CADTH Health Technology Review
Psychedelic-Assisted Psychotherapy for Post-Traumatic Stress Disorder, Anxiety Disorders, Mood Disorders, or Substance Use Disorders
Rapid Review
Authors: Yi-Sheng Chao, Jennifer Horton
Abbreviations
BDI
Beck Depression Inventory
CAPS
Clinician-Administered PTSD Scale
CBCT
cognitive-behavioural conjoint therapy
CBT
cognitive behavioural therapy
DMT
dimethyltryptamine
DSMV-IV
Diagnostic and Statistical Manual of Mental Disorders, fourth edition
HADS-A
Hospital Anxiety Depression Scale
HAM-D
Hamilton Rating Scale for Depression
LSD
lysergic acid diethylamide
MADRS
Montgomery-Åsberg Depression Rating Scale
MDD
major depressive disorder
MDMA
3,4-methylenedioxymethamphetamine
MET
motivational enhancement therapy
NEO-PI-R
Revised Neuroticism, Extraversion, Openness Personality Inventory
OCD
obsessive-compulsive disorder
PICO
population, intervention, comparator, and outcomes
PTSD
post-traumatic stress disorder
QIDS-SR
Quick Inventory of Depressive Symptomatology–Self
RCT
randomized controlled trial
SOWS
Subjective Opiate Withdrawal Scale
STAI-T/STAI-S
Spielberger State-Trait Anxiety Index
YBOCS
Yale-Brown Obsessive Compulsive Scale
Key Messages
Two systematic reviews, 3 randomized controlled trials, and 2 single-arm safety trials were identified that evaluated several combinations of psychedelic-assisted psychotherapy. Psilocybin was the psychedelic most tested. Other psychedelics identified in the systematic reviews and primary studies were 3,4-methylenedioxymethamphetamine (or MDMA), lysergic acid diethylamide (or LSD), ayahuasca (also named N,N-dimethyltryptamine [or DMT]), ibogaine, ketamine, and nitrous oxide.
Manualized therapy (not defined) and non-directive support (not defined) were the psychotherapies most studied in the relevant primary studies in the 2 systematic reviews. Other psychotherapies identified included integrative psychotherapy, cognitive behavioural therapy (CBT), CBT and motivational enhancement therapy, psychosocial interventions, non-directive support, group talk therapy, and guided support.
Clinical effectiveness lasting weeks to months was observed in 1 systematic review that reviewed primary studies examining various combinations of psychedelics and psychotherapy in patients with various mental health conditions. Significant improvement in symptom scores related to mental illnesses and no serious and long-term adverse events were reported in the other systematic review.
Various combinations of psychedelics and psychotherapies were evaluated in 3 randomized controlled trials (RCTs) and 2 safety studies. Ketamine-assisted psychotherapies were associated with improvements in the symptoms related to substance use disorder in 2 RCTs. Psilocybin-assisted psychotherapy was reported to be efficacious in treating MDD in 1 RCT. No serious adverse effects were reported in the RCTs or in 2 safety trials using MDMA-assisted psychotherapy.
There were several limitations to the included studies, including small sample sizes (less than 20 in the majority of primary studies), relatively short follow-ups (1 week to 3 years; less than or equal to 1 year in 27 out of 31 relevant publications), differences in psychotherapy classification between systematic reviews, considerable heterogeneity between studies, and unclear generalizability and availability of the interventions in Canadian contexts. Therefore, findings should be interpreted with caution. No relevant guidelines were identified.
Context and Policy Issues
Hallucinogens include many different drugs, which are often called “psychedelic” drugs.1 The US National Institute on Drug Abuse categorizes these drugs into 2 categories: classic hallucinogens and dissociative drugs.2 Both types of psychedelics can lead to hallucinations — sensations and images that seem real although they are imaginary.2 In addition, an individual using dissociative drugs can feel out of control or disconnected from their body and environment.2 Classic serotonergic psychedelics act primarily by a complete or partial agonist action on brain serotonin 5-hydroxytryptamine 2A receptors.3 Examples of classic psychedelics are LSD, mescaline, psilocybin, and ayahuasca (also identified as N,N- dimethyltryptamine [DMT]).3 Examples of dissociative drugs are phencyclidine, ketamine, dextromethorphan, and Salvia (Salvia divinorum).2
Psychedelics were tested for clinical use prior to the 1960s.4 However, methodological issues in clinical trials and political concerns have prevented the use of psychedelics in mainstream medicine.4 In 2010, it was reported that psychedelics were used by more than 30 million consumers in the US.4 Clinically, researchers acknowledge psychedelics as a potential effective drug for mental health conditions.4 Researchers and clinicians are testing the clinical effectiveness of psychedelics for mental illness treatment due to the improvement in research methods that reduce ethical and methodological concerns toward psychedelic trials.4 The wider application of psychedelics has also been motivated by a perceived lack of innovation in mental illness treatment.5 The number of new molecular entities for psychiatric conditions approved by the US FDA decreased from 13 in 1996 to 1 in 2016.5 One example of the psychedelics adopted for treatment is ketamine (not used in combination with psychotherapies) that has been used for the treatment of depression6 and post-traumatic stress disorder (PTSD),7 as reviewed in 2 CADTH reports. Other psychedelics, such as psilocybin and ayahuasca are increasingly being tested for their efficacy in treating mental illnesses.4
In addition to their use as stand-alone agents,6 psychedelics can be used in combination with psychotherapy (i.e., psychedelic-assisted psychotherapy).8 There are a wide variety of psychotherapies that may be used for the treatment of mental health conditions, including guided support that helps patients focus inward on their thoughts and better facilitate participant introspection4 and cognitive behavioural therapy (CBT) that combines different types of cognitive therapy and behavioural therapy.9 Psychedelic-assisted psychotherapy is often led by licensed professionals with training in administering psychedelics and monitoring their use.4 Psychedelics may work by altering a patient’s consciousness. They may also affect a patient’s subjective perspectives and approaches to processing thoughts, emotions, and behaviours, thereby providing an alternative therapeutic experience to psychotherapy alone.4 While psychedelic-assisted psychotherapy has been recently tried in patients with anxiety, depression, substance use disorder, and PTSD,4 some researchers consider the treatment response to be unsatisfactory in patients with mood disorder.10
This report aims to summarize the clinical effectiveness and safety of psychedelic drug-assisted psychotherapy for PTSD, anxiety disorders, mood disorders, or substance use disorders, in addition to clinical guidelines for the use of psychedelic drug-assisted psychotherapy.
Research Questions
What is the clinical effectiveness of psychedelic-assisted psychotherapy in the treatment of post-traumatic stress disorder, anxiety disorders, mood disorders, or substance use disorders?
What are the evidence-based guidelines regarding psychedelic-assisted psychotherapy for the treatment of post-traumatic stress disorder, anxiety disorders, mood disorders, or substance use disorders?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, PsycINFO, the Cochrane Database of Systematic Reviews, the international health technology assessment database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were psychotherapy and psychedelics. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016 and May 4, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Adults with post-traumatic stress disorder, anxiety disorders, mood disorders (e.g., depression), or substance use disorders |
Intervention | Psychedelic-assisted psychotherapy (i.e., psychotherapy is provided while the patient is under the influence of a psychedelic drug) Examples of psychedelic drugs: ketamine, psilocybin, LSD, MDMA, and ibogaine |
Comparator | Q1. Usual care, no treatment (e.g., wait list), placebo No comparator (safety outcomes only) Q2. Not applicable |
Outcomes | Q1. Clinical benefits (e.g., resolution and/or reduction of PTSD, anxiety, or mood disorder symptoms; quality of life; improvement in dysfunction or impairment) and harms (e.g., hypertension, tachycardia, toxicity, addiction, confusion, withdrawal symptoms, sleep problems, psychosis, hallucinogen-persisting perceptive disorder, memory impairments, short-term depression) Q2. Recommendations for best practices (e.g., dosage, contraindications, duration of treatment, how many administrations, method of administering) |
Study designs | Health technology assessments and systematic reviews, randomized controlled trials, non-randomized studies, and guidelines |
LSD = lysergic acid diethylamide; MDMA = 3,4-methylenedioxymethamphetamine; PTSD = post-traumatic stress disorder.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2016. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)11 for systematic reviews and the Downs and Black checklist12 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
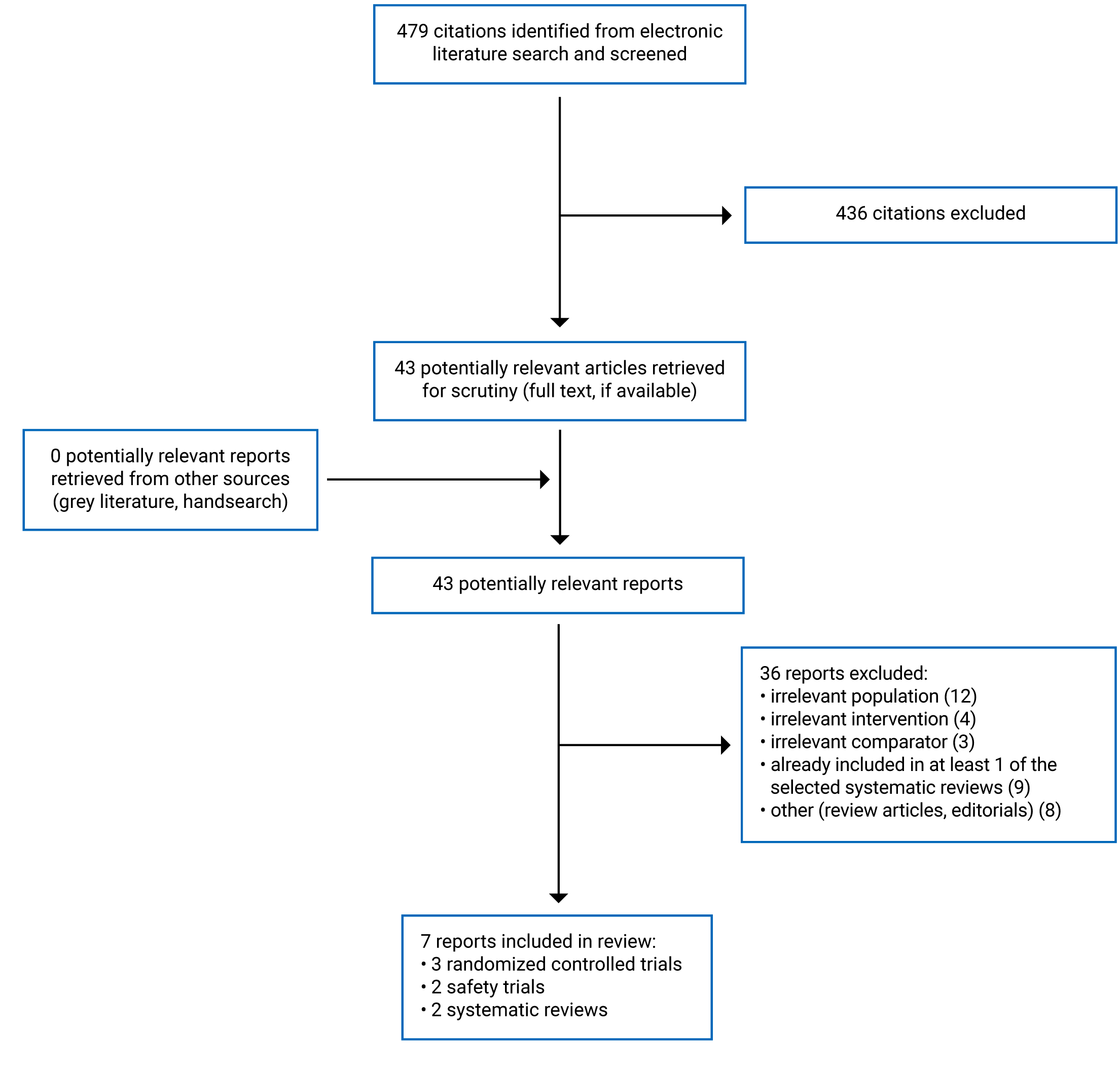
A total of 479 citations were identified in the literature search. Following the screening of titles and abstracts, 436 citations were excluded and 43 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 36 publications were excluded for various reasons, and 7 publications met the inclusion criteria and were included in this report. These comprised 2 systematic reviews, 3 RCTs, and 2 single-arm safety trials. Appendix 1 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)13 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Seven relevant publications were identified for this report, including 2 systematic reviews,4,14 3 RCTs,10,15,16 and 2 single-arm safety trials.17,18 No relevant evidence-based guidelines were identified. The 2 included systematic reviews had broader inclusion criteria than the present review.4,14 Specifically, both systematic reviews searched for studies using psychedelic drugs in patients with any mental health conditions.4,14 Andersen et al. (2021) included studies using psychedelics in combination with psychotherapy or alone.14 Only the characteristics and results of the subset of relevant studies will be described in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Systematic Reviews
In the 2 systematic reviews included in this report, primary studies were qualitatively summarized and there were no meta-analyses conducted.4,14 Various combinations of psychedelics and psychotherapy were identified.4,14
Andersen et al. (2021) searched for single-blind and double-blind placebo-controlled randomized trials, open-label trials, and proof-of-concept trials published between January 2000 and May 2020.14 Based on the 10 psychedelic-assisted trials identified, 16 articles were published; of those, 8 trials published in 12 publications were relevant to the population, intervention, comparator, and outcomes (PICO) criteria in this report.14
Wheeler and Dyer (2020) searched for any studies published after 1990, excluding case studies only, and included 43 studies, 30 of which were relevant to this report.4
A table depicting the overlap of relevant RCTs included within the systematic reviews is provided in Appendix 5. Only RCTs providing direct evidence of relevance to this report were included in the overlap table. There was a total of 31 relevant publications identified in the 2 systematic reviews. One primary study, Garcia-Romeu et al., was uniquely identified by Andersen et al. (2021).14
Randomized Controlled Trials
Three relevant RCTs were identified.10,15,16 Dakwar et al. (2020) conducted a randomized, controlled, double-blinded trial to test the efficacy of ketamine-assisted psychotherapy (motivational enhancement therapy [MET]) in patients with alcohol dependence.15 Dakwar et al. (2019) conducted a randomized double-blinded trial on the efficacy of ketamine-assisted therapy on cocaine dependence.16 Davis et al. (2020) assessed psilocybin-assisted therapy in a randomized, clinician-blinded, waiting list–controlled trial.10
Safety Trials
Sessa et al. (2021) and Monson et al. (2020) conducted single-arm, before-and-after trials on the feasibility, safety, and tolerability of MDMA-assisted psychotherapy.17,18
Country of Origin
Systematic Reviews
The authors of the 2 systematic reviews were based in the UK14 and Canada.4
Randomized Controlled Trials
Dakwar et al. (2020), Davis et al. (2020), and Dakwar et al. (2019) were conducted by researchers in the US.10,15,16
Safety Trials
Sessa et al. (2021) and Monson et al. (2020) were conducted by researchers based in the UK17 and Canada,18 respectively. In addition, there were researchers from the US contributing to Monson et al. (2020).18
Patient Population
Systematic Reviews
Andersen et al. (2021) and Wheeler and Dyer (2020) searched for studies recruiting adults diagnosed with any mental illnesses.4,14The populations in the primary studies identified by Andersen et al. (2021) were patients diagnosed with cancer-related anxiety and depression disorders (3 trials relevant to this report), illness-related anxiety and depressive disorders (1 relevant trial), depressive disorders (1 relevant trial), obsessive-compulsive disorder (OCD; 1 relevant trial), and substance use disorders (2 relevant trials).14 There were 4 additional publications reporting follow-up results of relevant trials.14 Wheeler and Dyer (2020) summarized results from patients with anxiety and depression (3 relevant publications), anxiety and depression associated with terminal illness (5 relevant publications), substance use disorders (9 relevant publications), PTSD (7 relevant publications), treatment-resistant depression (5 publications), and OCD ((1 relevant publication).4
Randomized Controlled Trials
Dakwar et al. (2020) recruited 40 treatment-seeking adults with alcohol dependence, 52.5% of who were female.15 The mean age of the participants was 53 years.15 The average number of drinks per day during the 7 days before consent to participate in the study was 6.6.15 Davis et al. (2020) included 24 patients diagnosed with major depressive disorder (MDD), who on average had depression for 21.5 years.10 The mean age of the patients was 39.8 years and 16% of them were female.10 Dakwar et al. (2019) enrolled 55 patients with cocaine dependence, 14% of which were female.16 The mean age of the patients was 47 years and the median baseline cocaine use was US$34.3 per day.16 The unit cost of cocaine was not reported.16
Safety Trials
Sessa et al. (2021) recruited 14 patients with alcohol use disorder who had recent detoxification.17 The mean age of the patients was 48 years and 6 (43%) of them were female.17 Monson et al. (2020) recruited 6 patients with PTSD and their 6 partners; the average age of the patients was 47 years.18 Partners also assessed patients’ symptoms using standardized questionnaires (such as the PTSD Checklist).18 Four of the patients were male and all of them were Canadian.18
Interventions and Comparators
Systematic Reviews
There were several combinations of psychedelic drugs and psychotherapies identified in the 2 systematic reviews.4,14 Andersen et al. (2021) included 8 primary studies relevant to this report, evaluating psilocybin (7 trials, 10 relevant publications) or LSD (1 trial, 2 relevant publications).14 The psychotherapies identified in relevant studies were integrative non-directive support (4 publications), brief support (3 publications), CBT (3 publications), motivational enhancement therapy (MET, 1 publication), and unspecified psychotherapy (1 publication).14 Comparators included baseline (7 publications), low-dose psychedelic drugs (3 publications), and niacin (2 publications).14
Wheeler and Dyer (2020) reported the types of psychedelic drugs in relevant primary studies: psilocybin (10 relevant publications), MDMA (9 relevant), ibogaine (3 relevant), ketamine (4 relevant), ayahuasca (1 relevant), LSD (2 relevant), and nitrous oxide (1 relevant).4 The psychotherapies identified were non-directive support (6 relevant publications), manualized therapy for PTSD (6 relevant), CBT (5 relevant), brief support (3 relevant), group talk therapy (1 relevant), MET (1 relevant), ibogaine support guidelines (1 relevant), existential psychotherapy (2 relevant), mindfulness-based therapy (1 relevant), and unspecified psychotherapies (4 relevant).4 The comparators were baseline (13 relevant), low-dose psychedelic drugs (7 relevant publications), placebo (6 relevant), niacin (2 relevant), and unspecified (2 relevant).4
Randomized Controlled Trials
Dakwar et al. (2020) adopted MET (various strategies to promote motivation and self-directed change) and compared ketamine (0.11 mg/kg bolus in saline, followed by a 50-minute slow-drip IV infusion of 0.6 mg/kg, once in the second week of the study) with midazolam (0.025 mg/kg, once in the second week).15 MET included 6 sessions in 5 weeks that engaged participants to explore goals and elicit motivations.15 Davis et al. (2020) used supportive psychotherapy over a total of 11 hours within 8 weeks during at least 18 visits, in combination with 2 doses of psilocybin (20 mg/70 kg in session 1 and 30 mg/kg in session 2), compared with delayed treatment (i.e., wait list control) in the other group.10 Dakwar et al. (2019) compared ketamine (0.5 mg/kg, once on study day 2) with midazolam (0.025 mg/kg, once on study day 2) and used mindfulness-based relapse prevention that cultivated attitudes of deliberate, present-centred awareness with training in behaviours, cognitive associations, judgments, and distortions.16 Mindfulness-based relapse prevention was offered after an infusion of ketamine or midazolam (daily sessions for 4 days during the inpatient phase, then weekly sessions for the remainder of the study).16
Safety Trials
Sessa et al. (2021) treated 14 patients with 8-week recovery-based therapy including 10 sessions and MDMA administration (twice, sessions 3 and 7; 125 mg MDMA with a booster dose of 62.5 mg in 2 hours).17 Monson et al. (2020) treated 6 couples with cognitive-behavioural conjoint therapy (CBCT) and MDMA (twice during the intervention, 75 mg and 100 mg, respectively; with optional supplemental half-dose 1.5 hours later).18 CBCT included face-to-face and online psychoeducation for trauma and relationships, and there were various activities in 15 sessions within 7 weeks.18
Outcomes
Systematic Reviews
Various outcomes were reported in the primary studies summarized in the 2 systematic reviews.4,14 Andersen et al. (2021) reported outcome measures for depression, patient-rated anxiety, clinician-rated anxiety, substance use or dependence, subjective experiences, and side effects.14 Depression outcomes were measured with several tools in primary studies, including the Beck Depression Inventory (BDI), Montgomery-Åsberg Depression Rating Scale (MADRS), Hamilton Rating Scale for Depression (HAM-D), GRID Hamilton Depression Rating Scale 17, Snaith-Hamilton Pleasure Scale, and Quick Inventory of Depressive Symptomatology–Self Report (QIDS-SR) in primary studies.14 Anxiety measures included Spielberger State-Trait Anxiety Index (STAI-T and STAI-S), the anxiety subscale of the Hospital Anxiety Depression Scale (HADS-A).14 The follow-up time in primary studies ranged from 3 months to 3 years, if reported.14
Wheeler and Dyer (2020) reported measures for anxiety (including HADS-A, BDI, STAI-S, and STAI-T), depression (including QIDS-SR, STAI-T, BDI, Snaith-Hamilton Pleasure Scale, and MADRS), substance use (including Hallucinogen Rating Scale, Five-Dimension Altered States of Consciousness profile(5D-ASC), Mystical Experience Questionnaire, Yale-Brown Obsessive Compulsive Scale [YBOCS]), and PTSD (clinician-administered continuous measures of PTSD symptom severity such as the Clinician-Administered PTSD Scale [CAPS]).4 Self-rated PTSD symptom scales were eligible if no clinician-administered scales were available.4 The follow-up time in the primary studies ranged from 1 week to 30 months.4
Randomized Controlled Trials
The outcomes reported by Dakwar et al. (2020) included self-reported drinking days and reduction in heavy drinking days (more than 4 drinks per day for men or more than 4 drinks per day for women) up to 21 days after infusion.15 Davis et al. (2020) measured depression and depressive symptoms using the Depression Rating Scale, BDI-II, the 9-item Patient Health Questionnaire, and the Columbia Suicide Severity Rating Scale through 1-month follow-up.10 Dakwar et al. (2019) reported outcomes in cocaine dependence using abstinence and time to relapse (defined as first use within 28 days or dropout) and cocaine use assessed through self-reporting and urine toxicology within 5 weeks.16
Safety Trials
The primary outcomes assessed by Sessa et al. (2021) were the completion of the 8-week psychotherapy program, the acceptance of the second booster dose of MDMA on drug-assisted days, and adverse events.17 The secondary outcomes were changes in drinking behaviour, mental well-being, psychosocial functioning, quality of life (measured by Subjective Units of Distress Scale and the Severity of Alcohol Questionnaire), and concomitant drug use.17 Monson et al. (2020) reported primary outcomes including adverse events, the CAPS-5 for PTSD symptoms, the PTSD Checklist (Posttraumatic Stress Disorder Checklist for DSM-5, patient and partner versions), and the Couples Satisfaction Index. The secondary outcomes were the Beck Depression Inventory-II for depression, the Pittsburgh Sleep Quality Index for sleep disturbances, the Emotion Regulation Questionnaire for emotion regulation strategies, and the Traumatic and Attachment Belief Scale for trauma-related beliefs.18
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
Both systematic reviews by Andersen et al. (2021) and Wheeler and Dyer (2020) described the study objectives, study design, and methods, with sufficient details.4,14 PICO components and the eligibility of primary study designs for inclusion were described.4,14 However, the protocols of both systematic reviews were not published a priori.4,14 Comprehensive literature searches were reported.4,14 Study selection and data extraction were conducted in duplicate.4,14 This helped to minimize human errors. Meta-analyses were not conducted due to heterogeneity between studies.4,14 Wheeler and Dyer (2020) described the included studies in detail,4 whereas Andersen et al. (2021) listed all included studies in supplemental materials.14 Andersen et al. (2021) described the heterogeneity between primary studies,14 but Wheeler and Dyer (2020) did not discuss the heterogeneity between primary studies in detail.4 There were several limitations common to both systematic reviews. Neither provided a list of the excluded studies.4,14 The risk of bias and the sources of funding in primary studies were not assessed.4,14 The risk of bias in primary studies was not considered while interpreting the results.4,14 Publication bias was not assessed in both systematic reviews.4,14 It was therefore not clear whether primary studies subject to biases were more likely to be included or used for interpretation. Neither reported review authors’ conflicts of interest.4,14
Randomized Controlled Trials
The 3 RCTs described their studies in sufficient detail, including study objectives, outcomes to be measured, patient characteristics, interventions of interest, distributions of principal confounders, main findings, random variabilities of the data for the main outcomes, adverse events, and patients lost to follow-up.10,15,16
The biases to the study design seemed to be minimized. Outcome assessors in the 3 RCTs were blinded to the treatment.10,15,16 This helped to maintain an unbiased assessment of the outcomes. Selective reporting of the patient data were not likely in the 3 RCTs.10,15,16 The time between the intervention and outcome measurement was the same for both study groups.10,15,16 The adherence to the interventions was reliable because patients were encouraged to participate in face-to-face interactions.10,15,16 The outcomes were measured with validated questionnaires.10,15,16 The statistical tests used to assess the outcomes seemed appropriate.10,15,16 However, Davis et al. (2020) could not blind the patients because of the waiting list control design, though outcome assessors were blinded.10 The other 2 RCTs blinded patients to the treatment.15,16
The selection bias might have been minimized in the 3 RCTs. Participants in both study groups were recruited from the same populations during similar time periods.10,15,16 Subjects were randomized to different groups.10,15,16 Patients lost to follow-up were described.10,15,16 However, allocation concealment was not reported.10,15,16
Safety Trials
Sessa et al. (2021) and Monson et al. (2020) reported study objectives, main outcome measures, patient characteristics, interventions of interest, main findings, estimates of random variability in the data for the main outcomes, adverse events, and patients lost to follow-up.17,18 The statistical tests used to assess the outcomes were appropriate.17,18 The adherence to interventions was reliable because patients had face-to-face interactions.17,18 The main outcome measures were accurate.17,18 Monson et al. (2020) reported actual P values18 and Sessa et al. (2021) reported 95% confidence intervals of the statistics.17 However, Sessa et al. (2021) and Monson et al. (2020) conducted safety trials that lacked comparison groups and features to prevent biases that threatened study validity.17,18 The patients and outcome assessors were not blinded.17,18 There was no power analysis for sample sizes in both studies.17,18 It was unclear whether small sample sizes led to insignificant findings by Sessa et al. (2021).17 Whether the patients were representative of the populations and whether the treatment in the trials was representative of the care the majority of patients received were not reported in both studies.17,18
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Psychedelic-Assisted Psychotherapy
There was extensive overlap in the primary studies that were included in the systematic reviews; 30 of the 31 unique primary studies were identified by Wheeler and Dyer (2020).4,14 One primary study was uniquely identified by Andersen et al. (2021).14 A citation matrix illustrating the degree of overlap is presented in Appendix 5.
Psilocybin-Assisted Psychotherapy for Anxiety and Depression Associated With Life-Threatening Cancer Diagnoses
Three relevant RCTs identified by Wheeler and Dyer (2020)4 were also identified by Andersen et al. (2021).14 In 1 RCT of patients with anxiety or depression associated with life-threatening diseases, Grob et al. (2011), significant reductions in trait anxiety at 1 and 3 months and in depression at a 6-month follow-up were observed in patients after receiving psilocybin compared with baseline.4,14 However, no significant between-group differences in outcome measures were reported compared with active placebo (i.e., niacin).4,14 In the RCT by Griffiths et al. (2016), response rates of 83% for anxiety and 78% for depression were reported after 6 months of follow-up compared with baseline.4,14 In the other RCT, Ross et al. (2016) found significantly greater symptom reductions in the psilocybin-first group than in the niacin-first group for anxiety outcome measures, until crossover.4,14
Psilocybin-Assisted Psychotherapy for Mood and Anxiety Disorders
Three relevant primary studies (5 relevant publications) were identified by Wheeler and Dyer (2020),4 2 of which (3 publications) were also identified by Andersen et al. (2021).14 Two of the publications included by Wheeler and Dyer (2020) — Carhart-Harris et al. (2018) and Erritzoe et al. (2018) — were the follow-up of subjects from 1 single-arm study — Carhart-Harris et al. (2016) — and reported that psilocybin-assisted psychotherapy was associated with a significant decrease in depressive symptom scores measured with the 16-item QIDS-SR that lasted up to 6 months and observed significant improvement in personality measures (Revised Neuroticism, Extraversion, Openness Personality Inventory, or NEO-PI-R, scores) compared with baseline.4 The other primary study, Stroud et al. (2018), concluded that emotional face processing became significantly faster in the psilocybin group compared to baseline, but not in the control group.4 Both systematic reviews also identified an RCT, Moreno et al. (2006), that found psilocybin-assisted psychotherapy was significantly associated with decreases in OCD symptoms score (YBOCS) in 9 subjects at sessions treating OCD compared with those taking placebo-like doses of psilocybin.4,14
In the waiting list–controlled RCT by Davis et al. (2020), psilocybin-assisted therapy (supportive psychotherapy) was associated with significantly fewer depression symptoms measured with validated tools (GRID-HAMD and QIDS-SR) at week 4.10 Davis et al. (2020) concluded that psilocybin-assisted psychotherapy was efficacious in treating MDD.10
Psilocybin-Assisted Psychotherapy for Substance Use Disorders
Two relevant primary studies (3 publications) were identified by Wheeler and Dyer (2020)4 and also identified by Andersen et al. (2021).14 One relevant single-arm study was reported in 2 publications, Johnson et al. (2014) and Johnson et al. (2017), evaluating psilocybin-assisted CBT for people with nicotine dependence and found 80% smoking abstinence 6 months after the intervention.4 In the other single-arm study, Bogenschutz et al. (2015), psilocybin-assisted MET was associated with significant reductions in drinking days and heavy drinking days throughout this 32-week follow-up compared with baseline.4
N-Methyl-D-Aspartate Receptor Antagonist-Assisted Psychotherapy for Anxiety and Depression
Three relevant primary studies were identified by Wheeler and Dyer (2020),4 none of which were identified by Andersen et al. (2021).14 In the single-arm study by Wilkinson et al. (2017), ketamine-assisted CBT was significantly associated with lower depression scores measured by MADRS, compared with non-responders.4 In another single-arm study, Dore et al. (2019), ketamine-assisted psychotherapy was associated with significant decreases in depression and anxiety scores measured by BDI and HAM-A scores compared with baseline.4 In the placebo-controlled crossover study by Nagele et al. (2015), nitrous oxide-assisted psychotherapy was associated with significant improvement in depressive symptoms measured by the Hamilton Depression Scale-21 compared with placebo.4
Ketamine-Assisted Psychotherapy for Substance Use Disorder
Wheeler and Dyer (2020) identified 2 primary studies, Krupitsky et al. (2002) and Krupitsky et al. (2007), that found ketamine-assisted psychotherapy (existential approach) with a high dose of ketamine and 3 sessions of high-dose ketamine-assisted psychotherapy, were each associated with significantly greater rates of heroin abstinence than their comparators (low-dose ketamine and 1 session of ketamine-assisted psychotherapy, respectively).4
In the RCT by Dakwar et al. (2019), ketamine-assisted mindfulness-based behavioural modification was associated with significantly higher abstinence rates, less likelihood to relapse, and lower craving scores in patients with cocaine dependence receiving mindfulness-based relapse prevention compared with midazolam.16 Dakwar et al. (2019) observed that the intervention was well-tolerated and there was no patient attrition due to adverse events.16
In the other RCT, Dakwar et al. (2020) found that ketamine-assisted MET was associated with significantly higher rates of abstinence, delayed relapse, and a reduction in the likelihood of heavy drinking days compared with midazolam.15 The ketamine-assisted psychotherapy was well-tolerated, without adverse event-related patient attrition.15 Dakwar et al. (2020) also observed that the intervention was well-tolerated and there was no patient attrition due to adverse events.16
MDMA-Assisted Psychotherapy for Post-traumatic Stress Disorder
Seven relevant publications were identified by Wheeler and Dyer (2020),4 none of which were identified by Andersen et al. (2021).14 Of those, 5 publications relating to 4 phase II studies were included in a pooled analysis, Mithoefer et al. (2019), which was discussed but not formally included in the systematic review by Wheeler and Dyer (2020). This led to the FDA granting breakthrough therapy designation (not defined) for MDMA-assisted psychotherapy for PTSD.4 Mithoefer et al. (2019) analyzed the data from 74 participants and found that PTSD symptoms measured by the CAPS-5 scores were significantly lower in the experimental group than in the control group (lower-dose MDMA).4 In the RCT by Bouso et al. (2008) that followed up patients for 6 months, better outcome measure scores were observed in the MDMA 75 mg group compared to the other 2 groups (50 mg MDMA and placebo).4 In the other RCT by Wagner et al. (2017) that evaluated patients who received MDMA-assisted psychotherapy and were followed up for 3.5 years on average, a significant increase in openness and a significant decrease in PTSD symptoms were reported (comparator not specified).4
Monson et al. (2020) observed no serious adverse events while patients with PTSD were treated with MDMA-assisted CBCT in the 1-arm safety trial.18 Monson et al. (2020) also observed significant improvements from baseline in clinician-assessed, patient-rated, and partner-rated, PTSD symptoms.18
MDMA-Assisted Psychotherapy for Substance Use Disorder
In the 1-arm safety trial by Sessa et al. (2021), MDMA-assisted psychotherapy (psychological support) was well-tolerated and participants’ psychosocial functioning improved in patients with alcohol use disorder.17
MDMA-Assisted Psychotherapy for Mood Disorder
Wheeler and Dyer (2020) identified 1 RCT that found MDMA-assisted mindfulness-based therapy was associated with significantly greater improvements in anxiety scores measured by Leibowitz Social Anxiety Scale (LSAS) scores in autistic adults compared with the control group taking placebo.4
Ibogaine-Assisted Psychotherapy for Substance Use Disorders
Three relevant primary studies were identified by Wheeler and Dyer (2020),4 none of which were identified by Andersen et al. (2021).14 In 1 retrospective study, Schenberg et al. (2014), ibogaine-assisted CBT was associated with a significant increase in the period of substance use abstinence compared with days before the first session.4 In 1 observational study, Brown and Alper (2018), the intervention referred to as “ibogaine treatment guidelines” was significantly associated with less opioid withdrawal symptoms measured by Subjective Opiate Withdrawal Scale (SOWS) scores at all time points compared with baseline.4 In the other observational study, Noller et al. (2018), ibogaine-assisted psychotherapy was associated with a significant reduction in withdrawal symptoms compared with baseline.4
Lysergic Acid Diethylamide–Assisted Psychotherapy for Mood Disorder
Both systematic reviews identified an RCT with 2 publications, Gasser et al. (2014) and Gasser et al. (2015), that reported that LSD-assisted psychotherapy was associated with significant reductions in anxiety symptoms measured by the STAI trait in patients with life-threatening disease compared with LSD at an active placebo dose.4,14
Ayahuasca-Assisted Psychotherapy for Mood Disorder
Wheeler and Dyer (2020) identified 1 observational study, Thomas et al. (2013), in which ayahuasca-assisted group talk therapy was associated with a significant reduction in cocaine use in 60% of the sample compared with baseline.4
Guidelines
No relevant guidelines were identified and thus no summary was provided.
Limitations
There were several limitations to the clinical evidence identified in the literature search. The overall sample sizes in the individual trials or the primary studies in both systematic reviews were small, with more than half of the included studies with 20 or fewer participants.4,14 There was considerable heterogeneity between studies due to the differences in study design, populations, interventions, psychotherapy classification, comparators, and outcome measures. Psychotherapy was not classified in the same manner in the 2 systematic reviews.4,14 Many combinations of psychedelic drugs, psychotherapy, and outcomes were identified. Five mental disorders, 7 psychedelic drugs, and 9 types of psychotherapies were identified in the systematic review by Wheeler and Dyer (2020).4 The patient characteristics might not be comparable across time because of changes in diagnostic criteria and medical practice. For example, there were different versions of diagnostic criteria for the same mental illnesses over time. Andersen et al. only included primary studies using DSM-IV criteria for diagnosis in the literature search.14 In contrast, DSM-5 criteria were used in 2 recent trials that were not identified in the systematic reviews.10,18 More than 10 types of psychotherapy were identified in the 2 systematic reviews, but it remained unclear whether the same type of psychotherapy was implemented with similar quality or intensity.4,14 Due to the heterogeneity between studies, it was difficult to quantitatively summarize the results across studies and only 1 pooled analysis of 6 trials using MDMA-assisted psychotherapy for treating PTSD by the same group of researchers was identified in 1 of the 2 systematic reviews.4,14 Moreover, 12 of the 31 uniquely identified publications in the 2 systematic reviews were single-arm or observational studies that lacked control groups to assess between-group effectiveness.4,14
There was a lack of long-term safety and efficacy studies in the identified systematic reviews, because most studies — 27 out of 31 primary relevant studies — followed up participants for less than or equal to 1 year.4,14
One primary study was conducted in Canada18 and the applicability of the findings in other studies to Canadian contexts was unclear. Currently, there is a demand for legalizing the use of psychedelic drugs in Canada.19 The availability of psychedelic-assisted therapy in Canada was also unclear, as there was only 1 included primary study that was conducted in Canada.
Conclusions and Implications for Decision or Policy-Making
Two systematic reviews,4,14 3 RCTs,10,15,16 and 2 safety trials17,18 that adopted any psychedelic-assisted psychotherapy for mood disorder, substance use disorder, and PTSD were identified.
Two systematic reviews included 31 unique relevant publications.4,14 Wheeler and Dyer (2020) identified 30 of the relevant publications.4 Several combinations of psychedelic drugs, psychotherapy, and mental illnesses were identified. Psilocybin was the psychedelic substance most tested in the primary studies in the 2 systematic reviews.4,14 Manualized therapy (not defined) and non-directive support (not defined) were the psychotherapies most frequently evaluated in the primary studies included in the systematic reviews by Andersen et al. (2021)14 and Wheeler and Dyer (2020),4 respectively. Anxiety and depression were the medical conditions that most primary studies evaluated.4,14 Different measures for PTSD symptoms, depression symptoms, anxiety symptoms, substance dependence, patients’ subjective experiences, and adverse events were used in primary studies.4,14 Patients were followed up for 1 week to 3 years, if reported.4,14
Overall, MDMA-assisted psychotherapy for PTSD (8 primary studies) and psilocybin-assisted psychotherapy for treatment-resistant depression (7 primary studies) were the strategies most tested in the primary studies in the systematic reviews.4,14 Andersen et al. (2021) concluded that, in general, the therapeutic effects seemed to last for week or months after 1 to 3 treatment sessions and no severe adverse events were reported in the primary studies.14 Wheeler and Dyer (2020) concluded that, in general, psychedelic drugs were associated with significant improvement in outcomes related to mental illnesses and no serious and long-term adverse events were reported in the primary studies.4 Wheeler and Dyer (2020) also discussed a separately published pooled analysis of 6 primary studies examining MDMA-assisted psychotherapy for PTSD that led to FDA-designated breakthrough therapy.4
Two of the 3 RCTs identified used ketamine-assisted psychotherapy for substance use or dependence and were published by the same first author.15,16 Dakwar et al. (2020) concluded that a single dose of ketamine infusion was associated with significant improvement in patients with alcohol dependence receiving motivational enhancement therapy compared with midazolam infusion.15 Dakwar et al. (2019) concluded that ketamine-assisted psychotherapy (mindfulness-based relapse prevention) was associated with higher rates of abstinence in cocaine-dependent adults 6 months later.16 The third RCT by Davis et al. (2020) concluded that psilocybin-assisted supportive psychotherapy was efficacious in treating MDD.10
Two single-arm safety trials used MDMA-assisted psychotherapy to treat patients with alcohol use disorder or PTSD.17,18 MDMA-assisted psychotherapy was well-tolerated and no serious adverse effects were reported.17,18
Despite some signals of possible effectiveness of psychedelic-assisted psychotherapy in the identified literature, there were several limitations to the clinical evidence that reduce certainty in the findings. The sample sizes in the primary studies included in the systematic reviews were mostly small, with fewer than 20 participants in more than half of the primary studies.4,14 The follow-up after intervention was relative short (i.e., 1 week to 3 years; less than or equal to 1 year in 27 out of 31 relevant publications), if reported.4,14 There was considerable heterogeneity between studies due to differences in study design, populations, interventions, psychotherapy, and outcome measures. Psychotherapy was not classified in the same manner in the 2 systematic reviews.4,14 The systematic review authors reported that quantitative synthesis of effectiveness data were not feasible for most psychedelic-assisted psychotherapy and only 1 pooled analysis of 6 trials by the same group of researchers was identified within 1 included systematic review.4 The generalizability of the interventions examined in the literature to Canadian contexts was unclear. The availability of psychedelic-assisted psychotherapy was not clear in Canada.
With respect to future research, RCTs sufficiently powered to assess the clinical effectiveness of psychedelic-assisted psychotherapy, compared to other active interventions or placebo, would reduce uncertainty. The long-term effectiveness of psychedelic-assisted psychotherapy also remains uncertain.
References
1.Centre for Addiction and Mental Health. Hallucinogens. Toronto, ON: Centre for Addiction and Mental Health; 2009: https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/hallucinogens. Accessed May 22, 2021.
2.National Institute on Drug Abuse. Hallucinogens DrugFacts. Bethesda (MD): National Institute on Drug Abuse; 2019: https://www.drugabuse.gov/publications/drugfacts/hallucinogens. Accessed May 22, 2021.
3.Nichols DE. Psychedelics. Pharmacol Rev. 2016;68(2):264-355. PubMed
4.Wheeler SW, Dyer NL. A systematic review of psychedelic-assisted psychotherapy for mental health: An evaluation of the current wave of research and suggestions for the future. Psychol Conscious (Wash D C). 2020;7(3):279-315.
5.Schenberg EE. Psychedelic-Assisted Psychotherapy: A Paradigm Shift in Psychiatric Research and Development. Front Pharmacol. 2018;9:733. PubMed
6.Kim J, Mierzwinski-Urban M. Ketamine for treatment-resistant depression or post-traumatic stress disorder in various settings: A review of clinical effectiveness, safety, and guidelines. Ottawa (ON): CADTH; 2018.
7.Li KX, Loshak H. Intravenous Ketamine for Adults with Treatment-Resistant Depression or Post-Traumatic Stress Disorder: A Review of Clinical Effectiveness, Cost-Effectiveness and Guidelines. Ottawa (ON): CADTH; 2019.
8.Trope A, Anderson BT, Hooker AR, Glick G, Stauffer C, Woolley JD. Psychedelic-Assisted Group Therapy: A Systematic Review. J Psychoactive Drugs. 2019;51(2):174-188. PubMed
9.Chao Y-S, Ford C. Cognitive Behavioural Therapy for Chronic Non-Cancer Pain: A Review of Clinical Effectiveness. Ottawa (ON): CADTH; 2019.
10.Davis AK, Barrett FS, May DG, et al. Effects of Psilocybin-Assisted Therapy on Major Depressive Disorder: A Randomized Clinical Trial. JAMA Psychiatry. 2020;04:04.
11.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
12.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Andersen KAA, Carhart-Harris R, Nutt DJ, Erritzoe D. Therapeutic effects of classic serotonergic psychedelics: A systematic review of modern-era clinical studies. Acta Psychiatr Scand. 2021;143(2):101-118. PubMed
15.Dakwar E, Levin F, Hart CL, et al. A Single Ketamine Infusion Combined With Motivational Enhancement Therapy for Alcohol Use Disorder: A Randomized Midazolam-Controlled Pilot Trial. Am J Psychiatry. 2020;177(2):125-133. PubMed
16.Dakwar E, Nunes EV, Hart CL, et al. A Single Ketamine Infusion Combined With Mindfulness-Based Behavioral Modification to Treat Cocaine Dependence: A Randomized Clinical Trial. Am J Psychiatry. 2019;176(11):923-930. PubMed
17.Sessa B, Higbed L, O'Brien S, et al. First study of safety and tolerability of 3,4-methylenedioxymethamphetamine-assisted psychotherapy in patients with alcohol use disorder. J Psychopharmacol. 2021;35(4):375-383. PubMed
18.Monson CM, Wagner AC, Mithoefer AT, et al. MDMA-facilitated cognitive-behavioural conjoint therapy for posttraumatic stress disorder: an uncontrolled trial. Eur J Psychotraumatol. 2020;11(1):1840123. PubMed
19.Zeidler M. Growing popularity of psychedelic therapy creates demand for underground guides. CBC News 2021; https://www.cbc.ca/news/canada/british-columbia/therapeutic-psychedelics-underground-guides-1.5929751. Accessed May 20, 2021.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Andersen et al. (2021),14 UK Funding not reported | 10 psychedelic- assisted therapy studies (16 papers) in total; 12 publications relevant to this report Relevant studies: 1 randomized, placebo-controlled, crossover trial, 2 open-label pre-post trials; 1 pre-post trial 1 RCT without between-group comparison, and 3 others not specified Eligibility criteria: single-blind and double-blind placebo-controlled randomized trials, open-label trials, and proof-of-concept trials Search time frame: January 1st, 2000 to May 1st, 2020 | Sample sizes ranging from 10 to 29 participants in relevant studies Patients with cancer-related anxiety and depression disorders (3 trials, 3 relevant), illness-related anxiety and depressive disorders (2 trial, 1 relevant), depressive disorders (2 trials, 1 relevant), obsessive-compulsive disorder (1 trial, 1 relevant), and substance use disorders (2 trials, 2 relevant) 4 additional publications included follow-up results for relevant trials Eligibility criteria: adults (18 years and older) diagnosed with a psychiatric disorder by their general practitioners and/or by structured clinical interviews using DSM or ICD criteria | Psychedelics Treated with psilocybin (7 trials, 10 publications relevant) or LSD (1 trial, 2 relevant publications) Psychotherapies Non-directive support: 4 publications Brief support: 3 publications CBT: 3 publications MET: 1 publication Psychotherapy not specified: 1 publication Comparators: Baseline (7 publications), low-dose psychedelic drugs (3 publications), and niacin (2 publications) | Depression outcomes: BDI, MADRS, HAM-D, GRID-HAM-D-17, SHAPS, QIDS-SR, POMS, and the depression subscale of the HADS-D Patient-rated anxiety outcomes: STAI-T and STAI-S, anxiety subscale of the HADS-A Clinician-rated anxiety outcome: HAM-A Substance use/dependence disorders outcome: TLFB Subjective experience rating scales: MEQ30 and 43-item version MEQ43, 11D-ASC, 5D-ASC, HRS, and SOCQ Follow-up: 3 months to 3 years, if reported |
Wheeler and Dyer (2020),4 Canada Funding not reported | 43 studies included, 30 relevant to this report Among relevant publications:
Case studies excluded Search time frame: 1990 to search date (not reported) | Patients with anxiety and depression (3 relevant publications), anxiety and depression associated with terminal illness (5 relevant publications), substance use disorders (9 relevant publications), PTSD (7 relevant publications), treatment-resistant depression (5 relevant publications), and OCD (1 relevant publication) Eligibility criteria: adults (at least 18 years of age) for a mental health condition Sample sizes: 25 relevant publications with a sample size of < 31 participants. 4 with a sample size of between 31 and 75 participants 1 with a sample size of 235 participants | Psychedelics Psilocybin (10 relevant publications), MDMA (9 relevant), ibogaine (3 relevant), ketamine (4 relevant), ayahuasca (1 relevant), LSD (2 relevant), and nitrous oxide (1 relevant) Psychotherapies Non-directive support: 6 relevant publications Manualized therapy for PTSD: 6 relevant CBT: 5 relevant Brief support: 3 relevant Group talk therapy: 1 relevant MET: 1 relevant Ibogaine support guidelines: 1 relevant Existential psychotherapy: 2 relevant Mindfulness-based therapy: 1 relevant Not specifying the type of psychotherapy: 4 relevant Comparators: baseline (13 relevant), low-dose psychedelics (7 relevant), placebo (6 relevant), niacin (2 relevant), and unspecified (2 relevant) | Primary outcomes: questionnaires for anxiety (including HADS-A, BDI, STAI-S, and STAI-T), depression (including QIDS-16, STAI-T, BDI, SHAPS, MADRS), substance use disorder (including HRS, 5D-ASC, MEQ, and YBOCS), PTSD (clinician-administered continuous measures of PTSD symptom severity such as CAPS). Self-rated PTSD symptom scales eligible if no clinician-administered scales Follow-up: 1 week to 30 months, if reported |
11D-ASC = 11-Dimensional Altered States of Consciousness rating scale; 5D-ASC = 5-Dimensional Altered States of Consciousness rating scale; BDI = Beck Depression Inventory; CAPS = Clinician-Administered PTSD Scale; CBT = cognitive behavioural therapy; DMT = dimethyltryptamine; DSM = Diagnostic and Statistical Manual of Mental Disorders; GRID-HAM-D-17 = GRID Hamilton Rating Scale for Depression 17 items; HADS-A = Hospital Anxiety Depression Scale; HADS-D = Hospital Anxiety and Depression Scale subscale; HAM-A = Hamilton Anxiety Rating Scale; HAM-D = Hamilton Depression Rating Scale; HRS = Hallucinogen Rating Scale; ICD = International Classification of Diseases; LSD = lysergic acid diethylamide; MADRS = Montgomery-Åsberg Depression Rating Scale; MDMA = 3,4-methylenedioxymethamphetamine; MEQ = Mystical Experience Questionnaire; MET = motivational enhancement therapy; OCD = obsessive-compulsive disorder; POMS = Profile of Mood States; PTSD = post-traumatic stress disorder; QIDS-SR = Quick Inventory of Depressive Symptomatology-Self; RCT = randomized controlled trial; SHAPS = Snaith-Hamilton Pleasure Scale; SOCQ = State of consciousness questionnaire; STAI-T/STAI-S = Spielberger's State-Trait Anxiety Index; TLFB = Timeline Followback tool; YBOCS = Yale-Brown Obsessive Compulsive Scale.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
RCTs | ||||
Dakwar et al. 2020,15 US Funding: National Institute on Alcohol Abuse and Alcoholism, the National Institute on Drug Abuse, and New York State Psychiatric Institute | Randomized controlled, double-blinded, single-centre trial Registration: NCT02539511 | 40 treatment-seeking adults with alcohol dependence Mean age = 53 years Female = 52.5% Average number of drinks per day 7 days before consent = 6.6 Inclusion criteria: < 70 years old, no medical illness or psychiatric comorbidity, DSM-IV criteria for alcohol dependence and minimum use daily (at least 4 heavy drinking days over the past 7 days) or weekly (35 drinks per week for men and 28 drinks per week for women), and not using other substances | Psychedelics Ketamine hydrochloride (a 2-minute 0.11 mg/kg bolus in saline followed by a 50-minute slow-drip IV infusion of 0.6 mg/kg) Psychedelic drugs provided in the second week of the 5-week trial Psychotherapies Motivational enhancement therapy for both groups (various strategies to promote motivation and self-directed change): 6 sessions in 5 weeks; engaging participants to explore goals and elicit motivations in both groups Comparator Active control (a 2-minute saline bolus followed by a 50-minute slow-drip IV infusion of midazolam, 0.025 mg/kg) with MET | Primary outcome: self-reported drinking days by timeline followback after the infusion Secondary outcomes: reduction in heavy drinking days (more than 4 drinks per day for men and more than 3 drinks per day for women) and others Follow-up: 6 months after the trial |
Davis et al. (2020),10 US Funding: a crowd-sourced funding campaign organized by Tim Ferriss, the Riverstyx Foundation; Tim Ferriss, Matt Mullenweg, Craig Nerenberg, Blake Mycoskie, the Steven and Alexandra Cohen Foundation, and NIDA | Randomized, clinician-blinded, waiting list–controlled, single-centre clinical trial | N = 24, mean age = 39.8 years, female = 16%, mean time with depression = 21.5 years Inclusion criteria: adults aged 21 to 75 years with an MDD diagnosis (DSM-5), not currently using antidepressant medications, and without histories of psychotic disorder, serious suicide attempt, or hospitalization | Immediate Treatment Condition 8 weeks, with at least 18 in-person visits (supportive psychotherapy, 11 hours), including 2 day-long psilocybin administration sessions Psilocybin dose: moderately high (20 mg/70 kg) in session 1 and high (30 mg/70 kg) in session 2 Delayed Treatment Condition 8-week delay period of the delayed treatment group | Primary outcomes: 17-item Hamilton Rating Scale for Depression (0 to 7: no depression; 8 to 16: mild depression; 17 to 23: moderate depression; ≥ 24: severe depression) Secondary outcomes: depressive symptoms measured using Beck Depression Inventory II (score range: 0 to 63, higher = severe) and the 9-item Patient Health Questionnaire (score range: 0 to 27, higher = severe); the Columbia Suicide Severity Rating Scale (range: 0 to 5, higher = more intents to die); anxiety symptoms measured using the clinician-administered Hamilton Rating Scale for Anxiety (score range: 0 to 56, higher = severe anxiety) and the State-Trait Anxiety Index (score range: 0 to 80, higher = greater anxiety); and blood pressure and heart rates Follow-up: 1 month |
Dakwar et al. (2019),16 US Funding: NIDA | Randomized, double-blinded, single-centre trial Registration: NCT01535937 | 55 cocaine-dependent individuals Mean age = 47 years Female = 14% Median baseline cocaine use = 34.3 US dollars/day Inclusion criteria: medically healthy treatment-seeking adults younger than age 70; DSM-IV criteria for cocaine dependence, with no psychiatric comorbidity; minimum cocaine use criteria over the 4-week period preceding screening (1 occasion of cocaine use per week at $200; 2 occasions of cocaine use per week at $40 each time; or 3 or more occasions of cocaine use a week at any amount; and urine toxicology indicative of cocaine use on at least 1 occasion during screening) | Psychedelics 40-minute IV infusion of ketamine (0.5 mg/kg, once) or midazolam (the control condition, 0.025 mg/kg, once) Psychotherapies Both groups receiving ketamine or midazolam during a 5-day inpatient stay, during which they also initiated a 5-week course of mindfulness-based relapse prevention (daily sessions on study days 2 to 5 during inpatient phase, then weekly sessions from study week 2 to 5) that “cultivate “mindfulness,” an attitude of deliberate, present-centred awareness, coupled with a suspension of behavioural reactivity and of cognitive associations, judgments, and distortions” (p. 924)16 | Primary outcomes: end-of-study abstinence and time to relapse (defined as first use or dropout); cocaine use assessed through self-report and urine toxicology Follow-up: 6 months |
Safety trials | ||||
Sessa et al. (2021),17 UK Funding and support statements: “sponsored and approved by Imperial College London” (p. 376); “The authors are grateful to the Alexander Mosley Charitable Trust for the entire funding of the study” (p. 383) | Open-label, 1-arm, within-subjects, proof-of-concept, safety and tolerability, feasibility, single-centre study No trial registration reported | 14 patients aged 18 to 65 years with alcohol use disorder (DSM-IV), who had recently undergone detoxification Mean age = 48 years Female = 6/14 | Psychedelic-assisted psychotherapies MDMA-assisted therapy for all patients 8-week course of recovery-based therapy comprising 10 psychotherapy sessions 1-hour psychotherapy sessions, employing aspects of motivational interviewing and “third-wave” cognitive behavioural approaches MDMA administration during a 6- to 8-hour assisted therapy session at sessions 3 and 7 MDMA dose: an initial oral dose of 125 mg MDMA and a booster dose of 62.5 mg MDMA 2 hours later | Primary outcomes: number of patients completing the 8-week psychotherapy course, the number accepting the second booster dose of MDMA on drug-assisted days, and adverse events Secondary outcomes: changes in drinking behaviour (measured by units per week consumed at 3, 6, and 9 months since completion of detoxification), measures of mental well-being, psychosocial functioning, quality of life and concomitant drug use (Subjective Units of Distress and Severity of Alcohol Dependence questionnaires) Follow-up: 9 months |
Monson et al. (2020),18 Canada Authors from Canada and the US Funding: Multidisciplinary Association for Psychedelic Studies | Single-arm, uncontrolled trial for safety, tolerability, and efficacy of MDMA-facilitated CBCT Trial registration: NCT02876172 | 6 patients with their 6 partners Average age of the patients = 47 years, 66.6% male (n = 4), all Caucasian, and all heterosexual couples, 5 with a history of multiple traumatic events Inclusion criteria: 1 partner with a current PTSD diagnosis according to CAPS-5, with a duration of at least 6 months, at least 18 years old; generally healthy per physical examination and medical history | Psychedelic-assisted psychotherapy CBCT for PTSD: psychoeducation about trauma and relationships, increasing relational safety, communication skills, tools for behavioural approach, and dyadic cognitive intervention related to problematic trauma-related and relationship cognitions 15 sessions with various activities in 7 weeks MDMA: 2 sessions (6- to 8-hours-long) timed to synergize with the CBCT interventions (i.e., provided after CBCT sessions 5 and 11 during 2 intensive treatment weekends) MDMA dose: 75 mg MDMA in the first MDMA session and 100 mg in the second MDMA session, with an optional supplemental half- dose 1.5 hours later in both sessions | Primary outcomes: adverse events; SCID-5 at baseline; the CAPS-5 for PTSD symptoms; the PCL-5, patient and partner versions; CSI Secondary outcomes: self-report measures of the BDI-II for depression; the Pittsburgh Sleep Quality Questionnaire for sleep disturbances; the Emotion Regulation Questionnaire for emotion regulation strategies; and the Traumatic and Attachment Belief Scale for trauma-related beliefs Follow-up: 6 months |
BDI = Beck Depression Inventory; CAPS-5 = Clinician- Administered PTSD Scale-5; CBCT = cognitive-behavioural conjoint therapy; CSI = Couples Satisfaction Index; DSM = Diagnostic and Statistical Manual of Mental Disorders (IV and 5 are fourth and fifth editions); MDD = major depressive disorder; MDMA = 3,4-methylenedioxymethamphetamine; MET = motivational enhancement therapy; NIDA = National Institute on Drug Abuse; PCL-5 = PTSD Checklist for DSM-5; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; SCID-5 = Structured Clinical Interview for DSM-5.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 211
Strengths | Limitations |
Andersen et al. (2021)14 | |
PICO components described in the research questions and inclusion criteria Selection of study design explained Comprehensive literature searches Study selection in duplicate Data extraction in duplicate Heterogeneity in the results explained | Review methods not published before the conducting of the review A list of excluded studies not provided Included studies not described in detail Risk of bis in primary studies not assessed Sources of funding for primary studies not reported Meta-analysis not conducted because of study heterogeneity Risk of bias in primary studies not accounted for while interpreting the results Publication bias not assessed Review authors’ conflict of interest not reported |
Wheeler and Dyer (2020)4 | |
PICO components described in the research questions and inclusion criteria Selection of study design explained Comprehensive literature searches Study selection in duplicate Data extraction in duplicate Included studies described in detail | Review methods not published before the conducting of the review A list of excluded studies not provided Risk of bias in primary studies not assessed Sources of funding for primary studies not reported Meta-analysis not conducted because of study heterogeneity Risk of bias in primary studies not accounted for while interpreting the results Heterogeneity in the results not explained Publication bias not assessed Review authors’ conflict of interest not reported |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PICO = population, intervention, comparator, and outcomes.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black checklist12
Strengths | Limitations |
RCTs | |
Dakwar et al. (2020)15 | |
Study objectives described Outcomes described in the methods The characteristics of the included patients described Interventions of interest described Distributions of principal confounders compared between groups Main findings clearly described Random variability for the results of the main outcomes provided Adverse events reported Patients lost to follow-up reported 95% CIs reported and P values not reported Patients blinded to the treatment Outcome assessors blinded to the treatment Selective reporting of patient data not likely The time period between intervention and outcome the same for cases and controls Appropriate statistical tests used to assess the outcomes Reliable compliance with the treatment Accurate outcome measures Participants in both study groups recruited from the same population and the same period of time Subjects randomized to groups | Whether the patients invited or included were representative of the entire population was not clear Whether the clinical settings in the trial were representative of the treatment the majority of patients received was unclear Treatment concealment not reported |
Davis et al. (2020)10 | |
Study objectives described Outcomes described in the methods The characteristics of the included patients described Interventions of interest described Distributions of principal confounders compared between groups Main findings clearly described Random variability for the results of the main outcomes provided Adverse events reported Patients lost to follow-up reported Actual P values reported Outcome assessors blinded to the treatment Selective reporting of patient data not likely The time period between intervention and outcome the same for cases and controls Appropriate statistical tests used to assess the outcomes Reliable compliance with the treatment Accurate outcome measures Participants in both study groups recruited from the same population and the same period of time Subjects randomized to groups Power analysis for sample sizes conducted | Whether the patients invited or included were representative the entire population was not clear Whether the clinical settings in the trial were representative of the treatment the majority of patients received was unclear Treatment concealment not reported Patients not blinded to the treatment |
Dakwar et al. (2019)16 | |
Study objectives described Outcomes described in the methods The characteristics of the included patients described Interventions of interest described Distributions of principal confounders compared between groups Main findings clearly described Random variability for the results of the main outcomes provided Adverse events reported Patients lost to follow-up reported 95% CIs reported and P values not reported Patients blinded to the treatment Outcome assessors blinded to the treatment Selective reporting of patient data not likely The time period between intervention and outcome the same for cases and controls Appropriate statistical tests used to assess the outcomes Reliable compliance with the treatment Accurate outcome measures Participants in both study groups recruited from the same population and the same period of time Subjects randomized to groups | Whether the patients invited or included were representative of the entire population was not clear Whether the clinical settings in the trial were representative of the treatment the majority of patients received was unclear Treatment concealment not reported |
Safety trials | |
Sessa et al. (2021)17 | |
Study objectives described Outcomes described in the methods The characteristics of the included patients described Interventions of interest described Main findings clearly described Random variability for the results of the main outcomes provided Adverse events reported Patients lost to follow-up reported 95% CIs reported and P values not reported Selective reporting of patient data not likely Appropriate statistical tests used to assess the outcomes Reliable compliance with the treatment Accurate outcome measures | Whether the patients invited or included were representative of the entire population was not clear Whether the clinical settings in the trial were representative of the treatment the majority of patients received was unclear Power analysis for sample sizes not conducted Distributions of principal confounders not compared because of single-arm design Patients not blinded to the treatment Outcome assessors not blinded to the treatment |
Monson et al. (2020)18 | |
Study objectives described Outcomes described in the methods The characteristics of the included patients described Interventions of interest described Main findings clearly described Random variability for the results of the main outcomes provided Actual P values reported Adverse events reported Patients lost to follow-up reported Selective reporting of patient data not likely Appropriate statistical tests used to assess the outcomes Reliable compliance with the treatment Accurate outcome measures | Whether the patients invited or included were representative of the entire population was not clear Whether the clinical settings in the trial were representative of the treatment the majority of patients received was unclear Power analysis for sample sizes not conducted Distributions of principal confounders not compared because of single-arm design Patients not blinded to the treatment Outcome assessors not blinded to the treatment |
CI = confidence interval; RCT = randomized controlled trial.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Included Systematic Reviews
Andersen et al. (2021)14
Main Study Findings
Twelve included publications were individually described, 1 [Garcia-Romeu et al. (2014)] of which was uniquely identified by Andersen et al. (2021).14
No meta-analysis was identified.
Mental illness diagnoses were studied: cancer, or illness-related anxiety and depression disorders, major depressive disorder, obsessive-compulsive disorder, or substance use disorder.
Interventions: psilocybin (n = 10) and lysergic acid diethylamide (LSD) (n = 2).
Mood and anxiety disorders (4 publications, 3 relevant)
Carhart-Harris et al. (2018) and Carhart-Harris et al. (2016)
Open-label, uncontrolled, including subjects from Carhart- Harris et al. (2016)
20 patients with moderate (2/20) or severe (18/20) unipolar major treatment-resistant depression
2 doses of psilocybin: a moderate [safety test] dose (10 mg), and 1 week later followed by a high dose (25 mg) versus baseline
Significant short to mid-term reductions in Quick Inventory of Depressive Symptoms–Self-Report (QIDS-SR16) scores 1 to 5 weeks post-therapy (P < 0.001), 3 months (P < 0.001), and 6 months (P = 0.004)
Moreno et al. (2006)
Modified double-blind
9 patients with obsessive-compulsive disorder (OCD), Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria
Up to 4 administrations of psilocybin separated by at least 1 week in an escalating dosage sequence of 100 mcg/kg, 200 mcg/kg, and 300 mcg/kg
Active placebo-like dose (25 mcg psilocybin) randomly assigned once at any of the last 3 sessions
Decreases in OCD symptoms score (Yale-Brown obsessive-compulsive scale [YBOCS]) in 9 subjects at 1 or more of the testing sessions (decreases from 23% to 100%)
End-of-life anxiety and depression (4 relevant studies, 5 publications)
Grob et al. (2011)
Double-blind, placebo-controlled
12 subjects with a life-threatening cancer diagnosis and a DSM-IV diagnosis of either acute stress disorder, generalized anxiety disorder (GAD), anxiety disorder because of cancer, or adjustment disorder with anxiety
Active placebo session (niacin 250 mg) versus 1 psilocybin session (0.2 mg/kg dose)
No significant between-group differences were found on any of the outcome measures: Beck Depression Inventory (BDI), Spielberger State-Trait Anxiety Index, Trait scale and State scale (STAI-T, and STAI-S). Comparing means of the whole group at baseline with scores at follow-up (after both groups received the psilocybin) shows significant reduction in trait anxiety at 1 and 3 months, and in depression at 6-month follow-up (t = 2.71, within-group comparison).
Gasser et al. (2014) and Gasser et al. (2015)
Double-blind, randomized, crossover, active placebo-controlled trial
12 patients with a baseline STAI trait or state score of higher than 40 and meeting DSM-IV criteria for an anxiety (n = 6) or depression disorder (n = 7) associated with life-threatening diseases
2 doses of active LSD (200 mcg) versus LSD at an active placebo dose (20 mcg) separated 2 to 3 weeks apart
Crossover 2 months after experiment: placebo group and additional open-label to the LSD (200 mcg) treatment
2-month follow-up: significant between-group differences in state anxiety (P = 0.021, data not reported)
After crossover, post hoc within-group analysis: significant reductions of trait and state anxiety at 2 and 12-month follow-up, compared to baseline (data not reported)
Griffiths et al. (2016)
Randomized crossover
Patients with life-threatening cancer diagnosis and DSM-IV mood disorder: chronic adjustment disorder with anxiety (n = 11) or with mixed anxiety and depression (n = 11), major depressive disorder (MDD) (n = 14), dysthymic disorder (n = 6), GAD (n = 5), or a combination of GAD and MDD (n = 4)
Placebo-like low-dose first group (1 or 3 mg/70 kg) versus a high-dose first group (22 or 30 mg/70 kg), with a crossover after 5 weeks
6-month follow-up: “an average clinical response rate of 83% for anxiety and 78% for depression among the whole group, with remission rates of 57% and 65%, respectively” (p. 108)14
Ross et al. (2016)
Randomized, double-blind, placebo-controlled, crossover
29 patients with anxiety of either adjustment disorder (90%) or GAD (10%)
Psilocybin first (dose not specified) versus active placebo (niacin) first, with a crossover at 7 weeks
Significant between-group reductions in the psilocybin-first group at 7 weeks: “clinical anti-depressive response rate in 83% of the patients (using BDI) and a 58% anxiolytic response rate by measure of HADS-A (vs. a 14% response rate in the placebo group for both measures)” (p. 108)
Significant symptom reductions in the psilocybin-first group than the niacin-first group for all clinical outcome measure assessments (Hospital Anxiety Depression Scale and subscales [HADS-A, HADS-D, HADS-T] and BDI) up until the crossover
“For both groups, all clinical outcome scores were significantly reduced at the 8 months’ follow-up in comparison with baseline” (p. 108)14
Substance use disorders (2 relevant studies, 3 publications)
Bogenschutz et al. (2015)
Open-label, single-arm
10 patients with DSM-IV–established diagnosis of alcohol dependence
Psilocybin administered first at week 4 (moderate-high dose of 21 mg/70 kg) and second at week 8 (high dose 28 mg/70 kg)
“Significant reductions in drinking days and heavy drinking days were observed at all assessment time points throughout this 32-week follow-up period” (p. 109)14
Johnson et al. (2014) and Johnson et al. (2017)
Also included in Wheeler and Dyer (2020)4
Single-arm
15 nicotine-dependent smokers
Psilocybin: week 5 (moderate dose, 20 mg/70 kg), week 7 (high dose, 30 mg/70 kg), and week 13 (moderate or high dose, 30 mg/70 kg)
6-month follow-up: 80% of the participants (12/15) abstinent; significant reductions in both self-reported daily smoking, urine cotinine, and breath carbon monoxide, compared to baseline
Long-term follow-up: 9 abstinent (mean 30 months post-first psilocybin session)
Quality of the subjective experience as clinical predictor
Garcia-Romeu et al. (2014)
Mystical/peak experience predicted long-term clinical outcome (30 months) in 1 trial (psilocybin for smoking cessation), statistics not reported in Andersen et al. (2021)14
Author’s Conclusion
“For a majority of patients, the therapeutic effects appeared to be long-lasting (weeks-months) after only 1 to 3 treatment session(s). All studies were conducted in line with guidelines for the safe conduct of psychedelic therapy, and no severe adverse events were reported.” (p. 101)14
Wheeler and Dyer (2020)4
Main Study Findings
Forty-three studies included; 30 publications relevant
Psilocybin for anxiety and depression associated with life-threatening cancer diagnoses
3 relevant studies, summarized in Andersen et al. (2021)14
Grob et al. (2011): summarized in Andersen et al. (2021)14
Griffiths et al. (2016): summarized in Andersen et al. (2021)14
Ross et al. (2016): summarized in Andersen et al. (2021)14
Psilocybin for treatment-resistant depression
4 relevant publications, 2 also identified and summarized by Andersen et al. (2021)14
Carhart-Harris et al. (2016) and Carhart-Harris et al. (2018): summarized in Andersen et al. (2021)14
Erritzoe et al. (2018): changes in personality measures (Revised Neuroticism, Extraversion, Openness Personality Inventory [NEO-PI-R]) for patients undergoing psychedelic therapy for depression; follow-up of Carhart-Harris et al. (2016). “NEO-PI-R domain scores changed significantly from baseline to 3 months post-psilocybin; Neuroticism scores decreased (T score change: –5.7, p =.002), both Extraversion and Openness increased (t = 6.5, p <.001, and 4.9, p =.012, respectively).” (p. 10)4
Stroud et al. (2018): compared to baseline, emotional face processing faster in the psilocybin group (P = 0.004, Cohen's d effect size statistic = 0.876), but not in the control group (P = 0.263, Cohen's d effect size statistic = 0.302)
Psilocybin for substance use disorders
2 relevant studies (3 publications) included; summarized by Andersen et al. (2021)14
Johnson et al. (2014): summarized in Andersen et al. (2021)14
Bogenschutz et al. (2015): summarized in Andersen et al. (2021)14
Johnson et al. (2017): summarized in Andersen et al. (2021)14
N-methyl-d-aspartate (NMDA) receptor antagonists for anxiety and depression
3 studies, 3 relevant
Wilkinson et al. (2017): “Of 16 patients, 8 achieved response, and 7 achieved remission; ketamine responders had lower baseline MADRS scores compared to non-responders (29.6 vs. 33.9, t = 2.34, p =.035)”(p. 13); ketamine with CBT associated with “sustained improvements in depression scores, and relapse occurred at a median duration of 12 weeks, which was longer than ketamine without psychotherapy” (p. 24)4
Dore et al. (2019): “Significant decrease in BDI and HAM-A scores from baseline to followup; BDI scores decreased and average of 11.24 points and HAM-A scores decreased an average of 5.5 points (p <.0001);” (p. 14);4 ketamine-assisted psychotherapy associated with significant decreases in depression and anxiety scores
Nagele et al. (2015): “At 2 hr and 24 hr after receiving nitrous oxide, depressive symptoms improved significantly compared with placebo (HDRS-21 difference at 2 hr, M = –4.8 points, 95% CI [–1.8, –7.8] points, p =.002; at 24 hr, M = –5.5 points, 95% CI [–2.5, –8.5] points, p <.001; comparison between nitrous oxide and placebo, p ” 0.001).” (p. 13)4; nitrous oxide-assisted psychotherapy associated with significant decreases in depression symptoms within 24 hours of administration
3,4-methylenedioxymethamphetamine (MDMA) for post-traumatic stress disorder (PTSD)
7 relevant publications, 5 analyzed in a primary study [Mithoefer et al. (2019)]
Mithoefer et al. (2019): a pooled analysis of 6 phase III randomized controlled trials (RCTs); 4 of which were published in 5 publications [Mithoefer et al. (2011), Mithoefer et al. (2013), Mithoefer et al. (2018); Oehen et al. (2013); Ot’alora et al. (2018)]. This pooled analysis led to 2 phase III trials (not included) and FDA-designated breakthrough therapy for MDMA-assisted psychotherapy for PTSD; “74 participants in the experimental group (75–125 mg of MDMA, 2 sessions) and 31 participants in the active control group (0–40 mg of MDMA, 2 sessions). The [Clinician-Administered PTSD Scale] CAPS-5 (Weathers, Keane, & Davidson, 2001) total scores were significantly different after the second experimental session, t(95) = –4.25, p <.0001, with the experimental group reporting a greater estimated mean drop in scores (M = –30.4, SE = 3.20) compared to the active control group (M = –10.5, SE = 4.46). Between-groups Cohen’s d effect size was 0.8, indicating a large treatment effect.” (p. 24 to 25)4
Bouso et al. (2008): “The 75 mg group obtained better scores on outcome measures compared to other 2 groups (50 mg and placebo), and the 50 mg group obtained better scores on outcome measures compared to placebo; statistical analysis was not performed.” (p. 15)4
Wagner et al. (2017): “ Significant interaction between change in Openness and CAPS scores, a greater increase in Openness correlated with a greater decrease in PTSD symptoms as measured by the CAPS, F(1, 17) = 5.68, p =.029; when Neuroticism was used as a covariate, there was a significant main effect of decreased CAPS scores regardless of treatment condition, F [statistic] (1, 17) = 20.48, p <.001.” (p. 16)4
Ibogaine for substance use disorders
3 relevant studies
Schenberg et al. (2014): retrospective study: “All of the women reported that they were abstinent at the time of contact, with 2 reporting a relapse, then remaining abstinent after a second ibogaine session; 38 men (57%) remained abstinent with no other treatments; there were significant increases in the period of abstinence achieved when comparing days before the first session (M [mean] = 88.30, SD [standard deviation] = 15.92, Mdn [median] = 60.00), after the first ibogaine session (M = 298.76, SD = 42.26, Mdn = 165.00), and after all sessions combined (M = 419.15, SD = 52.86, Mdn = 252.00; Friedman X2 = 23.471; p <.001.” (p. 18)
Noller et al. (2018): “ SOWS [Subjective Opiate Withdrawal Scale] scores showed a significant reduction in withdrawal symptoms from baseline (M = 25.2, SD = 12.57) to up to 24-hr post-treatment (M = 14.21, SD = 14.08; n = 14, p =.015).” (p. 18)4
Brown and Alper (2018): observational: “SOWS scores decreased from M = 31.0, SD = 11.6 pre-treatment to M = 14.0, SD = 9.8 at M = 76.5, SD = 30 hr post-treatment, t = 7.07, df = 26, p <.001; at 1-month follow-up, 15 patients (50%) reported no opioid use within the last 30 days; ASIC [Addiction Severity Index Composite] Drug Use and Legal and Family/Social Status scores were improved relative to baseline at all time points (p <.001).” (p. 19)4
Miscellaneous studies
7 relevant studies, 3 of which were identified and summarized in Andersen et al. (2021)14
Krupitsky et al. (2002): “…greater rate of abstinence in heroin addicts within first 2 years of follow-up, with roughly 16% of subjects remaining abstinent, compared with roughly 3% remaining abstinent in the low-dose group (p <.05).” (p. 20);4 ketamine-assisted psychotherapy (existential approach) with “a high dose of ketamine producing significantly greater rates of abstinence compared to a low dose” (heroin addiction). (p. 25)4
Krupitsky et al. (2007): “At 1-year follow-up, 13 out of 26 patients (50%) remained abstinent from the multiple ketamine therapies group, 6 out of 27 patients (22.2%) remained abstinent from the single ketamine therapy group (p <.05)” (p. 20);4 multiple ketamine sessions with greater abstinence rates compared with a single session at a 1-year follow-up (heroin addiction)
Moreno et al. (2006): summarized in Andersen et al. (2021)14
Gasser et al. (2014): summarized in Andersen et al. (2021)14
Thomas et al. (2013): ayahuasca group therapy for treating substance use disorders (including cocaine and cannabis): “Findings demonstrate decreases in 4WSUS [4 Week Substance Use Scale] scores for 40% of the participants, there was no change in cannabis use, and a statistically significant reduction was seen in cocaine use with 60% of the sample having used cocaine at baseline and 0% having used cocaine at the last follow-up.” (p. 21)4
Danforth et al. (2018): “At 1 month, the MDMA group had significantly greater improvements in Leibowitz Social Anxiety Scale scores compared to the control group, t(9) = 2.451, p =.037, 95% confidence interval [CI; 1.92, 47,87], placebo-subtracted Cohen’s d effect size was 1.4, 95% CI [0.074, 2.874]; similar results were observed from baseline to 6 months, t(9 = 2.454, p =.036, 95% CI [1.92, 47.01],” (p. 22)4; reductions in participants’ Liebowitz Social Anxiety Scale scores using MDMA-assisted psychotherapy for treating social anxiety in autistic adults.
Gasser et al. (2015): summarized in Andersen et al. (2021)14
Adverse events
Noller et al. (2018): “SOWS scores showed a significant reduction in withdrawal symptoms from baseline (M = 25.2, SD = 12.57) to up to 24-hr posttreatment (M = 14.21, SD = 14.08; n = 14, p =.015)” (p. 18)4; 1 death due to cardiac arrhythmia during an ibogaine session, without clear causes
“Mild adverse events were reported in 59% of the studies” (p. 25),4 concluded by Wheeler and Dyer (2020)4
Author’s Conclusion
“…psychedelics can significantly reduce clinical outcomes associated with these mental health conditions.” (p. 1)4
“Common themes identified from qualitative reports included increased acceptance and processing of emotions, connectedness to others, forgiveness, self-compassion, insights into the self, peak or mystical experiences, ego dissolution, positive changes in worldview, motivation and commitment to change, changes in the relationship to the substance of abuse for those with substance use disorder, and acceptance of death for those with terminal illness.” (p. 1)4
“No serious, long-term adverse events were reported directly attributable to drug ingestion.” (p. 1)4
Table 6: Summary of Findings of Included Primary Clinical Studies
Main study findings | Authors’ conclusion |
RCTs | |
Dakwar et al. (2020)15 | |
IV ketamine (0.71 mg/kg, n = 17) vs. midazolam (0.025 mg/kg, n = 23) with MET for patients with alcohol use disorder consuming an average of 5 drinks per day Clinical effectiveness
Safety
| “A single ketamine infusion was found to improve measures of drinking in persons with alcohol dependence engaged in motivational enhancement therapy.” (p. 125)15 |
Davis et al. 202010 | |
Immediate vs. delayed treatment of psilocybin-assisted therapy (supportive psychotherapy) in patients with MDD Completion
Depression rating
|
|
Dakwar et al. (2019)16 | |
Ketamine (0.5 mg/kg) vs. midazolam (control) with mindfulness-based relapse prevention in patients with cocaine dependence Abstinence
Relapse (dropout or use of cocaine)
Craving scores
Safety
| “A single ketamine infusion improved a range of important treatment outcomes in cocaine-dependent adults engaged in mindfulness-based behavioral modification, including promoting abstinence, diminishing craving, and reducing risk of relapse.” (p. 923)16 |
Safety trials | |
Sessa et al. (2021)17 | |
Patients with AUD experiencing 2 sessions with MDMA (187.5 mg each session) with psychological support, no control Safety
Alcohol use
| “This study provides preliminary support for the safety and tolerability of a novel intervention for AUD post detox.” (p. 375)17 |
Monson et al. (2020)18 | |
CBCT and MDMA for PTSD Completion
Safety
PTSD-related symptoms
Relationship adjustment
| “Our initial data indicates that MDMA delivered in combination with CBCT for PTSD appears to be safe, does not appear to be treatment-interfering, and may potentiate the treatment effects for PTSD and the larger relationship context in which it exists.” (p. 5)18 |
AUD = alcohol use disorder; CBCT = cognitive-behavioural conjoint therapy; CI = confidence interval; GAD-7 = Generalized Anxiety Disorder 7; GRID-HAMD = GRID Hamilton Depression Rating Scale; MDD = major depressive disorder; MDMA = 3,4-methylenedioxymethamphetamine; MET = motivational enhancement therapy; PHQ-9 = Patient Health Questionnaire 9; PTSD = post-traumatic stress disorder; QIDS-SR = Quick Inventory of Depressive Symptomatology-Self; vs. = versus.
Appendix 5: Overlap Between Included Systematic Reviews
Table 7: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Andersen et al. (2021)14 | Wheeler and Dyer (2020)4 |
Bogenschutz MP, et al. Journal of Psychopharmacology. 2015;29:289–299. | Yes | Yes |
Bouso JC, et al. Journal of Psychoactive Drugs. 2008;40:225–236. | No | Yes |
Brown TK, Alper K. The American Journal of Drug and Alcohol Abuse. 2018;44:24–36. | No | Yes |
Carhart-Harris RL, et al. The Lancet Psychiatry. 2016;3:619– 627. | Yes | Yes |
Carhart-Harris RL, et al. Psychopharmacology. 2018;235:399–408. | Yes | Yes |
Danforth AL, et al. Psychopharmacology. 2018;235:3137–3148. | No | Yes |
Dore J, et al. Journal of Psychoactive Drugs. 2019;51:189–198. | No | Yes |
Erritzoe D, et al. Acta Psychiatrica Scandinavica. 2018;138:368–378. | No | Yes |
Garcia-Romeu A, et al. Current Drug Abuse Reviews. 2014;7(3):157-164. | Yes | No |
Gasser P, et al. J Nerv Ment Dis. 2014;202(7):513-520. | Yes | Yes |
Gasser P, et al. J Psychopharmacol (Oxford, England). 2015;29(1):57-68. | Yes | Yes |
Griffiths R, et al. J Psychopharmacol. 2016;30(12):1181-1197. | Yes | Yes |
Grob CS, et al. Arch Gen Psychiatry. 2011;68(1):71-78. | Yes | Yes |
Johnson MW, et al. J Psychopharmacol. 2014;28(11):983-992. | Yes | Yes |
Johnson MW, et al. Am J Drug Alcohol Abuse. 2017;43(1):55-60. | Yes | Yes |
Krupitsky E, et al. Journal of Substance Abuse Treatment. 2002;23:273–283. | No | Yes |
Krupitsky EM, et al. Journal of Psychoactive Drugs. 2007;39:13–19. | No | Yes |
Mithoefer MC, et al. Journal of Psychopharmacology. 2011;25:439– 452. | No | Yes |
Mithoefer MC, et al. Journal of Psychopharmacology. 2013;27:28–39. | No | Yes |
Mithoefer MC, et al. The Lancet Psychiatry. 2018;5:486–497. | No | Yes |
Moreno FA, et al. J Clin Psychiatry. 2006;67(11):1735-1740. | Yes | Yes |
Nagele P, et al. Biologic Psychiatry. 2015;78:10–18. | No | Yes |
Noller GE, et al. The American Journal of Drug and Alcohol Abuse. 2018;44:37– 46. | No | Yes |
Oehen P, et al. Journal of Psychopharmacology. 2013;27:40– 52. | No | Yes |
Ot’alora GM, et al. Journal of Psychopharmacology. 2018;32:1295–1307. | NI | Yes |
Ross S, et al. J Psychopharmacol. 2016;30(12):1165-1180. | Yes | Yes |
Schenberg EES, et al. Journal of Psychopharmacology. 2014;28:993–1000. | No | Yes |
Stroud JB, et al. Psychopharmacology. 2018;235 :459– 466. | No | Yes |
Thomas G, et al. Current Drug Abuse Reviews. 2013;6:30– 42. | No | Yes |
Wagner MT, et al. Journal of Psychopharmacology. 2017;31:967–974. | No | Yes |
Wilkinson ST, et al. Psychotherapy and Psychosomatics. 2017;86:162–167. | No | Yes |
Appendix 6: References of Potential Interest
Systematic Reviews With Primary Studies Captured in More Comprehensive Reviews
1.Bahji A, Forsyth A, Groll D, Hawken ER. Efficacy of 3,4-methylenedioxymethamphetamine (MDMA)-assisted psychotherapy for posttraumatic stress disorder: A systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. 2020;96:109735. PubMed
2.Hoskins MD, Sinnerton R, Nakamura A, et al. Pharmacological-assisted Psychotherapy for Post-Traumatic Stress Disorder: a systematic review and meta-analysis. Eur J Psychotraumatol. 2021;12(1):1853379. PubMed
3.Trope A, Anderson BT, Hooker AR, Glick G, Stauffer C, Woolley JD. Psychedelic-Assisted Group Therapy: A Systematic Review. J Psychoactive Drugs. 2019;51(2):174-188. PubMed
4.Jerome L, Feduccia AA, Wang JB, et al. Long-term follow-up outcomes of MDMA-assisted psychotherapy for treatment of PTSD: a longitudinal pooled analysis of six phase 2 trials. Psychopharmacology (Berl). 2020;237(8):2485-2497. PubMed
5.Goldberg SB, Shechet B, Nicholas CR, et al. Post-acute psychological effects of classical serotonergic psychedelics: a systematic review and meta-analysis. Psychol Med. 2020;50(16):2655-2666. PubMed
6.Illingworth BJ, Lewis DJ, Lambarth AT, et al. A comparison of MDMA-assisted psychotherapy to non-assisted psychotherapy in treatment-resistant PTSD: A systematic review and meta-analysis. J Psychopharmacol. 2020:269881120965915. PubMed
7.Luoma JB, Chwyl C, Bathje GJ, Davis AK, Lancelotta R. A Meta-Analysis of Placebo-Controlled Trials of Psychedelic-Assisted Therapy. J Psychoactive Drugs. 2020;52(4):289-299. PubMed
Review Articles
8.Gorman I, Belser AB, Jerome L, et al. Posttraumatic Growth After MDMA-Assisted Psychotherapy for Posttraumatic Stress Disorder. J Trauma Stress. 2020;33(2):161-170. PubMed
9.Feduccia AA, Jerome L, Yazar-Klosinski B, Emerson A, Mithoefer MC, Doblin R. Breakthrough for Trauma Treatment: Safety and Efficacy of MDMA-Assisted Psychotherapy Compared to Paroxetine and Sertraline. Front Psychiatr. 2019;10:650. PubMed
10.Mithoefer MC, Feduccia AA, Jerome L, et al. MDMA-assisted psychotherapy for treatment of PTSD: study design and rationale for phase 3 trials based on pooled analysis of six phase 2 randomized controlled trials. Psychopharmacology (Berl). 2019;236(9):2735-2745. PubMed
11.Reiff CM, Richman EE, Nemeroff CB, et al. Psychedelics and Psychedelic-Assisted Psychotherapy. Am J Psychiatry. 2020;177(5):391-410. PubMed
12.Morgan L. MDMA-assisted psychotherapy for people diagnosed with treatment-resistant PTSD: what it is and what it isn't. Ann Gen Psychiatry. 2020;19:33. PubMed
Additional References
13.Barone W, Beck J, Mitsunaga-Whitten M, Perl P. Perceived Benefits of MDMA-Assisted Psychotherapy beyond Symptom Reduction: Qualitative Follow-Up Study of a Clinical Trial for Individuals with Treatment-Resistant PTSD. J Psychoactive Drugs. 2019;51(2):199-208. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca