CADTH Health Technology Review
Strategies to Reduce Alternate Level of Care
Environmental Scan
Key Messages
What Is the Issue?
Alternate level of care (ALC) is when a patient is occupying a bed in a hospital and does not require the intensity of resources or services provided in that hospital. ALC is a persistent barrier to providing efficient health care in Canada, as it is in most health systems worldwide (where ALC is referred to as delayed discharge).
Older adults (aged 65 years or older) who require placement in residential care are the largest subgroup of the ALC patient population.
Analyzing ALC use data can inform decision-makers about data trends and which jurisdictions have reduced ALC times.
By understanding the strategies, policies, or other interventions that have been used to reduce ALC in Canada, and which have been successful at minimizing ALC, decision-makers can consider which strategies to implement in their health jurisdictions.
What Did We Do?
We analyzed Canadian Institute for Health Information data related to ALC and average length of ALC in older adults in the provinces and territories of Canada.
We conducted an environmental scan of the academic and grey literature to:
identify strategies to address ALC in older adults in Canada
identify strategies that have been effective in reducing ALC in older adults in Canada.
What Did We Find?
In 2022 to 2023, Canada (excluding Quebec) had 15 ALC hospitalizations per 1,000 population, 369 total ALC days per 1,000 population, and a mean of 25 ALC days per hospitalization in patients aged 65 and older awaiting admission to residential care or elsewhere.
While there were variations across jurisdictions, the trends in ALC over time for adults aged 55 years and older were relatively consistent.
Patients with more ALC days were aged 75 years and older, had lower incomes, and were admitted to the hospital as urgent.
We identified 19 strategies that addressed ALC in older adults in Canada. These included input, throughput, and system-level interventions, which we categorized as live information sharing, recommended initiatives, tools and guidelines, practice changes, and infrastructure and finance.
We identified 4 studies that reported a favourable effect of a throughput or system-level strategy compared to no strategy or standard care on ALC hospitalizations, length of stay, or discharge to home.
Two throughput strategies may be effective: the Subacute Care for the Frail Elderly (SAFE) Unit improved ALC length of stay (LOS), hospital LOS, and discharge to home, and the Transitional Care Unit improved discharge to home.
Two system-level strategies may be effective: Home First improved ALC hospitalizations, ALC LOS, and discharge to home, and Behavioural Supports Ontario improved ALC hospitalizations and ALC LOS.
What Does This Mean?
We found common themes in our environmental scan that decision-makers may incorporate into strategies for addressing ALC in older adults waiting for residential care, including the provision of integrated care, promotion of age-friendly care, early identification of patients at risk of ALC, sharing of tools and resources, transitional care, and inclusion of families and caregivers in care planning.
This report may serve as the first step for future systematic reviews or other evidence syntheses with a broader scope. Future research might investigate the factors that contribute to ALC and interventions to address those factors.
Abbreviations
ALC
alternate level of care
CIHI
Canadian Institute for Health Information
ED
emergency department
IQR
interquartile range
LHIN
Local Health Integration Network
LOS
length of stay
LTC
long-term care
SAFE
Subacute Care for the Frail Elderly
Background and Context
What Is Alternate Level of Care?
Alternate level of care (ALC) is a designation used in Canada that is applied by clinical staff to that portion of a patient’s hospital stay when the patient is occupying a bed in a facility (e.g., acute care hospital) and does not require the intensity of resources or services provided in that care setting.1 There are several reasons that patients designated as ALC continue to occupy a hospital care bed or use hospital resources. People may present to a hospital emergency department (ED) — which then leads to hospitalization and ALC — for nonacute medical or social reasons because of a (real or perceived) lack of access to more appropriate services (e.g., primary care, long-term care [LTC], community supports).2-6 Patients who have an ALC designation may require new or additional services and are waiting for availability, such as home care or specialized care.2,3 Other factors contributing to ALC include the underestimation of the potential for patient independence, the deconditioning of patients as a consequence of inactivity and bedrest while in the hospital, and a lack of awareness by hospital staff about available resources for patients to receive care at home and in the community.4,7
As in most health systems worldwide (where ALC is referred to as delayed discharge), ALC is a current challenge in Canada. Since 2017, the rate of ALC and length of stay (LOS) in ALC has increased across jurisdictions in Canada. In 2022 to 2023, 6.2% of hospitalizations had ALC, with a provincial and territorial range of 1.0% to 8.3%;8 and 17.0% of hospital days were for patients in ALC, with a provincial and territorial range of 6.8% to 26.0%.8
Who Is Impacted?
ALC directly negatively impacts patients with an ALC designation.9 ALC has been associated with mortality, adverse events, hospital-acquired infections, and mental and physical deterioration.4,7,10-13 Patients, family, and caregivers have reported poor experiences with ALC, including confusion, stress, uncertainty, and frustration.4,7,14
ALC also impacts hospitals, as well as the entire health care system, and thus all other patients indirectly.9 ALC contributes to ED and hospital overcrowding.15 It is an inefficient use of finite and costly hospital resources and restricts the capacity to provide appropriate acute care.2 Higher hospital costs are due in part to patients occupying beds after they are medically fit for discharge, delays in hospital admissions that may occur when beds are still occupied by patients with an ALC designation, backlogs in ED and patient flow, deferred surgeries, hospital staff time, and administration costs.10
Attention to ALC in Canada may support health care systems to function with improved resource allocation, clinical outcomes, and quality of care for patients.16
Patient Population
People who require placement in residential care make up a significant proportion of the patient population with an ALC designation, with estimates ranging from 42% to 90%.17-21
In 2019, there were 6.6 million older adults aged 65 years and older and 838,200 people aged 85 and older in Canada.22 By 2040, one-quarter of people (10.7 million) in the country will be older adults, with the number of those aged 85 and older expected to triple to more than 2 million by 2050.22,23 People may experience health challenges and the need for care and support during their years lived at older age.22 Rates of chronic disease and neurodegenerative disorders are also increasing in Canada.16 These factors lead to increased demands for acute episodic care at the hospital level and within the community for residential care, which include LTC homes or facilities, nursing homes, private care homes, and special care homes.16 Unless these demands can be supported in alternate settings, such as community-based care settings, ALC rates are expected to increase.24
Purpose and Objectives
Analyzing real-world ALC use data can inform decision-makers about data trends and which jurisdictions have reduced ALC times. Implementing strategies targeted at avoiding or reducing ALC rates are key priorities for health care facilities and health regions in Canada. Because the largest subgroup of patients with an ALC designation are older adults (aged 65 years and older) waiting for residential care, this population group is a priority.20 By understanding the strategies, policies, or other interventions that have been used to reduce ALC in Canada, and which have been successful at minimizing ALC, decision-makers can consider which strategies to implement in their health jurisdictions.
The purpose of this evidence report is to present real-world data on ALC across jurisdictions, as well as to present health care decision-makers in Canada with an overview of strategies that have been recommended, implemented, and evaluated for effectiveness to reduce ALC in older people who are approved for and waiting for placement in residential care.
The key objectives are to:
analyze Canadian Institute for Health Information (CIHI) data related to ALC in older adults in the provinces and territories of Canada
identify strategies that have been effective in decreasing hospital LOS and/or improving patient flow in older adults waiting for placement in residential care
identify and describe how health care centres or regions in Canada are handling ALC in older adults waiting for placement in residential care.
Methods
To meet the key objectives and support decision-making, we conducted an analysis of real-world data and an environmental scan.
Analysis of Real-World Data
We worked collaboratively with CIHI to obtain hospitalizations and lengths of stay of patients with an ALC designation in Canada from the Discharge Abstract Database for the 5 most recent fiscal years (2018–2019 to 2022–2023).25,26 We obtained patient characteristics and ALC days by characteristics of patients with an ALC designation for 2022 to 2023. We used publicly available population data from Statistics Canada to calculate rates per 1,000 population.27,28 We reported descriptive statistics and produced narrative summaries of the findings by jurisdiction. We did not perform any hypothesis testing (i.e., calculating P values).
The Discharge Abstract Database has 1 field for the reporting of days in ALC, although some jurisdictions may capture a waiting period to assess the needs of patients (i.e., waiting for “panelling” or the process for assessing and approving applications for personal care homes or LTC) and a separate waiting period once patients are approved for residential care (i.e., “panelled” or assessed and approved for a personal care home or LTC and waiting for placement). These data are not available in the data held by CIHI; therefore, we reported on patients with an ALC designation who had an ALC diagnosis Z-code to identify that they were awaiting admission to an adequate facility elsewhere. This included patients waiting for residential care, chronic care, a private facility, complex continuing care, hospice for palliative care, or an addictions program.
Further details about the real-world data analysis are described in Appendix 1.
Environmental Scan
We searched key information and data sources — including journal databases — and conducted focused internet searches for relevant evidence on ALC strategies, policies, plans, models, or guidelines.
We included articles on strategies to address ALC in older adults in Canada that were published in the past 5 years (i.e., 2019 to 2024). Because of the small number of studies evaluating the effectiveness of ALC strategies published in the past 5 years, we expanded our time frame and included clinical studies published in the past 10 years (i.e., 2014 to 2024).
One reviewer conducted a descriptive analysis and produced a narrative synthesis of the findings. One reviewer collected and extracted the data for the included literature. The strategies were initially organized using a modified version of the input-throughput-output conceptual model15,29 that is presented in Figure 1.
The strategies were then organized using a modified version of Doern and Phidd’s conceptual framework for classifying policy instruments or tools along a continuum from those that are least coercive (e.g., information sharing) to those that are more coercive (e.g., public ownership or new infrastructure).6,30 The 4 modified categories were information sharing (i.e., live sharing or documented initiatives); tools and guidelines; practice changes; and infrastructure and finance. The category descriptions and strategies for each category are presented in Table 4.
We recognize that several strategies may fit into multiple categories and several categories are overlapping in each model; however, for reporting simplicity, we selected 1 category from each model for the included strategies.
Figure 1: Organization of Strategies to Reduce ALC
ALC = alternate level of care.
Note: Based on the conceptual model developed by Asplin et al. (2003)29 and the CADTH report on emergency department overcrowding (2023).15
Details regarding the literature search strategy and selection criteria for the environmental scan are described in Appendix 1.
Peer Review
A draft version of this report was reviewed by 1 content expert with experience in practice and policy research related to optimizing delivery and outcomes for individuals with complex needs.
Findings
What Is the Real-World Data on ALC in Older Patients in Canada?
All ALC data should be interpreted with caution. There may be differences in data collection and reporting across jurisdictions and the findings may not be comparable.
ALC Hospitalizations
The number of hospitalizations with ALC days per 1,000 population in patients aged 65 and older awaiting admission to residential care or another facility elsewhere is presented by jurisdictions across Canada in Table 1. In the 2022 to 2023 fiscal year, the number of ALC hospitalizations for Canada (excluding Quebec) was 15 per 1,000 population of those 65 years and older, and varied by jurisdiction. The jurisdictions with the lowest rate of ALC hospitalizations were the combined data for Nunavut, the Northwest Territories, and Yukon; British Columbia; and Saskatchewan.
Total ALC Days
Total ALC days per 1,000 population in patients aged 65 and older awaiting admission to residential care or another facility elsewhere is presented in Table 2. In the 2022 to 2023 fiscal year, Canada (excluding Quebec) had 369 total ALC days per 1,000 population. Total ALC days was lowest in Saskatchewan, followed by British Columbia, and then the combined data from Nunavut, the Northwest Territories, and Yukon.
Table 1: Number of ALC Hospitalizations per 1,000 Population Aged 65 and Older in 2022 to 2023a
Jurisdiction | Number of ALC hospitalizations per 1,000 populationb |
|---|---|
Canada (excluding Quebec) | 15 |
Alberta | 17 |
British Columbia | 9 |
Manitoba | 14 |
New Brunswick | 14 |
Newfoundland and Labrador | 14 |
Nova Scotia | 12 |
Ontario | 18 |
Prince Edward Island | 14 |
Saskatchewan | 9 |
Territoriesc | 7 |
ALC = alternate level of care.
aThis covers the fiscal year of April 1, 2022, to March 31, 2023.
bThis is the number of ALC hospitalizations in patients aged 65 and older with an ALC designation and reason for ALC of Z75.1 per 1,000 population of those aged 65 years and older.
cCombined data for Nunavut, the Northwest Territories, and Yukon.
Table 2: Total ALC Days per 1,000 Population Aged 65 and Older in 2022 to 2023a
Jurisdiction | ALC days per 1,000 populationb |
|---|---|
Canada (excluding Quebec) | 369 |
Alberta | 411 |
British Columbia | 231 |
Manitoba | 469 |
New Brunswick | 492 |
Newfoundland and Labrador | 549 |
Nova Scotia | 661 |
Ontario | 370 |
Prince Edward Island | 829 |
Saskatchewan | 189 |
Territoriesc | 258 |
ALC = alternate level of care.
aThis covers the fiscal year of April 1, 2022, to March 31, 2023.
bThis is the total number of ALC days for patients aged 65 and older with an ALC designation and reason for ALC of Z75.1 per 1,000 population of those aged 65 years and older.
cCombined data for Nunavut, the Northwest Territories, and Yukon.
Average ALC Days
Average ALC days per hospitalization in patients aged 65 and older awaiting admission to residential care or another facility elsewhere are presented in Table 3 and provide an assessment of patient experiences. In the 2022 to 2023 fiscal year, Canada (excluding Quebec) had a mean of 25 ALC days per hospitalization. Despite a relatively large volume of ALC hospitalizations per capita (18 per 1,000 population of those aged 65 and older), Ontario had the shortest mean ALC days per hospitalization at 21. Saskatchewan also had a mean of 21 ALC days per hospitalization, but with a relatively smaller volume of ALC hospitalizations per capita (9 per 1,000 population of those aged 65 and older). Standard deviations were not available. Means, standard deviations, medians, and interquartile ranges for ALC days in adults aged 55 and older are available in Appendix 4.
Table 3: Mean ALC Days per Hospitalization in Patients Aged 65 Years and Older in 2022 to 2023a
Jurisdiction | Mean ALC days per hospitalizationb |
|---|---|
Canada (excluding Quebec) | 25 |
Alberta | 25 |
British Columbia | 27 |
Manitoba | 34 |
New Brunswick | 36 |
Newfoundland and Labrador | 39 |
Nova Scotia | 54 |
Ontario | 21 |
Prince Edward Island | 60 |
Saskatchewan | 21 |
Territoriesc | 37 |
ALC = alternate level of care.
Note: Standard deviations were not available.
aThis covers the fiscal year of April 1, 2022, to March 31, 2023.
bThis is the mean number of ALC days per hospitalization with an ALC in patients aged 65 years and older with an ALC designation and reason for ALC of Z75.1.
cCombined data for Nunavut, the Northwest Territories, and Yukon.
What Strategies, Policies, Plans, Models, or Guidelines Exist to Address ALC in Older People in Canada?
We included 19 strategies identified from the published and grey literature published between 2019 and 2024.
The strategies are organized by categories in Table 4. The details of each strategy are presented in Appendix 2.
Table 4: Categories,a Descriptions,a and Included Strategies to Reduce ALC
Category name | Category description | Input strategies | Throughput strategies | Output strategies | System-level strategies |
|---|---|---|---|---|---|
Information sharing: Live sharing | Information sharing through in-person or technology-based communication | — | — | — | Implementing ALC leading practices31 |
Information sharing: Recommended initiativesb | Information sharing through documents that share strategies (calls to action), suggestions, recommendations, or for informational purposes (motivation) | Virtual LTC @ Home32 | — | ||
Tools and guidelines | A tangible and concrete guide to inform practice; an implemented tool or guidance document that is being used in the health care system | Supporting OHTs to influence ALC37 | — | — | |
Practice changes | A change in how care is delivered | — | — | ||
Infrastructure and finance | Tangible structural or financial changes | New seniors’ housing complex44 | — | — |
ALC = alternate level of care; LTC = long-term care; OHT = Ontario Health Team; SAFE = Subacute Care for the Frail Elderly.
aBased on the modified version of Doern and Phidd’s conceptual framework30 used by Cadel et al. (2021).6
bRecommended initiatives often combine other categories.
Input Strategies
We identified 5 strategies that focused on preventing older adults from presenting to the hospital and subsequently waiting for a residential care placement as an ALC.
Information Sharing: Recommended Initiatives
A Virtual LTC @ Home Program proposal for Ontario recommends that older patients are cared for in their homes by a coordinated and integrated teams of providers.32
Tools and Guidelines
Supporting Ontario Health Teams to Influence ALC provides lead practices in community-based early identification, assessment, delivery of interventions, and transition, with links to resources and tools.37
Practice Changes
Two different types of strategies altered how usual care was delivered:
The Complex Care Hub program provides hospital-at-home services (as an alternate to hospital admission) in Alberta.40
The Community Paramedicine for LTC program is pioneered by community paramedics in 5 Ontario communities to help people waiting for LTC stay safely in their homes.41
Infrastructure and Finance
In 2022, the Ontario government committed to building a new seniors’ housing complex with 56 independent living suites as well as dedicated health spaces to provide a range of specialized services and supports onsite to postpone and reduce the demand for hospital care and ALC designation.44
Throughput Strategies
We identified 7 strategies that aimed to reduce ALC time for older patients so that waiting for residential care does not need to happen in the hospital.
Information Sharing: Recommended Initiatives
Three articles recommended strategies to decrease ALC LOS:
Molnar (2021)33 presented the required elements of a comprehensive Acute Care Dementia Strategy for hospitals in Canada.
The report ALC and Delayed Discharge: Lessons Learned from Abroad recommends multicomponent, tailored approaches for Canada based on a rapid scoping review and jurisdictional review of programs in the UK.34
Personal support homes are the homes of trained personnel where patients who have been discharged and do not require any specialized needs or supports would receive temporary personal support rather than waiting in Ontario hospitals as patients with an ALC designation.35
Infrastructure and Finance
Transitional or intermediate level of care interventions vary, but the key element is the concept of transition, usually from the hospital to a posthospital destination with the aim of reducing ALC time by speeding up discharge and preventing readmissions.49
Four transitional care programs were available for older ALC patients in Ontario:
The Harbour Light Integrated Transitional Services Program is for patients designated as ALC with bariatric or mental health and addiction needs in Toronto.45
The Subacute Care for the Frail Elderly (SAFE) Unit is a 20-bed program with a strong emphasis on a restorative, collaborative, and integrated approach; it is located within a large nursing home.46
The Pine Villa Reintegration Unit is a 69-bed program that provides therapeutic recreation and specialized supports for patients with dementia, mental health, additions, and social determinants of health needs, and responsible behaviours.47
The Reactivation Care Centres in Toronto specialize in activation therapies for patients with an ALC designation.48
Output Strategies
Output strategies focus on enabling older adults to return home to wait for residential care placement, rather than remain in the hospital as ALC until a transfer to residential care. While we did not identify any strategies that were primarily output strategies, several system-level strategies incorporated the goal of facilitating return to home following discharge for older patients with an ALC designation.
System-Level Strategies
We identified 7 resources that incorporated input, throughput, and output strategies to address ALC.
Information Sharing: Living Sharing
Provincial Geriatrics Leadership Ontario cohosted an event with The Centre for Implementation to bring together health planners and representatives from specialized geriatric services to discuss roles in the system and inner and outer factors affecting change, and to provide high-level recommendations to support implementation of ALC leading practices.31
Information Sharing: Recommended Initiatives
Confronting the Alternate Level of Care (ALC) Crisis with a Multifaceted Policy Lens36 proposed:
upstream (input) interventions to overtly reduce ALC admissions and ALC inpatient days directly and avoid unnecessary admissions likely to result in ALC inpatient days
midstream (throughput) interventions to target improving patient flow, improving efficiency, and reducing the length of an ALC stay
downstream (output) interventions that focus on facilitating effective, timely, and durable discharges.36
In the commentary on Scenarios for Seniors’ Care: Future Challenges, Current Gaps and Strategies to Address Them, Wyonch (2024)2 proposed strategies to apply in the different settings that provide care for older people in Canada.
Tools and Guidelines
Essential Role of Caregivers in Improving Transitions and Addressing Alternate Level of Care is a guide, with tools and resources, to help Ontario Health teams proactively include and support caregivers across health care sectors to alleviate ALC.38
The Alternate Level of Care (ALC) Leading Practices Guide: Preventing Hospitalization and Extended Stays for Older Adults provides evidence-based leading practices, with tools and resources, for the care and proactive management of older adults at risk of ALC.39
Practice Changes
We categorized Home First in Ontario42 and Home First – Quick Response Project in Saskatchewan43 as system-level strategies because the programs focus on:
keeping older people safe in their homes for as long as possible with community supports (input)
improving workflow and communication when acute care is required (throughput)
supporting patients with an ALC designation to return to their own homes to wait for a residential care placement by providing needed supports (output).42,43
Which Strategies Implemented in Canada to Address ALC in Older People Have Been Effective?
Summary of Study Characteristics
Six studies published between 2014 and 2024 met our inclusion criteria. These were 1 randomized controlled trial50 and 5 nonrandomized studies.42,46,51-53
Three studies evaluated throughput strategies,46,51,53 1 study assessed an output strategy,50 and 2 studies evaluated system-level strategies.42,52
The 3 throughput strategies46,51,53 were transitional care strategies that involved tangible structural and financial changes. The output strategy50 focused on practice changes. One system-level strategy focused on practice changes.42 The other system-level strategy52 fit into the tools and guidelines category and incorporated practice changes.
The ages of the older adults in the study populations ranged from 60 to 96 years.42,46,50-53
Three studies specified that their study sample included patients needing residential care.46,50,51
Four studies took place in Ontario.42,46,50,52 Two Ontario studies took place in 1 Local Health Integration Network (LHIN)42,50 and another Ontario study took place across all LHINs in Ontario.52 The fourth study took place in 1 urban setting.43
One study took place in British Columbia53 and another study took place in Newfoundland and Labrador.51 Both studies took place in urban settings.49,51
Equity Characteristics
In addition to study characteristics, we also extracted data about additional equity-deserving group characteristics.
Three of 6 studies reported the medical conditions (e.g., frailty, hypertension, osteoarthritis, diabetes, renal disease) of the study population.46,50,53
Four of 6 studies reported the mental health conditions (e.g., dementia, responsive behaviours, mood disorders) of the population.46,50,52,53
Five of 6 studies reported the “sex” of the population, although it is unclear whether it was sex or gender identity as this was poorly defined and reported in the literature.42,46,50,51,53
Two of 6 studies reported the place of residence (e.g., private residence, living alone, independent dwelling with family or friends, houseless) for the study population.50,53
One of 6 studies reported the socioeconomic status (i.e., material deprivation quintiles) of the population.42
None of the 6 studies reported any information about race, ethnicity or country of origin, language, gender or gender identity, newcomer status, or sexual orientation.
The study characteristics for each included study are presented in Appendix 3.
Evidence of Favourable Effect
We considered a strategy to have a favourable effect when the direction of the effect was positive in favour of the intervention versus a comparator. Four of the 6 included studies reported evidence of favourable effect of an ALC strategy versus a comparator on at least 1 relevant outcome.42,46,52,53
We did not formally critically appraise the evidence or rate the certainty of the evidence. For the nonrandomized observational studies, we have low confidence in the quality and low certainty in the findings based on study design and methodological rigour (e.g., statistical analyses were not conducted for all outcomes). Therefore, the evidence should be interpreted with caution and not be considered conclusive.
Detailed study findings are presented in Appendix 3. The 4 studies42,46,52,53 on strategies with evidence of favourable effect are presented in Table 5.
Table 5: Evidence of Favourablea Effect by Outcome
Outcome | Strategy | Intervention | Comparator | Population |
|---|---|---|---|---|
ALC hospitalizations | System | Home First42 | No intervention | Patients aged ≥ 65 years at risk of ALC |
System | Behavioural Supports Ontario52 | No intervention | Older peopleb with responsive behavioursc | |
ALC LOS | Throughput | SAFE Unit46 | Patients who have an ALC designation in local hospitals | Patients with frailty aged ≥ 60 years |
System | Home First42 | No intervention | Patients aged ≥ 65 years at risk of ALC | |
System | Behavioural Supports Ontario52 | No intervention | Older peopleb with responsive behavioursc | |
Hospital LOS | Throughput | SAFE Unit46 | Patients who have an ALC designation in local hospitals | Patients with frailty aged ≥ 60 years |
Discharge to home | Throughput | SAFE Unit46 | Patients who have an ALC designation in local hospitals | Patients with frailty aged ≥ 60 years |
Throughput | Transitional Care Unit53 | Standard cared | Patients with an ALC designation who are aged ≥ 70 years | |
System | Home First42 | No intervention | Patients aged ≥ 65 years at risk of ALC |
ALC = alternate level of care; LOS = length of stay; SAFE = Subacute Care for the Frail Elderly; vs. = versus.
aThe direction of the effect was positive in favour of the intervention vs. the comparator.
bThe ages of the study population were not reported.52
cResponsive behaviours included aggression, disruptive behaviours, disinhibition, apathy, depression, anxiety, and agitation.52
dThe effect was statistically significant, P < 0.01.53
ALC Hospitalization
The Home First strategy was implemented in the province of Ontario to encourage keeping older people safe at their homes with community support.42 It includes services such as nursing, personal support, physiotherapy, occupational therapy, speech therapy, social work, adult day programs, assisted livings, and convalescent care beds, equipment, and supplies. When patients are hospitalized, Home First aims to support their discharge to home instead of an LTC facility by changing the workflow and communication. In a before-and-after study using real-world data and a study population of 6,058,426, Home First resulted in a 26% reduction (from 10.1% to 7.5%) of ALC hospitalizations at 13 years after its introduction (statistical significance was not reported).42
The Behavioural Supports Ontario program is a quality improvement project, using mixed methods, for older adults with responsive behaviours through the identification of change strategies and knowledge translation best practices that lead to system redesign.52 The strategies include system coordination and management (e.g., geriatric cooperatives), intersectoral and interdisciplinary service delivery (e.g., geriatric mental health outreach teams), and knowledge care teams and capacity development (e.g., educational opportunities). Following the implementation of the program by the South West LHIN, the mean number of ALC cases was 36% lower over 6 months (the study population and statistical significance were not reported).52
ALC LOS
The SAFE Unit is a 20-bed transitional care program located within a large nursing home in Ontario that primarily services aging veterans in Canada.46 Medical and restorative function-focused care is provided by an interdisciplinary team. Patients spend a mean LOS of 20.8 days (standard deviation = 13.3 days) in the SAFE Unit. In a case-control study of older patients with frailty and medical complexity, significant differences were observed in LOS of ALC days. Patients in the SAFE Unit (n = 153) spent fewer days in an ALC bed, with a median LOS of 0 days (interquartile range [IQR], 0 to 1 day) compared with 5 days (IQR, 3 to10 days) for the comparison group (patients with an ALC designation in Ottawa hospitals, n = 1,773; statistical significance was not reported).46
Following the implementation of the Home First strategy, the percentage of ALC days for enrolled patients decreased by 13% (from 19.7% to 17.2%; statistical significance was not reported).42
The Behavioural Supports Ontario program reported an approximately 36% decrease in number of ALC days over a 6-month period, followed by a levelling over the next 6 months (data were presented graphically by the study authors).52
Hospital LOS
Patients in the SAFE Unit spent an average of 3.2 less days in the hospital than the comparison group, with a median LOS of 13 days (IQR, 8 to19 days) compared to 15 days (IQR, 10 to 24 days) in the comparison group (statistical significance was not reported).46
Discharge to Home
Two throughput strategies may be effective for increasing discharge to home:
Patients in the SAFE Unit were more likely to be discharged to home (64.1%) compared to those in the control group (46.3%).46 More patients in the SAFE Unit (53%) were discharged home without support (or support not needed) compared to those in the control group (4.6%) and fewer patients in the SAFE Unit (13.7%) were discharged home with support compared to patients with an ALC designation (41.6%; statistical significance was not reported).46
The Transitional Care Unit at St. Joseph’s Hospital in British Columbia is a 22-bed inpatient unit designed to provide an age-friendly geriatric rehabilitation–style environment.53 The model uses family physicians trained in the care of patients; with similar staffing to a residential care setting (e.g., family physicians, home care and residential care liaisons, medical directors, nutritionist, pharmacist, and social worker), enhanced nursing (by a care aide, licensed practical nurse, and registered nurse care coordinator lead), and rehabilitation services (by activity aides, occupational therapist, and rehabilitation aide). There are weekly interdisciplinary care conferences, during which medical care and discharge planning are reviewed. In a before-and-after study, patients in the Transitional Care Unit (N = 138) were more likely to be discharged home or to assisted-living facilities (30% postintervention group [n = 86] versus 12% preintervention group [n = 49]; P < 0.01).53
Home First resulted in the percentage of patients with an ALC designation who were discharged home with support services increasing by 17% (from 14.3% to 28.4%) following its implementation (statistical significance was not reported).42
Evidence of Neutral or Unfavourable Effect
We considered a strategy to have a neutral effect on an outcome when there was no effect of the intervention versus a comparator. A strategy had an unfavourable effect when the direction of the effect was negative in favour of a comparator versus the intervention.
Following the implementation of the Restorative Care Unit, a 14-bed inpatient unit in a LTC home in Newfoundland and Labrador, there was an increase in ALC cases and ALC LOS at 1 year, despite improvements in function (i.e., great likelihood of being able to live at home with a degree of independence). The authors of this before-and-after study suggested that increased wait time for access to LTC, the duration of the study, and its small sample size may have contributed to these findings.51
The study on the Restorative Care Unit also reported additional data (i.e., 74% of patients were discharged to their preadmission living arrangements and unplanned acute transfers and readmissions within 60 days were 2% and 11%, respectively). However, because similar outcomes data were not collected in a comparison group, the effectiveness is unknown.51
The Transitional Care Unit resulted in a statistically nonsignificant reduction in hospital LOS.53
The Virtual Ward is an output strategy that incorporates many elements of hospital care that are appreciated by patients or clinicians (e.g., interprofessional team, daily team meeting, single point of contact for patients) into community-based care.50 Patients are admitted into the Virtual Ward on the day they are discharged home from hospital. In a randomized controlled trial of 1,923 older patients, there was no effect of the Virtual Ward compared to usual care on ED visits at follow-up or hospital readmissions in older adults at high risk of hospital readmission.50
There was no effect of the SAFE Unit on ED visits at 30 days, hospital readmissions at 30 days, or follow-up with a family physician in older adults with frailty.46
There was no effect of Home First42 or the Transitional Care Unit53 on percentage of patients discharged to residential care.
Limitations
Real-World Evidence
This analysis was limited to patients with an ALC designation who were waiting for admission to an “adequate facility elsewhere,” which includes LTC homes, complex continuing care, hospice palliative care, and inpatient addictions treatment. The population in these analyses was larger than the target population of those waiting for residential care but did not include patients with an ALC designation and a reason for ALC code of waiting for home care, with an ALC designation because of inadequate housing, or an ALC designation because of other reasons.
While there are guidelines to support ALC designation,1,54 it is unclear whether the variations seen across jurisdictions reflect differences in patient care or differences in data collection or reporting. CIHI has noted that ALC service varies among hospitals and patient populations and does not necessarily intend for their ALC measure to be comparable across jurisdictions.3
Counts and rates were based on number of hospitalizations, not unique patients. If a patient had more than 1 separate hospitalization that met inclusion criteria, each hospitalization was included, which may result in a slight overestimation of calculated rates if considering unique patients.
Data were not available for Quebec because of differences in the way ALC is defined.3 Results from Yukon, the Northwest Territories, and Nunavut were grouped to avoid data suppression for privacy reasons. Results for the territories should be interpreted with caution because of incomplete data for some years.
Environmental Scan of the Literature
The literature-based environmental scan was limited to available information, the extent of which varied widely. Information available from websites was typically not as comprehensive as that in published literature. Sixteen of the 19 (79%) identified strategies were specific to Ontario, 2 strategies (10.5%) were specific to Alberta, and 2 strategies (10.5%) were specific to Saskatchewan. Therefore, the transferability of the strategies to other provinces and territories is unknown.
We did not find evidence on the effectiveness of any input strategies. We found only 1 study that evaluated an output strategy. We found no evidence on the effectiveness of any strategies on ALC capacity or outcomes related to the residential care admission process (e.g., time from screening, approval, or waiting list to placement in residential care). We did not critically appraise the evidence; therefore, the quality of the studies and certainty of the findings is unclear.
Six of the 19 (26%) strategies specifically targeted adults waiting for residential care, specifically a LTC placement. None of the 6 studies of clinical effectiveness reported how many people in their study samples were waiting for residential care; therefore, the directness of the findings to patients waiting for residential care is uncertain. Four of the 6 (67%) included studies took place in Ontario, 1 study was set in British Columbia, and another study was in Newfoundland and Labrador. Therefore, the transferability of the findings to other provinces or territories is unknown.
We found a lack of information about equity-deserving group characteristics, including race, ethnicity or country of origin, language, gender or gender identity, newcomer status, or sexual orientation.
Conclusions and Implications for Decision- or Policy-Making
Real-World Evidence
In 2022 to 2023, the jurisdictions with the lowest number of hospitalizations with ALC days per 1,000 population in people aged 65 and older who were awaiting admission to residential care or elsewhere were the combined data for Nunavut, the Northwest Territories, and Yukon; British Columbia; and Saskatchewan. Total ALC days per 1,000 population in older adults who were awaiting admission to residential care or elsewhere were lowest in Saskatchewan and British Columbia.
The literature and analyses of real-world data typically defines “older adults” as people aged 65 years and older.55 For this reason, the patient population for this report was people aged 65 years and older. We also recognize the diversity of older adults, experiences of aging, and eligibility criteria for various programs and services in Canada.27,56-60 Therefore, we consider people aged 55 years and older to be a more inclusive age group. In Appendix 4, we present additional real-world data findings on ALC in patients aged 55 years and older.
While there were jurisdictional variations, the trends in ALC over time for people aged 55 years and older were relatively consistent. The jurisdictions with the lowest number of hospitalizations with ALC days per 1,000 population in patients 55 years of age and older were the combined data for Nunavut, the Northwest Territories, and Yukon; and British Columbia (since the 2018 to 2019 fiscal year). Total ALC days per 1,000 population in patients aged 55 years and older were lowest in British Columbia; Saskatchewan; and the combined data for Nunavut, the Northwest Territories, and Yukon (for the 2022 to 2023 fiscal year). Metrics such as number of patients designated with ALC and number of ALC days per 1,000 population demonstrate system impact. Median ALC LOS per hospitalization reflects the patient experience (e.g., what is meaningful to patients). The median ALC LOS for Canada (excluding Quebec) in patients 55 years and older was 11 days in the 2022 to 2023 fiscal year. The lowest median ALC LOS per hospitalization was 9 days in Ontario and 12 days each in British Columbia and Saskatchewan.
A number of risk factors for ALC designation in patients of all ages have been identified in the literature, including advanced age (e.g., older than 80 years), being female, diagnosis of dementia, falls, social vulnerability, and need for residential care.13,61-64 Several studies found the average age of patients with an ALC designation in Canada was approximately 83 years.13,18,61 Using CIHI data, we identified key characteristics of patients aged 55 years and older with an ALC designation in jurisdictions across Canada. The findings are presented in Appendix 4. The mean age of patients in Canada aged 55 years and older with an ALC designation and awaiting admission to adequate facility elsewhere was 80 years and more were female (55%), consistent with the literature. At least 70% of ALC days across jurisdictions came from patients aged 75 and older. Patients who lived in rural areas had longer LOS in ALC than patients living in urban areas in most jurisdictions. We found that the majority of patients with ALC started as an urgent admission (86%). Dementia was identified in 23% of patients with ALC but data limitations may have underestimated the true prevalence; patients with dementia had a median ALC LOS almost twice the overall ALC LOS. Patients with lower incomes had a larger contribution to ALC days in hospitals compared to patients with higher incomes. These characteristics can help clinicians and decision-makers identify patients who are at risk of ALC and recommend strategies to prevent ALC or improve patient flow as ALC.
We were aware that the COVID-19 pandemic had a great impact on the health care systems in Canada and could potentially affect ALC data and their interpretation. However, an interrupted time series using linked administrative data in Ontario found that ALC rates remained high during the pandemic despite efforts to reduce hospital occupancy.65 According to the study, there were no significant changes in the average level of ALC rates per month or monthly rate of change after the onset of the pandemic. There were also no meaningful differences of individuals with discharges by ALC designation before the pandemic and after the onset of the pandemic.65
Environmental Scan of the Literature
This report is, to our knowledge, the first to present and describe strategies to address ALC in older adults awaiting residential care in Canada. We included 23 articles in total from the literature-based environmental scan.
We identified 19 strategies that addressed ALC in older people in Canada. The strategies were primarily throughput (37%; 7 of 19) and system-level (37%; 7 of 19), followed by input (26%; 5 of 19) interventions. The most frequent intervention category was recommended initiatives (32%; 6 of 19), then infrastructure and finance (26%; 5 of 19), followed by practice changes (21%; 4 of 19), and tools and guidelines (16%; 3 of 19). Personnel involved in the strategies were mostly health care professionals (74%; 14 of 19), and many included multidisciplinary teams (58%; 11 of 19). Two of the 19 (10.5%) strategies were also evaluated for clinical effectiveness.42,46
We identified 6 studies on the clinical effectiveness of interventions implemented in Canada to address ALC in older people. Four of the 6 studies reported a favourable effect of the intervention compared to no strategy or standard care.
Two throughput interventions may be effective:
The SAFE Unit demonstrated a favourable effect on ALC LOS, hospital LOS, and discharge to home.46
The Transitional Care Unit demonstrated a favourable effect on discharge to home.51
Two system-level interventions may be effective:
Home First demonstrated a favourable effect on ALC hospitalizations, ALC LOS, and discharge to home.42
Behavioural Supports Ontario demonstrated a favourable effect on ALC hospitalizations and ALC LOS.52
We recognize that there may be other approaches to addressing ALC in older people in Canada. However, we did not include any articles or studies that did not meet our inclusion criteria. One example of an approach is increasing residential care capacity. For example, Alberta and Ontario have committed to building new, and replacing older, LTC or continuing care beds.66,67 While we can assume that more residential care beds will reduce ALC LOS and facilitate discharge of patients waiting for residential care, these articles did not specify the target population or indicate that the increased bed policy would address ALC. Also, building more acute care and postacute care beds has been viewed as a temporary and expensive solution.5,16,68
Considerations for Future Research
This report may be a helpful precursor for future systematic reviews or other evidence syntheses with a broader scope. Future work may focus on the development and evaluation of output strategies. Randomized studies on the effectiveness of interventions to address ALC are needed and could specifically include older adults waiting for residential care and assess patient-important outcomes, such as quality of life and patient preferences. Future research might investigate the causes, as well as the individual, organizational, and structural factors, that contribute to ALC and interventions to address those factors.
To help address health equity concerns in future studies, researchers might consider collecting equity-relevant population characteristics (e.g., race, ethnicity or country of origin, language, gender or gender identity, newcomer status, and sexual orientation) to assess potential health inequities related to ALC in Canada.
Considerations for Decision-Making
We found some common themes in our environmental scan, which decision-makers may incorporate into strategies for addressing ALC in older adults waiting for residential care:
increase the scope and provision of services across different health sectors (e.g., integrated care)
promote age-friendly care
concentrate on the early identification of patients at risk of ALC
share and increase the accessibility of tools and resources
include families and caregivers in care planning
focus on transition planning and transitional care.
Decision-makers may also consider factors such as acceptability, feasibility, and resource implications of the interventions identified in this report.
References
1.Definitions and guidelines to support ALC designation in acute inpatient care. Ottawa (ON): Canadian Institute for Health Information; 2016: https://www.cihi.ca/sites/default/files/document/acuteinpatientalc-definitionsandguidelines_en.pdf. Accessed 2024 May 15.
2.Wyonch R. Scenarios for seniors’ care: future challenges, current gaps and strategies to address them. Health Policy. Toronto (ON): C.D. Howe Institute; 2024: https://www.cdhowe.org/public-policy-research/scenarios-seniors-care-future-challenges-current-gaps-and-strategies-address. Accessed 2024 Jun 12.
3.Patient days in alternate level of care (percentage). Ottawa (ON): Canadian Institute for Health Information; 2023: https://www.cihi.ca/en/indicators/patient-days-in-alternate-level-of-care-percentage. Accessed 2024 May 15.
4.Bender D, Holyoke P. Why some patients who do not need hospitalization cannot leave: a case study of reviews in 6 Canadian hospitals. Healthc Manage Forum. 2018;31(4):121-125. PubMed
5.Bobrowski D, Elfassy MD, Bobrowski A. Hallway healthcare: solving acute care overflow from the community. Univ Toronto Med J. 2018;95(3):50-53.
6.Cadel L, Guilcher SJ, Kokorelias KM, et al. Initiatives for improving delayed discharge from a hospital setting: a scoping review. BMJ Open. 2021;11(2):e044291. PubMed
7.Abdelhalim A, Zargoush M, Archer N, Roham M. Decoding the persistence of delayed hospital discharge: an in‐depth scoping review and insights from two decades. Health Expect. 2024;27(2):e14050. PubMed
8.Inpatient hospitalization, surgery and newborn statistics, 2022–2023. Ottawa (ON): Canadian Institute for Health Information; 2024: https://www.cihi.ca/en/hospital-stays-in-canada-2022-2023. Accessed 2024 Jun 12.
9.Chuang YT, Zargoush M, Ghazalbash S, Samiedaluie S, Kuluski K, Guilcher S. From prediction to decision: optimizing long‐term care placements among older delayed discharge patients. Production and Operations Management. 2023;32(4):1041-1058.
10.Rojas‐García A, Turner S, Pizzo E, Hudson E, Thomas J, Raine R. Impact and experiences of delayed discharge: a mixed‐studies systematic review. Health Expect. 2018;21(1):41-56. PubMed
11.Everall AC, Guilcher SJT, Cadel L, Asif M, Li J, Kuluski K. Patient and caregiver experience with delayed discharge from a hospital setting: a scoping review. Health Expect. 2019;22(5):863-873. PubMed
12.Jones A, Lapointe-Shaw L, Brown K, et al. Short-term mortality and palliative care use after delayed hospital discharge: a population-based retrospective cohort study. BMJ support. 2024;09:09.
13.Lim Fat GJ, Gopaul A, Pananos AD, Taabazuing MM. Healthcare-associated adverse events in alternate level of care patients awaiting long-term care in hospital. Geriatrics. 2022;7(4):08.
14.Kuluski K, Im J, McGeown M. “It's a waiting game” a qualitative study of the experience of carers of patients who require an alternate level of care. BMC Health Serv Res. 2017;17(1):318. PubMed
15.Haas R, Brundisini F, Barbara A, et al. Emergency department overcrowding: an environmental scan of contributing factors and a summary of systematic review evidence on interventions. Canadian Journal of Health Technologies. 2023;3(11).
16.Durante S. The demography and policies of alternate levels of care: a selection of Canadian case studies [unpublished master's project]. Calgary (AB): University of Calgary; 2021: https://prism.ucalgary.ca/server/api/core/bitstreams/a40f0bb5-e775-482b-be2d-4f62b01c7578/content. Accessed 2024 Jun 12.
17.Seniors in transition: exploring pathways across the care continuum. Ottawa (ON): Canadian Institute for Health Information; 2017: https://www.cihi.ca/sites/default/files/document/seniors-in-transition-report-2017-en.pdf. Accessed 2024 May 15.
18.Costa AP, Hirdes JP. Clinical characteristics and service needs of alternate-level-of-care patients waiting for long-term care in Ontario hospitals. Healthc Policy. 2010;6(1):32. PubMed
19.Costa AP, Poss JW, Peirce T, Hirdes JP. Acute care inpatients with long-term delayed-discharge: evidence from a Canadian health region. BMC Health Serv Res. 2012;12(1):172. PubMed
20.Fransoo R, Martens P, Prior H, Burchill CA, Koseva I, Rajotte L. Who is in our hospitals--and why? Winnipeg (MB): Manitoba Centre for Health Policy; 2013.
21.Nuernberger K, Atkinson S, MacDonald G. Seniors in transition: exploring pathways across the care continuum. Healthc Q. 2018;21(1):10-12. PubMed
22.Aging and chronic diseases: a profile of Canadian seniors. Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/content/dam/hc-sc/documents/services/publications/diseases-and-conditions/aging-chronic-diseases/canadian-seniors-report_2021-eng.pdf. Accessed 2024 Jun 5.
23.Iciaszczyk N, Arulnamby A, Brydges M, et al. Ageing in the right place: supporting older Canadians to live where they want. Toronto (ON): National Institute of Ageing; 2022: https://www.niageing.ca/airp. Accessed 2024 Jun 12.
24.Jutan N, Langlois L, Damiano N. Seniors and alternative level of care: building on our knowledge. Healthc Q. 2013;16(3):7-10. PubMed
25.CIHI portal - DAD metadata dictionary. Ottawa (ON): Canadian Institure for Health Information; 2022: https://www.cihi.ca/sites/default/files/document/DAD-metadata-dictionary-2022-en.pdf. Accessed 2024 May 24.
26.DAD data elements, 2023–2024. Ottawa (ON): Canadian Institute for Health Information; 2023: https://www.cihi.ca/sites/default/files/document/dad-data-elements-2023-2024-en.pdf. Accessed 2024 Jun 12.
27.Statistics Canada. Population estimates on July 1, by age and gender. 2024; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2024 Jun 12.
28.Statistics Canada. Population estimates on July 1, by health region and peer group. 2023; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710013401. Accessed 2024 Jun 12.
29.Asplin BR, Magid DJ, Rhodes KV, Solberg LI, Lurie N, Camargo Jr CA. A conceptual model of emergency department crowding. Ann Emerg Med. 2003;42(2):173-180. PubMed
30.Doern GB PR. Canadian public policy: ideas, structure, process. Toronto (ON): Nelson Canada; 1992.
31.Provincial Geriatrics Leadership Ontario. Implementing alternative levels of care leading practices. 2024; https://geriatricsontario.ca/wp-content/uploads/2024/05/PGLO-Report-March-2024-V12.04.2024.pdf. Accessed 2024 May 15.
32.Kokorelias K, Flanagan A. Bringing long-term care home. Toronto (ON): The Hub; 2023: https://thehub.ca/wp-content/uploads/2023/09/HunterPrize_Kokerelias_BringingLongtermCareHome_v1.pdf. Accessed 2024 May 24.
33.Molnar FJ. Hospitals “failing to plan for dementia is planning to fail”: All Canadian hospitals must launch acute care dementia strategies if they are serious about decreasing hospital overcrowding, decreasing alternate level of care (alc), and thereby increasing hospital capacity to permit pandemic recovery and to meet future escalating needs. Canadian Geriatrics Society Journal of CME. 2021:1-8.
34.Bhatia D, Peckham A, Abdelhalim R, et al. Alternate level of care and delayed discharge: lessons learned from abroad. NAO rapid review. Toronto (ON): North American Observatory on Health Systems and Policies; 2020: https://naohealthobservatory.ca/wp-content/uploads/2020/03/NAO-Rapid-Review-22_EN.pdf. Accessed 2024 Jun 12.
35.Nauenberg E. Personal support homes: an innovative approach to reduce the alternative level of care population in Ontario hospitals. Healthc Policy. 2021;17(1):91. PubMed
36.Durante S, Fyie K, Zwicker J, Carpenter T. Confronting the alternate level of care (ALC) crisis with a multifaceted policy lens. The School of Public Policy Publications. 2023;16(1).
37.Provincial Geriatrics Leadership Ontario, Senior Friendly Care. Supporting Ontario health teams to influence alternate level of care. 2022; https://geriatricsontario.ca/wp-content/uploads/2023/06/2022-April-1-ALC-Community-_-FINAL.pdf. Accessed 2024 Jun 12.
38.Essential role of caregivers in improving transitions and addressing alternate level of care. Toronto (ON): The Ontario Caregiver Organization; 2023: https://ontariocaregiver.ca/wp-content/uploads/2023/12/6.-Essential-Role-of-Cgs-in-Improving-Transitions-and-Addressing-Alternate-Level-of-Care-EN-2.pdf. Accessed 2024 May 15.
39.The alternate level of care (ALC) leading practices guide: Preventing hospitalization and extended stays for older adults. Toronto (ON): Ontario Health; 2021: https://scholar.google.ca/scholar?hl=en&as_sdt=0%2C5&q=Ontario+Health.+%22The+Alternate+Level+of+Care+%28ALC%29+Leading+Practices+Guide%22&btnG=. Accessed 2024 Apr 22.
40.Alberta Health Services. Complex care hub: enhancing care in the community. 2024; https://www.albertahealthservices.ca/about/Page13602.aspx. Accessed 2024 May 24.
41.Payne E. Community paramedics will be deployed to deal with Ottawa's growing long-term care wait lists. Ottawa Citizen 2020; https://ottawacitizen.com/news/local-news/community-paramedics-will-be-deployed-to-deal-with-ottawas-growing-long-term-care-wait-lists. Accessed 2024 May 21.
42.Ahmed D. The challenge of alternate level of care (ALC) facing older adults in Ontario: implications for government and policy makers using a descriptive data analytics approach [thesis]. Hamilton (ON): McMaster University; 2019: https://macsphere.mcmaster.ca/bitstream/11375/24951/2/Ahmed_Didi_MH_201909_MSc.eHealth.pdf. Accessed 2024 Jun 12.
43.Compton RM, Owilli AO, Caine V, et al. Home first: exploring the impact of community-based home care for older adults and their family caregivers. Can J Aging. 2020;39(3):432-442. PubMed
44.Ontario Newsroom. Ontario building new seniors' housing complex in Kenora. 2022; https://news.ontario.ca/en/release/1002387/ontario-building-new-seniors-housing-complex-in-kenora Accessed 2024 May 21.
45.Egbujie BA, Tran J, Hirdes JP. Multistate competing risk analysis of transition back to the community among long-term care home (LTC) destined patients: a brief report. J Prim Care Community Health. 2023;14:21501319231220742. PubMed
46.Robert B, Sun AH, Sinden D, Spruin S, Hsu AT. A case-control study of the sub-acute care for frail elderly (SAFE) unit on hospital readmission, emergency department visits and continuity of post-discharge care. J Am Med Dir Assoc. 2021;22(3):544-550.e542. PubMed
47.Cheng I, Atzema CL, Carew D, et al. Using case costing to evaluate the potential impact of a reintegration unit on an acute-care hospital's capacity and resources. Healthc Q. 2022;24(4):27-33. PubMed
48.A Central LHIN Hospitals Collaborative. Reactivation care centre. https://www.reactivationcarecentre.ca/. Accessed 2024 May 24.
49.Coffey A, Leahy-Warren P, Savage E, et al. Interventions to promote early discharge and avoid inappropriate hospital (re) admission: a systematic review. Int J Environ Res Public Health. 2019;16(14):2457. PubMed
50.Dhalla IA, O'Brien T, Morra D, et al. Effect of a postdischarge virtual ward on readmission or death for high-risk patients: a randomized clinical trial. JAMA. 2014;312(13):1305-1312. PubMed
51.O’Brien K, Welsh D, Barnable A, Wiseman G, Colbourne A. The impact of introducing restorative care on client outcomes and health system effectiveness in an integrated health authority. Home Health Care Manag Pract. 2017;29(1):13-19.
52.Gutmanis I, Speziale J, Van Bussel L, Girard J, Hillier L, Simpson K. The South West Local Health Integration Network Behavioural Supports Ontario experience. Healthc Q. 2016;18 Spec No:50-56. PubMed
53.Manville M, Klein MC, Bainbridge L. Improved outcomes for elderly patients who received care on a transitional care unit. Can Fam Physician. 2014;60(5):e263-271. PubMed
54.Alternate level of care diagnosis list: clarification of use. Ottawa (ON): Canadian Institute for Health Information; 2022: https://www.cihi.ca/sites/default/files/document/alternate-level-care-diagnosis-list-job-aid-en.pdf. Accessed 2024 Jun 12.
55.Rosenberg MW, Puxty J, Crow B. Enabling older adults to age in community. Ottawa (ON): Federal/Provincial/Territorial Ministers Responsible for Seniors; 2022: https://www.canada.ca/content/dam/canada/employment-social-development/corporate/seniors/forum/reports/enabling-age-community-en.pdf. Accessed 2024 May 1.
56.Omolulu E. Benefits for seniors aged 55 and older in Canada. Savvy New Canadians 2024; https://www.savvynewcanadians.com/benefits-for-seniors-55-and-older-in-canada/. Accessed 2024 May 24.
57.Our right to health: First Nations’ perspectives across the generations. Ottawa (ON): Assembly of First Nations; [no date][no date]: https://afn.bynder.com/m/30591953bdc679f3/original/Our-Right-to-Health-First-Nations-Perspectives-Across-the-Generations.pdf. Accessed 2024 May 1.
58.Aging with dignity: elders and seniors strategy. Iqaluit (NU): Government of Nunavut; 2024: https://assembly.nu.ca/sites/default/files/2024-03/EIA%20Elder%20Strategy%20EN%20FINAL_print.pdf. Accessed 2024 May 24.
59.Métis vision for health. Ottawa (ON): Métis National Council; 2021: https://www.metisnation.ca/uploads/documents/3-1)Me%CC%81tis%20Vision%20for%20Health-July%2012%20update.pdf. Accessed 2024 May 24.
60.Hillier S, Al-Shammaa H. Indigenous peoples experiences with aging: a systematic literature review. Can J Disabil Stud. 2020;9:146-179.
61.Bai AD, Dai C, Srivastava S, Smith CA, Gill SS. Risk factors, costs and complications of delayed hospital discharge from internal medicine wards at a Canadian academic medical centre: retrospective cohort study. BMC Health Serv Res. 2019;19(1):935. PubMed
62.Arthur SA, Hirdes JP, Heckman G, Morinville A, Costa AP, Hebert PC. Do premorbid characteristics of home care clients predict delayed discharges in acute care hospitals: a retrospective cohort study in Ontario and British Columbia, Canada. BMJ Open. 2021;11(2):e038484. PubMed
63.Barnable A, Welsh D, Lundrigan E, Davis C. Analysis of the influencing factors associated with being designated alternate level of care. Home Health Care Manag Pract. 2015;27(1):3-12.
64.Dementia in hospitals. Ottawa (ON): Canadian Institute for Health Information: https://www.cihi.ca/en/dementia-in-canada/dementia-care-across-the-health-system/dementia-in-hospitals. Accessed 2024 May 22.
65.Guilcher SJT, Bai YQ, Wodchis WP, Bronskill SE, Kuluski K. An interrupted time series study using administrative health data to examine the impact of the COVID-19 pandemic on alternate care level acute hospitalizations in Ontario, Canada. CMAJ Open. 2023;11(4):E621-E629. PubMed
66.Ontario Newsroom. Ontario on track to build 30,000 new long-term care beds. 2022; https://news.ontario.ca/en/release/1002083/ontario-on-track-to-build-30000-new-long-term-care-beds. Accessed 2024 May 21.
67.Von Scheel E. Alberta promises to create and replace 6000 continuing care beds. CBC News 2021; https://www.cbc.ca/news/canada/calgary/alberta-continuing-care-beds-funding-1.6096916. Accessed 2024 Jun 12.
68.Sutherland JM, Crump RT. Alternative level of care: Canada's hospital beds, the evidence and options. Healthc Policy. 2013;9(1):26. PubMed
69.Geographic location stratifier: guidance on measuring and reporting health inequalities. Ottawa (ON): Canadian Institute for Health Information; 2022: https://www.cihi.ca/sites/default/files/document/measuring-health-inequalities-toolkit-geographic-location-stratifier-en.pdf. Accessed 2024 Jun 12.
70.Income stratifier: guidance on measuring and reporting health inequalities. Ottawa (ON): Canadian Institute for Health Information; 2022: https://www.cihi.ca/sites/default/files/document/measuring-health-inequalities-toolkit-income-stratifier-en.pdf. Accessed 2024 Jun 12.
71.Better quality hospital data for identifying patients experiencing homelessness. Ottawa (ON): Canadian Institute for Health Information; 2023: https://www.cihi.ca/en/better-quality-hospital-data-for-identifying-patients-experiencing-homelessness. Accessed 2024 Jun 12.
72.Privacy and security. Ottawa (ON): Canadian Institute for Health Information: https://www.cihi.ca/en/about-cihi/privacy-and-security#section5. Accessed 2024 Jun 12.
73.Murmann M, Sinden D, Hsu AT, et al. The cost-effectiveness of a nursing home-based transitional care unit for increasing the potential for independent living in the community among hospitalized older adults. J Med Econ. 2023;26(1):61-69. PubMed
74.Cheng I, Baker GR, Carew D, et al. Improving the use of healthcare resources in Canadian hospitals: the impact of a reintegration unit in expanding acute care capacity and resource use in Sunnybrook Health Sciences Centre. V1. Research Square. 2020.
75.Privacy policy on the collection, use, disclosure and retention of personal health information and de-identified data, 2010 — updated November 2022. Ottawa (ON): Canadian Institute for Health Information; 2022: https://www.cihi.ca/sites/default/files/document/privacy-policy-en.pdf. Accessed 2024 Jun 26.
Appendix 1: Detailed Methods
Note that this appendix has not been copy-edited.
Real-World Data Analysis
Inclusion Criteria
The relevant components for the real-world analysis are presented in Table 6. Patients were included in the aggregated dataset if they were aged 65 years and older and assigned an ALC designation with an ALC Z-code reason of Z75.1 (Person awaiting admission to adequate facility elsewhere). An ALC designation is assigned when a patient is occupying a bed in a facility and does not require the intensity of resources/services provided in that care setting.1 ALC designation is coded within the Discharge Abstract Database if the ALC LOS is at least 24 hours.1 An additional analysis of patients aged 55 and older was also conducted and presented in Appendix 4.
Table 6: Components for Real-World Data Analysis
Criteria | Description |
|---|---|
Population | Adults aged 65 years and older (main report); adults aged 55 years and older (Appendix 4) |
Data source | CIHI Discharge Abstract Database |
Exposure factor | ALC designation with an ALC Z-code reason of Z75.1 (Person awaiting admission to adequate facility elsewhere) |
Setting | Acute care inpatient hospitalization |
Outcomes | RQ 3: ALC by jurisdiction in Canada, patients aged 65 years and older (main report)
RQ 4: Trends in ALC over time by jurisdiction in Canada, patients aged 55 and older (Appendix 4)
RQ 5: Description of patients experiencing ALC by jurisdiction across Canada (Appendix 4)
RQ 6: Investigation of potential factors associated with ALC LOS (Appendix 4)
|
Time frame | RQ 3: 2022 to 2023 RQ 4, 2018 to 2019, 2022 to 2023 RQ 5: 2022 to 2023 |
ALC = alternate levels of care; CIHI = Canadian Institute for Health Information; ICD-10-CA = International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada; LOS = length of stay; RQ = research question.
Notes: Main report research question —
3What is the real-world data on ALC in older patients in jurisdictions across Canada?
Appendix 4: Additional research questions —
4What are the trends in ALC over time for older adults in jurisdictions across Canada?
5What are the characteristics of older adults experiencing ALC in jurisdictions across Canada?
6What factors are associated with ALC length of stay (LOS) in patients who are in jurisdictions across Canada?
aThe number of ALC days is calculated based on the date the patient is ready for ALC and the date of discharge.
Counts and rates were based on number of hospitalizations, not unique patients. If a patient had 2 or more separate hospitalizations meeting inclusion criteria, each hospitalization was included. To comply with privacy and confidentiality policies for personal health information,72 small cells (counts of 1 to 4) were suppressed and represented with “NR”. When secondary suppression was required to avoid recalculation of suppressed cells, “NR” was also used. Cells with counts of zero were represented with “0”. Reporting of findings from Yukon, the Northwest Territories and Nunavut were combined to reduce the likelihood of small cell suppression.
We used the July 1 populations for 2022 from Statistics Canada27 to calculate ALC hospitalizations and ALC days per 1,000 population in the main report on patients aged 65 years and older. We used the July 1 populations for 2018, 2019, 2020, 2021 and 2022 from Statistics Canada27 for the results reported in Appendix 4 on populations aged 55 and above.
Inpatient hospitalizations for mental health services in Ontario, 3 facilities in Newfoundland and Labrador and 1 facility in Manitoba were not included in the analyses because data from these facilities are reported to the Ontario Mental Health Reporting Service, and the analysis was restricted to data from the Discharge Abstract Database.
Environmental Scan of the Literature
Literature Search Strategy
An information specialist conducted a literature search on key resources including MEDLINE, CINAHL, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was alternate level of care. CADTH-developed search filters were applied to limit retrieval to the Canadian context. The search was completed on April 16, 2024, and limited to documents published since January 1, 2014.
One author also did a manual search of the reference lists of all included articles to identify other relevant information.
Study Selection
One author screened the literature search results and reviewed the full texts of all potentially relevant information, using the criteria presented in Table 7.
While our main interest was older people waiting for placement in residential care, initial scoping revealed that many articles did not report whether (or how many in) the population were waiting for residential care. We felt that strategies aimed at avoiding or reducing alternate level of care (ALC) in all older adults (except for those to be transferred to assisted living or retirement homes, which is beyond the scope of this project) would be relevant to those waiting for residential care. Therefore, we revised our criteria to include people aged 65 years and older or people waiting for residential care placement.
Table 7: Components for Literature Screening and Information Gathering
Criteria | Inclusion | Exclusion |
|---|---|---|
Population | Older adults (aged 65 years and older) or people who are approved for and waiting for placement in residential carea Subgroups of interest:
| Patients to be transferred to assisted livingb |
Interventions |
| — |
Comparator | RQ 1: NA RQ 2: Current practice, no intervention | — |
Outcomes | RQ 1: NA RQ 2:
| — |
Setting | Jurisdictions across Canada | Outside Canada |
Types of Information | RQ 1: Published and unpublished primary clinical studies; jurisdictional information; government documents; organizational guidance documents; policies, guides, or tools to inform practice RQ 2: Published and unpublished primary clinical studies | Conference abstracts; non-English language; modelling studies |
Time frame | RQ 1: 2019 to present RQ 2: 2014 to present | — |
ALC = alternate level of care; ED = emergency department; LOS = length of stay; NA = not applicable; RQ = research question.
Notes: Research questions —
1What strategies, policies, plans, models, or guidelines exist to address ALC in older people in Canada?
2Which strategies implemented in Canada to address ALC in older people have been effective?
aResidential care is available for seniors who are no longer able to function independently and require full-time facility-based long-term care (LTC) with 24-hour nursing supervision. Residential care includes LTC homes or facilities, nursing homes, private care homes, and special care homes. Residential care does not include assisted living.17
bAssisted living provides housing and personal care services for individuals who can live independently (without continuous medical care) but require a supportive environment due to physical and functional health challenges. Assisted living includes supportive living, supportive housing, and retirement homes.17
Appendix 2: Strategies to Reduce ALC
Table 8: Summary of Input Strategies
Strategy Name First Author, Year URL | Strategy Category Brief Strategy Description | Setting Province(s) | Target Population | Objective(s) | Relevant Personnel | Implementation Considerations |
|---|---|---|---|---|---|---|
Complex Care Hub Alberta Health Services 202440 | Practice changes Hospital-at-home services: Patients are admitted as they would be under a conventional hospital admission, but are sent home where they receive daily care and monitoring | Personal home; Calgary Zone Alberta | Older patients who come into Rockyview General Hospital’s ED for non-urgent treatment. | To allow patients recover within the comfort of their home and improve the health care system through more efficient use of resources. | Clinical team; including community paramedic; nurse navigator; general internist. | NR |
Virtual LTC @ Home Kokorelias and Flanagan 202332 https://thehub.ca/wp-content/uploads/2023/09/HunterPrize_Kokerelias_BringingLongtermCareHome_v1.pdf | Information sharing: Recommended initiatives Proposed program to provide LTC home-equivalent care in people’s own home the creation of highly coordinated and integrated teams of care providers. | Personal home Ontario | Individuals who are eligible for LTC; e.g., individuals already on or eligible to be added to an LTC home waitlist. | To optimize the utilization of existing LTC beds for those who need them most, while addressing issues of hallway medicine, wait times, surgical backlogs, and unprecedented ALC rates by more strongly focusing on delivering care within people’s own homes; to promote an opportunity for more seamless transitions from the community to LTC homes. | Community paramedics; home care service providers; primary care providers; staff at local community support services agencies. | Propose 10 demonstration programs to support up to 150 clients per year with up to $67,510 per enrollee per year for initial 3-year period in Ontario. Several OHTs have the potential to lead program implementation. Propose nation-wide implementation. |
New Seniors’ Housing Complex Ontario Newsroom 202244 http://news.ontario.ca/en/release/1002387/ontario-building-new-seniors-housing-complex-in-kenora | Infrastructure and finance Dedicated spaces for health care at a new seniors’ housing complex with 56 independent living suites in Kenora. | Community (Kenora) Ontario | Older adults | To postpone and reduce the demand for LTC and hospital services, including reducing the number of hospital patients who go on to be designated as ALC; to improve access to supportive and culturally sensitive services by having onsite, coordinated services that consider the unique needs of the population; and to help seniors remain in their home community by providing affordable housing. | NR | Ontario government is investing $4.5 million in the project. The housing complex is being developed by the Kenora District Services Board, together with the All Nations Health Partners, which includes Indigenous partners and organizations, who provided input into the design of the complex and the supports and services to be offered there. |
Supporting OHTs to Influence ALC Provincial Geriatrics Leadership Ontario & Senior Friendly Care 202237 http://geriatricsontario.ca/wp-content/uploads/2023/06/2022-April-1-ALC-Community-_-FINAL.pdf | Tools and guidelines Information to assist OHTs to pursue services in community settings; including early identification and assessment (to facilitate proactive identification and promote practices in care and self-management that prevent, slow or reverse declines in the physical and mental capacities of older adults); care plan development and ongoing re-assessment; delivery of interventions/senior friendly care; proactive transitions. | Community Ontario | Older adults at risk of ALC | To support OHTs with activities to help individuals at risk for protracted hospital stays (e.g., ALC designation). | Emergency services; health workers; OHTs; social care workers; voluntary sector workers. | Ontario’s network of socialized geriatric services provides further assistance to support implementation of services and supports for older adults with complex health conditions. |
Community Paramedicine for LTC Payne 202041 | Practice changes Enhanced paramedic and home-based services: Pilot program that expands the numbers and scope of what paramedics do, offering 24/7 access to health services, ongoing monitoring for those at highest risk. | Community; Brant County, Cochrane District, Ottawa, Renfrew Country, and York Region Ontario | People waiting for LTC | To help people waiting for LTC to stay safely in their homes. | Community paramedics; family doctors; home care nurses. | $5 million pilot program initially targets 5 communities to allow monitoring of around 200 patients per community. The program builds on existing community paramedic programs. It is expected to be expanded to other communities. |
ALC = alternate level of care; OHT = Ontario Health Team; NR = not reported; LTC = long-term care.
Note: This table has not been copy-edited.
Table 9: Summary of Throughput Strategies
Strategy Name First Author, Year URL | Strategy Category Brief Strategy Description | Setting Province(s) | Target Population | Objective(s) | Relevant Personnel | Implementation Considerations |
|---|---|---|---|---|---|---|
Harbour Light Integrated Transitional Care Program Egbujie et al. 202345 http://www.torontograce.org/programs-services/integrated-transitional-services/ | Infrastructure and finance Transitional care program in a community setting, with 15 rooms, each equipped with a modern bathroom, a meal serving pantry, and care station. | Urban hospital; Toronto Grace Health Center Ontario | Patients designated as ALC with a current LTC placement application; and bariatric or mental health and addiction needs as barriers to placement. | To support return to the community of acute hospital patients designated for LTC placement. | Chaplain; nurses; mental health case manager; PSWs; occupational or physical therapist; social worker; unit clerk. | NR |
Subacute Care for the Frail Elderly (SAFE) Unit Murmann 2023;73 Robert 202146 | Infrastructure and finance Transitional care unit with 20 beds that that focuses on preventing deconditioning that can happen in hospital. Patients can access the medical and rehabilitative supports needed to recover fully and return to their place of residence. | Urban nursing home (Ottawa) Ontario | Older patients with frailty who are at risk of deconditioning and/or disability due to surgery, illness, or accident. | To serve older patients with frailty at risk of deconditioning and/or disability, caused by prolonged hospitalization; to address the persisting capacity issue within Ontario’s hospitals. | Creative art instructors; dietitians; family physician; nurses; internists; geriatricians; physiotherapists; PSWs; recreational therapists; resident care liaisons; social workers. | 3-year pilot project. Collaboration between an acute-care hospital and a LTC home. |
Pine Villa Reintegration Unit Cheng et al. 2022;47 Cheng et al. 202074 | Infrastructure and finance Supportive site with 69 beds, providing specialized supports, therapeutic recreation, case management, and assistance with personal care. | Urban site (previous retirement home) Ontario | Older patients designated as ALC that are medically stable and can be discharged within 3 months, including patients awaiting placement in a LTC facility. | To alleviate hospital occupancy and emergency department crowding; to transfer patients with ALC designation out of hospital and transition them back into the community. | Case managers; doctor; nurse practitioner; practical nurses; PSWs; recreation therapists. | Sunnybrook Health Sciences Centre, SPRINT Senior Care, and LOFT Community Services oversee governance and quality together. Finding is from the Toronto Central LHIN. Sunnybrook served as operational lead, and SPRINT Senior Care and LOFT are service providers for up to 68 patients. Reintegration units are less intensive and expensive ($190 per day) than reactivation centres ($424 per day). |
Acute Care Dementia Strategy Molnar 202133 No URL | Information sharing: Recommended initiatives Proposed elements for an in-hospital comprehensive acute care dementia strategy; including hospital-level data, strong leadership and corporate commitment, documentation, person-centred, staff education an ongoing training, dementia care expertise, non-pharmacological prevention, management of responsive behaviours, individualized proactive discharge planning, supportive physical environment. | Acute care hospitals All provinces | Older adults with dementia. | To identify the required elements for an in-hospital comprehensive acute care dementia strategy for Canadian hospitals that are serious about decreasing hospital overcrowding and ALC. | Hospital boards; hospital CEOs; hospital HCPs; hospital staff; hospital VPs. | While implementation across proposed elements may be incremental, success rests on making progress across all elements. Detection and documentation, and valuing and supporting families as essential care partners are essential to support the remaining elements of the strategy. |
Personal Support Homes Nauenberg 202135 No URL | Information sharing: Recommended initiatives Proposed policy concept that allows people to leverage their empty bedrooms to temporarily house patients awaiting hospital by remunerating homeowners (certified either as a PSW or with a lower level of certification with outside PSW support). | Private homes Ontario | Older patients with ALC designation without dementia, complex medical needs, or impaired mobility issues. | To reduce ALC days in Ontario hospitals. | Homeowners; PSWs. | Heatmap by census division of Ontario’s spare bedroom supply in single-story detached homes. Proposed remuneration would be $120 to $150 per day. Recommend careful roll-out of the program: slow initiation with pilot programs in rural and remote areas. |
ALC and Delayed Discharge: Lessons Learned from Abroad Bhatia et al. 202034 http://naohealthobservatory.ca/wp-content/uploads/2020/03/NAO-Rapid-Review-22_EN.pdf | Information sharing: Recommended initiatives Strategies should be multi-component, tailored to the local context, and employ high-level policy implementation; expert transition navigators and assessment procedures; cross-sectoral access to information; facilitating partnerships; and expanding supply and use of ambulatory and community care settings. | Community; private home; hospital Ontario | Patients with ALC designation, including older patients at risk of prolonged hospitalization due to complex psychological needs. | To draw on published academic and grey literature from outside Canada to develop insight into some of the policy options governments may consider as they address delayed discharge and ALC. | Specialized transition coordinators | Policy level interventions should be implemented while also allowing for local innovations in adapting both within organizational approaches (e.g., specialized transition coordinators and interdisciplinary collaborations), and cross-organizational and health sector approaches (e.g., shared accountability and cross-sectoral communication). |
Reactivation Care Centres48 | Infrastructure and finance Collaborative and innovative approach that specialize in activation therapies. | Urban hospitals; Finch and Church sites Ontario | Patients who no longer need acute care services, but are waiting for an alternate care facility, such as LTC. | To deliver patient care in the most appropriate setting where patient privacy, dignity and safety are a top priority. | Hospital clinical staff | NR |
ADL = activities of daily living; ALC = alternate level of care; CEO = chief executive officer; HCP = health care provider; NR = not reported; LTC = long-term care; PSW = personal support worker; RN = registered nurse; VP = vice president.
Note: This table has not been copy-edited.
Table 10: Summary of System-Level Strategies
Strategy Name First Author, Year URL | Strategy Category Brief Strategy Description | Setting Province(s) | Target Population | Objective(s) | Relevant Personnel | Implementation Considerations |
|---|---|---|---|---|---|---|
Supporting the Implementation of Alternate Levels of Care Leading Practices The Centre for Implementation 202431 http://geriatricsontario.ca/wp-content/uploads/2024/05/PGLO-Report-March-2024-V12.04.2024.pdf | Information sharing: Live sharing Report summarizing activities and discussions from 2024 workshop on roles in the system; inner and outer setting factors affecting change; and 7 recommendations to support the implementation of ALC leading practices. | Health system Ontario | Older adults | To collaborate with others engaged in ALC related work, understand and identity levers for change, and learn how to support implementation. | Community partners; funders; hospital implementation teams; hospital leadership; OHTs; policymakers; researchers; quality improvement leads; secondary implementation supports. | The Interactive Systems Framework described a functioning implementation infrastructure, and the roles that contribute to the infrastructure. Recommendations to support implementation were: sharing tools, knowledge, and documents; tackling ageism; sharing information about patients; local roles in the implementation system; consider chains of support; clearly define the role of PGLO; and strategically consider diverse sources of change. |
Scenarios for Seniors’ Care: Future Challenges, Current Gaps and Strategies to Address Them Wyonch 20242 http://cdhowe.org/sites/default/files/2024 to 04/FinalCommentary_656.pdf | Information sharing: Recommended initiatives Proposed opportunities to reduce ALC patient days in the hospital setting, community and support services, seniors’ care spaces, home care, primary care access; proposed policy changes; and key recommendations for provinces. | Community; hospital LTC; primary care; private home All provinces | Older patients with ALC designation | To examine the availability of different housing and care options for seniors, the costs of providing care in different settings, and government policies that subsidize support services in homes, retirement communities, and LTC. | Front-line clinical staff; physicians | Incentives for physicians, families, and hospitals encourage ALC designations in most provinces (except Quebec). |
Confronting the ALC Crisis with a Multifaceted Policy Lens Durante et al. 202336 http://policyschool.ca/wp-content/uploads/2023/06/HSP112-Brief.ConfrontCareCrisis.pdf | Information sharing: Recommended initiatives Proposed upstream interventions (early recognition and intervention; improving community care and supports; and improving outpatient supports and medical management), midstream interventions (change perceptions of risk and increase tolerance of risk; early and enhanced discharge planning; reformed and increased bed charges; stricter policies for choosing discharge destinations and improved LTC wait-list management; increased use of activity-based funding models; and increased provision of ALC-specific inpatient units and reactivation centres), and downstream strategies (increased provision of transitional care settings and increased provision of LTC). | Community; hospital; LTC; private home Alberta, Ontario, Saskatchewan | Patients with unnecessary hospital admissions, e.g., older patients with frailty experiencing declines in function and independence; patients with ALC designation, especially older patients. | To present a paradigm of policy options to address the continuum of ALC challenges. | NR | Strategies can be devised and implemented either locally or at the system level. Local adaptation allows organizations to build their plan accounting for their own quality challenges, strategic goals and values, which supports a more effective alignment with operations. Risk management is likely one of the broadest and most difficult interventions to implement in the health-care system but is arguably one of the most important overall for ALC mitigation |
Essential Role of Caregivers in Improving Transitions and Addressing ALC The Ontario Caregiver Organization 202338 | Tools and guidelines Actions or best practices for OHTs organized by inform, implement, access (ALC Leading Practices, self-assessment, engage caregivers in planning); and implement (build processes to formally identify and include caregivers in care planning, communication about ALC designation, roles across settings, and provide caregivers with resources to prevent caregiver burnout). | Variety of settings; including community, hospital, LTC, primary care, private home Ontario | Patients at risk of ALC; e.g., people over 65 years; admitting diagnoses of general medical illness, falls and dementia; functional or cognitive impairments and multiple comorbidities; experience adverse events during hospital admission (i.e., functional decline, delirium, falls, social isolation). | To address ALC in Ontario; to mitigate the risk of ALC. | OHTs | Action steps and resources for OHTs to implement caregiver focused strategies. |
The ALC Practices Guide: Preventing Hospitalization and Extended Stays for Older Adults Ontario Health 202139 | Tools and guidelines Evidence-based leading practices for the care and proactive management of hospitalized older adults at risk of delayed transition to an appropriate setting that can be implemented in the emergency department, acute care, and post-acute care settings. | Hospital Ontario | Older adults at risk of delayed transitions in care. | To integrate senior-friendly care as the foundation of care across the organization; to ensure practices and structures are in place in the ED to avoid unnecessary admission; to avoid hospital-acquired harm and enhance well-being in facility-based acute and post-acute care areas. | Behavioural support clinician; geriatric emergency management nurse; geriatric physician specialist; home and community case manager; hospital staff; hospital volunteers; occupational therapist; pharmacist; physiotherapist; senior leadership team; social workers. | The leading practices describe what care should look like. Organizations determine how to implement these practices on their own, by prioritizing change ideas and developing action plans, and are encouraged to ensure that integrated care is woven into improvement plans by co-developing their quality improvement plans with organizations in other sectors. |
Home First Ahmed 201942 | Practice changes A transition management strategy that focuses on providing patients with the support needed stay safe in their homes for as long as possible with community supports. If acute hospital care is required, Home First facilitates return to home on discharge with or without community services. | Community; hospital; personal home Ontario | Patients with ALC designation, especially older adults | To keep patients (especially seniors with high needs) safe in their homes for as long as possible with community supports; to ensure successful transition from hospital back to a home or community setting. | Nursing; occupational therapist; PSW; physiotherapist, speech therapist; social worker. | Home First was implemented as a system-wide approach (14 LHINs across the province). The Home First implementation guide described the program and explained how to evaluate and monitor its performance. |
Home First – Quick Response Project Compton 201943 No URL | Practice changes Distinct program under the umbrella of home care in response to an increasing need for better integration of service supports to respond to the complex care needs required by older adults and by their family caregivers. | Community; hospital; personal home Saskatchewan | Patients with ALC designation over 75 years of age | To improve outcomes for older adults living with complex care needs within their community by providing care and support beyond regular home care services. | Community care aids; dietitian; home maintenance worker; nurse practitioner; occupational therapist; pharmacists; physiotherapist; RNs; social worker; volunteers. | Home First staff were assigned 5 to 6 patients per a 5.5 hours-of-service per day, compared to home care’s 8 to 12 patients. Home First staff utilized the additional time to educate patients and caregivers about resources to maintain health and well-being, promote independence and self-management, and perform more intensive monitoring of health conditions. |
ALC = alternate level of care; LHIN = Local Health Integrated Network; LTC = long-term care; OHT = Ontario Health Teams; PGLO = Provincial Geriatrics Leadership Ontario; PSW = personal support worker; RN = registered nurse.
Note: This table has not been copy-edited.
Appendix 3: Studies of Clinical Effectiveness
Table 11: Summary of Clinical Effectiveness Findings of Throughput Strategies
Author, Year Intervention Name Strategy Category Intervention Description Province | Study Design Comparison Setting | Inclusion Criteria Study Population | Findings | Author Conclusions |
|---|---|---|---|---|
Robert et. al. 202146 Subacute Care for the Frail Elderly (SAFE) Unit Infrastructure and finance A 20-bed transitional care program with a strong emphasis on a restorative, collaborative and integrated approach. Ontario | Case control study using population-based data from ICES, NACRS, DAD, Registered Persons Database, and OHIP claims database. Comparison: Patients designated as ALC in local (Ottawa) hospitals. Urban nursing home, Ottawa. | Patients with frailty aged ≥ 60 yearsa at risk of deconditioning to the point of requiring care in a nursing home. N: SAFE: n = 153 ALC: n = 1,773 Sex: SAFE: male 44%, female 56% ALC: male 42%, female 58% Age:a SAFE: 60 to 69 years 13%; 70 to 79 years 26%; 80 to 89 years 38%; ≥ 90 years 23% ALC: 60 to 69 years 17%; 70 to 79 years 28%; 80 to 89 years 37%; ≥ 90 years 18% Comorbidities: SAFE: hypertension, 86%; osteoarthritis 75%; CCS 44%; diabetes 43%; CHD 38%; LRTI 35%; arrhythmia 31%; renal disease 28%; asthma 26%; cancer 23%; stroke 18%; osteoporosis 16%; non-psychotic mood and anxiety disorders 15%; dementia 5%; ≥ 5 conditions 54% ALC: hypertension 76%; osteoarthritis 76%; diabetes 38%; CCS 30%; asthma 20%; CHD 20%; renal disease 20%; arrhythmia 19%; osteoporosis 19%; cancer 17%; dementia 16%; non-psychotic mood and anxiety disorders 15%; LRTI 12%; stroke 11%; ≥ 5 conditions 38% | Median index hospitalization LOS (days) SAFE: 13 (IQR 8 to 19) ALC: 15 (IQR 10 to 24) Median ALC LOS (days) SAFE: 0 (IQR 0 to 1) ALC: 5 (IQR 3 to 10) Total length of care per episode (days) SAFE: 36 (SD 17.9) ALC: 23 (SD 32.9) Discharge to home (all) SAFE: 64.1% ALC: 46.3% Discharge to home without support SAFE: 50.3% ALC: 4.7% Discharge to home with support SAFE: 13.7% ALC: 41.6% 30-day hospital readmission Adjustedb OR 1.41 (95% CI 0.86 to 2.31) 30-day ED visit Adjustedb OR 1.13 (95% CI 0.74 to 1.73) Follow-up with family physician Adjustedb OR 1.42 (95%CI 0.901 to 2.24) | Transitional care programs supplemented with function-focused care for older adults living with frailty are proving to offer a more effective, person-centred approach to care, leading to an improved likelihood of independence post-acute care discharge. The SAFE Unit, which leverages shared resources within the nursing home where it is situated, is an innovative model of care that has shown to be effective in decreasing LOS in hospital and helping restore independence so patients can return home following an acute care episode. |
O’Brien et al. 201751 Restorative Care Unit Infrastructure and finance A 14-bed inpatient unit providing restorative care to support the transition from hospital to community for older adults. Newfoundland and Labrador | Single group, pre- and post-study, using standardized clinical assessments. Comparison: No intervention (patients with ALC designation before program implementation). Urban LTC home, Corner Brook. | Patients ≥ 65 years with acute care LOS ≥ 10 days; BRASS score > 9 but < 25; medically stable; sitting tolerance of 1 to 2 hours, 2 to 3 times per day; able to tolerable 30 minutes of low to moderate intensity therapy 5 days per week; waiting for alternate services or for nursing home placement; not eligible for intensive inpatient rehabilitation. N: Pre: NR Post: n = 49 Sex (post group only): Male 29%, female 71% Age (post group only, years): Mean 83, range 66 to 96 | ALC cases Pre 194 Post 205 ALC LOS (days) Pre 10,986 Post 13,146 19.7% increase % inpatient days designated as ALC Pre 30.5 Post 35.5 6% increase | There was no reduction in ALC days in acute care 1 year following introduction of restorative care. |
Manville et al. 201453 Transitional Care Unit Infrastructure and finance A 22-bed inpatient unit designed to provide an age-friendly, geriatric rehabilitation–style environment. British Columbia | Before-and-after structured retrospective chart audit. Comparison: Standard care (patients with ALC designation in preintervention group who received care on acute medical, surgical, or psychiatric wards). Urban hospital, Comox. | Patients with ALC designation ≥ 70 years. N = 135 Pre: n = 49 Post: n = 86 Sex: Pre: male 37%, female 63% Post: male 44%, female 56% Age, mean years: Pre: 86.4 Post: 85.6 Known dementia: Pre: 51% Post: 52% Reason for hospitalization: Pre: dementia, delirium, or confusion 43%; fall, fracture, or injury 45%; frailty or failure to thrive 25%; infection 14%; cardiac condition 18%; psychiatric or neurologic condition 20% Post: dementia, delirium, or confusion 44%; fall, fracture, or injury 41%; frailty or failure to thrive 31%; infection 13%; cardiac condition 8%; psychiatric or neurologic condition 12% Reason for ALC designation: Pre: dementia 65%; immobility, falls, fracture, or postoperative rehab 41%; frailty 35%; caregiver burden or unable to care for self 29%; cancer 14% Post: dementia 57%; immobility, falls, fracture, or postoperative rehab 47%; frailty 35%; caregiver burden or unable to care for self 31%; cancer 10% Residence before admission: Pre: private residence 78%, assisted living 20%, residential care 1%; lives alone 55% Post: private residence 74%, assisted living 24%, residential care 1%; lives alone 60% | Total LOS (days) Difference −9.3 (pre 74.8 vs. post 65.5), P = 0.137 Acute (hospital) LOS (days) Difference −8.5 (pre 22.5 vs. post 14.0), P < 0.01 ALC LOS (days) Difference −1.1 (pre 52.6 vs. post 51.5), P = 0.446 Dischare to home or assisted-living facility Difference + 18 (pre 12% vs. post 30%), P < 0.01 Discharge to residential care facility Difference −12 (pre 59% vs. post 47%), P = 0.078 | This study demonstrates that caring for elderly post-acute hospital patients on an interdisciplinary TCU managed by FPs, with COE-trained physicians in leadership roles, can improve health outcomes, decrease LOS, and improve discharge disposition. A hospital- based unit as described in this study appears to provide better care at less cost. |
ALC = alternate level of care; BRASS = Baylock Risk Screening Assessment; CCS = chronic coronary syndrome; CHF = chronic heart failure; COE = care of the elderly; DAD = Discharge Abstract Database; FP = family physician; ICES = formerly known as the Institute for Clinical Evaluative Sciences; IQR = inter-quartile range; LOS = length of stay; LRTI = lower respiratory infections; NACRS = National Ambulatory Care Reporting System; NR = not reported; OHIP = Ontario Health Insurance Plan; SAFE = Subacute Care for the Frail Elderly; TCU = transitional care unit.
Note: This table has not been copy-edited.
aWe included this study because most of the population are 65 years of age and older, i.e., approximately > 85% of the study population were aged 70 years and older.
bAdjusted for sociodemographic characteristics.
Table 12: Summary of Clinical Effectiveness Findings of Output Strategies
Author, Year Intervention Name Strategy Category Intervention Description Province | Study Design Comparison Setting | Inclusion Criteria Study Population | Findings | Author Conclusions |
|---|---|---|---|---|
Dhalla et al. 201450 Post-Discharge Virtual Ward Practice changes Patients were admitted to a virtual ward on the day they were discharge home and received direct care and care coordination via a combination of telephone, home visits, or clinic visits for several weeks after hospital discharge; and individualized management plans. The virtual ward takes many elements of hospital care (e.g., interprofessional team, daily team meeting, single point of contact for patients) and incorporates them into community-based care. Ontario | Parallel-group, unblinded RCT. Comparison: Usual care (typed, structured discharge summary, prescription if necessary, counseling from physician, home care as needed, and recommendation or appointments for follow-up as required). Community, Toronto Central LHIN. | Patients aged ≥ 18 years,a discharged from general internal medicine ward of 4 hospitals, and at high risk of readmission based on LACE score ≥ 10. N = 1,923 Virtual ward: n = 963 Usual care: n = 960 Sex: Virtual ward: female 49% Usual care: female 49% Age, mean (SD) years:a Virtual ward: 71 (16) Usual care: 71 (16) Location patient was discharged to: Virtual ward: Independent dwelling with family or friends 49%; independent dwelling alone 32%; nursing home 10%; retirement home or supportive housing 7%; houseless 2% Usual care: Independent dwelling with family or friends 49%; independent dwelling alone 33%; nursing home 9%; retirement home or supportive housing 8%; houseless 1% Heart failure (reason for admission to hospital): Virtual ward: 9% Usual care: 8% “Risky” alcohol use: Virtual ward: 13% Usual care: 15% Illicit drug use: Virtual ward: 8% Usual care: 7% | Hospital readmission (at 30 days) Virtual ward: 18.9% Usual care: 21.3% Absolute difference 2.4%; 95% CI −1.2 to 5.9; P = 0.22 Hospital readmission (at 90 days) Virtual ward: 33.4% Usual care: 33.7% Absolute difference 0.4%; 95% CI −3.9 to 4.6; P = 0.91 Hospital readmission (at 1 year) Virtual ward: 59.2% Usual care: 58.4% Absolute difference 0.8%; 95% CI −5.4 to 3.7; P = 0.76 ED visit (at 30 days) Virtual ward: 28.1% Usual care: 29.6% Absolute difference 1.5%; 95% CI −2.5 to 5.6; P = 0.49 ED visit (at 90 days) Virtual ward: 46.1% Usual care: 46% Absolute difference −0.1%; 95% CI −4.6 to 4.4; P > 0.99 ED visit (at 1 year) Virtual ward: 71.8% Usual care: 70.6% Absolute difference −1.2%; 95% CI −5.4 to 2.9; P = 0.60 | Our study showed that the virtual ward model of care did not reduce the primary outcome of readmission or death, or either component individually, in a diverse group of high-risk patients being discharged from hospital. |
ALC = alternate level of care; ED = emergency department; LACE = length of stay, acuity of the admission, comorbidities, and emergency department visits in the previous 6 months; LHIN = Local Health Integration Network; RCT = randomized controlled trial.
Note: This table has not been copy-edited.
aWe included this study because most of the population are 65 years of age and older, i.e., mean age of the study population was 71 years.
Table 13: Summary of Clinical Effectiveness Findings of System-Level Strategies
Author, Year Intervention Name Strategy Category Intervention Description Province | Study Design Comparison Setting | Inclusion Criteria Study Population | Findings | Author Conclusions |
|---|---|---|---|---|
Ahmed 201942 Home First Practice changes A transition management strategy that focuses on providing patients with the support needed to facilitate their discharge to home with or without receiving community services. Ontario | Uncontrolled, before-and-after study using ICES data. Comparison: No intervention (before strategy implementation). 14 LHINS in Ontario. | Ontario citizens aged ≥ 65 years admitted to an Ontario acute care facility identified as at risk of becoming ALC. N = 6,058,426 Sex: Male 49%, female 51% Age: 65 to 74 years 49%; 75 to 84 years 36%; 85 to 94 years 13%; ≥ 95 years 1% Geographic location: Urban 83%, rural 17% Income quintiles: 1 (lowest) = 22%; 2 = 21%, 3 = 20%, 4 = 19%, 5 (highest) = 19% Material deprivationa quintiles: 1 (least deprived) = 17%; 2 = 18%, 3 = 20%, 4 = 22%, 5 (most deprived) = 24% | ALC hospitalizations Decrease of 26% (from 10.1% in 2011 to 7.5% in 2016) ALC days (all patients) Decrease of 13% (from 19.7% in 2011 to 17.2% in 2016) Discharge home without support services Minimum reduction (from 5.7% in 2011 to 3.6% 2016) Discharge home with support services Increase of 17% (from 24.3% in 2011 to 28.4% in 2016) Discharge to LTC Remained almost constant (from 56.8% in 2011 to 56.5% in 2016) ALC days (patients discharged home without support) Minimum reduction (from 3.2% in 2011 to 1.4% in 2016) ALC days (patients discharged home with support) Minimum reduction (from 14.0% in 2011 to 12.9% in 2016) ALC days (patients discharged to LTC) Remained almost constant (from 40.2% in 2011 to 39.7% in 2016) | Although the implementation of the Home First strategy in Ontario resulted in a 26% reduction of ALC hospitalizations and a 13% decrease in ALC days, the percentage of patients discharged to long-term care did not change. Being the subgroup having the highest percent of ALC hospitalizations and ALC days, this reflects some failure of this strategy achieving its main objectives and may require a review of the strategy's implementation policies and procedure. |
Gutmanis et al. 201652 Behavioural Supports Ontario Tools and guidelines; practice changes Change strategies, executed in strategies, that lead to system redesign, including system coordination and management, intersectoral and interdisciplinary service delivery, and knowledge care teams and capacity development. Ontario | Quality improvement project, using mixed methods. Comparison: Periods of time since implementation. South West LHIN (including adult programs offering overnight respite, community centres, LTC facilities, psychiatric facilities, and tertiary hospitals). | Older people with responsive behaviours (behavioural and psychological symptoms, including aggression, disruptive behaviours, disinhibition, apathy, depression, anxiety, and agitation). NR | Mean ALC cases Oct 2013: 58 Nov 2013: 55 Apr 2014: 36 Sept 2014: 24 36% lower over 6 months in 2014 to 2015 ALC LOS (days) A similar decrease as ALC cases was observed in number of ALC days of open cases between Nov 2013 and April 2014, with a similar levelling off between Nov 2014 and Apr 2015 (data presented graphically) | The observed reduction in ALC days, though likely attributable to the combined efforts of several LHIN-wide initiatives, suggest improved client flow. By honouring people, honouring partners and honouring possibilities, person- and family-centred care is and will continue to be the foundation on which we build a better system of care for those living with responsive behaviours. |
ALC = alternate level of care; ED = emergency department; LHIN = Local Health Integration Network; LOS = length of stay; LTC = long-term care; NR = not reported.
Note: This table has not been copy-edited.
aMaterial deprivation describes to what extent patients are deprived of accessing and attaining basic material needs.
Appendix 4: Real-World Evidence Findings for Patients 55 Years and Older
Note that this appendix has not been copy-edited.
What Are the Trends in ALC Over Time for People Who Are 55 Years and Older in Jurisdictions Across Canada?
ALC Hospitalizations
The number of hospitalizations with ALC days per 1,000 population of those aged 55 years and older is presented annually and by jurisdiction in Figure 2 and Table 14. Across Canada (excluding Quebec), the rate of ALC hospitalizations remained relatively stable from 8 ALC hospitalizations per 1,000 population in 2018 to 2019 to 9 ALC hospitalizations per 1,000 population in 2022 to 2023. Several jurisdictions had a small increase in ALC hospitalizations in 2019 to 2020, followed by a slight decrease in 2020 to 2021, and then increased slightly in 2022 to 2023.
Figure 2: Number of ALC Hospitalizations per 1,000 Population Aged 55 Years and Older,a by Fiscal Yearb and Jurisdictionc
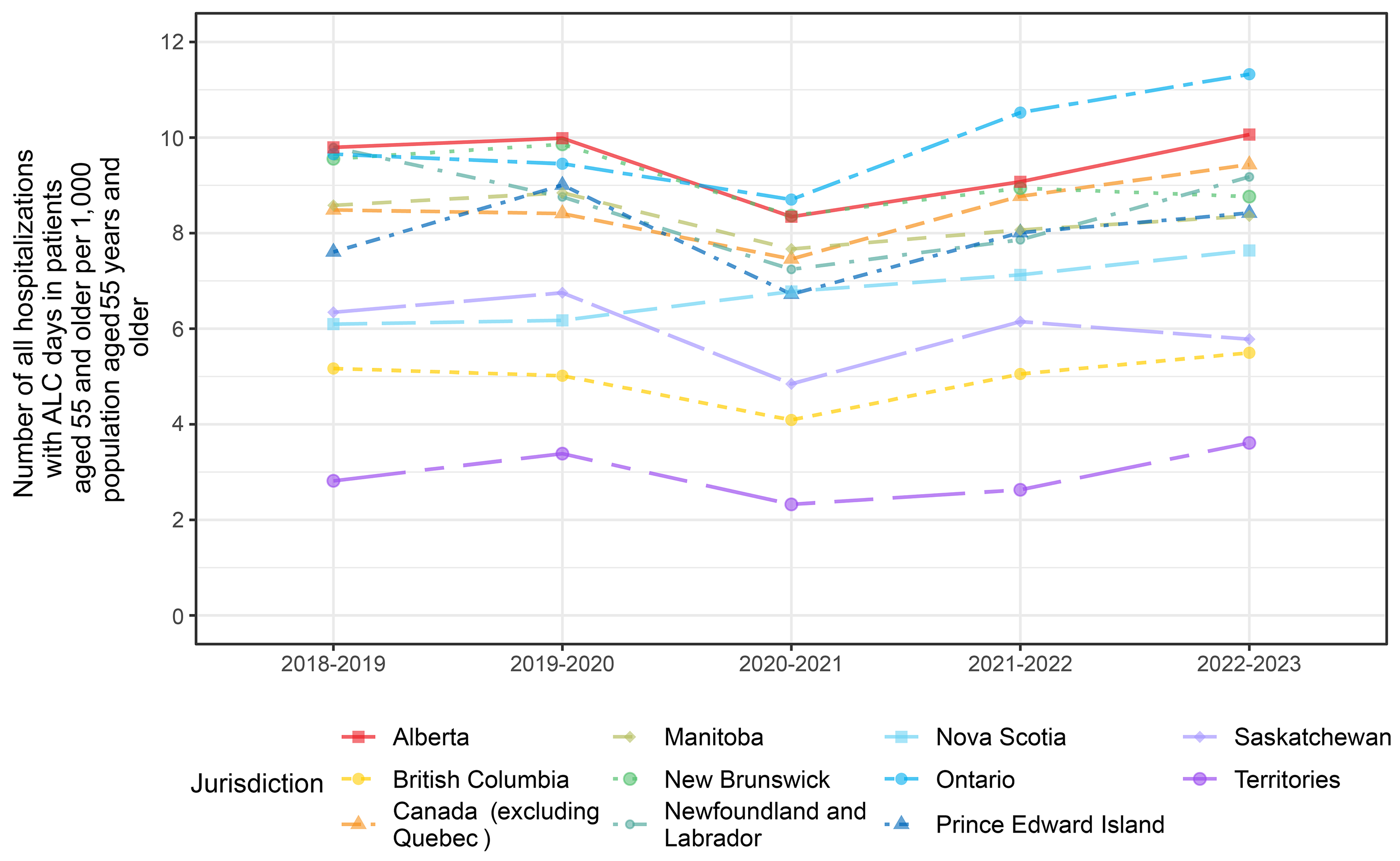
ALC = alternate level of care.
a Number of ALC hospitalizations per 1,000 population of those aged 55 years and older = number of ALC hospitalizations in patients 55 years and older with ALC designation and a reason for ALC of Z75.1 divided by the population of those aged 55 years and older, multiplied by 1,000.
b Fiscal year = April 1 to March 31.
c Combined data for Nunavut, the Northwest Territories, and Yukon.
Table 14: Number of ALC Hospitalizations per 1,000 Population Aged 55 Years and Older,a by Fiscal Yearb and Jurisdictionc
Fiscal Year | Canada (excluding Quebec) | AB | BC | MB | NB | NL | NS | ON | PEI | SK | Territoriesc |
|---|---|---|---|---|---|---|---|---|---|---|---|
2018 to 2019 | 8 | 10 | 5 | 9 | 10 | 10 | 6 | 10 | 8 | 6 | 3 |
2019 to 2020 | 8 | 10 | 5 | 9 | 10 | 9 | 6 | 9 | 9 | 7 | 3 |
2020 to 2021 | 7 | 8 | 4 | 8 | 8 | 7 | 7 | 9 | 7 | 5 | 2 |
2021 to 2022 | 9 | 9 | 5 | 8 | 9 | 8 | 7 | 11 | 8 | 6 | 3 |
2022 to 2023 | 9 | 10 | 5 | 8 | 9 | 9 | 8 | 11 | 8 | 6 | 4 |
AB = Alberta; ALC = alternate level of care; BC = British Columbia; MB = Manitoba; NB = New Brunswick; NL = Newfoundland and Labrador; NS = Nova Scotia; ON = Ontario; PEI = Prince Edward Island; SK = Saskatchewan.
aNumber of ALC hospitalizations per 1,000 population of those aged 55 years and older = number of ALC hospitalizations in patients aged 55 years and older with ALC designation and a reason for ALC of Z75.1 divided by the population of those aged 55 years and older, multiplied by 1,000.
bFiscal year = April 1 to March 31.
cCombined data for Nunavut, the Northwest Territories, and Yukon.
Total ALC days
Total ALC days per 1,000 population of those aged 55 years and older is presented in Figure 3 and Table 15. Overall, it appears that ALC days remained relatively stable over 5 years. In Canada (excluding Quebec), the rate was 233 ALC days per 1,000 population in 2018 to 2019 and 235 ALC days per 1,000 population in 2022 to 2023. There were variations in trends across jurisdictions. Alberta, Manitoba and the combined data for Nunavut, the Northwest Territories, and Yukon had declines of more than 20% over the five-year period and Saskatchewan declined by 11%. .
Figure 3: Total ALC Days Per 1,000 Population Aged 55 Years and Older,a by Fiscal Yearb and Jurisdictionc
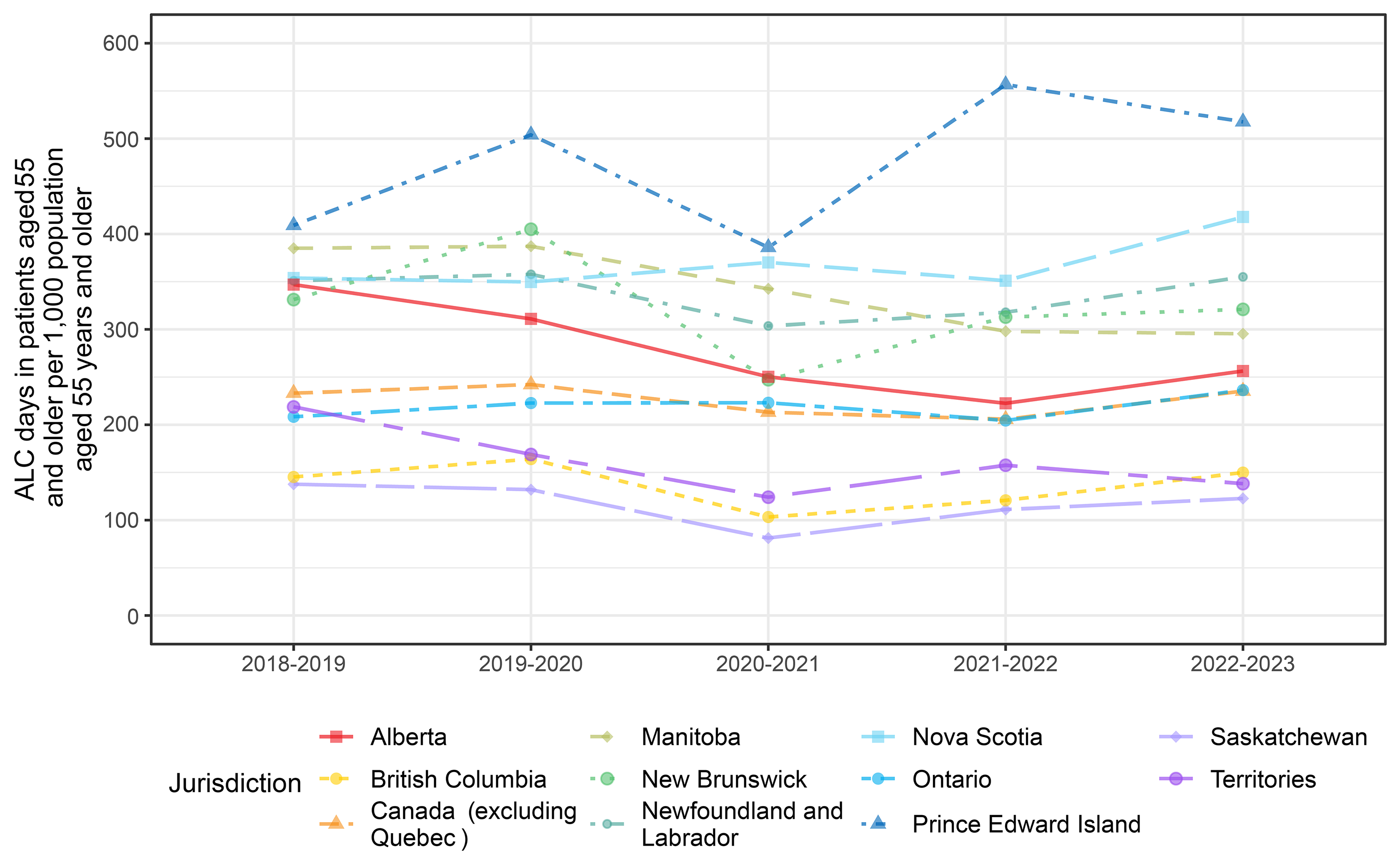
ALC = alternate level of care
a Total ALC days per 1,000 population of those aged 55 years and older = total ALC days in patients aged 55 years and older with ALC designation and a reason for ALC of z75.1 divided by the population of those aged 55 years and older, multiplied by 1,000.
b Fiscal year = April 1 to March 31.
c Combined data for Nunavut, the Northwest Territories, and Yukon.
Table 15: Total ALC Days per 1,000 Population in Patients 55 Years and Older,a by Fiscal Yearb and Jurisdictionc
Fiscal Year | Canada (excluding Quebec) | AB | BC | MB | NB | NL | NS | ON | PEI | SK | Territoriesc |
|---|---|---|---|---|---|---|---|---|---|---|---|
2018 to 2019 | 233 | 347 | 145 | 385 | 331 | 351 | 354 | 208 | 409 | 138 | 219 |
2019 to 2020 | 242 | 311 | 164 | 387 | 405 | 358 | 350 | 223 | 504 | 132 | 169 |
2020 to 2021 | 213 | 250 | 103 | 342 | 247 | 304 | 370 | 223 | 386 | 81 | 124 |
2021 to 2022 | 206 | 222 | 121 | 298 | 313 | 318 | 351 | 204 | 557 | 111 | 158 |
2022 to 2023 | 235 | 256 | 150 | 295 | 321 | 355 | 418 | 236 | 518 | 123 | 138 |
AB = Alberta; ALC = alternate level of care; BC = British Columbia; MB = Manitoba; NB = New Brunswick; NL = Newfoundland and Labrador; NS = Nova Scotia; ON = Ontario; PEI = Prince Edward Island; SK = Saskatchewan.
aTotal ALC days per 1,000 population of those aged 55 years and older = total ALC days in patients aged 55 years and older with ALC designation and a reason for ALC of Z75.1 divided by the population of those aged 55 years and older, multiplied by 1,000.
bFiscal year = April 1 to March 31.
cCombined data for Nunavut, the Northwest Territories, and Yukon.
Median ALC LOS
The median ALC LOS days per hospitalization in patients aged 55 years and older is presented in Figure 4 and Table 16 and provides information about patient experience. Overall, it appears that median ALC LOS days increased from 9 days in 2018 to 2019 to 11 days in 2022 to 2023, with variations in trends across jurisdictions. Median ALC LOS and 25th and 75th percentiles, and means and standard deviations are presented in Table 16. When there are outliers in the data, medians are a better reflection of the average patient experience. The median ALC LOS in Canada (excluding Quebec) was 11 days (25th to 75th percentile, 4 to 27) in 2022 to 2023, meaning 50% of patients waited with ALC designation for 11 days or fewer, and 50% of patients waited with ALC designation for longer than 11 days.
Figure 4: Median ALC LOS (in Days) in Patients Aged 55 Years and Older,a by Fiscal Yearb and Jurisdictionc
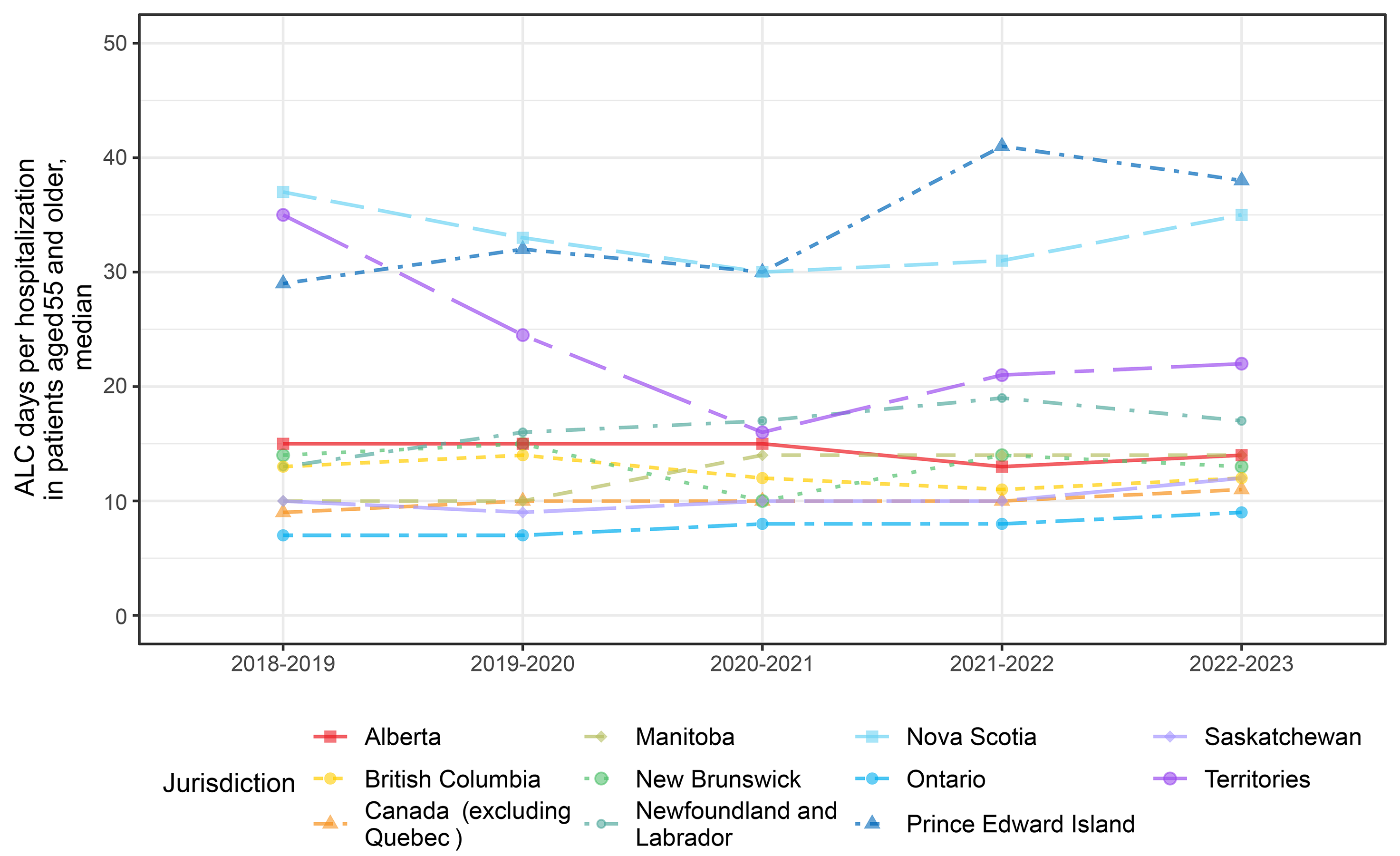
ALC = alternate level of care
a Median ALC days in patients aged 55 years and older = the 50th percentile of ALC days in patients aged 55 years and older with ALC designation and a reason for ALC of Z75.1.
b Fiscal year = April 1 to March 31.
c Combined data for Nunavut, the Northwest Territories, and Yukon.
Table 16: Mean and Median ALC LOS (in Days) in Patients Aged 55 Years and Older,a by Fiscal Yearb and Jurisdictionc
Fiscal Year | Canada (excluding Quebec) | AB | BC | MB | NB | NL | NS | ON | PEI | SK | Territoriesc |
|---|---|---|---|---|---|---|---|---|---|---|---|
Mean (SD) | |||||||||||
2018 to 2019 | 27 (59) | 35 (63) | 28 (43) | 45 (90) | 35 (63) | 36 (60) | 58 (63) | 22 (57) | 54 (63) | 22 (39) | 78 (96) |
2019 to 2020 | 29 (60) | 31 (50) | 33 (52) | 44 (90) | 41 (78) | 41 (64) | 57 (65) | 24 (59) | 56 (70) | 20 (30) | 50 (76) |
2020 to 2021 | 29 (62) | 30 (48) | 25 (45) | 45 (89) | 30 (59) | 42 (65) | 55 (75) | 26 (65) | 57 (74) | 17 (21) | 53 (118) |
2021 to 2022 | 23 (46) | 25 (38) | 24 (41) | 37 (76) | 35 (64) | 40 (57) | 49 (62) | 19 (43) | 69 (75) | 18 (24) | 60 (96) |
2022 to 2023 | 25 (48) | 25 (35) | 27 (49) | 35 (99) | 37 (67) | 39 (58) | 55 (62) | 21 (40) | 61 (74) | 21 (60) | 38 (60) |
Median (25th to 75th percentile) | |||||||||||
2018 to 2019 | 9 (4 to 26) | 15 (6 to 40) | 13 (5 to 34) | 10 (3 to 43) | 14 (5 to 37) | 13 (4 to 36) | 37 (14 to 78) | 7 (3 to 18) | 29 (12 to 68) | 10 (5 to 24) | 35 (16 to 122) |
2019 to 2020 | 10 (4 to 28) | 15 (6 to 36) | 14 (5 to 40) | 10 (3 to 42) | 15 (6 to 39) | 16 (6 to 43) | 33 (14 to 77) | 7 (3 to 19) | 32 (12 to 70) | 9 (5 to 22) | 25 (14 to 45) |
2020 to 2021 | 10 (4 to 28) | 15 (6 to 36) | 12 (4 to 27) | 14 (4 to 47) | 10 (4 to 29) | 17 (6 to 47) | 30 (14 to 69) | 8 (3 to 22) | 30 (11 to 76) | 10 (5 to 20) | 16 (9 to 33) |
2021 to 2022 | 10 (4 to 25) | 13 (6 to 30) | 11 (4 to 26) | 14 (5 to 35) | 14 (5 to 35) | 19 (7 to 52) | 31 (14 to 60) | 8 (3 to 20) | 41 (15 to 101) | 10 (5 to 21) | 21 (12 to 67) |
2022 to 2023 | 11 (4 to 27) | 14 (6 to 32) | 12 (4 to 29) | 14 (3 to 32) | 13 (5 to 36) | 17 (7 to 42) | 35 (16 to 73) | 9 (4 to 22) | 38 (18 to 77) | 12 (6 to 24) | 22 (10 to 45) |
AB = Alberta; ALC = alternate level of care; BC = British Columbia; MB = Manitoba; NB = New Brunswick; NL = Newfoundland and Labrador; NS = Nova Scotia; ON = Ontario; PEI = Prince Edward Island; SK = Saskatchewan; SD = standard deviation.
aMean ALC days in patients aged 55 years and older = total ALC days in patients aged 55 years and older with ALC designation and a reason for ALC of Z75.1 divided by the number of hospitalizations in patients aged 55 years and older with ALC designation and a reason for ALC of Z75.1.
bFiscal year = April 1 to March 31.
cCombined data for Nunavut, the Northwest Territories, and Yukon.
What Are the Characteristics of Patients 55 Years and Older Who Experienced ALC in Jurisdictions Across Canada?
Characteristics of patients aged 55 years and older with ALC designation and reason for ALC of Z75.1 are presented in Table 17. The mean age of patients was 80 years and 55% were female. Seventy 1 percent were aged 75 years and older. Nine percent were aged 55 to 64. Across Canada (excluding Quebec), 85% lived in urban centres but there was substantial variation across jurisdictions. The proportion of patients in the lowest neighbourhood income quintile (a measure of low socioeconomic status) was greater than expected (20% per category would be seen if there was no association between socioeconomic status and having an ALC hospitalization), and there was variation across jurisdictions. Most of the patients (86%) were admitted as an urgent admission. Twenty 3 percent had a diagnosis of dementia on the hospital record, with variation across jurisdictions.
What Factors Are Associated With ALC Days per 1,000 Population in Patients 55 Years and Older in Jurisdictions Across Canada?
Patients aged 55 years and older with ALC designation and a reason for ALC of Z75.1 had 235 days of ALC per 1,000 population of those aged 55 years and older (Table 15) for Canada (excluding Quebec). When looking at subgroups of the overall population, a larger number of days per 1,000 population provides an indication of where there is greater system burden and suggests potential targets for interventions. Table 18 provides ALC days per 1,000 population by subgroup. When a complete subgroup is reported, the total adds to 235 days. Patients aged 75 to 84 and 85 to 95 are the 2 largest contributing age groups, with 76 and 75 days per 1,000 population, respectively. Females had a slightly larger burden than males (122 and 113 ALC days per 1,000 population, respectively). There was variation in the impact of sex across jurisdictions. Urban patients contributed most of the ALC days (178 ALC days per 1,000 population) but this varied across jurisdictions; Manitoba, Newfoundland and the combined data for Nunavut, the Northwest Territories and Yukon had greater burden from rural and remote patients. Patient experience in Canada, reflected in the median LOS was worse in the rural population compared to the urban population (19 days (IQR 7 to 46) versus 10 days (IQR 4 to 24), data not shown in table). Patients in the lowest income quintile (a measure of socioeconomic status) were the largest contributing income group, with 75 ALC days per 1,000 population. The next lowest income quintile was the next largest contributor with the trend continuing through all income groups. There was variation across jurisdictions with respect to the effect of income quintile on ALC days per 1,000 population. Patients who were unhoused at admission had very low system impact, measured by ALC days per 1,000 population, but their experience, measured by the median length of stay was worse than those with housing, (median length of stay per hospitalization in unhoused patients was 21 ALC days (IQR 7 to 55) versus 11 ALC days (IQR 4 to 27) for patients with housing, data not shown in table). Patients who had an urgent admission contributed 187 ALC days per 1,000 population. Patients with a diagnosis of dementia on their hospital record contributed 89 ALC days per 1,000 population and their median length of stay was longer than typical at 21 ALC days (IQR 9 to 47, data not shown in table).
Table 17: Patient Characteristics of Patients Aged 55 and Older With ALC Days, by Jurisdiction, 2022 to 2023a
Characteristic | Canada (excluding Quebec) | AB | BC | MB | NB | NL | NS | ON | PEI | SK | Territoriesb |
|---|---|---|---|---|---|---|---|---|---|---|---|
N | 90,153 | 12,258 | 9,735 | 3,427 | 2,722 | 1,961 | 2,914 | 54,513 | 491 | 2,033 | 99 |
Mean age (SD), years | 80 (10) | 80 (10) | 81 (10) | 82 (10) | 80 (10) | 79 (10) | 81 (9) | 80 (10) | 82 (9) | 80 (11) | 77 (10) |
Age group, n (%) | |||||||||||
55 to < 65 years | 8,013 (8.9) | 1,189 (9.7) | 713 (7.3) | 187 (5.5) | 215 (7.9) | 162 (8.3) | 159 (5.5) | 5,173 (9.5) | 14 (2.9) | 190 (9.3) | 11 (11.1) |
65 to < 75 years | 17,621 (19.5) | 2,514 (20.5) | 1,800 (18.5) | 538 (15.7) | 589 (21.6) | 406 (20.7) | 530 (18.2) | 10,719 (19.7) | 82 (16.7) | 413 (20.3) | 30 (30.3) |
75 to < 85 years | 29,045 (32.2) | 3,852 (31.4) | 3,041 (31.2) | 1,108 (32.3) | 973 (35.7) | 749 (38.2) | 1,046 (35.9) | 17,454 (32.0) | 186 (37.9) | 604 (29.7) | 32 (32.3) |
85 to < 95 years | 29,978 (33.3) | 4,029 (32.9) | 3,501 (36.0) | 1,316 (38.4) | 826 (30.3) | 580 (29.6) | 1,008 (34.6) | 17,837 (32.7) | NR | 676 (33.3) | NR |
95 years and older | 5,496 (6.1) | 674 (5.5) | 680 (7.0) | 278 (8.1) | 119 (4.4) | 64 (3.3) | 171 (5.9) | 3,330 (6.1) | NR | 150 (7.4) | NR |
Male | 40,592 (45.0) | 5,523 (45.1) | 4,421 (45.4) | 1,446 (42.2) | 1,214 (44.6) | 852 (43.4) | 1,272 (43.7) | 24,686 (45.3) | 220 (44.8) | 895 (44.0) | 63 (63.6) |
Femalec | 49,561 (55.0) | 6,735 (54.9) | 5,314 (54.6) | 1,981 (57.8) | 1,508 (55.4) | 1,109 (56.6) | 1,642 (56.3) | 29,827 (54.7) | 271 (55.2) | 1,138 (56.0) | 36 (36.4) |
Location of residence | |||||||||||
Urban | 76,435 (84.8) | 10,138 (82.7) | 8,820 (90.6) | 2,475 (72.2) | 1,603 (58.9) | 904 (46.1) | 1,642 (56.3) | 49,116 (90.1) | 280 (57.0) | 1,410 (69.4) | 47 (47.5) |
Rural or remote | 12,847 (14.3) | 2,059 (16.8) | 841 (8.6) | 942 (27.5) | NR | 1,034 (52.7) | 1,250 (42.9) | 4,754 (8.7) | NR | 607 (29.9) | 52 (52.5) |
Missing | 871 (1.0) | 61 (0.5) | 74 (0.8) | 10 (0.3) | NR | 23 (1.2) | 22 (0.8) | 643 (1.2) | NR | 16 (0.8) | 0 |
Neighbourhood income quintilesd | |||||||||||
Quintile 1 (lowest income) | 27,602 (30.6) | 4,017 (32.8) | 3,351 (34.4) | 991 (28.9) | 828 (30.4) | 420 (21.4) | 710 (24.4) | 16,486 (30.2) | 146 (29.7) | 612 (30.1) | 41 (41.4) |
Quintile 2 | 20,077 (22.3) | 2,844 (23.2) | 2,094 (21.5) | 701 (20.5) | 555 (20.4) | 455 (23.2) | 723 (24.8) | 12,147 (22.3) | 129 (26.3) | 409 (20.1) | 20 (20.2) |
Quintile 3 | 15,932 (17.7) | 2,044 (16.7) | 1,858 (19.1) | 574 (16.7) | 581 (21.3) | 409 (20.9) | 606 (20.8) | 9,398 (17.2) | 81 (16.5) | 365 (18.0) | 16 (16.2) |
Quintile 4 | 13,617 (15.1) | 1,696 (13.8) | 1,317 (13.5) | 697 (20.3) | 413 (15.2) | 442 (22.5) | 471 (16.2) | 8,166 (15.0) | 71 (14.5) | 330 (16.2) | 14 (14.1) |
Quintile 5 (highest income) | 11,999 (13.3) | 1,595 (13.0) | 1,035 (10.6) | 452 (13.2) | 326 (12.0) | 197 (10.0) | 382 (13.1) | 7,654 (14.0) | NR | 294 (14.5) | NR |
Quintile missing | 926 (1.0) | 62 (0.5) | 80 (0.8) | 12 (0.4) | 19 (0.7) | 38 (1.9) | 22 (0.8) | 662 (1.2) | NR | 23 (1.1) | NR |
Unhoused at admission | 748 (0.8) | 153 (1.2) | 109 (1.1) | 11 (0.3) | 20 (0.7) | 5 (0.3) | 27 (0.9) | 405 (0.7) | NR | 14 (0.7) | NR |
Urgent admission | 77,884 (86.4) | 11,346 (92.6) | 8,353 (85.8) | 2,765 (80.7) | 2,247 (82.5) | 1,831 (93.4) | 2,757 (94.6) | 46,489 (85.3) | 416 (84.7) | 1,585 (78.0) | 95 (96.0) |
Dementia on hospitalization recorde | 20,964 (23.3) | 2,706 (22.1) | 2,280 (23.4) | 1,283 (37.4) | 869 (31.9) | 420 (21.4) | 1,412 (48.5) | 11,491 (21.1) | 174 (35.4) | 307 (15.1) | 22 (22.2) |
AB = Alberta; ALC = alternate level of care; BC = British Columbia; MB = Manitoba; NB = New Brunswick; NL = Newfoundland and Labrador; NR = not reported: suppressed in accordance with the Canadian Institute for Health Information privacy policy; NS = Nova Scotia; ON = Ontario; PEI = Prince Edward Island; SD = standard deviation; SK = Saskatchewan.75
aFiscal year = April 1 to March 31.
bCombined data for Nunavut, the Northwest Territories, and Yukon.
cFemale sex also includes “other and unknown” in one or more provinces and the Canada total. Each number is between 1 and 4 patients.
dIncome quintiles function as a measure of socioeconomic status.
eDementia in the ALC population may be greater than what is coded on hospitalization records because only those diagnoses that significantly affect the patient’s hospitalization are coded, and only the current hospitalization record was used.
Table 18: ALC Days per 1,000 Population in Patients Aged 55 Years and Older by Patient Characteristics
Measures | Canada (excluding Quebec) | AB | BC | MB | NB | NL | NS | ON | PEI | SK | Territoriesa |
|---|---|---|---|---|---|---|---|---|---|---|---|
Age (years) | |||||||||||
55 to < 65 | 22 | 31 | 12 | 24 | 27 | 28 | 27 | 24 | 26 | 13 | 18 |
65 to < 75 | 49 | 55 | 30 | 53 | 70 | 69 | 89 | 49 | 111 | 32 | 48 |
75 to < 85 | 76 | 79 | 48 | 95 | 118 | 141 | 149 | 75 | 186 | 34 | 40 |
85 to < 95 | 75 | 79 | 51 | 99 | 95 | 107 | 132 | 75 | NR | 36 | NR |
95 and older | 13 | 14 | 9 | 23 | 11 | 10 | 21 | 14 | NR | 8 | NR |
Male | 113 | 126 | 73 | 130 | 157 | 157 | 198 | 114 | 245 | 55 | 97 |
Femaleb | 122 | 131 | 77 | 165 | 164 | 198 | 220 | 122 | 273 | 68 | 41 |
Location of residence | |||||||||||
Urban | 178 | 197 | 127 | 141 | 140 | 170 | 212 | 201 | 224 | 91 | 42 |
Rural or remote | 55 | 58 | 21 | 153 | NR | 182 | 201 | 31 | NR | 31 | 96 |
Missing | 3 | 2 | 2 | 1 | NR | 2 | 4 | 4 | NR | 1 | 0 |
Neighbourhood income quintiles | |||||||||||
Quintile 1, lowest income | 75 | 91 | 51 | 90 | 111 | 59 | 102 | 76 | 143 | 42 | 69 |
Quintile 2 | 52 | 60 | 31 | 60 | 61 | 108 | 100 | 52 | 133 | 20 | 32 |
Quintile 3 | 41 | 40 | 29 | 49 | 63 | 80 | 93 | 38 | 97 | 22 | 17 |
Quintile 4 | 35 | 32 | 22 | 59 | 46 | 69 | 67 | 34 | 106 | 23 | 11 |
Quintile 5, highest income | 29 | 31 | 15 | 37 | 38 | 33 | 51 | 31 | NR | 15 | NR |
Quintile missing | 3 | 2 | 3 | 1 | 1 | 5 | 4 | 4 | NR | 1 | NR |
Unhoused at admission | 4 | 5 | 4 | 2 | 4 | 2 | 8 | 3 | NR | 1 | NR |
Urgent admission | 187 | 234 | 129 | 169 | 253 | 332 | 395 | 176 | 400 | 93 | 132 |
Dementia diagnoses at admission | 89 | 85 | 55 | 138 | 170 | 115 | 230 | 84 | 234 | 21 | 47 |
AB = Alberta; ALC = alternate level of care; BC = British Columbia; MB = Manitoba; NB = New Brunswick; NL = Newfoundland and Labrador; NR = not reported: suppressed in accordance with the Canadian Institute for Health Information privacy policy; NS = Nova Scotia; ON = Ontario; PEI = Prince Edward Island; SK = Saskatchewan.75
Note: Values from cells with low volumes may be unreliable; interpret with caution.
aCombined data for Nunavut, the Northwest Territories, and Yukon.
bFemale sex also includes “other and unknown” in one or more provinces and the Canada total.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Parts of this material are based on data and information provided by the Canadian Institute for Health Information. However, the analyses, conclusions, opinions, and statements expressed herein are those of CADTH and not necessarily those of the Canadian Institute for Health Information.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.