CADTH Horizon Scan
The Paige Prostate Suite: Assistive Artificial Intelligence for Prostate Cancer Diagnosis
Key Messages
What Is the Paige Prostate Suite?
The Paige Prostate Suite is a set of artificial intelligence (AI) applications that works alongside pathologists reviewing prostate biopsy samples. The suite is not available in Canada as of this writing (June 2024), but international counterparts have authorized it for clinical use.
The system requires pathology slides to be digitized for the suite to be able to highlight areas of suspicion for pathologist review. Pathologists can use Paige Prostate Detect as a “second set of eyes” on biopsy slides scanned into the digital system.
What Issue Does the Paige Prostate Suite Intend to Address?
In Canada, prostate cancer accounted for 20% of new cancers in 2022. It is the most common cancer found in people who have a prostate.
Unlike many other cancers, the disease progresses slowly and early diagnosis results in a 5-year survival rate close to 100%. However, health systems are faced with more cancer cases without an increased capacity in pathology.
What Is the Potential Impact?
Paige Prostate aims to improve pathologists’ ability to detect prostate cancer in less time by allowing pathologists to focus on positive cases. However, the time-saving benefits of the suite require further validation that reflects real world settings and applications.
The Paige Prostate Suite has the potential to optimize pathology workflow and prevent delays in diagnosis. Pathologists can use the suite to supplement their review instead of sending biopsy slides to the lab for additional staining or to experts for a second consultation. It does, however, require the added the step of digitizing slides to the workflow.
The Paige Prostate Suite aims to improve consistency by helping pathologists grade tumours.
What Else Do We Need to Know?
Canada is in the early stages of implementing technology to produce digital images of biopsies. To adapt to the uptake of AI, pathology departments will need to adopt new digital workflows and processes. They could leverage this infrastructure for telepathology to improve access in rural and remote areas.
Clinicians expect the Paige Prostate Suite to cost more than current practice. Costs will vary depending on the case load, system readiness for AI, and use case for the suite. Cost-effectiveness of the suite requires in-depth investigation that considers the cost-benefit from productivity changes.
Upcoming prospective studies will assess the benefits of the Paige Prostate Suite from a clinical utility and cost impact perspective. It is also important to further understand the diagnostic performance and impact of Paige Prostate in the context of race, ethnicity, and other equity considerations, as those in equity-deserving groups may be underrepresented in algorithm development and trials, or have different levels of prostate cancer risk.
Purpose and Scope
This Horizon Scan provides health care decision-makers in Canada an overview of the Paige Prostate Suite, an assistive AI diagnostic tool for pathology. The suite is not available in Canada as of this writing (June 2024), but international counterparts have authorized it for clinical use. This report describes the technology and how it was produced, its availability, some cost considerations, the clinical evidence, and some considerations related to its implementation in Canada.
This report is not a systematic review and does not involve critical appraisal or include a detailed summary of study findings of the Paige Prostate Suite. It is not intended to provide recommendations for or against the use of the technology.
Background: What Is the Issue?
Prostate cancer is 1 of the most common cancers worldwide in individuals with a prostate.1,2 In Canada, prostate cancer accounted for 20% of new cancers in 2022.3 Unlike many other cancers, the disease progresses slowly and early diagnosis results in a 5-year survival rate close to 100%.1
Effective screening practices — such as the prostate specific antigen test and digital rectal exam — facilitate early detection of prostate cancer, even for individuals without symptoms.1 These tests identify individuals who require a biopsy for diagnosis. During the biopsy, a clinician extracts a sample from the prostate to send to a laboratory to produce glass slides.1 Pathologists use a microscope to detect cancer on the glass slides. With complex cases, pathologists delay diagnosis by sending the glass slides for additional work-up (i.e., immunohistochemistry staining) or a second opinion to validate their findings.4
Health systems are experiencing increasing cases of cancer without a proportionate increase in the number of pathologists.
The media has reported wait times for biopsy results that exceed expected turnaround times amid the pathologist shortage.5,6 In March 2017, samples from “nonurgent” cases in Quebec were in queue to be analyzed for up to 4 months versus the typical 1-month turnaround time.5 Individuals may experience undue stress due to long wait times for diagnosis.5 Further, the number of new cancer cases per pathologist grew to 116.89 from 109 between 2007 and 2017.7 While updated statistics were not identified, the media has reported that pathology shortages in some regions persisted into 2023.8 High workloads with increasing demand can cause physician burnout, especially in an already overburdened health workforce.9,10
AI offers a potential solution to optimize clinical workflows by promising faster and more accurate diagnosis.11 Pathologists using AI may spend less time reviewing slides, potentially through focusing on samples that have been identified by AI as potentially cancerous (e.g., AI as a “second set of eyes”). However, in pathology, a limiting factor is in the manual processes and glass slides viewed using microscopes, as AI requires digital information. The advent of digital pathology has enabled the use of AI in pathology.12 The algorithms use digital images of biopsy slides, referred to as whole-slide images (WSIs), for training and analyzing cases.12
In 2021, Paige Prostate Detect received the first FDA authorization for AI in pathology.13 This has been described as a landmark authorization for assistive AI diagnostics in pathology.14 The Paige Prostate Suite, inclusive of Paige Prostate Detect, aims to streamline the diagnosis of prostate cancer and accelerate the adoption of digital pathology.15
What Is the Paige Prostate Suite? How Does It Work?
The Paige Prostate Suite is a set of AI applications that works alongside pathologists reviewing prostate biopsy samples.15 The AI applications and their functions are as follows:15
Paige Prostate Detect assists in detecting prostate cancer.
Paige Prostate Grade and Quantify grades areas suspicious for cancer using the Gleason scoring system and quantifies overall tumour percentage and length.
Paige Prostate Perineural Invasion identifies perineural invasion in the prostate.
Paige Prostate Biomarker Panel detects biomarkers relevant to prostate cancer (e.g., TP53 mutations).
The company, Paige, offers the suite through a platform compatible with any slide scanner and laboratory information system.16 The platform houses the image viewer, Full Focus, and the software that prioritizes and processes images.16 Pathology departments can integrate third-party AI into the platform for use. Paige provides users with a “1-stop shop” product that includes all the software pathologists need to operate AI.
Pathology departments create WSIs by scanning biopsy slides using a slide scanner. The AI applications analyze the WSIs and flag areas of suspicion for pathologists. Using the image viewer, pathologists can view the WSI and Paige Prostate’s findings to inform their review.
Paige also offers scalable cloud-based storage to assist with the challenges related to the storage of WSIs.16 A single case, inclusive of several WSIs, can take up at least 20 gigabytes of digital space.17
How Was the Algorithm Developed?
Typically, pathologists annotate tumours on WSIs to create a training dataset for AI, which is an expensive and time-consuming process that results in curated data that limits performance.18 The developers of the Paige algorithm labelled each WSI as “positive” or “negative” instead of annotating tumours.19 A positive WSI was defined as the presence of at least 1 tumour, whereas a negative WSI indicates no tumours.19 This method is known as “multiple instance learning.”19
The developers used a large volume of WSIs, including 12,727 prostate biopsy samples from laboratories across 45 countries.19 They validated the algorithm using an additional 12,000 slides.17,19 The developers used the slides as-is, without curation, rendering differences in slide preparation negligible to performance and avoiding the need for the suite’s calibration per site.19
Place in Care: How Could Paige Change Care?
The Paige Prostate Suite aims to improve diagnostic accuracy while preventing delays in diagnosis. The suite can be used as a quality assurance tool to confirm pathology findings or to inform a pathologist’s reviews in real time. This can allow pathologists to spend less time on negative cases and reduce potential delays associated with more complex cases, such as requests for secondary consultation or additional work-up of slides. Ideally, the Paige Prostate Suite will support the overburdened pathology workforce dealing with rising cases,8,20,21 and also reduce stress related to long wait times.5,6
Pathologists use the Gleason score to grade prostate tumours.22,23 They rely on human eyes to analyze biopsy samples with microscopes and WSIs. Hence, a certain level of inconsistency and subjectivity when grading tumours will always exist. The literature has noted considerable differences in Gleason grading between pathologists.22,24,25 AI aims to improve consistency in pathology,24,26 for example through the Paige Prostate Grade and Quantify function, which can standardize grading tumours to help pathologists.27
Regulatory Status and Availability
The Paige Prostate Suite is not available in Canada as of this writing (June 2024).
In 2021, the FDA authorized Paige Prostate Detect for clinical use with the Philips Ultrafast Scanner and FullFocus.13 Paige Prostate Detect received class II designation through the FDA’s de novo classification pathway.13 Pathologists in the US use Paige Prostate Detect to confirm their initial findings without the algorithm.13 The authorized version of the software will not be continually trained and improved with each cohort analyzed in clinical practice.13 The Paige Prostate Suite is also authorized for clinical use in Europe and the UK.15 The suite holds Conformité Européene in vitro device (CE-IVD) and UK conformity assessed (UKCA) marks with Leica Aperio AT2 and Philips Ultrafast Scanners.15
Cost and Administration
The cost of the Paige Prostate Suite varies based on the volume of cases and needs of the pathology department.27 Paige bills users on a subscription basis for services and the software required to run the algorithm.27 NICE reported that users pay Paige at least £1 per case, inclusive of detection, grading, and quantification services of the suite.27 The price per case increases based on the number of biopsies per slide, number of slides per case, and cloud storage and archiving needs.27 The subscription fee covers initial in-person or remote training for all users of the platform.27 Additionally, the startup cost includes a 1-time fee to integrate the software into the laboratory information system. This fee typically starts at £15,000.27
Adopters need to invest in the IT infrastructure, such as slide scanners and computers, to support the operation of the suite and the platform in pathology departments.
The Paige Prostate Suite aims to decrease productivity costs related to sending slides for second review (e.g., pathologist, shipping the slide) or for additional staining.27
What Is the Evidence?
We found 5 retrospective studies28-32 that assessed Paige Prostate’s diagnostic performance. Additionally, we found 1 conference abstract regarding the findings of a study evaluating the algorithm’s diagnostic performance on samples from individuals previously given treatment.33 One of the retrospective studies informed the FDA’s decision to grant Paige Prostate Detect de novo authorization.29 The evidence accepted the consensus of pathologists or diagnosis received at the diagnosing institution as ground truth.28-33 None of the studies were performed at an institution in Canada.
Two studies reported on Paige Prostate 1.028,29 and 2 studies reported on Paige Prostate Alpha.30,31 The studies described Paige Prostate 1.0 as the mature version of Paige Prostate Alpha,28,29 but they did not report the difference in function and capabilities between the 2 versions.
All studies listed at least 1 author that was a Paige consultant, employee, or equity holder.28-32 Paige funded 2 of the 5 studies.29,30
Overall, the evidence suggests that Paige Prostate improves pathologists' ability to detect cancer. However, limited evidence also suggests that it does not offer pathologists additional benefits for grading and quantifying tumours or identifying perineural invasion. The suite's benefits on patient outcomes and pathology workloads require further validation through rigorous clinical studies that replicate real-world application.
Paige Prostate as a Stand-Alone Diagnostic Tool
Four studies reported the sensitivity and specificity of Paige Prostate as indicators of its diagnostic performance as a stand-alone tool. Sensitivity measures Paige Prostate’s ability to yield a positive result for an individual with prostate cancer.34 Paige Prostate exhibited high sensitivity when detecting tumours from WSIs. The reported sensitivity ranged from 96% to 99.2% across studies with WSIs ranging from 232 to 610.28,29,31 Specificity measures Paige Prostate’s ability to yield a negative result for a person without prostate cancer.34 The specificity at the WSI level ranged from 93% to 98% across the same studies.28,29,31
In 1 study with 100 consecutive and archived cases, Paige Prostate identified all individuals with cancer, displaying a sensitivity of 100% at the case level.28 It also reported a positive predictive value (PPV) of 0.99 and negative predictive value (NPV) of 1.0,28 which highlights Paige Prostate’s ability to identify true positives and true negatives at the individual level.
The conference abstract reported an evaluation of Paige Prostate’s ability to detect tumours in 64 slides extracted from individuals given neoadjuvant treatment.33 The results revealed a sensitivity of 91% and a specificity of 94%,33 indicating good performance in identifying residual tumours after treatment.33
Paige Prostate as an Adjunct to Pathologists
As a prescreening tool, Paige Prostate correctly categorized 1,796 of 1,876 WSIs in 1 study.30 The pathologists, blinded to Paige Prostate’s results, reviewed 80 WSIs misclassified by the algorithm.30 Pathologists reduced misclassified WSIs to 21 from 80.30
Four studies evaluated the difference between the diagnostic accuracy of pathologists alone and assisted by Paige Prostate.28,29,31,32 The periods between unassisted and assisted review varied across studies. Refer to Table 1 for a detailed summary of study characteristics.
Detecting Tumours
One study found that assisted review resulted in similar sensitivity, specificity, PPV, and NPV as unassisted review of 105 WSIs.32 The agreement in diagnosis across pathologists remained the same between assisted and unassisted review.32 A similar effect was found between the findings of the same pathologist in unassisted and assisted review of WSIs.32
Other studies reported the following findings:
An increase in sensitivity ranging from 2.9% to 16% from unassisted to assisted review was reported.28,29,31 The assisted review of WSIs resulted in a sensitivity ranging from 90% to 96.9%.28,29,31 One study observed improvement in sensitivity across tumour grades and sizes in assisted review.29
Specificity remained relatively similar between unassisted and assisted review of WSIs.28,29,31 The largest decrease was 2.0%,28 whereas 1 study reported an increase of 0.7%.29 Assisted review resulted in specificity ranging from 96.6% to 99.8%.28,29,31
One study reported a 4.5% decrease to 94.9% in PPV at the WSI level and a 5.6% decrease to 92.3% at the individual or case level.28
The same study found a decrease of 1.2% to 98.5% in NPV at the WSI level and an increase of 1.6% to 95.8% at the individual or case level.28
Grading and Quantifying Tumours
As previously mentioned, pathologists use the Gleason score to grade prostate tumours.22 In 1 study, researchers found that pathologists graded tumours similarly with Paige Prostate’s insight.32 Pathologists’ mean Gleason score aligned with the ground truth at similar rates between unassisted and assisted review of 105 WSIs.32 Researchers found a similar effect when they compared mean Gleason score across pathologists.32 The pathologists’ median tumour size remained similar between reviews.32
Identifying Perineural Invasion
One study found no significant differences in the detection of perineural invasion between assisted and unassisted reviews of 105 slides.32 Perineural invasion indicates a high likelihood that the cancer has spread outside the prostate.35
Clinical Efficiency
Paige Prostate proposes to save pathologists time when reviewing cases. Clinical evidence suggests pathologists spend less time reviewing WSIs with Paige Prostate.28,32 However, 1 study ignored images that took more than 5 minutes to review.29 Another study proposes using Paige Prostate as a screening tool, given its optimal NPV.28 Pathologists in this study only reviewed slides Paige identified as suspicious, and ignored benign WSIs.28 Pathology departments may not all use Paige Prostate in the same way. Furthermore, some studies dismissed the time spent scanning and computer or platform processing.31,32 The adopters of telepathology in Quebec found 1 glass slide could be scanned every 3 minutes.36
Two factors that prolong diagnosis are additional staining of glass slides and requesting a second opinion. Pathologists in 1 study requested significantly less immunohistochemistry staining and second opinions with Paige Prostate.32 In another study, pathologists with Paige Prostate correctly diagnosed 287 (99.7%) of 288 WSIs initially deferred in unassisted review. Investigators defined this as an efficiency gain, or avoiding additional work-ups or consultation.29 However, assisted review led to the deferral of 112 (98.2%) of 114 images initially correct in unassisted review, representing some efficiency loss.29 Clinicians experienced with Paige Prostate cautioned adopters of AI’s influence on diagnostic patterns, potentially leading to unnecessary care or follow-up.27 They recommended monitoring the impact of AI, including Paige Prostate on reporting patterns.27
Clinician Perspectives and Experiences
Pathologists in 1 study answered a survey about their experience with and without Paige Prostate.31 The results indicated that pathologists would consider digital review of slides if the system included Paige Prostate after their experience with the platform.31 The pathologists became more confident with their results in assisted compared to unassisted review.31
Additional Considerations
Generalizability
Of the 5 studies we included, 3 assessed Paige Prostate’s diagnostic performance using archived slides from a single institution.28,30,32 None were performed at institutions in Canada.28,30,32 The remaining 2 studies included slides prepared from different laboratories, but it is unclear if investigators included slides prepared in Canada.29,31
Digital Pathology Infrastructure
Whole-Slide Scanners
Whole-slide scanning is a key component of digital and AI-enabled pathology. Limited adoption of whole-slide scanners is a barrier to implementing AI in pathology.26 In 2003, the Multi-Jurisdictional Telepathology Project aimed to facilitate diagnosis, especially in rural areas, by linking a network of pathologists for WSI review.37 An update in 2018 reported that telepathology remains in the early phase of implementation in Canada.38 The IT infrastructure for telepathology, such as slide scanners and data storage, overlaps with the infrastructure needed for WSIs and AI in pathology.
Whole-slide scanners impact an algorithm’s performance.39,40 The scanner determines the quality of the WSI, sets the limits to magnification, and impacts the time and effort required for scanning (e.g., some allow multiple slides to be scanned at a time).39 Most algorithms are trained using data from 1 type of scanner, including Paige Prostate (i.e., Leica Biosystems AT2).19,41 However, an unpublished, small-scale study by Paige reported excellent performance of Paige’s algorithms across 6 scanners.41
Whole-slide scanners require approval from regulatory bodies. The FDA’s de novo authorization for Paige Prostate Detect limits clinical use with WSIs from the Philips UltraScan scanner.13 In Canada, Philips IntelliSite Pathology Solution, inclusive of the Philips UltraScan, is approved for in vitro diagnostic use.42 Clinical centres with existing digital pathology infrastructure may find switching to an authorized whole-slide scanner a barrier to implementation.
Pathology Workflow
WSIs and AI require pathologists to adjust to new workflows and clinical processes.24,40,43 The results of a 2013 survey revealed 90% of pathologists and pathology residents see a need for digital pathology in practice.44 The 2014 guideline by the Canadian Association of Pathologists highlighted the need to develop a suitable workflow for the intended WSI application.40 An internal validation exercise can confirm that the digital pathology system meets its intended purpose and produces expected results before implementation.24,40,43 Adopters should also consider how the dependability of systems (i.e., scheduled and unscheduled downtime) and availability of technical support impacts workflow efficiency.45 The intention to use Paige Prostate determines its place in a pathology workflow.45 Figure 1 illustrates 1 potential use case for pathology departments. An alternative use case for Paige Prostate is to filter negative cases given its optimal NPV,28 whereas the FDA allows pathologists to use Paige Prostate for second consultation.13 The former allows pathologists to focus on cases that require immediate attention, whereas the latter aims to reduce second consultation and additional slide workup. The benefits of adopting Paige Prostate depend on how it is integrated into the pathology department’s workflow.
Figure 1: Pathology Workflow With Paige Prostate Versus Manual Review
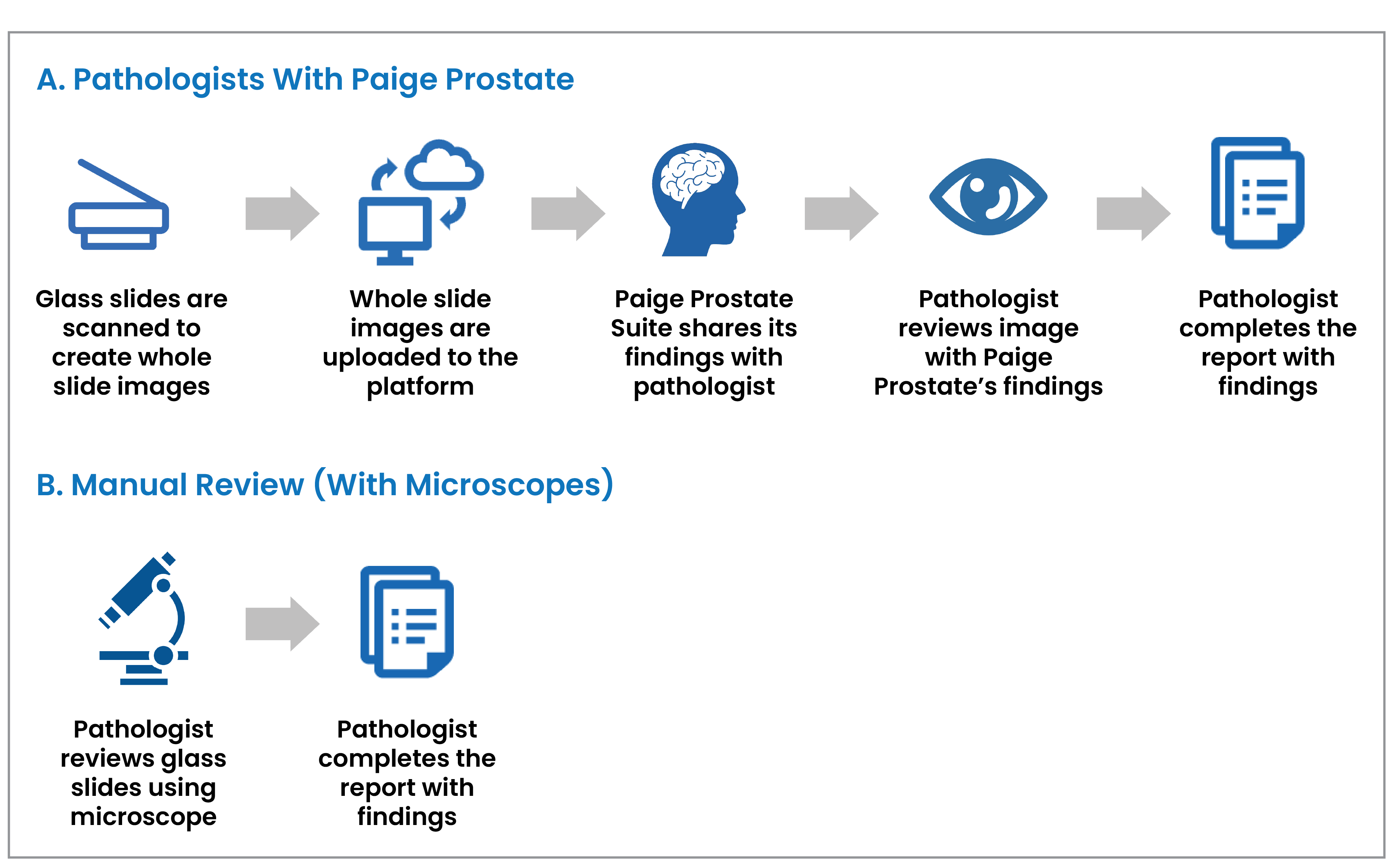
AI = artificial intelligence.
Note: Pathologists may use the Paige Prostate Suite for other uses (e.g., prescreening, second opinion) that may result in a different workflow from what is shown in part A of this figure.
Cloud-Based Storage
WSIs occupies large amounts of digital storage at risk for privacy breaches.17 Paige’s cloud storage complies with the Health Insurance Portability and Accountability Act (HIPAA) in the US and the General Data Protection Regulations (GDPR) in the European Union.15 In recent years, health organizations in Canada have had privacy breaches, especially with the rise of digital health during COVID-19.46-48 Health care data appeal to cyber criminals due to their vital, personal, and profitable nature.49 Individuals affected by privacy breaches can suffer discrimination, stigmatization, and financial and psychological distress.47 Given this risk, adopters of digital pathology tools should consider the cybersecurity systems and safeguards needed to ensure personal health data are safe and remain private.
The cloud and AI require extensive physical infrastructure and energy.50
For example, data centres rely on high-energy cooling systems to offset the heat produced by the technology.50 The cloud’s IT infrastructure contributes to carbon emissions and results in physical waste.50
Patient Safety
We did not identify studies evaluating the impact of Paige Prostate on individuals suspected to have prostate cancer. In general, AI in health care lacks studies evaluating its clinical benefits, especially for individuals seeking routine diagnostic care.24 The extent of Paige Prostate’s clinical value could be realized with evidence from prospective multicentre clinical trials.24,51
Training
Pathologists with less trust in AI could spend more time double-checking results generated by algorithms.26 Clinicians in the UK highlighted the importance of training pathology departments on the Paige Prostate Suite and AI to ensure proper use and to support patient understanding around diagnosis and treatment.27 They expect a learning curve with pathologists before seeing improvements in clinical efficiency.27 Paige provides initial training on the Paige Prostate platform for users as part of the standard subscription fee.27 Users can request additional training if needed.27
Ethical Considerations
AI in health care raises ethical concerns given its influence on clinical decision-making. The concerns include legal accountability, a lack of standards and regulations for developing and training models, consent, data security, and data ownership.39,52-54 The obscurity around how algorithms operate and make decisions challenges transparency and communication with users and individuals seeking diagnosis.39,52-55 Clinicians using Paige Prostate should be able to explain to their patients how it works, as well as its risks.54 They should be clear about the storage of WSIs, the safeguards in place to protect their personal health data, and if WSIs are used for other purposes, such as research.56
Costs
We did not identify any studies assessing the cost-effectiveness of Paige Prostate. The total cost will vary across pathology departments, depending on their need, use, and level of digital pathology readiness.27 Clinicians expect Paige Prostate to cost more than pathologists alone.27 Pathology departments will have to invest in IT infrastructure (e.g., WSI scanners, reliable internet and computers, laboratory information systems) and pay fees to Paige, in addition to paying pathologists. Future cost-effectiveness research needs to account for the productivity costs Paige Prostate purports to prevent.27,29,32
Funding for Paige Prostate and needed WSI technology will likely be a barrier to adoption.24,36
The telepathology network project in Canada found limited funding to finance equipment and new service modalities.36,37 This infrastructure overlaps with AI in pathology.
Paige promises competitive pricing of its cloud-based storage in comparison to other clouds in the market.16 However, this claim requires exploration outside the scope of this report. Further, pathology departments must retain glass slides even with WSIs, and are not exempt from associated costs.37
Inclusion, Diversity, Equity, and Accessibility
Race and Ethnicity
AI needs a large volume of diverse data to develop and train algorithms. This ensures equitable distribution of benefits and optimal performance across subgroups.52-54,57,58 The data should reflect the population, including individuals who are disproportionately affected by the condition or disease.52-54,57,58 The developers of the Paige Prostate Suite used a large number of biopsy slides from institutions around the world.19 However, the FDA reported that 82.2% of the training data comprised biopsy slides from patients who were white.13
One study reported no difference in the diagnostic performance of Paige Prostate by ethnicity or race.29 Of the WSIs, 7% were from individuals who identified as Black.29 Underrepresentation of individuals who are Black is common in prostate cancer trials, even though they are at higher risk of developing prostate cancer.2,59,60
Place of Residence
Investment in WSI infrastructure enables telepathology, which enhances access to diagnostic care, especially in rural and remote areas.36 One study concluded that there was no significant difference between the performance of onsite and remote pathologists reviewing WSIs with Paige Prostate.29
Gender
Transgender and nonbinary individuals with a prostate can develop prostate cancer.2 None of the included studies distinguished sex from gender. Further, studies did not report on gender or they reported their study population as “men.” We acknowledge that such language is not inclusive of trans and nonbinary individuals. It is unknown whether any of the studies included or excluded samples from trans or nonbinary people. The prevalence of prostate cancer and prostate cancer screening in transgender people is largely unknown.61 Many transgender and gender-diverse people experience and fear discrimination when accessing health services.62 This can influence their decision to seek care, including cancer screening and diagnosis.62
Funding for Cancer Research
Prostate cancer received the second largest proportion (16%) of Canada’s cancer research funding in 2015, following breast cancer.63 Prostate cancer research was overfunded relative to its disease burden in Canada, specifically incidence and mortality.63 The Paige Prostate Suite may benefit the landscape of prostate cancer diagnosis, but its adoption will not directly benefit other types of cancer.
Future Developments
An upcoming study plans to assess the benefit Paige Prostate brings to the clinical workflow of a pathology department.64 Paige and Oxford University will examine the impact of Paige Prostate with pathologists on individuals suspected to have prostate cancer.65 Paige and the Ohio State Wexner Medical Center will conduct a multiarm trial to compare the clinical utility and cost-savings impact with and without Paige Prostate.66
There are at least 2 other AI products, DeepDx67 and Inify,68 that support prostate cancer detection.26 Both products have CE-IVD marking (indicating that they can be commercialized for clinical use in Europe).26
AI can optimize other areas of prostate cancer diagnosis and care, such as treatment planning in oncology.69-71 There is a growing body of research evaluating AI’s ability to detect and classify prostate cancer through radiology, specifically MRI.72-74 The Canadian Urological Association recognizes multiparametric MRI (a type of MRI that produces a more detailed scan of the prostate than a standard MRI) as an adjunctive tool to improve prostate cancer diagnosis for select individuals.75 However, Canada is experiencing increasing demand for medical imaging with limited resources.76 As new and optimal technologies become available for diagnostics, their use will depend on the context and availability.75
Paige Breast Suite
The Paige Breast Suite leverages the same AI technology and platform as the Paige Prostate Suite to diagnose breast cancer.77 The algorithm used a large training dataset, inclusive of slides with macrometastases, micrometastases, and isolated tumour cells.77 The Paige Breast Suite holds CE-IVD (for Europe) and UKCA (for the UK) marks for clinical use with Leica Aperio AT2 and GT450 scanners.77 In October 2023, the FDA granted 1 of the Paige Breast Suite’s applications, Paige Lymph Node, breakthrough designation for breast cancer detection.78
Precision Medicine
Advances in AI for pathology, like the Paige Prostate Suite, make the potential for multiomic approaches for clinical decision-making in oncology a reality. With this approach, algorithms use genomic and molecular data, along with histopathology and radiology findings, to predict risk, assess prognosis, and personalize treatments.51,55,79,80 An algorithm using data from multiple sources can improve accuracy compared to when data are evaluated separately.80 Prostate cancer could benefit from such an approach, as clinicians find the diversity of cellular alterations difficult for prognosis and disease management.81
Final Remarks
The Paige Prostate Suite includes a set of AI applications to help pathologists detect and quantify prostate cancer. Its algorithm identifies and analyzes areas of suspicion on WSIs for pathologist review. The suite aims to improve accuracy, reduce time spent reviewing cases, prevent delays in diagnosis, and standardize diagnostic practices.77 The FDA authorized 1 of the suite’s applications, Paige Prostate Detect, for clinical use with the Philips UltraScan in 2021.13 The Paige Prostate Suite is not available in Canada as of this writing.
Supporting the widespread adoption of AI in pathology requires further investment in digital pathology. Pathologists continue to use microscopes because of limited IT infrastructure needed to produce digital WSIs.38 Given this, the suite is expected to cost more than current practice. Pathology departments will also have to navigate workflow changes when adopting digital pathology and AI.24,43
Early retrospective studies suggest that Paige Prostate improves pathologists’ ability to detect cancer.28-32 Studies in the US are under way to assess the cost impact and clinical value Paige Prostate brings to pathology departments.64,65 However, their findings should be validated in Canada. The cost-effectiveness of the suite also requires evaluation,24,57 with consideration of costs related to changes in productivity.27 Future prospective trials should consider the impact and diagnostic performance of the suite across race and ethnicity, especially with people who are Black, who are at higher risk of prostate cancer.
The use of AI in pathology and oncology is expanding. Other AI tools, such as the Paige Breast Suite, Deep Dx, and Inify, are available in other jurisdictions to support pathologists in diagnosing cancer. AI products are also being developed and tested to inform other areas of the clinical care pathway in oncology.69-74 Some experts anticipate machine learning soon being capable of leveraging different types of clinical data (e.g., molecular, genetic, histopathologic, and radiologic) to better inform clinical decision-making.51,55,79,80
References
1.What you need to know about prostate cancer. Toronto (ON): Canadian Cancer Society: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/what-you-need-to-know-about-prostate-cancer/what-you-need-to-know-about-prostate-cancer-en.pdf. Accessed 2023 Sep 18.
2.Canadian Cancer Society. What is prostate cancer? 2021; https://cancer.ca/en/cancer-information/cancer-types/prostate/what-is-prostate-cancer. Accessed 2023 Sep 18.
3.Canadian Cancer Society. Prostate cancer statistics. 2023; https://cancer.ca/en/cancer-information/cancer-types/prostate/statistics. Accessed 2023 Sep 18.
4.Mandel P, Wenzel M, Hoeh B, et al. Immunohistochemistry for prostate biopsy-impact on histological prostate cancer diagnoses and clinical decision making. Curr Oncol. 2021;28(3):2123-2133. PubMed
5.Molina K. Pathologist shortage in Outaouais has patients waiting months for biopsy results. Ottawa (ON): CBC; 2017: https://www.cbc.ca/news/canada/ottawa/biopsy-backlog-outaouais-region-1.4353979. Accessed 2023 Sep 22.
6.Garn N. ‘It’s not OK’: Regina woman waits months for breast cancer biopsy. Regina (SK): 980 CJME; 2023: https://www.cjme.com/2023/10/25/sask-breast-cancer-screening-biopsy-delays-a-growing-concern/. Accessed 2023 Oct 24.
7.Metter DM, Colgan TJ, Leung ST, Timmons CF, Park JY. Trends in the US and Canadian pathologist workforces from 2007 to 2017. JAMA Netw Open. 2019;2(5):e194337. PubMed
8.MacKinnon B. Vitalité hit with 'critical shortage' of pathologists. Fredericton (NB): CBC; 2023: https://www.cbc.ca/news/canada/new-brunswick/pathologists-new-brunswick-vacant-positions-vitalite-horizon-shortage-1.6888850. Accessed 2023 Sep 19.
9.Canadian Medical Association (CMA). Physician wellness: new 2021 National Physician Health Survey findings - burnout, short-staffing and an overburdened system take their toll. Physician Wellness Hub 2022; https://www.cma.ca/physician-wellness-hub/content/physician-wellness-new-2021-national-physician-health-survey. Accessed 2023 Dec 18.
10.Berg S. Work overload triples the risk of burnout in health care. Chicago (IL): American Medical Association; 2023: https://www.ama-assn.org/practice-management/physician-health/work-overload-triples-risk-burnout-health-care. Accessed 2023 Dec 18.
11.Ailia MJ, Thakur N, Abdul-Ghafar J, Jung CK, Yim K, Chong Y. Current trend of artificial intelligence patents in digital pathology: a systematic evaluation of the patent landscape. Cancers (Basel). 2022;14(10):2400. PubMed
12.Niazi MKK, Parwani AV, Gurcan MN. Digital pathology and artificial intelligence. Lancet Oncol. 2019;20(5):e253-e261. PubMed
13.Evaluation of automatic class III designation for Paige Prostate (DEN200080). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2021: https://www.accessdata.fda.gov/cdrh_docs/reviews/DEN200080.pdf. Accessed 2023 Sep 19.
14.Paige. Paige receives first ever FDA approval for AI product in digital pathology. 2021; https://paige.ai/paige-receives-first-ever-fda-approval-for-ai-product-in-digital-pathology/. Accessed 2023 Sep 18.
15.Paige. AI to support prostate cancer. 2023; https://paige.ai/diagnostic-ai/prostate-suite/. Accessed 2023 Sep 18.
16.Fuchs T. Understanding the use of AI in digital pathology [webinar]. New York (NY). Paige AI, Inc.2022: https://paige.ai/resources/#webinars. Accessed 2023 Sep 21.
17.Bhattacharya I, Khandwala YS, Vesal S, et al. A review of artificial intelligence in prostate cancer detection on imaging. Ther Adv Urol. 2022;14:17562872221128791. PubMed
18.Ayyad SM, Shehata M, Shalaby A, et al. Role of AI and histopathological images in detecting prostate cancer: a survey. Sensors (Basel). 2021;21(8):2586. PubMed
19.Campanella G, Hanna MG, Geneslaw L, et al. Clinical-grade computational pathology using weakly supervised deep learning on whole slide images. Nat Med. 2019;25(8):1301-1309. PubMed
20.Government of Canada. Job prospects: general pathologist in Canada. (Job Bank: labour market information) 2024; https://www.jobbank.gc.ca/marketreport/outlook-occupation/4070/ca. Accessed 2023 Oct 17.
21.MacKinnon B. N.B. urged to consider interprovincial licensing of pathologists to deal with 'critical' shortage. Fredericton (NB): CBC; 2023: https://www.cbc.ca/news/canada/new-brunswick/pathologists-shortage-new-brunswick-licensing-interprovincial-national-association-jason-karamchandani-1.6897067. Accessed 2023 Sep 19.
22.Munjal A, Leslie SW. Gleason Score. Treasure Island (FL): StatPearls Publishing; 2023: https://www.ncbi.nlm.nih.gov/books/NBK553178/. Accessed 2023 Sep 18.
23.van Leenders GJLH, van der Kwast TH, Grignon DJ, et al. The 2019 International Society of Urological Pathology (ISUP) consensus conference on grading of prostatic carcinoma. Am J Surg Pathol. 2020;44(8):e87-e99. PubMed
24.Oszwald A, Wasinger G, Pradere B, Shariat SF, Comperat EM. Artificial intelligence in prostate histopathology: where are we in 2021? Curr Opin Urol. 2021;31(4):430-435. PubMed
25.Bhattacharya I, Lim DS, Aung HL, et al. Bridging the gap between prostate radiology and pathology through machine learning. Med Phys. 2022;49(8):5160-5181. PubMed
26.Frewing A, Gibson AB, Robertson R, Urie PM, Corte DD. Don't fear the artificial intelligence: a systematic review of machine learning for prostate cancer detection in pathology. Arch Pathol Lab Med. 2023. PubMed
27.National Institute for Health and Care Excellence. Paige Prostate for prostate cancer. (Medtech innovation briefing MIB280) 2021; https://www.nice.org.uk/advice/mib280. Accessed 2023 Sep 18.
28.da Silva LM, Pereira EM, Salles PG, et al. Independent real-world application of a clinical-grade automated prostate cancer detection system. J Pathol. 2021;254(2):147-158. PubMed
29.Raciti P, Sue J, Retamero JA, et al. Clinical validation of artificial intelligence-augmented pathology diagnosis demonstrates significant gains in diagnostic accuracy in prostate cancer detection. Arch Pathol Lab Med. 2023;147(10):1178-1185. PubMed
30.Perincheri S, Levi AW, Celli R, et al. An independent assessment of an artificial intelligence system for prostate cancer detection shows strong diagnostic accuracy. Mod Pathol. 2021;34(8):1588-1595. PubMed
31.Raciti P, Sue J, Ceballos R, et al. Novel artificial intelligence system increases the detection of prostate cancer in whole slide images of core needle biopsies. Mod Pathol. 2020;33(10):2058-2066. PubMed
32.Eloy C, Marques A, Pinto J, et al. Artificial intelligence-assisted cancer diagnosis improves the efficiency of pathologists in prostatic biopsies. Virchows Arch. 2023;482(3):595-604. PubMed
33.Dogdas B, Kanan C, Raciti P, et al. Computational pathological identification of prostate cancer following neoadjuvant treatment. J Clin Oncol. 2020;38(15_suppl):e14052-e14052.
34.Shreffler J, Huecker MR. Diagnostic testing accuracy: sensitivity, specificity, predictive values and likelihood ratios. Treasure Island (FL): StatPearls Publishing; 2023: https://www.ncbi.nlm.nih.gov/books/NBK557491/. Accessed 2023 Nov 06.
35.The American Cancer Society. Your prostate pathology report: cancer (adenocarcinoma). Kennesaw (GA): The American Cancer Society; 2023: https://www.cancer.org/cancer/diagnosis-staging/tests/biopsy-and-cytology-tests/understanding-your-pathology-report/prostate-pathology/prostate-cancer-pathology.html. Accessed 2023 Oct 31.
36.Alami H, Fortin JP, Gagnon MP, Pollender H, Tetu B, Tanguay F. The challenges of a complex and innovative telehealth project: a qualitative evaluation of the Eastern Quebec Telepathology Network. Int J Health Policy Manag. 2018;7(5):421-432. PubMed
37.Background summary: evaluation of the Multi-jurisdictional Telepathology Project. Ottawa (ON): Canada Health Infoway; 2020: https://www.infoway-inforoute.ca/en/component/edocman/3827-evaluation-of-the-multi-jurisdictional-telepathology-project-background-summary/view-document?Itemid=101. Accessed 2023 Sep 18.
38.Evaluation of the Multi-jurisdictional Telepathology Project. (Final evaluation report). St. John's (NL): Newfoundland and Labrador Centre for Health Information; 2018: https://www.infoway-inforoute.ca/en/component/edocman/3825-evaluation-of-the-multi-jurisdictional-telepathology-project/view-document?Itemid=101. Accessed 2023 Oct 10.
39.Asif A, Rajpoot K, Graham S, Snead D, Minhas F, Rajpoot N. Unleashing the potential of AI for pathology: challenges and recommendations. J Pathol. 2023;260(5):564-577. PubMed
40.Canadian Association of Pathologists Telepathology Guidelines Committee, Bernard C, Chandrakanth SA, et al. Guidelines from the Canadian Association of Pathologists for establishing a telepathology service for anatomic pathology using whole-slide imaging. J Pathol Inform. 2014;5(1):15. PubMed
41.Rothrock B. Developing clinical-grade AI for healthcare with Paige [video]. San Bruno (CA): YouTube, uploaded by Ai4; 2020: https://www.youtube.com/watch?v=CeqcoXcfCPU&t=1211s. Accessed 2023 Sep 14.
42.Philips. Ultra Fast Scanner: digital pathology slide scanner. https://www.usa.philips.com/healthcare/product/HCNOCTN442/ultra-fast-scanner-digital-pathology-slide-scanner. Accessed 2023 Oct 10.
43.Chong Y, Kim DC, Jung CK, et al. Recommendations for pathologic practice using digital pathology: consensus report of the Korean Society of Pathologists. J Pathol Transl Med. 2020;54(6):437-452. PubMed
44.Bellis M, Metias S, Naugler C, Pollett A, Jothy S, Yousef GM. Digital pathology: attitudes and practices in the Canadian pathology community. J Pathol Inform. 2013;4:3. PubMed
45.Lau F, Hagens S, Muttitt S. A proposed benefits evaluation framework for health information systems in Canada. Healthc Q. 2007;10(1):112-116, 118. PubMed
46.Webster P. Canadian digital health data breaches: time for reform. Lancet Digit Health. 2020;2(3):e113-e114.
47.Securing public trust in digital healthcare: resolution of the Federal, Provincial and Territorial Privacy Commissioners and Ombudspersons with responsibility for privacy oversight. Ottawa (ON): Office of the Privacy Commissioner of Canada; 2022: https://www.priv.gc.ca/en/about-the-opc/what-we-do/provincial-and-territorial-collaboration/joint-resolutions-with-provinces-and-territories/res_220921/. Accessed 2023 Oct 11.
48.Woods M. Major data breach at Queensway Carleton Hospital could affect 100,000 patients. Ottawa (ON): CTV News; 2023: https://ottawa.ctvnews.ca/major-data-breach-at-queensway-carleton-hospital-could-affect-100-000-patients-1.6376140. Accessed 2023 Oct 11.
49.Thompson C. Moving forward for cybersafe healthcare: insights from the Canadian summit on healthcare cybersecurity. Ottawa (ON): HealthCareCAN; 2018: https://www.healthcarecan.ca/wp-content/themes/camyno/assets/document/Reports/2018/HCC/EN/CyberReport_finalweb.pdf. Accessed 2023 Sep 03.
50.Monserrate SG. The cloud is material: on the environmental impacts of computation and data storage. Cambridge (MA): MIT Schwarzman College of Computing; 2022: https://mit-serc.pubpub.org/pub/the-cloud-is-material/release/1. Accessed 2023 Oct 11.
51.Kartasalo K, Bulten W, Delahunt B, et al. Artificial intelligence for diagnosis and Gleason grading of prostate cancer in biopsies-current status and next steps. Eur Urol Focus. 2021;7(4):687-691. PubMed
52.Jackson BR, Ye Y, Crawford JM, et al. The ethics of artificial intelligence in pathology and laboratory medicine: principles and practice. Acad Pathol. 2021;8:2374289521990784. PubMed
53.Allen TC. Regulating artificial intelligence for a successful pathology future. Arch Pathol Lab Med. 2019;143(10):1175-1179. PubMed
54.Chauhan C, Gullapalli RR. Ethics of AI in pathology: current paradigms and emerging issues. Am J Pathol. 2021;191(10):1673-1683. PubMed
55.Busby D, Grauer R, Pandav K, et al. Applications of artificial intelligence in prostate cancer histopathology. Urol Oncol. 2023:S1078-1439(1022)00487-00482.
56.Sorell T, Rajpoot N, Verrill C. Ethical issues in computational pathology. J Med Ethics. 2022;48(4):278-284. PubMed
57.Shreve JT, Khanani SA, Haddad TC. Artificial intelligence in oncology: current capabilities, future opportunities, and ethical considerations. Am Soc Clin Oncol Educ Book. 2022;42:1-10. PubMed
58.Rariy C. We know how to regulate new drugs and medical devices - but we're about to let health care AI run amok. New York (NY): Fortune Media IP Limited; 2023: https://fortune.com/2023/10/03/how-to-regulate-new-drugs-medical-devices-health-care-ai-artificial-intelligence-run-amok-chevon-rariy/. Accessed 2023 Oct 24.
59.Otiono K, Nkonge B, Olaiya OR, Pierre S. Prostate cancer screening in Black men in Canada: a case for risk-stratified care. CMAJ. 2022;194(41):E1411-E1415. PubMed
60.Lee KM, Bryant AK, Lynch JA, et al. Association between prediagnostic prostate-specific antigen and prostate cancer probability in Black and non-Hispanic White men. Cancer. 2024;130(2):224-231. PubMed
61.Nik-Ahd F, Jarjour A, Figueiredo J, et al. Prostate-specific antigen screening in transgender patients. Eur Urol. 2023;83(1):48-54. PubMed
62.Scime S. Inequities in cancer care among transgender people: recommendations for change. Can Oncol Nurs J. 2019;29(2):87-91. PubMed
63.Coronado AC, Finley C, Badovinac K, Han J, Niu J, Rahal R. Discrepancies between Canadian cancer research funding and site-specific cancer burden: a spotlight on ten disease sites. Curr Oncol. 2018;25(5):338-341. PubMed
64.Flach RN, Stathonikos N, Nguyen TQ, Ter Hoeve ND, van Diest PJ, van Dooijeweert C. CONFIDENT-trial protocol: a pragmatic template for clinical implementation of artificial intelligence assistance in pathology. BMJ Open. 2023;13(6):e067437. PubMed
65.University of Oxford. ISRCTN91685765: Examining the impacts of pathologists using the assistance of computer technology (artificial intelligence software) on the diagnosis of prostate cancer biopsies. ISRCTN Registry. London (UK): BioMed Central Limited; 2023: https://trialsearch.who.int/Trial2.aspx?TrialID=ISRCTN91685765. Accessed 2023 Oct 17.
66.Business Wire. Paige and Ohio State Wexner Medical Center collaborate to study how AI tools can bring accuracy and efficiency to prostate cancer diagnosis in a community hospital setting. New York (NY): Paige; 2023: https://paige.ai/paige-and-ohio-state-wexner-medical-center-collaborate-to-study-how-ai-tools-can-bring-accuracy-and-efficiency-to-prostate-cancer-diagnosis-in-a-community-hospital-setting/. Accessed 2023 Sep 21.
67.Deep Bio Inc. DeepDx Prostate: AI software for prostate cancer. 2022; https://www.deepbio.co.kr/page/products/prostate/. Accessed 2023 Oct 17.
68.Inify Laboratories. Inify Prostate shown to accurately outline suspicious prostate cancer in study with two prominent medical centers. 2021; https://www.inify.com/inify-prostate-shown-to-accurately-outline-suspicious-prostate-cancer-in-study-with-two-prominent-medical-centers/. Accessed 2023 Oct 17.
69.University College, London. NCT05653063: ARCHERY - artificial intelligence based radiotherapy treatment planning for cervical, head and neck and prostate cancer. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/study/NCT05653063. Accessed 2023 Oct 17.
70.Dartmouth-Hitchcock Medical Center. NCT04441775: Artificial intelligence for prostate cancer treatment planning. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://clinicaltrials.gov/study/NCT04441775. Accessed 2023 Oct 17.
71.Region Örebro County. NCT04879563: Artificial intelligence Supporting CAncer Patients across Europe - the ASCAPE Project (ASCAPE). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://clinicaltrials.gov/study/NCT04879563. Accessed 2023 Oct 17.
72.Norwegian University of Science and Technology. NCT06000046: Proviz - a machine learning software, to support targeting of prostate biopsies on MR images in biopsy-naive patients. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2024: https://classic.clinicaltrials.gov/ct2/show/NCT06000046. Accessed 2023 Oct 17.
73.Radboud University Medical Center. NCT05489341: Artificial intelligence and radiologists at prostate cancer detection in MRI: The PI-CAI challenge. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Health; 2023: https://clinicaltrials.gov/study/NCT05489341. Accessed 2023 Oct 17.
74.Jonsson Comprehensive Cancer Center. NCT04765150: Integrating quantitative MRI and artificial intelligence to improve prostate cancer classification. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://classic.clinicaltrials.gov/ct2/show/NCT04765150. Accessed 2023 Oct 17.
75.Mason RJ, Marzouk K, Finelli A, et al. UPDATE - 2022 Canadian Urological Association recommendations on prostate cancer screening and early diagnosis Endorsement of the 2021 Cancer Care Ontario guidelines on prostate multiparametric magnetic resonance imaging. Can Urol Assoc J. 2022;16(4):E184-E196. PubMed
76.The Canadian Medical Imaging Inventory: 2022-2023. Evidence preview. (CADTH health technology review). Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/hta-he/HC0024_cmii_2022_2023_evidence_preview.pdf. Accessed 2023 Dec 19.
77.Paige. AI to support breast cancer diagnosis. https://paige.ai/diagnostic-ai/breast-suite/. Accessed 2023 Oct 16.
78.Business Wire. U.S. FDA grants Paige breakthrough device designation for cancer detection in breast lymph nodes. 2023; https://www.businesswire.com/news/home/20231026045607/en/U.S.-FDA-Grants-Paige-Breakthrough-Device-Designation-for-Cancer-Detection-in-Breast-Lymph-Nodes. Accessed 2023 Oct 26.
79.Luchini C, Pea A, Scarpa A. Artificial intelligence in oncology: current applications and future perspectives. Br J Cancer. 2022;126(1):4-9. PubMed
80.Cimadamore A, Lopez-Beltran A, Scarpelli M, Cheng L, Montironi R. Artificial intelligence and prostate cancer: advances and challenges. Urologia. 2022;89(3):388-390. PubMed
81.George RS, Htoo A, Cheng M, et al. Artificial intelligence in prostate cancer: definitions, current research, and future directions. Urol Oncol. 2022;40(6):262-270. PubMed
Appendix 1: Methods
Note that this appendix has not been copy-edited.
Literature Search Strategy
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was Paige Prostate. The search was completed on September 19, 2023, and limited to English-language documents published since January 1, 2018. A supplemental search was completed in MEDLINE on September 19, 2023, for literature on the implementation and utilization of AI in prostate cancer assessment.
Study Selection
One author screened the literature search results and reviewed the full text of all potentially relevant studies. Studies were considered for inclusion if the intervention was Paige Prostate Suite. Conference abstracts and grey literature were included when they provided additional information to that available in the published studies.
Peer Review
A draft version of this bulletin was reviewed by a clinician with expertise in prostate cancer and experience with AI. The manufacturer was also given the opportunity to comment on an earlier draft.
Appendix 2: Summary of Study Characteristics
Note that this appendix has not been copy-edited.
Table 1: Characteristics of Studies Evaluating the Diagnostic Performance of Paige Prostate as an Adjunct to Pathologists
First author (year) | Number of WSIs (total paired readsa) | Population | Ground truth | First review of WSIs | Second review of WSIs | Time between reads |
|---|---|---|---|---|---|---|
Eloy (2023)32 | 105 (420) | 41 individuals seen at an institution in Portugal | Agreement between 4 pathologists or 2 independent pathologists with access to IHC | 4 pathologists | The same 4 pathologists assisted by Paige Prostate | 2 weeks |
Raciti (2022)29 | 610 (9,760) | Individuals seen at MSKCC and external institutions | Diagnosis given in pathology reports at the diagnosing institution | 16 pathologists | The same 16 pathologists assisted by Paige Prostate 1.0 | None (immediate assisted review) |
Da Silva (2021)28 | 579 (1,158) | 100 individuals seen at an institution in Brazil | Agreement between pathologists and Paige Prostate; if not met, pathologists re-reviewed slides with additional IHC staining | 2 pathologists | The same pathologists assisted by Paige Prostate 1.0 | None (immediate assisted review) |
Perincheri (2021)30 | 1,876 (NA)b | 118 individuals seen at Yale Medicine | Clinical diagnosis from archived pathology reports with additional IHC as needed | Paige Prostate Alpha | 2 pathologists blinded to Paige’s initial read (WSIs incorrectly classified by Paige Prostate Alpha) | NA |
Raciti (2020)31 | 232 (696) | Individuals seen at MSKCC and external institutions | Clinical diagnosis from archived pathology reports | 3 pathologists | The same 2 pathologists assisted by Paige Prostate Alpha | 4 weeks |
IHC = immunohistochemistry; MSKCC = Memorial Sloan Kettering Cancer Center; NA = not assessed; WSI = whole-slide image.
aNumber of WSIs multiplied by the number of pathologists.
bPaige Prostate was used as a prescreening tool and second opinion.
Note: Paige Prostate 1.0 is a later version of Paige Prostate Alpha.28,29,31
ISSN: 2563-6596
Contributors: Andrea Smith; Eric C Belanger, MD, Genitourinary Pathologist, Vancouver General Hospital/University of British Columbia
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca