CADTH Health Technology Review
Risk of Sexual Transmission of HIV With Antiretroviral Therapy and Variable or Suppressed Viral Load
Technology Review
Authors: Sara Khangura, Anusree Subramonian, Melissa Severn
External Reviewers
This document was externally reviewed by content experts who have granted permission to be cited.
Dr. Marissa L Becker, MSc (Public Health), MD, FRCPC
Associate Professor
University of Manitoba
Dr. Sharon Walmsley, MSc, MD, FRCPC
Professor of Medicine, University of Toronto
University Health Network
Abbreviations
ART
antiretroviral therapy
HSSD
heterosexual serodiscordant
LWH
living with HIV
MA
meta-analysis
MSM
men who have sex with men
PHAC
Public Health Agency of Canada
PLWH
people living with HIV
PrEP
pre-exposure prophylaxis
SR
systematic review
Key Messages
The absolute risk of HIV transmission through sexual activity, reported as incidence rates of observed seroconversions across person-years of follow-up, ranged widely across the included studies of sex partners living with HIV with variable (or unreported) viral loads.
Two studies included sex partners living with HIV with suppressed viral loads of less than 200 copies/mL, reporting no phylogenetically linked seroconversions in either study.
Most studies in this report included data from heterosexual serodiscordant sex partners and did not report follow-up viral loads of sex partners living with HIV.
The included studies incorporated variable methods, investigated a broad variety of populations and exposures, and demonstrated a wide range of methodological strengths and limitations.
Context and Policy Issues
HIV has been a major public health issue since the recognition of AIDS, and the discovery of the virus in the early 1980s.1 Globally, HIV continues to be 1 of the most common causes of death in low-income countries, though the rates are decreasing significantly.2 WHO reports that there were 1.5 million new HIV infections worldwide in 2021.3 In Canada, it is estimated that there were 62,700 people living with HIV (PLWH) at the end of 2020 and 1,520 new infections occurred in 2020.4 The majority of those new infections are estimated to have occurred through sexual transmission.4
Current clinical guidelines recommend that antiretroviral therapy (ART) should be started in all PLWH, ideally within 7 days of diagnosis, if the patient is ready and there are no concomitant opportunistic infections.5 ART drugs act by inhibiting various levels of the viral life cycle, thereby suppressing the viral replication in human plasma.6 Several studies among serodiscordant couples (where 1 partner is living with HIV and the other partner is HIV negative) have shown that early initiation of ART can prevent sexual transmission of HIV.7-9 This led to the development of the global campaign “Undetectable = Untransmittable,” which seeks to build scientific consensus behind growing evidence that PLWH who are adherent to treatment and maintain an undetectable viral load are unable to transmit the virus through sexual activity.10
Disclosure of HIV status by a PLWH to a sexual partner is legally required in Canada where there is a “realistic possibility” of HIV transmission. Nondisclosure of HIV status has rendered consent to sexual activity “not obtained in law” when the sex partner living with HIV (LWH) is found to have not been clear and transparent about their status.11
A systematic review (SR) published in 2018 by the Public Health Agency of Canada (PHAC)12 found that when the sex partner LWH takes ART and maintains a viral load of < 200 copies/mL (i.e., a suppressed viral load) on consecutive viral load testing, the risk of sexually transmitting HIV is “negligible.”12 The authors also concluded that the risk of sexual transmission is “low” when the sex partner LWH takes ART and has variable levels of viral load. The findings of the review were based on studies among serodiscordant couples conducted from 2007 to 2017.12 With the emergence of new evidence since then, especially in the men-who-have-sex-with-men (MSM) population,13,14 an updated review of the evidence is warranted.
The purpose of this report is to identify evidence that has been published since the 2018 PHAC SR12 regarding the risk of HIV transmission associated with sex when the sex partner LWH takes ART with variable levels of viral load as well as with a suppressed viral load.
Research Questions
What are the absolute risks of HIV transmission associated with sex when the following preventive measures are taken to reduce the risk of transmission between a PLWH and a sex partner who is HIV negative:
the sex partner living with HIV takes ART with variable levels of viral load?
the sex partner living with HIV takes ART and has a suppressed viral load of less than 200 copies/mL on consecutive measurements every 4 to 6 months?
Methods
Literature Search Methods
The literature search strategy used in this report was developed for a previous SR.12 For the current report, search terms were added to the search strategy to expand the identification of articles relevant to the LGBTQ2S+ community.
For this update, published literature was identified by searching the following bibliographic databases: MEDLINE All via Ovid, Embase via Ovid, the Cochrane Central Register of Controlled Trials (CENTRAL) via Ovid, and Scopus. Duplicates were removed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were antiretroviral therapy, sex partners, and HIV. The following clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov and Health Canada’s Clinical Trials Database.
CADTH-developed search filters were applied to limit retrieval to health technology assessments, SRs, meta-analyses (MAs), indirect treatment comparisons, and any types of clinical trials or observational studies. Conference abstracts and preprints were excluded from the search results. Retrieval was not limited by language.
The update search was run on November 22, 2022, to capture any articles published or made available since the initial search dates.
Grey literature (literature that is not commercially published) was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature reference.15 Google was used to search for additional internet-based materials.
Selection Criteria
Titles and abstracts for all citations were screened by 2 independent reviewers, with full-text articles retrieved for any citation identified as potentially relevant by either independent reviewer. The full text of each potentially relevant study was read by 1 reviewer and assessed for eligibility. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Sex partners who are HIV serodiscordant Exclude: studies where HIV is not primarily transmitted through sex |
Exposures | Q1: Sex partner living with HIV takes antiretroviral therapy Subgroups: variable levels of viral load Q2: Sex partner living with HIV takes antiretroviral therapy and has a suppressed viral load (i.e., < 200 copies/mL on consecutive measurements every 4 to 6 months) |
Comparator | Any or none |
Outcomes | Absolute risks of HIV transmission during sex to a partner who is HIV negative |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2017.12 SRs in which all relevant studies were captured in either the PHAC review,12 or other more recent or comprehensive SRs, were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more of the included SRs.
Synthesis Approach
Relevant data from eligible studies were abstracted into tables and organized by 2 reviewers, with the information used to inform the narrative summary of findings. The narrative summary of findings was structured and presented by the research questions posed in this report, with a focus on absolute risk of HIV transmission in serodiscordant sex partners for whom the partner LWH is treated with ART. The limitations of the included studies were also summarized, as observed by the reviewers and as reported by the study authors.
Critical Appraisal of Individual Studies
Each included study was critically appraised by 1 reviewer using either the AMSTAR 2 (A MeaSurement Tool to Assess Systematic Reviews 2)16 tool for SRs, or the Downs and Black checklist17 for randomized and nonrandomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
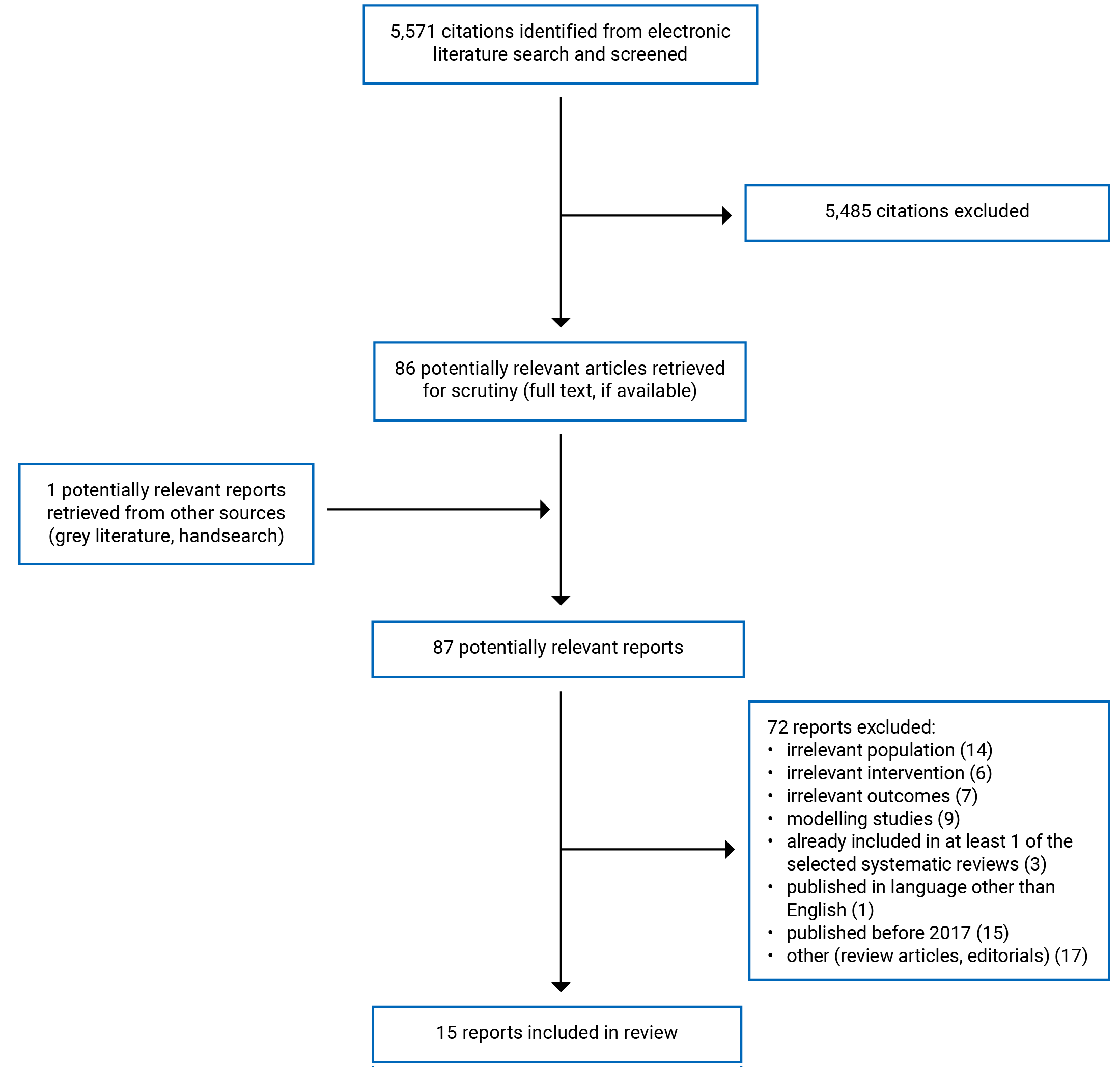
A total of 5,571citations were identified in the electronic database search. Following screening of titles and abstracts, 5,485 citations were excluded and 86 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 72 publications were excluded for various reasons, while 15 studies met the inclusion criteria and were included in this report.13,14,18-30 These comprised 1 overview of SRs and/or MAs,18 and 14 nonrandomized studies.13,14,19-30 Appendix 1 presents the PRISMA31 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The overview of reviews18 included 10 SRs and/or MAs — 2 of which were not described in the SR by PHAC.12 Overview of reviews or “umbrella review” refers to evidence synthesis of existing systematic reviews.32 Results of the 2 relevant SRs included in the overview are summarized in the current report. Of the 14 primary studies,13,14,19-30 only data describing characteristics and findings relevant to the current report were abstracted and summarized herein.
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
The overview of reviews was published in 2021, and sought SRs and MAs published between 2007 and 2019; there was no description of overlap between the studies included in the overview.18 The 14 primary studies were published between 2018 and 2022, all of which employed nonrandomized study designs.13,14,19-30 Seven of the nonrandomized studies used a prospective cohort design13,14,19,21-23,25 and 7 used a retrospective method.20,24,26-30
Country of Origin
The lead author of the included overview of the reviews was from Iran.18 Countries represented by the eligible primary studies included Brazil,13,27 China,19,24,26,28-30 Ethiopia,20 India,22,23 Kenya,25 Rwanda,21 and 2 international studies, 1 of which was conducted in 14 European countries,14 and the other which including participants from Australia, Brazil, and Thailand.13
Patient Populations
The overview sought SRs and MAs that described adult couples and/or sex partners who were HIV serodiscordant, including both couples and/or sex partners who were heterosexual as well as MSM.18 No other characteristics of the study participants described in the included SRs and MAs were reported.
The 14 primary studies also included couple were HIV serodiscordant and/or sex partners who were either heterosexual and/or MSM.13,14,19-21,23-30 None of the studies identified specified investigation of women who have sex with women. Whereas 11 of the studies included data for couples with only heterosexual serodiscordant (HSSD) sex partners,19-21,23-30 2 reported data only for MSM sex partners.13,14 One study did not specify whether participant couples were heterosexual or MSM.22 Of the heterosexual study cohorts, the sex composition of couples and/or sex partners who are serodiscordant by HIV status varied across 8 of the studies, with either the male or female sex partner LWH.19,21,25-30 Two of the heterosexual study cohorts included only males LWH,23,24 and 1 included only females LWH.20 The ages of the study participants were not reported consistently across the included studies, with some studies reporting age only for sex partners LWH,13,19,26,28-30 others reporting age for all study participants,14,20-22,24,25,27 and others not reporting on age at all.18,23
Study settings included local, hospital, government and/or university-based clinics;13,19,21,24,26 clinics specializing in the treatment of HIV, AIDS, and/or ART;22,23,27 hospitals;26 clinical research sites and facilities;14,25 and public health institutions.20 Three of the retrospective cohort studies reported the use of data from Guangxi, China, but did not provide detail describing the setting(s) from which participants were recruited.28-30 Finally, the presence or extent of potential overlap between patient populations across these studies (given their proximity in setting and jurisdiction) was unclear.
Exposures and Comparators
All included studies reported data on serodiscordant sex partners in whom the sex partner LWH was treated with ART.13,14,18-30 Types of ART regimens were not specified in most of the studies,13,14,18,20-23,25-30 although 2 studies did provide this information, describing lopinavir and ritonavir-based, raltegravir-based, efavirenz-based, and other (unspecified) regimens.19,24 For sex partners LWH and already using ART at baseline, the duration of use was described in 4 studies.14,21,24,25 Data describing ART use and adherence across follow-up were reported in 5 studies.13,14,20,23,25
Six of the primary studies reported data describing viral load at baseline in sex partners LWH,13,14,19,23,25,27 with 5 of these further specifying subgroups of participants with lowered viral loads.13,14,19,25,27 Studies describing subgroups of participants with a low viral load characterized participants at thresholds of either 200 copies/mL13,14 or 400 copies/mL,19,25 with 1 study reporting genital viral load in female sex partners LWH at a threshold of 40 copies/mL.27 Notably, 1 of the studies reporting viral load at a threshold of 400 copies/mL also included a definition of viral load at a threshold of 1,000 copies/mL, with a lack of clarity as to how these apparently variable thresholds were applied.25 Of the studies reporting any data describing viral load, 2 provided data at both baseline and follow-up,13,25 whereas 4 provided baseline data only.14,19,23,27 Per the research questions and study eligibility criteria for this report, data from studies describing findings in study participants LWH who demonstrated viral loads of less than 200 copies/mL across study follow-up were used to answer the second research question; those who did not specify study participants LWH who demonstrated a viral load of less than 200 copies/mL, or did not specify viral load clearly or at all, were used to answer the first research question.
Pre-exposure prophylaxis (PrEP) is a preventive therapy taken by sex partners who are HIV negative that can reduce the risk of HIV transmission in serodiscordant couples,33 and was featured in 4 of the studies included in this report.13,14,24,25. One of the studies included sex partners who were HIV negative, all of whom initiated PrEP across study follow-up.25 Two studies separated outcomes data for serodiscordant couples in whom the sex partner who was HIV negative received PrEP from those who did not.13,24 Another study measured the use of PrEP among study participants and excluded outcomes data for serodiscordant couples in whom the participants who were HIV negative were receiving PrEP.14
Eight studies included a comparison group18,19,21,24,25,28-30 and 7 studies did not.13,14,20,22,23,26,27 Of the 8 studies describing a comparator, 5 bore relevance to the current report (i.e., use of ART versus no use of ART)18,21,28-30 and 3 did not present comparative data of relevance (i.e., comparisons with exposures of no direct relevance to the research questions).19,24,25 Relevant comparison groups included those in which the sex partner LWH was not receiving ART,18,21 or was ART treatment-naive at baseline.28-30 Irrelevant comparison groups included those in which the sex partners LWH were both receiving ART, but the partners who were HIV negative either did or did not have hepatitis C virus,19 or were or were not receiving PrEP.24 Another study used a hypothetical comparison cohort.25
Outcomes
All 15 studies included in this report described seroconversions observed in serodiscordant sex partners.13,14,18-30 Seven studies summarized follow-up time using total person- or couple-years accrued,13,14,19,25,26,28,30 and 3 summarized follow-up time using the mean or median years observed per participant couple.20,21,27 Five studies did not report a summary value describing observed follow-up time.18,22-24,29 Exposure data of relevance to the research questions posed in this report included describing viral load in sex partners LWH across study follow-up, using consecutive measurement of viral load across a 3 to 12 month time frame, which was reported by 3 of the included studies.13,14,25
Thirteen of the included studies described the absolute risk of HIV transmission as seroconversions observed across follow-up in person- or couple-years, reported using incidence rates expressed as number of seroconversions observed per 100 person- or couple-years.13,14,18-23,25-29 One study did not report incidence rates, describing the absolute number of seroconversions observed over a 24-week course of follow-up per participant couple.24 Another study reported incidence rates across person-years of follow-up for serodiscordant couples among whom the sex partner LWH either was or was not receiving ART (i.e., combined results),30 which were not relevant to the current report. However, this study did report numbers of seroconversions observed at both 6- and 12-month intervals of follow-up in sex partners LWH who were receiving ART (comparing these with seroconversions observed among those who were not receiving ART),30 and these findings are included in this report.
Single-arm studies described the absolute risk of HIV transmission across serodiscordant couples in whom those with HIV all received ART,13,14,19,20,22,23,26,27 whereas comparative studies reported and compared data on the transmission risk across serodiscordant couples in whom those with HIV did or did not receive ART.18,21,28-30
In addition, viral or phylogenetic linkage among observed seroconversions was assessed by 3 studies,13,14,21 providing confirmatory information supporting the occurrence of HIV transmission between the sex partners under study (as opposed to another source of transmission).
Additional outcome measures bearing some relevance to this report included those describing relative risk of HIV transmission, often comparing groups with or without exposure to ART;18,21,28-30 and sexually transmitted infections observed during follow-up.13 One study described severe adverse events associated with ART use,25 but these data were not directly related to the research questions posed by this report.
Summary of Critical Appraisal
Overview of Systematic Reviews
The overview of SRs and MAs demonstrated both strengths and limitations,18 as assessed using the AMSTAR checklist,16 as well as additional items of particular relevance to overviews of reviews. Strengths included clearly reported eligibility criteria to judge the inclusion or exclusion of SRs, information on reasons for exclusion, sources of funding and conflict of interest statements for the overview study, and a published protocol, registered a priori with the PROSPERO database. Clarity in reporting is essential to ensure that readers can assess and judge the validity and reliability of the study’s findings. Methodological strengths included a comprehensive electronic literature search strategy, duplicate study selection, risk of bias assessments, and appropriate assessments of heterogeneity between the SRs, including a discussion of the impact of heterogeneity on the interpretation of the findings. Methodological rigour in SRs (including overviews of SRs) is critical to ensuring that confidence can be placed in the validity and reliability of the findings.
The overview of SRs and MAs study also demonstrated important limitations.18 As it concerned clarity in reporting, SRs excluded from the overview were not listed or described, and there were insufficient details describing the included SRs, making interpretation of the overview challenging. Furthermore, there was no mention of the risk of transitivity or publication bias, and the sources of funding for the included SRs were not reported. Methodological and other limitations included no mention of a search of grey literature, no description of an assessment of overlap between the included SRs, no description of duplicate data abstraction, and considerable heterogeneity identified among the included SRs. These missing details and methodological features make it difficult for the reader to assess the extent to which the findings of the overview are reliable and/or valid.
Primary Studies
Critical appraisal of the nonrandomized cohort studies summarized in this report focused on assessing the clarity of reporting, external and internal validity, and study power.17 All 14 studies demonstrated some strengths and limitations in either reporting or methodological rigour,13,14,19-30 and these are summarized in the following.
Clarity of Reporting
Clarity and completeness in reporting of empirical data collection and analyses are critical for the reader to assess the extent to which a study was conducted rigorously, and whether the findings are valid and reliable. A description of the study objectives and main outcomes were included in all 14 primary study reports.13,14,19-30 Details describing study participants and exposures were reported with sufficient detail in 6 studies,13,14,19,20,24,25 whereas 8 studies had relevant information missing on either 1 or more sex partner(s) of the serodiscordant couples, or with regard to the exposure of interest (i.e., the specific details of ART use, including regimens and/or adherence across study follow-up).21-23,26-30 Study participant loss to follow-up (including characteristics of participants) was not clearly described by most studies;14,20-28,30 though, 2 studies did report these data appropriately, including numbers and characteristics of those lost to follow-up and/or appropriate adjustments to account for follow-up losses.13,29 The lack of a clear description of participant loss to follow-up limits the extent to which the internal validity of the study can be assessed, as it remains unclear whether participants who did not complete the study follow-up were or were not similar to those for whom data collection were complete. Similarly, all but 1 study25 did not report information describing any adverse effects caused by ART,13,14,19-24,26-30 which, while not a particular focus of the current report, poses a limitation on the reader’s ability to assess the possible impact of this variable on the exposure of interest for these included studies.
Other descriptions of the exposure of interest (i.e., ART use across time, regimens, and/or adherence) were provided with variable levels of detail across the included studies.13,14,19-30 A sufficient description of the use of ART is essential to interpreting the findings of the studies, as the numbers of participants, their use over time, and their adherence to ART are critical details needed to answer the research questions concerning transmission of HIV. While 7 studies provided some or clear information describing ART use, regimens, and/or adherence,13,14,19-21,24,25 7 studies provided no or few details describing this exposure.22,23,26-30
Other study features (including participant characteristics and study outcomes) were generally included in and/or reported clearly across most of the studies;13,14,19-29 however, 1 study report was missing — or provided unclear descriptions of — critical information necessary to interpret the study findings (e.g., missing denominators and unclear HIV status of the partners who were not LWH), which limits the interpretation and utility of the study findings.30
External Validity
Establishing external validity is important to ensuring that the findings from a study are generalizable to the broader population (i.e., outside of the study context). The representativeness of the study populations and the care they received was variable across the included studies.13,14,20-30 Whereas 6 studies demonstrated some or clear evidence of external validity (e.g., recruitment of consecutive patients from clinics or health facilities used by most or all of the population of interest [i.e., serodiscordant sex partners]),14,19-22,28 the representativeness of the study populations and/or settings was unclear for 8 of the included studies,13,23-27,29,30 limiting the generalizability of their findings. Examples of these limitations included a study population that was older and cohabitating and may not bear generalizability to a broader and more representative population;19 study settings that were limited to research activities and may not be generalizable to a real-world health care setting;25 patient recruitment that was limited to urban settings with patients who were generally well-connected to adequate health care resources, and may not therefore bear sufficient generalizability to nonurban or disadvantaged populations;13 and, a lack of sufficient detail needed to assess the extent to which the health care settings were representative of the broader population of interest.30
Notably, information describing numbers and/or characteristics of patients who chose not to participate in the research during recruitment was either not reported or not clearly reported for all of the 14 primary studies.13,14,20-30 Data describing nonparticipants is important to an understanding of external validity (i.e., these ensure that the study population bears characteristics that are sufficiently similar to the source population to render findings that are representative and generalizable).
Internal Validity
Internal validity is necessary to establish confidence in the findings, demonstrated by methods that increase confidence in an association between the effect(s) observed with the exposures and/or interventions under study. None of the 14 primary studies summarized in this report used either randomization or blinding in their methods;13,14,19-30 though, these methodological limitations are necessary features of cohort studies investigating the exposure of interest (i.e., ART in serodiscordant couples). Nonetheless, the absence of randomization and blinding introduce a limitation to the internal validity of the studies, as the effects observed on the outcomes of interest cannot be isolated from any possible effects imposed by the researchers’, clinicians’, and study participants’ knowledge of the exposures and interventions experienced by the participants.
The effect of viral load in sex partners LWH is critical to understanding risk of transmission in couples in serodiscordant relationships. Viral load measured at either baseline and/or across follow-up was reported by 6 of the primary studies,13,14,19,23,25,27 but was missing or not clearly described in the report of findings for 8 of the included studies.20-22,24,26,28-30 Furthermore, of the 6 studies reporting any data on viral load, 3 did not report, or clearly report, data across follow-up, describing viral load at baseline only19,23,27 (with 1 of these including data on viral load for the entire study cohort, and no data specific to the subgroup of study participants relevant to this report23). This lack of data describing viral load across follow-up introduces an important limitation to understanding its effect on the risk of HIV transmission.
Viral, or phylogenetic, linkage of HIV transmission for serodiscordant couples in whom seroconversion is observed is critical to understanding whether transmission occurred between the sex partners under study or not.34 This variable was investigated and reported in 3 of the 14 studies,13,14,21 but was absent from the others.19,20,22-30 While self-report of exclusivity or monogamous sex partnerships may mitigate the limitations imposed by the absence of this variable, confirmation of transmission between the couple and/or sex partners under study cannot otherwise be validated, representing an important limitation to the internal validity, and thus interpretation, of the study findings.
The use of PrEP in 3 of the studies included in this report13,24,25 introduces a potential threat to their internal validity with regard to reported estimates of the effect of ART on the risk of HIV transmission (i.e., serodiscordant couples in whom the partner who is HIV negative is using PrEP may demonstrate different rates of seroconversion than couples in whom no PrEP is being used). Nonetheless, 2 of the studies reported outcomes data separately for participants who were HIV negative who were or were not administered PrEP, which allows for a clearer assessment of how this exposure may or may not have impacted the findings of the studies.13,24 One study included participants who were HIV negative and were were administered PrEP, which introduces an important risk of confounding with regard to the findings on HIV transmission in these serodiscordant couples.25 Of the remaining studies summarized in this report, 1 excluded participant data with any exposure to PrEP (increasing confidence in the internal validity of the findings),14 whereas the others made no mention of exposure (or no exposure) to PrEP, leaving uncertainty as to whether the findings may or may not have been impacted by this potentially confounding factor.18-23,26-30
For the 3 studies that reported actual losses to follow-up, proportions of participants lost or not completing follow-up ranged from between 11% and 35%.13,21,25 Significant loss to, or failure to complete, study follow-up can introduce a risk of confounding, potentially introducing limitations on the internal validity of the studies.
Study Power
Sample size and/or study power is critical to understanding a study's capacity to detect clinically important effect(s).35 Study power was not addressed (or not clearly described) by most of the included studies;19-21,23,25-27 though, 3 of the studies did provide information addressing and/or describing study power.13,14,22,24 Of these, 1 study acknowledged that it was underpowered due to an insufficiently small sample size24 and 2 studies reported an insufficient number of accrued couple-years to demonstrate a clinically meaningful effect.13,14
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Thirteen of the 15 included studies in this report presented data describing the absolute risk of HIV transmission associated with sex among serodiscordant couples when the sex partner LWH takes ART with variable (or unreported) levels of viral load.18-21,23-30 One of the 15 studies presented data describing the absolute risk of HIV transmission associated with sex among serodiscordant couples when the sex partner LWH takes ART and has a suppressed viral load of less than 200 copies/mL on consecutive measurements every 4 to 6 months.14 One of the 15 studies presented data of relevance to both research questions.13
Appendix 4 presents detailed and tabulated study findings.
Absolute Risk of HIV Transmission Associated With Sex Among Serodiscordant Couples When the Sex Partner LWH Takes ART With Variable Levels of Viral Load
Overview of SRs and MAs
Of the 2 SRs summarized in the overview study that were not previously included in the 2018 SR by PHAC,12 1 described eligible data on absolute risk, reporting a pooled incidence rate of 2.13 (95% confidence interval [CI], 0.00 to 4.63) seroconversions across an unspecified number of person-years in an unreported number of serodiscordant heterosexual couples for whom the sex partner LWH was receiving ART.18 The findings from the second SR did not include data describing absolute risk of seroconversion.18
Primary Studies
Incidence of HIV transmission reported as seroconversions observed across 100 person-years of follow-up in serodiscordant couples for whom the sex partner LWH was receiving ART and demonstrating variable (or unspecified) levels of viral load ranged widely across 12 of the 13 included primary studies,13,19-30 with the rate of seroconversions ranging between 0 (upper limit of 95% CI = 0.84)13 and 6.4 (95% CI, 4.64 to 8.76)20 seroconversions per 100 person-years of follow-up reported for all patients included in the studies (i.e., subgroup findings not included).
Three cohort studies in which the sex partner LWH was receiving ART with variable (or unreported) levels of viral load described observing no seroconversions (or, no phylogenetically linked seroconversions) across study follow-up.13,24,25 Two of these studies were prospective13,25 and 1 was retrospective,24 with 2 investigating HSSD pursuing pregnancy through natural conception24,25 and 1 investigating MSM sex partners.13 Sample sizes ranged from between 74 couples with 146.4 years of person follow-up25 to 343 couples with 588.4 couple-years of follow-up.13 In all 3 of these studies, some or all of the sex partners who were HIV negative were receiving PrEP during the study follow-up13,24,25 (with 2 studies reporting findings separately by PrEP status of the partner who was HIV negative and reporting zero seroconversions in both subgroups).13,24 Viral load was also monitored in sex partners LWH across study follow-up in 2 of the studies reporting no observed seroconversions,13,25 with 1 study reporting 75% of participants consistently demonstrating a viral load of less than 200 copies/mL.13 The other study reporting on viral load across follow-up (and reporting no observed seroconversions) indicated that suppressed viral load (described variably across the study report as either < 400 copies/mL and < 1,000 copies/mL) was demonstrated during 74.3% of follow-up clinic visits in serodiscordant couples who achieved pregnancy, and during 64.6% of follow-up clinic visits in couples who did not achieve pregnancy.25 Phylogenetic linkage analysis of observed seroconversions was conducted in 1 of the studies (with nonlinked seroconversions not included in the findings).13 HIV prevention methods included encouraging participants to limit condomless sex to the periovulatory period only,24,25 monitoring of adherence to ART in the sex partner LWH,13,25 and the sex partner who was HIV negative taking PrEP.13,24,25 Another retrospective cohort study of 186 heterosexual couples across a total of 507.7 person-years also reported an observation of no seroconversions among the subgroup of 119 participants who received ART within 1 month of HIV diagnosis.26
Of the 6 studies reporting at least 1 or more observed seroconversion(s) (but less than 2 seroconversions per 100 person-years of follow-up) across all study participant couples for whom the sex partner LWH was receiving ART with variable (or unreported) levels of viral load,19,21-23,26,28 3 studies found incidence rates of less than 1 per 100 person-years of follow-up19,21,26 and 3 studies reported incidence rates greater than 1 but less than 2 per 100 person-years of follow-up.22,23,28 Four of these 6 studies were prospective in their design,19,21-23 and 2 used retrospective study methods,26,28 with eligible data reported from a range of 9022 to 7,71328 study participants, and a range of study follow-up between a median of 1.4 years (standard deviation = 1.2)21 and 18,985.29 person-years.28 None of the 6 studies reporting observed seroconversions of greater than 0 but less than 2 per 100 person-years of follow-up reported information on the use of PrEP in sex partners who were HIV negative,19,21-23,26,28 and 1 reported information on viral linkage of seroconversions,21 whereas the remaining 5 did not.19,22,23,26,28 Of the 1 study that demonstrated viral linkage for a proportion of all seroconversions observed across the study follow-up, 19 seroconversions were observed among 2,032 serodiscordant couples for whom the sex partner LWH was receiving ART, with 14 of these 19 found to demonstrate viral linkage. An incidence rate of 0.63 (95% CI, 0.38 to 1.00) was reported for these 19 seroconversions (which comprised a combination of seroconversions with and without demonstrated viral linkage [i.e., no incidence rate was reported for the subgroup of 14 virally linked seroconversions]).21 One additional study reported a finding of 1.6 (95% CI, 1.0 to 2.2) observed seroconversions per 100 person-years in the subgroup of serodiscordant couples in whom the sex partner LWH received early ART.29
Of the remining 4 primary studies providing data in answer to the first research question posed in this report, 2 studies reported overall incidence rates exceeding 2 per 100 person-years of follow-up.20,27 Another study did not report incidence rates for the overall study cohort; rather, only for subgroups of participants LWH by timing of ART initiation, finding rates of seroconversion per 100 person-years ranging from between 1.6 (95% CI, 1.0 to 2.2) and 6.7 (95% CI, 5.0 to 8.4) for participants with early to late ART initiation, respectively.29 One additional retrospective study30 reported that there were 573 seroconversions among sex partners and/or couples in whom the sex partner LWH was receiving ART across 12 months of follow-up per couple; however, the number of sex partners LWH and receiving ART (among the overall 5,544 individuals in the study) was unclear from the publication, making any interpretation of the findings challenging. None of these studies reported whether the partners who were HIV negative were receiving PrEP during the study follow-up. Of these 4 studies that described the highest numbers of observed seroconversions (i.e., more than 2 per 100 person-years of follow-up), all were retrospective and investigated heterosexual sex partner couples.20,27,29,30 Sample sizes and follow-up ranged from between 200 couples with a median of 4.5 years of follow-up (range = 0.3 years to 21.7 years)27 and 13,132 couples accrued and followed from 2003 to 2014.29 ART adherence in sex partners LWH was measured by 1 of the studies,20 and measurement of viral load in sex partners LWH was reported in 1 of the studies.27 There was no viral linkage of seroconversions described by the 4 studies.20,27,29,30 One study reported on condom use as an HIV-preventive measure used by some participants,20 and another reported findings stratified by timing of ART initiation,29 but no other preventive measures were reported in the 4 studies.20,27,29,30 Of note, the extent to which the findings were interpretable in 1 of these studies was limited by inconsistent reporting and missing denominators for at least 1 outcome.30
Absolute Risk of HIV Transmission Associated With Sex Among Serodiscordant Couples When the Sex Partner LWH Takes ART and Has a Suppressed Viral Load of Less Than 200 Copies/mL on Consecutive Measurements Every 4 to 6 Months
Overview of SRs and MAs
No novel data (i.e., not previously included in the 2018 PHAC SR)12 describing the absolute risk of HIV transmission associated with sex among serodiscordant couples when the sex partner LWH takes ART and has a suppressed viral load of less than 200 copies/mL on consecutive measurements every 4 to 6 months were identified in the overview of SRs and MAs.18
Primary Studies
Two studies were identified describing the absolute risk of HIV transmission in serodiscordant couples with a sex partner LWH demonstrating a suppressed viral load of less than 200 copies/mL on consecutive measurements across study follow-up. Both studies included MSM participant couples only, representing a combined total of 1,049 study participants and 1,370.4 couple-years of follow-up, and reporting no observed transmissions that were phylogenetically linked.13,14 Notably, the findings for both of these studies did not include data on participant couples in whom the partner who was HIV negative was receiving PrEP.13,14
Relative Risk of HIV Transmission Among Serodiscordant Couples When the Sex Partner LWH Does Versus Does Not Take ART
Though not a focus of this report, 5 of the included studies reported relative risks of HIV transmission in serodiscordant couples for whom the sex partner LWH did or did not receive ART.
Overview of SR and MA
Neither of the 2 SRs and MAs included in the overview and eligible for inclusion in this report described incidence rates comparing groups of serodiscordant sex partners for whom the participants LWH did or did not receive ART.18
Primary Studies
Four studies provided effect estimates describing relative risk rates of HIV transmission in serodiscordant couples, comparing those for whom the sex partner LWH did or did not receive ART.21,28-30 Hazard ratios in 2 large, retrospective studies ranged from between 0.30 (95% CI, 0.18 to 0.50)29 and 0.48 (95% CI, 0.40 to 0.59),28 demonstrating a statistically significant benefit of ART, with 1 study specifying a 45% reduction in the risk of transmission observed in participants receiving ART.28 Another large prospective study compared incidence rates of seroconversion across groups receiving or not receiving ART, and reported an adjusted rate ratio of 6.9 (95% CI, 3.8 to 12.4), demonstrating a statistically significant effect of ART on reducing the risk of transmission.21 Finally, a large retrospective study compared seroconversions across groups of serodiscordant heterosexual couples receiving and not receiving ART at 12 months of follow-up, reporting an odds ratio of 0.50 (95% CI, 0.42 to 0.60), suggesting a statistically significant benefit of not taking ART (i.e., P < 0.0001).30 The authors of the study conceded that this finding is discordant with others in the literature and postulate that uncertainty of the HIV status of the nonindex partners at baseline may have contributed to the unexpected findings.30
HIV seroconversions and rates were also reported across multiple additional subgroup and stratified analyses that are tabulated and detailed in Appendix 4.
Limitations
This review identified 15 studies describing exposure to ART in sex partners LWH and the risk of HIV transmission in serodiscordant sex partners, but is limited by the quality of available evidence, as well as limited available data addressing the various populations and/or exposures.
Regarding the 14 studies addressing absolute risk of HIV transmission associated with sex among serodiscordant couples when the sex partner LWH takes ART with variable (or unreported) levels of viral load, all 14 studies had some methodological limitations, and some had considerable limitations.13,18-21,23-30 The overview of SRs and MAs included in this report was limited by a lack of clarity in its report of findings, a low quality of included SRs relevant to this review, and the degree of overlap with previous work.18 Specifically, the overview did not describe study characteristic details or absolute risk data for 1 of the SRs relevant to this review, which described an MSM population, and the quality of the other SR, for which a small amount of relevant data were available, was rated as low by the authors of the overview, demonstrating wide CIs and a limited degree of certainty in its results.18 Data overlap were also identified between those describing the PARTNER 1 study, as summarized in the 2018 SR,12 and those reported in 1 study included in this report.14 Study quality for the 13 primary studies addressing absolute risk of HIV transmission associated with sex among serodiscordant couples when the sex partner LWH takes ART with variable (or unreported) levels of viral load was also limited by the nonrandomized and unblinded methods employed, which limit the internal validity of study findings and the confidence that can be placed in the interpretation and conclusions of their results.13,18-30 Critical appraisal of the 13 cohort studies rendered variable findings, with some studies demonstrating more (and different) strengths and/or limitations than others.13,19-30 In particular, limitations were observed for some methodological features that demonstrate internal and external validity,13,19-30 introducing limitations on the confidence that can be placed in the representativeness, generalizability, reliability, and validity of the findings summarized herein. Nonetheless, particular limitations identified for each study are important to consider when interpreting their findings, including acknowledgement of how these may impact the confidence that can be placed in the conclusions that have been drawn, as well as their utility. For instance, while a larger sample size is an important contributor to the confidence that can be placed in the findings, other study features, such as a retrospective study design, lack of clarity in reporting, and missing data — as was seen in 1 study summarized in this report30 — reduce the confidence that can be placed in the findings and conclusions.
Evidence describing populations of interest was variable in 14 studies included in this report (i.e., 12 of the studies identified and summarized in this report focused only on HSSD,19-30 with 1 primary study providing data specific to MSM,13 and 1 overview of SRs and MAs that provided no data of relevance regarding MSM).18 The 2018 SR by PHAC also included a limited number of studies describing MSM populations;12 while the number of studies describing MSM populations has since increased, and now includes relatively large sample sizes as well as mostly robust study methods, there are still a limited number of available studies examining these groups.
Exposures of interest were represented and/or described with various levels of detail and relevance across the studies included and summarized in this report. While all of the included studies described use of ART in at least some of the sex partners LWH,13,18-30 details concerning use of ART across follow-up, types of ART regimens used, and duration of and adherence to therapy were not described — or not described clearly — in many of the studies, limiting the extent to which the role of ART exposure on the rates of HIV transmission can be considered. Additional exposures described may have introduced a risk of confounding to the observed association between ART and HIV transmission risk (e.g., use of PrEP13,24,25 or hepatitis C virus–positive status19 among sex partners who are HIV negative) and other exposures, such as condom use and/or timing of unprotected sex, may limit the internal validity of the findings with regard to the outcome of interest.
Viral load data for sex partners LWH were not reported by most studies included in this report, and for those that included these data, the availability and/or relevance was variable (e.g., viral load reported at baseline only and not across follow-up,19,23,27 or viral load across follow-up by subgroups of participants who did or did not achieve pregnancy using natural conception, as opposed to HIV transmission and/or ART use).25
Finally, data describing phylogenetic or viral linkage among observed seroconversions were not reported by 12 of the 14 included studies addressing the first research question concerning variable viral load.18-20,22-30 As demonstrated in 2 of the included studies in this report, observed seroconversions may not always demonstrate a linkage between sex partners in the study,13,14 which could introduce a risk to the internal validity of studies that do not include this information (e.g., overcounting of seroconversions may be assumed between the serodiscordant couples in the study where this information is missing).
Regarding the 2 studies reporting data in answer to the question concerning absolute risk of HIV transmission associated with sex among serodiscordant couples when the sex partner who is HIV positive takes ART and has a suppressed viral load of less than 200 copies/mL on consecutive measurements every 4 to 6 months (1 of which contributed data to the first question, as well), both contributed data from MSM populations, limiting the generalizability of the findings summarized in this report to other populations.13,14 While this lack of data specific to HSSD that met the criteria for this report represents a gap in recent literature (i.e., published since 2017), it is notable that earlier studies identified and summarized in the 2018 PHAC SR did describe HSSD with sex partners who were HIV positive and receiving ART with a viral load of less than 200 copies/mL.12 Both studies were affected by considerable participant loss to follow-up, failing to accrue the necessary number of couple-years specified by their respective study protocols, and limiting the study power required to demonstrate an effect.13,14 In addition, both studies received funding from pharmaceutical companies, which can introduce potential for conflict of interest and risk of bias.13,14
Overall, a limitation common to all 14 primary studies included in this report was external validity, which was either limited or unclear in many of the primary studies in this report.13,14,19-21,23-30 Generalizability of the 15 included studies to the Canadian context was also limited, with no available data generated in Canada, and a broad variety of populations and health care settings with unclear representativeness to a Canadian context.13,14,18-30 Finally, none of the available evidence in this report described women who have sex with women.
Conclusions and Implications for Decision- or Policy-Making
This aim of this report was to provide a summary of evidence that has been published since 2017 and not previously captured in the 2018 PHAC SR.12 This report identified 15 eligible studies addressing the risk of sexual transmission of HIV in serodiscordant couples for whom the sex partner LWH was treated with ART.13,14,18-30 One study was an overview of SRs and MAs18 and 14 were nonrandomized cohort studies.13,14,19-30 Fourteen included studies provided data in answer to the first research question posed by this report,13,14,18-30 and 2 studies provided evidence in answer to the second research question13,14 (1 of which also contributed data to the first research question13).
Regarding the absolute risk of HIV transmission associated with sex among serodiscordant couples in whom the sex partner LWH takes ART with variable (or unreported) measure of viral load, a wide range of seroconversions was observed across the 14 eligible studies reporting relevant data,13,18-30 with incidence rates from all patients included in the studies ranging between 0 (upper limit of 95% CI = 0.84)13 and 6.4 (95% CI, 4.64 to 8.76)20 seroconversions per 100 person-years of follow-up. Of the included studies, 3 studies reported no seroconversions;13,24,25 7 studies observed rates between 0 and 2 per 100 person-years,19,21-23,26,28,29 and 5 studies reported rates exceeding 2 per 100 person-years18,20,27,29,30 (with 1 study reporting rates across subgroups only and reporting both rates between 0 and 2, and exceeding 2, per 100 person-years29). Of the 3 studies with no seroconversions reported, 1 was affected by the potentially confounding effect of PrEP in all included participants.25 The 2018 PHAC SR reported a pooled incidence rate of 0.22 (95% CI, 0.14 to 0.33) seroconversions per 100 person-years.12 It is notable that the majority of included studies in this report describing serodiscordant couples in whom the sex partners LWH had variable (or unreported) viral loads also reported incidence rates ranging between greater than 0 and less than 1 seroconversion per 100 person-years,19,21-23,26,28,29 with smaller proportions of included studies reporting rates above18,20,27,29,30 or below13,24,25 this range.
The range of observed seroconversions and rates across studies included in this report among couples for whom patients who were HIV positive had variable (including unreported) viral loads may, in part, be associated with multiple differences across study methods, populations, and exposures, including performance and reporting of phylogenetic linkage analyses that support the observed seroconversions having occurred between the sex partners under study. Additional methodological differences contributing to this broad range of findings may include retrospective versus prospective studies; study sample sizes and the representativeness of the study participants to other populations; duration of and/or adherence to ART (including measurement of the latter); and use of additional HIV-preventive interventions, such as PrEP, condoms, and/or timing of unprotected sex.13,18-30
Regarding the absolute risk of HIV transmission associated with sex among serodiscordant couples in whom the sex partner LWH was takes ART and has a suppressed viral load of less than 200 copies/mL on consecutive measurements every 4 to 6 months, 2 studies met the inclusion criteria for this report, both of which investigated MSM populations and observed no seroconversions that were phylogenetically linked.13,14 This finding was consistent with that generated by the 2018 PHAC SR, which reported pooled results from 2 earlier studies that reported no seroconversions across 1,327 observed person-years of follow-up (upper limit of 95% CI = 0.28); a finding that was later updated with additional data to 0 seroconversions (upper limit of 95% CI = 0.13).12
While the nonrandomized and unblinded methods of the studies included in this report limit the interpretation, randomized and/or blinded study designs are likely not feasible in the context of investigating association between ART use in sex partners LWH and the risk of HIV transmission associated with sex. Consequently, consideration of the methodological strengths and limitations for available studies is a critical feature of assessing the utility of evidence in this area. For instance, while only 2 studies investigating HIV transmission between serodiscordant MSM sex partners were identified (both of which provided data in answer to this report’s second research question),13,14 both studies demonstrated important strengths that were not observed in many of the studies reporting data of relevance to the first question, including representation of populations across variable national contexts, and measurement of important exposure variables, such as ART adherence, viral load, and phylogenetic linkage of observed seroconversions.13,14
Extending from this, populations represented by the available studies are an important consideration when weighing the generalizability of the evidence. Differences in HIV transmission patterns between various populations36 make the need for robust data describing these populations essential to understanding the role of ART and any associated risk of HIV transmission associated with sex between serodiscordant couples. Furthermore, differences in the use and measurement of ART and other exposures across studies are important considerations; for instance, the timing of ART initiation following diagnosis of HIV is an important variable for understanding and assessing the risk of transmission.37,38 In addition, demonstration of viral linkage is important information that can supplement self-reported data describing sexual and other risk behaviours, providing confirmatory evidence for observed seroconversions that have occurred between the sex partners under study (as opposed to those having occurred from another source).
The limitations of the included literature should be considered when interpreting the findings of this report. Furthermore, it is important to consider that this report does not provide a comprehensive summary of all available evidence addressing both research questions as it only summarizes evidence published since 2017. Future research will benefit the existing evidence base and help to inform consensus and policy by considering current gaps (i.e., high-quality, prospective studies with sufficient study power — that is, large sample sizes — representing participant characteristics, including measurement and consideration of viral load across study follow-up), critical exposure and outcomes data (including phylogenetic linkage of observed HIV transmissions), settings, and health care systems that can be generalized to broader populations and real-world contexts.
References
1.Sharp PM, Hahn BH. Origins of HIV and the AIDS pandemic. Cold Spring Harb Perspect Med. 2011;1(1):a006841-a006841. PubMed
2.World Health Organization. The top 10 causes of death. 2020; https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death. Accessed 2023 Jan 23.
3.World Health Organization Global HIV Programme. Key Facts HIV 2022; https://cdn.who.int/media/docs/default-source/hq-hiv-hepatitis-and-stis-library/key-facts-hiv-2021-26july2022.pdf?sfvrsn=8f4e7c93_5. Accessed 2023 Jan 20.
4.Public Health Agency of Canada. Estimates of HIV incidence, prevalence and Canada’s progress on meeting the 90-90-90 HIV targets, 2020. Ottawa, Canada: Public Health Agency of Canada; 2022: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/estimates-hiv-incidence-prevalence-canada-meeting-90-90-90-targets-2020.html. Accessed 2023 Jan 19.
5.Gandhi RT, Bedimo R, Hoy JF, et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2022 Recommendations of the International Antiviral Society–USA Panel. JAMA. 2023;329(1):63-84. PubMed
6.Aquaro S, Borrajo A, Pellegrino M, Svicher V. Mechanisms underlying of antiretroviral drugs in different cellular reservoirs with a focus on macrophages. Virulence. 2020;11(1):400-413. PubMed
7.Cohen MS, Chen YQ, McCauley M, et al. Antiretroviral Therapy for the Prevention of HIV-1 Transmission. N Engl J Med. 2016;375(9):830-839. PubMed
8.Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493-505. PubMed
9.Rodger AJ, Cambiano V, Bruun T, et al. Sexual Activity Without Condoms and Risk of HIV Transmission in Serodifferent Couples When the HIV-Positive Partner Is Using Suppressive Antiretroviral Therapy. JAMA. 2016;316(2):171-181. PubMed
10.Prevention Access Campaign. https://preventionaccess.org/. Accessed 2023 Mar 14.
11.Department of Justice Canada. HIV Non-Disclosure. 2022; https://www.justice.gc.ca/eng/cons/hiv-vih/nd.html#:~:text=The%20Supreme%20Court%20of%20Canada,will%20not%20constitute%20a%20crime. Accessed 2023 Jan 20.
12.LeMessurier J, Traversy G, Varsaneux O, et al. Risk of sexual transmission of human immunodeficiency virus with antiretroviral therapy, suppressed viral load and condom use: a systematic review. CMAJ. 2018;190(46):E1350-E1360. PubMed
13.Bavinton BR, Pinto AN, Phanuphak N, et al. Viral suppression and HIV transmission in serodiscordant male couples: an international, prospective, observational, cohort study. Lancet HIV. 2018;5(8):e438-e447. PubMed
14.Rodger AJ, Cambiano V, Bruun T, et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet. 2019;393(10189):2428-2438. PubMed
15.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Nov 22.
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
18.Davari M, Giwa HB, Nabizade A, Taheri F, Giwa A. Antiretroviral therapy and the risk of sexual transmission of HIV: a systematic review and meta-analysis. HIV Med. 2020;21(6):349-357. PubMed
19.Chen F, Tang H, Han J, et al. Association of HCV Prior Infection and Unprotected Sex on Subsequent HIV Acquisition Risk in the Era of Treatment as Prevention. Front Med (Lausanne). 2022;9:902271. PubMed
20.Bantigen K, Kitaw L, Negeri H, et al. Rate of HIV Seroconversion Among Seronegative Male Partners Living with HIV Positive Women in Addis Ababa, Ethiopia, 2019: A Retrospective Cohort Study. HIV AIDS (Auckl). 2021;13:125-134. PubMed
21.Nyombayire J, Ingabire R, Mukamuyango J, et al. Antiretroviral Therapy Use and HIV Transmission Among Discordant Couples in Nonresearch Settings in Kigali, Rwanda. Sex Transm Dis. 2021;48(6):424-428. PubMed
22.Arjun Bal KP, Singh LR, Singh SK, et al. Seroprevalence and seroconversion rates of human immunodeficiency virus discordant couples attending a tertiary care center: A prospective cohort study. JMS - Journal of Medical Society. 2020;34(2):91-95.
23.Dieckhaus KD, Ha TH, Schensul SL, Sarna A. Modeling HIV Transmission from Sexually Active Alcohol-Consuming Men in ART Programs to Seronegative Wives. J Int Assoc Provid AIDS Care. 2020;19. PubMed
24.Sun L, Liu A, Li J, et al. Is PrEP necessary during natural conception in HIV-1-serodiscordant couples on ART with suppressed viral load? A retrospective cohort analysis. BMC Infect Dis. 2020;20(1):195. PubMed
25.Heffron R, Ngure K, Velloza J, et al. Implementation of a comprehensive safer conception intervention for HIV-serodiscordant couples in Kenya: uptake, use and effectiveness. J Int AIDS Soc. 2019;22(4):e25261. PubMed
26.Ma G, Chen H, Chen J, Jiang Z, Ma T. HIV transmission between spouses living in Lu'an city, Anhui province, China: a longitudinal study. Epidemiol Infect. 2019;147:e205. PubMed
27.Melo MGD, Sprinz E, Gorbach PM, et al. HIV-1 heterosexual transmission and association with sexually transmitted infections in the era of treatment as prevention. Int J Infect Dis. 2019;87:128-134. PubMed
28.Chen H, Yang X, Zhu Q, et al. Treatment for HIV prevention study in southwestern areas of China. Infect Dis Model. 2018;3:249-255. PubMed
29.Liu P, Tang Z, Lan G, et al. Early antiretroviral therapy on reducing HIV transmission in China: strengths, weaknesses and next focus of the program. Sci Rep. 2018;8(1):3431. PubMed
30.Zheng Z, Li Y, Jiang Y, Liang X, Qin S, Nehl EJ. Population HIV transmission risk for serodiscordant couples in Guangxi, Southern China: A cohort study. Medicine (Baltimore). 2018;97(36):e12077. PubMed
31.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
32.Pollock M, Fernandes RM, Becker LA, Pieper D, Hartling L. Chapter V: Overviews of Reviews. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook. 2022.
33.Ayerdi Aguirrebengoa O, Vera Garcia M, Portocarrero Nunez JA, et al. Implementing pre-exposure prophylaxis could prevent most new HIV infections in transsexual women and men who have sex with men. Rev Clin Esp (Barc). 2019;219(7):360-366. PubMed
34.Grabowski MK, Redd AD. Molecular tools for studying HIV transmission in sexual networks. Current opinion in HIV and AIDS. 2014;9(2):126-133. PubMed
35.Serdar CC, Cihan M, Yücel D, Serdar MA. Sample size, power and effect size revisited: simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochemia medica. 2021;31(1):010502. PubMed
36.UNAIDS. Global HIV & AIDS statistics — Fact sheet. 2022; https://www.unaids.org/en/resources/fact-sheet. Accessed 2023 Jan 23.
37.Nanditha NGA, Dong X, Tafessu HM, et al. A province-wide HIV initiative to accelerate initiation of treatment-as-prevention and virologic suppression in British Columbia, Canada: a population-based cohort study. CMAJ Open. 2022;10(1):E27-E34. PubMed
38.Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. 2019. https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/initiation-antiretroviral-therapy. Accessed 2023 Jan 20.
39.Rodger A, Bruun T, Weait M, et al. Partners of people on ART - a New Evaluation of the Risks (The PARTNER study): design and methods. BMC Public Health. 2012;12(1):296. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Overview of Systematic Reviews
Study citation, country, funding source, search methods | Study designs and numbers of included studies | Population characteristics | Exposure | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Overview of reviews | ||||
Davari et al. (2020)18 Iran Funding source: Tehran University of Medical Sciences Search methods: Databases searched: Cochrane Library, Web of Science, EMBASE, Scopus, PubMed Central Search dates: 2007 to 2019 ROB assessment: AMSTAR | Overview of SR/MAs Number of included SRs: 10 Number of relevant SRs: 10a | Adult (> 18 years) HIV-serodiscordant couples/sex partners Population characteristics: HSSD and MSM (no other characteristics reported) | Eligible exposure: Sex partner LWH and treated with ART Eligible Comparator: Sex partner LWH not treated with ART | Outcome: HIV transmission Measures: Relative risk, incidence rate (person years) Follow-up: NR |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ART = antiretroviral therapy; HSSD = heterosexual serodiscordant; ; LWH = living with HIV; MA = meta-analysis; MSM = men who have sex with men; NR = not reported; ROB = risk of bias; SR = systematic review.
aOnly 2 of the included SRs were not overlapped by other sources in this report; thus, data from these 2 SRs are summarized herein.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design, setting, study period | Population characteristics | Exposure and comparator | Clinical outcomes, length of follow-up, testing frequency |
|---|---|---|---|---|
Chen et al. (2022)19 China Funding source: NR | Prospective cohort Setting: Local clinics and hospitals in Zhumadian Study period: 2008 to 2014 | Heterosexual HIV-serodiscordant couples/sex partners (HIV-negative partners with or without HCV) Number of participant couples, n = 4,196 Baseline characteristics (sex partners LWH only): Age, n (%): < 50 year = 3,152 (75.12) ≥ 50 year = 1,044 (24.99) Sex, n (%): Male = 1,803 (42.97) Viral load (measure NR) copies/mL, n (%)*: ≤ 400 = 2,584 (64.49) > 400 = 1,423 (35.51) CD4 count cells/µL, n (%): ≤ 350 = 2,087 (50.54) > 350 = 2,043 (49.47) *Data on baseline viral load missing for 189 participants | Exposure: Sex partner LWH takes ART; HIV-negative partner does not have HCV Viral load in sex partner LWH across follow-up: NR ART regimen, n (%): AZT + 3TC+NVP/EFV = 819 (20.31) D4T + 3TC+NVP/EFV = 1,581 (39.20) TDF + 3TC+NVP/EFV = 148 (3.67) Other = 1,485 (36.82) ART use, n (%): Prevalent = 3,439 (81.96) New = 757 (18.04) Use of PrEP in HIV-negative partner: NR Comparator: No relevant comparator | Outcome: HIV seroconversion in the HIV-negative partner Follow-up: Until the first of 2 end points: (i) HIV seroconversion (date of last HIV-negative visit for HIV-negative partners) or (ii) 31 December 2014 Total person years of follow-up = 18,370.39 |
Bantigen et al. (2021)20 Ethiopia Funding source: Addis Ababa University, Ethiopia | Retrospective cohort study Setting: PMTCT units of Addis Ababa public health institutions Study period: 2013 to 2018 | Heterosexual serodiscordant couples where sex partners LWH are female with seronegative male partners Number of participants, n = 227 couples Age of participants: Mean age of participants when identified as discordant = 26.85 years (SD 4.205) Median time to initial testing of the partner after diagnosis of index case = 8 months Last CD4 count: ≥ 350 cells/µL, n = 165 (72.7%) 250 to 350 cells/µL, n = 37 (16.3%) ≤ 200 cells/µL, n = 25 (11.0%) Number of participants with STIs, n (%): HIV positive partner = 21 (9.3%) HIV negative partner: NR | Exposure: Sex partner LWH takes ART ART in sex partner LWH: ART regimen: NR ART initiation status: Early (CD4 between 350 to 500 cells/µL), n = 125 (55.1%) Late (CD4 < 350 cells/µL), n = 102 (44.9%) ART adherence: Good, n = 187 (82.4%) Fair, n = 20 (8.8%) Poor, n = 7 (3.1%) Condom use: Consistent, n = 65 (28.6%) Inconsistent, n = 55 (24.2%) Not used, n = 59 (26%) Viral load in sex partner LWH: NR Use of PrEP in HIV-negative partner: NR Comparator: none | Outcomes: Rate of HIV seroconversion (number of seronegative partners who became positive in 100 person-year follow-up) Follow-up: till the end of the study (May 2019). Median follow up time 32 months |
Nyombayire et al. (2021)21 Rwanda Funding sources: National Institutes of Health, AIDS International Training and Research Program Fogarty International Center, Emory Center for AIDS Research, Sub-Saharan African Network for TB/HIV Research Excellence, International AIDS Vaccine Initiative, US Agency for International Development, Global Fund | Prospective cohort Setting: Government clinics in Kigali Study period: 2010 to 2014 | Heterosexual HIV-serodiscordant couples/sex partners Number of couples recruited, n = 3,777 Baseline characteristics: Number of couples with male sex partners LWH (M+/F-):1,947 Number of couples with female sex partners LWH (M-/F+): 1,830 Age by sex overall, mean (SD): Male = 35.3 (9.3) Female = 29.6 (8.7) CD4 of sex partners LWH (units NR)*, mean (SD): M+/F- = 472.5 (234.6) M-/F+ = 525.4 (269.7) Couples with current ART use in sex partner LWH at baseline, n (%): 1,684 (44.6) M+/F- couples with no contraceptive/ condom use, n (%): 640 (80.7) M-/F+ couples with no contraceptive/ condom use, n (%): 570 (76.8) *Data were available for 36% of sex partners LWH, only | Exposure: Sex partner LWH receiving ART ART regimen: NR ART adherence: NR Viral load in sex partner LWH across follow-up: NR Duration of ART in sex partners LWH at baseline, mean year (SD): 3.1 (2.3) Use of PrEP in HIV-negative partner: NR Comparator: Sex partner LWH not receiving ART | Outcomes: HIV seroconversion in the HIV-negative partner; virological linkage analysis (for couples with seroconversion in the HIV-negative partner) Follow-up: Quarterly clinic visits for HIV-negative partners Median (SD) follow-up = 1.4 (1.2) |
Arjun Bal et al. (2020)22 India Funding source: non-funded study | Prospective cohort study with a cross sectional component Setting: ART Centre of Excellence, Northeastern India Study period: 2017 to 2019 | Serodiscordant couples (age > 18 years) who had been in a stable relationship for ≥ 3 months. Number of participants, n = 90 couples Age group of couples: 64.4% (n = 58) couples were between 41 and 50 years of age. Additional details NR. CD4 cell count in the sex partners LWH: < 200 cells/µL, n = 52/80 Baseline CD4 cell count (cells/µL), mean (SD, range) = 204.88 (160.32, 13 to 769) Number of participants with STIs: NR | Exposure: Sex partner LWH takes ART ART regime: NR ART adherence: NR Viral load: NR Condom use: Consistent, n = 58 (55.29%) Seldom, n = 32 (30.6%) Use of PrEP in HIV-negative partner: NR Comparator: None | Outcomes: Rate of seroconversion Follow-up: 2 years HIV negative partner: HIV testing at every 6 months |
Dieckhaus et al. (2020)23 India Funding source: National Institute on Alcohol Abuse and Alcoholism (U01AA0219909 to 01) | Prospective cohort study with mathematical modelling. Note: only the characteristics and results relevant to the current report are summarized here. Setting: ART centers in Maharashtra, India Study period: 2015 to 2018 | Married men (≥ 18 years of age) who are LWH, who are on ART ≥ 6 months or more, and have consumed alcohol in the previous 30 days. Relevant population: Serodiscordant couples from the above cohort. Total number of participants, n = 419 Number of serodiscordant couples, n = 233 Baseline characteristics of the relevant participants: NR Viral load at baseline: NR for the relevant population (80% of the overall cohort had < 1000copies/mL at baseline) | Exposure: Male sex partner LWH takes ART ART regimen: NR ART adherence: NR (95.5% of the overall cohort had > 50% adherence) Viral load across study follow-up: NR Condom use: NR (71.4% of the overall cohort “never used” condoms) Use of PrEP in HIV-negative partner: NR Comparator: None | Outcomes: Rate of seroconversion Follow-up: 3 years |
Sun et al. (2020)24 China Funding source: Reported as “Not applicable” (p. 5 of 5) | Retrospective cohort study Setting: Hospital- and University-based clinics Study period: January 2008 to January 2018 | Heterosexual HIV-serodiscordant couples/sex partners (sex partners LWH were male) pursuing pregnancy through natural conception Number of participant couples, n = 246 HIV-negative participants who voluntarily received PrEP, n (%): PrEP = 104 (42) No PrEP = 142 (58) Baseline characteristics: Seronegative women: Age, median year (IQR): PrEP = 28 (23, 30) No PrEP = 27 (24, 31) Men LWH: Age, median year (IQR): PrEP = 30 (26, 35) No PrEP = 30 (27, 35) CD4 (summary statistics NR), cells/µL: PrEP = 543 (442, 637) No PrEP = 560 (426, 690) Viral load in sex partner LWH: Natural conception was advised for couples when the HIV positive partner had demonstrated a sustained plasma viral load of < 50 copies/mL for at least 6mo | Exposure: Male sex partner LWH receiving ART; HIV-negative female partner voluntarily receiving PrEP Comparator: Male sex partner LWH receiving ART; HIV-negative female partner voluntarily not receiving PrEP PrEP regimens: AZT + 3TC, TDF/FTC, TDF/FTC + RAL, LPV/r-based ART regimens, n (%): LPV/r based PrEP = 3 (2.9) No PrEP = 11 (7.8) RAL based PrEP = 0 (0.0) No PrEP = 1 (0.7) EFV based PrEP = 94 (92.2) No PrEP = 126 (88.7) Other PrEP = 5 (4.9) No PrEP = 4 (2.8) ART treatment duration (summary statistics NR) at baseline, year (IQR): PrEP = 3.5 (2.7, 4.5) No PrEP = 4.2 (3.3, 5.7) Condom use: At all times except for the peri-ovulatory period Viral load in sex partners LWH: NR across follow-up | Outcomes: Primary: HIV seroconversion in the HIV-negative partner Measure: HIV testing in HIV-negative partners at 6, 12 and 24 week after the last occurrence of condom-less intercourse Follow-up: 24 week* *Overall study follow-up time is not explicitly reported, but is indicated vis-à-vis the timing of HIV testing in HIV-negative partners |
Heffron et al. (2019)25 Kenya Funding sources: Eunice K. Shriver Institute for Child Health and Human Development, Fogarty International Center, National Institute of Mental Health, Gilead Sciences LLC | Prospective cohort study Setting: Clinical research facility Study period: March 2016 to April 2018 | Adult (≥ 18yr for all; ≤ 49 year for women) heterosexual HIV-serodiscordant couples/sex partners pursuing pregnancy Number of participant couples, n = 74 Baseline characteristics (all): Age, median year (IQR): 32.8 (28.0, 38.3) Education, median year (IQR): 10.0 (8.0, 12.0) Couples with male sex partner LWH (M+/F-), n (%): 40 (54) Couples with female sex partner LWH (M-/F+), n (%): 34 (46) Baseline characteristics (sex partner LWH): CD4 count, median cells/µL (IQR): 568 (389, 735) Plasma HIV RNA, median log10 copies/mL (IQR): 1.6 (1.6, 1.9) Viral suppression (plasma) < 400 copies/mL, n (%): 58 (78.4) Baseline characteristic (HIV-negative partner): PrEP initiated, n (%): 74 (100) | Exposure: Multi-component intervention including counselling to encourage ART adherence for sex partners LWH ART regimens: NR Self-reported ART use > 3mo in sex partners LWH, n (%): 53 (71.6) Visits with ART use reported in sex partners LWH, (%): Couples achieving pregnancy = 100 Couples not achieving pregnancy = 99.3 Visits with viral suppression measured in sex partner LWH, (%): Couples achieving pregnancy (in the 3mo before pregnancy) = 74.3 Couples not achieving pregnancy (across all of follow-up) = 64.6 Comparator: None | Outcomes: Primary: HIV seroconversion in the HIV-negative partner Follow-up: Monthly (including HIV testing for HIV-negative partners) until the latest of 2 end points: (i) 12 months; (ii) end of pregnancy Total person years of follow up = 146.4 |
Ma et al. (2019)26 China Funding source: Non-funded | Retrospective cohort study Setting: Local clinics and hospitals in Lu’an Study period: 1999 to 2016 | Serodiscordant heterosexual married couples who had been in a stable relationship for > 6 months.a Total study cohort, n = 231 couples Relevant study cohort,a number of participants, n = 186 couples Characteristics of the total study cohort (N = 231): Age of sex partners LWH, mean (SD): Males = 41.86 (11.09) years Females = 34.54 (10.01) years P < 0.001 Sex: Males, n (%) = 167/231 (72.29%) Baseline characteristics of the relevant subgroup: NR | Exposure: Sex partner LWH takes ART ART in sex partner LWH: Started on ART within a month of diagnosis, n = 119/186 (63.98%) No ART initiation within a month of diagnosis, n = 67/186 (36%) ART regimen: NR ART adherence: NR Viral load in sex partner LWH: NR Condom use: NR Use of PrEP in HIV-negative partner: NR Comparator: None | Outcomes: Rate of seroconversion during follow-up period Follow-up: Till the end of the study (December 2016). There were 507.7 person years HIV negative partner: HIV testing at every 6 months |
Melo et al. (2019)27 Brazil Funding source: UCLA AIDS Institute and UCLA CFAR, NAID, NIH | Retrospective cohort study Setting: HIV/AIDS couples clinic in Porto Alegre, Brazil. Study period: 2014 to 2016 | Heterosexual serodiscordant couples/sex partners who had been in a stable relationship for ≥ 3 months. Number of participants, n = 200 couples Among the sex partners LWH: 140 (70%) were female. Age, mean (SD) years: sex partner LWH = 38.2 (9.8) years HIV negative partner = 39.9 (11.9) years Viral load in sex partner LWH at baseline: Measured viral load in copies/mL, median (range) = 0 (0 to 153,992) Genital viral load in HIV positive female partners (n = 140) Undetectable viral load (< 40 copies/mL), n (%) = 133 (95%) Detectable viral load, n (%) = 7 (5%) CD4 cell count in the sex positive partner LWH: < 350 cells/µL, n = 39 (19.5%) CD4 cell count, median (range), cells/µL = 602.5 (41.0 to 1658) Number of participants with STIs, n (%): sex partner LWH = 56 (28%) HIV negative partner = 29 (14.5%) | Exposure: Sex partner LWH takes ART and on regular follow-up ART in sex partner LWH: ART Regimen: NR Years on ART: NR ART adherence: NR Viral load across study follow-up: not clearly reported Condom use: Unprotected vaginal sex reported in 37.2 to 37.9 participants. Unprotected anal sex reported in 6 to 10.2% participants. Use of PrEP in HIV-negative partner: NR Comparator: None | Outcomes: Transmission incidence rate (in person-months) Follow-up: Every 6 months until the end of the study (December 2016) Median follow up per couple = 4.5 years (range 0.3 to 21.7 years) HIV negative partner: HIV testing at every 6 months |
Rodger et al. (2019)14 PARTNER2 UK (14 European countries) Funding source: NIHR, BHIVA, Danish National Research Foundation, Viiv health care, Gilead sciences, Augustinus Fonden and AP Moller Fonden. | Single arm prospective cohort study Setting: 75 sites across 14 European countries Study period: 2010 to 2017 | Gay male serodiscordant couples Inclusion criteria: both partners were ≥ 18 years of age, had penetrative sex with or without condoms in the month before enrolment, expected to have sex together again after enrolment, consent of both partners obtained. Exclusion criteria (for analysis): HIV negative partner using PEP or PrEP, reported no condomless sex, viral load of the sex partner LWH > 200 copies/mL, absence of viral load data, absence of HIV testing in the HIV negative partner. Number of participants, n = 782 couples (340 of whom were from PARTNER1)9 Age, median (IQR), years: sex partner LWH = 40.0 (33.3 to 46.1) years HIV negative partner = 37.6 (30.9 to 45.3) years CD4 cell count in the sex partner LWH: > 350 cells/µL, n = 730 (93%) ≤ 350 cells/µL, n = 51 (7%) Number of participants with STIs, n (%): sex partner LWH = 214 (27%) HIV negative partner = 185 (24%) | Exposure: Sex partner LWH takes suppressive ART and has viral load < 200 copies/mL ART Regimen: NR ART in sex partner LWH: Years on ART, median (IQR) = 4.3 (1.8 to 9.3) Self-reported ART adherence, n (%): ≥ 90% = 739 (98%) < 90% = 14 (2%) Viral load in sex partner LWH at baseline: Undetectable viral load (< 50 copies/mL), n (%) = 754 (97%) Measured viral load: < 200 copies/mL, n (%) = 774 (99%) ≥ 200 copies/mL, n (%) = 7 (< 1%) Condom use: NR, only condomless acts were included in the analysis. Use of PrEP in HIV-negative partner: data for participants exposed to PrEP were removed from the analyses Comparator: None | Outcomes: Rate of phylogenetically linked HIV infections. (Number of linked HIV infections / couple years of follow up) Follow-up: 1593 couple years. Median follow up per couple = 2 years (IQR 1.1 to 3.5 years) HIV negative partner: HIV testing baseline and every 6 to 12 months Sex partner LWH: Viral load tested baseline and every 6 to 12 months. |
Bavinton et al. (2018)13 Australia, Brazil, Thailand Funding source: National Health and Medical Research Council; amfAR, The Foundation for AIDS Research; ViiV Health care; and Gilead Sciences | Prospective cohort study Setting: 13 Australian clinics; 1 Brazilian clinic; 1 Thai clinic (no other information reported) Study period: May 2012 to March 2016 | HIV serodiscordant male same-sex couples/sex partners Number of participant couples, n = 343 Baseline characteristics (sex partner LWH): Age, median year (IQR): 34.4 (27,7, 43.9) Sex with outside partner(s), n (%): Any = 136 (40) CLAI = 59 (17) Viral load (measure NR) in the sex partner LWH, copies/mL, n (%): < 200 = 267 (78) ≥ 200 = 76 (22) Daily PrEP use by the HIV-negative partner in the past 3mo, n (%): 26 (8) ART use at baseline in sex partner LWH, n (%): 274 (80) ≥ 90% adherence to ART in the past 3mo at baseline (among 274 sex partners LWH and taking ART): 241 (88) Condom use/CLAI in the past 3mo, n (%): Always condoms/no CLAI = 156 (45) Some condoms/CLAI = 126 (37) Always CLAI = 61 (18) Any STI, n (%): Sex partner LWH = 46 (13) HIV-negative partner = 39 (11) | Exposure: Sex partners LWH were virally suppressed (most of whom were using ART) ART regimens: NR ART use in sex partner LWH during follow-up, n (%): Never = 6 (2) Initiated during follow-up = 85 (25) Always = 252 (73) Viral load in sex partner LWH during follow-up, n (%): Consistently < 200 copies/mL = 258 (75) Variably > / < 200 copies/mL = 78 (23) Consistently ≥ 200 copies/mL = 7 (2) Daily PrEP use by the HIV-negative partner anytime during follow-up, n (%): 115 (34) Comparator: None | Outcomes: Primary: HIV seroconversion in the HIV-negative partner with viral load monitoring and phylogenetic linkage demonstrated Follow-up: At least 2 clinic visits per year Viral load monitoring was every 3 to 6 months Total couple years of follow-up = 588.4 Median follow-up/couple (IQR) = 1.7 (0.9, 2.2) |
Chen et al.(2018)28 China Funding sources: Guangxi Medical and Health Project (Z20170126), Guangxi Science and Technology Bureau (Grant AB16380213), National Natural Science Foundation of China (Grants 81502862, 81460510 and 81360442), Guangxi Bagui Honour Scholarship, Ministry of Science and Technology of China (2017ZX10201101, 2018ZX10721102 to 006), and Chinese State Key Laboratory of Infectious Disease Prevention and Control | Retrospective cohort study Setting: China CDC database from Guangxi, China Study period: 2003 to 2014 | Heterosexual serodiscordant couples Number of participants, n = 7,713 couples Age of sex partner LWH, years, n 18 to 24 years, n = 578 ≥ 25 years, n = 6726 Sex of sex partner LWH: Males, n = 5432 Females, n = 1872 CD4 cell count in the sex partner LWH: ≥ 500cells/µL, n = 824 < 500 cells/µL, n = 5648 Missing, n = 832 Number of participants with STIs: NR | Exposure: Sex partner LWH takes ART (On ART group, N = 5828 couples) ART in sex partner LWH: ART regimen: NR Years on ART: NR ART adherence: NR Viral load in sex partner LWH: NR Condom use: NR analysis. Use of PrEP in HIV-negative partner: NR Comparator: Treatment naïve HIV positive partner (ART naïve group), n = 1885 couples | Outcomes: Rate of seroconversion, time to seroconversion Follow-up: Till end of the study in 2014. Overall, 18985.29 person years of follow-up. HIV negative partner: HIV testing baseline and every 6 months Sex partner LWH: Follow up every 6 months. |
Liu et al. (2018)29 China Funding source: National Natural Science Foundation of China (81502862, 81360442, 81460510), Guangxi Science and Technology Bureau (AB16380213), Guangxi Bagui Honour Scholars, Ministry of Science and Technology of China (2012ZX10001 to 002), Chinese State Key Laboratory of Infectious Disease Development Grant, and the International Development Research Center of Canada (grant #104519 to 010). | Retrospective cohort study Setting: Guangxi, China, data source NR Study period: 2003 to 2014 | Heterosexual serodiscordant couples Number of participants, n = 13,132 couples Based on baseline CD4 cell counts and time of initiation of ART in the sex partner LWH, participants were of 3 groups: Late ART group, n = 1339 Mid-ART group, n = 7496 Early ART group, n = 4297 Age of sex partner LWH, years, n(%) Late ART group: ≤ 30 = 456 (34.06) 31 to 40 = 494 (36.89) 41 to 50 = 257 (19.19) > 50 = 132 (9.86) Mid-ART group: ≤ 30 = 1899 (25.33) 31 to 40 = 2088 (27.85)) 41 to 50 = 1430 (19.08) > 50 = 2079 (27.73) Early ART group: ≤ 30 = 665 (15.48) 31 to 40 = 1129 (26.27) 41 to 50 = 1068 (24.85) > 50 = 1435(33.4) Sex of sex partner LWH, n (%): Late ART group: Male = 924 (69.01) Female = 415 (30.99) Mid ART group: Male = 5488 (73.21) Female = 2008 (26.79) Early ART group: Male = 3423 (79.66) Female = 874 (20.34) Number of participants with STIs: NR | Exposure: Sex partner LWH takes ART. Years on ART: NR Type of ART: NR Viral load in the sex partner LWH: NR Use of PrEP in HIV-negative partner: NR Comparator: Sex partner LWH not taking ART (estimated from the group of participants not receiving ART from clinic based on attrition rates in a 6-month cohort) including the pre-treatment group Late ART group: On ART, n = 636 Non-ART, n = 703 Mid-ART group: On ART, n = 3079 Non-ART, n = 4417 Early ART group: On ART, n = 2113 Non-ART, n = 2184 | Outcomes: Rate of seroconversion Follow-up: Till the end of the study (December 2014). HIV negative partner: HIV testing baseline and every 6 months Sex partner LWH: Clinical follow up every 6 months. |
Zheng et al. (2018)30 China Funding source: Guangxi Medical Project of Appropriate Technology Development and Applied Fund, code: S2016 82 | Retrospective cohort study Setting: Guangxi, China Study period: January 1, 2010 to December 31, 2010 | Heterosexual couples/sex partners (≥ 15yr) with 1 sex partner LWH (HIV status of the 2nd partner was either negative or unknown at baseline) Number of couples, n = 5,544 Baseline characteristics (sex partner LWH): Sex, n (%): Male = 4,095 (73.86) Age in year, n (%): 15 to 34 = 1,749 (31.55) 35 to 64 = 2,833 (51.64) 65* = 927 (16.72) Unknown = 5 (0.09) HIV testing status of HIV-negative partner at baseline as described in Table 1 (p. 3), n (%)**: Ever tested = 1,207 (21.77) Never tested = 4,337 (78.23) HIV testing status of HIV-negative partner at baseline as described in the narrative report of findings (p. 4), n (%)**: Ever tested = NR (49.9) Never tested = NR (51.1) Use of ART at baseline, n (%): Yes = NR No = NR CD4 count (summary statistic NR) cell/µL, n (%)***: ≤ 500 = 2,121 (38.25) > 500 = 334 (6.02) Missing = 3,084 (55.72) *Authors do not specify whether this age category included > 65yr **Discordant findings are described for this variable within the report ***Data do not sum to 100%; the reason for this is NR | Exposure*: Sex partner LWH using ART: ART regimen: NR Duration of ART: NR Adherence to ART: NR Viral load in sex partner LWH: NR Use of PrEP in HIV-negative partner: NR Comparator: Sex partner LWH ART-naïve: *ART is not a primary exposure of interest in the study and few data are reported describing this exposure | Outcomes: HIV seroconversion in the HIV-negative partner Follow-up: 6mo and 12mo from baseline Total person years of follow-up = 2,731.85 |
3TC = lamivudine; AIDS = AIDS; ART = antiretroviral therapy; AZT = zidovudine; CD4 = cluster of differentiation 4; CDC = Center for Disease Control and Prevention; CLAI = condomless anal intercourse; D4T = stavudine; EFV = efavirenz; FTC = emtricitabine; HCV = hepatitis C virus; IQR = Interquartile range; LPV/r = lopinavir/ritonavir; M+/F- = male partner positive, female partner negative; LWH = living with HIV; M-/F+ = male partner negative, female partner positive; n = number; NR = not reported; NVP = nevirapine; PEP = post-exposure prophylaxis; PMTCT = Prevention of Mother to Child Transmission; PrEP = pre-exposure prophylaxis; RAL = raltigravir; SD = standard deviation; RNA = ribonucleic acid; STI = sexually transmitted infections; TDF = tenofovir.
aThe study cohort included serodiscordant and seroconcordant couples (where both partners were HIV positive at the time of diagnosis and one partner was determined to be infected from the other). Only the characteristics and results of the relevant population i.e., serodiscordant couples where the sex partner LWH takes ART is summarized in the current report.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Overview of Systematic Reviews Using AMSTAR 216
Strengths | Limitations |
|---|---|
Davari et al. (2020)18 | |
Study eligibility criteria were clearly described. Authors developed a protocol describing the methods a priori and registered it within the PROSPERO database A comprehensive electronic literature search strategy was described Study selection at the title and abstract stage was performed in duplicate The rationales for exclusion of sources were reported aggregately in the PRISMA diagram Risk of bias for included SRs was assessed using the AMSTAR-2 checklist Appropriate tests of heterogeneity were conducted Heterogeneity and risk of bias were discussed in the interpretation of results, including description of sensitivity analyses The source of funding and COIs for the overview were clearly reported | There was no mention of a grey literature search The description of some included studies was sufficiently unclear, requiring review of the included study to support interpretation of the findings of the overview report Excluded studies were not listed Overlap between the primary studies of included SRs was not discussed; no citation matrix was presented; no methods for avoiding over-representation of overlapped studies were described Duplicate data abstraction was not clearly described Heterogeneity among included studies was identified as being significant There was no mention of the risk of transitivity The risk of publication bias was not mentioned Sources of funding for included studies were not reported |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; COI = conflict of interest; PRISMA = Preferred Reporting Items in Systematic Reviews and Meta-Analyses; PROSPERO = International prospective register of systematic reviews; SR = systematic review
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist17
Strengths | Limitations |
|---|---|
Chen et al. (2022)19 | |
The objective of the study was clearly described. The main study outcome was described in the methods section. It was valid and appropriate for the study objective. The definitions of various terms used in the study were provided. Baseline characteristics of the sex partners LWH including baseline viral load and information describing exposures were reported. While there was no randomization or blinding used in this observational study, the authors report enrollment of all eligible couples in the jurisdiction across follow up. The study outcome (rate of seroconversion) was clearly described. Estimates of random variability (e.g., confidence intervals) were provided. | Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. Characteristics of HIV-negative participants (other than HCV status) were not provided, limiting the extent to which the potential impact of these variables can be assessed Authors note that the population under study was largely older, cohabiting, and monogamous; thus, findings of the study may bear limited generalizability to other populations. While the authors indicate that informed consent was sought and obtained for all participants, numbers of patients who refused to provide consent to participate are not reported. Since no description of viral/phylogenetic linkage-testing was reported, it is not possible to confirm whether cases of seroconversion were transmitted from the sex partner LWH. Since no information concerning the use of PrEP in HIV-negative partners was reported, it is unclear whether this may have been a potentially confounding exposure. Characteristics of participants lost to follow-up were not reported. Adverse effects were not described. Study power was not addressed |
Bantigen et al. (2021)20 | |
The objective of the study was clearly described. The main study outcome was described in the methods section. It was valid and appropriate for the study objective. The definitions of various terms used in the study were provided. Baseline characteristics of the sex partners LWH were reported. Parameters such as timing of ART initiation, ART adherence, CD4 levels, time to testing of the seronegative partner, and sociodemographic variables were reported. Most sex partners LWH had good or fair ART adherence. The study outcome (rate of seroconversion) was clearly described. Estimates of random variability (e.g., confidence intervals) were provided. Participant couples were identified from multiple hospitals and clinics that provided ART service. The staff places and facilities where they were treated is likely representative of the treatment majority of people might receive in a similar country. | This was a single group retrospective cohort study using medical records. There was no randomization or blinding. Among the 628 serodiscordant couples screened for inclusion, 63.8% (n = 401) did not meet inclusion criteria due to lack of partner follow-up, or lost or incomplete medical records. Therefore, it is not known whether the excluded serodiscordant couples had a different outcome compared to those included. Viral load of the sex partners LWH was not reported. It was also not clear whether the HIV negative partner were exposed to PreP. These are potential confounding factors which were not considered in the study. Since no phylogenetic linkage-testing was undertaken, it is not possible to confirm whether the cases of seroconversion were transmitted from the index partner. Since no information concerning the use of PrEP in HIV-negative partners was reported, it is unclear whether this may have been a potentially confounding exposure. Since follow-up data was collected until the end of the study, participants were followed up for different durations depending on the time of entering the cohort. It was unclear whether there were seroconversions outside of the study period, which could affect the findings. |
Nyombayire et al. (2021)21 | |
The objective of the study was clearly described. Baseline characteristics of the recruited couples were reported. The main study outcomes were described in the methods section. They were valid and appropriate to the study objective. The primary exposure (i.e., ART) was sufficiently described. External validity was supported by the prospective method and real-world setting from which participants were recruited i.e., participant couples were identified from multiple, non-research government clinics that provided testing, counselling, and ART services The study findings were clearly described. Estimates of random variability (e.g., confidence intervals) were provided. Virological linkage analyses were used to indicate whether HIV transmission did or did not occur between the participant couple | Blinding/randomization were not possible, due to the real world setting in which the study was conducted Information on non-participants (i.e., those who chose not to participate in the study) was not provided Viral load of the sex partners LWH was not reported. Use of ART by sex partners LWH was self-reported and levels of adherence could not otherwise be validated Since no information concerning the use of PrEP in HIV-negative partners was reported, it is unclear whether this may have been a potentially confounding exposure. There was considerable loss to follow up (i.e., 35%) which could introduce the risk of confounding and compromise the internal validity of the study findings The characteristics of participants lost to follow up were not detailed Adverse effects were not described. Study power was not addressed |
Arjun Bal et al. (2020)22 | |
The objective of the study was clearly described. The definitions of various terms used in the study were clearly described. They were appropriate. The main study outcome was described in the methods section. It was valid and appropriate for the study objective. The inclusion and exclusion criteria for the participants were also reported. Around 98% participants were followed up to the end of the study (2 years). Thus, the study had good retention rates. The source population comprised of all serodiscordant couples (n = 135) attending the study centre. Thus, the patients asked to participate were likely representative of the entire population from which they were recruited. The staff, facilities, and places where the participants were treated were likely representative of the treatment majority of patients in a similar setting would receive. According to the sample size calculation reported, the study had sufficient power to detect a clinically important effect. | This was a single arm prospective cohort study. Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. Summary statistics were not specified for baseline characteristics (e.g., age), making interpretation difficult. The details of the ART (type of regime, adherence) were not reported, making the interpretation of results challenging. This could also affect the external validity of the results. Viral load of the sex partners LWH was not measured and reported. Estimates of random variability (e.g., 95% CI) were not reported for the main study outcome. It was unclear whether the HIV negative partner were exposed to PreP. PrEP use is a potential confounding factor which could affect transmission of HIV. Potential confounding factor such as condom use, and the frequency of sexual contact was reported. However, an adjusted analysis accounting for these factors were not available in the publication. Since no phylogenetic linkage-testing was undertaken, it is not possible to confirm whether the cases of seroconversion were transmitted from the index partner. The characteristics of patients lost to follow up (albeit few) were not reported. It is unclear whether there were incidences of seroconversion in among them. |
Dieckhaus et al. (2020)23 | |
The objective of the study was clearly described. Baseline characteristics of the sex partners LWH (study participants) were reported. The main study outcomes were described in the methods section. They were valid and appropriate to the study objective. The definitions of various terms used in the study were provided. | This was a mathematical modelling study with retrospective data. Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. Due to limited reporting and lack of details regarding methodology of the analysis relevant to the current report, a detailed critical appraisal was not possible. Some of the key limitations are listed below. The study enrolled men LWH were on ART. (not serodiscordant couples). HIV negative spouses were identified based on self-reporting. Characteristics of the seronegative partners were not reported. The seronegative partners were not followed up in the study. Incidences of seroconversion among them were mentioned as “reported to have”. Without objective testing of the partners, an accurate picture of seroconversions is unable to portray. Additionally, since no phylogenetic linkage-testing was undertaken, it is not possible to confirm whether the cases of seroconversion were transmitted from the index partner. Even though factors such as condom use, and viral load is presented, an adjusted analysis accounting for these was not available in the publication. Since no information concerning the use of PrEP in HIV-negative partners was reported, it is unclear whether this may have been a potentially confounding exposure. |
Sun et al. (2020)24 | |
The objective of the study was clearly described. Baseline characteristics of the recruited couples were reported. The main study outcomes were described in the methods section. They were valid and appropriate to the study objective. The study exposures and outcomes were described in sufficient detail Data describing HIV-negative partners who were or were not using PrEP were reported separately, enabling assessment of the extent to which this may have been a potentially confounding exposure. Study power was addressed by the authors | Blinding/randomization were not possible, due to both the program/exposure under study, as well as the retrospective methods used in the study Summary statistics were not specified for some baseline characteristics, making interpretation difficult Information on non-participants (i.e., those who may not have continued with the program/exposure, or those who chose not to participate in the study) was not provided Information on compliance (or lack thereof) with the intervention(s) was not explicated The time frame within which couples were studied spanned 10 years; no information was provided concerning any differences across time that may have been present in the care and/or treatment being provided External and internal validity (including generalizability and representativeness) are unclear due to the retrospective method used in the study and the potential for selection bias imposed by the limitation of data from certain clinics and couples Since no description of viral/phylogenetic linkage-testing was reported, it is not possible to confirm whether cases of seroconversion were transmitted from the sex partner LWH. Adverse effects were not described. Study power was acknowledged as being low by virtue of the small sample size analyzed. |
Heffron et al. (2019)25 | |
The objective of the study, main study outcomes and baseline characteristics of study participants were clearly described. Outcomes and measures were valid and appropriate to the study objective. Use of and levels of adherence to ART by sex partners LWH was described The study outcomes were clearly described. Estimates of random variability (e.g., confidence intervals) were provided. Adverse effects of ART were described. | Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. Information on non-participants (i.e., those who chose not to participate in the study) was not provided Representativeness of the study population and intervention provided were unclear, due to the research setting within which the study was conducted. Use of ART by sex partners LWH were self-reported and levels of adherence could not otherwise be validated Since no description of viral/phylogenetic linkage-testing was reported, it is not possible to confirm whether cases of seroconversion were transmitted from the sex partner LWH. All HIV-negative partners initiated PrEP during study follow up, constituting a potentially confounding exposure. There was considerable loss to follow up (i.e., > 13%) which could introduce the risk of confounding and compromise the internal validity of the study findings The characteristics of participants lost to follow up were not detailed Study power was not addressed |
Ma et al. (2019)26,a | |
The objective of the study was clearly described. The main study outcome was described in the methods section. It was valid and appropriate for the study objective. The inclusion and exclusion criteria for the participants were also reported. The study outcome (rate of seroconversion) was clearly described. Estimates of random variability (e.g., confidence intervals) were provided. | This was a single arm retrospective cohort study. Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. Baseline characteristics of the relevant population was not reported. Details about ART regimen, adherence, condom use and viral load were not reported. Since these are potential confounders, the internal validity of the results could be low due to lack of reporting. Since no phylogenetic linkage-testing was undertaken, it is not possible to confirm whether the cases of seroconversion were transmitted from the index partner. Since no information concerning the use of PrEP in HIV-negative partners was reported, it is unclear whether this may have been a potentially confounding exposure. The numbers and characteristics of patients lost to follow up were not reported. It is unclear whether there were incidences of seroconversion in among them. Since follow-up data was collected till the end of the study, participants were followed up for different durations depending on the time of entering the cohort. It was unclear whether there were seroconversions outside of the study period, which could affect the findings. It was unclear whether the study participants were representative of the source population. Details on loss to follow-up were also not reported. It was unclear whether the staff, places, and facilities where the patients were treated were representative of the care majority of patients would receive. Since the study cohort was from 1999 to 2016, it is possible that ART availability and coverage were different from the present day. Therefore, the external validity of the results is likely low. Study power was not addressed. |
Melo et al. (2019)27 | |
The objective of the study was clearly described. The main study outcome was described in the methods section. It was valid and appropriate for the study objective. The inclusion and exclusion criteria for the participants were also reported. The study outcome (rate of seroconversion) was clearly described. Estimates of random variability (e.g., confidence intervals) were provided. Baseline characteristics of the recruited couples were reported. Potential confounders like viral load, condom use, and STI were reported. Adjusted analyses were conducted. It was likely that the staff, places, and facilities where the patients were treated were representative of the care majority of patients would receive in a similar setting. | This was a single arm retrospective cohort study. Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. It was unclear whether the study participants were representative of the source population as the details were not reported. Only the individuals who answered the questionnaires were included in the study. Details on missing data was not reported. Details about ART such as the regimen, adherence, and duration of ART were not reported. Viral load of the sex partners LWH was not reported. Since follow-up data was collected till the end of the study, participants were followed up for different durations depending on the time of entering the cohort. It was unclear whether there were seroconversions outside of the study period, which could affect the findings. Since no phylogenetic linkage-testing was undertaken, it is not possible to confirm whether the cases of seroconversion were transmitted from the index partner. Since no information concerning the use of PrEP in HIV-negative partners was reported, it is unclear whether this may have been a potentially confounding exposure. Study power was not addressed. |
Rodger et al. (2019)14 (PARTNER2) | |
The objective of the study was clearly described. The study protocol (for PARTNER1 trial) was published a priori and was available for review.39 Inclusion and exclusion criteria for study participants were clear. Baseline characteristics of the included participants (both sex partners LWH and HIV negative partners) were reported. Use of ART by sex partners LWH were validated using measurement of viral load. Only couples in which the sex partner LWH had a viral load < 200 copies/mL were included in the analysis. The main study outcomes were described in the methods section. They were valid and appropriate to the study objective. Main findings of the study were clearly described, with simple outcome data, estimates of random variability, as well as adjusted analysis accounting for possible potential confounding factors. Some potential confounding factors (such as PrEP use in the HIV negative partner, condom use) were considered in the inclusion criteria, and were excluded from the analysis. This could increase the internal validity of the study. Phylogenetic linkage testing of the transmitted cased was undertaken to ensure whether the transmission was within-couple. This increased the internal validity of the results. The study was conducted in 75 centers across 14 European countries. All patients receiving ART were screened for study eligibility. Thus, the patients asked to participate were likely representative of the entire population from which they were recruited. The staff, facilities, and places where the participants were treated were likely representative of the treatment majority of patients in a similar setting would receive. The authors declared that the funders had no role in study design, conduct, analysis or writing of the report. | This was a single arm prospective cohort study. Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. The study population (n = 782 couples) included those enrolled in the first part of the trial (340 couples from PARTNER1) which was published earlier.9 Thus, there is some overlap of data between the 2 studies. From all couples recruited for the study (N unclear), 499 couples dropped out of the study due to various reasons (e.g., couple broke up, consent withdrawn). They were not included in the analysis. Additionally, 479 couple years of follow-up (23%) were deemed ineligible for analysis due to reasons such as use of PrEP, condom use, lack of viral load data and missing data. It is unclear whether the study outcomes would have been different for those excluded from the analysis. Their characteristics were not reported. According to the sample size calculation reported, sufficient number of participants were enrolled to ensure adequate power to detect a clinically important effect. However, the expected number of couple-years of follow-up was not met. The study received funding from pharmaceutical companies. |
Bavinton et al. (2018)13 | |
The objective of the study was clearly described. The study outcomes were described in the methods section and were valid and appropriate to the study objective. Baseline characteristics of the both sex partner LWH and HIV-negative partner were reported. The primary exposure (i.e., ART) was sufficiently described. Use of ART by sex partners LWH were validated using measurement of viral load While there was considerable loss to follow up (i.e., > 30%) authors report that participant characteristics did not differ across those that completed vs. those that did not complete follow-up The study outcome (rate of seroconversion) was clearly described. Estimates of random variability (e.g., confidence intervals) were provided. Phylogenetic linkage testing of the transmitted cased was undertaken to ensure whether the transmission was within-couple. This increased the internal validity of the results. Data describing HIV-negative partners who were or were not using PrEP were reported separately, enabling assessment of the extent to which this may have been a potentially confounding exposure. Study power calculations were clearly described. | Blinding/randomization were not possible Authors note that the population under study was largely older, cohabiting, and monogamous; thus, findings of the study may bear limited generalizability to other populations. Numbers and characteristics of patients who refused to provide consent to participate were not reported. Representativeness of the study participants could not be ascertained from the description of the study recruitment procedures; authors concede this as a limitation of their study i.e., that recruitment occurred in urban settings with patients connected to adequate health care resources. Recall bias may have affected self-reporting of some variables e.g., treatment adherence, number/type of sex acts Loss to follow-up may have impacted the number of linked transmissions observed Adverse effects were not described. The study was not able to accrue the required number of person years of follow-up to achieve sufficient power The study received funding from pharmaceutical companies. |
Chen et al.(2018)28 | |
The objective of the study was clearly described. The main study outcome was described in the methods section. It was valid and appropriate for the study objective. The inclusion and exclusion criteria for the participants were also reported. Main findings of the study were clearly described, with simple outcome data, estimates of random variability, as well as adjusted analysis accounting for possible potential confounding factors (e.g., age, time of initial ART, sociodemographic factors). Source population from which the study participants were identified was clear. It was likely that the staff, places, and facilities where the patients were treated were representative of the care majority of patients would receive in a similar setting. | This was retrospective cohort study. Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. The numbers and characteristics of patients lost to follow up were not reported. It is unclear whether there were incidences of seroconversion in among them. Baseline characteristics of the relevant population was not reported. Details about ART regimen, adherence, condom use, viral load of the sex partner LWH, and PrEP use in the HIV negative partner were not reported. Since these are potential confounders, the internal validity of the results could be low due to lack of reporting. Since no phylogenetic linkage-testing was undertaken, it is not possible to confirm whether the cases of seroconversion were transmitted from the index partner. Since follow-up data was collected till the end of the study, participants were followed up for different durations depending on the time of entering the cohort. It was unclear whether there were seroconversions outside of the study period, which could affect the findings. Study power was not addressed. |
Liu et al. (2018)29 | |
The objective of the study was clearly described. The main study outcome was described in the methods section. It was valid and appropriate for the study objective. The inclusion and exclusion criteria for the participants were also reported. The study outcome (rate of seroconversion) was clearly described. Estimates of random variability (e.g., confidence intervals) were provided. Main findings of the study were clearly described, with simple outcome data, estimates of random variability, as well as adjusted analysis accounting for possible potential confounding factors. Participants who were lost to follow up were right-censored on the date of last contact and included in the analysis. | This was retrospective cohort study. Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. Baseline characteristics of study participants were reported. However, distribution of potential confounding factors (e.g., condom use) and demographic factors between exposure and comparator groups were not reported. Viral load of the sex partners LWH was not reported. Comparator group (Non-ART group) was defined based on attrition in a 6 month cohort, who were no longer receiving ART at their treatment centre. The validity of that definition was unclear. Details about ART such as the regimen, adherence, and duration of ART were not reported. Since no phylogenetic linkage-testing was undertaken, it is not possible to confirm whether the cases of seroconversion were transmitted from the index partner. Since no information concerning the use of PrEP in HIV-negative partners was reported, it is unclear whether this may have been a potentially confounding exposure. Since follow-up data was collected till the end of the study, participants were followed up for different durations depending on the time of entering the cohort. It was unclear whether there were seroconversions outside of the study period, which could affect the findings. It was unclear whether the staff, places, and facilities where the patients were treated were representative of the care majority of patients would receive. Since the study cohort was from 2003 to 2016, it is possible that ART availability and coverage were difference from the present day. Therefore, the external validity of the results is likely low. Study power was not addressed |
Zheng et al. (2018)30 | |
The objective of the study was clearly described The main study outcome and measurement were described in the methods section. It was valid and appropriate to the study objective The study outcome (rate of seroconversion) was described Estimates of random variability (e.g., confidence intervals) were provided | Blinding/randomization were not possible, due to both the study design and the nature of exposure of the study. No information was reported describing patients who did not agree to participate in the study Participant loss to follow up is mentioned in the methods but actual loss to follow-up is NR External validity could not be ascertained i.e., the representativeness of the participants, staff, and settings where the patients were treated was unclear due to insufficient detail reported HIV-status of non-HIV-positive partners at baseline was not clear for > 78% of couples/sex partners; there are variable reports of numbers of participants with HIV-negative or unknown testing status across the report. Viral load of the sex partners LWH was not reported. Imputation of data for HIV-status is reported as having been input for some participants in the methods, but actual values are not reported in the results The report is unclear as to which partner is HIV-positive vs. HIV-negative, with multiple unspecified references simply to 'spouse/partner' Few relevant exposure data that may affect HIV transmission are reported e.g., ART adherence, duration of ART use, ART regimens Since no description of viral/phylogenetic linkage-testing was reported, it is not possible to confirm whether cases of seroconversion were transmitted from the sex partner LWH. Since no information concerning the use of PrEP in HIV-negative partners was reported, it is unclear whether this may have been a potentially confounding exposure. Denominators are missing for some key outcome data Adverse effects were not described. Study power was not addressed |
ART = antiretroviral therapy; CD4 = cluster of differentiation 4; CI = confidence interval; HCV = hepatitis C virus; LWH = living with HIV; NR = not reported; PrEP = pre-exposure prophylaxis; STI = sexually transmitted infection
aThe study cohort included serodiscordant and seroconcordant couples (where both partners were HIV positive at the time of diagnosis and one partner was determined to be infected from the other). Only the characteristics and results of the relevant population i.e., serodiscordant couples where the sex partner LWH takes ART is summarized in the current report.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — HIV Seroconversion in Single-Arm Studies of Those With Any Viral Load
Study citation and study design | Baseline viral load (copies/mL) of sex partners LWH, participants, n (%) | Population, sample size and follow-up | Number of seroconversions | Rate of seroconversions (95%CI) per 100 py |
|---|---|---|---|---|
Chen et al. (2022)19 Prospective cohort | ≤ 400,n = 2,584 (64.49%) > 400, n = 1,423 (35.51%) | HSSD N = 4,196 18370.39 py of follow-up | 81 | 0.44 (0.43 to 0.45) |
Bantigen et al. (2021)20 Retrospective cohort | NR | HSSD N = 227 | 38 (16.7%) | 6.4 (4.64 to 8.76) |
Arjun Bal et al. (2020)22 Prospective cohort | NR | N = 88 | 2 | 1.14 (95% CI NR) |
Dieckhaus et al. (2020)23 Prospective cohort | NR | HSSD N = 233 | 1 | 1.43 (95% CI NR)a |
Sun et al. (2020)24 Retrospective cohort | NR | HSSD, HIV-negative partner not receiving PrEP N = 142 | 0 | — |
HSSD, HIV-negative partner receiving PrEP N = 104 | 0 | — | ||
Heffron et al. (2019)25 Prospective cohort | < 400, n = 58 (78.4%) | HSSD, HIV-negative partners all initiated PrEP during study follow-up N = 74 146.4 py of follow up | 0 | — |
Ma et al. (2019)26 Retrospective cohort | NR | HSSD N = 186 | 2 | 0.39 (95%CI NR) |
Bavinton et al. (2018)13 Prospective cohort | < 200, n = 267 (78) ≥ 200, n = 76 (22) | MSM, HIV-negative partner not receiving PrEP N = NR 440.9 couple years of follow-up | 0 (phylogenetically linked seroconversions) | 0 (upper limit of 95% CI 0.84) |
MSM, HIV-negative partner receiving PrEP N = 115 117.5 couple years of follow-up | 0 (phylogenetically linked seroconversions) | 0 (upper limit of 95% CI 3.14) | ||
Melo et al. (2019)27 Retrospective cohort | NR | HSSD N = 200 | 5 | 2.5 (0.8 to 5.7) |
CI = confidence interval; HSSD = heterosexual serodiscordant; LWH = living with HIV; MSM = men who have sex with men; N = number; NR = not reported; py = person-years
Note: Results of subgroup analysis are presented in Table 9 and Table 10
aRates of seroconversion was reported in the publication as “per 1000 person years.”
Table 7: Summary of Findings by Outcome — HIV Seroconversion in Single-Arm Studies of Those With a Viral Load of < 200 copies/mL
Study citation and study design | Population, sample size and follow-up | Number of seroconversions | Rate of serconversions (95%CI) per 100 py | Notes |
|---|---|---|---|---|
Rodger et al. (2019)14 (PARTNER2) Prospective cohort | MSM, HIV-negative partner not receiving PrEP N = 782 1593 couple years of follow-up | 15 Phylogenetically linked transmissions, n = 0 | 0 (upper limit of 95% CI 0.23)a | 1 transmission per 435 years of condomless sex. 6 other seroconversions were reported outside of eligible couple years follow-up: Number of phylogenetically linked seroconversions = 0 There were 19.3 couple years of follow up in which the viral load of the sex partner LWH was > 200 copies/mL for at least 1 day. Number of phylogenetically linked seroconversions = 0 |
Bavinton et al. (2018)13 Prospective cohort | MSM, HIV-negative partner not receiving PrEP N = NR 232.2 couple years of follow-up | 0 (phylogenetically linked seroconversions) | 0 (upper limit of 95% CI 1.59) | 3 seroconversions were reported among study participants, but were not phylogenetically linked. |
MSM, no information on PrEP use in HIV-negative partner N = NR 560.0 couple years of follow-up | 0 (phylogenetically linked seroconversions) | 0 (upper limit of 95% CI 0.66) |
CI = confidence interval; LWH = living with HIV; MSM = men who have sex with men; N = number; py = person-year
Note: Results of subgroup analysis are presented in Table 9 and Table 10
aResults for condomless anal sex, phylogenetically linked transmissions only.
Table 8: Summary of Findings by Outcome — HIV Seroconversion in Comparative Studies of Those Receiving ART vs. No ARTa With Any Viral Load
Study citation and study design | Population and sample size | Number of seroconversions | Rate of seroconversion | Effect estimate (95% CI) | Notes | |||
|---|---|---|---|---|---|---|---|---|
ART group | No ART group | ART group | No ART group | Overall | Adjusted | |||
Davari et al. (2020)18 Overview of reviews Results from 1 SR (Baggaley et al. [2018]) | MSM NR | NR | NR | Receptive AI: Pooled RR = 1.67 (0.44 to 3.67) | Receptive AI: Pooled RR = 0.14 (0.04 to 0.29) | NR | Due to unclear number of participants, lack of data regarding the use and compliance of ART in the ART group, and concerns regarding use of “pooled RR” as a measure of risk of transmission the findings presented above are highly uncertain. | |
Insertive AI: Pooled RR = 0.14 (0.04 to 0.29) | Insertive AI: Pooled RR = 0.18 (0.09 to 0.31) | |||||||
Davari et al. (2020)18 Results from 1 SR (Zang et al. [2018]) | HSSD NR | NR | NR | Pooled IR: 2.13 (0.00 to 4.63) | Pooled IR: 1.44 (0.62 to 2.26) | NR | — | |
Nyombayire et al. (2021)21 Prospective cohort | HSSD N = 2,472b | 19/2032c | 31/440 | 0.63 (0.38 to 1.00) | 5.51 (3.73 to 7.83) | — | Rate Ratiod = 6.9 (3.8 to 12.4) | Decrease in seroconversion (ART vs. no ART) = 88.6% |
Chen et al.(2018)28 Retrospective cohort | HSSD N = 7,304 | 208/5828 | 239/1885 | 1.6 (1.3 to 1.8) | 4.2 (3.7 to 4.8) | HR = 0.48 (0.40 to 0.59) | AHR = 0.55 (0.44 to 0.69) | ART was associated with a 45% reduction in risk of transmission. |
Liu et al. (2018)29 Retrospective cohort | Late ART, n = 1,339 | 61/636 | 45/703 | 6.7 (5.0 to 8.4) | 11.2 (8.0 to 14.5) | HR = 0.60 (0.40 to 0.89) | AHR = 0.62 (0.42 to 0.94)e | — |
Mid-ART, n = 7,496 | 120/3079 | 156/4417 | 3.1 (2.5 to 3.6) | 5.9 (5.0 to 6.9) | HR = 0.51 (0.40 to 0.65) | AHR = 0.53 (0.41 to 0.68)d | — | |
Early ART, n = 4,297 | 27/2113 | 38/2184 | 1.6 (1.0 to 2.2) | 5.3 (3.6 to 7.0) | HR = 0.30 (0.18 to 0.50) | AHR = 0.32 (0.19 to 0.54)d | — | |
Zheng et al. (2018)30 Retrospective cohort | HSSD N = 5,544 At 6 months: | 278 | 152 | NR | NR | OR = 1.14 (0.91 to 1.43); P = 0.25 | — | Denominators for this finding appear to be reported variably across the study report, making interpretation unclear. |
Zheng et al. (2018)30 Retrospective cohort | HSSD N = 5,544 At 12 months: | 295 | 272 | NR | NR | OR = 0.50 (0.42 to 0.60) P < 0.0001 | — | Denominators for this finding appear to be reported variably across the study report, making interpretation unclear |
AHR = adjusted hazard ratio; AI = anal intercourse; ART = antiretroviral therapy; CI = confidence interval; HSSD = heterosexual serodiscordant; HR = hazard ratio; IR = incidence rate; LWH = living with HIV; MSM = men who have sex with men; N = number; OR = odds ratio; py = person-year; RR = relative risk; SR = systematic review
Note: Results of subgroup analysis are presented in Table 11
aData on viral load of participants LWH were not reported in any studies.
bThis is the number of participant couples who completed study follow-up
cOf 54 overall seroconversions observed, 4 were demonstrated to not be virologically linked and were removed from the analyses; of 50 seroconversions remaining, 36 were demonstrated to have viral linkage and 14 had unknown viral linkage status (i.e., not measured); 19 of 50 seroconversions observed occurred in couples for whom the sex partner LWH was exposed to ART; 14 of these 19 seroconversions demonstrated viral linkage (with an incidence rate reported only for the 19 seroconverting couples for whom the sex partner LWH was exposed to ART, and no incidence rate reported for the subgroup of 14 participant couples with both exposure to ART in the sex partner LWH and viral linkage demonstrated)
dAdjusted for man’s age
eAdjusted for age, sex, level of education, marital status, occupation, and route of HIV transmission in the sex partner LWH
Table 9: Summary of Findings by Outcome — HIV Seroconversion in HSSD Couples With Any Viral Load Stratified by Subgroups
Study citation and study design | Subgroup | Sample size, n | Number of seroconversions, n (%) | Risk of seroconversion |
|---|---|---|---|---|
HR or AHR (95% CI) | ||||
Single arm studies, no comparator | ||||
Chen et al. (2022)19 Prospective cohort | Unprotected sexa | |||
Unprotected sex and HCV- HIV-negative partner | 170 | 8 (4.71) | HR = 4.31 (1.93 to 9.59) P < 0.001b | |
Unprotected se and HCV+ HIV-negative partner | 216 | 22 (10.19) | HR = 8.78 (4.92 to 15.67) P < 0.001b | |
No unprotected sex and HCV- HIV-negative partner | 2,532 | 24 (0.95) | Reference | |
No unprotected sex and HCV+ HIV-negative partner | 1,278 | 27 (2.11) | HR = 1.86 (1.07 to 3.22) P < 0.001b | |
Age | ||||
> 50 years | NR | NR | HR = 1.71 (1.01 to 2.89) | |
Viral load | ||||
> 400 copies/mL | NR | NR | HR = 2.24 (1.35 to 3.70) | |
No AIDS defining illness in the sex partner LWH | NR | NR | HR = 1.80 (1.06 to 3.06) | |
Sex partner LWH is a new ART user | NR | NR | HR = 2.41 (1.16 to 5.01) | |
Bantigen et al. (2021)20 Retrospective cohort | ART initiation | |||
Delayed vs. early ART | NR | NR | AHR = 2.551 (1.009 to 6.451)c | |
Condom use | ||||
Inconsistent vs. consistent | NR | NR | AHR = 4.665 (1.593 to 13.659)c | |
CD4 of sex partner LWH, cells/µL | ||||
≤ 200 vs. > 350 | NR | NR | AHR = 3.121 (1.204 to 8.091)c | |
History of pregnancy | ||||
History of pregnancy during the relationship vs. no pregnancy | NR | NR | AHR = 4.061 (1.696 to 9.722)c | |
Ma et al. (2019)26 Retrospective cohort | Time of ART initiation | |||
Received ART within a month of diagnosis | 119 | 0 | NR | |
No ART within a month of diagnosis | 67 | 2 (2.99) | NR | |
AHR = adjusted hazard ratio; AIDS = AIDS; ART = antiretroviral therapy; CD4 = cluster of differentiation 4; CI = confidence interval; HCV = hepatitis C virus; HR = hazard ratio; HSSD = heterosexual serodiscordant; LWH = living with HIV; NR = not reported
aUnprotected sex was defined as inconsistent condom use in the previous year.
bCumulative 7-year risk of seroconversion.
cAdjusted analysis including significant and non-significant predictors: Significant factors: delayed ART initiation, inconsistent or no condom use, last CD4 cell count of the sex partner LWH, and history of pregnancy in the sex partner LWH during the discordant relationship. Non-significant factors: Age, educational status, employment status, STs, CD4 count at detecting discordancy, alcohol use
Table 10: Summary of Findings by Outcome — HIV Seroconversion in MSM Couples Stratified by Subgroups
Study citation and study design | Subgroup | Couple years of follow-up | Rate of transmission (upper limit of 95% CI) per 100 couple years of follow up |
|---|---|---|---|
Viral load < 200 copies/mL | |||
Rodger et al. (2019)14 (PARTNER2) Prospective cohort | Sex acts | ||
Condomless anal sex | 1593 | 0 (0.23) | |
Insertive condomless anal sex | 1343 | 0 (0.27) | |
Receptive condomless anal sex with ejaculation | 650 | 0 (0.57) | |
Receptive condomless anal sex without ejaculation | 865 | 0 (0.43) | |
Any condomless anal sex with an STI | 116 | 0 (3.17) | |
Variable viral loads | |||
Bavinton et al. (2018)13 Prospective cohort | Viral load of sex partner LWH (copies/mL) | ||
> 200 | 28.4 | 0 (12.99) | |
< 200 | 560 | 0 (0.66) | |
Combination prevention | |||
Viral load < 200 and/or daily PrEP use and/or no CLAI | 582.5 | 0 (0.63) | |
Viral load > 200 and/or no daily PrEP use and/or CLAI | 5.8 | 0 (63.32) | |
Commencement of ART | |||
Started since last clinic visit | 27.1 | 0 (13.63) | |
Did not start since last clinic visit | 561.3 | 0 (0.66) | |
CLAI | |||
No CLAI | 242.3 | 0 (1.52) | |
Any CLAI | 317 | 0 (1.16) | |
Sexual position for CLAI | |||
Insertive | 278.5 | 0 (1.32) | |
Receptive with withdrawal | 153.8 | 0 (2.40) | |
Receptive with ejaculation | 99.6 | 0 (3.70) | |
STIs | |||
Any, either partner | 76.9 | 0 (4.80) | |
Any, sex partner LWH | 56.4 | 0 (6.55) | |
Any, HIV-negative partner | 32.4 | 0 (11.37) | |
CLAI, viral load < 200 and no PrEP, overall and stratified by exposure variables | |||
Overall | 232.2 | 0 (1.59) | |
Commencement of ART | |||
Started since last clinic visit | 6.1 | 0 (60.07) | |
Did not start since last clinic visit | 226.1 | 0 (1.63) | |
Sexual position for CLAI | |||
Insertive | 202.2 | 0 (1.82) | |
Receptive with withdrawal | 102.6 | 0 (3.60) | |
Receptive with ejaculation | 66.7 | 0 (5.53) | |
STIs | |||
Any, either partner | 21.1 | 0 (17.48) | |
Any, sex partner LWH | 15.4 | 0 (23.97) | |
Any, HIV-negative partner | 8.95 | 0 (41.23) | |
ART = antiretroviral therapy; CI = confidence interval; CLAI = condomless anal intercourse; LWH = living with HIV; MSM = men who have sex with men; PrEP = pre-exposure prophylaxis; STI = sexually transmitted infections
Table 11: Summary of Findings by Outcome — HIV Seroconversion ART vs. No ART Stratified by Subgroups With Any Viral Load
Study citation and study design | Subgroup | Rates of seroconversion | Risk of seroconversion, | ||
|---|---|---|---|---|---|
ART group | No ART group | HR (95% CI) | AHR (95% CI) | ||
ART vs. No ART | |||||
Nyombayire et al. (2021)21 Prospective cohort | Sex of sex partner LWH | ||||
Males (M+/F-) | 0.67 (0.33 to 1.20) | 6.79 (4.57 to 9.72) | — | 6.5 (3.1 to 13.4)a | |
Females (M-/F+) | 0.60 (0.26 to 1.21) | 0.83 (0.02 to 4.63) | — | 1.3 (0.1 to 8.3)a | |
Liu et al. (2018)29 Retrospective cohort | CD4 cell counts at baseline (cells/µL) | ||||
0 to 199 | 1.5 (1.3 to 1.7) | 5.4 (4.0 to 6.9) | 0.44 (0.32 to 0.61) | 0.47 (0.34 to 0.65)b | |
200 to 349 | 1.1 (0.8 to 1.5) | 4.8 (3.5 to 6.1) | 0.35 (0.23 to 0.54) | 0.36 (0.24 to 0.55)b | |
350 to 499 | 1.0 (0.4 to 1.6) | 4.6 (3.5 to 5.7) | 0.36 (0.19 to 0.68) | 0.33 (0.17 to 0.64)b | |
≥ 500 | 1.0 (0.1 to 1.9) | 3.0 (2.2 to 3.8) | 0.67 (0.27 to 1.70) | 0.62 (0.24 to 1.58)b | |
Chen et al.(2018)28 Retrospective cohort | Duration of follow-up | ||||
≤ 3 years | 1.8 (1.6 to 2.1) | 4.5 (3.9 to 5.0) | 0.49 (0.41 to 0.60) | 0.57 (0.45 to 0.71) | |
> 3 years | 0.6 (0.3 to 0.9) | 1.9 (0.7 to 3.1) | 0.33 (0.15 to 0.73) | 0.31 (0.11 to 0.84) | |
Sex | |||||
Males | 1.4 (1.2 to 1.7) | 3.8 (3.2 to 4.4) | 0.49 (0.39 to 0.63) | 0.57 (0.43 to 0.75) | |
Females | 2.0 (1.5 to 2.4) | 5.2 (4.1 to 6.3) | 0.51 (0.37 to 0.70) | 0.54 (0.37 to 0.79) | |
Age | |||||
18 to 24 years | 1.4 (0.6 to 2.1) | 4.1 (2.7 to 5.5) | 0.38 (0.19 to 0.78) | 0.52 (0.24 to 1.15) | |
≥ 25 years | 1.6 (1.4 to 1.8) | 4.3 (3.7 to 4.8) | 0.50 (0.41 to 0.61) | 0.56 (0.44 to 0.71) | |
Education | |||||
Below high school | 1.6 (1.4 to 1.9) | 4.3 (3.7 to 4.9) | 0.49 (0.40 to 0.60) | 0.54 (0.43 to 0.69) | |
Above high school | 1.2 (0.7 to 1.7) | 3.7 (2.3 to 5.0) | 0.48 (0.28 to 0.84) | 0.62 (0.33 to 1.19) | |
Marital status | |||||
Living with partner | 1.3 (0.6 to 2.1) | 3.7 (2.1 to 5.4) | 0.47 (0.22 to 0.99) | 0.40 (0.17 to 0.96) | |
Married | 1.6 (1.4 to 1.8) | 4.3 (3.7 to 4.8) | 0.49 (0.40 to 0.59) | 0.60 (0.45 to 0.72) | |
Occupation | |||||
Farmer | 1.7 (1.4 to 1.9) | 4.5 (3.9 to 5.1) | 0.47 (0.38 to 0.59) | 0.52 (0.40 to 0.66) | |
Other | 1.3 (0.9 to 1.7) | 3.3 (2.3 to 4.3) | 0.56 (0.36 to 0.87) | 0.75 (0.44 to 1.28) | |
Route of HIV transmission | |||||
Heterosexual intercourse | 1.5 (1.5 to 2.1) | 4.4 (3.8 to 5.0) | 0.45 (0.37 to 0.55) | 0.50 (0.40 to 0.64) | |
Injecting drug use | 1.7 (0.7 to 2.2) | 3.4 (1.8 to 5.0) | 0.63 (0.32 to 1.23) | 1.07 (0.42 to 2.75) | |
Other or unknown | 1.6 (0.8 to 2.9) | 1.7 (0.0 to 3.5) | 1.82 (0.58 to 5.77) | 2.18 (0.52 to 9.11) | |
CD4 cell count (cells/µL): | |||||
< 500 | 1.6 (1.3 to 1.8) | 4.1 (3.4 to 4.9) | 0.56 (0.44 to 0.71) | 0.57 (0.45 to 0.72) | |
≥ 500 | 1.7 (0.2 to 3.2) | 2.9 (2.0 to 3.9) | 0.69 (0.27 to 1.75) | 0.66 (0.26 to 1.71) | |
CD4 count missing | 1.4 (–0.6 to 3.4) | 5.6 (4.4 to 6.8) | 0.25 (0.06 to 1.01) | 0.24 (0.06 to 0.97) | |
AHR = adjusted hazard ratio; ART = antiretroviral therapy; CD4 = cluster of differentiation 4; CI = confidence interval; HR = hazard ratio; LWH = living with HIV; M+/F- = male partner positive, female partner negative; M-/F+ = male partner negative, female partner positive
aAdjusted for man’s age
bAdjusted for age, sex, level of education, marital status, occupation, and route of HIV transmission in the sex partner LWH
Table 12: Summary of Findings by Outcome — Incidence of STI
Study citation and study design | Outcomes | Results |
|---|---|---|
Bavinton et al. (2018)13 Prospective cohort | STIs | STIs diagnosed during follow-up, n (%)
|
LWH = living with HIV; STI = sexually transmitted infection.
Appendix 5: References of Potential Interest
Scoping Review
Knight J, Kaul R, Mishra S. Risk heterogeneity in compartmental HIV transmission models of ART as prevention in Sub-Saharan Africa: A scoping review. Epidemics. 2022 09;40:100608.
Non-randomized studies
Le Guillou A, Cabie A, Delpierre C, et al. Dramatic decline in new HIV diagnoses in persons born in France in a large nationwide HIV cohort. Public Health. 2021;196():129-134.
Lima VD, Brumme ZL, Brumme C, et al. The Impact of Treatment as Prevention on the HIV Epidemic in British Columbia, Canada. Curr HIV/AIDS Rep. 2020;17(2)():77-87.
Woodson E, Goldberg A, Michelo C, et al. HIV transmission in discordant couples in Africa in the context of antiretroviral therapy availability. AIDS. 2018;32(12)():1613-1623.
Modelling Studies
Zhu J, Rozada I, David J, et al. The potential impact of initiating antiretroviral therapy with integrase inhibitors on HIV transmission risk in British Columbia, Canada. EClinicalMedicine. 2019;13():101-111.
Supervie V, Breban R. Brief Report: Per Sex-Act Risk of HIV Transmission Under Antiretroviral Treatment: A Data-Driven Approach. J Acquir Immune Defic Syndr. 2018 12 01;79(4):440-444.
Additional References
Patterson S, Nicholson V, Milloy MJ, et al. Awareness and Understanding of HIV Non-disclosure Case Law and the Role of Healthcare Providers in Discussions About the Criminalization of HIV Non-disclosure Among Women Living with HIV in Canada. Aids Behav. 2020;24(1):95-113. PubMed
Kesler MA, Kaul R, Loutfy M, et al. Prosecution of non-disclosure of HIV status: Potential impact on HIV testing and transmission among HIV-negative men who have sex with men. PLoS One. 2018;13(2):e0193269. PubMed
Patterson S, Kaida A, Ogilvie G, et al. Awareness and understanding of HIV non-disclosure case law among people living with HIV who use illicit drugs in a Canadian setting. Int J Drug Policy. 2017;43():113-121.
Acknowledgements: Kendra Brett, Shannon Hill, Lindsay Ritchie, Weiyi Xie
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.