CADTH Horizon Scan
Interventions Intended to Alleviate Emergency Department Overcrowding
A Compilation of New and Emerging Health Technologies and Interventions From Around the World
Jeff Mason
Sean Secord
Danielle MacDougall
Key Messages
Why Is This an Issue?
Emergency department (ED) overcrowding is a known issue in Canada that puts patients’ lives and health at risk when treatment needs within the ED exceed the resources required to address them.1
The causes and consequences of ED overcrowding are complex, varied, and extend beyond the ED.1-3 Left unchecked, ED overcrowding contributes to a deteriorating standard of care as staff become overworked and burned out.2
What Are the Potential Interventions to Address ED Overcrowding?
This roundup of 87 new and emerging interventions intended to alleviated ED overcrowding complements CADTH’s Emergency Department Overcrowding: An Environmental Scan of Contributing Factors and a Summary of Systematic Review Evidence on Interventions.4
Interventions were included in this report if they are not captured in CADTH’s complimentary report Emergency Department Overcrowding: An Environmental Scan of Contributing Factors and a Summary of Systematic Review Evidence on Interventions4 because they are either new or are not yet in wide use in EDs and health systems across Canada and could be reasonably be expected to affect ED overcrowding (e.g., by improving patient flow through the ED or reducing the number of people seeking care in the ED). Interventions that could address multiple causal factors (e.g., e-consult services) were also included.
What Is the Potential Impact?
Decreasing ED overcrowding has the potential to improve the standard of care delivered to those accessing EDs and contribute to decreasing the burden on ED staff, regardless of the intervention or which contributing factor it aims to act upon.
Some interventions that can alleviate ED overcrowding also have an impact on primary and community care; bolstering preventive care, increasing access to diagnostic testing for those who need it, and improving access to health care supports can improve health outcomes.
What Else Do We Need to Know?
The pan-Canadian issue of ED overcrowding calls for real solutions. CADTH is examining the evidence and expert-informed considerations and producing a series of publications about the causes and consequences of, and solutions to, ED overcrowding in health care systems across the country.
The interventions identified in this report may be of interest to senior health care decision-makers who are anticipating health system innovation and transformation.
Introduction
CADTH’s Horizon Scanning Service identifies and monitors new and emerging health technologies likely to have a significant impact on health care in Canada. The service scans and monitors health information sources to identify potentially important health technologies not yet widely used in Canadian health care systems. Summaries of current information about the use, effectiveness, cost, and implementation of these technologies are published regularly in CADTH Horizon Scan reports.
Purpose
This report complements CADTH’s Emergency Department Overcrowding: An Environmental Scan of Contributing Factors and a Summary of Systematic Review Evidence on Interventions.4 It identifies interventions intended to alleviate ED overcrowding not captured in the summary of systematic review evidence documented in this complementary report because they are new to, or are not yet in wide use in, EDs and health systems across Canada. The evidence behind the interventions included in this report was not assessed for quality. When available, research findings related to the interventions identified are reported; however, the purpose of this report is primarily the identification of new and emerging interventions.
The resulting report is a compilation of 87 new and emerging interventions published in articles, reports, conference abstracts, clinical trial registries, and other public sources of information (e.g., hospital websites) between 2018 and the first 7 months of 2023. This report uses a conceptual model developed by Asplin et al. (2003)5 that divides the emergency care system into 3 interdependent parts: input (arrival to the ED), throughput (flowing through the ED), and output (leaving the ED). The interventions are organized by the contributing factor to ED overcrowding (as reported in CADTH’s environmental scan),4 they are most intended to address. Eighty of the new and emerging interventions are distributed across 26 of the 42 categories of contributing factors. The remaining 7 interventions potentially address more than 1 factor. Figure 1 shows the percentage of interventions identified for each of 5 broad categories of factors contributing to ED overcrowding:
input factors (those that influence the need for ED services and relate to patient access to the ED5)
throughput factors (those that are focused within the ED5 and aim to encourage the appropriate and efficient flow of people and care throughout the ED)
output factors (those that concern patient disposition5 or the efficient discharge of people from the ED)
contextual factors (those that exist outside of the input, throughput, output groups)
interventions addressing multiple contributing factors.
Interventions from Canada are identified with a maple leaf icon throughout this report.
Figure 1: Percentage of New and Emerging Interventions Intended to Alleviate ED Overcrowding by Broad Contributing Factor
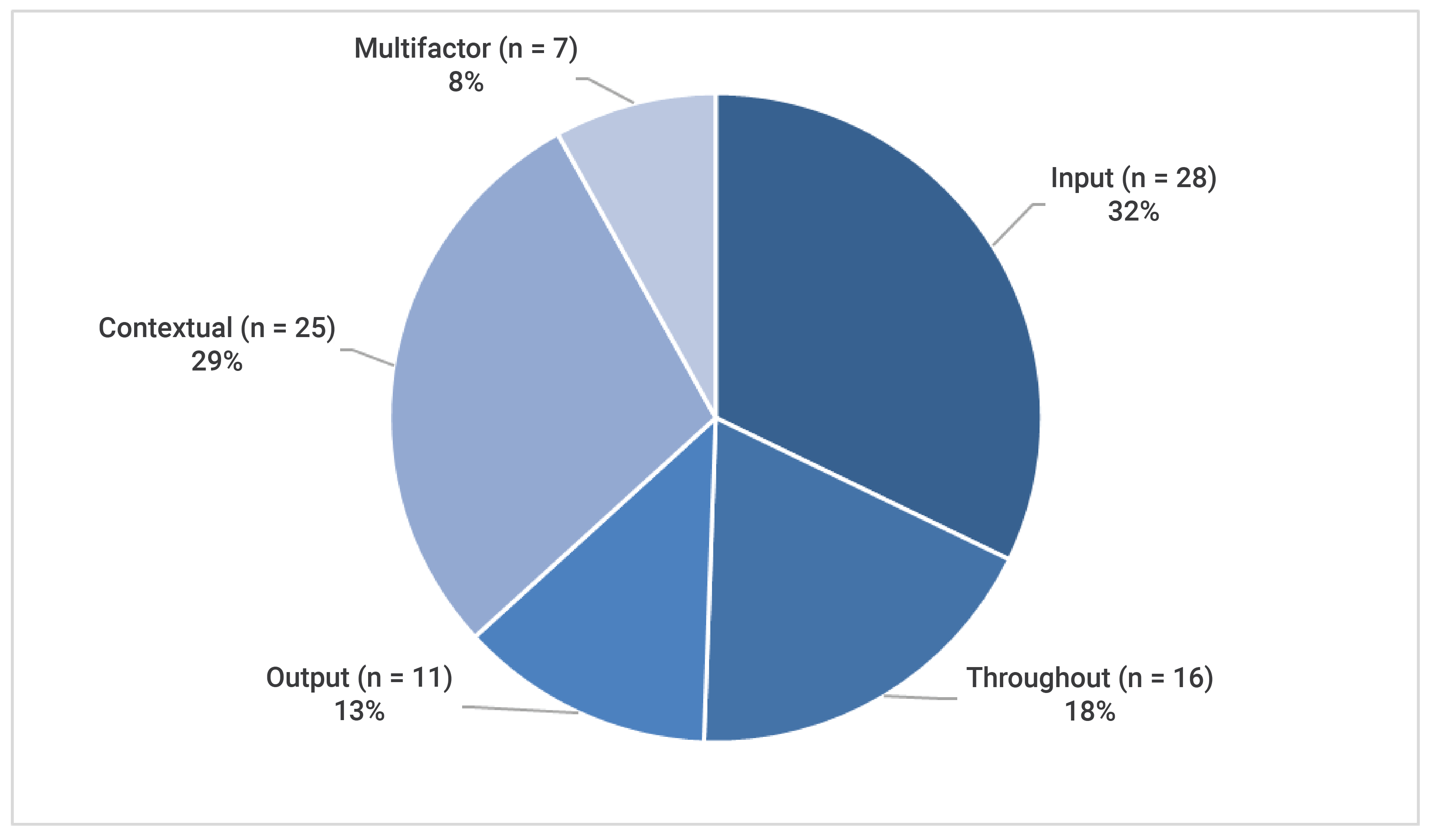
ED = emergency department.
Inclusion, Equity, Diversity, and Accessibility
As part of CADTH’s commitment to inclusion, equity, diversity, and accessibility, an equity lens is applied to CADTH reports and work. People from equity deserving groups may be disproportionately impacted by the effects of ED overcrowding. Some of the interventions identified in this report were intended to support the health and wellness of some equity deserving groups, including people experiencing houselessness, people with mental health needs, people with disabilities, children and youth, older adults (including residents of long-term care facilities), people without access to a primary care provider, and people living in rural and remote communities. CADTH recognizes that there are equity deserving groups who were not represented in the interventions identified in this report.
Not all equity deserving groups that may be disproportionately impacted by the effects of ED overcrowding were clearly represented in the interventions identified in this report. This does not mean people in these groups were not being served by the programs and services identified or included in the studies reviewed. Rather, they were not clearly identified as a group the intervention was intended to support. Equity deserving groups that do not appear to be supported by the interventions identified in this report include Indigenous people, Black people, people of colour, newcomers to Canada, members of the 2SLGBTQ+ community, people for whom English or French is not their first language, and people living in lower income households.
Input Factors Contributing to ED Overcrowding
Input factors are those that influence the need for ED services and relate to patient access to the ED.5 They are also described as factors that cannot be controlled by the ED.6 CADTH’s environmental scan categorized input factors into the following themes: primary care and community health services, repeated visits and low acuity visits to the ED, growing patient volume and complexity of needs (e.g., increasingly severe or complicated care needs of people attending the ED), and access via multiple avenues.4 Using this framework, 28 interventions were identified across 8 input factors contributing to ED overcrowding (Figure 2).
Primary Care and Community Health Services
Community and Outpatient Care Service Issues
Mobile Integrated Health Response Teams
In Thorold, Ontario, paramedics at the Niagara Emergency Medical Services formed an integrated interdisciplinary health team that works with local community groups to deliver patient-centred visits at home 24 hours a day, 7 days a week. The goal of this program is reduce the number of patients visiting the ED with low acuity needs, avoid using ambulance services when possible, and reduce or delay the need for long-term care or hospitalization.7,8 In Alberta, community paramedics are receiving extra training in areas such as gerontology, palliative care, and transfusion medicine to provide short-term management of low-acuity illnesses safely and effectively in the community.9 A similar approach is being studied in Italy where researchers are seeking to prevent ED visits and hospital admissions of people living in long-term care homes.10
Neighbourhood Model
The neighbourhood model is an approach to personal support care where personal support workers (PSWs) are employed on a full-time salary to deliver care in the community. This approach allows PSWs to provide care more frequently, based on individual needs, while also reducing missed visits and staff turnover.8 In Hamilton, the St. Joseph’s Home Care Neighbourhood Model for Seniors at Risk offers an onsite team of PSWs and cleaners to work with seniors living in a City of Hamilton–managed apartment building to offer services such as housekeeping, personal support (e.g., dressing and undressing, help with premeasured medications), crisis intervention, and personal care (e.g., bathing).11
Community Support Teams
In Alberta, CONNECT is a community support for to people in the province’s northern communities who are living with intellectual and developmental disabilities and mental illness, as well as their caregivers and care providers. The program’s services include crisis support, assessments, relationship building between families and services, supporting individuals who are moving from the hospital to the community, and helping clients access the services they need.12
Figure 2: New and Emerging Interventions That Address Input Factors Contributing to ED Overcrowding
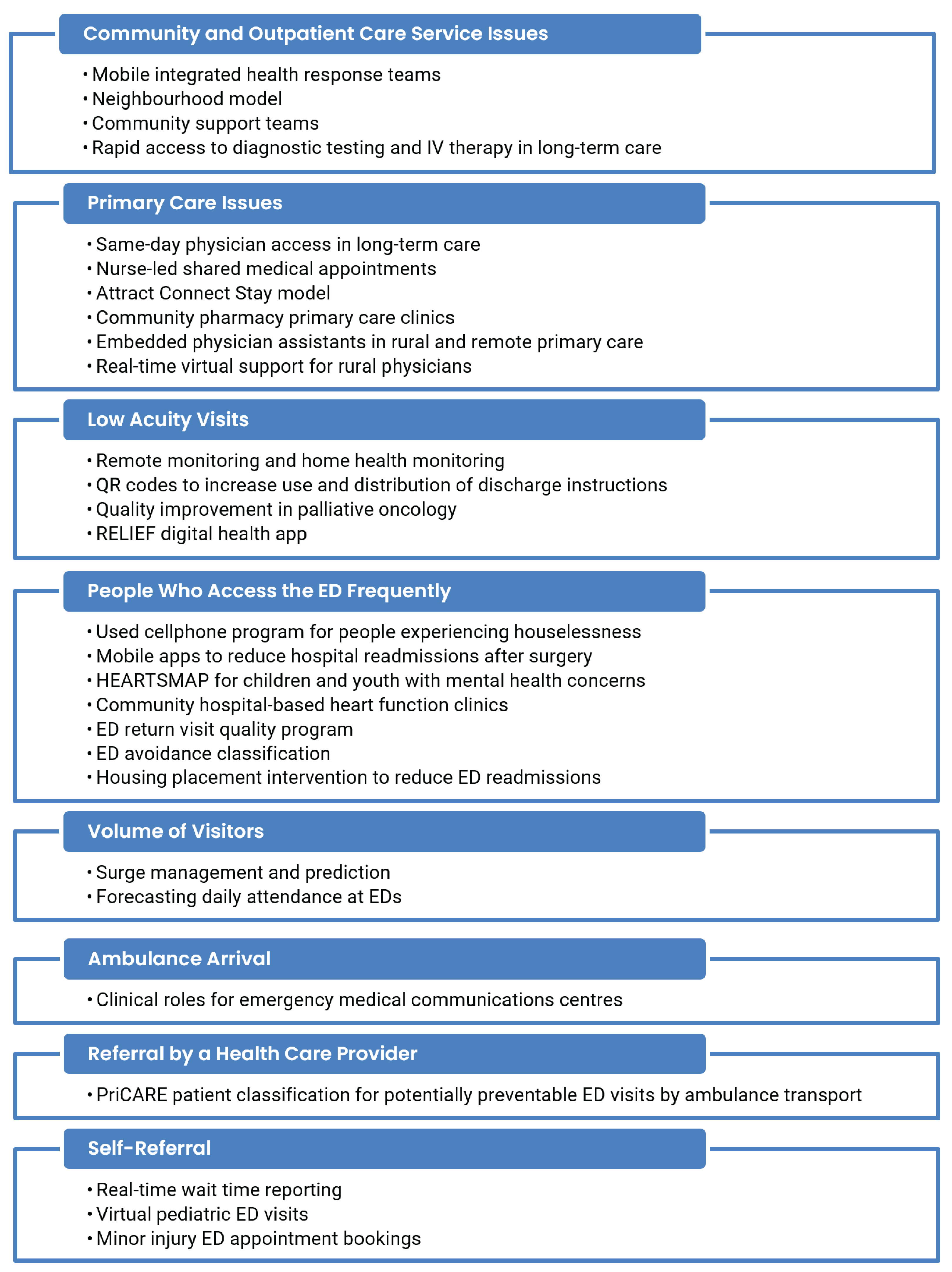
ED = emergency department; PriCARE = Primary Care–like Ambulance transports following Response for 911-Emergencies.
Rapid Access to Diagnostic Testing and IV Therapy in Long-Term Care
Timely access to diagnostic testing and IV therapy may help reduce the need for ED services for people living in long-term care. To understand the potential impact of long-term care homes providing rapid access to services such as blood tests, X-rays, urine culture, and IV therapy, researchers in Ontario surveyed long-term care homes and looked for associations between the services they offered and health administration database data. Rapid access to these services was found to reduce ED visits and expanding access could help more long-term care residents stay at home.13 Pilot projects that are meant to provide faster and more convenient access to diagnostic services such as X-rays and ultrasounds have also been announced by the government of Ontario at Humber River Hospital (Toronto) and the Royal Victoria Regional Health Centre (Barrie).14
Primary Care Issues
Same-Day Physician Access in Long-Term Care
Timely access to physicians may help reduce the need for ED services by people living in long-term care. To understand the potential impact of same-day physician access in Ontario long-term care homes, researchers in Ontario surveyed long-term care homes and looked for associations between the services they offered and health administration database data. They estimated that 1 in 6 ED visits could be avoided if long-term care homes had same-day physician access.15
Nurse-Led Shared Medical Appointments
With the goal of improving access to care and reducing health resource use by people with gastroesophageal reflux disease, dyspepsia, and irritable bowel syndrome, researchers in Calgary explored the potential impact shared medical appointments could have on patient care.16 Compared with usual care, the researcher found that patients who received nurse-led shared medical appointments had shorter wait times, fewer endoscopic exams, fewer re-referrals to gastroenterology, and reduced ED visits.
Attract Connect Stay Model
Developed in Marathon, Attract Connect Stay is an approach to rural clinician recruitment and retention. The model focuses on creating community-centred strengths-based approaches to recruitment and retention; it is supported by a Health Workforce Recruiter Connector hired by the local community to provide supports to interested candidates.17
Community Pharmacy Primary Care Clinics
In a pilot project, a partnership between the government, Nova Scotia Health, and the Pharmacy Association of Nova Scotia is working together to offer community pharmacy-based primary care clinics in areas of the province with the highest number of people without a family doctor. The pharmacist-led clinics will provide assessment and prescribing services for conditions such as strep throat, pink eye, diabetes, and chronic obstructive pulmonary disease. Prescription renewals and vaccinations will also be offered.18
Embedded Physician Assistants in Rural and Remote Primary Care
As part of its rural and remote clinician retention strategy, Ongomiizwin Health Services (Winnipeg) developed the physician extender program, which embeds physician assistants in primary health care teams in 1 hospital and several fly-in communities in remote areas of the province.19
Real-Time Virtual Support for Rural Physicians
In British Columbia, the Rural Coordination Centre of British Columbia connects rural care providers, including physicians, nurses, and midwives, to a network of on-call peers using real-time virtual care services (e.g., Zoom or phone). The Instant Access and Quick Reply pathways are provided at no cost to practitioners in rural, remote, and First Nations communities across the province for all urgent and low acuity cases, and offer peer support for specialist consultations, second opinions, and ongoing patient support. The potential benefits of the program include improved recruitment and retention, strengthened community practice, and reduced isolation of health care providers.20
Repeated Visits and Low Acuity Visits to the ED
Low Acuity Visits
Please note that while CADTH’s environmental scan identified low acuity visits in the literature as a factor contributing to ED overcrowding, we acknowledge that there is also evidence that patients with low acuity presentations have minimal impact on ED overcrowding. We also understand that low acuity visits to the ED are valid and varied.
Remote Monitoring and Home Health Monitoring
TEC4HOME Heart Failure is a remote monitoring program for people living with heart failure in British Columbia that is part of a 4 year research initiative to understand the impact of the program on ED visits, hospital admissions, and quality of life.21 People enrolled in a feasibility study for the program received a home health monitoring kit provided by Telus Health that includes a touch screen tablet computer and connected devices to measure blood pressure, oxygen saturation, and body weight. People enrolled in the program submit daily biometric measurements and responses to questions about their symptoms to a monitoring platform that alerts a monitoring nurse to changes such as rapid weight gain that may indicate a need for medication adjustments. The monitoring nurse also provides self-management education and advance care planning.22 A similar program for people living with chronic obstructive pulmonary disease is also being evaluated.23
QR Codes to Increase Use and Distribution of Discharge Instructions
Effective ED discharge instructions can support patient safety and satisfaction and help reduce the number of preventable ED return visits but may not be provided to all patients. To increase the provision of discharge instructions and reduce barriers for staff, the Vancouver General Hospital placed QR codes linked to relevant discharge instructions in treatment rooms throughout the unit. The QR codes could be used by staff to help patients access the resources directly or send them to the patient via a deidentified text or email service.24
Quality Improvement in Palliative Oncology
To reduce ED visits by people receiving palliative care and improve their end-of-life care, the Odette Cancer Centre in Toronto implemented a model for improvement intervention intended to reduce monthly ED visits by patients enrolled in the centre’s palliative care clinic by 20% over 1 year. By improving access to after-hours hospital and home care, researchers found the quality improvement intervention reduced the rate of ED visits by 24%.25
RELIEF Digital Health App
The RELIEF (Remote Self-Reporting of Symptoms by Patients with Palliative Care Needs) app is web-based application that allows patients receiving palliative care to self-report daily symptoms with the goal of improving communication between the patient and their care team to ensure they can remain at home and receive timely adjustments in their care. Alerts triggered by the app can also be used by the care team to determine if a visit to the ED is needed. Use of the app has been studied at the Brampton Civic Hospital.26
People Who Access the ED Frequently
Used Cellphone Program for People Experiencing Houselessness
Seeking to improve access to follow-up care and reduce the need for return ED visits, ED physicians at University Health Network (Toronto) started a program called Phone Connect that collects prepaid cell phone donations and provides them to people who visit the ED and are houseless, struggling with mental health or substance use, or socially isolated.27
Mobile Apps to Reduce Hospital Readmissions After Surgery
ED visits and hospital readmissions often occur following surgeries. Mobile apps may help avoid these additional visits. To improve patient care after hospital discharge, the thoracic surgery team at St. Joseph’s Health Care Hamilton developed a mobile app to support patients and their families during the initial discharge phase of their home care. The app provides users with education resources, self-care reminders (e.g., for upcoming appointments, daily exercises), and asks them to complete a daily symptom survey. Survey results are monitored by a program nurse who is alerted to any concerning symptoms for follow-up.28 Researchers at The Ottawa Hospital plan to study how2trak, a mobile app for self-assessing signs of surgical site infection following colorectal surgery.29 A similar study is also planned by researchers at Mount Sinai Hospital (Toronto).30
HEARTSMAP for Children and Youth With Mental Health Concerns
To help reduce variability in the assessment and management of children presenting to the pediatric ED with mental health concerns, researchers at the BC Children’s Hospital (Vancouver) implemented HEARTSMAP, an electronic tool to support physicians with psychosocial assessments and disposition decision-making. Use of HEARTSMAP was found to reduce ED length of stay and return visits for pediatric mental health concerns.31
Community Hospital–Based Heart Function Clinics
Heart function clinics for people living with heart failure may help improve care and avoid ED visits and hospital readmissions. A cohort study of people in central Ontario living with heart failure reported that individuals referred to the local community hospital heart function clinic had better fewer all-cause and heart failure–related ED visits compared with individuals who were not referred to the clinic, despite living with more comorbidities than their peers.32
ED Return Visit Quality Program
Ontario’s Emergency Department Return Visit Quality Program is a continuous quality improvement program that mandates that the largest EDs in the province conduct chart audits of some patients who return within 72 hours of being admitted to the hospital and all patients who return within 7 days with acute myocardial infarction, subarachnoid hemorrhage, and pediatric sepsis who are admitted to hospital. The purpose of the program is for hospitals to identify the underlying causes of the return visits to develop interventions to address and prevent them in the future.33,34 Seventy-two–hour readmission audit and feedback has also been evaluated in Calgary.35
ED Avoidance Classification
These authors outline a study that has taken place in 2019 in Hamilton, Ontario, (not published at the time of this writing) in which ED charts are retroactively assessed through a standardized tool to determine which patient who were seen in the ED could have been effectively assessed and cared for virtually or in an alternative subacute setting.36
Housing Placement Intervention to Reduce ED Readmissions
To understand how housing placement may impact the frequency of ED readmissions by people with mental health needs who are experiencing houselessness, a researcher in California evaluated a program that connected individuals to housing (e.g., shelters, room and board, or board and care) upon their discharge from the ED. Over a 3-month period, the program reduced readmissions for the 30 individuals enrolled.37
Growing Patient Volume and Complexity of Needs
No interventions intended to address the complexity of needs or increase in older adult patients input factors were identified.
Volume of Visitors
Surge Management and Prediction
High uncertainty about demand for ED services can make planning appropriate resource levels in the ED very challenging. Surge management and prediction tools and strategies may offer ED administrators solutions to the ongoing causes of ED overcrowding.38-40 At sites across Newfoundland and Labrador researchers are using SurgeCon,41 a home-grown quality improvement initiative using ED and hospital data to apply real-time protocols to manage surges in ED visits before they occur, reducing ED length of stay.42,43 At Niagara Health – St. Catherine’s Site (Ontario) patient flow simulation exercises were used to help an interdisciplinary team decide where to offload ambulance arrivals and transfer patients needing a bed.44 In Toronto the Hospital for Sick Children and St. Michael’s Hospital have both used forms of machine learning and artificial intelligence to understand when surges will happen in their EDs.45,46
Forecasting Daily Attendance at EDs
To help plan for the best use of ED resources and manage patient flow, researchers at a hospital in Lille, France, used time-series analysis to develop forecasting models based on retrospective daily pediatric ED attendance with the goal of accurately predicting daily demand for ED services.47 Moving these models from theory to practice, researchers in Finland developed a prospective ED crowding warning system to provide real-time hourly predictions.48 As more examples of predictive models emerge, researchers in Finland are also seeking to understand their accuracy.49
Access Via Multiple Avenues
Ambulance Arrival
Clinical Roles for Emergency Medical Communications Centres
Through a rapid scoping review, researchers from Dalhousie University (Halifax) sought to understand how clinicians are supporting the work of emergency medical communications centres matching resources to patients’ needs. Roles for nurses, paramedics, and physicians were identified. These clinicians supported emergency medical services staff with patient triage, advice, referral to nonemergency care, and peer-to-peer counselling. Alternatives to emergency care included self-care and referrals to general practitioners, pharmacists, and outreach programs.50
Referral by a Health Care Provider
PriCARE Patient Classification for Potentially Preventable ED Visits by Ambulance Transport
The PriCARE (Primary Care–like Ambulance transports following Response for 911-Emergencies) classification system is being developed by researchers in Ontario to help inform ED diversion protocols for ambulances transporting patients with nonemergent conditions who may be suitable for care at facilities offering subacute care (i.e., facilities providing primary care or multidisciplinary care for patients without immediate or acute care needs) rather than EDs.51
Self-Referral
Real-Time Wait Time Reporting
Reporting and displaying real-time ED wait times is a strategy that may help manage the expectations of people waiting in the ED for low acuity care or encourage patients to attend neighbouring EDs with shorter wait times.52,53 A 2022 scoping review looking at reporting of ED wait times in facilities across Canada to understand how widespread the practice is across the country and document the features of and information shared by wait time reporting systems used in Canada. The authors of this review concluded that wait time reporting is emerging as a practice in Canadian health systems and research into its effectiveness is needed.54
Virtual Pediatric ED Visits
During the early days of the COVID-19 pandemic, virtual care options emerged for services where they had not previously been used, including emergency care. At the Children’s Hospital of Eastern Ontario (Ottawa) a virtual pediatric ED was developed using secure video conferencing software embedded into the hospital’s EMR.55 Similarly, the Montreal Children’s Hospital’s pediatric ED implemented the WAVE (Waiting Room Assessment to Virtual Emergency Department) pathway using video-based telemedicine for some patients who were not critical, which was found to be both feasible and an acceptable way to deliver care.56
Minor Injury ED Appointment Bookings
The Royal Victoria Regional Health Centre (Barrie) announced a pilot project that allows the public to book a same-day or next-day arrival time with the ED to be assessed and treated for minor injuries such a sprains, strains, or potential simple fractures to a limb. The project uses an online booking system and offers multiple booking times from Monday to Friday following completion of an assessment questionnaire. The goal of the pilot project is to reduce wait times for these services and avoid overcrowding during busy times.57
Throughput Factors Contributing to ED Overcrowding
Throughput factors are those that are focused within the ED.5 CADTH’s environmental scan categorized throughput factors into the following themes: consultation, testing, and decision delays; staffing considerations; and operational inefficiencies.4 Using this framework, 16 interventions were identified across 6 throughput factors contributing to ED overcrowding (Figure 3).
Consultation, Testing, and Decision Delays
No interventions intended to address the consultations for people visiting the ED throughput factor were identified.
Diagnostic Testing and Procedures
Evidence-Informed Practice Change
A multisite study was conducted at 6 centres in Western Canada to determine an evidence-based approach to treating atrial fibrillation, the most common heart arrhythmia seen in EDs. A stringent research strategy was employed to ensure the validity of the results, which showed that using the sedated synchronized cardioversion approach was equally safe but resulted in twice as many patients being ready for discharge from the ED within 4 hours.58
Disposition Decision Delays
Group-Facilitated Audit and Feedback
This study, conducted in Calgary, sought to increase quality of care in EDs for pediatric patients with bronchiolitis through chart audits and pediatrician feedback. An assessment of pre- and post-intervention care revealed a statistically significant improvement in quality of care in EDs.59
Canadian Syncope Risk Score
Ottawa-based clinics are validating the Canadian Syncope Risk Score, which has been in development for more than a decade. This tool helps to differentiate serious from benign causes of syncope when patients arrive at the ED after a loss of consciousness, as well as assess the impact on ED wait times, resources, and patient safety.60
Barriers to Optimal Operational Efficiency
No interventions intended to address the patient processing throughput factor were identified.
Patient Triaging
Triage Kiosks
A review of 9 articles studied the use of patient-accessed ED kiosks to assist with self-triage to help alleviate ED pretriage wait times. Six of the 9 articles showed positive findings related to this strategy, with the main negative finding of the other 3 articles being low patient uptake.61
Machine Learning to Predict 30-Day Readmissions
These researchers investigated the accuracy and applicability of a decision tree-based machine learning model to predict patient readmission to the hospital and found a 94% accuracy for 30-day admissions. With this model, hospital administrators and decision-makers are better able to allocate resources to help reduce ED overcrowding through the reduction of patients returning to the ED after hospital discharge.62
Machine Learning Decision Support System for Patient Triage
A clinical trial conducted in New Zealand in 2021 and 2022 examined a decision support system at ED triage to predict hospital admission and longer ED length of stay using routinely collected data. This tool can help decision-makers and caregivers with resource allocation to improve efficiencies and quality of ED care.63
Artificial Intelligence-Assisted Triage
A proposed study of the Mediktor hospital tool to validate its ability to consistently and accurately triage patients with gynecological and obstetrical needs to help reduce the resource demands of triage on nursing staff.64
Machine Learning to Predict Patient Admission Status
These authors explore a framework for optimizing machine learning algorithms and forecast its applicability and practicality in predicting patients’ needs for hospital admission. Fifty-four models are developed and compared and found to show great promise in predicting patient needs, possibly alleviating crowding issues.65
Mobile Self-Triage
In conjunction with an Ottawa hospital, an app called Symptoms Pal was developed and studied. The app guides the user through a series of questions to help differentiate who needs immediate help through an ED and who can wait for a primary care appointment or attend to their symptoms through self-care.66
Figure 3: New and Emerging Interventions That Address Throughput Factors Contributing to ED Overcrowding
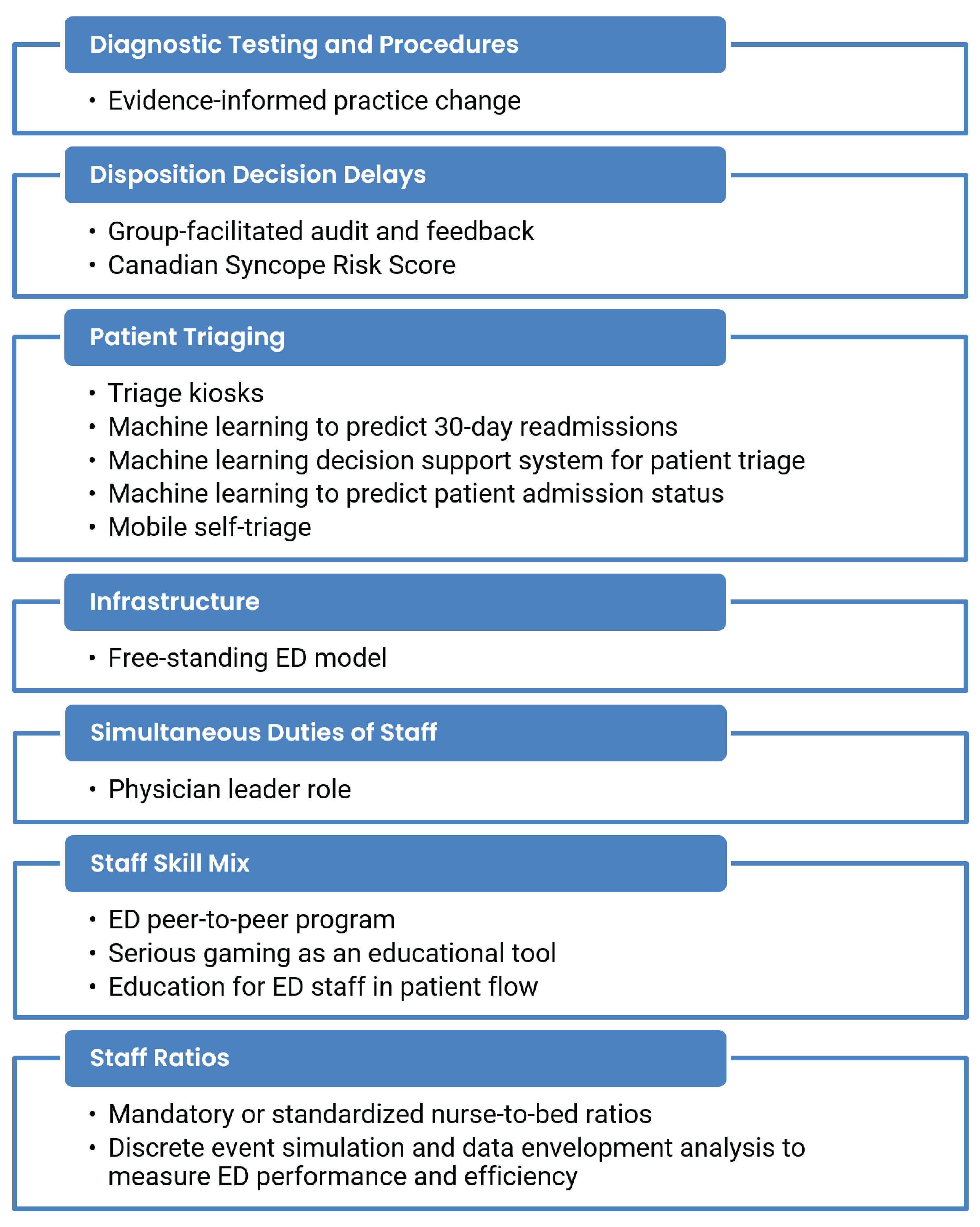
ED = emergency department.
Infrastructure
Free-Standing ED Model
With the effects of ED overcrowding on the whole hospital system in mind, these authors explored the free-standing ED model (i.e., an ED that is not structurally connected to a hospital with inpatient services) through the review of 23 papers and 12 case studies. Several structural and functional layouts are explored, analyzed, and compared among free-standing ED units in France, Spain, Sweden, Italy, and the US. The strengths and limitations are reviewed through this explorative study.67
Simultaneous Duties of Staff
Physician Leader Role
Pre- and post-physician lead role implementation was studied in 2 tertiary Alberta hospital EDs, examining ED length of stay, emergency medical services hallway length of stay, physician initial assessment time, 72-hour readmission rates, and left without being seen rates. Themes in provider feedback were related to facilitated patient flow, provider workload impacts, and patient safety, but varied between the 2 sites studied.68
Staffing Considerations
Staff Skill Mix
ED Peer-to-Peer Program
The ED peer-to-peer program exists to provide ED physicians with immediate on-demand coaching and support for all types of patient presentations, ages, and acuity across Ontario. This resource was initiated in October 2022 for rural and remote physicians, and then expanded to all departments in June 2023. ED peer physicians are available 24 hours a day, 7 days a week to assist ED physicians with problem solving, approach, assessments, diagnosis, and treatments.69
Serious Gaming as an Educational Tool
As EDs evolve, clinicians may need to develop new skills and competencies to manage the demands of higher patient volumes and patients with increasingly complex needs. Serious games (a genre of gaming intended to be both fun and educational) is an approach to training that could be adopted by new emergency clinician educators to help ensure they have the skills needed to work in today’s ED environment. One example is McMaster University’s (Hamilton) GridLockED, a serious game designed to help teach medical learners about teamwork and communication, patient flow, and roles in the ED.70,71
Education in Patient Flow for ED Staff
Patient flow through the emergency department is known to be important, but there has been limited academic inquiry into the skills and training needed for ED staff related to patient flow. Through a modified Delphi approach, the authors of this study reviewed the literature to identify 19 skills, 9 training strategies, and 12 training modalities, and included 39 and 28 participants in 2 rounds of study, respectively. They concluded that ED staff education on patient flow includes focusing on decisions that improving flow, managing patient backlog and surge, improving leadership skills and situational awareness, and allowing staff to work more effectively as a team.72
Staff Ratios
Mandatory or Standardized Nurse-to-Bed Ratios
As a global independent authority on health care technology and safety, ECRI released a postpandemic report on nurse-to-patient ratios in the ED and their effect on patient safety and outcomes. Six studies were reviewed, and the authors concluded that the evidence consistently showed a relationship between nurse staffing levels and patient care quality. However, the authors noted that, because the evidence is limited, the relationships between staffing levels and outcomes is unclear.73
Discrete Event Simulation and Data Envelopment Analysis to Measure ED Performance and Efficiency
This study uses a discrete event simulation model to explore various resource allocation configurations for the ED environment and their impacts on desirable versus undesirable outcomes. Thirty-five potential configurations were examined and 21 were found to increase efficiencies or capabilities and/or decrease undesirable outcomes. The authors suggested this model and approach may assist health care decision-makers with resource and facility management.74
Output Factors Contributing to ED Overcrowding
Output factors are those that concern patient disposition (e.g., to inpatient or outpatient care).5 CADTH’s environmental scan categorized output factors into the following themes: access block (when patients are unable to access appropriate hospital resources75) and boarding (the practice of holding admitted patients in the ED75,76), strained hospital-wide resources, and impediments to exiting the ED.4 Using this framework, 11 interventions were identified across 5 output factors contributing to ED overcrowding (Figure 4).
Access Block and Boarding
Access Block
Discharge Lounges
A discharge lounge is a place for patients to wait for a final treatment, transfer, or other intervention before leaving the hospital. Establishing this space allows ED rooms to become available sooner. A computer simulation study conducted with data from the Al-Zahra hospital (Iran) shows promise in making more efficient use of ED space and resources.77 The London Health Sciences Centre (London, Ontario) announced the opening of a discharge lounge at its University Hospital site in 2019.78
Changing Time of Discharge
The Sax Institute was commissioned to review published literature for solutions to access block, allowing expediency for patients requiring admission to the hospital from the ED. One such intervention is to orchestrate hospital resources and processes toward the expedited discharge of patients ready to leave the hospital, and doing so early in the day.79
Figure 4: New and Emerging Interventions That Address Output Factors Contributing to ED Overcrowding
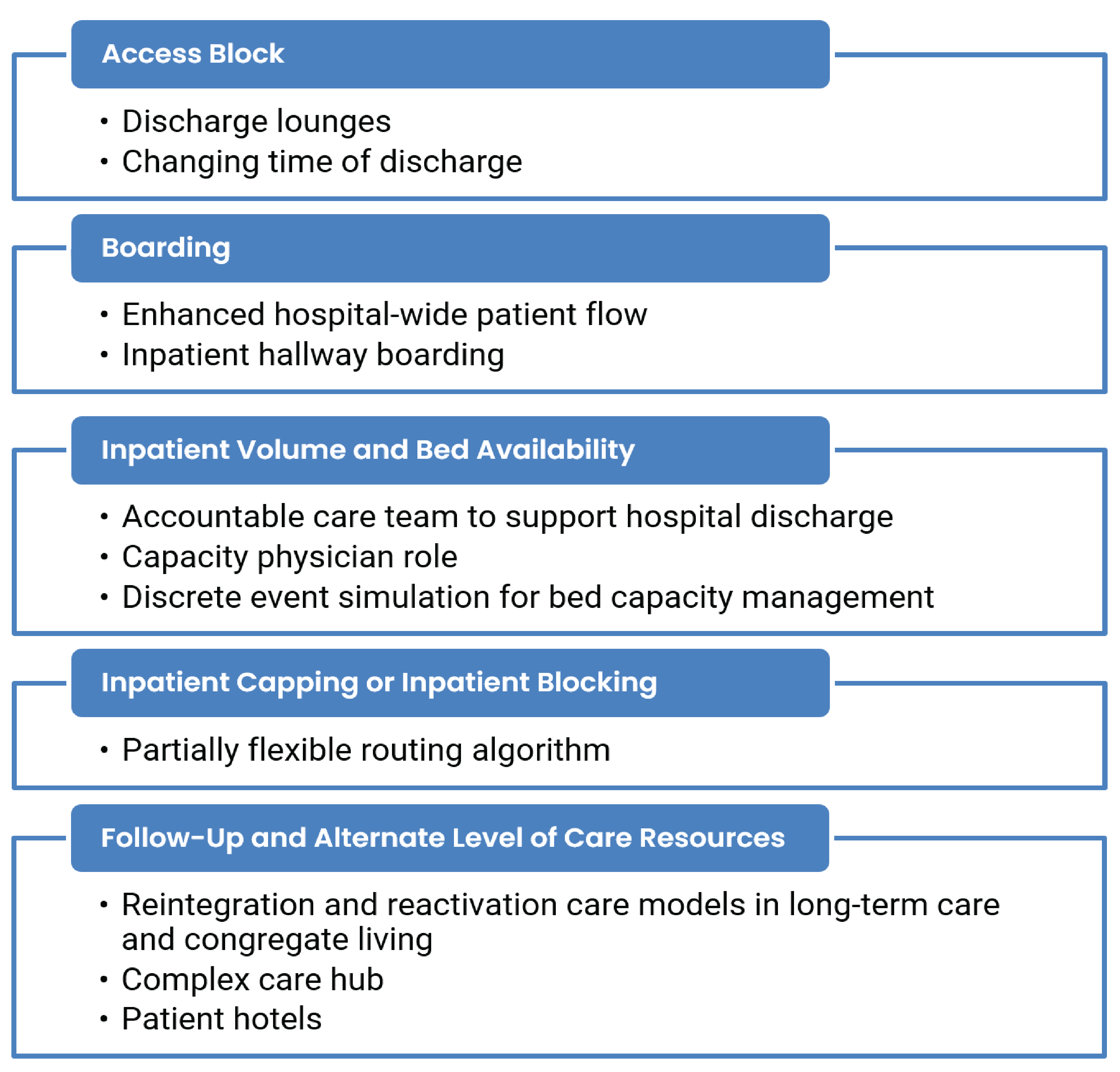
ED = emergency department.
Boarding
Enhanced Hospital-Wide Patient Flow
Multidisciplinary rounding was found to improve communication and collaboration in a large level 1 trauma, tertiary, regional transfer centre located in the southeastern US. This led to increased hospital-wide patient throughput by expediting discharges and helping prevent access block to ED admissions.80
Inpatient Hallway Boarding
This commentary related to the US system asserts that the cause of ED overcrowding is misaligned health care economics and financial pressures. Through a review of the literature, the authors list several solutions to remedy ED overcrowding, including temporary boarding of patients on the ward as opposed to within the ED, which frees up ED space and resources, and is preferred by the patients, according to these authors.75
Demand on Hospital Resources Outside the ED
No interventions intended to address the gravity of inpatient care needs or staffing resources outside of the ED output factors were identified.
Inpatient Volume and Bed Availability
Accountable Care Team to Support Hospital Discharge
This is a pilot study of an Accountable Care Team aimed at taking a multidisciplinary, unit-based approach to identifying quality improvement opportunities, addressing inefficiencies, and assuring progress on hospital throughput to timely, effective, patient-centred discharge. The pre- and post-implementation study showed significant improvements in the use of this team with earlier discharges from the unit, allowing rooms and resources for ED admissions.81
Capacity Physician Role
A prospective observational study of the implementation of a capacity physician — a role to aid in patient access, progress of care, and discharge. This role was created because of capacity levels in the ED, communication and coordination gaps across clinical services, and capacity issues on the wards. Implementation of the role reduced patient length of stay, facilitated hospital transfers, helped reduce waiting times for ED admissions, and was deemed to be a success.82
Discrete Event Simulation for Bed Capacity Management
Simulation scenario testing was undertaken to optimize hospital bed numbers, reduce length of stay, reduce discharge delays, and evaluate alternative solutions to bed management. Over occupancy and bottlenecks on the wards, particularly the surgical ward, was found to be a problem affecting hospital flow and ED overcrowding. The optimal solution was deemed to be an inpatient bed occupancy of 70% to 85%.83
Impediments to Exiting the ED
No interventions intended to address the transport delays and inefficient care transfer processes output factor were identified.
Inpatient Capping or Inpatient Blocking
Partially Flexible Routing Algorithm
A partially flexible routing algorithm is a model to assist in assigning patients admitted to the ED to inpatient wards. The partially flexible system, as examined through this simulation study, expedites admissions while preserving quality care and staff satisfaction.84
Follow-Up and Alternate Level of Care Resources
Reintegration and Reactivation Care Models in Long-Term Care and Congregate Living
Pine Villa is a supportive transitional home in Toronto geared toward patients who no longer need acute care hospital resources, but lack home or community supports or are awaiting long-term care facility availability.8,85 “Reactivation care centres” in the Greater Toronto Area specialize in activation therapies that are meant to support patients who no longer require acute care in their transition back to home or who are moving to an alternate level of care.86
Complex Care Hub
The complex care hub is a service that supports patients who need care and monitoring by providing it in their homes with the support of a community paramedic, a nurse navigator, and a general internist, as well as safety protocols and communication channels.87
Patient Hotels
With a hotel room costing far less than an acute care hospital bed, patients residing in the latter who no longer need hospital services but are awaiting a long-term care facility or other arrangement could take advantage of supportive care provided in hotel beds, as has been implemented in some countries.88
Contextual Factors Contributing to ED Overcrowding
Contextual factors are those that exist outside of the input-throughput-output categories. These factors may be applicable at the ED level (micro-level factors); hospital- or health system–wide level (meso-level factors); or broader socioeconomic, sociocultural, and institutional level (macro-level factors). Using this framework, 25 interventions intended to address meso-level contextual contributing factors were identified (Figure 5).
No interventions intended to address micro-level contextual factors (i.e., ED closures and crisis fatigue) or macro-level contextual factors (i.e., insurance policies, lack of political will, population growth and shift, and seasonality and temporal patterns) were identified.
Meso-Level Contextual Factors
Meso-level contextual factors are those that are applicable at the hospital-wide and the health system levels. CADTH’s environmental scan used the Consolidated Framework for Implementation Research (CFIR) construct of the Outer Setting domain to help inform this category. As defined in the CFIR, the Outer Setting is “the setting in which the inner setting exists, and that there can be more than one level within the Outer Setting.”89 The environmental scan identified 2 levels belonging to the Outer Setting: the hospital and the health system. The ED exists within both settings. Nine categories of meso-level contextual factors were identified in the environmental scan: limited post-acute care and alternate level of care resources, elective surgeries, limited health resources, entrenched hospital culture, limited resources for mental health and substance use, community hospital closures, limited inpatient workforce, limited care hours, and misalignment of leadership and priorities.4
No interventions intended to address the community hospitals closures or misalignment of leadership and priorities meso-level contextual factors were identified.
Figure 5: New and Emerging Interventions That Address Meso-Level Contextual Factors Contributing to ED Overcrowding
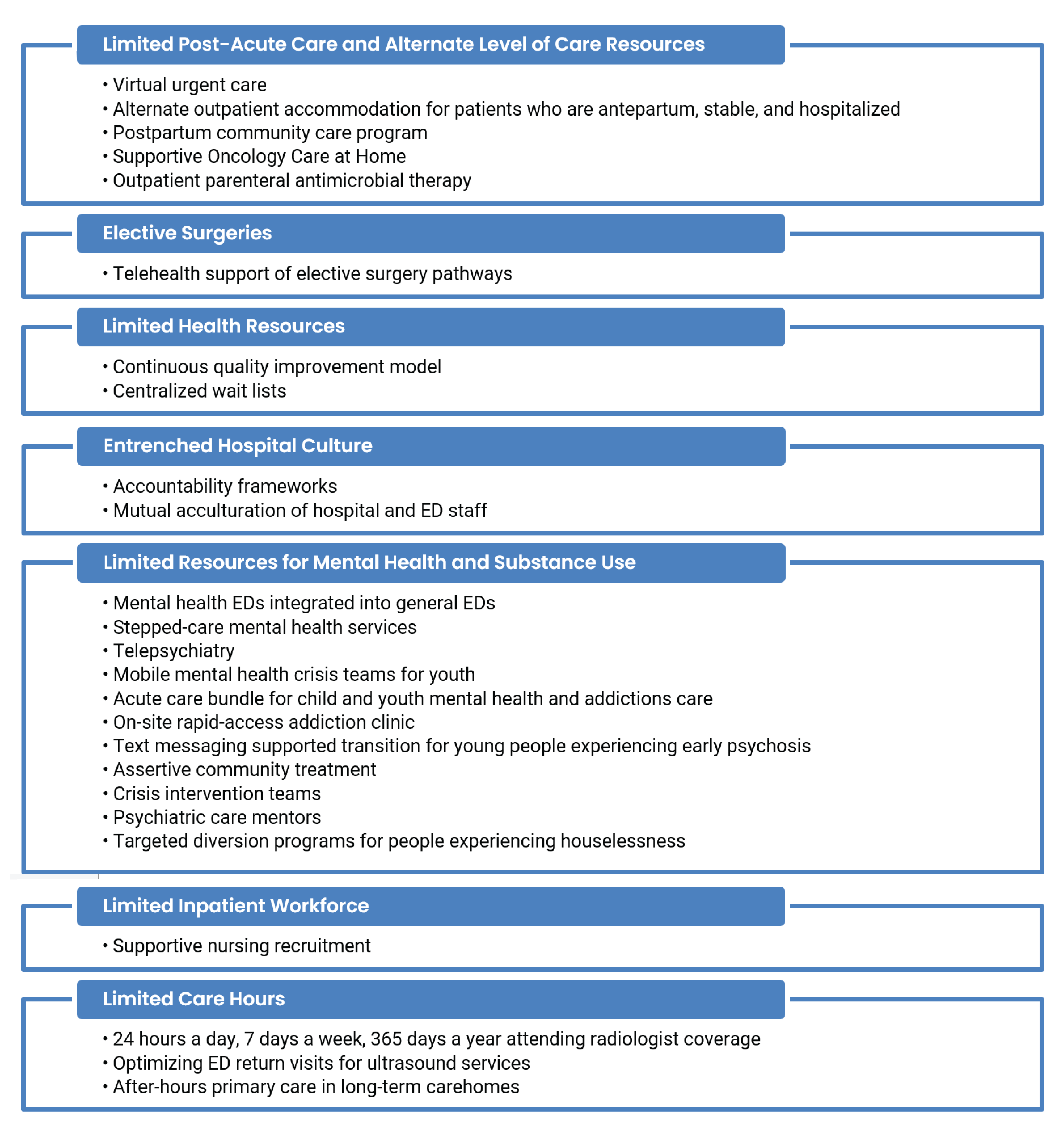
ED = emergency department.
Limited Post-Acute Care and Alternate Level of Care Resources
Virtual Urgent Care
In response to the COVID-19 pandemic, 14 virtual urgent care initiatives were funded as pilot projects by the Ontario Ministry of Health. Researchers in Toronto compared 30-day health care utilization and outcomes of patients accessing virtual urgent care to similar patients who accessed traditional in-person ED services; they concluded that virtual urgent care may be an alternative for people with minor medical concerns but cautioned that people discharged from these services may be more likely to have return ED visits within 30 days compared to patients who accessed in-person ED services.90
Alternate Outpatient Accommodation for Patients Who Are Antepartum, Stable, and Hospitalized
Pregnant people at risk of premature delivery who live in remote communities are often transferred to tertiary care centres for care. While continuing care and monitoring can often be provided in outpatient facilities, patients from remote communities who are stabilized may remain in hospital if their home community does not have neonatal intensive care facilities. Using a quality improvement approach, researchers in Edmonton sought to understand the barriers and facilitators to establish alternative accommodations for people who are pregnant and hospitalized in an out-of-town facility.91
Postpartum Community Care Program
Postpartum hypertension programs are uncommon in Canada but could be a solution to help avoid complications that lead to ED and clinic visits. Researchers in Calgary used the administrative data and chart reviews of pregnant people followed by the Calgary Antenatal Community Care Program for hypertensive disorders to understand risk factors for postpartum ED visits and determine if a postpartum program would be cost-effective.92
Supportive Oncology Care at Home
New ways of managing nonmetastatic pancreatic cancer using multidrug chemotherapy may lead patients to more frequently seek emergent care or become hospitalized to manage cancer symptoms or treatment side effects. The Supportive Oncology Care at Home pilot study offered patients with pancreatic cancer receiving care at Massachusetts General Hospital or Newton-Wellesley Hospital in Boston access to a dedicated oncology-trained multidisciplinary hospital-at-home team that worked collaboratively with the patient and their primary oncology team to provide remote monitoring, hospital-at-home care, and communication of important information. The program was reported to decrease ED visits and hospitalizations.93
Outpatient Parenteral Antimicrobial Therapy
Outpatient parenteral antimicrobial therapy (OPAT) is recognized as a safe and effective patient-centred alternative to hospitalization. In 2016, a dedicated OPAT clinic was established at Sunnybrook Health Sciences Centre (Toronto) as part of a quality improvement initiative to provide centralized follow-up to people receiving OPAT. The clinic operates 5 days a week during regular business hours and is staffed by a rotating group of infectious disease physicians supported by a specialist nurse and an administrative assistant whose services are shared with other clinics. With the aim of preventing unnecessary ED visits, the OPAT clinic offers guaranteed access to an infectious disease physician and a single point of contact for any OPAT-related issues.94
Elective Surgeries
Telehealth Support of Elective Surgery Pathways
The number of outpatient elective surgeries in Canada is increasing and cancellations and complications occur frequently. Digital health interventions may help improve care pathways for patients affected by these issues. To understand the potential cost benefits of implementing a dedicated telemedicine service for perioperative patients undergoing day surgeries, researchers at the University of Montreal will collaborate with LeoMed, a telemedicine provider, on a clinical trial that will provide patients with personalized support using a digital app.95
Limited Health Resources
Continuous Quality Improvement Model
Continuous quality improvement initiatives may be a helpful strategy for making the most of limited health care resources. At the Juravinski Hospital and Cancer Centre (Hamilton), staff in the oncology day services unit used continuous quality improvement tools to allow more same-day appointments for the growing number of patients requiring ongoing support, helping them avoid visits to the ED and hospital admissions.96 In Brampton, quality improvement initiatives for the care of children and adults living with sickle cell disease were used to implement a new adult clinic and develop new educational resources for patients and staff with the goal of reducing hospital admissions.97
Centralized Wait Lists
Centralized wait lists that are used by many health systems to assign patients to the next available provider to improve access to care. Researchers in Canada seeking to understand how the design and implementation of centralized wait lists affect access to health care services conducted a realist review. The authors concluded that provider behaviour and preferences may limit the effect of centralized wait lists on access to care and may also lead to inequitites.98
Entrenched Hospital Culture
Accountability Frameworks
Timely, quality care received at the right time from the right health care providers is a goal of any high-performing health care system. Accountability frameworks are when all parts of the health care system (including programs and specialists) explicitly understand that they are responsible for ensuring their target populations can access and receive care. Adopting such a framework may help reduce ED overcrowding by ensuring patients do not have to wait unreasonable amounts of time for primary care, surgeries, diagnostic imaging, and so forth.99
Mutual Acculturation of Hospital and ED Staff
Conflicts during patient handoff from the ED to other hospital services can negatively impact quality of care. To understand these conflicts and their potential solutions, researchers in Boston conducted focus groups with ED and internal medicine staff. In additional to pragmatic solutions, such as clearer documentation and pathways for patient disposition, participants suggested mutual acculturation activities such as developing joint training and leadership meetings and hosting social events.100
Limited Resources for Mental Health and Substance Use
Mental Health EDs Integrated Into General EDs
The General and Civic campuses of The Ottawa Hospital provide specialized services to assess people who present to the ED with a psychiatric illness and are in crisis. The hospital’s Psychiatric Emergency Service is located in the ED in a small, low stimulation, secure space with other design features such as closed-circuit TVs and panic alarms to help minimize risks to patients and staff. Patients are assessed by a multidisciplinary team and those requiring additional care are referred to other programs, as required.101
Stepped-Care Mental Health Services
The Ontario Structured Psychotherapy Program offers a stepped-care pathway delivered across 4 mental health hospital hubs and multiple community-based sites to treat depression and anxiety.8 Depending on their needs, the stepped-care model offers people in the program access to a variety of services, including group psychoeducation, clinician-supported internet-based cognitive behaviour therapy, self-management workbooks, or in-person psychotherapy. Adults accessing the program at CAMH (Toronto) are offered coach- or clinician-supported self-led resources or face-to-face cognitive behaviour therapy sessions delivered in person or virtually, depending on what best matches the person’s needs.102
Telepsychiatry
In response to decreasing access to emergency psychiatric services in Winnipeg, an emergency telepsychiatry service was established using the province’s secure MBTelehealth network.103 Using feedback from a survey exploring perceived barriers to such a service, a hub-and-spoke emergency telepsychiatry service opened in 2017. Daytime coverage was provided by a core team of salaried psychiatrists with after-hours service managed by a pool of psychiatrists and psychiatry residents. The Vitalité Health network in New Brunswick has also implemented telepsychiatry services to ensure access to psychiatric services in community hospitals.104
Mobile Mental Health Crisis Teams for Youth
Access to youth mental health services in Canada is limited despite interventions in childhood being critical to long-term mental health. Through a systematic review of the literature, researchers from Sunnybrook Hospital (Toronto) looked at the use of mobile mental health crisis teams for youth and explored team composition, interventions offered, outcomes measured, and impact on the communities the teams served. Despite sparse evidence, the authors concluded mobile mental health crisis teams for youth had a positive impact compared with traditional care, including reducing ED visits, and should be considered as an enhancement to the mental health system.105
Acute Care Bundle for Child and Youth Mental Health and Addictions Care
Researchers in Alberta plan to evaluate a novel, acute care bundle to help standardize a patient-centred approach to caring for children and youth experiencing a mental health or addictions crisis who have been brought to the pediatric ED. The bundle consists of 3 components intended for use as a whole or in part, as appropriate:
using the Ask Suicide-Screening Questionnaire (ASQ) to standardized assessment of self-harm risk at triage and allow risk stratification
using the HEADS-ED mental health and addiction screening tool to evaluate the mental health of those screened at high risk of self-harm on the ASQ
implementing the Choice and Partnership Approach to shared decision-making during follow-up care.106
Onsite Rapid-Access Addiction Clinic
In response to increased substance-related ED visits, researchers in Edmonton evaluated the need for a rapid-access addiction clinic that would offer onsite addictions medicine assessment, medical therapy such as opioid agonist treatment, counselling, harm reduction, and social stabilization. The authors concluded that if such a service were made available at least 4 people would be referred to an onsite clinic each day.107
Text Messaging–Supported Transition for Young People Experiencing Early Psychosis
In a study protocol, researchers at CAMH (Toronto) evaluated the use of a text messaging–supported intervention to improve the transition of young people presenting to the ED with psychosis to early psychosis intervention services. Text messages will be used to send reminders and psychoeduction resources, and for check-ins, with the goal of supporting first attendance at consultation appointments.108
Assertive Community Treatment
Since 2012, the Centre Hospitalier de l’Université de Montréal has provided outreach services, housing support, and integrated care to people experiencing early psychosis and substance use disorder through its intensive assertive community intervention team (EQIIP SOL). The approach, which uses a team of psychiatrists, nurses, social workers, and occupational therapists to provide intensive case management, may particularly benefit youth who are houseless and experiencing early psychosis and substance use disorder, who are at a higher risk of poor outcomes than their housed counterparts when combined with other early intervention services.109
Crisis Intervention Teams
People waiting for access to community mental health services are often housed in the ED, a phenomenon sometimes called psychiatric boarding. In countries like Canada, psychiatric boarding has increased as care for people living with mental health issues continues away from institutionalization and underresources other mental health services. Crisis interventions teams are community-based partnerships that include dedicated resources for assessment, crisis response, and referral that may help reduce length of stay for people with mental health issues being housed the ED.110
Psychiatric Care Mentors
Individuals experiencing houselessness and living with mental illness may experience high rates of hospital readmission. Seeking to understand the potential impact of connecting people experiencing houseless and mental illness to peer mentors on hospital readmission rates, 1 study looked at how a team of psychiatric care mentors could support individuals experiencing houselessness in receiving the health care services they need.111
Targeted Diversion Programs for People Experiencing Houselessness
People experiencing houselessness with drug or alcohol intoxication are often taken to the ED for low acuity and nonacute care because alternative options do not exist. Opportunities to divert individuals to more appropriate and supportive settings are being explored. The University Health Network (Toronto) opened an 11-bed, 24-hour stabilization and connection centre staffed by harm reduction workers, peer support workers, case workers, and an on-call physician to offer an alternative to the ED for people experiencing houselessness who have alcohol intoxication but do not require urgent or acute medical care.112 In Ottawa, Ottawa Inner City Health operates the Targeted Emergency Diversion program to allow people experiencing houselessness to detox in the community.8 Similar diversion strategies have also been evaluated at Health Sciences North (Sudbury).113
Limited Inpatient Workforce
Supportive Nursing Recruitment
Recognizing that current recruitment processes did not meet the London Health Sciences Centre’s (Ontario) COVID-19 recovery needs, a multidisciplinary team of administration, professional practice, human resources, corporate education, and front-line charge nurses developed a new approach to critical care nursing recruitment and retention over 6 months. In collaboration with new, current, and retired nurses, the team designed new processes focused on mentorship, education, job-sharing, and flexibility that recognize prior work experience, respond to individual learning needs, and are supportive of new graduates entering critical care nursing practice.114
Limited Care Hours
24 Hours a Day, 7 Days a Week, 365 Days a Year Attending Radiologist Coverage
Providing access to hospital services so patient access is available year-round, 7 days a week and 24 hours a day are potentially helpful and high-impact solutions to ED overcrowding.75 At the Vancouver General Hospital researchers evaluated pilot projects offering 24 hours a day, 7 days a week, 365 days a year coverage by an attending radiologist to understand the impact of expanding services on ED length of stay, disposition time, and other outcomes that affect patient flow through the ED.115-117
Optimizing ED Return Visits for Ultrasound Services
Because access to after-hours services is often limited, ED physicians may have patients return to the ED for next-day ultrasound services. With the goal of reducing return visits for next-day ultrasound by 50% over 6 months, researchers in Saskatchewan developed and implemented a new clinical pathway help guide physicians to determine the appropriate location (e.g., community ultrasound clinics) and timing of ultrasound services. Working collaboratively with ED physicians, the new clinical pathway saw a 54% reduction in next-day return visits 6 months after implementation in January 2022.118
After-Hours Primary Care in Long-Term Care Homes
People living in Ontario long-term care homes may be at increased risk of low acuity, evening ED visits on the same day they have a visit from a home care nurse. Hypothesizing that these increased ED visits could be reduced when long-term care home residents have access to after-hour primary care, researchers conducted a case-crossover study of residents of Ontario long-term care homes and concluded that increasing after-hours access to primary care could reduce some low acuity visits in this population.119
Interventions Addressing Multiple Contributing Factors to ED Overcrowding
The 7 interventions identified in this category may potentially impact or address more than 1 input, output, throughput, or contextual factor contributing to ED overcrowding (Figure 6).
Hospital Command Centre Model
Humber River Health (Toronto) employs a command centre centralized operating system that combines advanced technology with dedicated staff to function as a nerve centre for the organization. The centre has expanded several times from an initial focus on hospital flow to improving diagnostics and clinical outcomes, and is now extended into home and community care. The improvements of this arrangement include a culture of quality improvement, financial benefits, better workflow, better clinical outcomes, and increased hospital capacity, which assists with the problem of ED overcrowding.120 The feasibility of establishing a hospital capacity command centre has also been studied by McGill University’s Health Technology Assessment Unit (Montreal).121
NICE Recommendations for Research for Emergency and Acute Medical Care in over 16s
The National Institute for Health and Care Excellence’s (UK) guideline 94 is a recommendation for research into 17 areas sure to have an impact on ED access and overcrowding. These include extended access to general practitioners, community nursing, and social care services; expedient access and results from diagnostic services; adjuncts like clinical call handlers and decision support technologies; and minor injury units and urgent care centres.122
Rapid-Access Chest Pain Clinics
This retrospective observational study based in Regina and Saskatoon examined whether patients with chest pain, a common ED presentation that requires many ED resources, could be safely managed in an alternative way. The results of the study were positive, with the majority of those studied deemed to be eligible for care outside the ED environment.123
e-Consultations
Electronic clinician-to-clinician communication may help alleviate the need for face-to-face visits to specialists and improve access to care for patients with a variety needs. An Eastern Ontario study examined the feasibility, safety, and satisfaction of e-consultations with pediatric orthopedic specialists using the BASE eConsult service. E-consultations led to 68% of cases avoiding in-person appointments, and 97% of the primary care providers found the value of the care good or excellent. This innovation saved time and resources for patients and providers.124 An analysis of data collected from participants in the pan-Canadian Connected Medicine collaboration concluded that virtual consultation services (e.g., BASE eConsult and RACE) were widely used and impacted the referral practices of primary care providers and could be effectively scaled and spread across Canadian jurisdictions.125 Evidence about the clinical outcomes of international e-consultation services has also been reported in a 2021 systematic review.126
Figure 6: New and Emerging Interventions That Address Multiple Factors Contributing to ED Overcrowding
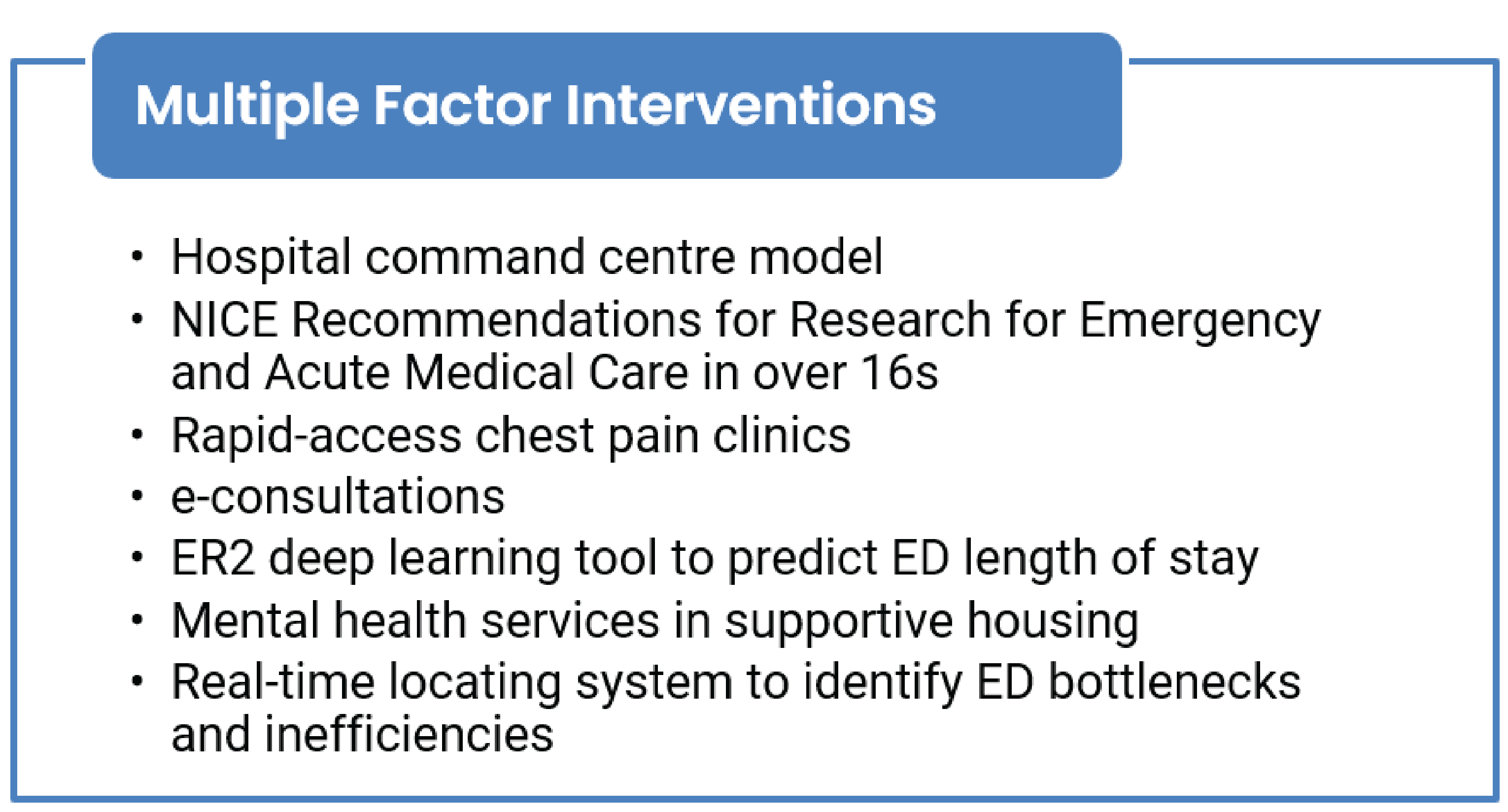
ED = emergency department; ER2 = Emergency Room Evaluation and Recommendations; NICE = The National Institute for Health and Care Excellence.
ER2 Deep Learning Tool to Predict ED Length of Stay
This Montreal-based study examined how the implementation of an Emergency Room Evaluation and Recommendations (ER2) tool affected hospital admissions and ED length of stay for older people with major neurocognitive disorders. While the tool led to fewer hospital admissions, it was associated with longer ED length of stay.127
Mental Health Services in Supportive Housing
This study evaluated the success of implementing an outpatient collaborative mental health care initiative in supportive housing that included multidisciplinary support for tenants, tenant engagement, and staff capacity-building. This supportive, preventive approach stands to decrease incidents of mental health instability that may require those affected to seek help in EDs.128
Real-Time Locating System to Identify ED Bottlenecks and Inefficiencies
This descriptive, retrospective study examined the use of real-time location system data in combination with other traditional data to track patient flow through the ED. Bottlenecks and delays were identified along with the finding that traditional tracking data are insufficient to study this flow for the purpose of quality improvement initiatives.129
Methods
CADTH’s Horizon Scanning Service identifies and monitors new and emerging health technologies likely to have a significant impact on health care in Canada. The service scans and monitors health information sources to identify potentially important health technologies not yet widely used in Canadian health care systems. Summaries of current information about the use, effectiveness, cost, and implementation of these technologies are published regularly in CADTH Horizon Scan reports.
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were overcrowding, emergency medicine (emergency departments, emergency medical services, and emergency medicine personnel), and interventions. CADTH-developed search filters were applied to limit retrieval to the Canadian context. The search was completed on July 17, 2023, and limited to English-language documents published since January 1, 2018. Conference abstracts were included in the search; the abstracts were limited to English-language results published since January 01, 2021. A supplemental literature search was conducted in Scopus and PsycINFO, as well as a focused internet search, for literature in the engineering, management, and operations fields. The search was conducted between June 20 and 23, 2023, and limited to English-language documents published since January 1, 2018. Additional potential interventions for inclusion were identified by the report authors, members of CADTH’s ED overcrowding project team, and members of the Health Technology Expert Review Panel (HTERP). Due to the number of search results and project time constraints, database search results, clinical trial results, and engineering search results where only screened back to those published since January 1, 2020. All grey literature search results and conference abstract results were screened.
Potential new and emerging interventions were screened by 1 report author and reviewed by the 1 project team member to ensure none of the potential interventions overlapped with the findings of CADTH’s summary of systematic review evidence.4 A final list of new and emerging interventions was categorized by 1 report author according to the contributing factor to ED overcrowding they were most intended to address. Categorization of the final list of interventions was reviewed by 1 project team member to ensure they matched the contributing factors as reported in CADTH’s environmental scan.4
The completeness of the interventions included in this roundup was validated through an engagement exercise with 1 ED physician with a known interest in the intersection of ED overcrowding and health care innovation, digital health, virtual care, artificial intelligence, learning health systems, quality improvement, and so forth.
What Else Is CADTH Doing?
This report is part of a series of publications that CADTH will produce on the topic of ED overcrowding in Canada as an update to the 2006 publications.130-133 Separate publications not described in this report were published in October of 2023 to address:
the factors contributing to ED overcrowding in Canada
which interventions effectively alleviate ED overcrowding (summary of systematic review evidence)
the impact ED overcrowding has on quality of care and patient safety (i.e., the risks of overcrowding), and on health professional learner experience and staff well-being
how ED overcrowding in Canada has changed since the last series of reports
a summary of CADTH’s multistakeholder dialogue sessions.
HTERP will use the CADTH deliverables as inputs into deliberations that will result in the development of guidance and response to addressing the decision problem of what evidence-informed solutions should be considered to guide decision- and policy-making to effectively alleviate overcrowding of adult and pediatric ED services in urban, rural, and remote health care settings in Canada?
References
1.Affleck A, Parks P, Drummond A, Rowe BH, Ovens HJ. Emergency department overcrowding and access block. CJEM. 2013;15(6):359-384. PubMed
2.Position statement on over-crowded emergency departments. West Melbourne (AU): International Federation for Emergency Medicine; 2022: https://assets.nationbuilder.com/ifem/pages/546/attachments/original/1670806966/IFEM_Position_Statement_on_Emergency_Department_Overcrowding_December_2022.pdf?1670806966. Accessed 2023 Apr 06.
3.Canadian emergency care is being crushed - and why that matters for all of us. Ottawa (ON): Canadian Association of Emergency Physicians; 2023: https://caep.ca/wp-content/uploads/2023/01/Letter-Canadian-Emergency-Care-is-Being-Crushed-Jan-2023.pdf. Accessed 2023 Apr 06.
4.Emergency department overcrowding: an environmental scan of contributing factors and a summary of systematic review evidence on interventions [in-progress]. (CADTH health technology review). Ottawa (ON): CADTH; 2023: https://www.cadth.ca/emergency-department-overcrowding-canada-update. Accessed 2023 Oct 05.
5.Asplin BR, Magid DJ, Rhodes KV, Solberg LI, Lurie N, Camargo CA, Jr. A conceptual model of emergency department crowding. Ann Emerg Med. 2003;42(2):173-180. PubMed
6.Savioli G, Ceresa IF, Gri N, et al. Emergency department overcrowding: understanding the factors to find corresponding solutions. J Pers Med. 2022;12(2):279. PubMed
7.Niagara Region. Mobile integrated health model of care. https://www.niagararegion.ca/living/health_wellness/ems/mobile-integrated-health.aspx. Accessed 2023 Aug 16.
8.Premier’s Council on Improving Healthcare and Ending Hallway Medicine. A healthy Ontario: building a sustainable health care system: 2nd report from the Premier’s Council on Improving Healthcare and Ending Hallway Medicine Toronto (ON): Queen’s Printer for Ontario; 2019: https://files.ontario.ca/moh-healthy-ontario-building-sustainable-health-care-en-2019-06-25.pdf. Accessed 2023 Aug 17.
9.Alberta Health Services. EMS mobile integrated healthcare: Community Paramedicine. 2023; https://www.albertahealthservices.ca/ems/Page16487.aspx. Accessed 2023 Aug 17.
10.Azienda Ospedaliero-Universitaria di Parma. NCT04085679: Multidisciplinary mobile unit for preventing hospitalization of nursing home residents. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://classic.clinicaltrials.gov/show/NCT04085679. Accessed 2023 Jul 17.
11.St. Joseph's Home Care. Neighbourhood Model for Seniors at risk. https://www.stjosephshomecare.ca/client-services/assisted-living-in-supportive-housing/neighbourhood-model-for-seniors-at-risk. Accessed 2023 Aug 16.
12.Alberta Health Services. Programs and services: CONNECT - Community Support Team. https://www.albertahealthservices.ca/findhealth/service.aspx?Id=1067017. Accessed 2023 Aug 16.
13.Kunkel E, Tanuseputro P, Hsu A, et al. Diagnostic testing in long-term care and resident emergency department visits: a retrospective cohort study. J Am Med Dir Assoc. 2021;22(4):901-906.e904. PubMed
14.Ontario connecting long-term care home residents to more diagnostic services. (News release). Toronto (ON): Government of Ontario; 2023: https://news.ontario.ca/en/release/1002675/ontario-connecting-long-term-care-home-residents-to-more-diagnostic-services. Accessed 2023 Aug 15.
15.Kobewka DM, Kunkel E, Hsu A, Talarico R, Tanuseputro P. Physician availability in long-term care and resident hospital transfer: a retrospective cohort study. J Am Med Dir Assoc. 2020;21(4):469-475.e461. PubMed
16.Novak KL, Halasz J, Andrews C, et al. Nurse-led, shared medical appointments for common gastrointestinal conditions-improving outcomes through collaboration with primary care in the medical home: a prospective observational study. J Can Assoc Gastroenterol. 2020;3(2):59-66. PubMed
17.Attract Connect Stay. About. 2023; https://attractconnectstay.com.au/about-attract-connect-stay/. Accessed 2023 Aug 16.
18.Pharmacy Association of Nova Scotia (PANS). Community Pharmacy Primary Care Clinics. 2023; https://pans.ns.ca/cppcc. Accessed 2023 Aug 16.
19.Promising practices to support retention of the healthcare workforce in northern, rural and remote communities in Canada. Ottawa (ON): Healthcare Excellence Canada; 2023: https://www.healthcareexcellence.ca/media/wofdrciy/20230224_implementing-a-physician-assistant-program-to-promote-retention-within-ongomiizwin-health-services.pdf. Accessed 2023 Aug 16.
20.Rural Coordination Centre of British Columbia. Real-time virtual support. 2023; https://rccbc.ca/initiatives/rtvs/. Accessed 2023 Aug 16.
21.TEC4Home Heart Failure: a randomized controlled trial of home health monitoring for patients with heart failure. Vancouver (BC): Digital Emergency Medicine, Department of Emergency Medicine, UBC: https://digem.med.ubc.ca/projects/tec4home-telehealth-for-emergency-community-continuity-of-care-connectivity-via-home-tele-monitoring/. Accessed 2023 Aug 16.
22.Ho K, Novak Lauscher H, Cordeiro J, et al. Testing the feasibility of sensor-based home health monitoring (TEC4Home) to support the convalescence of patients with heart failure: pre-post study. JMIR Form Res. 2021;5(6):e24509. PubMed
23.TEC4Home COPD. Vancouver (BC): Digital Emergency Medicine, Department of Emergency Medicine, UBC: https://digem.med.ubc.ca/projects/tec4home-copd/. Accessed 2023 Aug 17.
24.Cheng T, Lockington J, Lindsay H. MP26: Quality improvement in emergency department discharge via QR codes. In: CAEP/ACMU 2023 Scientific Abstracts. CJEM. 2023;25(Suppl 1):S41-S42. https://link.springer.com/content/pdf/10.1007/s43678-023-00508-z.pdf. Accessed 2023 Jul 17.
25.Huynh L, Nolen A, Bonares M, et al. OA02:03: Reducing emergency department use for ambulatory oncology patients requiring palliative care: a quality improvement initiative. In: Abstracts from the 12th World Research Congress of the European Association for Palliative Care. Palliat Med. 2022;36(1 Suppl):19. https://journals.sagepub.com/doi/epub/10.1177/02692163221093145. Accessed 2023 Aug 10.
26.Bhargava R, Keating B, Isenberg SR, Subramaniam S, Wegier P, Chasen M. RELIEF: a digital health tool for the remote self-reporting of symptoms in patients with cancer to address palliative care needs and minimize emergency department visits. Curr Oncol. 2021;28(6):4273-4280. PubMed
27.Dubois S. ER physician's project uses donated cellphones to connect vulnerable with ongoing medical care. Toronto (ON): CBC; 2023: https://www.cbc.ca/news/health/hospital-er-visits-reduce-cellphones-1.6773332. Accessed 2023 Aug 16.
28.Minervini F, Taylor J, Hanna WC, et al. Can a mobile app technology reduce emergency department visits and readmissions after lung resection? A prospective cohort study. Can J Surg. 2022;65(6):E798-E804. PubMed
29.Valk HA, Garcia-Ochoa C, Fontaine Calder J, et al. A mobile app for wound and symptom surveillance after colorectal surgery: protocol for a feasibility randomized controlled trial. JMIR Res Protoc. 2022;11(1):e26717. PubMed
30.Anpalagan T, Schmocker S, Raval M, et al. Home to Stay: a randomized controlled trial protocol to assess use of a mobile app to reduce readmissions following colorectal surgery. Colorectal Dis. 2022;24(12):1616-1621. PubMed
31.Ishikawa T, Chin B, Meckler G, Hay C, Doan Q. Reducing length of stay and return visits for emergency department pediatric mental health presentations. CJEM. 2021;23(1):103-110. PubMed
32.Gangbar E, Li Q, Saskin R, Candido E, Niu D. A propensity-matched cohort study to assess the effectiveness of a community hospital based Heart Function Clinic. Can J Cardiol. 2022;38(10 Suppl 2):S153-S154.
33.Chartier LB, Ovens H, Hayes E, et al. Improving quality of care through a mandatory provincial audit program: Ontario's Emergency Department Return Visit Quality Program. Ann Emerg Med. 2021;77(2):193-202. PubMed
34.Emergency Department Return Visit Quality Program. Toronto (ON): Health Quality Ontario (HQO); 2023: https://www.hqontario.ca/Quality-Improvement/Quality-Improvement-in-Action/Emergency-Department-Return-Visit-Quality-Program. Accessed 2023 Aug 17.
35.Kennedy W, Dowling S, Lonergan K, Rich T, Patocka C. A realist evaluation of a 72-hour readmission audit and feedback (A&F) intervention in emergency medicine. Cureus. 2021;13(9):e18402. PubMed
36.Strum RP, Mondoux S, Mowbray F, et al. Validation of a classification to identify emergency department visits suitable for subacute and virtual care models: a randomised single-blinded agreement study protocol. BMJ Open. 2022;12(12):e068488. PubMed
37.Anakor N. Housing intervention and placement to reduce the frequency of emergency room readmissions among the middle-aged homeless mentally ill population: dissertation. Irvine (CA): Marybelle and S. Paul Musco School of Nursing and Health Professions, University of Massachusetts Global; 2022.
38.Hu Y, Chan CW, Dong J. Prediction-driven surge planning with application in the emergency department. New York (NY): Columbia University; 2021: http://www.columbia.edu/~cc3179/SurgeStaffing_2021.pdf. Accessed 2023 Aug 16.
39.Jewer J. Investigating a work system approach to implement an emergency department surge management system: case study. J Med Internet Res. 2022;24(8):e37472. PubMed
40.Zaerpour F, Bischak DP, Menezes MBC, McRae A, Lang ES. Patient classification based on volume and case-mix in the emergency department and their association with performance. Health Care Manag Sci. 2020;23(3):387-400. PubMed
41.Mobia Health Innovations. SurgeCon emergency care capacity management. 2023; https://mobiahealth.io/surgecon. Accessed 2023 Aug 16.
42.Mariathas HH, Hurley O, Anaraki NR, et al. A quality improvement emergency department surge management platform (SurgeCon): protocol for a stepped wedge cluster randomized trial. JMIR Res Protoc. 2022;11(3):e30454. PubMed
43.Memorial University of Newfoundland. NCT04789902: SurgeCon: an emergency department surge management platform. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://classic.clinicaltrials.gov/show/NCT04789902. Accessed 2023 Jul 17.
44.Health Standards Organization (HSO). Leading practices: utilizing patient flow simulation to alleviate emergency department overcrowding. 2019; https://healthstandards.org/leading-practice/utilizing-patient-flow-simulation-alleviate-emergency-department-overcrowding/. Accessed 2023 Aug 16.
45.Varner C. Can artificial intelligence predict emergency department crowding? Toronto (ON): Healthy Debate; 2020: https://healthydebate.ca/2020/03/topic/predicting-emergency-department-crowding-artificial-intelligence-mar2020/. Accessed 2023 Aug 16.
46.Invest Ontario. Spotlights: Toronto hospital prescribes AI to cure ER wait times. 2020; https://www.investontario.ca/spotlights/toronto-hospital-prescribes-ai-cure-er-wait-times. Accessed 2020 Aug 17.
47.Kadri F, Harrou F, Chaabane S, Tahon C. Time series modelling and forecasting of emergency department overcrowding. J Med Syst. 2014;38(9):107. PubMed
48.Tuominen J, Koivistoinen T, Kanniainen J, Oksala N, Palomäki A, Roine A. Early warning software for emergency department crowding. J Med Syst. 2023;47:66. PubMed
49.Tampere University Hospital. NCT05174481: Forecasting ED overcrowding with statistical methods: a prospective validation study. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://classic.clinicaltrials.gov/show/NCT05174481. Accessed 2023 Jul 17.
50.Greene J, Goldstein J, Stirling J, et al. LO37: Clinical roles in the medical communications centre: a rapid scoping review by the prehospital evidence based practice program. In: CAEP/ACMU 2023 Scientific Abstracts. CJEM. 2023;25(Suppl 1):S20. https://link.springer.com/content/pdf/10.1007/s43678-023-00508-z.pdf. Accessed 2023 Jul 17.
51.Strum RP, Tavares W, Worster A, Griffith LE, Rahim A, Costa AP. Development of the PriCARE classification for potentially preventable emergency department visits by ambulance: a RAND/UCLA modified Delphi study protocol. BMJ Open. 2021;11(1):e045351. PubMed
52.Born K, Tierney M. Should hospitals post emergency department waits online? Toronto (ON): Healthy Debate; 2012: https://healthydebate.ca/2012/07/topic/innovation/real-time-emergency-dept-wait-time/. Accessed 2023 Aug 16.
53.Xie B, Youash S. The effects of publishing emergency department wait time on patient utilization patterns in a community with two emergency department sites: a retrospective, quasi-experiment design. Int J Emerg Med. 2011;4(1):29. PubMed
54.Rathagirishnan R, Birchall I, Latimer-Cheung A, Tse S, Cheung K. About time! A scoping review of public-facing emergency department wait time displays in Canada. CJEM. 2022;24(5):503-508. PubMed
55.Reid S, Bhatt M, Zemek R, Tse S. Virtual care in the pediatric emergency department: a new way of doing business? CJEM. 2021;23(1):80-84. PubMed
56.Osmanlliu E, Gagnon I, Weber S, Bach CQ, Turnbull J, Seguin J. The Waiting Room Assessment to Virtual Emergency Department pathway: initiating video-based telemedicine in the pediatric emergency department. J Telemed Telecare. 2022;28(6):452-457. PubMed
57.Royal Victoria Regional Health Centre. RVH’s Emergency Department launches pilot project booking system for minor limb injuries. 2023; https://www.rvh.on.ca/2023/05/rvhs-emergency-department-launches-pilot-project-booking-system-for-minor-limb-injuries/. Accessed 2023 Aug 24.
58.Reducing emergency department length-of-stay through practice change. Vancouver (BC): Centre for Advancing Health Communications; 2019: https://www.advancinghealth.ubc.ca/research-in-action/reducing-emergency-department-length-of-stay-through-practice-change/. Accessed 2023 Aug 16.
59.Dowling SK, Gjata I, Solbak NM, et al. Group-facilitated audit and feedback to improve bronchiolitis care in the emergency department. CJEM. 2020;22(5):678-686. PubMed
60.Ottawa Hospital Research Institute. NCT04790058: CSRS implementation - a pilot study. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://classic.clinicaltrials.gov/show/NCT04790058. Accessed 2023 Aug 16.
61.Joseph MJ, Summerscales M, Yogesan S, Bell A, Genevieve M, Kanagasingam Y. The use of kiosks to improve triage efficiency in the emergency department. NPJ Digit Med. 2023;6(1):19. PubMed
62.Ali U, Abdolkhani A, Rasheed HJ, Zhao J. Predicting patient readmission for improved resource allocation using machine learning. Presented at the STEM Fellowship Big Data Challenge 2022. Toronto (ON): STEM Fellowship; 2022: https://umarali.ca/files/Predicting%20Patient%20Readmission%20for%20Improved%20Resource%20Allocation%20using%20Machine%20Learning.pdf. Accessed 2023 Aug 16.
63.The Health Research Council of New Zealand (HRC). ACTRN12621001567819: Developing a Decision Support System at Emergency Room triage (DESSERT) for predicting health outcomes. Camperdown (AU): Australian New Zealand Clinical Trials Registry (ANZCTR); 2022: https://anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12621001567819. Accessed 2023 Aug 16.
64.Fundació Institut de Recerca de l'Hospital de la Santa Creu i Sant Pau. NCT05382000: Artificial intelligence (IA) advanced triage tool for G&O emergencies (TIAGO). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://classic.clinicaltrials.gov/show/NCT05382000. Accessed 2023 Jul 17.
65.Ahmed A, Ashour O, Ali H, Firouz M. An integrated optimization and machine learning approach to predict the admission status of emergency patients. Expert Syst Appl. 2022;202:117314.
66.Ziabari MK, Amyot D, Michalowski W, Bouattane EM, Hafez N. Creating mobile self-triage applications: requirements and usability perspectives. Notre Dame (IN): 2021 IEEE 29th International Requirements Engineering Conference Workshops (REW); 2021 Sep 20-24.
67.Brambilla A, Mangili S, Das M, Lal S, Capolongo S. Analysis of Functional layout in emergency departments (ED). Shedding light on the free standing emergency department (FSED) model. Appl Sci (Basel). 2022;12(10):5099.
68.Crowder K, Domm E, Lipp R, et al. The multicenter impacts of an emergency physician lead on departmental flow and provider experiences. CJEM. 2023;25(3):224-232. PubMed
69.Ontario Health. Emergency department peer-to-peer program. 2023; https://www.ontariohealth.ca/providing-health-care/clinical-resources-education/emergency-peer-program. Accessed 2023 Aug 16.
70.Hale SJ, Wakeling S, Bhalerao A, et al. Feeling the flow with a serious game workshop: GridlockED as Medical Education 2 study (GAME2 study). AEM Educ Train. 2021;5(3):e10576. PubMed
71.Fiala C, Ragothaman S, Johl G, Sabbineni M, Chan T. MP18: ExpandED: the GridlockED game expansion pack. In: CAEP/ACMU 2023 Scientific Abstracts. CJEM. 2023;25(Suppl 1):S38. https://link.springer.com/content/pdf/10.1007/s43678-023-00508-z.pdf. Accessed 2023 Jul 17.
72.Young C, Patey C, Norman P, et al. Identifying relevant topics and training methods for emergency department flow training. CJEM. 2022;24(8):837-843. PubMed
73.ED Nurse-to-patient ratios to optimize patient outcomes, safety, and efficiency and avoid staff burnout. (Clinical Evidence Assessment). Plymouth Meeting (PA): ECRI; 2022: www.ecri.org. Accessed 2023 Apr 06.
74.Taleb M, Khalid R, Ramli R, Nawawi MKM. An integrated approach of discrete event simulation and a non-radial super efficiency data envelopment analysis for performance evaluation of an emergency department. Expert Syst Appl. 2023;220:119653.
75.Kelen GD, Wolfe R, D’Onofrio G, et al. Emergency department crowding: the canary in the health care system. NEJM Catalyst. 2021. https://catalyst.nejm.org/doi/abs/10.1056/CAT.21.0217. Accessed 2023 Jun 30.
76.Savioli G, Ceresa IF, Novelli V, Ricevuti G, Bressan MA, Oddone E. How the coronavirus disease 2019 pandemic changed the patterns of healthcare utilization by geriatric patients and the crowding: a call to action for effective solutions to the access block. Intern Emerg Med. 2022;17(2):503-514. PubMed
77.Nasr Isfahani M, Davari F, Azizkhani R, Rezvani M. Decreased emergency department overcrowding by discharge lounge: a computer simulation study. Int J Prev Med. 2020;11:13. PubMed
78.London Health Sciences Centre. Discharge lounge opens on 5th floor UH. 2019; https://www.lhsc.on.ca/news/discharge-lounge-opens-on-5th-floor-uh. Accessed 2023 Aug 17.
79.Frommer M, Marjanovic S. Access block: a review of potential solutions. Glebe (AU): Sax Institute; 2022: https://acem.org.au/getmedia/d7ad79ba-0956-4dc1-8a17-461867c9c835/Access-block-A-review-of-potential-solutions-FINAL. Accessed 2023 Aug 16.
80.Hammer C, DePrez B, White J, Lewis L, Straughen S, Buchheit R. Enhancing hospital-wide patient flow to reduce emergency department crowding and boarding. J Emerg Nurs. 2022;48(5):603-609. PubMed
81.Orewa GN, Feldman SS, Hearld KR, Kennedy KC, Hall AG. Using accountable care teams to improve timely discharge: a pilot study. Qual Manag Health Care. 2021;31(1):22-27. PubMed
82.Safavi KC, Bravard MA, Yun BJ, Levine WC, Dunn PF. Design, implementation and impact of a new physician role to address capacity challenges at a large academic medical center. J Hosp Manag Health Policy. 2022;6:17.
83.Makarem D, Sarraj F, Alkandarie F, Thuwaini S, Tafesh Y, Kula U. A simulation study on bed capacity management in a public hospital: Systems simulation and probability and statistics in engineering applications. Dubai (UAE): Proceedings of the International Conference on Industrial Engineering and Operations Management; 2020 March 10-12: http://www.ieomsociety.org/ieom2020/papers/798.pdf. Accessed 2023 Aug 15.
84.Shakeri M, Haji B, Farrokhvar L. A partially flexible routing strategy for assigning emergency department patients to inpatient wards. Comput Ind Eng. 2023;176:108810.
85.PineVilla. About us. http://pinevilla.ca/. Accessed 2023 Aug 16.
86.Reactivation Care Centre. Home page. https://www.reactivationcarecentre.ca/. Accessed 2023 Sep 12.
87.Alberta Health Services. Complex Care Hub: enhancing care in the community. 2023; https://www.albertahealthservices.ca/about/Page13602.aspx. Accessed 2023 Aug 16.
88.Whatley S. Patient hotels: an established transitional solution to overcrowding – Shawn Whatley in the Hill Times. Ottawa (ON): Macdonald Laurier Institute; 2020: https://macdonaldlaurier.ca/patient-hotels-established-transitional-solution-overcrowding-shawn-whatley-hill-times/. Accessed 2023 Aug 16.
89.Consolidated Framework for Implementation Research. Ann Arbor (MI): CFIR Research Team-Center for Clinical Management Research; 2022: https://cfirguide.org/. Accessed 2023 Apr 06.
90.McLeod S, Tarride J, Mondoux S, et al. Healthcare utilization and outcomes of patients seen by virtual urgent care compared to traditional in-person emergency department care. In: CAEP/ACMU 2023 Scientific Abstracts. CJEM. 2023;25(Suppl 1):S68. https://link.springer.com/content/pdf/10.1007/s43678-023-00508-z.pdf. Accessed 2023 Aug 09.
91.Sullivan MB, Rentz A, Mathura P, et al. Establishing an alternative accommodation for stable hospitalised antepartum patients: barriers and challenges. BMJ Open Qual. 2022;11(1):e001625. PubMed
92.Luo FY, Crawford S, Drouin O, Chadha R. Can we predict and prevent emergency department visits for postpartum hypertensive complications in patients with hypertensive disorders in pregnancy? J Matern Fetal Neonatal Med. 2020;33(13):2241-2245. PubMed
93.Nipp RD, Gaufberg E, Vyas C, et al. Supportive Oncology Care at Home Intervention for patients with pancreatic cancer. JCO Oncol Pract. 2022;18(10):e1587-e1593. PubMed
94.Yan M, Lam PW, Andany N, et al. Assessing the utilization and impact of a newly established outpatient parenteral antimicrobial therapy (OPAT) program. J Assoc Med Microbiol Infect Dis Can. 2020;5(2):70-76. PubMed
95.Robin F, Roy M, Kuftedjian A, et al. A medicoeconomic evaluation of a telehealth platform for elective outpatient surgeries: protocol for a randomized controlled trial. JMIR Res Protoc. 2023;12:e44006. PubMed
96.Making room for more patients in Oncology Day Services. Hamilton (ON): Hamilton Health Sciences; 2019: https://www.hamiltonhealthsciences.ca/share/oncology-day-services/. Accessed 2023 Aug 16.
97.Binding A. Bringing sickle cell disease care closer to home: feasibility and efficacy of a quality improvement initiative at a community hospital. Hemoglobin. 2022;46(2):91-94. PubMed
98.Breton M, Smithman MA, Sasseville M, et al. How the design and implementation of centralized waiting lists influence their use and effect on access to healthcare - a realist review. Health Policy. 2020;124(8):787-795. PubMed
99.Atkinson P, Innes G. Patient care accountability frameworks: the key to success for our healthcare system. CJEM. 2021;23(3):274-276. PubMed
100.Kanjee Z, Beltran CP, Smith CC, et al. “Friction by Definition”: conflict at patient handover between emergency and internal medicine physicians at an academic medical center. West J Emerg Med. 2021;22(6):1227-1239. PubMed
101.The Ottawa Hospital. Psychiatric Emergency Services (PES) at the General and Civic Campuses. 2021; https://www.ottawahospital.on.ca/en/clinical-services/deptpgrmcs/departments/mental-health/our-services/psychiatric-emergency-services-pes/. Accessed 2023 Aug 16.
102.Ontario Structured Psychotherapy (OSP) Program. Toronto (ON): CAMH; 2023: https://www.camh.ca/en/your-care/programs-and-services/ontario-structured-psychotherapy-osp-program. Accessed 2023 Aug 16.
103.Hensel J, Graham R, Isaak C, Ahmed N, Sareen J, Bolton J. A novel emergency telepsychiatry program in a Canadian urban setting: identifying and addressing perceived barriers for successful implementation: Un nouveau programme de telepsychiatrie d'urgence en milieu urbain canadien: identifier et aborder les obstacles percus d'une mise en oeuvre reussie. Can J Psychiatry. 2020;65(8):559-567. PubMed
104.Vitalité, your health care network: quarterly report to the community, March 2023. Bathurst (MB): Réseau de Santé Vitalité Health Network; 2023: https://www.vitalitenb.ca/sites/default/files/documents/perf_dashboard/vitalite_-_rapport_communaute_2023-03-en.pdf. Accessed 2023 Aug 16.
105.Wang K, Samuels H, Bahadur A. 45.2 Mobile mental health crisis teams for youth: a systematic review. J Am Acad Child Adolesc Psychiatry. 2021;60(10S):S241.
106.Freedman S, Thull-Freedman J, Lightbody T, et al. Introducing an innovative model of acute paediatric mental health and addictions care to paediatric emergency departments: a protocol for a multicentre prospective cohort study. BMJ Open Qual. 2020;9(4):e001106. PubMed
107.Hann J, Wu H, Gauri A, et al. Identification of emergency department patients for referral to rapid-access addiction services. CJEM. 2020;22(2):170-177. PubMed
108.Polillo A, Foussias G, Wong AHC, et al. ED to EPI: protocol for a pragmatic randomised controlled trial of an SMS (text) messaging intervention to improve the transition from the emergency department to early psychosis intervention for young people with psychosis. BMJ Open. 2020;10(12):e042751. PubMed
109.Dore-Gauthier V, Miron JP, Jutras-Aswad D, Ouellet-Plamondon C, Abdel-Baki A. Specialized assertive community treatment intervention for homeless youth with first episode psychosis and substance use disorder: a 2-year follow-up study. Early Interv Psychiatry. 2020;14(2):203-210. PubMed
110.Hooks KP. The impact of a crisis intervention team program on psychiatric boarding. Norfolk (VA): Doctor of Philosophy (PhD), Dissertation, Counseling & Human Services, Old Dominion University; 2021: https://digitalcommons.odu.edu/cgi/viewcontent.cgi?article=1135&context=chs_etds. Accessed 2023 Aug 15.
111.Odutola TO. Reducing hospital readmission and emergency department revisits by homeless psychiatric patient through support from a psychiatric care mentor: dissertation. Irvine (CA): Marybelle and S. Paul Musco School of Nursing and Health Professions, University of Massachusetts Global; 2022.
112.Casey L. New hospital program helps Toronto's homeless, cuts ambulance offload time. Toronto (ON): CBC; 2022: https://www.cbc.ca/news/canada/toronto/toronto-homeless-hospital-program-1.6698229. Accessed 2023 Aug 16.
113.Roney M, Prpic J. Mental health and addictions emergency department diversion strategies. Sudbury (ON): City of Greater Sudbury; 2019: https://pub-greatersudbury.escribemeetings.com/FileStream.ashx?DocumentId=1897. Accessed 2023 Aug 17.
114.De Campos I, Gajasan J, Caslick T, et al. Critical care nursing resource recovery strategy: not just about recruitment, responding with a focus on retention and tailored education programs at London Health Sciences. In: Critical Care Canada Forum 2022 Abstracts. Can J Anaesth. 2023;70(Suppl 1):S63-S65. https://link.springer.com/content/pdf/10.1007/s12630-023-02445-y.pdf. Accessed 2023 Jul 17.
115.Jalal S, Ante Z, Ouellette H, Peters S, Munk P, Nicolaou S. Impact of 24/7/365 attending radiologist coverage on the turnaround time of trauma-related imaging studies being finalized within 48 hours in an emergency radiology department, offering a perspective from a tertiary care hospital. Can Assoc Radiol J. 2021;72(4):862-870. PubMed
116.Jalal S, Ouellette H, Ante Z, Munk P, Khosa F, Nicolaou S. Impact of 24/7/365 attending radiologist coverage on the turnaround time in an emergency and trauma radiology department. Can Assoc Radiol J. 2021;72(3):548-556. PubMed
117.Macri F, Niu BT, Erdelyi S, et al. Impact of 24/7 onsite emergency radiology staff coverage on emergency department workflow. Can Assoc Radiol J. 2022;73(1):249-258. PubMed
118.Nair R, Hon BS, Mondal P, et al. LO56: Optimizing ED return visits for ultrasound imaging: a quality improvement initiative. In: CAEP/ACMU 2023 Scientific Abstracts. CJEM. 2023;25(Suppl 1):S27. https://link.springer.com/content/pdf/10.1007/s43678-023-00508-z.pdf. Accessed 2023 Aug 09.
119.Jones A, Bronskill SE, Schumacher C, Seow H, Feeny D, Costa AP. Effect of access to after-hours primary care on the association between home nursing visits and same-day emergency department use. Ann Fam Med. 2020;18(5):406-412. PubMed
120.Humber River Health. Command Centre: a digital revolution for delivering care. 2022: https://www.humbercommandcentre.ca/. Accessed 2023 Aug 16.
121.Suarthana E, Almeida N. The feasibility and clinical value of establishing hospital capacity command centres. (Report no. 92). Montreal (QC): Technology Assessment Unit (TAU) of the McGill University Health Centre (MUHC); 2023: https://muhc.ca/sites/default/files/micro/m-TAU/tau-report-2023-02-20.pdf. Accessed 2023 Aug 17.
122.National Institute for Health and Care Excellence. Recommendations for research: Emergency and acute medical care in over 16s: service delivery and organisation. (NICE guideline NG94) 2018; https://www.nice.org.uk/guidance/ng94/chapter/recommendations-for-research#recommendations-for-research. Accessed 2023 Aug 16.
123.Moustapha A, Mah AC, Roberts L, et al. Can ED chest pain patients with intermediate HEART scores be managed as outpatients? CJEM. 2022;24(7):770-779. PubMed
124.Chang Y, Carsen S, Keely E, Liddy C, Kontio K, Smit K. Electronic consultation systems: impact on pediatric orthopaedic care. J Pediatr Orthop. 2020;40(9):531-535. PubMed
125.Liddy C, Boulay E, Crowe L, et al. Impact of the Connected Medicine collaborative in improving access to specialist care: a cross-sectional analysis. CMAJ Open. 2021;9(4):E1187-E1194. PubMed
126.Vimalananda VG, Orlander JD, Afable MK, et al. Electronic consultations (E-consults) and their outcomes: a systematic review. J Am Med Inform Assoc. 2020;27(3):471-479. PubMed
127.Beauchet O, Afilalo M, Allali G, Lubov J, Galery K, Launay CP. “Emergency Room Evaluation and Recommendations” and incident hospital admissions in older people with major neurocognitive disorders visiting emergency department: results of an experimental study. Dement Geriatr Cogn Disord. 2022;51(3):291-296. PubMed
128.Barker LC, Lee-Evoy J, Butt A, et al. Delivering collaborative mental health care within supportive housing: implementation evaluation of a community-hospital partnership. BMC Psychiatry. 2022;22(1):36. PubMed
129.von Wagner M, Queck A, Beekers P, et al. Towards accurate and automatic emergency department workflow characterization using a real-time locating system. Int J Healthc Manag. 2023.
130.Ospina MB, Bond K, Schull M, et al. Measuring overcrowding in emergency departments: a call for standardization (CADTH Technology report no. 67.1). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320a_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 May 05.
131.Bond K, Opsina M, Blitz S, et al. Interventions to reduce overcrowding in emergency departments. (CADTH Technology report no. 67.4). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320d_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Aug 29.
132.Rowe B, Bond K, Opsina M, et al. Data collection on patients in emergency departments in Canada. (CADTH Technology report no. 67.2). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320b_overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Aug 29.
133.Rowe B, Bond K, Opsina M, et al. Frequency, determinants, and impact of overcrowding in emergency departments in Canada: a national survey of emergency department directors. (CADTH Technology report no. 67.3). Ottawa (ON): CADTH; 2006: https://www.cadth.ca/sites/default/files/pdf/320c_Overcrowding_tr_e_no-appendices.pdf. Accessed 2023 Aug 29.
Authors: Jeff Mason, Sean Secord, Danielle MacDougall
Acknowledgements: Angela Barbara, Nazia Darvesh, Gino De Angelis, Robyn Haas, Amil Reddy, Carolyn Spry, Jennifer Skuce, Yan Wang, and Tasleem Nimjee, MSc, MD CCFP (EM), CPHIIMS-CA, Emergency Medicine Staff Physician, Humber River Hospital
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.