CADTH Horizon Scan
Objective Assessment System for Cognitive Function
Health Technology Update
Authors: Weiyi Xie, Sarah C. McGill
Key Messages
Horizon Scan reports provide brief summaries of information regarding new and emerging health technologies; these technologies are identified through the CADTH Horizon Scanning Service as topics of potential interest to health care decision-makers in Canada.
Identifying cognitive conditions allows health professionals to develop tailored rehabilitation strategies and track treatment effects for people with functional impairment.
This Horizon Scan summarizes the available information regarding an emerging technology, VoxNeuro CORE, and its software for the objective evaluation of cognitive performance, the cognitive health assessment management platform (CHAMP).
The Cognitive Health Assessment Management Platform System
Cognitive dysfunction can occur in conditions such as traumatic brain injuries (TBIs)1 (e.g., concussion) and cognitive impairment associated with conditions such as dementia.2 As an alternative or adjunct to cognitive behavioural assessments, VoxNeuro CORE can objectively evaluate brain performance using neurophysiological data captured by an electroencephalography (EEG) recording that can be used to inform clinical decision-making in treatment and rehabilitation.3
How It Works
VoxNeuro CORE is a noninvasive cognitive health assessment system designed to detect brain function using computerized cognitive and neuropsychological tests with simultaneous EEG recording of brain electrical activity.3 Event-related potentials (ERPs), which are biomarkers of cognitive processes,4 are captured by EEG and analyzed against a normative database to score cognitive function, including attention and concentration, information processing, and memory.5 Figure 1 illustrates the different amplitudes of ERP components (i.e., N100, N200, and P300) as seen in EEG waveforms of a person with cognitive impairment compared with the normative database, which reflect differences in brain responses to stimuli and tasks. Decreased amplitude of a wave component can indicate impairment in attention and concentration, information processing, or memory. Using the normative database allows assessment at any time without the need for baseline cognitive scores.
VoxNeuro CORE consists of standard stationary EEG equipment with 6 electrodes attached to the head, including 1 ground electrode and 1 reference electrode (Douglas Martin, Brand Manager, VoxNeuro Inc., Toronto, ON: personal communication, April 20, 2023). The lead-based EEGs can be easily applied to patients with various hair textures, head shapes, and head sizes. The 31-minute assessment includes a 5-minute awake and drowsy test, a 3.5-minute auditory evoked potential test, a 3.5-minute visual evoked potential test, a 10.5-minute attention and concentration as well as information processing test, and an 8.5-minute memory test (Douglas Martin, Brand Manager, VoxNeuro Inc., Toronto, ON: personal communication, April 20, 2023).
VoxNeuro CORE is intended as an adjunct to standard clinical assessment. The cloud-based software compares test results against the normative database and reports patient scores for each cognitive function, providing objective data to inform rehabilitation, develop personalized treatment plans, and track recovery over time.5
Figure 1: Hypothetical Event-Related Potential Waveforms of a Person With Cognitive Dysfunction Compared With the Normative Database
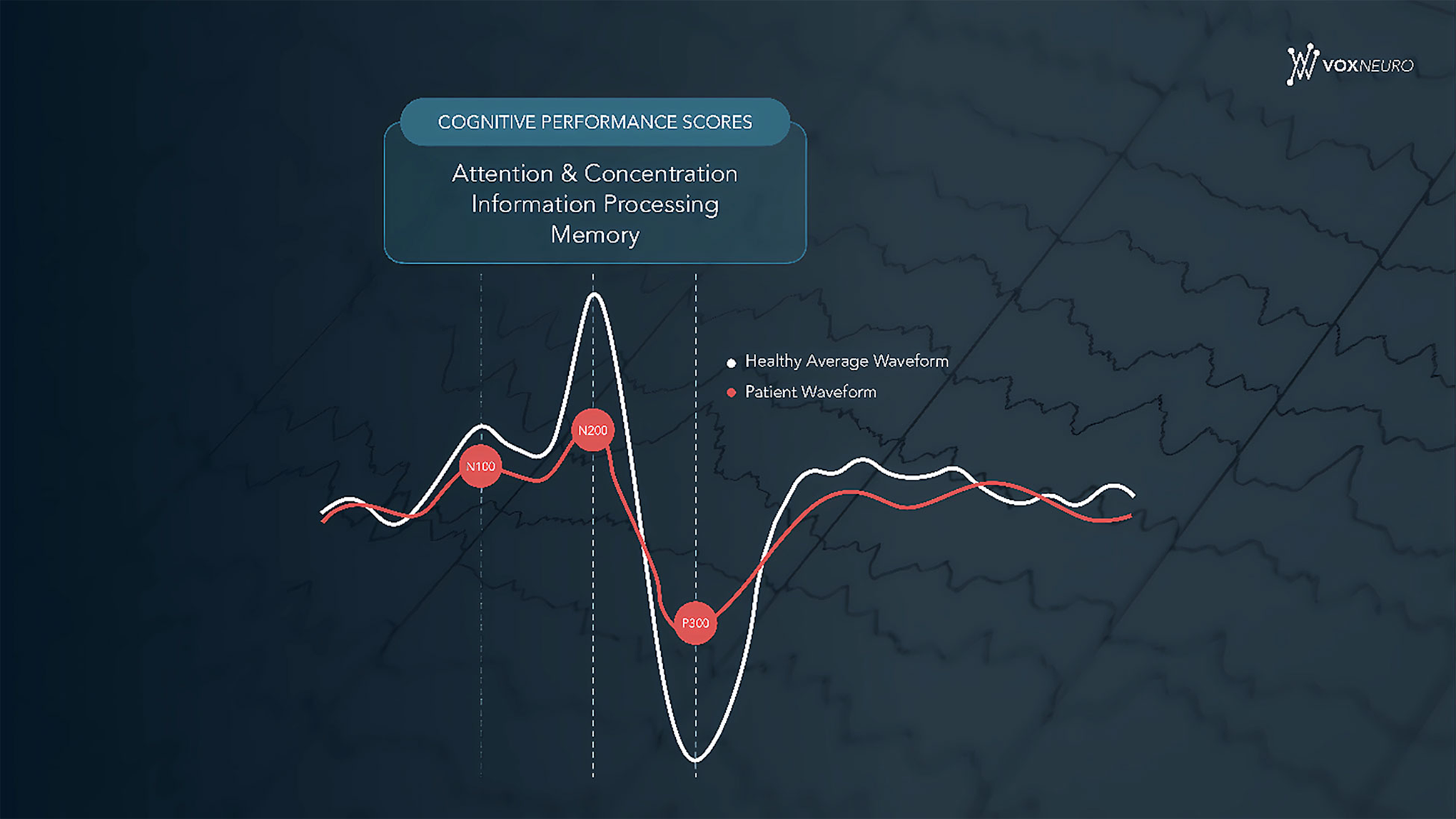
Source: Reproduced with permission from Douglas Martin, Brand Manager, VoxNeuro Inc.
Who Might Benefit?
VoxNeuro CORE is intended for use for individuals aged 12 to 90 years experiencing functional brain impairment resulting from neurological conditions such as TBI, and cognitive impairment, including dementia. Based on microsimulation models, the Public Health Agency of Canada estimated that TBI and dementia would be 2 of the 7 most prevalent neurological conditions in Canada between 2011 and 2031.6 In Canada, more than 6.7% of people aged 65 and older were reported to be living with dementia in 2016 to 2017.7 VoxNeuro CORE could be used repeatedly over time to track functional brain changes and treatment effects for individuals with dementia.
More than 20,000 people are hospitalized for mild-to-severe TBI every year in Canada, and emergency department visits related to TBI increased between 1990 to 2018.8 In addition, a 2018 publication from the Public Health Agency of Canada reported that approximately 20% of people aged 12 years and older who experienced a TBI did not seek care within 48 hours of their injury.9 Mild TBI, including concussion, can be difficult to diagnose due to the subtle signs and symptoms that patients experience10 and the self-reported nature of neurocognitive tests11 guiding the triage decision for further image investigation of brain injuries.12 Emerging objective tests have the potential to improve the evaluation of mild TBI.13 Moreover, patients who are in a coma, who cannot be evaluated with traditional behavioural assessments due to inability to communicate may benefit greatly from the EEG-based VoxNeuro CORE measure because it requires no verbal or behavioural responses.5
Other people who might benefit from VoxNeuro CORE include people with cognitive impairments caused by psychiatric disorders, such as major depressive disorder, attention-deficit/hyperactivity disorder (ADHD), and schizophrenia.5 Psychiatric disorders contribute to the disease burden in Canada; 4.7% of people were affected by major depressive disorder in 2012,14 8.7% of children and youth aged 4 to 17 years were affected by ADHD in 2015,15 2.9% of adults aged 20 to 64 years were affected by ADHD in 2012,16 and 1% of people aged 10 years or older were affected by schizophrenia in 2016 to 2017.17 Cognitive impairment was reported as a symptom of major depressive disorder 18 and ADHD.19 In addition, people with schizophrenia were found to have clinically significant greater estimated cognitive decline compared with participants without schizophrenia.20
Availability in Canada
Health Canada licensed CHAMP as a Class II Medical Device in 2021.21 FDA licensed CHAMP as a Class II Exempt Medical Device in 2021.21
What Does It Cost?
Information on the cost of the VoxNeuro CORE was unavailable. Main economic considerations for using the assessment include leasing fees for the hardware as well as costs for equipment setup and training, and pay-per-use software subscription fees, the price of which will become lower for VoxNeuro-certified clinics as the number of assessments performed increases (Douglas Martin, Brand Manager, VoxNeuro Inc., Toronto, ON: personal communication; March 9, 2023). Time associated with online and in-person training is also part of the cost to implement VoxNeuro CORE. Additional costs for patients may include charges for the assessment used as a complement to standard cognitive assessments,22 especially for repeated testing to track cognitive changes. According to the manufacturer, the assessment is covered by workplace insurance and the Treatment and Assessment Plan (OCF-18) in Ontario,5 but it is unclear whether the cost is covered by other jurisdictions in Canada, thus it is likely that patients need to pay out-of-pocket or seek support from other resources.23
Current Practice
Assessment of cognitive performance is usually conducted using validated neuropsychological screening tools such as the Mini-Mental State Examination, the Montreal Cognitive Assessment, and the cognitive subscale of the Alzheimer’s Disease Assessment Scale.24 Validated cognitive measures recommended by the National Institute for Health and Care Excellence guideline for patients suspected of dementia include the 10-point cognitive screener, 6-item cognitive impairment test, 6-item screener, Memory Impairment Screen, Mini-Cog, and the Test Your Memory test.25 Some of these measures detect various functions, such as attention, concentration, orientation, and memory,26-28 while others assess specific cognitive domains by using word recall and object naming tasks.29-31 These performance-based measures cannot be used in behaviourally unresponsive patients with conditions such as communication barriers, acute brain injury, and coma.
What Is the Evidence?
No published evidence for the use of VoxNeuro CORE or CHAMP to assess cognitive function was identified. The application of ERPs for cognitive assessment is well-documented;4 1 study was found that investigated the long-term cognitive consequences of concussion using ERPs, which was a 2019 cohort study led by the cofounder and chair of the VoxNeuro advisory board.1 However, no data were collected about the effectiveness VoxNeuro CORE itself.
Safety
No evidence about the safety of VoxNeuro CORE or CHAMP was identified in published literature. VoxNeuro CORE is a noninvasive measure using EEG, which is generally considered safe and painless.32
Issues to Consider
The clinical utility and clinical effectiveness of VoxNeuro CORE have not been compared with other cognitive assessment measures. In addition, there are no evidence-based recommendations regarding the use of objective cognitive measures for screening or diagnosing patients suspected of cognitive dysfunction. If found to be effective, other challenges in implementation could include the upfront cost of the device and software, training of staff, and the time associated with the assessment. Although VoxNeuro CORE is designed to be easily administered by individuals with limited knowledge of EEG, training is still required for the health staff to do the assessment. Additionally, administering the assessment in combination with standard cognitive measures would add time to the clinical evaluation, especially in the long-term rehabilitation process. Finally, if cost coverage mainly relies on out-of-pocket payment and private insurance, inequitable access to the device would be an important issue to consider, particularly for equity-deserving groups.
Related Developments
Other Objective Cognitive Assessment Devices
Most EEG-based cognitive assessment systems are primarily designed to diagnose patients with cognitive impairments, such as the BrainScope,33,34 Evoke Neuroscience and eVox Brain Health System,35 and NeuroCatch Platform.36 For example, BrainScope is intended to assist in the diagnosis of traumatic brain injury.33,34
Cognision37 is an EEG-based device used to monitor disease progression and treatment outcomes and measure cognitive domains, including working memory, focal attention, executive function, and brain processing speed.5,37 According to the manufacturer’s website, it requires the use of specially designed hardware.37
The Evoke Neuroscience and eVox Brain Health System,35 NeuroCatch Platform,36 and Cognision37 use a headset unlike VoxNeuro CORE, which makes them less accessible to individuals with coarse and curly hair textures, cornrows, and braids; above or below average head sizes; or severe brain injuries. Other objective cognitive assessment devices include WAVi,38 which combines EEG and heart rate variability measures,38 and the virtual reality–based Neuroflex.39
VoxNeuro CORE Used for Active Military Personnel
VoxNeuro is collaborating with the Canadian Armed Forces to investigate the cognitive consequences of intense military combat training regimens using VoxNeuro CORE before and after training.40 The study will also explore the extent to which VoxNeuro CORE assessment results could inform clinical decision-making.40
Assisting in Disease Diagnosis and Prognosis
Although VoxNeuro CORE is intended to inform rehabilitation, it also has the potential to aid in diagnosis. A research team at Boston University is studying the diagnostic accuracy of ERPs for Alzheimer disease and mild cognitive impairment in collaboration with VoxNeuro.41 In addition, researchers at VoxNeuro are investigating the application of machine learning to better identify neurophysiological biomarkers and improve disease prognosis for conditions such as coma.42
Looking Ahead
If proven to be effective, EEG-based cognitive assessments such as VoxNeuro CORE can be valuable tools in evaluating brain function by providing objective data independent of behavioural responses. However, further clinical studies comparing it with other cognitive assessments are needed to develop evidence-based guidelines regarding the use of such objective measures either on their own or as an adjunct to existing clinical cognitive assessments. Additionally, information on the cost of VoxNeuro CORE, including cost-effectiveness of the system compared with current behavioural assessments and/or other objective assessments, is essential to address cost and coverage issues, ensuring equitable access to people who can benefit from objective cognitive measures.
References
1.Ruiter KI, Boshra R, Doughty M, Noseworthy M, Connolly JF. Disruption of function: neurophysiological markers of cognitive deficits in retired football players. Clin Neurophysiol. 2019;130(1):111-121. PubMed
2.Paitel ER, Samii MR, Nielson KA. A systematic review of cognitive event-related potentials in mild cognitive impairment and Alzheimer's disease. Behav Brain Res. 2021;396:112904. PubMed
3.VoxNeuro. Healthcare provider brochure. 2022; https://nursing.queensu.ca/sites/default/files/inline-files/VoxNeuro%20Healthcare%20Providers%20Brochure%20%28additional%20resource%20%232%29.pdf Accessed 2023 Mar 10.
4.Connolly JF. Clinical neurophysiology: research methods and event-related potential components as assessment tools. Handb Clin Neurol. 2020;174:277-287. PubMed
5.VoxNeuro. 2023; https://voxneuro.com/. Accessed 2023 Mar 27.
6.Mapping Connections: An understanding of neurological conditions in Canada. The National population health study of neurological conditions. Ottawa (ON): Public Health Agency of Canada; 2014, updated 2018: https://www.canada.ca/en/public-health/services/reports-publications/mapping-connections-understanding-neurological-conditions.html. Accessed 2023 Mar 27.
7.Aging and chronic diseases: a profile of Canadian seniors. Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/aging-chronic-diseases-profile-canadian-seniors-report.html#a3_7a. Accessed 2023 Mar 10.
8.Injury in review, 2020 edition: spotlight on traumatic brain injuries across the life course. Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/en/public-health/services/injury-prevention/canadian-hospitals-injury-reporting-prevention-program/injury-reports/2020-spotlight-traumatic-brain-injuries-life-course.html. Accessed 2023 Mar 10.
9.Rao DP, McFaull S, Thompson W, Jayaraman GC. Traumatic brain injury management in Canada: changing patterns of care. Health Promotion and Chronic Disease Prevention in Canada. 2018;38(3):147-150. https://www.canada.ca/en/public-health/services/reports-publications/health-promotion-chronic-disease-prevention-canada-research-policy-practice/vol-38-no-3-2018/traumatic-brain-injury-management-canada.html. Accessed 2023 Apr 27. PubMed
10.Centers for Disease Control and Prevention. Symptoms of mild TBI and concussion. 2023; https://www.cdc.gov/traumaticbraininjury/concussion/symptoms.html. Accessed 2023 Apr 27.
11.Non-pharmacological interventions for the management of concussion. (CADTH scoping summary). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/pdf/de0100-concussion-scoping-summary.pdf. Accessed 2023 Apr 27.
12.Guideline for concussion/mild traumatic brain injury & prolonged symptoms. Adults 18+, healthcare professional version, third ed. Toronto (ON): Ontario Neurotrauma Foundation; 2018: https://braininjuryguidelines.org/concussion/fileadmin/media/Concussion_guideline_3rd_edition_final.pdf. Accessed 2023 Apr 27.
13.Marchand DK, Severn M. Biomarker-based point-of-care tests for the evaluation of mild traumatic brain injury. (CADTH Issues in Emerging Health Technologies, issue 188). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/biomarker-based-point-care-tests-evaluation-mild-traumatic-brain-injury. Accessed 2023 May 2.
14.Palay J, Taillieu TL, Afifi TO, et al. Prevalence of mental disorders and suicidality in Canadian Provinces. Can J Psychiatry. 2019;64(11):761-769. PubMed
15.Morkem R, Handelman K, Queenan JA, Birtwhistle R, Barber D. Validation of an EMR algorithm to measure the prevalence of ADHD in the Canadian Primary Care Sentinel Surveillance Network (CPCSSN). BMC Med Inform Decis Mak. 2020;20(1):166. PubMed
16.Hesson J, Fowler K. Prevalence and correlates of self-reported ADD/ADHD in a large national sample of Canadian adults. J Atten Disord. 2018;22(2):191-200. PubMed
17.Canadian Chronic Disease Surveillance System. Schizophrenia (aged 10+); and use of health services for schizophrenia (aged 1+). 2019; https://health-infobase.canada.ca/datalab/schizophrenia-blog.html?=undefined&wbdisable=true#fn1. Accessed 2023 Mar 27.
18.Perini G, Cotta Ramusino M, Sinforiani E, Bernini S, Petrachi R, Costa A. Cognitive impairment in depression: recent advances and novel treatments. Neuropsychiatr Dis Treat. 2019;15:1249-1258. PubMed
19.Das D, Cherbuin N, Anstey KJ, Easteal S. ADHD symptoms and cognitive abilities in the midlife cohort of the PATH Through Life Study. J Atten Disord. 2015;19(5):414-424. PubMed
20.Fujino H, Sumiyoshi C, Yasuda Y, et al. Estimated cognitive decline in patients with schizophrenia: a multicenter study. Psychiatry Clin Neurosci. 2017;71(5):294-300. PubMed
21.McGilp K. VoxNeuro receives Health Canada Class II Medical Device designation. 2021; https://www.businesswire.com/news/home/20210728005255/en/VoxNeuro-receives-Health-Canada-Class-II-Medical-Device-designation.
22.Professor John F. Connolly – Breaking Through Barriers: Assessing cognitive function in patients unable to communicate and those with invisible injuries. Scientia. 2020 Oct 2. https://www.scientia.global/professor-john-f-connolly-breaking-through-barriers-assessing-cognitive-function-in-patients-unable-to-communicate-and-those-with-invisible-injuries/. Accessed 2023 Mar 2.
23.Livelong Wellness Clinic. 2023; https://www.livelongwellness.ca/voxneuro.
24.Pottie K, Rahal R, Jaramillo A, et al. Recommendations on screening for cognitive impairment in older adults. Can Med Assoc J. 2016;188(1):37-46. PubMed
25.National Institute for Health and Care Excellence. Dementia: assessment, management and support for people living with dementia and their carers. (NICE guideline NG97). 2018; https://www.nice.org.uk/guidance/ng97, 2023 Mar 27.
26.Arevalo-Rodriguez I, Smailagic N, Roqué IFM, et al. Mini-Mental State Examination (MMSE) for the detection of Alzheimer's disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev. 2015;2015(3):Cd010783. PubMed
27.Rosen WG, Mohs RC, Davis KL. A new rating scale for Alzheimer's disease. Am J Psychiatry. 1984;141(11):1356-1364. PubMed
28.Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53. PubMed
29.Buschke H, Kuslansky G, Katz M, et al. Screening for dementia with the memory impairment screen. Neurology. 1999;52(2):231-238. PubMed
30.Brooke P, Bullock R. Validation of a 6 item cognitive impairment test with a view to primary care usage. Int J Geriatr Psychiatry. 1999;14(11):936-940. PubMed
31.Hancock P, Larner A. Test Your Memory test: diagnostic utility in a memory clinic population. Int J Geriatr Psychiatry. 2011;26(9):976-980. PubMed
32.National Health Service. Electroencephalogram (EEG). 2022; https://www.nhs.uk/conditions/electroencephalogram/. Accessed 2023 Mar 27.
33.BrainScope. 2023; https://www.brainscope.com/. Accessed 2023 Mar 27.
34.Jones S, Loshak H. An overview of new and emerging technologies for the pre-hospital identification of ischemic stroke. CADTH Issues in Emerging Health Technologies, issue 186. Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/hs-eh/eh0080-pre-hospital-identification-of-ischemic-stroke.pdf. Accessed 2023 May 2.
35.Evoke Neuroscience and eVox Brain Health System. 2023; https://evokeneuroscience.com/. Accessed 2023 Mar 27.
36.NeuroCatch Platform. 2023; https://www.neurocatch.com/. Accessed 2023 Mar 27.
37.Cognision. 2023; https://www.cognision.com/. Accessed 2023 Mar 27.
38.WAVI. 2023; https://wavimed.com/. Accessed 2023 Mar 27.
39.Neuroflex. 2023; https://www.neuroflex.io/. Accessed 2023 Mar 27.
40.Martin D. VoxNeuro announces collaboration with the Canadian Armed Forces and launch of clinical study measuring impact of training-related sub-concussive exposure. Business Wire. 2022 Sep 27. https://www.businesswire.com/news/home/20220927005172/en/VoxNeuro-Announces-Collaboration-with-the-Canadian-Armed-Forces-and-Launch-of-Clinical-Study-Measuring-Impact-of-Training-Related-Sub-Concussive-Exposure.
41.Boston University. NCT05673759: Event-Related Potential (ERP) components in clinical diagnosis. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://clinicaltrials.gov/ct2/show/NCT05673759?term=katherine+turk&draw=2&rank=2. Accessed 2023 Mar 27.
42.Connolly JF, Reilly JP, Fox-Robichaud A, et al. Development of a point of care system for automated coma prognosis: a prospective cohort study protocol. BMJ Open. 2019;9(7):e029621. PubMed
Appendix 1: Methods
Literature Search Strategy
An information specialist conducted a literature search on key resources including MEDLINE, Embase, and PsycInfo via Ovid; Scopus; the International HTA Database; and a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were cognitive health assessment software platforms or the device names VoxNeuro or CHAMP. The search was completed on March 9, 2023, and was limited to English- or French-language documents published since January 1, 2018. Regular alerts updated the search until April 24, 2023.
Study Selection
One author screened the literature search results and reviewed the full text of all potentially relevant studies. Studies were considered for inclusion if the intervention was VoxNeuro CORE or a cognitive health assessment management platform. Conference abstracts and grey literature were included when they provided additional information to that available in the published studies. These searches were supplemented by reviewing bibliographies of key papers and through contacts with industry.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca