CADTH Health Technology Review
Cost-Effectiveness of Nirsevimab for the Prevention of Respiratory Syncytial Virus Infection in Infants
Technology Review
Authors: Ramon Brown, Sean Tiggelaar, Bernice Tsoi, Ian Cromwell
Abbreviations
ED
emergency department
ICER
incremental cost-effectiveness ratio
ICU
intensive care unit
IP
immunization during pregnancy
mAb
monoclonal antibody
MV
mechanical ventilation
NIP
national immunization program
OECD
Organization for Economic Cooperation and Development
PHAC
Public Health Agency of Canada
QALY
quality-adjusted life-year
RSV
respiratory syncytial virus
SoC
standard of care
Key Messages
During CADTH’s search of the economic literature, 3 economic studies were identified that assessed the cost-effectiveness of a long-acting monoclonal antibody, nirsevimab, as an intervention to prevent respiratory syncytial virus in infants in high-income countries, including 1 study set in Nunavik.
The 3 studies were conducted for different geographical locations: Canada, the US, and England and Wales. While each study conducted an economic evaluation, their approaches differed: 1 was a cost-consequence analysis and the other 2 were cost-utility analyses.
The results from the 3 studies varied considerably, and the nirsevimab programs differed (e.g., in terms of patients eligible for immunization). In general, nirsevimab was generally more effective and associated with lower total costs than comparator programs. The results were sensitive to the modelled region, source of efficacy data, price of nirsevimab, and severity of the respiratory syncytial virus season.
The generalizability of the identified studies to Canadian policy-making may be limited given the population compositions and cost parameters included in the models. To understand the potential cost-effectiveness of nirsevimab, a de novo economic evaluation would be required that compared nirsevimab with the existing preventive strategies employed in Canada (which may include monoclonal antibodies for infants) and is conducted in a Canadian setting.
Introduction and Rationale
Background and Rationale
Respiratory syncytial virus (RSV) infections are a common cause of respiratory illness in infants (i.e., the period of time between birth to 2 years of age),1 particularly during the winter months.2 Infants who contract RSV may experience symptoms such as coughing, wheezing, and difficulty breathing, and can experience serious complications, including bronchiolitis, pneumonia, and hospitalizations.3 According to the Public Health Agency of Canada (PHAC), RSV is responsible for an estimated 2,500 hospitalizations and 20 to 30 deaths among children under the age of 5 every year in Canada.4
Palivizumab (Synagis) is a monoclonal antibody (mAb) indicated for the prevention of serious lower respiratory tract disease caused by RSV in pediatric patients at a high risk of RSV disease.5 Since its approval, it has become the standard of care (SoC).6 The recommended dosage of palivizumab typically consists of 4 injections given monthly at the onset of and continuing throughout the RSV season.5 However, administration of palivizumab does not result in a 100% reduction in infant hospitalization for RSV.7 Therefore, there remains a need to have more efficacious products to prevent RSV infection in infants.7 Furthermore, immunization with palivizumab requires monthly injections throughout the RSV season, which can reduce access, particularly for families in rural regions or for those with lower socioeconomic status.5
Nirsevimab (Beyfortus) is a long-acting mAb that has been developed to aid in the prevention of RSV infections in infants.8 Nirsevimab was recently approved by Health Canada7 for the prevention of lower respiratory tract infections caused by RSV in neonates and infants during their first RSV season, or children up to 24 months of age who remain vulnerable to severe RSV disease through their second RSV season.9 Nirsevimab can be given as a single dose at birth, or just before (or at) the commencement of the RSV season.5,10 Clinical trials have shown that nirsevimab is highly effective at preventing RSV infections in infants, reducing the burden of RSV infections in infants, and decreasing the need for hospitalization and other medical treatments.11 It can provide protection against RSV for up to 6 months.12
While nirsevimab shows promise as an alternative immunization option for the prevention of RSV infections, its cost-effectiveness in the infant population remains uncertain.
Research Question
What is the cost-effectiveness of nirsevimab for the prevention of RSV infection in infants?
Methods
A review of the economic literature was undertaken to identify previously published economic evidence regarding the cost-effectiveness of using nirsevimab for the prevention of RSV infection in infants in high-income countries.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were nirsevimab (Beyfortus) or RSV vaccines or prophylaxis. CADTH-developed search filters were applied to limit retrieval to economic studies, citations related to health utilities or quality of life, and for background, health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons. The search was completed on April 10, 2023, and limited to English- or French-language documents published since January 1, 2013. Regular alerts updated the search until June 13, 2023.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Infants |
Intervention | Nirsevimab |
Comparator | Any comparator (e.g., placebo, no intervention, alternative RSV prevention interventions [e.g., other mAb]) |
Outcomes | Quality-adjusted life-years, disability-adjusted life-years, incremental costs and incremental cost-effectiveness ratio (e.g., cost per quality-adjusted life-year gained or incremental cost per event or event avoided), net monetary benefit, net health benefit |
Study designs | Full economic evaluations (e.g., cost-minimization analysis, cost-consequence analyses, cost-effectiveness analyses, cost-utility analyses) |
mAb = monoclonal antibody; RSV = respiratory syncytial virus.
Exclusion Criteria
Studies were excluded if they:
did not meet the selection criteria outlined in Table 1
were duplicate publications
were published in languages other than English and French
were not conducted in countries identified as high income by the World Bank13
were systematic reviews whose primary cost-effectiveness studies were otherwise captured or excluded
were published before 2013
were summarized in a previous CADTH technology review that compared RSV prefusion F to nirsevimab.14
Data Extraction and Critical Appraisal
During data extraction, the following were collected: author, publication year, country, currency, source of funding, study design, modelling approach, study perspective, discounting, time horizon, outcomes, source of clinical efficacy, study population characteristics, and results. The quality of the included studies was critically appraised by 1 reviewer using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Economic Evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Cost-effectiveness outcomes were reported as unadjusted and adjusted. Where adjusted, outcomes were adjusted to 2023 Canadian dollars using Organization for Economic Cooperation and Development (OECD) purchasing power parity rates15 and inflation rates from the Bank of Canada.16
Summary of Evidence
Quantity of Research Available
A total of 395 citations were identified in the literature search. Following the screening of titles and abstracts, 332 citations were excluded and 63 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 61 were excluded for various reasons, leading to 3 publications that met the inclusion criteria and were included in the report. Appendix 1 presents the PRISMA flow chart of the study selection.
Of the 3 economic evaluations identified, all were model-based studies. There was 1 each of an age-stratified dynamic compartmental transmission model, a decision tree, and a drug-based transmission model.17-19 The studies were set in England and Wales,9,18 the US,19 and Canada.17 In terms of funding sources, 1 study reported direct industry funding for editorial support.19 The remaining studies reported funding either through the European Union’s Horizon 2020 research and innovation program and the European Federation of Pharmaceutical Industries and Associations, or the Canadian Institute of Health Research (CIHR) and PHAC through the Canadian Immunization Research Network (CIRN), the latter which reports some funding from industry.17,18 Table 3 of Appendix 1 provides an overview of the characteristics of the 3 included studies.
Summary of Critical Appraisal
All of the studies met more than 50% of the Joanna Briggs Institute (JBI) Critical Appraisal Checklist criteria (please refer to Appendix 1).20 Across all 3 studies, it was unclear if costs and outcomes were measured accurately.17-19 Specifically, none of the studies discussed the potential limitations associated with the costs and outcome measures used or the accuracy of the measurement. The Canadian study did not conduct any sensitivity analyses, whereas the remaining 2 studies conducted a sensitivity analysis to explore uncertainties on select parameters. None of the studies included in this review discussed how they validated the key sources or assumptions that informed their estimates.
Although 1 Canadian study was identified (i.e., set in Nunavik), it is unclear whether this would be generalizable to the whole Canadian population because of the high rates of RSV infections and associated hospitalizations in this region, as well as the high costs associated with potential medical transport from remote Arctic regions. These transport costs accounted for a meaningful portion of the reported hospitalization costs, which may not be generalizable to regions of the country where the populace lives in close proximity to a hospital.17 Two non-Canadian studies set in high-income OECD countries were further identified. However, due to differences in their national health care systems and infant RSV immunization strategies, it is unclear whether the studies would be generalizable to the Canadian population.18,19
Summary of Findings
The base-case analyses for all studies were conducted from a health care payer perspective.17-19 The identified models considered a cohort of infants born within 1 year until they reached 6 months, 1 year, or 10 years of age.17-19 Two of the studies did not have discounting due to their 6-month and 1-year time horizons.17,19 The remaining study applied a discount rate of 3.5% over a 10-year time horizon.9,18 One of the studies reported disaggregated costs and health outcomes separately.9,19 Two studies reported cost-effectiveness as incremental cost-effectiveness ratios (ICERs), calculated as the incremental cost per additional QALY.17,18 For the remainder of this review, costs, ICERs, and cost-effectiveness thresholds are adjusted to 2023 Canadian dollars. A summary table of the main findings of each identified economic study, including original and unadjusted results, is available in Table 4 in Appendix 1.
One study evaluated the impact of RSV prevention strategies (i.e., immunization programs, RSV prophylactics) on the reduction in medically attended (outpatient) visits and hospitalizations for infants in Nunavik.17 The study authors noted that Nunavik’s health authorities previously piloted a passive immunization program in which high-risk and eligible healthy full-term infants (aged 0 to 2 months) received 5 doses of palivizumab during the RSV season (January to June); this pilot has since been terminated.17 Two scenarios were relevant — the first scenario compared no intervention against multiple RSV prevention strategies, including the previous pilot program, a seasonal immunization during pregnancy (IP) strategy, a seasonal IP plus nirsevimab strategy for infants who were preterm and chronically ill, and, nirsevimab strategy for infants who were preterm (0 to 5 months of age) and chronically ill (< 1 years of age).17 The second scenario compared different populations in which to offer nirsevimab: in preterm (0 to 5 months of age) and chronically ill (< 1 years of age) versus an expanded population that further included healthy full-term infants (0 to 2 months of age). While this study used a pairwise approach to compare various RSV prevention strategies, the focus of this report will be on nirsevimab-based strategies as IP outcomes have been reported in a previous CADTH review.14
These strategies were evaluated over mild, moderate, and severe RSV seasons.17 Only direct medical costs were considered, including outpatient, pediatric, and intensive care unit (ICU) visit costs and drug costs for palivizumab, nirsevimab, and maternal vaccines. The severity of RSV seasons was defined by the proportion of households with at least 1 infant infected with RSV within the season (i.e., 30% to 50%, 50% to 70%, and 70% to 90% for mild, moderate, and severe seasons, respectively). The efficacy of nirsevimab was assumed to be equal to the efficacy of palivizumab in terms of proportion of infants who require pediatric ward or ICU care. For the proportion of patients requiring outpatient visits, rates slightly differed as nirsevimab was based on the MELODY trial (i.e., nirsevimab = 47% versus palivizumab = 48%).17 It was found that administration of nirsevimab to preterm and chronically ill infants under 1 year of age was always cost saving compared to administration of palivizumab. In the scenario where the eligible population was expanded to include healthy infants between the ages of 0 to 2 months and preterm and chronically ill infants under 1 year of age, nirsevimab was cost-effective at a threshold of $50,000 per QALY and even cost saving when compared to existing palivizumab-based strategies across all scenarios of mild, moderate, and severe seasons.17
The study conducted in England and Wales used an age-stratified dynamic transmission model to directly compare the existing SoC for RSV (i.e., palivizumab) to 5 different nirsevimab-administration programs: very-high risk, seasonal, year-round, seasonal with catch-up, and seasonal with national immunization program (NIP)-integrated catch-up.18 In the SoC arm, palivizumab was defined as administration to infants born at less than 34 weeks of gestational age with bronchopulmonary dysplasia and/or congenital heart disease and less than 9 months at the start of the RSV season between October and February.18 In the very-high risk strategy, nirsevimab was administered to all infants who were eligible for palivizumab at birth.18 In the seasonal and year-round strategies, nirsevimab was administered to all infants at birth during the RSV season (October to February) or year-round, respectively.18 In the seasonal with catch-up strategy, nirsevimab was administered at birth to all infants born between September and February in addition to all infants younger than 7 months of age in October.18 In the seasonal with NIP-integrated catch-up strategy, nirsevimab was administered to all infants at birth who were born in the months of September to February in addition to infants at either 8,12, or 16 weeks of age at the closest time to the start of the RSV season.18 It was assumed that either nirsevimab or palivizumab would be administered to 90% of all eligible infants in England and Wales through NIPs.18 The RSV protection efficacy of both nirsevimab and palivizumab was 74% among those who received immunization through NIPs, per the MELODY trial. The efficacy of nirsevimab was assumed to be equal to that of nirsevimab; however, no citation was given to support this assumption.11 In the SoC arm, those in the palivizumab program were provided protection throughout the entire RSV season (i.e., October to February) while those in all 5 of the nirsevimab programs were protected from RSV for 150 days following administration. The authors noted that following initial administration of nirsevimab, infants would experience an exponential loss of protection with a lambda parameter (rate) of 1 out of 150 days, The results demonstrate that nirsevimab is likely cost-effective, although the choice of strategy is dependent on the price of nirsevimab. If the price per dose was less than or equal to £32, the seasonal with catch-up program would be optimal; if it was between £33 to £63, the seasonal program would be optimal, and if it was over £63, the very-high risk program would be optimal. Across the price range of nirsevimab studied, seasonal with NIP-integrated catch-up and year-round programs were always dominated (i.e., more costly, less effective).18 Several scenario analyses were conducted on the following parameters: coverage rate, average age of first administration, age-specific efficacy, and duration of nirsevimab-conferred RSV protection (i.e., protection lasting 100 days, 250 days, and 360 days). They reported that, at 360 days of protection, the year-round program went from never being optimal to being optimal if the price of nirsevimab was £16 or less.18
The study based in the US compared the existing SoC for RSV to a nirsevimab immunization program.19 Three distinct infant populations were considered: term and late preterm infants, preterm infants not eligible for palivizumab, and infants eligible for palivizumab (i.e., born at fewer than 29 weeks of gestational age or those with chronic lung disease of prematurity or congenital heart disease).19 SoC for RSV consisted of 5 monthly administrations of palivizumab during the RSV season for eligible infants only, and no prophylaxis for the other infant groups.19 The first dose of palivizumab was administered at the start of the RSV season or at birth for those born within the RSV season.19 The passive nirsevimab immunization program was a universal immunization program in which infants received a single dose of nirsevimab at birth or at the start of the RSV season. The study reported in disaggregate the direct health care costs and health outcomes. Health care costs included in the study were inpatient hospitalization, ICU stays, mechanical ventilation (MV), emergency department (ED) visits, and primary care visits.19 Intervention costs were not considered in the analysis. The efficacy and protection associated with nirsevimab and palivizumab were derived from the MEDLEY trial. The model assumed the current palivizumab would have uptake rates of 58% and, under this immunization program, the model estimated that 14% of the US birth cohort population would be infected with RSV. Among those infected, 67% would require a primary care visit, 24% would require an ED visit, and 9% would be hospitalized.19 Of the hospitalized population, 28% would be treated in the ICU and 7% would require MV. Based on this, the estimated direct health care burden of RSV under the SoC was $1.2 billion.19 Even though hospitalized cases made up less than 10% of the overall infected population, their associated costs represented 91% of the direct medical cost burden associated with RSV.19 The model assumed nirsevimab uptake rates ranging from 71% to 80%. Based on these inputs, the model predicted a 55% reduction in health-related events compared to the SoC population.19 Specifically, a nirsevimab program was estimated to produce a 55% reduction in both primary care visits and ED visits, and a 53% reduction in hospitalizations. Among patients who were hospitalized, there was an estimated 52% reduction in ICU admissions and a 51% reduction in MV relative to the palivizumab SoC.19 A deterministic sensitivity analysis was performed to assess the impact of incidence rates of health events.19 The number of avoided hospitalizations predicted by the model was found to be sensitive to changes in the estimated coverage rate for nirsevimab. When using an upper bound of an 86.8% nirsevimab coverage rate, 15,817 additional ED visits and 43,267 additional primary care visits were avoided compared to the mean coverage rate. When using the lower bound of a 68% nirsevimab coverage rate, the number of ED visits and primary care visits avoided was reduced by 3,113 and 8,516, respectively, compared to the mean nirsevimab coverage rate.19 Palivizumab had a coverage rate of 58%, derived from IQVIA data. Sensitivity analysis was performed on nirsevimab coverage rates (71% to 80%) across all infant groups and was not broken down across population groups.19
Discussion
The review identified 3 economic evaluations conducted in high-income countries that assessed the costs and consequences of nirsevimab for the prevention of RSV infection in infants in Canada, the US, and England and Wales.17-19 All of the studies assessed and reported the costs and clinical benefits associated with nirsevimab in an infant population but only 2 conducted a cost-effectiveness analysis.17-19 In the study that reported an ICER, nirsevimab was cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained, or was cost saving, depending on the structure of the program.
Limitations
None of the 3 studies provided sufficient information related to the potential logistic or resource-based challenges associated with the implementation of the different programs, which could impact feasibility and the cost-effectiveness of the programs’ implementation. Specifically, concerns and challenges among health care workers were reported with respect to the pilot palivizumab RSV immunization program in Nunavik as a result of limited human resources, as well as ethical and communication challenges with the Inuit population. These may impact both the costs and the uptake rate associated with any immunization-based program.
Nirsevimab has only been shown to provide protection for 1 RSV season (5 months).11 Both the Canadian and US studies only considered RSV protection during a single season, which limits the information available on the potential long-term cost-effectiveness outcomes of nirsevimab immunization on a longitudinal open cohort over a longer period of time. One of the studies noted that, when analyses are performed for a single RSV season, waning would only affect the final month for infants born outside of the season and, as such, would not be expected to impact the study conclusions.18 Furthermore, the cost-effectiveness of nirsevimab and the optimal immunization schedule may depend on the severity of the RSV season, as demonstrated by the Nunavik study.17 To assess the long-term clinical efficacy across multiple seasons, a long-term modelling approach would be optimal, and only 1 of the included studies assessed long-term efficacy.
Non–peer-reviewed studies were excluded from the literature review based on discussions with the PHAC. These studies included several economic evaluations published by government agencies that did not have corresponding peer-reviewed manuscripts in the literature. These studies evaluated the cost-effectiveness of nirsevimab compared to no intervention and to palivizumab in US pediatric populations.21,22
Generalizability
Despite all 3 studies being conducted in high-income OECD countries, including 1 in Canada (Nunavik), none of the included studies are broadly applicable to the Canadian health care system.
The economic evaluation set in Canada considered the population of Nunavik. The study population of remote northern communities may not be generalizable to other regions of Canada. While highly relevant to decision-makers in Nunavik and similar regions, the high rates of RSV infections and associated hospitalizations, as well as the potential higher costs with delivering care in remote Arctic regions,2 likely reduce the generalizability of the study’s cost-effectiveness results to urban regions of Canada.
The economic evaluation conducted in England and Wales considered cost-effectiveness at a range of prices for nirsevimab. The acquisition price of nirsevimab was not firmly established in this study and is yet to be determined in Canada. Nevertheless, the cost-effectiveness conclusions would likely be similar in Canada if compared against a similar program. However, if the palivizumab program varies between Canada and England and Wales, it would be harder to infer conclusions regarding the cost-effectiveness of nirsevimab from this study given the reduced generalizability to a Canadian setting. The costs parameters considered in the model (i.e., GP consultations, hospital admissions, hospital bed days) are UK-specific parameters that may not reflect Canadian clinical practice or health care costs. As the research team did not conduct sensitivity analyses on any other costs parameters, it is uncertain how sensitive the model is to costs (such as the impact of Canadian costs on the results).
The study conduct for the US population may not be generalizable to a Canadian health care setting given differences in the structure of the health care system, as well as health care costs. Specifically, US-specific cost parameters for inpatient hospitalization, ICU, and MV were derived from a database of claims data, which may not reflect expected Canadian costs. It should also be noted that the costs associated with purchasing and administering nirsevimab were excluded, which further reduces the generalizability of the study to the Canadian setting. Moreover, differences in the criteria to access palivizumab and nirsevimab further reduce the generalizability of this study.
Conclusions
Three published cost-effectiveness analyses of nirsevimab as a preventive intervention for RSV infection in infants were identified. However, the generalizability of the findings to a Canadian setting may be limited.
When compared to existing interventions (e.g., palivizumab), nirsevimab was consistently less costly and more clinically efficacious. However, ICERs varied across studies depending on the modelled region, the comparator immunization program, the source and/or assumptions for the clinical efficacy data, the price of nirsevimab, and the severity of the RSV season. Specifically, the assumed price per dose of nirsevimab varied widely in the included studies, ranging from $125 to $1,736 (adjusted to 2023 Canadian dollars). At the time of this review, the price of nirsevimab in Canada is unknown. As such, the generalizability of the published economic evaluations to a Canadian health care setting is unknown.
References
1.Public Health Agency of Canada. Infancy (birth - two years of age). In: Stages of childhood. 2016; https://www.canada.ca/en/public-health/services/health-promotion/childhood-adolescence/stages-childhood/infancy-birth-two-years.html. Accessed 2023 Jun 7.
2.Lavoie PM, Reicherz F, Solimano A, Langley JM. Potential resurgence of respiratory syncytial virus in Canada. CMAJ. 2021;193(29):E1140-E1141. PubMed
3.Canadian Pediatric Society. RSV (Respiratory syncytial virus). 2021; https://caringforkids.cps.ca/handouts/health-conditions-and-treatments/respiratory_syncytial_virus. Accessed 2023 Jul 14.
4.Public Health Agency of Canada. Respiratory syncytial virus (RSV): for health professionals. 2023; https://www.canada.ca/en/public-health/services/diseases/respiratory-syncytial-virus-rsv/health-professionals.html. Accessed 2023 Jul 14.
5.Synagis (palivizumab): sterile solution for intramuscular (50 mg/0.5 mL and 100 mg/1 mL) [product monograph]. Mississauga (ON): AstraZeneca Canada Inc; 2021 Jul 9: https://pdf.hres.ca/dpd_pm/00062121.PDF. Accessed 2023 Jul 14.
6.Public Health Agency of Canada. Respiratory syncytial virus (RSV): prevention and risks. 2023; https://www.canada.ca/en/public-health/services/diseases/respiratory-syncytial-virus-rsv/prevention-risks.html. Accessed 2023 Jun 7.
7.Public Health Agency of Canada. Recommended use of palivizumab to reduce complications of respiratory syncytial virus infection in infants. 2022 Jun 1; https://www.canada.ca/en/public-health/services/publications/vaccines-immunization/palivizumab-respiratory-syncitial-virus-infection-infants.html#a9. Accessed 2023 Jun 7.
8.Canadian Lung Association. Respiratory syncytial virus (RSV). [2023]; https://www.lung.ca/lung-health/lung-disease/respiratory-syncytial-virus-rsv. Accessed 2023 Jul 14.
9.Beyfortus (nirsevimab injection): solution for injection, 100 mg/mL, intramuscular use (50 mg and 100 mg single use, pre-filled syringe) [product monograph]. Mississauga (ON): AstraZeneca Canada Inc; 2023 Apr 19: https://pdf.hres.ca/dpd_pm/00070439.PDF. Accessed 2023 May 17.
10.Product information: beyfortus (nirsevimab). Annex I summary of product characteristics. (European public assessment report, EPAR). Amsterdam (Netherlands): European Medicines Agency; 2022; updated 2023: https://www.ema.europa.eu/en/documents/product-information/beyfortus-epar-product-information_en.pdf. Accessed 2023 May 18.
11.Hammitt LL, Dagan R, Yuan Y, et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N Engl J Med. 2022;386(9):837-846. PubMed
12.AstraZeneca. Nirsevimab US regulatory submission accepted for the prevention of RSV lower respiratory tract disease in infants and children up to age 24 months [press release]. 2023 Jan 5; https://www.astrazeneca.com/media-centre/press-releases/2023/nirsevimab-us-regulatory-submission-accepted-for-the-prevention-of-rsv-lower-respiratory-tract-disease-in-infants-and-children.html. Accessed 2023 May 23.
13.World Bank Group. The world by income and region, 2021. 2023; https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html. Accessed 2023 Apr 17.
14.CADTH. Cost-effectiveness of RSVpreF for Prevention of RSV Outcomes in Infants [in progress]. 2023; https://www.cadth.ca/cost-effectiveness-rsvpref-prevention-rsv-outcomes-infants. Accessed 2023 Jul 14.
15.Organisation for Economic Co-operation and Development. Purchasing power for GDP and related indicators. In: OECD.Stat. 2023; https://stats.oecd.org/Index.aspx?DataSetCode=PPPGDP. Accessed 2023 Apr 24.
16.Bank of Canada. Inflation calculator. 2023; https://www.bankofcanada.ca/rates/related/inflation-calculator/.
17.Nourbakhsh S, Shoukat A, Zhang K, et al. Effectiveness and cost-effectiveness of RSV infant and maternal immunization programs: A case study of Nunavik, Canada. EClinicalMedicine. 2021;41:101141. PubMed
18.Hodgson D, Koltai M, Krauer F, Flasche S, Jit M, Atkins KE. Optimal respiratory syncytial virus intervention programmes using nirsevimab in England and Wales. Vaccine. 2022;40(49):7151-7157. PubMed
19.Kieffer A, Beuvelet M, Sardesai A, et al. Expected impact of universal immunization with nirsevimab against RSV-related outcomes and costs among all US infants in their first RSV season: a static model. J Infect Dis. 2022;226(Suppl 2):S282-S292. PubMed
20.JBI. Critical appraisal tools (JBI checklist). [2023]; https://jbi.global/critical-appraisal-tools. Accessed 2023 Jul 14.
21.Ortega-Sanchez IR. Economics of preventing respiratory syncytial virus lower respiratory tract infections (RSVLRTI) among US infants with nirsevimab. Presentation at: Advisory Committee on Immunization Practices (ACIP) Meeting; 2023 Feb 22-24; Atlanta (GA). 2023; https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-02/slides-02-23/RSV-Pediatric-03-Sanchez-508.pdf. Accessed 2023 Jul 14.
22.Hutton DW. Economic analysis of nirsevimab in pediatric populations. Presentation at: Advisory Committee on Immunization Practices (ACIP) Meeting; 2023 Feb 22-24; Atlanta (GA). 2023; https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-02/slides-02-23/RSV-Pediatric-02-Hutton-508.pdf. Accessed 2023 Jul 14.
Appendix 1: Included Studies’ Results
Note that this appendix has not been copy-edited.
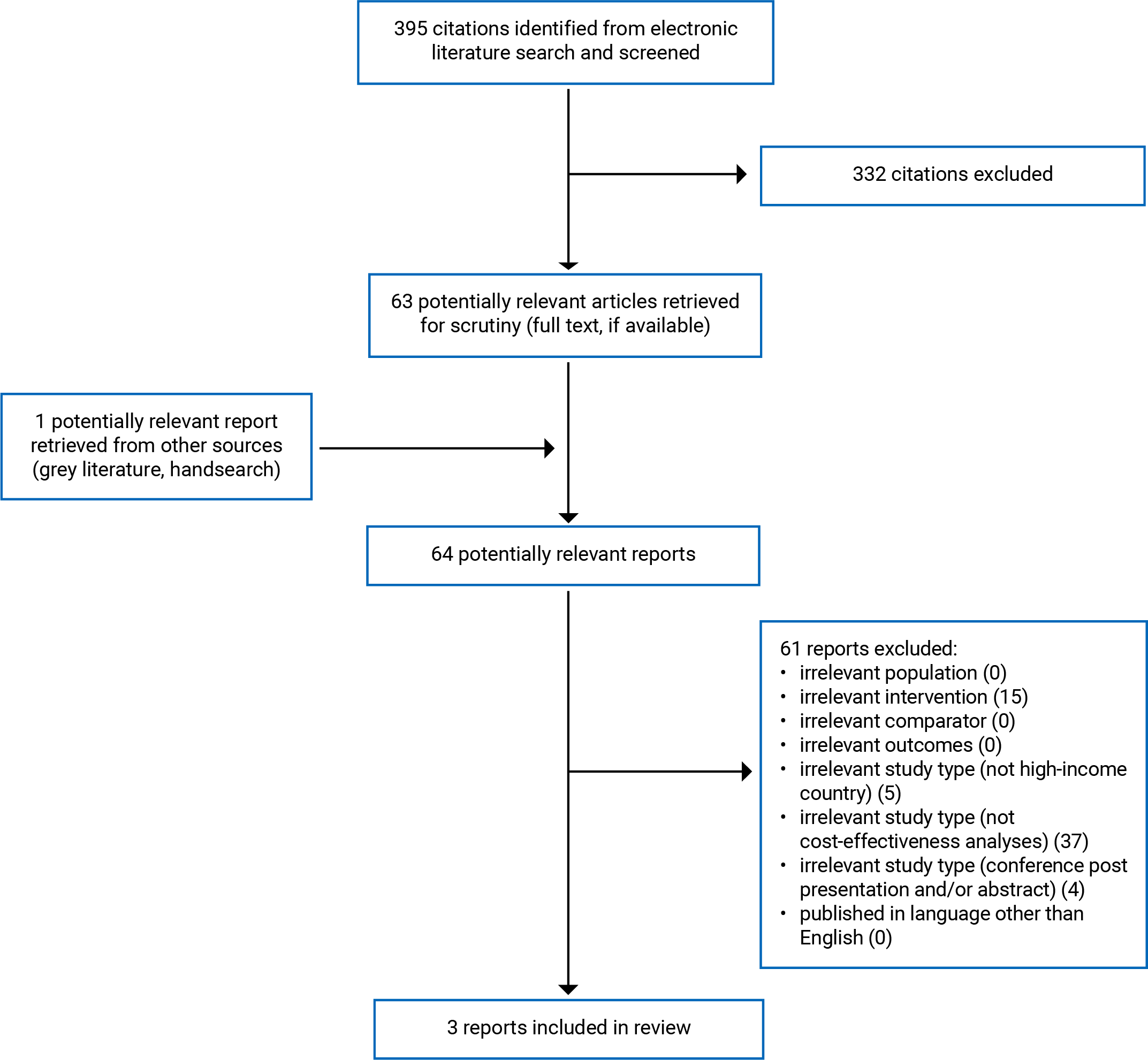
Table 2: Characteristics of Included Economic Evaluation
Author; year | Country | Type of analysis, perspective | Time horizon, discount rate | Population | Intervention and Comparators | Modelling Approach | Source of Clinical Efficacy | Price of nirsevimab | Industry Funding |
|---|---|---|---|---|---|---|---|---|---|
Hodgson et al 202218 | England and Wales | Cost-effectiveness analysis; health care payer | 10-year time horizon, 3.5% discount rate | New-born and infants | Comparator: Palivizumab Programmea Intervention: Five programmes that administers a single dose of nirsevimab: Very high-riskb, Seasonalc, Year-roundd, Seasonal with catch-upe, Seasonal with NIP-integrated catch-upf | Age-stratified compartmental dynamic transmission model 5 health outcomes associated with RSVg | MELODY Clinical Trial | £1–£4,600 | European Union’s Horizon 2020 research and innovation program and the European Federation of Pharmaceutical Industries and Associations. |
Kieffer et al 202219 | United States of America | Cost Consequence Analysis; health care payer | First RSV Season (6 months), No discounting | US birth cohort, separated into 3 Infant Groups:
| Comparator: 5 monthly administrations of palivizumab during RSV season for eligible patients only Intervention: Passive Immunization with nirsevimab | Decision tree | MELODY Clinical Trial | Not reported | AstraZeneca and Sanofi. |
Nourbaskhsh et al 202217 | Canada (Nunavik) | Cost-effectiveness analysis; health care payer | 1 year; No discounting | Infants (under 1 year of age) | Seasonal IP given to pregnant persons due Nov through Jun Seasonal IP plus long-acting mAb for preterm/ chronically ill infants No intervention Other interventions not directly compared to IP:
| Agent-based simulation | IPa: Derived from ResVax PREPARE trial data Short-acting mAb: palivizumab data from the literature Long-acting mAb assumed same as palivizumab | $1,560 (CAD $1,736 2023)b | CIHR and PHAC through CIRN, the latter of which reports some industry funding. |
mAB = monoclonal antibody, IP = immunization during pregnancy, CIHR = Canadian Institute of Health Research, CIRN = Canadian Immunization Research Network, PHAC = Public Health Agency of Canada
aPalivizumab has an efficacy of 74% is currently administered to 90% Palivizumab-eligible infants at birth between October to February, inclusive. Infants are eligible for Palivizumab if they are born at less than 34 weeks gestational age and Bronchopulmonary dysplasia (BPD) and/or congenital heart disease (CHD) and are < 9 months at the start of RSV season.
bVery High-Risk: Administration of nirsevimab to all infants who are currently eligible for Palivizumab at birth.
cSeasonal: Administration of nirsevimab to all infants born from October to February at birth.
dYear-Round: Administration of nirsevimab to all children at birth year-round.
eSeasonal with Catch-Up: Administration of nirsevimab to all infants born September to February at birth in addition to all infants less than 7 months of age in October.
fSeasonal with NIP-Integrated catch-up: Administration of nirsevimab to all infants born September to February at birth in addition to infants at either 8,12, or 16 weeks of age (to coincide with the existing National-Immunization Programme (NIP) in England) at the closest time to the start of the RSV season.
gRSV-associated health outcomes were: Symptomatic Infection, GP Consultations, Hospital Admissions, Hospital Bed Days, Deaths
hTerm and Late preterm infants: Born at or after 35 wGA (weeks’ gestational age)
iPreterm not eligible for Palivizumab: Preterm infants born between 29 wGA and 34 weeks, 6 days GA (gestational age) not eligible for palivizumab.
jPalivizumab-eligible: Infants born before 29 weeks wGA or those born with CLDP (chronic lung disease of prematurity) or CHD per the latest American Academy of Pediatrics recommendations.
Table 3: Quality Appraisal Results
Author; year | Critical appraisal: Joanna Briggs Institute (JBI) checklista | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
Hodgson et al 202218 | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes (limited) | Yes | Yes |
Kieffer et al 202219 | Yes | No | Yes | Yes | Unclear | Unclear | NA | No | Yes (limited) | Yes | Yes |
Nourbakhsh et al 202217 | Yes | Yes | Yes | Yes | Unclear | Unclear | NA | Yes | No | No | Yes |
aThe Joanna Briggs Institute (JBI) Checklist is a standardized tool used to assist in the critical appraisal of published economic evaluations that includes the following questions:
1Is there a well-defined question?
2Is there comprehensive description of alternatives?
3Are all important and relevant costs and outcomes for each alternative identified?
4Has clinical effectiveness been established?
5Are costs and outcomes measured accurately?
6Are costs and outcomes valued credibly?
7Are costs and outcomes adjusted for differential timing?
8Is there an incremental analysis of costs and consequences?
9Were sensitivity analyses conducted to investigate uncertainty in estimates of cost or consequences?
10Do study results include all issues of concern to users?
11Are the results generalizable to the setting of interest in the review?
Table 4: Main Results of Included Economic Evaluations
Authors, year | Country, currency | ICER nirsevimab vs. no intervention (original) | ICER nirsevimab vs no intervention (2023 CAD$)a | ICER nirsevimab vs. active comparator (specified) | Cost-effectiveness frontier (original) | Cost-effectiveness frontier (2023 CAD$) |
|---|---|---|---|---|---|---|
Hodgson et al 202218 | England and Wales 2018 Pound Sterling | Not considered in economic evaluation | Not considered in economic evaluation | Based on a willingness-to-pay threshold of £20,000 per QALY: If price < £63, there would be a 50% chance that optimal would be cost-effective relative to the current program with palivizumab. | Not reported but would depend on price of nirsevimab | Not reported but would depend on price of nirsevimab |
Kieffer et al 202219 | United States 2021 USD | Not considered in economic evaluation | Not considered in economic evaluation | Not reporteda | Not applicable | Not applicable |
Nourbakhsh et al 202117 | Canada (Nunavik) 2021 CAD$ | Mild season: $227,286/QALYd Moderate season: Dominant; -$587,402 Severe season: Dominant; -$809,332 | Mild: $252,856/QALYd Moderate: Dominant;-$587,402/QALY Severe: Dominant; -$900,382/QALY | Not compared. ICERs for long-acting mAb for preterm/chronically ill infants vs no intervention were lower than seasonal IP vs no intervention. In scenarios where healthy infants aged 0 to 2 were included, immunization with nirsevimab remained cost effective in mild, moderate and severe seasons of RSV compared to palivizumab with ICER values of $39,414 per QALY, $5,255 per QALY and cost savings of $7,049 per QALY, respectively | Not reported | Not reported |
mAB = monoclonal antibody, ICER = incremental cost-effectiveness ratio, QALY = quality-adjusted life-year
aAs this was a cost-consequence analysis, study reported that nirsevimab program would cost less and results in better health outcomes (fewer hospitalizations).
Appendix 2: Literature Search Strategy
Note that this appendix has not been copy-edited.
Economic Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: April 10, 2023
Alerts: Bi-weekly search updates until project completion June 12, 2023.
Search filters applied: Systematic reviews; meta-analyses; network meta-analyses; health technology assessments; economic evaluations; costs and cost analysis studies, and quality of life studies.
Limits:
Publication date limit: 2013-present
Language limit: English- and French-language
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
freq = # | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Respiratory Syncytial Virus Vaccines/
Respiratory Syncytial Virus Infections/dt, pc [Drug Therapy, Prevention & Control]
(nirsevimab* or nirsevumab* or beyfortus* or medi 8897* or MEDI8897* or medi8897* or MED-I8897* or “sp 0232*” or “sp 232*” or sp0232* or sp232* or VRN8S9CW5V*).ti,ab,kf,rn,nm.
((“respiratory syncytial” or RSV) adj3 (vaccin* or prophylaxis)).ti,kf.
or/1-4
Economics/
exp “Costs and Cost Analysis”/
Economics, Nursing/
Economics, Medical/
Economics, Pharmaceutical/
exp Economics, Hospital/
Economics, Dental/
exp “Fees and Charges”/
exp Budgets/
budget*.ti,ab,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ti,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ab. /freq=2
(cost* adj2 (effective* or utilit* or benefit* or minimi* or analy* or outcome or outcomes)).ab,kf.
(value adj2 (money or monetary)).ti,ab,kf.
exp models, economic/
economic model*.ab,kf.
markov chains/
markov.ti,ab,kf.
monte carlo method/
monte carlo.ti,ab,kf.
exp Decision Theory/
(decision* adj2 (tree* or analy* or model*)).ti,ab,kf.
or/6-27
“Value of Life”/
Quality of Life/
quality of life.ti,kf.
((instrument or instruments) adj3 quality of life).ab.
Quality-Adjusted Life Years/
quality adjusted life.ti,ab,kf.
(qaly* or qald* or qale* or qtime* or life year or life years).ti,ab,kf.
disability adjusted life.ti,ab,kf.
daly*.ti,ab,kf.
(sf36 or sf 36 or short form 36 or shortform 36 or short form36 or shortform36 or sf thirtysix or sfthirtysix or sfthirty six or sf thirty six or shortform thirtysix or shortform thirty six or short form thirtysix or short form thirty six).ti,ab,kf.
(sf6 or sf 6 or short form 6 or shortform 6 or sf six or sfsix or shortform six or short form six or shortform6 or short form6).ti,ab,kf.
(sf8 or sf 8 or sf eight or sfeight or shortform 8 or shortform 8 or shortform8 or short form8 or shortform eight or short form eight).ti,ab,kf.
(sf12 or sf 12 or short form 12 or shortform 12 or short form12 or shortform12 or sf twelve or sftwelve or shortform twelve or short form twelve).ti,ab,kf.
(sf16 or sf 16 or short form 16 or shortform 16 or short form16 or shortform16 or sf sixteen or sfsixteen or shortform sixteen or short form sixteen).ti,ab,kf.
(sf20 or sf 20 or short form 20 or shortform 20 or short form20 or shortform20 or sf twenty or sftwenty or shortform twenty or short form twenty).ti,ab,kf.
(hql or hqol or h qol or hrqol or hr qol).ti,ab,kf.
(hye or hyes).ti,ab,kf.
(health* adj2 year* adj2 equivalent*).ti,ab,kf.
(pqol or qls).ti,ab,kf.
(quality of wellbeing or quality of well being or index of wellbeing or index of well being or qwb).ti,ab,kf.
nottingham health profile*.ti,ab,kf.
sickness impact profile.ti,ab,kf.
exp health status indicators/
(health adj3 (utilit* or status)).ti,ab,kf.
(utilit* adj3 (valu* or measur* or health or life or estimat* or elicit* or disease or score* or weight)).ti,ab,kf.
(preference* adj3 (valu* or measur* or health or life or estimat* or elicit* or disease or score* or instrument or instruments)).ti,ab,kf.
disutilit*.ti,ab,kf.
rosser.ti,ab,kf.
willingness to pay.ti,ab,kf.
standard gamble*.ti,ab,kf.
(time trade off or time tradeoff).ti,ab,kf.
tto.ti,ab,kf.
(hui or hui1 or hui2 or hui3).ti,ab,kf.
(eq or euroqol or euro qol or eq5d or eq 5d or euroqual or euro qual).ti,ab,kf.
duke health profile.ti,ab,kf.
functional status questionnaire.ti,ab,kf.
dartmouth coop functional health assessment*.ti,ab,kf.
or/29-65
28 or 66
(systematic review or meta-analysis).pt.
meta-analysis/ or systematic review/ or systematic reviews as topic/ or meta-analysis as topic/ or “meta analysis (topic)”/ or “systematic review (topic)”/ or exp technology assessment, biomedical/ or network meta-analysis/
((systematic* adj3 (review* or overview*)) or (methodologic* adj3 (review* or overview*))).ti,ab,kf.
((quantitative adj3 (review* or overview* or synthes*)) or (research adj3 (integrati* or overview*))).ti,ab,kf.
((integrative adj3 (review* or overview*)) or (collaborative adj3 (review* or overview*)) or (pool* adj3 analy*)).ti,ab,kf.
(data synthes* or data extraction* or data abstraction*).ti,ab,kf.
(handsearch* or hand search*).ti,ab,kf.
(mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab,kf.
(met analy* or metanaly* or technology assessment* or HTA or HTAs or technology overview* or technology appraisal*).ti,ab,kf.
(meta regression* or metaregression*).ti,ab,kf.
(meta-analy* or metaanaly* or systematic review* or biomedical technology assessment* or bio-medical technology assessment*).mp,hw.
(medline or cochrane or pubmed or medlars or embase or cinahl).ti,ab,hw.
(cochrane or (health adj2 technology assessment) or evidence report).jw.
(comparative adj3 (efficacy or effectiveness)).ti,ab,kf.
(outcomes research or relative effectiveness).ti,ab,kf.
((indirect or indirect treatment or mixed-treatment or bayesian) adj3 comparison*).ti,ab,kf.
(meta-analysis or systematic review).md.
(multi* adj3 treatment adj3 comparison*).ti,ab,kf.
(mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf.
umbrella review*.ti,ab,kf.
(multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multiparamet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
or/68-90
67 or 91
5 and 92
93 use medall
*respiratory syncytial virus vaccine/
*respiratory syncytial virus infection/dt, pc [Drug Therapy, Prevention]
nirsevimab/
(nirsevimab* or nirsevumab* or beyfortus* or medi 8897* or MEDI8897* or medi8897* or MED-I8897* or “sp 0232*” or “sp 232*” or sp0232* or sp232*).ti,ab,kf,dq.
((“respiratory syncytial” or RSV) adj3 (vaccin* or prophylaxis)).ti,kf.
or/95-99
Economics/
Cost/
exp Health Economics/
Budget/
budget*.ti,ab,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ti,kf.
(economic* or cost or costs or costly or costing or price or prices or pricing or pharmacoeconomic* or pharmaco-economic* or expenditure or expenditures or expense or expenses or financial or finance or finances or financed).ab. /freq=2
(cost* adj2 (effective* or utilit* or benefit* or minimi* or analy* or outcome or outcomes)).ab,kf.
(value adj2 (money or monetary)).ti,ab,kf.
Statistical Model/
economic model*.ab,kf.
Probability/
markov.ti,ab,kf.
monte carlo method/
monte carlo.ti,ab,kf.
Decision Theory/
Decision Tree/
(decision* adj2 (tree* or analy* or model*)).ti,ab,kf.
or/101-118
socioeconomics/
exp Quality of Life/
quality of life.ti,kf.
((instrument or instruments) adj3 quality of life).ab.
Quality-Adjusted Life Year/
quality adjusted life.ti,ab,kf.
(qaly* or qald* or qale* or qtime* or life year or life years).ti,ab,kf.
disability adjusted life.ti,ab,kf.
daly*.ti,ab,kf.
(sf36 or sf 36 or short form 36 or shortform 36 or short form36 or shortform36 or sf thirtysix or sfthirtysix or sfthirty six or sf thirty six or shortform thirtysix or shortform thirty six or short form thirtysix or short form thirty six).ti,ab,kf.
(sf6 or sf 6 or short form 6 or shortform 6 or sf six or sfsix or shortform six or short form six or shortform6 or short form6).ti,ab,kf.
(sf8 or sf 8 or sf eight or sfeight or shortform 8 or shortform 8 or shortform8 or short form8 or shortform eight or short form eight).ti,ab,kf.
(sf12 or sf 12 or short form 12 or shortform 12 or short form12 or shortform12 or sf twelve or sftwelve or shortform twelve or short form twelve).ti,ab,kf.
(sf16 or sf 16 or short form 16 or shortform 16 or short form16 or shortform16 or sf sixteen or sfsixteen or shortform sixteen or short form sixteen).ti,ab,kf.
(sf20 or sf 20 or short form 20 or shortform 20 or short form20 or shortform20 or sf twenty or sftwenty or shortform twenty or short form twenty).ti,ab,kf.
(hql or hqol or h qol or hrqol or hr qol).ti,ab,kf.
(hye or hyes).ti,ab,kf.
(health* adj2 year* adj2 equivalent*).ti,ab,kf.
(pqol or qls).ti,ab,kf.
(quality of wellbeing or quality of well being or index of wellbeing or index of well being or qwb).ti,ab,kf.
nottingham health profile*.ti,ab,kf.
nottingham health profile/
sickness impact profile.ti,ab,kf.
sickness impact profile/
health status indicator/
(health adj3 (utilit* or status)).ti,ab,kf.
(utilit* adj3 (valu* or measur* or health or life or estimat* or elicit* or disease or score* or weight)).ti,ab,kf.
(preference* adj3 (valu* or measur* or health or life or estimat* or elicit* or disease or score* or instrument or instruments)).ti,ab,kf.
disutilit*.ti,ab,kf.
rosser.ti,ab,kf.
willingness to pay.ti,ab,kf.
standard gamble*.ti,ab,kf.
(time trade off or time tradeoff).ti,ab,kf.
tto.ti,ab,kf.
(hui or hui1 or hui2 or hui3).ti,ab,kf.
(eq or euroqol or euro qol or eq5d or eq 5d or euroqual or euro qual).ti,ab,kf.
duke health profile.ti,ab,kf.
functional status questionnaire.ti,ab,kf.
dartmouth coop functional health assessment*.ti,ab,kf.
or/120-158
119 or 159
100 and 160
(systematic review or meta-analysis).pt.
meta-analysis/ or systematic review/ or systematic reviews as topic/ or meta-analysis as topic/ or “meta analysis (topic)”/ or “systematic review (topic)”/ or exp technology assessment, biomedical/ or network meta-analysis/
((systematic* adj3 (review* or overview*)) or (methodologic* adj3 (review* or overview*))).ti,ab,kf.
((quantitative adj3 (review* or overview* or synthes*)) or (research adj3 (integrati* or overview*))).ti,ab,kf.
((integrative adj3 (review* or overview*)) or (collaborative adj3 (review* or overview*)) or (pool* adj3 analy*)).ti,ab,kf.
(data synthes* or data extraction* or data abstraction*).ti,ab,kf.
(handsearch* or hand search*).ti,ab,kf.
(mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab,kf.
(met analy* or metanaly* or technology assessment* or HTA or HTAs or technology overview* or technology appraisal*).ti,ab,kf.
(meta regression* or metaregression*).ti,ab,kf.
(meta-analy* or metaanaly* or systematic review* or biomedical technology assessment* or bio-medical technology assessment*).mp,hw.
(medline or cochrane or pubmed or medlars or embase or cinahl).ti,ab,hw.
(cochrane or (health adj2 technology assessment) or evidence report).jw.
(comparative adj3 (efficacy or effectiveness)).ti,ab,kf.
(outcomes research or relative effectiveness).ti,ab,kf.
((indirect or indirect treatment or mixed-treatment or bayesian) adj3 comparison*).ti,ab,kf.
(meta-analysis or systematic review).md.
(multi* adj3 treatment adj3 comparison*).ti,ab,kf.
(mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf.
umbrella review*.ti,ab,kf.
(multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multiparamet* adj2 evidence adj2 synthesis).ti,ab,kf.
(multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kf.
or/162-184
100 and 185
161 or 186
189 use oemezd
94 or 188
limit 189 to yr=”2013-current”
limit 190 to (english or french)
remove duplicates from 191
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.