Drugs, Health Technologies, Health Systems
Health Technology Review
Optimizing Hospital Diagnostic Ultrasound Scheduling: A Brief Survey
Key Messages
Diagnostic imaging departments in general hospitals located in rural or remote settings experience unique examination demands and challenges compared to their urban counterparts. To gain insight into their scheduling methods and strategies used to optimize capacity for diagnostic ultrasound, a brief survey was developed targeting these facilities.
Various administrative, human resource, and booking related strategies have been implemented to optimize ultrasound scheduling. The effectiveness of these strategies is dependent on the unique characteristics and capacity of each hospital.
All survey respondents indicated that their diagnostic imaging department’s ultrasound booking templates incorporate dedicated time for prioritizing emergency, urgent, and inpatient examination requests. About 25% of ultrasound examinations per day are reserved for emergency or urgent bookings.
Most diagnostic imaging departments have established systems to prioritize ultrasound examinations. These systems may involve consultations with the radiologist, and prioritizing patients requiring emergency care, patients travelling from out of town, or those with complex needs.
Each week, a median of 25% of patients travel from out of town for their diagnostic ultrasound appointments. This means that out of all the hospitals, one-half reported more than 25% of patients were from out of town, and one-half reported less than 25% of patients were from out of town. However, in some hospitals as many as 85% of patients came from out of town.
Most examination requests received by the diagnostic imaging department come from referring primary care practitioners. Less commonly, individuals may contact the imaging department directly to schedule appointments, or primary care practitioners may use the hospital’s central intake office.
The most common methods for scheduling appointments include individual time slot booking, block booking, and clustering appointments based on examination type or duration.
Context
Canada’s Drug Agency (CDA-AMC) received a request related to diagnostic ultrasound booking scheduling processes in general hospitals located in small-to-medium–sized population centres. Diagnostic ultrasound is a noninvasive imaging method that uses soundwaves to visualize internal organs, structures, and systems within the body in real time.1-3 Ultrasound plays an integral role in the clinical management of patients in Canada, facilitating the diagnosis of medical conditions and treatment planning. Ultrasound examinations are primarily conducted by sonographers (ultrasound technicians) in various settings within hospitals and clinics.4
A current labour shortage in medical sonographers in Canada has been exacerbated by a number of factors, such as the increasing volume and complexity of ultrasound examinations, as well as an increasing demand for services to support an aging population.5 On average, a sonographer may complete 11.25 examinations (range, 9 to 14 examinations) during an 8-hour shift in Canada.6 Increased sonographer workload demands have been linked to worsening mental and physical well-being and work-related injuries, and consequently, increased staff turnover rates that impact timely patient access to imaging services.7-11
General hospitals (acute care) located in small-to-medium–sized population centres (less than 100,000 people)12 experience unique examination scheduling and workload demands and challenges compared to large urban centres, often operating with less resources and expertise.13,14 Less than 28% of rural emergency departments have inhouse access to ultrasound imaging, requiring patient transfers to facilities with capacity.15 The limited availability of imaging resources and qualified professionals in these areas can affect examination scheduling and workload capacity. With a smaller workforce in these areas, sonographer workloads may increase as wait times increase.9,10,16
As jurisdictions consider enhancing ultrasound imaging capacity to accommodate the increased demand for these services, decision-makers may be interested in different types of scheduling systems that may help to enhance operational efficiencies, improve patient care, optimize resource allocation, and support the physical and mental well-being of sonographers.
Objective
The purpose of this report is to summarize ultrasound scheduling practices at hospitals located in small-to-medium–sized population centres in Canada, and to provide information on booking strategies used to manage examination workload.
Methods
A brief survey consisting of 10 multiple choice and open-ended questions was sent to contacts located at hospital diagnostic imaging departments across Canada. Contacts were asked to provide information on ultrasound scheduling practices.
Contacts were identified using the Canadian Medical Imaging Inventory’s network of more than 450 hospitals across all provinces and territories, and included self-reported data collected at advanced imaging facilities in Canada. A total of 119 facilities were screened for inclusion and included on a short list if the following criteria were met:
the facility is a general hospital
the facility operates in either a rural or remote setting (according to self-report) and is in a population centre with less than 50,000 people. A threshold of 50,000 was applied for comparability with the requesting hospital.
Hospitals that provide specialized care (e.g., tertiary and quaternary centres) were excluded, as were hospitals located in urban centres with populations of 50,000 or more. Contacts located in Quebec were not included on the short list, based on the rapid timelines for this report which did not allow for translation services.
Seventy-five hospitals met the inclusion criteria. To estimate the number of contacts needed to achieve the target 10 responses, as defined by the requestor, a 30% response rate was used, which represents the standard email-based survey response rate reported in the literature.17 After site randomization, 50 hospitals were selected, and 42 contacts were invited to participate. In some instances, the survey was sent to a single jurisdictional contact, who distributed the survey to hospitals that met the inclusion criteria. The requester was invited to contribute data to this report for jurisdictional representation. Therefore, the survey was sent to 43 contacts across 12 provinces and territories on August 7, 2024, and responses were collected until September 12, 2024. The survey questions are included in Appendix 1.
Results
Imaging Facility Overview
Participating Facilities
A total of 13 of 43 hospitals (30.2%) located in 4 provinces and all 3 territories volunteered information on their ultrasound scheduling practices. One survey respondent answered on behalf of a network of hospitals.
Overall, approximately 70% (9 of 13) of responding contacts were located in British Columbia, Alberta, and Ontario, and the remaining 30% (4 of 13) were located in Manitoba, the Northwest Territories, Nunavut, and Yukon. The number of hospital contacts that participated in the survey are presented in Figure 1.
Figure 1: Location of Participating Hospital Respondents
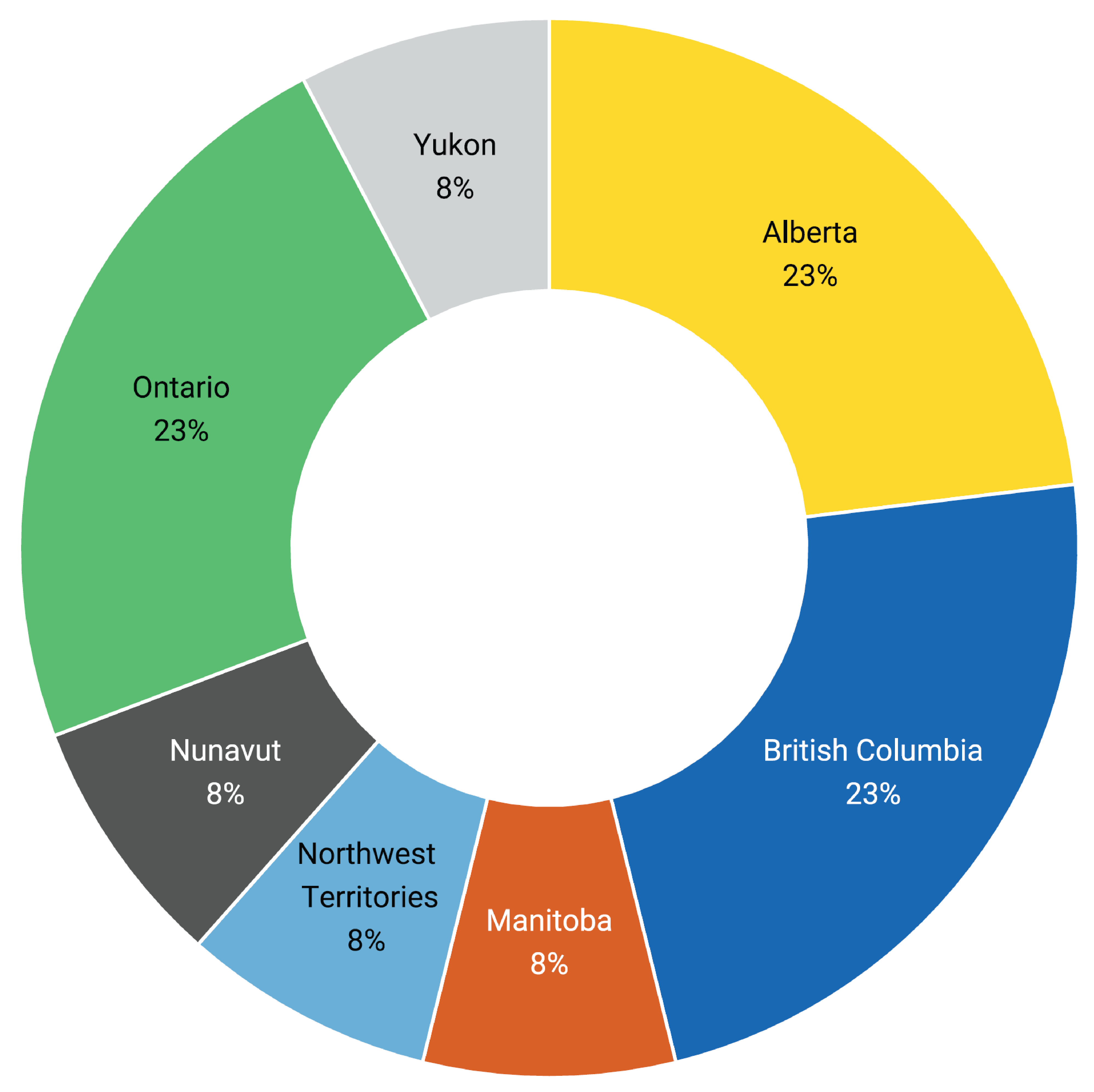
Note: Data are from 13 respondents located across 7 provinces and territories: Alberta (3 respondents), British Columbia (3 respondents), Manitoba (1 respondent), the Northwest Territories (1 respondent), Nunavut (1 respondent), Ontario (3 respondents), and Yukon (1 respondent).
Ultrasound Services Offered
All 13 survey respondents reported that general ultrasound services were provided, which included examinations of the abdomen, pelvis, peripheral veins, superficial structures, and obstetrics.
Four of 13 survey respondents indicated that dedicated ultrasound equipment was used to conduct vascular or cardiac examinations.
Four of 13 survey respondents reported the use of ultrasound equipment for other types of examinations, such as breast and inpatient transthoracic echocardiogram.
Patients Travelling From Out of Town
Survey respondents were asked to provide information on the percentage of individuals, in an average week, that travel from out of town for an ultrasound appointment. A total of 11 of 13 respondents provided information for this question.
A median of 25% of individuals were reported to travel from out of town each week. There was a broad range of responses (2% to 85%) to this question, suggesting differences in the types of populations served among the included hospitals, with 1 respondent commenting that air travel is common.
A total of 11 of the 13 respondents provided a response to this question and the distribution of responses are presented in Figure 2. One respondent, who reported on behalf of a network of hospitals, indicated that large examination volumes are conducted for patients who travelled from out of town and that a percentage could not be provided due to high geographic variability among hospitals.
Figure 2: Percentage of Weekly Examinations Scheduled for Patients Travelling From Out of Town, Distributed by Respondent
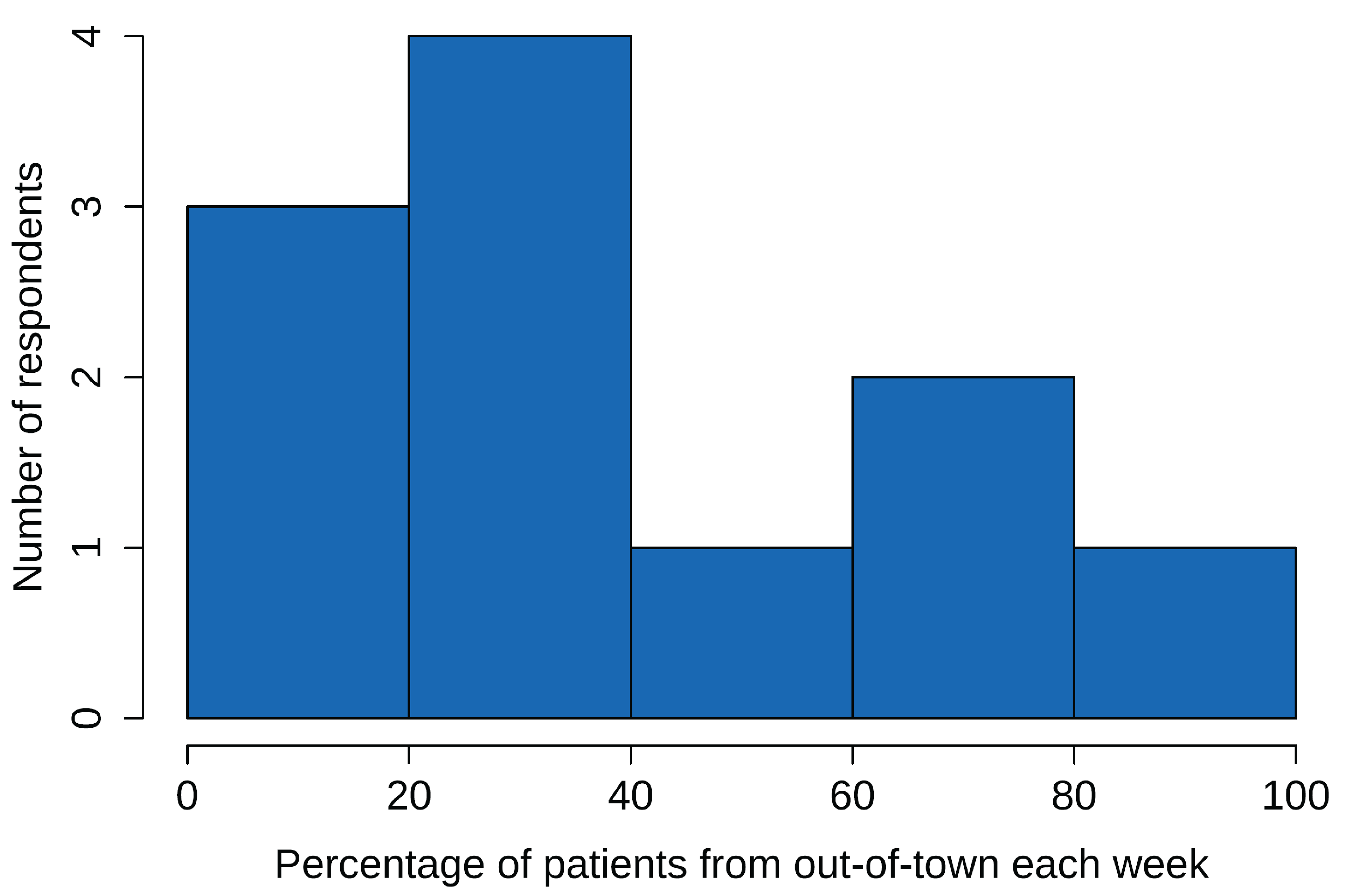
Notes: Data available for 11 of the 13 respondents.
No single definition was provided to respondents for out of town to allow for flexible responses.
Receiving Examination Requisitions
Survey respondents were asked to report how ultrasound examination requisitions are received by the hospital’s diagnostic imaging department. Figure 3 presents the methods through which ultrasound examination requisitions are submitted.
All 13 respondents indicated that a referring primary care practitioner sends examination requisitions to the diagnostic imaging department by fax, telephone, or computerized order entry.
Two of 13 survey respondents indicated that patients may also call the department directly to schedule an appointment. At another hospital the referring primary care practitioner may use the hospital’s central intake booking service to submit the requisition.
Figure 3: Methods of Receiving Ultrasound Examination Requisitions by Diagnostic Imaging Departments, Reported by Percentage
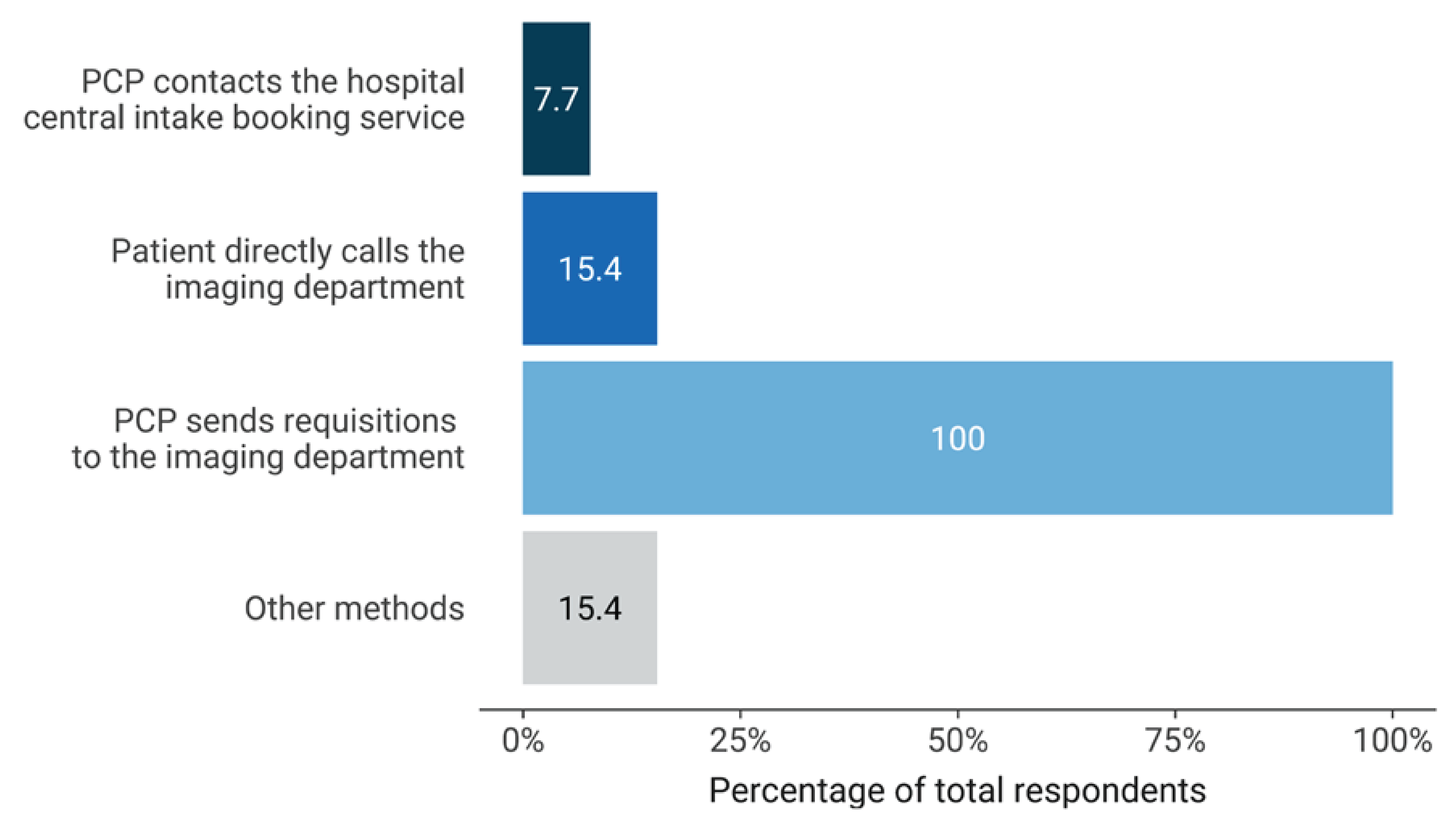
PCP = primary care practitioner.
Note: Data available for all 13 respondents.
Scheduling Examination Methods
Eleven of 13 survey respondents reported the use of a site-specific scheduling tool to book patient ultrasound examinations in the hospital diagnostic imaging department.
Booking Model
Survey respondents were asked to provide information relating to the specific booking model used to schedule ultrasound examinations to manage patient flow. Respondents were asked to choose from any of the following common booking models (Figure 4):
block of time (i.e., blocks of 15-minute bookings, appointment time adjusted for the examination being performed)
clustering (i.e., patients with similar needs are scheduled for a specific time slot)
open booking (a flexible window of time where a patient can attend their appointment, e.g., booking window: anytime between 2 p.m. and 4 p.m.)
time slot (i.e., patient is provided with a dedicated time slot)
other (respondent to specify).
The use of dedicated time slots was the most reported method for scheduling ultrasound examination appointments, reported by 11 of the 13 survey respondents. This was followed by the block of time model, reported by 4 of the 13 survey respondents, and clustering, reported by 1 respondent. Respondents did not specify any other method.
Figure 4: Type of Booking Models Used for Scheduling Ultrasound Examinations by Percentage
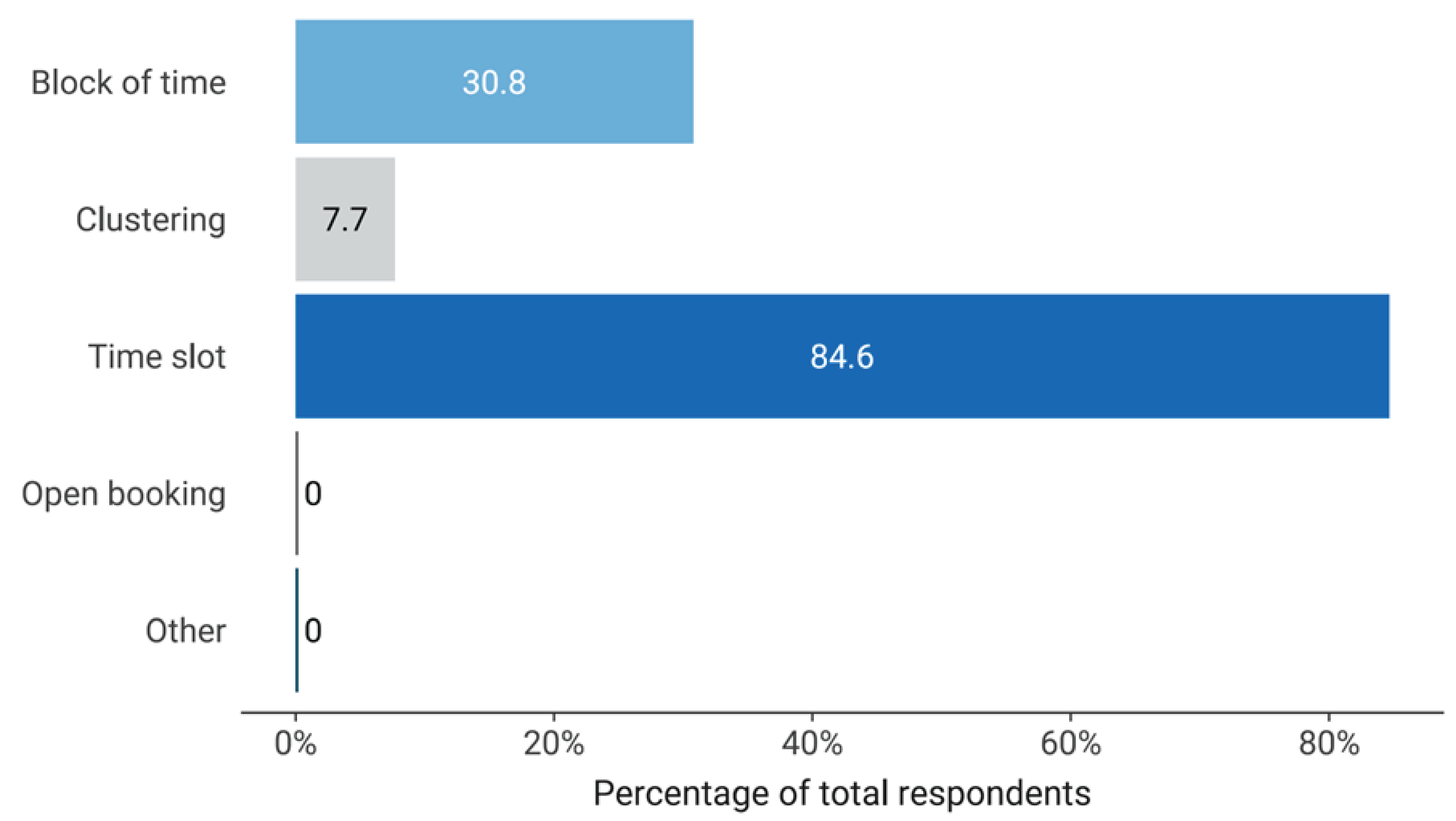
Note: Data available for all 13 respondents.
Prioritizing Examination Bookings
The hospital diagnostic imaging department oversees the diverse ultrasound imaging needs of the facility, including inpatient, emergency, specialist clinics, outpatient services, and patient follow-up. Respondents were invited to share their insights on how ultrasound examinations are prioritized.
All 13 respondents indicated that the diagnostic imaging department reserved appointment slots each day to accommodate emergency or urgent bookings.
A median of 25% of ultrasound examination slots were reported to be reserved for emergency or urgent bookings each day, as reported by 9 respondents across 6 provinces and territories. One respondent indicated that 2 slots are reserved for emergency ultrasound examinations each day.
Eleven of 13 survey respondents reported that the diagnostic imaging department has a system in place to assist with the prioritization or triaging of ultrasound examinations, to balance examination demands with patient priority.
Factors That Influence Scheduling Priorities
Survey respondents were asked to identify factors that the diagnostic imaging department considers when determining the scheduling priority of an ultrasound examination. Responses were received from 11 of the 13 respondents (Figure 5):
Nine of 11 survey respondents reported that examination requisitions received from the emergency or inpatient departments of the hospital are prioritized.
Seven of 11 survey respondents reported that the radiologist may prioritize an examination.
Six of 11 survey respondents reported that examinations are prioritized for patients travelling from out of town.
Three of 11 survey respondents indicated that examinations are prioritized for either inpatients or outpatients with medically complex conditions that require diagnostic imaging.
Figure 5: Considerations for Prioritizing Ultrasound Examination Scheduling by Percentage
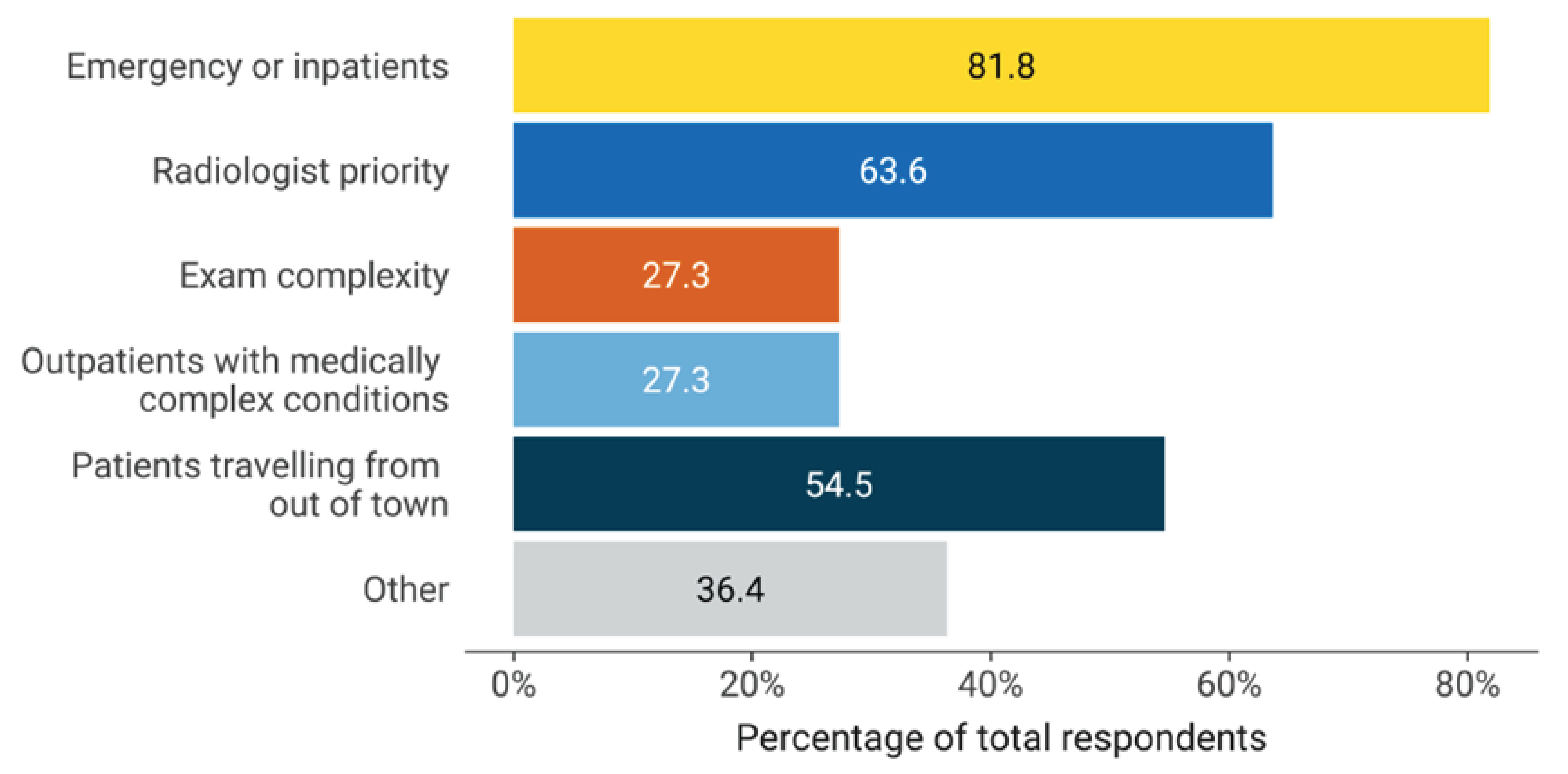
Note: Data available for 11 of the 13 respondents.
Additionally, 4 of the 11 respondents indicated that other factors or resources are used to guide ultrasound prioritization. For instance, 2 respondents reported that an examination may be prioritized if flagged as an urgent request or when ideal imaging timelines are provided by the referring primary care practitioner. Two respondents referenced jurisdictional ultrasound prioritization guidelines.
Templates for Scheduling Examinations
All 13 respondents reported that the imaging department uses a booking template to schedule ultrasound examinations throughout the day.
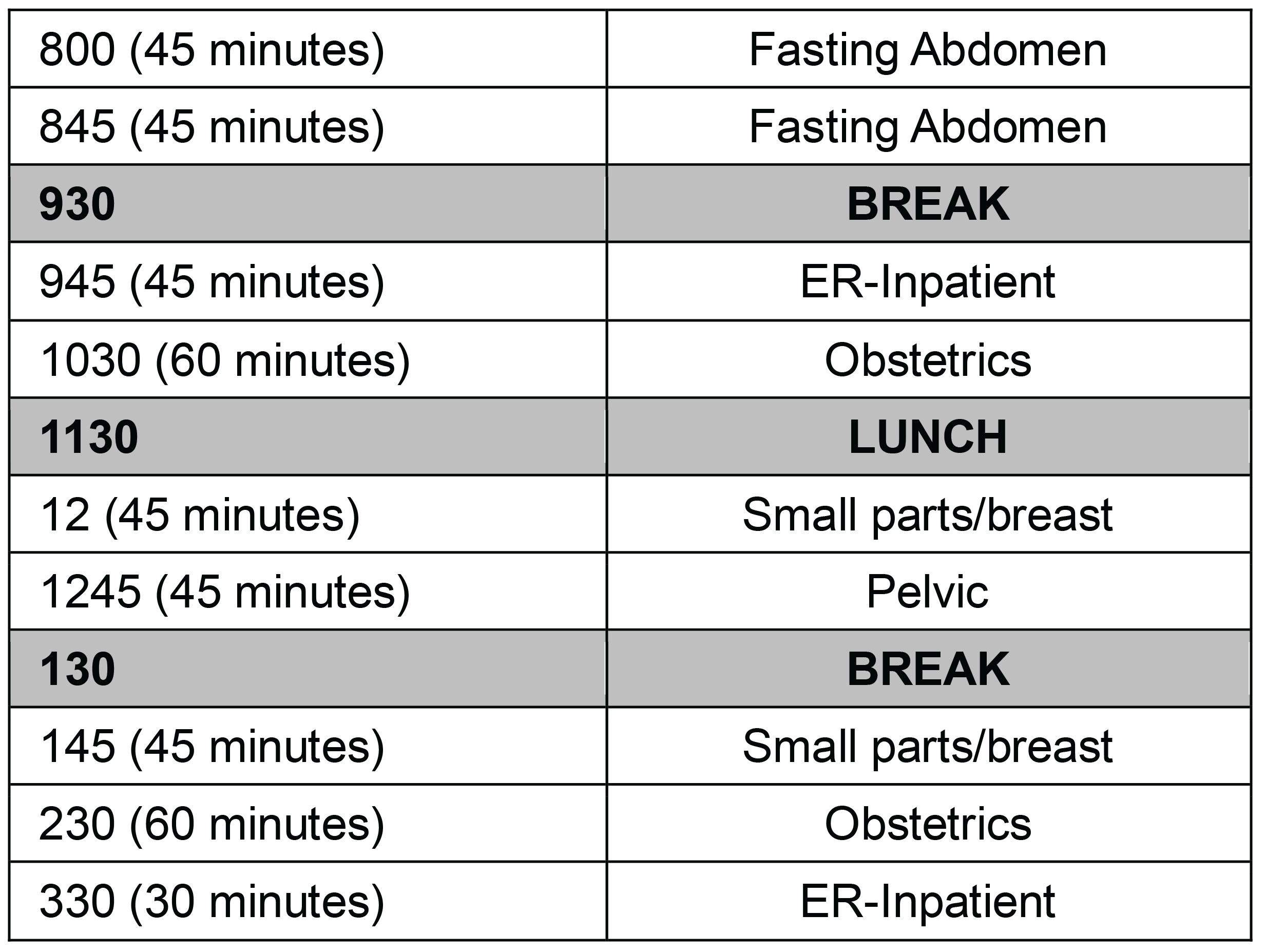
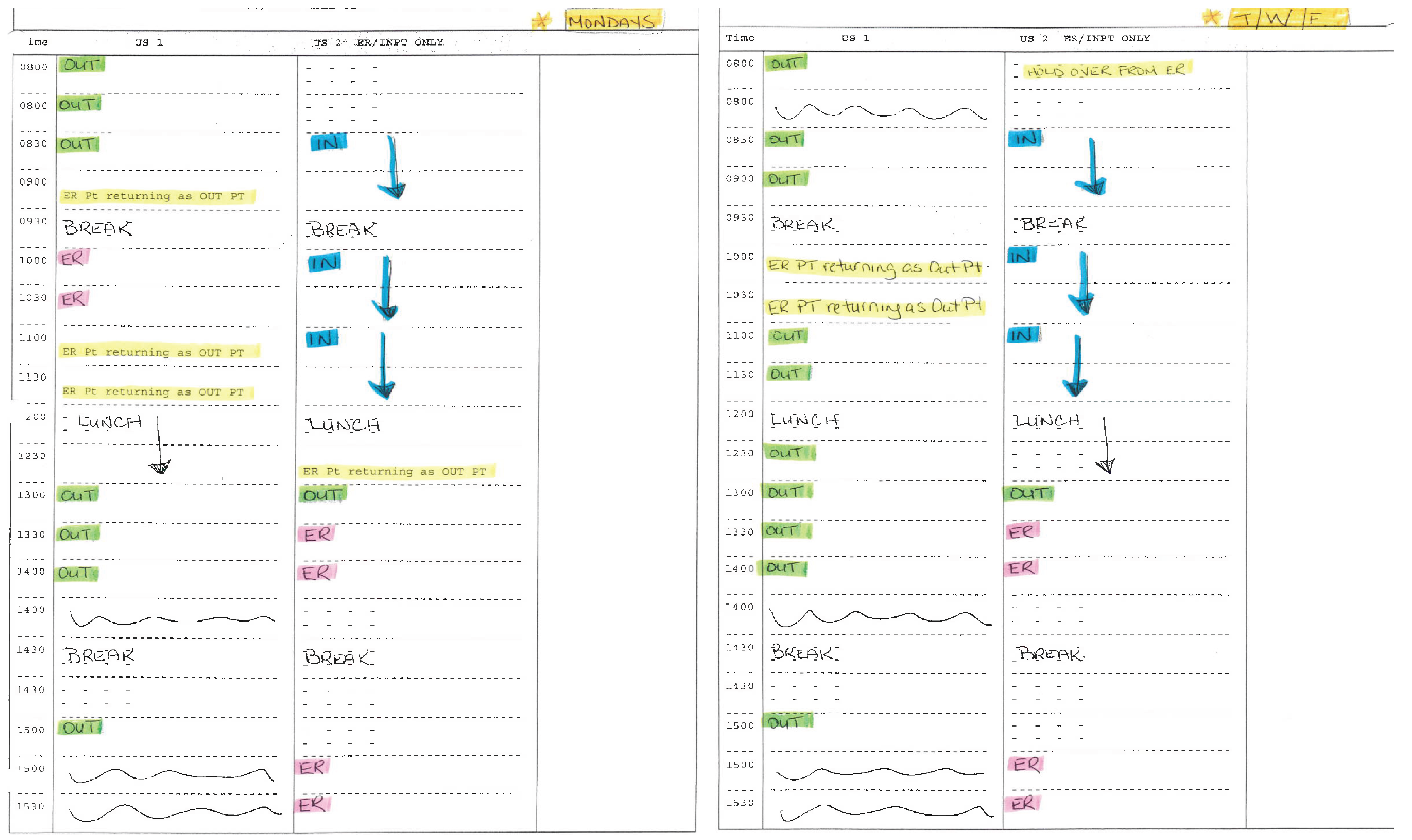
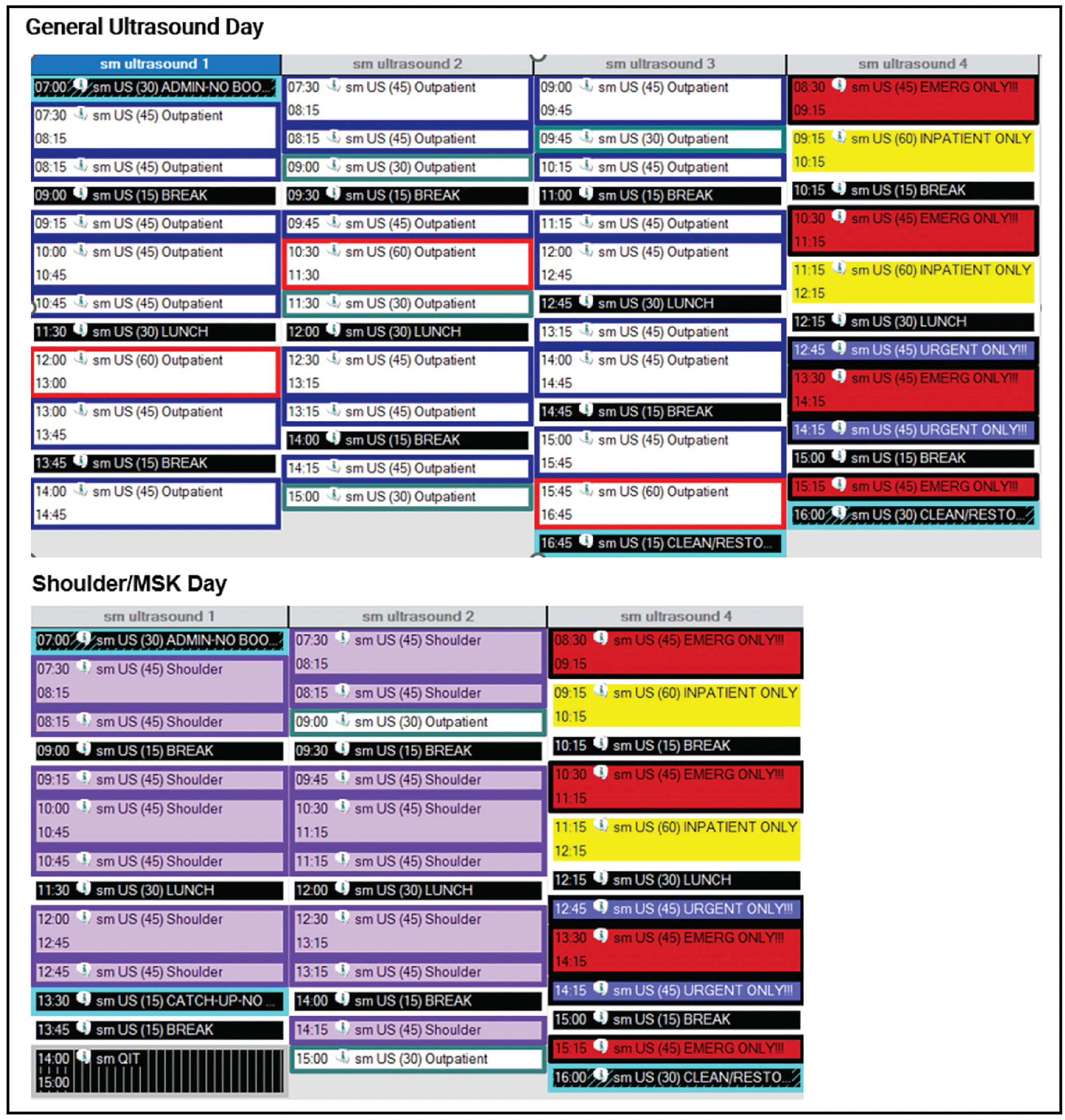
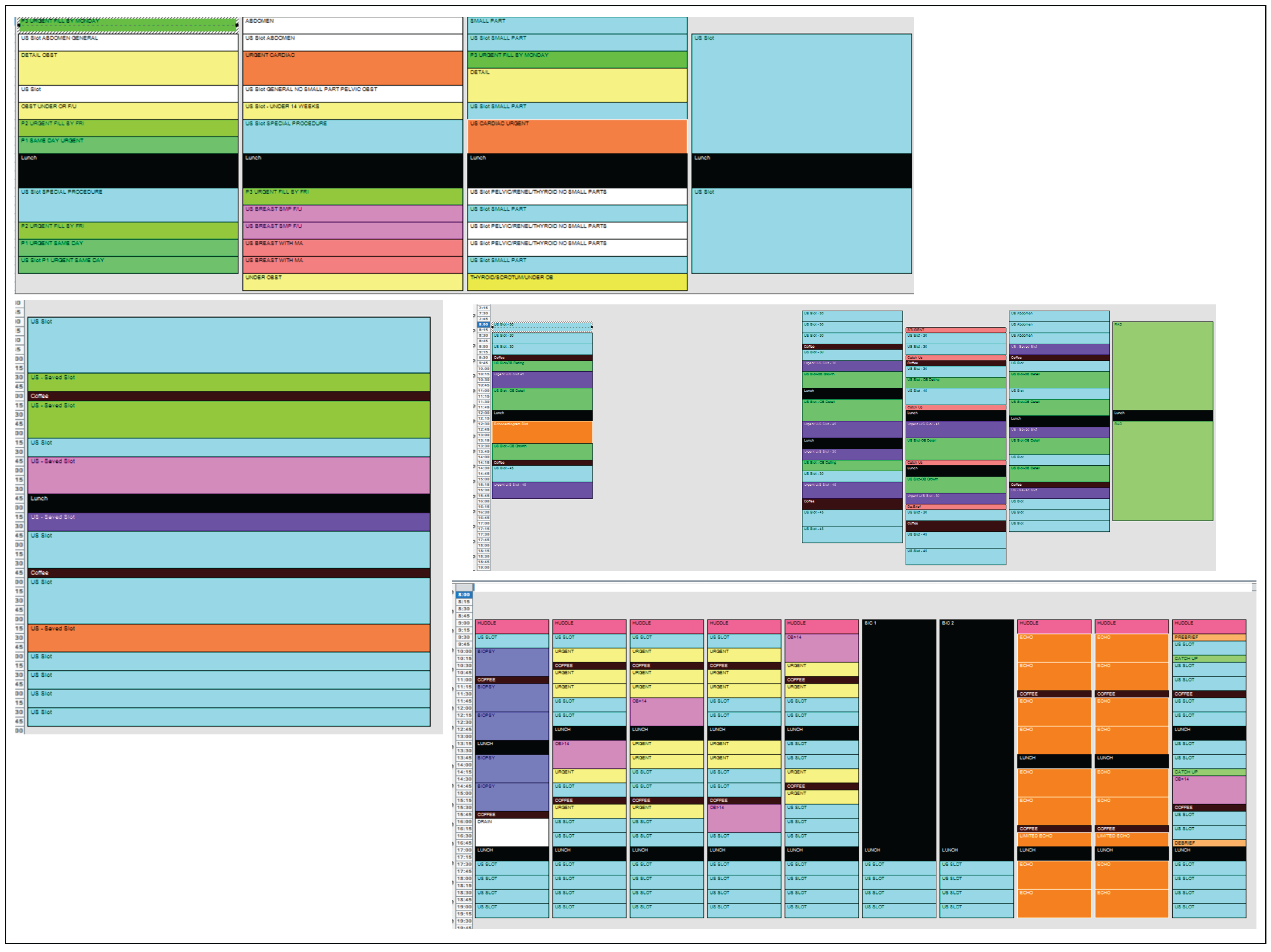
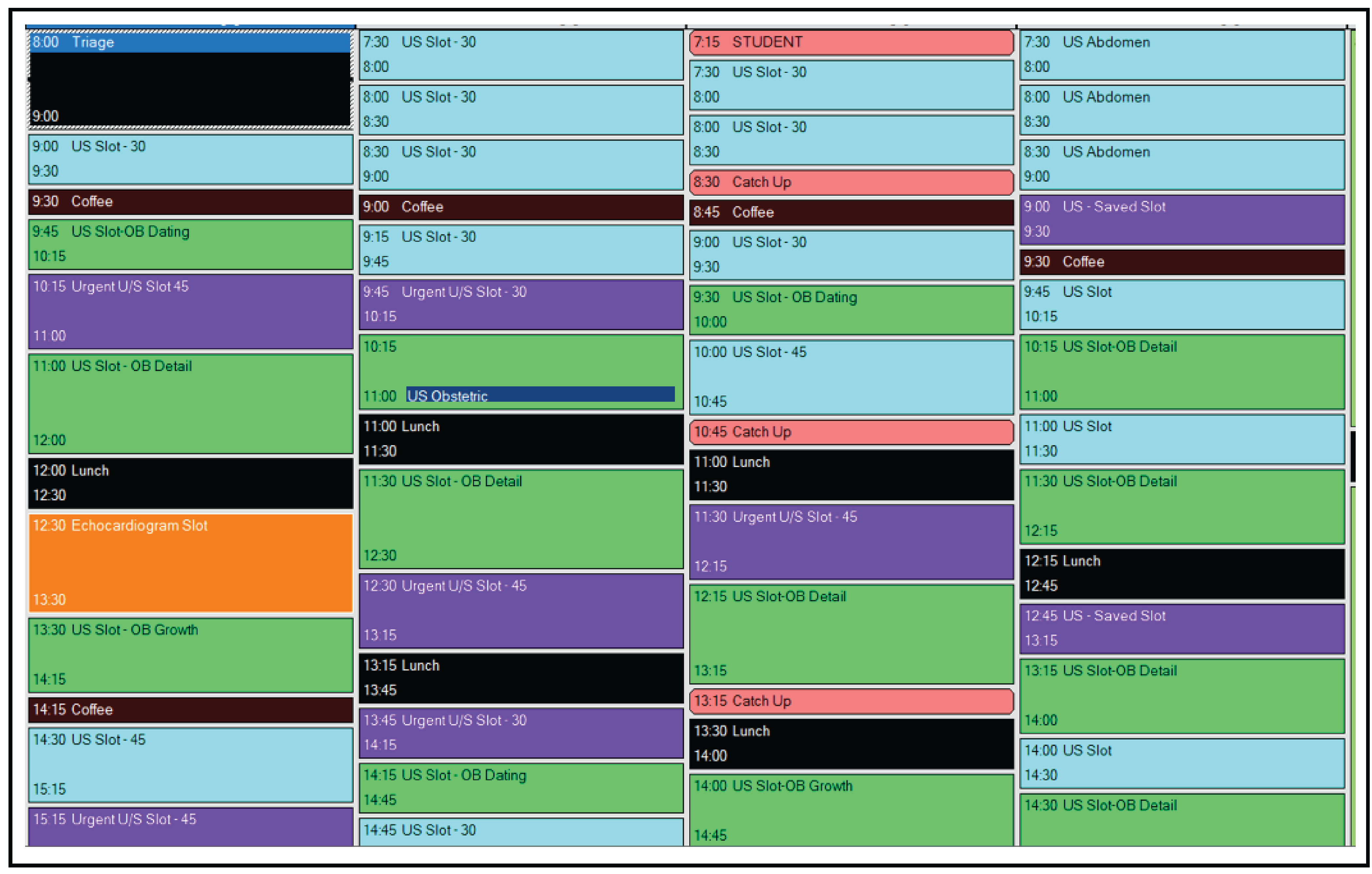
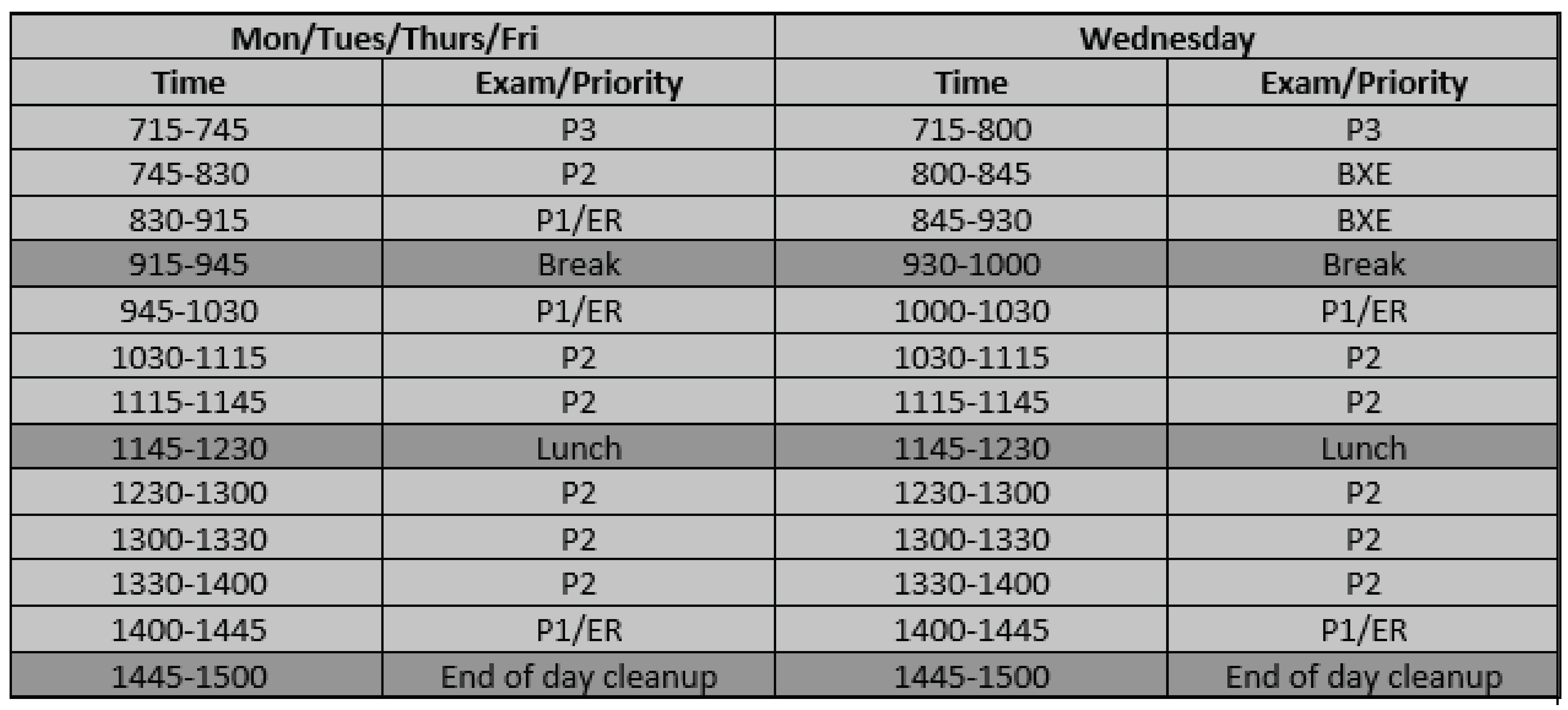
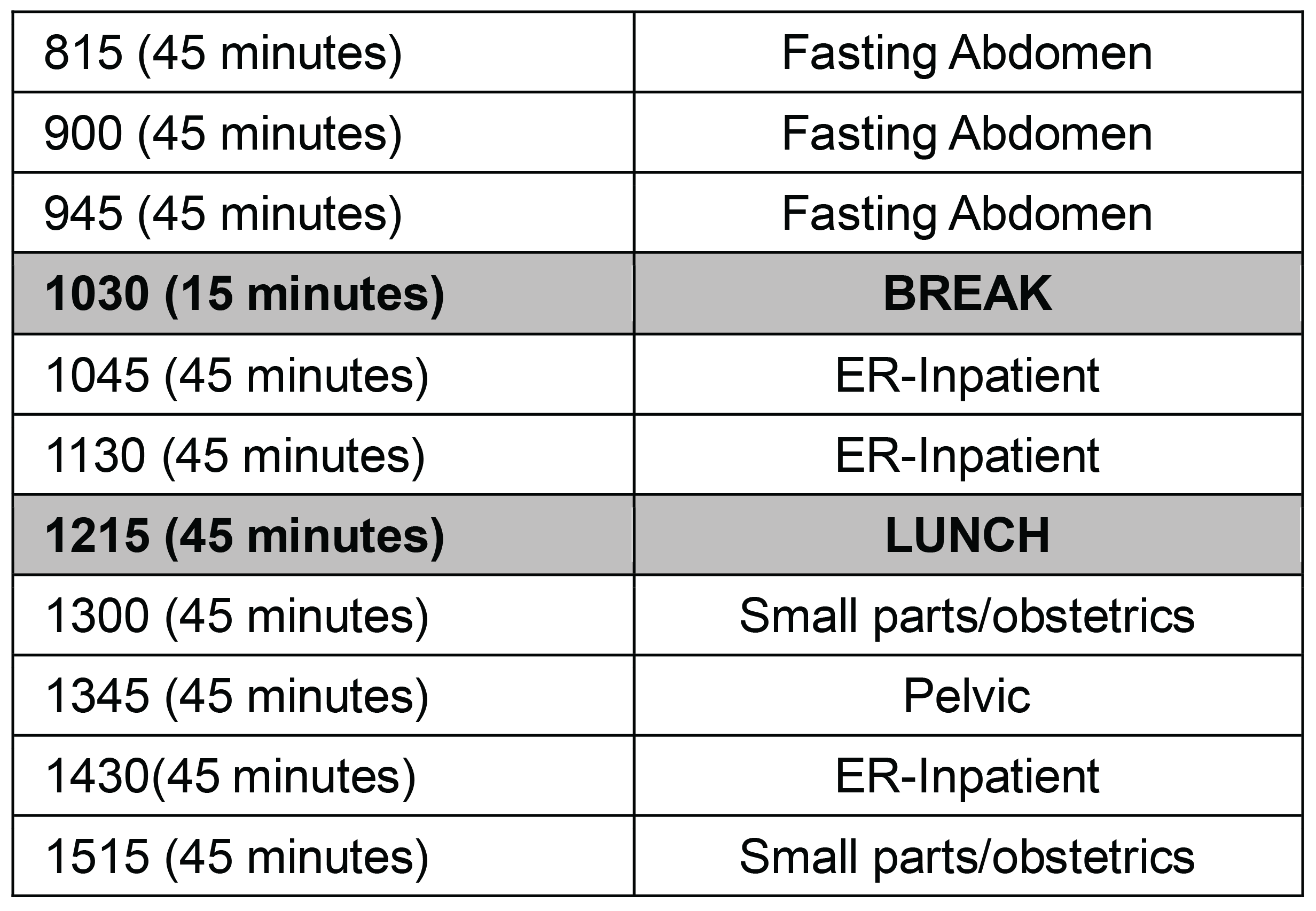
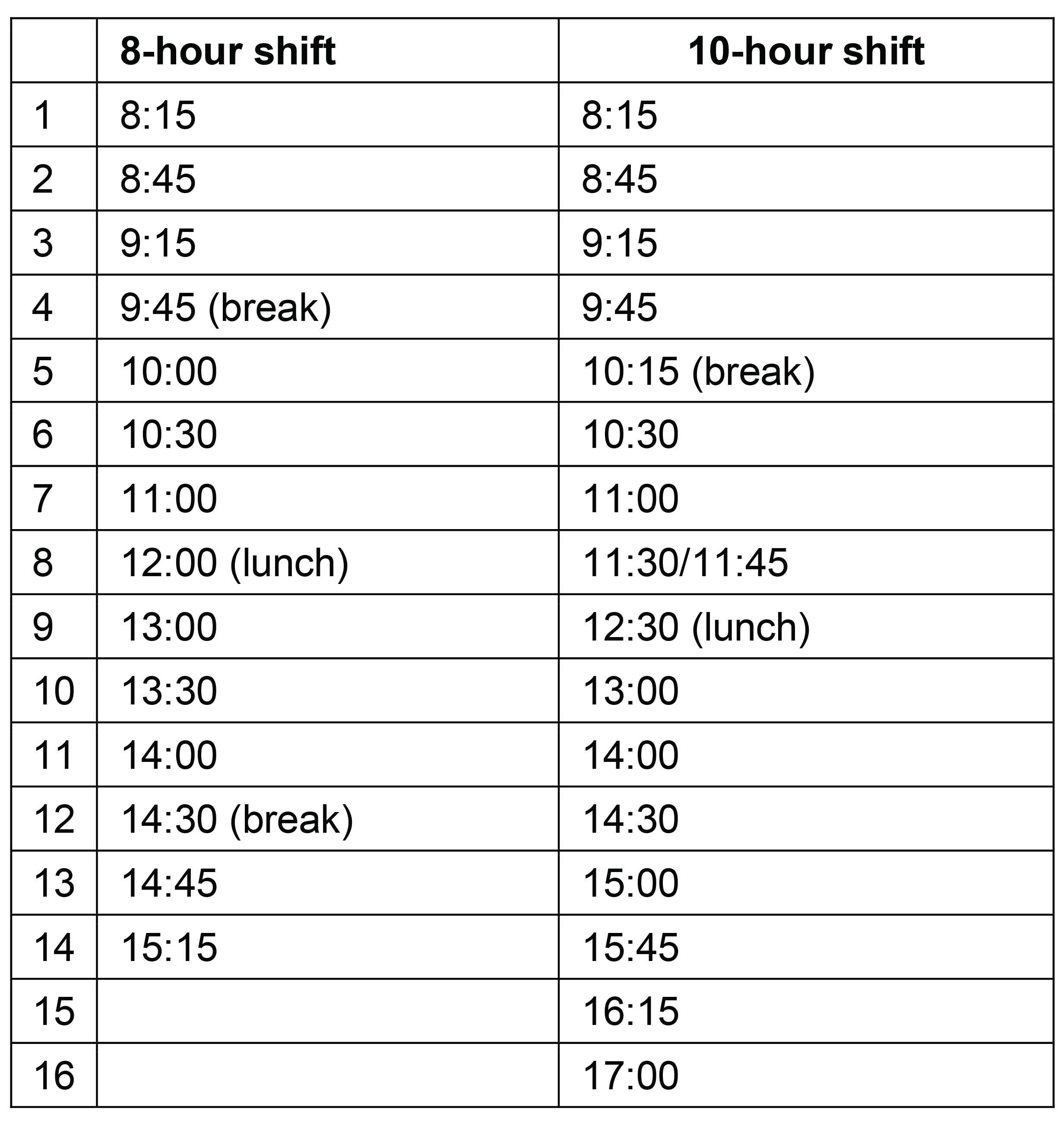
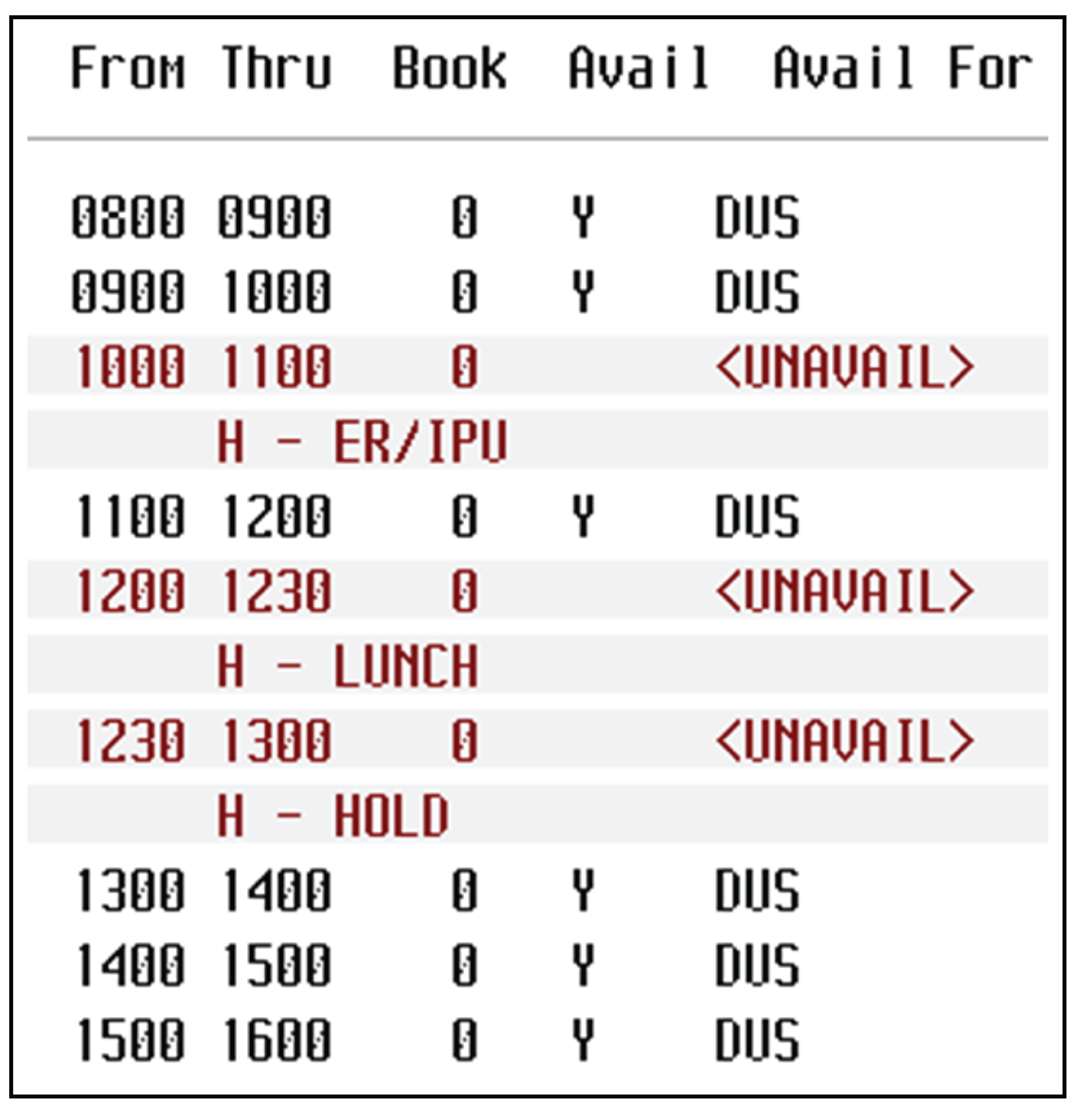
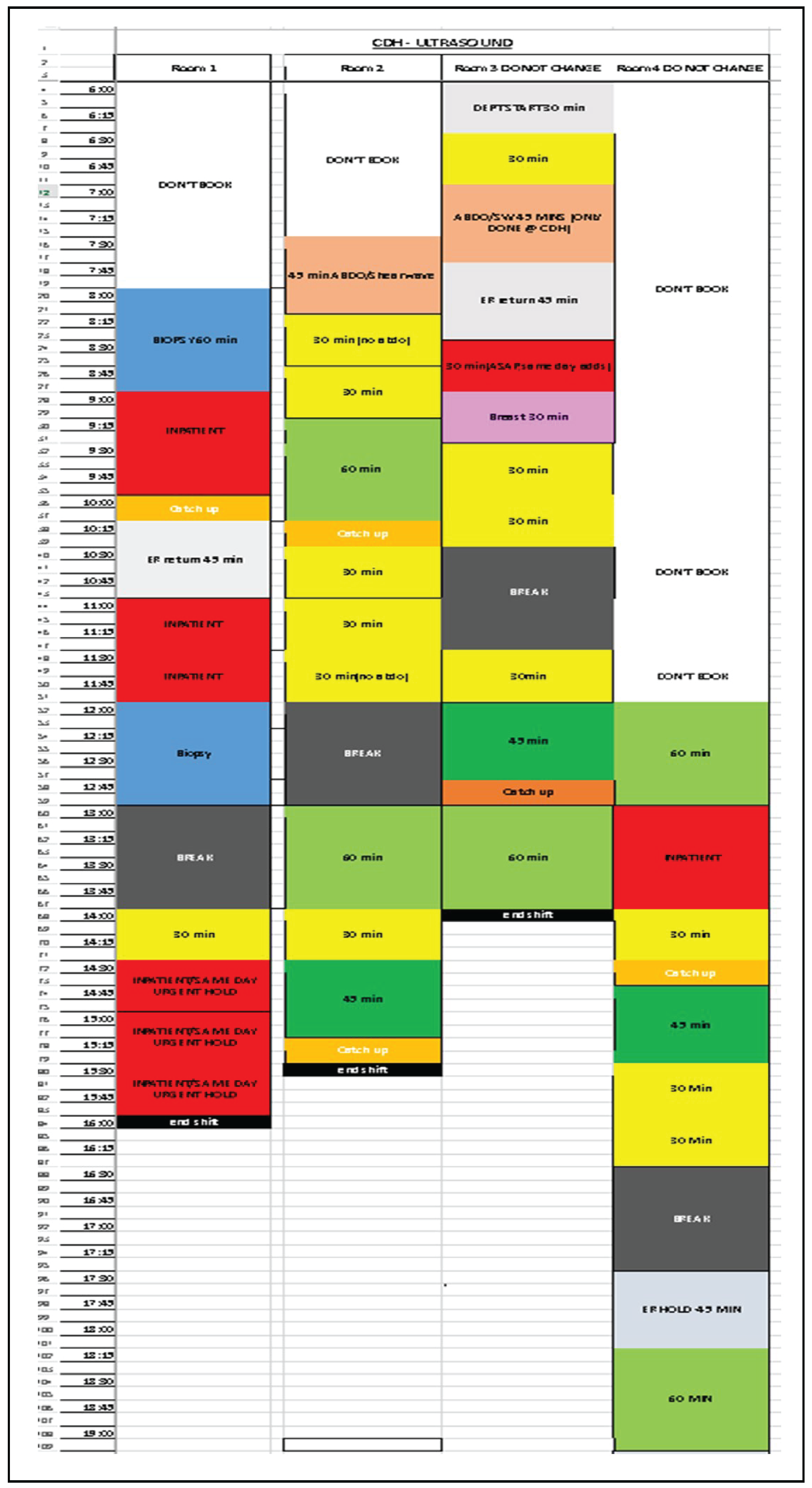
Eleven of the 13 survey respondents shared examples of the standard scheduling template used by the department to book daily ultrasound appointments. Appendix 2 includes several scheduling template examples used for booking daily ultrasound examinations at participating hospitals.
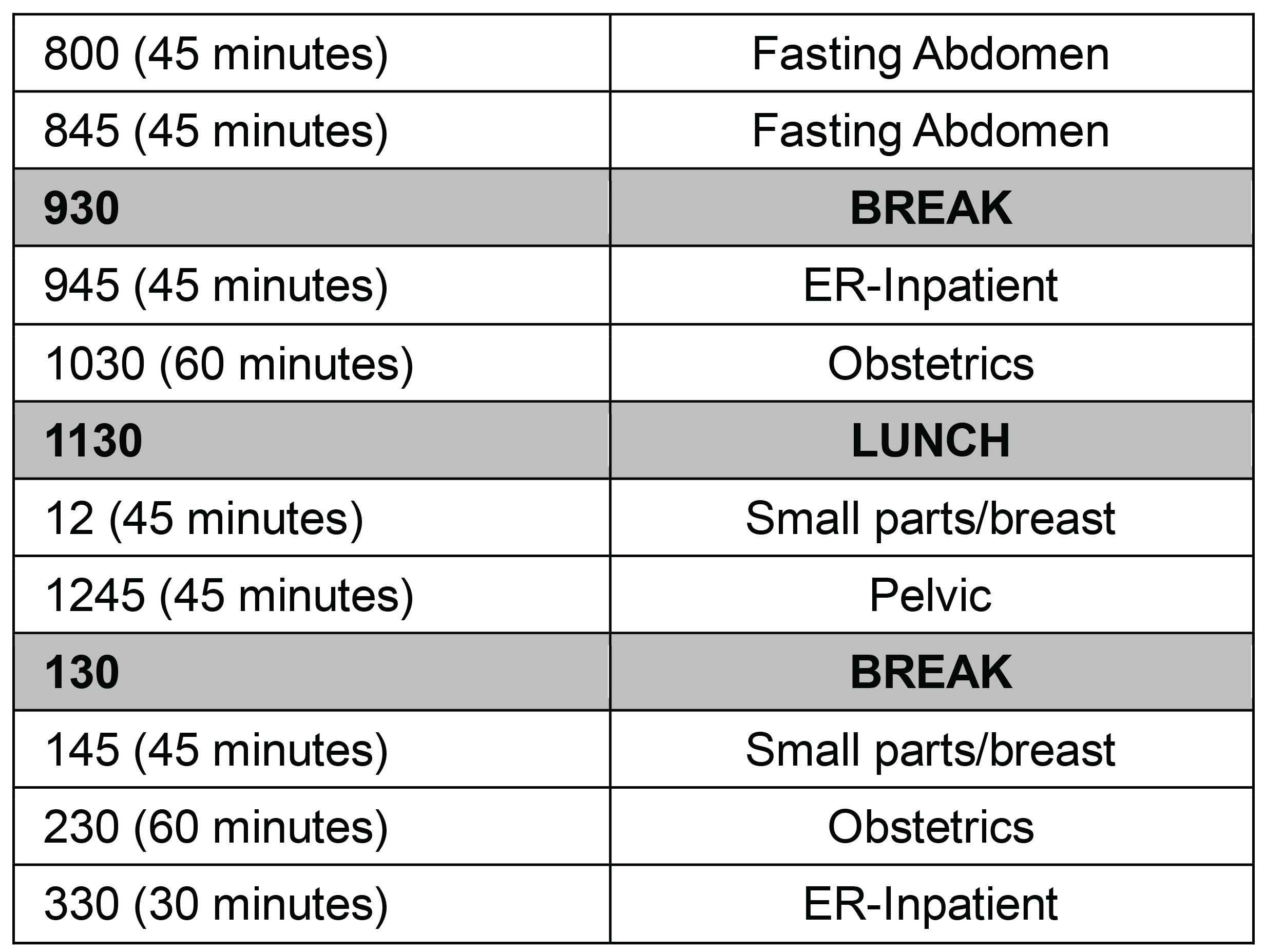
Overall, various responses were received regarding the methods used to schedule appointment slots. Some hospitals book examination slots according to examination type (e.g., pelvis or abdomen), while others schedule according to the time required by the sonographer to complete the examination. Additionally, others used fixed time slots of either 30 minutes or 1 hour. In all instances, standard booking templates included built-in time to prioritize emergency, inpatient, or urgent examination requests.
The number of examinations performed daily by each sonographer may not directly correspond to the booking slots available in the scheduling templates. For instance, 1 respondent noted that each outpatient examination is allocated a 1-hour slot to accommodate extra patients from the emergency department. This approach enables an additional 7 to 14 patients to receive imaging alongside the scheduled outpatients. Similarly, another respondent mentioned that it is common to fit 2 patients into a single time slot, depending on the type of examination requested.
The administrative responsibilities of a sonographer (e.g., scheduling patient appointments, coordinating urgent requests, and appointment preparation) was noted to vary across hospitals and is influenced by the number of available examination slots per day. One respondent reported that because sonographers were largely responsible for scheduling their own examinations, time was allocated to the start and end of each shift for administrative duties. Comparatively, another respondent highlighted that a medical imaging aid is an important team contributor for managing workflow, administrative tasks, and examination preparations, allowing sonographers to maximize scanning time.
Scheduling Strategies
Eleven of 13 survey respondents shared scheduling strategies used by their hospital’s imaging department to manage the fluctuating ultrasound examination workload.
Administrative Duties and Human Resources
Four respondents indicated that administrative support is necessary to maximize appointment times, especially in departments with multiple examination rooms. Administrative support included:
managing ultrasound examination bookings and requests
communicating with hospital departments and external referring physician offices
completing other routine paperwork.
Other human resource strategies used to manage workflow that were mentioned by survey respondents include the following:
stagger staff breaks and work shifts
limit the number of patient examinations per day per technologist to ensure capacity
limit comprehensive examinations to 2 to 3 patients per day and include a variety of examinations allowing for sonographers to not perform 1 type of scan repeatedly, which may cause increased physical strain
management may pursue additional staff coverage or increase staffing levels, including temporary staff, when short-staffed or when responding to high workloads and long wait times
sonographers may work through breaks, after-hours, or on weekends to accommodate urgent scans and reduce examination wait times.
Scheduling and Prioritizing Bookings
Overall, respondents emphasized that incorporating urgent slots into the scheduling process creates availability for patients referred by primary care providers and those on waitlists. One respondent mentioned that examinations are typically scheduled no more than 4 to 6 weeks in advance to reduce the need for rebooking due to urgent priority scans.
Other scheduling and prioritization related strategies that were mentioned by survey respondents include:
sonographers may consult with radiologists daily to triage appointments and offer priority to examinations most urgently needed
add additional examination slots
double book time slots according to the type of examination requested
exchange time slots for patients that arrive early for their scheduled appointment time
rebooking examination appointments to another day if capacity does not exist
use 1 hour booking slots for outpatient appointments to provide capacity for patients requiring emergency department care during the day
if an examination is completed early, then fill the remaining time with an emergency request
for patients who do not arrive for their appointments, fill in last minute vacancies with examination referrals from the emergency department, operation room, or a hospital inpatient department
examinations may be referred elsewhere if no capacity exists, and scan time frame is not feasible.
Limitations
This report is limited by the number of respondents that reported information on ultrasound scheduling practices. The results presented in this report are not representative of all scheduling practices at the provincial or territorial level, but rather represent a snapshot of practices. Additionally, the facilities included in this report varied in characteristics including the population served, geographic location, patients access to services, and administrative resources. For example, hospitals were located in population centres of varying sizes, ranging from those with fewer than 10,000 people to those with more than 40,000 people. Similarly, 31% of hospitals were reported to have dedicated ultrasound machines, with 1 hospital conducting nearly exclusive breast imaging 1 day a week.
Finally, there are no standard definitions for small or large population centres or rural or remote geographies. Instead, various classification approaches exist, and each approach, including those used in this report, have particular reporting implications and limitations.18
Conclusions
Based on the results of this survey, most diagnostic imaging departments in hospitals located in small-to-medium–sized population centres, have a system in place to aid with prioritizing ultrasound examinations, which most often are requested by primary care practitioners.
Between one-half to three-quarters of patients travel from out of town for their hospital ultrasound appointment, and the use of dedicated time slots is the most common method used to schedule an appointment.
All hospitals use a standard booking template to schedule ultrasound examinations, with time reserved for prioritizing emergency or urgent examinations each day. Various administrative, human resource, and examination prioritization strategies were identified to help with managing examination volumes, improving operational efficiency, and supporting staff well-being and patient care.
References
1.Shah AB, Bhatnagar N. Ultrasound imaging in musculoskeletal injuries-What the Orthopaedic surgeon needs to know. J Clin Orthop Trauma. 2019;10(4):659-665. PubMed
2.National Institute of Biomedical Imaging and Bioengineering. Ultrasound. 2023; https://www.nibib.nih.gov/science-education/science-topics/ultrasound. Accessed 2024 Sep 11.
3.Diagnostic Ultrasound. Schedule of Facility Fees for Independent Health Facilities. Toronto (ON): Ontario Ministry of Health; 2023: https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-facility-costs-2024-01-24.pdf. Accessed 2024 Sep 11.
4.Guidelines for Professional Ultrasound Practice. London (GB): Society and College of Radiographers and British Medical Ultrasound Society; 2017: https://www.bmus.org/static/uploads/resources/SCoR__BMUS_Guidelines_for_Professional_Ultrasound_Practice_Revised_Jan_2018.pdf. Accessed 2024 Sep 11.
5.Government of Canada. Canadian Occupation Projection System. 2022; https://occupations.esdc.gc.ca/sppc-cops/.4cc.5p.1t.3onsummaryd.2tail@-eng.jsp?tid=116. Accessed 2024 Sep 11.
6.General Ultrasound Examination Volumes per Sonographer 8-Hour Workday. Can J Health Technol. 2024;4(2). https://www.cda-amc.ca/sites/default/files/pdf/htis/2024/CM0012-000-Ultrasound-Exam-Volume-Per-Day.pdf.
7.Zhang D, Huang H. Prevalence of work-related musculoskeletal disorders among sonographers in China: results from a national web-based survey. J Occup Health. 2017;59(6):529-541. PubMed
8.Hogan A. Pain Levels and Injuries by Sonographic Specialty: A Research Study. J Diagn Med Sonogr. 2022;38(1):53-58.
9.Younan K, Walkley D, Quinton AE, Alphonse J. Burnout in the sonographic environment: The identification and exploration of the causes of sonographer burnout and strategies for prevention and control. Sonography. 2022;9:175 - 185.
10.Johnson J, Arezina J, McGuinness A, Culpan AM, Hall L. Breaking bad and difficult news in obstetric ultrasound and sonographer burnout: Is training helpful? Ultrasound. 2019;27(1):55-63. PubMed
11.Kawai K, Kawai AT, Wollan P, Yawn BP. Adverse impacts of chronic pain on health-related quality of life, work productivity, depression and anxiety in a community-based study. Fam Pract. 2017;34(6):656-661. PubMed
12.Statistics Canada. Population centre (POPCTR). 2022; https://www150.statcan.gc.ca/n1/pub/92-195-x/2021001/geo/pop/pop-eng.htm. Accessed 2024 Sep 9.
13.Review of Ultrasound in BC. Victoria (BC): British Columbia Ministry of Health; 2015: https://www2.gov.bc.ca/assets/gov/health/practitioner-pro/medical-services-plan/2015-03-23_final_ultrasound_report_for_msc_april_1_2015.pdf. Accessed 2024 Sep 9.
14.Davidson M, Kielar A, Tonseth RP, Seland K, Harvie S, Hanneman K. The Landscape of Rural and Remote Radiology in Canada: Opportunities and Challenges. Can Assoc Radiol J. 2024;75(2):304-312. PubMed
15.Micks T, Sue K, Rogers P. Barriers to point-of-care ultrasound use in rural emergency departments. CJEM. 2016;18(6):475-479. PubMed
16.Institute of Medicine Committee on the Future Health Care Workforce for Older Americans. Retooling for an Aging America: Building the Health Care Workforce. 2008: https://www.ncbi.nlm.nih.gov/books/NBK215400/. Accessed 2024 Sep 11.
17.Menon V, Muraleedharan A. Internet-based surveys: relevance, methodological considerations and troubleshooting strategies. Gen Psychiatr. 2020;33(5):e100264. PubMed
18.Rural Ontario Facts: Rural Classification Factsheet. Guelph (ON): Rural Ontario Institute; 2023: https://www.ruralontarioinstitute.ca/uploads/userfiles/files/Rural%20Ontario%20Facts%20-%20Rural%20Classification%20Factsheet%20-%20V2_0.pdf. Accessed 2024 Sep 11.
Appendix 1: Survey Questions
Please note that this appendix has not been copy-edited.
CMII: Survey — Optimizing Ultrasound Booking Schedules
The survey consists of 10 questions and may take between 5 to 10 minutes to complete.
Data confidentiality: The results of the survey will be included in a report that will be published on the CMII website. Data will be aggregated and presented at the provincial and/or territorial level. No site-level identifying information will be included in the report.
Facility Name (not included in report)
What kind of ultrasound services are provided by the imaging department:
Generalist ultrasound exams (e.g., abdomen, pelvis, obstetrics, peripheral veins, superficial structures).
Dedicated vascular or cardiac ultrasound exams
Other (please specify):
How are ultrasound exams scheduled (select all that apply):
Central intake booking service for patient to call
Central intake booking service for health care practitioner to call/send requisition
Patient calls in to book an appointment directly with the DI department identified by their health care practitioner
Patient books online (self-scheduling system)
Referring health care practitioner sends requisitions to DI department (e.g., fax, phone, computerized order entry)
Other (please specify):
Do you have a site-specific booking system?
Yes
No
Don’t know
What type of booking model is used for scheduling ultrasound exams:
“Block of time” model (i.e., block of 15 minutes, appointment time adjusted for the exam being performed.)
Clustering (i.e., patients with similar needs are scheduled for a specific time slot)
Open booking (a flexible window of time where a patient can attend their appointment, e.g., booking window: anytime between 2pm and 4pm)
Time slot (i.e., patient is provided with a dedicated time slot)
Other (please specify):
Does the imaging department use a template for scheduling exams throughout the day.
Yes
No
Don’t know
If possible, please attach/include a screenshot of your ultrasound booking schedule template (if applicable).
Scheduling comments
Are appointment slots reserved each day to accommodate emergency or urgent/last minute bookings?
Yes
No
Don’t know
If yes, what percentage of slots are reserved for emergency/urgent appointments an average day:
Do you have an ultrasound booking prioritization/triaging system?
Yes
No
Don’t know
If yes, how are ultrasound bookings prioritized (select all the apply)
Emergency/inpatient department
Radiologist prioritizing
Exam complexity
Outpatient medical complexity
Out-of-town patients, coordination of care
Other (please specify):
In an average week, what is the percentage of patients that travel from out-of-town for an ultrasound exam (if applicable)?
Please share any strategies that are used to manage the fluctuating workload, both in volume and type of exams requested:
Appendix 2: Scheduling Template Examples
Please note that this appendix has not been copy-edited.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.