Drugs, Health Technologies, Health Systems
Health Technology Review
Canada’s Early Experiences With Low-Field MRI: Insights From a Cross-Country Survey
Key Messages
What Is the Issue?
Canada’s Drug Agency (CDA-AMC) received a request to investigate the experiences of health care institutions with their low-field MRI units, including portable or point-of-care units, to support facilities that are considering this technology.
Low-field MRI systems operate using lower-strength magnetic fields and have seen a resurgence due to recent innovations improving image quality. They can supplement existing MRI capacity, expand access in resource-limited settings, and may be an option for patients who have certain contraindications or cannot tolerate conventional MRI systems.
We identified 1 previous study that examined portable MRI use in a remote hospital in Ontario. Our findings build on that work, incorporating data from facilities across a range of settings and jurisdictions, and providing a broader view of how these units were being used in the Canadian context at the time the survey was conducted.
What Did We Do?
CDA-AMC conducted a survey of the 6 known health care facilities identified through the 2022–2023 Canadian Medical Imaging Inventory National Survey as having low-field MRI units.
The report summarizes the experiences of 5 respondents to the survey, which explored the following themes:
technical specifications and operations
staffing and training needs
clinical applications
perceived impacts on patient care experiences
perceived benefits and challenges.
What Did We Find?
Respondents provided valuable insights into low-field MRI use in Canada. According to the survey:
4 of 5 respondents said they had access to a conventional MRI unit, and 1 respondent indicated that low-field MRI units are often used to complement existing imaging services
all respondents reported few technical issues with low-field MRI units and no adverse events that affect patients or staff
4 of 5 respondents said that minimal training was required to operate low-field MRI units, whereas 1 respondent indicated that more extensive training was required
all respondents said that the body areas most commonly imaged with low-field MRI are the head and neck
3 of 5 respondents reported improved imaging capabilities with low-field MRI, whereas 2 indicated no improvement
4 of 5 respondents cited portability and compact size as advantages of low-field MRI units over conventional MRI units
2 of 5 respondents mentioned image resolution as a challenge for low-field MRI units, with another respondent reporting challenges with staffing capacity.
What Does This Mean?
This report covers 5 of 6 facilities known to have low-field MRI systems at the time of this survey, providing the first national-level examination of their use in a variety of settings and jurisdictions, and encompassing both research and clinical practice. The findings highlight how low-field MRI units are being used — not as replacements for conventional MRI systems, but as complementary tools suited to specific clinical needs or use in space-limited or high-acuity environments.
An understanding of the perceived strengths and weaknesses of these units may help decision-makers make planning decisions regarding new imaging capacity.
Context
Canada’s Drug Agency (CDA-AMC) received a request to investigate the use of low-field MRI units in different health care settings. The units are designed to be smaller and more portable and use low magnetic field strengths to enable convenient bedside or outpatient imaging, thereby reducing the need to transport patients to conventional MRI suites.1,2
Low-field MRI units — such as portable and point-of-care (POC) systems — which were first commercially introduced around 2020, represent a growing area of innovation in medical imaging.3 Terminology in the literature is still evolving, with some sources distinguishing between categories like “ultra-low-field MRI” (typically below 0.01 T) and others using terms like “portable MRI” or “POC MRI” interchangeably.4 These terms are not always consistently applied, and not all POC systems meet strict criteria for portability. For the purposes of this report, “low-field MRI unit” refers to any MRI system with a magnetic field strength below the conventional 1.5 T used in standard full-sized scanners. This includes portable and POC systems.
Full-sized, conventional MRI units require purpose-built spaces to support their weight, maintain a constant power supply, and ensure appropriate shielding to protect staff and patients from high magnetic fields.5-7 These infrastructure requirements, along with the procurement of the full-size MRI unit, require substantial capital investment and ongoing maintenance costs. Low-field MRI units, because of their portability and relative affordability, could improve access to imaging in underserved communities such as rural and remote settings where the necessary infrastructure and support may not be in place.8 The smaller size of low-field MRI units also allows for more responsive and flexible uses, especially in emergent situations that require rapid imaging for assessments, such as in an intensive care unit (ICU) or emergency department.2
Low-field MRI units are still an emerging technology, and their role in clinical practice continues to evolve. While real-world evidence from Canada is limited, we identified 1 study from a remote hospital in Ontario that offers meaningful insight, contributing to the growing understanding of how these systems can be used in specific settings.9 That study reported that the implementation of a portable MRI unit was feasible and was associated with cost savings compared to acquiring a conventional MRI unit. While the portable MRI produced diagnostic-quality images in most cases, some limitations in image resolution were noted, with a subset of patients still requiring conventional imaging for further evaluation. Our study builds on that early work by exploring adoption and use across a broader range of clinical and institutional contexts nationwide.
CDA-AMC is uniquely positioned to provide a broader examination of low-field MRI use by leveraging site identification data collected by the Canadian Medical Imaging Inventory (CMII) national survey.10 While the original CMII survey did not capture detailed facility-level experience with low-field MRI units, it enabled targeted follow-up with identified sites. This follow-up survey offers valuable insights into the real-world deployment and clinical use of low-field MRI units (including portable or POC units) to help inform decision-makers within the Canadian health care system.
Objectives
This report summarizes survey responses examining the experiences of representatives from health care facilities and research institutions operating low-field MRI units, including portable or POC units. The survey explored the rationale for adopting this technology, as well as users’ overall experiences with its implementation and use. It covered the following key areas:
technical specifications and operations
staffing and training
clinical applications and observed outcomes
perceived impacts on patient care and experience
overall perceptions of the benefits and challenges of low-field MRI units.
Methods
A targeted survey consisting of 35 multiple-choice and open-ended questions was developed using Microsoft Forms and was distributed to the 6 sites in Canada known to have low-field MRI units. These sites were identified through the CMII or from publicly available news articles. Representatives from 5 of 6 facilities responded to our survey on their low-field MRI units.
Respondents were asked to share their experiences with low-field MRI units to inform a wide range of facilities about potential benefits and practical considerations related to patient care, workflow, and service delivery. The survey was disseminated on April 28, 2025, and remained open until May 15, 2025 (refer to Appendix 1 for the survey questions).
Results
This section presents the findings of the 5 facilities from which we received responses to the survey.
Facility Overview
Participating Facilities
Based on available data from the CMII and public sources, there are 6 sites in Canada that operate low-field MRI units. Out of 6 surveys distributed, 5 responses were received, representing 4 provinces, including Nova Scotia, Ontario, Saskatchewan, and British Columbia, and 1 territory, Nunavut. Respondents included a mix of small and large hospitals, as well as a research institute with 4 facilities located in an urban setting and 1 facility in a remote setting. The length of time low-field MRI units have been operated in these facilities ranged from 1 to 5 years.
Four of 5 respondents reported access to at least 1 full-sized conventional MRI unit, whereas 1 reported no onsite access to such a system.
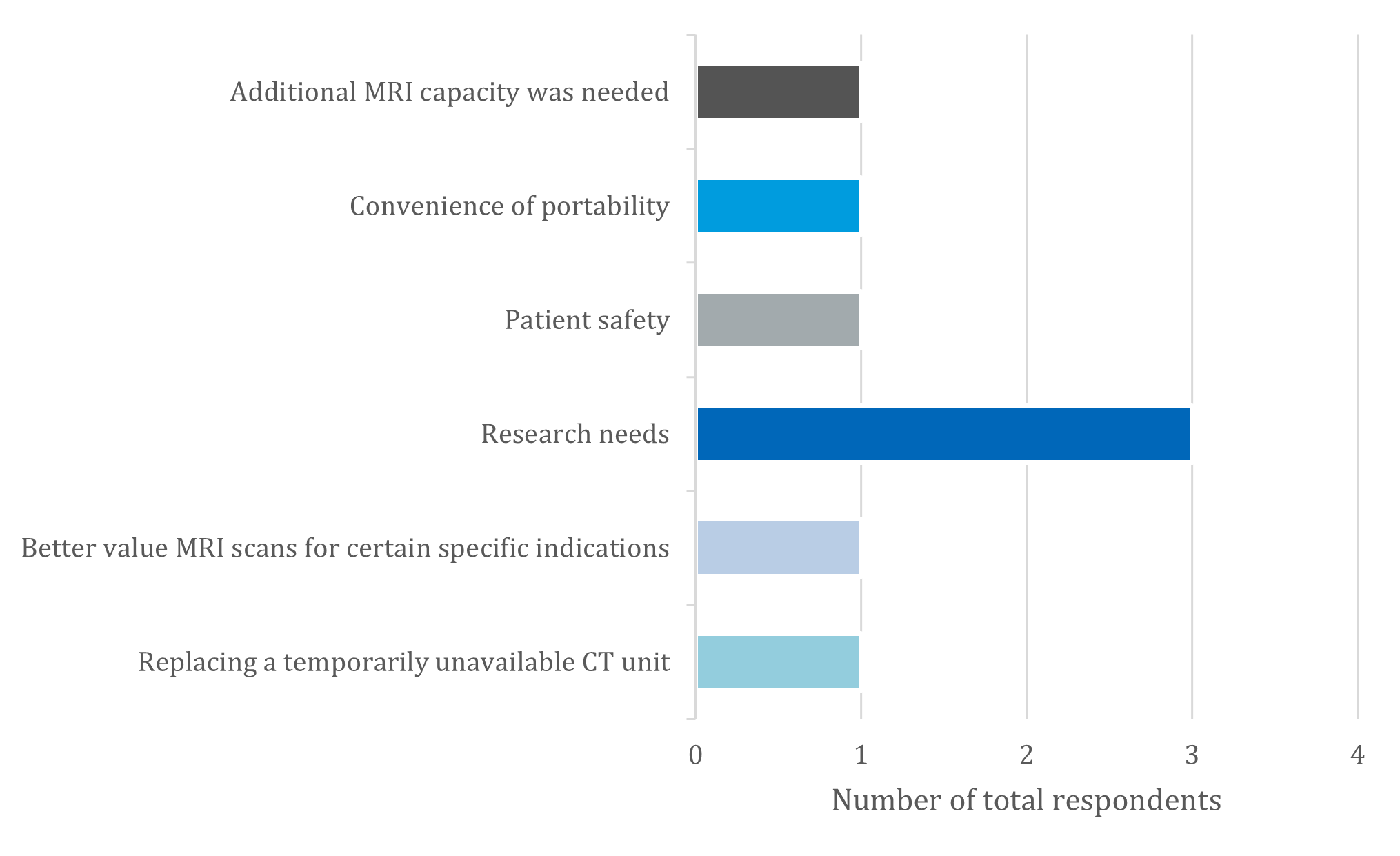
The primary reason for considering the adoption of a low-field MRI unit was for research needs, which was reported by 3 out of 5 respondents. Additional factors for adopting this technology are shown in Figure 1.
Technical Specifications, Operations, and Unit Location
Survey respondents were asked to report on the technical specifications of their low-field MRI units, including the make and model, field strength, and safety protocols.
Four of 5 respondents reported operating a portable MRI unit, and the remaining respondent reported operating a POC MRI unit.
The portable MRI units had a field strength of 64 mT.
The POC MRI unit had a field strength of 0.5 T.
These field strengths are relatively low compared to full-sized, conventional MRI units, which typically have a field strength of 1.5 T or 3.0 T.
All respondents reported that their units experienced very few technical issues.
All respondents confirmed that specific safety protocols for both patients and staff were established for their low-field MRI units.
One respondent commented that their POC MRI unit operated faster than a conventional, fixed MRI unit when performing ear, nose, and throat exams.
The units were deployed in a variety of settings, including research facilities, ICUs, and emergency departments. None were reported as being restricted solely to diagnostic imaging departments.
Staffing and Operating Low-Field MRI Units
Survey respondents were asked to provide information on staffing and operations related to their low-field MRI units.
Staff Roles and MRI Unit Operation
Four of 5 respondents reported that medical radiation technologists (MRTs) operate the low-field MRI units at their facilities.
One respondent noted that radiologists and physicians are also able to operate their MRI unit.
Another indicated that expert users can be trained to operate their portable MRI unit.
Patient and Staff Safety
All respondents confirmed that no adverse events related to staff operation or patient diagnosis from low-field MRI unit use were observed.
Training Requirements and Approaches
Four of 5 respondents reported that minimal training was required to operate the units, whereas 1 noted that more extensive training was necessary.
Training methods varied across facilities:
Some relied on manufacturer-led training, designating initial trainees as “super users” who subsequently trained others.
One facility developed and implemented its own internal training program.
Another engaged medical imaging physicists with MRI expertise to train staff.
Regulatory and Credentialing Considerations
All respondents reported no regulatory or scope-of-practice concerns related to staff operation of their low-field MRI unit.
Each facility reported employing staff certified by the Canadian Association of Medical Radiation Technologists (CAMRT) or consulting CAMRT before implementation.
Staff Acceptance and Use
Four of 5 respondents reported minimal to no resistance among staff when adopting the low-field MRI units.
One respondent observed some resistance among staff regarding the adoption of low-field MRI technology.
Clinical and Research Uses
Survey respondents were asked to identify the clinical uses of their low-field MRI unit, including the most commonly imaged body areas as well as specific neuroimaging applications.
Clinical Uses
Four of 5 respondents reported that the primary use of their low-field MRI unit was for diagnostic purposes, such as stroke evaluation and other neuroimaging applications.
All respondents indicated that the head and neck were the most commonly imaged body areas.
One respondent noted that their facility used their unit for imaging the upper extremities (e.g., the arms) in addition to the head and neck.
The 4 respondents who reported neuroimaging as their primary use for their unit provided further detail on the use of their units:
Three reported using the unit primarily for stroke-related imaging.
Additional diagnostic indications included follow-up for an intracranial bleed or mass in the brain; ventricular assessment; and imaging for ear, nose, and throat conditions (e.g., paranasal sinus imaging).
Research Uses
Two respondents indicated that their low-field MRI units were used for research purposes.
One respondent reported that research was the primary use for their portable MRI unit.
The other respondent reported that their unit was shared between research and diagnostic uses.
Among the 4 respondents who reported using their unit for neuroimaging applications, 2 respondents also used their unit for neuroimaging research.
Patient Experiences
Survey respondents were asked about patient-reported experiences with their low-field MRI units, including health-related outcomes and adverse events:
Among the 4 units used in clinical settings, 3 out of 4 respondents reported that low-field MRI use had improved patient outcomes, and the remaining respondent reported that it had not. Some respondents noted that further research is needed to fully understand the scope of benefit to patients.
In addition, 3 of 5 respondents relayed experiences from some patients who indicated that they found the low-field MRI units to be quieter than full-sized MRI units. It was observed that some patients fell asleep during the exam.
Additionally, 2 respondents commented that patients reported feeling less claustrophobic with the low-field MRI unit compared to full-sized, conventional MRI units.
An anecdote shared by Dr. Kolind at the University of British Columbia described a First Nations person who felt nervous about undergoing an MRI exam due to prior experiences with full-sized, conventional MRI units. The portable MRI unit enabled them to remain in their own clothing instead of changing into a hospital gown and allowed a support person to be present during the exam, creating a culturally safe and supportive environment (Dr. Shannon Kolind, Djavad Mowafaghian Centre for Brain Health, University of British Columbia, Vancouver, BC: personal communication, Jun 19, 2025).
No respondents reported any adverse events for patients related to the use of low-field MRI units.
General Experiences
Survey respondents were also asked about their general experience with their low-field MRI units. This provided insights into the key advantages and limitations encountered in clinical practice, how the units have expanded imaging capacity, and other recommendations from the responding facilities.
Advantages of Low-Field MRI
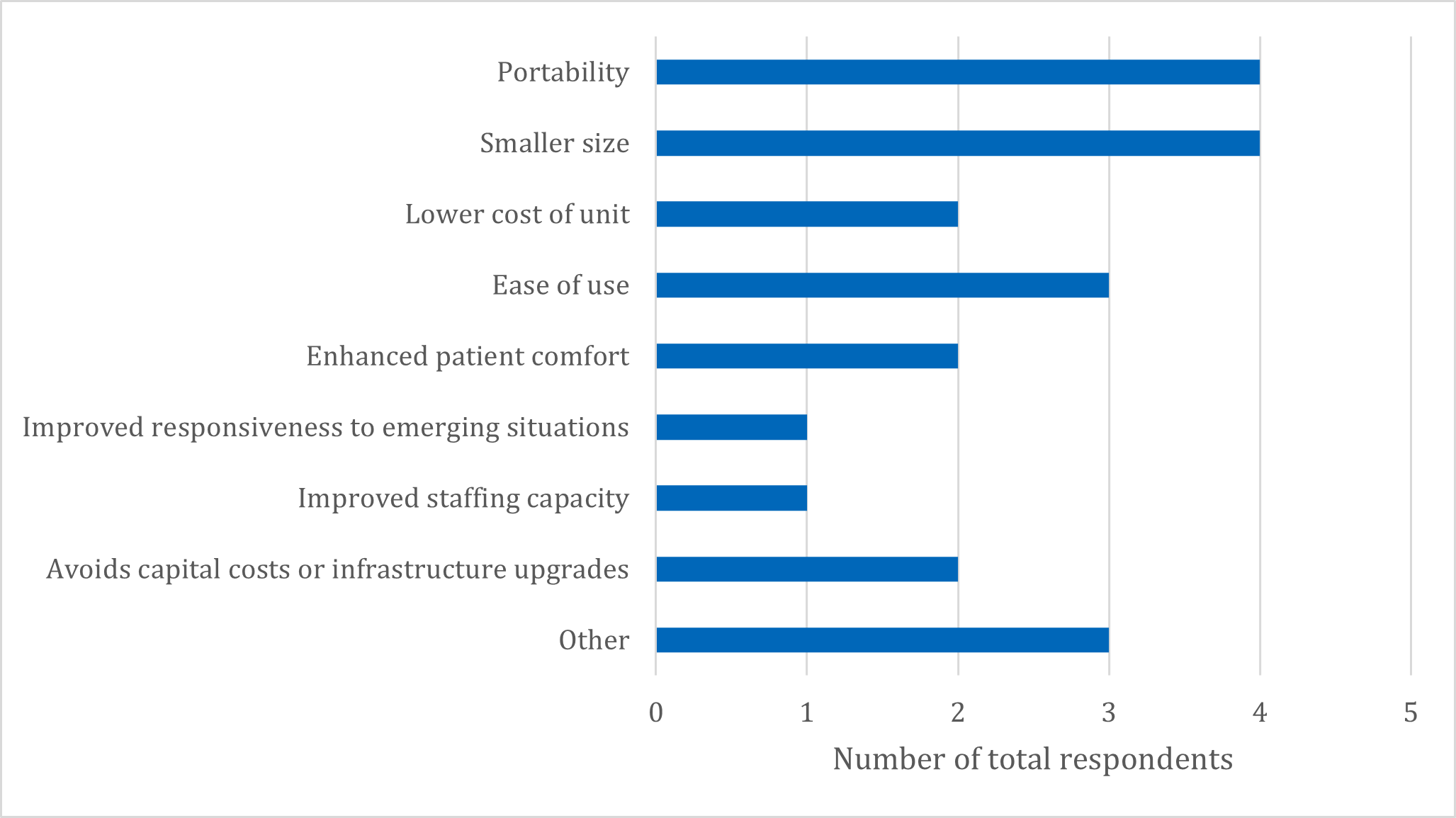
When asked about the key advantages of low-field MRIs, 4 of 5 respondents identified portability and the units’ compact size as the primary benefits. Additional advantages, mentioned by a smaller number of participants, included:
ease of use (n = 3)
enhanced patient comfort (n = 2)
cost savings (n = 2)
reduced infrastructure requirements (n = 2)
improved responsiveness in clinical settings (n = 1)
improved staffing capacity (n = 1).
A full list of reported advantages and their response frequencies is provided in Figure 2.
Two of 5 respondents reported that they would consider the acquisition of an additional low-field MRI unit. The other 3 respondents reported they would not consider acquiring an additional low-field MRI unit. However, no follow-up questions were asked to determine their reasons, so it is unclear whether their responses were based on factors such as patient volume, clinical need, or other considerations.
One respondent described a potential future scenario in which multiple low-field MRI units are assigned to image different body areas in parallel. According to Dr. Shannon Kolind, these units could be operated by noncredentialed staff with a credentialed MRT supervising and providing oversight over the units and staff (Dr. Shannon Kolind, Djavad Mowafaghian Centre for Brain Health, University of British Columbia, Vancouver, BC: personal communication, Jun 19, 2025).
Additional Comments From Respondents
Respondents also provided the following qualitative insights regarding the benefits of low-field MRI units:
“Provides access for patients who cannot tolerate or have contraindications to conventional field MRIs.”
“The usefulness of a dedicated imaging unit for a specific body part (e.g., head), allowing for multiple safer, low-interaction scanners and more skilled technologists.”
“The ability to triage exams to the best-suited field strength, as certain aspects of MRI physics lend advantages to lower field strengths.”
“Avoiding the transfer of unstable patients to a fixed MRI unit.”
“Rapid developments in image quality and disease-specific imaging protocols are broadening the range of applications, including multiple sclerosis, stroke, headaches, and dementia.”
“Ideal for pediatric use where it is desirable to avoid sedation or intubation for the purpose of acquiring an MRI.”
“The ability to deploy the unit for research.”
Challenges of Low-Field MRI
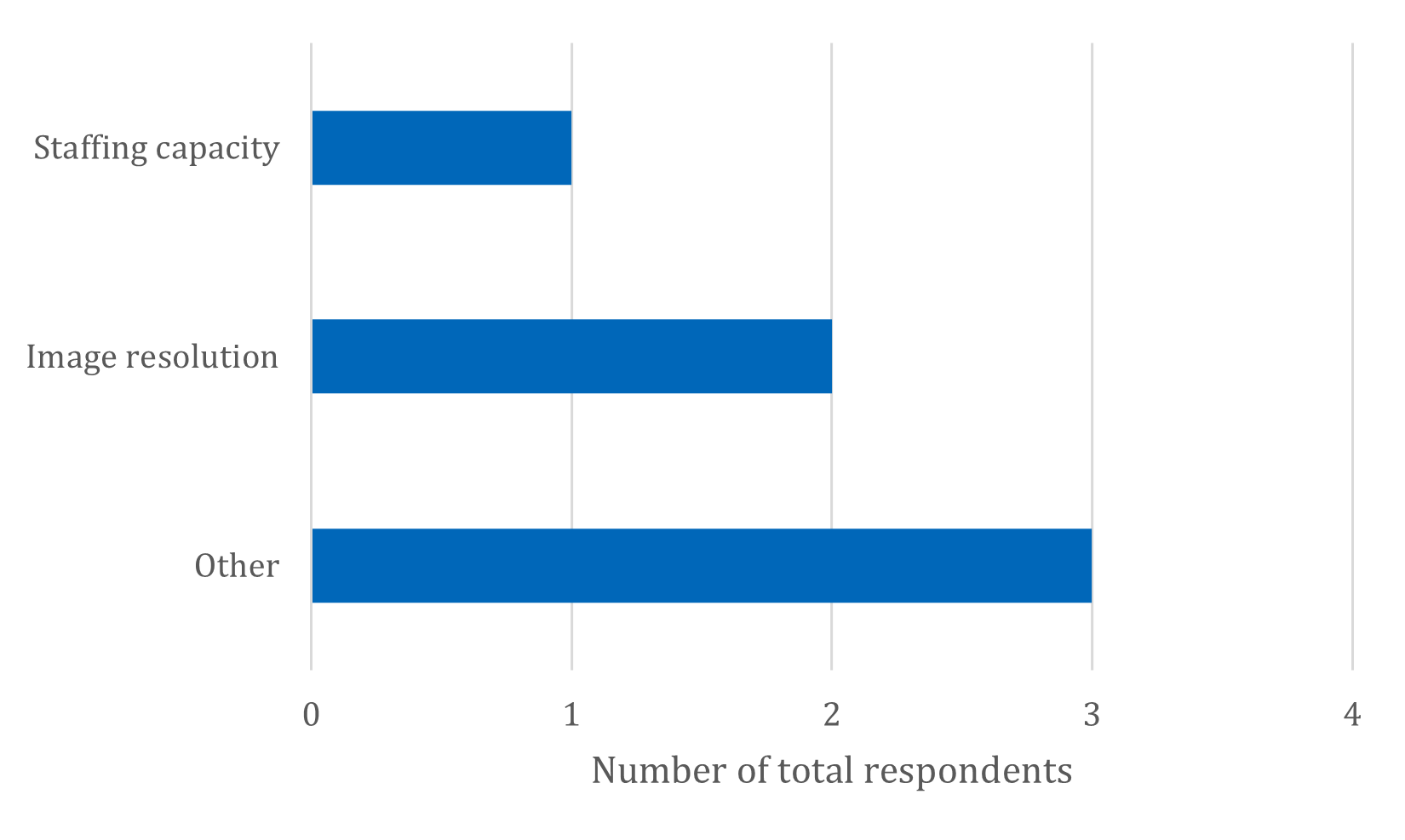
When asked about the primary challenges associated with low-field MRI, 2 of 5 respondents cited image resolution, and 1 respondent identified staffing capacity as an operational challenge (refer to Figure 3).
Additional Comments From Respondents
Respondents also provided the following qualitative insights regarding the challenges of low-field MRI units in the “Other” category:
“Overly narrow [patient selection] criteria for deploying the unit.”
“Many [medical] devices are not tested for MRI safety at 0.5 T, despite it being actually safe, requiring collaboration between MRTs and radiologists in clearing an exam [on the low-field unit].”
“While portable MRI has great potential, it may be less than ideal for imaging pediatric patients, but research possibilities remain open for this patient group.”
“A need to establish clinical indications and role with regard to conventional imaging.”
“MRI safety considerations specific to low field (i.e., regulatory and implant documentation/regulations may not have caught up).”
“Staffing shortage [of MRTs] and operational funding limits use of the device.”
“Some radiologists did not find the image to be sufficient for diagnostics.”
“Default imaging protocols limited initial images to thick slices, but further refinement of protocols has improved this.”
Imaging Capacity
Three of 5 respondents reported that the acquisition of their portable MRI unit helped improve imaging capabilities at their facility. Anecdotally, it was noted that this also helped ease capacity pressures on their CT services. The other 2 respondents reported no improvement to the imaging capabilities in their respective facilities.
Integration and Clinical Adoption
One respondent noted initial integration difficulties between their low-field MRI unit and the electronic health information system, which were later resolved with a software update.
Among the 3 respondents using portable MRI units, 2 reported that the portability outweighed potential imaging limitations — particularly for neuroimaging. One of these respondents additionally commented that they found the unit to be complementary to conventional imaging. The remaining respondent who had experience with a portable MRI unit indicated that concerns about potential imaging limitations outweighed the perceived benefits of portability, ultimately reducing the unit’s overall utility in their practice.
However, it was also observed that ongoing technological and software advancements are contributing to improvements in image quality. These developments suggest that low-field MRI units may be approaching readiness for broader clinical application in Canada.
Recommendations and Broader Adoption
Two of 5 respondents indicated they would recommend that other facilities consider acquiring a low-field MRI unit, with 1 of the respondents highlighting the unit’s potential for use in underserved areas, clinical trials, and research in addition to routine clinical use, based on their experience and positive patient feedback. In contrast, the remaining 3 respondents did not recommend acquisition, though their reasons varied:
One respondent stated they would have recommended acquisition only if a full-sized CT or MRI scanner was unavailable.
Another respondent suggested that low-field MRI units be limited to tertiary neurology centres until clinical indications and operational funding are clearly established.
A third respondent believed that, although portable MRI units held significant potential, they were not ideal for imaging pediatric patients at that time. However, they noted that future research applications could prove advantageous.
Limitations
This report is based on a targeted survey distributed to all 6 known Canadian facilities operating low-field MRI units at the time of data collection. Five facilities responded, representing 83% of this defined group. As such, while the total number of respondents is small, the report provides a near-complete picture of early implementation experiences in Canada. The results presented in this report should be viewed as a brief overview of facilities and their current use of their low-field MRI units, information that can be used by facilities considering their own acquisition of a low-field MRI unit.
One respondent reported that they have not used their portable MRI unit yet due to strict patient selection criteria. Their responses were based on intended, rather than actual use. Additionally, as mentioned by another respondent, more rigorous systematic research on the use of low-field MRI units in a clinical setting to better quantify long-term outcomes and benefits for patients and health care system efficiencies will clarify the role of low-field MRI as more units come into use.
This survey was intended to capture early implementation experiences rather than conduct a comprehensive clinical evaluation. As such, no patient demographic or imaging volume data were collected, and results are largely based on subjective feedback from institutional representatives.
Implications for Decision-Making
Low-field MRI units may offer a promising way to expand access to diagnostic imaging — for example, in underserved and rural areas where conventional full-sized MRI systems are often unavailable. For health system planners, these units may provide a lower-cost alternative for select clinical needs and could function in environments that do not demand infrastructural modifications or high capital investment.
Clinical Applications
Given the novelty of low-field MRI units, continued evidence-based exploration of appropriate clinical applications is important. Some systems are purpose-built for specific anatomic areas, whereas others are more versatile, enabling imaging across various body regions such as the musculoskeletal system or supporting intraoperative MRI-guided procedures.1,4 Notably, portable MRI units are most commonly used for neuroimaging, and their mobility allows them to be deployed beyond conventional diagnostic imaging departments.1,4 While 1 respondent raised concerns about image quality being insufficient for diagnosis — which may limit the utility of portable MRI — another noted that software updates have already led to noticeable improvements in resolution over a relatively short period.
Improved Accessibility for Critical Care
The compact size and lower weight of the equipment enable placement directly in patient care areas — such as ICUs and emergency departments — without the need for specialized infrastructure like reinforced floors, upgraded electrical systems, or magnetic shielding.1,4,11,12 This proximity improves accessibility for critically ill or unstable patients, allowing imaging to occur without the risks associated with transport to a centralized imaging suite — a process that can be logistically challenging and, in some cases, life-threatening.1,4
Preparing an ICU patient for transport to a conventional MRI scanner can be time-intensive due to the need to transport, manage, and monitor life-sustaining equipment. During this time, the medical team involved is unavailable to assist other patients.2 In contrast, portable low-field MRI units reduce the burden on staff and patients. By enabling safer and more immediate access to diagnostic information, low-field MRI units may support earlier diagnosis and treatment — potentially improving patient outcomes. However, this technology may not yet be appropriate for all clinical applications; for example, 1 respondent noted that their portable MRI unit was not ideal for imaging pediatric patients at this time.
Patient Experience
The compact design of low-field MRI units may improve the overall patient experience. Patients have often reported that these units are quieter and less likely to induce feelings of claustrophobia compared to conventional MRI units, and some low-field systems allow individuals to remain in their own clothing, contributing to a more culturally safe and comfortable environment.1 Some units can also accommodate a support person in the room during scanning, which may be particularly valuable for pediatric patients or those with anxiety.1,4 The lower field strength also minimizes risks associated with device interference, further supporting their use in nontraditional environments and expanding patient eligibility. However, in some clinical scenarios, repeat imaging on a higher-field scanner may be required if initial images are insufficient for diagnosis, potentially increasing patient burden or anxiety.
Workforce and Regulatory Considerations
Some low-field MRI systems have been designed with simplified, user-friendly interfaces and may not require extensive training for basic operation.13 This has enabled their use in certain settings by noncredentialed staff, expanding operational flexibility.14
However, in the Canadian context, regulatory requirements typically restrict the operation of MRI units — including low-field systems — to credentialed MRTs. These requirements are informed by provincial or territorial legislation and scope-of-practice standards set by professional bodies such as CAMRT and are in place to ensure consistently high standards of care.
As a result, even with simplified controls, facilities are generally required to ensure that qualified professionals with appropriate training in imaging, patient safety, and clinical protocols operate low-field MRI units.
Rural Deployment
Low-field MRI units have already been deployed in several low- and middle-income countries that lack the capital for conventional MRI infrastructure and ongoing maintenance (Dr. Sean Deoni, Gates Foundation, Seattle, WA: personal communication, Jul 2, 2025). These international implementations offer valuable lessons for deploying similar models in remote or rural communities in Canada and could also inform strategies to improve access for pediatric populations where appropriate.15 Such strategies could reduce patient travel and enhance timely access to care for some clinical indications and patient populations while potentially lowering system-wide costs related to imaging facility development and equipment upkeep. The 2024 Ontario study of a portable MRI unit deployed in a remote location found that 56% of patients scanned — most commonly for acute stroke — did not require transfer to a conventional MRI centre. Based on this, the study projected cost savings of $854,841 over 1 year, modelling 56% transfer avoidance among 50 patients receiving portable MRI scans.9
Urban Integration
In urban settings, integrating low-field MRI units into nontraditional care areas may also help alleviate demand on high-resolution imaging systems. A recent review highlights how low-field MRI units are already being used for neurologic applications across emergency, ICU, and outpatient environments.16 This redistribution of imaging volume for certain clinical scenarios (e.g., emergent situations in ICUs or emergency departments) may reduce wait times for conventional MRI and CT scans, improving system throughput and optimizing use of existing resources.
However, while this integration can enhance access, it also requires careful coordination to ensure appropriate clinical triaging. If low-field MRI is used in cases where higher-resolution imaging is warranted, there is a risk of delayed or incomplete diagnosis, which could offset the intended efficiencies. Therefore, clear clinical guidelines and appropriate oversight are essential to maximize benefit without compromising diagnostic accuracy.
Complementary Role and Future Considerations
Low-field MRI units are not intended to replace conventional MRI systems but to serve as complementary tools. They may be particularly valuable in settings where traditional MRI units are unavailable or when rapid, POC imaging is needed. To fully leverage their potential, institutions may need to adopt a new mindset regarding where and how low-field MRI units are deployed. This includes developing specific protocols and workflows tailored to their unique capabilities and clinical applications.
Guidelines, Safety, and Scalability
Finally, broader adoption will depend on the establishment of clear clinical guidelines, safety protocols specific to low-field operation, and standardized reimbursement models. As this emerging technology continues to evolve, ongoing evaluation, operational research, and feedback from early adopters will be crucial to supporting responsible, effective scalability.
Conclusions
This report presents early insights from 5 of the 6 known Canadian facilities operating low-field MRI units, offering a near-complete snapshot of their implementation. Experiences ranged from small to large hospitals, including ICU deployment and research settings. Respondents highlighted the size and portability of these units as advantages that often enhanced imaging capabilities and expanded access, particularly in underserved or remote regions.
Low-field MRI units are promising innovations that can expand imaging capacity and improve patient comfort; however, they are not replacements for full-sized, conventional MRI systems. Instead, they are best used as complementary tools to offload select cases — such as emergent stroke imaging or ICU diagnostics — from fixed systems, potentially reducing wait times. While some concerns remain about image resolution and clinical indications, ongoing software advancements are rapidly improving diagnostic utility without requiring hardware changes.
Facilities should carefully weigh the strengths and limitations of low-field MRI based on their unique contexts. This includes considering potential infrastructure savings, such as reduced space and power requirements, alongside operational factors like workflow integration and ongoing maintenance needs. Staffing considerations are critical, including the availability of trained operators and radiologists comfortable interpreting low-field images. Image quality, while improving rapidly, may still pose challenges for certain diagnostic applications and should be evaluated relative to clinical needs.
While these units offer a promising opportunity to broaden imaging access — especially in underserved or remote areas — instead of requiring the significant capital and operational costs associated with conventional MRI systems, their successful deployment requires thoughtful planning and alignment with facility capabilities and patient care priorities.
As low-field MRI technology continues to evolve, these findings may help inform decision-makers evaluating its role in the broader imaging landscape. Future research and policy development will be critical in guiding effective, equitable, and evidence-informed adoption across health care settings in Canada.
Acknowledgements
CDA-AMC would like to thank Dr. Steven Beyea at QEII Health Sciences Centre, Dr. Aditya Bharatha at St. Michael’s Hospital, and all the other respondents who took the time to fill out the survey. A very special thank-you to Dr. Shannon Kolind and Dr. Sharada Balaji from the University of British Columbia for taking the time to provide insight into their work with low-field MRI units. Also, thanks to Dr. Sean Deoni at the Gates Foundation for providing insight into the international use of low-field MRI units.
References
1.Agency CsD. Portable MRI for Use at the Bedside. 2022. Canadian Medical Imaging Inventory Service Report. Accessed 2025 Apr 30. https://www.cda-amc.ca/sites/default/files/attachments/2022-01/portable_MRI_for_use_at_the_bedside.pdf
2.Islam O, Lin LA, Bharatha A. Potential application of ultra-low field portable MRI in the ICU to improve CT and MRI access in Canadian hospitals: a multi-center retrospective analysis. Front Neurol. 2023;14. doi: 10.3389/fneur.2023.1220091 PubMed
3.Hori M, Hagiwara A, Goto M., Wada A., Aoki S. Low-Field Magnetic Resonance Imaging. Invest Radiol. 2021;56(11):669-679. doi: 10.1097/RLI.0000000000000810 PubMed
4.Arnold TC, Freeman CW, Litt B, Stein JM. Low-field MRI: Clinical promise and challenges. J Magn Reson Imaging. 2022;57(1):25-44. doi: 10.1002/jmri.28408 PubMed
5.Bronskill MJ, Carson PL, Einstein S, Koshinen M., Lassen M., Mun SK, Pavlicek W, Price RR, Wright A, Amari E, Erickson J. Site Planning for Magnetic Resonance Imaging Systems. Vol. 20. 1987:1-59. American Association of Physicists in Medicine Report. Accessed 2025 Jun 6. https://www.aapm.org/pubs/reports/rpt_20.pdf
6.CAMRT. MRI facility design (RTMR). CAMRT. 2018. Accessed Jun 6. https://camrt-bpg.ca/patient-safety/mri-safety/mri-facility-design-rtmr/
7.Jimeno MM, Vaughan JT, Geethanath S. Superconducting magnet designs and MRI accessibility: A review. NMR Biomed. 2023:e4921. doi: 10.1002/nbm.4921
8.Birly S. Teeple A, Illes J. The Realization of Portable MRI for Indigenous Communities in the USA and Canada. J Law Med Ethics. 2025;52(4):816-823. doi: 10.1017/jme.2024.159 PubMed
9.DesRoche CN, Johnson AP, Hore EB, Innes E, Silver I, Tampieri D, Kwan BYM, Jimenez JO, Boyd JG, Islam O. Feasibility and Cost Analysis of Portable MRI Implementation in a Remote Setting in Canada. Can J Neurol Sci. 2024 May;51(3):387-396. doi: 10.1017/cjn.2023.250. PubMed
10.Agency CsD. Canadian Medical Imaging Inventory 2022–2023: MRI. Canadian Journal of Health Technologies. 2024;4(8):1-65.
11.DesRoche C, Innes E, Silver I, Tampieri D, Kwan BYM, Jimenez JO, Boyd JG, Islam O. Utility of Novel Ultra-Low-Field Portable MRI in a Remote Setting in Canada. Can J Neurol Sci. 2024:1-7. doi: 10.1017/cjn.2024.346 PubMed
12.Shoghli A, Chow D, Kuoy E, Yaghmai V. Current role of portable MRI in diagnosis of acute neurological conditions. Front Neurol. 2023;14. doi: 10.3389/fneur.2023.1255858 PubMed
13.Prabhat A.M. CAL, Mazurek M.H., Yuen M.M., Chavva I.R., Ward A., Hofmann Jr W.V., Timario N., Qualls S.R., Helland J., Wira C., Sze G., Rosen M.S., Kimberly W.T., Sheth K.N. Methodology for Low-Field, Portable Magnetic Resonance Neuroimaging at the Bedside. Front Neurol. 2021;12. doi: 10.3389/fneur.2021.760321 PubMed
14.Commission IA. IAC Standards and Guidelines for MRI Accreditation. Personnel and Supervision. Ellicott City, MD: Intersocietal Accreditation Commission; 2025.
15.Abate F, Adu-Amankwah A, Ae-Ngibise KA, Agbokey A, Agyemang VA, Agyemang CT, Akgun C, Ametepe J, Arichi T, Asante KP, Balaji S, Baljer L, Basser PJ, Beauchemin J, Bennallick C, Berhane Y, Boateng-Mensah Y, Bourke NJ, Bradford L, Bruchhage MMK, Williams SCR. UNITY: A low-field magnetic resonance neuroimaging initiative to characterize neurodevelopment in low and middle-income settings. Dev Cogn Neurosci. 2024;69. 2024 May 31. doi:10.1016/j.dcn.2024.101397 Accessed 2025 Aug 11. https://www.sciencedirect.com/science/article/pii/S1878929324000586
16.Balaji S, Wiley N, Poorman ME, Kolind SH. Low-field MRI for use in neurological diseases. Curr Opin Neurol. 2024;37(4):381-391. doi: 10.1097/WCO.0000000000001282 PubMed
Appendix 1: Survey Questions
Please note that this appendix has not been copy-edited.
Introductory Questions
What is the name of your facility?
What is your contact email should we need to reach out for feedback?
Did your facility have other MRI imaging capacity prior to acquiring your portable MRI unit? (If other, please describe)
No MRI imaging capacity on site at all
Had a conventional, fixed MRI unit operating at maximum capacity
Had a conventional, fixed MRI unit operating within capacity
Other
What prompted your facility to acquire a portable MRI unit? (Please select all that apply and if “Other” is selected, please describe)
Additional MRI capacity was needed
Convenience of portability
Budgetary reasons
Patient safety
Research needs
Other
How long have you had your portable MRI unit?
Technical Specifications and Operations
What is the make or model of your portable MRI unit, if known?
What is the field strength of your portable MRI unit, if known?
What is the frequency of technical issues arising from your portable MRI unit?
Is the operation of the portable MRI unit faster than a conventional, fixed MRI unit?
Yes
No
Does your facility have specific safety protocols for your portable MRI unit? (This applies for both patients and staff)
Yes
No
Don’t know
Staffing and Operating the Portable MRI
Who can operate your portable MRI unit at your facility? (If other, please describe)
Radiologists
Medical Radiation Technologists (MRTs)
Other
Was specific training required for staff to operate the portable MRI unit prior to it becoming operational?
Yes, extensive training
Yes, minimal training
No
Please describe how medical staff were trained to use your portable MRI unit (e.g., directly hired trained staff, in-person training, online training)
Were there any regulatory or scope-of-practice considerations related to requirements set by governing bodies for staff? (e.g., Canadian Association of Radiologists or Canadian Association of Medical Radiation Technologists)
Have you encountered staff resistance to the use of portable MRIs?
Significant resistance
Minimal resistance
No resistance
Were there any adverse events for staff related to your portable MRI unit? (if applicable)
Clinical Uses and Outcomes
What is the main use of your portable MRI unit? (If other, please describe)
Research
Diagnostic
Interoperative or interventional scanning
Other
What is the most commonly imaged body part or area when using your portable MRI unit? (If other, please describe)
Head/neck
Upper extremities (i.e., arms)
Upper body (i.e., chest, shoulders)
Lower body (i.e., abdomen, pelvis)
Lower extremities (i.e., legs)
Neonatal
Whole body
Other
Which body areas have you used your portable MRI unit to image? (Please select all that apply and if “Other” is selected, please describe)
Head/neck
Upper extremities (i.e., arms)
Upper body (i.e., chest, shoulders)
Lower body (i.e., abdomen, pelvis)
Lower extremities (i.e., legs)
Neonatal
Whole body
Other
If your portable MRI unit is primarily used for neuroimaging, what is the most common application for it? (Please select all that apply and if “Other” is selected, please describe)
Research
Stroke-related
Dementia-related
Other
What location is the portable MRI unit most used in? (If other, please describe)
Emergency department
ICU
Inpatient wards
Radiology or medical imaging department
Critical care
Other
Patient Outcomes
Has the use of your portable MRI unit improved overall patient outcomes? (If other, please describe)
Yes
No
Other
What is the patient experience with your portable MRI unit compared to a conventional, fixed MRI? (if applicable)
Were there any adverse events for patients related to your portable MRI unit? (if applicable)
Concluding Questions
Has the acquisition of the portable MRI unit improved imaging capabilities of your facility? (If other, please describe)
Yes
No
Other
What are some advantages of the portable MRI unit? (Please select all that apply and if “Other” is selected, please describe)
Portability
Size
Cost of unit
Ease of use
Patient comfort
Responsiveness to emerging situations
Staffing capacity
Image resolution
Avoids capital costs or infrastructure upgrades
Image storage and network considerations
Other
Do you have any further comments on the advantages of your portable MRI unit?
What are some challenges encountered with the portable MRI unit? (Please select all that apply and if “Other” is selected, please describe)
Transporting the unit
Size
Cost of unit
Difficulty of use
Staffing capacity
Image resolution
Unexpected costs or maintenance
Image storage and network considerations
Other
Did you encounter any challenges when integrating the portable MRI unit into your existing health information systems? (e.g., transferring scans from the portable MRI unit into the patient electronic medical record)
Do you have any further comments on the challenges of your portable MRI unit?
Do you think the portability of the unit outweighs potential imaging resolution issues? (If other, please describe)
Yes
No
Other
Would you consider acquiring an additional portable MRI unit?
Yes
No
Based on your experiences, would you recommend other hospitals or facilities acquire a portable MRI unit? (If other, please describe)
Yes
No
Other
Do you have any other comments regarding your experience with a portable MRI unit?
Would you like to be publicly acknowledged in the final report? (This would waive the anonymity of your facility)
Yes
No
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.