CADTH Health Technology Review
Perspectives and Experiences Regarding the Impacts of Emergency Department Overcrowding: A Rapid Qualitative Review
Technology Review
Authors: Jamie Anne Bentz, Francesca Brundisini, Danielle MacDougall
Abbreviations
CASP
Critical Appraisal Skills Programme
ECHTA
Equity Checklist for Health Technology Assessment
ED
emergency department
Key Messages
This review used a rapid best-fit framework analysis approach to synthesize 9 included studies exploring how people who engage with emergency department (ED) services experience and understand the impacts of ED overcrowding, access block, and boarding on quality of care, patient safety, and the well-being of health care professional learners and staff working in the ED. None of the included studies were conducted in Canada.
The included studies detailed how people who engage with ED services understand the ED as a location that is appropriate for providing short-term treatment to people requiring critical or emergent care, but inappropriate for providing care to patients for extended lengths of time. Study participants described experiencing ED overcrowding, boarding, and access block as transforming the ED into an unsafe environment where the risk of avoidable patient harm increased due to the accelerated depletion of available equipment, space, and human resources. They observed that this unsafe environment led to patients experiencing delayed, missed, and inappropriate care, resulting in potential or actual physical harm, threats to their human rights and dignity, exposures to secondary suffering, reduced satisfaction, and worsening emotional and psychological states.
Participants reported that ED overcrowding, access block, and boarding had, for the most part, negative impacts on health care professional learners and staff working in the ED. Some ED staff reported that these phenomena led them to experience increased exposure to violence and physical harm, emotional and moral distress, dimensions of burnout, and/or missed learning opportunities for health care professional learners. Some ED staff reported experiences of camaraderie and collaboration necessarily forged as a coping mechanism to manage adversity in the context of overcrowding. Amid the challenges experienced within their practice setting, some experienced staff also perceived overcrowding as providing opportunities to exercise and expand their existing knowledge and skills.
Considering these findings, decision-makers seeking to address the adverse impacts of ED overcrowding, access block, and boarding on quality of care and patient safety may explore facilitating the integration of routine preventive care into ED processes; enhancing communication within the ED; optimizing available equipment and space; giving patients information before and during their stay to manage their expectations; and enhancing staff’s access to education and resources necessary to better address the needs of patients who frequently experience extended stays in the ED and require specialized care beyond that which ED staff typically have the training and experience to provide. They may prioritize interventions that alleviate, rather than add to, the workload of ED staff. Additionally, they may assess and explore working conditions in the ED with a lens of promoting the well-being and retention of ED staff. By drawing on the findings of this review, they may, for example, consider exploring how to incentivize senior staff to remain in their positions, enhance learning opportunities for health care professional learners, and promote interprofessional collaboration. They may also consider investigating and addressing systemic factors contributing to overcrowding, access block, and the recruiting and retaining of health care providers in their jurisdictions.
Decision-makers may also further explore how proposed interventions might address or exacerbate ethical and equity issues raised by ED overcrowding, including: the fair and equitable allocation of scarce resources; harms and forgone benefits to patients, health care providers, and other hospital staff; and inequitable access to and experience of ED care by patients, including impacts on patients’ dignity, relationships with care providers, and trust in EDs or health care systems. They may consider providing targeted support to groups identified as disproportionately at risk of harm in overcrowded EDs, including but not limited to: those requiring extended lengths of stay, those with limited agency to self-advocate or gain appropriate attention and care, those who are unable to perform activities of daily living, or those experiencing mental health emergencies. They also may consider that the included studies provided limited or no insight into the perspectives of people belonging to equity-deserving groups with a history of harm and lack of agency in the ED, including but not limited to: Indigenous people, Black people, and other people of colour; people with disabilities; people experiencing houselessness; those experiencing language barriers without access to a professional interpreter; and members of the 2SLGBTQ+ community. More research is needed to understand how these and other equity-deserving groups experience overcrowding, access block, and boarding as impacting their quality of care and safety.
What Is the Issue?
Emergency departments (EDs) across Canada are under strain and experiencing overcrowding, a situation in which the demand for health services in the ED exceeds the capacity of the ED, hospital, or community to deliver quality care in a reasonable amount of time.1,2 Between April 2021 and March 2022, approximately 14 million patients visited EDs in Canada.3 Recent evidence suggests that ED overcrowding is worsening in jurisdictions across Canada,4 and there is an increasing trend of unexpected temporary ED closures or reduction of services across the country.5,6
Overcrowding is intricately related to access block and boarding, distinct but connected concepts sometimes referred to interchangeably in the literature and in practice. Hospital access block (hereafter, access block) is a phenomenon characterized by patients being unable to access appropriate hospital resources (e.g., inpatient beds) within a reasonable amount of time.7 Access block causes excessive boarding, which is the practice of holding admitted patients in the ED after they have been admitted to the hospital because inpatient beds are not available, which limits available ED beds for new patients requiring assessment and management and, in turn, worsens overcrowding.7,8
The causes and consequences of ED overcrowding are complex, varied, and extend beyond the ED.1,9,10
What Did CADTH Do?
This report provides a nuanced understanding and synthesis of the perspectives and experiences of those engaged with ED services regarding the impacts of ED overcrowding, access block, and boarding. It intends to support decision-making by providing context on the value of evidence-based interventions to alleviate overcrowding and insights into which interventions may or may not best address the problem in practice.
From the project’s outset, we considered how to explore and understand Indigenous Knowledges and the perspectives and experiences of Indigenous people who engaged with (or faced barriers to accessing) health care services in overcrowded EDs in Canada. We understand that Indigenous Peoples’ experiences, values, needs, and priorities are important for understanding and improving the state of health services provided in EDs and informing decision-making around the potential solutions to ED overcrowding in Canada. Ultimately, after careful deliberation with CADTH’s Strategic Partner, Indigenous Engagement and Partnerships, we decided that, in the interest of fostering culturally safe practices, it would not be possible to appropriately seek input from Indigenous Peoples regarding their perspectives and experiences for several reasons. CADTH set the project timelines and research design to respond to short-term decision-making needs, which precluded the ability to engage with Indigenous Peoples and Knowledges appropriately. Without adequate time to develop respectful and meaningful relationships with Indigenous Peoples to inform this work, CADTH is aware that any attempt to reflect Indigenous Knowledges and voices would not be culturally appropriate or safe and could further perpetuate harm. CADTH acknowledges the lack of engagement with and inclusion of Indigenous perspectives and voices as a major limitation and gap. In the spirit of reconciliation, CADTH is committed to engaging with Indigenous partners to explore the importance of this topic and future CADTH work in this area, which would involve the development of a strengths-based approach and process to conduct the work respectfully and rigorously.
Research Question
How do people who engage with ED services experience and understand the impacts of ED overcrowding, access block, and boarding on quality of care, patient safety, and the well-being of health care professional learners and staff working in the ED?
In addition to the primary research question, the reviewer paid particular attention to equity considerations regarding accessing, using, and experiencing benefit from care provided within overcrowded EDs, as detailed by people engaging with ED services.
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, CINAHL, and Scopus. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were overcrowding; emergency medicine (EDs, emergency medical services, and emergency medicine personnel); and quality of care, patient safety, and staff well-being. CADTH-developed search filters were applied to limit retrieval to qualitative studies. The search was completed on June 5, 2023, and limited to English-language documents published since January 1, 2013.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, they reviewed titles and abstracts and retrieved potentially relevant articles. They based their final selection of full-text articles on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Sample | People of any age engaging with pediatric or adult ED services provided in urban, rural, or remote health care settings, including patients, their families and caregivers, and learners and staff working in the ED |
Phenomenon of interest | Experiences and understandings of the impacts of ED overcrowding, access block, and boarding on quality of patient care, patient safety, and the well-being of health care professional learners and staff working in the ED |
Design | Any qualitative design |
Evaluation | Perspectives on, experiences of, and understandings regarding the impacts of ED overcrowding, access block, and boarding on quality of patient care, patient safety, and the well-being of learners and staff working in the ED |
Research type | Qualitative studies or mixed-methods studies with a qualitative component (excluding surveys) |
ED = emergency department.
In this review, the impacts of ED overcrowding refer to how the experience of ED overcrowding affects the perceptions and understandings of quality of care, patient safety, and the well-being of health care professional learners and staff working in the ED. After engaging with the literature on overcrowding, and developing an understanding of its intricate relationship with access block and boarding, the reviewer included all 3 concepts as phenomena of interest to ensure the review captured the experience of those engaging with ED services in the context of overcrowding. Health care professional learners refer to people working in the ED to fulfill requirements for their undergraduate or postgraduate education as health care professionals, newly hired staff orientating in the ED, and novice staff with under 2 years of experience working in an ED. Benner’s “from novice to expert” model suggests that new graduate nurses generally transition from having the clinical judgment and skills of a novice to those of a competent practitioner after 2 to 3 years of practice in an analogous clinical setting.11
Exclusion Criteria
The reviewer excluded articles if they did not meet the selection criteria outlined in Table 1. Additionally, they excluded citations published in languages other than English, grey literature, and duplicate publications.
To ensure the sample of included studies would remain small enough to allow for prolonged engagement with the data in the context of a rapid review, the reviewer also excluded studies with aims and objectives that did not focus explicitly on exploring experiences and understandings of ED overcrowding, access block, and boarding. This purposeful sampling strategy aimed to capture citations that would provide a comprehensive understanding of the phenomena of interest.12
Critical Appraisal of Individual Studies
The reviewer used the optimized version of the Critical Appraisal Skills Programme (CASP) tool to critically appraise the included studies.13 This tool promotes an efficient and systematic appraisal that acknowledges, accepts, and considers the diverse philosophical underpinnings of qualitative inquiry and the varied approaches and methods they inform.13 The reviewer used the optimized CASP tool’s 11 items as prompts for engaged and critical reflection about the trustworthiness and rigour of the included studies. They did not exclude articles based on their quality but instead critically appraised the included studies to provide readers with insight into their limitations and strengths.
Data Analysis
One reviewer independently analyzed and synthesized the qualitative data using methods informed by the “rapid best-fit framework” synthesis approach.14 The analysis, which aimed at synthesizing qualitative findings in the included studies, followed a 3-stage approach, which included the development of an initial analytical framework informed by the research questions and familiarization with the included literature, a deductive and inductive extraction and analysis of the data informed by the initial framework, and the iterative refinement of the framework to reflect inductively identified content and relationships among data and themes.
The reviewer developed the initial framework based on 2 sensitizing categories drawn from the research questions, remaining open to refinement in the following analytical stages. The categories aimed to capture experiences and understandings regarding the impacts of ED overcrowding, access block, and boarding on:
quality of patient care, initially conceptualized as the timely provision of effective and safe health care, resulting in the attainment of optimal or desired physical, psychosocial, and spiritual health as perceived, understood, or experienced by patients, their families, and ED health care professional learners and staff.15 The reviewer also paid particular attention to the concept of patient safety, initially conceptualized as a component of quality of care and characterized by the reduced risk and absence of avoidable errors and harm to the physical, psychosocial, or spiritual wellness of patients and their families, as perceived, experienced, or understood by patients, families, and ED health care professional learners and staff.16
the well-being of health care professional learners and staff working in the ED, initially conceptualized as the physical, psychosocial, spiritual, and moral wellness of, and the educational quality and support received by, health care professional learners and staff working in the ED.
The reviewer also used considerations detailed in the Scoping and Evaluation phases of Benkhalti et al.’s Equity Checklist for Health Technology Assessment (ECHTA) to inform which concepts to remain sensitive to during the analysis to capture equity considerations.17 The reviewer conceptualized health equity as fair and just opportunity to access, use, and experience benefit from ED care to achieve or maintain the best possible health.17,18 They conceptualized equity of access as fair and just opportunity to receive and offer timely care throughout all stages of a patient’s journey through the ED. They conceptualized equity of use as patients’ and families’ fair and just opportunities to experience care that appropriately addresses their physical, psychosocial, cultural, and spiritual needs. Finally, the reviewer conceptualized equity of benefit as fair and just opportunity for patients, families, and ED health care professional learners and staff to achieve or maintain the best possible physical, psychosocial, cultural, and spiritual health while engaged in ED care.
The reviewer remained attuned to potential inequities in access, utilization, and benefit, and whether distribution disparities or institutional biases and care processes may have contributed to these inequities in the context of ED overcrowding.17 Instead of using dimensions of equity as a coding framework, however, they used these elements as concepts to prompt sensitivity to data, allowing for the exploration, description, and reporting of how equity considerations relate to the experience of ED overcrowding.
To begin the analysis, the reviewer first familiarized themselves with the studies by reading and rereading them in their entirety while making marginal notes and memos on initial thoughts and insights in a Microsoft Word document. These initial notes and memos included: thoughts to promote reflexivity, descriptions prompting familiarization with the content and how it could be mapped onto the preliminary framework, and preliminary equity considerations related to the experience of ED overcrowding. The reviewer also annotated reflections on methodological considerations as prompted by the optimized CASP tool to facilitate critical appraisal.
The reviewer then used NVivo 1419 to begin line-by-line coding of the text under the Findings sections of the included citations into categories of the preliminary framework. After noting similarities in the content and meaning of data that were relevant to the research question but did not fit under the preliminary categories, the reviewer added an additional category to the framework. They inductively assigned codes to data falling under the overarching categories based on content and meaning and considered connections between these codes, resulting in additional subcategories refining the preliminary framework. They mapped inductively identified equity considerations into the categories and emerging subcategories. The reviewer only coded text relevant to the perspectives on, experiences of, and understandings regarding the impacts of ED overcrowding, access block, and boarding on quality of patient care, patient safety, and the well-being of learners and staff working in the ED. During the analysis, they remained attuned to connections between the subcategories, and these connections formed the basis of an outline from which they synthesized descriptive themes. Drawing on their growing familiarity with the dataset built through iterative readings, the reviewer returned to their analytical memos and the primary studies to further develop connections within the data and between the subcategories and categories. By doing so, they continued to refine the framework while writing the findings.
Reflexivity
To uphold qualitative best practice, before screening the citations and throughout the analytical process, the reviewer practised reflexivity by creating memos about their prior experiences, assumptions, and knowledge relevant to the impacts of ED overcrowding, access block, and boarding on quality of care, patient safety, and the well-being of learners and staff working in the ED.20 They used these memos to reflect upon how their previous understandings might influence and inform their analysis and challenged assumptions or interpretations not grounded in the data.
Summary of Evidence
Quantity of Research Available
A total of 1,754 citations were identified in the literature search. Following screening of titles and abstracts, 1,718 citations were excluded and 36 potentially relevant reports from the electronic search were retrieved for full-text review. Of these potentially relevant articles, 27 publications were excluded for various reasons, and 9 publications met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA21 flow chart of the study selection.
Summary of Study Characteristics
Characteristics of the included studies are summarized below, and additional details are provided in Appendix 2.
Study Designs
The 9 included studies comprised 8 primary qualitative studies22-29 and 1 mixed-methods study.30 The authors of 7 studies reported specific qualitative methodologies underpinning their studies, including Chen et al.,22 Lin et al.,26 and Van de Ruit et al.29 using constructivist grounded theory; Kongcheep et al.25 and Rantala et al.28 using interpretive phenomenology; Han et al. using phenomenography;24 and Eriksson et al.23 using qualitative description. While Leong-Nowell et al.30 reported that their overall study had a convergent parallel mixed-methods design, neither they nor McCarty et al.27 specified a qualitative methodology informing their methods of data collection and analysis. Appendix 2 details the methods used for data collection and analysis.
Settings and Participant Characteristics
Three of the included studies were conducted in Taiwan,22,24,26 2 in Sweden,23,28 and 1 in Thailand,25 all of which have universal health care. One study each was conducted in the US,27 South Africa,29 and Samoa,30 within the context of health care systems funded through a mix of private and public funding. None of the included studies were conducted in Canada. Appendix 2 provides additional information on the study settings.
Sample sizes for the qualitative studies and qualitative component of the mixed-method study ranged from 13 participants26 to 4329 participants. The studies included the perspectives of a combined total of 215 participants, including:
12 parents or guardians of youth who had experienced mental health boarding in the ED or an inpatient unit27
123 nurses22,23,25,26,29,30 and 40 medical officers or physicians (including 6 medical residents)27,29,30
2 licensed nursing assistants27
1 child life specialist.27
Of note, McCarty et al.27 were the only authors to include hospital staff working in departments outside of the ED in their study; however, they did not separately report the demographic characteristics of these staff members versus other staff.
Across all studies, the reported ages of the included participants ranged from 25 years24 to 86 years28 for patients and family members, and 23 years to 52 years22 for hospital staff. Overall, 51.4% (n = 19) of the combined total of included patients,24,28 91.7% (n = 11) of the parents or guardians,27 and 81.9% (n = 122) of the included 149 hospital staff who disclosed their sex or gender reported identifying as female or women. McCarty et al.27 (who recruited participants from the northeastern US) reported that 100% (n = 12) of the parents and guardians and 94.1% (n = 16) of the health care providers included in their study were non-Hispanic white. Van de Ruit et al.29 reported that 46.5% (n = 20) of their clinician participants recruited from Cape Town, South Africa identified as Coloured [wording from original source; note that this is a racial classification commonly used in South Africa to refer to members of multiracial ethnic communities who may have ancestry from various populations], 32.6% (n = 14) as white, 18.6% (n = 8) as Black, and 2.3% (n = 1) as Asian. However, no other authors reported the race or ethnicity of their participants, and no authors explicitly reported including the perspectives of Indigenous people, members of the 2SLGBTQ+ community, or people experiencing houselessness. Of note, in the South African study, the authors did not indicate including people identifying as Indigenous people, and it is not possible to determine whether they included Indigenous Peoples within any of the 4 reported groups.
Reported ED boarding times experienced by patients ranged from 8.45 hours28 to 28.1 hours.24 Reported practice experience in the ED for the included health care providers ranged from 1 year23,30 to 2430 years. Of note, 4 studies23,27,29,30 reported including medical residents, staff with under 2 years of experience, or staff “new to emergency medicine” in their sample, but no study separately considered and reported the experiences of these ED learners.
Summary of Critical Appraisal
Of the 9 included studies, all but 130 were of moderate to high quality. Appendix 1 includes a narrative summary and Table 3 details the strengths and limitations of the included studies.
Findings
The findings of this synthesis consist of 3 overarching, interrelated categories, which included participants’ experiences and understandings regarding how ED overcrowding, access block, and boarding transform the ED into an unsafe environment, impact quality of care and patient safety, and impact the well-being of health care professional learners and staff working in the ED. The studies in this review primarily detailed the perspectives and experiences of ED staff, with less exploration of the experiences of people who received care in the ED and their families. As a result, the findings likewise have a similar focus.
Transformation of the ED Into an Unsafe Environment
People engaging with ED services perceived that ED overcrowding, boarding, and access block transformed the ED — a location staff understood as appropriate for providing short-term treatment to people requiring critical or emergent care but inappropriate for patients requiring extended stays — into an unsafe environment wherein the potential for avoidable harms increased due to the depletion of available equipment, physical space, and staff.22-29
The ED as an Environment Inappropriate for Extended Stays or Boarding
ED staff understood their practice setting as intended for providing initial, short-term treatment to people requiring critical and emergent medical care but inappropriate for patients requiring extended stays or boarding.22,23,27 Working in an environment designed to respond to unscheduled patient presentations, staff perceived the ED as lacking routines necessary for supporting the provision of regular essential and preventive care to patients with extended stays, which, in turn, caused difficulties in their scheduling, timing, and tracking of medications, meals and hydration, medical rounding, interprofessional handovers, documentation, and basic nursing interventions (e.g., repositioning, mobilization, and toileting) for each patient.23 Since these types of care were not embedded into ED processes or procedures, their completion depended on the “personal responsibility” and “common sense” of staff, some of whom felt unable to engage with or benefit from interventions or protocols intended to prompt care or elevate patients’ safety (e.g., checklists or commitments to daily rounding) that increased their workloads, and reported lacking consensus about their professional duties and obligations toward patients with extended stays.22,23,26 Patients experiencing ED boarding were attuned to this lack of ownership of their care, with 1 patient noting, “You are put into no man’s land. You’re not supposed to be admitted to the A & E [Accident and Emergency Department] and because I’m not at any ward, nobody is responsible for me.”28
In addition to an observed lack of routines supportive of regular essential and preventive care, some participants reported concerns that the specialization of human resources and physical environment within the ED were inappropriate for accommodating the needs of patients requiring extended stays or boarding.23,24,27,28 Some ED staff perceived themselves as lacking the skills necessary to provide care beyond the initial treatment and stabilization of patients (e.g., specialized psychotherapeutic interventions for patients requiring mental health services).23,27 Additionally, patients, their family members, and staff alike reported that the ED’s characteristic perpetual bright lighting, noise, and lack of secure locations to store personal belongings caused patients to feel anxious and disoriented and disrupted their ability to sleep or rest.23,24,27,28
Finally, participants reflected on how standard communication practices within the ED (e.g., the oral sharing of information between staff with minimal written documentation) could lead to communication breakdown in the context of extended stays or boarding.23 For example, staff perceived that they risked losing important data with each oral information exchange.23 This problem became increasingly apparent the longer patients boarded in the ED, as more providers became involved in their care.23 ED staff also described instances where sparse written documentation in the ED did not capture essential information, with 1 nurse noting, “There have been episodes when patients have deteriorated…and then you’ve noticed that the patient came in at six yesterday…and there is not a single note or vital signs have not been documented.”23 Additionally, patients boarding in the ED reported that staff did not share adequate information with them, particularly regarding the expected timing of their transfer to another unit.28
Accelerating the Depletion of Equipment, Space, and Human Resources
While perceiving the ED as inappropriate for people requiring extended stays or boarding at baseline, participants in the included studies experienced that overcrowding, boarding, and access block accelerated the depletion of equipment, space, and human resources available to respond to patients’ needs.22,23,25,26,29 As an unlimited number of patients with conditions of varying degrees of complexity and urgency continued to enter the ED while others remained boarded due to access block, staff reported that equipment and space quickly became occupied, necessitating that they triage less mobile or more critical patients to stretchers and others to chairs, and physically move patients to isolated areas of the department or closer together.23,25,26,29 The depletion of equipment to facilitate care increased the workload of ED staff, who already perceived that the demands of caring for each patient were growing alongside boarding times and worsening overcrowding.23,26 Staff noted that patients required more routine care the longer they boarded, and were more likely to “bother [staff] repeatedly” as staff became increasingly overworked and thus unable to tend to their needs promptly.23,26 With depleted equipment, an unrestricted number of patients requiring increasingly demanding care, and a finite and — as reported by ED staff — sometimes insufficient baseline number of available care providers, staff often perceived their assignments as overwhelming or unmanageable.22,23,25,26,28,29 Overwhelmed staff, who sometimes reported knowing “nothing about” the increasing number of patients assigned to them, perceived their ability to recognize and respond to the needs of each person as becoming depleted.22,23,25,26,28,29 As 1 nurse recounted, “The workload is beyond our potential. While 5 nurses were providing care for 50 patients, there were two cardiac arrest cases simultaneously. It was an unbearable task.”25 For reasons detailed later in this report, overcrowding could also motivate staff to leave their positions, thus further contributing to the loss of staff available to share these increasing workloads.22,29
Impacts on Quality of Care and Patient Safety
Delayed, Missed, or Inappropriate Care Resulting in Actual or Potential Physical Harm
Participants of the included studies described how they experienced the perceived unsafe environment of an overcrowded ED as leading to delayed, missed, or inappropriate care that resulted in patients experiencing potential or actual clinical deterioration, physical harm, or exposure to infection.22,23,25-29 Staff noted that the lack of routines supporting the provision of regular essential and preventive care, communication breakdown, physical isolation from their patients moved to locations without call bells, and unmanageable workloads left them without the processes, resources, time, or mental cues necessary for conducting timely and thorough patient investigations and assessments.23,29 Patients, at times, reported being acutely aware of this reality.28 Staff also noted that when patients were placed in chairs rather than beds or stretchers, the quality and completeness of the assessments they could conduct were inadequate.22,29 Some staff recalled instances in which missed, delayed, or inadequate assessments led them to missing key findings and resulted in their patients’ clinical deterioration, with 1 nurse recalling “a patient with [an] ileus who was placed in a very secluded room and got worse, had respiratory failure and became septic, and just because everyone had forgotten about him.”23,28,29
Staff also perceived their ability to provide interventions necessary for preventing patients’ deterioration, discomfort, and harm as limited during ED overcrowding, access block, and boarding.23,25-29 They reported instances in which a lack of available equipment rendered them unable to meet the needs of patients requiring life support or demanded they keep patients in chairs or stretchers for prolonged periods without necessary devices to facilitate their turning or repositioning.22,26,28,29 Prolonged care in chairs and stretchers increased patients’ risk of experiencing pressure-related injuries to the skin, falls, and physical discomfort, and required staff to amend how they provided care (e.g., kneeling instead of standing while starting an IV line).22,26,28,29 Patients and ED staff also perceived that staff were unable to effectively prevent the spread of infection because of ED overcrowding, as they had to move patients closer together to create space, could not place symptomatic patients in already-occupied isolation rooms or provide them with separate toilets, and needed to wait longer for laboratory results confirming infections.23,25,28
Additionally, ED staff who identified as being overworked reported experiencing limited time to care for each patient and frequent interruptions and distractions during overcrowding, all of which could lead to adverse outcomes.25,26,29 Some staff noted that lacking sufficient time to care for each patient and experiencing frequent interruptions led to impaired clinical judgment and increased their risk of making omissions or errors.26,29 Staff who felt overwhelmed also reported a pressure to quickly and sometimes inappropriately discharge patients to free up beds in the ED, which they observed could cause patients to deteriorate in the community and require readmission.29 Nurses reported that lacking routine and being overworked inhibited their ability to provide regular nursing interventions during overcrowding, including: administering medications and interventions to alleviate pain, providing hydration and nutrition, and repositioning and toileting.23,28,29 Unable to tend to the needs of everyone, 1 nurse described the reality of needing to triage care within their patient load: “Critically ill patients, they always come first, so if the old lady in the hallway is screaming that she needs to go to the bathroom, then I have to say, ‘You’ll have to wet yourself, because I don’t have the time.’”23 Delaying or missing essential nursing care, however, could lead to patients’ physical discomfort, pressure-related injuries to the skin, or clinical deterioration, which, aside from being harmful and potentially life-threatening, could prolong lengths of stay in the ED and worsen overcrowding.23,28,29
Threatened Rights, Dignity, and Psychological Well-Being
In the context of ED overcrowding, access block, and boarding, ED staff and patients alike not only described patients as being at risk of physical harm due to delayed, missed, and inappropriate care but also as experiencing threats to their rights, dignity, and psychological well-being.22-24,27,28 Participants in the included studies perceived that staff could not protect patients’ right to privacy during periods of overcrowding, given that they needed to share or collect personal information or receive and provide sensitive care (e.g., medical tests, examinations, and personal hygiene) in physically crowded or inappropriate locations such as corridors.23,28 Some ED staff also acknowledged that they could not work as caring professionals appropriately responding to their patients’ needs in the context of depleted resources, with 1 noting they instead worked “as a machine.”22 Perceiving that ED staff did not acknowledge or value their needs or desires, some patients felt they were treated as objects without autonomy, subjected to the will and decisions of health care providers.28 When physically isolated from staff experiencing overwhelming workloads, some patients even perceived themselves as being neglected, secluded, and abandoned in their time of suffering with nobody to talk to, update them, or tend to their needs.28 As 1 patient recalled, “Nobody cared that I was lying there, whimpering and that I gasped for air.”28
Due to physical crowding and a general lack of privacy, patients reported experiencing direct exposure to other patients’ narratives and displays of pain and discomfort.28 Witnessing the suffering of others provided some patients with a helpful point of comparison that made their own illness or injury feel bearable.28 Often, however, the empathy elicited because of these exposures added to patients’ distress by causing secondary suffering.28 As 1 patient described, “At the same time you deal with your own suffering, you also suffer for them.”28 Alongside an awareness of the suffering of fellow patients, some people receiving care were also attuned to the suffering of ED staff, whom they perceived as being overworked, doing their best in an “impossible situation,” stressed, and exposed to the same unsafe and anxiety-provoking setting they were.28 In an attempt to alleviate staff’s suffering, some patients reported refraining from voicing their needs so they would not add to their workload.28 Secondary suffering, then, not only could worsen patients’ psychological discomfort, but also further diminish the likelihood that staff would promptly meet their physical needs.
For many patients, the experience of ED overcrowding and boarding overwhelmed their ability to cope and maintain a state of emotional or psychological wellness.27,28 Some patients reported protecting themselves from such harm by mentally preparing themselves before arriving at the ED and setting realistic expectations for the quality of care they would receive, based, for example, on information gleaned about overcrowding from the news.28 Others radically accepted their situation, consciously practised patience, and hoped for the best, or ascribed meaning to their experience by conceptualizing it as an inevitable step toward their recovery or a challenge that would strengthen them.24,28 However, when feeling abandoned, neglected, and treated as objects in an unsafe setting, many patients experienced anxiety-provoking uncertainty about their security, health status, and how long they would be in the ED.28 With this uncertainty, patients waiting for long periods while exposed to the suffering of others had little distraction from negative thoughts regarding worst-case scenarios, including the possibility of their death in the ED.28 As patients perceived that staff did not have the time to notice or tend to them, some envisioned dying alone in the department: “Will they try to save me if I have seizures? What happens if nobody noticed me? The worst thing is the fear that I will lie here and die unnoticed.”28
Disparities in Exposure to Potential or Actual Harms
ED staff’s perspectives and experiences provided insight into inequities in patients’ accessing, using, and benefiting from or avoiding harm related to care in overcrowded EDs.23,27,29 Specifically, some staff noted that patients who could vocalize their needs or perform behaviours to garner attention, or those with loved ones who could do so for them, were more likely to access timely care addressing their needs.23,29 However, they experienced these people as diverting staff attention and time away from those lacking the agency to voice and advocate for their needs, including, according to some ED staff, patients with more severe illness and medical vulnerability.23,29 Additionally, staff narratives illustrating difficulties in providing regular essential and preventive nursing care due to ED overcrowding, access block, and boarding, and the adverse outcomes resulting from missing or delaying these cares, provides insight into how patients that depend on others for activities of daily living (e.g., feeding, mobility, and toileting), including some older adults, may disproportionately experience harm because of these phenomena.23
As previously detailed, ED staff also noted that patients required increasingly demanding care the longer they boarded, which ED staff often could not provide.23 For this reason, patients experiencing prolonged boarding may have a disproportionately high risk of experiencing delayed, missed, or inappropriate care and resulting harm. Notably, ED staff described patients requiring admission to mental health units as being especially at risk of prolonged boarding in the ED due to access block.27,29 Of concern, perspectives and experiences reported by ED staff and patient family members illuminated additional reasons why this population may be at a disproportionate risk of harm during ED overcrowding, access block, and boarding. They noted, for example, that adolescents boarding in the ED while awaiting admission to a mental health unit were already experiencing psychological vulnerability, which made them especially prone to experiencing adverse psychological impacts related to prolonged exposure to an anxiety-provoking setting.27 Additionally, ED staff voiced not having the expertise to provide specialized care to patients experiencing mental health emergencies, which they perceived caused some members of this population to have delayed access to optimal care and increased exposure to potentially harmful interventions like heavy sedation.27,29 As 1 ED staff member emphasized, “I would not want my child in psychiatric crisis boarding for days in the ED. In some ways, we worry it makes them worse. It’s really not a therapeutic environment in any way, shape, or form, both in a physical layout [and] to the services they get.”27
Impacts on the Well-Being of Health Care Professional Learners and Staff Working in the ED
The stress of exposure to the unsafe environment of an overcrowded ED, alongside the experience of being involved in the provision of poor-quality and unsafe patient care (i.e., that associated with an increased risk of potential or actual avoidable errors and harm) had, with some exceptions, negative impacts on the well-being of health care professional learners and staff.
Adverse Impacts on Physical Well-Being
ED staff perceived that working in an overcrowded ED threatened their physical safety and well-being.22,23,25,26,29,30 Some patients and their caregivers exposed to an unsafe environment and feeling abandoned and unsatisfied with their care experienced anger and frustration toward ED staff.23,26,29,30 Some staff expressed empathy and understanding regarding these frustrations and attempted to explain triage decisions or long wait times.26,30 However, these explanations were sometimes not enough to calm patients experiencing heightened emotions, which could make staff feel uneasy about their physical safety.30 As 1 ED staff member described, “There are different kinds of people, there are some who will understand when we explain the delay but there are some who just look like they are ready to come at you.”30 Staff members noted instances where patients’ anger and frustration manifested into physical violence.22,25,30 Alongside more frequent instances of threatened or actual violence against them, staff working in overcrowded EDs also reported experiencing: exposures to infections due to the previously detailed difficulties in identifying and isolating patients with contagious conditions; being hit or injured by equipment as a result of physical crowding; missing meal breaks for the entirety of their shifts due to unmanageable workloads; and living with physical manifestations of psychological stress, such as dyspepsia.25,26
Emotional and Moral Distress
ED staff reported experiencing psychological and moral distress due to the demands and risks posed by their working conditions, which they perceived as caused by factors beyond their control, such as hospital access block and short staffing.22,23,25,26 Staff experienced overcrowding as stressful and frustrating, and some described being acutely aware that their patients were receiving poor-quality and unsafe care and that the likelihood of them forgetting essential assessments or interventions was high.22,23,26 The stress and anxiety experienced because of this awareness remained with staff (who understood themselves as responsible for patient safety), even after they transferred the responsibility of care to others.23,26 One nurse recalled, “I was still feeling like I was at work when I was off duty and tried to recall any omission I may have made during my shift. I would regret it if any careless action was made. But I did not know how to do it better because there were too many patients in the ED.”26
Staff reported that hospital-level procedures and processes temporarily enacted during overcrowding and access block provided them with optimism that the issue had been recognized.26 However, these processes could sometimes have unintended consequences with the potential to add to their distress.26 For example, overhead announcements notifying patients and staff of access block made ED staff acutely aware that their workload would increase.26 As 1 nurse described, “We often heard broadcasts from the hospital saying ‘no bed available in this hospital’ when an overcrowded ED occurred. When I heard that news, I felt desperate because that meant the beginning of more patients in the ED.”26 Similarly, staff reported that prioritizing the treatment of patients with minor and easily managed conditions initially improved throughput and provided immediate relief from stress experienced due to large patient volumes.26 However, they also perceived such interventions as encouraging more people to seek care in the ED, ultimately adding to their workloads.26 In contrast, staff perceived hospital policies enacted during ED overcrowding that prioritized patients in the ED for admission to hospital wards as more effectively reducing their workloads and providing them with a sense of hope.26
Staff understood their professional duty was to provide safe, quality, holistic care that protected patients from harm and optimized their well-being.25,26 They valued caring for others in their professional role, and their desire to help people in need motivated them to practice in the ED.26 These staff perceived value in, and maintained a commitment to, their work when they could use external feedback (e.g., from patients and their families) or self-reassurance to affirm they did or could uphold this desire.26 At the same time, however, many experienced overcrowding as preventing them from acting on what they ought to do according to their moral and professional values, and developed a heightened awareness of this limitation as patients voiced their displeasures with increasing frequency.22,23,25,26 Exemplifying this conflict, 1 nurse noted, “You are supposed to take good care of patients. When there are too many patients with an emergency and critical status at a time, I feel I don’t have enough time to manage that situation.”26 ED staff used words such as “awful” and “painful” to describe these situations, which resulted in moral distress emotionally manifesting as sadness, guilt, and shame.22,23,26
Burnout and Turnover Intention
Some ED staff reported that frequent exposure to interpersonal tension, violence and physical harm, perceived powerlessness over their working conditions, and psychological and moral distress led them to experience dimensions of burnout, including professional dissatisfaction, emotional exhaustion, and cynicism.22,23,25,26 Chronically stressed staff perceiving themselves as unable to uphold their professional obligations and feeling inadequately supported by hospital administrators or respected and appreciated by patients reported feeling professionally inadequate, questioning the value of their work, and experiencing reduced satisfaction in their role.22,26 Working in an overcrowded ED also precipitated experiences of emotional exhaustion, especially because some staff felt “mentally tired when [they] go home, cause [they] have mainly been occupied sitting and defending why [they] don’t help [the patients]…why [patients] don’t get help.”23,25 ED staff working in overcrowded EDs also described experiencing cynicism and reduced empathy in their interactions with patients, which could worsen their experience of professional dissatisfaction.22 Experiencing these dimensions of burnout could cause staff to contemplate leaving their position.22,29 As 1 nurse disclosed, “I feel discouraged myself and become impatient. My sympathy is almost gone…My passion to work in the ED will be worn away.”22
Impacts on Learning and Professional Growth
The experiences captured in the included literature provided insight into how ED overcrowding impacted the professional growth and development of health care professional learners and experienced staff differently.25,26 Some ED staff described valuing and needing skilled and knowledgeable colleagues able to assume tasks and share workloads during overcrowding.26 Experienced ED staff, however, reported not having time to actively teach or exchange knowledge with health care professional learners in these contexts, which they acknowledged resulted in missed learning opportunities.25 For this reason, they noted that health care professional learners in the ED could only learn through observation.25 Unfortunately, however, even role modelling could be overwhelming for overworked experienced staff, with 1 nurse noting, “It’s very busy. Sometimes I tell novice nurses to stop, give me a moment, and leave me alone. They [novice nurses] were confused and didn’t know what to do next.”25
While the overcrowded ED could hinder the professional development of health care professional learners, some experienced staff perceived working in an overcrowded ED as enhancing opportunities for exercising and expanding upon their baseline knowledge, skills, prioritization techniques, and patient advocacy, which made them feel professionally accomplished and proud.26 Compared to health care professional learners, more experienced staff were better able to adjust their work priorities and adapt to a rapidly changing and demanding practice environment.26 When able to learn from their work and respond quickly to situations in their setting, some staff reported optimism regarding their ability to ultimately uphold “a promise of th[eir] professional role to patients” despite adversity in their practice setting.26 Feeling accomplished and proud when successfully adjusting work priorities during adversity and optimistic about the ability to uphold their professional responsibilities could consolidate staff’s commitment to their field despite the challenges of overcrowding.26 However, staff members acknowledged that experiencing overcrowding in this way depended on having a “distinct and orderly mind” and tacit knowledge or “instinct” that was challenging to describe but developed through previous practice experience.26 As 1 nurse working in an overcrowded ED articulated, “Working in the ED requires flexibility and a quick response with a brave work attitude…it is difficult to describe and explain that feeling. Let’s call it an instinct. You [a nurse] needed an accurate instinct to do your work.”
Camaraderie and Collaboration
Some ED staff also reported experiences of camaraderie and professional collaboration necessarily forged as a coping mechanism to manage and overcome adversities experienced while working in an overcrowded ED.25-27 These staff perceived limited or no institutional solutions or support from other hospital units during ED overcrowding.26 For this reason, they described relying heavily on their fellow teammates and noted the importance of flexibly modifying individual priorities to support the work of others.25,26 Some staff described how experiencing and managing the stress of overcrowding together could forge camaraderie and friendship that incentivized some to stay, despite what they perceived as a stressful and, at times, dangerous practice setting.26 Collaboration and communication between ED staff and staff outside the ED (e.g., inpatient staff and mental health professionals) could also ensure that patients boarding in the ED received consistent care of the highest possible quality.27
Limitations
This review has limitations that may reduce the trustworthiness and relevance of some of its findings. The reviewer deemed all but 130 of the included citations to be of moderate to high quality; however, the included studies focused primarily on the experiences of ED staff rather than patients and their families, with none separately examining and detailing the experiences of health care professional learners. Additionally, only 1 study27 reported the experiences of family members and health care providers of pediatric patients, and this study provided limited findings specifically on the experiences of receiving or providing care in the ED. Furthermore, none of the included studies were conducted in Canada. These factors may limit the transferability of the findings of this synthesis to the experiences of patients and their families, health care professional learners, and people who engage with ED services in Canada or pediatric care. Therefore, this report may be missing impacts of ED overcrowding that are important, relevant, or unique to patients and their families, health care professional learners, and Canadian or pediatric health care settings. Additionally, most of the authors of the included studies did not report the race or ethnicity of their participants, and none explicitly reported including Indigenous people, members of the 2SLGBTQ+ community, people experiencing houselessness, people living with a disability, or people experiencing language barriers without access to a professional interpreter. Therefore, this review may not adequately capture impacts relevant and important to members of groups disproportionately at risk of experiencing barriers to accessing, using, and benefiting from (or avoiding harms associated with) ED care or experiencing discrimination while working in the ED.31-38
Further limitations relate to the methods used to complete the review within a rapid time frame. Its narrowed scope does not capture perspectives of people not directly engaging in ED care, nor the impacts of ED overcrowding, access block, and boarding beyond quality of care, patient safety, and the well-being of health care professional learners and staff working in the ED. For this reason, it does not detail possible impacts on other hospital units, paramedical services, community resources, and the overall health care system and broader society. Finally, a single reviewer screened and selected the citations, conducted the analysis, and reported the results, and did so within a rapid time frame. These methods increased the likelihood of missing eligible citations or analytical findings. Taken together, these constraints limited the ability to produce an in-depth analysis, although the presented results raise relevant considerations to contemplate within the context of decision-making. The ethical implications of some of these limitations are detailed in the Ethical and Equity Considerations section.
Conclusions and Implications for Decision- or Policy-Making
This review used a rapid best-fit framework synthesis approach to explore how people who engage with ED services experience and understand the impacts of ED overcrowding, access block, and boarding on quality of care, patient safety, and the well-being of health care professional learners and staff working in the ED. It included 9 publications that a single reviewer synthesized within a framework comprising 3 categories: 1 inductively derived category (i.e., the transformation of the ED into an unsafe environment), and 2 a priori categories drawn from our research question (i.e., quality of patient care, and the well-being of health care professional learners and staff working in the ED).
The findings of this review highlight considerations relevant to decision-making aimed at addressing the impacts of ED overcrowding, access block, and boarding. This review described how people engaged with ED services experienced overcrowding, boarding, and access block that transformed the ED — a location described as inappropriate for providing care to patients for extended lengths of time — into an unsafe environment characterized by the accelerated depletion of available equipment, space, and human resources. Participants perceived this unsafe environment as leading to delayed, missed, and inappropriate care, resulting in potential or actual physical harm to patients, threats to their human rights and dignity, exposures to secondary suffering, reduced satisfaction with care, and worsening emotional and psychological states. These findings provide a nuanced understanding and corroboration of the extant literature reporting that ED staff are less able to adhere to best practices in the context of ED overcrowding, which poses risks to patients and increases the risk of exposure to medical errors; delays in assessment and care for life-threatening or altering conditions; and, ultimately, poorer outcomes and mortality.9,39-41
Given that this review focused on the experiences of people engaging directly with ED services, its findings point largely toward potential interventions to implement within the ED. Reflecting on these findings, decision-makers may consider promoting the integration of preventive and routine care (e.g., medication administration, nutrition and hydration, repositioning) and interprofessional rounding into ED processes. They may also consider interventions aimed at enhancing oral and written communication among ED staff and providing patients with the information necessary for managing their expectations to alleviate their anxiety and empower them to maximize their physical comfort and safety. Additionally, they may provide ED staff with education and supports to better address the needs of patients who frequently experience extended stays in the ED but require specialized care beyond that which staff in the department typically have training and experience to provide (e.g., those with mental health conditions who require specialized psychotherapeutic interventions). They may also optimize the availability of baseline equipment (e.g., stretchers, supplies facilitating repositioning, and call bells) and use of space within the ED in a manner that accounts for patients requiring increasingly complex care and prolonged stays, and minimizes potential risks for staff and patients while protecting patients’ rights to privacy. When considering these and other interventions, decision-makers may prioritize those that account for and alleviate, rather than add to, the workload of ED staff.
Finally, this review also found that ED overcrowding, access block, and boarding had, for the most part, negative impacts on the well-being of health care professional learners and staff working in the ED. Reported negative impacts included exposure to violence and physical harm; perceived powerlessness, negative emotional experiences, and moral distress; dimensions of burnout (i.e., professional dissatisfaction, emotional exhaustion, and cynicism and depersonalization); and reduced learning opportunities for health care professional learners. Findings in this review also supported those in the extant literature reporting that experiencing or witnessing violence, medical errors, moral distress, and burnout is associated with turnover intention in ED staff and that professional resilience (i.e., the ability to maintain well-being to cope with stress and adversity in the workplace) may be more common among ED staff with greater job satisfaction and professional experience or tenure in the ED.42-48 After reflecting on these findings, decision-makers may consider assessing and exploring working conditions in the ED with a lens of promoting the well-being and retention of ED staff. Examples of strategies for consideration may include incentivizing senior staff to remain in their positions, enhancing learning opportunities for health care professional learners in a manner that does not increase the workload of others, and promoting interprofessional collaboration. Drawing on the findings of this review focused on the impacts of ED overcrowding, access block, and boarding in the ED, decision-makers may also consider investigating and addressing broader, enduring systemic factors contributing to overcrowding, access block, and difficulties recruiting and retaining health care providers in their jurisdictions.
Ethical and Equity Considerations
The findings of this review also highlight ethical and equity considerations relevant to decision-making related to the impacts of ED overcrowding, access block, and boarding on patients, families, and health care professionals, learners, and other staff working in the ED. While the harms of ED overcrowding to patients and care providers entail ethical considerations related to human dignity, vulnerability, and professional roles and responsibilities, attending specifically to equity considerations within these highlights how these potential harms may be experienced differently or disproportionately by certain groups. Decision-makers involved in addressing ED overcrowding may explore how proposed interventions help address or exacerbate ethical and equity issues raised by ED overcrowding, including: the fair and equitable allocation of scarce resources; harms and forgone benefits to patients; and inequitable access to and experience of ED care by patients, including impacts on patients’ dignity, relationships with care providers, and trust in EDs or health care systems. In tandem, decision-makers may consider harms and forgone benefits to health care providers and other hospital staff, including moral distress and barriers to fulfilling ethical and professional obligations. They may also further investigate data gaps that limit understandings of diverse experiences and perspectives.
The perspectives and experiences detailed in this review indicate that ED overcrowding, access block, and boarding can negatively impact the quality and safety of care in the ED, which, in turn, can be harmful for patients and their families. In particular, the accelerated depletion of resources and perceived overwhelming demands placed on ED staff in the context of these phenomena can limit their abilities to offer safe, appropriate, personalized, and patient-centred care, which may lead to patients experiencing physical and psychological harm and dehumanizing care that threatens their dignity, at a time when they are inherently vulnerable.
It is important to consider whether and which patients may experience inequities and disproportionate burdens in accessing timely, appropriate, and high-quality ED care, and may thus be at increased risk of experiencing adverse outcomes in the ED due to ED overcrowding, access block, and boarding. This review found that patients with extended stays, with limited agency to self-advocate or gain appropriate attention and care (e.g., people experiencing medical vulnerability or without family at the bedside), experiencing the inability to perform activities of daily living (e.g., some older adults), or experiencing mental health emergencies may be at greater risk of harm due to ED overcrowding, access block, and boarding. Decision-makers may consider providing targeted supports to these and other groups at a disproportionate risk of harm in overcrowded EDs to promote equitable and effective ED care. Further groups or individuals not represented in this review who may face disparities in accessing, using, or benefiting from care within overcrowded EDs are discussed below. Moreover, while the present review was unable to speak explicitly to the impacts of ED overcrowding on patient and health care provider trust in EDs or the health care system more broadly, it is important to consider whether the quality of, and disparities in, care experienced by patients might impact their trust in health care providers and systems and willingness to seek future care, and how this may have future, negative implications for health outcomes and health inequities.
The review also highlighted that health care providers and staff working in the context of ED overcrowding, access block, and boarding also reported experiencing adverse impacts because of the phenomena, including dimensions of burnout and emotional and moral distress attributed to institutional and systemic barriers perceived to limit their abilities to fulfill their ethical and professional duties and obligations as health care providers. While some health care providers described experiencing dimensions of burnout, further research is required to understand whether emotionally and morally distressed care providers or other hospital staff also experienced lasting and clinically significant anxiety and depression, posttraumatic or secondary traumatic stress, and moral injury due to their experiences with ED overcrowding, access block, and boarding. Some health care providers also reported how ED overcrowding required greater triaging of limited personnel and resources in the ED but did not specify whether they received adequate support in making difficult resource allocation decisions in a fair and equitable manner that did not risk disadvantaging patients who may already experience poorer quality care or adverse outcomes at baseline.
Finally, decision-makers may consider that due to the limitations of this review, it does not provide insight into the full extent and impacts that ED overcrowding, access block, and boarding have on the health care system or people living and working in Canada. Although conducting primary research or an in-depth exploration of a wider breadth of literature were beyond the scope of this review, further research may be beneficial to understand how various, diverse groups impacted by ED overcrowding understand and experience proposed interventions to alleviate the phenomenon. This research may be important to helping protect patients from harm and ensuring that the benefits and burdens associated with proposed interventions are distributed and experienced equitably across patient groups. This review likely inadequately details experiences and impacts important to patients, their families, learners, people engaging in pediatric care, health care providers, or those closely affected by but not directly engaged with ED services (e.g., paramedics and other first responders, staff in other areas of the hospital, hospital management and administrators, and people providing community services to groups who frequently rely on the ED for health care). Further, there may be additional groups at disproportionately greater risk of harm due to ED overcrowding, access block, and boarding, including groups that currently experience reduced quality of care and adverse outcomes in the ED at baseline due to systemic and often intersecting factors such as racism, colonialism, and discrimination (e.g., Indigenous people, Black people, and other people of colour; those experiencing houselessness; those living with disability; those experiencing language barriers without access to a professional interpreter; and members of the 2SLGBTQ+ community).31-34,36-38 Notably, the perspectives and experiences of these groups are largely missing from the literature used to inform this review. Going forward, it is important to consider how data and evidence infrastructure can be improved to collect and analyze evidence required to better understand diverse perspectives and experiences of ED overcrowding, access block, and boarding, and the full range of associated ethical and equity considerations, to better inform decision-making about interventions to address ED overcrowding.
What Else Is CADTH Doing?
This report is part of a series of publications that CADTH has produced on the topic of ED overcrowding in Canada as an update to our 2006 publications.2,49-51 Separate publications not described in this report address:
the factors contributing to ED overcrowding in Canada
which interventions effectively alleviate ED overcrowding
how ED overcrowding in Canada has changed since the last series of reports
the identification of new and emerging interventions to alleviate ED overcrowding (those not captured in the summary of systematic review evidence)
a summary of CADTH’s multistakeholder dialogue sessions.
CADTH’s Health Technology Expert Review Panel will use the CADTH deliverables as inputs into deliberations that will result in the development of guidance in response to addressing the decision problem of what evidence-informed solutions should be considered to guide decision- and policy-making to alleviate overcrowding of adult and pediatric ED services in urban, rural, and remote health care settings in Canada.
For more information on CADTH’s work on this topic, visit: Emergency Department Overcrowding in Canada: An Update | CADTH
References
1.Affleck A, Parks P, Drummond A, Rowe BH, Ovens HJ. Emergency department overcrowding and access block. Can J Emerg Med. 2013;15(6):359-384. PubMed
2.Ospina MB, Bond K, Schull M, et al. Measuring overcrowding in emergency departments: a call for standardization. (CADTH Technology report no. 67.1). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320a_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 May 05.
3.Canadian Institute for Health Information. NACRS emergency department visits and lengths of stay. 2023; https://www.cihi.ca/en/nacrs-emergency-department-visits-and-lengths-of-stay. Accessed 2023 Apr 06.
4.Rowe BH, McRae A, Rosychuk RJ. Temporal trends in emergency department volumes and crowding metrics in a western Canadian province: a population-based, administrative data study. BMC Health Serv Res. 2020;20(1):356. PubMed
5.Cecco L. Emergency room death highlights Canadian healthcare crisis. London (UK): The Guardian; 2023: https://www.theguardian.com/world/2023/jan/11/canada-healthcare-crisis-emergency-room-death. Accessed 2023 May 04.
6.Canadian Association of Emergency Physicians expresses concerns over summer closures of emergency departments across Canada. Ottawa (ON): Canadian Association of Emergency Physicians; 2023: https://caep.ca/wp-content/uploads/2023/06/CAEP_Summer-Press-Release.pdf. Accessed 2023 Aug 14.
7.Kelen GD, Wolfe R, D’Onofrio G, et al. Emergency department crowding: the canary in the health care system. NEJM Catalyst. 2021. https://catalyst.nejm.org/doi/abs/10.1056/CAT.21.0217. Accessed 2023 Jun 30.
8.Savioli G, Ceresa IF, Novelli V, Ricevuti G, Bressan MA, Oddone E. How the coronavirus disease 2019 pandemic changed the patterns of healthcare utilization by geriatric patients and the crowding: a call to action for effective solutions to the access block. Intern Emerg Med. 2022;17(2):503-514. PubMed
9.Position statement on over-crowded emergency departments. West Melbourne (AU): International Federation for Emergency Medicine; 2022: https://assets.nationbuilder.com/ifem/pages/546/attachments/original/1670806966/IFEM_Position_Statement_on_Emergency_Department_Overcrowding_December_2022.pdf?1670806966. Accessed 2023 Apr 06.
10.Canadian emergency care is being crushed - and why that matters for all of us. Ottawa (ON): Canadian Association of Emergency Physicians; 2023: https://caep.ca/wp-content/uploads/2023/01/Letter-Canadian-Emergency-Care-is-Being-Crushed-Jan-2023.pdf. Accessed 2023 Apr 06.
11.Benner P. From novice to expert: excellence and power in clinical nursing practice. American J Nurs. 1984;84(12):1480.
12.Suri H. Purposeful sampling in qualitative research synthesis. Qual Res J. 2011;11(2):63-75.
13.Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods Med Health Sci. 2020;1(1):31-42.
14.Shaw L, Nunns M, Briscoe S, Anderson R, Thompson Coon J. A “Rapid Best-Fit” model for framework synthesis: using research objectives to structure analysis within a rapid review of qualitative evidence. Res Synth Methods. 2021;12(3):368-383. PubMed
15.Allen-Duck A, Robinson JC, Stewart MW. Healthcare quality: a concept analysis. Nurs Forum. 2017;52(4):377-386. PubMed
16.World Health Organization. Patient safety 2019; https://www.who.int/news-room/fact-sheets/detail/patient-safety. Accessed 2023 Jun 01.
17.Benkhalti M, Espinoza M, Cookson R, Welch V, Tugwell P, Dagenais P. Development of a checklist to guide equity considerations in health technology assessment. Int J Technol Assess Health Care. 2021;37:e17. PubMed
18.Braveman P. A new definition of health equity to guide future efforts and measure progress. Washington (DC): Health Affairs Blog; 2017: https://www.healthaffairs.org/content/forefront/new-definition-health-equity-guide-future-efforts-and-measure-progress. Accessed 2023 Jun 16.
19.NVivo qualitative data analysis, version 14 [computer program]. Doncaster (AU): QRS International Pty Ltd.; 2022.
20.Charmaz K. Constructing grounded theory 2nd ed. London (UK): Sage Publications Ltd; 2014.
21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
22.Chen LC, Lin CC, Han CY, Hsieh CL, Wu CJ, Liang HF. An interpretative study on nurses' perspectives of working in an overcrowded emergency department in Taiwan. Asian Nurs Res (Korean Soc Nurs Sci). 2018;12(1):62-68. PubMed
23.Eriksson J, Gellerstedt L, Hilleras P, Craftman AG. Registered nurses' perceptions of safe care in overcrowded emergency departments. J Clin Nurs. 2018;27(5-6):e1061-e1067. PubMed
24.Han CY, Lin CC, Goopy S, Hsiao YC, Barnard A, Wang LH. Waiting and hoping: a phenomenographic study of the experiences of boarded patients in the emergency department. J Clin Nurs. 2017;26(5-6):840-848. PubMed
25.Kongcheep S, Arpanantikul M, Pinyopasakul W, Sherwood G. Thai nurses' experiences of providing care in overcrowded emergency rooms in tertiary hospitals. Pac Rim Int J Nurs Res Thail. 2022;26(3):533-548.
26.Lin CC, Liang HF, Han CY, Chen LC, Hsieh CL. Professional resilience among nurses working in an overcrowded emergency department in Taiwan. Int Emerg Nurs. 2019;42:44-50. PubMed
27.McCarty EJ, Nagarajan MK, Halloran SR, Brady RE, House SA, Leyenaar JK. Healthcare quality during pediatric mental health boarding: a qualitative analysis. J Hosp Med. 2022;17(10):783-792. PubMed
28.Rantala A, Nordh S, Dvorani M, Forsberg A. The meaning of boarding in a Swedish Accident & Emergency department: a qualitative study on patients' experiences of awaiting admission. Healthcare (Basel). 2021;9(1):66. PubMed
29.van de Ruit C, Lahri S, Wallis LA. Clinical teams' experiences of crowding in public emergency centres in Cape Town, South Africa. Afr J Emerg Med. 2020;10(2):52-57. PubMed
30.Leong-Nowell TA, Tamani L, Kaspar A. Access block and overcrowding at the emergency department at Tupua Tamasese Meaole Hospital in Samoa. Int J Emerg Med. 2023;16(1):32. PubMed
31.Owens A, Holroyd BR, McLane P. Patient race, ethnicity, and care in the emergency department: a scoping review. CJEM. 2020;22(2):245-253. PubMed
32.Franco A, Meldrum J, Ngaruiya C. Identifying homeless population needs in the Emergency Department using Community-Based Participatory Research. BMC Health Serv Res. 2021;21(1):428. PubMed
33.Young R, Ayiasi RM, Shung-King M, Morgan R. Health systems of oppression: applying intersectionality in health systems to expose hidden inequities. Health Policy Plan. 2021;36(5):819. PubMed
34.McLane P, Mackey L, Holroyd BR, et al. Impacts of racism on First Nations patients' emergency care: results of a thematic analysis of healthcare provider interviews in Alberta, Canada. BMC Health Serv Res. 2022;22(1):804. PubMed
35.Kaltiso SO, Seitz RM, Zdradzinski MJ, et al. The impact of racism on emergency health care workers. Acad Emerg Med. 2021;28(9):974-981. PubMed
36.Fields A, Abraham M, Gaughan J, Haines C, Hoehn KS. Language matters: race, trust, and outcomes in the pediatric emergency department. Pediatr Emerg Care. 2016;32(4):222-226. PubMed
37.Flores G, Abreu M, Barone CP, Bachur R, Lin H. Errors of medical interpretation and their potential clinical consequences: a comparison of professional versus ad hoc versus no interpreters. Ann Emerg Med. 2012;60(5):545-553. PubMed
38.Hemsley B, Georgiou A, Hill S, Rollo M, Steel J, Balandin S. An integrative review of patient safety in studies on the care and safety of patients with communication disabilities in hospital. Patient Educ Couns. 2016;99(4):501-511. PubMed
39.Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316. PubMed
40.Darraj A, Hudays A, Hazazi A, Hobani A, Alghamdi A. The association between emergency department overcrowding and delay in treatment: a systematic review. Healthcare (Basel). 2023;11(3):385. PubMed
41.Pearce S, Marchand T, Shannon T, Ganshorn H, Lang E. Emergency department crowding: an overview of reviews describing measures causes, and harms. Intern Emerg Med. 2023;18(4):1137-1158. PubMed
42.Feng J, Li L, Wang C, et al. The prevalence of turnover intention and influencing factors among emergency physicians: a national observation. J Glob Health. 2022;12:04005. PubMed
43.Park JE, Song MR. Effects of emergency nurses' experiences of violence, resilience, and nursing work environment on turnover intention: a cross-sectional survey. J Emerg Nurs. 2023;49(3):461-469. PubMed
44.Witton N, Goldsworthy S, Phillips LA. Moral distress: does this impact on intent to stay among adult critical care nurses? Nurs Crit Care. 2023;28(2):211-217. PubMed
45.Clark P, Crawford TN, Hulse B, Polivka BJ. Resilience, moral distress, and workplace engagement in emergency department nurses. West J Nurs Res. 2021;43(5):442-451. PubMed
46.Sánchez-Zaballos M, Mosteiro-Díaz MP. Resilience among professional health workers in emergency services. J Emerg Nurs. 2021;47(6):925-932.e922. PubMed
47.Vagni M, Maiorano T, Giostra V, Pajardi D. Protective factors against emergency stress and burnout in healthcare and emergency workers during second wave of COVID-19. Soc Sci. 2021;10(5):178.
48.Schablon A, Kersten JF, Nienhaus A, et al. Risk of burnout among emergency department staff as a result of violence and aggression from patients and their relatives. Int J Environ Res Public Health. 2022;19(9):4945. PubMed
49.Bond K, Opsina M, Blitz S, et al. Interventions to reduce overcrowding in emergency departments. (CADTH Technology report no. 67.4). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320d_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Aug 29.
50.Rowe B, Bond K, Opsina M, et al. Data collection on patients in emergency departments in Canada. (CADTH Technology report no. 67.2). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320b_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Aug 29.
51.Rowe B, Bond K, Opsina M, et al. Frequency, determinants, and impact of overcrowding in emergency departments in Canada: a national survey of emergency department directors. (CADTH Technology report no. 67.3). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320c_Overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Aug 29.
52.Lincoln YS, Guba EG. But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Dir Program Eval. 1986;1986(30):73-84.
53.Tracy SJ. Qualitative quality: eight “big-tent” criteria for excellent qualitative research. Qual Inq. 2010;16(10):837-851.
Appendix 1: Selection of Included Studies
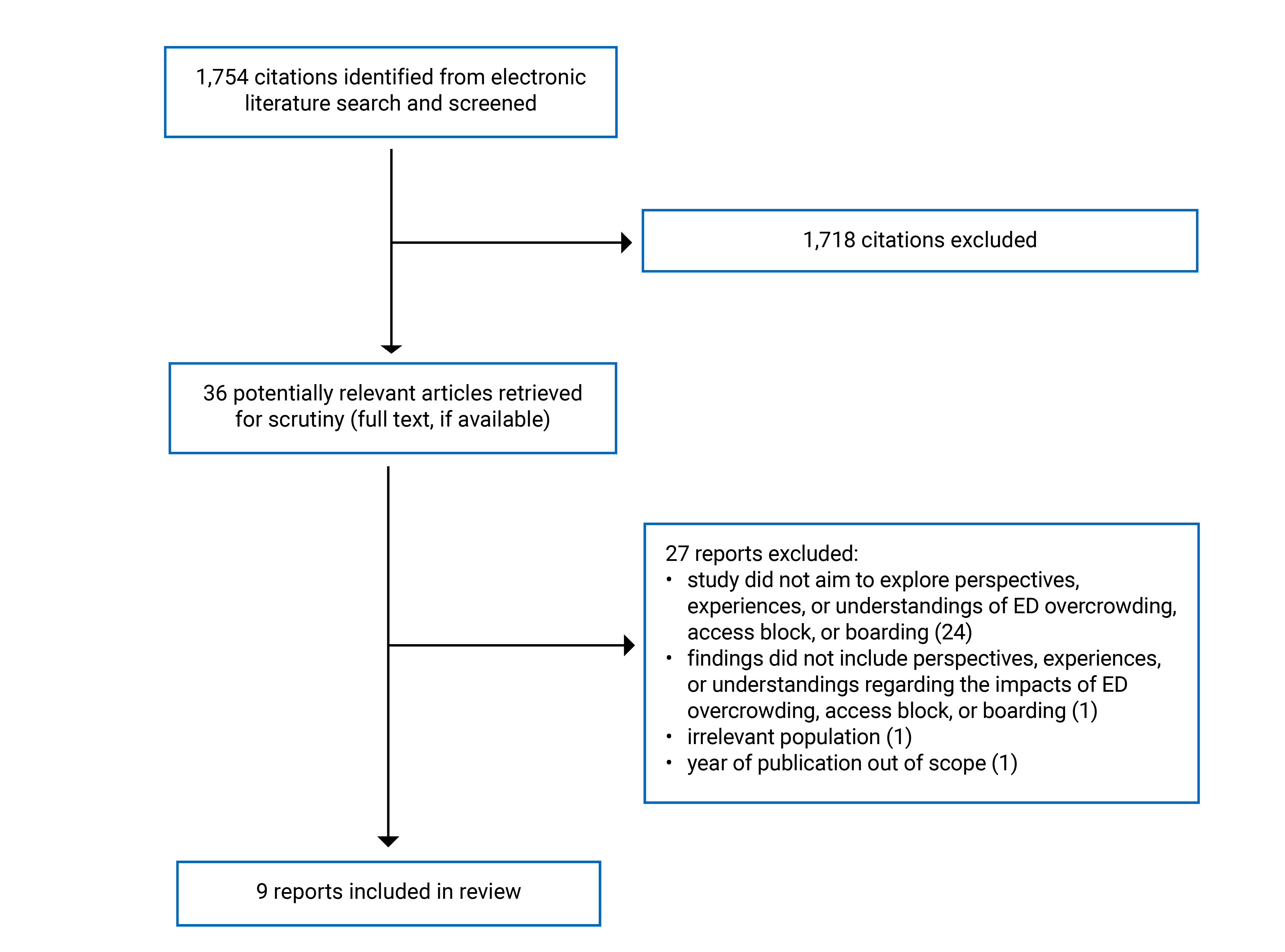
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Studies
Author, year, country | Aims or objectivesa | Methodology or design, sampling, data collection method, data analysis method | Setting | Inclusion criteria and sample size | Participant characteristicsb |
|---|---|---|---|---|---|
Chen et al., 201822 Taiwan | To gain an in-depth understanding of nurses’ perspectives of working in an overcrowded ED | Constructivist grounded theory Purposeful, theoretical, and snowball sampling; theoretical sampling then proceeded via snowball sampling until reaching “saturation of the data” Semistructured interviews (45 minutes to 1 hour) conducted in person Analytical methods informed by constructivist grounded theory | An ED in a tertiary care hospital with 3,338 ward beds and 233 emergency beds | Registered nurses (N = 40) employed by the participating ED with at least 1 year of full-time working experience in an ED | Age: Range, 23 years to 52 years Sex or gender: 100% (N = 40) female; male 0%; gender diverse NR Health literacy and education: 92.5% (n = 37) had completed a Bachelor of Nursing degree; 7.5% (n = 3) had completed a diploma in nursing Race or ethnicity (self-reported): NR Practice experience (HCPs): Years working in the ED ranged from 2 to 20 |
Eriksson et al., 201823 Sweden | To explore registered nurses’ perceptions of safe practice in care for patients with an extended length of stay in the ED | Qualitative description Purposeful sampling Semistructured interviews (26 minutes to 56 minutes) conducted in person Content analysis | 5 EDs located in 4 hospitals in a conurbation in Sweden, including: 3 university hospitals, 2 of which were connected and ranked as 1 of the largest university hospitals in Europe with “1,600 beds” and “1,609,000 patient visits” per year; 1 hospital with “85,000 acute seeking patients” (time frame NR); and 1 hospital described as having “one of the country’s largest numbers of emergency patients, with 82,000 visits in the ED” (time frame NR) | Registered nurses (N = 14) with a minimum of 1 year’s work experience in an ED | Age: NR Sex or gender: 78.6% (n = 11) women; 21.4% (n = 3) men; gender diverse NR Health literacy and education: NR Race or ethnicity (self-reported): NR Practice experience (HCPs): Years working in the ED ranged from 1 to 18 |
Han et al., 201724 Taiwan | To understand the experiences and concerns of patients in the ED during inpatient boarding | Phenomenography Purposeful sampling; participants were “recruited sequentially” until “data saturation was met” Semistructured interviews (45 to 68 minutes) conducted in person 7 steps of data analysis for a phenomenographic study, as articulated by Dahlgren and Fallsberg | Patients had received care in an ED in a hospital with more than 3,000 beds and approximately 15,000 ED presentations each month | People (N = 20) aged 20 years or older who had been waiting in the ED for a bed for more than 8 hours and were conscious, capable of communicating in Mandarin Chinese, and classified as non-trauma patients | Age: Mean 60.7 years (range, 25 years to 82 years) Sex or gender: 50% (n = 10) female; 50% (n = 10) male; gender diverse NR Health literacy and education: NR Race or ethnicity (self-reported): NR Boarding time: Mean 18.7 hours (range, 11.2 hours to 28.1 hours) |
Kongcheep et al., 202225 Thailand | To explore Thai nurses’ experiences in providing care for patients in overcrowded emergency rooms in tertiary hospitals | Interpretive phenomenology Purposeful, maximum variation sampling; interviews continued “until data saturation was reached” Open-ended, in-depth interviews (60 minutes to 120 minutes) conducted in person; some participants had a second interview intended “to verify data”; field notes and written reflections collected during and after the interviews Benner’s interpretive thematic analysis | The EDs of 5 public tertiary hospitals in Bangkok with “constant [emergency room] congestion,” including reporting at least 50 patients waiting in the ED each shift and having patients boarded in the ED for at least 2 days | Nurses (N = 20) with 2 or more years of experience working in the ED, able to communicate in Thai, and willing to participate | Age: Mean 38.2 years (range, 31 years to 50 years) Sex or gender: 100% (N = 20) female; 0% male; gender diverse NR Race or ethnicity: NR Health literacy and education: 80% (n = 16) had a bachelor’s degree Practice experience (HCPs): Average 15 years (range NR) experience working in the ED |
Leong-Nowell et al., 202330 c Samoa | The overall aim of the mixed-methods study was to provide preliminary data on access block and overcrowding in the ED of the national tertiary hospital of Samoa The qualitative component of the study aimed to explore the perspectives of front-line ED staff on access block and overcrowding | Qualitative component of a convergent parallel mixed-methods study (qualitative design NR) Purposeful sampling Semistructured focus groups (for junior nursing staff members) and in-depth interviews (for medical officers and senior nursing staff members); length and medium of data collection sessions NR; whether focus groups and interviews were semistructured or structured NR Thematic analysis | The ED of a hospital described as “the major centre for national emergency health services” in Samoa with 21 treatment bays | Nurses (n = 14) and medical officers (n = 3) working in the participating ED | Age: NR Sex or gender: NR Health literacy and education: NR Race or ethnicity (self-reported): NR Practice experience (HCPs): 7 junior nurses with 1 to 2 years of ED work experience; 5 junior nurses with more than 5 years of ED experience; 2 senior nurses with 19 to 24 years of ED experience The practice experience of the included medical officers was NR |
Lin et al., 201926 Taiwan | To explore and understand the experiences of resilience among nurses in an overcrowded ED and increase knowledge about what nurses identified as protective factors, which may be useful for future planning | Constructivist grounded theory Purposeful and theoretical sampling; sampling continued until achieving theoretical saturation In-depth, semistructured interviews (30 to 45 minutes) conducted in person Analytical methods informed by constructivist grounded theory | An ED in a tertiary hospital in Taiwan with more than 3,000 ward beds and 180 observation beds in the ED; the ED provides care to more than 2 million patients annually, with an ideal nurse to patient ratio of 1 to 6 or 8 | Nurses (N = 13) working full-time in the participating ED who were willing to participate in an interview and consented to being audiotaped | Age: Mean 28.8 years (range, 23 years to 39 years) Sex or gender: 100% (N = 13) female; male 0%; gender diverse NR Health literacy and education: 100% (N = 13) had a bachelor’s degree Race or ethnicity (self-reported): NR Practice experience (HCPs): Mean 5.4 years (range, 2 years to 17 years) experience working in the ED |
McCarty et al., 202227 US | To explore the perspectives and experiences of multidisciplinary clinicians and parents regarding mental health boarding and to develop a conceptual model to inform quality improvement efforts | Qualitative design (specific approach NR) Purposeful, maximum variation sampling; sampling continued until attaining “data saturation” Semistructured interviews (length NR) conducted in person (n = NR) or via video conference (n = NR) “A general inductive approach” incorporating methods borrowed from grounded theory (e.g., axial coding) and framework analysis | A tertiary care academic medical centre in the Northeastern US with a general (nonpediatric) ED and 22 licensed medical-surgical pediatric beds and no pediatric psychiatric beds | Clinicians (i.e., nurses, licensed nursing assistants, residents, physicians, and child life specialists; n = 19) who had cared for youth experiencing mental health boarding in the ED or an inpatient unit Parents or guardians (n = 12) of youth aged 18 years or younger who had experienced mental health boarding in the ED or an inpatient unit, and who themselves were aged older than 18 years, had English language proficiency, and were present at the bedside or available by phone to give consent | Cliniciansd Agee: Median 34.5 years (interquartile range, 29.75 years to 46.25 years) Sex or gender: 63.2% (n = 12) female; 36.8% (n = 7) male; gender diverse NR Health literacy and education: NR Race or ethnicity (self-reported)f: 94.1% (n = 16) non-Hispanic white; otherwise NR Practice experience (HCPs): NR Department of practice: 57.9% (n = 11), pediatric inpatient unit; 31.6% (n = 6), ED; 10.5% (n = 2) child and adolescent psychiatry Primary roles: 31.6% (n = 6) attending physician; 31.6% (n = 6) resident physician; 21.1% (n = 4) nurse; 10.5% (n = 2) licensed nursing assistant; 5.3% (n = 1) child life specialist Parents and guardiansd Ageg: Median 45.0 years (interquartile range, 39.5 years to 46.5 years) Sex or gender: 91.7% (n = 11) female; 8.3% (n = 1) male; gender diverse NR Health literacy and education: 33.3% (n = 4), more than 4-year college degree; 33.3% (n = 4), some college or 2-year degree; 16.7% (n = 2), 4-year college graduate; 16.7% (n = 2), high school or general educational development Race or ethnicity (self-reported): 100% (N = 12) non-Hispanic white Boarding time: Median 4.5 days (interquartile range, 3.25 days to 6.75 days) Location of boarding: NR |
Rantala et al., 202128 Sweden | To explore the meaning of being subjected to boarding at an A and E department, as experienced by patients | A phenomenological-hermeneutic approach Purposeful sampling Interviews (mean 48.5 minutes; range, 28 minutes to 72 minutes) conducted in person (n = 16) or by phone (n = 1); interview questions were described as “reflective and open-ended” Thematic structural analysis | An A and E department located in a general county hospital in the South of Sweden, which handles 75,200 A and E visits annually | People (N = 17) aged 18 years or older who experienced a decision to be admitted to the hospital but did not have a bed available within the past 14 days, were medically stable, and had knowledge of the Swedish language | Age: Median 64 years (range, 35 years to 86 years) Sex or gender: 52.9% (n = 9) women; 47.1% (n = 8) men; gender diverse NR Health literacy and education: NR Race or ethnicity: NR Boarding time: Median 18 hours and 10 minutes (range, 8 hours and 27 minutes to 22 hours and 55 minutes) |
van de Ruit et al., 202029 South Africa | To understand front-line staff’s perspectives on crowding in Cape Town public emergency centres to learn how they cope in such high-pressure working conditions, determine what they see as the factors contributing to crowding, and obtain their recommendations for reform | Constructivist grounded theory Purposeful, maximum variation, and theoretical sampling; sampling continued “until redundancy was accomplished” Semistructured interviews (15 to 30 minutes) conducted in person; data also included observations collected over 2 visits to each of the 5 included EDs Analytical methods inspired by constructivist grounded theory and interpretive description | 5 public emergency centres in Cape Town linked to “high-volume acute hospitals” | Staff working in the ED (N = 43), including physicians with varying levels of experience (n = 25) and registered or enrolled nurses (n = 18) | Age: NR Sex or gender: 60.5% (n = 26) women; 39.5% (n = 17) men; gender diverse: NR Health literacy and education: NR Race or ethnicity (as reported by the authors): 46.5% (n = 20) Coloured [wording from original source]h; 32.6% (n = 14) white; 18.6% (n = 8) Black; 2.3% (n = 1) Asian Practice experience (HCPs): The researchers sought “a mix of staff who were experienced and specialists emergency clinicians as well as staff who were generalist, new to emergency medicine, and less qualified”; specific proportion of each classification of staff NR |
A and E = accident and emergency; ED = emergency department; HCP = health care provider; NR = not reported.
Note: All non-integers have been rounded to the nearest 10th.
aThe aims and objectives of the studies are reported in the words of their authors.
bThe reporting of participant characteristics in this table uses the terms used by the authors of the included citations. Of note, while none of the authors reported including gender diversity beyond men or women, it is possible this was because of limitations in how they collected and reported their demographic data.
cOnly information relevant to the qualitative component of this mixed-methods study is reported here.
dBesides reporting the number of included clinicians practising in each department, the authors did not separately report the characteristics of participants working or having their youth boarded in different locations of the hospital.
eData missing for 3 participants.
fData missing for 2 participants; 1 participant preferred not to answer.
gData missing for 1 participant.
hThis is a racial classification commonly used in South Africa to refer to members of multiracial ethnic communities who may have ancestry from various populations.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Narrative Summary of the Findings of the Critical Appraisal
The authors of 5 of the 9 included studies clearly stated the philosophical assumptions underpinning their study, and these assumptions aligned with their stated methodologies and methods.22,25,26,28,29 The authors of 1 included study did not state their philosophical assumptions but used a pragmatic methodology agnostic to particular worldviews (i.e., qualitative description).23 The authors of the 3 remaining included studies did not report their philosophical underpinnings and/or their qualitative methodology.24,27,30 Congruence between philosophical underpinnings, methodologies, and methods enhances the credibility of a study’s findings, as it indicates that researchers have the knowledge and skills necessary to conduct qualitative inquiry.52
A qualitative approach was appropriate for addressing the stated objectives of all 9 studies.
By transparently reporting the methods they used, researchers enhance the rigour of their study by providing readers insights into whether their methods were sufficiently reasonable and appropriate.53 All authors explicitly reported methods used to recruit and select their participants and used a purposeful sampling approach appropriate for gaining access to relevant experiential experts. Additionally, all authors reported the number and characteristics of their participants. This enhanced the theoretical transferability of the studies’ findings by providing information allowing readers to compare settings and participants to their own context.
All authors reported methods of data collection, although the authors of 1 study did not report the length, structure, or medium of their interviews and focus groups and why they conducted in-depth interviews with some participants and focus groups with others.30 The same authors were the only ones not to report a particular analytical approach guiding the methods used for data analysis and did not provide sufficient detail to show that the methods used were appropriately rigorous and aligned with the cited approach.30
All authors provided a statement of ethical approval or ethical considerations except in 1 case27 where a research ethics board determined the study did not require further review. The authors of 3 studies22,25,29 detailed the nature of the relationship between the researchers and participants, and the authors of 4 studies24,25,28,29 explicitly reported using reflexive practices or examining their preconceptions. The authors of all but 1 study30 explicitly discussed methods used to enhance the credibility of their findings.
Table 3: Critical Appraisal Using the Optimized CASP Tool13
Strengths | Limitations |
|---|---|
Chen et al. (2018)22 | |
|
|
Eriksson et al. (2018)23 | |
|
|
Han et al. (2017)24 | |
|
|
Kongcheep et al. (2022)25 | |
| |
Leong-Nowell et al. (2023)30 | |
|
|
Lin et al. (2019)26 | |
|
|
McCarty et al. (2022)27 | |
|
|
Rantala et al. (2021)28 | |
|
|
van de Ruit et al. (2020)29 | |
|
|
CASP = Critical Appraisal Skills Programme; vs. = versus.
Acknowledgements: Ana Komparic, Renata Axler, Amil Reddy
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.