Drugs, Health Technologies, Health Systems
Health Technology Review
Planning for the Introduction of New CT Services in Rural and Remote Communities in Canada
Key Messages
CT services are essential for diagnosing various conditions in Canada. There are existing challenges with access to these services due to the limited availability of machines, high demand for services, and long wait times. Rural and remote communities may experience additional challenges, as these services are often located in large urban centres.
Canada’s Drug Agency (CDA-AMC) conducted an informal survey among senior medical imaging decision-makers to determine the factors that influence planning for new CT services in rural and remote communities in Canada. To better understand current access to CT services and support future planning, the average population served by CT services in rural and remote communities was also calculated.
When establishing a population-based threshold for CT capacity in rural and remote areas, CDA-AMC found that, on average, a hospital with CT capabilities serves a population of approximately 56,100 people, with a catchment area of a 100 km radius.
There are various factors that influence decision-making when planning for the placement of new CT services in rural and remote communities, some of which include the size of the community served, patient travel time to a primary care centre or travel distance to the nearest available CT facility, and the resources and costs associated with interfacility transfers and delayed scan times.
The volume of exams and the clinical needs of hospitals are other important factors that influence CT planning in rural and remote communities. This demand and need for CT services informs decision-making around staffing and maintaining professional competency.
Context
CDA-AMC received a request related to considerations for placing new CT units in rural and remote settings across Canada. CT exams are essential to individuals in Canada, with around 6.3 million exams performed in publicly funded health care facilities during 2022–2023.2 CT is used to detect cancers, injury, and disease, in areas of the body such as the head, spine, cardiovascular system, and heart.2 The main advantages of CT compared to other imaging modalities are its speed, which enables rapid imaging and diagnosis in urgent situations, and its ability to visualize fine details in bone, soft tissue, lungs, and other organs.2
Access to CT in rural hospitals across Canada is less than 20%1 and in some jurisdictions, as little as 3% of rural hospitals are equipped with local CT services.1 As a result, patients in these communities are often transferred hundreds of kilometres for imaging exams. The exception to this is Quebec, where more than 70% of rural emergency departments are equipped with CT units.1
Establishing new CT capacity in small communities can improve patient outcomes and overall satisfaction with care delivery.2,3 Reduced travel distances can facilitate quicker diagnoses and enable earlier intervention, ultimately benefiting patient health.1-4 However, placing CT units in small communities poses challenges, including the high costs of equipment purchase, maintenance, and operation,4 along with potential underutilization due to limited demand and staff.1,3,5
The absence of a local CT unit in rural and remote settings can complicate the physician decision-making process, as they must consider the risks associated with transporting patients over long distances, including the potential for delayed diagnoses, prolonged treatment times, and increased health care costs.1
As jurisdictions seek to enhance access to imaging services in small communities, insight into the practices and considerations for placing new CT units in rural and remote settings across Canada can provide valuable guidance for decision-making. Understanding the implications of these considerations may help to ensure that investments in CT infrastructure result in meaningful improvements to care delivery, ultimately reducing health inequities across the country.
Objective
This report aims to outline key considerations for deploying new CT units in rural and remote areas across Canada. The objectives include the following:
to identify the criteria used by senior medical imaging decision-makers across Canada when determining the introduction of new CT services in rural or remote communities
to report on the average population served by existing CT services within these communities.
Methods
First, the Canadian Medical Imaging Inventory (CMII) national 2022–2023 database7 and Statistics Canada 2021 census dataset8 were used to estimate the current average population served by existing CT services across all 13 provinces and territories. Census subdivisions (CSDs) were used to calculate average population estimates, which may more reliably represent populated rural or remote communities and cover larger geographic areas compared to the use of population centres.9
Statistics Canada developed an index to provide the relative remoteness of nearly all communities in Canada, which considers road network travel distances and proximity to and size of population centres within a given radius (e.g., proximity to and access to services at large urban centres).9 This index was used to determine the eligibility of CSDs for inclusion in this report.
A 100 km radius was calculated for each included CSD to estimate the average population served by existing CT services located in rural or remote CSDs.
Second, a brief survey consisting of a multiple-choice question and an open-ended question was sent to senior medical imaging decision-makers in all 10 provinces, identified through the CMII network of contacts. A 90% response rate to the survey was received. The survey excluded territorial decision-makers, as it was assumed that the territories are not considering expanding CT services to rural and remote areas at this time. Contacts were asked to provide information on criteria and considerations used to determine CT planning in rural or remote settings within their jurisdiction (refer to Appendix 1). The responses reflect general practices across either a region or province.
Inclusion
A total of 115 CT facilities across Canada were screened for inclusion, including both hospital-based and community-based sites, and were selected if both of the following criteria were met:
the CT facility operates in either a rural or remote setting (as self-reported by participants in the CMII 2022–2023 national survey)7
the CSD in which the CT facility operates is classified as either “less accessible,” “remote,” or “very remote,” according to Statistics Canada’s index.9
Exclusion
CT facilities were excluded if either of the following criteria were met:
the CT facility operates in urban settings (as self-reported by participants in the CMII national survey)7
the CSD in which the CT facility operates is classified as either “easily accessible” or “accessible” (e.g., populations greater than 100,000) according to Statistics Canada’s index.9
Results
Average Population Served by CT Equipment in Canada in the Rural and Remote Setting
To understand current access to CT services in small communities, the average population served by existing CT services in rural and remote communities in Canada was calculated.
Of the 115 CSDs with CT capacity, a total of 59 CSDs located across 12 provinces and territories met the inclusion criteria presented in the map (Figure 1). This map excludes CT facilities operating in urban settings and those classified by Statistics Canada as being either “easily accessible” or “accessible” (e.g., populations greater than 100,000). Data from these 59 CSDs were used to calculate average population estimates across Canada.
Figure 1: Location of CT Facilities and 100 km Radius by Census Subdivisions Operating in Rural or Remote Settings
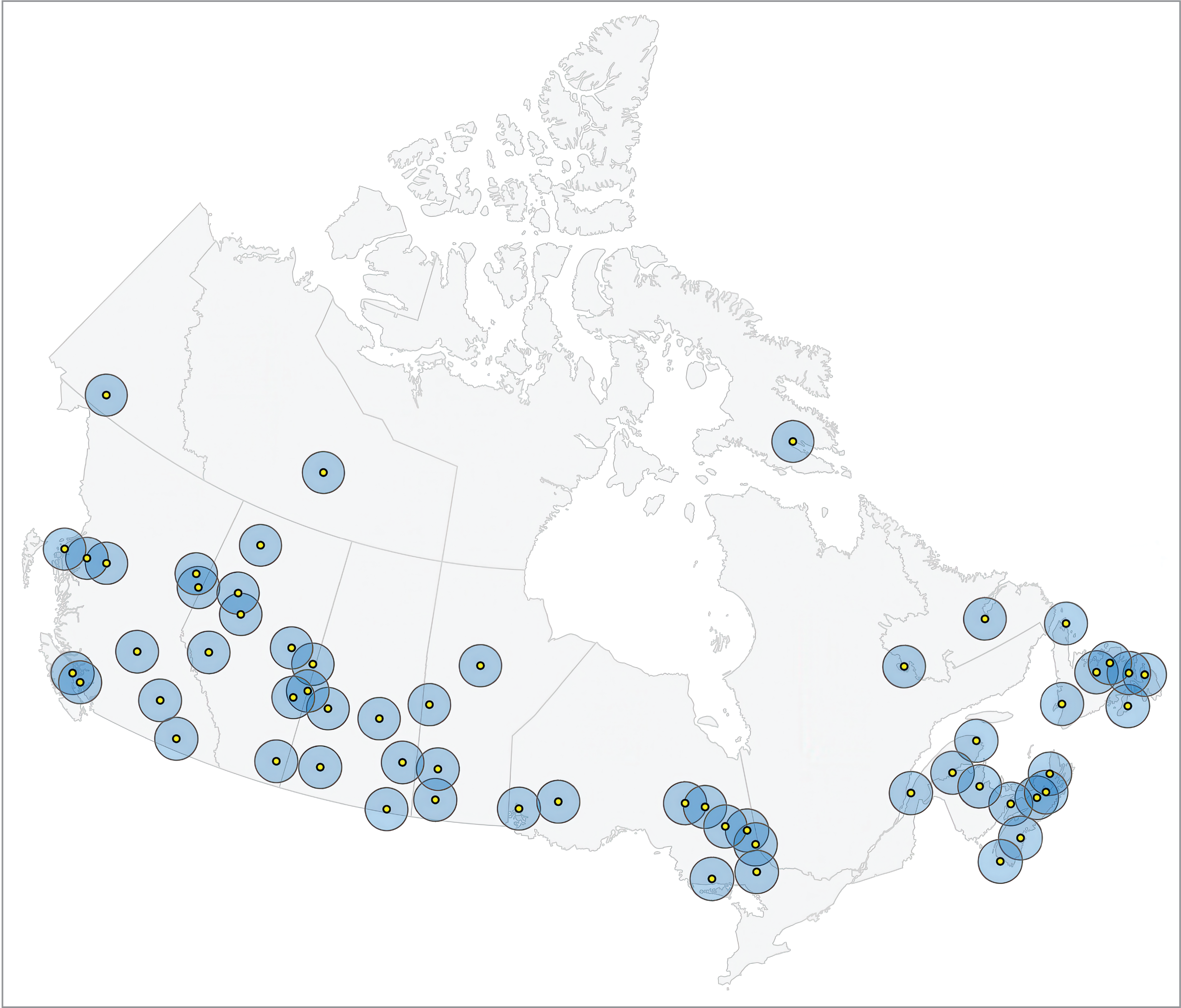
CSD = census subdivision.
Notes: CT location data are presented for 59 CSDs (populated communities) located across 12 provinces and territories: Newfoundland and Labrador (9 CSDs), Nova Scotia (6 CSDs), New Brunswick (2 CSDs), Quebec (2 CSDs), Ontario (9 CSDs), Manitoba (4 CSDs), Saskatchewan (6 CSDs), Alberta (8 CSDs), British Columbia (10 CSDs), Yukon (1 CSD), Northwest Territories (1 CSD), and Nunavut (1 CSD).
Each yellow circle represents a CSD with established CT services.
Each blue circle represents a 100 km radius around the centre of each CSD with established CT services.
On average, existing CT services located in rural and remote communities serve approximately 56,100 people. Table 1 summarizes the average number of people located in rural or remote CSDs across Canada that are served by CT equipment.
Table 2 (Appendix 2) presents the total population served within a 100 km radius for each rural or remote community with existing CT services.
Table 1: Average Rural or Remote Population in Canada Served by CT Equipment Within a 100 km Radius
Measure | Overall (N = 59) | Less accessible (N = 20) | Remote area (N = 38) | Very remote (N = 1) |
|---|---|---|---|---|
Population served within a 100 km radius | ||||
Mean (SD) | 56,100 (38,000) | 87,400 (29,800) | 40,800 (31,300) | 10,100 (NA) |
Median (range) | 50,300 (7,430 to 171,000) | 81,200 (47,100 to 144,000) | 35,100 (7,430 to 171,000) | 10,100 (10,100 to 10,100) |
CSD = census subdivision; NA = not applicable; SD = standard deviation.
Note: N refers to the number of CSDs (populated communities).
Criteria Used for CT Planning in the Rural and Remote Setting
The survey achieved a 90% response rate, with 10 senior decision-makers from 9 provinces participating. One respondent noted that historically, CT planning decisions are made at the facility level rather than with provincial government involvement. Two survey responses were received from 1 province.
The following criteria were reported as factors that are considered when making decisions on introducing new CT services to rural and remote communities:
Population Size of Rural Area
The size of the community served was the most reported criterion considered in planning for new CT services, as noted by 6 respondents.
One respondent specifically reported that a population threshold of 20,000 people or more within the catchment area was a requirement when considering introducing new CT services to rural and remote communities.
Patient Travel Time and Distance
Overall, 5 respondents indicated that patient travel time to a primary care centre or travel distance to the nearest available CT facility are key factors in planning for new CT placements in rural and remote settings.
One respondent reported a target patient travel time of less than 2 hours for rural areas.
Another respondent stated that a radius of 100 km from the nearest CT facility has been used historically, although they noted that this practice was evolving.
A different respondent noted that patient travel time is secondary to the number of CT exams ordered for patients in rural communities and surrounding areas. The respondent indicated that the threshold for the number exams ordered for patients in a rural area is between 12,500 and 13,000.
One respondent reported that the mode of transportation is an important consideration, as certain modes of transportation can be more costly or add travel time. For instance, patients in rural communities located off the mainland may need to rely on ferry services to reach the nearest CT facility.
Population Demographics
Five respondents reported that the demographics and medical needs of the population were important considerations when planning for new CT placements in rural and remote settings.
Initial and Ongoing Costs
Four respondents indicated that capital and operational costs associated with establishing CT services and imaging budgets were important factors when planning for new CT placements in rural and remote settings.
Referral Patterns
Four respondents indicated that CT referral patterns, including the type and volume of exams requested by physicians, are important factors when planning for new CT placements in rural and remote settings.
Interfacility Travel Costs
Overall, 3 respondents indicated that resources and costs associated with interfacility transfers and delayed scan times are considerations when planning for new CT placements in rural and remote settings. No set cost threshold was reported.
One respondent indicated that the most important consideration is the distance to the nearest available CT facility and the costs associated with transferring patients back to their home community.
Another respondent reported that hospital trauma and stroke care pathways have set time frames for CT exams, necessitating access to CT services across the province to meet these mandated time frames.
Staffing and Training
Three respondents indicated that investment in staffing and ensuring the ongoing maintenance of professional competency are important factors when planning for new CT placements in rural and remote settings.
Equipment Mobility
One respondent highlighted that the ability of CT equipment to function as a mobile unit serving multiple communities is a key consideration when planning new CT placements in rural and remote settings.
Limitations
The estimated average population served by existing CT services located in rural or remote communities does not consider the various community-specific factors that may influence access to CT services. For example, a radius of 100 km was used to estimate the average population served by existing CT services, which may underrepresent the population served, particularly in remote or highly rural areas where patients travel distances greater than 100 km to receive CT services.
The survey results presented in this report are limited by the number of respondents that reported information on the provision of CT services in rural or remote communities across Canadian jurisdictions. Therefore, the survey results presented in this report are not representative of all decision-making considerations or reported thresholds used at the provincial level. Territorial decision-making was not included in the survey.
Finally, various classifications exist to define “rural” and “remote,” each with its own reporting implications and limitations.9,10 For instance, this report excluded communities with small populations that were located in close proximity to large urban geographic areas, as it was assumed that these areas have better access to CT services due to their proximity to urban centres.
Conclusions
This analysis highlights factors that influence decision-makers when planning for new CT services across Canada’s rural and remote communities. By examining the average population within a 100 km radius of communities with existing CT capacity, we found that, on average, each CT facility serves approximately 56,100 people in these areas.
The survey responses from decision-makers across 9 of the 10 provinces underscore the importance of considering various criteria in CT planning. Notably, factors such as community size, patient travel time, distance to nearest available CT equipment, and interfacility transfer costs play significant roles in decision-making.
The clinical needs of a hospital and local demand for CT services are other important factors that also inform decision-making, along with an investment in staffing and ensuring the ongoing maintenance of professional competency. Additional considerations include the demographics of the rural population, capital and operational costs, referral patterns, and the potential for mobile CT units to serve multiple communities.
References
1.Merkens BJ MR, Creeden L, Engels PT, Rothwell DM, Chan BT, Tu K. A rural CT scanner: evaluating the effect of local health care. Can Assoc Radiol J. 2006;57(4):224-31.
2.Davidson M KA, Tonseth RP, Seland K, Harvie S, Hanneman K. The Landscape of Rural and Remote Radiology in Canada: Opportunities and Challenges. Can Assoc Radiol J. 2024;75(2):304-312.
3.Fleet R, Brochu, P. & Blanchard, PG. Is it time for a CT scanner in every Canadian rural hospital? Can J Emerg Med. 2021;23:579-580.
4.Watchorn A, Curran, J., Evans, Z., Wong, V. How long is too long for emergent CT imaging in rural communities? 2021. Accessed 2025 Feb 25. https://med-fom-rhsrnbc.sites.olt.ubc.ca/files/2021/06/Infographic_Rural-CT-and-Interfacility-transport.pdf
5.CDA-AMC. Canadian Medical Imaging Inventory 2022-2023: CT. 2024. Accessed 2025 Feb 25. https://www.cda-amc.ca/sites/default/files/hta-he/HC0024-05-CMII4-CT-Report.pdf.
6.Loria K. Accessible Care: Challenges and Opportunities Related to Radiology Services in Rural Areas. Radiology Today. 2021;20(19):22. .
7.CDA-AMC. Canadian Medical Imaging Inventory: About CMII. 2024. Accessed 2024 Dec 10. https://www.cda-amc.ca/canadian-medical-imaging-inventory-cmii..
8.Statistics Canada. Census of Population 2021. 2021. Accessed 2024 Dec 10. https://www12.statcan.gc.ca/census-recensement/index-eng.cfm
9.Statistics Canada. Developing Meaningful Categories for Distinguishing Levels of Remoteness in Canada. 2020. Accessed 2025 Feb 25. https://www150.statcan.gc.ca/n1/pub/11-633-x/11-633-x2020002-eng.htm
10.Institute RO. Rural Wellbeing: Rural Classification Factsheet. 2023. Accessed 2024 Dec 10. https://www.ruralontarioinstitute.ca/uploads/userfiles/files/Rural%20Wellbeing%20-%20Rural%20Classification%20Factsheet.pdf
Appendix 1: Survey Questions
Please note that this appendix has not been copy-edited.
CMII: Survey – CT Planning in Rural Communities
What criteria are used to determine the provision of CT services for rural areas within your jurisdiction?
Population size of rural area. If yes, please comment on the population threshold.
Patient travel time to primary care centre/hospital. If yes, please indicate average distance/travel time.
Resources and costs associated with interfacility transfers and delayed scan times. If yes, please indicate if there is a threshold used.
CT referral patterns (the type and volume of exams requested by physicians).
Capital and operational cost considerations.
Patient demographics and medical needs of rural population (e.g., age, prevalence of disease requiring imaging, or urgency of scans).
Other (please specify).
Please elaborate on the methods used to assess the need for adding CT services in rural areas.
The survey consists of 2 questions and may take approximately 5 minutes to complete.
Data confidentiality: The results of the survey will be included in a report that will be published on the CMII website. Data will be aggregated and anonymously presented.
Appendix 2: Estimated Population Served by CT Services, by Census Subdivision
Please note that this appendix has not been copy-edited.
Table 2: Total Population Served for Each Rural or Remote CSD With CT Services, 100 km Radius
CSD | Estimated population served | Remote classification |
|---|---|---|
1 | 7,429 | Remote area |
2 | 9,006 | Remote area |
3 | 9,376 | Remote area |
4 | 9,879 | Remote area |
5 | 10,054 | Very remote |
6 | 13,419 | Remote area |
7 | 13,737 | Remote area |
8 | 15,432 | Remote area |
9 | 16,059 | Remote area |
10 | 18,939 | Remote area |
11 | 19,349 | Remote area |
12 | 19,720 | Remote area |
13 | 22,278 | Remote area |
14 | 23,507 | Remote area |
15 | 26,647 | Remote area |
16 | 28,968 | Remote area |
17 | 32,555 | Remote area |
18 | 32,610 | Remote area |
19 | 33,355 | Remote area |
20 | 33,387 | Remote area |
21 | 36,716 | Remote area |
22 | 37,346 | Remote area |
23 | 39,029 | Remote area |
24 | 40,480 | Remote area |
25 | 41,970 | Remote area |
26 | 42,286 | Remote area |
27 | 42,614 | Remote area |
28 | 45,933 | Remote area |
29 | 47,123 | Less accessible |
30 | 50,297 | Remote area |
31 | 52,016 | Remote area |
32 | 52,779 | Remote area |
33 | 53,810 | Less accessible |
34 | 54,350 | Less accessible |
35 | 55,583 | Less accessible |
36 | 55,728 | Remote area |
37 | 57,297 | Remote area |
38 | 58,662 | Remote area |
39 | 62,087 | Remote area |
40 | 64,301 | Less accessible |
41 | 64,427 | Less accessible |
42 | 68,924 | Less accessible |
43 | 77,976 | Less accessible |
44 | 79,233 | Less accessible |
45 | 79,850 | Less accessible |
46 | 81,615 | Remote area |
47 | 82,513 | Less accessible |
48 | 83,614 | Less accessible |
49 | 84,846 | Less accessible |
50 | 93,868 | Less accessible |
51 | 97,589 | Remote area |
52 | 99,419 | Remote area |
53 | 101,875 | Less accessible |
54 | 115,683 | Less accessible |
55 | 122,414 | Less accessible |
56 | 128,657 | Less accessible |
57 | 143,869 | Less accessible |
58 | 144,155 | Less accessible |
59 | 170,598 | Remote area |
CSD = census subdivision.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.