CADTH Health Technology Review Recommendation
Advisory Panel Guidance on Minimum Retesting Intervals for Lab Tests
Appropriate Use Recommendation
Key Messages
What Is the Issue?
Lab test overuse can contribute to further unnecessary follow-up and testing, negative patient experiences, potentially inappropriate treatments, and the inefficient use of health care resources. One review of lab testing in Canada found that around 22% of blood tests were likely unnecessary.
One strategy to address lab test overuse is to establish minimal retesting intervals that can be implemented in medical laboratories to help identify and manage potentially inappropriate lab test requests.
Minimum retesting intervals suggest the minimum time before a test should be repeated based on the biochemical properties of the test and the clinical situation in which it is used. They are intended to inform clinical decisions about repeat testing.
The importance of lab resource stewardship is being addressed by Choosing Wisely Canada through Using Labs Wisely, a consortium of more than 150 hospitals committed to driving the appropriate use of lab testing in Canada. The hospitals participating in Using Labs Wisely identified a need for guidance on minimum retesting intervals for commonly used lab tests.
What Did We Do?
Choosing Wisely Canada and CADTH partnered to convene an independent time-limited advisory panel to develop consensus-based recommendations for minimum retesting intervals for 7 commonly used lab tests (antinuclear antibody [ANA], B-type natriuretic peptide [BNP] and N-terminal pro b-type natriuretic peptide [NT-proBNP], Hemoglobin A1C, lipase, lipid panel, serum protein electrophoresis [SPEP], and thyroid stimulating hormone [TSH]) in prespecified patient populations.
The advisory panel included core and specialist members who were recruited from across Canada. The 7 core advisory panel members brought together expertise in laboratory medicine, family practice, and patient lived experience. Seven additional specialist members brought expertise in endocrinology, cardiology, pediatric cardiology, rheumatology, hematology oncology, gastroenterology, and general internal medicine.
The Advisory Panel on Minimum Retesting Intervals considered patient group input, evidence from focused literature reviews, equity considerations, and clinical expertise. Through facilitated discussion, they reached consensus on the recommendations for minimum retesting intervals. Following external feedback, the recommendations for BNP and NT-proBNP and lipid panels were removed, and this document includes recommendations for minimum retesting intervals for 5 lab tests.
These are not recommendations for repeat testing. They are recommendations that if testing is undertaken, it should not be repeated sooner than the indicated intervals. They are not intended to replace clinical judgment as there may be exceptions in which the recommendations do not apply.
What Is the Potential Impact?
The recommendations on minimum retesting intervals can support the hospitals participating in Choosing Wisely Canada’s Using Labs Wisely program in their effort to reduce unnecessary lab tests and their impact on patients, providers, health systems, and the environment.
The recommendations may also be relevant to community and hospital lab stewardship efforts and may address the appropriate use of the 5 lab tests by enabling changes in lab test ordering in both inpatient and outpatient settings.
About the Panel Members
An independent time-limited advisory panel of 7 core and 7 specialist members developed recommendations on minimum retesting intervals for lab tests.
The 7 core panel members were recruited from across Canada and brought together expertise in laboratory medicine, family practice, and patient lived experience. The core panel helped draft and develop consensus-based recommendations.
The 7 specialist panel members brought expertise in endocrinology, cardiology, pediatric cardiology, rheumatology, hematology oncology, gastroenterology, and general internal medicine and participated in developing consensus-based recommendations for the tests that corresponded to their clinical area.
The names and biographies of the 14 panellists are on the CADTH website. Declarations of conflicts of interest can be found in Appendix 3.
Core Panel Members
Dr. Daniel Beriault, PhD, FCACB
Head of Biochemistry, Department of Laboratory Medicine, Unity Health Toronto; Associate Professor, University of Toronto, Ontario
Dr. Manal Elnenaei, MBChB, PhD, FRCPath, EuSpLM
Head of the Medical Biochemistry Division, Department of Pathology and Laboratory Medicine, Nova Scotia Health Authority; Professor, Dalhousie University, Nova Scotia
Dr. Rosilene Kraft, MBA, MSc, PhD, P.Eng.
Patient Partner, British Columbia
Dr. Janet Simons, FRCPC, Internal Medicine; FRCPC, Medical Biochemistry
Medical Biochemist and Internist, Providence Health Care; Assistant Clinical Professor, University of British Columbia, British Columbia
Dr. Alexander Singer, MB BAO BCh, CCFP, FCFP
Family Physician, Associate Professor, Clinician-Teacher and Director of Research and Quality Improvement, Department of Family Medicine, University of Manitoba, Manitoba
Dr. Li Wang, MD, MSc, FRCPC
Medical Biochemist, BC Children's and Women's Hospital and Health Centre; Clinical Associate Professor, University of British Columbia, British Columbia
Dr. Yan Yu, MD, MPP, MBA, CCFP
Family Physician, Alberta and Northwest Territories
Specialist Panel Members
Dr. Natalia Calo, MD
Therapeutic Endoscopist, St. Michael's Hospital Division of Gastroenterology; Assistant Professor of Medicine, University of Toronto, Ontario
Dr. Matthew Cheung, SM, MD, FRCP(C)
Clinician-Investigator and Clinical Hematologist, Odette Cancer Centre/Sunnybrook Health Sciences Centre; Professor, University of Toronto, Ontario
Dr. Nowell Fine, MD, SM, FRCPC, FACC, FCCS, FASE, FHFSA
Heart Failure Cardiologist and Echocardiologist and Associate Clinical Professor, University of Calgary, Alberta
Dr. Michael Khoury, MD
Pediatric Cardiologist and Assistant Professor, Stollery Children’s Hospital, University of Alberta, Alberta
Dr. Ferhan Siddiqi, MD FRCPC MScHQ
Endocrinologist, Queen Elizabeth II Health Sciences Centre; Associate Professor, Dalhousie University; Chair, Canadian Society of Endocrinology and Metabolism Quality Improvement Committee, Nova Scotia
Dr. William Silverstein, MD
General Internist, Sunnybrook Health Sciences Centre; Chair, Canadian Society of Internal Medicine’s Choosing Wisely Committee; Assistant Professor, University of Toronto, Ontario
Dr. Carter Thorne, MD, FRCPC, FACP, MACR
Consultant Staff Rheumatologist, Southlake Regional Health; Assistant Professor, University of Toronto, Ontario
In Partnership
Choosing Wisely Canada is the national voice for reducing unnecessary tests and treatments in Canada. Using Labs Wisely is a national consortium of more than 150 hospitals committed to making a measurable impact on reducing low-value lab testing in Canada.
CADTH is a not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs and medical devices in our health care system.
CADTH and Choosing Wisely Canada have partnered to host the Advisory Panel on Minimum Retesting Intervals for Lab Tests in support of Using Labs Wisely.
Acknowledgements
We wish to thank the following patient groups for their time and insights on the impact of the frequency of testing for patients: Arthritis Consumer Experts (ACE) Joint Health, Canadian Arthritis Patient Alliance, Cassie and Friends Society, Diabetes Canada, Gastrointestinal (GI) Society, JDRF Canada, Lupus Canada, Myeloma Canada, Pulmonary Hypertension Association Canada, Thyroid Foundation of Canada, and Thyroid Patients Canada.
We are grateful to the panel members who shared their time and expertise to develop these recommendations to support reducing unnecessary lab testing and thereby contributing to the quality of health care services in Canada.
We also wish to thank Dr. Doug Helmersen and Dr. Jason Weatherald for generously sharing their clinical expertise with the advisory panel on BNP and NT-proBNP retesting for pulmonary arterial hypertension. While the advisory panel's recommendation for this lab test was ultimately removed from the report due to strong differences of clinical opinion, the additional expertise deepened the panel's perspective.
Setting the Context
Overuse of Laboratory Tests
Laboratory testing is a critical component of effective patient care, and provides health care professionals and patients with important information to make decisions regarding the diagnosis, treatment, and management of many diseases.1 As a high-volume medical activity in Canada, it is estimated that more than $5 billion is spent annually on lab testing by the provincial and territorial governments.1
Inappropriate lab testing can occur when tests are underused, misused, or overused.1,2 Lab test overuse — which is the focus of Choosing Wisely Canada’s (CWC) Using Labs Wisely program — can occur in situations when they are not indicated, when there is the potential that patient harm exceeds the possible benefit, or when the test results are unlikely to inform the course of treatment or management of conditions (e.g., the test results may not reflect a clinically meaningful change).2 Other practices that can substantially contribute to the overuse of lab tests include repeat ordering of the same tests on the same patient before the indicated test interval or unnecessary duplicate testing (i.e., when a test is ordered even if there is valid result on file).2 A 2022 systematic review on inappropriately used clinical practices in Canada reported that approximately 22% of blood tests met the criteria for overuse (i.e., the potential harms exceeded the potential benefits).2 Lab test overuse can contribute to further unnecessary follow-up and testing, negative patient experiences, inaccurate diagnoses, potentially inappropriate treatments, and the inefficient use of health care resources.1-3
What Are Minimum Retesting Intervals?
One strategy to support the appropriate use of lab tests is to establish minimum retesting intervals. Minimum retesting intervals specify the minimum time before a test should be repeated, based on the biochemical properties of the test and the clinical situation in which it is used.4 They can help identify and manage lab test requests that are potentially inappropriate (i.e., if a test is ordered within a time frame that would likely not provide clinically meaningful information). They can reduce patient harm from potentially unnecessary testing and treatment and enable the creation of automated rules in laboratory information systems.
Rationale and Objectives for the Guidance
CWC, a national campaign focused on tests and treatments, is reducing unnecessary lab testing through Using Labs Wisely.5 Using Labs Wisely is a consortium of more than 150 hospitals committed to making a measurable impact on reducing low-value lab testing in Canada so that lab resources can be used more appropriately, and reduce the impact of unnecessary lab testing on patients, providers, health systems, and the environment.6
The hospitals participating in Using Labs Wisely identified a need for guidance on the minimum retesting intervals for 7 commonly repeated lab tests. CWC surveyed a small sample of the hospitals participating in Using Labs Wisely and identified heterogeneity in the retesting intervals for these lab tests.
In partnership with CWC, CADTH convened a time-limited advisory panel to support hospital labs by developing guidance on minimum retesting intervals for the following commonly repeated lab tests in in prespecified patient populations or clinical scenarios:
antinuclear antibody (ANA)
B-type natriuretic peptide (BNP) and N-terminal pro b-type natriuretic peptide (NT-proBNP)
hemoglobin A1C
lipase
lipid panel
serum protein electrophoresis (SPEP)
thyroid stimulating hormone (TSH).
This report includes a summary of the advisory panel discussions, the recommendations for minimum retesting intervals, and implementation advice for 5 of the 7 tests (excludingBNP and NT-proBNP and lipid panel). We received external feedback on our draft guidance report during our open call for feedback that revealed strong differences in clinical opinion over the proposed recommendations for BNP and NT-proBNP and lipid panel retesting. Given the significant difference of opinion, we felt the more prudent course of action was to remove these recommendations from the final report. Appendix 1 presents the recommendations and implementation advice for the remaining 5 tests.
Developing the Guidance
An overview of the approach used to develop consensus-based recommendations and the guidance report is provided in Figure 1. Appendix 2 presents a detailed description of the approach we used to develop this guidance.
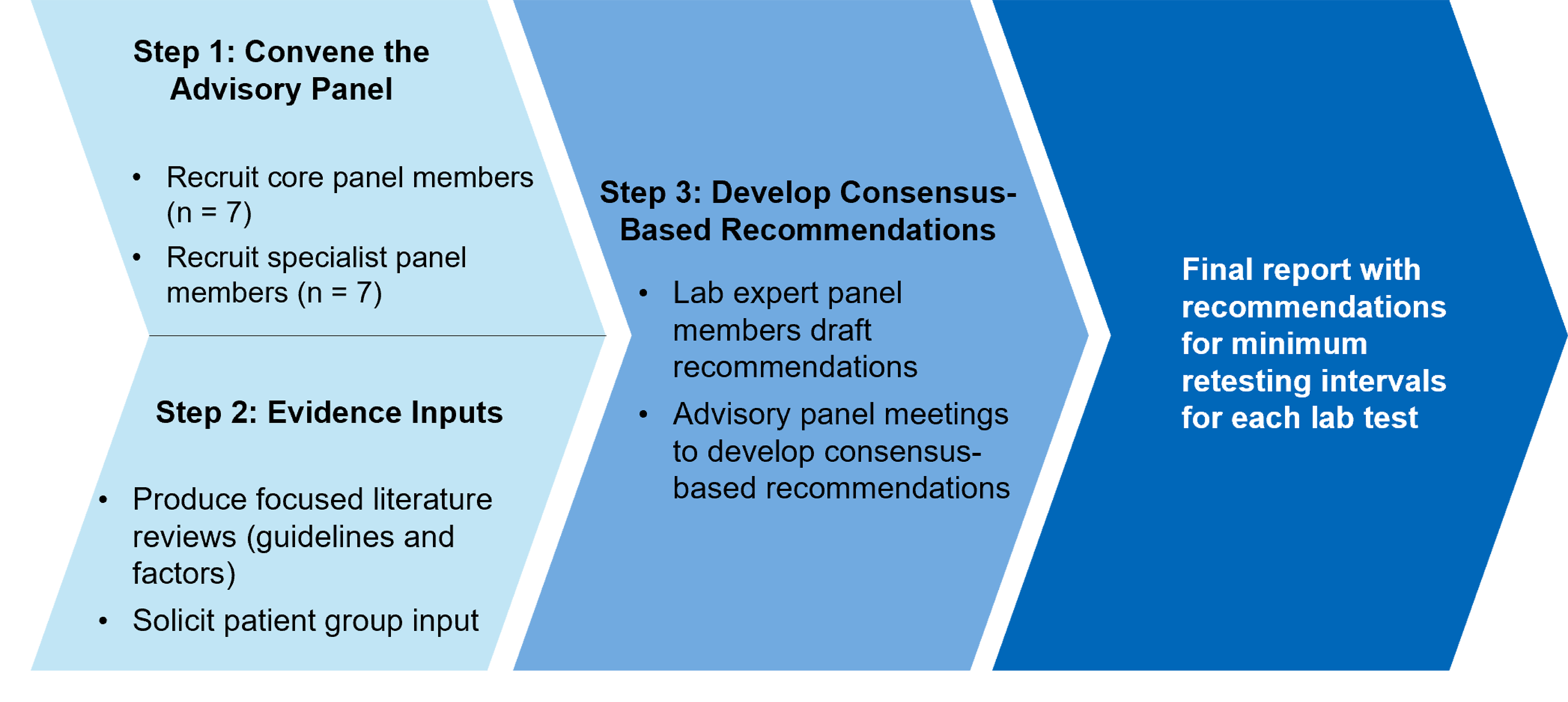
Step 1: Advisory Panel
CADTH and CWC coconvened an independent time-limited advisory panel that included specialists with expertise in the clinical areas covered by each test to develop recommendations for retesting and implementation advice. The core advisory panel comprised 4 lab experts, 1 of whom was the CWC Using Labs Wisely clinical lead; 2 family doctors; and a patient member. For each test, the core advisory panel was joined by 1 or 2 specialist panel members who brought relevant clinical expertise that related to each test (i.e., endocrinology, cardiology, rheumatology, hematology oncology, gastroenterology, and general internal medicine). Table 7 in Appendix 2 identifies the specialist panel members who participated in developing the guidance for each test.
Step 2: Evidence Inputs
CADTH solicited input from patient groups that represent people with the prespecified main condition(s) who could receive repeat testing with the lab tests of interest. We produced focused literature reviews for each test7 and summarized the existing guidance and evidence on factors that may impact the minimum retesting interval, as well as equity considerations.
Step 3: Developing Consensus-Based Recommendations
The advisory panel developed consensus-based guidance on minimum retesting intervals for lab tests through a series of synchronous and asynchronous approaches.
Before meeting, all advisory panel members received the literature reviews, a summary of patient group input, and a discussion guide to inform the development of preliminary and consensus-based recommendations. The discussion guide included questions to consider relating to the literature reviews (e.g., variation in the included evidence on repeat testing), patients’ experiences and perspectives from the patient group input, barriers and facilitators to implementation, and issues related to equity and equity-deserving groups.
First, the 4 lab experts independently prepared preliminary recommendations for each test. They met once (virtually) and through facilitated discussion developed a single consolidated draft recommendation for each test to be used as a starting point for the advisory panel discussions.
Next, the advisory panel, composed of the core advisory panel and applicable specialists, met virtually for a 1-hour facilitated, structured discussion of each lab test during which they generated consensus-based guidance (i.e., recommendations and implementation advice). In each discussion, the facilitator prompted the panel members to consider the evidence from the focused literature reviews, patient group input, equity considerations, and the expertise of the attending specialists to inform the panel’s revisions to the draft recommendations.
At the end of the discussion for each test, the advisory panel voted on accepting the recommendations as revised. Consensus (i.e., 70% agreement or higher) was reached on the recommendations for the 7 lab tests. All advisory panel members expressed agreement with the revised recommendations, with the exception of lipid panel, for which there were dissenting opinions. The panel's recommendations were consistent with or reflected the input of the patient groups in the majority of situations. When they may not have been perfectly aligned, it was generally because the patient group input was more detailed and specific (e.g., a specific clinical scenario that was outside the scope of the guidance) than could have been incorporated into a recommendation on minimum retesting intervals.
We posted the draft guidance document on the CADTH website for open feedback for 10 working days. We invited patient groups and others interested in the project to provide feedback through an online survey. A summary of the feedback we received and our responses to it, including the decision to remove the recommendations made for BNP and NT-proBNP and lipid panels, can be found in the Seeking and Responding to Feedback section in Appendix 2.
Advisory Panel Guidance
General Guidance for Implementing the Recommendations
Interpreting Recommendations for Minimum Retesting Intervals
The advisory panel developed recommendations on minimum retesting intervals, which are the suggested minimum times before the tests should be reordered, should repeat testing be clinically appropriate. They are not endorsements of repeat testing or direction that a test should be reordered at the recommended minimum retesting interval. They are recommendations that any repeat testing should not be done more frequently than the indicated intervals.
Implementation Advice by Lab Test
To support the adoption of minimum retesting interval recommendations, the panel developed specific implementation advice for several included tests with the intent of providing practical advice for labs, including suggested timing for hard stops (i.e., automated rules for laboratory information systems that could signal the lab to send the request back to the clinician because of it was requested before the minimum retesting interval). The panel recognized the need to balance the recommendations with the workflow of the labs. For example, during their discussions, the panel members noted how different timings of hard stops would likely affect the number of override requests, which could in turn impact their effectiveness at reducing unnecessary retesting.
General Implementation Advice
While recognizing that implementation will need to be tailored to the local context (e.g., care landscape, populations cared for, laboratory information systems, health system organization), the panel developed general guidance for recommendations:
For minimum retesting intervals to be applied effectively and for unnecessary repeat testing to be avoided, previous test results must be easily accessible for requesting physicians.
While the recommendations cannot account for all clinical scenarios, they were designed by the panel to apply to most cases for populations covered by the recommendations. Clinicians should always be able to discuss their test order with a lab professional if they feel repeat or more frequent testing is clinically appropriate, or if there are issues with a previous test result (e.g., interference, unexpected test results for the clinical context, a missing result).
When a lab test order is automatically rejected because an order is requested within the minimum retesting interval, the requesting physician should be notified that their test was not completed, and the existing test result should be provided to them.
When implementing these minimum retesting interval recommendations, in addition to considering local context, lab specialists can also explore options such as:
Opportunities for education can be embedded within laboratory information systems to support the uptake of recommendations for minimum retesting intervals and help change ordering behaviours. These can include education on what the minimum retesting interval is, reasons why a test does not need to be reordered, or why it is rejected, and can be included in orders and lab reports as comments or prompts, depending on the laboratory information system. For standard test panels, there can be educational prompts that direct the ordering of individual tests as opposed to the full panel.
Rules and algorithm suggestions for laboratory information systems: Options for implementing recommendations can, depending on the laboratory information system, include developing logic rules that account for previous test results. Labs can also consider promoting minimum retesting intervals for repeat tests based on specific levels of care, settings, or providers.
Advisory Panel Recommendations for Lab Tests
ANA
About the Test
ANAs are autoantibodies that bind to cellular components in the nucleus, cytoplasm, or mitotic apparatus, and are useful diagnostic biomarkers for autoimmune diseases.8,9 The ANA test measures the quantity (i.e., the titre) and the staining pattern of the antibodies.9 ANA testing is commonly used in the diagnosis of systemic autoimmune diseases such as systemic lupus erythematosus, systemic sclerosis, Sjogren disease, autoimmune hepatitis, and other rheumatic diseases.9
Recommendations
The clinical scenario in scope for the guidance is using ANA to monitor people with suspected or confirmed systemic autoimmune disease. The recommendations specific to ANA are in Table 1.
Table 1: Recommendations on Repeat ANA Testing
Recommendation and exceptions | Implementation advice |
|---|---|
1. If a previous ANA test is positive, do not reorder ANA for monitoring patients with suspected or confirmed systemic autoimmune disease. | To support reductions in unnecessary retesting, labs may consider implementing a 5-year hard stop minimum retesting interval. |
2. If a previous ANA test is negative or borderline positive, do not reorder ANA for monitoring patients with suspected or confirmed systemic autoimmune disease. An exception to this recommendation is if the clinical status of the patient significantly changes with newly developed symptoms, in which case ANA may be retested. | To support reductions in unnecessary retesting, labs may consider implementing a 24-month hard stop minimum retesting interval. |
ANA = antinuclear antibody.
Note: Minimum retesting intervals are recommendations that if testing is undertaken, it is not repeated sooner than indicated. They are not endorsements of repeat testing or a direction that a test should be reordered at the recommended minimum retesting interval. Clinicians should use clinical judgment as there may be exceptions in which the recommendations do not apply.
Developing the Guidance
The advisory panel for ANA was composed of the 7 core panel members plus a rheumatologist. They considered evidence from the ANA literature review7 and patient input from the Canadian Arthritis Patient Alliance, Cassie and Friends Society, Lupus Canada, and Arthritis Consumer Experts.
Key Discussion Points
The panel members discussed the following points when developing their recommendations:
The panel discussed the clinical guidance from the literature review that supported not repeating ANA following a previously positive test result in people with suspected or confirmed systemic autoimmune disease, as well as guidance from the literature review that it is only with a change in symptoms that a patient whose previous ANA test result is negative or borderline positive would warrant repeat ANA testing.
The panel noted the importance of the titre being provided by labs or within referrals to rheumatology alongside a positive or borderline positive ANA test result so that the results can be considered in conjunction with the patient’s symptoms to help guide clinical decisions.
Patient experiences with ANA testing were discussed, including instances where patients have newly developed symptoms following a borderline titre or test result and the need for retesting in these situations.
The panel discussed how more frequent testing may be warranted in those who are pregnant and pediatric patients with newly developed symptoms because of heightened potential risk to the person who is pregnant, the developing fetus, or the pediatric patient. The panel discussed that separate retesting intervals were not required for these populations, as the exception of retesting following newly developed symptoms applies to these populations.
There was alignment between the patient group input and the panel’s concerns around populations that may be more likely to have autoimmune diseases (e.g., people who are Black, Indigenous people, women) and who may experience additional barriers to accessing rheumatology care. The patient group input raised the issue of equity in terms of the impact and burden of repeat ANA testing on patients. The panel recognized that increasing the intervals between tests or removing the need to repeat previously positive results, and thus reducing unnecessary ANA testing and follow-up appointments, could benefit patients who experience barriers to accessing care, such as those living in rural and remote locations or those without access to a rheumatologist or primary care provider.
The panel reflected on the value of reducing unnecessary repeat testing for ANA, and that recommendations against reordering ANA tests in patients with suspected or confirmed autoimmune disease could reduce the time rheumatologists spend delivering low-value care (e.g., not spending time requesting ANA tests and following up about the ANA test results for patients who do not have a change in their clinical status) and potentially increase their capacity to better serve equity-deserving populations or underserved populations.
When developing the implementation advice for these recommendations, the panel considered whether shorter hard stops for the labs (e.g., 12 months) were needed to help limit the volume of requests from clinicians to override the minimum retesting interval. However, the panel aimed to strike a balance between the best clinical advice and what is reasonable for labs to implement (e.g., it may be challenging for laboratory information systems to implement a recommendation to never repeat a specific test).
After a previous positive ANA test result, the panel felt that the 5-year hard stop is sensible given the “do not reorder” recommendation, and that a hard stop of this length implies to the clinician that reordering after a previous positive result is not likely to provide useful clinical information. This was supported by evidence reported in the literature review that changes in ANA titres are not associated with autoimmune disease activity and that repeat ANA testing is not useful in determining disease progression.
Evidence reported in the literature review showed that repeat ANA testing after a negative ANA test result has low clinical utility. The panel felt that a 2-year hard stop after a previous negative ANA test result (in the absence of newly developed symptoms) was appropriate considering the “do not reorder” recommendation and to allow for clinical situations in which there might be a need to repeat ANA testing following a negative test result. This is shorter than the 5-year hard stop for a previously positive ANA test result given that repeat ANA testing after a previous positive result is not likely to provide useful clinical information.
Hemoglobin A1C
About the Test
The hemoglobin A1C test measures chronic glycemia and is useful for diagnosing diabetes and monitoring the overall effectiveness of diabetes treatments.10,11 Hemoglobin A1C is relatively unaffected by acute changes in blood glucose levels and is used to evaluate a person’s overall level of glucose control over time.10,11
Recommendations
The clinical scenario in scope for the guidance was using hemoglobin A1C to monitor people with an established diagnosis of type 1 or type 2 diabetes who are on either lifestyle modification, glucose lowering drugs, or insulin. The recommendations specific to hemoglobin A1C are in Table 2.
Table 2: Recommendations on Repeat Hemoglobin A1C Testing
Recommendation and exceptions | Implementation advice |
|---|---|
3. The recommended minimum retesting intervals for hemoglobin A1C in people who are being treated for diabetes are:
Exceptions to this recommendation that may warrant more frequent testing include children and adolescents with type 1 diabetes, people with diabetes who are planning to become pregnant, and people with rapidly changing blood glucose levels because of significant recent changes to lifestyle and/or medications | To support reductions in unnecessary retesting, labs may consider implementing a 60- to 86-day hard stop minimum retesting interval. This allows for practical considerations such as accommodating patient schedules for retesting appointments. |
4. Do not reorder hemoglobin A1C tests for assessing glycemic control in people with diabetes who have conditions that alter red blood cell turnover (e.g., iron deficiency anemia) or for people with diabetes who are in their second or third trimester of pregnancy. | To support reductions in unnecessary retesting, labs may consider implementing a 60- to 86-day hard stop minimum retesting interval. |
Note: Minimum retesting intervals are recommendations that if testing is undertaken, it is not repeated sooner than indicated. They are not endorsements of repeat testing or a direction that a test should be reordered at the recommended minimum retesting interval. Clinicians should use clinical judgment as there may be exceptions in which the recommendations do not apply.
Developing the Guidance
The advisory panel for hemoglobin A1C was composed of the 7 core panel members and an endocrinologist. The panel considered evidence from the focused literature review7 and patient input from the Juvenile Diabetes Research Foundation and Diabetes Canada.
Key Discussion Points
The panel members discussed the following points when developing their recommendations:
The panel discussed the clinical evidence from the literature review that supported a 3-month minimum retesting interval for adults who do not have stable glycemic levels and are still adjusting their diabetes therapy, as it related to the life cycle of red blood cells. The panel also noted that the clinical guidance from the literature review supports a 6-month minimum retesting interval for people with diabetes who have stable glycemic control.
Patient experiences with hemoglobin A1C testing were discussed, including the frequency of testing reported by patients every 3 to 6 months. Patient group input raised the issue of some people requiring more frequent testing, such as those who are actively undergoing changes in their treatment for their diabetes.
The panel recognized that there are exceptions for when more frequent hemoglobin A1C testing may be warranted, such as when an individual is experiencing rapid changes in their blood glucose because of changes in lifestyle or therapies. In these cases, retesting at 2 months would be appropriate.
The experts also discussed the importance of good glycemic control in people who are trying to become pregnant and noted that evidence from the literature review supported more frequent monitoring of hemoglobin A1C in the preconception period.
The panel considered whether there should be separate minimum retesting intervals for adults and children, but to simplify implementation they opted to have general recommendations that apply to both adults and children, except for the specific populations listed.
The panel considered equity issues, and recognized the importance of hemoglobin A1C testing for individuals who are not able to access technologies to monitor more frequent changes in blood glucose (e.g., continuous glucose monitoring).
The panel considered evidence from the literature review that there are several conditions (e.g., iron deficiency anemia, the second and third trimesters of pregnancy) that can result in invalid hemoglobin A1C test results (i.e., the hemoglobin A1C test result does not accurately reflect the person’s overall level of glycemic control) because of their impact on the rate of red blood cell turnover.
Based on their experiences, the panel members felt that much of the overuse of repeat hemoglobin A1C tests happened at less than 2 months, so using a 2-month cut off would be effective in reducing the majority of unnecessary lab tests. This approach is also supported by the evidence in the literature review regarding the clinical properties of the test and the clinical recommendations. They discussed labs’ experiences with implementation, where labs could have a 60- to 86-day hard stop with exceptions (these values are reflected in the literature review and based on expert experience). In particular, the panel wanted to enable access to hemoglobin A1C testing for individuals who have follow-up appointments scheduled before 3 months, and a hard stop between 60 to 86 days would provide flexibility to accommodate patient schedules.
Lipase
About the Test
Lipase is a digestive enzyme primarily produced in the pancreas to break down fats.12 When the pancreas becomes damaged or swollen due to inflammation, large amounts of lipase are released. Serum lipase testing can be used as part of the diagnostic criteria for acute pancreatitis.12,13
Recommendations
The clinical scenario in scope for the guidance was on using repeat lipase testing to monitor patients with acute or chronic pancreatitis. The recommendations specific to lipase are in Table 3.
Table 3: Recommendations on Repeat Lipase Testing
Recommendation and exceptions | Implementation advice |
|---|---|
5. Do not reorder lipase tests for monitoring patients with an established diagnosis of acute pancreatitis. | Not applicable |
6. Do not reorder lipase tests for monitoring patients with an established diagnosis of chronic pancreatitis. An exception to this recommendation is if there is clinical suspicion of acute-on-chronic pancreatitis, where lipase testing is required for diagnostic purposes. | To support reductions in unnecessary retesting, in outpatient or community settings, labs may consider implementing a 6-month hard stop minimum retesting interval. This recommendation is based on the experience of the advisory panel as no relevant information for serum lipase retesting for chronic pancreatitis was identified in the literature review. |
Note: Minimum retesting intervals are recommendations that if testing is undertaken, it is not repeated sooner than indicated. They are not endorsements of repeat testing or a direction that a test should be reordered at the recommended minimum retesting interval. Clinicians should use clinical judgment as there may be exceptions in which the recommendations do not apply.
Developing the Guidance
The advisory panel for lipase was composed of the 7 core panel members plus an internal medicine specialist and a gastroenterologist. The panel considered evidence from the focused literature review7 and patient input from the GI Society.
Key Discussion Points
The panel members discussed the following points when developing their recommendations:
The panel discussed that the utility of lipase testing is for the diagnosis of acute pancreatitis, and that it does not have prognostic value in patients with acute or chronic pancreatitis, even if lipase levels are persistently elevated or if levels return to normal.
In patients with an established diagnosis of acute pancreatitis, the consensus is that repeat lipase testing does not add clinical value, and that repeat testing in this population is unnecessary. Even in the presence of newly developed symptoms, the panel noted that repeat lipase testing does not add value once a diagnosis of acute pancreatitis is established. This is reflected in the literature review in the statements against repeat lipase testing and the consistent pattern of lipase levels after the onset of acute pancreatitis. Patient input also supports that lipase is important for diagnostic purposes but not for monitoring.
The experts noted that the diagnostic criteria for acute pancreatitis include lipase levels that are 3 times the upper limit of normal and suggested that labs may consider restricting repeat lipase testing if the previous result was greater than or equal to 3 times the upper limit of normal.
The experts discussed that the diagnosis of chronic pancreatitis is not based on lipase levels, and that lipase should not be retested in patients with a diagnosis of chronic pancreatitis as it has no prognostic value in patients with chronic pancreatitis. However, it was noted that acute episodes of pancreatitis can occur in patients with chronic pancreatitis (i.e., acute-on-chronic pancreatitis). Retesting lipase in patients with chronic pancreatitis is only relevant if the patient presents with symptoms of acute-on-chronic pancreatitis. In this case, the panel members discussed that these patients may seek urgent care, where lipase can be used in the acute care setting to confirm the diagnosis.
Based on panel members’ experience, lipase can be mildly elevated for multiple conditions, including chronic pancreatitis and health conditions unrelated to the pancreas. However, there is no clinical utility of repeating lipase in these patients and the test results can lead to patient distress due to a lack of prognostic value. It was suggested that lipase should not be tested in the absence of pain suggestive of acute pancreatitis.
The potential harms of repeating lipase testing in patients with an established pancreatitis diagnosis were discussed, including increased health care system costs with no added clinical value, and the potential for additional unnecessary tests being ordered for patients (e.g., imaging, endoscopy) due to persistently elevated lipase.
The panel acknowledged that there are certain equity-deserving populations that may be at higher risk for pancreatitis (e.g., people with alcohol use disorders), but that the same guidance regarding retesting would apply to these populations.
The panel considered that in outpatient settings some providers may repeat lipase testing to ensure lipase levels return to normal, and that education (i.e., lipase does not have prognostic value and serial lipase tests should not be ordered) is needed to help change inappropriate reordering behaviours. To support labs and care providers to reduce unnecessary retesting, the panel proposed implementing a 6 month hard stop for outpatient settings.
SPEP
About the Test
SPEP detects the presence or absence of monoclonal immunoglobulin (M protein) in the serum and provides a measurement of M protein concentration (or size).14 The M protein presentation, concentration and region from the SPEP sample can support the diagnosis and subsequent monitoring of patients with suspected or confirmed plasma cell dyscrasias (e.g., multiple myeloma, monoclonal gammopathy of undetermined significance [MGUS]).14,15
Recommendations
The clinical scenario in scope for the guidance is using SPEP for monitoring patients with confirmed plasma cell dyscrasias. The recommendation specific to SPEP is in Table 4.
Table 4: Minimum Retesting Interval Recommendations for SPEP
Recommendation and exceptions | Implementation advice |
|---|---|
7. The recommended minimum retesting intervals for SPEP for monitoring patients with an established diagnosis of plasma cell dyscrasias are:
Exceptions to this recommendation that may require more frequent testing include patients who are at high risk for plasma cell dyscrasias, those who are at high risk of poor outcomes or disease progression, those who recently completed therapy, or when there is biochemical progression that suggests impending clinical progression of the disease. | To support reductions in unnecessary retesting, labs may consider implementing these recommendations by specialty (e.g., hematology oncology, internal medicine, family medicine), by location of care (e.g., primary care, outpatient, oncology clinic), or by asking providers to specify the reason for ordering in the request form, based on the capabilities of their lab information system and/or which providers are monitoring patients and ordering SPEP. |
SPEP = serum protein electrophoresis.
Note: Minimum retesting intervals are recommendations that if testing is undertaken, it is not repeated sooner than indicated. They are not endorsements of repeat testing or a direction that a test should be reordered at the recommended minimum retesting interval. Clinicians should use clinical judgment as there may be exceptions in which the recommendations do not apply.
Developing the Guidance
The advisory panel for SPEP was composed of the 7 core panel members plus a specialist in hematology oncology. The panel considered evidence from the focused literature review7 and patient input from Myeloma Canada.
Key Discussion Points
The panel members discussed the following points when developing their recommendations:
The experts discussed that plasma cell dyscrasias are a heterogenous group of diseases that cover a spectrum of nuanced conditions ranging from asymptomatic and premalignant plasma cell disorders (e.g., monoclonal gammopathy of undetermined significance [MGUS]) to symptomatic and malignant diseases (e.g., multiple myeloma). The level of risk to the patient varies both across (e.g., smouldering myeloma versus MGUS) and within (e.g., high-risk versus low-risk MGUS) the different conditions.
The panel noted that the SPEP minimum retesting interval applies to all plasma cell dyscrasias, but that some conditions (e.g., MGUS) may require less frequent follow-up (as supported by the clinical guidance in the literature review).
For patients with acute or actively treated disease, the panel considered that most patients have treatment regimens on a monthly cycle so a 1-month interval would be appropriate for most patients. The recommended minimum retesting interval of 25 days would provide flexibility to accommodate patient schedules and allow testing to align with appointments for treatment.
The experts discussed that disease progression varies by patient (e.g., very rapid or very slow disease progression) and that, based on their experiences, it is unlikely that SPEP test results would change substantially on a weekly basis in the majority of patients. It was noted that when starting therapy, there may not even be a change in SPEP after the first month of therapy, and that providers may choose to wait 2 to 3 months before making treatment adjustments based on SPEP results.
For patients without actively treated disease, patients may not need to be monitored as frequently as those who have actively treated disease. A 3-month minimum retesting interval was discussed as appropriate for patients without actively treated disease.
The panel acknowledges that because of the variation across the disease spectrum there may be some exceptions to both recommendations and care providers should consider the patient’s specific clinical situation, such as the disease, the level of risk, biochemical changes, or the amount of time since the patient completed treatment.
The patient group input raised the issue that some plasma cell dyscrasias disproportionately affect equity-deserving groups (e.g., Black populations, older adults). The panel acknowledged that access to testing should be equitable, including considerations for race, ethnicity, and location, and recognized that testing should aim to be patient centric and aligned with the patient’s treatment cycle.
The panel considered that the approach that labs use to operationalize the 2 different recommendations will depend on how their institution differentiates between patients with actively treated disease and without actively treated disease (e.g., by specialty, by location of care) and the capabilities of their lab information system.
To support the implementation of the minimum retesting interval, labs can provide educational material on the different plasma cell dyscrasia conditions, including the nuances within each condition and the different levels of risk. This would assist providers with determining the SPEP retesting requirements for their patients.
TSH
About the Test
Thyroid hormones T4 (thyroxine) and T3 (triiodothyronine) are regulated by pituitary TSH.16 Serum TSH testing is used to evaluate thyroid dysfunction, primarily for the detection and treatment monitoring of hyperthyroidism and hypothyroidism.17
Recommendations
The clinical scenario in scope for the guidance is using TSH to monitor people who are being treated with thyroid replacement therapy for hypothyroidism and people who are being treated for hyperthyroidism. The recommendation specific to TSH is in Table 5.
Table 5: Minimum Retesting Interval Recommendations for TSH
Recommendation and exceptions | Implementation advice |
|---|---|
8. The recommended minimum retesting interval for TSH for monitoring people with known thyroid disease who have had an adjustment to their treatment (i.e., are under active investigation or management) is 6 weeks. Exceptions to this recommendation that may require more frequent testing include people with overt hyperthyroidism because of the risk of life-threatening conditions (e.g., acute thyrotoxicosis), children and adolescents, and people who are pregnant. | Because of variation in clinical cases, labs may consider creating test codes for specific clinical exceptions to support automatic bypasses to the recommended minimum retesting interval. |
TSH = thyroid stimulating hormone.
Note: Minimum retesting intervals are recommendations that if testing is undertaken, it is not repeated sooner than indicated. They are not endorsements of repeat testing or a direction that a test should be reordered at the recommended minimum retesting interval. Clinicians should use clinical judgment as there may be exceptions in which the recommendations do not apply.
Developing the Guidance
The advisory panel for TSH was composed of the 7 core panel members plus an endocrinologist. The panel considered evidence from the focused literature review7 and patient input from the Thyroid Foundation of Canada and Thyroid Patients Canada.
Key Discussion Points
The panel members discussed the following points when developing their recommendations:
In adults with known thyroid disease who are not pregnant and have had an adjustment to their treatment (e.g., recently initiated therapy or had a dose adjustment), 6 weeks was selected as the recommended minimum retesting interval as it is appropriate for most patients (with the exception of those with overt hyperthyroidism). This is consistent with the recommendations included in the literature review.
While the recommendation is for the minimum retesting interval for those who have had an adjustment to their treatment, the panel noted that for people with stable primary hypothyroidism (i.e., those with stable TSH levels), the testing frequency may be longer depending on the clinical situation and could vary by patient needs.
The panel considered whether there should be different intervals based on different clinical scenarios (e.g., hypothyroidism, hyperthyroidism, pregnancy) but noted that it may be challenging for labs to implement recommendations by condition, and that it is easier to have a single minimum retesting interval when clinically appropriate or different cut offs by age. For simplicity and to support appropriate implementation, the panel opted to recommend 1 minimum retesting interval that would apply to most situations and to specify the exceptions.
The panel recognized that there are exceptions in which retesting TSH at shorter intervals (e.g., 2 to 4 weeks) may be warranted, such as for pediatric patients, patients who are pregnant, and those with overt hyperthyroidism because of the risk of life-threatening conditions (e.g., acute thyrotoxicosis). This is supported by the literature review.
The patient group input raised the issue of some people requiring more frequent TSH monitoring due to sex hormone changes, such as people in perimenopause or menopause, or those taking hormone therapy (e.g., people who are transgender). The experts noted that the physiology of TSH would not be different in these populations and that the minimum retesting interval would still apply; however, the experts acknowledged that these individuals may require more frequent adjustments to their therapy.
Patient experiences with TSH testing were discussed, including the value of T3 and T4 testing. The experts discussed that TSH is the most sensitive test for monitoring people with primary hypothyroidism, and that T3 and T4 testing may be considered when required. The panel considered that most labs have reflex testing for thyroid hormones (i.e., the lab automatically adds the T4 test to the blood sample based on an abnormal TSH result) and that there are established guidelines and algorithms for thyroid hormone testing.
When considering the implementation advice for this recommendation, the panel discussed that it would be difficult to suggest hard stops for laboratory information systems given the variety of clinical scenarios and testing requirements for different populations that fall outside the recommended minimum retesting interval. Based on the capabilities of the lab information system and the patient populations, the panel suggested that institutions consider creating separate test codes for clinical exceptions (e.g., pregnancy) or implementing hard stops based on patient age.
Future Considerations
Across their discussions of the 7 included lab tests for which they made recommendations, the advisory panel returned to common themes about the overuse of lab tests.
The Importance of Prior Test Results Being Available
The advisory panel noted the need to have prior test results available in the General Guidance for Implementing the Recommendations section on minimum retesting intervals. Their availability is critical to reducing unnecessary retesting and improving the efficient use of lab tests. Increased connection and coordination between labs, providers, and health care facilities alongside improvements in the ability to access and share medical information across the health system can support the availability of prior lab test results.
The Importance of Education
Educational materials can be used to support the uptake of the recommendations, to help change ordering behaviours, and to support discussions between care providers and lab professionals. Educational materials can also be used to support communication between patients and care providers when discussing the value of repeat testing. When provided in combination with other strategies, such as hard stops in laboratory information systems, education can help support the reduction in unnecessary repeat testing.
The Value of Reducing Unnecessary Lab Testing
Unnecessary repeat testing comes at a cost to the health care system, both in terms of cost of the test and extra time to provide the low-value care. It also impacts patients in terms of potential harms from unnecessary follow-up, potentially inappropriate treatments, and having to travel and take time for unnecessary repeat testing, which can be significant particularly for those patients who do not live in close proximity to laboratory testing services. The panel members also noted that unnecessary repeat testing has an environmental impact, including producing carbon emissions and environmental waste.
Reflecting on Equity Considerations and Who Is Affected By Minimum Retesting Intervals
When developing recommendations to reduce the overuse of repeat lab tests, the advisory panel reflected on whether and how different populations would be affected by its recommendations. This included subgroups that were at higher risk of a condition or worsening outcomes, but also those who had less ready access to health care, particularly specialist care, based on their location of residence. The panel members discussed how, from an equity perspective, unnecessary repeat testing takes time and resources away from other valuable treatments or patients.
The Need for Guidance on Screening Tests
During the discussion for several tests (e.g., TSH, lipid panel) the panellists raised that a likely source of overuse was for screening purposes. Although the repeat use of lab tests for screening scenarios was out of scope for this work, it highlights future opportunities to provide guidance to clinicians and labs to support appropriate use of lab testing.
The Importance of Communication
The panel acknowledged that these recommendations cannot account for all clinical scenarios, and that clinicians and lab professionals need to be able to communicate to discuss exceptions to the recommendations to ensure patients receive appropriate care. This is consistent with the input from patient groups, which highlighted the importance of patient-centred care.
References
1.Naugler C, Wyonch R. What the Doctor Ordered: Improving the Use and Value of Laboratory Testing. (Commentary No. 533). Toronto (ON): C.D. Howe Institute; 2019: https://www.cdhowe.org/public-policy-research/what-doctor-ordered-improving-use-and-value-laboratory-testing. Accessed 2024 Feb 05.
2.Squires JE, Cho-Young D, Aloisio LD, et al. Inappropriate use of clinical practices in Canada: a systematic review. CMAJ. 2022;194(8):e279-e296. PubMed
3.Identifying Overused Lab Tests in Hospital Settings: A Delphi Study. Can J Health Technol. 2023;3(1). https://canjhealthtechnol.ca/index.php/cjht/article/view/ES0362. Accessed 2023 Nov 09.
4.Lang T, Croal B. National minimum retesting intervals in pathology. London (GB): The Royal College of Pathologists; 2021: https://www.rcpath.org/static/253e8950-3721-4aa2-8ddd4bd94f73040e/g147_national-minimum_retesting_intervals_in_pathology.pdf. Accessed 2023 Nov 10.
5.Choosing Wisely Canada. About. 2024; https://choosingwiselycanada.org/about/. Accessed 2024 Jan 24.
6.Choosing Wisely Canada. Using Labs Wisely. 2024; https://choosingwiselycanada.org/hospitals/using-labs-wisely/. Accessed 2024 Jan 24.
7.Minimum retesting intervals for lab tests [in progress]. (CADTH Heath Technology Review). Ottawa (ON): CADTH; 2024: https://www.cadth.ca/minimum-re-testing-intervals-lab-tests.
8.HealthLinkBC. Antinuclear Antibodies (ANA) Test. 2023; https://www.healthlinkbc.ca/tests-treatments-medications/medical-tests/antinuclear-antibodies-ana. Accessed 2023 Nov 30.
9.Bonroy C, Vercammen M, Fierz W, et al. Detection of antinuclear antibodies: recommendations from EFLM, EASI and ICAP. Clin Chem Lab Med. 2023;61(7):1167-1198. PubMed
10.Sacks DB, Arnold M, Bakris GL, et al. Guidelines and Recommendations for Laboratory Analysis in the Diagnosis and Management of Diabetes Mellitus. Diabetes Care. 2023;46(10):e151-e199. PubMed
11.Eyth E, Naik R. Hemoglobin A1C. StatPearls. Treasure Island (FL): StatPearls Publishing; 2023: https://www.ncbi.nlm.nih.gov/books/NBK549816/. Accessed 2023 Nov 14.
12.MedlinePlus. Lipase Test. Bethesda (MD): National Library of Medicine; 2022: https://medlineplus.gov/lab-tests/lipase-tests/. Accessed 2023 Dec 14.
13.Beyer G, Hoffmeister A, Lorenz P, Lynen P, Lerch MM, Mayerle J. Clinical Practice Guideline-Acute and Chronic Pancreatitis. Dtsch Arztebl Int. 2022;119(29-30):495-501. PubMed
14.Boccadoro M, Pileri A. Plasma cell dyscrasias: classification, clinical and laboratory characteristics, and differential diagnosis. Baillieres Clin Haematol. 1995;8(4):705-719. PubMed
15.Booth RA, McCudden CR, Balion CM, et al. Candidate recommendations for protein electrophoresis reporting from the Canadian Society of Clinical Chemists Monoclonal Gammopathy Working Group. Clin Biochem. 2018;51:10-20. PubMed
16.McDermott MT. Hypothyroidism. Ann Intern Med. 2020;173(1):ITC1-ITC16. PubMed
17.National Institute for Health and Care Excellence. Thyroid disease: assessment and management. (NICE guideline NG145). London (GB): NICE; 2023: https://www.nice.org.uk/guidance/ng145/resources/thyroid-disease-assessment-and-management-pdf-66141781496773. Accessed 2023 Nov 23.
Appendix 1: Advisory Panel Recommendations for Minimum Retesting Intervals
Note that this appendix has not been copy-edited.
The Advisory Panel on Minimum Retesting Intervals for Lab Tests developed recommendations for 6 commonly repeated lab tests for monitoring patients (refer to Table 6). Minimum retesting intervals are recommendations on the minimum time before a test should be repeated, based on the biochemical properties of the test and the clinical situation in which it is used.
How a minimum retesting interval recommendation is implemented by labs will depend on the local context, for example, if the patients with the condition are cared for within their facility or catchment, and the capacity of their laboratory information system to provide educational prompts and place limits on requests. Clinicians should have the option to override a minimum retesting interval or discuss options with a laboratory professional if they feel repeat or more frequent testing is clinically appropriate, or if there are issues with a previous test result (e.g., interference, unexpected test results for the clinical context, missing result).
Table 6: Advisory Panel Recommendations for Minimum Retesting Intervals
Recommendation and exceptions | Implementation advice |
|---|---|
ANA | |
1. If a previous ANA test is positive, do not reorder ANA for monitoring patients with suspected or confirmed systemic autoimmune disease. | To support reductions in unnecessary retesting, labs may consider implementing a 5-year hard stop minimum retesting interval. |
2. If a previous ANA test is negative or borderline positive, do not reorder ANA for monitoring patients with suspected or confirmed systemic autoimmune disease. An exception to this recommendation is if the clinical status of the patient significantly changes with newly developed symptoms, in which case ANA may be retested. | To support reductions in unnecessary retesting, labs may consider implementing a 24-month hard stop minimum retesting interval. |
Hemoglobin A1C | |
3. The recommended minimum retesting intervals for hemoglobin A1C in people who are being treated for diabetes are:
Exceptions to this recommendation that may warrant more frequent testing include children and adolescents with type 1 diabetes, people with diabetes who are planning to become pregnant, and people with rapidly changing blood glucose levels due to significant recent changes to lifestyle and/or medications. | To support reductions in unnecessary retesting, labs may consider implementing a 60- to 86-day hard stop minimum retesting interval. This allows for practical considerations such as accommodating patient schedules for retesting appointments. |
4. Do not reorder hemoglobin A1C tests for assessing glycemic control in people with diabetes who have conditions that alter red blood cell turnover (e.g., iron deficiency anemia) or for pregnant people with diabetes who are in their second or third trimester. | To support reductions in unnecessary retesting, labs may consider implementing a 60- to 86-day hard stop minimum retesting interval. |
Lipase | |
5. Do not reorder lipase tests for monitoring patients with an established diagnosis of acute pancreatitis. | Not applicable |
6. Do not reorder lipase tests for monitoring patients with an established diagnosis of chronic pancreatitis. An exception to this recommendation is if there is clinical suspicion of an episode of acute-on-chronic pancreatitis, where lipase testing is required for diagnostic purposes. | To support reductions in unnecessary retesting, in outpatient or community settings, labs may consider implementing a 6-month hard stop minimum retesting interval. This recommendation is based on the experience of the advisory panel as no relevant information for serum lipase retesting for chronic pancreatitis was identified in the literature review. |
SPEP | |
7. The recommended minimum retesting intervals for SPEP for monitoring patients with an established diagnosis of plasma cell dyscrasias are:
Exceptions to this recommendation that may require more frequent testing include patients who are at high risk for plasma cell dyscrasias, those who are at high risk of poor outcomes or disease progression, those who recently completed therapy, or when there is biochemical progression that suggests impending clinical progression of the disease. | To support reductions in unnecessary retesting, labs may consider implementing this recommendation by specialty (e.g., hematology oncology, internal medicine, family medicine), by location of care (e.g., primary care, outpatient, oncology clinic), or by asking providers to specify the reason for ordering in the request form, based on the capabilities of their lab information system and/or which providers are monitoring patients and ordering SPEP. |
TSH | |
8. The recommended minimum retesting interval for TSH for monitoring people with known thyroid disease who have had adjustment to their treatment (i.e., are under active investigation or management) is 6 weeks. Exceptions to this recommendation that may require more frequent testing include people with overt hyperthyroidism because of the risk of life-threatening conditions (e.g., acute thyrotoxicosis), children and adolescents, and people who are pregnant. | Because of variation in clinical cases, labs may consider creating test codes for specific clinical exceptions to support automatic bypasses to the recommended minimum retesting interval. |
ANA = antinuclear antibody; SPEP = serum protein electrophoresis; TSH = thyroid stimulating hormone.
Note: Minimum retesting intervals are recommendations that if testing is undertaken, it is not repeated sooner than indicated. They are not endorsements of repeat testing or a direction that a test should be reordered at the recommended minimum retesting interval. Clinicians should use clinical judgment as there may be exceptions in which the recommendations do not apply.
Appendix 2: Detailed Approach
Note that this appendix has not been copy-edited.
Scope
CWC identified 7 frequently used lab tests that would benefit from guidance to reduce unnecessary retesting. Our selection of tests was supported in part by a 2022 systematic review of inappropriate clinical practices in Canada that reported the percentage of overuse for TSH, hemoglobin A1C, and ANA lab tests as 3.0% to 35.1%, 22.9% to 28.1%, and 30.6%, respectively.2 In addition, a 2023 CADTH Delphi study to support CWC’s Using Labs Wisely program identified that hemoglobin A1C, TSH, lipase, BNP, and the lipid panel were highly used lab tests in Canada and potential candidates for reduction.3 To have the greatest impact on reducing unnecessary repeat testing, we limited the scope to the main conditions or populations that are tested and retested and where minimum retesting intervals could be applied. For each lab test, CWC, CADTH, and lab experts worked together to further specify the patient populations and/or clinical situations in which these tests are regularly used. For tests with broad populations (e.g., autoimmune diseases), we identified primary populations of interest.
Out of scope for this guidance were other lab tests, conditions, patient populations, and clinical scenarios (e.g., screening).
Step 1: Forming the Advisory Panel
CADTH and CWC co-led the recruitment of the time-limited advisory panel to develop recommendations for minimum retesting intervals for the 7 included lab tests.
We formed a core advisory panel with additional specialists to bring clinical expertise appropriate for each test and prespecified patient population or clinical scenario. We recruited potential panel members and specialists through CADTH’s and CWC’s networks (e.g., clinical societies). We consulted with the IDEA Strategic Partner at CADTH and sought advice on the importance of inclusion, diversity, equity and accessibility in the panel’s composition (e.g., diverse representation and geographic distribution). We consulted with the Engagement Team at CADTH on developing an approach to engage patients and patient groups throughout the course of the project.
Core Advisory Panel
The core advisory panel was composed of 4 lab specialists, 1 of whom was a CWC Using Labs Wisely Lead, 2 family doctors, and 1 patient panel member. Panel members participated in the consensus generating discussions and provided their perspective by sharing knowledge and insight on minimum retesting intervals for the lab test(s).
Specialist Panel Members
For each lab test, the core advisory panel was joined by 1 to 3 specialist physicians for each clinical area (i.e., endocrinology, cardiology, rheumatology, hematology oncology, gastroenterology, internal medicine) to provide their expertise to the panel and participate in consensus generation (refer to Table 7).
Table 7: List of Specialist Panel Members Who Participated in Each Test Discussion
Lab tests | Specialist(s) |
|---|---|
ANA | Dr. Carter Thorne, Rheumatologist |
BNP and NT-proBNP | Dr. Nowell Fine, Cardiologist Dr. Michael Khoury, Pediatric Cardiologist |
Hemoglobin A1C | Dr. Ferhan Siddiqi, Endocrinologist |
Lipase | Dr. William Silverstein, General Internist Dr. Natalia Calo, Gastroenterologist |
Lipid Panel | Dr. Nowell Fine, Cardiologist Dr. Ferhan Siddiqi, Endocrinologist Dr. Michael Khoury, Pediatric Cardiologist |
SPEP | Dr. Matthew Cheung, Clinical Hematologist |
TSH | Dr. Ferhan Siddiqi, Endocrinologist |
ANA = antinuclear antibody; BNP = B-type natriuretic peptide; NT = N-terminal; SPEP = serum protein electrophoresis; TSH = thyroid stimulating hormone.
Step 2: Panel Inputs
Focused Literature Reviews
CADTH conducted focused literature reviews for each of the included lab tests to support the development of recommendations. For each test, we searched for existing recommendations on retesting in prespecified patient populations or clinical scenarios. After the initial search, a research information specialist screened the results to prioritize guidance from countries similar to Canada (e.g., US, UK, Western Europe). We also searched for evidence on biological or physiological factors that might impact the minimum retesting interval for each test. We summarized equity considerations that may influence the minimum retesting interval when they were identified within the relevant clinical guidelines and other literature. Further details can be found in the Technology Review on Minimum Retesting Intervals for Lab Tests.7
Engaging Patient Groups
CADTH sought the expertise of patient groups to provide valuable insights into the impact of frequency of testing on patients when developing recommendations for minimum retesting intervals for selected lab tests. The purpose of the engagement was to broaden the patient perspectives available for the panel’s consideration during their consensus generation and mitigate the risks of a small panel.
We solicited the experiences and perspectives from patient groups of each of the prespecified main conditions or populations who receive repeat testing using the lab tests of interest. These groups have expertise in clinical areas of interest and were able to share the lived experience of patients and caregivers. We reached out to 18 patient groups in total with the initial invitation sent on December 11, 2023, and subsequent reminder emails on December 19, 2023, and January 9, 2024. We received responses from 11 patient groups and recognize that some groups may not have been able to participate due to the timing of our request (i.e., over the December holidays).
We requested patients’ lived experiences from patient groups through a set of survey questions which aimed to better understand the current burden of testing and gather insights on the potential impact of changing testing frequency. The survey questions also included the impact of frequency of testing on those subgroups with special considerations, such as pediatric patients and patients who are pregnant. We also consulted with the IDEA Strategic Partner at CADTH on developing questions related to the impact of frequency of testing for equity-deserving groups which include but are not limited to: women, racialized groups, Indigenous Peoples, people with disabilities, and 2SLGTBQ+ community members.
We collated, summarized, and shared the patient group information with the advisory panel members in advance of meetings. The patient representative on the panel also received the complete unedited patient group feedback and their role included sharing this input during the consensus-based discussions to represent and bring to life the patient voice.
Step 3: Developing Recommendations
Draft Recommendations
Draft recommendations were prepared in advance of the full panel meetings to serve as starting points for discussion. Two lab experts from the core panel were assigned to each test, and independently developed draft recommendations using the literature reviews, input from patient groups, and questions for consideration (including equity considerations). We consolidated the 2 independent draft recommendations for each test. The 4 lab experts from the core panel met through a 2 hour, virtual, facilitated discussion of all 7 lab tests on Jan 31, 2024. The objective of the virtual discussion was to revise the consolidated draft recommendations for clarity and so they reflected the lab experts’ opinions so that they were ready for consensus generation by the full advisory panel.
Developing Consensus-Based Recommendations
Prior to meeting, the advisory panel received background materials that included the draft recommendations, summaries of patient input, the literature reviews, and a discussion guide. The discussion guide included prompts for reflection and consideration, including general equity considerations and those that were raised by patient group input or in the literature review. It also included questions about the implications of limited or discordant identified guidance, barriers and facilitators to implementing the draft recommendations, and whether the panel was aware of additional evidence that should be considered. We consulted with the IDEA Strategic Partner at CADTH to develop questions to prompt panel members to consider equity-deserving groups during their discussions and included these in the background materials.
CADTH facilitated the discussion and consensus generation, and each lab test was discussed by the panel for 1 hour. We supported the development of robust consensus-based recommendations by using an experienced facilitator who prompted the advisory panel to consider the range of evidence and experience and ensured space for all voices and perspectives.
One of the lab experts who prepared the draft recommendations started the discussion by presenting their rationale. The patient panel member then shared patient group input and patients’ perspectives and experiences, after which the invited specialists had an opportunity to share their perspective on the draft recommendations.
Through facilitated discussion (approximately 60 minutes), the advisory panel developed recommendations for the minimum retesting interval(s) for the lab tests in prespecified population(s). Recommendations were also developed against repeat testing for certain lab tests in specific populations when supported by the evidence and clinical expertise. To support the process of developing consensus, we made live edits in a Word document which was shared on the screen during the meeting. This enabled advisory panel members to see suggested changes to the recommendations, as well as to implementation advice, and additional considerations. The facilitator also prompted the advisory panel to ensure that equity considerations and patient groups’ perspectives were discussed. Once the facilitator saw that the group had moved toward convergent thinking and was approaching consensus, the revised draft recommendations were put to a vote. Consensus was defined as 70% agreement and was reached on the recommendations for 7 lab tests. All advisory panel members voted in agreement with the revised recommendations at the end of the discussions with the exception of lipid panels.
In our project plan, we had allowances for members to provide asynchronous contributions to the development of the draft recommendations if panel members were not able to participate in the scheduled discussions. One core panel member was not able to participate in the discussion on a test (lipid panel) due to technical difficulties. We arranged a 30 minute virtual meeting to hear their perspectives. Some of their perspective was reflected in points raised by other panel members. Based on the importance of the perspective, we added detail to the discussion section for lipid panels incorporating this panel member’s feedback.
Over the course of the panel meetings, the advisory panel reached consensus on recommendations on all tests except for BNP and NT-proBNP testing in adults and children being treated for pulmonary arterial hypertension. The advisory panel felt it was necessary to consult with specialists in pulmonary arterial hypertension and deferred voting on the draft recommendations for this indication. We recruited 2 specialists who treat adults with pulmonary arterial hypertension (Table 8) and shared the draft recommendations and background materials for BNP for pulmonary arterial hypertension with them. The CWC Using Labs Wisely clinical lead and CADTH team facilitated a half hour virtual discussion with the attending specialists and documented their suggestions to the recommendations and rationale. We then revised the draft recommendations, and then sent them and their rationale to the advisory panel for an asynchronous electronic vote for which consensus was reached.
We sent the revised recommendations and implementation advice developed by the advisory panel to members for optional validation before incorporating them into the draft guidance report.
Table 8: List of Specialists Consulted for BNP and NT-proBNP Recommendations
Name | Role |
|---|---|
Dr. Jason Weatherald | Respirologist with the University of Alberta Pulmonary Hypertension Program, and Associate Professor in the Department of Medicine at the University of Alberta |
Dr. Doug Helmersen | Respirologist with the Southern Alberta Pulmonary Hypertension Program and Clinical Associate Professor at the University of Calgary |
Writing the Guidance Report
Once the consensus-based recommendations were developed, we summarized the key discussion points that arose during the development of the recommendations, including discussions of relevant information from the literature reviews, how the patient input informed the panel discussions, and clinical experience from the specialist experts.
The advisory panel had an opportunity to review the guidance report to ensure it appropriately and accurately captured their discussion and rationale for the recommendations and the implementation advice.
Seeking and Responding to Feedback
We posted the draft guidance document on the CADTH website for a 10-day feedback period. Patient groups engaged in the project and other interested parties were notified when the draft was posted and invited to provide feedback through an online survey which included a mix of closed and open-ended questions on agreement with and clarity of the recommendations and implementation advice.
We received 14 unique submissions from 10 from individual respondents, 2 patient groups, and 2 submissions from 3 clinical societies. Of the 14 submissions, 4 commented on ANA, 4 on BNP and NT-proBNP, 4 on SPEP, 3 on lipase, 3 on lipid panel, 2 on TSH, and 2 on hemoglobin A1C.
Of the 14 submissions, 8 disagreed with 1 or more aspects of 1 or more recommendations, ranging from word changes to exceptions for specific patient populations or indications. Five submissions disagreed with an aspect of the implementation advice for 1 or more tests, such as the timing of the hard stops. One respondent did not agree with the approach used to develop the guidance.
We considered and reviewed each of the feedback submissions we received. We made the following changes:
Revised the descriptions of minimum retesting intervals throughout the document to support their accurate interpretation.
Revised text in the document, including the key discussion points and added details, to support clarity in interpretation.
Revised our description of our approach used to developing the guidance to make clear our use of techniques consistent with rigour in consensus-based decision-making.
Revised language in the recommendations and implementation advice that was consistent with the panel’s intention that improved their clarity and to support their adoption.
Removed the minimum retesting interval recommendations made for BNP and NT-proBNP because of the strong differences in clinical opinion over approaches to retesting for BNP and NT-proBNP.
Removed the minimum retesting interval recommendations made for lipid panel because of the strong differences in clinical opinion over approaches to lipid panel retesting.
We noted that some comments were suggestions for future work that was out of scope for this project (e.g., additional tests, cost implications of minimum retesting intervals). We provided individual responses to each of the individuals or organizations who provided feedback.
Limitations
We acknowledged the potential limitations related to the breadth of the scope of this work (i.e., number of tests and clinical scenarios) and practical challenges to hosting the panel and developing recommendations.
We aimed to reduce biases in and improve the rigour of the recommendations by ensuring that the advisory panel had diverse clinical and expert representation. We addressed potential conflicts of interest by having panel members declare their conflicts of interest in accordance with the CADTH Conflict of Interest Policy. We considered a range of inputs and evidence, including patients’ perspectives and experiences, and existing guidance on minimum retesting intervals and biochemical properties of and equity considerations related to the tests.
We did not find any published evidence on the minimum retesting interval or testing frequency for lipase to monitor chronic pancreatitis, meaning that this recommendation was developed based on expert opinion.
Patient group input was intended to support the development of the recommendations, address limitations in published evidence, and raise equity considerations. We received patient input for all tests except for lipid panel, which did not have direct presentation of the experiences and perspectives of people on lipid-lowering therapy.
We worked to address equity considerations within the scope of the included tests and clinical scenarios when emergent from the literature reviews, patient group input, and panel discussions. We recognize there are likely considerations that were not raised or that relate to but are outside the scope of this project. Our exploration of equity considerations was preliminary in some cases and there remains work to be done. We specifically recognize that we did not seek concerns related to First Nations, Metis, and Inuit peoples.
Appendix 3: Advisory Panel Members Declarations of Conflict of Interests
The following are the declared conflicts of interests for each of the advisory panel members as per the CADTH Conflict of Interest Policy:
Drs. Daniel Beriault, Dr. Natalia Calo, Dr. Manal Elnenaei, Dr. William Silverstein, and Dr. Janet Simons reported no conflicts of interests.
Dr. Matthew Cheung is the Chair of Economics Committee for the Canadian Cancer Trials Group and Chair of Guidelines Subcommittee for the American Society of Hematology.
Dr. Nowell Fine received consulting honorariums from Pfizer, AstraZeneca, and Alnylan.
Dr. Michael Khoury received payment for attending an advisory board meeting from Ultragenyx.
Dr. Rosilene Kraft received access to oncology drugs through clinical trials and patient access programs from BC Cancer and Canadian Cancer Trials Group and Hoffman-La Roche, BC Cancer, and Astra Zeneca’s Oncology Patient Support Program. She received honorariums, waived registration fees, and travel funding for her role as a patient partner in research projects and reviewing grant applications from the Canadian Cancer Society, Rethinking Breast Cancer, the Marathon of Hope Cancer Centre and TRIF, and Canadian Cancer Research Alliance. She received payment for organizing the Canadian Cancer Research Conference.
Dr. Ferhan Siddiqi received travel payment from the Canadia Society for Endocrinology and Metabolism.
Dr. Carter Thorne received payment for attending advisory board meetings from Abbvie, Biogen, JAMP, Medexus, Nordic Pharma, Pfizer, Roche, Sandoz, and Sanofi, and grant funding from Pfizer and JAMP.
Dr. Li Wang received a travel grant and speaking fees for attending the 12th Oriental Congress of Laboratory Medicine.
Dr. Yan Yu received travel funding and speaking fees from CMA Joule, Immunize.io, and the College of Family Physician of Canada. He also received payment for his work as a faculty coordinator at the Department of Medicine at the University of Calgary and for participating in an advisory board meeting from Moderna.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.