVANCE (Pneumococcal 15-valent Conjugate Vaccine [CRM197 Protein], adsorbed), suspension for intramuscular injection [product monograph]. Kirkland (QC): Merck Canada Inc.; 2023: https://pdf.hres.ca/dpd_pm/00071531.PDF. Accessed 2024 Mar 14.
37.PREVNAR 20, Pneumococcal 20-valent Conjugate Vaccine (Diphtheria CRM197 Protein), suspension for intramuscular injection, one-dose syringe (0.5 mL) [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2023: https://pdf.hres.ca/dpd_pm/00073367.PDF. Accessed 2024 Mar 14.
38.PNEUMOVAX 23 (pneumococcal vaccine, polyvalent, MSD Std.) solution for injection [product monograph]. Kirkland (QC): Merck Canada Inc.; 2023: https://pdf.hres.ca/dpd_pm/00072367.PDF. Accessed 2024 Mar 14.
39.Scientific Committee on Vaccine Preventable Diseases: Updated recommendations on the use of pneumococcal vaccines for high-risk individuals. Hong Kong: Center for Health Protection. Department of Health. The Government of the Hong Kong Special Administrative Region; 2016: https://www.chp.gov.hk/files/pdf/updated_recommendations_on_the_use_of_pneumococcal_vaccines_amended_120116_clean_2.pdf. Accessed 2024 Apr 1.
40.Pneumococcal vaccination: summary of who and when to vaccinate. Atlanta (GA): U.S. Centers for Disease Control and Prevention; 2023: https://www.cdc.gov/vaccines/vpd/pneumo/hcp/who-when-to-vaccinate.html. Accessed 2024 Apr 8.
Appendix 1: Background Information
Note that this appendix has not been copy-edited.
Table 2: High-Risk Factors for IPD
Nonimmunocompromising conditions | Immunocompromising conditionsa | Other risk factors |
|---|---|---|
|
| Individuals
|
aConditions considered to result in the highest risk of IPD.
bGenerally, asplenia (functional or anatomic), sickle cell disease, and other hemoglobinopathies are not considered immunocompromising conditions, but for the purposes of pneumococcal vaccine recommendations, they are included in this category.
cHematopoietic stem cell transplant recipients have specific pneumococcal vaccination recommendations.
dCan include long-term care facilities.
Source: Public Health Agency of Canada.7
Table 3: Comparison of Pneumococcal Vaccines Authorized for Use in Adults in Canada
Vaccine | PCV13 (PREVNAR 13)35 | PCV15 (VAXNEUVANCE)36 | PCV20 (PREVNAR 20)37 | PPSV23 (PNEUMOVAX 23)38 |
|---|---|---|---|---|
Manufacturer | Pfizer | Merck | Pfizer | Merck |
Date of initial authorization in Canada | December 21, 2009 | November 16, 2021 | May 9, 2022 | December 23, 1983 |
Type of vaccine | Conjugate vaccine | Conjugate vaccine | Conjugate vaccine | Polysaccharide vaccine |
Adult dosage | Single 0.5 mL injection given intramuscularly | Single 0.5 mL injection given intramuscularly | Single 0.5 mL injection given intramuscularly | Single 0.5 mL injection given subcutaneously or intramuscularly |
Indicated age | Adults 18 years of age and older | Individuals 6 weeks of age and older | Adults 18 years of age and older | Individuals 2 years of age and older with IPD risk factors and all individuals 50 years of age and older. |
Health Canada indication | For the prevention of pneumonia and invasive pneumococcal disease (including sepsis, meningitis, bacteremic pneumonia, pleural empyema and bacteremia) caused by Streptococcus pneumoniae serotypes 1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, and 23F. | For the prevention of invasive disease (including sepsis, meningitis, bacteremic pneumonia, pleural empyema and bacteremia) caused by Streptococcus pneumoniae serotypes (1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, 22F, 23F, and 33F). | For the prevention of pneumonia and invasive pneumococcal disease (including sepsis, meningitis, bacteremic pneumonia, pleural empyema and bacteremia) caused by Streptococcus pneumoniae serotypes 1, 3, 4, 5, 6A, 6B, 7F, 8, 9V, 10A, 11A, 12F, 14, 15B, 18C, 19A, 19F, 22F, 23F, and 33F. | For pneumococcal disease caused by those pneumococcal types included in the vaccine (serotypes 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F, and 33F). |
Price per dose ($)a | 99.91 | 99.90 | 109.90 | 35.24 |
Note: at the time of this review, the Health Canada product monograph for PCV21 is not publicly available.
aAll prices are wholesale prices retrieved from IQVIA DeltaPA (accessed May 2024) and do not include dispensing fees.31
Table 4: Comparison of Serotypes Included In Pneumococcal Vaccines Authorized for Use in Canada
Serotype | PCV13 | PCV15 | PCV20 | PPSV23 |
|---|---|---|---|---|
1 | Yes | Yes | Yes | Yes |
2 | No | No | No | Yes |
3 | Yes | Yes | Yes | Yes |
4 | Yes | Yes | Yes | Yes |
5 | Yes | Yes | Yes | Yes |
6A | Yes | Yes | Yes | No |
6B | Yes | Yes | Yes | Yes |
7F | Yes | Yes | Yes | Yes |
8 | No | No | Yes | Yes |
9N | No | No | No | Yes |
9V | Yes | Yes | Yes | Yes |
10A | No | No | Yes | Yes |
11A | No | No | Yes | Yes |
12F | No | No | Yes | Yes |
14 | Yes | Yes | Yes | Yes |
15B | No | No | Yes | Yes |
17F | No | No | No | Yes |
18C | Yes | Yes | Yes | Yes |
19A | Yes | Yes | Yes | Yes |
19F | Yes | Yes | Yes | Yes |
20 | No | No | No | Yes |
22F | No | Yes | Yes | Yes |
23F | Yes | Yes | Yes | Yes |
33F | No | Yes | Yes | Yes |
Note: vaccine serotypes were sourced from the respective product monographs.35-38
Table 5: Currency Conversion Rates
Author, year | Country, currency | PPP rate | Inflation rate |
|---|---|---|---|
Choi et al., 201811 | South Korea, 2015 USD | 1.248042 | 1.2663477 |
Heo et al., 201712 | South Korea, 2015 USD | 1.248042 | 1.2663477 |
Ishigami et al., 201913 | US, 2018 USD | 1.206524 | 1.1984906 |
Rodriguez Gonzalez-Moro et al., 201614 | Spain, 2015 Euros | 1.877489a | 1.2663477 |
Shami et al., 202015 | Hong Kong, 2017 USD | 1.212304 | 1.2243639 |
Smith et al., 201316 | US, 2006 USD | 1.205365 | 1.4703704 |
CAD = Canadian dollar; PPP = purchasing power parity; USD = US dollar.
Note: Monetary amounts were first converted to CAD using OECD PPP rates9 for the respective currency year and then inflated to 2024 CAD using the Bank of Canada inflation calculator (accessed April 3, 2024).10
aRate obtained by dividing the Canadian 2015 PPP rate for CAD per USD (1.248042) by the Spanish 2015 PPP rate for Euro per USD (0.664740).9
Appendix 2: Included Peer-Reviewed Study Results
Table 6: Characteristics of Included Peer-Reviewed Studies
Author, Year | Choi et al., 201811 | Heo et al., 201712 | Ishigami et al., 201913 | Rodriguez Gonzalez-Moro et al., 201614 | Shami et al., 202015 | Smith et al., 201316 |
|---|---|---|---|---|---|---|
Country | South Korea | South Korea | US | Spain | Hong Kong | US |
Perspective | Health care payer | Societal | Health care payer | Health care payer | Societal | Societal |
Modelling approach | Markov model | Markov model | Markov model | Markov model | Sequential deterministic model (model structure not specified) | Markov model |
Time horizon | Lifetime | 15-years | Lifetime | Lifetime | Lifetime | 15-years |
Discount rate | 3% | 5% | 3% | 3% | 4% | 3% |
Study population | Primary analysis: Adults aged ≥ 65 years and at-riska adults aged ≥ 65 years Secondary analysis: At-riska adults aged 18 to 64 years | Primary analysis: Adults aged ≥ 65 years Secondary analysis: Low-, moderate-, and high-riskb adults aged 50 to 64 years | Adults with CKD aged 50 to 64 and 65 to 79 years | Adults with COPD aged ≥ 50 years | Adults aged 20 to 64 years with high-risk conditionsd and adults ≥ 65 years | Immunocompromisede adults aged 19 to 64 years |
Relevant population | At-riska adults aged 18 to 64 years | Moderate- and high-riskb adults aged 50 to 64 years | Adults with CKD aged 50 to 64 years | Adults with COPD aged 50 to 64 years | Adults aged 20 to 64 years with high-riskd conditions | Aligned with study population |
Relevant intervention(s) | PCV13 + PPSV23 | PCV13 | PCV13 | PCV13 | PCV13 + PPSV23 | PCV13 2 doses of PCV13 PCV13 + 2 doses of PPSV23 |
Comparator(s) | PPSV23 | No vaccination PPSV23 | No vaccination | PPSV23 | PPSV23 | No vaccination PPSV23 2 doses of PPSV23 |
Cost per dose (original currency) | PCV13 = US$50.48 PPSV23 = US$16.74 | PCV13 = US$50.31 PPSV23 = US$14.13 | PCV13 = US$132c | PCV13 = €47.04 PPSV23 = €8.70 | NR | PCV13 = US$128c PPSV23 = US$43c |
Cost per dose (CA$ 2024)f | PCV13 = $79.78 PPSV23 = $26.46 | PCV13 = $79.51 PPSV23 = $22.33 | PCV13 = $191c | PCV13 = $111.84 PPSV23 = $20.68 | NA | PCV13 = $226.86c PPSV23 = $76.21c |
Industry funding | Pfizer | None | None | Pfizer | Pfizer | None |
CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; NA = not applicable; NR = not reported; PCV13 = pneumococcal conjugate 13-valent; PPSV23 = pneumococcal polysaccharide 23-valent.
Notes: All studies were cost-utility analyses. Relevant interventions and comparators assume 1 dose per vaccine unless otherwise specified.
Note: This table has not been copy-edited.
aAt-risk conditions, as defined by the authors, include any of the following: chronic heart disease, chronic liver disease, chronic respiratory disease, diabetes, asthma, alcohol abuse and smoking, chronic renal disease, nephrotic syndrome, malignant tumour (hematologic malignancy, solid tumour), and immune deficiency (HIV, organ or bone marrow transplant, low immunoglobulin, asplenia, sickle cell disease, or immunosuppressive therapy).11
bAs defined by the authors, individuals are considered low-risk if they do not satisfy the criteria for high- or moderate-risk. Individuals are considered moderate-risk if they have any of the following: diabetes mellitus, chronic liver disease, chronic pulmonary disease, such as asthma or chronic obstructive lung disease, or chronic cardiovascular disease, such as heart failure, cardiomyopathy, or other chronic conditions affecting cardiac function. Individuals are considered high-risk if they have any of the following: splenic dysfunction including postsplenectomy status, hematologic malignancy such as multiple myeloma, leukemia, or lymphoma, a condition affecting the bone marrow or lymphatic system, such as chemotherapy with alkylating drugs or antimetabolites, or radiation within the previous 3 months, solid organ or stem cell transplant, chronic renal disease such as nephrotic syndrome or chronic renal failure, HIV infection, high-dose corticosteroid use (≥ 20 mg/day of prednisone or an equivalent) lasting 2 or more weeks, or treatment with a recombinant human immunomodulator.12
cCost is inclusive of administration costs. Vaccine costs are not presented separately.
dAs defined by the authors, individuals are considered high-risk if they have any of the following: history of invasive pneumococcal disease, immunocompromised states (asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to use of immunosuppressive drugs/systemic steroid), chronic disease (chronic cardiac, pulmonary, liver, or renal disease), diabetes mellitus, or CSF leakage, with cochlear implants.39
eAs defined by the authors, immunocompromising conditions include any of the following: HIV infection, Hodgkin disease, leukemia, lymphoma, myeloma, generalized malignancy, chronic renal failure, nephrotic syndrome, solid organ or bone marrow transplant, immunoglobulin deficiency, asplenia, sickle cell disease, or current immunosuppressive therapy (including radiation, systemic steroids, or chemotherapy).16
fReported monetary amounts were converted to CAD using OECD purchasing price parity rates9 for the respective currency year and then inflated to 2024 CAD using the Bank of Canada inflation calculator.10 Appendix 1, Table 5 details the PPP and inflation rates used to adjust monetary amounts to 2024 Canadian dollars.
Table 7: Quality Appraisal Results
Author, year | Critical appraisal: Joanna Briggs Institute checklista | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total criteria met | |
Peer-reviewed studies, broad population | ||||||||||||
Choi et al., 201811 | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | No | No | 6 |
Heo et al., 201712 | Yes | Yes | Yes | No | No | No | Yes | Yes | No | No | No | 5 |
Shami et al., 202015 | Yes | Yes | No | No | No | No | Yes | Yes | Yes | No | No | 5 |
Smith et al., 201316 | Yes | Yes | No | No | No | No | Yes | Yes | Yes | No | No | 5 |
Peer-reviewed studies, narrow population | ||||||||||||
Ishigami et al., 201913 | No | No | Unsure | No | No | No | Yes | Yes | Yes | No | No | 3 |
Rodriguez Gonzalez-Moro et al.,14 2016b | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | No | No | 6 |
NA = not applicable.
Note: This table has not been copy-edited.
a.Questions:
1Is there a well-defined question?
2Is there a comprehensive description of alternatives?
3Are all important and relevant costs and outcomes for each alternative identified?
4Has clinical effectiveness been established?
5Are costs and outcomes measured accurately?
6Are costs and outcomes valued credibly?
7Are costs and outcomes adjusted for differential timing?
8Is there an incremental analysis of costs and consequences?
9Were sensitivity analyses conducted to investigate uncertainty in estimates of cost or consequences?
10Do study results include all issues of concern to users?
11Are the results generalizable to the setting of interest in the review?
Table 8: Key Clinical Parameters of Included Peer-Reviewed Studies of Adults at Least 18 Years to 64 Years
Parameter | Author, year | Choi et al., 201811 | Shami et al., 202015 | Smith et al., 201316 |
|---|---|---|---|---|
Source of Clinical Efficacy | Vaccine uptake | 100% | PCV13 + PPSV23: 10% PPSV23: 0% | 33.9% |
Indirect Effects | Yes (relative reduction in IPD incidence) | No | Yes (relative reduction in PD incidence) | |
PCV13 | Moderate-risk: Expert panel High-risk: RCT investigating the VE of PCV9 in infants21 | CAPiTA clinical trial20 | Expert panel | |
PPSV23 | Moderate-risk: Expert panel and assumption High-risk: Expert panel and assumption | Assumption | Assumption | |
VE: IPD | PCV13 | Moderate-risk: 63.8% High-risk: 58.5% | 75.8% | Year 1: 50% Year 3: 45% Year 5: 35% Year 10: 25% Year 15: 5% |
PPSV23 | Moderate-risk: 65.6% High-Risk: 20.0% | NR | 50% of base IPD VE for PCV13 | |
VE: Pneumonia | PCV13 | Adults aged 18 to 49 Moderate-risk: 5.6%a High-risk: 3.7%a Adults aged 50 to 54 Moderate-risk: 5.4%a High-risk: 3.5%a | 41.1%b | Year 1: 35%d Year 3: 32%d Year 5: 25%d Year 10: 18%d Year 15: 4%d |
PPSV23 | 0%a | 0%c | 0%b | |
Serotype coverage | PCV13 | IPD: 35.1% NPP: 35.2% | Adults aged 20 to 64: 65% | Adults aged 19 to 49: 51.9% Adults aged 50 to 59: 48.3% |
PPSV23 | IPD: 59.5% NPP: 49.8% | Adults aged 20 to 64: 76% | Adults aged 19 to 49: 78.0% Adults aged 50 to 59: 73.3% | |
PCV13 + PPSV23 | NR | NA | NR |
IPD = invasive pneumococcal disease; NA = not applicable; NBP = nonbacteremic pneumonia; NR = not reported; NPP = nonbacteremic pneumococcal pneumonia; PCV13 = pneumococcal conjugate 13-valent; PD = pneumococcal disease; PPSV23 = pneumococcal polysaccharide 23-valent; RCT = randomized controlled trial; VE = vaccine effectiveness.
Notes: only inputs specific to the at-risk population, as defined by Table 2, are reported (i.e., inputs pertaining to adults 65 and older or adults who are not at high risk are not reported).
Note: This table has not been copy-edited.
aRate is specific to all-cause pneumonia.
bRate is specific to NBP.
cRate is specific to all-cause NBP.
dRate is specific to NPP.
Table 9: Key Clinical Parameters of Included Peer-Reviewed Studies of Adults 50 to 64 Years
Parameter | Author, year | Heo et al., 201712 | Ishigami et al., 201913 | Rodriguez Gonzalez-Moro et al., 201614 |
|---|---|---|---|---|
Source of Clinical Efficacy | Vaccine uptake | 60% | With clinical indication: 28.5% Without clinical indication: 9.7% | 41% |
Indirect Effects | Yes (relative reduction in IPD and NPP incidence) | No | Yes (relative reduction in IPD and NBP incidence) | |
PCV13 | CAPiTA clinical trial20 and RCT investigating the VE of PCV9 in infants21 | CAPiTA clinical trial20 | CAPiTA clinical trial20 | |
PPSV23 | Cochrane meta-analysis,22 expert survey, and assumption | NA | Cochrane meta-analysis,22 an observational study in adults ≥ 65,23 and assumption | |
VE: IPD | PCV13 | Year 1: 79.4% Year 3: 70.6% Year 5: 61.8% Year 7: 52.9% Year 10: 44.1% Year 15: 39.7% | 51.8% | Year 0: 82.0% Years 1 to 5: 82.9% Years 6 to 10: 53.3% Years 11 to 15: 21.0% Years 15+: 19.3% |
PPSV23 | Year 1: 95.3% Year 3: 91.2% Year 5: 87.2% Year 7: 61.5% Year 10: 20.5% Year 15: 0.0% | NA | Year 0: 87.3% Years 1 to 5: 69.0% Years 6 to 10: 22.8% Years 11 to 15: 2.7% Years 15+: 0.7% | |
VE: Pneumonia | PCV13 | Year 1: 52.0%a Year 3: 46.6%a Year 5: 39.9%a Year 7: 32.4%a Year 10: 28.6%a Year 15: 25.9%a | 30.6%b | Year 0: 9.5%c Years 1 to 5: 9.4%c Years 6 to 10: 6.2%c Years 11 to 15: 2.4%c Years 15+: 2.2%c |
PPSV23 | 0%a | NA | 0%c | |
Serotype coverage | PCV13 | IPD: 35.1% NPP: 35.2% | NR | IPD: 70.0% NBP: 19.4% |
PPSV23 | IPD: 59.5% NPP: 49.8% | NR | IPD: 76.5% NBP: NR | |
PCV13 + PPSV23 | IPD: 60.8% NPP: 53.4% | NA | NA |
IPD = invasive pneumococcal disease; NA = not applicable; NBP = nonbacteremic pneumonia; NR = not reported; NPP = nonbacteremic pneumococcal pneumonia; PCV13 = pneumococcal conjugate 13-valent; PPSV23 = pneumococcal polysaccharide 23-valent; RCT = randomized controlled trial; VE = vaccine effectiveness.
Notes: only inputs specific to the at-risk population, as defined by Table 2, are reported (i.e., inputs pertaining to adults 65 and older or adults who are not at high risk are not reported). Shami et al. report the results for the population aged 50 to 64; parameters are presented in Table 8.
Note: This table has not been copy-edited.
aRate is specific to NPP.
bRate is specific to noninvasive pneumococcal pneumonia.
cRate is specific to NBP.
Table 10: Original ICERs of Included Peer-Reviewed Studies of Adults at Least 18 Years to 64 Years
Author, year | Country, currency | Population | Original ICER (monies/QALY) | ||||
|---|---|---|---|---|---|---|---|
PCV13 vs. no vaccination | 2 doses PCV13 vs. PCV13 + 2 doses PPSV23 | PCV13 + PPSV23 vs. no vaccination | PCV13 + 2 doses PPSV23 vs. PCV13 | PCV13 + PPSV23 vs. PPSV23 | |||
Choi et al., 201811 | South Korea, 2015 USD | 18 to 64 and at riska | NA | NA | 6,643 | NA | 3,629 |
Shami et al., 202015 | Hong Kong, 2017 USD | 20 to 49 with chronic conditionsb | NA | NA | NA | NA | 26,677c |
20 to 49 and immunocompromisedd | NA | NA | NA | NA | Dominantc | ||
20 to 49 and high riske | NA | NA | NA | NA | 16,700c | ||
Smith et al., 201316 | US, 2006 USD | 19 to 64 and Immunocompromisedf,g | 70,937 | Dominated | NA | 136,724 | NA |
19 to 64 and HIV positiveg | 44,316 | Dominated | NA | 89,391 | NA | ||
HIV = HIV; ICER = incremental cost-effectiveness ratio; NA = not applicable; PCV13 = pneumococcal conjugate 13-valent; PPSV23 = pneumococcal polysaccharide 23-valent; QALY = quality-adjusted life-year; USD = US dollar.
Notes: ICERs assume 1 dose per vaccine unless otherwise specified.
Note: This table has not been copy-edited.
aAs defined by the authors, individuals at-risk have one or more of the following “chronic heart disease, chronic liver disease, chronic respiratory disease, diabetes, asthma, alcohol abuse and smoking...chronic renal disease, nephrotic syndrome, malignant tumour (hematologic malignancy, solid tumour), and immune deficiency (HIV, organ or bone marrow transplant, low immunoglobulin, asplenia, sickle cell disease, or immunosuppressive therapy)”.11
bAs defined by the authors, chronic conditions include chronic cardiac, pulmonary, liver or renal disease, diabetes mellitus, or CSF leakage.15
cWhile Shami et al. assert that the sequential strategy is being compared to PPSV23, as uptake of PPSV23 is 0% among adults less than 65, it is likely more appropriate to state that the sequential strategy is being compared to no vaccination in adults 20 to 49 years of age.15
dAs defined by the authors,15 immunocompromised individuals include those with asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to the use of immunosuppressive drugs/systemic steroids.39
eAs defined by the authors,15 high-risk individuals have a history of invasive pneumococcal diseases, immunocompromised conditions (asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to use of immunosuppressive drugs/systemic steroid), chronic diseases (chronic cardiac, pulmonary, liver or renal disease, diabetes mellitus, or CSF leakage), or cochlear implants.39
fAs defined by the authors, immunocompromised individuals include those with any of the following: HIV infection, Hodgkin disease, leukemia, lymphoma, myeloma, generalized malignancy, chronic renal failure, nephrotic syndrome, solid organ or bone marrow transplant, immunoglobulin deficiency, asplenia, sickle cell disease, or current immunosuppressive therapy (including radiation, systemic steroids, or chemotherapy).16
gIn both the immunocompromised and HIV-positive populations, 2 doses of PCV13 was dominated by PCV13 plus 2 doses of PPSV23.16 Additionally, both PPSV23 and 2 doses of PPSV23 were subject to extended dominance through no vaccination and PCV13.16
Table 11: Original ICERs of Included Peer-Reviewed Studies of Adults 50 to 64 Years
Author, year | Country, currency | Population | Original ICER (currency/QALY) | ||
|---|---|---|---|---|---|
PCV13 vs. no vaccination | PCV13 vs. PPSV23 | PCV13 + PPSV23 vs. PPSV23 | |||
Heo et al., 201712 | South Korea, 2015 USD | Moderate-riska | 16,782 | 10,545 | NA |
High-riskb | 7,188 | 3,761 | NA | ||
Ishigami et al., 201913 | US, 2018 USD | Moderate-riskc CDK | 25,000 | NA | NA |
High-riskd CKD | 17,000 | NA | NA | ||
Kidney failure or nephrotic-range UACRe | 1,000 | NA | NA | ||
Rodriguez Gonzalez-Moro et al., 201614 | Spain, 2015 Euros | COPD | NA | 9,800 | NA |
Shami et al., 202015 | Hong Kong, 2017 USD | Chronic conditionsf | NA | NA | Dominantg |
Immunocompromisedh | NA | NA | Dominantg | ||
High riski | NA | NA | Dominantg | ||
CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; eGFR = estimated glomerular filtration rate; ICER = incremental cost-effectiveness ratio; NA = not applicable; PCV13 = pneumococcal conjugate 13-valent; PPSV23 = pneumococcal polysaccharide 23-valent; QALY = quality-adjusted life-year; UACR = urinary albumin-creatinine ratio; USD = US dollar.
Notes: ICERs assume 1 dose per vaccine unless otherwise specified.
Note: This table has not been copy-edited.
aAs defined by the authors, individuals must have at least one of the following: diabetes mellitus, chronic liver disease, chronic pulmonary disease, or chronic cardiovascular or other chronic conditions affecting cardiac function.12
bAs defined by the authors, individuals must have at least one of the following: splenic dysfunction including postsplenectomy status, hematologic malignancy, a condition affecting the bone marrow or lymphatic system, solid organ or stem cell transplant, chronic renal disease, HIV infection, high-dose corticosteroid use (≥ 20 mg/day of prednisone or an equivalent) lasting 2 or more weeks, or treatment with a recombinant human immunomodulator.12
cCKD with moderate-risk is defined by the authors as having an “eGFR of 45 to 59 mL/min/1.73 m2 and UACR < 30 mg/g or eGFR ≥ 60 mL/min/1.73 m2 and UACR of 30 to 299 mg/g.”13
dCKD with high-risk is defined by the authors as having an “eGFR of 15 to 44 mL/min/1.73 m2 regardless of UACR, eGFR of 45 to 59 mL/min/1.73 m2 and UACR of 30 to 299 mg/g, or UACR of 300 to 1,999 mg/g regardless of eGFR.”13
eKidney failure or nephrotic-range UACR is defined by the authors as having an “eGFR < 15 mL/min/1.73 m2 and nephrotic-range albuminuria was UACR ≥ 2,000 mg/g.”13
fAs defined by the authors, chronic conditions include chronic cardiac, pulmonary, liver or renal disease, diabetes mellitus, or CSF leakage.15
gWhile Shami et al. assert that the sequential strategy is being compared to PPSV23, as uptake of PPSV23 is 0% among adults less than 65, it is likely more appropriate to state that the sequential strategy is being compared to no vaccination in adults 20 to 49 years of age.15
hAs defined by the authors,15 immunocompromised individuals include those with asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to the use of immunosuppressive drugs/systemic steroids.39
iAs defined by the authors,15 high-risk individuals have a history of invasive pneumococcal diseases, immunocompromised conditions (asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to use of immunosuppressive drugs/systemic steroid), chronic diseases (chronic cardiac, pulmonary, liver or renal disease, diabetes mellitus, or CSF leakage), or cochlear implants.39
Table 12: ICERs (2024 $CA) of Included Peer-Reviewed Studies of Adults at Least 18 Years to 64 Years
Author, year | Country, currency | Population | ICER (2024 $CA/QALY) | ||||
|---|---|---|---|---|---|---|---|
PCV13 vs. no vaccination | 2 doses PCV13 vs. PCV13 + 2 doses PPSV23 | PCV13 + PPSV23 vs. no vaccination | PCV13 + 2 doses PPSV23 vs. PCV13 | PCV13 + PPSV23 vs. PPSV23 | |||
Choi et al., 201811 | South Korea, 2015 USD | 18 to 64 and at riska | NA | NA | 10,499 | NA | 5,735 |
Shami et al., 202015 | Hong Kong, 2017 USD | 20 to 49 with chronic conditionsb | NA | NA | NA | NA | 39,597c |
20 to 49 and immunocompromisedd | NA | NA | NA | NA | Dominantc | ||
20 to 49 and high riske | NA | NA | NA | NA | 24,788c | ||
Smith et al., 201316 | US, 2006 USD | 19 to 64 and Immunocompromisedf,g | 125,724 | Dominated | NA | 242,320 | NA |
19 to 64 and HIV positiveg | 78,543 | Dominated | NA | 158,431 | NA | ||
HIV = HIV; ICER = incremental cost-effectiveness ratio; NA = not applicable; PCV13 = pneumococcal conjugate 13-valent; PPSV23 = pneumococcal polysaccharide 23-valent; QALY = quality-adjusted life-year; USD = US dollar.
Note: ICERs assume 1 dose per vaccine unless otherwise specified. Reported USD amounts were converted to CAD using OECD purchasing price parity rates9 for the respective currency year and then inflated to 2024 CAD using the Bank of Canada inflation calculator.10 Appendix 1, Table 5 details the PPP and inflation rates used to adjust monetary amounts to 2024 Canadian dollars.
Note: This table has not been copy-edited.
aAs defined by the authors, individuals at-risk have one or more of the following “chronic heart disease, chronic liver disease, chronic respiratory disease, diabetes, asthma, alcohol abuse and smoking...chronic renal disease, nephrotic syndrome, malignant tumour (hematologic malignancy, solid tumour), and immune deficiency (HIV, organ or bone marrow transplant, low immunoglobulin, asplenia, sickle cell disease, or immunosuppressive therapy)”.11
bAs defined by the authors, chronic conditions includes chronic cardiac, pulmonary, liver or renal disease, diabetes mellitus, or CSF leakage.15
cWhile Shami et al. assert that the sequential strategy is being compared to PPSV23, as uptake of PPSV23 is 0% among adults less than 65, it is likely more appropriate to state that the sequential strategy is being compared to no vaccination in adults 20 to 49 years of age.15
dAs defined by the authors,15 immunocompromised individuals include those with asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to the use of immunosuppressive drugs/systemic steroids.39
eAs defined by the authors,15 high-risk individuals have a history of invasive pneumococcal diseases, immunocompromised conditions (asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to use of immunosuppressive drugs/systemic steroid), chronic diseases (chronic cardiac, pulmonary, liver or renal disease, diabetes mellitus, or CSF leakage), or cochlear implants.39
fAs defined by the authors, immunocompromised individuals include those with any of the following: HIV infection, Hodgkin disease, leukemia, lymphoma, myeloma, generalized malignancy, chronic renal failure, nephrotic syndrome, solid organ or bone marrow transplant, immunoglobulin deficiency, asplenia, sickle cell disease, or current immunosuppressive therapy (including radiation, systemic steroids, or chemotherapy).16
gIn both the immunocompromised and HIV-positive populations, 2 doses of PCV13 was dominated by PCV13 + 2 doses of PPSV23.16 Additionally, both PPSV23 and 2 doses of PPSV23 were subject to extended dominance through no vaccination and PCV13.16
Table 13: ICERs (2024 $CA) of Included Peer-Reviewed Studies of Adults 50 to 64 Years
Author, year | Country, currency | Population | ICER (2024 $CA/QALY) | ||
|---|---|---|---|---|---|
PCV13 vs. no vaccination | PCV13 vs. PPSV23 | PCV13 + PPSV23 vs. PPSV23 | |||
Heo et al., 201712 | South Korea, 2015 USD | Moderate riska | 26,523 | 16,666 | NA |
High riskb | 11,360 | 5,944 | NA | ||
Ishigami et al., 201913 | US, 2018 USD | Moderate riskc CKD | 36,150 | NA | NA |
High riskd CKD | 24,582 | NA | NA | ||
Kidney failure or nephrotic-range UACRe | 1,446 | NA | NA | ||
Rodriguez Gonzalez-Moro et al., 201614 | Spain, 2015 Euros | COPD | NA | 23,300 | NA |
Shami et al., 202015 | Hong Kong, 2017 USD | Chronic conditionsf | NA | NA | Dominantg |
Immunocompromissedh | NA | NA | Dominantg | ||
High riski | NA | NA | Dominantg | ||
CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; eGFR = estimated glomerular filtration rate; ICER = incremental cost-effectiveness ratio; NA = not applicable; PCV13 = pneumococcal conjugate 13-valent; PPSV23 = pneumococcal polysaccharide 23-valent; QALY = quality-adjusted life-year; UACR = urinary albumin-creatinine ratio; USD = US dollar.
Note: ICERs assume 1 dose per vaccine unless otherwise specified. Reported monetary amounts were converted to CAD using OECD purchasing price parity rates9 for the respective currency year and then inflated to 2024 CAD using the Bank of Canada inflation calculator.10 Appendix 1, Table 5 details the PPP and inflation rates used to adjust monetary amounts to 2024 Canadian dollars.
Note: This table has not been copy-edited.
aAs defined by the authors, individuals must have at least one of the following: diabetes mellitus, chronic liver disease, chronic pulmonary disease, or chronic cardiovascular or other chronic conditions affecting cardiac function.12
bAs defined by the authors, individuals must have at least one of the following: splenic dysfunction including postsplenectomy status, hematologic malignancy, a condition affecting the bone marrow or lymphatic system, solid organ or stem cell transplant, chronic renal disease, HIV infection, high-dose corticosteroid use (≥ 20 mg/day of prednisone or an equivalent) lasting 2 or more weeks, or treatment with a recombinant human immunomodulator.12
cCKD with moderate-risk is defined by the authors as having an “eGFR of 45 to 59 mL/min/1.73 m2 and UACR < 30 mg/g or eGFR ≥ 60 mL/min/1.73 m2 and UACR of 30 to 299 mg/g.”13
dCKD with high-risk is defined by the authors as having an “eGFR of 15 to 44 mL/min/1.73 m2 regardless of UACR, eGFR of 45 to 59 mL/min/1.73 m2 and UACR of 30 to 299 mg/g, or UACR of 300 to 1,999 mg/g regardless of eGFR.”13
eKidney failure or nephrotic-range UACR is defined by the authors as having an “eGFR < 15 mL/min/1.73 m2 and nephrotic-range albuminuria was UACR ≥ 2,000 mg/g.”13
fAs defined by the authors, chronic conditions include chronic cardiac, pulmonary, liver or renal disease, diabetes mellitus, or CSF leakage.15
gWhile Shami et al. assert that the sequential strategy is being compared to PPSV23, as uptake of PPSV23 is 0% among adults less than 65, it is likely more appropriate to state that the sequential strategy is being compared to no vaccination in adults 20 to 49 years of age.15
hAs defined by the authors,15 immunocompromised individuals include those with asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to the use of immunosuppressive drugs/systemic steroids.39
iAs defined by the authors,15 high-risk individuals have a history of invasive pneumococcal diseases, immunocompromised conditions (asplenia, HIV/AIDS, primary immunodeficiency, immunodeficiencies related to malignancy and transplant, immunodeficiencies related to use of immunosuppressive drugs/systemic steroid), chronic diseases (chronic cardiac, pulmonary, liver or renal disease, diabetes mellitus, or CSF leakage), or cochlear implants.39
Appendix 3: Included Grey Literature Economic Evaluations
Note that this appendix has not been copy-edited.
Table 14: Characteristics of Included Grey Literature Economic Evaluations
Author, year | Kobayashi et al., 202317 (Merck model) | Kobayashi et al., 202317 (Pfizer model) |
|---|---|---|
Country | US | US |
Perspective | Societal | Health care payer and societala perspective |
Modelling approach | Multicohort model | Multicohort model |
Time horizon | Lifetime | Lifetime |
Discount rate | NR | NR |
Study population | Adults aged 19 to 64 with certain risk conditionsb | Adults aged 42 years (age selected to represent adults aged 19 to 64 years) with certain risk conditionsb |
Relevant population | Aligned with study population | Aligned with study population |
Relevant intervention(s) |
| Single dose of PCV20 |
Comparator | Previous CDC recommendationc | Previous CDC recommendationc |
Cost per dose | NR | NR |
Source of clinical efficacy | NR | NR |
Industry funding | Merckd | Pfizerd |
CDC = US Centers for Disease Control and Prevention; NR = not reported; PCV15 = pneumococcal 15-valent conjugate vaccine; PCV20 = pneumococcal 20-valent conjugate vaccine; PPSV23 = pneumococcal polysaccharide 23-valent vaccine.
Note: Limited details were provided in Kobayashi et al. regarding modelling inputs and assumptions. The models are described in greater detail elsewhere.7
aThe report does not specify the perspective from which the presented results are reported.
bAs defined by the CDC, risk conditions includes any of the following: alcoholism or cigarette smoking, CSF leak, chronic heart disease, including congestive heart failure and cardiomyopathies, excluding hypertension, chronic liver disease, chronic lung disease, including COPD, emphysema, and asthma, cochlear implant, decreased immune function from disease or drugs (i.e., immunocompromising conditions), diabetes mellitus, chronic renal failure or nephrotic syndrome, congenital or acquired asplenia, or splenic dysfunction, congenital or acquired immunodeficiency (includes B-(humoral) or T-lymphocyte deficiency; complement deficiencies, particularly C1, C2, C3, and C4 deficiency; and phagocytic disorders [excluding chronic granulomatous disease]), diseases or conditions treated with immunosuppressive drugs or radiation therapy (includes Hodgkin disease, leukemias, lymphomas, malignant neoplasms, and solid organ transplant), HIV infection, sickle cell disease, or other hemoglobinopathies).40
cThe previous CDC recommendation pneumococcal vaccination strategy was defined by the authors as “PPSV23 only for adults aged 19–64 years with chronic medical conditions; PPSV23 with an option to receive PCV13 on the basis of shared clinical decision-making for adults aged ≥ 65 years without an immunocompromising condition, a CSF leak, or a cochlear implant; and both PCV13 and PPSV23 for adults with an immunocompromising condition, a CSF leak, or a cochlear implant.”17
dConflict of interest statements are provided in Leidner et al.18
Table 15: ICERs of Included Grey Literature Economic Evaluations
Author, year | Country, currencya | Population | Original ICER (US$/QALY) | ICER (2024 $CA/QALY) | ||
|---|---|---|---|---|---|---|
PCV15 + PPSV23 vs. PR | PCV20 vs. PR | PCV15 + PPSV23 vs. PR | PCV20 vs. PR | |||
Kobayashi et al., 202317 (Merck model) | US, 2022 USD | At-risk adults aged 19 to 64 | $274,000 to $342,000 | $63,000 to $201,000 | $345,161 to $430,821 | $79,362 to $253,202 |
Kobayashi et al., 202317 (Pfizer model) | Adults aged 42 years (age selected to represent adults aged 19 to 64 years) | NA | $13,000 | NA | $16,376 | |
ICER = incremental cost-effectiveness ratio; NA = not applicable; PCV15 = pneumococcal conjugate 15-valent; PCV20 = pneumococcal conjugate 20-valent; PPSV23 = pneumococcal polysaccharide 23-valent; PR = previous recommendation; QALY = quality-adjusted life-year; USD = US dollar.
Note: all ICERs are presented relative to the previous CDC recommendation pneumococcal vaccination strategy, defined by the authors as “PPSV23 only for adults aged 19–64 years with chronic medical conditions; PPSV23 with an option to receive PCV13 on the basis of shared clinical decision-making for adults aged ≥ 65 years without an immunocompromising condition, a CSF leak, or a cochlear implant; and both PCV13 and PPSV23 for adults with an immunocompromising condition, a CSF leak, or a cochlear implant.”17 The reported ranges for the Merck model cover encompass 2 scenarios: one with indirect effects considered, and one without indirect effects considered. Reported USD amounts were converted to CAD using OECD purchasing price parity rates9 for 2022 (1.164518) and then inflated to 2024 CAD using the Bank of Canada inflation calculator (inflation rate = 1.0817439).10
Appendix 4: Literature Search Strategy
Note that this appendix has not been copy-edited.
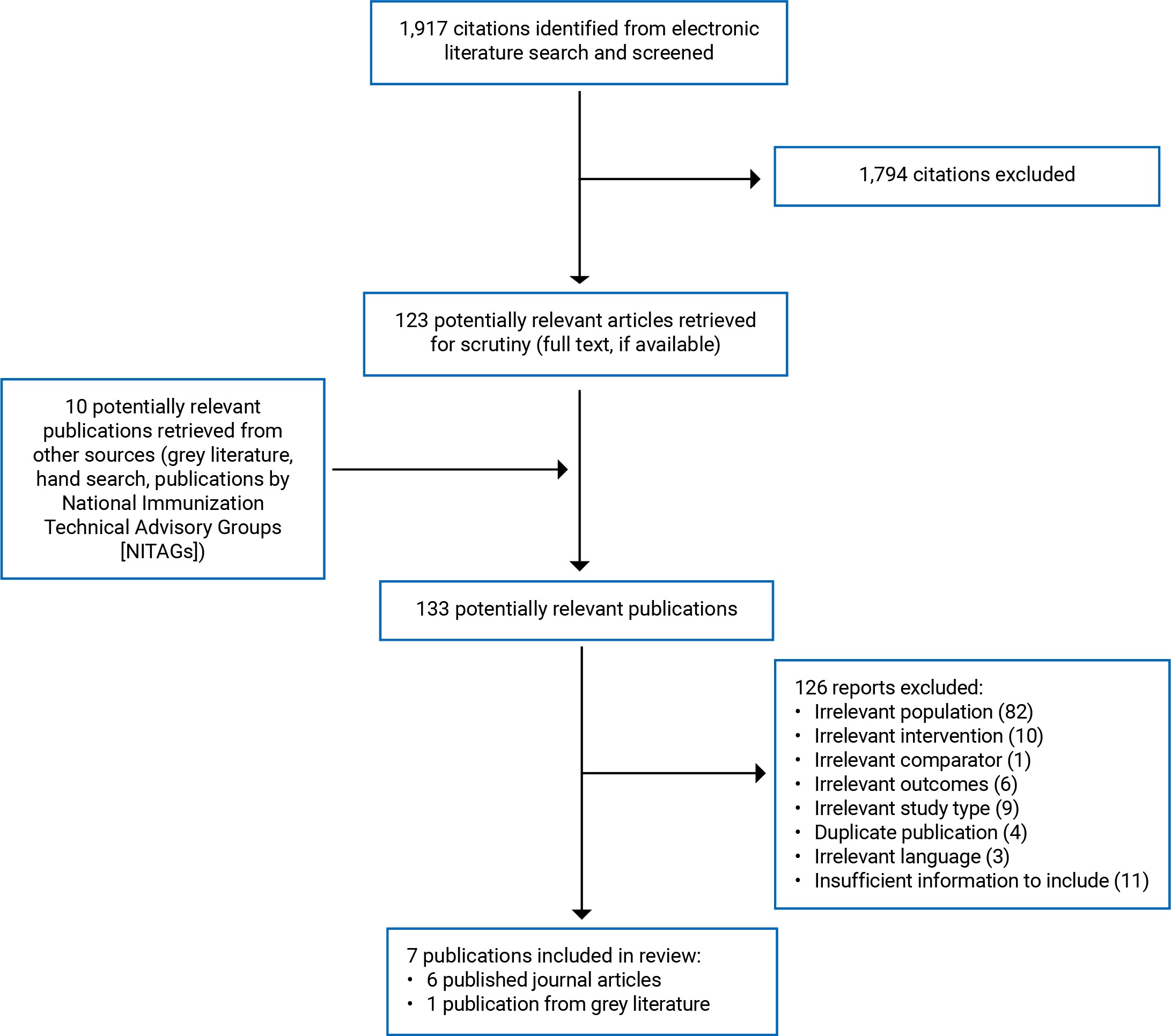
Economic Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database.
Date of search: February 22, 2024
Alerts: Bi-weekly search updates until project completion (May 13, 2024)
Search filters applied: Systematic reviews; meta-analyses; network meta-analyses; health technology assessments; economic evaluations; and costs and cost analysis studies.
Limits:
Publication date limit: 2011-present
Language limit: English- and French-language
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
Exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.pt | Publication type |
.mp | Mapped term |
.jw | Journal title word (MEDLINE) |
freq = # | Requires terms to occur # number of times in the specified fields |
Medal | Ovid database code: MEDLINE All, 1946 to present, updated daily |
Oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
exp Pneumococcal Vaccines/
(Vaccines/ or Vaccines, Conjugate/) and Pneumococcal Infections/
(PCV13 or PCV15 or PCV20 or PCV21 or PPV23 or PPSV23 or PPSV 23 or PNEU-C-15 or PNEU-P-23 or Pneu23 or Prevnar* or Prevenar* or PncOMPC or MnCC or PCV7 or PNCRM7 or pneumovax* or pneumorix* or Vaxneuvance* or synflorix* or pnu immune or pneu immune or pnu imune or pneuimmune or pnuimunne or pnuimune or apexxnar* or moniarix* or pneumopur* or streptopur* or streptorix* or 13 vpnc or 13vpnc or 20 vpnc or 20vpnc or SIIPL-PCV or PHiD-CV or pneumo 23).ti,ab,kf.
((Pneumoco* or pneumonia* or Streptococc* or strep or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23 or V116 or v 116 or v 110 or v 114 or v110 or v114) adj5 (vaccin* or immunis* or immuniz*)).ti,ab,kf.
((Pneumoco* or pneumonia* or Streptococc* or strep or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23 or V116 or v 116 or v 110 or v 114 or v110 or v114) and (vaccin* or immunis* or immuniz*)).ti.
((Pneumoco* or pneumonia* or Streptococc* or strep) and (13-valent or 15 valent or 20 valent or 21 valent or 23 valent or PCV21 or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23)).ti,ab,kf.
1 or 2 or 3 or 4 or 5 or 6
(Adolescent/ or exp Child/ or exp Infant/ or Pediatrics/ or (child or children or childhood or infant or infants or baby or babies or newborn or newborns or neonate or neonatal or neonates or preemie or preemies or infancy or paediatric or pediatric or girl or girls or boy or boys or kid or kids or teen or teens or teenage or teenager or teenagers or youngster or youngsters or youth or youths or adolescent or adolescents or adolescence or preadolescent or preadolescence or pre adolescent or pre adolescence or preschooler or school age or school aged or schoolchildren).ti,ab.) not (exp Adult/ or (adult or adults or adulthood or middle age or middle aged or elderly or senior or seniors or man or men or woman or women).ti,ab.)
7 not 8
(afghan* or albania* or algeria* or angola* or argentin* or armenia* or aruba* or azerbaijan* or bahrain* or bangladesh* or bengal* or bangal* or bajan or bajans or belarus* or belorus* or byelarus* or byelorus* or belize* or benin* or dahomey or bhutan* or bolivia* or bosnia* or herzegovin* or botswan* or batswan* or bechuanaland* or brazil* or brasil* or bulgaria* or burkina* or burkinese* or upper volta* or burundi* or urundi* or cabo verde* or cape verde* or cambodia* or kampuchea* or khmer* or cameroon* or cameroun* or ubangi shari* or chad or Chadian or (china* not (China National Infrastructure or China National Knowledge Infrastructure)) or beijing or shanghai or colombia* or comoro* or comore* or comorian* or mayotte* or congo* or zaire* or costa rica* or “cote d'ivoir*” or “cote d' ivoir*” or cote divoir* or cote d ivoir* or ivory coast* or ivorian* or cuba or cuban or cubans or “cuba's” or djibouti* or french somaliland* or dominica* or ecuador* or egypt* or united arab republic* or el salvador* or salvadoran* or guinea* or equatoguinea* or eritrea* or eswatini* or swaziland* or swazi* or swati* or ethiopia* or fiji* or gabon* or gabonese* or gabonaise* or gambia* or ghana* or grenada* or grenadian* or guatemala* or haiti* or hispaniola* or hondura* or ((india or indian or indians) not american india*) or delhi or indonesia* or iran* or iraq* or jamaica* or jordan* or kazakh* or kenya* or karabati* or kosovo* or kosova* or kyrgyz* or kirgiz* or kirghiz* or laos or lao or laotian* or lebanon* or lebanese* or lesotho* or lesothan* or lesothonian* or basutoland* or mosotho* or basotho* or liberia* or libya* or jamahiriya* or macedonia* or madagasca* or malagasy* or malawi* or nyasaland* or malaysia* or malay* federation or maldives* or maldivian* or mali or malian* or “mali's” or micronesia* or marshallese* or kiribati* or marshall island* or nauru or nauran or nauruans or “naurian's” or mariana or marianas or palau or paluan* or tuvalu* or mauritania* or mauritan* or mauritius* or mexico* or mexican* or moldova* or moldovia* or mongol* or montenegr* or morocco* or moroccan* or ifni or mozambique* or mozambican* or myanmar* or burma* or burmese or namibia* or nepal* or netherlands antill* or nicaragua* or niger* or pakistan* or palestin* or gaza* or west bank* or paraguay* or peru or peruvian* or “peru's” or philippine* or philipine* or phillipine* or phillippine* or filipino* or filipina* or russia* or ussr* or soviet* or rwanda* or rwandese or ruanda* or ruandese or samoa* or navigator island* or polynesia* or sao tome* or santomean* or senegal* or serbia* or sierra leone* or melanesia* or solomon island* or norfolk island* or somali* or south africa* or sri lanka* or ceylon* or saint lucia* or st lucia* or saint vincent* or st vincent* or vincentian* or grenadine* or sudan* or surinam* or syria* or tajik* or tadjik* or tadzhik* or tanzania* or tanganyika* or thai* or timor leste* or east timor* or timorese* or togo or togoles* or “togo's” or tonga* or tunisia* or turkiy* or turkey* or turk or turks or turkish or turkmen* or uganda* or ukrain* or uzbek* or vanuatu* or new hebrides* or venezuela* or vietnam* or viet nam* or yemen* or yugoslav* or zambia* or zimbabwe* or rhodesia* or global south or sahara* or subsahara* or magreb* or maghrib*).ti,ab,hw,kf.
(developing countr* or developing nation* or developing world or less developed countr* or less developed nation* or less developed world or lesser developed countr* or lesser developed nation* or lesser developed world or under developed countr* or under developed nation* or under developed world or underdeveloped countr* or underdeveloped nation* or underdeveloped world or middle income countr* or middle income nation* or low income countr* or low income nation* or lower income countr* or lower income nation* or underserved countr* or underserved nation* or under served nation* or deprived countr* or high burden countr* or high burden nation* or countdown countr* or countdown nation* or poor countr* or poor nation* or poor world or poorer countr* or poorer nation* or poorer world or developing econom* or less developed econom* or underdeveloped econom* or under developed econom* or middle income econom* or low income econom* or lower income econom* or low gdp or low gnp or low gross domestic or low gross national or lower gdp or lower gnp or lower gross domestic or lower gross national or lmic or lmics or third world or lami countr* or transitional countr* or emerging econom* or emerging nation*).ti.
(“Georgia (Republic)”/ or (georgia or georgian or georgians).ti,ab,kf.) not (Georgia/ or (atlanta or california or florida).ti,ab,kf.)
10 or 11 or 12
(American Samoa or Andorra* or Antigua* or Aruba* or Australia* or Austria* or Baham* or Barbuda* or Bahrain* or Barbad* or Belgium or Belgian or Bermud* or Brunei or Darussalam or Canad* or Cayman Islands or Channel Islands or Chile or Chilean* or Croatia* or Curacao or Cyprus or cypriot* or Czech* or Denmark or Danish or Estonia* or Faroe Islands or Finland or Finnish or France or French or Guyan* or guiana* or guyanese* or German* or Gibraltar or Greece or Greek* or grecian* or Greenland* or Guam or Hong Kong or Hungar* or Iceland* or Ireland or Irish or “Isle of Man” or Israel* or Ital* or Japan* or Korea* or Kuwait* or Latvia* or Liechtenstein or Lithuania* or Luxembourg or Macao or Malta or Maltese or “malta's” or Monaco or Nauru or Netherland* or Dutch or New Caledonia* or New Zealand* or Northern Mariana Islands or Norway or Norwegian* or oman or omani or omanis or “oman's” or Panam* or Poland or Polish or Portug* or Puerto Ric* or Qatar or Romania* or San Marino or Saudi Arabia* or Saudis or Seychelles or Singapor* or Sint Maarten or Slovak* or Slovenia* or Spain or Spanish or “St Kitts and Nevis” or saint kitts or st kitts or kittian* or nevisian* or St Martin or Swed* or Switzerland or Swiss or Taiwan* or Trinidad* or Tobago or “Turks and Caicos” or United Arab Emirates or UAE or United Kingdom or UK or England or Wales or Welsh or Scotland or Scottish or Great Britain or British or US or USA or “the us” or Uruguay* or Virgin Islands or high income or higher income or industrialized or industrialised or developed countr* or british columbia* or alberta* or saskatchewan* or manitoba* or ontario* or quebec* or new brunswick* or prince edward island* or nova scotia* or labrador* or newfoundland* or nunavut* or northwest territor* or yukon* or toronto* or montreal* or vancouver* or ottawa* or calgary* or edmonton* or winnipeg* or Appalachia* or great lakes or midwestern-us* or Midwest-us* or great plains or northeastern-us* or northeast-us* or pacific northwest or northwestern-us* or northwest-us* or southeast-us* or southeastern-us* or southern-us* or southwest-us* or southwestern-us* or “district of Columbia” or Washington dc or Alabama* or Alaska* or Arizona* or Arkansas or California* or Colorad* or Connecticut or Delaware or Florid* or Hawaii* or Hawai'i* or Idaho or Illinois or Indiana* or Iowa* or Kansas or Kansan or Kentucky or Louisiana* or Maine or Maryland or Massachusetts or Michigan or Minnesota* or Mississippi* or Montana* or Nebraska* or Nevada* or New Hampshire or New Jersey or New Mexico or New York or North Carolin* or Dakota* or Ohio or Ohian or Oklahoma* or Oregon* or Pennsylvania* or Rhode Island* or South Carolin* or Tennessee* or Texas or Texan or Utah or Vermont or Virginia or West Virginia* or Wisconsin or Wyoming).ti,ab,hw,kf.
13 not 14
9 not 15
Economics/
exp “Costs and Cost Analysis”/
Economics, Nursing/
Economics, Medical/
Economics, Pharmaceutical/
exp Economics, Hospital/
Economics, Dental/
exp “Fees and Charges”/
exp Budgets/
budget*.ti,ab,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ti,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ab. /freq=2
(cost* adj2 (effective* or utilit* or benefit* or minimi* or analy* or outcome or outcomes)).ab,kf.
(value adj2 (money or monetary)).ti,ab,kf.
exp models, economic/
economic model*.ab,kf.
markov chains/
markov.ti,ab,kf.
monte carlo method/
monte carlo.ti,ab,kf.
exp Decision Theory/
(decision* adj2 (tree* or analy* or model*)).ti,ab,kf.
or/17-38
(systematic review or meta-analysis).pt.
meta-analysis/ or systematic review/ or systematic reviews as topic/ or meta-analysis as topic/ or “meta analysis (topic)”/ or “systematic review (topic)”/ or exp technology assessment, biomedical/ or network meta-analysis/
((systematic* adj3 (review* or overview*)) or (methodologic* adj3 (review* or overview*))).ti,ab,kf.
((quantitative adj3 (review* or overview* or synthes*)) or (research adj3 (integrati* or overview*))).ti,ab,kf.
((integrative adj3 (review* or overview*)) or (collaborative adj3 (review* or overview*)) or (pool* adj3 analy*)).ti,ab,kf.
(data synthes* or data extraction* or data abstraction*).ti,ab,kf.
(handsearch* or hand search*).ti,ab,kf.
(mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab,kf.
(met analy* or metanaly* or technology assessment* or HTA or HTAs or technology overview* or technology appraisal*).ti,ab,kf.
(meta regression* or metaregression*).ti,ab,kf.
(meta-analy* or metaanaly* or systematic review* or biomedical technology assessment* or bio-medical technology assessment*).mp,hw.
(medline or cochrane or pubmed or medlars or embase or cinahl).ti,ab,hw.
(cochrane or (health adj2 technology assessment) or evidence report).jw.
(comparative adj3 (efficacy or effectiveness)).ti,ab,kf.
(outcomes research or relative effectiveness).ti,ab,kf.
((indirect or indirect treatment or mixed-treatment or bayesian) adj3 comparison*).ti,ab,kf.
(multi* adj3 treatment adj3 comparison*).ti,ab,kf.
(mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf.
umbrella review*.ti,ab,kf.
(multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multiparamet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
or/40-61
39 or 62
16 and 63
64 use medall
*Pneumococcus vaccine/
(PCV13 or PCV15 or PCV20 or PCV21 or PPV23 or PPSV23 or PPSV 23 or PNEU-C-15 or PNEU-P-23 or Pneu23 or Prevnar* or Prevenar* or PncOMPC or MnCC or PCV7 or PNCRM7 or pneumovax* or pneumorix* or Vaxneuvance* or synflorix* or pnu immune or pneu immune or pnu imune or pneuimmune or pnuimunne or pnuimune or apexxnar* or moniarix* or pneumopur* or streptopur* or streptorix* or 13 vpnc or 13vpnc or 20 vpnc or 20vpnc or SIIPL-PCV or PHiD-CV or pneumo 23 or pneumo23).ti,ab,kf.
((Pneumoco* or pneumonia* or Streptococc* or strep or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23 or V116 or v 116 or v 110 or v 114 or v110 or v114) adj5 (vaccin* or immunis* or immuniz*)).ti,ab,kf.
((Pneumoco* or pneumonia* or Streptococc* or strep or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23 or V116 or v 116 or v 110 or v 114 or v110 or v114) and (vaccin* or immunis* or immuniz*)).ti. 20055
((Pneumoco* or pneumonia* or Streptococc* or strep) and (13-valent or 15 valent or 20 valent or 21 valent or 23 valent or PCV21 or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23)).ti,ab,kf.
66 or 67 or 68 or 69 or 70
(exp *Adolescent/ or exp *Child/ or exp *Infant/ or exp *Pediatrics/ or (child or children or childhood or infant or infants or baby or babies or newborn or newborns or neonate or neonatal or neonates or preemie or preemies or infancy or paediatric or pediatric or girl or girls or boy or boys or kid or kids or teen or teens or teenage or teenager or teenagers or youngster or youngsters or youth or youths or adolescent or adolescents or adolescence or preadolescent or preadolescence or pre adolescent or pre adolescence or preschooler or school age or school aged or schoolchildren).ti.) not (exp Adult/ or (adult or adults or adulthood or middle age or middle aged or elderly or senior or seniors or man or men or woman or women).ti,ab.)
71 not 72
(afghan* or albania* or algeria* or angola* or argentin* or armenia* or aruba* or azerbaijan* or bahrain* or bangladesh* or bengal* or bangal* or bajan or bajans or belarus* or belorus* or byelarus* or byelorus* or belize* or benin* or dahomey or bhutan* or bolivia* or bosnia* or herzegovin* or botswan* or batswan* or bechuanaland* or brazil* or brasil* or bulgaria* or burkina* or burkinese* or upper volta* or burundi* or urundi* or cabo verde* or cape verde* or cambodia* or kampuchea* or khmer* or cameroon* or cameroun* or ubangi shari* or chad or Chadian or (china* not (China National Infrastructure or China National Knowledge Infrastructure)) or beijing or shanghai or colombia* or comoro* or comore* or comorian* or mayotte* or congo* or zaire* or costa rica* or “cote d'ivoir*” or “cote d' ivoir*” or cote divoir* or cote d ivoir* or ivory coast* or ivorian* or cuba or cuban or cubans or “cuba's” or djibouti* or french somaliland* or dominica* or ecuador* or egypt* or united arab republic* or el salvador* or salvadoran* or guinea* or equatoguinea* or eritrea* or eswatini* or swaziland* or swazi* or swati* or ethiopia* or fiji* or gabon* or gabonese* or gabonaise* or gambia* or ghana* or grenada* or grenadian* or guatemala* or haiti* or hispaniola* or hondura* or ((india or indian or indians) not american india*) or delhi or indonesia* or iran* or iraq* or jamaica* or jordan* or kazakh* or kenya* or karabati* or kosovo* or kosova* or kyrgyz* or kirgiz* or kirghiz* or laos or lao or laotian* or lebanon* or lebanese* or lesotho* or lesothan* or lesothonian* or basutoland* or mosotho* or basotho* or liberia* or libya* or jamahiriya* or macedonia* or madagasca* or malagasy* or malawi* or nyasaland* or malaysia* or malay* federation or maldives* or maldivian* or mali or malian* or “mali's” or micronesia* or marshallese* or kiribati* or marshall island* or nauru or nauran or nauruans or “naurian's” or mariana or marianas or palau or paluan* or tuvalu* or mauritania* or mauritan* or mauritius* or mexico* or mexican* or moldova* or moldovia* or mongol* or montenegr* or morocco* or moroccan* or ifni or mozambique* or mozambican* or myanmar* or burma* or burmese or namibia* or nepal* or netherlands antill* or nicaragua* or niger* or pakistan* or palestin* or gaza* or west bank* or paraguay* or peru or peruvian* or “peru's” or philippine* or philipine* or phillipine* or phillippine* or filipino* or filipina* or russia* or ussr* or soviet* or rwanda* or rwandese or ruanda* or ruandese or samoa* or navigator island* or polynesia* or sao tome* or santomean* or senegal* or serbia* or sierra leone* or melanesia* or solomon island* or norfolk island* or somali* or south africa* or sri lanka* or ceylon* or saint lucia* or st lucia* or saint vincent* or st vincent* or vincentian* or grenadine* or sudan* or surinam* or syria* or tajik* or tadjik* or tadzhik* or tanzania* or tanganyika* or thai* or timor leste* or east timor* or timorese* or togo or togoles* or “togo's” or tonga* or tunisia* or turkiy* or turkey* or turk or turks or turkish or turkmen* or uganda* or ukrain* or uzbek* or vanuatu* or new hebrides* or venezuela* or vietnam* or viet nam* or yemen* or yugoslav* or zambia* or zimbabwe* or rhodesia* or global south or sahara* or subsahara* or magreb* or maghrib*).ti,ab,hw,kf.
(developing countr* or developing nation* or developing world or less developed countr* or less developed nation* or less developed world or lesser developed countr* or lesser developed nation* or lesser developed world or under developed countr* or under developed nation* or under developed world or underdeveloped countr* or underdeveloped nation* or underdeveloped world or middle income countr* or middle income nation* or low income countr* or low income nation* or lower income countr* or lower income nation* or underserved countr* or underserved nation* or under served nation* or deprived countr* or high burden countr* or high burden nation* or countdown countr* or countdown nation* or poor countr* or poor nation* or poor world or poorer countr* or poorer nation* or poorer world or developing econom* or less developed econom* or underdeveloped econom* or under developed econom* or middle income econom* or low income econom* or lower income econom* or low gdp or low gnp or low gross domestic or low gross national or lower gdp or lower gnp or lower gross domestic or lower gross national or lmic or lmics or third world or lami countr* or transitional countr* or emerging econom* or emerging nation*).ti.
(“Georgia (Republic)”/ or (georgia or georgian or georgians).ti,ab,kf.) not (atlanta or california or florida).ti,ab,kf.
74 or 75 or 76
(American Samoa or Andorra* or Antigua* or Aruba* or Australia* or Austria* or Baham* or Barbuda* or Bahrain* or Barbad* or Belgium or Belgian or Bermud* or Brunei or Darussalam or Canad* or Cayman Islands or Channel Islands or Chile or Chilean* or Croatia* or Curacao or Cyprus or cypriot* or Czech* or Denmark or Danish or Estonia* or Faroe Islands or Finland or Finnish or France or French or Guyan* or guiana* or guyanese* or German* or Gibraltar or Greece or Greek* or grecian* or Greenland* or Guam or Hong Kong or Hungar* or Iceland* or Ireland or Irish or “Isle of Man” or Israel* or Ital* or Japan* or Korea* or Kuwait* or Latvia* or Liechtenstein or Lithuania* or Luxembourg or Macao or Malta or Maltese or “malta's” or Monaco or Nauru or Netherland* or Dutch or New Caledonia* or New Zealand* or Northern Mariana Islands or Norway or Norwegian* or oman or omani or omanis or “oman's” or Panam* or Poland or Polish or Portug* or Puerto Ric* or Qatar or Romania* or San Marino or Saudi Arabia* or Saudis or Seychelles or Singapor* or Sint Maarten or Slovak* or Slovenia* or Spain or Spanish or “St Kitts and Nevis” or saint kitts or st kitts or kittian* or nevisian* or St Martin or Swed* or Switzerland or Swiss or Taiwan* or Trinidad* or Tobago or “Turks and Caicos” or United Arab Emirates or UAE or United Kingdom or UK or England or Wales or Welsh or Scotland or Scottish or Great Britain or British or United States or USA or “the us” or Uruguay* or Virgin Islands or high income or higher income or industrialized or industrialised or developed countr* or british columbia* or alberta* or saskatchewan* or manitoba* or ontario* or quebec* or new brunswick* or prince edward island* or nova scotia* or labrador* or newfoundland* or nunavut* or northwest territor* or yukon* or toronto* or montreal* or vancouver* or ottawa* or calgary* or edmonton* or winnipeg* or Appalachia* or great lakes or midwestern-us* or Midwest-us* or great plains or northeastern-us* or northeast-us* or pacific northwest or northwestern-us* or northwest-us* or southeast-us* or southeastern-us* or southern-us* or southwest-us* or southwestern-us* or “district of Columbia” or Washington dc or Alabama* or Alaska* or Arizona* or Arkansas or California* or Colorad* or Connecticut or Delaware or Florid* or Hawaii* or Hawai'i* or Idaho or Illinois or Indiana* or Iowa* or Kansas or Kansan or Kentucky or Louisiana* or Maine or Maryland or Massachusetts or Michigan or Minnesota* or Mississippi* or Montana* or Nebraska* or Nevada* or New Hampshire or New Jersey or New Mexico or New York or North Carolin* or Dakota* or Ohio or Ohian or Oklahoma* or Oregon* or Pennsylvania* or Rhode Island* or South Carolin* or Tennessee* or Texas or Texan or Utah or Vermont or Virginia or West Virginia* or Wisconsin or Wyoming).ti,ab,hw,kf.
77 not 78
73 not 79
Economics/
Cost/
exp Health Economics/
Budget/
budget*.ti,ab,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ti,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ab. /freq=2
(cost* adj2 (effective* or utilit* or benefit* or minimi* or analy* or outcome or outcomes)).ab,kf.
(value adj2 (money or monetary)).ti,ab,kf.
Statistical Model/
exp economic model/
economic model*.ab,kf.
Probability/
markov.ti,ab,kf.
monte carlo method/
monte carlo.ti,ab,kf.
Decision Theory/
Decision Tree/
(decision* adj2 (tree* or analy* or model*)).ti,ab,kf.
or/81-99
62 or 100
80 and 101
102 use oemezd
65 or 103
exp animals/
exp animal experimentation/ or exp animal experiment/
exp models animal/
nonhuman/
exp vertebrate/ or exp vertebrates/
or/105-109
exp humans/
exp human experimentation/ or exp human experiment/
or/111-112
110 not 113
104 not 114
limit 115 to (english or french)
limit 116 to yr=”2011 -Current”
117 use medall
*Pneumococcus vaccine/
(PCV13 or PCV15 or PCV20 or PCV21 or PPV23 or PPSV23 or PPSV 23 or PNEU-C-15 or PNEU-P-23 or Pneu23 or Prevnar* or Prevenar* or PncOMPC or MnCC or PCV7 or PNCRM7 or pneumovax* or pneumorix* or Vaxneuvance* or synflorix* or pnu immune or pneu immune or pnu imune or pneuimmune or pnuimunne or pnuimune or apexxnar* or moniarix* or pneumopur* or streptopur* or streptorix* or 13 vpnc or 13vpnc or 20 vpnc or 20vpnc or SIIPL-PCV or PHiD-CV or pneumo 23 or pneumo23).ti,ab,kf.
((Pneumoco* or pneumonia* or Streptococc* or strep or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23 or V116 or v 116 or v 110 or v 114 or v110 or v114) adj5 (vaccin* or immunis* or immuniz*)).ti,ab,kf.
((Pneumoco* or pneumonia* or Streptococc* or strep or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23 or V116 or v 116 or v 110 or v 114 or v110 or v114) and (vaccin* or immunis* or immuniz*)).ti.
((Pneumoco* or pneumonia* or Streptococc* or strep) and (13-valent or 15 valent or 20 valent or 21 valent or 23 valent or PCV21 or PCV 13 or PCV 15 or PCV 20 or PCV 21 or PPV 23)).ti,ab,kf.
119 or 120 or 121 or 122 or 123
(exp *Adolescent/ or exp *Child/ or exp *Infant/ or exp *Pediatrics/ or (child or children or childhood or infant or infants or baby or babies or newborn or newborns or neonate or neonatal or neonates or preemie or preemies or infancy or paediatric or pediatric or girl or girls or boy or boys or kid or kids or teen or teens or teenage or teenager or teenagers or youngster or youngsters or youth or youths or adolescent or adolescents or adolescence or preadolescent or preadolescence or pre adolescent or pre adolescence or preschooler or school age or school aged or schoolchildren).ti.) not (exp Adult/ or (adult or adults or adulthood or middle age or middle aged or elderly or senior or seniors or man or men or woman or women).ti,ab.)
124 not 125
(afghan* or albania* or algeria* or angola* or argentin* or armenia* or aruba* or azerbaijan* or bahrain* or bangladesh* or bengal* or bangal* or bajan or bajans or belarus* or belorus* or byelarus* or byelorus* or belize* or benin* or dahomey or bhutan* or bolivia* or bosnia* or herzegovin* or botswan* or batswan* or bechuanaland* or brazil* or brasil* or bulgaria* or burkina* or burkinese* or upper volta* or burundi* or urundi* or cabo verde* or cape verde* or cambodia* or kampuchea* or khmer* or cameroon* or cameroun* or ubangi shari* or chad or Chadian or (china* not (China National Infrastructure or China National Knowledge Infrastructure)) or beijing or shanghai or colombia* or comoro* or comore* or comorian* or mayotte* or congo* or zaire* or costa rica* or “cote d'ivoir*” or “cote d' ivoir*” or cote divoir* or cote d ivoir* or ivory coast* or ivorian* or cuba or cuban or cubans or “cuba's” or djibouti* or french somaliland* or dominica* or ecuador* or egypt* or united arab republic* or el salvador* or salvadoran* or guinea* or equatoguinea* or eritrea* or eswatini* or swaziland* or swazi* or swati* or ethiopia* or fiji* or gabon* or gabonese* or gabonaise* or gambia* or ghana* or grenada* or grenadian* or guatemala* or haiti* or hispaniola* or hondura* or ((india or indian or indians) not american india*) or delhi or indonesia* or iran* or iraq* or jamaica* or jordan* or kazakh* or kenya* or karabati* or kosovo* or kosova* or kyrgyz* or kirgiz* or kirghiz* or laos or lao or laotian* or lebanon* or lebanese* or lesotho* or lesothan* or lesothonian* or basutoland* or mosotho* or basotho* or liberia* or libya* or jamahiriya* or macedonia* or madagasca* or malagasy* or malawi* or nyasaland* or malaysia* or malay* federation or maldives* or maldivian* or mali or malian* or “mali's” or micronesia* or marshallese* or kiribati* or marshall island* or nauru or nauran or nauruans or “naurian's” or mariana or marianas or palau or paluan* or tuvalu* or mauritania* or mauritan* or mauritius* or mexico* or mexican* or moldova* or moldovia* or mongol* or montenegr* or morocco* or moroccan* or ifni or mozambique* or mozambican* or myanmar* or burma* or burmese or namibia* or nepal* or netherlands antill* or nicaragua* or niger* or pakistan* or palestin* or gaza* or west bank* or paraguay* or peru or peruvian* or “peru's” or philippine* or philipine* or phillipine* or phillippine* or filipino* or filipina* or russia* or ussr* or soviet* or rwanda* or rwandese or ruanda* or ruandese or samoa* or navigator island* or polynesia* or sao tome* or santomean* or senegal* or serbia* or sierra leone* or melanesia* or solomon island* or norfolk island* or somali* or south africa* or sri lanka* or ceylon* or saint lucia* or st lucia* or saint vincent* or st vincent* or vincentian* or grenadine* or sudan* or surinam* or syria* or tajik* or tadjik* or tadzhik* or tanzania* or tanganyika* or thai* or timor leste* or east timor* or timorese* or togo or togoles* or “togo's” or tonga* or tunisia* or turkiy* or turkey* or turk or turks or turkish or turkmen* or uganda* or ukrain* or uzbek* or vanuatu* or new hebrides* or venezuela* or vietnam* or viet nam* or yemen* or yugoslav* or zambia* or zimbabwe* or rhodesia* or global south or sahara* or subsahara* or magreb* or maghrib*).ti,ab,hw,kf.
(developing countr* or developing nation* or developing world or less developed countr* or less developed nation* or less developed world or lesser developed countr* or lesser developed nation* or lesser developed world or under developed countr* or under developed nation* or under developed world or underdeveloped countr* or underdeveloped nation* or underdeveloped world or middle income countr* or middle income nation* or low income countr* or low income nation* or lower income countr* or lower income nation* or underserved countr* or underserved nation* or under served nation* or deprived countr* or high burden countr* or high burden nation* or countdown countr* or countdown nation* or poor countr* or poor nation* or poor world or poorer countr* or poorer nation* or poorer world or developing econom* or less developed econom* or underdeveloped econom* or under developed econom* or middle income econom* or low income econom* or lower income econom* or low gdp or low gnp or low gross domestic or low gross national or lower gdp or lower gnp or lower gross domestic or lower gross national or lmic or lmics or third world or lami countr* or transitional countr* or emerging econom* or emerging nation*).ti.
(“Georgia (Republic)”/ or (georgia or georgian or georgians).ti,ab,kf.) not (atlanta or california or florida).ti,ab,kf.
127 or 128 or 129
(American Samoa or Andorra* or Antigua* or Aruba* or Australia* or Austria* or Baham* or Barbuda* or Bahrain* or Barbad* or Belgium or Belgian or Bermud* or Brunei or Darussalam or Canad* or Cayman Islands or Channel Islands or Chile or Chilean* or Croatia* or Curacao or Cyprus or cypriot* or Czech* or Denmark or Danish or Estonia* or Faroe Islands or Finland or Finnish or France or French or Guyan* or guiana* or guyanese* or German* or Gibraltar or Greece or Greek* or grecian* or Greenland* or Guam or Hong Kong or Hungar* or Iceland* or Ireland or Irish or “Isle of Man” or Israel* or Ital* or Japan* or Korea* or Kuwait* or Latvia* or Liechtenstein or Lithuania* or Luxembourg or Macao or Malta or Maltese or “malta's” or Monaco or Nauru or Netherland* or Dutch or New Caledonia* or New Zealand* or Northern Mariana Islands or Norway or Norwegian* or oman or omani or omanis or “oman's” or Panam* or Poland or Polish or Portug* or Puerto Ric* or Qatar or Romania* or San Marino or Saudi Arabia* or Saudis or Seychelles or Singapor* or Sint Maarten or Slovak* or Slovenia* or Spain or Spanish or “St Kitts and Nevis” or saint kitts or st kitts or kittian* or nevisian* or St Martin or Swed* or Switzerland or Swiss or Taiwan* or Trinidad* or Tobago or “Turks and Caicos” or United Arab Emirates or UAE or United Kingdom or UK or England or Wales or Welsh or Scotland or Scottish or Great Britain or British or United States or USA or “the us” or Uruguay* or Virgin Islands or high income or higher income or industrialized or industrialised or developed countr* or british columbia* or alberta* or saskatchewan* or manitoba* or ontario* or quebec* or new brunswick* or prince edward island* or nova scotia* or labrador* or newfoundland* or nunavut* or northwest territor* or yukon* or toronto* or montreal* or vancouver* or ottawa* or calgary* or edmonton* or winnipeg* or Appalachia* or great lakes or midwestern-us* or Midwest-us* or great plains or northeastern-us* or northeast-us* or pacific northwest or northwestern-us* or northwest-us* or southeast-us* or southeastern-us* or southern-us* or southwest-us* or southwestern-us* or “district of Columbia” or Washington dc or Alabama* or Alaska* or Arizona* or Arkansas or California* or Colorad* or Connecticut or Delaware or Florid* or Hawaii* or Hawai'i* or Idaho or Illinois or Indiana* or Iowa* or Kansas or Kansan or Kentucky or Louisiana* or Maine or Maryland or Massachusetts or Michigan or Minnesota* or Mississippi* or Montana* or Nebraska* or Nevada* or New Hampshire or New Jersey or New Mexico or New York or North Carolin* or Dakota* or Ohio or Ohian or Oklahoma* or Oregon* or Pennsylvania* or Rhode Island* or South Carolin* or Tennessee* or Texas or Texan or Utah or Vermont or Virginia or West Virginia* or Wisconsin or Wyoming).ti,ab,hw,kf.
130 not 131
126 not 132
(systematic review or meta-analysis).pt.
meta-analysis/ or systematic review/ or systematic reviews as topic/ or meta-analysis as topic/ or “meta analysis (topic)”/ or “systematic review (topic)”/ or exp technology assessment, biomedical/ or network meta-analysis/
((systematic* adj3 (review* or overview*)) or (methodologic* adj3 (review* or overview*))).ti,ab,kf.
((quantitative adj3 (review* or overview* or synthes*)) or (research adj3 (integrati* or overview*))).ti,ab,kf.
((integrative adj3 (review* or overview*)) or (collaborative adj3 (review* or overview*)) or (pool* adj3 analy*)).ti,ab,kf.
(data synthes* or data extraction* or data abstraction*).ti,ab,kf.
(handsearch* or hand search*).ti,ab,kf.
(mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab,kf.
(met analy* or metanaly* or technology assessment* or HTA or HTAs or technology overview* or technology appraisal*).ti,ab,kf.
(meta regression* or metaregression*).ti,ab,kf.
(meta-analy* or metaanaly* or systematic review* or biomedical technology assessment* or bio-medical technology assessment*).mp,hw.
(medline or cochrane or pubmed or medlars or embase or cinahl).ti,ab,hw.
(cochrane or (health adj2 technology assessment) or evidence report).jw.
(comparative adj3 (efficacy or effectiveness)).ti,ab,kf.
(outcomes research or relative effectiveness).ti,ab,kf.
((indirect or indirect treatment or mixed-treatment or bayesian) adj3 comparison*).ti,ab,kf.
(multi* adj3 treatment adj3 comparison*).ti,ab,kf.
(mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf.
umbrella review*.ti,ab,kf.
(multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multiparamet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
or/134-155
Economics/
Cost/
exp Health Economics/
Budget/
budget*.ti,ab,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ti,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ab. /freq=2
(cost* adj2 (effective* or utilit* or benefit* or minimi* or analy* or outcome or outcomes)).ab,kf.
(value adj2 (money or monetary)).ti,ab,kf.
Statistical Model/
exp economic model/
economic model*.ab,kf.
Probability/
markov.ti,ab,kf.
monte carlo method/
monte carlo.ti,ab,kf.
Decision Theory/
Decision Tree/
(decision* adj2 (tree* or analy* or model*)).ti,ab,kf.
or/157-175
156 or 176
133 and 177
exp animals/
exp animal experimentation/ or exp animal experiment/
exp models animal/
nonhuman/
exp vertebrate/ or exp vertebrates/
or/179-183
exp humans/
exp human experimentation/ or exp human experiment/
or/185-186
184 not 187
178 not 188
limit 189 to (english or french)
limit 190 to yr=”2011 -Current”
191 use oemezd
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.