CADTH Health Technology Review
Formulary Management of Targeted Immune Modulators in Ulcerative Colitis
Environmental Scan
Authors: Sirjana Pant, Kim Le, Chris Vannabouathong, Peter Dyrda
Abbreviations
5-ASA
5-aminosalicylic acid
6-MP
6-mercaptopurine
AZA
azathioprine
CAF
Canadian Armed Forces
CSC
Correctional Services Canada
ES
Environmental Scan
IBD
inflammatory bowel disease
LOI
Letter of Intent
NIHB
Non-Insured Health Benefits
NOC
Notice of Compliance
pCPA
pan-Canadian Pharmaceutical Alliance
PLA
Product Listing Agreement
SC
subcutaneous
TIM
targeted immune modulator
VAC
Veterans Affairs Canada
Key Messages
Health Canada has approved 7 targeted immune modulators for the treatment of adults with moderate to severe ulcerative colitis, which include 5 biologics (adalimumab, infliximab, golimumab, ustekinumab, and vedolizumab) and 2 small molecules (tofacitinib and ozanimod). Biosimilars for adalimumab and infliximab and generics for tofacitinib are currently available in the Canadian market; however, although their patent protection has expired, there are no biosimilars for golimumab and ustekinumab.
All targeted immune modulators have undergone pan-Canadian Pharmaceutical Alliance negotiations and concluded with a Letter of Intent except for ustekinumab, which is the only targeted immune modulator not included on any public formularies for ulcerative colitis. Coverage is consistent across all drug plans except for golimumab and tofacitinib, which is not covered by all jurisdictions for ulcerative colitis.
Most public drug plans have implemented or have announced a biosimilar policy to promote the use of biosimilars over originator biologics. The listing status for targeted immune modulators in ulcerative colitis is similar across public drug plans; however, there is heterogeneity in criteria requirements for prior treatments and diagnosis definitions.
Considering these factors and the emergence of new data, it would be important to reassess these drugs and evaluate their place in therapy. Further research, such as horizon scanning, utilization analyses, and long-term effectiveness and safety studies, is warranted for targeted immune modulators to ensure the appropriate use of these drugs in the treatment of moderate to severe ulcerative colitis.
Summary
Objective
This Environmental Scan was conducted to gain a better understanding of the current landscape of targeted immune modulators (TIMs) used for treating moderate to severe ulcerative colitis (UC) in Canada. The scan focuses on the regulatory, exclusivity, and reimbursement statuses of these drugs across Canadian public formularies.
Regulatory Status
The landscape of UC treatment is rapidly expanding with the development of novel therapies, and biosimilar and generic entrants. Health Canada has approved 7 TIMs for the treatment of adults with moderate to severe UC, which include 5 biologics and 2 small molecules:
Biologics (5): Tumour necrosis factor antagonists (adalimumab, infliximab and golimumab), an anti-interleukin 12/23 drug (ustekinumab), and an anti-integrin drug (vedolizumab).
Small molecules (2): A Janus kinase inhibitor (tofacitinib) and a sphingosine-1-phosphate receptor modulator (ozanimod).
Adalimumab and infliximab have a total of 8 and 3 biosimilars available in the Canadian market, respectively. Nine of these biosimilars have been in the market since 2020. Tofacitinib has 3 generic versions that became available in the Canadian market in November 2022.
Exclusivity Status
Of the 7 approved drugs, patent protection for infliximab, golimumab, and ustekinumab has expired.
Despite the expiration of both patent and data protection for ustekinumab and golimumab, with data protection having ended over 5 years ago and patents expiring in 2021, there are presently no biosimilar versions available in Canada. A lack of a biosimilar entrant in Canada could be attributed to various factors, including clinical trial development based on exclusivity timelines in the US, where data protection is 4 years longer than it is in Canada. Seven biosimilar versions of ustekinumab have recently completed phase III trials or have an estimated study completion date in 2023.
Adalimumab still has active patents and predates data protection, and its biosimilar versions were marketed for UC approximately 3 years after the initial Notice of Compliance (NOC) was issued. This delay can be attributed to various factors, including litigation and global agreements between manufacturers.
Tofacitinib’s data protection expired in 2022 and generic versions are currently available, whereas vedolizumab’s data protection is approaching expiry in 2023.
CADTH Review Status
All TIMs, including biosimilars, used in UC have had comparable recommendations from CDEC, which were informed by placebo-controlled trials.
Reimbursement Status
All TIMs, including biosimilars, have undergone pan-Canadian Pharmaceutical Alliance negotiations for UC except for 3 biosimilar versions of infliximab (Remsima, Renflexis, and Inflixi). All negotiations concluded with a Letter of Intent (LOI) except for ustekinumab, which is the only targeted immune modulator not included on any public formularies for UC.
Coverage is consistent across all drug plans except for golimumab, which is not covered by British Columbia and Prince Edward Island, and tofacitinib, which is not covered by Yukon and Correctional Services Canada (CSC).
Biosimilar policies in British Columbia, Alberta, New Brunswick, and Newfoundland and Labrador mandate that all patients be administered biosimilar versions of adalimumab or infliximab if they are treatment-naive or switch to these biosimilars even if they are taking the originator biologic. Similar biosimilar initiatives were recently announced by Nova Scotia (effective February 2023), Saskatchewan (effective April 2023), and Ontario (effective December 2023). Currently, Ontario, Saskatchewan, Manitoba, New Brunswick, Newfoundland and Labrador, Prince Edward Island, Yukon, Non-Insured Health Benefits (NIHB), CSC, and Canadian Armed Forces (CAF) drug plans mandate the use of biosimilars for treatment-naive patients only for adalimumab or infliximab.
Two public drug plans (Manitoba and CSC) currently employ 2-tiered formularies, which require a trial of a tier 1 drug before reimbursement of a tier 2 drug. The second-tier drugs generally include the originator biologics for which a biosimilar version is available and funded.
The initial coverage criteria for TIMs in UC include an objective diagnosis based on the Mayo Score with a rectal bleeding subscore or an endoscopic subscore, which varies across jurisdictions. Except for Yukon and Ontario, which require a Mayo Score of at least 6 and endoscopic subscore of at least 2, all other jurisdictions require a Mayo Score of at least 4 with or without a rectal bleeding subscore of at least 2. Criteria for adalimumab differs from that of infliximab, golimumab, and vedolizumab in New Brunswick, which does not require a Mayo Score for coverage of adalimumab, and in Yukon, which accepts a lower Mayo Score for coverage of adalimumab.
Conclusion
In summary, the results of this Environmental Scan have revealed that access criteria for TIMs for UC are broadly similar in terms of being restricted for use in patients with moderate to severe UC after failure of a conventional therapy; however, there is considerable heterogeneity in other criteria related to TIM coverage, including requirements for prior treatments and diagnosis definitions. A tiered approach to ensure optimal sequencing of these drugs, supported by an appropriate drug class review, can seek payers greater value from TIMs that have demonstrated superiority as well as from equally effective drugs that have cheaper generic or biosimilar versions. There may also be opportunities to harmonize requirements for prior therapy as well as coverage criteria between public payers, based on recent evidence on best treatment practices and objective diagnosis.
Considering these factors and the emergence of new data, it would be important to reassess these drugs and evaluate their place in therapy. Further research, such as horizon scanning, utilization analyses, and long-term effectiveness and safety studies, is warranted for TIMs to ensure the appropriate use of these drugs in the treatment of moderate to severe UC.
Disease and Treatments
UC is an inflammatory bowel disease (IBD) that causes inflammation and ulcers in the digestive tract, affecting the mucosa of the large intestine (colon) and rectum.1,2 Although the etiology of UC is not completely understood, there is growing evidence to suggest that genetic and environmental factors may contribute to the irregular immune response that aberrantly recruits activated immune cells to the colon,3 which results in chronic inflammation that damages the colon and causes UC symptoms. UC generally develops in young adulthood4-6 and persists throughout life, marked by periods of spontaneous remission and relapse.7 The most common initial manifestation of UC is bloody diarrhea with or without mucus. In addition to frequent evacuations with blood and mucus, other symptoms include urgency or tenesmus of evacuations, fever, abdominal pain, and weight loss.3,8
UC has a worldwide incidence rate of 1.2 cases per 100,000 to 20.3 cases per 100,000 and a prevalence of 7.6 cases per 100,000 to 246.0 cases per 100,000.3 In 2017, the highest age-standardized prevalence rate of IBD occurred in high-income countries in North America,9 with Canada having 1 of the highest rates of in the world.4 The incidence rate for UC in Canada ranges from a low of 8.4 per 100,000 people in Alberta to a high of 21.4 per 100,000 people in Nova Scotia.4-6 There are an additional 15,000 individuals living with IBD in Canada who are not clearly classified as Crohn disease or UC (termed indeterminate colitis).10 Since 1990, the incidence of UC has remained stable in Manitoba (UC incidence: 10.8 per 100,000 people) while it has decreased in Alberta, Nova Scotia, and Quebec (UC incidence: 10.7 per 100,000 people) and increasing in Ontario (UC incidence: 11.1 per 100,000 people).4-6
The majority of individuals living with UC have a mild to moderate disease course, generally most active at diagnosis and then in varying periods of remission or mild activity.11 However, aggressive disease course is experienced in 10% to 15% of patients, with a cumulative risk of relapse between 70% to 80% at 10 years postdiagnosis.11 Regardless of severity, UC is associated with high morbidity, with high rates of fatigue, inferior health-related quality of life, and high disability, with approximately half of all patients hospitalized for UC at some point during the disease course. Moreover, approximately 1.5% of patients with UC are diagnosed with colorectal cancer, typically after prolonged active inflammation. Although UC is not associated with increased risk of all-cause mortality in the first year after diagnosis,12 gastrointestinal-specific mortality may be increased.11,12 Indeed, data from Manitoba suggest that, compared to the general population, individuals with UC are more likely to die from colorectal cancer or respiratory disease with the greatest risk of death being in the first 30 days following gastrointestinal surgery.12 In Ontario, the leading cause of death in seniors with UC is solid malignancies;13 in Quebec, mortality from digestive, respiratory, and infectious conditions, as well as all-cause mortality, is increased for individuals with UC.14
In Canada, approximately $1.2 billion is spent on health care utilization costs in patients with IBD, and an estimated indirect cost of $1.5 billion is borne due to loss of work and productivity, disability coverage, and premature retirement or death.15,16 In fact, the annual cost due to medical absenteeism is approximately $88 million,17 while the estimated lifetime lost wages due to premature retirement due to UC is $994,760 per person.17 Furthermore, 56% to 74% of people living with IBD in Canada have reported paying out of pocket for complementary and alternative medicines;18-20 with no difference between patients with Crohn disease versus those with UC.18 A US national survey estimated that the annual per-person out-of-pocket cost of using complementary and alternative medicine was US$1,236 for patients with UC.21
Treatment strategies have traditionally followed a step-up approach. Mild UC is typically managed using orally or rectally administered sulfasalazine and 5- aminosalicylic acids (5-ASAs). Conventional pharmacotherapy for moderate to severe UC entails an initial induction of remission with a corticosteroid; however, due to the side effects associated with corticosteroid, they should be reserved for induction therapy and not considered for long-term maintenance therapy. For patients who do not have an adequate response on a 5-ASA or corticosteroid, conventional immunosuppressants, such as azathioprine, mercaptopurine, and methotrexate, are treatment options. Should either drug class fail to provide durable effects, TIMs, such as biologics and small molecule drugs, can be used. Biologics for UC include tumour necrosis factor antagonists (infliximab, adalimumab, and golimumab), an anti-integrin antibody (vedolizumab), and an anti-interleukin (IL)-12/23 inhibitor (ustekinumab). The small molecules include a Janus kinase inhibitor (tofacitinib) and a sphingosine-1-phosphate receptor modulator (ozanimod). Biologics may lose effectiveness over time. One cause is the development of antidrug antibodies. In this situation, another biologic of the same class may be given. If loss of response persists or is not attributable to antidrug antibodies, patients may be switched to a different class.23 Because UC is a lifelong disease, management can become complex and can require multiple drugs in sequence or colectomy. The costs of these drugs can be substantial over time.
Objectives
Given the significant expenditures in Canada on biologic drugs, as well as the changing dynamics regarding loss of exclusivity, market entry of new drugs, biosimilars and generics, and availability of new evidence, an Environmental Scan (ES) was warranted for this treatment class. This ES assessed the regulatory, exclusivity, CADTH review, and reimbursement status of TIMs used to treat adults with moderate to severe UC relevant to Canadian federal, provincial, and territorial public drug plans.
The objectives of this ES were to provide a summary of the following for TIMs in the treatment of moderate to severe UC:
Regulatory status: including date of NOC, first marketed date, and indication with regards to UC
Exclusivity status: data protection and patent expiry dates, including potential biosimilar or generic entrants
CADTH review status: studies assessed and reasons for recommendation
Reimbursement status: listing status and coverage criteria across federal, provincial, and territorial public drug plans.
Methods
This ES provides information on the regulatory and reimbursement status and CADTH reviews on TIMs used in patients with moderate to severe UC. The components of the information presented in this scan are presented in Table 1. In this report, the term “drug” is used to refer to biologics and their biosimilar version (if available) and small molecule originators used in the treatment of UC, as listed in Table 1.
Table 1: Components for Literature Screening and Information Gathering
Component | Description |
|---|---|
Population | Adults (> 18 years old) with moderate to severe UC |
Intervention | Biologic (and biosimilars, if available):
Small molecules (and generics, if available):
|
Settings | Canadian publicly funded drug plans
|
Types of information |
|
CDR = CADTH Common Drug Review; JAK = Janus kinase; UC = ulcerative colitis.
aOmvyence (infliximab, Janssen Inc.) was approved on December 29, 2020, by Health Canada. This product is not a biosimilar. The NOC submission was made for an Additional Product Name for Remicade. The product is approved by Health Canada but not yet marketed in Canada.32,33
bInflixi is approved, not yet marketed. “Approved” refers to an active Drug Identification number (DIN) for a product that has been reviewed and authorized for sale in Canada but has not yet been marketed in Canada. ‘Marketed’ refers to an active DIN for a product that is currently being sold in Canada. “Dormant” refers to an active DIN for a product that was previously marketed in Canada but for which there have been no sales for period of at least 12 consecutive months.34
cNunavut and the Northwest Territories follow the coverage category and criteria of the Non-Insured Health Benefits program.30,31
Literature Search
A grey literature search was conducted on key resources, including the websites of Health Canada’s drug product database, patent register, and data protection register; CADTH website (CADTH Common Drug Review [CDR] records); Canadian public drug plan formulary databases; and clinicaltrials.gov database. No bibliographic literature searches were performed. The public drug plan databases were searched between April 10, 2022, and June 10, 2022. Other databases were searched between April 10, 2022, and December 21, 2022.
Some information presented in this report was not available in the public domain and was obtained through personal communication with members of the CADTH Formulary Working Group Health Technology Assessment (FWG-HTA) committee.29 In these cases, permission was obtained to publish this information in this report, and all details obtained through personal communication were referenced accordingly. Information from 4 federal public drug plans was included: NIHB, CSC, VAC, and CAF. Publicly reimbursed medications for residents of Nunavut and the Northwest Territories follow the coverage category and reimbursement criteria of the NIHB program.30,31
Exclusions
Private payers and Quebec’s public drug program, the Régie de l’assurance maladie du Québec (RAMQ), were excluded. The drugs included in this report are also indicated for medical conditions other than UC; however, relevant information related only to the UC indication are presented in this report. In addition to coverage criteria for the specific drugs, other relevant formulary policies are presented in this report, such as policies on the use of biosimilar drugs and biosimilar switching. Although the clinical basis and economic basis for a CADTH recommendation for the drugs (biologics and their biosimilar versions and small molecule TIMs) for UC are presented, this ES did not assess the comparative clinical effectiveness or the relative cost-effectiveness of the drugs used in the treatment of patients with UC. Thus, any conclusions or recommendations about the value of these medications or their place in therapy were outside of the scope of the ES.
Findings
A summary of findings related to the regulatory, exclusivity, CADTH review, and reimbursement status of TIMs used in the treatment of patients with UC is presented in the sections that follow.
Regulatory Status
Health Canada has approved 7 TIMs for the treatment of moderate to severe UC. These include 5 biologics and 2 small molecules. Of the 5 biologics for UC, 2 have biosimilar versions (adalimumab and infliximab) available in the Canadian market. Health Canada has approved 8 and 5 biosimilar versions of adalimumab and infliximab, respectively. All 8 biosimilars of adalimumab are marketed in Canada. Among the 5 infliximab biosimilars, 3 are marketed in Canada. Three generic versions of tofacitinib have recently been marketed in Canada. Although all 7 TIMs are indicated for the adult population, only 2 are indicated for pediatrics (adalimumab and infliximab).33,35-39
Currently, all biologic and biosimilar drugs for UC are available as IV and/or subcutaneous (SC) formulations. Adalimumab is available in SC formulation only.45,46,49 to 53,60,64. Infliximab is available in IV formulation only. One of the biosimilar versions of infliximab (Remsima IV) is indicated in UC, but the product is no longer marketed in Canada. There is an SC formulation of the product (Remsima SC) marketed in Canada; however, it is not considered a biosimilar to the SC formulation of Remicade (originator biologic for infliximab) and is not approved for use in UC.47,54,56-59 Golimumab, vedolizumab, and ustekinumab are available in both SC and IV formulations; however, the IV formulation of golimumab is not approved for use in UC.48,61,62 Both the small molecule drugs, tofacitinib and ozanimod, are available in oral formulations.63,65
The approval timeline in Figure 1 indicates the date of NOC for each drug for the UC indication. Some drugs received NOC for the UC indication after receiving their first NOC (for indications other than UC). Among the originator biologics, adalimumab (Humira), infliximab (Remicade), golimumab (Simponi), vedolizumab (Entyvio SC only), and ustekinumab (Stelara) received their NOC for UC in 2013 (versus 2004 for first NOC), 2006 (versus 2001 for first NOC), 2013 (versus 2009 for first NOC), 2020 (versus 2015 for first NOC), and 2020 (versus 2008 for first NOC), respectively.40-49 Both infliximab biosimilars, Inflectra and Remsima, received their NOC for UC in 2016 (versus 2014 for first NOC).42,43,50,51 Among the small molecules, tofacitinib (Xeljanz) and ozanimod (Zeposia) received their NOC for UC in 2018 (versus 2014 for first NOC) and 2022 (versus 2020 for first NOC), respectively.52-55 Figure 2 in Appendix 1 presents the approval timeline for the date of first NOC regardless of the indication, and Table 7 in Appendix 1 presents the regulatory information, including manufacturer, date of NOC, first marketed date, and indication with regards to UC for each drug.
Exclusivity Status
Exclusivity status is a function of patent and data protection. Patent protection is a 20-year period offered to innovative drugs from the date of filing that can be applied in various manners (e.g., chemical, change in use). Data protection regulations in Canada are governed by regulations under the Food and Drug Regulations published in 2006.95,96 These regulations provide data protection for an 8-year term with a possibility of adding 6 more months for submissions that include pediatric studies. During this time, only the owner or generator of preclinical and clinical trial data can use these data to obtain marketing authorization for drugs, effectively preventing a second-entry manufacturer from filing a submission for a copy of that innovative drug. Data protection begins from the time of issuance of NOC by Health Canada and when the drug is added to the Health Canada’s Register of Innovative Drugs.95,96 Data protection for biologics in the US is 12 years from approval.97
Patent protection is still valid for most TIMs except for 4; patent protection for infliximab expired in August 2017, both golimumab and ustekinumab expired in August 2021, and tofacitinib expired in 2022. The other 3 TIMs (adalimumab, vedolizumab, and ozanimod) have existing registered patents in Canada. Of these, the earliest patent to expire will be adalimumab in 2023 and the last patent to expire will be for vedolizumab in 2032.98
Figure 1: Health Canada Approval Timeline for Targeted Immune Modulators by NOC Date for UC Indication
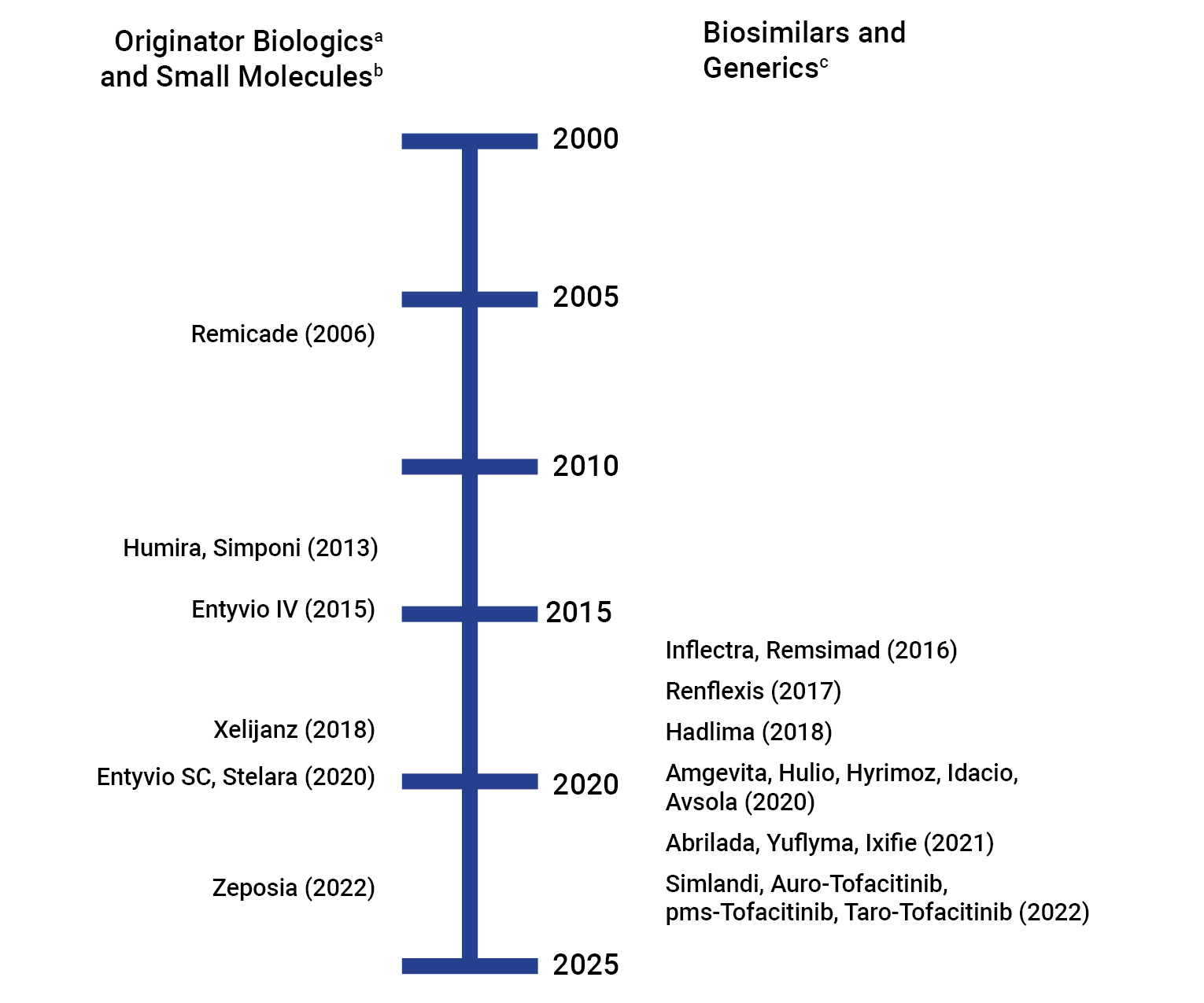
NOC = Notice of Compliance; UC = ulcerative colitis.
a Originator biologics: Remicade (infliximab), Humira (adalimumab), Simponi (golimumab), Entyvio (vedolizumab), and Stelara (ustekinumab).
b Small molecules: Xeljanz (tofacitinib) and Zeposia (ozanimod).
c Biosimilars: Adalimumab biosimilars (Amgevita, Hadlima, Hulio, Hyrimoz, Idacio, Abrilada, Simlandi, Yuflyma) and infliximab biosimilars (Inflectra, Remsima, Renflexis, Avsola, Ixifi). Generics: Tofacitinib (Auro-Tofacitinib, PMS-Tofacitinib, and Taro-Tofacitinib.
d Remsima IV is indicated in adult and pediatric UC; however, the product is “dormant,” and not marketed in Canada. Remsima SC is marketed in Canada but is not indicated in adult or pediatric UC. “Approved” refers to an active Drug Identification number (DIN) for a product that has been reviewed and authorized for sale in Canada but has not yet been marketed in Canada. “Marketed” refers to an active DIN for a product that is currently being sold in Canada. Dormant refers to an active DIN for a product that was previously marketed in Canada but for which there have been no sales for period of at least 12 consecutive months.34
e Only approved but not yet marketed.
Sources: Information was collected from Health Canada’s Drug Product Database and Notice of Compliance Database.32,33,37-46,48-54,56-94
Of the 7 TIMs approved for UC, all biologics except for vedolizumab have had their data protection status expire or have predated the enactment of the data protection regulations of 2006. Vedolizumab’s data protection will expire in July 2023. Data protection for tofacitinib expired in 2022 and ozanimod will expire in October 2026.94 Table 2 presents the status of data protection and patent expiry for the TIMs.
Biosimilars are approved for adalimumab despite registered patents for the originator biologic because the approval of adalimumab predated data protection regulations, thus data protection does not apply. However, it has been more than 8 years since the NOC date for the UC indication for adalimumab and more than 15 years since the NOC date for the UC indication for infliximab (Table 7). There was almost a 3-year delay between the NOC approval and marketed date for the first adalimumab biosimilar, Hadlima The delay is likely the result of litigation and/or agreements between the originator and biosimilar manufacturers.99,100 Despite the expiry of data and patent protection for both ustekinumab and golimumab, no biosimilar versions are currently available in Canada. Because the US market presents the largest opportunity for biosimilar developers,101 global development timelines for biosimilars may be based around US exclusivity timelines. The fact that the US applies a longer period of data exclusivity for biologics compared with Canada97 may explain some of the previous delays and the future delays that may occur for biosimilar launches in Canada.
A search on the clinical studies database, clinicaltrials.gov, for clinical trials on biosimilar versions of golimumab, ustekinumab, and vedolizumab found 7 biosimilar versions of ustekinumab in phase III (Appendix 2, Table 8). All these clinical studies were on plaque psoriasis. Of the 7 biosimilars, 4 were completed in 2022 and the remaining 3 have an estimated completion date for 2023. No clinical trials on biosimilar versions of golimumab or vedolizumab were identified on clinicaltrials.gov, indicating that biosimilar versions for these biologics are not yet in development.102 A 2021 CADTH report noted that a generic version of tofacitinib is undergoing a regulatory review for approval in rheumatoid arthritis, psoriatic arthritis, and UC in Canada.103 In November 2022, 3 generic versions of tofacitinib entered the Canadian market.37-39
Table 2: Status of Data Protection and Patent Expiry for Targeted Immune Modulators
Generic name | Brand name | Data protection expiry date | Pediatric extension | Data protection ended (yes/no) | Patent end date (for longest filed) | Patent expired (yes/no) |
|---|---|---|---|---|---|---|
Adalimumab | Humira | NAa | NA | NAa | November 11, 2031 | No |
Infliximab | Remicade | NAa | NA | NAa | August 1, 2017b | Yes |
Ustekinumab | Stelara | December 12, 2016 | NA | Yes | August 7, 2021 | Yes |
Golimumab | Simponi | April 7, 2017 | NA | Yes | August 7, 2021 | Yes |
Tofacitinib | Xeljanz | October 17, 2022 | Yes | Yes | November 25, 2022c | Yes |
Vedolizumab | Entyvio | July 29, 2023 | Yes | No | May 2, 2032 | No |
Ozanimod | Zeposia | October 2, 2026 | NA | No | November 15, 2030 | No |
NA = not available.
aNotices of Compliance for adalimumab, and infliximab were issued before the enactment of the data protection regulations in 2006.79,84,96
bThe longest patent that was filed for the originator infliximab was found to be infringed by the biosimilar launch. The only other patent filed for infliximab expired March 18, 2012.104
cThe patent expiry date for Xeljanz XR is March 12, 2034. However, Xeljanz XR is not indicated for UC.
Sources: Dates for data protection expiry and patent end date are from Health Canada databases.72,94,98,105,106
CADTH Review Status
For the indication of moderate to severe UC, CADTH has reviewed 5 originator biologics (adalimumab, infliximab, golimumab, ustekinumab, and vedolizumab), and 2 small molecules (tofacitinib and ozanimod).94 Of the 5 originator biologics, only 2 infliximab biosimilars (Inflectra and Renflexis) were reviewed. Biosimilars approved in Canada after 2019 were not reviewed due to a policy change by CADTH to no longer review files completed after June 1 of that year.92
Infliximab biosimilars, Inflectra and Renflexis, and vedolizumab, ustekinumab, and tofacitinib were recommended to be listed with criteria and conditions.107-112 Remicade (infliximab originator biologic) was recommended to be not listed, and Humira (adalimumab originator biologic) and golimumab were recommended to not be listed at the submitted price.113-115
Table 3 provides an overview of the CADTH review status and CDEC recommendations of the TIMs for UC; a summary of the evidence and clinical and/or economic rationale for the recommendations by CDEC are presented in Appendix 3, Table 9.
Table 3: CADTH Review Status and CDEC Recommendations for UC
Generic name | Brand name | CADTH review (yes/no) | CDEC recommendation for UC (date of publication) |
|---|---|---|---|
Adalimumab | Humira | Yes | Do not list at the submitted price (April 15, 2016) |
Amgevita (biosimilar) | NAa | — | |
Hadlima (biosimilar) | NAa | — | |
Hulio (biosimilar) | NAa | — | |
Hyrimoz (biosimilar) | NAa | — | |
Idacio (biosimilar) | NAa | — | |
Abrilada (biosimilar) | NAa | — | |
Simlandi (biosimilar) | NAa | — | |
Yuflyma (biosimilar) | NAa | — | |
Infliximab | Remicade | Yes | Do not list (April 22, 2009) |
Avsola (biosimilar) | NAa | — | |
Inflectra (biosimilar) | Yes | Reimburse with clinical criteria and/or conditions (October 25, 2016) | |
Remsima (biosimilar) | NAa | — | |
Renflexis (biosimilar) | Yes | Reimburse with clinical criteria and/or conditions (February 20, 2018) | |
Golimumab | Simponi | Yes | Do not list at the submitted price (March 19, 2014) |
Vedolizumab | Entyvio | Yes | Reimburse with clinical criteria and/or conditions (May 19, 2020) (SC) List with clinical criteria and/or conditions (October 28, 2015) (IV) |
Ustekinumab | Stelara | Yes | Reimburse with clinical criteria and/or conditions (July 16, 2020) |
Tofacitinib | Xeljanz | Yes | Reimburse with clinical criteria and/or conditions (February 27, 2019) |
Ozanimod | Zeposia | Yes | Reimburse with clinical criteria and/or conditions (December 1, 2022) |
CDEC = CADTH Canadian Drug Expert Committee; NA = not applicable; SC = subcutaneous; UC = ulcerative colitis.
aAs of June 1, 2019, CADTH stopped any work on any biosimilar reviews that would have been completed after June 1, 2019.116
Sources: Data were extracted from published CADTH reports.107-117
Reimbursement Status
Negotiated Agreements
The pan-Canadian Pharmaceutical Alliance (pCPA) was formed in 2010 for public drug plans to work together when entering negotiations with manufacturers for pharmaceuticals, from which, if successful, an LOI was created. The LOI lists the terms and conditions for funding a drug and are used to create a Product Listing Agreement (PLA) between each participating member jurisdiction and the manufacturer.118
The following TIMs have undergone pCPA negotiations for UC that resulted in an LOI: adalimumab (Humira), including 8 of its biosimilars; infliximab (Remicade), including 2 of its biosimilars; golimumab (Simponi); vedolizumab (Entyvio IV and SC); and tofacitinib (Xeljanz). The negotiation for ustekinumab (Stelara) concluded without an agreement. Negotiations have not been held for 2 infliximab biosimilars (Remsima and Renflexis) for UC. Further, negotiation has not been held for ozanimod (Zeposia) for UC because the drug had just received a reimbursement recommendation from CADTH at the time of publication of this report.119 Information on the pCPA negotiation status of TIMs for UC are presented in Appendix 4, Table 10.
Formulary Listing Status
The current process for formulary listings begins with an LOI, which leads to PLAs with individual drug plans. However, not all drugs achieve the LOI stage; when they do, not all LOIs lead to successful PLAs with jurisdictions. Some jurisdictions can choose to not participate in a negotiation, or formulary listings may take longer if the drug is not a priority.97
Most jurisdictional drug plans currently provide coverage for almost all the drugs included in this report, except for ustekinumab which concluded without an agreement. Golimumab is not publicly reimbursed by British Columbia and Prince Edward Island. All jurisdictions except Yukon and CSC provide coverage for tofacitinib.
Biosimilar Policies
Most public drug plans have implemented a biosimilar policy to promote the use of biosimilars over originator biologics. Some jurisdictions no longer provide coverage for originator biologics, and only provide coverage for biosimilars of adalimumab (Alberta, British Columbia, New Brunswick) and infliximab (Alberta, British Columbia, New Brunswick, Newfoundland and Labrador). Patients on originator biologics had to switch to the biosimilars versions to maintain coverage under the public drug plan. However, British Columbia (infliximab only) may allow access to originator biologics under exceptional circumstances on a case-by-case basis, and only for those currently treated with originator biologics.120-141
Most jurisdictions apply their biosimilar policy for treatment-naive patients only for adalimumab (Ontario, Saskatchewan, Manitoba, Nova Scotia, Newfoundland and Labrador, Prince Edward Island, Yukon, NIHB, CSC) and infliximab (Ontario, Saskatchewan, Manitoba, New Brunswick, Nova Scotia, Yukon, NIHB, CSC, CAF). These public drug plans allow patients currently undergoing treatment with originator biologic to continue their treatment with the originator biologic, with an option to switch to biosimilar versions.142,143 However, Nova Scotia, Saskatchewan, and Ontario have announced that effective February 2023, April 2023, and December 2023, respectively, these drug plans will no longer provide coverage for originator biologics, and only provide coverage for biosimilars of adalimumab and infliximab.141-143
Manitoba and CSC apply their biosimilar policy for the reimbursement of biologics for UC as a part of their 2-tiered biologics reimbursement policy. As opposed to other drug plans, Manitoba and CSC have an explicit policy to allow access to originator biologics if a patient fails on biosimilars. The policy requires patients to trial and fail the first tier of biologics to be eligible for coverage of the second tier. Manitoba’s policy applies to new patients (biologic naive) and existing patients who have previously trialled and been deemed unresponsive to biologic therapy. Patients must fail to respond to more than 2 tier 1 drugs to be eligible for coverage for tier 2 drugs. Tier 1 drugs include biosimilar versions of adalimumab (Abrilada, Amgevita, Hadlima, Hulio, Hyrimoz, Idacio, Simlandi, and Yuflyma) and infliximab (Avsola, Inflectra, Renflexis), and originator products Entyvio (vedolizumab), Simponi (golimumab), and Xeljanz (tofacitinib). Tier 2 drugs include originator biologics, Humira (adalimumab), and Remicade (infliximab).120,121,144 CSC also requires existing patients deemed unresponsive to biologic therapy to switch to a tier 1 biologic. Once all options on tier 1 are exhausted, options on tier 2 can be made available for coverage. Tier 1 drugs include biosimilar versions of adalimumab (Abrilada, Amgevita, Hadlima, Hulio, Hyrimoz, Idacio, Simlandi, and Yuflyma) and infliximab (Inflectra, Renflexis) and originator biologic Entyvio (vedolizumab). Tier 2 drugs include originator biologic, Humira (adalimumab).122 Additional details on these biosimilar policies are presented in Appendix 4, Table 11.
Type of Listing Status
Public drug plans list prescription medicines according to specific coverage categories that can be broadly classified as a restricted or unrestricted benefit. “Unrestricted benefit” refers to drugs with usage that is not limited by clinical criteria requiring authorization before drug plan coverage. Depending on the public drug plan, this type of formulary benefit status (coverage category) is referred to as open benefit, full benefit, or regular benefit. “Restricted benefit” refers to drugs with usage limited by specific clinical criteria or to a defined patient subgroup. Depending on the public drug plan, this type of formulary benefit status is categorized under Special Authorization, Exceptional Access Program (EAP), Exceptional Drug Status or Exception Status drug, Limited Use, Limited Coverage Drug, or Prior Authorization.145 The “restricted benefit” categories can be further classified by the following reimbursement processes:
Restricted Benefit–Active: Applicable to the following coverage categories for biologics for UC: Special Authorization or Limited Coverage Drug (British Columbia), Special Authorization (Alberta, New Brunswick, Newfoundland and Labrador, Prince Edward Island, VAC, CAF), Exceptional Drug Status or Exception Status drug (Saskatchewan, Manitoba, Nova Scotia, Yukon), EAP (Ontario), or Limited Use (NIHB). Application for public reimbursement with the required clinical details must be made by the authorized prescriber using established processes (e.g., use of specific authorization forms). Each request is subject to a medication review by staff responsible for claims adjudication for the public drug plan.123-136
Restricted Benefit–Passive: Applicable to the following coverage categories for biologics for UC: Limited Use (Ontario) and benefit with criteria medications (CSC). In comparison with Restricted Benefit–Active, the use of specific authorization forms and a medication review is not a requirement. Rather, a Limited Use code (Ontario) or a Reason for Use code (CSC) must be specified in the prescription.122,136,137
Table 4 provides an overview of the listing status of TIMs for UC across public drug plans. Appendix 4, Table 11 and Table 12, provides additional details of the coverage criteria. Given that ozanimod (Zeposia) just received a reimbursement recommendation from CADTH, it is not yet covered by any public drug plan and not included in this table. Given that tofacitinib generics have just entered the Canadian market, it is not yet covered by any public drug plan and not included in this table.
Clinical Criteria
All TIMs for UC are categorized as a restricted benefit, in which patients are required to meet specific clinical criteria to be eligible for reimbursement. These clinical criteria could vary between drug plans and between TIMs within a given drug plan. In general, initial coverage criteria for TIMs in UC currently includes some form of the following: objective diagnosis of UC (Mayo Score with a rectal bleeding or endoscopic subscore) and failure to respond to, contraindication to, or intolerance to conventional therapy (5-ASA, mesalamine, corticosteroids, AZA, 6-mercaptopurine [6-MP]). Most of the public drug plans explicitly state that the TIM must be prescribed by a “gastroenterologist” or a “physician with a specialty in gastroenterology.”120-140 Details on the requirements for diagnosis and prior therapy for each TIM are presented in Appendix 4, Table 11.
Diagnosis Requirements
TIMs are generally eligible for coverage for patients with moderate to severe UC, though some variation was noted between jurisdictions in the diagnosis definitions that are used. British Columbia, Yukon and Ontario require a diagnosis with a full Mayo Score; British Columbia requires a Mayo Score greater than 4, whereas Ontario and Yukon require a score greater than 6 (except for adalimumab, for which Yukon requires a Mayo Score of 4 or greater). In addition, all 3 of these plans require a rectal bleeding subscore (British Columbia) or an endoscopic subscore (Ontario and Yukon) of 2 or greater. To be eligible for initial coverage of a TIM, Alberta, New Brunswick, Nova Scotia, Newfoundland and Labrador, Prince Edward Island, NIHB, CSC, CAF require a diagnosis with a partial Mayo Score of 4 or greater, except for adalimumab in New Brunswick which does not require a score at all. Of the plans that require a partial Mayo Score, New Brunswick, Nova Scotia, Newfoundland and Labrador, Prince Edward Island, and CAF require a rectal bleeding subscore greater than 2.
Prior Therapy Requirements
TIMs for UC are currently only reimbursed if patients are deemed refractory, intolerant, or to have failed to respond to conventional therapy (5-ASA, mesalamine, AZA, or 6-MP). “Refractory” is defined as a lack of effect at the recommended doses and for a specified duration of treatment. “Intolerant” is defined as demonstrating serious adverse effects or contraindications to treatments, as defined in the product monographs. Previous therapy that included corticosteroids alone or in combination with other conventional therapy was applicable to all public drug plans and for all drugs unless contraindicated or not tolerated. Clinical criteria varied between drug plans, with regards to the number of conventional therapy combination regimens that needed to be trialled before requesting reimbursement for the TIM. The minimum dose and duration of treatment with prior conventional therapies may also vary by jurisdiction.
Table 4: Overview of Listing Status of TIMs for UC in Public Drug Plans
Generic name | Brand name | AB | BC | SK | MB | ON | NB | NS | NL | PE | YT | NIHBa,b | VAC | CSC | CAF |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Adalimumab | Humira | NAB | NAB | EDSb | EDS Tier 2c | EAPd | NAB | ESDe | SA | SA | EDS | LU | SA | CM Tier 2b | SA |
Amgevita (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | EDS | LU | SA | CM | NAB | |
Hadlima (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | NAB | LU | SA | CM | SA | |
Hulio (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | EDS | LU | SA | CM | NAB | |
Hyrimoz (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | EDS | LU | SA | CM | NAB | |
Idacio (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | EDS | LU | SA | CM | NAB | |
Abrilada (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | EDS | LU | SA | CM | NAB | |
Simlandi (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | EDS | LU | SA | CM | SA | |
Yuflyma (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | NAB | LU | SA | CM | SA | |
Infliximab | Remicadef | NAB | NAB | EDS | EDS Tier 2c | EAPd | NAB | ESDe | NAB | SA | EDS | LU | SA | CM | SA |
Avsola (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | NAB | NAB | LU | SA | NAB | SA | |
Inflectra (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | EDS | LU | SA | CM | SA | |
Remsima (biosimilar)g | NAB | ||||||||||||||
Renflexis (biosimilar) | SA | LCD/SA | EDS | EDS | LU | SA | ESD | SA | SA | EDS | LU | SA | CM | SA | |
Golimumab | Simponi | SA | NAB | EDS | EDS | EAP | SA | ESD | SA | NAB | EDS | LU | SA | CM | SA |
Vedolizumab | Entyvio | SA | LCD/SA | EDS | EDS | EAP | SA | ESD | SA | SA | EDS | LU | SA | CM | SA |
Ustekinumab | Stelara | NAB | |||||||||||||
Tofacitinib | Xeljanz | SA | LCD/SA | EDS | Part 2 Benefit | LU | SA | ESD | SA | SA | NAB | LU | SA | NAB | SA |
AB = Alberta; BC = British Columbia; CAF = Canadian Armed Forces; CM = Criteria Medicine; CSC = Correctional Services Canada; EDS = Exception Drug Status; ESD = Exception Status Drug; LU = Limited Use; MB = Manitoba; NAB = not a benefit; NB = New Brunswick; NIHB = Non-Insured Health Benefits; NL = Newfoundland and Labrador; NS = Nova Scotia; ON = Ontario; PA = prior approval; PE = Prince Edward Island; SA = Special Authorization; SC = subcutaneous; SK = Saskatchewan; TIM = targeted immune modulator; UC = ulcerative colitis; VAC = Veterans Affairs Canada; YT = Yukon.
Note: Because ozanimod (Zeposia) for UC has only recently received a reimbursement recommendation from CADTH and has not undergone pCPA negotiations at the time of publishing this report, it has not yet been added to any public drug plan, and hence, it is not included in this table.
aAlso applicable to Nunavut and the Northwest Territories.30,31
bAfter April 30, 2023, coverage of the originator biologic will no longer be provided. Refer to details in Appendix 4, Table 11.
cTier 2 refers to reimbursement only after tier 1 drugs have been trialled.
dAfter December 29, 2023, coverage of the originator biologic will no longer be provided. Refer to details in Appendix 4, Table 11.
eAfter February 3, 2023, coverage of the originator biologic will no longer be provided, unless an exemption is granted. Refer to details in Appendix 4, Table 11.
fIxifi is another biosimilar product for infliximab. However, the product is only Approved but not yet marketed in Canada. Hence, the listing status is not yet available. “Approved” refers to an active Drug Identification number (DIN) for a product that has been reviewed and authorized for sale in Canada but has not yet been marketed in Canada.34
gRemsima IV is indicated in adult and pediatric ulcerative colitis; however, the product is dormant, and not marketed in Canada. Remsima SC is marketed in Canada but is not indicated in adult or pediatric ulcerative colitis. “Dormant” refers to an active DIN for a product that was previously marketed in Canada but for which there have been no sales for period of at least 12 consecutive months.34
Sources: Listing statuses are from payer formulary websites.120-141
Table 5: Details on Diagnosis of UC
Public drug plan | Disease Activity Index score | Disease Activity Index subscore | Notes |
|---|---|---|---|
BC | Mayo Score ≥ 4 | Rectal bleeding subscore ≥ 2 | — |
AB | Partial Mayo Score > 4 | — | — |
ON | Mayo Score > 4 | Endoscopic subscore = 2 | Severe UC specified as Mayo Score > 10 |
NB | Partial Mayo Score > 4 (for infliximab, golimumab, vedolizumab) No score required for adalimumab | Rectal bleeding subscore ≥ 2 | Severe UC specified as Partial Mayo Score > 6 |
NS | Partial Mayo Score > 4 | Rectal bleeding subscore ≥ 2 | — |
NL | Partial Mayo Score > 4 | Rectal bleeding subscore ≥ 2 | Severe UC specified as Partial Mayo Score > 6 |
PE | Partial Mayo Score > 4 | Rectal bleeding subscore ≥ 2 | Severe UC specified as Partial Mayo Score > 6 |
YT | Mayo Score ≥ 4 (for adalimumab) Mayo Score > 6 (for infliximab, golimumab, vedolizumab) | Endoscopic subscore ≥ 2 | — |
NIHB | Partial Mayo Score > 4 | — | — |
CSC | Partial Mayo Score > 4 | — | Severe UC specified as Mayo Score > 10 |
CAF | Partial Mayo Score > 4 | Rectal bleeding subscore ≥ 2 | — |
AB = Alberta; BC = British Columbia; CAF = Canadian Armed Forces; CSC = Correctional Services Canada; MB = Manitoba; NIHB = Non-Insured Health Benefits; NL = Newfoundland and Labrador; NS = Nova Scotia; ON = Ontario; PE = Prince Edward Island; SK = Saskatchewan; VAC = Veterans Affairs Canada; UC = ulcerative colitis; YT = Yukon.
Note: Requirement for an objective diagnosis for UC was not identified in SK, MB, and VAC.
Sources: Canadian public drug plan formularies.120-140
For biologics, Saskatchewan requires failure of a corticosteroid only. Thirteen of 14 drug plans (Alberta, British Columbia, Manitoba, Ontario, Manitoba, New Brunswick, Nova Scotia, Newfoundland and Labrador, Prince Edward Island, Yukon, NIHB, VAC, CSC, CAF) require failure of a corticosteroid in combination with at least 1 other conventional therapy option before being eligible for biologic coverage. Among these plans, British Columbia, Alberta, Manitoba, NIHB, CSC, New Brunswick, Nova Scotia, Newfoundland and Labrador, Prince Edward Island, and CAF specify failure of a corticosteroid and a 5-ASA product for all biologics listed except for adalimumab, for which CSC specifies failure of a corticosteroid and a thiopurine (AZA or 6-MP) and New Brunswick does not specify prior conventional therapy failure. Ontario and Yukon specify failure of a corticosteroid and a thiopurine (AZA or 6-MP) for all biologics listed except for adalimumab, for which Yukon specifies failure of a corticosteroid and a 5-ASA product. Prior therapy requirements for tofacitinib are similar to biologics within each jurisdiction, except for Ontario which requires failure of a corticosteroid only (as opposed to requiring failure of 2 conventional therapies for biologics). VAC requires failure of a corticosteroid and another conventional therapy (unspecified) before being eligible for coverage for any of the TIMs listed. Additionally, patients who are deemed corticosteroid dependent are also eligible for TIM coverage in Nova Scotia, Newfoundland and Labrador, Prince Edward Island, CAF, Yukon, and New Brunswick (excluding adalimumab, where the conventional therapy is unspecified) regardless of the number of previously trialled conventional therapies.
Table 6: Requirement for Failure to Prior Line of Therapy
Drug | Provinces that require failure of 1 prior therapy with a corticosteroid | Provinces that require failure of 2 prior therapies or corticosteroid dependenta | Provinces that do not specify failed prior therapy | ||
|---|---|---|---|---|---|
Corticosteroid and 5-ASA | Corticosteroid and AZA/6-MP | Corticosteroid and conventional therapy (unspecified) | |||
Biologics: Adalimumab, infliximab, golimumab, vedolizumab | SK | BC, AB, MB, NIHB, PE,a CAF,a NS,a,b NL,a,b CSC (for infliximab, golimumab, vedolizumab), YTa (for adalimumab), NBa,b (for infliximab, golimumab, vedolizumab) | ON,a YT (for infliximab, golimumab, vedolizumab), CSCa (for adalimumab) | VAC | NB (for adalimumab only) |
Small molecules: Tofacitinib | SK, ON | BC, AB, MB, NIHB, NB,a CAF,a NS,a,b NL,a,b PEa,b | — | VAC | — |
6-MP = 6-mercaptopurine; 5-ASA = 5-aminosalicylic acid; AB = Alberta; AZA = azathioprine; BC = British Columbia; CAF = Canadian Armed Forces; CSC = Correctional Services Canada; MB = Manitoba; NB = New Brunswick; NIHB = Non-Insured Health Benefits; NL = Newfoundland and Labrador; NS = Nova Scotia; ON = Ontario; PE = Prince Edward Island; SK = Saskatchewan; UC = ulcerative colitis; VAC = Veterans Affairs Canada; YT = Yukon.
aFor AB, corticosteroid dependence refers to failure to taper off corticosteroids without recurrence of disease or disease requiring a second dose of corticosteroids within 12 months of previous dose. For BC, NB, NS, NL, and CAF corticosteroid dependence refers to unable to withdraw oral corticosteroid within 3 months of initiation without a recurrence of symptoms, a symptomatic relapse within 3 months of stopping, or the need for 2 or more courses of corticosteroids within 1 year). In ON and YT, corticosteroid dependence refers to stabilized with 2 weeks of oral prednisone at daily doses greater than or equal to 40 mg (or 1 week of IV equivalent) but the corticosteroid dose cannot be tapered despite 3 months of AZA or 6-MP or disease-modifying antirheumatic drugs (DMARDS).
bPrior therapy could vary for patients with severe UC. NB, NL, and PE specify severe UC with a partial Mayo Score of > 6. ON and CSC specify severe UC with a Mayo Score of > 10. For patients with severe UC; ON, NB, NS, NL, PE, and CSC only require failure of corticosteroid.
Sources: Canadian public drug plan formularies.120-140
Conclusion
The treatment landscape for UC continues to expand with the development of novel therapies with diverse mechanisms of action. Additionally, with the expiration of data protection for some existing treatments, the market is expected to further expand with the emergence of biosimilars and generics. Considering these factors and the emergence of new data, it would be important to reassess these drugs and evaluate their place in therapy. Further research, such as horizon scanning, utilization analyses, and long-term effectiveness and safety studies, is warranted for TIMs to ensure the appropriate use of these drugs in the treatment of moderate to severe UC.
References
1.Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. a randomized study. N Engl J Med. 1987;317(26):1625-1629. PubMed
2.Stenson WF. Inflammatory bowel diseaes. In: Cecil RL, Goldman I, Bennett JC, eds. Cecil Textbook of Medicine, 21st ed. Philadephia (PA): W.B. Saunders; 2000.
3.Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med. 2011;365(18):1713-1725. PubMed
4.Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769-2778. PubMed
5.Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46-54.e42; quiz e30. PubMed
6.Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis. 2011;17(1):423-439. PubMed
7.Cosnes J, Gower-Rousseau C, Seksik P, Cortot A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology. 2011;140(6):1785-1794. PubMed
8.Travis SP, Stange EF, Lémann M, et al. European evidence-based consensus on the management of ulcerative colitis: current management. J Crohns Colitis. 2008;2(1):24-62. PubMed
9.Alatab S, Sepanlou SG, Ikuta K, et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17-30. PubMed
10.Coward S, Clement F, I BE, al e. The rising prevalence of inflammatory bowel disease in Canada: Analyzing the past to predict the future [abstract] In: Abstracts presented to 2018 Canadian Diseases Week. J Can Assoc Gastroenterol. 2018;1(Suppl 2).
11.Fumery M, Singh S, Dulai PS, Gower-Rousseau C, Peyrin-Biroulet L, Sandborn WJ. Natural history of adult ulcerative colitis in population-based cohorts: a systematic review. Clin Gastroenterol Hepatol. 2018;16(3):343-356.e343. PubMed
12.Bernstein CN, Nugent Z, Targownik LE, Singh H, Lix LM. Predictors and risks for death in a population-based study of persons with IBD in Manitoba. Gut. 2015;64(9):1403-1411. PubMed
13.Nguyen GC, Bernstein CN, Benchimol EI. Risk of surgery and mortality in elderly-onset inflammatory bowel disease: a population-based cohort study. Inflamm Bowel Dis. 2017;23(2):218-223. PubMed
14.Bitton A, Vutcovici M, Sewitch M, Suissa S, Brassard P. Mortality trends in Crohn's disease and ulcerative colitis: a population-based study in Québec, Canada. Inflamm Bowel Dis. 2016;22(2):416-423. PubMed
15.Kawalec P, Malinowski KP. Indirect health costs in ulcerative colitis and Crohn's disease: a systematic review and meta-analysis. Expert Rev Pharmacoecon Outcomes Res. 2015;15(2):253-266. PubMed
16.Longobardi T, Jacobs P, Wu L, Bernstein CN. Work losses related to inflammatory bowel disease in Canada: results from a National Population Health Survey. Am J Gastroenterol. 2003;98(4):844-849. PubMed
17.Kuenzig ME, Lee L, El-Matary W, et al. The impact of inflammatory bowel disease in Canada 2018: indirect costs of IBD care. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S34-S41. PubMed
18.Rawsthorne P, Clara I, Graff LA, et al. The Manitoba Inflammatory Bowel Disease Cohort Study: a prospective longitudinal evaluation of the use of complementary and alternative medicine services and products. Gut. 2012;61(4):521-527. PubMed
19.Nguyen GC, Croitoru K, Silverberg MS, Steinhart AH, Weizman AV. Use of complementary and alternative medicine for inflammatory bowel disease is associated with worse adherence to conventional therapy: the COMPLIANT study. Inflamm Bowel Dis. 2016;22(6):1412-1417. PubMed
20.Weizman AV, Ahn E, Thanabalan R, et al. Characterisation of complementary and alternative medicine use and its impact on medication adherence in inflammatory bowel disease. Aliment Pharmacol Ther. 2012;35(3):342-349. PubMed
21.Gunnarsson C, Chen J, Rizzo JA, Ladapo JA, Lofland JH. Direct health care insurer and out-of-pocket expenditures of inflammatory bowel disease: evidence from a US national survey. Dig Dis Sci. 2012;57(12):3080-3091. PubMed
22.IBD treatments. Vienna (AT): European Crohn’s and Colitis Organization; 2013: https://www.ecco-ibd.eu/images/1_About_ECCO/1_8_ECCO/IBDTreatments.pdf. Accessed 2022 Jul 19.
23.Cohen RD, Stein AC. Management of moderate to severe ulcerative colitis in adults. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: https://www.uptodate.com. Accessed 2022 Dec 20.
24.Schroeder KW. Mayo Score / Disease Activity Index (DAI) for ulcerative colitis. New York (NY): MD+ Calc; n.d.: https://www.mdcalc.com/calc/3675/mayo-score-disease-activity-index-dai-ulcerative-colitis#pearls-pitfalls. Accessed 2022 Jun 9.
25.Sands BE, Peyrin-Biroulet L, Loftus EV, Jr., et al. Vedolizumab versus adalimumab for moderate-to-severe ulcerative colitis. N Engl J Med. 2019;381(13):1215-1226. PubMed
26.Ollendorf DA, Bloudek L, Carlson JJ, et al. Targeted immune modulators for ulcerative colitis: effectiveness and value: evidence report. Boston (MA): Institute for Clinical and Economic Review (ICER); 2020: https://icer.org/wp-content/uploads/2020/08/ICER_UC_Evidence_Report_091120-002.pdf. Accessed 2022 Dec 20.
27.FDA approves boxed warning about increased risk of blood clots and death with higher dose of arthritis and ulcerative colitis medicine tofacitinib (Xeljanz, Xeljanz XR). Silver Spring (MD): US Food and Drug Administration; 2019. Accessed 2022 Jul 19.
28.Summary Safety Review - Xeljanz/Xeljanz XR (tofacitinib) - assessing the potential risks of serious heart-related problems and cancer. Ottawa (ON): Health Canada; 2022: https://hpr-rps.hres.ca/reg-content/summary-safety-review-detail.php?lang=en&linkID=SSR00278. Accessed 2022 Jul 19.
29.Pharmaceutical Advisory Committee Formulary Working Group for Health Technology Assessments. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/collaboration-and-outreach/advisory-bodies/dpac-fwg-hta. Accessed 2022 Apr 15.
30.Extended health benefits for specified disease conditions program. Yellowknife (NT): Government of the Northwest Territories (GNWT); 2019: https://www.hss.gov.nt.ca/en/services/supplementary-health-benefits/extended-health-benefits-specified-disease-conditions. Accessed 2022 Apr 15.
31.EHB full coverage plan. Iqaluit (NU): Government of Nunavut; 2022: https://www.gov.nu.ca/health/information/ehb-full-coverage-plan. Accessed 27 April 2022.
32.Notice of Compliance information - OMVYENCE. Ottawa (ON): Health Canada; 2021: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2021 Apr 11.
33.Product information - RINVOQ. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=98509. Accessed 2022 Jun 9.
34.Drug Product Database (DPD): terminology. Ottawa (ON): Health Canada; 2022: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/drug-product-database/terminology.html. Accessed 2022 Apr 16.
35.Reimbursement review: upadacitinib (Rinvoq). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/upadacitinib-2. Accessed 2022 Dec 19.
36.About EORLA. Ottawa (ON): Eastern Ontario Regional Laboratory Association (EORLA); 2021: https://www.eorla.ca/about-us/. Accessed 2022 Jul 18.
37.Product information - TARO-TOFACITINIB. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=100052. Accessed 2022 Dec 20.
38.Product information - PMS-TOFACITINIB. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=101191. Accessed 2022 Dec 20.
39.Product information - AURO-TOFACITINIB. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=101923. Accessed 2022 Dec 20.
40.Notice of Compliance information - HUMIRA. Ottawa (ON): Health Canada; 2004: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
41.Notice of Compliance information - HUMIRA (UC). Ottawa (ON): Health Canada; 2013: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
42.Notice of Compliance information - INFLECTRA. Ottawa (ON): Health Canada; 2014: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
43.Notice of Compliance information - INFLECTRA (UC). Ottawa (ON): Health Canada; 2016: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
44.Notice of Compliance information - REMICADE. Ottawa (ON): Health Canada; 2001: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
45.Notice of Compliance information - REMICADE (UC). Ottawa (ON): Health Canada; 2006: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
46.Notice of Compliance information - SIMPONI. Ottawa (ON): Health Canada; 2009: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
47.Notice of Compliance information - SIMPONI (UC). Ottawa (ON): Health Canada; 2013: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
48.Notice of Compliance information - STELARA. Ottawa (ON): Health Canada; 2008: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
49.Notice of Compliance information - STELARA (UC). Ottawa (ON): Health Canada; 2020: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
50.Notice of Compliance information - REMSIMA. Ottawa (ON): Health Canada; 2014: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
51.Notice of Compliance information - REMSIMA (UC). Ottawa (ON): Health Canada; 2016: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
52.Notice of Compliance information - XELJANZ. Ottawa (ON): Health Canada; 2014: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
53.Notice of Compliance information - XELJANZ (UC). Ottawa (ON): Health Canada; 2018: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
54.Notice of Compliance information - ZEPOSIA. Ottawa (ON): Health Canada; 2020: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Jun 9.
55.Notice of Compliance information - ZEPOSIA (UC). Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Jun 9.
56.Notice of Compliance information - ADALIMUMAB INJECTION. Ottawa (ON): Health Canada; 2021: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
57.Notice of Compliance information - AMGEVITA. Ottawa (ON): Health Canada; 2020: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
58.Notice of Compliance information - AVSOLA. Ottawa (ON): Health Canada; 2020: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
59.Notice of Compliance information - ENTYVIO. Ottawa (ON): Health Canada; 2015: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
60.Notice of Compliance information - ENTYVIO (UC - sc). Ottawa (ON): Health Canada; 2020: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
61.Notice of Compliance information - HADLIMA. Ottawa (ON): Health Canada; 2018: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
62.Notice of Compliance information - HULIO. Ottawa (ON): Health Canada; 2020: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
63.Notice of Compliance information - HYRIMOZ. Ottawa (ON): Health Canada; 2020: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
64.Notice of Compliance information - IDACIO. Ottawa (ON): Health Canada; 2020: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
65.Notice of Compliance information - IXIFI. Ottawa (ON): Health Canada; 2021: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
66.Notice of Compliance information - RENFLEXIS. Ottawa (ON): Health Canada; 2017: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
67.Notice of Compliance information - SIMLANDI. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
68.Notice of Compliance information - YUFLYMA. Ottawa (ON): Health Canada; 2021: https://health-products.canada.ca/noc-ac/?lang=eng. Accessed 2022 Apr 27.
69.Health Canada approves new indications for Xeljanz in ulcerative colitis (UC) & psoriatic arthritis (PsA) [press release]. Kirkland (ZC): Pfizer; 2018: https://www.newswire.ca/news-releases/health-canada-approves-new-indications-for-xeljanz-in-ulcerative-colitis-uc--psoriatic-arthritis-psa-696193771.html. Accessed 2022 Apr 28.
70.Health Canada approves new indication for STELARA®* (ustekinumab) for the treatment of adults with moderately to severely active ulcerative colitis [press release]. Toronto (ON): Janssen Pharmaceuticals; 2020: https://www.bloomberg.com/press-releases/2020-01-27/health-canada-approves-new-indication-for-stelara-ustekinumab-for-the-treatment-of-adults-with-moderately-to-severely-acti. Accessed 2022 Apr 28.
71.Notice of Compliance search. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/noc-ac/index-eng.jsp. Accessed 2022 Jun 22.
72.Drug Product Database online query. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/index-eng.jsp. Accessed 2021 Apr 22.
73.Product Information - ABRILADA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=100029. Accessed 2022 Apr 12.
74.Product information - AMGEVITA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=94649. Accessed 2022 Apr 12.
75.Product information - AVSOLA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=98681. Accessed 2022 Apr 12.
76.Product information - ENTYVIO. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=92117. Accessed 2022 Apr 27.
77.Product information - HADLIMA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=96243. Accessed 2022 Apr 12.
78.Product information - HULIO. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=99197. Accessed 2022 Apr 12.
79.Product information - HUMIRA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=74379. Accessed 2022 Apr 12.
80.Product information - HYRIMOZ. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=99460. Accessed 2022 Apr 12.
81.Product information - IDACIO. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=99222. Accessed 2022 Apr 12.
82.Product information - INFLECTRA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=90410. Accessed 2022 Apr 12.
83.Product information - IXIFI. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=101230. Accessed 2022 Apr 27.
84.Drug and Health Product Submissions Under Review (SUR): supplemental submissions under review. Ottawa (ON): Health Canada; 2022: https://www.canada.ca/en/health-canada/services/drug-health-product-review-approval/submissions-under-review/supplemental-submissions-under-review.html. Accessed 2022 Dec 19.
85.Product information - REMSIMA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=90411. Accessed 2022 Apr 12.
86.Product information - REMSIMA SC. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=100076. Accessed 2022 Apr 12.
87.Product information - RENFLEXIS. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=95936. Accessed 2022 Apr 12.
88.Product information - SIMLANDI. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=101300. Accessed 2022 Apr 27.
89.Product information - SIMPONI. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=81020. Accessed 2022 Apr 27.
90.Product information - STELARA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=80608. Accessed 2022 Apr 12.
91.Product information - XELJANZ. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=90863. Accessed 2022 Apr 27.
92.Product information - YUFLYMA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=101284. Accessed 2022 Apr 27.
93.Product Information - ZEPOSIA. Ottawa (ON): Health Canada; 2022: https://health-products.canada.ca/dpd-bdpp/info.do?lang=en&code=99535. Accessed 2022 Jun 9.
94.Register of innovative drugs. Ottawa (ON): Health Canada; 2022: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/applications-submissions/register-innovative-drugs.html. Accessed 2022 Apr 10.
95.Guidance document: data protection under C.08.004.1 of the Food and Drug Regulations. Ottawa (ON): Health Canada; 2011: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/applications-submissions/guidance-documents/guidance-document-data-protection-under-08-004-1-food-drug-regulations.html. Accessed 2022 Apr 20.
96.Kendall M, D. H. A decade of data protection for innovative drugs in Canada: issues, limitations, and time for a reassessment. Biotechnol Law Rep. 2016;35(6). https://www.liebertpub.com/doi/full/10.1089/blr.2016.29030.mk. Accessed 2021 Jun 22. PubMed
97.Reducing data protection for biologics would slow medical procgress and chill R&D investment in the U.S. Washington (DC): Pharmaceutical Research and Manufacturers of America (PhRMA); 2015: http://phrma-docs.phrma.org/sites/default/files/pdf/data-exclusivity-for-biologics-fact-sheet.pdf. Accessed 2022 Apr 12.
98.Patent register. Ottawa (ON): Health Canada; 2021: https://pr-rdb.hc-sc.gc.ca/pr-rdb/index-eng.jsp. Accessed 2022 Apr 14.
99.Courage N, Shivakumar S. The biosimilar landscape in Canada. London (UK): Lexology; 2018: https://www.lexology.com/library/detail.aspx?g=bc06ea65-d2bc-4ffe-bf04-9b497b10fce0. Accessed 2022 Jun 10.
100.Mathias T. AbbVie, Samsung Bioepis in deal; Humira biosimilar U.S. release in 2023 [press release]. Canary Wharf (UK): Reuters 2018: https://www.reuters.com/article/us-abbvie-biogen-idUSKCN1HC1SP. Accessed 2022 Jun 10.
101.Blackstone EA, Joseph PF. The economics of biosimilars. Am Health Drug Benefits. 2013;6(8):469-478. PubMed
102.ClinicalTrials.gov. 2022; https://www.clinicaltrials.gov/ct2/home, Accessed 2022 Jun 10.
103.Tadrous M, Shakeri A, Hayes KN, et al. Canadian trends and projections in prescription drug purchases: 2001–2023. Can J Health Technol. 2021;1(11). https://canjhealthtechnol.ca/index.php/cjht/article/view/mt0001/mt0001. Accessed 2022 Jun 10.
104.Lee K, Wojtyra U. New Use Patent for Janssen’s REMICADE valid and infringed by Hospira’s biosimilar INFLECTRA. Ottawa (ON): Smart & Biggar; 2018: https://www.smartbiggar.ca/insights/publication/new-use-patent-for-janssen-s-remicade-valid-and-infringed-by-hospira-s-biosimilar-inflectra. Accessed 2022 Apr 18.
105.Search for expired patents. Ottawa (ON): Health Canada; 2021: https://pr-rdb.hc-sc.gc.ca/pr-rdb/search_expiration-recherche_expires.do. Accessed 2022 Apr 14.
106.Lexchin J. Increase in drug spending in Canada due to extension of data protection for biologics: a descriptive study. Healthc Policy. 2019;14(3):10-18. PubMed
107.CADTH Canadian Drug Expert Committee final recommendation: vedolizumab (Entyvio). Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/cdr/complete/SR0421_cdr_complete_Entyvio_Nov-2-15_e.pdf. Accessed 2022 Apr 18.
108.CADTH. CADTH Canadian Drug Expert Committee final recommendation: infliximab (Inflectra). Common Drug Review2016: https://www.cadth.ca/sites/default/files/cdr/complete/SE0483_IBD_Inflectra-Oct-28-16.pdf. Accessed 2022 Apr 10.
109.CADTH Canadian Drug Expert Committee recommendation: infliximab (Renflexis). Common Drug Review. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/cdr/complete/SE0532%20Renflexis%20-%20CDEC%20Final%20Recommendation%20February%2020%2C%202018%28redacted%29_for%20posting.pdf. Accessed 2022 Apr 10.
110.CADTH Canadian Drug Expert Committee recommendation: tofacitinib (Xeljanz). Common Drug Review. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/cdr/complete/SR0572-Xeljanz_UC-Mar-1-19.pdf. Accessed 2022 Apr 18.
111.CADTH Canadian Drug Expert Committee recommendation: ustekinumab (Stelara). Common Drug Review. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/complete/SR0627%20Stelara%20-%20CDEC%20Final%20Recommendation%20July%2020%2C%202020_for%20posting.pdf. Accessed 2022 Apr 18.
112.CADTH Canadian Drug Expert Committee recommendation: vedolizumab (Entyvio). Common Drug Review. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/cdr/complete/SR0635%20Entyvio%20-%20CDEC%20Final%20Recommendation%20%E2%80%93%20May%2021%2C%202020_for%20posting.pdf. Accessed 2022 Apr 18.
113.CEDAC final recommendation and reasons for recommendation: infliximab (Remicade) for ulcerative colitis. Common Drug Review. Ottawa (ON): CADTH; 2009: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_Remicade_Final_April_24_2009.pdf. Accessed 2022 Apr 18.
114.CDEC final recommendation: golimumab (Simponi) for ulcerative colitis. Common Drug Review. Ottawa (ON): CADTH; 2014: https://www.cadth.ca/sites/default/files/cdr/complete/SR0341_complete_Simponi_Mar-28-14.pdf. Accessed 2022 April 18.
115.CADTH Canadian Drug Expert Review Committee final recommendation: adalimumab (Humira) for ulcerative colitis. Common Drug Review. Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/cdr/complete/SR0450_complete_Humira-Apr-19-16_e.pdf. Accessed 2022 Apr 10.
116.CADTH pharmaceutical reviews update — Issue 8. Reimbursement review. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/cadth-pharmaceutical-reviews-update-issue-8. Accessed 2022 Apr 20.
117.Reimbursement review: ozanimod (Zeposia). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/ozanimod-0. Accessed 2022 Jun 9.
118.FAQs. Accessed 2022 Apr 27.
119.pCPA. Brand name drug negotiations status. Toronto (ON): pan-Canadian Pharmaceutical Alliance; 2022: https://www.pcpacanada.ca/negotiations. Accessed 2022 Apr 27.
120.Tiered biologics reimbursement policy by specialty. Winnipeg (MB): Manitoba Health; 2022: https://www.gov.mb.ca/health/pharmacare/profdocs/tiered_biologics_specialty.pdf. Accessed 2022 Apr 27.
121.Tiered biologics reimbursement policy overview. Winnipeg (MB): Manitoba Health; 2022: https://www.gov.mb.ca/health/pharmacare/profdocs/tiered_biologics_overview.pdf. Accessed 2022 Apr 27.
122.CSC National Formulary. Ottawa (ON): Correctional Services Canada; 2022.
123.Interactive Drug Benefit List (iDBL). Edmonton (AB): Government of Alberta; 2021: https://www.ab.bluecross.ca/dbl/publications.php. Accessed 2022 Apr 15.
124.Drug benefit list. Non-Insured Health Benefits. Toronto (ON): Express Scripts Canada; 2020: https://nihb.express-scripts.ca/dbl. Accessed 27 April 2022.
125.Veterans Affairs Canada drug formulary search form. Ottawa (ON): Government of Canada; 2022: https://www.veterans.gc.ca/eng/financial-support/medical-costs/treatment-benefits/poc10/search. Accessed 2022 Apr 22.
126.Canadian Armed Forces drug benefit list. Ottawa (ON): Government of Canada; 2022: http://www.cmp-cpm.forces.gc.ca/hs/en/drug-benefit-list/index.asp. Accessed 2022 Apr 27.
127.Formulary. Halifax (NS): Nova Scotia Department of Health; 2022: https://novascotia.ca/dhw/pharmacare/documents/formulary.pdf. Accessed 2022 Apr 27.
128.Special Authority drug list. Victoria (BC): British Columbia Ministry of Health; 2022: https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/pharmacare/prescribers/special-authority/sa-drug-list. Accessed 2022 Apr 19.
129.Manitoba drug benefits formulary. Winnipeg (MB): Manitoba Health; 2022: https://residents.gov.mb.ca/forms.html?d=details&pub_id=10541&filter_keyword=drug+benefits#page=46. Accessed 2022 Apr 18.
130.PEI pharmacare formulary. Charlottetown (PE): Health PEI; 2022: https://www.princeedwardisland.ca/sites/default/files/publications/pei_pharmacare_formulary.pdf. Accessed 2022 Apr 27.
131.Saskatchewan Online Formulary Database. Regina (SK): Government of Saskatchewan; 2022: https://formulary.drugplan.ehealthsask.ca/SearchFormulary/BG/682840. Accessed 2022 Apr 19.
132.Appendix A: exception drug status program. Regina (SK): Government of Saskatchewan; 2022: https://formulary.drugplan.ehealthsask.ca/PDFs/APPENDIXA.pdf. Accessed 2022 Apr 19.
133.NLPDP drug product database. St. John's (NL): Newfoundland and Labrador Health and Community Services; 2022: https://www.health.gov.nl.ca/health/prescription/newformulary.asp. Accessed 2022 Apr 27.
134.Yukon drug formulary. Whitehorse (YT): Government of Yukon; 2022: https://ihs.gov.yk.ca/drugs/f?p=161:9000 Accessed 2022 Apr 27.
135.New Brunswick drug plans formulary. Fredricton (NB): Government of New Brunswick; 2022: https://www2.gnb.ca/content/dam/gnb/Departments/h-s/pdf/en/NBDrugPlan/NewBrunswickDrugPlansFormulary.pdf. Accessed 2022 Apr 15.
136.Exceptional Access Program reimbursement criteria for frequently requested drugs. Toronto (ON): Ontario Ministry of Health; 2022: https://health.gov.on.ca/en/pro/programs/drugs/docs/frequently_requested_drugs.pdf. Accessed 2022 Apr 19.
137.Ontario drug benefit formulary search. Toronto (ON): Ontario Ministry of Health; 2022: https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Apr 19.
138.Adalimumab / infliximab / vedolizumab / tofactinib for ulcerative colitis: renewal coverage. Special authority request. Victoria (BC): British Columbia Ministry of Health; 2022: https://www2.gov.bc.ca/assets/gov/health/forms/5497fil.pdf. Accessed 2022 Apr 19.
139.Adalimumab / infliximab / vedolizumab / tofactinib for ulcerative colitis: initial/switch coverage. Special authority request. Victoria (BC): British Columbia Ministry of Health; 2022: https://www2.gov.bc.ca/assets/gov/health/forms/5388fil.pdf. Accessed 2022 Apr 19.
140.Part 3 Exception Drug Status (EDS). Winnipeg (MB): Manitoba Health; 2022: https://www.gov.mb.ca/health/mdbif/docs/edsnotice.pdf. Accessed 2022 Apr 18.
141.Ontario expanding safe use of biosimilars [press release]. Toronto (ON): Government of Ontario; 2022: https://news.ontario.ca/en/release/1002611/ontario-expanding-safe-use-of-biosimilars. Accessed 2022 Dec 22.
142.Saskatchewan formulary bulletin: Saskatchewan biosimilars initiative announced October 20, 2022. Bulletin #221. Regina (SK): Government of Saskatchewan; 2022: https://formulary.drugplan.ehealthsask.ca/Bulletins/Bulletin-0221-Oct-2022.pdf. Accessed 2022 Dec 19.
143.Nova Scotia Pharmacare: information for prescribers about the Nova Scotia biosimilar initiative. Halifax (NS): Government of Nova Scotia; 2022: https://novascotia.ca/dhw/pharmacare/information-for-prescribers-about-biosimilars.asp#:~:text=The%20Government%20of%20Nova%20Scotia,unless%20an%20exemption%20is%20granted. Accessed 2022 Dec 19.
144.Notice – tiered biologics reimbursement policy. Winnipeg (MB): Manitoba Health; 2018: https://www.gov.mb.ca/health/pharmacare/profdocs/notice_tiered_biologics.pdf. Accessed 2022 Jun 25.
145.Alignment among public formularies in Canada part 1: general overview. Ottawa (ON): Patented Medicine Prices Review Board; 2017: http://www.pmprb-cepmb.gc.ca/view.asp?ccid=1327#a1. Accessed April 2022 Apr 16.
Appendix 1: Regulatory
Note that this appendix has not been copy-edited.
Figure 2: Health Canada Approval Timeline for TIMs by First NOC Date
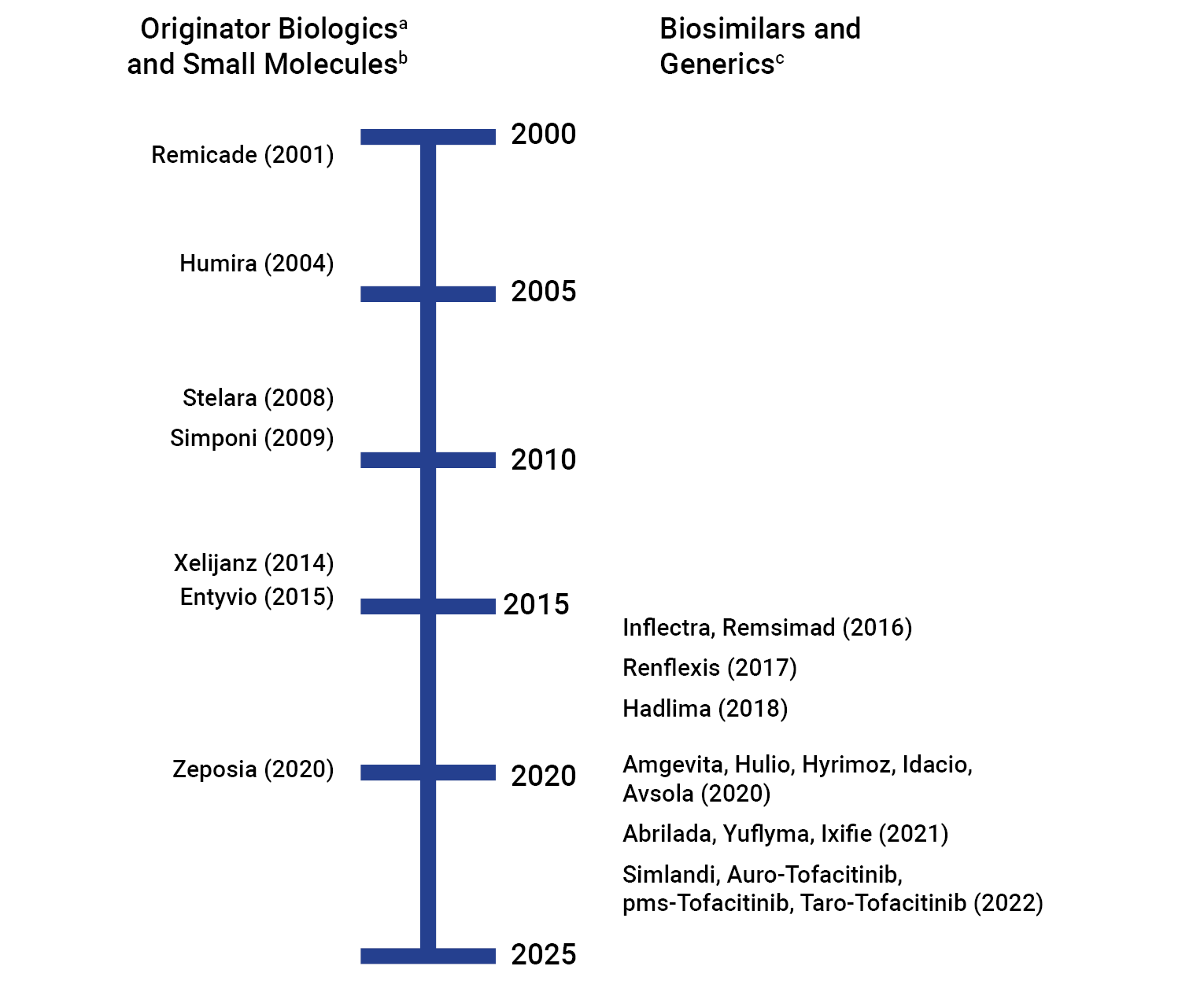
NOC = Notice of Compliance; UC = ulcerative colitis
a Originator biologics: Remicade (infliximab), Humira (adalimumab), Simponi (golimumab), Entyvio (vedolizumab) and Stelara (ustekinumab).
b Small molecules: Xeljanz (tofacitinib) and Zeposia (ozanimod).
c Biosimilars: Adalimumab biosimilars (Amgevita, Hadlima, Hulio, Hyrimoz, Idacio, Abrilada, Simlandi, Yuflyma) and infliximab biosimilars (Inflectra, Remsima, Renflexis, Avsola, Ixifi); Generics: Tofacitinib (Auro-Tofacitinib, pms-Tofacitinib, Taro-Tofacitinib).
d Remsima IV is indicated in adult and pediatric UC, however, the product is ‘dormant,’ and not marketed in Canada. Remsima SC is marketed in Canada but is not indicated in adult or pediatric UC. “Approved” refers to an active Drug Identification number (DIN) for a product that has been reviewed and authorized for sale in Canada but has not yet been marketed in Canada. ‘Marketed’ refers to an active DIN for a product that is currently being sold in Canada. ‘Dormant’ refers to an active DIN for a product that was previously marketed in Canada but for which there have been no sales for period of at least 12 consecutive months.34
e Only approved but not yet marketed.
Sources: Information was collected from Health Canada’s Drug Product Database and Notice of Compliance Database.32,33,37-46,48-54,56-66,68-82,84-87,90,93,94
Table 7: Regulatory Information for TIMs in UC
Generic name | Brand name / route of administration | Manufacturer | First NOC date | NOC date for UC (if different from first NOC date) | Marketed date | Indication for UC |
|---|---|---|---|---|---|---|
Adalimumab | Humira, SC | AbbVie Corporation | September 24, 2004 | November 21, 2013 | September 24, 2004 | Adult: Treatment of adult patients with moderately to severely active UC who have had an inadequate response to conventional therapy including corticosteroids and/or AZA or 6-MP or who are intolerant to such therapies. Efficacy in patients who have lost response to or were intolerant to TNF blockers has not been established. Pediatric: [only for Humira, and not for any biosimilars]: For inducing and maintaining clinical remission in pediatric patients 5 years of age and older with moderately to severely active UC who have had an inadequate response to conventional therapy including corticosteroids and/or AZA or 6-MP or who are intolerant to such therapies. Humira has not been studied in pediatric patients with ulcerative colitis less than 5 years of age. |
[B] Amgevita, SC | Amgen Canada Inc. | November 4, 2020 | Same as first NOC date | February 19, 2021 | ||
[B] Hadlima, SC | Samsung Bioepis Co., Ltd. | May 8, 2018 | February 19, 2021 | |||
[B] Hulio, SC | BGP Pharma ULC | November 24, 2020 | February 16, 2021 | |||
[B] Hyrimoz, SC | Sandoz Canada Inc. | November 4, 2020 | February 15, 2021 | |||
[B] Idacio, SC | Fresenius Kabi Canada Ltd. | October 30, 2020 | February 16, 2021 | |||
[B] Abrilada, SC | Pfizer Canada ULC | January 14, 2021 | February 24, 2022 | |||
[B] Simlandi, SC | Jamp Pharma Corporation | January 5, 2022 | April 13, 2022 | |||
[B] Yuflyma, SC | Celltrion Healthcare Co., Ltd. | December 24, 2021 | March 3, 2022 | |||
Infliximab | Remicadea,b,c IV | Janssen Inc. | June 6, 2001 | March 10, 2006 | June 14, 2001 | Adult: For reduction of signs and symptoms, induction and maintenance of clinical remission and mucosal healing, and reduction or elimination of corticosteroid use in adult patients with moderately to severely active UC who have had an inadequate response to conventional therapy (i.e., ASA and/or corticosteroid and/or an immunosuppressant). Pediatric: For reduction of signs and symptoms, induction and maintenance of clinical remission, and induction of mucosal healing in pediatric patients with moderately to severely active UC who have had an inadequate response to conventional therapy (i.e., ASA and/or corticosteroid and/or an immunosuppressant). The safety and efficacy of infliximab have not been established in patients less than 6 years of age. |
[B] Avsola IV | Amgen Canada Inc. | March 12, 2020 | Same as first NOC date | June 1, 2020 | ||
[B] Inflectra IV | Celltrion Healthcare Co., Ltd. | January 15, 2014 | June 10, 2016 | September 4, 2014 | ||
[B] Renflexis IV | Samsung Bioepis Co., Ltd. | December 1, 2017 | Same as first NOC date | March 22, 2018 | ||
[B] Ixifi IV | Pfizer Canada ULC | December 21, 2021 | Same as first NOC date | Approved Not yet Marketedb | ||
[B] Remsima SC, IV | Celltrion Healthcare Co., Ltd. | January 15, 2014 | August 5, 2016 | June 4, 2021 | Remsima IV is indicated in adult and pediatric UC, however, the product is ‘dormant’b, and not marketed b in Canada. Remsima SC is marketed in Canada but is not indicated in adult or pediatric UC. | |
Golimumab | Simponi SC, IV | Janssen Inc. | April 7, 2009 | September 19, 2013 | June 22, 2009 | Adult: For the treatment of adult patients with moderately to severely active UC who have had an inadequate response to, or have medical contraindications for, conventional therapy including corticosteroids, amino salicylates, AZA, or 6-MP, for inducing and maintaining clinical response (reduction in signs and symptoms); inducing clinical remission; achieving sustained clinical remission in induction responders; and improving endoscopic appearance of the mucosa during induction Simponi I.V. is not indicated for ulcerative colitis |
Vedolizumab | Entyvio SC, IV | Takeda Canada Inc. | January 29, 2015 | January 29, 2015 (IV) April 7, 2020 (SC) | April 21, 2015 | Adult: For the treatment of adult patients (≥ 18 years) with moderately to severely active UC who have had an inadequate response, loss of response to, or were intolerant to either conventional therapy or infliximab, a TNFα antagonist. Both IV and SC formulations are indicated for UC |
Ustekinumab | Stelara SC, IV | Janssen Inc. | December 12, 2008 | January 23, 2020 | January 5, 2009 | Adult: For the treatment of adult patients with moderately to severely active UC who have had an inadequate response with lost response to, or were intolerant to either conventional therapy or a biologic or have medical contraindications to such therapies. Both IV and SC formulations are indicated for UC |
Tofacitinib | Xeljanz / Xeljanz XR Oral | Pfizer Canada Inc. | April 17, 2014 | October 4, 2018 | June 3, 2014 | Adult: For the treatment of adult patients with moderately to severely active UC with an inadequate response, loss of response or intolerance to either conventional UC therapy or a TNFα inhibitor. XELJANZ XR is not indicated for UC0. |
[G] Auro-Tofacitinib | Auro Pharma Inc. | November 28, 2022 | Same as first NOC date | November 28, 2022 | Adult: For the treatment of adult patients with moderately to severely active UC with an inadequate response, loss of response or intolerance to either conventional UC therapy or a TNFα inhibitor. | |
[G] PMS-Tofacitinib | Pharmascience Ince | November 25, 2022 | Same as first NOC date | November 25, 2022 | Adult: For the treatment of adult patients with moderately to severely active UC with an inadequate response, loss of response or intolerance to either conventional UC therapy or a TNFα inhibitor. | |
[G] Taro-Tofacitinib | Taro Pharmaceuticals | November 28, 2022 | Same as first NOC date | November 28, 2022 | Adult: For the treatment of adult patients with moderately to severely active UC with an inadequate response, loss of response or intolerance to either conventional UC therapy or a TNFα inhibitor. | |
Ozanimod | Zeposia | Celgene Inc. | October 2, 2020 | April 8, 2022 | November 12, 2020 | Adult: For the treatment of adult patients with moderately to severely active UC with an inadequate response, loss of response or intolerance to either conventional UC therapy or a biologic drug. |
6-MP = 6-mercaptopurine; 5-ASA = 5-aminosalicylic acid; AZA = azathioprine; IV = Intravenous; NA = not applicable; NOC = Notice of Compliance; SC = subcutaneous; TNF = tumour necrosis factor; UC = Ulcerative Colitis.
*Marked [B] if biosimilar; [G] for generic.
aOmvyence (infliximab, Janssen Inc.) was approved on 29 December 2020 by Health Canada. This product is not a biosimilar. The NOC submission was made for an ‘Additional Product Name’ for Remicade. The product is approved by Health Canada but not yet marketed in Canada.32,33
b“Approved” refers to an active Drug Identification number (DIN) for a product that has been reviewed and authorized for sale in Canada but has not yet been marketed in Canada. ‘Marketed’ refers to an active DIN for a product that is currently being sold in Canada. ‘Dormant’ refers to an active DIN for a product that was previously marketed in Canada but for which there have been no sales for period of at least 12 consecutive months.34
Sources: Information was collected from Health Canada’s Drug Product Database and Notice of Compliance Database.32,33,37-46,48-54,56-66,68-82,84-87,90,93,94
Appendix 2: Clinical Trials
Note that this appendix has not been copy-edited.
Table 8: Clinical Trials Registered on Clinical Trials for Ustekinumab (Phase III)
Name | NCT | Condition | Completion Date |
|---|---|---|---|
ABP-654 | NCT04761627 NCT04607980 | Psoriasis | March 20, 2023 June 3, 2022 |
AVT-04 | NCT04930042 | Psoriasis | September 29, 2022 |
BAT-2206 | NCT04728360 | Psoriasis | May 30, 2023 |
BMAB-1200 | NCT05335356 | Psoriasis | October 30, 2023 |
CT-P43 | NCT04673786 | Psoriasis | May 12, 2022 |
DMB-3115 | NCT04785326 | Psoriasis | November 2022 |
FYB-202 | NCT04595409 | Psoriasis | March 2022 |
Appendix 3: CADTH Review
Table 9: Summary of CDEC Recommendations for TIMs in UC
Drug recommendation | Clinical rationale study details | Clinical reasons for recommendation | Economic rationale | |
|---|---|---|---|---|
Humira (adalimumab) Recommended not be listed at the submitted price for the treatment of adults with moderately to severely active UC who have had an inadequate response to conventional therapy including corticosteroids, AZA, and/or 6-MP or who are intolerant to such therapies. | Three phase III RCTs ULTRA1 [N = 576]: multinational, double-blind, placebo-controlled trial with 8-week treatment period, and open-label extension period. Primary outcomes: Proportion of patients achieving clinical remissiona at 8 weeks. ULTRA 2 [N = 518]: multinational, double-blind, placebo-controlled, with 8-week induction period and 44-week maintenance period. M10-447 [N = 274]: single country (Japan), double-blind, placebo-controlled, with 8-week induction period and 44-week maintenance period Co-primary outcomes: (for ULTRA 2 and M10): proportion of patients achieving clinical remissiona at 9 weeks and 52 weeks. | Adalimumab vs. placebo The proportion of patients achieving clinical remissiona at 8-weeks was statistically significantly greater with adalimumab in ULTRA 1 (19% versus 9%) and ULTRA 2 (17% versus 9%); however, there was no statistically significant difference in M10- 447. Both ULTRA 2 and M10-447 demonstrated a statistically significantly greater proportion of adalimumab-treated patients achieving clinical remissiona at 52 weeks (17% versus 9% in ULTRA 2 and 23% versus 7% in M10-447). | At the submitted marketed price of $740.36 per 40 mg/0.8 mL syringe or autoinjector, adalimumab ($22,211 in year 1, $19,249 thereafter) is priced similarly to golimumab ($22,803 in year 1, $19,763 thereafter), and less expensive than infliximab ($31,602 in year 1, $25,677 thereafter) and vedolizumab ($26,320 in year 1, $21,385 thereafter). Based on CADTH reanalysis the ICUR for adalimumab + SOC compared with SOC alone ranged from $67,000 to $130,000 per QALYb,c | |
[B] Inflectra (infliximab) Recommended to be reimbursed in accordance with the Health Canada–approved indications for the treatment of UC, if the following clinical criterion and conditions are met. Clinical Criterion: For use in patients for whom infliximab is considered to be the most appropriate treatment option. Conditions:
| Two RCTs PLANET-RA [N = 606] phase III, double-blind, multicentre, multinational, parallel-group clinical equivalence study; comparing efficacy and safety of Inflectra with Remicade Population: patients with active RA who had an inadequate response to treatment with MTX Primary end point: Proportion of patients with an ACR 20 response at week 30. Therapeutic equivalence of clinical response according to ACR20 criteria would be demonstrated if the 95% CI for the treatment difference was within ± 15%. PLANET-AS [N = 250] was a phase I, randomized, double-blind, multicentre, multinational, parallel-group study designed to compare the PK, safety, and efficacy of Inflectra and Remicade. Population: patients with active AS. Primary end point: demonstrate PK equivalence at a steady state of area under the concentration-time curve and observed maximum steady state serum concentration between Inflectra and Remicade between weeks 22 and 30. Equivalence was demonstrated if the 90% CIs lay within the equivalence margin of 80% to 125%. CT-P13 4.1 [N = 20] phase IV, a 4-year, open-label, single arm study in South Korea Population: Treatment-naive, adult patients with CD or UC in South Korea. Primary Outcome: not-stated | Inflectra vs. Remicade Inflectra and Remicade have similar efficacy and safety profiles in patients with RA and similar PK profiles in patients with AS. Extrapolation of the data from RA and AS to UC was also granted by Health Canada based on physiochemical and biological data. Results from CT-P13PMS:
Based on a complete case analysis: Among UC infliximab-naive patients, 9/13 (69.2%) experienced mucosal healing at week 30 while 6/9 (66.7%) patients who were switched from Remicade to CT-P13 [Inflectra in Canada] experienced mucosal healing throughout visits 2 to 5. | At the submitted price ($525.00 per 100 mg vial), Inflectra is less costly than Remicade ($987.56 per 100 mg vial) for use in accordance with the Health Canada approved indications for UC. | |
Remicade (infliximab) Recommended to be not listed | SR with 5 RCTs [N = 827]; the SR focused on 2 RCTs (ACT1 and ACT 2) ACT1 [N = 364]: double-blind, placebo-controlled, 46-weeks treatment period with follow-up at 54-weeks ACT 2 [N = 364]: double-blind, placebo-controlled, 22-weeks treatment period with 30-weeks duration of follow-up; and a 24-week extension period (continued in double-blind RCT groups) Population: moderate to severe UC Primary outcome: clinical responsea at week 8 | Infliximab vs. placebo Infliximab demonstrated statistically significant improvement in clinical responsea at week 8, relative to placebo. | At the recommended maintenance dose of 70 kg patient, the annual cost of infliximab 5mg//kg is $30,080 in the first year and $22,440 thereafter. | |
[B] Renflexis (infliximab) Recommended to be reimbursed in accordance with the Health Canada–approved indications for the treatment of adult and pediatric ulcerative colitis, if the following criterion and condition are met: Criterion: For use in patients for whom infliximab is considered to be the most appropriate treatment option. Condition: The cost of treatment with Renflexis should provide significant cost savings for jurisdictions compared with the cost of treatment with existing infliximab products. | Two RCTs Study SB2-G11-NHV [N = 159], phase I 3-arm, single-blind study, comparing Renflexis with EU-Remicade and US Remicade. Primary end point: PK profile (AUCinf, AUClast, Cmax), considered to be met if the 90% CI for the geometric mean was within the equivalence margin of 80% to 125% Study SB2-G31-RA [N = 584], phase III double-blind, multinational study, comparing efficacy, safety, immunogenicity, and PK of Renflexis with EU-Remicade Primary end point: ACR 20 response at Week 30. The primary end point was considered met if the 95% CI of the adjusted treatment difference was within the equivalence margin of −15% to 15%. For both RCTs Population: patients with moderate to severe RA despite MTX therapy | Renflexis vs. Remicade Renflexis has similar PK, efficacy, safety, and immunogenicity as the reference product, Remicade. Extrapolation of the data from RA to UC is reasonable given the demonstrated similarities between Renflexis and Remicade in the included trials, and the role that TNF-alpha drugs play in these indications. | At a manufacturer-submitted price of $525.00 per vial (100 mg/vial lyophilized powder), Renflexis is less costly than Remicade based on the Ontario Public Drug Plan price ($987.56 per 100 mg vial of lyophilized powder) for use in accordance with the Health Canada–approved indications. Renflexis is the same price as Inflectra, the first infliximab biosimilar approved by Health Canada, based on the Ontario Public Drug Plan price ($525.00 per 100 mg vial of lyophilized powder). | |
Simponi (golimumab) SCc Recommended not be listed at the submitted price for the treatment of ulcerative colitis (UC). | Two RCTs PURSUIT-SC: double-blind, placebo-controlled 2-part study (Part 1 dose finding phase [N = 169] and Part 2 [N = 896 new patients] for 6-weeks. PURSUIT-MAINTENANCE [N=464]: double-blind, placebo-controlled, included patients who were responders in PURSUIT-SC and in PURSUIT-IV (not included in this review due to the route of administration) for 52 weeks. Primary Outcome: Clinical response a through end of treatment | Golimumab vs. placebo Golimumab was superior to placebo for achieving clinical responsea and clinical remissiona in patients with UC. | Golimumab is available in 50 mg/0.5 mL and 100 mg/1.0 mL prefilled syringes at a price of $1,490.41 per syringe regardless of strength. The annual cost of golimumab is $22,356 in the first year and $19,375 in subsequent years (200 mg week 0, 100 mg week 2, and 50 or 100 mg every 4 weeks thereafter) and the annual cost of infliximab is $29,046 in the first year and $23,600 in subsequent years (5 mg/kg at weeks 0, 2, and 6, and every 8 weeks thereafter) - assuming a patient weight of 75 kg. Based on CADTH reanalyses, the ICUR for golimumab compared with conventional therapy could be as high as $104,000 per QALY when the time horizon is reduced to 1.25 years (15 months) from $52,000 for a time horizon of 2.5 yearsb,c | |
Entyvio (vedolizumab) (IV) Recommended to be listed for the treatment of adult patients with moderately to severely active UC who have had an inadequate response, loss of response to, or were intolerant to either conventional therapy or infliximab, a tumour necrosis factor (TNF) alpha antagonist, if the following clinical criterion and condition are met: Clinical criterion: Treatment with vedolizumab should be discontinued if a clinical responsea is not achieved within 6 weeks. Condition: Reduction in price to improve the cost-effectiveness of vedolizumab to a level acceptable to the drug plans. | One RCT GEMINI 1: double-blind, placebo-controlled with induction phase [N = 895] (6 weeks) and maintenance phase [N = 373] (52 weeks) Primary Outcome: clinical responsea at 6-weeks (induction phase) and clinical remissiona at 52-weeks (maintenance phase). | Vedolizumab IV versus placebo Vedolizumab was statistically superior to placebo for achieving clinical responsea at 6 weeks (induction) and clinical remissiona at 52 weeks (maintenance). | At the submitted price of $3,290 per 300 mg vial and the recommended dosing (300 mg every 8 weeks), the cost of vedolizumab in the first year ($26,320) and subsequent years ($21,385) is lower than infliximab ($31,602 and $25,677, respectively), but higher than golimumab ($22,803 and $19,763, respectively). Bases on CADTH reanalyses, the ICUR ranged from $60,000 (manufacturer’s base case) to $150,000 per QALY (CDR revised base case) for vedolizumab compared with conventional therapyb,c | |
Entyvio (vedolizumab) (SC) Recommended to be reimbursed for the treatment of adult patients with moderately to severely active UC who have had an inadequate response, loss of response, or were intolerant to either conventional therapy or infliximab, TNF-alpha antagonist, only if the following conditions are met. Conditions for Reimbursement:
| One RCT VISIBLE 1 [N=383]: double-blind, placebo-controlled, with induction by vedolizumab IV Responders to IV [N = 216] randomized to receive the vedolizumab IV [N = 54], vedolizumab SC [N = 106] and placebo [N = 54] for a 52 week follow-up period Population: Moderately to severely active UC Primary Outcome: clinical remissiona at Week 52 | Vedolizumab SC versus placebo More patients in the vedolizumab SC group showed clinical remissiona at week 52 when compared to the placebo group. The findings were consistent in both anti-TNF-naive and -experienced populations. | At the submitted price of $822.50 per prefilled syringe or pen, the annual cost per patient at the recommended dose is estimated to be $25,501 in the first year (including 2 initial IV doses priced at $3,291.00 per 300 mg vial) and $21,385 thereafter. Based on CADTH reanalyses, vedolizumab SC had an ICER of $1,152,959 per QALY gained compared with tofacitinibb,c | |
Stelara (ustekinumab) (SC and IV.) Recommended to be reimbursed for the treatment of adult patients with moderately to severely active ulcerative colitis who have had an inadequate response with lost response to or were intolerant to either conventional therapy or a biologic, or have medical contraindications to such therapies, only if the following conditions are met. Conditions for Reimbursement
| One RCT UNIFI [N = 961]: double-blind, 2 phase (8-week induction [N = 961] and 44-week maintenance phase [N = 783] (783 out of the 961 from induction phase)] Primary outcome: Clinical remissiona at week 8 (induction) and week 52 (maintenance) based on global definitiona, and US definition (an absolute stool number of 3 or lower, a Mayo rectal bleeding subscore of zero, and a Mayo endoscopy subscore of zero or 1). | Ustekinumab vs. placebo Ustekinumab was more effective than placebo at inducing (at 8 weeks) and maintaining (for another 44 weeks) clinical remissiona of UC, including corticosteroid-free remission and endoscopic healing. | At the sponsor-submitted price of $2,080 per 130 mg/26 mL solution vial for IV infusion and $4,593 for a prefilled syringe of 90 mg/1 mL for SC injection, the annual cost of treatment per patient with ustekinumab is estimated to be $33,798 in the first year and $32,152 annually thereafter. Based on CADTH reanalyses of the biologic-naive population determined that conventional therapy would be the optimal therapy if the willingness-to-pay threshold is up to $53,546 per QALY; thereafter, ustekinumab would be the optimal therapyb,c | |
Xeljanz (tofacitinib)e Recommended to be reimbursed for the treatment of adult patients with moderately to severely active UC with an inadequate response, loss of response, or intolerance to either conventional UC therapy or a TNFi, if the following conditions are met: Conditions:
| Three phase III RCTs OCTAVE Induction 1 (N = 614) and OCTAVE Induction 2 (N = 547) placebo-controlled for 8 weeks. Primary Outcome: Clinical remissiona at Week 8. OCTAVE Sustain (N = 593): placebo-controlled for 52 weeks. Primary Outcome: Clinical remissiona at Week 52 Population (all 3 RCTs): patients with moderately to severely active UC. | Tofacitinib vs. placebo Tofacitinib was associated with statistically significant differences in the proportion of patients who achieved remission at Week 8 (OCTAVE Induction 1 and OCTAVE induction 2), and at Week 52 (OCTAVE Sustain). | At the manufacturer-submitted price of $23.96 per 5 mg tablet and $42.34 per 10 mg tablet, the annual cost of tofacitinib is $19,501 in the first year and $17,442 every year thereafter based on recommended dosing for induction and 5 mg twice daily in the maintenance phase. This cost could increase significantly, up to $30,181 per year, in certain populations requiring tofacitinib 10 mg twice daily in the maintenance phase. Based on CADTH reanalyses, for biologic-naive patients, conventional therapy is the optimal therapy where the decision-maker is willing to pay less than $166,608 per QALY and infliximab biosimilar is the optimal therapy where the decision-maker is willing to pay more than $166,608 per QALY. Tofacitinib was dominated by infliximab biosimilar (i.e., tofacitinib is more costly and associated with less QALYs than infliximab biosimilar). For biologic-exposed patients, conventional therapy is the optimal therapy where the decision-maker is willing to pay less than $143,710 per QALY and tofacitinib is the optimal therapy where the decision-maker is willing to pay more than $143,710 per QALYb,c | |
Zeposia (ozanimod) Recommended to be reimbursed for the treatment of adult patients with moderately to severely active UC who have had an inadequate response, a loss of response, or intolerance to conventional therapy or a biologic drug. Conditions:
| One phase III RCT TRUE NORTH (N = 645) placebo-controlled for 10 weeks induction and 52 weeks maintenance period Primary outcome: clinical remissiona measured at week 10 and week 52 Population: adult patients with moderately to severe UC | Ozanimod vs. placebo Greater percentages of patients in the ozanimod group compared with the placebo group had clinical remission during the induction period at week 10 (18.4% versus 6.0%; between-group difference of 12.4%; 95% confidence interval [CI], 7.5% to 17.2%; P | At the manufacturer-submitted price of $68.49 per capsule (multiple strengths: 0.25 mg; 0.5 mg, and 1 mg), the annual cost of ozanimod is $25,000. Results from the CADTH base case were similar to the sponsor’s results, as ozanimod was not among the optimal treatments in the biologic-naivef or biologic-experiencedf populations. The probability that ozanimod is cost-effective at a willingness-to-pay threshold of $50,000 per QALY was 0% in both analyses. Price reductions of 73% and 66% would be necessary for ozanimod to be cost-effective at this threshold in biologic-naivef and biologic-experiencedf populations, respectively. | |
6-MP = 6- mercaptopurine; 5-ASA = 5-aminosalicylic acid; ACR = American College of Rheumatology; AS = ankylosing spondylitis; AZA = azathioprine; CD = Crohn Disease; CDR = CADTH Common Drug Review CI = Confidence Interval; ICUR = incremental cost-utility ratio; IV = Intravenous; MTX = methotrexate; NA = not applicable; NOC = Notice of Compliance; PK = pharmacokinetic; QALY = quality-adjusted life-year; RA = rheumatoid arthritis; RCT = randomized controlled trials; SC = Subcutaneous; SOC = standard of care; SR = Systematic Review; TNF = tumour necrosis factor; UC = ulcerative colitis; WTP = willingness-to-pay.
Note that this appendix has not been copy-edited.
aClinical response is defined as a decrease in partial Mayo scores from baseline of at least 2 points and at least 30%, with an accompanying decrease in the subscore for rectal bleeding of at least 1 point or an absolute subscore for rectal bleeding of 0 or 1 for patients with UC. Clinical remission is defined as a total partial Mayo Score of 2 points or lower, with no individual subscore exceeding 1 point. The Mayo scoring system consists of stool frequency subscore (from 0 [normal number of stools] to 3 [≥ 5 stools above normal]); rectal bleeding subscore (RBS) (from 0 [no blood seen] to 3 [blood alone passed]); endoscopy subscore (from 0 [normal] to 3 [severe]); and Physician's Global Assessment subscore (from 0 [normal] to 3 [severe]). A score of 3 to 5 points indicates mildly active disease, a score of 6 to 10 points indicates moderately active disease, and a score of 11 to 12 points indicates severely active disease.
bBased on CDR’s reanalyses to account for limitations in the manufacturer’s economic model.
cThe results should be interpreted with caution as CADTH reanalysis was not able to address all the limitations of the manufacturer-submitted economic analysis.
dSimponi IV is not indicated in UC.
eXeljanz XR is not indicated in UC.
fIn line with the sponsor submission, the term biologic was used to refer to anti-TNF therapies (i.e., infliximab, adalimumab, and golimumab), tofacitinib, ustekinumab, and vedolizumab.
Sources: Data were extracted from published CADTH reports.107-117
Appendix 4: Reimbursement
Note that this appendix has not been copy-edited.
Table 10: Overview of the pCPA Negotiation Status of TIMs
Generic name | Brand name | Status of UC indication (date negotiation concluded) | Status of other indication (date negotiation concluded) |
|---|---|---|---|
Adalimumab | Humira | Concluded with LOI (May 23, 2017)a | Plaque psoriasis: Concluded without agreement (April 16, 2020) Hidradenitis suppurativa: Concluded with LOI (October 23, 2017) |
[B] Amgevita | Concluded with LOI (January 20, 2021) | Plaque psoriasis, rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn disease, hidradenitis suppurativa, and uveitis: Concluded with LOI (January 20, 2021) | |
[B] Hadlima | Concluded with LOI (January 22, 2021) | Plaque psoriasis, rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn disease, hidradenitis suppurativa, and uveitis: Concluded with LOI (January 22, 2021) | |
[B] Hulio | Concluded with LOI (January 20, 2021) | Plaque psoriasis, rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn disease, hidradenitis suppurativa, and uveitis: Concluded with LOI (January 20, 2021) | |
[B] Hyrimoz | Concluded with LOI (January 20, 2021) | Plaque psoriasis, rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn disease, hidradenitis suppurativa, and uveitis: Concluded with LOI (January 20, 2021) | |
[B] Idacio | Concluded with LOI (January 26, 2021) | Plaque psoriasis, rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn disease, hidradenitis suppurativa, and uveitis: Concluded with LOI (January 26, 2021) | |
[B] Abrilada | Concluded with LOI (February 28, 2022) | Rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn disease, hidradenitis suppurativa, plaque psoriasis, uveitis: Concluded with LOI (February 28, 2022) | |
[B] Simlandi | Concluded with LOI (March 03, 2022) | Rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn disease, hidradenitis suppurativa, plaque psoriasis, uveitis: Concluded with LOI (March 03, 2022) | |
[B] Yuflyma | Concluded with LOI (March 01, 2022) | Rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn disease, hidradenitis suppurativa, plaque psoriasis, uveitis: Concluded with LOI (March 01, 2022) | |
Infliximab | Remicade | Concluded with LOI (February 23, 2015) | Rheumatoid arthritis, and Crohn disease: Concluded with LOI (February 23, 2015) |
[B] Avsola | Concluded with LOI (November 02, 2020) | Ankylosing spondylitis, psoriatic arthritis, rheumatoid arthritis, and Crohn disease: Concluded with LOI (November 02, 2020) | |
[B] Inflectra | Concluded with LOI (October 31, 2016) | Plaque psoriasis, ankylosing spondylitis, psoriatic arthritis, Rheumatoid arthritis, and Crohn disease: Concluded with LOI (October 31, 2016) | |
[B] Remsima | negotiations not held | Rheumatoid arthritis: Negotiations were not pursued (March 10, 2022) | |
[B] Renflexis | negotiations not held | Rheumatic conditions: Concluded with LOI (July 27, 2018) | |
[B] Ixifi | NAb | — | |
Golimumab | Simponi SC Simponi IV | Concluded with LOI (SC) (August 12, 2016) | Rheumatoid Arthritis (IV): Concluded without agreement (April 19, 2016) |
Vedolizumab | Entyvio SC Entyvio IV | Concluded with LOI (SC) (August 13, 2021) Concluded with LOI (IV) (March 03, 2017) | Crohn disease (SC): Concluded with LOI (August 13, 2021) Crohn disease (IV): Concluded with LOI (March 03, 2017) |
Ustekinumab | Stelara | Concluded without agreement (July 28, 2021) | Crohn disease: Concluded without agreement (March 29, 2019) Psoriatic arthritis: Negotiations were not pursued (November 27, 2014) |
Tofacitinib | Xeljanz Xeljanz XR | Concluded with LOI (July 24, 2020) | Rheumatoid Arthritis (Xeljanz XR): Concluded with LOI (July 09, 2019) Rheumatoid Arthritis (Xeljanz): Concluded with LOI (April 26, 2016) |
Ozanimod | Zeposia | NAc | Relapsing-Remitting Multiple Sclerosis: Negotiations were not pursued (July 29, 2021) |
LOI = Letter of Intent; NA = not applicable; NOC = Notice of Compliance, pCPA = pan-Canadian Pharmaceutical Alliance; SC = subcutaneous; UC = ulcerative colitis.
*Marked [B] if biosimilar
aFor Humira (citrate-free) and negotiated for multiple indications (details of indications not specified). Negotiation concluded (without an agreement) on March 16, 2020.
bIxifi had received NOC from Health Canada for UC, but the drug is not yet marketed in Canada.
cZeposia (Ozanimod) has only recently received CADTH recommendation for UC (December 1, 2022). Given that pCPA negotiations are considered after CADTH review is complete, a pCPA negotiation for Zeposia could be expected to begin in near future.
Source: Data are from LOI timelines published on the pCPA website.117-119
Table 11: Summary Coverage Criteria for TIMs Across Public Drug Plans
Drug plan | Drugs covered | Initial coverage criteria | Renewal criteria | Notes |
|---|---|---|---|---|
AB | Adalimumab Infliximab Golimumab Vedolizumab Tofacitinib | For ALL For the reduction in signs and symptoms and induction and maintenance of clinical remission of UC in adult patients (≥18 years of age) with active disease (partial Mayo scorea >4 prior to initiation of biologic therapy) and who are refractory or intolerantb to:
Immunosuppressive therapy as follows may also be initiated if in the clinician's judgment a trial is warranted:
Must be prescribed by a Specialist in Gastroenterology or a physician appropriately trained by the University of Alberta or the University of Calgary and recognized as a prescriber by Alberta Blue Cross ('Specialist'). FOR tofacitinib ONLY: Coverage cannot be provided for tofacitinib when intended for use in combination with a biologic drug. | For ALL For continued coverage beyond the initial coverage period, the patient must meet the following criteria: The patient must be assessed by a Specialist
after the initiation of therapy to determine response. The Specialist must confirm in writing that the patient is a 'responder' that meets the following criteria:
Ongoing coverage may be considered only if the following criteria are met at the end of each 12-month period:
| Biosimilar Policy Adalimumab: All new request for adalimumab-naive patients will be assessed for biosimilars only. Adult patients currently on the originator drug must switch to the biosimilar prior to May 1, 2022. During the switching period, both the originator drug and biosimilar(s) will be covered. As of May 1, 2022, the authorization will only cover the biosimilar(s). Infliximab: Remicade, the originator drug is no longer a benefit Switching policy:
Others: Patients are limited to receiving 1 biologic drug at a time regardless of the condition for which it is being prescribed. |
BC | Adalimumab Infliximab Vedolizumab Tofacitinib | For ALL
FOR tofacitinib ONLY: Coverage cannot be provided for tofacitinib when intended for use in combination with a biologic drug. | For ALL: Requires a score reduction from baseline ≥ 2 with a decrease in baseline from rectal bleeding subscore of ≥1, or a bleeding subscore of 0 or 1 | Biosimilar Policy Adalimumab: All new requests including renewals for adalimumab will only be assessed for biosimilars. Infliximab: All new requests including renewals for infliximab will only be assessed for biosimilars. Special Authority requests for patients who are unable to transition from Remicade (originator drug) to biosimilars will be considered on an exceptional case-by-case basis. |
SK | Adalimumab Infliximab Golimumab Vedolizumab Tofacitinib | For ALL
| For ALL Ongoing coverage will only be provided for those who respond to therapy. Initial clinical response should be assessed after
Confirmation of response required for ongoing coverage. Golimumab, Tofacitinib only: Patients undergoing this treatment should be reviewed every 6 months by a specialist in this area. | Biosimilar Policy: Established patients already receiving a reference biologic drug (or “originator” biologic) with an available biosimilar version will be required to use a biosimilar version by April 30, 2023, in order to maintain coverage under the Saskatchewan Drug Plan. During the period from now until April 30, 2023, established patients will have access to Saskatchewan Drug Plan coverage of both the reference biologic and the available biosimilar options listed on the Formulary. After April 30, 2023, coverage of the reference biologic will no longer be provided. Biosimilar products are not interchangeable. Prescriber must specify the specific biosimilar when requesting coverage. |
MB | Adalimumab Infliximab Golimumab Vedolizumab Tofacitinib | For ALL
| — | Biosimilar Policy Adalimumab: All new request for adalimumab-naive patients will be assessed for biosimilar only. Infliximab: All new request for infliximab-naive adult and pediatric patients will be assessed for biosimilar only. Tiered Approach:
Switching Policy: Switching between biologics or biosimilar is not permitted previously trialled and deemed unresponsive. |
ON | Adalimumab Infliximab Golimumab Vedolizumab Tofacitinib | For ALL: For the treatment of UC disease in patients who meet the following criteria: Induction Criteria
*The endoscopy procedure must be done within the 12 months prior to initiation of treatment. For Adalimumab, golimumab, vedolizumab ONLY: Mild disease (Mayo Score a <6 AND) and pediatric coverage will be considered on a case-by-case basis | For ALL: Maintenance therapy is funded for patients who meet the Ministry initiation criteria and whose disease is maintained at Mayo Score less than 6 AND who demonstrate at least 50% reduction in the dose of prednisone compared with the starting dose following the first 6 months of treatment or be off corticosteroids after the first year of treatment. | Biosimilar Policy:
Infliximab and Adalimumab: All new request for naive patients will be assessed for biosimilars only. |
NB | Adalimumab Infliximab Golimumb Vedolizumab Tofacitinib | For Adalimumab:
For Infliximab, Vedolizumab, tofacitinib:
| For Adalimumab: Confirmation of response is required. For Infliximab, Vedolizumab, tofacitinib:
. | Biosimilar Policy Adalimumab, Infliximab: All new requests will be assessed for biosimilar. Originator biologics are not covered. Others: Combined use of more than 1 biologic drug will not be reimbursed. |
NS | Adalimumab Infliximab Golimumab Vedolizumab Tofacitinib | For ALL For the treatment of patients with moderately to severely active UC who have a partial Mayo Score > 4, and a rectal bleeding subscore ≥ 2 and are:
Clinical Notes:
| For ALL Renewal requests must include information demonstrating the beneficial effects of the treatment, specifically:
| Biosimilar Policy Adalimumab: All new request for adalimumab-naive pediatric and adult patients whose adalimumab therapy is initiated after December 15, 2021, will be assessed for biosimilar. Infliximab: All new request for infliximab-naive patients whose infliximab therapy is initiated after December 1, 2016, will be assessed for biosimilar. For pediatric patients whose infliximab therapy is initiated after October 1, 2019, will be assessed for biosimilar. Starting 3 February 2023, some original biologic medications won’t be covered by Pharmacare if a biosimilar version is approved and available, unless an exemption is granted. Others: Combined use of more than 1 biologic DMARD will not be reimbursed. |
NL | Adalimumab Infliximab Golimumab Vedolizumab Tofacitinib | For ALL For the treatment of patients with moderately to severely active UC who have a partial Mayo Score > 4, and a rectal bleeding subscore ≥ 2 and are:
Clinical Notes: Consideration will be given for patients who have not received a 4-week trial of aminosalicylates if disease is severe (partial Mayo Score > 6). Must be prescribed by a gastroenterologist or physician with a specialty in gastroenterology. | For ALL Renewal requests must include information demonstrating the beneficial effects of the treatment, specifically:
| Biosimilar Policy Adalimumab: All new request for adalimumab-naive will be assessed for biosimilar. Patients whose initial Special Authority was received before April 17, 2021 will be eligible for coverage of Humira (originator drug) and will also be eligible for coverage of adalimumab biosimilars. Infliximab: All requests will be assessed for biosimilars. Requests for Remicade will not be considered. Switching Policy: Switching between biosimilars or biologics is not permitted if previously trialled and deemed unresponsive to therapy. Others: Combined use of more than 1 biologic DMARD will not be reimbursed. |
PE | Adalimumab Infliximab Vedolizumab Tofacitinib | For ALL For the treatment of adult patients with moderately to severely active UC who have a partial Mayo Score > 4, and a rectal bleeding subscore ≥ 2 and are:
Clinical Notes: Patients with severe disease (partial Mayo > 6) do not require a trial of 5-ASA. Must be prescribed by a gastroenterologist or physician with a specialty in gastroenterology. | For ALL Renewal requests must include information demonstrating the beneficial effects of the treatment, specifically:
| Biosimilar Policy Adalimumab: All request for Adalimumab-naive patients will be assessed for biosimilar. Others: Combined use of more than 1 biologic DMARD will not be reimbursed. |
YT | Adalimumab Infliximab Golimumab Vedolizumab | For ALL For patients with a Mayo Score > 6 AND an endoscopic subscore ≥ 2 within the last 12 months, AND failed 2 weeks of oral prednisone ≥ 40mg (or 1 week IV equivalent) AND 3 months of azathioprine or 6-mercaptopurine. OR stabilized on prednisone as above but the prednisone dose cannot be tapered despite 3 months of DMARDS. Must be prescribed by a specialist. | — | Biosimilar Policy Adalimumab and Infliximab: All new requests will be assessed for biosimilars. |
NIHB | Adalimumab Infliximab Golimumab Vedolizumab Tofacitinib | For ALL For the treatment of adult patients with moderately to severely active UC.
Must be prescribed by expert in gastroenterology. | For ALL: Coverage beyond initial approval and for continuous approval after 1 year will be based on a decrease in the partial Mayo Score of ≥ 2 points. | Biosimilar Policy Adalimumab: All new request for adalimumab-naive patients and whose therapy is initiated on or after June 11, 2021, will be assessed for biosimilar. Clients who received approval for Humira (originator drug) before June 11, 2021, will continue to have this brand covered and will also be eligible for coverage of adalimumab biosimilars. Infliximab: All new request for infliximab-naive patients and whose therapy is initiated on or after May 01, 2007, will be assessed for biosimilar. Clients who received approval for Remicade (originator drug) before May 01, 2017, will continue to have this brand covered and will also be eligible for coverage of infliximab biosimilars. Coverage for Inflectra or Renflexis will be approved indefinitely. |
VACc | Adalimumab Infliximab Golimumab Vedolizumab Tofacitinib | For Adalimumab, infliximab, golimumab, vedolizumab: When started while in hospital for fulminant UC OR when prescribed by a gastroenterologist for patients with moderate to severely active UC (UC) who have had an inadequate response, loss of response to, were intolerant to or where there is a contraindication to an adequate course of corticosteroid (i.e., prednisone) AND conventional therapy (i.e., 5-ASA, AZA, or 6-MP). For Tofacitinib: when started while in hospital for fulminant UC OR when prescribed by a gastroenterologist for patients with moderate to severely active UC who have had an inadequate response, loss of response to, were intolerant to or where there is a contraindication to an adequate course of either conventional UC therapy (i.e., corticosteroids, 5-ASA, azathioprine or 6-mercaptopurine) OR a tumour necrosis factor-alpha inhibitor (TNFi) | — | — |
CSC | Adalimumab Infliximab Golimumab Vedolizumab | For Adalimumab: Treatment of adults with moderately to severely active UC (UC) who: a) have a partial Mayo Score > 4, AND b) have had an inadequate response to conventional therapy including corticosteroids, AZA, and/or 6-MP or who are intolerant to such therapies. For Infliximab, golimumab, vedolizumab
Patients with severe disease (Mayo Score >10) do not require a trial of 5- ASA. For Vedolizumab only: Treatment with vedolizumab should be discontinued if a clinical response is not achieved prior to the administration of a fourth dose of vedolizumab. | For adalimumab: To obtain yearly approval after initial coverage, gastroenterologist must confirm that the patient’s symptoms have improved. The following is an example of what may be used to demonstrate improvement: Mayo scorea ≤ 2 with no subscore > 1. For Infliximab, golimumab: Maintenance/Renewal: Maintenance therapy is approved for patients who meet the initiation criteria and whose disease is maintained at Mayo Score less than 6 AND who demonstrate at least 50% reduction in the dose of prednisone compared with the starting dose following the first 6 months of treatment or be off corticosteroids after the first year of treatment. For Vedolizumab:
| Biosimilar Policy Adalimumab and infliximab: All new request will be assessed for biosimilars. Patients who are well maintained on a biologic (originator drug) and are considered responders can continue to receive their current medication at this time, but prescribers are encouraged to discuss with their patient the option of a switch from a biologic to a biosimilar drug. Tiered Approach: CSC’s Tiered Biologics Policy (existing patients): Patients deemed unresponsive to biologic therapy are required to switch to biosimilar/ biologic therapy on a CSC defined list (Tier 1). Once all options on tier 1 are exhausted, options on tier 2 list can be made available. Tier 1 drugs include biosimilars versions of adalimumab (Abrilada, Amgevita, Hadlima, Hulio, Hyrimoz, Idacio, Simlandi and Yuflyma) and infliximab (Inflectra, Renflexis), and originator drug Entyvio (vedolizumab). Tier 2 drugs include originator biologics Humira (adalimumab). |
CAF | Adalimumab Infliximab Golimumab Vedolizumab | For ALL For moderately to severely active UC who have a partial Mayo Score > 4, and a rectal bleeding subscore ≥ 2 who have had an inadequate response to conventional therapies as follows:
OR
Must be prescribed by an expert in gastroenterology | — | Biosimilar Policy Infliximab: All new request will be assessed for biosimilars. Patients that have previously received coverage for Remicade (originator drugs) may continue to receive coverage for this drug. |
6-MP = 6-mercaptopurine; 5-ASA = 5-aminosalicylic acid; AB = Alberta; AZA = azathioprine; BC = British Columbia; CAF = Canadian Armed Forces; CM = Criteria Medicine; CSC = Correctional Services Canada; EAP = Exceptional Access Program; EDS = Exception Drug Status; ESD = Exception Status Drug; IV = Intravenous; LU = Limited Use; MB = Manitoba; NA = not applicable; NAB = not a benefit; NB = New Brunswick; NIHB = Non-Insured Health Benefits; NL = Newfoundland and Labrador; NS = Nova Scotia; ODB = Ontario Drug Benefit; ON = Ontario; PA = Prior Approval; PE = Prince Edward Island; SA = Special Authorization; SC = subcutaneous; SK = Saskatchewan; TNF = tumour necrosis factor; UC = ulcerative colitis; VAC = Veterans Affairs Canada; YT = Yukon.
aThe Mayo scoring system consists of stool frequency subscore (from 0 [normal number of stools] to 3 [≥ 5 stools above normal]); rectal bleeding subscore (RBS) (from 0 [no blood seen] to 3 [blood alone passed]); endoscopy subscore (from 0 [normal] to 3 [severe]); and Physician's Global Assessment subscore (from 0 [normal] to 3 [severe]). A score of 3 to 5 points indicates mildly active disease, a score of 6 to 10 points indicates moderately active disease, and a score of 11 to 12 points indicates severely active disease.
b'Refractory' is defined as lack of effect at the recommended doses and for duration of treatments specified above. 'Intolerant' is defined as demonstrating serious adverse effects or contraindications to treatments as defined in product monographs. Nature of intolerance must be documented.
cInformation is based on a personal communication with the jurisdictional representative (Anne Bastarache: personal communication, December 2022).
Sources: Listing statuses are from payer formulary websites.120-141
Table 12: Dose and Duration of Therapy and Supply Limits for TIMs in UC
Dose and duration of therapy | Jurisdiction |
|---|---|
Adalimumab | |
Initial dose: 160 mg, then 80 mg at week 2, then 40 mg every 2 weeks | AB, BC, ON, NB, NL, PE, NIHB, CSC |
Initial approval period: 8 weeks | AB,a NB, NL, PE |
Initial approval period: 12 weeks | BC, NIHB, CSC |
Initial approval period: 16 weeks | NS |
Initial approval period: 6 month | VAC |
Initial approval period: 1 year | ON, YT |
Maintenance dose: 40 mg every 2 weeks | AB, BC, ON, NB, NL, PE, NIHB, CSC |
Renewal approval duration: 1 Year | AB, BC, ON, NS, NL, PE, YT, VAC, CSC |
Renewal approval duration: long term (not specified) | NB |
Supply limit: 28 day / 1 month supply per fill | AB, BC, YTb |
Infliximab | |
Initial dose: 5 mg/kg at week 0, 2, and 6 | AB, BC, ON, NL, PE, CSC |
Initial approval period: 6 weeks (3 doses) | AB, BC, ON, PE |
Initial approval period: 12 weeks | NBd, NL |
Initial approval period: 16 weeks | NS |
Initial approval period: 6 month | VAC |
Initial approval period: 1 year | ON, CSC |
Maintenance dose: 5 mg/kg every 8 weeks | ABc, BC, ON, NL, PE, CSC |
Renewal approval duration: 1 year | AB, BC, ON, NS, NL, PE, YT, VAC, CSC |
Renewal approval duration: long-term /continued coverage (duration not specified) | NB,d PE, NIHB |
Supply limit: 1 dose per prescription | AB, BC |
Supply limit: 1 month supply per fill | YT |
Golimumab | |
Initial dose: 200 mg (SC) at week 0 followed by 100 mg (SC) at week 2 | ABe, BC, NB, NL, YT, NIHB, CSC |
Initial approval period: | |
Initial approval period: 12 weeks | NB, NIHB |
Initial approval period: 16 weeks | NS, NL, CSC |
Initial approval period: 6 month | BC |
Initial approval period: 1 year | AB, YT |
Maintenance dose: 50 mg every 4 weeks | NL |
Maintenance dose: 50-100 mg every 4 weeks | ABf, BCg, NB, YT, NIHB, CSC |
Renewal approval duration: 1 year | AB, BC (if completely off steroids), NB, NS, NL, YT, NIHB, CSC |
Subsequent Renewal approval duration: 2 years | BC (if completely off steroids)h |
Renewal approval duration: long-term /continued coverage (duration not specified) | |
Supply limit: 1 dose per prescription | — |
Supply limit: 1 month supply per fill | AB, YT |
Vedolizumab | |
Initial dose: 300 mg IV at 0, 2 and 6 weeks | ON, YT, NIHB, CSC |
Initial dose: 300 mg IV at 0, 2 and 6 weeks or 2 doses of 300 mg IV with 1 dose dispensed at 0 and 2 weeks, followed by 108 mg SC at 6, 8, 10 and 12 weeks | AB, BC, NB, NL, PE |
Initial approval period: 3 doses (IV only) | BC, CSC |
Initial approval period: 14 weeks | NB, NL, NIHB |
Initial approval period: 16 weeks | NS |
Initial approval period: 6 month | ON, VAC |
Initial approval period: 1 year | ON (if completely off steroids), NL, YT, NB |
Maintenance dose: 300 mg IV every 8 weeks or 108 mg SC every 2 weeks | AB, BC, ON, NB, NL, PE, YT, NIHB |
Renewal approval duration: 1 year | AB, BC, ON (if completely off steroids), NS, PE, YT, NIHB, VAC, CSC |
Subsequent Renewal approval duration: 2 years | ON (if completely off steroids)h |
Supply limit: 1 dose IV or 2 doses SC per prescription | AB |
Supply limit: 1 month supply per fill | YT |
Supply limit: 56 days per fill for IV and 28 days for SC | BC |
Tofacitinib | |
(Initial and Maintenance) Dose: 10 mg twice daily | AB, BC, ON,i NB, NS, NL, PE, NIHB |
Initial approval period: 8 weeks | ABj, BC, ON, NIHB |
Initial approval period: 16 weeks | NB, NS, NL, PE |
Initial approval period: 6 month | VAC |
Renewal approval duration: 1 year | AB, BC, ON, NB, NS, NL, PE, VAC |
Supply limit: 1 month supply per fill | AB |
AB = Alberta; BC = British Columbia; CAF = Canadian Armed Forces; CSC = Correctional Services Canada; MB = Manitoba; NB = New Brunswick; NIHB = Non-Insured Health benefit; NL = Newfoundland and Labrador; NS = Nova Scotia; PE = Prince Edward Island; SK = Saskatchewan; VAC = Veterans Affairs Canada; YT = Yukon.
Note: Information on VAC is based on a personal communication with the jurisdictional representative (Anne Bastarache: personal communication, April 2022).
aAs an interim measure, an additional 40 mg dose of adalimumab will be provided at week 10 to allow time to determine whether the New Patient meets coverage criteria for maintenance dosing, for a total of 6 doses.
bFor the first 4 months.
cFor patients who showed a response to induction therapy then experienced secondary loss of response while on maintenance dosing with 5 mg/kg, the maintenance dose may be adjusted from 5 mg/kg to 10 mg/kg by making an additional special authorization request to Alberta Blue Cross for the increased dose.
dClaims that exceed the maximum claim amount of $9,999.99 must be divided and submitted as separate transactions as outlined here.
eAs an interim measure, an additional dose of 50 mg of golimumab will be provided at weeks 6 and 10 to allow time to determine whether the patient meets coverage criteria for maintenance dosing.
fFor patients who showed a response to induction therapy then experienced secondary loss of response while on maintenance dosing with 50 mg, the maintenance dose may be adjusted from 50 mg to 100 mg by making an additional special authorization request to Alberta Blue Cross for the increased dose.
gThe maintenance dose of 100mg every 4 weeks can be considered at the discretion of the treating physician.
hPatients who remain on steroids will be considered on a case-by-case basis.
IRecommends 5 mg twice daily for maintenance dose. But depending on therapeutic response; 10mg twice daily may also be used for maintenance in some patients. However, the lowest effective dose possible should be used for maintenance therapy to minimize adverse effects.
jAs an interim measure, coverage will be provided for additional doses of 5 mg twice daily for 4 weeks, to allow time to determine whether the New Patient meets coverage criteria for maintenance dosing.
Source: Listing statuses are from payer formulary websites.120-140
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca