CADTH Health Technology Review
Considerations of Access and Inclusion in Adolescent Eating Disorder Care: A Custom Rapid Report
Technology Review
Authors: Elijah Herington, Robyn Butcher, Danielle MacDougall
Abbreviations
LGBTQ2S+
lesbian, gay, bisexual, transgender, queer, 2-spirited, and others
CBT
cognitive behavioural therapy
CBT-E
enhanced cognitive behavioural therapy
CEDA
Canadian Eating Disorder Alliance
CIHI
Canadian Institute for Health Information
DBT
dialectical behavioural therapy
DSM
Diagnostic and Statistical Manual of Mental Disorders
ED
eating disorder
EDE-Q
Eating Disorder Evaluation Questionnaire
FBT
family based therapy
GAC
gender-affirming care
GAHT
gender-affirming hormone therapy
NEDIC
National Eating Disorders Information Centre
SGM
sexual and gender minority
Key Messages
This custom rapid report provides insight into some challenges of equitable access to and inclusion in specialized eating disorder care for racialized, LGBTQ2S+, and male adolescents living with distress related to body image, eating, and food. To do this work, this custom report is engaged with empirical and conceptual literature around adolescent eating disorders and investigates how access and inclusion have been conceptualized in that literature.
Equitable access to specialized and inclusive eating disorder care for racialized, LGBTQ2S+, and male adolescents can be hampered by reductive understandings of these adolescents’ needs and experiences of distress around eating and body image. Similarly, diagnostic categories, diagnostic assessment tools, and treatments designed with and for the archetype of the young, white, cisgender woman living with an eating disorder, reduce the understanding of adolescents not fitting this archetype. Cultural competency training and practising cultural humility were both described as supportive elements in working toward providing equitable access to inclusive eating disorder care.
A series of sensitizing questions are provided at the end of this report and are meant to support the CADTH team in remaining attentive to considerations of equity of access and inclusivity as they assess early intervention programs for adolescents living with eating disorders in an upcoming health technology assessment.
Context and Policy Issues
In the Canadian Eating Disorder Alliance’s (CEDA) 2019 to 2029 national strategy and recommendations document, they note the importance of publicly reaffirming that “all Canadians, including those living with an ED [eating disorder], must have equitable access to medically necessary services” regardless of who they are or where they live.(p.17)1 This reminder follows their description of the fragmentation of eating disorder (ED) care in Canada, where equitable access is hampered not only by location (e.g., rural versus urban) and limited availability of multidisciplinary care teams, but can also be challenged when the local services available promote treatment philosophies or modalities that are not matched with the developmental or symptomatic needs of the people engaging with those services.1
This fragmentation is particularly challenging in the light of utilization statistics emerging since the onset of the COVID-19 pandemic, where programs across Canada have indicated dramatic surges in hospitalizations and referrals since early 2020. The pediatric ED program at Hamilton Health Sciences’ McMaster Children’s Hospital reported a 90% increase in referrals throughout the pandemic2 and Eating Disorders Nova Scotia reported a 400% increase in demand for their services over the first year of the pandemic.3 These claims are supported by Canadian Institute for Health Information (CIHI) data, indicating an increase of nearly 60% in ED-related hospitalizations of young women ages 10 to 17 across Canada between March 2020 and May 2022.4
While these are certainly alarming statistics, they may be under-representative of actual systemic need. Psychiatric Director of the Child and Adolescent Eating Disorders Program at the Children’s Hospital of Eastern Ontario (CHEO), Dr. Leanna Isserlin has noted, for example, that, “many young people from marginalized and less-affluent neighbourhoods have difficulty accessing treatment for EDs and would not be reflected in the [CIHI] data.”4 So, while we can see a dramatic surge in ED-related hospitalizations for some adolescents (i.e., “young women” 10 to 17 years old) throughout the pandemic, we are unaware of what the impact has been for youth who are marginalized and less affluent who already had difficulty accessing ED-related services.
The underrepresentation of youth who are marginalized and less affluent has not been co-emergent with the pandemic, however. CEDA’s national strategy and recommendations were published in 2019 (just before the onset of the COVID-19 pandemic in Canada), and highlighted that there was an “alarmingly high number of under-resourced populations (e.g., rural, LGBTQ2S+ people, males, Indigenous and Northern communities, cultural and ethnic minorities)”(p.14)1 As such, it is likely that CIHI’s data and the absences noted by Dr. Isserlin tie into long-standing stereotypes around EDs as diseases of affluence5 primarily affecting young, white, cisgender, females.6
Despite the persistence of this stereotype, however, there is wide acknowledgement within the ED field (research and clinical practice) that ED affects people of all ages, races, gender identities, and cultural backgrounds.1 Some populations outside of the archetypal ED patient, like adolescents who identify as transgender and nonbinary, have even been identified as being more likely to report higher rates of ED symptoms than cisgender adolescents.7 How is it that these adolescents, and others not fitting the archetypal ED patient, remain alarmingly under-resourced in ED care in Canada?
This CADTH custom rapid report is an attempt to address just this question. In what follows, we sought to provide insight into the spaces and time points at which exclusions may be perpetuated for those populations identified above as being undercounted in hospitalization statistics in Canada and under-serviced by current ED care programming. Additionally, we sought to identify and articulate some suggestions from the literature on how best to address and push back against these exclusions.
This report was designed and completed in response to an internal CADTH request for early work identifying considerations around the equity components of access and inclusion in adolescent ED care broadly. The reason for this request, and thus its overarching purpose, was to provide an early sense of some of these equity considerations so that they could feed into an upcoming CADTH HTA assessing the use of early intervention programming for adolescents with EDs. As such, a primary output of this report is a series of questions that the CADTH project team can ask when considering early intervention programs for assessment in the HTA before finalizing the research protocol and as the team proceeds with the assessment. This, we imagined, would help CADTH position itself in a way that is responsive to its strategic plan objective of “fostering health systems that reflect the diverse people of Canada” and increase CADTH’s focus on equity in our work. To clarify, the purpose of this report is to provide a series of considerations that may be helpful to a future CADTH HTA on early intervention programs for adolescents; we have not focused on early interventions in this report.
Research Question
How have the problems of access and inclusivity been conceptualized, and imagined as being remediated, in literature focused on the identification of, or care for, adolescents living with an eating disorder?
Methods
Literature Search Methods
Information specialists completed a preliminary iterative search, trying to identify the main topics related to equity issues in eating disorders, from August 30, 2022 to September 2, 2022.
With feedback from the reviewer on these preliminary results, information specialists conducted a full literature search on key resources, including MEDLINE, PsycINFO, CINAHL, and Scopus, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were eating disorders and health care access. To address the topic of inclusivity, search concepts for ethnicity and race, Indigenous Peoples, sexual orientation and gender identity, socioeconomic status, and geographic disparities were also included. The MEDLINE and CINAHL searches were completed on October 6, 2022, while the PsycINFO and Scopus searches were completed on October 7, 2022. All searches were limited to English-language documents published since January 1, 2012.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first screening level, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. Grey literature was screened by skimming through the full publication to determine relevance for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adolescents living with an eating disorder Based on preliminary scoping, we are particularly interested in literature that is focused on adolescents who identify as LGBTQ2S+, are from racialized populations, are Indigenous, or are male These are not the ONLY populations of consideration, but they have been identified in scoping as populations we ought to pay attention to, as detailed in the background information before this table |
Phenomenon of interest | Considerations (e.g., theories, models, conceptualizations) or practices that foster accessible and inclusive care for adolescents living with eating disorders |
Types of information | We are interested in finding published or grey literature that:
|
LGBTQ2S+ = lesbian, gay, bisexual, transgender, 2-spirited, and others.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2012.
Additionally, once we began to review the literature, we made the decision to exclude studies that were primarily focused on the prevalence of, or risks for, developing EDs among males, Indigenous peoples, 2SLGBTQ+ peoples, and racialized peoples.
Prevalence studies certainly play a role in providing inclusive and accessible eating disorder care as they often provide valuable information countering common misunderstandings and stereotypes of EDs as primarily diseases of affluence5 affecting young, white, cisgender girls.6 However, given that 1 of the key understandings driving this review is the reality that adolescents not fitting this mould are systemically underrepresented in ED care, the reviewer decided that prevalence studies could not contribute further to understanding how the problems of access and inclusivity have been conceptualized and remediated.
Excluding publications focused on identifying or highlighting the risks adolescents of different subject positions run in developing an ED was a practical decision given the time constraints associated with this report and limited expertise in the ED field. Studies focused on identifying risk factors are challenging to critically engage with if you are not an expert in the field, as it could be easy to miss nuances. As such, rather than focusing on individual risk studies, this review focuses on how publications described and critiqued studies focused specifically on identifying discreet risk factors.
Approach
One reviewer conducted a rapid narrative review of the literature to understand and clarify how the concepts of accessible and inclusive care have been conceptualized in literature focused on care for adolescents living with an ED.8 To do so, the reviewer adopted an interpretative and questioning approach, guided by underlying key assumptions, to iteratively identify and explore the empirical, theoretical, and descriptive published and grey literature.
Key Assumptions
To better understand how theoretical and practical knowledge define concepts of accessible and inclusive ED care in the literature, our engagement with the literature was guided by the 2 following underlying assumptions around access and inclusion or exclusion.
For the purposes of this review, we followed Andersen and colleagues’ understanding of the concept of access as indicating the “actual use of personal health services and everything that facilitates or impedes their use …[including] not only visiting a medical provider but also getting the right services at the right time to promote improved health outcomes.”9 We paid particular attention throughout this custom report to the relationship and tension between 2 dimensions of access described by Andersen and colleagues – potential versus realized.9
Potential access is concerned with things that affect one’s ability to engage with care services at “both the contextual (health policy, financing) and individual (regular source of care, health insurance, income) levels.”(p.10)9 In the context of this work, paying attention to the “potential” of access to ED care involved being particularly attuned to how the historic or ongoing impact of colonialism, racism, sexism, and class struggle are articulated in the literature the reviewer found.
Realized access deals with the actual use of services. So, if potential access involves those factors that may help or hinder one’s ability to engage with (in this case) ED care, realized access is focused on when individuals use existing ED care services. We did not detail utilization statistics given what has been highlighted above regarding increases in referrals to specialized ED care and hospitalizations since the onset of COVID-192-4 and the “alarmingly high number of under-resourced populations”1 who have likely not been captured in these statistics.4 Instead, the author took improvements to realized access as an obvious end goal for ED care providers hoping to close gaps in care for these under-resourced populations. As such, the idea of realized access is active in this work through its absence.
To engage with how inclusive care has been conceptualized in ED care specifically, we drew from a previous CADTH rapid review10 that examined how to build inclusive health care services with Indigenous peoples as a starting point. From this review, we took 2 primary insights – considering inclusive care necessarily involves attending to its opposite, exclusion, and the importance of practices aimed are remediating exclusions rather than simply adding on inclusive practices.
Thinking about inclusive health care necessarily involves considering its opposite – exclusionary health care. This implies the need to focus on the assumptions, norms, or stereotypes that might foster an environment of exclusionary care and relates to the importance of attending to the contextual/individual factors of potential access described above. So, for this work, this implies focusing on the who of inclusion and exclusion (as noted in populations described as alarmingly under-resourced), and the how (or why) of this inclusion and exclusion.
Identifying or describing what might be fostering an environment of exclusionary care needs to be connected to the development and uptake of practices directed at remediating this exclusion. We then paid particular attention to what approaches focused on remediation and what they sought to do, how they do it, what their assumptions are, and how they converge and gel with broader thinking around equitable and inclusive access in health care more broadly.
Analysis
We conducted an iterative and interpretative analysis, drawing on the tenets of qualitative constant comparison11 and thematic synthesis techniques12 to analyze and question the identified empirical, theoretical and descriptive published and grey literature. The iterative, interpretative, and questioning approach allowed us to comprehensively understand what is currently known and where further knowledge offered novel insights or add clarity.
We began the analysis by reading and re-reading the eligible studies and making initial notes and memos to reflect on preliminary insights and thoughts. Throughout this process, the author explored, reflected on, and questioned theoretical frameworks, conceptual and practice descriptions and considerations as identified across various components of the eligible publications and grey literature (e.g., design or method, positioning of study authors, reported findings, commentary in the discussion section). To do so, we identified, described and problematized theories, norms and descriptions addressing how access, inclusion and exclusion, and remediations are defined, envisioned and applied to ED practice. We adopted this questioning approach guided by the underlying assumptions described above to move away from popular understandings of access, inclusion and exclusion, and remediations, and identify and clarify the conceptual underpinnings that guide and frame research and practice. Throughout the review process, we also noted the potential exclusions from ED care for racialized, LGBTQ2S+, and male adolescents struggling with disordered eating or a fully diagnosed ED. By disordered eating, we simply mean eating behaviours and patterns that may not (or not yet) warrant a diagnosis.
We then began to form initial descriptive themes by inductively making connections across the data and preliminary insights. Through ongoing readings, memoing, discussions with team members, and returning to the reviewer’s initial memos and original papers, we further developed the connections between the data and themes to form refined conceptual themes. In the context of this rapid review, the analysis stopped when the finalized thematic categories included the meaningful concepts, theories, and descriptions identified across the included literature and answered the review’s research question.
Summary of Evidence
Quantity and Characteristics of Included Literature
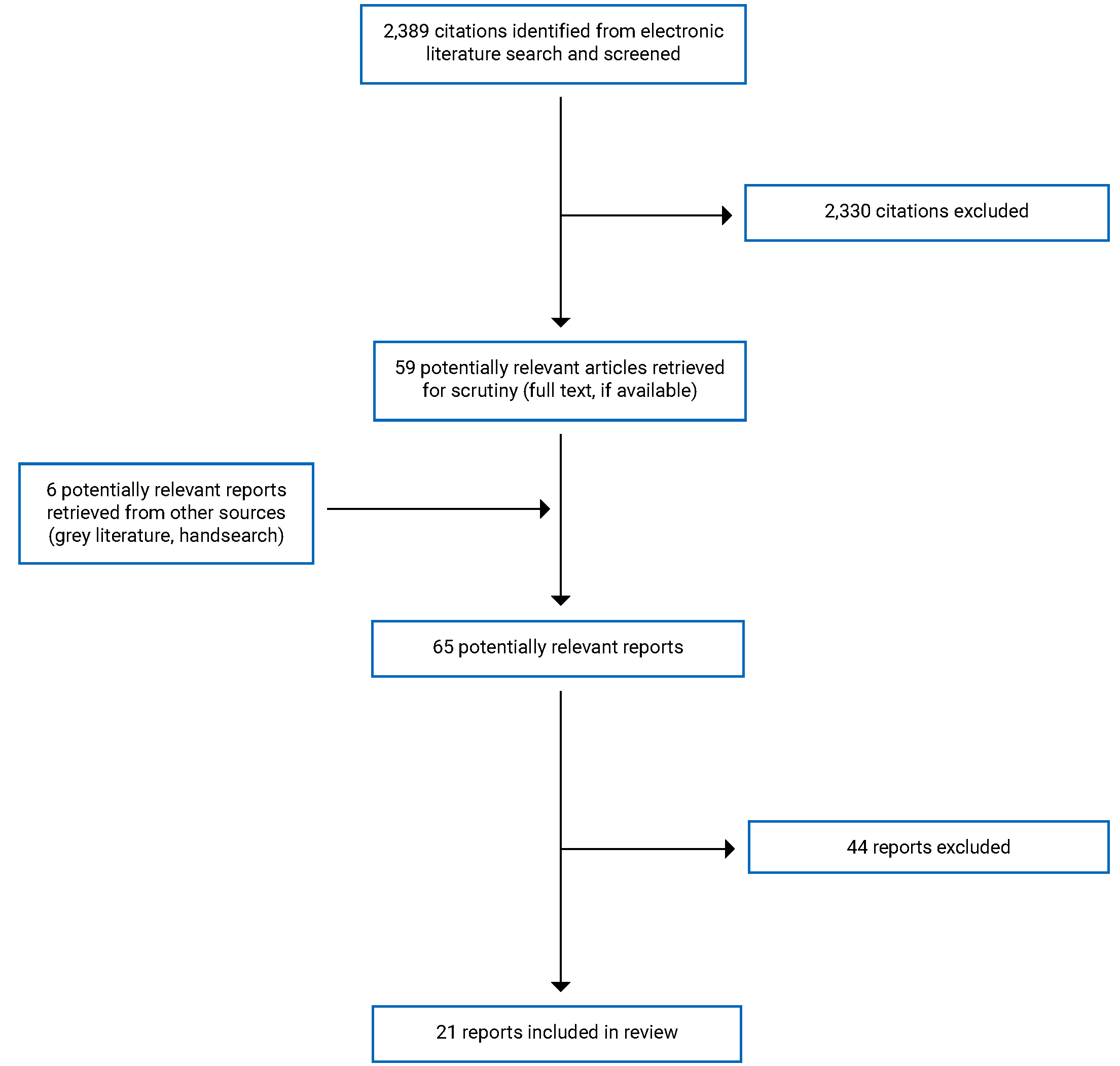
A total of 2,389 citations were identified in the literature search. After screening titles and abstracts, 2,330 citations were excluded, and 59 potentially relevant reports from the electronic search were retrieved for full-text review. 6 potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 38 publications were excluded, and 21 publications met the inclusion criteria and were included in this report. Of the 21 publications included in this report, 6 were primary qualitative studies,13-18 6 were literature reviews with recommendations,19-23,34 4 were commentaries with recommendations,24-27 2 were narrative reviews,28,29 1 is a systematic reviews,30 1 was a survey study,31 and one was a guidance document. Publications included the following populations: LGBTQ2S+ adolescents,15,17,21,24,25,27,33 broadly defined racial and ethnic minorities,14,16,18,22,30,31 and Asian Americans specifically,13,19,23 Latinx [as written in the literature],20 and male adolescents.26,28 Appendix 1 presents the PRISMA32 flow chart of the study selection.
Summary of Findings
We have organized the findings of this review into 4 overarching categories consisting of what we understand as 2 foundational elements of inclusive care and 2 broadly defined steps along the care pathway that may be reinforcing exclusionary care practices. The 2 foundational elements of inclusive care detailed throughout are found under the headings “exclusionary care is reductive” and “cultural competency and cultural humility.” To note, the 2 elements we are identifying as foundational are split by care pathway considerations identified under the headings of “diagnosis and assessment” and “treatment.” We have organized the findings in this way in an attempt to provide readers with a sense of progression from the more exclusionary (and, therefore, inaccessible or non-inclusive) elements of current ED care to some practices that may help mitigate the impact of these exclusions.
With this progression in mind, the reader will notice that we have used the language of exclusion or exclusionary care more frequently throughout this report than inclusive or accessible. This intentional approach reflects the details under Key Assumptions earlier in this document. By attending to the ways in which current ED care is, or may become, exclusionary for racialized, LGBTQ2S+, and male adolescents, this report provides a broadened, more structurally oriented, picture of what equitable access and inclusive care could look like. What we mean by this is that had we focused only on the positive practices of access and inclusion (e.g., cultural competency training), we may have missed some of the more structural and conceptual considerations, making it challenging for those positive practices to achieve their desired effect. This could, for example, have missed the possibility that diagnostic categorizations of eating disorders may not be inclusive of the distress around eating and body image that some adolescents outside of the archetype of the young, white, cisgender, affluent, woman experience.
However, the reader will also note that the exclusions, and potential mitigating factors described below, are neither always exclusionary nor will they always improve access to inclusive care. Instead, details that follow provide a series of considerations for our readers to engage with when considering developing or implementing new ED care programming. In particular, as already mentioned in our introduction, this report has been prepared with the specific intention of supporting an upcoming CADTH HTA assessing the implementation of early intervention programs for adolescents living with eating disorders. As such, we have provided both a brief discussion on 2 forms of inclusion identified throughout the included literature for their consideration and a series of questions they may find helpful as a sensitizing tool to ensure they remain attentive to how access and inclusion present in the context of early intervention programming.
Exclusionary Care Is Reductive
A foundational element to identifying (and working against) exclusionary practice rests on understanding that shared demographic or social identity does not imply sameness or uniformity of experience.17,19,21-23,25,33 This is a sentiment that was repeated numerous times throughout included publications as a way of tempering findings or recommendations oriented toward a particular shared identity (e.g., LGBTQ2S+ or Asian American).
For example, the National Eating Disorder Information Centre’s (NEDIC) guidance document on disordered eating among people in the LGBTQ2S+ community notes that in North American White supremacy culture, there can be differential experiences of discrimination or access to care for queer and transgender people based on the colour of their skin.33 In this case, while there is a common connection to the LGBTQ2S+ community (which carries its potential of discrimination and exclusion due to things like transphobia or homophobia), Black transgender or queer people may have additional layers of discrimination to navigate due simply to their “blackness.”33 Reducing the experiences of all LGBTQ2S+ people living with disordered eating to a single, common experience, and then developing treatments or supporting options out of this single experience, can reinforce existing structural and systemic exclusions for the diversity of people belonging to this community.33 This is not to suggest that all Black transgender or queer people will have shared experiences either, but simply to point to the importance of approaching inclusive care with an understanding that being part of a racialized or LGBTQ2S+ community does not imply shared experiences or needs around eating disorder care.
Treating each adolescent presenting with distressed eating or body image concerns as an individual with unique experiences is a simple concept. And while it is certainly clear from our review of the included publications that there is a growing focus on inclusive and accessible care in ED research and practice, being attentive to the possible variety of experiences and needs of adolescents dealing with ED remains challenging.
We then call attention to the ways in which reductive thinking and practice may continue to work their way into ED research and care for diverse adolescents. In the following subsections, we point to 2 particularly challenging areas in which reductive thinking may creep in, as noted in the included publications – that is, theoretical frameworks of risk and research on help-seeking behaviours. In the first, we use the term diagnostic tropes16 to identify misguiding conceptualizations that providers and researchers may adopt when attempting to identify people from various backgrounds as living with an eating disorder. We then briefly point to how the dissonance between help-seeking and structural barrier research might indicate a process of reducing adolescents as responsible for not looking for help or understanding when something is wrong. In both cases, the identified literature focuses on diverse adolescents, yet some literature also includes adult populations. We have decided to keep the literature that did not specifically focus on adult or adolescent populations as the challenges described below were discussed in this literature as relevant to both. As such, we have used the language of people to designate when publications were speaking to both adult and adolescent populations.
Diagnostic Tropes
In this section, we briefly highlight some prominent theoretical frameworks (i.e., minority stress model, objectification theory, and acculturation theory) used to detail risk relationships between eating disorder development and racialized, gendered, or cultural identities. Based on our review of the included publications, these theoretical frameworks may be practised as both helpful heuristics for thinking through an individual’s personal experiences of distress, and/or as diagnostic trope(s)16 that reduce a person’s distress to a series of pre-established origins found among others from similar racialized, gendered, or cultural backgrounds. As a heuristic, these frameworks may spur provider curiosity and encourage them to engage in personalized, open conversations with their patients that build off the potential risks identified in those frameworks. However, as diagnostic tropes, these frameworks remove the possibility of curiosity and act as surrogates for adolescents’ expressions of distress, experience, and need. This can be further disempowering29 for adolescents experiencing disordered eating and work against broader goals of providing more inclusive and accessible care.14,16,17,21,27 With this in mind, it may be helpful to understand these frameworks as neither wholly inclusive nor as wholly exclusionary, but rather dependent upon how they are put into practice.
Among prominent theoretical frameworks that address ED risk factors related to racialized, gendered, or cultural identities, acculturation is typically understood as a process of adaptation and assimilation when conflicting cultural practices meet.16,18-20,30 At its root, there is the assumption that adolescents from non-Western cultures (e.g., second-generation immigrants), but living in Western society, are vulnerable. Though primarily described as a unilateral move where dominant “Western” culture overruns and challenges non-Western cultural practices around food and eating or bodily ideals,16,19 acculturation can also be understood as having multiple pivot points that do not imply straightforward assimilation into Western cultural practice.18,19 In either case, the processes involved in acculturation are seen as creating a byproduct, acculturative stress, that can make adolescents managing the appeals of multiple cultures more likely to develop mental health issues like eating disorders.18
A basic premise of both minority stress and objectification theory is that persistent experiences of discrimination (whether based on gender, sexuality, or race) contribute to the development of eating disorders in adolescents (or adults) who identify outside of white cisgender heteronormativity. In their commentary and recommendations for providing care to sexual and gender minority (SGM) youth, as described by Golhammer et al. They described minority stress theory as purporting that SGM youth’s consistent experiences of stigma, discrimination, and victimization due to their sexuality or gender, “create stressors that negatively influence behavioural and physical health.”(p. 318)25 Other publications engaged in empirical work both seeking to understand transgender adolescents experiences of ED care15 and develop recommendations for how to provide inclusive ED care to SGM adolescents24 noted minority stress theory’s explanatory power for how these adolescents become “vulnerable to poor health outcomes including disordered eating behaviors.”(p. 8)15 Relatedly, objectification theory posits that the sexualization of some peoples’ bodies (e.g., Asian women,19,23 and gay adolescents25) encourages those in these bodies to understand their value as largely tied to their appearance. This, in turn, fosters an environment of increased body self-surveillance and image concern.19,23,25
At the root of all 3 theoretical models is an assumption of vulnerability. Vulnerability, here, can be understood as an internal deficit an adolescent may bring when navigating the world as a racialized person or someone whose sexual orientation and gender identity are outside of cisgender heteronormativity. Similarly, that vulnerability may be understood to exist within adolescents who are, for example, second-generation immigrants to North America navigating the boundaries between conflicting cultural practices and body ideals. Regardless, someone occupying any 1 of these subject positions is assumed to be at risk for developing an eating disorder.
Though this assumption may lead providers to engage with the adolescents presenting to them in a way that is curious and open to exploring whether this assumption is valid, others may apply the framework and assumption of vulnerability as a surrogate for individual experiences. In their systematic review of literature focused on eating disorders among racial and ethnic minorities, Acle et al. note that the literature has repeatedly pointed to the importance of attending to acculturation and acculturative stress among these populations as they are “essential to understanding ED presentation and case conceptualization”(p.482)30 They suggest including measures of acculturation at assessment and that the results of these measures can “provide a framework for eliciting dialogue about the meaning of one’s ED and addressing cognitive distortions that maintain ED symptoms.”(p.482)30 Yet, as other scholars note, if these measurements and the ascription of a theoretical framework for one’s etiological journey to disordered eating are meant to inform treatment and care provision, these broadly held theories may incidentally disempower people.29
We argue then that this move to include measures like acculturation implies that it is possible for notions like “ethnic identity” and “acculturative stress” to become placeholders for the person’s conception of what is going on. We take Channa et al.’s16 case example of a female, Southeast Asian adolescent, living in the UK as a helpful way of problematizing a move toward broad theories like “acculturation” or even “minority stress.” In their case study, it is evident to the authors that Reeya, their adolescent, has indeed been influenced by Western body ideals and media. They note that these elements have certainly informed the development of her diagnosis with bulimia and even her move to seek help. However, they also clearly point out that acculturation is not the sole determinant in developing bulimia. They talk about the multiple and complex ways that Reeya came to be living with bulimia. They even go so far as to say that “what Reeya’s narrative does show is that we cannot assume that we know either the meaning or etiology of an individual’s disordered eating practices from the fact that they may appear to present with diagnostic tropes.”(p.377)16
Papathomas and Lavalee34 point out that experts tend to understand ED as multicausal and tied up into various biopsychosocial factors that change from person to person. They draw on other literature to note that if any number of biopsychosocial factors may be considered supportive of the development of eating disorders then it is challenging to identify any generally predictive theories.34 They suggest that it may be more beneficial to focus on the individual circumstances of the person presenting with distress rather than how well they align with predictive theories.34 Lamarre et al. similarly point to the challenges of winnowing away individual context and replacing it with socialized, racialized, or gendered categories.29 While, as NEDIC has said, people may share common understandings of gender, society, race, and so forth., this is not the same as assuming their experiences are in common.33
These “diagnostic tropes” may be helpful to some degree — in an effort to find some sort of foundation to work from — it is also problematic to assume that these can explain why, or even how someone is living with the condition in question.
Structural Challenges of Access
Conversations around the gaps between potential and realized access to care for adolescents (and, at times, adults) with eating disorders were described along 2 lines of responsibility in the included publications – that is, individual help-seeking behaviours and provider-referral practices.
When discussing challenges that could be affecting an individual’s decision to seek help, published literature noted both cultural and personal barriers. Cultural barriers tended to include stigma, shame and guilt,13,14,16,20,30 while personal factors described included denial, ambivalence, or poor health literacy.13,16,20 However, given the wide variety of personal and cultural factors that may affect one’s willingness to seek out care for disordered eating, some publications focused more on identifying structural challenges affecting access to care. When examining these structural challenges, studies included dismissive primary care providers,13,14,21 and persistence of stereotype of eating disorders as problems only for straight, cisgender, white women and girls.15 Channa et al. noted that studies evaluating the differences between prevalence, risk and access may be missing a broader investigation and understanding of structural challenges like referral patterns.16 In the introduction to their case study, the authors highlight several studies that point to broad disparities in referral patterns for “ethnic minorities” to eating disorder specialist services in the UK.16 This was also identified and described as important for gatekeepers to specialist eating disorder care spaces like general practitioners.14
Referral and stigma may overlap where providers who are unfamiliar with how disordered eating might present in non-normed populations (in people who do not fit the archetype of eating disorder patient) and thus could miss the experience of distress.13-15,21,24,28 For example, when describing challenges of male eating disorders in their critical narrative review of the literature on male eating disorders, Murray et al.28 note that the presentation of disordered eating and concerns about body image may be different in males (e.g., muscle oriented) and this could lead to misdiagnosis. They note that this external, clinically reinforced form of stigmatization marks males as outside the purview of eating disorder care and may prevent males from seeking help.28 Similarly, in Calzo et al.’s review of the research on what is referred to as sex and gender minorities, they address similar concerns, as they report the following participant quote: “People won’t seek resources if they’re nonbinary for fear of being misgendered or misunderstood and doctors not knowing how to talk to trans people.”(p.53)21
Rather than focusing the attention on how to change adolescents’ understanding of disordered eating as a way of correcting poor help-seeking behaviours, 1 publication suggested finding ways to integrate screening and assessment into services these adolescents may already be accessing.25 In particular, this publication focused on finding better ways to support LGBTQ2S+ adolescents dealing with disordered eating and suggested integrating screening services into sexual health clinics, since LGBTQ2S+ youth may already be accessing these services.25 To be a successful pipeline, eating disorder specialist services would need to engage with and have relationships with other spaces their absent clientele may be visiting already.25
Diagnosis and Assessment
Diagnostic Categories
Though less common in the literature than other exclusions being highlighted throughout this review, some publications pointed to the diagnostic categories of EDs themselves as potentially exclusionary. A primary critique across these publications was that diagnostic categories currently used in the DSM-V (or previously in other DSM iterations) have been built through observation of the archetypal patient with an eating disorder – young, white, cisgender, heterosexual women and girls.23,28,29 Understanding EDs through these categories alone can have the effect of excluding from care those who exist outside the bounds of this idealized patient. This may further entrench people’s (adolescents and adults) understandings of themselves as “abnormal”29 and reinforce experiences of structural oppression.
The problem is that diagnostic categorizations, and the “ability” to fit within 1 of them, are often the gateways to care.29 As such, diagnostic categories meant for, or built upon, a particularized version of who it is that can be living with an ED, and what an ED is, limit who has access to specialized treatment. The boundaries around diagnostic categories are, of course, intentional and purposefully developed to work as an organizational tool. However, when practising inclusive care, the literature suggests being attentive to the foundations of these categories and how they reinforce structural exclusion.23,28,29
This may involve providers moving away from exclusively focusing on their knowledge and expertise27,29 to limit the risk of reductive interpretations of the adolescent in front of them (e.g., diagnostic tropes described above) and expand the intention of finding the right diagnostic fit to creating a space that supports hearing “each person as they experience themselves in their gendered, sociohistorical and cultural contexts.”(p.8)29 Grounded in their critical feminist approach to eating disorders and care, LaMarre et al. suggest that this may help resist the exclusionary force of diagnostic categories that can “disempower and disembody people whose EDs express and represent issues of helplessness, subjectivity, and loss.”(p. 9)29 This does not mean that DSM-V categories are altogether unhelpful, but consideration needs to be made in light of an understanding that these categories are likely to be limiting the sorts of people who can gain access to care.
Rather than attempting to identify where an adolescent’s thoughts or behaviours indicate a discrete diagnostic category, then, practising inclusive care may involve pushing back against these categories and making space to focus on the adolescent’s distress without honing in on a particular diagnosis. In their literature review and recommendations for multiculturally informed feminist therapy with Asian American women, Yokoyama et al.23 argue that disordered eating behaviours and concerns with body image are best seen as situated along a continuum rather than as always indicative of discrete diagnostic categories. They suggest that allowing for distress to exist along a continuum may be particularly supportive of inclusive care with Asian American women and girls as “studies indicate that there are high numbers of women who do not fit the traditional DSM categories and who exhibit subclinical eating disorder behaviours.”(p. 184)23 This resonates with others’ calls to expand the boundaries around ED in an effort to be more attentive to the multiplicity of distress possible for adolescents (and adults) traditionally excluded from ED care spaces (e.g., LGBTQ2S+ and adolescents who are racialized, as well as cisgender males).27-29
As such, we might suggest that broadening out from diagnostic categories to an understanding that distress happens along a continuum could be helpful, and inclusive, practice. The goal is not to encourage an increased medicalization of distress, but rather to find ways to support people in their distress and find ways of counteracting that distress.
Assessment for Diagnosis
If diagnostic categories built around young, white, cisgender women’s experiences with disordered eating have the potential to exclude the experiences of distress for adolescents outside of this archetypal patient, it follows that assessment tools built to identify people fitting these categories may involve similar challenges to access and inclusive care. In this section, we engage with the challenges to access caught up with diagnostic assessment tools and practices.
Assessment tools can help streamline and standardize the process of seeking out whether the individual being assessed fits pre-existing diagnostic categories. These tools are built on what are considered to be the core constructs, or primary features, of the condition under examination.26 As such, in their review of ED assessment measures and their applicability to men or boys, Lavendar et al.26 note that these measures are only as valuable as the constructs upon which they are built. If, for example, a measure intended to identify anorexia was built using only data and input from young, white, hetero and cisgender women, then the specificities of anorexia for this group of people is likely to be reflected in the measurement tool itself. As such, it is possible that this measure would be unable to capture nuances that are more applicable or relevant for adolescent, hetero and cisgender boys, or Black transgender girls.
While Lavendar et al.’s review attempts to mark out which sort of tools have been developed with cisgender and heterosexual boys or men in mind,26 it is important that we consider these exclusions at all levels. This re-implies the importance of providers getting to know the person before them rather than assuming they understand where they are coming from. In other words, this concern with construct remains relevant across all metrics used to assess whether 1 is living with an ED and, if so, with what severity.
Another publication centred on the eating disorder evaluation questionnaire (EDE-Q), that is, 1 of the more common assessment tools available in the ED space.31 The authors conducted a study to determine whether this tool could remain invariant across white/non-white Latin American people (as described in the study). They found that some subset of the EDE-Q could identify more accurately those living with an ED, given its focus on a different construct of what might be happening for someone. However, they also noted in their discussion that “recent evidence suggests that even measures that display invariance may be less sensitive for minority populations.”(p. 109)31 With this in mind, the authors suggest that rather than privilege the form of ED clinicians think may be present for their patients, that they, instead, focus on the function of what the distressed eating patterns point to. This seems to relate, again, to what LaMarre and colleagues are pointing toward when considering feminist approaches to ED care.29 As such, LaMarre’s presentation of feminist approaches to ED care they lay out how diagnosis and assessment are done matter. In their review, LaMarre et al. suggest staying away from framing “what’s wrong” with the person being identified as living with ED/disordered eating. They suggest “mainstream” care practices focus on the taxonomy of EDs and might ask what to do about the ED someone has. Instead, they note that feminist approaches might focus on what the distress someone is living with feels like and what these feelings of distress might lead to in particular social contexts, and what “therapists and people seeking help can do together to generate, that is, embody, constructive changes”(p.8).29 These are both different ways of imagining what work should be done. Is the work to take a diagnostic category and work specifically on that category or is it to step back from the category and work on how that person relates to the category, social context, selves.
Given these challenges around assessment tools, some publications suggest that focusing on assessment as a practice rather than a tool could be helpful. In their review of ED care for transgender adolescents, Giordano discusses the importance of distinguishing between transgender adolescents with disordered eating patterns and other people living with EDs.27 Their goal is to ensure that the identification of disordered eating patterns does not automatically place 1 inside of disordered eating care. While this may seem counterintuitive, they describe that this could be important for adolescents who identify as transgender, as they may have a different reason as to why they are engaged in disordered eating behaviours. As such, the authors emphasize that what is important in these assessment interactions is determining where the distress is coming from and what the goals of eating behaviour are. Understanding these goals could be helpful in determining the sorts of care that are likely to be more supportive. For instance, it could be possible that adolescents who identify as transgender are engaging in their disordered eating patterns as a way of making their bodies fit the gender for those who are dealing with body dysmorphia. What might be more supportive, and helpful for these adolescents is referring them on to people who can support decision-making around gender-affirming hormone therapy.24,27 In the absence of this, it is possible that any ED care will not be good care but may further entrench habits and how these adolescents see themselves.
This relates to those challenges around diagnostic tropes. Included literature suggested that adolescents who identify as transgender and gender non-conforming are increasingly being identified as living with some form of disordered eating.15,24,25,27 While it could be as beneficial to some degree as it helps to raise recognition that disordered eating is not just a problem for women who are young, white, affluent and cisgender, it could also reinforce clinicians to seek and find EDs among adolescents who identify as transgender. For example, Giordano notes that “it would be simplistic to read the correlation found in the literature to indicate that many gender nonconforming adolescents are afflicted by psychopathology, in addition to gender dysphoria. At worst, seeking alternative psychopathological reasons for the disordered eating may blind professionals to the fact that the medical care provided may be inadequate, and that this delay or failure to treat the gender dysphoria may be the direct cause of the disordered eating.”(p.49).27
Again, as noted earlier, what is at stake here is a devaluing of the lived experience of the person in distress in favour of the generalizability of the expert knowledge. Perhaps, rather than privileging expert knowledge and diagnostic categories as the first step in identifying disordered eating, it would be helpful to first focus on what the distress is meant to be working toward and could be serving as fallout from.27,29 In a sense then, “inclusive care” might be able to be characterized as spending concerted effort to understand whether “ED care” is the most important and necessary treatment for the adolescent in question. Inclusive care might involve then referring on to another form of care like gender-affirming hormone therapy (GAHT).
Treatment
As with previous stages, another way that exclusions might happen in ED care for adolescents is at the stage of treatment. As with diagnostic categories, assessment measures, and diagnostic tropes, particular visions of what is at stake are evident in different treatment approaches. Studies that did engage with treatment often suggested that it would be possible to simply find ways of adapting existing approaches to the population of interest. As such, standard treatment approaches like cognitive behavioural therapy (CBT), dialectical behavioural therapy (DBT), and family-based therapy (FBT) were all described as adaptable.
For example, in their study focused on EDs among adolescents who identify as a “sexual minority” and gender non-conforming, Goldhammer et al.25 suggested that the effectiveness of these standard therapies may be enhanced by attending to “unique minority stressors and sociocultural factors that amplify risk in SGMs…”(p. 319) As such, inclusion is imagined as happening at the stage of adaptation or representation. What’s challenging about this notion, however, is that in our previous conversation on these diagnostic tropes of minority stressors or sociocultural factors that amplify risk, these “unique stressors” have the possibility of becoming explanatory devices, rather than just prompts for further investigation.
Acle et al. also suggest that an approach to enhanced CBT (CBT-E) using the transdiagnostic view to understand what’s at stake may be helpful when considering care for “minority ethnic populations.”30 The transdiagnostic view understands ED diagnoses as overlapping symptomology, where patients can transition across diagnoses as the ED progresses, and the mechanism thought to be maintaining symptoms are the focus of the treatment. This suggests that previous possibilities for diagnostic creep are attenuated using a transdiagnostic model and may even be supportive of people who do not meet the clinical thresholds of an ED.
Similarly, Yu et al. note in their review of Asian American’s that the individualizing therapies like CBT or DBT may never be appropriate for this population.19 In this review, the authors describe how important it can be to both understand that many people who identify as “Asian American” may be coming from a cultural space that privileges collectivism over individualism, but simultaneously acknowledge the diversity of this category and not make assumptions.19 Though providers may be better off focusing on treatment choices that focus on “individual” healing or wellness over “collective” understandings of healing or wellness may be less beneficial and supportive in these populations.
Cultural Competency and Cultural Humility
This brings us to a second foundational point of “inclusion” across health care spaces. Several scholars and practitioners in the field of EDs indicated that providers, nonclinical staff, and the system broadly need education and training on cultural competency and cultural humility.14,15,19,21,23-25 A broad sense of what qualifies as “cultural” was evident in the literature, and it should be noted that we are not speaking exclusively of race or ethnicity, but also of gender identity and sexual orientation.
Several of the studies pointed to the importance of cultural competency. This could involve being aware that other people may be coming from a different background and what that different background might be. In some ways, this is as simple as asking for people’s pronouns to avoid misgendering them,15,21,24,25 but it was often described as needing more in-depth training and education.21,24 For example, some publications described the importance of providers training in gender-affirming care for adolescents who identify as transgender and gender non-conforming, so these adolescents do not feel the burden of needing to “teach” their providers how to provide gender-affirming care.21,24 If providers don’t have a deeper level of competency than just repeating the correct pronouns, it could lead a person to not pursue care and act as a form of “exclusion.”21
As we have already described above, primary care providers are often the gatekeepers to access and they are not always trained in how to engage with and identify disordered eating among adolescents who are racialized, gender non-binary, transgender, and sexually diverse. If primary care providers are not trained to hear the concerns of the diverse adolescents or their families due to pre-existing stereotypes, assumptions, or disagreements, adolescents will not even be able to gain access to specialist care.14 Given this there is a need for training beyond specialist care centres.
However, without a commitment and openness to change through learning from mistakes, researchers suggest competency-based educational material alone was likely to be insufficient at fostering inclusive care environments.21 This is where cultural humility may come into play to encourage self-reflection and understanding one’s own positionality.19,21,23 In their recommendations for how to provide inclusive care to SGM adolescents, Calzo et al. note at 1 point the importance that providers be able to and institutions incorporate “cultural humility approaches to pedagogy and practice that encourage self-evaluation and critique, acknowledgement of power imbalances, and a commitment to lifelong learning.”(p.55)21 This takes a different tack from cultural competency in that it is less focused on making sure everything about the other is known ahead of time and is, instead, focused on cultural practices fostered by the providers or care institutions themselves. So, while it is certainly important to be aware of the languages and backgrounds people may be coming from, it cannot exist in isolation from self-reflection. What Calzo et al. point to is that rather than placing importance on knowing the culture the other comes from, the provider is required to understand where and how they are situated. This may help with situations of multiple and overlapping identities and encourage the clinical interactions to remain open, flexible, and curious.
This is not to discourage practices of cultural competency, either, as it can be important to learn how others operate and what needs they may have when it comes to caring for them and from their specific place. However, doing this without reflecting on how one’s “knowledge” is interfering with the other’s ability to be different than what one might expect has the potential to create further exclusions.
Limitations
There are several limitations affecting this report. For one, time has been a limiting factor affecting the analytical and conceptual depth of this report. While we had initially planned to conduct a full narrative review, timelines needed to be adapted to conduct a rapid narrative review. In and of itself this is not a problem as this work will help inform the HTA assessment of early intervention for ED programs; however, abbreviated timelines have limited the depth with which we were able to analyze included publications. This means that our arguments have remained necessarily loose and some connections between publications only briefly touched on.
Similarly, while we had initially planned to return to the literature in an iterative manner, limited time frames made that challenging and we were only able to go back to the literature once. We are confident that the included publications are relevant to our overall research question and that our findings will be supportive to the CADTH team’s assessment of early intervention programs for EDs. However, having the opportunity to return to the literature multiple times, perhaps with the support of experts in the ED field, may have helped us refine the breadth of our analysis and focus on only what is most relevant to CADTH’s upcoming assessment.
Relatedly, CADTH librarians continue to test out search strategies around how best to capture and incorporate literature that focuses on questions of equity. Again, while we are confident in the literature that we do have, we are aware that, as a learning project, there may be other literature that could have been similarly helpful to our work or introduced us to new ideas.
Finally, as already alluded to, it has been quite challenging proceeding with this work in the absence of expert support. Throughout this review, there were several situations where we may have benefited from asking experts their thoughts on what we were seeing in the publications. One hallmark of a full narrative review is in identifying the central, or most relevant literature of the field. This has been challenging without expert guidance due to the time limitations of this review.
Discussion and Questions for Consideration
Discussion
In response to CADTH’s growing interest in “fostering health systems that reflect the diverse people of Canada” and in supporting the equitable implementation of accessible and inclusive health technologies, this custom report was developed to provide early insight into some equity considerations that may be relevant to an upcoming CADTH HTA assessing the role of early intervention programs in the care of adolescents living with EDs. To do this, this custom report has engaged with both empirical and conceptual literature around adolescent EDs and asked how access and inclusion have been conceptualized in that literature. We have focused primarily on conceptualizations relevant to the disparities of access that have already been noted regarding racialized, LGBTQ2S+, and cisgender male adolescents.1,4
This discussion is organized as a reflection on the broader findings that highlights 1 overarching tension noticed across the literature. Following this, we provide a series of questions the CADTH team may ask when assessing early interventions for adolescents with EDs.
A primary tension in the literature we have engaged with stems from what we read as dissonance over what qualifies as “inclusion.”
On the 1 hand, inclusive care (and access to that care) seems to pivot primarily around the practices of recognition and representation. In this understanding, it is well-acknowledged that any adolescent can be living with an ED and that what is primarily at stake is ensuring that diverse adolescents dealing with disordered eating are captured and brought into the fold of pre-existing care spaces and practices. This form of inclusion is visible in theoretical frameworks identifying persistent experiences of discrimination as increasing the possibility that adolescents may engage in harmful practices around food and eating.14-21,23,25,27,29,30 It is also present in literature highlighting personal and cultural barriers to help-seeking that need to be accounted for when attempting to develop inclusive care spaces.13,14,16,20,30 It can also be seen in literatures focused on identifying assessment tools that remain invariant across diverse populations or expanding existing treatment approaches to be more culturally responsive.31 Continuing education in cultural competency that, for example, improves providers’ awareness of transgender health needs and teaches them the importance of using the correct pronouns may also fit within this understanding of inclusion. These practices all have the potential to be positive moves toward inclusive and accessible care. However, positive they may be, we suggest that without a more intensive, structural engagement with the exclusions detailed throughout this report, these moves may fall short of broader goals of improving equitable (e.g., inclusive and accessible) care.
We say this based on our “read” of another form of inclusion identified in this review. In this second form, we see authors promoting a thorough interrogation of the conceptual and structural underpinnings of eating disorder research and practice. In some instances, this appeared as a counterweight to those understandings of inclusion noted in the previous paragraph. For instance, in response to literature promoting the value of theoretical frameworks as heuristic devices detailing risk relationships between ED development and racialized, gendered, or cultural identities, we also pointed to literature warning how these could easily slip into the domain of “diagnostic trope.”16 In this case, these frameworks can be helpful to understand how these individuals stand at a different relationship to risk than those who do not consistently experience discrimination or deal with challenges of navigating multiple cultural inputs of how to live and eat. However, as these theoretical frameworks are meant to speak broadly across all adolescents (or adults) within the framework’s targeted population, they also run the risk of reducing personal experience, circumstance and behaviour to a generalizable norm. This slippage between heuristic and diagnostic trope, we note, can find (at least partial) remediation through care practices that centre the individual and their own context within the clinical encounter.
At first glance, this may simply seem to reinforce standard calls for “tailoring” common throughout medical literature, increasingly focused on “patient-centred” and “personalized” care. However, the importance of attending to individual context appears again in our engagement with literature critiquing the potential exclusions of current diagnostic categories. Lamarre et al. identify this as a tension between critical feminism’s engagements with ED that attend to the ways in which structural and systemic factors may impact experiences around food, exercise, and embodied distress; and more “mainstream” approaches that acknowledge the existence of these factors, but places them in a secondary position to biomedical understandings of disease.(p.5)29 While inclusive care does involve attending to individual needs, this other form of inclusive practice also attends to the structural elements that may be acting as exclusions for diverse adolescents dealing with eating disturbance and challenges around body image. These structural elements may include, among others, the diagnostic categories and assessment criteria developed using bodies and experiences so focused on an idealized image of eating disordered patient (i.e., young, white, cisgender, heterosexual women) that people not fitting this definition go undiagnosed and unable to access specialized care for the distress around eating and body image. This view does not aim to diminish the distress and needs of young, white, cisgender, heterosexual women living with an ED, but signals that improving access and inclusive care for all adolescents may require rethinking, or engaging differently, with existing diagnostic, assessment and treatment practices.
Questions for Consideration
As the CADTH team prepares to assess early intervention programs for adolescents with ED, this report aims to clarify and support awareness around the challenges of access and inclusion to ED care for racialized, LGBTQ2S+, and male adolescents detailed throughout this report. We have prepared a series of questions that are reflective of these challenges and aim to be a sensitizing tool that can help the CADTH HTA team remain attuned to the considerations around equitable access and inclusion to care.
How does this program or intervention engage adolescents with disordered eating or a diagnosed eating disorder who either self-identify, or read, as a person from a systemically excluded population? For example, does this program approach these adolescents as unique individuals with needs and experiences around ED that may be different from their peers occupying similar identities?
How does this program or intervention receive potentially eligible patients (e.g., who is able to refer)?
How does this program or intervention define eligibility? Are their specific diagnostic criteria that need to be met before a person gains entry to care? If so, how might the diagnostic categories exclude adolescents from care?
Does this program or intervention have any language identifying a specific focus on some populations? What does this language look like, and what sort of understandings of populations outside of the woman being young, White, cisgender, affluent archetype are being articulated? Are there any diagnostic tropes that may be coming into play – acculturation, minority stress, objectification? While these may not necessarily be negative, how might they limit the sorts of experiences and needs one is expected to have around ED or how they can appear in care?
How might the assessment tools and procedures that area used to determine eligibility for this program perpetuate exclusions for adolescents outside of the young, White, affluent woman archetype?
References
1.The Canadian eating disorders strategy: 2019-2029. Toronto (ON): Canadian Eating Disorders Alliance; 2019: http://edfc.ca/wp-content/uploads/2019/11/Canadian-Eating-Disorders-Strategy-Nov-2019-English.pdf. Accessed 2023 Feb 13.
2.Hamilton Health Sciences. “It's no one's fault”: exploring the complexity of eating disorder diagnoses. 2022; https://www.hamiltonhealthsciences.ca/share/complexity-of-eating-disorder-diagnoses/. Accessed 2023 Feb 17.
3.Stoodley C. Nova Scotia sees 400% rise in demand for eating disorder services. 2021; https://halifax.citynews.ca/local-news/nova-scotia-sees-400-rise-in-demand-for-eating-disorder-services-3361443. Accessed 2023 Feb 17.
4.Canadian Institute for Health Information. Hospitalizations for eating disorders among young women jumped by more than 50% during the COVID-19 pandemic. 2022; https://www.cihi.ca/en/news/hospitalizations-for-eating-disorders-among-young-women-jumped-by-more-than-50-during-the. Accessed 2023 Feb 17.
5.Huryk KM, Drury CR, Loeb KL. Diseases of affluence? A systematic review of the literature on socioeconomic diversity in eating disorders. Eat. 2021;43:101548. PubMed
6.Halbeisen G, Brandt G, Paslakis G. A plea for diversity in eating disorders research. Front Psychiatry. 2022;13:820043. PubMed
7.Coelho JS, Suen J, Clark BA, Marshall SK, Geller J, Lam PY. Eating disorder diagnoses and symptom presentation in transgender youth: a scoping review. Curr Psychiatry Rep. 2019;21(11):107. PubMed
8.Greenhalgh T, Thorne S, Malterud K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur J Clin Invest. 2018;48(6):e12931. PubMed
9.Andersen RM, Davidson PL. Improving access to care in America: individual and contextual indicators. Changing the U.S. health care system: key issues in health services policy and management. 3rd ed. San Francisco (CA): Jossey-Bass; 2007:3-31.
10.Building inclusive health care services: a rapid qualitative review. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RC1293%20ICHS%20Final.pdf. Accessed 2023 Feb 13.
11.Charmaz K. Constructing grounded theory. 2nd ed. Thousand Oaks (CA): Sage Publications Ltd; 2014: https://us.sagepub.com/en-us/nam/constructing-grounded-theory/book235960. Accessed 2023 Feb 8.
12.Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45. PubMed
13.Wales J, Brewin N, Raghavan R, Arcelus J. Exploring barriers to South Asian help-seeking for eating disorders. Ment Health Rev (Brighton). 2017;22(1):40-50.
14.Chowbey P, Salway S, Ismail M. Influences on diagnosis and treatment of eating disorders among minority ethnic people in the UK. J Public Ment Health. 2012;11(2):54-64.
15.Hartman-Munick SM, Silverstein S, Guss CE, Lopez E, Calzo JP, Gordon AR. Eating disorder screening and treatment experiences in transgender and gender diverse young adults. Eat. 2021;41:101517. PubMed
16.Channa S, Lavis A, Connor C, Palmer C, Leung N, Birchwood M. Overlaps and disjunctures: a cultural case study of a British Indian young woman's experiences of bulimia nervosa. Cult Med Psychiatry. 2019;43(3):361-386. PubMed
17.Miraglia KA. Treating disordered eating patterns in trans-identified individuals. Dissertation abstracts international B: the sciences and engineering. 2022;83(10-B):No pagination specified.
18.Mustafa N, Khanlou N, Kaur A. Eating disorders among second-generation Canadian South Asian female youth: an intersectionality approach toward exploring cultural conflict, dual-identity, and mental health. Today's youth and mental health: hope, power, and resilience. Cham (CH): Springer International Publishing AG; 2018:165-184.
19.Yu KY, Pope SC, Perez M. Clinical treatment and practice recommendations for disordered eating in Asian Americans. Prof Psychol Res Pr. 2019;50(5):279-287.
20.Cachelin FM, Gil-Rivas V, Vela A. Understanding eating disorders among Latinas. Adv Eat Disord. 2014;2(2):204-208. PubMed
21.Calzo JP, Lopez EE, Silverstein S, Brown TA, Blashill AJ. Where is the evidence of evidence-based treatment for LGBTQIA+ individuals experiencing eating disorders? Adapting evidence-based eating disorder treatments for novel populations and settings: a practical guide. New York (NY): Routledge; 2021:50-73.
22.Reyes-Rodriguez ML, Franko D. Cultural adaptations of evidence-based treatments for eating disorders. Adapting evidence-based eating disorder treatments for novel populations and settings: a practical guide. New York (NY): Routledge; 2021:3-30.
23.Yokoyama K. The double binds of our bodies: multiculturally-informed feminist therapy considerations for body image and eating disorders among Asian American women. Feminist reflections on growth and transformation: Asian American Women in therapy. Vol 30. New York (NY): Taylor and Francis; 2013:177-192.
24.Geilhufe B, Tripp O, Silverstein S, Birchfield L, Raimondo M. Gender-affirmative eating disorder care: clinical considerations for transgender and gender expansive children and youth. Pediatr Ann. 2021;50(9):e371-e378. PubMed
25.Goldhammer HB, Maston ED, Keuroghlian AS. Addressing eating disorders and body dissatisfaction in sexual and gender minority youth. Am J Prev Med. 2019;56(2):318-322. PubMed
26.Lavender JM. Using eating disorder and body image assessment questionnaires with boys/men. Eating disorders in boys and men. Cham (CH): Springer International Publishing AG; 2021:83-101.
27.Giordano S. Eating yourself away: reflections on the ‘comorbidity’ of eating disorders and gender dysphoria. Clin Ethics. 2017;12(1):45-53.
28.Murray SB, Nagata JM, Griffiths S, et al. The enigma of male eating disorders: a critical review and synthesis. Clin Psychol Rev. 2017;57:1-11. PubMed
29.LaMarre A, Levine MP, Holmes S, Malson H. An open invitation to productive conversations about feminism and the spectrum of eating disorders (part 1): basic principles of feminist approaches. J Eat Disord. 2022;10(1). PubMed
30.Acle A, Cook BJ, Siegfried N, Beasley T. Cultural considerations in the treatment of eating disorders among racial/ethnic minorities: a systematic review. J Cross Cult Psychol. 2021;52(5):468-488.
31.McEntee ML, Serier KN, Smith JM, Smith JE. The Sum Is greater than its parts: intersectionality and measurement validity of the Eating Disorder Examination Questionnaire (EDE-Q) in Latinx undergraduates in the United States. Sex Roles. 2021;84(1-2):102-111.
32.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
33.Affirming care for every body. A guide to eating disorders in the 2SLGBTQ+ community by individuals with lived experience for community members and carers. Toronto (ON): National Eating Disorder Information Centre: https://nedic.ca/2slgbtq/. Accessed 2023 Feb 21.
34.Papathomas A, Lavallee D. Eating disorders in sport: a call for methodological diversity. Rev Psicol Deporte. 2012;21(2):387-392.
Appendix 1: Selection of Included Studies
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca