Drugs, Health Technologies, Health Systems
Health Technology Review
Comparative Effectiveness of Real-Time Teleultrasound Versus In-Person Ultrasound
Key Messages
What Is the Issue?
Ultrasound imaging requires highly trained professionals for accurate diagnostic exams and interpretation.1,2
Ultrasound is more affordable and portable than CT and MRI and does not expose patients to radiation. This makes ultrasound the preferred method for real-time assessment and soft tissue imaging. For more detailed or complex imaging, or when clinically indicated, CT and MRI may be more appropriate.3
In Canada, less than 28% of rural hospitals have in-house access to ultrasound, leading to patient transfers.4
Ultrasound exams are often conducted by sonographers, and there is a notable shortage of sonographers both in Canada and worldwide.5,6
Limited access to skilled ultrasound professionals has led to the development of teleultrasound (TUS), which supports remote clinical decision-making.2,5
TUS can be delivered in real time with remote guidance from a sonographic expert.
TUS can be used by a variety of health care professionals with minimal ultrasound training. However, as the use of real-time TUS continues to expand to different clinical areas, its clinical effectiveness compared with traditional in-person ultrasound remains unclear.
What Did We Do?
We received a request related to the use of real-time TUS to support policy decision-making.
A literature search was conducted to identify studies examining the clinical effectiveness of real-time TUS compared with conventional in-person ultrasound and any evidence-based guidelines for TUS use in clinical practice.
We also report some of the advantages and challenges of TUS as described in the literature.
What Did We Find?
Real-time TUS was comparable to conventional in-person ultrasound for exam image quality and diagnostic consistency.
Exams took, on average, more than 25% (or 6 minutes) longer to complete compared with in-person ultrasound.
Real-time TUS was associated with high clinician satisfaction for comfortability, telecommunication quality, exam duration and quality, and accessibility.
Several studies reported transient safety-related complications (e.g., increased pressure, pain), patient discomfort or fear, and technical difficulties during 10% of robotic-assisted TUS exams.
Real-time TUS was studied in a wide range of clinical indications in various settings, highlighting its growing role and potential for expanded application in clinical practice.
No evidence-based guidelines were identified for the use of TUS in clinical practice.
Abbreviations
ECG
electrocardiogram
SR
systematic review
TUS
teleultrasound
Background
Ultrasonography is a portable and noninvasive imaging method that uses soundwaves to visualize internal organs, structures, and systems within the body in real time. According to the WHO, ultrasound and/or X-ray is sufficient for 80% to 90% of patients that require medical imaging for diagnosis.5 WHO considers ultrasound an essential diagnostic imaging technology, and access to ultrasound has been declared a minimal global standard. However, two-thirds of the world’s population lack access to medical imaging services.1
Ultrasound imaging is a highly operator-dependent imaging modality that requires well-trained professionals to provide accurate diagnostic exams and interpretation of exam images.1,2 The quality of an ultrasound exam varies depending on the sonographer’s experience with operating the equipment, whereas the image quality of CT or MRI exams are less dependent on the operator’s performance.2 As well, ultrasound is much more affordable and portable than CT and MRI and, unlike CT, does not expose patients to radiation.3 As a result, ultrasound is the preferred method for soft tissue imaging in cases in which the higher image quality of CT and MRI is not crucial.3
Access to ultrasound services in rural or underserved regions is often limited by the lack of qualified professionals, appropriate equipment, and insufficient infrastructure or resources.1,5,9 In Canada, less than 28% of rural emergency departments have in-house access to ultrasound, requiring patient transfers to facilities with capacity.4
Ultrasound exams are conducted by imaging professionals, and a shortage of these professionals both in Canada and in many countries worldwide has been reported.10,11 Poor job satisfaction is cited as 1 reason for high turnover rates of these health care professionals.10 As well, recruitment and retention challenges have exacerbated existing staff shortages and contribute to wait times.10,11
Limited access to ultrasound professional expertise has led to the development of TUS, an imaging technique that utilizes advances in information technology and ultrasound to support remote clinical decision-making.2,7 TUS allows for the electronic transmission of ultrasound images from 1 location to another, so images are obtained at a distance from where the interpreting ultrasound professional is located.2,9
TUS is intended to enhance patient care by offering access to specialized expertise, either to complement existing services or to provide care in resource-limited settings. By expanding access to these services, TUS has the potential to improve time to diagnosis, reduce costs for both patients and the health care system, and decrease patient travel time.1,12-14
How Is TUS Delivered?
TUS involves either real-time (synchronous) or asynchronous (“store and forward”) video transmission.5,15
Real-time “supervised” transmission: The ultrasound exam occurs with real-time supervision by an imaging expert, often a radiologist or sonographer. The imaging expert is located in a remote location and provides guidance to an onsite ultrasound operator. In some cases, the imaging expert will remotely perform the exam using robotic ultrasound technology with the assistance of an in-person assistant to help position the equipment. Real-time TUS is often used in emergency settings, where valuable contextual information is needed to aid interpretation and the operator may have limited ultrasound experience.2,16
Asynchronous transmission: The ultrasound images are captured locally, stored, and sent to the remote expert later for review and interpretation. Using this method, individuals with limited or no imaging experience (e.g., medical students, nonimaging health care professionals) can be trained to obtain images of the body using basic scanning protocols, which are sent to the expert without degradation in image quality.2,5,15,17
Purpose of This Review
With rapid advances in diagnostic imaging technology, various TUS systems exist, such as robotic-assisted ultrasound, portable pocket-sized hand-held ultrasound scanners (i.e., point-of-care ultrasound), and AI-integrated solutions.2,14,18,19 TUS systems support decision-making across a wide range of clinical settings, and examinations can be conducted at point-of-care, in emergency or community settings, or in dedicated imaging facilities.
Real-time TUS, which allows the remote expert to be virtually present during the ultrasound scan, has gained greater use with the changing health care landscape, access to new technologies, and its utility for mentoring and training. More recently, the unprecedented demand on the health care system during the COVID-19 pandemic led to the rapid development and use of innovative tools to provide urgently needed ultrasound services in a minimal-contact setting for screening and diagnosing symptoms.35
Real-time TUS can be used by a variety of health care professionals with minimal to no ultrasound training when guided by an imaging professional. However, as the use of real-time TUS continues to expand to different clinical areas, the clinical effectiveness of real-time TUS compared with traditional in-person ultrasound remains uncertain.7,8
The current report aims to provide a summary of the clinical effectiveness of real-time TUS (i.e., synchronous remotely supervised ultrasound) compared with ultrasound delivered using the traditional in-person model. This report also aims to summarize the relevant recommendations from evidence-based guidelines relating to TUS.
Research Questions
What is the comparative effectiveness of real-time TUS (remotely supervised ultrasound) compared with the traditional service model of ultrasound with an in-person imaging specialist insofar as patient care quality, service quality, and access to care are concerned?
What are the evidence-based guidelines regarding the use of TUS in clinical practice?
What are some reported perceived strengths and challenges associated with the use of TUS in clinical practice?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were telemedicine or remote supervision and ultrasound. The search was completed on August 27, 2024, and was limited to English-language documents published since January 1, 2019.
Selection Criteria
One reviewer screened citations and selected studies. In the first level of screening, the titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Articles published before 2019 were excluded due to the rapid timelines for this report and focus on current literature.
Criteria | Description |
|---|---|
Population | Patients seeking ultrasound exams, of any age |
Intervention | Real-time TUS (remotely supervised ultrasound) |
Comparator | Traditional service model (standard ultrasound delivered in-person by an imaging specialist) |
Outcomes | Q1: Clinical effectiveness (e.g., patient care quality, service quality, access to care) Q2: Recommendations related to the appropriate use of TUS in clinical practice Q3: Strengths and challenges associated with the use of TUS in clinical practice |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies with a control group, evidence-based guidelines |
Exclusion criteria |
|
TUS = teleultrasound.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: The Downs and Black checklist20 for primary studies, the A Measurement Tool to Assess Systematic Review 2 (AMSTAR 2)21 for systematic reviews (SRs), and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument22 for guidelines. The strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
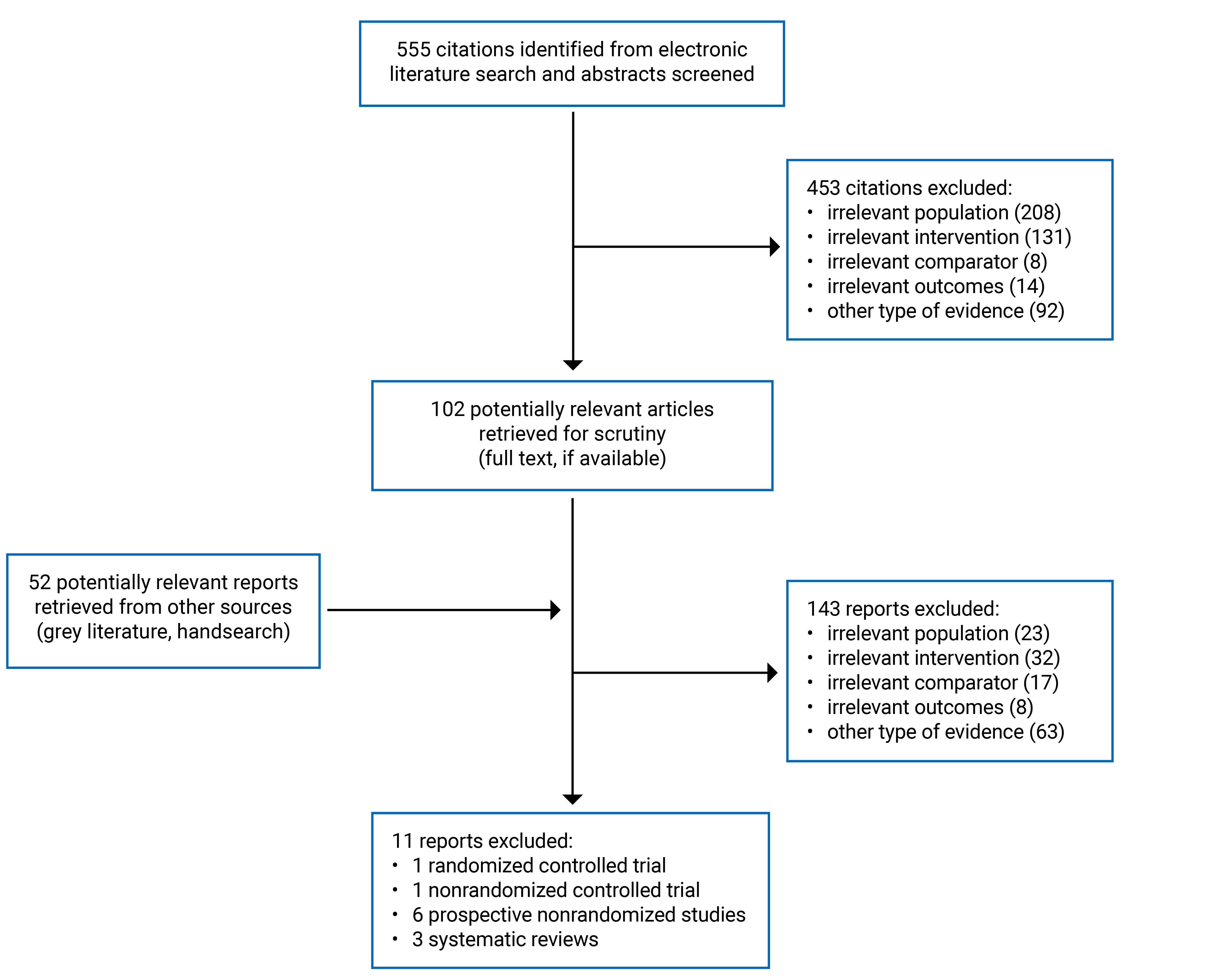
A total of 555 citations from the literature search were identified. Following screening of titles and abstracts, 453 citations were excluded and 102 potentially relevant reports from the electronic search were retrieved for full-text review. Fifty-two potentially relevant publications from the grey literature search were also retrieved. Of these potentially relevant articles, 143 were excluded for various reasons. Overall, 11 publications met the inclusion criteria. These comprised 6 prospective nonrandomized studies, 1 nonrandomized controlled trial, 1 randomized noninferiority trial, and 3 SRs. Appendix 1, Figure 3 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)23 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Eight primary studies and 3 SRs were included in this report, totalling 1,591 participants across 7 countries who underwent TUS or traditional in-person ultrasound.
No relevant evidence-based guidelines for TUS were identified.
Detailed characteristics of the 11 included studies are presented in Table 4 and Table 5 in Appendix 2.
Study Design
Primary Studies and Systematic Reviews
Eight primary studies24-31 (6 prospective nonrandomized studies;1 randomized noninferiority trial; 1 prospective, parallel, nonrandomized controlled trial) were published between 2019 and 2024.
Three SRs9,32,33 were published between 2020 and 2024 and included 4 relevant primary studies published between 1996 and 2017. Only results of the relevant studies from the following SRs are included in the present report:
the SR by Alhussein et al. (2024)32 included 9 publications, of which 1 validation study was relevant to the present report
the SR by Duarte et al. (2021)9 included 10 publications, of which 1 prospective nonrandomized controlled trial was relevant to the present report
the SR by Salerno et al. (2020)33 included 15 publications, of which 2 feasibility studies were relevant to the present report.
Evidence-Based Guidelines
No relevant evidence-based guidelines were identified for TUS.
Country of Origin
The included primary studies were conducted by authors in China, France, Poland, and the US.24-31 The SRs9,32,33 were conducted by authors in Brazil and the US, and the 4 studies included in the SRs originated from France, Norway, and 2 from Korea.
Patient Population
A summary of the patient population and clinical setting are provided in Table 4 (primary studies) and Table 5 (SRs).
The 8 primary studies included 1,337 adult and pediatric participants. All studies compared real-time TUS with conventional ultrasound.
A total of 254 participants from the relevant studies included in the 3 SRs comprised of both adult or pediatric populations who were referred for an electrocardiogram (ECG) or abdominal exam for various reasons.
Interventions and Comparators
The intervention used in all studies included in this report was real-time TUS delivered through various methods:
6 primary24-27,30,31 studies and 1 SR32 reported the use of robotic-assisted TUS
1 study29 reported on the use of a hand-held pocket-sized ECG
1 primary study28 and 2 SRs9,33 reported on the use of real-time telementored ECG.
In all cases, the comparator was the use of conventional in-person ultrasound delivered by a trained imaging professional.
A summary of the intervention, comparator, and operator characteristics are provided in Table 4 (primary studies) and Table 5 (SRs).
Outcomes
The relevant outcomes reported by the included studies are summarized in Table 2.
Table 2: Outcomes Reported by the Included Studies
Type of outcome | Description |
|---|---|
Procedural effectiveness outcomes | |
Care and service quality outcomes |
TUS = teleultrasound.
Real-time TUS was comparable to conventional in-person ultrasound in relation to exam image quality and diagnostic consistency for various types of exams, as determined by expert review. However, real-time TUS exams took significantly longer to complete in most studies, averaging 6 minutes longer.
Patients expressed a high level of satisfaction with real-time TUS regarding comfortability, telecommunication quality, exam duration, and accessibility for various types of exams. However, in some studies where robotic-assisted TUS systems were used, up 10% of patients reported feeling discomfort, pain, or fear, although no serious adverse events were reported.
Clinicians and operators expressed a high level of satisfaction with real-time TUS in terms of the quality of exam images, telecommunication quality, and scan duration. However, some clinicians and operators reported that they experienced physical discomfort with using the system and technical difficulties for a subset of exams.
Three evidence-based guidelines were included in this review to provide clinical guidance on the use of point-of-care ultrasound for central venous catheter insertion in the acute care setting (i.e., emergency department and intensive care unit).
Appendix 3 presents the main study findings by outcome.
Summaries of the outcomes related to procedural effectiveness (i.e., image quality, scan duration, diagnostic consistency) are presented in Figure 1 and Table 6.
Summaries of outcomes related to care and service quality (i.e., safety and complications, patient satisfaction, clinician satisfaction, accessibility) are presented in Figure 2 and Table 7.
Real-Time TUS in Clinical Practice: Procedural Effectiveness
Figure 1: Summary of Findings Related to Procedural Effectiveness
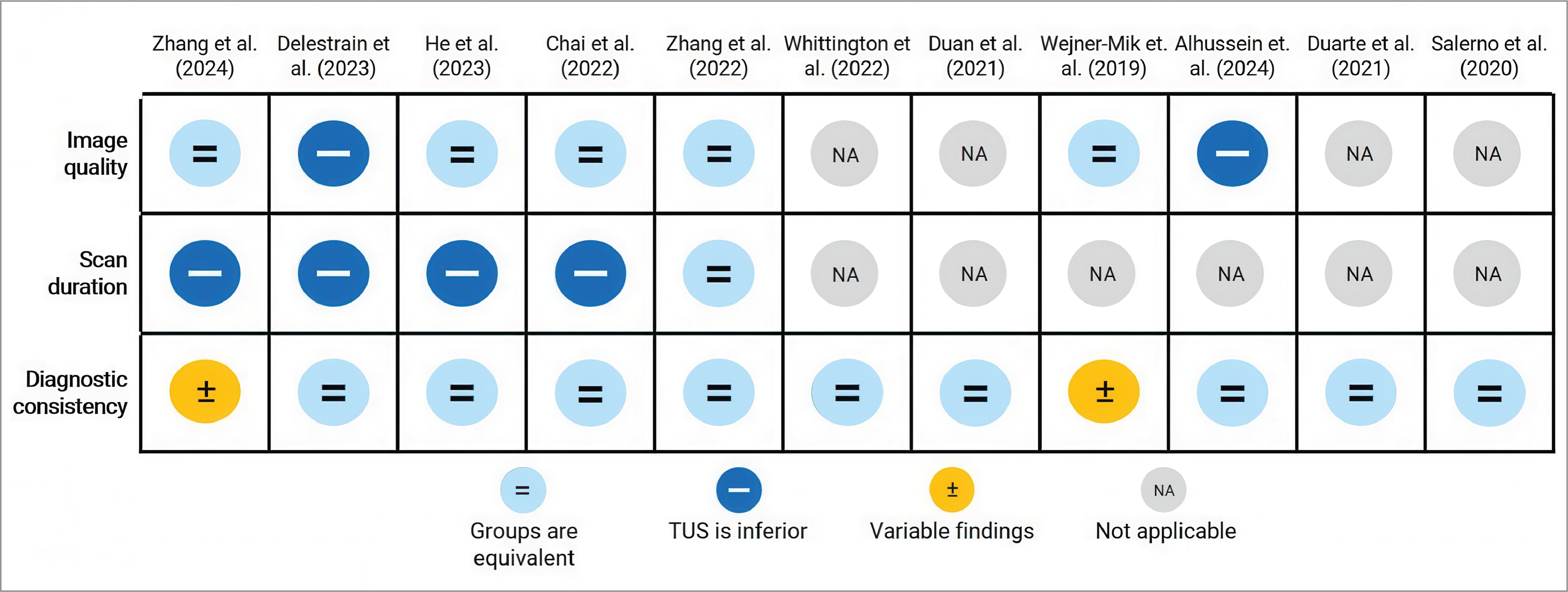
NA = not applicable; TUS = teleultrasound.
Notes: The coloured circles and symbols represent the findings from studies that compared procedure-related outcomes between real-time TUS and conventional ultrasound groups.
Light blue with equal sign = Real-time TUS and conventional ultrasound findings were equivalent or not significantly different (P ≥ 0.05).
Blue with minus sign = TUS was inferior to conventional ultrasound.
Orange with ± sign = Variable findings were reported for the outcome (equivalence and differences between groups).
Grey with NA = The study did not report on this outcome or no comparisons were made between groups.
Exam Image Quality
Overall, the image quality of the ultrasound exams was not statistically significantly different between TUS and conventional ultrasound groups (Table 6). Seven of the 11 studies reported this outcome:
Five24,27,28,30,31 of the 8 primary studies reported that the quality of images obtained for real-time TUS were comparable to images obtained using conventional ultrasound, with no statistically significant differences between groups (P > 0.05).
Delestrain et al. (2023)25 and Alhussein et al. (2024)32 reported that the image quality was significantly higher for the conventional ultrasound group than the TUS group (P < 0.05).
The remaining 2 primary studies26,29 and 2 SRs9,33 either did not report on this outcome or did not report on image quality for the conventional ultrasound group.
Scan Duration
Overall, the mean length of time to complete the ultrasound was statistically significantly longer for the TUS group compared with the conventional ultrasound group (Table 6). Five primary studies24,25,27,30,31 reported this outcome:
The average scan time ranged from 5.6 minutes to 26 minutes for the TUS group, and 5.2 minutes to 13.9 minutes for the conventional ultrasound group. Four studies24,25,27,30 reported significantly longer average scan times for the TUS group compared to the conventional ultrasound group (P < 0.05), while 1 study31 did not find significant differences between groups.
The remaining 3 primary studies26,28,29 and all 3 SRs9,32,33 either did not report on this outcome or did not report on scan duration for the conventional ultrasound group.
Diagnostic Consistency
Overall, TUS and the conventional ultrasound groups did not show statistically significant differences in diagnostic consistency (e.g., agreement, correlation), although the results were mixed (Table 6). This outcome was reported by all 11 studies:
Six primary studies24-27,29,31 and all 3 SRs9,32,33 reported “good” to “excellent” agreement, with similar diagnostic values and no statistically significant differences between the TUS and conventional ultrasound groups.
Two primary studies reported variable findings for diagnostic consistency.28,30 Zhang et al. (2024)30 reported “very good” consistency in the diagnosis of 29 types of disease and most structural measurements between the 2 ultrasound methods. Zhang reported that TUS underestimated the transverse diameter of the kidney compared with conventional ultrasound (P = 0.024 to 0.006). Similarly, Wejner-Mik et al. (2019)28 reported good correlation for cardiac anatomical dimensions and agreement on cardiac abnormalities between groups but reported weaker correlation on the measurement of the right ventricle’s systolic function (r = 0.52; P = 0.0037).
Complications and Safety
Findings related to patient-reported complications and safety were mixed across the 6 primary studies that reported this outcome (Table 7). Reported complications included temporary pain and discomfort during the exam.
Three primary studies reported no injuries,24,27 complications,26 or significant changes in vital signs26 for patients who underwent TUS.
Three other studies25,30,31 reported complications or adverse events relating to robotic-assisted TUS:
Zhang et al. (2024)30 reported that 8.4% of patients experienced mild pain during the abdominal exam.
Zhang et al. (2022)31 reported that 7.2% of patients experienced neck discomfort or temporary suffocation during the thyroid exam.
Delestrain et al. (2023)25 reported that 5.3% of patients reported temporary pain during the exam, although no severe adverse events occurred.
Real-Time TUS in Clinical Practice: Care and Service Quality
Figure 2: Summary of Findings Related to Care and Service Quality
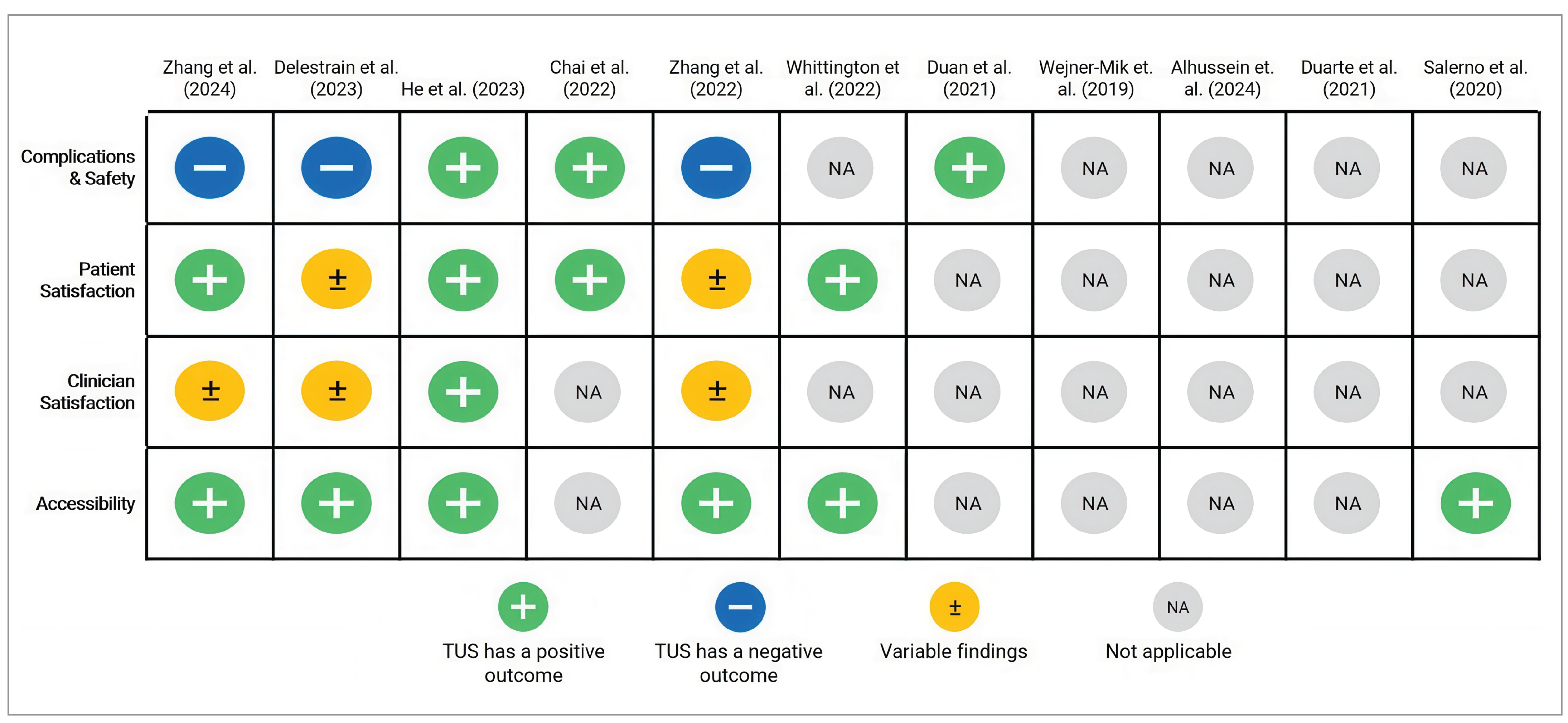
NA = not applicable; TUS = teleultrasound.
Notes: The coloured circles and symbols represent the findings from studies that examined care and service quality–related outcomes for real-time TUS.
Green with plus sign = A positive experience with TUS relating to the outcome of interest was reported.
Blue with minus sign = A negative experience with TUS relating to the outcome of interest was reported.
Orange with ± sign = Variable findings were reported for the outcome of interest.
Grey with NA = The study did not report this outcome.
Patient Satisfaction
Overall, patients indicated a high level of satisfaction with TUS according to several domains captured in self-reported questionnaires, although there were variable findings relating to comfort with TUS (Table 7). Six24,25,27,29-31 of the 11 studies reported this outcome.
Acceptance
In 3 studies27,30,31 that assessed patient acceptance, 85.6% to 95.3% of patients indicated acceptance of the TUS system.
Comfort
In 5 studies24,25,27,30,31 that assessed patient comfort, 90% to 100% of patients indicated no discomfort during the TUS exam or indicated comfort in knowing the robotic TUS device was controlled from elsewhere.
In a study25 that used robotic TUS in a pediatric population, 45% of parents reported that the child felt less pressure with the system compared with conventional ultrasound. Conversely, 16% of parents reported that their child felt increased pressure from the robotic system.
Fear
In 3 studies27,30,31 that assessed patient fear, 89.2% to 96% of patients reported no fear of the robotic TUS system.
Telecommunications
Three studies25,29,30 assessed patient satisfaction with communicating with the TUS sonographer during the TUS exam or during remote consultation or image interpretation after the TUS exam. For each of the 3 studies, more than 90% of patients and parents were either satisfied or comfortable with the remote procedure and consultation.
Scan Duration
In 3 studies27,30,31 that assessed patient satisfaction with TUS exam duration, 85.8% to 94.3% of patients indicated acceptance or satisfaction with the length of time.
Clinician Satisfaction
Overall, both teleclinicians (i.e., teleradiologists, telesonographers) and patient site assistants indicated a high level of satisfaction with real-time TUS, although there were variable findings relating to comfort and technical performance (Table 7). Four25,27,30,31 of the 11 studies reported this outcome.
Comfort
Delestrain et al. (2023)25 assessed comfort levels in the telesonographers’ handling of the remote robotic ultrasound probe and patient site assistants holding the robotic system. The authors reported that 34% of telesonographers experienced more physical strain than conventional ultrasound, and 16% of site assistants experienced significant physical strain.
Exam Satisfaction
In 2 studies30,31 that assessed overall satisfaction with exam quality, 83.3% to 98.6% of exams were considered satisfactory and accepted by the teleclinicians.
Technical Performance
In 3 studies27,30,31 that assessed satisfaction with the technical performance of the TUS system, teleclinicians reported difficulty during 11.8% to 18.1% of exams. Additionally, some telesonologists (a sonographer that provides remote ultrasound services) expressed concern in the scope of scanning of study participants with large breasts.
Telecommunications
In 3 studies27,30,31 that assessed communication quality between the remote and patient sites, telesonographers reported no obvious transmission delays in 84.3% to 97.6% of exams.
In the study by Delestrain et al. (2023),25 98% of telesonographers felt the audio was sufficient to communicate with the site assistants. Similarly, all patient site assistants reported feeling comfortable communicating with the remote sonographer using the TUS system.
Scan Duration
In 3 studies27,30,31 that assessed clinician satisfaction with TUS scan duration, on average, 85.7% of exams (range, 84.9% to 86.7%) were reported as satisfactory in duration by the teleclinicians.
Accessibility
The accessibility of TUS was assessed most frequently by studies that used patient- and clinician-completed questionnaires to examine the following areas: patient willingness to pay for TUS as a service, patient willingness to undergo TUS in the future, and the use of TUS in routine clinical practice (Table 7). Six of the 11 studies reported this outcome:
In 3 studies,27,30,31 87.1% to 90% of patients were willing to pay a certain amount of extra money to undergo TUS by an expert compared with conventional ultrasound.
In the same 3 studies, 88.3% to 100% of teledoctors accepted TUS as a routine ultrasound tool in clinical practice.
Delestrain et al. (2023)25 reported that 87% of parents agreed to the use of TUS in the future for their child.
Whittington et al. (2022)29 found that patient satisfaction with TUS was not significantly associated with age, race, parity, body mass index, rurality, or external referral practice. However, the patient satisfaction analysis was focused on remote exam interpretation following the real-time TUS procedure.
The relevant study included in the SR by Alhussein et al. (2024)32 reported that successful clinical application of TUS used social network video call technology, indicating a free and widely available telecommunication tool can be used for TUS application in clinical practice.
Advantages and Challenges of Teleultrasonography
Some potential advantages and challenges associated with TUS application in clinical practice, as reported and perceived by various authors that reviewed the current literature are summarized in Table 3.12,14,34
Table 3: Potential Strengths and Challenges Associated With Teleultrasonography
Potential strengths | Potential challenges |
|---|---|
Health care system and clinical practice | |
|
|
Technical implementation | |
|
|
TUS = teleultrasound.
Summary of Critical Appraisal
Appendix 4 provides details regarding the strengths and limitations of the included primary studies24-31 (Table 8) and SRs9,32,33 (Table 9).
Primary Studies
The included studies were explicit in terms of reporting the methodological characteristics required for critical appraisal but had several limitations related to the external and internal validity that may reduce the certainty and generalizability of the findings.
For reporting, the authors of all included studies24-31 clearly described the objective of the study, the main outcomes to be measured, the intervention of interest, and the main findings. Most authors reported on the characteristics of the participants,24,26,27,29-31 and the randomized controlled trial compared group differences (i.e., potential confounders) in demographics of the randomized participants. Of the 8 studies, 7 reported adverse events of the intervention and 6 reported patient-related experiences.24,25,27,29-31 The actual P values for the main outcomes were reported in all studies. All the predefined outcomes were relevant and valid and adequately reported.
For external validity, the studies were conducted in both inpatient and outpatient hospital or clinic settings (i.e., hospital, disability care centre, mobile car) located in urban and rural or remote areas, representing high ecological validity. However, TUS can require technological (e.g., 5G internet connectivity, robotic system) and human-related resources that may not be widely accessible and, therefore, not representative of the imaging mode received by most patients in rural or remote settings. Furthermore, the patients included in the studies may not be representative of the entire population from which they were selected, which may limit the generalizability of findings to different settings or patient groups outside the study settings; 7 of the 8 primary studies24-28,30,31 recruited patients from a single centre, and half of the studies24-26,28 had small sample sizes of less than 50 patients.
For internal validity related to bias, there were potential risks of selection, performance, and detection biases because 7 of the 8 studies were not randomized controlled trials by design.24-28,30,31 Four studies reported a lack of operator masking (an unawareness of group assignment).26,28-30 Additionally, 2 studies26,30 that used robotic TUS excluded certain exams due to limitations with the robotic arm, which may have increased the risk of performance and detection bias to favour TUS. Similarly, robotic-assisted TUS was limited to scanning specific organs due to limitations of the robotic probe, which may have resulted in selection and performance bias.24-27,30,31 However, statistical tests were used appropriately, and the main outcome measures were valid and reliable.
For internal validity related to confounding, there were some differences between groups in recruitment strategies and in the experience of operators who performed the procedures. The work experience and clinical expertise of the various teleclinicians and TUS operators differed across the studies, and often the exact level of experience was not reported.24-31 It is possible that lower-skilled teleclinicians and operators could negatively impact procedure-related outcomes. Similarly, each study used a different protocol and length of time to train the teleclinician and operators, particularly with the use of robotic-assisted TUS. Individual differences in learning and mastering the technology may have significantly influenced the interpretation of ultrasound findings.
None of the authors of the included studies identified and adjusted for potential confounding factors in the analyses. None of the authors of the included studies reported whether sample size calculations were performed, leaving it unclear whether any nonsignificant differences in certain outcomes were due to insufficient power in the studies. Similarly, clinical and patient satisfaction assessments were collected only for patients who underwent real-time TUS.25,27,30,31 Satisfaction with service and care quality was not assessed in the conventional ultrasound group; therefore, no direct or statistical comparisons could be made for these outcomes.
Systematic Reviews
Overall, the 3 SRs met a limited number of the AMSTAR 2 criteria, indicating low to moderate quality of the evidence.
The authors of all 3 SRs9,32,33 included components of the PICO (population, intervention, comparison, outcome) process that were clearly defined in research questions and inclusion criteria. The reviews were comprehensive in their search strategies, clearly defined their inclusion criteria and objectives, and included a variety of study designs. The literature search strategy was comprehensive and clearly described in all SRs and it used multiple combinations of keywords, enhancing the reproducibility of the reviews. The authors of 1 SR9 searched the reference lists of the included studies for additional potentially relevant studies. All review authors disclosed the funding sources and potential conflicts of interest but did not report the funding sources or conflicts of interest for the included studies.
One of the 3 SRs33 reported that study selection was performed in duplicate, and it is unclear if data extraction and quality assessment were also conducted in duplicate for any of the SRs. The SRs did not include a list of excluded studies or reasons for study exclusion.
The review authors of all 3 SRs narratively summarized the findings from the included studies, with limited numerical results, thereby reducing the clarity of findings. Alhussein et al. (2024)32 noted that a meta-analysis was not conducted due to the heterogeneity of included study designs. None of the SRs included an assessment of methodological quality or heterogeneity among the included studies.
Limitations
This report is limited by the quantity and quality of research identified that met our inclusion criteria. First, the primary studies and SRs identified are at risk of bias due to several important limitations outlined in the Summary of Critical Appraisal section. Only 4 of the 32 studies in the included SRs were relevant to this report, and all showed low to moderate quality of evidence. Additionally, no evidence-based guidelines concerning the use of TUS in clinical practice were identified.
Second, the literature search was limited to English-language articles and articles published within the past 5 years. Therefore, the strength of the conclusions in this report may be limited by the exclusion of relevant articles published before 2019.
Third, this report was limited by clinical scope, which focused on real-time TUS. Although real-time and asynchronous (“store and forward”) methods of TUS are both widely used, this report did not examine the use of asynchronous TUS and its effectiveness compared with in-person ultrasound.
Finally, 6 of the 8 primary studies examined robotic-assisted real-time TUS, which may limit the generalizability of findings to other types of TUS systems. However, this report includes studies published through the height of the COVID-19 pandemic when remote robotic-assisted TUS systems were proposed for screening or diagnosing COVID-19 symptoms.25 The unprecedented demand on the health care system during that time led to the rapid development and clinical expansion of innovative tools to provide urgently needed ultrasound services in a minimal-contact setting.35 Therefore, it is possible that the high representation of robotic-assisted TUS systems in this report is reflective of the changing landscape of real-time TUS.
Conclusions and Implications for Decision- or Policy-Making
We reviewed the clinical evidence from 8 primary studies (6 prospective nonrandomized controlled trials;1 randomized noninferiority trial; 1 prospective, parallel, controlled nonrandomized trial) and 3 SRs, all comparing real-time TUS systems (i.e., robotic-assisted, pocket hand-held ECG, general) with conventional in-person ultrasound. The role of ultrasound imaging specialists and the scope of practice varies globally, and this review included various imaging professionals (i.e., sonographer, sonologist, radiologist, specialist physician) that reflect the practices relevant to each study’s setting.
The 8 primary studies identified in this report showed high-quality evidence, although most were limited by a single-centre nonrandomized controlled study design and small sample size. The 3 SRs met a limited number of the AMSTAR 2 criteria, showing low to moderate methodological rigour.
Overall, real-time TUS was found to be comparable to conventional in-person ultrasound with regards to diagnostic consistency and exam image quality, and it was well tolerated and accepted by patients and clinicians. However, real-time TUS took, on average, more than 25% (or 6 minutes) longer to complete than in-person ultrasound. For some studies that used robotic-assisted TUS, temporary safety-related complications or discomfort was reported by up to 10% of patients, and technical difficulties occurred in up to 20% of exams. Notably, the included studies performed a wide range of exam types (i.e., abdominal, thyroid, obstetrics, renal, cardiac, pulmonary, and breast exams) and included both comprehensive and point-of-care exams, highlighting the growing role and expanding application of TUS in clinical practice.
To date, most studies report outcomes relating to the technical feasibility and image interpretation of real-time TUS. When there is acceptable variability in population and intervention characteristics, conducting a systematic review with network meta-analysis, when appropriate, may be helpful to understand the relevant differences between real-time TUS and conventional in-person ultrasound.
Considering the current limitations of the body of evidence, future well-controlled larger studies are needed to evaluate care quality beyond feasibility and safety of TUS. This includes examining patient perspectives relating to accessibility (equitable access to services, financial burden) and personal preference and expectations. This may include designing studies that incorporate surveys into both study arms or into the preintervention and postintervention design. Studies that examine the real-world community and health system impact of real-time TUS are also needed to determine the benefit of TUS for increasing access to services and providing timely and accurate diagnoses, particularly in resource-limited settings.
As many real-time TUS devices are more portable and reportedly less expensive and easier to use than traditional ultrasound, they are increasingly available globally. Real-time TUS has been shown to be an effective, accessible, and safe method of imaging patients, which may lead to improved patient outcomes. Other studies have found that TUS is associated with reduced wait times, patient care load, and system-level costs, as well as improved treatment planning and intervention.1,12-14 Studies that evaluate current clinical unmet needs and training programs with well-defined procedural competencies are needed.1,12 Finally, regulations supporting the adoption of real-time TUS in clinical practice and development of data-sharing agreements across different legislative spaces are also needed.12,36
References
1.Adams SJ, Burbridge B, Obaid H, Stoneham G, Babyn P, Mendez I. Telerobotic Sonography for Remote Diagnostic Imaging: Narrative Review of Current Developments and Clinical Applications. J Ultrasound Med. 2021;40(7):1287-1306. PubMed
2.Pian L, Gillman LM, McBeth PB, et al. Potential Use of Remote Telesonography as a Transformational Technology in Underresourced and/or Remote Settings. Emerg Med Int. 2013;2013(1):986160. PubMed
3.Bhide A, Datar S, Stebbins K. Ultrasound Imaging - Cheap, Versatile, and Safe (Working Paper 20-003). Case Histories of Transformational Advances. Boston (MA): Harvard Business School; 2020: https://www.hbs.edu/ris/Publication%20Files/20-003_8157a0c0-71c9-4f6a-88c7-98cba5294123.pdf. Accessed 2024 Oct 17.
4.Micks T, Sue K, Rogers P. Barriers to point-of-care ultrasound use in rural emergency departments. CJEM. 2016;18(6):475-479. PubMed
5.Dowdy DL, Harris RD. Tele-Ultrasound: Meeting Global Imaging Challenges. Applied Radiology. 2024;53(1):38-41.
6.Canada Go. Canadian Occupation Projection System (2022-2031). 2022; https://occupations.esdc.gc.ca/sppc-cops/.4cc.5p.1t.3onsummaryd.2tail@-eng.jsp?tid=116, 2024 Nov 26.
7.Dearing E, Boniface K. Tele-Ultrasound. In: Sikka N, ed. A Practical Guide to Emergency Telehealth. New York (NY): Oxford University Press; 2021.
8.Li XL, Sun YK, Wang Q, et al. Synchronous tele-ultrasonography is helpful for a naive operator to perform high-quality thyroid ultrasound examinations. Ultrasonography. 2022;41(4):650-660. PubMed
9.Duarte ML, Dos Santos LR, Iared W, Peccin MS. Telementored ultrasonography: a narrative review. Sao Paulo Med J. 2022;140(2):310-319. PubMed
10.Executive Summary. Recommendation Report: Diagnostic Medical Sonographers – August 31, 2016. New Westminster (BC): Health Sciences Association of British Columbia; 2016: https://www.hsabc.org/sites/default/files/uploads/Executive%20Summary_1.pdf. Accessed 2024 Oct 8.
11.Strategic Plan 2023-2025. Ottawa (ON): Sonography Canada; 2022: https://sonographycanada.ca/app/uploads/2022/11/Sonography-Canada-Strategic-Plan-2023-2025-Member-version.pdf. Accessed 2024 Oct 8.
12.Barberato SH, Lopes M. Echoes of Telecardiology Guideline. Arq Bras Cardiol. 2020;114(1):130-132. PubMed
13.Hanna TN, Steenburg SD, Rosenkrantz AB, Pyatt RS, Jr., Duszak R, Jr., Friedberg EB. Emerging Challenges and Opportunities in the Evolution of Teleradiology. AJR Am J Roentgenol. 2020;215(6):1411-1416. PubMed
14.Uschnig C, Recker F, Blaivas M, Dong Y, Dietrich CF. Tele-ultrasound in the Era of COVID-19: A Practical Guide. Ultrasound Med Biol. 2022;48(6):965-974. PubMed
15.Chen RJ. Teleultrasound in Remote and Austere Environments. Journal of Mobile Technology in Medicine. 2023;9(1):43-47.
16.Marsh-Feiley G, Eadie L, Wilson P. Telesonography in emergency medicine: A systematic review. PLoS ONE. 2018;13(5):e0194840. PubMed
17.Salerno A, Tupchong K, Verceles AC, McCurdy MT. Point-of-Care Teleultrasound: A Systematic Review. Telemed J E Health. 2020;26(11):1314-1321. PubMed
18.Constantinescu EC, Nicolau C, Săftoiu A. Recent Developments in Tele-Ultrasonography. Curr Health Sci J. 2018;44(2):101-106. PubMed
19.Tenajas R, Miraut D, Illana CI, Alonso-Gonzalez R, Arias-Valcayo F, Herraiz JL. Recent Advances in Artificial Intelligence-Assisted Ultrasound Scanning. Applied Sciences. 2023;13(6):3693.
20.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
21.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
22.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Oct 8.
23.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
24.Chai HH, Ye RZ, Xiong LF, et al. Successful Use of a 5G-Based Robot-Assisted Remote Ultrasound System in a Care Center for Disabled Patients in Rural China. Front Public Health. 2022;10:915071. PubMed
25.Delestrain C, Jung C, Malterre A, et al. Comparison of telerobotic and conventional ultrasonography in children: a crossover bicentric pilot study. Transl Pediatr. 2023;12(5):816-826. PubMed
26.Duan S, Liu L, Chen Y, et al. A 5G-powered robot-assisted teleultrasound diagnostic system in an intensive care unit. Crit Care. 2021;25(1):134. PubMed
27.He T, Pu YY, Zhang YQ, et al. 5G-Based Telerobotic Ultrasound System Improves Access to Breast Examination in Rural and Remote Areas: A Prospective and Two-Scenario Study. Diagnostics (Basel). 2023;13(3):18. PubMed
28.Wejner-Mik P, Teneta A, Jankowski M, et al. Feasibility and clinical utility of real-time tele-echocardiography using personal mobile device-based pocket echocardiograph. Arch Med Sci. 2019;18(4):998-1003. PubMed
29.Whittington JR, Hughes DS, Rabie NZ, et al. Detection of Fetal Anomalies by Remotely Directed and Interpreted Ultrasound (Teleultrasound): A Randomized Noninferiority Trial. Am J Perinatol. 2022;39(2):113-119. PubMed
30.Zhang YQ, Sun LP, He T, et al. A 5G-based telerobotic ultrasound system provides qualified abdominal ultrasound services for patients on a rural island: a prospective and comparative study of 401 patients. Abdom Radiol. 2024;49(3):942-957. PubMed
31.Zhang YQ, Yin HH, He T, Guo LH, Zhao CK, Xu HX. Clinical application of a 5G-based telerobotic ultrasound system for thyroid examination on a rural island: a prospective study. Endocrine. 2022;76(3):620-634. PubMed
32.Alhussein M. Use of Real-Time Remote Tele-mentored Ultrasound Echocardiography for Cardiovascular Disease Diagnosis in Adults: A Systematic Review. Ultrasound Med Biol. 2024;50(6):779-787. PubMed
33.Salerno A, Kuhn D, El Sibai R, Levine AR, McCurdy MT. Real-Time Remote Tele-Mentored Echocardiography: A Systematic Review. Medicina (Kaunas). 2020;56(12):02.
34.Recker F, Höhne E, Damjanovic D, Schäfer VS. Ultrasound in Telemedicine: A Brief Overview. Applied Sciences. 2022;12(3):958.
35.Adams SJ, Burbridge B, Chatterson L, McKinney V, Babyn P, Mendez I. Telerobotic ultrasound to provide obstetrical ultrasound services remotely during the COVID-19 pandemic. J Telemed Telecare. 2022;28(8):568-576. PubMed
36.Villani S, Pana J, Madubuobi H, Browne IL, Kimbrow LA, Reece SCM. Telerobotic Sonography for Remote Diagnostic Imaging. J Ultrasound Med. 2023;42(6):1375-1376. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Characteristics of Included Primary Studies
Study citation, country, funding source | Study design, outcomes | Population characteristics | Intervention and comparator(s) |
|---|---|---|---|
Zhang et al. (2024)30 Country: China Funding source: Various | Prospective non-RCT design Type of ultrasound: Robotic Sample size: 401 Relevant Outcomes:
| Patients scheduled for an abdominal ultrasound examination. Mean age, years ± SD: 54.96 ± 15.43 (range: 12 to 88 years) Sex, %:
| Intervention: 5G-based telerobotic abdominal ultrasound (MGIUS-R3, MGI Tech Co., Ltd., Shenzhen, China). Teleultrasound Operator: Onsite assistant who received training session; tele-radiologist guided. Comparator: Conventional in-person ultrasound with the Wisconic Clover 60. Conventional ultrasound operator: Onsite radiologist with 5 to 15 years of clinical experience in abdominal ultrasound. |
Delestrain et al. (2023)25 Country: France Funding source: Grant from European Space Agency | Prospective interventional crossover design Type of ultrasound: Robotic Sample size: 38 Relevant Outcomes:
| Children aged 1 to 10 years in 2 regional hospitals in the pediatric department, requiring lung, abdominal, or cardiac ultrasound Mean age, years ± SD: 5.7 ± 2.7 | Intervention: MELODY telerobotic ultrasound system Teleultrasound Operator: Pediatric caregivers with specific skills in using the MELODY system with children; expert sonographer guided. Comparator: Conventional in-person ultrasound with the Mindray TE7 system. Traditional ultrasound operator: Senior expert sonographers |
He et al. (2023)27 Country: China Funding source: Various | Prospective non-RCT design Type of ultrasound: Robotic Scenario A: Teleultrasound exam and conventional exam conducted at a rural hospital Scenario B: Teleultrasound exam conducted in mobile car setting in remote setting. Sample size: 83 (Scenario 1: 63; Scenario 2: 20) Relevant Outcomes:
| Patients referred for breast examinations. Mean age, years ± SD:
Sex, %:
| Intervention: 5G based telerobotic ultrasound- MGIUS-R3; MGI Tech Co., Ltd., Shenzhen, China Teleultrasound Operator: Onsite assistant- hospital auxiliary personnel with 1 year experience; expert sonographer guided. Comparator: Conventional in-person ultrasound onsite sonologist with 15 years of experience. Traditional ultrasound operator: Sonologist with 15 years of experience. |
Chai et al. (2022)24 Country: UK Funding source: Zhejiang Medicine Scientific and Technology Project | Prospective non-RCT Type of ultrasound: Robotic Sample size: 49 Relevant Outcomes:
| Adult patients located at a remote long-term care centre requiring abdominal ultrasound. Mean age, years (range): 61 (19 to 91) Sex, %:
| Intervention: 5G-base robot-assisted remote ultrasound Teleultrasound Operator: Sonographers with 5-year experience Comparator: Conventional bedside ultrasound Traditional ultrasound operator: Sonographers with 5 years of experience |
Zhang et al. (2022)31 Country: China Funding source: Various | Prospective, parallel, and controlled study non-RCT design Type of ultrasound: Robotic Sample size: 139 Relevant Outcomes:
| Patients undergoing thyroid ultrasound. Mean age, years ± SD: 58.6 ± 12.7 Sex, %:
| Intervention: 5G-based telerobotic ultrasound (MGIUS-R3, MGI Tech Co., Ltd., Shenzhen, China) Teleultrasound Operator: Onsite assistant who received systematic training session; expert sonographer guided. Comparator: Conventional ultrasound examination with the Wisonic Clover 60 system. Traditional ultrasound operator: Doctor with 15 years of clinical experience in thyroid ultrasound |
Whittington et al. (2022)29 Country: US Funding source: Centers for Disease Control and Prevention National Center on Birth Defects and Developmental Disabilities | Randomized noninferiority study design Type of ultrasound: General Sample size: 585 Relevant Outcomes:
| Women referred to a maternal-fetal medicine clinic to assess fetal abnormalities. Mean age, years ± SD:
Race, %:
No significant differences in demographics between groups. | Intervention: Teleultrasound and telemedicine counselling; remotely directed and interpreted ultrasound (n = 294) Teleultrasound Operator: Registered diagnostic medical sonographers. Comparator: Conventional in-person ultrasound and counselling (n = 291) Traditional ultrasound operator: Registered diagnostic medical sonographers. |
Duan et al. (2021)26 Country: China Funding source: Medical Research Council | Prospective non RCT Type of ultrasound: Robotic Sample size: 32 Relevant Outcomes:
| Patients in the intensive care unit with stable conditions requiring ultrasound to assess for pleural and abdominal effusion. Mean age, years (range): 61 ± 20 (13 to 94)
| Intervention: 5G powered robot-assisted teleultrasound (MGIUS-R3) Teleultrasound operator: Ultrasound physician Comparator: conventional in-person ultrasound Teleultrasound operator: Ultrasound physician |
Wejner-Mik et al. (2019)28 Country: UK Funding source: Medical Research Council | Prospective non RCT Type of ultrasound: Pocket-sized hand-held ECG Sample size: 30 Relevant Outcomes:
| Patients admitted to various hospital departments (i.e., infectious diseases, internal medicine, and cardiology) for TTE. Mean age, years (range): 54 ± 14 (24 to 74) Sex, %:
BMI, kg/m2: 27 ± 6 | Intervention: Inexperienced operator performed focused TTE using Lumify with real-time collaboration with an experienced cardiologist Teleultrasound operator: Either a nurse or 2 students trained in using the device Comparator: Conventional bedside TTE Traditional ultrasound operator: Experienced cardiologist |
BMI = body mass index; ICU = intensive care unit; RCT = randomized controlled trial; RTMUS = real-time telementored echocardiography; SD = standard deviation; SR = systematic review; TTE = transthoracic echocardiographic examination.
Table 5: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study design, outcomes | Population characteristics | Intervention and comparator(s) | Included studies |
|---|---|---|---|---|
Systematic reviews | ||||
Alhussein et al. (2024)32 Country: US Funding source: None | SR of various study designs (i.e., feasibility, evaluation, pilot, experimental) Type of ultrasound: RTMUS Sample size: 30 (from relevant study included) Relevant Outcomes:
| Use of RTMUS in adult population. | Intervention: Various RTMUS modalities Comparator: Various | 1 of 9 studies relevant to present report. Arbille et al. (2014) Intervention: Robotic ultrasound Teleultrasound Operator: Nonsonographer operator; sonographer guided Comparator: Conventional TTE. Traditional ultrasound operator: Sonographer |
Duarte et al. (2021)9 Country: Brazil Funding source: None | SR of various study designs (e.g., prospective, RCT, cohort, cross-sectional) Type of ultrasound: Various but all requiring synchronous transmission and real-time oversight. Sample size: 115 (from relevant study included) Relevant Outcomes: Diagnostic confidence | Use of teleultrasound in various settings with experience ultrasound physician as distant mentor. | Intervention: Various teleultrasound methods Comparator: Various | 1 of 10 studies relevant to present report. Kim et al. (2015) Population: Pediatric cases with suspected acute appendicitis in the emergency department Intervention: Telementored real-time ultrasound with a resident and expert sonographer Teleultrasound operator: Emergency medicine residents; sonographer guided Comparator: Expert-performed conventional ultrasound. Traditional ultrasound operator: Expert |
Salerno et al. (2020)33 Country: US Funding source: None | SR of various study designs (e.g., prospective, RCT, cohort, cross-sectional) Type of ultrasound: Various but all requiring synchronous transmission and real-time oversight. Sample size: 98 (from relevant study included) Relevant Outcomes: Diagnostic confidence | Use of RTMUS in various settings in adults | Intervention: Various teleultrasound methods Comparator: Various | 2 of 15 studies relevant to present report. #1.# Afset et al. (1996) Country: Norway Population: Patients with known or suspected heart disease (n = 38) Intervention: Learner's measurement with real-time remote telementored echocardiography Teleultrasound Operator: learner (inexperienced doctor); sonographer guided Comparator: Expert-performed conventional ultrasound. Traditional ultrasound operator: expert sonographer #2.# Kim et al. (2017) Population: Patients presenting to the ICU and requiring an ECG exam (n = 60). Intervention: Novice sonographer performing ECG with a remote offsite expert. Teleultrasound operator: Novice sonographer; sonographer guided Comparator: Expert-performed conventional ultrasound. Traditional ultrasound operator: onsite cardiologist |
RTMUS = real-time telementored echocardiography; SR = systematic review; TTE = transthoracic echocardiographic examination.
Appendix 3: Main Study Findings
Table 6: Summary of Findings — Procedural Effectiveness–Related Outcomes
Citation study | Primary study | Image quality, score | Mean scan duration, minutes | Diagnostic consistency | ||
|---|---|---|---|---|---|---|
TUS | Conventional ultrasound | TUS | Conventional ultrasound | |||
Primary studies | ||||||
— | Zhang et al. (2024)30 | 4.54 ± 0.63 Each scanned organ was visible in 97.9% of the ultrasound exams using TUS. | 4.57 ± 0.61 P = 0.112 Image quality scores were similar between groups.a | 12.54 ± 3.20b (range 6 to 25) | 7.23 ± 2.10 (range 5 to 16) P = 0.001 TUS took significantly longer than conventional ultrasound.b |
|
— | Delestrain et al. (2023)25 | 18.9 ± 3.6 | 23.1 ± 10.5 P = 0.011 Image quality score was significantly higher for the conventional ultrasound group.c | 26 ± 12.5 (range 18 to 30) | 13.9 ± 11.2 P < 0.0001 TUS took significantly longer than conventional ultrasound. |
|
— | He et al. (2023)27 | 4.86 | 4.90 P = 0.159 Image quality did not differ significantly between groups.e | 10.3 +/− 3.3 (range 5 to 22) | 7.6 +/− 3.0 (range 4 to 16) P = 0.017 TUS took significantly longer than conventional ultrasound. |
|
— | Chai et al. (2022)24 | 4.7g (IQR 4.5 to 5.0) 68.7% images were scored 5/5 | 5g P = 0.176 73.1% of images were scored 5/5 Image quality did not differ significantly between groups.a | 12.2 ± 4.5 (range: 5 to 26) | 7.5 ± 1.8 (range: 5 to 13) P < 0.001 TUS took significantly longer than conventional ultrasound. |
|
— | Zhang et al. (2022)31 | 4.63 ± 0.60 69.8% images were scored 5/5 | 4.65 ± 0.61 P = 0.102 Image quality did not differ significantly between groups.h | 5.57 ± 2.20 (range 2 to 13) | 5.23 ± 2.1 (range 2 to 15) P = 0.164 No significant difference in scan duration between groups. |
|
— | Whittington et al. (2022)29 | — | — | — | — |
|
— | Duan et al. (2021)26 | 4.73a (Expert 1: 4.75 Expert 2: 4.71) 70% images were scored 5/5 | NR | 17 +/− 7b (range 9 to 37) | NR |
|
— | Wejner-Mik et al. (2019)28 | Acceptable image quality sufficient for diagnostic use was obtained in over 70% of patients for all the basic views and showed good correlation with conventional ultrasound.k | — | 12 ± 4 | — |
|
Systematic reviews | ||||||
Alhussein et al. (2024)32 | Arbeille et al. (2014) | Quality of cardiac views was lower than that of the reference | — | — | — |
|
Duarte et al. (2021)9 | Kim et al. (2015) | — | — | — | — |
|
Salerno et al. (2020)33 | Afset et al. (1996) | — | — | — | — |
|
Kim et al. (2017) | — | — | — | — |
| |
ACR TI-RADS = American College of Radiology Thyroid Imaging Reporting and Data System; Bi-RADS = Breast Imaging Reporting and Data System, fTTE = focused transthoracic echocardiographic examination; NPV = negative predictive value; NR = not reported; PPV = positive predictive value; TAPSE = tricuspid annular plane systolic excursion; TTE = transthoracic echocardiographic examination; TUS = teleultrasonography.
Note: This table has not been copy-edited.
aThe subjective quality scoring method (MOS: Mean Opinion Score) was used to score the quality of the transmitted ultrasound images on the basis of an internationally prescribed 5-level absolute evaluation scale (5 points: No deterioration in the image quality is observed at all, very good; 4 points: a change in image quality can be seen but viewing is unhindered, good; 3 points: it can be clearly seen that the image quality has deteriorated, which hinders viewing slightly, fair; 2 points: viewing is hindered, poor; 1 point: viewing is severely hindered, very poor.
bScan duration included diagnosis consultation time.
cThe image quality was qualitatively scored from 1 (very poor) to 5 (excellent), and a visualization score, expressed as a percentage, was calculated with respect to the reference ECG.
dA total lung ultrasound (LUS) score was calculated: 6 lung regions of interest, delineated by a parasternal line, anterior axillary line, posterior axillary line, and paravertebral line, were examined on each side. All regions were characterized, and a score based on aeration from normal (0 score) to complete loss of lung aeration (3 scores) was calculated. The LUS score was calculated as the sum of the 12 regional scores.
eThe scoring was as follows: 1 point: very poor (image quality is severely impaired); 2 points: poor (image quality is impaired); 3 points: fair (image quality hinders viewing slightly but acceptable for interpretation); 4 points: excellent (minor suggestions for improvement but viewing is unhindered); 5 points: perfect (no suggestion for improvement).
fThe ultrasound characteristics and categories of the breast nodules were assessed based on the BI-RADS of the American College of Radiology.
gMedians were reported for image quality scores.
hThe quality of the ultrasound images was scored using a five-point Likert scale (5 points: perfect, no suggestions for improvement of ultrasound image quality; 4 points: excellent, minor suggestions for improvement of ultrasound image quality; 3 points: fair, ultrasound image quality is acceptable for interpretation; 2 points: poor, ultrasound image quality may affect the interpretation; 1 point: meaningless, ultrasound images were not meaningful or undiagnosable).
iThe levels of agreement (kappa) are characterized by Landis and Koch (1977) as slight agreement (0 to 0.20), fair (0.21 to 0.40), moderate (0.41 to 0.60), substantial (0.61 to 0.80), and almost perfect agreement (0.81 to 1.00).
jKappa ≥ 0.75 indicated there was good consistency between the 2; 0.75 > kappa ≥ 0.4 indicated there was general consistency between the 2; kappa < 0.4 indicated poor consistency.
kQuality (the possibility of interpretation) of acquired images was graded as acceptable or unacceptable.
lRight ventricular function was assessed using TAPSE.
Table 7: Summary of Findings — Care and Service Quality–Related Outcomes
Citation study | Primary study | Complications/safety | Patient satisfaction | Clinician satisfaction | Accessibility |
|---|---|---|---|---|---|
Primary studies | |||||
— | Zhang et al. (2024)30 |
|
|
|
|
— | Delestrain et al. (2023)25 |
|
|
|
|
— | He et al. (2023)27 |
|
|
|
|
— | Chai et al. (2022)24 |
|
| — | — |
— | Zhang et al. (2022)31 |
|
|
|
|
— | Whittington et al. (2022)29 | — |
| — |
|
— | Duan et al. (2021)26 |
| — | — | — |
— | Wejner-Mik et al. (2019)28 | — | — | — | — |
Systematic Reviews | |||||
Alhussein et al. (2024)32 | Arbeille et al. (2014) | — | — | — | — |
Duarte et al. (2021)9 | Kim et al. (2015) | — | — | — | — |
Salerno et al. (2020)33 | Afset et al. (1996) | — | — | — | — |
Kim et al. (2017) | — | — | — |
| |
TUS = teleultrasonography.
Note: This table has not been copy-edited.
Appendix 4: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 8: Strengths and Limitations of the Included Primary Studies Using the Downs and Black Checklist20
Strengths | Limitations |
|---|---|
Zhang et al. (2024)30 | |
|
|
Delestrain et al. (2023)25 | |
|
|
He et al. (2023)27 | |
|
|
Chai et al. (2022)24 | |
|
|
Zhang et al. (2022)31 | |
|
|
Whittington et al. (2022)29 | |
|
|
Duan et al. (2021)26 | |
|
|
Wejner-Mik et al. (2019)28 | |
|
|
BMI = body mass index; ICU = intensive care unit; IQR = interquartile range.
Table 9: Strengths and Limitations of the Included Systematic Reviews Using AMSTAR 221
Strengths | Limitations |
|---|---|
Alhussein et al. (2024)32 | |
|
|
Duarte et al. (2021)9 | |
|
|
Salerno et al. (2022)33 | |
|
|
SR = systematic review.
Appendix 5: References of Potential Interest
Please note that this appendix has not been copy-edited.
This is a list of studies from the literature search that were excluded from this report but may be of interest to decision-makers working in the field of TUS.
Primary Articles
Jensen SH, Weile J, Aagaard R, et al. Remote real-time supervision via tele-ultrasound in focused cardiac ultrasound: A single-blinded cluster randomized controlled trial. Acta Anaesthesiol Scand. 2019;63(3):403-409. PubMed
Kaneko T, Kagiyama N, Nakamura Y, et al. Effectiveness of real-time tele-ultrasound for echocardiography in resource-limited medical teams. J Echocardiogr. 2022;20(1):16-23. PubMed
Kory PD, Pellecchia CM, Shiloh AL, Mayo PH, DiBello C, Koenig S. Accuracy of ultrasonography performed by critical care physicians for the diagnosis of DVT. Chest. 2011;139(3):538-542. PubMed
Li XL, Sun YK, Wang Q, et al. Synchronous tele-ultrasonography is helpful for a naive operator to perform high-quality thyroid ultrasound examinations. Ultrasonography. 2022;41(4):650-660. PubMed
Liu L, Duan S, Zhang Y, Wu Y, Zhang L. Initial Experience of the Synchronized, Real-Time, Interactive, Remote Transthoracic Echocardiogram Consultation System in Rural China: Longitudinal Observational Study. JMIR Med Inform. 2019;7(3):e14248. PubMed
Olivieri PP, Verceles AC, Hurley JM, Zubrow MT, Jeudy J, McCurdy MT. A Pilot Study of Ultrasonography-Naive Operators' Ability to Use Tele-Ultrasonography to Assess the Heart and Lung. J Intensive Care Med. 2020;35(7):672-678. PubMed
Siu M, Dan J, Cohen J, et al. Impact of Telemedicine on Extended Focused Assessment With Sonography for Trauma Performance and Workload by Critical Care Transport Personnel. Air Med J. 2023;42(2):105-109. PubMed
Sun YK, Li XL, Wang Q, et al. Improving the quality of breast ultrasound examination performed by inexperienced ultrasound doctors with synchronous tele-ultrasound: a prospective, parallel controlled trial. Ultrasonography. 2022;41(2):307-316. PubMed
Reviews
Adams SJ, Burbridge B, Obaid H, Stoneham G, Babyn P, Mendez I. Telerobotic Sonography for Remote Diagnostic Imaging: Narrative Review of Current Developments and Clinical Applications. J Ultrasound Med. 2021;40(7):1287-1306. PubMed
Salerno A, Tupchong K, Verceles AC, McCurdy MT. Point-of-Care Teleultrasound: A Systematic Review. Telemed J E Health. 2020;26(11):1314-1321. PubMed
Shi R, Rosario J. Paramedic-Performed Prehospital Tele-Ultrasound: A Powerful Technology or an Impractical Endeavor? A Scoping Review. Prehospital Disaster Med. 2023;38(5):645-653. PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.