CADTH Health Technology Review
Canadian Medical Imaging Inventory 2022–2023: The Medical Imaging Team
CMII Report
Abbreviations
CIHI
Canadian Institute for Health Information
CMII
Canadian Medical Imaging Inventory
FTE
full-time equivalent
MRT
medical radiation technologist
Key Messages
A workforce comprising medical radiation technologists (MRTs), radiologists, nuclear medicine specialists, medical imaging physicists, and other medical staff is essential for the delivery of medical imaging services.
There is wide variation in the numbers of staff in each profession in Canada, ranging from 45 positions located in 6 provinces for medical imaging physicists to 25,000 positions located across all provinces and territories for MRTs.
Data from 2022–2023 suggest that the number of full-time staff has not grown at the same pace as the volume of exams. Sufficient staffing is needed to ensure the sustainable operation and delivery of medical imaging services that is supported by investment in the workforce through equitable education and training opportunities.
According to a Canadian Medical Imaging Inventory (CMII) report on wait time strategies, staffing shortages may extend wait times and may lead to disruptions in service delivery.
Managing the growing demand for imaging services and clearing the backlog of exams deferred during the pandemic has exacerbated existing staffing shortages and contributed to increased workloads and decreased staff well-being.
The adoption of supportive tools and technologies — such as clinical decision support tools, automated order entry, and AI-driven solutions — may assist the workforce by creating efficiencies, improving image quality, and increasing access to medical imaging.
What Is the Context?
Medical imaging has transformed the delivery of health care by enabling the early detection of disease and improving patient outcomes.1-3 The medical imaging team, comprising physicians, technologists, physicists, sonographers, and other medical staff, is responsible for providing essential imaging services within the health care system in Canada.1,4 These services include the use of routine advanced medical imaging technologies, such as CT, MRI, PET-CT, SPECT, SPECT-CT, and PET-MRI (Appendix 1).5,6
Demand for imaging exams has been shown to exceed capacity in some settings, leading to long wait times.3,7 Factors such as expanding clinical indications, aging of the population, and increasing incidence of diseases such as cancer have contributed to the greater demand for imaging.8 Excessive wait times can result in adverse outcomes for patients, and lead to inefficiencies and increased costs.9
In 2023, wait times for medically necessary elective CT exams exceeded the recommended 30-day maximum target3 in all provinces (data for territories were not available), apart from Quebec, with a national average wait time of 46 days.7 Similarly, for MRI, wait times exceeded the 30-day recommended maximum target in all provinces (data for territories were not available), with a national average wait time of 90 days.7 This is consistent with trends over time which show an ongoing challenge in timely access to imaging.7
The COVID-19 pandemic exacerbated existing challenges in imaging departments. Reports of increased workloads, high stress, exhaustion, and reported decreased well-being among health care professionals are believed to contribute to an observed trend in staffing shortages.10-13 These human resource shortages limit the hours that machines can operate and, in some instances, have led to shutdowns and service disruptions.14-16
As demand for imaging services increases, decision-makers, administrators, and regulators face complex health human resource decisions, with a focus on strong recruitment and retention policies and strategies to build a resilient and sustainable workforce.
The CMII was created in 2015 to better understand the medical imaging landscape in Canada and to track, compare, and map trends over time related to the availability, distribution, technical specifications, and use of advanced imaging equipment in Canada (i.e., CT, MRI, PET-CT, PET-MRI, SPECT, and SPECT-CT). This is the fourth iteration of the CMII since CADTH resumed the collection of these data in 2015.17-19 Previously, the Canadian Institute for Health Information (CIHI) collected data on medical imaging technologies in Canada from 2003 to 2012.20-23
The CMII collects data through a survey conducted approximately once every 2 years and, among other data elements, reports on the use of strategies for improving appropriate imaging, enhancing system efficiencies, reducing wait lists, and addressing other systemic challenges. Through this work, the CMII provides health care decision-makers with information on the imaging landscape in Canada that may be used to identify and address service and medical equipment gaps and inform strategic planning.
This report summarizes medical imaging team–related findings from the 2022–2023 national CMII survey and other sources.
What Did We Do?
The purpose of this CMII report is to present data on the current medical imaging team and health human resource landscape in Canada for 2022–2023. This report is a component of a series of publications produced as part of the CMII national survey, which includes CT, MRI, PET-CT, SPECT-CT, SPECT, and PET-MRI.
Why Did We Do This?
The CMII provides information on the medical imaging landscape across Canada to help support health care decision-making. Robust data are required to ensure health systems can deliver the imaging required to provide timely, safe, patient-centred care; improve health outcomes; and deliver health care efficiencies. The CMII also reports on data relating to the health human resources and wait times for advanced imaging equipment in Canada. Further details on the purpose of the CMII is described in the Canadian Medical Imaging Inventory 2022–2023: Provincial and Territorial Overview report located on the CMII website.
Methods Overview
Data were collected on 6 imaging modalities, primarily using a web-based self-report survey that was sent to all identified health care facilities with advanced imaging equipment in Canada (refer to Canadian Medical Imaging Inventory 2022–2023: Methods). Data were supplemented with information from provincial and territorial validators who are senior medical imaging–related health care decision-makers. As well, data from peer reviewers, literature searches, CIHI, and previous iterations of CMII data were incorporated into the report. Both English and French versions of the survey were provided.
The CMII survey collected the following data:
number and location of imaging equipment
volume of exams
hours of equipment operation
age of imaging equipment
technical specifications of machines
adoption of new and emerging supportive tools and technologies
imaging storing and communication services.
The survey opened on May 5, 2023, and primary data collection and validator responses were collected up until October 31, 2023. The full data collection and analysis strategy, including survey development, respondent identification, sources of data used, and data validation procedures can be found in the Canadian Medical Imaging Inventory 2022–2023: Methods report on the CMII website.
The CMII also presents data from both the survey and other sources relating to human resources, funding structures, ordering and referral practices, and the adoption of tools that may support appropriate imaging, system efficiencies, and wait list reductions.
Comparisons between data from Canada and data from other Organisation for Economic Co-operation and Development countries are reported, as are trends and projections on imaging capacity.
Response Rate for the 2022–2023 National Survey
A total of 504 sites were invited to participate in the survey. Data on modalities and unit counts were available for 467 sites (92.7%).
A 100% participation rate was received from publicly funded facilities (i.e., hospitals) in 7 provinces and all territories. The participation rate for the remaining provinces ranged from 51% to 93% for publicly funded facilities.
A complete response rate was received for unit counts and exam volumes by provincial and territorial validators, while the response rate varied for other survey questions. A total of 308 sites provided updated or new information (72%), reflecting an increased response rate of 34% since the CMII 2019–2020 survey.
While the overall survey participation rate was high, in some instances, not all survey questions were answered. This may lead to a nonresponse bias, which may result in the overgeneralization of some findings. To enable readers to assess the representativeness of each data point, the number of sites that responded to each question are included with the reported data.
Provincial and territorial validators provided high-level information for nonresponding publicly funded health facilities. Data obtained from the previous survey iteration, and from other sources (e.g., personal communications, websites of health care facilities), were used to inform the status of the remaining sites. Data from free-standing sites with private imaging capacity supplemented data for public capacity; detailed information for private imaging facilities is limited due to the low number of survey responses.
The survey questions and full data collection and analysis strategy, including survey development, respondent identification, sources of data used, and data validation procedures can be found in the Canadian Medical Imaging Inventory 2022–2023: Methods report on the CMII website.
Medical Imaging Team Overview
Advanced medical imaging teams usually comprise multidisciplinary professionals, including MRTs, radiologists, nuclear medicine specialists, medical imaging physicists, biomedical engineers, and other support staff. These skilled professionals work collaboratively to provider numerous services, including:9,21,24-26
evaluating exam appropriateness
preparing patients for exams
image acquisition
reading and interpreting exams and reporting findings
radiation safety and quality assurance
designing, installing, operating, and maintaining equipment
managing the day-to-day operations of an imaging department.
Close collaboration between team members is required to deliver optimal patient care; advance a better understanding of the policies, protocols, and practices for specific exams; promote appropriate imaging; and ensure patient safety. The size, composition, distribution, and interrelationships of these professionals varies depending on the type of imaging facility, its size, its geographical location, and the expertise required to perform specific exams.6,26
Role in Assessing Appropriate Imaging
More than 9.5 million advanced imaging exams were conducted in Canada in 2022–2023, reflecting a 12% increase since the 2019–2020 CMII survey.27 As imaging exam volumes continue to increase in Canada, so too does the rate of low-value exam referrals, which can impact exam wait times.28
An imaging exam referral may be considered inappropriate (i.e., low value) for several reasons:4,29-31
referring physician practice patterns
an exam’s inability to contribute to patient management
the performance of an exam at the incorrect time in a patient’s care pathway
failure to obtain imaging when indicated
inadequate referral information.
One of the responsibilities of the medical imaging team is to evaluate exam requests to ensure there is appropriate alignment between the requested imaging and a patient’s clinical history. Evidence has indicated the following:4,29-35
Between 10% and 25% of medical imaging exams conducted annually are considered unnecessary or low value.
Low-value scanning may result in unnecessary exposure to ionizing radiation and/or contrast material as well as increased health spending costs.
Radiologists consulting with referring providers may reduce low-value scanning by at least 20%.
In Canada, the estimated 5-year cost associated with low-value scanning in early-stage breast cancer was estimated between $4.4 million and $6.8 million.
Ensuring patients receive an appropriate examination at the most appropriate time is critical for patient care and safety, and to reduce health care system costs.29,30,36
Scope of Practice
The CMII reports on data relating to the main professionals working in imaging department: MRTs, radiologists, nuclear medicine specialists, and medical imaging physicists.
Medical Radiation Technologist Practice
There are 4 different subspecialties of MRTs, including magnetic resonance technologists, nuclear medicine technologists, radiation therapists, and radiological technologists.37,38
MRTs produce high-quality diagnostic images or carry out diagnostic procedures using ionizing radiation. They use their scientific knowledge, technical competence, and patient interaction skills to provide safe and accurate imaging procedures.39 The scope of practice of MRTs includes, but is not limited to, the following:37-39
deliver high-quality care to ensure optimal patient outcomes through the acquisition of images or the planning and delivery of ionizing radiation for therapeutic purposes
collaborate with other health care professionals to optimize patient diagnostic and treatment services through the gathering of information to plan for the exam or treatment, adapting protocols to accommodate patient needs, and ensuring optimal patient positioning
apply knowledge of radiation protection and safety for patients, families, and other health care colleagues and providers
evaluate images for technical quality and determine if additional images are necessary
identify, prepare, and/or administer prescribed pharmaceuticals under the supervision of a physician
monitor patient status and respond to any change in condition
demonstrate ongoing commitment to education and training.
Radiologist Practice
Radiologists are physicians who specialize in the field of medical imaging to diagnose and treat illness.40 Radiologists interpret imaging procedures including MRI, CT, nuclear medicine, ultrasound, and X-ray. There are also numerous interventions performed by radiologists — from biopsies throughout the body to locoregional therapies for cancer to vascular interventions, such as aortic aneurysm repairs and uterine fibroid embolization. Radiologists are integral in population screening programs (e.g., for breast cancer and lung cancer) in appropriately selected patients.40 Using a variety of follow-up imaging, they monitor efficacy of ongoing patient therapies. The scope of a radiologist’s practice varies depending on their provincial regulatory bodies or authorities and their area of specialization; however, they often include:40-42
review of medical histories to chose best imaging for a patient's symptoms
prioritize requests for investigation and liaise with referring physicians
supervise technologists in performing imaging exams
analyse medical images to find abnormalities or provide a diagnosis
correlate medical image findings with other examinations and prior tests
direct patient care as part of their medical report or when participating in multidisciplinary case conferences
recommend further appropriate examinations or treatments when necessary and confer with referring physicians
establish radiation safety protocols for patients and staff.
Nuclear Medicine Specialist Practice
Nuclear medicine specialists are medical physicians who use their knowledge of radiation biology, radiopharmacy, and nuclear physics to diagnose and treat a broad spectrum of conditions in patients.43 The main imaging modalities used by these specialists include planar imaging, SPECT, SPECT-CT, PET-CT, and PET-MRI.
The scope of practice of nuclear medicine specialists includes but is not limited to the following:43,44
advise physicians on the appropriate nuclear medicine diagnostic exam to address the clinical investigation
perform clinical assessment of patients, correlate the results with other clinical investigations, and select the optimal procedural protocol
supervise and support technologists in performing nuclear medicine exams, interpret results, and provide a timely report
advise on the therapeutic use of nuclear medicine by assessing patients, developing treatment plans, administering treatment, and assessing treatment safety and efficacy
provide emergency medicine to patients related to nuclear medicine diagnosis or treatment
manage the activities and oversee the workflow of nuclear medicine departments
establish radiation safety protocols and for isotope generation, storage, dosage, use, and disposal
advise facilities on the purchase of new equipment and isotopes and develop new protocols for diagnosis and treatment
identify, prepare, and/or administer prescribed pharmaceuticals
demonstrate ongoing commitment to education and training.
Imaging Medical Physicist Practice
There are 3 certifications for imaging medical physicists in Canada: diagnostic radiological physics (X-ray), MRI, and nuclear medicine physics. Certified imaging medical physicists specialize in optimizing the use and functionality of medical imaging equipment. They work with X-ray, fluoroscopy, mammography, CT, MRI, nuclear medicine, and ultrasound.45 Most certified imaging medical physicists work in hospital imaging departments.
Their main responsibilities may include:
accreditation of imaging equipment
equipment selection and purchasing
acceptance testing to ensure that equipment specifications are met and are safe to use
periodic performance audits of imaging equipment
equipment safety testing for patient and staff dose estimates and radiation protection.
Number of Full-Time Imaging Professionals in Canada
The rising demands for imaging services has placed greater emphasis on understanding the availability of full-time equivalent (FTE) positions in the medical imaging profession in Canada.
The number of FTE advanced imaging professionals by province and territory for MRTs, radiologists, nuclear medicine specialists, and imaging medical physicists is presented in Table 1. The latest publicly available data for the number of practising professionals for radiology and nuclear medicine is from 2019; given reports of current staffing shortages, this number is likely underestimated.3,46,47 The number of full-time trained professionals per million people (i.e., per capita) was calculated using 2023 population estimates.48
The overall counts of FTE positions included in this report represent the number of total available positions reported in Canada, which may not reflect the total number of filled or vacant positions at the time of this report. In addition, the counts do not capture the geographical disparity that exists in the distribution of positions throughout Canada, particularly in provinces and territories with large rural and remote areas.
In 2022–2023, MRTs comprised the largest professional group within the advanced imaging workforce, followed by radiologists, nuclear medicine specialists, and imaging medical physicists.
MRTs and radiologists practiced in all provinces and territories, while nuclear medicine specialists practiced in 9 provinces and imaging medical physicists practiced in 6 provinces.
Number of Trained MRTs
A total of 25,752 FTE MRTs were reported to practice in all 13 provinces and territories, ranging from 40 to 11,174. The highest number of FTE MRTs was in Ontario, Quebec, and Alberta.
There were approximately 646 FTE MRTs per million people in Canada, ranging from 305.8 per million people to 779.5 per million people. The jurisdictions with the greatest density of MRTs per capita were Quebec, Newfoundland and Labrador, and Nova Scotia.
Number of Radiologists
A total of 2,602 radiologists were reported to practice in all 13 provinces and 1 territory, ranging from 1 to 933. The highest number of radiologists were in Ontario, Quebec, and British Columbia.
There were approximately 65 radiologists per million people in Canada, ranging from 7.6 per million people to 103.1 per million people. The jurisdictions with the greatest density of radiologists per capita were Newfoundland and Labrador, Nova Scotia, and Quebec.
Number of Nuclear Medicine Specialists
A total of 284 nuclear medicine specialists were reported to practice in 9 provinces, ranging from 3 to 116. The highest number of nuclear medicine specialists were in Quebec, Ontario, and Alberta.
There were approximately 7 nuclear medicine specialists per million people in Canada, ranging from 3.6 per million people to 13.1 per million people. The jurisdictions with the greatest density of nuclear medicine specialists per capita were Quebec, Nova Scotia, and Newfoundland and Labrador.
There may be some overlap with individuals identified as both radiologists and nuclear medicine specialists due to a trend in hiring doctors with dual Royal College of Physicians and Surgeons of Canada fellowships in nuclear medicine and radiology.
Number of Imaging Medical Physicists
A total of 45 imaging medical physicists were reported to practice in 6 provinces, ranging from 2 to 17. The highest number of imaging medical physicist were in Ontario, Alberta, British Columbia, and Quebec.
There was approximately 1 imaging medical physicist per million people in Canada, ranging from 0.7 per million people to 2.8 per million people. The jurisdictions with the greatest density of imaging medical physicists per capita were Manitoba, Alberta, and Nova Scotia.
The number of imaging medical physicists was low across Canada; there were no designated imaging medical physicists in 4 provinces and in all territories.
Table 1: Numbers of Medical Radiation Technologists, Radiologists, Nuclear Medicine Specialists, and Imaging Medical Physicists in Canada, 2022–2023
Province or territory | Medical radiation technologists | Radiologists | Nuclear medicine specialists | Imaging medical physicistsa | ||||
|---|---|---|---|---|---|---|---|---|
Count | Per million populationb | Count | Per million populationb | Count | Per million populationb | Count | Per million populationb | |
Alberta | 2,411 | 512.6 | 293 | 62.3 | 29 | 6.2 | 10 | 2.1 |
British Columbia | 1,838 | 338.0 | 316 | 58.1 | 28 | 5.1 | 6 | 1.1 |
Manitoba | 893 | 618.3 | 90 | 62.3 | 7 | 4.8 | 4 | 2.8 |
New Brunswick | 604 | 726.3 | 56 | 67.3 | 3 | 3.6 | 0 | 0.0 |
Newfoundland and Labrador | 391 | 732.6 | 55 | 103.1 | 4 | 7.5 | 0 | 0.0 |
Nova Scotia | 767 | 732.4 | 84 | 80.2 | 9 | 8.6 | 2 | 1.9 |
Ontario | 11,174 | 720.9 | 933 | 60.2 | 82 | 5.3 | 17 | 1.1 |
Prince Edward Island | 108 | 613.2 | 9 | 51.1 | 0c | 0.0 | 0d | 0.0 |
Quebec | 6,884 | 779.5 | 686 | 77.7 | 116 | 13.1 | 6 | 0.7 |
Saskatchewan | 642 | 525.6 | 79 | 64.7 | 6 | 4.9 | 0 | 0.0 |
Territoriese | 40 | 305.8 | 1 | 7.6 | 0 | 0.0 | 0 | 0.0 |
Canada | 25,752 | 646.1 | 2,602 | 65.3 | 284 | 7.1 | 45 | 1.1 |
aKhadija Cutcher, Membership and Education Coordinator, Canadian Organization of Medical Physicists, ON: personal communication, Aug 21, 2023.
bThe population (estimated) as of first quarter, 2023.48
cAlthough not reported by the Canadian Medical Association, there is 1 radiologist practising in Prince Edward Island who is fellowship trained in nuclear medicine (Grant McKenna, Health PEI, Queen Elizabeth Hospital, PE: personal communication, Oct 20, 2020).
dThere is 1 imaging medical physicist practising in Prince Edward Island who is certified in mammography (Grant McKenna, Health PEI, Queen Elizabeth Hospital, PE: personal communication, Oct 20, 2020).
eTerritories = Northwest Territories, Nunavut, and Yukon.
Sources: CIHI (2021),12 CADTH (2019),10 CADTH (2019).11
MRTs in Canada: Results From the CMII National Survey
The CMII national survey asked the 467 participating facilities to provide information on the number of FTE MRTs assigned to each of the following advanced imaging modalities at the site level: CT, MRI, PET-CT, SPECT-CT, SPECT, and PET-MRI. Data from CMII 2022–2023 were compared with the CMII 2019–2020 survey results.27
An FTE position for a MRT is considered to amount to an 8-hour workday, 5 days per week. The reported number of FTE MRTs may not reflect the total number of filled FTE MRTs for a specific modality, but rather the total number of budgeted positions. Data were derived from the survey question: “How many FTE technologists are assigned to all units (collective number of FTEs for all units)?” Although most jurisdictions reported fewer FTE MRTs per capita since 2019–2020 for most modalities, the low response rate to this question, along with some jurisdictions reporting higher MRT counts for 2022–2023, limits the reliability of these findings.
FTE MRTs for CT Units
Number of CT MRTs per Site in Canada, 2022–2023
For CT, there was an average of 6 FTE MRTs reported to be employed per site, ranging from 1 to 28 (Table 2).
On average, there were approximately 31 FTE MRTs operating CT equipment per million people in Canada. The jurisdictions with the greatest density of MRTs per million people were Yukon (112.6 per million people), Nunavut (73.7 per million people), and Newfoundland and Labrador (65.6 per million people).
Table 2: Numbers of FTE MRTs for CT Units, 2022–2023
Province or territory | Number of reporting sites | Total FTE MRTs | Average FTE MRTs per site (minimum to maximum) | FTE MRTs per million populationa | Populationa |
|---|---|---|---|---|---|
Alberta | 37 | 187 | 5.1 (1 to 19) | 39.8 | 4,703,772 |
British Columbia | 35 | 246 | 7 (1 to 26) | 45.2 | 5,437,722 |
Manitoba | 16 | 85.2 | 6.2 (3 to 20.6) | 59.0 | 1,444,190 |
New Brunswick | 8 | 47 | 5.9 (3 to 12) | 56.5 | 831,618 |
Newfoundland and Labrador | 11 | 35 | 3.2 (1 to 7) | 65.6 | 533,710 |
Northwest Territories | 1 | 2 | 2 (2 to 2) | 43.8 | 45,668 |
Nova Scotia | 8 | 51 | 6.4 (3 to 16) | 48.7 | 1,047,232 |
Nunavut | 1 | 3 | 3 (3 to 3) | 73.7 | 40,715 |
Ontario | 54 | 357 | 6.6 (1 to 18) | 23 | 15,500,632 |
Prince Edward Island | 2 | 8 | 4 (3 to 5) | 45.4 | 176,113 |
Quebec | 21 | 140 | 6.7 (1 to 28) | 15.9 | 8,831,257 |
Saskatchewan | 13 | 70 | 5.4 (2 to 12) | 57.3 | 1,221,439 |
Yukon | 1 | 5 | 5 (5 to 5) | 112.6 | 44,412 |
Canada | 208 | 1,236.2 | 6 (1 to 28) | 31 | 39,858,480 |
FTE = full-time equivalent; MRT = medical radiation technologist.
Notes: Data were available for 208 of 394 sites across all jurisdictions with CT capacity.
Data derived from the survey question: “How many full-time equivalents (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
aThe population (estimated) as of first quarter, 2023.48
Change in the Number of CT MRTs Since the 2019–2020 CMII Survey
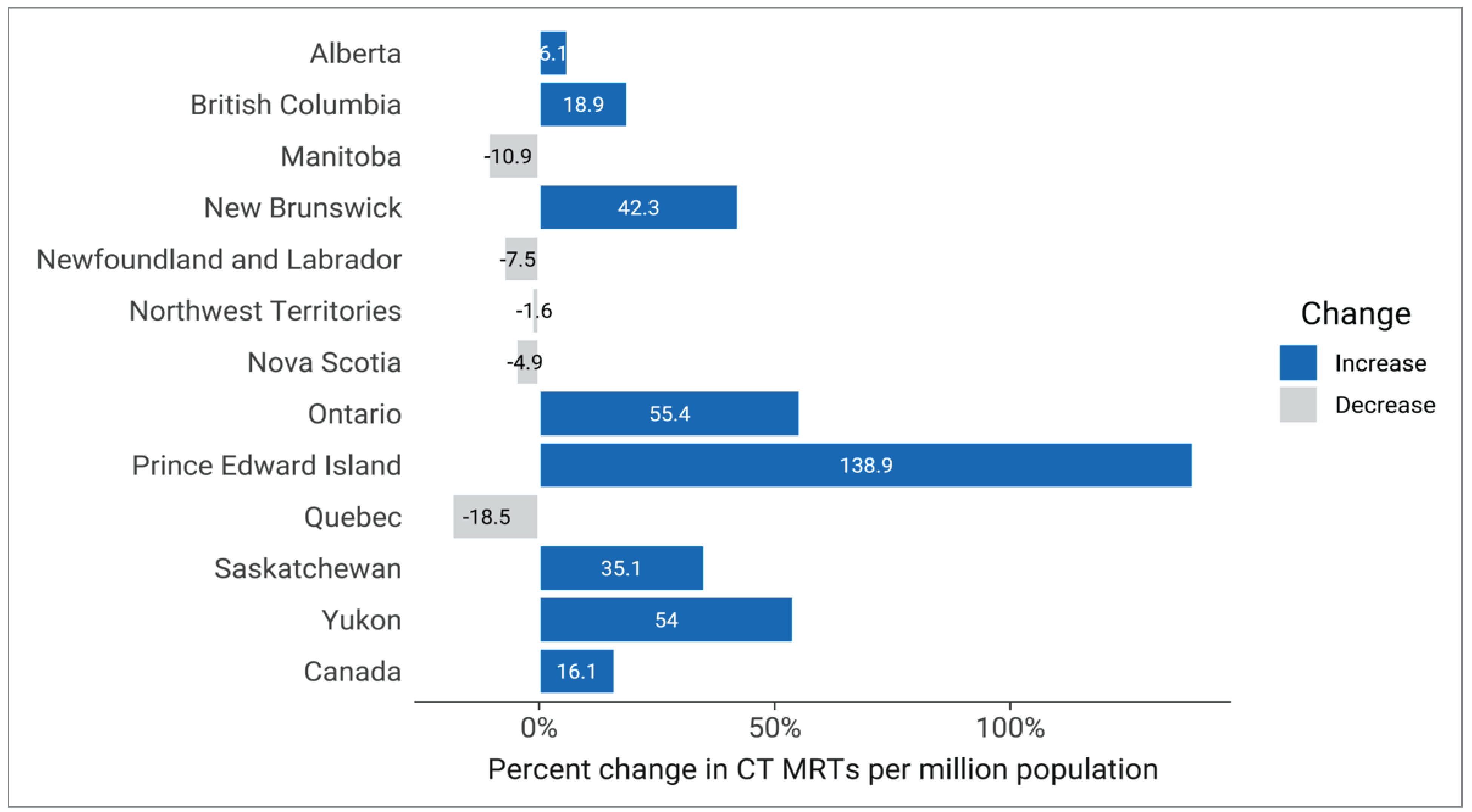
Since 2019–2020, the number of reported FTE MRTs operating CT equipment in Canada has increased by 22.5%, from 1,009 to 1,236.
Since 2019–2020, the estimated density of FTE CT MRTs per capita has increased by 16.1% in Canada (Figure 1). Prince Edward Island, Ontario, and Yukon have experienced the highest increase in number of MRTs per million people of all jurisdictions with CT capacity, increasing by 138.9%, 55.4%, and 54%, respectively.
Figure 1: Percentage Change in FTE MRTs for CT Units per Million Population, 2019–2020 to 2022–2023
FTE = full-time equivalent; MRT = medical radiation technologist.
Notes: For 2022–2023, data were available for 208 of 394 sites across all jurisdictions with CT capacity. For 2019–2020, data were available for 191 of 338 sites with CT capacity.
No data were available for Nunavut in the 2019–2020 survey.
Data derived from the survey question: “How many full-time equivalent (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
Sources: CADTH (2020),27 CADTH (2024).
FTE MRTs for MRI Units
Number of MRI MRTs per Site in Canada, 2022–2023
For MRI, there were approximately 7 FTE MRTs reported to be employed per site, ranging from 2 to 23 (Table 3).
On average, there were approximately 22 FTE MRTs operating MRI equipment per million people in Canada. The jurisdictions with the greatest density of MRTs per million people were Manitoba (54.7 per million people), Yukon (45 per million people), and British Columbia (38.8 per million people).
Table 3: Numbers of FTE MRTs for MRI Units, 2022–2023
Province or territory | Number of reporting sites | Total FTE MRTs | Average FTE MRTs per site (minimum to maximum) | FTE MRTs per million populationa | Populationa |
|---|---|---|---|---|---|
Alberta | 19 | 142 | 7.5 (2 to 22) | 30.2 | 4,703,772 |
British Columbia | 27 | 211 | 7.8 (3 to 23) | 38.8 | 5,437,722 |
Manitoba | 9 | 79 | 5.8 (2 to 13) | 54.7 | 1,444,190 |
New Brunswick | 7 | 31 | 4.4 (2 to 8) | 37.3 | 831,618 |
Newfoundland and Labrador | 3 | 12 | 4 (4 to 4) | 22.5 | 533,710 |
Northwest Territories | — | — | — | — | 45,668 |
Nova Scotia | 5 | 20 | 4 (2 to 5) | 19.1 | 1,047,232 |
Nunavut | — | — | — | — | 40,715 |
Ontario | 36 | 261 | 7.2 (2 to 19) | 16.8 | 15,500,632 |
Prince Edward Island | 1 | 3 | 3 (3 to 3) | 17 | 176,113 |
Quebec | 13 | 80 | 6.2 (2 to 22) | 9.1 | 8,831,257 |
Saskatchewan | 5 | 45 | 9 (3 to 18) | 36.8 | 1,221,439 |
Yukon | 1 | 2 | 2 (2 to 2) | 45 | 44,412 |
Canada | 126 | 886 | 6.8 (2 to 23) | 22.2 | 39,858,480 |
— = not applicable; FTE = full-time equivalent; MRT = medical radiation technologist.
Notes: Data were available for 126 of 296 sites across all jurisdictions with MRI capacity.
Data derived from the survey question: “How many full-time equivalent (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
aThe population (estimated) as of first quarter, 2023.48
Change in the Number of MRI MRTs Since the 2019–2020 CMII Survey
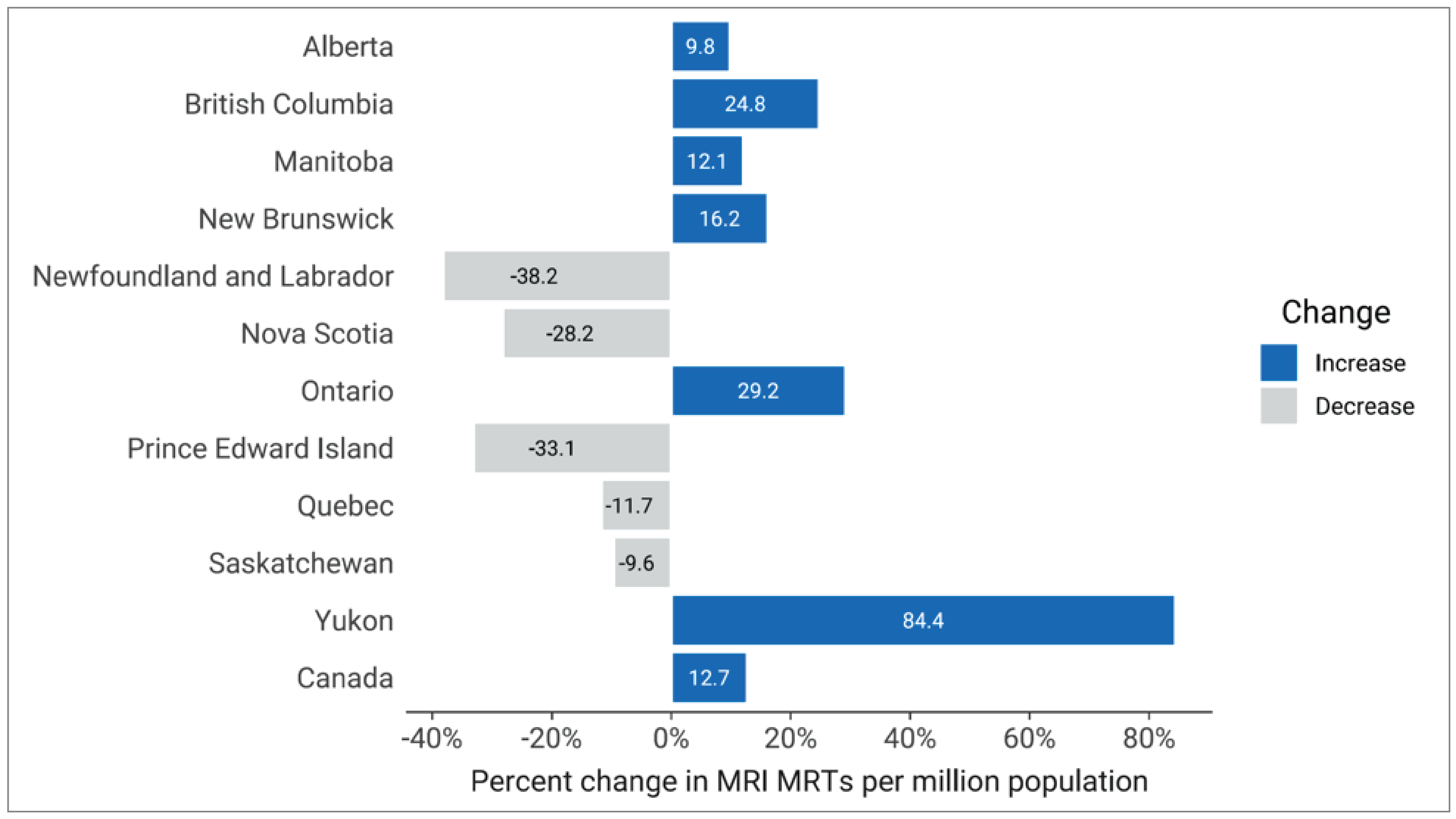
Since 2019–2020, the number of reported FTE trained MRTs operating MRI equipment in Canada has increased by 18.4%, from 748 to 886.
Since 2019–2020, the estimated density of FTE MRI MRTs per capita has increased by 12.7% in Canada (Figure 2). Yukon, Ontario, and British Columbia have experienced the highest increase in number of MRTs per million people of all jurisdictions with MRI capacity, increasing by 84.4%, 29.2%, and 24.8%, respectively.
Figure 2: Percentage Change in FTE MRTs for MRI Units per Million Population, 2019–2020 to 2022–2023
FTE = full-time equivalent; MRT = medical radiation technologist.
Notes: For 2022–2023, data were available for 126 of 296 sites across all jurisdictions with MRI capacity. For 2019–2020, data were available for 118 of 214 sites with MRI capacity.
No data were available for Nunavut in the 2019–2020 survey. There is no MRI capacity reported in the Northwest Territories.
Data derived from the survey question: “How many full-time equivalent (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
Sources: CADTH (2020),27 CADTH (2024).
FTE MRTs for PET-CT and PET-MRI Units
Number of PET-CT and PET-MRI MRTs per Site in Canada, 2022–2023
For PET-CT, there were approximately 4 FTE MRTs reported to be employed per site, ranging from 1 to 9 (Table 4).
On average, there were approximately 2 FTE MRT operating PET-CT equipment per million people in Canada. The jurisdictions with the greatest density of MRTs per million people were Saskatchewan (6.5 per million people), Newfoundland and Labrador (5.6 per million people), and Nova Scotia (3.8 per million people).
For PET-MRI, 2 FTE MRTs were assigned to the 1 site that reported information for FTE.
Table 4: Numbers of FTE MRTs for PET-CT Units, 2022–2023
Province or territory | Number of reporting sites | Total FTE MRTs | Average FTE MRTs per site (minimum to maximum) | FTE MRTs per million populationa | Populationa |
|---|---|---|---|---|---|
Alberta | 4 | 16 | 4 (3 to 5) | 3.4 | 4,703,772 |
British Columbia | NR | NR | NR | NR | 5,437,722 |
Manitoba | 1 | 3 | 3 (3 to 3) | 2.1 | 1,444,190 |
New Brunswick | 1 | 2 | 2 (2 to 2) | 2.4 | 831,618 |
Newfoundland and Labrador | 1 | 3 | 3 (3 to 3) | 5.6 | 533,710 |
Northwest Territories | — | — | — | — | 45,668 |
Nova Scotia | 1 | 4 | 4 (4 to 4) | 3.8 | 1,047,232 |
Nunavut | — | — | — | — | 40,715 |
Ontario | 10 | 36 | 3.6 (1 to 7) | 2.3 | 15,500,632 |
Prince Edward Island | — | — | — | — | 176,113 |
Quebec | 6 | 22 | 3.7 (2 to 9) | 2.5 | 8,831,257 |
Saskatchewan | 1 | 8 | 8 (8 to 8) | 6.5 | 1,221,439 |
Yukon | — | — | — | — | 44,412 |
Canada | 25 | 94 | 3.8 (1 to 9) | 2.4 | 39,858,480 |
— = not applicable; FTE = full-time equivalent; MRT = medical radiation technologist; NR = not reported.
Notes: Survey response data were available for 25 of 52 sites across 8 of 9 jurisdictions with PET-CT capacity. No data were available for British Columbia.
Data derived from the survey question: “How many full-time equivalent (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
aThe population (estimated) as of first quarter, 2023.48
Change in the Number of PET-CT MRTs Since the 2019–2020 CMII Survey
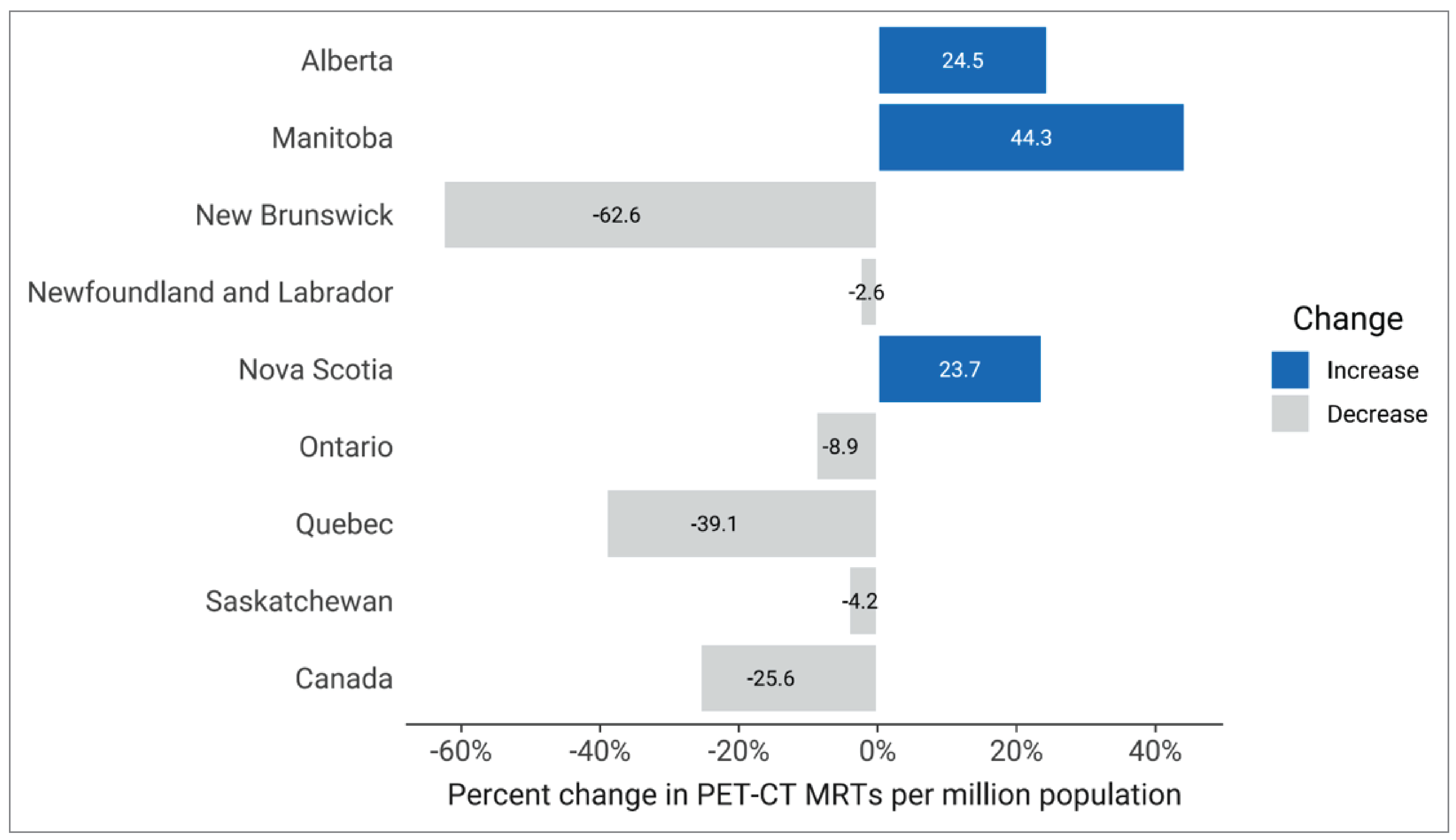
Since 2019–2020, the reported number of FTE trained MRT operating PET-CT equipment in Canada has decreased by 23%, from 122 to 94.
Since 2019–2020, the estimated density of FTE PET-CT MRTs per capita has decreased by 25% in Canada, from 3.2 to 2.4 (Figure 3). Manitoba, Alberta, and Nova Scotia reported an increase in the number of MRT per million people, increasing by 40%, 25.9%, and 22.6%, respectively. All other jurisdictions with PET-CT capacity reported a decrease.
Figure 3: Percentage Change in FTE MRTs for PET-CT Units per Million Population, 2019–2020 to 2022–2023
FTE = full-time equivalent; MRT = medical radiation technologist.
Notes: For 2022–2023, data were available for 25 of 52 sites with PET-CT capacity. For 2019–2020, data were available for 24 of 44 sites with PET-CT capacity.
No responses were received from British Columbia for the 2022–2023 survey. There is no PET-CT capacity reported in Yukon, the Northwest Territories, Nunavut, and Prince Edward Island.
Data derived from the survey question: “How many full-time equivalent (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
Sources: CADTH (2020),27 CADTH (2024).
FTE MRTs for SPECT-CT Units
Number of SPECT-CT MRTs per Site in Canada, 2022–2023
For SPECT-CT, there were approximately 4 FTE MRTs reported to be employed per site, ranging from 1 to 18 (Table 5).
On average, Canada has an estimated 10 FTE MRT operating SPECT-CT equipment per million people. The jurisdictions with the greatest density of MRTs per million people were Newfoundland and Labrador (28.1 per million people), Manitoba (25.6 per million people), and New Brunswick (18 per million people).
Table 5: Numbers of FTE MRTs for SPECT-CT Units, 2022–2023
Province or territory | Number of reporting sites | Total FTE MRTs | Average FTE MRTs per site (minimum to maximum) | FTE MRTs per million population | Populationa |
|---|---|---|---|---|---|
Alberta | 19 | 76 | 4 (1 to 9) | 16.2 | 4,703,772 |
British Columbia | 18 | 85 | 4.7 (2 to 10) | 15.6 | 5,437,722 |
Manitoba | 5b | 37 | 7.4 (3 to 14) | 25.6 | 1,444,190 |
New Brunswick | 4 | 15 | 3.8 (2 to 6) | 18 | 831,618 |
Newfoundland and Labrador | 3 | 15 | 5 (2 to 10) | 28.1 | 533,710 |
Northwest Territories | — | — | — | — | 45,668 |
Nova Scotia | 3 | 7 | 2.3 (2 to 3) | 6.7 | 1,047,232 |
Nunavut | — | — | — | — | 40,715 |
Ontario | 28 | 97 | 3.5 (1 to 12) | 6.3 | 15,500,632 |
Prince Edward Island | 1 | 3 | 3 (3 to 3) | 17 | 176,113 |
Quebec | 12 | 58 | 4.8 (1 to 18) | 6.6 | 8,831,257 |
Saskatchewan | 3 | 17 | 5.7 (1 to 8) | 13.9 | 1,221,439 |
Yukon | — | — | — | — | 44,412 |
Canada | 96 | 410 | 4.3 (1 to 18) | 10.3 | 39,858,480 |
— = not applicable; FTE = full-time equivalent; MRT = medical radiation technologist.
Notes: Data were available for 96 of 180 sites with SPECT-CT capacity.
Data derived from the survey question: “How many full-time equivalents (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
aThe population (estimated) as of first quarter, 2023.48
bCombined SPECT and SPECT-CT FTE MRT count.
Change in the Number of SPECT-CT and SPECT MRTs Since the 2019–2020 CMII Survey
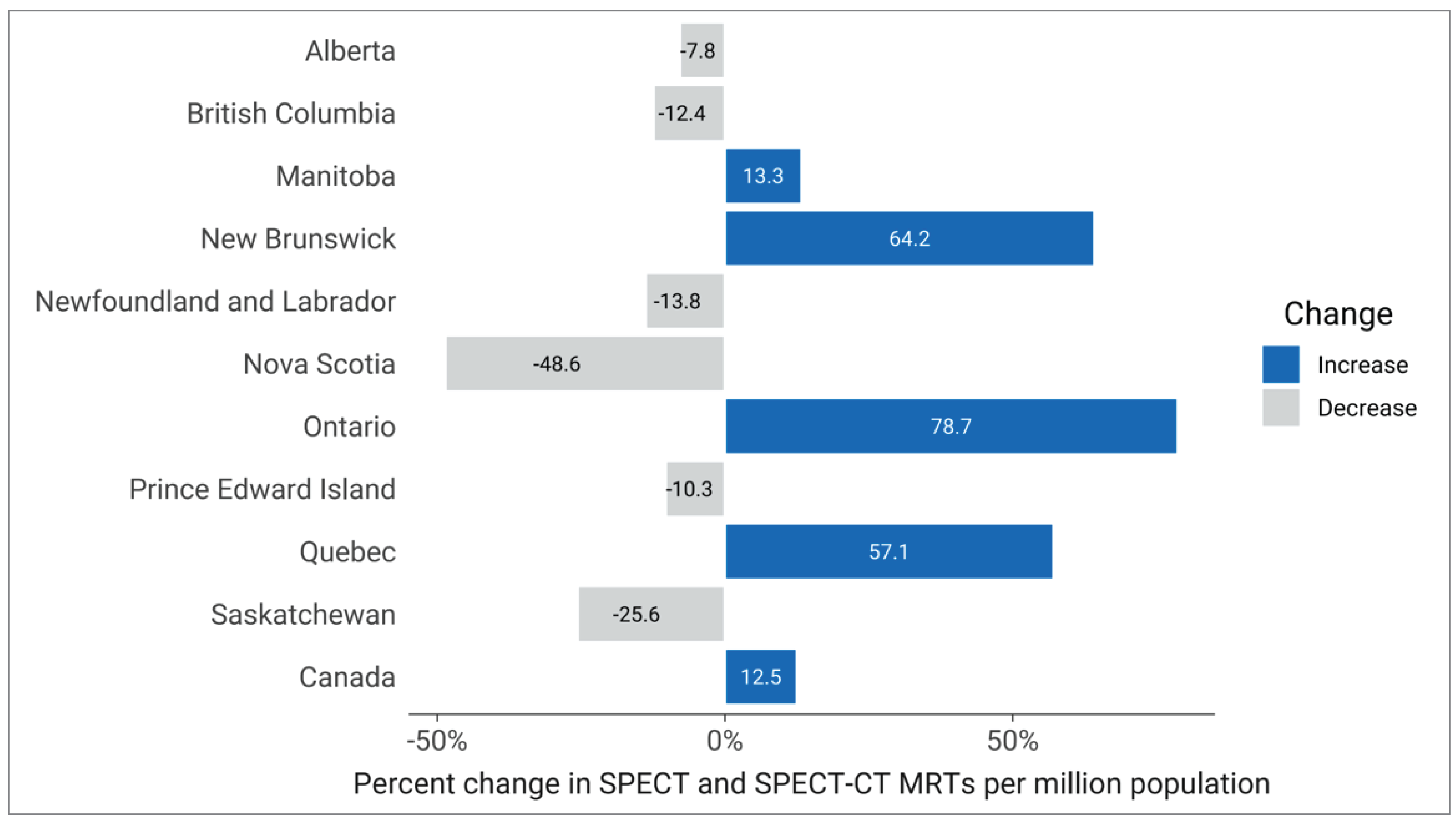
In the 2019–2020 CMII survey, FTE MRTs for SPECT and SPECT-CT were reported as a combined total. For consistency, the 2022–2023 FTE MRT counts for SPECT-CT and SPECT have been combined and are summarized in this section on SPECT-CT.
Since 2019–2020, the number of reported FTE trained MRTs operating SPECT-CT and SPECT equipment in Canada has increased by 18.5%, from 546 to 647.
Since 2019–2020, the estimated density of FTE SPECT MRTs per capita has increased by 12.5% in Canada, although most provinces experienced a decrease in the number of MRTs per capita (Figure 4). Manitoba, New Brunswick, Ontario, and Quebec reported increased MRT density per capita.
Figure 4: Percentage Change in FTE Trained MRTs for SPECT-CT and SPECT Units per Million Population, 2019–2020 to 2022–2023
FTE = full-time equivalent; MRT = medical radiation technologist.
Notes: For 2022–2023, data were available for 96 of 180 sites with SPECT-CT capacity and for 62 of 138 sites with SPECT capacity. For 2019–2020, data were available for 87 of 138 sites with SPECT-CT or SPECT capacity.
There is no SPECT-CT or SPECT capacity reported in Yukon, the Northwest Territories, and Nunavut.
Data derived from the survey question: “How many full-time equivalent (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
Sources: CADTH (2020),27 CADTH (2024).
FTE MRTs for SPECT Units
Number of SPECT MRTs per site in Canada, 2022–2023
For SPECT, there were approximately 4 FTE MRTs reported to be employed per site, ranging from 1 to 18 (Table 6).
On average, there were approximately 6 FTE trained MRT operating SPECT equipment per million people in Canada. The jurisdictions with the greatest density of MRTs per million people were Saskatchewan (16.4 per million people), New Brunswick (15.6 per million people), and Alberta (14.5 per million people).
Table 6: Numbers of FTE Trained MRTs for SPECT Units, 2022–2023
Province or territory | Number of reporting sites | Total FTE MRTs | Average FTE MRTs per site (minimum to maximum) | FTE MRTs per million population | Populationa |
|---|---|---|---|---|---|
Alberta | 14 | 68 | 4.9 (2 to 9) | 14.5 | 4,703,772 |
British Columbia | 5 | 16 | 3.2 (1 to 10) | 2.9 | 5,437,722 |
Manitoba | 0b | — | — | — | 1,444,190 |
New Brunswick | 4 | 13 | 3.2 (2 to 6) | 15.6 | 831,618 |
Newfoundland and Labrador | 0 | NR | NR | NR | 533,710 |
Northwest Territories | — | — | — | — | 45,668 |
Nova Scotia | 4 | 9 | 2.2 (2 to 3) | 8.6 | 1,047,232 |
Nunavut | — | — | — | — | 40,715 |
Ontario | 24 | 83 | 3.5 (1 to 12) | 5.4 | 15,500,632 |
Prince Edward Island | — | — | — | — | 176,113 |
Quebec | 9 | 28 | 3.1 (2 to 11) | 3.2 | 8,831,257 |
Saskatchewan | 2 | 20 | 10 (2 to 18) | 16.4 | 1,221,439 |
Yukon | — | — | — | — | 44,412 |
Canada | 62 | 237 | 3.8 (1 to 18) | 5.9 | 39,858,480 |
— = not applicable; FTE = full-time equivalent; MRT = medical radiation technologist; NR = not reported.
Note: Survey response data available for 62 of 138 sites across 8 of 9 jurisdictions with SPECT capacity. No data were available for Newfoundland and Labrador.
Data derived from the survey question: “How many full-time equivalent (FTE) technologists are assigned to all units (collective number of FTEs for all units)?”
aThe population (estimated) as of first quarter, 2023.48
bCombined SPECT-CT and SPECT FTE MRT count are reported in Table 5.
Trends in Practising MRTs Relative to CT and MRI Exam Volumes
Imaging exam volumes are increasing in Canada, as is the demand for highly skilled MRTs that support these diagnostic procedures that are often central to a patient’s care journey.39,49 Identifying trends in exam and MRT patterns over time can help inform planning and decisions around human resources, service delivery, and equipment investments.50
Trend data are drawn from current and previous iterations of the CMII national survey. Before 2015, data on exams were from CIHI. CIHI data were also used for MRT staffing counts. Total volumes of public CT and MRI examinations, MRT counts, and totals per capita for Canada for the years 2004 to 2022–2023 are presented subsequently.
Volume of Exams and Number of MRTs, 2004 to 2022–2023
Since 2004, there has been a rapid increase in the volume of publicly funded CT and MRI exams in Canada. The number of available FTE MRT positions in Canada has experienced a slower stable increase over time, suggesting that the number of full-time MRT positions in Canada has not kept pace with exam growth. Since 2004, Canada’s population has increased by 24.4%, from 32,039,959 to 39,858,480 people in 2022–2023.20,48
The overall volume of CT exams in Canada increased by 130.7%, from 2,767,849 exams in 2004 to 6,385,665 exams in 2022–2023 (Figure 5).
The overall volume of MRI exams in Canada increased by 188.2%, from 768,302 exams in 2004 to 2,214,157 exams in 2022–2023 (Figure 5).
The overall number of MRT positions in Canada increased by 64.4%, from 15,667 positions in 2004 to 25,752 positions in 2022–2023 (Figure 5).
Figure 5: Total Reported CT and MRT Exam Volumes and Number of Trained MRTs in Canada, 2004 to 2022–2023
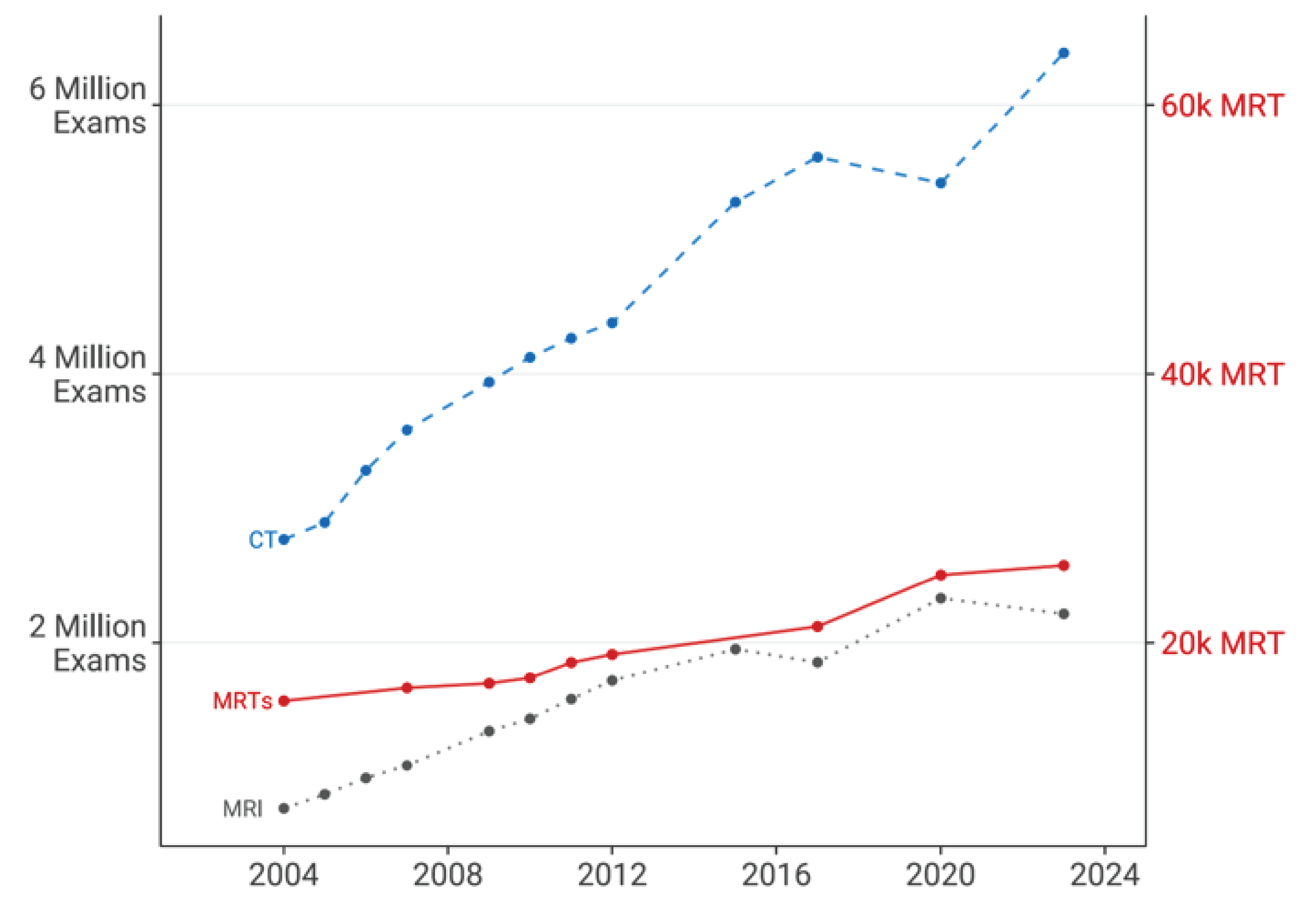
k = thousand; MRT = medical radiation technologist.
Exam sources: CIHI (2003),20 CIHI (2007),21 CIHI (2012),51 CADTH (2015),17 CADTH (2017),19 CADTH (2020),27 CADTH (2024).
Changes per Capita in Volume of CT and MRI Exams Relative to the Number of MRTs
Since 2004, there has been a rapid increase in the volume of publicly funded CT and MRI exams per 1,000 people in Canada.17-23 The number of available full-time MRT positions per million people in Canada has experienced a slower increase over time, keeping similar pace with population growth during this period.12,52-54
CT exam volume in Canada has experienced an 85.4% growth rate, increasing from 86.4 exams per 1,000 people in 2004 to 160.2 exams per thousand people in 2022–2023 (Figure 6).
MRI exam volume in Canada has experienced a 131.7% growth rate, increasing from 24.0 exams per 1,000 people in 2004 to 55.6 exams per thousand people in 2022–2023 (Figure 6).
The number of MRT positions Canada has experienced a 32.1% growth rate, increasing from 489.0 positions per million people in 2004 to 646.1 positions per million people in 2022–2023 (Figure 6).
Figure 6: Percentage Increase in CT and MRI Exam Volumes and the Number of MRTs per Capita in Canada Since 2004
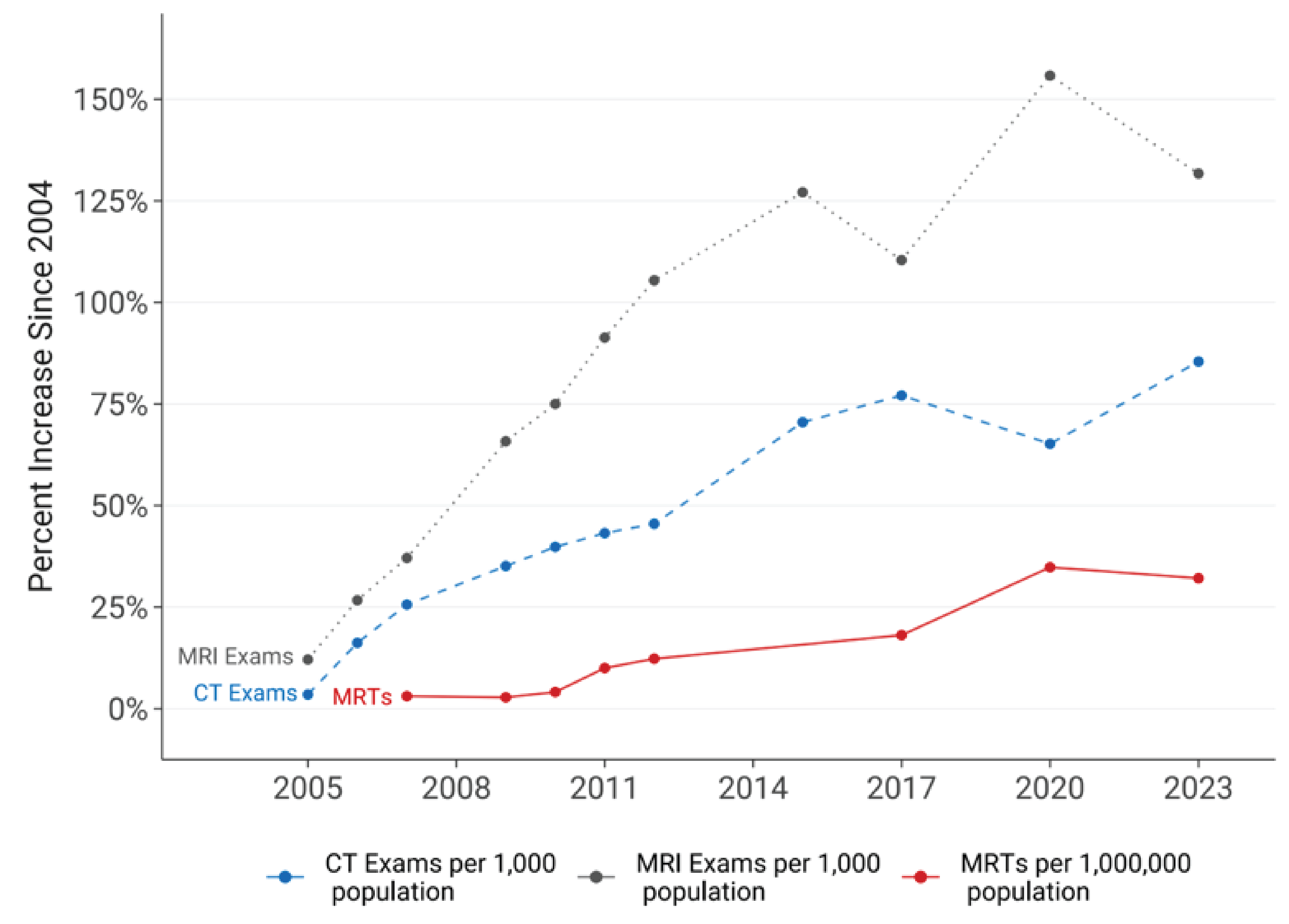
MRT = medical radiation technologist.
Exam sources: CIHI (2003),20 CIHI (2007),21 CIHI (2012),51 CADTH (2015),17 CADTH (2017),19 CADTH (2020),27 CADTH (2024).
Health Human Resources
Without considering health human resources, investing in new equipment may not achieve the increased capacity required to meet growing imaging demand. Reported medical imaging staff shortages in the context of increasing service demand has contributed to extended wait times, limited access to services, poor staff well-being, and reduced quality of patient care.33,34
Staffing
There have been reports of an increasing shortage of trained medical imaging staff in Canada.55 The following factors, among others, have been identified through a literature review as contributing to the shortage, which has also been described as negatively impacting staff well-being:13,56
COVID-19–Related Factors
The COVID-19 pandemic exacerbated existing staff shortages within the health care system in Canada.10-13,56 Postponed diagnostic imaging and resulting medical treatment during this time put increased strain on medical imaging teams in Canada.57
When compared to the prepandemic period, there are now fewer full-time professionals in practice across Canada (Figure 7), with medical physicists experiencing the largest decline per million people (9.7%).10-12,27
There are now fewer MRTs in practice per million population, while the volume of CT and MRI exams per technologist has increased since 2019.12,27,58
Population-Related Factors
Older adults often have complex health care needs that require more health care services than younger patients. In 2020, it was estimated that older adults represented 47%, 22%, and 46% of total exams volumes in Canada for CT, MRI, and PET-CT, respectively.59
The older adult population along with an increasing incidence of diseases such as cancer may exacerbate the already rising need for additional medical imaging equipment in Canada.59,60
An older workforce has also led to a loss of expertise as radiologists and technologists retire.47
Equipment and Innovation Factors
Less efficient and older equipment or a lack of access to imaging equipment, especially in remote or rural areas, can lead to long wait times and increased patient load.61,62
Limited innovative technological, diagnostic screening, and radiation therapy enhancements, including digital solutions and teleradiology, can lead to less efficient workflows and higher imaging staff workloads.63-65
Training, Hiring, and Retention Factors
Some of the identified training, hiring, and retention factors identified in the literature include:
increased hiring demand, prompted by installation of new imaging equipment, as well as expanding clinical indications for imaging equipment3,7
geographical and organizational financial constraints to support employing and retaining highly trained professionals61
limited recruitment and retention incentives, career and promotion opportunities, and investment in positions outside of urban areas46,62,66
education and training opportunities that are limited to larger urban centres and may have limited funding, training incentives, or insufficient accessibility supports for students to complete training15,66
limited intraprofessional backup and support in rural or remote areas as well as health care infrastructure constraints and isolated work environments.62
Professional Well-Being Factors
Stress and mental health concerns among medical imaging staff are reported to have worsened compared to the prepandemic period.13,14,33,40,67-70 A national mental health survey of a sample of MRTs in 2023 found that compared to 2018:71
emotional exhaustion increased by 94%, depersonalization increased by 106%, and feelings of reduced personal accomplishment grew by 21%
there was a 2-fold increase in the number of participants that reported having a serious mental health issue.
Staff well-being may be linked to increased workloads, health and safety considerations, management practices, and workflow protocols.66,72,73
Organizational factors have been linked to staff mental and physical well-being:66,72,73
Since 2018, medical imaging team professionals have reported a 42% increased workload and up to 25% decrease in feelings of trust, respect, and safety in the workplace.71
Stress and poor mental and/or physical health contribute to overall decreased well-being, increased absenteeism, and underperformance, and have a potential negative impact on patient care.13,67,68
An increasing number of staff are reportedly leaving the profession in Canada, thus exacerbating existing shortages of imaging staff:71
Since 2018, the reported vacancy rates for MRT positions have increased more than 2-fold, 3-fold, and 4-fold for CT, nuclear medicine, and MRI, respectively.
Figure 7: Percentage Change in Staff per Million Population, 2019 to 2022–2023
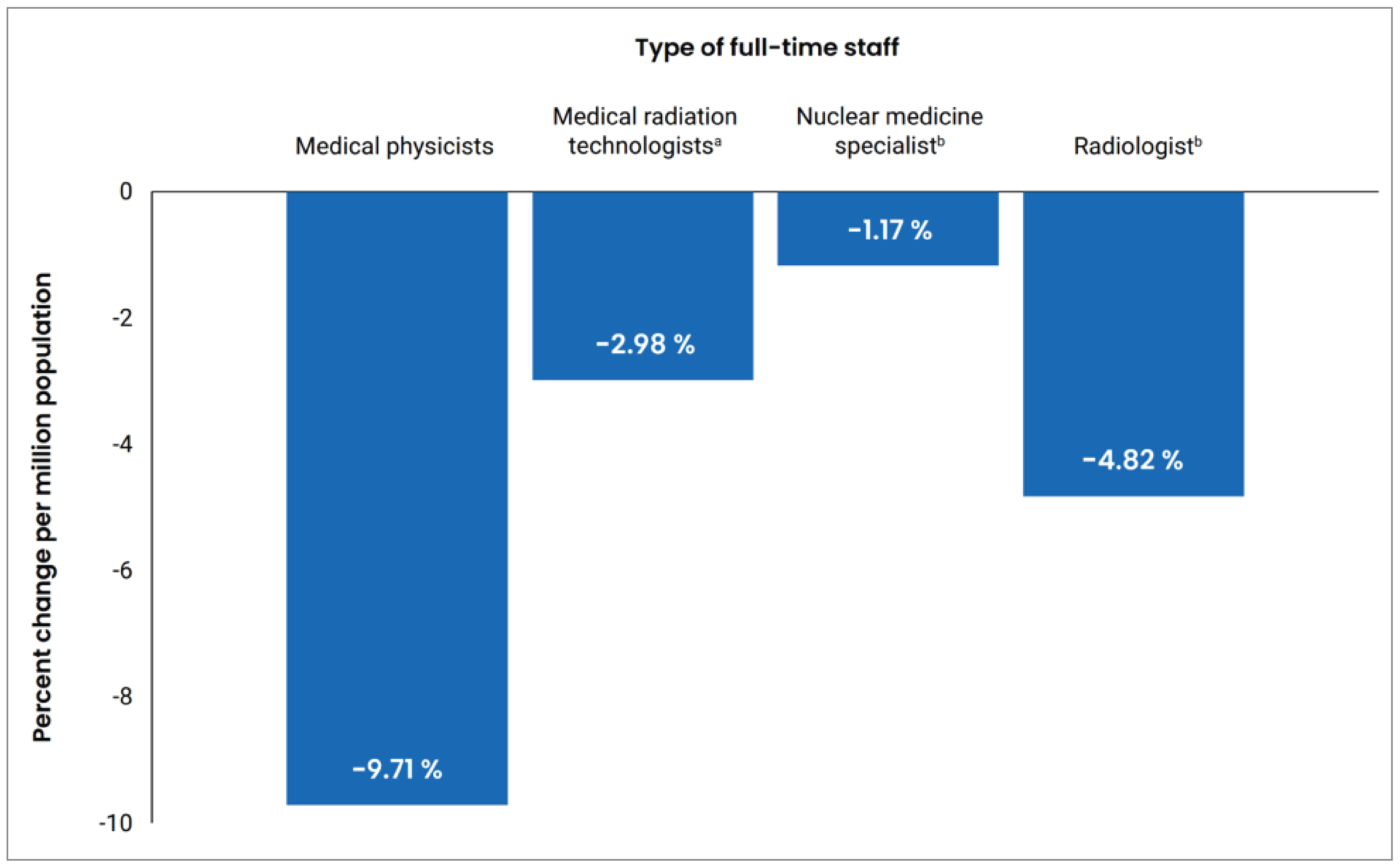
a Medical radiation technologist data from 2021.
b Nuclear medicine specialist and radiologist data from 2019. Assumed unchanged staff retention since 2019 and increased population growth.10,11
Wait Times in Canada
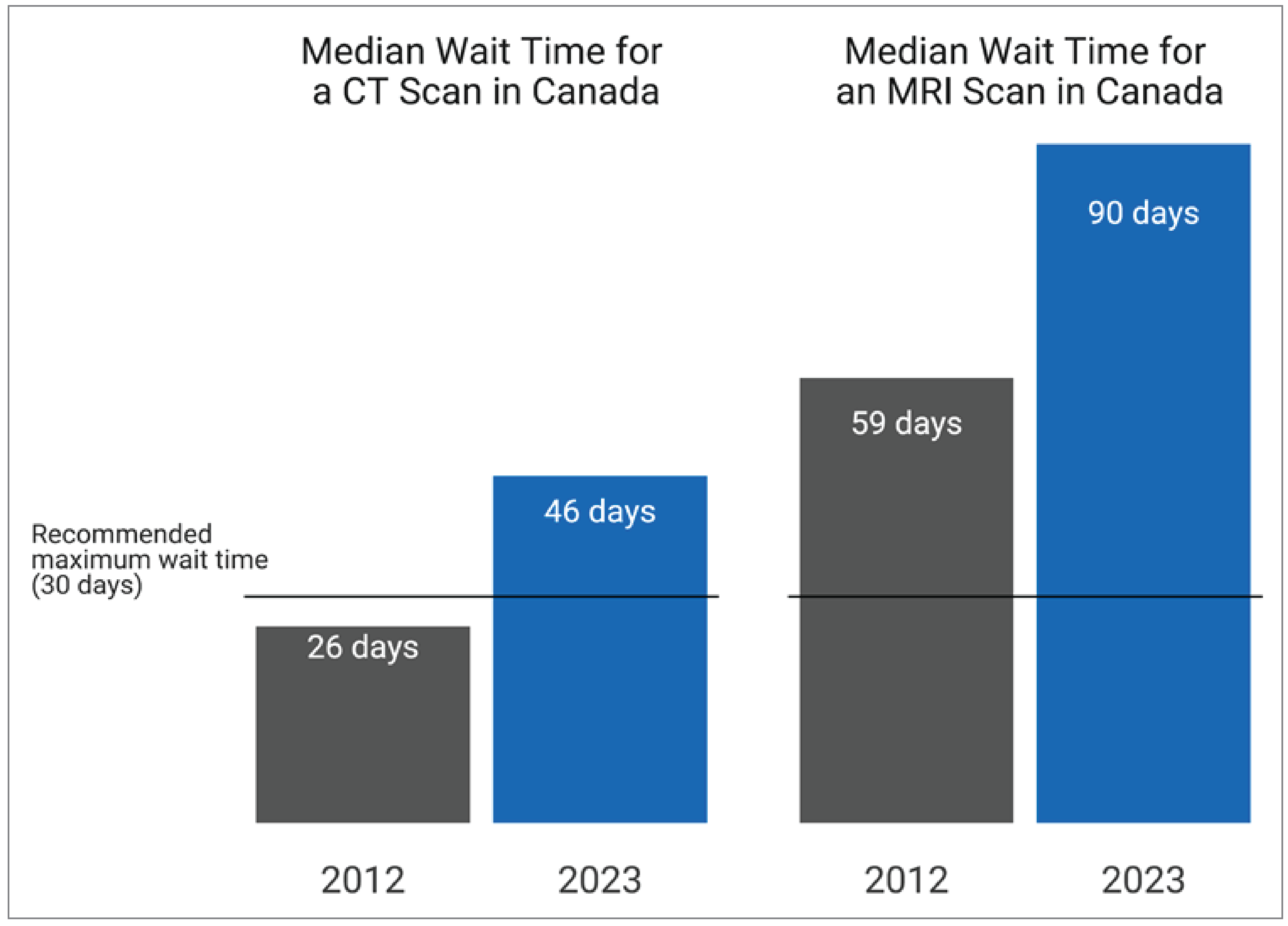
Wait times for medical imaging appear to be exacerbated by increased service demand and reduced staffing.74 There are several reports of patients waiting beyond the recommended wait times for CT and MRI of 30 days.7,75-77
Between 2012 and 2023, the median wait time for CT increased by 77% (from 26 to 46 days) and the wait time for MRI increased by 53% (from 59 to 90 days) (Figure 8).7,75
Funding challenges, less efficient equipment, and low-value exam volumes are reported to contribute to growing wait times.25,74,78
Strategies to Support Health Human Resources
Several strategies have been recommended by organizations in Canada and internationally as well as studies to help support health and human resourcing. These include:3,62,67,73,74,79-82
investment in innovative medical technologies and replacement of obsolete equipment
developing a robust health human resources strategy for medical imaging departments
prioritize enhancing management practices and leadership training to promote a healthy, safe, and respectful workplace environment to improve staff well-being and retention
invest in the hiring and retention and training practices to improve diversity and cultural competency in the workforce
ensure equitable distribution of equipment and incentivize professionals to practice in underserved regions
increase rural and remote education opportunities during radiology training
implement clinical decision support systems, appropriateness criteria, and other tools to streamline referral and scheduling processes and communication (e.g., referral pathway, booking, intake).
Limitations of Findings
Counts for the number of imaging professional by discipline were limited to the most recent publicly available year. Although count data for imaging medical physicists were available for 2023, most recent data for MRTs were limited to 2021, and counts from 2019 were retrieved for both radiologists and nuclear medicine professionals. It was presumed that the number of professionals in these disciplines remained constant over time and population growth increased, which may not accurately reflect the rapidly changing imaging team environment.
The counts were limited to the number of posted or available positions for imaging professionals or the number of professionals actively registered with a professional association. This does not account for the number of filled or vacant positions, or the number of professionals on leave, listed as inactive, or retired. Consequently, this approach may not accurately represent the current number of professionals in practice, potentially leading to overestimated staffing values.
This report includes self-reported survey and questionnaire data from multiple sources and therefore sampling bias, response bias, and low response rates for some questions may limit the generalizability of findings.
For specific survey questions, the accuracy of the data in this report relies in part on the survey participants’ personal knowledge of their particular health care setting (e.g., number of FTE MRT). For these survey questions, recall bias cannot be avoided because we were unable to assess whether all information was visually verified and based on real-time observations or whether questions were answered from memory. As a result, the accuracy and completeness of the reporting may be impacted.
Since 2015, the CMII national survey forms have been prepopulated with responses from sites that participated in previous CMII national survey iterations. Invited survey respondents are asked to update their data to reflect the status at the time of responding to the survey. If the survey was not updated for this iteration, it was assumed that no changes had been made from the previous CMII survey response. Although this method improved survey respondent engagement and reduced fatigue, not all data may be up-to-date in some instances for some sites.
For feasibility, the CMII survey has been restricted to 6 advanced imaging modalities, creating a bias toward urban areas. This focus bias does not capture alternative imaging options, such as ultrasound or X-ray, that are available outside these regions, especially in remote or rural areas where patients would otherwise need to travel or be transferred significant distances for imaging.
What Else Are We Doing?
This Canadian Medical Imaging Inventory 2022–2023: The Medical Imaging Team report is part of a series of publications that is part of a series of publications produced based on the CMII national survey.
The following additional publications, which can be found on the CMII website, are available to provide jurisdiction-level information on medical imaging modalities and resources:
Canadian Medical Imaging Inventory 2022–2023: Provincial and Territorial Overview
Canadian Medical Imaging Inventory 2022–2023: CT
Canadian Medical Imaging Inventory 2022–2023: MRI
Canadian Medical Imaging Inventory 2022–2023: PET-CT and PET-MRI
Canadian Medical Imaging Inventory 2022–2023: SPECT and SPECT-CT
provincial and territorial summaries
What Else Have We Done?
The following are other CMII-related reports released in 2023 to 2024 in response to specific decision-maker needs and are published on the CMII website:
General Ultrasound Examination Volumes per Sonographer 8-Hour Workday
Average Volume of MRI Exams Conducted per Hour Across Canada
Use of MRI and CT in Private Imaging Facilities in Canada: Service Report
Imaging Implementation Advice Panel: Guidance for PSMA-PET Implementation
Individuals’ Access to Medical Imaging Results via Patient Portals
References
1.Rehani MM. Challenges in radiation protection of patients for the 21st century. Am J Roentgenol. 2013;200(4):762-764. PubMed
2.Canadian Cardiovascular Society Position Statement on radiation exposure from cardiac imaging and interventional Pprocedures. Can J Cardiol. 2013;29(11):1361-1368. https://www.onlinecjc.ca/article/S0828-282X%2813%2900363-2/abstract. Accessed 2024 Jan 27. PubMed
3.Addressing the medical imaging dilemma in Canada: Restoring timely access for patients post-pandemic. Ottawa (ON): Canadian Association of Radiologists; 2022: https://car.ca/wp-content/uploads/2021/07/CAR-PreBudgetSubmission-2022-e-web-FINAL.pdf. Accessed 2023 Nov 9.
4.Appropriate Use of Medical Imaging in Canada. Ottawa (ON): The Medical Imaging Team; 2012: https://imagingteam.ca/Appropriate_use_of_Medical_Imaging_in_Canada.pdf. Accessed 2024 Apr 26.
5.Crowell MS, Dedkam EA, Johnson MR, et al. Diagnostic imaging in a direct-access sports physical therapy clinic: a 2-year retrospective practice analysis. Int J Sports Phys Ther. 2016;11(5):708-717. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5046964/. Accessed 2024 Jan 27. PubMed
6.Canadian Institute for Health Information. Medical imaging in Canada 2007. Ottawa (ON): CIHI; 2008: https://publications.gc.ca/collections/collection_2008/cihi-icis/H118-13-2007E.pdf. Accessed 2024 Jan 10.
7.Moir M, Barua B, Wannamaker H. Waiting your turn: Wait times for health care in Canada, 2023 Report. Vancouver (BC): Fraser Institute; 2023: https://www.fraserinstitute.org/sites/default/files/waiting-your-turn-2023.pdf. Accessed 2024 Jan 10.
8.Smith-Bindman R, Kwan ML, Marlow EC, et al. Trends in Use of Medical Imaging in US Health Care Systems and in Ontario, Canada, 2000-2016. JAMA. 2019;322(9):843-856. PubMed
9.Value of Radiology Part II Advocacy Toolkit. Ottawa (ON): Canadian Association of Radiologists: https://car.ca/wp-content/uploads/2019/07/Value-of-Radiology-Advocacy-Toolkit-2019.pdf. Accessed 2024 Apr 26.
10.Diagnostic radiology profile. Ottawa (ON): Canadian Medical Association; 2019: https://cma.ca/sites/default/files/2019-01/diagnostic-radiology-e.pdf. Accessed 2023 Nov 9.
11.Nuclear medicine profile. Ottawa (ON): Canadian Medical Association; 2019: https://www.cma.ca/sites/default/files/2019-01/nuclear-e.pdf. Accessed 2023 Nov 9.
12.Health workforce in Canada, 2017 to 2021: Overview — Data tables. Ottawa (ON): Canadian Institute for Health Information (CIHI); 2022: https://www.cihi.ca/sites/default/files/document/health-workforce-canada-2017-2021-overview-data-tables-en.xlsx. Accessed 2023 Nov 10.
13.The mental health of medical radiation technologists in Canada: 2021 survey. Ottawa (ON): Canadian Association of Medical Radiation Technologists 2021: https://www.camrt.ca/wp-content/uploads/2021/10/CAMRT-National-Mental-Health-Survey-2021.pdf. Accessed 2023 Nov 9.
14.May K. HSC cancer-diagnostic scanner sits idle due to lack of staff. The Free Press. 2023: https://www.winnipegfreepress.com/breakingnews/2023/04/12/no-staff-to-operate-hsc-cancer-diagnostic-scanner-since-purchase-two-years-ago. Accessed 2024 Apr 27.
15.Daflos P. CT scanner disruptions grow as B.C. medical imaging hangs by a thread. CTV News Vancouver. 2024: https://bc.ctvnews.ca/ct-scanner-disruptions-grow-as-b-c-medical-imaging-hangs-by-a-thread-1.6823901. Accessed 2024 Apr 26.
16.Written Submission for the Pre-Budget Consultations in Advance of the 2024 Budget. Ottawa (ON): The Canadian Association of Medical Radiation Technologists (CAMRT): https://www.ourcommons.ca/Content/Committee/441/FINA/Brief/BR12565053/br-external/CanadianAssociationOfMedicalRadiationTechnologists-e.pdf. Accessed 2024 Apr 28.
17.Sinclair A, Quay T, Pyke L, Morrison A. The Canadian Medical Imaging Inventory 2015. CADTH Optimal use report. Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/pdf/canadian_medical_imaging_inventory_2015_e.pdf. Accessed 2024 Jan 10.
18.The Canadian medical imaging inventory, 2019-2020. CADTH health technology review. Ottawa: CADTH; 2021: https://www.cadth.ca/sites/default/files/ou-tr/op0546-cmii3-final-report.pdf. Accessed 2023 Nov 9.
19.Sinclair A, Morrison A, Young C, Pyke L. The Canadian medical imaging inventory, 2017. CADTH Optimal use report. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pdf/canadian_medical_imaging_inventory_2017.pdf. Accessed 2024 Jan 10.
20.Medical imaging in Canada. Ottawa (ON): Canadian Institute for Health Information; 2003: https://publications.gc.ca/Collection/H118-13-2003E.pdf. Accessed 2024 Jan 10.
21.Medical imaging in Canada 2007. Ottawa (ON): Canadian Institute for Health Information (CIHI); 2008: https://publications.gc.ca/collections/collection_2008/cihi-icis/H118-13-2007E.pdf. Accessed 2024 Jan 10.
22.Canadian Institute for Health Information (CIHI). QuickStats. Selected medical imaging equipment in Canada. 2012.
23.Canadian Institute for Health Information. Medical imaging in Canada 2012 (executive summary). Ottawa (ON): CIHI; 2013.
24.Information for health care professionals Ottawa (ON): The Medical Imaging Team: https://imagingteam.ca/information-resources/information-for-health-care-professionals/ Accessed 2024 Apr 26.
25.Team Working in Clinical Imaging. London (UK): The Society and College of Radiographers: https://www.sor.org/learning-advice/professional-body-guidance-and-publications/documents-and-publications/policy-guidance-document-library/team-working-in-clinical-imaging. Accessed 2024 Apr 26.
26.The Medical Imaging Team https://imagingteam.ca/the-medical-imaging-team/. Accessed 2024 Apr 26.
27.Chao Y-S, Sinclair A, Morrison A, Hafizi D, Pyke L. The Canadian medical imaging inventory 2019-2020. CADTH Health Technology Review. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/ou-tr/op0546-cmii3-final-report.pdf. Accessed 2024 Jan 10.
28.Decisions, Decisions: Family Doctors as Gatekeepers to Prescription Drugs and Diagnostic Imaging in Canada. Toronto (ON): Health Council of Canada; 2010: https://publications.gc.ca/collections/collection_2011/ccs-hcc/H174-19-2010-eng.pdf. Accessed 2024 Mar 22.
29.Appropriateness of requisition, order or prescription. Ottawa (ON): Canadian Association of Medical Radiation Technologists; 2024: https://camrt-bpg.ca/quality-of-care/appropriate-care/appropriateness-of-requisition/. Accessed 2024 Jan 10.
30.Walther F, Eberlein-Gonska, M., Hoffmann, RT et al. Measuring appropriateness of diagnostic imaging: a scoping review. Insights Imaging. 2023;14. PubMed
31.Bianco A, Zucco R, Lotito F, Pavia M. To what extent do hospitalised patients receive appropriate CT and MRI scans? Results of a cross-sectional study in Southern Italy. BMJ Open. 2018;8(2):e018125. PubMed
32.Kjelle E, Brandsaeter IO, Andersen ER, Hofmann BM. Cost of Low-Value Imaging Worldwide: A Systematic Review. Appl Health Econ Health Policy. 2024;22(4):485-501. PubMed
33.Madden Yee K. Radiologist' expertise cuts inappropriate imaging. AuntMinnie.com: Science and Medicine Group; 2016: https://www.auntminnie.com/practice-management/administration/economics/article/15615407/radiologists-expertise-cuts-inappropriate-imaging. Accessed 2024 Apr 26.
34.Rao VM, Levin DC. The overuse of diagnostic imaging and the Choosing Wisely initiative. Ann Intern Med. 2012;157(8). PubMed
35.Thavorn K, Wang Z, Fergusson D, van Katwyk S, Arnaout A, Clemons M. Cost implications of unwarranted imaging for distant metastasis in women with early-stage breast cancer in Ontario. Curr Oncol. 2016;23(Suppl 1):S52-55. PubMed
36.Choosing Wisely Canada. Imaging Wisely: Communicating and Collaborating to Improve Imaging Services. 2017; https://choosingwiselycanada.org/imaging-wisely/. Accessed 2024 Jan 11.
37.Canadian Association of Medical Radiation Technologists. See me as I see you. 2020.
38.Description of practice. Ottawa (ON): Canadian Association of Medical Radiation Technologists; 2020: https://www.camrt.ca/mrt-profession/description-of-practice-2/. Accessed 2024 Apr 15.
39.Medical radiation technologist. Ottawa (ON): Canadian Institute for Health Information: https://www.cihi.ca/en/medical-radiation-technologists. Accessed 2024 Apr 15.
40.Diagnostic radiology profile. Ottawa: Canadian Medical Assocation; 2018: https://www.cma.ca/sites/default/files/2019-01/diagnostic-radiology-e.pdf. Accessed 2024 Apr 15.
41.Canadian Association of Radiologists. Patient resources: who are radiologists. 2020; https://car.ca/patient-care__trashed/patient-resources/. Accessed 2024 Apr 15.
42.American College of Radiology. What does a radiologist do? 2019; https://www.radiologyinfo.org/en/info.cfm?pg=article-your-radiologist. Accessed 2024 Apr 15.
43.Nuclear medicine profile. Ottawa: Canadian Medical Association; 2018: https://www.cma.ca/sites/default/files/2019-01/nuclear-e.pdf. Accessed 2024 Apr 15.
44.Owen MA, Pickett MW, Christian PE, et al. Nuclear medicine practitioner competencies. J Nucl Med Technol. 2007;35(1):39-41. PubMed
45.Scope of practice for Canadian certified medical phycisists. Kanata (ON): Canadian Organization of Medical Physicists; 2015: https://comp-ocpm.ca/_uploads/53jbyv2t9.pdf. Accessed 2024 Apr 15.
46.Pickrell A. Advocates speak out about radiation therapist shortage in New Brunswick. CTV News Atlantic 2023: https://atlantic.ctvnews.ca/advocates-speak-out-about-radiation-therapist-shortage-in-new-brunswick-1.6680059. Accessed 2024 Apr 26.
47.Fleishon HB. The Radiology Labor Shortage. Bulletin. Reston (VA): American College of Radiology; 2022: https://www.acr.org/Practice-Management-Quality-Informatics/ACR-Bulletin/Articles/March-2022/The-Radiology-Labor-Shortage.
48.Statistics Canada. Canada's population estimates, first quarter 2023. The Daily. Ottawa (ON): Government of Canada; 2023: https://www150.statcan.gc.ca/n1/daily-quotidien/230628/dq230628c-eng.htm. Accessed 2024 Jan 5.
49.Canada’s Medical Radiation Technologists: A Case for Investment in Health Workforce. Ottawa (ON): The Canadian Association of Medical Radiation Technologists (CAMRT); 2022: https://www.ourcommons.ca/Content/Committee/441/HESA/Brief/BR11654747/br-external/CanadianAssociationOfMedicalRadiationTechnologists-e.pdf Accessed 2024 Apr 26.
50.Radiology Resilience Now and Beyond. Ottawa (ON): Canadian Association of Radiologists; 2020: https://car.ca/wp-content/uploads/2020/10/RAD_Resilience-Report_2020_ENG_FINAL-2.pdf. Accessed 2023 Nov 9.
51.QuickStats: Selected medical imaging equipment in Canada. Ottawa (ON): Canadian Institute for Health Information (CIHI); 2012.
52.Medical Radiation Technologists in Canada, 2010. Ottawa (ON): Canadian Institute for Health Information; 2012: https://publications.gc.ca/collections/collection_2012/icis-cihi/H115-58-2010-eng.pdf. Accessed 2024 Apr 26.
53.Canada's health care providers, 2014 to 2018 - data tables. Ottawa (ON): Canadian Institute for Health Information; 2018.
54.Canada’s Health Care Providers, 1997 to 2011— A Reference Guide. Ottawa (ON): Canadian Institute for Health Information: https://publications.gc.ca/collections/collection_2013/icis-cihi/H118-1-4-2011-eng.pdf. Accessed 2024 Apr 26.
55.Canadian Association of Radiologists. Addressing the Health Human Resource Crisis in Radiology Departments Across Canada. CISION: CNW Group; 2023: https://www.newswire.ca/news-releases/addressing-the-health-human-resource-crisis-in-radiology-departments-across-canada-842727175.html. Accessed 2023 Nov 9.
56.Wright T. ‘Requests are just piling up’: Patients continue to suffer long waits for medical imaging. Global News. 2022. https://globalnews.ca/news/9125436/medical-imaging-canada-backlogs-covid/. Accessed 2023 Nov 9.
57.Improving Access to Lifesaving Imaging Care for Canadians. Ottawa (ON): Canadian Association of Radiologists: https://car.ca/wp-content/uploads/2022/11/CAR_Multistakeholder_Brief_FINAL_2022_Nov.pdf. Accessed 2024 Apr 26.
58.Morrill S, Baerlocher MO, Patlas MN, Kanani S, Kantarevic J, van der Pol CB. CT, MRI, and Medical Radiation Technologist Trends in Ontario. Can Assoc Radiol J. 2023:8465371231209923. PubMed
59.Advanced Medical Imaging Equipment for Older Adults Across Canada. Canadian Medical Imaging Inventory Service Report. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/attachments/2022-11/advanced_medical_imaging_equipment_for_older_adults_across_canada_cmii_service_report.pdf.
60.Public Health Agency of Canada. Cancer in Canada. Ottawa (ON): Government of Canada; 2018: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/fact-sheet-cancer-canada/fact-sheet-cancer-canada.pdf. Accessed 2024 May 1.
61.Expanded and upgraded interventional radiology suites open in Regina. Regina (SK): Government of Saskatchewan; 2022: https://www.saskatchewan.ca/government/news-and-media/2022/march/15/expanded-and-upgraded-interventional-radiology-suites-open-in-regina. Accessed 2023 Feb 22.
62.Davidson M, Kielar A, Tonseth RP, Seland K, Harvie S, Hanneman K. The Landscape of Rural and Remote Radiology in Canada: Opportunities and Challenges. Can Assoc Radiol J. 2023:8465371231197953. PubMed
63.Job prospects: Medical Radiation Technologist (MRT) in Ontario. Ottawa (ON): Government of Canada Job Bank; 2023: https://www.on.jobbank.gc.ca/marketreport/outlook-occupation/18254/ON. Accessed 2024 Jan 5.
64.Workforce Challenges in Radiology. Oakville (ON): Siemens Healthcare Limited: https://www.siemens-healthineers.com/en-ca/radiologys-workforce-crisis. Accessed 2024 Apr 26.
65.Kalidindi S, Gandhi S. Workforce Crisis in Radiology in the UK and the Strategies to Deal With It: Is Artificial Intelligence the Saviour? Cureus. 2023;15(8):e43866. PubMed
66.Gerwing M. New PET scanner sits idle at Winnipeg hospital without staff to operate it. CTV News Winnipeg.2023: https://winnipeg.ctvnews.ca/new-pet-scanner-sits-idle-at-winnipeg-hospital-without-staff-to-operate-it-1.6346224#:~:text=New%20PET%20scanner%20sits%20idle%20at%20Winnipeg%20hospital%20without%20staff%20to%20operate%20it,-Michelle%20Gerwing&text=The%20installation%20of%20a%20new,to%20show%20the%20body's%20metabolism. Accessed 2024 Apr 26.
67.Canadian Association of Radiologists. Addressing the health human resource crisis in radiology departments across Canada. Newswire.2023: https://www.newswire.ca/news-releases/addressing-the-health-human-resource-crisis-in-radiology-departments-across-canada-842727175.html. Accessed 2023 Nov 9.
68.Cao DJ, Hurrell C, Patlas MN. Current Status of Burnout in Canadian Radiology. Can Assoc Radiol J. 2023;74(1):37-43. PubMed
69.Huizinga R. New Brunswick medical imaging suffering from pandemic burnout. CBC News. 2022 Mar 10. https://www.cbc.ca/news/canada/new-brunswick/new-brunswick-medical-imaging-technologists-burnout-1.6379322. Accessed 2024 Jan 11.
70.Axelrod G. More MRI techs needed to combat wait times as burnout figures rise, association says. CBC News. 2024: https://www.cbc.ca/news/canada/manitoba/more-mri-techs-need-to-combat-wait-times-1.7157863. Accessed 2024 Apr 26.
71.Addressing the Health Human Resource Crisis within the MRT Professions [unpublished internal document]. Ottawa (ON): Canadian Association of Medical Radiation Technologists (CAMRT); 2024.
72.The mental health of medical radiation technologists in Canada. Ottawa (ON): Canadian Association of Medical Radiation Technologists 2021: https://www.camrt.ca/wp-content/uploads/2021/10/CAMRT-National-Mental-Health-Survey-2021.pdf. Accessed 2023 Nov 9.
73.Nurturing the Radiology Workplace. Bulletin. Reston (VA): American College of Radiology; 2022: https://www.acr.org/Practice-Management-Quality-Informatics/ACR-Bulletin/Articles/June-2022/Nurturing-the-Radiology-Workplace.
74.Wait list strategies for CT and MRI exams. Can J Health Technol. 2023;3(1). https://www.cadth.ca/sites/default/files/attachments/2023-01/CM0002-HC0052-Wait-List%20Strategies-for-CT-and-MRI-Scans.pdf. Accessed 2024 Jan 10.
75.Waiting your turn: Wait times for health care in Canada 2012 report. Studies in health policy. Vancouver (BC): Fraser Institute; 2012: https://www.fraserinstitute.org/sites/default/files/waiting-your-turn-2012-rev.pdf. Accessed 2023 Nov 9.
76.Canadian Institute for Health Information (CIHI). Explore wait times for priority procedures across Canada. 2023; https://www.cihi.ca/en/explore-wait-times-for-priority-procedures-across-canada. Accessed 2024 Jan 5.
77.Canadian Institute for Health Information (CIHI). Wait Times for Priority Procedures in Canada, 2014. 2014; https://secure.cihi.ca/free_products/2014_WaitTimesAiB_EN.pdf. Accessed 2024 Jan 5.
78.Fine B, Dhanoa D. Imaging appropriateness criteria: why Canadian family physicians should care. Can Fam Physician. 2014;60(3):217-218. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3952750. Accessed 2020 Sep 30. PubMed
79.Fraser J, Reed M. Appropriateness of imaging in Canada. Can Assoc Radiol J. 2013;64(2):82-84. PubMed
80.A national plan to re-invest in radiology through people, technology and equipment. Ottawa (ON): Canadian Association of Radiologists; 2023: https://car.ca/wp-content/uploads/2023/08/CAR_2024_PreBudgetSubmission_FINAL.pdf. Accessed 2024 Apr 26.
81.Cho A. MRI for all: Portable low-field scanners could revolutionize medical imaging in nations rich and poor—if doctors embrace them. Science. 2023 Feb 23. https://www.science.org/content/article/mri-all-cheap-portable-scanners-aim-revolutionize-medical-imaging. Accessed 2023 Nov 9.
82.Lacson R, Laroya R, Wang A, et al. Integrity of clinical information in computerized order requisitions for diagnostic imaging. J Am Med Inform Assoc. 2018;25(12):1651-1656. PubMed
83.Canadian Coordinating Office for Health Technology Assessment (CCOHTA). Computed tomography scanners in Canadian hospitals. Ottawa (ON): CCOHTA; 2000: https://www.cadth.ca/sites/default/files/pdf/ct_report_01.pdf. Accessed 2024 Feb 29.
84.Organisation for Economic Co-Operation and Development. Computed tomography (CT) scanners. 2022; https://data.oecd.org/healtheqt/computed-tomography-ct-scanners.htm. Accessed 2024 Feb 29.
85.Canadian Coordinating Office for Health Technology Assessment (CCOHTA). Magnetic resonance imaging scanners in Canadian hospitals. Ottawa (ON): CCOHTA; 2001: https://www.cadth.ca/sites/default/files/pdf/mri_report_01.pdf. Accessed 2024 Feb 29.
86.Ghadimi M, Sapra A. Magnetic resonance imaging contraindications. Treasure Island (FL): StatPearls Publishing; 2023: https://www.ncbi.nlm.nih.gov/books/NBK551669/. Accessed 2024 Jan 10.
87.Mayfair Diagnostics. How private MRI fits into public health care. 2018; https://www.radiology.ca/article/how-private-mri-fits-public-health-care. Accessed 2024 Feb 29.
88.National Institute of Biomedical Imaging and Bioengineering. Nuclear medicine. Washington (DC): U.S. Department of Health & Human Services; 2024: https://www.nibib.nih.gov/science-education/science-topics/nuclear-medicine. Accessed 2024 Jan 10.
89.HealthLink BC. Single Photon Emission Computed Tomography (SPECT). 2022; https://www.healthlinkbc.ca/tests-treatments-medications/medical-tests/single-photon-emission-computed-tomography-spect#:~:text=Results-,Single%20photon%2Demission%20computed%20tomography%20(SPECT)%20is%20a%20test,you%20right%20after%20the%20test. Accessed 2024 Jan 10.
90.Statistics Canada. Indigenous peoples - 2021 Census promotional material. Ottawa (ON): Government of Canada; 2021: https://www.statcan.gc.ca/en/census/census-engagement/community-supporter/indigenous-peoples. Accessed 2024 Jan 10.
91.John Hopkins Medicine. Positron Emission Tomography (PET). 2024; https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/positron-emission-tomography-pet. Accessed 2024 Jan 10.
92.Diagnostic imaging: nuclear medicine. Geneva (CHE): World Health Organization; 2016.
93.Canadian Association of Medical Radiation Technologists. Breastfeeding and lactation in nuclear medicine (RTNM). 2013; https://camrt-bpg.ca/patient-safety/radiation-safety-patients/breastfeeding-in-rtnm/. Accessed 2024 Jan 10.
94.Hricak H CB, Scott AM, Sugimura K, Muellner A, von Schulthess GK, et al. Global trends in hybrid imaging. Radiology. 2010;257(2):498-506. PubMed
95.Couillard F. Anticipating a problem, proposing solutions. Ottawa (ON): Canadian Association of Medical Radiation Technologists; 2014: https://www.camrt.ca/blog/2014/11/25/anticipating-a-problem-proposing-solutions/. Accessed 2024 Jan 10.
96.Natural Resources Canada. Medical isotopes. Ottawa (ON): Government of Canada; 2020: https://natural-resources.canada.ca/our-natural-resources/energy-sources-distribution/nuclear-energy-uranium/medical-isotopes/23060. Accessed 2024 Jan 10.
97.Weber WA. ET/MR imaging: a critical appraisal. J Nucl Med. 2014;55(6):(Suppl 2):56S-58S.
98.Delso G, Voert E.T., Barbosa F.G., Veit-Haibach P. Pitfalls and limitations in simultaneous PET/MRI. Seminars in Nuclear Medicine. 2015;45(6):552-559. PubMed
99.Positron emission tomography in oncology. Policy forum: health technology policy information. Ottawa (ON): CADTH; 2009: https://www.cadth.ca/sites/default/files/policy_forum_section/PET_Policy_Information_Document_e.pdf. Accessed 2024 Jan 10.
100.Shellock F, Crues J. MRI: Bioeffects, safety and patient management. Los Angeles (CA): Biomedical Research Publishing Company; 2014.
101.MRIsafety.com. Safety information article list. 2024; https://www.mrisafety.com/SafetyInformation_list.php. Accessed 2024 Jan 11.
Appendix 1: Introduction to Imaging Modalities Collected in 2022–2023
Note that this appendix has not been copy-edited.
CT
CT employs X-rays as a source of ionizing radiation, sensitive radiation detectors, and computer analysis to create cross-sectional images of the body, including the head, heart, lungs, cardiovascular system, musculoskeletal system, abdomen, pelvis, and spine.83 Specialties that routinely employ CT include neurology, cardiology, oncology, internal medicine, orthopedics, and emergency trauma care.
The main advantages of CT are its speed, which enables rapid imaging and diagnosis in urgent situations, and its ability to visualize fine details in bone, lungs, and other organs.83,84 CT involves exposure to ionizing radiation, which means that the risks and benefits of its use in pregnancy, in young children, and of repeated use must be assessed.83
MRI
MRI uses powerful electromagnetic and radiofrequency fields and computation to produce cross-sectional images of the body, including the head, neck, cardiovascular system, breast, abdomen, pelvis, musculoskeletal system, and spine.85 Specialties that commonly employ MRI include neurology, gastroenterology, cardiology, oncology, internal medicine, orthopedics, and emergency services.85
MRI does not use ionizing radiation, and therefore may be preferred when CT and MRI would provide comparable information, for example, when imaging children.85 MRI provides high sensitivity and soft-tissue details, especially in the abdomen and pelvis, allowing for visualization of anatomy and pathologies. In oncology, this assists early diagnosis, staging and re-staging, identification of treatment response, and detection of recurrence in various cancers.85
A challenge of MRI is that exams can take up to an hour or more, and patients must remain motionless within a narrow enclosure. It may not be suitable for people with claustrophobia, those who cannot lie flat for prolonged periods, or those who are obese.85 The magnetic fields and radiofrequencies used in MRI are incompatible with many common implantable medical devices, such as deep brain stimulators, cochlear implants, and pacemakers.85,86 All people undergoing an MRI exam must be screened beforehand to identify any potentially contraindicated devices or metallic foreign bodies.85-87
Nuclear Medicine (SPECT and PET)
SPECT
In nuclear medicine imaging, trace amounts of radiopharmaceuticals are administered to patients intravenously or by injection (e.g., subcutaneously or intradermally), ingestion, or inhalation to visualize areas of radioisotope uptake within the body.11,88 Depending on the radiopharmaceutical administered, the function (i.e., physiology) of almost any organ system can be observed. Nuclear medicine gamma cameras detect the gamma rays emanating from the radioisotope and form flat images; most cameras are also capable of cross-sectional imaging (SPECT).89
Nuclear medicine exams identify and evaluate a variety of pathologies, including cancer, heart disease, as well as gastrointestinal, endocrine, and neurological disorders. Medical specialties that commonly use SPECT imaging include oncology, neurology, cardiology, internal medicine, orthopedics, pediatrics, pneumology, and infectious disease.11,88
PET
PET uses injection of a sugar or other metabolic tracer labelled with a positron-emitting radioisotope, sensitive radiation detector cameras, and powerful computers to detect and visualize areas of increased metabolism, such as tumours. It creates three-dimensional images of regions of interest, such as brain, bone, and heart.90,91
The main advantage of PET (and its successor PET-CT) imaging is the ability to precisely quantify metabolic processes (e.g., the rate of glucose metabolism) and, depending on the pathology, to more accurately localize abnormalities. PET-radiolabelled sugar (i.e.,18F-FDG) is the most common PET tracer currently used in Canada, but other tracers are becoming available, especially for cardiac and neurological imaging. Another advantage of PET-CT imaging is that the whole body can be imaged, which is useful for assessing tumour spread or recurrence.
Medical specialties that commonly use PET imaging include oncology, neurology, psychiatry, cardiology, pediatrics, and infectious disease.
Hybrid Medical Imaging Technologies (SPECT-CT, PET-CT, and PET-MRI)
Hybrid imaging combines 2 or more imaging modalities to take advantage of the characteristics of each. Therefore, hybrid imaging can simultaneously provide high anatomic detail and metabolic and/or physiological function, enabling more accurate diagnosis, better care pathways, refined treatment regimes, and improved patient outcomes.92
SPECT-CT
SPECT-CT combines SPECT and CT to create three-dimensional images of the body part of interest, such as brain, bone, and heart. Its main advantage is that it offers both metabolic and physiologic information, coupled with the resolution of CT. During a hybrid SPECT-CT, both scans are performed in sequence; the images are then computationally aligned with each other to show anatomic and functional detail, and to enable attenuation correction of the SPECT signal. Medical specialties that commonly use SPECT-CT imaging include oncology, neurology, cardiology, internal medicine, and orthopedics.
The challenges of SPECT-CT are those of the component modalities, both of which involve exposure to ionizing radiation,93 and concerns about availability of radioisotopes.
PET-CT
PET-CT combines the modalities of PET and CT, creating three-dimensional images of the body part of interest, such as brain, bone, and lung. Both scans are performed in sequence during a single session, and the images are computationally aligned.94 PET-CT is commonly used in oncology to diagnose and stage various cancers, such as lung, gastrointestinal, colorectal, breast, and thyroid cancer. Additionally, PET-CT is commonly employed to diagnose neurologic, cardiovascular, infectious, and inflammatory pathologies, and the CT component is used to detect coronary artery calcification, a marker of coronary atheroscleosis.92
The main advantage of PET-CT is the ability to demonstrate metabolic information with the precise anatomic detail of multislice high resolution CT images; as a result, PET-CT has replaced PET in Canada. Medical specialties that commonly use PET-CT imaging include oncology, neurology, cardiology, internal medicine, and orthopedics.
The challenges of PET-CT are those of the component modalities, both of which involve exposure to ionizing radiation.92,95,96 The radioisotopes used in PET-CT have a half-life measured in hours, so imaging depends on availability of a cyclotron and transportation.
PET-MRI
PET-MRI combines PET with MRI,97 permitting high-sensitivity metabolic imaging with high resolution of soft-tissue detail, enabling visualization of anatomy and pathologies not commonly attainable with other modalities. The 2 scans are performed in tandem, and the images are then computationally aligned. PET-MRI is the newest combination to reach clinical use and has applications in oncology, neurology, cardiology, internal medicine, and orthopedics.98,99
PET-MRI requires injection of radioisotope tracers and therefore requires the same risk-benefit assessment as other nuclear medicine imaging modalities for females of reproductive age and children.100,101 Since the CT component is replaced by MRI, X-ray exposure is avoided; however, the hazards of magnetic fields remain.100,101 The radioisotopes have a short half-life, requiring proximity to a cyclotron. The units and their infrastructure requirements are extremely expensive.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments, or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca