CADTH Health Technology Review
Trends in Public Drug Plan Expenditures for Patients With Crohn Disease and Ulcerative Colitis Initiating Targeted Immune Modulator Therapy
Technology Review
Abbreviations
CD
Crohn disease
CIHI
Canadian Institute for Health Information
DAD
Discharge Abstract Database
IBD
inflammatory bowel disease
ICD-10-CA
International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canada
NPDUIS
National Prescription Drug Utilization Information System
pCPA
pan-Canadian Pharmaceutical Alliance
TIM
targeted immune modulator
UC
ulcerative colitis
Key Messages
The objective of this analysis was to examine the changes in drug expenditures with the initiation of targeted immune modulator (TIM) treatment in patients diagnosed with Crohn disease (CD) and ulcerative colitis (UC).
Patient cohorts for CD and UC were identified from hospitalizations in Canada. Expenditure data for TIMs with a Health Canada–approved indication for the treatment of CD or UC were extracted from all provincial drug plans (except Quebec) and Yukon from 2016 to 2021, and a descriptive analysis was performed to assess the expenditure patterns.
Annual expenditures on TIMs for patients with CD increased each year from 2016 to 2019 before decreasing in 2020 and 2021, whereas expenditures on TIMs in UC increased each year, generally by a greater percentage than was observed in CD (peak percentage growth of 92.5% for UC versus 15.9% for CD in 2018).
Expenditures associated with TIM initiation among patients with CD and UC were driven by infliximab and adalimumab, with the 2 drugs accounting for nearly all expenditures in both indications in 2016 and most expenditures in 2021.
In both CD and UC, vedolizumab expenditures increased over time, as did the proportions of TIM expenditures on ustekinumab in CD and tofacitinib in UC, albeit to a lesser extent than vedolizumab.
Background
CD and UC, the 2 predominant types of inflammatory bowel disease (IBD), involve chronic inflammation of the gastrointestinal tract.1,2 CD most commonly affects the small intestine, with the inflammation often spreading to the deep layers of the bowel; UC causes inflammation and ulcers in the mucosa of the large intestine.3,4 Both types of IBD cause diarrhea, abdominal pain, rectal bleeding, nausea, vomiting, reduced appetite, and weight loss.5,6 Patients with CD may also develop mouth sores, pain or drainage near or around the anus due to fistula formation, and extraintestinal manifestations (e.g., inflammation in other organs and systems, kidney stones, anemia), whereas patients with UC commonly experience severe, frequent, and bloody diarrhea, as well as tenesmus and urgency (feeling of the need to defecate immediately).3-5 The prevalence of CD and UC in Canada is among the highest in the world,7-11 and is expected to increase from 259 per 100,000 persons in 2008 to 487 per 100,000 persons in 2030 for CD and from 210 per 100,000 persons to 408 per 100,000 persons during the same time period for UC.12 In a recently published 2023 report on the impact of IBD in Canada, the prevalence of IBD was estimated to be approximately 322,600 people (0.8% of the population), with a projected growth to 470,000 people in Canada (1.1% of the population) by 2035.13 IBD is associated with a substantial burden to patients, caregivers, and the health care system; in 2023, it was estimated that IBD resulted in $5.38 billion in combined direct and indirect costs in Canada.13
Approximately 1 in 5 adults with CD and 1 in 8 adults with UC are hospitalized each year based on data from Ontario, with more hospitalized patients with CD than with UC undergoing a surgical procedure during their initial hospitalization.14 The frequency and costs of hospitalizations for IBD have decreased over the past 2 decades, possibly because of increased use of biologic therapies (with associated improvements in disease control) and advances in management strategies.14 As such, there has been a shift away from hospitalization costs and toward drug costs as the main driver of the economic impact of IBD.14
Treatment approaches for CD and UC are determined by the site and extent of disease, risk factors for poor prognosis, and the severity of inflammation and symptoms.15-20 Patients with moderately to severely active CD or UC who have either not responded to or lost response to a corticosteroid and/or conventional immunosuppressant are often recommended a TIM, such as a biologic or small molecule drug.15-20 TIMs currently marketed in Canada for the treatment of moderately to severely active CD and UC are listed in Table 1. Most of the available TIMs are listed on public provincial drug plans across Canada with limited use, special authorization, or exception drug status coverage.21
Table 1: Marketed Targeted Immune Modulators for Moderately to Severely Active CD or UC
Drug | Year approved for CD | Year approved for UC | Biosimilar or generic available | Funded by at least 1 public drug plan |
|---|---|---|---|---|
Tumour necrosis factor-alpha inhibitor | ||||
Adalimumab | 2007 | 2013 | Yes | Yes |
Golimumab | — | 2013 | No | Yes |
Infliximab | 1998 | 2006 | Yes | Yes |
Anti-integrin antibody | ||||
Vedolizumab | 2016 | 2015 | No | Yes |
Interleukin-23 inhibitor | ||||
Mirikizumab | — | 2023 | No | No |
Risankizumab | 2022 | — | No | Yes |
Interleukin-12/23 inhibitor | ||||
Ustekinumab | 2016 | 2020 | Yes | Yes |
Janus kinase inhibitor | ||||
Tofacitinib | — | 2018 | Yes | Yes |
Upadacitinib | 2023 | 2022 | No | No |
Sphingosine-1-phosphate receptor modulator | ||||
Ozanimod | — | 2022 | No | Yes |
Note: Dash indicates that it is not indicated.
Purpose of This Report
The objective of this analysis was to examine the expenditures for TIM treatment initiation in patients diagnosed with CD and UC in Canada from 2016 to 2021.
Policy Issues
There are several TIMs currently marketed for the treatment of CD and UC in Canada, as well as emerging agents that will expand the therapeutic options for these conditions. Public health administrative claims databases provide a valuable source of real-world data to assess trends in therapy. Given the evolving landscape for TIMs used to treat CD and UC and the potential impact on public drug spending, we conducted an analysis using public claims data to estimate the expenditure patterns of these therapies to help inform public drug plan formulary management and funding considerations.
Research Question
What was the expenditure distribution for each of the publicly funded TIMs initiated in patients with CD and UC in Canada from 2016 to 2021, including:
annual expenditures for initial TIMs for CD and UC
changes in expenditures for each of the approved TIMs initiated among patients with CD and UC in Canada from year to year?
Methods
Data Sources and Time Frame
Data from the Canadian Institute for Health Information (CIHI), including the Discharge Abstract Database (DAD)22 and the National Prescription Drug Utilization Information System (NPDUIS),23 from January 1, 2016, until December 31, 2021, were used to conduct this analysis.
Discharge Abstract Database
The DAD contains clinical, demographic, and administrative information relating to hospital acute care admissions from Yukon and all provinces in Canada except Quebec.22 Medical conditions experienced by the patient during each hospital admission are captured in the DAD using the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada (ICD-10-CA) classification codes. Patients with a diagnosis of CD or UC were identified from the DAD based on a definition of 2 hospitalizations for either CD (ICD-10-CA code K50.X) or UC (ICD-10-CA code K51.X) from January 1, 2016, until December 31, 2021. Patients who had diagnostic codes for both UC and CD in the DAD during the study period were excluded from the analysis.
National Prescription Drug Utilization Information System Database
The NPDUIS database was used to determine expenditures for a patient’s first TIM dispensed for the treatment of CD and/or UC between January 1, 2016, until December 31, 2021 The NPDUIS database contains information on medication use and expenditures for Yukon and provincial drug plans, with the exception of Quebec.23 For the purpose of this analysis, data for the calendar year 2021 were not available for New Brunswick and were only available up until September for Alberta.
Patients identified from the DAD with UC or CD were then selected if they had at least 1 claim for a conventional UC or CD treatment, including corticosteroids, anti-inflammatory agents, and immunosuppressive therapies (Appendix 2). Conventional therapies were first identified because patients are generally required to be intolerant or refractory to conventional therapies to meet the funding criteria for TIMs. Following the selection of patients with at least 1 conventional therapy claim, the first index dispensation of a relevant TIM (adalimumab, golimumab, infliximab, tofacitinib, ustekinumab, or vedolizumab, or any available biosimilars) was then identified (Appendix 2), along with its associated expenditure for the analysis period of January 1, 2016, until December 31, 2021. All medications were identified based on Drug Identification Numbers (DINs) assigned by Health Canada and by the WHO Anatomical Therapeutic Chemical (ATC) classification codes (Appendix 2).
Exclusion
Claims for drugs administered outside of public drug plans are not submitted to NPDUIS; therefore, expenditures for such claims were not included.23 The NPDUIS database does not include information regarding prescriptions that were written but never dispensed; prescriptions that were dispensed but for which the associated drug costs were not submitted to, or not accepted by, the public drug program; or diagnoses or conditions for which prescriptions were written.23 In addition, ozanimod (Zeposia), upadacitinib (Rinvoq), risankizumab (Skyrizi), and mirikizumab (Omvoh) were not available during the time frame of this analysis; therefore, these agents were not included. A timeline detailing the conclusion dates of pan-Canadian Pharmaceutical Alliance (pCPA) negotiations for the molecules of interest is presented in Appendix 3. These dates serve as indicative markers for the subsequent potential listings on public provincial plans.
Data Analysis
The total public drug plan expenditures for the first index TIM dispensed among patients with either CD or UC in each year from 2016 to 2021 were aggregated from province-level data and presented at the national level. Expenditures were calculated based on the total dollar amount of a prescription accepted by the drug plan as eligible toward a deductible or for reimbursement, which includes the drug cost as well as the associated professional fees and markup, if applicable. Total annual expenditures were calculated and reported based on diagnosis (UC or CD) for all TIMs as well as for each TIM from 2016 to 2021. Finally, the proportion of TIMs expenditures for either CD or UC was calculated.
Findings
Expenditures of TIMs Initiated in Patients With Crohn Disease and Ulcerative Colitis
The cumulative expenditures of initial TIM therapy for patients with CD was $272,959,998 from 2016 to 2021. During this time period, the annual expenditures of initial TIM therapy increased by 17.2% from $39,315,956 in 2016 to $46,063,174 in 2021. The largest total expenditure for TIMs in patients with CD was in 2019 ($49,273,431). The total expenditures for initial TIMs in patients with CD are listed in Table 2.
From 2016 to 2021, the cumulative expenditures of initial TIM therapy for patients with UC was $70,386,523. Similar to patients with CD, the annual expenditures for initial TIM therapy increased over time, from $5,834,016 in 2016 to $15,326,161 in 2021. The largest year-over-year increase in expenditures was observed in 2018 ($6,928,190 in 2017 to $13,334,468 in 2018). The total expenditures for initial TIMs by year in patients with UC are listed in Table 2.
Most of the expenditures on initial TIMs from 2016 to 2021 was for CD (79.4% versus 20.6% for UC) (Table 3). However, the proportion of expenditures for UC increased over time (87.1% for CD and 12.9% for UC in 2016; 75.0% for CD and 25.0% for UC in 2021); the ratio of expenditures for CD relative to UC decreased each year from 6.74 in 2016 to 3.01 in 2021.
Table 2: Year-Over-Year Change in Public Expenditures for Initial TIMs in Patients With CD or UC
TIM | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | Total |
|---|---|---|---|---|---|---|---|
CD | $39,315,956 | $41,062,347 | $47,571,427 | $49,273,431 | $48,673,662 | $46,063,174 | $271,959,998 |
Year-over-year change | — | 4.4% | 15.9% | 3.6% | −1.2% | −5.4% | — |
UC | $5,834,016 | $6,928,190 | $13,334,468 | $14,287,271 | $14,675,706 | $15,326,872 | $70,386,523 |
Year-over-year change | — | 18.8% | 92.5% | 7.1% | 2.7% | 4.4% | — |
CD = Crohn disease; TIM = targeted immune modulator; UC = ulcerative colitis.
Table 3: Proportion and Ratio of Public Expenditures for TIMs for CD or UC by Year
TIM | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 6-year total |
|---|---|---|---|---|---|---|---|
CD | 87.1% | 85.6% | 78.1% | 77.5% | 76.8% | 75.0% | 79.4% |
UC | 12.9% | 14.4% | 21.9% | 22.5% | 23.2% | 25.0% | 20.6% |
Ratio (CD:UC) | 6.74 | 5.93 | 3.57 | 3.45 | 3.32 | 3.01 | 3.85 |
CD = Crohn disease; TIM = targeted immune modulator; UC = ulcerative colitis.
Individual TIM Distribution
In patients with CD, infliximab (54.9%; $149,271,728) accounted for more than half of total expenditures associated with public claims for initial TIMs from 2016 to 2021, followed by adalimumab (32.5%; $88,344,086), vedolizumab (9.4%; $25,543,536), ustekinumab (2.9%; $7,917,427), golimumab (0.3%; $717,514), and tofacitinib (0.06%; $165,707) (Table 4). Adalimumab and infliximab accounted for the majority of public expenditures for initial TIMs in each year included in the study period, contributing to 99.7% of costs in 2016 (adalimumab: 35.6% [$13,997,887]; infliximab: 64.1% [$25,210,289]) and 76.3% of costs in 2021 (adalimumab: 30.3% [$13,947,719]; infliximab: 46.0% [$21,190,430]) (Figure 1; Table 5). The proportion of expenditures for vedolizumab claims increased from 0% in 2016 ($0) to 17.1% ($7,865,743) in 2021. The proportion of expenditures attributable to ustekinumab also increased throughout the study period from 0.1% ($34,339) in 2016 to 6.4% ($2,927,401) in 2021. Expenditures associated with golimumab (0.2% in 2016 and 2021; peak of 0.4% in 2018) and tofacitinib (0% in 2016 to a peak of 0.06% in 2021) remained low throughout the study period.
In UC, infliximab (60.2%; $42,398,002) accounted for the majority of total expenditures associated with public claims for initial TIMs among patients from 2016 to 2021, followed by vedolizumab (23.3%; $16,392,608), adalimumab (13.4%; 9,393,357), golimumab (1.6%; $1,145,849), tofacitinib (1.4%; $960,962), and ustekinumab (0.1%; $95,745) (Table 4). Infliximab accounted for most of the public expenditures on initial TIMs in 2016 (94.1%; $5,491,676) (Figure 1; Table 5). Although the proportion of expenditures attributable to infliximab decreased from 2016 to 2021 (94.1% to 48.8%), infliximab still accounted for more expenditures than any other TIM in UC. The proportions of public TIM expenditures in UC for vedolizumab (0% [$0] in 2016; 28.2% in 2021 [$4,326,161]; peak of 30% [$4,410,340] in 2020), adalimumab (4.9% [$285,756] in 2016; 15.8% [$2,419,075] in 2021), and tofacitinib (0% [$0] in 2016; 5.6% [$853,825] in 2021) increased throughout the study period. The proportions of annual public expenditures for golimumab (0.6% [$37,752] in 2016; 1.5% [$225,928] in 2021; peak of 2.0% [$261,310] in 2018) and ustekinumab (0.3% [$18,832] in 2016; 0.2% [$27,161] in 2021) were low throughout the study period.
Year-over-year changes in public expenditures for TIMs among patients with CD, UC, and IBD overall by molecule are presented in Table 5. The greatest year-over-year percent increases in expenditures for adalimumab, golimumab, and infliximab were observed in 2017 and 2018 in CD and UC, followed by subsequent year-over-year decreases or reduced rates of growth for these molecules between 2019 and 2021. Year-over-year percent increases for tofacitinib were greatest in 2018 for CD (in which it is not indicated) and in 2021 for UC. The greatest year-over-year percent increases in expenditures for ustekinumab were observed in 2018 for CD and IBD overall, and in 2020 for UC. Similarly, the greatest increase in expenditures for vedolizumab across CD, UC, and IBD overall was observed in 2018, followed by decreasing rates of growth in each subsequent year of the analysis.
Table 4: Proportion of Public Expenditures for Each Initial TIM for CD or UC Over the Full Study Period (2016 to 2021)
Drugs | CD | UC |
|---|---|---|
Adalimumab | ||
Expenditures | $88,344,086 | $9,393,357 |
Proportion of total | 32.5% | 13.4% |
Golimumab | ||
Expenditures | $717,514 | $1,145,849 |
Proportion of total | 0.3% | 1.6% |
Infliximab | ||
Expenditures | $149,271,728 | $42,398,002 |
Proportion of total | 54.9% | 60.2% |
Tofacitinib | ||
Expenditures | $165,707 | $960,962 |
Proportion of total | 0.1% | 1.4% |
Ustekinumab | ||
Expenditures | $7,917,427 | $95,745 |
Proportion of total | 2.9% | 0.1% |
Vedolizumab | ||
Expenditures | $25,543,536 | $16,392,608 |
Proportion of total | 9.4% | 23.3% |
CD = Crohn disease; TIM = targeted immune modulator; UC = ulcerative colitis.
Table 5: Public Expenditures and Year-Over-Year Changes for Initial TIMs for CD or UC
Public expenditures and year-over-year changes | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|---|
Adalimumab | ||||||
CD expenditures | $13,997,887 | $14,659,009 | $15,677,266 | $15,001,714 | $15,060,491 | $13,947,719 |
CD year-over-year change | — | 4.7% | 6.9% | −4.3% | 0.4% | −7.4% |
UC expenditures | $285,756 | $584,331 | $1,653,264 | $2,087,934 | $2,362,997 | $2,419,075 |
UC year-over-year change | — | 104.5% | 182.9% | 26.3% | 13.2% | 2.4% |
Golimumab | ||||||
CD expenditures | $73,441 | $107,667 | $193,131 | $135,799 | $127,570 | $79,905 |
CD year-over-year change | — | 46.6% | 79.4% | −29.7% | −6.1% | −37.4% |
UC expenditures | $37,752 | $126,141 | $261,310 | $265,296 | $229,422 | $225,928 |
UC year-over-year change | — | 234.1% | 107.2% | 1.5% | −13.5% | −1.5% |
Infliximab | ||||||
CD expenditures | $25,210,289 | $25,723,149 | $27,457,502 | $26,180,771 | $23,509,588 | $21,190,430 |
CD year-over-year change | — | 2.0% | 6.7% | −4.6% | −10.2% | −9.9% |
UC expenditures | $5,491,676 | $5,934,639 | $8,146,072 | $7,760,748 | $7,590,146 | $7,474,722 |
UC year-over-year change | — | 8.1% | 37.3% | −4.7% | −2.2% | −1.5% |
Tofacitinib | ||||||
CD expenditures | $0 | $4,585 | $18,361 | $29,342 | $61,442 | $51,977 |
CD year-over-year change | — | — | 300.4% | 59.8% | 109.4% | −15.4% |
UC expenditures | $0 | $0 | $22,823 | $24,793 | $59,521 | $853,825 |
UC year-over-year change | — | — | — | 8.6% | 140.1% | 1,334.5% |
Ustekinumab | ||||||
CD expenditures | $34,339 | $72,640 | $524,140 | $1,920,500 | $2,438,407 | $2,927,401 |
CD year-over-year change | — | 111.5% | 621.6% | 266.4% | 27.0% | 20.1% |
UC expenditures | $18,832 | $9,502 | $0 | $16,970 | $23,280 | $27,161 |
UC year-over-year change | — | −49.5% | −100% | — | 37.2% | 16.7% |
Vedolizumab | ||||||
CD expenditures | $0 | $495,296 | $3,701,027 | $6,005,305 | $7,476,164 | $7,865,743 |
CD year-over-year change | — | — | 647.2% | 62.3% | 24.5% | 5.2% |
UC expenditures | $0 | $273,577 | $3,251,001 | $4,131,530 | $4,410,340 | $4,326,161 |
UC year-over-year change | — | — | 1,088.3% | 27.1% | 6.7% | −1.9% |
CD = Crohn disease; TIM = targeted immune modulator; UC = ulcerative colitis.
Figure 1: Proportion of Public Expenditures for Initial TIM for CD or UC per Year
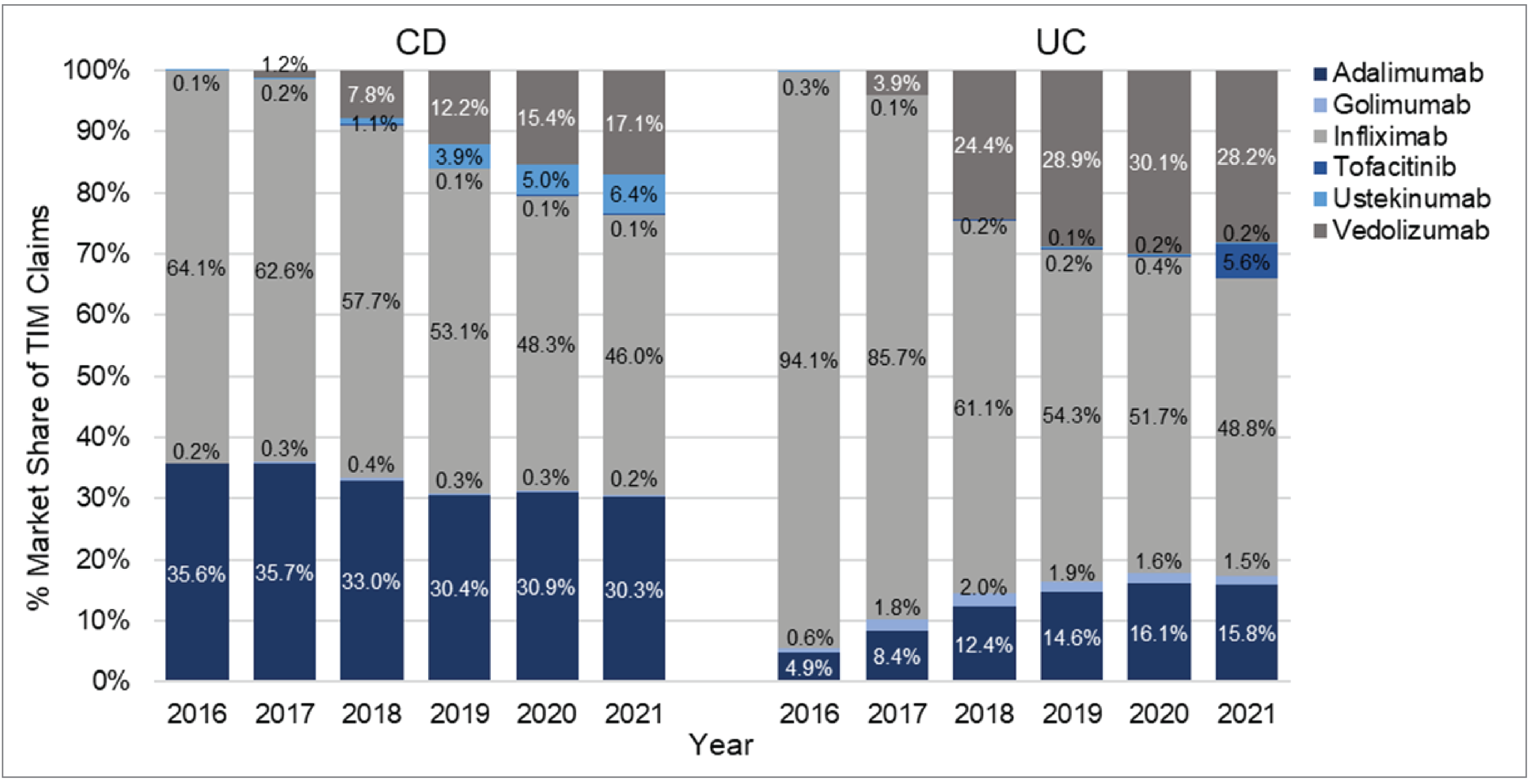
CD = Crohn disease; TIM = targeted immune modulator; UC = ulcerative colitis.
Discussion
This study sought to determine the expenditures for initial TIMs among patients with CD and UC in Canada by assessing expenditures associated with public drug claims from the NPDUIS database. Patients with CD or UC initiating a TIM were identified by linking claims from the NPDUIS database to a patient cohort from the DAD using ICD-10-CA coding for CD and UC, which was necessary because several of the TIMs of interest are approved for other indications. Because only 1 in 5 patients with CD and 1 in 8 patients with UC are hospitalized each year,14 most patients with IBD are treated in an ambulatory setting, and these patients were not included in this analysis. In addition, patients with IBD who require hospitalization are likely to have more severe and potentially more complicated disease than patients managed in other settings; as such, the expenditures should be interpreted as initial TIM costs among patients with a history of hospitalization for CD or UC. These points should be considered when interpreting the findings of this analysis.
Annual expenditures on initial TIMs for patients with CD increased each year from 2016 to 2019 before decreasing in 2020 and 2021, whereas expenditures on initial TIMs in UC increased in each year of the analysis, generally by a greater percentage than was observed in CD (peak percentage growth of 92.5% for UC versus 15.9% for CD in 2018). This was reflected in the ratio of TIM expenditures attributable to CD relative to UC, which decreased each year from 6.74 in 2016 to 3.01 in 2021. Nonetheless, initial TIM expenditures remained substantially higher in CD than in UC, which may be due in part to the higher prevalence of CD than UC in Canada12 and a greater proportion of patients with CD are hospitalized than those with UC.14
Expenditures associated with TIMs among patients with CD and UC were largely driven by infliximab and adalimumab, with the 2 agents accounting for nearly all expenditures in both indications in 2016 and most expenditures in 2021. These findings are in line with previous real-world treatment pattern data collected during an overlapping time period, which showed that physicians largely preferred infliximab and adalimumab as first-line biologic therapy for moderate to severe CD and UC.24 In this report, the proportion of expenditures attributable to infliximab decreased over time for both types of IBD, particularly in patients with UC. Adalimumab accounted for a greater proportion of expenditures in CD than in UC, with a small year-over-year decline in CD and more than a 3-fold increase in percentage growth in UC throughout the study period. The increase in adalimumab expenditures among patients with UC appeared to align with the conclusion of pCPA negotiations for the branded product (Humira) in 2017, whereas pCPA negotiations for Humira were not conducted in CD.21 The findings may also be partially explained by the timelines for biosimilar introduction in Canada because pCPA negotiations were concluded for the first infliximab and adalimumab biosimilars in 2016 and 2021, respectively.21 However, this is challenging to discern from the present findings because policies related to nonmedical switching from originator biologics to biosimilars vary in terms of process and timing from province to province.25
In both CD and UC, vedolizumab expenditures increased over time after pCPA negotiations were concluded and the product was subsequently added to public drug plans as an IV formulation in 2017.21,26 By 2021, it accounted for a greater percentage of TIM expenditures compared to 2016, especially in UC. A subcutaneous formulation of vedolizumab was also added to provincial plans in August 2021;21 however, the effect of this addition was not fully captured in this analysis because the study period ended in December 2021. Notably, results of the phase IIIb VARSITY trial showing vedolizumab was more efficacious than adalimumab in UC were published in 2019,16 leading several international organizations to recommend consideration of vedolizumab over adalimumab in updated treatment guidelines for moderate to severe UC.16,17 These findings and changes in clinical practice guidelines may have potentially contributed to the increased uptake of vedolizumab in UC compared with CD.
The proportions of TIM expenditures on ustekinumab in CD and tofacitinib in UC also increased over time, albeit to a lesser extent than vedolizumab. For tofacitinib, the increase in expenditures in 2021 occurred after the conclusion of its pCPA negotiations in July 2020.21 However, although ustekinumab received positive reimbursement recommendations from CADTH for CD in 2017 and UC in 2020,27,28 pCPA negotiations were concluded without agreement for both indications, and ustekinumab was not listed as a benefit by public drug plans for either CD or UC at the time of conducting this analysis and writing this report.21 Golimumab expenditures were also low in both CD (in which it is not indicated) and UC throughout the study period, with little change from year to year aside from a slight increase in UC expenditures after pCPA negotiations were concluded in August 2016.21
Limitations
There are several notable limitations of the current analyses:
In all jurisdictions captured by the NPDUIS database, people covered by provincial workers’ compensation boards or federal drug programs are not eligible for provincial public coverage. In Ontario, individuals who have coverage through the First Nations and Inuit Health Branch (FNIHB) have their drug claims first covered by the Ontario Drug Benefit, with remaining costs covered by FNIHB. In several provinces, including Alberta, Nova Scotia, and Prince Edward Island, claims dispensed through certain plans are not included in the NPDUIS database (refer to Appendix 1 for full details).
The NPDUIS database does not capture public claims from all age groups in all jurisdictions. For example, the Ontario dataset only includes the Ministry of Community and Social Services and the Ontario Ministry of Health and Long-Term Care Drug Benefit Program, meaning that a sizable proportion of adult patients aged between 25 and 65 years would not have been captured in this province.
The annual costs reported in the NPDUIS database are not adjusted for inflation; therefore, year-over-year changes in expenditures should be interpreted with this limitation in mind.
As with any analysis of prescription claims data, there is uncertainty regarding the actual use of the prescriptions claimed and expensed in the current analysis. Therefore, any interpretations of the findings presented herein should be limited to the context of expenditures associated with initial TIM claims for CD and UC as opposed to actual use of these drugs and whether they were taken as prescribed.
Because the claims data for TIMs from the NPDUIS database were linked to patients with diagnoses of CD or UC identified using ICD-10-CA codes in the DAD, it is possible that some patients with relevant diagnoses and claims for TIMs were not captured in the analysis. In addition, because patients with CD and UC were defined as having 2 hospitalizations with relevant ICD-10-CA codes, the results only reflect patients hospitalized for CD or CD. Many patients with IBD are diagnosed and treated in community gastroenterology clinics without being hospitalized; therefore, the results of this analysis must be interpreted within the context of patients hospitalized at least twice for CD or UC with a relevant initial TIM claim through public insurance.
This analysis did not assess expenditures for different dosage strengths of TIMs. Although this was outside the scope of the research question for this analysis, understanding the expenditures associated with different dosage strengths of TIMs in CD and UC may be valuable to inform policy decisions and is a worthwhile consideration for future studies, especially considering the regular use of dose escalation of biologic therapies in clinical practice.29-32
Although ozanimod (Zeposia) and risankizumab (Skyrizi) are currently funded by some public drug plans, they were not publicly funded during the analysis time frame. As such, expenditures associated with ozanimod and risankizumab for CD and UC are not included in this analysis.
Finally, the COVID-19 pandemic may have affected hospitalizations for CD and UC, which would result in an underestimation of the public drug plan expenditures for initial TIMs in 2020 and 2021.
Conclusions and Implications for Decision- or Policy-Making
Overall, public expenditures on TIMs among patients with CD and UC increased from 2016 to 2021. Although TIM expenditures were considerably higher for CD than for UC throughout the study period, the percentage increase was higher for UC than for CD, which is notable because the prevalence and proportion of patients hospitalized are greater in CD than in UC.14 In addition, there are a greater number of TIMs currently available for UC than for CD in Canada, and the changes in expenditure patterns for individual TIMs during the study period were more pronounced in UC than in CD. The most prominent trends in UC were a greater percentage decrease in infliximab expenditure and greater percentage increases in vedolizumab and adalimumab expenditures between 2016 and 2021, although infliximab continued to account for the greatest proportion of public TIM expenditures among patients with either CD or UC. It will be important for jurisdictions to monitor the trends reported herein, especially considering several new TIMs (ozanimod, upadacitinib, risankizumab, and mirikizumab) have been approved by Health Canada since the end of the study period, and the introduction of these new therapies may result in further changes in expenditure patterns. In addition, there have been several recent changes in exclusivity status for the TIMs included in this analysis: patents expired for ustekinumab and golimumab in 2021, and data protection expired for tofacitinib and vedolizumab in 2022 and July 2023, respectively. Although it is unclear whether these developments may affect expenditure patterns with the expected introduction of additional biosimilars and generics into the market over the next several years, the situation is worth monitoring. Overall, the findings of this analysis may help inform jurisdictions in formulary management and funding considerations for initial TIMs indicated for patients with CD and UC.
References
1.Lamb CA, Kennedy NA, Raine T, et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1-s106. PubMed
2.Ordás I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ. Ulcerative colitis. Lancet. 2012;380(9853):1606-1619. PubMed
3.Mayo Clinic. Crohn's disease. 2022; https://www.mayoclinic.org/diseases-conditions/crohns-disease/symptoms-causes/syc-20353304. Accessed 2023 Jun 02.
4.Mayo Clinic. Ulcerative colitis. 2022; https://www.mayoclinic.org/diseases-conditions/ulcerative-colitis/symptoms-causes/syc-20353326. Accessed 2023 Jun 02.
5.Crohn's and Colitis Canada. About Crohn's and colitis. 2019; https://crohnsandcolitis.ca/About-Crohn-s-Colitis/Signs-Symptoms. Accessed 2023 Jun 02.
6.Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114(3):384-413. PubMed
7.Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769-2778. PubMed
8.Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46-54.e42; quiz e30. PubMed
9.Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis. 2011;17(1):423-439. PubMed
10.Kaplan GG, Bernstein CN, Coward S, et al. The impact of inflammatory bowel disease in Canada 2018: epidemiology. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S6-S16. PubMed
11.Kuenzig ME, Fung SG, Marderfeld L, et al. Twenty-first century trends in the global epidemiology of pediatric-onset inflammatory bowel disease: systematic review. Gastroenterology. 2022;162(4):1147-1159.E4. PubMed
12.Coward S, Clement F, Benchimol EI, et al. A29 The rising prevalence of inflammatory bowel disease in Canada: analyzing the past to predict the future. J Can Assoc Gastroenterol. 2018;1(Suppl 2):47-48.
13.Impact of inflammatory bowel disease in Canada report. Toronto (ON): Crohn's and Colitis Canada; 2023: https://crohnsandcolitis.ca/Crohns_and_Colitis/documents/reports/2023-IBD-Report-English-LR.pdf?ext=.pdf. Accessed 2023 Jun 02.
14.Kuenzig ME, Benchimol EI, Lee L, et al. The impact of inflammatory bowel disease in Canada 2018: direct costs and health services utilization. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S17-S33. PubMed
15.Bressler B, Marshall JK, Bernstein CN, et al. Clinical practice guidelines for the medical management of nonhospitalized ulcerative colitis: the Toronto consensus. Gastroenterology. 2015;148(5):1035-1058.e3. PubMed
16.Raine T, Bonovas S, Burisch J, et al. ECCO guidelines on therapeutics in ulcerative colitis: medical treatment. J Crohns Colitis. 2022;16(1):2-17. PubMed
17.Feuerstein JD, Isaacs KL, Schneider Y, et al. AGA clinical practice guidelines on the management of moderate to severe ulcerative colitis. Gastroenterology. 2020;158(5):1450-1461. PubMed
18.Lichtenstein GR, Loftus EV, Isaacs KL, Regueiro MD, Gerson LB, Sands BE. ACG clinical guideline: management of Crohn's disease in adults. Am J Gastroenterol. 2018;113(4):481-517. PubMed
19.Feuerstein JD, Ho EY, Shmidt E, et al. AGA clinical practice guidelines on the medical management of moderate to severe luminal and perianal fistulizing Crohn's disease. Gastroenterology. 2021;160(7):2496-2508. PubMed
20.Panaccione R, Steinhart AH, Bressler B, et al. Canadian Association of Gastroenterology clinical practice guideline for the management of luminal Crohn's disease. Clin Gastroenterol Hepatol. 2019;17(9):1680-1713. PubMed
21.Pant S, Le K, Vannabouathong C, Dyrda P. Formulary management of targeted immune modulators in ulcerative colitis. Can J Health Technol. 2023;3(3). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/ES0366/ES0366. Accessed 2024 Jun 17. PubMed
22.Canadian Institute for Health Information. Discharge Abstract Database (DAD) metadata. 2024; https://www.cihi.ca/en/discharge-abstract-database-dad-metadata. Accessed 2024 Jun 14.
23.Canadian Institute for Health Information. National Prescription Drug Utilization Information System (NPDUIS) metadata. 2024; https://www.cihi.ca/en/national-prescription-drug-utilization-information-system-metadata. Accessed 2024 Jun 14.
24.Huynh L, Hass S, Peyrin-Biroulet L, et al. Real-world treatment patterns and physician preferences for biologics in moderate-to-severe inflammatory bowel disease: Retrospective chart review in Europe. Crohns Colitis 360. 2022;4(1):otac001. PubMed
25.Zhang Y, Peterson C. Biosimilars in Canada: building momentum in the wake of recent switching policies. Presented at 2021 CADTH Symposium, November 2021, virtual. Ottawa (ON): Patented Medicine Prices Review Board; 2021: https://www.canada.ca/content/dam/pmprb-cepmb/documents/npduis/analytical-studies/slide-presentations/biosimilars-cadth/Biosimilars%20in%20Canada_CADTH%20Nov%202021.pdf. Accessed 2023 Aug 22.
26.Crohn's and Colitis Canada. Provincial drug plans make Entyvio (vedolizumab) available to treat Crohn's and colitis. 2017; https://crohnsandcolitis.ca/News-Events/News-Releases/Provincial-drug-plans-make-ENTYVIO-vedolizumab-a. Accessed 2023 Jun 02.
27.Drug Reimbursement Expert Review Committee final recommendation: ustekinumab (Stelara — Janssen Inc.). Ottawa (ON): CADTH; 2017 Mar 21: https://www.cadth.ca/sites/default/files/cdr/complete/SR0501_complete_Stelara_Mar-23-17.pdf. Accessed 2023 Jun 02.
28.Drug Reimbursement Expert Review Committee final recommendation: ustekinumab (Stelara/Stelara I.V. — Janssen Inc.). Ottawa (ON): CADTH; 2020 Jul: https://www.cadth.ca/sites/default/files/cdr/complete/SR0627%20Stelara%20-%20CDEC%20Final%20Recommendation%20July%2020%2C%202020_for%20posting.pdf. Accessed 2023 Jun 02.
29.Kathe N, Umashankar K, Mirchandani K, et al. Dose escalation of biologic therapies in biologic treatment-naïve adult patients with ulcerative colitis: results from the Odessa Database Study. Inflamm Bowel Dis. 2022;28(Supplement_1):S9-S10.
30.Vaughn BP, Yarur AJ, Graziano E, et al. Vedolizumab serum trough concentrations and response to dose escalation in inflammatory bowel disease. J Clin Med. 2020;9(10):3142. PubMed
31.Ylisaukko-Oja T, Puttonen M, Jokelainen J, et al. Dose-escalation of adalimumab, golimumab or ustekinumab in inflammatory bowel diseases: characterization and implications in real-life clinical practice. Scand J Gastroenterol. 2022;57(4):415-423. PubMed
32.Jasurda JS, McCabe RP, Vaughn BP. Adalimumab concentration changes after dose escalation in inflammatory bowel disease. Ther Drug Monit. 2021;43(5):645-651. PubMed
Appendix 1: List of Public Plans and Programs Included in Analysis
Note that this appendix has not been copy-edited.
Table 6: List of Public Plans and Programs Included in Analysis23
Jurisdiction | Plan/Program Description |
|---|---|
Albertaa | Non-Group Seniors Palliative Care |
British Columbia | Permanent Residents of Licensed Residential Care Facilities Recipients of B.C. Income Assistance Cystic Fibrosis Children in the At Home Program No-Charge Psychiatric Medication Program Fair PharmaCare BC Palliative Care Drug Plan Smoking Cessation |
Manitoba | Employment and Income Assistance Personal Home Care/ Nursing Homes Palliative Care Pharmacare |
New Brunswick | New Brunswick Prescription Drug Program
New Brunswick Drug Plan Medical Abortion Plan |
Newfoundland and Labrador | The Foundation Plan The 65Plus Plan The Access Plan Assurance Plan Select Needs/Cystic Fibrosis Plan Select Needs/Change Hormone Plan |
Nova Scotiab | Diabetic Assistance Pharmacare Program Drug Assistance for Cancer patients Family Pharmacare Program Palliative Drug Care Program Under 65 – Long-Term Care Pharmacare Plan Seniors' Pharmacare Program |
Ontario | Ministry of Community and Social Services (MCSS) Ontario Ministry of Health and Long-Term Care (MOHLTC) Drug Benefit Program (ODB) |
Prince Edward Islandc | Diabetes Control Program Family Health Benefit Program Immunization Program High Cost Drugs Program Nursing Home Seniors Drug Cost Assistance Program Sexually Transmitted Diseases (STD) Children-In-Care/Financial Assistance Smoking Cessation Program Catastrophic Drug Program Opioid Replacement Therapy Drug Program Generic Drug Program |
Saskatchewan | Universal Program |
Yukon | Children's Drug and Optical Plan Chronic Disease Program Pharmacare |
NPDUIS = National Prescription Drug Utilization Information System.
Note: In all jurisdictions, people covered by provincial workers’ compensation boards or federal drug programs are not eligible for provincial public coverage. In Ontario, individuals who have coverage through the First Nations and Inuit Health Branch (FNIHB) first have their drug claims covered by the Ontario Drug Benefit, with remaining costs covered by FNIHB.
aClaims financed through the Income Support, Alberta Adult Health Benefit, Assured Income for the Severely Handicapped, and Alberta Child Health Benefit programs, are not submitted. Claims financed to residents of long-term care facilities are not submitted.
bClaims dispensed through the Department of Community Services Drug Programs are not submitted.
cClaims dispensed through the Child in Care/Financial Assistance, Seniors Cost Assistance, Diabetes Control, Family Health Benefits, High Cost Drugs, Nursing Home, Quit Smoking, and Sexually Transmitted Diseases programs are included. Claims for all other plans are not submitted.
Appendix 2: Drugs Included in the NPDUIS Database Search
Note that this appendix has not been copy-edited.
Table 7: Drugs Included in the NPDUIS Database Search
Chemical (Generic Name) | ATC Code |
|---|---|
Conventional therapy | |
Anti-inflammatory agents | |
5-aminosalicylic acid/mesalamine/mesalazine | A07EC02 |
Olsalazine | A07EC03 |
Sulfasalazine | A07EC01 |
Corticosteroids | |
Betamethasone | A07EA04 |
Budesonide | A07EA06 |
Hydrocortisone | C05AA01 |
Methylprednisolone | H02AB04 |
Prednisone | H02AB07 |
Immunosuppressive agents | |
6-mercaptopurine | L01BB02 |
Azathioprine | L04AX01 |
Methotrexate | L01BA01 |
Targeted Immune modulators | |
Adalimumab | L04AB04 |
Infliximab | L04AB02 |
Golimumab | L04AB06 |
Tofacitinib | L04AA29 |
Ustekinumab | L04AC05 |
Vedolizumab | L04AA33 |
ATC = Anatomical Therapeutic Chemical; NPDUIS = National Prescription Drug Utilization Information System.
Appendix 3: Timeline for Conclusion of pCPA Negotiations for TIMs Approved for CD and UC Before or During the Study Period
Note that this appendix has not been copy-edited.
Figure 2: Timeline for Conclusion of pCPA Negotiations for TIMs Approved for CD and UC Before or During the Study Period
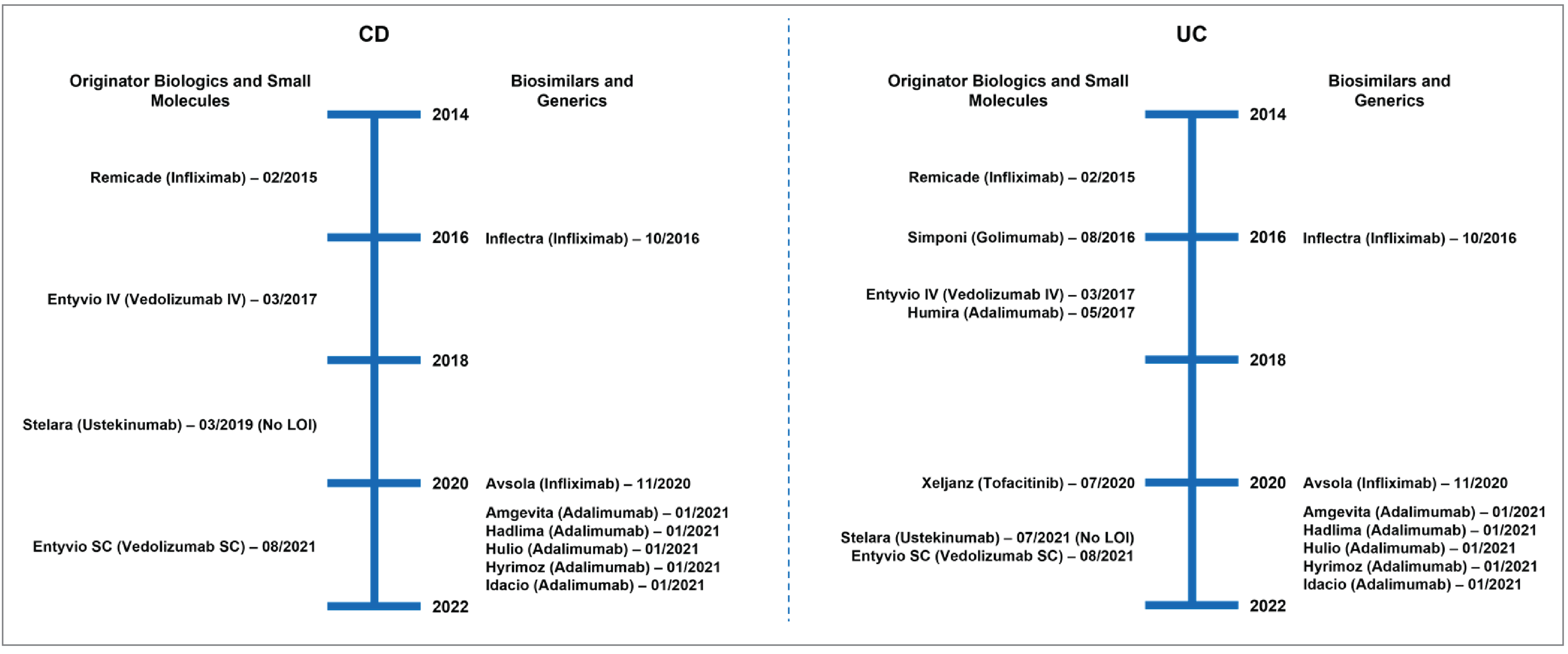
CD = Crohn disease; LOI = letter of intent; pCPA = pan-Canadian Pharmaceutical Alliance; SC = subcutaneous; UC = ulcerative colitis.
Note: Remicade (infliximab) was approved for the treatment of CD and UC and Humira (adalimumab) was approved for the treatment of CD by Health Canada before pCPA was established. In addition, pCPA negotiations were concluded for Stelara (ustekinumab) without an agreement for both CD and UC.
ISSN: 2563-6596
Acknowledgement: Canadian Institute for Health Information
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.