CADTH Health Technology Review
Drug Shortages and Patient Harms
Technology Review
Key Messages
What Is the Issue?
Drug shortages are a global issue with complex dynamics. Shortages can occur because of disruption at any point along the drug supply chain. Several strategies are used in Canada to prevent or alleviate the effects of drug shortages, including mandatory reporting by drug manufacturers.
An understanding of the amount and types of real or potential harms caused to patients can inform policy decisions around drug shortage management and prevention.
What Did We Do?
We searched for literature providing evidence on patient outcomes associated with supply chain disruptions of pharmaceuticals and vaccines. An information specialist conducted a search of peer-reviewed literature sources published between January 1, 2003, and September 13, 2023.
Documents were excluded if the objective was to investigate the potential effects of a drug shortage in the absence of an actual drug shortage or if the outcomes were not direct patient harms.
What Did We Find?
One scoping review and 33 nonrandomized studies were identified that evaluated patient outcomes associated with supply chain disruptions of pharmaceuticals and vaccines.
We identified a wide variety of drug classes experiencing shortages. The most frequently reported shortages were anesthetics, oncology drugs, vaccines, drugs for the treatment of COVID-19, antimicrobials, and small-volume parenteral solutions.
Most of the included primary studies concluded that the replacement drug or protocol was a safe or acceptable alternative to the shortage drug. The subset of primary studies that concluded that the replacement drug or protocol was not a safe or acceptable alternative to the shortage drug reported worse outcomes in health system use (including length of hospital stay), adverse events, disease progression, and mortality.
What Does This Mean?
Drug shortages have the potential to cause harm to patients and some drug shortages may have a greater impact on patients than others. The ability to predict which drugs could cause the greatest harm during a supply disruption would be a great benefit for future planning.
The diversity of drugs experiencing shortages and their associated harms emphasizes that decision-makers may need to take a case-by-case approach when developing policies meant to lessen the impact of drug shortages.
Context and Policy Issues
What Is the Problem?
Drug shortages are a global issue with complex dynamics. Between 2022 and 2023, more than 2,700 drug shortages were reported to Health Canada, lasting an average of 98 days.1 Of these, 34 were considered high impact — shortages with the greatest potential consequences to people and health care systems (e.g., no therapeutic alternatives available).1,2
There are multiple steps along the drug supply chain, including:
drug development and regulatory approval
manufacturing
purchase and distribution
delivery to hospitals, pharmacies, and patients.3
Interruptions to any of these phases can cause a shortage. For example:
good manufacturing practices noncompliance leading to recalls
nonprofitable drugs leading to decisions to cease production
stockpiling of medication
In addition, weak points in the supply chain, such as relying on the supply of drugs from a single source or not having protocols in place to respond to increases in demand, can also cause or worsen existing drug shortages.3,4
What Is the Current Practice?
Strategies currently used in Canada to attempt to prevent or alleviate drug shortages include:
an expedited drug review process to accelerate Health Canada approval of substitute drugs in urgent circumstances
drug manufacturing quality assurance protocols
the development of ethical frameworks for resource allocation
compounding drugs
rationing protocols at the hospital and pharmacy level.3
Furthermore, mandated reporting of drug shortages went into effect in 2017,2 Drug manufacturers are required to report anticipated shortages or discontinuations, ideally 6 months in advance, to allow time to put mitigation plans into place. Manufacturers are also required to report actual shortages as soon as they are aware of them.2
Why Is It Important to Do This Review?
People can experience clinical harm as a result of drug shortages. This can take several forms:
inadequate treatment or management of health conditions
withdrawal-related side effects
adverse or safety events associated with replacement drugs
medication errors.4
Some drugs have the potential for much greater patient harm if they become difficult to obtain. For example, shortages of drugs with life-saving benefits or strict dosing schedules might have more impact on patient outcomes, especially if there are no alternative options available.2,4
This report is the first in a series of CADTH-published initiatives that aims to emphasize potential priority medications and to ultimately support decision-making during drug shortages.
Objective
The purpose of this report is to summarize the evidence on patient outcomes associated with supply chain disruptions of pharmaceuticals and vaccines.
Research Question
What is the evidence on patient outcomes associated with supply chain disruptions of pharmaceuticals and vaccines?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE and the Cochrane Database of Systematic Reviews. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was drug shortages. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons; any types of clinical trials or observational studies; real-world evidence using routinely collected data; or to the context in Canada. The search was completed on September 13, 2023, and limited to documents published since January 1, 2003.
Selection Criteria and Summary Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Information from the relevant studies was extracted into summary tables and organized into broad clinical indication categories by 1 reviewer. Data were extracted on the study characteristics; shortage drug and its substitute, if applicable; findings that related to direct patient harms; and overall conclusion. Outcome results and their direction of effect were briefly summarized as reported by the study’s authors and categorized into the following: no difference, worse, improved, or mixed between groups (e.g., in studies with multiple comparator groups, an outcome may improve in 1 group but worsen in another). No formal critical appraisal (e.g., risk of bias assessment) of the included studies was conducted.
Criteria | Description |
|---|---|
Population | General population |
Concept | Supply chain disruptions of pharmaceuticals and vaccines |
Outcomes | Patient harms (e.g., mortality, emergency department visits, hospitalization rates, adverse events) |
Study designs | Health technology assessments, systematic reviews, scoping reviews, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2003.
Studies were excluded if:
the natural effects of a drug shortage could not be observed because of the study design (e.g., randomized controlled trial)
the shortage product was a multivitamin, supplement, homeopathic medication, or device
the purpose of the study was to investigate the potential effects of a drug shortage in the absence of an actual drug shortage (e.g., anticipatory)
the primary or secondary outcomes were not direct patient harms (e.g., studies that reported treatment delays without describing a direct measurable effect to patients were excluded).
Because of the large volume of potentially relevant articles identified for full-text review, those published before January 1, 2018, were excluded. A list of the articles published before 2018 that were identified for full-text review, but not screened for inclusion and exclusion criteria, can be found in Appendix 2.
Overall Summary
Quantity of Research Available
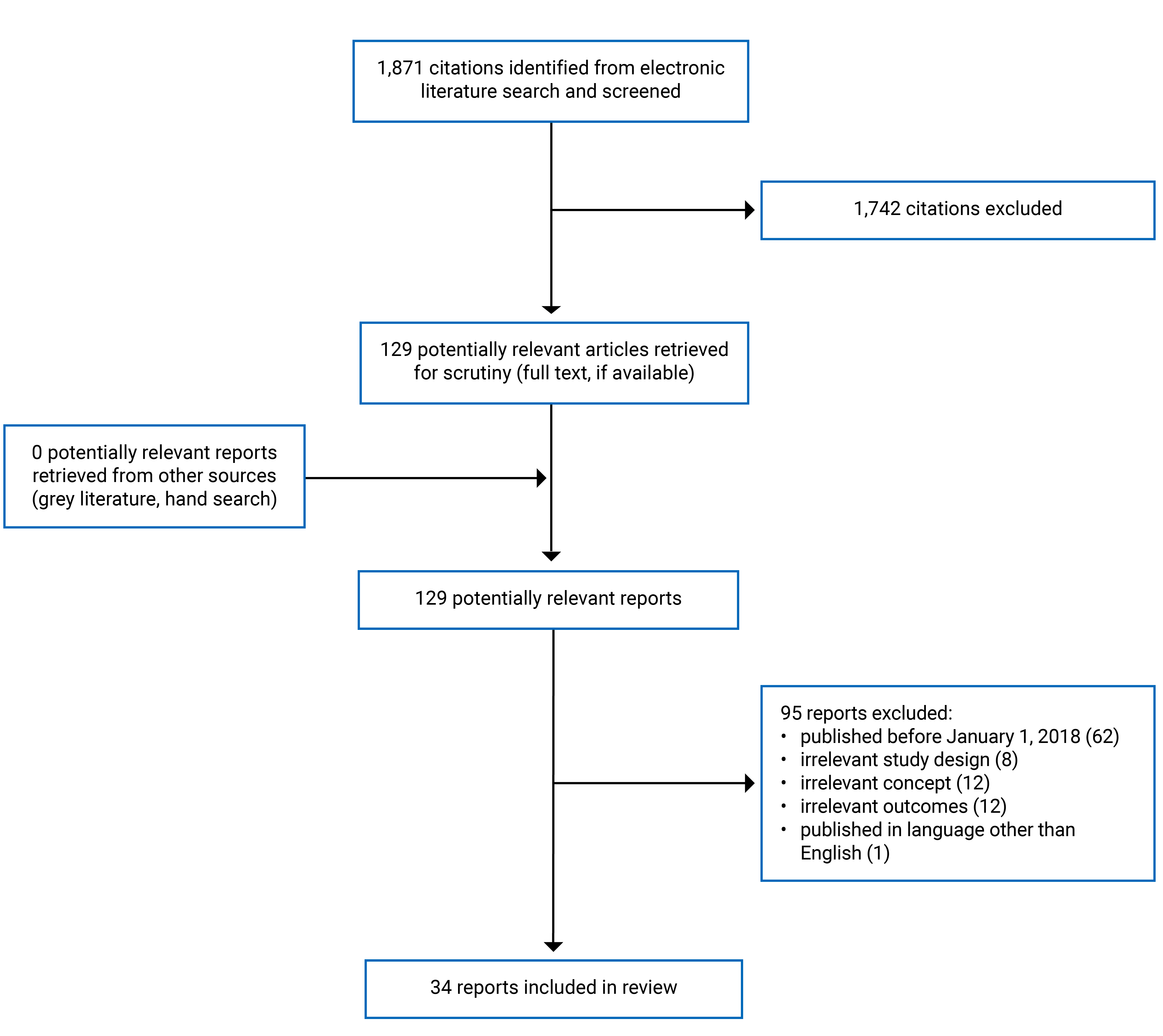
A total of 1,871 citations were identified in the literature search. Following screening of titles and abstracts, 1,742 citations were excluded and 129 potentially relevant reports from the electronic search were retrieved for full-text review. Of these potentially relevant articles, 95 publications were excluded for various reasons, and 34 publications met the inclusion criteria and were included in this report. These comprised 1 scoping review (SR) and 33 nonrandomized studies (NRSs).
Appendix 1 presents the PRISMA5 flow chart of the study selection. Additional references of potential interest are provided in Appendix 2.
Summary of Study Characteristics
The SR by Phuong et al. (2019)6 included 40 studies. Sixteen primary studies published between 2006 and 2017 met the inclusion criteria for this report. Of these, 3 were prospective cohort studies and 13 were retrospective cohort studies. The authors of the SR were from Australia.6
Of the 16 relevant primary studies in the SR, 4 were conducted in a surgical setting, 2 in a nonspecific hospital setting, 1 in the intensive care unit, 1 in an air medical setting, and 8 did not specify a setting.6
The 33 included primary clinical studies comprised 1 registry study,7 5 prospective cohort studies,8-12 and 27 retrospective cohort studies.13-39 Two studies were published as research letters.8,30 The studies were published between 2018 and 2023. The primary clinical studies were conducted by authors from Australia,11,12 Brazil,23 Canada,13,20,30,33 the Democratic Republic of the Congo,38 France,7,14,27 Japan,8 the Netherlands,39 and the US.9,10,15-19,21,22,24-26,28,29,31,32,34-37
Twenty of the included primary studies compared outcomes between the shortage drug and its substitute before and during a drug shortage period.13-22,24,26,27,31-35,37,39 Of these, 3 studies had at least 1 substitute drug group that had a supply disruption and was further compared to an additional substitute drug group.14,34,39 In Cole et al. (2021), the intervention and comparator groups flipped partway through when supply of the shortage drug resumed, and the substitute drug went into shortage.10 In Li and Cimino (2020), the study occurred during the drug shortage period and compared patients who continued receiving the shortage drug to those who switched to a substitute drug.28 In van Langenberg et al. (2020), for long-term outcomes, the intervention group was the substitute drug and was compared to patients who switched back to the shortage drug when supply resumed.11 In this same study, there was no comparator group for short-term outcomes.11 Nine studies did not have a comparator group.8,9,12,23,25,29,30,36,38 The registry study aimed to identify adverse drug reactions related to drug shortages and describe the types of drugs and harms involved.7
Nine of the included primary studies were conducted in a nonspecific hospital setting,13,18,22,24,25,29,35,36,39 6 in the emergency department (ED),10,15,26,32-34 5 in the intensive care unit,17,20,21,27,31 5 in the community,8,9,12,30,38 3 in a surgical setting,16,19,37 3 in a hospital outpatient setting,11,14,28 and 1 in dialysis clinics.23
Summary of Findings
The 16 relevant primary studies from the SR are summarized in Table 2. The registry study and 32 NRSs are summarized in Table 3.
There was considerable variability in the types of drugs experiencing shortages. Broadly defined categories by clinical indication were identified as follows:
anesthetic, analgesic, or sedative medications (SR: 3 studies; NRS: 7 studies)6,10,17-19,26,34,37
oncology drugs and drugs used in conjunction with oncology drugs (SR: 4 studies; NRS: 5 studies)6,13,14,28,35,36
antimicrobials, including antibiotics and antivirals, and drugs used in conjunction with antimicrobials (SR: 3 studies; NRS: 3 studies)6,22,31,33
drugs specific to the treatment or management of COVID-19 (NRS: 3 studies)20,27,39
drugs that did not fit into the previously mentioned categories (SR: 6 studies; NRS: 6 studies)6,11,16,21,23,30,32
nondrug, specifically, small-volume parenteral solutions, which are used to administer IV drugs (NRS: 4 studies).15,24,25,29
Strategies used to manage drug shortages:
alternative drug (SR: 13 studies; NRS: 14 studies)6,8-14,16,26,30-32,34,37
dose-sparing strategies (e.g., fixed dose) (SR: 1 study; NRS: 3 studies)6,20,22,38
alternative route of administration (e.g., oral formulations) (NRS: 4 studies)18,21,35,36
alternative method of administration (e.g., infusion technique) (SR: 1 study; NRS: 4 studies)6,15,24,25,29
none (e.g., no suitable replacement available) (SR: 1 study; NRS: 2 studies)6,23,33
a combination of the previously mentioned categories, either at the same time or in sequence (NRS: 5 studies).17,19,27,28,39
Outcomes related to patient harms and the direction of effect during a drug shortage period:
Mortality: no difference (SR: 5 studies; NRS: 9 studies);6,11,15-17,21,22,24,27,31 worse (SR: 1 study; NRS: 1 study);6,20 improved (NRS: 1 study);13 mixed results between groups (NRS: 1 study)39
Hospital admission: no difference (NRS: 1 study);30 worse (NRS: 1 study);11 mixed results between groups (NRS: 1 study)34
Intensive care unit (ICU) admission: no difference (SR: 1 study; NRS 1 study);6,34 worse (NRS: 2 studies)13,39
ED visit: no difference (NRS: 2 studies);18,37 worse (NRS: 1 study)30
Hospital readmission: no difference (NRS: 1 study);33 improved (NRS: 2 studies)18,24
Hospital length of stay (LOS): no difference (SR: 3 studies; NRS: 7 studies);6,17,18,20,22,24,31,35 worse (NRS: 1 study);13 mixed results between groups (NRS: 2 studies)34,39
Postanesthetic care unit LOS: worse (NRS: 1 study)37
Adverse events: no difference (SR: 8 studies; NRS: 17 studies);6,8,9,12,14-16,25-29,31,33-36,38 worse in at least 1 safety outcome (SR: 2 studies; NRS: 5 studies);6,11,13,19,24,37 improved in at least 1 safety outcome (SR: 2 studies; NRS: 1 study);6,32 mixed results between groups (NRS: 1 study)10
Disease progression: no difference (SR: 1 study; NRS: 2 studies);6,27,28 worse (SR: 2 studies; NRS: 3 studies);6,11,23,31 improved (NRS: 1 study)13
Duration of mechanical ventilation: no difference (SR: 1 study; NRS: 2 studies);6,17,20 worse (SR: 1 study);6 improved (NRS: 1 study)21
Pain: no difference (NRS: 1 study)17
Primary study author’s conclusions:
The replacement drug or protocol was a safe or acceptable alternative to the shortage drug (NRS: 26 studies).8-10,12-18,20-22,24-30,32-36,38
The replacement drug or protocol was considered not safe or at increased risk of harmful outcomes (NRS: 6 studies).11,19,23,31,37,39 The shortage drug class differed for all 6 studies11,19,23,31,37,39 and was compared to an alternative drug or protocol in 5 studies.11,19,31,37,39 There was no suitable replacement therapy available in 1 study.23 For these 6 studies, worsening direct patient harms were reported for the following outcome categories: health system use (3 studies),11,37,39 adverse events (3 studies),11,19,37 and disease progression (3 studies).11,23,31 Swets et al. (2023) reported lower survival in 2 of the 3 replacement drug groups compared to the shortage drug.39
Context in Canada
Four primary studies investigated drug shortages occurring in Canada.13,20,30,33 The shortage drugs were carmustine, tocilizumab, probenecid (in conjunction with an antibiotic), and generic valsartan.13,20,30,33 Lachance et al. (2023) reported that the alternative drug, bendamustine, had worse outcomes in adverse events and ICU admissions and better outcomes in survival and disease progression.13 Stukas et al. (2022) reported that the decreased dose of tocilizumab had worse outcomes in mortality, but no difference in hospital LOS, ICU LOS, or duration of mechanical ventilation.20 Landry et al. (2019) reported that using the antibiotic without addition of the shortage drug had no difference in readmissions or adverse events.33 McAlister and Youngson (2020) reported worse outcomes for ED and outpatient visits, but no difference in hospital admissions.30 Three studies concluded that the replacement drug or protocol was an acceptable alternative to the shortage drug.13,20,33 The fourth study concluded that there were no long-term adverse effects because of the shortage.30
Table 2: Summary of Included Scoping Review — Phuong et al. (2019)6
Study citation | Study characteristics | Drug characteristics | Relevant outcomes | Outcome results |
|---|---|---|---|---|
Anesthetics | ||||
Romito B, et al. Hosp Pharm. 2015;50(9):798-805. US | Study design: retrospective cohort Population: NR Setting: surgery | Drug class: general anesthetic, systemic Shortage: propofol Replacement: alternative agents | Mortality | No difference |
Price B, et al. Am J Emerg Med. 2013;31(7):1124-32. US | Study design: retrospective cohort Population: people requiring endotracheal intubation Setting: air medical | Drug class: general anesthetic, systemic Shortage: etomidate Replacement: ketamine | Adverse drug reaction | No difference |
Hemodynamics | No difference | |||
Roberts R, et al. Crit Care Med. 2012;40(2):406-11. US | Study design: retrospective cohort Population: noncardiac patients in the ICU Setting: ICU | Drug class: general anesthetic, systemic Shortage: propofol Replacement: alternative anesthetic drugs | Duration of mechanical ventilation | Increased with alternative anesthetic drugs (NSS) |
Oncology drugs and adjuncts | ||||
Duan F, et al. Radiology. 2016;278(2):612-21. US | Study design: prospective cohort Population: people undergoing transcatheter arterial chemoembolization for hepatocellular carcinoma Setting: NR | Drug class: NR Shortage: NR Replacement: alternative vehicles of oncology medications | Adverse drug reaction | No difference |
Berger JL, et al. Onco Targets Ther. 2014;7:1409-13. US | Study design: retrospective cohort Population: people with recurrent epithelial ovarian carcinoma Setting: NR | Drug class: antineoplastic Shortage: pegylated liposomal doxorubicin (Doxil) Replacement: non–FDA-approved second-generation liposomal doxorubicin | Treatment response | No patients had a complete or partial response with alternative therapy |
Nickel RS, et al. Pediatr Blood Cancer. 2014;61(5):810-4. US | Study design: retrospective cohort Population: people with newly diagnosed lymphoblastic leukemia and lymphoma Setting: hospital | Drug class: antineoplastic Shortage: daunorubicin Replacement: mitoxantrone | Mortality | No difference |
ICU admission | No difference | |||
Adverse events: fever, bacteremia, invasive fungal disease | No difference | |||
Hospital LOS | No difference | |||
Trifilio S, et al. Leuk Res. 2013;37(8):868-71. US | Study design: retrospective cohort Population: people with acute myeloid leukemia Setting: NR | Drug class: antineoplastic Shortage: daunorubicin Replacement: idarubicin | Mortality | No difference |
Adverse drug reaction | No difference | |||
Complete remission | No difference | |||
Antimicrobials and adjuncts | ||||
McLaughlin MM, et al. Infect Dis Ther. 2017;6(2):259-64. US | Study design: retrospective cohort Population: NR Setting: NR | Drug class: antiviral Shortage: IV acyclovir Replacement: high-dose oral valacyclovir | Adverse drug reaction | 40% of patients experienced at least 1 adverse drug reaction to high-dose oral valacyclovir |
Dilworth TJ, et al. J Manag Care Pharm. 2014;20(12):1246-54. US | Study design: retrospective cohort Population: people with HIV Pneumocystis jirovecii pneumonia Setting: hospital | Drug class: sulfonamide Shortage: IV trimethoprim-sulfamethoxazole Replacement: alternative agents | Mortality | Equal number of deaths in both groups |
Clinical status | Worsened in the shortage group | |||
Treatment failure | No difference | |||
Adverse events | No difference | |||
Hospital LOS | No difference | |||
Mendez MN, et al. Pharmacotherapy. 2006;26(1):61-7. US | Study design: retrospective cohort Population: NR Setting: NR | Drug class: penicillin; beta-lactamase inhibitor Shortage: piperacillin-tazobactam Replacement: alternative antimicrobials | Adverse drug reaction |
|
Other | ||||
Vail E, et al. JAMA. 2017;317(14):1433-42. US | Study design: retrospective cohort Population: people with septic shock Setting: NR | Drug class: vasopressor Shortage: norepinephrine Replacement: alternative vasopressors | Mortality | Increased with alternative vasopressors |
Blaine KP, et al. Clin Anesth. 2016;35:516-23. US | Study design: retrospective cohort Population: people undergoing cardiac surgery Setting: surgery | Drug class: antifibrinolytic Shortage: epsilon-aminocaproic acid Replacement: tranexamic acid | Adverse drug reaction | Decreased with tranexamic acid |
Cho S, et al. nn Pharmacother. 2016;50(9):718-24. US | Study design: retrospective cohort Population: people with acute subarachnoid hemorrhage Setting: NR | Drug class: calcium channel blocker Shortage: nimodipine Replacement: shortened course of treatment | Mortality | No difference |
Adverse drug reaction | No difference | |||
Hospital LOS | No difference | |||
Duration of mechanical ventilation | No difference | |||
Neurologic outcomes | No difference | |||
Malone C, et al. Ulster Med J. 2016;85(3):174-7. UK | Study design: prospective cohort Population: people undergoing nonemergent caesarean section Setting: surgery | Drug class: uterotonic Shortage: IV oxytocin Replacement: Syntometrine | Transfusions, blood loss | No difference |
Adverse drug reaction | Increased intraoperative antiemetics with Syntometrine | |||
Ladha KS, et al. Anesth Analg. 2015;121(2):404-9. US | Study design: retrospective cohort Population: NR Setting: surgery | Drug class: vasopressor Shortage: pharmacy-prepared ephedrine syringes Replacement: alternative vasopressors | Hemodynamics | No difference |
Goldblatt J, et al. Blood Cells Mol Dis. 2011;46(1):107-10. Australia | Study design: prospective cohort Population: people with Gaucher disease Setting: NR | Drug class: metabolic enzyme Shortage: imiglucerase Replacement: None | Clinical complications | Most patients had no significant clinical complications |
ICU = intensive care unit; LOS = length of stay; NR = not reported; NSS = not statistically significant.
Table 3: Summary of Included Nonrandomized Studies by Clinical Indication
Study citation, location | Study characteristics | Drug characteristics | Relevant outcomes | Outcome results |
|---|---|---|---|---|
General | ||||
Borneau-Martin et al. (2023),7 France | Study design: registry Population: drug shortage–related ADRs reported to a pharmacovigilance database (N = 462) Setting: any | Drug class: any Most frequently reported: nervous system drugs, cardiovascular drugs, anti-infectives for systemic use; replacement drug used in 96% of reported ADR cases | Number of ADR cases related to drug shortages | Increased at a greater rate than total reported ADRs over the study period |
ADRs | 84% of cases related to drug shortages | |||
Serious ADRs: hospitalization, medically significant or life-threatening events, death | 46% of cases related to drug shortages | |||
Death | 2% of cases related to drug shortages | |||
Disease worsening | 16% of cases related to drug shortages | |||
Medication errors | 11% of cases related to drug shortages | |||
Anesthetics, analgesics, and sedatives | ||||
John et al. (2022),17 US | Study design: retrospective cohort Population: adults receiving mechanical ventilation (N = 100) Setting: ICU | Drug class: opioid analgesic Shortage: IV opioids Replacement: oral opioids or alternative nonopioid drugs | Hospital LOS | No difference |
ICU LOS | No difference | |||
Mortality | No difference | |||
Duration of mechanical ventilation | No difference | |||
Pain level | No difference | |||
Katsivalis et al. (2022),18 US | Study design: retrospective cohort Population: adults with sickle cell disease (N = 89) Setting: hospital | Drug class: opioid analgesic Shortage: IV opioid medications Replacement: oral opioids | Hospital LOS | No difference |
Readmission | Fewer 30-day readmissions during the shortage period | |||
ED visits | No difference | |||
Rodriguez-Monguio et al. (2022),19 US | Study design: retrospective cohort Population: adults with cancer (N = 3,906) Setting: surgery | Drug class: Opioid analgesic Shortage: any opioid analgesic in shortage during the study period Replacement: any, including drug substitutions, dose conversions, and alternative administration routes | Adverse event: post-operative hypoxemia | Increased in patients exposed to opioid shortages (NSS) |
Adverse event: post-operative hypoxemia reversed by IV naloxone | Increased in patients exposed to opioid shortages (NSS) | |||
Cole et al. (2021),10 US | Study design: prospective cohort Population: patients with acute agitation (N = 1,257) Setting: ED | Drug class: antipsychotic Shortage: droperidol; olanzapine Replacement: droperidol; olanzapine | ED LOS | Longer ED LOS in the olanzapine group |
Adverse event: extrapyramidal | Extrapyramidal adverse events were more common with droperidol | |||
Adverse events: cardiovascular, respiratory, intubation | No difference | |||
Farrell et al. (2020),26 US | Study design: retrospective cohort Population: adults requiring rapid sequence intubation (N = 82) Setting: ED | Drug class: general anesthetic, systemic Shortage: etomidate Replacement: ketamine; methohexital | Complications: dental trauma, airway trauma, esophageal intubation, new onset seizures | No occurrences in either group |
Complications: aspiration | Two aspirations occurred in the etomidate group | |||
Nelson et al. (2019),34 US | Study design: retrospective cohort Population: adults with acute alcohol withdrawal syndrome (N = 300) Setting: ED | Drug class: benzodiazepine Shortage: IV diazepam; IV lorazepam Replacement: IV lorazepam with IV phenobarbital; IV phenobarbital alone | ICU admission | No difference |
Overall admission |
| |||
LOS, total | LOS was shortest with lorazepam + phenobarbital compared to diazepam and phenobarbital only | |||
LOS, ED | ED LOS was shortest with diazepam compared to lorazepam + phenobarbital and phenobarbital only | |||
LOS, floor and ICU | No difference | |||
Intubation | No difference | |||
Neff et al. (2018),37 US | Study design: retrospective cohort Population: adults undergoing general anesthesia (N = 2,090) Setting: surgery | Drug class: general anesthetic, systemic Shortage: propofol Replacement: inhaled volatile drugs | Postoperative nausea and vomiting | Greater incidence of postoperative nausea and vomiting during the propofol shortage period |
PACU LOS | Longer duration of stay in the PACU during the propofol shortage period | |||
Readmit to ED | No difference | |||
Oncology drugs and adjuncts | ||||
Lachance et al. (2023),13 Canada | Study design: retrospective cohort Population: patients undergoing autologous stem cell transplant for relapsed-refractory lymphoma (N = 227) Setting: hospital | Drug class: antineoplastic Shortage: carmustine Replacement: bendamustine | Febrile neutropenia | No difference |
Mucositis | Increased development of grade ≥ 3 mucositis with bendamustine | |||
Toxicity: cardiac, pulmonary, liver | No difference | |||
Toxicity: renal | Increased with bendamustine | |||
ICU admission | Increased with bendamustine | |||
Transfusion |
| |||
Hospital LOS | Increased with bendamustine | |||
Mortality |
| |||
Disease progression | Better progression-free survival with bendamustine | |||
Strobbe et al. (2023),14 France | Study design: retrospective cohort Population: patients receiving paclitaxel-based chemotherapy (N = 831) Setting: outpatient | Drug class: H2A Shortage: ranitidine; famotidine Replacement: alternative H2A (famotidine); no H2A (H1A, corticosteroid, or combined H1A and corticosteroid) | Hypersensitivity reactions | No difference |
Li and Cimino (2020),28 US | Study design: retrospective cohort Population: patients receiving chemotherapy (N = 22) Setting: outpatient | Drug class: antineoplastic Shortage: etoposide injection Replacement: alternative therapy (e.g., oral etopisode or etopophos injection) | Adverse drug events | No difference |
Disease progression | No difference | |||
Medication errors | None recorded | |||
Roy et al. (2019),35 US | Study design: retrospective cohort Population: adults receiving HDTMX as inpatients (N = 18) Setting: hospital | Drug class: alkalinizing drugs Shortage: IV sodium bicarbonate and IV sodium acetate Replacement: oral sodium bicarbonate with oral or IV acetazolamide as needed | Hospital LOS | No difference |
Adverse events: acute kidney injury, hepatotoxicity, myelosuppression | No difference | |||
Adverse events: pneumonitis, mucositis, rash | No occurrences in either group | |||
Visage et al. (2019),36 US | Study design: retrospective cohort, uncontrolled Population: pediatric patients receiving HDTMX (N = 102) (HDTMX cycles) Setting: hospital | Drug class: alkalinizing drug Shortage: IV sodium bicarbonate Replacement: oral sodium bicarbonate and oral sodium citrate-citric acid | GI side effects | The incidence of GI side effects was not drastically impacted by use of an oral alkalinizing drug |
Vaccines | ||||
Miyazato et al. (2023),8 Japan | Study design: prospective cohort, uncontrolled Population: people at risk of yellow fever (N = 1,1279) Setting: community | Drug Class: live vaccine, viral Shortage: YF-Vax Replacement: alternative 17D-204 yellow fever vaccine (Stamaril) | Adverse events | The alternative vaccination was shown to be generally safe |
Serious adverse events | Three participants developed serious adverse events that may have been related to vaccination | |||
Rojas et al. (2023),9 US | Study design: prospective cohort, uncontrolled Population: people at high risk of yellow fever (N = 627,079) Setting: community | Drug class: live vaccine, viral Shortage: YF-Vax Replacement: Stamaril | Adverse events | No safety issues were identified |
Serious adverse events | Serious adverse events were very rare and consistent with the known safety profile | |||
Wong et al. (2020),12 Australia | Study design: prospective cohort, uncontrolled Population: children (N = 6,779) Setting: community | Drug class: live vaccine, bacterial Shortage: Sanofi-Pasteur BCG strain Replacement: BCG-10 (derived from the Moreau strain) | Adverse events following immunization | BCG-10 had a similar safety profile to that reported for other BCG strains |
Nzolo et al. (2018),38 DRC | Study design: retrospective cohort, uncontrolled Population: people receiving preventative fractional dose yellow fever vaccination during an outbreak (N = 7,466,998) Setting: community | Drug class: live vaccine, viral Shortage: 17DD yellow fever vaccine, full dose Replacement: 17DD yellow fever vaccine, fractional dose | Adverse events following immunization | Fractional dose vaccination had an acceptable safety profile |
Serious adverse events following immunization | Serious adverse events were reported by 5 individuals | |||
Antimicrobials and adjuncts | ||||
Haiduc et al. (2021),22 US | Study design: retrospective cohort Population: adults in hospital with febrile neutropenia (N = 150) Setting: hospital | Drug class: cephalosporin Shortage: cefepime Replacement: cefepime (dose sparing) | Hospital LOS | No difference |
Mortality, all-cause, infection-related | No difference | |||
Patel et al. (2020),31 US | Study design: retrospective cohort Population: neonates (N = 101) Setting: neonatal ICU | Drug class: cephalosporin Shortage: cefotaxime Replacement: ceftazidime | Culture positive late-onset sepsis | Increased with the use of ceftazidime (NSS) |
Multidrug-resistant organism infection | Increased with the use of ceftazidime (NSS) | |||
Stage II to III necrotizing enterocolitis | Increased with the use of ceftazidime | |||
Urinary tract infection | No difference | |||
Mortality | No difference | |||
Hospital LOS | No difference | |||
Adverse events | No occurrences in either group | |||
Landry et al. (2019),33 Canada | Study design: retrospective cohort Population: adults with uncomplicated cellulitis requiring IV therapy (N = 203) Setting: ED | Drug class: uricosuric drug Shortage: probenecid (in combination with IV cefazolin) Replacement: IV cefazolin only, continuous infusion | Recurrence (admission or ED visit for cellulitis within 30 days of treatment end) | No difference |
Adverse events: rash, nausea | No difference | |||
COVID-19 | ||||
Swets et al. (2023),39 the Netherlands | Study design: retrospective cohort Population: adults hospitalized for COVID-19 (N = 5,485) Setting: hospital | Drug class: monoclonal antibody (interleukin-6 inhibitor) Shortage: tocilizumab (IV) Replacement: tocilizumab (fixed dose and low dose); sarilumab | Mortality | • Lower survival with fixed-dose tocilizumab and sarilumab • No difference in survival with low-dose tocilizumab |
Hospital LOS | • Shorter LOS with low-dose tocilizumab and sarilumab • No difference in LOS with fixed-dose tocilizumab | |||
ICU admission or mortality | Higher ICU admissions or death with fixed-dose tocilizumab, low-dose tocilizumab, and sarilumab | |||
Stukas et al. (2022),20 Canada | Study design: retrospective cohort Population: adults with a diagnosis of pneumonia secondary to SARS-CoV-2 infection (N = 153) Setting: ICU | Drug class: monoclonal antibody (interleukin-6 inhibitor) Shortage: tocilizumab (IV), weight-based dose Replacement: tocilizumab (IV), fixed dose | Duration of mechanical ventilation | No difference |
ICU LOS | No difference | |||
Hospital LOS | No difference | |||
Mortality | Higher mortality in the fixed-dose group (NSS) | |||
Lecronier et al. (2020),27 France | Study design: retrospective cohort Population: patients with severe SARS-CoV-2 pneumonia (N = 80) Setting: ICU | Drug class: protease inhibitor Shortage: lopinavir-ritonavir Replacement: hydroxychloroquinine | Treatment escalation: intubation, ECMO, RRT | No difference |
Mortality | No difference | |||
Safety and tolerance outcomes: neutropenia, anemia, thrombocytopenia, increased ASP and ALT, acute renal failure, prolonged QT interval | No difference | |||
Other | ||||
Dannemiller et al. (2022),16 US | Study design: retrospective cohort Population: adults undergoing cardiac surgery (N = 1,544) Setting: surgery | Drug class: antifibrinolytic drug Shortage: epsilon-aminocaproic acid Replacement: tranexamic acid | Safety events: mortality, cardiovascular, renal, seizure | No difference |
Freeman et al. (2021),21 US | Study design: retrospective cohort Population: adults who qualified for general or continuous renal replacement therapy electrolyte replacement protocol (N = 288) Setting: ICU | Drug class: electrolytes Shortage: IV electrolyte replacement products Replacement: enteral electrolyte replacement | ICU LOS | No difference |
Mortality | No difference | |||
Duration of mechanical ventilation | Decreased in the shortage period group | |||
Neto et al. (2021),23 Brazil | Study design: retrospective cohort, uncontrolled Population: patients with atypical hemolytic uremic syndrome (N = 24) Setting: dialysis clinic | Drug class: monoclonal antibody Shortage: eculizumab Replacement: None | Disease relapse | Increased after unplanned eculizumab interruption |
McAlister and Youngson (2020),30 Canada | Study design: retrospective cohort, uncontrolled Population: adults dispensed any of the recalled valsartan products (N = 34,726) Setting: community | Drug class: angiotensin receptor blocker Shortage: generic valsartan Replacement: alternative angiotensin receptor blocker; brand name valsartan | Outpatient visits | Increased immediately after generic valsartan recall |
ED visits | Increased immediately after generic valsartan recall (older patients only) | |||
ED visits, hospitalizations for stroke or TIA | No difference | |||
van Langenberg et al. (2020),11 Australia | Study design: prospective cohort Population: people with mild to moderate ulcerative colitis (N = 31) Setting: outpatient | Drug class: 5-ASA Shortage: balsalazide Replacement: alternative 5-ASA formulations (e.g., multimatrix mesalazine) | Clinical activity | Higher than expected proportion of patients with worsening disease with alternative 5-ASA |
Adverse events | Higher than expected proportion of patients with significant side effects with alternative 5-ASA | |||
Remission | No difference | |||
Treatment escalation | No difference | |||
Mortality | No difference | |||
Flares requiring hospitalization | Increased with alternative 5-ASA | |||
Yang et al. (2020),32 US | Study design: retrospective cohort Population: adult patients with hyperkalemia receiving IV insulin (N = 134) Setting: ED | Drug class: glucose-elevating drug Shortage: dextrose 50% Replacement: dextrose 10% | Symptomatic hypoglycemia | Lower incidence in the dextrose 10% group (NSS) |
Adverse events, including extravasation | No occurrences in either group | |||
Non-drug | ||||
Acadamia et al. (2022),15 US | Study design: retrospective cohort Population: adults (N = 696) Setting: ED | Drug class: small-volume parenteral solutions Shortage: IV piggyback administration of penicillins and carbapenems Replacement: IV push administration of penicillins and carbapenems | Drug-related adverse events | No difference |
Mortality | No difference | |||
Tschumper et al. (2021),24 US | Study design: retrospective cohort Population: adults (N = 90) Setting: hospital | Drug class: small-volume parenteral solutions Shortage: prolonged infusion (4 hour) of piperacillin-tazaobactam Replacement: continuous infusion of piperacillin-tazobactam | Hospital LOS | No difference |
Mortality | No difference | |||
Safety: thrombocytopenia | Higher incidence with continuous infusion (NSS) | |||
Safety: Clostridioides difficile infection, acute renal failure | No difference | |||
Safety: seizure | No occurrences in either group | |||
Readmission | Fewer readmissions with continuous infusion (NSS) | |||
Blair and Covington (2020),25 US | Study design: retrospective cohort, uncontrolled Population: adults (N = 120) Setting: hospital | Drug class: small-volume parenteral solutions Shortage: 4-hour extended infusion of piperacillin-tazobactam Replacement: continuous infusion of piperacillin-tazobactam | Acute kidney injury | Incidence with continuous infusion similar to previously reported results with extended infusion |
Marsh et al. (2020),29 US | Study design: retrospective cohort, uncontrolled Population: adults (N = 1,000) Setting: hospital | Drug class: small-volume parenteral solutions Shortage: IV piggyback administration of beta-lactam antibiotics Replacement: IV push administration of beta-lactam antibiotics | Adverse events | Safety of IV push administration similar to previously reported results with IV piggyback administration |
5-ASA = 5-aminosalicylate; ADR = adverse drug reaction; ALT = alanine aminotransferase; AST = aspartate aminotransferase; BCG = Bacillus Calmette-Guérin; DRC = Democratic Republic of the Congo; ECMO = extracorporeal membrane oxygenation; ED = emergency department; GI = gastrointestinal; H1A = histamine-1 antagonist; H2A = histamine-2 antagonists; HDTMX = high-dose methotrexate; ICU = intensive care unit; LOS = length of stay; NSS = not statistically significant; PACU = post-anesthetic care unit; RRT = renal replacement therapy; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; TIA = transient ischemic attack.
Conclusions
The development of a preventive approach could possibly help mitigate the impacts of drug shortages. To achieve this, first, drugs that are potentially the highest impact need to be identified. Anticipating which drugs are likely to be most impactful during a shortage involves identifying those most at risk of supply chain disruptions and those most likely to cause patient harm. Ranking drugs based on their risk of shortage and their risk of harm during a shortage can help decision-makers put into place pre-emptive strategies. This report supports this objective by summarizing types of harms that may occur during drug shortages, and, although not the primary intent of this report, by identifying the types of drugs experiencing shortages studied in the literature. Most of the published trials examined the effectiveness and safety of alternative drugs during drug shortages. The harms outcomes that were most frequently reported were adverse events or safety-related outcomes and health system use, including length of stay, mortality, and disease progression. Similarly, a French registry study described the types of adverse drug reactions related to drug shortages as reported to a pharmacovigilance database.7 The authors described harms from adverse drug reactions; serious adverse drug reactions, including hospitalization, life-threatening events, or death; and disease progression.7 The primary studies that concluded that the examined drug shortage had negative consequences reported health system use, adverse events, disease progression, and mortality as harms outcomes.11,19,23,31,37,39
This report summarizes the available evidence on the effect of drug shortages on patient outcomes and will be used in combination with other CADTH work to support future decision-making regarding drug shortages, including:
an environmental scan of existing clinical tools or scoring systems available for drug shortage or supply chain disruptions
facilitation of a Delphi panel to support the identification of high-priority drugs based on their supply chain risk and clinical risk.
References
1.Drug Shortages in Canada. Ottawa (ON): Health Canada; 2023: https://www.canada.ca/content/dam/hc-sc/documents/services/drugs-health-products/drug-products/drug-shortages/2022-2023-review/2022-2023-review-en.pdf. Accessed 2023 Nov 9.
2.Protocol for the Notification and Communication of Drug Shortages. Drug Shortages Canada; 2017: https://www.drugshortagescanada.ca/files/MSSC_Protocol_2017.pdf. Accessed 2023 Nov 9.
3.A Toolkit for Improved Understanding and Transparency of Drug Shortage Response in Canada. Drug Shortages Canada; 2017: https://www.drugshortagescanada.ca/files/MSSC_Toolkit_2017.pdf. Accessed 2023 Nov 9.
4.Aronson JK, Heneghan C, Ferner RE. Drug shortages. Part 1. Definitions and harms. Br J Clin Pharmacol. 2023;16:16. PubMed
5.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst. 2021;10(1):89. PubMed
6.Phuong JM, Penm J, Chaar B, Oldfield LD, Moles R. The impacts of medication shortages on patient outcomes: A scoping review. PLoS ONE. 2019;14(5):e0215837. PubMed
7.Bourneau-Martin D, Babin M, Grandvuillemin A, et al. Adverse drug reaction related to drug shortage: A retrospective study on the French National Pharmacovigilance Database. Br J Clin Pharmacol. 2023;89(3):1080-1088. PubMed
8.Miyazato Y, Terada M, Ujiie M, et al. A nationwide prospective cohort study on safety of the 17D-204 yellow fever vaccine during a vaccine shortage in Japan. J Travel Med. 2023;30(2):05.
9.Rojas A, Hachey W, Kaur G, Korejwo J, Muhammad R. Enhanced safety surveillance of STAMARIL R yellow fever vaccine provided under the expanded access investigational new drug program in the United States. J Travel Med. 2023;31:31. PubMed
10.Cole JB, Stang JL, DeVries PA, Martel ML, Miner JR, Driver BE. A Prospective Study of Intramuscular Droperidol or Olanzapine for Acute Agitation in the Emergency Department: A Natural Experiment Owing to Drug Shortages. Ann Emerg Med. 2021;78(2):274-286. PubMed
11.van Langenberg DR, Cheng RK, Garg M. Outcomes of a drug shortage requiring switching in patients with ulcerative colitis. World J Gastrointest Pathophysiol. 2020;11(2):32-42. PubMed
12.Wong NX, Buttery J, McMinn A, Azhar Z, Crawford NW. Safety of the Polish BCG-10 Vaccine During a Period of BCG Vaccine Shortage: An Australian Experience. Pediatr Infect Dis J. 2020;39(6):e66-e68. PubMed
13.Lachance S, Bourguignon A, Boisjoly JA, et al. Impact of Implementing a Bendamustine-Based Conditioning Regimen on Outcomes of Autologous Stem Cell Transplantation in Lymphoma while Novel Cellular Therapies Emerge. Transplant Cell Ther. 2023;29(1):34.e31-34.e37. PubMed
14.Strobbe G, Gaboriau L, Abele M, et al. Impact of histamine-2 antagonist shortage on the incidence of hypersensitivity reactions to paclitaxel: a reconsideration of premedication protocols in France (PACLIREACT Study). Eur J Clin Pharmacol. 2023;79(9):1229-1238. PubMed
15.Academia EC, Jenrette JE, Mueller SW, McLaughlin JM. Evaluation of First-Dose, Intravenous Push Penicillins and Carbapenems in the Emergency Department. J Pharm Pract. 2022;35(3):369-376. PubMed
16.Dannemiller RE, Knowles DM, Cook BM, Goodberlet MZ, Kelly JM, Malloy R. Comparison of trauma-dosed tranexamic acid versus aminocaproic acid in cardiac surgery in the setting of drug shortage. J Card Surg. 2022;37(10):3243-3249. PubMed
17.John K, Cape K, Goodman L, Elefritz J. Impact of the Injectable Opioid Drug Shortage on Analgesia and Sedation Management in the Medical Intensive Care Unit: A Retrospective Cohort Study. Hosp Pharm. 2022;57(1):160-166. PubMed
18.Katsivalis KV, Kosacz J, Austin Szwak J. Opioid Use in Vaso-Occlusive Crisis During Intravenous Opioid Drug Shortage. Hosp Pharm. 2022;57(6):721-726. PubMed
19.Rodriguez-Monguio R, Lun Z, Bongiovanni T, Chen CL, Seoane-Vazquez E. Postoperative Respiratory Events in Surgical Patients Exposed to Opioid Analgesic Shortages Compared to Fully Matched Patients Non-exposed to Shortages. Drug Saf. 2022;45(4):359-367. PubMed
20.Stukas S, Goshua G, Kinkade A, et al. Reduced fixed dose tocilizumab 400 mg IV compared to weight-based dosing in critically ill patients with COVID-19: A before-after cohort study. Lancet Reg Health Am. 2022;11:100228. PubMed
21.Freeman L, Newsome AS, Huang E, Rowe E, Waller J, Forehand CC. Assessment of Electrolyte Replacement in Critically Ill Patients During a Drug Shortage. Hosp Pharm. 2021;56(4):296-301. PubMed
22.Haiduc M, Patel M, Walsh TL, Moffa MA, Bremmer DN. Impact of a cefepime shortage on dosing regimens and outcomes in hospitalized adults with febrile neutropenia. J Oncol Pharm Pract. 2021;27(2):297-304. PubMed
23.Neto ME, de Moraes Soler L, Vasconcelos HVG, et al. Eculizumab interruption in atypical hemolytic uremic syndrome due to shortage: analysis of a Brazilian cohort. J Nephrol. 2021;34(4):1373-1380. PubMed
24.Tschumper E, Dupuis K, McCrory K, Pitts W. Evaluation of Prolonged Versus Continuous Infusions of Piperacillin/Tazobactam During Shortages of Small Volume Parenteral Solutions. J Pharm Technol. 2021;37(6):271-277. PubMed
25.Blair K, Covington EW. Incidence and Risk Factors of Acute Kidney Injury in Patients Receiving Concomitant Vancomycin and Continuous-Infusion Piperacillin/Tazobactam: A Retrospective Cohort Study. Ann Pharmacother. 2020;54(11):1096-1101. PubMed
26.Farrell NM, Killius K, Kue R, Langlois BK, Nelson KP, Golenia P. A Comparison of Etomidate, Ketamine, and Methohexital in Emergency Department Rapid Sequence Intubation. J Emerg Med. 2020;59(4):508-514. PubMed
27.Lecronier M, Beurton A, Burrel S, et al. Comparison of hydroxychloroquine, lopinavir/ritonavir, and standard of care in critically ill patients with SARS-CoV-2 pneumonia: an opportunistic retrospective analysis. Crit Care. 2020;24(1):418. PubMed
28.Li H, Cimino SK. Clinical impact of the etoposide injection shortage. J Oncol Pharm Pract. 2020;26(1):187-192. PubMed
29.Marsh K, Ahmed N, Decano A, et al. Safety of intravenous push administration of beta-lactams within a healthcare system. Am J Health-Syst Pharm. 2020;77(9):701-708. PubMed
30.McAlister FA, Youngson E. Impact of the Generic Valsartan Recall in Alberta, Canada. J Am Coll Cardiol. 2020;75(15):1860-1862. PubMed
31.Patel PD, Bhagat P, Bartlett AH, Bondi DS. Comparison of Neonatal Outcomes With the Use Cefotaxime Versus Ceftazidime in a Neonatal Intensive Care Unit. The Journal of Pediatric Pharmacology & Therapeutics. 2020;25(2):117-123. PubMed
32.Yang I, Smalley S, Ahuja T, Merchan C, Smith SW, Papadopoulos J. Assessment of dextrose 50 bolus versus dextrose 10 infusion in the management of hyperkalemia in the ED. Am J Emerg Med. 2020;38(3):598-602. PubMed
33.Landry DL, Eltonsy S, Jalbert LP, Girouard G, Couture J, Belanger M. Continuous cefazolin infusion versus cefazolin plus probenecid for the ambulatory treatment of uncomplicated cellulitis: A retrospective cohort study. J Assoc Med Microbiol Infect Dis Can. 2019;4(2):108-112. PubMed
34.Nelson AC, Kehoe J, Sankoff J, Mintzer D, Taub J, Kaucher KA. Benzodiazepines vs barbiturates for alcohol withdrawal: Analysis of 3 different treatment protocols. Am J Emerg Med. 2019;37(4):733-736. PubMed
35.Roy AM, Lei M, Lou U. Safety and efficacy of a urine alkalinization protocol developed for high-dose methotrexate patients during intravenous bicarbonate shortage. J Oncol Pharm Pract. 2019;25(8):1860-1866. PubMed
36.Visage R, Kaiser N, Williams M, Kim A. Oral Methods of Urinary Alkalinization for High-dose Methotrexate Administration: Alternatives to Intravenous Sodium Bicarbonate During a Critical Drug Shortage. J Pediatr Hematol Oncol. 2019;41(5):371-375. PubMed
37.Neff MP, Wagner D, Phillips BJ, et al. Propofol Drug Shortage Associated With Worse Postoperative Nausea and Vomiting Outcomes Despite a Mitigation Strategy. Aana J. 2018;86(2):147-154. PubMed
38.Nzolo D, Engo Biongo A, Kuemmerle A, et al. Safety profile of fractional dosing of the 17DD Yellow Fever Vaccine among males and females: Experience of a community-based pharmacovigilance in Kinshasa, DR Congo. Vaccine. 2018;36(41):6170-6182. PubMed
39.Swets MC, Moss RJ, Kor F, et al. A comparison of the effectiveness of different doses of tocilizumab and sarilumab in the treatment of severe COVID-19: a natural experiment due to drug shortages. Int J Infect Dis. 2023;129:57-62. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
Scoping Reviews
Unclear Outcomes
Tucker EL, Cao Y, Fox ER, Sweet BV. The Drug Shortage Era: A Scoping Review of the Literature 2001-2019. Clin Pharmacol Ther. 2020;108(6):1150-1155. PubMed
Nonrandomized Studies
Not Direct Patient Harm Outcomes
Chun B, He M, Jones C, et al. Variation in Statewide Intravesical Treatment Rates for Non-Muscle Invasive Bladder Cancer During the Bacillus Calmette-Guerin Drug Shortage. Urology. 2023;177():74-80.
N'Kaoua E, Attarian S, Delmont E, et al. Immunoglobulin shortage: Practice modifications and clinical outcomes in a reference centre. Rev Neurol (Paris). 2022;178(6):616-623. PubMed
Zhang B, Yeh DD, Ortiz-Reyes LA, Chang Y, Quraishi SA. Impact of nationwide essential trace element shortages: A before-after, single-center analysis of hospitalized adults receiving home parenteral nutrition therapy. Nutr Clin Pract. 2022;37(2):442-450. PubMed
Martei YM, Grover S, Bilker WB, et al. Impact of Essential Medicine Stock Outs on Cancer Therapy Delivery in a Resource-Limited Setting. J Global Oncol. 2019;5():1-11.
Hedlund NG, Isgor Z, Zwanziger J, et al. Drug Shortage Impacts Patient Receipt of Induction Treatment. Health Serv Res. 2018;53(6):5078-5105. PubMed
Additional References
Potentially Relevant Studies Published Before January 1, 2018
Alhogbani MM, Picard JA, Fassi-Fehri MH, Badet JL, Colombel CM. Prognostic impact of Bacillus Calmette-Guerin interruption at the time of induction and consolidation. Urol Ann. 2017;9(4):315-320. PubMed
Gross AE, Johannes RS, Gupta V, Tabak YP, Srinivasan A, Bleasdale SC. The Effect of a Piperacillin/Tazobactam Shortage on Antimicrobial Prescribing and Clostridium difficile Risk in 88 US Medical Centers. Clin Infect Dis. 2017;65(4):613-618. PubMed
Howard J, Wigley J, Rosen G, D'Mello J. Glycopyrrolate: It's time to review. J Clin Anesth. 2017;36():51-53.
Hsueh K, Reyes M, Krekel T, et al. Effective Antibiotic Conservation by Emergency Antimicrobial Stewardship During a Drug Shortage. Infect Control Hosp Epidemiol. 2017;38(3):356-359. PubMed
McLaughlin MM, Sutton SH, Jensen AO, Esterly JS. Use of High-Dose Oral Valacyclovir During an Intravenous Acyclovir Shortage: A Retrospective Analysis of Tolerability and Drug Shortage Management. Infect. 2017;6(2):259-264. PubMed
Vail E, Gershengorn HB, Hua M, Walkey AJ, Rubenfeld G, Wunsch H. Association Between US Norepinephrine Shortage and Mortality Among Patients With Septic Shock. JAMA. 2017;317(14):1433-1442. PubMed
VanderWeide LA, Abdel-Rasoul M, Gerlach AT. The Incidence of hypotension with continuous infusion atracurium compared to cisatracurium in the Intensive Care Unit. Int J Crit Illn Inj Sci. 2017;7(2):113-118. PubMed
Barber KE, Bell AM, Travis King S, Parham JJ, Stover KR. Impact of piperacillin-tazobactam shortage on meropenem use: implications for antimicrobial stewardship programs. Braz J Infect Dis. 2016;20(6):631-634. PubMed
Blaine KP, Press C, Lau K, Sliwa J, Rao VK, Hill C. Comparative effectiveness of epsilon-aminocaproic acid and tranexamic acid on postoperative bleeding following cardiac surgery during a national medication shortage. J Clin Anesth. 2016;35():516-523.
Cho S, Bales J, Tran TK, Korab G, Khandelwal N, Joffe AM. Effects of 14 Versus 21 Days of Nimodipine Therapy on Neurological Outcomes in Aneurysmal Subarachnoid Hemorrhage Patients. Ann Pharmacother. 2016;50(9):718-24. PubMed
Dotson B, Larabell P, Patel JU, et al. Calcium Administration Is Associated with Adverse Outcomes in Critically Ill Patients Receiving Parenteral Nutrition: Results from a Natural Experiment Created by a Calcium Gluconate Shortage. Pharmacotherapy. 2016;36(11):1185-1190. PubMed
Duan F, Wang EQ, Lam MG, et al. Superselective Chemoembolization of HCC: Comparison of Short-term Safety and Efficacy between Drug-eluting LC Beads, QuadraSpheres, and Conventional Ethiodized Oil Emulsion. Radiology. 2016;278(2):612-21. PubMed
Gawronski CA, Gawronski KM. Vitamin A Supplementation for Prevention of Bronchopulmonary Dysplasia: Cornerstone of Care or Futile Therapy?. Ann Pharmacother. 2016;50(8):680-4. PubMed
Kesteman T, Rafalimanantsoa SA, Razafimandimby H, et al. Multiple causes of an unexpected malaria outbreak in a high-transmission area in Madagascar. Malar J. 2016;15():57.
Malone C, Acheson JR, Hinds JD, McComiskey MH. Uterotonics for Non-emergent Caesarean Section: Protocol Change During UK-Licensed Drug Shortage. Ulster Med J. 2016;85(3):174-177. PubMed
Reed BN, Fox ER, Konig M, et al. The impact of drug shortages on patients with cardiovascular disease: causes, consequences, and a call to action. Am Heart J. 2016;175():130-41.
Storey MA, Weber RJ, Besco K, Beatty S, Aizawa K, Mirtallo JM. Evaluation of Parenteral Nutrition Errors in an Era of Drug Shortages. Nutr Clin Pract. 2016;31(2):211-7. PubMed
Chhim RF, Crill CM. Premixed Parenteral Nutrition Solution Use in Children. Journal Pediatr Pharmacol Ther. 2015;20(5):378-84. PubMed
Clothier HJ, Hosking L, Crawford NW, et al. Bacillus Calmette-Guerin (BCG) vaccine adverse events in Victoria, Australia: analysis of reports to an enhanced passive surveillance system. Drug Saf. 2015;38(1):79-86. PubMed
Hughes KM, Goswami ES, Morris JL. Impact of a Drug Shortage on Medication Errors and Clinical Outcomes in the Pediatric Intensive Care Unit. Journal Pediatr Pharmacol Ther. 2015;20(6):453-61. PubMed
Ladha KS, Nanji KC, Pierce E, Poon KT, Hyder JA. The Impact of a Shortage of Pharmacy-Prepared Ephedrine Syringes on Intraoperative Medication Use. Anesth Analg. 2015;121(2):404-9. PubMed
Romito B, Stone J, Ning N, et al. How Drug Shortages Affect Clinical Care: The Case of the Surgical Anesthetic Propofol. Hosp Pharm. 2015;50(9):798-805. PubMed
Shah S, Theodossiades J, Chapman K, Murdoch I. Impact of supply problems of preservative-free glaucoma medications on patients and hospital staff. Ophthalmic Physiol Opt. 2015;35(2):236-41. PubMed
Shahabi S, Fazlalizadeh H, Stedman J, Chuang L, Shariftabrizi A, Ram R. The impact of international economic sanctions on Iranian cancer healthcare. Health Policy (New York). 2015;119(10):1309-18. PubMed
Van Berkel MA, Fuller LA, Alexandrov AW, Jones GM. Methylene blue, midodrine, and pseudoephedrine: a review of alternative agents for refractory hypotension in the intensive care unit. Crit Care Nurs Q. 2015;38(4):345-58. PubMed
Anger KE, Belisle C, Colwell MB, et al. Safety of compounded calcium chloride admixtures for peripheral intravenous administration in the setting of a calcium gluconate shortage. J Pharm Pract. 2014;27(5):474-7. PubMed
Berger JL, Smith A, Zorn KK, et al. Outcomes analysis of an alternative formulation of PEGylated liposomal doxorubicin in recurrent epithelial ovarian carcinoma during the drug shortage era. Onco Targets Ther. 2014;7():1409-13.
Bible JR, Evans DC, Payne B, Mostafavifar L. Impact of drug shortages on patients receiving parenteral nutrition after laparotomy. JPEN J Parenter Enteral Nutr. 2014;38(2 Suppl):65S-71S. PubMed
Davis C, Javid PJ, Horslen S. Selenium deficiency in pediatric patients with intestinal failure as a consequence of drug shortage. JPEN J Parenter Enteral Nutr. 2014;38(1):115-8. PubMed
Dill S, Ahn J. Drug shortages in developed countries--reasons, therapeutic consequences, and handling. Eur J Clin Pharmacol. 2014;70(12):1405-12. PubMed
Dilworth TJ, Ibrahim OM, Mercier RC. Impact of an intravenous trimethoprim/sulfamethoxazole shortage on treatment outcomes among HIV-infected patients with Pneumocystis jirovecii pneumonia. J Manag Care Spec Pharm. 2014;20(12):1246-54. PubMed
Mazer-Amirshahi M, Pourmand A, Singer S, Pines JM, van den Anker J. Critical drug shortages: implications for emergency medicine. Acad Emerg Med. 2014;21(6):704-11. PubMed
Miller JL, Thomas AN, Johnson PN. Use of continuous-infusion loop diuretics in critically ill children. Pharmacotherapy. 2014;34(8):858-67. PubMed
Morgan KP, Snavely AC, Wind LS, et al. Rates of Renal Toxicity in Cancer Patients Receiving Cisplatin With and Without Mannitol. Ann Pharmacother. 2014;48(7):863-869. PubMed
Nickel RS, Keller F, Bergsagel J, et al. Mitoxantrone as a substitute for daunorubicin during induction in newly diagnosed lymphoblastic leukemia and lymphoma. Pediatr Blood Cancer. 2014;61(5):810-4. PubMed
Stollings JL, Diedrich DA, Oyen LJ, Brown DR. Rapid-sequence intubation: a review of the process and considerations when choosing medications. Ann Pharmacother. 2014;48(1):62-76. PubMed
Thoma BN, Li J, McDaniel CM, Wordell CJ, Cavarocchi N, Pizzi LT. Clinical and economic impact of substituting dexmedetomidine for propofol due to a US drug shortage: examination of coronary artery bypass graft patients at an urban medical centre. Pharmacoeconomics. 2014;32(2):149-57. PubMed
Tolia VN, Murthy K, McKinley PS, Bennett MM, Clark RH. The effect of the national shortage of vitamin A on death or chronic lung disease in extremely low-birth-weight infants. JAMA, Pediatr. 2014;168(11):1039-44. PubMed
Wiggins BS, Nappi J, Fortier CR, Taber DJ. Cardiovascular Drug Shortages: Predominant Etiologies, Clinical Implications, and Management Strategies. Ann Pharmacother. 2014;48(9):1177-1186. PubMed
Krisl JC, Fortier CR, Taber DJ. Disruptions in the supply of medications used in transplantation: implications and management strategies for the transplant clinician. Am J Transplant. 2013;13(1):20-30. PubMed
Nappi JM. A retrospective evaluation of the efficacy of intravenous bumetanide and comparison of potency with furosemide. Pharm Pract. 2013;11(1):44-50. PubMed
Neavyn MJ, Boyer EW, Bird SB, Babu KM. Sodium acetate as a replacement for sodium bicarbonate in medical toxicology: a review. J Med Toxicol. 2013;9(3):250-4. PubMed
Price B, Arthur AO, Brunko M, et al. Hemodynamic consequences of ketamine vs etomidate for endotracheal intubation in the air medical setting. Am J Emerg Med. 2013;31(7):1124-32. PubMed
Rider AE, Templet DJ, Daley MJ, Shuman C, Smith LV. Clinical dilemmas and a review of strategies to manage drug shortages. J Pharm Pract. 2013;26(3):183-91. PubMed
Trifilio S, Zhou Z, Mehta J, et al. Idarubicin appears equivalent to dose-intense daunorubicin for remission induction in patients with acute myeloid leukemia. Leuk Res. 2013;37(8):868-71. PubMed
Briere EC, Jackson M, Shah SG, et al. Haemophilus influenzae type b disease and vaccine booster dose deferral, United States, 1998-2009. Pediatrics. 2012;130(3):414-20. PubMed
Golembiewski J. Drug shortages in the perioperative setting: causes, impact, and strategies. J Perianesth Nurs. 2012;27(4):286-92. PubMed
Ipema HJ. Use of oral vitamin K for prevention of late vitamin k deficiency bleeding in neonates when injectable vitamin K is not available. Ann Pharmacother. 2012;46(6):879-83. PubMed
Kwak GY, Kwon HJ, Kim JH, et al. The immunogenicity and safety of DTaP interchangeable immunization among Korean children. Vaccine. 2012;30(31):4644-7. PubMed
Lowther SA, Shinoda N, Juni BA, et al. Haemophilus influenzae type b infection, vaccination, and H. influenzae carriage in children in Minnesota, 2008-2009. Epidemiol Infect. 2012;140(3):566-74. PubMed
Metzger ML, Billett A, Link MP. The impact of drug shortages on children with cancer--the example of mechlorethamine. N Engl J Med. 2012;367(26):2461-3. PubMed
Ralls MW, Blackwood RA, Arnold MA, Partipilo ML, Dimond J, Teitelbaum DH. Drug shortage-associated increase in catheter-related blood stream infection in children. Pediatrics. 2012;130(5):e1369-73. PubMed
Goldblatt J, Fletcher JM, McGill J, Szer J, Wilson M. Enzyme replacement therapy “drug holiday”: results from an unexpected shortage of an orphan drug supply in Australia. Blood Cells Mol Dis. 2011;46(1):107-10. PubMed
Johnson PN, Miller J, Gormley AK. Continuous-infusion neuromuscular blocking agents in critically ill neonates and children. Pharmacotherapy. 2011;31(6):609-20. PubMed
Kranzer K, Ford N. Unstructured treatment interruption of antiretroviral therapy in clinical practice: a systematic review. Trop Med Int Health. 2011;16(10):1297-313. PubMed
Thomas JD, Jackson ML, Sharma D, et al. Haemophilus influenzae type b carriage among young children in metropolitan Atlanta in the context of vaccine shortage and booster dose deferral. Clin Vaccine Immunol. 2011;18(12):2178-80. PubMed
Jo YM, Song JY, Hwang IS, et al. Dose sparing strategy with intradermal influenza vaccination in patients with solid cancer. J Med Virol. 2009;81(4):722-7. PubMed
Anonymous. Continued shortage of Haemophilus influenzae Type b (Hib) conjugate vaccines and potential implications for Hib surveillance--United States, 2008. MMWR Morb Mortal Wkly Rep. 2008;57(46):1252-5. PubMed
Hrynash Y, Nadraga A, Dasho M. Effectiveness of a vaccination program against mumps in Ukraine. Eur J Clin Microbiol Infect Dis. 2008;27(12):1171-6. PubMed
Abuelreish M, Subedar A, Chiu T, Wludyka P, Rathore M. Increase in invasive pneumococcal disease in children associated with shortage of heptavalent pneumococcal conjugate vaccine. Clin Pediatr (Phila). 2007;46(1):45-52. PubMed
Sheth HS, Verrico MM, Skledar SJ, Towers AL. Promethazine adverse events after implementation of a medication shortage interchange. Ann Pharmacother. 2005;39(2):255-61. PubMed
Kiromat M, Vince JD, Oswyn G, Tefuarani N. The management of children with cancer in Papua New Guinea: a review of children with cancer at Port Moresby General Hospital. P N G Med J. 2004;47(3-4):138-45. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein do not necessarily reflect the views of Health Canada, Canada’s provincial or territorial governments, other CADTH funders, or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to requests@cadth.ca.