CADTH Health Technology Review
Thrombopoietin Receptor Agonists as Second-Line Treatment in Children With Ongoing Immune Thrombocytopenia
PROSPERO Registration Number: CRD42023429164
Technology Review
Key Messages
What Is the Issue?
Immune thrombocytopenia (ITP) is an autoimmune disorder characterized by low platelets and an increase in bleeding risk; in the pediatric population, the reported incidence rate varies between 2 and 5 per 100,000 children per year. Spontaneous remission may be observed in up to 70% of patients, while 20% of patients may experience severe bleeding symptoms.
In children whose ITP does not respond to first-line corticosteroids, IV immunoglobulin (IVIG), or anti-D immunoglobulin, guidelines recommend the use of thrombopoietin receptor agonists (TPO-RAs), i.e., eltrombopag or romiplostim (avatrombopag did not have a marketing authorization and Notice of Compliance at the time that the review was initiated). Rituximab is considered a subsequent-line of therapy. Splenectomy is not usually considered an appropriate treatment option in children.
The goal of therapy in pediatric patients with ITP is to reduce bleeding and improve quality of life. Platelet response is considered a valid and appropriate surrogate end point in studies and routine assessment in clinical practice.
Children whose ITP does not respond to available first-line drugs may require subsequent treatment with off-label drugs because they do not have access to TPO-RAs.
What Did We Do?
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence.
A systematic review of the literature identified 5 studies (4 randomized controlled trials [RCTs] and 1 observational study), which were synthesized narratively.
The review addressed the following policy questions:
In children with ongoing, active ITP, what is the overall body of evidence supporting the use of TPO-RAs and rituximab after failure of first-line therapies?
Based on the level and quality of clinical evidence, should TPO-RAs be reimbursed for use earlier in the treatment sequencing for children with ongoing, active ITP, instead of being reimbursed only after a course of rituximab?
What Did We Find?
Evidence from 2 RCTs (n = 159) suggests that eltrombopag likely increases and maintains platelet response over time, in addition to decreasing the use of rescue medication and clinically significant bleeding compared to placebo, which were considered clinically meaningful outcomes for pediatric patients with ITP. There was a low risk of bias in the studies, but uncertainty was introduced due to the small sample sizes.
Evidence from 1 RCT (n = 62) suggests that romiplostim may also increase and maintain platelet response, as well as reduce clinically significant bleeding compared to placebo. However, there was some concern due to a high risk of bias in the studies and uncertainty due to the small sample size, which suggests a need for caution in the interpretation of the findings.
The effectiveness of rituximab was inconclusive due to the lack of evidence, as no comparative RCTs could be identified, while the observational study included presented only descriptive comparisons. No evidence was identified in support of trying rituximab before accessing TPO-RAs.
What Does This Mean?
Given that ITP is rare in children, there is a gap in available relevant evidence, and robust evidence from large RCTs in this patient population are unlikely to be conducted.
Jurisdictions may consider requesting an implementation advice panel for use of eltrombopag and romiplostim after failure of first-line therapies in children with ongoing, active ITP.
Abbreviations
AE
adverse event
CI
confidence interval
DB
double blind
HRQoL
health-related quality of life
HTA
health technology assessment
ITP
immune thrombocytopenia
ITT
intention to treat
IVIG
IV immunoglobulin
KIT
Kid’s ITP Tools
MCID
minimal clinically important difference
OR
odds ratio
PDSA
Platelet Disorder Support Association
PICOS
participants, intervention, comparator or control, outcomes, and study design
RCT
randomized controlled trial
ROBINS-I
Risk of Bias in Nonrandomized Studies – Interventions
SAE
serious adverse event
TPO-RA
thrombopoietin receptor agonist
Executive Summary
Background and Policy Context
ITP is an autoimmune disorder characterized by low platelets and an increase in bleeding risk.1-4 In the pediatric population, the reported incidence rate varies between 2 and 5 per 100,000 children per year.5 ITP differs between the adult and pediatric populations; both spontaneous remission and severe bleeding are substantially more frequent in children than in adults.6-8
First-line therapy may include observation, but, in the presence of non–life-threatening mucosal bleeding or bleeding that impacts quality of life, first-line therapy is a short course of corticosteroids.9,10 Alternatively, IVIG and anti-D immunoglobulin may be used in patients whose ITP does not respond or have a contraindication to taking corticosteroids.9,10 Considering the balance of benefits and harms, costs, patient preference, and feasibility, guidelines suggest that TPO-RAs (eltrombopag or romiplostim) are the preferred second-line therapy in pediatric patients whose ITP does not respond to first-line treatment; rituximab would be considered a subsequent-line therapy.9,10 Splenectomy is not usually considered an appropriate treatment option in children.9,10
A systematic review was undertaken at the request of public drug plans to help inform which treatment(s) should be used in pediatric patients with ITP who have failed first-line treatments. For jurisdictions, knowing the level of evidence for, and efficacy of, TPO-RAs will add to what is currently known and may help inform decision-making regarding the reimbursement of these drugs.
Clinical Evidence
The research protocol was developed a priori, by engaging with patient groups and clinical experts, and the systematic review used robust methodology. Eight publications were identified, reporting findings from 5 unique studies. The populations in the studies contributing to the evidence were considered generalizable to most children with ITP in the clinical setting. A narrative synthesis was conducted due to clinical and methodological heterogeneity between studies that precluded an indirect treatment comparison. Avatrombopag was not included, as it did not have a marketing authorization and Notice of Compliance at the time this review was initiated.
Evidence from 2 double-blind (DB) RCTs (n = 159) suggests that eltrombopag likely results in a clinically important, long-lasting platelet response when compared to placebo (at least 6 weeks and up to 12 months) in pediatric patients with ITP in whom first-line treatments have failed. Eltrombopag also likely results in a reduction in the use of rescue medication and clinically significant bleeding compared to placebo, which were considered clinically meaningful outcomes for patients. There was a low risk of bias in the studies, but uncertainty was introduced due to the small sample sizes. Evidence from 1 DB RCT (n = 62) suggests that romiplostim may result in a clinically important, long-lasting platelet response and reduction in clinically significant bleeding when compared to placebo (at least 24 weeks and up to 12 months). However, there is some concern that a high risk of bias and uncertainty was introduced due to the small sample size, which suggests a need for caution in the interpretation of the findings.
Due to the scarcity of evidence in the patient population, conclusions could not be drawn for the impact of TPO-RAs on health-related quality of life (HRQoL) and function in children. Assessment of the effectiveness of rituximab was inconclusive due to the lack of evidence, as no comparative RCTs could be identified, while the 1 observational study included presented only descriptive within-arm data (i.e., no direct comparisons). In addition, no evidence was identified in support of trying rituximab before accessing TPO-RAs.
Limitations
The review was based on limited availability of evidence. No head-to-head RCT in the target patient population was identified in the literature, and methodological considerations prevented a meaningful indirect treatment comparison from being conducted. As a result, direct comparisons of effectiveness between treatments cannot be made. Most included studies had a relatively small sample size, which limited the level of precision and affected the certainty in the findings. We acknowledge that ITP is a rare disease in children and that large RCTs in this patient population may be unfeasible. One observational study was included in the review; however, the authors did not present comparative effect estimates. Results of this study should be interpretated with caution, and findings should be viewed as complementary to those from RCTs.
Conclusions and Implications for Decision- or Policy-Making
Public drug programs may consider requesting an implementation advice panel for use of eltrombopag and/or romiplostim in children with ITP after failure of first-line treatments.
Introduction
Background and Rationale
ITP is an autoimmune disorder characterized by low platelets and an increase in bleeding risk due to increased platelet destruction and impaired platelet production.1-4 It was previously called idiopathic thrombocytopenic purpura but is no longer considered an idiopathic disease.3,4 The specific cause of ITP is unknown but may be a mix of genetic and environmental factors.11 In addition, not all patients will experience bleeding symptoms such as purpura.11
Primary ITP is defined as isolated thrombocytopenia, i.e., peripheral blood platelet count below 100 × 109/L, in the absence of other causes or disorders that may be associated with thrombocytopenia.4 The disorder falls into 1 of the following 3 disease groups according to disease duration:4
Newly diagnosed ITP: active disease duration of 0 to 3 months
Persistent ITP: active disease duration of 3 to 12 months, including those patients not reaching spontaneous remission or not maintaining complete response of therapy
Chronic ITP: ongoing, active disease lasting longer than 12 months.
ITP differs between the adult and pediatric populations. Spontaneous remission, which occurs when there is an improved platelet count in the absence of ongoing or recent therapy, may be observed in around 70% of children,6,7 which is substantially more frequent than in the adult population (45% of adults achieve spontaneous remission at 6 months, 49% at 12 months, and 56% at 24 months).6,7
ITP has a reported incidence rate varying between 2 and 5 per 100,000 children per year according to various epidemiological studies around the world.5 Bleeding symptoms are often present, including severe bleeding (such as in the gastrointestinal tract or in the brain) in approximately 20% of children.7,8
Pediatric patients newly diagnosed with ITP with no or minor bleeding may undergo observation according to the American Society of Hematology 2019 Guidelines for Immune Thrombocytopenia9 and the 2019 International Consensus Report on the Investigation and Management of Primary Immune Thrombocytopenia.10 In the presence of non–life-threatening mucosal bleeding or bleeding that impacts quality of life, first-line therapy is a short course (up to 7 days) of corticosteroids. For patients with ITP whose ITP does not respond or have a contraindication to taking corticosteroids, other first-line therapies include IVIG and anti-D immunoglobulin.9 According to the international standardized definition, a platelet count response may be defined as a platelet count of 30 × 109/L or higher, with at least a 2-fold increase in platelet count from baseline, combined with the absence of bleeding; a complete platelet response would typically be defined as a platelet count of 100 × 109/L or higher, as long as there is an absence of bleeding.4
In pediatric patients whose ITP does not respond to first-line treatment, which is often simplified in the literature as a platelet count below 50 × 109/L,10 guidelines recommend the use of TPO-RAs, i.e., eltrombopag or romiplostim (avatrombopag was not included in this review as at the time the review was initiated, it did not have a marketing authorization and Notice of Compliance).9,10 Considering the balance of benefits and harms, costs, patient preference, and feasibility, the American Society of Hematology suggests the use of TPO-RAs rather than rituximab, which would be considered a subsequent-line therapy.9,10 Issues such as the scarcity of evidence, however, led to this recommendation being conditional, based on very low certainty in the evidence of effects.9 Based on the body of evidence, the guideline panel concluded that the potential benefits of TPO-RAs were high, especially with regard to the reduction of bleeding events and reduction or discontinuation of corticosteroids. Additionally, the risks of TPO-RAs were considered low.9 These drugs were also favoured over immunosuppressants, as a high value is placed on avoiding immunosuppression in children.9 The importance of avoiding immunosuppression in the pediatric population was emphasized by the clinical experts consulted for this review. For example, the clinical experts mentioned the issue of delay in the standard immunization schedule because of the use of immunosuppressive therapies, which has been described in the literature12-14 and became even more serious in clinical practice during the recent COVID-19 pandemic.
Other subsequent-line therapies include azathioprine, cyclophosphamide, cyclosporine, danazol, dapsone, mycophenolate mofetil, and vinca alkaloids used off-label; however, guidelines such as that of the American Society of Hematology did not prioritize a review of these drugs due to limited availability of data, lack of direct comparisons, and large variability in outcome measures.9 The clinical experts also confirmed that there is now only a very limited role for immunosuppressants in children with ITP in clinical practice, that is, in patients who do not respond to TPO-RAs.
Based on major guidelines9,10 and clinical expert opinion, splenectomy is not usually considered an appropriate treatment option in children with ITP. The clinician feedback received emphasized that splenectomy would not be considered an appropriate criterion for reimbursement purposes given that it is major surgery, other therapies are recommended as prior lines of treatment, and splenectomy has many negative effects for children, including lifetime immune suppression, posing a risk of life-threatening infections (i.e., loss of protection against Streptococcus pneumoniae, Neisseria meningitidis, and Hemophilus spp.).15-17 Immune suppression due to splenectomy also results in prolonged use of antibiotics, both for prophylaxis and treatment of pyrexia which may be because of an unknown cause, which can contribute to antibiotics resistance. In addition, splenectomy cannot be considered a guaranteed cure for ITP. As there are no predictive factors to determine who is more likely to respond to splenectomy, making the decision to have a child undergo major surgery remains challenging. Hence, feedback highlighted that physicians and surgeons would be best placed to make this clinical decision. For these reasons, splenectomy was not one of the interventions assessed in this systematic review.
Before being authorized to access a TPO-RA, children who require second-line pharmacotherapy may be required, in some jurisdictions, to try another drug such as rituximab. As TPO-RAs are not reimbursed as second-line options, there remains a need for ITP treatments for the few patients who do not respond to first-line therapy.
Therefore, we performed a systematic review assessing the efficacy and safety of TPO-RAs (i.e., eltrombopag and romiplostim) and other relevant drugs identified by the jurisdictions (i.e., rituximab for children with ITP in whom first-line therapies have failed) to help inform decision-making regarding place in therapy and public reimbursement of TPO-RAs.
Of note, only eltrombopag has a Health Canada indication in children with ITP;18 romiplostim holds an indication in adult patients, but Health Canada has not authorized an indication for pediatric use.19 Avatrombopag did not hold a Notice of Compliance from Health Canada at the time this review was performed. A Notice of Compliance was granted on November 3, 2023, for the use of avatrombopag in adult patients. However, a placebo-controlled, phase III RCT evaluating the use of avatrombopag in children with ITP was ongoing at the time of this review and has since been completed;20 it may provide further insights on the use of TPO-RAs in this patient population once results become available.
The final scope of this health technology assessment (HTA) project was informed by feedback received following publication of our HTA on the comparative effectiveness and cost-effectiveness of treatments for ITP in the adult population after failure of first-line therapies.21
Clinical Review Objectives
The objective of this HTA was to review the clinical effectiveness and safety of TPO-RAs eltrombopag and romiplostim as second-line treatments in pediatric patients with ITP when compared to current second-line drugs.
Policy Questions
To assist jurisdiction in making local decisions, the systematic review aimed to address the following policy questions:
In children with ongoing, active ITP, what is the overall body of evidence supporting the use of TPO-RAs (i.e., eltrombopag and romiplostim) and rituximab after failure of first-line therapies?
Based on the level and quality of clinical evidence, should TPO-RAs be reimbursed for use earlier in the treatment sequencing for children with ongoing, active ITP, instead of being reimbursed only after a course of rituximab?
Research Questions
The project will address the following research question:
What are the clinical efficacy and safety of TPO-RAs (i.e., eltrombopag and romiplostim) and rituximab for children with ITP in whom first-line therapies have failed?
What are the comparative clinical efficacy and safety of TPO-RAs (i.e., eltrombopag and romiplostim) and rituximab for children with ITP in whom first-line therapies have failed?
Opportunities for Stakeholder Feedback
Patient Engagement
We involve patients, families, and patient groups to improve the quality and relevance of our assessments, ensuring that those affected by the assessments have an opportunity to contribute to them. We have adopted a Framework for Patient Engagement in HTA. The framework includes Standards for Patient Involvement in Individual HTAs and is used to support and guide our activities involving patients and patient groups. For this HTA on pediatric ITP, the belief that individuals who have experience with ITP have knowledge, perspectives, and experiences that are unique and contribute to essential evidence for HTA guided our patient engagement activities.
Engagement Activities
Patient Group Input
We received a patient group input submission from the Platelet Disorder Support Association (PDSA) for an earlier report on adult ITP, outlining patient priorities and concerns.
Patient Advocacy Group Dialogue
PDSA was approached about participating in this report, after its input was received on a previous report. A Patient Engagement Officer gave an overview of the purpose and scope of the project and the purpose of the engagement.
PDSA outlined several areas of particular interest to the pediatric population, as distinct from the adult population with ITP. With consent, the dialogue was recorded for notetaking purposes and for sharing with members of the project team.
Team Presentation
A presentation, developed by the Patient Engagement Officer and reviewed by PDSA, was shared at a project team meeting to enhance the team’s understanding of the issues surrounding pediatric ITP from patients’ and caregivers’ perspectives. This presentation occurred during the protocol drafting phase, so that patients’ perspectives could be considered during the drafting of the protocol and the development of the report from the start.
Stakeholder Feedback
The draft report was released to the public for a 10-day stakeholder feedback period. Members of the public, including patients, patient groups, and clinicians, may review and submit their written feedback on the findings of the report during this period.
Stakeholder feedback was also solicited at key steps throughout the systemic review process. Thus, stakeholders were given the opportunity to provide feedback on the draft list of included studies and the draft report.
Several key themes were identified as specific to the pediatric population with ITP.
As there are different disease courses between pediatric and adult ITP, PDSA felt that it is important to focus research on the smaller percentage of children who have more frequent, severe bleeding than on those who spontaneously recover within a short period of time. Children are typically treated very conservatively, with limited focus on the prevention of bleeding, and PDSA was concerned about this tendency continuing in the treatment of children who develop chronic ITP and those who experience serious bleeding beyond mild skin bleeding. PDSA reported that children are usually not treated for a low platelet count, whereas adults would be treated at those same levels, regardless of their bleeding symptoms. It felt that the guidelines for treating children are less clear than those for treating adults.
Due to the heterogeneity of pediatric ITP, PDSA felt strongly about the need for multiple forms of treatment and for patients to have the ability to try different therapies according to their symptoms, rather than be forced to follow a stepwise order of treatment, since everyone (adults and children) responds differently to ITP treatments. The heterogeneity is not only seen in the clinical symptoms, but also in treatment response, duration of response, and other aspects of the natural history of the disorder. There are also concerns about requiring splenectomy, with its inherent risks, before accessing second-line treatments. The adult HTA identified that there wasn’t strong evidence to suggest a splenectomy must be performed before other access to treatment, which the patient group felt may also hold true for children. Children with ITP also have fewer treatment options than adults.
PDSA reflected that there are barriers to treatment, including the requirement for parental insurance that ends when children are no longer in school, patient-borne costs, invasiveness of treatment, time-consuming nature of some treatments, and method of delivery. For example, infusions performed in hospitals or clinics necessitate taking time away from work and school, affecting job performance and academic achievement. Most patients would choose oral medication over an infusion for many hours.
Quality of life was an important concern for PDSA. Having frequent bleeds in public, including visible bleeds such as dense petechiae, large ugly bruises, and oral blood blisters in mouth and lips can be humiliating and can contribute to poor self-esteem and mental health. Spending significant amounts of time in clinics or hospitals can impact school and social participation.
Ultimately, PDSA reported that patients want treatments that won’t cause them to go into financial debt, have minimal side effects, work long-term, reduce their fatigue, and are convenient.
Clinical Review Methods
To inform the conduct of this systematic review, a preliminary informal scoping of the existing literature was conducted. Stakeholder feedback was solicited at key steps. The systematic review protocol was developed a priori22 and was registered in the PROSPERO international prospective registry of systematic review as project number CRD42023429164.23 The protocol was followed throughout the study process, without deviations. The project is an HTA that includes a clinical evaluation only; although jurisdictions mentioned potential interest in an economic evaluation, this was not deemed feasible due to the limited evidence available.
Eligibility Criteria
Prespecified selection criteria for inclusion of studies in this systematic review are presented in Table 1. To be included, studies had to meet all the eligibility criteria.
Criteria | Description |
|---|---|
Population | Pediatric patients (< 18 years) with ongoing, active ITP who have failed first-line treatment (i.e., observation, corticosteroids, IVIG, or anti-D immunoglobulin) |
Interventionsa | Question 1 (clinical efficacy and safety) and Question 2 (comparative clinical efficacy and safety):
|
Comparatorsb | Question 1 (clinical efficacy and safety):
Question 2 (comparative clinical efficacy and safety):
|
Outcomes | Efficacy outcomes
Harms outcomes
|
Study Design | Published phase II, phase III, and phase IV RCTs If no RCTs are available to adequately inform a particular comparison: Published nonrandomized controlled trials and comparative prospective cohort studies |
HRQoL = health-related quality of life; ITP = immune thrombocytopenia; IVIG = IV immunoglobulin; RCT = randomized controlled trial; SC = subcutaneous.
Note: Relevant comparisons do not include different doses of the same drug.
aOnly eltrombopag has a Health Canada indication in children with ITP.18 Romiplostim holds an indication in adults with ITP; Health Canada has not authorized an indication for pediatric use.19 Rituximab does not have a Health Canada indication for ITP.24
bHealth Canada–recommended dosage for pediatric ITP or clinically relevant dosage based on expert advice or on relevant ITP guidelines.
cReported as a composite outcome, i.e., total numbers and proportions of patients with AEs or SAEs.
The following was considered when selecting studies for inclusion:
For research question 1 (clinical efficacy), evidence was sought from placebo-controlled RCTs. We discourage the use of informal naive indirect comparisons (i.e., observational comparisons across the results of separate trials or groups of trials), because they do not preserve the within-trial randomization. Such comparisons are likely to be affected by bias and confounding.
For research question 2 (comparative clinical efficacy), direct head-to-head evidence from RCTs was sought first, since well-designed and conducted RCTs typically offer the highest internal validity to inform causal inferences. When no such head-to-head RCTs could be identified for any given outcome-comparison, then eligible evidence included the following:
Nonrandomized controlled trials and comparative prospective cohort studies. To be considered prospective, comparative cohort studies must have clearly defined a hypothesis before the enrolment of patients and collection of outcomes data.
Full texts of titles or abstracts describing potentially relevant studies in a wider patient population were retrieved for assessment and included in the systematic review if appropriate subgroup results were reported.
Drug regimens eligible for inclusion in the systematic review for interventions and comparators were those that have been approved by Health Canada for ITP or were considered clinically relevant based on expert advice or on the major ITP guidelines.9,10
This review was limited to studies reported in English or French, as there is capacity for reviewing in both languages. No eligible studies were excluded for being published in a language other than English or French.
If multiple reports were identified for the same study, they were all included and cited; however, only unique data were extracted without duplication and the reports were considered as 1 single study in the analysis. The first complete report of a study was identified as the primary report; others were referred to as “associated reports.”
Abstracts, conference proceedings, or results posted on clinicaltrials.gov were not considered a complete report, as they typically do not provide sufficient information to properly assess risk of bias or generalizability. Therefore, studies reporting findings only though these means of publication were not included in the systematic review. However, we reported on ongoing trials registered in clinicaltrials.gov at the time the final report for this project was published.
Literature Search Methods
An information specialist performed the literature search for clinical studies, using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.25 The complete search strategy is presented in Appendix 1.
Published literature was identified by searching the following bibliographic databases: MEDLINE via Ovid and Embase via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the PICOS (population, interventions, comparators, outcomes, and study designs) framework and research questions. The main search concepts were pediatrics, ITP, and eltrombopag, romiplostim, or rituximab. The following clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, the European Union Clinical Trials Register, and the European Union Clinical Trials Information System.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 contains the detailed search strategies.
The initial search was completed May 2, 2023. Regular alerts to update the search were run until project completion.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from Grey Matters: A Practical Tool for Searching Health-Related Grey Literature. Included in this search are the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers (i.e., the included studies and relevant systematic reviews) and through contacts with appropriate experts. In addition, a list of included studies was posted on our website for feedback, where stakeholders were welcome to highlight any potentially relevant studies that could have been missed.
Study Selection Process
Before beginning screening, 2 reviewers conducted a pilot round by independently screening 50 randomly selected articles in duplicate, after which they met to resolve disagreements. No additional pilot round was needed. Then, the 2 reviewers independently (in duplicate) screened the titles and abstracts of all the citations retrieved from the literature search for relevance to the clinical research question in Microsoft Excel workbooks. Full texts of titles or abstracts that were judged to be potentially relevant by at least 1 reviewer were retrieved and independently assessed by 2 reviewers for possible inclusion based on the predetermined selection criteria outlined in Table 1. The 2 reviewers then compared their chosen included and excluded studies; disagreements at the full-text level were discussed until consensus was reached. If consensus could not be reached, a third reviewer was consulted. The study selection process is presented in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 flow chart.26 Studies excluded at the full-text screening stage, along with reasons for exclusion, were recorded and reported. Reference lists of included studies and relevant systematic reviews identified during screening were screened following the same selection process. Reviewers did not attempt to retrieve further information from study investigators, as it was not deemed necessary.
Studies identified via stakeholder feedback and reference list scanning were reviewed following the previously outlined process.
Data Extraction
All relevant data were extracted directly into a standardized data abstraction form, which was part of a review-specific Microsoft Excel workbook. It was planned that the form would be piloted before beginning full data extraction to ensure that it was usable and that it completely and reliably captured the items of interest, while avoiding redundancies. However, this was not deemed necessary due to the small number of included studies.
Formal data extraction was performed by 1 reviewer and independently checked for accuracy and completeness by a second reviewer. Any disagreements in the assessment of these data were resolved through discussion until consensus was reached or through involvement of a third reviewer, if required.
Relevant information to be extracted included details of the study characteristics (study design, enrolment dates, length of follow-up, funding source), population (number randomized, setting and region, inclusion and exclusion criteria, baseline characteristics), intervention and comparator (dose, route of administration, timing and frequency, description of co-interventions, adherence), outcomes (definitions and assessment methods, details of any scales used, timing of assessment) as well as relevant results (number randomized; analysis perspective; e.g., intention-to-treat [ITT]; analysis method; within and between-group results), and conclusions regarding the outcomes listed in Table 1. Where possible, data reporting on the ITT effect were preferentially extracted. All numerical data, including data presented in text or in figures, were extracted.
Where multiple variations of the same outcome were reported in the included studies, we collected the most clinically relevant definitions and time points for each outcome (based on clinical expert input, where needed), which facilitated later synthesis of the findings. Wherever possible, we prioritized data reported according to established definitions, as suggested by Rodeghiero and colleagues.4
If data were not reported for an outcome, no assumption was made about their presence or absence. Due to resource constraints, reviewers did not routinely contact authors of included studies to clarify any information or retrieve missing information.
Risk of Bias Assessment
The reviewers used the following risk of bias assessment tools, according to the study design of the included studies:
Outcome-level risk of bias of relevant RCTs, based on the effect of assignment to the intervention (i.e., ITT effect), was assessed using the Cochrane Risk of Bias tool, version 2.27 This assessment tool facilitates the evaluation of potential biases across 5 domains: the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results. A judgment of low risk of bias, some concerns regarding the risk of bias, or high risk of bias was assigned for each domain.
Outcome-level risk of bias in nonrandomized studies were assessed using the Risk of Bias in Nonrandomized Studies – Interventions (ROBINS-I) tool.28 This tool was chosen for ease of comparison to assessment of the risk of bias in RCTs. ROBINS-I facilitates the assessment of the risk of bias across 7 domains: confounding, selection bias, measurement of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported results. A judgment of low, moderate, serious, or critical risk of bias was assigned for each domain.
For each tool, the overall risk of bias of each study was rated and designated based on the domain-level assessments. Where possible, attempts were made to predict the direction of the potential bias. A rationale is provided for decisions about the risk of bias for both the domain-level and overall assessments.
It was planned that all reviewers involved in the risk of bias assessment would independently pilot the selected tools across a few studies and meet to resolve disagreements, to ensure a mutual understanding of the tool and methodological intricacies across studies. However, this was not deemed necessary due to the small number of included studies. The risk of bias was evaluated in duplicate by 2 independent reviewers. Any disagreements were resolved through discussion, with involvement of a third reviewer if consensus could not be reached.
In addition to the risk of bias, a generalizability assessment of the findings was also performed (i.e., patient population, choice of outcomes, treatment regimen, and length of follow-up). Throughout the critical appraisal process, reviewers included clinical input from experts consulted for this review.
Studies were not excluded from the systematic review based on the results of the risk of bias assessment. However, the critical appraisal results and how they affect study findings were used to inform conclusions about the body of evidence for each outcome-comparison.
Data Analysis and Synthesis
Before embarking on synthesis, the team considered the clinical and methodological heterogeneity of the relevant studies (i.e., with respect to methodology, outcomes definition and measurement, timing of assessment, and populations). We tabulated the characteristics of the included studies and presented these in a table with accompanying textual summary. We then charted the available studies and considered whether they were similar enough in their PICOS elements (including time point of outcome measurement) to be grouped in the synthesis.
The included studies were deemed too heterogeneous to combine statistically, mainly due to heterogeneity in the outcome measures that were reported. Findings were therefore synthesized narratively, considering the guidance by Popay et al.29 There were only 2 studies for eltrombopag versus placebo and 2 for romiplostim versus placebo. For these comparisons, we developed preliminary conclusions by organizing the studies by direction and size of effect. We intended to explore within- and between-study relationships and factors (including the a priori subgroups) that might have influenced the direction and magnitude of observed effects. However, this was unfeasible due to the small number of studies. We considered the robustness of the findings (e.g., impact of risk of bias) and drew a single, final conclusion about our best estimate of the size and direction of the anticipated effect across studies.
Interpretation and Drawing Conclusions
Conclusions were drawn for each outcome-comparison. The following items were considered: the risk of bias of the contributing studies, the precision of the effect estimates, the consistency of the evidence (in cases where more than 1 study contributes evidence for an outcome-comparison), and the generalizability (or applicability) of the findings. The risk of publication bias could not be formally appraised due to the small number of studies in each synthesis.
Results of Clinical Evaluation
Selection of Primary Studies
A total of 733 records were identified in the literature searches. Following screening of titles and abstracts, 43 reports were identified as potentially relevant and retrieved for full-text review. No report retrieved from other sources (i.e., grey literature, handsearch, and search alerts) was included as potentially relevant. Of these 43 potentially eligible reports, a total of 8 reports of 5 studies met the inclusion criteria and were included for review: 6 reports30-35 presenting data from 4 unique RCTs and 2 reports36,37 presenting data from 1 unique observational study. No relevant ongoing studies were identified.
The study selection process is illustrated in Appendix 2. Lists of included and excluded studies, with details describing the rationale for those excluded, are presented in Appendix 3 and Appendix 4, respectively.
Study and Patient Characteristics
Study and patient characteristics are shown in Appendix 5 and outlined in Table 2. Two of the included RCTs compared eltrombopag to placebo, and 2 RCTs compared romiplostim to placebo. No RCTs evaluating rituximab were identified. A prospective cohort study with eltrombopag, rituximab, and romiplostim arms was included in attempt to fill the gap in comparative evidence. However, the study provided only within-arm data without formal direct comparisons.
Table 2: High-Level Study Characteristics
Criteria | Bussel et al.30 PETIT | Grainger et al.32 PETIT2 | Tarantino et al.35 | Elalfy et al.33 | Grace et al. (2019)36 ICON1 |
|---|---|---|---|---|---|
Design | RCT | RCT | RCT | RCT | Cohort study |
Population | Patients < 18 years with diagnosis of ITP who have active disease, i.e., whose ITP relapsed or was refractory, after having tried ³ 1 prior treatment option | Patients with ITP who failed to maintain response to ≥ 2 prior treatment options | Patients < 18 years with diagnosis of ITP starting second-line treatments as monotherapy | ||
N | 67 | 92 | 62 | 18 | 120 |
Key baseline characteristics |
|
|
|
|
|
Interventions | Eltrombopag (dose to be adjusted according to platelet response) | Romiplostim (dose to be adjusted according to platelet response) | Rituximab Romiplostim Eltrombopag | ||
Comparators | Matching placebo | Matching placebo | Matching placebo | Placebo | Interventions compared to one another (descriptive comparisons only) |
Primary outcome | Platelet count response — various definitions were used across the studies | ||||
Time point for key measures | 6 weeks | 12 weeks | 24 weeks | NR | 1, 6, and 12 months |
Other key outcomes |
|
|
|
|
|
HRQoL = health-related quality of life; IBLS = ITP Bleeding Scale; ITP = immune thrombocytopenia; IVIG = IV immunoglobulin; KIT = Kid's ITP Tools; NR = not reported; RCT = randomized controlled trial.
Eltrombopag Versus Placebo — RCTs
In the 2 RCTs comparing eltrombopag to placebo,30,32 eltrombopag was administered orally once daily at a prespecified starting dosage, then adjusted based on platelet response; the target platelet count was 50 to 200 × 109/L. The mean age of patients was 9 to 10 years across treatment groups at baseline; patients were well distributed among age cohorts. Between 82% and 91% of patients in 1 RCT30 and all patients in the other RCT32 had ITP that lasted for at least 12 months (i.e., chronic ITP). Between 50% and 66% of patients across treatment groups had a baseline platelet count of 15 × 109/L or lower. The proportions of patients using concomitant ITP medication ranged from 3% to 21%; some imbalance between arms could be observed in 1 of the studies.32 Almost all patients had received previous ITP medication, but details of the specific therapies received were not consistently reported.
Both RCTs reported platelet count response as the primary outcome and used a minimal platelet count threshold of 50 × 109/L as part of the platelet response definition, in addition to the absence of rescue therapy. However, there were differences as to the conditions observed for patients to be considered responders, such as the time needed to be spent above the threshold value (ranging from at least once during the study to throughout the last 6 weeks of study follow-up). Both RCTs also reported on the use of concomitant ITP medications and/or rescue therapies, as well as bleeding as an outcome for efficacy assessment using the WHO bleeding scale, which has been validated in adults with ITP.38 One RCT30 reported findings on HRQoL using the Kid's ITP Tool (KIT) questionnaire, which is a validated measure used in pediatric patients with ITP.31 The score ranges from 0 to 100, with higher scores being associated with a better state. Using data from the PETIT study, the within-group minimal clinically important difference (MCID) was estimated as ranging from 5.9 to 8.4 points by parent report and 6.9 to 9.2 points by child report, using a distribution-based approach.31 No data were reported for the outcomes of function.
Romiplostim Versus Placebo — RCTs
In the 2 RCTs comparing romiplostim to placebo,33,35 romiplostim was administered by subcutaneous injection once weekly at a starting dosage of 1 mcg/kg. However, there were substantial differences between the 2 studies in their respective designs, patient populations (age, disease duration, and prior treatments), time points for outcome assessment, and outcome definitions; as a result, we opted to describe them separately.
In the DB RCT,35 the dose was titrated weekly in 1 mcg/kg increments based on platelet response; the target platelet count was 50 to 200 × 109/L. The median age of patients was 7.5 to 10 years across treatment groups at baseline; patients were well distributed among age cohorts. The median time since diagnosis averaged 2 years (interquartile range 1.0 to 4.2), which was consistent with chronic ITP. The median baseline platelet count was 17.8 × 109/L. Twelve percent to 20% of patients received concomitant ITP medication, suggesting some imbalance; as for previous first-line ITP medication, 76% of patients had received corticosteroids, 82% had received IVIG, and 31% had received anti-D immunoglobulin. The primary outcome was platelet count response, using a minimal platelet count threshold of 50 × 109/L that needed to be maintained for at least 6 of the final 8 weeks, in addition to the absence of rescue therapy. The RCT also reported on the use of concomitant ITP medications and/or rescue therapies, as well as bleeding using bleeding-related adverse events (AEs) of grade 2 or higher. Findings on HRQoL were reported using the KIT questionnaire in a separate publication;34 no data were reported for the outcomes of function.
In the small, single-blinded pilot RCT,33 the dose was escalated to 5 mcg/kg, then tapered; no detail was provided in the publication as to the target platelet count or regarding the escalation and tapering regimen. The median age of patients was 7 to 9.5 years across treatment groups at baseline (range not reported). The median disease duration was 2 to 3 years across treatment groups at baseline, with substantial variability, as shown by the interquartile range between 1 to 7 years. The median baseline platelet count was 10.5 × 109/L; no patient had a platelet count above 20 × 109/L. Details were not reported regarding the use of concomitant or previous ITP medication received, apart from the fact that all patients received prior corticosteroids. The study provided no detail as to how response to treatment was assessed. No data were reported for the use of concomitant ITP medications and/or rescue therapies or for the outcomes of bleeding, HRQoL, and function.
Rituximab Versus Placebo — RCTs
Assessment of the effectiveness of rituximab compared to placebo was inconclusive due to the lack of evidence, as no comparative RCTs could be identified, while the observational study included presented only descriptive comparisons with TPO-RAs.
Rituximab, Romiplostim, and Eltrombopag — Observational Evidence
In the prospective cohort study evaluating the comparative effectiveness of rituximab, romiplostim, and eltrombopag given as monotherapy,36 medications were administered according to physicians’ best judgment. No details were reported on whether there were any prespecified target platelet counts to achieve, or to inform on the doses of medication patients actually received. The mean age of patients ranged from 9.8 to 12.2 years across treatment groups at baseline. Approximately 50% of patients had chronic ITP in every study group, with approximately 30% having persistent ITP and between 15% to 20% having newly diagnosed ITP. The vast majority of patients had primary ITP. Between 40% and 58% of patients had a baseline platelet count that was below 10 × 109/L; the proportions of patients with a platelet count of no less than 30 × 109/L ranged from 7% to 20% of patients across treatment groups. The baseline grade 2 bleeding scores reported were consistent with the conclusion that substantial proportions of patients were experiencing clinically significant skin and nonskin bleeding at baseline; however, these proportions varied across treatment groups and bleeding category. Information about the use of concomitant treatments was not reported.
The primary outcome was platelet count response, using a minimal platelet count threshold of 30 to 100 × 109/L depending on the outcome definition, which needed to be attained at least half the time; there was no criterion related to the use of rescue medication. The cohort study did not report on the use of concomitant ITP medications and/or rescue therapies; however, bleeding was assessed as an efficacy outcome using the ITP Bleeding Scale and findings on HRQoL were reported using the KIT questionnaire. No data were reported for the outcomes of function.
Summary of Risk of Bias and External Validity Assessment
The risk of bias appraisal of all the included trials is presented for each domain in Table 3 and Table 4 and described in detail in Appendix 6. The key limitations, i.e., those having an impact on the interpretation of the findings, are summarized in this section for each treatment comparison.
Eltrombopag Compared to Placebo
Eltrombopag was compared to placebo in 2 DB RCTs of 7 weeks’30 and 12 weeks’ duration.32 Of these, both were rated as having a low risk of bias for all outcomes, with the exception of HRQoL, which was rated as having a high risk of bias. More specifically, there were large amounts of missing data for HRQoL in PETIT,30 large enough to have the potential to bias the outcome. In terms of generalizability, both study populations appear to be representative of clinical practice in Canada.
Romiplostim Compared to Placebo
Romiplostim was compared to placebo in 2 RCTs with substantial heterogeneity in methodology. Of these, Tarantino et al.35 was a DB RCT of 24 weeks’ duration rated as having some concern for the risk of bias for all efficacy outcomes, and at low risk of bias for the harms outcomes. No information was reported regarding missing efficacy outcome data and how they were handled; based on patient withdrawals, it is possible that missing data amount to proportions sufficiently high to introduce a risk of bias. In terms of generalizability, the study population appears to be representative of clinical practice in Canada.
Elalfy et al.33 was a single-blinded pilot RCTs of 15 weeks’ duration rated as having a high risk of bias for all outcomes assessed in the study. In addition, the trial publication has poor reporting. Platelet response was not defined, and, therefore, it is not possible to assess whether the threshold used and conditions required to be considered as having a platelet response were valid and relevant according to the definitions described in the guidelines and used in clinical practice. In addition, there is the possibility that multiple and inconsistent definitions could have been used by assessors, again affecting precision and confidence in the findings. No information was reported regarding missing outcome data and how they were handled. No prespecified analysis plan was reported and, considering the overall setting and trial conduct, it was impossible to determine whether investigators were blinded to outcome data. The trial was performed exclusively in Egypt; it is possible that the standard of care is different in other countries, which would affect generalizability of the results to the population in Canada. The fact that the study included some patients who had ongoing disease for up to 7 years and who had a platelet count that still did not exceed 20 × 109/L raises questions concerning generalizability of the population, i.e., whether these patients had been appropriately treated according to current practice standards in Canada before entering the study.
Rituximab, Romiplostim, and Eltrombopag — Observational Evidence
The use of rituximab, romiplostim, and eltrombopag was evaluated in a prospective, longitudinal cohort study of 12 months’ duration. ICON136 was rated using the ROBINS-I tool28 as having a serious risk of bias for all outcomes assessed in the study.
More specifically, the study was considered at increased risk of bias due to confounding, especially considering the fact that the authors did not attempt to control for postintervention variables that could have affected the interventions; the direction of potential bias cannot be predicted. Interventions were well defined and based on information obtained before the start of follow-up; however, there is the possibility that the choice of treatment may have been influenced by disease characteristics. There was an increased risk of bias due to significant patient attrition, with proportions differing between treatment groups and reasons for missing outcomes data not detailed in the publications. This suggests that patients contributing to the analyses at further time points are likely to be more representative of responders. The outcome of HRQoL was subject to additional bias, considering the subjectivity of the outcome, making it vulnerable to influence by knowledge of the intervention received, as assessors were aware of the intervention received. These issues introduce uncertainty around the true treatment effect; thus, results from the study should be interpretated with caution and findings should be viewed as complementary to those from RCTs. In terms of generalizability, the study population appears to be representative of clinical practice in Canada.
Table 3: Risk of Bias Assessment Per Outcome Within Each RCT Using Cochrane Risk of Bias Tool, Version 227
Study | Randomization process | Deviations from intended interventions (assignment) | Deviations from intended interventions (adherence) | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall |
|---|---|---|---|---|---|---|---|
Platelet response | |||||||
Bussel et al.30 (PETIT) | Low | Low | Low | Low | Low | Low | Low |
Grainger et al.32 (PETIT2) | Low | Low | Low | Low | Low | Low | Low |
Tarantino et al.35 | Low | Some concern | Low | Some concern | Low | Low | Some concern |
Elalfy et al.33 | Some concern | High | High | High | Low | Some concern | High |
Use of concomitant or rescue medication | |||||||
Bussel et al.30 (PETIT) | Low | Low | Low | Low | Low | Low | Low |
Grainger et al.32 (PETIT2) | Low | Low | Low | Low | Low | Low | Low |
Tarantino et al.35 | Low | Some concern | Low | Some concern | Low | Low | Some concern |
Elalfy et al.33 | Some concern | High | High | High | Low | Some concern | High |
Bleeding | |||||||
Bussel et al.30 (PETIT) | Low | Low | Low | Low | Low | Low | Low |
Grainger et al.32 (PETIT2) | Low | Low | Low | Low | Low | Low | Low |
Tarantino et al.35 | Low | Some concern | Low | Some concern | Low | Low | Some concern |
HRQoL | |||||||
Bussel et al.30 (PETIT) | Low | High | Low | High | Low | Low | High |
Tarantino et al.35 (Mathias et al.34 reporting on HRQoL) | Low | Some concern | Low | Some concern | Low | Low | Some concern |
Harms | |||||||
Bussel et al.30 (PETIT) | Low | Low | Low | Low | Low | Low | Low |
Grainger et al.32 (PETIT2) | Low | Low | Low | Low | Low | Low | Low |
Tarantino et al.35 | Low | Low | Low | Low | Low | Low | Low |
Elalfy et al.33 | Some concern | High | High | High | High | Some concern | High |
HRQoL = health-related quality of life.
Table 4: Risk of Bias Assessment Per Outcome for the ICON1 Observational Study Using ROBINS-I28
Grace et al. (2019)36 (ICON1) | Confounding | Patient selection | Classification of interventions | Deviations from intended interventions | Missing data | Outcome measurement | Selection of reported results | Overall |
|---|---|---|---|---|---|---|---|---|
Platelet response | Serious | Low | Moderate | Low | Serious | Low | Moderate | Serious |
Use of rescue medication | Low | Low | ||||||
Bleeding | Serious | Low | ||||||
HRQoL | Serious | Low |
HRQoL = health-related quality of life; ROBINS-I = Risk of Bias in Nonrandomized Studies – Interventions.
Data Analysis and Synthesis
Results
Detailed outcome results for studies included in the narrative synthesis are outlined in Table 5 and Table 6 and presented in Appendix 7. All the studies included in the systematic review reported platelet count response as the primary outcome; however, the definitions used to assess platelet response varied substantially across the studies. According to the international standardized definition, a platelet count response may be defined as a platelet count of 30 × 109/L or higher, with at least a 2-fold increase in platelet count from baseline, combined with the absence of bleeding; a complete platelet response would typically be defined as a platelet count of 100 × 109/L or higher, as long as there is an absence of bleeding.4 In addition to the platelet count thresholds, there were differences among all the studies as to the conditions observed for patients to be considered responders, such as the time needed to be spent above the threshold value (ranging from at least once during the study to throughout the last 6 weeks of study follow-up), as well as criteria related to the use of rescue medication.
Eltrombopag Compared to Placebo
Platelet Response
In PETIT (n = 67),30 the proportions of patients achieving a platelet count of 50 × 109/L or more at least once over 6 weeks, in the absence of rescue therapy, were 62% in the eltrombopag arm and 32% in the placebo arm (odds ratio [OR] = 4.31; 95% confidence interval [CI], 1.39 to 13.34; P = 0.011). The outcome definition was consistent with a basic measure by only requiring patients to achieve an adequate platelet count threshold once throughout 6 weeks. A more stringent outcome definition was used as a secondary outcome; the proportions of patients achieving a platelet count of 50 × 109/L or more in at least 60% of assessments were 36% in the eltrombopag arm and 0% in the placebo arm (OR = 5.84; 95% CI, 1.18 to 28.90; P = 0.0017) versus placebo. The magnitude of the point estimate for the between-group difference may be considered clinically meaningful according to the clinical experts consulted.
In PETIT2 (n = 92),32 the proportions of patients achieving a platelet count of 50 × 109/L or more in the absence of rescue therapy for at least 6 weeks from week 5 to 12 were 40% in the eltrombopag arm and 3% in the placebo arm (OR = 18.0; 95% CI, 2.3 to 140.9; P = 0.0004) versus placebo. The magnitude of the point estimate for the between-group difference may be considered clinically meaningful, according to the clinical experts consulted. The outcome definition was considered stringent, meaning that patients who were counted as responders had to achieve an adequate platelet count threshold and maintain response for at least 6 of the last 8 weeks of study duration, which was 12 weeks. Results for the secondary outcome of likelihood of maintaining a response during 12 weeks (repeated-measures analysis of platelet response) were consistent with these findings, as the use of eltrombopag was associated with an OR of 25.3 (95% CI, 8.2 to 78.7); P < 0.0001) versus placebo; no absolute effect estimates were reported.
Need for Rescue Medication
In PETIT (n = 67),30 the proportions of patients initiating rescue medication was 13% in the eltrombopag arm and 50% in the placebo arm over 6 weeks (OR = 0.1; 95% CI, 0.04 to 0.49; P = 0.0020). The between-group difference was of much smaller magnitude in PETIT2 (n = 92),32 where the corresponding proportions were 19% in the eltrombopag arm and 24% in the placebo arm over 12 weeks (OR = 0.44; 95% CI, 0.2 to 0.9; P = 0.032). This is consistent with the findings from platelet response, suggesting that more patients in the placebo group failed to achieve platelet response and therefore required the use of rescue therapy.
Bleeding
Clinically significant bleeding was assessed in the studies using the WHO bleeding scale. In PETIT (n = 67),30 the proportions of patients with WHO grade 2 to 4 bleeding, estimated with the use of a logistic regression model, were 27% in the eltrombopag arm and 59% in the placebo arm over 6 weeks, yielding an OR of 0.21 (95% CI, 0.06 to 0.72; P = 0.013). In PETIT2 (n = 92),32 5% of patients in the eltrombopag group and 7% of patients in placebo had WHO grade 2 to 4 bleeding at week 12; no comparison between groups was reported. The magnitude of the point estimate for the between-group difference may be considered clinically meaningful, according to the clinical experts consulted.
Health-Related Quality of Life
HRQoL was assessed in PETIT (n = 62)30 using the KIT questionnaire (range 0 to 100, higher scores indicate a better state) but was not assessed in PETIT2.32 The mean difference between treatment groups for change from baseline to week 6 was –1.5 points (95% CI, –8.1 to 5.1 points; P = 0.64) in favour of eltrombopag. The magnitude of the between-group difference was not considered clinically meaningful according to the MCID identified in the literature.31
Function
No data were reported for the outcome of function.
Harms Outcomes
High proportions of patients experienced AEs throughout the studies, and proportions were relatively similar between treatment groups. The proportions of patients who experienced serious AEs (SAEs) ranged between 8% and 14% across treatment groups and were overall not higher with eltrombopag than with placebo. No deaths were reported in the studies.
Romiplostim Compared to Placebo
Platelet Response
In Tarantino et al. (n = 62),35 the proportions of patients achieving a platelet count of 50 × 109/L or more at least 6 of the final 8 weeks (out of a total of 24 weeks), without rescue medication within the prior 4 weeks, were 52% in the romiplostim arm and 10% in the placebo arm (OR = 9.1; 95% CI, 1.9 to 43.2; P = 0.002). The magnitude of the point estimate for the between-group difference may be considered clinically meaningful according to current clinical practice standards. The outcome definition was considered stringent, meaning that patients who were counted as responders had to achieve an adequate platelet count threshold and maintain response for at least 6 of the last 8 weeks of study duration, which was 24 weeks. Results for a less stringent secondary outcome measure were consistent with those findings. The proportions of patients achieving at least 4 weekly platelet counts of 50 × 109/L or more without rescue medication during the 24-week follow-up were 71% in the romiplostim arm and 20% in the placebo arm (OR = 9.0; 95% CI, 2.5 to 32.3; P = 0.0002).
In Elalfy et al. (n = 18),33 the proportions of patients achieving a platelet response was 83% in the romiplostim arm and 0% in the placebo arm. No statistical comparison between groups was reported. Platelet response was not defined, and, therefore, it is not possible to assess whether the threshold used and conditions required to be considered as having a platelet response were valid and relevant according to the definitions described in the guidelines and used in clinical practice.
Need for Rescue Medication
The proportions of patients initiating rescue medication were similar between treatment groups in Tarantino et al. (41% versus 45%; P = 0.7103; n = 62).35 In Elalfy et al. (n = 18),33 the corresponding proportions were 8% in the romiplostim arm and 33% in the placebo arm; however, no statistical comparison between groups was reported.
Bleeding
Clinically significant bleeding was assessed and reported in Tarantino et al. (n = 62),35 using the grade ≥ 2 AEs of bleeding; the rate of events (i.e., the total number of events/100 patient-weeks) was 8% in the romiplostim arm and 18% in the placebo arm over 24 weeks (P = 0.0006). The magnitude of the point estimate for the between-group difference may be considered clinically meaningful according to current clinical practice standards. This outcome was not collected in Elalfy et al.33
Health-Related Quality of Life
HRQoL was assessed in Tarantino et al. (n = 62)35 and reported in Mathias et al.34 using the KIT questionnaire, which was completed by both children and parents. For Child Self-Report, the mean difference within treatment groups for change from baseline to week 25 was 13.7 points (standard deviation [SD] 16.7 points) in the romiplostim arm and 9.8 points (SD 15.7 points) in the placebo arm. The between-group difference in change from baseline was not reported, and the P value was reported as nonsignificant. For Parent Impact, the mean change from baseline was 17.5 points (SD 16.7 points) in the romiplostim arm and 12.8 points (SD 16.3 points) in the placebo arm (between-group difference not reported, P = 0.015). Considering the MCID estimates identified in the literature,31 the point estimates for the between-group differences would not be considered clinically meaningful.
Function
No data were reported for the outcome of function.
Harms Outcomes
High proportions of patients experienced SAEs in Tarantino et al. (n = 62),35 and proportions were higher with romiplostim than with placebo (24% versus 5%, respectively). In Elalfy et al. (n = 18),33 AEs were experienced by 50% of patients in both groups, and the proportion of patients experiencing SAEs was not reported. No deaths were reported in the studies.
Rituximab Versus Placebo — RCTs
Assessment of the effectiveness of rituximab compared to placebo was inconclusive due to the lack of evidence, as no comparative RCTs could be identified, while the observational study included presented only descriptive comparisons with TPO-RAs.
Rituximab, Romiplostim, and Eltrombopag — Observational Evidence
Platelet Response
ICON1 (n = 120)36 assessed platelet response as the within-group change from month 1 to month 6; findings for these comparisons are reported as descriptive information as a result of the lack of statistical between-group comparisons. The proportions of patients with either a complete or a partial response to treatment were 79% at 6 months versus 55% at 1 month with rituximab (P = 0.0003), 83% at 6 months versus 52% at 1 month with romiplostim (P = 0.0001), and 67% at 6 months versus 55% at 1 month with eltrombopag (P value reported as not meeting the a priori defined threshold for statistical significance). The thresholds set in the study for achieving a complete or partial platelet response were consistent with the international standardized definition4 but had to be met for at least 50% of the platelet counts over the time period. One limitation of the interpretation of this outcome assessment is that the effect of the medications would already be observed by month 1. Therefore, the within-group change from month 1 to month 6 should not be viewed as the true treatment effect. Findings speak to the capacity of the drug to maintain efficacy over time rather than informing on the proportions of patients who responded to the drugs compared to before it was initiated.
Need for Rescue Medication
The reduction in use of rescue therapy from 1 to 6 months was 6.1% with rituximab, 12.5% with romiplostim, and 40% with eltrombopag. No confidence intervals were reported. This suggests that response to treatment in patients who received eltrombopag was achieved while requiring less rescue medication over time. Further interpretation of the results is limited by the fact that the use of concomitant ITP drugs at baseline and throughout the study was not reported. Differential use of rescue medications has the potential to impact other outcome results, the direction of which would be against eltrombopag.
Bleeding
The proportions of patients with grade 1 to 2 bleeding decreased from baseline to 6 months within each individual treatment. In patients who received rituximab, the proportions of patients experiencing skin bleeding were 81.4% at baseline versus 36.4% at 6 months (P < 0.0001), and the proportions of patients experiencing nonskin bleeding were 53.5% at baseline versus 15.2% at 6 months (P = 0.003). In patients who received romiplostim, the corresponding proportions for skin bleeding were 83.9% at baseline versus 50.0% at 6 months (P = 0.024), and for nonskin bleeding were 58.1% at baseline versus 33.3% at 6 months (P = 0.264). Finally, in patients who received eltrombopag, the corresponding proportions for skin bleeding were 85.0% at baseline versus 26.7% at 6 months (P = 0.005), and for nonskin bleeding were 50.0% at baseline versus 20.0% at 6 months (P = 0.276).
Health-Related Quality of Life
HRQoL was assessed using the KIT questionnaire. Median and range were reported both at baseline and at 12 months; differences within treatment groups were calculated. The median within-group change from baseline to 12 months was 18.5 with rituximab (P < 0.0001), 11.9 with romiplostim (P = 0.0001), and 15.1 with eltrombopag (P = 0.0003). It should be noted that there was significant patient attrition at 12 months and that these results are therefore based on a limited sample of the initial study population. The magnitude of the within-group differences appears consistent with that reported in 1 RCT,35 suggesting that there might be clinically meaningful improvement in HRQoL after 12 months of treatment with all 3 drugs.
Function
No data were reported for the outcome of function.
Harms Outcomes
No harms data were reported.
Table 5: Outcomes Assessing Platelet Count Response
Interventions | Eltrombopag versus placebo | Romiplostim versus placebo | Rituximab versus romiplostim versus eltrombopag | ||
|---|---|---|---|---|---|
Bussel et al.30 (PETIT) | Grainger et al.32 (PETIT2) | Tarantino et al.35 | Elalfy et al.33 | Grace et al. (2019)36 (ICON1) | |
Primary outcome | Proportion of patients achieving a platelet count of ≥ 50 × 109/L at least once from weeks 1 to 6, in the absence of rescue therapy Eltrombopag (N = 45): 62% Placebo (N = 22): 32% At week 6 OR = 4.31 (95% CI, 1.39 to 13.34) P = 0.011 | Proportion of patients achieving a platelet count of ≥ 50 × 109/L, in the absence of rescue therapy for ≥ 6 weeks from weeks 5 to 12 Eltrombopag (N = 63): 40% Placebo (N = 29): 3% At week 12 OR = 18.0 (95% CI, 2.3 to 140.9) P = 0.0004 | Proportions of patients achieving weekly platelet counts of ≥ 50 × 109/L in at least 6 of the final 8 weeks (no rescue medication within 4 weeks) Romiplostim (N = 42): 52% Placebo (N = 20): 10% At 24 weeks OR = 9.1 (95% CI, 1.9 to 43.2) P = 0.002 | Not defined in the publication Romiplostim (N = 12): 83% Placebo (N = 6): 0% No statistical comparison reported | Proportions of patients with platelet response (complete + partial)a — within-group change from 1 to 6 months Rituximab: 79% at 6 months (N = 33) versus 55% at 1 month (N = 42) Romiplostim: 83% at 6 months (N = 24) versus 52% at 1 month (N = 29) Eltrombopag: 67% at 6 months (N = 15) versus 55% at 1 month (N = 20) |
Relevant secondary outcome | Proportion of patients achieving a platelet count of ≥ 50 × 109/L in at least 60% of assessments from weeks 2 to 6 Eltrombopag (N = 45): 36% Placebo (N = 22): 0% At week 6 OR = 5.84 (95% CI, 1.18 to 28.90) P = 0.0017 | Likelihood of maintaining a response (repeated-measures analysis of platelet response during 12 weeks) Eltrombopag (N = 63) versus placebo (N = 29) Over 12 weeks: OR = 25.3 (95% CI, 8.2 to 78.7) P < 0.0001 | Proportions of patients achieving at least 4 weekly platelet counts ≥ 50 × 109/L (no rescue medication) during study Romiplostim (N = 42): 71% Placebo (N = 20): 20% At 24 weeks OR = 9.0 (95% CI, 2.5 to 32.3) P = 0.0002 | NR | Proportions of patients with complete response / Proportions of patients with partial response Rituximab: 19% / 36% at 1 month (N = 42) 52% / 27% at 6 months (N = 33) 55% / 26% at 12 months (N = 31) Romiplostim: 21% / 31% at 1 month (N = 29) 71% / 15% at 6 months (N = 24) 56% / 25% at 12 months (N = 16) Eltrombopag: 30% / 25% at 1 month (N = 20) 27% / 40% at 6 months (N = 15) 42% / 33% at 12 months (N = 12) |
CI = confidence interval; NR = not reported; OR = odds ratio.
aComplete platelet response: ≥ 50% of platelet counts > 100 × 109/L. Partial platelet response: ≥ 50% of platelet counts > 30 × 109/L and twice the baseline value.
Interventions | Eltrombopag versus placebo | Romiplostim versus placebo | Rituximab versus romiplostim versus eltrombopag | ||
|---|---|---|---|---|---|
Bussel et al.30 (PETIT) | Grainger et al.32 (PETIT2) | Tarantino et al.35 | Elalfy et al.33 | Grace et al. (2019)36 (ICON1) | |
Initiation of rescue therapy | Eltrombopag (N = 45): 13% Placebo (N = 22): 50% Over 6 weeks OR = 0.1 (95% CI, 0.04 to 0.49) P = 0.0020 | Eltrombopag (N = 63): 19% Placebo (N = 29): 24% Over 12 weeks OR = 0.44 (95% CI, 0.2 to 0.9) P = 0.032 | Romiplostim (N = 42): 41% Placebo (N = 20): 45% Over 24 weeks P = 0.7103 | Romiplostim (N = 12): 8% Placebo (N = 6): 33% | Reduction from 1 to 6 months in the use of rescue medication Rituximab (N = 33): 6.1% Romiplostim (N = 24): 12.5% Eltrombopag (N = 15): 40% |
Clinically significant bleeding | WHO grade 2 to 4 Logistic regression model Eltrombopag (N = 45): 27% Placebo (N = 22): 59% Over 6 weeks OR = 0.21 (95% CI, 0.06 to 0.72) P = 0.013 | WHO grade 2 to 4 Proportions Baseline Eltrombopag (N = 63): 25% Placebo (N = 29): 21% End of study (week 12) Eltrombopag (N = 63): 5% Placebo (N = 29): 7% | Grade ≥ 2 AEs of bleeding Rate (events per 100 patient-weeks) Romiplostim (N = 42): 8 Placebo (N = 20): 18 Over 24 weeks P = 0.0006 | NR | NR |
HRQoL, change from baseline in KIT scores | Change from baseline to week 6, mean (SD) Eltrombopag (N = 20): 3 (10) Placebo (N = 22): 2 (8) Mean difference –1.5 (95% CI, –8.1 to 5.1) P = 0.64 | NR | Change from baseline to week 25, mean (SD) Child self-report Within-group change: Romiplostim (N = 28): 13.7 (16.7) Placebo (N = 11): 9.8 (15.7) Between-group: NS Parent impact Within-group change: Romiplostim (N = 37): 17.5 (16.7) Placebo (N = 16): 12.8 (16.3) Between-group: P = 0.015 | NR | Within-group change from baseline to 12 months, median (range) Rituximab Baseline (N = 43): 66.7 (32.7 to 96.2) 12 months (N = 31): 85.2 (47.1 to 100.0) Romiplostim Baseline (N = 31): 75.6 (51.0 to 98.1) 12 months (N = 16): 87.5 (70.2 to 99.0) Eltrombopag: Baseline (N = 20): 69.9 (43.3 to 94.2) 12 months (N = 12): 85.0 (61.5 to 97.1) |
Harms outcomes | AEs Eltrombopag (N = 45): 82% Placebo (N = 22): 95% SAEs Eltrombopag (N = 45): 9% Placebo (N = 22): 10% Deaths NR | AEs Eltrombopag (N = 63): 81% Placebo (N = 29): 72% SAEs Eltrombopag (N = 63): 8% Placebo (N = 29): 14% Deaths NR | AEs NR SAEs Romiplostim (N = 42): 24% Placebo (N = 20): 5% Deaths NR | AEs Romiplostim (N = 12): 50% Placebo (N = 6): 50% SAEs NR Deaths NR | NR |
AE = adverse event; CI = confidence interval; HRQoL = health-related quality of life; KIT = Kid's ITP Tools; OR = odds ratio; NR = not reported; NS = not significant (did not meet the a priori defined threshold for statistical significance); SAE = serious adverse event; SD = standard deviation.
Discussion
Summary of Evidence
The aim of this HTA was to review the clinical effectiveness and safety of TPO-RAs (i.e., eltrombopag and romiplostim) and rituximab in children with ongoing, active ITP after failure of first-line therapies. The project scope and research protocol were informed by engaging with patient groups to better understand the challenges associated with pediatric ITP and current treatments. A total of 8 publications met the final inclusion criteria, reporting findings from 5 unique studies on the use of eltrombopag, romiplostim, and rituximab as second-line treatments in pediatric patients with ITP.
Overall, the studies included in the systematic review were performed in pediatric patients (< 18 years of age) with a confirmed diagnosis of ITP of various duration, who still had active disease after having tried at least 1 prior treatment option. Most studies required patients to have chronic ITP (ongoing, active disease lasting longer than 12 months), with a platelet count of < 30 × 109/L before study entry. Two DB RCTs compared eltrombopag to placebo over 6 or 12 weeks; both were rated as having a low risk of bias for most outcomes. Two studies evaluated the use of romiplostim; 1 had some concern for the risk of bias, and the other had a high risk of bias. Of these, 1 DB RCT compared romiplostim to placebo over 24 weeks, while 1 small single-blinded pilot RCT compared romiplostim to placebo over 15 weeks. Finally, 1 prospective, longitudinal cohort study assessed the efficacy of rituximab, romiplostim, and eltrombopag given as monotherapy over a maximum of 12 months; the study was rated as having a serious risk of bias. The populations in the studies contributing to the evidence were considered generalizable to most children with ITP in the clinical setting. The primary efficacy outcome was platelet response. Considering the clinical and methodological heterogeneity of the included studies with respect to methodology, outcomes definition and measurement, timing of assessment, and populations, the studies were deemed too heterogenous to combine statistically and findings were synthesized narratively.
Interpretation of Clinical Results
Eltrombopag Versus Placebo — RCTs
Evidence from 2 DB RCTs (n = 159) with a low risk of bias suggests that eltrombopag likely results in a clinically important increase in the proportions of patients achieving a platelet response at 6 weeks and at 12 weeks compared to placebo. At least 1 outcome definition for platelet response in each study was considered stringent, meaning that patients who were counted as responders had to achieve an adequate platelet count threshold and maintain the response over time. Eltrombopag likely results in a clinically important reduction in the use of rescue therapy throughout the study durations compared to placebo, therefore preventing exposure of patients to the numerous harmful AEs associated with the use of IVIG or prednisone. In addition, eltrombopag likely results in a clinically important reduction in clinically significant bleeding compared with placebo. However, uncertainty was introduced due to the small sample sizes of the studies, resulting in wide confidence intervals for between-group comparisons and suggesting a large range of possible effects for eltrombopag versus placebo. One DB RCT assessed the impact of eltrombopag on HRQoL; findings suggest that the drug may not result in a clinically important improvement compared to placebo after 6 weeks, but the evidence is very uncertain due to several limitations. It should be noted that large amounts of missing data for HRQoL had the potential to bias the outcome and that differential use of rescue therapy may overestimate measures of efficacy in the placebo group. The magnitude and direction of the sum of all sources of bias are uncertain and significantly affect our confidence in the findings. The harms profile of eltrombopag was similar to that of placebo in the studies and did not raise new safety concerns.
Romiplostim Versus Placebo — RCTs
Evidence from 1 DB RCT (n = 62) that has raised some concern for the risk of bias suggests that romiplostim may result in a clinically important increase in the proportions of patients achieving a platelet response at 24 weeks compared to placebo. The key outcome definition for platelet response was considered stringent, as, once again, patients who were counted as responders had to achieve an adequate platelet count threshold and maintain the response over time. However, the lack of information reported regarding missing outcome data and how they were handled introduced uncertainty across all outcomes, as the missing data may reach proportions sufficiently high to impact the results. The magnitude and direction of potential bias is uncertain. Findings suggest that romiplostim may also result in a clinically important reduction in clinically significant bleeding compared with placebo. Once again, uncertainty was introduced due to the small sample sizes of the study, resulting in wide confidence intervals for between-group comparisons and suggesting a large range of possible effects for romiplostim versus placebo. Romiplostim may not result in a clinically important reduction in the use of rescue therapy in the study compared to placebo, or in between-group improvement in HRQoL compared to placebo at 25 weeks. Within-group improvements in HRQoL were observed with both romiplostim and placebo, the magnitude of which was not considered clinically significant; this may be indicative of a confounder, leading to overestimating treatment effect in the placebo group. Finally, romiplostim was associated with additional toxicity in the study compared with placebo. Overall, uncertainty suggests the need for some caution in the interpretation of efficacy and safety findings.
One small, single-blinded, pilot RCT comparing romiplostim to placebo was included in the systematic review but contributed only minimally to the available evidence. The high risk of bias, combined with the small sample size of 18 patients and concerns regarding generalizability of the population to the setting in Canada, introduced substantial uncertainty and considerably diminished our confidence in the findings. Poor reporting regarding key outcome definitions and lack of statistical comparison between groups also limited the conclusions that could be drawn from this study.
Romiplostim and Eltrombopag — Observational Evidence
As part of the overall body of evidence, findings from 1 observational study that included eltrombopag, romiplostim, and rituximab arms may help to inform decision-making regarding the optimal use of ITP medications in children who failed to respond to first-line therapy in the context of limited evidence. Findings were, however, reported only as descriptive information as a result of the lack of statistical between-group comparisons, which constitutes a major limitation to the evidence. Additionally, the lack of randomization and other methodological limitations place the study at serious risk of bias. The observational cohort study supports the conclusions drawn from the RCTs, suggesting that romiplostim and eltrombopag may result in a clinically important, long-lasting platelet response, as assessed within each treatment group, as well as in a clinically important improvement in HRQoL over up to 12 months, providing that the uncertainty surrounding the results is taken into account when interpreting the findings. As reasons for missing outcome data were not detailed in the publications, it is not possible to assess whether patients discontinued due to nonresponse or whether some patients may have experienced spontaneous remission; therefore, the magnitude and direction of potential bias cannot be ascertained. Romiplostim and eltrombopag may also be effective at reducing bleeding; however, interpretation of the results is difficult because of the absence of details on the evaluation tool used to assess bleeding, as grade 1 to 2 AEs of bleeding or WHO grade 1 to 2 bleeding would not be considered clinically meaningful bleeding events. Therefore, although the findings suggest a substantial reduction in some types of bleeding, there is uncertainty as to whether this corresponds to clinically relevant events that have a negative impact on patients.
As part of the overall body of evidence, findings from this observational study may help inform decision-making regarding the optimal use of second-line ITP medications in children in the context of limited RCT evidence in this patient population, as long as the uncertainty surrounding the results is taken into account when interpreting the results.
Rituximab — RCTs and Observational Evidence
No RCT was identified in the literature comparing rituximab to placebo and the within-arm evidence from the observational study alone is too uncertain to adequately inform the use of rituximab in the patient population. The study was at serious risk of bias, and there were no formal between-group comparisons. In addition, the study did not assess harms outcomes, which constitutes the main drawback of using rituximab in children. Therefore, assessment of the effectiveness and safety of rituximab was inconclusive due to the lack of evidence.
Strengths and Limitations of the Systematic Review
Strengths
The systematic review was developed using robust methodology. The research protocol was developed a priori and registered with the PROSPERO database; a detailed scoping plan was posted publicly for stakeholder input. Input from those with lived experience was used to inform the research protocol. The literature search was comprehensive and the list of included studies was also publicly posted for stakeholder feedback. Evidence collection and evaluation of the quality of the studies were completed using methods that reduced the risk of bias and error.
Limitations
The systematic review was based on limited evidence available. No head-to-head RCT in the target patient population was identified in the literature; therefore, the evidence relied on placebo-controlled trials. We discourage the use of informal, naive, indirect comparisons (i.e., observational comparisons across the results of separate trials or groups of trials), because they do not preserve the within-trial randomization. Such comparisons are likely to be affected by bias and confounding. Most included studies had a relatively small sample size, introducing some uncertainty in the findings, which were affected by wide variability. We acknowledge that ITP is a rare disease in children and that large RCTs in this patient population may be impractical. One comparative observational study was included in the review, but only descriptive comparisons across drugs could be made, as the study authors performed no formal comparisons. Due to serious risk of bias, results from the study should be interpretated with caution and findings should be viewed as complementary to those from RCTs.
Conclusions and Implications for Decision- or Policy-Making
There is an unmet need in children with ITP who did not respond to first-line therapy; input from clinical experts suggests that, without access to TPO-RAs, patients are being exposed to subsequent-line off-label therapies, with uncertainty surrounding their effectiveness and numerous potential harms, such as immunosuppression. Considering the balance of benefits and harms, costs, patient preference, and feasibility, guidelines9,10 recommend the use of TPO-RAs in this patient population rather than rituximab or other subsequent-line treatments. A high value is being placed on avoiding immunosuppression in the pediatric population,9 which was also emphasized in the literature12-14 and by the clinical experts consulted for this review. The clinical experts noted that splenectomy is not considered an appropriate treatment option in children with ITP, considering the unclear efficacy, the risks associated with such major surgical procedure, equity concerns, and long-term harms such as permanent immunosuppression, posing a risk of life-threatening infections and leading to prolonged antibiotic prophylaxis.15-17
To determine which treatment(s) should be used in pediatric patients with ITP who have failed first-line treatments, a systematic review of the efficacy of treatments was undertaken at the request of public drug plans. A narrative review of 8 publications, reporting findings from 4 RCTs and 1 observational cohort study, informed the conclusions. Evidence from 2 DB RCTs with a low risk of bias and 1 comparative cohort study suggests that eltrombopag likely increases and maintains platelet response over time compared to placebo. Eltrombopag also likely reduces the use of rescue medication and clinically significant bleeding compared to placebo, which were considered clinically meaningful outcomes for patients. Evidence from 1 DB RCT and 1 comparative cohort study suggests that romiplostim may also increase and maintain platelet response, as well as reduce clinically significant bleeding compared to placebo; as the evidence was scarce and potentially subject to bias, uncertainty suggests a need for caution in the interpretation of the findings. Due to the scarcity of evidence in the patient population, conclusions could not be drawn for the impact of TPO-RAs on HRQoL and function in children. Assessment of the effectiveness of rituximab, and its use before accessing TPO-RAs, was inconclusive due to the lack of evidence.
As highlighted by feedback received, ITP is a rare disease in children, and thus large RCTs in this patient population may not be feasible. If deemed appropriate, public drug plans may explore requesting an implementation advice panel for further support.
References
1.Provan D, Stasi R, Newland AC, et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood. 2010;115(2):168-186. PubMed
2.Neunert C, Lim W, Crowther M, et al. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood. 2011;117(16):4190-4207. PubMed
3.Michel M. Immune thrombocytopenia nomenclature, consensus reports, and guidelines: what are the consequences for daily practice and clinical research? Semin Hematol. 2013;50 Suppl 1:S50-54. PubMed
4.Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113(11):2386-2393. PubMed
5.Terrell DR, Beebe LA, Vesely SK, Neas BR, Segal JB, George JN. The incidence of immune thrombocytopenic purpura in children and adults: A critical review of published reports. Am J Hematol. 2010;85(3):174-180. PubMed
6.Despotovic JM, Grimes AB. Pediatric ITP: is it different from adult ITP? Hematology Am Soc Hematol Educ Program. 2018;2018(1):405-411. PubMed
7.Schifferli A, Holbro A, Chitlur M, et al. A comparative prospective observational study of children and adults with immune thrombocytopenia: 2-year follow-up. Am J Hematol. 2018;93(6):751-759. PubMed
8.Kuhne T, Berchtold W, Michaels LA, et al. Newly diagnosed immune thrombocytopenia in children and adults: a comparative prospective observational registry of the Intercontinental Cooperative Immune Thrombocytopenia Study Group. Haematologica. 2011;96(12):1831-1837. PubMed
9.Neunert C, Terrell DR, Arnold DM, et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019;3(23):3829-3866. PubMed
10.Provan D, Arnold DM, Bussel JB, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019;3(22):3780-3817. PubMed
11.Swinkels M, Rijkers M, Voorberg J, Vidarsson G, Leebeek FWG, Jansen AJG. Emerging Concepts in Immune Thrombocytopenia. Front Immunol. 2018;9:880. PubMed
12.Nazi I, Kelton JG, Larche M, et al. The effect of rituximab on vaccine responses in patients with immune thrombocytopenia. Blood. 2013;122(11):1946-1953. PubMed
13.Government of Canada. Immunization of immunocompromised persons: Canadian Immunization Guide. 2023: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-3-vaccination-specific-populations/page-8-immunization-immunocompromised-persons.html. Accessed 2024 Mar 25.
14.Centers for Disease Control and Prevention (CDC). Altered Immunocompetence: General Best Practice Guidelines for Immunization. Vaccine Recommendations and Guidelines of the ACIP 2023: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/immunocompetence.html. Accessed 2024 Mar 25.
15.Canadian Paediatric Society. Position Statement: Preventing and treating infections in children with asplenia or hyposplenia. 2019: https://cps.ca/en/documents/position/preventing-treating-infections-in-children-with-asplenia. Accessed 2024 Mar 25.
16.Madenci AL, Armstrong LB, Kwon NK, et al. Incidence and risk factors for sepsis after childhood splenectomy. J Pediatr Surg. 2019;54(7):1445-1448. PubMed
17.Lee GM. Preventing infections in children and adults with asplenia. Hematology Am Soc Hematol Educ Program. 2020;2020(1):328-335. PubMed
18.Revolade (eltrombopag): film-coated tablets, 25 mg and 50 mg, oral use [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc; 2021: https://pdf.hres.ca/dpd_pm/00063465.PDF. Accessed 2024 Mar 25.
19.Nplate (romiplostim): lyophilized powder for solution, 250 mcg/0.5 mL and 500 mcg/1 mL [product monograph]. Mississauga (ON): Amgen Canada Inc; 2021: https://pdf.hres.ca/dpd_pm/00062536.PDF. Accessed 2024 Mar 25.
20.Sobi Inc. NCT04516967: Avatrombopag for the Treatment of Thrombocytopenia in Pediatric Subjects With Immune Thrombocytopenia for ≥6 Months. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2024: https://clinicaltrials.gov/study/NCT04516967. Accessed 2024 Mar 25.
21.Treatment of adult patients with immune thrombocytopenia after failure of first-line therapies. Can J Health Technol. 2023;3(7). https://www.cadth.ca/treatment-adult-patients-immune-thrombocytopenia-after-failure-first-line-therapies. Accessed 2024 Mar 25.
22.CADTH Health Technology Review: Thrombopoietin Receptor Agonists as Second-Line Treatment in Children With Ongoing Immune Thrombocytopenia - Project Protocol. Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/hta-he/HC0033-Drugs-for-Ped%20ITP-Protocol.pdf. Accessed 2024 Mar 25.
23.Shivji F, Gates M, Gauthier K. Thrombopoietin Receptor Agonists as Second-Line Treatment in Children With Ongoing Immune Thrombocytopenia (CRD42023429164). PROSPERO: International prospective register of systematic reviews. York (GB): University of York Centre for Reviews and Dissemination; 2023: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=429164. Accessed 2024 Apr 15.
24.Rituxan (rituximab): 120 mg/mL solution for subcutaneous injection [product monograph]. Mississauga (ON): Hoffmann-La Roche Ltd; 2018: https://pdf.hres.ca/dpd_pm/00044394.PDF. Accessed 2024 Mar 25.
25.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40-46. PubMed
26.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. PubMed
27.Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. PubMed
28.Sterne JA, Hernan MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. PubMed
29.Popay J, Roberts H, Sowden A, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. Lancaster (GB): Lancaster University; 2006: https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf. Accessed 2024 Mar 1.
30.Bussel JB, de Miguel PG, Despotovic JM, et al. Eltrombopag for the treatment of children with persistent and chronic immune thrombocytopenia (PETIT): a randomised, multicentre, placebo-controlled study. Lancet Haematol. 2015;2(8):e315-325. PubMed
31.Grainger JD, Blanchette VS, Grotzinger KM, Roy A, Bussel JB. Health-related quality of life in children with chronic immune thrombocytopenia treated with eltrombopag in the PETIT study. Br J Haematol. 2019;185(1):102-106. PubMed
32.Grainger JD, Locatelli F, Chotsampancharoen T, et al. Eltrombopag for children with chronic immune thrombocytopenia (PETIT2): a randomised, multicentre, placebo-controlled trial. Lancet. 2015;386(10004):1649-1658. PubMed
33.Elalfy MS, Abdelmaksoud AA, Eltonbary KY. Romiplostim in children with chronic refractory ITP: randomized placebo controlled study. Ann Hematol. 2011;90(11):1341-1344. PubMed
34.Mathias SD, Li X, Eisen M, Carpenter N, Crosby RD, Blanchette VS. A Phase 3, Randomized, Double-Blind, Placebo-Controlled Study to Determine the Effect of Romiplostim on Health-Related Quality of Life in Children with Primary Immune Thrombocytopenia and Associated Burden in Their Parents. Pediatr Blood Cancer. 2016;63(7):1232-1237. PubMed
35.Tarantino MD, Bussel JB, Blanchette VS, et al. Romiplostim in children with immune thrombocytopenia: a phase 3, randomised, double-blind, placebo-controlled study. Lancet. 2016;388(10039):45-54. PubMed
36.Grace RF, Shimano KA, Bhat R, et al. Second-line treatments in children with immune thrombocytopenia: Effect on platelet count and patient-centered outcomes. Am J Hematol. 2019;94(7):741-750. PubMed
37.Grace RF, Klaassen RJ, Shimano KA, et al. Fatigue in children and adolescents with immune thrombocytopenia. Br J Haematol. 2020;191(1):98-106. PubMed
38.Fogarty PF, Tarantino MD, Brainsky A, Signorovitch J, Grotzinger KM. Selective validation of the WHO Bleeding Scale in patients with chronic immune thrombocytopenia. Curr Med Res Opin. 2012;28(1):79-87. PubMed
39.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res Involv Engagem. 2017;3:13. PubMed
Appendix 1: Flow Diagram
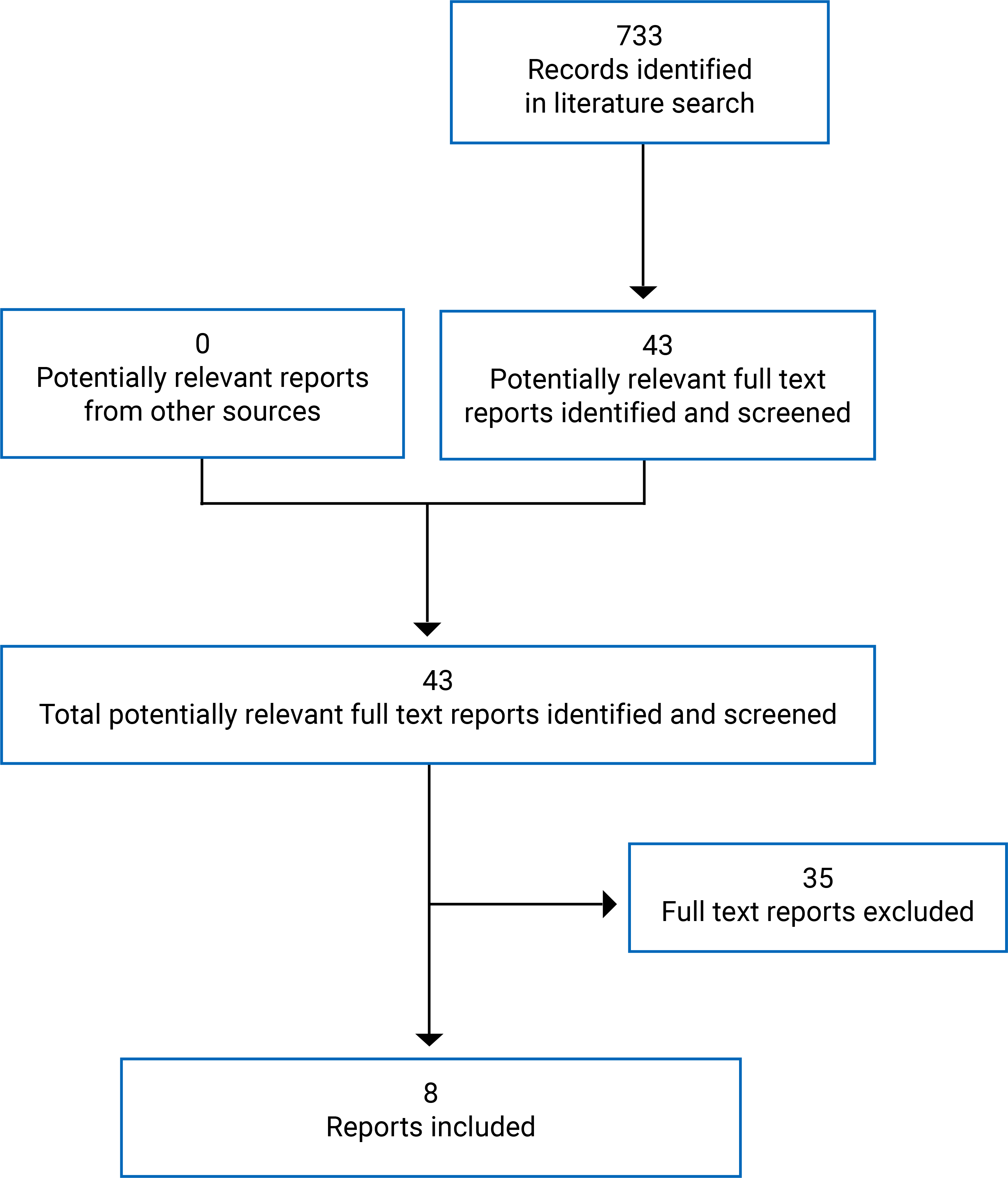
Appendix 2: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: May 2, 2023
Alerts: search updates until project completion
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Purpura, thrombocytopenic/ or purpura, thrombocytopenic, idiopathic/
((autoimmune* or immun* or idiopathic* or purpur*) adj2 thrombocytop*).ti,ab,kf.
(Werlhof* disease* or morbus werlhof*).ti,ab,kf.
ITP.ti,ab,kf.
or/1-4
Pediatrics/ or Hospitals, Pediatric/ or Intensive Care Units, Pediatric/ or Adolescent/ or exp Child/ or exp Infant/ or Pediatric Nursing/ or Child, Hospitalized/ or Adolescent, Hospitalized/
(child* or infant* or baby or babies or newborn* or newborns or neonate or neonates or neonatal or preemie? or infancy or paediatric* or pediatric* or toddler* or girl? or boy? or kid? or teen or teens or teenage* or youngster? or youth* or preteen* or adolescent* or adolescence or preschooler* or pre-schooler* or nursery school* or daycare* or school age? or (months adj2 age) or (month? adj2 old) or preadolescen* or juvenile* or prepubescen* or prepubert* or pre-pubescen* or pre-pubert* or pre-adolescen*).ti,ab,kf.
(pediat* or paediat* or child* or adolescen* or juvenile*).jw.
or/6-8
(TPO RA* or TPORA* or thrombopoietin receptor agonist*).ti,kf.
(eltrombopag* or revolade* or promacta* or alvaiz* or DDL701 or DDL 701 or SB497 115 or SB 497 115 or SB 487115 or SB497115 or SSS20 or SSS 20 or ETB115 or ETB 115 or S56D65XJ9G).ti,ab,kf,rn,nm,hw,ot.
(romiplostim* or Nplate* or romiplate* or AMG531 or AMG 531 or GN5XU2DXKV).ti,ab,kf,rn,nm,hw,ot.
Rituximab/
(rituximab* or mabthera* or Rituxan* or GP2013 or GP 2013 or IDEC102 or IDEC 102 or “PF 05280586” or PF05280586 or RG105 or RG 105 or IDEC C2B8 or IDECC2B8 or truxima* or riximyo* or ruxience* or CTP10 or CT P10 or blitzima* or riabni* or ritemvia* or rituenza* or rixathon* or 4F4X42SYQ6).ti,ab,kf,rn,nm,hw,ot.
or/10-14
and/5,9,15
16 use medall
Thrombocytopenic purpura/ or idiopathic thrombocytopenic purpura/
((autoimmune* or immun* or idiopathic* or purpur*) adj2 thrombocytop*).ti,ab,kf,dq.
(Werlhof* disease* or morbus werlhof*).ti,ab,kf,dq.
ITP.ti,ab,kf,dq.
or/18-21
exp pediatrics/ or pediatric hospital/ or pediatric intensive care unit/ or exp adolescent/ or exp child/ or exp pediatric nursing/
(child* or infant* or baby or babies or newborn* or newborns or neonate or neonates or neonatal or preemie? or infancy or paediatric* or pediatric* or toddler* or girl? or boy? or kid? or teen or teens or teenage* or youngster? or youth* or preteen* or adolescent* or adolescence or preschooler* or pre-schooler* or nursery school* or daycare* or school age? or (months adj2 age) or (month? adj2 old) or preadolescen* or juvenile* or prepubescen* or prepubert* or pre-pubescen* or pre-pubert* or pre-adolescen*).ti,ab,kf,dq.
(pediat* or paediat* or child* or adolescen* or juvenile*).jx.
or/23-25
(TPO RA* or TPORA* or thrombopoietin receptor agonist*).ti,kf.
*Eltrombopag/
(eltrombopag* or revolade* or promacta* or alvaiz* or DDL701 or DDL 701 or SB497 115 or SB 497 115 or SB 487115 or SB497115 or SSS20 or SSS 20 or ETB115 or ETB 115).ti,ab,kf,dq.
*Romiplostim/
(romiplostim* or Nplate* or romiplate* or AMG531 or AMG 531).ti,ab,kf,dq.
*Rituximab/
(rituximab* or mabthera* or Rituxan* or GP2013 or GP 2013 or IDEC102 or IDEC 102 or “PF 05280586” or PF05280586 or RG105 or RG 105 or IDEC C2B8 or IDECC2B8 or truxima* or riximyo* or ruxience* or CTP10 or CT P10 or blitzima* or riabni* or ritemvia* or rituenza* or rixathon*).ti,ab,kf,dq.
or/27-33
and/22,26,34
35 use oemezd
conference abstract.pt.
36 not 37
or/17,38
remove duplicates from 39
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | eltrombopag, romiplostim, pediatric ITP]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- eltrombopag, romiplostim, pediatric ITP]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- eltrombopag, romiplostim, pediatric ITP]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- eltrombopag, romiplostim, pediatric ITP]
EU Clinical Trials Information System (CTIS)
European Union Clinical Trials Information System, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- eltrombopag, romiplostim, pediatric ITP]
Grey Literature
Keywords: eltrombopag, romiplostim, pediatric ITP
Limits: None
Relevant websites from the following sections of the grey literature checklist searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 3: List of Included Studies
Note this appendix has not been copy-edited.
Randomized Controlled Trials
PETIT Main Publication
Bussel JB, de Miguel PG, Despotovic JM, et al. Eltrombopag for the treatment of children with persistent and chronic immune thrombocytopenia (PETIT): a randomised, multicentre, placebo-controlled study. Lancet Haematol. 2015;2(8):e315-325. PubMed
Related Publication
Grainger JD, Blanchette VS, Grotzinger KM, Roy A, Bussel JB. Health-related quality of life in children with chronic immune thrombocytopenia treated with eltrombopag in the PETIT study. Br J Haematol. 2019;185(1):102-106. PubMed
PETIT2 Main Publication
Grainger JD, Locatelli F, Chotsampancharoen T, et al. Eltrombopag for children with chronic immune thrombocytopenia (PETIT2): a randomised, multicentre, placebo-controlled trial. Lancet. 2015;386(10004):1649-1658. PubMed
Main Publication
Tarantino MD, Bussel JB, Blanchette VS, et al. Romiplostim in children with immune thrombocytopenia: a phase 3, randomised, double-blind, placebo-controlled study. Lancet. 2016;388(10039):45-54. PubMed
Related Publication
Mathias SD, Li X, Eisen M, Carpenter N, Crosby RD, Blanchette VS. A Phase 3, Randomized, Double-Blind, Placebo-Controlled Study to Determine the Effect of Romiplostim on Health-Related Quality of Life in Children with Primary Immune Thrombocytopenia and Associated Burden in Their Parents. Pediatr Blood Cancer. 2016;63(7):1232-1237. PubMed
Main Publication
Elalfy MS, Abdelmaksoud AA, Eltonbary KY. Romiplostim in children with chronic refractory ITP: randomized placebo controlled study. Ann Hematol. 2011;90(11):1341-1344. PubMed
Observational Studies
Main Publication
Grace RF, Shimano KA, Bhat R, et al. Second-line treatments in children with immune thrombocytopenia: Effect on platelet count and patient-centered outcomes. Am J Hematol. 2019;94(7):741-750. PubMed
Related Publication
Grace RF, Klaassen RJ, Shimano KA, et al. Fatigue in children and adolescents with immune thrombocytopenia. Br J Haematol. 2020;191(1):98-106. PubMed
Appendix 4: List of Excluded Studies
Note this appendix has not been copy-edited.
Author (year) | Reason for exclusion | Reference |
|---|---|---|
RCT | ||
Grainger 2023 | Design | Blood Advances 2023 7(3):396-405 |
Shimano 2021 | Population | BMJ Open 2021 11(8):e044885 |
White 2020 | Design | British Journal of Haematology 2020 191(1)15-16 |
Gurlek Gokcebay 2018 | Design | Transfusion and Apheresis Science 2018 57(3):416-417 |
Anonymous 2017 | Unavailable | Blood. Conference: 59th Annual Meeting of the American Society of Hematology, ASH 2017 130(Supplement 1): |
Uhl 2017 | Population | Transfusion 2017 57(10):2532-2538 |
Chaturvedi 2016 | Design | Lancet 2016 388(10039):4-6 |
Anonymous 2015 | Design | The Lancet Haematology 2015 2(10): |
Grainger et al. | Design | The Lancet 2015 386(10004)1630 |
Neunert 2015 | Design | Lancet 2015 386(10004):1606-9 |
Bussel et al. | Design | Pediatric Blood & Cancer 2015 62(2):208-213 |
Seidel 2014 | Design | British Journal of Haematology 2014 165(3):419-21 |
Kluter 2012 | Population | American Journal of Hematology 2012 87(5):558-61 |
Citak 2011 | Design | Journal of Tropical Pediatrics 2011 57(1):71-2 |
Anonymous 2010 | Unavailable | Annals of Hematology. Conference: 3rd Intercontinental Cooperative ITP Study Group 2010 89(SUPPL. 1): |
Bay 2006 (J Peds) | Design | Journal of Pediatrics 2006 148(3):423 to 4; author reply 424 |
Bay 2006 (Peds Int) | Design | Pediatrics International 2006 48(5):514-6 |
Bennett 2006 | Design | Blood 2006 107(7):2639-42 |
Taube 2006 | Design | Journal of Pediatrics 2006 148(3):423 |
Roganovic 2005 | Design | European Journal of Pediatrics 2005 164(5):334 |
Observational studies | ||
Fang 2023 | Design | Expert Opinion on Drug Safety 2023 1 to 8 |
Chaudhury 2021 | Intervention | Archives of Disease in Childhood 2021 106(9):929-931 |
Yasser 2020 | Design | Pediatric Hematology/Oncology and Immunopathology 2020 19(3):26-30 |
Depre 2018 | Design | PLoS ONE [Electronic Resource] 2018 13(6):e0198184 |
Neunert 2016 | Design | Pediatric Blood & Cancer 2016 63(8):1407-13 |
Weide 2016 | Design | Oncology Research and Treatment 2016 39(1 to 2):41-4 |
Ghanima 2014 | Design | Haematologica 2014 99(5):937-44 |
Ramaswamy 2014 | Design | Journal of Pediatrics 2014 165(3):600 to 5.e4 |
Saleh 2013 | Population | Blood 2013 121(3):537-45 |
Grace 2012 | Outcome | Pediatric Blood & Cancer 2012 58(2):221-5 |
Perel 2012 | Design | Archives de Pediatrie 2012 19(6 SUPPL. 1):H168-H169 |
Wang 2005 | Design | Journal of Pediatrics 2005 146(2):217 to 21 |
Appendix 5: Summary of Study Characteristics
Note this appendix has not been copy-edited.
Table 9: Details of Included RCTs
Detail | Bussel et al.30 (PETIT) | Grainger et al.32 (PETIT2) | Tarantino et al.35 | Elalfy et al.33 |
|---|---|---|---|---|
Designs and populations | ||||
Study design | DB phase II RCT | DB phase III RCT | DB phase III RCT | Single-blind pilot RCT |
Enrolment dates | March 17, 2010 to January 15, 2013 | March 15, 2012 to January 2, 2014 | January 24, 2012 to February 19, 2015 | March 2010 to July 2010 |
Locations | Multicentre: 22 centres in US, Canada, UK, and Europe | Multicentre: 38 centres US, UK, Europe, and Asia | Multicentre: 27 centres in US, Canada, and Australia | Single centre: Egypt |
Randomized | N = 67 Randomized in a 2:1 ratio. Stratified by age cohort. | N = 92 Randomized in a 2:1 ratio. Stratified by age cohort. | N = 62 Randomized in a 2:1 ratio. Stratified by age cohort. | N = 18 Randomization was not described |
Place in therapy | Patients < 18 years with diagnosis of ITP who have active disease, i.e., who relapsed or are refractory, after having tried ≥ 1 prior treatment option. | Patients with ITP who failed to maintain response to ≥ 2 prior treatment options. | ||
Inclusion criteria |
|
|
|
|
Exclusion criteria |
|
|
|
|
Drugs | ||||
Intervention | Eltrombopag orally once daily | Romiplostim SC injection once weekly | ||
Starting Dose | Starting dose according to age. | Starting dose of 1 mcg/kg. | ||
Dose Adjustments | Based on target platelet count 50 to 200 × 109/L. | Dose escalated to 5 mcg/kg/week, then tapered. | ||
Maximal Dose | Maximum dose of 75 mg per day. | Maximum dose of 10 mcg/kg. | ||
Comparator(s) | Matching placebo | Placebo | ||
Concomitant medications | Stable dose of maintenance ITP medication. | Standard of care therapy at stable dose. | NR | |
Duration | ||||
Length of follow-up | 7 weeks | 12 weeks | 24 weeks | 15 weeks |
Outcomes | ||||
Primary outcome | Platelet count response Outcome measure: Proportion of patients achieving a platelet count of ≥ 50 × 109/L in the absence of rescue therapya at least once from weeks 1 to 6. | Platelet count response Outcome measure: Proportion of patients achieving a platelet count of ≥ 50 × 109/L in the absence of rescue therapya for ≥ 6 weeks throughout weeks 5 to 12. | Platelet count response Outcome measure: Incidence of durable platelet response, i.e., achieving weekly platelet responses (≥ 50 × 109/L with no rescue therapyb in prior 4 weeks) in ≥ 6 of the final 8 weeks. | Platelet count response Outcome measure: NR |
Secondary / exploratory outcomes |
|
|
|
|
Notes | ||||
Funding source | GlaxoSmithKline | Amgen | NR | |
Publications | Bussel et al.30 Related publication: Grainger 201931 | Grainger et al.32 | Tarantino et al.35 Related publication: Mathias 201634 | Elalfy et al.33 |
AEs = adverse events; DB = double blind; HRQoL = health-related quality of life; ITP = immune thrombocytopenia; IVIG = IV immunoglobulin; KIT = Kid's ITP Tools; NR = not reported; RCT = randomized controlled trials; SC = subcutaneous; VTE = venous thromboembolism.
aRescue therapy was defined in the studies as any new ITP drug, dose increase in a concomitant ITP drug, platelet transfusion, or splenectomy.30,32
bRescue therapy was defined in the study as either: any medication intended to increase platelet count or to treat or prevent bleeding; or any increase in dose or frequency of concomitant ITP therapy; or addition of a new ITP therapy.35
Table 10: Details of Included Cohort Study
Study characteristics | Grace et al. (2019)36 (ICON1) |
|---|---|
Designs and populations | |
Study design | Prospective, longitudinal cohort study |
Enrolment dates | September 2013 to December 2015 |
Locations | Multicentre: 21 centres in US and Canada |
N | 120 |
Place in therapy | Patients < 18 years with diagnosis of ITP starting second-line treatments as monotherapy. |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Interventions | Any ITP treatment based on physician and patient preference. A minimum of 15 evaluable patients was required for a treatment to be included in the study cohort |
Concomitant medications | NR |
Duration | |
Length of follow-up | 12 months (primary analyses were performed at 1 month and at 6 months) |
Outcomes | |
Primary outcome | Platelet count response Outcome measure: Change in response category from baseline visit (within-group and between-group):
|
Secondary / exploratory outcomes |
|
Notes | |
Funding source | Pediatric ITP Consortium of North America (ICON) |
Publications | Grace et al. (2019)36 Related publication: Grace 202037 |
IBLS = ITP Bleeding Scale; ITP = immune thrombocytopenia; IVIG = IV immunoglobulin; KIT = Kid's ITP Tools; NR = not reported.
Table 11: Summary of Baseline Patient Characteristics — RCTs
Baseline Characteristics | Bussel et al.30 (PETIT) | Grainger et al.32 (PETIT2) | Tarantino et al.35 | Elalfy et al.33 | ||||
|---|---|---|---|---|---|---|---|---|
Eltrombopag N = 45 | Placebo N = 22 | Eltrombopag N = 63 | Placebo N = 29 | Romiplostim N = 42 | Placebo N = 20 | Romiplostim N = 12 | Placebo N = 6 | |
Age in years | Mean (95% CI) 9 (8 to 10) | Mean (95% CI) 10 (8 to 12) | Mean (95% CI) 9.4 (8.2 to 10.5) | Mean (95% CI) 9.8 (8.3 to 11.3) | Median (IQR) 10 (6 to 14) | Median (IQR) 7.5 (6.5 to 13.5) | Median (range) 9.5 (2.5 to 16) | Median (range) 7 (4 to 15) |
Age cohorts, n (%) | ||||||||
12 to 17 years | 16 | 8 | 23 | 10 | 16 (38) | 7 (35) | NR | NR |
6 to 11 years | 19 | 9 | 26 | 13 | 18 (43) | 9 (45) | NR | NR |
1 to 5 years | 10 | 5 | 14 | 6 | 8 (19) | 4 (20) | NR | NR |
Sex, n (%) | ||||||||
Boys | 18 (40) | 9 (41) | 33 (52) | 15 (52) | 18 (43) | 9 (45) | 10 (83) | 3 (50) |
Girls | 27 (60) | 13 (59) | 30 (48) | 14 (48) | 24 (57) | 11 (55) | 2 (17) | 3 (50) |
Ethnic origin, n (%) | ||||||||
White | 40 (89) | 20 (91) | NR | NR | NR | NR | NR | NR |
Caucasian | NR | NR | NR | NR | 26 (62) | 15 (75) | NR | NR |
African-American | NR | NR | NR | NR | 6 (14) | 2 (10) | NR | NR |
Asian | NR | NR | NR | NR | 3 (7) | 2 (10) | NR | NR |
East Asian | NR | NR | 20 (32) | 10 (34) | NR | NR | NR | NR |
Other | 5 (11) | 2 (9) | 43 (68) | 19 (66) | 7 (17) | 1 (5) | NR | NR |
Weight in kg | Mean (95% CI) 39 (34 to 45) | Mean (95% CI) 43 (33 to 53) | Mean (range) 41.0 (35.5 to 46.4) | Mean (range) 42.7 (33.2 to 52.3) | NR | NR | NR | NR |
Average duration of ITP | NR | NR | Time in months since diagnosis, mean (SD) 41 (34.1) | Time in months since diagnosis, mean (SD) 53 (40.3) | Time in years since diagnosis, median (IQR) 1.9 (1.0 to 4.2) | Time in years since diagnosis, median (IQR) 2.2 (1.5 to 3.7) | Disease duration in years, Median (range) 2.3 (1.2 to 7.0) | Disease duration in years, Median (range) 3.0 (1.5 to 6.5) |
Disease duration – category, n (%) | ||||||||
6 to 12 months | 8 (18) | 2 (9) | NR | NR | NR | NR | NR | NR |
3 12 months | 37 (82) | 20 (91) | NR | NR | NR | NR | NR | NR |
Baseline platelet count ( × 109/L) | Mean (SD) 15.5 (8.0) | Mean (SD) 12.4 (8.8) | NR | NR | Median (IQR) 17.8 (7.5 to 24.5) | Median (IQR) 17.7 (9.8 to 24.1) | Median (range) 10.5 (2 to 20) | Median (range) 10.5 (6 to 20) |
≤ 15 × 109/L, n (%) | 23 (51) | 11 (50) | 38 (60) | 19 (66) | NR | NR | NR | NR |
Baseline concomitant ITP drug use | ||||||||
Any, n (%) | 5 (11) | 2 (9) | 13 (21) | 1 (3.4) | 5 (12) | 4 (20) | NR | NR |
Previous ITP medication, n (%) | ||||||||
Any | 43 (96) | 22 (100) | 60 (95) | 28 (97) | NR | NR | NR | NR |
> 2 previous treatments | 38 (84) | 19 (86) | 46 (73) | 26 (90) | NR | NR | NR | NR |
Type, n (%) | ||||||||
Corticosteroids | NR | NR | NR | NR | 32 (76) | 15 (75) | 12 (100) | 6 (100) |
Anti-D immunoglobulin | NR | NR | 13 (21) | 3 (10) | 12 (29) | 7 (35) | NR | NR |
IV immunoglobulin | NR | NR | NR | NR | 35 (83) | 16 (80) | NR | NR |
Rituximab | NR | NR | 9 (14) | 6 (21) | 11 (26) | 7 (35) | NR | NR |
Other | NR | NR | NR | NR | 10 (23) | 6 (30) | NR | NR |
CI = confidence interval; IQR = interquartile range; ITP = immune thrombocytopenia; nr = not reported; RCT = randomized controlled trial; SD = standard deviation.
Appendix 6: Risk of Bias Assessment
Table 12: Risk of Bias Assessment Per Outcome Within Each RCT Using RoB227
Study | Randomization process | Deviations from intended interventions (assignment) | Deviations from intended interventions (adherence) | Missing outcome data | Measurement of the outcome | Selection of the reported results | Overall |
|---|---|---|---|---|---|---|---|
Bussel et al.30 (PETIT) | |||||||
Platelet Response | Low Central, random component in the sequence generation process (telephone-based interactive voice). No apparent baseline imbalances. | Low Patients and study personnel blinded (matching placebo / no apparent differential toxicity). ITT analysis, patients with missing data included as nonresponders (small amount that is unlikely to cause bias). | Low Patients and study personnel blinded to study treatment. | Low Small amount of missing data unlikely to cause bias. | Low Outcomes measured appropriately and similarly between groups. Outcome assessors unaware of treatment received. | Low Data appeared to have been analyzed according to a prespecified plan. Outcomes were assessed using one measurement tool. | Low risk of bias |
Use of Concomitant / Rescue Medication | |||||||
Bleeding | |||||||
Harms | |||||||
HRQoL | High Large amount of missing data having the potential to bias the outcome. | High Large amount of missing data with potential of bias. | High risk of bias | ||||
Grainger et al.32 (PETIT2) | |||||||
Platelet Response | Low Central, random component in the sequence generation process (telephone-based interactive voice). Baseline imbalances not incompatible with chance. | Low Patients and study personnel blinded to study treatment (matching placebo / no apparent differential toxicity). ITT analysis, patients with missing data included as having a negative response (small amount of missing data that is unlikely to cause bias). | Low Patients and study personnel blinded to study treatment. | Low Small amount of missing data unlikely to cause bias. | Low Outcomes measured appropriately and similarly between groups. Outcome assessors unaware of treatment received. | Low Data appeared to have been analyzed according to a prespecified plan. Outcomes were assessed using one measurement tool. | Low risk of bias |
Use of Rescue Medication | |||||||
Bleeding | |||||||
Harms | |||||||
HRQoL | NR | ||||||
Tarantino et al.35 (related publication: Mathias 201634 reporting on HRQoL) | |||||||
Platelet Response | Low Central, random component in the sequence generation process (interactive voice response system). No apparent baseline imbalances. | Some concern Patients and study personnel blinded (matching placebo / no apparent differential toxicity). Type of analysis not reported. No information on the number of patients with missing data and how they were handled. | Low Patients and study personnel blinded to study treatment. | Some concern Though few in number, 2% and 15% withdrew from the romiplostim and placebo groups; it is not clear how missing data were handled. | Low Outcomes measured appropriately and similarly between groups. Outcome assessors unaware of treatment received. | Low Data appeared to have been analyzed according to a prespecified plan. Outcomes were assessed using one measurement tool. | Some concern for the risk of bias |
Use of Rescue Medication | |||||||
Bleeding | |||||||
Harms | |||||||
HRQoL | |||||||
Elalfy et al.33 | |||||||
Platelet Response | Some concern No details reported on randomization process / placebo. | High Single-blinded, no further detail on who was blinded, or on the appearance of placebo. No information on how missing data were handled. | High Single-blinded, no further detail. No analysis estimating the effect on bias. | High No information reported on missing outcome data and how they were handled. | Low Objective outcome; appropriate and similar measure between groups. | High No prespecified analysis plan reported. Investigators may not have been blinded to outcome data. | High risk of bias |
Harms | High Vulnerable to influence by knowledge of the intervention. | ||||||
Use of Concomitant / Rescue Medication | NR | ||||||
Bleeding | |||||||
HRQoL | |||||||
HRQoL = health-related quality of life; RoB2 = Cochrane Risk of Bias tool, version 2; NR = not reported.
Note: This table has not been copy-edited.
Table 13: Risk of Bias Assessment Per Outcome for the ICON1 Observational Study Using ROBINS-I28
Grace et al. (2019)36 (ICON1) | Confounding | Patient selection | Classification of interventions | Deviations from intended interventions | Missing data | Outcome measurement | Selection of reported results | Overall |
|---|---|---|---|---|---|---|---|---|
Platelet response | Serious Potential for confounding of the effect of interventions; no evidence from the publications that authors controlled for postintervention variables that could have affected the intervention. | Low Treatment was initiated based on physician / patient preference after enrolment. All eligible patients expected to be included in the study; start of follow-up and start of intervention coincided. | Moderate Interventions well defined and based solely on information collected at time of intervention. Choice of treatment may however be influenced by disease characteristics. | Low Deviations from intended interventions reflected usual practice (no information suggested otherwise). | Serious Significant patient attrition reported. Proportions differed across interventions. Missingness reasons not detailed. No analyses intended to mitigate the risk of bias. | Low Comparable methods of assessment. Objective outcomes. No evidence of systematic error relative to intervention status. | Moderate No indication of selection of reported analysis; though possible, as multiple measurements likely for platelet counts. | Serious Uncontrolled for confounding. Missing data due to attrition. |
Use of Rescue Medication | Low Reported results correspond to all intended outcomes, analyses, and subcohorts. | |||||||
Bleeding | Serious Outcomes vulnerable to influence by knowledge of the intervention received; assessors aware of intervention received. | Serious Uncontrolled for confounding. Missing data due to attrition. Subjective outcome assessed while aware of intervention received. | ||||||
HRQoL |
HRQoL = health-related quality of life; ROBINS-I = Risk of Bias in Nonrandomized Studies – Interventions tool.
Note: This table has not been copy-edited.
Appendix 7: Detailed Outcome Data
Table 14: Detailed Outcome Data — RCTs
Outcomes | Bussel et al.30 (PETIT) | Grainger et al.32 (PETIT2) | Tarantino et al.35 | Elalfy et al.33 | ||||
|---|---|---|---|---|---|---|---|---|
Eltrombopag N = 45 | Placebo N = 22 | Eltrombopag N = 63 | Placebo N = 29 | Romiplostim N = 42 | Placebo N = 20 | Romiplostim N = 12 | Placebo N = 6 | |
Primary outcome in the study | Proportion of patients achieving a platelet count of ≥ 50 × 109/L at least once from weeks 1 to 6, in the absence of rescue therapy | Proportion of patients achieving a platelet count of ≥ 50 × 109/L, in the absence of rescue therapy for ≥ 6 weeks from Week 5 to 12 | Proportions of patients achieving weekly platelet counts of ≥ 50 × 109/L in ≥ 6 of the final 8 weeks (no rescue medication within 4 weeks) | Platelet response not defined in the publication | ||||
n (%) | 28 (62) | 7 (32) | 25 (40) | 1 (3) | 22 (52) | 2 (10) | 10 (83) | 0 |
OR (95% CI); p value | 4.31 (1.39 to 13.34); P = 0.011 | 18.0 (2.3 to 140.9); P = 0.0004 | 9.1 (1.9 to 43.2); P = 0.002 | NR | NR | |||
Relevant secondary outcomes in the study | Proportion of patients achieving a platelet count of ≥ 50 × 109/L in ≥ 60% of assessments from weeks 2 to 6 | Likelihood of maintaining a response (repeated-measures analysis of platelet response during 12 weeks) | Proportions of patients achieving at least 4 weekly platelet counts ≥ 50 × 109/L (no rescue medication) during weeks 2 to 25 | NR | NR | |||
n (%) | 16 (36) | 0 | NR | NR | 30 (71) | 4 (20) | NR | NR |
OR (95% CI); p value | 5.84 (1.18 to 28.90); P = 0.0017 | 25.3 (8.2 to 78.7); P < 0.0001 | 9.0 (2.5 to 32.3); P = 0.0002 | NR | NR | |||
Relevant additional measures of platelet response in the study | NR | NR | Weighted mean platelet change up to week 12 | Weighted mean platelet change up to week 12 | Median number of weeks with platelet response (primary outcome) | Median number of weeks with platelet response (primary outcome) | NR | NR |
Mean area under the curve | NR | NR | 63.9 | 23.7 | NR | NR | NR | NR |
Median (IQR) in weeks | NR | NR | NR | NR | 12 (3 to 20) | 1 (0 to 2.5) | NR | NR |
p value | NR | NR | P < 0.0001 | P = 0.0004 | NR | NR | ||
Use of Concomitant and/or Rescue Medication | ||||||||
Initiation of rescue therapy, n (%) | 6 (13) | 11 (50) | 12 (19) | 7 (24) | 17 (41) | 9 (45) | 1 (8) | 2 (33) |
OR (95% CI); p value | 0.1 (0.04 to 0.49); P = 0.0020 | 0.44 (0.2 to 0.9); P = 0.032 | P = 0.7103 | NR | NR | |||
Concomitant and/or rescue ITP medications received throughout study duration, n (%) | ||||||||
IV immunoglobulin | 6 (13) | 8 (36) | NR | NR | 9 (21) | 4 (20) | NR | NR |
Corticosteroids | 4 (9) | 7 (32) | NR | NR | 5 (12) | 6 (30) | NR | NR |
Anti-D | 3 (7) | 2 (9) | NR | NR | 3 (7) | 2 (10) | NR | NR |
Vincristine or vinblastine | 0 | 1 (5) | NR | NR | NR | NR | NR | NR |
Antifibrinolytic | NR | NR | NR | NR | 6 (14) | 2 (10) | NR | NR |
Platelets | NR | NR | NR | NR | 1 (2) | 1 (5) | NR | NR |
Bleeding | ||||||||
Clinically significant bleeding | WHO Grade 2 to 4 Logistic regression model | WHO Grade 2 to 4 Logistic regression model | WHO Grade 2 to 4 Proportions | WHO Grade 2 to 4 Proportions | Grade ≥ 2 AEs of bleeding | Grade ≥ 2 AEs of bleeding | NR | NR |
Baseline, n (%) | 9 (20) | 6 (27) | 16 (25) | 6 (21) | NR | NR | NR | NR |
End of study, n (%) | 4 (9) | 7 (32) | 3 (5) | 2 (7) | NR | NR | NR | NR |
n (rate)a | NR | NR | NR | NR | 80 (8) | 79 (18) | NR | NR |
Logistic regression model, n (%) | 12 (27) | 13 (59) | NR | NR | NR | NR | NR | NR |
OR (95% CI); p value | 0.21 (0.06 to 0.72); P = 0.013 | NR | NR | P = 0.0006 | NR | NR | ||
Other bleeding measures | NR | NR | NR | NR | Composite bleeding and/or rescue therapy | NR | NR | |
Duration-adjusted rates per 100 patient-weeks | NR | NR | NR | NR | 5.9 | 17.9 | NR | NR |
p value | NR | NR | NR | NR | P < 0.0001 | P < 0.0001 | NR | NR |
Health-Related Quality of Life | ||||||||
Change from Baseline in KIT Total Score | ||||||||
Patients contributing to the analysis | n = 20 | n = 15 | NR | NR | NR | NR | NR | NR |
Baseline, mean (SD) | 74 (14) | 76 (17) | NR | NR | NR | NR | NR | NR |
Change from baseline to week 6 in KIT total score, mean (SD) | 3 (10) | 2 (8) | NR | NR | NR | NR | NR | NR |
Model-adjusted change from baseline to week 6 in KIT total score,b mean (SE) | 3 (2) | 2 (2) | NR | NR | NR | NR | NR | NR |
Difference from placebo, mean (95% CI); p value | –1.5 (–8.1 to 5.1); P = 0.64 | NR | NR | NR | NR | NR | NR | |
Change from Baseline in KIT Total Score by Child Self-Report and Parent Impact | ||||||||
Child self-report | ||||||||
N | NR | NR | NR | NR | N = 28 | N = 12 | NR | NR |
Baseline | NR | NR | NR | NR | 66.8 (16.0) | 68.9 (16.8) | NR | NR |
N | NR | NR | NR | NR | N = 30 | N = 13 | NR | NR |
Week 8 | NR | NR | NR | NR | 76.3 (14.8) | 77.2 (17.4) | NR | NR |
N | NR | NR | NR | NR | N = 28 | N = 11 | NR | NR |
Change from baseline to week 8 | NR | NR | NR | NR | 9.4 (13.9) | 9.1 (12.8) | NR | NR |
N | NR | NR | NR | NR | N = 29 | N = 12 | NR | NR |
Week 16 | NR | NR | NR | NR | 78.1 (14.4) | 76.9 (17.3) | NR | NR |
N | NR | NR | NR | NR | N = 27 | N = 10 | NR | NR |
Change from baseline to week 16 | NR | NR | NR | NR | 10.7 (14.3) | 8.4 (15.6) | NR | NR |
N | NR | NR | NR | NR | N = 30 | N = 13 | NR | NR |
Week 25 | NR | NR | NR | NR | 80.2 (14.8) | 78.0 (18.9) | NR | NR |
N | NR | NR | NR | NR | N = 28 | N = 11 | NR | NR |
Change from baseline to week 25 | NR | NR | NR | NR | 13.7 (16.7) | 9.8 (15.7) | NR | NR |
Between-group difference in mean change from baseline,c p value | NR | NR | NR | NR | Reported as nonsignificant | Reported as nonsignificant | NR | NR |
Parent impact | ||||||||
N | NR | NR | NR | NR | N = 40 | N = 18 | NR | NR |
Baseline | NR | NR | NR | NR | 34.4 (19.0) | 35.5 (17.0) | NR | NR |
N | NR | NR | NR | NR | N = 42 | N = 17 | NR | NR |
Week 8 | NR | NR | NR | NR | 48.3 (22.5) | 39.2 (20.7) | NR | NR |
N | NR | NR | NR | NR | N = 40 | N = 16 | NR | NR |
Change from baseline to week 8 | NR | NR | NR | NR | 13.3 (11.7) | 3.6 (17.3) | NR | NR |
N | NR | NR | NR | NR | N = 41 | N = 18 | NR | NR |
Week 16 | NR | NR | NR | NR | 50.1 (22.9) | 48.3 (18.9) | NR | NR |
N | NR | NR | NR | NR | N = 39 | N = 17 | NR | NR |
Change from baseline to week 16 | NR | NR | NR | NR | 15.4 (16.4) | 12.3 (15.4) | NR | NR |
N | NR | NR | NR | NR | N = 39 | N = 17 | NR | NR |
Week 25 | NR | NR | NR | NR | 53.7 (25.4) | 49.4 (18.2) | NR | NR |
N | NR | NR | NR | NR | N = 37 | N = 16 | NR | NR |
Change from baseline to week 25 | NR | NR | NR | NR | 17.5 (16.7) | 12.8 (16.3) | NR | NR |
Between-group difference in mean change from baseline,c p value | NR | NR | NR | NR | P = 0.015 | NR | NR | |
Harms | ||||||||
AEs | 36 (82) | 20 (95) | 51 (81) | 21 (72) | NR | NR | 6 (50) | 3 (50) |
SAEs | 4 (9) | 2 (10) | 5 (8) | 4 (14) | 10 (24) | 1 (5) | NR | NR |
Deaths | 0d | 0d | 0 | 0 | NR | NR | 0 | 0 |
AEs = adverse events; CI = confidence interval; IQR = interquartile range; ITP = immune thrombocytopenia; KIT = Kid's ITP Tools; NR = not reported; RCT = randomized controlled trial; SAEs = serious adverse events; SD = standard deviation; SE = standard error.
Note: This table has not been copy-edited.
aRate = total number of events/100 patient-weeks.
bANCOVA.
cMixed-effects repeated-measures analysis.
dFatal AEs.
Note this appendix has not been copy-edited.
Table 15: Detailed Outcome Data — Cohort Study
Outcomes | Grace et al. (2019)36 (ICON1) | ||
|---|---|---|---|
Rituximab N = 43 | Romiplostim N = 31 | Eltrombopag N = 20 | |
Patients Contributing to the Analyses | |||
At 1 month | N = 42 | N = 29 | N = 20 |
At 6 months | N = 33 | N = 24 | N = 15 |
At 12 months | N = 31 | N = 16 | N = 12 |
Platelet Response | |||
Patients with Complete Platelet Response, n (%) | |||
At 1 month | 8 (19) | 6 (21) | 6 (30) |
At 6 months | 17 (52) | 17 (71) | 4 (27) |
At 12 months | 17 (55) | 9 (56) | 5 (42) |
Patients with Partial Platelet Response, n (%) | |||
At 1 month | 15 (36) | 9 (31) | 5 (25) |
At 6 months | 9 (27) | 3 (15) | 6 (40) |
At 12 months | 8 (26) | 4 (25) | 4 (33) |
Proportions of Patients with Platelet Response (Complete + Partial) – Change from 1 to 6 Months | |||
At 1 month | 55% | 52% | 55% |
At 6 months | 79% | 83% | 67% |
p value for within-group change | P = 0.0003 | P = 0.0001 | reported as nonsignificant |
Average Platelet Count × 109/L, Median (range) | |||
At 1 month | 65 (4 to 230) | 67 (1 to 357) | 89 (10 to 402) |
At 6 months | 151 (3 to 412) | 160 (6 to 598) | 97 (6 to 301) |
At 12 months | 156 (4 to 408) | 147 (29 to 408) | 106 (15 to 300) |
Reduction in the Use of Rescue Medication | |||
Change from 1 to 6 months, % | 6.1% | 12.5% | 40% |
Bleeding | |||
Proportions of Patients with Grade 1 to 2 Skin Bleeding, % | |||
Baseline | 81.4% | 83.9% | 85.0% |
At 1 month | 42.9% | 48.3% | 65.0% |
At 6 months | 36.4% | 50.0% | 26.7% |
At 12 months | 34.5% | 18.8% | 33.3% |
Within-Group Change from Baseline | |||
p value at 1 month | P = 0.0004 | P = 0.011 | P = 0.33 |
p value at 6 months | P < 0.0001 | P = 0.024 | P = 0.005 |
Proportions of Patients with Grade 1 to 2 Nonskin Bleeding, % | |||
Baseline | 53.5% | 58.1% | 50.0% |
At 1 month | 16.7% | 13.8% | 20.0% |
At 6 months | 15.2% | 33.3% | 20.0% |
At 12 months | 24.1% | 6.3% | 16.7% |
Within-Group Change from Baseline | |||
p value at 1 month | P = 0.0006 | P = 0.0001 | P = 0.067 |
p value at 6 months | P = 0.003 | 0 = 0.264 | P = 0.276 |
Health-Related Quality of Life – Change from Baseline in KIT Scores, median (range) | |||
Baseline | 66.7 (32.7 to 96.2) | 75.6 (51.0 to 98.1) | 69.9 (43.3 to 94.2) |
At 1 month | 75.2 (35.6 to 97.1) | 83.7 (57.0 to 98.1) | 80.8 (32.7 to 97.1) |
At 12 months | 85.2 (47.1 to 100.0) | 87.5 (70.2 to 99.0) | 85.0 (61.5 to 97.1) |
Within-Group Change from Baseline | |||
p value at 1 month | P = 0.0001 | P = 0.0003 | P = 0.0008 |
p value at 12 months | P < 0.0001 | P = 0.0001 | P = 0.0003 |
Notes: No data were reported in the publication for harms outcomes.
This table has not been copy-edited.
Appendix 8: Patient Engagement
Note this appendix has not been copy-edited.
Table 16: Patient Engagement in Drugs to Treat Children With Immune Thrombocytopenia report
Section and Topic | Item | Section |
|---|---|---|
Aim | The Platelet Disorder Support Association contributed to this HTA. This engagement offered insights to the project team, highlighting key issues and priorities of the patient population and contextualizing the information gleaned from the literature. | — |
Methods | A previous patient group submission on adult ITP was reviewed, and a patient group participated in a dialogue with staff. A Patient Engagement Officer presented the key themes to the project team during the protocol development phase. | — |
Results of Engagement | The Platelet Disorder Support Association contributed thoughts and perspectives on the nuances of pediatric ITP compared to adult ITP, highlighting some important distinctions and priorities for the treatment of pediatric ITP. Refer to Patient Engagement section. | Patient Engagement |
Discussion and Conclusions | There were many distinctions between pediatric and adult ITP that the patient group highlighted as their priorities. They wanted to ensure that we considered these nuances when reviewing the literature. The project team benefited from these insights and appreciated understanding patient priorities when developing the protocol, reviewing the literature, and drafting the report. | — |
Critical Reflections | The success of this engagement was related to several factors. First, there was an existing relationship with an active and involved patient group who was familiar with CADTH’s mandate and earlier work with adult ITP. Second, the patient group representative was supported in the engagement by a Patient Engagement Officer who acted as a liaison between the project team and the patient group. Third, the project team was receptive to patient group involvement. The Platelet Disorder Support Association was informed about the Stakeholder Feedback period, advising them that the draft report would be going out for public review and that they would have an opportunity to provide feedback. That way, they could both submit feedback as a patient group, and could disseminate the link to their members for individual patients to provide feedback. | NA |
Based on GRIPP2 Reporting Checklist39
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.